Radicalization leading to violence in Quebec schools: issues ...
Upload
independentCategory
view
1download
0
At the Intersection of Health, Health Care and Policy
doi: 10.1377/hlthaff.2011.0656
, 30, no.11 (2011):2080-2089Health AffairsHomes For Children
Neighborhood Characteristics Associated With Access To Patient-Centered MedicalJaya Aysola, E. John Orav and John Z. Ayanian
Cite this article as:
http://content.healthaffairs.org/content/30/11/2080.full.html
available at: The online version of this article, along with updated information and services, is
For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php
http://content.healthaffairs.org/subscriptions/etoc.dtlE-mail Alerts : http://content.healthaffairs.org/subscriptions/online.shtmlTo Subscribe:
written permission from the Publisher. All rights reserved.mechanical, including photocopying or by information storage or retrieval systems, without prior
may be reproduced, displayed, or transmitted in any form or by any means, electronic orAffairs HealthFoundation. As provided by United States copyright law (Title 17, U.S. Code), no part of
by Project HOPE - The People-to-People Health2011Bethesda, MD 20814-6133. Copyright © is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600,Health Affairs
Not for commercial use or unauthorized distribution
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

By Jaya Aysola, E. John Orav, and John Z. Ayanian
Neighborhood CharacteristicsAssociated With AccessTo Patient-Centered MedicalHomes For Children
ABSTRACT Understanding social determinants of health, such as the socialand physical conditions under which children and their families live,work, and play, is essential to reducing disparities and improving thequality of primary care. We studied the relationship between perceptionsof neighborhood characteristics such as cohesion, safety, physicalenvironment, and whether children receive care from a patient-centeredmedical home. We found that place matters. Children were less likely tohave access to a medical home if they were from less socially cohesiveneighborhoods, less safe neighborhoods, or neighborhoods with feweramenities. These associations persisted even after adjustment forsocioeconomic factors and proved to be more strongly associated thanrace and income. Our findings underscore the need to foster medicalpractice models that make use of trusted community partners, such aschurches and schools, expand care teams to include community healthworkers, and identify additional ways to build collaborative relationshipsbetween providers and their patients and their families from less cohesiveneighborhoods.
The concept of the patient-centeredmedical home first emerged in thepediatric literature in 1967.1 In 1992the American Academy of Pediat-rics promoted the medical home
model as a way to provide cost-effective, high-quality care to children with special health careneeds.2 In 2002 the academy expanded its con-cept of themedical home and recommended thatall children, not just childrenwith special needs,be served by one.3
By 2007 four primary care professional soci-eties—the American Academy of Pediatrics,American College of Physicians, American Acad-emy of Family Physicians, and American Osteo-pathic Association—endorsed the model and is-sued the Joint Principles of the Patient CenteredMedical Home. In this document, the conceptwas expanded again to incorporate quality im-provement initiatives and health information
technology, as well as new models of paymentto compensate medical home providers.4 The Af-fordable Care Act of 2010 promotes evaluation,implementation, and expansion of patient-centered care models to improve quality and re-duce disparities in primary care.Despitewidening support for patient-centered
medical homes, several studies have revealeddisparities in access to thismodel for low-incomeanduninsured populations.5–7 In addition,majorgeographic8 and racial and ethnic disparities9
exist in access to patient-centered medicalhomes for the pediatric population. However,it is not yet fully understoodor establishedwhichfactors contribute to these disparities.Ecological evidence has linked neighborhood
characteristics, such as social cohesion, commu-nity safety, and the physical environment, tohealth outcomes—including birthweight,10 coro-nary artery disease11 and subclinical athero-
doi: 10.1377/hlthaff.2011.0656HEALTH AFFAIRS 30,NO. 11 (2011): 2080–2089©2011 Project HOPE—The People-to-People HealthFoundation, Inc.
Jaya Aysola ([email protected]) is a research fellow inthe Department of HealthCare Policy at HarvardMedical School and atBrigham and Women’sHospital, in Boston,Massachusetts.
E. John Orav is an associateprofessor of biostatistics atthe Harvard School of PublicHealth and an associateprofessor of medicine(biostatistics) at HarvardMedical School.
John Z. Ayanian ([email protected]) is aprofessor of medicine andhealth care policy at HarvardMedical School and aprofessor of health policy andmanagement at the HarvardSchool of Public Health.
2080 Health Affairs November 2011 30:1 1
Health Centers & Health Homes
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

sclerosis,12 obesity,13,14 mental health,15–17 sexu-ally transmitted diseases,18 cancer,19 andasthma20—and academic performance.21 Socialcohesion reflects community solidarity, whichis often measured by levels of trust and mutualsupport perceived between communitymembers.Moreover, prior studies indicate that social
determinants, such as the social and physicalenvironment in which people live, their schools,their incomes, and their neighborhoods, mayaffect health disparities.22–24 However, little isknown about the interplay between social deter-minants ofhealthandaccess to innovativehealthcare services such as patient-centered medi-cal homes.How neighborhood factors relate to one an-
other and exert their influence on health is anarea of ongoing debate25 and evaluation. Accessto health care services within a neighborhoodhas been proposed as one potential mechanismfor understanding the relationship betweenhealth and where a person lives.22,26 Perceptionsof community safety and cohesion among pa-tients has been shown to be associatedwith trustand satisfactionwith health care providers.27 Thepresence of neighborhood disorder, such as di-lapidated housing, has been shown to be asso-ciatedwith self-ratedhealth andhealthbehavior,even after adjustment for many individual- andarea-level socioeconomic variables.28 Moreover,in a comparison of neighborhoods, the presenceofmore schools and churches has been shown tobe independently associated with increasedhealth care use and lower health care costs forlow-income adolescents.29
To determine whether such social determi-nants contribute to disparities in access topatient-centered medical homes, we exam-ined—using a nationally representative sur-vey—whether neighborhood characteristics areassociated with children’s likelihood of havingaccess to this primary care model.
