
NEPHROTOXIC POTENTIAL OF HERBAL DRUGS
216
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of NEPHROTOXIC POTENTIAL OF HERBAL DRUGS


Message
Dear Friends,
East Delhi Physician Association is well known for its dedication in providing regular medical update to all its members and other physicians, which was well planed by our visionary founder members and has been carried out by our past executive committees year after year. EDPA's unity and excellent co-ordination among all executives and senior member has always been a good example to follow.
This year we have had two major events 'Family get together' and 'Mid Term CME' Family Get Together is a platform where all members and their families meet enjoy and share their experiences. The Bollywood's theme was extraordinary.
Mid Term CME on 'Infections Update' under chairmanship of Dr. Anil Motta and organizing secretary Dr. Vikas Jain and Dr. Jaya Jain was well appreciated by everyone.
Annual CME EDPACON 2014 is our most prestigious activity of the year. I am grateful to the chairman Dr. Rajiv Bansal and Organising Secretary Dr. Anirudh Lochan for their hard work to make EDPACON 2014 a success.
This time we have invited National level Speakers and also delegates from other parts of Delhi besides East Delhi and also from NCR including Noida, Gurgaon and Ghaziabad.
I am thankful to the 'Scientific Committee' of Dr. Ashok Grover, Dr. Rajiv Gupta, Dr. Vimal Nakra, Dr. Navin Atal and Dr. Nitin Sinha who have worked round the year. Our monthly CME's have been very successful and rich in scientific contents under their able guidance.
I am grateful to my 'Executive Committee' of Dr. Ajay Gupta (Secretary), Dr. Pankaj Choudhary, Dr. Naresh Aggarwal (Vice-Presidents), Dr. B.K. Tiwari (Finance Secretary) who have supervised all functions of EDPA around the year.
I am specially grateful to Dr. Paras Gangwal who has worked single handedly to bring out this excellent bulletin cum souvenir which has been designated as EDPA YEAR BOOK 2014. This is a compilation of more than 30 clinically relevant chapters including latest updates and guidelines for our day to day practice.
I am thankful to all the members for giving me all the support during my tenure as president of EDPA. All the work that we have done during the last two years would not have been possible without their support.
I wish EDPA to reach its epitome of a strong organization, with the same continuing support and active involvement of all the members.
Dr. LAlit
President, EDPA

Message
I wish all executives of EDPA good luck for the success of annual CME (EDPACON) 2014 who have been working hard for its success. This year conference is being taken to another level by the organising commitee.
I also hope the souvenir also is as good as last yrs.
Finally I wish for the sucess of the conference .
Dr N.K. GovilImm. Past President, EDPA

Message
Dear Friends,
I feel privileged and honored that I have been given the responsibility of organizing the 15th Annual Conference of EDPA 2014 (EDPACON 2014) to be held at Hotel Le Meridien, New Delhi on 7th Dec. 2014.
The aim of this scientific extravaganza is to upgrade ourselves with the latest developments in the field of Internal Medicine.
We have tried our best to cover the most latest and burning clinical topics through Sessions, Panel Discussions, Oration & Clinical Case Presentations.
For the very first time we are introducing the Clinical Case presentations by the PG students.
In the field of Diabetes we have two latest topics of -- Role Of Kidney in The Management of Type 2 Diabetes and Management of Post Prandial Hyperglycemia.
We are also conducting a session on EBOLA VIRUS INFECTION which is a major global threat to mankind.
This year's Bela Devi Oration has been conferred to the renowned Gastroenterologist Dr Prof. S K Sarin who will be speaking on Portal Hypertension.
We have two Panel Discussions , Acute Kidney Injury and Management of Haemoptysis.
Like previous years we have tried to get the best Speakers of National and International repute who are Masters in their respective fields.
For the first time , We have tried to involve big no of our fellow Physicians from other parts of Delhi & NCR .
In the end I would say that it's a Mega Conference and a Mega Scientific Event & I am sure that everyone will enjoy it.
I am really thankful to everyone and the organising committee for their continuous guidance and support.
I look forward to meet you at Hotel Le Meridien on 7th Dec 2014. Your valuable feedback and suggestions are most desired for future and keeping the scientific standards of the conference at highest levels.
Dr Rajeev BansalChairman, EDPACON 2014

Message
It gives me immense pleasure to welcome you all to our 15th Annual conference - EDPACON 2014. The conference has been meticulously planned and like previous years promises to be rich in Scientific knowledge. Over the years EDPACON has become an annual event that has been accepted and appreciated by medical fraternity.
I congratulate the organizing committee under the leadership of Dr Rajeev Bansal in making huge efforts to make this event a memorable one. They have been able to bring the top brass national experts as faculty for this conference.
This Annual conference being organised on such a large scale is thanks to the Vision, Dynamism and untiring efforts of our president Dr Lalit, Chairman Scientific committee Dr Ashok Grover, & Advisors Dr Vimal Nakra, Dr N K Govil, Dr M K Seth, Dr Vijay Arora.
I express my sincere thanks to Dr Pankaj Choudhry , Dr Naresh Agrawal Vice Presidents, Dr Anirudh Lochan Conference Secretary, and Dr B K Tiwari Treasurer for designing and execution of the scientific program.
This year apart from the regular monthly meeting we organised a hands on certificate workshop on ECHO in association with FORTIS Escorts.
My thanks & appreciation to Dr Anil Motta, Dr Jaya Jain, & Dr Vikas Jain for organising the INFECTIONS UPDATE 2014 (MIDCON) which again was a great success.
True to our commitment to bring a informative and educational Souvenir, Dr Paras Gangwal has been working day and night. I congratulate him for bringing the souvenir in this shape.
No conference can be successful without the active participation of the delegates, so a big thanks to all.
Dr. Ajay Kumar Gupta
Secretary EDPA

Message
Greetings to all my seniors!
Being the youngest organising secretary in the history of EDPACON has been a learning and nerve-wracking experience for me.
All over Delhi-NCR, EDPA is known as a body of physicians that is committed solely to academics, a reputation that has been well earned and maintained.
At EDPA, it is our costant endeavour to keep all our members, associates and students updated about the latest developments in medicine.
It is with this purpose in mind that EDPACON is held. It is perhaps the only conference where the topics, speakers, faculty and itenary are planned and decided by practicing physicians.
EDPACON has one sole purpose, and that is to address the questions that a physician is likely to face in his practice.
Given my inexperience, organising EDPACON would have been impossible, but for the continued support of Dr Pankaj Choudhary, Dr Rajiv Bansal, Dr Ajay Kumar Gupta, Dr Lalit Khari, Dr B.K.Tiwari, Dr Paras Gangwal, Dr Vimal Nakra, Dr Nitin Sinha,Dr NK Govil, Dr Anil Motta, Dr Rajiv lochan, Dr Naresh Aggarwal, Dr Vikas Jain,Dr Navin Atal and Dr Rajiv Gupta.
Last, but not the least, i would like to thank Shambhoo for his efficient and reliable support.
I would also like to apologise for any mistakes that i may have inadvertantly committed.
Thanking you
Yours sincerelyDr Anirudh LochanOrganising Secretary
EDPACON 2014

Message
Dear FRIENDS
It has always been a proud feeling and a great pleasure to be part of a vibrant organization Like “EAST DELHI PHYSICIAN ASSOCIATION”, where members and executives are in so much of unison and everything scientific or cultural is done with so much of enthusiasm and vigor, that bigger tasks look smaller and tough is made to look easier, where seniors cuddle juniors and would do anything to accommodate the request made by the fellow executive and colleague.
I am thankful to the Executives and Association to bestow me with responsibility, as an EDITOR to bring out it's NEWS AND VIEWS BULLETIN, which for practical reasons has been merged with our earlier activity of 'souvenir release' at our annual conference .This year we are going a step ahead to bring out a landmark publication in form of this booklet which is embraced in your hands as “EDPA YEAR BOOK 2014”, a concept which has long been in minds of earlier EDPA Executives and it's founder members, which further got a push again during HT SOCIETY ANNUAL CONFERENCE MEETING organized by Dr N.P. Singh ,where our senior founder members Dr Parkash Gera, Dr Ashok Grover expressed the desire and we took that hint and suggestion further with a always encouraging consent and go ahead and promise of all support in this project as always, of Current EDPA president Dr Lalit , past president Dr N.K. Govil , organizing chairman of EDPACON 2014 Dr Rajiv Bansal, secretary EDPA Dr Ajay Gupta, man in action Dr Pankaj Chaudhary and other executives and other senior members who were present there.
With kind cooperation of EDPA Executives, All the Authors & contributions from the invited faculty we have been able to compile more than 30 clinically relevant chapters, guidelines which should surely help us in keeping ourselves abreast with latest in fast evolving advances in field of clinical medicine, my heart filled thanks are due to all my authors and writers, who took out time from there busy schedules, to write such crisp write-ups, rich in scientific content and also for accommodating and acknowledging my requests of urgency.
I am highly thankful to my seniors Dr. Ashok Grover, Dr.Rajiv Gupta, Dr Rajiv Lochan, Dr. S.C. Chhabra, Dr. N.P. Singh, Dr. N.K. Govil, Dr. Lalit who has always supported and guided me by all means & also greatful to my close friends and colleagues Dr. Rajiv Bansal, Dr Pankaj Chaudhary, Dr. Aman Rohatgi, Dr. Amitabh Yaduvanshi, Dr. Ajay Gupta, Dr. Naresh Agarwal, Dr. Navin Atal, Dr. Vikas Jain, Dr. Jaya Jain, Dr. Kapil Khanna, Dr. Sri Ram Kabra, Dr.Amit Chhabra, Ms. Pragati, and last but not the least our newly found Gem of association Dr. Anirudh Lochan; all have always assured and extended there timely support, which has helped me to complete this mammoth task without much twinge.
To conclude I will request you all, to read all the inputs and give us your valuable feedback, which can be encouraging or learning for our team and can be accommodated in next edition. Also we wish to invite scientific inputs from all EDPA members and all the specialist physicians across Delhi and The Nation, as we would finally have a circulation to all physicians in Delhi and NCR & also EDPA YEARBOOK 2014 will be made available through a link at EDPA website (www.edpadelhi.com) and would be made available as soft version via Email on request.
Wishing a GREAT SUCCESS to all 'THE TEAM', for this EDPA YEAR BOOK 2014, and extra specially to our esteemed EDPACON 2014.!!
Dr. Paras GangwalEditor –in-chief : EDPA YEARBOOK 2014 News & Views Bulletin
Chairman, Souvenir Committee EDPACON 2014








PatronsDr Saroj Prakash, Dr G D Gupta, Dr Parkash Gera, Dr A S Dave,
Dr S C Chhabra, Dr Rajiv Lochan
Editor-in-chiefDr Paras Gangwal
EditorsDr Rajiv Bansal, Dr Navin Atal, Dr Aman Rohatagi, Dr Pankaj Choudhary
Editorial BoardInternal Medicine
Dr Ashok Grover, Dr N P Singh, Dr Lalit, Dr Nitin Sinha, Dr Jaya JainDr Vijay Arora, Dr. Subhash Tyagi
Cardiology
Dr Rajiv Passey, Dr Ajay Mittal, Dr Amitabh Yaduvanshi
GastroenterologyDr Neeraj Jain, Dr Deepak Lahoti, Dr Naresh Agarwal, Dr Vibhu Mittal
NeurologyDr B K Gupta, Dr Nitin Jain, Dr Rajesh Gupta
NephrologyDr Dilip Bhalla, Dr Neeru P Aggarwal, Dr Sriram Kabra
DiabetologyDr Rajeev Gupta, Dr Gulab Gupta, Dr Anil Motta
EndocrinologyDr R K Prasad, Dr Saptrishi
Oncology & HematologyDr Sameer Khatri, Dr Amit Upadhyay
PulmonologyDr Rajesh Gupta, Dr K K Pandey, Dr Praveen Pandey
Drug ReviewDr N K Govil, Dr Ajay Gupta, Dr Kapil Khanna, Dr Sunil Bhardwaj
Images in MedicineDr Vikas Jain, Dr Vimal Nakra, Dr Rajiv Gupta, Dr KJS Narula
Case ReportsDr Amit Chhabra, Dr Vijay Arora
Medical EthicsDr Anil Chaturvedi, Dr R K Gupta
1

EDPACON 2014Executive Members EDPA
President
Vice President
Imm Past President
Past President
Secretary
Jt. Secretary
Treasurer
Editor (News & Views)
Dr. Lalit
Dr. Pankaj Choudhry
Dr. Naresh Agarwal
Dr. N.K. Govil
Dr. B.K. Gupta
Dr. Ajay Kumar Gupta
Dr. Anirudh Lochan
Dr. B.K. Tiwari
Dr. Paras Gangwal
Scientific CommitteeChairman
Convener
Advisor
Dr. Ashok Grover
Dr. Nitin Sinha
Dr. Rajiv Gupta
Dr. Vimal Nakra
Dr. Navin Atal
Reception CommitteeDr. Anita Sehgal
Dr. Anupam Zutshi
Dr. Arjun Singh
Dr. Banarsi
Dr. Bharat Bhushan
Dr. Kartar Ahuja
Dr. L.M. Singh
Dr. Nirmala Lahoti
Dr. Praveen Roy
Dr. R.K. Gupta
Dr. Rajeev Garg
Dr. S.K. Johri
Dr. Sushil Garg
Dr. Sunil Arora
Dr. T.M. Agarwal
Dr. V.K. Gupta
Dr. Vijay Kumar
Dr. V.R. Sood
Souvenir CommitteeDr. A.K. Gupta
Dr. Amitabh Yadurvanshi
Dr. Amit Upadhyaya
Dr. Aman Rohtagi
Dr. Chako George
Dr. Harshita Tyagi
Dr. Jaya Jain
Dr. K.J.S. Narula
Dr. Kunaldas
Dr. Kapil Khanna
Dr. Mukesh Ajmera
Dr. Neeru P Agarwal
Dr. Nitin Sinha
Dr. Nitin Jain
Dr. Paras Gangwal
Dr. Rajesh Gupta (Pulmo)
Dr. Rajesh Gupta (Neuro)
Dr. Satish Goel
Dr. Saptrishi
Dr. Sameer Khatri
Dr. Sunil Bhardwaj
Dr. Vikas Jain
Dr. Sriram Kabra
Advisory CommitteeDr. A.S. Dave
Dr. Ajay Mittal
Dr. Anand Pandey
Dr. Anil Chaturvedi
Dr. Anil Motta
Dr. B.K. Gupta
Dr. Deepak Lahoti
Dr. N.P. Singh
Dr. Naresh Agarwal
Dr. Dilip Bhalla
Dr. G.D. Gupta
Dr. Gulab Gupta
Dr. K.S. Chaddha
Dr. M.K. Seth
Dr. Manoj Singhal
Dr. Mukesh Mehra
Dr. Rajesh Gupta
Dr. Rajiv Lochan
Logistics CommitteeDr. Pankaj Choudhry
Dr. Paras Gangwal
Registration CommitteeDr. Vijay Arora
Dr. Vikas Jain
Dr. L.M. Singh
Dr. Naresh Dang
Dr. Neeraj Jain
Dr. P.C. Bhalla
Dr. Parkash Gera
Dr. Rajesh Chawla
Dr. S.C. Chhabra
Dr. Saroj Prakash
Dr. S.N.A. Rizvi
Dr. S.K. Agarwal
Dr. Vijay Arora
2

ContentsSmt. Bela Devi OrationDr. S.K. Sarin
Scrub TyphusDr. N.K. Govil
Frequently asked questions on RabiesDr. Pankaj Nand Choudhry
Post Op FeverDr. Neeraj Goel
Primaquine: A must know Molecule for Ideal Malaria Management and ControlDr. Paras Gangwal
Diagnosis and Treatment of MalariaDr. Paras Gangwal
Approach to EosinophiliaDr. Ashok Grover
Approach to Patient with ThrombocytopeniaDr Amit Upadhyay
Management of Depression in Primary CareDr. Rajesh Kumar, Dr. Paramjeet Singh, Dr. Prerna Kukreti
Management of Alcohol withdrawal in Medical SettingsDr Pankaj Kumar, Dr Prerna Kukreti, Dr Amit Garg
Approach to the Patient & Pleural EffusionDr. Kamal Kumar Pandey
Pulmonary Fungal InfectionsDr. Praveen Pandey
Pulmonary Arterial HypertensionDr. Ashok Grover
Algorithm of 2014 Hypertension Management GuidelinesInput by Dr. Rajeev Bansal
Resistant HypertensionDr. Ajay U. Mahajan
Acute Coronary SyndromeDr Rajiv Passey, Dr Dileep K. Tiwari
Anticoagulation Update on the new oral Anticoagulants (NOACs)Dr Amitabh Yaduvanshi, Dr Mohan Nair
3
6
15
16
20
24
31
38
41
48
60
66
70
77
79
80
84
89

ContentsThrombolysis in Acute Ischemic StrokeDr. Vivek Kumar
Cerebral Granulomatous DiseaseSumanto Chatterjee, Bipin Kumar Gupta, Seema M. Maheshwari, Arushi Nautiyal, Chitra Yadav
Practical Tips in Management of a Patient with CKDDr Samir Tawakley
Anemia Management in CKD KDIGO Guidelines revisitedDr. Shri Ram Kabra, Dr Satish Chhabra, Dr Aditya Jayraman
Nice Guidelines for Management of Anemia in CKDInput by Dr. Rajeev Bansal, MD
Dialysis Interventions for Treatment of AKI Analyzing the KDOQI GuidelinesDr. Shri Ram Kabra, Dr Satish Chhabra, Dr Aditya Jayraman
Nephrotoxic Potential of Herbal DrugsNarinder P Singh Anupam Prakash Anish Gupta, ,
Management of Liver AbscessDr Naresh Agarwal
Acute Pancreatitis-Early Phase: Management DecisionsDr Vibhu Mittal
Recent Advances in the Treatment of Hepatitis CDr Deepak Lahoti, Dr Rohit Goyal, Dr Rajan Dingra
Consensus Statement and Proposed Guidelines by API for Insulin Therapy in Type2DMDr Rajiv Gupta
Premix Insulin Initiation & Patient Self Titration: Recent StudiesDr Indranil Bhattacharya
PPG and CVD RiskDr. Banshi Saboo
SGLT2 Inhibitors: A New Treatment Option for Type 2 DiabetesDr. Abdul Hamid Zargar
Subclinical Hypothyoidism Clinical Importance and Newer guidelines of ManagementDr. Amit Chhabra
Preventive Health Care: Why is it Important?Dr. Vikas Jain
Common age related Medical ProblemsDr. B. K. Tiwari
4
97
105
113
118
123
126
130
136
141
144
146
149
151
160
161
165
168
library
Highlight
library
Highlight

ContentsNuclear Medicine in Everyday Clinical PracticeDr Ashwani Gupta
Clinical Application of Magnetic Resonance Imaging: Current StatusDr. Suchit Aggarwal
Nutrition in ICUDr Kamal Lashkari, Dr Ashutosh Garg
Vasopressors and Inotropes in ICUDr. Ashutosh Garg, Dr. Sanjay Nihalani
A case of common but rarely thought of Urinary InfectionDr. Nitin Sinha
Deep Vein Thrombosis in Patients of Pulmonary Tuberculosis & Therapeutic ImplicationsDr. Nitin Sinha
Interesting Case of Thrombocytopenia Encountered during Antitubercular TherapyDr Ashok Grover, Dr. Arushi Notiyal, Dr. Pankaj Nand Choudhary
5
171
174
180
184
188
192
195
Smt. Bela Devi Oration
Smt. Bela Devi (1907-1995) was a great visionary, a lady of the future, who had long ago
realized the value of higher education. Inspire of being educated only upto third
standard, it did not deter her to think ahead of her time.
She was born in 1907 in a middle class family of Khurja, then a small town of district
Bulandshahr. UP married at a very young age of 15 years, she shifted to Shahdara, Delhi.
She was blessed with eight daughters and one son.
Educating her children was always a prime concern and objective of her life. This she
achieved against all odds. She was an ardent advocate of "Girls Education" ad was of the
firm belief that girls should be independent.
Shahdara was a small satellite town of Delhi. It was separated from it by the River Yamuna
and a thick forest. Only a Primary School existed for girls on this side of Yamuna. The only
mode of transportation available to further pursue their education (Middle and High
School and College) was a tonga or a train. One could only imagine the obstacles and
hardships faced by her children in those difficult times of pre-independence and
immediately after freedom.
Delhi was not her limit. She was also willing to encourage her children to go abroad if they
so desired. One can only imagine the odds against which she must have carried on. Her
life exemplifies that female foeticide is a big mistake which is depriving the society of
potentially great women. Thanks to her, that we have Dr. Saroj Prakash, one of her very
able daughters who rose to such heights that will make any mother proud. She is a
renowned physician and a great academician. She is also a founder member of our
association.
Rightly so, that her daughter has dedicated this oration in the memory of a legendary
lady, a loving and caring mother.
Smt. Bela Devi(1907-1995)
6

Beladevi Oration consists of a talk on a specified, unrivalled and unparalleled topic in
International Medicine of 30 minutes duration. The members of the association express
their reverence in the form of a medallion and a token money of rupees five thousand.
This is the 12th successive year in which this Oration is being delivered. Previously we
have been honoured with eminent dignitaries of great repute in their respective field.
Speaker Year Speciality Topic
Dr. Savitri Srivastava 2000 Paediatric Cardiologist Congenital Heart Diseases
Dr. Harbans S. Wasir 2001 Cardiologist Preventive Cardiology
Dr. P.S. Gupta 2002 Physician & Gastroenterologist PUO
Dr. G.K. Ahuja 2003 Neurologist Single CT Lesion
Dr. J.S. Guleria 2004 Cardiologist & Chest Physician Sarcoidosis
Dr. J.N. Pande 2005 Physician and Chest Specialist Interstitial Lung Disease
Dr. V.S. Sukhija 2006 Nephrologist Management of Renal Failure
Dr. B.N. Tondon 2007 Gastro Enterolgist Issues in Management Hepatitis B
Dr. A.N. Malviya 2008 Rheumatologist Distinction Between inflammatory
& Mechanical Arthritis
Dr. K.K. Malhotra 2009 Nehrologist Approach to CRF
Diagnostic Considerations and
Principles of Management
Dr. S.N. Chugh 2010 Professor of Medicine Medicosocial Implications of Pesticide (Aluminium Phosphide) Poisoning
Dr. M. Khallilulla 2011 Senior Interventional Cardiologist Journey of a Cardiologist- Goals Achieved & What's New on Horizon
Dr. Neena Valecha 2012 Director, National Institute of Current Perspective on Diagnosis & Malaria Research (ICMR), N. Delhi Treatment of Malaria
Dr. P.D. Gulati 2013 Sr. Consultant, Nephrologist Cardiovascular Morbidity in CKD Tirath Ram Shah Hospital, N. Delhi
This year's Bela Devi Orartion is being conferred on Dr. S.K. Sarin, Director, ILBS Hospital, Delhi, who is delivering
the oration on "Overview of Portal Hypertension".
7

Curruculum Vitae of
Prof. (Dr.) S.K. SarinMD, DM, FNA, FNASc
Senior Professor and Head, Department of Hepatology
D irector, Institute of Liver and Biliary Science (ILBS)
Adjunct Prof. Molecular Medicine, Jawahar Lal Nehru Univ., New Delhi
Prof. S.K. Sarin, is a Senior Professor of Hepatology and Director, Institute of Liver and Biliary Sciences (ILBS), New Delhi, a Deemed to be University, in the field of Liver and Biliary Diseases.
His research interests include Portal hypertension, Chronic hepatitis B and C, Liver Regeneration, Acute-On-Chronic Liver Failure and Liver Cancer.
He has published over 370 original articles in prestigious journals like New England Journal of Medicine, The Lancet, Annals of Internal Medicine, Gastroenterology and Hepatology. He has edited 9 books. He led the development of five major global guidelines for the Asian Pacific Association for the Study of the Liver (APASL).
He has received several awards including the Shanti Swarup Bhatnagar Award, Third World Academy of Medical Sciences (TWAS) International Prize, Om Prakash Bhasin Award, Ranbaxy Medical Sciences Award, The Dhanvantri Medical Award and the 'Best Teacher' Award, Amrut Mody Research Foundation Award, Fogarty International Fellowship, Dr. Dharamveer Datta Memorial Oration of ICMR, Mike Moshal Lecture of SAGES, South Africa, Silver Jubilee Research Award of MCI, Dr. Kunti Om Prakash Award of ICMR, Bhagwan Mahaveer Award, Malaysia Liver Foundation Award, Most Distinguished Physicians from India by American Association of Physicians of Indian origin USA. He was awarded the Padma Bhushan in 2007 for his overall seminal contributions to the Medical field in India.
He is the founding Chief Editor of a prestigious international Journal, Hepatology International (Springer International). Dr Sarin served as the President of Asian Pacific Association for the Study of the Liver (APASL).
8

Curruculum Vitae of
Dr. Parkash Chandra GeraLIFE TIME ACHIEVEMENT AWARD
Name : Dr. Prakash Chandra Gera
Address : 184, Ram Vihar, Opposite Yamuna Sports Complex, Vikas Marg, Extension, Delhi-110092.
Date of Birth : 15.10.1949
Qualifications : M.B.B.S (1972) & M.D. (Medicine) (1977) From Institute of Medical Sciences, B.H.U., Varanasi.
Medical Registration : Medical Council of India Delhi Medical Council. General Medical Council
Professional Experience : Worked as junior resident in Medicine form 03.02.1975 to 02.02.1977 at Institute of Medical Sciences, B.H.U., Varanasi. Thesis entitled "Study of coronary Arteries in Ischaemic Heart Disease (Clinical & Postmortem)" accepted during this period.
Worked as senior resident in Psychiatry from May 1977 to December 1977 at Lady Hardinge Medical College & Hospital.
Worked as senior resident in Medicine from December 1977 to June 1980 at Dr. R.M.L Hospital, New Delhi.
Worked in Chest Medicine in NHS, UK (1980-81).
Working as consultant Physician & Cordiologist in East Delhi since 1982. Actively involved in management of all type of cases of various fields of medicine, providing them Indoor and OPD service. Presently working as Senior Consultant & HOD, Department of Medicine with Pushpanjali Group of Hospital.
9

1) Pushpanjali Crosslay Hospital, NABH Accredited W-3, Sec-1 Vaishali Ghaziabad, NCR UP-201012
2) Pushpanjali Medical Centre A-14, Pushpanjali Vikas Marg Extn. Delhi-110092
Active Organiser Have been participating/ Organizing conferences/ seminars/ Workshops in the field of medicine for the last about 40 years at State Level & National Level
Editor Edited a book entitled "Manual of Medical Emergencies" of which 10,000 books have already been sold.
Founder Member East Delhi Physician Association
Member Life member - East Delhi Physician Association Life member- BHU Medical Association Life member- Association Physicians of India Life member- National academy of Medical Specialties Life member- Geriatric society of India Life member - Indian Society of Electrocardiography Life member- Indian Society of Critical Care Medicine. Life member Indian Society of Hypertension. Life member- Indian Medical Association. Life member - RSSDI
Extra Curricular Activities : Represented college in Cricket, Badminton and table Tennis
Actively involved in the activities of IMA & DMA since 1978. Member of DMA Executive for approximately 25 years. I have worked as Chairman/ co-chairman/ Convenor of various Committees / Sub- Committees for the last 30 years.
Founder Chairman - Children Welfare Society which is actively involved in betterment of children of trans-yamuna.
Other attachments Retired as Divisional Medical Referee LIC of India (Division II) Delhi after working of approximately 25 years
Medical Advisor to, i. MECON Ltd. (Govt. of India Enterprise) ii NALCO Delhi (Govt. of India Enterprises) iii Hindustan Copper Ltd. (Govt. of India Enterprise)
10

8.00 am - 8.30am Registration
8.30am -9.30amCase presentation by Post Graduate Students Chairpersons Dr N P Singh, Dr N K Govil, Dr Rajeev Bansal,Dr Pankaj Choudhary
9.30am-10.10amPostprandial hyperglycemia Speaker Dr Banshi SabooChairpersons Dr Anupam Prakash, Dr Vijay Arora, Dr Saptarshi Bhattacharya
10.10am-10.50amEmerging concepts in the management of dyslipidemiaSpeaker Dr Rajesh RajputChairpersons Dr Rajeev Lochan, Dr Subhash Chandra, Dr Anil Chaturvedi
10.50am-11.20am Tea Break
11.20pm-12.00pm Role of Kidney in the management of type II Diabetes MellitusSpeaker Dr A H ZargarChairpersons Dr Rajiv Gupta, Dr Rajeev Chawla,, Dr Anil Motta
12.00pm -12.40pm Panel discussion on AKIModerator Dr N P SinghPanelists Dr S C Chhabra, Dr Naresh Dang, Dr Manoj Arora, Dr Ravi Bansal
12:40pm-1.00pmLifetime Achievement Award & Souvenir Release
1.00pm-1.40pmGuest Oration "Overview of Portal Hypertension" Speaker Dr S K Sarin
1.40pm -2.30pm Lunch
2.30pm -3.10pmWhat we should know about Ebola VirusSpeaker Dr A K GadpayleChairpersons Dr (Prof) Rajendra Kapila, Dr (Prof) S Anuradha, Dr Ashok Grover, Dr Vimal Nakra
3.10pm-3.50pmManagement of Resistant hypertensionSpeaker Dr Ajay MahajanChairpersons Dr Parkash Gera, Dr M P S Chawla, Dr Sandeep Garg
3.50pm-4.30pmRole of Ketoanalogues in Renal Failure Speaker Dr Ashwani GuptaChairpersons Dr Dilip Bhalla, Dr Neeru Agarwal, Dr Himanshu Mahapatra
4.30pm-5.00pm Tea Break
5.00pm-5.40pmPanel discussion on the management of HemoptysisModerator Dr Praveen PandeyPanelists Dr Rajesh Gupta, Dr K K Pandey, Dr Deepak Hans, Dr L M Darlong
5.40pm-6.00pmValedictory Ceremony
11
Scie
ntif
ic P
rogr
amm
e

Dear Friends
Our guru's have always tought us prevention is better than cure. Also Louis Pasteur said “When meditating over a disease I never think of finding a remedy for it but instead a means of prevention”.
The very reason that we immunize our children, is that they are naïve, frail and vulnarable and we are cocerned for their morbidity and mortality and surely we love them; also applies to adult practices, then what makes us less smarter than our paediatric collegues who always talk of universal immunization and we as adult practitioner are always in a dilemma, when we think about vaccination in adults, is because of our mind set and training 'not to practice it' and lack of conviction and comfort within us ,which is mainly because of lack of fine details of our knowledge about vaccines, that we have not even seen those vials and syringes live and we have no idea about their schedule, indications and contra indications.
Friends it is time that we catch up with our deficiencies and realise that even in adults, immunity wanes over time and we are vulnerable to serious life threatening infections like pneumococcus, influenza and many other vaccine preventable diseases (VPD)
Which are causing almost 200 times more deaths as compared to children.
When we so commonly use aspirin for CVD prevention based on guidelines then despite being from so premier institutes and so many guidelines on VPD we do not adapt it in our practice. We know that those age less than 60 years are prescribed only 25 to 30% vaccination and even in more vulnerable groups above age 65 years vaccination coverage is only 60 % even in U.S.
So in lieu of high prevalance of VPD,we have a reason
to be convinced & it is our responsibility to practice it with full force.
Through this editorial I wish to enlighten all of us with respect to our comforts in prescribing by means of indepth understanding of the vaccination schedule and vaccine prescribing information of each vaccine which can be grasped to a significant understanding by a glance at vaccination chart for adults (table on page no 202). I am covering pneumococcal vaccination and hepatitis vaccination in detail in this part of editorial and remaining will be continued as some chapter in later edition of the EDPA YEAR BOOK.
Editorial
Dr. Paras GangwalMD (Medicine)Editor-in-Chief, EDPA Year Book 2014
Let's make Adult Immunization a Habit: Be Convinced & Ready to Prescribe
12

PNEUMOCOCCAL CONJUGATE (PCV13) VACCINATIONNot all our Internal Medicine Practice Patients need this only 20% May Need
• Adults aged 19 years or older with immuno-compromising conditions (including chronic renal failure and nephrotic syndrome), functional or a n a t o m i c a s p l e n i a , cerebrospinal fluid leaks, or cochlear implants who have not previously received PCV13 or PPSV23 should receive a single dose of PCV13 followed by a dose of PPSV23 at least 8 weeks later.
- RENAL PATIENTS
- ASPLEENIC
- CSF LEAKS
- COCHLEAR IMPLANTS
WOULD NEED BOTH PCV13 --------------PPSV23
IF FRESH :
FIRST PCV 13 8 WEEKS LATER PPSV23
• Adults aged 19 years or older with the aforementioned conditions who have previously received 1 or more doses of PPSV23 should receive a dose of PCV13 one or more years after the last PPSV23 dose was received. For adults who require additional doses of PPSV23, the first such dose should be given no sooner than 8 weeks after PCV13 and at least 5 years after the most recent dose of PPSV23.
PPSV23 ALREADY RECEIVED
1 OR MORE YEARS LATER PCV13
PPSV23 FIRST DOSE GIVENND
5 YEARS LATER PPSV 2 DOSE
• When indicated, PCV13 should be administered to patients who are uncertain of their vaccination status history and have no record of previous vaccination.
• Although PCV13 is licensed by the U.S. Food and Drug Administration for use among and can be administered to persons aged 50 years or older, ACIP recommends PCV13 for adults aged 19 years or older with the specific medical conditions noted above.
FDA APPROVES
PCV 13 TO ANY PERSON ABOVE 50 YEARS
ACIP RECOMMENDS
ADULTS AGED 19+ YEARS IF HAVE SPECIFIC MEDICAL CONDITIONS
PCV 13 DOSAGE AND ADMINISTRATION
Preparation for Administration
Since this product is a suspension containing an adjuvant, shake vigorously immediately prior to use to obtain a homogenous, white suspension in the vaccine container. Do
not use the vaccine, if it cannot be resuspended. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration. This product should not be used if particulate matter or discoloration is found. Do not mix Prevnar 13 with other vaccines/products in the same syringe.
Administration Information
For intramuscular injection only.
Each 0.5ml dose is to be injected intramuscularly using a sterile needle attached to the supplied prefilled syringe. The preferred sites for injection are the anterolateral aspect of the thigh in infants and the deltoid muscle of the upper arm in toddlers, children and adults. The vaccine should not be injected in the gluteal area or areas where there may be a major nerve trunk and/or blood vessel.
PNEUMOCOCCAL POLYSACCHARIDE (PPSV23) VACCINATION• When PCV13 is also indicated, PCV13 should be given
first .
• Vaccinate all persons with the following indications:
(ALMOST 80% OF THOSE IN A INTERNAL MEDICINE CONSULTANT CLINIC)
all adults aged 65 years or older;
adults younger than 65 years with chronic lung disease (including chronic obstructive pulmonary disease, emphysema, and asthma), chronic cardiovascular diseases, diabetes mellitus, chronic renal failure, nephrotic syndrome, chronic liver disease (including cirrhosis), alcoholism, cochlear i m p l a n t s , c e r e b r o s p i n a l f l u i d l e a k s , immunocompromising conditions, and functional or anatomic asplenia (e.g., sickle cell disease and other hemoglobinopathies, congenital or acquired asplenia, splenic dysfunction, or splenectomy [if elective splenectomy is planned, vaccinate at least 2 weeks before surgery]);
residents of nursing homes or long-term care facilities; and
adults who smoke cigarettes.
• Persons with immunocompromising conditions and other selected conditions are recommended to receive PCV13 and PPSV23 vaccines. See above notes for information on timing of PCV13 and PPSV23 vaccinations.
• Persons with asymptomatic or symptomatic HIV infection should be vaccinated as soon as possible after their diagnosis.
• When cancer chemotherapy or other immuno-suppressive therapy is being considered, the interval between vaccination and initiation of immuno-suppressive therapy should be at least 2 weeks. Vaccination during chemotherapy or radiation therapy should be avoided.
13

VACCINE 2 WEEKS LATER CHEMO OR IMMUNOSUPPRESSIVE THERAPY
• Routine use of PPSV23 vaccine is not recommended for American Indians/Alaska Natives or other persons younger than 65 years unless they have underlying medical conditions that are PPSV23 indications. However, public health authorities may consider recommending PPSV23 for American Indians/Alaska Natives who are living in areas where the risk for invasive pneumococcal disease is increased.
• When indicated, PPSV23 vaccine should be administered to patients who are uncertain of their vaccination status and have no record of vaccination.
Rule: Not Sure of Vaccination Status? Vaccinate if Indicated..!!!
PNEUMOVAX 23 PRESCRIBING INFORMATION
PNEUMOVAX 23 (Pneumococcal Vaccine Polyvalent) is a sterile, liquid vaccine for intramuscular or subcutaneous injection. It consists of a mixture of highly purified capsular polysaccharides from the 23 most prevalent or invasive pneumococcal types of Streptococcus pneumoniae, including the six serotypes that most frequently cause invasive drug-resistant pneumococcal infections among children and adults in the United States. The 23-valent vaccine accounts for at least 90% of pneumococcal blood isolates and at least 85% of all pneumococcal isolates from sites which are generally sterile as determined by ongoing surveillance of U.S. data.
PNEUMOVAX 23 is manufactured according to methods developed by the Research Laboratories. Each 0.5 ml dose of vaccine contains 25 μg of each polysaccharide type in isotonic saline solution containing 0.25% phenol as a preservative.
Pneumovax 23 Dosage and Administration
Do not inject intravenously or intradermally.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. PNEUMOVAX 23 is a clear, colorless solution. The vaccine is used directly as supplied. No dilution or reconstitution is necessary. Phenol 0.25% has been added as a preservative.
It is important to use a separate sterile syringe and needle for each individual patient to prevent transmission of infectious agents from one person to another.
Withdraw 0.5 mL from the vial using a sterile needle and syringe free of preservatives, antiseptics, and detergents.
Administer a single 0.5 mL dose of PNEUMOVAX 23 subcutaneously or intramuscularly (preferably in the deltoid muscle or lateral mid-thigh), with appropriate precautions to avoid intravascular administration.
Store unopened and opened vials at 2-8°C (36-46°F). All vaccine must be discarded after the expiration date.
Use With Other Vaccines
The ACIP states that pneumococcal vaccine may be administered at the same time as influenza vaccine (by separate injection in the other arm) without an increase in side effects or decreased antibody response to either vaccine. In contrast to pneumococcal vaccine, influenza vaccine is recommended annually, for appropriate populations.
Revaccination and Understanding sequential usage of pcv13 and ppsv23
Editorial continue end of all articles (at page no. 201 & 202)14

Scrub Typhus
Introduction
This illness was first detected in Japan in 1899. Actually word typhus is a greek word meaning fever with stupor. It is a reemerging disease in India in which all ages are affected. It is caused by a bacteria known as ricketsia tsutsugamushi which has been renamed as orientia tsutsugamushi. Tt is transmitted to humans by arthopod vector of trombiculidae family commonly as mites. This disease is endemic in an area starting from northen Japan to Pakistan in West, East Russia in north to northen Australia in South. This is also known as tsutsugamushi triangle.it is prevalent in many parts of India in subhimalayan region but has also been reported from south. Pathogen orientia tsutsugamushi is a intracellular gram negative bacteria with multiple serotypes which makes it difficult to make vaccines against this bacteria as no single strain conforms immunity against all sero types. Mites also known as chiggers are primary reservoir for this disease. Once infected by bacteria they remain infectious throughout thier life span. Incubation period of the disease is from 7-21 days mean 10-12 days clinical features first sign of illness is usally a eschar (vesicular) lesion at the sight of bite or an ulcer it is usually seen in axilla, groin, genitalia, this is followed by fever, severe headache, myalgias, all of which starts very abrubtly. Spotted rash may also appear on trunk. Headache is important criterion for suspicion of disease if the disease is not detected or treated properly serious complications may follow which include pneumonitis, ards ac hepatic failure meningitis dic myocarditis it may also involve git tract, manifesting as bleeding diagnosis haemogram m a y b e n o r m a l o r s h o w l e u c o c y t o s i s , thrombocytopenia increase in level of transaminases in around 75%- 90% cases decrease in albumin levels in
50%. USG may show hepatosplenomegaly, xray chest will show peumonitis, or pleural effusion. Specific test weil felix test 50 % pts have +ve test during 2nd week. indirect immunofluroescence antibody can be performed if available. Elisa for igm antibody to o.tsutsugamushiis also available pcr from skin lesion,lymph node biopsiesoe blood (edta) culture studies can also be done but time taken is around 27 days.
Treatment
Recommended treatment duration is from 7 to 14 days treatment should be started early if the suspicion is strong. Doxycycline is drug of choice given in 2 doses as 100 mg each. In children and pregnant patients azithromycin in dose of 500mg daily can be given rifampicin is also can be used but can be given in combination with either of the 2 drugs, for fear of development of ressistance fever disappears rapidly,which is chacterstic, supportive treatment has to be good to prevent progression to dic or septic shock. Mortality is 0% to 30% in untreated pts. But tend to vary, depending on time of diagnosis, age of pt, or development of complications prevention avoidance of mite infestaed area. Use of protective clothing, use of clothes impregnted with benzyl benzoate or permethrin. Application of repellants on exposed areas of body use of chemicals in soil infested with mites chemoprophylaxis in form of doxycycline 200mg once a wk is effective.
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Dr. Neeraj GovilMD (Medicine)Sr. Consultant Medicine, Goel Hospital
Dilshad Garden, Delhi Timings: 9.00am-10.30am, 6.00pm-8.00pmPanchsheel Garden, Shahdara Timings: 10.30am-12.30amDr. Roshan Lal Hospital, Naveen Shahdara, Delhi Timings: 12.30pm-1.30pm, 8.00-9.00pmGoyal Hospital Centre, Krishna Nagar, Delhi Timings: [email protected]
Q 1: HOW DOES ONE TREAT AN ANIMAL BITE?
If a person is bitten by an animal:
● Wounds should be washed and flushed immediately with soap and water for 10–15 minutes. If soap is not available, flush with water alone. This is the most effective first-aid treatment against rabies.
● Wounds should be cleaned thoroughly at the health care facility with 70% alcohol or povidoneiodine.
● Assess the vaccination status: e.g. whether diphtheria, pertussis, tetanus (DPT) or tetanus toxoid vaccination has been given in the past. Tetanus toxoid should be inoculated when necessary.
● Antimicrobials should be prescribed to prevent possible bacterial infection.
Q 2: WHAT SHOULD NOT BE DONE WITH AN ANIMAL BITE WOUND?
Avoid:
● Covering the wound with dressings or bandages.
● Suturing which facilitates further inoculation of rabies virus.
— If necessary for closing large wounds, suturing should be done after infiltration of wound with rabies immunoglobulin (RIG). Rabies immunoglobulin of human origin (HRIG) is expensive and only limited amounts are available. Rabies immunoglobulin of equine origin (ERIG) is available in many countries and is considerably cheaper than HRIG.— The sutures should be loose and not interfere with free bleeding and drainage. It is well established that secondary suture of bite wounds results in better cosmetic outcomes.
Q 3: WHAT ARE THE INDICATIONS FOR POST-EXPOSURE RABIES PROPHYLAXIS (PEP)?
The WHO Expert Consultation on Rabies (2013) has categorized rabies risk based on category of exposure and made recommendations for PEP
1. Touching or feeding animals. Liicks on intact skin. Contact of intact skin with secretions or excretions of a rabid animal or human case
Recommendation: None, if reliable history is available
II. Nibbling of uncovered skin Minor scratches or abrasions without bleeding
R e c o m m e n d a t i o n : A d m i n i s t e r v a c c i n e immediately. Stop treatment if animal remains healthy throughout an observation period of 10 days or is proven to be negative for rabies by a reliable laboratory using appropriate diagnostic techniques.
III. Single or multiple transdermal bitesd or scratches, licks on broken skin Contamination of mucous membrane with saliva (i.e. licks) Exposure to bats.
Recommendation: Administer rabies vaccine immediately and rabies immunoglobulin, preferably as soon as possible after initiation of p o s t - e x p o s u r e p r o p h y l a x i s . R a b i e s immunoglobulin can be injected up to 7 days after first vaccine dose administration. Stop treatment if animal remains healthy throughout an observation period of 10 days or is proven to be negative for rabies by a reliable laboratory using appropriate diagnostic techniques
Q 4: CAN THE RABIES VACCINE AND I M M U N O G L O B U L I N B E G I V E N TO A PREGNANT WOMAN OR A LACTATING MOTHER?
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Frequently asked questions on Rabies
Dr. Pankaj Nand ChoudhryMD(Medicine)Associate ConsultantPushpanjali Crosslay Hospital, Vaishali,Ghaziabad(U.P.)

Yes. All modern rabies vaccines are inactivated, safe and potent and can be given to pregnant women or lactating mothers. It has no effect on fetal development during pregnancy or breastfed infants during lactation. The rabies virus is not known to cross the placental barrier in women and healthy babies have been born via caesarean section.
Q 5: WHAT TYPES OF RABIES VACCINES ARE AVAILABLE?
Rabies vaccines in use can be categorized on the basis of their origin, as follows:
● tissue culture origin
● embryonated egg origin.
Modern rabies vaccines are commercially available as human diploid cell vaccine (HDCV), purified Vero cell rabies vaccine (PVRV), purified chick-embryo cell vaccine (PCECV) and purified duck embryo vaccine (PDEV).
Q 6: WHAT IS THE STANDARD VACCINATION SCHEDULE FOR RABIES PROPHYLAXIS?
Modern rabies vaccines are administered for pre-exposure and post-exposure prophylaxis and the
vaccination schedule is determined accordingly.
Pre-exposure prophylaxis
Intramuscular administration: One dose of vaccine is administered intramuscularly on each of days 0, 7 and 21 or 28.
Intradermal administration: One intradermal injection of 0.1 ml is given on each of days 0, 7 and 21 or28. To maximize savings, sessions of intradermal pre-exposure prophylaxis should involve enough individuals to use all opened vials within 6 hours.Three doses/three visits
IM or ID one dose each on day 0, day 7, and day 21 or 28.Day 0 means day of first vaccination, not necessarily day of bite.
Post-exposure prophylaxis (PEP)
There are three vaccination schedules for this purpose:
Five- versus four-doses IM regimen (“Essen” regimen)
One dose of vaccine is administered intramuscularly on days 0, 3, 7, 14 and 28. Injections must be given in the upper arm (deltoid region) or, in small children, into the anterolateral thigh muscle. Vaccines should never be administered into the gluteal region or the buttocks, where absorption is unpredictable.
The reduction in doses (four doses IM regimen) for PEP recommended by the Centers for Disease Control and Prevention (CDC) in Atlanta, USA, was based in part on studies that indicated that four vaccine doses in combination with rabies immune globulin (RIG) elicited adequate immune responses, and that a fifth dose of vaccine did not contribute to more favourable o u t c o m e s . ( h t t p : / / w w w . c d c . g o v / mmwr/preview/mmwrhtml/rr5902a1.htm)
Full Essen regimen (five visits/with or without RIG)
IM one dose each on day 0, day 3, day 7, day 14 and day 28.
IM one dose each on day 0, day 3, day 7 and day 14.18Shortened Essen regimen (four visits/four doses with or without RIG)
IM one dose each on day 0, day 3, day 7 and day 14.
Rabies PEP should be administered using a five-dose IM regimen for persons with immunosuppression.
The first dose should be administered as soon as possible after exposure (day 0).
Day 0 means day of first vaccination, not necessarily day of bite.
Abbreviated multisite IM regimen (Zagreb regimen), four doses/three visits (2-1-1) regimen
One dose of vaccine is administered intramuscularly into the left and one into the right upper arm (deltoid region) on day 0 followed by one dose into the upper arm (deltoid region) on days 7 and 21. This schedule saves two clinic visits and one vaccine dose.
Multisite intradermal (ID) vaccination schedule
Updated Thai Red Cross (TRC) regimen/twosite ID schedule (2-2-2-0-2)
One dose each (0.1 ml) is given at two sites, on both arms (over deltoids) on day 0, day 3, day 7 and day 28.The standard schedule is recommended in designated health-care facilities by trained health professionals under the supervision of a medical officer.
Q 7 . A R E T H E R E A N Y S H O R T E R INTRADERMAL (ID) PEP REGIMENS?
There are clinical trials to shorten PEP in order to improve patient compliance for the full course of vaccination. A four-site one-week PEP regimen (4-4- 4) has been proposed to replace the Thai Red Cross (TRC) regimen, given by four-site ID injections on days 0, 3 and 7. The immunogenicity study results are promising. WHO has recommended further assessment of this regimen through a well-designed study.
17
Q 8.WHAT ARE THE IMPORTANT POINTS TO BE CONSIDERED WHILE ADMINISTERING MODERN RABIES VACCINES?
All rabies vaccines are available as single-dose vials for IM use and must be given in the deltoid region (i.e. upper arm, near the shoulder) or, in small children, into the anterolateral area of the thigh
muscle (on the upper thigh). As with other injections, the rabies vaccine should not be given in the gluteal region (buttocks) because of low absorption due to the presence of adipose (fat) tissue.
● The IM or ID dose is same for all age groups.
● It is desirable to use the same type of modern rabies vaccine for the full course of vaccination, such as HDCV, PVRV, PCECV or PDEV.
● All the rabies vaccines can be used for IM regimen, but only PVRV and PCECV are approved for ID.
● Antibody response to ID regimen has been unsatisfactory in some groups receiving chloroquine for anti-malarial chemoprophylaxis, therefore an IM regimen should be used in such cases.
Q 9: WHAT IS RABIES IMMUNOGLOBULIN (RIG) AND HOW IT IS USED?
RIG is a biological product which is used to provide immediate readymade antibodies until the patient's own immune system responds to immunization. RIG may be of human or animal origin.
● Equine rabies immunoglobulin (ERIG)
● Human rabies immunoglobulin (HRIG).
The dose calculation is done as follows:
● ERIG – 40 IU/kg body weight with a maximum of 3000 units
● HRIG – 20 IU/kg body weight with a maximum of 1500 units.For all category III bites, RIG should be given immediately after the incident. RIG should be infiltrated as much as possible in and around all wounds. After infiltration of the wounds, if there is any remaining RIG, i t should be g iven intramuscularly on the anterolateral region or deltoid region. Anti-rabies vaccines should then be administered, preferably on the same day, but at a different site (right arm for vaccine and left arm for serum, or vice versa).
● RIGs remain in short supply throughout the world, but new technology capable of producing monoclonal antibodies (MAbs) against rabies might help increase the supply of RIGs globally.
Q10: WHAT PRECAUTIONS SHOULD BE TAKEN WHILE ADMINISTERING RIGS?
All emergency drugs and facilities for managing any adverse reactions must be available.
● The RIG vial(s) taken out from refrigerator should be kept outside for a few minutes before administration to the patient (to warm to room/ body temperature).
● RIG should preferably be administered before administering the anti-rabies vaccination. It should, however, never be administered later than 7 days after start of vaccination as it then will suppress native antibody production.
● RIG should not be administered in the same syringe as the vaccine, or at the same site as the vaccine.
● While infiltrating RIG into bite wounds, care must be taken to avoid injecting into blood vessels and nerves. Anatomical feasibility must always be kept in mind while injecting RIG.
● While injecting into finger tips, care must be taken to avoid compartment syndrome*.
● In small children with multiple bites, if the volume is insufficient for infiltration in and around all wounds, RIG should be diluted with sterile normal saline to double or three times the volume.
● Keep the patient under observation for at least 1 hour after ERIG administration before sending him or her home.
● The patient should not be given RIG on an empty stomach.
● Pregnancy is not a contraindication for RIG and anti-rabies vaccination.
Q 11: IS IT NECESSARY TO PERFORM AN A N T I B O D Y T E S T O N T H E PAT I E N T FOLLOWING ANTI-RABIES VACCINATION?
It is not necessary on a routine basis when human rabies vaccines are properly stored and given according to the approved schedule in a healthy individual. It is recommended only under special medical conditions, such as for immunocompromised patients, or in cases of delayed vaccination, or cases of frequent exposure to the rabies virus. Such patients require special wound care and careful immunoglobulin infiltration into the wounds.
Q 12:ARE THERE ANY CONTRAINDICATED DRUGS OR DIETARY RESTRICTIONS DURING ANTI-RABIES VACCINATION?
All immunosuppressive drugs are contraindicated
18

during vaccination such as steroids, chloroquine (anti-malarial drug) and anti-cancer drugs. If thesedrugs cannot be avoided and the patient is in an immunocompromised state, the IM regimen must be followed by infiltration of site of bite wound with RIG. Monitoring of antibody titration is recommended in such patients where possible.
There are no dietary restrictions during the course of vaccination.
Q.13: IS THERE ANY POSSIBILITY OF FAILURE AFTER PEP?
There are occasional human rabies cases reported despite PEP, due to various factors related to negligence and individual health status. Most cases have been reported due to delayed vaccination, or non-use of rabies immunoglobulin in category III exposure, or incomplete course of vaccination. Some cases are related to immunocompromised status such as HIV/AIDS, cirrhosis or use of chloroquine, steroids or anti-cancer drugs. Unexplained failure in cases where everything was apparently done correctly have also been documented.
Q 14: IF A PREVIOUSLY IMMUNIZED PERSON IS BITTEN BY A RABID DOG AGAIN, WHAT IS T H E R E - E X P O S U R E VA C C I N AT I O N SCHEDULE?
If a person has been previously fully vaccinated against rabies using a modern rabies vaccine, either for pre-exposure or post-exposure vaccination by IM or ID route, only two doses of vaccines are given on days 0 and 3. (However, a full vaccination course is recommended for those previously vaccinated with nerve tissue vaccine.)
Persons previously immunized against rabies have two distinct comparative advantages.
● It is not necessary to administer RIG, even in a category III exposure.
Pre-vaccination leads to added protection by inducing memory cells causing an accelerated immune response when a booster dose of vaccine is administered. This is the reason why parents are encouraged to vaccinate their children against rabies, because they are most vulnerable to dog bites and category III exposure.
Q 15: ARE THERE ANY ADVERSE EFFECTS OF RABIES VACCINATION?
Mild symptoms such as pain, redness, irritation or swelling at the site of injection may occur. Generalized
symptoms such as headache, fever and influenza-like illness might be observed in some patients.
All these adverse effects are temporary and self- limiting and rarely need medication. All patients should be told about the possible adverse effects, but they must be advised that it is essential to continue vaccination – even if there are local or mild systemic adverse reactions.
Q 16: IS THERE ANY POSSIBILITY OF FAILURE AFTER PEP?
There are occasional human rabies cases reported despite PEP, due to various factors related to negligence and individual health status. Most cases have been reported due to delayed vaccination, or non-use of rabies immunoglobulin in category III exposure, or incomplete course of vaccination. Some cases are related to immunocompromised status such as HIV/AIDS, cirrhosis or use of chloroquine, steroids or anti-cancer drugs. Unexplained failure in cases where everything was apparently done correctly have also been documented.
Q 17: DO WE NEED TO CONSIDER SPECIFIC VACCINE POTENCY FOR ID VACCINATION?
No. There has been concern as single IM doses are reconstituted in different volumes depending on manufacturers. The WHO-recommended minimum potency is 2.5 IU per IM dose and the WHO- recommended volume of a single dose of rabies vaccine administered per ID site is 0.1 ml.
Q 18: IS IT NECESSARY TO PERFORM A SKIN SENSITIVITY TEST WHILE USINGERIIG?
Most ERIG products currently being manufactured are highly purified and the occurrence of adverse events has been significantly reduced. There are no scientific grounds for performing a skin test prior to administering ERIG because testing does not predict reactions, and it should still be given whatever the result of the test.
The treating physician should be prepared to manage anaphylaxis which, although rare, could occur during any stage of administration. However, some manufacturers of ERIG still recommend performing a skin test. It should be kept in mind that a negative skin test does not guarantee that anaphylaxis would not occur.
19

INTRODUCTION — Fever above 38ºC (100.4ºF) is common in the first few days after major surgery. Most early postoperative fever is caused by the inflammatory stimulus of surgery and resolves spontaneously but my as well be caused by infectious etiologies which may require aggressive antibiotic therapy. So it is pertinent for treating physicians to know the “ABC” of post operative fever to avoid unnecessary tests, antibiotics and undue harassment to oneself and the patient.
PATHOPHYSIOLOGY OF POSTOPERATIVE FEVER — Fever is a manifestation of cytokine release in response to a variety of stimuli. Fever-associated cytokines are released by tissue trauma and do not necessarily signal infection. The magnitude of the trauma is correlated with the degree of the fever response. For example, laparoscopic cholecystectomy is associated with less tissue trauma and fewer episodes of postoperative fever than is open cholecystectomy.
DIFFERENTIAL DIAGNOSIS BASED ON THE TIMING OF FEVER — The timing of fever after surgery is one of the most important factors to consider in generating a prioritized differential diagnosis of postoperative fever (figure 1). The timing of postoperative fever can be usefully described as:· Immediate — onset in the operating suite or within
hours after surgery· Acute — onset within the first week after surgery· Subacute — onset from one to four weeks following
surgery· Delayed — onset more than one month after
surgery
Immediate — The potential causes of fever in the immediate operative and postoperative period are
mainly limited to: medications or blood products to which the patient was exposed during preoperative care; trauma suffered as part of surgery. The vasodilation that often accompanies these reactions makes hypotension a common presenting sign. Fever due to the trauma of surgery usually resolves within two to three days. It is strongly advised against considering infectious etiology during this phase. Malignant hyperthermia — Malignant hyperthermia is an inherited disorder most commonly manifesting as hypermetabolism during general anesthesia. MH-susceptible patients have genetic skeletal muscle receptor abnormalities allowing excessive calcium accumulation in the presence of certain anesthetic triggering agents. Prompt recognition of the initial clinical signs and treatment with dantrolene limits the morbidity and mortality associated with this disorder.
Acute — There are many causes of fever in the first week after surgery. Nosocomial infections are common during this period. Patients receiving mechanical ventilation during surgery are at risk for ventilator-associated pneumonia (VAP). UTI is a frequent cause of postoperative fever in patients with indwelling urethral catheters. UTI is more common in patients who have undergone a genitourinary procedure and in those who have chronic, indwelling catheters prior to surgery. Acute fever can also be caused by noninfectious conditions. Pancreatitis, myocardial infarction, pulmonary embolism, thrombophlebitis can complicate the acute postoperative period.
Subacute — SSI is a common cause of fever more than one week after surgery. Fever from antibiotic-associated diarrhea, typically attributed to Clostridium difficile, also occurs more commonly during this
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Post Op FeverDr. Neeraj GoelAssoc. Professor & ConsultantDepartment of Clinical Microbiology and ImmunologySir Ganga Ram Hospital

period. Febrile drug reactions are a frequent cause of subacute fever. Beta-lactam antibiotics and sulfa-containing products, H2-blockers, procainamide, and hepar in , a re common incr iminat ing drugs . Thrombophlebitis should be considered as a cause of subacute fever in a patient with impaired mobility. Deep venous thrombosis and pulmonary embolism can cause fever and are more frequent in patients who are debilitated either by chronic medical problems or by the surgery.
Delayed — Most delayed postoperative fevers are due to infection.Viral infections from blood products, including cytomegalovirus (CMV), hepatitis viruses, and human immunodeficiency virus (HIV), can arise late in postoperative patients. SSIs due to more indolent m i c r o o r g a n i s m s ( e g , c o a g u l a s e - n e g a t i v e staphylococci) can cause delayed fever, especially in patients with implanted medical devices. Patients can also develop delayed cellulitis when surgery has disrupted venous or lymphatic drainage; this type of cellulitis can be recurrent.
Infective endocarditis due to perioperative bacteremia is also more likely to present weeks or months after surgery.
SPECIAL CASE SCENARIOCardiothoracic surgery Pneumonia is most common cause of fever after cardiac surgery and may occur in more than five percent of patients. This is followed by sternal wound infection occurs in 1 to 5 percent of patients after median sternotomy. It is detected at a median of seven postoperative days. A positive blood culture in a persistently febrile patient can be the first manifestation of a sternal wound infection, occurring before apparent wound inflammation.
Neurosurgery — Meningitis is a frequent and serious cause of fever after neurosurgery. Classic symptoms and signs of meningeal inflammation, such as headache, photophobia, and nuchal rigidity, are usually not helpful because they can be caused either by infection or by hemolyzed blood from the surgery irritating the meninges. Microscopic and analytical examination of the cerebrospinal fluid (CSF) is indicated in patients with fever, because, combined with specific clinical findings. Patients with all of the following criteria can probably be safely observed without administration of antimicrobials: fever less than 39.4ºC (102.9ºF); CSF
WBC less than 7,500/µL; CSF glucose above 10 mg/dL; no delirium, seizure, or surgical site inflammation.Neurosurgical procedures that impact the hypothalamus can lead to disorders of thermoregulation and cause postoperative fever [96].
Abdominal surgery — The primary cause of postoperative fever that is unique to abdominal surgery is deep abdominal abscess. Distinguishing between abscess, hematoma, and a benign peritoneal fluid collection can be difficult. Imaging studies and needle aspiration may be helpful, but exploration is sometimes necessary. Empiric antimicrobial treatment should be directed at the combination of aerobic Gram negative enteric bacilli and anaerobes.
Splenoportal thrombosis may cause fever following splenectomy, and is recognized with increased frequency since the availability of CT scanning. Risk factors include massive splenomegaly, and myeloproliferative and hemolytic disorders.
Pancreatitis more frequently causes postoperative fever after upper abdominal surgeries than after other surgeries. Diagnosis can be made by elevated serum amylase and l ipase concentrations with the considerations that salivary glands also produce amylase, and macro variants of amylase can produce elevated serum concentrations.
Obstetric and gynecologic surgery — Postpartum endometritis, manifested by fever, pelvic pain and purulent vaginal discharge, is more common in patients with preexisting medical problems, after premature rupture of membranes, difficult deliveries, and after the use of internal fetal monitoring.
The differential diagnosis of fever after gynecologic surgery includes urinary tract infection (UTI), cellulitis, necrotizing fasciitis, superficial abscess, deep abscess, and pelvic thrombophlebitis. As with other major surgeries, fever in the first day or two after gynecologic surgery usually resolves spontaneously. Extensive laboratory testing is not beneficial; fever evaluation should be targeted to the individual patient, based on repeated assessment of symptoms and signs. Similar to abdominal surgery, identifying a fluid collection and distinguishing between abscess, hematoma, and a benign fluid collection, though difficult, can be critically important.
Urologic surgery — Infection of the urinary tract at any level is the major consideration in evaluating
21

patients with fever after urologic surgery. Although bacteriuria due to a urethral catheter is common, culture alone is not as revealing as the combination of urine culture findings and urine analysis for pyuria and bacteriuria. Deep infections, such as prostatic and perinephric abscess, may present with fever and pain, but relatively benign urine findings. Infection can also spread from the lower urinary tract through Batson's venous plexus to the lumbar spine and present after the UTI is resolved.
Orthopedic surgery — As with other major surgeries, self-limited fever is the rule after major orthopedic surgery. The dominant special considerations in the differential diagnosis of persistent fever are surgical site infection (SSI), infected prosthesis, hematoma, and DVT. Repeat clinical assessment, imaging, and sometimes needle aspiration may be required to adequately assess the surgical site.
APPROACH TO THE PATIENT WITH FEVER AFTER SURGERY — A detailed history and physical examination remains, taking into account the timing of the onset of fever is essential for coming to a diagnosis in a febrile postoperative patients
A useful initial screen for the more common causes of postoperative fever is represented by the four-part mnemonic "Wind, Water, Wound, What did we do?” "Wind" refers to pulmonary causes of fever including pneumonia, aspiration, and pulmonary embolism. "Water" refers to UTI, and "Wound" refers to SSI. "What did we do?" is a reminder to consider treatments as a cause of fever and includes medications, blood product transfusions, and intravascular, urethral, nasal, and abdominal catheters.
Further investigation may be indicated depending upon the clinical assessment.· Respiratory specimen – BAL/ET/Sputum Gram
stain and culture are indicated for febrile patients with suspected pneumonia. It is recommended to correlate findings of microbiology findings with clinical features- a new or progressive pulmonary infiltrate; an increased respiratory rate; an increased minute volume; a decreased tidal volume; decreased oxygenation; needing more ventilatory support; or requiring more inspired oxygen.
· Urine – Urinalysis and urine culture are indicated for patients with a urethral catheter, urinary obstruction, renal calculi, recent genitourinary surgery or trauma.
· Blood: A positive blood culture in a persistently febrile patient can be the first manifestation of infection in febrile post-op patients. Culture of Staphylococcus aureus from the blood in cardiothoracic surgery patients raises the possibility of mediastinitis, even if the wound appears uninfected. Endocarditis should be considered in patients who develop positive blood cultures after undergoing valve replacement.
· Procalcitonin (PCT) assay are adjunctive diagnostic tools for distinguishing fever due to infection from noninfectious fever. Currently, the body of evidence for PCT testing is conflicting. The value of serum p r o c a l c i t o n i n ( P C T ) c o n c e n t r a t i o n f o r differentiating bacterial infection from other causes of postoperative fever has been explored in a few studies. PCT is a more specific marker of bacterial infection than CRP. However, postoperative PCT concentrations vary substantially following different types of surgery, and from patient to patient following the same type of surgery. Therefore the use of PCT in the evaluation of postoperative fever is not clear, pending additional clinical evidence.C-reactive protein (CRP) has also been studied as a biomarker for identifying infection, but it appears less promising because it lacks specificity, rises later than PCT, doesn't correlate as well with severity of disease, and tends to be lower among patients with liver disease [49]. Both PCT and CRP predict mortality in ICU patients.
· Chest imaging – A chest radiograph is easily obtainable in the ICU and worthwhile in many patients with respiratory symptoms or signs. It may detect a new or progressive pulmonary infiltrate, distinguish pneumonia from tracheobronchitis, or identify a respiratory source of fever other than pneumonia or tracheobronchitis that would otherwise be missed because it is not associated with sputum production. Computed tomography (CT) should be reserved for the clarification of abnormal chest radiographic findings.
· Abdominal imaging – Abdominal imaging is indicated for patients with symptoms or signs of an intraabdominal process, but for whom the laboratory testing has not identified the cause of the symptoms or signs. It is also indicated for patients who have a reason to have an intraabdominal infection (eg, recent abdominal surgery) and no alternative source of the fever has been identified, even if there are no symptoms or signs of an
22

abdominal process. Finally, abdominal imaging may be indicated if laboratory testing suggests a possible intraabdominal process, but the results are insufficient to identify the exact abnormality. As an example, in a patient with fever, transaminitis, and hyperbilirubinemia, a right upper quadrant ultrasound exam may determine whether there is acalculous cholecystitis, choledocholithiasis, or a primary hepatic condition.
TREATMENT — Any unnecessary treatments, including medications and catheters, should be discontinued in patients with postoperative fever. It is probably appropriate to suppress the fever in most patients with one or two days of scheduled acetaminophen to minimize patient discomfort and the physiologic stress and metabolic demands of fever and shivering. This approach is unlikely to mask a significant pathologic condition. Additional treatment depends upon the cause of the fever.
The decision to administer antibiotics to a patient with postoperative fever depends upon careful clinical assessment including an appraisal of the patient's stability. Patients who have undergone major surgery and are receiving intensive care and patients with hemodynamic instability generally should be treated empirically with broad-spectrum antibiotics after cultures have been obtained. For example, a patient
with a suspected intraabdominal or pelvic infection should be treated with a regimen effective against aerobic Gram negative enteric bacilli and anaerobes. Empiric antifungal therapy should not be included unless the patient is at high risk for fungal infection.
Nosocomial pathogens are often resistant to many antimicrobials; hospital antibiograms can be useful for selecting an appropriate broad-spectrum regimen. If a source of fever is not apparent and blood cultures show no growth after 48 hours, then discontinuation of antimicrobials should be seriously considered.
If a site of infection is identified and/or cultures are positive, the broad-spectrum regimen should be focused to cover the probable or known causative organism(s). Antimicrobial treatment beyond the empiric period of 48 hours should be reserved for patients in whom an infection has been identified. Gram stain findings and hospital antibiograms can be used to guide empiric antimicrobial selection, but definitive treatment should be based upon antimicrobial susceptibility results from cultured organisms. Carefully selecting antimicrobial treatment can help to avoid adverse medication reactions and can help to minimize the prevalence of resistant organisms in the hospital.
23

