National Training Manual and Training Plan for Men and Boys ...
208
National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS Republic of Namibia Ministry of Gender Equality and Child Welfare
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of National Training Manual and Training Plan for Men and Boys ...

National Training Manual and Training Plan for Men and Boys
on GBV, SRH and HIV/AIDS
Republic of Namibia
Ministry of Gender Equality and Child Welfare

1National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Table of ContentsAcknowledgements
Preface
Introduction
About the Manual
i. How it was developed
ii. Target Audience
iii. Objectives of the manual
iv. How it is organized
v. How to use it
vi. Training Materials
vii. Training Agenda
Section 1: Workshop Prelude
Overview
Activity 1.1 Welcoming and Introductions
Activity 1.2 Review of Workshop objectives and Agenda
Activity 1.3 Pre-Test
Section 2: Understanding Gender
Overview
Activity 2.1 Looking at our Attitudes
Activity 2.2 Learning about Gender
Activity 2.3 The Gender Roles we play
Section 3: HIV Risks and Prevention
Overview
Activity 3.1 HIV and AIDS Myths and Facts
Activity 3.2 Levels of HIV Risk
Activity 3.3 Positive or Negative
Activity 3.4 Multiple Concurrent Partnerships, Cross-generational Sex and
Transactional Sex
Activity 3.5 Alphabets of Prevention
Activity 3.6 Getting Tested for HIV

2 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Section 4: Gender and Power Relations
Overview
Activity 4.1 Power Relations and Gender Implications
Activity 4.2 Persons and Things
Activity 4.3 Gender Fishbowl
Activity 4.4 Healthy and Unhealthy Relationships
Section 5: Gender Based Violence
Overview
Activity 5.1 What is Gender Based Violence?
Activity 5.2 Sexual Violence in the Daily Routine
Activity 5.3 Men as Victims of Violence
Activity 5.4 Understanding the Causes and Effects of Violence
Activity 5.5 Domestic Violence Cycle
Section 6: Sexual and Reproductive Health
Overview
Activity 6.1 Understanding Sexuality
Activity 6.2 Sexual Reproductive Health and its Determinants
Activity 6.3 Understanding STI’s
Activity 6.4 Sexual Reproductive Health Rights
Activity 6.5 Men’s Health
Section 7: Gender Norms and Violence
Overview
Activity 7.1 Digital Stories
Section 8: Alternatives to Violence
Overview
Activity 8.1 Effective Communication
Activity 8.2 Going Deeper: How feelings can trick us
Activity 8.3 Going Deeper: Managing my anger

3National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Section 9: Taking Action
Overview
Activity 9.1 The Legal framework in Namibia
Activity 9.2 Community Mapping
Activity 9.3 Identifying Community Engagement Activities
Activity 9.5 Developing Action Plans
Activity 9.6 Post-test and Evaluation
Appendices
Appendix A: Optional Sessions
Appendix B: Workshop Energizers
Appendix C: Pre and Post Test Questionnaire
Appendix D: Training Evaluation
Appendix E: Resources

4 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Preface
Numerous reports have stated that one of every three women has, at some point in her life been the victim of sexual, physical or psychological violence perpetrated by men. This is of concern, especially in light of the many thousands of programs
that have been developed to assist these women, from shelters and legal aid groups, to support groups and counselling services. These services are an absolute essential, but are insufficient because they do not distinctly address the plight of men and the many social challenges they face. Additionally, improving the health and wellbeing of adult and young women requires the engagement of boys and men.
Historically, it has been assumed that men and boys are not so concerned about their health, and this can possibly be attributed to societal expectations that men ought to be tough; and as a result, seeking help related to their health is seen as a sign of weakness. Most health services, especially those related to sexual and reproductive health, are geared primarily towards women, and women are socialized to access these services while men are not. This is a key rationale for seeking to understand and respond to the sexual and reproductive needs and realities of men and boys.
In seeking to address these issues, a thorough understanding of men and boys and the behaviours they engage in that may culminate in increased risk for women (violence and increased HIV risk specifically), is of high importance. It is imperative to highlight that these behaviours do not exist in a vacuum, but that, to a large extent, men and boys are socialized in a way that perpetuates their aggression, and even condones it. A potent mixture of the cultural and gender norms that are harmful, have engrained behaviours which are difficult to counter without a process that assists individuals unpack these.

5National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
The need to correct these misconceptions has in recent years been more visible than ever before. Disturbing news of violence and the high level of HIV infection rates is a common occurrence in the media in Namibia. It calls stakeholders to task, and challenges decision making bodies and organizations geared towards social action to remedy a dire situation. This requires a gender-transformative approach which must seek to identify those gender and cultural norms which are harmful, and based on this, promote more gender-equitable relationships between men and women.

6 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Introduction
Numerous reports have stated that one of every three women has, at some point in her life been the victim of sexual, physical or psychological violence perpetrated by men. This is of concern, especially in light of the many thousands of programs
that have been developed to assist these women, from shelters and legal aid groups, to support groups and counselling services. These services are an absolute essential, but are insufficient because they do not distinctly address the plight of men and the many social challenges they face. Additionally, improving the health and wellbeing of adult and young women requires the engagement of boys and men.
Historically, it has been assumed that men and boys are not so concerned about their health, and this can possibly be attributed to societal expectations that men ought to be tough; and as a result, seeking help related to their health is seen as a sign of weakness. Most health services, especially those related to sexual and reproductive health, are geared primarily towards women, and women are socialized to access these services while men are not. This is a key rationale for seeking to understand and respond to the sexual and reproductive needs and realities of men and boys.
In seeking to address these issues, a thorough understanding of men and boys and the behaviours they engage in that may culminate in increased risk for women (violence and increased HIV risk specifically), is of high importance. It is imperative to highlight that these behaviours do not exist in a vacuum, but that, to a large extent, men and boys are socialized in a way that perpetuates their aggression, and even condones it. A potent mixture of the cultural and gender norms that are harmful, have engrained behaviours which are difficult to counter without a process that assists individuals unpack these.
The need to correct these misconceptions has in recent years been more visible than ever before. Disturbing news of violence and the high level of HIV infection rates is a common occurrence in the media in Namibia. It calls stakeholders to task, and challenges decision making bodies and organizations geared towards social action to remedy a dire situation. This requires a gender-transformative approach which must seek to identify those gender and cultural norms which are harmful, and based on this, promote more gender-equitable relationships between men and women.

7National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
The challenge is not only to involve men in the response to HIV/AIDS, but also to engage them as friends, community members, caring partners, fathers and leaders. Men must partake fully in dialogues, actions and policies to deal effectively with gender inequalities and the resulting vulnerability that fuels the spread of HIV (WHO 2003)
The number of programmes focusing on women empowerment has far outweighed those focused on men and boys. By leaving men and boys out of the equation, the potential for women alone to make changes in gender relations is limited. Thus, initiatives geared towards giving men and boys the opportunity to unpack and re-align gender norms are an absolute necessity and promise to yield very good results in the quest for HIV risk reduction, HIV infection alleviation and reduction of harmful gender practices. They are long overdue.
This Training manual is directly designed to fill these gaps, with a male-centric approach. It looks more specifically at Gender Based Violence (GBV), HIV/AIDS and Sexual and Reproductive Health issues. The interplay between these issues is explored herein, and it also looks at how the consequences affect the health outcomes for both men and women in society. The manual highlights actions that can be taken in order to alleviate, if not to eradicate GBV and HIV/AIDS, thus resulting in better sexual and reproductive health outcomes for both men and women.

8 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
About the Manual
i. How it was developed
This manual was compiled using various existing materials and tools that incorporate gender, HIV/AIDS and sexual reproductive health components. This compilation was informed by the Behaviour Determinant Logic (BDI) Model. This is a graphic
depiction that shows clearly and concisely the causal mechanisms through which specific interventions can affect behaviour and thereby achieve a health goal. One might think of them as road maps specifying the causal pathways between programs and behaviours (Kirby 2004). BDI models must also include the causal linkages among the health goal, the behaviours affecting that goal, their determinants, and their respective intervention components. That is, they specify which particular intervention components affect which determinants that, in turn, affect which behaviours that achieve the health goal.BDI models can serve a variety of useful functions. In general, they provide a framework for the development of more effective programs and for the evaluation of those programs. More specifically, if developed properly and used properly, BDI models can:
Link key intervention components and activities to key determinants of important •
behaviours, the behaviours themselves, and health goals. Make explicit the implicit theories behind programs and thereby provide a clear •
rationale for program activities, a rationale that will facilitate funding and provide guidance to program staff or to different organizations involved in the initiative. Encourage program designers • and program implementers to not only recognize the complexity of reality, but also to focus on the most important program elements, determinants and behaviours. Help determine what additional information needs to be gathered or what research •
needs to be conducted in order to design or improve a program. Guide both the design of a program and the refinement of an existing program. •
(Kirby 2004).
The BDI logic model1 for this training manual is depicted graphically as follows:
1 Kirby, D. (2004). Logic Models: A Useful Tool for Designing, Strengthening and Evaluating Programs to Reduce Adolescent Sexual Risk-Taking, Pregnancy, HIV and Other STDs.Resource Center for Adolescent Pregnancy Prevention (ReCAPP). ETR Associates.

9National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
10
Behavio
urDete
rmin
antLo
gicM
odelfo
rNationalTrainingM
anualonGBV,SRHandHIV/A
IDS
Reduce
dincidence
anda
ccepta
bilityo
f
GBV
Incr
ease
dp
ract
ices
ofaltern
ativesto
vio
lence
Incr
ease
dd
isclosu
re
andreportin
go
f
GBV
Incr
ease
d
know
ledgea
nd
utiliza
tiono
fGBV
serv
ices
Incr
ease
d
willingness
toa
ct
andspeako
ut
again
stG
BV
Reduct
ionintheN
ational
Pre
vale
nce
ofGBVin
Nam
ibia
Increase
dknowledgeonG
ender
base
dviolence
andits
conse
quence
s
Increase
dknowledgeandskills
ofaltern
ative
ways
ofre
solving
conflict
Decrease
inthebelief(a
mongst
menandw
om
en)th
atth
ere
are
reaso
nsth
atjustifyviolence
againstpartnersandchildre
n
Increase
dknowledgeofse
rvices
andlawspertainingtoG
BV
Decrease
inthePerceptionthat
violence
isanorm
alandnatu
ral
occ
urrence
Goal
Behavio
urs
Dete
rmin
ants
Curr
iculu
mA
ctiv
itie
s
•
DigitalStories
•
UnderstandingtheCausesandEffectsof
Violence
•
DomesticViolenceCycle
•
TheNamibianLegalFramework
•
DigitalStories
•
UnderstandingtheCausesandEffectsof
Violence
•
DomesticViolenceCycle
•
EffectiveCommunication
•
GoingDeeper:Howfeelingscantrickus
•
GoingDeeper:Managingmyanger
•
LookingatourAttitudes
•
LearningaboutGender
•
TheGenderRolesweplay
•
PowerRelations:PersonsandThings
•
GenderFishbowl
•
HealthyandUnhealthyRelationships
•
WhatisGenderBasedViolence?
•
SexualViolenceintheDailyRoutine
•
MenasVictimsofViolence
•
UnderstandingtheCausesandEffectsof
Violence
•
DomesticViolenceCycle

10 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
11
Incr
ease
d
know
ledgea
nd
aw
are
ness
ofSRH
dete
rmin
ants
Incr
ease
d
willingness
for
test
inga
nd
treatm
entofSTI’s
ando
ther
repro
duct
ivetra
ct
infe
ctio
nsand
disease
s
Incr
ease
dm
ale
involv
em
entin
SRH
issu
esth
ataffect
both
mena
nd
wom
en
Incr
ease
da
ndim
pro
ved
sexualandrepro
duct
ive
healtho
utc
om
esfo
rm
en
andw
om
eninN
am
ibia
Increase
dknowledgeofSR
H
issu
essu
chasm
ate
rnaland
infa
nthealthandm
ortality
,
fam
ilyplanning,abortionetc.
andm
aleinvo
lvem
entinthese
issu
es
Increase
dknowledgeand
understa
ndingofth
erisks
of
contractinganSTIandthe
conse
quence
sofanundiagnose
d
anduntreate
dSTI
Increase
dknowledgeofth
e
ava
ilabilityofco
nfidentialand
afford
abletestingandtre
atm
ent
serv
icesaswellasSR
Hpolicies
Increase
dskillsfo
reffective
com
municationasam
eansto
healthyco
uplerelationsh
ips,fam
ily
stru
cture
sandthecom
munityat
larg
e
Goal
Behavio
urs
Dete
rmin
ants
Curr
iculu
mA
ctiv
itie
s
•
UnderstandingSTI’s
•
SexualReproductiveHealthRights
•
Men’sHealth
•
GettingTestedforHIV
•
CommunityMapping
•
DevelopingPersonalActionPlans
•
EffectiveCommunication
•
SexualReproductiveHealthandits
Determinants
•
IdentifyingCommunityEngagementActivities
•
DevelopingActionPlans
CommunityActionTeams
•
UnderstandingSexuality
•
SexualReproductiveHealthandits
Determinants

11National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
12
Incr
ease
dcorrect
andconsist
ent
condom
use
Reduct
ionin
multip
lea
nd
concu
rrent
partners
hip
s,
transa
ctio
naland
cross
‐genera
tional
sex
Incr
ease
dH
IV
volu
nta
ry
counse
llin
ga
nd
test
ing
Reduct
ionintheN
ational
Pre
vale
nce
ofHIV
infe
ctio
n
inN
am
ibia
Decrease
harm
fulgendernorm
sth
at
disco
ura
getheuse
ofco
ndom
s
Decrease
barriers/increase
positive
attitudesto
obta
iningcondom
s
Increase
skillandefficacy
touse
condom
sco
rrectly
Increase
dknowledgeaboutHIV
includinghowitistra
nsm
itte
d,its
conse
quence
sandpre
vention.
Increase
positive
attitudeabout
havingm
utu
allyfa
ithfu
l/re
spectfu
l,
monogam
ousre
lationsh
ips.
Decrease
harm
fulgendernorm
sth
at
supporthavingM
CP(e.g.m
en’s
sexu
aldesire
isunco
ntrollable)
•
MultipleConcurrentPartnerships,Cross‐
generationalSexandTransactionalSex
•
PositiveorNegative
•
HIVandAIDSMythsandFacts
•
LevelsofHIVRisk
•
AlphabetsofPrevention
•
GettingTestedforHIV
•
Thegenderrolesweplay
•
Communitymapping
•
Developingpersonalactionplan
•
HIVandAIDSMythsandFacts
•
LevelsofHIVRisk
•
Learningaboutcondoms
•
AlphabetsofPrevention
Increase
selfefficacy
toacc
ess
counse
llingandtestingserv
ices
Increase
understa
ndingof
reluctance
ofm
ostm
entogette
sted
Increase
understa
ndingofth
e
benefitsofkn
owingone’ssta
tus
Goal
Behavio
urs
Dete
rmin
ants
Curr
iculu
mA
ctiv
itie
s

12 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
ii. Target Audience
The manual will be utilized by professionals and community based groups who work with different groups of men and boys on GBV, SRH, HIV and AIDS. This includes teachers, religious leaders, football coaches, caregivers and facilitators. Training participants are envisioned to be adult men and boys (ideally 14 year olds and above), though the course content can work well with mixed groups of not more than 20 participants at a time.
iii. Training Objectives
The Training will be guided by the following objectives, as informed by the BDI Logic Model:
To provide an extensive understanding of the key concepts of GBV, SRH and HIV/AIDS as relating to men and boys in the Namibian context,
To increase awareness that fosters a reduction or eradication in participants’ acceptability of GBV practices,
To create awareness of and consequently increase participants’ practices of alternatives to violence and help seeking behaviours that are linked to HIV/AIDS and sexual reproductive health,
To equip participants with skills in order to encourage them to willingly act and stand up against GBV and be advocates for better health outcomes for both men and women.
Help participants develop a personal and community plan for the next steps to build prevention and response to GBV for follow-up and continuing action after the workshop, as well as act to reduce HIV infection risks.
iv. How it is organized
This manual is a compilation of relevant activities from various curricula. The manual is set out with 8 sections, and each section has its specific objectives. There are 3-6 sessions in each section; which directly speak to the section objective. The manual presents information for each session in a standardized format. This includes information on:
Objectives of the activityThis describes what participants should learn as a result of doing the activity. It is a good idea to begin each activity by telling participants about its learning objectives. This helps participants to understand why they are doing the activity and what they can hope to

13National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
get out of it. Unless otherwise specified in the directions, sharing the learning objectives with participants also helps in reviewing the activities at the end of each day. This review helps one determine if the workshop is making progress in terms of what participants are learning.
Resources: Low (no need for flipchart, markers, or other resources outside of a few handouts that can be prepared in advance); medium (flipchart or writing surface and markers); high (PowerPoint projector or DVD player; large number of handouts)
Time required for the activityThis is how long the activity should take, based on past experience. Depending on certain factors, such as the number of participants, the time for doing each activity could vary. The activities in the manual are designed for sessions as short as 45 minutes or as long as two hours, and in some cases, a range of time is provided. It is most important to work at the pace of the participants. But in general, sessions should not be longer than two hours. It is also important to remember that any agenda for a workshop is usually a full one. Taking too long with one activity may mean you do not have time to complete others. Try to stick to the time suggested.
Materials needed for the activityThese are the materials necessary for each activity. You will need to prepare some of them before the workshop begins. For the most part, these include basic materials, such as flipchart paper and markers. In cases where the materials listed cannot be easily accessed, you should feel free to improvise. For example, flipchart and markers can be substituted with chalkboard and chalk.
Advance preparation This section will inform you about any preparation that needs to be done before the activity is implemented.
Steps for implementing the activityThese are the steps you should follow in order to use the activity well. These instructions are numbered and should be followed in order. For the most part, the activities are written to be easily adapted to groups with different reading and writing levels, but you should be attentive to whether the steps are feasible and appropriate for the participants. For example, where the procedure calls for reading a text, you can instead read the text aloud.
The steps will often also include suggested questions to help guide the discussion on the activity topic. You should feel free to add to them or to rephrase them, based on the local context. Moreover, it is not necessary that the group discuss all of the suggested questions or that you adhere strictly to the order in which they are listed in the activity. Rather, you should focus on encouraging as many participants as possible to express

14 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
their opinions. It is important to be patient, since some participants may be shy in the beginning or may not feel comfortable discussing these topics with each other. You should never force anybody to speak.
Notes on the process of the activityThese notes will help you to facilitate the activity better. They point out important aspects of the process and background information and tips to help you prepare for the activity. Make sure you have read these notes before you begin.
Key learning points (Closing)The section highlights the key points that participants should learn as a result of doing the activity. It may be helpful to refer to these key points while you are facilitating the discussion. You can also use them in summing up the discussion at the end of the activity.
Handouts that may be given out during the activitySome activities have handouts. These are included at the end of the activity. The handouts include information for participants to take away with them or for you to review with them. If possible, you should make enough copies of handouts for all participants. Another possibility is to write out the information on the sheets of flipchart paper for the participants to refer to during the activity.
Resource Sheets for reference by the facilitatorThis is additional information for the facilitator to review when preparing an activity. Not all activities will have resource sheets.
The appendices at the end of the manual highlight the following:
Appendix A: Optional Sessions
This appendix covers sessions that may be used provided there is enough time for the original sessions to be done comfortably. Alternatively, they may be used to enrich sessions and also to provide additional resources for the facilitator. They are by no means meant to replace the original sessions. The facilitator should assess the knowledge levels of the participants and decide on which may be applicable.
Appendix B: Workshop Energizers
This is a list of various warm-ups/energizers that can simply be lively exercises to bring the energy back into the group when they are feeling tired or concentration seems poor.
Appendix C: Pre and Post Test Questionnaires
This questionnaire assesses the knowledge prior to and after the training in order to determine its impact. It should be administered at the onset of training before any session

15National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
is conducted and again after the all the sessions have been done. Where possible, this test can also be administered at the least 1 month after training has ended. This will allow the facilitator to assess whether your training has had a sustainable impact on participants’ knowledge, attitudes, and behaviours.
Appendix D: Training Evaluation Form
This evaluation form assesses the overall training content, facilitation methods and training facilities. It is used for improvements for future trainings.
v. How to use itBefore beginning the work with men, it is important that the facilitator and/or trainer read the entire manual to understand how it is organized and what it contains. Due to the nature of the activities which are designed to explore individual experiences, it is advised that the facilitator/trainer has outstanding interpersonal communication skills and a basic understanding of counselling skills.
The activities draw on an experiential learning model in which men are encouraged to question and analyze their own experiences and lives to understand how gender can perpetuate unequal power in relationships, and make both women and men vulnerable to reproductive health problems as well as HIV and AIDS. Most importantly, the activities engage men to think about how they can make positive changes in their lives and communities. This process of questioning and change takes time. Experience has shown that it is preferable to use the activities as a complete set (or using groups of activities from the different sections), rather than using just one or two activities. Many of the activities complement each other and when used together, contribute to richer and more rewarding reflections than if used alone. Since most of the activities are participatory, they are most effective when carried out with small groups of 10 to 20 participants.
Before the facilitator begins many of the activities, especially those dealing specifically with HIV and AIDS, it is suggested that he/she gather together all the most up-to-date information that can be found. You will discover a list of printed resources in the ‘References’ section at the end of this Manual; there is useful information on relevant material and organizations.
Men or Women Facilitators?•
Who should facilitate the group activities with men and boys? Should only men be facilitators? Common experience is that in some settings men and boys appreciate the opportunity to work with and interact with a male facilitator who can listen to them in a thoughtful way and who can serve as a role model for thinking about what it means to be a man. However, collective experience suggests that the qualities of the facilitator –

16 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
the ability of a facilitator, man or woman, to engage a group, to listen to them, to inspire them – are far more important than the sex of the facilitator. It may also be useful to have facilitators work in pairs, and sometimes male-female pairs, which have the important benefit of showing the ways that men and women, can interact as equals.
vi. Materials for Training
STATIONERY EQUIPMENT OTHER
Flipchart paper (at least two pads)
1 Ream of A4 blank paper A4 Notepads (3) A5 Notebooks (1 for each
participant) Coloured paper cards Plastic pocket folders Nametags Permanent Markers (different
colours) Prestick Pens/pencils Colour pencils/crayons/oil
pastels A roll of string Old magazines
Flipchart stand DVD: Matlakala’s Story DVD Player and Sound
System/Projector and Screen
DVD: Male Engagement Initiative: Digital Stories
Digital Stories Facilitator’s Guide
DVD Player and Sound System/Projector and Screen/TV
Take Control Flannelgram A jug of water
Training Agenda Copies of Handouts Pre/Post Test
Questionnaires Evaluation Forms IEC Materials e.g.
relevant fliers/leaflets from different organizations

