North West Local Health Integration Network
95
975 Alloy Dr., Suite 201 Thunder Bay, ON, P7B 5Z8 • Tel: 807-684-9425 • Fax: 807-684-9533 • Toll Free: 1-866-907-5446 | www.northwestlhin.on.ca 975, prom. Alloy, Bureau 201 Thunder Bay, ON, P7B 5Z8 • Tél: 807 684 9425 • Télécopieur : 807 684 9533 • Sans frais : 1 866 907 5446 BOARD OF DIRECTORS Open Session Meeting Package Date: Tuesday, September 25, 2018 9:00 a.m. (Eastern) Location: North West LHIN 975 Alloy Drive First Floor Boardroom Thunder Bay, ON Teleconference: 1-855-392-2520 Access Code: 4252308#
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of North West Local Health Integration Network
975 Alloy Dr., Suite 201 Thunder Bay, ON, P7B 5Z8 • Tel: 807-684-9425 • Fax: 807-684-9533 • Toll Free: 1-866-907-5446 | www.northwestlhin.on.ca
975, prom. Alloy, Bureau 201 Thunder Bay, ON, P7B 5Z8 • Tél: 807 684 9425 • Télécopieur : 807 684 9533 • Sans frais : 1 866 907 5446
BOARD OF DIRECTORS
Open Session Meeting Package
Date: Tuesday, September 25, 2018 9:00 a.m. (Eastern)
Location: North West LHIN 975 Alloy Drive First Floor Boardroom Thunder Bay, ON
Teleconference: 1-855-392-2520 Access Code: 4252308#

The following were identified during the June, 2007 Board of Directors retreat and adopted as Behavioural
Expectations at the Board of Directors Meeting of November 20, 2007.
Rules–of–the-Road: Behavioural Expectations
of the
North West LHIN Board of Directors
(adopted November 20, 2007
Reviewed: September 9, 2008)
be evidence-based; be courageous; share the workload; open mind & open heart; celebrate diversity; be collaborative; be empathetic; lead by example; create safe/supportive environment; maintain a sense of humour; build trust/demonstrate respect; celebrate innovation/success; focus on the issue – not the person; maintain confidentiality; speak with one voice; be prepared to be engaged; hold ourselves and others accountable for following these rules.

Triple Aim
Framework

North West Local Health Integration Network
Decision Making Framework
Description
1Advancement of the NW LHIN's IHSP or ASP goals (exclude Access and Integration, which are separate criteria)
Degree of impact on advancing IHSP and/or ASP goals and priorities. IHSP priorities include: Access to Primary Care; Access to Specialty Care; Chronic Disease Prevention and Management; Mental Health and Addictions; Seniors' Services; Integration of Services Along the Continuum of Care; Engagement with Aboriginal People; Ensuring French Language Services; Integration of e-Health; and Regional Health Human Resources Plan. (Refer to NW LHIN IHSP for more details.)
2 Alignment with Ministry strategic direction
Degree of impact on advancing the Ministry's strategic directions. These include:• ED/ALC• Mental Health & Addictions services• Diabetes•eHealth.
3 Alignment with MLPA
Extent to which progam/initiative improves MLPA indicators. These include:•Cancer •Cataracts
•Hip & knee joint replacement
•MRI & CT diagnostic imaging,
•Cardiac Biyass
•ALC days
•CCAC In-Home Service
•ED Wait Times
•Mental Health and Addictions unplanned readmissions
4 Advancement of HSP role/mandate
Extent to which program/initiative is consistent with the provider(s) vision, mission, values and capacity, and extent to which there is an alignment compared to other providers in the health system (local community, regional or Ontario, as appropriate).
5improvement in population health status (clinical outcomes and quality of life)
Extent to which program/initiative is expected to improve (short or long term) clinical outcomes for the patient/client, reduce risk of adverse events, and/or improve physical, mental or social quality of life, as compared to current practice/ service. Determination as to whether there will be an impact should be based on evidence/best practice, where available. (Note: The application of this definition will need to be tailored to the objectives of the specific investment, and the definition may therefore require further clarification.)
6 Potential population impact
Magnitude of the disease/ condition that will be directly impacted by the program/initiative as measured by prevalence (i.e., number of individuals with the condition in the defined population at a given point in time). Determination as to whether there will be a direct impact should be based on evidence/best practice, where available.
7 Project scope
Outreach in the North West LHIN (sub-community; community; specific region; or NW LHIN-wide outreach). The five regions are:•Kenora
•Northern Communities
•Rainy River
•City of Thunder Bay
•Thunder Bay District
8Improvement in health promotion/disease prevention
Impact on illness/injury prevention and/or promotion of health and well-being as measured by projected longer term improvements in health and/ or likelihood of downstream service. Includes impacts on determinants of health. Determination as to whether there will be an impact should be based on evidence/best practice, where available.
Stra
tegi
c Fi
t / S
yste
m A
lignm
ent
Popu
latio
n H
ealth
Criteria
1 of 3

North West Local Health Integration Network
Decision Making Framework
DescriptionCriteria
9 Improvement in client-focused service
Extent to which program/initiative is expected to meet the health needs of a defined population and the population in general, and the degree to which patients/clients are expected to have choice and satisfaction in the type and delivery of care (the planned service is client centered).
10 Partnerships and collaboration
Degree to which appropriate level of partnerships/collaborations and/ or appropriateness of partnerships/collaborations will be achieved/leveraged in order to ensure service quality enhancement, improved comprehensiveness, optimal resource use, minimal duplication, and/or increased coordination. Role of partners should be clearly explained.
11 Community engagement
Level of appropriate involvement of target population and other key stakeholders in defining the project andplanned involvement in evaluating its impact on population health and key system performance.
12 Innovation
Impact on generation, transfer, and/or application of new knowledge to solve health or health system problems, including potential for broader scale implementation; encouraging leading practices, building on evidence and application of leading practices. Evidence of evaluation plan should be provided. Innovation includes new services, as well as process redesign for existing services.
13 Improvement in equity across NW
Improves the health status and/or access of service of recognized sub-populations where there is a known health status gap between this specific population and the general population as compared to current practice/ service. The absence of systematic and potentially remediable differences in one or more aspects of health across populations or population groups, defined socially, economically, demographically, culturally, linguistically or geographically.
Some areas of equity can include:•Aboriginal•Age related groups (Children and youth)•Disabled•Ethno-racial•Francophone•Homeless•Low Income•Religious/Fath communities•Rural/remote•Sex/gender, e.g. women, men, tansgender, transsexual, two-spirited•Sexual orientation
14Improvement in overall HSP efficiency (clinical, human resources, financial)
Extent to which program/initiative contributes to efficient utilization of clinical, financial, and/or human resources capacity to optimize health and other benefits within the system. Includes achieving improved outcomes with same or less resources; reducing overuse, inappropriate use or waste; and exceeding benchmarks that are based on best practices. Assessment will be based on gains in efficiency.
Syst
em V
alue
s
2 of 3

North West Local Health Integration Network
Decision Making Framework
DescriptionCriteria
15 Sustainability of project into future
Impact on health service delivery, financial, and human resources capacity over time. Considers whether the initiative is viable and sustainable after the initial investment, and whether new resource capacity is created in the health system. The health system should have enough qualified providers, funding, information, equipment, supplies and facilities to look after people’s health needs.
16 Integration (IHSP priority)
Extent to which program/initiative improves coordination of health care among health service providers, including LHIN funded and nonfunded providers and community providers to ensure continuity of care in the local health system and provision of care in the most appropriate setting as determined by patient/client's needs.
17 Improvement in quality of services
Extent to which program/initiative improves appropriateness, safety, effectiveness and client experience related to health service(s) provided, based on standards (including cultural standards) and best evidence for clinical care. Includes prevention of system errors/failures.
18Improvement in access to services (IHSP priority)
Extent to which program/initiative improves physical, cultural, linguistic and timely access to appropriate level of health services for defined population(s) in the local health system.
Syst
em P
erfo
rman
ce
3 of 3

Item # To Be Accomplished Lead Time Supporting Material
1.0 PROCEDURAL ITEMS For Approval:
1.1 Call to Order
Chair 5 min
1.2 Declaration of Conflict of Interest
1.3 Approval of Agenda Att. 1.3
1.4 Business Arising
2.0 BOARD EDUCATION
3.0 BOARD LINKAGES (Community Engagement, Consultations, Meetings)
3.1 Chair Report G. Labine 10 min Verbal
4.0 CONSENT AGENDA (Regular routine items such as Board of Director Minutes, Committee Packages, Declaration of Compliance, final approval of proposals)
4.1 Board of Director Meeting Minutes:
June 27, 2018
August 8, 2018
G. Labine 2 min Att. 4.1A-B
5.0 BOARD ENDS DISCUSSION
5.1 ENDS Education
5.2 ENDS Discussion
5.3 ENDS Monitoring
5.3-1 2017/18 Board of Directors Meeting Evaluation Summary G. Labine 5 min Att. 5.3-1
5.4 Generative Discussion
6.0 BOARD DECISIONS/PROCESSES (Approval of Policy, Committee Reports and Capital Approval)
North West Local Health Integration Network Board of Directors Meeting Agenda
OPEN Session
Date: September 25, 2018 Location: North West LHIN Boardroom 975 Alloy Drive, Thunder Bay, ON Teleconference: 1-855-392-2520 / Access Code 4252308 Time: 9:00 am (Eastern)
Agenda Item 1.3

North West Local Health Integration Network Board of Directors Meeting Agenda September 25, 2018
Page 2 of 2
Item # To Be Accomplished Lead Time Supporting Material
6.1 Committee Reports
6.1-1 Audit and Finance (A&F) Committee: No Report T. Berube
6.1-2 Governance and Nominations Committee: September 5, 2018
Leadership Awards
September 5, 2018 Draft Minutes (for information)
C. Farrell 10 min Att. 6.1-2
6.2 Policy Review
6.3 LHIN Operations
6.3-1 North West LHIN Planning (approval) B. Ktytor 5 min Att. 6.3-1
6.3-2 TBRHSC – Pre-Capital Submission – Pharmacy Services (approval) S. Pilatzke 5 min Att. 6.3-2
6.3-3 Health Links
Expenditures
S. Pilatzke 5 min Att. 6.3-3
7.0 MONITORING REPORTS (Executive Limitations and Board Process Policies)
7.1 EL-103 Enterprise Risk Management (approval) T. Berube 5 min Att. 7.1
8.0 QUALITY & ETHICS
8.1 Quality Report B. Ktytor 15 min Att.
9.0 INFORMATION
9.1-1 CEO Report: R. Crocker Ellacott
10 min Att. 9.1-1
9.1-2 Ministry LHIN Accountability Agreement (MLAA) Indicator Report B. Ktytor 5 min Att. 9.1-2
10.0 CLOSED SESSION
10.1 Report out of Closed Session
11.0 ADJOURNMENT
11.1 Meeting Evaluation Att. 11.1
11.2 Future Agenda Items
11.3 Date of Next Meeting – October 23, 2018
11.4 Adjourn
Agenda Item 1.3

Page 1 of 6
BOARD OF DIRECTORS MEETING MINUTES
North West LHIN Office June 26, 2018 975 Alloy Drive, Thunder Bay ON 9:00 am (Eastern)
Present Regrets
Gil Labine, Chair Cathy Farrell t/c Tina Copenace Carol Neff Dorothy Piccinin Cindy Jarvela Beatrice Metzler Darryl Allan Tim Berube Francois Hastir
Staff Recording Secretary
Rhonda Crocker Ellacott Susan Pilatzke Brian Ktytor Rakib Mohammed Petty Ndebele Sarah Newbery t/c Betty-Anne Grey
Item # To Be Accomplished Action
1.0 PROCEDURAL ITEMS
1.1 Call to Order The meeting was called to order at 9:00 am (Eastern) by Chair G. Labine. Guests and North West LHIN staff were welcomed to the meeting.
1.2 Declaration of Conflict of Interest G. Labine declared conflict of interest as a family member is employed with Thunder Bay Regional Health Sciences Centre in the Pediatric ward
1.3 Approval of Agenda The agenda was approved as presented.
1.4 Business Arising None.
2.0 BOARD EDUCATION
2.1 Home and Community Care R. Mohammed provided an overview of the North West LHIN Home and Community Care division as outlined in the previously distributed presentation. Highlights included:
History and background
Home and Community Care services
Home and Community Care patient
Patient’s journey
Care coordination
2017-18 Facts and Figures
Agenda Item 4.1A

North West Local Health Integration Network Board of Directors Meeting Minutes June 26, 2018
Page 2 of 6
Item # To Be Accomplished Action
Contracted Service Provider Organizations
Direct Nursing Programs
Future Goals and Priorities o Patients First: A Roadmap to Strengthen Home
and Community Care Discussion ensued, questions were addressed.
3.0 BOARD LINKAGES
3.1 Chair Report The Chair provided an update on recent activities including:
Dr. Bob Bell, Deputy Minister, will be retiring effective July 1, 2018.
The LHINs have received a Ministry expenditure directive effective immediately. G. Labine noted that he will attend the PAN LHIN meetings by teleconference until further notice.
G. Labine, F. Hastir and S. Pilatzke attended the Réseau du mieux-être francophone du Nord de l’Ontario Annual General Meeting on May 30, 2018. The meeting was very informative.
G. Labine attended a number of meetings with R. Crocker Ellacott.
4.0 CONSENT AGENDA
4.1 4.2
Board of Directors Meeting Minutes May 29, 2018 Declaration of Compliance: April 1, 2018 to June 30, 2018 G. Labine presented the consent agenda for approval. Resolution #2018 - 67 Moved by C. Neff and seconded by D. Allan that the North West LHIN Board of Directors approve the Consent Agenda as presented. CARRIED
5.0 BOARD ENDS DISCUSSION
5.1 ENDS Education None.
5.2 ENDS Discussion None.
5.3 ENDS Monitoring
5.4 Generative Discussion None.
6.0 BOARD DECISIONS/PROCESSES
6.1 Committee Reports
6.1-1 Audit and Finance (A&F) Committee The Audit and Finance meeting package for June 18, 2018 was pre-distributed to the Board. A brief overview of the meeting was
Agenda Item 4.1A

North West Local Health Integration Network Board of Directors Meeting Minutes June 26, 2018
Page 3 of 6
Item # To Be Accomplished Action
provided. The Audited Financial Statements were reviewed at the Audit and Finance Committee meeting June 18, 2018. Deloitte issued an audit opinion that the financial statements present fairly in all material respects and confirmed that the audit was a clean audit. The Board was asked to support a motion to approve the financial statements of the North West LHIN for the year ending March 31, 2018. Resolution #2018 - 68 Moved by D. Allan and seconded by D. Piccinin that the North West LHIN Board of Directors approve the North West LHIN Financial Statements for the year ending March 31, 2018 as presented. CARRIED A brief overview of the Audit and Finance Committee meeting was provided as follows:
The process of procuring audit services for the LHINs is underway.
The committee discussed the Board Quality Committee structure and reporting. The committee will review further and bring this back to the September Board meeting.
The Office of the Auditor General of Ontario Survey has been submitted.
FIN 434 Board of Directors Per Diem policy recommendations for revisions was distributed to the Board. There were no further revisions required.
EL-103 Enterprise Risk Management was reviewed and discussed and will be brought to the September Board meeting for approval.
6.1-2 Governance and Nominations (G&N) Committee The Governance and Nominations Committee meeting package from June 18, 2018 was pre-distributed to the Board. A brief overview of the meeting was provided. It was noted that only the relevant material from the meeting will be included in the Board meeting package. The following amended policies were brought forward for Board approval: GP-106 Board Education and Development Policy Resolution #2018 - 69 Moved by C. Neff and seconded by T. Copenace that the North West LHIN Board of Directors approve Policy GP-106 Board Education and Development as amended. CARRIED GP-110 CEO Succession Plan Process Policy
Agenda Item 4.1A