Study Data And MethodsData We used data from the National Survey ofChildren’s Health, conducted by the NationalCenter for Health Statistics in 2007 and 2008.This survey provides national and state-specificestimates on a broad range of indicators forchildren’s health and well-being.Random-digit-dial sampling was used to iden-
tify households with children ages 0–17 fromeach of the fifty states and the District of Colum-bia. After households with children were identi-fied, one child from each household—the so-called index child—was randomly selected asthe subject of the survey.
Telephone interviews were conducted in En-glish, Spanish, or one of four Asian languages,between April 2007 and July 2008, with the pa-rent or guardian most familiar with the indexchild’s care. The total sample included 91,642children from birth through age seventeen, witha range of 1,725 to 1,932 children per state. Theinterview completion rate, measuring the per-centage of completed interviews among knownsampled households with children, was 66 per-cent. Methodological details of the survey aredescribed elsewhere.30,31 Because we analyzedpublicly available deidentified data, the studywas deemed exempt by the Human Studies Com-mittee at Harvard Medical School.Key Predictors The primary predictors in
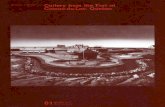
our study were derived from the perceptions ofparents and guardians of their children’s socialand physical environment (Exhibit 1), includingthe following factors: neighborhood cohesion(social cohesion); perceived neighborhoodsafety; the number of neighborhood amenitiespresent, such as parks and sidewalks; and thenumber of neighborhood detractors present,such as vandalism or dilapidated housing. Thesurvey questions used to assess these neighbor-hoodmeasures, detailed in Exhibit 1, were origi-nally developed for the Longitudinal Studies ofChild Abuse and Neglect. They have also beenused in the Survey of Income and ProgramParticipation and were derived from validatedmeasures.21,32,33
Neighborhood cohesion was characterized bya composite score derived from four survey itemsfocused on positive aspects of social cohesionrelating to children.We categorized this continu-ous composite score into quartiles labeled “notcohesive,” “somewhat cohesive,” “cohesive,”and “very cohesive.”Perceived neighborhood safety was derived
from a four-point scale response by parents orguardians regarding their perceptions of safetyin their community or neighborhood. We di-chotomized the perceived safety variable bygrouping “never safe” and “sometimes safe” as“unsafe,” and “usually safe” and “always safe”as “safe.”The assessment of the neighborhood built
environment, or positive aspects of the physicalenvironment, included data from the neighbor-hood amenities measure, which was derivedfrom four dichotomous questions on the pres-ence or absence of physical amenities within thechild’s neighborhood. Affirmative responsesfrom these four questions were combined to cre-ate four categories (fewer than two, two, three,or four amenities).The presence of negative aspects of the physi-
cal environment was characterized by the num-
November 2011 30: 1 1 Health Affairs 2081
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

ber of neighborhood detractors, derived fromthree dichotomous questions assessing the pres-ence of factors that detract from the child’s envi-ronment. Affirmative responses from thesequestions were combined to create three catego-ries (zero, one, or two or more detractors).Other Covariates Other covariates included
age (0–5, 6–11, or 12–17 years), sex, race or eth-nicity, type of insurance coverage, consistency ofinsurance over a twelve-month period, parentaleducation, household income level, family struc-ture, primary language, household employmentstatus, geographic region, and presence of spe-cial health care needs. The latter were identifiedin the survey with the aid of questions from avalidated screening tool.30,34
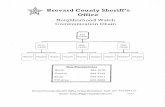
Primary Outcome The primary outcome var-iable was whether children had a usual source ofprimary care that satisfied the criteria of a pa-tient-centered medical home. To make this de-termination, we used a robust medical homemeasure, based on the American Academy ofPediatrics’ definition of medical home that wasincluded in the data set30,31 and operationalizedin previous national studies.5,35,36 Exhibit 2shows the algorithm, based on eighteen ques-tions from the National Survey of Children’sHealth, that was used to determine this outcomemeasure.Satisfying the medical home criteria required
the report of both a personal doctor and usual
source of care and the presence of three sub-components: patient- or family-centeredness, ef-fective care coordination, and “no referral prob-lems.” The criteria required to achieve each ofthese subcomponents are detailed in Exhibit 2.This outcome measure is broadly defined to en-compass both the availability and the use ofservices.Statistical Analysis For the entire sample,
percentages were tabulated for each of the pre-dictors and covariates for thosewith andwithouta medical home, weighted according to the sam-pling design. The unadjusted analysis evaluateddifferences in those characteristics between chil-dren with a medical home and those without,using a chi-square test.The adjusted analysis using multivariable lo-
gistic regression included all four predictors ofinterest and all other covariates. We report ad-justed rates for each covariate at average valuesof the remaining covariates. Subjects with miss-ing values for our four predictors and outcomewere omitted from the analysis; however, indi-cator variables for missing responses for ourother covariates were used so that subjects withmissing responses for these variables could beincluded in the adjusted analysis.The final analytic sample included responses
for 83,142 children, representing 91 percent ofthe original sample.To better understand the relation between the
Exhibit 1
Predictors Derived From The 2007 National Survey Of Children’s Health, By Variable
Variable Survey question Response options
Perceived neighborhood safety How often do you feel the child is safe in your communityor neighborhood?
