
Neural Structures
120
CHAPTER 17 Diagnosis of Nonodontogenic Toothache 685 The peripheral axons of the trigeminal ganglion run in three divisions—the ophthalmic (V1), maxillary (V2), and mandib- ular (V3)—which innervate most of the oral mucosa, the tem- poromandibular joint, the anterior two thirds of the tongue, the dura of the anterior and middle cranial fossae, the tooth pulp, the gingiva, and the periodontal membrane. In the peripheral nervous system, these neurons or nerves are referred to as primary afferent (i.e., sensory) fibers. The primary afferent fibers can broadly be divided into A-beta fibers, which transmit light touch or proprioceptive informa- tion, and A-delta and C fibers, which encode pain. The tooth is densely innervated by afferent nerve fibers, which are believed to transmit mainly pain in response to thermal, mechanical, or chemical stimuli. The majority of dental nerves are C fibers that innervate the central pulp, most of which terminate beneath the odontoblasts. 23 A-beta Fibers The rapidly conducting myelinated neurons that respond to light touch are called A-beta fibers. Under normal conditions, activation of the A-beta fibers by high-intensity stimulation results in low-frequency output in the central nervous system. Activation of A-beta fibers normally is interpreted as nonpain- ful mechanical stimulation 133 or, under certain conditions, can be perceived as a “prepain” sensation. 23 A-beta fibers also have been shown to undergo phenotypic changes that allow them to encode painful stimuli under certain inflammatory conditions. 98 A-delta Fibers The A-delta fibers are lightly myelinated, have a faster conduc- tion velocity than C fibers, and are believed to transmit a sharp or pricking sensation. A-delta fibers respond primarily to noxious mechanical stimuli rather than to chemical or thermal stimuli. Other A-delta fibers may be polymodal (responding to mechanical, chemical, and thermal stimuli) 13 or respond only to cold/mechanical 78 or hot/mechanical noxious stimuli. 39 In the tooth pulp, A-delta fibers traverse the odontoblastic layer and terminate in the dentinal tubules. 25 Because of their location and their sensitivity to mechanical stimulation, A- delta fibers are believed to respond to stimuli that result in into two broad categories: somatic and neural structures. Somatic structures are those that make up the different non- neural tissues and organs. The somatic structures can be further anatomically divided into superficial and deep struc- tures. Superficial structures include the skin, mucosa, and gingiva; pain that arises from these superficial structures is usually well localized (e.g., a sharp explorer penetrating the gingiva results in well-localized pain). Deep structures include musculoskeletal and visceral tissues. Pains from these deep structures are typically poorly localized and diffuse in nature. Neural Structures Neural structures involved in the perception of pain include the afferent (toward the brain) and efferent (away from the brain) regulation of somatic structures. Nerve impulses are transmitted from orofacial structures to the brain via the peripheral nervous system, whereas modulation and interpre- tation of these impulses into what we feel as pain occurs in the central nervous system. Pain can arise solely from either central or peripheral nervous tissue but heterotopic pain, which is often involved with nonodontogenic toothache, likely requires central modulation to occur. Peripheral Nervous System Pain arises as a result of tissue damage, or the potential for tissue damage, and is transmitted via terminal nerve fibers known as primary afferent nerve fibers. Two major classes of nociceptive (or pain-sensing) primary afferent nerve fibers can detect potentially damaging noxious stimuli: the A-delta and C fibers. Both fiber types have a wide distribution throughout the skin, oral mucosa, and tooth pulp. In addition, separate classes of nerve fibers exist that are involved in detecting non- noxious stimuli such as vibration and in proprioception. These fibers can be found in the periodontal ligament, skin, and oral mucosa and include the A-beta fibers. Primary Afferent Neurons Primarily the trigeminal, or fifth cranial, nerve detects and encodes noxious stimuli for the orofacial region. The majority of cell bodies of the trigeminal sensory fibers are in the trigemi- nal ganglion located on the floor of the middle cranial fossa. FIG. 17-1 Pantomogram of a patient who has undergone several endodontic procedures without resolution of her chief complaint. (Courtesy Dr. Jeffrey Okeson, Lexington, Kentucky.)
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Neural Structures
CHAPTER 17 Diagnosis of Nonodontogenic Toothache 685
The peripheral axons of the trigeminal ganglion run in three divisions—the ophthalmic (V1), maxillary (V2), and mandib-ular (V3)—which innervate most of the oral mucosa, the tem-poromandibular joint, the anterior two thirds of the tongue, the dura of the anterior and middle cranial fossae, the tooth pulp, the gingiva, and the periodontal membrane.
In the peripheral nervous system, these neurons or nerves are referred to as primary afferent (i.e., sensory) fibers. The primary afferent fibers can broadly be divided into A-beta fibers, which transmit light touch or proprioceptive informa-tion, and A-delta and C fibers, which encode pain. The tooth is densely innervated by afferent nerve fibers, which are believed to transmit mainly pain in response to thermal, mechanical, or chemical stimuli. The majority of dental nerves are C fibers that innervate the central pulp, most of which terminate beneath the odontoblasts.23
A-beta FibersThe rapidly conducting myelinated neurons that respond to light touch are called A-beta fibers. Under normal conditions, activation of the A-beta fibers by high-intensity stimulation results in low-frequency output in the central nervous system. Activation of A-beta fibers normally is interpreted as nonpain-ful mechanical stimulation133 or, under certain conditions, can be perceived as a “prepain” sensation.23 A-beta fibers also have been shown to undergo phenotypic changes that allow them to encode painful stimuli under certain inflammatory conditions.98
A-delta FibersThe A-delta fibers are lightly myelinated, have a faster conduc-tion velocity than C fibers, and are believed to transmit a sharp or pricking sensation. A-delta fibers respond primarily to noxious mechanical stimuli rather than to chemical or thermal stimuli. Other A-delta fibers may be polymodal (responding to mechanical, chemical, and thermal stimuli)13 or respond only to cold/mechanical78 or hot/mechanical noxious stimuli.39
In the tooth pulp, A-delta fibers traverse the odontoblastic layer and terminate in the dentinal tubules.25 Because of their location and their sensitivity to mechanical stimulation, A- delta fibers are believed to respond to stimuli that result in
into two broad categories: somatic and neural structures. Somatic structures are those that make up the different non-neural tissues and organs. The somatic structures can be further anatomically divided into superficial and deep struc-tures. Superficial structures include the skin, mucosa, and gingiva; pain that arises from these superficial structures is usually well localized (e.g., a sharp explorer penetrating the gingiva results in well-localized pain). Deep structures include musculoskeletal and visceral tissues. Pains from these deep structures are typically poorly localized and diffuse in nature.
Neural StructuresNeural structures involved in the perception of pain include the afferent (toward the brain) and efferent (away from the brain) regulation of somatic structures. Nerve impulses are transmitted from orofacial structures to the brain via the peripheral nervous system, whereas modulation and interpre-tation of these impulses into what we feel as pain occurs in the central nervous system. Pain can arise solely from either central or peripheral nervous tissue but heterotopic pain, which is often involved with nonodontogenic toothache, likely requires central modulation to occur.
Peripheral Nervous SystemPain arises as a result of tissue damage, or the potential for tissue damage, and is transmitted via terminal nerve fibers known as primary afferent nerve fibers. Two major classes of nociceptive (or pain-sensing) primary afferent nerve fibers can detect potentially damaging noxious stimuli: the A-delta and C fibers. Both fiber types have a wide distribution throughout the skin, oral mucosa, and tooth pulp. In addition, separate classes of nerve fibers exist that are involved in detecting non-noxious stimuli such as vibration and in proprioception. These fibers can be found in the periodontal ligament, skin, and oral mucosa and include the A-beta fibers.
Primary Afferent NeuronsPrimarily the trigeminal, or fifth cranial, nerve detects and encodes noxious stimuli for the orofacial region. The majority of cell bodies of the trigeminal sensory fibers are in the trigemi-nal ganglion located on the floor of the middle cranial fossa.
FIG. 17-1 Pantomogram of a patient who has undergone several endodontic procedures without resolution of her chief complaint. (Courtesy Dr. Jeffrey Okeson, Lexington, Kentucky.)
686 PART II The Advanced Science of Endodontics
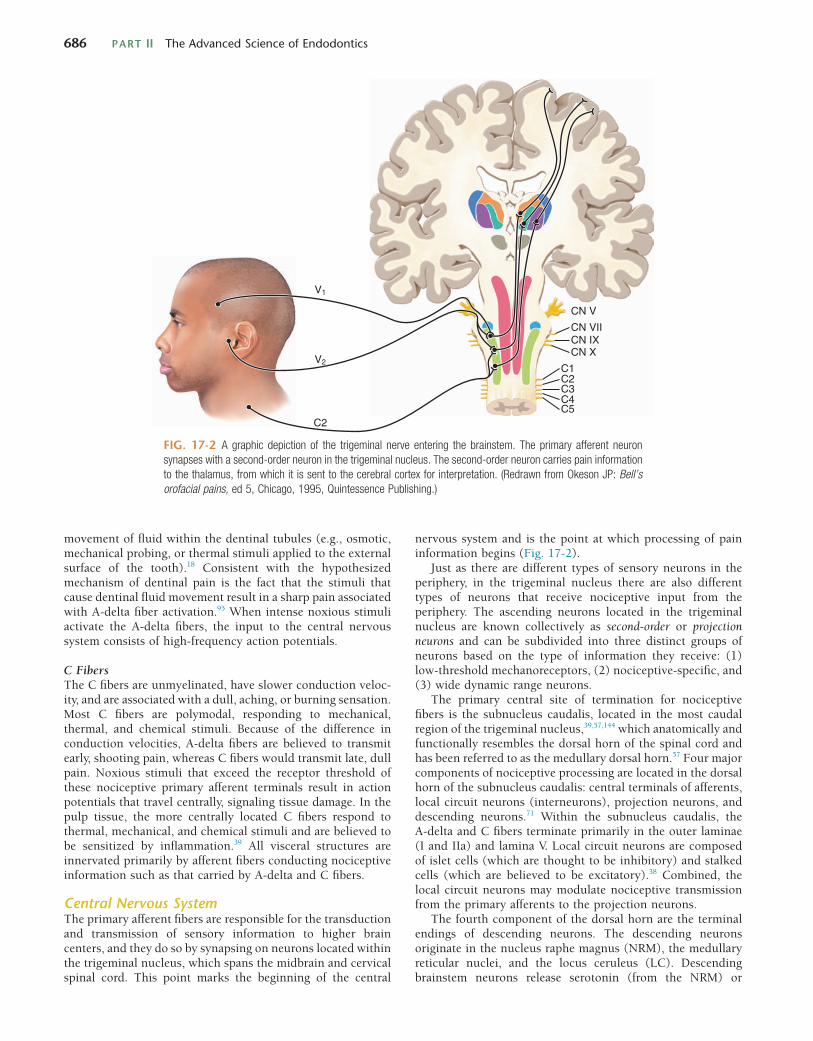
nervous system and is the point at which processing of pain information begins (Fig. 17-2).
Just as there are different types of sensory neurons in the periphery, in the trigeminal nucleus there are also different types of neurons that receive nociceptive input from the periphery. The ascending neurons located in the trigeminal nucleus are known collectively as second-order or projection neurons and can be subdivided into three distinct groups of neurons based on the type of information they receive: (1) low-threshold mechanoreceptors, (2) nociceptive-specific, and (3) wide dynamic range neurons.
The primary central site of termination for nociceptive fibers is the subnucleus caudalis, located in the most caudal region of the trigeminal nucleus,39,57,144 which anatomically and functionally resembles the dorsal horn of the spinal cord and has been referred to as the medullary dorsal horn.57 Four major components of nociceptive processing are located in the dorsal horn of the subnucleus caudalis: central terminals of afferents, local circuit neurons (interneurons), projection neurons, and descending neurons.71 Within the subnucleus caudalis, the A-delta and C fibers terminate primarily in the outer laminae (I and IIa) and lamina V. Local circuit neurons are composed of islet cells (which are thought to be inhibitory) and stalked cells (which are believed to be excitatory).38 Combined, the local circuit neurons may modulate nociceptive transmission from the primary afferents to the projection neurons.
The fourth component of the dorsal horn are the terminal endings of descending neurons. The descending neurons originate in the nucleus raphe magnus (NRM), the medullary reticular nuclei, and the locus ceruleus (LC). Descending brainstem neurons release serotonin (from the NRM) or
movement of fluid within the dentinal tubules (e.g., osmotic, mechanical probing, or thermal stimuli applied to the external surface of the tooth).18 Consistent with the hypothesized mechanism of dentinal pain is the fact that the stimuli that cause dentinal fluid movement result in a sharp pain associated with A-delta fiber activation.95 When intense noxious stimuli activate the A-delta fibers, the input to the central nervous system consists of high-frequency action potentials.
C FibersThe C fibers are unmyelinated, have slower conduction veloc-ity, and are associated with a dull, aching, or burning sensation. Most C fibers are polymodal, responding to mechanical, thermal, and chemical stimuli. Because of the difference in conduction velocities, A-delta fibers are believed to transmit early, shooting pain, whereas C fibers would transmit late, dull pain. Noxious stimuli that exceed the receptor threshold of these nociceptive primary afferent terminals result in action potentials that travel centrally, signaling tissue damage. In the pulp tissue, the more centrally located C fibers respond to thermal, mechanical, and chemical stimuli and are believed to be sensitized by inflammation.39 All visceral structures are innervated primarily by afferent fibers conducting nociceptive information such as that carried by A-delta and C fibers.
Central Nervous SystemThe primary afferent fibers are responsible for the transduction and transmission of sensory information to higher brain centers, and they do so by synapsing on neurons located within the trigeminal nucleus, which spans the midbrain and cervical spinal cord. This point marks the beginning of the central
FIG. 17-2 A graphic depiction of the trigeminal nerve entering the brainstem. The primary afferent neuron synapses with a second-order neuron in the trigeminal nucleus. The second-order neuron carries pain information to the thalamus, from which it is sent to the cerebral cortex for interpretation. (Redrawn from Okeson JP: Bell’s orofacial pains, ed 5, Chicago, 1995, Quintessence Publishing.)
CN V
V1
V2
CN VIICN IXCN X
C1C2
C2
C3C4C5

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 687
norepinephrine (from the LC), which may inhibit the activity of projection neurons directly or by activating local opioid interneurons. These neurons are responsible for the endoge-nous abatement of pain; blockade of their activity increases pain transmission and reduces pain thresholds.
Second-Order NeuronsProjection neurons have axons that cross to the contralateral medulla to ascend in the trigeminothalamic tract and project to the ventral posterior medial and intralaminar nuclei of the thalamus, where additional neurons project to the cortex. Pro-jection neurons involved in the transmission of painful stimuli can be divided into two classes: wide dynamic range and nociceptive-specific neurons. Wide dynamic range neurons receive input from mechanoreceptors, thermoreceptors, and nociceptors, whereas nociceptive-specific neurons are excited solely by nociceptors. These two types of projection neurons may be responsible for signaling the severity and location of pain, respectively.79
Multiple primary afferent neurons may synapse on a single projection (i.e., convergence). This occurs to a much greater degree in deep tissues as opposed to cutaneous tissues. Primary afferent fibers of nontrigeminal origin such as those derived from vagus, glossopharyngeal, facial, and cervical spinal ganglia have been shown to converge and synapse onto tri-geminal projection neurons located as far caudal as spinal level C4.74 This phenomenon of convergence may result in the clini-cal finding of pain that radiates beyond an area of tissue injury. Convergence may also explain why pain appears to be associ-ated with a site other than the injured area. Interestingly, when projection neurons receive input from superficial and deep structures, the more superficial inputs usually predominate.121 Thus, pain originating from deep structures would typically be referred to superficial areas (e.g., pain originating from the jaw muscles would typically be referred to the face rather than deeper structures).
Autonomic Nervous SystemThe stellate ganglia supply the entire sympathetic innervation of the orofacial region, which is located bilaterally at the level of the seventh cervical vertebra. Under normal conditions, sympathetic stimulation has no influence on sensory function. However, afferent sympathetic fibers in an area of trauma may become involved in the response to pain and may also play a role in chronic pain states. Specifically, C fibers in the area of partial nerve injury may become responsive to sympathetic nerve stimulation. The modulation of nociception by the sym-pathetic nervous system has been shown such that release of pain neurotransmitters may be altered in the presence of sym-pathetic agonists and by blockade of the sympathetic nervous system, using antagonists.70 Whether the effects of sympathetic nerve fibers on pain transmission are direct (via homeostatic regulation) or indirect remains unclear. The parasympathetic division of the autonomic nervous system has not been shown to be involved in the development or modulation of pain.
REVIEW OF NEUROPHYSIOLOGY
Peripheral SensitizationAfter tissue insult there is an inflammatory reaction that often produces pain. The severity of pain that follows is related to several aspects of the injury, such as the type, extent, and
location; the innervation of the tissue; and the phase of the inflammation. In the nociceptive system, tissue injury can manifest itself as increased responsiveness or reduced thresh-olds to a noxious stimulus, referred to as hyperalgesia. Hyper-algesia can be partially accounted for by sensitization of nociceptors (primary hyperalgesia) and by central nervous system mechanisms (secondary hyperalgesia).
In the absence of tissue damage, activation of C or A-delta fibers produces a transient pain. This pain is believed to serve as a physiologic warning. When there is tissue injury, afferent fibers may be activated by lower intensity stimuli than usual, and the quality of pain may be more persistent and intense. This phenomenon is due, in part, to the sensitization of noci-ceptors, including an increase in spontaneous activity.
At the site of tissue injury, there are a number of inflamma-tory mediators that can directly or indirectly sensitize primary afferent nociceptors (see Chapter 12 for more details). These inflammatory mediators may be released from the local tissue cells, circulating and resident immune cells, vasculature and endothelial smooth muscle cells, and peripheral nervous system cells.
Central SensitizationAfter peripheral tissue injury there is an afferent barrage from C fibers resulting from peripheral tissue inflammation, decreased afferent thresholds, and spontaneous firing of affer-ent fibers. When a second-order neuron receives a prolonged barrage of nociceptive input, the second-order neuron may also become sensitized. This results in a phenomenon referred to as central sensitization.17 The result of central sensitization is enhanced processing (i.e., amplification) of neural impulses that are being transmitted to higher brain centers. Two effects of central sensitization are secondary hyperalgesia and referred pain.
Secondary hyperalgesia is an increased response to painful stimulation at the site of pain resulting from central nervous system changes. This is in contrast to primary hyperalgesia, which is a lowered pain threshold resulting from sensitization of peripheral neurons. Secondary hyperalgesia might be felt in superficial (e.g., gingiva or skin) or deep structures (e.g., muscles or teeth).
TerminologyIn general, as research progresses and uncovers new ways for us to look at pain, the terminology changes. This can introduce some confusion, especially when older terms are used. There-fore, it may be helpful to present contemporary definitions of some of the basic terms and review some of the previously mentioned terms (Box 17-1).
CLINICAL ENTITIES THAT CAN PRESENT AS TOOTHACHE
Sources of Odontogenic ToothacheBefore considering heterotopic pains that may present as tooth-ache, it is important to fully understand odontogenic pain as a primary source for toothache. Only two structures serve as sources for primary odontogenic pain: the pulp–dentin complex and the periradicular tissues. The innervation of the pulp is similar to that of other deep visceral tissues, and in various states of pathosis will have pain characteristics similar to deep
688 PART II The Advanced Science of Endodontics
BOX 17-1
Types of Pain
PainAn unpleasant sensory and emotional experience associated with
actual or potential tissue damage or described in terms of such damage.86
Nociceptive PainPain arising from activation of nociceptors.86
Neuropathic PainPain arising as a direct consequence of a lesion or disease affecting
the somatosensory system.86,135
Peripheral SensitizationIncreased responsiveness and reduced thresholds of nociceptors to
stimulation of their receptive fields.86
Central SensitizationIncreased responsiveness of nociceptive neurons in the central
nervous system to their normal or subthreshold afferent input.86
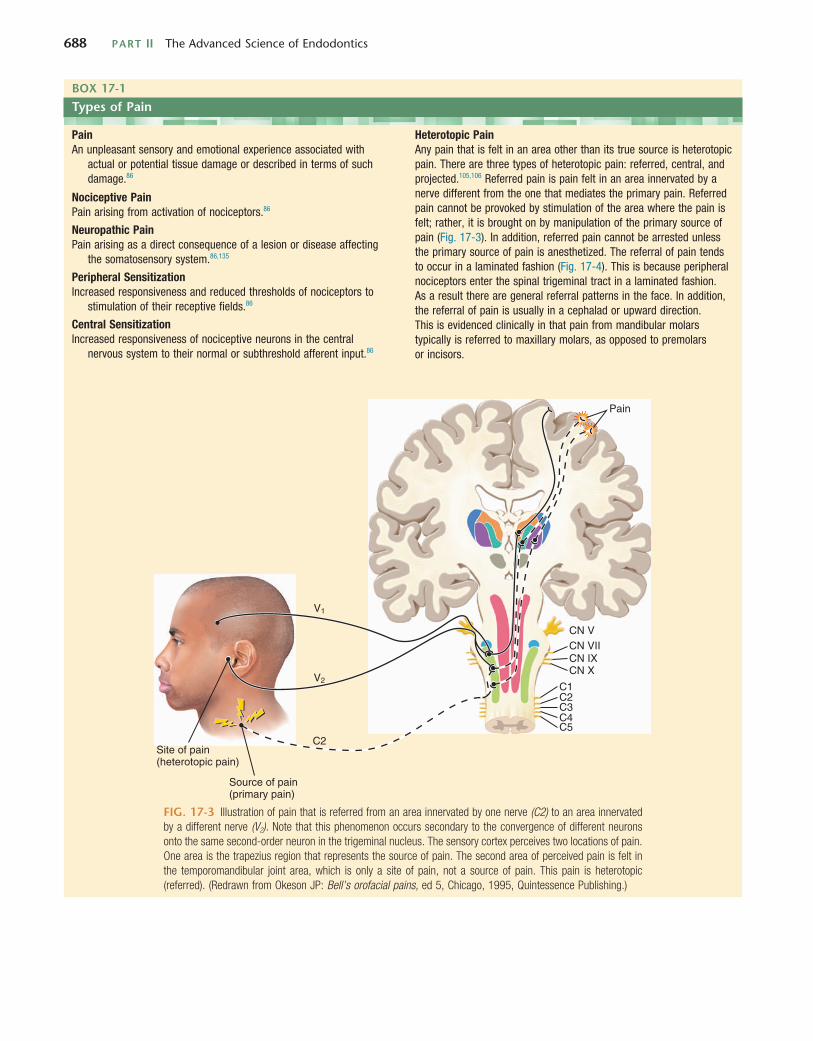
Heterotopic PainAny pain that is felt in an area other than its true source is heterotopic pain. There are three types of heterotopic pain: referred, central, and projected.105,106 Referred pain is pain felt in an area innervated by a nerve different from the one that mediates the primary pain. Referred pain cannot be provoked by stimulation of the area where the pain is felt; rather, it is brought on by manipulation of the primary source of pain (Fig. 17-3). In addition, referred pain cannot be arrested unless the primary source of pain is anesthetized. The referral of pain tends to occur in a laminated fashion (Fig. 17-4). This is because peripheral nociceptors enter the spinal trigeminal tract in a laminated fashion. As a result there are general referral patterns in the face. In addition, the referral of pain is usually in a cephalad or upward direction. This is evidenced clinically in that pain from mandibular molars typically is referred to maxillary molars, as opposed to premolars or incisors.
FIG. 17-3 Illustration of pain that is referred from an area innervated by one nerve (C2) to an area innervated by a different nerve (V2). Note that this phenomenon occurs secondary to the convergence of different neurons onto the same second-order neuron in the trigeminal nucleus. The sensory cortex perceives two locations of pain. One area is the trapezius region that represents the source of pain. The second area of perceived pain is felt in the temporomandibular joint area, which is only a site of pain, not a source of pain. This pain is heterotopic (referred). (Redrawn from Okeson JP: Bell’s orofacial pains, ed 5, Chicago, 1995, Quintessence Publishing.)
Pain
Site of pain(heterotopic pain)
Source of pain(primary pain)
CN V
V1
V2
CN VIICN IXCN X
C1C2
C2
C3C4C5

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 689
BOX 17-1
Types of Pain—cont’d
FIG. 17-4 Illustration of the laminated pattern of innervation from orofacial structures into the trigeminal nucleus. These laminated patterns commonly reflect the patterns of referred pains felt in the orofacial structures. (Redrawn from Okeson JP: Bell’s orofacial pains, ed 5, Chicago, 1995, Quintessence Publishing.)
112345
23
45
12
34
5
visceral tissues. The primary nociceptors of the pulp that respond to inflammation are the slow-conducting, high-threshold C fibers. Because their threshold is high and they rarely terminate in dentinal tubules, C fibers do not respond to normal or nonpathologic dentinal stimulation. C fibers typi-cally conduct pain that is associated with tissue damage. In addition, C fibers respond in a threshold manner that can be termed “all or nothing.” For example, a slightly cold stimulus that is below the C fiber threshold will fail to produce any sensation. Only when a stimulus is intense enough to reach the threshold will the C fiber fire, resulting in the sensation of pain.
Pulpal pain is mediated by C fibers and is dull, aching, or throbbing in nature. This is in contrast to the quick, short, sharp sensation produced by A-delta fibers that mediate den-tinal pain. Therefore, when pulp testing, it is meaningful to note not only whether the patient perceived the stimulus but also the nature of the stimulus perceived. A simple notation would be to use an “s” (short) to indicate a response more typical of an A-delta fiber (dentinal pain) or a “p” (prolonged) to indicate the response was more indicative of a C fiber response (pulpal pain).
Tissue inflammation can result in sensitization of nerve fibers. When peripheral nociceptors (e.g., pulpal C fibers) are sensitized, the threshold of firing in response to a given stimu-lus (e.g., temperature and pressure) is lowered. In states of sensitization these nociceptors can be provoked with a less intense stimulus. The threshold for excitation is still “all or nothing” but the required level of stimulation has decreased. These fibers can become so sensitized that they may fire at as
low a temperature threshold as body temperature,95 normally not sufficient to stimulate a C fiber. In fact, they can become so sensitized that they will fire in response to the normal pulse pressure of cardiac contraction, eliciting a complaint of “I can feel my heartbeat in my tooth” or “my tooth is throbbing.” Sensitized C fibers can even fire without provocation, resulting in spontaneous pain.
Similar to deep visceral tissues, the pulpal nociceptors demonstrate a high degree of convergence in the central nervous system. In a study of cat brain, 74% of the neurons tested in the subnucleus caudalis showed convergence from multiple tooth pulps.22 In addition, the dental pulp has little to no proprioceptive neurons. The high degree of con-vergence from pulp tissue and the lack of proprioceptive information provided are the key factors in why purely pulpal pain can be so difficult for patients to localize. In addition to reducing localization of pain, convergence increases the refer-ral of pain to tissues not actually affected by the inflamma-tion. The fact that neurons from the pulps of mandibular teeth converge with those of maxillary teeth can result in pain from a mandibular pulpitis being referred to the maxil-lary arch. Because the patient may poorly localize pulpal pain, it is important for the clinician to localize the source of the pain. This is often accomplished through the use of tests that are employed in an attempt either to reproduce the elic-iting stimulus of a patient’s pain or to eliminate the pain. For example, pulpal pain should be aggravated with hot or cold stimulation and should be eliminated or significantly reduced with local anesthetic.

690 PART II The Advanced Science of Endodontics
disorder characterized either as intense, intermittent lightning bolt–type pain within one or more distributions of the trigemi-nal nerve, or as continuous pain that is often mild to moderate in intensity that arises in association with injury to a specific branch of the trigeminal nerve. Efforts have resulted in a working diagnostic framework for neuropathic pains.135 Our classification scheme uses this framework to enhance the clarity of communication and follows the American Academy of Orofacial Pain’s guidelines for assessment, diagnosis, and management for orofacial pain,30 even though the application of these criteria to pains that present in the orofacial region is known to be associated with misclassification.35
Overall, one can classify the nonodontogenic reasons for toothache into five broad groups of pain disorders:1. Musculoskeletal and other nonprogressive pains arising
from somatic structures2. Neurovascular pain, otherwise known as headache
disorders3. Neuropathic pains4. Pain of purely psychologic origin, otherwise known as psy-
chogenic toothache5. Pain associated with a pathologic process
Musculoskeletal and Somatic PainMyofascial PainAlthough any deep somatic tissue type in the head and neck has the propensity to induce central excitatory effects and therefore cause referral of pains to teeth, pains of muscular origin appear to be the most common.46 Myofascial pain (MFP) emanates from small foci of hyperexcitable muscle tissue. Clin-ically these areas feel like taut bands or knots and are termed trigger points.134 Typically the pain is described as a diffuse, constant, dull, aching sensation; this may lead the clinician to a misdiagnosis of pulpal pain. Another potentially misleading characteristic of masticatory muscle pain is that patients may report pain when chewing. This feature is similar to pain that is periradicular, not pulpal, in origin. On further investigation, it should become clear that the pain is triggered by contraction of masticatory muscles rather than loading of periodontal liga-ments. Palpation of the muscles of mastication should repro-duce the pain, whereas percussion of the teeth should not. The intensity of the pain will increase and can be perceived in a distant site. Myofascial pain that is perceived to emanate from a tooth is a referred type of heterotopic pain—that is, the pain is felt in an area other than the nerve branch that innervates the trigger point. Typically muscles that refer pain to teeth are the masseter, temporalis, and lateral pterygoid; muscles of the neck and nonmuscular deep structures of the face can also be a source for this type of pain.134,142
Although the definitive pathogenesis of MFP is unknown, authors have theorized that muscles may become disturbed through injury or sustained contraction such as clenching.45,105 Clinically this muscular contraction might occur as a parafunc-tional habit or as a protective response by localized muscle to an ongoing deep noxious input such as dental pain. Consider-ing this theory and what is witnessed clinically, trigger points appear to be induced or aggravated by toothache. It also appears that trigger points can persist after the toothache has been resolved. This can be confusing for the clinician and frustrating for the patient. It is important to realize the relation-ship of these two entities. MFP can mimic toothache, and toothaches may induce the development of MFP.
Unlike pulpal pain, pain of periradicular origin is easier to localize. Mechanoreceptors are numerous in the periodontal ligament (PDL) and are most densely concentrated in the apical one third.87 Once inflammation from pulpal disease extends into the periodontal ligament, patients are able to locate the source of the pain much more readily. As a muscu-loskeletal structure, the PDL responds to noxious stimulation in a graded fashion—that is, the degree of discomfort a patient feels in relation to periradicular pain depends on the degree of peripheral sensitization and the amount of provoca-tion to this structure. A sensitized PDL will be uncomfortable to a patient if percussed lightly but more uncomfortable if percussed heavily. This is known as a graded response. It is, therefore, appropriate to record periradicular testing such as percussion and palpation in terms of degrees of tenderness (versus “all or nothing”). As with pulpal pain, pain of perira-dicular origin should also have an identifiable etiology. Peri-radicular pain tends to be dull, aching, or throbbing and should resolve completely with local anesthesia. If pain of suspected periradicular origin is nonresponsive to local anes-thetic, it is a strong indication that the pain may be nonodon-togenic in origin.
The tooth is unique in the human body in that it has a visceral-like component, the pulp, and a musculoskeletal com-ponent, the periodontal ligament. Therefore, odontogenic pain can have a wide variety of presentations. Tooth pain can be diffuse or well localized, mild or intense, or spontaneous or provoked with various stimuli applied at various intensities. The quality can vary between sharp and dull and aching or throbbing. This potential for extreme variability makes it pos-sible for toothaches to mimic or be mimicked by many other types of pain that occur in the head and neck. In addition, because both the pulp tissue and periodontal ligament can be categorized as deep somatic tissue, continued nociceptive input from odontogenic pain has a great propensity to produce central excitatory effects such as secondary hyperalgesia, referred pain, secondary co-contraction of muscles, myofascial trigger points, and autonomic changes. These effects add to the complexity of diagnosing odontogenic pain and differentiating tooth pain from other sources in the region.
Sources of Nonodontogenic ToothacheThis chapter provides information that will help the dental clinician to identify toothaches with a nonodontogenic etiol-ogy. The clinician must have a thorough knowledge of all possible causes of orofacial pain, which includes both odonto-genic and nonodontogenic conditions. This knowledge pre-vents misdiagnosis and allows for proper treatment selection and referral if necessary. For information about treatment of these disorders, other references should be used.
Consensus on the exact taxonomy with diagnostic criteria and their interrelationships among various orofacial pain dis-orders has not been established. Various health care profes-sions involved in the diagnosis and treatment of such pains have used different terms in the literature. This, of course, can and has led to confusion, especially within what we refer to as neuropathic pain. The terms used in the literature are diverse, and they overlap in meaning to an unknown degree; for example, phantom tooth pain and atypical odontalgia are used interchangeably. At other times the literature uses the same terms to describe seemingly different disorders; for example, trigeminal neuralgia has the connotation of an idiopathic pain

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 691
endoscopes, in addition to imaging tests such as radiology and computed tomographic imaging.36,125 Treatment of sinus/nasal mucosal pain is dependent on the etiology (e.g., bacterial, viral, allergic, or obstructive).
Salivary Gland PainPain referred from one or more of the salivary glands may be perceived as tooth pain; the authors have not encountered this response in clinical practice, but it has been reported to present as a nonodontogenic toothache.80,115 Because the primary somatosensory innervation of the major salivary glands comes from the mandibular branch, it is conceivable that such a pre-sentation will occur most often in mandibular teeth.
Neurovascular PainNeurovascular pains, otherwise and interchangeably referred to as headache disorders, have qualities similar to pulpal pain. These types of pain can be intense, often pulsatile, and are known to occur only in the head. The International Headache Society (Oxford, UK) has developed a classification system that is widely accepted even though validation studies of these criteria have yet to be published. The interested reader should consult the classification system for more details on this topic.56 Primary neurovascular pain disorders are thought to be a referred pain phenomenon, meaning that intracranial branches of the trigeminal nerve become sensitized via incompletely understood mechanisms and the associated pain and symp-toms are perceived in the somatic structures of the head. Most commonly people report pain presenting in the forehead, back of the head, and temples but also in the sinuses, jaws, and teeth.
The current understanding of the pathophysiology of head-aches implies that dental disease and treatments are not likely to be a cause of a person developing a headache disorder, but rather, because the same neuroanatomic circuitry is involved, these aspects of dentistry can be thought of as an inciting event, similar to the analogy that exercise producing increased demands on the cardiovascular system can be an inciting event for an acute myocardial infarction. For this reason, dental clini-cians should be aware of the diagnostic status of their patients, because patients with headache disorders are likely to experi-ence more peritreatment pain complications that are related to the innate hyperexcitability of the trigeminal nervous system in these people.
Of most interest to the dental clinician are the primary headache disorders, which make up the bulk of the headache disorders that occur within the population and have been reported to present as nonodontogenic toothache. To simplify thinking, these primary headache disorders can be grouped into three major subdivisions: (1) migraine, (2) tension-type headache, and (3) cluster headache and other trigeminal auto-nomic cephalalgias (TACs).
Migraine is a common headache experienced by about 18% of females and 6% of males.82,128 It is associated with significant amounts of disability, which is the motivating factor that brings the patient to seek care and the reason why this type of head-ache is the one most often seen in medical clinics.131 Migraine has been reported to present as toothache4,26,34,52,96,103 and is likely the most common neurovascular disorder to do so. In addition, people with migraine headaches are thought of as having increased regional pain sensitivity that has diagnostic and treatment implications for the clinician.102
Toothaches of myofascial origin may arise with or without evidence of pulpal or periapical pathosis. Definitive diagnosis is based on lack of symptoms after pulp testing and percussion or palpation sensitivity, or failure to resolve symptoms with local anesthetic blockade. In contrast, jaw function and palpation of the masticatory muscle(s) elicit toothaches of myofascial origin. Typically, local anesthetic infiltration into the trigger point(s) will resolve symptoms.
Common therapeutic modalities used to treat myofascial pain include deep massage, relaxation techniques, “spray and stretch,” muscle relaxants, and trigger point injections. Deep massage and relaxation techniques have the advantage of being noninvasive and easily administered. Spray and stretch involves an application of a vapor coolant spray to the skin overlying the trigger point, followed by a gentle stretching of the muscle. Trigger point injections are used for both the diagnosis and treatment of myofascial pain. Specifically, if the pain complaint is diminished on injection of the trigger point(s), then the source of the pain has been confirmed. The therapeutic efficacy of a trigger point injection varies. Some patients might experi-ence lasting relief with one injection or several, whereas others may not. See the Additional Tests section for further informa-tion about trigger point injections.
Pain of Sinus or Nasal Mucosal OriginSinus/nasal mucosal pain is another source of pain that can mimic toothache.1,2,28,138 Sinus pain can exhibit symptoms of fullness or pressure below the eyes but is generally not particu-larly painful unless the nasal mucosa is also affected.37 Pain from the nasal mucosa tends to be dull and aching and can also have a burning quality typical of visceral mucosal pain. In general, these pains are of viral, bacterial, or allergic etiology. Other symptoms consistent with these types of disease (e.g., congestion or nasal drainage) should be noted in the patient history.
Typical of deep visceral-like tissues, sinus/nasal mucosal pain can induce central excitatory effects such as secondary hyperalgesia, referral of pain, and autonomic changes. It is this tendency that gives sinus/nasal pain the ability to mas-querade as toothache. Secondary hyperalgesia, seen clinically as a concentric spread of pain beyond the area of tissue injury, results in tenderness of the mucosa in the area of the maxillary sinuses as well as tenderness to percussion of several maxil-lary teeth. Teeth tender to percussion and palpation suggest periradicular inflammation. Autonomic sequelae might present as edema or erythema in the area, which could suggest a dental abscess. However, when an etiology for pulpal and therefore periradicular pathosis is absent, sinus/nasal mucosal disease should be suspected. The three cardinal symptoms of acute rhinosinusitis are (1) purulent nasal discharge, (2) nasal obstruction, and (3) facial pain-pressure-fullness.118 Other symptoms of sinus disease include sensitivity to palpation of structures overlying sinuses (i.e., paranasal tenderness) and a throbbing or increased pain sensation when the head is placed lower than the heart. Dental local anesthetic blockade will not abate sinus/nasal mucosal pain, although topical nasal anes-thetic will.
Patients with suspected sinus/nasal mucosal disease should be referred to an otolaryngologist for further diagnosis and treatment. Physical examination as well as adjunctive tests may be necessary for a definitive diagnosis. Tests may include nasal cytologic and ultrasound studies and the use of nasal

692 PART II The Advanced Science of Endodontics
complete remission between episodes, whereas toothache pain usually has at least some background pain that stays between any exacerbations. Provocation of the tooth should not result in a clear increase in pain but cause a slight alteration because this tissue has become hypersensitized. Local anesthetic is unpredictable in these cases and can mislead the clinician. Management by the typical clinician is to determine that the pain is not of odontogenic origin and then to refer the patient to an appropriate care provider. Other neurovascular disorders not classified as primary headaches have been reported to present as nonodontogenic toothache, such as cough head-ache.91 One would not expect a dental clinician who does not have a specific focus on orofacial pain to arrive at such a spe-cific diagnosis but rather to be aware of and sensitive to the fact that more obscure headache disorders exist and should be considered in the differential diagnosis of a nonodontogenic toothache that is not easily classified.
Neuropathic PainAll previously described pain entities can be classified as somatic pain. That is, they are a result of noxious stimulation of somatic structures. These impulses are transmitted by normal neural structures, and their clinical characteristics are related to stimulation of normal neural structures. Neuropathic pain actually arises from abnormalities in the neural structures themselves, specifically the somatosensory system. The clinical examination generally reveals no somatic tissue damage, and the response to stimulation of the tissue is disproportionate to the stimulus. For this reason, neuropathic pains can be misdi-agnosed as psychogenic pain simply because a local cause cannot be readily identified. There are many ways to categorize neuropathic pain in the orofacial region. For the purposes of this chapter and ease of discussion, neuropathic pain is divided into four subcategories: neuralgia, neuroma, neuritis, and neu-ropathy. It should be acknowledged that these subcategories are arbitrary and are not mutually exclusive.
NeuralgiaAs alluded to previously, not all uses of the term neuralgia refer to what is often thought of as the classic trigeminal neuralgia or tic douloureux. Sometimes the term neuralgia is used to describe pain felt along a specific peripheral nerve distribution, such as with postherpetic neuralgia and occipital neuralgia, as opposed to a focus of pain disorders that have similar charac-teristics and are thought to have common underlying patho-physiologic mechanisms. When used in the generic sense to describe pains that present intraorally, the term can lead to a great deal of confusion.
Although deviations are not uncommon, trigeminal neural-gia is characteristically an intense, sharp shooting pain that is most often unilateral. Ipsilateral to the perceived location of the symptoms is an area that, on stimulation such as light touch, elicits sharp shooting pain. The area that elicits the pain is referred to as a trigger zone, and it can be in the distribution of the resultant pain or in a different distribution—but is always ipsilateral. Although most patients present with a char-acteristic trigger zone, not all patients will present with this finding. An important characteristic of trigger zones is that the response to the stimulus is not proportional to the intensity of the stimulus—that is, slight pressure on a trigger zone results in severe pain. In addition, once triggered, pain typically subsides within a few minutes until triggered again. This is in
Migraine headaches typically last between 4 and 72 hours. They tend to be unilateral in presentation and pulsatile in quality, with a moderate to severe intensity to the pain. Patients may also experience nausea or vomiting, as well as photopho-bia or phonophobia, which are different from toothache. The headache is usually aggravated with routine physical activity, such as walking up stairs. Caffeine/ergotamine compounds have been used widely in the past as abortive agents for migraine headaches, but in contemporary times they have been replaced with triptans, such as sumatriptan and rizatriptan.93 Of note, migraine headaches may partially or fully abate with the use of nonsteroidal anti-inflammatory medications in a similar fashion as toothaches.
Tension-type headache is the most frequent headache dis-order experienced, with a wide range of reported prevalence (41% to 96%).117,123 The concept of tension-type headache pain presenting as toothache has not been reported in the literature to our knowledge, likely because the construct of what a tension-type headache is has not been clearly defined. Some research supports the notion that a tension-type headache has a significant musculoskeletal component to the pain,129 whereas other research suggests otherwise. Tension-type headaches are likely a heterogeneous group of similarly presenting head pains that have overlapping pathophysiologic mechanisms, which has led some researchers to consider aspects of tension-type headache to be the same as musculoskeletal orofacial pain, otherwise known as temporomandibular disorders (TMDs).55 This has further been supported by data from a TMD valida-tion study to derive criteria for such headaches that are of TMD origin.6,122
Cluster headaches and other TACs are rare neurovascular disorders that are strictly unilateral pains defined by the con-current presentation of at least one ipsilateral autonomic symptom—such as nasal congestion, rhinorrhea, lacrimation, eyelid edema, periorbital swelling, facial erythema, ptosis, or miosis—that occurs with the pain. The major distinguishing features between these headache disorders are the duration and frequency of the pain episodes, as well as the gender most often afflicted. Cluster headache is the most common of the group, occurring in men three to four times more often than in women, with pain episodes lasting between 15 minutes and 2 hours that occur at a frequency of eight episodes per day to one every other day. These headaches come in clusters, with active periods of 2 weeks to 3 months,56 thus the name. Elimi-nation of pain after 10 minutes with inhalation of 100% oxygen is diagnostic for cluster headache,49 whereas sublingual ergota-mine and sumatriptan are also effective acute treatments for cluster headache.42 Paroxysmal hemicrania, which has a 3 : 1 female predilection, presents with characteristics similar to those of cluster headache but with a frequency of more than five per day and a duration lasting 2 to 30 minutes.56 This headache disorder has a 100% response to indomethacin but is refractory to other treatments,65 thus underscoring the need for obtaining an accurate diagnosis from an experienced clinician.
From a nonodontogenic perspective, cluster headache4,14,21,51 and almost all the other TACs have been reported in the litera-ture to present as nonodontogenic toothache.4,11,12,31,92,110,120 The concurrent autonomic features, such as discoloration or swelling in the anterior maxilla, might compound the diagnos-tic problem by suggesting tooth abscess. It is important to note that neurovascular headaches tend to be episodic with

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 693
variable periods of remission.48 The subsequent onset of true neuralgic pain may be sudden or may appear several years later,105 which emphasizes the need for long-term follow-up of these patients to obtain an accurate final diagnosis.
NeuromaThe term neuroma has been around for many years and is often overused in an attempt to describe other types of neuropathic pain. A traumatic neuroma, also known as an amputation neuroma, is a proliferative mass of disorganized neural tissue at the site of a traumatically or surgically transected nerve. A part of the diagnosis, therefore, is confirmation of a significant event that would account for the damage to the nerve. Symp-toms will not develop until the neural tissue on the proximal stump has had time to proliferate, typically about 10 days after the event. Tapping over the area of a neuroma elicits volleys of sharp electrical pain (i.e., Tinel sign) similar to trigeminal neuralgia. In contrast to trigeminal neuralgia, there should be a zone of anesthesia peripheral to the area of the neuroma111 that can be identified by checking for loss of pinprick sensibil-ity, such as with the use of an explorer.
Treatment of a neuroma involves pharmacologic manage-ment, often via local measures, and may involve surgical coap-tation of the nerve with prognosis being variable and dependent on adequate distal nerve tissue and the time interval between injury and reconstruction.148 Therefore, early recognition and referral are of key importance to prevent significant distal nerve degeneration.76 Although neuromas most commonly develop in the area of the mental foramen, lower lip, and tongue, there is some evidence that they can also form in extraction sites and after pulpal extirpation. Neuromas were found to form in extraction sites between 4 and 6 months after removal of the tooth in an experimental animal model.69 Although not all neuromas that form are painful, this could be a potential expla-nation for ongoing pain in extraction sites after healing has appeared to occur.111 It is interesting to ponder the possibility of neuroma formation in deafferentation injuries such as pul-pectomy and the implications this might have on continued PDL sensitivity after adequate root canal treatment. For treat-ment of neuromas that are not amenable to surgical correction, see the Neuropathy section of this chapter.
NeuritisNeuritis is a condition caused by inflammation of a nerve or nerves secondary to injury or infection of viral or bacterial etiology. In general, pain from a virally induced neuritis, such as recurrent herpes simplex or herpes zoster, is associated with skin or mucosal lesions (Fig. 17-5). This presentation does not result in much of a diagnostic challenge, but pain can precede the vesicular outbreak by many days or even weeks.47 Because neuritic disorders are caused by reactivation of a virus that has been dormant in the trigeminal ganglion, they are considered projected pain with distribution within the dermatomes inner-vated by the affected peripheral nerves. The nerves affected by the virus may solely supply deeper tissues and therefore may not produce any cutaneous lesions. In the absence of skin or mucosal lesions, a viral neuritis can be difficult to diagnose47,60,67 and should be considered in the differential diagnosis of a patient with a history of primary herpes zoster infection. Bacte-rial infection of the sinuses or dental abscess can also cause neural inflammation that may result in pain. This pain occurs simultaneously with pain of the infected tissues and usually
contrast to odontogenic pain, which may come and go but does not do so in such a predictable and repeatable manner. Finally, the trigger for odontogenic pain is an area that has no sensory abnormalities (e.g., dysesthesia or paresthesia).
Trigger zones for trigeminal neuralgia tend to be related to areas of dense somatosensory innervation, such as the lips and teeth. For this reason, triggers that elicit this type of pain may include chewing and may lead both the patient and clinician to think of a diagnosis of odontogenic pain. In addition, because the trigger involves peripheral input, anesthetizing the trigger zone may diminish symptoms. This can be very mis-leading to the clinician if the assumption is that local anes-thetic blocks only odontogenic pain.
Because symptoms can be quite severe, patients may consent to or even insist on treatment even though the clinical findings do not definitively support an odontogenic etiology. The pos-sibly misleading symptoms, along with the willingness of the patient to consent to what may seem to be desperate measures, emphasize the importance of a thorough history and clinical evaluation. The absence of a dental etiology for the symptoms (e.g., large restorations, dental trauma, or recent dental treat-ment) in the presence of the characteristic sharp shooting pain should alert the clinician to consider trigeminal neuralgia in the differential diagnosis. In general, these individuals should be referred to a neurologist or orofacial pain/oral medicine clinician for a complete diagnostic workup and treatment, because case series have suggested 15% to 30% of patients have secondary reasons for their pain,58,143 such as brain tumors and multiple sclerosis.
Trigeminal neuralgia typically presents in individuals older than 50 years of age. The etiology is thought to be irritation/compression of the root of the trigeminal nerve, prior to the gasserian ganglion, possibly as a result of carotid artery pres-sure. Individuals with multiple sclerosis develop trigeminal neuralgia more frequently than the general population. For this reason, a person younger than 40 years of age who develops trigeminal neuralgia should also be screened for multiple scle-rosis147 or other intracranial pathosis.58
The two general treatment options for trigeminal neuralgia are pharmacologic and surgical procedures. Because of the possible complications associated with surgery, this form of treatment is usually considered only after attempting pharma-cologic therapies. Several medications, including carbamaze-pine, baclofen, gabapentin, and more recently pregabalin and oxcarbazepine, have been used to treat trigeminal neuralgia. Drugs aimed at relieving nociception, such as nonsteroidal antiinflammatory agents, have no significant benefit in these patients, nor do opioid-based analgesics. Clinical trials support carbamazepine as a first-line drug for treating trigeminal neu-ralgia.8 In patients who experience pain relief from carbamaze-pine, the effect is usually rapid; most will report a decrease in severity of symptoms within the first couple of days.
What is thought to be a variation of trigeminal neuralgia, and may also mimic toothache, is pretrigeminal neuralgia. Pretrigeminal neuralgia, as the name suggests, has been described as symptoms that are different from those of classic trigeminal neuralgia but that respond to pharmacotherapy like classic trigeminal neuralgia and, over time (usually weeks to 3 years), take on the classic characteristics of trigeminal neu-ralgia. The definitive features include the presence of a dull aching or burning pain that is less paroxysmal in nature but still triggered by a light touch within the orofacial region, with
694 PART II The Advanced Science of Endodontics
Additional surgical insult further traumatizes the nerve, pro-longing the already present nociceptive barrage, which puts the patient at an increased risk of developing central hyperalgesia. Undiagnosed and mistreated cases of acute neuritis not only lead to unnecessary dental procedures but may also aggravate the neuritis and, therefore, the neuritic pain has a greater chance of becoming chronic, something that is often referred to as neuropathic pain.
Neuritic pain typically is a persistent, nonpulsatile burning often associated with sensory aberrations such as paresthesia, dysesthesia, or anesthesia. The pain can vary in intensity, but when stimulated, the pain provoked is disproportionate to the stimulus.
Treatment of acute neuritis is based on its etiology. In instances of chemical trauma (e.g., Sargenti paste) where an obvious irritant is present, surgical debridement of the nerve to remove any substance that can continue to irritate the nerve is an important aspect of treatment. With neuritis secondary to mechanical compression (e.g., implant placement) of a nerve, nerve decompression by removal of the implant fixture is indicated. Such localized, acute, traumatically induced neu-ritis is inflammatory in nature and, therefore, can also benefit from supportive pharmacotherapies such as steroids. For man-agement of neuritis that is not responsive to the previously cited treatments, medications used to treat neuropathic pain may be used (see Neuropathy). For neuritis occurring second-ary to an infection, such as one of odontogenic or viral etiology, treatment is directed at eliminating the offending pathogen and minimizing injury to the afferent nerves.
NeuropathyIn this chapter we use the word neuropathy as the preferred term for localized, sustained nonepisodic pain secondary to an injury or change in a neural structure. Historically, other terms have been used including atypical facial pain. This term sug-gests pain that is felt in a branch of the trigeminal nerve and that does not fit any other pain category. Pain of an unknown source that is perceived in a tooth may be labeled atypical odontalgia. Pain that persists after the tooth has been extracted
dissipates once the etiology is addressed. In susceptible indi-viduals, virally or bacterially induced neuritis may produce a postinfection neuropathy of the infected nerve. The pain is fairly constant and can be dull, aching, and burning. Also, the pain may be accompanied by allodynia, a painful response to normally non-noxious stimulation such as light brushing of the skin. Oral acyclovir has become the most common treat-ment for acute herpetic outbreaks and has been shown to be efficacious in decreasing the duration and severity of pain after herpes zoster infection. Efficacy is based only on administra-tion in the prevesicular, not the vesicular, stage. The addition of prednisolone to acyclovir produces only slight benefits over acyclovir alone. Neither acyclovir alone nor its combination with prednisolone appears to reduce the frequency of posther-petic neuralgia.140
Localized traumatic injury can also induce neuritis. This injury can be chemical, thermal, or mechanical in nature. A classic endodontic example of a chemical injury to a nerve is the overextension of a highly neurotoxic paraformaldehyde-containing paste (e.g., Sargenti paste) onto the inferior alveolar nerve canal. Chemical trauma can be due to certain toxic components of the endodontic filling materials (such as eugenol), irrigating solutions (such as sodium hypochlorite), or intra canal medicaments (such as formocresol) (Fig. 17-6).94 Mechanical compression, in addition to thermal trauma, may be a factor when thermoplasticized material is overextended, using an injectable50 or carrier-based technique. Mechanical nerve trauma is more commonly associated with oral surgical procedures, such as orthognathic surgery, and third molar extraction.
Neuritic complications have also been documented after mandibular implant surgery at a rate of 5% to 15%, with permanent neuropathies, which are discussed later, resulting in approximately 8% of these cases.66 It is unfortunate that traumatic neuritis is often misdiagnosed as a posttreatment chronic infection and that the area is reentered and debrided.
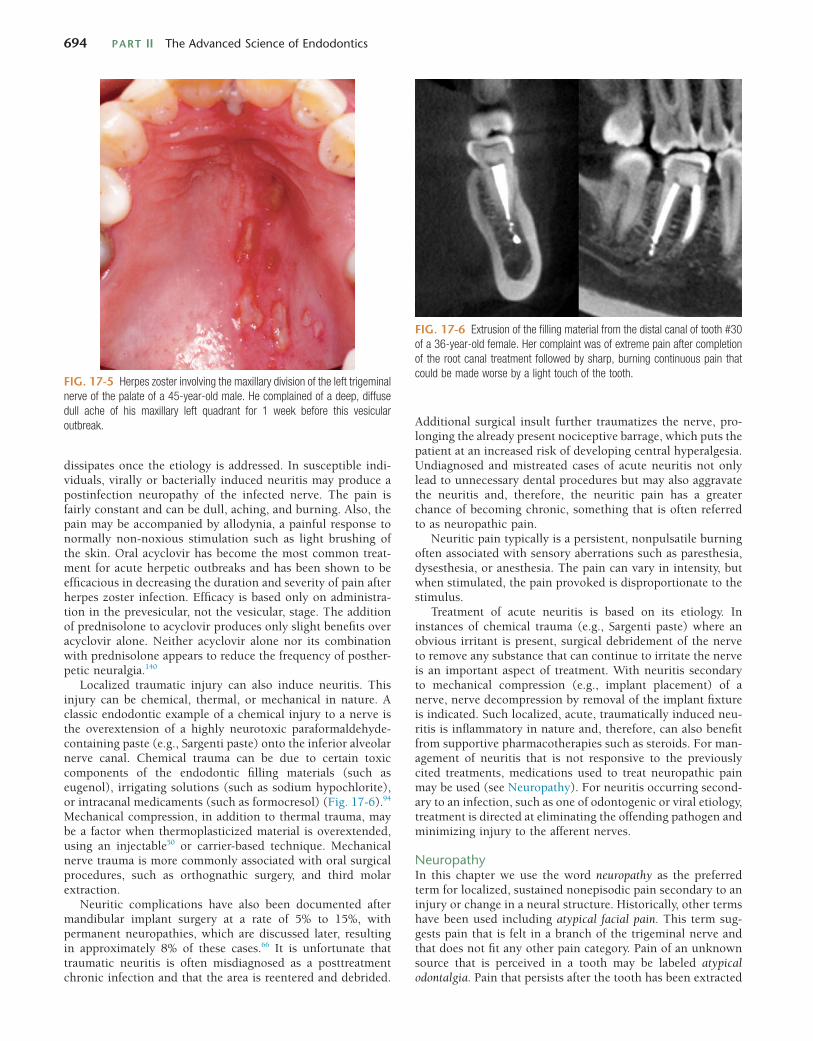
FIG. 17-5 Herpes zoster involving the maxillary division of the left trigeminal nerve of the palate of a 45-year-old male. He complained of a deep, diffuse dull ache of his maxillary left quadrant for 1 week before this vesicular outbreak.
FIG. 17-6 Extrusion of the filling material from the distal canal of tooth #30 of a 36-year-old female. Her complaint was of extreme pain after completion of the root canal treatment followed by sharp, burning continuous pain that could be made worse by a light touch of the tooth.

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 695
is referred to as phantom tooth pain. The major limitation in the use of all these terms is that they merely suggest an area where a pain of unknown etiology exists and completely lack any information regarding the pathophysiology. Although each of these terms has been extensively described in the literature,88,89 probably none actually represents one discrete condition but rather a collection of various conditions. Based on these thoughts, a consensus process resulted in proposing new ter-minology, persistent dentoalveolar pain disorder (PDAP), and diagnostic criteria (Fig. 17-7).99
Once a nerve has been sensitized via injury or disease it may remain so and present as a peripherally sensitized nerve. This peripheral sensitization and the ongoing pain (nociceptive barrage) that accompanies it can induce changes in the central nervous system. Peripheral sensitization and central sensitiza-tion can potentially impact the clinical presentation of a neuropathy. A typical clinical course of someone with an undiagnosed neuropathy might consist of treatment for a toothache. When the pain does not resolve with nonsurgical root canal treatment, it might then be followed by apical surgery and then perhaps an extraction. The extraction site might then be explored and debrided in a misguided attempt to remove any potential source of the patient’s ongoing pain. After each treatment, there tends to be a reduction of the pain for a short time and then a return to its original, or even increased, level of pain intensity. It is likely that this is a result of a new neural injury consisting of reorganization and resprouting that increases the inhibition of nerve firing for a time. Surgical approaches to neuropathies are not effective because they do not desensitize the nerve. On the contrary, surgical intervention may aggravate the situation by inflicting an additional neural injury in the periphery and contributing to the already present nociceptive input. This intervention therefore puts the patient at increased risk of developing
FIG. 17-7 Diagnostic criteria for persistent dentoalveolar pain disorder (PDAP).
Criteria12 Persistent, meaning pain present at least 8 hours/day ≥15 days or more per month for ≥3 months Pain is defined as per IASP criteria (includes dysesthesia)
3 Localized, meaning the maximum pain defined within an anatomic area4 Extent of evaluation non-specified (dental, neurologic exam ± imaging, such as intraoral, CT and/or MRI)
PDAP
A. Persistent1 pain,2 andB. Localized3 in the dentoalveolar region(s), andC. Not caused by another disease or disorder4
SecondaryIn close temporal relationship
to a causal event(e.g., dental procedures,facial trauma, infection)
PrimaryNot in close temporal
relationship to a causal event(e.g., dental procedures,facial trauma, infection)
Sensory abnormalitypresent
Sensory abnormalityabsent
persistent pain, which is supported by a couple of long-term observational studies3,113 and further supported by the observa-tion that patients with pain following root canal therapy did not uniformly experience elimination of this pain with apico-ectomy surgery.108
A diagnosis of neuropathy is based primarily on history and examination with the use of selected diagnostic tests to rule out other potential etiologies. The history should reveal some inflammation-inducing event (see the earlier sections Neuritis and Neuroma), although the nature of the initial insult is not always identified, as seemingly spontaneous development of such pains has been reported.99 Typically, the examination is grossly unremarkable with no evidence of local tissue damage, leaving the clinician to rely mainly on the patient’s report of symptoms. Although quality of pain is no longer thought to be capable of distinguishing neuropathic pains from others, patients repeatedly reported several features that may be key for identification purposes (Box 17-2).40 Regarding examina-tion features, the area where the pain is perceived may be hyperalgesic or allodynic—that is, noxious stimulation to the area will be perceived as more painful or non-noxious stimula-tion will now be perceived as painful. This phenomenon is documented by reports where standardized applications of stimuli to the affected tissue are performed and demonstrate exaggerated responses.85,90,146 Besides gain in sensory function, loss of function has also been observed,85 which is more in line with a general definition for neuropathic pain.135 Furthermore, maintenance of pain following local anesthesia to the affected region83 and a lack of pain reduction with fentanyl and ketamine7 all suggest the role of a central pain-related mechanism.
Research related to the diagnostic imaging of cases that may be PDAP suggests two roles: first, to identify pathosis contrib-uting to the pain presentation and, second, as a means of

696 PART II The Advanced Science of Endodontics
The clinical presentation of a central neuropathy is similar to that of a peripheral neuropathy. After sensitization of periph-eral nerves and the accompanying nociceptive barrage, the pain is nonremitting and lacks evidence of tissue insult. Unlike its peripheral counterpart, allodynia and secondary hyperalge-sia are clearly present—that is, the area of pain is significantly larger than the initial site of injury. The most telling sign that a neuropathy has taken on a more central component is that local anesthetics are no longer effective. Therefore, the treat-ment must be directed toward the central processing of pain. This is done with medications such as NMDA receptor agonists (ketamine), gabapentin, tricyclic antidepressants, and opioids. The prognosis for a central neuropathy is not as good as for a peripheral neuropathy, as central neuropathic pain tends to become more refractory with time. Treatment is often based on the management of pain, rather than its cure, and sometimes is best performed in a multidisciplinary chronic pain clinic facility.
The last variation of neuropathic pain is sympathetically enhanced or maintained pain. In cases of sympathetically maintained pain (SMP), peripheral nerve fibers upregulate the expression of adrenergic receptors, making them responsive and sensitive to sympathetic input. SMP may also have a central component, whereby the constant sympathetic drive alters neuronal excitability. Neuronal injury may induce sprouting of sympathetic axons into the trigeminal spinal nucleus because basket-like formations of sympathetic fibers have been reported around the cell bodies of sensory neurons in the dorsal root ganglia.141 Increases in sympathetic drive, such as with stress and fever, may aggravate SMP. Diagnosis of sympathetically maintained pain is based on blocking sympa-thetic outflow to the affected region via sympathetic nerve blocks. In the orofacial region this would require a stellate ganglion block. The block is considered diagnostic for SMP if it effectively decreases the patient’s pain. Multiple blocks can also be used as a form of therapy. Other therapies include drugs that target peripheral α2-adrenoceptors (agonists) or α1-adrenoceptors (antagonists), such as guanethidine, phentol-amine, and clonidine. SMP presenting in the orofacial region is extremely rare54 and therefore makes clinicians prone to deriving a falsely positive diagnosis of this condition.101 Fur-thermore, researchers have failed to produce SMP-type pain in animals,10 something that is presumed to be due to the fact that the efferent nerve fibers in the head and neck region run with the blood vessels as opposed to the afferent nerves, as they do elsewhere in the human body. For these reasons, the likelihood of this type of pain presenting as “toothache” is extremely low and thus does not require much discussion here.
Psychogenic ToothachePsychogenic toothache falls within a group of mental disorders known as somatoform disorders. The name is derived from the fact that the patient has somatic complaints yet lacks a physical cause. Because these patients lack a physical cause for pain, they also present without local tissue changes. Patients with somatoform disorders are not fabricating the symptoms, nor are they consciously seeking benefit. It is important to make a distinction between somatoform disorders and factitious pain or malingering behavior.5 In factitious pain there are physical or psychological symptoms that are produced by the individual and are under voluntary control. Malingering is similar to facti-tious pain with the added characteristic that the symptoms are
obtaining a positive finding for this enigmatic chronic pain disorder. As for the first role, diagnostic imaging is recom-mended to assess for odontogenic-related pathosis and other regionally presenting disease, as most pain in the dentoalveolar region is tooth-related. For patients suspected of having PDAP, the diagnostic yield of cone-beam computed tomography (CT) was reported to be superior to PA radiograph, but the findings were of questionable significance.112 For patients without local pathosis and PDAP, magnetic resonance imaging (MRI) of the brain revealed several cases of intracranial findings thought to be related to the pain presentation (e.g., cysts, tumors, infarcts).104 This is consistent with the clinical experience of one of the authors, which has led to brain imaging being routine prior to a diagnosis of PDAP being rendered. As for the second role of diagnostic imaging, conventional dental radio-graphic techniques have consistently been found not to be able to identify patients with PDAP, thus prompting pilot investiga-tion into other imaging techniques. Results suggest high levels of sensitivity and specificity can be reached using thermogra-phy64 revealing a “cold” image profile.63 On the contrary, results suggest that a technetium-99 bone scan had low sensitivity and specificity for detecting dentoalveolar regions with chronic pain,32 and MRI techniques do not seem to have been studied.
Neuropathic disorders have a predilection for women but can affect both genders. These patients are usually older than 30 years of age and may have a history of migraine.126 In the orofacial region, neuropathies are most commonly seen in the maxillary premolar area and molar region.61,108
Neuropathies can be classified on the basis of their clinical presentation and response to therapies. Peripheral neuropathy may develop after sensitization of a peripheral nerve and pre-sents clinically as described previously. Diagnosis of peripheral neuropathy is based on its favorable response to peripheral neural blockade. Treatment is directed at decreasing the sensi-tization of peripheral nerves and reducing ectopic neuronal firing. Topical as well as systemic medications can be used to treat cutaneous peripheral neuropathies. Topical medications include topical anesthetics, capsaicin-containing compounds, and anticonvulsants, as well as nonsteroidal anti-inflammatory drugs (NSAIDs), sympathomimetic agents, and N-methyl-D-aspartate (NMDA) receptor-blocking agents109 with encourag-ing results.72
BOX 17-2
Recurrent Patient-Reported Themes Regarding Their Persistent Dentoalveolar Pain Disorder (PDAP)
♦ Difficult for patients to respond to history taking because their words do not adequately describe what they feel; therefore time may be needed to obtain the necessary information
♦ Well localized to a region within the dentoalveolar structures♦ Pain is perceived to be deep in the tissues, rather than on
the surface♦ Continuous pain, one that never stops and seems to always
be there♦ Pain has the sensation of feeling pressure with a dull ache
quality♦ Complex and confounding descriptors, such as itching, tingling,
or pricking, are sometimes present

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 697
of food.9 Cardiac pain cannot be aggravated by local provoca-tion of teeth. Anesthetizing the lower jaw or providing dental treatment will not reduce the pain. It can be decreased with rest or a dose of sublingual nitroglycerin. Diagnosis of cardiac pain, along with immediate referral, is mandatory to avoid impending myocardial infarction.
Besides pain of cardiac origin, other chest structures have been reported to produce nonodontogenic toothache pain. Various cancerous lesions of the lungs have been described to present a mandibular pain, with the pain being both ipsilateral and contralateral to the side where the tumor is present.24,59 Furthermore, diaphragmatic pain is mediated via the phrenic nerve and may present as nonodontogenic tooth pain.15
Intracranial StructuresSpace-occupying lesions within and around the brain are known to impinge on structures innervated with somatosen-sory fibers, such as the dural and perivascular tissues, causing pain. These pains are highly variable, with a common com-plaint being headache or head pain. Just as intracranially derived pain may be referred to the face and jaws in neurovas-cular disorders, it may also present as a toothache.137 To outline the vast differences in clinical features of such pain, intracra-nial lesions have also been reported to cause trigeminal neu-ralgic pain in response to treatment of what was first thought to be toothache.29 This extreme variability has been observed by one of the authors, which leads to the recommendation that if local etiologic factors are not readily identified in a patient with toothache symptoms, magnetic resonance brain imaging should be considered.
Throat and Neck StructuresNonodontogenic toothache has been reported to arise from various structures of the neck, but these reports are sparse and hence it is not possible to draw conclusions regarding how patients with these pain-provoking disorders may present. Squamous cell carcinoma of the lateral pharyngeal surface pre-senting as ipsilateral mandibular molar pain has been observed by one of the authors. This finding is consistent with previous reports of nonodontogenic pain being associated with smooth muscle tumors of a similar location.139 Vascular structures of the neck have also been implicated in the production of tooth-ache symptoms, with a report of a patient initially presenting for dental care when pain was from the result of a life-threatening carotid artery dissection.119
Craniofacial StructuresClinically, pain from other craniofacial structures has been observed as being the most common reason for organic pathologies presenting as nonodontogenic toothache, likely because these structures are innervated by branches of the trigeminal nerve. Tumors in the maxillary sinus27,43,145 and jaw,132 as well as metastatic disease, particularly within the mandible,33,53,114,124 have been reported. The clinical presenta-tion of symptoms is highly variable, but a common feature is sensory loss along the distribution of the nerve, the result of pain arising from nerve impingement. This underscores the need for regional imaging techniques, such as pantomography or computed tomography (CT) (as opposed to just periapical radiographs). This is especially true in patients who have a history of cancer. One must also not forget that nerve impinge-ment anywhere along the distribution of the trigeminal nerve,
presented for obvious and recognizable benefit. This category poses a significant diagnostic challenge. Lacking evidence of local tissue damage is typical of heterotopic pain entities previously discussed in this chapter. It is important to empha-size that psychogenic pain is rare. When arriving at this diag-nosis it is critical that all other potential diagnoses have been ruled out.
The diagnosis of psychogenic toothache is one of exclusion and is based on the clinician’s awareness of other heterotopic pain characteristics and behavior. Of particular note are cen-trally emanating pains, cardiac pain, neurovascular pain, and neuropathic pain. Adding to the diagnostic difficulty is that comorbid psychological disorders are commonly present with chronic intraoral pain disorders, including those erroneously presenting as toothache.84,130 This has led to the current think-ing that psychological disorders (i.e., depression, anxiety, somatization) may not be related to the initiation or perpetu-ation of chronic pain disorders but rather are a consequence of living with chronic pain.
Psychogenic pain is known to be precipitated by severe psychologic stress. These pains present a general departure from the characteristics of any other pain condition—that is, they may not fit normal anatomic distributions or physiologi-cally plausible patterns. The pain may be felt in multiple teeth and may jump around from one tooth to another. The intensity of pain reported tends to be more severe than is reflected by the patient’s level of concern about the condition. Patients’ responses to therapy are variable and include a lack of response or an unusual or unexpected response. Early identification of psychogenic pain and referral to a psychologist or psychiatrist is necessary to avoid irreversible and unnecessary dental treatment.
Toothache Referred from a Distant Organic SourceA variety of pathologies that seem to be unrelated have been reported to present as nonodontogenic toothache.107,115 The only common link that can be identified is that branches of cranial nerves innervate the involved tissues, and hence the trigeminal nucleus processes nociceptive input. Therefore, conceivably, any somatic structure with cranial nerve innerva-tion has the potential to cause pain that the patient perceives as a toothache. For this reason, once dentoalveolar etiologies for such pain have been ruled out, all possible sources of non-odontogenic pain including distant pathology should be con-sidered in the differential diagnosis. Several of these types of organic pathologies that have been reported to present as toothache are described in the following sections.
Cardiac and Thoracic StructuresCardiac pain has been cited as the cause of nonodontogenic toothache in a number of case reports.9,41,62,77,97,136 Classically, cardiac pain presents as a crushing substernal pain that most commonly radiates to the left arm, shoulder, neck, and face. Although not as common, anginal pain may present solely as dental pain, generally felt in the lower left jaw.16 Similar to pain of pulpal origin, cardiac pain can be spontaneous and diffuse, with a cyclic pattern that fluctuates in intensity from mild to severe. The pain can also be intermittent and the patient may be completely asymptomatic at times. The quality of cardiac pain when referred to the mandible is chiefly aching and some-times pulsatile. Cardiac pain may be spontaneous or increased with physical exertion, emotional upset, or even the ingestion

698 PART II The Advanced Science of Endodontics
all descriptors that apply and then filling in the remaining blanks. As the details of a patient’s pain complaint are gathered, the clinician should be mentally progressing through an algo-rithm of possible diagnoses, as each detail should lend itself to one type of pain over another. After completing a thorough and accurate history of the complaint(s) (Fig. 17-9), often the diag-nosis has already been narrowed down to one particular pain entity. This is particularly true with odontogenic pain. The only question that will remain is “which tooth is it?” It is critical to keep in mind that whereas patients will provide information about the perceived site of pain, it is the clinician’s examination that will reveal the true source of their pain. With more com-plicated pain complaints, the clinician may have a list of pos-sible diagnoses. This is known as a differential diagnosis. This differential will guide the examination and testing in an effort to confirm one diagnosis while ruling out all others. If after completing the subjective examination all items on the differ-ential are outside the clinician’s scope of practice, then the clini-cian should continue the examination until he or she has a firm idea of the possible diagnosis so that a proper referral can be made. In addition, it is paramount that all odontogenic sources have been ruled out and that this information is communicated to the health care provider to which the patient is referred. If no differential can be formulated after the history has been
even within the cranial vault itself,20 can elicit nonodonto-genic tooth pain.
Vascular structures within the craniofacial region have also been reported to present as nonodontogenic toothache, with arteritis being the pain-provoking pathology.68,73 These pains have been described as a continuous dull pain that can some-times be made worse with jaw function. The stereotypical presentation includes a history of eyesight changes, such as blurred vision, and the examination feature of pulseless, indu-rated temporal arteries that are painful to palpation. A labora-tory finding of an elevated erythrocyte sedimentation rate (ESR) is suggestive of the disorder, and diagnosis is confirmed by temporal artery biopsy. Treatment includes administration of corticosteroids; therefore, because permanent blindness is a possible sequela if cranial arteries are left unmanaged, immedi-ate referral to the appropriate medical colleague is indicated.
Frequency of Nonodontogenic ToothacheThe prevalence of nonodontogenic toothache in the popula-tion is unknown, as is the prevalence of such a presentation for dental care. Specific to endodontics, pain is thought to be present in 5.3% of patients 6 or more months following treat-ment,100 with about half of those individuals being estimated to have nonodontogenic etiologies accounting for their com-plaint of that pain.100 At present, the proportion of such patients having the aforementioned nonodontogenic pain diagnosis is unknown. It remains unclear how this nonodontogenic pain is related to the endodontic diagnosis and subsequent treatment.
TAKING A PATIENT’S HISTORYPain diagnosis is largely based on the patient’s subjective history; however, patients rarely give all pertinent diagnostic information about their pain of their own accord. Often it is necessary to carefully extract the details of the patient’s pain complaint through systematic and thorough questioning. This is known as “taking a history,” and it involves both careful listening and astute questioning. Fig. 17-8 is an example of a basic diagnostic workup for odontogenic pain. It can be easily used to obtain histories of typical odontogenic pain by circling
FIG. 17-8 Example of a form to evaluate odontogenic pain.
Sufficient for pain of odontogenic origin.
Subjective
Pain: (Circle all appropriate) Level (0-10)
Well-localized
Spontaneous
Constant
Dull ache
Onset
Progression (F/I/D)
Aggravating factors
Relieving factors
Diffuse
Elicited (cold, hot, chewing)
Fluctuant
Sharp shooting
Intermittent
Throbbing
FIG. 17-9 Example of a form to evaluate pain history.
Chief complaintPrioritize complaintsSpecify locationVAS 0-10Initial onsetWhen did you first notice this?ProgressionFrequencyIntensityDurationPrevious similar complaintsHave you ever had this type of pain before?Characterize complaintDaily, not dailyConstant, fluctuant, intermittentDurationTemporal patternQualityAggravating factorsWhat makes this pain worse? Be specific!Alleviating factorsWhat makes this pain better?How much better?Associated factorsSwellingDiscolorationNumbnessRelationship to other complaintsWould your jaw hurt if your tooth didn’t hurt?Prior consults/treatmentWho?When?What was the diagnosis?What was done?How did it affect the pain?