North West Local Health Integration Network Board of Directors Meeting Minutes June 26, 2018
Page 4 of 6
Item # To Be Accomplished Action
Resolution #2018 - 70 Moved by C. Neff and seconded by B. Metzler that the North West LHIN Board of Directors approve Policy GP-110 CEO Succession Plan Process as amended. CARRIED BC-103 CEO Compensation Policy Resolution #2018 - 71 Moved by C. Neff and seconded by T. Copenace that the North West LHIN Board of Directors approve Policy BC-103 CEO Compensation as amended. CARRIED
6.2 Policy Review
6.2-1 BC-102 Performance Evaluation Policy BC-102 Performance Evaluation was reviewed; no changes were recommended.
6.2-2 BC-103 CEO Compensation Policy BC-103 CEO Compensation was reviewed; no changes were recommended.
6.3 LHIN Operations
6.3-1 Equipment Rental Contract B. Ktytor provided an overview of the proposed approach to address requirements for equipment rental service to support North West LHIN Home and Community Care clients as detailed in the previously distributed briefing note. Resolution #2018 - 72 Moved by C. Jarvela and seconded by B. Metzler that the North West LHIN Board of Directors authorize the Chief Executive Officer to execute a contract with Medigas for the provision of equipment rentals for home and community care clients leveraging the standard provincial template. CARRIED
6.3-2 Short Term Transitional Care Models Funding Program S. Pilatzke provided an overview of the proposed Short Term Transitional Care Models Funding Program. It was noted that the North West LHIN will wait for further implementation until further guidelines are received from the Ministry of Health and Long-Term Care. Questions ensued and were answered. Resolution #2018 - 73 Moved by D. Piccinin and seconded by C. Neff that the North West LHIN Board of Directors approve in principle the Short
Agenda Item 4.1A

North West Local Health Integration Network Board of Directors Meeting Minutes June 26, 2018
Page 5 of 6
Item # To Be Accomplished Action
Term Transitional Care Models Funding Program subject to expenditure restraints. CARRIED
7.0 MONITORING REPORTS
8.0 QUALITY AND ETHICS
9.0 INFORMATION
9.1 Transition Update S. Pilatzke noted that the North West LHIN is one-year post transition and is currently moving through transition to transformation. The following items were highlighted:
Work in progress with IT.
Policies and procedures continue to be reviewed.
French Language Services alignment is underway.
Human Resources processes in progress.
Continuing to work on business processes.
Working on and beyond on the 32 projects.
Accreditation is under review and work is underway across all LHINs.
9.2-1 CEO Report The CEO Report was distributed to the Board for information. The document is a compilation of all of the North West LHIN divisions. R. Crocker Ellacott provided an overview of her activities since the last Board meeting.
Board members were allotted time for questions.
9.2-2 Ministry LHIN Accountability Agreement (MLAA) Indicator Report The Q4 Ministry LHIN Accountability Agreement Indicator Report was provided to the Board. Discussion ensued with focus on the following indicators:
Percent of Home Care Clients Receiving Personal Support Service Within 5 Days
Home and Community Care Services Wait Time – From Community
Rate of Repeat ED Visits for Mental Health
Rate of Repeat ED Visits for Substance Abuse A break was observed at 10:30 am to 10:40 am prior to commencing the Closed session.
10.0 CLOSED SESSION Resolution #2018 - 74 Moved by B. Metzler and seconded by D. Piccinin that at 10:40 am (Eastern) the Board members attending the meeting, specified above, move into a Closed Session pursuant to the following exception(s) set out in s. 9 (5) of the Local Health System Integration Act (LHSIA), 2006: (a) Personal or Public Interest
Agenda Item 4.1A

North West Local Health Integration Network Board of Directors Meeting Minutes June 26, 2018
Page 6 of 6
Item # To Be Accomplished Action
(g) Personnel Matters And further that the following persons be permitted to attend: R. Crocker Ellacott, B. Ktytor, S. Pilatzke, P. Ndebele, R. Mohammed, S. Newbery and B. Grey. CARRIED
Report out of Closed Session The following motions were brought from the closed session. Resolution #2018 - 79 Moved by C. Neff and seconded by B. Metzler that the North West LHIN Board of Directors approve the May 28, 2018 Governance to Governance Report as presented and approve that the report be released to the public and posted to the North West LHIN website. CARRIED
11.0 ADJOURNMENT
11.1 Meeting Evaluation Completed evaluations to be provided to B. Grey.
10.2 Future Agenda Items Agenda items to be forwarded to the Chair or to B. Grey by September 4, 2018.
All members
11.3 Date of Next Meeting The next meeting is scheduled for September 25, 2018.
11.4 Adjournment Resolution #2018 - 80 Moved by C. Neff and seconded by C. Jarvela that at 3:26 pm (Eastern) the meeting be adjourned. CARRIED
Chair
Secretary
Agenda Item 4.1A

Page 1 of 3
SPECIAL BOARD OF DIRECTORS MEETING TELECONFERENCE
MINUTES North West LHIN Office August 8, 2018 975 Alloy Drive, Thunder Bay ON 11:30 am (Eastern)
Present
Gil Labine, Chair Cathy Farrell, Vice-Chair Tim Berube t/c
Staff Recording Secretary
Rhonda Crocker Ellacott t/c Susan Pilatzke Byron Ball Chrysta Burns Petronilla Ndebele Betty-Anne Grey
Item # To Be Accomplished Action
1.0 PROCEDURAL ITEMS
1.1 Call to Order The meeting was called to order at 11:30 am (Eastern) by Chair G. Labine.
1.2 Approval of Agenda The agenda was approved as presented
1.3 Declaration of Conflict of Interest None declared
2.0 LHIN OPERATIONS: Executive Limitations – Funding for Approval
2.1 2018/19 BSO Community Funding Enhancement Recommendations S. Pilatzke provided an overview of the draft plan for the allocation of base funding for Behavioural Supports Ontario (BSO) at home and in the community intended to expand services and continue central coordination or services as detailed in the briefing note. Background information on the process and recommendation was provided. The LHIN was required to submit an implementation plan to the ministry by July 31, 2018. Upon Board approval of the proposed plan and Ministry feedback is provided, the LHIN staff will immediately start working with the system partners to executive the implementation plan.
Agenda Item 4.1B

North West Local Health Integration Network Special Board of Directors Meeting Minutes August 8, 2018
Page 2 of 3
Item # To Be Accomplished Action
Resolution #2018 - 81 Moved by C. Farrell and seconded by T. Berube that the North West LHIN Board of Directors approve the draft plan as listed below for allocation of base funding of up to $425,900 (2018/19) for Behavioural Supports Ontario (BSO) at home and in the community. Additionally, the North West LHIN Board of Directors approves an allocation of $145,000 of the funding on a one-time basis to support the ongoing development of consistent processes across the North West LHIN. Carried
2.2 2018/19 BSO Long-Term Care Funding Enhancement Recommendations S. Pilatzke provided an overview on the proposed allocation of additional base funding of up to $431,520 for enhancing Behavioural Supports Ontario (BSO) services in Long-Term Care (LTC) sector across the region. Background information was provided as outlined in the previously distributed briefing note. The LHIN was required to submit an implementation plan to the ministry by July 31, 2018. Upon Board approval of the proposed plan and Ministry feedback is provided, the LHIN staff will immediately start working with the system partners to executive the implementation plan. Resolution #2018 - 82 Moved by C. Farrell and seconded by T. Berube that the North West LHIN Board of Directors approve the preliminary proposed plan for 2018/19 Behaviours Supports Ontario Long Term Care Funding Enhancement expenditure of the $431,520. The amounts are listed below as the Base Funding Allocation; allocation of $8,630 for staff retention and $4,422 for training and supplies. Carried
2.3 2018/19 Dementia Program Funding Recommendations S. Pilatzke provided an overview on the draft recommendations for allocation of base funding of up to $326,000 (2018/19) for community dementia programs across the region. Background information was provided as outlined in the previously distributed briefing note. Upon Board approval the North West LHIN will immediately start working with the system partners to execute the recommendation. Resolution #2018 - 83 Moved by T. Berube and seconded by C. Farrell that the North West LHIN Board of Directors approve the expenditure of up to $326,000 for Dementia Programs as outlined in the briefing note based on the initial evaluation of the proposed
Agenda Item 4.1B

North West Local Health Integration Network Special Board of Directors Meeting Minutes August 8, 2018
Page 3 of 3
Item # To Be Accomplished Action
initiatives. Carried
3.0 CLOSED SESSION Resolution #2018 - 84 Moved by C. Farrell and seconded by T. Berube that at 11:41 am (Eastern) the Board members attending the meeting, specified above, move into a Closed Session pursuant to the following exception(s) set out in s. 9 (5) of the Local Health System Integration Act (LHSIA), 2006: (a) Personal or Public Interest (g) Personnel Matters And further that the following persons be permitted to attend: R. Crocker Ellacott, S. Pilatzke, C. Burns, P. Ndebele, B. Ball and B. Grey. CARRIED
4.0 ADJOURNMENT
4.1 Adjournment Resolution #2018 - 89 Moved by C. Farrell and seconded by T. Berube that at 12:26 pm (Eastern) the meeting be adjourned. CARRIED
Chair
Secretary
Agenda Item 4.1B

BOARD OF DIRECTORS MEETING EVALUATION ANNUAL SUMMARY
April 2017 – March 2018
Please rate the following on a scale of 1 to 5. Strongly Disagree
Disagree Neutral Agree Strongly Agree
1 2 3 4 5
1. The members met the Behavioural Expectations outlined in the "Rules of the Road".
15% 85%
2. The members focused on the Board's mandate and strategic priorities.
39% 61%
3. The members avoided getting into operational details. 1.6% 3% 24% 71%
4. The agenda was clear, supported by the necessary documents, and circulated prior to the meeting.
2% 15% 84%
5. All members came prepared to discuss materials sent in advance. 2% 35% 61%
6. Reports were clear and contained needed information. 16% 84%
7. Presenters were concise and ensured sufficient time for discussion. 2% 24% 76%
8. A diversity of opinions was expressed and issues were dealt with in a respectful manner.
20% 82%
9. There was adequate opportunity for generative discussion. 2% 2% 20% 75%
10. The education sessions were strategic and informative. (Select N/A if an Education Session was not provided at this meeting)
14% 86%
11. The Chair guided the meeting effectively. 1.64% 3% 14% 83%
12. Board members participated responsibly (see “Rules of the Road”. 20% 80%
13. Next steps were identified and responsibly assigned. 26% 74%
1. What aspect of this meeting was most valuable to you?
Board Education Sessions o Policy Review o Non-urgent transportation o Very comprehensive, informative presentations o Home and Community presentation o Education presentation o Pre-capital planning presentation o Indigenous Health presentation o Political Activity presentation
Strong Communication from Management and Chair on Direction and Updates o LHIN funding arrangements and reporting o Staff open to answering questions o Board reports o Verbal reports from Board Chair on events
Agenda Item 5.3-1

Board of Directors Meeting Evaluation Annual Summary - 2017-2018
2
o CEO report o ALC pressures, discussion re reclassification of LTC beds to acute care at HRM o J. Simser, legal advisor at Board meeting was beneficial o Generative discussion on MLAA and Wait Time level 1
Excellent CEO Report and CEO Interpretation Document 2. What aspect of the meeting could have been better / be improved?
Technical Issues o Access to Portal / Email on and off site
Board Materials o Lots of materials to cover but people need to be encouraged by the Chair to participate
rather that feeling they are delaying the process
Board Meeting Process o More time allowed for Legal Education o Afternoon break would be nice o Shorter meetings
Agenda Item 5.3-1

Page 1 of 3
GOVERNANCE & NOMINATIONS COMMITTEE MEETING Minutes
North West LHIN Office, North West LHIN, Board Room September 5, 2018 975 Alloy Drive, Thunder Bay, ON 2:30 p.m. Eastern
Present
Regrets
Cathy Farrell, Chair
Gil Labine
Beatrice Metzler
Tina Copenace (t/c)
Francois Hastir
Carol Neff
Staff Recording Secretary
Rhonda Crocker Ellacott Susan Pilatzke Linda Molenda
Item # To Be Accomplished Action:
1.0 PROCEDURAL ITEMS
1.1 Call to Order The meeting was called to order at 2:38 p.m. (Eastern) by Chair, C. Farrell.
1.2 Declaration of Conflict of Interest None declared.
1.3 Approval of Agenda The agenda was reviewed and approved as circulated. MOTION Moved by T. Copenace and seconded by G. Labine that the Governance and Nominations Committee meeting agenda of September 5, 2018 be approved as presented. CARRIED
Moved by: T. Copenace Seconded: G. Labine
1.4 Approval of Minutes The Governance and Nominations Committee minutes of June 18, 2018 were presented for approval and accepted as circulated.
Agenda Item 6.1-2

North West Local Health Integration Network Governance and Nominations Committee Meeting Minutes September 5, 2018
Page 2 of 3
Item # To Be Accomplished Action:
MOTION Moved by B. Metzler and seconded by G. Labine that the Minutes of the Governance and Nominations Committee Meeting held on June 18, 2018 be approved as circulated. CARRIED
Moved by: B. Metzler Seconded: G. Labine
1.5 Business Arising from Minutes not Covered on Agenda None
2.0 BOARD LINKAGES / EDUCATION
2.1 Governance-to-Governance Session – October 18, 2018 Webinar The date of the Governance-to-Governance Session was discussed. On consensus the Committee agreed to change the date of the Governance-to-Governance Session to Wednesday October 24, 2018, 10:00 a.m. to 3:00 p.m. Further discussion was held regarding the agenda, presenters and attendees.
3.0 BOARD ENDS DISCUSSION
4.0 BOARD DECISIONS/PROCESSES
5.0 G& N COMMITTEE ITEMS
6.0 CLOSED SESSION MOTION Moved by G. Labine and seconded by B. Metzler that at 2:55 p.m. the Committee Members attending the meeting specified above move into a closed session pursuant to the following exception(s) set out in s.9 (5) of the Local Health System Integration Act (LHSIA) 2006: (i) Personal or Public Interest (vii) Personnel Matters And further that the following persons be permitted to attend: R. Crocker Ellacott, S. Pilatzke and L. Molenda CARRIED Meeting reconvened following the Closed Session.
Moved by: G. Labine Seconded: B. Metzler
7.0 NEW BUSINESS
8.0 ADJOURNMENT
8.1 Date of Next Meeting – October 9, 2018 2-4 p.m.
Agenda Item 6.1-2

North West Local Health Integration Network Governance and Nominations Committee Meeting Minutes September 5, 2018
Page 3 of 3
Item # To Be Accomplished Action:
8.2 Adjourn MOTION Moved by T. Copenace and seconded by B. Metzler that the meeting was adjourned at 3:26 p.m. CARRIED
Moved by: T. Copenace Seconded: B. Metzler
Agenda Item 6.1-2

Briefing Note Topic/Issue: North West LHIN Workplace Planning Project Expenditure Approval Submitted to: North West LHIN Board of Directors Submitted by: Brian Ktytor, Vice President Corporate Services Date Submitted: September 25, 2018
Priority Level: X High Action Level: None
Medium
Information Only
Low Input
Policy Development
X Decision
Purpose: To provide background and recommendation to approve an $89,000 expenditure, given the Ministry of Health and Long Term Care (MOHLTC) expenditure restraint directives, for the North West LHIN Thunder Bay offices “Future-state Workplace Project” work plan provided by Infrastructure Ontario. Background Information: When the North West LHIN transitioned with the NW CCAC on June 21, 2017 the two offices in Thunder Bay (975 Alloy Drive and 961 Alloy Drive) became the home offices for the organization. The leases for the two Thunder Bay offices expire June 30, 2020 and there is a requirement to review the current space needs and explore opportunities for amalgamating the two offices into one, or exploring an alternative office location. Integrating the two offices into one will result in significant benefit to the organization. It will allow for improved productivity, more team collaboration, effective use of space, and improved employee morale. Furthermore, it is expected to significantly reduce accommodation expenses.
Agenda Item 6.3-1