17National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
vi
i. Tr
aini
ng A
gend
a
Tim
eD
ay 1
Day
2D
ay 3
Day
4D
ay 5
08h0
0 - 1
0h30
Wel
com
e &
In
trod
uctio
nsEx
pect
ation
s/G
roup
ru
les
Cour
se O
bjec
tives
Pre-
test
Chec
k In
:M
CP, T
S, C
GS
Chec
k In
Wha
t is
GBV
?
Sexu
al V
iole
nce
Chec
k In
SRH
and
its
dete
rmin
ants
Chec
k In
Expl
orin
g Fe
elin
gs
Man
agin
g m
y A
nger
10h3
0-10
h50
Bre
akBr
eak
Brea
kBr
eak
Brea
k
10h5
0-13
h00
Look
ing
at o
ur
Attitu
des
Lear
ning
abo
ut
Gen
der
The
Gen
der
Role
s w
e pl
ay
Alp
habe
ts o
f Pr
even
tion
Getti
ng T
este
d fo
r H
IV
Men
as
Victi
ms
of
Viol
ence
Dom
estic
Vio
lenc
e Cy
cle
Und
erst
andi
ng S
TIs
SRH
Rig
hts
The
Lega
l fra
mew
ork
in N
amib
ia
Com
mun
ity M
appi
ng
13h0
0-14
h00
Lunc
hLu
nch
Lunc
hLu
nch
Lunc
h
14h0
0-15
h30
HIV
/AID
S M
yths
and
Fa
cts
Leve
ls o
f HIV
Ris
k
Pow
er R
elati
ons:
Pe
rson
s an
d Th
ings
Gen
der
Fish
bow
l
Caus
es a
nd E
ffect
s of
Vi
olen
ce
Men
’s H
ealth
Dig
ital S
tori
es
Iden
tifyi
ng
Com
mun
ity
Enga
gem
ent a
ctivi
ties
Dev
elop
ing
Acti
on
Plan
s15
h30-
15h4
5 B
reak
Brea
kBr
eak
Brea
kBr
eak
15h4
5-17
h00
Posi
tive
or N
egati
ve?
Hea
lthy/
Unh
ealth
y Re
latio
nshi
psU
nder
stan
ding
Se
xual
ity
Effec
tive
Com
mun
icati
on
Post
- Te
stEv
alua
tion
Wra
p - u
p

work
shop
Prel
ude
Section1

19National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objectives:1. To become acquainted with each other.2. To clarify the workshop plan, including schedule, agenda and workshop.3. To encourage dialogue based on respect and to establish ground rules for the
workshop4. To assess participants’ prior knowledge and skills using the pre-test
Total Time 1–2 hours, depending on the size of the group
Materials:• Flipchart paper• Markers• Nametags• Agenda• Pre-test Questionnaire• Handouts
Activity 1.1 Welcoming and Introductions
Objective1. To provide an interactive way for participants to get to know each other
Time30 minutes
Materials• Flipchart paper• Markers• Nametags
Advance Preparation• Prepare a flipchart with the heading, “Expectations.”• Identify an introductory energizer (See Appendix B) that may work with the
participants

20 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps1. Welcome the group to the workshop. Explain that this workshop will focus on
understanding how engaging boys and men can contribute to a reduction in GBV incidence, HIV infection risk and enhanced sexual and reproductive health.
2. Introduce yourself and explain your role in the workshop. Have other facilitators do the same.
3. Divide the group into pairs. Have them introduce themselves to each other, looking at the following:
• Name• Where they work• One interesting thing about themselves• One expectation they have for this workshop
Allow 15 minutes for the exercise.After the pairs have found each other and exchanged information, ask them to BRIEFLY introduce each other to the larger group. Record their expectations on flipchart paper to use during the review of the agenda. 4. Have the group come up with ground rules that will ensure that learning will be done
in a conducive environment and that the group’s expectations will be met to a large extent. (Note: you may want to raise cellphone use, punctuality, and participation etc. if these are not brought up.) Don’t take too much time on this!
Activity 1.2: Review of Workshop Objectives and Agenda
Objective1. To review workshop objectives and discuss the agenda
Time20 minutes
Materials• Flipchart paper• Markers• Enough copies of the agenda for all participants• Resource Sheet 1: Training Objectives

21National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Advance Preparation• Prepare a flipchart paper listing the workshop objectives• Prepare a flipchart paper entitled, “Parking Lot”
Steps1. Review the workshop objectives using the flipchart paper prepared earlier. Pass out
copies of the agenda and review with participants. Link participant expectations discussed during the introductions to the objectives and activities of the workshop.
2. Write any expectations that do not fall within the scope of the workshop on the flipchart paper entitled “Parking Lot.” Explain that you will identify ways to meet participant expectations if they are not addressed in the training.
3. Ask participants if they have any questions about the workshop objectives and agenda.
Facilitator Notes 1: Training Objectives
The training will be guided by the following objectives:
To provide an extensive understanding of the key concepts of GBV, SRH and HIV/AIDS as relating to men and boys in the Namibian context
Reduction in acceptability of GBV Increased practices of alternatives to violence Increased willingness to act and stand up against GBV
By the end of the training workshop, participants will be able to:
Understand key concepts of GBV, SRH and HIV/AIDS as relating to men and boys in the Namibian context
Reduce acceptability of GBV Increase practices of alternatives to violence Increase willingness to act and stand up against GBV

22 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 1.3: Pre-Test
Objective1. To conduct an assessment of participants’ knowledge and attitudes regarding gender,
reproductive health, HIV/AIDS and GBV before the workshop
Time30 minutes
Materials• Enough copies of the Pre-test (see Appendix C) for all participants• Pens and pencils
Steps1. Explain to the participants that the purpose of the pre-test and post-test is to help
facilitators determine how well the objectives of the training were achieved.2. Distribute the pre-test to each participant. Ask them not to put their names on the
test papers.3. Allow 25 minutes for participants to complete the test.4. After 25 minutes, collect the pre-tests for review later. If the participants have
questions about the answers, let them know that their questions will be addressed during the training.
5. Mark the tests and compare the results with the post-test in order to evaluate the effectiveness of the training.

Understanding GenderSection
2

24 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objectives:1. Increase knowledge and understanding of gender issues.
Total Time 2-3 hours
Changing Attitudes for Gender Equality
Throughout this manual there is a need to alter behaviours to reflect more gender equity, increased help seeking behaviours for SRH services, a reduction in the incidence of gender based violence and a reduced HIV infection rate. However, at the foundation of changing gender behaviour is changing attitudes. This section looks at why attitude change is necessary and how it can come about.
What is an Attitude? Attitudes represent an individual's degree of like or dislike, or judgment, for something and this usually falls in the spectrum of positive, undecided and negative views.
Attitudes are said to develop on the ABC model (affect, behaviour, and cognition) through experiences and observations. The affective response is emotional and expresses an individual's preference. The behavioural response indicates the preference verbally or through behaviour. The cognitive response involves an evaluation on the individual's beliefs about the object. Attitudes change with experiences, through persuasion.
Implicit attitudes, which are often relevant when considering people’s attitudes towards gender are outside of awareness, but are real and have effects.
Attitudes involve feelings, beliefs and behaviours that are formed, nurtured and perpetuated by society, institutions, religions and families, among others. They form the basis of one’s perception of what is right or wrong, the way men and women relate to each other within the home and in society, reflect the beliefs and behaviour they observe as children growing up and receive as instruction at school, in religious organizations or in the community. It is therefore apparent that attitudes form the basis of gender inequality and any change towards equality will need to focus on changing attitudes that society has about different groups. That is quite a feat! How can a goal like that be achieved?

25National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
If an attitude is comprised of three elements: feelings, beliefs and behaviour, then the change can occur at any one or all of the levels. According to psychological theory, feelings and beliefs are much easier to change than behaviour.
An example of attitude change is a conversation with a gentleman who considered himself gender sensitive. In a bid to illustrate the difficulty in changing behaviour, even though feelings and beliefs have changed, the gentleman was asked if he would carry his wife’s handbag. The response was a definitive “no” because a man cannot be seen carrying a woman’s handbag. In trying to persuade the gentleman to accept that he was not as gender sensitive as he thought he was, it was explained that a lady’s handbag is so small and presents no inconvenience and the refusal to carry it was a mere function of our socialization and conditioning. By carrying a woman’s handbag, nothing would biologically change and alter the man’s features. The gentleman eventually accepted the challenge to carry his wife’s handbag, but could not visualize himself actually doing it. This exchange confirms the difficulty in changing behaviour, though feelings and beliefs can easily change.
Our attitudes are greatly embedded in our value system, and therefore to change them will necessitate a critical look at this value system, and more importantly, a significant mind shift.
Activity 2.1 Looking At Our Attitudes2
ObjectivesTo explore attitudes about gender differences, roles, and inequalities
Time: 45 minutes
Materials• Four signs (“Strongly Agree,” “Strongly Disagree,” “Agree,” and “Disagree”)• Markers• Prestik• Handout 1: Namibian Trends and Statistics
2 Adapted from the Manual:Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

26 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Advance preparationBefore the activity begins, place the four signs around the room. Leave enough space between them to allow a group of participants to stand near each one. Review the statements provided below. Choose five or six that you think will help the discussion most.
Statements• It is easier to be a man than a woman.• When a woman is pregnant, preventing HIV infection to her child is her responsibility
since she carries the child.• A man is more of a “man” if he has many sexual partners.• Sex is more important to men than to women.• It is okay for a man or woman to have sex outside of relationship, if his partner does
not know about it.• A woman who carries a condom in her purse is “easy.”• A man and a woman should decide together what type of contraceptive to use.• GBV prevention and SRH programmes are only for women and girls.• A woman should tolerate violence in order to keep her family together.• A man should have the final word about decisions in his home.• There are times when a woman deserves to be beaten.• Women who wear revealing clothing are asking to be raped.• It is compulsory for a partner to disclose any STIs, including HIV to their partner.
Facilitator’s notesIf all the participants agree about any of the statements, play the role of “devil’s advocate” by walking over to the opposite side of the room and asking, “Why would someone be standing on this side of the room?” (i.e., what values would they have that would put them here?)
Some participants may say that they don’t know whether they agree or disagree and don’t want to stand beside any of the four signs. If this happens, ask these participants to say more about their reactions to the statement. Then encourage them to choose a sign to stand beside. If they still don’t want to, let these participants stand in the middle of the room as a “don’t know” group.
Steps1. Explain to the participants that this activity is designed to give them a general
understanding of their own and each other’s values and attitudes about gender. It is designed to challenge some of their current thinking about gender issues and help them clarify how they feel about certain issues. Remind the participants that everyone has a right to his or her own opinion, and everyone’s opinions should be respected.

27National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
2. Read aloud the first statement you have chosen. Ask participants to stand near the sign that says what they think about the statement. After the participants have moved to their sign, ask for one or two participants beside each sign to explain why they are standing there. Ask them to say why they feel this way about the statement.
3. After a few participants have talked about their attitudes towards the statement, ask if anyone wants to change their mind and move to another sign. Then bring everyone back together to the middle of the room and read the next statement.
4. Repeat Steps 2 and 3. Continue with each of the statements you have chosen.5. After reading all of the statements, lead a discussion by asking the following
questions:What statements, if any, did you have strong opinions and not very strong •opinions about? Why?What benefits does gender equality bring to men’s lives?•How did it feel to talk about an opinion that was different from that of some of •the other participants?How do you think people’s attitudes about the statements might affect the way •they deal with men and women in their lives?How do you think people’s attitudes about the statements help or do not help •to reduce the spread of HIV and AIDS?
6. Illustrate this flow chart on the flipchart: Values/Beliefs ® Attitudes ® Behaviour Explain to the group what each term means and that behaviour is a result of attitudes
which are determined by our values. 7. Explain that it is often difficult to change behaviour if we still have the same attitude
and we don’t challenge our value system in order for the behaviour change to occur.
8. End the activity by reminding participants about the importance of thinking about their own attitudes towards gender. Encourage people to continue to challenge their own personal values and beliefs about gender throughout this workshop, and beyond.
9. Give Handout 1: Namibian Trends and Statistics to participants. Have the group members read a statement aloud; explain that this workshop will try to contribute to a reduction in the statistics that are written.
ClosingEveryone has their own attitudes about gender. Often, our attitudes may be in conflict with others. It is important to respect other people’s attitudes about gender, but to also challenge them if their attitudes and values can be harmful to them and to others. As you do gender-related work, it is equally important to challenge your own personal values and beliefs about gender.

28 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 2.1: Namibian Trends and Statistics3
According to Namibian Police crime statistics of 2008, there were 939 reported cases of rape for that year, of which 541 were perpetrated against adult females, 17 against young men and 375 against young females. Still the same report shows that there were 10 917 reported cases of assault with intent to do grievous bodily harm; 3756 of these where committed by adult women, 172 by male juveniles and 118 by female juveniles. The rest of that figure (6827) is accounted for by men.
Over 40% of all women aged 18-49 in Namibia had been subject to physical gender based violence, compared to 27.6% for males.
17% of all women aged 18-49 in Namibia had experienced sexual violence sometime in their life.
Emotional violence affected a higher 59%, and was higher for males than females. Overall, combining physical and emotional violence, 69.7% of females and 68.9% of males had ever experienced violence.
Attitudes towards domestic violence: Adolescents aged 15-19 who think that a husband/partner is justified in hitting or beating his wife/partner under certain circumstances (2002-2009*) Female 38% and Male 44%.
HIV knowledge: adolescents aged 15-19 who have comprehensive knowledge of HIV (2005-2009*) Female 62% and Male 58%.
Estimated number of people (all ages) living with HIV (2009) - 180 000 (13.7% of population)
Prevention among young people: % who have comprehensive knowledge of HIV, 2005-2009*, Female 65% and Male 62%
Prevention among young people: % who used condom at last higher-risk sex, 2005-2009*, Male 81% and Female 64%
51 percent of women have ever been tested for HIV and received their results compared to 32 percent of men.
Namibia’s relatively small population of 2.1 million has one of the highest HIV prevalence rates in the world.
On average, 13 foetuses are found in the City of Windhoek’s sewerage system per month.
3 UNICEF (2009) www.unicef.org/infobycountry/namibia_statistics.html Ministry of Health and Social Services (MoHSS) (2010) UNGASS Country Report Ministry of Health and Social Services (MoHSS) and Macro International Inc. (2008). Namibia Demographic and
Health Survey 2006-07. Ministry of Health and Social Services (MoHSS) (2004). An Assessment of the Nature and Consequences of
Intimate Male-Partner Violence in Windhoek Police Statistics were sourced from the UNICEF Library. Children and Adolescents in Namibia, A situation analysis 2010. National Planning Commission

29National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
What is Gender? Gender refers to the social attributes and opportunities associated with being male and female and the relationships between women and men and girls and boys, as well as the relations between women and those between men. These attributes, opportunities and relationships are socially constructed and are developed through socialization processes. They are context/ time-specific and changeable.
Gender determines what is expected, allowed and valued in a woman or a man in a given context. In most societies there are differences and inequalities between women and men in responsibilities assigned, activities undertaken, access to and control over resources, as well as decision-making opportunities.
http://www.itu.int/gender/about/gender.html
What then, is the difference between Gender and Sex?"Sex" refers to the biological and physiological characteristics that define men and women."Gender" refers to socially constructed roles, behaviors, activities, and attributes that a given society considers appropriate for men and women.To put it another way:"Male" and "female" are sex categories, while "masculine" and "feminine" are gender categories.Aspects of sex will not vary substantially between different human societies, while aspects of gender may vary greatly.
Some examples of sex characteristics:Women menstruate while men do not •
Men have testicles while women do not •
Women have developed breasts that are capable of lactating, while men do not•
Men generally have more massive bones than women•
•
Some examples of gender characteristics:Women get paid less than a man for doing the same amount of work •
Women in Namibia carry the brunt of childcare and caring for people living with •
HIV and AIDS More men than women are represented in the Namibian parliament•

30 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Gender Equality and Gender Equity Gender Equality means equality between men and women; the freedom to develop and make choices unrestricted by gender stereotypes, roles and prejudices; that the different behaviours, aspirations and needs of women and men are considered, valued and favoured equally. It does not mean that women and men have to become the same, but that their rights, responsibilities and opportunities do not depend on whether they are born male or female.
Gender Equity means fairness and it is also a route to principles of justice to correct or enhance the law. It is in this sense that specific measures must be designed to remove inequalities between women and men, discrimination and to ensure equal opportunities. Gender equity leads to equality.
http://portal.unesco.org/ci/en/ev.php-URL_ID=3443&URL_DO=DO_TOPIC&URL_SECTION=201.html
Activity 2.2 Learning About Gender4
Objectives1. To understand the difference between the terms “sex” and “gender”2. To understand the terms “gender equity” and “gender equality”
Time40 to 60 minutes
Materials• Flipchart• Marker• Prestik • Enough copies of Handout 2: The Gender Game for all participants
Steps1. Explain that this session will help clarify some of the terminology that we will be
using in the workshop. It will also help us understand what these terms mean in our own lives.
2. Ask participants if they can explain the difference between “sex” and “gender.” After getting feedback from the group, provide the following definitions:
4 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

31National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Sex refers to physiological attributes that identify a person as male or female.• Gender refers to widely shared ideas and expectations concerning women and
men. These include ideas about typically feminine/female and masculine/male characteristics and abilities, and commonly shared expectations about how women and men should behave in various situations. These are not universal, but are learnt and acquired. They vary from one society to another and change over time.
(These definitions are based on those used by WHO)
3. Distribute the handout and ask the participants to indicate if the statements are referring to “sex” or “gender.” After giving the participants a chance to read and answer the statements on their own, discuss each of the answers with the entire group.
4. Explain that there are several terms related to the word “gender” that also need to be explained. Ask the group if they have ever heard the term “gender equality.” Ask them what they think it means. Allow plenty of time for discussion.
5. After getting their feedback provide the following definition:• Gender Equality means that men and women enjoy the same status. They share the
same opportunities for realizing their human rights and potential to contribute and benefit from all spheres of society (economic, political, social, and cultural).
6. Ask the group if the definition makes sense. Allow them to ask questions about it. 7. Ask the group to discuss whether or not gender equality actually exists in Namibia.As the group discusses this, write down any statements that explain why women do not share equal status with men in all spheres of society. Be sure to include some of the following points if they are not mentioned by the group:• Women in many countries are more likely than men to experience sexual and
domestic violence.• Men are paid more than women for the same work (in most cases).• Men are in more positions of power within the business sector.• Women bear the brunt of the AIDS epidemic, both in terms of total infections and in
care and support for those living with HIV.8. Ask the group if they have ever heard the term “gender equity.” Ask them what they
think it means and how it is different from gender equality. Allow plenty of time for discussion. After getting their feedback provide the following definition:

32 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Gender Equity is the process of being fair to men and women. Gender equity leads to gender equality. For example, an affirmative action policy that promotes increased support to female-owned businesses may be gender equitable because it leads to ensuring equal rights among men and women. After clarifying the definitions of gender equality and gender equity, ask the group the following questions:
Why should men work towards achieving gender equality? What benefits does gender equality bring to men’s lives? How does gender inequity contribute to HIV infection? How can gender equity contribute to preventing HIV?
10. Ask the group to identify gender-equitable actions that men can take to help create gender equality.
ClosingA major goal of engaging men and boys is to encourage communities to be more gender sensitive, so that men and women can live healthier and happier lives, and to prevent HIV infection.
To achieve this, we must encourage gender-equitable behaviours such as men and women making joint decisions about their health, a man respecting a woman’s right to say no to sex, men and women settling differences without violence, and men and women sharing responsibility for parenting and care for others.

33National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 2.2: The Gender Game
Identify if the statement refers to gender or sex.
Gender Sex
1. Women give birth to babies, men don’t.
2. Girls should be gentle, boys should be tough.
3. Globally, women or girls are the primary caregivers for those sick with
AIDS-related illnesses in more than two-thirds of households.
4. Women can breastfeed babies, men can bottle feed babies.
5. Many women do not make decisions with freedom, especially regarding
sexuality and couple relationships.
6. The number of women with HIV (human immunodeficiency virus) infection
and AIDS (acquired immunodeficiency syndrome) has increased steadily
worldwide.
7. More men than women die of suicide in Namibia.
8. Women get paid less than men for doing the same work.

34 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Answers to the Gender Game1. Sex – a women’s reproductive system (i.e. womb) is capable of carrying a baby.2. Gender – this is a socially assigned role3. Gender – women are socialized to be the caregivers in the home4. Sex – women’s breasts are capable of lactating and producing milk5. Gender – the socially assigned gender roles prescribe that women should be meek
and not initiate sexual activity or make decisions.6. Sex and Gender – a woman’s vagina has a larger surface area that makes it more
vulnerable to tears and bruises and also because most women do not generally exercise freedom when it comes to negotiating safer sex.
7. Gender – due to the socially constructed rule that men must be tough and brave, they are likely not to talk about their feelings or problems. Unfortunately, some men will see suicide as the only solution to their problems.
8. Gender – In some instances, women are considered to not equally contribute or work as hard as men.
Gender SocializationWhy do men and women act the way they do? Society expects different attitudes and behaviours from boys and girls. Gender is considered a social construction. Gender socialization begins at birth once an infant’s sex becomes known. From birth infants learn attitudes, thoughts, and behaviour patterns that have been established by society based on an individual’s sex.
Gender socialization is the tendency for boys and girls to be socialized differently. Boys are raised to conform to the male gender role, and girls are raised to conform to the female gender role. A gender role is a set of behaviors, attitudes, and personality characteristics expected and encouraged of a person based on his or her sex. Boys learn to be boys and girls learn to be girls. This "learning" happens by way of many different agents of socialization. The family is certainly important in reinforcing gender roles, but so are one’s friends, school, work and the mass media.
Girls in traditional cultures typically work alongside their mothers from a young age and by adolescence they can contribute equal amounts of work. Girls typically maintain a close relationship with their mothers. In adolescence, socialization stays narrow or becomes even narrower for girls, their budding sexuality is likely to be tightly restricted, and there is a focus on preparing for marriage or gender-specific adult work.
For boys, manhood is something that has to be achieved and the attainment of manhood is often fraught with peril and carries a possibility of failure. In most cultures an adolescent

35National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
boy must demonstrate three capacities before he can be considered a man: provide, protect, and procreate. Manhood requirements involve not just the acquisition of skills in these three areas but also the development of certain character qualities that must accompany the skills.
In general terms, femininity is associated with expressive traits such as being nurturing and compliant while masculinity is associated with instrumental traits such as being independent and aggressive.
Activity 2.3: The gender roles we play5
Objectives1. To identity the differences between rules of behaviour for men and for women2. To understand how these gender rules affect the lives of women and men
Time45 to 60 minutes
Materials• Flipchart• Markers• Prestick• Resource Sheet 2: Example of Flipcharts for The Gender Roles We Play
Facilitator’s notes
This activity is a good way to understand perceptions of gender norms. Remember that these perceptions may also be affected by class, race, ethnicity, and other differences.It is also important to remember that gender norms are changing in many countries. It is getting easier, in some places, for men and women to step outside of their “boxes.” If there is time, discuss with the group what makes it easier in some places for women and men to step outside of the box.
5 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

36 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps
1. Ask the male participants if they have ever been told to “Act like a Man.” Ask them to share some experiences of someone saying this or something similar to them. Ask: “Why do you think they said this?” “How did it make you feel?”
2. Now ask the female participants if they have ever been told to “Act like a woman.” Ask them to share some experiences of someone saying this or something similar. Ask: “Why do you think they said this?” “How did it make you feel?”
3. Tell the participants that you want to look more closely at these two phrases. Explain that by looking at them, we can begin to see how society creates very different rules for how men and women are supposed to behave. Explain that these rules are sometimes called “gender norms” because they define what is “normal” for men and women to think, feel, and act. Explain that these rules restrict the lives of both women and men by keeping men in their “Act like a Man” box and women in their “Act like a Woman” box.
4. In large letters, print on one sheet of flipchart paper the phrase “Act Like a Man.” Ask participants what men are told in their community about how they should behave.
Write these on the sheet. Check the examples in the resource sheet to see the kinds of messages that are often listed and introduce them into the discussion if they have not been mentioned.
5. When the group has no more to add to the list, ask the discussion questions listed below. Which of these messages can be potentially harmful? Why? (Place a star next to
each message and discuss one by one.) How does living in the box impact a man’s health and the health of others,
especially in relation to HIV and AIDS? How does living in the box limit men’s lives and the lives of those around
them? What happens to men who try not to follow the gender rules (e.g. “living outside
the box”)? What do people say about them? How are they treated? How can “living outside the box” help men to positively address HIV and AIDS?
6. Print on another sheet of flipchart paper the phrase “Act Like a Woman.” Ask participants what women are told in their community about how they should behave.

