
Regional age-related effects in the monkey brain measured with 1H magnetic resonance spectroscopy
Upload
independentCategory
view
5download
0
doi:10.1182/blood-2002-03-0701Prepublished online July 5, 2002;
Jesus F San Miguel and Stephen MackinnonAngel Leon, Kwee Yong, Ana Sureda, Ann Hunter, Jordi Sierra, Anthony H Goldstone, David C Linch,Chopra, Javier Garcia-Conde, Don W Milligan, Stephen Schey, Alvaro Urbano-Ispizua, Anne Parker, Jose A Perez-Simon, Panagiotis D Kottaridis, Rodrigo Martino, Charles Craddock, Dolores Caballero, Raj disordersbetween two prospective studies in patients with lymphoproliferative Non-myeloablative transplants with or without CAMPATH-1H: comparison
(1922 articles)Transplantation � (3779 articles)Clinical Trials and Observations �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom For personal use only. by guest on October 30, 2013. bloodjournal.hematologylibrary.orgFrom

1
NON-MYELOABLATIVE TRANSPLANTS WITH OR WITHOUT CAMPATH-1H: COMPARISON BETWEEN TWO PROSPECTIVE
STUDIES IN PATIENTS WITH LYMPHOPROLIFERATIVE DISORDERS.
Jose A Pérez-Simón, Panagiotis D Kottaridis, Rodrigo Martino, Charles Craddock, Dolores Caballero, Raj Chopra, Javier García-Conde, Don W Milligan, Stephen Schey, Alvaro Urbano-Ispizua, Anne Parker, Angel Leon, Kwee Yong, Ana Sureda, Ann Hunter, Jordi Sierra, Anthony H Goldstone, David C Linch, Jesus F San Miguel, Stephen Mackinnon.
Spanish and UK Collaborative Groups for non-myeloablative transplantation.
Correspondence to:Dr José A Pérez SimónServicio de HematologíaHospital Universitario de SalamancaPaseo de San Vicente s/n, 37007Spain FAX: 34-923-294624 e-mail: [email protected]
Acknowledgement:To Jose Manuel García de Cecilia, Statistician of the SEK University (Segovia) for
his support in the statistical analysis.
Key-words: Non-myeloablative transplants, comparative study, CAMPATH-1H
Copyright 2002 American Society of Hematology
Blood First Edition Paper, prepublished online July 5, 2002; DOI 10.1182/blood-2002-03-0701

2
Summary:Although non-myeloablative conditioning regimen transplants (NMT)
induce engraftment of allogeneic stem cells with a low spectrum of toxicity, GVHD
remains a significant cause of morbidity and mortality. In vivo-T cell depletion, using
CAMPATH-1H, has been shown to reduce the incidence of GVHD . However this type of
maneuvers whilst reducing GVHD may have an adverse impact on disease response, since
NMT exhibit their antitumour activity by relying on a graft versus malignancy effect. In
order to explore the efficacy of CAMPATH-1H as compared to methotrexate (MTX) for
GVHD prophylaxis we have compared the results of 129 recipients of a sibling NMT
enrolled in two pospective studies for chronic lymphoproliferative disordersBoth NMT
were based on the same combination of fludarabine and melphalan but the UK regimen
(group A) used Cyclosporine A plus CAMPATH-1H whilst the Spanish regimen (group B)
used Cyclosporine A plus MTX for GVHD prophylaxis.
Patients receiving CAMPATH-1H had a higher incidence of CMV reactivation
(85% vs 24%, p<0.001) and a significantly lower incidence of aGVHD (23.1% vs 45.1% ,
p=0.006) and cGVHD (5% vs 66.7% , p<0.001). Twenty one percent (group A) and 67.5%
(group B) of patients achieved CR or PR 3 months after transplant (p<0.001). Eighteen
patients in group A received donor lymphocyte infusions (DLI) in order to achieve disease
control. At last follow up there was no difference in disease status between the groups with
71% vs 67.5% (p=0.43) of patients reaching CR or PR in groups A and B, respectively. No
significant differences were observed in event free or overall survival between both groups.
In conclusion, CAMPATH-1H significantly reduced GVHD but its use was associated with
a higher incidence of CMV reactivation. Patients receiving CAMPATH-1H often required
DLI in order to achieve similar tumour control but the incidence of GVHD was not
significantly increased after DLI.
Introduction:
Non-myeloablative transplants (NMT) are currently being evaluated in patients with
hematological malignancies considered poor candidates for conventional allogeneic
transplantation due to advanced age or other concurrent medical conditions. The rationale

3
for NMT relies on previous observations that adoptive transfer of allo-reactive donor
lymphocytes may eradicate refractory or recurrent disease.1-5 Therefore, in an effort to
reduce the toxicity associated with high dose chemotherapy,6-11 several groups have
designed less toxic regimens that might exhibit their antitumor effect relying on a graft
versus malignancy effect rather than on myeloablative chemotherapy.12-16 Although these
regimens have been shown to permit engraftment of allogeneic haemopoietic stem cells
with a low spectrum of toxicity, GVHD remains a significant cause of increased morbidity
and mortality.4-16, 17-20 The ideal approach for GVHD prophylaxis remains uncertain and
several agents have been introduced to reduce incidence and severity. The UK
Collaborative group has incorporated CAMPATH-1H as part of a fludarabine-based
protocol and a low incidence of GVHD has been reported in both related and unrelated
donor transplants.21 However, this type of intervention to reduce the incidence and severity
of GVHD may have an adverse impact on disease response, since several studies have
suggested a positive correlation between GVHD and GVL effect,6, 15, 16, 19, 22-25 both in
myeloid and also in lymphoid malignancies18,20,25,26 and higher relapse rates have been
reported after syngeneic or T-cell depleted transplants.27,28 Thus the ideal approach is to
establish the optimum balance between the risk/benefit of decreasing GVHD versus an
increase in the risk of relapse.
In order to explore the efficacy of CAMPATH-1H in comparison to methotrexate
(MTX) (both in combination with cyclosporine) for GVHD prophylaxis and its impact on
the outcome of patients transplanted for lymphoproliferative disorders, we have
retrospectively compared the results of two prospective studies carried out in the United
Kingdom21 and Spain.29 Both NMT schedules were based on the same combination of
fludarabine and melphalan but the UK regimen (group A) used cyclosporine A plus
CAMPATH-1H whilst the Spanish regimen (group B) used cyclosporine A plus MTX.
Patients included in this study underwent transplantation from February 1998 to January
2001 (group A) and from February 1999 to May 2001 (group B).
PATIENTS AND METHODS:

4
Patient characteristics:
We have analyzed 129 patients with chronic lymphoproliferative disorders who were
included in both registries and underwent a peripheral blood stem cell transplant from HLA
matched siblings. Both studies included patients considered candidates to receive a
transplant from a related donor but who had a high risk of transplant related mortality
(TRM) due to advanced age (≥45 years old, n=77) or other concurrent medical condition
(relapse after a previous autologous transplantation, n=30; severe organ disfunction, active
fungal infection or heavily pretreated patients; n=22).. Patients gave written informed
consent for inclusion in the protocols, which were approved by all local ethical review
boards as well as the Spanish (protocol 99-0151) and the UK (study number 974/0127)
Drug Agencies.
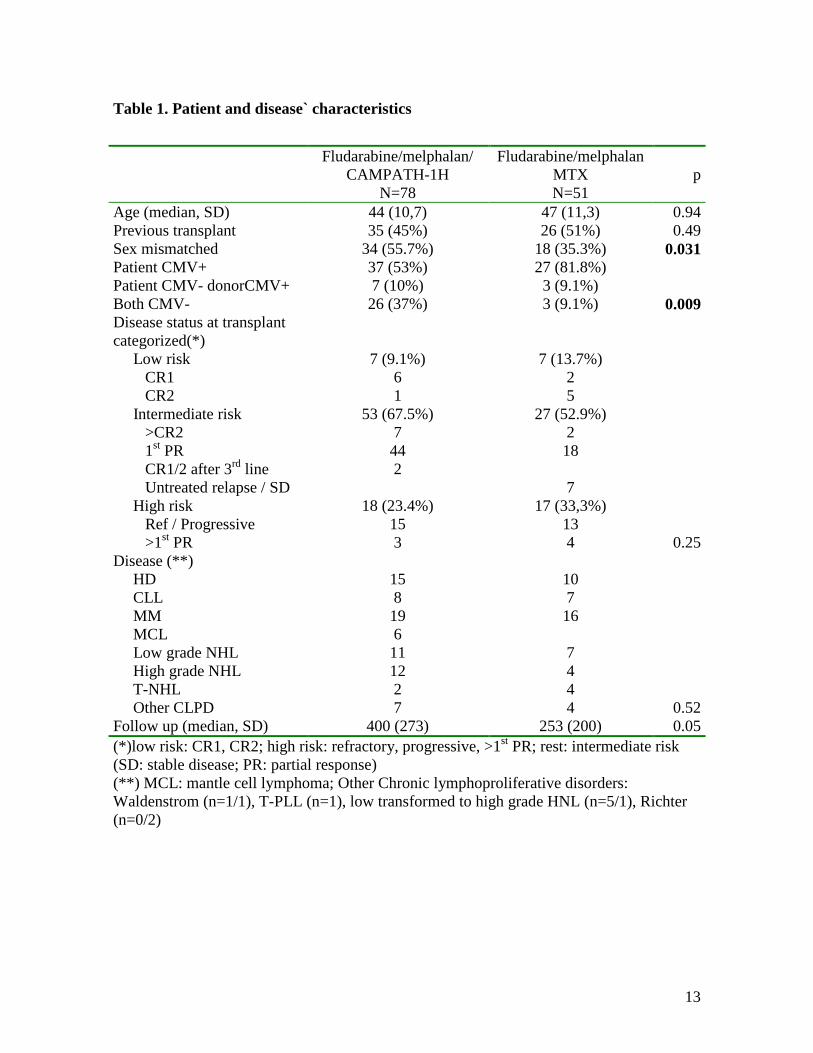
No significant differences were observed between the two groups in median age,
diagnosis or previous transplant. Disease status at transplant was categorized as low risk
(patients in CR1 and CR2), high risk (patients with refractory or progressive disease and
>1st partial response) and intermediate risk (the rest of cases, ie. >2nd CR); no differences
were observed in terms of disease status. In contrast, there was a sex mismatch in 56% of
the CAMPATH-1H group (A) compared to 35% in MTX group (B) (p=0.031). In addition,
in 37% of cases in group A both donor and recipient were CMV negative compared to only
9% in group B (p=0.009). Other patient characteristics are specified in Table 1.
Mobilisation regimens and peripheral blood stem cell collection procedures were
similar in both trials. 21, 29
Conditioning regimen and GVHD prophylaxis:
In both trials the conditioning regimen consisted of fludarabine 30mg/m2
intravenously (IV) for 5 days followed by melphalan 140mg/m2 intravenously in one dose
or divided in two doses: fludarabine 30mg/m2 days –7 to –3 plus melphalan 140mg/m2 on
day –2 in group A and fludarabine 30mg/m2 days –8 to –4 plus melphalan 140mg/m2
divided in two doses on days –3 and –2 in group B. 21,29