BN to North West LHIN Board of Directors North West LHIN Workplace Planning Project Expenditure Approval September 25, 2018
2
Direction was received from MOHLTC on January 31, 2017 for the LHINs to use Infrastructure Ontario for all workplace solutions which includes real estate options analysis, workplace change management, space planning etc. The project plan and costing that Infrastructure Ontario provided is their requirement to assess and develop a future state solution to the NW LHIN’s Thunder Bay office accommodation needs beyond June 2020. Activities to Date: Given the complexity of developing a future-state Thunder Bay office solution, and as directed by MOHLTC, the North West LHIN began discussions with Infrastructure Ontario in July 2017 regarding their services and the need for analysis of our current and future office needs in the city of Thunder Bay. A mutually agreeable proposal to meet the North West LHIN’s needs was developed with Infrastructure Ontario. The estimated costing for phase one work plan cost is $49,000 and phase two work plan is $40,000 for a total of $89,000. This expenditure was budgeted for in this fiscal year. On June 20, 2018 an expenditure restriction memo was received by the LHINs requesting an immediate freeze of any new discretionary spending. It referred to a memo from the Cabinet Office that included any expense that can be placed on hold without putting government service delivery or the public at risk. As a result we inquired of Infrastructure Ontario how long we could delay or postpone the required work without putting the project at risk of non-completion by the lease expiry date. Infrastructure Ontario indicated that September 2018 is the latest we could postpone the project. If the project does not proceed, the North West LHIN would not be in a position to occupy an optimal office solution in June 2020, and in all likelihood would be re-negotiating a sub-optimal accommodation solution in the existing two-office location configuration. On September 10, 2018, a Briefing Note was brought forward to the North West LHIN Senior Leadership Team requesting approval to move forward with expenditure on the project. The Senior Leadership Team approved this proposal on the basis that it be brought forward to the Board of Directors for approval.
Agenda Item 6.3-1

BN to North West LHIN Board of Directors North West LHIN Workplace Planning Project Expenditure Approval September 25, 2018
3
Next Steps:
Request expenditure approval from the North West LHIN Board of Directors.
Once Board of Directors approval is received, sign comfort agreement and begin the planning process with Infrastructure Ontario.
Recommendation: That the North West LHIN Board of Directors approve the $89,000 expenditure with respect to the Infrastructure Ontario proposal for the North West LHIN Thunder Bay Office Future-state Accommodation project to ensure adherence to the Thunder Bay offices June 2020 lease expiration timeline.
Agenda Item 6.3-1

Briefing Note
Topic/Issue: Thunder Bay Regional Health Sciences Centre – Pre-
Capital Submission re: Pharmacy Services
Submitted to: North West LHIN Board of Directors
Submitted by: Susan Pilatzke, Vice President, Health System Strategy, Integration and Planning
Date Submitted: September 25, 2018
Priority Level: High
x Medium
Low
Action Level: None
Information Only
Input
Policy Development
x Decision
Purpose: To obtain a recommendation from the North West LHIN Board of Directors, for endorsement of Part A of a Pre-Capital Submission from Thunder Bay Regional Health Sciences Centre (TBRHSC) to fund facility upgrades, new equipment and renovations to comply with the National Association of Pharmacy Regulatory Authorities (NAPRA) standards. The funds are being requested through the Ministry of Health and Long-term Care (MOHTLC) capital process, with a proposal for Ministry cost sharing. The estimated cost of this project is approximately $2.41M. The endorsement of further stages of the capital ask will be contingent on the findings and final regional pharmacy plan that is currently underway with all hospital sites and is expected to be completed in Fall 2018.
Agenda Item 6.3-2

2
Background Information: The capital planning process is a joint review process between the Ministry of Health and Long-Term Care (MOHLTC) and the Local Health Integration Networks (LHIN). There are three stages of the capital planning process:
1. Pre-Capital Submission is intended to provide a high level description of the role of the HSP in the local health system and describes the initiative being proposed including program rationale, evidence of alignment with local health system priorities and the development concept.
2. Stage 1 Proposal Submission is intended to further articulate both program/service planning and physical infrastructure planning. Comprehensive documentation is required to support the proposal for new or renovated capital infrastructure.
3. Stage 2 Functional Program Submission is intended to provide detailed articulation of the relationship between program planning and facility planning. The Functional Program also describes associated workload, staffing, major equipment and space requirements, as well as required departmental adjacencies and relationships.
Each of the three stages above is further broken down into two parts. Part A (LHIN review) includes the program and service elements. Part B (MOHLTC review) includes the physical and cost elements of the capital project.
The pre-capital submission proposes to fund facility upgrades, new equipment and renovations to comply with the Ontario College of Pharmacists (OCP) hospital accreditation program. The OCP has stipulated that hospitals become compliant, or have sufficient mitigation strategies in place for compliance, with National Association of Pharmacy Regulatory Authorities (NAPRA) standards for sterile compounding of hazardous and non-hazardous drugs by January 2019. TBRHSC requires significant facility upgrades to meet the NAPRA standards regarding environmental air quality control and ISO clean-room requirements.
Activities to Date: The North West LHIN has reviewed the Pre-Capital Submission Form, Part A submitted by TBRHSC and has been in discussion with the hospital Manager of Pharmacy to seek additional clarification and information about the submission. Adequate information has been received for this stage of the capital process. The North West LHIN, together with the twelve hospitals within the region, is currently working to develop an approach that the LHIN and the hospitals can use to make decisions on how to coordinate and manage pharmacy services throughout the region to ensure compliance with the NAPRA standards and ensure quality pharmacy services across the region. The resulting regional pharmacy plan will outline how the hospitals in the North West LHIN will collectively provide medication management services according to the National Association of Pharmacy Regulatory Authorities (NAPRA) standards – to meet critical elements for hazardous and non-
Agenda Item 6.3-2

3
hazardous compounding by January 1, 2019, as well as all standards and quality in the longer term. The Ministry capital branch is aware of the regional planning that the LHIN and hospitals are undergoing and has requested that all capital requests be submitted per usual process in the immediate term, with final endorsement (in alignment with the regional plan) to be communicated once the plan is finalized. As such, endorsement of further stages of this capital ask is contingent on the findings and final regional pharmacy plan to be complete in Fall 2018.
Overall, the following summarizes the review of the submission:
The proposed renovation work is required to meet NAPRA standards
There are no changes contemplated to services delivered or service volumes
There are no additional operating costs associated with the physical renovations, since there will be no change is services
The above is predicated on the assumption that the regional planning work underway does not determine that there should be any change in services delivered by TBRHSC
Assessment of Alignment to LHIN strategy: This proposal supports the North West LHIN’s strategic direction of “Continuous Quality Improvement”. The project deliverables are to ensure TBRHSC, as a regional site, can continue to deliver necessary chemotherapies to patients in Thunder Bay and the region, through compliance with NAPRA standards.
Next Steps: If the North West LHIN Board of Directors supports Part A of this Pre-Capital Submission for the program and service elements of the proposal, written confirmation and feedback is provided to the hospital to consider for the subsequent stages, if necessary. The LHIN also provides confirmation of support to the MOHLTC which includes rationale and advice, if necessary. The hospital then completes Part B of the Pre-Capital Submission Form, attaches the LHINs confirmation and submits it to the MOHLTC for their review. In parallel the North West LHIN will continue to work with all hospital sites to develop a regional pharmacy plan. Pending the results of this plan, the LHIN will advise the Ministry and sites if there is any change to the status of this endorsement for the capital ask.
Recommendations: That the North West LHIN Board of Directors endorse Part A of the Pre-Capital Submission Form submitted by Thunder Bay Regional Health Science Centre (TBRHSC) for facility upgrades, new equipment and renovations to comply with the National Association of Pharmacy Regulatory Authorities (NAPRA) standards. This endorsement is contingent on the final results of the regional pharmacy plan that is currently under development with all hospital sites. At this time, the Board of Directors recommends that the hospital continue to the next stage of the capital process.
Agenda Item 6.3-2

MEMORANDUM Date: September 25, 2018
To: Chair and Members of the Board of Directors From: CEO, North West Local Health Integration Network Subject: MONITORING REPORT – EL-103 ENTERPRISE RISK MANAGEMENT
Board policy is indicated in bold typeface throughout. I hereby present the monitoring report on our Executive Limitations policy “Enterprise Risk Management” according to the schedule set out. I certify that the information contained in this report is true, and represents compliance with all aspects of the policy, unless specifically stated otherwise. Signed: Date: “The CEO shall not cause or allow conditions, procedures or decisions which fail to identify, measure, monitor and manage within established risk tolerances, potential events that may affect achievement of the ENDS, or allow conditions which interfere with an environment that fosters learning, innovation, responsible risk taking, continuous improvements and addresses underlying system issues that contribute to risk.” CEO INTERPRETATION: I submit that the Board has comprehensively interpreted this policy in its subsequent policy provisions. My interpretation and data will be attached to those provisions below. I submit that the data to follow demonstrates compliance with this global provision. Accordingly, the CEO shall not: 1. Fail to establish and maintain an enterprise risk management policy and process
that is well communicated and implemented by staff.
Agenda Item 7.1

CEO INTERPRETATION: Compliance will be demonstrated when an Enterprise Risk Management (ERM) policy and ERM processes are documented and reviewed annually with all management and staff. Implementation will be demonstrated by quarterly and annual Ministry and North West LHIN Board risk reporting requirements being met, which necessarily requires all staff to take responsibility for risk management in day to day decision making processes, which are aligned with Board ENDS. EVIDENCE: An ERM operational policy has been developed, FIN 301 Enterprise Risk Management. It is aligned with the Ministry of Finance Risk Management Policy for the Province of Ontario as required in the LHIN’s Memorandum of Understanding with the Ministry of Health and Long Term Care (MOHLTC). This policy has been implemented at the North West LHIN. All new staff to the organization go through an orientation process and are required to confirm that they have read and understood all policies of the North West LHIN including Enterprise Risk Management policies FIN 301 and EL 103 (both attached). The North West LHIN Enterprise Risk Management process is comprised of a comprehensive process and tools to identify, measure, and mitigate risks that may face the organization. The tools used include an Enterprise Risk Register, a Risk Mitigation Plan and Action Tracker, and Risk Universe Definitions The Enterprise Risk Register is populated and it provides a comprehensive view of all risks facing the North West LHIN including recommended actions where the risk level exceeds the risk tolerance level of the organization. Risks are actively managed accordingly. The North West LHIN System Quality and Performance Department has incorporated risk analysis and reporting into the project management processes and software. All North West LHIN projects are required to identify, monitor, and mitigate risks. North West LHIN staff are involved in the identification and mitigation of health care system level risks in the North West LHIN. These risks are submitted quarterly for Quarters 1 through 3 to the MOHLTC. North West LHIN staff are involved in the identification and mitigation of government agency level risks. This information is provided quarterly through the Agencies and Appointments Directive Risk Assessment Report which is submitted quarterly to the MOHLTC LHIN Liaison Branch (LLB).
Agenda Item 7.1

North West LHIN staff are involved in the identification and mitigation of LHIN operational level risks for the preparation and reporting of this assessment. This assessment is presented to the North West LHIN senior team as required. Finally, the North West LHIN utilized the provincial Risk Management Framework (as noted, largely based on the North West LHIN ERM framework) to manage LHIN-CCAC transition risks. All the above assessments and mitigation strategies are conducted to help maximize the achievement of North West LHIN Board ENDS. 2. Fail to establish risk management strategies for identified and/or known risks.
CEO INTERPRETATION: Compliance will be demonstrated when there is a risk register (quarterly and annual risk reports) prepared which identifies known risks and there is a risk mitigation strategy identified for each respective risk based on risk tolerance. EVIDENCE: The risk reports are submitted to the MOHLTC as required. All registered risks have mitigation strategies established to address same. 3. Neglect to identify risks or fail to report these risks in a timely manner to the
Board.
CEO INTERPRETATION Compliance will be demonstrated when all known material risks are identified to the Board on a regular and/or urgent basis by the CEO and/or designate(s). EVIDENCE: All material risks identified through the LHIN’s ERM framework have been brought to the attention of the Board in a timely manner from the CEO office.
Agenda Item 7.1

4. Fail to present the quarterly CEO Compliance Report for Board review and approval.
CEO INTERPRETATION Compliance will be demonstrated when the CEO provides the Compliance Reports to the Board and they are subsequently approved. EVIDENCE: The Declaration of Compliance is presented and approved as part of the Board of Director’s consent agenda. The Board motion below was approved in each quarter as follows: June 27, 2017 October 24, 201 January 30, 2018 April 24, 2018 That the North West LHIN Board of Directors approve the Declaration of Compliance for the period (April 1 - June 30, 2017, July 1 - September 30, 2017, October 1 - December 31, 2017, and January 1 - March 31, 2018) as presented, and give direction to the Board Chair to certify that this attestation has been approved by the Board of the North West LHIN. 5. Neglect to provide expertise and advice to the strategic planning process.
CEO INTERPRETATION: Compliance will be demonstrated by having the CEO present and actively participating in the Boards Strategic Planning process. The CEO will also engage the right expertise to help the Board through the development of all strategic planning documents.
Agenda Item 7.1

EVIDENCE:
The Board conducts strategic planning retreat in the fall each year. These retreats result in an annual refresh of the Board’s ENDS and CEO interpretation of same. The CEO was present and actively participated in the planning exercise in fiscal 2017-2018. Furthermore, various preparatory research, environmental scans and expertise was provided to the Board for the strategic planning process through the CEO’s office. The CEO provides ongoing environmental scanning information throughout the year through a variety of formats (i.e., external Health Service Provider presentations, research reports, articles, staff presentations, etc.) to provide regular expertise and advice to inform the Board’s strategic planning process.
Agenda Item 7.1

Board Report September 2018
Agenda Item 8.1

2
Introduction
What is Quality?
Quality can mean different things depending on one’s involvement in the health care system. To the health system planners and clinicians providing front line care, quality is measured by indicators such as performance, patient satisfaction and outcomes. To patients and families who receive care, quality is reflected in how, where, and the timeliness in which they receive care; goals and input are respected and care is effective and efficient. Continuous quality improvement applies to both viewpoints, and is an integral characteristic of the designing for value priority that the North West Local Health Integration Network seeks to build.1
The North West Local Health Integration Network has adopted the Health Quality Ontario quality definition and the health system quality definition:2
Health Quality Ontario’s System Quality Advisory Committee defines a health system that delivers world-leading safe, effective, patient-centred services, efficiently, and in a timely fashion, resulting in optimal health status for communities.3
How can the North West Local Health Integration Network improve the health of our population? How can the North Local Health Integration Network improve both patient and provider experiences. Quality is how we design and deploy improvement initiatives. Quality is how we achieve outcomes.3
1 North West Local Health Integrated Network Integrated Health Services Plan 2016-2018 p.16 2 Health Quality Ontario, What is Health Quality. www.hqontario.ca/what-is-health-quality 3 Quality Matters; Realizing Excellent Care for All; A Report by Health Quality Ontario Advisory Committee p. 27
Health Quality Ontario: Health quality is achieving better health outcomes and experiences for every person living in Ontario; because better has no limit.
Agenda Item 8.1

3
Purpose of the Quarterly Quality of Care Board Report
This report supports the provision of governance oversight with respect to quality issues, overall quality of health services delivered by the Corporation, and quality improvement initiatives and policies. The table below outlines select monitoring considerations with related monitoring material that augments this report.
Oversight Considerations
Related Monitoring Support Material
Overall quality of the healthcare system in the North West Local Health Integration Network
Health Quality Ontario Annual Quality Report Canadian Institute for Health Information (CIHI)
Overall quality of patient care services provided by the North West Local Health Integration Network
Quality Monitoring Infographics (Appendices A and B)
Risk Management; patient services, patient safety, privacy, performance of contracted service providers, ethics, appeals and other matters
Six Quality Dimensions, Patient Safety Dashboard
Appropriate system to capture, respond and report on patient and service provider complaints, including critical incidents and adverse event reports or their equivalent,
Events Tracking Management System, reported via Patient Safety Dashboard
Appropriate patient and caregiver surveys to measure the patient care experience and satisfaction with care delivery and reports the results to the Board of Directors
NRC Health Client and Caregiver Experience Survey
Annual Quality Improvement Plan for approval by the Board of Directors
Quality Improvement Plan update and direction for 2018-2019
Regular reports on Patient Safety and Quality Measures to the Board of Directors
Patient Safety Dashboard
Agenda Item 8.1