37National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Write these messages on the sheet. Check the examples to see the kinds of messages that are often listed. Feed these in to the discussion if they have not been mentioned.
7. When the group has no more to add to the list, ask the discussion questions listed below. Which of these messages can be potentially harmful? Why? (Place a star next to
each message and discuss one by one). How does living in the box impact a woman’s health and the health of others,
including in relation to HIV and AIDS? How does living in the box limit women’s lives and the lives of those around
them? What happens to women who try not to follow the gender rules? What do
people say about them? How are they treated? How can “living outside the box” help women to positively address HIV and
AIDS?
8. Next, draw another table that has both a column for men and women. Label it “Transformed Men/Women.” Ask the participants to list characteristics of men who are “living outside the box.” Record their answers. Once you get seven or so responses, ask the same about women who are “living outside the box.” Help the participants recognize that, in the end, characteristics of gender equitable men and women are actually similar.
9. Ask participants the following questions: Are your perceptions about the roles of men and women affected by what your
family and friends think? How? Do the media have an effect on gender norms? If so, in what way(s)? How do the
media portray women? How do the media portray men? How can you, in your own lives, challenge some of the nonequitable ways men
are expected to act? How can you challenge some of the nonequitable ways that women are expected to act?
10. Ask each participant to draft a personal action plan that will help them to stay out of the gender box. This can have such headings such as: what I will do differently, who will support me/be accountable to, and how I will make this change known.
11. Participants can also revisit their individual action plan towards the end of the workshop in order to include other aspects of the course content.

38 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Closing
Throughout their lives, men and women receive messages from family, media, and society about how they should act as men and women and how they should relate to each other. As we have seen, many of these differences are constructed by society and are not part of our nature or biological make-up. Many of these expectations are completely fine, and help us enjoy our identities as either a man or a woman. However, we all have the ability to identify unhealthy messages as well as the right to keep them from limiting our full potential as human beings. As we become more aware of how some gender stereotypes can negatively impact our lives and communities, we can think constructively about how to challenge them and promote more positive gender roles and relations in our lives and communities. Therefore, we are all free to create our own gender boxes and how we choose to live our lives as men and women.

39National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 2.3:Example of Flipcharts for The gender roles we play
Act Like a Man Act Like a Woman
• Be tough • Be passive and quiet
• Do not cry • Be the caretaker and homemaker
• Be the breadwinner • Act sexy, but not too sexy
• Stay in control and do not back down • Be smart, but not too smart
• Have sex when you want it • Follow men’s lead
• Have sex with many partners• Keep your man, provide him with sexualpleasure
• Get sexual pleasure from women • Don’t complain
• Produce children • Produce children
• Get married • Don’t discuss sex
• Take risks • Get married
• Don’t ask for help • Be pretty
• Use violence to resolve conflicts • Be seen, not heard
• Drink
• Smoke
• Ignore pain
• Don’t talk about problems
• Be brave
• Be courageous
• Make decisions for others
Transformed Men Transformed Women
• Be loving • Be loving
• Act caring • Act caring
• Be an assertive communicator • Be an assertive communicator
• Express emotions constructively and whenappropriate
• Express emotions constructively and whenappropriate
• Remain faithful to one partner • Remain faithful to one partner
• Get tested for HIV regularly • Get tested for HIV regularly
• Use condoms regularly • Use condoms regularly
• Delay sexual activities until both partnersare ready
• Delay sexual activities until both partnersare ready
• Speak out in favour of gender equality • Speak out in favour of gender equality
• Challenge others to recognise their harmful gender norms and change themselves
• Challenge others to recognise their harmful gender norms and change themselves

HIV Risks and Prevention
Section3

41National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objectives:1. Increased understanding and knowledge on HIV&AIDS and how GBV perpetuates
risk for HIV infection
Total Time 3-4 hours
Materials:Flipchart paper•Markers•Handouts •
What is HIV? HIV is the virus that causes AIDS. The first cases of AIDS were identified in the United States in 1981, but the virus probably existed here and in other parts of the world for many years before that. In 1984, scientists proved that HIV causes AIDS. The first case of AIDS in Namibia was diagnosed in 1986.
What is the difference between HIV and AIDS? A person infected with HIV may remain healthy for several years with no physical signs or symptoms of infection. A person with the virus, but no symptoms, is “HIV-infected” or “HIV-positive.” After a person has been infected with HIV for a period of time (often many years), symptoms caused by the virus begin to develop. At this stage, people with HIV are likely to contract opportunistic infections. When an HIV-positive person contracts one or more specific infections (including tuberculosis, rare cancers, and eye, skin, and nervous system conditions), she or he is defined as having “AIDS.”
When HIV enters your body, it infects specific cells in your immune system. These cells are called CD4 cells or helper T cells. They are important parts of your immune system and help your body fight infection and disease. When your CD4 cells are not working well, you are more likely to get sick.
Usually, CD4 cell counts in someone with a healthy immune system range from 500 to 1,800 per cubic millimeter of blood. AIDS is diagnosed when your CD4 cell count goes below 200. Even if your CD4 cell count is over 200, AIDS can be diagnosed if you have HIV and certain diseases such as tuberculosis or Pneumocystis carinii [pneumonia (PCP).

42 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
There are general stages of HIV infection that one may go through before AIDS develops.
Infection The earliest stage is right after you are infected. HIV can infect cells and copy itself before your immune system has started to respond. You may have felt flu-like symptoms during this time.
Response The next stage is when your body responds to the virus. Even if you don’t feel any different, your body is trying to fight the virus by making antibodies against it. This is called sero-conversion, when you go from being HIV negative to HIV positive.
No symptoms You may enter a stage in which you have no symptoms. This is called asymptomatic infection. You still have HIV and it may be causing damage that you can’t feel.
Symptoms Symptomatic HIV infection is when you develop symptoms, such as certain infections, including PCP.
AIDS AIDS is diagnosed when you have a variety of symptoms, infections, and specific test results. There is no single test to diagnose AIDS.
Activity 3.1: HIV&AIDS Myths and Facts6
Objectives 1. To understand the basic facts about HIV&AIDS
Time 60 minutes
Materials • Flipchart • Markers• Statement cards (see Advance Preparation below)• Enough copies of Handout 3: The Facts About HIV and AIDS for all participants
6 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

43National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Advance preparation Before you begin, write each statement on a separate piece of paper:• You can become infected with HIV from mosquito bites. • Anal sex is the riskiest form of sexual contact.• People can contract HIV if they perform oral sex on a man.• When used consistently and correctly, condoms can reduce the risk of HIV
transmission.• Circumcised men do not need to use condoms.• HIV is a disease that affects only poor people.• If you stay with only one partner, you cannot contract HIV.• People with STIs are at higher risk for becoming HIV-infected than people who do
not have STIs. • A man can transmit HIV to his partner during sex, even if he withdraws before
ejaculation. • A man can be cured of HIV by having sex with a virgin. • HIV is transmitted more easily during dry sex than wet sex.• You cannot contract AIDS by living in the same house as someone who has the
infection.• You can always tell if a person has HIV by his or her appearance.• Traditional healers can cure HIV.• HIV can be transmitted from one person to another when sharing needles during
drug use.
Steps 1. Give out the statement cards to the participants. Draw two columns on a flipchart.
Write “True” at the top of the left-hand column and “False” at the top of the right-hand column.
2. Ask one of the participants to read aloud the statement on his card. Ask whether he thinks it is true or false. Have him place it in the correct column on the flipchart and to explain his reasons. Then ask the group if they agree. Discuss, using the information in the Handout.
3. Repeat step 2 for all of the cards. Then give the Handout, and if there is time, review its information with the group.
Closing HIV stands for human immunodeficiency virus. This virus attacks the body’s immune system, which protects the body against illness. HIV infects only humans. Becoming infected with HIV leads to a weakened immune system. This makes a person who has HIV vulnerable to a group of illnesses that a healthy person without HIV probably would not contract.

44 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
A person infected with HIV may remain healthy for several years with no physical signs or symptoms of infection. A person with the virus but no symptoms is “HIV-infected”or “HIV-positive.” After a person has been infected with HIV for a period of time (often many years), symptoms caused by the virus begin to develop. At this stage, people with HIV are likely to contract opportunistic infections. When a HIV-positive person contracts one or more specific infections (including tuberculosis, rare cancers, and eye, skin, and nervous system conditions), she or he is defined as having Acquired Immune Deficiency Syndrome (AIDS).
HIV is found in an infected person’s blood (including menstrual blood), breast milk, semen, and vaginal fluids.

45National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 3.1: The Facts about HIV&AIDS
You can become infected with HIV from mosquito bites. – FALSE. It has been extensively researched and proven that HIV cannot be transmitted this way. In Africa, where malaria is common (and spread through mosquito bites), the only people infected with HIV are sexually-active men and women, babies born to HIV-infected mothers, and people who became infected due to blood transfusions or sharing needles.
Anal sex is the riskiest form of sexual contact. – TRUE. Anal sex carries a higher risk for HIV transmission than other types of sexual contact. During anal sex, the penis can tear the mucous membrane of the anus, which provides the virus with an entry point into the bloodstream. Dry vaginal sex also causes tearing of the mucous membrane and, therefore, is a high-risk behaviour for HIV transmission.
People can become infected with HIV if they perform oral sex on a man. – TRUE. HIV is present in the semen of infected men. Therefore, HIV may be transmitted if semen enters the person’s mouth. A man can reduce the risk for transmitting HIV by wearing a condom and ensuring that no semen enters his partner’s mouth.
When used correctly and consistently, condoms can protect men and women from becoming infected with HIV. – TRUE. Latex condoms are not 100% effective, but after abstinence, they are the most effective way of preventing STIs, including HIV infection. Some groups have reported inaccurate research suggesting HIV can pass through latex condoms, but that is not true. In fact, standard tests show that water molecules, which are five times smaller than HIV molecules, cannot pass through latex condoms.
Circumcised men do not need to use condoms. – FALSE. In the recent past, research has indicated that men who are circumcised may have a lower risk for HIV transmission than those who are uncircumcised. But this does not mean that circumcised men cannot contract HIV. It only means their chances of infection are lower. They still need to use condoms correctly every time they have intercourse.
HIV is a disease that affects only poor people. – FALSE. Anyone can become infected with HIV. A person’s risk for HIV is not related to the type of person he or she is (e.g., whether they’re wealthy), but rather to the behaviour he or she engages in.
If you stay with only one partner, you cannot become infected with HIV. – FALSE. Individuals who are faithful to their partner may still be at risk for HIV if their partner has sex with other people. In addition, individuals who have sex only with their partner may have been infected with HIV from someone else in the past. They may have the infection without knowing it, and without their current partner knowing it. Only a long-term, faithful relationship with someone who has not been previously infected can be considered “safe.”

46 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
People with STIs are at higher risk for becoming HIV-infected than people who do not have STIs. – TRUE. Infections in the genital area provide HIV with an easy way to enter the bloodstream.
A man can transmit HIV to his partner during sex, even if he withdraws before ejaculation. – TRUE. Withdrawal does not eliminate the risk for HIV. Pre-ejaculatory fluid from the penis can contain the virus, which can then be transmitted to another person. However, withdrawing is better than ejaculating inside the sexual partner, since it reduces the amount of exposure to semen.
A man can be cured of HIV by having sex with a girl who is a virgin. – FALSE. This is a misconception. Virgins do not have any power to heal HIV-infected individuals. There is no way to cure HIV once a person is infected.
HIV is transmitted more easily during dry sex than wet sex. – TRUE. HIV can be transmitted more easily during dry sex because the lack of lubrication causes cuts and tearing of the skin and the mucous membranes of both men and women’s genitals. These cuts provide the virus with an easy way to enter the bloodstream.
You cannot contract AIDS simply by living in the same house as someone who has the infection. – TRUE. HIV is transmitted through exposure to infected blood and other infected bodily secretions. Living in the same house with someone who is infected with HIV does not put those in contact with him or her at risk unless they share items that have been exposed to the infected person’s blood or genital secretions (e.g., shared toothbrushes, razors, or douching equipment).
You can always tell if a person has HIV by his or her appearance. – FALSE. Most people who become infected with HIV do not show any signs of illness for years. However, the virus remains in their body and can be passed on to other people. People with HIV look ill only during the last stages of AIDS, when they are near death.
Traditional healers can cure HIV. – FALSE. Over the years, many indigenous healers have claimed to be able to cure AIDS. To this day, no treatments by traditional healers have proven to cure HIV infection. We often hear people say they have developed a cure for AIDS. People with HIV are a vulnerable group because they desperately want to get rid of their life-threatening illness and will often pay large amounts of money for what they believe is a chance at a cure. Many see these vulnerable people as an easy source of money and try to exploit them. People with AIDS often feel better and seem to recover a little after taking useless treatments just because they have the hope of a longer life. Unfortunately, there is no cure at the moment for HIV infection.
HIV can be transmitted from one person to another when they share needles while using drugs. – TRUE. Sharing needles during injection drug use carries a very high risk for HIV transmission. Infected blood is easily passed from one person to another via an infected needle or other equipment used to prepare or inject

47National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
How is HIV Transmitted?Ways in which you can contract HIV:HIV is found in an infected person’s blood (including menstrual blood), breast milk, semen, and vaginal fluids. HIV can be transmitted in the following ways:• During unprotected vaginal, oral, or anal sex. HIV can pass from someone’s infected
blood, semen, or vaginal fluids directly into another person’s bloodstream, through the thin skin lining the inside of the vagina, mouth, or anus.
• Through HIV-infected blood transfusions or contaminated injecting equipment or cutting instruments.
• During pregnancy, delivery, and breastfeeding. About one-third of all babies born to HIV-infected women become infected. But it can take 12 to 18 months until it is known whether or not the child has HIV.
Ways you cannot get (and no one else can get) HIV:just working with or being around someone who has HIV •
being stung or bitten by an insect •
sitting on toilet seats •
doing everyday things like sharing a meal •
According to the Behavioural and Contextual Factors Driving the Epidemic report, a number of factors are likely contributing to the high levels of HIV in Namibia. The report identified the following behavioural and contextual factors:1. Multiple and concurrent partnerships - increases the odds of passing the virus to
several other persons. At the population level, each infected individual needs only infect one new person for the epidemic to be sustained
2. Inter-generational sex - exposes adolescents and young adults to partners who, by virtue of their age, are more likely to be HIV positive
3. Transactional sex - In these types of relationships, sex is exchanged for food, money, gifts, drinks, transportation, or other favours. These relationships may be long- or short-term, casual or stable.
4. HIV risk perceptions - People’s behaviours often depend on their perceptions of risk. Two aspects of HIV risk are relevant - a. the perceived likelihood of acquiring the infection and b. the expected impact that the disease will have on one’s life
5. Low and inconsistent condom-use 6. Male circumcision - Male circumcision itself is not driving the epidemic, but low
levels of circumcision combined with frequent concurrent partnerships and low condom use, is likely to be an important contributor to high prevalence of HIV in the country.

48 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
7. Alcohol abuse - High levels of alcohol consumption and alcohol abuse are likely to be contributing to the spread of HIV/AIDS in Namibia by increasing sexual risk behaviours
8. Mobility and migration patterns - High levels of population mobility further accelerate the spread of HIV. Travel away from home is associated with an increase in multiple partnerships in Namibia
9. Norms regarding partnerships - Across Namibia, two notable and inter-related trends are taking place that have important repercussions for the HIV/AIDS epidemic. The first is the marked decline in marriage and cohabitation rates. The second has been the widespread adoption of sex as a currency for acquiring otherwise unattainable goods and services.
Activity 3.2: Levels of HIV Risk7
Objectives 1. To identify the level of HIV risk of various behaviours and sexually-pleasurable
behaviours
Time 60 minutes
Materials • “Levels of Risk” cards (“Higher Risk,” “Medium Risk,” “Lower Risk,” and “No Risk”) –
see facilitator’s notes• “Sexual Behaviour” cards (16) – see facilitator’s notes• Enough copies of Handout 4: Levels of Risk for HIV Infection for all participants
Facilitator’s notes In large letters, print each of the following titles on cards (or pieces of paper), one title per card: “Higher Risk,” “Medium Risk,” “Lower Risk,” and “No Risk.”
In large letters, print each of the following sexual behaviours (or other behaviours that are relevant to your area or client population) on cards (or pieces of paper). Write one behaviour per card. • Abstinence• Masturbation• Vaginal sex without a condom
7 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

49National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Vaginal sex with a condom• Hugging a person who has AIDS• Fantasizing• Kissing• Dry sex without a condom• Massage• Anal sex with a condom • Performing oral sex on a man without a condom• Performing oral sex on a man with a condom• Performing oral sex on a woman without protection• Performing oral sex on a woman with protection• Infant breastfeeding from an HIV-infected mother• Anal sex without a condom
Steps 1. Explain to participants that they are going to do an activity about behaviours that
carry a risk for HIV infection. Lay out the four “Levels of Risk” cards in a line on the floor. Start with “No Risk,” then “Lower Risk,” then “Medium Risk,” and finally “Higher Risk.”
2. Give out the “Sexual Behaviour” cards to participants. Ask one of the participants to read his/her card and to place it on the floor under the correct category (“Higher Risk,” “Medium Risk,” “Lower Risk,” or “No Risk”) for HIV transmission. Ask the participant to explain why he/she has placed it there.
3. Repeat step 2 until all of the cards have been placed on the floor. Once all of the cards are down, ask the participants to review where the cards have been placed. Then ask whether they:
• Disagree with the placement of any of the cards • Do not understand the placement of any of the cards • Had difficulty placing any of the cards4. Discuss the placement of cards that are not clear-cut in terms of risk. Also discuss
cards that are clearly in the wrong place. Use the information in the closing and the handout to guide you on the correct placement.
5. Ask the participants to look at the behaviours in the “Lower Risk” and “No Risk” categories. Ask the group to identify other behaviours that could fit in these categories. Emphasize the idea that some pleasurable sexual behaviour involves low or no risk.
6. Finish the activity by emphasizing that risk depends on the context of the behaviour, and review the handout.

50 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Closing HIV risk depends on the context of the behaviour. This includes: • How much HIV the infected person has in their body• Whether or not the person is the “giver” or “receiver” of the sexual behaviour• How weak are the immune systems of the people involved • The presence of cuts or openings on the skin where contact with HIV is likely (for
example, as a result of STIs) • The presence of sores or bloody gums during oral sex• How well condoms and other protections are used

51National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 3.2: Levels of Risk for HIV Infection
Level BehaviourNo Risk =
No contact with infected body fluids. HIV is transmitted in body fluids. If there is no contact with such fluids, there is no risk for HIV being passed from an infected person to an uninfected person.
• Abstinence• Masturbation• Hugging a person who has AIDS• Kissing• Fantasizing• Massage
Lower Risk =
The possibility of contact with HIV because of the failure of protection. Using a condom still carries some risk because no protective method is 100% effective.
• Vaginal sex with a condom• Anal sex with a condom (the chances of
breakage are higher than for vaginal sex, so could be placed in next category.)
• Performing oral sex on a man with a condom• Performing oral sex on a woman with
protectionMedium Risk =
Medium possibility of HIV transmission. This can be due to a lack of protection in situations where there is some chance of HIV-infected fluids entering another person’s body (oral sex without a condom). Or it can be because protection is used, but there is a very strong chance that HIV-infected fluids will enter another person’s body (anal sex with condom).
• Performing oral sex on a man without a condom
• Performing oral sex on a woman without protection
• Infant breastfeeding from an HIV-infected mother
Higher Risk =
High probability of HIV transmission. This is because no protection is used and there is a very strong chance that HIV-infected fluids will enter another person’s body.
• Vaginal sex without a condom• Anal sex without a condom• Dry sex without a condom

52 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 3.3: Positive or Negative?8
Objectives 1. To discuss the factors that makes men and women vulnerable
to HIV and AIDS
Time 90 minutes
Materials • Small pieces of paper with selected profiles from Facilitator
Notes 3.3: HIV Profiles
• Pieces of paper with positive and negative symbols written on them
Advance preparation Prior to the session, choose five profiles from the Resource Sheet or create five profiles that would best fit the context in which you are working. Write these phrases on small pieces of paper (one per paper). Note: The facilitator should not include the HIV and AIDS test results on these pieces of paper. These results are only to be revealed later in the activity.
Steps 1. Explain to the participants that this activity is to discuss men’s and women’s
vulnerability to HIV and AIDS. 2. Review with the participants what HIV and AIDS is and how it is transmitted. Note:
The time necessary for this review will be based on the background knowledge of the group related to HIV and AIDS. It is important, however, that the participants have a clear understanding of how HIV is transmitted before they start this activity.
3. Ask for five volunteers. Distribute the profiles you have written on the small pieces of paper or for low-literacy groups, whisper a profile to each participant. Tell the volunteers they are going to put themselves in the shoes of the person whose profile they received.
4. Ask each volunteer to introduce himself to the larger group, according to the profile that s/he received. Each volunteer should give his or her character a name and feel free to incorporate mannerisms and behaviours into the presentation of the character.
8 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

53National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
5. Explain to the other participants that they should ask questions to get to know these five characters better. Emphasize to the volunteers playing the characters that they should be creative in answering the questions, while always keeping the profile descriptions in mind.
6. After approximately 20 to 25 minutes of introductions and questions, the facilitator should tell the group that these five volunteers have gone in for an HIV and AIDS test and are about to receive the results. Ask them what they think will be the results of each test.
7. Distribute the test results to each participant playing a role (these should be based on the results provided in the Resource Sheet alongside each profile), and then share these with the larger group.
8. Use the questions below to facilitate a discussion about the group’s reactions to the results and the complexities of men’s and women’s vulnerability to HIV and AIDS: To the volunteers: How did you feel representing these characters? How did
you feel when you received the test result? Was the result what you expected based on the description of your character? If not, why not?
Are these men’s and women’s experiences common? Does anyone know of any similar situations?
What characteristics are often associated with these men and women? What are some explanations for the different results these men and women
received? Were men or women more vulnerable in the sexual situations discussed in the
case studies? How could the men in the case studies have used their privilege and power
differently? What kinds of factors (social, economic, political) make men and women more
vulnerable to HIV infection? How can men and women protect themselves from HIV? Do couples generally talk about HIV and AIDS? Why or why not? What factors might inhibit a man from talking to his partner about HIV and
AIDS? What factors might inhibit a woman from talking to her partner about HIV and AIDS?
What support do couples need to protect themselves from STIs and HIV? Is this kind of support available in the community?
What have you learned in this activity? Have you learned anything that could be applied to your own life and relationships?