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 699
taken, then the history should be redirected to the patient to confirm that the information is complete and accurate. If the patient is unable to provide sufficient information regarding the pain complaint, then it may be helpful to have the patient keep a pain history, detailing the aspects of the pain on a daily basis. Of utmost importance is to avoid treatment when the diagnosis is uncertain. Diagnostic therapy (i.e., “let’s do a root canal treat-ment and see if it helps”) may result in costly treatment that does not improve the patient’s condition and could be a factor in aggravating and perpetuating a patient’s pain. Treatment should always specifically address a diagnosis.
A complete medical history along with current medications and drug allergies should always be ascertained. It is also important to make note of demographic information, as patients of certain genders and ages are more at risk for some disorders compared with others.
Recording a patient’s chief complaint in the patient’s own words is a medical legal necessity but falls short of constituting a thorough pain history. A complete history begins with a patient’s general pain complaint—for example, “My tooth hurts.” Patients may have more than one pain complaint—for example, “My tooth hurts and it is starting to make my jaw hurt.” All pain complaints should be noted and investigated separately. Understanding the specific components of the com-plaints makes it possible to discern the relationship between them—that is, either the complaints are wholly separate and two types of pathosis are present, or one source of pain is merely creating a heterotopic pain that is wholly secondary to the first.
Begin with determining the location at which the patient perceives the pain. Aspects of the location involve localization and migration. Pain should be definable as either well localized or diffuse and either superficial or deep. Easily localized super-ficial pain tends to be cutaneous or neurogenic. Musculoskel-etal pain is felt deeply and is more localizable once it is provoked. Deep, diffuse pain is suggestive of deep somatic pain, be it visceral or musculoskeletal. Both tissue types are involved in a high degree of nociceptor convergence in the trigeminal nucleus and, therefore, much more likely to be involved in creating heterotopic pain. Typical referral patterns of deep somatic pain tend to follow peripheral dermatomes that reflect the laminations in the trigeminal nucleus. Referred pain also tends to occur in a cephalad direction. Therefore, referred pain from a deep somatic tissue such as tooth pulp, cardiac tissue, or skeletal muscle will respect this pattern. Pain that spreads distally along a nerve branch is much more indica-tive of a projected type of heterotopic pain. Projected pains imply a neurogenic source and possibly one that is secondary to impingement from intracranial pathosis. Recall that super-ficial sources of pain are not likely to be involved in referral, so if a patient is indicating that the pain is superficial and spreading, this is highly suggestive of a neurogenic rather than a cutaneous source.
Assessment of the intensity of pain is easily accomplished using a verbal analog scale. This question is best phrased, “On a scale of one to ten, zero being no pain and ten being the worst pain you can imagine, how bad is your pain?” Not only can intensity provide insight about pain type; it can also help guide posttreatment pain management as well as provide a baseline for response to therapies.
Identifying the onset of pain may provide information regarding etiology. Question if the onset followed a particular
event such as a dental appointment or a traumatic injury. Beware of these relationships, as they can be misleading. Having a temporal correlation does not necessarily ensure a cause-and-effect relationship. The onset of pain may be either gradual or sudden. Severe pain of sudden onset can signal a more serious problem. Pain that has been present over a protracted period of time, particularly if the pain has been unchanging, is highly suggestive of a nonodontogenic pain source.
Other temporal aspects of pain include frequency and dura-tion. The clinician should ask the patient, “How often does the pain occur and how long does it last?” These temporal aspects may establish patterns that point more clearly to one condition over another.
Progression of the patient’s pain over time should be noted. Whether pain is better, worse, or unchanging since its onset should be broken down into three factors: frequency, intensity, and duration. Static pain that does not change over time is typically not odontogenic in origin.
The quality of pain—that is, “what it feels like”—is a critical aspect of a pain history. Knowledge of pain characteristics as they relate to tissue types is essential. Pain quality can be dif-ficult for patients to describe, and it is often necessary to provide them with a list of descriptors from which to choose. In instances of odontogenic pain, the list is fairly short. The deep visceral and musculoskeletal components of a tooth limit true odontogenic pain to having qualities that are dull, aching, or throbbing. If there is an aspect of sharpness to the pain, it is helpful to understand whether the sharpness is stabbing in nature, which would indicate A-delta fiber–mediated dentinal pain, or whether it is electrical in nature, which would indicate neuralgia. Common examples of pain descriptors and their respective pain types are listed in Table 17-1.
Factors that precipitate or aggravate the patient’s pain com-plaint are of key importance in diagnosis. Not only do aggra-vating factors suggest the tissue types that may be involved, but they also aid in directing the objective tests. When gather-ing information, it is important to be specific. If a patient reports pain while eating, keep in mind that many structures are stimulated during mastication, such as muscles, temporo-mandibular joints (TMJs), mucosa, PDLs, and, potentially, pulps. Be specific as to the aggravating factor. The lack of any aggravating factors indicates that the pain is not of odonto-genic origin.
Alleviating factors can provide insight as to the nature of the pain. If a medication relieves the pain, it is critical to know the specific medication, its dosage, and the degree to which the pain was attenuated. It is equally important to know what has no effect on the intensity of the pain. For example, if a pain of midlevel intensity is completely unresponsive to anti-inflammatory drugs, then it is probably not inflammatory in origin.
TABLE 17-1
Examples of Pain Descriptors
Origin Quality of Pain
Muscular Dull, aching
Neurogenic Shocking, burning
Vascular Throbbing, pulsatile

700 PART II The Advanced Science of Endodontics
Associated factors such as swelling, discoloration, and numbness must be ascertained, as well as their correlation with symptoms. Swelling of acute onset suggests an infection, and its concurrent pain would be of inflammatory origin. Swelling that comes and goes with the intensity of pain suggests an autonomic component. The same can be said for discoloration, such as redness. Numbness or any other type of sensory aber-rations should be recorded. If the altered sensation is a major component of the pain complaint, then it should be investi-gated separately and its relationship to the pain determined. Pains that occur with sensory aberrations tend to have a strong neurogenic component.
If the patient complains of more than one pain, an effort should be made during the subjective history to determine the relationship of the complaints. One pain might serve as an aggra-vating factor to the other. There may be a correlation as to the onset, intensity, or progression of the complaints. Also, keep in mind that patients may actually have more than one type of pathosis occurring concurrently and there may be no relation-ship whatsoever. Ask whether there have been any previous similar complaints and, if so, what happened. Recurrence of similar pains might reveal a pattern that lends itself to a par-ticular pain diagnosis.
It is critical to gain knowledge of any prior consultations that have occurred. Details regarding the type of clinician, actual workup performed, and diagnosis rendered will help to narrow down a differential. Any treatment that was performed should be ascertained along with its effect on the chief complaint.
PATIENT EXAMINATIONAs stated previously, the purpose of the history is to gather information about a patient’s pain complaint in order to for-mulate a list of possible diagnoses based on specific pain char-acteristics. Poor or improper symptom analysis will lead to a false differential, and any testing will therefore have limited meaning. Performing a general examination including an extraoral, intraoral, and hard and soft tissue assessment is requisite to confirm the health of various structures and to identify possible pain-producing etiologies. When a patient presents with a toothache, the pain is usually of odontogenic origin. Diagnostic procedures are often limited to confirming a suspect tooth rather than identifying a nonodontogenic source of pain. Standard pulpal and periradicular tests serve to aid in both ruling in odontogenic pain and therefore ruling out nonodontogenic pain as a diagnosis. Remember that the site of pain is determined by patient history, but the true source of the pain should be revealed with testing. If the chief complaint cannot be reproduced with standard tests then additional tests may be necessary to narrow down a differential diagnosis. For details on general examinations and standard tests, please refer to Chapter 1.
Additional TestsFurther tests should be chosen with forethought in an effort to develop a workable differential that can guide the clinician toward a meaningful consultation or an appropriate referral for the patient. These tests may consist of palpation or provocation of various structures, sensory testing, or diagnostic blocks. The application of these tests is not covered in detail in this chapter. For more information about the application and interpretation of these tests, please consult other sources.
Palpation and percussion are common tests to differentiate odontogenic pain from pain of sinus origin. Palpation of the sinuses consists of firm pressure placed over the involved sinus (usually maxillary). In addition, pain of sinus origin may be provoked with a lowering of the patient’s head.
If pain of muscular origin is suspected, then an attempt to reproduce this pain can be done by palpation of the muscles of mastication or provocation via functional manipulation. The temporalis, deep and superficial masseter, medial pterygoid, and digastric muscles should be palpated in an effort to dis-cover tenderness or trigger points that reproduce the pain complaint. The medial pterygoid is only partially accessible to palpation and may need to be functionally tested by stretching the muscle (opening wide) or contracting the muscle (biting firmly). The lateral pterygoid may be difficult if not impossible to palpate intraorally and therefore is more appropriately assessed by functional manipulation. Pain emanating from this muscle may be increased by protruding the jaw against resis-tance. Exacerbating the chief complaint by muscular function provides a strong indication of a myofascial source of pain.
Because of the complexity of innervation and the occur-rence of heterotopic pain in the orofacial region, it may be difficult to definitively determine the origin of pain by testing alone. It cannot be stressed enough that primary pain should not only be provoked by local manipulation but also be relieved by anesthetic blocking. In diagnostic anesthesia the relief of pain has a typical onset and duration, depending on the par-ticular anesthetic used. In addition, the pain should be com-pletely diminished or else suspicion of a central component or a coexisting disorder should arise. The use of diagnostic anes-thesia may be necessary and useful in augmenting the diagnos-tic workup (Fig. 17-10). Topical anesthetic can be helpful in the investigation of cutaneous pain and peripheral neuropa-thies. Anesthetic injection including peripheral nerve blocks can be used to determine whether the etiology of the pathosis is peripheral to the area of the block. Pain that persists after the onset of usual signs of anesthesia suggests a central com-ponent. The patient’s history and general examination are of key importance in differentiating between the pain of a central neuropathy and the central pain emanating from an intracra-nial mass.
Pain that is primarily muscular, as suggested by trigger points discovered on examination, can be further investigated by local anesthetic injection into the trigger point. Trigger point injections are typically performed with either a 27- or a 25-gauge needle and a minimally myotoxic anesthetic such as 2% lidocaine or 3% mepivacaine without a vasoconstrictor. Myofascial trigger point injections may temporarily relieve pain at the trigger point as well as at the site of referral.
Sympathetic efferent activity can play a role in the enhance-ment or maintenance of chronic pain. In the head and neck, sympathetic activity flows through the stellate ganglion located bilaterally near the first rib. When there is suspicion of a sym-pathetic component to a patient’s pain, a stellate ganglion block can be used to provide diagnostic insight. A trained anesthesi-ologist usually performs this procedure. An effective block delivered to the stellate ganglion will interrupt sympathetic outflow to the ipsilateral side of the face, resulting in a partial Horner syndrome. This is evidenced by flushing, congestion, lacrimation, miosis of the pupil, ptosis, and anhidrosis.75 A sympathetic blockade that diminishes or eliminates a pain state may guide future treatment such as repeated blocks or systemic
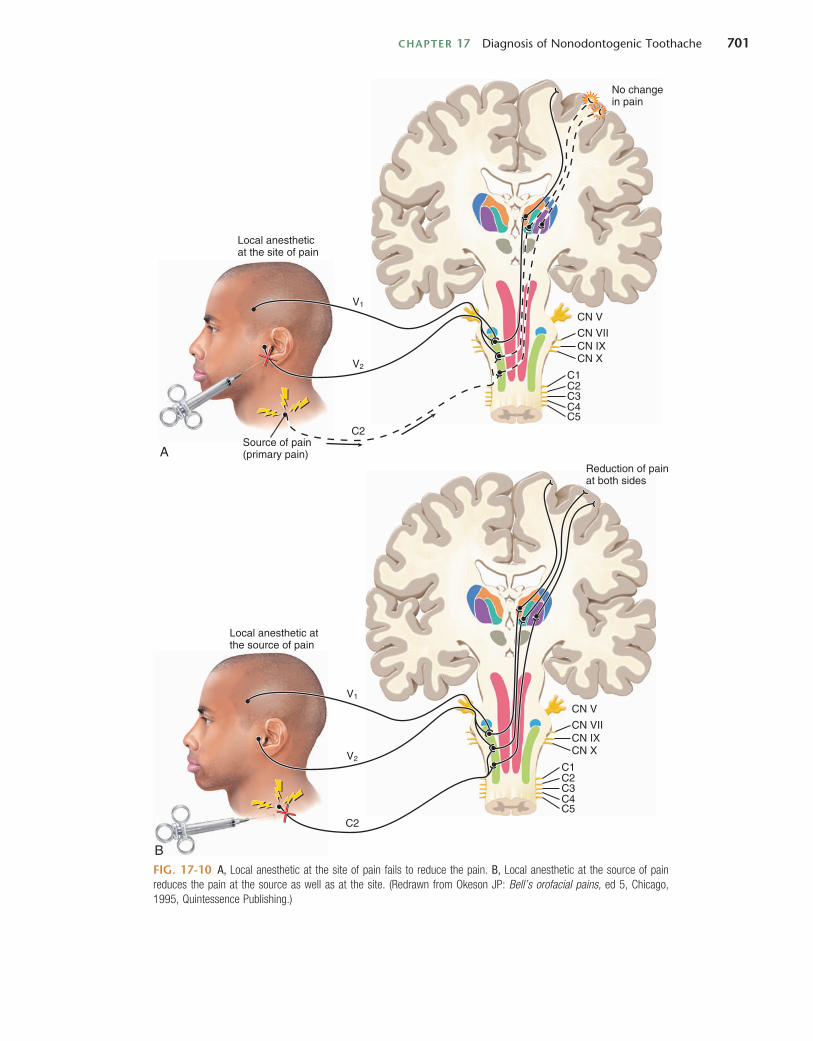
CHAPTER 17 Diagnosis of Nonodontogenic Toothache 701
FIG. 17-10 A, Local anesthetic at the site of pain fails to reduce the pain. B, Local anesthetic at the source of pain reduces the pain at the source as well as at the site. (Redrawn from Okeson JP: Bell’s orofacial pains, ed 5, Chicago, 1995, Quintessence Publishing.)
Source of pain(primary pain)A
CN VV1
V2
CN VIICN IXCN X
C1C2
C2
C3C4C5
No changein pain
Local anestheticat the site of pain
CN V
Reduction of painat both sides
Local anesthetic atthe source of pain
V1
V2
CN VIICN IXCN X
C1C2
C2
C3C4C5
B

702 PART II The Advanced Science of Endodontics
A periapical radiograph (Fig. 17-11) shows evidence of prior nonsurgical root canal treatment and mesiobuccal root amputation of tooth #3. Mild to moderate horizontal bone loss is evident in the quadrant. No radiographic evidence of caries or apical radiolucencies is noted.
Additional TestsIn the absence of a clear etiology, a more extensive extraoral examination is performed. Cranial nerves II through XII are intact. The sharp shooting pain is predictably produced with light brushing of the skin over the area of tooth #3. This examination increases the patient’s subjective complaint of a dull ache associated with tooth #3. With the likelihood of two possible sources of pain existing, a diagnostic anesthetic block of tooth #3 is performed: buccal infiltration of tooth #3 with 27 mg of 3% mepivacaine without epinephrine. After 3 minutes the patient no longer reports a dull ache at tooth #3 and he is nontender to percussion. His sharp shooting pain can still be initiated with light brushing of the skin over the area of tooth #3 and continues to cause a dull ache in the area of tooth #3. Diagnoses of trigeminal neuralgia and advanced localized adult periodontitis of tooth #3 are made. The patient is referred to a neurologist for evaluation and treatment. The diagnosis of trigeminal neuralgia is confirmed and he is placed on carba-mazepine at 100 mg/day.
Case 2A 28-year-old male presents with a chief complaint of “My teeth on the right side hurt.” His medical history is not signifi-cant. He denies any systemic disease and has no known drug
treatment with sympathetically active drugs (e.g., clonidine and prazosin).116
Neurologic conditions, both peripheral and central, can present as pain in the orofacial region. A role of the clinician is to help rule out gross neurologic conditions secondary to intracranial pathosis. Systemic complaints such as nausea, diz-ziness, or changes in one of the special senses should raise suspicion of intracranial pathosis. A neurologic screening examination including a gross sensory and motor evaluation of cranial nerves II through XII should be performed. For details on cranial nerve examination, please refer to other sources.44 Investigation of sharp/dull differentiation as well as light touch discrimination between the different branches of the trigeminal nerve can provide insight as to the location and etiology of the pathosis.
Case StudiesCase 1A 56-year-old male presents with a chief complaint of “This tooth still hurts and it’s getting worse. It even hurts when I smile.” He has a history of angina secondary to a 70% occlu-sion of his right coronary artery. He also reports a history of hypercholesterolemia. He has no history of myocardial infarc-tion and denies any other significant medical history. The patient is taking lovastatin (Mevacor, 400 mg/day), nifedipine (Procardia, 60 mg once per day), and atenolol (50 mg once per day). He has no known drug allergy.
The patient was referred by a periodontist for evaluation of continued pain associated with tooth #3. He had been receiv-ing periodontal maintenance therapy for generalized moderate adult periodontitis for more than 5 years. He had root canal treatment and a mesial buccal root amputation of tooth #3 as treatment for a localized area of advanced periodontitis 6 months ago.
Subjective HistoryAfter careful questioning, it becomes apparent that the patient is experiencing pain of two different qualities: an intermittent ache associated with tooth #3 and an intermittent sharp shoot-ing pain also associated with tooth #3. The intermittent dull ache was of gradual onset 9 months ago. This pain was unaf-fected by the nonsurgical root canal treatment and root ampu-tation. This pain has increased in frequency, intensity, and duration over the past 3 months. There is no temporal com-ponent. The dull ache is aggravated by biting and by the occur-rence of the sharp shooting pain. The sharp shooting pain had a sudden onset 6 months ago. It has also increased in fre-quency, intensity, and duration without a temporal component. It can occur spontaneously or when the patient is “smiling big.” The patient reports that the sharp shooting pain can also be aggravated by pressing lightly on his face in the area overly-ing #3, but not by pressing intraorally on #3.
ExaminationThe coronal portion of the amputated mesiobuccal root had been restored with IRM (Intermediate Restorative Material; DENTSPLY Caulk, Milford, DE). No cracks, fractures, sinus tracts, or swelling is detected. There are generalized probing depths of 4 mm throughout the upper right sextant. Tooth #3 has an 8-mm-broad probing defect mesially with bleeding on probing. For the results of clinical testing, see Table 17-2.
FIG. 17-11 Periapical radiograph showing prior nonsurgical root canal treatment and mesiobuccal root amputation of tooth #3.
TABLE 17-2
Case 1: Clinical Results of Testing
Tooth
Test #2 #3 #4
Endo Ice* + (s)† − + (s)
Percussion − + −Palpation − − −
*Endo Ice (Coltène/Whaledent, Cuyahoga Falls, Ohio) is used to detect pulp vitality.†s, pain of short duration.

CHAPTER 17 Diagnosis of Nonodontogenic Toothache 703
the muscles of mastication reveal a trigger point in the patient’s right deep masseter. Palpation of this trigger point immediately intensifies his “toothache.” A trigger point injection of 3% mepivacaine without epinephrine is done in an effort to clarify a diagnosis. After a trigger point injection, all tests are repeated. Palpation of the trigger point no longer produces pain. The bite test and cold test still produce a short sharp pain but are no longer followed by a dull ache.
Diagnoses of reversible pulpitis secondary to a cracked tooth #31 and myofascial pain of the right masseter are made. The patient is given home care instructions for treatment of his myofascial pain, and he is referred to his general clinician for cuspal coverage of both teeth #3 and #30.
SUMMARYAs clinicians who are frequently called on to diagnose and treat complaints of orofacial pain, it is important to have a thorough knowledge of the odontogenic and nonodontogenic causes. The basis for this knowledge begins with an understanding of the anatomy and physiology of the pain system, and how alterations in this system can result in pain that is poorly local-ized and therefore misdiagnosed. A realization that pain does not always originate in the structures in which they are felt, along with an understanding of the neurobiologic basis of heterotopic pain, is necessary to ensure accurate diagnosis of orofacial pain.
There are several indicators that a toothache may be non-odontogenic in origin. Red flags for nonodontogenic pain include toothaches that have no apparent etiology for pulpal or periradicular pathosis; pain that is spontaneous, poorly localized, or migratory; and pain that is constant and nonvari-able. In addition, pain that is described as burning, pricking, or “shocklike” is less likely to be pulpal or periradicular in origin.
A thorough pain history and an examination of dental and nondental structures are essential to differentiate between odontogenic and nonodontogenic sources of pain. Examples of key components of the pain history and examination are included in this chapter for reference. In addition, the chapter has focused on the more common nonodontogenic sources of orofacial pain. As stated previously, the role of the dental clini-cian is to diagnose and treat disorders of the oral cavity and masticatory structures. In the event that a nondental pathosis is suspected, a differential diagnosis of probable disorders is essential as part of a referral to a more appropriate health care provider. In addition, an understanding of any potential role or interaction of dental structures in the patient’s pain com-plaint should be communicated as part of the referral.
allergies. He is currently taking 600 mg of ibuprofen as needed for pain. He is taking no other medications. The patient was referred by his general clinician for evaluation of pain associ-ated with his teeth on the right side.
Subjective HistoryAfter careful questioning, it is determined that the patient is experiencing pain of two different types. The most distressing pain to the patient is a diffuse, right-sided, constant low-grade dull ache (3/10 on a verbal analog scale [VAS]). The onset was gradual, beginning 2 years ago. The pain has recently increased in intensity and duration. This pain is aggravated by opening wide and increases in intensity after the occurrence of a sharp pain that is induced by biting down. There is no notable tem-poral component, and the patient has made no attempts to obtund the pain.
His other pain type had a sudden onset approximately 4 months ago. This pain is localized to the area of the right first molars. It is an intermittent sharp shooting pain (8/10 on VAS) that occurs when biting.
ExaminationTooth #3 has an occlusal amalgam with cracks evident on the mesial marginal ridge and the buccal groove. Tooth #30 has an occlusal amalgam, and cracks are noted on the mesial and distal marginal ridges of the tooth. There are no swellings or sinus tracts and no probing greater than 4 mm on the right side. A periapical radiograph demonstrates no evidence of caries or apical radiolucencies. The patient’s sharp pain is reproduced with a bite test applied to the mesial lingual cusp of tooth #30. After the bite test, the patient reports that his dull ache has intensified. For the results of clinical testing see Table 17-3. Thirty seconds after pulp testing has been completed, the patient again reports that his dull ache has intensified.
Additional TestsIn consideration of an uncertain diagnosis, a more extensive examination is performed. Palpation and provocation tests of
TABLE 17-3
Case 2: Clinical Results of Testing
Tooth
Test #2 #3 #4 #31 #30 #29
Endo Ice + (s) + (s) + (s) + (s) + (s) + (s)
Percussion − − − − − −Palpation − − − − − −
REFERENCES1. Abu-Bakra M, Jones NS: Prevalence of nasal mucosal
contact points in patients with facial pain compared with patients without facial pain, J Laryngol Otol 115:629, 2001.
2. Albin R, Wiener J, Gordon R, Willoughby JH: Diagnosis and treatment of pansinusitis: report of case, J Oral Surg 37:604, 1979.
3. Allerbring M, Haegerstam G: Chronic idiopathic orofacial pain: a long-term follow-up study, Acta Odontol Scand 62:66, 2004.
4. Alonso AA, Nixdorf DR: Case series of four different headache types presenting as tooth pain, J Endod 32:1110, 2006.
5. American Psychiatric Association: Diagnostic and statistical manual of mental disorders (DSM-IV), Washington, DC, 1994, American Psychiatric Association, p 447.
6. Anderson GC, John MT, Ohrbach R, et al: Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain, Pain 152:765, 2011.
7. Baad-Hansen L, Juhl GI, Jensen TS, et al: Differential effect of intravenous S-ketamine and fentanyl on atypical odontalgia and capsaicin-evoked pain, Pain 129:46, 2007.
8. Backonja M: Use of anticonvulsants for treatment of neuropathic pain, Neurology 59(5 suppl 2):S14, 2002.
9. Batchelder B, Krutchkoff DJ, Amara J: Mandibular pain as the initial and sole clinical manifestation of coronary insufficiency, J Am Dent Assoc 115:710, 1987.

704 PART II The Advanced Science of Endodontics
10. Benoliel R, Eliav E, Tal M: No sympathetic nerve sprouting in rat trigeminal ganglion following painful and non-painful infraorbital nerve neuropathy, Neurosci Lett 297:151, 2001.
11. Benoliel R, Sharav Y: Paroxysmal hemicrania: case studies and review of the literature, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85:285, 1998.
12. Benoliel R, Sharav Y: SUNCT syndrome: case report and literature review, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85:158, 1998.
13. Besson J, Chaouch A: Peripheral and spinal mechanisms of nociception, Physiol Rev 67:67, 1987.
14. Bittar G, Graff-Radford SB: A retrospective study of patients with cluster headaches, Oral Surg Oral Med Oral Pathol 73:519, 1992.
15. Blows WT: Diaphragmatic cramp as a possible cause of noncardiac chest pain and referred mandibular pain, J Neurosci Nurs 31:187, 1999.
16. Bonica J: The management of pain with special emphasis on the use of analgesic block in diagnosis, prognosis and therapy, Philadelphia, 1953, Lea & Febiger.
17. Bonica J: The management of pain, Philadelphia, 1990, Lea & Febiger, 1990.
18. Brannstrom M, Johnson G, Nordenvall KJ: Transmission and control of dentinal pain: resin impregnation for the desensitization of pain, J Am Dent Assoc 99:612, 1979.
19. Brattberg J, Thorslund M, Wickman A: The prevalence of pain in a general population. The results of a postal study in a county in Sweden, Pain 37:215, 1989.
20. Brazis PW, Wharen RE, Czervionke LF, et al: Hemangioma of the mandibular branch of the trigeminal nerve in the Meckel cave presenting with facial pain and sixth nerve palsy, J Neurophthalmol 20:14, 2000.
21. Brooke RI: Periodic migrainous neuralgia: a cause of dental pain, Oral Surg Oral Med Oral Pathol 46:511, 1978.
22. Broton J, Hu JW, Sessle BJ: Effects of temporomandibular joint stimulation on nociceptive and nonnociceptive neurons of the cat’s trigeminal subnucleus caudalis (medulla dorsal horn), J Neurophysiol 59:1575, 1988.
23. Brown A, Beeler WJ, Kloka AC, Fields RW: Spatial summation of pre-pain and pain in human teeth, Pain 21:1, 1985.
24. Buddery DJ: Mandible pain, Br Dent J 194:121, 2003.25. Byers M: Dental sensory receptors, Int Rev Neurobiol
25:39, 1984.26. Campbell JK: Facial pain due to migraine and cluster
headache, Semin Neurol 8:324, 1988.27. Chan YW, Guo YC, Tsai TL, et al: Malignant fibrous
histiocytoma of the maxillary sinus presenting as toothache, J Chin Med Assoc 67:104, 2004.
28. Chen YH, Tseng CC, Chao WY, et al: Toothache with a multifactorial etiology: a case report, Endod Dent Traumatol 13:245, 1997.
29. Cirak B, Kiymaz N, Arslanoglu A: Trigeminal neuralgia caused by intracranial epidermoid tumor: report of a case and review of the different therapeutic modalities, Pain Physician 7:129, 2004.
30. de Leeuw R: Differential diagnosis of orofacial pain. In de Leeuw R, editor: Orofacial pain: guidelines for assessment, diagnosis, and management, Hanover Park, IL, 2008, Quintessence Publishing, p 49.
31. Delcanho RE, Graff-Radford SB: Chronic paroxysmal hemicrania presenting as toothache, J Orofac Pain 7:300, 1993.
32. DeNucci DJ, Chen CC, Sobiski C, Meehan S: The use of SPECT bone scans to evaluate patients with idiopathic jaw pain, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90:750, 2000.
33. Dewan K, Owens J, Silvester K: Maintaining a high level of suspicion for recurrent malignant disease: report of a case with periapical involvement, Int Endod J 40:900, 2007.
34. Dodick DW: Migraine with isolated face pain: a diagnostic challenge, Cephalalgia 27:1199, 2007.
35. Drangsholt MT, Svennson P, Nguyen KL: Which orofacial pain conditions are neuropathic? A systematic review using NEUPSIG ’08 criteria, World Congress on Pain, International Association for the Study of Pain, August 2008.
36. Druce H: Diagnosis of sinusitis in adults: History, physical examination, nasal cytology, echo, and rhinoscope, J Allergy Clin Immunol 90:436, 1992.
37. Druce H, Slavin RG: Sinusitis: critical need for further study, J Allergy Clin Immunol 88:675, 1991.
38. Dubner R, Bennet G: Spinal and trigeminal mechanisms of nociception, Ann Rev Neurosci 6:381, 1983.
39. Dubner R, Hayes RL, Hoffman DS: Neural and behavioral correlates of pain in the trigeminal system, Res Publ Assoc Res Nerv Ment Dis 58:63, 1980.
40. Durham J, Exley C, John MT, Nixdorf DR: Persistent dentoalveolar pain: the patient’s experience, J Orofac Pain 27:6, 2013.
41. Durso BC, Israel MS, Janini ME, Cardoso AS: Orofacial pain of cardiac origin: a case report, Cranio 21:152, 2003.
42. Ekborn K: Treatment of cluster headache: clinical trials, design and results, Cephalalgia 15:33, 1995.
43. Ellinger RF, Kelly WH: Maxillary sinus lymphoma: a consideration in the diagnosis of odontogenic pain, J Endod 15:90, 1989.
44. Evans RW: Saunders manual of neurologic practice, Philadelphia, 2003, Elsevier Science.
45. Fricton J: Masticatory myofascial pain: an explanatory model integrating clinical, epidemiological and basic science research, Bull Group Int Research Sci Stomatol Odontol 41:14, 1999.
46. Fricton JR: Critical commentary: A unified concept of idiopathic orofacial pain: clinical features, J Orofac Pain 13:185, 1999.
47. Fristad I, Bardsen A, Knudsen GC, Molven O: Prodromal herpes zoster: a diagnostic challenge in endodontics, Int Endod J 35:1012, 2002.
48. Fromm GH, Graff-Radford SB, Terrence CF, Sweet WH: Pre-trigeminal neuralgia, Neurology 40:1493, 1990.
49. Gallagher R, Mueller L, Ciervo CA: Increased prevalence of sensing types in men with cluster headaches, Psychol Rev 87:555, 2000.
50. Gatot A, Peist M, Mozes M: Endodontic overextension produced by injected thermopolasticized gutta-percha, J Endod 15:273, 1989.
51. Gaul C, Gantenbein AR, Buettner UW, et al: Orofacial cluster headache, Cephalalgia 28:903, 2008.
52. Gaul C, Sandor PS, Galli U, et al: Orofacial migraine, Cephalalgia 27:950, 2007.
53. Gaver A, Polliack G, Pilo R, et al: Orofacial pain and numb chin syndrome as the presenting symptoms of a metastatic prostate cancer, J Postgrad Med 48:283, 2002.
54. Giri S, Nixdorf D: Sympathetically maintained pain presenting first as temporomandibular disorder, then as parotid dysfunction, Tex Dent J 124:748, 2007.
55. Glaros A, Urban D, Locke J: Headache and temporomandibular disorders: evidence for diagnostic and behavioural overlap, Cephalalgia 27:542, 2007.
56. Goadsby PJ: The international classification of headache disorders, ed 2, Cephalalgia 24(suppl 1):1-106, 2004.
57. Gobel S, Falls W, Hockfield S: The division of the dorsal and ventral horns of the mammalian caudal medulla into eight layers using anatomic criteria. In Anderson D, Matthews B, editors: Pain in the trigeminal region, proceedings of a symposium held in the Department of Physiology, University of Bristol, England, on July 25-27, 1977, Amsterdam, 1977, Elsevier Press, p 443.
58. Goh B, Poon CY, Peck RH: The importance of routine magnetic resonance imaging in trigeminal neuralgia diagnosis, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:424, 2001.
59. Goldberg HL: Chest cancer refers pain to face and jaw: a case review, Cranio 15:167, 1997.
60. Goon WW, Jacobsen PL: Prodromal odontalgia and multiple devitalized teeth caused by a herpes zoster
infection of the trigeminal nerve: report of case, J Am Dent Assoc 116:500, 1988.
61. Graff-Radford SB, Solberg WK: Atypical odontalgia, J Craniomandib Disord 6:260, 1992.
62. Graham LL, Schinbeckler GA: Orofacial pain of cardiac origin, J Am Dent Assoc 104:47, 1982.
63. Gratt BM, Graff-Radford SB, Shetty V, et al: A 6-year clinical assessment of electronic facial thermography, Dentomaxillofac Radiol 25:247, 1996.
64. Gratt BM, Pullinger A, Sickles EA, Lee JJ: Electronic thermography of normal facial structures: a pilot study, Oral Surg Oral Med Oral Pathol 68:346, 1989.
65. Greenberg DA, Aminoff MJ, Simon RP: Clinical neurology, New York, 2002, McGraw-Hill, p 390.
66. Gregg J: Neuropathic complications of mandibular implant surgery: review and case presentations, Ann R Australas Coll Dent Surg 15:176, 2000.
67. Gregory WB Jr, Brooks LE, Penick EC: Herpes zoster associated with pulpless teeth, J Endod 1:32, 1975.
68. Guttenberg SA, Emery RW, Milobsky SA, Geballa M: Cranial arteritis mimicking odontogenic pain: report of case, J Am Dent Assoc 119:621, 1989.
69. Hansen H: Neuro-histological reactions following tooth extractions, Int J Oral Surg 9:411, 1980.
70. Hargreaves K, Bowles WR, Jackson DL: Intrinsic regulation of CGRP release by dental pulp sympathetic fibers, J Dent Res 82:398, 2003.
71. Hargreaves K, Dubner R: Mechanisms of pain and analgesia, Amsterdam, 1991, Elsevier Press.
72. Heir G, Karolchek S, Kalladka M, et al: Use of topical medication in orofacial neuropathic pain: a retrospective study, Oral Surg Oral Med Oral Path Oral Radiol Endod 105:466, 2008.
73. Hellmann DB: Temporal arteritis: a cough, toothache and tongue infarction, JAMA 287:2996, 2002.
74. Jacquin MF, Renehan WE, Mooney RD, Rhoades RW: Structure-function relationships in rat medullary and cervical dorsal horns. I. Trigeminal primary afferents, J Neurophysiol 55:1153, 1986.
75. Kisch B: Horner’s syndrome, an American discovery, Bull Hist Med 25:284, 1951.
76. Kraut R, Chahal O: Management of patients with trigeminal nerve injuries after mandibular implant placement, J Am Dent Assoc 133:1351, 2002.
77. Kreiner M, Okeson JP, Michelis V, et al: Craniofacial pain as the sole symptom of cardiac ischemia: a prospective multicenter study, J Am Dent Assoc 138:74, 2007.
78. Lamotte R, Campbell JN: Comparison of responses of warm and nociceptive C-fiber afferents in monkey with human judgements of thermal pain, J Neurophysiol 41:509, 1978.
79. LeBars D, Dickenson AH, Besson JM, Villaneuva L: Aspects of sensory processing through convergent neurons. In Yaksh TL, editor: Spinal afferent processing, New York, 1986, Plenum Press.
80. Li Y, Li HJ, Huang J, et al: Central malignant salivary gland tumors of the jaw: retrospective clinical analysis of 22 cases, J Oral Maxillofac Surg 66:2247, 2008.
81. Lipton J, Ship JA, Larach-Robinson D: Estimated prevalence and distribution of reported orofacial pain in the United States, J Am Dent Assoc 124:115, 1993.
82. Lipton RB, Stewart WF, Diamond S, et al: Prevalence and burden of migraine in the United States: data from the American Migraine Study II, Headache 41:646, 2001.
83. List T, Leijon G, Helkimo M, et al: Effect of local anesthesia on atypical odontalgia—A randomized controlled trial, Pain 122:306, 2006.
84. List T, Leijon G, Helkimo M, et al: Clinical findings and psychosocial factors in patients with atypical odontalgia: a case-control study, J Orofac Pain 21:89, 2007.
85. List T, Leijon G, Svensson P: Somatosensory abnormalities in atypical odontalgia: a case-control study, Pain 139:333, 2008.
86. Loeser JD, Treede RD: The Kyoto protocol of IASP basic pain terminology, Pain 137:473, 2008.
CHAPTER 17 Diagnosis of Nonodontogenic Toothache 705
87. Long A, Loeschr AR, Robinson PP: A quantitative study on the myelinated fiber innervation of the periodontal ligament of cat canine teeth, J Dent Res 74:1310, 1995.
88. Marbach J, Raphael KG: Phantom tooth pain: a new look at an old dilemma, Pain Med 1:68, 2000.
89. Melis M, Lobo SL, Ceneviz C, et al: Atypical odontalgia: a review of the literature, Headache 43:1060, 2003.
90. Moana-Filho EJ, Nixdorf DR, Bereiter DA, et al: Evaluation of a magnetic resonance-compatible dentoalveolar tactile stimulus device, BMC Neurosci 11:142, 2010.
91. Moncada E, Graff-Radford SB: Cough headache presenting as a toothache: a case report, Headache 33:240, 1993.
92. Moncada E, Graff-Radford SB: Benign indomethacin-responsive headaches presenting in the orofacial region: eight case reports, J Orofac Pain 9:276, 1995.
93. Mondell B: A review of the effects of almotriptan and other triptans on clinical trial outcomes that are meaningful to patients with migraine, Clin Ther 25:331, 2003.
94. Morse D: Infection-related mental and inferior alveolar nerve paresthesia: literature review and presentation of two cases, J Endod 23:457, 1997.
95. Nahri M: The neurophysiology of the teeth, Dent Clin North Am 34:439, 1990.
96. Namazi MR: Presentation of migraine as odontalgia, Headache 41:420, 2001.
97. Natkin E, Harrington GW, Mandel MA: Anginal pain referred to the teeth: report of a case, Oral Surg Oral Med Oral Pathol 40:678, 1975.
98. Neumann S, Doubell TP, Leslie T, Woolf CJ: Inflammatory pain hypersensitivity mediated by phenotypic switch in myelinated primary sensory neurons, Nature 384:360, 1996.
99. Nixdorf DR, Drangsholt MT, Ettlin DA, et al: International RDC-TMD Consortium: Classifying orofacial pains: a new proposal of taxonomy based on ontology, J Oral Rehabil 39:161, 2012.
100. Nixdorf DR, Moana-Filho EJ, Law AS, et al: Frequency of persistent tooth pain after root canal therapy: a systematic review and meta-analysis, J Endod 36:224, 2010.
101. Nixdorf DR, Sobieh R, Gierthmuhlen J: Using an n-of-1 trial to assist in clinical decision making for patients with orofacial pain, J Am Dent Assoc 143:259, 2012.
102. Nixdorf DR, Velly AM, Alonso AA: Neurovascular pains: implications of migraine for the oral and maxillofacial surgeon, Oral Maxillofac Surg Clin North Am 20:221, vi, 2008.
103. Obermann M, Mueller D, Yoon MS, et al: Migraine with isolated facial pain: a diagnostic challenge, Cephalalgia 27:1278, 2007.
104. Ogutcen-Toller M, Uzun E, Incesu L: Clinical and magnetic resonance imaging evaluation of facial pain, Oral Surg Oral Med Oral Path Oral Radiol Endod 97:652, 2004.
105. Okeson J: Orofacial pain: guidelines for assessment, diagnosis and management, Chicago, 1996, Quintessence Publishing.
106. Okeson JP: Bell’s orofacial pains: the clinical management of orofacial pain, ed 6, Chicago, 2005, Quintessence Publishing.
107. Okeson JP, Falace DA: Nonodontogenic toothache, Dent Clin North Am 41:367, 1997.
108. Oshima K, Ishii T, Ogura Y, et al: Clinical investigation of patients who develop neuropathic tooth pain after endodontic procedures, J Endod 35:958, 2009.
109. Padilla M, Clark GT, Merrill RL: Topical medications for orofacial neuropathic pain: a review, J Am Dent Assoc 131:184, 2000.
110. Pareja JA, Antonaci F, Vincent M: The hemicrania continua diagnosis, Cephalalgia 21:940, 2001.
111. Peszkowski M, Larsson AJ: Extraosseous and intraosseous oral traumatic neuromas and their association with tooth extraction, J Oral Maxillofac Surg 48:963, 1990.
112. Pigg M, List T, Petersson K, et al: Diagnostic yield of conventional radiographic and cone-beam computed tomographic images in patients with atypical odontalgia, Int Endod J 44:1092, 2011.
113. Pigg M, Svensson P, Drangsholt M, List T: 7-year follow-up of patients diagnosed with atypical odontalgia: a prospective study, J Orofac Pain 27:151, 2013.
114. Pruckmayer M, Glaser C, Marosi C, Leitha T: Mandibular pain as the leading clinical symptom for metastatic disease: nine cases and review of the literature, Ann Oncol 9:559, 1998.
115. Quail G: Atypical facial pain: a diagnostic challenge, Aust Fam Physician 34:641, 2005.
116. Raja S, Davis KD, Campbell JN: The adrenergic pharmacology of sympathetically-maintained pain, J Reconstr Microsurg 8:63, 1992.
117. Rasmussen BK, Jensen R, Schroll M, Olesen J: Epidemiology of headache in a general population–a prevalence study, J Clin Epidemiol 44:1147, 1991.
118. Rosenfeld RM, Andes D, Bhattacharyya N, et al: Clinical practice guideline: adult sinusitis, Otolaryngol Head Neck Surg 137(suppl):S1, 2007.
119. Roz TM, Schiffman LE, Schlossberg S: Spontaneous dissection of the internal carotid artery manifesting as pain in an endodontically treated molar, J Am Dent Assoc 136:1556, 2005.
120. Sarlani E, Schwartz AH, Greenspan JD, Grace EG: Chronic paroxysmal hemicrania: a case report and review of the literature, J Orofac Pain 17:74, 2003.
121. Schaible HG: Basic mechanisms of deep somatic tissue. In McMahon SB, Koltzenburg M, editors: Textbook of pain, Philadelphia, 2006, Elsevier, p 621.
122. Schiffman E, Ohrbach R, List T, et al: Diagnostic criteria for headache attributed to temporomandibular disorders, Cephalalgia 32(9):683, 2012.
123. Schwartz BS, Stewart WF, Simon D, Lipton RB: Epidemiology of tension-type headache, JAMA 279:381, 1998.
124. Selden HS, Manhoff DT, Hatges NA, Michel RC: Metastatic carcinoma to the mandible that mimicked pulpal/periodontal disease, J Endod 24:267, 1998.
125. Setzen G, Ferguson BJ, Han JK, et al: Clinical consensus statement: appropriate use of computed tomography for paranasal sinus disease, Otolaryngol Head Neck Surg 147(5):808, 2012.
126. Sicuteri F, Nicolodi M, Fusco BM, Orlando S: Idiopathic pain as a possible risk factor for phantom tooth pain, Headache 31:577, 1991.
127. Stewart W, Ricci JA, Chee E, et al: Lost productive time and cost due to common pain conditions in the US workforce, JAMA 290:2443, 2003.
128. Stewart WF, Lipton RB, Celentano DD, Reed ML: Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors, JAMA 267:64, 1992.
129. Svennson P: Muscle pain in the head: overlap between temporomandibular disorders and tension-type headaches, Curr Opin Neurol 20:320, 2007.
130. Takenoshita M, Sato T, Kato Y, et al: Psychiatric diagnoses in patients with burning mouth syndrome and atypical odontalgia referred from psychiatric to dental facilities, Neuropsychiatr Dis Treat 6:699, 2010.
131. Tepper SJ, Dahlof CG, Dowson A, et al: Prevalence and diagnosis of migraine in patients consulting their physician with a complaint of headache: data from the Landmark Study, Headache 44:856, 2004.
132. Thomas G, Pandey M, Mathew A, et al: Primary intraosseous carcinoma of the jaw: pooled analysis of world literature and report of two new cases, Int J Oral Maxillofac Surg 30:349, 2001.
133. Torebjork H, Lundberg LE, LaMotte RH: Pain, hyperalgesia and activity in nociceptive C units in humans after intradermal injection of capsaicin, J Physiol 448:749, 1992.
134. Travell JG, Simons DG: Myofascial pain and dysfunction: the trigger point manual, Baltimore, 1983, Williams & Wilkins, p 1.
135. Treede RD, Jensen TS, Campbell JN, et al: Neuropathic pain: redefinition and a grading system for clinical and research purposes, Neurology 70:1630, 2008.
136. Tzukert A, Hasin Y, Sharav Y: Orofacial pain of cardiac origin, Oral Surg Oral Med Oral Pathol 51:484, 1981.
137. Uehara M, Tobita T, Inokuchi T: A case report: toothache caused by epidermoid cyst manifested in cerebellopontine angle, J Oral Maxillofac Surg 65:560, 2007.
138. Webb DJ, Colman MF, Thompson K, Wescott WB: Acute, life-threatening disease first appearing as odontogenic pain, J Am Dent Assoc 109:936, 1984.
139. Wertheimer-Hatch L, Hatch GF 3rd, Hatch KF, et al: Tumors of the oral cavity and pharynx, World J Surg 24:395, 2000.
140. Wood M, Johnson RW, McKendrick MW, et al: A randomized trial of acyclovir for 7 days or 21 days with and without prednisolone for treatment of acute herpes, N Engl J Med 330:896, 1994.
141. Woolf C: Phenotype modification of primary sensory neurons: the role of nerve growth factor in the production of persistent pain, Philos Trans R Soc Lond B Biol Sci 351:441, 1996.
142. Wright EF: Referred craniofacial pain patterns in patients with temporomandibular disorder, J Am Dent Assoc 131:1307, 2000.
143. Yang J, Simonson TM, Ruprecht A, et al: Magnetic resonance imaging used to assess patients with trigeminal neuralgia, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81:343, 1996.
144. Yokota T: Neural mechanisms of trigeminal pain, Pain, New York, 1985, McGraw-Hill.
145. Yoon JH, Chun YC, Park SY, et al: Malignant lymphoma of the maxillary sinus manifesting as a persistent toothache, J Endod 27:800, 2001.
146. Zagury JG, Eliav E, Heir GM, et al: Prolonged gingival cold allodynia: a novel finding in patients with atypical odontalgia, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 111:312, 2011.
147. Zakrzewska JM: Diagnosis and differential diagnosis of trigeminal neuralgia, Clin J Pain 18:14, 2002.
148. Zuniga J: Surgical management of trigeminal neuropathic pain, Atlas Oral Maxillofac Surg Clin North Am 9:59, 2001.
706
Emergency ClassificationsEmergency Endodontic Management
Teeth with Vital PulpsReversible PulpitisIrreversible PulpitisPulpal Necrosis with Acute Apical Abscess
Fascial Space InfectionsManagement of Abscesses and CellulitisIncision for Drainage
Symptomatic Teeth with Previous Endodontic TreatmentLeaving Teeth OpenSystemic Antibiotics for Endodontic InfectionsAnalgesicsLaboratory Diagnostic AdjunctsFlare-UpsCracked and Fractured TeethSummary
Management of Endodontic EmergenciesSAMUEL O. DORN | GARY SHUN-PAN CHEUNG
CHAPTER 18
CHAPTER OUTLINE
EMERGENCY CLASSIFICATIONSThe proper diagnosis and effective management of acute dental pain are possibly the most rewarding and satisfying aspects of providing dental care. An endodontic emergency is defined as pain or swelling caused by various stages of inflammation or infection of the pulpal or periapical tissues. The cause of dental pain is typically from caries, deep or defective restorations, or trauma. Sometimes occlusion-related pain can also mimic acute dental pain (Fig. 18-1). Bender8 stated that patients who manifest severe or referred pain almost always had a previous history of pain with the offending tooth. Approximately 85% of all dental emergencies arise as a result of pulpal or periapical disease, which would necessitate either extraction or endodon-tic treatment to relieve the symptoms.38,68 It has also been estimated that about 12% of the U.S. population experienced a toothache in the preceding 6 months.65
Determining a definitive diagnosis can sometimes be chal-lenging and even frustrating for the clinician; but a methodical, objective, and subjective evaluation, as described in Chapter 1, is imperative before developing a proper treatment plan. Unfortunately, on the basis of the diagnosis, there are conflict-ing opinions on how to best clinically manage various end-odontic emergencies. According to surveys of board certified endodontists by Dorn and associates in 197722,23 and 199031 and by Lee in 2009,63 there are seven clinical presentations that are considered endodontic emergencies:1. Irreversible pulpitis with normal periapex2. Irreversible pulpitis with symptomatic apical periodontitis3. Necrotic pulp with symptomatic apical periodontitis, with
no swelling
4. Necrotic pulp, fluctuant swelling, with drainage through the canal
5. Necrotic pulp, fluctuant swelling, with no drainage through the canal
6. Necrotic pulp, diffuse facial swelling, with drainage through the canal
7. Necrotic pulp, diffuse facial swelling, with no drainage through the canalThere are other endodontic emergencies that were not dis-
cussed in these surveys. These emergencies pertain to trau-matic dental injuries, as discussed in Chapter 20, to teeth that have had previous endodontic treatment, as discussed in Chapters 8 and 19, and endodontic flare-ups that may occur between treatment sessions. Of course, there are also many types of facial pain that have a nonodontogenic origin; these are described in detail in Chapter 17.
In the decades between the previously cited surveys, there have been several changes pertaining to the preferred clinical management of endodontic emergencies. Many of these treatment modifications have occurred because of the more contemporary armamentarium and materials as well as new evidence-based research and the presumption of empirical clinical success.
EMERGENCY ENDODONTIC MANAGEMENTBecause pain is both a psychological and biologic entity, as discussed in Chapters 4 and online Chapter 28, the manage-ment of acute dental pain must take into consideration both the physical symptoms and the emotional status of the
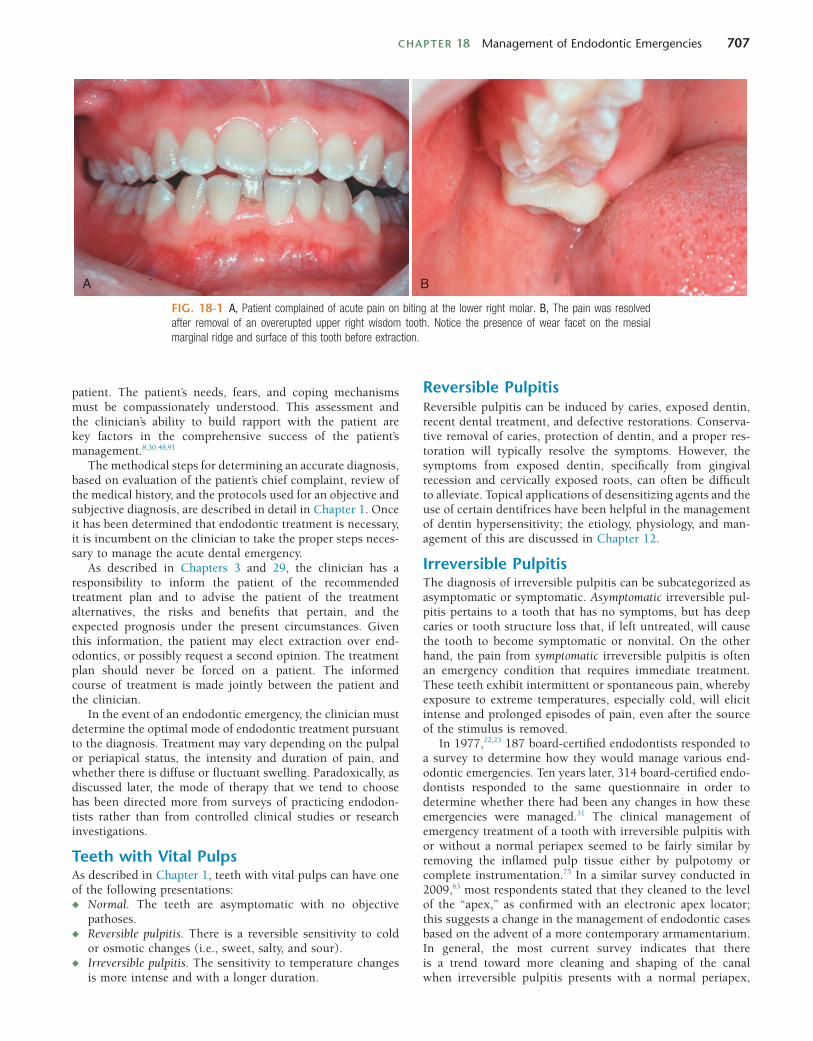
CHAPTER 18 Management of Endodontic Emergencies 707
Reversible PulpitisReversible pulpitis can be induced by caries, exposed dentin, recent dental treatment, and defective restorations. Conserva-tive removal of caries, protection of dentin, and a proper res-toration will typically resolve the symptoms. However, the symptoms from exposed dentin, specifically from gingival recession and cervically exposed roots, can often be difficult to alleviate. Topical applications of desensitizing agents and the use of certain dentifrices have been helpful in the management of dentin hypersensitivity; the etiology, physiology, and man-agement of this are discussed in Chapter 12.
Irreversible PulpitisThe diagnosis of irreversible pulpitis can be subcategorized as asymptomatic or symptomatic. Asymptomatic irreversible pul-pitis pertains to a tooth that has no symptoms, but has deep caries or tooth structure loss that, if left untreated, will cause the tooth to become symptomatic or nonvital. On the other hand, the pain from symptomatic irreversible pulpitis is often an emergency condition that requires immediate treatment. These teeth exhibit intermittent or spontaneous pain, whereby exposure to extreme temperatures, especially cold, will elicit intense and prolonged episodes of pain, even after the source of the stimulus is removed.
In 1977,22,23 187 board-certified endodontists responded to a survey to determine how they would manage various end-odontic emergencies. Ten years later, 314 board-certified endo-dontists responded to the same questionnaire in order to determine whether there had been any changes in how these emergencies were managed.31 The clinical management of emergency treatment of a tooth with irreversible pulpitis with or without a normal periapex seemed to be fairly similar by removing the inflamed pulp tissue either by pulpotomy or complete instrumentation.75 In a similar survey conducted in 2009,63 most respondents stated that they cleaned to the level of the “apex,” as confirmed with an electronic apex locator; this suggests a change in the management of endodontic cases based on the advent of a more contemporary armamentarium. In general, the most current survey indicates that there is a trend toward more cleaning and shaping of the canal when irreversible pulpitis presents with a normal periapex,
patient. The patient’s needs, fears, and coping mechanisms must be compassionately understood. This assessment and the clinician’s ability to build rapport with the patient are key factors in the comprehensive success of the patient’s management.8,30,48,91
The methodical steps for determining an accurate diagnosis, based on evaluation of the patient’s chief complaint, review of the medical history, and the protocols used for an objective and subjective diagnosis, are described in detail in Chapter 1. Once it has been determined that endodontic treatment is necessary, it is incumbent on the clinician to take the proper steps neces-sary to manage the acute dental emergency.
As described in Chapters 3 and 29, the clinician has a responsibility to inform the patient of the recommended treatment plan and to advise the patient of the treatment alternatives, the risks and benefits that pertain, and the expected prognosis under the present circumstances. Given this information, the patient may elect extraction over end-odontics, or possibly request a second opinion. The treatment plan should never be forced on a patient. The informed course of treatment is made jointly between the patient and the clinician.
In the event of an endodontic emergency, the clinician must determine the optimal mode of endodontic treatment pursuant to the diagnosis. Treatment may vary depending on the pulpal or periapical status, the intensity and duration of pain, and whether there is diffuse or fluctuant swelling. Paradoxically, as discussed later, the mode of therapy that we tend to choose has been directed more from surveys of practicing endodon-tists rather than from controlled clinical studies or research investigations.
Teeth with Vital PulpsAs described in Chapter 1, teeth with vital pulps can have one of the following presentations:◆ Normal. The teeth are asymptomatic with no objective
pathoses.◆ Reversible pulpitis. There is a reversible sensitivity to cold
or osmotic changes (i.e., sweet, salty, and sour).◆ Irreversible pulpitis. The sensitivity to temperature changes
is more intense and with a longer duration.
FIG. 18-1 A, Patient complained of acute pain on biting at the lower right molar. B, The pain was resolved after removal of an overerupted upper right wisdom tooth. Notice the presence of wear facet on the mesial marginal ridge and surface of this tooth before extraction.
A B