NeverSometimesUsuallyAlwaysDon’t knowRefused to answer
Neighborhood cohesion People in my neighborhood help each other outWe watch out for each other’s children in this neighborhoodThere are people I can count on in this neighborhoodIf my child were outside playing and got hurt or scared, thereare adults nearby who I trust to help my child
Definitely agreeSomewhat agreeSomewhat disagreeDefinitely disagreeDon’t knowRefused to answer
Neighborhood amenities Presence of sidewalks or walking pathsPresence of a park or playground areaPresence of a recreation center, community center, or boys’or girls’ club
Presence of a library or bookmobile
YesNoDon’t knowRefused to answer
Neighborhood detractors Presence of litter or garbage on the street or sidewalksPresence of poorly kept or dilapidated housingPresence of vandalism such as broken windows or graffiti
YesNoDon’t knowRefused to answer
SOURCE National Survey of Children’s Health 2007; see Note 30 in text.
Health Centers & Health Homes
2082 Health Affairs November 2011 30:1 1
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

predictors and specific elements of the medicalhome model, we conducted secondary analysesexamining each predictor’s association witheach of the five subcomponents of the medicalhome composite measure. These were measuredsequentially with a series of logistic regressionmodels following the algorithm (Exhibit 2) andadjusted for the same sociodemographic covari-ates used in our primary analysis.We also com-pared the multivariable logistic regressionmodel with and without neighborhood predic-tors to evaluate if neighborhood characteristicsaccounted for differences in access to medicalhomes by race or ethnicity or by income. In addi-tional secondary analyses we explored the inter-
actions of income, insurance status, and race orethnicity with each of our four neighborhoodpredictors.All analyses wereweighted to represent theUS
populationofnoninstitutionalized childrenages0–17. To account for the complex survey design,SUDAAN software version 10.0.1 was used in thedescriptive and adjusted analyses. Two-tailed pvalues and 95 percent confidence intervals arereported for all covariates; p < 0:05 was consid-ered statistically significant.Limitations Our study had some limitations.
We were unable to assess causality, given thecross-sectional design. Our outcome variable,the medical home composite measure, lacked
Exhibit 2
The Subcomponent Criteria And Algorithm Of The Medical Home Composite Measure
Personal provider
Usual source of care
Yes: a medical home
Family or patient centereda Health care providers usually or always:•listened to the family/child•spent enough time with the family/child•were sensitive to family’s needs and customs•provided needed information•made the family feel like a partner in the
child’s care, and•provided interpreter services, if needed
Medical home subcomponent Criteria needed to meet subcomponent
No referral problemsa,b
No to one or both:no medical home
No: no medical home
No: no medical home
No: no medical home
SOURCE National Survey of Children’s Health 2007; see Note 30 in text. aBased on responses to survey questions asking family orpatient to describe their experience over the past twelve months. bChildren who did not require a referral and/or did not have two typesof services requiring care coordination and communication among providers were characterized as legitimate skips and met the cri-teria for the subcomponent.
November 2011 30: 1 1 Health Affairs 2083
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

two well-established components: continuity ofcare, which is difficult to measure with cross-sectional data, and accessibility of care. Ques-tions requiring respondents to recall what tran-spired over the past twelve months may havebeen subject to recall bias. The National Surveyof Children’sHealthdata sampling structure is atthe state and national level, so we were not able
to assess our ecological predictors at the neigh-borhood level in order to evaluate this effect inourmodels.Ourpredictors arebasedonpeoples’perceptions. However, the individual-level cor-relations among our four neighborhoodpredictors were relatively weak (Cronbach’salpha ¼ 0:42), which suggests that respondentswere able to discriminate among various neigh-borhood characteristics rather than reflectingmore general positive or negative attitudes.Ourmedical homecompositemeasurewasbasedon self-reported data; however, there are studiesdemonstrating the reliability of self-report forsimilar measures.37–39
The ability to assess the goals of this primarycare model from the end user or consumer per-spective could also be viewed as a strength. Addi-tional strengths of our study include a large,nationally representative sample and a compre-hensive set of questions on both neighborhoodcharacteristics and patient-centered medi-cal homes.