4
System Quality Dimensions The North West Local Health Integration Network adopted the Six Quality Dimensions below created by The National Academy of Medicine (NAM), previously the Institute of Medicine (IOM) to align to the North West Local Health Integration Network Board Policy, Health Quality Ontario, and the North West Local Health Integration Network Quality Strategy.
In the pages and infographics to follow the North West Local Health Integration Network system quality is reported by high level indicators which align to the quality dimensions.
North West Local Health Integration Network Quality Dimensions
Community
Partnership
Patient Safety
and Clinical
Quality
Continuous
Improvement
Measure/
Monitor /
Feedback
Patient - centered
Equita
ble
Tim
ely
Efficie
nt
Safe
Effective
Safe
Avoiding harm to patients from the care that is intended to help them.
Effective
Providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit (avoiding underuse and misuse, respectively).
Patient-Centred
Providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions. Timely Reducing waits and sometimes harmful delays for both those who receive and those who give care. Efficient Avoiding waste, including waste of equipment, supplies, ideas, and energy. Equitable Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.
BOARD QUALITY DIMENSIONS
Agenda Item 8.1

5
A full copy of this infographic is attached as Appendix A
Agenda Item 8.1

6
Quality Dimension – Safety
The overarching goal in this Quality Domain is avoiding harm to patients from the care that is
intended to help them.
Health System - Safety 1. In-Hospital Sepsis The following table provides comparative data for the rate of cases of In-Hospital Sepsis (risk adjusted after admission) recorded in the North West Local Health Integration Network compared to the Provincial average.
North West LHIN Average
Provincial Average
In-hospital sepsis*
2 per (1,000)
4 per (1,000)
*Canadian Institute for Health Information (CIHI) 2016-2017
Trend Over Time: In-Hospital Sepsis (per 1,000)
Agenda Item 8.1

7
Sepsis is a clinical syndrome that occurs as a complication of infections. Sepsis is a leading cause of mortality and is linked to increased hospital resource utilization and prolonged stays in intensive care units. Appropriate preventive and therapeutic measures during a hospital stay can reduce the rate of infections and / or progression of infection to sepsis. The indicator addresses the extent to which acute care hospitals are effective in preventing the development of sepsis. It will help hospitals improve patient safety and learn from their peers regarding best practice methods for appropriate treatment of infections and prevention of sepsis.4 The North West Local Health Integration Network experienced improvement with the Safety Dimension specifically for in-hospital sepsis over a four year period. The North West Local Health Integration Network is in dialog with Clinical Leaders to understand this change and critical success factor for sustaining the improvement to build knowledge and process-spread opportunities into future quality improvement planning. 2. Falls in Long-Term Care The following table provides comparative data for the percentage of falls experienced by patients in long-term care recorded in the North West Local Health Integration Network compared to the Provincial average. This indicator looks at how many long-term care residents fell in the 30 days leading up to the date of their quarterly clinical assessment. Falls are the leading cause of injury for seniors and contribute to a significant burden on the health care system. Residents are at a higher risk of falling if they have a history of falls or are taking certain medications. Preventing falls increases the safety and quality of care of residents.
North West LHIN
Provincial
Falls in Long-Term Care*
16.9 per cent
15.8 per cent
*Canadian Institute for Health Information (CIHI) 2016-2017
4 Canadian Institute of Health Information (CIHI) Indicator Library
Agenda Item 8.1

8
Trend Over Time: Falls in the Last 30 Days in Long-Term Care (Percentage)
The above indicator is a part of Continuing Care Reporting System (CCRS) quality indicators developed by interRAI (www.interrai.org), an international research network, to provide organizations with measures of quality across key domains, including physical and cognitive function, safety, and quality of life. Each indicator is adjusted for resident characteristics that are related to the outcome and independent of quality of care. This is a measure in the Safety dimension the North West Local Health Integration Network will continue to monitor closely. Statistically, the North West Local Health Integration Network trend is considered on par with the province. This is a measure that requires discussion with the Long-Term Care sector to understand if there are changes happening on the ground that have led to the one year increase and to determine the quality improvement work that may be required.
Agenda Item 8.1

9
Home and Community Care - Safety 1. Safety
The following table provides comparative data for the Key Performance Indicator – Safety experienced by patients receiving Home and Community Care recorded in the North West Local Health Integration Network compared to the Provincial average.
North West LHIN
Provincial
Safety*
93.3 per cent
90.8 per cent
*NRC Health Patient Survey October to December 2017 April to September 2017
The North West Local Health Integration Network conducts phone Patient and Caregiver Experience Surveys monthly via the Provincial vendor NRC Health. The Key Performance Indicators (KPIs) used above and throughout this document are October to December 2017 unweighted positive scores. The Provincial aggregate scores used for benchmarking are available semi-annually with the next release anticipated in September 2018.
Weighted reports are used for the benchmarking purposes, ensuring distribution in overall reports is representative of the service population and not those responding. When reporting up to the aggregate level, up weight/down weight results to represent the actual population.
Quality improvement should be based on unweighted results. Please note the weighted verse unweighted results have very little change and as such why the most recent unweighted results are included in this report. Overall, our patients agree or strongly agree they were satisfied with the support received from the Care Coordinator to address safety concerns at home. Additionally, the patients were satisfied with the support received from the service provider to address safety concerns at home. Safety in the home as well as falls for home care patients (listed on next page) are areas of focused effort. A Home and Community improvement team worked collaboratively with the largest therapy provider to create joint education about safety and how to prevent falls in the home. The Care Coordinators and Therapist use the same documentation and speak the same language in an effort to deliver consistent messages to our patients. The elements from the successful pilot in the City of Thunder Bay will be spread to the rest of the region.
Agenda Item 8.1

10
2. Falls for Home Care Patients The following table provides comparative data for the percentage of falls experienced by patients receiving home care recorded in the North West Local Health Integration Network as compared to the Provincial average.
North West LHIN
Provincial
Falls for Home Care
Patients*
37.3 per cent
39.4 per cent
*Health Shared Services Organization (HSSO) Members Portal Q4 2017-2018
This indicator is a part of Continuing Care Reporting System (CCRS) quality indicators developed by interRAI (www.interrai.org), an international research network, to provide organizations with measures of quality across key domains, including physical and cognitive function, safety and quality of life. Each indicator is adjusted for resident characteristics that are related to the outcome and independent of quality of care. The fall indicator will be used to drive continuous improvement efforts in Home and Community Care. The percentage of in-home falls in the North West Local Health Integration Network continues to be one of the lowest in the province.
Agenda Item 8.1

11
Quality Dimension – Effective The Effective Quality Dimension relates to providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit, thus avoiding underuse and misuse respectively.
Health System – Effective 1. Follow up Primary Care
The following table provides comparative data for the percentage of patients in the North West Local Health Integration Network who receive follow-up with primary care after being discharged from hospital as compared to the Provincial average.
North West LHIN
Provincial
Follow up with Primary Care
post-hospital*
29 per cent
34 per cent
*Health Quality Ontario, Health System Performance -2016
This indicator shows the follow-up rate with a family doctor in the North West Local Health Integration Network within seven days of discharge after hospitalization for any of the following:
Pneumonia
Diabetes
Stroke
Gastrointestinal Disease
Congestive Heart Failure
Chronic Obstructive Pulmonary Disease
Heart Attack
other cardiac conditions. A higher rate is considered better as this follow-up can help smooth patient transition from hospital to home or community. A total of 29 per cent of patients in the North West Local Health Integration Network receive a primary care appointment following discharge from hospital. There is growing evidence that follow-up care with a primary care provider post-hospital decreases the risk of further decline or readmission.
Agenda Item 8.1

12
The North West Local Health Integration Network explored this indicator in the Primary Care Capacity work conducted in the summer of 2017. This exploration included dialogue with over 100 physicians and Nurse Practitioners to understand local primary care capacity, including timely access to primary care and post-discharge access. This capacity assessment information has informed investment decisions in interdisciplinary primary care teams across the North West Local Health Integration Network and continues to drive planning. 2. Worsened Physical Function in Long-Term Care
This indicator looks at how many long-term care residents worsened or remained completely dependent in transferring and locomotion. An increased level of dependence on others to assist with transferring and locomotion may indicate deterioration in the overall health status of a resident. The following table provides comparative data for the percentage of patients living in Long-Term Care in the North West Local Health Integration Network with worsened physical function compared to the Provincial average.
North West LHIN
Provincial
Worsened Physical Function
in Long Term Care *
31.per cent
34.7per cent
*Canadian Institute for Health Information (CIHI) 2016-2017
The above indicator is a part of Continuing Care Reporting System (CCRS) quality indicators developed by interRAI (www.interrai.org), an international research network, to provide organizations with measures of quality across key domains, including physical and cognitive function, safety and quality of life. Each indicator is adjusted for resident characteristics that are related to the outcome and independent of quality of care. Worsened Physical Function in Long term Care indicator will be used to drive continuous improvement efforts across the North West Local Health Integration Network Long Term Care homes. This is an area where performance in Long Term Care Homes in the North West Local Health Integration Network improved compared to 2015-2016 at 44 per cent. A lower rate is desirable as it indicates that a lower percentage of residents worsened or remained dependent in transferring and locomotion. This is a measure in the effective dimension that the North West Local Health Integration Network will continue to monitor closely. This measure requires continued monitoring and discussion with the Long-Term Care sector to understand if there are changes happening on the ground and to determine what changes to make the improvement and if further quality improvement work is required.
Agenda Item 8.1

13
3. All Patients Readmitted
The following table provides comparative data for the percentage of all patients readmitted to hospital in the North West Local Health Integration Network compared to the Provincial average.
North West LHIN
Provincial
All Patients Readmitted*
9.9 per cent
9.2 per cent
*Canadian Institute for Health Information (CIHI) 2016-2017
Trend Over Time: All Patients Readmitted to Hospital (Percentage)
*Canadian Institute for Health Information (CIHI) 2016-2017
This indicator measures the risk-adjusted rate of urgent readmissions within 30 days of discharge for episodes of care for the following patient groups:
Obstetric
Patients age 19 years and younger
Surgical
Medical.
Agenda Item 8.1

14
Readmission rates can be influenced by a variety of factors, including the quality of inpatient and outpatient care, the effectiveness of care transition and coordination, and the availability and use of effective disease management community-based programs. While not all unplanned readmissions are avoidable, interventions during and after a hospitalization can be effective in reducing readmission rates. Urgent readmissions to acute care facilities are increasingly being used to measure institutional or regional quality of care and care coordination. A lower rate is desirable. Work on this measure will be a priority in the North West Local Health Integration Network Quality Improvement Plan (QIP) and will be a focus of system-level work throughout the region as well. This is a measure in the Effective dimension the North West Local Health Integration Network will continue to monitor closely. This measure requires discussion with multiple sectors and stakeholders to understand if there are changes happening on the ground and to determine if any quality improvement work is required. 4. Mental Health and Addictions – Hospital Readmission
The table below provides North West Local Health Integration Network comparative data for the percentage of all patients readmitted to hospital for a mental illness or addiction in the North West Local Health Integration Network as compared to the Provincial average.
North West LHIN
Provincial
Hospital Readmission for a
Mental Illness or an Addiction*
9.7 per cent
12.7 per cent
* Canadian Institute for Health Information (CIHI) 2016-2017
Agenda Item 8.1

15
Trend Over Time: Repeat Hospital Stays for Mental Illness (Percentage)
It is important to note this indicator is different than the indicator reported in the North West Local Health Integration Network Board of Directors Score Card. The indicator above is for readmission for mental health and addictions while other indicators report on the rate of repeat Emergency Room visits (mental health and substance abuse, separately).
While the results for this indicator in the North West Local Health Integration Network is reported as being below the Provincial average, we will maintain a focus on this Quality indicator and will continue to monitor closely. This measure requires discussion with multiple sectors and stakeholders to understand what is happening on the ground to determine if quality improvement work may be required. Work is underway to formalize a Regional Mental Health and Addictions Plan which will support standardized, equitable access to care. Additionally, the North West Local Health Integration Network is continuing to invest in areas where service gaps have been identified, including support with housing and high support housing. 5. Quality Based Procedures
Quality Based Procedures (QBPs) are specific groups of patient services that offer opportunities for health care providers to share best practices that will allow the system to achieve even better quality and system efficiencies.
Agenda Item 8.1
16
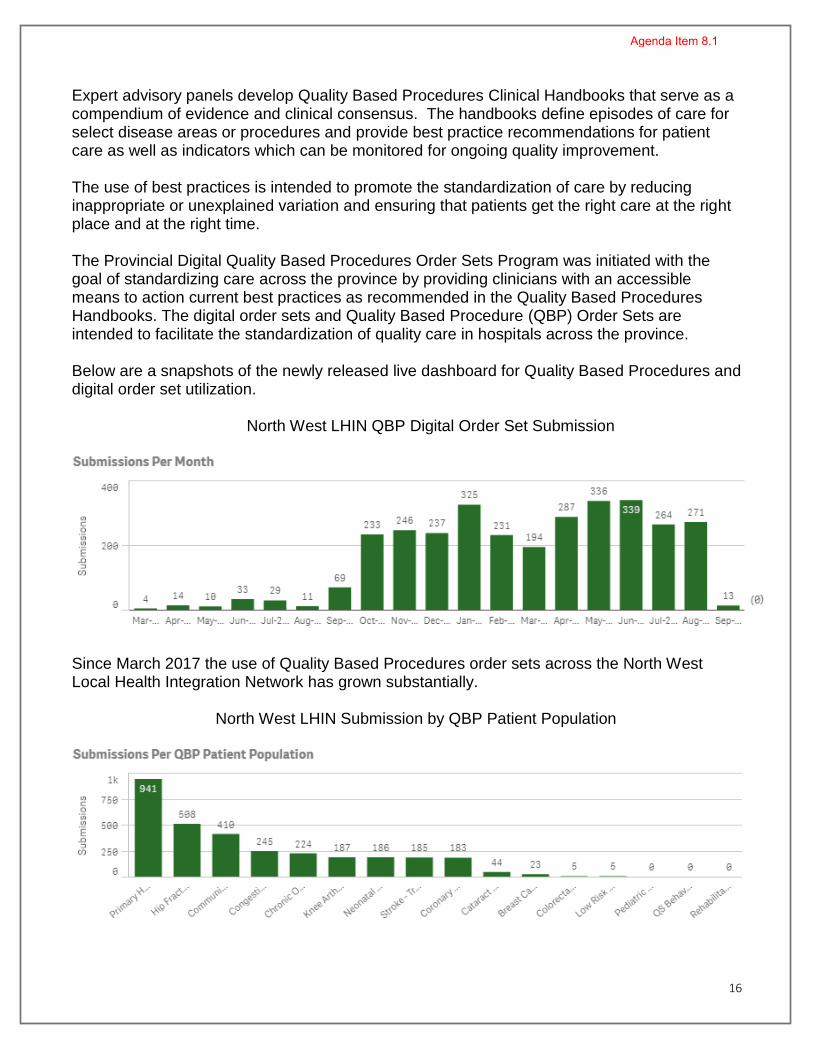
Expert advisory panels develop Quality Based Procedures Clinical Handbooks that serve as a compendium of evidence and clinical consensus. The handbooks define episodes of care for select disease areas or procedures and provide best practice recommendations for patient care as well as indicators which can be monitored for ongoing quality improvement. The use of best practices is intended to promote the standardization of care by reducing inappropriate or unexplained variation and ensuring that patients get the right care at the right place and at the right time. The Provincial Digital Quality Based Procedures Order Sets Program was initiated with the goal of standardizing care across the province by providing clinicians with an accessible means to action current best practices as recommended in the Quality Based Procedures Handbooks. The digital order sets and Quality Based Procedure (QBP) Order Sets are intended to facilitate the standardization of quality care in hospitals across the province. Below are a snapshots of the newly released live dashboard for Quality Based Procedures and digital order set utilization. North West LHIN QBP Digital Order Set Submission
Since March 2017 the use of Quality Based Procedures order sets across the North West Local Health Integration Network has grown substantially.
North West LHIN Submission by QBP Patient Population
Agenda Item 8.1