5
Acute and chronic GVHD were similarly graded by established criteria in both trials 30,31. In group A GVHD prophylaxis consisted of cyclosporine A (CsA) 3 mg / kg iv
starting on day -1 and switched to an oral dose as soon as the patient could tolerate oral
medications.. The median duration of administration was 4 months for the first 40 patients,
however the observed low incidence of GVHD led physicians to taper the dose by the end
of the second month in the rest of the patients. In patients without evidence of GVHD CsA
was discontinued by the end of the third month. CAMPATH-1H was administered at a dose
of 20 mg / day iv infusion over 8 hours on days -8 to -4.
In group B, CsA was started on day –7. In the absence of grade II or greater acute GVHD,
CsA was tapered 10% weekly starting on day +90 and discontinued by day +150. In both
groups CsA levels were monitored starting on day +1 and were maintained in the
therapeutic range (150-300 ng / mL) until tapering. MTX in group B was given at a dose of
10 mg/m2 IV on days +1,+3 and +6, followed by folinic acid rescue ( 10 mg IV every 6
hours for 4 doses starting 24 hours after each dose of MTX).
Patients with relapsed / progressive disease post-transplant or those not evolving to
100% donor chimerism after discontinuing immunosupression were considered eligible for
DLI in both studies.
An escalated dose regimen starting at 1x106 CD3+ T-cells/kg with dose escalation
at 3 monthly intervals, was used in group A. The median interval from transplant to the first
DLIwas 230 days (182-781). Overall, eighteen patients received DLI in group A. Fifteen
patients received DLI for persistent disease post transplant and 3 for mixed chimerism.In
group B, also an escalated dose regimen at 3 monthly intervals was used, however the
starting dose was 1 x 107 CD3+ T-cells / kg. In this group, 4 patients received DLI due to
persistent disease (n=3) or progression (n=1). The median interval to start DLI after
transplant was +210 days (120-243).Data on chimerism analysis and DLI (manuscript
under preparation) have already been reported.21, 29. Protocols for the prevention and
treatment of transplant complications and supportive care were similar in both groups 21,29.
Finally, patients were monitored for CMV reactivation by weekly CMV
antigenemia (group B) or PCR assay (group A) and pre-emptive therapy with ganciclovir (32,33) was started after one positive antigenemia (group A) or after 2 consecutive positive
PCR assays (group B).

6
Statistical methods:
Comparison of relapse rate and GVHD between groups was performed by using the Chi
square and Fisher’s exact test. Events analyzed were calculated from the time of
transplantation using Kaplan-Meier product-limit estimates. For transplant related mortality
(TRM) patients were censored at last follow-up. Disease free survival (DFS) was calculated
from transplant until disease progression for those patients reaching CR after transplant and
also for those reaching CR after DLI. Patients who suffered TRM and those who were still
alive without progression at the time of reporting were censored at death and last follow-up,
respectively. Event free survival (EFS) was calculated from transplant until disease
progression or death and those patients who did not reach disease response (CR or PR) any
time after transplant were considered events. Overall survival (OS) was calculated from
transplant until death from any cause, and surviving patients were censored at last
follow-up. The incidence and time to onset of chronic GVHD were calculated in patients
followed for at least 90 days.
Results:
Engraftment:
Both regimens induced an early and sustained engraftment.21,28 As shown in Table
2, granulocyte recovery was faster in group A ; the median time for > 500 granulocytes /
mm3 was 12.8 vs 14.7 days (p<0.001) and for > 1,000 granulocytes / mm3 13.7 vs 17.6 days
(p<0.001) for groups A and B, respectively. In contrast, the use of CAMPATH-1H was
associated with a significant delay in platelet recovery: median of 14.4 vs 11.2 days to
reach > 20 x 109 / L platelets (p=0.009) and 21.7 vs 14.1 days to reach > 50 x 109 / L
platelets (p=0.001) in groups A and B, respectively.
GVHD and infectious complications:
Patients receiving CAMPATH-1H had a significantly lower incidence of aGVHD
(17.9%) when compared to patients receiving MTX (45.1%) (p=0.001). In addition, in
patients receiving CAMPATH-1H the incidence of grades II-IV and III-IV aGVHD was
significantly lower in comparison to patients receiving MTX: 6.4% vs 43.1% grades II-IV
aGVHD in groups A and B, respectively (p<0.001) and 2.6% vs 13.7% grades III-IV

7
aGVHD in groups A and B, respectively (p=0.015). Interestingly, eighteen patients
received DLI in group A due to relapse / persistence of disease or mixed chimerism and
only 3 of these patients developed GVHD (one grade I, one grade IV and one limited
cGVHD), so that a significantly lower incidence of aGVHD persisted in patients receiving
CAMPATH-1H even after DLI. However, there was no significant difference in terms of
severe aGVHD (grades III and IV) after DLI (p=0.09) (Table 2).
There were also differences in the incidence of chronic GVHD between the
groups.Only two patients receiving CAMPATH-1H developed cGVHD (1 limited, 1
extensive) in contrast to 22 (66.7% of patients at risk) patients receiving MTX (13 cases of
extensive cGVHD) (p<0.001).
Patients were monitored for CMV reactivation by weekly CMV antigenemia (group
B) or PCR assay (group A). Statistically significant differences were observed in the
incidence between both groups. Although a lower percentage of patients in group B were
CMV negative, only 22.7% developed CMV reactivation as compared to 47% in group A
(p=0.018). Even more strikingly, amongst CMV positive patients, 85% had CMV
reactivation in group A vs 24% in group B (p<0.001). Despite the high incidence of
reactivation only one patient died of CMV disease in group A vs none in group B.
Transplant related mortality:
No significant differences were observed in terms of TRM between both groups
although a trend towards a higher mortality rate was observed in group B [10.2% vs 20%
for groups A and B, respectively (p=0.12; log rank: p=0.06, fig 1)].
Overall 25.6% of patients in group A died compared to 29.4% in group B (p=0.6).
33.4% of deaths in group B were related to GVHD compared to 5% in group A. By
contrast, the most frequent cause of death in patients receiving CAMPATH-1H was disease
relapse / progression (60% of deaths vs 20%). Data concerning morbidity and mortality are
specified in table 2.
Disease response:
Disease status was evaluated three months after transplant (table 3). After three
months 21.1% of patients in group A were in CR/PR in contrast to 67.5% in group B
(p<0.001). Interestingly, disease status at transplant significantly influenced response to