54 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Closing Men’s and women’s vulnerability to HIV and AIDS is largely determined by gender norms about sexuality. It is often assumed that “real men” have lots of sexual relations and that women should be coy and passive in sexual matters. As a result, women might not always have the power and/or skills to communicate and negotiate sexual behaviors and methods of prevention. Other factors, such as poverty, make it even less likely that men and women will be able to negotiate protection or even access important health information and services. Promoting women’s rights to be free from discrimination, coercion, and violence is an important step toward reducing vulnerability to HIV and AIDS. It is just as important to involve men in discussions about the role of negative gender norms and encourage them to discuss HIV and AIDS prevention with their partners.
Facilitator Notes 3.3: HIV Profiles
Woman, 30 years old, homemaker. She is married and has a five-year-old daughter and a three-year-old son. Recently discovered that her husband has sex with other people.
POSITIVE
Woman, 28 years old, sex worker. She is married. NEGATIVE
Woman, 17 years old, dropped out of school at 12 years old. She works to help her family pay the bills. Currently dating a man who is 26 years old.
POSITIVE
Woman, 15 years old, student. Likes to help her mom, has several friends, and is dating a 17-year-old guy. He is the first person with whom she has had sex.
POSITIVE
Woman, 26 years old, homemaker and wife of a gold miner. Her husband only visits a few times a year and in order to help feed her children, she began to have unprotected sex with a man who brought her food and a little money.
POSITIVE
Man, 32 years old, gold miner working 300 kilometres from his rural home. He lives in a hostel and sees his wife only a few times a year. After living away from his wife for a while, he starts to have sex with women in the nearby townships.
NEGATIVE
Man, 23 years old, student, who has been sexually active with girls his age and younger, and is currently in a monogamous relationship with a young woman.
NEGATIVE
Man, 25 years old, schoolteacher. He is married but still has other sex partners. He recently found out that he has a STI and decides to wait for it to go away before going to a doctor.
POSITIVE

55National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 3.4: Multiple Sexual Partners, Cross-Generational Sex, and Transactional Sex9
9 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.
10 Ms Libet Malony, Intrahealth: MCP Flannelgram, 2010
Objectives1. To define concurrent multiple sexual partnerships, cross-generational sex, and
transactional sex2. To explore how rigid gender norms drive these high-risk sexual behaviours 3. To identify risks and costs associated with these sexual behaviours
Time 60 minutes
Materials • Flipchart Paper • Markers• MCP Flannelgram10

56 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps 1. Explain that this session will explore three issues related to gender and sexual
activity: 1) men with concurrent multiple sexual partners, 2) men engaging in cross-generational sex, and 3) men engaging in transactional sex.
2. Divide the participants into three groups and assign one of the following issues to each.
• Group 1: Concurrent Multiple Sexual Partners • Group 2: Cross-Generational Sex • Group 3: Men Engaging in Transactional Sex3. Ask each group to provide a definition of their term. If they prefer, they can simply
provide an example of their term. 4. Ask someone from each group to share their definition and/or example. As each
group presents its definition, ask participants to provide additional examples. The definitions should be similar to the following:
• Concurrent Multiple Sexual Partners—this means a person is involved in more than one sexual relationship at the same time (for example, a man who is sexually active with his wife, but also has a girlfriend with whom he has sex).
• Cross-Generational Sex—this refers to two sexually-involved individuals with at least a 10-year difference in their ages (for example, a 30-year-old man who is in a sexual relationship with a 15-year-old girl).
• Transactional Sex—this refers to a sexual relationship or sexual act in which the exchange of gifts, services, or money is an important factor (for example, an older man buys a younger girl a cell phone or pays her school fees in exchange for sex).
5. After they have written their definitions, ask each group to discuss the following question:
Why does your issue put men, women, and communities at risk for HIV? 6. When they are ready, have someone from each group share their response to the
question. Be sure to include the following points if they are not mentioned: • Concurrent Multiple Sexual Partners—A person is much more likely to pass on HIV
if he or she has more than one sexual partner. It is easiest to transmit HIV when a person is first infected. Therefore, if someone is infected by one person, and has unprotected sex soon after with a second person, that second person will likely become infected, too.
• Cross-Generational Sex—When a man has sex with a person who is at least 10 years younger than he, there is a major imbalance in power. As a result, the younger person may find it difficult to say no to sexual activity and may be unable to negotiate safer sex.
• Transactional Sex—A person who is receiving money, gifts, or services may find it difficult to say no to sexual activity and may be unable to negotiate safer sex.

57National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
7. After discussing the risk factors, ask the participants to return to their groups. Remind them of the “Act Like A Man” box that was discussed earlier in the workshop. Ask each group to explore how societal messages about masculinity perpetuate the issue they are examining.
8. Ask someone from each group to share their response. Allow other participants to make additional comments.
9. Conclude the activity with the following discussion questions: Why do you think men are more likely than women to have multiple sexual
partnerships? Why do you think men are more likely than women to engage in sex with
partners at least 10 years younger than they? Why do you think men are more likely than women to provide gifts, services, or
money for sex? What are the costs and negative outcomes that come from men engaging in
multiple sexual partnerships, cross-generational sex, and transactional sex? How can men challenge other men to stop engaging in multiple sexual
partnerships, cross-generational sex, and transactional sex? What did you learn from this session?
Training Option:For low literacy groups, you can introduce the MCP Flannelgram to illustrate the three concepts with a visual aid. Follow the instructions on the cue card that you will find included in the materials provided.
Closing Rigid gender norms often drive the HIV epidemic by facilitating unsafe behaviour such as concurrent multiple sexual partnerships, cross-generational sex, and transactional sex. It is important for both men and women to realize this and identify ways that these norms can be changed and/or addressed.
HIV Prevention and TreatmentHIV counselling and testing are fundamental for HIV prevention. People living with HIV are less likely to transmit the virus to others if they know they are infected and if they have received counselling about safer behaviour. For example, a pregnant woman who has HIV will not be able to benefit from interventions to protect her child unless her infection is diagnosed. Those who discover they are not infected can also benefit, by receiving counselling on how to remain uninfected.
The availability and accessibility of antiretroviral treatment is crucial; it enables people living with HIV to enjoy longer, healthier lives, and as such acts as an incentive for HIV

58 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
testing. Continued contact with health care workers also provides further opportunities for prevention messages and interventions. Studies suggest that HIV-positive people may be less likely to engage in risky behaviour if they are enrolled in treatment programmes.
Someone can eliminate or reduce their risk of becoming infected with HIV during sex by choosing to:
Abstain from sex or delay first sex •
Be faithful to one partner or have fewer partners •
Condomize, which means using male condoms or female condoms consistently and correctly
There is now very strong evidence that male circumcision reduces the risk of HIV transmission from women to men by around 50%, which is enough to justify its promotion as an HIV prevention measure in some high-prevalence areas. However, studies of circumcision and HIV suggest that the procedure does not reduce the likelihood of male-to-female transmission, and the effect on male-to-male transmission is unknown.
Activity 3.5: Alphabets of Prevention11
Objectives 1. To explore different HIV and AIDS prevention options
Time 60 minutes
Materials • Flipchart• Markers
Advance preparation Write out the following on a flipchart: A – Abstain, delay sexual debut, say no to sexB – Be faithful, reduce number of partners C – Condom useD – Do it yourself (masturbation)
11 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

59National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
E – Enquire if your partner has been tested for HIV F- Find other ways of giving and receiving sexual pleasureG – Get testedMC – Male Circumcision
Facilitator notesReview the optional sessions and try to incorporate key sections in the Alphabets of Prevention session. Alternatively, write down the closing remarks of those sessions on a flipchart after the discussions on abstinence, condom use and male circumcision respectively.
Steps 1. Begin by asking if everyone in the group if they have heard of the ABC’s of HIV
prevention? Have them explain what they know about abstinence, faithfulness, and condoms.
2. Explain that many people feel that ABC is a good strategy, but that it might not be sufficient. Ask if anyone can think of additional meanings for D, E, F, and G?
3. After a few people have shared, show them the flipchart you prepared before the session.
4. Discuss each “letter” and its key components as a group.5. Divide the group into eight teams and have them develop a one-minute “commercial”
advertising their form of the Prevention Alphabet. Allow the groups 10 minutes to prepare and then ask each group to perform its commercial.
6. Discuss the following questions with the whole group: How do messages about gender and masculinity make it difficult for men to
carry out these strategies? How do messages about gender and masculinity make it difficult for women to
carry out these strategies? What other factors (e.g., economic class, marital status, religious beliefs) can
make it difficult to carry out these strategies? How can men and women be empowered to carry out HIV prevention in their
lives and relationships? What have you learned from this activity? Have you learned anything that could
be applied to your own life and relationships?
Closing Many men put themselves in situations of risk because they feel pressure to be “real men.” They feel they have to be masculine and that they cannot express their true emotions and feelings. Likewise, women may face situations of risk because of social norms that they be passive, or because of inadequate access to information and services.

60 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Both men and women need opportunities for open and honest discussions about HIV and AIDS and prevention strategies, as well as social supports that extend beyond mere information provision.
Training OptionIf there is ample time available, the facilitator can briefly explore abstinence and condom use further as a prevention method. See Appendix A: Optional Sessions.
Activity 3.6: Getting Tested for HIV12
Objectives 1. To discuss the importance
of HIV and AIDS counselling and testing and its related benefits and challenges
Time 40 minutes
Materials • Flipchart Paper• Markers• Prestick
Advance preparation Prior to the session, gather information on local centres for voluntary counselling and testing (VCT) in that specific area, and, if possible, arrange for a staff person to participate in this session. It is also important to be aware of policies and services related to the provision of antiretroviral drugs (ARV) for people who have HIV and AIDS.
12 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

61National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps 1. Ask the group if any of them have ever been for an HIV test. 2. If any did, follow up with these questions:
• What made you want to take the test? • How long did it take you to decide to take the test? • What were your feelings at the time? Why? • Who did you tell that you will be going for the test?
3. Wrap-up the discussion with the questions below. • Do people in your community know where they can go for HIV counselling and
testing? Do they trust it will be done safely and anonymously? • How do you think people are treated when they seek HIV counselling and
testing?• How do you think they should be treated? • Do you think men are more or less likely than women to seek out HIV counselling
and testing? Why? • What do you think are the biggest factors that hinder men from seeking HIV
counselling and testing? • What can be done to address these factors? • What should a man do if his test result is positive? • What should a man do if his test result is negative? • How can you encourage more men in your community to be tested?
Closing Men are often less likely than women to seek health services, including counselling and testing for HIV, since they often see themselves as invulnerable to illness or risk, or may just want to “tough it out” when they are sick. However, as has been discussed, men face many risks, and HIV testing is an important part of taking care of themselves and their partners. It is important for men to know where in their community they can get these services and to seek them out, when appropriate. The participants should think together about how to support those men who test negative so that they continue to protect themselves and how to encourage those men who test positive so that they live positively, that is, to seek out appropriate services and protect themselves and their partners from reinfection.

Gend
er an
d Pow
er Re
latio
nsSection
4

63National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objective: Decrease in the belief (amongst men and women) that there are reasons that justify violence against partners and children
Total Time 3-4 hours
Materials:Flipchart paper•Markers•Handouts •
What is power? Power is the ability to articulate personal goals and influence others to achieve those goals. It is the ability to get what we want, to hold on to what we get, and to shape events the way we want to shape them. At the collective level, power is the ability to combine different resources of individual power to bring about desired change that benefits groups rather than individuals.
Generally, men tend to have more economic, social and political power than women. This starts from the household, community, organisational, national all the way to international levels.
The Canadian International Development Agency (CIDA) has developed a classification of power that is helpful from a gender perspective. The four categories of power are “power to”, “power with”, “power within” and “power over”.
· Power to. This power is creative and enabling. It is the essence of an individual’s aspect of empowerment. It is associated with knowledge and ability e.g. ability to solve a problem, to understand issues, to learn a skill etc.
· Power with. This involves a sense of collective action. It is collective, democratic and interactive power, which enables people to feel empowered, through being organized and united to achieve common goals.
· Power within. This is innate power e.g. talent, born with. It resides in each of us and is the basis for self-acceptance and self- respect that in turn extends to respecting and accepting others as equals.
· Power over. This power entails relationship of domination and subordination. It is based on social sanctions and threats of violence and intimidation. It is coercive and often invites active and passive resistance. It creates dualities such as good/evil, man/woman, rich/poor, black/white, and us/them.

64 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity: 4.1 Power relations and gender implications
Objective1. To develop a better understanding of power and how it relates to gender
Time 40 minutes
Materials Flipchart •Markers•Enough copies of Handout 4.1: Power relations and gender implications•
Steps:1. Ask participants what they understand by the term power. Note down all the
responses on the Flipchart2. Present ‘Power relations and gender implications’ (Handout 5).3. Divide participants into 2 groups. Group 1 should analyze issues at household level.
Group 2 should analyze issues at community level • Identify unequal power relations that exist between men and women in Namibia
in social, economic and political life.• What are the consequences of the identified power relationships?• Propose 1-2 strategy for addressing each of the identified unequal power
relation.4. Let the groups report back in plenary using flip charts.

65National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 4.1: Power Relations and Gender Implications
1. Power relationsGender is about power relations that create differences between men and women.Gender relations are based on ideologies that attribute unequal power, authority and control of resources. Such relations are not easily negotiated. Women, in particular, are socially constructed to accept and perpetuate these power imbalances.Power is of different types.
1. Power Over – This refers to where one person is inferior to another.2. Power With – this refers to collective power, and is experienced when a
group tackles problems together and creates energy that is greater than the sum of its parts.
3. Power Within – this type of power resides within the individual and represents internal strength. It is based on self acceptance and self respect, which in turn extends to respect for others and acceptance of others as equals.
4. Power To – This type of power refers to the individual aspect of empowerment. It enables the individual to control or manage the situation to his/her benefit.
Source: Gender Training Manual and Resource Guide: Ministry of Gender Equality and Child Welfare
2. Gender implications of the unequal power relations: gender biasesThe main consequence of power relations is that there is continued exclusion of women from many social, economic and political opportunities. In the process, development is negatively affected because of the gender gaps created by the unequal power relations. Transforming power relations is thus important to achieving gender equality and empowerment.
3. Strategies for dealing with unequal power relationsStrategies for dealing with unequal power relations between men and women have to focus on gender equality and empowerment. It should be noted that gender equality and empowerment are not straightforward concepts and often create confusions. Gender equality means that there is no discrimination in terms of access to and control of resources, opportunities and benefits on the basis of sex. It refers to a principle of same status, rights and responsibility for men and women. Gender equality embraces the notion that ‘all people are created equal’ and no individual should be less privileged than the other. Achieving gender equality, therefore, entails identifying and removing all the underlying causes of discrimination. For this to happen, empowerment is a requirement.
Empowerment refers to a process of providing capacity for critical thinking; a process of challenging existing power relations; and a process of gaining greater decision making capacity on issues that affect one self and power sharing. This includes power relations in all spheres of life – political, cultural, economic etc.

66 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 4.2: Persons and Things13
Objectives 1. To increase awareness about the existence of power in relationships and its impact
on individuals and relationships
Time 30 minutes
Materials None
Facilitator’s notes Some of the participants might not feel comfortable with the role-play in this activity. It is important to be sensitive to how participants react to being assigned the role of “persons” or “things” and to be prepared to make the necessary accommodations or changes. For example, rather than have the participants actually carry out the role-play, the facilitator might invite the participants to discuss in pairs how “persons” might treat “things” and the feelings that this might generate for the “persons” and “things.” The facilitator should also be prepared to make referrals to counselling or other services for those participants who might be especially affected by the activity.
Steps 1. Divide the participants into three groups. Each group should have the same number
of participants. (Note: If the number of participants does not allow for an even distribution, assign the “extra” participants to the third group which, as described below, will be the observers.)
2. Tell the participants that the name of this activity is: Persons and Things. Choose, at random, one group to be the “things,” another to be “persons,” and a third to be “observers.”
3. Read the following directions to the group: • THINGS: You cannot think, feel, or make decisions. You have to do what the
“persons” tell you to do. If you want to move or do something, you have to ask the person for permission.
• PERSONS: You can think, feel, and make decisions. Furthermore, you can tell the objects what to do.
• OBSERVERS: You just observe everything that happens in silence.
13 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

67National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
4. Assign each “person” a “thing” and tell them that they can do what they want with them (within the space of the room).
5. Give the group five minutes for the “people” and “things” to carry out their designated roles.
6. After five minutes, tell the persons and things that they will switch and that now the “persons” will be “things” and “things” will be “persons.” Give them another five minutes to carry out the new roles.
7. Finally, ask the groups to go back to their places in the room and use the questions below to facilitate a discussion. • How did your “persons” treat you? What did you feel? Did you feel powerless?
Why or why not? • How did you treat your “things”? How did it feel to treat someone this way? Did
it make you feel powerful? Why or why not? • Why did the “things” obey the instructions given by the “persons”? • Were there “things” or “persons” who resisted the exercise? • In your daily lives, do others treat you like “things”? Who? Why? • In your daily lives, do you treat others like “things”? Who? Why? • For the “observers”: How did you feel not doing anything? Did you feel like
interfering with what was happening? If yes, what do you think you could have done?
• In our daily lives, are we “observers” of situations in which some people treat others like things? Do we interfere? Why or why not?
• If you had been given a chance to choose between the three groups, which would you have chosen to be in and why?
• Why do people treat each other like this? • What are the consequences of a relationship where one person might treat
another person like a “thing?” • How would being treated like a “thing” impact a person’s vulnerability to HIV? • In your communities, do men most often belong to one of these three groups?
Which group? Do women most often belong to one of these three groups? Which group? Why do you think this is?
• How does society/culture perpetuate or support these kinds of relationships?• What can we do to make sure that different groups such as men and women
live in an equitable world where they can enjoy the same opportunities, equal treatment, and equal rights?
Closing There are many types of relationships in which one person might have more power over another. As you will discuss throughout many of the activities in this manual, the unequal power balances between men and women in intimate relationships can have

68 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
serious repercussions for the risk for STIs, HIV and AIDS, and unplanned pregnancy. For example, a woman often does not have the power to say if, when, and how sex takes place, including whether a condom is used, because of longstanding beliefs that men should be active in sexual matters and women should be passive (or that women “owe” sex to men). In other cases, a woman who is dependent on a male partner for financial support might feel that she does not have the power to say no to sex. In cases of cross-generational sex, the age and class differences between men and women can further create unequal power relations that can lead to risk situations.
Activity 4.3: Gender Fishbowl14
14 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.
Objective1. To share experiences related to gender issues2. To develop a better understanding of and empathy for the experience of the other
sex
Time 60 minutes

69National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Materials • None
Facilitator’s notes This activity works best with a mixed-gender group of participants. However, you can run it with an all-male group. Simply divide the male participants into two groups. Ask the first to answer the top five questions from the list of questions for men. Then ask the other group to answer the last five questions from the list of questions for men.
In some communities (especially when both husbands and wives are attending the session), it might be difficult for women to truly express themselves because they’re afraid to publicly speak in front of their husbands. It might be more appropriate to conduct these discussions separately and have someone take notes to later share with the other gender.
Questions for Women
1. What is the most difficult thing about being a woman in Namibia? 2. What do you want to tell men that will help them better understand women? 3. What decisions do you typically make concerning your household? 4. How does your culture view men and women? Why?5. At family or community gatherings/events, what does the typical set up look like
with regard to men and women?6. What kinds of power do women have over men?7. How does this power contribute positively or negatively in relationships with the
opposite sex?8. How have gender roles influenced your life?9. How can men support and empower women? 10. How can women support and empower men?
Questions for Men
1. What is the most difficult thing about being a man in Namibia? 2. What do you want to tell women to help them better understand men? 3. What decisions do you typically make concerning your household? 4. How does your culture view men and women? Why?5. At family or community gatherings/events, what does the typical set up look like
with regard to men and women?6. What kinds of power do men have over women?

70 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
7. How does this power contribute positively or negatively in relationships with the opposite sex?
8. How have gender roles influenced your life?9. How can women support and empower men? 10. How can men support and empower women?
Steps 1. Divide the male and female participants.2. Ask the women to sit in a circle in the middle of the room and the men to sit around
the outside of the circle, facing in. 3. Begin a discussion by asking the women the questions listed in the facilitator’s notes
above. The men’s job is to observe and listen to what is being said. They are not allowed to speak.
4. After 30 minutes, close the discussion and have the men and women switch places. Lead a discussion with the men, while the women listen. The questions for the men are also in the facilitator’s notes.
5. Discuss the activity after both groups have taken a turn. Use the following questions: What surprised you about this activity? How did it feel to talk about these things with others listening? What did you learn?
Closing Often, our opinions and perspectives about the other sex are informed by stereotypes and gender and social norms that are reinforced over time by many sources, such as the media or our peers. This often makes it difficult for us to understand the other sex and their needs and concerns. By having a better understanding of the opposite sex and their needs and experiences, we are able to have greater empathy of how they experience gender and how it affects them. There are other examples of power relationships in our lives and communities. Think of relationships between youth and adults, students and teachers, employees and bosses. Sometimes the power imbalances in these relationships can lead one person to treat another person like an object. As you discuss gender and relationships between men and women, it is important to remember the connection between how you might feel oppressed or treated like “objects,” in some of your relationships and how you, in turn, might treat others, including women, like “objects.” Thinking about these connections can help motivate you to construct more equitable relationships with women in your homes and communities.

71National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 4.4: Healthy and Unhealthy Relationships15
Objectives1. To be able to identify healthy and unhealthy behaviours that exists within
relationships
Time 45-60 minutes
Materials• Three “Relationship Range” cards (see advance preparation)• A set of “Relationship Situation” cards (see advance preparation)• Flipchart paper, pens, and tape• Handout 4.4: Healthy and Unhealthy Relationships
Advance preparation Before the activity, write the following in large letters on separate pieces of paper: “Very Healthy,” “Very Unhealthy” and “Depends.” Also write each of the following Relationship Situations on a separate card (or piece of paper):• The most important thing in the relationship is sex.• You never disagree with your partner.• You spend some time by yourself without your partner.• You have fun being with your partner.• Your partner is still close to his or her ex-boyfriend or ex-girlfriend.• You feel closer and closer to your partner as time goes on.• You will do anything for your partner.• Sex is not talked about.• One person usually makes every decision for the couple.• You stay in the relationship because it is better than being alone.• You are in control of yourself and you are able to do what you want to do.• One person hits the other to make him or her obey.• You talk about problems when they arise in the relationship.• You argue and fight often.• Your partner usually starts calling you names if he/she does not agree with what
you say or do.• A man using violence against his wife/partner is a private matter that shouldn’t be
discussed outside the couple.
15 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

72 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• My partner dictates who I spend time with• My partner has more say than I do about important decisions that affect us • If you do not have cards/paper, you can simply read aloud each situation to the
participants.
Facilitator’s notes In healthy relationships, both partners are happy to be with the other person. In unhealthy relationships, one or both partners are unhappy because of continuing problems with the relationship that are not being addressed. Gender has an impact on people staying in unhealthy relationships. In general, women find it harder to leave unhealthy relationships than men. Women earn less money than men and have less control over economic resources (land, credit). This makes many women economically dependent on their husbands. Socially, women are more stigmatized for being divorced or separated. There is huge social pressure on women to preserve the family.
Men need skills and support to talk with their wives and girlfriends about creating healthier relationships. There is little support for either men or women in making their relationships healthier. But gender rules for women allow them to ask each other for support and to talk about their feelings. The gender rules for men make it difficult for them to ask for support on personal matters or to show their emotions. The first step toward healthier relationships is to challenge these gender rules. Men need more opportunities and permission to ask for support. Men also need specific training on how to talk about their feelings and their relationships.
Steps 1. On the wall in front of the group, place the “Very Unhealthy” sign on the left and
the “Very Healthy” sign on the right. Explain that this is the “Relationship Range” that will be used to discuss behaviours in relationships. Make clear that romantic relationships can be anywhere on this range between healthy and unhealthy.
2. Break the group into pairs. Ask each person to share with their partner an example of a healthy relationship and an unhealthy relationship. The examples can be from their own lives or from people that they know. Allow each person five minutes to share their examples.
3. Bring everyone back together. Ask the group to define healthy and unhealthy romantic relationships. Share the definition included in the facilitator’s notes section. Ask the group to brainstorm the qualities of a healthy relationship. Write these under the “Very Healthy” sign. Emphasize these key qualities: respect, equality, responsibility, and honesty. Make clear that the qualities of an unhealthy relationship are the opposite of those for a healthy relationship.