17
The predominate Quality Based Procedure order set being utilized is for Primary Hip and Knee Replacement with 941 order sets submitted since March 2017. All 941 digital order set submission originated from Thunder Bay Regional Health Sciences. The three other acute care facilities performing hips or knee are not live with the Quality Based Procedures Hip and Knee Digital order set. Work is actively underway to align regional physician practices with orthopedic surgeons. Future quality work will include further analysis on each Quality Based Procedure, linking with other system data bases to understand where variation remains.
Home and Community Care - Effective 1. Links to Other Services
The following table provides comparative data for the percentage of home care patients who responded favorably to being linked to services by the North West Local Health Integration Network as compared to the Provincial average.
North West LHIN
Provincial
Link to Other Services*
77.6 per cent
77.7 per cent
*NRC Health Annual Patient Survey October to December 2017 April 2017 to September 2017
Home care is one of the few care settings in Ontario that has already implemented a standardized patient experience survey. Results from the survey are made available through a centralized data-collection and reporting mechanism. Local Health Integration Networks have used longitudinal data from the Client and Caregiver Experience Evaluation survey to inform decision-making5. Data from the surveys is used to evaluate how patients are linked to other services both while they are receiving home care and following discharge as this speaks to system continuity (or lack thereof). This data is also used to determine if patients feel they received the service they needed next in their care journey. According to our Home and Community Care patients, 77.6 per cent replied positively that they were linked to further support in their community. Additionally, if our patients needed further support they were linked after home care services ended. This is a decrease in positive response from April to September 2017, when 80.6 per cent of patients replied positively to being linked to other services.
5 HQO Ontario Patient Experience Measuring Strategy, August 2016
Agenda Item 8.1

18
2. Hospital Readmissions The following table provides comparative data for the percentage of home care patients who are readmitted to hospital in the North West Local Health Integration Network compared to the Provincial average.
North West LHIN
Provincial
Hospital Readmissions*
22.5 per cent
18.3 per cent
*Health Shared Services Ontario (HSSO) Members Portal Q2 2017-2018
Measuring the readmission of home care patients with an unplanned readmission within 30 days of discharge allows for review of effectiveness of service(s) and considerations for improvements.
The Hospital Readmissions rate for home care patients is above the Provincial average. This will be an area of focus for the 2018-2019 Home and Community Care Quality Improvement Plan. The Q2 2017-2018 readmission rate was 22.5 per cent, an increase from 18.3 per cent in the previous quarter. It is important to note the Provincial readmission data is delayed by nine months. The North West Local Health Integration Network local data projects an improvement in readmission rates beginning in Q4 2017–2018. Local data can be found on the Quality Improvement Plan scorecard.
Agenda Item 8.1

19
Quality Dimension – Timely The Quality Dimension focuses on reducing waits and sometimes harmful delays for both those who receive and those who provide care.
Health System – Timely 1. Emergency Room – Physician Initial Assessment
This indicator measures the time between the arriving in the Emergency Room (date and time), to the date and time of the initial assessment by a physician.
North West LHIN
Provincial
Emergency Room –
Physician Initial Assessment (PIA)*
2.6 hours
3 hours
* Canadian Institute Health Information (CIHI) 2016-2017
Time is crucial to the effectiveness and outcome of patient care, especially for patients seeking treatment in the Emergency Room. In conjunction with other indicators, this can be used to monitor the time patients spend in the Emergency Room in an effort to improve the efficiency and, ultimately, the outcome of patient care. Multiple factors can influence the indicator results, including:
triage level
patient population
availability of resources. In the North West Local Health Integration Network, the Physician Initial Assessment (PIA) indicator is continually monitored in each Emergency Room. Additionally, through the pay-for-results program at Thunder Bay Regional Health Sciences Centre, several initiatives have impacted the Physician Initial Assessment. These initiatives include:
establishment of Rapid Assessment Zones
Triage Enhancements during daily peak times
Staffing changes to facilitate patient flow.
Agenda Item 8.1

20
2. Same day / next day Appointment with Primary Care
The following table provides comparative data for the percentage of patients who are able to be seen by their primary care provider same day or next day in the North West Local Health Integration Network compared to the provincial average.
North West LHIN
Provincial
Same day / next day
appointment with Primary Care*
30 per cent
43.1 per cent
*Health Quality Ontario, System Performance 2016
The results for the North West Local Health Integration Network are significantly lower than the Provincial results when comparing data for same day / next day appointments with primary care. We are working with physicians through the Clinical Division to understand these results and to identify best local practices that could be utilized or developed.
The North West Local Health Integration Network explored this indicator in the Primary Care Capacity work conducted in the summer of 2017. This exploration included dialogue with over 100 physicians and Nurse Practitioners to understand local primary care capacity, including timely access to primary care and post-discharge access. The capacity assessment information has informed investment decisions in interdisciplinary primary care teams across the North West Local Health Integration Network and continues to drive planning.
Home and Community Care – Timely 1. Five Day Wait for Services
With a specific emphasis on reducing wait times for patients with the greatest need, the Ministry of Health and Long-Term Care introduced new measures for access to timely care, including five-day wait times for home nursing visits and personal support visits for patients with complex care needs.
Agenda Item 8.1

21
The following table provides comparative data for the percentage of North West Local Heath Integration Network complex home care patients requiring personal support and all nursing patents who receive their first visit within five days as compared to the Provincial average.
North West LHIN
Provincial
Five Day Wait for Services
(Personal Support)*
86.84 per cent
85.34 per cent
Five Day Waits
(Nursing)*
96.45 per cent
95.77per cent
* Stocktake Q4 2017-2018
This indicator measures our ability to provide care within five days of assessment by a Care Coordinator. This measurement is made for all patients who require nursing, as well as for complex patients who require personal support.
The five day wait for personal support services increased from the previous quarter to from 68.75 per cent to 86.48 per cent. The small volume of patients in the North West Local Health Integration Network impacts this indicator significantly and also increases the volatility of percentage.
This indicator is up by 18.09 per cent when compared to the previous quarter and up by 20.17 per cent when compared to the same quarter one year ago. For Q3 2017-2018, this indicator contains 38 clients of which five did not receive service within the access target. The small volume of clients impacts this indictor significantly and increases the volatility. As an example, one of the 10 clients included in the indicator received service within five days but was not properly captured as a pre-planned service which reduced performance by three per cent. Given this indicator is influenced by data quality and small case counts, the North West Local Health Integration Network is planning to analyze this indicator at a detailed level on a monthly basis.
In this particular period it was noted that clients that did not receive service within the access required either respite service or were part of the Wait at Home Program. Service provider capacity is a challenge which impacts the ability to provide service on a timely basis for those requiring Wait at Home services. To mitigate this risk, in cases where the demand for Wait at Home activity surges, the North West Local Health Integration Network meets with all personal support service providers to collaborate with all providers and develop action plans to provide service to clients on a timely basis.
Agenda Item 8.1

22
Based on internal data reviewed, the North West Local Heath Integration Network anticipates performance for Q1 2018-2019 to be in alignment with the performance of Q4. As noted previously, due to the low volume of cases included in this indicator (approximately 30 per quarter), it is anticipated volatility in performance will be experienced.
The five-day wait indicator for nursing service continues to perform above the Provincial target of 95 per cent, which is an ongoing improvement when compared to the previous year.
This indicator is continuing to perform above the 95 per cent Provincial target and has been generally consistent over time. The North West Local Health Integration continues to monitor this indicator to maintain performance. The North West Local Health Integration Network has implemented several strategies to achieve current performance levels. These are related to properly undertaking and coding pre-planned service. The North West Local Health Integration Network works with the client to determine the most beneficial time to begin service as not all nursing interventions are not required to occur within five days such as assessments for long-term care or certain palliative care services. Appointments are scheduled at a mutually agreeable time between patient, family and nursing provider after the coordinator authorizes nursing service. Where this occurs it is important for this pre-planned activity to be captured. The Home and Community Care Division continues to monitor both indicators to maintain the performance goal, which is the Provincial Target. In the event performance is not kept, several strategies are available to pinpoint the cause and assign resources as required.
Agenda Item 8.1

23
2. Community Setting to Home Care Services The table below provides comparative data at the 90th percentile of North West Local Heath Integration Network referrals originating in the community setting (excluding acute care) to first service as compared to the Provincial average.
North West LHIN
Provincial
Community Setting to First
Service*
21 days
28 days
* Stocktake Q4 2017-2018
There are three time periods that impact this indicator:
time required for assessment during intake
time required for assessment in home to authorize service
time required for the provider to visit the patient. Our performance during the fourth quarter of 2017-2018 was between the target of 21 days and the Provincial average of 28 days. The North West Local Health Integration Network performance this quarter is three days better than the previous quarter and we are outperforming the province by seven days. Improvements were realized through intense monitoring of this indicator to ensure staffing levels were maintained or augmented to process the referrals in a timely manner. This indicator is comprised of two components: assessment wait time (first two bullets above) and service initiation wait time (third bullet above). For Q4 2017-2018, the wait time for assessment was 13 days which is four days better than the Provincial average of 17 days. For this same time period the wait time for service initiation was eight days, which is four days better than the Provincial average. Home and Community Care continues to focus on a strategic approach to improve this indicator and will continue to work to identify which time periods impact performance negatively and which time periods can be improved. It is expected this indicator will further improve.
Agenda Item 8.1

24
Quality Dimension – Equitable The goal of the Equitable Quality Dimension is to ensure that the care that is provided does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status. Health equity will be achieved when all people living in Ontario are able to reach their full health potential. This means all people are able to receive quality care that is fair and appropriate to them – regardless of where they live, their economic or social status, language, culture, gender, or religion. This also means all people are able to access appropriate housing, education, and earn fair incomes. To this end, achieving health equity is complex. Things like housing, education, and income greatly influence people’s health and fall outside the walls of the health care system.
Health System – Equitable 1. Life Expectancy at Birth
The indicator table below is the number of years a person would be expected to live, starting at birth, if the age- and gender-specific mortality rates for a given reference period were held constant over his or her life span in the North West Local Health Integration Network compared to the province.
North West LHIN
Provincial
Life Expectancy at Birth *
78.3 years
82.3 years
* Canadian Institute for Health Information (CIHI) 2012-2014
Agenda Item 8.1

25
Trend Over Time: Life Expectancy at Birth (Years)
Used worldwide, life expectancy at birth is understood as a measure of the general health of a population. By definition, life expectancy is affected by age- and gender-specific mortality rates in a particular reference period. Life expectancy is shorter in the north. People in the North West Local Health Integration Network region have a life expectancy of 78.3 years which remains basically the same compared to 2009 (78.6 years), compared to 82.3 years (an improvement since 2009 at 81.5 years in Ontario).
2. Avoidable Deaths
Avoidable mortality refers to untimely deaths that should not occur in the presence of timely and effective health care, including prevention. It serves to focus attention on the portion of population health attainment that can potentially be influenced by the health system. Potentially avoidable mortality includes premature deaths that could potentially have been avoided through all levels of prevention (primary, secondary, tertiary).
Agenda Item 8.1

26
This table compares the rate of avoidable deaths in the North West Local Integration Network to the province.
North West LHIN
Provincial
Avoidable Deaths*
307 (per 100,000)
190 (per 100,000)
*Canadian Institute for Health Information (CIHI) 2013-2015
Trend Over Time: Avoidable Deaths (per 100,000)
The Northwest also has a high avoidable death rate compared to the province and Canada. An analysis of avoidable mortality highlights the need for prevention.6 The avoidable death rate in the north remains static since 2006.
Avoidable death indicators provide additional insight into the North West Local Health Integration Network and subsequently Ontario and Canadian health systems. These measures can be used to assess the impact of prevention strategies and the outcomes of health policy decisions and health care provision. Lower rates are desirable.
6 Canadian Institute for Health Information (CIHI) Indicator Library, Avoidable Deaths
Agenda Item 8.1

27
The potentially avoidable mortality indicator includes premature deaths that could be avoidable through all levels of prevention. Mortality from preventable causes focuses on premature deaths from conditions that could potentially be avoided through primary prevention efforts, such as lifestyle modifications or population-level interventions (for example, vaccinations and injury prevention). The indicator informs efforts aimed at reducing the number of initial cases, or incidence reduction, as deaths are prevented by avoiding new cases altogether. Mortality from treatable causes focuses on premature deaths that could potentially be avoided through secondary and tertiary prevention efforts, such as screening for and effective treatment of an existing disease. The indicator informs efforts aimed at reducing the number of people who die once they have the condition, or case-fatality reduction. Home and Community Care – Equitable 1. Patient Goals at Discharge
The table below indicates the percentage of patients who have met their care goal(s) on discharge of home care service. The percentage excludes those patients who stopped their service and those who died.
North West LHIN
Provincial
Patient goal(s) met at
discharge *
92 per cent
-
*Health Shared Services Organization (HSSO) Members Portal Reporting Site: Q1 2018-2019
This is an internal Home and Community Care indicator used to ensure we are measuring care goal(s) and advancing patient goal(s) and progression to discharge where appropriate.
Agenda Item 8.1

28
2. Levels of Care
The Levels of Care Framework is an approach to ensure that Ontarians receive consistent, high quality home and community care, regardless of where they live, through a standardized approach to assessing need, and the transparent and understandable assignment of home and community care services.
North West LHIN
Provincial
Levels of Care
(Measurement currently in Development)
-
-
As the Levels of Care work heads into implementation we will be looking to develop / add a measure to demonstrate equitable service.
Agenda Item 8.1

29
Quality Dimension – Patient-Centred The emphasis of this Quality Dimension is the provision of care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions.
Health System – Patient-Centred 1. Hospital Survey (Acute Care Experience Survey)
The patients in the North West Local Health Integration Network report a 77 per cent satisfaction with the acute care hospital experience. This measure must, however, be interpreted with caution since only seven of 11 hospitals used this measure on their Quality Improvement Plans.
North West LHIN
Provincial
Acute Care Experience
Survey *
77 per cent
62.6 per cent
*Health Quality Ontario, Quality Improvement Plan (HQO QIP) 2016-2017
The data above will be used to inform the 2018-2019 North West Local Health Integration Network Quality Plan. A review of the 2018-2019 Acute Care Quality Improvement Plan is forthcoming to further develop this measure.
Home and Community Care – Patient-Centred
1. Overall Experience The table below is the measurement of Overall Experience for patients receiving North West Local Health Integration Network home care services compared to the province.
North West LHIN
Provincial
Overall Experience*
91.35 per cent
90.8 per cent
*NRC Health Annual Patient Survey October to December 2017 April to September 2017
Agenda Item 8.1

30
Home and Community Care patients responded positively at a rate of 91.35 per cent when asked to rate the services they received from the North West Local Health Integration Network and any of the individuals who have provided care. While this measure continues to be above the 90 per cent, improvement opportunities remain. The majority of patients respond to the three questions making up this key performance indicator as ‘good’ instead of ‘very good’ or ‘excellent’. The response proportions between the three answers signals it is time to stretch the indicator and focus on ‘very good’ and ‘excellent’, which requires a deeper understand of what is driving overall experience. 2. Quality of Care The table below is the measurement of the quality of care received by patients served by North West Local Health Integration Network home care services compared to the Provincial average.
North West LHIN
Provincial
Quality of Care*
95.31 per cent
93.3 per cent
*NRC Health Annual Patient Survey October to December 2017 April to September 2017
Home and Community Care patients responded positively about the quality of care they received when asked if they felt their plan was right for their needs. The survey responses included specific feedback with regards to how the Care Coordinator helped arrange the services that were required and if the service provider understood their needs. Although performance in this indicator continues to be above 90 per cent, there is still room for collaborative improvement and work with our Service Provider Organizations.
Agenda Item 8.1

31
3. Client-Centred Care
The following table is the measurement of Client-Centred Care received by patients supported by North West Local Health Integration Network home care services as compared to the Provincial results.
North West LHIN
Provincial
Client-Centred Care
91.3 per cent
87.5 per cent
*NRC Health Annual Patient Survey October to December 2017 April to September 2017
When Home and Community Care patients were asked if they received all the information about services and that they felt included in the care plan, the positive response was 91.3 per cent compared to 87.1 per cent in April to September 2017. Opportunities continue to exist for improvement, specifically for patients to feel included in developing their care plan.
Agenda Item 8.1