Primaquine:A must know Molecule for Ideal
Malaria Management and ControlDr. Paras GangwalMD (Medicine)Critical Care Consultant & Internist PhysicianEast Delhi Medical Centre & Max Patparganj, Delhi
Primaquine is an 8-aminoquinoline, a descendant of the first generally available synthetic anti-malarial plasmoquine (plasmochin, pamaquine).
THE 8-AMINOQUINOLINES HAVE UNIQUE ANTI-MALARIAL PROPERTIES
They have multipronged action
1. The 8-aminoquinolines kill mature gametocytes of Plasmodium falciparum.
2. They kill developing parasites of all species in the liver (causal prophylactic activity),
3. Also kill the dormant hypnozoites of Plasmodium vivax and Plasmodium ovale (radical curative activity), and
4. They have weak asexual stage activity (very weak for P. falciparum).
Their pertinent issue is that they cause haemolysis in people who are glucose-6-phosphate dehydrogenase (G6PD) deficient. This X-linked abnormality is very common in tropical areas with gene frequencies typically ranging from 3 to 30%.
RENEWED INTEREST IN PRIMAQUINE
1. The rising concern that spread of artemisinin-resistant falciparum malaria which could again reverse the recent decrease in malaria morbidity and mortality
2. There is a evolving understanding that repeated relapse in vivax malaria is a major cause of morbidity and mortality in areas of high transmission.
EXTENSIVE TRACK RECORD IN HISTORY : BUT STILL WHETHER , WHEN N HOW !?
Primaquine in history has extensive track record of usages
The Korean War……. Over 250,000 US soldiers received 14-day radical curative.
The Chinese Provinces …….100 million people.
In Azerbaijan, Tajikistan, Northern Afghanistan, and North Korea (DPR Korea) ………………. eight million people received mass treatments with primaquine to prevent or eliminate P. vivax infections.
In Nicaragua…… 1.9 million people received a three day regimen of chloroquine and primaquine to control and eliminate vivax and falciparum malaria .
Although radical five- to 14-day primaquine regimens have been recommended widely for over 50 years in tropical regions where P. vivax is prevalent and As a gametocytocide in P. falciparum infections, only one dose of primaquine is given (traditionally 0.5-0.75 mg base/kg, recently reduced to 0.25 mg base/kg) , Despite all these recommendations and administration of primaquine to some 200 million people, arguments continue about whether, when and how to give it!
India, bears the majority of the global burden of vivax malaria and here we have approximately three million malaria cases reported annually, over half caused by P. vivax.
RADICAL CURE DOSE IN VIVAX : THE HYPNOZOITOCIDAL ACTIVITY
HYPNOZOINTICIDAL activity of primaquine is predominantly a function of total dose administered:
1. adult dose :15 mg/day for 14 days
prevents >90% of long latency P. vivax relapses
2. adult dose :30 mg/day for 14 days
twice the dose (total 7 mg base/kg; adult dose 30 mg/day for 14 days) is required for short latency
Dr. Paras Gangwal's Clinic17RPS, DDA Flat Mansarover Park, Delhi Ph.: 011-22576000, 9811305970East Delhi Medical Centre1/550, Under G.T. Road Flyover, Mansarover Park, Shahdara, Delhi-32 Ph.: 22596736Max Pataparganj, Delhi Ph.: 4303-3333
YEAR BOOK & SOUVENIR 2014
Timings:1.00pm to 8.00pm9.00pm to 10.30pm
Wednesday : 8.00am to 9.30am

25
frequently relapsing infections in east Asia and Oceania.
DETERMINANTS OF EFFICACY
Poor adherence is an important cause of reduced effectiveness. There is no evidence for acquired resistance to the liver stage activity.
Both the parasite burden (number of hypnozoites in the liver) and degree of acquired immunity are important determinants of the therapeutic response.
R O L E I N FA L C I PA R U M I N F E C T I O N : GAMETOCYDAL DRUG AS STERILIZATION OF INFECTIVITY TO OTHERS—15 mg SINGLE ADULT DOSE
Primaquine has potent gametocytocidal activity in P. falciparum infections and rapidly sterilizes the treated infection . Provided a drug with adequate asexual stage activity is given as well, this substantially reduces onward transmission. In a recent trial in uncomplicated falciparum malaria and normal G6PD enzyme function, patients were randomized to receive three different dose regimens to reduce infectivity period along with artemether–lumefantrine combination
(1) a single dose of 0.1 mg/kg, (2) 0.4 mg/kg, or(3) 0.75 mg/kg primaquine base. The mean duration of gametocyte carriage a) was 6.6 days (95% CI 5.3-7.8) in the 0.75 mg/kg reference groupb) 6.3 days (5.1-7.5) in the 0.4 mg/kg primaquine group (p = 0.74)c) 8.0 days (6.6-9.4) in the 0.1 mg/kg primaquine group (p = 0.14)d) 12.4 days (9.9-15.0) in the placebo group (p <0.0001)Thus 0.4 mg/kg was non-inferior to 0.75 mg/kg.
Primaquine is substantially more active in reducing infectivity to mosquitos. Data from direct transmission blocking assessments from mosquito feeding studies suggests that, given together with an effective artemisinin combination treatment (ACT), a single 0.25 mg base/kg dose (15 mg for adult) gives maximal gametocytocidal effects, and this is now the recommended dose .
TOXICITY OF PRIMAQUINE
Main side effects are as follows:
1. Abdominal discomfort
Generally occurs at doses over 1 mg/kg but is well
tolerated at individual doses ≤0.5 mg base/kg if given together with food.
2. Methaemoglobinaemia
is common, but very seldom is dangerous.
3. Oxidant haemolysis
is the main adverse effect of primaquine . Although some red cell loss may occur in normal subjects, patients who are G6PD deficient are particularly vulnerable.
CONCEPTS ABOUT G6PD DEFICIENCY
It is the potential for toxicity in G6PD deficiency that has limited the use of primaquine. There are over 180 different genetic G6PD variants, nearly all conferring an unstable enzyme, which degrades more rapidly than the normal variant thereby rendering older red cells vulnerable to oxidant damage .
The extent of haemolysis depends on
a) the degree of G6PD deficiency and
b) the dose and duration of exposure to primaquine.
Two of the most prevalent G6PD variants represent ends of the severity spectrum.
1. Mediterranean variant
(the main variant found in Europe, west and central Asia, and northern India)
being amongst the most profound deficiencies.
2. African A- variant
(found in sub-Saharan Africa and in African-Americans)
being amongst the mildest. Severe haemolytic reactions can still occur in G6PDA-, but they are much less frequent.
HAEMOLYTIC RISKS VARY WIDELY
1. As there is also substantial variability in G6PD activity between individuals with the same genotype, and even within the same individual over time
2. In less severe G6PD variants, primaquine-induced haemolysis typically becomes evident after one or two days' exposure, when all the older erythrocytes' oxidant defences (mainly reduced glutathione) have been depleted .
If primaquine is continued in subjects with the African A- variant then haemolysis lessens, and the haemoglobin starts to rise again despite further drug administration, as reticulocytes enter the circulation to replace the haemolysed cells (Figure 1). These young red cells contain five times more G6PD than the oldest

26
red cells and so are relatively resistant to the haemolytic effect.
However, further haemolysis does occur if higher doses of primaquine are given .
In the severe Mediterranean variant, haemolysis continues if primaquine is not stopped and life-threatening anaemia may result (Figure 1)
SEVERAL OUTSTANDING QUESTIONS REMAIN DESPITE KNOWING THE PATHOPHYSIOLOGY OF PRIMAQUINE HAEMOLYSIS
1. Are patients with malaria at greater or lesser risk of haemolysis than healthy subjects?
2. Does pre-existing hookworm or malaria-related anaemia reduce haemolysis?
3. What exactly are the risks associated with the different therapeutic regimens?
4. What reductions in haemoglobin are life threatening?
5. There are also uncertainties over P. vivax relapse rates and latency intervals across much of the tropics which complicate therapeutic assessments, the methods for assessing gametocytocidal effects and their interpretation in clinical evaluations are disputed.
6. the community benefits from deployment of primaquine as a single dose gametocytocide have not been well characterized.
Primaquine-induced haemolysis in adults with different G6PD variants during daily dosing. Primaquine was given daily for 14 days at a dose of 30 mg/day in individuals with Mediterranean and African A-variants and 15 mg/day ...
SAFETY & DEATHS RELATED TO PRIMAQUINEDeathsTotal Only 14 deaths associated with primaquine have been reported in last sixty years.
A) 12 were from severe haemolysis B) one was due to hepatic necrosis, C) and the cause of another was not CLARIFIED.
One fatality may have followed a single 45-mg dose . All the other deaths followed multiple dose administrations.
Haemolytic Adverse Effects(but no deaths) were reported from the mass treatments (MDA) in Jiangsu (>28 million treated) and from the combined experience in Azerbaijan, Afghanistan, Tajikstan, and DPR Korea (>eight million treated).
G6PD screening was not performed during these MDAs but haemolysis was anticipated, and so education was provided and health services reinforced during the drug administrations.
T H E E S T I M AT E D R I S K F O R D E AT H ASSOCIATED WITH PRIMAQUINE from all these reports(excluding Chinese data) is one in 621,428 with an upper 95% CI of one in 407,807. If Chinese data is included it would make the risk four times lower.
The reported deaths occurred mainly in countries with a minority of the global malaria burden.
SEVERE ADVERSE EVENTS1. Severe Intravascular haemolysis is most common serious adverse event (SAE)
presenting with dark or black urine and mild jaundice.
2. Allergic reactions and3. Neuropsychiatric symptoms Have also been reported rarely in association with
primaquine use.
THERE ARE TWO SERIOUS CONSEQUENCES OF SEVERE HAEMOLYSIS1. Life-threatening anaemia and2. Haemoglobinuric renal failure.
INCIDENCE OF PRIMAQUINE RELATED SAEs IS VERY LOW & IS MAINLY IN THOSE WHO ARE G6PD DEFICIANT In various studies which evaluated primaquine
Figure 1

27
adverse events, no SAEs were reported in G6PD-normal individuals, with the possible exception of one psychotic reaction. Total 191 SAEs have been reported ,of which25 were in individuals likely to have been G6PD deficient, and 166in those with proven G6PD deficiency .The incidence of SAEs in the known G6PD-deficient group was 11.2%.
Of all SAEs, 11.5% occurred after a probable overdose of primaquine, 75.9% with radical curative regimens for vivax malaria and 12.6% after administration of 30 or 45 mg primaquine in weekly prophylactic or radical curative regimens, or as a single-dose gametocytocide.
Almost all the probable primaquine overdose (95.5%) SAEs were in children; most from a single case series of 21 Sri Lankan children aged two to 12 years hospitalized with acute intravascular haemolysis. All those tested for G6PD activity (17 children) were deficient .
SAEs IN MDA PROGRAMMESIn a TOTAL of 12 MDA PROGRAMMES 27 SAEs were reported, an estimated incidence of three SAEs per million. The majority of the SAEs were haemolysis, giving an estimated incidence of 1.8 episodes of severe haemolysis per million people receiving radical curative regimens of primaquine as MDA.
SAEs CAN BE AVOIDED BY INTERRUPTED REGIMENIn some MDA programmes given to almost 300,000 people in Azerbaijan (where the prevalence of G6PD deficiency, presumed Mediterranean variant, varied between 0 and 38.7%) and Kunduz Province, northern Afghanistan (Mediterranean variant prevalence 5-10%), an interrupted regimen was used, designed specifically so that haemolytic toxicity could be detected and managed.
This was 15 mg primaquine (adult dose) once daily for four days, followed by three days without drug, then primaquine for a further ten days .
HAEMOLYSIS FOLLOWING SINGLE-DOSE PRIMAQUINEHaemolysis is self-limiting as primaquine is eliminated rapidly (t five hours). This is exploited in the once 1/2
weekly 0.75-mg base/kg radical cure regimen recommended for patients with vivax malaria and 'mild' G6PD variants and the interrupted MDA regimens.
Reticulocytosis following each dose compensates for haemolysis and the progressively younger red cell population becomes increasingly resistant to primaquine's haemolytic effects.
THE EFFECT OF SINGLE-DOSE PRIMAQUINE ON ANAEMIAHas been specifically examined in Few reports ,in the treatment of malaria, partly because malaria itself causes anaemia with a similar time course to that caused by oxidant haemolysis.
Primaquine as a gametocytocide has usually been recommended in areas of low transmission where the haemoglobin nadir from malaria occurs around day 7. This coincides with the nadir following primaquine haemolysis.
the usual recommended dose (0.75 mg/kg) for the past 50 years has been exactly the same as that recommended weekly for radical cure in G6PD-deficient patients .
know with newly recommended dose of 0.25-mg/kg gametocytocidal dose the risk is assumed to be three times lower . G6PD testing has almost never been performed in this context.
AMPLE EVIDENCE IN MANY INSTANCES,IN LITERATURE ALL ACROSS THE GLOBE : SINGLE WEEKLY DOSE HAS BEEN SAFE EVEN IN MILD G6PD DEFICIENCY BUT CAUTION IS ALWAYS BETTER ADVISED1. IN Thailand (G6PD-deficiency prevalence mainly
Mahidol variant ~10%) no fatalities and no serious haemolysis was reported
WITH 45 mg doose .
2. Tanzania With use of 0.75 mg/kg primaquine single dose
with ACT , 15 children who were homo or hemizygous for G6PDA- deficiency there was a mean [95% CI] fall in haemoglobin on day 7 of -2.5 g/dL [-1.2 to -3.8 g/dL].
In one child, a G6PD A- heterozygote, the haemoglobin concentration fell from 8.3 to 4.8 g/dL.
3. Myanmar (G6PD-deficiency prevalence 10-20%), in a randomized comparison of different ACTs in acute falciparum malaria, 397 patients received a single 0.75 mg base/kg dose of primaquine. Overall

28
30% of patients had pre-treatment haemoglobins <10 g/dL but no serious haemolysis (Hb ≤5 g/dL) was observed .
4. Uganda: In a recent randomized trial of 468 children with uncomplicated malaria who received artemether-lumefantrine followed by a single dose of primaquine 0.1, 0.4 or 0.75 mg/kg or placebo of whom 27% had some degree of G6PD deficiency, no children developed symptomatic anaemia .
SARDINIA V/S IRAN STORYSARDINIA19 healthy individuals with presumed Mediterranean type G6PD deficiency were given primaquine 45 mg and chloroquine 300 mg; the median [range] fall in haematocrit was 8% [6-19%] .
IRAN a single primaquine 0.33 mg/kg dose was given with chloroquine to six subjects with confirmed G6PD deficiency (likely Mediterranean variant but not genotyped) without malaria.
All developed haemoglobinuria. The median [range] haemoglobin reduction was 2.3 [0.7-3.4] g/dL. None required a blood transfusion. DOSE-RESPONSE RELATIONSHIP FOR HAEMOLYSISPRIMAQUINES ACTIVE INTERMEDIATESPrimaquine is metabolized in vivo via cytochrome P450 to reactive intermediates (mainly through CYP2D6).These reactive intermediates though have not been characterized definitively but are thought to mediate both anti-malarial and haemolytic effects .Individuals with CYP2D6 genetic polymorphisms conferring reduced enzyme activity may have reduced primaquine efficacy .
THE RELATIONSHIPS BETWEEN PRIMAQUINE DOSE, DURATION AND HAEMOLYSISHave been characterized in detail for the G6PD A-variant in healthy adult volunteers. A clear dose-response relationship was evident:a) increasing daily doses up to 45 mg progressively
shortened red cell survival (Figure 2) . b) Dosing 45 mg daily could cause severe anaemia
whilst 15 mg daily caused only mild anaemia. c) Taking 30 mg/day for 14 day in the African A- variant resulted in approximately
the same degree of haemolysis
v/s 15 mg/day in the Mahidol or Viengchan variants,
with no further decline in haemoglobin during the second week of drug administration (Figure 1).
These and other data are consistent with a 'GENE DOSAGE' EFFECT as the African A- G6PD deficiency is less severe than the Mahidol and Viengchan variants, which in turn are less severe than the Mediterranean variant.
G6PD-deficient red cell survival following daily primaquine dosing. G6PD-deficient red cell survival
51was assessed by Cr labelling and transfusion into G6PD-normal healthy recipients (15 mg/day or 45 mg single dose in Mahidol or Viengchan ...
DISCUSSION 1.Primaquine is a very valuable anti-malarial drug, which is under-used.Concerns over potentially dangerous haemolytic toxicity along with the general unavailability of a simple test to identify patients at risk have substantially limited its deployment, and continue to do so.
2.All patients with malaria haemolyse andall G6PD-deficient patients haemolyse additionally with primaquine treatment. The extent of haemolysis depends on the dose, duration and severity of deficiency.
3. a single low dose is very likely to be safe, BUT daily primaquine dosing for the radical cure of vivax malaria
Figure 2

29
in a patient with severe deficiency risks potentially life-threatening haemolysis.
Still primaquine has good safety track record & only 12 deaths from severe haemolysis have been documented over the past 60 years. More may have gone unreported, although millions of people, many thousands of whom must have had severe variants of G6PD deficiency, received such regimens in MDAs without reported loss of life. The most likely explanation is simply that MDA recipients who suddenly felt ill and passed dark urine stopped taking primaquine.
4.For the physician contemplating radical curative treatment of P. vivax or P. ovale malaria, the correct approach is to test for G6PD deficiency. The NADPH 'spot' test identifies <30% of normal activity and should therefore identify all G6PD male hemizygotes and most female heterozygotes at high risk. Heterozygous females are genetic mosaics due to random X chromosome inactivation, also known as 'Lyonisation'; as a consequence they may by chance have a predominance of deficient erythrocytes. Point-of-care tests with similar performance characteristics to the “spot test” have been developed recently .
5.For G6PD-deficient individuals the recommended options are to
a) withhold primaquine, orb) in 'mild deficiency' to give 0.75 mg/kg once weekly for eight weeks.
6. WHAT SHOULD BE RECOMMENDED IN THE MAJORITY OF P. VIVAX-ENDEMIC AREAS WHERE G6PD-DEFICIENCY TESTING IS NOT READILY AVAILABLE? Multiple relapses cause substantial morbidity, interfering with development and educational performance in children, causing abortion and intra-uterine growth retardation in pregnancy and contributing to life-threatening anaemia in young children in higher transmission settings . When relapse rates exceed 50% (e.g., in east Asia and Oceania), effective radical curative treatment more than halves the incidence of vivax malaria.
The benefits of radical cure are substantial for all patients, while the risks of iatrogenic haemolytic anaemia are borne by the minority who are G6PD deficient. If there is no available G6PD test the correct approach to patient management depends on the risks and the benefits i.e. the prevalence and severity of
G6PD deficiency in the area and the dose regimen required for radical cure, the degree of anaemia and the availability of blood transfusion (i.e., the risk) as well as the probability and health impact of relapses (the benefit).
7 .RECOMMENDING PRIMAQUINE AS A GAMETOCYTOCIDE IN FALCIPARUM MALARIA in this scenario the assessment of risk is easier, whilst that of benefit is more difficult. The currently recommended 0.25 mg/kg dose is 14 to 28 times lower than the radical curative dose and two to three times lower than previously recommended gametocytocidal doses . This low dose is associated with a red cell survival in the G6PD A- variant five times longer than with the previously recommended 0.75 mg/kg dose.
Direct dose-response assessments of infectivity to anopheline mosquito vectors suggest that primaquine 0.25 mg base/kg produces maximum gametocytocidal effects when given with an ACT. The issue is that the treatment provides benefit to the community but no direct benefit to the treated patient
THE USUAL MEDICAL RESPONSE TO UNCERTAINTY IS CAUTION. However the struggle to contain and eliminate artemisinin-resistant falciparum malaria is a race against time, with potentially catastrophic consequences if we lose, so every approach to preventing the transmission of artemisinin-resistant parasites should be taken. It is essential to distinguish clearly the real risks of dangerous haemolytic anaemia associated with radical curative regimens of primaquine in vivax malaria from the considerably lower risk associated with giving a single small dose in falciparum malaria. This is why it is recommended that a gametocytocidal dose of primaquine should be added now to ACTs as part of regional elimination efforts .
TAKE HOME MESSAGE1. Primaquine is very important drug because of its
multi dimensional capability in Malaria control and management, both for individual and community.
2. Concerns regarding it's adverse effects are genuine but are exagerated; seeing evidence of it's commendable track record moreover, with clear applications of principles of hemolysis related to this drug, this risk can always be minimised.

30
3. Must get G6PD where availability and affordability is not an issue.
4. Where availability and affordability is an issue, primaquine still can be used
a) caution to patient about lowering of hemoglobin menifested as weakness and smoky black urine as sign of hemoglobinuria must be explained:in these events should stop the drug and seek medical help.
b) single gametocydal dose 0.25 mg/kg, in falciparum do not generally warrant G6PD order and invariably is likely to be safe ,though informing patients signs of hemolysis, which even because of malaria can happen, is always prudent.
c) concepts of interrupted regimen or weekly regimen may be applied for vivax radical cure.
5. In Vivax and Ovale for Radical cure: dosage 0.25 mg / kg (15 mg for 60 kg) for 14 days or 0.75 mg /kg weekly for 8 weeks (for those with mild
G6PD deficiency) or 0.25 mg/kg(15 mg/day for adults) for 4 days and
wait for 3 days and complete remaining 10 doses if no clinical evidence of hemolysis
6. In falciparum malaria As gametocydal role, which helps community not
the individual and is important to prevent evolution of Artemisinin Resistance
0.25mg/kg as single dose.
7. Do not hesitate and do use it and play your learned role in malaria treatment and control for both individual and community!!
ReferencesMalar J. 2014; 13(1): 418.Primaquine: the risks and the benefitsElizabeth A Ashley, Judith Recht, and Nicholas J White

Diagnosis and Treatment of MalariaGuidelines from
Directorate of National Vector Borne Disease Control Programme
Input by:Dr. Paras GangwalMD (Medicine)Critical Care Consultant & Internist PhysicianEast Delhi Medical Centre & Max Patparganj, Delhi
Diagnosis &TreatmentAll fever cases diagnosed as malaria by either RDT or microscopy should be promptly given effective treatment. The medicine chosen will depend upon whether the patient has vivax malaria or falciparum malaria as diagnosed by the blood test. The flow charts in different settings for diagnosis and drug selection for the treatment of malaria are as under:
ACT-AL - Artemisinin-based Combination Therapy- Artemether - LumefantrineACT-SP- Artemisinin-based Combination Therapy (Artesunate+Sulfadoxine-Pyrimethamine)CQ - ChloroquinePQ - Primaquine
YEAR BOOK & SOUVENIR 2014
Dr. Paras Gangwal's Clinic17RPS, DDA Flat Mansarover Park, Delhi Ph.: 011-22576000, 9811305970East Delhi Medical Centre1/550, Under G.T. Road Flyover, Mansarover Park, Shahdara, Delhi-32 Ph.: 22596736Max Pataparganj, Delhi Ph.: 4303-3333
Timings:1.00pm to 8.00pm9.00pm to 10.30pm
Wednesday : 8.00am to 9.30am

32
Note: 1) However, if malaria is strongly suspected, prepare & send slide for microscopy
2) If a patient has severe symptoms at any stage, then immediately refer to a nearest PHC or
other health facility with indoor patient management or a registered medical doctor.
3) PQ is contra-indicated in pregnancy and in children under 1 year (Infant).
ACT-AL - Artemisinin-based Combination Therapy- Artemether - Lumefantrine
ACT-SP- Artemisinin-based Combination Therapy (Artesunate+Sulfadoxine-Pyrimethamine)
CQ - Chloroquine
PQ - Primaquine
Treatment of Vivax Malaria
Diagnosis of vivax malaria may be made by the use of RDT (Bivalent) or microscopic
examination of the blood smear. On confirmation following treatment is to be given:
Drug schedule for treatment of P vivax malaria:
1. Chloroquine: 25 mg/kg body weight divided over three days i.e.
10 mg/kg on day 1,
10 mg/kg on day 2 and
5 mg/kg on day 3.

33
2. Primaquine*: 0.25 mg/kg body weight daily for 14 days.Primaquine is contraindicated in infants, pregnant women and individuals withG6PD deficiency.14 day regimen of Primaquine should be given under supervision.
Note: CQ 250mg tablet is having 150 mg base
Treatment of Falciparum MalariaDiagnosis of falciparum malaria may be made by the use of RDT (Monovalent or Bivalent) or microscopic examination of the blood smear. It is imperative to start the treatment for falciparum malaria immediately on diagnosis. The treatment for falciparum malaria is as follows:
In North-Eastern States (NE States):1. ACT-AL Co-formulated tablet of ARTEMETHER( 20 mg) - LUMEFANTRINE (120 mg)(Not recommended during the first trimester of pregnancy and for children weighing < 5 kg)

34
2. Primaquine*: 0.75 mg/kg body weight on day 2In other States:1. Artemisinin based Combination Therapy (ACT-SP)*Artesunate (AS), available as 50 mg tablets are given for three days, and Sulfadoxine- Pyrimethamine (S-P) tablets, containing 500 mg Sulfadoxine and 25 mg pyrimethamine are given for one day, as shown in the dosage chart below. All tablets for a day should be taken together, swallowed with water. In addition, Primaquine (PQ Large) tablets should be given on the second day.
Dose schedule for Treatment of uncomplicated P.falciparum cases:1. Artemisinin based Combination Therapy (ACT-SP)*Artesunate 4 mg/kg body weight daily for 3 days PlusSulfadoxine (25 mg/kg body weight) – Pyrimethamine (1.25 mg/kg body weight) on first day.* ACT is not to be given in 1st trimester of pregnancy.
2. Primaquine*: 0.75 mg/kg body weight on day 2.With the introduction of different coloured Blister Packs for different age groups, treatment by the field level staff has been made easy. The colour code for different age groups for Packing of Tablet ACT+SP has been given as follows:
Dosage Chart for Treatment of falciparum Malaria with ACT-SP
Treatment of uncomplicated P.falciparum cases in pregnancy:1st Trimester : Quinine salt 10mg/kg 3 times daily for 7 days.Quinine may induce hypoglycemia; pregnant women should not start taking quinine on an empty stomach and should eat regularly, while on quinine treatment.

35
2nd and 3rd trimester: Area-specific ACT as per dosage schedule given above.i.e. ACT-AL in North Eastern StatesACT-SP in Other StatesPrimaquine (PQ) prevents transmission of falciparum malaria to others by its ability to killgametocytes. PQ tablets should be taken after a meal; not on an empty stomach. Childrenless than the age of one year and pregnant women should not be given Primaquine. As pregnant women having falciparum malaria require different medicines, they should be directed to go to the nearest PHC or hospital immediately, without delay.
Treatment of mixed infections (P.vivax + P.falciparum) cases:All mixed infections should be treated with full course of ACT and Primaquine 0.25 mg per kg body weight daily for 14 days.
In North-Eastern States: Treat with: Age-specific ACT-AL for 3 days + Primaquine 0.25 mg per kg body weight daily for 14 days.
In Other States: SP-ACT 3 days + Primaquine 0.25 mg per kg body wt. daily for 14 days.
Dosage Chart for Treatment of mixed (vivax and falciparum) Malaria with ACT-SP
Treatment of severe malaria casesSevere malaria is an emergency and treatment should be given as per severity and associated complications which can be best decided by the treating physicians. Before admitting or referring patients, the attending doctor or health worker, whoever is able to do it, should do RDT and take blood smear; give a parenteral dose of artemisinin derivative or quinine in suspected cerebral malaria cases and send case sheet, details of treatment history and blood slide with patient. The guidelines for specific antimalarial therapy is as follows:
Parenteral artemisinin derivatives or quinine should be used irrespective of chloroquine resistance status of the area with one of the following options:

36
Note: The parenteral treatment in severe malaria cases should be given for minimum of 24 hours once started(irrespective of the patient’s ability to tolerate oral medication earlier than 24 hours).

37
After parenteral artemisinin therapy, patients will receive a full course of Area-specific oral ACT for 3 days. Those patients who received parenteral Quinine therapy should receive oral Quinine 10 mg/kg body weight three times a day for 7 days (including the days when parenteral Quinine was administered) plus Doxycycline 3 mg/kg body weight once a day or Clindamycin 10 mg/kg body weight 12-hourly for 7 days (Doxycycline is contraindicated in pregnant women and children under 8 years of age) or area-specific ACT as described.
ChemoprophylaxisChemoprophylaxis should be administered only in selective grips in high P.falciparum endemic areas. Use of personal protection measures including Insecticide Treated bed Nets (ITN) / Long Lasting Insecticidal Nets (LLIN) should be encouraged for pregnant women and other vulnerable population including travelers for longer stay. However, for longer stay of Military and Para-Military forces in high Pf endemic areas, the practice of chemoprophylaxis should be followed wherever appropriate e.g troops on night patrol duty and decisions oftheir Medical Administrative Authority should be followed.
Short term chemoprophylaxis (up to 6 weeks)Doxycycline : 100 mg once daily for adults and 1.5 mg/kg once daily for children(contraindicated in children below 8 years). The drug should be started 2 days before travel and continued for 4 weeks after leaving the malarious area.Note : It is not recommended for pregnant women and children less than 8 years
Chemoprophylaxis for longer stay (more than 6 weeks)Mefloqiune: 250 mg weekly for adults and should be administered two weeks before, during and four weeks after exposure.
Note : Mefloquine is contraindicated in individuals with history of convulsions, neuropsychiatric problems and cardiac conditions. Therefore, necessary precautions should be taken and all should undergo before prescription of the drug.
Use of chemoprophylaxis is limited to following situations:Short term travelers/tourists (less than 6 weeks) from non-malarious areas to malarious areas. Drug of choice is Doxycycline 100 mg daily in adults and 1.5 mg/kg bwt in children above 8 years; beginning 2 days before travel – 4 weeks after leaving a malarious area.
Doxycycline is contraindicated in children under 8 years and pregnant women, in whom personal protection should be used In long term travelers where appropriate e.g. military & paramilitary troops on night patrol duty etc. in malarious areas, the decision of respective medical administrative authority is to be followed. Drug of choice in such cases is Mefloquine 250 mg weeky for adults and 5 mg/kg for children once a week; beginning 2 weeks before to 4 weeks after exposure.
References:1. National Drug Policy for Malaria 2010, NVBDCP, MoH&FW, Govt. of India, 2010.2. Operation Manual for Malaria Control for District level Officers. NVBDCP, 2008.3. Website of National Vector Borne Disease Control Programmehttp://www.nvbdcp.gov.in/malaria-new.html4. World Health Organization (2006). WHO Guidelines for the Treatment of Malaria. GenevaWorld Health Organization

Ashok Kumar Grover, Sr. Consultant PhysicianAbhinav Mohabey, Sr. DNB StudentDepartment of Medicine, Pushpanjali Crosslay Hospital, Vaishali, Ghaziabad
INTRODUCTIONElevations in the levels of peripheral blood and tissue eosinophils can occur in a wide variety of disease processes that include infectious, allergic, neoplastic, primary hematologic disorders, and other, often less well-defined entities. Worldwide, multicellular helminth (worm) parasites are most commonly associated with significant eosinophilia, followed in frequency by drug hypersensitivity and atopic diseases. Hypereosinophilic syndromes (HES), in contrast, are a set of relatively rare, heterogeneous disorders characterized by persistent eosinophilia (defined as >1500/ul for 6 months) and organ involvement/ dysfunction in which other clinical entities have been excluded . The approach to defining these non-HES causes of persistently elevated eosinophilia is the focus of this review.
BIOLOGY OF THE EOSINOPHIL AND EOSINOPHILIAEosiniophill are produced in the bone marrow. Its funct ion is to combat parasi t ic in fect ions , ectoparasites, certain viral infections, and amplify responses of mast cells in atopy This is largely accomplished by generating ribonucleases, oxidative species and inducing degranulation of basophils and mast cells.Eosinophils are attracted to tissues by
cer ta in chemok ines (RANTES, CCL11/24) and leukotrienes.They require IL-5 (Eosinophil growth factor, secreted b y T - c e l l s ) f o r proliferation and to prevent apoptosis.They are very sensitive to steroids.
EOSINOPHILLIA- Eosinophilia is defined as a peripheral blood eosinophil count > 500/μL. Eosinophilia can be -
1. Primary (i.e. hematologic disorders such as leukemias and myeloproliferative disorders)
2. Secondary to numerous nonhematologic disorders
Most common cause world wise is parasitic infections followed by drug hypersensitivity reaction, atophic disease.
CONDITION ASSOCIATED WITH MARKED PERIPHERAL BLOOD EOSINOPHILLIA-Infectious Diseases• Parasitic infections primarily with helminths • N o n p a r a s i t i c i n f e c t i o n s ( A l l e r g i c
b r o n c h o p u l m o n a r y a s p e r g i l l o s i s , Coccidiomycosis,mycobacterial disease)
• Infestations – Scabies Allergic or Atopic Diseases• Drug hypersensitivity or medication-associated
eosinophilias • Atopic diseases
Hematologic and Neoplastic Disorders• Hypereosinophilic syndromes (HES) including
chronic eosinophilic leukemia • Leukemia (Acute myelogenous leukemias, B cell
ALL)• Lymphomas ( Hodgkin's, T- and B-cell lymphomas)• Tumor associated— Adenocarcinomas — Squamous carcinomas— Large cell lung carcinomas— Transitional cell carcinoma of the bladder• Systemic mastocytosis Connective tissue, vasculitic, granulomatous
disorders
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Approach to Eosinophillia

39
• Dressler syndrome• Eosinophilic fasciitis• Idiopathic eosinophilic synovitis • Inflammatory bowel disease• Polyarteritis nodosa • Churg strauss syndrome • Progressive systemic sclerosis (scleroderma)• RA• Sarcoidosis • Sjögren syndrome• SLE
Immunologic• Primary Immunodeficiency Diseases (HyperIgE
syndrome, Omenn's syndrome)• Graft-versus-host-Disease
Endocrinologic Disorders• Hypoadrenalism
Other• Irradiation• Atheroembolic Disorders• Sarcoidosis
History The medical history of a patient with eosinophilia
should first involve evaluation of the presenting complaint, followed by a systematic review.
Allergy· A history of hay fever, eczema, asthma, or urticaria
should be sought.
Geographic factors· Residence in or travel to an area where parasitic
infestation or coccidioidomycosis is endemic should be ascertained.
· If the patient has lived in or travelled to a tropical region, he or she should be questioned about exposure to soil or freshwater and about any symptoms suggestive of parasitic disease during the visit.
· All travel experiences (not only recent) are important (e.g., strongyloidiasis can present many decades after leaving an endemic area, particularly when immunity is suppressed).
HIV infection· Risk factors for HIV infection should be sought,
because HIV-positive patients are more likely to have disseminated parasitic or fungal infections that promote eosinophilia.
Drug history· A drug history should be taken (particularly of non-
prescription drugs, newly given drugs [usually s t a r t e d 2 - 6 w e e k s p r e v i o u s l y ] , a n d immunosuppressive drugs).
· A history of recent administration of corticosteroids or other immunosuppressive agents is relevant, because immunosuppressive treatment may lead to hyperinfestation with Strongyloides stercoralis.
· It should be noted whether the patient is taking any drugs often associated with adverse reactions (e.g., sulphonamides, cephalosporins, penicillin, nitrofurantoin, carbamazepine, allopurinol, phenytoin, or gold). Fever, rash, lymphadenopathy, and impaired liver function tests may indicate an adverse drug reaction.
History of rash or lymphadenopathy· Previous rash or lymphadenopathy is relevant, not
only in relation to a drug reaction but also to primary skin diseases that can cause eosinophilia. Leukaemia, lymphoma, or systemic mastocytosis can all cause both a rash and lymphadenopathy.
Cardiac history· Cardiac symptoms (e.g., dyspnoea, chest pain,
palpitations) in a patient with marked or prolonged eosinophilia could indicate cardiac damage by eosinophil products. Eosinophilic cardiac disease is a clinically urgent situation.
Other organ-related symptoms· Symptoms related to specific organ systems may
indicate a specific inflammatory disease, such as dysphagia in eosinophilic oesophagitis, or abdominal pain and diarrhoea in eosinophilic gastroenteritis.
Symptoms of lymphoma· Fever, night sweats, weight loss, itch, and alcohol-
induced pain, all possible symptoms of lymphoma, should be specifically enquired about.
Episodic symptoms· Symptoms such as episodic weight gain and
episodic angio-oedema should be sought, as they occur in the rare condition of Gleich's syndrome (episodic angio-oedema with eosinophilia).
Physical examination The temperature should be recorded. Fever may
indicate parasitic infestation, infection, or a drug reaction.

40
The skin should be examined for erythema, eczematous rash, oedema, urticaria, or skin infiltration. This could indicate primary skin disease, a drug reaction, some parasitic infections, eosinophilic leukaemia, urticaria pigmentosa associated with systemic mastocytosis, cutaneous T-cell lymphoma, or cyclic angio-oedema with eosinophilia.
Signs of vasculitis or peripheral ischaemia should be looked for. These could indicate a primary vasculitic condition such as Churg-Strauss syndrome or be a feature of hypereosinophilia itself, in either case indicating possible clinical urgency.
Bronchospasm can be a feature of asthma, allergic bronchopulmonary aspergillosis, or a severe drug reaction. Other abnormalities (such as cough, dyspnoea, or wheeze) in the lungs could indicate a lifecycle-related pulmonary migration of parasites, a d rug r eac t ion , o r eos inoph i l i c l eukaemia . Schistosomiasis can cause pulmonary hypertension, and Churg-Strauss syndrome can cause pulmonary infiltrates.
All lymph node areas should be examined for lymphadenopathy. If nodes are enlarged, the size and texture of the nodes should be assessed, because this may suggest a possible neoplasm (e.g., lymphoma or either lymphoid or myeloid leukaemia): hard, fixed, non-tender nodes are more likely to be due to malignancy.
Hepatomegaly and splenomegaly may be features of lymphoma or eosinophilic leukaemia.
Cardiomegaly, arrhythmia, or cardiac failure may indicate cardiac damage by eosinophils and a clinically urgent situation.
Neuropathy could inIdicate damage by eosinophil proteins.
INVESTIGATION • Haemogram-
—Cytopenia- haematological malignancy
—Thrombocytosis-infection, inflammation, malignancy
—Lymphocytosis-haematological malignancy
• Stool R/M – for ova,cyst ,parasite and hookworm infestation
• Serology for filaria ,coccidioidomycosis
• Sputum,BAL to identify parasites
• Skin biopsy for pemphigus and bullous pemphigoid
• In ABPA- raised IgE level,Positive aspergillus skin test,bronchiectasis in X-ray,CT
• Churg Strauss Syndrome-
—Sinus x ray – features of sinusitis
—Normocyti normochromic anemia,raised ESR,CRP
—Chest Xray- reticulo nodular infilteration,pleural effusion,lymphadenopathy
—P-ANCA positive in 40 %
• Leukemia diagnosed with blood film and bone marrow
· MANAGEMENT-
-Treatment tackles the underlying cause of the condition, whether it is an allergy, a medicine reaction, or a parasitic infection. These treatments are usually effective, and fairly non-toxic.
- Studies indicate that up to 50 % of patients never have a cause of their eosinophilia identified despite exhaustive evaluation. Others have suggested a strategy of using empiric anti-helminthic therapies on the basis of cost-effectiveness
-Treatment for hypereosinophilic syndrome is oral corticosteroid therapy, usually starting with prednisolone at single daily doses of 30-60mg.

Dr Amit Upadhyay, MDConsultant Hematology & Medical OncologyMax Super Specialty Hospital, Patparganj, New Delhi
YEAR BOOK & SOUVENIR 2014
Physicians often see patients who present with a low platelet count. Although further inquiry may elicit additional signs and symptoms of systemic disease, the etiology of thrombocytopenia usually is not immediately apparent. A low platelet count may be the only hematologic abnormality. In adults, thrombocyto-penia is defined as a platelet count of less than 150 ×
910 /L. Cases are considered mild if counts are between
9 970 and 150 × 10 /L and severe if less than 20 × 10 /L.1 9
Patients with a platelet count greater than 50 × 10 /L (50 9× 10 /L) often are asymptomatic. Patients with a count
9from 30 to 50 × 10 /L) rarely present with purpura, although they may have excessive bleeding with
9trauma. However, counts from 10 to 30 × 10 /L) may cause bleeding with minimal trauma, and counts less
9than 10 × 10 /L increase the risk of spontaneous bleeding, petechiae, and bruising. Spontaneous bleeding (i.e., mucosal, intracranial, gastrointestinal, and genitourinary bleeding) is more likely in patients
9 9with platelet counts less than 5 × 10 /L (5 × 10 /L), and is considered a hematologic emergency.
Initial EvaluationThrombocytopenia can result from decreased platelet production, increased platelet consumption, or sequestration (Table 1). A systematic approach should be used to evaluate incidental thrombocytopenia. During the patient history, physicians should inquire about easy bruising or petechiae, melena, rashes, fever and bleeding. They should also inquire about medication use, immunizations, recent travel or transfusion history, family history, and medical history. A history of acute and chronic alcohol use should be obtained. Any recent hospitalization or heparin exposure should raise the possibility of heparin-induced thrombocytopenia. Pregnant patients with visual symptoms, headaches, abdominal pain, or influenza-like symptoms may have preeclampsia or HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome.( Table 2)
The physical examination should include the eyes (e.g., hemorrhage is suggestive of central nervous system
Approach to Patient withThrombocytopenia
9 Thrombocytopenia is defined as a platelet count of less than 150 × 10 / . It is often discovered incidentally when obtaining a complete blood count on routine testing. The etiology usually is not obvious, and additional investiga-
9tions are required. Patients with platelet counts greater than 50 × 10 /L rarely have symptoms. A platelet count from
9 930 to 50 × 10 /L occasionally manifests as purpura. A count from 10 to 30 × 10 /L may cause bleeding with minimal 9trauma. A platelet count less than 5 × 10 /L may cause spontaneous bleeding and constitutes a hematologic
emergency. Patients who present with thrombocytopenia as part of a multisystem disorder usually are ill and require urgent evaluation and treatment. These patients most likely have an acute infection, heparin-induced thrombocyto-penia, liver disease, thrombotic thrombocytopenic purpura/hemolytic uremic syndrome, disseminated intravascular coagulation, or a hematologic disorder. During pregnancy, preeclampsia and the HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome are associated with thrombocytopenia. Patients with isolated thrombocytopenia commonly have drug-induced thrombocytopenia, immune thrombocytopenic purpura, pseudothrombocytopenia, or if pregnant, gestational thrombocytopenia. A history, physical examination, and laboratory studies can differentiate patients who require immediate intervention from those who can be treated in the outpatient setting. Treatment is based on the etiology and, in some cases, treating the secondary cause results in normalization of platelet counts. Consultation with a hematologist should be considered if patients require hospitalization, if there is evidence of systemic disease, or if thrombocytopenia worsens despite initial treatment

42
bleeding), abdomen (e.g., splenomegaly, hepatomeg-aly), lymph nodes (e.g., lymphadenopathy), skin (e.g., petechiae, purpura, bruising), and neurologic system. Bleeding (e.g., epistaxis, mucosal, gastrointestinal, g e n i t o u r i n a r y ) a l s o s h o u l d b e a s s e s s e d . Thrombocytopenia can be classified as emergent (usually requires inpatient management) or nonemergent (outpatient management). Some syndromes may fall in either category based on the severity of thrombocytopenia.
A peripheral blood smear can provide diagnostic information on a variety of white blood cell disorders, hemolytic anemia, and thrombocytopenia. A blood smear should be obtained during the initial evaluation. Table 3 lists common findings on peripheral blood smear and their associated diagnoses.
Factitious/ Pseudo ThrombocytopeniaPseudothrombocytopenia is secondary to platelet clumping and has no clinical significance. It occurs in one in 1,000 persons in the general population, and can be confirmed by a peripheral blood smear. Causes i n c l u d e u s e o f a b c i x i m a b ( R e o p r o ) o r ethylenediaminetetraacetic acid (EDTA) dependent agglutinins. The platelet count should be repeated by c o l l e c t i n g b l o o d i n a t u b e w i t h a n o n -ethylenediaminetetraacetic acid anticoagulant, such as heparin or sodium citrate. If the complete blood count still shows thrombocytopenia, other causes should be investigated.
IMMUNE (IDIOPATHIC) THROMBOCY TOPENIC PURPURAImmune thrombocytopenic purpura is an acquired immune-mediated disorder characterized by isolated thrombocytopenia and the absence of other conditions or agents known to induce thrombocytopenia. The inci-dence is 10 cases per 1 Lac persons annually, and approximately 50 percent of cases occur in children. Immune thrombocytopenic purpura in children often resolves spontaneously but tends to be more insidious and chronic in adults. The risk of bleeding correlates to the severity of thrombocytopenia. Patients may present without symptoms, with minimal bleeding, or with serious hemorrhage (e.g., mucosal, intracranial, gastro-intestinal, genitourinary). Older patients, patients on antiplatelet therapy, and patients with comorbid condi-tions may have more severe bleeding manifestations.
Secondary immune thrombocytopenic purpura is associated with other underlying conditions, such as autoimmune disorders (e.g., systemic lupus erythema-
tosus, antiphospholipid syndrome, Graves disease, sar-coidosis), lymphoproliferative disorders, and infections (e.g., human immunodeficiency virus, Epstein-Barr virus, cytomegalovirus, varicella-zoster virus, hepatitis C virus, Helicobacter pylori). Testing to rule out other causes should be performed as clinically indicated. Treatment is generally restricted to those with severe thrombocytopenia and is rarely indicated
9when platelet counts are greater than 50 × 10 /L unless there is evidence of active bleeding. Corticosteroids are considered first-line treatment and increase platelet counts usually within one week of initiation. Intravenous immune globulin, anti Rh D globulin and Rituximab also have been used for initial treatment of immune thrombocytopenic purpura. Second-line treatment includes thrombopoietin receptor agonists and splenectomy. Any patient older than 60 years pre-senting with isolated thrombocytopenia should be evaluated for myelodysplastic syndrome and lympho-proliferative disorders.
HEPARIN-INDUCED THROMBOCYTOPENIAHeparin-induced thrombocytopenia should be sus-pected in patients recently treated with heparin. Platelet counts decline within five to 10 days in patients with no previous exposure to heparin and may decline pre-cipitously (within hours) in patients with recent heparin exposure . This l i fe- threatening disorder i s characterized by the presence of platelet-activating antibodies recognizing multimolecular complexes bound to unfractionated heparin or low-molecular-weight heparin. Patients with heparin-induced thrombocytopenia present with mild thrombocytopenia or a 50 percent decrease in platelet count from baseline. The incidence is higher among surgical patients than medical patients. Thrombotic complications (termed heparin-induced thrombocytopenia with thrombosis) develop in 20 to 50 percent of patients and may affect arterial and venous systems, even after heparin is discontinued.
Characteristic features are erythematous or necrotizing skin reactions at the site of injection or severe mani-festations, such as deep venous thrombosis, pulmonary emboli, stroke or myocardial infarction. The most widely available diagnostic test is an enzyme-linked immunosorbent assay with platelet factor 4/anion complex as the antigen. This test has a high sensitivity (greater than 97 percent) but a lower specificity (74 to 86 percent) because of the presence of platelet factor 4 antibodies in patients without heparin-induced thrombocytopenia. If the clinical diagnosis is suspected or confirmed by laboratory analysis, heparin should be

43
stopped immediately and treatment should be changed to a nonheparin anticoagulant. One study showed that p a t i e n t s w h o d e v e l o p e d h e p a r i n - i n d u c e d thrombocytopenia had a 20 percent in-hospital mortality rate, regardless of thrombosis development.
THROMBOTIC THROMBOCYTOPENIC PURPURAPatients presenting with thrombocytopenia and micro-angiopathic hemolytic anemia should be admitted to the hospital with a presumptive diagnosis of thrombotic thrombocytopenic purpura. Renal manifestations, neu-rologic changes and fever also may be present. Severity is reflected by the extent of microvascular aggregation of platelets resulting in ischemia and necrosis of tissue cells. The incidence of thrombotic thrombocytopenic purpura is four to 11 patients per 1 million annually in the United States. It is fatal without treatment. Prompt initiation of plasma exchange is critical. Thrombotic thrombocytopenic purpura occurs primarily in adults. Hemolyt ic uremic syndrome is thrombot ic thrombocytopenic purpura found in children presenting with acute renal failure, bloody diarrhea, and/or abdominal pain. Shiga toxin-producing Escherichia coli is the most common causative organism in hemolytic uremic syndrome.
PREECLAMPSIA AND HELLP SYNDROMEPregnant patients beyond 20 weeks' gestation with thrombocytopenia or signs and symptoms such as headache, visual disturbances, right upper quadrant abdominal pain, or elevated blood pressure should be evaluated for preeclampsia and HELLP syndrome. Laboratory abnormalities may include anemia, e l e v a t e d l i v e r e n z y m e s , e l e v a t e d l a c t a t e dehydrogenase, and proteinuria.Treatment is intravenous magnesium sulfate and active management to deliver the fetus. Pregnant patients also can present with other causes of thrombocytopenia, including disseminated intravascular coagulation (as seen with sepsis and placenta abruptio) and thrombotic thrombo-cytopenic purpura, which can mimic HELLP syndrome.DRUG-INDUCED THROMBOCYTOPENIAOne of the most common types of thrombocytopenia in the outpatient setting is drug-induced thrombocytope-nia. An epidemiologic study from Europe and the United States showed an annual incidence of 10 cases per 1 million persons, but numbers could be higher in older persons and in hospitalized patients. Drug-induced thrombocytopenia should be suspected in all patients presenting with an acute drop in platelet count.
Most patients with drug-induced thrombocytopenia have moderate to severe thrombocytopenia reaching a
9nadir platelet count of 20 × 10 /L .Physicians should ask specific questions about the use of any medications, including nutritional supplements and over-the-counter remedies.
Table 4 lists common medications that may cause thrombocytopenia. Drug-induced thrombocytopenia typically occurs within five to seven days of exposure to the causative agent and usually resolves within seven to 14 days after discontinuation. If drug-induced thrombocytopenia is suspected, the causative medication should be discontinued and the patient's platelet count should be repeated in one week.
INFECTIONSInfections may cause thrombocytopenia by direct bone marrow suppression or increased peripheral platelet consumption. Malaria, Typhoid are common infections which can cause thrombocytopenia. Common viruses inc lude hepat i t i s B and C, Dengue human immunodeficiency virus, Epstein-Barr, cyto-megalovirus, parvovirus B19, varicella-zoster, rubella, and mumps. Recent studies found thrombocytopenia in 14 percent of hospitalized patients with influenza A (H1N1) virus. Platelet counts usually recover in patients with a self-limited viral infection.
LIVER DISEASEChronic liver disease usually causes persistent thrombocytopenia, and manifests as cirrhosis, fibrosis and portal hypertension. The most common cause is chronic alcohol abuse. However, other etiologies include infectious hepatitis, drug-induced liver disease, nonalcoholic liver disease, and metabolic disorders. Thrombocytopenia results from direct toxic marrow suppression and splenic sequestration. Folic acid deficiency (related to malnutrition) often coexists with alcohol abuse. Abstinence and nutritional replacement often lead to platelet normalization in three to four weeks in the absence of chronic liver disease.
GESTATIONAL THROMBOCYTOPENIAGestational thrombocytopenia is the most common diagnosis of thrombocytopenia in pregnancy, occurring in 8 percent of pregnancies Its etiology is thought to be hemodilution and accelerated platelet clearance. Gestational thrombocytopenia is characterized by mild thrombocytopenia, no history of thrombocytopenia, no association of fetal thrombocytopenia, and spontaneous resolution after delivery. Gestational thrombocytopenia

44
is a benign clinical condition not associated with maternal or neonatal morbidity or mortality. Recommendations for the initial evaluation of throm-bocytopenia in pregnancy include a complete blood count and peripheral blood smear. Additional studies are done on the basis of history and physical exam-ination.
Mild immune thrombocytopenic purpura and ges-tational thrombocytopenia often are indistinguishable and cannot be differentiated; however, 12 to 15 percent of neonates delivered to women with immune thrombocytopenic purpura will develop platelet counts
9of less than 50 × 10 /L .The platelet count in infants should be monitored when immune thrombocytopenic purpura is suspected in the mother.
OTHER CAUSESAplastic anemia, chemotherapy, irradiation, acute leukemias, and myelodysplastic disorders may result in severe or symptomatic thrombocytopenia. Paroxysmal nocturnal hemoglobinuria is associated with hemolysis, renal disease and thrombosis complications. Hospitalized patients with comorbid conditions, such as sepsis, trauma, burns or malignancy, can develop disseminated intravascular coagulation with resultant thrombocytopenia.
MANAGEMENTSymptomatic patients require immediate evaluation. Patients with incidental thrombocytopenia (i.e., platelet
9counts of 50 to 150 × 10 /L ) who are asymptomatic should have a platelet count repeated in one to four weeks depending on the severity of thrombocytopenia. Reassessment should be performed immediately if patients become symptomatic during the surveillance period. Additional laboratory evaluation should be performed as clinically indicated, and a trial of discontinuing agents known to decrease platelet counts is recommended. Patients with unexplained severe thrombocytopenia, decreasing platelet counts, additional hematologic abnormalities or associated bleeding complications should be referred to a hematologist. ACTIVITY PARTICIPATION AND INVASIVE PROCEDURESGeneral recommendations for activity participation have been based on historical data from patients with chronic severe thrombocytopenia. A platelet count
9greater than 50 × 10 /L is adequate for hemostasis and is unlikely to be clinically recognized. Patients with a
9platelet count greater than20x10 /L can engage in most activities, but should use caution if participating in
contact sports. Patients with platelet counts less than 10 9× 10 /L should be restricted from contact sports and
other potentially traumatic activities. Most surgical and invasive procedures can be per-formed safely in patients with platelet counts greater
9than 50 × 10 /L . Other procedures, such as bone marrow biopsy, bronchoscopy, and endoscopy, can be completed safely in patients with platelet counts greater
9than 20 × 10 /L, provided that no other bleeding abnormalities are noted. The American College of Obstetricians and Gynecologists recommendations state that epidural anesthesia in pregnancy is safe in patients with platelet counts between 50 and 100 ×
910 /L .
CONCLUSION:-A low platelet count can result from a wider range of conditions and may be determined by multiple mechanisms. Prompt recognition of the cause of thrombocytopenia is often crucial for the correct management of patients, as in acute promyelocytic leukemia, heparin induced thrombocytopenia, or thrombotic thrombocytopenic purpura/hemolytic uremic syndrome. The initial approach to determine the cause of thrombocytopenia is based on taking careful history of any underlying diseases and drug treatment, on physical examination, and on careful examination of the peripheral blood smear. The 2 most common causes of a low platelet count in the absence of other hematologic abnormalities and absence of any multi system disease are ITP and DITP. The most common cause of a low platelet count in pregnancy is GT. In hospitalized and critically ill patients, the diagnosis of thrombocytopenia is often challenging due to the presence of several potential etiologies, including drugs and infections. Examination of the BM with aspiration and biopsy is warranted in patients with severe or worsening thrombocytopenia of unexplained nature. Thrombocytopenia in pregnancy deserves special consideration because of the possible consequences on the fetus.
SUGGESTED READING:-1. Arepally GM, Ortel TL. Clinical practice. Heparin
– induced thrombocytopenia. N Engl J Med. 2006:355 (8):809-817.
2. BainBJ. Diagnosis from the blood smear, N Engl J Med .2005:353(5): 498-507.
3. Chapman AS, Bakken JS, Folk SM, et al: Tickborne Rickettsial Diseases working Group: CDC. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted

45
fever, ehrilichioses, and anaplasmosis – united states: a practical guide for physicians and other health – care and public health professionals. MMWR Recomm Rep. 2006; 55(RR-4): 1-27.
4. C i n e s D B , B l a c h e t t e V S , I m m u n e thrombocytopenia purpura. N Engl J Med.2002: 346(13):995-1008.
5. F i n n i s h M e d i c a l S o c i e t y D u o d e c i m . Thrombocytopenia. In EBM Guidelines. Evidences –Based Medicines. Helsinki, Finland: Wiley Interscience john Wiley & Sons: April 27,2007.http://www.guideline.govt/content.
6. George JN. Evalatiuon and management of thrombocytopenia by primary care physicians U p t o d a t e . h t t p / / w w w. u p t o d a t e . c o m / contents/evaluation-and –management- of- thrombocytopenia-by-primary-care-physicians.
7. Lacey JV.Penner JA. Managemnt of idiopathic thrombocytopenia purpura in the adult. Semin thromb Hemost. 1977; 3 (3): 160-174
8. Landlaw SA, George JN. Approach to the adult patient with thrombocytopenia .up to date .http:// www.uptodate.com/contents/approch- to- the-adult-patient-with- thrombocytopenia.
9. Moake JL.Throbotic microangiopathies. N Engl J Med. 2002: 347(8):589-600.
10. Proven D, Stasi R, Newland AC, et al. In te rna t iona l consensus repor t on the investigations and management of primary i m m u n e t h r o m b o c y t o p e n i a . B l o o d .2010:115(2):168-186.
11. R e n n e y B , S t a c k G . D r u g i n d u c e d t h r o m b o c y t o p e n i a . A r c h p a t h o l L a b Med.2009:133(2):309-314
12. Veneri D, franchini M, Randon F, Nichele I, Pizzolo G, Ambrosetti A. Thrombocytopenia: A c l i n i c a l p o i n t o f v i e w . B l o o d Transfus.2009;7(2):75-85
TABLE .1 ETIOLOGIES OF THROMBOCYTOPENIA
DECREASED PLATELET PRODUCTION
Bone marrow failure (e.g., aplastic anemia, paroxysmal nocturnal hemoglobinuria, Shwachman-Diamond syndrome)
Bone marrow suppression (e.g., from medication, chemotherapy, or irradiation)
Chronic alcohol abuse*
Congenital macrothrombocytopenias (e.g., Alport syndrome, BernardSoulier syndrome, Fanconi anemia, platelet-type or pseudo von Willebrand disease, Wiskott-Aldrich syndrome)
Infection† (e.g., cytomegalovirus, Epstein-Barr virus, hepatitis C virus, HIV, mumps, parvovirus B19, rickettsia, rubella, varicella- zoster virus)
Myelodysplastic syndrome
Neoplastic marrow infiltration
Nutritional deficiencies (vitamin B12 and folate)
Sequestration/other
Chronic alcohol abuse*
Dilutional thrombocytopenia (e.g., hemorrhage, excessive crystalloid infusion)
Gestational thrombocytopenia
Hypersplenism (e.g., distributional thrombocytopenia)
Liver disease (e.g., cirrhosis, fibrosis, portal hypertension)
Pseudothrombocytopenia
Pulmonary emboli
Pulmonary hypertension
INCREASED PLATELET CONSUMPTION Heparin-induced thrombocytopenia
Immune thrombocytopenic purpura*
Infection† (e.g., cytomegalovirus, Epstein-Barr virus, hepatitis C virus, HIV, mumps, parvovirus B19, rickettsia, rubella, varicella-zoster virus)
Mechanical destruction (e.g., aortic valve, mechanical valve, extracorporeal bypass)
Preeclampsia/HELLP syndrome
Thrombotic thrombocytopenic purpura/hemolytic uremic syndrome
Increased platelet consumption
Alloimmune destruction (e.g. posttransfusion, neonatal, posttransplantation)
Autoimmune syndromes (e.g., antiphospholipid syndrome, systemic lupus erythematosus, sarcoidosis)
Disseminated intravascular coagulation*/severe sepsis*
Drug-induced thrombocytopenia
*indicates more than one mechanism of action

46
Table 2 : Clinical Considerations to Aid in Diagnosis of Thrombocytopenia
TIMINGS
Acute
Chronic
History
Family history
Liver disease
Pregnancy
Recent change in medication
Recent hospitalization
Recent immunization
Recent transfusion or high-risk behavior
Recent travel
Recent valve replacement surgery
Symptoms
Abdominal pain
Recent fever
Weight loss or night sweats
Physical examination
Acute rash
Generalized lymphadenopathy
Hepatomegaly
Neurologic
Splenomegaly*
Acute infection (primarily viral), acute leukemias, aplastic anemia, chemotherapy or irradiation,I DITP, HELLP syndrome/preeclampsia, HIT , ITP, malignancies with marrow infiltration, myelofibrosis, TTP/HUS
Chronic alcohol abuse, congenital syndromes, ITP, liver disease, myelodysplastic syndrome
Congenital thrombocytopenia
Chronic alcohol abuse, chronic liver disease
Gestational thrombocytopenia, HELLP /preeclampsia
Drug-induced thrombocytopenia(DITP)
Heparin-induced thrombocytopenia
MMR, varicella, influenza A (H1N1)
Alloimmune destruction, posttransfusion purpura, viral infection (HCV, HIV)
Dengue fever, malaria, rickettsial diseases
Mechanical destruction
HELLP syndrome/preeclampsia, HUS, platelet sequestration
Viral infections (CMV, EBV, HIV, influenza A [H1N1], parvovirus B19), TTP, rickettsial diseases
HIV, malignancies (acute leukemias, myelodysplasia)
Rickettsial diseases, SLE, viral infections
Viral infections (CMV, EBV, HIV), SLE, myeloproliferative or lymphoproliferative disorders
Chronic liver disease, acute leukemia, viral infections (CMV, EBV, HBV, HCV)
TTP
Autoimmune,SLE, hypersplenism, viral infections
CMV = cytomegalovirus; EBV = Epstein-Barr virus; HBV = hepatitis B virus; HCV = hepatitis C virus; HELLP = hemolysis, elevated liver enzymes, and low platelet count; HIV = human immunodeficiency virus; HUS = hemolytic uremic syndrome; ITP = immune thrombocytopenic purpura; MMR = measles, mumps, and rubella; SLE = systemic lupus erythematosus; TTP = thrombotic thrombocytopenic purpura.
*—Ultrasonography may be useful in patients who are obese.