Study ResultsThe study population was nationally rep-resentative of approximately 65.7 million chil-dren residing inUShouseholds during 2007 and2008. More than 93 percent of the populationreported access to a personal provider and usualsource of care, but these providers met the cri-teria for a patient-centered medical home foronly 58 percent of children. Unadjusted propor-tions of children with and without access tomedical homes are depicted in Exhibit 3.When compared with children who did not
receive care from medical homes, children whoreceived care from medical homes were morelikely to be non-Hispanic whites, from higher-incomehouseholds, and fromhouseholdswhereEnglishwas the primary language. Childrenwithprivate insurance weremore likely to havemedi-cal homes than those with public insurance orthose who were uninsured.About 60 percent of children with consistent
insurance coverage had access to medicalhomes, compared to 39 percent of children withgaps in their coverage. Children from house-holds with two biological parents were morelikely to havemedical homes, compared to thosefrom households with single mothers (63 per-cent versus 47 percent).More than 66 percent ofchildren of parents withmore than a high schooleducation had access to medical homes, com-pared to about 35 percent of children of parentswith less than a high school diploma. Amongchildren with special health care needs, forwhom the original medical home model was de-signed, only 50.1 percent had a medical home,
Exhibit 3
Baseline Characteristics Of US Children Without And With Access To A Medical HomeIn 2007
Characteristic
No medical home(n = 31,285, pop.estimate 27,428,702)
Medical home(n = 51,857; pop.estimate 38,287,542)
All children 41.8% 58.1%
Race or ethnicity
Hispanic 60.7 39.3White, non-Hispanic 31.8 68.2Black, non-Hispanic 55.7 44.3Multi or other, non-Hispanica 43.6 56.4
Household income level as percent of federal poverty level
Less than 100% 59.9 40.1100%–199% 50.3 49.7200%–399% 37.1 62.9400% or more 30.3 69.7
Insurance status/type
Public (Medicaid/CHIP) 53.8 46.2Private health insurance 33.3 66.7Uninsured 63.6 36.4
Primary language
English 38.0 62.0Language other than English 70.2 29.8
Neighborhood characteristics
Perceived neighborhood safetyUnsafe (never/sometimes) 61.5 38.5Safe (usually/always) 38.7 61.3
Neighborhood cohesionNot cohesive 58.6 41.4Somewhat cohesive 46.3 53.7Cohesive 40.3 59.7Very cohesive 32.0 68.0
Neighborhood amenitiesFewer than two 48.1 51.9Two 43.7 56.3Three 43.7 56.3Four 38.5 61.5
Neighborhood detractorsZero 38.7 61.3One 47.5 52.5Two or more 53.1 46.9
SOURCE Authors’ analysis of data from National Survey of Children’s Health 2007. NOTES Alldifferences were statistically significant (p < 0:001). Percentages total across rather than down,so “No medical home” and Medical home” equal 100 percent. CHIP is Children’s Health InsuranceProgram. aNon-Hispanic children reporting only one race category of Asian, American Indian,Alaska Native, Native Hawaiian, or Pacific Islander are grouped as “other, non-Hispanic” becauseof small sample sizes in many states. Non-Hispanic children who reported more than one raceare categorized as “multiracial.” Given the small frequencies in both of these categories, they arecombined here as “multi or other, non-Hispanic.”
Health Centers & Health Homes
2084 Health Affairs November 2011 30: 1 1
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

compared to 60.2 percent of children withoutspecial health care needs.In unadjusted analyses, the four neighbor-
hood predictors were each significantly associ-ated with having a medical home (all p < 0:001)(Exhibit 3; see Supplemental Exhibit 3, in theonline Appendix, for additional detail).40 Afteradjustment for all covariates detailed above,three of the four predictors studied—neighbor-hood cohesion, perceived community safety, andthe presence of neighborhood amenities—remained statistically significant predictors ofreceiving care from a medical home. (Exhibit 4;see Supplemental Exhibit 4 for additional de-tail).40 Children living in less cohesive (not co-hesive, somewhat cohesive, cohesive) neighbor-hoods were less likely to have a medical homecompared to those living in very cohesive neigh-borhoods. Children living in communities per-ceived as unsafe were also less likely to have amedical home compared to children living incommunities perceived as safe. Lastly, childrenliving in neighborhoods with fewer amenitieswere less likely tohave amedicalhomecomparedto those with four amenities.The fourth predictor, having detracting ele-
ments in the neighborhood, was found in ad-justed analysis to have a weak association withreceiving care from a medical home. Other co-variates in the adjusted analysis that had signifi-cant associations with having a medical homeincluded age, race or ethnicity, insurance typeand status, consistency of insurance, parentaleducation, primary language, household em-ployment status, geographic region, and specialhealth careneeds (Exhibit 4; not all data shown).Secondary analyses revealed no significant as-
sociation between predictors (neighborhood co-hesion, perceived safety, and neighborhoodamenities) and having a personal doctor, a usualsource of care, or difficulty obtaining referrals.Only one predictor, neighborhood cohesion,was found to have a significant association witheffective care coordination. Children from verycohesive neighborhoods were more likely to re-ceive effective care coordination compared tochildren from less-cohesive neighborhoods (ad-justed rates [standard error]: very cohesive:94.6 percent [0.3]; cohesive: 92.6 pecent[0.5]; somewhat cohesive: 91.5 percent [0.5];not cohesive: 89.2 percent [1.0]; p < 0:001).All three neighborhood characteristics were
significantly associated with family- or patient-centeredness. Parents or guardians of childrenfrom very cohesive neighborhoods were morelikely than those from less cohesive ones to re-port family- or patient centered-care (adjustedrates [standard error]: very cohesive: 76.4 per-cent [0.7]; cohesive: 72.1 percent [0.8]; some-
what cohesive: 69.6 percent [0.9]; not cohesive:64.2 percent [1.1]; p < 0:001). Parents or guard-ians of children from neighborhoods perceivedas safe were more likely to report family- or pa-tient-centered care than those from neighbor-hoods perceived as unsafe (adjusted rates [stan-dard error]: safe: 72.7 percent [0.5]; unsafe:65.3 percent [1.2]; p < 0:001). Children fromneighborhoodswith positive built environments(four amenities) were more likely to receivefamily- or patient-centered care compared withthose from poor built environments (fewer than