32
Quality Dimension – Efficient This Quality Dimension focuses on methods to avoid waste, including waste of equipment,
supplies, ideas, and energy.
Health System - Efficient 1. Per Capita Health Service Spending The table below provides the Per Capita North West Local Health Integration Network health services spending allocation as a percentage of the Provincial average Local Health Integration Network health care spending.
North West LHIN
Provincial
Percentage of health service
spending*
155 per cent
*CEO Interpretations Q2 Board ENDS Report Card October 2017
2. Cost of a Standard Hospital Stay
In the following table, the indicator measures the ratio of a hospital's total acute inpatient care expenses to the number of acute inpatient weighted cases related to the inpatients for which the hospital provided care.
North West LHIN
Provincial
Cost of a Standard Hospital
Stay*
$5,210
$5,360
* Canadian Institute for Health Information (CIHI) 2016-2017
Agenda Item 8.1

33
Trend Over Time: Cost of a Standard Hospital Stay (Dollars)
Canadian Institute for Health Information (CIHI) 2015
The cost of a standard hospital stay is an indicator that measures the relative cost-efficiency of a hospital's ability to provide acute inpatient care. This indicator compares a hospital's total acute inpatient care expenses to the number of acute inpatient weighted cases related to the inpatients that it provided care for. The result is the hospital's average full cost of treating the average acute inpatient. A high cost of a standard hospital stay indicates a relatively high cost of treating the average acute inpatient; a low cost of a standard hospital stay indicates that the cost of treating the average acute inpatient is relatively low. The average cost for a standard hospital stay in the North West Local Health Integration Network is right at the Provincial average. However, the percentage of per capita health care spending by the North West Local Health Integration Network continues to rise year over year.
Identifying additional indicators in the Healthcare System Level Efficiency Quality Domain will be included in the 2018-2019 North West Local Health Integration Network Quality Plan.
Agenda Item 8.1

34
Home and Community Care – Efficient The following table compares the percentage of Home and Community funding on purchased service and case management in the North West Local Health Integration Network to the province.
North West LHIN
Provincial
Percentage total of Home and Community funding spent on direct services*
80.9 per cent
80.0 per cent
Percentage total of Home and Community funding
spent on Case Management
19.1 per cent
20.0 per cent
Percentage of purchased
services with a unit cost at or below the Provincial average
82.66 per cent
*Health Data Branch: MIS Fiscal 2017 2018
In fiscal 2017-2018, the North West Local Health Integration Network spent 81.4 per cent of the Home and Community Care funding on purchased services, such as nursing, personal support, therapies, social work and nutrition. Additionally, the percentage of Home and Community funding spent on case management is below the Provincial average. Additionally the percentage of purchased services with a unit cost at or below the Provincial average is 82.66 per cent. This is a measure in the efficient dimension the North West Local Health Integration Network will continue to monitor closely.
Agenda Item 8.1

35
Home and Community Care Quality Improvement Plan 2018-2019
Status on Home and Community Care Quality Improvement Plan (QIP)
In the above table the status of each indicator is outlined. Each year the North West Local Health Integration Network reviews the year prior and plans for the year ahead. The intent and spirit of the Quality Improvement Plan is to always be pushing for improvement, even if the target is not achieved in a particular year.
Status
Q2 Q3 Q4* Q1* YTD Target Q2 Q3 Q4 Q1 YTD Target
11.0% 10.2% 15.6% 12.8% 12.9% 9.3% 11.5% 10.5% 10.2% 10.0% 10.5% 9.3%
22.7% 15.9% 22.8% 17.4% 20.2% 17.3% 18.9% 17.1% 18.9% 18.3% 18.3% 17.3%
Q3 Q4 Q1 Q2** YTD Target Q3 Q4 Q1 Q2 YTD Target
66.67% 62.50% 60.87% 54.55*** 63.40% 62.91% 44.83% 33.85% 34.21% 68.75% 44.87% 62.91%
33.6% 36.8% 34.4% 35.0% 35.0% 30.0% 30.6% 32.4% 34.3% 27.5% 31.4% 30.0%
96.3% 96.4% 95.8% 95.4% 96.3% 98.5% 95.7% 95.4% 95.6% 96.1% 95.7% 98.5%
71.9% 87.2% 85.7% 81.8% 81.8% 90.0% 73.8% 81.3% 89.7% 90.0% 82.7% 90.0%
YTD Target YTD Target
91.9% 93.0% 92.2% 93.0%
Q1 Q2 Q3 Q4 YTD Target Q1 Q2 Q3 Q4 YTD Target
CB CB CB CB CB CB N/A N/A N/A N/A N/A N/A
CB CB CB CB CB CB N/A N/A N/A N/A N/A N/A
CB CB CB CB CB CB N/A N/A N/A N/A N/A N/A
Q4 Q1 Q2** Q3 YTD Target Q4 Q1 Q2 Q3 YTD Target
42.9% 37.1% 38.2% N/A 38.6% 48.0% N/A 43.3% 35.3% 32.4% 35.0% 48.0%
Notes
Percentage of complaints acknowledged to the individual who made a
complaint within two business days
Post Emergency Department Visits (ED Visits)
Hospital Re-admissions
Percentage of patients diagnosed with a healable diabetic foot ulcer,
whose ulcer closed within 12 weeks
***Based on internal data. Not included in YTD
% Patients receiving their first Nursing visit within 5 days
92.2%
QIP Indicators
QIP Indicators StatusQIP Reporting Cycle - Q3 2017/18 - Q2 2018/19 QIP Reporting Cycle - Q3 2016/17 - Q2 2017/18
QIP Indicators
% Complex Patients receiving their first Personal Support within 5 days
StatusQIP Reporting Cycle - Fiscal 2018/19 QIP Reporting Cycle - Fiscal 2017/18
CCEE - KPI 1 - Overall Experience Rating
Q1-2 Combined
91.9%
Q1-4 Combined
N/A
Q1-2 Combined
*2017/18 Q4 & 2018/19 Q1 based on internal data. Official
results expected early 2019
5 Day Wait Time Indicators
End of Life - Preferred Place of Death
Falls for Long-Stay Home Care Clients - All Populations
2017/2018 QIP Workplan2018/2019 QIP Workplan
91.4%
StatusQIP Reporting Cycle - Fiscal 2017/18 QIP Reporting Cycle - Fiscal 2016/17
Q1-4 Combined
Cultural Competence & Diversity Training for staff.
QIP Indicators Status
QIP Reporting Cycle - Q4 2017/18 - Q3 2018/19 QIP Reporting Cycle - Q1 2017/18 - Q3 2017/18
Undetermined
Notes Notes
Undetermined
**2018/19 Q2 as of August 31st, 2018
Percentage of patients identified as meeting Health Link criteria who
are offered access to Health Links Approach
QIP for Home Care DashboardNot on track to meet target Not on track to meet target
North West Local Health Integration Network
QIP Indicators StatusQIP Reporting Cycle - Q2 2017/18 - Q1 2018/19 QIP Reporting Cycle - Q2 2016/17 - Q1 2017/18
On target to meet On target to meet
Agenda Item 8.1

36
It is important to note each indicator reporting period starts at a different point in time. Part of the 2018-2019 Quality Improvement Plan reports on historical data, for example Q3 and Q4 2017-2018. Improvements and changes planned and actioned on the indicators in 2018-2019 will be visible in Provincial data during the 2019-2020 Quality Improvement Plan cycle. Of the eight indicators, three are on track to meet target during the 2018-2019 Quality Improvement Plan cycle. For the post emergency room visits and re-admissions measure within 30 days of discharge from acute care. The North West Local Health Integration Network is targeting three pieces of work:
1. Emergency room discharge follow up phone call a. Identify change in care plan.
2. Implementation of Detection of Indicators and Vulnerabilities for Emergency Room
Trips (DIVERT) scale algorithm in the City of Thunder Bay. DIVERT Scale is a validated decision support system that identifies a patient's likelihood of future unplanned emergency use. The DIVERT scale is an empirically sound, visual representation of the predictors for Emergency Department visits among home care patients. It distinguishes six different risk categories (a score of 6 represents the highest level of risk). The DIVERT scale is intended to assist in targeting home and community care patients at risk of unplanned emergency department use.
3. Using the CRISIS Scale (CRISIS Identification and Situation Improvement Strategies)
a. The scale works within a framework of seven clinical risk categories and five risk levels with two outcomes:
i. Clinical Assessment Protocols (CAPs) to inform patient care planning interventions and avoid preventable crisis admissions
ii. Recommends a CRISIS Risk Level from 1 to 5 (where 5 is most risk) based on patient risk of crisis admission to long-term care placement within 90 days.
Given our high demand for long term care placement and limited supply many home care patients await placement in an acute care facility resulting in high Alternate Level of Care rates. Identifying home care patients on the tipping point prior to crisis can allow for a change in care plan and diverted hospital admission or readmission.
Agenda Item 8.1

37
Home and Community Care Event Tracking Management System
Safety is an area of focus within Home and Community Care and reviews of patient safety events are standard work. The Event Tracking Management System is an application used to create new and edit existing events, using a streamlined electronic management system. The Event Tracking Management System application provides a consistent, simple and quick way to create an accurate compliment, complaint or risk event. Once information is entered, forms are electronically sent to Service Provider Organizations that have been set up on the portal and the designated Manager. The Event Tracking Management System application is a vital tool in monitoring the abilities of organizations to deliver patient-driven care. Event management is part of an overall enterprise wide risk management and quality improvement approach to providing services to patients. Event management ensures timely notification to the North West Local Health Integration Network of real or potential risks that could adversely affect the health and safety of the patient, caregiver, service provider, or Local Health Integration Network staff, the environment, the functioning of the North West Local Health Integration Network business processes, or the North West Local Health Integration Network reputation, and includes the identification of opportunities to reduce or eliminate those risks through continuous Quality Improvement. This data is an internal pull from the Events Tracking Management System for each event entered and in all cases the most responsible Manger is notified to begin an investigation. There are a number of processes in effect to monitor, manage, and address all events entered. When comparing the data from the previous year, it is important to note that an increase in the number of events does not necessarily mean more harm. We follow a robust framework to monitor risk and address and action events. In the table below, the adherence to the process and mechanisms for escalation is standard. This dashboard is a reflection of customary practice and reporting.
Agenda Item 8.1

38
Part of the quality framework includes review of all adverse events and unexpected deaths. In April and May 2018, Home and Community Care experienced an unusual number of events leading to intensive review and follow up with system partners. It is important to highlight the current framework outlines investigation of all atypical events regardless of the level of care with the patient. The largest increase in risk event reporting continues to occur in the low- and medium-risk categories. This is exactly the category we would like to see increase as this indicates that we are now gathering information on low/no-harm and near-misses. Comparing Q2 2017-2018 to Q2 2018-2019 the number of reported events is consistent form year to year. We strongly encourage our patients, staff, and service providers to report concerns. This is part of the no blame culture we seek to foster. This data is a powerful tool that can be used to evaluate system level issues, new trends, clustered events, performance, and opportunities for improvement. An ideal system captures adverse events, when care harms patients, and near misses, when errors occur without any harm. Near misses signal system weaknesses and, because harm did not occur, may provide insight into solutions.7
7 The American Surgeon, Volume 72, Number 11, November 2006, pp. 1088-1091 (4)
Home and Community Patient Safety DashboardJune July August Total June July August Total
Number All Event Types (Risk Events,Complaint,Privacy,High-Adverse) 68 82 111 261 84 97 75 256
Number of All Unexpected Death 0 0 0 0 <5 <5 0 <5
Number of High-Adverse Events 0 0 0 0 0 0 0 0
Number of Unexpected Death 0 0 0 0 0 0 0 0
Number of all other High-Adverse events: Permanent harm/injury to Patient/LHIN or Service Provider 0 0 0 0 0 0 0 0
Number of Risk Events 50 70 91 211 70 79 60 209Number of High Risk Events: has actual potential for signif icant but not permanent harm/injury to
Patient/LHIN/ or Service Provider 13 26 22 61 6 9 7 22
Number of Medium Risk Events: Has actual potential for some harm/injury to Patient/LHIH/or Service
Provider 21 27 40 48 32 26 32 90
Number of Low Risk Events: Near miss, no harm, minimal harm/injury to Patient/LHIN or Service
Provider 16 17 29 62 32 44 21 97
Number of Complaints 14 11 19 25 6 7 10 23
Number of Privacy Events <5 <5 <5 6 8 <5 <5 8
Number of High Client Fall Risk Events 0 0 0 0 0 0 0 0
Number of High Medication Error Risk Events <5 <5 <5 7 <5 <5 0 <5
Number of Compliments 13 <5 <5 20 <5 8 6 17
17/18 18/19
Agenda Item 8.1

39
Home and Community Care Service Provider Organization – Quality Scorecard The purpose of the Quality Scorecard is to give a visual snapshot of how all of our current Service Provider Organizations and Vendors are performing in the key standard areas. These areas are identified within the contracts and by request from Health Quality Ontario. It is a tool that quickly highlights those areas in which particular Service Provider Organizations and Vendors are struggling in as well as those in which they are excelling. The Performance Management process has been undergoing many changes and will likely continue to transform and change to adapt the philosophy and vision of Quality Improvement.
Service Provider or Vendor Missed Care
On-Time
First Visits
Satisfaction
with
Appointment
Times
Satisfaction
with
Continuity
Acceptance
of
Referrals
Collaboration
and
Innovation
Report
Timeliness
Frequency of
Risk Events
Service Provider or Vendor 1 B D C C B B C D
Service Provider or Vendor 2 A A C C B B D B
Service Provider or Vendor 3 D C B B A B C B
Service Provider or Vendor 4 A C B A A A A A
Service Provider or Vendor 5 D A B B D B B B
Service Provider or Vendor 6 A A NA NA A B A A
Service Provider or Vendor 7 A A B A A A A A
Service Provider or Vendor 8 A A B B A B A A
Service Provider or Vendor 9 NA NA NA NA NA NA NA NAService Provider or Vendor 10 A A B A B A B A
Service Provider or Vendor 11 A B A A B C B A
Service Provider or Vendor 12 A A B A A B A A
Service Provider or Vendor 13 A B B B B A A A
Service Provider or Vendor 14 A A B A A A A A
Service Provider or Vendor 15 A A A A A B A A
Service Provider or Vendor 16 A A B A A A A A
Service Provider or Vendor 17 A A B A A A A A
Service Provider or Vendor 18 A A A A A B A A
Service Provider or Vendor 19 A A A A A B A A
Service Provider or Vendor 20 A A A A A B A A
Patient Experience System Experience
Provider Performance
Reporting
Contracted Service Provider Inventory and Perfromance North West LHIN
Updated as of August 27, 2018
Agenda Item 8.1

40
Quality Scorecard Key
Definitions Definitions A B C D
Acceptance of Referrals Acceptance of
Referrals Above target At target Band below target Well below target
Collaboration and Innovation
Collaboration and Innovation
Proactive in proposing
innovations & dealing with
service challenges
Willingness to try new service
delivery methods & take on challenges
No offer of help but not a
hindrance either
Difficult to deal with & lacks ability or willingness
to even improve
Report Timeliness Report Timeliness Above targets At targets Slightly below
target Requires reminders to complete or very late
Missed Care Missed Care Above target At target Band below target Well below target
On-Time First Visits On-Time First Visits Above target At target Band below target Well below target
Frequency of Risk Events Frequency of Risk
Events
No Events in past four months
One or two Events in past four months
Several Events in past four months
Many Events in past four months
Satisfaction with Appointment Times
Satisfaction with Appointment Times Above target At target Band below target Well below target
Satisfaction with Continuity
Satisfaction with Continuity Above target At target Band below target Well below target
Agenda Item 8.1