73National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
4. Next to the Relationship Range put up another sign marked “Depends.” Then give out the “Relationship Situation” cards to the participants. Choose one of the participants at random to read aloud what is on their card. Ask them to say how healthy or unhealthy this situation is in a relationship and why they think so. Tell them to place the card in the appropriate place on the Relationship Range, or in the “Depends” category.
5. Ask the group what they think about this placement. Allow time for discussion. If they don’t agree, remind them of the qualities of a healthy relationship (respect, equality, responsibility, honesty). Ask them if the situation shows these qualities.
6. Repeat steps 4 and 5 for each of the “Relationship Situation” cards. Then lead a general discussion by asking the following questions: • Why do you think some people stay in unhealthy relationships? • Are the reasons different for women and for men? Why?• How can friends and family help people in unhealthy relationships? • What skills and support do men need to create healthier relationships?
Closing Healthy relationships are based on communication and mutual respect. Decisions are made together and neither person dominates the relationship. Unhealthy relationships, on the other hand, can mean poor communication and unequal decision making, which makes open talk about sexual behaviour and contraception extremely difficult, and thus puts one or both partners at greater risk for STIs and HIV, and in some instances, violence.

74 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 4.4: Healthy vs. Unhealthy Relationships
Relationships are a necessary part of healthy living, but there is no such thing as a perfect relationship. Relationships, from acquaintances to romances, have the potential to enrich our lives and add to our enjoyment of life. However, these same relationships can cause discomfort, and sometimes even cause harm.
What makes a healthy relationship? A healthy relationship is when two people develop a connection based on:
♥ Mutual respect ♥ Trust ♥ Honesty ♥ Support ♥ Fairness/equality ♥ Separate identities ♥ Good communication ♥ A sense of playfulness/fondness
All of these things take work. Each relationship is most likely a combination of both healthy and unhealthy characteristics. Relationships need to be maintained and healthy relationships take work. This applies to all relationships; work relationships, friendships, family, and romantic relationships.
What are signs of a healthy relationship?A healthy relationship should bring more happiness than stress into your life. Every relationship will have stress at times, but you want to prevent prolonged mental stress on either member of the relationship.
While in a healthy relationship you:Take care of yourself and have good self-esteem independent of your •
relationship Maintain and respect each other's individuality •
Maintain relationships with friends and family •
Have activities apart from one another •
Are able to express yourselves to one another without fear of consequences •
Are able to feel secure and comfortable •
Allow and encourage other relationships •
Take interest in one another’s activities •
Do not worry about violence in the relationship •

75National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Trust each other and be honest with each other •
Have the option of privacy •
Have respect for sexual boundaries •
Are honest about sexual activity if it is a sexual relationship •
Accept influence. Relationships are give and take; allowing your partner to •
influence you is important; this can be especially difficult for some men. Resolve conflict fairly: Disagreement is part of even healthy relationships; the •
difference is how the conflict is handled.
What are the signs of an unhealthy relationship?At times all relationships will have some of the below characteristics. However, unhealthy relationships will exhibit these characteristics more frequently and cause you stress and pressure that is hard to avoid. This tension is unhealthy for both members and may lead to problems in other areas of your life.
While in an unhealthy relationship you:Put one person before the other by neglecting yourself or your partner •
Feel pressure to change who you are for the other person •
Feel worried when you disagree with the other person •
Feel pressure to quit activities you usually/used to enjoy •
Pressure the other person into agreeing with you or changing to suit you •
better Notice one of you has to justify your actions (e.g. where you go, who you see) •
Notice one partner feels obligated to have sex or has been forced •
Have a lack of privacy, and may be forced to share everything with the other •
person You or your partner refuse to use safer sex methods •
Notice arguments are not settled fairly •
Experience yelling or physical violence during an argument •
Attempt to control or manipulate each other •
Notice your partner’s attempts to control how you dress and criticizes your •
behaviours Do not make time to spend with one another •
Have no common friends, or have a lack of respect for each others’ friends and •
family Notice an unequal control of resources (food, money, home, car, etc.) •
Experience a lack of fairness and equality•

76 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
If some of your relationships have some of these characteristics it does not necessarily mean the end of that relationship. By recognizing how these characteristics affect you, you can begin to work on improving the negative aspect of your relationships to benefit both of you.
When should I seek help for my relationship?If a partner ever tries to harm you physically or force you to do something sexually that should be a clear sign for you that it is an unhealthy relationship. In that situation, you should consider getting help, or ending the relationship. Even if you believe the person loves you it does not make up for the harm they are putting you through. Other circumstances include:
When you are unhappy in a relationship, but cannot decide if you should •
accept it, try to improve the relationship, or end the relationship. When you have decided to leave a relationship, but find yourself still in the •
relationship. When you think you are staying in the relationship for the wrong reasons, •
such as fear of being alone or guilt. If you have a history of staying in unhealthy relationships.•

Gender Based ViolenceSection
5

78 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objective: Decrease in the perception that violence is a normal and natural occurrence in our society Total Time: 3 – 4 hours
What is violence? Violence can be defined as the use of force (or the threat of force) by one individual against another.
What is Gender Based Violence?According to the SADC Protocol on Gender and Development 2008-2015 GBV is defined as acts perpetrated against women, men, girls and boys on the basis of their sex which cause or could cause them physical, sexual, psychological, emotional or economic harm, including the threat to take such acts, or to undertake the imposition of arbitrary restrictions on or deprivation of fundamental freedoms in private or public life in peace time and during situations of armed or other forms of conflict.
Gender-based violence is related to the way men and women are expected to behave. It could be that a woman is beaten for failing to cook the dinner on time, or a man has to prove his manhood by showing aggression to a woman. Gender-based violence can be directed at children, adults or the elderly. A boy-child may be beaten if he cries because men are not supposed to show emotion. An elderly woman may be beaten if she fails to care for her children and her grandchildren, because traditionally elderly women are supposed to do this. Gender-based violence is common in Namibia. It is estimated that one in five women are in an abusive relationship. (LAC: addressing Gender Based Violence
through Community Empowerment).
The rights group Amnesty International has identified three distinct types of gender-based violence (GBV). The first is so-called ‘family violence’. The second type of GBV is ‘community violence’ and the third type is ‘state violence’, or violence committed or condoned by individuals employed by the state. (Refer to Handout 5: Gender Based Violence)

79National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 5: Gender Based Violence16
Types of Gender-Based Violence Sites of Gender-Based Violence
Overt physical abuse (includes battering, •sexual assault, at home or in the workplace)Psychological abuse (includes •deprivation of liberty, forced marriage, sexual harassment, at home or in the workplace)Deprivation of resources needed •for physical and psychological well-being (including health care, nutrition, education, means of livelihood)Treatment of women as commodities •(includes trafficking in women and girls for sexual exploitation)
FamilyIs one of the primary sites of gender violence.• Prepares its members for social life, forms gender •stereotypes and perceptions of division of labor between the sexes. Is the arena where physical abuses (spousal •battering, sexual assault, sexual abuse) and/or psychological abuses occur. (Domestic violence can also take such forms as confinement, forced marriage of woman arranged by her family without her consent, threats, insults and neglect; overt control of a woman’s sexuality through either forced pregnancy or forced abortion.)Because violence within the family and household •takes place in the home, it is often seen as a ‘private’ issue.
Community/SocietyAs a group sharing common social, cultural, •religious or ethnic belonging, it perpetuates existing family structure and power inequalities in family and society. justifies the behaviour of male abusers aimed •at establishing control over women in the family, and supports harmful traditional practices such as battering and corporal punishment Workplace can also be a site of violence. Either in •governmental service or in a business company, women are vulnerable to sexual aggression (harassment, intimidation) and commercialized violence (trafficking for sexual exploitation).
StateLegitimizes power inequalities in family and society •and perpetuates gender based violence through enactment of discriminatory laws and policies or through the discriminatory application of the law. Is responsible for tolerance of gender violence •on an unofficial level (i.e. in the family and in the community). To the extent that it is the State’s recognized role •to sanction certain norms that protect individual life and dignity and maintain collective peace, it is the State’s obligation to develop and implement measures that redress gender violence.
16 Prevention of Domestic Violence and Trafficking in Human Beings, Training Manual, Winrock International, Kyiv, Ukraine, 2001, available at http://www.winrock.org/GENERAL/Publications/Dos_manual.pdf.

80 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 5.1: Gender-Based Violence: Definitions and Perceptions17
Objectives1. To explore and define the concept of gender based violence2. To highlight perceptions prevalent in society regarding violence, and how these
perceptions may contribute to an increase in GBV.
Time 45 minutes
Materials • Flipchart • Markers
Steps:1. Lead a brainstorming session to create a list of words that describe gender-based
violence. Facilitator asks each of the participants to share their ideas randomly or in turn. The ideas are not criticized or discussed; participants may build on ideas voiced by others. The questions for brainstorming are:• What does the phrase ‘gender-based violence’ mean to you?• What acts do you qualify as ‘violence’?
Write down each answer as they are offered on a flipchart without any comments, notes or questions for 5-7 minutes. After discussing the ideas, post the list on the wall so it is visible throughout the training workshop.2. Summarize the results of the brainstorming and highlight the following definition:GBV is defined as acts perpetrated against women, men, girls and boys on the basis of their sex which cause or could cause them physical, sexual, psychological, emotional or economic harm, including the threat to take such acts.3. Divide participants into 4 groups and assign each group an example of gender
violence (e.g. physical, sexual, psychological/emotional and economic).4. Explain that each group must prepare a 5 minute role play that clearly depicts their
example of gender based violence. Emphasise that they should keep in mind the definition they got earlier. Preparation time should not be longer than 15 minutes.
17 Adapted from UNIFEM Gender Fact Sheet, available at http://www.unifemeseasia.org/Gendiss/downloads/UNIFEMSheet5.pdf.

81National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
5. Get the entire group together and ask participants to present their role plays. Correct any misconceptions that may have been depicted.
6. Ask participants about how society views GBV. What do culture, religion and gender norms say about GBV?
7. Do these views contribute to GBV, and if so, what can be done to lessen its incidence?
Our perceptions of gender based violence can greatly influence our actions, especially with regard to taking a stand or acting when we see this violence happening.
ClosingBoth men and women can be victims of gender-based violence. However, data shows that women are more likely than men to be victims of this kind of violence. There are several reasons for this:Men are often physically stronger than women. This can make it easier for a man to physically abuse a woman, than for a woman to physically abuse a man.
In many cultures in Namibia, the traditional role of a woman is to serve the man. If the woman fails to do what the man wants, it is considered acceptable that the man should beat the woman.
The Namibian Constitution protects all citizens against GBV and provisions are made to combat GBV in any form that it may occur. The Combating of Domestic Violence Act 4 (2003) (See Handout elsewhere in this manual) and the Combating of Rape Act are two legal documents that ensure that human rights are protected regarding gender based violence.

82 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 5.2: Sexual Violence in the Daily Routine18
18 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.
Objectives1. To better understand the many ways in which women’s (and men’s) lives are limited
by male violence, especially sexual violence
Time 60 minutes

83National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Materials • Flipchart • Markers
Facilitator’s notes This activity is critical for setting and establishing a clear understanding of the extent and impact of men’s violence against women. Be sure to allow ample time! This activity works best in mixed gender workshops where the ratio of men to women is reasonably balanced. But it can be included in any workshop. If men are defensive, make sure to look more closely at their reactions. Make it clear that you’re not accusing anyone in the room of having created such a climate of fear. Remind the group that you are trying to show how common and how devastating violence against women is.
Some people have strong emotional reactions to this activity. These reactions can include anger, outrage, astonishment, shame, embarrassment, and defensiveness. As workshop participants show their feelings, let them know that their reaction is normal and appropriate. Many people are shocked and become angry when they learn the extent and impact of violence against women. Remind them that anger can be a powerful motivating force for change. Encourage them to identify ways to use their anger and outrage usefully to prevent violence and to promote gender equity.
Be aware that some men may think that they need to protect women from violence. If some men in the group say this, remind the group that it is important for each of us to be working to create a world of less violence. Men and women need to work together as allies in this effort. The danger of saying that it is up to men to protect women is that we take away women’s power to protect themselves.
Steps 1. Ask participants what they understand by the term sexual violence. Write all the
responses on the flipchart. Don’t make this discussion too long, 5 minutes should be enough. You can clarify the definition to round this up:
Sexual violence is about power, control and manipulation on the part of a stranger, acquaintance, family member, friend or partner. It can happen to or be inflicted by women or men and includes the following, but is not limited to:Any unwanted touching or act of a sexual nature committed through physical force •
Being forced to watch or participate in unwanted sexual activity •
Any unwanted verbal comments of a sexual nature •
Rape (forced penetration of the vagina or anus) •
(Canadian Federation of Sexual Health)

84 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
2. After this discussion, draw a line down the middle of a flipchart paper from top to bottom. On one side, draw a picture of a man and on the other, a woman. Let the participants know that you want them to reflect on a question in silence for a moment. Tell them that you will give them plenty of time to share their answers once they have thought it over in silence. Ask the question: • “What do you do on a daily basis to protect yourself from sexual violence?”
3. Ask the men in the group to share their answers to the question. Most likely, none of the men will identify doing anything to protect themselves. If a man does identify something, make sure it is a serious answer before writing it down. Leave the column blank unless there is a convincing answer from a man. Point out that the column is empty or nearly empty because men don’t usually even think about having to protect themselves from sexual violence.
4. If there are women in the group, ask the same question. If there are no women, ask the men to think of their wives, girlfriends, sisters, nieces, and mothers and imagine what these women do on a daily basis to protect themselves from sexual violence.
5. Once you have captured ALL the ways in which women limit their lives to protect themselves from sexual violence, break the group into pairs and tell each pair to ask each other the following question. Each person has five minutes to answer: • What does it feel like to see all the ways that women limit their lives because of
their fear and experience of men’s violence?6. Bring the pairs back together after 10 minutes and ask people to share their
answers and their feelings. Allow plenty of time for this discussion, as it can often be emotional. Then ask each pair to find two other pairs (to form groups of six people) and discuss the following questions for 15 minutes:
How much did you already know about the impact of men’s violence on •
women’s lives? What does it feel like to have not known much about it before? How do you •
think you were able to not notice this, given its significant impact on women? How does men’s violence damage men’s lives as well? •
What are the consequences of sexual violence in relation to HIV? •
What do you think you can do to change this trend and to create a world in •
which women don’t live in fear of men’s violence?7. Bring the small groups back together after 15 minutes and ask each group to report
back on its discussion. Sum up the discussion, making sure all points in the closing are covered.

85National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Closing Sexual violence and the threat of violence is an everyday fact for women. Because most men do not live with the daily threat of sexual violence, they do not realize the extent of the problem women face. Most men usually do not understand how sexual violence—actual and threatened—is such a regular feature of women’s daily lives. However, men’s lives are damaged too by sexual violence against women. It is men’s sisters, mothers, daughters, cousins, and colleagues who are targeted—women that men care about are being harmed by sexual violence every day. Social acceptance of this violence against women gives men permission to treat women as unequal and makes it harder for men to be vulnerable with their partners, wives, and female friends. Sexual violence makes it impossible for a woman to negotiate condom use and eliminates any element of choice regarding the decision to have sex or not. Also, as mentioned in other activities, the tearing of tissue during rape dramatically increases the risk for HIV transmission. Therefore, the prevention of sexual violence is key to reducing HIV.
Activity 5.3: Men as Victims of Violence19
19 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.

86 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Objectives 1. To explore issues and challenges faced by men who are victims of violence
Time 45 minutes
Steps:1. Open the session by asking participants to find a partner and discuss the following
question: What are examples of how men can be victims of violence?2. Once the pairs have held discussions, list their ideas on a flipchart paper. Next, ask the participants to form groups of five to six people and discuss the
following questions: • Why would it be hard for men to talk about being victims of violence?• What effects would these experiences have on men? • What resources are available in the community to assist men who are victims of
violence?3. After the groups have discussed the questions for about 15 minutes, have them
present their ideas to the entire group. Sum up the discussion, making sure that all the points in the closing are covered.
Closing Men and boys are often victims of physical violence. However, men are socialized to disregard pain and to not show weakness. Thus, men who are victims rarely discuss or report to relevant authorities their problems with others. Men and boys can also be victims of sexual violence, which stigmatizes them. Few resources exist to assist, however. It is vital that men and boys are offered opportunities to share their experiences and work through their feelings. Emphasise strongly that provisions made in the law cater for both men and women. For example, the Combating of Domestic Violence Act (4 of 2003) is all inclusive and does not discriminate against men.

87National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 5.4: Understanding the Causes and Effects of Violence20
20 Adapted from the Manual: Engaging Boys and Men in Gender Transformation: The Group Education Manual. EngenderHealth/The Acquire Project/Promundo.
Objective1. To discuss the relationship between the violence that men suffer and the violence
they use against others
Time 60 minutes
Materials Flipchart •
Markers•
Pens/pencils•
Five small pieces of paper for each participant•
A roll of String•
Chairs•
Tables•

88 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator’s notes During this activity, you might notice that it is easier for participants to talk about the violence they have suffered outside their homes than the violence they have suffered inside their homes, or the violence they have used against others. They might not want to go into detail about these experiences, and it is important you do not insist they do. Being a victim of interpersonal violence is associated with committing acts of violence later in life. Moreover, in talking about violence they’ve committed, the participants might seek to justify themselves, blaming the other person for being the aggressor. Helping men grasp this connection and think about the pain that violence has caused them is a potential way of interrupting the victim-to-aggressor cycle of violence. Explain that experiencing violence over a period of time can lead to one also perpetuating it, as they may see violence as a way to resolve conflict.
Prior to the session, consult local and national laws regarding mandatory reporting procedures in the case that a minor (or individual under a certain age) reveals that he is suffering violence or abuse. It is also important to clarify with your organization any ethical and legal aspects related to dealing with situations that might come up during the discussions on violence. Also, Facilitators should be prepared to offer brief counselling to participants who may be traumatized during or after this session. Arrange this beforehand.
Advance preparation Before the session, create a clothesline with 5 lines using the string and chairs. Make sure that it is elevated (you can put the chairs on the tables) so that it is at face level. Ensure there is enough space to move between the chairs. Then hang one piece of card paper on each line. On each paper, write one of the five categories below: • Violence used against me • Violence that I use against others • Violence that I have witnessed • How I feel when I use violence • How I feel when violence is used against me
Steps 1. At the beginning of the session, explain to the participants that the purpose of this
activity is to talk about the violence in our lives and our communities. Review the flipchart with the meanings of violence from previous activities.
2. Ask the participants what reasons people have for committing violent acts. The group can think of any perpetuating/contributing factors.

89National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
3. For each of these, brainstorm actions that the group or individuals can take to address these causes. Brainstorm actions that others should take to address these causes.
4. After the discussion, give each participant five sheets of paper. 5. Ask the participants to think for a while about the five categories from above and
then to write a short reply to each on the pieces of paper that they have received. They should write one response on each paper, and they should not put their names on the paper.
6. Allow about 10 minutes for this task. Explain to them that they should not write much, just a few words or a phrase, and then hang it to the corresponding clothesline.
7. After hanging their papers on the clothesline, participants can move between the clotheslines to read the responses from each category in silence.
8. Open up the discussion with the following questions. • What is the most common type of violence used against us? • How do we feel about being a victim of this type of violence? • What is the most common type of violence we use against others? • How do we know if we are really using violence against someone? • How do we feel when we use violence against others? • Is there any connection between the violence we use and the violence that is
used against us? • Where do we learn violence? • Is any kind of violence worse than another? • Is there a link between violence and power? Explain. • In general, when we are violent or when we suffer violence, do we talk about
it? Do we report it? Do we talk about how we feel? If we do not, why not? • How do media (music, radio, movies, etc.) portray violence? • What is the link between violence in our families and relationships and other
violence that we see in our communities? • Some researchers say that violence is like a cycle, that is to say, someone who is
a victim of violence is more likely to commit acts of violence later. If this is true, how can we interrupt the cycle of violence?
After the discussion, ask the group what it was like for them to talk about the violence they have experienced. If anyone in the group shows a need for special attention due to an act of violence they have suffered, one facilitator should attend to her/him and you should consider referring the individual to appropriate services (See Resource Sheet 4: Referral Services).

90 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Closing When people talk about violence, they think mainly of physical aggression. It is important to think of other forms of violence besides the physical. It is also important to think about the acts of violence that you, as men, might perpetrate, because very often men think it is only other people who are violent, not themselves. It is important to also remember that violence is not about natural aggression and that it has many causes. All forms of violence share the same fundamental causes: the use of violence to maintain or claim power and control. Current social and economic problems are also an important context for understanding why violence happens, who suffers from it, and who commits it. However, as much as context may help to explain violence, it should not be used to excuse it. People, men mostly, still make a choice when they use violence. People need to be held accountable for the decision to use violence and for the suffering that they cause. The purpose of this session is to help you think about how you learn and express violence differently and how you can stop the cycle of violence in your lives and communities.
Activity 5.5: Domestic Violence Cycle21
ObjectivesTo understand the cyclical pattern of domestic violence in intimate relationships1.
Identify difficulties in helping those who are in abusive relationships.2.
Explore interventions for domestic violence3.
Time 1 hour and 30 minutes
Materials Flipchart •Markers•DVD: Matlakala’s Story•DVD Player and Sound System/Projector and Screen•Handout 8: Domestic Violence Cycle•Handout 9: Non-Violence Wheel•
21 Adapted from the Manuals: Violence against Women Training materials, Soul City, 2001 and Gender Training Manual and Resource Guide, MGECW.

91National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Advance PreparationEnsure that you have a working DVD machine or projector screen to play the video “Matlakala’s Story”. You must have watched it before the session to familiarize yourself with the content.
Before starting the video, write the following questions on a flipchart. These are questions for participants to think about during the video.
• What form did Matlakala’s abuse take?• What are some of the difficulties about helping someone who is a victim of
domestic violence? (What made it difficult for Matlakala to get help?)• What did Matlakala do to resolve the problem?
Draw the domestic violence cycle (Handout 8) on the flipchart
Facilitator’s notes Some people have strong emotional reactions to watching the video. These reactions can include anger, outrage, sadness, astonishment, shame, embarrassment, and defensiveness. As workshop participants show their feelings, let them know that their reaction is normal and appropriate. Many people are shocked and become angry when they learn the extent and impact of violence against women. Remind them that anger can be a powerful motivating force for change. Encourage them to identify ways to use their anger and outrage usefully to prevent violence and to promote gender equity.
Steps 1. Before the DVD, brainstorm examples of domestic violence Refer to Handout 7
Gender Based Violence.2. After watching the DVD ask the group to share their feelings and answers to the
questions written on the flipchart. Allow enough time for this discussion, as it can often be emotional. (See Resource Sheet 4: Matlakala’s Story)
3. Present the domestic violence cycle (Handout 8: Domestic Violence Cycle), and allow a short discussion of the Cycle
4. Give all participants Handout 9: Non-Violence Wheel.
ClosingDenial characterizes abuse, which makes it difficult to address domestic violence. Many people who are abused do not see themselves as victims. Also, many abusers do not see themselves as being abusive. Anyone can be a victim, regardless of age, sex, race, culture, education, employment or marital status.

92 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Some people only think of domestic violence as physical violence only, but it is much broader
than that. This can also make it difficult to identify.
Training Option:Where it is impossible to screen the DVD, you should just go directly to a discussion of the Domestic Violence Cycle.
Time 40 minutes
Steps:• Brainstorm examples of domestic violence and record these on the flipchart • Present the domestic violence cycle, and allow an extensive discussion of the Cycle

93National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 5.5.1: Domestic Violence Cycle22
Domestic violence has a typical pattern that is cyclical; it follows a pattern that goes around in a circle. This pattern makes it very difficult to intervene.
83
The cycle of violence is a recurring pattern where the offender swings between affectionate, remorseful and calm behaviour to periods of tension that grow into physical, sexual or emotional violence.
Handout5.5.2:Non‐ViolenceWheel23
23SourcedfromtheGenderTrainingManualandResourceGuide,MinistryofGenderEqualityandChildWelfare
The cycle of violence is a recurring pattern where the offender swings between affectionate, remorseful and calm behaviour to periods of tension that grow into physical, sexual or emotional violence.
22 Sourced from the Gender Training Manual and Resource Guide, Ministry of Gender Equality and Child Welfare

94 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 5.5.2: Non-Violence Wheel2384
The Non-Violence Wheel shows behaviours based on equality rather than power. It provides ideas for setting goals and boundaries in personal
relationships.
FacilitatorNotes5.5.1:Matlakala’sStory24
24 Adapted from the Community Counsellor Toolkit: Module 2 Basic Counselling. LifeLine/ChildLine and Violence Against Women Training Materials, Soul City 2001.
23 Sourced from the Gender Training Manual and Resource Guide, Ministry of Gender Equality and Child Welfare
The Non-Violence Wheel shows behaviours based on equality rather than power. It provides ideas for setting goals and boundaries in personal relationships.