47
Table 3 : Common Peripheral Blood Smear Findings and Possible Diagnoses
Smear Findings
Atypical lymphocytosis
Basophilic stippling
Cryoglobulin
Giant platelets
Megakaryocyte fragments
Nucleated red blood cells
Oval macrocytosis
Platelet agglutination
Platelet hypogranularity
Round macrocytosis
Schistocytosis
Target cells
Parasites
Possible Diagnosis
Viral infection (e.g., Epstein-Barr virus, cytomegalovirus)
Thalassemia, chronic alcohol use, lead or metal poisoning
Cryoglobulinemia, mycoplasma pneumonia, multiple myeloma, some autoimmune disorders
Congenital thrombocytopenias, immune thrombocytopenic purpura
Myelofibrosis
Severe hemolysis, myelofibrosis
Vitamin B12 and folate deficiencies
Pseudothrombocytopenia
Myelodysplastic syndrome, myelofibrosis
Myelodysplastic syndrome, myelofibrosis, chronic liver disease
Thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, disseminated intravascular coagulation, defective prosthetic heart valve
Chronic liver disease, hemoglobinopathies
Malaria, Kala-azar, Babesiosis
Table 4: Medications/Substances Commonly Associated with Drug-Induced Thrombocytopenia
Medications /SubstancesAbciximab (Reopro)AlcoholCarbamazepine (Tegretol)CephalosporinsChemotherapyCimetidine (Tagamet)Eptifibatide (Integrilin)Gold saltsHeparinHydrochlorothiazideInterferonMeasles, mumps, and rubella vaccineLinezolidPhenytoin (Dilantin)ProcainamideQuinidine/quinineRifampinSulfasalazine (Azulfidine)Trimethoprim/sulfamethoxazole (Bactrim, Septra)Vancomycin

Dr. Rajesh Kumar, Consultant Psychiatrist, Dr. Paramjeet Singh, Consultant Psychiatrist, Dr. Prerna Kukreti, Sr. Resident Psychiatry, Institute of Human Behaviour & Allied Sciences, Dilshad Garden, Delhi
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
IntroductionDepression is a common disorder. The World Health Organization speculates that as many as 121 million
1people worldwide suffer from depression. Estimates further suggest that the number is set to rise significantly over the next two decades and depression alone with constitute one of the largest health problems
2worldwide by the year 2020.
Despite a very high prevalence, depression is one of the most commonly under diagnosed and undertreated medical conditions, especially within the medical and primary care setting. Many people feeling depressed with some somatic symptoms will present to primary care physicians first and most treatments can be provided in the primary care settings. However, there is considerable evidence that depressive disorders are often not recognized in people presenting to primary healthcare workers (Goldberg 1984). It is estimated that 30-50% of cases of depression in primary care
3and medical settings are not detected .
This chapter is an attempt to empower general physicians in Indian setting to manage a significant number of depressed patients, which cannot be dealt by a limited number of psychiatrists. Furthermore, a large number of people are prescribed antidepressants without any need, creating a financial burden, exposure to side effects, and liability of abuse for those prescribed. As of now, 75% of antidepressant use is
4,5attributed to general physician. They can prevent this with:
· Scientific base to manage depression
· Rigorousness of diagnostic process
· Appropriate use of antidepressants and anxiolytics
· Monitoring for use of antidepressants and anxiolytics with watch for side effects and misuse
Some statistics highlighting treatment gap for 6
depressive disorders
· Nearly 20% of general population is affected by depression during their lifetime
· Fourth largest contributor to global burden of disease
· Nearly half of the patients have a missed diagnosis of depression in primary care settings
· DEPRES study involving 78,463 individuals found that only 4% of the depressed population received adequate antidepressant therapy
· A study in France showed that only 54% were recognized to be depressed and of there only 7% received adequate treatment
Need for Depression Management by general 7-13physicians
AvailabilityWith a limited strength of mental health professionals in the developing world, the patients would have an easier availability of mental health services if delivered through these sectors.
AcceptabilityStigma has been a major barrier for individuals and families with mental illness approaching psychiatric facilities. The widespread acceptability of general physicians would facilitate and enhance treatment seeking behavior in these illnesses.
AffordabilityThe involvement of these services for mental health issues would bring down cost and make treatment more affordable for general community.
Management of Depression in Primary Care

49
Therapeutic RelationshipThe patients and their families have been in contact with these doctors for a variety of health problems and for long have shared a rapport and therapeutic relationship, which is an essential ingredient of management of depression.
Barriers of managing depression by general physicians
· Less time is available with general physicians for accurate diagnosis
· There is limitation in understanding, diagnosis, and treatment of depression
· Patients often feel stigmatized on being diagnosed with depression and general physicians fear loss of patients by being scientifically rational
· Patient often want quick relief for their symptoms and are not inclined to provide details required for correct diagnosis and management
· Moreover depression may be undetected in many individuals presenting mostly with somatic symptoms of depression
· Option of collaborating with psychiatrist for management is not available for most of general physicians in Indian setting
Many drugs are available, which need not be and cannot be familiarized by a general physician. Latter are advised to just familiarize with pharmacology of 2-3 antidepressant drugs. We recommend using Fluoxetine, Escitalopram, and Sertraline by general physician in view of their safety.
Step wise approach in Assessment and Management
Differentiation between normal and abnormal sadness
Normal Sadness – The term depression is used to describe a normal emotional experience as well as a disorder. Normal sadness or unhappiness is however, different from the nature, experience and severity of depressive symptoms in a disorder. It is a part of normal fluctuations depending on the situations/context.
Abnormal Sadness - More severe and persistent sadness associated with other emotional changes such as anxiety, irritability or apathy. It cannot be explained by the situations/context. There are also cognitive, behavioral and somatic symptoms. It can also be observed by others and not just subjective feelings only. The symptoms associated cause clinically significant
distress and impairment in social, occupational and other areas of functioning.
Condition that present with less severe depressive symptoms are:-
a. Dysthymia – The depressive symptoms are chronic and long term but symptoms are less than major depressive disorder.
b. Adjustment disorder – There is distinct stressors that cause distress and give rise to mild symptoms. The symptoms of depression develop within 3 months of an identifiable stressor(s).
Step 1: Establishing a definitive diagnosis of depressive episodeSad/depressed mood present for at least 2 weeks period and representing a change from previous functioning, at least one of the symptoms is either, depressed mood or loss of interest or pleasure. Depressed mood most of the day, nearly every day, as indicated by either subjective report (feels sad or empty) or observations made by other (appears tearful), in children and adolescents it can be irritable mood. Patient can have other symptoms physical/somatic symptoms e.g. loss of weight, insomnia or hypersomnia, fatigue or loss of energy etc. In severe states, patient can have depressive cognition (worthlessness, helplessness and hopelessness) and also death wishes/suicidal wishes.
Assessment 1. Take a detailed history of the presenting symptoms
and determine the severity and duration of the depressive episode.
2. Establish history of prior episodes, prior manic or hypomanic episodes, substance abuse and other psychiatric illnesses.
3. Look out for coexisting medical conditions, family history of mental illness.
4. Do a mental state examination including evaluation of severity of depression.
5. Do a physical examination to exclude medical condition.
6. Laboratory testing may be indicated if there is a need to rule out medical conditions.
Psychiatric disorders associated with depression1. Bipolar disorder
2. Dysthymia
3. Grief, bereavement

50
4. Anxiety disorder
5. Post traumatic stress disorder
6. Somatoform disorders
7. Eating disorders
8. Sleep disorders
9. Substance abuse
Life situations associated with depression
1. Coping with chronic illnesses
2. Marital discord
3. Child rearing difficulties
4. Work stress
5. Abuse (domestic violence, physical or sexual abuse)
Step 2: Deciding whether the patient can be managed in general physician's settingIn the Indian healthcare system, where there is no statutory requirement for general physicians to treat mental health problems, physicians have differing levels of confidence of dealing with mental health problems including depression. The possible levels of management of depression by different general physicians can be:
· Diagnosis of depressed patients and referral to psychiatrist.
· Diagnosis of depressed patients and management of uncomplicated mild to moderately depressed patients.
· Diagnosis of depressed patients and management of most of the depressed patients.
· Collaborative care of all depressed patients in association with psychiatrist/mental health team.
Step 3: Choosing and optimizing an antidepressant and arranging follow upT h e g e n e r a l p r i n c i p l e s f o r p re s c r i b i n g antidepressants are:
· Do not prescribe antidepressant and just wait and watch when in doubt about diagnosis of depression and no urgent intervention is required.
· Refer to psychiatrist when in doubt about diagnosis of depression and urgent intervention is required.
· Almost all classes of antidepressants have similar efficacy in treating depression.
· Selective serotonin reuptake inhibitors are usual first choice in view of their safety in case of overdose and better adherence due to lesser side
14effects .
· Choose an antidepressant whose side effects can be beneficial for the patient (e.g. sedating effect of Mirtazepine can be comforting to patient experiencing insomnia, whereas, activating effect of Fluoxetine can be equally comforting for patients experiencing daytime lassitude.
· Choose an antidepressant that had been effective in earlier depressive episode in the given patient.
· Begin with low dose and gradually increase to therapeutic level over first week while monitoring for side effects.
· Avoid combinations.
· Expect for any response only after 2 weeks. Any early response within first few days should indicate wrong diagnosis or progression to mania. Antidepressants should be stopped immediately.
· Increase dose of antidepressant gradually up to maximum therapeutic dose only after waiting for 2-4weeks. Do not assume that antidepressant is not working if not given for adequate duration.
· Target for remission (complete resolution of depressive symptoms) rather than partial response (a significant reduction in depressive symptoms).
· Do ask for side effects of antidepressants on follow up. Most of the depressed patients do not spontaneously report side effects. This is more so for sexual side effects.
· Address side effects to improve compliance. Use Bupropion in case of sexual dysfunction. Initial anxiety symptoms may be managed with careful use of benzodiazepines for initial 2-4 weeks.
· Continue antidepressant for 12 months after ndremission of first episode, 3 years after 2 and
rdindefinitely after 3 or more episodes (Table –1).
Step 4: Patient information and patient-physician communicationGood communication between patient and physician is the key to success of any therapy and obviously this will be more so for treatment of depression. The depressed patient should be adequately explained about the condition according to his receptiveness and willingness, the medication to be used, other treatment options available and the expected response. Not too much information should be imparted in one go. Information that can be provided to patient includes:
1. Depression
a) Being depressed does not indicate being weak. Accepting the illness and getting treated effectively indicates strength only
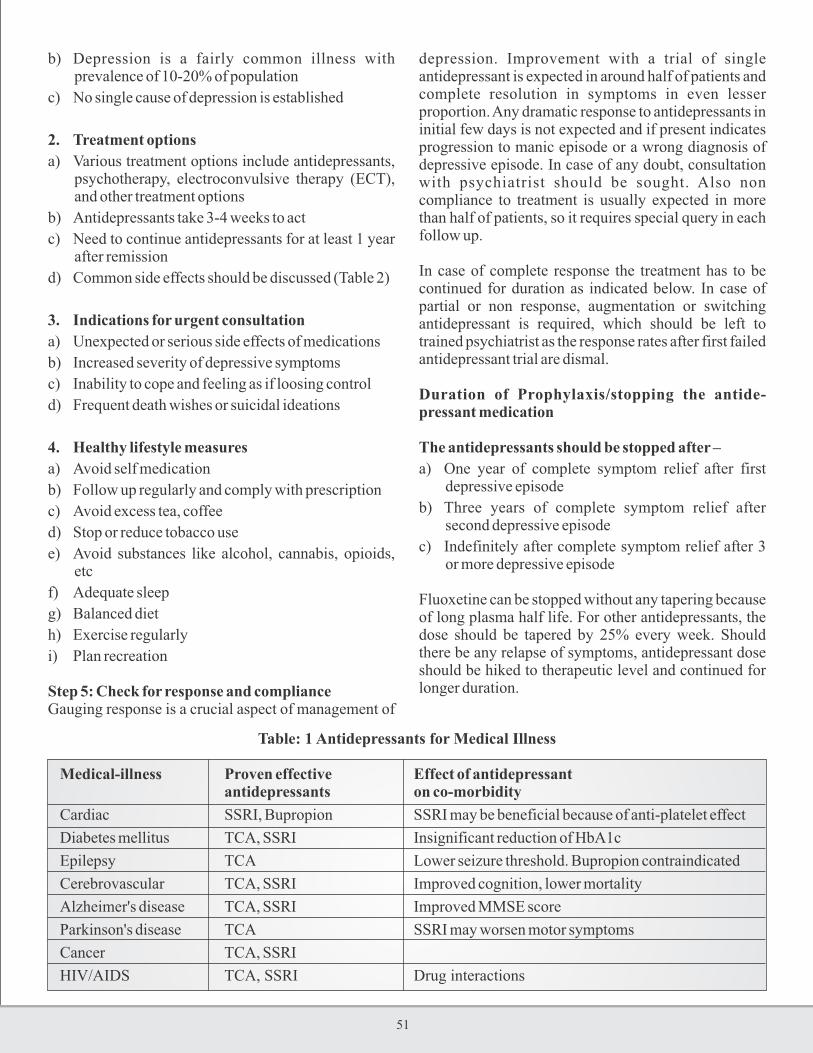
51
b) Depression is a fairly common illness with prevalence of 10-20% of population
c) No single cause of depression is established
2. Treatment options
a) Various treatment options include antidepressants, psychotherapy, electroconvulsive therapy (ECT), and other treatment options
b) Antidepressants take 3-4 weeks to act
c) Need to continue antidepressants for at least 1 year after remission
d) Common side effects should be discussed (Table 2)
3. Indications for urgent consultation
a) Unexpected or serious side effects of medications
b) Increased severity of depressive symptoms
c) Inability to cope and feeling as if loosing control
d) Frequent death wishes or suicidal ideations
4. Healthy lifestyle measures
a) Avoid self medication
b) Follow up regularly and comply with prescription
c) Avoid excess tea, coffee
d) Stop or reduce tobacco use
e) Avoid substances like alcohol, cannabis, opioids, etc
f) Adequate sleep
g) Balanced diet
h) Exercise regularly
i) Plan recreation
Step 5: Check for response and complianceGauging response is a crucial aspect of management of
depression. Improvement with a trial of single antidepressant is expected in around half of patients and complete resolution in symptoms in even lesser proportion. Any dramatic response to antidepressants in initial few days is not expected and if present indicates progression to manic episode or a wrong diagnosis of depressive episode. In case of any doubt, consultation with psychiatrist should be sought. Also non compliance to treatment is usually expected in more than half of patients, so it requires special query in each follow up.
In case of complete response the treatment has to be continued for duration as indicated below. In case of partial or non response, augmentation or switching antidepressant is required, which should be left to trained psychiatrist as the response rates after first failed antidepressant trial are dismal.
Duration of Prophylaxis/stopping the antide-pressant medication
The antidepressants should be stopped after –
a) One year of complete symptom relief after first depressive episode
b) Three years of complete symptom relief after second depressive episode
c) Indefinitely after complete symptom relief after 3 or more depressive episode
Fluoxetine can be stopped without any tapering because of long plasma half life. For other antidepressants, the dose should be tapered by 25% every week. Should there be any relapse of symptoms, antidepressant dose should be hiked to therapeutic level and continued for longer duration.
Table: 1 Antidepressants for Medical Illness
Medical-illness Proven effective Effect of antidepressant antidepressants on co-morbidity
Cardiac SSRI, Bupropion SSRI may be beneficial because of anti-platelet effect
Diabetes mellitus TCA, SSRI Insignificant reduction of HbA1c
Epilepsy TCA Lower seizure threshold. Bupropion contraindicated
Cerebrovascular TCA, SSRI Improved cognition, lower mortality
Alzheimer's disease TCA, SSRI Improved MMSE score
Parkinson's disease TCA SSRI may worsen motor symptoms
Cancer TCA, SSRI
HIV/AIDS TCA, SSRI Drug interactions

52
Table: 2 Commonly prescribed antidepressant medications
Drug Starting dose Therapeutic Maximum dose Common side
(mg) range (mg) (mg) effects
SSRI drugs
Fluoxetine 20 20-60 80 Gastritis
Escitalopram 10 10-20 40 Nausea
Paroxetine 10 20-50 60 Decreased libido
Sertaline 25 25-200 200 Sleep disturbances
TCAs
Amitryptiline 25 50-200 300 Dry mouth
Imipramine 25 50-200 300 Sedation
Clomipramine 25 50-200 300 Weight gain
Blurring of vision
Seizures (clomipramine)
SNRI
Venlafaxine 37.5 37.5-225 375 Hypertension
Discontinuation syndrome
Decreased libido
Duloxetine 30 30-90 120 Urinary obstruction
Desvenlafaxine 50 50-100 200 Same as venlafaxine,
less in frequency
Miscellaneous
Mirtazapine 7.5 15-45 45 Sedation
(serotonin Weight gain
antagonist)
Bupropion-SR 150 150-300 400 Agitation
(dopamine Seizures
reuptake (No sexual side effects)
inhibitor)
SSRI: Selective serotonin reuptake inhibitor, TCAs: Tricyclic antidepressants, SNRI: Serotonin norepinephrine reuptake inhibitor

53
Management algorithm for non-medically ill patient presenting with depressive symptoms

54
Conditions requiring referral to Psychiatrist
A. Special conditions
1. Bipolar depression (history of episode of inappropriate over cheerfulness in past)
2. Depression with psychotic symptoms (delusions, hallucinations, catatonia)
3. Atypical depression
4. Pregnancy/lactation
5. Severe postnatal depression
6. Child/adolescent depression
7. Onset within 6 weeks of child birth
8. Multiple prior episodes
9. Geriatric population
B. Psychiatric co-morbidity
1. History of chronic psychotic illness
2. Substance use disorders
3. Personality disorders
C. Psychosocial issues
1. Significant interpersonal issues
2. Need for detailed psychosocial therapies
D. Treatment related issues
1. Poor response to past treatment trials or current treatment
2. Medication intolerance (severe side effects)
3. Poor compliance or lack of motivation to initiate treatment
4. Drug interactions
Table – 3 Common side effects of antidepressants and management
Antidepressant side effect Offending agents Management
Dry mouth Anti-cholinergic side effects Reduce dose as these are dose-related,
Urinary retention with tricyclics and paroxetine build dose more slowly, consider
Blurred vision among SSRI changing the agent
Constipation
Sedation (can interfere with Tricyclics, Mirtazepine Give before going to sleep,
driving or operating reduce dose if required
machinery)
Sleep disruption Fluoxetine, Fluvoxamine Use in morning
Weight gain TCAs, Mirtazepine, SSRIs Lifestyle measures, diet review
Nausea Serotonergic effect. Prescribe after meals,
Gastrointestinal More with SSRIs divide the dose,
disturbance/diarrhea prescribe antacid if needed
Inability to achieve an SSRIs, most antidepressants Reduce dose, use cyproheptadine
erection/loss of libido except Bupropion Change to Bupropion
Anxiety More common during initial Build dose slowly
few weeks with most Use low dose benzodiazepines
antidepressants in some patients for initial 2-4 weeks
TCIs: Tricyclic antidepressants, SSRI: Serotonin specific reuptake inhibitors

55
Selective Serotonin Reuptake Inhibitors (SSRIs)
Contraindications to SSRI1. Hypersensitivity to SSRIs or any other component2. Manic phase 3. Concomitant used with MAOIs
Dosage of SSRIs1. Should be started low and adjusted to patient's
response2. Dose should be gradually reduced before stopping
therapy, do not stop treatment abruptly, risk of seizures or withdrawal syndrome
Some recommendations regarding pharmacotherapy1. There is no clinically significant difference in
effectiveness between selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs). Treatment decisions need to be based on considerations of relative patient acceptability, toxicity and cost.
2. For moderate and severe depressive disorders with melancholic features, TCAs are still the initial drug of choice providing they are prescribed at an adequate dose and the patient can tolerate the side effects.
3. When TCA is used in treatment of depression in adults, low dose tricyclics (typically 75-100 mg is justified.
4. In general practice, a starting dose less than 75mg could be tried and stepped up according to the clinical effect and tolerance of individual patients.
5. Medication should be maintained at the full dosage required to attain symptom remission in the acute treatment phase. Patient should be reviewed every 1-2 weeks at the start of antidepressant treatment.
6. Continuation of treatment for further 3-6 months for
first episode and for up to 3 years for recurrent episodes of depression are recommended.
7. Treatment should be continued for at least 4 weeks (6 weeks in the elderly) before considering whether to switch antidepressant due to lack of efficacy.
8. In cases of partial response, continue for a further 2 weeks (elderly patients may take longer to respond).
9. The use of Fluoxetine, Sertraline, Escitalopram and Paroxetine should be considered in patients with depression with concomitant anxiety symptoms.
10. In general all medications should be tailed off over a four week period. This is probably not necessary for Fluoxetine due to its extended half life.
11. The use of benzodiazepine may be considered for short term use in the management of anxiety symptoms which coexist with depression. It should be used judiciously in view of the risk of abuse/dependence in vulnerable patients. The use of benzodiazepines should be reserved for the management of anxiety symptoms only and sedatives/hypnotics should be used for the m a n a g e m e n t o f s l e e p p r o b l e m s . T h e benzodiazepines should not be used for hypnotic purpose including its use on SOS basis. The ideal hypnotics are “Z” group of drugs e.g. Zolpidem (5-10 mg), Zopiclon (7.5 mg) and Zaleplon (1-2 mg). These drugs are ideal as they don't have abuse/dependence potential and hangover effects and they facilitate the normalization of sleep architecture.
12. The medications must be started only after confirmation of the diagnosis and a brief information must be shared with the patient about the probable side effects, drug-drug interactions and tentative period of drug use as it will facilitate/ promote compliance.

56
Table – 4 Medications and Medical illnesses which can cause depressionTable – 4 Medications and Medical illnesses which can cause depression
Drugs Medical illnesses
Steroids Hypothyroidism/hyperthyroidism
Reserpine Addison's disease
Alfa methyldopa Cushing's syndrome
Anticholinergics, Sedatives/hypnotics, Anxiolytics Tertiary syphilis, Hepatitis, Influenza Beta-blockers Viral hepatitis
Phenothiazine antipsychotics AIDS
Vincristine, vinblastine SLE
Interferon, Chemotherapy agent, Levodopa Rheumatoid arthritis, Diabetes, Alcoholism or other substance abuse/dependence
Anticonvulsants Pellagra
Statins Pernicious anemia
Narcotics Multiple sclerosis
Calcium channel blockers Parkinson's disease Head trauma Cerebral tumors Cerebro-vascular accident Sleep disorders Malignancy Myocardial infarction
Table – 5 Common drug interactions with antidepressants
Antidepressant Drug interactions
MAOI Hypertensive crisis with cough and cold medications containing ephedrine or other sympathomimetics, reserpine, TCAs, levodopa, alcohol, opioids, pethidine
TCAs Potentiate sympathomimetics (asthma/cold medications), CNS depressants antihypertensive action of guanethidine and clonidine is abolished. SSRIs inhibit metabolism of TCAs and barbiturates and carbamazepine inhibit it. Phenytoin, aspirin displace from protein binding site, can cause toxicity
Bupropion Hypertensive crisis with MAOI Carbamazepine decreases plasma concentration delirium and
psychosis can occur when coadministered with dopaminergic agents like levodopa
Mirtazepine Excessive sedation with benzodiazepines Hypertensive crisis with MAOI
Venlafaxine Hypertensive crisis with MAOI Cimetidine inhibits metabolism
SSRIs Serotonin syndrome with MAOI Fluoxetine, sertraline and paroxetine increase level of TCA and
cause toxicity
MAOI: Monoamine oxidase inhibitors, CNS: Central nervous system, TCAs: Tricyclic antidepressants, SSRIs: Selective serotonin reuptake inhibitors

57

58
ConclusionThe prevalence of depression is very high in the community and is expected to rise in future in view of increasing stress of daily life, rapid urbanization, migration and changing family systems etc. The depression significantly affects the concerned individual, family and society because of its nature of symptoms. The major concerns are increasing prevalence, lack of detection and lack of adequate treatment. Depression if not treated early and adequately can give rise to significant morbidity and mortality in the form of suicide or by complicating the
coexistence medical illnesses. This is one problem that cannot be left only to be managed by psychiatrists considering its universal nature and severe dearth of trained mental health professionals. The general physicians/family physicians are strategically placed in the community and they can be very crucial in early detection and management of depression. This minimal effort by them will go a long way in decreasing the morbidity and mortality associated with depression including improving the quality of life of suffering individuals.

59
References:
1. The Mental Health Context: Mental health policy and service guidance package.
2. Murray CJL, Lopez A, D., editors. The global burden of disease: A comprehensive assessment of mortality and disability from disease, injuries and risk factors in 1990 and projected to 2020. USA: Harvard School of Public Health on behalf of the World Health Organization and the World Bank, distributed by Harvard University; 1996.
3. Ronalds C, Creed F, Stone K, Webb S, Tomenson B. The outcome of anxiety and depressive disorders in general practice. Br J Psychiatry 1997; 171:427-433.
4. Ali IM. Prescribing antidepressants in general practice. Prescription does not mean that major depression is being treated. BMJ 1997;314:827.
5. Rosholm JU, Hallas J, Gram LF. Outpatient utilization of antidepressants: a prescription database analysis. J Affect Disord 1993;27:21-8.
6. Lecrubier Y. The burden of depression and anxiety in general medicine. J Clin Psychiatry 2001;62:4-9.
7. Coyne JC, Schwenk TL, Fechner-Bates S. Nondetection of depression by primary care physicians reconsidered. Gen Hosp Psychiatry 1995;17:3-12.
8. Lecrubier Y. Recognizing and effectively treating depression. CNS Spectr 2008;13 (7 Suppl 11):5-9.
9. Coulehan JL, Schulberg HC, Block MR, et al. Treating depressed primary care patients improves their physical, mental and social functioning. Arch Intern Med 1997;157:1113-20.
10. Goldberg RJ. Depression in primary care: DSM-III diagnosis and other depressive syndromes. J Gen Intern Med 1988;3:491-7.
11. S imon GE, Vonkor ff M. Recogn i t ion , management, and outcomes of depression in primary care. Arch Fam Med 1995;4:99-105.
12. Schulberg HC, Katon W, Simon GE, Rush AJ. Treating major depression in primary care practice: an update of the agency for Health Care Policy and Research Practice Guidelines. Arch Gen Psychiatry 1998;55:1121-7.
13. Wells KB, Sherbourne C, Schoenbaum M, et al. Impact of disseminating quality improvement programs for depression in managed primary care: a randomized controlled trial. JAMA 2000;283:212-20.
14. Bostwick JM. A generalist's guide to treating patients with depression with an emphasis on using side effects to tailor antidepressant therapy. Mayo Clin Proc 2010;85:538-50.

Dr Pankaj Kumar, Assistant ProfessorDr Prerna Kukreti, Senior ResidentDr Amit Garg, Department of Psychiatry, Institute of Human Behaviour& Allied Sciences (IHBAS)
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
Management of Alcoholwithdrawal in Medical Settings
INTRODUCTIONAlcohol use disorders have a high prevalence in Indian population (Gururaj 2001).
General population
70-80% lifetime use
15-30% lifetime abuse
10-20% lifetime dependence
Special populations
20-40% medical inpatients
50% trauma and surgical patients
Chronic alcoholism is a panacea for diseases related to almost all systems of body, not only degenerative diseases but also many traumatic conditions. Hence, general medical practitioners come across clients with comorbid alcohol use problems frequently. Alcohol withdrawal syndromes are significant cause of morbidity and mortality,especially if missed in initial assessment. Thus, a sound knowledge base regarding assessment and management of alcohol withdrawal can be lifesaving. These guidelines aim to equip clinicians with evidence base practice in alcohol use disorder management, focusing mainly on withdrawal related complications.
I. IDENTIFY THE ALCOHOL USE PATTERNIdentify the pattern of Alcohol use disorder for appropriate treatment:
1. Acute Intoxication
2. Withdrawal State
3. Dependence Syndromes
4. Harmful Use
1. Acute Intoxication is a transient condition following the administration of alcohol resulting in disturbances in level of consciousness, cognition,
perception, affect or behavior, or other psycho-physiological functions and responses. This is usually associated with high blood levels of the drug. However, sometimes even a low dose of alcohol is sufficient to cause intoxication as an idiosyncratic reaction. The recovery is generally complete, as blood concentration decreases, except in cases where tissue damage or other complications have occurred.
2. Withdrawal Statecomprises a cluster of symptoms that develops on total or partial withdrawal of the drug usually after repeated and/or high-dose use. Withdrawal syndrome is generally short lasting ranging from few hours to few days. Withdrawal symptoms are relieved if the drug is taken. The withdrawal states are further classified as:
(i) Uncomplicated
(ii) With convulsions
(iii) With delirium
3. Dependence syndrome is a cluster of physiological, behavioral, cognitive phenomena in which the use of a substance takes much higher priority than other behaviors that once had greater value. The definite diagnosis of dependence should usually be made only if at least three of the following have been experienced at some time during the previous year;
(i) A strong desire or sense of compulsion to take the substance.
(ii) Difficulties in controlling substance-taking behavior in terms of its onset, termination or levels of use.
(iii) A physiological withdrawal state occurs when the substance use has ceased or reduced,
(iv) Evidence of tolerance is seen in dependent users. In order to achieve the effects of the drug

61
obtained with low doses initially, he person has to take the higher doses.
(v) Progressive neglect of alternative pleasures or interests because of substance use occurs and the individual spends more time in procuring and using the psychoactive drug.
(vi) There is persistence with the substance despite of harmful effects caused by the drug on various body organs
(vii) Harmful Useof a drug refers to a pattern of physically hazardous use of drug (i.e. driving during intoxication). It requires actual damage caused to the physical or the mental health of the user and client should not be fulfilling criteria for dependence syndrome.
II. ASSESSMENT OF ALCOHOL USE Screening: For effective early detection, brief history of alcohol use must be enquired in all clients presenting with alcohol use related medical disorders. But seeing the high frequency of hazardous drinking, it is encouraged to incorporate screening for alcohol use disorders as a routine practice in all patients getting admitted to general hospital setting. Alcohol misuse can be identified by various methods, clinical history, use of short structured questionnaires, medical examination and lab parameters.
1. BRIEF CLINICAL HISTORY
a. Use of alcohol, units of alcohol per day/ week (appendix one: alcohol units)
b. Use pattern in last few weeks
c. Last alcohol intake?''
d. Continuous use/ episodic use/ binge pattern
e. Craving, tolerance, withdrawal symptoms, use despite harmful consequences, neglect of other activities (s/o dependence pattern)
f. Past h/o complicated withdrawal e.g. sweating, tremor, autonomic instability, hallucination, seizure and delirium
g. Coexisting medical problems: screen for-
i. Cardiac disease (arrhythmia, CHF)
ii. GI bleed
iii. Cancer
iv. Liver/ pancreas disease
v. Neuropathy
vi. Cognitive/ amnestic disorder
vii. Movement disorderh. Reasons of current abstinence
i. History of head injury
j. Risk of harm to self or others
k. Motivation to leave alcohol
2. SHORT SCREENING QUESTIONNAIREa) Alcohol use disorder identification test (AUDIT) (appendix two)It is a 10 item questionnaire, takes less than two minutes to apply and is excellent screening tool to tell about the pattern of use e.g. hazardous drinking/ harmful use/ dependence. It assesses frequency, quantity, lack of control, guilt, blackouts etc. It can be self-administered and has 90%sensitivity and 85% specificity.
b) Fast Alcohol use screening test (FAST) (appendix three)It is a 4 item questionnaire, takes less than twenty seconds to apply and is excellent screening tool in time constrained emergency settings.
3. MEDICAL EXAMINATIONVirtually every system of body is affected by alcohol use (appendix four- physical health hazards of alcohol use). Thorough physical examination, especially of abdominal system, central nervous system and signs of nutritional deficiency should be done. A few physical signs are highly suggestive of alcohol use, should be sought and recorded:
· Spider naevi
· Telengeictasia
· Gynecomastia
· Dupytren s contracture
· Facial mooning
· Parotid enlargement
· Palmar erythema
4. LABORATOORY PARAMETERSFollowing tests after consent should be carried out:
i. Routine investigations
a) Hemogram with RBC Indices (especially MCV>100 is seen in chronic drinkers, but may be seen in other conditions too)
b) Liver function test (including ALT/AST>2:1 is suggestive of alcoholic liver disease AST is more specific for alcohol use, returns to normal after 48 hours)
c) Kidney function tests
d) Serum electrolytes
ii. Specific investigations
e) Gamma glutamyltransefrase ( it is a liver enzyme,

62
often raised {>35 U} in chronic alcoholics, return normal after 5 weeks of abstinence)
f) Ammonia (in cases of delirium)
g) Non contrast CT Head (to r/o head injury)
h) Magnesium (in cases of withdrawal seizure/ delirium)
i) Hepatitis and HIV (in selected high risk cases)
j) Blood/ Breath alcohol concentration
k) Carbohydrate deficient transferase (>20U, more for research use; most specific marker of recent use)
Laboratory markers only provide corroborative evidence in addition to clinical history. None is sensitive or specific to be used in isolation.
Summary of state markers of alcohol consumption
Marker Sensitivity (%) Diagnostic Specificity (%)
GGT 61 Data not available Chronic alcohol use
ALT Method dependent Data not available Chronic alcohol use
AST 56 Data not available Chronic alcohol use
CDT 26-83 91 Heavy alcohol use (> 60 grams per day
or > 4-5 standard unit of drink)
I. ACUTE ALCOHOL WITHDRAWAL SYNDROMMESAlcohol withdrawal may occur in alcohol dependent patients who suddenly stop alcohol or reduce their intake. It may range from mild tremors (most common), to increased autonomic activity, to hallucinations in clear sensorium, to seizures and to most life threatening delirium tremens. In medical settings, inadvertent
abstinence following admission for an unrelated condition or surgery can lead to precipitated withdrawal and worsen prognosis. So, early identification by asking clinical history at the outset and giving agonist therapy from starting can be beneficial and also prompt identification and management of acute withdrawal can be lifesaving. Alcohol withdrawal syndromes (AWS) can be grouped into four:
S.No ALCOHOL EXPECTED TIME SYMPTOMS/SIGNS WITHDRAWAL DURATION SYNDROMES (After last drink)
1 UNCOMPLICATED Onset: 6-8 hrs Tremors, anxiety, insomnia, restlessness, ALCOHOL Peak : 10-30 hrs agitation Sweating, tachycardia, WITHDRAWAL Subside: 40-50 hrs raised BP, hyper-reflexia
COMPLICATED ALCOHOL WITHDRAWAL SYNDROMMES
2 ALCOHOLIC Onset: 12-24 hrs Auditory hallucinations (derogatory/ accusatory), HALLUCINOSIS Subside: 48 hrs visual hallucinations (bugs crawling on bed) occurring in clear sensorium
3 ALCOHOL Onset: 24 hrs Generalized Tonic ClonicSeizure, WITHDRAWAL Rare beyond: 48 hrs Usually single; may be clusters SEIZURE (if focal seizure rule out,head injury) 30% seizures are followed by delirium tremens All seizures should be evaluated for possibility of underlying independent cause too
4 DELIRIUM TREMENS Onset: 48-72 hrs Disorientation, ill sustained attention, Mortality: 5% (in treated Rare beyond: 4-5 days marked autonomic instability, hallucinations, patients) to 20% agitation, insomnia, nausea, vomiting, (in untreated patients) motor incoordination
''PLEASE NOTE'': Any patient in withdrawal state has potential to develop seizure/ DT, manage alcohol withdrawal pre-emptively. If Delirium Tremens are not detected early and managed effectively, high chances of mortality
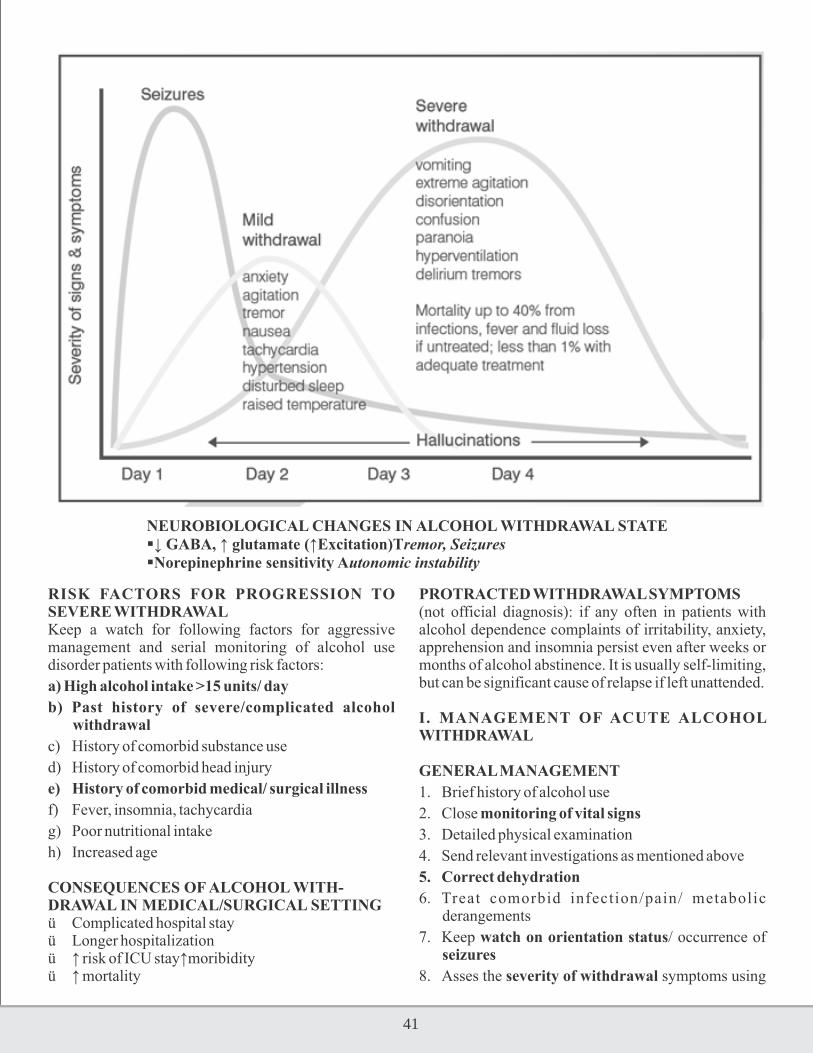
63
NEUROBIOLOGICAL CHANGES IN ALCOHOL WITHDRAWAL STATE↓ GABA, ↑ glutamate (↑Excitation)Tremor, SeizuresNorepinephrine sensitivity Autonomic instability
RISK FACTORS FOR PROGRESSION TO SEVERE WITHDRAWALKeep a watch for following factors for aggressive management and serial monitoring of alcohol use disorder patients with following risk factors:
a) High alcohol intake >15 units/ day
b) Past history of severe/complicated alcohol withdrawal
c) History of comorbid substance use
d) History of comorbid head injury
e) History of comorbid medical/ surgical illness
f) Fever, insomnia, tachycardia
g) Poor nutritional intake
h) Increased age
CONSEQUENCES OF ALCOHOL WITH-DRAWAL IN MEDICAL/SURGICAL SETTINGü Complicated hospital stayü Longer hospitalizationü ↑ risk of ICU stay↑moribidityü ↑ mortality
PROTRACTED WITHDRAWAL SYMPTOMS(not official diagnosis): if any often in patients with alcohol dependence complaints of irritability, anxiety, apprehension and insomnia persist even after weeks or months of alcohol abstinence. It is usually self-limiting, but can be significant cause of relapse if left unattended.
I. MANAGEMENT OF ACUTE ALCOHOL WITHDRAWAL
GENERAL MANAGEMENT
1. Brief history of alcohol use
2. Close monitoring of vital signs
3. Detailed physical examination
4. Send relevant investigations as mentioned above
5. Correct dehydration
6. Treat comorbid infection/pain/ metabolic derangements
7. Keep watch on orientation status/ occurrence of seizures
8. Asses the severity of withdrawal symptoms using

64
Clinical institute of withdrawal rating scale, revised(CIWA-r). It is a clinician administered scale, covers physiological/cognitive/perceptual changes and takes less than 5 minutes. Higher s c o r e s u g g e s t s g r e a t e r r i s k o f complications.(severity rating based on score of CIWA-r is mentioned in appendix-five)
9. Give multivitamin supplement, especially thiamine to avoid precipitating Wernicke's encephalopathy. Any glucose containing fluid supplementation to be given at least half an hour after thiamine supplementation.
SPECIFIC MANAGEMENTCHOICE OF MEDICATIONBenzodiazepines are the mainstay of alcohol withdrawal treatment.2 types:• Longer acting ( ½ life ~ 30 hours)
e.g. Diazepam, Chlordiazepoxide
• Shorter acting ( ½ life ~15 hours)
e.g.Lorazepam, Oxazepam
• Longer acting better for ↓ seizures, but sedation
• Liver disease and old age significantly affect the pharmacokinetics of benzodiazepines that undergo p h a s e I o x i d a t i v e m e t a b o l i s m ( e . g . chlordaizepoxide), but only mildly alter the kinetics of those that only go phase II glucoronidation (e.g. lorazepam, oxazepam). Metabolites of long acting Benzodaizepines accumulate; metabolism will be slower and will necessitate close monitoring.
• Shorter acting Benzodaizepines preferred (due to: No active metabolites, ease of monitoring& ↓ side effects) in:
- Elderly
- Hepatic impairment
- Renal impairment
- Pulmonary diseases
- Head injury
DOSING STRATEGYDose of Benzodiazepines should be individually determined according to severity of withdrawal and is a matter of clinical decision. However, following are the regimes as per suggested prescribing guidelines:
A. “Fixed schedule”
• Set doses at fixed intervals
• PRNs for breakthrough symptoms
• Tapered over 3-5 days
• Problems: over/under- medication
• Beneficial in: history of seizure/ sedation and pre operatively in surgical patients
Examples: • Lorazepam 2 mg q4h • Diazepam 10-20 mg q6h • Chlordiazepoxide 25-50 mg q6h • Oxazepam15 mg q6h
B. “Symptom- triggered” • Medication given when CIWAr>8 • ↓ Dose, side effects, treatment time • Problems: cost/staff time • Beneficial in: Elderly/ debilitating medical
illnesses
Examples • Lorazepam 2 mg q1h (CIWA-r 8-13) • Lorazepam 3 mg q1h (CIWA-r 14-20) • Lorazepam 4 mg q1h (CIWA-r>20)
II. TREATMENT(Appendix-six mentions flow chart of alcohol withdrawal management)
A. ACUTE PRESENTATIONPatients presenting in acute withdrawal can be prescribed chlordiazepoxide (if liver function normal) on a flexible dosing for initial 24-48 hours with 2-3 hourly clinical assessment of withdrawal signs and symptoms. Subsequently, patient can be put on a standardized reducing (20% daily reduction in dosages) regimen.
B. BREAKTHROUGH WITHDRAWALScreen for comorbid medical illness/infection/ metabolic abnormalities and repeat dosage of last days standard regime before starting scale on a daily based from this point.
C. SEVERE WITHDRAWAL/ DELIRIUM TREMENS
a) Non pharmacological management i. Shift patient to an optimal stimulation
environment ii. Reduce excessive stimulation iii. Provide orientation cues at regular interval (tell
time/ show calendar/ appraise of staff and family around)Keep limited familiar people around
iv. Well lit room v. Adequate hydration to be maintained

65
vi. Input/ output chartingvii. Vitals monitoringviii. Parenteral thiamine: 100-300 mg daily
b) Pharmacological managementBenzodiazepines are the main stay and objective is to make patient calm and sedated but easily arousable.Prefer parenteral route due to poor absorption from gastrointestinal tract
Diazepam - IV 5-10 mg, every 15-20 minutes (IM route to be
avoided, per rectal in rare cases can be given) - Should be given in a large vein, not exceeding at rate
of 5 mg/min - Limitation: long acting, metabolites with long half-
life, marked sedation, at times difficult to assess sensorium in patients with medical illnesses
Lorazepam- Preferred route: IV 2-4 mg, every 15-20 minutes
(can be given IM too)- Bypasses first pass metabolism and has no
metabolites, so drug of choice in patients with deranged liver function/ renal function/ compromised respiratory reserve and elderly.
• Psychotic symptoms or marked agitation unresponsive to benzodiazepines can be given low dose haloperidol 1.5-5 mg in divided doses (oral or parentral). however, caution needs to be exercised as antipsychotics have seizure lowering threshold.
D. WERNICKE ENCEPHALOPATHYIt is an acute life threatening condition presenting in alcoholics due to thiamine deficiency. Characterized by classic triad of:
i. Global confusion
ii. Ataxia
iii. External opthalmoplegia
But the classic triad is hardly seen in 10 % of the cases. Hence Wernicke s encephalopathy may not be recognized in routine clinical settings.
Signs Incidence (%)
Mental changes 82
Eye signs 29
Ataxia 23
Classic triad 10
Mental changes are non-specific and may be attributed to intoxication, withdrawal, head injury and other intercurrent illnesses. Thus a high index of suspicion is required; if any of the following signs are present:
i. Acute confusion
ii. Decreased consciousness/coma
iii. Memory disturbances
iv. Nystagmus
v. Opthalmoplegia
vi. Gait disturbances
vii. Unexplained hypotension with hypothermia
Treatment: High dose of parenteral thiamine 100-300 mg IV/IM daily for 7 days followed by 100-200 mg oral thiamine supplementation for next three months. After acute withdrawal state, higher cognitive functions (attention, concentration, memory) should be monitored.
I. DISCHARGE PLANNING AND AFTERCAREPatients who have been identified as requiring an unplanned detoxification as inpatient are those in severe withdrawal and possibly alcohol dependent and are likely to reinstate their drinking after abstinent. There is high risk of accidental overdose due to mixing of alcohol and their discharge benzodiazepine medications. Also these patients are at high risk of self-harm and may use discharge medications for the purpose. So, clinical team to ensure following before discharge:
1. Patients should have finished their detoxification regime before discharge
2. They have been prescribed adequate dose of benzodiazepine on discharge
3. Prescription for thiamine and vitamin B complex to be given
4. Referral to appropriate deaddiction services for long term relapse prevention

Exudate
Tuberculosis
Neoplastic disease
Pulmonary embolism
Para pneumonic effusion
Drug induced
Gasterointestinal due pancreatic disease,
subphrenic absum, Esophageal perforation
Post CABG/Dressloris synd.
Collogen Vasucalr disease
Chylothorax
Hemothorax
Transudate
CHF (Congestive heart failure)
Cirrhosis
Nephrotic Syndrom
CKD
Peritoneal dialysis
Myxedema
Hypoalbuminemic
Urinothorax
Dr. Kamal Kumar PandeySenior consultant, PulmonologyPushpanjali Crosslay Hospital
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
Approach to the Patient & Pleural Effusion
Pleural effusion is abnormal accumulation of fluid in pleural cavity which normally contains a very thin layer of fluids. A good history is very important in investigating any patient with pleural effusion. In investigating any patient with pleural effusion, always ask about:
(1) TB status(2) Trauma (Chest /Abd)(3) CABG surgery(4) Previous Pneumonic or Pleurisy(5) Prior Malignancy and treatment (6) Asbestos exposure(7) Residence & Travel history(8) Drugs(9) Time to Reaccumulation after thoracocentasis
When a patient presents to us with pleural effusion, the first step is to determine whether the effusion is a transudate or an exudate.
A transudate pleural effusion is mostly due to systemic factors and an exudates effusion is due to local factors.
Important causes of effusion
Lights's Criteria for distinguish Transudative pleural effusion from exudative pleural effusion.Exudate pleural effusion meets at least one of the following criteria , whereas transudate pleural effusion meet none:(1) Pleural fluid protein/Sr. Protein > 0.5(2) Pleural fluid LDH/Sr. LDH > 0.6
rd(3) Pleural fluid LDH more than 2/3 normal upper
limit for Serum LDH
These criteria misidentify or 25% of transudate as exudates. In such situation the difference between Sr. Protein & Plural fluid Protein should be measured. If this gradient is > 3.1 gm/dl, the effusion is definitely transudative.
If there is a significant possibility of transudative pleural effusion, the most cost effect Utilization of the laboratory is to only obtain the protein and LDH levels of pleural fluid at the initial diagnostic thoracocentasis. Pleural fluid sample should be kept aside for other test if the fluid proves to be an exudate Peternon & speichor reviewed the charts of 83 patients whose pleural fluid was transudate by protein and LDH level during a 1 year period. They found that 725 additional studies were performed on these 83 pleural fluids.
Only 9 of the 725 studies yielded positive results and the positive result was eventually proven to be false in 7 of the 9 patient. If no test other than the protein and LDH had been obtained in these 83 patient, there would have been a mean cost saving of $ 185 per patient.
RULE OF THUMBOnly send pleural fluid protein and LDH for initial evaluation of any pleural effusion. If Pleural effusion is transudative no further pleural fluid evaluation required

67
Cost of the Pleural fluid Analysis
Diagnostic Algorithm of pleural effusion. Pleural fluid nucleated cell. The TLC count of fluid is rarely helpful in establishing a definite diagnosis; however it may provide useful information. If the nucleated cell count is <500/ml, the fluid is usually a transudate. If the nucleated cell count is > 50000/ml, it usually represent emphysema Nucleated cell count between 25000-50000 are usually seen only with uncomplicated parapneumonic effusion, Acute pancreatitis & acute pulmonary infarction.
The D/D of an exudates pleural fluid with a lymphocyte count of > 80% includes:
(1) Tubercular pleurisy
(2) Lymphoma
(3) Chylothorax
(4) Ch Rheumatoid pleurisy
(5) Sarcodiosis
(6) Yellow naily syndrome
(7) The Post CABG
The D/D of pleural fluid eosinophila 10% of TLC) INCLUDES MOST COMMONLY
(1) Pneumothorex and hemothorax
(2) BAPE
(3) Pulmonary embolism & infraction
(4) Parasitic disease
(5) Fungal diseases
(6) Drug Induced (Nitrofuratoin, dantroline, proplythiouracil, valproic acid and bromocriptin, i so t re tenoin) Amiodarone , methot rexa te procarbezim) Clozapine, INH, Procanamide
(7) Hodgkin lymphoma & Carcionoma
Pleural fluid pH & Glucose.A Pleural fluid PH < 7.3, in the setting of a N blood pH narrows a D/D of the exudates effusion to:
(1) Emphyema/ Complicated para pneumonic effusion
(2) Ch rheumatoid pleurisy
(3) Malignancy
(4) Tuberculer pleurisy
(5) Lupus Pleuritiis
Urinothorex, most common caused by obstructive uropathy is the only cause of a low pH transudate. Emphyema & Rheumatoid Pleurisy are the only effusions that can present with glucose concentration of 0 mg/dl.
Complicated parapenumonic effusion, emphyema, rheumatoid pleurisy and pleural paragonimiasis are the only effusions with a triad of a pH <7.3, a glucose <60mg/dl & LDH > 1000 U/L.D/D of B/L effusion on chest radiograph.B/L effusions are commonly transudate due to
(1) CHF/(2) Nephrotlic syndrome
(2) Hypo albuminamie
(3) Peritonieal dialysis
(4) Constrictive pericarditis
Most common causes of B/L exudative pleural effusion are(1) Malignancy(2) Lupus Pleuritis (3) Yellow nail Syndrome
When effusion are associated with interstitial lung disease. the D/D includes:
(1) CHF
(2) Rheumatoid arthritis
(3) Lymphongitis carcinomatoses
(4) Asbesto-Induced disease (BAPE)
(5) LAM
(6) Viral & Mycoplasma pneumonia
(7) Sarcodiasis
(8) PCP Pneumonia
Causes of Spontaneous Resolution of pleural effusion(1) Patient with pulmonary embolism without
pulmonary infarct, the effusion resolves completely within 7-10 days. If associated with infarct it may talk 2-3 weeks.
(2) The pleural effusion associated with Ac pancreatitis resolves within 1-2 weeks.
Protein
LDH Rs. 335/-
Protein
Sugar
Cytology Cell Count
LDH
ADA
Cytospin for malignant cells
Genexpert
AFB Stain & AFB Culture
Rs. 5260/-

68
With continues HD, a exudative uremic pleural effusion resolves in 4-6 weeks.
Persistence of the uremic effusion suggests that either a trapped lung or fibrothorax has developed which can be successfully treated with decortication.
A tubucular effusion has a spontaneous resolution rate of 4 to 16 weeks, corticosteroids therapy will shorten resolution time. Rheumatoid effusion takes 4 to 6 month to resolves effusion that persist for >1 yr have a limited D/D that includes:
(1) Trapped lung
(2) Cytothorax
(3) Yellow nail syndrome
(4) Lymphangiectasia
(5) Rhematoid Pleuristy
(6) Malignancy
Diagnoses that can be definitively establish by pleural fluid analysis include:
(1) Emphyma (Pus)
(2) Malignancy cytology(+)
(3) Tuberculer effusion (AFB+)
ADA highly (+)
(4) Lupus Pleurit (Lupus cells ANA+ )
(5) Cylothorax (Milky effusion triglyceride > 110 mg/dl)
(6) Hemothorax (Blood effusion pleural fluid/Blood Hct >0.5
(7) Urinothoex (Pleural fluid/Sr creatine >1.0)
(8) Peritoneal Dialysis (Total protein <0.5 gm/dl & Glucose 200-400 mg/dl)
(9) Esophageal rupture (Increase Salivary amylase & pH<7.00)
(10) Rheumatoid pleurisity (Pleural fluid glucose < 60mg/dl & Pleural fluid cytology-tadpole/comet cells in background of necrotic material)
Common disease associated with Pleural Effusions(1) Congestive heart failure
Patient with Plerual effusion from CHF will provide H/o orthopnea/PND typical of LVF.
The CXR will demonstrate Cardiography, B/L effusion, interstiatial or alveolar infiltrate.
A diagnostic thoraxcorcentasis is indicated in suspected CHF when there is
(a) FEVER
(b) Pleuritic chest pain
(c) A unilateral effusion
(d) A left effusion greater than right effusion
(e) Effusione of disparate size.
With the typical presentation thoracocentasis can be withheld while observing the response to treatment.
Use of diuretics can transform a transudate into pseudo exudates. Pleural effusion N T pro BNP > 1500 pg/ml is virtually diagnostic of CHF.
HEPTATIC HYDROTHORAXPleural effusion occurs in 5% of patient with cirrhosis and ascitis. The predominate mechanim is the direct movement of the peritoneal fluid through small opening in a diaphragem into pleural space. The effusion is usually right-sided and frequently is large enough to produce severe dyspnea.
PARAPNEUMONIC EFFUSIONIt is associated with bacterial pneumonia /lung abscess or bronchiectasis. If a patient with pneumonic develops pleural effusions.
The following feature in effusion needs intervention.
(1) Loculated pleural fluid
(2) Pleura fluid pH <7.20
(3) Pleural fluid glucose <60 g/dL)
(4) Positive gram stain or culture of the Pleural Fluid
(5) Presence of gross pus in the pleural space
If any of these characteristic are present, a repeat thoracentesis should be performed. If the fluid cannot be completely removed , ICD insertion with fibrinolytic agent (tpa 10 mg) or thoracoscoy with breakdown of adhesions should be done. Decorticetion should be considered when these measures are ineffective.
Malignant effusions.The three tumors that cause > 75% of all malignant pleural effusion are lung and breast carcinome and lymphoma. the diagnosis usually is made via cytology of the pleural fluid. If the initial cytology examined is negative, thoracoscopy Is the best next procedure if malignancy is strongly suspected.
Patient with a malignant pleural effusion are treated symptomaticaly for the most part as they frequent

69
disseminatd malignancy and are not curable with chemotherapy . Symptomatic treatment includes:(a) Insertion of and small indewling catheter(b) ICD and pleurodesis
Mesothelioma: Malignant mesotheloma are primary tumor of pleura. Most are related to asbestos exposure.
Thoracoscopy or open pleural biopsy is usually necessory to establish the diagnosis.
Pulmonary embolizm:The diagnosis most commonly overlooked in the D/D of a patient with undiagnosed pleural effusion is PE. Dyspnea is the most common symptoms.Pleural fluid is almost always an exudative. Diagnosis is established by pulmonary angiography .
Tuberculer pleuritis In developing countries, including India, the most common cause of an exudative pleural effusion is tuberculosis (TB). But it is relatively uncommon in developed countries. Patient with TB pleuritis present with fever, weight loss, dyspnea and/or pleuritic chest pain.
The pleural fluid is exudative with d 90 – 95% lymphocyte.
The finding of >10% mesothelial cells & pleural fluid eosigititice makes the diagnosis unlikely. The exudates and predominantly lymphocytic effusion with high ADA (> 40) /interferon ϒ 140 pg/dl) is virtually diagnostic of tuberculosis pleural efficacy .
Alternatively , the diagnosis of can be established by AFB culture of the pleural fluid, needle biopsy of the pleurar or thorcoscopy.
Effussion sec to viral infection, viral infection are probable responsible for 20% OF undiagnosed exudate pleural effusism, These effusion resolve spontaneously therefore if the patient with undiagnosed exudates effusiasm is improving clinically it is probably for spontaneous resolution.
CHYLOTHORAX: A Chylothorax occurs when the thoracic dust is disrupted and chyle accumulates in the pleural space. The most common cause of chylothorax is trauma (most frequently thoracic surgery), but it also may result from tumors in the mediastinum. Thoracentiesis
reveals milky fluid, and biochemiscal analysis reveals a triglyceride level that exceeds 1.2 mmol/L (110 mg/dL).
The treatment of choice for most chylothoraxes is insertion of a chest tujbe plus the administration of octreotide. An alternative treatment is ligation of the thoracic duct.
HEMOTHORAX: When diagnosis thoracenteis reveals bloody pleural fluid, a hematocrit should be obtained on the pleural fluid. If the hematocrit is more than one half of that in the peripheral blood, the patient is considered to have a hemothorax. Most hemothorax should be treated with ICD drug…
If the pleural hemorrhage exceeds 200 mL/h, consideration should be given to thoracoscopy or thoracotomy.
Trappred Lung: Trapped lung occurs when a fibrous membrane covers the visceral pleura preventing lung expansion. Causes of trapped lung include.
(1) Emphysema
(2) Rhematoid Pleurisy
(3) Malignancy
(4) Uramic Pleuritis
(5) Hemothorax,
(6) P/CABH,
(7) BAPE.
The effusion recurs rapidly following thoracentesis to the pre-thoracentesis volume. Pleural fluid forms with trapped lung because failure of lung expansion creates a space and this negative pressure space fills with fluid . the fluid is typically between a transudate and exudates. The diagnosis of trapped lung by should be considered when an effusion has been presented for several months and longer.
Decortication is effective if the underlying lung is relatively normal. Only patient with large crapped-lung effusion who are symptomatic should be considered for Decortiation.

Dr. Praveen PandeySenior consultant, Pulmonology, critical care and sleep medicineMax Hospitals, Patparganj,Delhi
YEAR BOOK & SOUVENIR 2014
Fungi are a group of spore-bearing, often filamentous, organisms that lack chlorophyll and therefore obtain their food by either a saprophytic or a parasitic existence. Most live by breaking down dead organic matter and, in their turn, they or their spores may provide food for other organisms such as amoebae and insects. They reproduce by producing spores, either sexually or asexually, or by budding or fragmentation.
With very few exceptions, humans and the animal kingdom are incidental to the life history of fungi and pathogenic effects result from the accidental intrusion of fungal spores into the animal environment. Generally, therefore, fungal diseases affect the skin and the lungs, organs in direct contact with the air in which spores are carried. Occasionally soft tissue infections may occur as a result of penetrating injuries that introduce soil borne spores. The pulmonary syndromes associated with fungi in humans are asthma, hypersensitivity pneumonitis, saprophytic colonization and infection.
Among the pathogenic fungi, there are two distinct groups:(i) The primary pathogens that most frequently
infect healthy individuals. Fortunately, they are not commonly found in the Indian subcontinent and are natural inhabitants of North and South America. These include s p e c i e s l i k e B l a s t o m y c e s , C o c c i d i o i d e s , H i s t o p l a s m a a n d Paracoccidioides.
(ii) Opportunistic invaders: These fungi i n v a d e d e b i l i t a t e d o r immunocompromised individuals and those with a pre-existing, diseased and scarred lung parenchyma. In the days of i n c r e a s i n g n u m b e r o f
immunocompromised patients like HIV infected individuals, organ transplant recipients on immunosuppressive therapy, we have been encountering an increasing number of patients with fungal infections. These include species like Aspergillus, Candida, and Cryptococcus.
Sources of fungi are almost invariably that it was inhaled from the ambient air. The air is full of fungal spores, liberated from organisms growing on dead or living vegetable matter. Most of these spores are small and of appropriate size and shape to be respirable.
PULMONARY ASPERGILLOSISAspergillus is a ubiquitous saprophytic mold with worldwide distribution that plays an essential role in recycling carbon and nitrogen. This fungus has a simple biological cycle characterized by a high sporulating capacity, which results in the release of conidia at high concentrations (1 to100 conidia/m3) into the atmosphere. Aspergillus conidia have a diameter small enough (2 to 3μm) to reach the lung alveoli. However, despite the fact that humans constantly inhale Aspergillus conidia, such conidia are effectively eliminated in immunocompetent individuals.
Pulmonary Fungal Infections

71
Allergic Bronchopulmonary Aspergillosis (ABPA)Allergic bronchopulmonary aspergillosis (ABPA) is an idiopathic inflammatory lung disease characterized by an allergic inflammatory response to the colonization of Aspergillus or other fungi in the lung. It was first described in 1952 by Hinson and coworkers and then again in 1967, when Scadding recognized an association of this disease with proximal bronchiectasis in a reas previous ly a ffec ted by inf i l t ra tes (predominantly in the upper lobes)
Criteria for the Diagnosis of ABPAPrimary
Episodic bronchial obstruction (asthma)
Peripheral blood eosinophilia (>1000/mm3)
Immediate type skin reactivity to Aspergillus antigens
Precipitating serum antibodies (precipitins) against Aspergillus antigens
Elevated serum IgE concentrations (>1000 ng/ml)
Elevated serum IgE and/or IgG antibodies specific to A. fumigatus
History of pulmonary infiltrates (transient or fixed) on chest radiographs or CT scans
Central bronchiectasis on chest CT scans
Secondary
A. fumigatus in sputum (by repeated culture or microscopic examination)
History of expectoration of brown plugs or flecks
Arthus reactivity (late skin reactivityy) to Aspergillus antigen
Clinical Stages of ABPA
Stage I: Acute
Acute asthma symptoms
Elevated serum IgE (>1000 IU/ml)
Peripheral blood eosinophilia (may be absent in patients treated with oral coricosteroids)
Fleeting infiltrates on chest x-ray (may be absent in patients treated with oral coricosteroids)
Positive specific IgE, IgG, skin test reactivity, and precipitins to A. fumigatus
Responds to steroids/antifungal therapy
Stage II: Remission
Resolution of symptoms
Resolution of pulmonary infiltrates
Improvement in eosinophilia and A. fumigatus specific blood abnormalities
Stage III: Exacerbation/recurrence
Recurrence/worsenning of clinical symptoms
Recurrent pulmonary infiltrates
Rising IgE levels
Stage IV: Steroid-dependent-asthma
Refractory steriod-dependent asthma
Persistently elevated serum IgE levels
Persistently elevated A. fumigatus–specific blood abnormalities
Stage V: Fibrotic lung disease
Refractory steriod-dependent asthma
Fibrotic lung disease (irreversible obstructive and restrictive defects with impaired diffusing capacity)
Chronic bronchiectasis symptoms (sputrum production, frequent infections)
Management of ABPA:
Steroids, both inhalational and oral, have remained the sheet anchor of ABPA treatment. Some authorities also have used itraconazole with encouraging results. The accepted regimen for prednisolone therapy is as follows:
(1) Initiate treatment with 0.5 mg/kg per day for two weeks.
(2) This can be changed to alternate day therapy for next three months. This dose of prednisolone should be
sufficient to control asthmatic episodes and this can further be corroborated by a) disappearance of pulmonary opacities, (b) more than 35% reduction of serum IgE levels and (c) reduction of peripheral eosinophilia.
(3) In case the above criteria are met, then prednisolone is to be gradually reduced to about 7.5 mg on alternate days.
AspergillomaMycetoma is the name given to a mass of fungal hyphal material growing in a lung cavity. The usual organism is A. fumigatus and thus the lesion is usually called aspergilloma; however, other fungi and other species of Aspergillus may occasionally be found. In most patients there is pre-existing lung disease, although the condition may occasionally arise in apparently normal

72
lung or may be the consequence of an aspergillar pneumonia. The most common predisposing conditions are old tuberculous cavities and the bronchiectasis associated with upper lobe fibrosis in chronic sarcoidosis, allergic alveolitis, ankylosing spondylitis or rheumatoid disease. Other conditions in which Aspergilloma has occurred include pulmonary infarcts, pneumonia, lung abscess and bulla.
Clinical features:Hemoptysis is the typical manifestat ion of aspergilloma, as it is seen in 50 to 90 percent of patients. Hemoptysis is typically infrequent and mild but is occasionally massive or even fatal. The presence of any other symptoms, including dyspnea, fever, malaise, and weight loss, in patients with aspergilloma should be attributed to the underlying cavitary pulmonary disease or bacterial superinfection or suggest the presence of an overlapping IPA syndrome such as CNPA.
Diagnosis: The classical radiological picture is a mass within a cavity and an air crescent on top of the mass which goes by the name of Monod's sign. This mass can shift its position on change of posture. There may be surrounding infiltration or fibrosis. Though the location is usually in the upper lobes and at times multiple, it could be present in any place. Most of these patients do show positive precipitin test to Aspergillus antigen and disease can be confirmed by demonstration of fungal hyphae in respiratory secretions or tissue specimens. Skin hypersensitivity to fungus and raised IgE are unreliable pointers to the diagnosis.
Treatment: Treatment has remained both problematic as well as controversial24. Asymptomatic persons can be left undisturbed with reassurance that it may disappear by coughing out of fungal fragments. The dominant problem being haemoptysis, bronchial artery embolization by nonabsorbable materials, provides a good treatment option. But recurrence rates are high. Surgical resection is also a good option and at least, eliminates the risk of life-threatening haemoptysis in future, but results are variable. Some surgical authorities have grouped the cases to simple or complex, simple aspergillomas are those with thin walled cavity with minimal involvement of surrounding parenchyma and they do well with surgery.
Invasive AspergillosisInvas ive a spe rg i l lo s i s i s a d i sease o f the immunosuppressed, particularly of those with defective
granulocyte function. Thus it affects patients with acute leukaemia, patients on high doses of corticosteroids and children and young adults with chronic granulomatous disease. It is also seen in patients immunosuppressed after transplantation of bone marrow or solid organs. It is less common in AIDS, occurring as a late and usually fatal complication, sometimes manifesting as a necrotizing tracheobronchial infection [244–246]. It may also occur in a wide variety of other clinical situations, for example following influenza or other pneumonia, pulmonary infarction, treatment of chronic airflow obstruction with corticosteroids and resection of aspergilloma. Very occasionally it may appear to occur de novo.
Clinical presentation in an immunocompromised host could be with tracheitis, broncho pneumonia, or pneumonic consolidation. There is resultant patchy mucosal ulceration with pseudo membranous plaques of mucus and hyphae in bronchial channels. They may present with unremittent fever with poor response to broad spectrum antibacterial combination. X-ray chest can show patchy pneumonia or single or multiple areas of homogeneous consolidation in the form of so called “round pneumonia”. Cavitation can occur in 1-3 months' time. Unless treated aggressively, fatality can be the result.
The diagnosis is usually suspected on clinical grounds. Diagnosis should be suspected in seriously ill, febrile immunocompromised or neutropenic patients and can be confirmed by bronchoalveolar lavage or FNAC. Repeated culture of Aspergillus from sputum also gives strong support, although sputum may be culture-negative in invasive disease and there may not be time to wait for repeated cultures. Galactomannan is a polysaccharide cell wall component of Aspergillus spp. that is released into the circulation during fungal growth in tissues and can be detected in the serum of patients with IA. Sensitivity rates ranging from 67 to 100 percent and specificity rates ranging from 86 to 99 percent has been reported. A colorimetric assay for the detection of 1, 3-β-Dglucan, an integral cell-wall component in a number of pathogenic yeasts and filamentous fungi, recently became commercially available. The sensitivity and specificity rates for this test in limited studies thus far have ranged from 67 to 100 percent and from 84 to 100 percent, respectively. PCR detection of Aspergillus nucleic acids is a promising method for early detection of IA. The sensitivity of PCR is excellent, but its specificity for invasive infections can be problematic, and false-positive results are common.