Exhibit 4
Adjusted Rates For Access To Patient-Centered Medical Home, By Neighborhood PredictorsAnd Other Covariates
Medical home access
Variable Percent (SE) p valuePerceived neighborhood safety
Unsafe (never/sometimes) 52.1 (1.2) <0.001Safe (usually/always) 59.2 (0.5)
Neighborhood cohesion
Not cohesive 50.1 (1.1) <0.001Somewhat cohesive 56.2 (1.9)Cohesive 58.6 (0.8)Very cohesive 63.3 (0.7)
Neighborhood amenities
Fewer than two 54.9 (1.2) <0.001Two 57.1 (1.0)Three 56.7 (0.8)Four 60.3 (0.6)
Neighborhood detractors
Zero 59.0 (0.5) 0.03One 56.4 (0.9)Two or more 56.7 (1.3)
Race or ethnicity
Hispanic 53.8 (1.4) <0.001Black, non-Hispanic 49.0 (1.1)White, non-Hispanic 62.5 (0.6)Multi or other, non-Hispanica 55.6 (1.5)
Household income level as percent of federal poverty level
Less than 100% 57.3 (1.3) 0.12100%–199% 56.4 (1.0)200%–399% 58.7 (0.8)400% or more 59.7 (0.8)
Insurance status/type
Uninsured 53.1 (2.2) 0.02Public (Medicaid/CHIP) 57.4 (1.0)Private health insurance 59.3 (0.6)
Primary language
Language other than English 43.4 (2.0) <0.001English 60.1 (0.5)
SOURCE Authors’ analysis of data from the National Survey of Children’s Health 2007. NOTES SE isstandard error. CHIP is Children’s Health Insurance Program. aNon-Hispanic children reporting onlyone race category of Asian, American Indian, Alaska Native, Native Hawaiian, or Pacific Islander aregrouped as “other, non-Hispanic” because of small sample sizes in many states. Non-Hispanic childrenwho reported more than one race are categorized as “multiracial.” Given the small frequencies in bothof these categories, they are combined here as “multi or other, non-Hispanic.”
November 2011 30: 1 1 Health Affairs 2085
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

two amenities) (adjusted rates [standard error]:four amenities: 73.6 percent [0.6]; fewer thantwo amenities: 68.3 percent [1.3]; p < 0:001).Our analyses revealed that the addition of
neighborhood characteristics to our multi-variable logistic regression model reduced theincome-level differences in medical home accessby about half and the differences by race or eth-nicity to a much lesser degree (AppendixExhibit A).39
We found no significant interactions betweenrace and insurance status and our four predic-tors. We did find a significant interaction be-tween household income and both neighbor-hood cohesion and neighborhood detractors,with stronger effects of both neighborhood pre-dictorsonmedicalhomeaccess for children fromhigher-income households (more than 200 per-cent of the federal poverty level; see AppendixExhibit B).40
Discussion And ConclusionUsing data from the National Survey of Chil-dren’s Health, our analysis revealed that chil-dren were less likely to have access to a medicalhome if they were from less socially cohesiveneighborhoods, less safe neighborhoods, orneighborhoods with fewer amenities. Theseassociations persisted for each measure afteradjustment for people’s demographic and socio-economic characteristics and remaining neigh-borhood predictors. Moreover, adjusting forthese predictors reduced the income-related dis-parity in access to a medical home by half andreduced the racial or ethnic disparity in medicalhome access to a lesser degree.Our findings suggest that these neighborhood
characteristics are independently associatedwith access to patient-centered medical homesand contribute greatly to the socioeconomic dis-parity inmedical home access.More than 93per-cent of children surveyed had access to both apersonal provider and a usual source of care, soavailability of primary care services did not ap-pear to be the issue. However, our secondaryanalysis suggests that children from disadvan-tagedneighborhoodswere less likely thanothersto experience family- or patient-centered care.Thus, where a child resides may play a crucialrole in ensuring access to care that reflects acollaborative family or patient relationship withthe provider.Measuring how community factors influence
health is an evolving science. The interplay be-tween social determinants, health services suchas the patient-centered medical home, andhealth outcomes has not been well describedin the literature. Neighborhood characteristics
may improve health care access and use by influ-encing the availability of health services; peo-ple’s care-seeking behavior; and the effective-ness of outreach efforts by hospitals, clinics,or health care providers.22,26 Leveraging thisknowledge into policy that can be acted uponshould be the aim of practices trying to imple-ment patient-centered medical homes in re-source-poor neighborhoods.Examples include practice models in Seattle
and Los Angeles that feature community partici-pation in developing and evaluating health caredelivery and prevention programs,41,42 collabora-tive partnerships to promote health care serviceswith trusted community organizations such asschools43 and churches,44 and the use of commu-nity health workers.45,46
In addition, our findings underscore the needfor practices to implement initiatives that fostercollaborative relationships betweenpatients andtheir families and providers.47 Policy interven-tions may include training providers in patientcommunication and cultural effectiveness andproviding on-site language interpreters.48–50
Early studies of such interventions have demon-strated benefits in both better communicationand increased access to and use of healthcare.51–54
The concept of the patient-centered medicalhome has gained widespread support over thepast decade. Our study supports the call to betterdefine patient-centered medical homes and evalu-ate the model in different settings to determineits effects on improving quality and reducinginequities in care.36,55–58 Interventions that ad-dress social determinants of health have the po-tential to reduce socioeconomic and racial orethnic disparities.50,51 As the definition and as-sessments of the medical home model continueto develop, our findings support an emphasis onpatient-centered care and community engage-ment in efforts to redesignmedical practices.59,60
Understanding the role that social and environ-mental factors play in the uptake of new modelsof health care delivery is central to informingpolicy and ensuring that patient-centered medi-cal homes are accessible in all communities. ▪
Measuring howcommunity factorsinfluence health is anevolving science.