708 PART II The Advanced Science of Endodontics
To assist the clinician in assessing the level of difficulty of a given endodontic case, the American Association of Endo-dontists (Chicago, IL) has developed the “AAE Endodontic Case Difficulty Assessment Form and Guidelines” (Fig. 18-2). This form is intended to make case selection more efficient, more consistent, and easier to document, as well as to provide a more objective ability to determine when it may be necessary to refer the patient to another clinician who may be better able to manage the complexities of the case.
Pulpal Necrosis with Acute Apical AbscessNo SwellingOver the years, the proper methodology for the emergency endodontic management of necrotic teeth has been controver-sial. In a 1977 survey of board-certified endodontists,22,23 it was reported that, in the absence of swelling, most respondents would completely instrument the canals, keeping the file short of the radiographic apex. However, when swelling was present, the majority of those polled in 1977 preferred to leave the tooth open, with instrumentation extending beyond the apex to help facilitate drainage through the canals. Years later and again validated in a 2009 study, most respondents favored complete instrumentation regardless of the presence of swelling. Also, it was the decision of 25.2% to 38.5% of the clinicians to leave these teeth open in the event of diffuse swelling; 17.5% to 31.5% left the teeth open in the presence of a fluctuant swell-ing. However, as discussed later, there is currently a trend toward not leaving teeth open for drainage. There is also another trend: when treatment is done in more than one visit, most endodontists will use calcium hydroxide as an intracanal medicament.63
Care should be taken not to push necrotic debris beyond the apex during root canal instrumentation, as this has been shown to promote more posttreatment discom-fort.13,31,87,96 Crown-down instrumentation techniques have been shown to remove most of the debris coronally rather than pushing it out the apex. The use of positive-pressure irrigation methods, such as needle-and-syringe irrigation, also poses a risk of expressing debris or solution out of the apex.10,20 Improvements in technology, such as electronic apex locators, have facilitated increased accuracy in deter-mining working length measurements, which in turn may allow for a more thorough canal debridement and less apical extrusion. These devices are now used by an increased number of clinicians.56,63
TrephinationIn the absence of swelling, trephination is the surgical perfora-tion of the alveolar cortical plate to release, from between the cortical plates, the accumulated inflammatory and infective tissue exudate that causes pain. Its use has been historically advocated to provide pain relief in patients with severe and recalcitrant periradicular pain.22,23 The technique involves an engine-driven perforator entering through the cortical bone and into the cancellous bone, often without the need for an incision,16 in order to provide a pathway for drainage from the periradicular tissues. Although more recent studies have failed to show the benefit of trephination in patients with irreversible pulpitis with symptomatic apical periodontitis69 or necrotic teeth with symptomatic apical periodontitis,74 there remain some advocates who recommend trephination for managing acute and intractable periapical pain.45 The clinician should
compared with performing just pulpectomies as described in the 1977 survey. None of the individuals surveyed in the 1990 or 2009 poll stated that they would manage these emergencies by establishing any type of drainage by trephinating the apex, making an incision, or leaving the tooth open for an extended period of time.
In addition, for vital teeth, the 1977 survey did not even broach the concept of completing the endodontics in one visit, whereas in the 1988 study about one third of the respondents indicated that they would complete these vital cases in a single visit and the response rose to 79% in the most recent survey. Since the early 1980s, there seems to have been an increase in the acceptability of providing endodontic therapy in one visit, especially in cases of vital pulps, with most studies revealing an equal number, or fewer, flare-ups after single-visit endodon-tic treatment.24,78,83,88,90,98 However, this has not come without controversy, with some studies showing otherwise,111 contend-ing that there is more posttreatment pain after single-visit endodontics, and possibly a lower long-term success rate. Unfortunately, time constraints at the emergency visit often make the single-visit treatment option not practical.4
If root canal therapy is completed at a later date, medicating the canal with calcium hydroxide has been suggested to reduce the chances of bacterial growth in the canal between appoint-ments in most studies,17 but not all.13,17 One randomized clini-cal study showed that a dry cotton pellet was as effective in relieving pain as a pellet moistened with camphorated mono-chlorophenol (CMCP), metacresylacetate (Cresatin), eugenol, or saline.40 Sources of infection, such as caries and defective restorations, should be completely removed to prevent recon-tamination of the root canal system between appointments.40 The concept of single- versus multiple-visit endodontics is described in greater detail in Chapter 11.
For emergency management of vital teeth that are not ini-tially sensitive to percussion, occlusal reduction has not been shown to be beneficial.19,31 However, the clinician should be cognizant of the possibility of occlusal interferences and pre-maturities that might cause tooth fracture under heavy masti-cation. In vital teeth in which the inflammation has extended periapically, which will present with pretreatment pain to percussion, occlusal reduction has been reported to reduce posttreatment pain.31,74,89
Antibiotics are not recommended for the emergency man-agement of irreversible pulpitis53,99 (see Chapters 11 and 14), as placebo-controlled clinical trials have demonstrated that antibiotics have no effect on pain levels in patients with irre-versible pulpitis.72
Most endodontists and endodontic textbooks recommend the emergency management of symptomatic irreversible pulpi-tis to involve the initiation of root canal treatment,17,31,39,63,103 with complete pulp removal and total cleaning of the root canal system. Unfortunately, in an emergency situation, the allotted time necessary for this treatment is often an issue. Given the potential time constraints and inevitable differences in skill level between clinicians, it may not be feasible to complete the total canal cleaning at the initial emergency visit. Subsequently, especially with multirooted teeth, a pulpotomy (removal of the coronal pulp or tissue from the widest canal) has been advo-cated for emergency treatment of irreversible pulpitis.15,39,103 In a clinical study of various emergency procedures, it has been demonstrated that this treatment is highly effective for alleviat-ing acute dental pain due to irreversible pulpitis.15
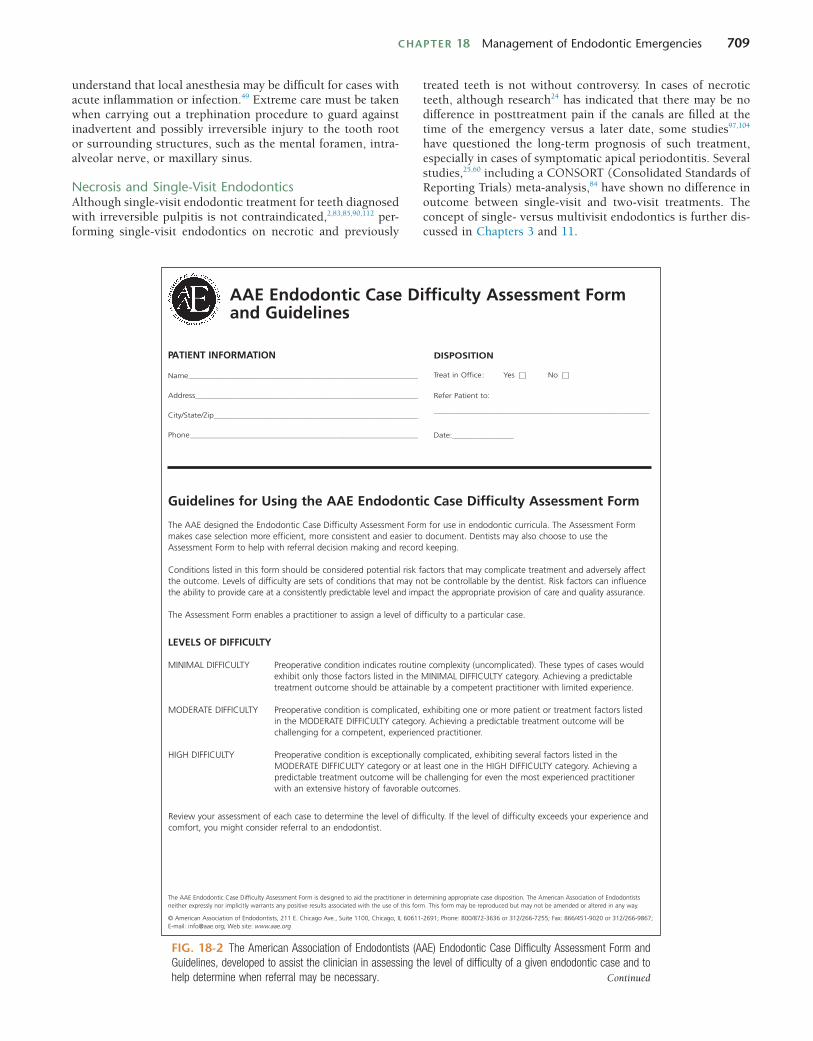
CHAPTER 18 Management of Endodontic Emergencies 709
understand that local anesthesia may be difficult for cases with acute inflammation or infection.49 Extreme care must be taken when carrying out a trephination procedure to guard against inadvertent and possibly irreversible injury to the tooth root or surrounding structures, such as the mental foramen, intra-alveolar nerve, or maxillary sinus.
Necrosis and Single-Visit EndodonticsAlthough single-visit endodontic treatment for teeth diagnosed with irreversible pulpitis is not contraindicated,2,83,85,90,112 per-forming single-visit endodontics on necrotic and previously
treated teeth is not without controversy. In cases of necrotic teeth, although research24 has indicated that there may be no difference in posttreatment pain if the canals are filled at the time of the emergency versus a later date, some studies97,104 have questioned the long-term prognosis of such treatment, especially in cases of symptomatic apical periodontitis. Several studies,25,60 including a CONSORT (Consolidated Standards of Reporting Trials) meta-analysis,84 have shown no difference in outcome between single-visit and two-visit treatments. The concept of single- versus multivisit endodontics is further dis-cussed in Chapters 3 and 11.
AAE Endodontic Case Difficulty Assessment Formand Guidelines
PATIENT INFORMATION
Name__________________________________________________________________________________
Address________________________________________________________________________________
City/State/Zip_________________________________________________________________________
Phone__________________________________________________________________________________
Guidelines for Using the AAE Endodontic Case Difficulty Assessment Form
The AAE designed the Endodontic Case Difficulty Assessment Form for use in endodontic curricula. The Assessment Formmakes case selection more efficient, more consistent and easier to document. Dentists may also choose to use theAssessment Form to help with referral decision making and record keeping.
Conditions listed in this form should be considered potential risk factors that may complicate treatment and adversely affectthe outcome. Levels of difficulty are sets of conditions that may not be controllable by the dentist. Risk factors can influencethe ability to provide care at a consistently predictable level and impact the appropriate provision of care and quality assurance.
The Assessment Form enables a practitioner to assign a level of difficulty to a particular case.
LEVELS OF DIFFICULTY
MINIMAL DIFFICULTY Preoperative condition indicates routine complexity (uncomplicated). These types of cases would exhibit only those factors listed in the MINIMAL DIFFICULTY category. Achieving a predictable treatment outcome should be attainable by a competent practitioner with limited experience.
MODERATE DIFFICULTY Preoperative condition is complicated, exhibiting one or more patient or treatment factors listed in the MODERATE DIFFICULTY category. Achieving a predictable treatment outcome will be challenging for a competent, experienced practitioner.
HIGH DIFFICULTY Preoperative condition is exceptionally complicated, exhibiting several factors listed in the MODERATE DIFFICULTY category or at least one in the HIGH DIFFICULTY category. Achieving a predictable treatment outcome will be challenging for even the most experienced practitioner with an extensive history of favorable outcomes.
Review your assessment of each case to determine the level of difficulty. If the level of difficulty exceeds your experience andcomfort, you might consider referral to an endodontist.
DISPOSITION
Treat in Office: Yes No
Refer Patient to:
_____________________________________________________________________________
Date:______________________
The AAE Endodontic Case Difficulty Assessment Form is designed to aid the practitioner in determining appropriate case disposition. The American Association of Endodontists neither expressly nor implicitly warrants any positive results associated with the use of this form. This form may be reproduced but may not be amended or altered in any way.
© American Association of Endodontists, 211 E. Chicago Ave., Suite 1100, Chicago, IL 60611-2691; Phone: 800/872-3636 or 312/266-7255; Fax: 866/451-9020 or 312/266-9867; E-mail: [email protected]; Web site: www.aae.org
FIG. 18-2 The American Association of Endodontists (AAE) Endodontic Case Difficulty Assessment Form and Guidelines, developed to assist the clinician in assessing the level of difficulty of a given endodontic case and to help determine when referral may be necessary. Continued
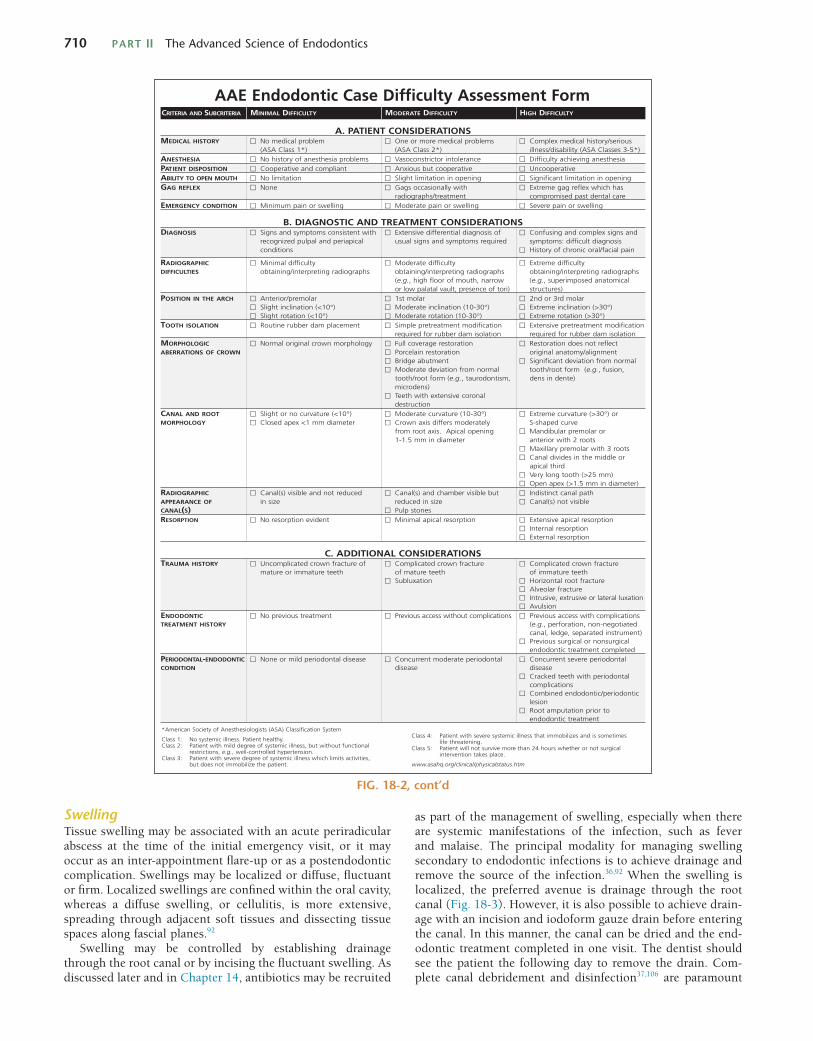
710 PART II The Advanced Science of Endodontics
SwellingTissue swelling may be associated with an acute periradicular abscess at the time of the initial emergency visit, or it may occur as an inter-appointment flare-up or as a postendodontic complication. Swellings may be localized or diffuse, fluctuant or firm. Localized swellings are confined within the oral cavity, whereas a diffuse swelling, or cellulitis, is more extensive, spreading through adjacent soft tissues and dissecting tissue spaces along fascial planes.92
Swelling may be controlled by establishing drainage through the root canal or by incising the fluctuant swelling. As discussed later and in Chapter 14, antibiotics may be recruited
AAE Endodontic Case Difficulty Assessment FormCRITERIA AND SUBCRITERIA MINIMAL DIFFICULTY MODERATE DIFFICULTY HIGH DIFFICULTY
*American Society of Anesthesiologists (ASA) Classification System
Class 1: No systemic illness. Patient healthy.Class 2: Patient with mild degree of systemic illness, but without functional
restrictions, e.g., well-controlled hypertension.Class 3: Patient with severe degree of systemic illness which limits activities,
but does not immobilize the patient.
Class 4: Patient with severe systemic illness that immobilizes and is sometimes life threatening.
Class 5: Patient will not survive more than 24 hours whether or not surgical intervention takes place.
www.asahq.org/clinical/physicalstatus.htm
A. PATIENT CONSIDERATIONSMEDICAL HISTORY No medical problem One or more medical problems Complex medical history/serious
)*5-3sessalCASA(ytilibasid/ssenlli)*2ssalCASA()*1ssalCASA(ANESTHESIA No history of anesthesia problems Vasoconstrictor intolerance Difficulty achieving anesthesiaPATIENT DISPOSITION Cooperative and compliant Anxious but cooperative UncooperativeABILITY TO OPEN MOUTH gnineponinoitatimiltnacifingiSgnineponinoitatimilthgilSnoitatimiloNGAG REFLEX sahhcihwxelfergagemertxEhtiwyllanoisaccosgaGenoN
radiographs/treatment compromised past dental careEMERGENCY CONDITION Minimum pain or swelling Moderate pain or swelling Severe pain or swelling
B. DIAGNOSTIC AND TREATMENT CONSIDERATIONSDIAGNOSIS Signs and symptoms consistent with Extensive differential diagnosis of Confusing and complex signs and
recognized pulpal and periapical usual signs and symptoms required symptoms: difficult diagnosisniaplaicaf/larocinorhcfoyrotsiHsnoitidnoc
RADIOGRAPHIC ytluciffidemertxEytluciffidetaredoMytluciffidlaminiMDIFFICULTIES obtaining/interpreting radiographs obtaining/interpreting radiographs obtaining/interpreting radiographs
(e.g., high floor of mouth, narrow (e.g., superimposed anatomical or low palatal vault, presence of tori) structures)
POSITION IN THE ARCH ralomdr3rodn2ralomts1ralomerp/roiretnASlight inclination (<10°) Moderate inclination (10-30°) Extreme inclination (>30°)Slight rotation (<10°) Moderate rotation (10-30°) Extreme rotation (>30°)
TOOTH ISOLATION Routine rubber dam placement Simple pretreatment modification Extensive pretreatment modificationrequired for rubber dam isolation required for rubber dam isolation
MORPHOLOGIC Normal original crown morphology Full coverage restoration Restoration does not reflect ABERRATIONS OF CROWN Porcelain restoration original anatomy/alignment
lamronmorfnoitaivedtnacifingiStnemtubaegdirBModerate deviation from normal tooth/root form (e.g., fusion,tooth/root form (e.g., taurodontism, dens in dente) microdens)Teeth with extensive coronal destruction
CANAL AND ROOT Slight or no curvature (<10°) Moderate curvature (10-30°) Extreme curvature (>30°) or MORPHOLOGY Closed apex <1 mm diameter Crown axis differs moderately S-shaped curve
from root axis. Apical opening Mandibular premolar or1-1.5 mm in diameter anterior with 2 roots
Maxillary premolar with 3 rootsCanal divides in the middle or apical thirdVery long tooth (>25 mm)Open apex (>1.5 mm in diameter)
RADIOGRAPHIC Canal(s) visible and not reduced Canal(s) and chamber visible but Indistinct canal pathAPPEARANCE OF elbisivton)s(lanaCezisnidecuderezisniCANAL(S) Pulp stonesRESORPTION No resorption evident Minimal apical resorption Extensive apical resorption
Internal resorption External resorption
C. ADDITIONAL CONSIDERATIONSTRAUMA HISTORY Uncomplicated crown fracture of Complicated crown fracture Complicated crown fracture
hteeterutammifohteeterutamfohteeterutammiroerutamerutcarftoorlatnoziroHnoitaxulbuS
Alveolar fractureIntrusive, extrusive or lateral luxationAvulsion
ENDODONTIC No previous treatment Previous access without complications Previous access with complications TREATMENT HISTORY (e.g., perforation, non-negotiated
canal, ledge, separated instrument)Previous surgical or nonsurgical endodontic treatment completed
PERIODONTAL-ENDODONTIC None or mild periodontal disease Concurrent moderate periodontal Concurrent severe periodontal CONDITION esaesidesaesid
Cracked teeth with periodontal complicationsCombined endodontic/periodontic lesionRoot amputation prior to endodontic treatment
FIG. 18-2, cont’d
as part of the management of swelling, especially when there are systemic manifestations of the infection, such as fever and malaise. The principal modality for managing swelling secondary to endodontic infections is to achieve drainage and remove the source of the infection.36,92 When the swelling is localized, the preferred avenue is drainage through the root canal (Fig. 18-3). However, it is also possible to achieve drain-age with an incision and iodoform gauze drain before entering the canal. In this manner, the canal can be dried and the end-odontic treatment completed in one visit. The dentist should see the patient the following day to remove the drain. Com-plete canal debridement and disinfection37,106 are paramount
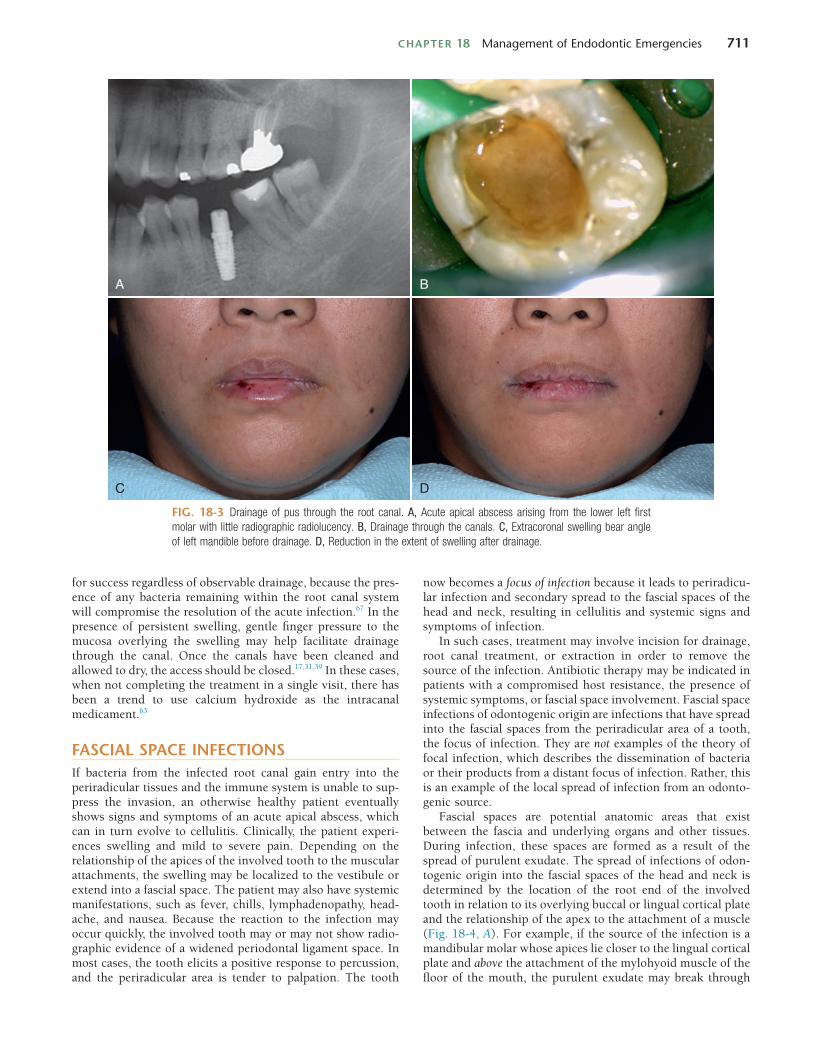
CHAPTER 18 Management of Endodontic Emergencies 711
now becomes a focus of infection because it leads to periradicu-lar infection and secondary spread to the fascial spaces of the head and neck, resulting in cellulitis and systemic signs and symptoms of infection.
In such cases, treatment may involve incision for drainage, root canal treatment, or extraction in order to remove the source of the infection. Antibiotic therapy may be indicated in patients with a compromised host resistance, the presence of systemic symptoms, or fascial space involvement. Fascial space infections of odontogenic origin are infections that have spread into the fascial spaces from the periradicular area of a tooth, the focus of infection. They are not examples of the theory of focal infection, which describes the dissemination of bacteria or their products from a distant focus of infection. Rather, this is an example of the local spread of infection from an odonto-genic source.
Fascial spaces are potential anatomic areas that exist between the fascia and underlying organs and other tissues. During infection, these spaces are formed as a result of the spread of purulent exudate. The spread of infections of odon-togenic origin into the fascial spaces of the head and neck is determined by the location of the root end of the involved tooth in relation to its overlying buccal or lingual cortical plate and the relationship of the apex to the attachment of a muscle (Fig. 18-4, A). For example, if the source of the infection is a mandibular molar whose apices lie closer to the lingual cortical plate and above the attachment of the mylohyoid muscle of the floor of the mouth, the purulent exudate may break through
for success regardless of observable drainage, because the pres-ence of any bacteria remaining within the root canal system will compromise the resolution of the acute infection.67 In the presence of persistent swelling, gentle finger pressure to the mucosa overlying the swelling may help facilitate drainage through the canal. Once the canals have been cleaned and allowed to dry, the access should be closed.17,31,39 In these cases, when not completing the treatment in a single visit, there has been a trend to use calcium hydroxide as the intracanal medicament.63
FASCIAL SPACE INFECTIONSIf bacteria from the infected root canal gain entry into the periradicular tissues and the immune system is unable to sup-press the invasion, an otherwise healthy patient eventually shows signs and symptoms of an acute apical abscess, which can in turn evolve to cellulitis. Clinically, the patient experi-ences swelling and mild to severe pain. Depending on the relationship of the apices of the involved tooth to the muscular attachments, the swelling may be localized to the vestibule or extend into a fascial space. The patient may also have systemic manifestations, such as fever, chills, lymphadenopathy, head-ache, and nausea. Because the reaction to the infection may occur quickly, the involved tooth may or may not show radio-graphic evidence of a widened periodontal ligament space. In most cases, the tooth elicits a positive response to percussion, and the periradicular area is tender to palpation. The tooth
FIG. 18-3 Drainage of pus through the root canal. A, Acute apical abscess arising from the lower left first molar with little radiographic radiolucency. B, Drainage through the canals. C, Extracoronal swelling bear angle of left mandible before drainage. D, Reduction in the extent of swelling after drainage.
A B
C D
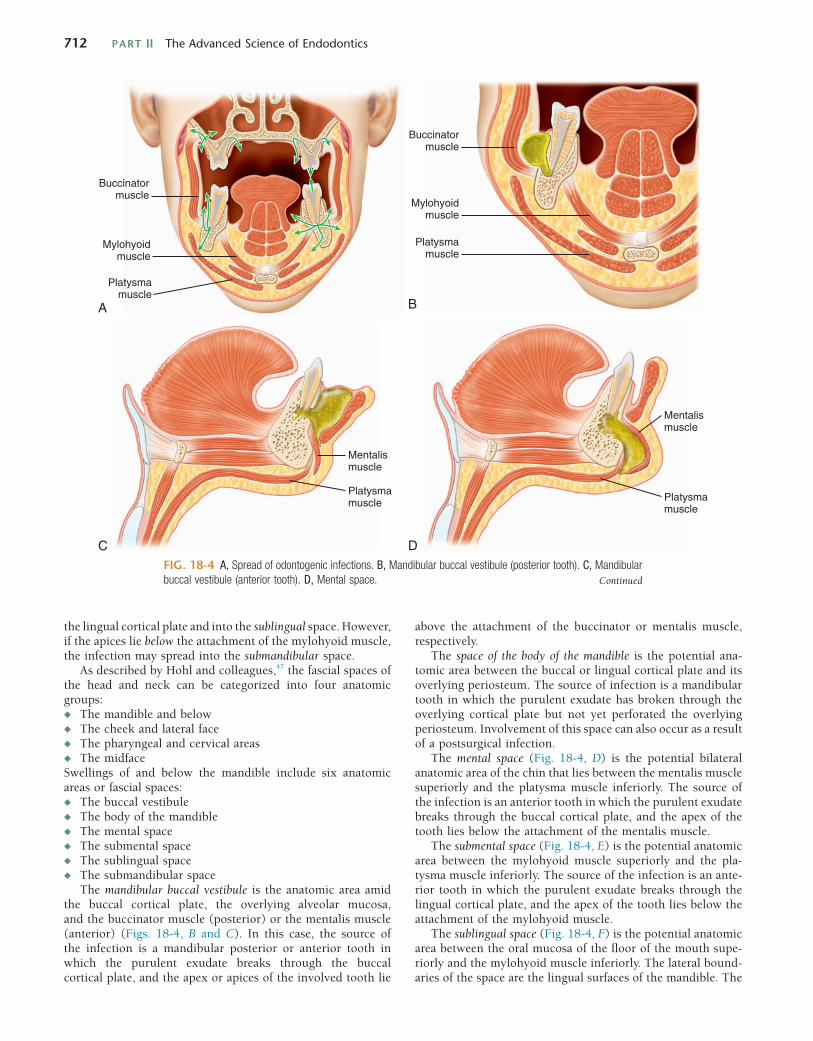
712 PART II The Advanced Science of Endodontics
above the attachment of the buccinator or mentalis muscle, respectively.
The space of the body of the mandible is the potential ana-tomic area between the buccal or lingual cortical plate and its overlying periosteum. The source of infection is a mandibular tooth in which the purulent exudate has broken through the overlying cortical plate but not yet perforated the overlying periosteum. Involvement of this space can also occur as a result of a postsurgical infection.
The mental space (Fig. 18-4, D) is the potential bilateral anatomic area of the chin that lies between the mentalis muscle superiorly and the platysma muscle inferiorly. The source of the infection is an anterior tooth in which the purulent exudate breaks through the buccal cortical plate, and the apex of the tooth lies below the attachment of the mentalis muscle.
The submental space (Fig. 18-4, E) is the potential anatomic area between the mylohyoid muscle superiorly and the pla-tysma muscle inferiorly. The source of the infection is an ante-rior tooth in which the purulent exudate breaks through the lingual cortical plate, and the apex of the tooth lies below the attachment of the mylohyoid muscle.
The sublingual space (Fig. 18-4, F) is the potential anatomic area between the oral mucosa of the floor of the mouth supe-riorly and the mylohyoid muscle inferiorly. The lateral bound-aries of the space are the lingual surfaces of the mandible. The
the lingual cortical plate and into the sublingual space. However, if the apices lie below the attachment of the mylohyoid muscle, the infection may spread into the submandibular space.
As described by Hohl and colleagues,47 the fascial spaces of the head and neck can be categorized into four anatomic groups:◆ The mandible and below◆ The cheek and lateral face◆ The pharyngeal and cervical areas◆ The midfaceSwellings of and below the mandible include six anatomic areas or fascial spaces:◆ The buccal vestibule◆ The body of the mandible◆ The mental space◆ The submental space◆ The sublingual space◆ The submandibular space
The mandibular buccal vestibule is the anatomic area amid the buccal cortical plate, the overlying alveolar mucosa, and the buccinator muscle (posterior) or the mentalis muscle (anterior) (Figs. 18-4, B and C). In this case, the source of the infection is a mandibular posterior or anterior tooth in which the purulent exudate breaks through the buccal cortical plate, and the apex or apices of the involved tooth lie
Buccinatormuscle
Mylohyoidmuscle
Platysmamuscle
A
Buccinatormuscle
Mylohyoidmuscle
Platysmamuscle
B
Mentalismuscle
Platysmamuscle
C
Mentalismuscle
Platysmamuscle
DFIG. 18-4 A, Spread of odontogenic infections. B, Mandibular buccal vestibule (posterior tooth). C, Mandibular buccal vestibule (anterior tooth). D, Mental space. Continued
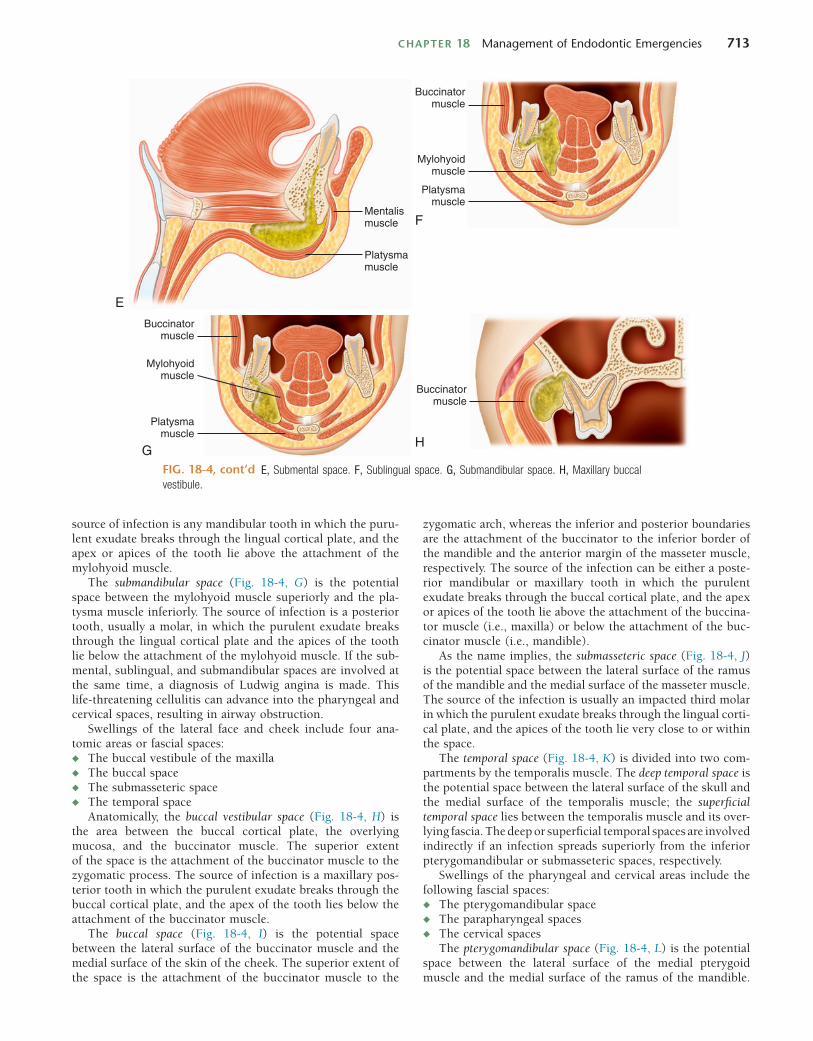
CHAPTER 18 Management of Endodontic Emergencies 713
Mentalismuscle
Platysmamuscle
E
Buccinatormuscle
Mylohyoidmuscle
Platysmamuscle
F
Buccinatormuscle
Mylohyoidmuscle
Platysmamuscle
G
Buccinatormuscle
H
source of infection is any mandibular tooth in which the puru-lent exudate breaks through the lingual cortical plate, and the apex or apices of the tooth lie above the attachment of the mylohyoid muscle.
The submandibular space (Fig. 18-4, G) is the potential space between the mylohyoid muscle superiorly and the pla-tysma muscle inferiorly. The source of infection is a posterior tooth, usually a molar, in which the purulent exudate breaks through the lingual cortical plate and the apices of the tooth lie below the attachment of the mylohyoid muscle. If the sub-mental, sublingual, and submandibular spaces are involved at the same time, a diagnosis of Ludwig angina is made. This life-threatening cellulitis can advance into the pharyngeal and cervical spaces, resulting in airway obstruction.
Swellings of the lateral face and cheek include four ana-tomic areas or fascial spaces:◆ The buccal vestibule of the maxilla◆ The buccal space◆ The submasseteric space◆ The temporal space
Anatomically, the buccal vestibular space (Fig. 18-4, H) is the area between the buccal cortical plate, the overlying mucosa, and the buccinator muscle. The superior extent of the space is the attachment of the buccinator muscle to the zygomatic process. The source of infection is a maxillary pos-terior tooth in which the purulent exudate breaks through the buccal cortical plate, and the apex of the tooth lies below the attachment of the buccinator muscle.
The buccal space (Fig. 18-4, I) is the potential space between the lateral surface of the buccinator muscle and the medial surface of the skin of the cheek. The superior extent of the space is the attachment of the buccinator muscle to the
zygomatic arch, whereas the inferior and posterior boundaries are the attachment of the buccinator to the inferior border of the mandible and the anterior margin of the masseter muscle, respectively. The source of the infection can be either a poste-rior mandibular or maxillary tooth in which the purulent exudate breaks through the buccal cortical plate, and the apex or apices of the tooth lie above the attachment of the buccina-tor muscle (i.e., maxilla) or below the attachment of the buc-cinator muscle (i.e., mandible).
As the name implies, the submasseteric space (Fig. 18-4, J) is the potential space between the lateral surface of the ramus of the mandible and the medial surface of the masseter muscle. The source of the infection is usually an impacted third molar in which the purulent exudate breaks through the lingual corti-cal plate, and the apices of the tooth lie very close to or within the space.
The temporal space (Fig. 18-4, K) is divided into two com-partments by the temporalis muscle. The deep temporal space is the potential space between the lateral surface of the skull and the medial surface of the temporalis muscle; the superficial temporal space lies between the temporalis muscle and its over-lying fascia. The deep or superficial temporal spaces are involved indirectly if an infection spreads superiorly from the inferior pterygomandibular or submasseteric spaces, respectively.
Swellings of the pharyngeal and cervical areas include the following fascial spaces:◆ The pterygomandibular space◆ The parapharyngeal spaces◆ The cervical spaces
The pterygomandibular space (Fig. 18-4, L) is the potential space between the lateral surface of the medial pterygoid muscle and the medial surface of the ramus of the mandible.
E, Submental space. F, Sublingual space. G, Submandibular space. H, Maxillary buccal vestibule. FIG. 18-4, cont’d
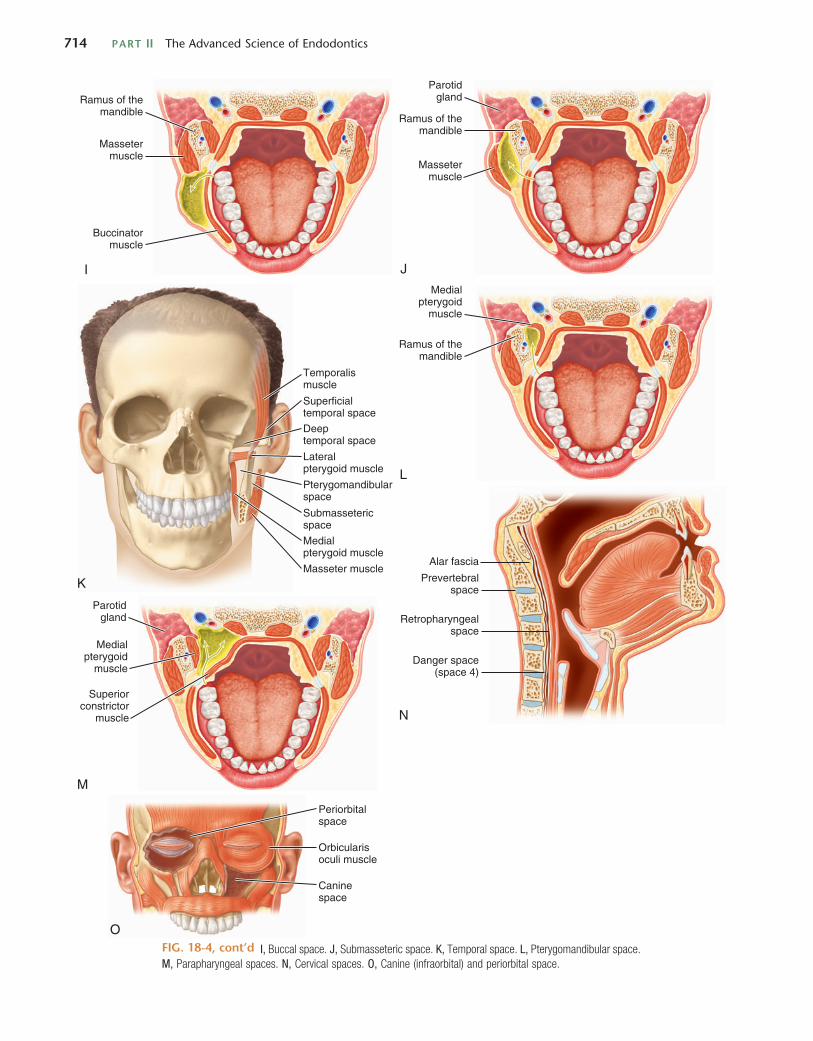
714 PART II The Advanced Science of Endodontics
Massetermuscle
Ramus of themandible
Buccinatormuscle
I J
Massetermuscle
Ramus of themandible
Parotidgland
Superficialtemporal space
Temporalismuscle
Deeptemporal space
Masseter muscle
Medialpterygoid muscle
Pterygomandibularspace
Lateralpterygoid muscle
Submassetericspace
K
Ramus of themandible
Medialpterygoid
muscle
L
Parotidgland
Medialpterygoid
muscle
Superiorconstrictor
muscle
M
Prevertebralspace
Alar fascia
Retropharyngealspace
Danger space(space 4)
N
Periorbitalspace
Orbicularisoculi muscle
Caninespace
OI, Buccal space. J, Submasseteric space. K, Temporal space. L, Pterygomandibular space.
M, Parapharyngeal spaces. N, Cervical spaces. O, Canine (infraorbital) and periorbital space. FIG. 18-4, cont’d

CHAPTER 18 Management of Endodontic Emergencies 715
The superior extent of the space is the lateral pterygoid muscle. The source of the infection is mandibular second or third molars in which the purulent exudate drains directly into the space. In addition, contaminated inferior alveolar nerve injec-tions can lead to infection of the space.
The parapharyngeal spaces comprise the lateral pharyngeal and retropharyngeal spaces (Fig. 18-4, M). The lateral pharyn-geal space is bilateral and lies between the lateral surface of the medial pterygoid muscle and the posterior surface of the supe-rior constrictor muscle. The superior and inferior margins of the space are the base of the skull and the hyoid bone, respec-tively, and the posterior margin is the carotid space, or sheath, which contains the common carotid artery, internal jugular vein, and the vagus nerve. Anatomically, the retropharyngeal space lies between the anterior surface of the prevertebral fascia and the posterior surface of the superior constrictor muscle and extends inferiorly into the retroesophageal space, which extends into the posterior compartment of the mediastinum. The pharyngeal spaces usually become involved as a result of the secondary spread of infection from other fascial spaces or directly from a peritonsillar abscess.
The cervical spaces comprise the pretracheal, retrovisceral, danger, and prevertebral spaces (Fig. 18-4, N). The pretracheal space is the potential space surrounding the trachea. It extends from the thyroid cartilage inferiorly into the superior portion of the anterior compartment of the mediastinum to the level of the aortic arch. Because of its anatomic location, odonto-genic infections do not spread to the pretracheal space. The retrovisceral space comprises the retropharyngeal space superi-orly and the retroesophageal space inferiorly. The space extends from the base of the skull into the posterior compartment of the mediastinum to a level between vertebrae C6 and T4. The danger space (i.e., space 4)26,33 is the potential space between the alar and prevertebral fascia. Because this space is composed of loose connective tissue, it is considered an actual anatomic space extending from the base of the skull into the posterior compartment of the mediastinum to a level corresponding to the diaphragm. It is not unknown for odontogenic infection to spread into this space, if left untreated and undiagnosed.32 The consequence can be fatal. The prevertebral space is the potential space surrounding the vertebral column. As such, it extends from vertebra C1 to the coccyx. A retrospective study showed that 71% of cases in which the mediastinum was involved arose from the spread of infection from the retrovis-ceral space (21% from the carotid space and 8% from the pretracheal space).64
Swellings of the midface consist of four anatomic areas and spaces:◆ The palate◆ The base of the upper lip◆ The canine spaces◆ The periorbital spacesOdontogenic infections can spread into the areas between the palate and its overlying periosteum and mucosa and the base of the upper lip, which lies superior to the orbicularis oris muscle, even though these areas are not considered actual fascial spaces. The source of infection of the palate is any of the maxillary teeth in which the apex of the involved tooth lies close to the palate. The source of infection of the base of the upper lip is a maxillary central incisor in which the apex lies close to the buccal cortical plate and above the attachment of the orbicularis oris muscle.
The canine, or infraorbital, space (Fig. 18-4, O) is the poten-tial space between the levator anguli oris muscle inferiorly and the levator labii superioris muscle superiorly. The source of infection is the maxillary canine or first premolar in which the purulent exudate breaks through the buccal cortical plate, and the apex of the tooth lies above the attachment of the levator anguli oris muscle. There is a chance for the infection to spread from the infraorbital space into the cavernous sinus in the cranium via the valveless veins of the face and anterior skull base.26
The periorbital space (see Fig. 18-4, O) is the potential space that lies deep to the orbicularis oculi muscle. This space becomes involved through the spread of infection from the canine or buccal spaces. Infections of the midface can be very dangerous because they can result in cavernous sinus thrombo-sis, a life-threatening infection in which a thrombus formed in the cavernous sinus breaks free, resulting in blockage of an artery or the spread of infection. Under normal conditions, the angular and ophthalmic veins and the pterygoid plexus of veins flow into the facial and external jugular veins. If an infec-tion has spread into the midfacial area, however, edema and the resultant increased pressure from the inflammatory response cause the blood to back up into the cavernous sinus. Once in the sinus, the blood stagnates and clots. The resultant infected thrombi remain in the cavernous sinus or escape into the circulation.77,115
MANAGEMENT OF ABSCESSES AND CELLULITISThe two most important elements of effective patient manage-ment for the resolution of an odontogenic infection are correct diagnosis and removal of the cause. When endodontic treat-ment is possible and preferred, in an otherwise healthy patient, chemomechanical preparation of the infected root canals and incision for drainage of any fluctuant periradicular swelling usually provide prompt improvement of the clinical signs and symptoms. The majority of cases of endodontic infections can be treated effectively without the use of systemic antibiotics. The appropriate treatment is removal of the cause of the inflammatory condition.
Antibiotics are not recommended for irreversible pulpitis, symptomatic apical periodontitis, draining sinus tracts, after endodontic surgery, to prevent flare-ups, or after incision for drainage of a localized swelling (without cellulitis, fever, or lymphadenopathy).28,46,72,86,110 When the ratio of risk to benefit is considered in these situations, antibiotic use may put the patient at risk for side effects of the antimicrobial agent and select for resistant microorganisms. Analgesics (not antibiot-ics) are indicated for controlling the pain.
Antibiotics in conjunction with appropriate endodontic treatment are recommended for progressive or persistent infec-tions with systemic signs and symptoms such as fever (over 100°F or 37°C), malaise, cellulitis, unexplained trismus, and progressive or persistent swelling (or both). In such cases, antibiotic therapy is indicated as an adjunct to debridement of the root canal system, which is a reservoir of microorganisms. In addition, aggressive incision for drainage is indicated for any infection marked by cellulitis. Incision for drainage is indicated whether the cellulitis is indurated or fluctuant. It is important to provide a pathway of drainage to prevent further spread of the abscess or cellulitis. An incision for drainage

716 PART II The Advanced Science of Endodontics
This will allow compartmentalized areas of inflammatory exudates and infection to be disrupted and evacuated.
◆ To promote drainage, the wound should be kept clean with warm saltwater mouth rinses. Intraoral heat application to infected tissues results in a dilation of small vessels, which subsequently intensifies host defenses through increased vascular flow.36,92
◆ A drain should be placed to prevent the incision from closing too early. The preferable type of drain is 1
2-inch iodoform gauze, which is more comfortable and less trau-matic to the patient.(Fig. 18-5). The patient should be seen the following day to remove the drain.
◆ In many cases, the endodontic treatment can be com-pleted in one visit after the drain is placed. The drainage allows for the ability to dry the instrumented canal, and completing the endodontic treatment eliminates the source of the infection, enabling the periapical lesion to heal quicker.A diffuse swelling may develop into a life-threatening
medical emergency. Because the spread of infection can tra-verse between the fascial planes and muscle attachments, vital structures can be compromised and breathing may be impeded. Two examples are Ludwig’s angina and cervical fasciitis.32 It is imperative that the clinician be in constant communica-tion with the patient to ensure that the infection does not worsen and that medical attention is provided as necessary. Antibiotics and analgesics should be prescribed, and the patient should be monitored closely for the next several days or until there is improvement. Individuals who show signs of toxicity, elevated body temperature, lethargy, central nervous system (CNS) changes, or airway compromise should be referred to an oral surgeon or medical facility for immediate care and intervention.
SYMPTOMATIC TEETH WITH PREVIOUS ENDODONTIC TREATMENTThe emergency management of teeth with previous endodontic treatment may be technically challenging and time consuming. This is especially true in the presence of extensive restorations, including posts and cores, crowns, and bridgework. However, the goal remains the same as for the management of necrotic teeth: remove contaminants from the root canal system and establish patency to achieve drainage.85 Gaining access to the periapical tissues through the root canals may require removal of posts and obturation materials, as well as negotiating blocked or ledged canals. Failure to complete root canal debridement and achieve periapical drainage may result in continued painful symptoms, in which case a trephination procedure or apicoectomy may be indicated. The ability, prac-ticality, and feasibility to adequately retreat the root canal system must be carefully assessed before the initiation of treat-ment, as conventional retreatment might not be the optimal treatment plan. This is further discussed in Chapter 8.
LEAVING TEETH OPENOn rare occasions, canal drainage may continue from the periapical spaces (Fig. 18-6). In these cases, the clinician may opt to step away from the patient for some time to allow the drainage to continue and hopefully resolve on the same treatment visit.103
allows decompression of the increased tissue pressure associ-ated with edema and provides significant pain relief. Further-more, the incision provides a draining pathway not only for bacteria and their products but also for the inflammatory medi-ators associated with the spread of cellulitis.
A minimum inhibitory concentration of antibiotic may not reach the source of the infection because of decreased blood flow and because the antibiotic must diffuse through the edem-atous fluid and pus. Drainage of edematous fluid and purulent exudate improves circulation to the tissues associated with an abscess or cellulitis, providing better delivery of the antibiotic to the area. Placement of a drain may not be indicated for localized fluctuant swellings if complete evacuation of the purulent exudate is believed to have occurred.
For effective drainage, a vertically oriented stab incision is made through the mucoperiosteum in the most dependent site of the swelling. The incision must be long enough to allow blunt dissection using a curved hemostat or periosteal elevator under the periosteum for drainage of pockets of inflammatory exudate. A rubber dam drain or a Penrose drain is indicated for any patient with a progressive abscess or cellulitis to main-tain an open pathway for drainage. A more detailed description is given later.
Patients with cellulitis should be followed on a daily basis to ensure that the infection is resolving. The best practical guide for determining the duration of antibiotic therapy is clinical improvement of the patient. When clinical evidence indicates that the infection is certain to resolve or is resolved, antibiotics should be administered for no longer than 1 or 2 days more.
Endodontic treatment should be completed as soon as pos-sible after the incision for drainage. The drain can usually be removed 1 or 2 days after improvement. If no significant clini-cal improvement occurs, the diagnosis and treatment must be reviewed carefully. Consultation with a specialist and referral may be indicated for severe or persistent infections. Likewise, patients requiring extraoral drainage should be referred to a clinician trained in the technique.
INCISION FOR DRAINAGEEstablishing drainage from a localized soft tissue swelling is sometimes necessary. This can be accomplished through the incision for drainage of the area.73 Incision for drainage is indi-cated whether the cellulitis is indurated or fluctuant,92 and it is used when a pathway for drainage is needed to prevent further spread of infection. Incision for drainage allows decom-pression from the increased tissue pressure associated with edema and can provide significant pain relief for the patient; noteworthy is that often pain decreases when the soft tissues swell due to the relief of pressure within the bone. The incision also provides a pathway not only for bacteria and bacterial by-products but also for the inflammatory mediators that are associated with the spread of cellulitis.
The basic principles of incision for drainage are as follows:◆ Anesthetize the area.◆ Make a vertically oriented incision at the site of greatest
fluctuant swelling.◆ Dissect gently, through the deeper tissues, and thoroughly
explore all parts of the abscess cavity, eventually extending to the offending roots that are responsible for the pathosis.

CHAPTER 18 Management of Endodontic Emergencies 717
SYSTEMIC ANTIBIOTICS FOR ENDODONTIC INFECTIONSA hundred years ago, infectious diseases were the major rec-ognized causes of death in the world. The advent of antibiotics resulted in a significant decline in the incidence of life-threatening infections and heralded a new era in the therapy of infectious diseases; but the enthusiasm generated turned out to be premature. Over the years, microbial evolutionary responses to the selective pressure exerted by antibiotics have resulted in microbial species resistant to virtually every known antibiotic agent.41 The rapid emergence of resistant microbial strains comes as a consequence of the astonishing power of natural selection among microorganisms. If a given member of
Historically, in the presence of acutely painful necrotic teeth with no swelling or diffuse swelling, 19.4% to 71.2% of sur-veyed endodontists would leave the tooth open between visits.22,23 However, the more current literature makes it clear that this form of treatment would impair uneventful resolution and create more complicated treatment.5,7,113 For this reason, leaving teeth open between appointments is not recommended. Foreign objects have been found in teeth left open for drainage (Fig. 18-7). There has even been a documented case report of a foreign object being found to enter the periapical tissues through a tooth that had been left open for drainage.95 In addi-tion, leaving a tooth open provides an opportunity for oral microorganisms to invade and colonize the root canal system if the tooth is left open for an extended period.
FIG. 18-5 A, Iodoform gauze cut to proper length. B, Iodoform gauze drain after 24 hours.
A B
FIG 18-6 Nonvital infected tooth with active drainage from the periapical area through the canal. A, Access opened and draining for 1 minute. B, Drainage after 2 minutes. C, Canal space dried after 3 minutes.
CBA

718 PART II The Advanced Science of Endodontics
among the beta-lactamase producers.34 Bacteria that produce beta-lactamases protect not only themselves but also other penicillin-susceptible bacteria present in a mixed community by releasing free beta-lactamase into the environment.11
Overuse and misuse of antibiotics has been considered the major cause for the emergence of multidrug-resistant strains. Improper use of antibiotics includes use in cases with no infec-tion, erroneous choice of the agent, dosage or duration of therapy, and excessive use in prophylaxis.80,81 Antibiotics are used in clinical practice far more often than necessary. Antibi-otic therapy is actually warranted in about 20% of the individu-als who are seen for clinical infectious disease, but they are prescribed up to 80% of the time. To complicate matters further, in up to 50% of cases, recommended agents, doses, or duration of therapy are incorrect.66
The appalling rise in the frequency of multidrug resistance among leading pathogens should cause great concern and incite a commitment to act carefully and responsibly. A single erroneous use of antibiotics can be a significant contribution to the current scenario of increasing microbial resistance. Dis-eases that were effectively treated in the past with a given antibiotic may now require the use of another drug, usually more expensive and potentially more toxic, to achieve effective antimicrobial treatment. Unfortunately, even the new drug may not be effective.
Antibiotics are defined as naturally occurring substances of microbial origin or similar synthetic (or semisynthetic) sub-stances that have antimicrobial activity in low concentrations and inhibit the growth of or kill selective microorganisms. The purpose of antibiotic therapy is to aid the host defenses in controlling and eliminating microorganisms that temporar-ily have overwhelmed the host defense mechanisms.80 Based on the earlier discussion, it becomes clear that the most important decision in antibiotic therapy is not so much which antibiotic should be employed but whether antibiotics should be used at all.79 One should bear in mind that antibiotics are very useful drugs classically employed to treat or help treat infectious disease and provide prophylaxis in carefully selected cases.
The majority of infections of endodontic origin are treated without the need for antibiotics. As mentioned, the absence of blood circulation in a necrotic pulp prevents antibiotics from reaching and eliminating microorganisms present in the root canal system; therefore, the source of infection is often unaffected by systemic antibiotic therapy. Antibiotics can, however, help impede the spread of the infection and devel-opment of focal infections in medically compromised patients and provide a valuable adjunct for managing selected cases of endodontic infection. In addition to the indications for systemic antibiotics discussed earlier for acute abscesses and cellulitis, antibiotics are also prescribed for prophylaxis in medically compromised patients during routine endodontic therapy, in some cases of persistent exudation not resolved after revision of intracanal procedures, and after the replanta-tion of avulsed teeth.
Selection of antibiotics in clinical practice is either empiri-cal or based on the results of microbial sensitivity tests. For diseases with known microbial causes, empirical therapy may be used. This is especially applicable to infections of end-odontic origin, because culture-dependent antimicrobial tests of anaerobic bacteria can take too long to provide results about their susceptibility to antibiotics (7 to 14 days).
a microbial community possesses genes of resistance against a certain antibiotic and the community is persistently exposed to the drug, the resistant microorganism is selected to emerge and multiply to the detriment of the susceptible portion of the community. Passing on the genes responsible for resistance via plasmids and quorum sensing41 has also been shown to encour-age the survival of the microbial community. The emergence of multidrug-resistant strains of several bacterial species capable of causing life-threatening infections has been reported.41,66,82,100,114 Antibiotic resistance among obligately anaerobic bacteria is increasing, with resistance to penicillins, clindamycin, and cephalosporins noted at community hospi-tals and major medical centers.42,43
Among oral bacteria, there have been reports on emerging resistance to commonly used antibiotics. Resistance has been found in F. nucleatum strains for penicillin, amoxicillin, and metronidazole, in P. intermedia for tetracycline and amoxicillin, and in A. actinomycetemcomitans for amoxicillin and azithro-mycin.59,107 Macrolides (erythromycin and azithromycin) have presented decreased activity against Fusobacterium and nonpig-mented Prevotella species.44,58,59 Production of beta-lactamase by oral bacteria has also been reported, with the most promi-nent beta-lactamase-producing bacteria belonging to the anaer-obic genus Prevotella.9,12,27,34,108 Kuriyama and colleagues58 revealed that beta-lactamase production was detected in 36% of the black-pigmented Prevotella and 32% of the nonpigmented Prevotella species isolated from pus samples of oral abscesses. Susceptibility of Prevotella strains to several cephalosporins, erythromycin, and azithromycin has been found to correlate with amoxicillin susceptibility; amoxicillin-resistant strains can be similarly resistant to these other antibiotics.59 This finding suggests that there is little value in the use of oral cephalosporins and macrolides in managing endodontic abscesses, particularly when penicillin-resistant strains are evident. Other enzyme-producing oral anaerobic species include strains of F. nucleatum, P. acnes, Actinomyces species, and Peptostreptococcus species.12,27,34,108 Facultative bacteria such as Capnocytophaga and Neisseria species have also been detected
FIG. 18-7 Foreign object in tooth left open to drain. Patient used a sewing needle to clear out food particles that were blocking the canal and broke the needle in the tooth.

CHAPTER 18 Management of Endodontic Emergencies 719
Because of their anti-inflammatory effect, NSAIDs can sup-press swelling to a certain degree after surgical procedures. The good analgesic effect combined with the additional anti-inflammatory benefit make NSAIDs, especially ibuprofen, the drug of choice for acute dental pain in the absence of any contraindication to their use. Ibuprofen has been used for more than 30 years and has been thoroughly evaluated.21 If the NSAID alone does not have a satisfactory effect in controlling pain, then the addition of an opioid may provide additional analgesia. However, in addition to other possible side effects, opioids may cause nausea, constipation, lethargy, dizziness, and disorientation.
LABORATORY DIAGNOSTIC ADJUNCTSChapter 14 discusses culturing techniques and indications. Because the results of culturing for anaerobic bacteria usually require at least 1 to 2 weeks, it is not considered routine in the management of an acute endodontic emergency. Thus, in an endodontic emergency, antibiotic treatment, when indicated (see Chapter 18), should begin immediately, because oral infections can progress rapidly.
FLARE-UPSAn endodontic flare-up is defined as an acute exacerbation of a periradicular pathosis after the initiation or continuation of nonsurgical root canal treatment.3 The incidence may be from 2% to 20% of cases.50,70,76,109 A meta-analysis of the literature, using strict criteria, showed the flare-up frequency to be about 8.4%.105 Endodontic flare-ups are more prevalent among females under the age of 20 years and may occur more in maxillary lateral incisors; in mandibular first molars, when there are large periapical lesions; and in the retreatment of previous root canals.102 The presence of pretreatment pain may also be a predictor of potential posttreatment flare-ups.50,102,109 Fortunately, there is no decrease in the endodontic success for cases that had a treatment flare-up.54
Endodontic flare-ups may occur for a variety of reasons, including preparation beyond the apical terminus, over-instrumentation, pushing dentinal and pulpal debris into the periapical area,36 incomplete removal of pulp tissue, overexten-sion of root canal filling material, chemical irritants (such as irrigants, intracanal medicaments, and sealers), hyperocclu-sion, root fractures, and microbiologic factors.94 Although many of these cases can be pharmacologically managed (see Chapter 18), recalcitrant cases may require periapical surgery, reentry into the tooth, the establishment of drainage either through the tooth or via trephination, or, at a minimum, adjustment of the occlusion.19,89,94 The prophylactic use of anti-biotics to decrease the incidence of flare-ups has been met with some controversy. Whereas earlier investigators71 found that antibiotic administration before treatment of necrotic teeth decreased the incidence of flare-ups, more recent studies found antibiotic use either less effective than analgesics or to have no effect in reducing interappointment emergencies or posttreat-ment symptoms.86,110,101
CRACKED AND FRACTURED TEETHDescribed in detail in Chapter 1 and Chapter 21, cracks and incomplete fractures can be difficult to locate and diagnose,
Therefore, it is preferable to opt for an antimicrobial agent whose spectrum of action includes the most commonly detected bacteria. Most of the bacterial species involved with endodontic infections, including abscesses, are susceptible to penicillins,6,51,55,59 which make them first-line drugs of choice. Because the use of antibiotics is restricted to severe infections or prophylaxis, it seems prudent to use amoxicillin, a semi-synthetic penicillin with a broad spectrum of antimicrobial activity and one that is well absorbed in the alimentary canal. In more serious cases, including life-threatening conditions, combining amoxicillin with clavulanic acid or metronidazole may be required to achieve optimum antimicrobial effects as a result of the extended spectrum of action to include penicillin-resistant strains.59 In patients allergic to penicillins or in cases refractory to amoxicillin therapy, clindamycin is indicated. Clindamycin has strong antimicrobial activity against oral anaerobes.55,57,59,61
The risk/benefit ratio should always be evaluated prior to prescribing antibiotics. Appropriately selected patients will benefit from systemically administered antibiotics. A restrictive and conservative use of antibiotics is highly recommended in endodontic practice. Indiscriminate use (including cases of a reversible or irreversible pulpitis) is contrary to sound clinical practice, as it may cause a selective overgrowth of intrinsically resistant bacteria, predisposing patients to secondary and super-infections, rendering drugs ineffective against poten-tially fatal medical infectious diseases.
ANALGESICSAs a more thorough description of pain medications can be found in Chapter 4, the following information is merely a summary of pain control using analgesics. Because pulpal and periapical pain involves inflammatory processes, the first choice of analgesics is nonsteroidal anti-inflammatory drugs (NSAIDs).63 However, no pain medication can replace the effi-cacy of thoroughly cleaning the root canal system to rid the tooth of the source of infection.35
Aspirin has been used as an analgesic for more than 100 years. In some cases, it may be more effective than 60 mg of codeine18; its analgesic and antipyretic effects are equal to those of acetaminophen, and its anti-inflammatory effect is more potent.21 However, aspirin’s side effects include gastric distress, nausea, and gastrointestinal ulceration. In addition, its analge-sic effect is inferior to that of ibuprofen, 400 mg. When NSAIDs and aspirin are contraindicated, such as in patients for whom gastrointestinal problems are a concern, acetaminophen is the preferred nonprescription analgesic. A recommended maximum daily dose of 4 g of acetaminophen is currently in force, and a further reduction of this dosage has been proposed to reduce the chance of acetaminophen-related liver toxicity.62,93
For moderate to severe pain relief, ibuprofen, an NSAID, has been found to be superior to aspirin (650 mg) and acet-aminophen (600 mg) with or without codeine (60 mg). Also, ibuprofen has fewer side effects than the combinations with opioid.18,52 The maximal dose of 3.2 g in a 24-hour period should not be exceeded. Patients who take daily doses of aspirin for its cardioprotective benefit can take occasional doses of ibuprofen; however, it would be prudent to advise such patients to avoid regular doses of ibruprofen.1 These patients would gain more relief by taking a selective cyclooxy-genase (COX)-2 inhibitor, such as diclofenac or celecoxib.

720 PART II The Advanced Science of Endodontics
teeth may be more challenging. In addition, it must be deter-mined whether the crack or fracture was the cause of pulpal necrosis and whether there has been extensive periodontal breakdown. If so, the prognosis for the tooth is generally poor; thus extraction is recommended.
SUMMARYThe management of endodontic emergencies is an important part of a dental practice. It can often be a disruptive part of the day for the clinician and staff, but it is an invaluable solution for the distressed patient. Methodical diagnosis and prognostic assessment are imperative, with the patient being informed of the various treatment alternatives.
ACKNOWLEDGMENTSThe authors acknowledge the outstanding work of Drs. J. Craig Baumgartner, Jeffrey W. Hutter, and Louis Berman in previous editions of this text.
but their detection can be an important component in the management of an acute dental emergency. In the early stages, cracks are small and difficult to discern. Removal of filling materials, applications of dye solutions, selective loading of cusps, transillumination, and magnification are helpful in their detection. As the crack or fracture becomes more extensive, it can become easier to visualize. Because cracks are difficult to find and their symptoms can be so variable, the name cracked tooth syndrome has been suggested,14 even though it is not truly a syndrome. Cracks in vital teeth often exhibit a sudden and sharp pain, especially during mastication. Cracks in nonvital or obturated teeth tend to have more of a “dull ache” but can still be sensitive to mastication.
The determination of the presence of a crack or fracture is paramount because the prognosis for the tooth may be directly dependent on the extent of the crack or fracture. Management of cracks in vital teeth may be as simple as a bonded restoration or a full coverage crown. However, even the best efforts to manage a crack may be unsuccessful, often requiring endodon-tic treatment or extraction. Fractures in nonvital or obturated
REFERENCES1. Abramowicz M, editor: Do NSAIDs interfere with the
cardioprotective effects of aspirin? Med Lett Drugs Ther 46:61, 2004.
2. Albahaireh ZS, Alnegrish AS: Postobturation pain after single and multiple-visit endodontic therapy: a prospective study, J Dent 26:227, 1998.
3. American Association of Endodontics: Glossary of endodontic terms, ed 7, Chicago, 2003, American Association of Endodontists.
4. Ashkenaz PJ: One-visit endodontics, Dent Clin North Am 28:853, 1984.
5. Auslander WP: The acute apical abscess, N Y State Dent J 36:623, 1970.
6. Baumgartner JC, Xia T: Antibiotic susceptibility of bacteria associated with endodontic abscesses, J Endod 29:44, 2003.
7. Bence R, Meyers RD, Knoff RV: Evaluation of 5,000 endodontic treatment incidents of the open tooth, Oral Surg Oral Med Oral Pathol 49:82, 1980.
8. Bender IB: Pulpal pain diagnosis: a review, J Endod 26:175, 2000.
9. Bernal LA, Guillot E, Paquet C, Mouton C: Beta-lactamase producing strains in the species Prevotella intermedia and Prevotella nigrescens, Oral Microbiol Immunol 13:36, 1998.
10. Boutsioukis C, Psimma Z, Kastrinakis E: The effect of flow rate and agitation technique on irrigant extrusion ex vivo, Int Endod J 47:487, 2014.
11. Brook I: beta-Lactamase-producing bacteria in mixed infections, Clin Microbiol Infect 10:777, 2004.
12. Brook I, Frazier EH, Gher ME Jr: Microbiology of periapical abscesses and associated maxillary sinusitis, J Periodontol 67:608, 1996.
13. Bystrom A, Claesson R, Sundqvist G: The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals, Endod Dent Traumatol 1:170, 1985.
14. Cameron CE: The cracked tooth syndrome, J Am Dent Assoc 93:971, 1976.
15. Carrotte P. Endodontics: part 3. Treatment of endodontic emergencies, Br Dent J 197:299, 2004.
16. Chestner SB, Selman AJ, Friedman J, Heyman RA: Apical fenestration: solution to recalcitrant pain in root canal therapy, J Am Dent Assoc 77:846, 1986.
17. Chong BS, Pitt Ford TR: The role of intracanal medication in root canal treatment, Int Endod J 25:97, 1992.
18. Cooper SA, Beaver WT: A model to evaluate mild analgesics in oral surgery outpatients, Clin Pharmacol Ther 20:241, 1976.
19. Creech JH, Walton RE, Kaltenbach R: Effect of occlusal relief on endodontic pain, J Am Dent Assoc 109:64, 1984.
20. Desi P, Himel V: Comparative safety of various intracanal irrigation systems, J Endod 35:545,2009.
21. Dionne RA, Phero JC, Becker DE: Management of pain and anxiety in the dental office, Philadelphia, 2002, Saunders.
22. Dorn SO, Moodnik RM, Feldman MJ, Borden BG: Treatment of the endodontic emergency: a report based on a questionnaire—part I, J Endod 3:94, 1977.
23. Dorn SO, Moodnik RM, Feldman MJ, Borden BG: Treatment of the endodontic emergency: a report based on a questionnaire—part II, J Endod 3:153, 1977.
24. Eleazer PD, Eleazer KR: Flare-up rate in pulpally necrotic molars in one-visit versus two-visit endodontic treatment, J Endod 24:614, 1998.
25. Field JW, Gutmann JL, Solomon ES, Rakuskin H: A clinical radiographic retrospective assessment of the success rate of single-visit root canal treatment, Int Endod J 37:70, 2004.
26. Flynn TR: Anatomy of oral and maxillofacial infections. In Topazian RG, Goldberg MH, Hupp JR, editors: Oral and maxillofacial infections, ed 4, Philadelphia, 2002, WB Saunders, pp 188-213.
27. Fosse T, Madinier I, Hitzig C, Charbit Y: Prevalence of betalactamase-producing strains among 149 anaerobic gram negative rods isolated from periodontal pockets, Oral Microbiol Immunol 14:352, 1999.
28. Fouad AF, Rivera EM, Walton RE: Penicillin as a supplement in resolving the localized acute apical abscess, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81:590, 1996.
29. Reference deleted in proofs.30. Gatchel RJ: Managing anxiety and pain during dental
treatment, J Am Dent Assoc 123:37, 1992.31. Gatewood RS, Himel VT, Dorn S: Treatment of the
endodontic emergency: a decade later, J Endod 16:284, 1990.
32. Goldberg MH, Topazian RG: Odontogenic infections and deep fascial space infections of dental origin. In Topazian RG, Goldberg MH, Hupp JR, editors: Oral and maxillofacial infections, ed 4, Philadelphia, 2002, WB Saunders, pp 158-187.
33. Grodinsky M, Holyoke EA: The fasciae and fascial spaces of the head, neck, and adjacent regions, Am J Anat 63:367, 1938.
34. Handal T, Olsen I, Walker CB, Caugant DA: Beta-lactamase production and antimicrobial susceptibility of subgingival bacteria from refractory periodontitis, Oral Microbiol Immunol 19:303, 2004.
35. Hargreaves KM, Keiser K: New advances in the management of endodontic pain emergencies, J Calif Dent Assoc 32:469, 2004.
36. Harrington GW, Natkin E: Midtreatment flare-ups, Dent Clin North Am 36:409, 1992.
37. Harrison JW: Irrigation of the root canal system, Dent Clin North Am 28:797, 1984.
38. Hasler JF, Mitchel DF: Analysis of 1628 cases of odontalgia: a corroborative study, J Indianap Dist Dent Soc 17:23 1963.
39. Hasselgren G: Pains of dental origin, Dent Clin North Am 12:263, 2000.
40. Hasselgren G, Reit C: Emergency pulpotomy: pain relieving effect with and without the use of sedative dressings, J Endod 15:254, 1989.
41. Hayward CMM, Griffin GE: Antibiotic resistance: the current position and the molecular mechanisms involved, Br J Hosp Med 52:473, 1994.
42. Hecht DW: Prevalence of antibiotic resistance in anaerobic bacteria: worrisome developments, Clin Infect Dis 39:92, 2004.
43. Hecht DW, Vedantam G, Osmolski JR: Antibiotic resistance among anaerobes: what does it mean? Anaerobe 5:421, 1999.
44. Heimdahl A, von Konow L, Satoh T, Nord CE: Clinical appearance of orofacial infections of odontogenic origin in relation to microbiological findings, J Clin Microbiol 22:299, 1985.
45. Henry BM, Fraser JG: Trephination for acute pain management, J Endod 29:144, 2003.
46. Henry M, Reader A, Beck M: Effect of penicillin on postoperative endodontic pain and swelling in symptomatic necrotic teeth, J Endod 27:117, 2001.
CHAPTER 18 Management of Endodontic Emergencies 721
47. Hohl TH, Whitacre RJ, Hooley JR, Williams B: A self instructional guide: diagnosis and treatment of odontogenic infections, Seattle, 1983, Stoma Press.
48. Holmes-Johnson E, Geboy M, Getka EJ: Behavior considerations, Dent Clin North Am 30:391, 1986.
49. Horrobin DF, Durnad LG, Manku MS: Prostaglandin E 1 modifies nerve conduction and interferes with local anesthetic action, Prostaglandins 14:103, 1997.
50. Imura N, Zuolo ML: Factors associated with endodontic flareups: a prospective study, Int Endod J 28:261, 1995.
51. Jacinto RC, Gomes BP, Ferraz CC, et al: Microbiological analysis of infected root canals from symptomatic and asymptomatic teeth with periapical periodontitis and the antimicrobial susceptibility of some isolated anaerobic bacteria, Oral Microbiol Immunol 18:285, 2003.
52. Jain AK, Ryan JR, McMahon G: Analgesic efficacy of low-dose ibuprofen in dental extraction, Pharmacotherapy 6:318, 1986.
53. Keenan JV, Farman AG, Fedorowica Z, Newton JT: A Cochrane Systematic Review finds no evidence to support the use of antibiotics for pain relief in irreversible pulpitis, J Endod 32:87, 2006.
54. Kerekes K, Tronstad L: Long-term results of endodontic treatment performed with a standardized technique, J Endod 5:83, 1979.
55. Khemaleelakul S, Baumgartner JC, Pruksakorn S: Identification of bacteria in acute endodontic infections and their antimicrobial susceptibility, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94:746, 2002.
56. Kim E, Lee SJ: Electronic apex locator [Review], Dent Clin North Am 48:35, 2004.
57. Kuriyama T, Karasawa T, Nakagawa K, et al: Bacteriologic features and antimicrobial susceptibility in isolates from orofacial odontogenic infections, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90:600, 2000.
58. Kuriyama T, Karasawa T, Nakagawa K, et al: Incidence of beta-lactamase production and antimicrobial susceptibility of anaerobic gram-negative rods isolated from pus specimens of orofacial odontogenic infections, Oral Microbiol Immunol 16:10, 2001.
59. Kuriyama T, Williams DW, Yanagisawa M, et al: Antimicrobial susceptibility of 800 anaerobic isolates from patients with dentoalveolar infection to 13 oral antibiotics, Oral Microbiol Immunol 22:285, 2007.
60. Kvist T, Molander A, Dahlen G, Reit C: Microbiological evaluation of one- and two-visit endodontic treatment of teeth with apical periodontitis: a randomized, clinical trial, J Endod 30:572, 2004.
61. Lakhassassi N, Elhajoui N, Lodter JP, et al: Antimicrobial susceptibility variation of 50 anaerobic periopathogens in aggressive periodontitis: an interindividual variability study, Oral Microbiol Immunol 20:244, 2005.
62. Larson AM, Polson J, Fontana RJ, et al: Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study, Hepatology 42:1364, 2005.
63. Lee M, Winkler J, Hartwell G, et al: Current trends in endodontic practice: emergency treatments and technological armamentarium, J Endod 35:35, 2009.
64. Levitt GW: The surgical treatment of deep neck infections, Laryngoscope 81:403, 1970.
65. Lipton JA, Ship JA, Larach-Robinson D: Estimated prevalence and distribution of reported orofacial pain in the United States, J Am Dent Assoc 124:115, 1993.
66. Madigan MT, Martinko JM, Parker J: Brock biology of microorganisms, ed 9, Upper Saddle River, NJ, 2000, Prentice-Hall.
67. Matusow RJ, Goodall LB: Anaerobic isolates in primary pulpal–alveolar cellulitis cases: endodontic resolutions and drug therapy considerations, J Endod 9:535, 1983.
68. Mitchell DF, Tarplee RE: Painful pulpitis: a clinical and microscopic study, Oral Surg 13:1360, 1960.
69. Moos HL, Bramwell JD, Roahen JO: A comparison of pulpectomy alone versus pulpectomy with trephination for the relief of pain, J Endod 22:422, 1996.
70. Morse DR, Koren LZ, Esposito JV, et al: Asymptomatic teeth with necrotic pulps and associated periapical radiolucencies: relationship of flare-ups to endodontic instrumentation, antibiotic usage and stress in three separate practices at three different time periods, Int J Psychosom 33:5, 1986.
71. Morse DR, Furst ML, Belott RM, et al: Infectious flare-ups and serious sequelae following endodontic treatment: a prospective randomized trial on efficacy of antibiotic prophylaxis in cases of asymptomatic pulpal–periapical lesion, Oral Surg 64:96, 1987.
72. Nagle D, Reader A, Beck M, Weaver J: Effect of systemic penicillin on pain in untreated irreversible pulpitis, Oral Surg Oral Med Oral Pathol 90:636, 2000.
73. Natkin E: Treatment of endodontic emergencies, Dent Clin North Am 18:243, 1974.
74. Nusstein J, Reader A, Nist R, et al: Anesthetic efficacy of the supplemental intraosseous injection, J Endod 24:487, 1998.
75. Nyerere JW, Matee MI, Simon EN: Emergency pulpotomy in relieving acute dental pain among Tanzanian patients, BMC Oral Health 6:1, 2006.
76. Oginni AO, Udoye CI: Endodontic flare-ups: comparison of incidence between single and multiple visit procedures in patients attending a Nigerian teaching hospital, BMC Oral Health 4:4, 2004.
77. Ogundiya DA, Keith DA, Mirowski J: Cavernous sinus thrombosis and blindness as complications of an odontogenic infection, Oral Maxillofac Surg 47:1317, 1989.
78. Oliet S: Single-visit endodontics: a clinical study, J Endod 24:614, 1998.
79. Pallasch TJ: Antibiotics in endodontics, Dent Clin North Am 23:737, 1979.
80. Pallasch TJ: Pharmacokinetic principles of antimicrobial therapy, Periodontol 2000 10:5, 1996.
81. Pallasch TJ, Slots J: Antibiotic prophylaxis and the medically compromised patient, Periodontol 2000 10:107, 1996.
82. Patel R: Clinical impact of vancomycin-resistant enterococci, J Antimicrob Chemother 51(suppl 3):iii13, 2003.
83. Pekruhn RB: The incidence of failure following single-visit endodontic therapy, J Endod 12:68, 1986.
84. Penesis VA, Fitzgerald PI, Fayad MI, et al: Outcome of one-visit and two-visit endodontic treatment of necrotic teeth with apical periodontitis: a randomized controlled trial with one-year evaluation, J Endod 34:251, 2008.
85. Peters LB, Wesselink PR: Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms, Int Endod J 35:660, 2002.
86. Pickenpaugh L, Reader A, Beck M, et al: Effect of prophylactic amoxicillin on endodontic flare-up in asymptomatic, necrotic teeth, J Endod 27:53, 2001.
87. Reddy SA, Hicks ML: Apical extrusion of debris using two hand and two rotary instrumentation techniques, J Endod 24:180, 1998.
88. Roane JB, Dryden JA, Grimes EW: Incidence of postoperative pain after single- and multiple-visit endodontic procedures, Oral Surg Oral Med Oral Pathol 55:68, 1983.
89. Rosenberg PA, Babick PJ, Schertzer L, Leung A: The effect of occlusal reduction on pain after endodontic instrumentation, J Endod 24:492, 1998.
90. Rudner WL, Oliet S: Single-visit endodontics: a concept and a clinical study, Compend Contin Educ Dent 2:63, 1981.
91. Rugh JD: Psychological components of pain, Dent Clin North Am 31:579, 1987.
92. Sandor GK, Low DE, Judd PL, Davidson RJ: Antimicrobial treatment options in the management of odontogenic infections, J Can Dent Assoc 64:508, 1998. Comment in J Can Dent Assoc 65:602, 1999.
93. Schilling A, Corey R, Leonard M, Eghtesad B: Acetaminophen: old drug, new warnings, Cleve Clin J Med 77:19, 2010, doi: 10.3949/ccjm.77a.09084.
94. Seltzer S, Naidorf IJ: Flare-ups in endodontics. 1. Etiological factors, J Endod 11:472, 1985.
95. Simon JH, Chimenti RA, Mintz GA: Clinical significance of the pulse granuloma, J Endod 8:116, 1982.
96. Siqueira JF, Rocas IN: Microbial causes of endodontic flareups, Int Endod J 36:433, 2003.
97. Sjogren U, Figdor D, Persson S, Sundqvist G: Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis, Int Endod J 30:297, 1997.
98. Southard DW, Rooney TP: Effective one-visit therapy for the acute periapical abscess, J Endod 10:580, 1984.
99. Sutherland S, Matthews DC. Emergency management of acute apical periodontitis in the permanent dentition: a systematic review of the literature, J Can Dent Assoc 69:160, 2003.
100. Tendolkar PM, Baghdayan AS, Shankar N: Pathogenic enterococci: new developments in the 21st century, Cell Mol Life Sci 60:2622, 2003.
101. Torabinejad M, Dorn SO, Eleazer PD, et al: The effectiveness of various medications on postoperative pain following root canal obturation, J Endod 20:427, 1994.
102. Torabinejad M, Kettering JD, McGraw JC, et al: Factors associated with endodontic interappointment emergencies of teeth with necrotic pulps, J Endod 14:261, 1988.
103. Torabinejad M, Walton R: Endodontics: principles and practice, ed 4, St. Louis, 2009, Saunders.
104. Trope ME, Delano EO, Orstavik D: Endodontic treatment of teeth with apical periodontitis: single vs. multivisit treatment, J Endod 25:345, 1999.
105. Tsesis I, Faivishevsky V, Fuss Z, Zukerman O: Flare-ups after endodontic treatment: a meta-analysis of literature, J Endod 34:1177, 2008.
106. Turkun M, Cengiz T: The effects of sodium hypochlorite and calcium hydroxide in tissue dissolution and root canal cleanliness, Int Endod J 30:335, 1997.
107. van Winkelhoff AJ, Herrera D, Oteo A, Sanz M: Antimicrobial profiles of periodontal pathogens isolated from periodontitis patients in The Netherlands and Spain, J Clin Periodontol 32:893, 2005.
108. van Winkelhoff AJ, Winkel EG, Barendregt D, et al: beta-Lactamase producing bacteria in adult periodontitis, J Clin Periodontol 24:538, 1997.
109. Walton R, Fouad A: Endodontic interappointment flare-ups: a prospective study of incidence and related factors, J Endod 18:172, 1992.
110. Walton RE, Chiappinelli J: Prophylactic penicillin: effect on posttreatment symptoms following root canal treatment of asymptomatic periapical pathosis, J Endod 19:466, 1993.
111. Weiger R, Axmann-Krcmar D, Löst C: Prognosis of conventional root canal treatment reconsidered, Endod Dent Traumatol 14:1, 1998.
112. Weiger R, Rosendahl R, Lost C: Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions, Int Endod J 33:219, 2000.
113. Weine FS, Healey HJ, Theiss EP: Endodontic emergency dilemma: leave tooth open or keep it closed? Oral Surg Oral Med Oral Pathol 40:531, 1975.
114. Whitney CG, Farley MM, Hadler J, et al: Increasing prevalence of multidrug-resistant Streptococcus pneumoniae in the United States, N Engl J Med 343:1917, 2000.
115. Yun MW, Hwang CF, Lui CC: Cavernous sinus thrombus following odontogenic and cervicofacial infection, Eur Arch Otorhinolaryngol 248:422, 1991.