73
Treatment is urgent and systemic antifungal agents of proved efficacy like parenteral amphotericin B, triazoles, echinocandins etc in appropriate dosage.
Chronic Necrotising AspergillosisChronic necrotizing pulmonary aspergillosis (CNPA) corresponds to an indolent process of lung destruction caused by the Aspergillus fungus, generally A. fumigates. This entity is different from an aspergilloma, as a pre-existing cavity is not needed, although a cavity may develop in the lung as a secondary phenomenon. In contrast to invasive aspergillosis, CNPA occurs over a period of months to years and there is no vascular invasion or dissemination to other organs. The main risk factors are: chronic obstructive pulmonary disease, sequelae of tuberculosis, pulmonary resection, r a d i a t i o n - i n d u c e d p u l m o n a r y f i b r o s i s , pneumoconiosis, cystic fibrosis, pulmonary infarction and sarcoidosis. Other immunosuppression conditions, such as diabetes mellitus, malnutrition, alcoholism, connective tissue diseases and prolonged corticosteroid therapy, are also situations of increased risk. Results from chest X-rays may reveal unilateral or bilateral infiltrates with or without cavitation and pleural thickness, especially in the upper lobes and in the upper segments of the lower lobes. In 50% of the cases an aspergilloma occurs simultaneously. The definite diagnosis is made through the his tological demonstration of tissue invasion by the fungus and the growth of Aspergillus species in a culture. Other helpful tests include serum IgG antibodies to Aspergillus and immediate skin reactivity for Aspergillus antigens. Due to the difficulty in confirming the diagnosis, the following diagnosis criteria were established and together are highly indicative of CNPA: characteristic clinical and radiological findings, elevation of inflammatory markers (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)) and either serological test results positive for Aspergillus or the isolation of Aspergillus from respiratory samples. Active tuberculosis, non-tuberculosis mycobacteriosis, cavitary histoplasmosis and coccidioidomycosis should be excluded. Galactomannan and polymerase chain reaction (PCR) tests from bronchoalveolar lavage, as well as cutaneous sensitivity tests for Aspergillus, do not have a confirmed use in diagnosis.Therapy with voriconazole or itraconazole has emerged as the first-line treatment and is safer than amphotericin B. The long-term prognosis for patients with CNPA is not well documented. The ideal treatment duration has not yet been defined and depends on the extension of the disease, the patient's response to treatment, the base disease and the patient's immunological condition. In
some cases, lifelong therapy may be required.
CANDIDIASISCandida spp. are imperfect forms of the ascomycete genera Saccharomyces and Pichia. Most species, including the most important, C. albicans, are commensals in the mouth and gastrointestinal tract of humans. Disease occurs as a result of local invasion of damaged skin or mucosa, aspiration into lung or introduction into the tissues or bloodstream. Thus, surgical operations and indwelling intravenous cannulae can lead to disseminated candidiasis, whereas local disease may manifest as thrush, oesophagitis, lung abscess or infection of skin burns. Infection is promoted by diabetes, malnutrition, and immunosuppression and, in the case of local infection, by the use of broad-spectrum antibiotics that remove competing bacteria.
The clinical manifestations of primary Candida pneumonia are nonspecific and mainly include persistent fever and tachypnea. Chest pain, cough, and sputum production occur occasionally. Also, physical examination and routine laboratory studies are nonspecific. Chest radiographs may demonstrate a local or diffuse infiltrate involving one or both lungs, which is most often associated with infection acquired by the endobronchial route .A miliary-nodular pattern is most often associated with hematogenous seeding of the lung in cases of disseminated candidiasis and often appears late in the clinical course of the disease.
Diagnosis of pulmonary candidiasis is challenging and depends on evidence of tissue invasion. Isolation of yeast from sputum does not prove invasive yeast infection of the respiratory tract because of contamination by commensals from the oropharynx. Candida is present in the oropharynx of approximately 20 to 40 percent of all patients, especially those with chronic lung disease and those receiving chronic antibacterial treatment. Bronchial washings and BAL specimens provide a more representative picture of the respiratory pathology compared with sputum. However, they can still be contaminated with mouth flora. Histopathological demonstration of tissue invasion by Candida spp. in open lung biopsy or fine-needle aspiration is definitive, although such biopsies are difficult to perform in pancytopenic patients with pneumonia. Transbronchial biopsy revealing tissue invasion by Candida spp. is also diagnostic.
Fortunately, most of them are amenable to oral-antifungal agents like ketoconazole or fluconazole. However, involvement of deeper or vital organs may

74
have to be managed by amphotericin B and echinocandins.
PNEUMOCYSTIS CARINII PNEUMONIA (PCP)Pneumocystis carinii pneumonia (PCP) is an o p p o r t u n i s t i c i n f e c t i o n t h a t o c c u r s i n immunosuppressed populations, primarily patients with advanced human immunodeficiency virus infection. Before the widespread use of prophylaxis, PCP was the AIDS-defining illness in 60 percent of cases and eventually affected 80 percent of patients with AIDS. The signs and symptoms of PCP can be subtle. The diagnosis requires a heightened index of suspicion because risk factors for HIV may be denied, remote or unknown. The classic presentation of nonproductive cough, shortness of breath, fever, bilateral interstitial infiltrates and hypoxemia does not always appear. Diagnostic methods of choice include sputum induction and bronchoalveolar lavage. P. carinii cannot be routinely cultured and is identified by stains demonstrating the cyst wall or the trophozoite. The drug of choice for treatment and prophylaxis is trimethoprim-sulfamethoxazole, but alternatives are often needed because of adverse effects or, less commonly, treatment failure. Patients with AIDS require three weeks of treatment for PCP, compared with two weeks in other populations. Adjunctive corticosteroid therapy improves survival in moderate to severe cases. Complications such as pneumothorax and respiratory failure lead to poorer survival. Prophylaxis dramatically lowers the risk of disease in susceptible populations. Although PCP has declined in incidence in the developed world as a result of prophylaxis and effective antiretroviral therapy, its diagnosis and treatment remain challenging.
PULMONARY CRYPTOCOCCOSISPulmonary cryptococcosis occurs in 'normal' hosts as well as those who are immunocompromised. Not surprisingly, the disease is generally more severe in those who have defects in immunity and often accompanied by disseminated infection, including CNS d i sease . In immunocompe ten t hos t s , cryptococcosis is more likely to be limited to the lung and occurs more commonly in patients with chronic lung disease. Immunocompetent subjects with pulmonary cryptococcosis usually are asymptomatic or have mild symptoms that include fever, malaise, cough with sputum production and perhaps dyspnoea. Immunocompromised patients are much more likely to present with fulminant infection with fever, dry cough and dyspnoea that can progress to acute respiratory distress syndrome (ARDS). The diagnosis of
pulmonary cryptococcal infection is confirmed if the organism is grown in culture from sputum or BAL fluid in a patient who has clinical symptoms and radiographic findings compatible with cryptococcosis. The cryptococcal antigen test is highly sensitive and specific and is routinely used to help establish the diagnosis of cryptococcal meningitis and disseminated cryptococcosis. Therapy is dependent upon whether the patient has isolated pulmonary infection or has dissemination to other organs, especially the CNS, and is also dependent on whether the patient is immunosuppressed.
PULMONARY MUCORMYCOSISPulmonary Mucormycos i s i s l e ss common opportunistic fungal disease, localized in the lungs or the mediastinum. Mucormycosis is found in patients of wide age range but with a male predominance. It
presents with fever, dyspnoea, cough and chest pain.Invasion of blood vessel by fungal hyphae, results in necrosis of tissue parenchyma, which may ultimately lead to cavitation and/or hemoptysis. Most common predisposing conditions for mucormycosis are uncontrolled diabetes mellitus, malignancy, chronic illnesses and transplants. Radiographically, a variety of findings may be present. In descending order of frequency these may include lobar consolidation, isolated masses, nodular disease, and cavitation. The most common method used for diagnosis is microscopic examination of specimens obtained via flexible fiber-optic bronchoscopy. Treatment of pulmonary mucormycosis is based on rapidity of diagnosis, reversal of the underlying predisposing factors (if possible) along with prompt institution of antifungal therapy and extensive surgical debridement. The mortality in this dreaded infection has been reported to be around 80%.
MYCOSIS NOT COMMON IN OUR COUNTRY:Some of these fungi are not usual inhabitants of this part of the world. They are usually found in North and South America and are known to cause invasive mycosis in vulnerable host. The clinical entities in this group include the following:
(a) Histoplasmosis
(b) Coccidioidomycosis
(c) Paracoccidioidosis

75

76

Dr Ashok Kumar Grover, Sr. Consultant PhysicianDr Anando Sengupta, DNB StudentDepartment of Medicine, Pushpanjali Crosslay Hospital, Vaishali, Ghaziabad
Pulmonary arterial hypertension (PAH) is a distinct subgroup of pulmonary hypertension that comprises idiopathic PAH, familial/heritable forms, and PAH associated with connective tissue disease, congenital heart disease, portal hypertension, human immunodeficiency virus (HIV) infection, and some other conditions. Pulmonary arterial hypertension (PAH) is defined by right-heart catheterization (RHC) showing precapillary pulmonary hypertension with a mean pulmonary artery pressure (mPAP) of >25 mmHg and a normal pulmonary artery wedge pressure
1(PCWP) of <15 mmHg .
Importance-
· One of the most common contributing cause of death in last decade
· Chronic and progressive disease leading to right heart failure and ultimately death if untreated
· Observed increases in reporting of PH might indicate an actual increase in the number of patients or greater awareness among physicians
· More prevalent among women, blacks, and older adults
· NIH reg (1980s)- The median survival 2.8 years, with 1, 3, and 25-year survival rates of 68%, 48%, and 34%, respectively
· French national multicenter registry(2002-03)- 39.2% of patients had idiopathic PAH and 3.9% familial PAH. In the subgroup of PAH, where PAH was associated with other conditions, 15.3% had connective tissue disease, 11.3% congenital heart diseases, 10.4% portal hypertension, 9.5%
3anorexigen-related PAH and 6.2% HIV infection .
· REVEAL registry- Variables independently associated with increased mortality-pulmonary vascular resistance >32 Wood units, NYHA functional class IV, men older than 60 years and family history of PAH
· Patients with CTD- and HIV-associated PAH tend to have a worse prognosis, whereas those with congenital heart disease–associated PAH tend to have a better prognosis
· Prognostic indicators in PAH- functional class [FC], exercise endurance, and hemodynamics
· Pregnancy is considered to be associated with high rate of mortality (30-50%) in PAH patients
Diagnostic classification of pulmonary hypertension
1. Pulmonary arterial hypertension (PAH)- idiopathic/heritable/ d rug induced /CTD as soc i a t ed / congen i t a l hea r t diseases/schistosomiasis
2. Pulmonary hypertension with left heart disease- systolic/diastolic dysfunction/ valvular HD
3. Pulmonary hypertension due to lung diseases and/or hypoxia- COPD/ILD
4. Chronic thromboembolic pulmonary hypertension
5. PH with unclear and/or multifactorial mechanism- myeloproliferative disoders, sarcoidosis, vasculitis, metabolic disorders
Genetics- · French PAH registry- cohort of 674 patients, prevalence of
familial PAH 3.9% of all cases of PAH and a proportion of 7.3% of familial PAH in the subgroup of idiopathic, familial or anorexigen-associated PAH
· Autosomal dominant trait with a markedly reduced penetrance, since only 10-20% of necessary carriers of the mutation will develop PAH
· Mutation of bone morphogenetic protein receptor type 2 gene (BMPR2)- 58-74% of PAH patients with a family history of the disease, and 3.5-40% of so called idiopathic PAH patients
· Mutation in ACVRL1 (Activin A receptor type II-like kinase 1) and ENG (endoglin) genes also shown to predispose
Pathophysiology- The right ventricle responds to an increase in pulmonary vascular resistance by increasing right ventricular (RV) systolic pressure to preserve cardiac output. In some patients, chronic changes occur in the pulmonary circulation, resulting in progressive remodeling of the vasculature, which can sustain or promote pulmonary hypertension even if the initiating factor is removed. Current hypothesis for development of pulmonary hypertension is genetic predisposition for PAH followed by a superimposed environmental factor (infection, inflammation, autoimmunity).
Intima and media proliferation and its consequent pulmonary vascular obstruction are key elements in pathogenesis.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Pulmonary Arterial Hypertension

78
Symptoms and signs-
· Persistant dyspnea on exertion
· Chest pain, light-headedness and syncope on exertion
· Palpitations
· Hemoptysis
· Hoarseness of voice – Ortner's syndrome
· H/O autoimmune disease
· Loud S2, systolic murmur of TR, diastolic murmur of PR(rare)
· Signs of right heart failure(severe cases)- venous jugular distension, hepato-jugular reflux, tender hepatomegaly, Lower limb edema, ascitis and generalized edema
Diagnosis-
· ECG- RVH with strain, and right atrial dilation
· Chest Xray-central pulmonary arterial dilatation which contrasts with loss of the peripheral blood vessels
· PFT- relatively preserved lung volumes and normal flows with impaired diffusion capacity
· Six minute walk test- clinical assessment of functional status, distance walked is inverse predictor of mortality
· Echo-RV and right atrial enlargement, a reduction in left ventricular (LV) cavity size, and a tricuspid regurgitant jet that can be used to estimate RV systolic pressure by Doppler, Transthoracic doppler-echocardiography (TTE).
· HRCT chest( for parenchymal disease), V/Q scan and CT pulmonary angiography- assess thromboembolic disesase, sleep study
· Right heart catheterization- resting mPAP of ≥25 mmHg and a normal PCWP, distinction between precapillary (normal PCWP ≤15 mmHg) and postcapillary PH (PCWP >15 mm Hg), measure at end expiration only
· Thyroid functions, ANA, HIV testing
Treatment- · General measures-low level graded aerobic exercises(eg
walking), avoid high altitudes
· Diuretics and O2
· Anticoagulants- in few trials INR 1.5-2.5, CTEPH- INR between 2 and 3
· Calcium channel blockers- recommended after positive vasodilatation challenge test after inhaled NO, nifedipine 90 to 240 mg/day or diltiazem 360 to 900 mg/day in acute vasodilatation response, C/I in PVOD
· Prostanoids- short half life
Epoprostanol(iv infusion)start 2-4 ng/kg/min and is gradually increased to 10-16 ng/kg/min- treatment of choice NYHA IV
Treprostinil- subcutaneous infusion
Iloprost- inhaled/iv- daily inhalation of 2.5 μg or 5.0 μg of iloprost 6 or 9 times a day
· Endothelin receptor antagonists-
Bosentan- started at 62.5 mg twice a day and increased to 125 mg twice daily after one month, s/e- raised liver enzymes
Ambrisentan- once daily at a dose of 5 mg or 10 mg
· Phosphodiesterase -5 inhibitors-
Sildenafil- 20 mg three times a day
Tadalafil- 40 mg once daily
· Combination therapy- addition of bosentan or sildenafil to epoprostenol, treprostinil or iloprost are being studies and combination therapy has been found to be better than single drug in few studies
· Drugs in the pipeline- macitentan, vardenafil, riociguat, selexipag, tyrosine kinase inh
· Non medical treatment- balloon atrial septostomy, lung transplant
4Algorithm for management of pulmonary hypertension
References-
1. R u b i n L J : P r i m a r y p u l m o n a r y hypertension.
N Engl J Med 1997, 336(2):111-7.
2. D'Alonzo GE, et al.: Survival in patients with primary pulmonary hypertension. Results from a national prospective r e g i s t r y. A n n I n t e r n M e d 1 9 9 1 , 115(5):343-9
3. Humbert M, et al.: Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med 2006, 173(9):1023-30.
4. Marc Humbert & Gérald Simonneau- Drug Insight: endothelin-receptor antagonists for pulmonary arterial hypertension in systemic rheumatic diseases. Nature Reviews Rheumatology 1, 93-101 (December 2005)
5. Montani D, et al.: pulmonary arterial hypertension. Orphanet Journal of Rare Diseases 2013, 8:97

Algorithm of 2014Hypertension Management Guidelines
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Input byDr. Rajiv Bansal, MD (Medicine)Sr. Consultant Physician Internist, Max Patparganj, DelhiGoel Hospital, Delhi
Krishna Nagar, Delhi Timings: 1.00am-2.00pm, 6.00pm-9.00pmGoyal Hospital & Urology Centre, Krishna Nagar, Delhi Timings: 9.00am-10.30amMax Balaji Hospital, Patparganj, Delhi Timings: 2.00pm-4.00pm (Wed & Fri)[email protected]
Adult aged> 18 years with hypertension
Set blood pressure goal and intiate blood pressure lowering-medication based on age,diabetes, and chronic kidney disease (CKD).
Implement lifestyle intervention (continue throughout management).
Blood pressure goalSBP > 140 mm HgDBP <90 mm Hg
Blood pressure goalSBP > 140 mm HgDBP <90 mm Hg
Blood pressure goalSBP > 140 mm HgDBP <90 mm Hg
Nonblack BlackAll races
Initiate thiazide- type diureticor ACEI or ARB or CCB, alone
or in combination.
Initiate thiazide- type diureticor CCB, alone
or in combination.
Initiate ACEI or ARB, aloneor in combination with other
drug class
Select drug treatment titration strategyA. Maximize first medication before adding second or
B. Add second medication before reaching maximum does of first medication or C. Start with 2 medication classes separately or as fixed-does combination
Reinforce medication and lifestyle adherence.For strategies A and B, add and titrate thiazide-type diuretic or ACEI or ARB or CCB (use
medication class not previously selected and avoid combined use of ACEI and ARB).For strategy C, titrate doses of initial medication to maximum.
Reinforce medication and lifestyle adherence.Add and titrate thiazide-type diuretic or ACEI or CCB (use medication class
not previously selected and avoid combined use of ACEI and ARB).
Reinforce medication and lifestyle adherence.Add additional medication class (eg. B-blcker, aldosterone antagonist, or others)
and/or refer to physician with expertise in hypertension management.
All agesDiabetes present
No CKD
All agesCKD present with
or without diabetesAge > 60years
At goal blood pressure?
At goal blood pressure?
At goal blood pressure?
General population(no diabetes or CKD) Diabetes or CKD present
Blood pressure goalSBP > 150 mm HgDBP <90 mm Hg
Age > 60years
No
No
No
Yes
Yes
Yes

Resistant HypertensionDr. Ajay U. MahajanM.D. (Medicine), D.M. (Cardiology), F.I.C.P., F.I.C.C, F.A.C.C. (USA), F.E.S.C.,(EUROPEAN UNION), F.S.C.A.I. (USA).Interventional Cardiologist,Professor, Department of Cardiology,Lokmanya Tilak Municipal Medical College & General Hospital, Sion, Mumbai 400 022
Hypertension is one of the leading cause of global burden of diseases. Approximately 7.6 Million deaths (13-15 %) of total deaths are attributed to hypertension. Bes ides Hyper tens ion doub les the r i sk o f cardiovascular disease including coronary heart disease, congestive heart failure, hemorrhagic stroke and peripheral vascular disease. Optimal blood pressure control is key to prevent complicat ions as cardiovascular risk doubles for every 20mm hg systolic and 10 mm hg diastolic blood pressure.
Resistant hypertension as defined by AHA is blood pressure remaining above goal (140/90)in spite of concurrent use of 3 antihypertensive agents of different classes. Ideally, 1 of the 3 agents should be a diuretic & all agents should be prescribed at optimal dose amounts.
The incidence of resistant hypertension in general population is low, but it accounts for 15% of cases of hypertension in specialized clinics and in trials like Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) after approximately 5 years of follow-up, 27% of participants were on 3 or more medications.
Resistant hypertension needs to be considered as different entity as it is a relatively common problem and to identify high-risk patients, identify patients with reversible cause who are likely to benefits from diagnostic tools and therapeutic interventions.
Resistant hypertension as a subset is more common in patients with obesity, diabetes mellitus, deranged renal functions and obstructive sleep apnea.
Causes of Resistant Hypertension:
PATIENT RELATED PHYSICIAN RELATED
High Sodium Intake Sub Clinical Volume Over Load
Poor adherence to Rx. plan Inadequate Use of Diuretics
Intake of Drugs that raise BP Progressive Renal Insufficiency
Lack of Life Style Adherence Unsuspected Secondary Cause
Clinical markers for resistant hypertension include:
1. Advancing age
2. High Base line Blood Pressure
3. Obesity and Over Weight
4. Excessive Dietary Salt Intake, Alcoholism
5. Chronic Kidney Disease (CKD)
6. Diabetes Mellitus (Type II)
7. Left Ventricular Hypertrophy (LVH)
8. Black Race, Female Gender
Algor i thm for management o f re s i s tan t hypertension includes the following steps:
1. Confirm treatment resistance
2. Exclude pseudo resistance
3. Identify and reverse contributing lifestyle factors
4. Screen and discontinue interfering substances
5. Screen for secondary hypertension
6. Pharmacological treatment
7. Referral to specialist
Step 1: Confirm treatment resistanceEnsure that the blood pressure of the patient is recorded as per standard guidelines with appropriate cuff size and patient meets the definition criteria for resistant hypertension.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

81
Step 2. Exclude pseudo resistanceCauses such as “White Coat” hypertension m can be excluded using home and ambulatory blood pressuremonitoring. Non-compliance with drug treatment and lack of life style modification are other c o m m o n c a v e a t s t h a t r e s u l t i n P S E U D O RESISTANCE.
STEP 3. Identify and reverse contributing lifestyle factors.Lifestyle Factors Contributing to Resistant Hypertension such as Obesity or overweight , high salt diet, Physical inactivity, Ingestion of low-fiber, high-fat diet, Heavy alcohol ingestion should be corrected.Non-Pharmacologic Recommendations include
• Weight loss
• Regular exercise (at least 30 min most days of the week)
• Low dietary salt ingestion (<100 mEq sodium/24-hr)
• Moderate alcohol ingestion (no more than 2 drinks per day for most men and 1 drink per day for women or lighter weight persons)
• Ingestion of low-fat, high-fiber diet
• Treat obstructive sleep apnea if present
Step 4. Screen & discontinue interfering substancesApart from medications for hypertension here is a list of medications and preparations which must be actively screened in patients as they interfere in optimal control of blood pressure.
• Non-Narcotic Analgesics
- Non-steroidal anti-inflammatory agents including aspirin
- Selective COX-2 inhibitors
• Sympathomimetic agents
- decongestants
- diet pills
- cocaine
• Stimulants
-methylphenidate
-dexmethylphenidate,
-dextroamphetamine
- amphetamine, methamphetamine
-modafinil
• Other subtances
- Alcohol
-Oral contraceptives
-Cyclosporine
-Erythropoietin
-Natural licorice
-Herbal compounds
Step 5: Screen for secondary hypertensionSecondary hypertension accounts for significant portion of cases of resistant hypertension, once conventional common causes are ruled out it is imperative to search for secondary hypertension, as it can be readily corrected.
Step 6. Pharmacological treatment: General Principles of treatment include:
1. If a correctable cause is found, treat it
2. Aggressive drug therapy – Optimizing the current treatment
3. Withdrawal or down titration of interfering substances as possible
4. Use of a long-acting thiazide diuretic, preferably chlorthalidone
5. Combine agents with different mechanisms of action
6. Recommended triple regimen of
-ACE inhibitor or ARB
- Calcium channel blocker
-Thiazide diuretic
Newer drugs for resistant hypertensionCilnidipine
• 4th generation Ca2+ channel blocker; dual L/N-type Ca2+ channel-blocking action.
• The blockade of N-type Ca2+ channels effectively suppresses neurohumoral regulation in the cardiovascular system, including sympathetic nervous system and renin-angiotensin-aldosterone system.
• cilnidipine is superior to amlodipine in preventing the progression of proteinuria in patients with hypertension and chronic renal disease (Fujita et al., 2007).
Common secondary causes of resistant hypertension
Obstructive sleep apnea
Renal parenchymal disease
Primary aldosteronism
Renal artery stenosis
uncommon secondary causes of resistant hypertension
Pheochromocytoma
Cushing's disease
Hyperparathyroidism
Aortic coarctation
Intracranial tumor

82
ALISKERIN;· Aliskerin is a direct renin inhibitor.
· Aliskiren may have reno protective effects independent of its blood pressure−lowering effect in patients with hypertension, type 2 diabetes, and nephropathy, who are receiving the recommended Reno protective treatment.
· AVOID study, researchers found that treatment with 300 mg of aliskiren daily, as compared with placebo, reduced the mean urinary albumin-to-creatinine ratio by 20%, with a reduction of 50% or more in 24.7% of the patients who received aliskiren as compared with 12.5% of those who received placebo.
Aldosterone antagonist
High prevalence of primary aldosteronism in patients with resistant HT have been studies demonstrating thatMineralocorticoid receptor antagonists provide significant antihypertensive benefit when added to existing multidrug regimens
• Spironolactone
• Used for resistant HT with normal aldosterone levels, 12.5-50mg/daily
• Additional benefits: antiproteinuric, improves heart failure survival (RALES)
• 10% gynecomastia
• Not when creatinine > 2.5, K > 5.0
• Eplerenone
• 10- to 20-fold lower affinity for the aldosterone receptor in vitro compared with spironolactone,
• Eplerenone is 50% to 75% as potent as spironolactone.
• There was no effect of eplerenone on heart rate.
• Eplerenone is a new selective aldosterone receptor antagonist with decreased progestational and antiandrogenic side effects compared with spironolactone.
ENDOTHELIAL RECEPTOR ANTAGONIST
Class of agents that may prove useful for resistant HT is endothelin-receptor antagonists (ERAs)
In patients with mild-to-moderate essential HT, both nonselective and selective (type A receptor) ERAs produce BP reductions comparable to those of common antihypertensive agents, but concerns about adverse events precluded their use as a treatment option for uncomplicated hypertension
DARUSENTAN
It is a selective ERA recently tested in 115 patients with resistant HT, demonstrated a dose-dependent decrease in BP. The largest reductions (11.5/6.3 mm Hg) were observed after 10 weeks of follow-up with the largest dose, and the drug was generally well tolerated. Ongoing phase III clinical trials with such agents are awaited to provide further information in this interesting field
Darusentan provides additional reduction in blood pressure in patients who have not attained their treatment goals with three or more antihypertensive drugs. As with other vasodilator drugs, fluid management with effective diuretic therapy might be required.
STEP 7. Referral to specialist
• If a specific secondary cause of hypertension is suspected in a patient with resistant hypertension, re fer ra l to the appropr ia te spec ia l i s t i s recommended as needed.
• In the absence of suspected secondary causes of hypertension, referral to a hypertension specialist is recommended if the blood pressure remains elevated in spite of 6 months of treatment
C AT H E T E R B A S E D T H E R A P E U T I C MODALITIES IN RESISTANT HYPERTENSION
1. BARORECEPTOR ACTIVATION THERAPY
Activation of the baroreceptors by pressure/stretching leads to buffer-like compensatory adjustments in the parasympathetic and sympathetic nervous system and in turn blood pressure.Electrical baroreceptor stimulation has been shown to decrease BP by attenuation of sympathetic activity and increase in parasympathetic activity.
The Rheos Baroreflex Activation Therapy System (CVRx) consists of a programmable pacemaker-like pulse generator implanted in the right infraclavicular space and connected to bilateral electrode leads that encompass the perivascular space of the carotid sinuses.
— US Rheos pivotal trial was a double-blind randomized clinical trial evaluating baroreflex activation therapy in 265 participants with resistant hypertension at baseline.
• Established safety and efficacy of procedure.
• Sustained BP reduction of 44 mm Hg in 63% of patients at follow-up of 6 months.
• In addition to BP reduction in patients with resistant

83
hypertension, the Rheos system has been shown to have potentially
Normalization of these key cardiac parameters suggests improvement of diastolic filling pressures, thus potentially improving diastolic dysfunction that is often seen in patients with chronic uncontrolled hypertension. Other desirable effects on cardiac structure and function:
— Reduction of left ventricular mass index, — Decreased left atrial dimensions.
2. RENAL SYMPATHETIC DENERVATIONSurgical Renal sympathetic denervation was utilized as treatment modality in 1950s, but was abandoned because of procedure related complications and increased availability of drug therapy.
Rena l Sympathe t i c Denerva t ion addresses uncontrolled hypertension by reducing the drive of the sympathetic nervous system. It is a minimally invasive procedure that modulates the output of the sympathetic nerves located outside the renal artery walls and represents a breakthrough approach and first-of-its-kind device-based treatment for resistant hypertension. Selective denervation of renal nerves by radiofrequency energy delivered into the renal artery lumen circumferentially and longitudinally.
This concept had promising early results as per trials Simplicity Hypertension 1 and 2 which showed significant decrease in systolic and diastolic blood pressure in subjects that had renal artery denervation.
Howsoever with advent of Simplicity Hypertension 3 trial, Prospective, single-blind, randomized, sham-controlled trial. In Simplicity Hypertension 3 trial though a significant change in office as well as ambulatory systolic blood pressure was noted at 6 months it did not meet the predetermined superiority margin.
There was also no significant difference in heart rate, renal function, glycated hemoglobin levels which were secondary endpoints. Thus Simplicity Hypertension 3 trial did not show a benefit of renal-artery denervation with respect to either of the efficacy end points for which the study was powered (reduction in office or ambulatory systolic blood pressure at 6 months).
Renal artery denervation has taken back seat since arrival of Simplicity Hypertension 3 results .
3. RENAL ANGIOPLASTY
Atherosclerotic RAS is the most common cause of secondary hypertension. Prevalence 6.8% in patients above 65 years of age. Nearly 19% in patients with
CAD and Hypertension. All patients with significant bilateral stenosis and solitary functioning kidney with stenosis are candidates for revascularization, regardless of renal insufficiency. When renal insufficiency is present, patients with unilateral stenosis are also possible candidates for revascularization. Procedural success rate is > 95%.Patency rates are 80-85% at 5 years. Restenosis requiring repeat angioplasty has been reported in 8-30% with atherosclerotic stenosis.
The CORAL trial, funded by the National Heart, Lung, and Blood Institute (NHLBI), was launched in 2005, 947 patients with renal-artery atherosclerosis (stenosis >60%) who had either systolic hypertension and were taking two or more blood pressure-lowering drugs or chronic kidney disease. They were randomized equally to medical therapy alone or medical therapy plus renal-artery stenting.At a median follow-up of 43 months, the rate of the primary composite end point (death from CV or renal causes, MI, stroke, hospitalization for congestive heart failure, progressive renal insufficiency, or need for kidney replacement) was no different between groups. In both groups, the primary end point occurred in 35% of patients.
• There were also no differences in rates of individual components of the end point or in rates of all-cause mortality.
• A "very modest difference" in systolic blood pressure was seen between groups (–2.3 mm Hg in the stenting group), but this clearly did not translate into clinically meaningful differences. Of note, 11 patients suffered an arterial dissection in the stenting group.
Thus the CORAL study did not support a preference for renal stenting as the initial treatment for presumed atherosclerotic renovascular hypertension.
Current American College of Cardiology and American Heart Association guidelines guidelines recommend renal artery stenting as a reasonable option for patients with one of the following:
1. An atherosclerotic severe renal artery stenosis (>70% angiographic diameter renal artery stenosis
2. 50% to 70% stenosis with hemodynamic confirmation of lesion severity) associated with
• resistant or uncontrolled hypertension and the failure of 3 antihypertensive drugs, 1 of which is a diuretic agent,
• and hypertension and intolerance to medication.
Thus resistant hypertension as a subgroup requires a dedicated holistic approach, it is with a systemic and hoilistic care that target blood pressure goals can be achieved and hypertension conquered.

Acute coronary syndrome (ACS) refer to a spectrum of clinical presentations ranging from those for ST segment elevation myocardial infarction (STEMI) to presentations found in non ST elevation myocardial infarction (NSTEMI) or in unstable angina (UA). It is almost always associated with rupture of an atherosclerotic plaque and complete or partial occlusion of infarct related artery.
Approximately 30% of patients presenting with ACS have STEMI and the remainder have NSTEMI or UA. NSTE ACS term refers to both NSTEMI and UA because both have similar clinical presentations.
INITIAL ASSESSMENT: Patients presenting with chest pain should be rapidly evaluated to determine if their symptoms are suggestive of acute ischemia, or some other potentially life-threatening illness i.e. aortic dissection, pulmonary thromboembolism, pericarditis, tension pneumothorex, perforating peptic ulcer etc.
The diagnosis of acute coronary syndrome depends upon the characteristics of the chest pain, specific a s s o c i a t e d s y m p t o m s , a b n o r m a l i t i e s o n electrocardiogram (ECG), and levels of serum markers of cardiac injury. A patient with a possible acute coronary syndrome (ACS) should be treated rapidly.
CLINICAL PRESENTATION: Ischemic chest pain - Ischemic pain is often characterized more as a discomfort than pain, and it may be difficult for the patient to describe. Terms frequently used by patients include squeezing, tightness, pressure, constriction, crushing, strangling, burning, heartburn, fullness in the chest, band-like
sensation etc. In some cases, the patient cannot qualify the nature of the discomfort but places his or her clenched fist in the center of the chest, known as the "Levine sign." ain is typically gradual in onset, Palthough the intensity of the discomfort may wax and wane. It is provoked by an activity and does not change with respiration or position. Classic anginal pain lasting more than 20 minutes suggests ACS.
ASSOCIATED SYMPTOMS - Ischemic pain is often associated with other symptoms. The most common is shortness of breath, which may reflect mild pulmonary congestion resulting from ischemia-mediated diastolic dysfunction. Other symptoms may include belching, nausea, indigestion, vomiting, diaphoresis, dizziness, lightheadedness, clamminess, and fatigue.
ATYPICAL SYMPTOMS - Some patients with acute coronary syndrome (ACS) present with atypical symptoms rather than chest pain. One-third of patients have no chest pain on presentation to the hospital. These patients often present with symptoms such as dyspnea alone, weakness, nausea and/or vomiting, palpitations, syncope, or cardiac arrest. They are more likely to be older, diabetic, and women.
PHYSICAL EXAMINATION:The initial physical examination should focus on findings that permit rapid triage and aid in immediate diagnosis and management and should include the following:
Responsiveness, airway, breathing and circulation – if patient in respiratory or cardiorpulmonary arrest, the appropriate resuscitation algorithms should be followed.
YEAR BOOK & SOUVENIR 2014
Acute Coronary Syndrome
Dr Rajiv Passey DM (Cardiology), MNAMS, FICPSenior Consultant Cardiologist, Dharma Vira Heart Center Sir Ganga Ram Hospital, New Delhi Contact No. +919810178588Dr Dileep K. Tiwari DNB (Cardiology)Attending Cardiologist, Dharma Vira Heart Center Sir Ganga Ram Hospital, New Delhi Contact No. +91996814793

85
Evidence of systemic hypoperfusion (Cardiogenic shock) - Hypotension; tachycardia; impaired cognition; cool and clammy extrimities complicating the acute MI, requires aggressive evaluation and management
Evidence of heart failure - Jugular venous distention, new or worsening pulmonary crackles, hypotension, tachycardia, new S3 gallop and new or worsening MR murmur. Aggressive management is needed for patients with heart failure complicating an acute MI.A screening neurologic examination should be performed to assess for focal lesions or cognitive deficits that might preclude safe use of thrombolytic therapy.
ELECTROCARDIOGRAM: In patients with chest pain or other symptoms suggestive of ACS, a 12 lead ECG should be performed and evaluated for ischemic changes within 10 minutes of patient arrival at emergency department. Serial ECGs (e.g., 15-to30-minute intervals during the first hour) should be performed to detect ischemic changes. I t i s r e a s o n a b l e t o o b t a i n s u p p l e m e n t a l electrocardiographic leads V7 to V9 in patients whose initial ECG is non diagnostic and who are at intermediate/high risk of ACS.
Findings consistent with ST elevation myocardial infarction (STEMI): New ST elevation at the J point in two anatomically contiguous leads using the following diagnostic thresholds: ≥0.1 mV (1 mm) in all leads other than V2-V3, where the following diagnostic thresholds apply: ≥0.2 mV (2 mm) in men ≥ 40 years; ≥0.25 mV (2.5 mm) in men <40 years, or ≥0.15 mV (1.5 mm) in women.
Findings consistent with Non ST elevation myocardial infarction or unstable angina: New horizontal or down-sloping ST depression ≥0.05 mV (0.5 mm) in two anatomically contiguous leads and/or T inversion ≥0.1 mV (1mm) in two anatomically contiguous leads with prominent R wave or R/S ratio >1.CARDIAC BIOMARKERS: Cardiac-specific troponin (troponin I or T) levels should be measured at presentation and 3 to 6 hours after symptom onset in all patients who present with symptoms consistent with ACS to identify a rising and/or falling pattern. If the initial troponin is elevated
th(defined as greater then 99 percentile of the upper value of the reference range), the diagnosis of MI is made if a >/=20% rise or fall in subsequent troponin occurs. Additional troponin levels should be obtained
beyond 6 hours after symptom onset in patients with normal troponins on serial examination when electrocardiographic changes and/or clinical presentation confer an intermediate or high index of suspicion for ACS. With contemporary troponin assays, creatine kinase myocardial isoenzyme (CK-MB) and myoglobin are not usefull for diagnosis of ACS.
The presence and magnitude of troponin elevations are useful for short- and long-term prognosis. It may be reasonable to remeasure troponin once on day 3 or day 4 in patients with myocardial infarction as an index of infarct size and dynamics of necrosis. Use of selected newer biomarkers, especially B-type natriuretic peptide (BNP) or NT-Pro BNP, may be reasonable to provide additional prognostic information.
High-risk patient — The patient has a high-risk ACS if ST segment depression (≥0.05 mV [0.5 mm]) is present in two or more contiguous leads, elevated serum biomarkers, and/or the TIMI risk score is ≥5. This patient is typically admitted to an intensive care unit. Those with persistent pain or hemodynamic compromise generally undergo urgent angiography and revascularization. Others with resolution of symptoms and stable hemodynamics are typically referred for early elective angiography and revascularization if appropriate.
MANAGEMENT:Management of NSTE-ACS will be discussed here.
EARLY HOSPITAL CARE: Oxygen: Supplemental oxygen should be administered to patients with ACS with arterial oxygen saturation less than 90%, respiratory distress, or other high-risk features of hypoxemia.
Secure IV access and blood investigation should be obtained.
Look for signs of hemodynamic compromise and left heart failure; determine baseline neurologic functions especially if fibrinolytic therapy is to be given.
Nitrates: Patients with NSTE-ACS with continuing ischemic pain should receive sublingual nitroglycerin (0.3mg–0.4mg) every 5minutes for up to 3 doses, after which an assessment should be made about the need for intravenous nitroglycerin if not contraindicated. Intravenous nitroglycerin is indicated for patients with ACS for the treatment of persistent ischemia, heart failure or hypertension.

86
Analgesic therapy: IV morphine sulfate 2-4 mg every 5-15 minute may be given for continued ischemic chest pain despite maximally tolerated anti-ischemic medications. NSAIDs (except aspirin) should not be initiated and should be discontinued during hospitalization for ACS.
Beta-blockers: Oral beta-blocker therapy should be initiated within the first 24 hours in patients who do not have signs of HF, evidence of low-output state, increased risk for cardiogenic shock, or other contraindications to beta blockade (e.g., PR interval >0.24second, second- or third-degree heart block without a cardiac pacemaker, active asthma, or reactive airway disease). In patients with concomitant ACS, stabilized HF, and reduced systolic function, it is recommended to continue beta-blocker therapy with 1 of the 3 drugs proven to reduce mortality in patients with HF: sustained-release metoprolol succinate, carvedilol, or bisoprolol.
Calcium Channel Blockers: In patients with NSTE-ACS, who have continuous or recurrent ischemia, and where beta blockers are contraindicated, a non dihydropyridine calcium channel blockers (CCB) (e.g., verapamil or diltiazem) should be given as initial therapy in the absence of clinically significant LV dysfunction, increased risk for cardiogenic shock, PR interval greater than 0.24 second, or second- or third-degree atrioventricular block without a cardiac pacemaker. Oral non dihydropyridine calcium antagonists are to be used in patients with NSTE-ACS who have recurrent ischemia after appropriate use of beta blockers and nitrates. Long-acting CCBs and nitrates are recommended in patients with coronary artery spasm. Immediate-release nifedipine should not be administered to patients with NSTE-ACS in the absence of beta-blocker therapy.
Cholesterol Management: High-intensity statin therapy should be initiated or continued in all patients with NSTE-ACS. It is reasonable to obtain a fasting lipid profile in patients with NSTE-ACS, preferably within 24hours of presentation. Atorvastatin 80 mg should be given to all patients as early as possible and preferably before percutaneous coronary intervention (PCI).
Inhibitors of Renin-Angiotensin-Aldosterone System: Angiotensin-convertingenzyme (ACE) inhibitors should be started and continued indefinitely in all patients with left ventricular ejection fraction (LVEF) less than 0.40 and in those with hypertension,
diabetes mellitus, or stable chronic kidney disease (CKD) unless contraindicated. Angiotensin receptor blockers are recommended if patients are ACE inhibitor intolerant. Aldosterone blockade is recommended in post–MI patients who are without significant renal dysfunction (creatinine >2.5 mg/dL in men or >2.0mg/dL in women) or hyperkalemia (K >5.0mEq/L) who are receiving therapeutic doses of ACE inhibitor and beta blocker and have a LVEF0.40 or less, diabetes mellitus, or HF.
Initial Antiplatelet Therapy: Non–enteric-coated, chewable aspirin (162mg to 325 mg) should be given to all patients with NSTE-ACS without contraindications as soon as possible after presentation, and a maintenance dose of aspirin (81mg/d to 162 mg/d) should be continued indefinitely. In patients with NSTE-ACS who are unable to take aspirin because of hypersensitivity or major gastrointestinal intolerance, a loading dose of clopidogrel (300-600 mg) followed by a daily main tenance dose (75mg da i ly ) should be administered.
A P2Y12 inhibitor (either clopidogrel or ticagrelor) in addition to aspirin should be administered for up to 12 months to all patients with NSTE-ACS without contraindications who are treated with either an early invasive or ischemia-guided strategy. It is reasonable to prefer Ticagrelor over clopidogrel.
Clopidogrel: 300-mg or600-mg loading dose, then75 mg daily.
Ticagrelor: 180-mg loading dose, then 90 mg twice daily.
Prasugrel, 60 mg loading dose followed by 10 mg once daily should be given to patients with NSTE-ACS prior to PCI and when coronary anatomy is known and there is no additional risk of bleeding, in patients who are <75 years of age, >60 Kg weight and no prior history of stroke.
In patients with NSTE-ACS treated with an early invasive strategy and dual antiplatelet therapy (DAPT) with intermediate/high-risk features (e.g., positive troponin), a glycoprotein (GP) IIb/IIIa inhibitor may be considered as part of initial anti platelet therapy. Eptifibatide or tirofiban are the preferred options over the abciximab.

87
Anticoagulant Therapy:In patients with NSTE-ACS, anticoagulation is recommended for all patients, in addition to antiplatelet therapy, irrespective of initial treatment strategy. Treatment options include:
Enoxaparin: 1mg/kg subcutaneous (SC) every 12 hours. Reduce the dose to 1 mg/kg SC once daily in patients with creatinine clearance [CrCl] <30 mL/min. I t should be cont inued for the durat ion of h o s p i t a l i z a t i o n o r u n t i l p e r c u t a n e o u s coronaryintervention (PCI) is performed. An initial intravenous loading dose is 30mg.
Bivalirudin: 0.10 mg/kg loading dose followed by 0.25 mg/kg per hour (only in patients managed with an early invasive strategy). It should be continued until diagnostic angiography or PCI, with only provisional use of GPIIb/IIIa inhibitor.
Fondaparinux: 2.5 mgSC daily, continued for the duration of hospitalization or until PCI is performed. If PCI is performed while the patient is on fondaparinux, an additional anticoagulant with either UFH or bivalirudin should be administered because of the risk of catheter thrombosis.
UFH IV: Initial loading dose of 60 IU/kg (maximum 4,000 IU)with initial infusion of 12 IU/kg per hour (maximum 1,000 IU/h) adjusted per activated partial thromboplastin time to maintain therapeutic anticoagulation according to the specific hospital protocol, continued for 48 hours or until PCI is performed.
In patients with NSTE-ACS (i.e.without ST elevation, true posterior MI, or left bundle-branch block not known to be old), intravenous fibrinolytic therapy is contraindicated.
Ischemia-Guided Strategy versus Early Invasive Strategies:An urgent/immediate invasive strategy (diagnostic angiography with intent to perform revascularization if appropriate based on coronary anatomy, PCI or CABG) is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability and also in initially stabilized patients with NSTE-ACS who have an elevated risk for clinical events. It is reasonable to choose an early invasive strategy (within 24 hours of admission) over a delayed invasive strategy (within24 to 72 hours) for initially stabilized high-risk patients with NSTE-ACS. For
those not at high/intermediate risk, a delayed invasive approach is reasonable.
In initially stabilized patients, an ischemia-guided strategy may be considered for patients with NSTE-A C S w i t h o u t s e r i o u s c o m o r b i d i t i e s o r contraindications who have an elevated risk for clinical events. The decision to implement an ischemia-guided strategy in initially stabilized patients without serious comorbidities or contraindications to this approach may be reasonable after considering clinician and patient preference.
In patients with extensive comorbidities (Organ failure or cancer) and in whom the likelihood of ACS is low (i.e. troponin -negative), an early invasive therapy is not recommended.
Risk Stratification before Discharge for Patients with an Ischemia-Guided Strategy of NSTE-ACS: Noninvasive stress testing should be done in low- and intermediate-risk patients who have been free of ischemia at rest or with low-level activity for a minimum of 12to 24 hours. Treadmill exercise testing is useful in patients who are able to exercise and in whom the ECG is free of resting ST changes that may interfere with interpretation. Stress testing with an imaging modality should be used in patients who are able to exercise but have ST changes on resting ECG that may interfere with interpretation. In patients undergoing a low-level exercise test, an imaging modality can add prognostic information. Pharmacological stress testing with imaging is recommended when physical limitations preclude adequate exercise stress. A noninvasive imaging test is recommended to evaluate LV function in patients with ACS.
Coronary Artery Bypass Graft in Relation to Use of Antiplatelet Agents:Non–enteric-coated aspirin (81mg to 325mg daily) should be administered preoperatively to the patients undergoing coronary artery bypass graft (CABG). In patients referred for elective CABG, clopidogrel and ticagrelor should be discontinued for at least 5 days and prasugrel for at least 7 days prior to surgery. In patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued for atleast 24 hours to reduce major bleeding. Short-acting intravenous GPIIb/IIIa inhibitors (eptifibatide ortirofiban) should be discontinued for atleast 2 to 4 hours before surgery and abciximab for at least 12 hours before surgery.

88
Posthospital Oral Antiplatelet Therapy: Aspirin should be continued indefinitely. The maintenance dose should be 81 mg daily in patients treated with ticagrelor and 81 mg to 325 mg daily in all other patients. In addition to aspirin, a P2Y12 inhibitor (either clopidogrel or ticagrelor) should be continued for up to 12 months in all patients who are treated with an ischemia-guided strategy. . Options include:Clopidogrel: 75 mg daily. OrTicagrelor: 90 mg twice daily
In patients receiving a stent (bare-metal stent or DES) during PCI for NSTE-ACS, P2Y12 inhibitor therapy should be given for at least 12 months. Options include:Clopidogrel: 75 mg daily. OrPrasugrel: 10 mg daily. OrTicagrelor: 90 mg twice daily
SECONDARY PREVENTION: All eligible patients with NSTE-ACS should be referred to a comprehensive cardiovascular rehabilitation program either before hospital discharge or during the first outpatient visit.
The pneumococcal vaccine is recommended for the patients 65 years of age and older and in high-risk patients with cardiovascular disease.
Patients should be educated about appropriate cholesterol management, blood pressure, smoking cessation, and lifestyle management.
Patients who have undergone PCI or CABG derive benefit from risk factor modification and should receive counseling that revascularization does not obviate the need for lifestyle changes.
Before hospital discharge, the patient's need for treatment of chronic musculoskeletal discomfort should be assessed, and a stepped-care approach should be used for selection of treatments.
Pain treatment before consideration of NSAIDs should begin with acetaminophen, non acetylated salicylates, tramadol, or small doses of narcotics if these medications are not adequate.An evidence-based plan of care that promotes medication adherence, timely follow-up with the health care team, appropriate dietary and physical activities, and compliance with interventions for secondary prevention should be provided to patients.
In addition to detailed instructions for daily exercise, patients should be given specific instruction on activities (e.g., lifting, climbing stairs, yard work, and household activities) that are permissible and those to avoid. Specific mention should be made of resumption of driving, return to work, and sexual activity.
REFERENCES:1. Amsterdam EA, et al. 2014 AHA/ACC Guideline for the
Management of Patients With Non–ST-Elevation Acute Coronary Syndromes: A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; Sept 23..
2. Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA 2000; 283:3223.
3. Swap CJ, Nagurney JT. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA 2005; 294:2623.
4. Pope JH, Aufderheide TP, Ruthazer R, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000; 342:1163.
5. Brieger D, Eagle KA, Goodman SG, et al. Acute coronary syndromes wi thout ches t pa in , an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest 2004; 126:461.
6. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomized trials of more than 1000 patients. Fibrinolytic Therapy Trialists'(FTT) Collaborative Group.Lancet.1994;343:311-22.
7. Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction. Results of the TIMI IIIB Trial. Thrombolysis in Myocardial Ischemia. Circulation.1994;89:1545-56.
8. Pfeffer MA, McMurray JJ, Velazquez EJ, et al. Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. NEngl JMed.2003;349:1893-906.

AnticoagulationUpdate on the new oral
Anticoagulants (NOACs)
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Background The acceptability of warfarin has been limited by mandatory laboratory monitoring. A number of new orally active anticoagulants (NOACs), which can be used as alternatives to warfarin, are now available.
ObjectiveWe review the clinical indications and considerations associated with the use of the NOACs.
DiscussionThe NOACs currently approved in Australia are dabigatran, rivaroxaban and apixaban. Indications include thromboprophylaxis in non-valvular atrial fibrillation and following hip and knee replacement surgery. Rivaroxaban is also approved for treatment and secondary prevention of deep venous thrombosis (DVT) and pulmonary embolus (PE).The NOACs differ from warfarin in that they do not require laboratory monitoring. They need to be used cautiously in patients with renal impairment and are contraindicated in patients with renal failure. Bleeding may require blood product replacement aided by haematological advice and specialist investigations. Antidotes to the NOACS are undergoing clinical trials.
Warfarin was orginally developed as a pesticide against rodents but has been used for the treatment of eembolic conditions since the 1950s. It is the most commonly used anticoagulant worldwide. Warfarin requires routine coagulation monitoring and dose adjustments to compensate for the many food-drug and drug-drug interactions that interfere with its effects.
This complicates treatment and is the stimulus for the development of a l ternat ive ant icoagulants . Ximelagatran, the first of the alternative agents to be
developled, is a direct thrombin inhibitor. It showed clinical efficacy in non-valvular atrial fibrillation and venous thromboembolic disease in studies conducted in 2000-2005. It was approved for both indications in a range of countries throughout Europe but it was associated with an unacceptable incidence of liver toxicity and was withdrawn from the market in 2006. Ximelagatran was never approved for use in India.
A number of new oral anticoagulants (NOACs) with properties that overcome the practical limitations of warfarin have recently become available. These agents have a more stable pharmacokinetic profile, have no significant food-drug interactions and fewer drug-drug interactions, and can be administered in a standard dose without the need for routine monitoring.
The NOACs have been evaluated for use in venous thromboembolic disease, non-valvular atrial fibrillation and several other cardiac indications. The purpose of this article is to provide a simple overview of the different agents and some rational guidance on their integration into our clinical practice.
Pharmacology of the NOACsThe NOACs fall into two broad categories: direct thrombin inhibitors and the factor Xa inhibitors (Fig. 1).
The direct thrombin inhibitors inactivate soluble and fibrin-bound thrombin and limit thrombogenesis and
1thrombus growth. Dabigatran, the second orally active direct thrombin inhibitor to be marketed after ximelagatran, is not associated with hepatotoxicity and has been approved for stroke prevention in atrial fibrillation and prevention of venous thromboembolism in at-risk populations. Factor Xa inhibitors directly inhibit the enzyme
Dr Amitabh Yaduvanshi MD, DMHead of CathlabDr Mohan Nair MD, DM Chairman, Cardiac Sciences, Saket City Hospital, New Delhi

90
2responsible for thrombin formation. Those available include apixaban and rivaroxaban.
The properties of the different NOACs are shown in Table 1.
Clinical indicationsVenous thromboembolic diseaseProphylaxisAlthough dabigatran,and apixaban are available in India for primary venous thromboembolism (VTE) prophylaxis(Table 2), approval is limited to the context of elective hip and kneereplacement surgery, where they have been extensively studied.
Dabigatran (150 mg and 220 mg once daily) was as effective asenoxaparin 40 mg daily at preventing any VTE and mortality ofany cause, with no significant
3difference in major bleeding rates.
Rivaroxaban 10 mg daily and apixaban 2.5 mg twice daily wereeach superior to enoxaparin 40 mg daily with
4-6no difference in majorbleeding rates. Currently, there
are no major studies evaluating theuse of NOACs in hip fracture surgery, minor orthopaedic proceduresand non-orthopaedic surgery. Consequently, they are not approved forthese uses.
NOACs do not have approval for prophylaxis in acutely illmedical inpatients at risk of VTE, although rivaroxaban (MAGELLANtrial) and apixaban
7,8(ADOPT trial) have been studied. Rivaroxaban10 mg given daily for 35 days was superior to enoxaparin 40 mg for6-14 days, and apixaban 2.5mg twice daily for 30 days was noninferiorto enoxaparin. Both NOACs showed increased bleeding riskwhen used for these
7,8extended periods of thromboprophylaxis.
Figure1. Sites of action of VKA (vitamin k antagonist/warfarin) & NOAC

91
Treatment and secondary preventionOnly rivaroxaban is currently approved for treatment of DVT and PE, but is not yet available in India. Its use offers a convenient, singledrugapproach to VTE treatment. Its efficacy is comparable tothat of warfarin for prevention of recurrent VTE but it has a lowerbleeding risk (Table 3). High-risk patients, such as those withantiphospholipid syndrome and recurrent thrombotic events,were excluded from clinical trials and warfarin should remainthe standard of care for t h e s e p a t i e n t s u n t i l N O A C s h a v e
9,10beenevaluated. Apixaban and dabigatran have also been studiedin VTE treatment and may eventually become available for thisindication (Table 3). All
NOACs are small molecules that cross theplacenta and a r e c o n t r a i n d i c a t e d i n p r e g n a n t a n d breastfeedingpatients.
Dabigatran, rivaroxaban and apixaban were evaluated forextended (6-12 months) treatment of VTE and, as expected, showedreduced risk of recurrence, compared with placebo. However, onlydabigatran was compared with warfarin, the current standard of care,and had comparable results for VTE recurrence and
1 0 - 1 2bleed ingra tes . The r i sk -benef i t r a t io o f continuedanticoagulant therapy should be re-assessed at least annually.
Figure2. Sites of action of the NOACs

92
Atrial fibrillationEach of the three NOACs has been evaluatedin patients with non-valvular atrial fibrillation and at least oneadditional risk factor for stroke in single, large
13-15multicentre trials(Table 4). A direct comparison of the results of the three majortrials is impeded by differences in trial design, patient populations, definitions of endpoints and availability of published data for someendpoints. Nevertheless, some consistent themes have emergedand can be summarised as follows:
• All NOACs are 'non-inferior' to warfarin in the primary efficacyendpoint of stroke and systemic embolism. Apixaban anddabigatran 150 mg are
superior to warfarin, although the numbersneeded to treat to show this benefit are large (number needed totreat with a NOAC rather than warfarin to prevent one stroke: 312for apixaban; 175 for dabigatran 150 mg).
• All NOACs are 'non-inferior' to warfarin for the primary safetyendpoint of major bleeding. Apixaban and dabigatran 110 mg aresuperior to warfarin. Intracranial haemorrhage, an infrequent butserious complication of warfarin, is significantly less frequentwith all NOACs. Again, the numbers needed to treat to reducethis important outcome are large (196 for dabigatran 110 mg; 500for rivaroxaban).

Choosing between warfarin and a NOACMany patients find the limitations of warfarin burdensome andattend their GP requesting a change to a NOAC. For patients onwarfarin whose INR levels are easily maintained within targetlevels, the clinical benefit of such a change is limited; the mainreason for choosing a NOAC under this circumstance is patientpreference. For patients in whom INR control is difficult, however,alternative strategies, such as home-monitoring of INR or change toa NOAC, should be considered.
All of the NOACs have some degree of renal excretion so forpatients with severe renal impairment or labile renal funct ion, warfarin should remain the anticoagulant of choice. The NOAC trialsincluded
patients with moderate chronic kidney disease and dose adjustment algorithms have been developed to optimise NOAC use in this population (Table 5).Clinical experience with NOACs is limited, compared with warfarin, and the role of NOACs in the broader range of patients than those included in the clinical trials is uncertain. Rare adverse events may yet be encountered and reporting of any events associated with the use of NOACs is important. Postmarketing surveillance will provide more information about this in the future.
Choosing between NOACsFactors to consider when deciding between the NOACs include the patient's likelihood to comply with twice daily (dabigatran, apixaban) versus single, daily
93

94
(rivaroxaban) treatment, and any concomitant chronic medications that may interfere with the metabolism of the drugs. For practical purposes, the most important interactions are with verapamil and amiodarone, which can increase the circulating concentrations of all three NOACs. This effect is minimised by ingestion of the anticoagulant drug at least 2 hours before ingestion of the other medications. Rivaroxaban and apixaban should not be co-administered with azone antifungals or HIV protease inhibitors.
In the atrial fibrillation studies, gastrointestinal bleeding was encountered more frequently with dabigatran and rivaroxaban than with warfarin; this was not the case for apixaban. If a patient has a predisposition to this condition (untreated ulcer symptoms, previous gastrointestinal bleeding with non-remediated cause), apixaban or warfarin may be more prudent options.
Other potential indicationsAtrial fibrillation in patients with valvular heart disease. Patients with atrial fibrillation and haemodynamically significant valvular heart disease were excluded from the trials evaluating the NOACs. Warfarin remains the standard of care for these patients and, until further
studies are performed, NOACs are not recommended for patients with atrial fibrillation and valvular heart disease.
Prosthetic valve thromboprophylaxisPatients with prosthetic valves represent a particularly high-riskgroup for whom warfarin has been the mainstay of therapy. To date,only dabigatran has been evaluated in this population. However, the study was terminated prematurely because of an increased rate ofthromboembolism and bleeding in patients receiving dabigatran.16 Itis important that patients in this group not be treated with a NOAC.
Laboratory testingAlthough NOACs do not require routine monitoring, laboratory testingis informative in the context of b l e e d i n g , u r g e n t s u r g e r y o r r e c u r r e n t -thromboembolism. Standard coagulation assays are variably affectedby NOACs but cannot provide drug quantification and results are notequivalent to INR
17-19testing for warfarin. At present, assays fordrug quantification (Table 6) are performed in specialised coagulat ionlaboratories with advice from a haematologist.
Management of bleedingThe cause of bleeding should be evaluated and the presence of residual or excessive anticoagulant effect assessed. Minor bleedingmay be managed with local measures and temporary drug cessation. Patients with clinically significant bleeding may be managed with charcoal, standard resuscitation measures and surgical, r a d i o l o g i c a l o r e n d o s c o p i c i n t e r v e n t i o n . Prohaemostatic agents may be used but have no proven efficacy. Dabigatran may be removed with dialysisbut factor Xa inhibitors are too highly protein-bound.
Vitamin K does not reduce the anticoagulant activity of NOACs and is of no benefit.Reversal agents have now been developed for NOACs but they are just entering clinical trial evaluation. Management of bleeding often requires expert haematological advice and GPs should ensure they have ready access to these services when commencing patients ona NOAC.
ConclusionsThe more selective mechanisms of action of the NOACs and the fact that they do not require routine

95
laboratory monitoring make them viable alternatives to warfarin for many, but not all, conditions requiring anticoagulant therapy. The NOACs are contraindicated inpatients with end-stage renal failure and should be used carefully in patients with renal impairment. Given that experience with these agents is limited, prescribers need to be vigilant for adverse events and report these. If required in cases of urgent surgery or bleeding, laboratory monitoring can be performed in specialised laboratories in most teaching hospitals. For currently approved indications, bleeding risk with NOACs is not increased when compared with warfarin. When clinically significant bleeding does occur, it should be managed in conjunction with specialist haematology advice. Currently, no antidotes are available; however, reversal agents for each drug have been developed and are undergoing evaluation in clinical trials.
Key points
o The main difference between the NOACs (apixaban, dabigatran and rivaroxaban) and warfarin is that routine laboratory monitoring of coagulation is not required for the NOACs.
o The NOACs are indicated for thromboprophylaxis in patients with non-valvular atrial fibrillation and should be considered in patients who are poorly controlled on warfarin or who express a strong preference for one of the newer drugs.
o All agents may be used for thromboprophylaxis following hip and knee replacement surgery and rivaroxaban can be used for treatment and secondary prevent ion fo l lowing venous thromboembolic events.
o The NOACs are not indicated for other conditions, including anticoagulation following mechanical prosthetic valve replacement, hip fracture surgery, minor orthopaedic procedures and non-orthopaedic surgery, or prophylaxis in acutely ill medical inpatients at risk of VTE
o Standard coagulation assays respond variably to the different NOACS and laboratory testing, if required is best done in specialised haematology laboratories with advice from a haematologist.
o Given the limited experience with NOACs, there is the potential for as yet unrecognised adverse events and reporting of suspected events is important with these new agents.
References
1. Weitz JI. Factor Xa or thrombin: is thrombin a better target? J ThrombHaemost 2007;5(Suppl 1):65-67.
2. Yong CM, Boyle AJ. Factor Xa inhibitors in acute coronary syndromes andvenous thromboembolism. CurrVascPharmacol 2010;8:5-11.
3. 3.Friedman RJ, Dahl OE, Rosencher N, et al. Dabigatran versus enoxaparinfor prevention of venous thromboembolism after hip or knee arthroplasty: apooled analysis of three trials. Thromb Res 2010;126:175-82.
4. Eriksson BI, Borris LC, Friedman RJ, et al. R i v a r o x a b a n v e r s u s e n o x a p a r i n forthromboprophylaxis after hip arthroplasty. N Engl J Med 2008;358:2765-75.
5. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban orenoxaparin for thromboprophylaxis after knee replacement. N Engl J Med2009;361:594-604.
6. Lassen MR, Ageno W, Borris LC, et al . R i v a r o x a b a n v e r s u s e n o x a p a r i n f o r thromboprophylaxis after total knee arthroplasty. N Engl J Med2008;358:2776-86.
7. Cohen AT, Spiro TE, Buller HR, et al. Rivaroxaban for thromboprophylaxis inacutely ill medical patients. N Engl J Med 2013;368:513-23.
8. Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. A p i x a b a n v e r s u s e n o x a p a r i n forthromboprophylaxis in medically ill patients. N Engl J Med 2011;365:2167-77.
9. Buller HR, Prins MH, Lensin AW, et al. Oral rivaroxaban for the treatment ofsymptomatic p u l m o n a r y e m b o l i s m . N E n g l J M e d 2012;366:1287-97.
10. Bauersachs R, Berkowitz SD, Brenner B, et al. Oral r i v a r o x a b a n f o r s y m p t o m a t i c v e n o u s thromboembolism. N Engl J Med 2010;363:2499-510.
11. Agnelli G, Buller HR, Cohen A, et al. Apixaban for extended treatment ofvenous thromboembolism. N Engl J Med 2013;368:699-708.
12. Schulman S, Kearon C, Kakkar AK, et al. Extended use of dabigatran, warfarin,or placebo in venous thromboembolism. N Engl J Med 2013;368:709-18.

96
13. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin inpatients with atrial fibrillation. [Erratum appears in N Engl J Med. 2010 N o v 4 ; 3 6 3 ( 1 9 ) : 1 8 7 7 ] . N E n g l J M e d 2009;361:1139-51.
14. Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin inpatients with atrial fibrillation. N Engl J Med 2011;365:981-92.
15. Mega JL, Braunwald E, Mohanavelu S, et al. Rivaroxaban versus placebo inpatients with acute coronary syndromes (ATLAS ACS-TIMI 46): a randomised,double-blind, phase II trial. Lancet 2009;374:29-38.
16. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarinin patients with mechanical heart valves. N Engl J Med 2013;369:1206-14.
17. Douxfils J, Mullier F, Robert S, Chatelain C, Chatelain B, Dogne JM. Impactof dabigatran on a large panel of routine or specific coagulation assays .Labora tory recommendat ions for monitoring of dabigatranetexilate.ThrombHaemost 2012;107:985-97.
18. Harenberg J, Erdle S, Marx S, Kramer R. Determination of rivaroxaban inhuman plasma samples. SeminThrombHemost 2012;38:178-84.
19. Douxfils J, Chatelain C, Chatelain B, Dogne JM, Mullier F. Impact of apixabanon routine and specific coagulation assays: a practical laboratory guide.ThrombHaemost 2013;110:283-94.
20. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban f o r t h e t r e a t m e n t o f a c u t e v e n o u s thromboembolism. N Engl J Med 2013;369:799-808.
21. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in thetreatment of acute venous thromboembolism. N Engl J Med 2009;361:2342-52.
22. Schulman S, Kakkar AK, Goldhaber SZ, et al. Treatment of acute venousthromboembolism with d a b i g a t r a n o r w a r f a r i n a n d p o o l e d analysis.Circulation 2014;129:764-72.
23. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvularatrial fibrillation. N Engl J Med 2011;365:883-91.
24. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS Guidelinefor the management of patients with atrial fibrillation: a report of theAmerican College of Cardiology/American Heart Association Task Force onPractice Guidelines and the Heart Rhythm Society. J Am CollCardiol. 2014; doi:10.1016/j.jacc.2014.03.022.

Dr. Vivek KumarAssociate Director – Neurology.M.D. in Medicine. D. M. In Neurology.
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
Thrombolysis in AcuteIschemic Stroke
Introductionrd
Brain stroke is the 3 leading cause of death and the leading cause of long term disability. Every year an estimated 16 lakhs Indians suffer a Brain Stroke. Brain attack kills more than 6 lakhs Indians annually. Of those who survive 30-45% have to cope with serious permanent impairment.
Though a disease of elderly, 20-30% of all strokes in India occurs in people under 45 years of age. Stroke risk increases with age. For every decade after the age of 55, risk of brain stroke doubles. However there has been a paradigm shift in management of acute stroke from nihilism and passive approach in the past to a more specific and targeted treatment strategies like thrombolytic therapies which can salvage the ischemic brain ( penumbra ) and thus prevent lifetime disability and save lives. This article will discuss the basis of thrombolytic therapies and the latest treatment guidelines.
Evolution of thrombolytic therapyThe December of 1995 was unlike any other month for stroke research; and not without reason. National Institute of Neurological Disorders and Stroke (NINDS) in United States of America had just reported its success in significantly improving the outcome of ischemic stroke by using intravenous recombinant t issue-type plasminogen activator (rtPA), if administered within 3 hours. on the basis of NINDS trial results , r-tpa got FDA approval for use in acute stroke upto 03 hrs in 1996. 18 years down the line, rtPA is the most effective treatment in ischemic stroke patients. However, there are still some barriers in delivering thrombolytic therapy to ischemic stroke patients as only 2-12% of stroke are able to get this treatment. Two subsequent European trials, the European Cooperative Acute Stroke Study (ECASS)
and ECASS II, investigated a time window of up to 6 hours but failed to show the efficacy of thrombolytic treatment, as defined by each trial.In 2008, results of ECASS III, a randomized, placebo-controlled, phase 3 trial showed that the efficacy of alteplase administered in patients with acute ischemic stroke can be safely extended to a time window of 3 to 4.5 hours after the onset of stroke symptoms. On the basis of this trial the window period for IV rTpa was extended to 4.5 hrs in Europe and also by Indian Stroke Association.
Basis of Thrombolytic TherapyIschemic stroke is caused by blockage of an artery supplying a particular area of brain, which results in rapid cell death forming a core of infracted area which cannot be regenerated. But beyond this core is a large area of potentially ischemic brain which can be salvaged if the blood supply can be restored immediately. Thrombolytic therapies try to restore blood supply by fibrinolysis thus salvaging the ischemic penumbra, limiting the size of infarct and thus result in better outcome.