8
transplant in patients receiving CAMPATH-1H but not in those receiving MTX. The most
important differences in response were observed in patients categorized as high risk
patients according to disease status pre-transplant with no patient reaching CR or PR in
group A vs 52.9% in group B (p<0.001). In the intermediate risk group of patients 18.8%
reached CR or PR in group A compared to 55.5% in group B (p<0.001). In contrast, no
significant differences were observed in the low risk group, although the number of patients
in this subgroup was too small to reach any conclusion. As previously stated, eighteen
patients received DLI in group A because of relapse / persistence of disease or mixed
chimerism vs four patients in group B. Disease status at last follow-up ( after cyclosporine
A taper and DLI) is summarized in Table 3. Disease status at last follow up was not
significantly different between both groups for the overall series of patients. In addition, no
significant differences were observed according to pre-transplant disease status, since in the
high risk group 53.8% of patients receiving CAMPATH-1H reached CR / PR vs 50% in the
group of patients receiving MTX (p=0.45). Also in the intermediate risk group 55.8% of
patients receiving CAMPATH-1H reached CR / PR as compared to 56.5% of patients
receiving MTX (p=0.76).
On analyzing all patients (Table 4) we found an association between development
of aGVHD and disease response (55.2% of patients developing aGVHD reached CR/PR as
compared to 29.5% for those who did not develop aGVHD, p=0.025) but this association
disappeared after DLI. The same occurred when we analyzed patients developing grades II
to IV aGVHD. In order to evaluate whether these results could be attributed to any of the
GVHD prophylaxis regimens both groups were separately analyzed. No clear relation
between aGVHD and response to transplant or disease status after DLI was observed in
neither group A or B, although this might be related to the lower number of cases included,
when both series were separately analyzed. In addition, 74% of patients developing
cGVHD achieved CR / PR as compared to 29% of patients who did not develop it
(p<0.001). In this case, the impact of DLI could not be evaluated since only two patients in
group A developed cGHVD.
Finally, results from both registries were analyzed according to the type of the
underlying disease: in multiple myeloma both response to transplant and disease status after
DLI was improved in patients receiving MTX (52.6% of patients in group A reached CR /
PR at last follow up as compared to 68.8% in group B, p=0.029). In MM patients there was

9
no clear relation between aGVHD and disease control, however 50% of those patients who
developed aGVHD reached CR/PR in comparison to 25% for those who did not develop
GVHD (p=0.25).
In Hodgkin´s disease patients, the initial response was better in group B, however disease
status after DLI was similar in both groups (53.3% of patients reached CR / PR in group A
as compared to 50% in group B, p=0.21). Finally, within patients diagnosed with high
grade NHL (n=21), only two were categorized as low risk disease at transplant whilst the
rest were categorized as intermediate (n=9) and high risk (n=10). Response to transplant
was significantly better for patients receiving MTX but, after examining disease status after
DLI no significant differences were observed between the two groups, although we
observed a trend towards a better disease control for patients in group B (26.7% of patients
receiving CAMPATH-1H in CR/PR vs 50% for those receiving MTX). In view of the low
number of patients no other disease categories were analyzed.
Overall survival and disease free survival:
Disease free survival was first calculated identifying only those patients reaching a
complete response after transplant. Median DFS was not reached for patients receiving
CAMPATH-1H and not computed for those receiving MTX since no relapses were
observed among patients reaching CR. No significant differences were found. When we
also considered patients achieving CR after DLI, DFS at 2 years was 76% for patients in
group A vs 100% in group B(p=0.19). When we compared both groups according to pre-
transplant disease status no significant differences were found for any of the risk categories
when we considered disease status after DLI.
Median event free survival (EFS) amongst patients receiving CAMPATH-1H was
438 days vs 267 days for patients receiving MTX. Event free survival at 2 years was 34%
in group A vs 39% in group B, p=0.14 (fig 2). When both groups were examined according
to pre-transplant disease status no significant differences were found for any of the risk
categories when we considered disease status after DLI. When we analyzed only those
patients achieving any response (CR, PR or stable disease), median EFS was not reached
for any of the two groups. For these patients EFS at 2 years was 72% and 76% for groups A
and B respectively, p=0.6 (Fig 3).

10
With regard to overall survival, at the present time the median survival has not been
reached for either of the two groups. No significant differences were observed between
both groups (72% OS at 2 years in group A vs 66% in group B, p=0.22) even when we
considered the different risk categories (Fig 4).
Discussion:
It has been well established that non-myeloablative transplants may offer a reduced
risk of procedure associated mortality,6, 14-16, 21, 29 compared to conventional transplants.8-10
However, despite the considerably lower toxicity, GVHD still remains a major limitation
for this strategy.6, 14-16, 29 In order to explore the impact of CAMPATH-1H on the
prevention of GVHD and the efficacy of NMT, we have performed the first comparative
study between two prospective national studies in patients diagnosed with
lymphoproliferative disorders.
Both conditioning regimens21,29 were based on the same doses of fludarabine and
melphalan, with the only difference being the use of CAMPATH-1H (group A) or MTX
(group B) in addition to CsA to prevent GVHD. Characteristics of patients at transplant
were similar, except for a higher incidence of sex mismatched pairs in the group of patients
receiving CAMPATH-1H and a lower percentage of CMV seronegativity in the group of
patients receiving MTX.
This comparative study has confirmed that CAMPATH-1H significantly reduces the
overall incidence of aGVHD when compared to MTX. In addition, this reduction can be
maintained even after DLI. Since the efficacy of this type of transplant relies primarily on
the graft versus tumor effect,6-10, 24 any attempt to decrease GVHD may be offset by a
higher risk of relapse and the results should be cautiously interpreted. Disease response at
three months was significantly better in the group of patients receiving MTX. In addition,
patients who developed GVHD obtained a better disease response after transplant.
Nevertheless, 18 patients in group A received DLI in order to generate a tumour response
and our analysis has shown that disease status at last follow up did not differ between both
groups. Interestingly, disease response after DLI was not associated with a significant
increase in GVHD since differences in GVHD incidence between both groups remained
even post DLI. In addition, correlation between GVHD and response was not significant
when we considered disease status after DLI. These results are in accordance with previous