722
Sodium Hypochlorite (NaOCl)Instrument Separation
Causes of Instrument SeparationManagement of Separated InstrumentsConditions for Separated Instrument Removal AttemptsSeparated Instrument Removal TechniquePrognosis
Ledge FormationCauses of Ledge FormationManagement of Ledge FormationBypassing a LedgePotential Complications of Removal or Bypassing a LedgePrevention of Ledge FormationPrognosis
Perforations (Nonsurgical)
Radicular Extrusion of Root Canal Filling MaterialsCauses of Extrusion of Obturation Materials Beyond
the Radicular ForamenManagement of Obturation Materials Extruded Beyond
the Radicular ForamenManagement of Tissue Damage Caused by Extrusion of Root
Canal Filling MaterialsSinus PerforationInferior Alveolar Nerve (IAN) Injury
Nonsurgical Causes of IAN InjurySurgical Causes of IAN InjuryPrognosisPrevention of Complications Due to Nerve Injury
Cervicofacial Subcutaneous Emphysema
Managing Iatrogenic Endodontic EventsYOSHITSUGU TERAUCHI
CHAPTER 19
CHAPTER OUTLINE
An iatrogenic event is defined as a procedure “induced inad-vertently by a physician or surgeon” (Merriam-Webster dic-tionary). This is true for dentistry as well, with cases of endodontic malpractice being among the most prevalent in dentistry.57,111,252 These occurrences are not limited to the United States, with other countries reporting similar percent-ages of endodontic malpractice claims.225
Although iatrogenic accidents cannot be prevented with absolute certainty, their occurrences can be greatly reduced with the aid of the “Three Ts”: training, technique, and tech-nology. Incumbent with the first (training) is expertise with the other two factors, especially regarding technology and, more specifically, the dental operating microscope. It has proved itself indispensable in locating canals,155,157,250,277 remov-ing separated instruments,279 repairing perforations,234 and enhancing the delivery of quality care.150 The superior visual-ization permits more accurate clinical evaluations, allowing for a precise assessment of the challenge and the appropriate treat-ment plan for its resolution. This instrument is indispensable for all of the treatment scenarios that follow, which are there-fore assumed to be performed with the aid of magnification.
SODIUM HYPOCHLORITE (NaOCl)Often happening without warning, the progression of events following sodium hypochlorite extrusion into periradicular
tissues is both rapid and startling to witness. In addition to the physical outcomes, the experience is likely to leave the patient wary of both the procedure and practitioner.
Although the properties and methods of delivering sodium hypochlorite are covered in Chapter 6, the gravity of the con-sequences of its misuse merits a brief highlight. Sodium hypo-chlorite is an effective irrigating solution in concentrations ranging from 0.5% to 6%127,317 and is able to disrupt the biofilm,45 dissolve necrotic tissues,184 and remove organic com-ponents of the smear layer.17 However, it is extremely cyto-toxic, irrespective of the tissue it contacts,202 with concentrations as low as 0.01% lethal to fibroblasts in vitro.116 NaOCl injection into vital tissue initiates hemolysis and ulceration, damages endothelial and fibroblast cells, and inhibits neutrophil migra-tion.89,91 A study investigating the physical effects of NaOCl on bone ex vivo found degradation of the organic matrix collagen and no sign of living cellular contents (Fig. 19-1).140
The majority of reported NaOCl complications appear to be due to an inaccurate working length, iatrogenic widening of the radicular foramen, lateral perforation of the root, or wedging of the irrigation needle.147,271 The pattern of facial distention is comparable to that encountered with a cervicofa-cial emphysema (discussed later), dissecting fascial spaces in a similar fashion, with the concomitant tissue destruction mag-nifsying the effect and impeding recovery. This swelling is further exacerbated by the presence of effervescing agents such

CHAPTER 19 Managing Iatrogenic Endodontic Events 723
In addition to sensory deprivation, motor nerve dysfunction secondary to irreversible chemical damage has been reported (Fig. 19-3).206 In this case, there was distinct loss of upper lip and cheek function, with problems in the musculature. In mandibular teeth, extension into the submandibular, submen-tal or sublingual regions can compromise the airway, compel-ling immediate hospitalization and surgical intervention to avert a life-threatening episode.30
Upon realizing that an extrusion event has occurred, it is imperative that the clinician cease further treatment and imme-diately engage in measures targeted at diminishing the effect of the chemical; ignoring the event reduces outcomes.162,223 Treatment protocols are empirical and are predicated on cause and severity. With the emphasis on pain control, local
as hydrogen peroxide, potentiating the effect of the hypochlo-rite and amplifying soft tissue involvement.20,161 The initial patient reaction to the fluid insult is severe and immediate pain, with marked edema or bruising that may continue to extend over the injured side of the face, cheek, or lips (Fig. 19-2). There may be spontaneous and profuse hemorrhaging from the canal space, and, in the case of maxillary posterior teeth, the patient may report periorbital pain,21,89 chlorine taste, or irritation of the throat.63 The amount that has been expressed into the periradicular area, the spatial location of the fluid introduction, and the proximity to sensitive anatomic structures will dictate the severity and duration of the reaction. Paresthesia, either transient21 or permanent,223 can occur, espe-cially if interventional treatment is not rendered immediately.
FIG. 19-1 Femur shaft cross sections (A) untreated bone section; (B) saline-treated bone; (C) NaOCl-treated bone section. Grossly, NaOCl caused significant changes in cancellous structure, leaving large structural craters of apparent demineralization. (From Kerbl FM, DeVilliers P, Litaker M, Eleazer PD: Physical effects of sodium hypochlorite on bone: an ex vivo study, J Endod 38:357, 2012.)
A B C
FIG. 19-2 A, Clinical presentation 3 days following the extrusion of NaOCl during treatment of the maxillary right canine. The patient had difficulty opening her right eye, and the swelling had extended to the submandibular/sublingual regions on the affected side; she also experienced limited mouth opening. There was altered sensation infraorbitally and in the region of the upper right lip, but no reported paresthesia of the alveolar or facial nerves. B, One month post extrusion, the ecchymosis had resolved, with a return of sensation and full function. Therapy was completed without incident. (From de Sermeño RF, da Silva LA, Herrera H: Tissue damage after sodium hypochlorite extrusion during root canal treatment, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108:e46, 2009.)
A B

724 PART II The Advanced Science of Endodontics
usually complete and uneventful, will ease their anxiety. They should be informed as to why it occurred and what to expect during their recovery. Recovery should be monitored and doc-umented daily until the resolution is imminent.
Prevention involves attention to detail and an appreciation for fluid dynamics. In summary, the clinician should do the following:◆ Establish an accurate working length and avoid overinstru-
mentation/enlargement of the radicular foramen.◆ If irrigating using positive pressure, employ a small side-
vented needle placed no closer than 2 mm from the working length. Express the fluid slowly and observe that it is venting through the access cavity.29
◆ Carefully assess the canal integrity for signs of perforation or other large portals of fluid egress.
◆ Avoid wedging the needle tip in the canal space or inserting it beyond the working length.
◆ Confirm the identity of the solution prior to injection or irrigation.104
INSTRUMENT SEPARATIONThe introduction of NiTi rotary instruments into endodontics revolutionized the way the root canal system is instrumented. However, with the advent of rotary NiTi files, there has also been a perceived increase in the occurrence of separated
anesthetics and analgesics can be administered, along with cold compresses, in an effort to moderate swelling and edema. Directed at diluting the effect of the extrusion, it has been sug-gested that the clinician immediately irrigate the canal with normal saline to encourage bleeding, both diluting the irritant and removing it from the site of the injury.63,179 In addition, clinicians may immediately irrigate the canal and periradicular areas of the extrusion with saline, using a negative pressure irrigation device with the cannula placed at the radicular foramen. In one report, the subsequent reaction was short lived with this approach.235
After one day, warm compresses are substituted for the cold, and warm oral rinses are prescribed to stimulate the local microcirculation. Antibiotics are usually prescribed, and their administration commensurate with the severity of hard and soft tissue destruction and necrosis; milder cases can be treated with oral medications, whereas severe presentations are better controlled and modulated in a hospital setting with intrave-nous routes of delivery. The use of corticosteroids is equivocal; the control of the spreading edema must be balanced with the increased risk of infection. The patient should be monitored closely; a marked increase in the size or extent of the swelling or signs of impending airway obstruction mandate immediate referral to the hospital or a maxillofacial surgeon for more aggressive treatment and management. Lastly, reassuring patients that recovery, in spite of their current appearance, is
FIG. 19-3 A, Radiograph of the maxillary left lateral incisor (#10, #22) before post removal. Radicular root resection had been completed, and the canal space is empty. Prior to re-cementation, the canal was irrigated with 3% NaOCl, precipitating the extrusion event. B, Twenty-four hours post extrusion, there was altered sensation infraorbitally and from the upper left lip to the left lip corner. In addition, the buccal branch of the facial nerve was affected, as evidenced by a distinct loss of upper lip and cheek function (the corner of the mouth could not be pulled up by the mimic musculature). The mouth opening was limited to 20 mm (C), 3 years post incident. The weakness of the mimic musculature of the left face side is clearly visible. Attempts to laugh resulted in a hanging left lip corner secondary to the weakness of the motor innervation by the facial nerve. In the gray-marked area there is a permanent hypoesthesia. (From Pelka M, Petschelt A: Permanent mimic musculature and nerve damage caused by sodium hypochlorite: a case report, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:e80, 2008.)
A B C

CHAPTER 19 Managing Iatrogenic Endodontic Events 725
visualized under the dental operating microscope (DOM) or become apparent on radiographs for the first time (Fig. 19-4).
Causes of Instrument SeparationA common cause for instrument separation is improper use.84,245 Typical examples of improper use include inadequate access, overuse of the instrument, too much radicular pressure during instrumentation,247,291 and the continuous use of a large
instruments,84,242 with some reports indicating that separation of NiTi rotary instruments occurs more frequently than hand instruments.294 On radiographic examination, separated instru-ments can usually be discerned by the distinct radiopacity within the canal. However, if the canal with a separated instru-ment is subsequently obturated with radiopaque materials, it may not be visualized in the radiograph. Upon removal of filling materials from the canal, a separated instrument may be
A
B1 B2
B3 B4
C
D
E
F
FIG. 19-4 A, Radiograph of the mandibular left first molar with a long indistinct separated instrument obviously longer than 4.5 mm in the mesial root that is extruded beyond the radicular foramen. B1, Sagittal view of CBCT showing the radicular end of the separated instrument is extended into the IAN and it measures 14 mm on it. B2, Sagittal view of CBCT showing root perforation in the distal canal (yellow arrow). B3, Axial view of CBCT showing the perforation in the distal canal (yellow arrow). B4, Coronal view of CBCT showing the radicular end of the separated instrument is in the IAN. C, Separated instrument in the mesiobuccal canal upon removal of root filling materials (red arrow) D, Radiograph showing removal of the root fillings in the mesiobuccal canal revealed the overall length of the separated instrument (red arrow). E, Retrieved separated instruments measuring 14 mm on the ruler. F, Radiograph showing completion of separated instrument removal. Continued

726 PART II The Advanced Science of Endodontics
instrument in a curved canal.107,219 Additional contributing factors are operator experience,200,285 rotational speed,53,169 canal curvature (radius),170,219 instrument design and tech-nique,33,152 torque setting,83 manufacturing process,5 the type of NiTi alloys used,88 the type of rotational motion (con-tinuous rotations versus reciprocating motions),205 the type of tooth,51,191,258 and absence of a glide path.204 Based on these factors, it is not surprising that the reported incidence of sepa-rated NiTi files ranges from 0.4% to 23%.5,7,210,221,248,272
Separated instruments seem to occur more frequently in molars than anterior teeth, especially in mandibular molars. This high incidence of instrument fracture in molars may be related to accessibility to the canal, diameter of the root canal, and root canal curvature.51,191,258 Endodontists have reported the incidence of instrument separation to be about 5%.5,200 The clinician must inform the patient of the instrument separation and treatment options as well as potential complications of both the separated instrument retention and its attempted removal.
Endodontic instruments fracture as a result of cyclic fatigue or torsional fatigue47 or a combination of both types of fatigue.245,257,296 Cyclic fatigue is caused by repetitive compres-sive and tensile stresses acting on the outer portion of a file rotating in a curved canal, leading to cyclic failure without previous signs of plastic deformation.200 Torsional failure occurs when the tip of the instrument binds but the shank of the file (driven by the handpiece) continues to rotate.245 Shear fracture of the material then occurs when the maximum strength of the material is exceeded.154 Clinically, cyclic fatigue seems to be more prevalent in curved root canals, whereas torsional failure might happen even in a straight canal.43,316 Cyclic-fatigued instruments are reported to become less resis-tant to torsional fatigue failure,145 whereas the use of rotary instruments at a high torque setting is reported to increase the risk of cyclic fatigue failure.84 Interestingly, the use of recipro-cal motions (as opposed to rotational motions) is reported to
extend the life span of an instrument56,315 and increase cyclic fatigue resistance.205 It is recommended that instruments designed for reciprocating motion be used for shaping a severely curved canal and that the instruments used to prepare such curved root canals be discarded after use to prevent instrument fracture.
Management of Separated InstrumentsManagement of separated instruments includes nonsurgical orthograde (mechanical or chemical) or surgical approaches. The mechanical removal involves the use of tools dedicated to separated instrument removal such as extractors, wire loops, post removal systems, ultrasonics, and laser irradiation (see also Chapter 8). The chemical removal involves the use of chemical solvents for instrument corrosion and electrochemi-cal process for instrument dissolution. Surgical approaches include radicular surgery, intentional replantation, root ampu-tation, or hemisection.
For a nonsurgical approach in removing a separated file, various methods and devices have been developed (see also Chapter 8). When a separated instrument extends above the root canal orifice, it can often be easily removed with a hemo-stat, Steiglitz forceps, a modified Castroviejo needle holder,78 or a Perry plier.304 A spoon excavator or a Caulfield retriever can also be used to engage and remove the separated instrument with coronally directed pressure. In the event that a hand file can bypass the separated instrument, a “braiding technique” can be used whereby several Hedstrom files are inserted along the bypassed instrument, the files are twisted to grasp the sepa-rated instrument, and it is then extracted as one unit. When a fractured instrument is below the canal orifice and cannot be bypassed, one basic method for removing the separated instru-ment requires the exposure of approximately 2 mm of the coronal portion of the separated file. This allows the use of an extracting device for engaging the file, securing it, and remov-ing it. The Masserann kit (Micro-Mega, Besancon, France) is a
I J K
G, Perforation site in the distal canal (yellow arrow). H, Perforation repaired with MTA (yellow arrow). I, Postoperative radiograph showing root canal fillings in all the canals and perforation repair (yellow arrow). J, One-month postoperative radiograph revealing the periradicular lesions still present. K, Three-month postoperative radiograph showing periradicular healing.
FIG. 19-4, cont’d
G H

CHAPTER 19 Managing Iatrogenic Endodontic Events 727
fragments of a separated file can often be pushed back into a more radicular and narrow level of the canal, which would eventually increase the risk of perforation and extra dentin sacrifice upon attempted fragment removal.
The success rate for removing separated files varies from 33% to 95%7,51,221,240,301 with the time required for using ultra-sonic techniques varying between 3 to over 60 minutes.9,185,285 The variations in success rates are due to the location of frac-tured instruments, the diameter of the root canal,258 the degree of canal curvature,9,220,268 the radius of curvature,9,219 operator experience,9,285 operator fatigue, and the length of the sepa-rated instrument.284 Visualization and accessibility to the sepa-rated instrument play a major role in file retrieval.51 In general, the success rate for removal is high for separated files located before the canal curvature, moderate for those located at the curvature, and low for those located beyond the curvature.170,305 The success rate is also more favorable when the canal curva-ture is less and the radius of curvature is longer.9 The com-bination of ultrasonic techniques and microscopes typically improves success rates in file removal.51,82,191,301
It has been recommended that removal attempts of sepa-rated instruments from root canals should not exceed 45 to 60 minutes because the success rates may drop with increased treatment time.279 The reduced success rate could be related to operator fatigue or overenlargement of the canal, which com-promises the integrity of the tooth and increases the risk of perforation. Any case where the separated instrument can be visualized under the DOM may be considered less challenging to manage. If the separated instrument is considered irretriev-able after a sufficient attempt, the case should be completed by having the separated file incorporated as part of the obtura-tion and kept under observation.74,79,221,269
Conditions for Separated Instrument Removal AttemptsFile removal can be attempted in either a dry or a wet environ-ment. Dry conditions provide better visibility when using the dental operating microscope, preventing fewer additional procedural accidents.242,268,279,300 However, heat generation by ultrasonics is inevitable,96,113,156,173,258,268,279,300 and a temperature rise above 10° C on the external root surface can damage the periodontal tissues.66,280 In addition, the separated instrument will be susceptible to secondary heat when ultrasonic tips are in contact with the file.286,300 Therefore, it is recommended that water or some other irrigant be used while the ultrasonic tip is activated at the lowest possible power setting.37,70,175,300 In addition, the irrigating solution used in the canal should be EDTA solution; the use of an ultrasonic tip as an adjunct with EDTA solution enhances the canal wall cleanliness.256
Separated Instrument Removal TechniqueThe majority of separated instruments are NiTi,272 with the mean length of separated instruments being 2.5 to 3.5 mm.135 Many NiTi rotary instruments used have a .04 to .08 taper range with a tip size of #20 to #30, resulting in a coronal diameter of about 0.30 mm to 0.58 mm. If the coronal diam-eter of the separated instrument is smaller than 0.45 mm, then a #3 modified Gates Gliden bur (#3 MGG bur from the FRK, DentalCadre, Seattle, WA) should be used to enlarge the canal to the separated instrument, followed by the micro-trephine bur (DentalCadre) for exposing the coronal portion of the
popular system for the removal of separated instruments located within the straight part of the canal. This kit involves the use of trephine burs to expose the coronal portion of the separated instrument and for creating a space for an extractor. An extractor is then used to grasp and remove the separated instrument. The limitation of this system is that it cannot be used for cases involving separated instruments located beyond the midroot or in a curved canal, as this technique involves a considerable amount of dentin sacrifice that can weaken the root structure and increase the risk of perforation.313 An alterna-tive to the Masserann kit is the Endo Safety System.306 This system differs from the Masserann kit in that it uses smaller diameter trephine burs and the extractor has its own unique mechanism for grasping instruments. The Endo Extractor (Brasseler Inc., Savannah, GA) can also be used in these types of cases. This system consists of a trephine bur to expose the coronal portion of the separated instrument and a hollow tube extractor that is threaded over the exposed portion of the sepa-rated instrument and bonded to it with cyanoacrylate adhe-sive.92 The Canal Finder System (FaSociété Endo Technique, Marseilles, France) or the EndoPuls System (EndoTechnic, San Diego, CA) provides a different approach to a separated instru-ment. The system is composed of a handpiece and files that are designed exclusively for the system.164 The system produces a vertical movement with a maximum amplitude of 1 to 2 mm, which decreases when the speed increases.126 This vertical movement of the file will also help bypass an instrument frag-ment. The flutes of the file can mechanically engage with the separated instrument, and with the vertical vibration, the instrument fragment can be loosened or even retrieved.125 The mechanical movement of the file can get aggressive, so the clini-cian must use caution to avoid root perforation, especially in a curved canal. These systems are technique sensitive and there-fore results can vary between cases.
Ultrasonic instruments are very effective for the removal of separated instruments.42,185,241 However, it is important to realize that separated NiTi files tend to fracture repeatedly when ultrasonics are applied to them for broken file removal, whereas stainless steel instruments are more resistant and more easily removed with ultrasonics than NiTi instruments.241,279,301 Small ultrasonic instruments allow continuous and improved vision of the field of operation. The use of ultrasonics, espe-cially when performed under the microscope, enhances the removal process and can provide relatively safe removal of separated instruments.191,279,300 The ultrasonic tip is placed on the staging platform between the exposed portion of the sepa-rated file and the canal wall, and it is vibrated around it in a counterclockwise direction, applying an unscrewing force to the separated file. This technique will help with removing most rotary instruments that have a clockwise cutting action. If it is known that the separated file has a counterclockwise cutting action, then a clockwise rotation will be needed. The energy applied will aid in loosening the file, and occasionally the file will suddenly exit out of the canal.
However, the use of ultrasonics does have some drawbacks. Upon ultrasonic activation, a separated file can be accidentally extruded into the bone, either radicularly or through a perfora-tion. In addition, the ultrasonic activation of a separated instrument has been reported to separate small fragments from the original fragment,41 further complicating the management of the case. Smaller fragments of a file are considered more difficult to remove than longer fragments.170,219,241 These smaller

728 PART II The Advanced Science of Endodontics
separated file. Therefore, the dentin wall contacting the coronal third of the separated file has to be eliminated to free it and facilitate its removal (Fig. 19-6). It is recommended that the ultrasonic tip be used in a counter clockwise direction to trough around the coronal aspect of a separated instrument.240 However, a fatigued separated instrument is already extremely susceptible to secondary fracture by ultrasonic activation.286,300
separated instrument, with less risk than ultrasonics for sec-ondary fracture of the separated instrument.285,286 The inner diameter of the micro-trephine bur is 0.45 mm and it is then used, in a counter clockwise rotation, with the intent of unscrewing the separated instrument. This bur should be used at 600 rpm in wet conditions; if the rotational speed exceeds 600 rpm, unintentional ledge formation may occur, especially in a curved canal.
If the coronal diameter of the separated instrument is larger than 0.45 mm or the canal curvature is greater than 15 degrees, a larger NiTi rotary instrument, with tip size 0.1 mm (two sizes) larger than the coronal diameter of the separated instru-ment, should be used to enlarge the canal coronal to the sepa-rated instrument, followed by ultrasonic instruments to expose the coronal portion.
Firstly, the spoon tip with the concave portion facing the separated instrument (DentalCadre) will be introduced into the thin gap between the separated instrument and the inside curve of the canal to create one quarter space of the circle around the separated instrument. Secondly, the straight tip (DentalCadre) is introduced to expand the space to complete the semicircular space on the inside curve. The ultrasonic tip should always be applied to the area on the inner canal curve being extended in the radicular direction (Fig. 19-5). If the ultrasonic tip is placed in the space outside the curve and ultrasonic energy is given to the separated instrument from the outside of the curve, the force applied will redirect the separated instrument in an apical direction, eventually pushing it more apically and making the instrument retrieval more difficult, whereas the force applied from the inside of the curve to the separated instrument will consequently reorient the separated instrument in a coronal direction. In most cases, the coronal one third of the separated file is the main portion engaged in the canal wall. This portion is typically resistant to mechanical force for disengagement due to the highly stressed concentration on the coronal one third of the
FIG. 19-5 A, Separated file around the curve after the canal enlargement with a NiTi rotary file. B, Space needs to be created on the inside curve with the spoon ultrasonic tip, followed by the straight tip. C, Thin space created on the inner curve. D, Ultrasonic forces applied to the separated instrument from the outside curvature will reorient it in a radicular direction. E, Ultrasonic forces applied to the separated instrument from the inside curvature will reorient it in a coronal direction rather than a radicular direction.
A B C D E
FIG. 19-6 The coronal one third of the file length is typically the part to be stuck in the canal wall, whereas the radicular portion of the file is typically not in contact with the canal wall. Stress is concentrated mostly on the coronal one third of the file length.

CHAPTER 19 Managing Iatrogenic Endodontic Events 729
For this reason it is safer to cut only a semicircular trough on one side of the separated instrument behind which there is dentin wall support,286 and a pulsing motion should be applied to it while ultrasonics is activated to prevent instrument frac-ture and temperature rise, especially in dry conditions.66,280,286,300 Just a thin space created on one side of the coronal third of the separated instrument is enough to free the separated instrument from being engaged in the canal wall. Especially in a curved canal, ultrasonic activation should always apply to the thin space created between the separated fragment and the inside curve, and the dentin wall supporting the separated file fragment must always be present behind the ultrasonic activation site to prevent secondary fracture. The radicular extent to be created along the separated instrument should be approximately as long as one third of the fragment length. For example, if the separated file fragment is 3 mm long, the semi-circular space needs to be extended radicularly about 1 mm on the inside curve to help the ultrasonic tip loosen it. This process of extending the space in an apical direction must continue until it is confirmed that the separated file is seen dancing with ultrasonics under the DOM. The root canal preparation for instrument retrieval is done when the move-ment of the separated instrument is confirmed. The ultrasonic tip used for this purpose should be as thin as possible, allow-ing the clinician to both visualize the operative field and prevent overenlargement of the canal wall. During this ultra-sonic preparation phase, the separated file may come out by ultrasonic activation at any moment (Fig. 19-7).
When the separated instrument is not visible upon the straight line access to it, instrument retrieval is considered challenging and it requires expertise and a little bit of guess-work to remove it. First, the microexplorer (DentalCadre) is precurved to meet the separated instrument, and then radio-graphs are taken with the microexplorer in the canal to confirm that it is in the space between the separated instrument and the inside curve. Next, the straight tip is precurved the same
FIG. 19-7 A, Separated file may accidentally come out with ultrasonic activation during a preparation phase. B, EDTA solution is put into the canal to take advantage of cavitation and acoustic streaming effects for instrument retrieval. C, Ultrasonics must be activated within the space created. D, Separated file is removed from the canal with ultrasonics in the presence of EDTA solution.
A B C D
way as the microexplorer was precurved to get into the inner thin space, and the ultrasonic tip is activated to extend the space apically until the separated instrument gets loosened (Fig. 19-8).
Once the root canal preparation for instrument retrieval is completed, it is important to confirm that the canal wall is smooth from the separated file to the coronal extent, with no protrusions on the outside canal wall. Following the ultrasonic loosening of the coronal portion of the separated instrument, the canal is filled with EDTA solution to enhance the ultrasonic effect (see Fig. 19-7, B). A retrospective study and the author’s empirical findings show that when the separated instrument is shorter than 4.5 mm, the clinician will most likely be able to retrieve it with ultrasonics alone (Fig. 19-9).284 Ultrasonic activation should be applied in push-pull motions in the space created between the separated file and the inside curva-ture of the canal until the separated file is removed (see Fig. 19-7, C and D).
If the separated instrument is longer than 4.5 mm, or if it is seen moving with ultrasonic activation, but the instrument retrieval with ultrasonics was not successful, then the loop device (DentalCadre, Seattle, WA) should be applied to it to capture the coronal portion of the separated file and pull the file fragment out of the canal.284 The probability is that an instrument fragment longer than 4.5 mm is touching all over the canal walls, which creates more friction as it is reoriented in a coronal direction and makes it more resistant to instru-ment retrieval with ultrasonics alone, requiring more mechani-cal force to pull it out of the canal. The coronal portion of the separated instrument needs to be peripherally exposed by at least 0.7 mm (see Fig. 19-10, A), and a semicircular space needs to be created and extended apically on the inside curva-ture of the canal the same way as in the root canal preparation for ultrasonic instrument retrieval until the separated instru-ment is seen dancing with ultrasonics. The loop size must be adjusted to fit the coronal diameter of the separated file using

730 PART II The Advanced Science of Endodontics
FIG. 19-8 A, Preoperative radiograph showing deep caries lesions underneath the crown with meager looking pulp-capping materials on the pulp chamber. The tooth was diagnosed with irreversible pulpitis. B, NiTi rotary instrument (ProTaper NEXT X1) was separated in the mesial canal during root canal instrumentation. C, Interop-erative radiograph showing an instrument fractured beyond the severe curve (red arrow). D, Separated instrument measured 1.94 mm on the axial view of CBCT. E, Interoperative radiograph showing the location of the curved microexplorer in relation to the separated instrument in the mesial canal. F, Interoperative radiograph showing the separated instrument was removed with the curved straight ultrasonic tip activated inside the curve. G, Retrieved separated instrument measured actually 2 mm on a ruler in contrast with the coronal portion of the fractured instrument. H, Postoperative radiograph showing the final root fillings, which reveals dentin sacrifice for removal of the separated instrument was minimum.
A B C
D E F
G H
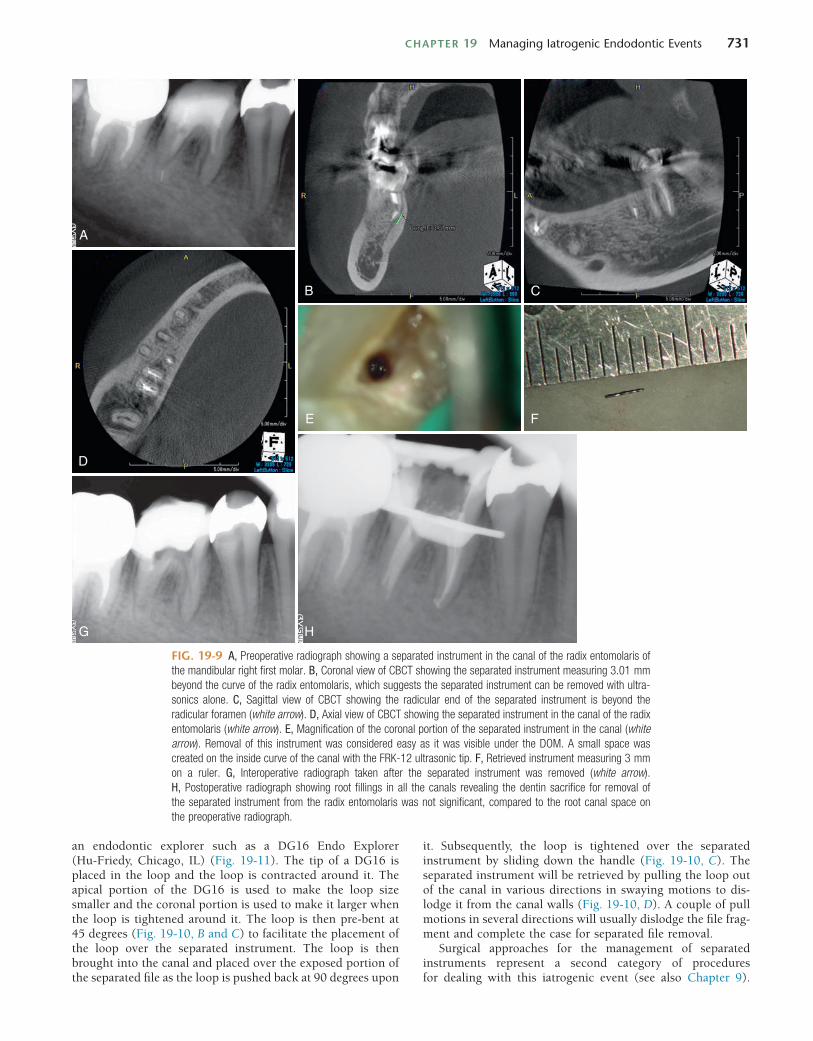
CHAPTER 19 Managing Iatrogenic Endodontic Events 731
FIG. 19-9 A, Preoperative radiograph showing a separated instrument in the canal of the radix entomolaris of the mandibular right first molar. B, Coronal view of CBCT showing the separated instrument measuring 3.01 mm beyond the curve of the radix entomolaris, which suggests the separated instrument can be removed with ultra-sonics alone. C, Sagittal view of CBCT showing the radicular end of the separated instrument is beyond the radicular foramen (white arrow). D, Axial view of CBCT showing the separated instrument in the canal of the radix entomolaris (white arrow). E, Magnification of the coronal portion of the separated instrument in the canal (white arrow). Removal of this instrument was considered easy as it was visible under the DOM. A small space was created on the inside curve of the canal with the FRK-12 ultrasonic tip. F, Retrieved instrument measuring 3 mm on a ruler. G, Interoperative radiograph taken after the separated instrument was removed (white arrow). H, Postoperative radiograph showing root fillings in all the canals revealing the dentin sacrifice for removal of the separated instrument from the radix entomolaris was not significant, compared to the root canal space on the preoperative radiograph.
A
B C
D
E F
G H
an endodontic explorer such as a DG16 Endo Explorer (Hu-Friedy, Chicago, IL) (Fig. 19-11). The tip of a DG16 is placed in the loop and the loop is contracted around it. The apical portion of the DG16 is used to make the loop size smaller and the coronal portion is used to make it larger when the loop is tightened around it. The loop is then pre-bent at 45 degrees (Fig. 19-10, B and C) to facilitate the placement of the loop over the separated instrument. The loop is then brought into the canal and placed over the exposed portion of the separated file as the loop is pushed back at 90 degrees upon
it. Subsequently, the loop is tightened over the separated instrument by sliding down the handle (Fig. 19-10, C). The separated instrument will be retrieved by pulling the loop out of the canal in various directions in swaying motions to dis-lodge it from the canal walls (Fig. 19-10, D). A couple of pull motions in several directions will usually dislodge the file frag-ment and complete the case for separated file removal.
Surgical approaches for the management of separated instruments represent a second category of procedures for dealing with this iatrogenic event (see also Chapter 9).

732 PART II The Advanced Science of Endodontics
FIG. 19-10 A, Coronal portion of the separated file should be exposed at least 0.7 mm above the bottom of the space created around it. B, Approaching the separated file with the loop bent at 45 degrees against it. C, Loop is pushed back at 90 degrees as it is placed over the separated file. Removal with the loop requires the diameters of the loop device (0.16 mm ~ 0.45 mm) and the separated instrument and a depth of at least 0.7 mm. D, Separated file is pulled out with the loop device in various directions.
A B C D
A B1
B2 C1
C2
D
FIG. 19-11 File retrieval kit (FRK). A, Modified #3 Gates Glidden bur that is also called GG-3M (upper) and microtrephine bur that is also called FRK-T (lower). B1, FRK-6 ultrasonic tip (the tip portion looks like a spoon and is also called a spoon tip. It has a micro-concave on the spoon, which turns toward the handpiece at the 6 o’clock position. B2, FRK-S ultrasonic tip (the tip portion looks like a sharp spear and is also called a straight tip). C1, Yoshi loop, which captures a separated instrument. This micro-lasso is comprised of a tiny wire loop at the end of a stainless steel cannula, with a sliding handle that tightens the loop when pulled. C2, Yoshi loop holding a separated file from an actual case. Note that the loop holding the files requires 0.7 mm in length and width. D, File retrieval kit (FRK) in an autoclavable cassette case. The kit includes a GG-3M, FRK-T, FRK-6 ultrasonic tip, FRK-12 ultrasonic tip, FRK-S ultrasonic tip, Yoshi loop, gutta-percha removal (GPR) instrument, and a microexplorer instrument.
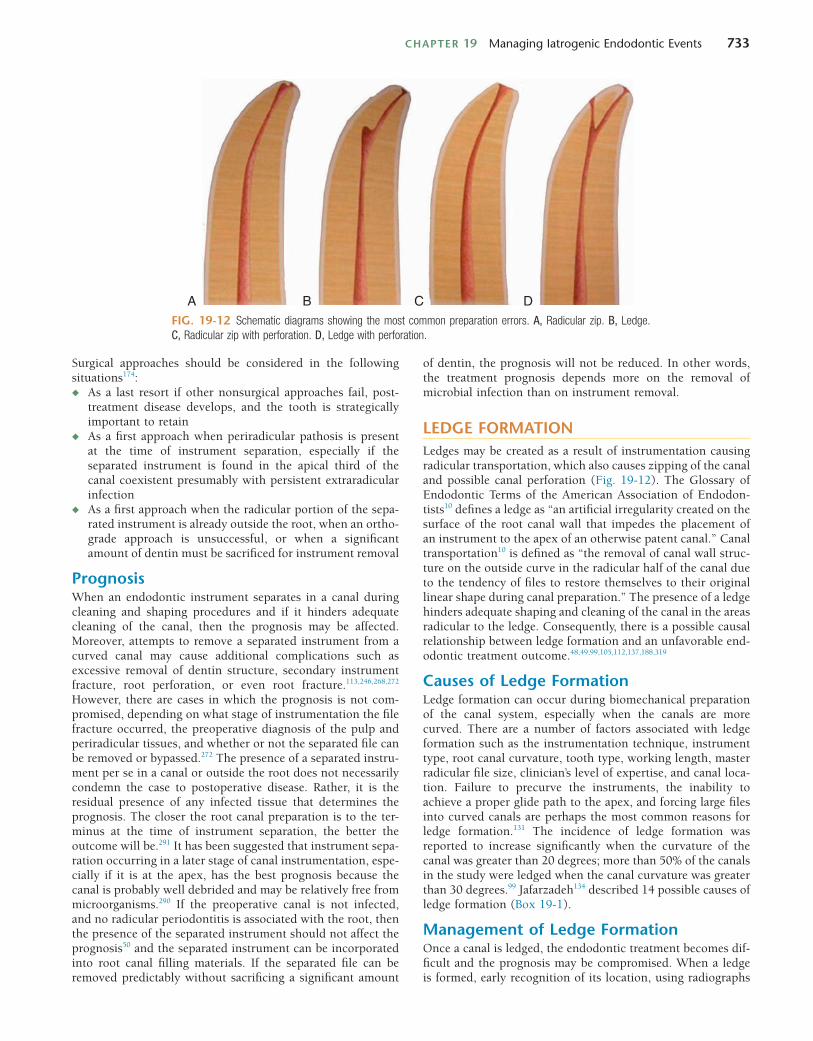
CHAPTER 19 Managing Iatrogenic Endodontic Events 733
of dentin, the prognosis will not be reduced. In other words, the treatment prognosis depends more on the removal of microbial infection than on instrument removal.
LEDGE FORMATIONLedges may be created as a result of instrumentation causing radicular transportation, which also causes zipping of the canal and possible canal perforation (Fig. 19-12). The Glossary of Endodontic Terms of the American Association of Endodon-tists10 defines a ledge as “an artificial irregularity created on the surface of the root canal wall that impedes the placement of an instrument to the apex of an otherwise patent canal.” Canal transportation10 is defined as “the removal of canal wall struc-ture on the outside curve in the radicular half of the canal due to the tendency of files to restore themselves to their original linear shape during canal preparation.” The presence of a ledge hinders adequate shaping and cleaning of the canal in the areas radicular to the ledge. Consequently, there is a possible causal relationship between ledge formation and an unfavorable end-odontic treatment outcome.48,49,99,105,112,137,188,319
Causes of Ledge FormationLedge formation can occur during biomechanical preparation of the canal system, especially when the canals are more curved. There are a number of factors associated with ledge formation such as the instrumentation technique, instrument type, root canal curvature, tooth type, working length, master radicular file size, clinician’s level of expertise, and canal loca-tion. Failure to precurve the instruments, the inability to achieve a proper glide path to the apex, and forcing large files into curved canals are perhaps the most common reasons for ledge formation.131 The incidence of ledge formation was reported to increase significantly when the curvature of the canal was greater than 20 degrees; more than 50% of the canals in the study were ledged when the canal curvature was greater than 30 degrees.99 Jafarzadeh134 described 14 possible causes of ledge formation (Box 19-1).
Management of Ledge FormationOnce a canal is ledged, the endodontic treatment becomes dif-ficult and the prognosis may be compromised. When a ledge is formed, early recognition of its location, using radiographs
Surgical approaches should be considered in the following situations174:◆ As a last resort if other nonsurgical approaches fail, post-
treatment disease develops, and the tooth is strategically important to retain
◆ As a first approach when periradicular pathosis is present at the time of instrument separation, especially if the separated instrument is found in the apical third of the canal coexistent presumably with persistent extraradicular infection
◆ As a first approach when the radicular portion of the sepa-rated instrument is already outside the root, when an ortho-grade approach is unsuccessful, or when a significant amount of dentin must be sacrificed for instrument removal
PrognosisWhen an endodontic instrument separates in a canal during cleaning and shaping procedures and if it hinders adequate cleaning of the canal, then the prognosis may be affected. Moreover, attempts to remove a separated instrument from a curved canal may cause additional complications such as excessive removal of dentin structure, secondary instrument fracture, root perforation, or even root fracture.113,246,268,272 However, there are cases in which the prognosis is not com-promised, depending on what stage of instrumentation the file fracture occurred, the preoperative diagnosis of the pulp and periradicular tissues, and whether or not the separated file can be removed or bypassed.272 The presence of a separated instru-ment per se in a canal or outside the root does not necessarily condemn the case to postoperative disease. Rather, it is the residual presence of any infected tissue that determines the prognosis. The closer the root canal preparation is to the ter-minus at the time of instrument separation, the better the outcome will be.291 It has been suggested that instrument sepa-ration occurring in a later stage of canal instrumentation, espe-cially if it is at the apex, has the best prognosis because the canal is probably well debrided and may be relatively free from microorganisms.290 If the preoperative canal is not infected, and no radicular periodontitis is associated with the root, then the presence of the separated instrument should not affect the prognosis50 and the separated instrument can be incorporated into root canal filling materials. If the separated file can be removed predictably without sacrificing a significant amount
FIG. 19-12 Schematic diagrams showing the most common preparation errors. A, Radicular zip. B, Ledge. C, Radicular zip with perforation. D, Ledge with perforation.
A B C D

734 PART II The Advanced Science of Endodontics
A rubber stopper with a directional indicator is valuable in this situation because the indicator can be pointed in the same direction as the bend placed in the instrument.131 A slight rotation of the file combined with a “pecking” motion can often help advance the instrument to the full working length of the canal.131,299 Whenever resistance to negotiation is met, the file should be retracted slightly, rotated, and then advanced again with the precurved tip facing in a different direction. This action should be repeated until the file consistently bypasses the ledge.131 If this technique is unsuccessful, the clinician should flare the canal coronal to the ledge in an anticurvature direction to obtain wider straight-line access to the original pathway of the canal beyond the ledge, followed by a #10 K-file with the tip precurved to bypass the ledge (see Fig. 19-13). Small hand files dedicated to the microscopic use (such as the micro-opener with #10/.06 taper) may help flare the orifice of the original pathway beyond the ledge. The use of such small micro–hand files under the DOM with magnifi-cation and illumination helps the clinician locate the original pathway and facilitate bypassing the ledge. The micro-opener is available only in 16 mm and it is short enough to provide tactile sensation and better control. However, in some cases a longer instrument is required to reach the ledge present in the radicular third of a long canal. In these instances, a hand instrument holder such as an EndoHandle (Venta, Logan, UT) may help the clinician easily negotiate the canal radicular to the ledge. Any hand files can be attached to the handle for microscopic use. Other hand instruments are available specifi-cally for this purpose (microexplorer instrument, DentalCadre and ELES instrument, DenMat Lompoc, CA) that are long enough to reach the ledge formed in the radicular third. Both of the instruments are made of stainless steel. The microex-plorer is used to explore the original canal and penetrate a narrow canal beyond the ledge, while the ELES is used to reduce the ledge as the tip portion is coated with fine diamond particles. They can be used in sequence to reduce or remove the ledge. The microexplorer instrument can be precurved as it has a smooth surfaced tip to get into the original pathway beyond the ledge (Fig. 19-14), whereas the ELES instrument has diamond coating on the tip to enlarge the original pathway (Fig. 19-15). The microexplorer instrument has a 0.1 mm biconical tip with a .08 taper for the first 1-mm portion from the radicular end and a .06 taper for the next 10-mm portion, which gives the instrument more stability in push-pull motions than a .02 tapered K-file, while the tip diameter of the ELES instrument is 0.2 mm with a .06 taper. The maximum diam-eter of the microexplorer instruments is 0.78 mm, which pro-vides stability and maintains a high visibility under the DOM when it is precurved. On the other hand, the maximum diam-eter of the ELES instrument is 0.68 mm, which provides flex-ibility and visibility even around a curve. Once the first microexplorer instrument has successfully bypassed the ledge, subsequently the ELES instrument can be used to enlarge and reestablish the original pathway (Fig. 19-16), followed by hand instruments (such as ProTaper S1 and S2 hand instru-ments, DENTSPLY Tulsa Dental Specialties, Tulsa, OK) to both reduce the ledge and complete the shape. #15/.04 and #15/.06 Vortex Blue rotary files (DENTSPLY Tulsa Dental Specialties) can also be precurved with ease and used as hand files in short pumping motions to reduce the ledge after the preliminary enlargement of the original pathway with the micro-hand instruments.
including CBCT and magnification, will facilitate its manage-ment.105 The canal is usually “straightened” at the point where the file stops negotiating the curve, and there is suddenly a looser feeling of the file within the canal, with no more tactile sensation of the tip of the instrument binding in the canal. If the radiograph reveals that the tip of the instrument deviates away from the canal curvature, then it is highly likely that a ledge formation has occurred on the canal wall.
When a ledge formation is identified, the shortest file pos-sible that can reach the working length should be selected to bypass the ledge. Shorter instruments have more stiffness and allow the clinician’s fingers to be placed closer to the tip of the instrument, which consequently provides greater tactile sensa-tion and more control over the instrument.134 It usually requires determination, perseverance, and patience to bypass a ledge once it is formed.48 The successful management of a ledge depends on whether both the ledge and the orifice of the origi-nal pathway can be visualized, reached, or felt with instru-ments.166 Any case where the ledge can be visualized under the DOM may be considered less complex to treat. Cases whereby the ledge is not directly visible are more difficult to treat, as tactile sensation and negotiation require patience and experi-ence.48 However, 3D radiographic images obtained from CBCT reveal the locations and the directions of both the ledge and the original pathway to the canal terminus, which provides additional information for diagnosis and therefore helps the clinician manage the ledge formation with a more predictable outcome and negotiate the original canal.203
Bypassing a LedgeUsing Hand InstrumentsPrecurving of a #8 or #10 hand file is a critical step in bypass-ing a ledge. The small file should have a distinct curve at the tip (that is, in the radicular 2 to 3 mm) (Fig. 19-13). This file should be used initially to negotiate past the ledge and explore the original pathway of the canal to the radicular foramen.48,131,299
BOX 19-1
14 Possible Causes of Ledge Formation
1. Not extending the access cavity sufficiently to allow adequate access to the radicular part of the root canal48,105,131,137,159,299
2. Loss of instrument control if endodontic treatment is attempted via a proximal surface cavity or through a proximal restoration131
3. Incorrect assessment of the root canal direction48,137,159
4. Incorrect root canal length determination48,137,159
5. Forcing the instrument into the canal wall303
6. Using a noncurved stainless steel instrument that is too large for a curved canal48,131,137,218,299
7. Failing to use the instruments in sequential order48,105,137,159
8. Rotating the file excessively at the working length105,303
9. Inadequate irrigation or lubrication during instrumentation299
10. Over-relying on chelating agents303
11. Attempting to retrieve separated instruments48,137,159
12. Removing root filling materials during endodontic retreatment48,137,159
13. Attempting to negotiate calcified root canals48,137,159
14. Inadvertently packing debris in the radicular portion of the canal during instrumentation48,299
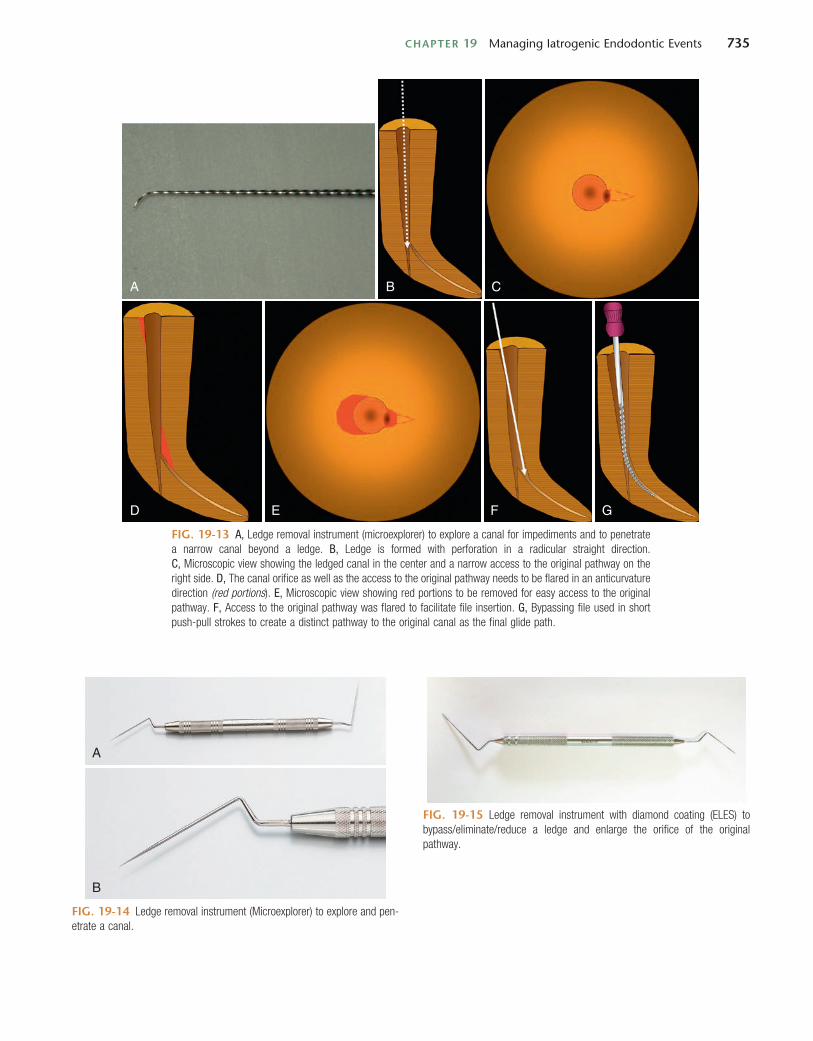
CHAPTER 19 Managing Iatrogenic Endodontic Events 735
FIG. 19-13 A, Ledge removal instrument (microexplorer) to explore a canal for impediments and to penetrate a narrow canal beyond a ledge. B, Ledge is formed with perforation in a radicular straight direction. C, Microscopic view showing the ledged canal in the center and a narrow access to the original pathway on the right side. D, The canal orifice as well as the access to the original pathway needs to be flared in an anticurvature direction (red portions). E, Microscopic view showing red portions to be removed for easy access to the original pathway. F, Access to the original pathway was flared to facilitate file insertion. G, Bypassing file used in short push-pull strokes to create a distinct pathway to the original canal as the final glide path.
A
D E F G
B C
FIG. 19-14 Ledge removal instrument (Microexplorer) to explore and pen-etrate a canal.
A
B
FIG. 19-15 Ledge removal instrument with diamond coating (ELES) to bypass/eliminate/reduce a ledge and enlarge the orifice of the original pathway.

736 PART II The Advanced Science of Endodontics
ultrasonic tip (such as the straight ultrasonic tip, DentalCadre, Seattle, WA) is selected and precurved in the direction of the original canal. Then it is simply placed in the orifice of the original pathway to the radicular foramen and activated, which will automatically enlarge the opening of the true canal in a few seconds. Ultrasonic tips can cut dentin faster than hand instruments and widen the orifice of the original pathway more easily so that files can consecutively be placed into the original canal for root canal preparation. Ultrasonics should be used on the lowest power setting to avoid overextending the ledge, as ultrasonics may get very aggressive in cutting.243 Once the orifice of the original pathway gets wide enough for file inser-tion, negotiation files need to be placed into the canal to establish patency and to smooth out the irregularities on the canal wall that may have been created with ultrasonics,
Using Ultrasonic TipsSmall diameter ultrasonic tips improve visibility with the added benefit of reducing the need for sacrificing sound dentin in bypassing or removing the ledge.167 The only drawback to the thinner tips could be that they are more prone to fracture during ultrasonic activation.298 Therefore, thinner ultrasonic tips should be activated in a pulsing fashion at the lowest pos-sible power setting to prevent fracture and heat generation.
The use of longer ultrasonic tips may also facilitate bypass-ing or reducing the ledge in the radicular third as long as it is performed under the DOM. The orifice of the original canal just coronal to the ledge should be enlarged. If the ledged portion of the canal can be visualized under the DOM, then ultrasonic instruments should be used over hand instruments (Fig. 19-17). First, an appropriate size of a small diameter
FIG. 19-16 Schematic diagrams showing bypassing the ledge with ledge removal hand instruments. A, Ledge is created in a radicular straight direction around a curve. B, Original pathway is explored and opened up with the microexplorer instrument in short push-pull strokes. C, Original pathway is widened with the ELES instrument. D, ELES instrument used in push-pull motions to reduce the ledge. E, Precurved straight ultrasonic tip can also be used here to reduce the ledge instead of the ELES instrument. F, File with a biconical tip is brought into the canal to eliminate/reduce the ledge and negotiate the original canal. The primary cone of the biconical tip has no cutting tip. As it hits the curve or irregularities on the canal wall, it will slip alongside the curve and scoot over the irregularities. G, Secondary cone of the biconical tip removes the points at the transition angles and provides a smooth surface that guides the tip portion into the original pathway. H, Orifice of the original canal beyond the ledge needs to be enlarged for easy file insertion after the ledge has been bypassed successfully. I, Orifice of the original canal can be efficiently widened with a precurved instrument such as a ProTaper S1 hand file and a #15/.04 Vortex Blue rotary file used as a hand file, and the apical patency established. J, Original canal can be sequentially prepared with more tapered NiTi files. K, Postoperative canal showing the ledge is significantly eliminated.
A B C
D E
F G
H I J K

CHAPTER 19 Managing Iatrogenic Endodontic Events 737
advantage of the step-back technique is that this method tends to minimize procedural errors such as transportation and ledge formation.298 Each file is used in sequence with circumferential filing to remove any irregularities before a larger diameter file is placed. The effective use of circumferential filing, especially with Hedström files, will ensure smoothness of the canal walls and flaring toward the coronal end of the canal, which will help to prevent the formation of ledges.105,299 Precurving the instruments and not forcing them into the canal is one of the most important considerations in the prevention of ledge formation.131
The use of NiTi files and instruments with noncutting tips helps to maintain original root canal curvatures.131 The concept of use of these instruments is that the rounded tip does not cut into the wall but will slip alongside it.130,131 In addition to the tip design, flexibility of an instrument also plays an impor-tant role for keeping the instrument centered in the canal, with NiTi instruments favored over stainless steel instru-ments.121,128,196 Compared to stainless steel instruments, NiTi instruments offered less canal transportation, more dentin con-servation, and reduced risk of zipping or stripping curved canals.69,95,201
PrognosisA ledge in a canal is analogous to any intracanal obstruction that hinders the cleaning and shaping of the root canal to the radicular terminus. The presence of a non-negotiated ledge may have a similar prognosis as a canal with a retained sepa-rated instrument. If the ledge can be bypassed or eliminated, and if the canal beyond the ledge can be cleaned without exces-sive enlargement or perforation, then the prognosis should not be that greatly reduced.290,291 The amount of debris and bacteria left in the canal apical to the ledge greatly influences the prognosis.
PERFORATIONS (NONSURGICAL)The topic of nonsurgical perforations, whether by caries, access bur, or post drill, and whether occurring in the furcation or
followed by root canal preparation with NiTi rotary or hand files (Figs. 19-18, 19-19).
Using Rotary InstrumentsPre-curved rotary PathFiles are also beneficial for negotiating past a ledge. First the radicular 2 to 3 mm of the #13 PathFile is precurved at 30 to 45 degrees and is rotated at 100 rpm or slower as it is brought slowly into the canal and moved radicu-larly. If a ledge or sharp radicular curvature is encountered, the instrument is withdrawn about 1 mm and immediately rein-serted. This allows the precurved tip to move to a different orientation within the canal as it is reinserted. This may require one or two withdrawals and re-insertions to negotiating the original canal. This procedure is followed in sequence by the #16 and #19 PathFiles to preliminarily enlarge the original pathway and reduce the ledge prior to the conventional root canal preparation with NiTi rotary instruments.
Potential Complications of Removal or Bypassing a LedgeDuring ledge removal or bypassing a ledge, complications can occur, including root fracture, root perforation, worsening the ledge, and instrument separation. Since a ledge is likely to form around a curve, attempts to bypass or eliminate it may often involve dentin sacrifice, which may eventually compromise the integrity of the tooth and increase the risk of perforation or root fracture. Care should be taken not to remove excessive root structure or overstress the instruments during the ledge removal process. If a ledge cannot be bypassed with any of the techniques described earlier, and if signs or symptoms of the periradicular lesion persist, then the treatment options are limited to surgical intervention such as periradicular surgery or intentional replantation.131
Prevention of Ledge FormationPassive step-back and balanced force techniques are two ben-eficial methods of canal preparation that reduce the chances of ledge formation.131,299 Moreover, it has been proposed that an
FIG. 19-17 Non-visible ledge removal with ultrasonics. A, Ledge formed beyond the curve. CBCT is taken to locate both the ledge and the original pathway. B, Canal coronal to the ledge is flared in an anticurvature direction with NiTi rotary files in brushing motions. Original pathway to the canal terminus is explored with a #10 precurved K-file or the precurved microexplorer instrument and radiographs are taken with it inserted in the canal to see if it is in the original canal beyond the ledge. C, Straight ultrasonic tip is precurved the same way as the hand instrument used and placed in the canal to eliminate/reduce the ledge. The red portion needs to be smoothed out to facilitate the insertion of an instrument into the original pathway. D, Postoperative canal showing the ledge is significantly reduced.
A B C D
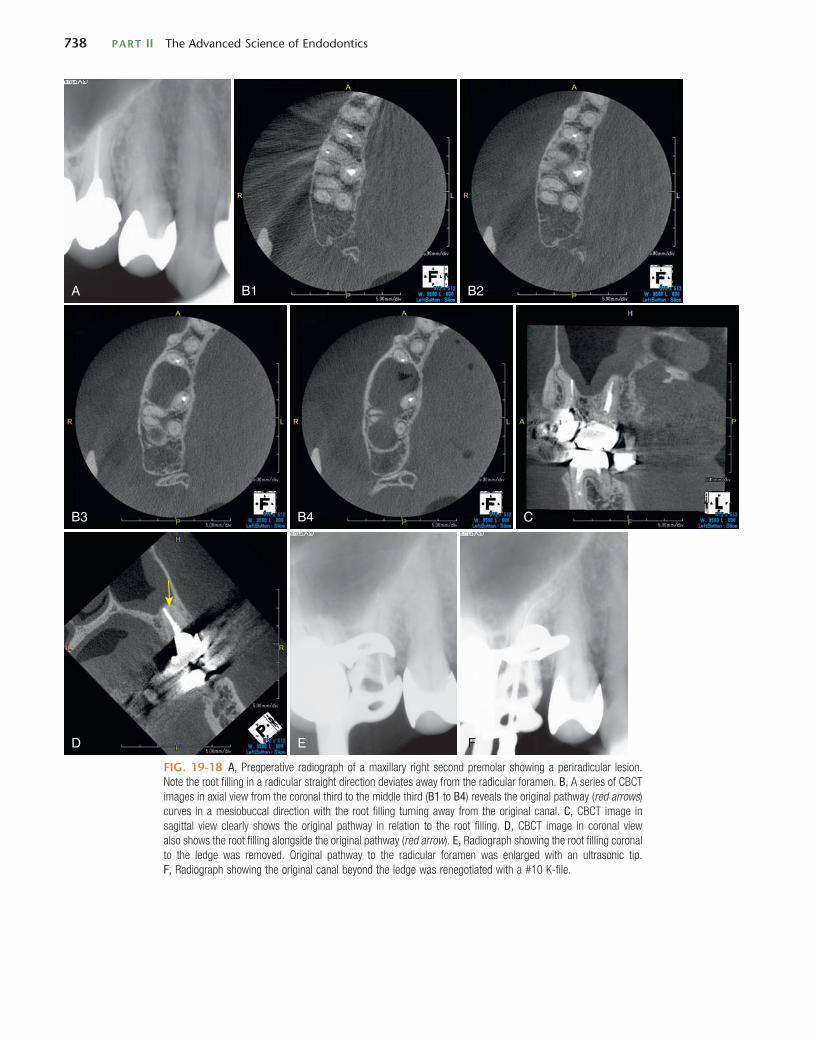
738 PART II The Advanced Science of Endodontics
A B1 B2
B3 B4 C
D E F
FIG. 19-18 A, Preoperative radiograph of a maxillary right second premolar showing a periradicular lesion. Note the root filling in a radicular straight direction deviates away from the radicular foramen. B, A series of CBCT images in axial view from the coronal third to the middle third (B1 to B4) reveals the original pathway (red arrows) curves in a mesiobuccal direction with the root filling turning away from the original canal. C, CBCT image in sagittal view clearly shows the original pathway in relation to the root filling. D, CBCT image in coronal view also shows the root filling alongside the original pathway (red arrow). E, Radiograph showing the root filling coronal to the ledge was removed. Original pathway to the radicular foramen was enlarged with an ultrasonic tip. F, Radiograph showing the original canal beyond the ledge was renegotiated with a #10 K-file.

CHAPTER 19 Managing Iatrogenic Endodontic Events 739
associated with posttreatment inflammation and flare-up or the lack of radicular healing.186,254,261,289 In vivo histologic studies show the most favorable histologic outcome when the root filling material remains within the radicular constriction. When gutta-percha is extruded into the periradicular tissue, there can be a severe inflammatory reaction.232 However, other materials such as ProRoot MTA (DENTSPLY Tulsa Dental Specialties) are more biocompatible1,98,144 and do not seem to produce much periradicular inflammation if extruded beyond the root of the tooth.75,267
Studies show that almost all instrumentation techniques promote the radicular extrusion of debris including root filling materials.8,122,283 Furthermore, gutta-percha and Resilon filling materials obtained from teeth associated with refractory radic-ular periodontitis have indicated the presence of bacterial biofilm and E. faecalis.102,187,196,255 Another study stressed the possibility of gutta-percha–centered E. faecalis biofilm as well as the role of tissue fluids such as saliva and serum in the biofilm formation.90 E. faecalis adheres well to gutta-percha with and without canal sealers, with the biofilm formation more effective when it is in contact with serum in periradicular tissues. Because bacterial biofilm is considered the primary cause of chronic and recurrent endodontic infections,292 it is crucial to keep gutta-percha filling materials within the canal system as much as possible to prevent potential periradicular periodontitis.
canal space, has been extensively discussed in other chapters of this text. For ease of reference, the various locations and topics are as follows:◆ Chapter 8: Nonsurgical Retreatment. Clinical examples of
nonsurgical repair of furcation and midlevel perforations, with descriptions of the latest techniques and materials, illustrated with clinical photographs and radiographs. Listed also are the appropriate literature references, indica-tions and contraindications for the repairs presented, and protocols for treatment management.
◆ Chapter 5: Tooth Morphology and Access Cavity Prepara-tion. Diagrams of perforations and repairs.
◆ Chapter 29: Endodontic Records and Legal Responsibilities. Legal implications and clinician responsibilities.
◆ Chapter 26: Effects of Age and Systemic Health on End-odontics. Radiographs of perforations secondary to end-odontic attempts in calcified canals.
RADICULAR EXTRUSION OF ROOT CANAL FILLING MATERIALSThe extrusion of root filling materials beyond the radicular foramen may occur either when the canal is obturated or during the removal of obturation materials. Radicularly extruded materials such as obturating materials, necrotic pulp tissue, bacteria, medicaments, and irrigants have been
G H I J
K L M
G, Radiograph showing the original canal was flared with a TF adaptive SM1 rotary file used as a hand file in push-pull motions. H, Radiograph showing the original canal was sequentially more tapered with a TF Adaptive SM2 rotary file used as a hand file. I, Radiograph showing the final root canal preparation of the original canal with a #20/.06 Vortex Blue rotary file used as a hand file. J, Postoperative radiograph showing the obturation of the original canal. K, Magnification of the original canal orifice side by side with the root filling in the ledged canal. Note the locations of the original canal and the ledge are exactly the same as shown on the axial view of CBCT B3. L, Magnification of the original canal showing it was flared with the precurved straight ultrasonic tip. M, Magnification of the original canal showing the original canal was completely shaped to the canal terminus with NiTi instruments.
FIG. 19-18, cont’d

740 PART II The Advanced Science of Endodontics
A B C
D E
F
G H I
FIG. 19-19 A, Preoperative radiograph of a mandibular right second molar showing periradicular lesions associated with the mesial and distal roots. Note the root filling in the mesial root deviates away from the center of the root. B, Schematic diagram showing gutta-percha root filling materials in the ledged canal of the mesial root. C, Root filling materials were removed chemomechanically from the mesial root. D, Original pathway to the radicular foramen was explored and enlarged with the microexplorer and a pre-curved FRK-S ultrasonic tip. E, Original canal beyond the ledge was renegotiated with a #10 K-file, followed by a #15 K file. F, Schematic diagram showing the original canal shaped to the canal terminus. G, Interoperative radiograph showing root canal preparation of the original canal with a ProTaper S1 file. H, Postoperative radiograph showing root canals filled with MTA both in mesial and distal roots. I, Three-month postoperative radiograph showing periradicular healing.
Uncontrolled obturation can cause the extrusion of root canal filling materials into the maxillary sinus67 or into the territory of the inferior alveolar nerve (IAN).214 Serious com-plications such as maxillary sinusitis, aspergillosis infection, paresthesia, dysesthesia, and similar neural complications may occur after extruding the root filling materials into such sensi-tive areas.176
Endodontic-related paresthesia can be caused mechanically or chemically via the passage of endodontic materials into the vicinity of the major nerves such as the IAN or its branches.3 These materials include root canal irrigants, sealers, and paraformaldehyde-containing pastes.297 Because of the potential
for chemical degeneration of the nerve axons, the use of paraformaldehyde-containing pastes is not recommended for endodontic obturation.183,217 The optimum pH of an endodontic medicament should be as close as possible to that of body fluids, which is around 7.35. Significantly higher or lower pHs are likely to cause cellular necrosis of tissues when they are in direct contact with these materials. The clinician must also consider the pH of some of the routinely used endodontic and related dental materials. It has been reported that an alkaline pH of root canal sealers could neutralize the lactic acid from osteoclasts and prevent dissolution of mineralized components of teeth; therefore, root canal sealers, especially calcium silicate–based

CHAPTER 19 Managing Iatrogenic Endodontic Events 741
as an opportunistic infection.143 Many studies have demon-strated that maxillary sinus aspergillosis is generally caused by extruded root canal filling material containing zinc oxide and formaldehyde.18,19,151,163,274 Besides maxillary sinus infections, the overextension of root filling materials such as gutta-percha into the maxillary sinus may also cause mechanical irrita-tion.149 When paresthesia is involved, it is thought to occur more from mechanical or thermal insult to the affected neurons.217 In addition, although such substances are not con-sidered toxic,270 they may cause an additional foreign body reaction. Inflammation caused by mechanical irritation is likely to persist until the extruded materials are removed, and it may become permanent secondary to the mechanical, thermal, or chemical insult.114 The incidence of IAN damage has been reported to be up to 1% of cases when performing a root canal filling of a lower premolar.148 This overextension may cause an unnecessary mechanical or chemical irritation, which hinders repair of the periradicular tissue and thus diminishes the prob-ability of a successful prognosis. The patient may also experi-ence sharp, localized posttreatment pain, which may or may not resolve. When the inferior alveolar nerve is injured, the pain is not only located in the immediate periradicular area but may radiate and refer to the surrounding or distant structures.195
cements or sealers, can contribute to hard tissue formation by activating alkaline phosphatase.276 Commonly used endodontic medicaments are as follows39,87,226,260:◆ Formocresol: pH 12.45 +/− 0.02◆ Sodium hypochlorite: pH 11 to 12◆ Calcium hydroxide (Calyxl): pH 10 to 14◆ ProRoot MTA: pH 11.7 to 7.12 at 3 hours to 28 days◆ Endosequence BC Sealer: pH 10.31 to 11.16 at 3 hours to
240 hours◆ MTA Fillapex: pH 9.68 to 7.76 at 3 hours to 168 hours◆ AH plus: pH 7.81 to 7.17 at 3 hours to 240 hours◆ Antibiotic-corticosteroid paste (Ledermix): pH 8.13
+/− 0.01◆ Eugenol: pH 4.34 +/−0.05◆ Iodoform paste: pH 2.90 +/−0.02Neural damage from these materials may be permanent and can cause neuropathic pain (i.e., dysesthesia) or anesthesia.
Orbital pain and headache may occur secondary to the local compression of overextended material into the maxillary sinus.311 Sinus infection caused by zinc-oxide-eugenol–based filling materials extruded into the maxillary sinus is often associated with aspergillus growth18,19,93,151,236 (Fig. 19-20). Although aspergillosis of the paranasal sinuses is a relatively rare finding in non-immunocompromised patients, it is known
FIG. 19-20 Maxillary sinus aspergillosis. A, Preoperative radiograph showing a lesion associated with the palatal root, from which the extrusion of the root filling materials occurred in the maxillary sinus. B, CBCT image in sagittal view showing the relation between mucositis on the maxillary sinus floor and the gutta-percha filling material. C, CBCT image in axial view showing the relation between mucositis on the mesial wall of the maxillary sinus and the extruded root filling materials. D, CBCT image in coronal view showing the relation between the palatal root and the extruded root filling materials. E, Postoperative radiograph of orthograde root canal retreat-ment on the maxillary left first molar showing the mesiobuccal, distobuccal, and palatal root canals were ade-quately filled without overextension of the filling materials. F, Aspergillus was found on the filling materials retrieved from the maxillary sinus.
AA
BB CC
DD EEF

742 PART II The Advanced Science of Endodontics
chloroform,46,132 although the extruded portion of root canal fillings will often remain in the periradicular tissue46 (Fig. 19-21). The relative ease of gutta-percha removal suggests a failure of previous endodontic treatment, possibly related to poor obturation compaction or canal shaping, which resulted in both radicular extrusion and failure of the radicular seal. Comparatively, well-filled canals with radicular extrusion do not appear to have a significant failure rate.13,132 On the other hand, the extrusion of the MTA root filling material into the periradicular tissues does not appear to negatively affect the periradicular healing due to the high biocompatibility and antibacterial properties that the calcium silicate–based cement possesses,171,281 compared to gutta-percha filling mate-rials (Fig. 19-22).
When gutta-percha is overextended into the periradicular space, removal can be attempted by inserting a new Hedstrom file, usually a #15 or #20, into the radicular obturation, using a gentle clockwise rotation to a depth of 0.5 to 1 mm beyond the radicular constriction. The file is then slowly and firmly withdrawn with no rotation, thereby engaging and removing the overextended material.180 This technique works frequently, but care must be taken not to force the instrument, or further extrusion of the gutta-percha or separation of the file may result. The overextended radicular portion of the gutta-percha should not be softened with heat or solvent, because this appli-cation can decrease the likelihood of the Hedstrom file engag-ing the obturation, hindering its retrieval.273 In addition, care should be taken not to overextend the file into the area of the inferior alveolar nerve canal, which could cause irreversible damage to the associated nerves.
The use of rotary NiTi files that are specifically designed for gutta-percha removal appears to be effective124,265 include Pro-Taper Universal Retreatment files (DENTSPLY Tulsa Dental Specialties), Mtwo R rotary files (VDW, Munich, Germany), R-Endo retreatment files (Micromega, Besancon, France), and hand instruments such Micro-debriders (DENTSPLY Maillefer, Ballaigues, Switzerland), EGPR-L/R/U/D (G. Hartzell & Son, Concord, CA), and the gutta-percha removal instrument (DentalCadre). The self-adjusting file (SAF) (ReDent-Nova, Ra’anana, Israel) is also effective in removing obturation mate-rial, especially the remaining gutta-percha after conventional retreatment. Its variable shape and scraping motion allow it to touch a higher percentage of root canal walls than rotary instru-ments, facilitating effective cleaning.181 Literature has shown that significantly less debris was extruded with the rotary retreatment files during endodontic retreatment compared with other traditional techniques using Hedström files with chloro-form,124 although all techniques resulted in some radicular extrusion.124,265 ProTaper Universal Retreatment files have been reported to remove gutta-percha from the canals in large pieces around the spirals of instruments, whereas Hedström files gen-erally remove gutta-percha in small increments.124 Further-more, a combination of both rotary instruments for initial quick removal of gutta-percha and hand instruments to refine and complete the cleaning of the canal, especially in the radicular third of the root, shows the better protocol for obtaining clean canal walls during endodontic retreatment.24,129
In difficult retreatment cases where root canal fillings per-sistently remain in the periradicular tissues, the use of a solvent, such as chloroform, may help to dissolve the remain-ing gutta-percha. In addition, chloroform has been reported to be capable of reducing the intracanal levels of Enterococcus
One study with a 10-year follow-up reported that the overall success rate of endodontic treatment was 91%, with the best prognosis achieved when the obturation was under 0 to 2 mm from the apex.262 Consequently, radicular extrusion of root canal filling materials must be avoided as much as possible to obtain optimal results.
Causes of Extrusion of Obturation Materials Beyond the Radicular ForamenThe extrusion of obturation material that was thought to be the cause of endodontic failure is reported to be as low as 3%,266 with the majority of causes thought to be more from coronal leakage. However, several researchers have seen a higher fre-quency of failure and unhealed periradicular lesions in cases where the root filling material had extruded beyond the radicu-lar foramen.23,34,209 Overextension of the root canal filling mate-rials occurs mainly for lack of material control.36,106 The degree of extrusion of obturation materials into periradicular tissues depends on the techniques used for root canal preparation and obturation,233 which include accidental overinstrumentation and incorrect canal working length measurement. Caution should also be taken when obturating a canal with open apices and larger minor foramen diameters, which are often found in cases with radicular inflammatory resorption. Warm vertical compaction techniques produce a homogeneous obturation that adapts well to the canal walls249,309 but may result in the extrusion of gutta-percha filling into the periradicular tissues.36 Carrier-based obturation was also found to have more radicular extrusion of gutta-percha when compared with warm vertical compaction.158 The type of canal shaping may also be a con-tributing factor. The canal shape created with the Profile GT system is more prone to extrusion of gutta-percha when obtu-rated with the carrier-based technique than the canal shape created using Profile 0.06 instruments. The Profile GT system created a more parallel preparation coronally and a tapered preparation radicularly, whereas the Profile 0.06 system created a preparation with uniform taper from the apex to its most coronal extent.233 Therefore, possibly the more continuously tapered the canal shape is, the less obturation material is extruded beyond the radicular foramen.
When endodontic retreatment is performed, irritants in the form of root filling materials can be extruded into the perira-dicular tissues.8,122,283 Techniques involving push-pull filing strokes usually create a greater mass of debris than those involving some sort of rotational motions.6,32,76,142,178,222
Management of Obturation Materials Extruded Beyond the Radicular ForamenNonsurgical Management of Extrusion of Obturation MaterialsMethods to remove the gutta-percha filling material from the root canal include the use of heat-carrying instruments, ultra-sonics, solvents, and rotary or hand files. Mechanized methods to remove filling materials are faster but possibly not more effective than manual methods.141,282 Heat-carrying instrument may damage the periradicular tissues if the removal attempts extend beyond the radicular foramen. The complete removal of gutta-percha from the root canal system has proven diffi-cult.108,282 Poorly compacted gutta-percha obturation can easily be removed with Hedstrom files and solvents such as

CHAPTER 19 Managing Iatrogenic Endodontic Events 743
FIG. 19-21 Root filling materials extruded beyond the radicular foramen. A, Preoperative radiograph showing overextension of the root filling material with a large lesion associated with the root. B, Root filling in the canal was mechanically removed, but the extruded portion of it remained in the periradicular tissues. C, MTA was filled in the canal with the extruded portion remaining in the lesion. D, Six-month postoperative radiograph showing the reduced size of the lesion, but the lesion surrounding the extruded portion stayed the same in size for the next 6 months, indicating infection of the extruded gutta-percha point. The extruded portion was surgically removed from the lesion at this point. E, 3-month follow-up radiograph after the surgery showing the healing lesion. F, 12-month follow-up radiograph after the surgery showing a more periradicular healing. G, Gutta-percha point retrieved from the lesion.
A B C D
E F G
faecalis.62,182 When chloroform is used during the early stages of gutta-percha removal, more filling material will remain in the canal and some of it may be extruded beyond the radicular foramen.124,172 Although the carcinogenicity of chloroform in humans is suspect, chloroform is regarded as a safe and effec-tive endodontic solvent, when used carefully.44,177
Unlike rotary instruments, the EGPR-L/R/U/D hand instru-ments and the gutta-percha removal instrument are 30 mm in length, allowing them to remove obturation material not only from the radicular third of the canal but also from the perira-dicular tissues through the radicular foramen. The micro-debriders are designed to be used in conjunction with a dental operating microscope. They have a Hedström cutting configu-ration with a standard .02 taper in sizes 20 and 30 with 16 mm of cutting flutes, which may not be long enough to reach the gutta-percha filling material beyond the radicular foramen. The EGPR instrument has a tiny projection on one side of the tip for scratching and engaging the gutta-percha filling left on the canal wall. The overall diameter of the tip is 0.3 mm and the length of the projection is 0.1 mm. This hand instrument
works like a scraper on the canal wall. First, a small hole is created with a small diameter ultrasonic tip between the canal wall and the root filling material, and the instrument is brought into the canal with the projection facing away from the gutta-percha filling. When the radicular portion comes down to the bottom of the hole created, the projection is turned back on the gutta-percha filling so that it can be hooked on the projec-tion pressed against it. Then the gutta-percha filling should be scraped and come apart in large pieces from the canal wall (Fig. 19-23, A to C).
The gutta-percha removal instrument has a tiny conical harpoon-shaped tip that is sharp and small enough to penetrate into a mass of gutta-percha filling and hook it on the rim on the return stroke. The tip portion of this instrument has a .40 taper with the minimum tip diameter of 0.1 mm and the maximum diameter of 0.3 mm with a 0.2-mm diameter shank supporting the tip portion. The 0.1-mm gap between the 0.3-mm and the 0.2-mm diameters works practically as a tiny circular projection over the shank portion that can hook a mass of gutta-percha fillings. Gutta-percha fillings can be separated

744 PART II The Advanced Science of Endodontics
FIG. 19-22 A, Preoperative radiograph showing a large periradicular lesion associated with the root of the man-dibular left incisor. B, Interoperative radiograph showing the cast post and the root filling in the canal was mechanically removed. Calcium hydroxide was placed as an intracanal dressing on the first appointment. C, Postoperative radio-graph on the second appointment showing the canal was obturated with MTA, which resulted in overextension of the material into the periradicular tissues. D, Six-month postoperative radiograph showing the significantly reduced size of the lesion. E, One-year postoperative radiograph showing a nice periradicular healing with a residual of the MTA root filling extruded into the periradicular tissues. F, Three-year postoperative radiograph showing the tooth has maintained healthy periradicular tissues with the extruded MTA filling reduced in size. G, Twelve-year postoperative radiograph showing the tooth has maintained healthy periradicular tissues with the extruded MTA filling completely absorbed in the bone.
A B C
D E F
G
from the canal wall by wedging the tip between the gutta-percha and the canal wall. The gutta-percha filling can also be hooked by pressing the projecting rim against it, and then the gutta-percha filling should be removed in large pieces from the canal wall.
It is recommended that a small hole be created in the center of the gutta-percha filling with a small diameter ultrasonic tip to facilitate the root filling removal with the hand gutta-percha removal instrument placed into the hole. If the gutta-percha filling is poorly adapted to the canal wall with a large radicular diameter, the insertion space for the hand instrument should be created between the canal wall and the gutta-percha filling to avoid radicular extrusion of the root filling materials with the hand instrument or an ultrasonic tip. When a small amount
of gutta-percha filling remains on the inside curve or in the radicular third of the canal after the mechanical removal attempts, chloroform should be filled in the canal and the gutta-percha removal instrument can be used to agitate it in short push-and-pull motions in the canal, or even outside the canal if root filling is extruded beyond the radicular foramen, to actively dissolve the residual root filling.
Management of Tissue Damage Caused by Extrusion of Root Canal Filling MaterialsWhen root canal filling material extends into the periradicular spaces, tissue damage may occur. The majority of these cases are managed by nonsurgical methods such as analgesics, cold

CHAPTER 19 Managing Iatrogenic Endodontic Events 745
root canal treated teeth with overextension of the root canal sealer into the maxillary sinus might be the main cause for aspergillosis in healthy patients.18,19 Surgical intervention is usually the most predictable method for removing extruded root canal filling material and allowing for adequate healing secondary to IAN or sinus complications.287
INFERIOR ALVEOLAR NERVE (IAN) INJURYPrior to considering any treatment to resolve IAN damage, the etiology must be first determined. Common causes of injury to the IAN are listed in Box 19-2.226 The IAN may be damaged when an increase in temperature proximal to the IAN is greater than 10° C.68 IAN damage has been suggested to occur in up to 1% of mandibular premolars that receive root canal treat-ment.68 The type of sealer cement used may influence the symptoms of IAN damage.189 If the patient exhibits neuro-pathic signs after the local anesthesia has worn off, posttreat-ment radiographs should be exposed to observe the possibility of any obturation material extending into the IAN canal.
packs, corticosteroids, and antibiotics.72 Dexamethasone is a corticosteroid that has been widely used in dentistry, and it seems to decrease periradicular inflammation caused by a foreign body183 with minimal side effects.52 If the tissue damage is extended to the IAN or maxillary sinus, a different approach may be necessary.
SINUS PERFORATIONThere is a close proximity of maxillary premolars and molars to the sinus, and the apices of these teeth can be less than 2 mm from the floor of the sinus.61 Pathologic destruction of the sinus floor may predispose a maxillary sinus communication,253 pro-ducing an oroantral communication,80,165,239,302 also known as an OAC. In general, exposure of the sinus lumen is well toler-ated,133,208 with no overt repercussions on healing. One investi-gator302 found no significant difference in the healing of the mucosa in patients with and without intraoperative perfora-tions and regeneration of the membrane, complete with cilia, in approximately 5 months following complete removal.22 However, introduction of foreign materials during the access or apical resection/manipulation can initiate thickening of the sinus mucosa with symptoms of maxillary sinusitis.65
Conventional radiographs appear to be of limited value in predicting the potential for OAC, with the position of the root tip, periapical lesion, or outline of the lesion not statistically significant in that respect.197 In contrast, a CBCT survey of the intended surgical field is much more informative, providing accurate measurements of the osseous thickness, distance to the sinus floor, and presence of pathosis.28
Maxillary sinus complications secondary to the extrusion of root canal filling material need to be managed differently. Approximately 10% of all patients with chronic sinusitis are found to have an aspergilloma.101,168 It has been suggested that
FIG. 19-23 Diagrams showing removal of gutta-percha filling materials extruded beyond the radicular foramen. A, Solid gutta-percha filling extruded beyond the radicular foramen. B, Small space is created between the canal wall and the gutta-percha filling with a thin ultrasonic tip (such as a FRK-S ultrasonic tip). C, Gutta-percha removal hand instrument, such as the GPR instrument and the EGPR instrument, is brought into the canal with the tiny projection pressed against the gutta-percha filling to pull it out. D, Extruded gutta-percha root filling portion sepa-rated from the coronal portion within the canal. E, Chloroform is filled in the canal using a gutta-percha removal hand instrument and agitating it to dissolve the extruded portion. F, Gutta-percha filling material is diluted and dissolved with the hand instrument in push-and-pull motions.
A B C D E F
BOX 19-2
Common Causes of Damage to the IAN
1. Local anesthetic injections2. Third molar surgery3. Implants4. Endodontics (extrusion of the materials used in endodontic
treatment, overinstrumentation, elevated temperatures)5. Ablative surgery6. Trauma7. Orthognathic surgery

746 PART II The Advanced Science of Endodontics
Management should be performed by immediate removal of endodontic materials within 24 to 48 hours via periapical surgery, tooth extraction, or surgical debridement, whichever will be the most effective option with the least potential damage to the IAN.59,153,214,226
Nonsurgical Causes of IAN InjuryTrigeminal nerve injury is the most challenging consequence of contemporary dental surgical procedures with significant medical-legal repercussions (see also Chapter 29).38 An approx-imate estimation places the incidence if IAN injury at 5%, with approximately one third of these patients afflicted with neu-ropathies, including neuropathic pain.228 Neuropathic pain is characterized by symptoms that differ significantly from other chronic pain states, including paresthesia, either as a tingling or formication (ants crawling on the skin), burning or shooting pain, electric shock and evoked pain in the form of hyperalge-sia, and mechanical allodynia. There is almost always an area of abnormal sensation, and the patient’s maximum pain is often coexistent with the site of sensory deficit.227 This is an impor-tant diagnostic feature, as the sensory deficit is usually to noxious and thermal stimuli, indicating damage to small diam-eter afferent fibers of the spinothalamic tract.224
The highest incidence of reported damage to the inferior alveolar and lingual nerves is associated with third molar extractions.15,118,119 Local anesthesia was the second most common cause of nerve injury, and its exact mechanism can be confusing. It may be physical (needle damage, epineural/perineural hemorrhage) or chemical (local anesthetic con-tents). Reports have implicated certain local anesthetics of high concentrations (prilocaine 4% and articaine 4%) with IAN neuropathies (see also Chapter 4).14,110,120,216
A relatively small percentage of IAN injury cases (8%) are associated with an endodontic procedure.229 Mandibular second molars are most commonly associated with this popula-tion, but cases involving treatment of mandibular first molars and premolars have also been reported.148 The three primary factors responsible for instigating IAN damage during end-odontic treatment are as follows:1. Chemical factors: cytotoxic materials employed either in
the preparation (e.g., irrigation liquids, intracanal medica-ments)2,91 or the obturation of the canal space238
2. Mechanical factors: repeated insertions of endodontic instruments through the apex into the IAN and surrounding tissues57
3. Thermal factors: inappropriate/prolonged heat application71
The presence of bone between the apices and the IAN canal does not necessarily protect against injury to the nerve. Research has provided an enlightening explanation to this puzzle (Figs. 19-24, 19-25, and 19-26).288 Using fresh cadaver specimens (mandibles), researchers examined the true ana-tomic relationship among the root apices, inferior alveolar nerve, and the artery. They drew the following conclusions:◆ There was never any compact layer of cortical bone sur-
rounding the mandibular nerve sheath. In some cases a slightly denser cancellous bone was found, but it was replete with multiple perforations that would not afford significant resistance to penetration.115
◆ The proximity of the IAN canal to the apices of the second molars was < 1 mm, and it was more variable (1 to 4 mm) with first molars. This could explain the higher percentages of paresthesias reported with these teeth.
FIG. 19-24 Cross section of mandible in the molar region showing the presence of bone vacuoles (yellow arrows). (From Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by endodontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.)
FIG. 19-25 Longitudinal mandible cross section in the molar region showing the spongy bone cover of the neurovascular bundle. Note the multiple fenestrations and honeycombed trabeculations. (From Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by end-odontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.)