98
This figure clearly defines the efficacy of thrombolytic therapy which is superior to even cardiac thrombolysis and much superior to use of aspirin alone in acute stroke.
Mechanism of Action of ThrombolyticsWith high affinity r –Tpa binds to and activates plasminogen attached to the fibrin netting of a blood clot. Plasminogen is converted to plasmin which catalyses breakdown of fibrin resulting in break up of the clot. The affinity for freely circulating plasminogen is low, so r-tpa has highly effective local fibrinolytic effects and relatively few systemic effects
Stroke is an emergencyEvery minute if stroke is untreated, the average patient loses 1.9 million neurons, 13.8 billion synapses, and 12 km (7 miles) of axonal fibers. Each hour in which treatment fails to occur, the brain loses as many neuron
as it does in almost 3.6 years of normal aging. Hence time is brain, time lost is brain lost. Even though the window period is 4.5hrs, best outcome is seen in those
stwho receive thrombolysis in 1 90minutes.IV Thrombolysis in Acute Ischemic StrokeRecommendation on thrombolytic therapy
Prerequisites and criteria for inclusion:
1. Diagnosis of acute ischemic stroke.
2. No evidence of hemorrhage on plain CT scan (NCCT) of brain.
3. Measurable neurological deficit (NIHSS 4-25)
4. Neurological deficits of low NIHSS score but significant functional disability:
Aphasias
Hemineglect
Hemianopia
5. Neurological signs should not be clearing up spontaneously in the evaluation period.
6. Onset of symptoms within 4.5 hours of beginning treatment.
7. Absence of major head trauma or major stroke in the previous 3 months.
8. N o m y o c a r d i a l i n f a r c t i o n r e q u i r i n g hospitalization in the past 3 months (to prevent hemopericardium)

99
9. No major gastrointestinal or urinary tract hemorrhage in the past 3 weeks.
10. No major surgery in the previous 14 days.
11. No history of previous intracranial hemorrhage due to aneurysm, angioma or arterio-venous malformations.
12. Diagnosed brain tumor.
13. Blood pressure should be less than 185/110 mm Hg.
14. No evidence of acute bleeding from any site or acute fracture on examination.
15. Not taking oral anticoagulants or if anticoagulants are being taken, INR to be ≤ 1.7
16. If receiving heparin in last 48 hours, a-PTT is to be performed and should be normal ( < 35 secs).
17. Platelet count to be assessed if there is clinical suspicion of thrombocytopenia. Platelet count should be ≥ 1,00,000 /μl. If there is no clinical suspicion, platelet count test is ordered, but need not wait for result to start thrombolysis.
18. Arterial puncture at a non-compression site < 7 days.
19. Blood glucose concentration ≥ 50 mg % and ≤ 300 mg%.
20. Seizure at onset to be ascertained whether due to stroke. If there is clinical suspicion of non-vascular postictal deficit, magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI) to CT with CT angiography (CTA) to be performed to document stroke.
21. NCCT head should not show a large or multilobar hypodensity involving more than 1/3 rd of arterial territory (limited literature suggests increased risk of hemorrhagic transformation).
22. Informed consent from patient or responsible care giver.
Eligibility criteria for treatment in the 3 to 4.5 hours after acute stroke are similar to those for treatment at earlier time periods, with any 1 of the following additional exclusion criteria:
· Patients older than 80 years
· All patients taking oral anticoagulants are excluded regardless of the international normalized ratio (INR)
· Patients with baseline NIHSS score > 25
· Patients with a history of stroke and diabetes
· Patients with imaging evidence of ischemic
damage to more than one third of the middle cerebral artery (MCA) territory[19]
Figure 1 is a visual decision aid that depicts the benefits and risks of intravenous thrombolytic therapy provided to patients within 3 hours of stroke onset. Overall, of every 100 patients treated, 32 will have a better and 3 will have a worse final global disability outcome as a result of therapy.
Treatment regime for IV thrombolysis with rt-PA in acute ischemic stroke
1. Infuse 0.9 mg/Kg (maximum dose of 90 mg) over 60 minutes with 10% of the dose given as a bolus over 1 minute.
2. Admit the patient to an intensive care unit or a dedicated stroke unit for monitoring.
3. Perform neurological assessments every 15 minutes during the infusion and every 30 minutes thereafter for next 6 hours, then hourly until 24 hours aft er treatment.
4. If the patient develops severe headache, acute hypertension, nausea or vomiting, discontinue the infusion (if the infusion is still on) and obtain emergency CT scan.
5. Measure blood pressure every 15 minutes for the first 2 hours and subsequently every 30 minutes for the next 6 hours, then hourly until 24 hours after treatment.
6. Increase the frequency of blood pressure measurements if a systolic blood pressure is ≥ 180

100
mmHg or if a diastolic blood pressure is ≥ 105 mmHg; administer antihypertensive medications to maintain blood pressure at or below these levels.
7. Delay placement of nasogastric tubes, bladder catheters or intra-arterial (IA) pressure catheters.
8. Obtain a follow-up CT scan at 24 hours before starting anticoagulants or antiplatelet agents.
Prethrombolysis Management
1. Start supplementary oxygen if unable to maintain O2 saturation > 92%. Treat any fever with acetominophen. NPO for any oral intake (e.g., food, medication, etc.).
2. Do not place Foley, nasogastric tube, arterial line or central venous line unless it is necessary for patient safety.
3. Do not place any femoral catheters (venous or arterial).
4. Do not lower blood pressure unless it is causing myocardial ischemia or exceeds 220/120. Use labetolol iv (5-20 mg iv q 10-20 mins). Monitor with non-invasive cuff pressures every 15 mins or continuous arterial pressure monitoring.
5. Do not administer heparin unless recommended by the Acute Stroke Team.
6. Alert interventional neuroradiology and anesthesia about possible case.
7. Alert neuro-ICU and check for bed availability. Consider bypassing CT Angio if risk is increased (e.g., renal failure, acute CHF) and it is unlikely to change treatment decision. Hold metformin 48 hrs after iodinated contrast. Check MRI exclusions (e.g., Severe claustrophobia, implanted pacemaker, metal fragments, s h r a p n e l ) . R e v i e w C T / C TA w i t h interventionalist and stroke team. Obtain written or verbal informed consent for endovascular procedure and general anesthesia from patient or appropriate caregiver. If no individual is available for consent, consider emergency consent procedures.
If time permits, obtain STAT DWI-MR imaging but do not delay time to treatment.
Guidelines for management of blood pressure prior and perithrombolysis:
• Pretreatment
• Systolic > 185 mmHg or diastolic > 110 mmHg
• Labetalol 10-20 mg IV over 1-2 min
• If labetalol is not available, oral captopril ( 12. 5 mg) and repeat at intervals of 15 minutes or clonidine ( 0.1 mg)
• if still elevated
• May repeat or double labetalol every 10 min to maximum dose of 300 mg, or give initial labetalol dose, then start labetalol drip at 2-8 mg/min
• Nicardipine 5 mg/h IV infusion as initial dose and titrate to desired eff ect by increasing 2.5 mg/h every 5 min to maximum of 15 mg/h
• If blood pressure is not controlled by labetolol or nicardipine, consider sodium nitroprusside or rule out other cause of acute hypertension such as hypertensive urgency
• During/aft er treatment
• Monitor blood pressure
• Check blood pressure every 15 min for 2 h, then every 30 min for 6 h, and finally every hour for 16 h
• Diastolic > 140 mmHg
• Sodium nitroprusside 0.5 mcg/kg/min IV infusion as initial dose and titrate to desired blood pressure
• Systolic > 230 mmHg or diastolic >121 – 140 mmHg
• Option 1
• Labetalol 10 mg IV for 1-2 min
• May repeat or double labetalol every 10 min to maximum dose of 300 mg, or give initial labetalol dose, then start labetalol drip at 2-8 mg/min
• Option 2
• Nicardipine 5 mg/h IV infusion as initial dose and titrate to desired eff ect by increasing 2.5 mg/h every 5 min to maximum of 15 mg/h; if blood pressure is not controlled by labetolol or nicardipine, consider sodium nitroprusside.
• Systolic 180 – 230 mmHg or diastolic 105 - 120 mmHg
• Labetalol 10 mg IV for 1 - 2 min
• May repeat or double labetalol every 10 - 20 min to maximum dose of 300 mg or give initial labetalol dose, then start labetalol drip at 2 - 8 mg/min
For acute stroke onset during or immediately after diagnostic or therapeutic angiography/ or coronary and cardiac interventions

101
If a femoral arterial sheath is still in place, DO NOT REMOVE IT. The sheath should remain sutured in place while t-PA is given. Consider IA urokinase if the sheath can be accessed and the Interventional Neuroradiology staff is available. If not, consider giving t-PA i.v. at full dose 0.9 mg/kg. In all cases, leave the sheath in place and check STAT a-PTT. Observe the groin site closely and follow hematocrit and vital signs for evidence of acute blood loss. If a hematoma forms or there is evidence of blood loss, notify vascular surgery and apply pressure until hemostasis is achieved. If bleeding continues, t-PA can be reversed with FFP, cryoprecipitate and platelets. Vascular surgery may choose to surgically repair the artery. If no bleeding occurs, the sheath can be removed after 24hours.
Bleeding due to Tpa
In a recent review by Mayo clinic, the overall mean SICH( symptomatic intracerebral hemorrhage ) and mortality rates of patients treated with intravenous thrombolysis were 5.6% (SD 2.3) and 14.7% (SD 4.8), respectively. Studies defined SICH as parenchymal hemorrhage with a neurological decline NIHSS ≥4 occurring within 36 h of intravenous thrombolysis .
1. For suspected symptomatic hemorrhage aft er t-PA:
• Hold administration of IV t-PA if still infusing until Brain CT completed and shows no evidence of bleeding.
• Exclude other possible causes of neurologic worsening or acute hemodynamic instability.
2. For confirmed symptomatic hemorrhage on head CT:
• Consult neurosurgery for possible intervention.
• Check STAT values: CBC, PT, a-PTT, platelets, fibrinogen and D-dimer.
• If fi brinogen < 100 mg/dL, then give cryoprecipitate 0.15 units/kg rounded to the nearest integer. If still bleeding at 1 hr and fibrinogen level still less than 100 mg/dL, repeat cryoprecipitate dose.
• Institute frequent neurochecks and therapy of acutely elevated ICP, as needed.
• Additional options or considerations, Fresh frozen plasma
• If platelet dysfunction suspected, give platelets 4 U.
• Monitor for signs of anaphylaxis; the risk is higher in diabetics who have received insulin.
• Follow-up with STAT a-PTT q1 hour for the next 4 hours, then q4 hours through 12 hours of hospitalization.
• Serious systemic hemorrhage should be treated in a similar manner. Manually compress and compressible sites of bleeding, and consult appropriate additional services to consider mechanically occluding arterial or venous sources of medically uncontrollable bleeding.
HYPERSENSITIVITY REACTIONS DUE TO r-TPA
• Orolingual angioedema occurs in about 2% of treated patients. (Nervenartz.2009)
• Risk is more in those taking ACE inhibitors. (J Neurology, 2005)
Anaphylaxis is a rare complication.
INTRA-ARTERIAL THROMBOLYSIS
Catheter-Based or intra-arterial (IA) thrombolysis or reperfusion strategies: IA thrombolysis is still under investigation and should be used in well-equipped centers within a framework of research protocol.
Indications
• A significant neurologic deficit expected to result in long term disability.
• Deficits attributable to large vessel occlusion (basilar, vertebral, internal carotid or MCA M1 or M2 branches).
• Non-contrast CT scan without hemorrhage or showing well-established infarct
• Acute ischemic stroke symptoms with known onset. Treatment initiated within 6-8 hours of established, nonfl uctuating defi cits due to Anterior Circulation (carotid/MCA) stroke. The window of opportunity for treatment is less well-defi ned in posterior circulation (Vertebral/Basilar) ischemia and patients may have fluctuating, reversible ischemic symptoms over many hours or even days and still be appropriate candidates for therapy.
Contraindications
1. Intracranial hemorrhage (ICH, SAH, subdural hematoma, etc.)
2. Well-established acute infarct on CT/MRI in the territory to be reperfused ***

102
3. Major infarction. ***
[e.g. > 1/3 cerebral hemisphere]
4. CNS lesion with high likelihood of hemorrhage s/p chemical thrombolytic agents (e.g., brain tumors, abscess, vascular malformation, aneurysm, contusion) ***
5. Suspicion of subarachnoid hemorrhage
T h e i t e m s m a r k e d w i t h * * * a r e n o t contraindications for mechanical clot lysis.
Warnings
These conditions may increase the risk of unfavorable outcomes but are not necessarily a contraindication to treatment:
1. Recent surgery/trauma (< 15 days) ***
2. Recent intracranial or spinal surgery, head trauma, or stroke (< 3 months) ***
3. History of intracranial hemorrhage or brain aneurysm or vascular malformation or brain tumor *** [may consider IA catheter-based repurfusion in patients with CNS lesions that have a very low likelihood of bleeding such as small unruptured aneurysms or benign tumors with low vascularity]
4. Active internal bleeding (< 22 days) ***
[including arterial puncture at a non-compressible site]
5. Platelets less than 100,000/μl, PTT > 40 sec aft er heparin use, or PT > 15 or INR > 1.7, or known bleeding diathesis ***
6. Left heart thrombus documented ***
7. Increased risk of bleeding due to any of the following: ***
• Acute pericarditis
• Subacute bacterial endocarditis (SBE)
• Hemostatic defects including those secondary to severe
• hepatic or renal disease
• Pregnancy (relative contraindication)
• Diabetic hemorrhagic retinopathy, or other hemorrhagic ophthalmic conditions
• Septic thrombophlebitis or occluded AV cannula at seriously infected site
• Patients currently receiving oral anticoagulants, e.g., Warfarin sodium and INR > 1.7
• Advanced age
• Status - post-full dose IV Tpa
Bleeding compl ica t ions wi th in t ra -ar te r ia l thrombolysis is around 10%.
MECHANICAL THROMBOLYSIS:
Subgroup analyses of the NINDS data showed that patients with severe strokes had only an 8% likelihood of achieving clinically significant improvement with tPA.[2] The poor outcome in these patients has inspired the search for acute-stroke treatments that are more effective than tPA.
Mechanical thrombolytic devices can remove a clot in a matter of minutes, whereas pharmaceutical thrombolytics, even those delivered intra-arterially, may take as long as 2 hours to dissolve a thrombus.[3, 4] Of concern, however, is the lack of a trial showing better outcomes with mechanical embolectomy plus IV tPA than with IV tPA alone.
Thrombolytic DevicesStryker Neurovascular Trevo Stent RetrieverThe Trevo stent retriever received US Food and Drug Administration (FDA) clearance in 2012 after a randomized, multicenter trial showed superior revascularization and patient outcomes with this device compared with the Merci Retriever.[5]
Covidien Solitaire Stent Retriever SystemThe Solitaire stent retriever system also received FDA clearance in 2012 after showing better outcomes, better revascularization, and an absence of symptomatic intracranial hemorrhage with this device compared with the Merci Retriever in a randomized, multicenter trial.[5]
Concentric Merci Retrieval SystemThe Concentric Merci Retrieval System is a corkscrewlike apparatus designed to remove clots from vessels in patients experiencing an ischemic stroke (Concentric Medical, Inc, Mountain View, Calif) (see the images below).[6, 7]
Concentric MERCI Retriever embedded in a clot. Courtesy of Concentric Medical, Inc, Mountain View, Calif. Clot retrieved from the basilar artery by using the MERCI Retriever. Courtesy of Concentric Medical, Inc, Mountain View, Calif, and Yu et al, 2003.
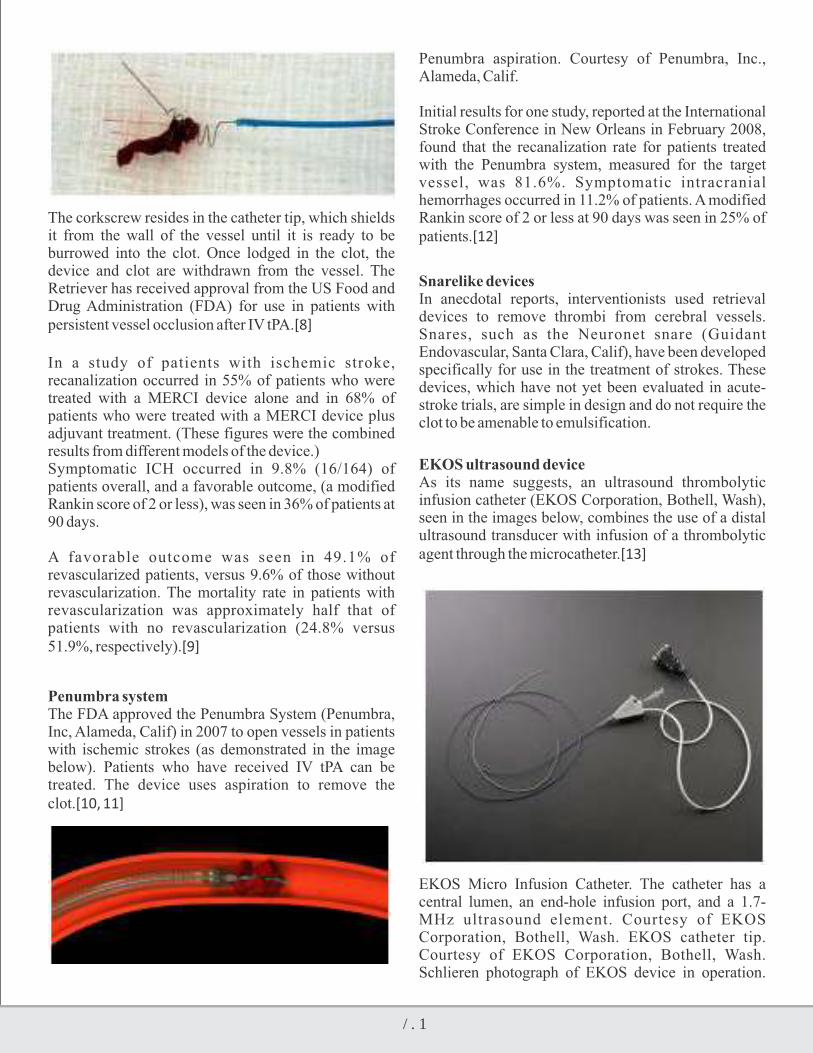
103
The corkscrew resides in the catheter tip, which shields it from the wall of the vessel until it is ready to be burrowed into the clot. Once lodged in the clot, the device and clot are withdrawn from the vessel. The Retriever has received approval from the US Food and Drug Administration (FDA) for use in patients with persistent vessel occlusion after IV tPA.[8]
In a study of patients with ischemic stroke, recanalization occurred in 55% of patients who were treated with a MERCI device alone and in 68% of patients who were treated with a MERCI device plus adjuvant treatment. (These figures were the combined results from different models of the device.) Symptomatic ICH occurred in 9.8% (16/164) of patients overall, and a favorable outcome, (a modified Rankin score of 2 or less), was seen in 36% of patients at 90 days.
A favorable outcome was seen in 49.1% of revascularized patients, versus 9.6% of those without revascularization. The mortality rate in patients with revascularization was approximately half that of patients with no revascularization (24.8% versus 51.9%, respectively).[9]
Penumbra systemThe FDA approved the Penumbra System (Penumbra, Inc, Alameda, Calif) in 2007 to open vessels in patients with ischemic strokes (as demonstrated in the image below). Patients who have received IV tPA can be treated. The device uses aspiration to remove the clot.[10, 11]
Penumbra aspiration. Courtesy of Penumbra, Inc., Alameda, Calif.
Initial results for one study, reported at the International Stroke Conference in New Orleans in February 2008, found that the recanalization rate for patients treated with the Penumbra system, measured for the target vessel, was 81.6%. Symptomatic intracranial hemorrhages occurred in 11.2% of patients. A modified Rankin score of 2 or less at 90 days was seen in 25% of patients.[12]
Snarelike devicesIn anecdotal reports, interventionists used retrieval devices to remove thrombi from cerebral vessels. Snares, such as the Neuronet snare (Guidant Endovascular, Santa Clara, Calif), have been developed specifically for use in the treatment of strokes. These devices, which have not yet been evaluated in acute-stroke trials, are simple in design and do not require the clot to be amenable to emulsification.
EKOS ultrasound deviceAs its name suggests, an ultrasound thrombolytic infusion catheter (EKOS Corporation, Bothell, Wash), seen in the images below, combines the use of a distal ultrasound transducer with infusion of a thrombolytic agent through the microcatheter.[13]
EKOS Micro Infusion Catheter. The catheter has a central lumen, an end-hole infusion port, and a 1.7-MHz ultrasound element. Courtesy of EKOS Corporation, Bothell, Wash. EKOS catheter tip. Courtesy of EKOS Corporation, Bothell, Wash. Schlieren photograph of EKOS device in operation.

104
Courtesy of EKOS Corporation, Bothell, Wash.
Ultrasound changes the structure of the clot to temporarily increase its permeability while providing an acoustic pressure gradient to move the drug into the clot to speed its dissolution. The EKOS product has not yet received FDA approval for use against acute stroke
Summary
• Time is brain, identify stroke and act fast.
• IV Thrombolysis is easy to administer, safe and effective.
• Proper selection of patients reduce the risk of bleeding.
• Ist 4.5 hrs are the golden hrs for IV Thrombolysis.
• Ensure door to needle time of <60 minutesst
• Best response is seen when given in 1 90 min.
• Those with severe deficits are less likely to respond to IV Thrombolysis.
• IA and Mechanical thrombolysis holds promise in selected group of patients.

Cerebral Granulomatous Disease
Bipin Kumar Gupta, Sumanto Chatterjee,Seema M. Maheshwari, Arushi Nautiyal, Chitra YadavDepartment of Neurology, Pushpanjali Crosslay Hospital
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Granuloma is a special type of chronic inflammation characterized by focal collection of macrophages, epithelioid cells and multinucleated giant cells , formed by the response of the mononuclear phagocytic system to a soluble antigen or irritant, which could be infective or non infective. It is the characteristic lesion of cerebral granulomatous diseases which can be defined as a space occupying lesion of non neoplastic origin.
CNS granulomatous infections usually result from hematogenous spread, most common source being the lung. Primary CNS involvement may be seen in sarcoidosis, as well in fungal infections spreading from sinuses especially in diabetics, immunocompromised individuals. Many granulomatous infections are accompanied with meningitis which can be detected on contrast imaging.
In the past few decades the cell mediated immune etiology and T lymphocyte-macrophage interaction have been established as the basis of the immune
granulomatous inflammatory response, and the essentially protective function of the lesions has been acknowledged. (Zulma and James, 1996).
Granulomas can be classified on basis of their microscopic appearance into necrotizing and non necrotizing. Non-necrotizing granulomas are characteristic of sarcoidosis, hypersensitivity pneumonitis, drug reactions, Crohn's disease and others. The presence of non-necrotizing granulomas is generally indicative of a non-infectious etiology. However, non-necrotizing granulomas may occur along with necrotizing granulomas in infectious diseases such as tuberculosis (TB) and may be the only finding in small biopsy specimen. Necrotizing granulomas are characteristic of infectious diseases such as TB and fungal infections as well as rheumatoid nodules, Wegener granulomatosis, necrobiotic post-surgical granulomas and others. (Metwally,2006-2).
INFECTIVE
• Tuberculosis
• Fungus infection
o Aspergillosis, candidiasis
coccidioidosis, and cryptococcosis
• Parasitic infection
o Toxoplasmosis
o Cvsticercosis
o Hydatid disease
o Schistosomiasis
paragonimiasis
NONINFECTIVE
• Sarcoidosis
• Wegener granulomatosis
• Histiocytosis
• Cholesteatoma
• Cholesterol Granuloma
• Granulomatous Angitis

106
The granulomatous disorders involving the CNS are a diverse confusing medical problem. The diseases often have non specific systemic and neurological clinical presentations, each disease has its own diagnostic workup and most of the non invasive investigations are non specific leading to difficult management decisions. Thus, the gold standard for definite diagnosis for most of these disorders is tissue biopsies and cultures, which is hindered by technical obstacle and even if a definite diagnosis is reached, treatment studies on neurological manifestations of granulomatous diseases are lacking.
It is worth mentioning the role of epidemiological distribution in the diagnosis of such overlapping conditions. This can be applied clinically when atypical cases are encountered. For example TB is endemic in developing countries especially in India. Yet recently it started spreading again in developed countries with migration. Cysticercosis is also prevalent in India and many developing countries due to poor sanitation. Hydatid disease is prevalent in Middle East, east Africa, parts of Russia and South America. Bilharziasis is endemic in parts of Asia, South America and Africa including Egypt, while absent in Europe and North America. Although some types of fungal infections are present worldwide, such as candida and Cryptococcus, yet others have a limited geographical distribution like Aspergillosis which is prevalent in the tropical zones and Mediterranean, and coccidioidomycosis is present only in Arizona in the United States of America.
Even the non infectious granulomas have a rather clinically significant pattern of distribution. For example, sarcoidosis is prevalent in northern Europe while almost absent in China and southern Asia.
In the last few decades, both the incidence and the prevalence of some of these disorders have increased. This is directly related to the increased prevalence of immunosuppressive states, due to the pandemic of HIV infection, use of immunosuppressive drugs, and organ transplantation. The most common granulomatous d i s o r d e r s e n c o u n t e r e d i n r e l a t i o n t o t h e immunesuppression are TB, Toxoplasmosis, Cryptococcus , candid ias i s , cocc id io idos is , aspergillosis and mucormycosis. Clinically, the above mentioned granulomatous disorders have an overlapping widely varied clinical presentation. Rarely the clinical picture may have some specific features according to the cause, for example, blindness is common in cryptococcal meningitis, while acute onset of focal neurologic deficits is more suggestive of aspergillosis, and CNS candidiasis usually present in
the context of systemic affection. Because of the aforementioned confusing clinical presentations we rely on investigations to reach a reliable diagnosis. The definitive diagnosis of CNS tuberculosis needs to be rapid as the prognosis differs radically depending on the time of start of treatment. Yet the gold standard (smear, culture) are time consuming and not sensitive. Lately PCR is showing promising results. In CNS toxoplasmosis radiological studies show multiple brain enhancing lesions which when combined with positive serology, empirical treatment should be started and if there is no response in 2 weeks, a tissue biopsy should be obtained. As regard fungal CNS granulomas, MRI may show multiple infarctions, with hemorrhage in 50%. The CSF exam and culture carries the main brunt for diagnosing the fungal etiology
On imaging, granulomas are most commonly seen as small, single or multiple, solid or discrete ring-enhancing lesions with surrounding edema at the cortical-subcortical junction, which could have variable intensities on T1W, T2W and DW1 in MRI. Due to lack of specificity, and absence of characteristic findings, they may mimic the appearance of each other, or of metastatic lesions (Robert, 2004).
Most granulomatous inflammations are associated with meningitis which is represented on CT and MRI as cisternal enhancement, usually following the vessel routes. Contrast enhanced images are critical in establishing the diagnosis of granulomatous meningitis.
Approach to a patient with cerebral granulomatous disease is described in the following algorithm.

107
The granulomatous disorders involving the CNS are a diverse confusing medical problem. The diseases often have non specific systemic and neurological clinical presentations, each disease has its own diagnostic workup and most of the non invasive investigations are non specific leading to difficult management decisions. Thus, the gold standard for definite diagnosis for most of these disorders is tissue biopsies and cultures, which is hindered by technical obstacle and even if a definite diagnosis is reached, treatment studies on neurological manifestations of granulomatous diseases are lacking.
It is worth mentioning the role of epidemiological distribution in the diagnosis of such overlapping conditions. This can be applied clinically when atypical cases are encountered. For example TB is endemic in developing countries especially in India. Yet recently it started spreading again in developed countries with migration. Cysticercosis is also prevalent in India and many developing countries due to poor sanitation. Hydatid disease is prevalent in Middle East, east Africa, parts of Russia and South America. Bilharziasis is endemic in parts of Asia, South America and Africa including Egypt, while absent in Europe and North America. Although some types of fungal infections are present worldwide, such as candida and Cryptococcus, yet others have a limited geographical distribution like Aspergillosis which is prevalent in the tropical zones and Mediterranean, and coccidioidomycosis is present only in Arizona in the United States of America.
Even the non infectious granulomas have a rather clinically significant pattern of distribution. For example, sarcoidosis is prevalent in northern Europe while almost absent in China and southern Asia.
In the last few decades, both the incidence and the prevalence of some of these disorders have increased. This is directly related to the increased prevalence of immunosuppressive states, due to the pandemic of HIV infection, use of immunosuppressive drugs, and organ transplantation. The most common granulomatous d i s o r d e r s e n c o u n t e r e d i n r e l a t i o n t o t h e immunesuppression are TB, Toxoplasmosis, Cryptococcus , candid ias i s , cocc id io idos is , aspergillosis and mucormycosis. Clinically, the above mentioned granulomatous disorders have an overlapping widely varied clinical presentation. Rarely the clinical picture may have some specific features according to the cause, for example, blindness is common in cryptococcal meningitis, while acute onset of focal neurologic deficits is more suggestive of aspergillosis, and CNS candidiasis usually present in
the context of systemic affection. Because of the aforementioned confusing clinical presentations we rely on investigations to reach a reliable diagnosis. The definitive diagnosis of CNS tuberculosis needs to be rapid as the prognosis differs radically depending on the time of start of treatment. Yet the gold standard (smear, culture) are time consuming and not sensitive. Lately PCR is showing promising results. In CNS toxoplasmosis radiological studies show multiple brain enhancing lesions which when combined with positive serology, empirical treatment should be started and if there is no response in 2 weeks, a tissue biopsy should be obtained. As regard fungal CNS granulomas, MRI may show multiple infarctions, with hemorrhage in 50%. The CSF exam and culture carries the main brunt for diagnosing the fungal etiology
On imaging, granulomas are most commonly seen as small, single or multiple, solid or discrete ring-enhancing lesions with surrounding edema at the cortical-subcortical junction, which could have variable intensities on T1W, T2W and DW1 in MRI. Due to lack of specificity, and absence of characteristic findings, they may mimic the appearance of each other, or of metastatic lesions (Robert, 2004).
Most granulomatous inflammations are associated with meningitis which is represented on CT and MRI as cisternal enhancement, usually following the vessel routes. Contrast enhanced images are critical in establishing the diagnosis of granulomatous meningitis.
Approach to a patient with cerebral granulomatous disease is described in the following algorithm.

108
Tuberculosis is still highly prevalent in developing nations and assuming importance in developed nations as well due to its reemergence with the AIDS pandemic and immigration. In the CNS, tuberculosis may present as meningitis, tuberculomas or cerebral abscesses. Meningeal tuberculosis is characterized by the presence of a dense gelatinous cisternal exudate, particularly in the interpeduncular fossa and suprasellar region, extending to the prepontine cistern and Sylvian fissures, involving local nerves and vessels. It may block CSF space and lead to hydrocephalus, exudates may cause arteritis, spasm and occlusion of vessels leading to infarcts most commonly around the sylvian region and basal ganglia. CSF study shows cells- 100-1000 cells/microlitre, lymphocytic in 65-75% cases, high protein levels may be seen, glucose being low to normal.
Tuberculomas are firm, avascular, spherical granulomatous masses, measuring about 2–8 cm in diameter. Surrounding brain tissue shows edema and gliosis. The inside of these masses may contain necrotic areas composed of caseous material, in which tubercle bacilli can be demonstrated. Intracranial tuberculomas can occur at any age. The symptoms produced are related to their location. Low-grade fever, headache vomiting, seizures, focal neurological deficit, and papilledema are characteristic clinical features of supra tentor ia l tuberculomas . Inf ra tentor ia l tuberculomas are more common in children and may present with brainstem syndromes, cerebellar manifestations, and multiple cranial nerve palsies. Symptoms are frequently chronic and slowly progressive, with a mean duration of weeks to months.
The diagnostic tests fall into three categories1. Biochemical tests detecting some other features of
the organism or products released as a result of the host's response.
• Tuberculostearic acid (TSA) • 3-(2'-ketohexyl)-indoline • Adenosine deaminase (ADA)
2. Immunological tests that detect mycobacterium antigen or antimycobacterial antibody in the CSF.
• Enzyme linked immuno sorbent assay (ELISA) • Immunofluorescent assay (IFA) • Radio immunoassay (RIA) • Immunoblot assays and T cell-based gamma-
interferon release assay
3. Molecular biological tests that detect DNA
fragments of the organism. • PCR assay
The non-caseating granulomas are hypointense on T1-weighted images and hyperintense on T2-weighted images. The tuberculoma with central liquefaction of the caseous material appears centrally hypointense on T1- and hyperintense on T2-weighted images with a peripheral hypointense ring which represents the capsule of tuberculoma. All the primary ATT drugs penetrate CNS well.
Fungal granulomas are increasing in occurrence with acquired infectious immunosupression and transplant procedures. Aspergillus is an opportunistic fungus with septate hyphae, found in soil and plants. CNS involvement may occur from haematogenous dissemination from lung focus or direct invasion from sinuses. It can cause meningitis, basal bone involvement leading to skull base osteomyelitis, vascular invasion leading to thrombosis- ischemia, infarcts and mycotic aneurysms. It should be suspected in cases with acute onset of focal neurological deficits resulting from a suspected vascular or space-occupying lesions especially in immunocompromised hosts. In patients with paranasal sinus disease, orbital extension with proptosis, ocular palsies, visual deterioration, and chemosis may occur. The symptoms frequently encountered are headache, vomiting, convulsions, hemiparesis, fever, cranial nerve deficits, paralysis, and sensory impairment of varying degree. Features typical of meningitis and subarachnoid or intracranial hemorrhage may manifest (Saravia, 1978; Hall, 1992; Sharma et al., 2000). In immunocompetent patients, the disease is usually slowly progressive and symptoms may persist for months. It may be isolated from spinal fluid analysis by staining using PAS, GMS (Gomori's methanamine) stains. However is rarely isolated from blood and CSF. The different neuroimaging patterns reported varied depending on the immune status of the patients and can be divided into infarcts, ring or nodular enhancing lesions consistent with abscesses or granulomas, and localized meningitis. Generally speaking, the more evident is the enhancement, the slower is the course of the illness which in turn implies a better immune status of the patient that is capable of encapsulating the organism and this correlates with a better clinical outcome. Amphotericin B combined with flucytosine and treatment of the source of infection should form the mainstay of the management. Surgical debridement maybe required in presence of abscesses.

109
Cryptococcus- The most common site of entry is via lungs, polysaccharide capsule prevents phagocytosis, remains dormant and reactivates with any period of immunesupression, hematogenus dissemination. Most commonly presenting with headache followed by fever, cranial neuropathies. Complications in form of raised ICT and blindnesss may occur. Diagnosis by demonstrating the yeasts in CSF study- india ink stain, cryptococcal antigen or culture.
The most common finding of cryptococcal infection is a communicating or noncommunicating hydrocephalus (Takasu et al., 1991). Hydrocephalus occurs less in the immunocompromised population which may be related to an inability to initiate an inflammatory response to the meningoencephalitis or the formation of adhesions within the basal cisterns, Leptomeningeal e n h a n c e m e n t i s a n u n c o m m o n f i n d i n g . Hypoattenuating nonenhancing lesions within the basal ganglia may be present on CT scan and represent dilated Virchow-Robin spaces. These areas are isointense to cerebrospinal fluid without surrounding edema on MR imaging. These spaces may become voluminous as the yeasts produce mucoid material that distends these areas.The presence of gelatinous pseudocysts suggests an immunocompromised state (Zheng et al., 1996). Other patterns of involvement include the miliary form or the presence of granuloma (cryptococcoma), which may be of low or high attenuation on CT scan. On MR imaging, these lesions are typically hypointense on Tl-weighted images and hyperintense on T2-weighted images. Immunocompetent patients more often present with cryptococcomas (Ostrow et al., 1994). Guidelines instruct initial induction therapy with amphotericin B at 0.7 mg/kg/day with flucytosine at 100 mg/kg/day for 2 weeks, and then switching to 400 to 800 mg /day of fluconazole for 8 weeks
Mucormycosis- Intracranial granuloma formation by mucormycosis is a rare occurrence. Rhinocerebral mucor infection usually presents as sinusitis, periorbital cellulitis, proptosis and chemosis. Angioinvasive nature of the fungus may result in cavernous sinus thrombosis and internal carotid artery thrombosis with extensive cerebral infarctions. Occasionally cerebral vascular invasion may lead to hematogenous dissemination of the infection. Because of its propensity for vascular structures, neuroradiologic findings associated with mucormycosis include arteritis, ischemic changes, bland or hemorrhagic infarction and aneurysm formation. Intracranial granuloma formation by mucormycosis is a rare
occurrence.Ring enhancement may be shown after the administration of contrast material.
Diagnosis usually requires histopathological evidence as isolation from body fluids is rarely positive. . High- dose liposomal amphotericin B (15 mg/kg/day) is treatment of choice.
Cysticercosis – It occurs following ingestion of taenia solium eggs from infected pork, vegetables, develop as larval cysts almost anywhere in the body.. Parenchymal cysts may present with seizures. Extraparenchymal may present with hydrocephalus from mechanical obstruction by cyst or surrounding inflammation. Patients may also present with symptoms and signs of raised ICP. Symptoms may include nausea or vomiting, visual changes, or dizziness. The patients with cysticercal encephalitis may have altered mental status raised ICP, or seizures (Rangel et al., 1987). Viable cysts do not enhance with contrast appear as 10 to 20 mm cysts, the wall is not visible and the fluid, isodense with the cerebrospinal fluid. when attacked by body immune defense and amidst mounting inflammation, the cysts appear as ring enhancing lesions, followed by calcification, presenting as solid masses and when found in absence of evidence of any other illness are highly suggestive of neurocysticercosis
Diagnostic criteria for neurocysticercosis (Del Brutto et al., 2001): History of frequent travel to disease-endemic areas. Individuals coming from or living in an area where cysticercosis is endemic , positive CSF ELISA for detection of anticysticercal antibodies or cysticercal antigens, minor resolution of intracranial cystic lesions after therapy with albendazole or praziquantel, positive serum immunoblot for the detection of anticysticercal antibodies
Praziquantel in a dosage of 50 mg/kg/day for 2 weeks or Albendazole- 15mg/kg/day for one week is the treatment of choice. Between the second and fifth days of antiparasitic therapy, there is usually an exacerbation of neurological symptoms, attributed to local inflammation due to the death of the larvae. For this reason, both albendazole and praziquantel are generally given simultaneously with steroids in order to control the edema and intracranial hypertension that may occur as a result of therapy (Hector et al., 2002). Antiepileptic drugs maybe required. Withdrawal of AEDs in patients with residual calcification are at an increased risk of seizures.

110
Toxoplasmosis: Toxoplasma gondii is an obligate intracellular protozoan parasite that causes the most common cerebral mass lesion encountered in HIV-positive patients. The occurence of neurotoxoplasmosis i s a ra re condi t ion , v i r tua l ly res t r ic ted to immunocompromised individuals. The extent of the hosts' immune response depends on their ability to establish effective humoral and cellular responses. It has beenspeculated that different patterns of presentation stem from the cause and intensity of immunocompromise.
The CNS symptoms are related to fever, headache, and confusion progressing to coma, focal neurologic signs, and seizures. Imaging patterns for focal lesions in toxoplasmosis will depend on the damage caused by T. Gondii and the host's immune response. It is thus possible to show multiple or isolated expanding lesions with intense enhancement and necrotic areas that mimic primary or metastatic CNS neoplasia as well as unenhanced diffuse lesions with an encephalitic aspect. MRI with intravenous contrast injection is more sensitive than CT to demonstrate all types of lesions in neurotoxoplasmosis. In MRI studies these lesions will have hyposignal on T1 and hypersignal on T2, with extensive perilesional edema and varying degrees of contrast enhancement. Practically whenever there is enhancement there will be some degree ofnecrosis, which must be sought systematically as a marker for this disease.
One well-known pattern in neurotoxoplasmosis lesions is called eccentric target sign. It is an annular enhanced area with an eccentric nodule along an irregular wall. Several criteria have been proposed to distinguish toxoplasmosis from other conditions such as CNS lymphoma, mainly in the context of AIDS. These criteria value the subcortical location of toxoplasmosis lesions, eccentric target sign, and the multiplicity of lesions and enhancement of a wall that is thinner than is observed in lymphomas.
Cerebral echinococcus:CNS disease typically presents as a mass lesion. In this case, the slowly enlarging lesion may cause headaches, seizures, or focal neurologic abnormalities (Altinors et al., 2000).
Diagnosis is primarily made by imaging studies. In the case of E. granulosus, CT or MRI scans of brain typically demonstrate a spherical cystic lesion with smooth borders. When the internal images from the
protoscolexes "hydatid sand" are seen, the image can be diagnostic. Midline shift and distortion of the ventricles are common. Lesions are usually not inflamed and thus do not have surrounding edema or enhancement. The cyst wall usually shows a rim of low signal intensity on both TI- and T2-weighted images. Cysts may be found outside the CNS, which suggests that the CNS lesion is also due to hydatid disease. The treatment of choice for CNS hydatid disease is surgical removal. In the case of E. granulosus, care must be taken not to rupture the cyst with resultant spread of the protoscolexes. Antiparasitic drugs, particularly albendazole, are routinely recommended before surgery in hepatic cases. However, the role of preoperative antiparasitic drugs in CNS infection has not been clearly defined. The dose of albendazole for patients weighing more than 60 kg is 400 mg PO twice daily for 28 days. A dose of 15 mg/kg of body weight daily in 2 divided doses (not to exceed total daily dose of 800 mg) has been suggested for patients weighing less than 60 kg. For CE, the 28-day course may be repeated after 14 days without treatment to a total of 3 treatment cycles.
Sarcoidosis- The cause is unkown and is considered to be due to an exaggerated immune response to self or foreign antigens. In neurosarcoidosis, the granulomas in the CNS, consists of lymphocytes and mononuclear phagocytes surrounding a noncaseating epithelioid cell granuloma (Metwally, 2006-5). It generally occurs in 5- 16% of cases usually if the disease has had substantial systemic involvement and signs of active disease usually within 2 years (Lower et al., 1997 and James, 1998). However, strictly neurological forms are seen in fewer than 10% of patients (Bourahoui et al., 2004). Neurosarcoidosis carries a mortality rate of 10%.
Those with an acute onset present with isolated cranial neuropathies (most commonly facial nerve) or aseptic meningitis, and those with chronic onset usually present with parenchymal involvement, hydrocephalus, multiple cranial neuropathies, or peripheral nervous system manifestations. Most common lesions on MRI include: multiple white matter lesions (43% of patients), meningeal enhancement (38% of patients), optic nerve enhancement (28% of patients) and mass lesions in brain parenchyma (Zajicek et al., 1999. Furthermore, it was found that these lesions recur frequently.
Disease enti t ies that can involve the basal leptomeninges and mimic leptomeningeal sarcoidosis on imaging include granulomatous disease (such as

111
TB), Wegener granulomatosis and fungal meningitis, pyogenic meningitis, leptomeningeal lymphoma, demyelination, meningoangiomatosis , acute lymphocyt ic leukemia, and leptomeningeal carcinomatos. Supratentorial granulomatous lesions are more common than infratentorial masses.. The most common intracranial sites of involvement are the hypothalamus, the third ventricle region, and the pituitary gland. Hypothalamic and pituitary gland granulomatous infiltration are well recognized. Hyperprolactinemia and inappropriate antidiuretic hormone secretion (SIADH) may occur, but hypothalamic hypothyroidism is rare. In addition, hypothalamic dysfunction can affect vegetative functions like appetite, temperature, sleep, and libido. Sarcoid mass lesions can be mistaken for meningiomas, intraventricular tumors, cerebellopontine angle tumors, and en plaque subdural lesions indistinguishable from meningiomas, and they may necessitate biopsies for definitive diagnosis
Serum Angiotensin Converting Enzyme (ACE) levels are elevated in 56% to 86% of patients (Israel et al., 1986). Levels may correlate with the disease activity post-treatment, but they have little prognostic value in the initial evaluation. Serum ACE levels are also elevated in patients with liver disease, diabetes mellitus, hyperthyroidism, systemic infection, malignancy, Gaucher's disease and in normal young individuals, but they are much higher in sarcoidosis (Consensus Conference, 1994).
CSF commonly shows a mononuclear pleocytosis, usually less than 50 white blood cell
(WBC)/mm.. Other abnormalities include elevated CSF pressure, increased protein (< 100 mg%), and hypoglycorrhachia. These abnormalit ies are nonspecific and other CSF tests to rule out infectious, inflammatory causes should be done.
The main goal of treatment is to salvage tissue function and prevent progression of the disease, especially fibrosis and ischemia. Corticosteroids should be started in high doses and, after a clinical response occurs, gradually tapered, similar to their use in other inflammatory conditions (Chapelon et al., 1990). Complete withdrawal can be attempted if the clinical course permits. In case of relapse, a repeat course of high-dose steroid treatment should be attempted.
Initial treatment with prednisolone 40 mg daily or 20
mg twice daily if fever is prominent, then 30 mg daily in single morning dose, then 25 mg daily. Then 20 mg daily, each dose level lasting 2 weeks. Daily maintenance (after 8 wk) 15 mg daily (10 mg may be adequate later). A small number of patients, specifically those with diffuse encephalopathy and vasculopathy, have undergone radiation treatment. These patients were treated with total nodal and craniospinal irradiation with some benefit (Chapelon et al., 1990). Newer immunomodulatory agents and other modalities of treatment under research include tacrolimus, sirolimus, anticytokine therapy, anticellular adhesion molecules, T-helper-2 cytokines, and gene therapy targeting proinflammatory cytokines.
Wegener granulomatosis:Wegener granulomatosis (WG) is characterized by necrotizing granulomatous vasculitis of the upper and lower respiratory tract, pauci-immune segmental necrotizing glomerulonephritis, and small vessel vasculitis. Neurological involvement, seen primarily as cranial neuropathies and peripheral neuropathies, occurs in about 34% of cases.
Primary angiitis of the CNS is a rare disease characterized by vasculitis of small and medium arteries in the brain and spinal cord. Presentations are highly variable, but the triad of headache, organic brain syndrome, and multifocal neurologic deficits is most suggestive. Most affected patients do not have systemic symptoms, signs, or abnormal routine blood tests, including ESR.
MRI is most sensitive, being abnormal in more than 80% of patients. Analysis of biopsy specimens of brain cortex and leptomeninges can help establish the diagnosis. The best therapy has not been established many patients are treated with prednisone and cyclophosphamide.
Histiocytosis is a rare blood disease that is caused by an excess of white blood cells called histiocytes. It mainly affects children. Clinically it affects the skin, bone, eyes, gastrointestinal tract, with diabetes insipidus being the hallmark of CNS affection. Others symptoms due to CNS affection include other endocrinal deficiencies and rarely behavioral changes or manifestations of increased ICT.
MRI findings in histiocytosis include thickening of the pituitary stalk, dura based masses, white matter lesions and cystic changes in pineal gland. Treatment strategy

112
is dependent on the type and site of the lesions and the state of LCH outside the CNS.
Cholesteatoma and cholesterol granuloma are two destructive lesions affecting the temporal bone, with possible CNS complication secondary to local invasion. They can be diagnosed by CT scan, differentiated by MRI, and treated by different surgical approaches.
To summarize, need of the hour is to establish treatment protocols specific for CNS granulomas, to replace those based on systemic granulomatous disorders. To facilitate research work for searching and testing new diagnostic tools and investigations that would provide better sensitivity and specificity and less time consuming. To look for new treatments that are more effective and less toxic, and last but not the least to perform more studies about the current and possible treatment regiments for CNS granulomatous disorders instead of focusing studies on the systemic aspects of these disorders.
REFERENCES1. Altinors N, Bavbek M, Caner HH, et al Central
nervous system hydatidosis in Turkey: a cooperative study and literature survey analysis of 458 cases. J Neurosurg; (2000). 93:1-8.
2. Bourahoui A., J. de Seze, R. Guttierez, B. Onraed, B. Hennache, D. Ferriby, T. Stojkovic, P. Vermersch; CSF isoelectrofocusing in a large cohort of MS and other neurological diseases; European Journa l o f Neuro logy 2004. 11(8):525–529.
3. Chapelon C, Ziza JM, Piet te JC, et al Neurosarcoidosis: Signs, course and treatment in 35 confirmed cases; Medicine (Baltimore). 1990. 69:261-276
4. Del Brutto O H, Rajshekhar V, White A C Jr et al P r o p o s e d d i a g n o s t i c c r i t e r i a f o r neurocysticercosis; Neurology. 2001; 57:177-183
5. Hall WA. Neurosurgical Infections in the Compromised Host in Haines SJ, Hall WA, editors, Neurosurgery Clinics of North America, Infections in Neurologic Surgery, Vol 3, Philadelphia: WB Saunders Co; 1992.435-42.
6. Metwally Y (2006-2).; Hydatid disease; Text book of Neuroimaging (web based e-book); Ver 7.2
7. Ostrow TD, Kudgins PA, Magnetic resonance imaging of intracranial fungal infections. Top Magn Reson Imaging,1994. 6:22-31.
8. Rangel R, Torres B, Del Brutto O, et al. Cysticercotic encephalitis: a severe form in young females. Am J Trop Med Hyg, 1987. 36:387-392.
9. Robert D. Zimmerman. Physiological imaging in infection, inflammation and demyelination; In: Clinical MR Neuroimaging; Jonathan H. Gillard, Adam D. Waldman, Peter B. Barker (eds). Cambridge University Press. 2004. 359-361
10. Saravia-Gomez J.; Aspergillosis of the Central Nervous System, in Vinken PJ, Bruyn GW, editors, Handbook of Clinical Neurology Vol, Holland: North-Holland Publishing Company. 1978. 35:395-400
11. Sharma RR, Lad SD, Desai AP, Lynch PG; Surgical Management of Fungal Infections of the Nervous System, Schmidek and Sweet Operative Neurosurgical Techniques: Indications, Methods and Results, 4th edn .Philadelphia.WB Saunders Company.2000. 1726
12. Zajicek JP. Neurosarcoidosis. Curr Opin Neurol. 2000. 13:323-325
13. Zulma A and James DG. Granulomatous infections: etiology and classification. Clin Infect Dis.1996. 23: 146–158

Dr. B. K. TiwariM.B.B.S., M.D. (Medicine), Senior Consltant Physician
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
Practical Tips in Management ofa Patient with CKD
Kidney disease is defined as an abnormality of kidney structure or function with implications for the health of an individual, which can occur abruptly, and either resolve or become chronic. CKD is a general term for heterogeneous disorders affecting kidney structure and function with variable clinical presentation, in part related to cause, severity and the rate of progression. The concept of CKD evolved after the recognition of the contribution of disordered kidney structure and function on the health of individuals across a wide range of severity.CKD is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health. CKD is classified based on cause, GFR category, and albuminuria category . Kidney failure is traditionally considered asthe most serious outcome of CKD. Symptoms are usually due to complications of decreased kidney function and when severe, they can be treated only by dialysis or transplantation.
The Kidney Disease: Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease (CKD) serves to update the 2002 KDOQI Clinical Practice Guidelines for Chronic Kidney Disease : Eva lua t ion , C lass i f i ca t ion , and Stratification following a decade of focused research and clinical practice in CKD. The document aims to provide state-of-the-art guidance on the evaluation, management and treatment for all patients with CKD.
In people with GFR <60 ml/min/1.73 m2 (GFR categories G3a-G5) or markers of kidney damage, review past history and previous measurements to determine duration of kidney disease. * If duration is >3 months, CKD is confirmed.
* If duration is not >3 months or unclear, CKD is not confirmed. Patients may have CKD or acute kidney diseases (including AKI) or both and tests should be repeated accordingly.
CKD progression can be defined based on the following :Decline in GFR category (>90 [G1], 60–89 [G2], 45–59 [G3a], 30–44 [G3b], 15–29 [G4], <15 [G5] ml/min/1.73 m2).
The management of progression of CKD is aimed at addressing a multiplicity of factors known to be associated with progression. There are general measures which have been shown to address cardiovascular health and CKD together, or each separately. Strategies include general lifestyle measures which improve cardiovascular health, BP control, and interruption of the RAAS. In addition, control of other metabolic parameters such as blood sugar, uric acid, acidosis, dietary/lifestyle manipulations and dyslipidemia may also be important.
PROTEIN INTAKEIt is suggested that lowering protein intake to 0.8 g/kg/day in adults with diabetes or without diabetes and GFR <30 ml/min/ 1.73 m2 (GFR categories G4-G5), with appropriate education.It is suggested avoiding high protein intake (<1.3 g/kg/day) in adults with CKD at risk of progression.
Excess dietary protein leads to the accumulation of uremic toxins, conversely insufficient protein intake may lead to loss of lean body mass, and malnutrition
Dr Samir TawakleyMBBS,DNB(Med),DNB(Nephro)Sr Consultant NephrologistSt Stephens hospital and Apollo hospital, Delhi and Noida

114
(the latter more frequent in the elderly). The benefits of dietary protein restriction include reduction of accumulation of metabolic waste products that may suppress the appetite and stimulate muscle protein wasting. The role of dietary protein restriction in slowing progression of CKD is more controversial and advanced CKD is associated with a protein wasting syndrome which is directly correlated with morbidity and mortality. Note that statements about reduction in dietary protein do not apply to pediatric populations given issues related to growth and nutrition.
Studies on protein restriction have not been widely tested in different ethnicities or within cultures with low baseline proten intake or purely vegetarian diets, like in India. Thus, the applicability of statements to all regions of the world is limited, including India. Clinicians should be aware of different sources of protein, and if lowering of protein is recommended, education and monitoring for malnutrition should be implemented. Appropriate dietary counseling for CKD patients may have healthcare resource implications, although as part of a combined strategy to manage obesity, salt intake, and diabetes may be considered cost-effective on a population basis in certain countries. Avoidance of malnutrition is important.
SALT INTAKE We recommend lowering salt intake to <90 mmol (<2 g) per day of sodium (corresponding to 5 g of s o d i u m c h l o r i d e ) i n a d u l t s , u n l e s s contraindicated.
We recommend restriction of sodium intake for children with CKD who have hypertension (systolic and/or diastolic blood pressure <95th percentile) or prehypertension (systolic and/or diastolic blood pressure <90th percentile and < 9 5 t h p e rc e n t i l e ) , f o l l o w i n g t h e a g e -basedRecommended Daily Intake. We recommend supplemental free water and sodium supplements for children with CKD and polyuria to avoid chronic intravascular depletion and to promote optimal growth.
In subjects with CKD, impaired excretion of sodium is often present. High sodium intake increases BP and proteinuria, induces glomerular hyperfiltration and blunts the response to RAAS blockade. Lowering salt
intake not only reduces BP, but also lowers albuminuria. There are some conditions in which salt restriction may be harmful, and hence the qualifier ''unless contraindicated.' These conditions include salt losing nephropathies and those prone to hypotension and volume contraction who do not have heart failure. Salt intake has been identified as an important driver of high BP in all countries and in adults, thus this recommendation is of international relevance and applicability. In most developed countries, a reduction in salt intake can be achieved by a gradual and sustained reduction in the amount of salt added to foods by the food industry. In other countries where most of the salt consumed comes from salt added during cooking or from sauces, a public health campaign is needed to encourage consumers to use less salt. The range of sodium intake associated with improved long-term outcomes is easily achievable and may have the potential to greatly improve health outcomes in patients with CKD around the world.
HYPERURICEMIA There is insufficient evidence to support or refute the use of agents to lower serum uric acid concentrations in people with CKD and either symptomatic or asymptomatic hyperuricemia in order to delay progression of CKD.
Hyperuricemia is common in people with CKD and is defined by urate concentrations above 7.0 mg/dl (420 mmol/l) as measured by automated enzymatic (uricase) laboratory methods. Concentrations ob t a ined w i th co lo r ime t r i c me thods a r e approximately 1 mg/dl (60 mmol/l) lower. Observational data had implicated uric acid in the progression of CKD suggesting that adverse outcomes in people with CKD may be improved by specific uric acid lowering therapy. Small studies using appropriate RCT design have shown reduced left ventricular mass, improved endothelial function, and reduced progression of CKD in people with either symptomatic or asymptomatic hyperuricemia and CKD.
The specific statement is intended to ensure and foster RCTs to properly assess the risk and benefits of uric acid lowering strategies in people with CKD. Presently,there is insufficient evidence to recommend the use of uric acid lowering agents in

115
asymptomatic individuals for the specific purpose of delaying CKD progression.
LIFESTYLEWe recommend that people with CKD be encouraged to undertake physical activity compatible with cardiovascular health and tolerance (aiming for at least 30minutes 5 times per week), achieve a healthy weight (BMI 20 to 25, according to country specific demographics), and stop smoking.
CKD patients have a reduced exercise capacity and impaired physical functioning. Moreover, reduced physical activity is associated with increased mortality and poor QOL in people with CKD. Regular exercise leads to increased exercise capacity, decreased morbidity, and improved health-related QOL. Exercise may reduce cardiovascular risk through its beneficial effects on BP, triglycerides, high-density lipoprotein cholesterol (HDL-C), insulin resistance, and glycemic control. In ESRD, exercise has been shown to improve arterial stiffness, BP, cardiorespiratory function, and QOL.
Exercise, weight loss and smoking cessation in CKD are equally important in all countries and thus this recommendation is of international relevance and a p p l i c a b i l i t y . I m p l e m e n t a t i o n o f t h i s recommendation has no public health cost but has the potential to make far-reaching public health gains both in terms of population health and healthcare economics.
C K D M E TA B O L I C B O N E D I S E A S E I N C L U D I N G L A B O R A T O R Y ABNORMALITIESChanges in bone mineral metabolism and alterations in calcium and phosphate homeostasis occur early in the course of CKD and progress as kidney function declines These changes are grouped under the umbrella term Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) which includes renal osteodystrophy and extraskeletal (vascular) calcification related to abnormalities of bone mineral metabolism. Renal osteodystrophy is the component of CKD-MBD that is identified and quantified through bone biopsy histomorphometry and includes osteitis fibrosa (hyperparathyroidism), osteomalacia, and adynamic bone disease.
We recommend measuring serum levels of calcium, phosphate, PTH, and alkal ine phosphatase activity at least once in adults with GFR <45 ml/min/1.73 m2 (GFR categories G3b-G5) in order to determine baseline values. Thereafter, for CKD Stage 3, it is recommended every 12 months, for CKD Stage 4 every 3 months, and for CKD Stage 5 every month except PTH which should be done every 3 months. Serum levels of corrected total calcium should be maintained within the normal range for the laboratory used, preferably towards the lower end(8.4 to 9.5 mg/dl).
In people with GFR <45 ml/min/1.73m2 (GFR categories G3b-G5), we suggest maintaining serum phosphate concentrations in the normal range according to local laboratory reference values.
In CKD patients(Stages 3 and 4), the serum level of phosphorus should be maintained at or above 2.7 mg/dl and no higher than 4.6 mg/dl. In CKD Stage 5 patients and those treated with haemodialysis or peritoneal dialysis, the serum levels of phosphorus should be maintained between 3.5 mg/dl and 5.5 mg/dl.
In people with GFR <45 ml/min/1.73m2 (GFR categories G3b-G5) the optimal PTH level is not known. We suggest that people with levels of intact PTH above the upper normal limit of the assay are f i r s t e v a l u a t e d f o r h y p e r p h o s p h a t e m i a , hypocalcemia, and vitamin D deficiency. Levels of intact PTH as determined by immunoradiometric assay(IRMA) or immunochemiluminometric assay(ICMA) are an adequate screening tool to separate high-turnover bone disease ( osteitis fibrosa ) from low-turnover bone disorders ( adynamic bone disease ). Blood levels of PTH begin to rise when GFR falls below 60ml/min/1.73m2, and evidence of bone disease due to hyperparathyroidism may be present at stage 3 of CKD. The target intact PTH levels at CKD Stage 3 should be 35-70 pg/ml, for CKD Stage 4 should be 70-110 pg/ml and for CKD Stage 5 should be 150-300 pg/ml.
We suggest not to routinely prescribe vitamin D supplements or vitamin D analogs, in the absence of suspected or documented deficiency, to suppress elevated PTH concentrations in people with CKD not on dialysis.

116
It is suggested not to prescribe bisphosphonate treatment in people with GFR<30 ml/min/1.73 m2 (GFR categories G4-G5) without a strong clinical rationale.
VACCINATIONSIt is recommended that all adults with CKD are offered annual vaccination with influenza vaccine, unless contraindicated.
We also recommend that all adults with eGFR <30 ml/min/1.73 m2 (GFR categories G4-G5) and those at high risk of pneumococcal infection (e.g., nephritic syndrome, diabetes, or those receiving immunosuppression) receive vaccination with polyvalent pneumococcal vaccine unless contraindicated. We recommend that all adults with CKD who have received pneumococcal vaccination are offered revaccination within 5 years.
We recommend that all adults who are at high risk of progression of CKD and have GFR <30 ml/min/1.73 m2 (GFR categories G4-G5) be immunized against hepatitis B and the response confirmed by appropriate serological testing. The available formulation of hepatitis B vaccine is administered at a double standard dose in a 4 dose schedule for CKD patients. Testing after vaccination is recommended to determine the response to the vaccine. Testing should be performed 1-2 months after administration of the last dose of the vaccine series by using a method that allows determination of the protective levels of anti-HBs(>10 mIU/ml). A booster dose should be administered when anti-HBs levels decline to <10 mIU/ml.
Consideration of live vaccine should include an appreciation of the patient's immune status and should be in line with recommendations from official or governmental bodies.
Pediatric immunization schedules should be followed according to official international and regional recommedations for children with CKD.
REFERRAL TO SPECIALIST SERVICESWe recommend referral to specialist kidney care services for people with CKD in the following circumstances :
* AKI or abrupt sustained fall in GFR;
* GFR o30 ml/min/1.73 m2 (GFR categories G4-G5);
* a consistent finding of significant albuminuria (ACR >300 mg/g [>30 mg/mmol] or AER>300 mg/24 hours, approximately equivalent to PCR >500 mg/g [>50 mg/mmol] or PER >500 mg/24 hours);
* progression of CKD
* urinary red cell casts, RBC>20 per high power field sustained and not readily explained;
* CKD and hypertension refractory to treatment with 4 or more antihypertensive agents;
* persistent abnormalities of serum potassium;
* recurrent or extensive nephrolithiasis;
* hereditary kidney disease.
We recommend timely referral for planning renal replacement therapy (RRT) in people with progressive CKD in whom the risk of kidney failure within 1 year is 10-20% or higher, as determined by validated risk prediction tools.
TIMING THE INITIATION OF RRTWe suggest that dialysis be initiated when one or more of the following are present: symptoms or signs attributable to kidney failure (serositis, acidbase or electrolyte abnormalities, pruritus); inability to control volume status or blood pressure; a progressive deterioration in nutritional status refractory to dietary intervention; or cognitive impairment.
This often but not invariably occurs in the GFR range between 5 and 10ml/min/1.73 m2.
Living donor preemptive renal transplantation in adults should be considered when the GFR is <20 ml/min/1.73 m2, and there is evidence of progressive and irreversible CKD over the preceding 6-12 months.
Appropriate planning allows for the initiation of dialysis therapy at the appropriate time with a permanent access in place at the start of dialysis therapy. Patients with a GFR<30 ml/min/ 1.73m2(CKD stage 4) should be educated on all modalities of renal replacement therapy(RRT) options. In patients with CKD stage 4 or 5, forearm and upper-arm veins suitable for placement of vascular access should not be used for venipuncture

117
or the placements of intravenous catheters.A fistula should be placed at least 6 months before the anticipated start of HD treatments. This timing allows for access evaluation and additional time for revision to ensure a working fistula is available at initiation of dialysis therapy.
A graft should, in most cases, be placed at least 3 to 6 weeks before the anticipated start of HD therapy. Some newer graft materials may be cannulated immediately after placement.
A peritoneal dialysis(PD) catheter ideally should be placed at least 2 weeks before the anticipated start of dialysis treatment.
The order of placement of various accesses should be as follows:1.) Fis tulae–wris t ( radiocephal ic) , e lbow
(brachicephalic), transposed brachial basilic vein
2.) AVG- forearm loop graft, preferable to a straight configuration; upper arm graft; chest wall or “necklace” prosthetic graft or lower-extremity graft.
Avoid if possible: Long term catheters. They should not be placed on the same side as a maturing AV
access, if possible.The preferred insertion site for tunneled cuffed venous dialysis catheters or port catheter systems is right internal jugular vein. Other options include the right external jugular vein, left internal and external jugular veins, subclavian veins, femoral veins, and translumbar and transhepatic access to the IVC. Ultrasound should be used in the placements of catheters. The position of the tip of any central catheter should be verified radiologically.
There is a need to ensure appropriate access to services and education surrounding quality care during terminal stages of a chronic condition. There is increasing attention to this in many societies but not in all. Appreciating the variability in the resources required and their availability to different groups of pat ients is important for implementat ion. Furthermore, involvement of religious and cultural leaders in recognition of these care practices can be enhanced if they are overtly recognized as part of the care continuum. There is a need for robust assessment of best practices in CKD and other chronic conditions so that we may provide best care throughout the continuum of life. Researchers around the world are actively pursuing this so that we may have better tools, programs, and ultimately, better outcomes for our patients.

Dr. Shri Ram Kabra, Senior ConsultantDr Satish Chhabra, Jr. Resident,Nephrology, Max Superspeciality Hospital, Patparganj, DelhiDr Aditya Jayraman, Jr. Resident,Nephrology, Max Superspeciality Hospital, Patparganj, Delhi
Prevalence of anemia severity stratified by stage of chronic kidney disease.
Anemia Management in CKDKDIGO Guidelines revisited
Burden of the diseaseIn patients with CKD not requiring dialysis, untreated anemia increases cardiovascular risk, hospitalization, and all-cause mortality, and diminishes health-related quality of life and exercise capacity. Heightened risk for progression of kidney failure has also been linked to untreated anemia of CKD. Thus, management of anemia throughout the CKD continuum is essential
Anemia is in fact a common problem in the chronic kidney disease population and increases in severity as the renal dysfunction gets worse. But please note that it occurs very early and over 25% of patients are anemic at levels of serum creatinine which would not be recognized by many practitioners as indicating the presence of chronic kidney disease. More than 30% of patients already have hemoglobin (Hb) levels <12 g/dL by Stage 3 CKD.Hence, individuals who have undiagnosed asymptomatic chronic kidney disease may have untreated anemia.
What is even more important and shows an area for potential improvement of patient management is that it is under-recognized and more importantly under-treated. As seen in the studies quoted below, in patients whose hemoglobin count is well under ten, less than 20% of the patients are getting erythropoietin therapy and even fewer are receiving iron.
Pathophysiology of anemia of CKDAnemia of CKD arises primarily from a progressive failure of kidney endocrine function. Peritubular cells in the kidneycortex function as oxygen sensors controlling red cell mass. Renal tissue hypoxia triggers hypoxia-inducible factorsignaling, which, in turn, up-regulates erythropoietin production to stimulate division and differentiation of red cell precursors. In anemic but otherwise healthy individuals, this feedback system restores red blood cell mass and tissue oxygenation; however, in patients with CKD, one or more of these processes become impaired. In early CKD, plasma erythropoietin levels may fall within the normal range, but show a blunted response to decreasing hematocrit. As CKD advances, the peritubular cells progressively diminish in number and function, producing insufficient erythropoietin to r e s to re and ma in ta in appropr i a t e r ed ce l l mass.Congestive heart failure (CHF) frequently complicates CKD and adversely affects erythropoiesis.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

119
Moderate-to severe CKD has been reported in 50% of patients with CHF; conversely, approximately 40% of patients with CKD have CHF . Untreated CHF may contribute to anemia of CKD both by enhancing chronic inflammation and by directly inducing kidney damage.
Consequences of untreated anemia of CKDAmong patients not requiring renal replacement, untreated anemia of CKD is strongly associated with cardiovascular and renal complications, resulting in increased hospitalizations and mortality.
Left Ventricular HypertrophyThe necessary adaptive changes to anemia in CKD– chronic vasodilation, volume and pressure overload, increased heart rate, and increased cardiac output – ultimately result in left ventricular hypertrophy (LVH), whose prevalence is estimated at 39% in Stage 2 CKD, 50% in Stage 3 CKD, and 60%-74% in Stage 4.
Congestive Heart FailureChronic LVH and mechanical heart stress resulting from anemia contribute to development of congestive heart failure (CHF). In the ANCHOR study of 59,772 adults with CHF, 42.6% had anemia at baseline (Hb<12 g/dL for women, <13 g/dL for men). In this cohort, anemia showed a graded, independent relationship to mortality in CHF patients, the risk of death rising from 16% for 12.0–12.9 g/dl to 248% for <9.0 g/dl.
Coronary Heart DiseaseIn the ARIC study, anemia independently predicted coronary heart disease in CKD patients. Elevated creatinine without anemia did not significantly increase coronary risk.
Progression to Renal ReplacementUntreated anemia of CKD is also associated with increased risk of progression to renal replacement. In a retrospective US Veterans' Affairs cohort, each 1.0 g/dL increase in time-averaged Hb conferred a 26% reduction in risk for renal replacement. Among diabetic nephropathy patients in the RENAAL study, Hb<11.3 g/dL roughly doubled the risk of renal replacement onset and every 1 g/dLHb decrease increased renal replacement risk by 11%.
Etiology of anemia in CKD: contributing factors· EPO insufficiency· Iron deficiency· Acute/ Chronic Inflammatory conditions· 2° Hyperparathyroidism· Aluminum toxicity· Folate deficiency· Decreased RBC survival· Hypothyroidism· Hemoglobinopoathies

120
Anemia workup in CKD· Hemoglobin and / or Hematocrit· Red blood cell indices· Reticulocyte count· Peripheral smear morphology· Iron parameters· S. Iron· TIBC (TSAT)· Ferritin· Test for occult blood in stool· B12 and Folate
Assessment of Iron Status· Frequently used tests:o Serum Ferritin > 100 < 500 ng/mlo Transferrin saturation (Iron/TIBC x100) > 20%· Additional Measurements:o Reticulocyte Hb Conc.o Erythrocyte ferritino % hypochromic RBCso Marrow iron stores
What does KDIGO Guidelines say?Frequency of testing for anemia1.1.1: For CKD patients without anemia (as defined
below in Recommendation 1.2.1 for adults and Recommendation 1.2.2 for children), measure Hb concentration when clinically indicated and (Not Graded):
· at least annually in patients with CKD 3· at least twice per year in patients with CKD 4–5ND· at least every 3 months in patients with CKD 5HD
and CKD 5PD1.1.2: For CKD patients with anemia not being treated
with an ESA, measure Hb concentration when clinically indicated and (Not Graded):
· at least every 3 months in patients with CKD 3–5ND and CKD 5PD
· at least monthly in patients with CKD 5HD [See Recommendations 3.12.1–3.12.3 for
measurement of Hb concentration in patients being treated with ESA.]
Diagnosis of anemia 1.2.1: Diagnose anemia in adults and children >15
years with CKD when the Hb concentration is <13.0 g/dl in males and <12.0 g/dl in females. (Not Graded)
1.2.2: Diagnose anemia in children with CKD if Hb concentration is <11.0 g/dl in children 0.5–5 years, <11.5
g/dl in children 5–12 years, and <12.0 g/dlin children 12–15 years. (Not Graded)
Investigation of anemia1.3: In patients with CKD and anemia (regardless of age
and CKD stage), include the following tests in initial evaluationof the anemia (Not Graded):
· Complete blood count (CBC), which should include Hb concentration, red cell indices, white blood cell counttotal and differential, and platelet count
· Absolute reticulocyte count· Serum ferritin level· Serum transferrin saturation (TSAT)· Serum vitamin B12 and folate levels
Treatment options for Anemia in CKD· I V / Oral Iron· Erythrocyte Stimulating Agents (ESAs)o EPOo Darbepoetin Alfao CERA· PRBC transfusionso For severe or acute anemia· Correction of nutritional deficiencies
Iron therapy- What does KDIGO Guidelines say?
Treatment with iron agents2.1.1: When prescribing iron therapy, balance the
potential benefits of avoiding or minimizing blood transfusions, ESA therapy, and anemia-related symptoms against the risks of harm in individual patients (e.g., anaphylactoid andother acute reactions, unknown long-term risks). (Not Graded)
2.1.2: For adult CKD patients with anemia not on iron or ESA therapy we suggest a trial of IV iron (or in CKD NDpatients alternatively a 1–3 month trial of oral iron therapy) if (2C):
an increase in Hb concentration without starting ESA treatment is desired andTSAT is <30% and ferritin is <500 ng/ml (<500 mg/l)
2.1.3: For adult CKD patients on ESA therapy who are not receiving iron supplementation, we suggest a trial of IV iron (or in CKD ND patients alternatively a 1–3 month trial of oral iron therapy) if (2C):
· an increase in Hb concentration or a decrease in ESA dose is desired and
· TSAT is <30% and ferritin is <500 ng/ml (<500 mg/l)
2.1.4: For CKD ND patients who require iron supplementation, select the route of iron administration based on the severity of iron deficiency, availability of venous access, response to prior oral iron therapy, side effects with prior oral or IV iron therapy, patient compliance, and cost. (Not Graded)

121
2.1.5: Guide subsequent iron administration in CKD patients based on Hb responses to recent iron therapy,as well as ongoing blood losses, iron status tests (TSAT and ferritin), Hb concentration, ESA responsivenessand ESA dose in ESA treated patients, trends in each parameter, and the patient's clinical status.(Not Graded)2.1.6: For all pediatric CKD patients with anemia not on iron or ESA therapy, we recommend oral iron (or IV iron in CKD HD patients) administration when TSAT is <20% and ferritin is <100 ng/ml (<100 mcg/l). (1D)
2.1.7: For all pediatric CKD patients on ESA therapy who are not receiving iron supplementation, we recommend oral iron (or IV iron in CKD HD patients) administration to maintain TSAT >20% and ferritin >100 ng/ml (>100 mcg/ l). (1D)
Iron status evaluation2.2.1: Evaluate iron status (TSAT and ferritin) at least every 3 months during ESA therapy, including the decision to start or continue iron therapy. (Not Graded)2.2.2: Test iron status (TSAT and ferritin) more frequently when initiating or increasing ESA dose, when there is blood loss, when monitoring response after a course of IV iron, and in other circumstances where iron stores may become depleted. (Not Graded)
Cautions regarding iron therapy2.3: When the initial dose of IV iron dextran is administered, we recommend (1B) and when the initial dose of IV nondextraniron is administered, we suggest (2C) that patients be monitored for 60 minutes after the infusion, and thatresuscitative facilities (including medications) and personnel trained to evaluate and treat serious adverse reactionsbe available.
Iron during infection2.4: Avoid administering IV iron to patients with active systemic infections. (Not Graded)
Use of ESAs and other agents to treat anemia in CKD : KDIGO Guidelines
ESA initiation3.1: Address all correctable causes of anemia (including iron deficiency and inflammatory states) prior to initiation ofESA therapy. (Not Graded)
3.2: In initiating and maintaining ESA therapy, we recommend balancing the potential benefits of reducing bloodtransfusions and anemia-related symptoms against the risks of harm in individual patients (e.g., stroke, vascularaccess loss, hypertension). (1B)
3.3: We recommend using ESA therapy with great caution, if at all, in CKD patients with active malignancy—inparticular when cure is the anticipated outcome—(1B), a history of stroke (1B), or a history of malignancy (2C).
3.4.1: For adult CKD ND patients with Hb concentration >10.0 g/dl , we suggest that ESA therapy not beinitiated. (2D)
3.4.2: For adult CKD ND patients with Hb concentration <10.0 g/dl we suggest that the decision whether toinitiate ESA therapy be individualized based on the rate of fall of Hb concentration, prior response to iron therapy,the risk of needing a transfusion, the risks related to ESA therapy and the presence of symptoms attributable toanemia. (2C)
3.4.3: For adult CKD 5D patients, we suggest that ESA therapy be used to avoid having the Hb concentration fall below9.0 g/dl by starting ESA therapy when the hemoglobin is between 9.0–10.0 g/dl (2B)
3.4.4: Individualization of therapy is reasonable as some patients may have improvements in quality of life at higher Hbconcentration and ESA therapy may be started above 10.0 g/dl. (Not Graded)
3.4.5: For all pediatric CKD patients, we suggest that the selection of Hb concentration at which ESA therapy is initiatedin the individual patient includes consideration of potential benefits (e.g., improvement in quality of life, schoolattendance/performance, and avoidance of transfusion) and potential harms. (2D)
ESA maintenance therapy3.5.1: In general, we suggest that ESAs not be used to maintain Hb concentration above 11.5 g/dl in adultpatients with CKD. (2C)
3.5.2: Individualization of therapy will be necessary as some patients may have improvements in quality of life at Hbconcentration above 11.5 g/dl and will be prepared to accept the risks.(Not Graded)
3.6: In all adult patients, we recommend that ESAs not be used to intentionally increase the Hb concentration above 13 g/dl. (1A)
3.7: In all pediatric CKD patients receiving ESA therapy, we suggest that the selected Hb concentration be in the range of11.0 to 12.0 g/dl . (2D)
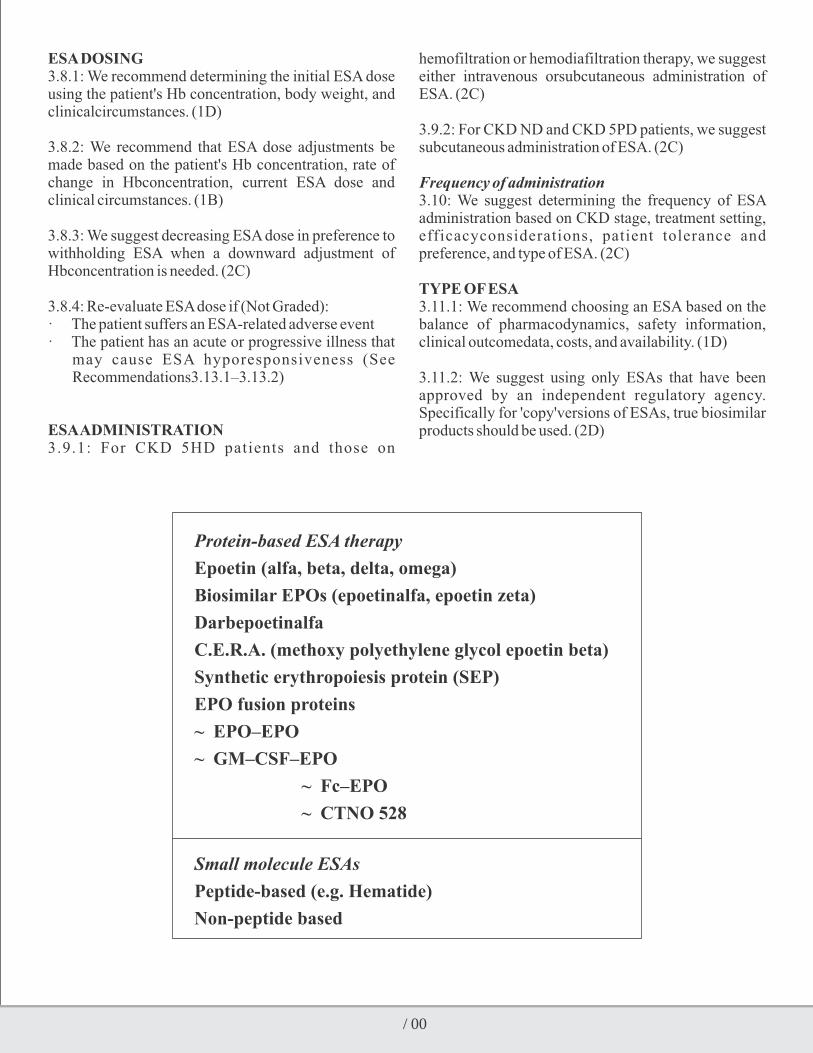
122
ESA DOSING3.8.1: We recommend determining the initial ESA dose using the patient's Hb concentration, body weight, and clinicalcircumstances. (1D)
3.8.2: We recommend that ESA dose adjustments be made based on the patient's Hb concentration, rate of change in Hbconcentration, current ESA dose and clinical circumstances. (1B)
3.8.3: We suggest decreasing ESA dose in preference to withholding ESA when a downward adjustment of Hbconcentration is needed. (2C)
3.8.4: Re-evaluate ESA dose if (Not Graded):· The patient suffers an ESA-related adverse event· The patient has an acute or progressive illness that
may cause ESA hyporesponsiveness (See Recommendations3.13.1–3.13.2)
ESA ADMINISTRATION3.9.1: For CKD 5HD patients and those on
hemofiltration or hemodiafiltration therapy, we suggest either intravenous orsubcutaneous administration of ESA. (2C)
3.9.2: For CKD ND and CKD 5PD patients, we suggest subcutaneous administration of ESA. (2C)
Frequency of administration3.10: We suggest determining the frequency of ESA administration based on CKD stage, treatment setting, efficacyconsiderations, patient tolerance and preference, and type of ESA. (2C)
TYPE OF ESA3.11.1: We recommend choosing an ESA based on the balance of pharmacodynamics, safety information, clinical outcomedata, costs, and availability. (1D)
3.11.2: We suggest using only ESAs that have been approved by an independent regulatory agency. Specifically for 'copy'versions of ESAs, true biosimilar products should be used. (2D)
Protein-based ESA therapy
Epoetin (alfa, beta, delta, omega)
Biosimilar EPOs (epoetinalfa, epoetin zeta)
Darbepoetinalfa
C.E.R.A. (methoxy polyethylene glycol epoetin beta)
Synthetic erythropoiesis protein (SEP)
EPO fusion proteins
~ EPO–EPO
~ GM–CSF–EPO
~ Fc–EPO
~ CTNO 528
Small molecule ESAs
Peptide-based (e.g. Hematide)
Non-peptide based