Health Centers & Health Homes
2086 Health Affairs November 2011 30: 1 1
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

The study on which this article is basedwas presented as an oral scientificabstract at the Annual Meeting of theSociety of General Internal Medicine inPhoenix, Arizona, May 5, 2011. Thiswork was supported by Grant No.T32HP10251 from the Health Resources
and Services Administration,Department of Health and HumanServices, to support the HarvardMedical School Fellowship in GeneralMedicine and Primary Care. The authorsthank Shimon Shaykevich (Division ofGeneral Medicine and Primary Care,
Brigham and Women’s Hospital) foradvice on statistical programming, andIchiro Kawachi (Department of Society,Human Development, and Health,Harvard School of Public Health) forguidance on the conceptual framework.
NOTES
1 Sia C, Tonniges TF, Osterhus E,Taba S. History of the medical homeconcept. Pediatrics. 2004;113(5 Suppl):1473–8.
2 American Academy of Pediatrics AdHoc Task Force on Definition of theMedical Home. The medical home.Pediatrics. 1992;90(5):774.
3 Medical Home Initiatives for Chil-dren with Special Needs Project Ad-visory Committee, American Acad-emy of Pediatrics. The medicalhome. Pediatrics. 2002;110(1 Pt 1):184–6.
4 Patient-Centered Medical HomeCollaborative. Joint principles of thepatient centered medical home [In-ternet]. Washington (DC): The Col-laborative; 2007 [cited 2011 Sep 27].Available from: http://www.pcpcc.net/content/joint-principles-patient-centered-medical-home
5 Strickland BB, Singh GK,Kogan MD, Mann MY, Van Dyck PC,Newacheck PW. Access to the medi-cal home: new findings from the2005–2006 National Survey ofChildren with Special Health CareNeeds. Pediatrics. 2009;123(6):e996–1004.
6 Stevens GD, Seid M, Pickering TA,Tsai KY. National disparities in thequality of a medical home for chil-dren. Matern Child Health J. 2010;14(4):580–9.
7 Beal A, Hernandez S, Doty M. Latinoaccess to the patient-centered medi-cal home. J Gen Intern Med. 2009;24(Suppl 3):514–20.
8 Singh GK, Strickland BB,Ghandour RM, van Dyck PC. Geo-graphic disparities in access to themedical home among US CSHCN.Pediatrics. 2009;124(Suppl 4):S352–60.
9 Raphael JL, Guadagnolo BA,Beal AC, Giardino AP. Racial andethnic disparities in indicators of aprimary care medical home for chil-dren. Acad Pediatr. 2009;9(4):221–7.
10 Buka SL, Brennan RT, Rich-EdwardsJW, Raudenbush SW, Earls F.Neighborhood support and the birthweight of urban infants. Am J Epi-demiol. 2003;157(1):1–8.
11 Kawachi I, Berkman LF. Neighbor-hoods and health. Oxford: OxfordUniversity Press; 2003.
12 Kim D, Diez Roux AV, Kiefe CI,Kawachi I, Liu K. Do neighborhoodsocioeconomic deprivation and low
social cohesion predict coronarycalcification? The CARDIA study. AmJ Epidemiol. 2010;172(3):288–98.
13 Singh GK, Siahpush M, Kogan MD.Neighborhood socioeconomic con-ditions, built environments, andchildhood obesity. Health Aff (Mill-wood). 2010;29(3):503–12.
14 Carter MA, Dubois L. Neighbour-hoods and child adiposity: a criticalappraisal of the literature. HealthPlace. 2010;16(3):616–28.
15 Barnes J, Belsky J, Frost M,Melhuish E. Neighborhood charac-teristics and mental health: the rel-evance for mothers of infants indeprived English neighborhoods.Soc Psychiatry Psychiatr Epidemiol.2010 Oct 6 [Epub ahead of print].
16 Truong KD, Ma S. A systematic re-view of relations between neighbor-hoods and mental health. J MentHealth Policy Econ. 2006;9(3):137–54.
17 Xue Y, Leventhal T, Brooks-Gunn J,Earls FJ. Neighborhood residenceand mental health problems of 5 to11-year-olds. Arch Gen Psychiatry.2005;62(5):554–63.
18 Cohen DA, Mason K, Bedimo A,Scribner R, Basolo V, Farley TA.Neighborhood physical conditionsand health. Am J Public Health.2003;93(3):467–71.
19 Freedman VA, Grafova IB,Rogowski J. Neighborhoods andchronic disease onset in later life.Am J Public Health. 2011;101(1):79–86.
20 Subramanian SV, Kennedy MH.Perception of neighborhood safetyand reported childhood lifetimeasthma in the United States (U.S.): astudy based on a national survey.PLoS One. 2009;4(6):e6091.
21 Milam AJ, Furr-Holden CM, Leaf PJ.Perceived school and neighborhoodsafety, neighborhood violence, andacademic achievement in urbanschool children. Urban Rev. 2010;42(5):458–67.
22 Kawachi I, Berkman L. Social cohe-sion, social capital, and health. In:Berkman L, Kawachi I, editors. So-cial epidemiology. Oxford: OxfordUniversity Press; 2000. p. 174–90.
23 Marmot MG, Bell R. Action onhealth disparities in the UnitedStates: commission on social deter-minants of health. JAMA. 2009;301(11):1169–71.
24 Keshavjee S. Medical anthropology:
insights into the social, political, andeconomic determinants of health.JAMA. 1996;276(13):1096–7.