CHAPTER 19 Managing Iatrogenic Endodontic Events 747
◆ The mandibular artery ran along the superomedial side of the IAN up to the first molar, and then crossed on the upper side until the mental foramen. Perforation of this vessel, with the concomitant hemorrhage exerting pressure on the pedicle, could feasibly produce a paresthetic event via the resulting ischemia.58
◆ Only with root apices in direct contact with the IAN canal were extrusions able to penetrate the nerve. If cancellous bone was interspersed between the apices and pedicle, the spread of the extrusion through the trabeculations remained at the periphery of the sheath.
◆ The low density of trabeculations and presence of numerous vacuoles provided an avenue for the diffusion of extruded irrigation fluids and obturation materials toward the IAN bundle. In a tooth with apical resorption, the foramen is frequently enlarged310; these two factors in concert could explain the occurrence of sensory symptoms in the absence
of clinical or radiographic signs of overexpression or close proximity to the mandibular nerve.Prevention is the key to successful treatment. Damage,
either directly to the IAN or to the vessel(s) that nourish it, will result in sensory events that may be transient or perma-nent. Pretreatment radiographic assessment using periapical images is mandatory; in critical cases, CBCT may be more appropriate and precise in establishing proximity (Fig. 19-27). Every attempt should be undertaken to confine the instrumen-tation and irrigation processes to within the canal space; damage from extrusions can be chemical or mechanical in origin,251 and toxic products can easily diffuse through the trabecular spaces and vacuoles surrounding the nerve bundle. This latency in diffusion, and the potential onset of paresthetic symptoms, dictates close monitoring for 72 hours postopera-tively in cases where extrusion is apparent.214 Imprudent heat application during thermoplastic compaction of gutta-percha may also lead to IAN injury.26
There is a strong correlation between duration, origin, sig-nificance of the injury, and the prognosis for resolution of the paresthesia. The longer the irritation persists, either chemical of mechanical, the more fibers are involved in a degenerative process and the more likely the paresthesia will become per-manent.244 If injury to the nerve is demonstrated by postopera-tive neuropathy and radiographs confirm the presence of a significant extrusion into the IAN canal, management entails the surgical removal of the offending material.214,226,228 However, in spite of the best efforts to eliminate the causative agent, the symptoms may persist because of the associated chemical damage to the nerve. If sensory improvement has not been evident after 2 months, with or without repair during inter-ventional surgery, then the prognosis for recovery is poor, and steps should be taken to alleviate the patient’s concerns through counseling and systemic medications for chronic pain.229
Surgical Causes of IAN InjurySurgical endodontic procedures need to be designed to mini-mize trauma to nerves including the IAN, mental nerve, and mental foramen. Although the mental foramen is most often
FIG. 19-26 Overfill of the distal root under direct observation. Note the proximity of the extruded material to the artery and nerve bundle (pedicle). (From Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by endodontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.)
FIG. 19-27 A, Panoramic radiograph demonstrating significant overfilling and extension in the radicular vacu-oles and overlying the mandibular canal. B, A coronal CT section demonstrating that the extruded material is lateral and below the mandibular bundle (arrows). The patient’s sensory complications were temporary. (From Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by endodontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.)
A B

748 PART II The Advanced Science of Endodontics
located apically to the second premolar,190,211–213 it can vary in anterior-posterior locations,139,193 coronal-apical locations,77 and number. Pogrel215 concluded that the severity of the injury was proportional to the process by which the injury was created, and these processes included scalpel blade wounding/transection, crushing, and stretching damages. These would be analogous to the dissection and reflection of the flap, improper retraction location/application, and postoperative edema.
If the transected ends are closely approximated following the injury, either naturally or surgically, proliferating axons will attempt to bridge the gap and, if they find a perineural tube to populate, gradually restore function. However, in cases where the gap is beyond a critical length, a neuroma may develop at the proximal end. Neuromas consist of dense fibrous tissue intermingled with nerve fascicles, with a disproportionate pro-liferation of unmyelinated fibers. Treatment, if initiated within 3 months of the initial event, often entails resection of the neuroma and repair by tension-free anastomosis or nerve grafting.
Careful presurgical assessment via radiographs and CBCT provides critical information on the size, location, and spatial relation of the planned surgery to nearby trigeminal nerves.27 Before exiting the mandibular canal, the nerve often loops anteriorly, then superior and posteriorly in the apical portion of the premolar region.100 If an apical procedure is planned in an area commensurate with this anatomic variant, then CBCT is warranted and strongly advised. Controlled reflection of the tissue overlying the suspected location of the foramen will diminish the incidence of transection. Cautious reflection of the flap will reveal evidence of tissue “funneling” at its base (Fig. 19-28); this is the telltale sign of the exiting nerve bundle.194 This exiting tissue, upon discovery, can be marked with a dot of gentian violet or methylene blue dye. By high-lighting it in this fashion, the surgeon can avoid unintentional impingement with a retractor. The tissues should be minimally distended and the underside of the flap kept well hydrated.
Transient paresthesia may occur in cases where a protracted surgical procedure, inadvertent stretching, or excessive post-
FIG. 19-28 Full-thickness reflection of the flap in the region of the premolar root apices reveals the mental nerve exiting the foramen; note how the tissue “funnels” from the reflected flap to the foramen. (From Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by end-odontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.)
operative edema has occurred. Appropriate reevaluation appointments include neurosensory testing and mapping the outline of the sensory deficit. Return of sensation within the first 4 weeks indicates a neuropraxia and implies an excellent prognosis.
PrognosisAlthough the prognosis in the case of the IAN damage caused by resorbable or inert material is favorable, as it is dissolved over time, the toxicity of the material, whether chemical or pH, may cause permanent damage if left in place.195 In addition, pressure from the material on the IAN may be caused by a hematoma or inflammatory, which can also contribute to tem-porary or permanent IAN damage.72,195
The prognosis of the IAN damage depends on the severity of the direct injury to the nerve, toxicity of the irritant, the amount and speed of its resorption, and how rapidly the caus-ative agent is removed.195,198,214 Because the paresthesia can be of both a mechanical and a chemical nature, removal of the excess material might not be sufficient if the nerve fibers have already undergone degeneration from a chemical irritant. Nevertheless, paresthesia caused by an instant irritation of the nerve, like a minor overinstrumentation or swelling from infection or minor inflammation, usually subsides within days. If no signs of healing are observed within 6 months, the chances of healing are considered much lower, although normal sensory function might still return after this time.94,288 Counseling and therapeutic management are indicated within 48 hours for injuries caused by endodontic treatment or local anesthetic injections.81
Radiographs, especially CBCT, are often useful in revealing the extent of tissue damage in relation to hard tissues (e.g., the size and location of the lesion or the location of extruded materials in relation to the mandibular canal or the maxillary sinus).26,85,94
Prevention of Complications Due to Nerve InjuryPrevention of complications during root canal treatment should be the main focus, as once permanent nerve injury has occurred the patient may not regain normal sensation.307 Careful consideration should also focus on the distance between the root apices and the mandibular canal. For man-dibular first molars, this distance varies between 1 and 4 mm, and for mandibular second and third molars, the distance can be less than 1 mm.288 With mandibular premolars, the proxim-ity of a mental foramen should always be considered.192 In addition, a study using CBCT has shown that the mesiobuccal root apex of maxillary second molars is frequently in very close proximity with the sinus floor199 (Fig. 19-29).
CERVICOFACIAL SUBCUTANEOUS EMPHYSEMASubcutaneous emphysema is defined as the penetration of air or other gases beneath the skin and submucosa, resulting in soft tissue distention. A specific type, termed cervicofacial subcutane-ous emphysema (CFSE), is a relatively rare occurrence and may be limited to traumatic, iatrogenic, or spontaneous events.
The first recorded instance was reported by Turnbull in 1900.293 It details the account of a musician inducing CFSE by
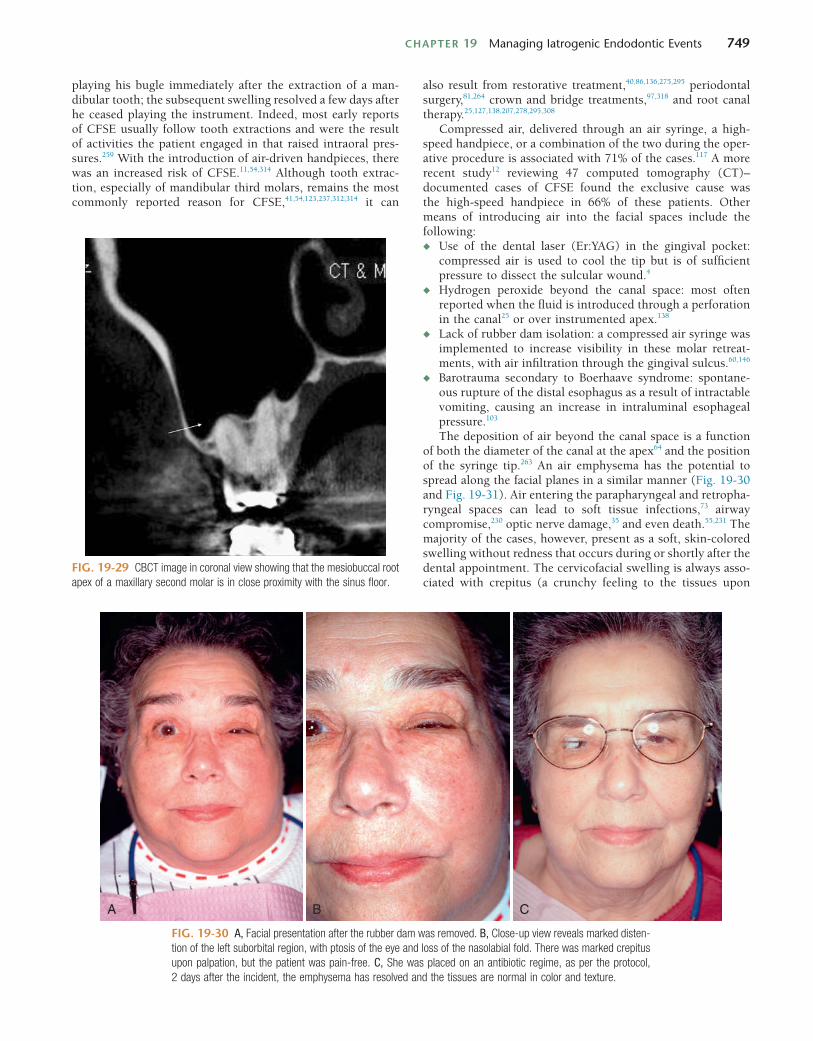
CHAPTER 19 Managing Iatrogenic Endodontic Events 749
also result from restorative treatment,40,86,136,275,295 periodontal surgery,81,264 crown and bridge treatments,97,318 and root canal therapy.25,127,138,207,278,295,308
Compressed air, delivered through an air syringe, a high-speed handpiece, or a combination of the two during the oper-ative procedure is associated with 71% of the cases.117 A more recent study12 reviewing 47 computed tomography (CT)–documented cases of CFSE found the exclusive cause was the high-speed handpiece in 66% of these patients. Other means of introducing air into the facial spaces include the following:◆ Use of the dental laser (Er:YAG) in the gingival pocket:
compressed air is used to cool the tip but is of sufficient pressure to dissect the sulcular wound.4
◆ Hydrogen peroxide beyond the canal space: most often reported when the fluid is introduced through a perforation in the canal25 or over instrumented apex.138
◆ Lack of rubber dam isolation: a compressed air syringe was implemented to increase visibility in these molar retreat-ments, with air infiltration through the gingival sulcus.60,146
◆ Barotrauma secondary to Boerhaave syndrome: spontane-ous rupture of the distal esophagus as a result of intractable vomiting, causing an increase in intraluminal esophageal pressure.103
The deposition of air beyond the canal space is a function of both the diameter of the canal at the apex64 and the position of the syringe tip.263 An air emphysema has the potential to spread along the facial planes in a similar manner (Fig. 19-30 and Fig. 19-31). Air entering the parapharyngeal and retropha-ryngeal spaces can lead to soft tissue infections,73 airway compromise,230 optic nerve damage,35 and even death.55,231 The majority of the cases, however, present as a soft, skin-colored swelling without redness that occurs during or shortly after the dental appointment. The cervicofacial swelling is always asso-ciated with crepitus (a crunchy feeling to the tissues upon
FIG. 19-29 CBCT image in coronal view showing that the mesiobuccal root apex of a maxillary second molar is in close proximity with the sinus floor.
FIG. 19-30 A, Facial presentation after the rubber dam was removed. B, Close-up view reveals marked disten-tion of the left suborbital region, with ptosis of the eye and loss of the nasolabial fold. There was marked crepitus upon palpation, but the patient was pain-free. C, She was placed on an antibiotic regime, as per the protocol, 2 days after the incident, the emphysema has resolved and the tissues are normal in color and texture.
A B C
playing his bugle immediately after the extraction of a man-dibular tooth; the subsequent swelling resolved a few days after he ceased playing the instrument. Indeed, most early reports of CFSE usually follow tooth extractions and were the result of activities the patient engaged in that raised intraoral pres-sures.259 With the introduction of air-driven handpieces, there was an increased risk of CFSE.11,54,314 Although tooth extrac-tion, especially of mandibular third molars, remains the most commonly reported reason for CFSE,41,54,123,237,312,314 it can

750 PART II The Advanced Science of Endodontics
which replaces the trapped air, is more readily absorbed at the site.146 More severe presentations warrant hospitalization with intravenous antibiotics, where the extent and regression of the CFSE can be closely monitored using CT scans and complications can be managed more effectively.31 Resolution, barring any severe complications, is characteristically rapid and uneventful, with the patients returning to their normal appear-ance within 4 to 7 days. A reevaluation of the cause of the emphysema should be examined and corrected before treat-ment resumes, especially in instances of a perforation.
From an endodontic perspective, minimizing compressed air at the site, from either a high-speed handpiece or an air syringe, is key to preventing this consequence. Isolation with a rubber dam, the use of paper points or high-volume aspira-tion for drying canal spaces, and avoiding the use of hydrogen peroxide during the procedure will also reduce the risk of introducing or entrapping air beneath the overlying tissues. For endodontic microsurgery, the use of a rear-exhausting high-speed handpiece for root resection as well as ultrasonics for root end preparation would decrease the likelihood of pre-cipitating a CFSE during root end procedures.16
palpation), which may not be palpable before a latency period of several hours. The more serious presentation of pneumome-diastinum is characterized by dyspnea with a brassy voice, chest or back pain, and Hamman sign (a bubbling or crunching sound caused by air or movement accompanied by cardiac pulsation).109 Secondary complications such as pyogenic medi-astinitis or necrotizing fasciitis must be considered, and appro-priate means taken to evaluate and manage them (blood cultures, broad-spectrum intravenous antibiotics).60 Differen-tial diagnosis should include an allergic reaction (more pro-nounced dermal signs prior to cardiac/respiratory symptoms), hematoma (a rapid accumulation of fluid without initial dis-coloration and without crepitation), and angioneurotic edema (a defined, circumscribed area of edema, often preceded by a burning sensation in the mucous membranes or skin).81
Treatment is largely empirical and dependent on the extent of the CFSE. Antibiotics are usually prescribed due to the non-sterility of the air supply and the possibility of necrotic debris or microorganisms forced into surrounding tissues.230 Admin-istration of 100% oxygen via a non-rebreather mask is reported to hasten the resolution of the emphysema because the oxygen,
FIG. 19-31 A, Preoperative radiograph tooth #10136; dystrophic calcification has obliterated the pulp chamber and the coronal half of the canal space. B, A #10 file inserted to estimated working length; the file is actually through a facial perforation of the root at the radicular extent of the ultrasonic excavation. Repeated drying of the canal space using an air syringe forced air through the perforation site and precipitated the emphysema seen in Fig. 19-26 (A and B). C, The radicular perforation site was sealed with mineral trioxide aggregate (MTA) before the canal space was obturated. The tooth has remained asymptomatic since the incident.
A B C
REFERENCES1. Abbasipour F, Rastqar A, Bakhtiar H, et al: The
nociceptive and anti-nociceptive effects of white mineral trioxide aggregate, Int Endod J 42:794, 2009.
2. Ahlgren FK, Johannessen AC, Hellem S: Displaced calcium hydroxide paste causing inferior alveolar nerve paraesthesia: report of a case, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:734, 2003.
3. Ahonen M, Tjaderhane L: Endodontic-related paresthesia: a case report and literature review, J Endod 37:1460, 2011.
4. Mitsunaga S, Iwai T, Aoki N, et al: Cervicofacial subcutaneous and mediastinal emphysema caused by air
cooling spray of dental laser, Oral Surg Oral Med Oral Pathol Oral Radiol 115:e13, 2013.
5. Alapati SB, Brantley WA, Svec TA, et al: SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical use, J Endod 31:40, 2005.
6. Albrecht LJ, Baumgartner JC, Marshall JG: Evaluation of apical radicular debris removal using various sizes and tapers of ProFile GT files, J Endod 30:425, 2004.
7. Al-Fouzan KS: Incidence of rotary ProFile instrument fracture and the potential for bypassing in vivo, Int Endod J 36:864, 2003.
8. Al-Omari MA, Dummer PM: Canal blockage and debris extrusion with eight preparation techniques, J Endod 21:154, 1995.
9. Alomairy KH: Evaluating two techniques on removal of fractured rotary nickel-titanium endodontic instruments from root canals: an in vitro study, J Endod 35:559, 2009.
10. American Association of Endodontists: Glossary of endodontic terms, ed 7, Chicago, 2003, American Association of Endodontists.
11. American Association of Oral and Maxillofacial Surgeons, Council on Dental Materials, Instruments and Equipment:

CHAPTER 19 Managing Iatrogenic Endodontic Events 751
Air-driven handpieces and air emphysema, J Am Dent Assoc 123:108, 1992.
12. Arai I, Aoki T, Yamazaki H, et al: Pneumomediastinum and subcutaneous emphysema after dental extraction detected incidentally by regular medical checkup: a case report, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107:e33, 2009.
13. Augsburge RA, Peters DD: Radiographic evaluation of extruded obturation materials, J Endod 16:492, 1990.
14. Bartling R, Freeman K, Kraut RA: The incidence of altered sensation of the mental nerve after mandibular implant placement, J Oral Maxillofac Surg 57:1408, 1999.
15. Bataineh AB: Sensory nerve impairment following mandibular third molar surgery, J Oral Maxillofac Surg 59:1012; discussion 7, 2001.
16. Battrum DE, Gutmann JL: Implications, prevention and management of subcutaneous emphysema during endodontic treatment, Endod Dent Traumatol 11:109, 1995.
17. Baumgartner JC, Mader CL: A scanning electron microscopic evaluation of four root canal irrigation regimens, J Endod 13:147, 1987.
18. Beck-Mannagetta J, Necek D, Grasserbauer M: Solitary aspergillosis of maxillary sinus, a complication of dental treatment, Lancet 2:1260, 1983.
19. Beck-Mannagetta J, Necek D, Grasserbauer M: Zahnaerztliche Aspekte der solitaeren Kieferhoehlen-Aspergillose, Z Stomatol 83:283, 1986.
20. Becker GL, Cohen S, Borer R: The sequelae of accidentally injecting sodium hypochlorite beyond the root apex: report of a case, Oral Surg Oral Med Oral Pathol 38:633, 1974.
21. Becking AG: Complications in the use of sodium hypochlorite during endodontic treatment: report of three cases, Oral Surg Oral Med Oral Pathol 71:346, 1991.
22. Benninger MS, Sebek BA, Levine HL: Mucosal regeneration of the maxillary sinus after surgery, Otolaryngol Head Neck Surg 101:33, 1989.
23. Bergenholtz G, Lekholm U, Milthon R, Engstrom B: Influence of apical overinstrumentation and overfilling on re-treated root canals, J Endod 5:310, 1979.
24. Betti LV, Bramante CM: Quantec SC rotary instruments versus hand files for gutta-percha removal in root canal retreatment, Int Endod J 34:514, 2001.
25. Bhat KS: Tissue emphysema caused by hydrogen peroxide, Oral Surg Oral Med Oral Pathol 38:304, 1974.
26. Blanas N, Kienle F, Sandor GK: Inferior alveolar nerve injury caused by thermoplastic gutta-percha overextension, J Can Dent Assoc 70:384, 2004.
27. Bornstein MM, Lauber R, Sendi P, von Arx T: Comparison of periapical radiography and limited cone-beam computed tomography in mandibular molars for analysis of anatomical landmarks before apical surgery, J Endod 37:151, 2011.
28. Bornstein MM, Wasmer J, Sendi P, et al: Characteristics and dimensions of the Schneiderian membrane and apical bone in maxillary molars referred for apical surgery: a comparative radiographic analysis using limited cone beam computed tomography, J Endod 38:51, 2012.
29. Boutsioukis C, Verhaagen B, Versluis M, et al: Evaluation of irrigant flow in the root canal using different needle types by an unsteady computational fluid dynamics model, J Endod 36:875, 2010.
30. Bowden JR, Ethunandan M, Brennan PA: Life-threatening airway obstruction secondary to hypochlorite extrusion during root canal treatment, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:402, 2006.
31. Breznick DA, Saporito JL: Iatrogenic retropharyngeal emphysema with impending airway obstruction, Arch Otolaryngol Head Neck Surg 115:1367, 1989.
32. Brown DC, Moore BK, Brown CE, Newton CW: An in vitro study of apical extrusion of sodium hypochlorite during endodontic canal preparation, J Endod 12:587, 1995.
33. Bryant ST, Thompson SA, al-Omari MA, Dummer PM: Shaping ability of ProFile rotary nickel-titanium
instruments with ISO sized tips in simulated root canals: part 1, Int Endod J 31:275, 1998.
34. Buckley M, Sprangberg LSW: The prevalence and technical quality of endodontic treatment in an American subpopulation, Oral Pathol Oral Radiol Endod 79:92, 1995.
35. Buckley MJ, Turvey TA, Schumann SP, Grimson BS: Orbital emphysema causing vision loss after a dental extraction, J Am Dent Assoc 120:421; discussion 423, 1990.
36. Budd CS, Weller RN, Kulild JC: A comparison of thermoplasticized injectable gutta-percha obturation techniques, J Endod 17:260, 1991.
37. Budd JC, Gekelman D, White JM: Temperature rise of the post and on the root surface during ultrasonic post removal, Int Endod J 38:705, 2005.
38. Caissie R, Goulet J, Fortin M, Morielli D: Iatrogenic paresthesia in the third division of the trigeminal nerve: 12 years of clinical experience, J Can Dent Assoc 71:185, 2005.
39. Candeiro GTM, Correia FC, Duarte MAH, et al: Evaluation of radiopacity, ph, release of calcium ions, and flow of a bioceramic root canal Sealer, J Endod 38:842, 2012.
40. Chan DC, Myers T, Sharaway M: A case for rubber dam application—subcutaneous emphysema after Class V procedure, Oper Dent 32:193, 2007.
41. Chen SC, Lin FY, Chang KJ: Subcutaneous emphysema and pneumomediastinum after dental extraction, Am J Emerg Med 17:678, 1999.
42. Chenail BL, Teplitsky PE: Orthograde ultrasonic retrieval of root canal obstructions, J Endod 13:186, 1987.
43. Cheung GS, Peng B, Bian Z, et al: Defects in ProTaper S1 instruments after clinical use: fractographic examination, Int Endod J 38:802, 2005.
44. Chutich MJ, Kaminski EJ, Miller DA, Lautenschlager EP: Risk assessment of the toxicity of solvents of gutta- percha used in endodontic retreatment, J Endod 24:213, 1998.
45. Clegg MS, Vertucci FJ, Walker C, et al: The effect of exposure to irrigant solutions on apical dentin biofilms in vitro, J Endod 32:434, 2006.
46. Cohen S, Burns RC: Pathways of the pulp, ed 3, St. Louis, 1984, CV Mosby, pp 291-292.
47. Cohen S, Burns RC: Pathways of the pulp, ed 5, St. Louis, 1991, Mosby.
48. Cohen S, Burns RC: Pathways of the pulp, ed 8, St Louis, 2002, Mosby, pp 94, 242-252, 530, 870, 910.
49. Cohen S, Hargreaves KM: Pathways of the pulp, ed 9, St Louis, 2006, Mosby, pp 992-994.
50. Crump MC, Natkin E: Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation, J Am Dent Assoc 80:1341, 1970.
51. Cuje J, Bargholz C, Hulsmann M: The outcome of retained instrument removal in a specialist practice, Int Endod J 43:545, 2010.
52. Dan AE, Thygesen TH, Pinholt EM: Corticosteroid administration in oral and orthognathic surgery: a systematic review of the literature and meta-analysis, J Oral Maxillofac Surg 68:2207, 2010.
53. Daugherty DW, Gound TG, Comer TL: Comparison of fracture rate, deformation rate, and efficiency between rotary endodontic instruments driven at 150 rpm and 350 rpm, J Endod 27:93, 2001.
54. Davies DE: Pneumomediastinum after dental surgery, Anaesth Intensive Care 29:638, 2001.
55. Davies JM, Campbell LA: Fatal air embolism during dental implant surgery: a report of three cases, Can J Anaesth 37:112, 1990.
56. De-Deus G, Moreira EJ, Lopes HP, Elias CN: Extended cyclic fatigue life of F2 Pro-Taper instruments used in reciprocating movement, Int Endod J 43:1063, 2010.
57. Dempf R, Hausamen JE: Lesions of the inferior alveolar nerve arising from endodontic treatment, Aust Endod J 26:67, 2000.
58. Denio D, Torabinejad M, Bakland LK: Anatomical relationship of the mandibular canal to its surrounding structures in mature mandibles, J Endod 18:161, 1992.
59. Dorn S, Garther A: Case selection and treatment planning. In Cohen S, Burns RC, editors: Pathways of the pulp, ed 7, St Louis, 1998, Mosby, p 60.
60. Durukan P, Salt O, Ozkan S, et al: Cervicofacial emphysema and pneumomediastinum after a high-speed air drill endodontic treatment procedure, Am J Emerg Med 30:2095.e3, 2012.
61. Eberhardt JA, Torabinejad M, Christiansen EL: A computed tomographic study of the distances between the maxillary sinus floor and the apices of the maxillary posterior teeth, Oral Surg Oral Med Oral Pathol 73:345, 1992.
62. Edgar SW, Marshall JG, Baumgartner JC: The antimicrobial effect of chloroform on Enterococcus faecalis after gutta-percha removal, J Endod 32:1185, 2006.
63. Ehrich DG, Brian JD Jr, Walker WA: Sodium hypochlorite accident: inadvertent injection into the maxillary sinus, J Endod 19:180, 1993.
64. Eleazer PD, Eleazer KR: Air pressures developed beyond the apex from drying root canals with pressurized air, J Endod 24:833, 1998.
65. Ericson S, Finne K, Persson G: Results of apicoectomy of maxillary canines, premolars and molars with special reference to oroantral communication as a prognostic factor, Int J Oral Surg 3:386, 1974.
66. Eriksson AR, Albrektsson T: Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit, J Prosthet Dent 50:101, 1983.
67. Erisen R, Yucel T, Kucukay S: Endomethasone root canal filling material in the mandibular canal: a case report, Oral Surg Oral Med Oral Pathol 68:343, 1989.
68. Escoda-Francoli J, Canalda-Sahli C, Soler A, et al: Inferior alveolar nerve damage because of overextended endodontic material: a problem of sealer cement biocompatibility? J Endod 33:1484, 2007.
69. Esposito P, Cunnington C: A comparison of canal preparation with nickel-titanium and stainless steel instruments, J Endod 21:173, 1995.
70. Ettrich CA, Labossiere PE, Pitts DL, et al: An investigation of the heat induced during ultrasonic post removal, J Endod 33:1222, 2007.
71. Fanibunda K, Whitworth J, Steele J: The management of thermomechanically compacted gutta percha extrusion in the inferior dental canal, Br Dent J 184:330, 1998.
72. Farren ST, Sadoff RS, Penna KJ: Sodium hypochlorite chemical burn: case report, N Y State Dent J 74:61, 2008.
73. Feinstone T: Infected subcutaneous emphysema: report of case, J Am Dent Assoc 83:1309, 1971.
74. Feldman G, Solomon C, Notaro P, Moskowitz E: Retrieving broken endodontic instruments, J Am Dent Assoc 88:588, 1974.
75. Felippe MC, Felippe WT, Marques MM, Antoniazzi JH: The effect of the renewal of calcium hydroxide paste on the apexification and periapical healing of teeth with incomplete root formation, Int Endod J 38:436, 2005.
76. Ferraz CC, Gomes NV, Gomes BP, et al: Apical extrusion of debris and irrigants using two hand and three engine-driven instrumentation techniques, Int Endod J 34:354, 2001.
77. Fishel D, Buchner A, Hershkowith A, Kaffe I: Roentgenologic study of the mental foramen, Oral Surg Oral Med Oral Pathol 41:682, 1976.
78. Fors UGH, Berg JO: A method for the removal of separated endodontic instruments from root canals, J Endod 9:156, 1983.
79. Fox J, Moodnik RM, Greenfield E, Atkinson JS: Filling root canals with files: radiographic evaluation of 304 cases, N Y State Dent J 38:154, 1972.
80. Freedman A, Horowitz I: Complications after apicoectomy in maxillary premolar and molar teeth, Int J Oral Maxillofac Surg 28:192, 1989.
752 PART II The Advanced Science of Endodontics
81. Fruhauf J, Weinke R, Pilger U, et al: Soft tissue cervicofacial emphysema after dental treatment: report of 2 cases with emphasis on the differential diagnosis of angioedema, Arch Dermatol 141:1437, 2005.
82. Fu M, Zhang Z, Hou B: Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome, J Endod 37:619, 2011.
83. Gambarini G: Rational for the use of low-torque endodontic motors in root canal instrumentation, Endod Dent Traumal 16:95, 2000.
84. Gambarini G: Cyclic fatigue of nickel-titanium rotary instruments after clinical use with low-and high-torque endodontic motors, J Endod 27:772, 2001.
85. Gambarini G, Plotino G, Grande NM, et al: Differential diagnosis of endodonticrelated inferior alveolar nerve paraesthesia with cone beam computed tomography: a case report, Int Endod J 44:176, 2011.
86. Gamboa Vidal CA, Vega Pizarro CA, Almeida Arriagada A: Subcutaneous emphysema secondary to dental treatment: case report, Medicina Oral, Patologia Oral y Cirugia Bucal 12:E76, 2007.
87. Gandolfi MG, Siboni F, Primus CM, Prati C: Ion release, porosity, solubility, and bioactivity of MTA plus tricalcium silicate, J Endod 40:1632, 2014.
88. Gao Y, Shotton V, Wilkinson K, et al: Effects of raw material and rotational speed on the cyclic fatigue of ProFile Vortex rotary instruments, J Endod 36:1205, 2010.
89. Gatot A, Arbelle J, Leiberman A, Yanai-Inbar I: Effects of sodium hypochlorite on soft tissues after its inadvertent injection beyond the root apex, J Endod 17:573, 1991.
90. George S, Basrani B, Kishen A: Possibilities of gutta-percha-centered infection in endodontically treated teeth: an in vitro study, J Endod 36:1241, 2010.
91. Gernhardt CR, Eppendorf K, Kozlowski A, Brandt M: Toxicity of concentrated sodium hypochlorite used as an endodontic irrigant, Int Endod J 37:272, 2004.
92. Gettleman BH, Spriggs KA, ElDeeb ME, Messer HH: Removal of canal obstructions with the endo extractor, J Endod 17:608, 1991.
93. Giardino L, Pontieri F, Savoldi E, Tallarigo F: Aspergillus mycetoma of the maxillary sinus secondary to overfilling of a root canal, J Endod 32:692, 2006.
94. Giuliani M, Lajolo C, Deli G, et al: Inferior alveolar nerve paresthesia caused by endodontic pathosis: a case report and review of the literature, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:670, 2001.
95. Glickman GN, Koch KA: 21st century endodontics, J Am Dent Assoc 131:39, 2000.
96. Gluskin AH, Ruddle CJ, Zinman EJ: Thermal injury through intraradicular heat transfer using ultrasonic devices: precautions and practical preventive strategies, J Am Dent Assoc 136:1286, 2005.
97. Goorhuis H, Rothrock SG: Cervicofacial and thoracic barotrauma following a minor dental procedure, Pediatr Emerg Care 9:29, 1993.
98. Gorduysus M, Avcu N, Gorduysus O, et al: Cytotoxic effects of four different endodontic materials in human periodontal ligament fibroblasts, J Endod 33:1450, 2007.
99. Greene KJ, Krell KV: Clinical factors associated with ledged canals in maxillary and mandibular molars, Oral Surg Oral Med Oral Pathol 70:490, 1990.
100. Greenstein G, Tarnow D: The mental foramen and nerve: clinical and anatomical factors related to dental implant placement: a literature review, J Periodontol 77:1933, 2006.
101. Grigorin D, Brambule J, Delacretaz J: La sinusite maxillaire fungique, Dermatologica 159:180, 1979.
102. Guerreiro-Tanomaru JM, De Faria-Jnior NB, Duarte MAH, et al: Comparative analysis of Enterococcus faecalis biofilm formation on different substrates, J Endod 39:346, 2013.
103. Gulati A, Baldwin A, Intosh IM, Krishnan A: Pneumomediastinum, bilateral pneumothorax, pleural effusion, and surgical emphysema after routine
apicectomy caused by vomiting, Br J Oral Maxillofac Surg 46:136, 2008.
104. Gursoy UK, Bostanci V, Kosger HH: Palatal mucosa necrosis because of accidental sodium hypochlorite injection instead of anaesthetic solution, International Endod J 39:157, 2006.
105. Gutmann JL, Dumsha TC, Lovdahl PE, Hovland EJ: Problem solving in endodontics, ed 3, St Louis, 1997, Mosby, pp 96-100, 117.
106. Gutmann JL, Rakusin H: Perspectives on root canal obturation with thermoplasticized injectable gutta-percha, Int Endod J 20:261, 1987.
107. Haikel Y, Serfaty R, Bateman G, et al: Dynamic and cyclic fatigue of engine-driven rotary nickel-titanium endodontic instruments, J Endod 25:434, 1999.
108. Hammad M, Qualtrough A, Silikas N: Three-dimensional evaluation of effectiveness of hand and rotary instrumentation for retreatment of canals filled with different materials, J Endod 34:1370, 2008.
109. Hamman L: Spontaneous mediastinal emphysema, Bull Johns Hopkins Hosp 54:46, 1961.
110. Handschel J, Figgener L, Joos U: [Forensic evaluation of injuries to nerves and jaw bone after wisdom tooth extraction from the viewpoint of current jurisprudence], Mund Kiefer Gesichtschir 5:44, 2001.
111. Hapcook CP Sr: Dental malpractice claims: percentages and procedures, J Am Dent Assoc 137:1444, 2006.
112. Harty FJ, Parkins BJ, Wengraf AM: Success rate in root canal therapy: a retrospective study of conventional cases, Br Dent J 128:65, 1970.
113. Hashem AA: Ultrasonic vibration: temperature rise on external root surface during broken instrument removal, J Endod 33:1070, 2007.
114. Hauman CH, Chandler NP, Tong DC: Endodontic implications of the maxillary sinus: a review, Int Endod J 35:127, 2002.
115. Heasman PA: Variation in the position of the inferior dental canal and its significance to restorative dentistry, J Dent 16:36, 1988.
116. Heling I, Rotstein I, Dinur T, et al: Bactericidal and cytotoxic effects of sodium hypochlorite and sodium dichloroisocyanurate solutions in vitro, J Endod 27:278, 2001.
117. Heyman SN, Babayof I: Emphysematous complications in dentistry, 1960-1993: an illustrative case and review of the literature, Quintessence Int 26:535, 1995.
118. Hillerup S: Iatrogenic injury to oral branches of the trigeminal nerve: records of 449 cases, Clin Oral Investig 11:133, 2007.
119. Hillerup S: Iatrogenic injury to the inferior alveolar nerve: etiology, signs and symptoms, and observations on recovery, Int J Oral Maxillofac Surg 37:704, 2008.
120. Hillerup S, Jensen R: Nerve injury caused by mandibular block analgesia, Int J Oral Maxillofac Surg 35:437, 2006.
121. Himel V, Ahmed K, Wood D, et al: An evaluation of nitinol and stainless steel files used by students during a laboratory proficiency exam, Oral Surg 79:232, 1995.
122. Hinrichs RE, Walker WA, Schindler WG: A comparison of amounts of apically extruded debris using handpiece-driven nickel-titanium instrument systems, J Endod 24:102, 1998.
123. Horowitz I, Hirshberg A, Freedman A: Pneumomediastinum and subcutaneous emphysema following surgical extraction of mandibular third molars: three case reports, Oral Surg Oral Med Oral Pathol 63:25, 1987.
124. Huang X, Ling J, Gu L: Quantitative evaluation of debris extruded apically by using ProTaper Universal Tulsa Rotare System in endodontic retreatment, J Endod 33:1102, 2007.
125. Hulsmann M: Removal of fractured root canal instruments using the Canal Finder System, Dtsch Zahnarztl Z 45:229, 1990.
126. Hulsmann M: Methods for removing metal obstructions from the root canal, Endod Dent Traumatol 9:223, 1993.
127. Hulsmann M, Hahn W: Complications during root canal irrigation: literature review and case reports, Int Endod J 33:186, 2000.
128. Hulsmann M, Peters OA, Dummer PMH: Mechanical preparation of root canals: shaping goals, techniques and means, Endod Topics 10:30, 2005.
129. Hülsmann M, Stotz S: Efficacy, cleaning ability and safety of different devices for gutta-percha removal in root canal retreatment, Int Endod J 30:227, 1997.
130. Ingle JI: PDQ endodontics, London, 2005, BC Decker, p 220.
131. Ingle JI, Bakland LK: Endodontics, ed 5, London, 2002, BC Decker, pp 412, 482-489, 525-538, 695, 729, 769, 776.
132. Ingle JI, Luebke RG, Zidell JD, et al: Obturation of the radicular space. In Ingle JI, Taintor JF, editors: Endodontics, ed 3, Philadelphia, 1985, Lea & Febiger, pp 223-307.
133. Ioannides C, Borstlap WA: Apicoectomy on molars: a clinical and radiographical study, Int J Oral Surg 12:73, 1983.
134. Jafarzadeh H, Abbott PV: Ledge formation: review of a great challenge in endodontics, J Endod 33:1155, 2007.
135. Jiang LM, Verhaagen B, Versluis M, van der Sluis LWM: The influence of the orientation of an ultrasonic file on the cleaning efficacy of ultrasonic activated irrigation, J Endod 36:1372, 2010.
136. Josephson GD, Wambach BA, Noordzji JP: Subcutaneous cervicofacial and mediastinal emphysema after dental instrumentation, Otolaryngol Head Neck Surg 124:170, 2001.
137. Kapalas A, Lambrianidis T: Factors associated with root canal ledging during instrumentation, Endod Dent Traumatol 16:229, 2000.
138. Kaufman AY: Facial emphysema caused by hydrogen peroxide irrigation: report of a case, J Endod 7:470, 1981.
139. Kekere-Ekun TA: Antero-posterior location of the mental foramen in Nigerians, Afr Dent J 3:2, 1989.
140. Kerbl FM, DeVilliers P, Litaker M, Eleazer PD: Physical effects of sodium hypochlorite on bone: an ex vivo study, J Endod 38:357, 2012.
141. Kfir A, Tsesis I, Yakirevich E, et al: The efficacy of five techniques for removing root filling material: microscopic versus radiographic evaluation, Int Endod J 45:35, 2012.
142. Khademi A, Yazdizadeh M, Feizianfard M: Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems, J Endod 32:417, 2006.
143. Khongkhunthian P, Reichart PA: Aspergillosis of the maxillary sinus as a complication of overfilling root canal material into the sinus: report of two cases, J Endod 27:476, 2001.
144. Kim EC, Lee BC, Chang HS, et al: Evaluation of the radiopacity and cytotoxicity of Portland cements containing bismuth oxide, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 105:e54, 2008.
145. Kim JY, Cheung GS, Park SH, et al: Effect from cyclic fatigue of nickel-titanium rotary files on torsional resistance, J Endod 38:527, 2012.
146. Kim Y, Kim MR, Kim SJ: Iatrogenic pneumomediastinum with extensive subcutaneous emphysema after endodontic treatment: report of 2 cases, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109:e114, 2010.
147. Kleier DJ, Averbach RE, Mehdipour O: The sodium hypochlorite accident: experience of diplomates of the American Board of Endodontics, J Endod 34:1346, 2008.
148. Knowles KI, Jergenson MA, Howard JH: Paresthesia associated with endodontic treatment of mandibular premolars, J Endod 29:768, 2003.
149. Kobayashi A: Asymptomatic aspergillosis of the maxillary sinus associated with foreign body of endodontic origin: report of a case, Int J Oral Maxillofac Surg 24:243, 1995.
150. Koch K: The microscope: its effect on your practice, Dent Clin North Am 41:619, 1997.

CHAPTER 19 Managing Iatrogenic Endodontic Events 753
151. Kopp W, Fotter R, Steiner H, et al: Aspergillosis of the paranasal sinuses, Radiology 156:715, 1985.
152. Kosti E, Zinelis S, Lambrianidis T, Margelos J: A comparative study of crack development in stainless-steel Hedström files used with step-back or crown-down techniques, J Endod 30:38, 2004.
153. Kothari P, Hanson N, Cannell H: Bilateral mandibular nerve damage following root canal therapy, Br Dent J 180:189, 1996.
154. Kramkowski TR, Bahcall J: An in vitro comparison of torsional stress and cyclic fatigue resistance of ProFile GT and ProFile GT Series X rotary nickel-titanium files, J Endod 35:404, 2009.
155. Krasner P, Rankow HJ: Anatomy of the pulp-chamber floor, J Endod 30:5, 2004.
156. Kremeier K, Pontius O, Klaiber B, Hulsmann M: Nonsurgical endodontic management of a double tooth: a case report, Int Endod J 40:908, 2007.
157. Kulild JC, Peters DD: Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars, J Endod 16:311, 1990.
158. Kytridou V, Gutmann JL, Nunn MH: Adaptation and sealability of two contemporary obturation techniques in the absence of the dentinal smear layer, Int Endod J 32:464, 1999.
159. Lambrianidis T: Ledge formation. In Iatrogenic complications during endodontic treatment. Thessaloniki, Greece, 1996, Univ Studio Press.
160. Reference deleted in proofs.161. Lee J, Lorenzo D, Rawlins T, Cardo VA Jr: Sodium
hypochlorite extrusion: an atypical case of massive soft tissue necrosis, J Oral Maxillofac Surg 69:1776, 2011.
162. Lee JS, Lee JH, Lee JH, et al: Efficacy of early treatment with infliximab in pediatric Crohn’s disease, World J Gastroenterol 16:1776, 2010.
163. Legent F, Billet J, Beauvillain C, et al: The role of dental canal fillings in the development of aspergillus sinusitis: a report of 85 cases, Arch Otorhinolaryngol 246:318, 1989.
164. Levy G: [Canal Finder System 89: improvements and indications after 4 years of experimentation and use], Rev Odontostomatol (Paris) 19:327, 1990.
165. Lin L, Chance K, Shovlin F, et al: Oroantral communication in periapical surgery of maxillary posterior teeth, J Endod 11:40, 1985.
166. Ling JQ, Wei X, Gao Y: Evaluation of the use of dental operating microscope and ultrasonic instruments in the management of blocked canals, Zhonghua Kou Qiang Yi Xue Za Zhi 38:324, 2003; review article 1162.
167. Liu R, Kaiwar A, Shemesh H, et al: Incidence of apical root cracks and apical dentinal detachments after canal preparation with hand and rotary files at different instrumentation lengths, J Endod 39:129, 2013.
168. Loidolt D, Mangge H, Wilders-Trushing M, et al: In vivo and in vitro suppression of lymphocyte function in aspergillus sinusitis, Arch Otorhinolaryngol 246:321, 1989.
169. Lopes HP, Ferreira AA, Elias CN, et al: Influence of rotational speed on the cyclic fatigue of rotary nickel-titanium endodontic instruments, J Endod 35:1013, 2009.
170. Lopes HP, Moreira EJ, Elias CN, et al: Cyclic fatigue of ProTaper instruments, J Endod 33:55, 2007.
171. Lovato KF, Sedgley CM: Antibacterial activity of EndoSequence Root Repair Material and ProRoot MTA against clinical isolates of Enterococcus faecalis, J Endod 37:1542, 2011.
172. Ma J, Al-Ashaw AJ, Shen Y, et al: Efficacy of ProTaper Universal Rotary Retreatment System for gutta-percha removal from oval root canals: a micro-computed tomography study, J Endod 38:1516, 2012.
173. Madarati A, Watts DC, Qualtrough AE: Opinions and attitudes of endodontists and general dental practitioners in the UK towards the intracanal fracture of endodontic instruments: part 2, Int Endod J 41:1079, 2008.
174. Madarati AA, Hunter MJ, Dummer PMH: Management of intracanal separated instruments, J Endod 39:569, 2013.
175. Madarati AA, Qualtrough AJ, Watts DC: Efficiency of a newly designed ultrasonic unit and tips in reducing temperature rise on root surface during the removal of fractured files, J Endod 35:896, 2009.
176. Manisal Y, Yücel T, Erişen R: Overfilling of the root, Oral Surg Oral Med Oral Pathol 68:773, 1989.
177. McDonald MN, Vire DE: Chloroform in the endodontic operatory, J Endod 18:301, 1992.
178. McKendry DJ: Comparison of balanced forces, endosonic and step-back filing instrumentation techniques: quantification of extruded apical debris, J Endod 16:24, 1990.
179. Mehdipour O, Kleier DJ, Averbach RE: Anatomy of sodium hypochlorite accidents, Compend Contin Educ Dent 28:544, 548, 550, 2007.
180. Metzger Z, Ben-Amar A: Removal of overextended gutta-percha root canal fillings in endodontic failure cases, J Endod 21:287, 1995.
181. Metzger Z, Teperovich E, Zary R, et al: The self-adjusting file (SAF). Part 1: respecting the root canal anatomy—a new concept of endodontic files and its implementation, J Endod 36:679, 2010.
182. Molander A, Reit C, Dahen G, Kvist T: Microbiological status of root-filled teeth with apical periodontitis, Int Endod J 31:1, 1998.
183. Morse DR: Endodontic-related inferior alveolar nerve and mental foramen paresthesia, Compend Contin Educ Dent 18:963, 1997.
184. Naenni N, Thoma K, Zehnder M: Soft tissue dissolution capacity of currently used and potential endodontic irrigants, J Endod 30:785, 2004.
185. Nagai O, Tani N, Kayaba Y, et al: Ultrasonic removal of separated instruments in root canals, Int Endod J 19:298, 1986.
186. Nair PN: On the causes of persistent apical periodontitis: a review, Int Endod J 39:249, 2006.
187. Nair PNR, Henry S, Cano V, Vera J: Microbial status of apical root canal system of human mandibular first molars with primary apicalr periodontitis after “one-visit” endodontic treatment, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:231, 2005.
188. Namazikhah MS, Mokhlis HR, Alasmakh K: Comparison between a hand stainless steel K file and a rotary NiTi 0.04 taper, J Calif Dent Assoc 28:421, 2000.
189. Neaverth E: Disabling complications following inadvertent overextension of a root canal filling material, J Endod 15:135, 1989.
190. Neiva RF, Gapski R, Wang HL: Morphometric analysis of implant-related anatomy in Caucasian skulls, J Periodontol 75:1061, 2004.
191. Nevares G, Cunha RS, Zuolo ML, et al: Success rates for removing or bypassing fractured instruments: a prospective clinical study, J Endod 38:442, 2012.
192. Ngeow WC: Is there a “safety zone” in the mandibular premolar region where damage to the mental nerve can be avoided if periapical extrusion occurs? J Can Dent Assoc 76:a61, 2010.
193. Ngeow WC, Yuzawati Y: The location of the mental foramen in a selected Malay population, J Oral Sci 45:171, 2003.
194. Niemczyk SP: Essentials of endodontic microsurgery, Dent Clin North Am 54:375, 2010.
195. Nitzan DW, Stabholz A, Azaz B: Concepts of accidental overfilling and overinstrumentation in the mandibular canal during root canal treatment, J Endod 9:81, 1983.
196. Noiri Y, Ehara A, Kawahara T, et al: Participation of bacterial biofilms in refractory and chronic periapical periodontitis, J Endod 28:679, 2002.
197. Oberli K, Bornstein MM, von Arx T: Periapical surgery and the maxillary sinus: radiographic parameters for clinical outcome, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103:848, 2007.
198. Ozkan BT, Celik S, Durmus E: Paresthesia of the mental nerve stem from periapical infection of mandibular canine tooth: a case report, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 105:e28, 2008.
199. Pagin O, Centurion BS, Rubira-Bullen LRF, Capelozza ALA: Maxillary sinus and posterior teeth: accessing close relationship by cone-beam computed tomographic scanning in a Brazilian population, J Endod 39:748, 2013.
200. Parashos P, Gordon I, Messer HH: Factors influencing defects of rotary nickel titanium endodontic instruments after clinical use, J Endod 30:722, 2004.
201. Park H: A comparison of greater taper files, profiles, and stainless steel files to shape curved root canals, Oral Surg Oral Med Oral Pathol Oral Radiol 9:715, 2001.
202. Pashley EL, Birdsong NL, Bowman K, Pashley DH: Cytotoxic effects of NaOCl on vital tissue, J Endod 11:525, 1985.
203. Patel S, Dawood A, Ford TP, Whaites E: The potential applications of cone beam computed tomography in the management of endodontic problems, Int Endod J 40:818, 2007.
204. Patino PV, Biedma BM, Liebana CR, et al: The influence of a manual glide path on the separation rate of NiTi rotary instruments, J Endod 31:114, 2005.
205. Pedull E, Grande NM, Plotino G, et al: Influence of continuous or reciprocating motion on cyclic fatigue resistance of 4 different nickel-titanium rotary instruments, J Endod 39:258, 2013.
206. Pelka M, Petschelt A: Permanent mimic musculature and nerve damage caused by sodium hypochlorite: a case report, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:e80, 2008.
207. Penna KJ, Neshat K: Cervicofacial subcutaneous emphysema after lower root canal therapy, N Y State Dent J 67:28, 2001.
208. Persson G: Periapical surgery of molars, Int J Oral Surg 11:96, 1982.
209. Petersson K, Petersson A, Olsson B, et al: Technical quality of root fillings in an adult Swedish population, Endod Dent Traumatol 2:99, 1986.
210. Pettiette MT, Conner D, Trope M: Procedural errors with the use of nickel-titanium rotary instruments in undergraduate endodontics, J Endod 28:259, 2002.
211. Phillips JL, Weller RN, Kulild JC: The mental foramen: 1. Size, orientation, and positional relationship to the mandibular second premolar, J Endod 16:221,1990.
212. Phillips JL, Weller RN, Kulild JC: The mental foramen: 2. Radiographic position in relation to the mandibular second premolar, J Endod 18:271, 1992.
213. Phillips JL, Weller RN, Kulild JC: The mental foramen: 3. Size and position on panoramic radiographs, J Endod 18:383, 1992.
214. Pogrel MA: Damage to the inferior alveolar nerve as the result of root canal therapy, J Am Dent Assoc 138:65, 2007.
215. Pogrel MA, Le H: Etiology of lingual nerve injuries in the third molar region: a cadaver and histologic study, J Oral Maxillofac Surg 64:1790, 2006.
216. Pogrel MA, Thamby S: Permanent nerve involvement resulting from inferior alveolar nerve blocks, J Am Dent Assoc 131:901, 2000.
217. Poveda R, Bagan JV, Diaz Fernandez JM, et al: Mental nerve paresthesia associated with endodontic paste within the mandibular canal: report of a case, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e46, 2006.
218. Powell SE, Wong PD, Simon JH: A comparison of the effect of modified and nonmodified instrument tips on apical canal configuration: part II, J Endod 14:224, 1988.
219. Pruett JP, Clement DJ, Carnes DL Jr: Cyclic fatigue testing of nickel-titanium endodontic instruments, J Endod 23:77, 1997.
220. Rahimi M, Parashos P: A novel technique for the removal of fractured instruments in the apical third of curved root canals, Int Endod J 42:264, 2009.
221. Ramirez-Salomon M, Soler-Bientz R, de la Garza-Gonzalez R, et al: Incidence of Lightspeed separation and the potential for bypassing, J Endod 23:586, 1997.
222. Reddy SA, Hicks ML: Apical extrusion of debris using two hand and two rotary instrumentation techniques, J Endod 24:180, 1998.
754 PART II The Advanced Science of Endodontics
223. Reeh ES, Messer HH: Long-term paresthesia following inadvertent forcing of sodium hypochlorite through perforation in maxillary incisor, Endod Dent Traumatol 5:200, 1989.
224. Rehm S, Koroschetz J, Baron R: An update on neuropathic pain, Eur Neur Rev 3:125, 2008.
225. Rene N, Owall B: Dental malpractice in Sweden, J Law Ethics Dent 4:16, 1991.
226. Renton T: Prevention of iatrogenic inferior alveolar nerve injuries in relation to dental procedures, Dent Update 37:350, 354, 358, passim, 2010.
227. Renton T, Dawood A, Shah A, et al: Post-implant neuropathy of the trigeminal nerve: a case series, Br Dent J 212:E17, 2012.
228. Renton T, Yilmaz Z: Profiling of patients presenting with posttraumatic neuropathy of the trigeminal nerve, J Orofac Pain 25:333, 2011.
229. Renton T, Yilmaz Z: Managing iatrogenic trigeminal nerve injury: a case series and review of the literature, Int J Oral Maxillofac Surg 41:629, 2012.
230. Reznick JB, Ardary WC: Cervicofacial subcutaneous air emphysema after dental extraction, J Am Dent Assoc 120:417, 1990.
231. Rickles NH, Joshi BA: A possible case in a human and an investigation in dogs of death from air embolism during root canal therapy, J Am Dent Assoc 67:397, 1963.
232. Ricucci D, Langeland K: Apical limit of root-canal instrumentation and obturation, Int Endod J 31:394, 1998.
233. Robinson MJ, McDonald NJ, Mullally PJ: Apical extrusion of thermoplasticized obturating material in canals instrumented with Profile 0.06 or Profile GT, J Endod 30:418, 2004.
234. Roda RS: Root perforation repair: surgical and nonsurgical management, Pract Proced Aesthet Dent 13:467; quiz 474, 2001.
235. Roda RS: Personal communication, 2013.236. Ross IS: Some effects of heavy metals on fungal cells,
Transactions of the British Mycology Society 64:175, 1975.
237. Rossiter JL, Hendrix RA: Iatrogenic subcutaneous cervicofacial and mediastinal emphysema, J Otolaryngol 20, 1981.
238. Rowe AH: Damage to the inferior dental nerve during or following endodontic treatment, Br Dent J 155:306, 1983.
239. Rud J, Rud V: Surgical endodontics of upper molars: relation to the maxillary sinus and operation in acute state of infection, J Endod 24:260, 1998.
240. Ruddle CJ: Micro-endodontic non-surgical retreatment, Dent Clin North Am 41:429, 1997.
241. Ruddle CJ: Nonsurgical retreatment. In Cohen S, Burns RC, editors: Pathways of the pulp, ed 8, St. Louis, 2002, CV Mosby, p 875.
242. Ruddle CJ: Nonsurgical retreatment, J Endod 30:827, 2004.
243. Sabala CL, Roane JB, Southard LZ: Instrumentation of curved canals using a modified tipped instrument: a comparison study, J Endod 14:59, 1988.
244. Sakkal S, Gagnon A, Lemian L: [Paresthesia of the mandibular nerve caused by endodontic treatment: a case report], J Can Dent Assoc 60:556, 1994.
245. Sattapan B, Nervo GJ, Palamara JE, Messer HH: Defects in rotary nickel-titanium files after clinical use, J Endod 26:161, 2000.
246. Saunders JL, Eleazer PD, Zhang P, Michalek S: Effect of a separated instrument on bacterial penetration of obturated root canals, J Endod 30:177, 2004.
247. Schafer E, Dzepina A, Danesh G: Bending properties of rotary nickel-titanium instruments, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:757, 2003.
248. Schafer E, Schulz-Bongert U, Tulus G: Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study, J Endod 30:432, 2004.
249. Schilder H: Filling root canals in three dimensions, Dent Clin North Am 11:723, 1967.
250. Schwarze T, Baethge C, Stecher T, Geurtsen W: Identification of second canals in the mesiobuccal root of maxillary first and second molars using magnifying loupes or an operating microscope, Aust Endod J 28:57, 2002.
251. Scolozzi P, Lombardi T, Jaques B: Successful inferior alveolar nerve decompression for dysesthesia following endodontic treatment: report of 4 cases treated by mandibular sagittal osteotomy, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 97:625, 2004.
252. Selbst AG: Understanding informed consent and its relationship to the incidence of adverse treatment events in conventional endodontic therapy, J Endod 16:387, 1990.
253. Selden HS: The endo-antral syndrome: an endodontic complication, J Am Dent Assoc 119:397, 401, 1989.
254. Seltzer S, Naidorf IJ: Flare-ups in endodontics. I. Etiological factors, J Endod 11:472, 1985.
255. Senges C, Wrbas KT, Altenburger M, et al: Bacterial and Candida albicans adhesion on different root canal filling materials and sealers, J Endod 37:1247, 2011.
256. Serafino C, Gallina G, Cumbo E, et al: Ultrasound effects after post space preparation: an SEM study, J Endod 32:549, 2006.
257. Setzer FC, Bohme CP: Influence of combined cyclic fatigue and torsional stress on the fracture point of nickel-titanium rotary instruments, J Endod 39:133, 2013.
258. Shen Y, Peng B, Cheung GS: Factors associated with the removal of fractured NiTi instruments from root canal systems, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98:605, 2004.
259. Shovelton DS: Surgical emphysema as a complication of dental operations, Br Dent J 102:125, 1957.
260. Silva EJ, Rosa TP, Herrera DR, et al: Evaluation of cytotoxicity and physicochemical properties of calcium silicate-based endodontic sealer MTA Fillapex, J Endod 39:274, 2013.
261. Siqueira JF: Microbial causes of endodontic flare-ups, Int Endod J 36:453, 2003.
262. Sjögren U: Success and failure in endodontics, Umeå University Dissertation N. 60 33, 1996.
263. Smatt Y, Browaeys H, Genay A, et al: Iatrogenic pneumomediastinum and facial emphysema after endodontic treatment, Br J Oral Maxillofac Surg 42:160, 2004.
264. Snyder MB, Rosenberg ES: Subcutaneous emphysema during periodontal surgery: report of a case, J Periodontol 48:790, 1997.
265. Somma F, Cammarota G, Plotino G: The effectiveness of manual and mechanical instrumentation for the retreatment of three different root canal filling materials, J Endod 34:466, 2008.
266. Song M, Kim HC, Lee W, Kim E: Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery, J Endod 37:1516, 2011.
267. Sousa CJ, Loyola AM, Versiani MA, et al: A comparative histological evaluation of the biocompatibility of materials used in apical surgery, Int Endod J 37:738, 2004.
268. Souter NJ, Messer HH: Complications associated with fractured file removal using an ultrasonic technique, J Endod 31:450, 2005.
269. Souyave LC, Inglis AT, Alcalay M: Removal of fractured endodontic instruments using ultrasonics, Br Dent J 159:251, 1985.
270. Spangberg L, Langeland K: Biologic effects of dental materials. 1. Toxicity of root canal filling materials on HeLa cells in vitro, Oral Surg 35:402,1973.
271. Spencer HR, Ike V, Brennan PA: Review: the use of sodium hypochlorite in endodontics—potential complications and their management, Br Dent J 202:555, 2007.
272. Spili P, Parashos P, Messer HH: The impact of instrument fracture on outcome of endodontic treatment, J Endod 31:845, 2005.
273. Stabholz A, Friedman S: Endodontic retreatment—case selection and technique. Part 2: treatment planning for retreatment, J Endod 14:607, 1988.
274. Stammberger H, Jakse R, Beaufort F: Aspergillosis of the paranasal sinuses: x-ray diagnosis, histopathology and clinical aspects, Ann Otol Rhinol Laryngol 93:251, 1984.
275. Steelman RJ, Johannes PW: Subcutaneous emphysema during restorative dentistry, International Journal of Paediatric Dentistry/the British Paedodontic Society [and] the International Association of Dentistry for Children 17:228, 2007.
276. Stock CJ: Calcium hydroxide: root resorption and perio-endo lesions, Br Dent J 158:325–34, 1985.
277. Stropko JJ: Canal morphology of maxillary molars: clinical observations of canal configurations, J Endod 25:446, 1999.
278. Sujeet K, Shankar S: Images in clinical medicine. Prevertebral emphysema after a dental procedure, New Engl J Med 356:173, 2007.
279. Suter B, Lussi A, Sequeira P: Probability of removing fractured instruments from root canals, Int Endod J 38:112, 2005.
280. Sweatman TL, Baumgartner JC, Sakaguchi RL: Radicular temperatures associated with thermoplastic gutta percha, J Endod 27:512, 2001.
281. Tahan E, Çelik D, Er K, Taşdemir T: Effect of unintentionally extruded mineral trioxide aggregate in treatment of tooth with periradicular lesion: a case report, J Endod 36:760, 2010.
282. Takahashi CM, Cunha RS, De Martin AS, et al: In vitro evaluation of the effectiveness of ProTaper Universal rotary retreatment system for gutta-percha removal with or without a solvent, J Endod 35:1580, 2009.
283. Tanalp J, Kaptan F, Sert S, et al: Quantitative evaluation of the amount of apically extruded debris using 3 different rotary instrumentation systems, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:252, 2006.
284. Terauchi Y: Separated file removal, Dentistry Today 31:110, 2012.
285. Terauchi Y, O’Leary L, Kikuchi I, et al: Evaluation of the efficiency of a new file removal system in comparison with two conventional systems, J Endod 33:585, 2007.
286. Terauchi Y, O’Leary L, Yoshioka T, Suda H: Comparison of the time required to create secondary fracture of separated file fragments using ultrasonic vibration under various canal conditions, J Endod 39:1300, 2013.
287. Thompson SA, Dummer PMH: Shaping ability of Quantec Series 2000 rotary nickel-titanium instruments in simulated root canals: part 2, Int Endod J 31:268, 1998.
288. Tilotta-Yasukawa F, Millot S, El Haddioui A, et al: Labiomandibular paresthesia caused by endodontic treatment: an anatomic and clinical study, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102:e47, 2006.
289. Tinaz AC, Alacam T, Uzun O, et al: The effect of disruption of apical constriction on periapical extrusion, J Endod 31:533, 2005.
290. Torabinejad M, Lemon RR: Procedural accidents. In Walton RE, Torabinejad M, editors: Principles and practice of endodontics, ed 3, Philadelphia, 2002, WB Saunders, p 310.
291. Torabinejad M, Walton RE, editors: Principles and practice of endodontics, ed 4, St. Louis, 2009, Saunders.
292. Tronstad L, Sunde PT: The evolving new understanding of endodontic infections, Endod Topics 6:57, 2003.
293. Turnbull A: Remarkable coincidence in dental surgery [letter], Br Med J 1:1131, 1900.
294. Tzanetakis GN, Kontakiotis EG, Maurikou DV, et al: Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: a five-year retrospective clinical study, J Endod 34:675, 2008.
295. Uehara M, Okumura T, Asahina I: Subcutaneous cervical emphysema induced by a dental air syringe: a case report, Int Dent J 57:286, 2007.
296. Ullmann CJ, Peters OA: Effect of cyclic fatigue on static fracture loads in ProTaper nickel-titanium rotary instruments, J Endod 31:183, 2005.