11
reports suggesting that the approach of using delayed DLI can induce disease response and
may be associated with less GVHD compared to early infusion34 and also support previous
reports showing that the use of DLI can contribute to overcome the negative effect on GVL
of in vitro T-cell depletion using CAMPATH-1 in myeloid as well as in lymphoid
malignancies35.
This study also confirmed that lymphomas, CLL and multiple myeloma are
susceptible to graft versus tumor effect.18, 20, 25, 26, 36-40 This effect is not equally potent
across tumor subtypes and disorders with low proliferative capacity may respond better
when compared to more aggressive forms of disease. We were also able to demonstrate a
correlation between disease response and severity of GVHD and, not surprisingly, in our
series of myeloma patients, response to transplant was significantly better in group B.
Interestingly, the improved outcome in group B remained even after DLI in group A,
suggesting that an early onset of GVHD might be more beneficial in multiple myeloma.
“Although the use of T-cell depletion combined with cyclosporine may have a
deletereous effect on transplant outcome41, recent reports have unexpectedly shown that
CAMPATH and cyclosporin can reduce the rik of death due to infections 6 months after the
transplant42. Therefore further studies will be needed to explore the mechanism of the
cyclosporin effect and the potential benefit in combination with T-cell depletion”
As previously reported, the use of less intensive regimens may have a beneficial effect on
infections.43 In the immediate post transplant period, the short duration of neutropenia may
result in reduced incidence of bacterial infections. In the present study, CAMPATH-1H
recipients experienced increased incidence of CMV reactivation in comparison to MTX
although only one patient in the former group died due to CMV disease. This difference in
terms of CMV reactivation can not be atributted to the different techniques used in both
trials since several studies have demonstrated that antigenemia and PCR assay have similar
predictive values and show a high linear correlation (44,45). According to this findings, the
CDC have recently recommended that any of both techniques should be selected to
determine the need for pre-emptive treatment (46). On the other hand, we were able to show
that the use of MTX, as expected, was associated with delayed neutrophil engraftment
although unexpectedly platelet engraftment was delayed in patients receiving CAMPATH-
1H although these differences were not clinically important. The delay in platelet
engraftment in group A, might be related to the in vivo T cell depletion induced by

12
CAMPATH-1H, since T lymphocytes may be an important element for platelet
engraftment,47 or in addition, CAMPATH-1H might have direct toxicity on megakaryocytic
progenitors.
Although a major concern about the use of anti-T monoclonal antibodies is the
increased incidence of post-transplant lymphoproliferative disorders (PTLD), in this study,
none of the patients developed PTLD. This is in contrast to previous reports on other anti-T
monoclonal antibodies 48,49 and is probably related to the anti-B cell effect induced by
CAMPATH-1H.
In conclusion, both non-myeloablative regimens offer good results in patients
considered poor candidates to undergo a conventional allogeneic transplantation, but a
different pattern of complications was observed: CAMPATH-1H significantly reduced
GVHD but it was related to a higher incidence of CMV reactivation. These findings have
prompted us to initiate a study to establish an optimum dose of CAMPATH-1H in order to
maintain its efficacy for GVHD prophylaxis without increasing CMV
reactivation.50However, patients receiving CAMPATH-1H required donor lymphocyte
infusion in order to achieve a similar response rate in comparison to those receiving MTX
but the incidence of GVHD did not significantly increase after DLI, thus suggesting the
possibility of separating GVHD from GVL. Finally, better responses were observed early
post transplant in patients with multiple myeloma or with active disease pre transplant
indicating that these patients may benefit from MTX containing regimens. Considering
these results a randomized trial comparing both protocols of GVHD prophylaxis is
warranted.
13
Table 1. Patient and disease` characteristics
Fludarabine/melphalan/CAMPATH-1H
N=78
Fludarabine/melphalanMTXN=51
p
Age (median, SD) 44 (10,7) 47 (11,3) 0.94Previous transplant 35 (45%) 26 (51%) 0.49Sex mismatched 34 (55.7%) 18 (35.3%) 0.031Patient CMV+Patient CMV- donorCMV+Both CMV-
37 (53%)7 (10%)26 (37%)
27 (81.8%)3 (9.1%)3 (9.1%) 0.009
Disease status at transplant categorized(*) Low risk CR1 CR2 Intermediate risk >CR2 1st PR CR1/2 after 3rd line Untreated relapse / SD High risk Ref / Progressive >1st PR
7 (9.1%)61
53 (67.5%)7442
18 (23.4%)153
7 (13.7%)25
27 (52.9%)218
717 (33,3%)
134 0.25
Disease (**) HD CLL MM MCL Low grade NHL High grade NHL T-NHL Other CLPD
158196111227
10716
7444 0.52
Follow up (median, SD) 400 (273) 253 (200) 0.05(*)low risk: CR1, CR2; high risk: refractory, progressive, >1st PR; rest: intermediate risk (SD: stable disease; PR: partial response)(**) MCL: mantle cell lymphoma; Other Chronic lymphoproliferative disorders: Waldenstrom (n=1/1), T-PLL (n=1), low transformed to high grade HNL (n=5/1), Richter (n=0/2)

14
Table 2: Transplant related morbidity and mortality
Fludarabine/melphalan/CAMPATH-1H
(n=78)
Fludarabine/melphalan/MTX(n=51) p
Days to reach >500 granulocytes >1000 granulocytes >20.000 platelets >50.000 platelets
12.88 (2.84)13.7 (3.89)14.49 (6.49)21.73 (14.1)
14.79 (2.14)17.68 (3.09)11.25 (5.34)14.14 (5.38)
<0.001<0.001
0.0090.001
aGVHD No Grade I Grade II-IV Grade III-IV
64 (82.1%)9 (11.5%)5 (6.4%)2 (2.6%)
28 (54.9%)1 (2%)
15 (29.4%)7 (13.7%)
Yes vs no: 0.001
0-1 vs 2-4: <0.001
0-2 vs 3-4: 0.015
Overall aGVHD(pre+postDLI) No Grade I Grade II-IV Grade III-IV
60 (76.9%)10 (12.8%)3 (3.8%)4 (5.1%)
28 (54.9%)1 (2%)
15 (29.4%)7 (13.7%)
Yes vs no: 0.006
0-1 vs 2-4: <0.001
0-2 vs 3-4: 0.092
cGVHD Limited Extensive
11
913 <0.001
CMV reactivation 27 (46.6%) 10 (22.7%) 0.018CMV reactivation CMV+patient or donor CMV-patient and donor
26 (86.7%)0
7 (25%)0
<0.001
TRM 8 (10.3%) 10 (20%) 0,12