25 Macinko J, Starfield B. The utility ofsocial capital in research on healthdeterminants. Milbank Q. 2001;79(3):387–427.
26 Derose KP, Varda DM. Social capitaland health care access: a systematicreview. Med Care Res Rev. 2009;66(3):272–306.
27 Ahern MM, Hendryx MS,Siddharthan K. The importance ofsense of community on people’sperceptions of their health-careexperiences. Med Care. 1996;34(9):911–23.
28 Franzini L, Caughy M, Spears W,Fernandez Esquer ME. Neighbor-hood economic conditions, socialprocesses, and self-rated health inlow-income neighborhoods in Texas:a multilevel latent variables model.Soc Sci Med. 2005;61(6):1135–50.
29 Youngblade LM, Curry LA, Novak M,Vogel B, Shenkman EA. The impactof community risks and resources onadolescent risky behavior and healthcare expenditures. J Adolesc Health.2006;38(5):486–94.
30 Child and Adolescent Health Meas-urement Initiative, Data ResourceCenter for Child and AdolescentHealth. National Survey of Chil-dren’s Health 2007: guide to topicsand questions asked [Internet].Portland (OR): CAHMI; [cited 2011Sep 27]. Available from: http://www.childhealthdata.org/learn/topics_questions/2007-nsch
31 Blumberg SJ, Foster EB, Frasier AM,Satorius J, Skalland BJ, Nysse-CarrisKL, et al. Design and operation of theNational Survey of Children’sHealth, 2007 [Internet]. Hyattsville(MD): National Center for HealthStatistics; [cited 2011 Aug 16]. (Vitaland Health Statistics, Series 1, Pro-gram and Collection Procedures).Available from: http://ftp.cdc.gov/pub/health_statistics/nchs/slaits/nsch07/2_Methodology_Report/NSCH_Design_and_Operations_052109.pdf
32 Sampson RJ, Raudenbush SW,Earls F. Neighborhoods and violentcrime: a multilevel study of collectiveefficacy. Science. 1997;277(5328):918–24.
33 Brownson RC, Hoehner CM, Day K,Forsyth A, Sallis JF. Measuring thebuilt environment for physical ac-
November 2011 30: 1 1 Health Affairs 2087
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

tivity: state of the science. Am J PrevMed. 2009;36(4 Suppl):S99–123.e12.
34 Newacheck PW, Strickland B,Shonkoff JP, Perrin JM,McPherson M, McManus M, et al.An epidemiologic profile of childrenwith special health care needs.Pediatrics. 1998;102(1):117–23.
35 Strickland BB, Jones JR, GhandourRM, KoganMD, Newacheck PW. Themedical home: health care accessand impact for children and youth inthe United States. Pediatrics. 2011;127(4):604–11.
36 Bethell CD, Read D, Brockwood K.Using existing population-baseddata sets to measure the AmericanAcademy of Pediatrics definition ofmedical home for all children andchildren with special health careneeds. Pediatrics. 2004;113(5 Suppl):1529–37.
37 Varni JW, Limbers CA,Burwinkle TM. Parent proxy-reportof their children’s health-relatedquality of life: an analysis of 13,878parents’ reliability and validityacross age subgroups using thePedsQL 4.0 Generic Core Scales.Health Qual Life Outcomes. 2007;5:2.
38 Shea S, Stein AD, Lantigua R,Basch CE. Reliability of the behav-ioral risk factor survey in a triethnicpopulation. Am J Epidemiol. 1991;133(5):489–500.
39 Co JP, Sternberg SB, Homer CJ.Measuring patient and family expe-riences of health care for children.Acad Pediatr. 2011;11(3 Suppl):S59–67.
40 To access the Appendix, click on theAppendix link in the box to the rightof the article online.
41 Krieger J, Allen C, Cheadle A,Ciske S, Schier JK, Senturia K, et al.Using community-based participa-tory research to address social de-terminants of health: lessonslearned from Seattle Partners forHealthy Communities. Health EducBehav. 2002;29(3):361–82.
42 Moreno G, Rodriguez MA,Lopez GA, Bholat MA, Dowling PT.Eight years of building communitypartnerships and trust: the UCLA
family medicine community-basedparticipatory research experience.Acad Med. 2009;84(10):1426–33.
43 Simmer-BeckM, Gadbury-Amyot CC,Ferris H, Voelker MA, Keselyak NT,Eplee H, et al. Extending oral healthcare services to underserved childrenthrough a school-based collabora-tion: part 1—a descriptive overview. JDent Hyg. 2011;85(3):181–92.
44 Campbell MK, Hudson MA,Resnicow K, Blakeney N, Paxton A,Baskin M. Church-based healthpromotion interventions: evidenceand lessons learned. Annu RevPublic Health. 2007;28:213–34.
45 Lewin S. Bridging the equity gap inmaternal and child health: lay healthworkers may help bridge equity gapin maternal and child health. BMJ.2005;331(7520):844.
46 Lewin SA, Dick J, Pond P,Zwarenstein M, Aja G, van Wyk B,et al. Lay health workers in primaryand community health care.Cochrane Database Syst Rev.2005;(1):CD004015.
47 Kilo CM, Wasson JH. Practiceredesign and the patient-centeredmedical home: history, promises,and challenges. Health Aff (Mill-wood). 2010;29(5):773–8.
48 Cooper LA. Health disparities. To-ward a better understanding of pri-mary care patient-physician rela-tionships. J Gen Intern Med. 2004;19(9):985–6.