CHAPTER 19 Managing Iatrogenic Endodontic Events 755
297. Vasilakis GJ, Vasilakis CM: Mandibular endodontic-related paresthesia, General Dent 52:334, 2004.
298. Walton RE: Current concepts of canal preparation, Dent Clin North Am 36:309, 1992.
299. Walton RE, Torabinejad M: Principles and practice of endodontics, ed 3, Philadelphia, 2002, WB Saunders, pp 184, 222-223, 319.
300. Ward JR, Parashos P, Messer HH: Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: an experimental study, J Endod 29:756, 2003.
301. Ward JR, Parashos P, Messer HH: Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical cases, J Endod 29:764, 2003.
302. Watzek G, Bernhart T, Ulm C: Complications of sinus perforations and their management in endodontics, Dent Clin North Am 41:563, 1997.
303. Weine F: Endodontic therapy, ed 5, St Louis, 1996, Mosby, pp 324-330, 545.
304. Weisman MI: The removal of difficult silver cones, J Endod 9:210, 1983.
305. Wilcox LR, Roskelley C, Sutton T: The relationship of root canal enlargement to finger-spreader induced vertical root fracture, J Endod 23:533, 1997.
306. Wong R, Cho F: Microscopic management of procedural errors, Dent Clin North Am 41:455, 1997.
307. Worthington P: Injury to the inferior alveolar nerve during implant placement: a formula for protection of the patient and clinician, Int J Oral Maxillofac Implants 19:731, 2004.
308. Wright KJ, Derkson GD, Riding KH: Tissue-space emphysema, tissue necrosis, and infection following use of compressed air during pulp therapy: case report, Pediatr Dentistry 13:110, 1991.
309. Wu MK, Kast’akova A, Wesselink PRL: Quality of cold and warm gutta-percha in oval canals in mandibular premolars, J Endod 24:223, 1998.
310. Wu MK, Wesselink PR, Walton RE: Apical terminus location of root canal treatment procedures, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89:99, 2000.
311. Yaltirik M, Berberoglu HK, Koray M, et al: Orbital pain and headache secondary to overfilling of a root canal, J Endod 29:771, 2003.
312. Yang SC, Chiu TH, Lin TJ, Chan HM: Subcutaneous emphysema and pneumomediastinum secondary to dental
extraction: a case report and literature review, Kaohsiung J Med Sci 22:641, 2006.
313. Yoldas O, Oztunc H, Tinaz C, Alparslan N: Perforation risks associated with the use of Masserann endodontic kit drills in mandibular molars, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 97:513, 2004.
314. Yoshimoto A, Mitamura Y, Nakamura H, Fujimura M: Acute dyspnea during dental extraction, Respiration 69:369, 2002.
315. You SY, Bae KS, Baek SH, et al: Lifespan of one nickel-titanium rotary file with reciprocating motion in curved root canals, J Endod 36:1991, 2010.
316. Yum J, Cheung GS, Park JK, et al: Torsional strength and toughness of nickel-titanium rotary files, J Endod 37:382, 2011.
317. Zehnder M: Root canal irrigants, J Endod 32:389, 2006.
318. Zemann W, Feichtinger M, Karcher H: Cervicofacial and mediastinal emphysema after crown preparation: a rare complication, Int J Prosthodont 20:143, 2007.
319. Zuolo ML, Walton RE, Imura N: Histologic evaluation of three endodontic instrument/preparation techniques, Endod Dent Traumatol 8:125, 1992.

This page intentionally left blank
757
CHAPTER 20The Role of Endodontics After Dental Traumatic Injuries
CHAPTER 21Cracks and Fractures
CHAPTER 22Restoration of the Endodontically Treated Tooth
CHAPTER 23Vital Pulp Therapy
EXPERT CONSULT CHAPTERS
CHAPTER 24Pediatric Endodontics: Endodontic Treatment for the Primary and Young Permanent Dentition
CHAPTER 25Endodontic and Periodontal Interrelationships
CHAPTER 26Effects of Age and Systemic Health on Endodontics
CHAPTER 27Bleaching Procedures
CHAPTER 28Understanding and Managing the Fearful Dental Patient
CHAPTER 29Endodontic Records and Legal Responsibilities
CHAPTER 30Key Principles of Endodontic Practice Management
Expanded Clinical Topics
PART III
758
Unique Aspects of Dental TraumaMost Common Types of Dental Trauma
Crown FracturesCrown-Root FracturesRoot FracturesLuxation Injuries and Avulsion
Follow-Up After Dental TraumaRadiographic Examinations
Cone Beam Computed Tomography and Dentoalveolar Trauma
Root ResorptionHorizontal (Transverse) Root FracturesLuxation Injuries
Crown FracturesCrown InfractionUncomplicated Crown FractureTreatmentComplicated Crown FractureTreatmentVital Pulp Therapy: Requirements for SuccessTreatment MethodsTreatment of the Nonvital Pulp
Crown-Root FractureRoot Fracture
Diagnosis and Clinical PresentationTreatmentHealing PatternsTreatment of Complications
Luxation InjuriesDefinitionsIncidenceTreatmentBiologic Consequences
Clinical Management of the Avulsed ToothConsequences of Tooth AvulsionTreatment ObjectivesClinical ManagementDiagnosis and Treatment Planning
Preparation of the RootExtraoral Dry Time Less Than 60 MinutesExtraoral Dry Time More Than 60 Minutes
Preparation of the SocketSplintingManagement of the Soft TissuesAdjunctive Therapy
Second VisitEndodontic Treatment
Extraoral Time Less Than 60 MinutesExtraoral Time More Than 60 Minutes
Temporary RestorationRoot Filling Visit
Permanent RestorationFollow-Up Care
The Role of Endodontics After Dental Traumatic InjuriesMARTIN TROPE | FREDERIC BARNETT | ASGEIR SIGURDSSON | NOAH CHIVIAN
CHAPTER 20
CHAPTER OUTLINE
A traumatic injury to the tooth results in damage to many dental and periradicular structures, making the management and consequences of these injuries multifactorial. Knowledge of the interrelating healing patterns of these tissues is essential. This chapter concentrates on the role of the dentinopulpal complex in the pathogenesis of disease subsequent to dentinal trauma and how treatment of this complex can contribute to favorable healing after an injury.
UNIQUE ASPECTS OF DENTAL TRAUMAMost dental trauma occurs in the 7- to 12-year-old age group and is mainly due to falls and accidents near home or school.23,143 It occurs primarily in the anterior region of the mouth, affecting the maxillary more than the mandibular jaw.28 Serious accidents, such as automobile crashes, can affect any tooth and can occur in all age ranges. In many cases, after a

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 759
pulp of a traumatized fully formed tooth. As circulation is restored, the responsiveness to pulp tests returns.73
The transition from a negative response to a positive response at a subsequent test may be considered a sign of a healing pulp. The repetitious finding of responses may be taken as a sign of a healthy pulp. The transition from a response to no response may be taken as an indication that the pulp is probably undergoing degeneration and therefore an inter-vention in the form of endodontic treatment might be indi-cated. The persistence of no response would suggest that the pulp has been irreversibly damaged, but even this is not absolute.32
Thermal and electrical pulp tests of all anterior teeth (canine to canine) of the maxillary and mandibular jaws should be performed at the time of the initial examination and carefully recorded to establish a baseline for comparison with subse-quent repeated tests in later months. These tests should be repeated at 3 weeks; at 3, 6, and 12 months; and at yearly intervals after the trauma. The purpose of the tests is to estab-lish a trend as to the physiologic status of the pulps of these teeth. Particularly in traumatized teeth, carbon dioxide snow (CO2, −78° C) or dichlorodifluoromethane (−40° C) placed on the incisal third of the facial surface gives more accurate responses than a water-ice pencil (Fig. 20-1).71,72 The intense cold seems to penetrate the tooth and covering splints or res-torations and reach the deeper areas of the tooth. Neither the dry ice nor the dichlorodifluoromethane spray forms ice water, which could disperse over adjacent teeth or gingiva to give a false-positive response. In trauma evaluation, there is no ques-tion that using water-ice pencils should be avoided because of this. Dichlorodifluoromethane spray is a very inexpensive alternative to CO2 snow; its coldness elicits much more reliable responses than water-ice. The electrical pulp test relies on electrical impulses directly stimulating the nerves of the pulp. These tests have limited value in young teeth but are useful when the dentinal tubules are closed and do not allow dentinal fluid to flow in them. This situation is typical of teeth in elderly patients or in traumatized teeth that are undergoing premature sclerosis. In these situations, the thermal tests that rely on fluid flow in the tubules cannot be used, and the electrical pulp test becomes important.
Laser Doppler flowmetry (LDF) was introduced in the early 1970s for measurement of blood flow in the retina.88 The tech-nique has also been used to assess blood flow in other tissue systems, such as the skin and renal cortex. It uses a beam of
traumatic dental injury, endodontic treatment is provided to caries-free, single-rooted, young permanent teeth. If quick and correct treatment for these teeth is provided after injury, the potential for a successful endodontic outcome is very good.
MOST COMMON TYPES OF DENTAL TRAUMA
Crown FracturesMost crown fractures occur in young, caries-free anterior teeth.95,107 This makes maintaining or regaining pulp vitality essential. Luckily, vital pulp therapy supports a good prognosis in these situations if correct treatment and follow-up proce-dures are carefully followed.
Crown-Root FracturesCrown-root fractures are first treated periodontally to ensure that there is a sufficient and good margin to allow restoration. If the tooth can be maintained from a periodontal point of view, then the pulp is treated as for a crown fracture.
Root FracturesA surprisingly large number of pulps in root-fractured teeth will survive this rather dramatic injury. In almost every case, the apical segment stays vital, and in many cases, the coronal segment stays vital or regains vitality subsequent to the injury. If the coronal segment permanently loses vitality, it should be treated as an immature permanent tooth with nonvital pulp. The apical segment rarely needs treatment.
Luxation Injuries and AvulsionLuxation injuries and avulsion often result in pulp necrosis and damage to the cemental protective layer of the root. The potential complication of pulp infection in a root that has lost its cemental protective layer makes these injuries potentially catastrophic. Correct emergency and follow-up evaluation, which may include timely endodontic treatment, is critical.
FOLLOW-UP AFTER DENTAL TRAUMAThe reader is referred to Chapter 1 for specific descriptions of pulp tests, but a few general statements about pulp tests on traumatized teeth may be helpful in trying to interpret the results.
For decades, controversy has surrounded the validity of thermal and electric tests on traumatized teeth. Only general-ized impressions may be gained from these tests following a traumatic injury. They are in reality sensitivity tests for nerve function and do not indicate the presence or absence of blood circulation within the pulpal space. It is assumed that subse-quent to traumatic injury, the conduction capability of the nerve endings and/or sensory receptors is sufficiently deranged to inhibit the nerve impulse from an electrical or thermal stimulus. This makes the traumatized tooth vulnerable to false-negative readings from such tests.123
Teeth that give a response at the initial examination cannot be assumed to be healthy and to continue to give a response over time. Teeth that yield no response cannot be assumed to have necrotic pulps because they may give a response at later follow-up visits. It has been demonstrated that it may take as long as 9 months for normal blood flow to return to the coronal
FIG. 20-1 Difluorodichloromethane (−40° F [−40° C]) gas is sprayed on a cotton pellet and then placed on the incisal edge of the maxillary incisor.
760 PART III Expanded Clinical Topics
image can be confounded by a number of factors, including the regional anatomy and superimposition of both the teeth and surrounding dentoalveolar structures. As a result of super-imposition, periapical radiographs reveal only limited aspects (i.e., a 2D view) of the true 3D anatomy.44,119 Additionally, there is often geometric distortion of the anatomic structures imaged with conventional radiographic methods.3 These problems can be overcome by using cone beam computed tomography (CBCT) imaging techniques, which produce accurate 3D images of the teeth and surrounding dentoalveolar structures and have shown promise in improving the clinician’s ability to properly diagnose luxation injuries, alveolar fractures, root fractures, and root resorption (Fig. 20-4).42,43
In instances of soft tissue laceration, it is advisable to radio-graph the injured area before suturing to be sure that no foreign objects have been embedded. A soft tissue radiograph with a normal-sized film briefly exposed at reduced kilovoltage should reveal the presence of many foreign substances, including tooth fragments (Fig. 20-5).
Cone Beam Computed Tomography and Dentoalveolar TraumaCBCT is accomplished by using a rotating gantry to which an x-ray source and detector are fixed (see Chapter 2). A divergent pyramidal or cone-shaped source of ionizing radiation is directed through the middle of the area of interest onto an area x-ray detector on the opposite side of the patient. The x-ray source and detector rotate around a fixed fulcrum within the region of interest. During the exposure sequence, hundreds of planar projection images are acquired of the field of view (FOV) in an arc of at least 180°. In this single rotation, CBCT provides precise, essentially immediate, and accurate 3D radio-graphic images. Because CBCT exposure incorporates the
infrared (780 to 820 nm) or near-infrared (632.8 nm) light that is directed into the tissue by optical fibers. As light enters the tissue, it is scattered by moving red blood cells and station-ary tissue cells. Photons that interact with moving red blood cells are scattered, and the frequency shifts according to the Doppler principle. Photons that interact with stationary tissue cells are scattered but not Doppler shifted. A portion of the light is returned to a photodetector, and a signal is produced (Fig. 20-2).
Attempts have been made to use LDF technology for pulp vitality diagnosis in traumatized teeth because this would provide a more accurate reading of the vitality status of the pulp.113,175,176 Studies have shown promising results, indicating that laser Doppler can detect blood flow more consistently and earlier than the standard vitality tests would be expected to render a response. In a study on young dogs, laser Doppler was able to correctly detect blood flow as early as 2 to 3 weeks after avulsion of an immature tooth and at the same time indicate no flow in those that would remain necrotic.176
Presently the cost of a laser Doppler flowmetry machine limits its use in private dental offices; these are used primarily in hospitals and teaching institutions.
RADIOGRAPHIC EXAMINATIONSRadiographic imaging is essential for thorough examination, diagnosis, and management of dentoalveolar trauma. Imaging may reveal root fractures, subgingival crown fractures, tooth displacements, bone fractures, root resorptions, and embedded foreign objects. A single radiograph, even a panoramic image, is insufficient to properly diagnose just about any dental trauma case. In its 2012 guidelines for the management of traumatic dental injuries, and in the current recommendations on its interactive website (www.dentaltraumaguide.org), the International Association of Dental Traumatology (IADT) has recommended taking at least four different radiographs for almost every injury65-67: a direct 90-degree on the axis of the tooth, two with different vertical angulations, and one occlusal film (Fig. 20-3).
Multiple radiographs increase the likelihood of diagnosing root fractures, tooth displacement, and other possible injuries. However, two-dimensional (2D) imaging methods have well-known inherent limitations, and their lack of three-dimensional (3D) information may prevent proper diagnosis and adversely affect long-term treatment outcomes. The interpretation of an
FIG. 20-2 Laser Doppler machine. (Courtesy Moor Instruments, Devon, United Kingdom.)
FIG. 20-3 An occlusal film of a luxation injury of central incisors. Both were diagnosed to be laterally luxated with apical translocation. Note that the left central is completely obliterated and has a history of being luxated some years prior.
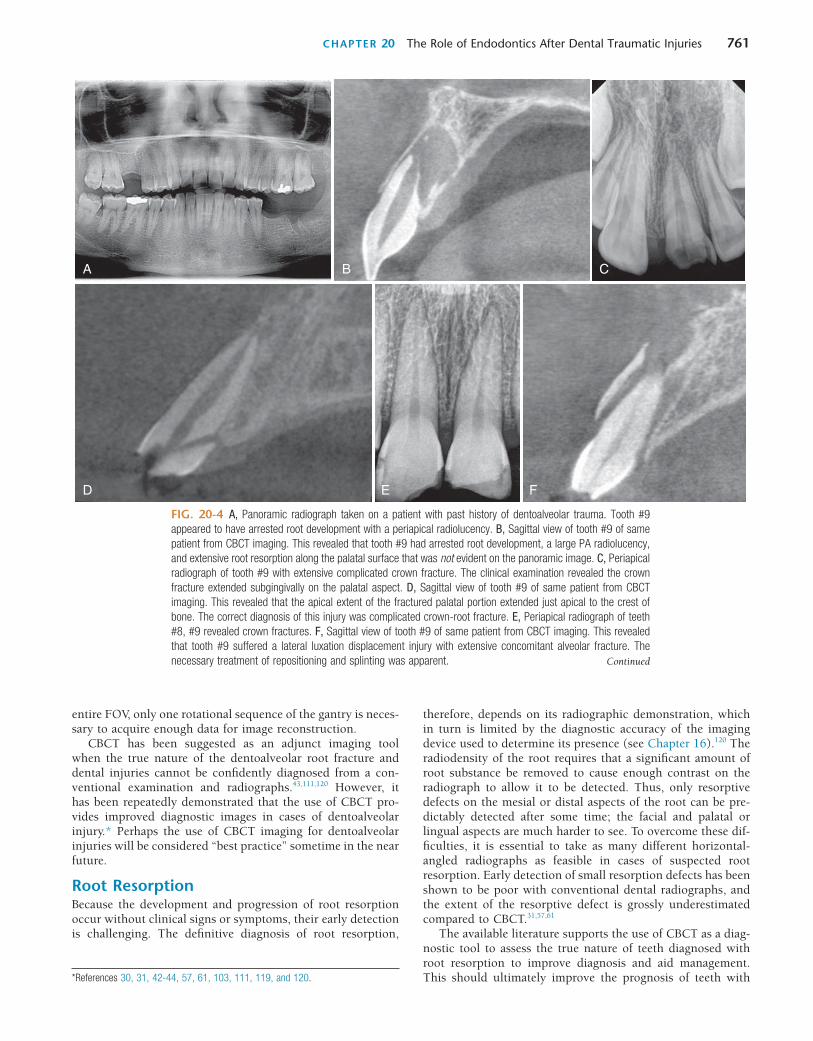
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 761
A
D E F
B C
entire FOV, only one rotational sequence of the gantry is neces-sary to acquire enough data for image reconstruction.
CBCT has been suggested as an adjunct imaging tool when the true nature of the dentoalveolar root fracture and dental injuries cannot be confidently diagnosed from a con-ventional examination and radiographs.43,111,120 However, it has been repeatedly demonstrated that the use of CBCT pro-vides improved diagnostic images in cases of dentoalveolar injury.* Perhaps the use of CBCT imaging for dentoalveolar injuries will be considered “best practice” sometime in the near future.
Root ResorptionBecause the development and progression of root resorption occur without clinical signs or symptoms, their early detection is challenging. The definitive diagnosis of root resorption,
*References 30, 31, 42-44, 57, 61, 103, 111, 119, and 120.
therefore, depends on its radiographic demonstration, which in turn is limited by the diagnostic accuracy of the imaging device used to determine its presence (see Chapter 16).120 The radiodensity of the root requires that a significant amount of root substance be removed to cause enough contrast on the radiograph to allow it to be detected. Thus, only resorptive defects on the mesial or distal aspects of the root can be pre-dictably detected after some time; the facial and palatal or lingual aspects are much harder to see. To overcome these dif-ficulties, it is essential to take as many different horizontal-angled radiographs as feasible in cases of suspected root resorption. Early detection of small resorption defects has been shown to be poor with conventional dental radiographs, and the extent of the resorptive defect is grossly underestimated compared to CBCT.31,57,61
The available literature supports the use of CBCT as a diag-nostic tool to assess the true nature of teeth diagnosed with root resorption to improve diagnosis and aid management. This should ultimately improve the prognosis of teeth with
FIG. 20-4 A, Panoramic radiograph taken on a patient with past history of dentoalveolar trauma. Tooth #9 appeared to have arrested root development with a periapical radiolucency. B, Sagittal view of tooth #9 of same patient from CBCT imaging. This revealed that tooth #9 had arrested root development, a large PA radiolucency, and extensive root resorption along the palatal surface that was not evident on the panoramic image. C, Periapical radiograph of tooth #9 with extensive complicated crown fracture. The clinical examination revealed the crown fracture extended subgingivally on the palatal aspect. D, Sagittal view of tooth #9 of same patient from CBCT imaging. This revealed that the apical extent of the fractured palatal portion extended just apical to the crest of bone. The correct diagnosis of this injury was complicated crown-root fracture. E, Periapical radiograph of teeth #8, #9 revealed crown fractures. F, Sagittal view of tooth #9 of same patient from CBCT imaging. This revealed that tooth #9 suffered a lateral luxation displacement injury with extensive concomitant alveolar fracture. The necessary treatment of repositioning and splinting was apparent. Continued
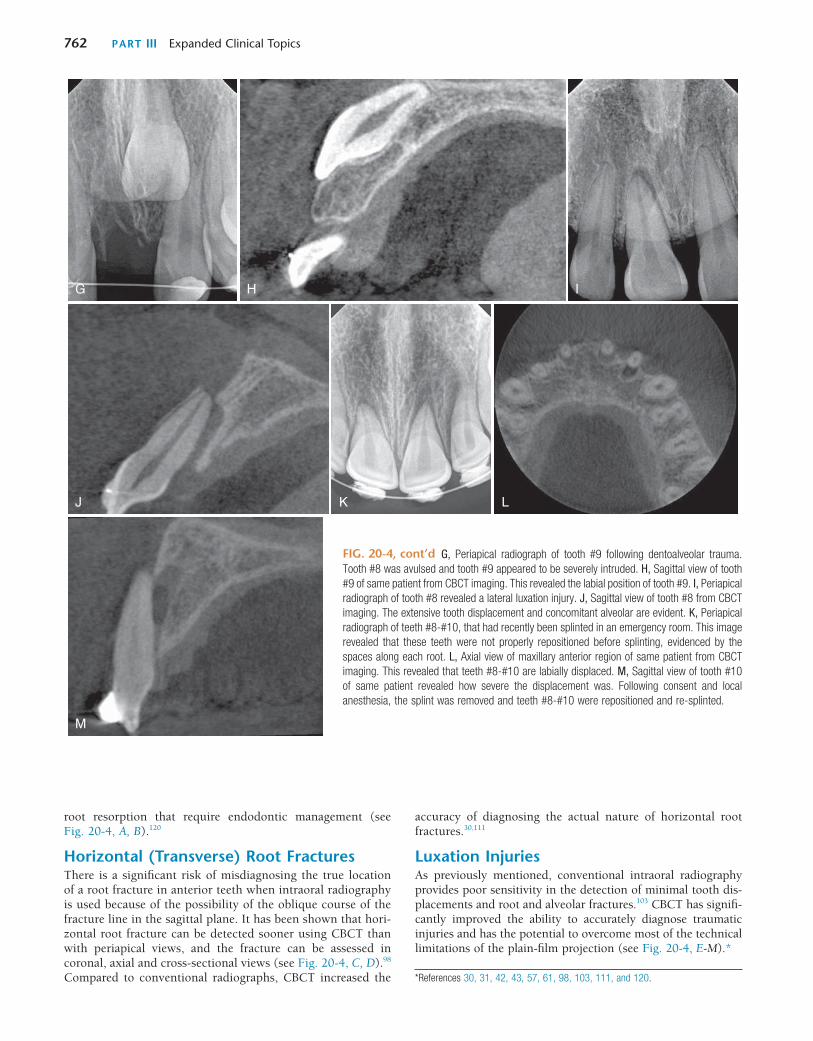
762 PART III Expanded Clinical Topics
M
G
J K L
H I
root resorption that require endodontic management (see Fig. 20-4, A, B).120
Horizontal (Transverse) Root FracturesThere is a significant risk of misdiagnosing the true location of a root fracture in anterior teeth when intraoral radiography is used because of the possibility of the oblique course of the fracture line in the sagittal plane. It has been shown that hori-zontal root fracture can be detected sooner using CBCT than with periapical views, and the fracture can be assessed in coronal, axial and cross-sectional views (see Fig. 20-4, C, D).98 Compared to conventional radiographs, CBCT increased the
accuracy of diagnosing the actual nature of horizontal root fractures.30,111
Luxation InjuriesAs previously mentioned, conventional intraoral radiography provides poor sensitivity in the detection of minimal tooth dis-placements and root and alveolar fractures.103 CBCT has signifi-cantly improved the ability to accurately diagnose traumatic injuries and has the potential to overcome most of the technical limitations of the plain-film projection (see Fig. 20-4, E-M).*
G, Periapical radiograph of tooth #9 following dentoalveolar trauma. Tooth #8 was avulsed and tooth #9 appeared to be severely intruded. H, Sagittal view of tooth #9 of same patient from CBCT imaging. This revealed the labial position of tooth #9. I, Periapical radiograph of tooth #8 revealed a lateral luxation injury. J, Sagittal view of tooth #8 from CBCT imaging. The extensive tooth displacement and concomitant alveolar are evident. K, Periapical radiograph of teeth #8-#10, that had recently been splinted in an emergency room. This image revealed that these teeth were not properly repositioned before splinting, evidenced by the spaces along each root. L, Axial view of maxillary anterior region of same patient from CBCT imaging. This revealed that teeth #8-#10 are labially displaced. M, Sagittal view of tooth #10 of same patient revealed how severe the displacement was. Following consent and local anesthesia, the splint was removed and teeth #8-#10 were repositioned and re-splinted.
FIG. 20-4, cont’d
*References 30, 31, 42, 43, 57, 61, 98, 103, 111, and 120.
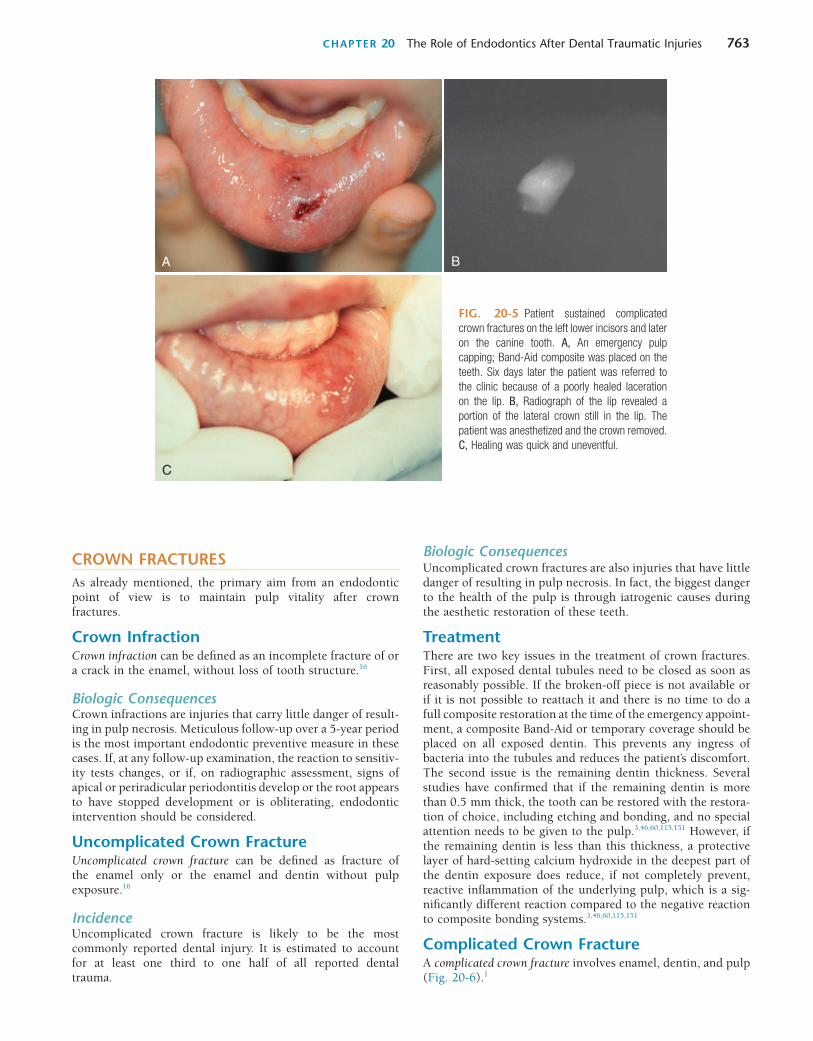
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 763
BA
C
FIG. 20-5 Patient sustained complicated crown fractures on the left lower incisors and later on the canine tooth. A, An emergency pulp capping; Band-Aid composite was placed on the teeth. Six days later the patient was referred to the clinic because of a poorly healed laceration on the lip. B, Radiograph of the lip revealed a portion of the lateral crown still in the lip. The patient was anesthetized and the crown removed. C, Healing was quick and uneventful.
CROWN FRACTURESAs already mentioned, the primary aim from an endodontic point of view is to maintain pulp vitality after crown fractures.
Crown InfractionCrown infraction can be defined as an incomplete fracture of or a crack in the enamel, without loss of tooth structure.16
Biologic ConsequencesCrown infractions are injuries that carry little danger of result-ing in pulp necrosis. Meticulous follow-up over a 5-year period is the most important endodontic preventive measure in these cases. If, at any follow-up examination, the reaction to sensitiv-ity tests changes, or if, on radiographic assessment, signs of apical or periradicular periodontitis develop or the root appears to have stopped development or is obliterating, endodontic intervention should be considered.
Uncomplicated Crown FractureUncomplicated crown fracture can be defined as fracture of the enamel only or the enamel and dentin without pulp exposure.16
IncidenceUncomplicated crown fracture is likely to be the most commonly reported dental injury. It is estimated to account for at least one third to one half of all reported dental trauma.
Biologic ConsequencesUncomplicated crown fractures are also injuries that have little danger of resulting in pulp necrosis. In fact, the biggest danger to the health of the pulp is through iatrogenic causes during the aesthetic restoration of these teeth.
TreatmentThere are two key issues in the treatment of crown fractures. First, all exposed dental tubules need to be closed as soon as reasonably possible. If the broken-off piece is not available or if it is not possible to reattach it and there is no time to do a full composite restoration at the time of the emergency appoint-ment, a composite Band-Aid or temporary coverage should be placed on all exposed dentin. This prevents any ingress of bacteria into the tubules and reduces the patient’s discomfort. The second issue is the remaining dentin thickness. Several studies have confirmed that if the remaining dentin is more than 0.5 mm thick, the tooth can be restored with the restora-tion of choice, including etching and bonding, and no special attention needs to be given to the pulp.3,46,60,115,151 However, if the remaining dentin is less than this thickness, a protective layer of hard-setting calcium hydroxide in the deepest part of the dentin exposure does reduce, if not completely prevent, reactive inflammation of the underlying pulp, which is a sig-nificantly different reaction compared to the negative reaction to composite bonding systems.3,46,60,115,151
Complicated Crown FractureA complicated crown fracture involves enamel, dentin, and pulp (Fig. 20-6).1
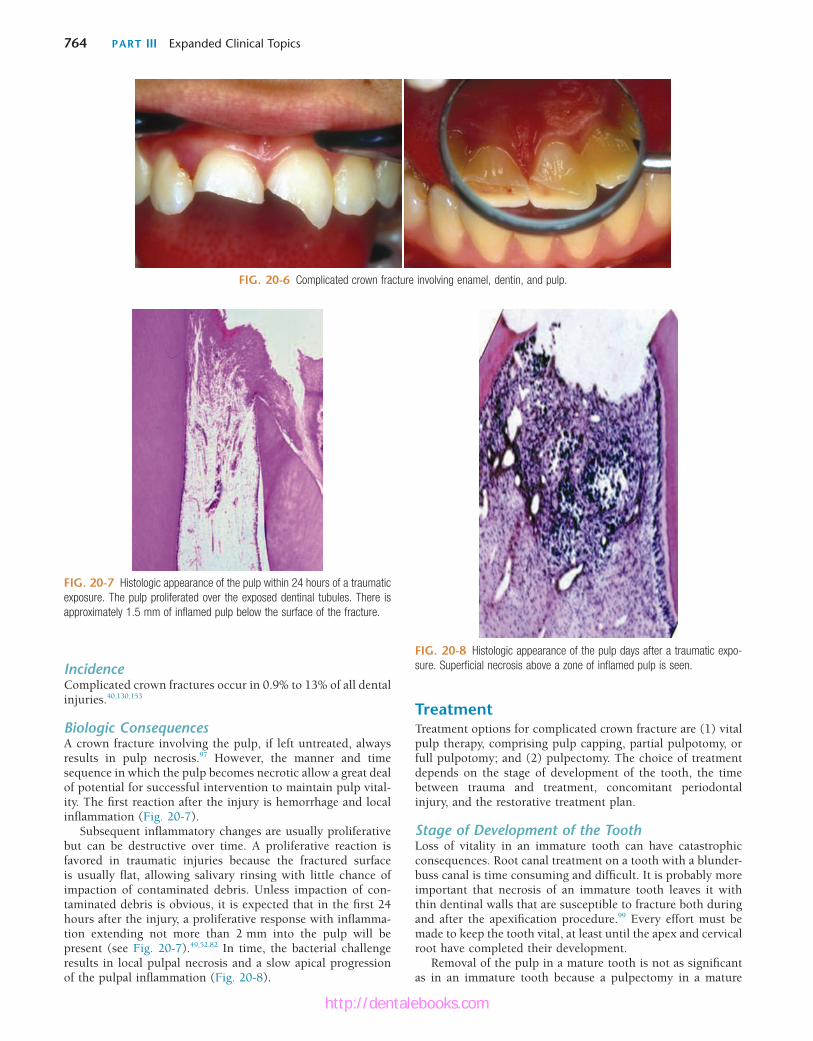
764 PART III Expanded Clinical Topics
FIG. 20-6 Complicated crown fracture involving enamel, dentin, and pulp.
FIG. 20-7 Histologic appearance of the pulp within 24 hours of a traumatic exposure. The pulp proliferated over the exposed dentinal tubules. There is approximately 1.5 mm of inflamed pulp below the surface of the fracture.
IncidenceComplicated crown fractures occur in 0.9% to 13% of all dental injuries.40,130,153
Biologic ConsequencesA crown fracture involving the pulp, if left untreated, always results in pulp necrosis.97 However, the manner and time sequence in which the pulp becomes necrotic allow a great deal of potential for successful intervention to maintain pulp vital-ity. The first reaction after the injury is hemorrhage and local inflammation (Fig. 20-7).
Subsequent inflammatory changes are usually proliferative but can be destructive over time. A proliferative reaction is favored in traumatic injuries because the fractured surface is usually flat, allowing salivary rinsing with little chance of impaction of contaminated debris. Unless impaction of con-taminated debris is obvious, it is expected that in the first 24 hours after the injury, a proliferative response with inflamma-tion extending not more than 2 mm into the pulp will be present (see Fig. 20-7).49,52,82 In time, the bacterial challenge results in local pulpal necrosis and a slow apical progression of the pulpal inflammation (Fig. 20-8).
TreatmentTreatment options for complicated crown fracture are (1) vital pulp therapy, comprising pulp capping, partial pulpotomy, or full pulpotomy; and (2) pulpectomy. The choice of treatment depends on the stage of development of the tooth, the time between trauma and treatment, concomitant periodontal injury, and the restorative treatment plan.
Stage of Development of the ToothLoss of vitality in an immature tooth can have catastrophic consequences. Root canal treatment on a tooth with a blunder-buss canal is time consuming and difficult. It is probably more important that necrosis of an immature tooth leaves it with thin dentinal walls that are susceptible to fracture both during and after the apexification procedure.99 Every effort must be made to keep the tooth vital, at least until the apex and cervical root have completed their development.
Removal of the pulp in a mature tooth is not as significant as in an immature tooth because a pulpectomy in a mature
FIG. 20-8 Histologic appearance of the pulp days after a traumatic expo-sure. Superficial necrosis above a zone of inflamed pulp is seen.
http://dentalebooks.com
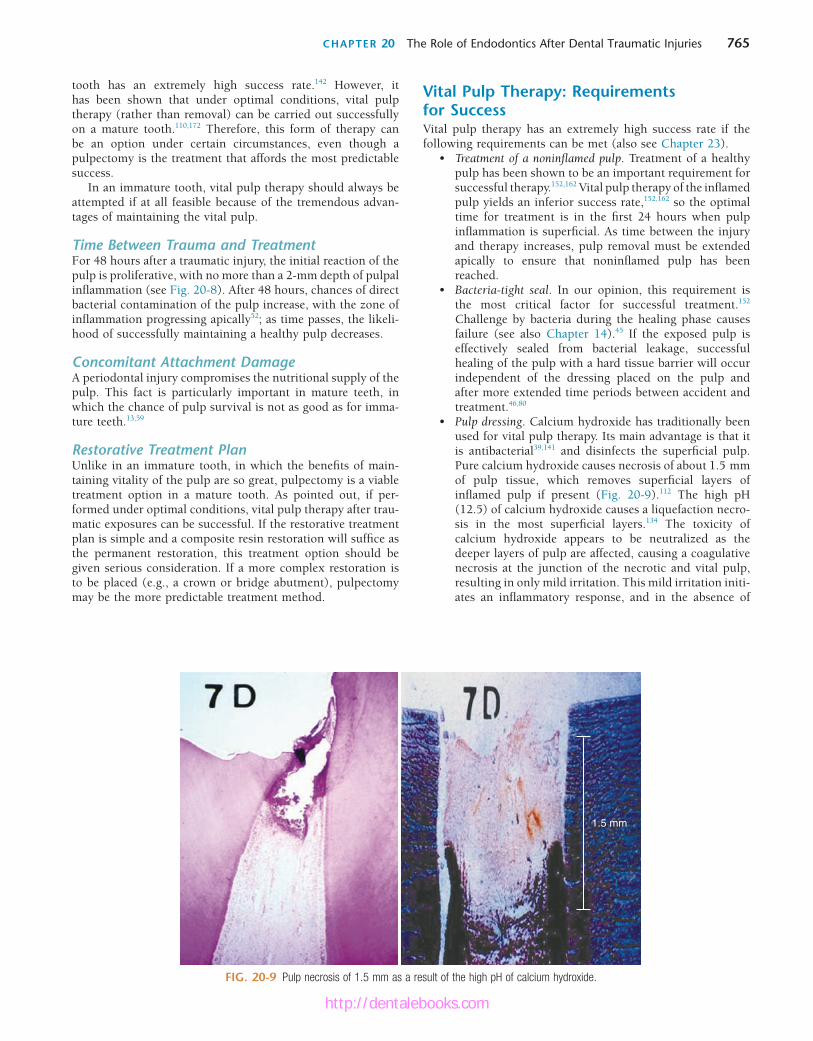
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 765
Vital Pulp Therapy: Requirements for SuccessVital pulp therapy has an extremely high success rate if the following requirements can be met (also see Chapter 23).
• Treatment of a noninflamed pulp. Treatment of a healthy pulp has been shown to be an important requirement for successful therapy.152,162 Vital pulp therapy of the inflamed pulp yields an inferior success rate,152,162 so the optimal time for treatment is in the first 24 hours when pulp inflammation is superficial. As time between the injury and therapy increases, pulp removal must be extended apically to ensure that noninflamed pulp has been reached.
• Bacteria-tight seal. In our opinion, this requirement is the most critical factor for successful treatment.152 Challenge by bacteria during the healing phase causes failure (see also Chapter 14).45 If the exposed pulp is effectively sealed from bacterial leakage, successful healing of the pulp with a hard tissue barrier will occur independent of the dressing placed on the pulp and after more extended time periods between accident and treatment.46,80
• Pulp dressing. Calcium hydroxide has traditionally been used for vital pulp therapy. Its main advantage is that it is antibacterial39,141 and disinfects the superficial pulp. Pure calcium hydroxide causes necrosis of about 1.5 mm of pulp tissue, which removes superficial layers of inflamed pulp if present (Fig. 20-9).112 The high pH (12.5) of calcium hydroxide causes a liquefaction necro-sis in the most superficial layers.134 The toxicity of calcium hydroxide appears to be neutralized as the deeper layers of pulp are affected, causing a coagulative necrosis at the junction of the necrotic and vital pulp, resulting in only mild irritation. This mild irritation initi-ates an inflammatory response, and in the absence of
tooth has an extremely high success rate.142 However, it has been shown that under optimal conditions, vital pulp therapy (rather than removal) can be carried out successfully on a mature tooth.110,172 Therefore, this form of therapy can be an option under certain circumstances, even though a pulpectomy is the treatment that affords the most predictable success.
In an immature tooth, vital pulp therapy should always be attempted if at all feasible because of the tremendous advan-tages of maintaining the vital pulp.
Time Between Trauma and TreatmentFor 48 hours after a traumatic injury, the initial reaction of the pulp is proliferative, with no more than a 2-mm depth of pulpal inflammation (see Fig. 20-8). After 48 hours, chances of direct bacterial contamination of the pulp increase, with the zone of inflammation progressing apically52; as time passes, the likeli-hood of successfully maintaining a healthy pulp decreases.
Concomitant Attachment DamageA periodontal injury compromises the nutritional supply of the pulp. This fact is particularly important in mature teeth, in which the chance of pulp survival is not as good as for imma-ture teeth.13,59
Restorative Treatment PlanUnlike in an immature tooth, in which the benefits of main-taining vitality of the pulp are so great, pulpectomy is a viable treatment option in a mature tooth. As pointed out, if per-formed under optimal conditions, vital pulp therapy after trau-matic exposures can be successful. If the restorative treatment plan is simple and a composite resin restoration will suffice as the permanent restoration, this treatment option should be given serious consideration. If a more complex restoration is to be placed (e.g., a crown or bridge abutment), pulpectomy may be the more predictable treatment method.
FIG. 20-9 Pulp necrosis of 1.5 mm as a result of the high pH of calcium hydroxide.
1.5 mm
http://dentalebooks.com

766 PART III Expanded Clinical Topics
probably three main reasons. The first is likely to be that because MTA needs a moist environment for at least 6 hours to set properly, the treatment becomes a two-step procedure, compared with a one-step procedure for other medicaments. Using MTA as a pulp capping agent thus necessitates that a wet cotton pellet be placed over it until it is set, and then the per-manent restoration can be fabricated at a later time. The second likely reason is that originally, MTA was gray in color and reported to cause discoloration in the tooth crown when used as a capping agent in anterior teeth.37 To counter this discol-oration problem, a new white version of MTA was marketed a few years ago. Initially there were some concerns that the pulp did not respond to the white version as favorably as it had to the gray one.121 Relatively few studies have been done compar-ing the white MTA to the gray one, but most have indicated that the pulp seems to react as well to one as the other.91,116,131 Unfortunately, the white MTA has been found to discolor in a similar fashion to the gray, presumably because of the bismuth oxide filler in the material.
The third likely reason is that recently, newer generation bioceramic materials have come to the market that have the same positive properties as MTA but not the disadvantages described previously. They set quickly enough for a one-visit procedure and do not discolor the tooth. These materials are now considered superior to calcium hydroxide as the capping agent for traumatic pulp exposures.
Treatment MethodsPulp CappingPulp capping implies placing the dressing directly on the pulp exposure without any removal of the soft tissue.24
IndicationsThere are few indications for pulp capping when traumatic pulp exposures are treated. The success rate of this procedure
bacteria,134 the pulp will heal with a hard tissue barrier (Fig. 20-10).133,134 Hard-setting calcium hydroxide does not cause necrosis of the superficial layers of pulp; it has also been shown to initiate healing with a hard tissue barrier.150,159
The major disadvantage of calcium hydroxide is that it does not seal the fractured surface. Therefore, an additional material must be used to ensure that bacteria do not challenge the pulp, particularly during the critical healing phase.
Many materials, such as zinc oxide eugenol,25,162 tricalcium phosphate,84 and composite resin,24 have been proposed as medicaments for vital pulp therapy. None to this date have afforded the predictability of calcium hydroxide used in con-junction with a well-sealed coronal restoration.60,102,139,151 In a dog study, for example, pulps capped directly with various adhesive agents showed moderate to severe inflammatory reac-tions, with progressive extension of tissue necrosis with time and total absence of continuous hard tissue bridge forma-tion.102 Application of a calcium hydroxide–based material was characterized by inflammatory cell infiltration, limited tissue necrosis, and partial to complete hard tissue bridging.102 In a similar study on human teeth in vivo, it was found that Scotch-bond Multi-Purpose Plus (3M, St. Paul, MN) caused inflam-matory changes when applied directly to exposed pulp tissue; however, direct capping with Dycal followed by sealing with Scotchbond Multi-Purpose Plus showed favorable results in pulp tissue.151
Currently, bioceramic materials are considered the pulp capping agents of choice.4 Mineral trioxide aggregate (MTA), a first-generation bioceramic material, has been shown to be a good pulp capping agent.62,116,118,174 It has a high pH, similar to that of calcium hydroxide, when unset156 and after setting creates an excellent bacteria-tight seal.157 It is also hard enough to act as a base for a final restoration.156 Yet MTA does not enjoy the same popularity as calcium hydroxide as a pulp capping agent in the treatment of traumatic exposures. There are
FIG. 20-10 Hard tissue barrier after calcium hydroxide partial pulpotomy. A, Histologic appearance of replace-ment odontoblasts and a hard tissue barrier. B, Clinical appearance of the barrier on removal of the coronal restoration 3 months after placement of the calcium hydroxide. C, Radiographic appearance of the hard tissue barrier.
A B C
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 767
anesthetic solution to a thick mix and carefully placed on the pulp stump. If the pulp size does not permit additional loss of pulp tissue, a commercial hard-setting calcium hydroxide can be used.150 The prepared cavity is filled with a material with the best chance of a bacteria-tight seal (zinc oxide eugenol or glass ionomer cement) to a level flush with the fractured surface. The material in the pulpal cavity and all exposed dentinal tubules are etched and restored with bonded composite resin. Alterna-tively, after hemostasis has been obtained, the pulp can be capped with MTA, a wet cotton pellet can be placed on top of it, and the access can be temporized for the appropriate time. The cotton pellet needs to be removed as early as possible and the tooth then restored with composite restoration.
Follow-UpThe follow-up is the same as for pulp capping. Emphasis is placed on evidence of maintenance of responses to sensitivity tests and radiographic evidence of continued root development (Fig. 20-12).
PrognosisThis method affords many advantages over pulp capping. Superficial inflamed pulp is removed during preparation of the pulpal cavity. Calcium hydroxide disinfects dentin and pulp and removes additional pulpal inflammation. Most important, space is provided for a material that can achieve a bacteria-tight seal to allow pulpal healing with hard tissue under optimal conditions. Additionally, coronal pulp remains, which allows sensitivity testing to be carried out at the follow-up visits. The prognosis is extremely good (94% to 96%).49,70
Full PulpotomyFull pulpotomy involves removal of the entire coronal pulp to a level of the root orifices. This level of pulp amputation is chosen arbitrarily because of its anatomic convenience. Because inflamed pulp sometimes extends past the canal orifices into the root pulp, many mistakes are made that result in treatment of an inflamed rather than a noninflamed pulp.
IndicationsFull pulpotomy is indicated when it is anticipated that the pulp is inflamed to the deeper levels of the coronal pulp. Traumatic exposures after more than 72 hours and carious exposure of a young tooth with a partially developed apex are two examples of cases in which this treatment may be indicated. Because of the likelihood that the dressing will be placed on an inflamed pulp, full pulpotomy is contraindicated in mature teeth. In the immature tooth, benefits outweigh risks for this treat-ment form only with incompletely formed apices and thin dentinal walls.
TechniqueThe procedure begins with administration of an anesthetic, rubber dam placement, and superficial disinfection, as for pulp capping and partial pulpotomy. The coronal pulp is removed as in partial pulpotomy, but to the level of the root orifices. A calcium hydroxide dressing, a bacteria-tight seal, and a coronal restoration are carried out as for partial pulpotomy.
Follow-UpFollow-up is the same as for pulp capping and partial pul-potomy. A major disadvantage of this treatment method is that
(80%),69,125 compared to partial pulpotomy (95%),49 indicates that a superficial pulp cap should not be considered after trau-matic pulp exposures. The lower success rate is not difficult to understand because superficial inflammation develops soon after the traumatic exposure. If the treatment is at the superfi-cial level, a number of inflamed (rather than healthy) pulps will be treated, lowering the potential for success. In addition, a bacteria-tight coronal seal is much more difficult to attain in superficial pulp capping because there is no depth to the cavity to aid in creating the seal, as there is with a partial pulpotomy.
It must be acknowledged that the studies suggesting that an inflamed pulp is contraindicated for an attempt at pulp capping were performed in the 1970s with amalgam as the standard coronal restoration. If we consider that amalgam leaks and calcium hydroxide washes out in the presence of moisture as the reasons for the poor results, then it may be poor coronal seal, rather than the inflamed pulp, that leads to the failure in these cases. More recent studies suggest that with the bio-ceramic as the pulp cap, the inflamed pulp is not the impedi-ment as previously thought, but rather that the seal seems to be the major factor for success. Thus this material used as a base in these situations may give us more leeway for capping the inflamed pulp.
However in a situation of a traumatic pulp exposure of a tooth (injuries in which most patients are young [large pulps]), the patient typically presents for treatment within 48 hours because of sensitivity and aesthetic concerns. There-fore, the pulpal inflammation is usually only superficial. In these cases, we still feel it is prudent to remove the superficial layer of inflammation and place a bioceramic agent for pulp capping.
Partial PulpotomyPartial pulpotomy implies the removal of coronal pulp tissue to the level of healthy pulp. Knowledge of the reaction of the pulp after a traumatic injury makes it possible to accurately determine this level. This procedure is commonly called the Cvek pulpotomy.
IndicationsAs for pulp capping.
TechniqueAdministration of an anesthetic (possibly without a vasocon-strictor), rubber dam placement, and superficial disinfection are performed. A 1- to 2-mm deep cavity is prepared into the pulp, using a high-speed handpiece with a sterile diamond bur of appropriate size and copious water coolant (Fig. 20-11).77 A slow-speed bur or spoon excavator should be avoided. If bleeding is excessive, the pulp is amputated deeper until only moderate hemorrhage is seen. Excess blood is carefully removed by rinsing with sterile saline, and the area is dried with a sterile cotton pellet. Use of 5% sodium hypochlorite (NaOCl; bleach) has been recommended to rinse the pulpal wound.46 The bleach causes chemical amputation of the blood coagulum; removes damaged pulp cells, dentin chips, and other debris; and provides hemorrhage control with minimal damage to the “normal” pulp tissue underneath.
Care must be taken not to allow a blood clot to develop because this would compromise the prognosis.49,133 A thin layer of pure calcium hydroxide is mixed with sterile saline or
http://dentalebooks.com
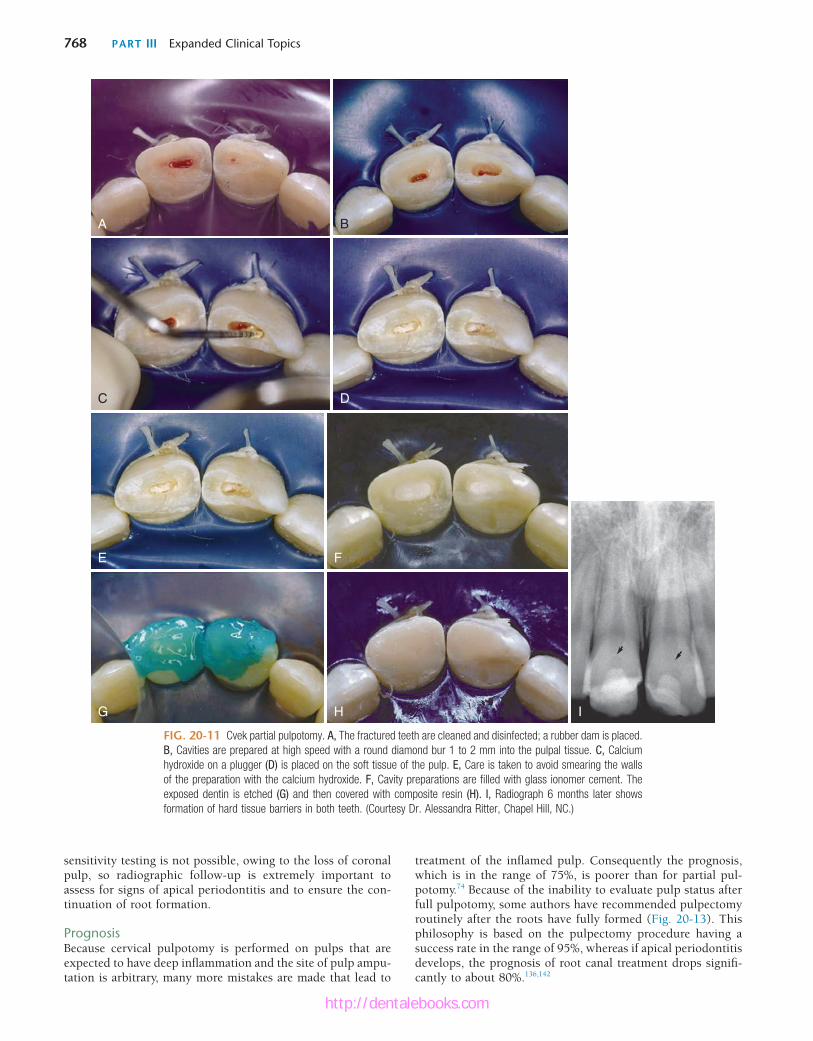
768 PART III Expanded Clinical Topics
treatment of the inflamed pulp. Consequently the prognosis, which is in the range of 75%, is poorer than for partial pul-potomy.74 Because of the inability to evaluate pulp status after full pulpotomy, some authors have recommended pulpectomy routinely after the roots have fully formed (Fig. 20-13). This philosophy is based on the pulpectomy procedure having a success rate in the range of 95%, whereas if apical periodontitis develops, the prognosis of root canal treatment drops signifi-cantly to about 80%.136,142
sensitivity testing is not possible, owing to the loss of coronal pulp, so radiographic follow-up is extremely important to assess for signs of apical periodontitis and to ensure the con-tinuation of root formation.
PrognosisBecause cervical pulpotomy is performed on pulps that are expected to have deep inflammation and the site of pulp ampu-tation is arbitrary, many more mistakes are made that lead to
FIG. 20-11 Cvek partial pulpotomy. A, The fractured teeth are cleaned and disinfected; a rubber dam is placed. B, Cavities are prepared at high speed with a round diamond bur 1 to 2 mm into the pulpal tissue. C, Calcium hydroxide on a plugger (D) is placed on the soft tissue of the pulp. E, Care is taken to avoid smearing the walls of the preparation with the calcium hydroxide. F, Cavity preparations are filled with glass ionomer cement. The exposed dentin is etched (G) and then covered with composite resin (H). I, Radiograph 6 months later shows formation of hard tissue barriers in both teeth. (Courtesy Dr. Alessandra Ritter, Chapel Hill, NC.)
A B
C D
E F
G H I
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 769
techniques cannot create an apical stop to facilitate effective root canal filling.
Biologic ConsequencesA nonvital immature tooth presents a number of difficulties for adequate endodontic treatment. The canal is often wider api-cally than coronally, necessitating the use of a filling technique with softened filling material to mold it to the shape of the apical part of the canal. Because the apex is extremely wide, no barrier exists to stop this softened material from moving into and traumatizing the apical periodontal tissues. Also, the lack of apical stop and extrusion of material through the canal might result in a canal that is underfilled and susceptible to leakage. An additional problem in immature teeth with thin dentinal walls is their susceptibility to fracture, both during and after treatment.50
PulpectomyPulpectomy implies removal of the entire pulp to the level of the apical foramen.
IndicationsPulpectomy is indicated in a complicated crown fracture of mature teeth if conditions are not ideal for vital pulp therapy or if it is foreseeable that restoring the tooth would require placement of a post. This procedure is no different from root canal treatment of a vital nontraumatized tooth.
Treatment of the Nonvital PulpImmature Tooth: ApexificationIndicationsApexification should be performed in teeth with open apices and thin dentinal walls in which standard instrumentation
FIG. 20-12 Continued root development after partial pulpotomy. A, Radiograph of immature tooth with a complicated crown fracture. B, At the time of placement of calcium hydroxide after partial pulpotomy. C, Follow-up radiograph confirming that the pulp maintained vitality and the root continued to develop.
A B C
FIG. 20-13 Successful pulpotomy followed by a pulpectomy at 18 months. (Courtesy Dr. Leif Tronstad, Oslo, Norway.)
0 6 m 18 m 18 m
http://dentalebooks.com

770 PART III Expanded Clinical Topics
calcium hydroxide is meticulously removed from the access cavity to the level of the root orifices, and a well-sealing, tem-porary filling is placed in the access cavity. A radiograph is taken; the canal should appear to have become calcified, indi-cating that the entire canal has been filled with the calcium hydroxide (Fig. 20-16). Because calcium hydroxide washout is evaluated by its relative radiodensity in the canal, it is prudent to use a calcium hydroxide mixture without the addition of a radiopaquer, such as barium sulfate. These additives do not wash out as readily as calcium hydroxide, so if they are present in the canal, evaluation of washout is impossible.
At 3-month intervals, a radiograph is exposed to evaluate whether a hard tissue barrier has formed and if the calcium hydroxide has washed out of the canal. This is assessed to have occurred if the canal can be seen again radiographically. If no washout is evident, the calcium hydroxide can be left intact for another 3 months. Excessive calcium hydroxide dressing changes should be avoided if at all possible because the initial toxicity of the material is thought to delay healing.104
When completion of a hard tissue barrier is suspected, the calcium hydroxide should be washed out of the canal with NaOCl. A file of a size that can easily reach the apex can be used to gently probe for a stop at the apex. When a hard tissue barrier is indicated radiographically and can be probed with an instrument, the canal is ready for filling.
Bioceramic BarrierThe creation of a physiologic hard tissue barrier, although quite predictable, takes anywhere from 3 to 18 months with calcium hydroxide. The disadvantages of this long time period are that the patient is required to present for treatment multiple times and the tooth may fracture during treatment before the thin, weak roots can be strengthened. In addition, one study has indicated that long-term treatment with calcium hydroxide may weaken the roots and make them even more susceptible to fracture.19
Bioceramic material has been used to create a hard tissue barrier quickly after disinfection of the canal (see earlier in the section Traditional Method) (Fig. 20-17). Calcium sulfate is pushed through the apex to provide a resorbable extraradicular barrier against which to pack the bioceramic material. The material is mixed and placed into the apical 3 to 4 mm of the canal in a manner similar to the placement of calcium hydrox-ide. A wet cotton pellet should be placed against the bio-ceramic material and left for at least 6 hours. After the material
These problems are overcome by stimulating the formation of a hard tissue barrier to allow for optimal filling of the canal and by reinforcing the weakened root against fracture, both during and after apexification.101,154
TechniqueDisinfection of the CanalIn most cases nonvital teeth are infected,29,138 so the first phase of treatment is to disinfect the root canal system to ensure periapical healing.39,53 The canal length is estimated with a parallel preoperative radiograph, and after access to the canals has been prepared, a file is placed to this estimated length. When the length has been confirmed radiographically, very light filing (because of the thin dentinal walls) is performed with copious irrigation with 0.5% NaOCl.54,147 A lower strength of NaOCl is used because of the increased danger of placing the agent through the apex in immature teeth. The increased volume of irrigant used compensates for this lower concentra-tion of NaOCl. An irrigation needle that can passively reach close to the apical length is useful in disinfecting the canals of these immature teeth. The canal is dried with paper points and a creamy mix of calcium hydroxide (toothpaste thickness) spun into the canal with a Lentulo spiral instrument (Fig. 20-14). Additional disinfecting action of calcium hydroxide is effective after its application for at least 1 week,141 so continu-ation of treatment can take place any time after 1 week. Further treatment should not be delayed more than 1 month because the calcium hydroxide could be washed out by tissue fluids through the open apex, leaving the canal susceptible to reinfection.
Hard Tissue Apical BarrierTraditional MethodFormation of the hard tissue barrier at the apex requires a similar environment to that required for hard tissue formation in vital pulp therapy: a mild inflammatory stimulus to initiate healing and a bacteria-free environment to ensure that inflam-mation is not progressive.
As with vital pulp therapy, calcium hydroxide is used for this procedure.50,83,85 Pure calcium hydroxide powder is mixed with sterile saline (or anesthetic solution) to a thick (powdery) consistency (Fig. 20-15). The calcium hydroxide is packed against the apical soft tissue with a plugger or thick point to initiate hard tissue formation. This step is followed by backfill-ing with calcium hydroxide to completely fill the canal. The
FIG. 20-14 Creamy mix of calcium hydroxide on a Lentulo spiral instrument ready for placement into the canal.
FIG. 20-15 Thick mix of calcium hydroxide.
http://dentalebooks.com
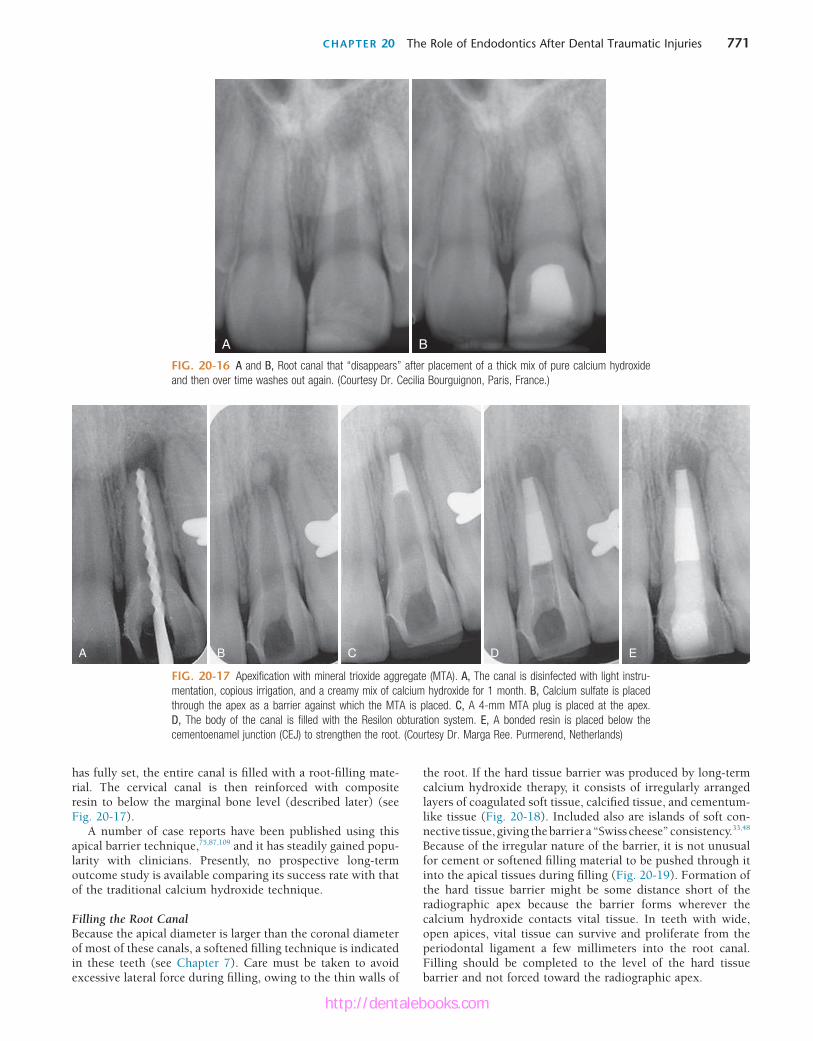
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 771
FIG. 20-16 A and B, Root canal that “disappears” after placement of a thick mix of pure calcium hydroxide and then over time washes out again. (Courtesy Dr. Cecilia Bourguignon, Paris, France.)
BA
FIG. 20-17 Apexification with mineral trioxide aggregate (MTA). A, The canal is disinfected with light instru-mentation, copious irrigation, and a creamy mix of calcium hydroxide for 1 month. B, Calcium sulfate is placed through the apex as a barrier against which the MTA is placed. C, A 4-mm MTA plug is placed at the apex. D, The body of the canal is filled with the Resilon obturation system. E, A bonded resin is placed below the cementoenamel junction (CEJ) to strengthen the root. (Courtesy Dr. Marga Ree. Purmerend, Netherlands)
A B D EC
has fully set, the entire canal is filled with a root-filling mate-rial. The cervical canal is then reinforced with composite resin to below the marginal bone level (described later) (see Fig. 20-17).
A number of case reports have been published using this apical barrier technique,75,87,109 and it has steadily gained popu-larity with clinicians. Presently, no prospective long-term outcome study is available comparing its success rate with that of the traditional calcium hydroxide technique.
Filling the Root CanalBecause the apical diameter is larger than the coronal diameter of most of these canals, a softened filling technique is indicated in these teeth (see Chapter 7). Care must be taken to avoid excessive lateral force during filling, owing to the thin walls of
the root. If the hard tissue barrier was produced by long-term calcium hydroxide therapy, it consists of irregularly arranged layers of coagulated soft tissue, calcified tissue, and cementum-like tissue (Fig. 20-18). Included also are islands of soft con-nective tissue, giving the barrier a “Swiss cheese” consistency.33,48 Because of the irregular nature of the barrier, it is not unusual for cement or softened filling material to be pushed through it into the apical tissues during filling (Fig. 20-19). Formation of the hard tissue barrier might be some distance short of the radiographic apex because the barrier forms wherever the calcium hydroxide contacts vital tissue. In teeth with wide, open apices, vital tissue can survive and proliferate from the periodontal ligament a few millimeters into the root canal. Filling should be completed to the level of the hard tissue barrier and not forced toward the radiographic apex.
http://dentalebooks.com

772 PART III Expanded Clinical Topics
Reinforcement of Thin Dentinal WallsThe apexification procedure has become a predictably success-ful procedure (see the section Prognosis),68 but thin dentinal walls still present a clinical problem. Should secondary injuries occur, teeth with thin dentinal walls are more susceptible to fractures that render them unrestorable.56,158 It has been reported that approximately 30% of these teeth will fracture during or after endodontic treatment.101 Consequently, some clinicians have questioned the advisability of the apexification procedure and have opted for more radical treatment proce-dures, including extraction followed by extensive restorative procedures, such as dental implants. Studies have shown that intracoronal bonded restorations can internally strengthen endodontically treated teeth and increase their resistance to fracture.76,99 Thus, after root filling, the material should be removed to below the marginal bone level and a bonded resin filling placed (see Fig. 20-17).
Follow-UpRoutine recall evaluation should be performed to determine success in the prevention or treatment of apical periodontitis.
FIG. 20-18 Histologic appearance of hard tissue barrier after calcium hydroxide apexification. The barrier is composed of cementum and bone with soft tissue inclusions.
FIG. 20-19 Root filing with a soft technique after calcium hydroxide apexi-fication. Sealer and softened filling material is expressed through the “Swiss cheese” holes in the barrier.
Restorative procedures should be assessed to ensure that they in no way promote root fractures.
PrognosisPeriapical healing and the formation of a hard tissue barrier occur predictably with long-term calcium hydroxide treatment (79% to 96%).50,101 However, long-term survival is jeopardized by the fracture potential of the thin dentinal walls of these teeth. It is expected that the newer techniques of internally strengthening the teeth described earlier will increase their long-term survivability.
Pulp RevitalizationRevitalization of a necrotic pulp has been considered possible only after avulsion of an immature permanent tooth that was reimplanted within 40 minutes (discussed later). The advan-tages of pulp revascularization lie in the possibility of further root development and reinforcement of dentinal walls by depo-sition of hard tissue, thus strengthening the root against frac-ture (see also Chapter 10). After reimplantation of an avulsed immature tooth, a unique set of circumstances exists that allows regeneration to take place. The young tooth has an open apex and is short, which allows new tissue to grow into the pulp space relatively quickly. The pulp is necrotic but usually neither degenerated nor infected, so it acts as a matrix into which the new tissue can grow. It has been experimentally shown that the apical part of a pulp may remain vital and after reimplantation proliferate coronally, replacing the necrotized portion of the pulp.26,117,145 Because in most cases the crown of the tooth is intact and caries free, bacterial penetration into the pulp space through cracks106 and defects will be a slow process. The race between new tissue growth and infection of the pulp space favors the new tissue.
Regeneration of pulp tissue in a necrotic infected tooth with apical periodontitis was thought to be impossible until about a decade ago.114 However, if it is possible to create an environ-ment similar to that described for the avulsed tooth, regenera-tion will probably occur. If the canal is effectively disinfected, a matrix into which new tissue can grow is provided, and coronal access is effectively sealed. Regeneration should occur as in an avulsed immature tooth.
Banchs and Trope25 wrote one of the first case reports that suggest it may be possible to replicate the unique circum-stances of an avulsed tooth. The case (Fig. 20-20) described the treatment of an immature second mandibular premolar that had radiographic and clinical signs of apical periodontitis, along with a sinus tract. The canal was disinfected without mechanical instrumentation but with copious irrigation with 5.25% NaOCl, followed by placement of an intracanal mixture of antibiotics consisting of equal amounts of ciprofloxacin, metronidazole, and minocycline for 3 weeks.89
The antibiotic mixture was rinsed out after 3 weeks, and a blood clot was produced to the level of the cementoenamel junction to provide a matrix for ingrowth of new tissue; this was followed by a deep coronal restoration to provide a bacteria-tight seal. Clinical and radiographic evidence of healing appeared as early as 22 days; the large radiolucency had disappeared within 2 months; and at the 24-month recall, it was obvious that the root walls were thick and development of the root below the restoration was similar to that of the adjacent and contralateral teeth. More recently, published cases and case series reports have further supported that it is possible
http://dentalebooks.com
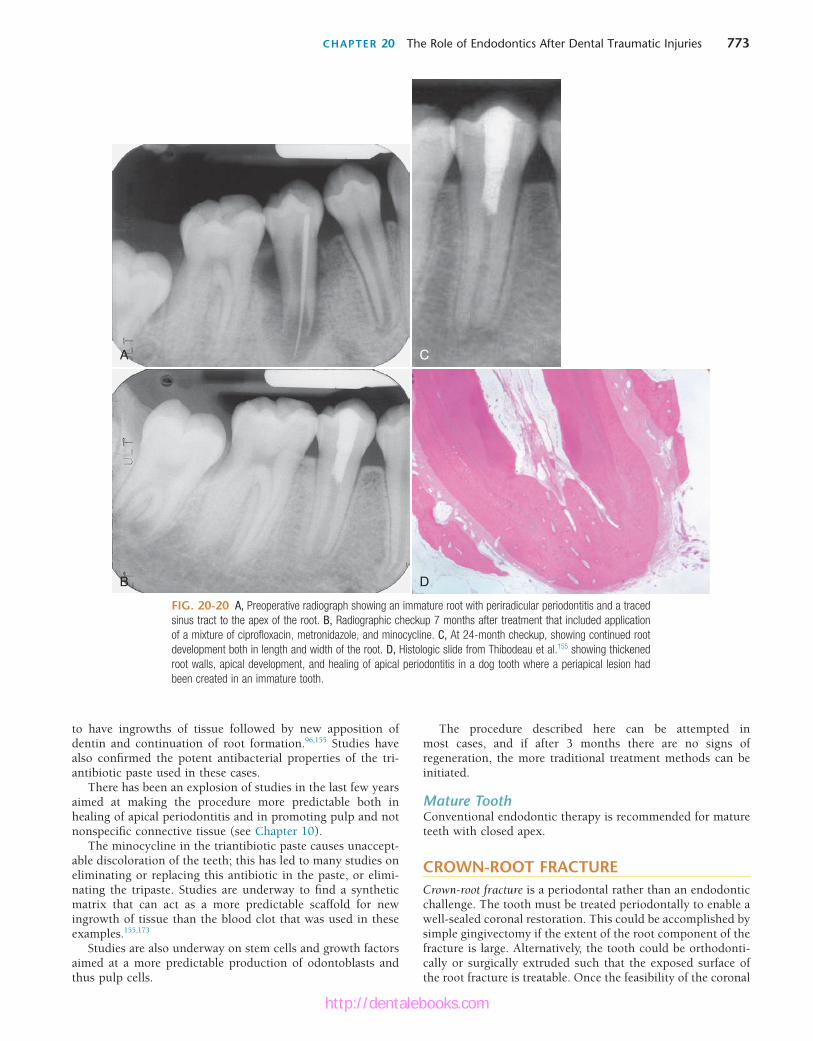
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 773
The procedure described here can be attempted in most cases, and if after 3 months there are no signs of regeneration, the more traditional treatment methods can be initiated.
Mature ToothConventional endodontic therapy is recommended for mature teeth with closed apex.
CROWN-ROOT FRACTURECrown-root fracture is a periodontal rather than an endodontic challenge. The tooth must be treated periodontally to enable a well-sealed coronal restoration. This could be accomplished by simple gingivectomy if the extent of the root component of the fracture is large. Alternatively, the tooth could be orthodonti-cally or surgically extruded such that the exposed surface of the root fracture is treatable. Once the feasibility of the coronal
to have ingrowths of tissue followed by new apposition of dentin and continuation of root formation.96,155 Studies have also confirmed the potent antibacterial properties of the tri-antibiotic paste used in these cases.
There has been an explosion of studies in the last few years aimed at making the procedure more predictable both in healing of apical periodontitis and in promoting pulp and not nonspecific connective tissue (see Chapter 10).
The minocycline in the triantibiotic paste causes unaccept-able discoloration of the teeth; this has led to many studies on eliminating or replacing this antibiotic in the paste, or elimi-nating the tripaste. Studies are underway to find a synthetic matrix that can act as a more predictable scaffold for new ingrowth of tissue than the blood clot that was used in these examples.155,173
Studies are also underway on stem cells and growth factors aimed at a more predictable production of odontoblasts and thus pulp cells.
FIG. 20-20 A, Preoperative radiograph showing an immature root with periradicular periodontitis and a traced sinus tract to the apex of the root. B, Radiographic checkup 7 months after treatment that included application of a mixture of ciprofloxacin, metronidazole, and minocycline. C, At 24-month checkup, showing continued root development both in length and width of the root. D, Histologic slide from Thibodeau et al.155 showing thickened root walls, apical development, and healing of apical periodontitis in a dog tooth where a periapical lesion had been created in an immature tooth.
A
B
C
D
http://dentalebooks.com