41
The How – North West Local Health Integration Network Quality Strategy
The North West Local Health Integration Network and systems partners have a plethora of opportunities for improvement. The data is compelling in the Equity and Effectiveness domains. The North West Local Health Integration Network Quality Strategy is the foundational building block and framework to how we improve quality for the residents of Northwestern Ontario. In alignment with governance expectations and the North West Local Health Integration Network Quality Strategy, the Regional Quality Committee (Operational), will develop a fiscal 2018-2019 quality work plan that includes analyzing all Quality Improvement Plans, reviewing published data, setting priorities, objectives, and targets. Additionally, the 2018-2019 Quality Plan will advance a system-wide, comprehensive and integrated approach to quality across all healthcare system sectors, North West Local Health Integration Network sub-regions and local health hubs, as well as non-Local Health Integration Network-funded organizations that contribute to the health of the population, wherever possible. The North West Local Health Integration Network Quality Strategy is aligned with the North West Local Integration Strategic Directions, priorities and goals as follows:
1. Improved health outcomes resulting in healthier people. 2. Access to health care that people need, as close to home as possible. 3. Continuous quality improvement. 4. A system-wide culture of accountability.
The Quality Strategy enables Health Service Providers to align local initiatives with regional priorities in order to advance quality improvement in our region. It outlines a framework which is designed to help us achieve the priorities for our region through to 2020. This Quality Strategy establishes three overarching priorities that will guide activities over the coming three years (2018-2020) to advance and improve health outcomes within the North West Local Health Integration Network region. These priorities are:
- Population Health of Sub-Regions - Design for Optimal Value - Health Equity
By focusing on these priorities and continuing to work with local Health Service Providers and key stakeholders, the North West Local Health Integration Network will build a quality framework to support a more integrated, safer, and efficient health care system. This will lead to value-designed, higher quality care throughout the region.
Agenda Item 8.1

42
Quality Goal By 2020 the North West LHIN will improve the quality of care for the residents in each sub-region by enegaging with clinicians and listening to patients and families.
By 2030 the North West LHIN will improve the health of people in each sub-region by targeting specific outcomes.
This will be possible as Sub-Region Planning Tables will set the Priority Health Outcomes and commensurate Quality Improvement goal(s) / indicator(s) for their specific sub region. Sub-region planning will shape health care transformation through community partnerships and through the adoption of a culture of continuous quality improvement. It will use measurement and feedback to inform both clinical quality work and patient safety initiatives.
Agenda Item 8.1

43
Appendices
Appendix A – North West LHIN Quality Scorecard September 2018 (infographic)
Appendix B - North West LHIN Home and Community Care September 2018 (infographic)
Agenda Item 8.1

Quality Dimensions
Safety
Effective
Timely
Equitable
Patient-centred
Efficient
Health System
Home and
Community Care
At Provincial AverageBetter Provincial Average
North West LHINQuality ScorecardSeptember 2018
The North West LHIN Quality Scorecard is based on the six Quality Dimensions. Within each dimensionhigh level indicators represent the overall maturity within the scope. These dimensions align to the Boardpolicy, Health Quality Ontario and the North West LHIN Quality Strategy. The scorecard is a baseline toolto evaluate progress towards a robust value-based model.
Avoiding harm topatients from the carethat is intended to help
Services based onscientific knowledge -which are beneficial
Reduce waits and sometimesharmful delays tothose receiving and providingcare
Care that does not vary in qualitybecause of characteristics suchas gender, ethnicity, geography,or socioeconomic status
Care that is respectful of andresponsive to individual patientpreferences, needs, and values
Avoiding waste, including wasteof equipment, supplies, ideas,and energy
Below Provincial Average
In-hospital sepsis(per 1000) Falls in the last 30days in Long TermCare
Follow up Primary Carepost-hospitalPhysical functioning in LongTerm Care All patient hospitalreadmissions Quality Based Procedures
Links to other services Hospital Readmissions
Emergency Department- Physician initialassessmentSame day/ next dayappointment withPrimary Care
5 - Day waits for serviceCommunity Setting toService
Life Expectancyat Birth AvoidableDeaths
Key Performance Indicator1: Overall Experience Key Performance Indicator2: Client Centred CareKey Performance Indicator4: Quality of Care
Hospital Survey(QualityImprovement Plan)Perceived Health(self reported)
Patient goal(s) met at
discharge
Measurement in
development - will link to
Levels of Care
Cost of a Standard HospitalStayPer Capita health servicespendingArea to advance Value-BasedHealth Care calcuation
Percent total of Homeand Community funding spend on purchase services
Falls: Q1 2018/19
5 Day Waits: Q4 2017/18
NRC: October to December 2017
Hospital Readmission
Q2 2017/18
CIHI: 2016-2017
Key PerformanceIndicator 9: Safety Falls for HomeCare Patients
Scores determined by composite data, not solely based on one indicator. Indicators above arehighlights for each dimension.
In Development
Agenda Item 8.1

Annual Patient Survey Highlights: October - December 2017
Quality of Care
Falls and Goals Met
Timely - 5 Day Wait
Nursing Complex PersonalSupport
Q4 2017/18 We measure our ability to provide care within five days of assessment by a CareCoordinator. We measure this for all patients who need nursing, as well as for complexpatients who need personal support. Nursing target 95%, Personal Support 87%.
Q4 2017/18 90th percentile - 9 out of 10 patients from the community wait 24 days for firstservice. Target 21 days.
96.4%
86.8%
21 days
28 days
91.3
95.3
93.893.3
Client Centred Care
91.3
77.6
Wait time from community setting to community home care service
North West LHIN Provincial Average
Missed Care Rate - Q1 2018/19
92%Patients with
Goals Met(on discharge)
35%Falls
Provincial 43%
North West LHIN
Home and Community Care
87.6
93.5
91.9
80.6
95.8
Overall Experience
Safety
Linking to Other Services
Willingness to Recommend
Overall percentage of how ourpatients rate the service andmanagement of care from theNorth West LHIN.Provincial: 90.8
Percentage of patients with apositive response that thecare plan met their needs.Provincial: 93.3
Positive responses to receivingsupport to address safety concernsat home. Provincial: 91.8
Percentage of our patientswho feel involved in their planand who were given theinformation they needed aboutservices.Provincial: 87.5
Positive response to beinglinked with further supportsand community services.Provincial: 77.7
Overall percentage of our patientswilling to recommend the NorthWest LHIN to family or friends.Provincial: 95.3
0.02%Nursing
0.10%Personal
Support Service
Patient Experience and Quality of Care
Q2 2018/19
Q1 2018/19
93.4
Results compared to April - September 2017 (local and provincial)
Agenda Item 8.1

September 25, 2018
Submitted by: Dr. Rhonda Crocker Ellacott
Agenda Item 9.1-1

2
This Board report provides information by Division on how the LHIN is advancing the goals of the Minister’s mandate letter and the work of the North West LHIN Board’s Strategic directions, the CEO Interpretation document, the LHIN’s Integrated Health Service Plan, the LHIN’s Annual Business Plan and the LHIN’s Health Services Blueprint.
CHIEF EXECUTIVE OFFICER UPDATE
In the past two months, I have continued to engage with our Leadership Team and staff to grow my learnings while discussing opportunities and challenges for the organization over the next three years. Also under the theme of engagement, I continue to work with system partners on health system transformation and meet regularly with Thunder Bay Regional Health Sciences Centre and St Joseph’s Care Group to discuss overcapacity issues. Over the summer period, I have both travelled to and met virtually with a number of health service providers, which continues to grow my understanding and knowledge of both operations, planning and other challenges we face. The following list includes the health service providers and service provider organizations that I have engaged with since the last Board meeting:
Atikokan General Hospital
Dryden Regional Health Centre
Patricia Region Senior Services Inc.
Fort Frances Tribal Area Health Services Inc.
Gizhewaadiziwin Health Access Centre
Riverside Health Care Facilities Inc.
CVH (No 2) LP (Southbridge) Long-Term Care Home (Birchwood Terrace)
Mary Berglund Community Health Centre
Changes Recovery Homes
Waasegiizhig Nanaandawe’iyewigamig
Board of Management of the District of Kenora Homes for the Aged
Kenora Association for Community Living
Kenora Chiefs Advisory Inc.
Kenora Sexual Assault Centre
Lake of the Woods District Hospital
Alzheimer Society of Kenora/Rainy River
Canadian Mental Health Association – Kenora
Canadian National Institute for the Blind
North of Superior Healthcare Group Long-Term Care Home (Wilkes Terrace)
NorWest Community Health Centres
People Advocating for Change through Empowerment (PACE) Inc.
Canadian Hearing Society
Upsala Volunteer Ambulance
Municipality of Machin
Indigenous Health Council
Winnipeg Regional Health Authority
Agenda Item 9.1-1

3
Externally, I continue to participate in Ministry of Health and Long-Term Care (MOHLTC) / LHIN Senior Leadership Team meetings, as well LHIN CEOs engagements. I want to thank our staff, for their support of assistance as we navigate the next Integrated Health Service Plan for the North West LHIN and to get our priorities for leading our health care system.
HEALTH SYSTEM STRATEGY, INTEGRATION AND PLANNING DIVISION Indigenous Health Council The Aboriginal Health Services Advisory Committee is currently being transitioned, and will be replaced with the formation of the North West LHIN Indigenous Council (IHC). The IHC will work closely with the Senior Leadership Team to strengthen partnerships that support an integrated health care system. This council will assist in shaping the North West LHIN’s programs, services and initiatives designed to improve care across the North West LHIN region for Indigenous patients. The IHC will aim to guide the development of the Indigenous Health Strategy. This strategy will address the diverse needs of the region’s Indigenous population, implement a harmonized governance structure of Indigenous cultural values and principles with LHIN organizational structures and mechanisms. It will also decrease the widening health disparity gap and social determinants of health. This past June, an expression of interest was sent out to all of LHIN funded health service providers, and phone calls were made to key leaders in the region to determine their interest in becoming a member of the IHC. The first meeting occurred on August 17, 2018, at Anishinabe Muskiki, and was facilitated by staff from the Ontario Indigenous Cultural Safety Program. Discussions focused on a proposed process to develop the IHC and to nurture the beginnings of a shared vision. It is important to acknowledge the contributions of Michelle Sault and her work on Indigenous councils in Toronto, across Ontario and nationally and her expertise in how to work collaboratively in defining Terms of Reference for these groups. Youth Inquest Recommendation #114 The North West LHIN continues to facilitate planning for a program in response to the Youth Inquest Recommendation #114 with partners. The three involved education authorities; Keewaytinook Okimakanak Board of Education (KOBE), Matawa Learning Centre (MLC), and Northern Nishnawbe Education Council (NNEC), have submitted their individual proposals to the North West LHIN for submission to both federal and provincial governments, as well as regulatory review. The proposals have adopted a multi-sited approach with shared services and protocols to best meet the needs of their respective student populations. The Ministry of Children, Community, and Social Services (MCCSS) has carried out a licensing review of all three programs and determined that as proposed, no licensing is required of the sites. Indigenous Services Canada has committed to funding approximately two-thirds of the required operating costs for the sites over the 2018-2019 fiscal year, and the remaining third of program funding is currently being considered by the Ministry of Health and Long-Term Care. As a result of implementing this program and providing safe sobering sites to youth, it is anticipated that health outcomes will be improved and health system utilization will be reduced.
Agenda Item 9.1-1

4
Chronic Disease Prevention and Management A forum was held June 29, 2018, with participants from 16 LHIN and non-LHIN funded regional chronic disease health service providers. The purpose of the engagement was to conceptualize an effective, ongoing communication exchange that will improve collaborative planning and strengthen a coordinated and integrated system of Chronic Disease Prevention and Management (CDPM) across the North West LHIN. Fifteen seats for the Michener Institute 10-week, online course The Foundations of Foot Management in Diabetes: A Holistic Approach, have been allocated to the North West LHIN to enhance the capacity of health care professionals to identify, prevent and treat diabetes-related complications of the feet based on a patient-centred, evidence-based model. Expressions of Interest (EOI) from 92 people were collected regionally with three candidates from each Sub-region were selected to participate in one of three cohort sessions being offered between September 2018 and March 2019. Base funding for offloading devices has been expanded to the Northern sub-region and the District of Thunder Bay in phase two of the Ministry of Health Offloading Devices Initiative. All five sub-regions are now receiving funding for offloading devices as a treatment option for individuals with diabetic foot ulcers. Mental Health and Addictions A regional psychiatry meeting was held on August 1, 2018, with participants from Thunder Bay Regional Health Sciences Centre (TBRHSC), Lake of the Wood District Hospital (LWDH), and St. Joseph’s Care Group (SJCG) present. The purpose of the engagement was to move forward the discussion that was started in the 2017-2018 fiscal year on how the Schedule 1 providers within the region can provide services in a more integrated, seamless manner. The result of the meeting was verbal acceptance by LWDH of the Higher Level of Care (HLOC) policy that was introduced by TBRHSC.
TBRHSC presented a draft Mental Health Emergency Services (MHES) proposal to the North West LHIN on August 17, 2018. The proposal outlines numerous positive impacts on the system, including decreased length of stay in the Emergency Department (ED) for admitted mental health patients, reduced inappropriate mental health admissions, and improved patient/family satisfaction. Next steps for TBRHSC are to submit a pre-capital submission, which they anticipate having completed by the end of September 2018.
Health Services Blueprint and Sub-region Planning As the North West LHIN Integrated Health Service Plan (IHSP) V work progresses, we are also clarifying and defining roles, responsibilities and accountabilities related to the Health Services Blueprint and sub-region planning. The North West LHIN remains committed to sub-region planning using a population health based planning approach that engages broader stakeholders. The North West LHIN appreciates the feedback that stakeholders have provided to inform the IHSP V, the Health Services Blueprint
Agenda Item 9.1-1

5
and sub-region planning; including what has been working well and what needs improvement. This feedback is helping to shape the way we will do things in the next three years. Over the fall period, the North West LHIN will engage all sub-region Planning Table members, as well as broader stakeholders throughout the region, to discuss the IHSP V, as well as future directions for the Health Services Blueprint and sub-region planning. Primary Care The North West LHIN continues to work with health service and primary care providers to advance coordinated care planning for complex patients within the region through the expansion of the Health Links approach to care. In the first quarter of this fiscal year, a total of 48 individuals received an individualized care plan, which outlines their personal goals and have a team of providers that are working together with them to ensure those goals are met. The North West LHIN is working with health service and primary care providers across the region to spread the implementation of coordinated care planning so that as many people as possible receive better, more coordinated care.
HOME AND COMMUNITY CARE DIVISION Home Care Strategies for Hospital Overcrowding and Alternate Level of Care Reduction Ontario’s hospitals are experiencing high occupancy rates and rising Alternate Level of Care (ALC) rates. One of the current provincial priorities is to reduce hospital overcrowding by creating additional care capacity outside of the hospital in community based settings. The North West LHIN Home and Community Care division is actively exploring all opportunities to not only increase capacity but also to optimize patient flow from hospital to community-based settings. In collaboration with Wesway, an innovative care model has been implemented to enhance home and community care capacity to support ALC patients outside of the hospital sectors. Home and Community Care will begin to enhance therapy services at home to minimize preventable hospital admissions and/or readmission to hospital. The social work therapy part of the enhanced therapy services, will focus on advanced care planning for patients who may need focused intervention. The North West LHIN has also expanded the Network of Individualized Community Enhancements (NICE) fund regionally to offer more equitable support for patients with short term needs and extraordinary circumstances. New Vendor for Medical Equipment
Effective July 16, 2018, the North West LHIN has secured a new medical equipment vendor called Medigas. The previous vendor, Shoppers Home Health Care, is no longer in the business of providing medical equipment, which has necessitated this change. The North West LHIN Home and Community Care division proactively worked with all hospital and community partners to ensure continuity of care. With advanced discharge planning and collaborative working relationships, the North West LHIN Home and Community Care were able to minimize impacts to patients and families. To date, there has been no delay in any hospital discharge because of the new equipment vendor.
Agenda Item 9.1-1