95National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 5.5.1: Matlakala’s Story24
Domestic violence: behaviours used by one person in a relationship to control the other. (Partners may be married or not married, heterosexual, gay, lesbian, living together, separated or dating).
Examples of domestic violence:• Name calling or putdowns• Keeping a partner from contacting their family or friends• Withholding money• Stopping a partner from getting or keeping a job• Actual or threatened physical harm• Sexual assault• Stalking• IntimidationNote: these can happen all the time or once in awhile.
Matlakala’s Story:1. Forms of abuse:
• Physical abuse• Emotional abuse – verbal putdowns• Not wanting her to work• Expecting her to be at his beck and call• Distrust when she is with friends• Stopping her contacting friends and family or speaking to others
2. Difficulties in helping someone who is a victim of domestic violence:• Secrecy: Secrecy is a key characteristic of domestic violence. There is so
much hiding and lies to cover up what it happening. Sometimes the secrecy is because of shame from what is happening, sometimes it can be because of denial, sometimes to protect the abuser (i.e. husband) and sometimes the secrecy is forced by the abuser.
• Cultural issues: how women are viewed in a culture. Women can be viewed as property of her husband because of dowry (Lobola) that is paid when married. Violence against women can be condoned in some cultures.
• Gender issues: unequal power relations• Communities not wanting to get involved: this includes friends, neighbours
and families. Domestic violence is seen as a private matter between husband and wife.
• Cyclical pattern of abuse: it may be confusing for those witnessing the abuse and the normalcy or honeymoon phase interchangeably
24 Adapted from the Community Counsellor Toolkit: Module 2 Basic Counselling. LifeLine/ChildLine and Violence Against Women Training Materials, Soul City 2001.

96 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 5.5.2: The Combating of Domestic Violence Act 4 of 2003
Types of domestic Violence• Physical Abuse• Sexual Abuse• Economic Abuse• Intimidation• Harassment• Trespass • Emotional, verbal or psychological abuse
What is a domestic relationship? People who are in the following relationships are in what is called domestic relationships in terms of the Combating of Domestic Violence Act:• People who are married (civil or customary marriage) or engaged to be married• People who are cohabiting (living together as husband and wife)• Two people who are the parents of a child – whether or not they have ever lived
together• Parents and their children• Other family members related by blood, marriage or adoption, IF they live in the
same house OR have some other connection between them, such as financial dependency
• Girlfriend and boyfriend• The domestic relationship continues for at least one year after separation
(divorce, moving out, etc.) – but if two people have a child together they have a domestic relationship as long as that child is alive or for at least one year after the child’s death.
What can you do if you are experiencing domestic violence?Under the law, someone who is experience domestic violence can:
Make an application for a protection order at a magistrate’s court•
If the abuse amounts to a crime (such as hitting which is assault, or stabbing •
which may be attempted murder, or rape), you can lay a charge with the police OR ask the police to give the abuser a formal warning.
You can do both of these things at the same time.

97National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Protection Orders:Who can apply for a protection order?Anyone who is experiencing domestic violence. If the person being abused is a minor (under age 21) anyone can ask for a protection order for them. If someone older than 21 is unable to apply for a protection order themselves (for example because they are unconscious or under the influence of alcohol or drugs), someone else can apply on their behalf.
How do you apply for a protection order?Go to the magistrate’s court. You do not need a lawyer, and the clerk of the court will help you to fill in the forms. You should take any witnesses or evidence (such as medical records) to the court. You may first get an interim (immediate but temporary) protection order and then can be called for an enquiry at which the magistrate will listen to both sides of the story and may then grant a final protection order.
Terms of a protection order: All protection orders will order the abuser to stop committing domestic violence. A protection order can be adapted to fit the problem. It may include the following provisions:
No weapons – an order to give the gun or other weapon to the police1.
No contact provisions – ordering the abuser not to come near the abused person 2.
or their home or work, or communicate with themMove out of the joint household – if there has been physical violence the abuser 3.
can be ordered to move out of the joint household, even if the house is owned by the abuser (in that case it can only be for a period of 6 months)Alternative accommodation – an order to the abuser to pay rent or arrange 4.
another place to stay for the abused personPossession and protection of property – an order to give the abused person 5.
possession of certain property (e.g. ID card, chequebook, clothes, children’s toys) and not to sell or damage any property in which the abused person has interestProtection of children and maintenance – the protection order can also 6.
include temporary orders for maintenance, or custody of children (day to day responsibility for their care) and access to them (visiting them).
Different parts of the protection order remain in force for different time periods. For example some provisions such as no contact, can remain in force for up to 3 years, while others, such as maintenance are only for 6 months.

98 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
For a full description of this Act, see Guide to the Combating of Domestic Violence Act 4 of 2003 available in English, Afrikaans, Oshiwambo, Otjiherero and Khoekhoegowab from LAC.
Adapted from the Gender Training Manual and Resource Guide, Ministry of Gender Equality and Child Welfare

Sexual and Reproductive Health
Section6

100 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objective:
1. Increased understanding of Sexual Reproductive Health issues that place men and women at risk of HIV and AIDS
Total Time 3-4 hours
What is sexual health?Sexual health means both physical and emotional health in matters relating to sex, sexuality and reproduction. Sexuality is more than just sexual acts or reproduction. It includes our desires, feelings, what we do, our values and attitudes.
What is Reproductive Health?Reproductive health includes safe development into adults, the avoidance of sexual and reproductive illnesses, and the ability to choose when to have children, to conceive safely and to avoid unwanted pregnancy. It also involves good health care to avoid the complications of childbirth, abortion, use of contraceptive methods and the long-term effects of sexually transmitted and reproductive tract infections.
People learn about their sexuality, and about sex and sexual health, from different sources: parents, friends, teachers, radio, newspapers and television, work colleagues, community elders. When people have a concern about sexual health, it may be possible to go to formal health care services, such as clinics or hospitals, or to traditional health healers. Anyone to whom people go for advice or treatment is a sexual health carer or educator.
Why work with men?Many sexual and reproductive health services focus only on the needs of women. In recent years, great effort has been made to improve women's health, including their sexual and reproductive health. This has involved challenging the view that women are less important than men, and that inequality between men and women is the nature of things and cannot be changed. Real improvements have been made, and yet many people working with women have found that there are limits to what can be achieved unless they also work with men.
Excluding men from sexual health promotion means that women often have to take all the responsibility for their own, and their partner's sexual health. If men and women

101National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
understand how each other's bodies work, they can understand each other better. Many men want to be involved in planning their families and looking after the health of their partners and their children. Benefits in women's and children's lives will be limited unless men are also involved in sexual and reproductive health activities. Working on sexual reproductive health may also encourage men to examine wider social issues such as the changing roles of men and women.
Before delving into the intricacies of SRH, let us first look at sexuality:
Men's sexual health matters @ Healthlink Worldwide, 1998
Activity 6.1: Understanding Sexuality25
Objectives1. To discuss human sexuality in a holistic and comprehensive way 2. To provide a framework for further discussions on sexuality and HIV
Time 60 minutes
Materials • Flipchart • Markers • Prestick• Enough copies of Handout 10: Definitions and Questions for Small Group Discussions about
Sexuality for all participants• Handout 11: Definitions for Circles of Sexuality
Advance preparation Prepare a flipchart with the circles of sexuality as illustrated in Handout 6.1.1: The Circles of Sexuality.
Steps 1. Explain that this session will explore the concept of “sexuality.” Ask participants to
share what they think sexuality means to them. 2. Explain that there are many long and complicated definitions of sexuality, but that
they are often confusing. Tell them we like to simplify the definition, by thinking of sexuality as comprising several circles.
3. Draw the diagram by referring to Handout 6.1.1. When drawing the circles, label

102 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
each, but do not add the information contained in the circles. Each circle represents one of the elements of sexuality. When all of the circles are placed together, they encompass the total definition of sexuality. Explain that one of the circles is in a different colour and is not linked to the others (Sexuality to Control Others) because it is a negative element of sexuality, even if it exists in many situations.
4. Divide the participants into four groups. Explain that each will take on a circle of sexuality and explore what they think it means (the Sexual Identity circle will be explained by the facilitator). Assign a circle to each group and ask them to describe what the circle entails using flipchart paper and markers. Pass out Handout 10: Definitions and Questions for Small Group Discussions about Sexuality and tell them to refer to the guiding questions related to their circle to help them with this activity.
5. Ask each group to present their four circles then explain the Circle of Sexual Identity. Once this has been done, pass out Handout 6.1.2: Definitions for Circles of Sexuality.
Make sure the key points of each circle are covered by referring to Handout 6.1.2. 6. After all of the circles are presented, conclude the activity with the following
discussion questions: • Is it easy to talk about sexuality? Why or why not? • Are the challenges of talking about sexuality different for men and women?
Why? What makes it hard for men to talk about this? What makes it hard for women?
• What would make it easier for men and women to talk about sexuality? • Where is “sexual intercourse” included within the definition of sexuality? Does
the term play a large or small role in the definition of sexuality? • What are some similarities in how men and women experience sexuality? • What are some differences? Why do you think these differences exist? • What have you learned from this exercise? How can you apply this in your own
lives and relationships?
Closing Sexuality is an important component of human life and while the sexual act for reproduction is similar for nearly all living creatures, only humans attribute values, customs, and meanings to sexuality that go beyond procreation. Sexuality also includes how we feel about our bodies, how we give and receive pleasure, and how we express romantic feelings, among other things. Unfortunately, in many cultures, men and women receive different messages about sexuality. Men’s sexuality is seen as impulsive and uncontrollable while women’s sexuality is seen as passive and controllable. These contrasting messages often have negative implications for how men and women relate to each other in intimate and sexual relationships. It is therefore important that both men and women have opportunities to comfortably talk about sexuality and develop skills to communicate about sexuality with partners.

103National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 6.1.1: Definitions and Questions for Small Group Discussions about Sexuality
Sensuality – Sensuality is how our bodies get and give pleasure. • What senses do our bodies use to get and give pleasure?• What types of activities involve pleasure?
Intimacy/relationships – Intimacy is the part of sexuality that deals with relationships.• What is needed for a healthy relationship?• Where do we learn how to love and care for a person?
Sexual health – Sexual health involves our behaviour related to producing children, enjoying sexual behaviours, and maintaining our sexual and reproductive organs. • What sexual health issues do men and women face?
Sexuality to control others – Unfortunately, many people use sexuality to violate someone else or to get something from another person. • How do people try to use sex to control other people? • How do the media try to use sex to control others?
Circles of Sexuality
92
Handout6.1.1:DefinitionsandQuestionsforSmallGroup
DiscussionsaboutSexuality
Sensuality–Sensualityishowourbodiesgetandgivepleasure.
•Whatsensesdoourbodiesusetogetandgivepleasure?
•Whattypesofactivitiesinvolvepleasure?
Intimacy/relationships–Intimacyisthepartofsexualitythatdealswithrelationships.
•Whatisneededforahealthyrelationship?
•Wheredowelearnhowtoloveandcareforaperson?
Sexual health – Sexual health involves our behaviour related to producing children,
enjoyingsexualbehaviours,andmaintainingoursexualandreproductiveorgans.
•Whatsexualhealthissuesdomenandwomenface?
Sexuality to control others – Unfortunately, many people use sexuality to violate
someoneelseortogetsomethingfromanotherperson.
•Howdopeopletrytousesextocontrolotherpeople?
•Howdothemediatrytousesextocontrolothers?
CirclesofSexuality
SexualitytoControlOthersUsing sex to violate someone’s rights or get something from another (e.g. advertisements, rape)

104 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 6.1.2: Definitions for Circles of Sexuality
Sensuality – Sensuality is how our bodies derive pleasure. It is the part of our body that deals with the five senses: touch, sight, hearing, smell, and taste. Any of these senses, when enjoyed, can be sensual. Ask the participants to provide examples of how a person might enjoy each of the five senses in a sensual manner. The sexual response cycle is also part of our sensuality because it is the mechanism that enables us to enjoy and respond to sexual pleasure. Our body image is part of our sensuality. Whether we feel attractive and proud of our bodies influences many aspects of our lives.
Our need to be touched and held by others in loving and caring ways is called skin hunger. Adolescents typically receive less touch from family members than do young children. Therefore, many teens satisfy their skin hunger through close physical contact with a peer. Sexual intercourse may result from a teen’s need to be held, rather than from sexual desire. Fantasy is part of sensuality. Our brain gives us the capacity to fantasize about sexual behaviours and experiences, without having to act upon them.
Intimacy/relationships – Intimacy is the part of sexuality that deals with relationships. Our ability to love, trust, and care for others is based on our levels of intimacy. We learn about intimacy from relationships around us, particularly those within our families. Emotional risk-taking is part of intimacy. In order to experience true intimacy with others, a person must open up and share feelings and personal information. We take a risk when we do this, but intimacy is not possible otherwise.
Sexual identity – Every individual has his or her own personal sexual identity. This can be divided into four main elements:Biological sex is based on our physical status of being either male or female. Gender identity is how we feel about being male or female. Gender identity starts to form at around age two, when a little boy or girl realises that he or she is different from the opposite sex. If a person feels like he or she identifies with the opposite biological sex, he or she often considers himself or herself transgender. In the most extreme cases, a transgender person will have an operation to change his or her biological sex (often called gender “re-assignment” surgery) so that it can correspond to his or her gender identity.

105National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Gender roles are society’s expectations of us based on our biological sex. Ask the group to think about what behaviours we expect of men and what behaviours we expect of women. These expectations are gender roles. Sexual orientation is the final element of sexual identity. Sexual orientation refers to the biological sex that we are attracted to romantically. Our orientation can be heterosexual (attracted to the opposite sex), bisexual (attracted to both sexes), or homosexual (attracted to the same sex). People often confuse sexual orientation and gender roles. For example, if a man is feminine or a woman is masculine, people often assume that these individuals are homosexual. Actually, they are expressing different gender roles. Their masculine or feminine behaviour has nothing to do with their sexual orientation. A gay man may be feminine, masculine, or neither. The same applies to heterosexual men. Also, a person may engage in same-sex behaviour and not consider himself or herself homosexual. For example, men in prison may have sex with other men but may consider themselves heterosexual.
Sexual health – Sexual health involves our behaviour related to producing children, enjoying sexual activities, and maintaining our sexual and reproductive organs. Issues like sexual intercourse, pregnancy, and sexually transmitted infections (STIs) are part of our sexual health. Ask the group to identify as many aspects of sexual health as possible.After discussing the four circles of sexuality, draw a fifth circle that is disconnected from the other four. This circle is a negative aspect of sexuality and can inhibit an individual from living a sexually healthy life. You can say that the circle can “cast a shadow” on the other four circles of sexuality. It is described as follows:Sexuality to control others – This element is not a healthy one. Unfortunately, many people use sexuality to violate someone else or get something from another person. Rape is a clear example of sex being used to control somebody else. Sexual abuse and forced prostitution are others. Even advertising often sends messages of sex in order to get people to buy products.

106 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 6.2: Sexual Reproductive Health and its determinants26
Objective1. Define sexual and reproductive health and list its components.2. List the broad range of factors that can affect sexual and reproductive health.
Time 60 minutes
Materials Flipchart•Markers•
Steps:1. Ask the participants what they understand by the term sexual and reproductive
health. You can break up this term and define it separately.2. Record all the responses on the flipchart3. After all responses have been exhausted, summarize and add any components that
were left out. Allow for questions.4. Ask participants to add any elements or components of sexual and reproductive
health based on the previous discussions. Record their responses on a flipchart. Reproductive health as described in the ICPD Programme of Action includes the following elements:• Family planning education, counselling, and services• Education and services for prenatal (antenatal) care, safe delivery, and postnatal
care, and infants’ and women’s health care• Prevention and management of abortion complications• Treatment of reproductive health conditions• Prevention and treatment of reproductive tract infections, including STI’s and
HIV/AIDS• Information, education, and counselling on human sexuality and responsible
parenthoodIf any of these are missing from the list the group compiled, add them.5. Divide the participants into six groups and assign each group a topic for discussion:
• Group 1: Family planning Discussion: - Define the term What does family planning entail? What methods of contraception are available? Which of these are typically used by men?

107National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Group 2: Maternal and Infant Health Discussion: - Define the term What barriers may limit male involvement in maternal health? What role should men play in improving maternal health?• Group 3: Maternal and Infant Mortality Discussion: - Define the term What are the causes of this? How can men get involved in decreasing this?• Group 4: Fertility Discussion: - Define the term What perceptions are attached to male and female fertility? What happens if one partner wants to have more children and
the other does not? • Group 5: Abortion Discussion: - Define the term In which instances is abortion legal in Namibia? What are some of the reasons that some women resort to illegal
abortions? How does an unsafe abortion affect a woman’s health? • Group 6: Reproductive Infections and Diseases Discussion: - What are some health problems that affect the reproductive
system that you are aware of? Which of those you listed typically affect men? What do people generally do to treat infections and diseases?
6. Allow 15-20 minutes for this discussion, after which the groups present their discussions for 5 minutes each.
7. Questions may be asked, and make sure to read all the information in this section.8. You may give the information in the resource sheet to round up.
ClosingSexual behaviour and the consequences that come with it should be a shared responsibility between both partners. SRH includes their right to make decisions concerning sexuality and reproduction free of discrimination, coercion and violence.

108 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 6.2: Determinants for Sexual and Reproductive Health
Family planning is the planning of when to have children, and the use of birth control and other techniques to implement such plans. Other techniques commonly used include sexuality education, prevention and management of sexually transmitted infections, pre-conception counseling, and management, and infertility management.
Family planning is sometimes used in the wrong way and can also be seen as a synonym for the use of birth control, though it often includes more. It is most usually applied to a female-male couple who wish to limit the number of children they have and/or to control the timing of pregnancy (also known as spacing children). Family planning may encompass sterilization, as well as pregnancy termination.
Maternal and Infant HealthMeasures that can prevent and reduce health risks to expectant mothers and their children are known as maternal and child care.
An expectant mother requires great support during and after delivery in terms of nutrition, exercise and not to be subjected to hard labour chores. This is one of the reasons for women dying every year due to lack of financial and physical support from their husbands and male partners.
There are various factors that affect maternal health such as:• Postnatal care services to treat any complications that may arise from birth and
deliveries• Birth spacing – short intervals between births are bad for maternal health and
also reduce the children’s chances of survival • Violence – beatings may result in complications during pregnancy and even
miscarriage.
Maternal and Infant MortalityMaternal death is the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. A maternal death is one for which the

109National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
certifying medical doctor has designated a maternal condition as the underlying cause of death.
Infant mortality is defined as the number of infant deaths (one year of age or younger) per 1000 live births.
Fertility Fertility is the capability of producing healthy offspring through normal sexual activity. Fertility preferences refer to how many children men and women would ideally like to have.
AbortionAbortion is the expulsion of the fetus before it is viable (the ability to live outside the womb). This could include spontaneous abortion (miscarriage) or induced abortion, in which someone (a doctor, the woman herself, or a layperson) causes the abortion. If done incorrectly and in unhygienic conditions, abortion may have serious negative consequences for women, in some cases, even resulting in death.
Abortion is regulated in Namibia by the Abortion and Sterilization Act 2 of 1975, which allows abortion only in certain narrowly defined situations – serious threat to the woman’s life or health, serious threat of permanent damage to the woman’s mental health, a serious risk that the child will suffer from a mental or physical defect that will result in serious and irreparable handicaps; or cases where the pregnancy is the result of rape, incest or intercourse with a woman who has a severe mental disorder.
Reproductive Infections and DiseasesLike all complex organ systems the human reproductive system is affected by many diseases. There are four main categories of reproductive diseases in humans. They are: 1) genetic or congenital abnormalities, 2) cancers, 3) infections which are often sexually transmitted and 4) functional problems cause by environmental factors, physical damage, psychological issues, autoimmune disorders, or other causes. The best known types of functional problems include sexual dysfunction and infertility which are both broad terms relating to many disorders with many causes.

110 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 6.3: Understanding Sexually Transmitted Infections27
Objective:1. To enable participants to describe how STIs are transmitted; how to prevent
transmitting them, and where to seek testing and treatment; 2. To recognise the signs and symptoms of STIs, and the importance of seeking
treatment 3. To increase participants’ awareness about the importance of seeking testing and
treatment.
Time 60 minutes
Materials • Flipchart• Markers
Handout 6.3.1: Key Information on STI’s •Handout 6.3.2: • Sexually Transmitted Infections

111National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps:1. Begin by asking participants what are some of the common diseases or infections
that they know about in their community (for example, colds; flu; measles)2. Explain that many infections are caused by viruses and bacteria passing from one
person to another; and that some diseases are caused by poor hygiene or poor general health
3. Ask the group – “What is a sexually transmitted infection?” Write up their answers. Explain that an STI is any infection that is passed from one person to another through sexual intercourse or other sexual contact with a person who has an STI
4. Ask the group to name any STI’s they are familiar with – write these up and add others (e.g. syphilis; herpes; gonorrhea; chlamydia; hepatitis A and B; HIV/AIDS) – ask them what names people use for some of these STI’s
5. Explain that some of these infections are caused by viruses or bacteria (see Handout 13)
6. Ask the group to brainstorm everything they have heard about STI’s (especially what people in their culture say about STI’s) under the following headings:
7. Write the answers up under the four headings8. Correct any wrong answers and provide correct information about STI’s. Give
participants Handout 6.3.1 and 6.3.2. 9. Ask the group where they would go for an STI test or treatment. Give information
about where people can go for an STI test and treatment in their community – e.g. doctors; nurses; community clinics (Note: this would be mapped out extensively in Section 8)
Closing
An STI is any infection that is passed from one person to another through sexual intercourse or other sexual contact with a person who has an STI. There are many types of STI’s such as syphilis, herpes, gonorrhoea, Chlamydia, hepatitis A and B, and HIV/AIDS.
Many STI’s have very few or no symptoms, so it is not easy to know if you are infected. If caught early enough, many STI’s, such as gonorrhoea and chlamydia, can be easily treated. There is a vaccine against hepatitis A and B. Other STD’s, such as HIV, cannot be vaccinated against or cured. If STIs are not treated, they can lead to serious health problems. One is also more likely to become infected with HIV if they are already infected with an STD. If anyone is concerned about having an STD, they should visit their local health care facility for advice, testing and treatment.