774 PART III Expanded Clinical Topics
way to accomplish reapproximation of the two segments is to release the coronal segment from the bone by gently pulling it slightly downward with finger pressure or extraction forceps and, once it is loose, rotating it back to its original position (Fig. 20-23). The traditionally recommended124 splinting pro-tocol has been changed from 2 to 4 months with rigid splinting to a semirigid splint to adjacent teeth for 2 to 4 weeks.18 If a long time has elapsed between the injury and treatment, repo-sitioning of the segments close to their original position prob-ably will not be possible; this compromises the long-term prognosis for the tooth.
Healing PatternsInvestigators21 have described four types of responses to root fractures.
1. Healing with calcified tissue. Radiographically, the frac-ture line is discernible, but the fragments are in close contact (Fig. 20-24, A).
2. Healing with interproximal connective tissue. Radiographi-cally, the fragments appear separated by a narrow radiolucent line, and the fractured edges appear rounded (Fig. 20-24, B).
3. Healing with interproximal bone and connective tissue. Radiographically, the fragments are separated by a dis-tinct bony ridge (Fig. 20-24, C).
4. Interproximal inflammatory tissue without healing. Radio-graphically, a widening of the fracture line and/or a developing radiolucency corresponding to the fracture line becomes apparent (Fig. 20-24, D).
The first three healing patterns are considered successful. The teeth are usually asymptomatic and respond positively to sensitivity testing. Coronal yellowing is possible because calcific metamorphosis of the coronal segment is not unusual (see Fig. 20-29).94,177
The fourth type of root fracture response is typical when the coronal segment loses its vitality. The infective products in the coronal pulp cause an inflammatory response and typical radiolucencies at the fracture line (see Fig. 20-24, D).21
Treatment of ComplicationsCoronal Root FracturesHistorically it had been thought that fractures in the cervical segment had a poor prognosis, and extraction of the coronal segment was recommended. Research does not support this treatment; in fact, if these coronal segments are adequately splinted, chances of healing do not differ from those for midroot or apical fractures (Fig. 20-25).177 However, if the fracture occurs at the level of or coronal to the crest of the alveolar bone, the prognosis is extremely poor.
If reapproximation of the fractured segments is not possible, extraction of the coronal segment is indicated. The level of fracture and length of the remaining root are evaluated for restorability. If the apical root segment is long enough, gentle orthodontic eruption of this segment can be carried out to enable fabrication of a restoration.
Midroot and Apical Root FracturesPermanent pulpal necrosis occurs in 25% of root fractures.48,93 Initially it is likely that in many cases the pulp in the coronal segment will become necrotic after the injury; however, because of a very large apical opening in the coronal segment, revascu-larization is possible if the segments are well reapproximated.
restoration is assured, the particular crown fracture is treated as previously described.
ROOT FRACTURERoot fracture implies fracture of the cementum, dentin, and pulp. These injuries are relatively infrequent, occurring in less than 3% of all dental injuries.177 Immature teeth with vital pulps rarely sustain horizontal root fractures.7 When a root fractures horizontally, the coronal segment is displaced to a varying degree, but generally the apical segment is not dis-placed. Because the apical pulpal circulation is not disrupted, pulp necrosis in the apical segment is extremely rare. Perma-nent pulpal necrosis of the coronal segment, requiring end-odontic treatment, occurs in about 25% of cases.8,9,93
Diagnosis and Clinical PresentationThe clinical presentation of a root fracture is similar to that of luxation injuries. The extent of displacement of the coronal segment is usually indicative of the location of the fracture and can vary from none, simulating a concussion injury (apical fracture), to severe, simulating an extrusive luxation (cervical fracture).
Radiographic examination for root fractures is extremely important. Because root fractures are usually oblique (facial to palatal) (Fig. 20-21), one periapical radiograph may easily miss it. It is imperative to take at least three angled radiographs (45°, 90°, and 110°) so that at least at one angulation, the x-ray beam passes directly through the fracture line to make it visible on the radiograph (Fig. 20-22).
TreatmentEmergency treatment involves repositioning the segments into close proximity as much as possible. In the case of severe dis-placement of the coronal segment, its apical extension is fre-quently lodged in (if not perforating through) the cortical bone facial to the tooth. Forcing the crown facially is not possible, and the two segments will not be properly aligned. The only
FIG. 20-21 Extracted root after a root fracture. Note the oblique angle of the fracture.
http://dentalebooks.com
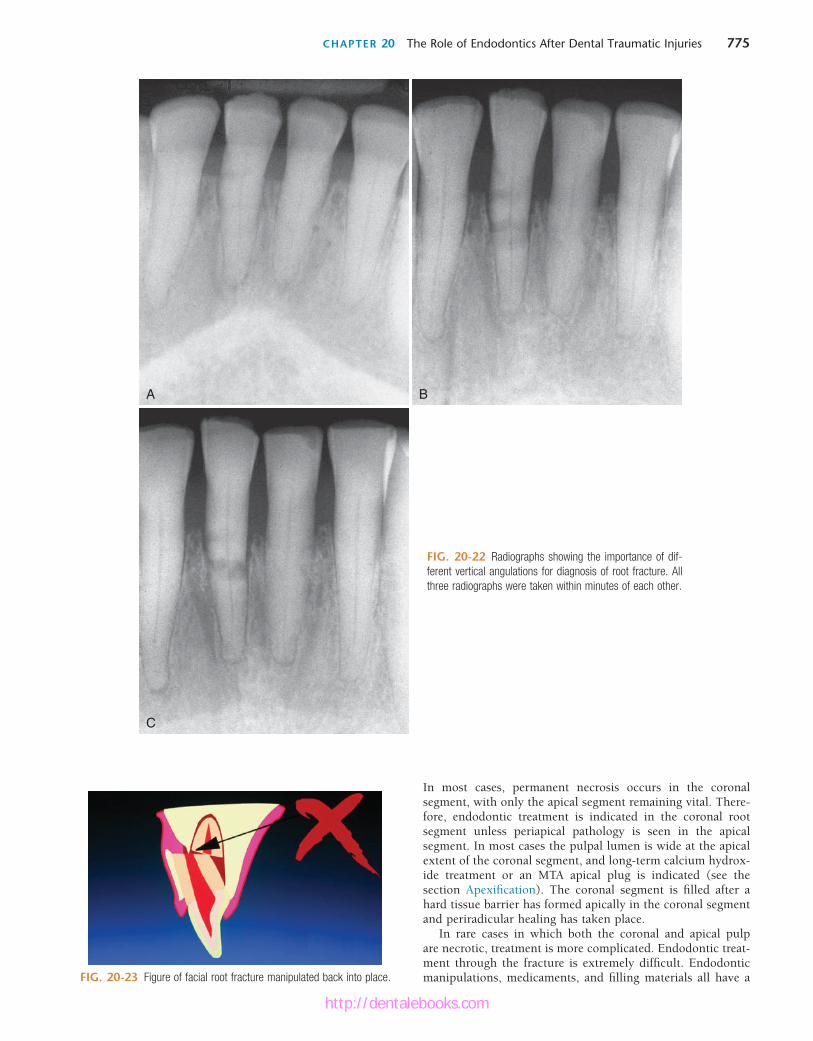
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 775
A
C
B
FIG. 20-22 Radiographs showing the importance of dif-ferent vertical angulations for diagnosis of root fracture. All three radiographs were taken within minutes of each other.
FIG. 20-23 Figure of facial root fracture manipulated back into place.
In most cases, permanent necrosis occurs in the coronal segment, with only the apical segment remaining vital. There-fore, endodontic treatment is indicated in the coronal root segment unless periapical pathology is seen in the apical segment. In most cases the pulpal lumen is wide at the apical extent of the coronal segment, and long-term calcium hydrox-ide treatment or an MTA apical plug is indicated (see the section Apexification). The coronal segment is filled after a hard tissue barrier has formed apically in the coronal segment and periradicular healing has taken place.
In rare cases in which both the coronal and apical pulp are necrotic, treatment is more complicated. Endodontic treat-ment through the fracture is extremely difficult. Endodontic manipulations, medicaments, and filling materials all have a
http://dentalebooks.com

776 PART III Expanded Clinical Topics
FIG. 20-24 Healing patterns after horizontal root fractures. A, Healing with calcified tissue. B, Healing with interproximal connective tissue. C, Healing with bone and connective tissue. D, Interproximal connective tissue without healing.
A B
C D
FIG. 20-25 Internal root resorption in the root fracture area; tooth was diagnosed with compound midroot fracture. A, Coronal portion was repositioned and then splinted to the lateral incisor with a composite splint. B, At 6-month recall, the pulp responded normally to cold, but an internal root-resorptive defect was noted on radiograph. No treatment was indicated, because the pulp did respond normally to vitality tests. C, At 42-month recall, the tooth was still asymptomatic, and the pulp still responded to vitality tests. The resorptive defect had healed, and signs of dystrophic calcifications were evident in the apical and coronal segments.
A B C
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 777
the pulp might be unresponsive to vitality tests for several weeks if not months.144 When the pulp is unresponsive initially after the trauma, patients should be recalled on a regular basis and monitored for any additional signs of infection of the root canal (discussed later).
Teeth with lateral and extrusive luxation should be reposi-tioned as soon as possible. In lateral luxation, the apex might be perforating the facial bone plate, and the tooth must be slightly and gently pulled down to loosen the hold before it is repositioned in its original position. Current IADT guidelines call for 2 weeks of physiologic splinting in cases of extrusion luxation and 4 weeks for lateral luxation. A decision on root canal therapy follows the guidelines for avulsion (discussed later). If the tooth has a fully formed apex and was diagnosed to have moved into (if not through) the cortical plate (apical translocation), there is a good likelihood of the pulp being devitalized; therefore, endodontic treatment should be initi-ated as early as 2 weeks after the injury. If the apex is still not fully formed, waiting for signs of revascularization is strongly recommended.
Permanent teeth that are intruded are not likely to sponta-neously re-erupt, especially if the apex is fully formed.100 Alter-native treatment, such as orthodontic extrusion or immediate surgical repositioning, should be considered. If orthodontic extrusion is planned for an intruded tooth, it should be initi-ated as soon as possible and should not be delayed longer than 2 to 3 weeks after the trauma. Only a few studies have evalu-ated the true efficacy of this approach. One study168 using a dog model indicated that severely intruded teeth showed signs of ankylosis as early as 11 to 13 days after the trauma, despite initiation of orthodontic movement 5 to 7 days after the injury.
For the surgical approach, one study47 (using a dog model) concluded that “a careful immediate surgical repositioning of a severely intruded permanent tooth with complete root forma-tion has many advantages with few disadvantages.” Another investigation,58 a retrospective study of 58 intruded human teeth, indicated that surgical repositioning resulted in a pre-dictable outcome, with only five of the teeth lost over the observation period. However, it was also observed that less surgical manipulation positively influenced the healing. If an intruded tooth is immediately reimplanted, it should be splinted for at least 4 weeks, but in most cases the splint needs to be left on the tooth longer.
Biologic ConsequencesLuxation injuries result in damage to the attachment apparatus (periodontal ligament and cemental layer), the severity of which depends on the type of injury sustained (concussion least, intrusion most). The apical neurovascular supply to the pulp is also affected to varying degrees, resulting in an altered or nonvital tooth.
Healing can be favorable or unfavorable. Favorable healing after a luxation injury occurs if the initial physical damage to the root surface and the resultant inflammatory response to the damaged external root surface are again covered with cemen-tum. An unfavorable response occurs when there is direct attachment of bone to the root, with the root ultimately being replaced by bone.
There are two resorption responses in which the pulp plays an essential role:
1. In external inflammatory root resorption, the necrotic infected pulp provides the stimulus for periodontal
detrimental effect on healing of the fracture site. If healing of the fracture has been completed and is followed by necrosis of the apical segment, the prognosis is much improved.
In more apical root fractures, necrotic apical segments can be surgically removed. This is a viable treatment if the remain-ing coronal root segment is long enough to provide adequate periodontal support. Removal of the apical segment in midroot fractures leaves the coronal segment with a compromised attachment; endodontic implants have been used to provide additional support to the tooth.
Follow-UpAfter the splinting period is completed, follow-up is as for all dental traumatic injuries: at 3, 6, and 12 months and yearly thereafter.
PrognosisThe following factors influence repair:
1. The degree of dislocation and mobility of the coronal fragment are extremely important in determining outcome.7,17,94,148,177 Increased dislocation and coronal fragment mobility result in a poorer prognosis.
2. Immature teeth are seldom involved in root fractures, but in the unlikely event they are, the prognosis is good.17,92
3. The quality of treatment is vital to successful repair. The prognosis improves with quick treatment, close reduc-tion of the root segments, and semirigid splinting for 2 to 4 weeks.18
Complications include pulp necrosis and root canal obliteration. Pulp necrosis can be treated successfully48,93 by treating the coronal segment with calcium hydroxide to stimulate hard tissue barrier formation. Root canal obliter-ation is common if the root segment (coronal or apical) remains vital.
LUXATION INJURIES
DefinitionsThe types of luxation injury can be defined as follows:
1. Concussion implies no displacement, normal mobility, and sensitivity to percussion.
2. Subluxation implies sensitivity to percussion, increased mobility, and no displacement.
3. Lateral luxation implies displacement labially, lingually, distally, or incisally.
4. Extrusive luxation implies displacement in a coronal direction.
5. Intrusive luxation implies displacement in an apical direc-tion into the alveolus.
Definitions 1 through 5 describe injuries of increasing mag-nitude in terms of intensity of the injury and subsequent sequelae.
IncidenceLuxation injuries as a group are the most common of all dental injuries, with a reported incidence ranging from 30% to 44%.55
TreatmentTeeth that are concussed or subluxated do not need any imme-diate treatment. Responses to vitality tests should be investi-gated and noted. Even after mild injury, such as subluxation,
http://dentalebooks.com

778 PART III Expanded Clinical Topics
radiograph is taken at a specific angle. It is important to avoid misinterpreting these cases as progressive. The pulp is not involved. If the pulp responds to sensitivity tests, this is a clue that no treatment should be performed. A wait-and-see attitude can allow spontaneous healing to take place. It is important to realize that in the initial stages, radiolucency could be followed by spontaneous repair, and endodontic treatment should not be initiated.
Diffuse Injury: Healing by Osseous ReplacementWhen the traumatic injury is severe (e.g., intrusive luxation or avulsion with extended dry time), involving diffuse damage on more than 20% of the root surface, an abnormal attachment can occur after healing takes place.105 The initial reaction, as always, is inflammation in response to the severe mechanical damage to the root surface. After the initial inflammatory response, a diffuse area of root surface devoid of cementum results. Cells in the vicinity of the denuded root now compete to repopulate it. Often cells that are precursors of bone, rather than the slower-moving periodontal ligament cells, move across from the socket wall and populate the damaged root. Bone comes into contact with the root without an intermediate attachment apparatus. This phenomenon is termed dentoalveo-lar ankylosis.105 However, the ankylosis and osseous replace-ment that follows cannot be reversed and can be considered a physiologic process because bone resorbs and reforms through-out life. Thus root is resorbed by osteoclasts, but in the reforming stage, bone is laid down instead of dentin, slowly replacing the root with bone. This process is termed osseous replacement (Fig. 20-27).164 The initial inflammation to remove the mechanical debris of the traumatic injury is a pathologic response that in the authors’ opinion may be reversed. In these traumatic cases, however, the resorptive phase includes the root (Fig. 20-28).
inflammation in the ligament space. If the cementum has been damaged, the inflammatory stimulators in the pulp space are able to diffuse through the dentinal tubules and stimulate an inflammatory response over large areas of the periodontal ligament. Because of the lack of cemental protection, the periodontal inflammation includes root resorption in addition to the expected bone resorption.
2. With internal inflammatory root resorption, the inflamed pulp is the tissue involved in resorbing the root struc-ture. The pathogenesis of internal root resorption is not completely understood. Here it is thought that coronal necrotic infected pulp provides a stimulus for a pulpal inflammation in the more apical parts of the remaining vital pulp.7 If the internal root surface has lost its prece-mental protection during an injury, internal root resorp-tion occurs in the area adjacent to the inflamed pulp. Thus, both the necrotic infected pulp and the inflamed pulp contribute to this type of root resorption.
External Root ResorptionCaused by an Injury (Alone) to the External Root SurfaceIf an injury harms the attachment, the by-products of this mechanical damage stimulate an inflammatory response. The healing response depends on the extent of the initial damage.
Localized Injury: Healing with CementumWhen the injury is localized (e.g., after concussion or sublux-ation injury), mechanical damage to the cementum occurs, resulting in a local inflammatory response and a localized area of root resorption. If no further inflammatory stimulus is present, periodontal healing and root surface repair occur within 14 days (Fig. 20-26).78 The resorption is localized to the area of mechanical damage, and treatment is not required because it is free of symptoms and not even visualized radio-graphically in most cases. In a minority of cases, however, small radiolucencies can be seen on the root surface if the
FIG. 20-26 Histologic section showing previous root resorptive defect healed with new cementum and periodontal ligament.
FIG. 20-27 Histologic appearance of osseous replacement. There is direct contact between bone and root structure. Resorptive defects are seen in the bone and root tissue, which is the normal physiologic process of bone turn-over. The resorptive defects are filled by new bone and additional areas resorbed. In this way the entire root is replaced by bone at a rate dependent on the metabolic rate of the patient.
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 779
FIG. 20-28 Radiographic appearance of osseous replacement. The root acquires the radiographic appearance of the surrounding bone (without a lamina dura). Note that radiolucencies typical of active inflammation are not present.
TreatmentTreatment strategies for limiting the effect of the traumatic injury to the periodontal structures are outside the scope of this chapter. However, in general they involve minimizing the initial inflammatory response to the injury. The initial inflam-mation is destructive in nature and increases the surface area of root to be covered in the healing phase.20 The smaller the surface area to be covered by new cementum, the higher the chances of favorable repair.
A study has indicated that if Ledermix, a drug combining corticosteroid and tetracycline, is placed in the root canal immediately after a severe trauma in which osseous replace-ment is expected, favorable healing occurs at a very high rate.38 In a more recent study, it was shown that triamcinolone (the corticosteroid portion of the Ledermix paste) was as effective as Ledermix at inhibiting external root resorption.41 Both of these studies were done on young dogs and need to be repli-cated in human studies.
Caused by an Injury to the External Root Surface and Inflammatory Stimulus in the Root CanalRecognized inflammatory stimuli that cause root resorption are pressure, pulp space infection, and sulcular infection. This chapter focuses on pulp space infection.
Consequences of Apical Neurovascular Supply DamagePulp Canal Obliteration (Calcification)Pulp canal obliteration is common after luxation injuries (Fig. 20-29). The frequency of pulp canal obliteration appears inversely proportional to pulp necrosis. The exact mechanism of pulp canal obliteration is unknown. It has been theorized that the sympathetic/parasympathetic control of blood flow to the odontoblasts is altered, resulting in uncontrolled reparative dentin.7,15 Another theory is that hemorrhage and blood clot formation in the pulp after injury form a nidus for subsequent calcification if the pulp remains vital.7,15 One study11 found that pulp canal obliteration could usually be diagnosed within the first year after injury and was more frequent in teeth with open
FIG. 20-29 A, Pulp canal calcification after a luxation injury. Radiographic appearance of a calcified maxillary lateral incisor; note that despite calcifica-tion, it has now become necrotic and infected, evident by the periapical lesion. B, The typical yellow appearance of the tooth caused by thickened dentin in the pulp chamber.
A
B
apices (>0.7 mm radiographically), those with extrusive and lateral luxation injuries, and those that had been rigidly splinted.11
Pulp NecrosisThe factors most important for the development of pulp necro-sis are the type of injury (concussion least, intrusion most) and the stage of root development (mature apex more than an immature apex).10 Pulp necrosis is most likely to lead to infec-tion of the root canal system, with problematic consequences.
Pulp Space InfectionPulp space infection in conjunction with damage to the exter-nal root surface results in periradicular root and bone resorp-tion and continues in its active state as long as the pulpal stimulus (infection) remains. When the root loses its cemental protection, lateral periodontitis with root resorption can result (Fig. 20-30).
To have pulp space infection, the pulp must first become necrotic. Necrosis occurs after a fairly serious injury in which displacement of the tooth results in severing of the apical blood vessels. In mature teeth, pulp regeneration cannot occur, and usually by 3 weeks, the necrotic pulp becomes infected. (For details of the typical bacterial contents of a traumatized necrotic pulp, the reader is referred to Chapter 14 or to Bergenholtz.29) Because a serious injury is required for pulp necrosis, areas of cemental covering of the root usually are also affected, resulting in loss of its protective (insulating) quality. Now bacterial toxins can pass through the dentinal tubules and
http://dentalebooks.com
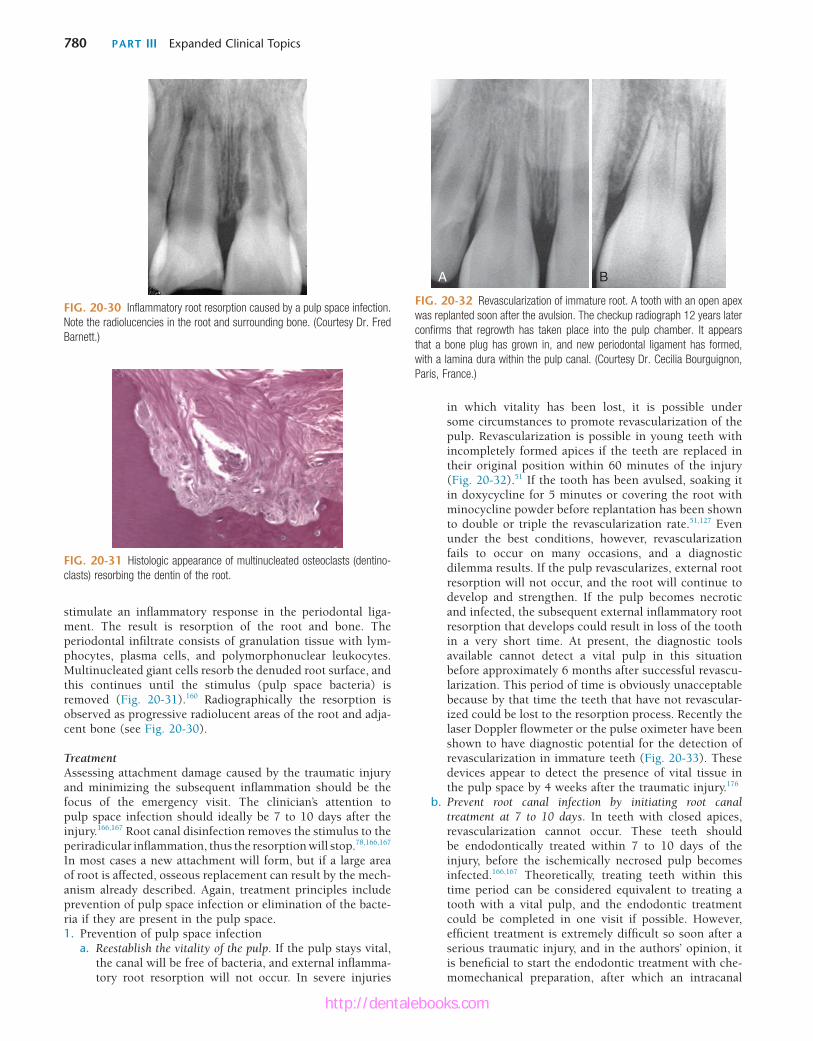
780 PART III Expanded Clinical Topics
stimulate an inflammatory response in the periodontal liga-ment. The result is resorption of the root and bone. The periodontal infiltrate consists of granulation tissue with lym-phocytes, plasma cells, and polymorphonuclear leukocytes. Multinucleated giant cells resorb the denuded root surface, and this continues until the stimulus (pulp space bacteria) is removed (Fig. 20-31).160 Radiographically the resorption is observed as progressive radiolucent areas of the root and adja-cent bone (see Fig. 20-30).
TreatmentAssessing attachment damage caused by the traumatic injury and minimizing the subsequent inflammation should be the focus of the emergency visit. The clinician’s attention to pulp space infection should ideally be 7 to 10 days after the injury.166,167 Root canal disinfection removes the stimulus to the periradicular inflammation, thus the resorption will stop.78,166,167 In most cases a new attachment will form, but if a large area of root is affected, osseous replacement can result by the mech-anism already described. Again, treatment principles include prevention of pulp space infection or elimination of the bacte-ria if they are present in the pulp space.1. Prevention of pulp space infection
a. Reestablish the vitality of the pulp. If the pulp stays vital, the canal will be free of bacteria, and external inflamma-tory root resorption will not occur. In severe injuries
FIG. 20-30 Inflammatory root resorption caused by a pulp space infection. Note the radiolucencies in the root and surrounding bone. (Courtesy Dr. Fred Barnett.)
FIG. 20-31 Histologic appearance of multinucleated osteoclasts (dentino-clasts) resorbing the dentin of the root.
in which vitality has been lost, it is possible under some circumstances to promote revascularization of the pulp. Revascularization is possible in young teeth with incompletely formed apices if the teeth are replaced in their original position within 60 minutes of the injury (Fig. 20-32).51 If the tooth has been avulsed, soaking it in doxycycline for 5 minutes or covering the root with minocycline powder before replantation has been shown to double or triple the revascularization rate.51,127 Even under the best conditions, however, revascularization fails to occur on many occasions, and a diagnostic dilemma results. If the pulp revascularizes, external root resorption will not occur, and the root will continue to develop and strengthen. If the pulp becomes necrotic and infected, the subsequent external inflammatory root resorption that develops could result in loss of the tooth in a very short time. At present, the diagnostic tools available cannot detect a vital pulp in this situation before approximately 6 months after successful revascu-larization. This period of time is obviously unacceptable because by that time the teeth that have not revascular-ized could be lost to the resorption process. Recently the laser Doppler flowmeter or the pulse oximeter have been shown to have diagnostic potential for the detection of revascularization in immature teeth (Fig. 20-33). These devices appear to detect the presence of vital tissue in the pulp space by 4 weeks after the traumatic injury.176
b. Prevent root canal infection by initiating root canal treatment at 7 to 10 days. In teeth with closed apices, revascularization cannot occur. These teeth should be endodontically treated within 7 to 10 days of the injury, before the ischemically necrosed pulp becomes infected.166,167 Theoretically, treating teeth within this time period can be considered equivalent to treating a tooth with a vital pulp, and the endodontic treatment could be completed in one visit if possible. However, efficient treatment is extremely difficult so soon after a serious traumatic injury, and in the authors’ opinion, it is beneficial to start the endodontic treatment with che-momechanical preparation, after which an intracanal
FIG. 20-32 Revascularization of immature root. A tooth with an open apex was replanted soon after the avulsion. The checkup radiograph 12 years later confirms that regrowth has taken place into the pulp chamber. It appears that a bone plug has grown in, and new periodontal ligament has formed, with a lamina dura within the pulp canal. (Courtesy Dr. Cecilia Bourguignon, Paris, France.)
A B
http://dentalebooks.com
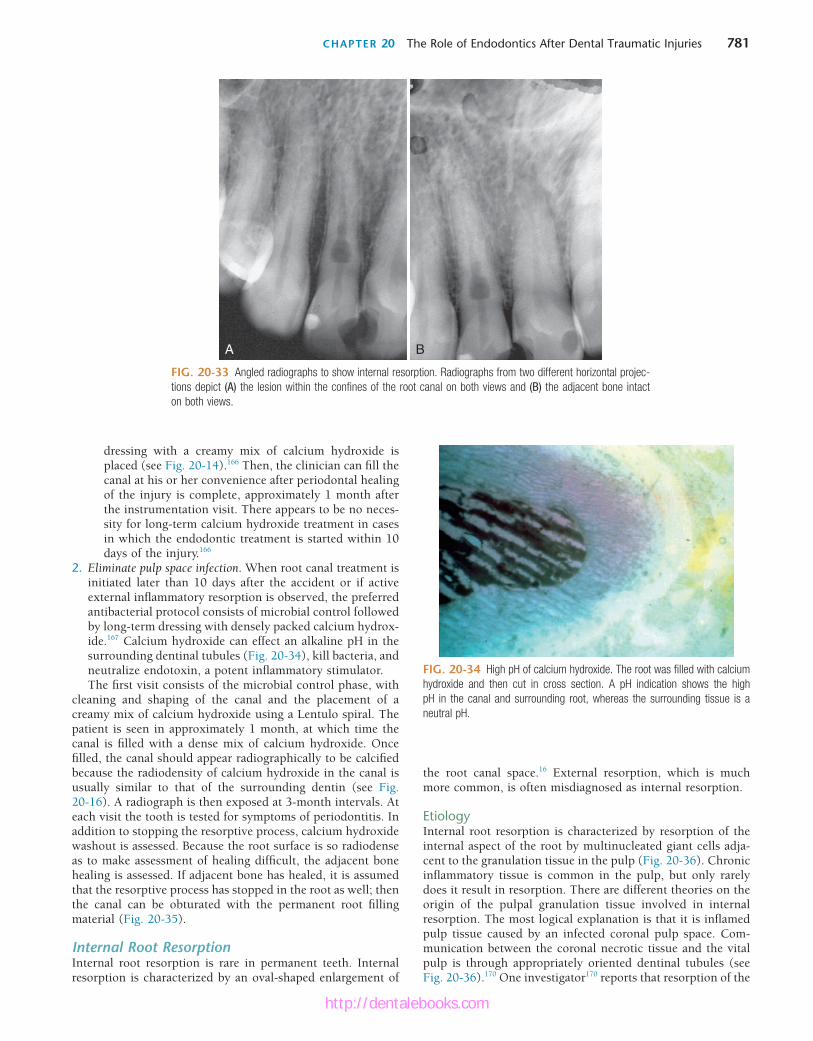
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 781
FIG. 20-33 Angled radiographs to show internal resorption. Radiographs from two different horizontal projec-tions depict (A) the lesion within the confines of the root canal on both views and (B) the adjacent bone intact on both views.
A B
dressing with a creamy mix of calcium hydroxide is placed (see Fig. 20-14).166 Then, the clinician can fill the canal at his or her convenience after periodontal healing of the injury is complete, approximately 1 month after the instrumentation visit. There appears to be no neces-sity for long-term calcium hydroxide treatment in cases in which the endodontic treatment is started within 10 days of the injury.166
2. Eliminate pulp space infection. When root canal treatment is initiated later than 10 days after the accident or if active external inflammatory resorption is observed, the preferred antibacterial protocol consists of microbial control followed by long-term dressing with densely packed calcium hydrox-ide.167 Calcium hydroxide can effect an alkaline pH in the surrounding dentinal tubules (Fig. 20-34), kill bacteria, and neutralize endotoxin, a potent inflammatory stimulator.The first visit consists of the microbial control phase, with
cleaning and shaping of the canal and the placement of a creamy mix of calcium hydroxide using a Lentulo spiral. The patient is seen in approximately 1 month, at which time the canal is filled with a dense mix of calcium hydroxide. Once filled, the canal should appear radiographically to be calcified because the radiodensity of calcium hydroxide in the canal is usually similar to that of the surrounding dentin (see Fig. 20-16). A radiograph is then exposed at 3-month intervals. At each visit the tooth is tested for symptoms of periodontitis. In addition to stopping the resorptive process, calcium hydroxide washout is assessed. Because the root surface is so radiodense as to make assessment of healing difficult, the adjacent bone healing is assessed. If adjacent bone has healed, it is assumed that the resorptive process has stopped in the root as well; then the canal can be obturated with the permanent root filling material (Fig. 20-35).
Internal Root ResorptionInternal root resorption is rare in permanent teeth. Internal resorption is characterized by an oval-shaped enlargement of
FIG. 20-34 High pH of calcium hydroxide. The root was filled with calcium hydroxide and then cut in cross section. A pH indication shows the high pH in the canal and surrounding root, whereas the surrounding tissue is a neutral pH.
the root canal space.16 External resorption, which is much more common, is often misdiagnosed as internal resorption.
EtiologyInternal root resorption is characterized by resorption of the internal aspect of the root by multinucleated giant cells adja-cent to the granulation tissue in the pulp (Fig. 20-36). Chronic inflammatory tissue is common in the pulp, but only rarely does it result in resorption. There are different theories on the origin of the pulpal granulation tissue involved in internal resorption. The most logical explanation is that it is inflamed pulp tissue caused by an infected coronal pulp space. Com-munication between the coronal necrotic tissue and the vital pulp is through appropriately oriented dentinal tubules (see Fig. 20-36).170 One investigator170 reports that resorption of the
http://dentalebooks.com

782 PART III Expanded Clinical Topics
Clinical ManifestationsInternal root resorption is usually asymptomatic and is first recognized clinically through routine radiographs. For internal resorption to be active, at least part of the pulp must be vital. The coronal portion of the pulp is often necrotic, whereas the apical pulp that includes the internal resorptive defect can remain vital. Therefore, a negative sensitivity test result does not rule out active internal resorption. It is also possible that the pulp becomes nonvital after a period of active resorption, giving a negative sensitivity test, radiographic signs of internal resorption, and radiographic signs of apical inflammation. Tra-ditionally, the pink tooth has been thought pathognomonic of internal root resorption. The pink color is due to the granula-tion tissue in the coronal dentin undermining the crown enamel. The pink tooth can also be a feature of subepithelial external inflammatory root resorption, which must be ruled out before a diagnosis of internal root resorption is made.
Radiographic AppearanceThe usual radiographic presentation of internal root resorption is a fairly uniform radiolucent enlargement of the pulp canal (Fig. 20-37). Because the resorption is initiated in the root canal, the resorptive defect includes some part of the root canal space, so the original outline of the root canal is distorted.
Histologic AppearanceLike that of other inflammatory resorptive defects, the histo-logic picture of internal resorption is granulation tissue with multinucleated giant cells (see Fig. 20-35). An area of necrotic pulp is found coronal to the granulation tissue. Dentinal tubules containing microorganisms and communicating between the necrotic zone and the granulation tissue can sometimes be seen (see Fig. 20-36).140,160,167,170 Unlike external root resorption, the adjacent bone is not affected with internal root resorption.
TreatmentTreatment of internal root resorption is conceptually very easy. Because the resorptive defect is the result of the inflamed pulp and the blood supply to the tissue is through the apical
FIG. 20-36 Histologic appearance of internal root resorption. A, Section stained with Brown and Brenn. Bacteria are seen (in the dentinal tubules) communicating between the necrotic coronal segment and the apical granu-lomatous tissue and resorbing cells. B, An area of active internal root resorp-tion. (Courtesy Dr. Leif Tronstad, Oslo, Norway.)
A B
dentin is frequently associated with deposition of hard tissue resembling bone or cementum and not dentin. He postulates that the resorbing tissue is not of pulpal origin but is “meta-plastic” tissue derived from the pulpal invasion of macrophage-like cells. Others149 concluded that the pulp tissue was replaced by periodontium-like connective tissue when internal resorp-tion was present. In addition to the requirement of the pres-ence of granulation tissue, root resorption takes place only if the odontoblastic layer and predentin are lost or altered.160
Reasons for the loss of predentin adjacent to the granulation tissue are not obvious. Trauma frequently has been suggested as a cause.135,171 Another reason for the loss of predentin might be extreme heat produced when cutting on dentin without an adequate water spray. The heat presumably would destroy the predentin layer, and if later the coronal aspect of the pulp becomes infected, the bacterial products could initiate the typical inflammation in conjunction with resorbing giant cells in the vital pulp adjacent to the denuded root surface. Internal root resorption has been produced experimentally by the appli-cation of diathermy.170
FIG. 20-37 A maxillary incisor with internal root resorption. Uniform enlargement of the pulp space is apparent. Outline of the canal cannot be seen in the resorptive defect.
FIG. 20-35 Healing of external inflammatory root resorption after calcium hydroxide treatment. The radiolucencies seen before treatment have disap-peared with the reestablishment of the lamina dura. (Courtesy Dr. Fred Barnett.)
http://dentalebooks.com
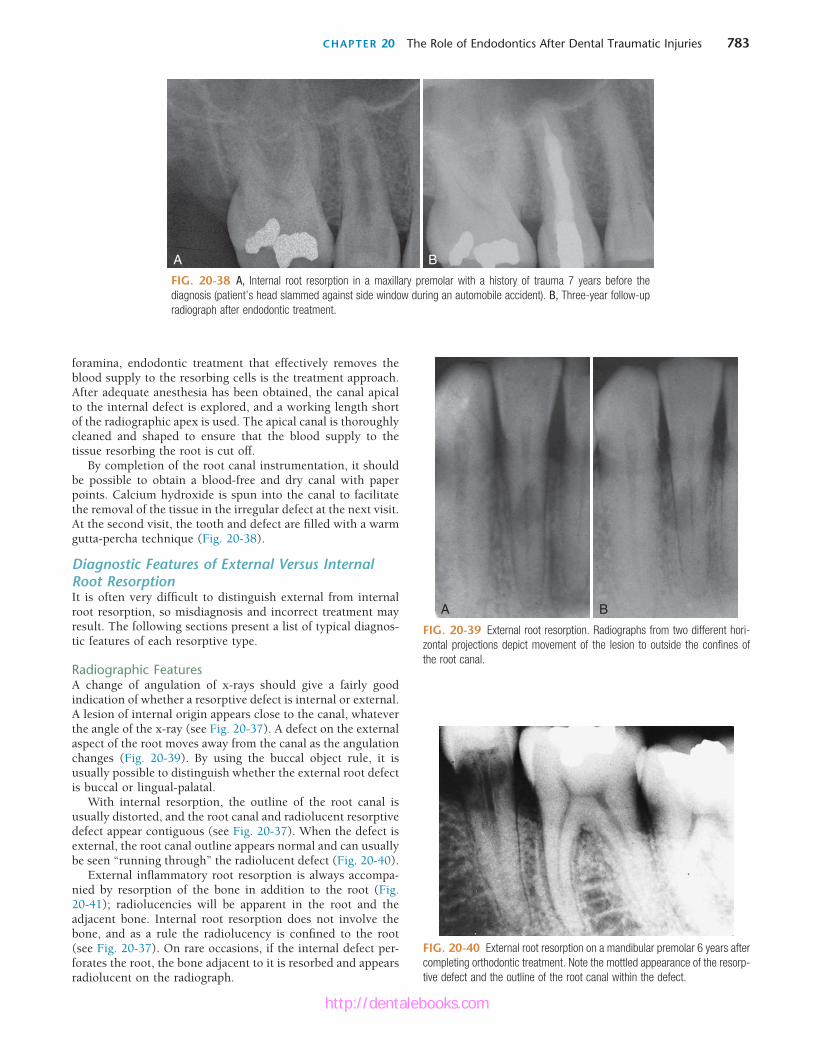
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 783
FIG. 20-38 A, Internal root resorption in a maxillary premolar with a history of trauma 7 years before the diagnosis (patient’s head slammed against side window during an automobile accident). B, Three-year follow-up radiograph after endodontic treatment.
BA
FIG. 20-39 External root resorption. Radiographs from two different hori-zontal projections depict movement of the lesion to outside the confines of the root canal.
A B
foramina, endodontic treatment that effectively removes the blood supply to the resorbing cells is the treatment approach. After adequate anesthesia has been obtained, the canal apical to the internal defect is explored, and a working length short of the radiographic apex is used. The apical canal is thoroughly cleaned and shaped to ensure that the blood supply to the tissue resorbing the root is cut off.
By completion of the root canal instrumentation, it should be possible to obtain a blood-free and dry canal with paper points. Calcium hydroxide is spun into the canal to facilitate the removal of the tissue in the irregular defect at the next visit. At the second visit, the tooth and defect are filled with a warm gutta-percha technique (Fig. 20-38).
Diagnostic Features of External Versus Internal Root ResorptionIt is often very difficult to distinguish external from internal root resorption, so misdiagnosis and incorrect treatment may result. The following sections present a list of typical diagnos-tic features of each resorptive type.
Radiographic FeaturesA change of angulation of x-rays should give a fairly good indication of whether a resorptive defect is internal or external. A lesion of internal origin appears close to the canal, whatever the angle of the x-ray (see Fig. 20-37). A defect on the external aspect of the root moves away from the canal as the angulation changes (Fig. 20-39). By using the buccal object rule, it is usually possible to distinguish whether the external root defect is buccal or lingual-palatal.
With internal resorption, the outline of the root canal is usually distorted, and the root canal and radiolucent resorptive defect appear contiguous (see Fig. 20-37). When the defect is external, the root canal outline appears normal and can usually be seen “running through” the radiolucent defect (Fig. 20-40).
External inflammatory root resorption is always accompa-nied by resorption of the bone in addition to the root (Fig. 20-41); radiolucencies will be apparent in the root and the adjacent bone. Internal root resorption does not involve the bone, and as a rule the radiolucency is confined to the root (see Fig. 20-37). On rare occasions, if the internal defect per-forates the root, the bone adjacent to it is resorbed and appears radiolucent on the radiograph.
FIG. 20-40 External root resorption on a mandibular premolar 6 years after completing orthodontic treatment. Note the mottled appearance of the resorp-tive defect and the outline of the root canal within the defect.
http://dentalebooks.com

784 PART III Expanded Clinical Topics
Summary of Possible Diagnostic Features♦ External inflammatory root resorption due to pulp
infection.• Apical: No response of the pulp to thermal or electric
stimuli, with or without a history of trauma.• Lateral: History of trauma, no response of the pulp to
thermal or electric stimuli, lesion moves on angled x-rays, root canal visualized radiographically overlying the defect, bony radiolucency also apparent.
♦ Subepithelial external inflammatory root resorption due to sulcular infection. History of trauma (often forgotten, or its long-term risks not appreciated by the patient); positive pulp sensitivity test; lesion located at the attachment level of the tooth; lesion moves on angled x-rays; root canal outline is undistorted and can be visualized radiographi-cally; crestal bony defect associated with the lesion; pink spot possible.
♦ Internal root resorption. History of trauma, crown prepara-tion, or pulpotomy; responsive pulp to thermal or electric stimuli likely, may occur at any location along the root canal (not only attachment level); lesion stays associated with the root canal on angled x-rays, radiolucency contained in the root without an adjacent bony defect; pink spot possible.Most misdiagnoses of resorptive defects are made between
subepithelial external and internal root resorptions. The diag-nosis should always be confirmed as treatment proceeds. If root canal therapy is the treatment of choice for an apparent inter-nal root resorption, the bleeding within the canal should cease quickly after pulp extirpation because the blood supply of the granulation tissue is the apical blood vessels. If bleeding con-tinues during treatment, and particularly if it is still present at the second visit, the source of the blood supply is external, and treatment for perforating external resorption should be carried out. On obturation, it should be possible to fill the entire canal from within in internal resorption. Failure to achieve this should make the clinician suspicious of an external lesion that perforates the root. Finally, if the blood supply of an internal resorption defect is removed on pulp extirpation, any continu-ation of the resorptive process on recall radiographs should alert the clinician to the possibility that an external resorptive defect was misdiagnosed.
CLINICAL MANAGEMENT OF THE AVULSED TOOTHFavorable healing after an avulsion injury requires quick emer-gency intervention followed by evaluation and possible treat-ment at decisive times during the healing phase. The urgency of the emergency visit and the multidisciplinary nature of follow-up evaluations require that both the public and clini-cians from many dental disciplines be knowledgeable about the treatment strategies involved.
Consequences of Tooth AvulsionTooth avulsion results in attachment damage and pulp necro-sis. The tooth is “separated” from the socket due mainly to tearing of the periodontal ligament that leaves viable periodon-tal ligament cells on most of the root surface. In addition, small and localized cemental damage occurs from the crushing of the tooth against the socket.
If the periodontal ligament left attached to the root surface does not dry out, the consequences of tooth avulsion are
Vitality TestingExternal inflammatory resorption in the apical and lateral aspects of the root involves an infected pulp space, so no response to sensitivity tests supports the diagnosis. However, because subepithelial external root resorption does not involve the pulp (the bacteria are thought to originate in the sulcus of the tooth), a normal response to sensitivity testing is usually associated with this type of resorption. Internal root resorption usually occurs in teeth with vital pulps and responses to sensi-tivity testing. In teeth that exhibit internal root resorption, it is common to register a no-response to sensitivity testing because often the coronal pulp has been removed or is necrotic, and the active resorbing cells are more apical in the canal. Also, the pulp might have become necrotic after active resorption took place.
Pink SpotWith apical and lateral external root resorption, the pulp is nonvital, so the granulation tissue that produces the pink spot is not present in these cases. For subepithelial external (Fig. 20-42) and internal root resorption, the pink spot due to the granulation tissue undermining the enamel is a possible sign.
FIG. 20-41 Mandibular molar with subepithelial external inflammatory resorption on its mesial aspect. Note the small opening into the root and the extensive resorption in the dentin; however, the pulp is not exposed. Also note that a resorptive defect is present in the adjacent bone, appearing on the radiograph as similar to an infrabony pocket.
FIG. 20-42 Pink spot of subepithelial external inflammatory root resorption. A, Radiographic appearance. B, Clinical appearance.
A B
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 785
during the initial injury is unavoidable but usually minimal. However, all efforts must be made to minimize necrosis of the remaining periodontal ligament while the tooth is out of the mouth. Pulpal sequelae are not a concern initially and are dealt with at a later stage of treatment.
The single most important factor to assure a favorable outcome after replantation is the speed with which the tooth is replanted.16,22 Of utmost importance is the prevention of drying, which causes loss of normal physiologic metabolism and morphology of the periodontal ligament cells.22,146 Every effort should be made to replant the tooth within the first 15 to 20 minutes.27 This usually requires emergency personnel at the site of the injury with some knowledge of treatment pro-tocol. The clinician should communicate clearly with the person at the site of the accident. Ideally this information should have been given at an earlier time; for example, as an educational offering to school nurses or athletic trainers. Failing this, the information can be given over the phone. The aim is to replant a clean tooth with an undamaged root surface as gently as possible, after which the patient should be brought to the office immediately. If doubt exists that the tooth can be replanted adequately, the tooth should quickly be stored in an appropriate medium until the patient can get to the dental office for replantation. Suggested storage media, in order of preference, are milk, saliva (either in the vestibule of the mouth or in a container into which the patient expectorates), physi-ologic saline, and water.86 Water is the least desirable storage medium because the hypotonic environment causes rapid cell lysis and increased inflammation on replantation.35,36
Cell culture media in specialized transport containers, such as Hank’s Balanced Salt Solution (HBSS), have shown superior ability to maintain the viability of the periodontal ligament fibers for extended periods.165 Presently they are considered impractical because they need to be present at the accident site before the injury occurs. However, if we con-sider that more than 60% of avulsion injuries occur close to home or school,81 it seems reasonable to assume that it would be beneficial to have these media available in emergency kits at these sites. It would also be advantageous to have them in ambulances and in the kits of emergency response personnel who are likely to treat the more serious injuries in which teeth might otherwise be sacrificed to a more serious life-threatening situation.
Management in the Dental OfficeEmergency VisitPrepare socket, prepare root, replant, construct a functional splint, and administer local and systemic antibiotics.
Recognizing that a dental injury might be secondary to a more serious injury is essential. The attending dental clinician is likely to be the first health care provider the patient sees after a head injury, so ruling out any injuries to the brain (e.g., concussion) and/or central nervous system (CNS) in general is paramount. If on examination a CNS injury is suspected, immediate referral to the appropriate expert is the first priority, above and beyond the dental injury. Once a CNS injury has been ruled out, the focus of the emergency visit is the attach-ment apparatus. The aim is to replant the tooth with a minimum of irreversibly damaged cells (that will cause inflammation) and the maximal number of periodontal ligament cells that have the potential to regenerate and repair the damaged root surface.
usually minimal.14,146 The hydrated periodontal ligament cells will maintain their viability and repair after replantation, with minimal destructive inflammation as a by-product. Because the areas of the crushing injury are localized, inflammation stimulated by the damaged tissues will be correspondingly limited, and favorable healing with new replacement cemen-tum is likely to occur after the initial inflammation subsides (see Fig. 20-26).
If excessive drying occurs before replantation, the damaged periodontal ligament cells elicit a severe inflammatory response over a diffuse area on the root surface. Unlike the situation described earlier, in which the area to be repaired after the initial inflammatory response is small, here a large area of root surface is affected that must be repaired by new tissue. The slower moving cementoblasts cannot cover the entire root surface in time, and it is likely that in certain areas, bone will attach directly onto the root surface. In time, through physio-logic bone recontouring, the entire root will be replaced by bone. As earlier noted, this has been termed osseous replacement or replacement resorption (see Figs. 20-27 and 20-28).20,163
Pulpal necrosis always occurs after an avulsion injury. Although a necrotic pulp itself is not of consequence, the necrotic tissue is extremely susceptible to bacterial contamina-tion. If revascularization does not occur or effective endodontic therapy is not carried out, the pulp space inevitably becomes infected. The combination of bacteria in the root canal and cemental damage on the external surface of the root results in an external inflammatory resorption that can be very serious and can lead to rapid loss of the tooth (see Fig. 20-30).160
The consequences after tooth avulsion appear to be directly related to the severity and surface area of the inflammation on the root surface and resultant damaged root surface that must be repaired. Treatment strategies should always be considered in the context of limiting the extent of the periradicular inflam-mation, thus tipping the balance toward favorable responses (cemental) rather than unfavorable ones (osseous replacement or inflammatory resorption).
Treatment ObjectivesTreatment is directed at avoiding or minimizing resultant inflammation due to the two main consequences of the avulsed tooth: attachment damage and pulpal infection.
Attachment damage as a direct result of the avulsion injury cannot be avoided. However, considerable additional damage can occur to the periodontal ligament in the time that the tooth is out of the mouth (primarily because of drying). Treatment is directed at minimizing this damage (and the resultant inflammation) so that the fewest possible complications result. When severe additional damage cannot be avoided and osseous replacement of the root is considered certain, steps are taken to slow the replacement of the root by bone to maintain the tooth in the mouth for as long as possible.
In the open apex tooth, all efforts are made to promote revas-cularization of the pulp, thus avoiding pulp space infection. When revascularization fails (in the open apex tooth) or is not possible (in the closed apex tooth), all treatment efforts are made to prevent or eliminate toxins from the root canal space.
Clinical ManagementEmergency Treatment at the Accident SiteReplant if possible or place in an appropriate storage medium. As mentioned, damage to the attachment apparatus that occurred
http://dentalebooks.com

786 PART III Expanded Clinical Topics
saline) for 5 minutes before replantation significantly enhanced complete revascularization. This result was confirmed later in dogs by other investigators.127,176 A study found that covering the root with minocycline (Arestin, OraPharma, Warminster, Pennsylvania), which attaches to the root for approximately 15 days, further increased the revascularization rate in dogs.127 Although animal studies do not provide us with a prediction of the rate of revascularization in humans, it is reasonable to expect that the same enhancement of revascularization that occurred in two animal species also will occur in humans. As for a closed apex tooth, the open apex tooth is gently rinsed and replanted.
Extraoral Dry Time More Than 60 MinutesClosed ApexRemove the periodontal ligament by placing in acid for 5 minutes, soak in fluoride, replant.
When the root has been dry for 60 minutes or more, sur-vival of the periodontal ligament cells is not expected.22,146 In such cases the root should be prepared to be as resistant to resorption as possible (attempting to slow the osseous replace-ment process). These teeth should be soaked in acid for 5 minutes to remove all remaining periodontal ligament and thus remove the tissue that would initiate the inflammatory response on replantation. The tooth should then be soaked in 2% stan-nous fluoride for 5 minutes and replanted.34,137 A few years ago, studies were published that indicated that an enamel matrix protein, Emdogain (Straumann USA, Andover, Massachusetts), could be beneficial in teeth with extended extraoral dry times, not only to make the root more resistant to resorption, but also, possibly, to stimulate the formation of new periodontal liga-ment from the socket (see Fig. 20-8).64,90 Unfortunately, more recent studies have shown that the positive effect of Emdogain is only temporary, and most of these teeth start to resorb after a few years.132
If the tooth has been dry for more than 60 minutes and no consideration is given to preserving the periodontal ligament, the endodontics may be performed extraorally. In the case of a tooth with a closed apex, no advantage exists to this addi-tional step at the emergency visit. However, in a tooth with an open apex, endodontic treatment performed after replanta-tion involves a long-term apexification procedure. In these cases, completing the root canal treatment extraorally, in which a seal in the blunderbuss apex is easier to achieve, may be advantageous. When endodontic treatment is per-formed extraorally, it must be performed aseptically with the utmost care to achieve a root canal system that is thoroughly disinfected.
Open ApexReplant? If yes, treat as with closed apex tooth. Endodontic treat-ment may be performed out of the mouth.
Because these teeth are in young patients in whom facial development is usually incomplete, many pediatric clinicians consider the prognosis to be so poor and the potential compli-cations of an ankylosed tooth so severe, they recommend that these teeth not be replanted. Considerable debate exists as to whether it would be beneficial to replant the root even though it will inevitably be lost due to osseous replacement. If the patients are followed carefully and the root submerged by decoronation procedure at the appropriate time,6,63,67 the height, and more important, the width of the alveolar bone will
Diagnosis and Treatment PlanningIf the tooth was replanted at the site of injury, a complete history is taken to assess the likelihood of a favorable outcome. The position of the replanted tooth is assessed and adjusted if necessary. On rare occasions, the tooth may be gently removed to prepare the root to increase the chances of a favorable outcome (discussed later).
If the patient presents with the tooth out of the mouth, the storage medium should be evaluated and the tooth placed in a more appropriate medium if required. HBSS is presently considered the best medium for this purpose. Milk or physi-ologic saline is also appropriate for storage purposes.
The medical and accident histories are taken, and a clinical exam is carried out, with emphasis on questions about when, how, and where the injury occurred.
The clinical examination should include an examination of the socket to ascertain whether it is intact and suitable for replantation. The socket is gently rinsed with saline, and when it has been cleared of the clot and debris, its walls are examined directly for the presence, absence, or collapse of the socket wall. The socket and surrounding areas, including the soft tissues, should be radiographed. Three vertical angulations are required for diagnosis of the presence of a horizontal root fracture in adjacent teeth.16 The remaining teeth in both the upper and lower jaws should be examined for injuries, such as crown fractures. Any soft tissue lacerations should be noted and, if tooth fragments are missing, explored.
PREPARATION OF THE ROOTPreparation of the root depends on the maturity of the tooth (open versus closed apex) and on the dry time of the tooth before it was placed in a storage medium. A dry time of 60 minutes is considered the point where survival of root peri-odontal ligament cells is unlikely.
Extraoral Dry Time Less Than 60 MinutesClosed ApexThe root should be rinsed of debris with water or saline and replanted in as gentle a fashion as possible.
If the tooth has a closed apex, revascularization is not possible,51 but because the tooth was dry for less than 60 minutes (replanted or placed in appropriate medium), the chance for periodontal healing exists. Most important, the chance of a severe inflammatory response at the time of replantation is lessened. A dry time of less than 15 to 20 minutes is considered optimal, and periodontal healing would be expected.14,27,146
A continuing challenge is the treatment of the tooth that has been dry for more than 20 minutes (periodontal cell sur-vival is assured) but less than 60 minutes (periodontal cell survival unlikely). In these cases, logic suggests that the root surface consists of some cells with the potential to regenerate and some that will act as inflammatory stimulators.
Open ApexGently rinse off debris, soak in doxycycline for 5 minutes or cover with minocycline, replant.
In an open apex tooth, revascularization of the pulp and continued root development are possible (see Fig. 20-32). Investigators51 found in monkeys that soaking the tooth in doxycycline (1 mg in approximately 20 mL of physiologic
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 787
If these lacerations are sutured, care must be taken to clean the wound thoroughly beforehand because dirt or even minute tooth fragments left in the wound affect healing and the aes-thetic result.
ADJUNCTIVE THERAPYSystemic antibiotics given at the time of replantation and before endodontic treatment are effective in preventing bacte-rial invasion of the necrotic pulp and therefore subsequent inflammatory resorption.79 Tetracycline has the additional benefit of decreasing root resorption by affecting the motility of the osteoclasts and reducing the effectiveness of collage-nase.128 The administration of systemic antibiotics is recom-mended, beginning at the emergency visit and continuing until the splint is removed.79 For patients not susceptible to tetracy-cline staining, the antibiotic of choice is doxycycline twice daily for 7 days at the appropriate dosage for patient age and weight.128,129 Penicillin V 1000 mg as a loading dose, followed by 500 mg 4 times daily for 7 days, has also been shown to be beneficial. The bacterial content of the sulcus also should be controlled during the healing phase. In addition to stressing to the patient the need for adequate oral hygiene, the use of chlorhexidine rinses for 7 to 10 days is helpful.
As stated previously, a recent series of studies by our research group found great benefit in removal of the pulp contents at the emergency visit and placing Ledermix or corticosteroid into the root canal.38,41 Apparently the use of the medicament was able to shut down the inflammatory response after replan-tation to allow for more favorable healing compared to those teeth that did not have the medicament.
The need for analgesics should be assessed on an individual case basis. The use of pain medication stronger than non-prescription nonsteroidal antiinflammatory drugs (NSAIDs) is unusual. The patient should be sent to a physician for con-sultation regarding a tetanus booster within 48 hours of the initial visit.
Second VisitThe second visit should take place 1 to 2 weeks after the trauma. At the emergency visit, emphasis was placed on the preservation and healing of the attachment apparatus. The focus of the second visit is the prevention or elimination of potential irritants from the root canal space. These irritants, if present, provide the stimulus for the progression of the inflam-matory response, bone and root resorption. Also at this visit, the course of systemic antibiotics is completed; the chlorhexi-dine rinses can be stopped. At this appointment the splint is removed; the tooth might still have class I or class II mobility after splint removal, but all indications are that it will continue to heal better without the splint.3
ENDODONTIC TREATMENT
Extraoral Time Less Than 60 MinutesClosed ApexInitiate endodontic treatment after 1 to 2 weeks. When endodontic treatment is delayed or signs of resorption are present, provide long-term calcium hydroxide treatment before obturation.
No chance exists for revascularization of teeth with closed apices; therefore, endodontic treatment should be initiated at
be maintained, allowing for easier permanent restoration at the appropriate time when the child’s facial development is complete.
PREPARATION OF THE SOCKETThe socket should be left undisturbed before replantation.16 Emphasis is placed on removal of obstacles in the socket to facilitate replacement of the tooth into the socket.78 It should be lightly aspirated if a blood clot is present. If the alveolar bone has collapsed or may interfere with replantation, a blunt instrument should be inserted carefully into the socket in an attempt to reposition the wall.
SPLINTINGA splint that allows for physiologic movement of the tooth during healing and that is in place for a minimal period results in a decreased incidence of ankylosis.3,12,78 Semirigid (physio-logic) fixation for 1 to 2 weeks is recommended.3,5,67 The splint should allow movement of the tooth, should have no memory (so the tooth is not moved during healing), and should not impinge on the gingiva and/or prevent maintenance of oral hygiene in the area. Many splints satisfy the requirements of an acceptable device. A new titanium trauma splint (TTS) has recently been shown to be particularly effective and easy to use (Fig. 20-43).169 After the splint is in place, a radiograph should be exposed to verify the positioning of the tooth and as a pre-operative reference for further treatment and follow-up. When the tooth is in the best possible position, adjusting the bite to ensure that it has not been splinted in a position causing trau-matic occlusion is important. One week is sufficient to create periodontal support to maintain the avulsed tooth in posi-tion.164 Therefore, the splint should be removed after 1 to 2 weeks. The only exception is with avulsion in conjunction with alveolar fractures, for which 4 to 8 weeks is the suggested time of splinting.164
MANAGEMENT OF THE SOFT TISSUESSoft tissue lacerations of the socket gingiva should be tightly sutured. Lacerations of the lip are fairly common with these types of injuries. The clinician should approach lip lacerations with some caution; a plastic surgery consult might be prudent.
FIG. 20-43 Titanium trauma splint (TTS) in place.
http://dentalebooks.com
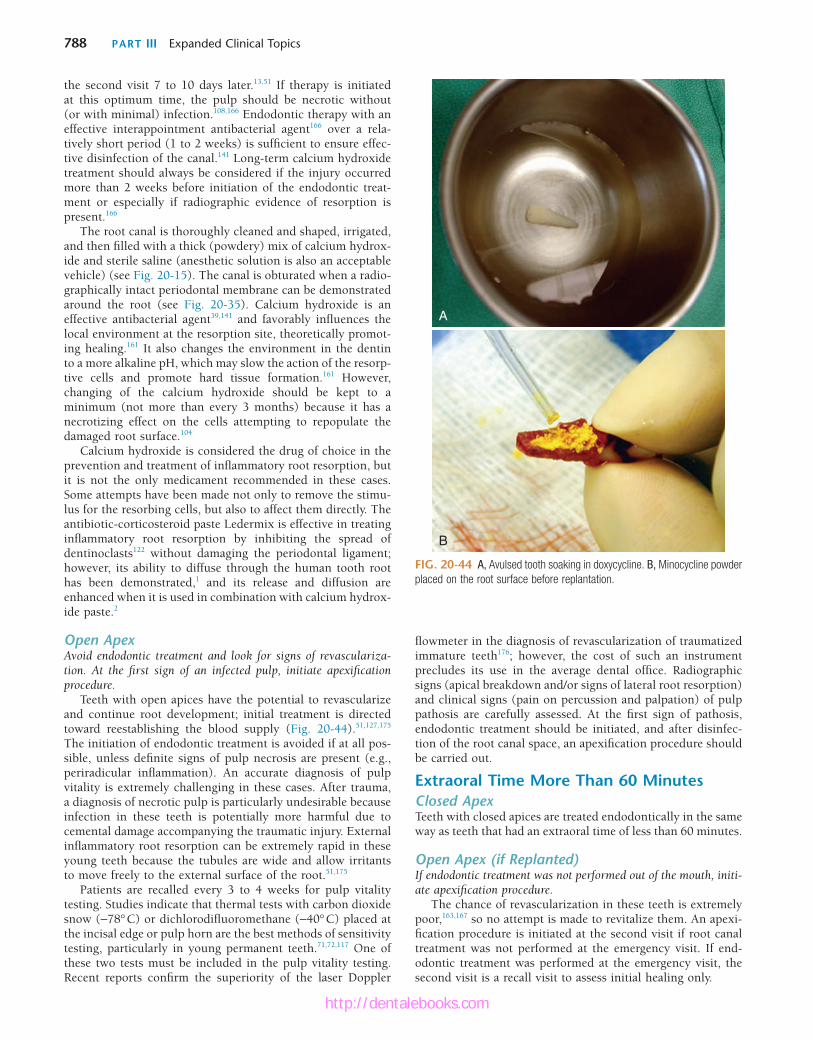
788 PART III Expanded Clinical Topics
flowmeter in the diagnosis of revascularization of traumatized immature teeth176; however, the cost of such an instrument precludes its use in the average dental office. Radiographic signs (apical breakdown and/or signs of lateral root resorption) and clinical signs (pain on percussion and palpation) of pulp pathosis are carefully assessed. At the first sign of pathosis, endodontic treatment should be initiated, and after disinfec-tion of the root canal space, an apexification procedure should be carried out.
Extraoral Time More Than 60 MinutesClosed ApexTeeth with closed apices are treated endodontically in the same way as teeth that had an extraoral time of less than 60 minutes.
Open Apex (if Replanted)If endodontic treatment was not performed out of the mouth, initi-ate apexification procedure.
The chance of revascularization in these teeth is extremely poor,163,167 so no attempt is made to revitalize them. An apexi-fication procedure is initiated at the second visit if root canal treatment was not performed at the emergency visit. If end-odontic treatment was performed at the emergency visit, the second visit is a recall visit to assess initial healing only.
the second visit 7 to 10 days later.13,51 If therapy is initiated at this optimum time, the pulp should be necrotic without (or with minimal) infection.108,166 Endodontic therapy with an effective interappointment antibacterial agent166 over a rela-tively short period (1 to 2 weeks) is sufficient to ensure effec-tive disinfection of the canal.141 Long-term calcium hydroxide treatment should always be considered if the injury occurred more than 2 weeks before initiation of the endodontic treat-ment or especially if radiographic evidence of resorption is present.166
The root canal is thoroughly cleaned and shaped, irrigated, and then filled with a thick (powdery) mix of calcium hydrox-ide and sterile saline (anesthetic solution is also an acceptable vehicle) (see Fig. 20-15). The canal is obturated when a radio-graphically intact periodontal membrane can be demonstrated around the root (see Fig. 20-35). Calcium hydroxide is an effective antibacterial agent39,141 and favorably influences the local environment at the resorption site, theoretically promot-ing healing.161 It also changes the environment in the dentin to a more alkaline pH, which may slow the action of the resorp-tive cells and promote hard tissue formation.161 However, changing of the calcium hydroxide should be kept to a minimum (not more than every 3 months) because it has a necrotizing effect on the cells attempting to repopulate the damaged root surface.104
Calcium hydroxide is considered the drug of choice in the prevention and treatment of inflammatory root resorption, but it is not the only medicament recommended in these cases. Some attempts have been made not only to remove the stimu-lus for the resorbing cells, but also to affect them directly. The antibiotic-corticosteroid paste Ledermix is effective in treating inflammatory root resorption by inhibiting the spread of dentinoclasts122 without damaging the periodontal ligament; however, its ability to diffuse through the human tooth root has been demonstrated,1 and its release and diffusion are enhanced when it is used in combination with calcium hydrox-ide paste.2
Open ApexAvoid endodontic treatment and look for signs of revasculariza-tion. At the first sign of an infected pulp, initiate apexification procedure.
Teeth with open apices have the potential to revascularize and continue root development; initial treatment is directed toward reestablishing the blood supply (Fig. 20-44).51,127,175 The initiation of endodontic treatment is avoided if at all pos-sible, unless definite signs of pulp necrosis are present (e.g., periradicular inflammation). An accurate diagnosis of pulp vitality is extremely challenging in these cases. After trauma, a diagnosis of necrotic pulp is particularly undesirable because infection in these teeth is potentially more harmful due to cemental damage accompanying the traumatic injury. External inflammatory root resorption can be extremely rapid in these young teeth because the tubules are wide and allow irritants to move freely to the external surface of the root.51,175
Patients are recalled every 3 to 4 weeks for pulp vitality testing. Studies indicate that thermal tests with carbon dioxide snow (−78° C) or dichlorodifluoromethane (−40° C) placed at the incisal edge or pulp horn are the best methods of sensitivity testing, particularly in young permanent teeth.71,72,117 One of these two tests must be included in the pulp vitality testing. Recent reports confirm the superiority of the laser Doppler
FIG. 20-44 A, Avulsed tooth soaking in doxycycline. B, Minocycline powder placed on the root surface before replantation.
A
B
http://dentalebooks.com

CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 789
TEMPORARY RESTORATIONEffectively sealing the coronal access is essential to prevent infection of the canal between visits. Recommended temporary restorations are reinforced zinc oxide eugenol cement, acid etch composite resin, or glass ionomer cement. The depth of the temporary restoration is critical to its sealability. A depth of at least 4 mm is recommended, so a cotton pellet should not be placed; the temporary restoration is placed directly onto the calcium hydroxide in the access cavity. Calcium hydroxide should be removed from the walls of the access cavity before the temporary restoration is placed because calcium hydroxide is soluble and washes out when it comes into contact with saliva, leaving a defective temporary restoration.
After initiation of the root canal treatment, the splint is removed. If time does not permit complete removal of the splint at this visit, the resin tacks are smoothed so as not to irritate the soft tissues; the remaining resin is removed at a later appointment.
At this appointment, healing is usually sufficient to allow a detailed clinical examination of the teeth surrounding the avulsed tooth. Pulp vitality tests, reaction to percussion and palpation, and periodontal probing measurements should be carefully recorded for reference at follow-up visits.
Root Filling VisitThis visit should take place at the clinician’s convenience or after long-term calcium hydroxide therapy, when an intact lamina dura is traced.
If the endodontic treatment was initiated 1 to 2 weeks after the avulsion and a thorough examination confirms normality, filling of the root canal at this visit is acceptable. Long-term use of calcium hydroxide is also a proven option for these cases. If endodontic treatment was initiated more than 2 weeks after the avulsion or active resorption is visible, the pulp space
must first be disinfected before root filling. Traditionally, the reestablishment of a lamina dura (see Fig. 20-35) is a radio-graphic sign that the canal bacteria have been controlled. When an intact lamina dura can be traced throughout, root filling can take place.
The canal is cleaned, shaped, and irrigated under strict asepsis (i.e., a rubber dam). After completion of cleaning and shaping, the canal can be filled.
PERMANENT RESTORATIONMuch evidence exists that coronal leakage caused by defective temporary and permanent restorations results in a clinically relevant amount of bacterial contamination of the root canal after root filling.126 Therefore, the tooth should receive a per-manent restoration as soon as possible. The depth of restora-tion is important for a tight seal, so the deepest restoration possible should be made. A post should be avoided if possible. Because most avulsions occur in the anterior region of the mouth where aesthetics is important, composite resins com-bined with dentin bonding agents are recommended in these cases.
Follow-Up CareFollow-up evaluations should take place at 3 months, 6 months, and yearly for at least 5 years. If osseous replacement is identified (see Fig. 20-28), a more closely monitored follow-up schedule is indicated. In the case of inflammatory root resorption (see Fig. 20-30), a new attempt at disinfection of the root canal space by standard retreatment might reverse the process. Teeth adjacent to and surrounding the avulsed tooth or teeth may show pathologic changes long after the initial accident, so these teeth, too, should be tested at follow-up visits and the results compared to those collected soon after the accident.
REFERENCES1. Abbott PV, Heithersay GS, Hume WR: Release and
diffusion through human tooth roots in vitro of corticosteroid and tetracycline trace molecules from Ledermix paste, Endod Dent Traumatol 4:55, 1988.
2. Abbott PV, Hume WR, Heithersay GS: Effects of combining Ledermix and calcium hydroxide pastes on the diffusion of corticosteroid and tetracycline through human tooth roots in vitro, Endod Dent Traumatol 5:188, 1989.
3. About I, Murray PE, Franquin JC, et al: The effect of cavity restoration variables on odontoblast cell numbers and dental repair, J Dent 29:109, 2001.
4. Accorinte L, Holland R, Reis A, et al: Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth, J Endod 34:1, 2008.
5. Andersson L, Friskopp J, Blomlof L: Fiber-glass splinting of traumatized teeth, ASDC J Dent Child 50:21, 1983.
6. Andersson L, Malmgren B: The problem of dentoalveolar ankylosis and subsequent replacement resorption in the growing patient, Aust Endod J 25:57, 1999.
7. Andreasen FM: Pulpal healing after luxation injuries and root fracture in the permanent dentition, Endod Dent Traumatol 5:111, 1989.
8. Andreasen FM, Andreasen JO: Resorption and mineralization processes following root fracture of permanent incisors. Endod Dent Traumatol 4:202, 1988.
9. Andreasen FM, Andreasen JO, Bayer T: Prognosis of root-fractured permanent incisors: prediction of healing modalities, Endod Dent Traumatol 5:11, 1989.
10. Andreasen FM, Pedersen BV: Prognosis of luxated permanent teeth: the development of pulp necrosis, Endod Dent Traumatol 1:207, 1985.
11. Andreasen FM, Zhijie Y, Thomsen BL, Andersen PK: Occurrence of pulp canal obliteration after luxation injuries in the permanent dentition, Endod Dent Traumatol 3:103, 1987.
12. Andreasen JO: Etiology and pathogenesis of traumatic dental injuries: a clinical study of 1,298 cases, Scand J Dent Res 78:329, 1970.
13. Andreasen JO: Luxation of permanent teeth due to trauma: a clinical and radiographic follow-up study of 189 injured teeth,. Scand J Dent Res 78:273, 1970.
14. Andreasen JO: Effect of extra-alveolar period and storage media upon periodontal and pulpal healing after replantation of mature permanent incisors in monkeys, Int J Oral Surg 10:43, 1981.
15. Andreasen JO: Review of root resorption systems and models: etiology of root resorption and the homeostatic mechanisms of the periodontal ligament. In Davidovitch Z, editor: The biological mechanisms of tooth eruption and resorption, Birmingham, Ala, 1989, EB-SCOP Media.
16. Andreasen JO, Andreasen FM, Andersson L: Textbook and color atlas of traumatic injuries to the teeth, ed 4, Hoboken, NJ, 2007, Wiley-Blackwell.
17. Andreasen JO, Andreasen FM, Mejare I, Cvek M: Healing of 400 intra-alveolar root fractures. Part 1. Effect of pre-injury and injury factors such as sex, age, stage of
root development, fracture type, location of fracture and severity of dislocation, Dent Traumatol 20:192, 2004.
18. Andreasen JO, Andreasen FM, Mejare I, Cvek M: Healing of 400 intra-alveolar root fractures. Part 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics, Dent Traumatol 20:203, 2004.
19. Andreasen JO, Farik B, Munksgaard EC: Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture, Dent Traumatol 18:134, 2002.
20. Andreasen JO, Hjorting-Hansen E: Replantation of teeth. I. Radiographic and clinical study of 110 human teeth replanted after accidental loss, Acta Odontol Scand 24:263, 1966.
21. Andreasen JO, Hjorting-Hansen E: Intraalveolar root fractures: radiographic and histologic study of 50 cases, J Oral Surg 25:414, 1967.
22. Andreasen JO, Kristerson L: The effect of limited drying or removal of the periodontal ligament: periodontal healing after replantation of mature permanent incisors in monkeys, Acta Odontol Scand 39:1, 1981.
23. Andreasen JO, Ravn JJ: Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample, Int J Oral Surg 1:235, 1972.
24. Arakawa M, Kitasako Y, Otsuki M, Tagami J: Direct pulp capping with an auto-cured sealant resin and a self-etching primer, Am J Dent 16:61, 2003.
http://dentalebooks.com
790 PART III Expanded Clinical Topics
25. Banchs F, Trope M: Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 30:196, 2004.
26. Barrett AP, Reade PC: Revascularization of mouse tooth isografts and allografts using autoradiography and carbon-perfusion, Arch Oral Biol 26:541, 1981.
27. Barrett EJ, Kenny DJ: Avulsed permanent teeth: a review of the literature and treatment guidelines, Endod Dent Traumatol 13:153, 1997.
28. Bastone EB, Freer TJ, McNamara JR: Epidemiology of dental trauma: a review of the literature, Aust Dent J 45:2, 2000.
29. Bergenholtz G: Micro-organisms from necrotic pulp of traumatized teeth, Odontol Revy 25:347, 1974.
30. Bernardes RA, de Moraes IG, Duarte MAH, Azevedo BC: Use of cone-beam volumetric tomography in the diagnosis of root fractures, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108:270, 2009.
31. Bernardes RA, de Paulo RS, Pereira LO, et al: Comparative study of cone beam computed tomography and intraoral periapical radiographs in diagnosis of lingual-simulated external root resorptions, Dent Traumatol 28:268, 2012.
32. Bhaskar SN, Rappaport HM: Dental vitality tests and pulp status, J Am Dent Assoc 86:409, 1973.
33. Binnie WH, Rowe AH: A histological study of the periapical tissues of incompletely formed pulpless teeth filled with calcium hydroxide, J Dent Res 52:1110, 1973.
34. Bjorvatn K, Selvig KA, Klinge B: Effect of tetracycline and SnF2 on root resorption in replanted incisors in dogs, Scand J Dent Res 97:477, 1989.
35. Blomlof L: Milk and saliva as possible storage media for traumatically exarticulated teeth prior to replantation, Swed Dent J Suppl 8:1, 1981.
36. Blomlof L, Lindskog S, Andersson L, et al: Storage of experimentally avulsed teeth in milk prior to replantation, J Dent Res 62:912, 1983.
37. Bortoluzzi EA, Broon NJ, Bramante CM, et al: Mineral trioxide aggregate with or without calcium chloride in pulpotomy, J Endod 34:172, 2008.
38. Bryson EC, Levin L, Banchs F, et al: Effect of immediate intracanal placement of Ledermix Paste on healing of replanted dog teeth after extended dry times, Dent Traumatol 18:316, 2002.
39. Bystrom A, Claesson R, Sundqvist G: The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals, Endod Dent Traumatol 1:170, 1985.
40. Canakci V, Akgul HM, Akgul N, Canakci CF: Prevalence and handedness correlates of traumatic injuries to the permanent incisors in 13 17-year-old adolescents in Erzurum, Turkey, Dent Traumatol 19:248, 2003.
41. Chen H, Teixeira FB, Ritter AL, et al: The effect of intracanal anti-inflammatory medicaments on external root resorption of replanted dog teeth after extended extra-oral dry time, Dental Traumatol 24:74, 2008.
42. Cohenca N, Simon JH, Roges R, et al: Clinical indications for digital imaging in dento-alveolar trauma. Part 1. Traumatic injuries, Dent Traumatol 23:95, 2007.
43. Cohenca N, Simon JH, Marhtur A, Malfaz JM: Clinical indications for digital imaging in dento-alveolar trauma. Part 2. Root resorption, Dent Traumatol 23:105, 2007.
44. Cotton TP, Geisler TM, Holden DT, et al: Endodontic applications of cone beam volumetric tomography, J Endod 33:1121, 2007.
45. Cox CF, Keall CL, Keall HJ, et al: Biocompatibility of surface-sealed dental materials against exposed pulps. J Prosthet Dent 57:1, 1987.
46. Cox CF, Tarim B, Kopel H, et al: Technique sensitivity: biological factors contributing to clinical success with various restorative materials, Adv Dent Res 15:85, 2001.
47. Cunha RF, Pavarini A, Percinoto C, et al: Influence of surgical repositioning of mature permanent dog teeth following experimental intrusion: a histologic assessment, Dent Traumatol 18:304, 2002.
48. Cvek M: Treatment of non-vital permanent incisors with calcium hydroxide. IV. Periodontal healing and closure of the root canal in the coronal fragment of teeth with intra-alveolar fracture and vital apical fragment: a follow-up, Odontol Revy 25:239, 1974.
49. Cvek M: A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture, J Endod 4:232, 1978.
50. Cvek M: Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha: a retrospective clinical study, Endod Dent Traumatol 8:45, 1992.
51. Cvek M, Cleaton-Jones P, Austin J, et al: Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisors, Endod Dent Traumatol 6:170, 1990.
52. Cvek M, Cleaton-Jones PE, Austin JC, Andreasen JO: Pulp reactions to exposure after experimental crown fractures or grinding in adult monkeys, J Endod 8:391, 1982.
53. Cvek M, Hollender L, Nord CE: Treatment of non-vital permanent incisors with calcium hydroxide. VI. A clinical, microbiological and radiological evaluation of treatment in one sitting of teeth with mature or immature root, Odontol Revy 27:93, 1976.
54. Cvek M, Nord CE, Hollender L: Antimicrobial effect of root canal debridement in teeth with immature root: a clinical and microbiologic study, Odontol Revy 27:1, 1976.
55. Da Silva AC, Passeri LA, Mazzonetto R, et al: Incidence of dental trauma associated with facial trauma in Brazil: a 1-year evaluation, Dent Traumatol 20:6, 2004.
56. Deutsch AS, Musikant BL, Cavallari J, et al: Root fracture during insertion of prefabricated posts related to root size, J Prosthet Dent 53:786, 1985.
57. Durack C, Patel S, Davies J, et al: Diagnostic accuracy of small volume cone beam computed tomography and intraoral periapical radiography for the detection of simulated external inflammatory root resorption, Int Endod J 44:136, 2011.
58. Ebeleseder KA, Santler G, Glockner K, et al: An analysis of 58 traumatically intruded and surgically extruded permanent teeth, Endod Dent Traumatol 16:34, 2000.
59. Eklund G, Stalhane I, Hedegard B: A study of traumatized permanent teeth in children aged 7-15 years. III. A multivariate analysis of post-traumatic complications of subluxated and luxated teeth, Sven Tandlak Tidskr 69:179, 1976.
60. Ersin NK, Eronat N: The comparison of a dentin adhesive with calcium hydroxide as a pulp-capping agent on the exposed pulps of human and sheep teeth, Quintessence Int 36:271, 2005.
61. Estrela C, Reis Bueno M, Alencar AHG: Method to evaluate inflammatory root resorption by using cone beam computed tomography, J Endod 35:1491, 2009.
62. Faraco IM Jr, Holland R: Response of the pulp of dogs to capping with mineral trioxide aggregate or a calcium hydroxide cement, Dent Traumatol 17:163, 2001.
63. Filippi A, Pohl Y, von Arx T: Decoronation of an ankylosed tooth for preservation of alveolar bone prior to implant placement, Dent Traumatol 17:93, 2001.
64. Filippi A, Pohl Y, von Arx T: Treatment of replacement resorption with Emdogain: preliminary results after 10 months, Dent Traumatol 17:134, 2001.
65. Flores MT, Malmgren B, Andersson L, et al: Guidelines for the management of traumatic dental injuries. I. Fractures and luxations of permanent teeth, Dent Traumatol 23:66, 2007.
66. Flores MT, Malmgren B, Andersson L, et al: Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth, Dent Traumatol 23:130, 2007.
67. Flores MT, Malmgren B, Andersson L, et al: Guidelines for the management of traumatic dental injuries. III. Primary teeth, Dent Traumatol 23:196, 2007.
68. Frank AL: Therapy for the divergent pulpless tooth by continued apical formation, J Am Dent Assoc 72:87, 1966.
69. Fuks AB, Bielak S, Chosak A: Clinical and radiographic assessment of direct pulp capping and pulpotomy in young permanent teeth, Pediatr Dent 4:240, 1982.
70. Fuks AB, Cosack A, Klein H, Eidelman E: Partial pulpotomy as a treatment alternative for exposed pulps in crown-fractured permanent incisors, Endod Dent Traumatol 3:100, 1987.
71. Fulling HJ, Andreasen JO: Influence of maturation status and tooth type of permanent teeth upon electrometric and thermal pulp testing, Scand J Dent Res 84:286, 1976.
72. Fuss Z, Trowbridge H, Bender IB, et al: Assessment of reliability of electrical and thermal pulp testing agents, J Endod 12:301, 1986.
73. Gazelius B, Olgart L, Edwall B: Restored vitality in luxated teeth assessed by laser Doppler flowmeter, Endod Dent Traumatol 4:265, 1988.
74. Gelbier MJ, Winter GB: Traumatised incisors treated by vital pulpotomy: a retrospective study, Br Dent J 164:319, 1988.
75. Giuliani V, Baccetti T, Pace R, Pagavino G: The use of MTA in teeth with necrotic pulps and open apices, Dent Traumatol 18:217, 2002.
76. Goldberg F, Kaplan A, Roitman M, et al: Reinforcing effect of a resin glass ionomer in the restoration of immature roots in vitro, Dent Traumatol 18:70, 2002.
77. Granath LE, Hagman G: Experimental pulpotomy in human bicuspids with reference cutting technique, Acta Odontol Scand 29:155, 1971.
78. Hammarstrom L, Lindskog S: General morphological aspects of resorption of teeth and alveolar bone, Int Endod J 18:93, 1985.
79. Hammarstrom L, Pierce A, Blomlof L, et al: Tooth avulsion and replantation: a review, Endod Dent Traumatol 2:1, 1986.
80. Hebling J, Giro EM, Costa CA: Biocompatibility of an adhesive system applied to exposed human dental pulp, J Endodontol 25:676, 1999.
81. Hedegard B, Stalhane I: A study of traumatized permanent teeth in children 7-15 years. I, Sven Tandlak Tidskr 66:431, 1973.
82. Heide S, Mjor IA: Pulp reactions to experimental exposures in young permanent monkey teeth, Int Endod J 16:11, 1983.
83. Heithersay GS: Calcium hydroxide in the treatment of pulpless teeth with associated pathology, J Br Endod Soc 8:74, 1962.
84. Heller AL, Koenigs JF, Brilliant JD, et al: Direct pulp capping of permanent teeth in primates using a resorbable form of tricalcium phosphate ceramic, J Endod 1:95, 1975.
85. Herforth A, Strassburg M: Therapy of chronic apical periodontitis in traumatically injuring front teeth with ongoing root growth. Dtsch Zahnarztl Z 32:453, 1977.
86. Hiltz J, Trope M: Vitality of human lip fibroblasts in milk, Hanks Balanced Salt Solution and Viaspan storage media, Endod Dent Traumatol 7:69, 1991.
87. Holland R, Bisco Ferreira L, de Souza V, et al: Reaction of the lateral periodontium of dogs’ teeth to contaminated and noncontaminated perforations filled with mineral trioxide aggregate, J Endod 33:1192, 2007.
88. Holloway GA Jr, Watkins DW: Laser Doppler measurement of cutaneous blood flow. J Invest Dermatol 69:306, 1977.
89. Hoshino E, Kurihara-Ando N, Sato I, et al: In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline, Int Endod J 29:125, 1996.
90. Iqbal MK, Bamaas N: Effect of enamel matrix derivative (Emdogain) upon periodontal healing after replantation of permanent incisors in beagle dogs, Dent Traumatol 17:36, 2001.
91. Iwamoto CE, Erika A, Pameijer CH, et al: Clinical and histological evaluation of white ProRoot MTA in direct pulp capping, Am J Dent 19:85, 2006.
92. Jacobsen I: Root fractures in permanent anterior teeth with incomplete root formation, Scand J Dent Res 84:210, 1976.
http://dentalebooks.com
CHAPTER 20 The Role of Endodontics After Dental Traumatic Injuries 791
93. Jacobsen I, Kerekes K: Diagnosis and treatment of pulp necrosis in permanent anterior teeth with root fracture, Scand J Dent Res 88:370, 1980
94. Jacobsen I, Zachrisson BU: Repair characteristics of root fractures in permanent anterior teeth, Scand J Dent Res 83:355, 1975.
95. Jarvinen S: Fractured and avulsed permanent incisors in Finnish children: a retrospective study, Acta Odontol Scand 37:47, 1979.
96. Jung IY, Lee SJ, Hargreaves KM: Biologically based treatment of immature permanent teeth with pulpal necrosis: a case series, J Endod 34:876, 2008.
97. Kakehashi S, Stanley HR, Fitzgerald RJ: The effect of surgical exposures on dental pulps in germ-free and conventional laboratory rats, Oral Surg 20:340, 1965.
98. Kamburoglu K, Ilker Cebeci AR, Grondahl HG: Effectiveness of limited cone-beam computed tomography in the detection of horizontal root fracture, Dent Traumatol 25:256, 2009.
99. Katebzadeh N, Dalton BC, Trope M: Strengthening immature teeth during and after apexification, J Endod 24:256, 1998.
100. Kenny DJ, Barrett EJ, Casas MJ: Avulsions and intrusions: the controversial displacement injuries. J Can Dent Assoc 69:308, 2003.
101. Kerekes K, Heide S, Jacobsen I: Follow-up examination of endodontic treatment in traumatized juvenile incisors, J Endod 6:744, 1980.
102. Koliniotou-Koumpia E, Tziafas D: Pulpal responses following direct pulp capping of healthy dog teeth with dentine adhesive systems, J Dent 33:639, 2005.
103. Kositbowornchai S, Nuansakul R, Sikram S, et al: Root fracture detection: a comparison of direct digital radiography with conventional radiography, Dentomaxillofac Radiol 30:106, 2001.
104. Lengheden A, Blomlof L, Lindskog S: Effect of delayed calcium hydroxide treatment on periodontal healing in contaminated replanted teeth, Scand J Dent Res 99:147, 1991.
105. Lindskog S, Pierce AM, Blomlof L, Hammarstrom L: The role of the necrotic periodontal membrane in cementum resorption and ankylosis, Endod Dent Traumatol 1:96, 1985.
106. Love RM: Bacterial penetration of the root canal of intact incisor teeth after a simulated traumatic injury, Endod Dent Traumatol 12:289, 1996.
107. Love RM, Ponnambalam Y: Dental and maxillofacial skeletal injuries seen at the University of Otago School of Clinicianry, New Zealand, 2000-2004, Dent Traumatol 24:170, 2008.
108. Lundin SA, Noren JG, Warfvinge J: Marginal bacterial leakage and pulp reactions in Class II composite resin restorations in vivo, Swed Dent J 14:185, 1990.
109. Maroto M, Barberia E, Planells P, Vera V: Treatment of a non-vital immature incisor with mineral trioxide aggregate (MTA), Dent Traumatol 19:165, 2003.
110. Masterton JB: The healing of wounds of the dental pulp: an investigation of the nature of the scar tissue and of the phenomena leading to its formation, Dent Pract Dent Rec 16:325, 1966.
111. May JJ, Cohenca N, Peters OA: Contemporary management of horizontal root fractures to the permanent dentition: diagnosis, radiologic assessment to include cone-beam computed tomography, Pediatr Dent 35:120, 2013.
112. Mejare I, Hasselgren G, Hammarstrom LE: Effect of formaldehyde-containing drugs on human dental pulp evaluated by enzyme histochemical technique, Scand J Dent Res 84:29, 1976.
113. Mesaros S, Trope M, Maixner W, Burkes EJ: Comparison of two laser Doppler systems on the measurement of blood flow of premolar teeth under different pulpal conditions, Int Endod J 30:167, 1997.
114. Myers WC, Fountain SB: Dental pulp regeneration aided by blood and blood substitutes after experimentally
induced periapical infection, Oral Surg Oral Med Oral Pathol 37:441, 1974.
115. Murray PE, Smith AJ, Windsor LJ, Mjor IA: Remaining dentine thickness and human pulp responses, Int Endod J 33:36, 2003.
116. Nair PN, Duncan HF, Pitt Ford TR, Luder HU: Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial, Int Endod J 41:128, 2008.
117. Ohman A: Healing and sensitivity to pain in young replanted human teeth: an experimental, clinical and histological study, Odontol Tidskr 73:166, 1965.
118. Parirokh M, Kakoei S: Vital pulp therapy of mandibular incisors: a case report with 11-year follow up, Aust Endod J 32:75, 2006.
119. Patel S, Dawood A, Pitt Ford T, Whaites E: The potential applications of cone beam computed tomography in the management of endodontic problems, Int Endod J 40:818, 2007.
120. Patel S, Durack C, Abella F, et al: Cone beam computed tomography in endodontics: a review, Int Endod J 48:3, 2015.
121. Perez AL, Spears R, Gutmann JL, Opperman LA: Osteoblasts and MG-63 osteosarcoma cells behave differently when in contact with ProRoot MTA and White MTA, Int Endod J 36:564, 2003.
122. Pierce A, Lindskog S: The effect of an antibiotic/corticosteroid paste on inflammatory root resorption in vivo, Oral Surg Oral Med Oral Pathol 64:216, 1987.
123. Pileggi R, Dumsha TC, Myslinksi NR: The reliability of electric pulp test after concussion injury, Endod Dent Traumatol 12:16, 1996.
124. Rabie G, Barnett F, Tronstad L: Long-term splinting of maxillary incisor with intra alveolar root fracture, Endod Dent Traumatol 4:99, 1988.
125. Ravn JJ: Follow-up study of permanent incisors with complicated crown fractures after acute trauma, Scand J Dent Res 90:363, 1982.
126. Ray HA, Trope M: Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration, Int Endod J 28:12, 1995.
127. Ritter AL, Ritter AV, Murrah V, et al: Pulp revascularization of replanted immature dog teeth after treatment with minocycline and doxycycline assessed by laser Doppler flowmetry, radiography, and histology, Dent Traumatol 20:75, 2004.
128. Sae-Lim V, Wang CY, Choi GW, Trope M: The effect of systemic tetracycline on resorption of dried replanted dogs’ teethl, Endod Dent Traumatol 14:127, 1998.
129. Sae-Lim V, Wang CY, Trope M: Effect of systemic tetracycline and amoxicillin on inflammatory root resorption of replanted dogs’ teeth, Endod Dent Traumatol 14:216, 1998.
130. Saroglu I, Sonmez H: The prevalence of traumatic injuries treated in the pedodontic clinic of Ankara University, Turkey, during 18 months, Dent Traumatol 18:299, 2002.
131. Sawicki L, Pameijer CH, Emerich K, Adamowicz-Klepalska B: Histological evaluation of mineral trioxide aggregate and calcium hydroxide in direct pulp capping of human immature permanent teeth, Am J Dent 21:262, 2008.
132. Schjott M, Andreasen JO: Emdogain does not prevent progressive root resorption after replantation of avulsed teeth: a clinical study, Dental Traumatol 21:46, 2005.
133. Schroder U: Reaction of human dental pulp to experimental pulpotomy and capping with calcium hydroxide (thesis), Odont Revy 24(Suppl 25):97, 1973.
134. Schroder U, Granath LE: Early reaction of intact human teeth to calcium hydroxide following experimental pulpotomy and its significance to the development of hard tissue barrier, Odontol Revy 22:379, 1971.
135. Seltzer S: Endodontology, Philadelphia, 1988, Lea & Febiger.
136. Seltzer S, Bender IB, Turkenkopf S: Factors affecting successful repair after root canal therapy, J Am Dent Assoc 52:651, 1963.
137. Selvig KA, Zander HA: Chemical analysis and microradiography of cementum and dentin from periodontically diseased human teeth, J Periodontol 33:103, 1962.
138. Shuping GB, Orstavik D, Sigurdsson A, Trope M: Reduction of intracanal bacteria using nickel-titanium rotary instrumentation and various medications, J Endod 26:751, 2000.
139. Silva GA, Lanza LD, Lopes-Junior N, et al: Direct pulp capping with a dentin bonding system in human teeth: a clinical and histological evaluation, Oper Dent 31:297, 2006.
140. Silverman S: The dental structures in primary hyperparathyroidism, Oral Surg 15:426, 1962.
141. Sjogren U, Figdor D, Spangberg L, Sundqvist G: The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing, Int Endod J 24:119, 1991.
142. Sjogren U, Hagglund B, Sundqvist G, Wing K: Factors affecting the long-term results of endodontic treatment, J Endod 16:498, 1990.
143. Skaare AB, Jacobsen I: Dental injuries in Norwegians aged 7-18 years, Dent Traumatol 19:67, 2003.
144. Skieller V: The prognosis for young teeth loosened after mechanical injuries, Acta Odontol Scand 18:171, 1960.
145. Skoglund A, Tronstad L: Pulpal changes in replanted and autotransplanted immature teeth of dogs, J Endod 7:309, 1981.
146. Soder PO, Otteskog P, Andreasen JO, Modeer T: Effect of drying on viability of periodontal membrane, Scand J Dent Res 85:164, 1977.
147. Spangberg L, Rutberg M, Rydinge E: Biologic effects of endodontic antimicrobial agents, J Endod 5:166, 1979.
148. Stalhane I, Hedegard B: Traumatized permanent teeth in children aged 7-15 years, Sven Tandlak Tidskr 68:157, 1975.
149. Stanley HR: Diseases of the dental pulp. In Tieck RW, editors: Oral pathology, New York, 1965, McGraw-Hill.
150. Stanley HR, Lundy T: Dycal therapy for pulp exposures, Oral Surg Oral Med Oral Pathol 34:818, 1972.
151. Subay RK, Demirci M: Pulp tissue reactions to a dentin bonding agent as a direct capping agent, J Endod 31:201, 2005.
152. Swift EJ Jr, Trope M: Treatment options for the exposed vital pulp, Pract Periodontics Aesthet Dent 11:735, 1999.
153. Tapias MA, Jimenez-Garcia R, Lamas F, Gil AA: Prevalence of traumatic crown fractures to permanent incisors in a childhood population: Mostoles, Spain, Dent Traumatol 19:119, 2003.
154. Teixeira FB, Teixeira EC, Thompson JY, Trope M: Fracture resistance of roots endodontically treated with a new resin filling material, J Am Dent Assoc 135:646, 2004.
155. Thibodeau B, Teixeira F, Yamauchi M, et al: Pulp revascularization of immature dog teeth with apical periodontitis, J Endod 33:680, 2007.
156. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR: Physical and chemical properties of a new root-end filling material, J Endod 21:349, 1995.
157. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR: Bacterial leakage of mineral trioxide aggregate as a root-end filling material, J Endod 21:109, 1995.
158. Trabert KC, Caput AA, Abou-Rass M: Tooth fracture: a comparison of endodontic and restorative treatments, J Endod 4:341, 1978.
159. Tronstad L: Reaction of the exposed pulp to Dycal treatment, Oral Surg Oral Med Oral Pathol 38:945, 1974.
160. Tronstad L: Root resorption: etiology, terminology and clinical manifestations, Endod Dent Traumatol 4:241, 1988.
161. Tronstad L, Andreasen JO, Hasselgren G, et al: pH changes in dental tissues after root canal filling with calcium hydroxide, J Endod 7:17, 1980.
http://dentalebooks.com

792 PART III Expanded Clinical Topics
162. Tronstad L, Mjor IA: Capping of the inflamed pulp, Oral Surg Oral Med Oral Pathol 34:477, 1972.
163. Trope M: Root resorption of dental and traumatic origin: classification based on etiology, Pract Periodontics Aesthet Dent 10:515, 1998.
164. Trope M: Clinical management of the avulsed tooth: present strategies and future directions, Dent Traumatol 18:1, 2002.
165. Trope M, Friedman S: Periodontal healing of replanted dog teeth stored in Viaspan, milk and Hank’s Balanced Salt Solution, Endod Dent Traumatol 8:183, 1992.
166. Trope M, Moshonov J, Nissan R, et al: Short vs long-term calcium hydroxide treatment of established inflammatory root resorption in replanted dog teeth, Endod Dent Traumatol 11:124, 1995.
167. Trope M, Yesilsoy C, Koren L, et al: Effect of different endodontic treatment protocols on periodontal repair and
root resorption of replanted dog teeth, J Endod 18:492, 1992.
168. Turley PK, Joiner MW, Hellstrom S: The effect of orthodontic extrusion on traumatically intruded teeth, Am J Orthod 85:47, 1984.
169. von Arx T, Filippi A, Buser D: Splinting of traumatized teeth with a new device: TTS (titanium trauma splint), Dent Traumatol 17:180, 2001.
170. Wedenberg C, Lindskog S: Experimental internal resorption in monkey teeth, Endod Dent Traumatol 1:221, 1985.
171. Wedenberg C, Zetterqvist L: Internal resorption in human teeth: a histological, scanning electron microscopic, and enzyme histochemical study, J Endod 13:255, 1987.
172. Weiss M: Pulp capping in older patients, N Y State Dent J 32:451, 1966.
173. Windley W, Teixeira F, Levin L, et al: Disinfection of immature teeth with a triple antibiotic paste, J Endod 31:439, 2005.
174. Witherspoon DE, Small JC, Harris GZ: Mineral trioxide aggregate pulpotomies: a case series outcomes assessment, J Am Dent Assoc 137:610, 2006.
175. Yanpiset K, Trope M: Pulp revascularization of replanted immature dog teeth after different treatment methods, Endod Dent Traumatol 16:211, 2000.
176. Yanpiset K, Vongsavan N, Sigurdsson A, Trope M: Efficacy of laser Doppler flowmetry for the diagnosis of revascularization of reimplanted immature dog teeth, Dent Traumatol 17:63, 2001.
177. Zachrisson BU, Jacobsen I: Long-term prognosis of 66 permanent anterior teeth with root fracture, Scand J Dent Res 83:345, 1975.
http://dentalebooks.com
793
Unobserved TraumaDiagnostic ChallengeFracture MechanicsCracked and Fractured Cusps
DefinitionDiagnosisEtiologyTreatment Planning
Cracked and Split TeethDefinitionDiagnosis
EtiologyTreatment Planning
Vertical Root Fracture (VRF)DefinitionDiagnosisEtiology
Treatment PlanningSummary
Cracks and FracturesZVI METZGER | LOUIS H. BERMAN | AVIAD TAMSE
CHAPTER 21
CHAPTER OUTLINE
Root cracks and fractures can be two of the most frustrating aspects of endodontic and restorative dentistry. The diagnosis can be difficult; the symptoms can be either vague or specific, yet they are often insufficient for a definitive diagnosis; the radiographic evaluation can be evasive. Clinical management of the crack or fracture depends on its extent. Prevention of a potential crack or fracture is a fundamental principle, and early detection is imperative.
UNOBSERVED TRAUMATooth fracture is commonly associated with impact trauma. A car accident, a fall from a bicycle, and an accidental blow to the face are among the common causes. These types of trau-matic fractures mainly occur in the anterior segment of the mouth and are covered elsewhere in this book (see Chapter 20). In contrast, the cracks and fractures described in this chapter are often not associated with a traumatic event that the patient can remember. These cracks and fractures are frequently the result of an accumulating, unobserved trauma resulting from either normal or excessive occlusal forces that are repetitively applied22,34,45,47,70,71,90 without the patient’s awareness.
DIAGNOSTIC CHALLENGEThree categories of cracks and fractures are discussed in this chapter: cracked and fractured cusps, cracked and split teeth, and vertical root fractures. Each is often undiagnosed or mis-diagnosed for a relatively long time.16,19,80 The astute clinician can usually diagnose a pulpitis, apical periodontitis, or an
abscess after appropriate diagnostic tests and clinical assess-ments are performed. However, because of the wide variety of clinical presentations from cracks and fractures, the diagnosis is less straightforward.16,18,78 To complicate the diagnosis, not one of the three entities necessarily exhibits a radiographic manifestation in the early stages, depriving the dentist of one of the most objective diagnostic tools.
Symptoms from one of these conditions may be present for several months before an accurate diagnosis is made,5,16,19 which may be frustrating for both the patient and the dentist, and often causes the patient to develop a subsequent loss of trust and confidence in the dentist.
The final diagnosis is typically reached at a relatively late stage of these conditions, often after complications have already occurred. Complications may include a catastrophic fracture of the tooth or cusp or significant periradicular bone loss associated with a vertical root fracture as seen by radio-graphic examination (see also Chapter 2). For this reason, this chapter emphasizes the early diagnosis of these conditions. The collection of signs and symptoms associated with each of the three categories of cracks and fractures may be confusing unless the clinician considers these indicators as representing a continuous process examined at a given time point.
FRACTURE MECHANICSFracture mechanics is the field of biomechanics concerned with the propagation of cracks in a given material until the forma-tion of the final catastrophic fracture.7,52 Many terms have been loosely used in the dental literature to describe the clinical entities that are the subject of this chapter.5,9,18,35 Here, the term
http://dentalebooks.com

794 PART III Expanded Clinical Topics
Clinical ManifestationEarly ManifestationThe typical characteristic of cracked cusps is a sharp pain upon chewing, although the affected tooth may not be sensitive, or only selectively sensitive, to percussion.70 The tooth is vital, and its response to a cold stimulus may be normal; but with time, this response may resemble a pulpitis, which may be either localized or referred to other odontogenic or nonodon-togenic locations.16,47,71
Cracked cusps are often associated with extensive occlusal restorations,3,29,71,78 which may undermine and weaken the cusp and predispose it to initiating or perpetuating a crack from occlusal forces. Nevertheless, cracked cusps may also be present in intact teeth or teeth with smaller restorations.13,70
Late ManifestationWith time, a crack may propagate and result in a fractured cusp. If the fracture line occurs coronally to the periodontal ligament the fractured portion will simply separate from the tooth. However, if the fracture line extends subgingivally, gin-gival fibers or the periodontal ligament will often retain the fractured cusp. Initially, it may be possible to move the cusp by wedging a sharp explorer into the fracture line, making the fractured cusp more visible. Often, from continued mastica-tion, a localized and more acute type of pain may emerge secondary to the movement of the fractured fragment in the coronal PDL. The pulpal pain that is typical at an earlier stage (the cracked cusp) will typically resolve once a complete frac-ture occurs.
DiagnosisA cracked cusp may be diagnosed, to a large extent, on the basis of the patient history. To locate the affected tooth, a biting test should be performed using a Tooth Slooth (Professional Results, Laguna Niguel, CA) or a similar device9,12 (Fig. 21-2). The device is composed of a small pyramid with a flattened top that is placed on a selective cusp, while the wider part of the device is applied to several opposing teeth while the patient occludes (see Fig. 21-2). The application of these forces to a cracked cusp will generate a sharp pain, which may occur upon pressure or released.3,34,43 The patient will typically state that this sensation has reproduced the sensation of the chief complaint.
Magnification with such devices as loupes or an operating microscope can be helpful when looking for a crack. If the tooth does not have an extensive intracoronal restoration, transillumination may also assist in revealing the crack line. If the tooth has a large restoration, the removal of the restoration may facilitate the effective use of this diagnostic tool (Fig. 21-3). The light source should be intense but with small dimensions (Fig. 21-4); it is applied to the tooth at the area of the suspected cusp fracture, with the lights of the dental unit, microscope, and room extinguished. The light penetrates the tooth structure up to the crack, leaving the part beyond the crack relatively dark (see Fig. 21-3). However, when large intracoronal restorations are present, this type of examination may be less effective.
Once the crack propagates, resulting in a fractured cusp, the diagnosis becomes more straightforward: the fractured cusp will either be missing or moved by wedging an explorer into the fracture line (Fig. 21-5).
crack will be used in the biomechanical sense: a partial discon-tinuity in a material that may propagate and eventually lead to a complete discontinuity, also known as a fracture.7,52 In this context, a cusp may be described as cracked, a condition leading with time to a fractured cusp. A cracked tooth may be so called until a final fracture occurs that separates the tooth into two parts, a condition termed a split tooth. Similarly, microcracks may appear in the radicular dentin of an endodon-tically treated tooth, and these cracks may propagate with time until a vertical root fracture occurs, at which point the full thickness of the dentinal wall shows discontinuity: a through-and-through fracture. Such a fracture may be incomplete, involving one wall of the root, or complete, separating the root into two parts80 (Fig. 21-1).
CRACKED AND FRACTURED CUSPS
DefinitionA cracked cusp is characterized by a crack between a cusp and the rest of the tooth structure, to the extent of allowing micro-scopic flexure upon mastication. This crack typically does not involve the pulp. With time, the crack may propagate, eventu-ally resulting in a fractured cusp.5
DiagnosisPatient HistoryIn the case of a cracked cusp, the patient history is the most important tool for making a diagnosis. The patient will likely complain about pain when chewing, to the extent of not being able to chew on the side on which the crack occurred.18,35,69 The patient will also often state that the condition existed for a relatively long time and that his or her dentist could not find the source or glean any information from radiography.3,16,47 When asked whether the pain is sharp or dull, patients will typically report a sharp pain that makes them immediately stop chewing on that side. The diagnostic challenge is attempting to determine which cusp of which tooth is involved, as patients often have difficulties determining the specific location of the discomfort.16,18,35,69 Because the pain has a pulpal origin, the patient’s proprioception may not be accurate, as no periodontal ligament is involved. Occasionally, the pain upon chewing may radiate to nondental locations on the same side of the face,16,47,71 as also described in Chapters 4 and 17.
FIG. 21-1 Complete vertical root fracture. A cross section of a mesial root of a mandibular molar with a complete vertical root fracture. The fracture is in the buccolingual plane and extends from the buccal convexity of the root to its lingual convexity.
M
http://dentalebooks.com
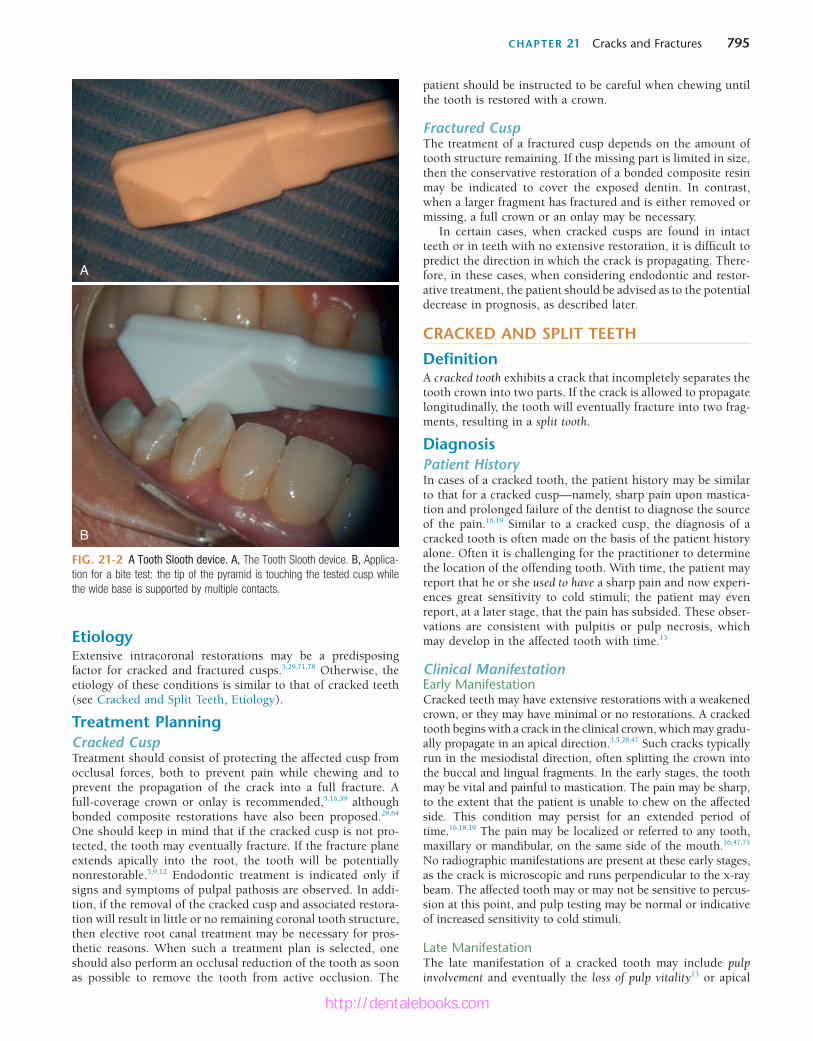
CHAPTER 21 Cracks and Fractures 795
FIG. 21-2 A Tooth Slooth device. A, The Tooth Slooth device. B, Applica-tion for a bite test: the tip of the pyramid is touching the tested cusp while the wide base is supported by multiple contacts.
A
B
EtiologyExtensive intracoronal restorations may be a predisposing factor for cracked and fractured cusps.3,29,71,78 Otherwise, the etiology of these conditions is similar to that of cracked teeth (see Cracked and Split Teeth, Etiology).
Treatment PlanningCracked CuspTreatment should consist of protecting the affected cusp from occlusal forces, both to prevent pain while chewing and to prevent the propagation of the crack into a full fracture. A full-coverage crown or onlay is recommended,5,16,39 although bonded composite restorations have also been proposed.28,64 One should keep in mind that if the cracked cusp is not pro-tected, the tooth may eventually fracture. If the fracture plane extends apically into the root, the tooth will be potentially nonrestorable.5,9,12 Endodontic treatment is indicated only if signs and symptoms of pulpal pathosis are observed. In addi-tion, if the removal of the cracked cusp and associated restora-tion will result in little or no remaining coronal tooth structure, then elective root canal treatment may be necessary for pros-thetic reasons. When such a treatment plan is selected, one should also perform an occlusal reduction of the tooth as soon as possible to remove the tooth from active occlusion. The
patient should be instructed to be careful when chewing until the tooth is restored with a crown.
Fractured CuspThe treatment of a fractured cusp depends on the amount of tooth structure remaining. If the missing part is limited in size, then the conservative restoration of a bonded composite resin may be indicated to cover the exposed dentin. In contrast, when a larger fragment has fractured and is either removed or missing, a full crown or an onlay may be necessary.
In certain cases, when cracked cusps are found in intact teeth or in teeth with no extensive restoration, it is difficult to predict the direction in which the crack is propagating. There-fore, in these cases, when considering endodontic and restor-ative treatment, the patient should be advised as to the potential decrease in prognosis, as described later.
CRACKED AND SPLIT TEETH
DefinitionA cracked tooth exhibits a crack that incompletely separates the tooth crown into two parts. If the crack is allowed to propagate longitudinally, the tooth will eventually fracture into two frag-ments, resulting in a split tooth.
DiagnosisPatient HistoryIn cases of a cracked tooth, the patient history may be similar to that for a cracked cusp—namely, sharp pain upon mastica-tion and prolonged failure of the dentist to diagnose the source of the pain.16,19 Similar to a cracked cusp, the diagnosis of a cracked tooth is often made on the basis of the patient history alone. Often it is challenging for the practitioner to determine the location of the offending tooth. With time, the patient may report that he or she used to have a sharp pain and now experi-ences great sensitivity to cold stimuli; the patient may even report, at a later stage, that the pain has subsided. These obser-vations are consistent with pulpitis or pulp necrosis, which may develop in the affected tooth with time.13
Clinical ManifestationEarly ManifestationCracked teeth may have extensive restorations with a weakened crown, or they may have minimal or no restorations. A cracked tooth begins with a crack in the clinical crown, which may gradu-ally propagate in an apical direction.3,5,28,47 Such cracks typically run in the mesiodistal direction, often splitting the crown into the buccal and lingual fragments. In the early stages, the tooth may be vital and painful to mastication. The pain may be sharp, to the extent that the patient is unable to chew on the affected side. This condition may persist for an extended period of time.16,18,19 The pain may be localized or referred to any tooth, maxillary or mandibular, on the same side of the mouth.16,47,71 No radiographic manifestations are present at these early stages, as the crack is microscopic and runs perpendicular to the x-ray beam. The affected tooth may or may not be sensitive to percus-sion at this point, and pulp testing may be normal or indicative of increased sensitivity to cold stimuli.
Late ManifestationThe late manifestation of a cracked tooth may include pulp involvement and eventually the loss of pulp vitality13 or apical
http://dentalebooks.com

796 PART III Expanded Clinical Topics
analysis. In each of these teeth, a longitudinal crack was observed, which extended to the pulp. Although the study had a limited sample size, the clinician should understand the potentially poor prognosis from cracked teeth, especially when the crack is suspected to be the cause of pulp necrosis.13
Pulp involvement occurs more often in cases of centrally located cracks (i.e., extending from marginal ridge to mar-ginal ridge through the central fossa) than in cracks with a more buccal or lingual location.18,90 These centrally located cracks commonly affect the roof of the pulp chamber at a later stage. Consequently, pulp vitality may be compromised and later lost due to bacterial penetration through the crack. The pulp may first become reversibly or irreversibly inflamed and later necrotic and infected. The sharp pain upon mastica-tion that is typical of the early stage may disappear once pulp vitality is lost. Moreover, apical periodontitis in an apparently intact molar may be a late manifestation of an untreated case of a cracked tooth.13 When pulp necrosis occurs, the radiographic manifestation may be an apical radiolucency, which is undistinguishable from that of apical periodontitis (Fig. 21-6).
A crack may propagate with time through the pulp chamber and into the root, resulting in a complete fracture that sepa-rates the tooth into two parts, a condition termed split tooth. When this split occurs, the resulting parts of the tooth may be movable by wedging a sharp explorer into the fissure.5,9 Later, more evident movement of the parts may be observed. The radiographic presentation at such a late stage may eventually develop into a diffuse radiolucency surrounding the root. At this late stage, narrow isolated deep periodontal pockets may be present.9 However, such pockets are typically located
FIG. 21-3 Transillumination for the detection of a cracked cusp/tooth. An intense but small light source is applied to the suspect tooth, preferably in relative darkness. The light is transmitted through the tooth structure but is reflected from the crack plane, leaving the area behind the crack in darkness.
A B
C D
FIG. 21-4 Light source for transillumination. The light source should be intense yet with small dimensions, such as the simple battery-operated device manufactured by Yeti Dental (Engen, Germany).
propagation of the fracture, resulting in a split tooth. In one investigation,13 27 nonvital molar and premolar teeth that had minimal or no restorations or caries were studied. Upon extrac-tion, these teeth were examined under a surgical operating microscope or using micro–computed tomography (CT)
http://dentalebooks.com

CHAPTER 21 Cracks and Fractures 797
FIG. 21-5 A fractured cusp. A, The mesiopalatal cusp of a maxillary first right molar was fractured. The fractured cusp was movable and was retained by the periodontal ligament. B, The cusp was removed, and the tooth was considered restorable. It was treated with root canal treatment and a crown.
A B
FIG. 21-6 A case of fracture-induced necrosis. A tooth with minimal or no restoration or caries is unlikely to become nonvital. A, This radiograph of a mandibular second molar shows a restoration that is distant from the pulp chamber, yet the tooth is nonvital and symptomatic. B, On occlusal examination, a slight crack is observed on the distal marginal ridge. C, After extraction, the mesial aspect of the crown and root shows no indication of a fracture. D, However, the distal aspect of the crown and coronal root shows the fracture. E, F, When the crown is sectioned, the crack can be observed to extend well into the pulp chamber.
A
B
C D
E
F
mesially or distally and, if adjacent teeth are present, they will be difficult, if not impossible, to detect.
Cracked and split teeth may present with a large and vari-able collection of signs and symptoms that are potentially confusing.16,18,78 Only by being aware of the process leading from early to late manifestations can clinicians interpret these signs and symptoms and identify the specific point they are encountering on the potential timeline of this process.
A definitive combination of factors, signs, and symptoms that, when collectively observed, allows the clinician to conclude the existence of a specific disease state is termed a syndrome. However, given the multitude of signs and symptoms that cracked roots can present with, it is often dif-ficult to achieve an objective definitive diagnosis. For this reason, the terminology of cracked tooth syndrome18 should be avoided.
DiagnosisAs in the case of a cracked cusp, early detection is imperative in order to resolve the patient’s symptoms as well as increasing the prognosis. However, the use of the Tooth Slooth device (see Fig. 21-2) may or may not provide as clear a result for a sym-metrically cracked tooth, as each of the parts of the tooth may be rather stable. Asking the patient to chew on a cotton roll9 or on the tip of a cotton-tip applicator placed at a particular site may reproduce the pain. Nevertheless this method may not indicate whether the source is a maxillary or mandibular tooth and need further measures to pinpoint the involved tooth. Magnification using either loupes or an operating microscope can be helpful for detecting a fracture line. In addition, dyes, such as methylene blue or tincture of iodine, which are applied either to the outer surface of the crown or to the dentin after the removal of an existing intracoronal restoration, can be
http://dentalebooks.com

798 PART III Expanded Clinical Topics
A root canal treatment followed by a permanent crown has the benefit of immediately eliminating the long-lasting, painful symptoms as well as early protection from occlusal forces that may cause propagation of a cracked tooth to become a split tooth. Nevertheless, when 127 cracked teeth with revers-ible pulpitis were treated with a crown alone, 20% of these teeth converted to irreversible pulpitis within 6 months and required root canal treatment.51 In contrast, none of the other teeth needed a root canal over a 6-year evaluation period.51 However, it should also be understood that varying percentages of crowned teeth, cracked or noncracked, may also require endodontic treatment, merely from the trauma of the crown preparation. By comparison, it has been shown that when suspected cracked teeth were restored with resin bonded res-torations, only 7% required subsequent endodontic treatment or extraction.64
After removal of an intracoronal restoration or when pen-etrating the dentin to prepare for endodontic access, one may observe discoloration along the crack in the dentin. Once the access cavity has been completed, the floor and the distal and mesial walls of the pulp chamber should be carefully inspected to check for the presence and extent of any cracks. Upon evaluating 245 restored teeth, cracks were observed preopera-tively in 23.3% of the teeth; however, when the restorations were removed, 60% of these teeth were found to have cracks.1 Methylene blue dye may be helpful in this type of examina-tion. If a crack is found that reaches from the mesial wall, through the floor of the pulp chamber and into the distal wall, then the prognosis for the tooth is poor, and extraction should be considered (see Fig. 21-6).5,9,12 If the crack does not reach the pulp chamber or is limited to the coronal parts of the mesial or distal wall, the subsequent protection of the tooth with a crown may save the tooth. Nevertheless, as men-tioned previously, the patient should be advised that the treatment success may be compromised and that long-term follow-up will be required.5,9,12
Given that such cracks occasionally occur in teeth with minimal or no restorations and that all of the pain may cease once the pulp is removed, it may be tempting to limit the final restoration to an intracoronal amalgam or composite restora-tion. This temptation should be resisted by all means, as the forces that caused the crack are still present, and the apical propagation of the crack and loss of the tooth is still likely.
Split ToothWhen the tooth is split either through its whole length or diagonally (Fig. 21-7), extraction is typically the only treat-ment option.5,9 However, if the fracture line is such that the split results in large and small segments, and if the removal of the small fragment preserves enough tooth structure that is restorable, then retention and restoration of the tooth may be considered.5
VERTICAL ROOT FRACTURE (VRF)
DefinitionA vertical root fracture (VRF) is a longitudinally oriented com-plete or incomplete fracture initiated in the root at any level and is usually directed buccolingually5 (Figs. 21-1 and 21-8 through 21-11). By definition, these types of fractures do not arise from the propagation of a fracture that originated in the crown. This definition separates a VRF from a split tooth,
helpful for visualizing the crack (see Fig. 21-3). Transillumina-tion can also be applied to the suspected tooth and, if the tooth has no restorations, this method may yield an impressively straightforward diagnosis (see Fig. 21-3). Anesthetizing the suspected tooth, followed by asking the patient to chew again on the cotton roll, may further confirm the diagnosis and finally differentiate the origin as a mandibular or maxillary tooth. At a later stage, when splitting of the tooth has occurred, wedging of a sharp explorer into the fracture line will provide a clear diagnosis of a split tooth.
Generally speaking, the diagnosis of a crack in a tooth can be difficult. When there are signs and symptoms of a pulpitis or necrosis, it is incumbent upon the clinician to determine the source that initiated the signs and symptoms. In the case of a problematic tooth with no apparent reason for the pulpitis or necrosis, like a tooth with minimal or no caries, restoration, or trauma, a crack or fracture must be considered.13 In some cases, an objective diagnosis may not be possible; however, with the possibility of a crack or fracture, the patient should be advised of a potential decrease in the endodontic or restor-ative prognosis.5,12
EtiologyMasticatory forces are the cause of cracked teeth.22,34,45,47,70,71,90 Thus, the dietary habit of chewing on coarse food has been proposed as a contributing factor.22,90 Bruxism or clenching of the teeth as well as occlusal prematurities are also frequent causes of cracked teeth.18,22,34,45,47,70,71,90 For this reason, certain teeth may be more prone to developing cracks, such as man-dibular second molars and maxillary premolars.18 Masticatory habits such as chewing ice may also predispose teeth to cracks. The term fatigue root fracture, proposed by Yeh,90 encompasses all of these causes.
In certain cases, traumatic injuries, such as a severe upward blow to the mandible (e.g., during a car or sports accident) can also cause a tooth crack or fracture. Another potential cause is the unexpected chewing of a hard object (e.g., a cherry pit or an unpopped corn kernel in popcorn). The occlusal forces applied by the first molars are as high as 90 kg,45 which, when fully applied unexpectedly, may damage the tooth structure. However, in most cases, a tooth crack can be attributed to no specific cause other than normal or excessive masticatory forces.22,34,45,47,70,71,90
Treatment PlanningCracked ToothWhen a cracked tooth is either suspected or determined, the patient should be informed that the prognosis is reduced and sometimes questionable.5,9,12 Protecting a tooth from the propa-gation of a crack and improving comfort while chewing are the principal goals in the treatment of cracked teeth. Both goals can often be immediately achieved by placing an orthodontic band around the tooth3,9,16 or by placing a provisional crown. These procedures allow the clinician to evaluate the extent of pulp involvement by checking whether the pulpal symptoms subside in response to the intervention.3,9,16
Protecting the tooth from further splitting forces by the placement of a permanent crown is essential in these cases.3,5,9,16,39 Unfortunately, a crown alone is often not suffi-cient to resolve symptoms, and endodontic treatment may be considered prior to the placement of the permanent crown, depending on the pulpal symptoms.9
http://dentalebooks.com
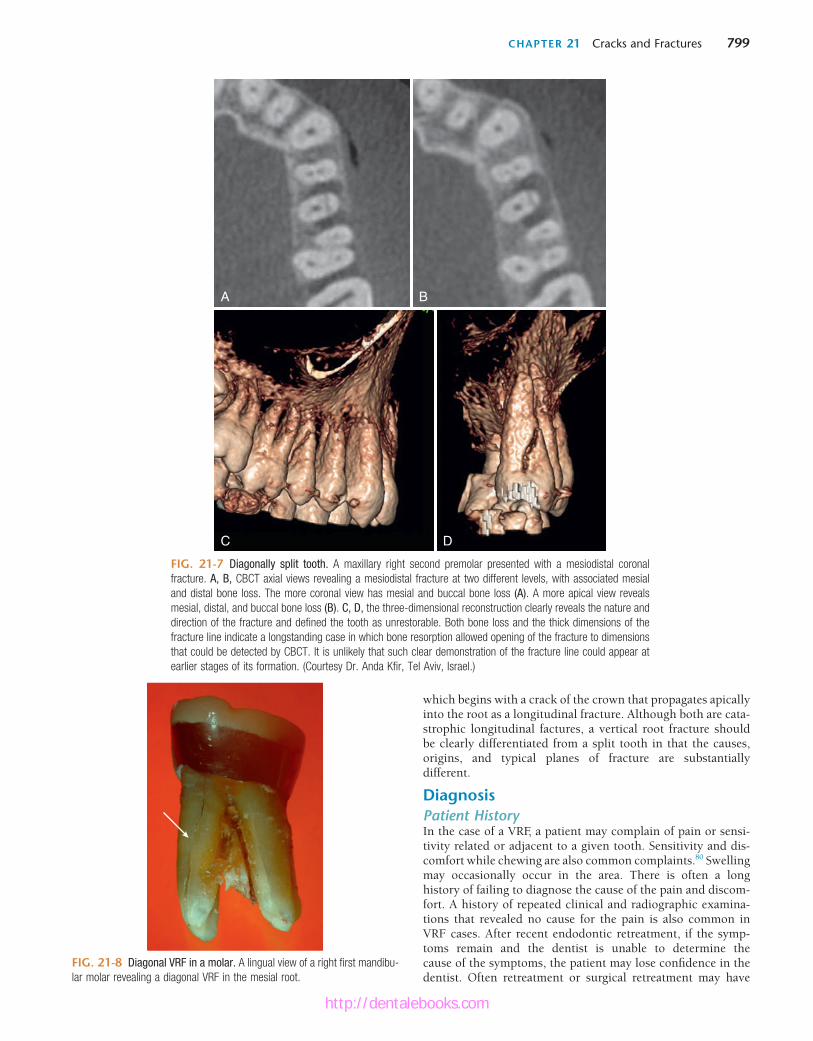
CHAPTER 21 Cracks and Fractures 799
FIG. 21-7 Diagonally split tooth. A maxillary right second premolar presented with a mesiodistal coronal fracture. A, B, CBCT axial views revealing a mesiodistal fracture at two different levels, with associated mesial and distal bone loss. The more coronal view has mesial and buccal bone loss (A). A more apical view reveals mesial, distal, and buccal bone loss (B). C, D, the three-dimensional reconstruction clearly reveals the nature and direction of the fracture and defined the tooth as unrestorable. Both bone loss and the thick dimensions of the fracture line indicate a longstanding case in which bone resorption allowed opening of the fracture to dimensions that could be detected by CBCT. It is unlikely that such clear demonstration of the fracture line could appear at earlier stages of its formation. (Courtesy Dr. Anda Kfir, Tel Aviv, Israel.)
A B
C D
FIG. 21-8 Diagonal VRF in a molar. A lingual view of a right first mandibu-lar molar revealing a diagonal VRF in the mesial root.
which begins with a crack of the crown that propagates apically into the root as a longitudinal fracture. Although both are cata-strophic longitudinal factures, a vertical root fracture should be clearly differentiated from a split tooth in that the causes, origins, and typical planes of fracture are substantially different.
DiagnosisPatient HistoryIn the case of a VRF, a patient may complain of pain or sensi-tivity related or adjacent to a given tooth. Sensitivity and dis-comfort while chewing are also common complaints.80 Swelling may occasionally occur in the area. There is often a long history of failing to diagnose the cause of the pain and discom-fort. A history of repeated clinical and radiographic examina-tions that revealed no cause for the pain is also common in VRF cases. After recent endodontic retreatment, if the symp-toms remain and the dentist is unable to determine the cause of the symptoms, the patient may lose confidence in the dentist. Often retreatment or surgical retreatment may have
http://dentalebooks.com

800 PART III Expanded Clinical Topics
FIG. 21-9 Three types of VRFs. A, A coronally located VRF extending apically as far as one third of the root. B, A midroot VRF extending along the middle third of the root. C, An apically located VRF extending coronally as far as the apical two thirds of the root.
A B C
FIG. 21-10 Radiographic presentation of VRF-associated bone loss. A second right mandibular bicuspid was endodontically treated and restored using a short post. Two years later the patient started experiencing discomfort and sensitivity upon chewing. Initially no radiographic signs were present. This lasted for 9 months until a radiograph (A) revealed an extensive bone resorp-tion and the tooth extracted. A, A large radiolucent lesion was present along the root on the distal side. B, The tooth was extracted, but the buccal VRF was not readily evident. C, Transillumination with an intense but small light source was used after extraction to clearly demonstrate the VRF. (Courtesy Dr. Ramy Levi, Israel.)
A
B C
been attempted to reveal the accurate diagnosis.1 Unfortu-nately, such ineffective treatment attempts may only worsen the dentist-patient relationship.
Clinical ManifestationsSusceptible Teeth and VRF LocationVertical root fractures are commonly associated with endodon-tically treated teeth with or without a post.5 Nevertheless, VRFs can also occur in teeth with no previous root canal treatment.22 The most susceptible sites and tooth groups are the maxillary and mandibular premolars, the mesial roots of the mandibular molars, the mesiobuccal roots of the maxillary molars, and the mandibular incisors.81 However, VRFs may occasionally occur in other teeth and roots as well.
Vertical root fractures may progress in the buccolingual direction in these teeth and roots, which are typically narrow mesiodistally and wide buccolingually.40 However, VRFs may also propagate diagonally, thus affecting the mesial or distal aspect of the root (see Fig. 21-8). VRFs may be initiated at any root level.5 They may be initiated at the apical part of the root and propagate coronally (see Fig. 21-9, C). Nevertheless, certain VRFs originate at the coronal, cervical part of the root and extend apically (see Fig. 21-9, A), and in other cases, a VRF may be initiated as a midroot fracture (see Figs. 21-9, B; 21-10, C; and 21-11, D).
It is commonly believed that VRFs begin as microcracks at the root canal surface of the radicular dentin and gradually propagate outward until the full thickness of the radicular dentin is fractured.5,10,21,56,87 Studies14,17,50,76,91 indicate that microcracks can also be initiated at the outer surface of the root and propagate inward. Therefore, the correlation between microcracks in the radicular dentin and the formation of VRFs should be further investigated.
Early ManifestationIn the early stages of a VRF, there may be pain or discomfort on the affected side of the tooth. In particular, the tooth may feel uncomfortable and sensitive upon chewing, although this pain is often of a dull nature, as opposed to the sharp pain typical of
http://dentalebooks.com

CHAPTER 21 Cracks and Fractures 801
FIG. 21-11 Small isolated radiographic presentation of VRF-associated bone loss. A second right mandibular bicuspid was end-odontically treated and restored with no dowel. A year later the patient started complaining about sensitivity on the lingual side. Three months later the radiograph (A) was taken and the tooth extracted. A small radiolucent lesion was present along the root on the distal side. The tooth was extracted, but the lingual VRF was not readily evident (B). Transillumination with an intense but small light source was used after extraction to clearly demonstrate the VRF (C, D). (Courtesy Dr. Ramy Levi, Israel.)
A B
C D
a cracked cusp or tooth with a vital pulp. As the fracture and subsequent infection progresses, swelling often occurs, and a sinus tract may be present at a location more coronal than a sinus tract associated with a case of chronic apical abscess79,81 (Fig. 21-12). These signs and symptoms are frequently similar to those encountered from nonhealing root canal treatment.57,86 In the early stages, radiographic findings are unlikely because (1) the root canal filling may obstruct the detection of the frac-ture (Fig. 21-13, A), and (2) the bone destruction (which still
has limited mesiodistal dimensions) may be obstructed by the superimposed root structure (Fig. 21-14).
A deep, narrow, and isolated periodontal pocket may be associated with the root, which often cannot be explained by, as it is inconsistent with, the surrounding periodontal exami-nation.79,81,85 This specific type of periodontal defect occurs secondary to the bony dehiscence caused by the vertical root fracture. It is substantially different from the pockets caused by advanced periodontitis (discussed later).
FIG. 21-12 Coronally located sinus tracts. A, A maxillary right lateral incisor with a sinus tract located at the attached gingiva, an uncommon location for sinus tract drainage from a chronic periapical abscess. Maxillary lateral incisors are not among the teeth with high prevalence of VRFs. B, A draining sinus tract at a coronal location originating from a buccal VRF in the first left maxillary premolar. C, A draining sinus tract at the gingival margin of a right first mandibular molar with a buccal VRF in the mesial root. (A and B, Courtesy Dr. Russ Paul, Zichron Yaakov, Israel.)
A B C
http://dentalebooks.com
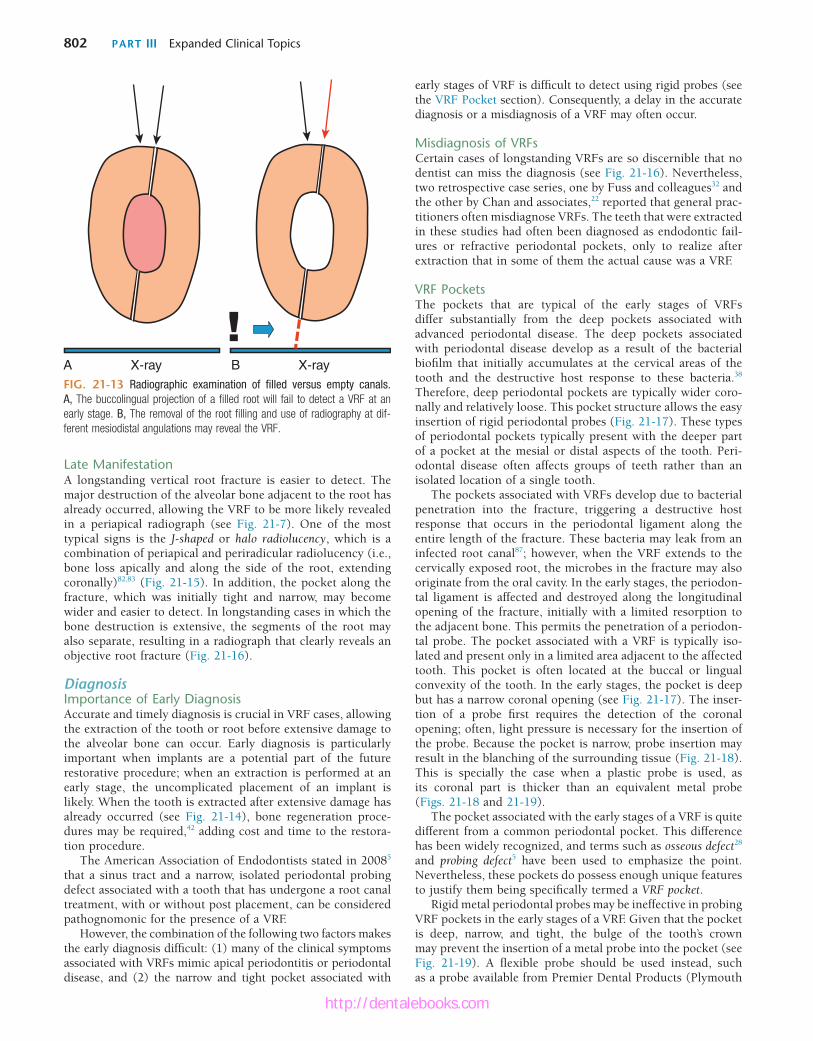
802 PART III Expanded Clinical Topics
Late ManifestationA longstanding vertical root fracture is easier to detect. The major destruction of the alveolar bone adjacent to the root has already occurred, allowing the VRF to be more likely revealed in a periapical radiograph (see Fig. 21-7). One of the most typical signs is the J-shaped or halo radiolucency, which is a combination of periapical and periradicular radiolucency (i.e., bone loss apically and along the side of the root, extending coronally)82,83 (Fig. 21-15). In addition, the pocket along the fracture, which was initially tight and narrow, may become wider and easier to detect. In longstanding cases in which the bone destruction is extensive, the segments of the root may also separate, resulting in a radiograph that clearly reveals an objective root fracture (Fig. 21-16).
DiagnosisImportance of Early DiagnosisAccurate and timely diagnosis is crucial in VRF cases, allowing the extraction of the tooth or root before extensive damage to the alveolar bone can occur. Early diagnosis is particularly important when implants are a potential part of the future restorative procedure; when an extraction is performed at an early stage, the uncomplicated placement of an implant is likely. When the tooth is extracted after extensive damage has already occurred (see Fig. 21-14), bone regeneration proce-dures may be required,42 adding cost and time to the restora-tion procedure.
The American Association of Endodontists stated in 20085 that a sinus tract and a narrow, isolated periodontal probing defect associated with a tooth that has undergone a root canal treatment, with or without post placement, can be considered pathognomonic for the presence of a VRF.
However, the combination of the following two factors makes the early diagnosis difficult: (1) many of the clinical symptoms associated with VRFs mimic apical periodontitis or periodontal disease, and (2) the narrow and tight pocket associated with
FIG. 21-13 Radiographic examination of filled versus empty canals. A, The buccolingual projection of a filled root will fail to detect a VRF at an early stage. B, The removal of the root filling and use of radiography at dif-ferent mesiodistal angulations may reveal the VRF.
A X-ray B X-ray
early stages of VRF is difficult to detect using rigid probes (see the VRF Pocket section). Consequently, a delay in the accurate diagnosis or a misdiagnosis of a VRF may often occur.
Misdiagnosis of VRFsCertain cases of longstanding VRFs are so discernible that no dentist can miss the diagnosis (see Fig. 21-16). Nevertheless, two retrospective case series, one by Fuss and colleagues32 and the other by Chan and associates,22 reported that general prac-titioners often misdiagnose VRFs. The teeth that were extracted in these studies had often been diagnosed as endodontic fail-ures or refractive periodontal pockets, only to realize after extraction that in some of them the actual cause was a VRF.
VRF PocketsThe pockets that are typical of the early stages of VRFs differ substantially from the deep pockets associated with advanced periodontal disease. The deep pockets associated with periodontal disease develop as a result of the bacterial biofilm that initially accumulates at the cervical areas of the tooth and the destructive host response to these bacteria.38 Therefore, deep periodontal pockets are typically wider coro-nally and relatively loose. This pocket structure allows the easy insertion of rigid periodontal probes (Fig. 21-17). These types of periodontal pockets typically present with the deeper part of a pocket at the mesial or distal aspects of the tooth. Peri-odontal disease often affects groups of teeth rather than an isolated location of a single tooth.
The pockets associated with VRFs develop due to bacterial penetration into the fracture, triggering a destructive host response that occurs in the periodontal ligament along the entire length of the fracture. These bacteria may leak from an infected root canal87; however, when the VRF extends to the cervically exposed root, the microbes in the fracture may also originate from the oral cavity. In the early stages, the periodon-tal ligament is affected and destroyed along the longitudinal opening of the fracture, initially with a limited resorption to the adjacent bone. This permits the penetration of a periodon-tal probe. The pocket associated with a VRF is typically iso-lated and present only in a limited area adjacent to the affected tooth. This pocket is often located at the buccal or lingual convexity of the tooth. In the early stages, the pocket is deep but has a narrow coronal opening (see Fig. 21-17). The inser-tion of a probe first requires the detection of the coronal opening; often, light pressure is necessary for the insertion of the probe. Because the pocket is narrow, probe insertion may result in the blanching of the surrounding tissue (Fig. 21-18). This is specially the case when a plastic probe is used, as its coronal part is thicker than an equivalent metal probe (Figs. 21-18 and 21-19).
The pocket associated with the early stages of a VRF is quite different from a common periodontal pocket. This difference has been widely recognized, and terms such as osseous defect28 and probing defect5 have been used to emphasize the point. Nevertheless, these pockets do possess enough unique features to justify them being specifically termed a VRF pocket.
Rigid metal periodontal probes may be ineffective in probing VRF pockets in the early stages of a VRF. Given that the pocket is deep, narrow, and tight, the bulge of the tooth’s crown may prevent the insertion of a metal probe into the pocket (see Fig. 21-19). A flexible probe should be used instead, such as a probe available from Premier Dental Products (Plymouth
http://dentalebooks.com

CHAPTER 21 Cracks and Fractures 803
FIG. 21-14 Early versus late radiographic presentation of a VRF-associated bone defect. At an early stage, a bone defect (red) is not likely to be detected in a periapical radiograph, as the root will overlap with the defect (A, B). At later stages, when major damage has occurred to the cortical plate (C), the bone defect may be large enough to extend beyond the silhouette of the root (C, D) and appear as a radiolucent defect along the root (E). (Surgical image courtesy Dr. Devora Schwartz-Arad, Ramat-Hasharon, Israel.)
Early
Late
Cortical bone
Cortical bone
A B
C
D E
Meeting, Pennsylvania) (see Fig. 21-19) or a similar device. This type of flexible probe should be included on every end-odontic examination tray and is an essential tool when check-ing for potential VRF pockets.
A typical VRF pocket was observed in 67% of the VRF cases reported by Tamse and colleagues.81 However, because the early detection of such pockets is technique sensitive and because traditional metal probes were used in the aforemen-tioned study, the incidence of these pockets may in fact be higher than reported. When a typical VRF pocket is located on the convex flank of the root on the buccal or lingual side, it is likely that the root has a VRF. In contrast, when such a pocket
is located at the furcation of a molar, the pocket may indicate either a VRF or a sinus tract from an apical abscess that found a point of least resistance at the furcation area. In cases with a furcation pocket, when a VRF diagnosis cannot be conclusively determined, a positive healing response to the elimination of infection by initiating root canal retreatment may differentiate between these two types of pathoses.
Coronally Located Sinus TractSinus tracts that originate from a chronic apical abscess are typically detected at the site of least bone resistance, against the apical part of the root or in the area of the junction of the
http://dentalebooks.com
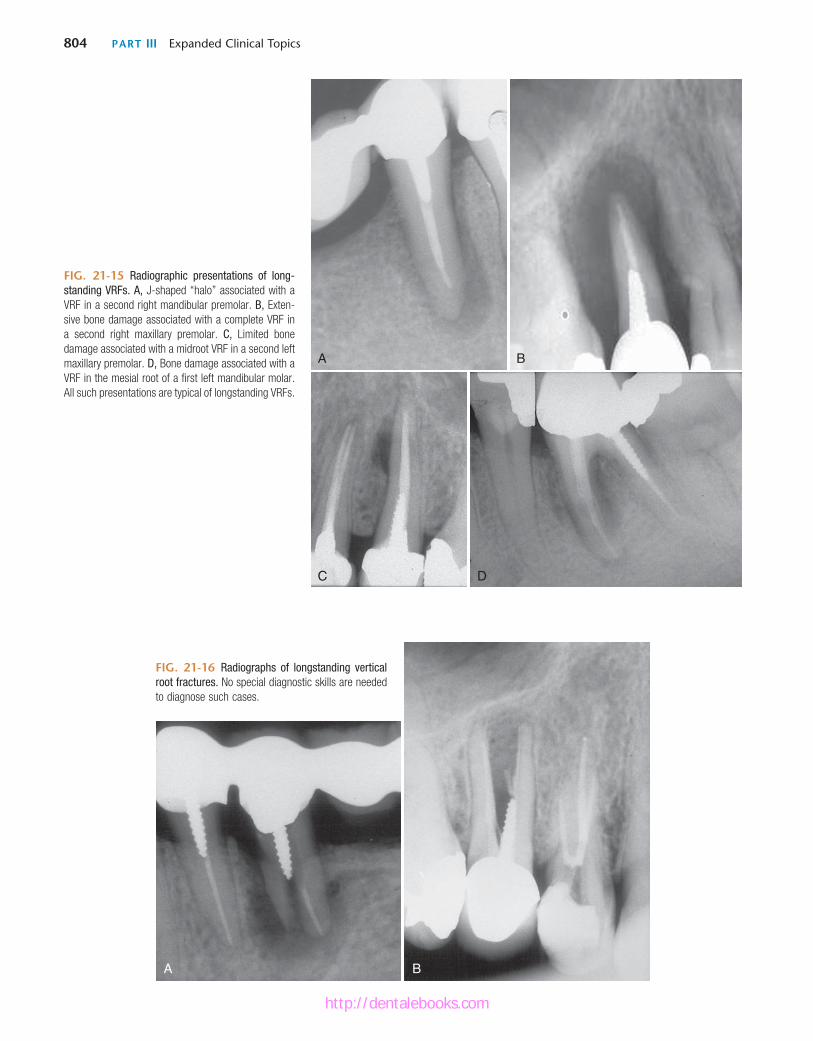
804 PART III Expanded Clinical Topics
FIG. 21-15 Radiographic presentations of long-standing VRFs. A, J-shaped “halo” associated with a VRF in a second right mandibular premolar. B, Exten-sive bone damage associated with a complete VRF in a second right maxillary premolar. C, Limited bone damage associated with a midroot VRF in a second left maxillary premolar. D, Bone damage associated with a VRF in the mesial root of a first left mandibular molar. All such presentations are typical of longstanding VRFs.
A B
C D
A B
FIG. 21-16 Radiographs of longstanding vertical root fractures. No special diagnostic skills are needed to diagnose such cases.
http://dentalebooks.com




