15
Table 3. Disease Response and Transplant Outcome
Fludarabine/melphalan/CAMPATH-1H
N=78
Fludarabine/melphalan/MTXN=51
p
Disease response 3 months after transplantResponse
CR PR Stable /prog free Progression
15 (21.1%)0
48 (67.6%)8 (11.3%)
19 (47.5%)8 (20%)
9 (22.5%)4 (10%) <0.001
Disease status at last follow up*Disease status CR PR Stable /prog free Progression
28 (47.4%)14 (23.7%)16 (27.1%)
1 (1.8%)
19 (47.5%)8 (20%)
9 (22.5%)4 (10%) 0.43
(*) Disease status after CsA taper and DLI
Table 4: Response to transplant according to GVHD development
aGVHDYes No
p
Response to transplantCR / PR
Stable / prog16 (55.2%)13 (44.8%)
26 (29.5%)56 (70.5%) 0.025
Dis.status at last follow up*CR / PR
Stable / prog21 (75%)7 (25%)
47 (67.1%)23 (32.9%) 0.61
cGVHDYes No
Response to transplant CR / PR Stable / prog
17 (74%)6 (23%)
23 (29%)57 (71%) 0.016
(*): disease status after CsA taper and DLI

16
REFERENCES:
1. Porter DL, Roth MS, McGarigle C, Ferrara JL, Antin JH. Induction of graft versus
host disease as immunotherapy for relapsed chronic myeloid leukemia. N Eng J
Med 1994; 330: 100-106
2. Collins RH Jr, Shpilberg O, Drobyski WR, Porter DL, Giralt S, Champlin R,
Goodman SA, Wolff SN, Hu W, Verfaillie C, List A, Dalton W, Ognoskie N,
Chetrit A, Antin JH, Nemunaitis J. Donor leukocyte infusions in 140 patients
relapsed with malignancy after allogeneic bone marrow transplantation. J Clin
Oncol 1997; 15: 433-444
3. Kolb HJ, Schattenberg A, Goldman JM, Hertenstein B, Jacobsen N, Arcese W,
Ljungman P, Ferrant A, Verdonck L, Niederwieser D. Graft versus leukemia effect
of donor lymphocyte transfusions in marrow grafted patients. Blood 1995; 86:
2041-2050
4. Lockhorst HM, Schattenberg A, Cornelissen JJ, Thomas LLM, Verdonk LF. Donor
leukocyte infusions are effective in relapsed multiple myeloma after allogeneic bone
marrow transplantation. Blood 1997; 90: 4206-4211
5. Kolb HJ, Schattenberg A, Goldman JM, Hertenstein B, Jacobsen N, Arcese W,
Ljungman P, Ferrant A, Verdonck L, Niederwieser D, van Rhee F, Mittermueller J,
de Witte T, Holler E, Anseri H. Graft versus myeloma effect of donor lymphocyte
transfusions in marrow grafted patients. European Group for Blood ad Marrow
Transplantation Working Party Chronic Leukemia. Blood 1995; 86: 2041-2050
6. Pérez-Simón JA, Caballero D, Lopez-Pérez R, Mateos G, Cañizo C, Vazquez L,
Vidriales B, Mateos MV, Gonzalez M, San Miguel JF. Chimerism and minimal
residual disease monitoring after reduced intensity conditioning (RIC) allogeneic
transplantation. Leukemia (in press)

17
7. Bortin MM, Horowitz MM, Gale RP, Barret AJ, Champlin RE, Dicke KA,
Gluckman E, Kolb HJ, Marmont AM, Mrsic M. Changing trends in allogeneic bone
marrow transplantation for leukemia in the 1980s. JAMA 1992; 268: 607-612
8. Armitage JO. Bone Marrow Transplantation. N Eng Med 1994, 330: 827-838
9. Klingemann HG, Storb R, Fefer A, Deeg HJ, Appelbaum F, Buckner CD, Cheever
MA, Greenberg PD, Stewart PS, Sullivan KM, Whitherspoon RP, Thomas ED.
Bone marrow transplantation in patients aged 45 years and older. Blood 1986; 65:
770-776
10. Ringden O, Horwitz MH, Gale RP, Biggs JC, Gajewski J, Rimm AA, Speck B,
Veum-Stone JA, de Witte T, Bortin MM. Outcome after allogeneic bone marrow
transplantation for leukemia in older patients. JAMA 193; 270: 5760
11. Blumme KG, Forman SJ, Nademanee AP, O´Donnell MR, Snyder DS, Fahey JL,
Findley DO, Lipsett JA, Zaia JA, Metter GE, Hill LR. Bone marrow transplantation
for hematologic malignancies in patients aged 30 years or older. J Clin Oncol 1986;
4: 1489-1492
12. Slavin S, Weiss L, Morecki S, Weigensberg M. Erradication of murine leukemia
with histoincompatible marrow grafts in mice conditioned with total lymphoid
irradiation. Cancer Immunother 1981; 11: 155-158
13. Storb R, Yu C, Wagner JL et al. Stable mixed hematopoietic chimerism in DLA-
identical littermate dogs given sublethal total body irradiation before and
pharmacological immunosuppression after marrow transplantation. Blood 1997; 89:
3048-3054
14. Slavin S, Nagler A, Naparstek E, Kapelushnik Y, Aker M, Cividalli G, Varadi G,
Kirschbaum M, Ackerstein A, Samuel S, Amar A, Brautbar C, Ben-Tal O, Eldor A,
Or R. Nonmyeloablative stem cell transplantation and cell therapy as an alternative
to conventional bone marrow transplantation with letal cytoreduction for the
treatment of malignant and nonmalignant hematologic diseases. Blood 1998; 91:
756-763
15. Giralt S, Estey E, Albitar M, van Besien K, Rondon G, Anderlini P, O´Brien S,
Khouri I, Gajewski J, Mehra R, Claxton D, Andersson B, Beran M, Przepiorka D,
Koller C, Kornblau S, Körbling M, Keating M, Kantarjian H, Champlin R.
Engraftment of allogeneic hematopoietic progenitor cells with purine analog-