6
Family-Managed Home Care The North West LHIN Home and Community Care continues to work with the provincial Family- Managed Home Care (FMHC) Working Group to further develop the program. Provincial templates and supporting documents have been developed to support a standardized approach to the implementation of FMHC. At this time, we are in the process of onboarding the first patient into this program and responding to expressions of interest from three caregivers. Special Needs Strategy for Children As a part of the Provincial Special Needs Strategy, the existing North West LHIN school health rehabilitation services for speech-language pathology, occupational therapy and physiotherapy services in publicly funded schools will be transitioned to the Children’s Treatment Centres (CTCs). As of June 15, 2018, the North West LHIN had been directed by the Ministry of Health and Long-Term Care to hold all work in this regard until further notice. The Ministry of Children and Youth Services has communicated the same request to the CTCs. In order to ensure continuity of care, the North West LHIN Home and Community Care will continue to deliver rehabilitation services in public schools for the upcoming school year starting in September, 2018. Care Coordination in Primary Care The integration of care coordination with primary care is a provincial priority to ensure smooth transitions of care between home and community care and other health and social services as required. The North West LHIN is working with physicians and partners at Harbourview Family Health Team and Fort William Family Health Team to build better working relationships between the North West LHIN Community Care Coordinators and the physicians and care team within the primary care clinics. Community Care Coordinators have been aligned to each of the two Family Health Teams as a pilot within the City of Thunder Bay, and will be working to ensure there is better coordinated care for patients, by developing better communication channels and sharing information on mutual patients. Similar work is happening within each community in the North West LHIN to better align Community Care Coordinators to primary care practices. As a result, patients will receive better care knowing their care team is working together. CarePartners Privacy Issue
The North West LHIN has returned to business as usual with CarePartners following the June 12, 2018, cyber-attack on their organization. On August 1, 2018, all LHINs received assurance from HSSO that it was safe to resume normal operational protocols for patient care services with CarePartners. ParaMed Nursing Clinics On August 17, 2018, Ontario LHINs were informed that the Middlesex-London Public Health Unit discovered that three Flex Clinics operated by ParaMed in London had lapses in infection prevention practices. The North West LHIN Home and Community Care division does not have nursing clinics operated by ParaMed, nor does it have a wound care clinic operated by a service provider organization (SPO). All of the North West LHIN’s wound care procedures occur within the patient’s home, with single use or patient specific wound care supplies.
Agenda Item 9.1-1

7
Levels of Care The Levels of Care Framework will help ensure that home and community care service assessments and care planning are consistent and transparent across the province. It will also provide a more caregiver- and patient-centered process, where caregivers and patients are partners with LHIN Care Coordinators in developing care plans. The North West LHIN has been participating at the Pan-LHIN Implementation Working Group lead by the Ministry and HSSO Ontario. The Ministry has begun to work with six LHIN demonstration sites to prepare for the province-wide implementation of the Levels of Care Framework. The North West LHIN will continue to inform the overall demonstration approach through the provincial working group and prepare for local implementation based on lessons learned from the demonstration sites. The demonstration is expected to continue throughout the Fall 2018 and the Winter 2019. Patient and Family Advisory Committee The North West LHIN hosted their Patient and Family Advisory Committee (PFAC) meeting on September 11, 2018. The Chair of the Minister’s Patient and Family Advisory Council is attending the meeting by videoconference to have an interactive discussion regarding PFAC priorities from the provincial prospective. The North West LHIN PFAC team is currently in the process of developing a work plan to ensure patient and family engagement across the organization.
CLINICAL DIVISION The Clinical Division continues to focus on local engagement and knowledge sharing with the goal of making it easier for clinicians in the community to provide care across the spectrum. The North West LHIN will be providing regular updates in Fall 2018 to share important information on emerging clinical topics with local clinicians. The Northern Physician Resources Task Force, chaired by the Vice Presidents, Clinical of the North West and North East LHINs, continues to advance the recommendations from the Health Human Resources Summit that was held in January, 2018. The Task Force has published the final summary report of the summit focused on ways to ensure that rural and remote communities in Northern Ontario will have a sustainable supply of well-trained physicians to meet their health care needs. The North West LHIN Clinical Leads continue to engage locally to identify local priorities and ensure the voice of clinicians is brought forward. A network of primary care clinicians within the City of Thunder Bay, along with the City of Thunder Bay recruiter and Health Force Ontario Regional Advisor, met in June 2018 to identify ways to improve recruitment and retention of primary care clinicians.
Agenda Item 9.1-1

8
CORPORATE SERVICES DIVISION System Information, eHealth, Management & Technology eHealth Health Report Manager eNotification Health Report Manager (HRM) eNotifications are now available to primary care providers in the North West LHIN. These notifications enable providers to be notified within their electronic medical record (EMR) when their patients are discharged from the Emergency Department or are admitted or discharged from in-patient units. eNotifications are augmented with Home and Community Care and Health Links information prior to being sent to the EMR. After receiving an eNotification, primary care will subsequently receive a discharge summary and/or other reports from the hospital after the hospital has prepared the report(s) for electronic transmission. OntarioMD is currently engaging with primary care providers in the region making them aware of this service.
eConsult Primary care providers within the North West LHIN have been utilizing eConsult over the past two years. Currently, there are over 250 providers registered in the program. eConsult enables primary care providers to engage in a secured, electronic dialogue with specialists to manage patient care without the need for a patient visit with specialist. The benefits include:
Faster access to specialist advice
Avoidance of unnecessary in-person specialist visits
Improved care coordination and enable collaboration between clinicians
More flexibility and auditability than traditional phone calls, pages, or hallway conversations
To ensure all Ontarians have equitable access irrespective of their region, the multiple eConsult programs that currently exist across the province will be blended and deployed together as a single unified service. This will enable providers to be able to access local communities of practice in addition to provincial-level service through eConsult. In addition, the newly created Ontario eConsult Centre of Excellence, housed at The Ottawa Hospital and Bruyère Research Institute, is now leading the Ontario eConsult Program. The North West LHIN currently engages with the Ontario eConsult Centre of Excellence to further advance meaningful use of eConsult within the region. Telehomecare Vivify Implementation The Telehomecare Program has implemented new hardware and software called Vivify to help streamline processes and to enable future direct video conferencing with patients from within the home. The new hardware replaced legacy equipment that was no longer meeting the requirements of the program. In addition, the new hardware utilizes a self-install/uninstall model which decreases the asset management costs for the program.
Agenda Item 9.1-1
9
Information Systems/Technology Enterprise Review
With the Community Care Access Centre (CCAC)/LHIN transition completed, LHINs are jointly exploring opportunities to further improve effectiveness and efficiencies through an independent third-party assessment of the HSSOntario and LHINs Information Technology (IT) back office and email/messaging services. The overarching objective of this project is to conduct an assessment of the current state of IT services of HSSOntario and the LHINs with a focus on improving efficiency and cost-effectiveness while continuing to support the goals of the health care system. The project deliverables will provide a provincial overview on:
Systems and processes used across the province to deliver IT service
IT operating models and governance
Aggregate IT costs
The North West LHIN has completed and submitted all required assessment information and interviews for the current state for the consultant firm conducting the assessment. The findings and recommendations are expected to be available in the Fall of 2018. Cybersecurity Due to the cybersecurity incident that impacted the service provider CarePartners, the North West LHIN was forced to adopt business continuity plans in relation to all interactions with CarePartners during the better part of June and July. Normal operational protocols resumed in August. In response to this incident, all North West LHIN IT/IS cybersecurity practices have been reviewed to ensure alignment with stated HSSOntario practices. Formalized emergency management procedures have also been reviewed and modified as required to better address Cybersecurity incidents if they are to occur again. In addition, the Ministry of Health and Long-Term Care (MOHLTC) is undertaking a cybersecurity assessment on all health sectors across the province. The North West LHIN has completed all cybersecurity questionnaires required by the MOHLTC to support this assessment. Privacy and Issues Management Privacy Between June 1 and August 30, 2018, there were 16 various audit reports completed on users of our electronic medical record (CHRIS). No malicious activity or breaches were identified for users of the system. Freedom of Information Requests Between April 1 and August 30, 2018 there was one Freedom of Information (FOI) request for which action is currently underway.
Agenda Item 9.1-1

10
Issues Management The Event Tracking Management System (ETMS) has been modified to provide a common operational method to report, manage, and resolve organizational events occurring across the North West LHIN. The legacy-CCAC ETMS application was leveraged to create a harmonized approach, thereby allowing for timely reporting, communication, and analysis of events. Digitization of these events is a critical component for quality improvement, risk management, excellent patient experience, effective planning, and sustainable partnerships. The application was adapted to reflect the pan-LHIN complaints management framework, compliance, and reporting requirements.
HUMAN RESOURCES AND ORGANIZATIONAL DEVELOPMENT DIVISION Recruitment Activity: June 10, 2018 – September 9, 2018
Non-Union: New Hires
Jesse Traer, Manager of Employee Relations
Melanie Cates, Manager of Home and Community Care
Adam Vinet, Senior Operations Director
*Pending/Underway
Administrative Assistant, Sub-regions
Administrative Assistant, System Information
Director of City of Thunder Bay Sub-region
Director of Kenora Sub-region
Performance, Funding and Contract Management Lead
Program Support
Public Relations Lead *Recruitment is on hold as per Expenditure Restriction Directive
Union (ONA): New Hires:
Nicole Bradley: Community Care Coordinator, Sioux Lookout
Leanne Hilhorst: Community Care Coordinator, Kenora
Pending/Underway – Internal Postings:
Community Care Coordinator (Community), Thunder Bay
Community Care Coordinator (Complex), Thunder Bay
Community Care Coordinator (Float), Thunder Bay
Community Care Coordinator (Schools), Thunder Bay
Community Care Coordinator (TBRHSC), Thunder Bay
Rapid Response Nurse, Thunder Bay
Agenda Item 9.1-1

11
Pending/Underway – External Postings:
NA
Union (UNIFOR): New Hires:
Rachelle Smart: Team Assistant
Pending/Underway – External Postings:
NA
COMMUNICATIONS AND ENGAGEMENT DIVISION Strategic communications and engagement activities continued to enhance the brand, reputation and image of the North West LHIN. Community Engagement In July, 336 participants took part in 86 engagement sessions, and in August 554 participants took part in 101 engagement sessions with the North West LHIN. The number of engagement sessions remains steady, which can be attributed to being in caretaker mode during the transition of government. Of the total number of participants engaged in July and August, 403 individuals were from LHIN-funded health service providers. Engagement sessions ranged from teleconferences, forums, webinars and face-to-face meetings with providers. Integrated Health Service Plan V 2019-2022
Between March 12 and May 7, 2018, the North West LHIN engaged with a total of 1,956 residents over 34 engagement sessions in 12 municipalities, resulting in a total of 4,105 comments. These comments identify areas of strength and improvement in the health care system. Top three priorities identified through engagement are mental health and addictions, home and community care, and long-term care. Internal and external validation of IHSP V priorities identified took
place in August and September. A summary report entitled What We Heard has been developed and will be posted to the website. Accomplishments 2017-2018 The North West LHIN has produced its public-facing document that celebrates the accomplishments of the Integrated Health Service Plan (IHSP) 2016-2019 year two and CEO Interpretation Goals. This report-back to the community publication which is based on the Annual Report 2017-2018 tells the story of a year in which the North West LHIN was able to effectively plan with health system partners, key stakeholders and the people of Northwestern Ontario to increase health system integration, improve health outcomes, and increase value for money. Once approved, the report is expected to be released end of September.
Agenda Item 9.1-1

12
Minister’s Medal The Minister’s Medal Honouring Excellence in Health Quality and Safety is an annual program designed to recognize the excellent work done by health care providers across the province. From the North West LHIN, 13 applications were received, reviewed internally and submitted to the Ministry of Health and Long-Term Care on August 30, 2018. Medal recipients will be officially recognized at Health Quality Transformation 2018, an annual event hosted by Health Quality Ontario on October 17, 2018. Leadership Award The call for nominations for the fourth annual North West LHIN Leadership Award was launched on August 8, 2018. LHIN-funded providers who submitted applications for the Minister’s Medal have been encouraged to enter the Leadership Award. As a result of the expenditure restrictions, recommendations are being made to the Board on the recognition format for the Award. Media Relations The media relations goal is to help create a better understanding of the North West LHIN’s mandate, vision, mission, values, and role as leader of the health system transformation. Earned Media - From April – August, 2018, the North West LHIN appeared in the mainstream media at least 99 times compared 16 mentions – during the same period last year as monitored by the Communications Team. This volume of media mentions is higher given the significant gain in awareness through the Picture Your Health campaign for the Integrated Health Service Plan V engagement sessions and supporting media attention during and after the sessions. North West LHIN spokespeople were interviewed seven times for this period, with interviews largely surrounding the IHSP V community engagement sessions, and an interview with the Registered Nurses Association of Ontario (RNAO) regarding best practice guidelines across the LHIN. Media coverage was positive. North West LHIN HSPs and SPOs have been in the media at least 206 times as monitored by the Communications Team during this five month period. Coverage was mostly positive with 84 positive mentions, along with 118 neutral mentions another four mentions that can be considered negative. Online Community Engagement The North West LHIN website continues to be a central hub of information for internal and external audiences in the Northwest region. Between April and August 2018, the number of total visitors was 13,360, compared to 13,919 during the same period in 2017 and the decrease can be attributed to limited new content to the website due to caretaker mode. The number of new visitors during this five month period was 11,508 compared to 8,358 last year. The number of returning visitors was 2,943 compared to 2,096 from last year.
Agenda Item 9.1-1

13
Analyzing user behaviour on the North West LHIN website describes the pages most visited for each period, representing the focus of interest for each visitor. The top five web pages between April – August, 2018 were as follows:
1. Careers 2. Contact Us 3. Senior Leadership Team 4. About Our LHIN 5. Joint Mobile Crisis Response News Release
Agenda Item 9.1-1

NORTH WEST LHIN
PROVINCIAL TARGET
PROVINCIAL PERFORMANCE
LEGEND
Meeting or exceeding the provincial target. Worse than target, but within 10% of target. Worse than target, more than 10%.
PERCENT OF HOME CARE CLIENTS RECEIVING PERSONAL SUPPORT SERVICE WITHIN 5 DAYS
PERCENT OF HOME CARE CLIENTS RECEIVING NURSING SERVICE WITHIN 5 DAYS
North West LHIN Board of Directors Scorecard: Performance Update 1st QUARTER 2018/19
HOME AND COMMUNITY CARE SERVICES WAIT TIME - FROM COMMUNITY
HOME AND COMMUNITY CARE SERVICES WAIT TIME - FROM HOSPITAL
PERFORMANCE INDICATOR
Home and Community Care
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
Provincial Target
Provincial Target
Provincial Target
All LHINs
All LHINs
All LHINs
All LHINs
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
86.84%
96.45%
21 Days
5 Days
Agenda Item 9.1-2

NORTH WEST LHIN
PROVINCIAL TARGET
PROVINCIAL PERFORMANCE
LEGEND
Meeting or exceeding the provincial target. Worse than target, but within 10% of target. Worse than target, more than 10%.
ED WAIT TIME - LOW ACUITY PATIENTS
PERCENT OF PATIENTS RECEIVING A HIP REPLACEMENT SURGERY WITHIN ACCESS TARGET
Patient Access & Outcomes
ED WAIT TIME - HIGH ACUITY PATIENTS
Emergency Department Wait Times
PERCENT OF PATIENTS RECEIVING A KNEE REPLACEMENT SURGERY WITHIN ACCESS TARGET
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
Provincial Target
Provincial Target
Provincial Target
Provincial Target
All LHINs
All LHINs
All LHINs
All LHINs
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
10.4 Hours
4.8 Hours
84.11%
76.99%
Agenda Item 9.1-2

NORTH WEST LHIN
PROVINCIAL TARGET
PROVINCIAL PERFORMANCE
LEGEND
Meeting or exceeding the provincial target. Worse than target, but within 10% of target. Worse than target, more than 10%.
PERCENT ALC DAYS
ALC RATE
RATE OF REPEAT ED VISITS FOR MENTAL HEALTH
Mental Health and Substance Abuse
RATE OF REPEAT ED VISITS FOR SUBSTANCE ABUSE
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
North West LHIN Performance Compared to:
Provincial Target
Provincial Target
Provincial Target
Provincial Target
All LHINs
All LHINs
All LHINs
All LHINs
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
North West LHIN Performance
27.48%
35.51%
22.43%
44.50%
Agenda Item 9.1-2

NORTH WEST LHIN
PROVINCIAL TARGET
PROVINCIAL PERFORMANCE
LEGEND
Meeting or exceeding the provincial target. Worse than target, but within 10% of target. Worse than target, more than 10%.
HOSPITAL READMISSION RATE SELECT HIG GROUPERS
Readmission Rates
North West LHIN Performance Compared to:
Provincial Target All LHINs
North West LHIN Performance
16.72%
Agenda Item 9.1-2