Nice Guidelines for Management of Anemia in CKD
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Input byDr. Rajiv BansalSr. Consultant Physician Internist, Max Patparganj, DelhiGoel Hospital, Delhi
Krishna Nagar, Delhi Timings: 1.00am-2.00pm, 6.00pm-9.00pmGoyal Hospital & Urology Centre, Krishna Nagar, Delhi Timings: 9.00am-10.30amMax Balaji Hospital, Patparganj, Delhi Timings: 2.00pm-4.00pm (Wed & Fri)[email protected]
Diagnosis
Iron Treatment
Is anaemia due to CKD?2Consider other causes if eGFR> 60 ml/min/1.73m
Iron correction should maintain
serum ferritin > 200 ug/ltransferrin saturation > 20% (unless ferritin > 800 ug/l)
% hypochromic red cells <6% (unless ferritin > 800 ug/l)
Optimise iron status:
before or when starting ESAsbefore deciding whether to use ESAs in non-dialysis patients
Iron deficiency anaemia:diagnosed when serum ferritin <100ug/l in stage 5 CKD
considered when serum ferritin < 100 ug/l in stage 3 and 4 CKD
Functional iron deficiency defined byserum ferritin > 100 ug/l and either % hypochromic red cells > 6%
(if test available), or transferrin saturation <20%
Determine iron status:
Consider treating anaemia when:
Hb falls to < 11 g/dL(or<10.5g/dL if younger than 2 years), orsymptoms attributable to anaemia develop

124
Maintenance Iron
Initiate ESAS:
• For patients likely to benefit in quality of life and physical function
• consider appropriateness of ESA use if comorbiditiesor prognosis negate benefit
• initiate ESA trial if benefit uncertain
Age alone should not be a determinant for treating anaemia of CKD
Adjust ESA dose and frequency:
• to maintain stable Hb between 10 and 12g/dl (or 9.5 and 11.5g/dlin children under 2 years
• to keep rate of Hb increase between 1 and 2 g/dl/month
• if Hb above 11.5 g/dl or below 10.5 g/dl
Give iron supplements to maintain:
• serum ferritin 200-500 ug/l in both haemodialysis and
non-haemodialysis patients
and either
• transferrin saturation > 20% (unless ferritin > 800ug/l), or
• %hypochromic red cells <6% (unless ferritin > 800 ug/l)
In practice it is likely this will require intravenous iron
Monitor:
• iron status no earlier than 1 week after receiving iv. iron
and at intervals of 4 weeks to 3 months routinely
• Hb every 2-4 weeks (induction phase) or 1-3 months
(maintenance phase) during ESA therapy
• Hb more actively after adjusting ESA dose
• in clinical setting agreed with patient

125
Maintenance ESAs
Adjust ESA dose and frequency:
• if Hb > 11.5 g/dl or < 10.5g/dl
• established rate of change in Hb, e.g.> 1g/dl/month
investigate cause of any unexpected change in Hb level
Review ESA use:• if ESA trial, review effectiveness
• discuss continued use with all patients after an agreed interval

Dialysis Interventions for Treatment of AKIAnalyzing the KDOQI Guidelines
KDOQI guidelines… the preludeThe optimal timing of dialysis for AKI is not defined. In current practice, the decision to start RRT is based most often on clinical features of volume overload and biochemical features of solute imbalance (azotemia, hyperkalemia, severe acidosis).
However, in the absence of these factors there is generally a tendency to avoid dialysis as long as possible, a thought process that reflects the decisions made for patients with CKD Stage 5.
Why do clinicians delay RRT???Dialysis is often delayed when the clinician suspect that patients may recover on their own and due to the concern for the well-known risks associated with the RRT procedure, including hypotension, arrhythmia, membrane bioincompatibility, complications of vascular access and anticoagulant administration. There are some concern that RRT may compromise recovery of renal function, and increase the progression of CKD.
Whether these risks outweigh the potential benefits of earlier initiation of RRT is still unclear
What does the Guideline say?
5.1.1: Initiate RRT emergently when life-threatening changes in fluid, electrolyte, and acid-base balanceexist. (Not Graded)
5.1.2: Consider the broader clinical context, the presence of Conditions that can be modified with RRT, and trends of lab tests—rather than single BUN and creatinine thresholds alone—when making the decision to start RRT. (Not Graded)
Rationale…There are no RCTs for dialysis in life threatening indications. It is widely accepted that patients with severe hyperkalemia, severe acidosis, pulmonary edema, and uremic complications should be dialyzed emergently.
HyperkalemiaIn the absence of significant kidney function, and when therapeutic measures that promote the intracellular shift of potassium are exhausted, an excess of potassium can only be eliminated with RRT.
When intermittent dialysis is used after these therapeutic interventions, the extracorporeal removal of potassium will be reduced and the post-treatment rebound of serum potassium will be more pronounced
Metabolic acidosisIt is a frequent clinical problem in severe AKI.MA associated with AKI can usually be corrected with
-HCO and should rarely require urgent dialysis if not 3
accompanied by volume overload or uremia. pH and -
HCO values to initiate dialysis for MA are not 3
supported by evidence- no standard criteria for initiating dialysis for acidosis exist.A variety of poisons, drug overdoses, and toxic compounds (e.g., salicylates, ethylene glycol, methanol, metformin) can contribute to acid-base problems and also lead to AKI. In these circumstances, RRT may also facilitate removal of the offending drug.
Studies Against Early RRTAn RCT by Bouman et al (n=106) found no difference in outcomes between early [within 12 hours of oliguria (<30 ml/h for 6 hours, not responding to diuretics or hemodynamic optimization), or CrCl<20 ml/min] Vs
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Dr. Shri Ram Kabra, Senior ConsultantDr Satish Chhabra, Jr. Resident,Nephrology, Max Superspeciality Hospital, Patparganj, DelhiDr Aditya Jayraman, Jr. Resident,Nephrology, Max Superspeciality Hospital, Patparganj, Delhi

127
late RRT in AKI. However, this study had a shortcoming – it wastoo small aand underpowered study to draw conclusive information.
Studies in favour of Early RRTThese are mostly observational studies as it is difficult to have a RCT given the criticality of the patients.1. Conger JD. A controlled evaluation of prophylactic
dialysis in posttraumatic acute renalfailure. J Trauma 1975; 15: 1056–1063.
2. Fischer RP, Griffen WO, Jr., Reiser M, et al. Early dialysis in the treatment of acute renal failure. SurgGynecolObstet 1966; 123: 1019–1023.
3. Kleinknecht D, Jungers P, Chanard J, et al. Uremic and non-uremic complications in acute renal failure: Evaluation of early and frequent dialysis on prognosis. Kidney Int 1972; 1: 190–196.
4. Parsons FM, Hobson SM, Blagg CR, et al. Optimum time for dialysis in acute reversible renal f a i l u r e . D e s c r i p t i o n a n d v a l u e o f a n improveddialyser with large surface area. Lancet 1961; 1: 129–134.
5. All these studies had evidences in favour of early renal replacement therapy in AKI. Then came a large study- Program to Improve Care in Acute Renal Disease (PICARD) which was a prospective multicenter observational cohort study (n=243) with sizable study cohort. The results of this study showed that initiation of RRT at higher BUN (>76 mg/dl [blood urea>27.1mmol/l]) was associated with an increased risk of death (RR 1.85; 95% CI 1.16–2.96)
6. Bagshaw SM, Uchino S, Bellomo R, et al. Timing of renal replacement therapy and clinical outcomes in critically ill patients with severe acute kidney injury. J Crit Care 2009; 24: 129–140.- this was a Prospective multicenter observationalstudy conducted at 54 ICUs in 23 countries which concluded that
a. Timing of RRT stratified into ''early'' or ''late'' by median urea at the time RRT started (24.2 mmol/l [BUN 67.8 mg/dl]),
b. Also categorized temporally from ICU admission into early (less than 2 days), delayed (between 2–5 days), or late (more than 5 days).
c. Timing by serum urea showed no significant difference in mortality.
d. However, when timing was analyzed in relation
to ICU admission, late RRT was associated with greater crude mortality (72.8% late vs. 62.3% delayed vs. 59% early, P¼0.001) and covariate-adjusted mortality (OR 1.95; 95% CI 1.30–2.92; P¼0.001).
e. Overall, late RRT was associated with a longer duration of RRT and stay in hospital, and greater dialysis dependence
7. Shiao CC, Wu VC, Li WY, et al. Late initiation of renal replacement therapy is associated with worse o u t c o m e s i n a c u t e k i d n e y i n j u r y a f t e r majorabdominal surgery. Crit Care 2009; 13: R171- The analysis of surgical ICU patients with AKI, showed that late initiation of RRT (defined as RIFLE-I or -F) was an independent predictor of mortality (HR 1.846; CI 1.07–3.18)
Indications and Goals of Dialysis in AKITraditional indications for RRT, developed for patients with advanced CKD, are not necessarily valid in the context of AKI. Consider a Case Scenario of a patient with massive volume overload resulting from volume resuscitation may be an indication for RRT even in the absence of significant elevations in BUN or SCr. In this instance, it may be more appropriate to consider dialytic intervention in the ICU patient as a form of renal support rather than renal replacement.
Here, I would like to introduce to you the concept of RENAL SUPPORT in AKI. Hence…, treatment of AKI with RRT has the following goals:i) to maintain fluid and electrolyte, acid-base, and
solute homeostasis;ii) to prevent further insults to the kidney; iii) to permit renal recovery; and iv) to allow other supportive measures (e.g.,
antibiotics, nutrition support) to proceed without limitation or complication
There is increasing evidence that fluid overload in critical illness and AKI is associated with adverse outcomes.
Payen D, de Pont AC, Sakr Y, et al. A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit Care 2008; 12: R74. This multicenter observational cohort showed that mean daily fluid balance in AKI patients was significantly more positive among non survivors than survivors.

128
Data from PICARD group further supports these findings. Survivors had lower fluid accumulation at dialysis initiation compared to non survivors (8.8% vs. 14.2% of baseline body weight). The adjusted OR for death associated with fluid overload at dialysis initiation was 2.07 (95% CI 1.27–3.37).
What should be the modality....CRRT or SLEDD???Let us analyze some studies to answer this question.1. Mehta RL, McDonald B, Pahl M, et al. Continuous
vs. intermittent dialysis for acute renal failure in the ICU: Results from a randomized multicenter trial (abstract). J Am SocNephrol 1996; 7: 1456.
a. Secondary analysis of this randomized trial comparing IHD to CRRT showed that patients receiving RRT predominantly for solute control experienced bet ter outcomes than those predominantly treated for volume overload.
b. Patients dialyzed for control of both azotemia and volume overload experienced the worst outcome
Factors that may influence the initiation of RRT in AKI• Severity of the underlying disease (affecting the
likelihood of recovery of kidney function),
• The degree of dysfunction in other organs (affecting the tolerance to e.g., fluid overload),
• The prevalent or expected solute burden (e.g., in tumor lysis syndrome), and
• The need for fluid input related to nutrition or drug therapy
Criteria for Stopping RRT- the guidelines 5.2.1: Discontinue RRT when it is no longer required, either because intrinsic kidney function has recovered to the point that it is adequate to meet patient needs, or because RRT is no longer consistent with the goals of care. (Not Graded)
5.2.2: We suggest not using diuretics to enhance kidney function recovery, or to reduce the duration or frequency of RRT. (2B)
Many, but not all, patients requiring RRT will recover. The mean duration of RRT in two recent large RCTs was 12–13 days. More than 50% of patients with severe AKI will not improve, despite appropriate therapy.RRT is one of the therapies most likely to be discontinued during withdrawal of life support. In general, decisions to withdraw therapy occur in 10% of all patients from general ICUs, and are responsible for roughly 40% of all deaths.
In general, an assessment of Residual renal function can guide us to the right time for terminating RRT.
Assessment of kidney function during RRT……NOT EASY!!!In Intermittent Hemodialysis (IHD), the fluctuations of solute levels prevent achieving a steady state and thus exclude the use of clearance measurements.IHD will be associated with post-treatment rebound in solute levels, and that changes in BUN and creatinine levels can also be modified by nonrenal factors, such as volume status and catabolic rate.
Native kidney function can only be assessed during the interdialytic period by:

129
• evaluating urine volume, • urinary excretion of creatinine• changes in SCr and/or BUN values
In CRRT, continuous solute clearance of 25–35 ml/min will stabilize serum markers after 48 hours. This allows more reliable measurements of CrCl by the native kidneys during CRRT.One small retrospective study demonstrated that a CrCl (measured over 24 hours) >15 ml/min was associated with successful termination of CRRT, defined as the absence of CRRT requirement for at least 14 days following cessation.
Urine output- Multivariate logistic regression identified urine output as the most significant predictor of successful termination (OR 1.078 per 100 ml/d).Predictive ability of urine output was negatively affected by the use of diuretics.
Independent predictors for restarting RRT within 30 days• Longer duration of RRT, • A higher Sequential Organ Failure Assessment
score, oliguria, and • Age >65 years
Switching from CRRT to IHD, or decreasing the frequency of IHD from daily to every other day, represents different methods of testing the ability of the patient's own kidney to take over
Whether too-early discontinuation of RRT, requiring reinstitution, is by itself harmful has not been properly investigated. Observational studies have found a higher mortality in patients who needed to be retreated with RRT (42.7% vs. 28.5% and 79.7% vs. 40%)
Narinder P SinghChairman, Medicine and Allied Specialities, Senior Consultant in Nephrology, Pushpanjali Crosslay Hospital Anupam PrakashAssociate Professor, Department of Medicine, Lady Hardinge Medical College, New Delhi. Anish GuptaResearch Associate, Dept. of Nephrology, Pushpanjali Crosslay Hospital.
YEAR BOOK & SOUVENIR 2014
Nephrotoxic Potential of Herbal Drugs
Ph (Off)91-120-4173000,4188000, (Res) 91-11-22723637Mob 09868446621
Timings: Only Appointment
IntroductionIn recent years, the use of herbal medicines and dietary supplements to promote health and to treat various chronic diseases has increased globallyand there always has been a belief about allopathic medicines that they are more toxic and have greater side-effects than medicines from other branches of sciences viz. Homeopathy, Unani, etc. The science of 'Ayurveda' and its medicines exist in India since time immemorial. The name of Dhanvantri vaidya is enshrined in the mythology and in ancient scriptures also one finds the mention of use of liniments, tamra leaves and turmeric on wounds and injuries. The Government of India has supported and opened ventures in the field of complementary and alternative medicine (CAM) in the last one decade and so, which is a welcome move, since it will promote research and standardisation of medications used in CAM. However, as has always been the practice, there are a number of persons in the society who are unqualified and/or incompetent to prescribe medicines in any branch of medicine whether it be allopathy or homeopathy or branches from CAM, but these faith-healers and quacks are inherently mingled with the society and prescribe medicines injudiciously causing more damage than good. In fact, recent studies have suggested that there has been a rise in usage of alternative therapies not only in the developing countries but also in the developed world and a significant number of these could be herbal medicines. An oft quoted survey of alternative medicine revealed that 42% Americans used alternative therapies with 12% of these therapies being use of herbal
1supplements . Almost, 70% modern medicines in India are derived from natural products. To date, there are at
least 11,000 species of plants for medicinal use, and about 500 of them are commonly used by various ethnic groups. In rural India, 70% of the population is dependent on the traditional system of medicine. In western world also the practitioner of herbal medicines is steadily growing and approximately 40% of the
2population is taking herbs to treat diseases . These herbal medicines and dietary supplements could be unstandardised or unresearched, lacking consistent requirements for rigorous safety, efficacy and purity testing resulting in varying amounts of active constituents from batch to batch; and thus may cause irreparable damage to the unsuspecting patients. Although the prevalence of toxicity of organs caused by traditional medicines is directly related to a combination of ignorance, poverty, lack of medical facilities, lack of legislation, and widespread belief in indigenous systems of medicine in rural areas, it has been realized recently that the problems and concerns of herbal medicines arise from intrinsic toxicity, adu l t e r a t i on , con tamina t ion , subs t i t u t i on , misidentification, mistaken labeling, unfavorable herb-drug interactions, lack of standardization, or poor quality control. In spite of this, the use of herbal medicines continues to grow in many disease conditions, but the risk from use may overshadow potential benefit, especially in vulnerable patients who may be in a compensated state and require minimal insult to their jeopardised systems to trip over in to a decompensated disease. Renal compromised patients constitute one such group. In the ensuing article, one will find herbs which are associated with renal injury in the acute or chronic setting in the healthy individuals and in kidney-disease individuals.
library
Highlight

131
Mechanism of NephrotoxicityA number of anatomical, physiological and biochemical features attributable to the kidney make it particularly sensitive to injury as a result of exposure to exogenous compounds viz. herbal agents. These include a large blood flow, high endothelial surface area, high metabolic activity, active uptake by tubular cells and medullary interstitial concentration, presence of a variety of xenobiotic transporters and metabolising enzymes, and concentration of solutes during urine production. Besides, the conjugation of exogenous agents to glutathione and/or cysteine targets these chemicals to the kidney where inhibition of renal function occurs through varied mechanisms. Agents like aristolochic acids can affect the renal cytochrome
P450 metabolism and induce renal injury. The toxins may injure the tubules directly, at the site of toxin transport or concentration, or by inducing renal
3 ,4ischemia, hemoglobinuria or myoglobinuria . Continued exposure and exposure to high doses can increase the severity of renal failure. Of the several lesions that have been described after nephrotoxic injury, acute tubular or cortical necrosis and acute interstitial nephritis is the most frequently encountered. However, other renal syndromes that have been associated with herbal drugs include Fanconi's syndrome, hypokalemia, hypertension, papillary necrosis, chronic interstitial nephritis, nephrolithiasis,
2urinary retention and carcinoma of the urinary tract .
Table 1. Kidney syndromes induced by herbal medicines
Hypertension • Glycyrrhiza species (Chinese herbal teas, gancao, boui-ougi-tou) • Ephedra species (ma huang)
Acute tubular necrosis • Traditional African medicine: toxic plants (Securidaca longepedunculata, Euphoria matabelensis, Callilepsis laureola, Cape aloes, or adulteration by dichromate) • Chinese medicine: Taxus celebica • Morocco: Takaout roumia (paraphenylenediamine)
Acute interstitial nephritis • Peruvian medicine (Uno degatta) • Tung Shueh pills (adulterated by mefenamic acid)
Fanconi syndrome • Chinese herbs containing AAs (Akebia species, Boui, Mokutsu) • Chinese herbs adulterated by cadmium
Papillary necrosis • Chinese herbs adulterated by phenylbutazone
Chronic interstitial renal fibrosis • Chinese herbs or Kampo containing AAs (Aristolochia species, Akebia species, Mutong, Boui, Mokutsu)
Urinary retention • Datura species, Rhododendron molle (atropine, scopolamine)
Kidney stones • Ma huang (ephedrine) • Cranberry juice (oxalate) Urinary tract carcinoma • Chinese herbs containing AAs
Nephrotoxic Herbal agentsVarious herbal agents that are known to be toxic can be
5classified into
1. Agents which are directly nephrotoxic,
2. Herbal drugs which result in electrolyte abnormalities by acting upon the kidney,
3. Agents which can predispose to formation of stones (oxalate stones),
4. Agents which act as diuretics,
5. Herbal drugs which contain heavy metals or other drugs and
6. Herbal agents which can interact with other drugs especially in the renal transplanted subject.

132
Herbs which are directly nephrotoxic-1. Chinese herb nephropathy or Aristolochic acid
6-10nephropathy - In Belgium between 1990-1992, nephrotoxicity was reported in over 100 persons consuming a Chinese weight loss herbal remedy containing aristolochic acid; and 70 of these required renal transplants or dialysis and 30 subsequently developed urothelial carcinoma. In fact, May 1990 witnessed a change in slimming therapy incorporating two Chinese herbs namely Stephania tetrandra and Magnolia officinalis. A specific type of fibrosing interstitial
10nephritis was observed with their usage . Aristolochic acid is a nitrophenanthrene carboxylic acid which forms DNA adducts in renal as well as other tissues after metabolic activation. The DNA adducts result in genotoxic mutations resulting in urothelial carcinoma as well as the characteristic renal interstitial fibrosis and extensive loss of cortical tubules. Several other plants particularly from the Asarum and Bragantia genera, contain aristolochic acid. Patients present with renal insufficiency, moderate increase in blood urea, mild proteinuria, severe anemia and urinary sediment. Glycosuria and sterile proteinuria are common and usually indicate tubular dysfunction. Disease usually progresses rapidly to end stage renal disease. No therapy has been found to be effective, although a beneficial effect with steroids has
11been suggested . Renal transplant is effective in patients who progress to end-stage renal disease and no recurrence has been reported in transplanted kidney.
2. Balkan endemic nephropathy has been reported from the Balkan states, resulting from plant products contaminated by the fungal mycotoxin ochratoxin A, which also forms mutagenic DNA adducts in kidney tissue. However, the exact aetiology of Balkan
12endemic nephropathy is still a mystery .
13-153. Djenkol bean poisoning (Djenkolism) - is a
cause of acute renal failure occurring in the tropics. Symptoms of poisoning occur soon after or up to 36 hours of ingestion. Symptoms include fever, leukocytosis, lower abdominal and bilateral lumbar pain, dysuria, haematuria, oligo-anuria, passage of sandy particles in the
urine and hypertension; manifesting as acute renal failure. High fluid intake and urinary alkalinisation with sodium bicarbonate helps in dissolving crystals; and majority of patients recover with in a few days. Djenkol bean is a pungent smelling edible fruit of the hardwood tree Pithecellobium labatum (Jering trees). These may be eaten raw, fried or roasted and contain djenkolic acid, a sulphur rich cysteine thioacetal of formaldehyde. Djenkolic acid produces severe tubular necrosis with a lesser degree of glomerular cell necrosis in animals. Djenkolic acid forms needle like crystals, specially in concentrated acidic urine in distal tubules, leading to obstruction, which acts as a nidus for stone formation.
4. Impila poisoning- It is a herb derived from the tuberous roots of the plant Callilepis laureola, and is used as a traditional remedy in South Africa to treat a number of conditions; often given during pregnancy to ensure easy childbirth, for sexually transmitted diseases for fertility and blood purification. It has marked hepatic and renal toxicity. In fact, it is one of the most common causes of ARF in black
16population of South Africa . Symptoms appear in 1-4 days in >70% cases manifesting as nausea and vomitings followed by hypoglycaemia leading to altered sensorium and convulsions. Patient has oliguric renal failure, oliguric phase lasting 8-12 days and serum creatinine rises 0.5-1.0 mg/day. Treatment is largely supportive, but the mortality is high (>50%). Renal damage caused is characteised by acute proximal convoluted tubule and loop of Henle necrosis resulting in renal failure.
5. Mushroom poisoning- Ingestion of wild mushrooms containing the nephrotoxin
17orellanine has resulted in acute renal failure . Kidney biopsy showed marked tubular interstitial nephritis and fibrosis.
6. Cat's claw (Uncaria tomentosa)- It is a Peruvian herbal preparation used for gastritis, rheumatism, cirrhosis, gonorrhoea and cancers of the female genital tract and has been associated with development of acute renal failure; kidney biopsy showing acute interstitial nephritis.

133
Herbal drugs that can alter serum potassium levels-1. Licorice root (Glycyrrhiza glabra)- in high doses
and when used for long durations causes aldosterone like effect resulting in sodium retention and consequent hypertension and hypokalemia. Licorice root contains glycyrrhizic acid which is hydrolysed to glycyrrhetenic acid which in turn inhibits renal 11-hydroxysteroid dehydrogenase thus preventing inactivation of cortisol to cortisone. Accumulation of cortisol in the kidney stimulates aldosterone receptors in cells of cortical collecting duct resulting in sodium reabsorption.
2. Laxative herbs- Senna (Senna Alexandria) and rhubarb ((Rheum officinale) which are used as laxatives can result in electrolyte imbalance particularly hypokalemia.
3. Noni juice (Morinda citrifolia) derived from the noni fruit is a popular herbal supplement which is also available in India and is used for its immune-boosting properties in many diseases and in convalescence and rehabilitation. However, it can result in serious hyperkalemia due to its high content of potassium (56.3 meq/L), which is similar
18to orange and tomato juices .
4. Dandelion (Taraxacum officinale), stinging nettle (Urtica dioica), horsetail (Equisetum arvense), and alfalfa (Medicago sativa) are other popular herbs which can also contribute to hyperkalemia.
Table 2. Herbal supplements containing potassium
Alfalfa, American Ginseng, Bai Zhi (root), Bitter Melon (fruit, leaf),Black Mustard (leaf), Blessed Thistle, Chervit (leaf),
Chicory (leaf), Chinese Boxthorn (leaf), Coriander (leaf), Dandelion (root, leaf), Dulse, Evening Primrose, Feverfew,
Garlic (leaf), Genipap (fruit), Goto Kola, Japanese Honeysuckle (flower), Kelp, Kudzu (shoot), Lemongrass, Mugwort,
Noni, Papaya (leaf, fruit), Purslane Sage (leaf), Safflower (flower), Sassafras, Scullcap, Shepherd's Purse, Stinging Nettle
(leaf), Turmeric (rhizome), Water Lotus.
Herbal drugs that have high content of oxalic acid-
1. Rhubarb (Rheum officinale)- It is a common herbal preparation but has high oxalate content and can promote the formation of renal calculi.
2. Star fruit (Averrhoa carambola)- ingestion has been reported to produce acute oxalate
19nephropathy .
Herbal drugs with diuretic activity-
1. Some herbal supplements that act like a diuretic or "water pill" may cause "kidney irritation" or damage. Juniper berry (Juniperus communis), parsley (Petroselinum crispum), dandelion (Taraxacum officinale), horsetail (Equisetum arvense), asparagus root (Asparagus officinalis), lovage root (Levisticum officinale), goldenrod (Solidago virgaurea), uva ursi (Arctostaphylos uva ursi), stinging nettle leaf (Urtica dioica), and alfalfa (Medicago sativa) have been traditionally used as diuretics in health and disease. These herbs have varying degrees of diuretic activity and their use requires caution in healthy individuals as well as in the renal- compromised patient. Some of these herbs act as irritants to the tubular cell while
some may alter serum electrolytes. Juniper berries contain terpine-4-ol which may cause kidney irritation and damage in excess. In Germany, parsley and goldenrod are indicated for systemic irrigation of the urinary tract and for preventing kidney stones. The diuretic effect of parsley leaf and root is due to its volatile oil components myristicin and apiole. Also in Germany, dandelion, horsetail, and uva ursi are licensed as standard medicinal teas to stimulate diuresis.
Herbal products containing heavy metals-
1. It is a widely known fact and well-corroborated that many herbal medications particularly Chinese and Ayurvedic herbal preparations contain nephrotoxic heavy metals viz. lead,
2mercury, cadmium and arsenic . Firstly many heavy metals are considered to have therapeutic effects in the CAM specialities. Secondly, the problem lies in the fact that their concentration is not standardised and there is great batch to batch variability. Thirdly, the presence of heavy metals and their concentrations are many a times not revealed on the labels of herbal medicines.

134
Table 1- Herbs implicated in causing renal injury
Herbs known to be unsafe Herbs that may be toxic Herbs that may be harmful for all people to the kidneys in chronic kidney disease
Chapparal, Pennyroyal, Comfrey, Artemisia absinthium (wormwood plant), Alfalfa, Buckthorn, Ginger, Nettle, Pokeroot, Ephedra (Ma Huang), Periwinkle, Autumn crocus, Sassafras, Vervain, Aloe, Capsicum, Ginseng, Sassafras, Lobelia, Senna, Chuifong tuokuwan (Black Pearl), Noni juice, Bayberry, Cascara, Mandrake, Yohimbine Tung shueh, Horse chestnut, Horsetail, Panax, Blue Cohosh, Vandelia cordifolia Coltsfoot, Licorice, Rhubarb, Broom, Dandelion, Mate, Senna
Herbal drugs containing other drugs-
1. I t has been recognised that many herbal formulat ions contain non-steroidal ant i -inflammatory drugs which inhibit renal vasodilator prostaglandins and can lead to renal failure.
2. Other drugs that have been reported to be present in herbal medications include ephedrine, steroids, fenfluramine, methyltestosterone, phenacetin and
2sildenafil .
Herbal drugs with immunomodulating properties (in the renal transplant patient)-
1. Echinacea (Echinacea purpurea)- is a herbal remedy which is promoted as an immune system stimulant.
Ingestion of this drug could seriously jeopardise the transplanted kidney of the patient taking immunosuppressant drugs.
2. St. John's wort (Hypericum perforatum)- causes a decrease in serum cyclosporine levels and again can compromise a successful organ transplant
The National Kidney Foundation (NKF) of the USA has prescribed guidelines under the head- Use of Herbal Supplements in Chronic Kidney Disease
2 0(CKD) . It mentions that “use of herbal supplements may be unsafe for CKD patients, since they are not able to clear waste products like a healthy person”. Table 1 enlists the various herbs
20which have been implicated in renal injury .
The guidelines of the NKF make it amply clear that even a healthy person should exercise a lot of caution before venturing to take herbal drugs. It mentions that “natural does not always mean safe”
Are some herbs Nephroprotective also?There is some evidence about herbs which are
5nephroprotective or beneficial to the kidneys , and this article shall conclude with a word about them. Silymarin derived from milk thistle (Silybum marianum) seeds contains several potent antioxidant flavonolignans. Silymarin has renal protective effects in animals due to its antioxidant effects against damaging free radicals and by virtue of stimulating RNA and protein synthesis which is important for renal & hepatic repair mechanisms. Silymarin also protects k idney ce l l s in cul ture f rom drug- induced
21nephrotoxicity and also protects against experimental 22
cyclosporine nephrotoxicity . Picroliv (Picrorhiza kurrooa), a popular medicinal Ayurvedic herb and its extracts from the roots and rhizomes protected the kidney in a renal ischemia-reperfusion induced injury
23model in rats . Astragalus (Astragalus membranaceus), a popular Chinese herb, is effective against
experimentally induced glomerulonephritis in rats, especially in reducing proteinuria. Cordyceps (Cordyceps sinensis), a fungus found growing in caterpillar larvae of certain moths, is valued as a kidney tonic in China. The Japanese traditional remedy Sairei-to, a 12 herb mixture, has also been found to be renoprotective. Extracts from the root of Salvia miltiorriza (Danshen) along with fructose 1-6 diphosphate prevented the decline of renal cortical Na-K-ATPase activity induced by ischemia and gentamicin in rats. Extracts of the plant Herniaria hirsute inhibit calcium oxalate crystal aggregation and thus may be useful in preventing kidney stone formation. However, similar benefits when demonstrated in human studies w i l l d e f i n e t h e p l a c e o f h e r b a l d r u g s i n nephroprotection.
Conclusion:This article is not in any way against herbal medicines but in this era of evidence-based medicine, it is pertinent for each of us to base our decisions on the available evidence. Although, the principles of Ayurveda were enunciated long time back and it were based on good scientific evidence, but as of today a lot

135
of research needs to be put and integration with the modern system of medicines is required to pave the way for evidence-based herbal medicine which could benefit all and sundry. Importantly, the inherent properties of the herb are not the only source of herb-associated renal disorders, as herb–drug interactions, mistakes in dosage and ident i f icat ion, and contaminants within the mixture are all issues of concern. Strict controls on the presence of adulterants within herbal medicines, labeling of dosages and contraindications, and manufacturing techniques must be maintained to ensure the safety of those consuming herbal medicines.
References-
1. Onopa J. Complementary and alternative medicine (CAM): a review for the primary care physician. Hawaii Med J 1999; 58(2): 9-19.
2. Shadma Wahab, Arshad Hussain, Parwez Ahamd and Aleza rizvi.Current Status of Herbal Drugs in the D e v e l o p m e n t o f N e w e r T h e r a p e u t i c s Agents.International Journal of Pharmaceutical and Chemical Sciences 2013;2 (3):1462-73.
3. Nand N, Aggarwal HK, Jai D, Sharma M. Indigenous drug induced nephropathy. In: Sahay BK (ed). Medicine Update 2006; vol. 16, 458-462.
4. Van Vleet TR, Schnellmann RG. Toxic nephropathy: environmental chemicals. Semin Nephrol 2003; 23(5): 500-508.
5. Combest W, Newton M, Combest A, Kosier JH. Effects of herbal supplements on the kidney. Urologic Nursing 2005; 25(5): 381-386, 403.
6. Lord GM, Tagore R, Cook T, Gower P, Pusey CD. Nephropathy caused by Chinese herbs in the UK. Lancet 1999; 354 (9177): 481-482.
7. Lord GM, Cook T, Arlt VM, Schmeiser HH, Williams G, Pusey CD. Urothelial malignant disease and Chinese herbal nephropathy. Lancet 2001; 358 (9292): 1515-1516.
8. Nortier JL, Martinez MC, Schmeiser HH, et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). NEJM 2000; 342 (23): 1686-1692.
9. Cosyns JP, Jadoul M, Squifflet JP, Wese FX, van Ypersele de Strihou C. Urothelial lesions in Chinese-herb nephropathy. AJKD 1999; 33 (6): 1011-7.
10. Vanherweghem JL, Depierreux M, Tielemans C, et al. Rapidly progressive interstitial renal fibrosis in young women: association with slimming regimen including Chinese herbs. Lancet 1993; 341(8842): 387-91.
11. Vanherweghem JL, Abramowicz D, Tielemans C. Effects of steroids on the progression of renal failure in chronic interstitial renal fibrosis: a pilot study in Chinese herb nephropathy. AJKD 1996; 27: 209-215.
12. Tatu CA, Orem WH, Finkelman RB, Feder GL. The etiology of Balkan endemic nephropathy: still more questions than answers. Environ Health Perspect 1998; 106(11): 689-700.
13. Segasothy M, Swaminathan M, Kong NC, Bennett WM. Djenkol bean poisoning (djenkolism): an unusual cause of acute renal failure. AJKD 1995; 25(1): 63-66.
14. Wong JS, Ong TA, Chua HH, Tan C. Acute anuric renal failure following jering bean ingestion. Asian J Surg 2007; 30(1):80-81.
15. H'ng PK, Nayar SK, Lau WM, Segasothy M. Acute renal failure following jering ingestion. Singapore Med J 1991; 32(2): 148-149.
16. Seedat VK, Acute renal failure among blacks and Indians in South Africa. S Afr Med J 1978; 54: 27-431.
17. Bednarova V, Bodlakova B, Pelclova D. Mushroom poisoning by Cortinarius orellanus. Cas Lek Cesk 1999; 138(4): 119-121.
18. Mueller BA, Scott MK, Sowinski KM, Prag KA. Noni juice (Morinda citrifolia): hidden potential for hyperkalemia? AJKD 2000; 35(2): 310-312.
19. Chen CL, Fang HC, Chou KJ, Wang JS, Chung HM. Acute oxalate nephropathy after ingestion of star fruit. AJKD 2001; 37(2):418-422.
http://www.kidney.org/ATOZ/atozitem.cfm?id=123
20. National Kidney Foundation website -Kidney Disease- A to Z health guide- Use of herbal supplements in Chronic Kidney Disease.
21. Sonnenbichler J, Scalera F, Sonnenbichler I, Weyhenmeyer R. Stimulatory effects of silibinin and silicristin from the milk thistle Silybum marianum on kidney cells. J Pharmacol Exp Ther 1999; 290(3): 1375-1383.
22. Zima T, Kamenikova L, Janebova M, Buchar E, Crkovska J, Tesar V. The effect of silibinin on experimental cyclosporine nephrotoxicity. Ren Fail 1998; 20(3): 471-479.
23. Seth P, Kumari R, Madhavan S, et al. Prevention of renal ischemia-reperfusion-induced injury in rats by picroliv. Biochem Pharmacol 2000; 59(10): 1315-1322.

Dr Naresh AgarwalMD, DM (Gastroenterology, Formerly at GB Pant Hospital, New Delhi)Consultant Gastroenterologist, Hepatologist and Therapeutic Endoscopist Rajdhani Gastro and Liver Clinic, 28, Vigyan Vihar, Delhi-110092Associated with Max Superspeciality Hospital, Patparganj, New Delhi-110092
Cell: 09810612415,email: [email protected]
Timings:
YEAR BOOK & SOUVENIR 2014
Management of Liver Abscess
Liver abscess (pus collection in liver parenchyma) is a common clinical situation and can sometimes complicate into multi organ failure. It is far more common in males, difference between sex being more obvious in cases of amebic liver abscess. Most of the liver abscesses are either pyogenic or amebic. However secondarily infected amebic liver abscess are also quite common and in fact, mode of presentation in substantial proportion of cases of amebic liver abscess. I will however discuss the management of liver abscess in two broad categories, Pyogenic and amebic
Pyogenic liver abscess Nowadays, pyogenic liver abscess are more common in later life and usually result from some focus of sepsis in
1portal system. Biliary tract disease is one of the commonest causes. A substantial proportion is now cryptogenic too (table 1). However, initially they were also noticed in younger age group because of pyelphlebitis brought about by acute appendicitis and colitis.
Hepatobiliary
Benign · Stone diseases · ERCP ?PTBD · Cholecyst itis · Bilio-enteric
anastomosis
Malignant
· Biliopancreatic malignancies (Peri-ampullary, pancreas, bile ducts)
Portal
Benign · Appendicitis · IBD · Post-operative
sepsis
· GI perforation
· Pancreatic infections
Malignant
· Colonic and gastric cancers
Arterial
· Endocarditis · Vascular sepsis · ENT infection · Dental infections
Traumatic
Benign · Abdominal trauma
Malignant · Tran arterial
chemoembolization · Percutaneous
ethanol injection
· Radio-frequency ablation of HCC
Table 1: Different causes of pyogenic liver abscess
Clinical symptomsPresentation is usually insidious. Characteristic presentation is malaise, dull pain upper abdomen, low fever, anorexia and weight loss. Symptoms are there for many weeks (average 4 weeks) before a diagnosis is made. Abscess near diaphragm may lead to chest pain, right shoulder pain and breathlessness because of pulmonary atelectesis.
Patient s may have sepsis or frank septic shock, particularly in case of biliary origin. Multiple liver abscesses are associated with more toxic state. Characteristically, pyogenic liver abscess are mostly multiple but solitary abscesses are not uncommon.
On examination, liver enlargement with tenderness if usually felt. Patient uncommonly have splenomegaly or

137
ascites. Jaundice if distinctly uncommon except for cholangitis and biliary communications.
InvestigationsHigh total leukocyte counts with polymor-phonucleocytosis is usually seen. Pus culture is positive only in 40% cases. Blood culture is positive in around 80% treatment naïve patients
Ultrasound is initial screening method and has sensitivity of 75-80%. On ultrasound, abscess may be completely missed if it is deep under diaphragm, or there are initial multiple abscesses. Initially it is hyperechoic, but as pus formation takes place, echoes reduce. Thick pus containing abscesses may be confused with a slid neoplastic lesion. Ultrasound exam is of particular importance because it also gives good delineation of biliary tract.
Computed tomography is more sensitive (up to 95%) in demonstrating nature, number and location of abscess (Figure 1). In an ideal setting, all patients with liver abscess should undergo a CT scan. Contrast enhanced CT scan reveals peripheral enhancement with central hypo density.
Figure 1. CECT of abdomen with liver abscess
Treatment2Treatment of pyogenic liver abscess is three pronged
· Institution of appropriate antibiotics depending on the organisms
· Drainage of pus
· Treatment of primary etiology of abscess
Antibiotics: Initially broad spectrum antibiotics to cover both gram negative and gram positive organisms should be chosen. A third generation cephalosporin plus metronidazole or ampicillin, and aminoglycoside plus metronidazole is god initial emipirical antibiotic.
As per standard recommendation, antibiotics should be given parentally for two weeks for initial 2 weeks and thereafter orally for 4 weeks. In few cases of culture positive streptococcal organism, longer duration of oral antibacterial, up to 6 month may be required.
Drainage: USG and CT guided drainage of pyogenic liver abscess is more important and necessary than amebic abscess. If multiple large abscesses are present, most should be drained. In cases of abscess with varying sizes, largest should be drained first. An indwelling catheter (PCD-
Percutaneous catheter drainage) may be kept inside the abscess and removed after drain has dried up. Few clinicians prefer percutaneous needle aspiration (PNA). PNA does not gives good results for large abscesses containing thick pus. Major advantages of PNA over PCD are being less invasive and less expensive, and that multiple abscesses can be drained at similar time. However success rate is only
377% as compared to PCD (table 2). PCD has distinct advantage of a more meticulous and complete drainage. PCD therefore is preferred in toxic patients, patients with large abscess, those with thick pus or abscesses with internal echoes suggesting debris. However PCD may be associated with complications like hemorrhage, pleural effusion / empyema, bile leak, catheter displacement and sepsis. Table 2: Head to head comparison between PNA and PCD (n=60)

138
Ten percent patients getting treated by aspiration fail to respond. Important causes of failure are smaller size catheter, displaced catheter, thick pus and septate cavity of abscess. Repositioning of catheter, upsizing the catheter may help increasing success of radiological treatment. Surgery is now rarely required for uncomplicated abscess.
Ruptured liver abscessSmaller multiple abscesses rarely rupture. However, larger abscesses, particularly situated at peripheral parenchyma tissue may rupture into adjoining organs and viscera. Left lobe abscess rupture particularly needs attention as it can rupture in pericardium causing acute temponade. Not all abscesses located in left lobe rupture. Risk is highest with abscesses larger than 3 cm in left lobe. Minute size pyogenic abscsess situated in left lobe need not be drained. Other situations which can arise because of ruptured liver abscess are peritonitis, paracolic collection, empyema, peritoneopleural fistula and subphrenic collection. Untreated ruptured liver abscess may rapidly complicate into multi organ failure and can be fatal.
USG / CT guides drainage of ruptured collection by PCD usually treats resulting sepsis, toxemia and shock. Uncommonly, surgery is required for drainage and lavage of resulting collection.
Amebic liver abscess (ALA)ALA is far more common in males. Most common age
rd thgroup for developing ALA is 3 and 4 decade. Presentation of ALA is more acute than PLA and two weeks the average time of diagnosis before symptom appear. Less than 10 % pts have recent history of amebic intestinal infection and in long latent period of many years lapse before liver lesion appear.
Pain is the most common symptom and is located in right upper quadrant (RUQ). Continuous high grade fever is common. Mayalgia, malaise and arthralgia are more common than PLA. Jaundice appears in 15 % cases and is usually because of biliary communication, but mild jaundice may appear without biliary communication. In a deeply jaundiced patient with ALA, biliary communication should be strongly considered.
Few conditions that predispose development of amebic liver abscess are · Alcoholism· Malnutrition and debility· HIV and AIDS complex· Corticosteroid use· Disorders of cell mediated immunity· Travel to tropical regions

139
Table 3: Major differences between Amebic and Pyogenic liver abscess
Character Pyogenic Amebic
Number Usually multiple Solitary
Location Both lobes Usually right t lobe
Presentations Insidious Acute
Jaundice Uncommon Moderate and more common
Diagnosis Radiology Radiological and serology
Treatment Antibacterial and drainage Anti amebic , antibacterial, requirement of drainage less than pyogenic
In contrast to PLA, biliary communication is usually a complication of abscess rather than cause. Biliary communication of ALA present with sudden increase in pain, increasing fever with chills and jaundice.
Serology is extremely sensitive (up to 95%) and it is as specific. PCR based tests to detect amebic DNA are available in research settings.
TreatmentNitro-Imidazoles (including Metronidazole, most commonly used drug is useful in more than 90% cases. In uncomplicated abscess, Metronidazole is usually
sufficient as single agent and should be continued for 2-4 weeks (table 4). Most clinicians prefer to use a luminal amebicide like Diloxanide Furoate, or Iodoquinol for another 7-10 days. Aspiration should be considered in following situations:
1. Left lobe abscess
2. Less than 1 cm live parenchyma around abscess
3. Failure of medical treatment for 48-72 hours
4. Sero-negative abscess
5. Too sick patients in whom failure of medical treatment may be life threatening
On exam, tender hepatomegaly is found, but may be missing if abscess is sub-diaphragmatic. Movements of right side of chest and diaphragm may be restricted in such aces. Patients are usually febrile and splenomegaly may be present, particularly in cases with initial portal hypertension. After development to cirrhosis, abscess however is uncommon.
InvestigationsTotal leukocyte count is high with increase in polymorphonulclear cells. Liver function (LFT) is
deranged in case of biliary communication of abscess. It suggests obstructive pattern. Frank cholangitis may be present. Positive blood culture is uncommon except in cholangitis.
Most of the ALA are located in right lobe and are solitary. Figure 2 depicts proportionate location of ALA. Ultrasound cannot distinguish between appearance of amebic and pyogenic liver abscess, apart from size, number and location (Table 3).

140
Chloroquine alone is uncommonly used but in cases of complicated ALA like ruptured ALA, Systemic toxicity, or in Cholangitis, it should be used ads as an adjunct to metronidazole. Chloroquine also is most useful tool in cases of Imidazole resistance.
Cases of ruptured ALA are treated in similar fashion as PLA. However, biliary communication of ALA requires early ERCP (endoscopic retrograde cholangio-pancreatography), endoscopic papillotomy and stenting. Response to ERCP in such cases is unusually dramatic.
Natural immunity after amebic infection is not long term. This is also the reason for failure to develop an affective vaccine against amebic infections.
References:1. Branum G, et al. Hepatic abscess: changes in
etiology, diagnosis and management. Ann Surg 1990;212:655-62
2. Sharma MP, et al. Management of amoebic and pyogenic liver abscess. Indian J Gastroenterol 2001; 20, supplement C33-36.
3. Yu SC, et al. Treatment of pyogenic liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Hepatology 2004; 39:932-8.
Table 4: Protocol treatment for ALA

Dr Vibhu MittalMD (Medicine), DM (Gastroenterology)Consultant at Pushpanjali Crosslay Hospital
Consultant at Pushpanjali Crosslay Hospital – 10:00am – 2: 00 pmDeepak Memorial Hospital – 5:00 pm – 6:00 pm
YEAR BOOK & SOUVENIR 2014
Acute pancreatitis is a disease which entails lots of physical, mental and emotional trauma to the patient and in severe cases also leads to significant morbidity and mortality.
There have been changes in the understanding of this entity with changes in previously used terminology. The revised Atlanta classification and guidelines proposed by American College of Gastroenterology and International Association of Pancreatology have proposed changes in how we assess severity and few management decisions.
Diagnosing Acute Pancreatitis
The diagnosis requires presence of 2 out of 3
· Typical abdominal pain, (Severe upper abdominal pain with or without radiation to back)
· Elevated pancreatic enzymes (S. Amylase or S. Lipase), >3 times the upper limit of normal. Lipase is more specific as compared to amylase but sensitivity and specificity of lipase is also not absolute.
· Cross sectional imaging in the form of CT scan or MRI abdomen can confirm the diagnosis in majority
CECT or MRI is not recommended as a routine in all patients. They are best used at admission in case of diagnostic dilemma to confirm the diagnosis of acute pancreatitis or to look for alternate diagnosis. Or they should be employed after 3-4 days in patients who fail to improve (persistent pain, fever, nausea and failure to initiate orally) to look for local complication. MRI may have to be used in biliary pancreatitis also with intent to look for choledocholithiasis.
Evaluation for EtiologyDetailed history looking at alcohol and drug use, previous biliary pain, recent H/o trauma, passage of worms, recent ERCP etc. should be taken. A USG abdomen is done in all patients with intent to look for gall stones. A lipid profilewith triglycerides of more than 1000mg/dl should be considered as etiology for pancreatitis. Further evaluation to look for etiology of pancreatitis using endoscopic interventions is not warranted in acute setting.
Initial Assesment and Risk StratificationUnlike in past these patients are now classified into mild, moderately severe and severe pancreatitis. Severe disease is based on presence of organ failure as assessed by modified Marshall Score.
Mild Pancreatitis: No organ failure or local complication
Moderately severe Pancreatitis: Local complication and/or transient organ failure
Severe Pancreatitis: Persistent (>48 hr) organ failure.
In severe pancreatitis now two distinct phases are identified. First week characterized with organ failure and late phase (after first 7 days) having local complications as the dominant problem. But the problem is that at presentation most patients of severe pancreatitis would not have organ failure and may be missed at evaluation. Here comes the age old question of predicting severe pancreatitis so that proper triage of these patients to an ICU setting in an institution capable of handling these patients can be made.
Acute Pancreatitis-Early Phase:Management Decisions
142
Predicting Severe PancreatitisThere are various scoring systems which have been proposed over the years, but unfortunately none of them predict severity at time of admission, are cumbersome to do and by the time they become accurate, the severity is clinically evident. No single laboratory test (even CRP) has also been able to be good enough in predicting severity.
Now the recommendation is to use SIRS (Systemic Inflammatory Response Syndrome), which has following components:
SIRS Presence of >2 of following
Pulse>90 bpm
RR >20 / min or pCO2 >32 mm Hg
Temperatures >38? C or <36?
WBC count >12000 cells/cc or <4000 cells/cc, or>10%immature neutrophils
During the early phase of the disease (within the first week), death occurs as a result of the development, persistence, and progressive nature of organ dysfunction. The development of organ failure appears to be related to the development and persistence of SIRS. The reversal of and early organ failure has been shown to be important in preventing morbidity and mortality in patients with AP. Although the presence of SIRS during the initial 24 h has a high sensitivity for predicting organ failure and mortality, the presence of SIRS lacks specificity for severe disease (41 %). The lack of specificity is due to the fact that the presence of SIRS is not as important as its persistence.
The approach to predict outcomes should be three pronged with following components
· Patient's characteristics : Age >55, BMI >30, Associated comorbidity
· Clinical risk stratification : SIRS presence and persistence
· Response to treatment: BUN, creatinine and hematocrit
INITIAL MANAGEMENTFluid resuscitationThis is the most effective medical intervention in acute pancreatitis alteringthe natural history of disease positively if used effectively. There is enough direct and
indirect data supporting this strategy. The rationale is already present hypovolemia in these patients due to poor intake (due to pain and vomiting), losses s e c o n d a r y t o v o m i t i n g a n d t h i r d s p a c e sequestration.Add to this hypovolemia,is the combination of microangiopathic effects and edema of the inflamed pancreas decreases blood flow, leading to increased cellular death, necrosis, and ongoing release of pancreatic enzymes activating numerous cascades. Early aggressive intravenous fluid resuscitation provides micro- and macrocirculatory support to prevent serious complications such as pancreatic necrosis. Hydration is important during first 12-24 hr after admission. Aggressive hydration beyond this is not as important.
· Ringer Lactate has proven to be superior to normal saline as the fluid of ideal choice in this setting in various trials. There is no role for colloids.
· Rate of fluid infusion is usually 5-10 ml/kg/hr for initial 6 hr. This is to be continually monitored.
· A total of 3.0 -4.5 L fluid in first 12-24 hr is usually used
· Be more circumspect in aggressive fluid resuscitation in elderly or those with preexisting cardio, pulmonary or renal pathologies to avoid fluid over load, pulmonary edema etc.
· In those not responding to aggressive fluid resuscitation in first 6 -12 hr are not likely to benefit from continued aggressive fluid resuscitation
Monitoring during fluid resuscitation – is important to prevent complications with fluid resuscitation· No invasive targets of PR < 120 beats/min, Mean
arterial pressure of 65-85 mm Hg and urine output >0.5 -1 ml/kg/hr
· Central venous pressure measurement is used as a marker for volume status. But recent studies show that this is not as reliable as thought of. Recently measurement of intra thoracic blood volume index is shown to be a better indicator of volume status
· Biochemical target of Hct<35% or fall in BUN.
AnalgesiaManaging pain effectively helps in symptomatic relief to patient and is also helpful in improving respiratory status by improving the splinting effect of painful abdomen. NSAIDs remain the first choice agents and

143
are safe if renal parameters are acceptable. Opioids in addition to NSAIDs or alone in cases of renal compromise are acceptable. In cases of hypoxemia opioid use need to be cautioned as they may increase respiratory compromise
AntibioticsInfection both pancreatic and extra pancreatic (cholangitis, catheter related, Urinary tract infection and pneumonia) are an important cause of mortality. Moreover in acute phase presence of SIRS secondary to pancreatic inflammation may make diagnosis of infection difficult. But the evidence till now suggest
· Prompt use of antibiotics if extrapancreatic infection is present. In cases where it was suspected but investigations came out to be negative, antibiotics should be withdrawn.
· No prophylactic use of antibiotics in early phase of pancreatitis
· No use of antibiotics to prevent infection of sterile necrosis
· Infected necrosis is considered a possibility if patient of pancreatic necrosis fail to improve after 7-10 d of hospitalization. In such scenario antibiotics with pancreatic penetration may be considered after sending all relevant cultures or CT guided FNA
· Routine antifungals are not recommended with antibiotics
No probiotics should be used in acute pancreatitis as their use was associated with increased mortality in a clinical trial
NutritionImportant as also shown to decrease sepsis related complications with enteral feeding.
· In mild acute pancreatitis, start enteral feeding after cessation of nausea, vomiting and decrease in pain. Feeds may be startd with soft diet directly
· In severe pancreatitis enteral feeds as tolerated needs to be initiated as soon as ileus improves.
· Parenteral route to be used if enteral feed not tolerated or not meeting the caloric requirement
· If oral feeding not tolerated due to gastroparesis, nasojejunal feeding is an option
Role of ERCPERCP should not be used for diagnostic purpose. MRCP or EUS are safer investigations to confirm the presence of CBD stone. ERCP is done to remove retained CBD stone.
ERCP is to be done as soon as possible in presence of cholangitis and in presence of CBD stone with pancreatitis. In severe acute pancreatitis without present CBD stone use of ERCP is not recommended
ConclusionWith these recent changes in the understanding and hence management of acute pancreatitis, changes on positive side of clinical end point are expected. In patients of severe disease or moderately severe disease who have an expected stormier course, management should be done at tertiary centers equipped with interventional radiology, endoscopic and surgical expertise with best intensive care.
Suggested reading· Banks PA ,Bollen TL , Dervenis C et al.
Classification of acute pancreatitis— 2012: revision of Atlanta classification and definitions by internationalconsensus. Gut 2013 ; 62 : 102 – 11 .
· Tenner S, Baille J et al. American college of gastroenterology guidelines – Management of acute pancreatitis. Am J Gastroenteroladvance online p u b l i c a t i o n , 3 0 J u l y 2 0 1 3 ; d o i : 10.1038/ajg.2013.218

Recent Advances in the Treatment of Hepatitis C
Dr Deepak Lahoti, Senior Consultant and Head, Deptt of GastroenterologyDr Rohit Goyal, Consultant Deptt of GastroenterologyDr Rajan Dhingra, Consultant Deptt of GastroenterologyMax Superspeciality Hospital, Patparganj, Delhi
Hepatitis C patients often present as chronic hepatitis. Patients with acute hepatitis C virus (HCV) infection are not common in clinical practice . When detected patients show good response to six months of standard therapy with interferon (IFN). Because spontaneous resolution is common, no definitive recommendation for timing of therapy initiation has been advocated; however, waiting 2-4 months after the onset of illness seems reasonable.Chronic hepatitis C
Treatment has two aims. The first is to achieve sustained eradication of HCV characterized by SVR which is defined as the persistent absence of HCV RNA in serum 6 months or more after completing antiviral treatment. The second aim is to prevent progression to cirrhosis, HCC, and decompensated liver disease requiring liver transplantation.
Peg interferon and ribavirin combination has been a standard of care for patients with chronic hepatitis C so far. However with advent of direct antiviral drugs the scenario is changing very fast. Though highly effective these drugs are very expensive and not available in every part of the world
Treatment with PEG-IFN alfa-2a and ribavirin depends on the genotype. Patients with HCV genotype 1 are treated for 48 weeks with Peg IFN and a standard dose of ribavirin; those with HCV genotype 2 or 3 require a low dose of ribavirin for 24 weeks. Viral kinetics during therapy provides information on how to individualize treatment. . Hepatitis C virus (HCV) RNA is measured at baseline, 4 weeks and 12 weeks. RVR is defined as undetectable HCV RNA at 4 weeks and EVR as >/=2 log(10) decrease in HCV RNA at 12 weeks. RVR is a strong predictor of SVR (PPV>96%)
and failure to achieve EVR is a strong predictor of non-SVR (NPV>75%), independent of pat ients ' pretreatment status. Response to therapy of HCV genotype 1 (i.e. achievement of SVR) can now be predicted by looking for patients with CC genotype of the IL-28B who have much more favorable response as compared to CT or TT genotype (70% vs 25-30%). Adverse effects Adverse effects are common with IFN and ribavirin combination therapy. Approximately 75% of patients experience one or more of adverse effects. Adverse effects of IFN include hematologic complications (ie, neutropenia, thrombocytopenia) neuropsychiatric complications (ie, memory and concentration disturbances, visual disturbances, headaches, depression, irritability),and flu-like symptoms
Adverse effects of ribavirin include hematologic complications (ie, hemolytic anemia)
Growth factors, such as granulocyte-stimulating factor (GSF) and erythropoietin, are frequently used to counteract the adverse hematologic effects of IFN and ribavirin, respectively. However they often prove to be very expensive. In November 2012, the US Food and Drug Admin i s t r a t ion (FDA) approved eltrombopag, an oral thrombopoietin agonist, for treatment of thrombocytopenia in patients with chronic hepatitis C to allow the initiation and maintenance of IFN-based therapy. Because of this, a significant improvement in virologic response was observed in the patients given eltrombopag
Direct antiviral drugsProtease and Polymerase InhibitorsDespite the improved results achieved with the addition
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

145
of ribavirin to PEG-IFN, the current available therapies for chronic HCV infection are effective in fewer than 50% of patients with HCV genotype 1.
A new class of direct-acting antiviral agents (DAAs) has revolutionized the treatment of HCV genotype 1 infection. These drugs target specific enzymes involved in viral replication. The addition of these new protease inhibitors to pegylated interferon and ribavirin is becoming the new standard of care for the treatment of chronic HCV infection.
The first protease inhibitor , boceprevir was approved by the FDA in May 2011 followed by approval of telaprevir. However these two protease inhibitors are no longer recommended due to the more recent availability of more effective options. A third protease inhibitor, simeprevir was approved in November 2013 and is recommended as a part of combination therapy for chronic hepatitis C infection. Most recently, HCV NS5B polymerase inhibitor sofosbuvir (Sovaldi) was shown to result in suppression of HCV replication and has emerged as an important component of currently recommended regimens. In November 2014, the FDA approved an all oral regimen of simeprevir plus sofosbuvir for treatment-naïve or treatment-experienced patients. The treatment duration is 12 weeks for patients without cirrhosis and 24 weeks for those with cirrhosis. Current treatment recommendations for chronic hepatitis C infection (American Association for the Study of Liver Diseases [AASLD] and the Infectious Disease Society of America [ISDA])Treatment-naïve patients:
Genotype 1: sofosbuvir (SOF) 400 mg daily with PEG IFN/RBV (weight-based, 1000 to 1200 mg daily) for 12 weeks or simeprevir (SMV) 150 mg with PEG IFN/RBV for 12 weeks followed by another 12 weeks of PEG IFN/RBV; an alternative for IFN-ineligible patients is combination SOF, SMV, and RBV for 12 weeks.
Genotype 2: SOF 400 mg daily with RBV (weight-based, 1000 to 1200 mg daily) for 12 weeks.
Genotype 3: SOF 400 mg daily with RBV (weight-based, 1000 to 1200 mg daily) for 24 weeks (an alternative is SOF with PEG IFN/RBV for 12 weeks).
Genotypes 4: Daily sofosbuvir (400 mg) and weight-based RBV (1000 mg [< 75 kg] to 1200 mg [≥75 kg]) plus weekly PEG for 12 weeks is recommended for IFN-eligible. Alternatively, Daily simeprevir (150 mg)
for 12 weeks and weight-based RBV (1000 mg [< 75 kg] to 1200 mg [≥75 kg]) plus weekly PEG for 24 to 48 weeks.
For IFN-ineligible patients, daily sofosbuvir (400 mg) plus weight-based RBV (1000 mg [< 75 kg] to 1200 mg [≥75 kg]) for 24 weeks is recommended.
Patients with prior PEG IFN/RBV treatment failure:
Genotype 1: SOF 400 mg daily, SMV 150 mg daily, and RBV (1000 to 1200 mg daily) for 12 weeks (an alternative is SOF for 12 weeks with PEG IFN/RBV for 12 to 24 weeks or SMV 150 mg for 12 weeks with PEG IFN/RBV for 48 weeks).
Genotype 2: SOF 400 mg daily with RBV (weight-based, 1000 to 1200 mg daily) for 12 weeks (an alternative is SOF 400 mg daily with PEG IFN/RBV [weight-based, 1000 to 1200 mg daily] for 12 weeks).
Genotype 3: SOF 400 mg daily with RBV (weight-based, 1000 to 1200 mg daily) for 24 weeks (an alternative is SOF 400 mg daily with PEG IFN/RBV [weight-based, 1000 to 1200 mg daily] for 12 weeks).
Genotypes 4 to 6: SOF 400 mg daily with PEG IFN/RBV (weight-based, 1000 to 1200 mg daily) for 12 weeks.
Patients with genotype 1 and prior TVR or BOC protease inhibitor failure: SOF for 12 weeks with PEG IFN/RBV for 12 to 24 weeks.
Direct antiviral drugs hold great promise for treatment of hepatitis C in near future
Suggested readings1 American Association for the Study of Liver Diseases and Infectious Diseases Society of America. Recommendations for Testing, Managing, and Treating Hepatitis C. Available at http://www.hcvguidelines.org/full-report-view. Accessed January 14, 2014
2 Osterwell N. Ledipasvir Sofosbuvir Combination Cuts Cirrhotic Hepatitis C. Medscape Medical News. Available at http://www.medscape.com/viewarticle/834869. Accessed November 17, 2014.

Consensus Statement and ProposedGuidelines by API for Insulin Therapy
in Type2DM
Type2 Diabetes Mellitus is characterised by progressive loss of insulin secretion from beta cells and increasing insulin resistance driven by obesity. It is estimated that by the time diagnosis is done, most patients have lost more than 50% of their beta cell function which steadily continues to decline at approximately 3-5% per year. Overtime even with multiple oral anti diabetic drugs patients fail to achieve glycemic control and need Insulin.
Several guidelines international, national and regional are available for diabetes management to assist physicians by providing stepwise treatment algorithm, but these guidelines cannot be widely used in Indian clinical practice. This current consensus guideline aims to provide recommendations for use in routine Indian clinical practice.
Traditionally, insulin treatment in type2DM patients is usually started when the oral therapy in double or triple combination and at maximal tolerated doses fails to achieve optimal glycemic control. However the recent recommendation is to initiate insulin early in the course of disease when the HbA1c remains above9%.Timely initiation of insulin therapy is crucial for optimal
glycemic control and improved patient outcome.
Targets Fasting plasma glucose <110 mg/dL Postprandialglucose < 180 mg/d
Initiation of insulinBoth Premixed insulin and basal insulin can be considered as a start insulin in patients with type2DM.
1. When Fasting plasma glucose (FPG) is high, consider initiating insulin therapy with Basal insulin and preferably basal analogue insulin over basal human insulin such as NPH, Lente insulin. The dose of insulin can be adjusted by increasing or decreasing by 2 units every 3 days to achieve the desired level.
2. When both FPG and PPG are high consider initiating insulin therapy with Premixed insulin. Since PPG contribution to hyperglycaemia is more in Asian population ,premixed insulin that improves PPG should be preferred method of insulin initiation in this population when both FPG and PPG are high. Premixed insulin can be started as once daily before breakfast or before dinner and later intensified twice daily to achieve the goals.
Intensification of insulinAlthough initiating basal insulin or once daily premixed insulin results in significant improvement in glycemic
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Dr Rajiv GuptaSr. Consultant Physician & DiabetologistAdvisor Delhi Diabetic Forum
Insulin Initiation & Intensification

147
control, therapy eventually needs to be intensified in due course of time. Basal insulin may require bolus therapy of prandial insulin in the form of rapid acting insulin with each meal.
In a fully optimised basal-bolus regimen,the total daily insulin dose will resemble a ratio of approximately 50% basal insulin and 50% divided into three equal bolus dose of rapid acting insulin.
When intensifying premixed insulin therapy from OD to BID, it is recommended to split the OD dose into into equal prebreakfast and predinner doses when total insulin dose crosses 30 units.When intensifying premixed insulin from BID to TID consider adding 2-6 units or 10% of total daily insulin before lunch? This may require reduction of the morning dose by 2-4 units.
Insulin in Critically ill patientsGlycemic targets in critically ill patients aim for a range of 140-180 mg/dL.
It is recommended to start intensive intravenous insulin therapy with a short acting regular human insulin, preferably using an infusion pump. It is recommended to start insulin infusion by dividing the blood glucose value by 100 and rounding off to the nearest decimal e.g. the blood glucose is 387mg/dL then start insulin infusion at a rate of 4 units per hour.
Administration of bolus dose is not recommended.It is recommended to monitor capillary blood glucose every hour and titrate the dose of insulin.If the capillary blood glucose does not show a declining trend then it is suggested to increase the dose according to the patient's response.
If the blood glucose value falls to 70mg/dL immediately stop infusion and manage hypoglycaemia and monitor blood glucose every 20-30minutes.If the blood glucose start rising restore infusion at a lower dose.Transition from IV to Subcutaneous insulinOnce the patient is stable and has been started on enteral or oral feeds switch over to SC insulin. It is recommended to start SC insulin 1 hour prior to discontinuing IV insulin. It is recommended to start basal-bolus regimen in such patients.
Sample conversion from IV insulin to SC insulinIf a patient is receiving 2units/hour insulin while NPO then his/her 24hour basal dose during stress is 24 multiplied by 2 equal to 48 units.Adjusting for stress reduce this by 2/3 basal rate for 24 hours I.e.32 units.
Total daily dose is multiplied by 2 I.e. 64 units.
As patient has just started to eat10% of the basal dose I.e.3units of rapid acting insulin can be started before each meal in addition to the basal insulin dose.

148
This article is based on the Special Issue on Consensus Statement on Insulin Therapy published as a supplement to JAPI July 2014 vol 62 issue No
7.Readers are requested to refer to the original publication for complete information.