18
containing chemotherapy: harnessing graft versus leukemia without myeloablative
therapy. Blood 1997; 89: 4531-4536
16. McSweeney P, Niederwieser D, Shizuru J, Sandmaier BM, Molina AJ, Maloney
DG, Chauncey TR, Gooley TA, Hegenbart U, Nash RA, Radish J, Wagner JL,
Minor S, Appelbaum F, Bensinger WI, Bryant E, Flowers ME, Georges GE,
Grumet FC, Kiem HP, Torok-Storb B, Yu C, Blume K, Storb R. Hematopoietic cell
transplantation in older patients with hematologic malignancies: replacing high dose
cytotoxic therapy with graft versus tumor effect. Blood 2001; 97: 3390-3400
17. Giralt S, Thall P, Khouri I, Wang X, Braunschweig I, Ippolitti C, Claxton D,
Donato M, Bruton J, Cohen A, Davis M, Andersson BS, Anderlini P, Gajewski J,
Kornblau S, Andreeff M, Przepiorka D, Ueno NT, Molldrem J, Champlin R.
Melphalan and purine analog-containing preparative regimens: reduced-intensity
conditioning for patients with hematologic malignancies undergoing allogeneic
progenitor cell transplantation. Blood 2001; 97: 631-637
18. Kouri IF, Keating M, Körbling M, Przepiorka D, Anderlini P, O`Brien S, Giralt S,
Ippoliti C, von Wolff B, Gajewski J, Donato M, Claxton D, Ueno N, Andersson B,
Gee A, Champlin R. Transplant-lite induction of graft-versus-malignancy using
fludarabine based nonablative chemotherapy and allogeneic blood progenitor cell
transplantation as treatment for lymphoid malignancies. J Clin Oncol; 16: 2817-824
19. Childs R, Clave E, Contentin N, Jayasekera D, Hensel N, Leitman S, Read EJ,
Carter C, Bahceci E, Young NS, Barret AJ. Engraftment kinetics after
nonmyeloablative allogeneic peripheral blood stem cell transplantation: full donor
T-cell chimerism precedes alloinmune responses. Blood 1999; 94: 3234-3241
20. Badros A, Barlogie B, Morris C, Desikan R, Martin S, Munshi N, Zangani M, Toor
A, Cottler-Fox M, Fasas A, Aniassie E, Schihman S, Tricot G. High response rate in
refractory and poor risk multiple myeloma after allotransplantation using a
nonmyeloablative conditioning regimen and donor lymphocyte infusions. Blood
2001; 97: 2574-2579
21. Kottaridis PD, Milligan D, Chopra R, Chakraverty R, Chakrabarti S, Robinson S,
Peggs K, Verfuerth S, Pettengell R, Marsh JC, Schey MS, Mahendra P, Morgan GJ,
Hale G, Waldmann H, Ruiz de Elvira C, Williams CD, Devereux S, Linch D. In

19
vivo CAMPATH-1H prevents graft – versus - host disease following non
myeloablative stem cell transplantation. Blood 2000; 96: 2419-2425
22. Weiden PL, Sullivan KM, Flournoy N, Storb R, Thomas ED. Antileukemic effect of
chronic graft versus host disease: contribution to improved survival after allogeneic
marrow transplantation. N Eng J Med 1981; 304: 1529-1533
23. Horowitz MM, Gale RP, Sondel PM, Goldman JM, Kersey J, Kolb HJ, Rimm AA,
Ringden O, Rozman C, Speck B. Graft versus leukemia reactions after bone marrow
transplantation. Blood 1990; 75: 555-562
24. Childs RW, Chernoff A, Contentin N, Bahceci E, Schrump D, Leitman S, Read E,
Tisdale J, Dunbar C, Linehan WM, Young NS, Barret J. Regression of metastatic
renal cell carcinoma after nonmyeloablative allogeneic peripheral blood stem cell
transplantation. N Eng J Med 2000; 343: 750-758
25. Bertz H, Burger JA, Kunzmann R, Mertelsmann R, Finke J. Adoptive
immunotherapy for relapsed multiple myeloma after allogeneic bone marrow
transplantation (BMT): evidence for a graft versus myeloma effect. Leukemia 1997;
11: 281-283
26. Nagler A, Slavin S, Varadi G, Naparstek E, Samuel S, Or R. Allogeneic peripheral
blood stem cell transplantation using a fludarabine based low intensity conditioning
regimen for malignant lymphomas. Bone Marow Transp 2000; 25: 1021-1028
27. Roux E, Helg C, Chapuis B. Mixed chimerism after bone marrow transplantation
and the risk of relapse. Blood 1994; 83: 4385-4386
28. Mackinnon S, Barnett L, Bourhis JH, Black P, Heller G, O´Reilly RJ. Myeloid and
lymphoid chimaerism after T-cell depleted bone marrow transplantation: evaluation
of conditioning regimens using the polymerase chain reacton to amplify human
minisatellite regions of genomic DNA. Blood 1992; 80: 3235-3241
29. Martino R, Caballero D, Canals C, Pérez-Simón JA, Solano C, A, Urbano-Ispízua A,
Bargay J, Rayón C, Sierra J, San Miguel J. Allogeneic peripheral blood stem cell
transplantation with reduced-intensity conditioning: results of a prospective
multicenter study. Br J Hematol 2001;115: 653-659
30. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatly P, Hows J, Thomas
ED. Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant
1995; 15: 825-830.