49 Barr JK, Kelvey-Albert M. Reducinghealthcare disparities: cultural di-versity training for primary carephysician office practice throughcontinuing medical education. ConnMed. 2008;72(1):45–8.
50 Williams DR, Costa MV,Odunlami AO, Mohammed SA.Moving upstream: how interven-tions that address the social deter-minants of health can improvehealth and reduce disparities. JPublic Health Manag Pract. 2008;14(Suppl):S8–17.
51 Bambra C, Gibson M, Sowden A,Wright K, Whitehead M,Petticrew M. Tackling the wider so-cial determinants of health andhealth inequalities: evidence fromsystematic reviews. J Epidemiol
Community Health. 2010;64(4):284–91.
52 Anderson LM, Scrimshaw SC,Fullilove MT, Fielding JE,Normand J. Culturally competenthealthcare systems. A systematic re-view. Am J Prev Med. 2003;24(3 Suppl):68–79.
53 Helitzer DL, Lanoue M, Wilson B,de Hernandez BU, Warner T,Roter D. A randomized controlledtrial of communication training withprimary care providers to improvepatient-centeredness and health riskcommunication. Patient EducCouns. 2011;82(1):21–9.
54 Sequist TD, Fitzmaurice GM,Marshall R, Shaykevich S,Marston A, Safran DG, et al. Culturalcompetency training and perfor-mance reports to improve diabetescare for black patients: a clusterrandomized, controlled trial. AnnIntern Med. 2010;152(1):40–6.
55 Barr MS. The need to test the pa-tient-centered medical home. JAMA.2008;300(7):834–5.
56 Friedberg MW, Lai DJ, Hussey PS,Schneider EC. A guide to the medicalhome as a practice-level interven-tion. Am J Manag Care. 2009;15(10 Suppl):S291–9.
57 Homer CJ. Health disparities and theprimary care medical home: could itbe that simple? Acad Pediatr. 2009;9(4):203–5.
58 Cooley WC, McAllister JW,Sherrieb K, Kuhlthau K. Improvedoutcomes associated with medicalhome implementation in pediatricprimary care. Pediatrics. 2009;124(1):358–64.
59 Berenson RA, Hammons T,Gans DN, Zuckerman S, Merrell K,Underwood WS, et al. A house is nota home: keeping patients at thecenter of practice redesign. HealthAff (Millwood). 2008;27(5):1219–30.
60 Rittenhouse DR, Thom DH,Schmittdiel JA. Developing a policy-relevant research agenda for thepatient-centered medical home: afocus on outcomes. J Gen InternMed. 2010;25(6):593–600.
Health Centers & Health Homes
2088 Health Affairs November 2011 30:1 1
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from

ABOUT THE AUTHORS: JAYA AYSOLA, E. JOHN ORAV &JOHN Z. AYANIAN
Jaya Aysola is aresearch fellow atHarvard MedicalSchool and Brighamand Women’sHospital.
In this month’s Health Affairs, JayaAysola, John Orav, and JohnAyanian write about theirexamination of the relationshipbetween neighborhoodcharacteristics—such as cohesion,safety, dilapidation, and availabilityof amenities—and the ease withwhich children can obtain healthcare through a patient-centeredmedical home.The authors found that children
from less cohesive or safeneighborhoods, or neighborhoodswith fewer amenities, were lesslikely than others to have access tomedical homes. They recommendfostering medical practice modelsthat enhance communityengagement, expand care teams toinclude community health workers,and identify additional ways tobuild collaborative relationshipsbetween providers and patientsfrom less cohesive communities.Aysola is a general medicine
research fellow in the Departmentof Health Care Policy at HarvardMedical School and the Division of
General Medicine and Primary Careat Brigham and Women’s Hospital,where she examines policysolutions to disparities in primarycare. She is a practicing internistand pediatrician with the BostonHealthcare for the Homelessprogram.Aysola earned her medical degree
from the University of PittsburghSchool of Medicine. She receivedher master of public health degreein health care policy from theHarvard School of Public Healthand completed the CommonwealthFund/Harvard University HealthMinority Health Policy Fellowship.
E. John Orav is anassociate professorof biostatistics atthe Harvard Schoolof Public Health.
Orav is an associate professor ofbiostatistics at the Harvard Schoolof Public Health and an associateprofessor of medicine(biostatistics) at Harvard MedicalSchool. He is also a biostatisticianin the Department of Medicine atBrigham and Women’s Hospital. Heis the primary statistician forNational Institutes of Health–funded studies to improve quality
and reduce medical errors in thehospital and in primary carepractices statewide. In addition, heis the primary statistician for astatewide project to evaluate andimprove electronic health recordsin primary care settings. Hisdoctorate in statistics is fromStanford University.
John Z. Ayanian isa professor ofmedicine and healthcare policy atHarvard MedicalSchool.
Ayanian is a professor ofmedicine and health care policy atHarvard Medical School and aprofessor of health policy andmanagement at the Harvard Schoolof Public Health. A generalinternist at Brigham and Women’sHospital, he provides primary careand teaches medical residents. Hehas published more than 200articles and book chapters onaccess to care, health disparitiesrelated to cancer, quality of care,and other topics. His medicaldegree is from Harvard MedicalSchool, and his master of publicpolicy degree is from Harvard’sKennedy School of Government.
November 2011 30: 1 1 Health Affairs 2089
at LIBRARY OF MEDICINE on December 7, 2011Health Affairs by content.healthaffairs.orgDownloaded from
Copyright © 2022 FDOKUMEN