Premix Insulin Initiation & Patient Self Titration: Recent Studies
Dr Indranil BhattacharyaMD (Medicine)Lilly India
Type 2 diabetes mellitus (T2DM) is a chronic illness that requires clinical recognitionand treatment of the dual pathophysiologic entities of altered glycemic control and insulin resistance to reduce the risk of long-term micro- and macrovascular complications. Although insulin is one of the most effective and widely used therapeutic options in the management of diabetes, it is used by less than one-half of patients for whom it is recommended. Clinician-, patient-, and health care system-related challenges present numerous obstacles to insulin use in T2DM. Clinicians must remain informed about new insulin products, emerging technologies, and treatment options that have the potential to improve adherence to insulin therapy while optimizing glycemic control and mitigating the risks of therapy. Patient-related challenges may be overcome by actively listening to the patient's fears and concerns regarding insulin therapy and by educating patients about the importance, rationale, and evolving role of insulin in individualized self-treatment regimens. Self-management of diabetes requires improved patient awareness regarding the importance of lifestyle modifications, self-monitoring, and/or continuous glucose monitoring, improved methods of insulin delivery (eg, insulin pens), and the enhanced convenience and safety provided by insulin analogs. To increase the success rate of treatment of T2DM, the 2012 position statement from the American Diabetes Association and the European Association for the Study of Diabetes focused on individualized patient care and provided clinicians with general treatment goals, implementation strategies, and tools to evaluate the quality of care.In patients with type 2 diabetes, glycaemic control typically deteriorates over time due to the progressive nature of the disease, and a significant proportion of
patients with type 2 diabetes will require exogenous insulin therapy to reach glycaemic goals.
There are several options available for starting and progressing with insulin therapy. Once-daily basal insulin is the most convenient strategy for insulin initiation because it is practical and simple to use, but its efficacy is limited since fewer than 40% of patients meet glycaemic targets.
At this time, intensification of insulin therapy is recommended and different approaches can be used. Theadministration of a rapid-acting analogue before the mealassociated with the largest postprandial glycaemic value in addition to basal insulin is considered to be more flexible and is usually recommended. Alternatively, a premixed insulin analogue twice daily (bid) may be used, although this strategy is considered to be less flexible and studied. There is a lack of head-to-head studies comparing the efficacy and safety of a premixed insulin analogue bid with that of once-daily basal insulin and once-daily prandial insulin as the second insulin therapy step after the initial basal insulin regimen has failed.
A recent multinational, randomized, open-label trial that compared insulin lispro low mixture (LM25; n=236) twice daily with a basal–prandial regimen of insulin glargine once daily and insulin lispro once daily (IGL; n=240) over 24weeks in patients with HbA1c 7.5–10.5% and fasting plasma glucose ≤6.7 mmol/l. The primary objective was to assess non-inferiority [per-protocol (PP) population], and then superiority [intention-to-treat (ITT) population], of LM25 versus IGL according to change in HbA1c after 24weeks (non-inferiority margin 0.4%, two-sided significance level 0.05). Estimated change [least squares (LS) mean (95%
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

150
CI)] in HbA1c after 24 weeks: −1.30 (−1.44, −1.16)% with LM25 and −1.08 (−1.22, −0.94)%with IGL. Non-inferioritywas shown [LSmean (95% CI) HbA1c treatment difference−0.21 (−0.38,−0.04) (PP population)]; gated superiority assessment showed a statistically significant advantage for LM25 (p=0.010; ITT population). Mean blood glucose, glycaemic variability, overall tolerability and hypoglycaemic episodes per patient-year did not show significant differences between treatments during the study. The study concluded that in patients with type 2 diabetes inadequately controlled on once-daily basal insulin glargine and metformin and/or pioglitazone, intensification with LM25 was superior to a basal–prandial approach in terms of reduction in HbA1c after 24 weeks and did not increase hypoglycaemia episodes.
Further, there is a need, particularly in the generalist setting, for evidence to support the implementation of simple approaches to prandial insulin therapy that empower the patient and promoteindividualized treatment. No randomized,controlled studies in patients withtype 2 diabetes have investigated treatment escalation with prandial (bolus) insulin using patient-driven treatment intensification. The AUTONOMY trial was designed to compare the efficacy and safety of two patient-basedselftitrationalgorithms for initiation and titration of prandial insulin lispro therapy in patients with type 2 diabetes who could not achieve adequate glycemic control on basal insulin plus OADs. The study provides the first comparison of two self-
titration insulin algorithms for the escalation of prandial insulin therapy in a large, multicountry, randomized, controlled trial.The trial was designed as two independent, multinational, parallel, open-label studies (A and B), identical in design, to provide substantial evidence of efficacy and safety in endocrine and generalist settings. Subjects were 18–85 years old (study A: N = 528; study B: N = 578), on basal insulin plus oral antidiabetic drugs for ‡3 months, and had an HbA1c 7.0% to £12.0% (>53.0 to £107.7 mmol/mol). Once optimized on insulin glargine, subjects were randomized to one of two self-titration algorithm groups adjusting lispro either every day (Q1D) or every 3 days (Q3D) for 24 weeks. The primary outcome was the change in HbA1c from baseline. The primary and secondary objectives were evaluated for the overall population and subjects ‡65 years old. The trial showed significant and equivalent reductions in HbA1c from baseline (study A: Q3D –0.96% [–10.49 mmol/mol], Q1D –1.00% [–10.93 mmol/mol], Q3D–Q1D 0.04% [0.44 mmol/mol] [95% CI –0.15 to 0.22 (–1.64 to 2.40)]; study B: Q3D –0.92% [–10.06 mmol/mol], Q1D –0.98% [–10.71 mmol/mol], Q3D–Q1D 0.06% [0.66 mmol/mol] [95% CI –0.12 to 0.24 (–1.31 to 2.62)]). The incidence and rate of hypoglycemia were similar for Q3D and Q1D in both studies. In general, no clinically relevant differences were found between the two algorithms in subjects ‡65 years old in either study. The study further concluded that prandial insulin lispro can effectively and safely be initiated, by either of two self-titratedalgorithms, in a variety of practice settings.

Dr. Banshi SabooDiabetologist and Endocrine Physcian
PPG and CVD riskDiabetes is a major metabolic disease with a worldwide prevalence of 366 million people in 2011 and an estimated to affect 552 million people by 2030. Uncontrolled/ poorly controlled diabetes is an independent risk factor for macrovascularand microvascular complications inwhich CVD alone accounts for almost 75% mortality in type 2 diabetes
1,2subjects . In diabetes patients, the CVD risk is almost
2atwo to four times than that of nondiabetics [Figure 1].
In a 7-year follow-up study that compared the incidence of CV events in 1069 diabetic and 1373 non-diabetic patients with or without prior MI, it was found that
diabetes had a similar risk for stroke, CV death and MI as that of prior MI (20.2% vs. 18.8%) and the incidence of CV events in prior MI patients were increased if diabetes was present (18.8% in non-diabetics vs. 45% in diabetics).This suggests that diabetes is an
2cindependent risk factor for CHD [Figure 1a].
p<0.001 for prior MI vs. no MI and diabetes vs. no diabetes; calculated with Cox proportional-hazards models, adjusted for age and sex
CVD risk factors associated with T2DMDiabetes patients with insulin resistance often present with a proatherogenic cardiovascular risk profile. Although the individual risk factors including metabolic syndrome can bring some CVD risk, these in combination can further enhance it. CVD risk factors associated with T2DM include hyperglycemia, hyperinsulinemia, obesity, dyslipidemia (low HDL levels, increased TGs and sdLDL formation), hypertension, microalbuminuria, high white WBC count, vascular inflammation markers (increased C-reactive protein, monocyte chemotactic protein-1 and proinflammatory cytokines), coagulation and thrombotic markers (increased von Wilebrand factor, plasminogen activator inhibitor-1, fibrinogen and matr ix metal loprote inase levels , decreased antithrombin III),endothelial dysfunction (decreased vascular reactivity, reduced release of prostacyclin, increased degradation of nitric oxide and impaired
2bflow-mediated dilation) .
Metabolic defects of T2DM that contribute to hyperglycaemiaAs per the pathophysiology of type 2 diabetes, three metabolic defects can contribute to hyperglycaemia besides increased glucose uptake. These include:1) Decreased glucose uptake by muscle cells and
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
PPG and CVD Risk

152
adipocytes due to decreased peripheral insulin sensitivity
2) Increased hepatic glucose output in the pre-meal or fasting state due to decreased insulin secretion by β-cells of pancreas
3) Decreased suppression of hepatic glucose output in post prandial state due to delayed and decreased insulin secretion by β-cells of pancreas in response
3,4to glucose stimulus [Figure 2]
Glycaemic contribution to HbA1CGlycaemia is combination of fasting plasma glucose (FPG) and postprandial plasma glucose (PPG) and thus HbA1c which reflects overall exposure of glycaemia is dependent on both FPG and PPG. HbA1c target levels are achieved only by using treatment strategies that target either FPG or PPG.
Though HbA1c reflects overall glycaemic control over last 2-3 months, it does not give a clear picture on daily glycaemic fluctuations. If only, FPG to be considered, a true fasting state is impossible as the person spends mostly in postprandial state (more than 12hr) and most
of the post prandial peaks might also be missed [Figure 3].
PPG is more prominent in diabetes due to decreases/ delayed first and second phases of insulin secretion. As glucose tolerance deteriorates (HbA1c exceeds 6.5%), the postprandial glucose rises much earlier (four times faster) than fasting glucose levels [Figure 4]. So, the patients with normal glycaemia at pre-breakfast time may result in elevated post meal glucose levels with highest peak at post-breakfast [Figure 4a]. Moreover large calories meals do prolong the duration of post prandial and further deteriorate the post meal glucose excursions [Figure 5]. Hence considering FPG alone might overlook the deleterious effects of PPG peaks 5,6,7,8, 9,9a
.
4aFig.2A: Impaired insulin secretion in type 2 diabetes
Fig.2: Metabolic defects of type 2 Diabetes
Fig.3: Duration of postprandial state
Fig.4: PPG rises much earlier than FPG

153
In patients with HbA1c < 7.3, almost 70% of the glycaemia is due to post prandial rise and in patients with HbA1c < 6, PPG contributes to nearly 90% which may be of clinical relevance in impaired glucose
10tolerance . But as the HbA1c value increases above 7, the FPG which inturn effects PPG dominates with a contribution of 70% at the highest range of HbA1c
11,12(10.2%) [Figure 6]. Moreover, Indians unlike other races like Caucasians have high contribution from PPG
13,14,15,16,17,18,19,20,21,22,23,24irrespective of the HbA1c value [Table 1].
Contribution of PPG to HbA1cClinical relevanceOverall glycaemic controlDetermines the A1C levels along with FPGEarly disease prognosis:PPG is the earliest abnormality that can be detected much before the actual diagnosis of T2DM, so is prominent sign of glycaemicdysregulation at early stages of diabetes progressionDecision with improvement in HbA1cAs HbA1c improves and FPG levels become normal, the contribution of PPG to A1C levels increases. So PPG lowering drugs should be started to achieve overall glycaemic control
How Indians are at more risk for PPG elevelation than that of Caucasians?Epigenetic effects:Asian Indian Phenotype makes Indians more prone to Type 2 Diabetes'Thrifty Phenotype' in Asians Indians• Poor nutrition in foetal and early infant life is
detrimental to the development and function of the Beta cells. A foetus growing in a malnourished mother will need to grab all the glucose it can for its development. It does this by making its muscles resistant to insulin
• Maternal under nutrition, infant's low birth weight, and rapid postnatal child growth are all associated with increased risk of diabetes in off spring in Indians
“A Thin- Fat Indian” · Have higher body fat composition · Great degree of central obesity · Lesser muscle mass · Increased insulin resistance
Fig.4a:Daily glycaemic variation withworsening diabetes.
Twenty-four hour recordings from the continuous glucose monitoring system in type 2 diabetes.
Curve 1 (blue): A1C <6.5%; curve 2 (red): ≤ 6.5% to <7%; curve 3 (green): ≤7% to <8%; curve 4 (orange): ≤8% to 9%; curve 5 (purple): ≥9%.
Fig.5: Duration of postprandial state based on size of meal
Fig.6: Contribution of FPG and PPG to HbA1c
Table 1: Relative contribution of PPG to HbA1cIndians vs. Caucasians
Type 2 Diabetes

154
Food habits:Asian Indians show higher glycemic response to the same food as compared to CaucasiansCarbohydrates are integral to asian Indian dietary traditions.In a typical Asian Indian Diet the carbohydrate intake is about 70%-80% while in typical American diet it is about 50%.
Disease and prevalence:nd· 2 highest diabetes population is of Indians
followed by china· Highest diabetes related deaths: –Indians-23.8% –Chinese-13.4% –United states-15.2%· Undiagnosed diabetes population –Indians-51.1% –Chinese-58.7% –United states-29.2%· Prevalence of diabetes in younger age –Diabetes occurs at a younger age in Indians
compared to caucasians
HYPERGLYCAEMIA AS CVD RISK FACTORData from MRFIT showed that diabetes has significantly increased the risk of CVD events in patients with other risk factors like hypertension, hyperlipidaemia and smoking more than that without diabetes. This shows that hyperglycaemia is an
25independent CVD risk factor [Figure 7].
Mechanism and pathogenesisEffect of PPG on oxidant stress and inflammationHyperglycemia increases the glucose uptake by cells and increases the protein kinase C and diacylglycerol activation thus resulting in decreased nitric oxide (NO) and increased endothelin-1 and plasminogen activator inhibitor-1. Acute glycaemic exacerbations decrease
acetylcholine induced vasodilation and thus increases the vascular tone. They are linked with endothelial damage due to decreased NO synthesis or increase the free radicals through over production of NO thus increasing the oxidative stress.
Linear correlation between post-prandial glucose excursions and urinary excretion of 8-iso prostaglandin
28F2 (PGF2), a measure of oxidant stress
They are also linked with increased thrombosis through alterations in coagulation such as shortening of fibrinogen half-life and increased platelet aggregation through increasing of fibrinopeptide, prothrombin, and factor VII. In addition, evidences show that 2-hr PPG is linked to increased plasma levels of ICAM-1 and cytokines like C-reactive protein which can initiate the atherosclerosis.In addition, increased oxidative stress and glycosylation of extracellular proteins like LDL, abnormal coaguability, vascular permeability, and matrix formation further worsens atherosclerosis. Recent evidences have also shown that hyperglycemia increases the apoptosis of myocytes, endothelial cells and fibroblasts through deposition of nitrotyrosine, an
26,27independent CVD risk factor [Figure 8].
Effect of PPG on post-meal lipidemiaPost prandial hyperglycaemia in diabetes is associated with postprandial hyperinsulinemia. Hyperinsulinemia
Fig.7: CVD death rate in Diabetes and Non-diabetes [MRFIT]
Fig.8: Mechanism and pathogenesis of hyperglycaemia in atherogenesis

155
in turn leads to higher plasma triglycerides, chylomicrons, plasma lipoproteins (LDL, VLDL) and free fatty acids. High triglycerides lead to improper lipid metabolism leading to sdLDL formation and low HDL levels. Thus apart from glycaemic peak variability, PPG's effect on post-meal lipidemia can also worsen atherosclerosis and contribute to CVD risk via increasing LDL oxidation, vasoconstriction and
27,28thromogenesis. [Figure 9] .
Epidemiological evidence for PPG related CVD riskAlthough no large scale interventional studies till date are available to confirm the target PPG for reduction of CV complications, emerging evidences state that PPG contributes to significant increase in CVD risk apart from overall glycaemia.
Paris Prospective Study on non-diabetic (FPG < 140 mg/ dl) showed that impaired glucose tolerance
(normal FPG but elevated PPG) had increased CV risk 29by 2-folds [Figure 10]. This suggests that PPG but not
FPG is a significant risk factor in prediabetics.Similar results were shown byFunagata Diabetes Study in which IGT but not IFG doubled the CVD risk when
30compared to that of NGT [Figure 11].
Helsinki Policeman Study showed that 1-2 hr PPG during OGTT is better CHD risk predictor than FBG. DECODE analysis showed that rise in 2-hr PPG in individuals with normal FPG increased the risk for mortality in previous non-diabetics when compared to that of individuals with normal glucose tolerance. It also showed that 2-hr PPG increases with age but FBG does not [Figure12, 13] .This suggests that measurement of FPG alone is not sufficient and further strengthened that PPG is better than FPG in predicting
31,32CVD risk . Two other studies: Islington Diabetes Study and Hoorn study confirmed that 2-hr PPG is
33better than HbA1c as a predictor of CHD .
Fig. 9: Within 2 to 4 h of 75 g glucose load, glucose and triglyceride levels double, causing immediate oxidant stress,
inflammation, resulting in deterioration in endothelial function
Fig.11: Glucose tolerance, from IGT to overt diabetes: a risk factor for CVD death [Funagata study]
Fig.12: The effect of PPG on mortality risk increases linearly and the risk that starts before the cut-point (11.1 mmol/L)
in asymptomatic people is almost high as in known diabetes [Decode analysis]

156
Honlolulu Heart Program has shown a linear relationship between incidence of fatal coronary heart diseases and post-challenge glycaemia and has established PPG as an independent risk factor for CVD. Framingham offspring study had shown that every 40 mg/dl rise in 2-hr PPG increases the CVD (CHD, stroke
33or PAD) risk by 12-42% . Diabetes intervention study mentioned PPG but not FPG as one of the independent
34risk factors for CV death . A 20-year follow-up for mortality of non-diabetic men in three European cohorts [Whitehall Study (n = 10,025), the Paris
Prospective Study (n = 6,629), and the Helsinki Policeman Study (n = 631)] showed that men in upper 20% of the 2-h post prandial and 2.5% of fasting plasma glucose distributions had significantly higher CHD
35mortality .
Effect of PPGmacrovascularcomplicationsMany evidences have shown that post challenge and post meal hyperglycemia is a better predictor of CV events (including myocardial infarction and stroke)and all-cause mortality than that of FPG. Apart from this, many studies have shown that PPG is associated with i n c r e a s e i n b i o m a r k e r s o f m a c r o v a s c u l a r complications.
A study on 403 non-diabetic subjects showed that individuals with higher PPG (8.24 > or = pp plasma glucose < 11.1 mmol/l) were significantly associated with higher BMI, waist-to-hip ratio, TGs, albuminuria and lower HDL-c with a parallel increase in carotid
36, 37intima media thickness CIMT) .
Another study showed that myocardial blood flow (MBF) and myocardial blood volume (MBV) were decreased significantly in postmeal state while unaltered in fasting state of diabetic patients.
Other studies on acute glucose fluctuations in post meal state have shown that post meal hyperglycemia triggers oxidative stress, elevates adhesion molecules and decreases NO release. It also impairs endothelium dependent vasodilation and may activate thrombosis thus intiating and progressing atherosclerosis.
All these confirm the fact that PPG is an independent risk factor for development of macrovascular
38complications .
Effect of PPG on microvascular complicationsThough PPG is not established as an independent risk factor, recent evidences favour the fact that PPG is a better predictor for development of all microvascular complications. An observational study demonstrated
Fig.13: 2-hr PPG increases with age but FPG does not [DECODE analysis]

157
that PPG is a better predictor of diabetic retinopathy than that of HbA1c. A multiregression analysis of a cross-sectional study showed that PPG rather than FPG or HbA1c correlates with the incidence of diabetic
39microangiopathy (neuropathy and nephropathy) .
Other effects of PPGThough a stronger association is seen for men in a large cohort study on 35658 men and women,PPG >11.1 mmol/L (200mg/dL) when compared to that of PPG <6.7 mmol/L (121mg/dL) was associated with an increased risk for developing pancreatic cancer (relative risk of 2.15). However, another larger study with 31304 men, 33293 women and 2478 incident cases of cancer showed that highest quartiles when compared to lowest quartiles of fasting and postmeal glucose increased the cancer risk in women over 10 years by 1.26 and 1.31 respectively. This data suggests that PPG can be implicated as a risk factor for pancreatic cancer.Another study in elderly type 2 diabetes patients has shown that significant postmealglycaemic excursions (>200mg/dL) were linked with disturbance in cognitive
38(global, executive and attention) functioning .
Benefits of targeting PPG: Effect on CIMT regression and surrogate markers of CV riskSTOP - NIDDM trial and a seminal study organized by the Campanian Post-prandial Hyperglycemia Study Group showed that reduction of PPG but not FPG significantly correlated with CIMT regression and reduction in IL-6 and CRP thus reducing the risk of
40MI .
STOP-NIDDM trial also showed that acarbose significantly reduced the risk of cardiovascular disease and hypertension in people with IGT. Another study in IGT people showed that acarbose significantly reduced the progression of carotid IMT along with a positive
41, 42effect on surrogate markers of CV risk .
CIMT regression with greater decreases in interleukin-6 and C-reactive protein and similar HbA1c levels was also observed after 12 months in 52% vs. 18% of people
40, 43receiving repaglinide and glyburide respectively .
Controlling PPG with rapid acting insulin showed an improvement in myocardial blood flow and decrease in CV markers such as nitrotyrosine, endothelial function, and methylglyoxal(MG) and 3-deoxyglucosone (3-
38, 44DG) in type 1 and type 2 diabetic patients .
Evidences are not available to show that PPG reduction
alone can reduce microvascular complications. But a study has showed that 2-h PPG <10 mmol/l (180 mg/dl) along with FPG <6.1 mmol/l (110 mg/dl) is strongly associates with reductions in retinopathy and
38nephropathy .
It was also shown that controlling PPG has been demonstrated to improve microvascular and macrovascular complications through improvement of endothelial function by reducing oxidative stress and
39,45inflammation .
Low risk of hypoglycaemiaHbA1c goals can be achieved by targeting FPG or PPG alone. But some studies demonstrated that even after achieving FPG target, HbA1c levels were still elevated(>7%). A study showed that only 64% vs. 94% of patients targeted to control FPG and PPG respectivelyhave achieved HabA1c goal (<7% &<7.8% respectively). It also showed that decrease in HbA1c with PPG reduction was almost twice than that
46observed with FPG reduction .On the other hand, tight control through FPG targeting alone can increase the risk of nocturnal hypoglycaemia which is significantly less when PPG alone is targeted. This shows that PPG targeting was associated with lower hypo glycaemic risk at similar HbA1c goal (<7%) than that of FPG
38, 47, 48targeting .
PPG: Harmful effects· Independent risk factor for macrovascular diseases (MI, stroke)· Associated with –Increased carotid-intima-media thickness –Increased oxidative stress, inflammation and
endothelial function –Decreased myocardial blood flow and volume –Impaired cognitive function in elderly T2DM· Associated with increased risk of –Retinopathy, neuropathy and nephropathy –Pancreatic cancer
Benefits of targeting PPG· Optimal glycaemic control· Reduction of vascular events· CIMT regression· Reduction of surrogate CV markers (interleukin-6, C-reactive protein, nitrotyrosine,
methylglyoxal (MG) and 3-deoxyglucosone (3-DG)· Improvement in myocardial blood flow· Low hypoglycaemia risk

158
PPG targetIn normal individuals, post prandial glycaemic levels peak after 60 minutes, rarely exceeding 7. 8 mmol/ L and up to10 mmol/ L followed by large meals. As per ADA recommendation in diabetic patients with high HbA1C but normal FPG, PPG target levels < 10 mmol/ L should be considered. However PPG target levels < 7.8 mmol/L, < 7.5 mmol/ L and < 7. 8 mmol/L are recommended by AACE, EASD and IDF
49respectively .
Clinical management strategy for glycaemic control
$*1-2 hrs after meals; 2 hrs after meals; IDF: International diabetes federation;ADA: American diabetes association; AACE: American association of clinical endocrinologists
Reasons to target PPG value
· Gold standard for diagnosis of diabetes
· Earliest abnormality that can be detected even before T2DM
· Frquent finding when optimal control is achieved
· Contributes to HbA1c along with FPG
· Reflects the premeal elevations (FPG)
· Better glycaemic control at HbA1c < 8.4%
· Targeting FPG alone is not sufficient to achieve HbA1c goal
· Targeting FPG alone may increase risk of nocturnal hypoglycaemia
· Must for gestational diabetes
· Independent risk factor for CV events
· Therapeutic monitoring of specifically PPG lowering drugs
Non-pharmacological managementDiets with different glycaemic index (GI) decide the glycaemic load on the post prandial levels. As any usual diet is a mixture of carbohydrates, proteins, fats and fibres; optimum diabetic diet should not be limited to carbohydrate counts but should contain foods with lower GI (eg. legumes, fruits). The foods, especially carbohydrates with high GI (eg. Rice, breakfast cereals, white and brown bread) should be limited or avoided. The foods should be rich in fibres or may be slowly digested and absorbed to prevent any sudden increase in
38post meal glycaemia . Observational studies have shown that diets with high GI increase the risk of diabetes mellitus, gestational diabetes and CV risk in
50, 51, 52, 53, 54non-diabetics . It also has been shown in a meta-analysis that diets with lower GI improve HbA1c
55levels . Thus, nutritional interventions based on GI can effectively reduce postprandial glycaemic excursions and reduce CV events.
Physical activity and weight control that occupy a cornerstone in the management of diabetes can also have a beneficial effect on postprandial levels through
38reduction of insulin resistance .
Pharmacological managementMany anti-diabetic drugs improve overall glycaemic control including both fasting and postprandial levels. But some drugs target specifically PPG levels by addressing deficiencies in pancreatic and gut hormones that in turn affect the levels of insulin and glucagon, satiety and gastric emptying. These include:Traditional therapies such as · insulin (rapid-acting insulin analogues, premixed
insulin, regular insulin, inhaled insulin)· glinides and · α-glucosidase inhibitors
Newer therapies such as· amylin analogues· glucagon-like peptide-1(GLP-1) derivatives
38· dipeptidyl peptidase-4 (DPP-4) inhibitors
InsulinRapid-acting insulin, premixed insulin and inhaled insulin control the PPG by mimicking normal physiological insulin response. They have a rapid onset and peak activity for a short duration. So, they can effectively lower the blood glucose post meal when
38, 56administered just before or with first bite of meal .
GlinidesGlinides (nateglinide and repaglinide) are rapid acting

159
secratogogues which can stimulate the insulin release from pancreatic beta cells. They control PPG with less chance of hypoglycaemia than that of sulfonylureas
57because of their short duration of action .
α-glucosidase inhibitorsα-glucosidase inhibitors (acarbose, miglitol and voglibose) are the oral antidiabetic drugs that can prevent postmeal plasma glucose excursions. These act by inhibiting the enzyme α-glucosidase that breaks down complex carbohydrates to monosacharides. As they delay gastrointestinal absorption of glucose, the
58risk of hypoglycaemia can also be decreased .
Among these drugs, vogliboseis well tolerable and effective at comparable doses. Voglibose, like acarbose, has been associated with an in increase in glucagon like peptide (GLP-1), which has insulinotrupic effect and which has inhibitory effects on glucagon secretion, which results in overall reduction post-prandial hyperglycaemia.In terms of inhibitory effect on maltose and sucrose, voglibose is 190-270 times more effective than acarbose and 100 times more effective than miglitol.But unlike acarbose, it is a selective dissacharidase inhibitor with a weak inhibitory effect on pancreatic amylase. On average it decreases elevated PPG by 50 mg/dL and FPG by 10-20 mg/dL. It has an additive effect with other antidiabetic drugs like sulfonylureas, meglitinides and gliptins. Combination therapy with vogliboseeffectively reduced the glycaemic excursions with a significant improvement in glycemic parameters.
In newly diabetic patients, voglibose along with diet has been effective in reducing excess visceral and subcutaneous adipose tissue fat and has shown to
improve obesity in diabetic and metabolic syndrome patients. Recently, it has been approved in Japan for management of prediabetic patients and is an effective alternative for metformin apart from lifestyle modifications for Indian patients also. It can also be helpful as an atherosclerotic drug as it effectively improves insulin sensitivity and dyslipidemic states and reduces the progression of carotid intima media thickness in non-diabetic patients.
Amylin analogueAmylin analogue like pramlintide are stable synthetic antidiabetics that mimic the role of physiological amylin cosecreted with insulin from β-cells. They assist the insulin in restoring postprandial glucose control and blunt postmeal glycaemic excursions by inhibiting glucagon secretion, delaying gastric emptying and
59increasing satiety .
Glucagon-like peptide-1 (GLP-1) derivativesGLP-1 derivatives like exenatide share a similar homology with GLP-1, an incretin hormone of the gut and mimic most of its effects. It lowers the glucose by stimulating insulin secretion, increasing neogenesis of β-cells, inhibition of β-cell apoptosis and glucagon secretion, delaying gastric emptying and inducing
60satiety .
Dipeptidyl peptidase-4 (DPP-4) inhibitorsDPP-4 inhibitors like sitaglipitin extend the active form of GLP-1 by inhibiting the DPP-4 enzyme that degrades it. This result in stimulation of glucose-dependent insulin secretion, suppression of glucagon release, delayed gastric emptying and increased satiety which in
61turn can control PPG .

Diabetes mellitus is a chronic disease often requiring complex treatment regimens to prevent long-term complications Treatment of type 2 diabetes (T2DM) continues to present challenges, with significant proportion of patients failing to achieve and maintain glycemic targets. Despite the availability of many oral antidiabetic agents, therapeutic efficacy is offset by side effects such as weight gain and hypoglycemia. Therefore, the search for novel therapeutic agents with an improved benefit-risk profile continues. Recent research has focused on the kidney as a potential therapeutic target, especially because maximal renal glucose reabsorption is increased in T2DM. Each day, approximately 180 g of glucose are filtered from the glomeruli of a healthy adult, and almost all of the filtered glucose is reabsorbed from the glomerular filtrate and returned to the circulation. Of the filtered glucose, 90% is reabsorbed in the bloodstream by the SGLT2, located primarily in the luminal membrane of the proximal renal tubules. Under n o r m a l p h y s i o l o g i c a l conditions, nearly all filtered glucose is reabsorbed in the proximal tubule of the nephron, principally via the sodium-g l u c o s e c o t r a n s p o r t e r 2 (SGLT2). SGLT2-inhibitors are a new class of oral antidiabetics, which reduce hyperglycemia by increasing urinary glucose
excretion independently of insulin secretion or action. Clinical results are promising with significant lowering of HbA1c without increased risk of hypoglycemia, reduction of body weight and reduction of systolic blood pressure. Dapagliflozin is the first highly selective SGLT2-inhibitor approved by the European Medicine Agency. Canagliflozin and empagliflozin are the other SGLT2 Inhibitors currenly in use. Actual safety issues are an increased risk for genital- and urinary tract infections.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
SGLT2 Inhibitors:A New Treatment Option for Type 2 Diabetes
Dr. Abdul Hamid Zargar, DMMember, Medical Council Of India.Member Institute Body, AIIMS, New DelhiPast-President,Endocrine Society of India
Former, Chairman, Department of Endocrinology,Director & Ex-Officio Secretary to Govt.,Sheri-Kashmir Institute of Medical Sciences,Srinagar - 190011, Kashmir, India

Dr Amit Chhabra, MD BHU Fellowship in EndocrinologyConsultant PhysicianDiabetologist & Endocrinologist
SAMARPAN HORMONES & HEALTH CLINIC2nd B-87, Sector 2, Vaishali, Ghaziabad 201010Dept of Diabetes & EndocrinologyPushpanjali Crosslay Hospital, Vaishali, GhaziabadMobile : 9871701699 Email : [email protected]
Timings 6 to 8 pm, Weekly off Thursday
YEAR BOOK & SOUVENIR 2014
Subclinical Hypothyoidism Clinical Importance and Newer guidelines of Management
Subclinical hypothyroidism (SCH) is biochemically diagnosed when there is a persistently high TSH level, while circulating free thyroid hormone levels are within range.[1,2] Other terms for this condition are mild hypothyroidism,early thyroid failure, preclinical hypothyroidism, and decreased thyroid reserve.[3] The prevalence of SCH is 3-8%, which increases with age, more prevalent in females; but it approaches to males after 6th decade.[4,5] Presence of thyroid antibody raises the risk of developing subclinical and then progressing to overt hypothyroidism.
Medical condition which can lead to biochemical diagnoses of SCH[1] [Table 1] Include. Chronic autoimmune thyroiditis, persistently elevated TSH in subacute thyroiditis, postpartum thyroiditis and painless thyroiditis, injury to thyroid, partial thyroidectomy (other neck surgery), radioactive iodine/external radiotherapy exposure, drugs causing impairment of thyroid function (iodine and iodine-con ta in ing medica t ions , e .g . , amiodarone , radiographic, contrast agents, lithium carbonate, cytokines (especially interferon-a), aminoglutethimide, ethionamide, sulfonamides, and sulfonylureas), i nadequa te r ep lacemen t t he rapy fo r ove r t hypothyroidism, (inadequate dosage, noncompliance, drug interact ions ( i ron, calcium carbonate, cholestyramine, fiber, dietary soy, etc.), increased thyroxine (T4) clearance (phenobarbital, phenytoin, carbamazepine, etc.), malabsorption), infiltration of thyroid, (amyloidosis, sarcoidosis, hemochromatosis, R i e d e l ' s t h y r o i d i t i s , c y s t i n o s i s , a c q u i r e d immunodeficiency syndrome (AIDS), primary thyroid lymphoma), central hypothyroidism, toxic substances, industrial and environmental agents, and mutations of TSH receptor gene like G a gene mutations. Transient rise in TSH levels can be seen in granulomatous, postpartum, and silent thyroiditis cases.[5]
Screening RecommendationAmerican Thyroid Association --Women and men >35 years of age should be screened every 5 years
Diagnosis FactsSingle high reading of TSH should be repeated after 4-6 weeks, as there is transient fluctuation in TSH in different medical /physiological condi t ions . Controversies surround the upper normal limit of TSH level too, while traditionally most of the laboratories consider 4 mU/L as upper limit, there are some expert/organization that are advocating levels of 2.5-3 mU/L as true upper limits. There is also a physiological rise in TSH with age and levels of 6-8 mU/L could be considered in individuals >80 years of age.[6]
Natural Progression of diseaseProgression from subclinical to overt hypothyroidism is very high, the incidence range from 33 to 55% in prospective studies with nearly 10-20 years of follow-up.[4,7,8] This progression rate is considered to be around 2.6-4.3% each year.[4] Presence of thyroid autoantibodies,[7,9,10] goiter, underlying autoimmune diseases, and prior exposure to radioactive iodine/radiation are considered high risk for conversion into overt hypothyroidism.
Clinical ImportanceSubclinical hypothyroidism and pregnancyThyroid hormone disturbances have known to have adverse effect in pregnancy outcomes. That is why thyroid function assessment is relevant in reproductive dysfunction.[11] Review of literature revealed that SCH increased the rate of miscarriage/fetal death and later it adversely affects the cognitive development of offspring. Though universal screening for thyroid hormone bnormalities in pregnancy is not routinely recommended at present, but thyroid function must be

162
assessed in those having reproductive dysfunction and treated as appropriate.
Subclinical hypothyroidism and bone healthThyroid hormone and TSH play an important role in bone mineral homeostasis and bone growth. Thyroid hormone has direct effect on stimulation of bone resorption through osteoclast function. Overt hyperthyroidism is associated with increased bone turnover and an increased risk of osteoporosis and fracture,[12] but SCH effects on bone are not well-established. Results of one study conducted to determine the impact of SCH on bone health in children demonstrated no significant impairment in bone health which is evaluated by lumbar spine dual-energy X-ray absorptiometry (DXA) and phalangeal quantitative ultrasound (QUS).[13]
Subclinical hypothyroidism and cardiovascular riskRisk of cardiovascular disease in overt hypothyroidism is more established than in SCH. Although, there are observational studies[14,15] that suggest increased risk of coronary heart disease in SCH.
In a meta-analysis involving 25,977 participants out of which 2,020 were with SCH (seven rospective cohort studies) revealed a significant trend of increased risk of coronary heart disease (CHD) events at higher serum TSH concentrations.[16] This increased risk was not affected based on gender, age, or presence of preexisting CVD.
There are other cardiovascular risk factors associated with SCH.Cardiovascular defects such as diastolic dysfunction and increased peripheral vascular resistance are seen both in overt as well as SCH.[17]
Subclinical hypothyroidism and cholesterol metabolismA cross-sectional study (25,862 participants, median age 56 years), revealed individuals with serum TSH between 5.1 and 10 mU/L had significantly higher mean total cholesterol concentrations compared with euthyroid individuals (5.6 versus 5.8 mmol/L).There are studies revealing a link between elevated TSH and cho l e s t e ro l concen t r a t i ons ( t o t a l and LDL cholesterol).[18]
Subclinical hypothyroidism and metabolic syndromeWeight gain or failure to lose weight is one of the most common fea tures of over t and subc l in ica l hypothyroidism. Role of thyroid hormone is vital in
lipid synthesis, mobilization, and metabolism. A trial conducted in Ege University Medical School, Izmir, Turkey revealed that metabolic syndrome frequency is increased in overt and subclinical hypothyroidism patients.[19]
Subclinical hypothyroidism and neuropsychiatric issuesThere are several reports linking SCH with neuropsychiatric diseases,[20] Link between SCH and some of the neuropsychiatric disorders are exhibited in these studies, higher frequency of neuromuscular symptoms (weakness, paresthesias, fatigue, and cramps),[21] defects in verbal memory and executive functioning, and increased risk of Alzheimer disease (AD) in women but not in men (in population-based study).[22]
Sub clinical and weight gainWeight changes remain the one of the most important manifestation of thyroid diseases. Weight loss in hyperthyroidism as well as weight gain in overt hypothyroidism is well-established. But only few studies look into weight fluctuation in SCH. There are three studies which reveal increasing serum TSH level within the normal range resulting in modest increase in body weight.[23]
Other important associationAlthough our knowledge regarding SCH remains limited due to lack of randomized clinical trials, but there are some date to show association of higher risk of unprovoked deep venous thrombosis (pilot study) and more likelihood of common bile duct stones, thought to be secondary to sphincter of Oddi dysfunction.[24]Another interesting finding was noted regarding replacement of iron in subclinical hypothyroid patient with coexisting iron deficiency anemia. Rise in hemoglobin was noted to be greater in patient when given both iron and thyroid hormone compared with those given iron alone.[25]
Management Recommendations as per 2013 ETA (European Thyroid Association)[26](1) In younger SCH patients (<65 years; serum TSH < 1 0 m U / l ) w i t h s y m p t o m s s u g g e s t i v e o f hypothyroidism, a trial of L -thyroxine replacement therapy should be considered.
(2) There is limited evidence for improvement in mental function with LT 4 treatment of SCH in younger individuals.(3) Following hemithyroidectomy, persistent SCH

163
should be treated with L -thyroxine to normalise TSH levels.
(4) Patients with persistent SCH and diffuse or nodular goitre should be treated with L -thyroxine replacement with the aim of normalising serum TSH levels.
(5) There is no evidence for a favourable effect of L -thyroxine therapy on body weight in obese subjects with serum TSH levels <10 mU/l and normal FT 4 concentrations.
(6) In patients with type 1 diabetes mellitus, serum TSH should be monitored, once yearly.
(7) In patients with type 2 diabetes mellitus and an unexplained change in glycaemic control, serum TSH and FT 4 should be measured.
(8) L -Thyroxine therapy of SCH is able to reduce the levels of both total and LDL cholesterol, although normalisation of serum lipids is seldom achieved. The effect of L -thyroxine replacement on serum lipid concentrations is more pronounced in patients with pretreatment serum TSH value >10 mU/l.
(9) Age-specific reference ranges for serum TSH should be considered in order to establish a diagnosis of SCH in older people. The oldest old subjects (>80–85 years) with elevated serum TSH ≤ 10 mU/l should be carefully followed with a wait-and-see strategy, generally avoiding hormonal treatment.
(10) If the decision is to treat SCH, then oral L -thyroxine, administered daily, is the treatment of choice. There is no evidence to support use of liothyronine (T 3 ) or combined L - Thyroxine or liothyronine in the treatment of SCH.
(11) For patients without cardiac disease, a weight-related dose of L -thyroxine should be used, approximating to 1.5 μg/kg/day (e.g. 75 or 100 μg/day for a woman, 100 or 125 μg for a man).
(12) For patients with cardiac disease and in the elderly,a small dose of L -thyroxine should be started, 25 or 50 μg daily. The dose of L -thyroxine should be increased by 25 μg/day every 14–21 days until a full replacement dose is reached.
(13) L -Thyroxine should be taken on an empty stomach, either first thing in the morning, an hour before food, or at bedtime, 2 h or more after the last
food. Medications causing interference with L -thyroxine absorption (calcium and iron salts, proton pump inhibitors, etc.) should be avoided, or taken 4 h or more after L -thyroxine ingestion.
(14) The serum TSH should be re-checked 2 months after starting L -thyroxine therapy, and dosage adjustments made accordingly. The aim for most adults should be to reach a stable serum TSH in the lower half of the reference range (0.4–2.5 mU/l). For older patients (>70–75 years), a higher treatment target for serum TSH (around 1–5 mU/l) is acceptable.
(15) For patients with mild SCH (serum TSH <10 mU/l) who have been started on L -thyroxine for symptoms attributed to SCH, response to treatment should be reviewed 3 or 4 months after a serum TSH within the reference range is reached. If there is no improvement in symptoms, L -thyroxine therapy should generally be stopped.
(16) If thyroid function has normalised following an initially abnormal serum TSH result, then no further testing is required in those who are asymptomatic, have negative thyroid autoantibodies or do not have goitre.
(17) In those who have persistent SCH but in whom treatment is not commenced, thyroid function should be tested 6 monthly for the first 2 years and then yearly thereafter.
(18) Once patients with SCH are commenced on L - thyroxine treatment, then serum TSH should be monitored at least annually thereafter.
References
1. Biondi B, Cooper DS. The clinical significance of subclinical thyroid dysfunction. Endocr Rev 2008;29:76-131.
2. Cooper DS, Biondi B. Subclinical thyroid disease. Lancet 2012;379:1142-54.
3. CooperDS. Subclinical hypothyroidism. NEngl J Med 2001;345:260-5.
4. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, Clark F, et al. The incidence of thyroid disorders in the community: A twenty year follow-up of the Whickham Survey. Clin Endocrinol (Oxf) 1995;43:55-68.
5. Fatourechi V. Subclinical hypothyroidism: An update for primary care physicians. Mayo Clin Proc 2009;84:65-71.

164
6. Surks MI, Hollowell JG. Age-specific distribution of serum thyrotropin and antithyroid antibodies in the US population: Implications for the prevalence of subclinical hypothyroidism. J Clin Endocrinol Metab 2007;92:4575-82.
7. Huber G, Staub JJ, Meier C, Mitrache C, Guglielmetti M, Huber P, et al. Prospective study of t h e s p o n t an eo u s co u r s e o f s u b c l i n i ca l hypothyroidism: Prognostic value of thyrotropin, thyroid reserve, and thyroid antibodies. J Clin Endocrinol Metab 2002;87:3221-6.
8. Kabadi UM. Subclinical hypothyroidism. Natural course of the syndrome during a prolonged f o l l o w - u p s t u d y . A r c h I n t e r n M e d 1993;153:957-61.
9. Rosenthal MJ, Hunt WC, Garry PJ, Goodwin JS. Thyroid failure in the elderly. Microsomal antibodies as discriminant for therapy. JAMA 1987;258:209-13.
10. Díez JJ, Iglesias P. Spontaneous subclinical hypothyroidism in patients older than 55 years: An analysis of natural course and risk factors for the development of overt thyroid failure. J Clin Endocrinol Metab 2004;89:4890-7.
11. Sarkar D. Recurrent pregnancy loss in patients with thyroid dysfunction. Indian J Endocrinol Metab 2012;16 (Suppl 2):S350-1.
12. Vestergaard P, Mosekilde L. Hyperthyroidism, bone mineral, and fracture risk: A meta-analysis. Thyroid 2003;13:585-93.
13. Di Mase R, Cerbone M, Improda N, Esposito A, Capalbo D, Mainolfi C, et al. Bone health in children with long-term idiopathic subclinical hypothyroidism. Ital J Pediatr 2012;38:56
14. Hak AE, Pols HA, Visser TJ, Drexhage HA, H o f m a n A , Wi t t e m a n J C . S u b c l i n i c a l hypothyroidism is an independent risk factor for atherosclerosis and myocardial infarction in elderly women: The Rotterdam Study. Ann Intern Med 2000;132:270-8.
15. Lindeman RD, Romero LJ, Schade DS, Wayne S, Baumgartner RN, Garry PJ. Impact of subclinical hypothyroidism on serum total homocysteine concentrations, the prevalence of coronary heart disease (CHD), and CHD risk factors in the New M e x i c o E l d e r H e a l t h S u r v e y. T h y r o i d 2003;13:595-600.
16. Monzani F, Caraccio N, KozàkowàM, Dardano A, Vittone F, Virdis A, et al. Effect of levothyroxine replacement on lipid profile and intima-media
thickness in subclinical hypothyroidism: A double blind, placebo controlled study. J Clin Endocrinol Metab 2004;89:2099-106
17. Iqbal A, Schirmer H, Lunde P, Figenschau Y, Rasmussen K, Jorde R. Thyroid stimulating hormone and left ventricular function. J Clin Endocrinol Metab 2007;92:3504-10.
18. Knapp M, Lisowska A, Sobkowicz B, Tycińska A, Sawicki R, Musiał W. Myocardial perfusion and intima-media thickness in patients with subclinical hypothyroidism. Adv Med Sci 2013;58:44-9.
19. Erdogan M, Canataroglu A, Ganidagli S, Kulaksızoglu M. Metabolic syndrome prevalence in subclinic and overt hypothyroid patients and the relation among metabolic syndrome parameters. J Endocrinol Invest 2011;34:488-92
20. Monzani F, Del Guerra P, Caraccio N, Pruneti CA, P u c c i E , L u i s i M , e t a l . S u b c l i n i c a l hypothyroidism: Neurobehavioral features and beneficial effect of L-thyroxine treatment. Clin Investig 1993;71:367-71.
21. Simonsick EM, Newman AB, Ferrucci L, Satterfield S, Harris TB, Rodondi N, et al. Health ABC Study. Subclinicalhypothyroidism and functional mobility inolder adults. Arch Intern Med 2009;169:2011-7.
22. Tan ZS, Beiser A, Vasan RS, Au R, Auerbach S, Kiel DP, et al. Thyroid function and the risk of Alzheimer disease: The Framingham Study. Arch Intern Med 2008;168:1514-20
23. Fox CS, Pencina MJ, D'Agostino RB, Murabito JM, Seely EW, Pearce EN, et al. Relations of thyroid function to body weight: Cross-sectional and longitudinal observations in a community-based sample. Arch Intern Med 2008;168:587-92.
24. Laukkarinen J, Kiudelis G, Lempinen M, Räty S, Pelli H, Sand J, et al. Increased prevalence of subclinical hypothyroidism in common bile duct stone patients. J Clin Endocrinol Metab 2007;92:4260-4.
25. Cinemre H, Bilir C, Gokosmanoglu F, Bahcebasi T. Hematologic effects of levothyroxine in iron-deficient subclinical hypothyroid patients: A randomized, doubleblind, controlled study. J Clin Endocrinol Metab 2009;94:151-6.
26. Pearce, Brabant, Duntas, Monzani, Peeters, Razvi, Wemeau Eur Thyroid J 2013;2:215–228 DOI: .10.1159/000356507

Dr. Vikas Jain, MD (Medicine)Sr. Consultant Physician, Non Invasive CardiologistArogya Clinic & East Delhi Medical Centre
Just as health encompasses a variety of physical and mental states, so do the disease and disability, which are affected by various environmental factors, genetic predisposition, disease agents, and lifestyle choices
Each year, millions of people die preventable deaths. According to estimates made by the World Health Organization (WHO), about 55 million people died worldwide in 2011, two thirds of this group from non-communicable diseases, including cancer, diabetes, and chronic cardiovascular and lung diseases.
In the age group 25-69, the mortality rate rises sharply. The leading causes ofdeath in this age group are:
• Cardiovascular diseases (25%),
• COPD, asthma, other respiratory (10.2%),
• Tuberculosis (10.1%),
• Malignant and other neoplasms (9%),
• Symptoms signs and ill-defined conditions (5.3%),
• Digestive diseases (5.1%),
• Diarrhoeal diseases (5%),
• Unintentional injuries: Other (4.6%),
• Intentional self-harm or suicide (3%), and
• Malaria (2.8%).
Preventive healthcare is especially important given the worldwide rise in prevalence of chronic diseases and deaths from these diseases.
There are many methods to prevention of disease. It is recommended that adults and children aim to visit
their doctor for regular check-ups, even if they feel healthy, to perform disease screening, identify risk factors for disease, discuss tips for a healthy and balanced lifestyle, stay up to date with immunizations and boosters, and maintain a good relationship with a healthcare provider. Some common disease screenings include checking for hypertension, hyperglycemia, hypercholesterolemia, screening for colon cancer, depression, HIV and other common types of sexually transmitted disease such as chlamydia, syphilis, and gonorrhea, mammography (to screen for breast cancer), colorectal cancer screening, a pap test (to check for cervical cancer), and screening for osteoporosis.
Genetic testing can also be performed to screen for mutations that cause genetic disorders or predisposition to certain diseases such as breast or ovarian cancer.
However, these measures are not affordable for every individual and the cost effectiveness of preventive healthcare is still a topic of debate.
One of the best ways to stay healthy is with preventive health care. Key screenings and tests can help finding medical problems early -- before they cause bigger problems that make them more complicated to treat.
• Blood pressure check. Most people have a heart attack, a stroke, and eye and kidney problems without ever knowing they have high blood pressure. It's a condition usually without symptoms. That's why it's important to screen blood pressure even in asymptomatic people.
Arogya Clinic, Dilshad Garden, Delhi Timings: 10.00am-2.00pmPanchsheel Hospital, Yamuna Vihar Timings: 6.00-7.00pmSamra Hospital, Yamuna Vihar Timings: [email protected]
YEAR BOOK & SOUVENIR 2014
Preventive Health Care: Why is it Important?

166
If blood pressure is lower than 120/80, at least once every two years is fine. If blood pressure is between 120/80 and 139/89, should be screened yearly.
• Cholesterol screening. Heart disease is the number one cause of death world wide. One of its main risk factors is a high blood cholesterol level.
It's recommended that one should start getting cholesterol tested at least once every five years at the age of 20. A simple blood test can predict risk for heart disease.
With age, risk for heart disease increases. So in 50s, it's vitally important to continue getting screened.
• Mammogram. As a screening test for breast cancer, experts agree that a mammogram is the best way to find breast cancer early. There's some debate about how often one should get one.
The U.S. Preventive Services Task Force recommends that all women between ages 50 and 74 have a mammogram once every 2 years.
The American Cancer Society recommends a mammogram each year for women after age 40.
• Colon cancer screening. Colon cancer is the second-leading cause of cancer deaths in the U.S. After age of 50, chance of developing colon cancer increases. So -- unless there is above average risk -- 50 is the age when screening should be done. The good news: there are several tests that can help detect colon cancer early. Some commonly performed screenings include:
o Colonoscopy, once every 10 years
o Fecal occult blood test, once a year
o Sigmoidoscopy, every 5 years, combined with a fecal occult blood test every 3 years
Sigmoidoscopy and colonoscopy are two cancer screenings that can also help prevent cancer from deve lop ing . Dur ing these sc reen ings , precancerous polyps can also be removed.
• Pap test. This test checks for cervical cancer, which is easy to treat when caught early. Although risk of cervical cancer decreases with age, need for routine Pap tests doesn't stop with menopause.
Pap test should be done every year. Can be done
every three years if person had three normal Pap test results for three years in a row (if there is no past history of a precancerous Pap test result, no HIV infection, no weakened immune system, and n o h i s t o r y o f i n u t e r o e x p o s u r e t o diethystilbestrol).
Women who have a higher risk of cancer may need a Pap test more often.
• Lung cancer screening: There is evidence that screening persons with low dose helical CT, aged 55 to 74 years who have cigarette smoking histories of 30 or more pack years and who, if they are former smokers, have quit within the last 15 years reduces lung cancer mortality by 20% and all cause mortality by 7 %. However screening with chest X ray or sputum cytology does not reduce mortality from lung cancer in the general population or in ever- smokers.
• Bone mineral density scan. This screening checks risk for osteoporosis. It's recommended for all women at age 65. For patients at high risk, this test may be recommended early.
Men, ages 70 and older, may also benefit from this screening.
• AAA screening. Experts recommend a one-time abdominal aortic aneurysm (AAA) screening for men ages 65 to 75 who have smoked at any point in their lives. This ultrasound screens for an enlarged blood vessel in the abdominal area that can cause severe bleeding and death if it ruptures. If blood vessel is enlarged, surgery can correct it.
• Depression is a common cause of disability in adults, although it's often overlooked. It frequently arises with chronic illness and aging. Depression isn't a normal part of aging, and can be treated. People start feeling sad, hopeless, or loose interest in their regular activities. Also can present as non specific somatic complaints. Depression can be screened by asking to fill a simple questionnaire or by asking them a few simple questions.
• Diabetes screening. Prevalence of diabetes in India is increasing very rapidly and it has become a important cause for mortality and morbidity.

167
Individuals with the following risk factors should be screened for diabetes
1. Hypertension
2. Dyslipidemia
3. Obesity.body mass index greater than or equal to 30 kg/m2
4. Prior identification of impaired fasting glucose or glucose intolerance.
5. Any two of the following characteristics:
i. Overweight(BMI grearer than 25 but less than 30 kg/m2
ii. A family history of diabetes
iii. 65 years of age or older
iv. A history of gestational diabetes mellitus
v. Delievery of a baby weighing more than 9 pounds.
Pre-diabetes is defined as an impaired fasting glucose level of 100-125 mg/dl or an impaired glucose tolerance level of 140-199mg/dl 2 hr post glucose challenge.
• Immunizations. With age, a few extra vaccines are required to stay healthy.1. Influenza Vaccine: Recommended yearly for
everyone, 6 months of age and older.
2. Pneumococcal vaccine: Two different vaccines are recommended in 65 or older age. The vaccine is also recommended in high risk groups i.e diabetes, liver disease, asthma, any other type of lung disease, or immune compromised patients.
3. Other immunizations with Hepatitis B, hepatitis A,HPV, meningococcal, shingles etc should also be considered according to adult immunization schedule.
Screening for STDs , HIV , alcohol misuse screening and counseling, tobacco- use and couselling, obesity screening and counseling should also be done at regular interval.
Preventing the disease before it appears or start damaging our body is always better than treating it at later stages.

Dr. B. K. TiwariM.B.B.S., M.D. (Medicine), Senior Consltant Physician
Max Super Speciality Hospital108 A, Indraprastha Extension, Patparganj, New Delhi- 110092.Phone : +91-11-4303 3333, Fax : +91- 11-2223 5563, www.maxhealthcare.inContact No:- +91 9811933661
Timings: Mon – Sat – 9:00 am to 5:00 pm..
YEAR BOOK & SOUVENIR 2014
Common age related Medical Problems
Most Common age related medical problems are Communicable diseases, non communicable diseases, osteoarthritis and joint deformity, sexual & urogenital problems and last but not the least are aesthetic problems like baldness, facial changes and skin changes. Some of these problems are inevitable but now a days we have their partial solution but without any doubt that ageing is still unconquered.
Among the communicable diseases, Respiratory disorder like: repeated sore throat, chest infection, chronic- bronchitis, emphysema, pneumonia and tuberculosis of lung, Digestive disorder like: hyper acidity, diarrhoeal diseases, Seasonal infection like: Malaria, Dengue, common cold, Kidney disorder like: nephritis,urinary tract Infection are the health issues encompasses with advancing age.
However another breed of the diseases has developed called life style (non communicable) diseases among which most common are Obesity,Type-2Diabetese Mellitus, Heart diseases like Hypertension and Heart Attack, Cancer, Stroke, diseases due to air pollution and water pollution, Alcoholic Liver Disorder, Depression &Dementia, Osteoporosis and vision loss due to Cataract.
Sexual and Urogenital Disorders like loss of libido, dyspareunia, recurrent urogenital infection, prolapsed of uterus and cystocoele, dryness of vagina, urinary incontinence and menopausal symptoms in females and Prostate enlargement (BPH), hernia in males are very common but due to shyness and hesitation what we see in society is a tip of iceberg and these diseases go without being disclosed and discussion.
Last but not the least aesthetic changes in the body
like hair loss and baldness, osteoarthritis(age related joint and bony deformities), age related skin & facial changes are the universal fact of the life but those who are conscious and concern of these situations can hope to maintain youth for much longer duration than what we did in the past.
As so many medical problems have been enumerated above it is difficult to recognize them at a personal level. But we can take certain precaution and preventive steps for these health issues. Coming to the infections (communicable diseases) we have certain symptoms and indicators which can help us in catching the diseases early: Feeling feverish and weak for more than couple of days, excessive sputum production during the chest infection specially if it is copious and yellow or green in colour, pain in throat with chills, cough & sputum for more than four weeks, development of new bowel habit like frequent loose stools or constipation, blood coming out from anywhere like nipple, rectum or from mouth, fever during epidemic season like dengue or malaria, burning and increase in frequency of urination or Sudden pain anywhere in the body parts should not be ignored and always be consulted with doctors.
Life style (non communicable) diseases mentioned above can be prevented at three levels : Primary prevention (preventing disease before it happens as well as identifying and modifying risk factors), secondary prevention(identifying disease early), or tertiary prevention (treating complications of the disease or limiting the impact of established disease). This includes the prevention of obesity by eating low calories diet and exercising regularly which also helps in preventing other diseases like Type-2Diabetese Mellitus, Heart diseases Hypertension and Heart

169
Attack. Regular checkups of breasts and genital system of females by a gynaecologist can prevent many cancers pertaining to these organs. Avoiding smoking and air pollution can reduce the incidence of lung cancer. Taking enough exposure of Sun light will prevent Vitamin- D deficiency and osteoporosis. Early cataract surgery by lens implant is the way of reducing the morbidity of cataract induced visual loss. Depression is now a day's very common problem. If someone is feeling low lethargic, loss of interest in any work, sudden irritability or anxiety, loss of mental concentration or thoughts of death it may be depression and one should not hesitate in consulting with an experienced physician or psychiatrist. Post menopausal depression is quite common in ladies. Depression due to the stress of modern life in a large majority of Senior Citizens can be tackled by keeping you active. Regular reading habits, playing chess games, remaining intellectually active with lots of human interaction will go a long way to help the aging persons. Using low doses of aspirin, antioxidants, fresh seasonal fruits and balanced diet is of utmost importance.
Sexual and Urogenital Disorders can be prevented by observing few Sexual Hygiene Habits. These habits are washing the genitals by a female from vagina to the anus to prevent the transfer of germs from the anus to the vagina and also avoid yeast or other infections. For uncircumcised men pull back the foreskin and wash the glans penis with soap & water which essential to remove bacteria and dead cells and body fluids from these parts. Both partners should wash their hands and nails before and after sex to prevent transfer of germs and bacteria from each other genitals. It is important to trim the pubic hair during summer as heat and sweat can result in infections. Avoid oral sex if your partner has sores around the mouth or near the genitals otherwise it can pass on to you. To avoid embarrassment or bad odor women should avoid having sex during their menstrual cycle. Loss of libido (sex desire) can be prevented by keeping yourself active sexually and having a youthful thinking irrespective of your age.
Walking is considered as one of the best exercise when your schedule is busy and you don't have much time for yourself and it prevents almost all the life style diseases. Make sure you do not eat an hour before going out for a walk. Exercise alone is difficult to continue for a very long and make sure that you have
exercise partner who also keeps you away from smoking and regular alcohol intake. It does not really matter when you do the walk though few acknowledge early morning walk better because air is significantly fresher and rich in oxygen. The speed of the walk should be 3 to 5 miles per hour and if your pace is brisk 30 minutes walk is sufficient but if you are walking leisurely then 45 minutes to 60 minutes, walking is required for at least five times a week. Hydrate yourself with lots of water. Advantage of walking are immense and gives you cardiovascular fitness, flexibility, muscular endurance, less desire of smoking, better control of blood pressure, helps to reduce cholesterol, hypertension, heart problems. Apart from these benefits it reduces stress and boosts the immune system. It gives you the self confidence, brain fitness, energy, weight control and last but not the least increases your sexual performance in the bed.
Referring our last group of age related aesthetic problems like skin changes (wrinkling, brownish pigmentation and loosening) facial changes like sagging of the skin folds at cheek, neck and forehead can be dealt now a days by minimally invasive procedures commonly available in cosmetic clinics, skin specialist and at big hospitals. These skin changes are due to loss of subcutaneous fat, gravitational changes, decreased cell turnover, and alterations in skin elasticity. Risk factors for premature skin aging include sun exposure, smoking, and sleeping positions. Facial rejuvenation procedures typically aim to restore facial symmetry, and thereby attractiveness; interventions focus on reducing wrinkles and folds, restoring volume loss, and smoothing the skin surface. Two procedures are very popular, firstly injecting Botox (BTX-A) which acts immediately and face remains wrinkle free for three to four months and secondly injecting Dermal fillers which are meant for restoring volume and the fullness of face. The effect of dermal filler lasts for 6 months to two years. Combination therapy of Botox and Dermal Filler is now commonly being used to achieve more satisfying cosmetic results.
Chemical peels are available to improve appearance of the skin surface and reduce uneven pigmentation. For baldness many hair transplant institutes are available all over Delhi and many of them are giving satisfactory results in the cost of one to two lakhs rupees for the required amount of hair transplantation. It may require one or two sittings.

170
1. Hair transplant
2.Knee transplant
3. Effect of injection Botox
4. Effects of injection dermal filler
(Note: Images published in this article are taken from Google images)
Bone and joint problems can be handled by replacing the defective or diseased joints by the artificial one (Arthoplasty) which is easily available and reliable technique to help those patients who are suffering from bad and painful joint deformity and arthritis. Many people with severe painful osteoarthritis of knees and hip had taken the advantage of these successful joint replacement surgeries.
However, it is always judicious to consult a doctor before taking invasive preventive measures. Living happily, working optimally, exercising regularly and giving sufficient time to yourself and family are the key points in the life.

Nuclear Medicine in Everyday Clinical Practice
Nuclear Medicine is the science of using radioisotopes for the diagnosis and therapy of various disorders. Though it has been in clinical practice for last many decades but it remains hitherto unknown discipline to most of us and still remains in confines of big corporate hospitals in major cities of India. In last few years it is making inroads to second tier cities also. The reason perhaps could be the non inclusion of this discipline in the curriculum of graduation and post graduation.
The beauty of this science lies in the fact that it is a functional imaging. Unlike the anatomical imaging which we all are largely familiar with like USG, CT and MRI, it images the physiology of the organs or organ systems. The disease manifests earlier with change in the physiology rather than the structural or morphological changes. So with nuclear medicine we can diagnose disease earlier than with anatomical imaging most of the times.
Initially nuclear medicine remained synonymous with diseases of thyroid and its treatment. But it extends beyond thyroid and is useful for diseases of almost all organ systems. The indications are vast and too many. But for my convenience, I would be talking majorly about its use in ischemic heart disease and cancer.
Ischemic Heart Disease:Radionuclide studies from an important part of non invasive evaluation of ischemic heart disease. In the presence of coronary artery stenosis detected on angiography, whether conventional or CT, assessment of resultant ischemia forms an important parameter in management of these patients. The study is known as myocardial perfusion study. The various agents used for the study are thallium (Tl-201) and technetium based
compounds like SestaMIBI or Tetrofosmin. The basic preparation includes fasting for 4-6 hours and off beta blockers for 48 hours.
Many of us are familiar with 'Stress Thallium'. Thallium is a radioisotope and is an analogue of potassium and its uptake in myocardial cells is suggestive of viability. The isotope upon injection distributes itself according to the perfusion status of the myocardial segment i.e. hypoperfused segments receive less thallium. Patient is subsequently imaged using the gamma Camera in SPECT mode. The images are then reformatted in short axis (like taking slices of left ventricle starting from apex towards the base), horizontal long axis (taking horizontal slices from inferior wall to anterior wall) and vertical long axis (taking slices from septum to lateral wall).
The usual protocol consists of two sets of imaging stress and rest/ redistribution. The stress can be either physiological with patient exercising on treadmill/ bicycle ergometer or pharmacological with drugs like dobutamine, adenosine or dipyridamaole. Besides thallium, technetium based agents are used more frequently nowadays. It gives better image quality and convenient for patient as they need not be fasting for entire duration of stress and rest imaging. GATED SPECT (RR gating) study can also be easily done with technetium agents which gives us information about end systolic ventricular wall thickness, wall motion and ejection fraction of left ventricle like ECHO.
Indications:Indications for an Radionuclide exercise stress test are:1. Detection of obstructive coronary artery
disease(CAD) in the following:
Action Cancer HospitalA-IV Paschim Vihar, Delhi 110032Mobile No: 9811069226 E mail: [email protected]
YEAR BOOK & SOUVENIR 2014
Dr Ashwani GuptaMBBS, DRM, CBNC (USA), Fellow EBNM (Europe)Sr Consultant & Head , Department of Nuclear Medicine & PET.CT
172
(a) Patients with an intermediate pretest probability of CAD based on age, gender, and symptoms.
(b) Patients with high-risk factors for CAD (e.g.,diabetes mellitus, peripheral, or cerebral vascular disease).
2. Risk stratification of post-myocardial infarction patients before discharge (submaximal test at 4-6 days), and early (symptom-limited at 14-21 days) or late (symptom-limited at 3-6 weeks) after discharge.
3. Risk stratification of patients with chronic stable CAD into a low-risk category that can be managed medically or into a high-risk category that should be considered for coronary revascularization.
4. Risk stratification of low-risk acute coronary syndrome patients (without active ischemia and/or heart failure 6-12 hours after presentation) and of intermediate-risk acute coronary syndrome patients 1-3 days after presentation (without active ischemia and/or heart failure symptoms).
5. Risk stratification before non cardiac surgery in patients with known CAD or those with high-risk factors for CAD.
6. To evaluate the efficacy of therapeutic interventions (anti-ischemic drug therapy or coronary revascularization) and in tracking subsequent risk based on serial changes in myocardial perfusion in patients with known CAD.
Contraindications:Absolute ContraindicationsAbsolute contraindications for exercise stress testing include:
1. High-risk unstable angina. However, patients with chest pain syndromes at presentation, who are otherwise stable and pain-free, can undergo exercise stress testing.
2. Decompensated or inadequately controlled congestive heart failure.
3. Uncontrolled hypertension (blood pressure [200/110 mm Hg).
4. Uncontrolled cardiac arrhythmias (causing symptoms or hemodynamic compromise).
5. Severe symptomatic aortic stenosis.
6. Acute pulmonary embolism.
7. Acute myocarditis or pericarditis.
8. Acute aortic dissection.
9. Severe pulmonary hypertension.
10. Acute myocardial infarction (<4 days).
11. Acutely ill for any reason.
Relative ContraindicationsRelative contraindications for exercise stress testing include:
1. Known left main coronary artery stenosis.
2. Moderate aortic stenosis.
3. Hypertrophic obstructive cardiomyopathy or other forms of outflow tract obstruction.
4. Significant tachyarrhythmias or bradyar-rhythmias.
5. High-degree atrioventricular (AV) block.
6. Electrolyte abnormalities.
7. Mental or physical impairment leading to inability to exercise adequately.
8. If combined with imaging, patients with complete left bundle branch block (LBBB), permanent pacemakers, and ventricular pre-excitation (Wolff-Parkinson-White syndrome) should preferentially undergo pharmacologic vasodilator stress test (not dobutamine stress test).
(reproduced from American Society of Nuclear Cardiology Guidelines)
Interpretation:Two sets of stress and rest images are analyzed simultaneously. If there is a defect seen in any segment of left ventricular wall on stress images and it shows improvement i.e. reversibility on rest images, it is suggestive of stress induced reversible ischemia. If hypoperfusion or perfusion defect on stress images persists on resting images, it suggests infarct which could further be analyzed to partial or full thickness infarct. Since it is being used for such a long time, it has been used for the prognostication of disease. It has been seen that if myocardial perfusion scan is normal, then chances of having a hard cardiac even is less than 1%.Now we make use of FDG (Flouro-deoxy glucose) PET imaging for diagnosis of myocardial viability. If FDG uptake is seen in the segments showing infarct on SPECT images, it suggests viable myocardium. FDG PET is considered as gold standard for detection of myocardial viability.
PET imagingPET (Positron Emmission tomography) has been available in India for almost a decade now. Most of the centres in India are doing FDG PET. FDG being a glucose analogue, it gets into the glucose cycle. FDG gets intracellular with the help of glucose transporters present in the cell membranes. It gets phosphorylated but cannot get further metabolized as enzymes donot recognize FDG, so in a way, it gets trapped in the cell. Since malignant cells over express glucose transporters

173
and phosphorylase enzymes, more of it gets trapped in the malignant cells. Therefore, benign and malignant lesions can be distinguished by the amount of uptake of FDG.
FDG PET imaging has proved to be boon for the oncology patients. PET imaging is being used at all stages of their management. Starting from the diagnosis, pretreatment staging, treatment response evaluation and restaging at the completion of treatment. It is then used for the follow up / disease surveillance. During the follow up, if the tumor markers show a rising trend even within normal limits, it is an indication of PET imaging to catch the recurrence at very early stage so as to treat it effectively.
With a large experience in cancer patients, PET is being used for almost all malignancies. It has been proved to be of immense use in cases of lymphoma, lung cancer, soft tissue sarcomas, breast cancer, gynaecological malignancies etc. It contributes by changing the staging of disease at the beginning. In gross terms, PET has been found to be altering the staging in about 20% cases either by upstaging or downstaging and therefore changing the treatment modality. It has been proved to be effective in reduction of treatment cost per patient and reduction in treatment related morbidities.
The treatment guidelines for cancer have taken into account the use of PET imaging. It has been incorporated in the assessment of treatment effectiveness and decision related to change in treatment regimen in various malignancies in very early course of treatment. As early as post 2 cycles of chemotherapy treatment, PET is used for interim staging. PERCIST 1.0 guidelines are there to assess treatment response for solid tumors. Similarly Deuville criteria are there for assessment of lymphoma. These guidelines help in standardization of interpretation rather than subjective perception.
There are certain limitations of PET imaging using FDG. Certain malignancies l ike prostate or neuroendocrine cancers show low glucose utilization and there FDG PET is not useful for their evaluation. Now Gallium 68 PET imaging is being used for these malignancies. Ga-PSMA (prostate specific membrane antigen) imaging is very useful for prostate cancer patients. It is highly specific and has found to be of great use in primary staging, radiotherapy planning and suspected cases of recurrence. The advantage with Gallium PET is that it can be produced in the department itself, so imaging is possible at all working hours. Similarly, for neuroendocrine malignancies Ga DOTANOC/ DOTATATE imaging is being done. These
receptors based imaging is being further followed to treatment with the help of Lu-PSMA and Lu-DOTATOC.
Word about MythsUsage of word radioisotope brings with it the fear of radiation exposure. But fact remains that the diagnostic doses used are so miniscule that they remain absolutely safe for all age groups and have been studied over decades. We the medical fraternity should discard all preconceived ill notions regarding radiation effects with these studies and should make use of it in all possible ways for the benefit of patients.
Picture1 : Reversible defect in distal LAD territory marked with yellow arrowPicture2: Normal Myocardial perfusion study.