112 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 6.3.1: Key Information on STIs
Sexually Transmitted Infections• STI’s are infections caused by bacteria or viruses (germs). They are passed from
one person to another by sexual contact or by sexual intercourse with a person who is infected with an STI
• These bacteria or viruses are carried by body secretions (semen, vaginal fluids, blood from an infected person)
• STI’s are not spread through casual contact (such as shaking hands), where there is no exchange of body secretions
• Sexually transmitted diseases are a major cause of ill health and infertility among both males and females
• The presence of an STI increases the person’s risk of HIV infection
Some facts about sexually transmitted diseases• A person can have an STI but not have any symptoms (signs)• Most STIs can be treated and cured with modern drugs• Some STIs cannot be cured, including herpes and HIV/AIDS, but can be treated
with drugs to reduce symptoms• STIs can cause damage to the reproductive system• If a person thinks they have an STI; they should go to a doctor or clinic for
treatment. Their partner must also be treated to avoid re-infection• STIs sometimes have no visible symptoms• Sometimes symptoms of STIs go away by themselves – but the STI is still there
and the person can still infect someone else• All STIs are preventable
Common symptoms of STIs• Unusually thick and strong and sometimes unpleasant smelling discharge from
the vagina or penis• Burning pain when urinating• Sores, rash or redness around the sexual organs, anus or mouth• Itching or discomfort in or around the sex organs• Painful swelling in the lymph glands in the groin

113National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 6.3.2: Sexually Transmitted Infections
Gonorrhoea
What is it?A bacterial infection that is sexually transmitted and can infect the cervix, urethra, rectum, anus and throat.
Signs and symptoms
Symptoms of infection may show up at anytime between 1 and 14 days after exposure. It is possible to be infected with gonorrhoea and have no symptoms. Men are far more likely to notice symptoms than women.Men• a yellow or white discharge from the penis• irritation and/or discharge from the anus• inflammation of the testicles and prostate glandWomen• a change in vaginal discharge. This may increase, change to a yellow
or greenish colour and develop a strong smell• a pain or burning sensation when passing urine• irritation and/or discharge from the anus
How it is spread
by penetrative sex (when the penis enters the vagina, mouth, or anus) and less often by:• rimming (where a person uses their mouth and tongue to stimulate
another person's anus)• inserting your fingers into an infected vagina, anus or mouth and then
putting them into your own without washing your hands in between
Complications
MenGonorrhoea can cause inflammation of the testicles and the prostate gland, which causes pain. Without treatment a narrowing of the urethra or abscesses can developWomenIf left untreated gonorrhoea can lead to pelvic inflammatory disease (PID). This is inflammation of the fallopian tubes which can cause fever, lower abdominal pain and backache. Sex may be uncomfortable. PID can cause a woman to become infertile or have an ectopic pregnancy
TreatmentYes: Antibiotics Cure: Yes

114 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Chlamydia
What is it?
Chlamydia is the most common treatable bacterial sexually transmitted infection. It infects the cervix in women. The urethra, rectum and eyes can be infected in both sexes. Occasionally Chlamydia lives in other parts of the body, including the throat, lungs and liver.
Signs and symptoms
MenSymptoms of infection may show up at anytime. Often this is between 1 to 3 weeks after exposure.• a discharge from the penis which may be white/cloudy and watery
and stain underwear• pain and/or a burning sensation when passing urine• a painful swelling and irritation in the eyes (if they are infected)
Chlamydia in the rectum rarely causes symptoms.Women• a slight increase in vaginal discharge - caused by the cervix becoming
inflamed• a need to pass urine more often/pain on passing urine• lower abdominal pain• pain during sex• irregular menstrual bleeding• a painful swelling and irritation in the eyes (if they are infected)
How it is spread
• having sex with someone who is infected• a mother to her baby at birth• occasionally, by transferring the infection on fingers from the
genitals to the eyes
Complications
MenComplications caused by Chlamydia in men are uncommon. But it may lead to painful inflammation of the testicles, which can cause infertility.Women• If untreated, Chlamydia can lead to pelvic inflammatory disease
(PID-inflammation of the fallopian tubes) PID can lead to problems with fertility: Rash on the soles of the feet and genitals, Appendicitis (inflammation of the appendix), risk of ectopic pregnancy (pregnancy outside the womb) or a premature birth. The infection can be passed on to the baby, giving it an eye or lung infection, and chronic (long-term) pelvic pain.
TreatmentYes: AntibioticsCure: Yes

115National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Syphilis
What is it?It is a bacterial infection caused by Treponema pallidium, which used to be known as the pox.
Signs and symptoms
The signs and symptoms of syphilis are the same in both men and women. They can be difficult to recognise and may take up to 3 months to show after having sexual contact with an infected person. Syphilis has several stages. The primary and secondary stages are very infectious.Primary stageOne or more painless sores appear at the place where the syphilis bacteria entered the body. On average, this will be after 21 days. You may not notice them.These sores can appear anywhere on the body but mainly: on the vulva (lips of the vagina), the clitoris and around the opening of the urethra, on the cervix (neck of the womb) in women and on the penis and foreskin in men, around the anus and mouth (both sexes)The sore (or sores) is very infectious and may take from 2 to 6 weeks to heal.Secondary stageIf the syphilis infection remains untreated the secondary stage usually occurs 3 to 6 weeks after the appearance of sores. The symptoms include:• a non-itchy rash covering the whole body or appearing in patches• flat, warty-looking growths on the vulva in women and around the
anus in both sexes• a flu-like illness, a feeling of tiredness and loss of appetite,
accompanied by swollen glands (this can last for weeks or months)
• white patches on the tongue or roof of the mouth• patchy hair lossWhen these symptoms are present, syphilis is very infectious and may be sexually transmitted to a partner. Treatment at any time during these first two stages of syphilis will cure the infection.Latent stageLatent syphilis refers to the presence of untreated syphilis. There may not be symptoms or signs of the infection, which is diagnosed by a positive blood test. If left untreated, it may develop symptomatic late syphilis. This would usually develop after more than 10 years. It is then that syphilis can affect the heart, and possibly the nervous system.If treatment for syphilis is given during the latent stage the infection can be cured. However, if there has been heart or nervous-system damage before treatment is started this may be irreversible.
How it is spreadSyphilis can be transmitted by:• having sex with someone who has the infection• a mother to her unborn baby
ComplicationsSyphilis may cause heart and nervous system damage if left untreated until the latent phase.Increased HIV susceptibility
TreatmentYes: Penicillin injections or, in some cases, antibiotic tablets or capsules.

116 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Hepatitis
What is it?
Hepatitis refers to viral infections that cause inflammation of the liver and can also be caused by alcohol and some drugs. Several different types of hepatitis virus exist (labeled A to G), with hepatitis A, B and C being the most common. Each of these viruses acts differently.
Signs and symptoms
People may have no symptoms at all, but they can still pass on the hepatitis virus to others.Symptoms may include:• a short, mild, flu-like illness• nausea and vomiting• diarrhoea• loss of appetite• weight loss• jaundice (yellow skin and whites of eyes, darker yellow urine and
pale faeces)• itchy skin.
How it is spread
The hepatitis A virus (HAV) is a common infection in many parts of the world. It is possible to become infected through eating or drinking contaminated food or water. The hepatitis A virus is found in faeces. It can be passed on if even a tiny amount of faeces from a person with hepatitis A comes into contact with another person's mouth.This means the virus can also be passed on sexually through practices such as rimming. Personal hygiene, with careful hand washing, can minimise the risk of the virus being passed on.• by unprotected penetrative sex with someone who is infected.
Also by sex which draws blood with someone who is infected- however, this is not a common way of becoming infected with hepatitis C
• by sharing contaminated needles or other drug-injecting equipment
• by using non-sterilised equipment for tattooing, acupuncture or body piercing
• through a blood transfusion where blood is not tested for the hepatitis virus.
• on rare occasions, from an infected mother to her baby, mainly during delivery. The risk may be greater if the mother is also infected with HIV
Complications
If a person continues to be infected over a number of years with the hepatitis virus, they could develop the following complications:• chronic hepatitis• liver cirrhosis• liver cancer.
Treatment
Yes: Immunization against HAV and HBV, at present there is no vaccine available to protect against hepatitis C.Those who have been in contact with the virus and have become infected may be given an injection to reduce the severity of the symptoms. If infected with hepatitis, limiting alcohol intake is crucial. One might be advised to avoid fatty foods and follow a low-salt diet. Your partner should also be immunised against hepatitis B (if not already infected).

117National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Genital Herpes
What is it?
Genital herpes is caused by the herpes simplex virus. The virus can affect the mouth, the genital area, the skin around the anus and the fingers. Once the first outbreak of herpes is over, the virus hides away in the nerve fibres, where it remains totally undetected and causes no symptoms. However, in some people, genital herpes may come back (recur) on the skin surface, at or near the place where it was caught. This may be when the person is ill. Some people never get another outbreak.There are two types of the genital herpes virus. Either type is infectious, but:• Type I infects the mouth or nose. It is more likely to recur than if Type
II infects this area.• Type II infects the genital and anal area, it is more likely to recur than
if Type I infects this area.
Signs and symptoms
Symptoms of the first infection usually appear 1 to 26 days after exposure and last two to three weeks. Both men and women may have one or more symptoms, including:• an itching or tingling sensation in the genital or anal area• small fluid-filled blisters. These burst and leave small sores which can
be very painful. In time they dry out, scab over and heal. With the first infection they can take between 2 and 4 weeks to heal properly
• pain when passing urine, if it passes over any of the open sores• a flu-like illness, backache, headache, swollen glands or feverAt this time the virus is highly infectious. Recurrent infections are usually milder. The sores are fewer, smaller, and less painful and heal more quickly, and there are no flu-like symptoms.
How it is spread
Genital herpes is passed on through skin contact with an infected person. The virus affects the areas where it enters the body. This can be by: • kissing (mouth to mouth)• penetrative sex • oral sex
Complications
If herpes first occurs in the first 3 months of pregnancy there is a small risk of a miscarriage. Catching herpes towards the end of pregnancy may cause the baby to be born early. However, most women who have several episodes of genital herpes during pregnancy have a normal delivery. A herpes infection in the eyes can lead to severe complications, including blindness.Increased HIV susceptibility

118 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Treatment
Currently there is no cure for herpes. However, medicine may be prescribed to treat the symptoms.Help during an outbreak• Take pain-killers (aspirin/paracetamol) if you have any pain.• Gently bathing the sore areas with a salt solution twice a day may
help: it is soothing and helps the sores to dry out.• Wear loose clothing so that the air can get to the sore areas.• Place an ice-pack wrapped in a clean cloth or towel on the affected
area.• If passing urine is painful, try urinating in a bath of water. Or try
pouring water over yourself as you pass urine.• Drink plenty of fluids, such as mineral water and soft drinks, to help
neutralise the urine. It is important not to hold back from passing urine as this can cause further problems.
Genital Warts
What is it?Genital warts are small fleshy growths which may appear anywhere on a man or woman's genital area. They are caused by a virus called human papilloma virus (HPV).
Signs and symptoms
After infection with the genital wart virus it usually takes between 1 and 3 months for warts to appear on the genitals.Pinkish/white small lumps or larger cauliflower-shaped lumps on the genital area. Warts can appear around the vulva, the penis, the scrotum or the anus. They may occur singly or in groups. They may itch, but are usually painless. Often there are no other symptoms, and the warts may be difficult to see. In women genital warts can develop inside the vagina and on the cervix. If a woman has warts on her cervix, this may cause slight bleeding or, very rarely, an unusual coloured vaginal discharge.Not everyone who comes into contact with the virus will develop warts.
How it is spreadSkin-to-skin contact. If you have sex or genital contact with someone who has genital warts you may develop them too. (It is possible for warts to spread to the area around the anus without having anal sex.)
Complications
Some types of the genital wart virus may be linked to changes in cervical cells which can lead to cancer. It is important that all women over 20 years of age have a regular cervical smear test.Also, genital warts may cause anal and penis cancer.Increased HIV susceptibility
TreatmentYes: A topical liquid which is painted on to the wart(s) and must be washed off. Another common treatment is freezing the warts or laser treatment.Never try to treat genital warts by yourself. Always seek medical advice.

119National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Human Immunodeficiency Virus (HIV)
What is it?A virus that attacks the immune system and weakens the body's natural way to fight infections.
Signs and symptoms
Soon after being infected with HIV, some people feel as if they have the flu. They may have a fever, headache, tiredness and a rash. Others may not. Sometimes people start getting illnesses two to seven years after they first get infected. People with HIV can look or feel healthy. Many don't realise they have it because they don't feel or see anything wrong. If a person goes for a blood test to see whether they have the virus, sometimes it can take up to three months (after infection) for the virus to show up on the blood test.
How it is spreadUnprotected penetrative sex with someone who has HIV Sharing needles, syringes or other injecting equipment. An infected mother to her baby through breastfeeding
ComplicationsWithout treatment, after many years, a person who has HIV can't fight off some infections and cancers. This stage of HIV is called AIDS (Acquired Immunodeficiency Syndrome).
TreatmentYes: Antiretroviral DrugsCure: No
Non-specific urethritis (NSU)
What is it?Non-specific urethritis (NSU) is an inflammation of a man's urethra. This
inflammation can be caused by several different types of infection, the most common being Chlamydia.
Signs and symptoms
• pain or a burning sensation when passing urine• a white/cloudy fluid from the tip of the penis. This may be more
noticeable first thing in the morning• feeling that you need to pass urine frequentlyOften there may be no symptoms, but this does not mean that one cannot pass the infection on to partner(s).
How it is spread NSU is almost always caused through sexual infection.
Complications
• NSU may recur. A recurrence may be triggered by excessive friction during sex or masturbation, or by excessive alcohol consumption. Serious complications are rare.
If they do occur you may experience:• inflammation of the testicles• reduced fertility• Reiters syndrome - which causes inflammation of the eyes, joints
and urethra, and sometimes sores on the penis or soles of the feet• Increased HIV susceptibility
TreatmentYes: AntibioticsCure: Yes

120 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Pubic lice (crabs)
What is it?Pubic lice, or crabs, are small parasites found in the pubic hair called Phthirus pubis. They are different to head lice. Condoms and dental dams do not protect against pubic lice.
Signs and symptoms Itching in the pubic hair and/or visible eggs or lice.
How it is spreadPubic lice are spread by direct skin-to-skin contact including sexual activity, and contact with towels, underclothing or bedding of an infected person.
Complications Increased HIV susceptibility
TreatmentYes: Insecticide lotions or shampoos. All bed linen, towels and clothing must be washed in hot water. You do not need to shave your pubic hair. Cure: Yes
Scabies
What is it?Scabies is caused by Sarcoptes scabiei (a mite which lays its eggs under the skin surface).
Signs and symptoms
ItchingA rash on the genitals, knees, buttocks, waistline, hands, wrists, and between the fingersSilvery lines where the mite has burrowed
How it is spreadDirect skin-to-skin contact with an infected personOral, anal and vaginal sex
Complications Increased HIV susceptibility
Treatment
Yes: Anti-scabies lotions. All bed linen, towels and clothing must be washed in hot water and dried well. The itch often lasts for four weeks after successful treatment. Cure: Yes
Trichomoniasis
What is it?Trichomoniasis is an infection caused by a parasite called Trichomonas vaginalis.
Signs and symptoms
Trichomoniasis only usually occurs in females.Some females don't have any symptoms of infection. Others may notice:Red, sore or itchy vulva (genital area). Vaginal discharge which is thin and foamy and may have an unpleasant 'fishy' odour. Burning or pain when passing urine or during sex. Symptoms in males are rare. Occasionally, males may notice:Slight discharge from the penis. Burning or pain when passing urine or during sex.

121National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
How it is spreadIt's passed on through unprotected vaginal, anal or oral sex with an infected person.
ComplicationsPremature delivery in pregnant women Increased HIV susceptibility
TreatmentYes: AntibioticsCure: Yes
Molluscum contagiosum
What is it?Molluscum contagiosum is a fairly common skin infection caused by the Molluscum contagiosum virus
Signs and symptoms
Molluscum contagiosum shows up as small, round, pearly lumps. They are often mistaken for warts. If passed on through sex, the spots tend to be found around the genitals. The spots usually show up several weeks after being infected.
How it is spreadIt is spread by skin-to-skin contact. In adults it is mainly spread by sexual contact (oral, anal and vaginal sex) with an infected person. Any spots not covered by a condom or dental dam can infect you.
Complications Increased HIV susceptibility
Treatment
Yes: Molluscum contagiosum is generally harmless and will disappear on its own in healthy people. The infection can last up to two years, although each spot generally goes after two or three months. If you are worried or uncomfortable, or have another medical condition, your doctor may treat the spots with cream or by freezing them. Cure: Yes

122 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 6.4: Sexual Reproductive Health Rights28
Objectives1. To discuss SRH related rights and responsibilities and how they are important in the
prevention of sexual coercion and abuse and HIV/STI infection
Time 30 minutes
Materials • Flipchart • Markers • Pieces of paper or cards
Steps 1. Brainstorm rights and responsibilities with the participants. Start with the question,
“What are some basic rights we have as individuals?” Some examples may include the right to free speech, the right to practice one’s own religion, the right to live where one wants, etc. Then ask, “What are some basic responsibilities we have as individuals?” Some examples may include respecting the property of others by not stealing, providing for family, obeying laws, etc.

123National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
2. Write the heading “My Sexual Rights” on a piece of flipchart paper. Ask the participants to list their sexual rights and write their responses on the paper. Be sure the following rights are included: • The right to sexual enjoyment • The right to protect yourself from the risk for infection • The right to avoid unintended pregnancy • The right to refuse unwanted sex • The right to express sexual orientation • The right to obtain information on sexuality and sexual health
3. On another piece of flipchart paper, write the title “My Sexual Responsibilities.” Ask the participants to list their sexual responsibilities and write their responses on the paper. Be sure the following sexual responsibilities are included:• Respecting a person’s right to say no• Informing a partner if you are infected with a STI, including HIV• Taking care of any children you have
4. Complete the session with the discussion questions below: In your communities, is it more common for women’s rights to be respected or
not respected? If not, why do you think this is? In your communities, is it more common for men’s rights to be respected or not
respected? If not, why do you think this is? What is the connection between sexual rights and sexual responsibilities? How can a person’s right to get information on sexuality and sexual health be
violated? How can the violation of a person’s sexual rights leave them more vulnerable to
HIV and AIDS? How does someone neglecting their sexual responsibilities put them at risk for
HIV and AIDS? What have you learned from this exercise? How can you apply this to your own
relationships?
Closing Respect for sexual rights is an integral part of respecting human rights in general. Though we are not obligated to agree with or approve of other people’s choices, we do have to respect everyone’s right to choose and to express their sexuality equally. When sexual rights are not respected, both women and men are more vulnerable to STIs and HIV and AIDS. It follows, therefore, that respecting sexual rights, as well as other rights, creates a more secure society for everyone.

124 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 6.5: Men’s Health29
Objectives 1. To discuss how gender norms influence the sexual and reproductive health problems
of men 2. To identify men’s SRH problems and where to seek help
Time 60 minutes
Materials • Flipchart• Small pieces of paper• Prestick• Markers• Handout 6.5: The Male Reproductive System and Genitalia
Facilitator’s notes If possible, it might be interesting to follow up this activity with a visit to a local health facility, where the men can meet and talk with health professionals.
Steps 1. Draw an outline of a body on two or three new sheets of flipchart paper. Ask for
a volunteer to sketch the male genitals on the body. If the participants are too embarrassed to do this, the facilitator can do so.
2. When the outline is finished, give the participants two small pieces of paper and ask them to write sexual and reproductive health problems/needs men face (one per piece of paper).
3. When they have finished, ask each participant to read aloud the health problems/needs, and place them on the part of the body where this health problem appears. It does not matter if some problems are repeated.
4. Probe to see if the participants identify STIs, erectile dysfunction, prostate and penile cancers, impotence, infertility, HIV and AIDS, and substance use as health problems. If they have not mentioned them, ask if these are problems men face in their community.
5. Use the questions below to facilitate a discussion: • What are some health problems/needs men face? (See Resource Sheet 7)• What are the causes of these health problems? What are the consequences of
these health problems? • How does a man’s role in his family or community affect his health?

125National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Do men and women take care of their bodies and health in the same way? How do men take care of their health?
• When men are ill or sick, what do they do? Do they usually look for help as soon as they feel ill, or do they wait? When women are ill or sick, what do they do? Do men get tested for HIV as frequently as women? Why?
• Where can men in your community go to ask questions about their health or to seek services for health problems?
• What can you do in your own lives to take better care of your health? What can you do to encourage other men to take better care of their health?
6. Round up the discussion using the information in the resource sheet, and encouraging men to seek medical help if they suspect any symptoms in their sexual and reproductive organs.
7. After this session has been exhausted explain to the participants that you have covered all the three key issues at hand. Ask them that after learning about GBV, HIV and SRH, what do they think the linkages are between these areas? Allow a short discussion of this and round up with the information contained in Facilitators Notes 6.5.2: Linkages between GBV, SRH and HIV &AIDS.
Closing As discussed in this and previous sessions, there is a clear relationship between how men are raised and if, and how, they worry about their health. Many men, as a way of showing their masculinity, do not worry about their health and may believe that taking care of the body or being overly concerned about health are female attributes. These kinds of attitudes and behaviours are learned at early ages and impact men’s health throughout their lives. For this reason it is important that men learn the importance of taking care of themselves, including basic hygiene practices. Doing so has positive benefits for both men and their partners. This is well addressed in the activities on safer sex and HIV and AIDS.

126 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 6.5: The Male Reproductive System and Genitalia
113
Handout6.5:TheMaleReproductiveSystemandGenitalia
Frompubertyon,spermarecontinuouslyproduced in the testicles (or testes),whichare
foundinsidethescrotum.Asthespermmature,theymoveintotheepididymis,wherethey
remaintomatureforabouttwoweeks.Thespermthenleavetheepididymisandenterthe
vasdeferens.Thesetubespassthroughtheseminalvesiclesandtheprostategland,which
releases fluids that mix with the sperm to make semen. During ejaculation, the semen
travels throughthepenisandoutof thebodybywayof theurethra, thesametubethat
carries urine. The urethral or urinary opening is the spot from which a man urinates or
ejaculates.
From puberty on, sperm are continuously produced in the testicles (or testes), which are found inside the scrotum. As the sperm mature, they move into the epididymis, where they remain to mature for about two weeks. The sperm then leave the epididymis and enter the vas deferens. These tubes pass through the seminal vesicles and the prostate gland, which releases fluids that mix with the sperm to make semen. During ejaculation, the semen travels through the penis and out of the body by way of the urethra, the same tube that carries urine. The urethral or urinary opening is the spot from which a man urinates or ejaculates.