20
31. Sullivan KM, Shulman HM, Storb R, Weiden PL, Witherspoon RP, McDonald GB,
Schubert MM, Atkinson K, Thomas ED. Chronic graft-versus-host disease in 52
patients: adverse natural course and successful treatment with combination
immunosuppression. Blood 1981; 57:267-276.
32. Boeckh M, Bowden RA, Gooley T, Myerson D, Corey L. Successful modification
of a pp65 antigenemia-based early treatment strategy for prevention of
cytomegalovirus disease in allgeneic marrow transplant recipients. Blood 1999; 93:
1781-1787
33. Boeckh M, Gooley TA, Myerson D, Cunningham T, Schoch G, Bowden RA.
Cytomegalovirus pp65 antigenemia-guided early treatment with ganciclovir versus
gancliclovir at engraftment after allogeneic marrow transplantation. A randomize
double-blind study. Blood 1996; 88: 4063-4071
34. Mackinnon S, Papadopoulos EP, Carabasi MH, Reich L, Collins NH, Poulad F,
Castro-Malaspina H, Childs BH, Gilio AP, Kernan NA, Small TN, Young JW,
O´Reilly RJ. Adoptive immunotherapy evaluating escalating doses of donor
leucocytes for relapse of chronic myeloic leukemia following bone marrow
transplantation: separation of graft versus leukemia responses from graft versus host
disease. Blood 1995; 86: 1261-1268
35. Naparstek E, Or R, Nagler A, Cividalli G, Engelhard D, Aker M, Gimon Z, Manny
N, Sacks T, Tochner Z, Weiss L, Samuel S, Brautbar C, Hale G, Wldmann H,
Steiberg SM, Slavin S. T-cell-depleted allogeneic bone marrow transplantation for
acute leukaemia using Campath-1 antibodies and postransplant administration of
donor `s peripheral blood lymphocytes for prevention of relape. Br J Hematol 1995;
89: 506-515
36. Van Besien K, Sobocinski KA, Rowlings PA, Murphy SC, Armitage JO, Bishop
MR, Chaekal OK, Gale RP, Klein JP, Lazarus HM, McCarthy PL Jr, Raemaekers
JM, Reiffers J, Phillips GL, Schattenberg AV, Verdonck LF, Vose JM, Horowitz
MM. Allogeneic bone marrow transplantation for low-grade lymphoma. Blood
1998 Sep 1;92(5):1832-6
37. Rondon G, Giralt S, Huh Y, Khouri I, Andersson B, Andreeff M, Champlin R.
Graft-versus-leukemia effect after allogeneic bone marrow transplantation for
chronic lymphocytic leukemia. Bone Marrow Transplant. 1996 Sep;18(3):669-72
21
38. Khouri IF, Przepiorka D, van Besien K, O´Brien S, Palmer JL, Lerner S, Mehra RC,
Vriesendorp HM, Andersson BS, Giralt S, Korbling M, Keating MJ, Champlin RE.
Allogeneic blood or marrow transplantation for chronic lymphocytic leukaemia:
timing of transplantation and potential effect of fludarabine on acute graft-versus-
host disease.Br J Haematol. 1997 May;97(2):466-73
39. Tricot G, Vesole DH, Jagannath S, Hilton J, Munshi N, Barlogie B. Graft-versus-
myeloma effect: proof of principle. Blood. 1996 Feb 1;87(3):1196-8.
40. Mackinnon S. Who may benefit from donor leucocyte infusions after allogeneic
stem cell transplantation? Br J Hematol 2000; 110: 12-17
41. Apperley JF, Mauro FR, Goldman JM, Gregory W, Arthur CK, Hows J, Arcese W,
Papa G, Mandelli F, Wardle D. Bone marrow transplantation for chronic myeloid
leukemia in first chronic phase: importance of a graft versus leukemia effect. Br J
Hematol 1998; 69: 239-245
42. Hale G, Cobbold S, Novitzky N, Bunjes D, Willemze R, Prentice HG, Milligan D,
Mackinnon S, Waldmann H on behalf of CAMPATH users. CAMPATH-1
antibodies in stem cell transplantation. Cytotherapy 2001; 3: 145-164
43. Martino R, Caballero D, Canals C, San Miguel J, Sierra J, Rovira M, Solano C,
Bargay J, Pérez-Simón J, León A, Sarra J, Brunet S, de la Cámara R. Reduced-
intensity conditioning reduces the risk of severe infections after allogeneic
peripheral Blood stem cell transplantation. Bone Marrow Transpl 28 (4): 341-347,
2001
44. Camargo LF, Uip DE, Simpson AA, Caballero O, Stolf NA, Vilasboas LS, Pannuti
CS. Comparison between antigenemia and a quantitative-competitive polymerase
chain reaction for the dagnosis of cytomegalovirus infection after heart
transplantation. Trnasplantation 2001; 71: 412-417
45. Guiver M, Fox AJ, Mutton K, Mogulkoc N, Egan J. Evaluation of CMV viral load
using TaqMan CMV quantitative PCR and comparison with CMV antigenemia in
heart an lung transplantation. Transplantation 2001; 71: 1609-1615
46. Dykewicz CA. Summary of the guidelines for preventing opportunistic infections
among hematopoietic stem cell transplant recipients. Clin Inf Diseases 2001; 33:
139-144

22
47. Martin PJ. Influence of alloreactive T cells on initial hematopoietic reconstitution
after marrow transplantation. Exp Hematol 1995; 23: 174-79.
48. Curtis RE, Travis LB, Rowlings PA, Socie G, Kingma DW, Banks PM, Jaffe ES,
Sale GE, Horowitz MM, Witherspoon RP, Shriner DA, Weisdorf DJ, Kolb HJ,
Sullivan KM, Sobocinski KA, Gale RP, Hoover RN, Fraumeni JF Jr, Deeg HJ. Risk
of lymphoproliferative disorders after bone marrow transplantation: a multi-
institutional study.Blood. 1999 ;94: 2208-16.
49. Gross TG, Steinbuch M, DeFor T, Shapiro RS, McGlave P, Ramsay NK, Wagner
JE, Filipovich AH. B cell lymphoproliferative disorders following hematopoietic
stem cell transplantation: risk factors, treatment and outcome. Bone Marrow
Transplant. 1999 ; 23: 251-8.
50. Chakrabarti S, Mackinnon S, Chopra R, Kottaridis P , Peggs K, O’ Gorman P,
Chakraverty R, Marshall T, Osman H, Mahendra P, Craddock C, Waldmann H, Hale
G, Fegan C, Yong K, Goldstone A, Linch D, and Milligan D. High Incidence Of
Cytomegalovirus Infection After Nonmyeloablative Stem Cell Transplantation:
Potential Role of CAMPATH-1H in Delaying Immune Reconstitution. Blood: in
press
Copyright © 2022 FDOKUMEN




