Clinical Application of MagneticResonance Imaging: Current Status
Dr Suchit Aggarwal, Sr. Consultant Radiologist, Platinum Imaging Centre, Dayanand Vihar, Delhi-110092
Magnetic resonance imaging has far reaching ,real , extensive and very valuable clinical applications. Magnetic resonance imaging is non-invasive and provides exquisite images with excellent contrast detail of soft tissue and anatomic structures like gray and white matter in the brain or small metastatic lesions (cancers) in the liver. It does not use ionizing radiation as in CT or radiograph. The contrast media (gadolinium) used in MRI has no absolute contraindication and very less complications. Contraindications to MRI include most cochlear implants and cardiac pacemakers, shrapnel and metallic foreign bodies in the orbits. The safety of MRI during the first trimester of pregnancy is uncertain, but it may be preferable to alternative options.
HOW MRI WORKS::To perform a study the patient is positioned within an MRI scanner which forms a strong magnetic field around the area to be imaged. In most medical applications protons (hydrogen atoms) in tissues containing water molecules are used to create a signal that is processed to form an image of the body. Exogenous contrast agents may be given intravenously, orally or intra-articularly
MRI requires a magnetic field that is both strong and uniform. The field strength of the magnet is measured in tesla – and the majority of systems operate at 1.5T. MRI at 1.5 T suffices most of the recent clinical needs.All patients are reviewed for contraindications prior to MRI scanning. Medical devices and implants are categorized as MR Safe, MR Conditional or MR Unsafe: · MR-Safe — The device or implant is completely
non-magnetic, non-electrically conductive, and non-RF reactive, eliminating all of the primary potential threats during an MRI procedure.
· MR-Conditional — A device or implant that may contain magnetic, electrically conductive or RF-reactive components that is safe for operations in proximity to the MRI, provided the conditions for safe operation are defined and observed (such as 'tested safe to 1.5 teslas' or 'safe in magnetic fields below 500 gauss in strength').
· MR-Unsafe — Objects that are significantly ferromagnetic and pose a clear and direct threat to persons and equipment within the magnet room.
The MRI environment may cause harm in patients with MR-Unsafe devices such as cochlear implants and most permanent pacemakers. Several deaths have been reported in patients with pacemakers who have undergone MRI scanning without appropriate precautions. Many implants can be safely scanned if the appropriate conditions are adhered to and these are available online (see www.MRIsafety.com). MR Conditional pacemakers are increasingly available for selected patients.
Ferromagnetic foreign bodies such as shell fragments, or metallic implants such as surgical prostheses and ferromagnetic aneurysm clips are also potential risks. Interaction of the magnetic and radio frequency fields with such objects can lead to heating or torque of the object during an MRI.
It is important to be aware of all this before entering MRI room.
The various popular applications of MRI are::NEUROIMAGING::MRI is the investigative tool of choice for neurological cancers as it is more sensitive than CT for small tumors and offers better visualization of the posterior fossa.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

175
Image 1. A case of neurocysticercosisImage 2. A case of intraventricular oligodendrglioma.
Image 2. A case of intraventricular oligodendrglioma Image 4. Sagital fat sat images in a patient
with neurogenic tumor.
The contrast provided between grey and white matter makes it the optimal choice for many conditions of the central nervous system including demyelinating diseases, dementia, cerebrovascular disease, infectious diseases and epilepsy.
MusculoskeletalApplications in the musculoskeletal system include spinal imaging, assessment of joint disease and soft tissue tumors. As we all know, it is the modality of choice for prolapsed disc detection. The latest application in musculoskeletal imaging include MR arthrohraphy which provide in depth knowledge about the articular cartilage, ligaments, tendons and joint capsule.

176
Image 5. A case of neurfibroma. Image 6. Hyperintense lesion seen on coronal fat sat images.
Biopsy suggestive of mesenchymal tumor.
Image 7. MRCP in a case of choledhocholithiasis.
Liver and gastrointestinal MRIHepatobiliary MR is used to detect and characterize lesions of the liver, pancreas and bile ducts. Focal or diffuse disorders of the liver may be evaluated using diffusion-weighted, opposed-phase imaging and dynamic contrast enhancement sequences. cholangiopancreatography (MRCP, Image 7). MR enterography provides non-invasive assessment of inflammatory bowel disease and small bowel tumors. MR-colonography can play a role in the detection of large polyps in patients at increased risk of colorectal cancer.
GENITOURINARY ::MR Urography(Image 8) provides extensive anatomical knowledge about the kidneys and the urinary tract. The ability to be performed in patients with compromised renal functions is additional benefit. MRI contrast media is also less nephrotoxic as compared to CT contrast media. MRI of prostate can detect the smallest of the prostatic cancers and target specific biopsies can be performed based on MRI. MR spectroscopy and dynamic contrast for evaluation of prostate gland is a boon to all urologists. However, MRI lacks in sensitivity to detect urolithiasis as compared to CT.
Image 8. Normal MR Urography.

177
BREAST: MRI of the breast compliments mammography and can be used as a problem solving tool where mammography is equivocal. Follow up in cases of cancer of breast using MRI is rewarding. High resolution dedicated breast coil provides excellent contrast resolution which in association with dynamic contrast study provides a very sensitive imaging tool in cases of suspected breast malignancies( ). Image 9A &9B
Image 9A & 9B MRI breast done on a dedicated breast coil in a case of carcinoma breast.
Specialized applications of MRI
Diffusion MR:
Image 10A. Diffusion tensor imaging . Image 10B Restricted diffusion in a case of posterior territory infarct

178
Diffusion MRI diffusion measures the of water molecules in biological t issues. The recent development of (( ) diffusion tensor imaging Image 10Aenables diffusion to be measured in multiple directions and the fractional anisotropy in each direction to be calculated for each voxel. Another application of diffusion MRI is (DWI, diffusion-weighted imagingImage 10B stroke). Following an ischemic , DWI is highly sensitive to the changes occurring in the lesion. The DWI enhancement appears within 5–10 minutes of the onset of (as compared to stroke symptomscomputed tomography, which often does not detect changes of acute infarct for up to 4–6 hours) and remains for up to two weeks. Coupled with imaging of cerebral perfusion, researchers can highlight regions of "perfusion/diffusion mismatch" that may indicate regions capable of salvage by reperfusion therapy.
A more sophisticated extension of diffusion imaging is diffusion tensor imaging or DTI. DTI is a non-invasive in-vivo method for mapping white matter fibre tract trajectories in the human brain and spinal cord. The demonstration of white matter tracts by DTI can provide critical information to the neurosurgeon in cases of brain tumours by displaying the relation of a tumour to an adjacent white matter tract.
Magnetic resonance angiographyMagnetic resonance (MRA) generates angiographypictures of the arteries to evaluate them for stenosis(abnormal narrowing) or (vessel wall aneurysmsdilatations, at risk of rupture). MRA is often used to evaluate the arteries of the neck and brain(Image 11,12,13), the thoracic and abdominal aorta, the renal arteries, and the legs (called a "run-off"). Magnetic resonance venography (MRV) is a similar procedure that is used to image veins.
Image 11. Normal non contrast
peripheral MR angiography of lower
limbs done using 2D inflow technique.
Image 12. Non contrast
carotid angiography.
Image 13. MR angiography of brain.
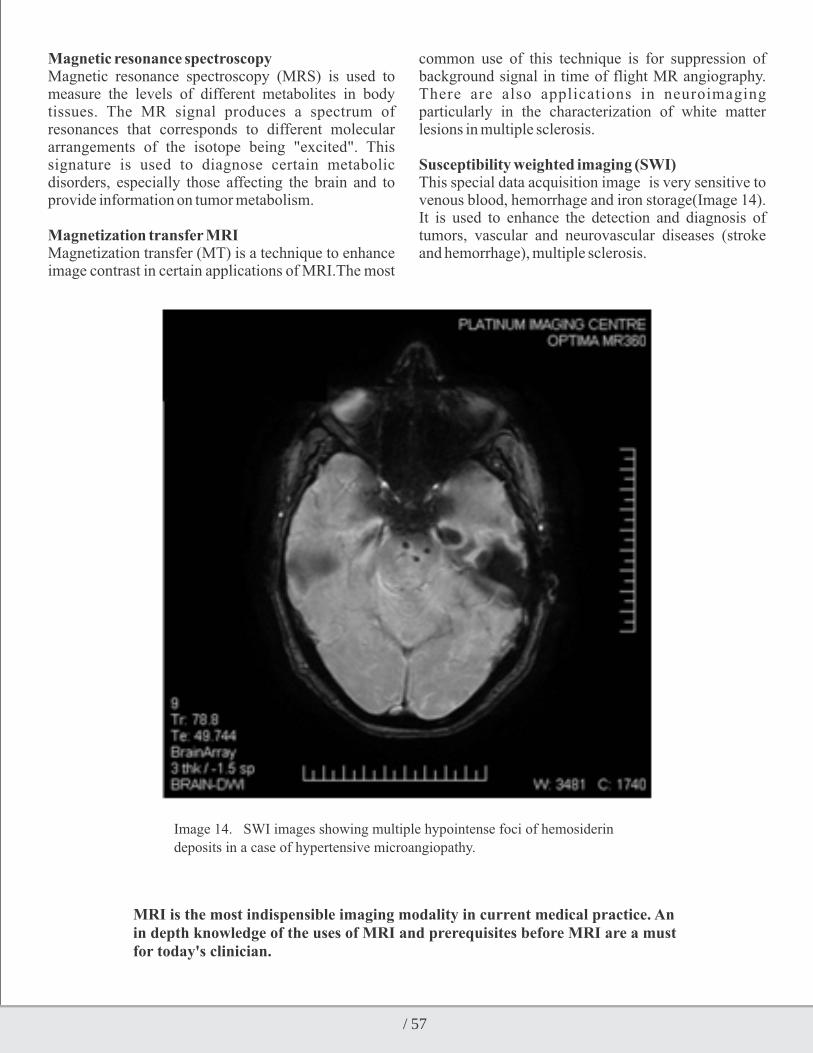
179
Magnetic resonance spectroscopy Magnetic resonance spectroscopy (MRS) is used to measure the levels of different metabolites in body tissues. The MR signal produces a spectrum of resonances that corresponds to different molecular arrangements of the isotope being "excited". This signature is used to diagnose certain metabolic disorders, especially those affecting the brain and to provide information on tumor metabolism. Magnetization transfer MRI Magnetization transfer (MT) is a technique to enhance image contrast in certain applications of MRI.The most
common use of this technique is for suppression of background signal in time of flight MR angiography. There are also applications in neuroimaging particularly in the characterization of white matter lesions in multiple sclerosis.
Susceptibility weighted imaging (SWI)This special data acquisition image is very sensitive to venous blood, hemorrhage and iron storage(Image 14). It is used to enhance the detection and diagnosis of tumors, vascular and neurovascular diseases (stroke and hemorrhage), multiple sclerosis.
Image 14. SWI images showing multiple hypointense foci of hemosiderin
deposits in a case of hypertensive microangiopathy.
MRI is the most indispensible imaging modality in current medical practice. An in depth knowledge of the uses of MRI and prerequisites before MRI are a must for today's clinician.

Nutrition in ICUDr Kamal Lashkari Associate Consultant, Critical Care Medicine Max Super Speciality Hospital, Patparganj New DelhiDr Ashutosh Garg, MD
The metabolic response to critical illness is characterized by the changes in carbohydrate, fat, and amino acid metabolism. Stressful condition of critical illness results in catabolic state, and hence increasednutritional requirement. The malnutrition can have negative impact on multiple organ system. Thisleads to poor outcome in terms of increased length of stay, ventilator dependence and mortality. Proper resuscitation and hemodynamic stability is of paramount importance before starting any typeof nutritional support. Despite being one of most discussed topics, practically it remains difficult to implement and neglected aspect in ICU.
Nutritional assessment of critically illThe goals of nutrition support in ICU patients are to provide adequate calorie and protein to keep upongoing losses, prevent and correct nutritional deficiencies, support wound healing and promoteimmune function.
Apart from Patients nutritional status at admission, nutritional history, functional capacity and Bodymass index(BMI) are also important for proper assessment. There are many other parameters like anthropometry and markers like albumin, prealbumin levels,but bedside clinical assessment & subjective global assessment by history & simple physical examination are more reliable.
Most of the calculations are based on ideal body weight; reason being actual body weight cannot bemeasured in critically ill patient.
Ideal body weightMale Ideal Body Weight = 50 kg + 2.3 kg × (Height (in) - 60)Female Ideal Body Weight = 45.5 kg + 2.3 kg × (Height (in) - 60)
· Usually 25-30 kcal/kg/day provides most patients requirement.
· In acute stage of illness lower calorie targets(20-25 kcal/kg/day).
· In recovery stage higher calorie targets(25-30 kcal/kg/day).
· 10% should beadded to energy needs for every degree of body temperature >37° C.
There are severalformulae like Harris - Benedict for calories calculations, butare impractical and time consuming. A more simple method forestimating calorie requirement in hospitalized patients has been developed using BMI.BMI Energy (kcal/kg/day)<15 35-4015-19 30-3520-25 20-2526-29 15-1729 15
· Carbohydrate should form 70-75% while fat should form 25-30 % of total energyrequirement.
· Protein intake should not be calculated as calorie source.
· Usually isocaloric feed is usedi.e. 1 ml/cal..· Micronutrient supplementation and electrolyte
correction should be done in each patient.· Indirectcalorimetery can also be reliably used for
calorie calculations
Protein requirement are based on ideal body weight and stress factor.In general 1.5 -2 g/kgIBW calculates approximate requirement of most patient.No stress 0.7-0.8 gm/kg/dayMild stress 0.8-1.0 gm/kg/day
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

181
Moderate stress 1-1.5 gm/kg/daySevere stress 1.5-2.0 gm/kg/day
Nitrogen balanceIt is difference between intake and output of nitrogen. Negative nitrogen balance is associated withpoor outcome. It should be performed in most critically ill patients at least once a week.Try to achieve at least equal nitrogen balance.· Nitrogen Intake=protein intake /6.25· Nitrogen Output=24 hr urinary urea nitrogen+4
(non urinary nitrogen).
Refeeding syndromePrecautions should be taken while prescribing a malnourished patient,as large amount of glucoseand calorie load can cause a massive shift of potassium, phosphate, and magnesium in tointracellular compartment,leading to severe fall of these electrolytes in plasma, resulting in cardiorespiratory failure. This phenomenon is called as refeeding syndrome. Phosphate,magnesium & potassium should be checked & replaced, and calories & glucose load should be gradually increased.
Route of deliveryAt present general consensus is to feed enterally whenever possible. It is natural way of feeding withleast complications especially in critically ill patients. It helps in preventing integrity of gutmucosa and hence prevents translocation of gut bacteria which may cause sepsis and multiorgandysfunction.
If use of enteral route is not feasible or if functioning of gut is uncertain, one should not reluctant tostart Total parenteral nutrition (TPN) at earliest.
Advantages of Enteral Nutrition (EN) Preserve intestinal villous integrity and function Maintains splanchnic blood flow Promotes gut motility, thus paving the way for oral feeding Reduces bacterial translocation from the gut Avoids infectious &metabolic complications associated with parenteral nutrition: Ease of administration & lesscostly
Advantages of parenteral nutrition (PN) Easy to perform at the initial phase of injury Ensures full delivery of specific nutritional needs Avoids risks of gastro esophageal reflux, aspiration pneumonia,diarrhea and GI intolerance.
Absolute Contraindications to enteral nutrition- Adequate oral intakes (more than 80% of the energy target) Non-functional gut, anastomotic disruption, lower GI obstruction,gutischaemia/necrosis Generalized peritonitis Uncontrolled severe shock states
Absolute Contraindications to parenteral nutrition- Adequate oral intake Enteral nutrition feasible and covering more than 60% of the energy target within the three days Uncontrolled severe shock states
E n t e r a l f e e d i n g m a y b e g i v e n t h r o u g h n a s o g a t r i c , n a s o j e j u n a l , g a s t r o s t o m y o r jejunostomytubes.Delivery of feeding into small bowel has been recommended as strategy to reduce risk ofaspiration; however most of studies have been inconclusive. Head of bed elevation by 30-45, continuous rather than bolus feeding and avoidance of frequent residual aspiration should be done.Initial aspiration should be done at 2 hr then 8 to 12 h r ly the rea f t e r. IV Metoc lopramide shou ld beconsidered in all patients showing intolerance(>250 ml aspiration, abdominal distention and emesis)
Types of enteral feedBlenderized kitchen feediscommonly used but nutritive value is highly unpredictive and absorptionsare also variable.it may not be balanced & complete. Synthetic polymeric dietcontains nitrogen as a whole protein and b a l a n c e d & c o m p l e t e . C a r b o h y d r a t e i s .hydrolysedstarch and fat contains long chain triglycerides.It is more balanced and digestible solution and preferred.Predigested dietare considered in presence of significantmalabsorption,which contains nitrogen as short peptides or as freeamino acids and rest of calorie as long and medium chain triglycerides and carbohydrate.
There are plenty of Disease specific formulaes are available.Like low carbohydrate content in type 2respiratoryfailure and modifiedprotein, electrolyte and volume in renal patients.Low protein intakeis not recommended in Hepatic encephalopathy patients & also no benefit of branched chain amino acid.
Immunonutrition :Glutamine should be added to standard enteral formulae in burn and trauma patients.Although nobenefit of immune modulating formulae (glutamine, arginine, omega-3 fatty acids and

182
antioxidants)has been established in patients with sepsis, in fact caution should be used while using arginine inthese patients.
Parenteral nutrition (PN)Recent guidelines suggest that when enteral feeding is not possible, parenteral nutrition shouldbe initiated within 7 days (ASPEN guideline) or within 3 days (ESPEN guideline).Among such patients who have protein-energy malnutrition at the timeof admission to the ICU, the American clinical practice guidelines suggest that parenteralnutrition should be initiated without delay.
TPN usually needs central venous catheter, as it may c a u s e p h l e b i t i s . B u t p e r i p h e r a l p a r e n t e r a l nutritionformulas can be used for purpose of partial or supplemental parenteral nutrition.TPN should begiven with dedicated lumen.Parenteral glutamine addition to TPN formulae is associated with improved outcome in burns andtrauma patients.Complications of TPN
· Sepsis
· Hyper-/hypoglycemia
· Hyperlipidemia
· Steatosis
· Macrophage dysfunction
· Electrolyte and acid base disorders
· Venous thrombosis
Summary of important recommendationsEuropean society for parenteral & enteral nutrition (ESPEN) has given Comprehensive clinical practice guidelines.
ESPEN Guidelines on Enteral Nutrition (Intensive Care 2006)
· All patients who are not expected to be on a full oraldiet within 3 days should receive enteral nutrition (C).
· Haemodynamically stable critically ill patientswho have a functioning gastrointestinal tract shouldbe fed early (<24 h) using an appropriate amount offeed.(C)
· Avoid additional parenteral nutrition in patients who tolerate EN and can be fed approximately to the target values.(A)
· There is no significant difference in the efficacy ofjejunal versus gastric feeding in critically ill patients(C)
· In burned patients trace elements (Cu, Se and Zn) should be supplemented in a higher than standarddose.(A)
· Glutamine should be added to standard enteral formula in burned patients and trauma patients(A)
· Immune-modulating formulae(formulae enriched with arginine, nucleotides and omega-3 fatty acids) are superior to standard enteral formulae: in trauma patients(A), elective upper GI surgical patients (A)& mild sepsis (APACHE II <15)(B)
· In patient with severe sepsis, immune modulating formulae may be harmful & so not recommended.
· No recommendation for immune-modulating formulae can be given for burned patients due to insufficient data.
· Formulae containing omega-3 fatty acids and antioxidants should be usedin patients with ARDS.(B)
· ICU patients with very severe illness who do not tolerate more than 700 ml enteral formulae per day should notreceive an immune-modulating formula enriched with arginine, nucleotides and omega-3 fatty acids.
ESPEN Guidelines on Parenteral Nutrition:( Intensive care2009)
· Patients should be fed because starvation or underfeeding in ICU patients is associated with increasedmorbidity and mortality (C )
· All patients who are not expected to be on normal nutrition within 3 days should receive PN within24 to 48 h if EN is contraindicated or if they cannot tolerate EN.(C)
· ICU patients receiving PN should receive a complete formulation to cover their needs fully. (C )
· During acute illness, the aim should be to provide energy as close as possible to the measured energy expenditure in order to decrease negative energy balance. (B )

183
· In the absence of indirect calorimetry, ICU patients should receive 25 kcal/kg/day increasing to target overthe next 2–3 days.(C )
· All patients receiving less than their targeted enteral feeding after 2 days should be considered for supplementary PN.©
· The minimal amount of carbohydrate required is about 2 g/kg of glucose per day. (B )
· Hyperglycemia (glucose >10 mmol/L) contributes to death in the critically ill patient and should also beavoided to prevent infectious complications.(B)
· There is a higher incidence of severe hypoglycemia in patients treated to the tighter limits.
· Lipids should be an integral part of PN for energy and to ensure essential fatty acid provision in long-term ICU patients.(B )
· Intravenous lipid emulsions (LCT, MCT or mixed emulsions) can be administered safely at a rate of 0.7 g/kg up to 1.5 g/kg over 12 to 24 h (B)
· The tolerance of mixed LCT/MCT lipid emulsions in standard use is sufficiently documented.© )
· Olive oil-based parenteral nutrition is well tolerated in critically ill patients. (B )
· Addition of EPA and DHA to lipid emulsions has demonstrable effects on cell membranes and inflammatory processes. Fish oil-enriched lipid emulsions probably decrease length of stay in critically ill patients. (B )
· When PN is indicated, a balanced amino acid mixture should be infused at approximately 1.3–1.5 g/kg ideal body weight/day in conjunction with an adequate energy supply. (B)
· When PN is indicated in ICU patients the amino acid solution should contain 0.2–0.4 g/kg/day of L-glutamine(e.g. 0.3–0.6 g/kg/day alanyl-glutamine dipeptide).(A)
· All PN prescriptions should include a daily dose of multivitamins and of trace elements.( C )
· A central venous access device is often required to administer the high osmolarity PN mixture
designed tocover the nutritional needs fully.(C )
· Peripheral venous access devices may be considered for low osmolarity (<850 mOsmol/L) mixtures designedto cover a proportion of the nutritional needs and to mitigate negative energy balance.(C )
· If peripherally administered PN does not allow full provision of the patient's needs then PN should be centrally administered (C)
· PN admixtures should be administered as a complete all-in-one bag (B)
References· ESPEN Guidelines on Enteral Nutrition:Intensive
care 2006· ESPEN Guidelines on Parenteral Nutrition:
Intensive care 2009· Pac t modu le . e s i cm,2010 ronan th ibau l t ,
claudepichard,brunoraynard,pierre singernd· Washington manual of critical care medicine 2
edition· ICU protocols,A stepwise approach,Chawla and
Todi 1 st edition

Alpha receptors Beta -1 receptors Beta -2 receptors
Vasoconstriction - rise in Increased cardiac contractility- Vasodilatation - fall in B.P.B.P. ↑ Cardiac output Bronchodilatation
Adrenergic receptors and associated response
Selection of inotropes or vasopressors:· Despite adequate fluid resuscitation,if patient is
hypotensive, vasoactive agents should be started to maintain cardiac output and blood pressure.
· 3 broad groups of vasoactive agents may be identified :
- Predominant β – agonis t ( dobutamine, dopexamine, isoprenaline)
- Predominant α – agonist (phenylephrine)
- Mixed β - & α – effects ( adrenaline & noradrenaline)
· In general when the heart is failing & peripheral
vascular resistance is normal, an agent with predominant inotropic effect (β-1 selective agents) would be good choice.
· If there is vasodilatation, a vasoconstrictor with predominant α-agonist activity is appropriate.
· Volume deficit should always be corrected as much as possible before resorting to vasopressors.
· All inotropes & vasopressors should be titrated so that tissue perfusion is restored with the lowest dose of drug & to the desired end points with minimal side effects. Titratevasopressors to MAP of 65-70 mmHg.
Vasopressors and Inotropes in ICUDr. Ashutosh Kumar GargAssoc. Consultant, Critical Care DepartmentMax Super Speciality Hospital, Patparganj, DelhiDr. Sanjay Nihalani (MD)
Pharmacological support of blood pressure & blood flow is one of the fundamental practices in care of critically ill patients. This chapter describes vasopressors & inotropes used for circulatory support in ICU.
Inotropic agents are defined as drugs that act on the heart by increasing the cardiac contractility & results in increased cardiac output and blood pressure.
Vasopressors are drugs that have a predominantly vasoconstrictive action on the peripheral vasculature, both arterial and venous. These drugs are used primarily to increase mean arterial pressure.
The distinction between these two groups of drugs is often confusing. Many of the commonly used agents such as the catecholamine have both inotropic &
variable effects on the peripheral vasculature that include vasoconstriction, arteriolar vasodilatation and constriction.
Vasoregulatory agents may modula te the responsiveness of the peripheral vasculature to vasoactive drugs in pathological states such as sepsis. These agents include vasopressin and corticosteroids. Given the overlap of pharmacodynamics effects of these drugs, the term 'vasoactive therapy' is a more appropriate description.
Catecholamines: These are drugs that promote blood flow & blood pressure by stimulating adrenergic receptors. Despite differences in adrenergic receptor activation & physiologic responses, no catecholamine drug has proven superior to the others for improving clinical outcomes.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014

185
· In patient with long standing hypertension, renal failure, recent cerebral infarct &increased intraabdominalpressure, a higher MAP is desirable.
· In trauma with active bleeding, a lower MAP till bleeding source is controlled is advisable.
Use of ionotropes& vasopressorsChoice of ionotropes& vasopressors may vary depending on clinical situation.

186
Agents used in septic shock–
· Noradrenaline centrally administered as initial vasopressors of choice.
· Useadrenaline as first alternative agent in septic shock when blood pressure is poorly responsive to noradrenaline.
· Vasopressin at dose of 0.03unit/min may be subsequently added to noradrenaline.
· Recommend not to use low dose dopamine for renal protection.
TIPS FOR MAKING INFUSION
1. Usually 2 ampules(double strength) of drug are dissolved in NS to total 50ml volume(Exception 1. Vasopressin 2 amp in total 40ml volume& 2. Dobutamine1 amp in total 50ml volume).
e.g .For Norepinephrine infusion-4mg (2amp) diluted to total 50ml volume with NS
4mg in 50ml =4000mcg/50 ml =80µg/ml
F o r 6 0 k g p a t i e n t , 0 . 0 5 µ g / k g / min=0.05×60×60=180µg/hr=2.25ml/hr
2. Rule of2ml/hr for starting vasopressor infusions usually fits andthen titrate infusion according to BP(Exception Vasopressin started at 1ml/hr and maximum infusion rate is 2ml/hr).
DOPAMINE
Dopamine is an endogenous catecholamine.
Actions-
At low infusion rates (<3 µg/kg/min), dopamine selectively activates dopamine receptors in renal & splanchnic circulations,which increases blood flow in these regions.Low dose dopamineincreases both urinary sodium excretion& urine output independent of changes in renal blood flow. The renal effects of low dose dopamine are minimal or absent in acute renal failure.
At moderate infusion rates(3-10 µg/kg/min)
Dopamine stimulates β- receptors in the heart & peripheral circulation, producing an increase in myocardial contractility & heart rate, along with peripheral vasodilatation.
At high infusion rates (>10 µg/kg/min) dopamine produces a dose dependent activation of α-receptors leading to pulmonary&systemic vasoconstriction.
Clinical uses:Dopamine can be used in management of
cardiogenic & septic shock but other measures are favoured in these conditions (Mechanical assist devices for cardiogenic shock & norepinephrine preferred for sept ic shock) . Low dose dopamine is NOT recommended as a therapy in acute renal failure.
Adverse effect:Sinus tachycardia &atrial fibrillation are reported in 25% of patients receiving dopamine infusion.Other adverse effects areincreased intraocular pressure, splanchnichypoperfusion, & delayed gastric emptying, which may lead to aspiration pneumonia.
NOREPINEPHRINE
Norepinephrine is an endogenous catecholamine that normally functions as excitatory neurotransmitter. When used as an exogenous drug, it acts as a vasopressor.
Actions – Principal action is α-mediated peripheral vasoconstriction. Norepinephrine infusions are accompanied by decrease in renal blood flow but in patients with septic shock, renal blood flow is increased. Similar with splanchnic blood flow (i.e. normally reduced but not in septic shock).
Clinical uses – Norepinephrine is the preferred catecholamine for circulatory support in patient with septic shock. This preference is not based on improved outcome but because of less adverse effect than dopamine or epinephrine.
Adverse effects – Local tissue necrosis may occur from drug extravasation& intense systemic vasoconstriction when high dose is required.
DOBUTAMINE
Dobutamine is a synthetic catecholamine that is classified as an inodilator because it has positive inotropic & vasodilator effects.
Actions –Primarily β -1 receptor agonist but also has weak β – 2 agonist activity.
Clinical Use –
· Dobutamine has been used to augment cardiac output in patients with decompensated heart failure due to systolic dysfunction
· Preferred inotropic agent for treatment of myocardial depression associated with septic shock

187
but i t usual ly must be combined with a vasoconstrictor agent to raise blood pressure.
Adverse effect –
· Dobutamine produces only mild increase in heart rate (5-15 beats/min) in most patients but sometimes it may cause significant tachycardia(>30 beats/min) which can be deleterious in patients with coronary artery disease.
EPINEPHRINE
Epinephrine is an endogenous catecholamine released by adrenal medulla in response to physiological stress.It is most potent natural β – agonist.
Actions-
Epinephrine is more potent β-1 agonist than dopamine & produces a greater increase in stroke volume & heart rate than comparable dose of dopamine.
Clinical use - Epinephrine has important role in resuscitation of cardiac arrest & it is the drug of choice for hemodynamic support in anaphylactic shock.
Adverse effects–It causes unwanted cardiac stimulation (which may be deleterious in coronary artery disease).Other adverse effects include hyperglycemia, splanchnic hypoperfusion& increase in serum lactate level.
VASOPRESSIN
Antidiuretic hormone (ADH) is an osmoregulatory hormone that is also called vasopressin because it produces vasoconstriction.
Actions – The vasoconstrictor effect are mediated by vasopressin (V1) receptors located on vascular smooth muscle.Exogenous vasopressin increases blood pressure in patient with hypotensioncaused by peripheral vasodilatation.This type of hypotension occurs in septic shock, anaphylactic shock, autonomic insufficiency & hypotension associated with spinal & general anaesthesia.
Clinical uses–
· In the resuscitation of cardiac arrest, vasopressin can be given as a single IV dose (40 units) to replace first or second dose of epinephrine.
· In cases of septic shock resistant to norepinephrine or dopamine, vasopressin infusion can be used to
raise the blood pressure & reduce catecholamine requirement (catecholamine sparing effect) unfortunately, there is no survival benefit with this practice.
· In cases of haemorrhage from esophageal or gastric varices, vasopressin infusion can be used to promote splanchnic vasoconstriction & reduce rate of bleeding.
Adverse effects – at higher infusion rates effects because of severe vasoconstriction (impaired renal & hepatic function) along with excessive water retention &hyponatremia.
References –
1. Holmes CL, Walley KR. Vasoactive drugs for vasodilatory shock in ICU. CurrOpinCrit care 2009;15:398-402.
2. Beale RJ,HollenbergSM, Vincent J-L, Parrilo JE. Vasopressor & inotropic support in septic shock . An evidence based review. Crit Care Med 2004:32(suppl):S455-S465.
3. Dobutamine hydrochloride. In McEvoy GK ed. AHFS Drug information,2012bethesda ,2012, 1314-1316.
4. Steen PA, Tinker JH, Pluth JR et al . Efficacy of dopamine, dobutamine, & epinephrine during emergence from cardiopulmonary bypass in man. Circulation 1978; 57:378-384.
5. De BackerD, Biston P, DevriendtJ,et al . Comparison of dopamine and norepinephrine in in the t r ea tment o f shock . N Engl J Med 2010;362:779-789.
6. Dopamine hydrochloride. In McEvoy GK ed. AHFS Drug information,2012 bethesda,2012: 1314-1316.
7. Epinephrine. In McEvoy GK ed. AHFS Drug information,2012 bethesda,2012: 1362-1368.
8. Levy B. Bench to bedside review: Is there a place for epinephrine in septic shock? Crit care 2005;9:561-565.
9. Norepinephrine bitartrate. In McEvoy GK ed. AHFS Drug information,2012 bethesda,2012: 1371-1374.
10. Phenylephrine hydrochloride. In McEvoy GK ed. AHFS Drug information,2012 bethesda,2012: 1306-1311.

Co-authors:-Dr. R S Tonk- Professor, Deptt of MedicineDr. A K Varshney- Professor, Deptt of MedicineDr. Madhubala Negi- Assistant Professor, Deptt of MedicineDr. Gurmeet Kaur- Assistant Professor, Deptt of MedicineDr. Prabhat Kumar- Senior Resident, Deptt of MedicineDr. Dinesh Meher- Second year Post Graduate, Deptt of Medicine
Dr. Nitin SinhaAssistant Professor (Medicine)Post Graduate Institute of Medical Education and Research (PGIMER) & Dr. R.M.L. Hospital, New Delhi-110001
INTRODUCTIONGenitourinary tuberculosis is the second most common site of extrapulmonary tuberculosis. Irritative bowel symptoms are the most common manifestation. Systemic symptoms are less frequently seen. Daignosis is done by demonstrating bacteria in the urine directly or by Polymerase Chain Reaction (PCR) method. Intravenous pyelography (IVP) and Voiding Cystourethrogram (VCU) are also helpful in diagnosing morbidity caused by this infection. Only one investigation is sometimes not suffice and diagnosis is made after assessing all the relevant investigations. Treatment is ATT and if given early can prevent significant morbidity. Steroids are also helpful in certain situations. Surgery becomes an important part of management in certain situations.
CASE SUMMARYMr. H, an engineer belonging to upper middle class, unmarried and resident of Indore, Madhya Pradesh, presented with complaints of pain in both the flanks intermittently for last 6 months and dysuria and increased frequency of micturation for last 3 months. Pain in flank was like that of a renal colic and used to get relieved on analgesics. There was no history of urethral discharge, perineal pain, suprapubic pain, hematuria, vomittings or fever. There was no history of any abdominal swelling palpable during last 6 months. There was no history of anorexia or weight loss. He had no significant past or family history of any chronic medical illness. He had no addictions and there was no history of any sexual promiscuity. He got evaluated at Indore for the first time around four
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
A case of common but rarelythought of Urinary Infection
Abstract:Mr. H a 28 year old engineer of upper middle class from Indore, Madhya Pradesh presented with complaints of pain in flanks intermittently over last six months and dysuria with increased urinary frequency for last three months. He was evaluated in Indore where he was diagnosed as having bilateral renal calculi with left hydronephrosis and left hydroureter. He then presented to our hospital for further management. His investigations in our hospital and previous reports showed sterile pyuria. Urinary tract tuberculosis was suspected and Urine Ziehl-Nelson (ZN) staining showed acid- fast bacilli suggestive of Mycobacterium tuberculosis infection. He has been started on anti tubercular therapy (ATT) with steroids and might require surgical intervention for left hydronephrosis and hydroureter if there is no response. Genitourinary tuberculosis needs to be thought of if there is persistent sterile pyuria. However, in common practice it is seen that patients are mostly managed as recurrent urinary tract infection with different antibiotics being given from time to time. Also, there is lack of knowledge regarding suspicion and diagnosing genitourinary tuberculosis. ATT is the mainstay of management but here surgical management also is required in most cases.

189
months prior to presentation to our hospital. His urine examination showed acidic urine with 15-20 pus cells with no RBC's or casts and no albuminuria. Ultrasound (USG) abdomen showed bilateral renal calculi (around 4mm calculus in upper calyx of right kidney and around 3-4 mm calculus in middle calyx of left kidney) with rest of sonography being normal. He was given a course of antibiotics alongwith some syrup but his symptoms did not improve. He then developed increased frequency of micturation and dysuria. After this, for the next two months, he consulted three more private practitioners who always got his urine examination done which showed similar findings a s t h e f i r s t r e p o r t . However, urine cultures were always sterile. He r e c e i v e d c o u r s e o f different antibiotics in these two months but his s y m p t o m s d i d n o t s u b s i d e . H e t h e n consulted a urologist who a d v i s e d h i m t o g e t Commuted Tomography (CT) of kidney-ureter-bladder (KUB) done. CT was done one month prior to presentation to our hospital which revealed bilateral renal calculi almost of the same size as s e e n i n t h e f i r s t ultrasound but there was left hydronephrisis and left hydroureter till lower third and a stone in the lower third of the ureter (Image 1 and 2). Subsequently, Intravenous Pyelography (IVP) was advised which was done a fortnight prior to presentation to our hospital and it showed normal functioning of both kidneys with left hydronephrosis with left hydroureter till the lower third of ureter with no evidence of filling defect in the left ureter. An ultrasound examination was done which showed findings similar to IVP with no calculus in left ureter. The patient, meanwhile, decided to come to our hospital for further management. His general physical and systemic examinations were normal. His
st investigations showed ESR-44 mm in 1 hour with rest
of haematological and biochemical examinations being normal. Urine routine examination showed an acidic urine with 40-50 pus cells with 10-15 RBC's with albumin(+) with no casts or crystals. Three urine samples showed Acid fast Bacilli (AFB) on ZN staining suggestive of Mycobacterium tuberculosis infection. Urine PCR for Mycobacterium tuberculosis also came positive. Urine AFB Culture report on Lowenstein-Jensen medium is awaited. Voiding cystourethrogram (VCU) showed no vesico-ureteric
reflux with a normal capacity bladder with any bladder ulcerations. Montaux was negative. HIV was non-reactive. There was no evidence of active tuberculosis at any other site on investigations. He has been started on ATT (Isoniazid, Rifampicin, Pyrazinamide and Ethambutol according to weight) along with steroids (40mg/day of Prednisolone). Plan is to taper steroid over next two months and repeat an IVP to look for resolution of hydroureter and hydronephrosis. However, if there would be persistence or increase in hydronephrosis and hydroureter, he will be taken up for surgical intervention.
Image 1: CT showing left hydronephrosis

190
DISCUSSIONGenitourinary tuberculosis is the second most common form of extrapulmonary tuberculosis after tubercular lymphadenopathy. Mycobacterium tuberculosis is the most common causative organism but Mycobacterium bovis can also involve the genitourinary tract. Spread to the genitourinary tract is through hematogenous route from an active site of infection. Usually, the infection becomes latent and flares up later. This is precisely why genitourinary tuberculosis commonly occurs after 20 years of age and is less commonly seen in the paediatric age group. Rarely, genitourinary tuberculosis is seen along with an active tubercular lesion elsewhere in the body. It has been seen that genitourinary tuberculosis complicates 3-4% cases of pulmonary tuberculosis. Entire genitourinary tract can be involved with kidney being involved most commonly. Further discussion will focus on genitourinary tract tuberculosis in males. Female genital tuberculosis is not covered here.
Cavitation, renal abscess, perirenal abscess, pseudocalculi, calyceal strictures, diffuse miliary
involvement can all be seen when kidneys are involved. Extensive involvement can lead to “Autonephrectomy”. Ureterovesical junction is the most common site of involvement in ureter with middle third being the second common. Strictures form at the site of involvement leading to back pressure changes. Bladder involvement occurs primarily at the ureterovesical orifice and later extensive involvement can lead to a low capacity bladder called “Thimble Bladder”. Epididymis and vas deferens can be involved leading to stricture formation. Prostate involvement can be in the form of cavitation and necrosis. “Autoprostatectomy” has also been reported. Uretheral involvement can lead to stricture. Penile involvement can be in the form of
1non-healing ulcer.
Irritative bowel symptoms are the most common. Microscopic hematuria is seen in 50% with overt hematuria being seen only in 5% cases. Recurrent bacterial infections can occur due to strictures leading to urinary tract obstruction. Hemospermia can be a manifestation. Infertility should always prompt doctor
Image 2 :- CT showing left hydroureter with left hydronephrosis

191
to look for tuberculosis. Scrotal swelling, perineal pain, perineal fistula, penile ulcer can all occur due to genitalia involvement. Flank pain can occur due to kidney swelling or perinephric abscess. Fistula to the adjacent organs (eg:- renocolic fistula) can also occur. Systemic symptoms are rare. Symptoms of
1,2tuberculosis elsewhere in the body can also be there.
Diagnosis can be made by examining atleast three, preferably five, early morning urine samples. 200-300 mL of early morning urine should be sent for ZN Staining. Yield is around 20-30%. Urine should also be sent for culture either on Lowenstein-Jensen Medium or BACTEC along with a culture on pyruvate egg medium containing penicillin for Mycobacterium bovis. Yield from culture is around 60%. PCR of urine for Mycobacteria can be employed for diagnosis. IS6110 sequence is species specific and carries 95% sensitivity and 98% specificity. 16s RNA is genus specific and carries 87% sensitivity and 99% specificity. Blood investigations may reveal elevated ESR. Kidney Function Tests may be deranged if there is concomitant renal failure. Montaux is positive in around 90% of cases. Semen analysis can show reduced sperm count, increased leucocytes and RBC's. Semen can also be sent for culture and PCR tests but yield is low. Active tuberculosis elsewhere in the body should be ruled out by appropriate investigations. IVP and nowadays, contrast CT of the KUB can demonstrate not only kidney functions but also structural changes in the genitourinary tract. VCU is helpful for delineating bladder pathology and also to look for vesicoureteric reflux. Ultrasound can demonstrate structural changes and can also be helpful in obtaining FNAC from a mass. Cystoscopy can also be used to assess bladder pathology and can also be used to take biopsies and collect urine from different
1,2ureters.
Treatment is ATT according to weight and Category as per the DOTS. Steroids are given if there is stenosis/stricture or there is extensive bladder
1involvement so as to prevent fibrosis.
Surgery is also a modality of treatment. Non functioning kidney can be removed. Nephro-colic or nephrocutaneous fistula needs removal. Perinephric abscess can be drained. Lower and middle ureteric strictures can be dealt with ureteric dilatations, stents and ureteroneocystotomy. Upper ureter strictures can be dealt with dilatations and percutaneous
nephrostomy. Urinary bladder augmentation surgery is done if bladder capacity is <100 mL and a new urinary bladder is created if there is Thimble Bladder (Bladder capacity <30 mL). Uretheral strictures require dilatation and sometimes urethroplasty. Orchidectomy, epididymectomy and penectomy
1(partial) may be required in appropriate cases.
Our patient had sterile pyuria and if early suspicion had been kept probably ureteric stricture could have been prevented.So, a high index of suspicion for genitourinary tuberculosis should be kept and investigations should be done promptly and in adequate manner. REFERENCES1. Hemal AK. Genitourinary Tuberculosis. In:
ndSharma SK, Mohan A, editors. Tuberculosis. 2 ed. New Delhi. Jaypee Brothers Medical Publishers (P) Ltd; 2009.
2. Lessnau KD. Tuberculosis of the Genitourinary System Overview of GUTB [Internet] [Updated 2013 Jul 7; cited 2014 Nov 21]. Available from: http://emedicine.medscape.com/article/450651-overview#aw2aab6b2

Dr. Nitin Sinha, Assistant Professor (Medicine),Post Graduate Institute of Medical Education and Research(PGIMER),Dr. R.M.L. Hospital, New Delhi-110001
Key words: Pulmonary tuberculosis, Deep vein thrombosis, Rifampicin and Warfarin Interaction INTRODUCTIONTuberculosis is associated with hypercoagulable state. This has been proved in different studies. There are certain case reports which have shown development of deep vein thrombosis in patients of pulmonary tuberculosis. We report here two cases of pulmonary tuberculosis that developed deep vein thrombosis with no other risk factors. We also highlight the implications of using rifampicin and warfarin concomitantly.
CASE SUMMARYCASE 1: A 30 year housewife presented with complaints of productive cough and sputum for seven months. She was diagnosed as a case of pulmonary tuberculosis six months back and was on category I {according to Directly Observed Treatment Short Course (DOTS) guidelines, India} anti tubercular therapy (ATT) [Isoniazid and Rifampicin in weight adjusted doses] and there was adequate compliance. She had developed swelling of the entire left lower limb for the last 3 days. Swelling was not associated with any redness or swelling any where else in the body. There w a s n o f a m i l y h i s t o r y o f t u b e r c u l o s i s o r hypercoagulable state and there was no history of any significant major illness in the past. There was no history of any recent surgery, immobilization, oral contraceptive use or any history of DVT in the past. She was not pregnant at the time of presentation. Her examination revealed inspiratory crackles in the right
infraclavicular area and left mammary, axillary and infraaxillary areas. There was hepatomegaly one centimeter below the right costal margin. There was pitting edema over left lower limb. Rest of the examination was essentially normal. Her investigations revealed hemoglobin of 10.5 gm/dL with TLC of
3 314,000/ mm . Platlet count was 2.6 lacs/ mm . ESR was
st40 mm in 1 hour. Rest of the hematological profile was essentially normal. The metabolic profile was essentially normal. The oxygen saturation in blood gas analysis was 95%. Prothrombin time at presentation was normal with an INR of 1.1. Montaux test revealed induration of 14 millimeters at 72 hrs. Acid fast bacilli (AFB) were present in all the three sputum samples examined. Chest X-ray P.A. view revealed fibroinfiltrative opacities in the right upper zone and non homogenous opacities along with fibroinfiltrative opacities in the left middle and lower zones. A thin walled irregular cavity was also seen in the left upper zone. CECT chest revealed bronchiectatic changes in left lower lung. There was a large air filled irregular cavity, occupying the upper two thirds of the left lung. Similar destructive changes involving the apical and anterior segment of the right upper lobe were seen. Mediastinal lymphadenopathy was also noted. Ultrasonography of the abdomen was essentially normal. Doppler left lower limb venous system revealed thrombus in the left common iliac, external iliac, femoral and popliteal veins. She was started on category II ATT (Isoniazid, rifampicin, pyrazinamide, ethambutol and streptomycin in weight adjusted doses) considering her to be a treatment failure along with low
1-B-183, Surya Nagar, Ghaziabad, U.P. E-mail: [email protected]
Timings: Only Appointment
YEAR BOOK & SOUVENIR 2014
Deep Vein Thrombosis in Patients ofPulmonary Tuberculosis & Therapeutic Implications
AbstractTwo cases of lower limb proximal deep vein thrombosis (DVT) in young patients without any risk factors are reported here. Patients also had concomitant pulmonary tuberculosis. The cause-effect relationship between pulmonary tuberculosis and DVT is discussed in these cases. This is a rare association with significant therapeutic implications.

193
molecular weight heparin and warfarin. LMWH was continued till therapeutic INR was reached. She achieved an INR of 1.7 on 10 milligram warfain once a day. She has not followed after discharge.
CASE 2: 14 year old young unmarried girl a student of class VIII presented with complaints of productive cough with sputum for 1 month and swelling in left lower limb for last 3 days. There was no swelling elsewhere in the body. She had fever for last 1 month which was 99-100˚F with an evening rise. She also had anorexia. There was no history of any recent surgery, immobilization or history of use of oral contraceptives. There was no family history of tuberculosis or hypercoagulable state and there was no history of DVT in the patient in past. Her examination revealed crackles in the right infraclavicular and axillary areas and in left infraclavicular, axillary, infraaxillary and left interscapular areas. There was pitting edema over left lower limb with a positive Homan's sign. Rest of the examination was essentially within normal limits. Her investigations revealed hemoglobin of 8.5 gm/dL, TLC
3 3of 12,400/ mm and platelet count of 3.3 lacs/ mm . ESR was 39 mm in 1st hour. Rest of the hematological and metabolic parameters was within normal limits. Prothrombin time at presentation was within normal limits with INR of 1.2. Montaux test revealed induration of 13 mm at 72 hrs. Sputum examination revealed AFB in all the three sputum samples. Chest X-ray P.A. view revealed fibroinfiltrative opacities with areas of breakdown in bilateral lung fields with relative sparing of left lower zone. Ultrasonogram of the abdomen was normal. Doppler left lower limb venous system revealed thrombus in left common iliac, external iliac, superficial femoral and popliteal veins. Doppler right lower limb venous system was normal. Patient was started on intensive phase of category I ATT (Isoniazid, rifampicin, pyrazinamide and ethambutol in weight adjusted doses for 2 months), low molecular weight heparin and warfarin. LMWH was continued with warfarin till therapeutic INR was achieved. Patient required twelve milligram warfarin once a day to maintain an INR between 1.5- 2.5. Patient is on regular followup for last three months and is maintaining INR between 1.5-2.5 and is currently on maintainence ATT (Isoniazid and Rifampicin).
Both the patients belonged to low socio-economic strata. Protein C, protein S, antithrombin III levels were within normal range. Anti-phospholipid antibody was negative. Serum fibrinogen levels were within normal limits in both the patients.
DISCUSSIONPulmonary tuberculosis (PTB) is one of the most common infections seen in India. Pulmonary tuberculosis is caused by Mycobacterium tuberculosis. This disease can lead to significant morbidity and
1mortality. Severe pulmonary tuberculosis can be associated with hypercoagulable state. Decreased anti thrombin III, decreased protein C and elevated plasma fibrinogen levels, thrombocytosis and increased platelet aggregation appear to induce a hypercoagulable state seen in pulmonary tuberculosis and improve with
2treatment. In another study, similar findings were observed but it was seen that fibrinogen levels increased during first two weeks of therapy but along with other
3parameters normalized in twelve weeks. In a study which was done to look for incidence of venous thromboembolism (VTE) in patients of tuberculosis who had been treated showed that the overall incidence of VTE in these patients was 0.6% and all the cases occurred among new pulmonary tubeculosis patients
4with rifampicin being part of initial treatment. Also, in patients with pulmonary tuberculosis antiphospholipid
5antibodies are found in higher frequency. There have been few reported associations between PTB and
6,7disseminated intravascular coagulation. Studies have shown subtle changes in blood rheologic properties and in the haemostatic system in patients with PTB. A study by Kaminiskia et al showed erythrocyte edema, their more rapid depletion, lower resistance, and higher aggregation which is accompanied by increased
8haematocrit and normal erythrocyte count. Studies have demonstrated association between deep venous
9thrombosis and use of rifampicin. However, this does not contraindicate the use of this drug.
Case reports of occurrence of deep vein thrombosis in patients of pulmonary tuberculosis are there but, are
5,10very few. Cases of deep vein thrombosis in patients of 11
abdominal tuberculosis have also been reported. Cases of inferior vena cava obstruction in patient of pulmonary tuberculosis and case of aseptic cerebral venous thrombosis in patient of abdominal tuberculosis
12,13have also been reported.
Both of our cases had pulmonary tuberculosis along with proximal DVT. In the event of absence of any known risk factors and in the light of case reports of pulmonary tuberculosis patients developing deep vein thrombosis, we believe that our patients developed deep vein thrombosis as a complication of pulmonary tuberculosis. Although, we do agree that none of the hematological abnormalities noted in previous case reports and studies were noted in our patients. Probably,

194
some other factors could be playing some role and it is difficult to comment upon them right now. A longitudinal study of active tuberculosis patients (of any site) studying the various coagulation parameters before during and after treatment is required.
So, in patients of pulmonary tuberculosis, deep vein thrombosis can be one of the complication and high index of suspicion should be kept in symptomatic patients.
Rifampicin is one of the mainstays of treatment in patients of tuberculosis. Rifampicin induces metabolism of warfarin and hence, higher doses of warfarin are required in patients receiving concomitant
14,15,16rifampicin and warfarin. Discontinuation of rifampicin can result in over anticoagulation. Adequate monitoring is required at this time and warfarin should
17be tapered over 4-5 weeks. Extensive changes in warfarin dosage are required to attain and maintain a therapeutic INR during the initiation, maintenance, and discontinuation of rifampin.
REFERENCES
1. Sharma RR, Acharya KV, Poornima V:A rare complication of pulmonary tuberculosis. JIACM 2007; 8(2):179-181.
2. Turken O, Kunter E, Sezer M, Solmazgul E, Cerrahoglu K, Bozkanat E, Ozturk A, Ilvan A: Hemostatic changes in active pulmonary tuberculosis. Int J Tuberc Lung Dis 2002 Oct; 6(10): 927-32.
3. Robson SC, White NW, Aronson I, Woollgar R, Goodman H, Jacobs P. Acute-phase response and the hypercoagulable state in pulmonary tuberculosis. Br J Haematol 1996 Jun; 93(4): 943-49.
4. Ambrosetti M, Ferrarese M, Codecasa LR, et al: Frequency of venous thromboembolism among patients with tuberculosis during short course c h e m o t h e r a p y . S o u r c e : meeting.chestjournal.org/cgi/content/abstract/128/4/404S-b. Accessed May 12, 2008.
5. Suárez Ortega S, Artiles Vizcaíno J, Balda Aguirre I, Melado Sánchez P, Arkuch Saade ME, Ayala Galán E et al: Tuberculosis as risk factor for venous thrombosis. Ann Med Interna 1993 Aug; 10(8): 398-400.
6. Wa n g J Y, H s u e h P R , L e e L N , e t a l : M y c o b a c t e r i u m t u b e r c u l o s i s i n d u c i n g disseminated intravascular coagulation. Thromb Haemost 2005; 93: 729-34.
7. Ip M, Cheng KP, Cheung WC: Disseminated intravascular coagulopathy associated with rifampicin. Tubercle 1991; 72: 291-93.
8. Kaminskaia GO, Serebrianaia BA, Martynova EV, Mishin VI: Intravascular coagulation as a typical concomitant of acute pulmonary tuberculosis. Probl Tuberk 1997; 3: 42-46.
9. White NW: Venous thrombosis and rifampicin. Lancet 1989; 2: 1397.
10. Naithani R, Agrawal N, Choudhary VP: Deep venous thrombosis associated with tuberculosis. Blood Coagulation & Fibrinolysis 2007 Jun;18(4): 377-80.
11. Gogna A, Pradhan GR, Sinha RS, Gupta B: Tuberculosis presenting as deep vein thrombosis. Postgrad Med J 1999; 75: 104-05.
12. Raj M, Agarwal A: Inferior vena cava thrombosis complicating tuberculosis. N Z Med J 2006 Oct; 119(1244): 2279.
13. Kakkar N, Banerjee AK, Vasishta RK, et al. Aseptic cerebral venous thrombosis associated with abdominal tuberculosis. Neurol India 2003; 51: 128–29.
14. Heimark LD, Gibaldi M, Trager WF, O'Reilly RA, Goulart DA. The mechanism of the warfarin-rifampin drug interaction in humans. Clin Pharmacol Ther 1987; 42: 388-94.
15. O'Reilly RA. Interaction of Chronic Daily Warfarin Therapy and Rifampin. Ann Internal Medicine 1975; 83: 506-08.
16. Casner PR. Inability to attain oral anticoagulation: Warfarin-Rifampin interaction revisited. Southern Medical Journal 1996; 89(12): 1200-03.
17. L e e C R , Tr a s h e r K A . D i f f i c u l t i e s i n Anticoagulation Management during co-administration of Warfarin and Rifampin. Pharmacotherapy 2001; 21(10): 1240-46.

Interesting Case of Thrombocytopenia Encountered
during Antitubercular Therapy
Treatment of tuberculosis can be quite challenging as it requires use of multiple drugs and for a long duration. Problems often encountered are the side effects of the drugs, non compliance and resistance. Thrombo-cytopenia is a complication which has been reported with regard to all the primary antitubercular drugs. Though ATT induced thrombocytopenia is an uncommonly reported adverse effect, it is potentially fatal1.
Here we present a case of a young male presenting with thrombocytopenia following.
Mr. X, 28 years old ,male, resident of Indirapuram, Ghaziabad presented to Pushpanjali Crosslay Hospital with complaints of rashes all over body since one week. The rash was first seen on lower limbs, then spread to the trunk. Patient also complained of black colored stools for last two days. There was no history of fever, epistaxis, bleeding gums, hematemesis, hematuria, headache. No previous history of prolonged bleeding from wounds.
Two weeks prior to this presentation patient had complained of a swelling in his right supraclavicular region. The swelling was not associated with pain, fever, sore throat, there had been no change in the size of the swelling in that period. FNAC performed from outside was inconclusive, CT chest showed mediastinal lyphadenopathy. Patient was advised a core biopsy which revealed a necrot izing granulomatous lymphadenitis suggestive of tuberculosis. Patient was initiated on anti tubercular
sttherapy on 1 july 2014 with tablets Rcinex (600/300), Ethambutol (1200mg), Pyrazinamide (1500).
Complete blood count and liver function tests performed at initiation of ATT and were found to be within normal range. Platelet count- 1,70,000 . On examination, patient was conscious, oriented to time, place, person, PR: 84/ min, normal volume, regular rhythm, BP: 110/80 right arm supine position, afebrile, no pallor, icterus , clubbing, cyanosis, lymphadenopathy, edema. Petechial spots were detected all over the body. No abnormality was detected on systemic examination.
Differential diagnosis under consideration were drug induced thrombocytopenia, infection Induced or immune thrombocytopenia.
Investigations revealed the following results- Hb: 15, TLC: 4.7, platelets: 5000, SGOT: 52.1, Uric acid:15, folate: 20, Vit. B12: 630. Ps for MP: negative, dengue NS1: negative, PT/ INR: 11.8/ 0.97, APTT: 2 5 , U l t r a s o u n d a b d o m e n r e v e a l e d m i l d splenomegaly, normal liver, no other abnormality.
During the course of hospitalization, anti tubercular treatment was stopped. Patient was transfused one unit of single donor platelets. Following transfusion platelets were monitored twice daily initially. A steady rise was observed (50- 55- 100- 77- 121- 160). Bone marrow aspiration and biopsy were done which revealed a hypocellular bone marrow. Patient was started on T. levoflox, Inj. Streptomycin for two weeks. Patient was restarted on Tablet Isoniazid and Pyrazinamide, Ethambutol while monitoring platelets closely, Inj. Streptomycin was discontinued. On follow up patient does not report recurrence of rashes, fall in platelet count.
[email protected]@gmail.comMobile:9350290527
YEAR BOOK & SOUVENIR 2014
Ashok Kumar Grover, Consultant PhysicianPankaj N Choudhary, Consultant PhysicianArushi Nautiyal, DNB StudentDepartment of Medicine, Pushpanjali Crosslay Hospital, Vaishali, Ghaziabad
196
Discussion: As the patient did not have fever, no other cell line apart from platelets were affected, no organomegaly and an increase in counts following withdrawal of ongoing drugs, thus the provisional diagnosis of drug induced thrombocytopenia was made. Drug induced thrombocytopenia is a frequently encountered complication in medical practice. Detection of the offending drug can be a challenge when the patient is on multiple concurrent drugs. Timely detection however is important to prevent the complications that can result from severe thrombocytopenia if the drug is not stopped. It is usually a result of either bone marrow suppression or immune mediated, wherein antibodies develop which bind to glycoproteins on platelets and cause their destruction , but do so only in the presence of the offending drugs. These antibodies can be detected by using radiolabeled IgG, ELISA or flow cytometry.
Standard criteria to establish association between drug and thrombocytopenia :1. Drug administration preceded thrombocytopenia; recovery from thrombocytopenia completed and sustained after drug discontinued 2 . O t h e r d r u g s a d m i n i s t e r e d p r i o r t o thrombocytopenia were continued or reintroduced after discontinuation of the suspected drug 3. Other etiologies of thrombocytopenia excluded 4. Reexposure to the drug resulted in recurrent thrombocytopenia
On the basis of these criteria, studies can be stratified into the following levels of evidence:1. Definite: all 4 criteria met. 2. Probable: criteria 1-3 met. 3.
2Possible: criterion 1 met
In our case the drug Rifampicin was administered prior to the thrombocytopenia, its discontinuation was accompanied by a sustained recovery of platelet counts, other drugs also being taken by the patient were reintroduced without any effect on counts, other etiologies of thrombocytopenia were also excluded, t h u s a d i a g n o s i s o f R i f a m p i c i n i n d u c e d thrombocytopenia was made.
Thrombocytopenia has been reported with almost all the primary antitubercular drugs, but the most common o ff end ing agen t i s R i f amp ic in . Thrombocytopenia associated with rifampicin is usually occurs with intermittent regimen, though has
3been reported with daily administration as well .
During reinitiation of Antitubercular treatment, three drugs not used in the previous regimen should be started comprising of two oral and one parenteral drug (polypeptide or aminoglycoside). The offending drug should be avoided for future use as even small
4amounts may lead to immune reactions . Conclusion: ATT induced thrombocytopenia can become a diagnostic and therapeutic conundrum. This potentially fatal complication requires immediate withdrawal of all ongoing drugs and careful reintroduction and follow up.
REFERENCES1. Verma AK, Singh A, Chanra A, Kumar S, Gupta
RK . Rifampicin induced thrombocytopenia. Indian J Pharmacol. Aug 2010; 42(4): 240–42
2. George JN, Raskob GE, Shah SR, Rizvi MA, Hamilton SA, Osborne S, et al. Drug induced thrombocytopenia a systematic review of published case reports. Ann Intern Med 1998;129:886-90
3. George JN, Raskob GE, Shah SR, Rizvi MA, Hamilton SA, Osborne S, et al. Drug induced thrombocytopenia a systematic review of published case reports. Ann Intern Med 1998;129:886-90.
4. Kant S, Verma SK, Gupta V, Anand SC, Prasad R. Pyrazinamide induced thrombocytopenia. Indian J Pharmacol. Apr 2010; 42(2): 108–109

OFFICE BEARERS OF EDPA
YEAR PRESIDENT SECRETARY TREASURER
1995-1997 Dr. Saroj Prakash Dr. Parkash Gera Dr. Lalit
1997-1999 Dr. G.D. Gupta Dr. Neeraj Jain Dr. Ashok Grover
1999-2001 Dr. Parkash Gera Dr. Vijay Arora Dr. Ashok Grover
2001-2003 Dr. A.S. Dave Dr. Rajiv Lochan Dr. B.K. Gupta
2003-2005 Dr. Neeraj Jain Dr. Lalit Dr. Navin Atal
2005-2007 Dr. Ashok Grover Dr. R.K. Gupta Dr. Paras Gangwal
2007-2009 Dr. Rajiv Lochan Dr. N.K. Govil Dr. Paras Gangwal
2010-2011 Dr. B.K. Gupta Dr. Pankaj Choudhary Dr. Ajay Kr. Gupta
2011-2013 Dr. N.K. Govil Dr. Vikas Jain Dr. Ajay Kr. Gupta
2013-2015 Dr. Lalit Dr. Ajay Kr. Gupta Dr. B.K. Tiwari
197

The Office Bearers &
The Organising Committee of
EDPACON 2014Thanks
to all our Affiliates for their
Academic
&
Publication Grants
198

Academic Grants1. ERIS LIFE SCIENCES
2. ASTRA ZENECA DIABETES
3. ELI LILLY
4. ZYDUS GROUP
5. EMCURE PHARMA
6. INTAS CARDIODIABETES
7. LUPIN PHARMA
8. UNISEARCH
9. SUN PHARMA
10. USV
11. GLENMARK DIBETES
12. ZYDUS CADILLA
13. TORRENT PHARMA
14. ARISTO PHARMA
15. BIOCON DIABETES
16. DR REDDY
17. CIPLA
199

Publication Grants1. Lilly & BI (Humalog & Trajenta)
2. Dios Life Sciences
3. Jain Hospital (Jain Neuro Centre)
3. Goel Medicos
4. Alkem (Euclide-M; TSart)
5. Max Neuro Sciences
6. Glenmark Respiratory
7. Pharmed
8. USV (Roseday, Tazloc & Glycomet GP)
9. Ranbaxy (Cepodem XP)
10. Quest Diagnostic
11. Platinum Imaging Centre
12. Ronyd Pharma
13. Lupin (Rablet)
14. HOD (House of Diagnostics)
15. CDC (Clinical Diagnostic Centre)
16. Brygon (Tauroven)
17. Vestal Health Care
18. Intas Pharma
19. Reddy's Lab (Glimy & Metsmall)
20. Eris Pharma
21. LG Life Sciences
22. Shrea Neutraceuticals
200

Revaccination with PPSV23· One-time revaccination 5 years after the first dose of
PPSV23 is recommended for persons aged 19 through 64 years with
1. chronic renal failure or nephrotic syndrome, 2. functional or anatomic asplenia (e.g., sickle cell
disease or splenectomy), or 3. immunocompromising conditions.· Persons who received 1 or 2 doses of PPSV23 before age 65
years for any indication should receive another dose of the vaccine at age 65 years or later if at least 5 years have passed since their previous dose.
· No further doses of PPSV23 are needed for persons vaccinated with PPSV23 at or after age 65 years.
REVACCINATE ALL AFTER 65 &ONLY ONCE IN 65+ KEEP 5 YEARS GAP FROM PREVIOUS PPSV23
HEPATITIS A VACCINATIONITS ALMOST A UNIVERSAL RECOMMENDATION· Vaccinate any person seeking protection from hepatitis A
virus (HAV) infection and · VACCINATE persons with any of the following
indications: – MSM (men who have sex with men) and persons who use
injection or noninjection illicit drugs; – persons working with HAV-infected primates or with
HAV in a research laboratory setting; – persons with chronic liver disease and persons who
receive clotting factor concentrates; – persons traveling to or working in countries that have high
or intermediate endemicity of hepatitis A; and – unvaccinated persons who anticipate close personal
contact (e.g., household or regular babysitting) with an international adoptee during the first 60 days after arrival in the United States from a country with high or intermediate endemicity. (Seefootnote 1 for more information on travel recommendations.) The first dose of the 2-dose hepatitis A vaccine series should be administered as soon as adoption is planned, ideally 2 or more weeks before the arrival of the adoptee.
· Single-antigen vaccine formulations should be administered in a 2-dose schedule at either 0 and 6 to 12 months (Havrix), or 0 and 6 to 18 months (Vaqta). If the
combined hepatitis A and hepatitis B vaccine (Twinrix) is used, administer 3 doses at 0, 1, and 6 months; alternatively, a 4-dose schedule may be used, administered on days 0, 7, and 21 to 30 followed by a booster dose at month 12.
HBV VACCINATIONIT IS ALSO ALMOST A UNIVERSAL VACCINATION STATUS FOR ADULTS
· Vaccinate persons with any of the following indications and any person seeking protection from hepatitis B virus (HBV) infection:
–sexually active persons who are not in a long-term, mutually monogamous relationship (e.g., persons with more than 1 sex partner during the previous 6 months); persons seeking evaluation or treatment for a sexually transmitted disease (STD); current or recent injection drug users; and men who have sex with men;
–health care personnel and public safety workers who are potentially exposed to blood or other infectious body fluids;
–persons with diabetes who are younger than age 60 years as soon as feasible after diagnosis; persons with diabetes who are age 60 years or older at the discretion of the treating clinician based on the likelihood of acquiring HBV infection, including the risk posed by an increased need for assisted blood glucose monitoring in long-term care facilities, the likelihood of experiencing chronic sequelae if infected with HBV, and the likelihood of immune response to vaccination;
–persons with end-stage renal disease, including patients receiving hemodialysis, persons with HIV infection, and persons with chronic liver disease;
–household contacts and sex partners of hepatitis B surface antigen–positive persons, clients and staff members of institutions for persons with developmental disabilities, and international travelers to countries with high or intermediate prevalence of chronic HBV infection; and
–all adults in the following settings: STD treatment facilities, HIV testing and treatment facilities, facilities providing drug abuse treatment and prevention services, health care settings targeting services to injection drug users or men who have sex with men, correctional facilities, end-stage renal disease programs and facilities for chronic hemodialysis patients, and institutions and nonresidential day care facilities for persons with developmental disabilities.
· Administer missing doses to complete a 3-dose series of hepatitis B vaccine to those persons not vaccinated or not completely vaccinated. The second dose should be administered 1 month after the first dose; the third dose should be given at least 2 months after the second dose (and at least 4 months after the first dose). If the combined hepatitis A and hepatitis B vaccine (Twinrix) is used, give 3 doses at 0, 1, and 6 months; alternatively, a 4-dose Twinrix schedule, administered on days 0, 7, and 21 to 30 followed by a booster dose at month 12 may be used.
TWINRIX ACCELARATED allows fast achievement of immunity in around 30 days agaist the standard regimen which confers protection in around 6 months. Also Twinrix comes at a
Notes:Vaccine indicated for HAV-susceptible patients with any of the following: chronic liver disease, injection-drug use, men who have sex with men, or persons with planned travel to countries that have high or intermediate endemicity for hepatitis A virus
3Certain specialists might delay vaccination until CD4+ count >200 cells/mm
201





