127National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 6.5.1: Problems Affecting the Male Sexual and Reproductive System
Men may sometimes experience reproductive system problems. Below are some examples of disorders that affect the male reproductive system:
Male genital problems and injuries Male genital problems and injuries can occur fairly easily since the scrotum and penis are not protected by bones. Genital problems and injuries most commonly occur during:
• Sports or recreational activities, such as mountain biking, soccer, or rugby.
• Work-related tasks, such as exposure to irritating chemicals.• Falls.
A genital injury often causes severe pain that usually goes away quickly without causing permanent damage. Home treatment is usually all that is needed for minor problems or injuries. Pain, swelling, bruising, or rashes that are present with other symptoms may be a cause for concern.Male genital conditionsTesticular cancer: This is the most common cancer in men 15 to 35 years old. Testicular cancer is more common in white men than in black men. Many growths in the scrotum or testicles are not cancer (benign). However, a painless lump in a testicle may be a sign of cancer.An erection problem: This may occur when blood vessels that supply the penis are injured. A man may not be able to have an erection (erectile dysfunction), or the erection may not go away naturally (priapism), which is a medical emergency. Torsion of a testicle: This occurs when a testicle twists on the spermatic cord and cuts off the blood supply to the testicle. This is a medical emergency. Scrotal problems: These problems may include a painless buildup of fluid around one or both testicles (hydrocele) or an enlarged vein (varicose vein) in the scrotum (varicocele). Usually these are minor problems but may need to be evaluated by your doctor. Problems with the foreskin of an uncircumcised penis: Conditions that makes it difficult to pull the foreskin back from the head of the penis (phimosis) or that prevent a tightened, retracted foreskin from returning to its normal position over the head of the penis (paraphimosis) need to be evaluated.Hypospadias: This is a common birth defect where the urethra does not extend to the tip of the penis.
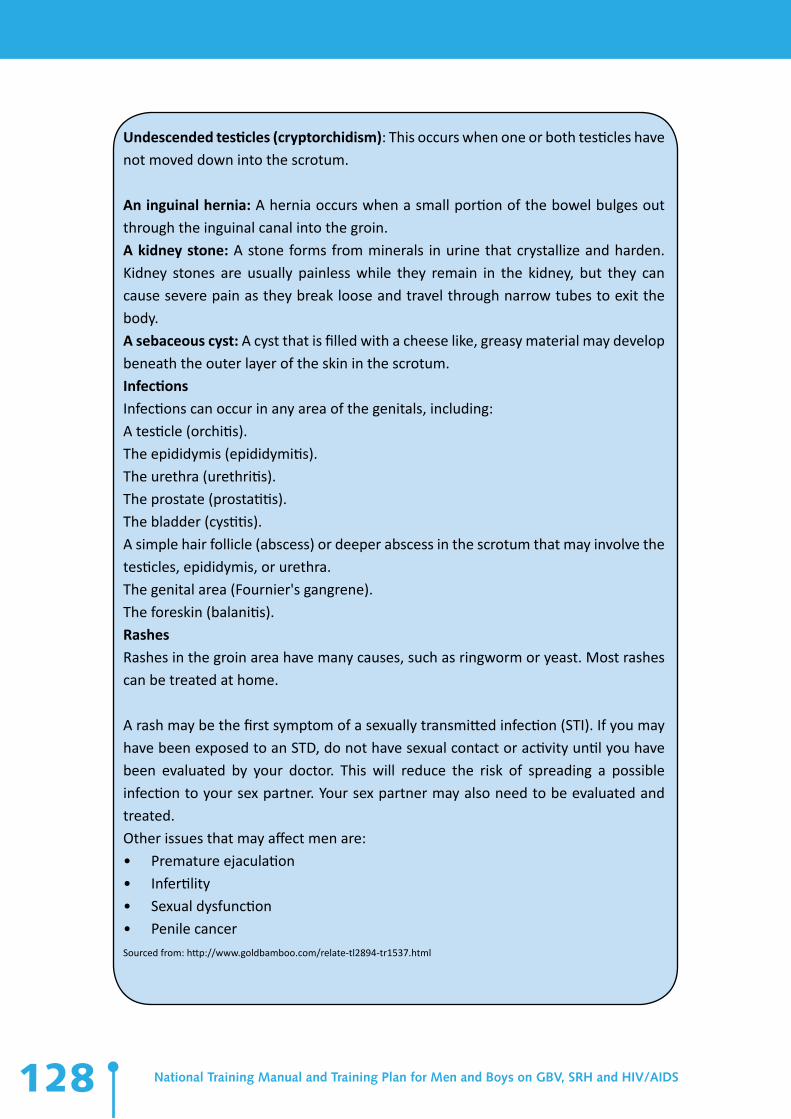
128 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Undescended testicles (cryptorchidism): This occurs when one or both testicles have not moved down into the scrotum.
An inguinal hernia: A hernia occurs when a small portion of the bowel bulges out through the inguinal canal into the groin.A kidney stone: A stone forms from minerals in urine that crystallize and harden. Kidney stones are usually painless while they remain in the kidney, but they can cause severe pain as they break loose and travel through narrow tubes to exit the body.A sebaceous cyst: A cyst that is filled with a cheese like, greasy material may develop beneath the outer layer of the skin in the scrotum.InfectionsInfections can occur in any area of the genitals, including:A testicle (orchitis).The epididymis (epididymitis).The urethra (urethritis).The prostate (prostatitis).The bladder (cystitis). A simple hair follicle (abscess) or deeper abscess in the scrotum that may involve the testicles, epididymis, or urethra.The genital area (Fournier's gangrene).The foreskin (balanitis). RashesRashes in the groin area have many causes, such as ringworm or yeast. Most rashes can be treated at home.
A rash may be the first symptom of a sexually transmitted infection (STI). If you may have been exposed to an STD, do not have sexual contact or activity until you have been evaluated by your doctor. This will reduce the risk of spreading a possible infection to your sex partner. Your sex partner may also need to be evaluated and treated. Other issues that may affect men are:• Premature ejaculation• Infertility• Sexual dysfunction• Penile cancerSourced from: http://www.goldbamboo.com/relate-tl2894-tr1537.html

129National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Facilitator Notes 6.5.2: The linkages between GBV, SRH and HIV/AIDS
GBV is intimately linked to the transmission of HIV, due to the unequal power relations between men and women where violence is used or threatened. GBV fosters the spread of HIV/AIDS because it limits women’s and girls’ ability to negotiate safe sexual practices, to disclose HIV status and to access services due to fear of GBV.
Boys and men are more likely to engage in unprotected sexual activity in order to prove their masculinity, thus putting them at risk of HIV infection and endangering their sexual and reproductive health. Not using protection during sexual intercourse/activity can itself be seen as a form of exercising power. Rigid gender norms often drive the HIV epidemic by facilitating unsafe behaviour such as multiple concurrent partnerships, cross-generational and transactional sex. There is thus an apparent vicious circle between GBV, HIV and SRH.
HIV infection is primarily acquired through sexual relations, which themselves are greatly influenced by socio-cultural factors, underlying which are gender power imbalances. Gender based violence, or the fear of it, may interfere with the ability to negotiate safer sex or refuse unwanted sex.
The physiology of the female genital tract makes women—especially young women— inherently more vulnerable to HIV infection than men. Women are twice as likely to acquire HIV from men during sexual intercourse than vice versa. And forced or violent intercourse can cause scratches and cuts, which facilitate entry of HIV through vaginal mucosa. Furthermore, violence against a woman can interfere with her ability to access treatment and care and maintain adherence to ARV treatment. Evidence also exists that living with HIV can represent a risk factor for GBV, with many people reporting experiences of violence following disclosure of HIV status, or even following admission that HIV testing has been sought. Fear of violence is an undermining factor in terms of seeking treatment. Women may hesitate to be tested for HIV or fail to return for the results because they are afraid that disclosing their HIV-positive status may result in physical violence, expulsion from their home or social isolation. Sexual and reproductive health is therefore compromised by the presence of GBV.

Alte
rnat
ives t
o Vio
lenc
eSection
7

131National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objectives: 1. Increased level of understanding and knowledge regarding harmful Gender norms
that perpetuate the use of violence and places men and women at risk of HIV and AIDS
2. Increased understanding, knowledge and skills on effective communication as a means of resolving conflict within intimate relationships, family structures and the community at large
Total Time: 2-3 hoursMost of the violence that occurs is usually a result of poor communication and lack of knowledge about other ways of resolving misunderstandings and conflicts. This section will explore how people can communicate effectively in order to reduce and eradicate violence. In addition to this, it is worth exploring the concept of emotional intelligence as a way of dealing with our emotions effectively. Emotional intelligence refers to the ability to perceive, control and evaluate emotions. In doing so, we are better able to regulate and respond appropriately to our own and others’ emotions.
The Digital Stories in this section tell stories related to forms of injustice and pain, as well as how the men and women overcame this and their transformation into gender activists. The stories challenge myths and stereotypes about how men can act and live, showing that men can change to build a more just, gender equitable and healthy society.
Activity 7.1: Digital Stories30
Objectives 1. To convey messages on gender equitable activities by men2. To challenge myths and stereotypes about how men can live, showing that men can
act and live, showing that men can change to build a more just, gender equitable and healthy society.
Time 60 minutes
Materials • Flipchart• Markers

132 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Prestick• DVD: Male Engagement Initiative: Digital Stories• Digital Stories Facilitator’s Guide• DVD Player and Sound System/Projector and Screen
Advance PreparationEnsure that the equipment is in good working order before the session. Review the stories of Ngamane, Henry, Ephraim and James prior to the screening to familiarise yourself with each one of them.
Facilitator’s notes These sessions are meant to help the participants see that change is possible, especially for people who have faced challenges or have not behaved in very gender equitable ways in the past. Take the time to process how these transformations happen and challenge participants to think about how these stories apply to their lives or people they know. You may face some resistance from people who recognize that change is hard to come by, but always use your digital story heroes as a point of reference for positive transformation and messages. During and after viewing the stories, make sure that all the participants are still engaged and feel prepared emotionally to continue on with the discussion.
Steps 1. It is important that you prepare participants with a short introduction regarding
the nature of the stories, and offer your assistance to anyone who may find them difficult to watch.
2. Watch one of the four stories at a time 3. After the story, follow up with the relevant questions as outlined in the Digital Stories
Facilitator guide for each story. 4. Share the key points of each story after the discussion5. Follow all these steps for each of the four stories
Closing The storytellers entrust you, the facilitator, to honour their stories, and use them for educational and motivational purposes. Many of the stories are quite personal; however the storytellers have chosen to share them, to assist in reducing violence and the spread and impact of HIV/AIDS. As many of the stories stress, we must break the silence to confront these twin epidemics.
Ensure that the key points of each story are emphasised at the end of it.

133National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Training OptionIf it is impossible to screen the digital stories, the facilitator can ask 4 participants to each read a story in the large group and then follow up with Steps 3-5 above.Alternatively, the participants can be divided into 4 groups, and each group can be given a story along with the discussion questions. Facilitator can make copies of each story, but ensure that the key points are not copied until the end of the discussion.
The four small groups can then share their stories at the end of their discussion. Allow for 30 minutes for small group discussions and about 20 minutes in the large group.
Activity 7.2: Effective Communication31
Objective 1. To develop skills to communicate assertively
Time 45 minutes
Materials • Flipchart • Markers

134 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Advance Preparation Before the session, prepare the following three flipcharts:Flipchart 1:Passive CommunicationAgressive CommunicationAssertive Communication
Flipchart 2: Assertive CommunicationFormula = ACTION + RESPONSE + REASON + SUGGESTIONS
“I” Statements—CLEAR (to the point) and CLEAN (free of blame or judgment)The Action: “When….” Be specific and nonjudgmentalMy Response: “ I feel….” Keep it to your own feelingsReason: “….because…..” (optional)Suggestions: “What I’d like is……” (ask but not demand)
Flipchart 3:What do you say when someone tries to persuade you?
Refuse: Say no clearly and firmly, and if necessary, leave • “No, no, I really mean no” • “No, thank you” • No, no—I’m leaving”
Delay: Put off a decision until you can think about it • “I am not ready yet” • “Maybe we can talk later” • “I’d like to talk to a friend first”
Bargain: Try to make a decision that both people can accept• “Let’s do…. instead” • “I won’t do that, but maybe we could do…” • “What would make us both happy?”
Facilitator’s notes When we teach people to be assertive, we need to also teach them to assess situations and to consider their personal safety. In some situations, speaking up and communicating assertively can be dangerous (if someone has a weapon, has been drinking or taking drugs, is extremely angry, etc.).

135National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
When you introduce the topic of assertiveness, keep in mind that communicating assertively, especially for women, is not considered the norm in some cultures. Individual cultural teachings regarding assertiveness will vary among participants. Some will come from families in which speaking up for oneself or refusing a request, especially from an adult or a male, is considered inappropriate.
You do not want to encourage people to behave in a way that could have unpleasant consequences for them in their culture or family circles. It is important, however, that all participants understand there are certain situations in which assertive behaviour will often yield positive results (examples include resisting pressure from romantic partners or peers to have sex, use alcohol, or other drugs, etc.).
Steps 1. First, ask the group to describe “assertive communication.” After a few responses,
show participants the first flipchart and explain that there are three types of communication: passive, aggressive, and assertive.
2. Tell the group that it is very important that we assess a situation and consider our personal safety before using assertive communication. For example, if someone is on drugs, is drunk, or has a weapon, it probably is not the best time to speak up. However, in relationships, especially romantic relationships, it is important to be assertive.
3. Tell participants that one way to make communication more effective in difficult situations, is to choose the appropriate kind of communication. Read the following scenario aloud:
Simon and Selma have been dating for three months. During that time, they never had sex. One afternoon, Simon wanted them to go out for a movie, but Selma suggested that they spend quality time at Simon’s place. Simon thought at last Selma was ready to have sex, and started making sexual advances. Selma made it clear that she was not ready for sex, but Simon continued to pressure her.
Have the participants write one sentence describing what Selma should do in this situation. Allow about three minutes, and then ask participants to form three groups, based on the following criteria:Group 1: Get angry at Simon and leaveGroup 2: Submit to his advances and have sex Group 3: Explain that you do not want to have sex but would like to continue spending
“quality time”

136 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
4. Once the three groups have been formed, ask them to answer the following questions as a group: Why do you think this response is appropriate? What results may happen because of this response?
5. Allow five minutes for each discussion, then ask everyone to be seated.6. Ask one participant from each group to share group responses to the questions.
Record the major points in three separate columns on flipchart paper.7. Use flipchart 1 and ask participants to match each term to the list of outcomes for
the responses.8. Review Selma’s choices for action one more time, and illustrate why assertiveness is
usually the best choice in a situation like this. • Passive Response: Behaving passively means not expressing your own needs
and feelings, or expressing them so weakly that they will not be heard. • Aggressive Response: Behaving aggressively is asking for what you want or
saying how you feel in a threatening, sarcastic, or humiliating way that may offend the other person(s).
• Assertive Response: Behaving assertively means asking for what you want or saying how you feel in an honest and respectful way, so that it does not infringe on another person’s rights or put the individual down.
9. Next, ask for two volunteers who can role-play the scenario in which Selma responds assertively.
10. Conclude the activity with the following discussion points: Were you surprised by anyone’s response in this exercise? Why or why not? How did it feel to think about speaking assertively? Would it have been different if the roles were reversed (Simon did not want to
have sex and Selma was pushing Simon)? Why is it so hard for some people to be assertive? Do you think there are differences in gender that affect how assertive a person
is? How can the lack of assertive communication put people at risk for unsafe sex
and sexually transmitted infections? What have you learned from this exercise?
11. In closing this activity, review ways that participants can be assertive by reviewing flipcharts 2 and 3 with them.

137National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
ClosingAlthough being assertive may not come naturally to you, it is important to think about when it might be important for you to be assertive since it can often yield important benefits. However, you need to determine when that behavior might be most appropriate, and you need to ensure that you can be safe. In some situations, speaking up and communicating assertively can be dangerous (if someone has a weapon, has been drinking or taking drugs, is extremely angry, etc.)
If you feel uncomfortable being assertive, you can practice being assertive in “mock” situations with people you feel safe with, such as friends or family members.
Activity 7.3: Going Deeper: How feelings can trick us32
Objectives1. T o help the participants identify when some of the more “acceptable” emotions (like
anger for men) are hiding some of the less acceptable emotions (like hurt) in order to communicate feelings more accurately to others.
Time 60 minutes
Materials • Flipchart • Paper• Pens• Prestick• Copies of handout 15: Reflection Sheet
Advance preparationBefore the workshop, draw a picture of an onion on the flipchart – it should be a cross section, showing the different layers of the onion.

138 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps Mention that in the last session we learnt how important it is to identify our feelings, •
even the ones that are considered socially “unacceptable” (eg anger for women, fear for men).Identifying feelings can be quite challenging though because of this. Just because •
we are a man does not mean we do not feel fear. We do in some situations. Just because we are a woman and it is considered not so socially acceptable for woman to get angry and shout, does not mean that we do not feel anger. We do in some situations.Because of these complicated pressures we feel from the outside (society, our •
community, our family etc) we can sometimes try to hide the feelings we are not comfortable feeling – we try to cover them with other emotions. And to make things even more complicated, ANGER, is often the emotion that we let •
people see, when at our core, what we are really feeling is hurt or fear.One way of helping us to understand this is to think of our emotions as an onion •
– there are various layers, and if we peel these back we can find the feeling that is right at the centre of our beings. Show the diagram of an onion and explain that the feeling we see from the outside •
(the skin of the onion) are not always the heart of what we really feel. Sometimes we have to pull back the layers to understand how we, and others, feel about something.
Consider this scenario – facilitator to read:Tangeni and Selma have been dating for 3 months. They decide they will go to the local cuca shop for a drink on Saturday night. The vibe is great, and they know lots of people there. An old boyfriend of Selma’s from high school is there. When they were a couple in matric, they were known as the hottest dancers in their school. Selma’s ex-boyfriend, Cleo is there with a girlfriend, Tjipee, and she is very beautiful too. Everyone is chatting and laughing, and drinking and then the dancing starts. Tangeni and Selma hit the dance floor and impress everyone with their moves. Cleo and Tjipee join them. Then Cleo asks
124
Materials
• Flipchart
• Paper
• Pens
• Prestick
Advancepreparation
Before the workshop, draw a picture of an onion on the flipchart – it should be a cross
section,showingthedifferentlayersoftheonion.
Steps
1. In order for us to communicate honestly and openly, particularly in couple
relationships, it is important to identify our feelings, even the ones that are
consideredsocially“unacceptable”(egangerforwomen,fearformen).
2. Identifyingfeelingscanbequitechallengingthoughbecauseofthis.Justbecausewe
are a man does not mean we do not feel fear. We do in some situations. Just
becauseweareawomananditisconsiderednotsosociallyacceptableforwoman
togetangryandshout,doesnotmeanthatwedonotfeelanger. Wedoinsome
situations.
3. Because of these complicated pressures we feel from the outside (society, our
community, our family etc)we can sometimes try to hide the feelingswe are not
comfortablefeeling–wetrytocoverthemwithotheremotions.
4. Andtomakethingsevenmorecomplicated,ANGER,isoftentheemotionthatwelet
peoplesee,whenatourcore,whatwearereallyfeelingishurtorfear.
5. Onewayofhelpingustounderstandthis istothinkofouremotionsasanonion–
there are various layers, and ifwepeel thesebackwe can find the feeling that is
rightatthecentreofourbeings.
6. Showthediagramofanonionandexplainthatthefeelingweseefromtheoutside
(theskinoftheonion)arenotalwaystheheartofwhatwereallyfeel. Sometimes
we have to pull back the layers to understand how we, and others, feel about
something.

139National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Selma to dance, for old time’s sake. Their dancing is stunning – it takes people’s breath away, and it is very, very sexy. Everyone else moves off the dance floor to watch, clap with the movement and cheer for the talented couple on the floor. At the end of the second song, Selma looks around for Tangeni. He is gone. She returns to his place to find him and he is very drunk and very angry. He accuses her of being a whore, of two-timing him with Cleo. He says their relationship is over and he never wants to see her again. He comes towards her holding a chair, threatening to hit her with it and looks at her with hate in his eyes. She feels he could kill her in this moment so she runs away to go and sleep at her sister’s house.
While asking these questions, the feelings can be identified and drawn on the onion.What feeling does Tangeni show Selma on the outside? (Anger, hate)•
What other feelings do you think he might have had? (• Hurt/Embarrassment – that she had somehow made him look foolish in public by dancing in this way with another man. Fear – that her feelings for Cleo might come back and she might leave him. Embarrassed in front of the community)Why would the • anger have been the feeling that Tangeni was most comfortable showing?
(Society says it is okay for men to be angry – especially with women. If a woman somehow makes a man look foolish in public, he then has the right to be angry and punish her – he has to prove he is a man)
What feelings would Selma have experienced in this situation? (Perhaps Excitement at dancing with Cleo and being the centre of attention, Worried when she discovered Tangeni had left the Cuca shop, Confused, Hurt and Fearful at Tangeni’s reaction later because she knows she is not a whore, or unfaithful to him.)
Important Point: If these feelings are not better understood, this scenario could end in disaster. Selma and Tangeni’s new relationship could come to an end. Tangeni could become a very angry man who does not trust women – and he could move into another relationship like this. Selma could remain very confused about why her actions had provoked such a reaction.
Rewind If we rewind this story to the point when Selma came to find Tangeni, how could things be different? Divide the participants into two groups and ask them to write a short dialogue on a flipchart paper that could have saved this situation (using what they have learnt in the previous session). Let each group read these out. If they are a less literate

140 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
audience, they can act this scenario differently. If you would like to, you can also read the following example of how things could have ended differently:
Tangeni: I feel very angry with you right now (using an “I” statement to express his feelings).
Selma: I am so sorry – I did not mean to make you angry. Please help me to understand why you feel this way. (Apologises – seeks to understand more)
Tangeni: I felt like a fool in public – I was embarrassed Selma, in front of the whole community, because of your sexy dancing with Cleo tonight. (Again owns another feeling – embarrassment – feeling a fool in public and explains when he felt like this)
Selma: But it did not mean anything – we danced a dance we used to dance in high school. When the dance finished I was looking for you to see if you liked my dancing – I was dancing for you. I don’t care about Cleo anymore. I was worried when I could not find you. (Selma has the chance to clarify how she was feeling and how she still feels about Cleo AND Tangeni)
Tangeni: I could just imagine all your old feelings for Cleo coming right back as you danced with him. I felt afraid that I was just losing you in that moment. (expresses another feeling – fear - as his thoughts ran away with him)
Selma: Tangeni – it is you I love. It is you I want to be with. Cleo is an old friend who no longer means a lot to me. You are the man I want to be with. (Again Selma clarifies feelings and is able to reassure)
Tangeni: Eish Selma, I feel very relieved now to hear you say this! But I would prefer it in future that you don’t dance with another man in that way when we are out in public. I felt hurt and it was confusing for me, and I am sure it was confusing for others watching you. I want people to know we are a couple – I am proud to be out with you. (Expresses relief that she has clarified the situation but asks that it does not happen again)
Selma: Tangeni, I understand what you are saying and I will make sure that does not happen again. You are also a great dancer, and if we practice we can also enjoy dancing together in that way. (Accepts his request and comes up with a good suggestion instead)
Closing What we feel can be way more complicated than just one simple feeling. It is important that we learn to identify all the feelings we feel and sometimes to explain those to others step-by-step. In this way we all gain clarity, and conflict is avoided. Relationships can then be restored. Anger is a deceptive emotion and it often hides other feelings that are less socially acceptable, particularly for men.

141National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 7.4: Going Deeper: Managing my Anger33
Objectives1. To help participants better regulate their destructive feelings.
Time 40 minutes
Materials • Flipchart • Paper• Pens• Prestick• Handout 15: Reflection Sheet
Advance PreparationBefore the workshop, draw a picture of a jug on the flipchart. Alternatively have 2 jugs
with water in one and place where you can pour the water into the other jug where it won’t matter if the water spills.
127
Closing
Whatwefeelcanbemorecomplicatedthanjustonesimplefeeling.Itisimportantthatwe
learntoidentifyallthefeelingswefeelandsometimestoexplainthosetoothersstep‐by‐
step. In this way we all gain clarity, and conflict is avoided. Relationships can then be
restored.Angerisadeceptiveemotionanditoftenhidesotherfeelingsthatarelesssocially
acceptable,particularlyformen.
Activity7.4:GoingDeeper:ManagingmyAnger33
Objectives
1.Tohelpparticipantsbetterregulatetheirdestructivefeelings.
Time
40minutes
Materials
•Flipchart
•Paper
•Pens
•Prestick
� Handout7.4:ReflectionSheet
AdvancePreparation
Beforetheworkshop,drawapictureofajugontheflipchart.Alternativelyhave2jugswith
water in one and placewhere you can pour thewater into the other jugwhere itwon’t
matterifthewaterspills.
33 CommunityCounsellorToolkit:module1:PersonalGrowth.LifeLine/ChildLineNamibia
Steps 1. Remind participants that they have already learnt a lot about anger. They have
learnt that it can be the feeling that hides a lot of other feelings that society finds unacceptable (particularly for men). They have learnt that anger is not the same as violence, and they have learnt some alternative ways of expressing anger.
2. This session is about how to recognise anger and other destructive emotions before they get out of hand, and what to do about this.
3. Explain that it is almost like we have a jug inside us where our emotions are stored over time. We need to learn to monitor and keep these emotions under some control, otherwise we can end up – literally - exploding.

142 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
4. Use the following scenario to help people understand how our negative emotions can build up and then we can have an almighty explosion that often impacts on one person, but is not their fault.
Scenario: A Bad Day You wake up late for work, rush off without having any tea or breakfast and struggle •
to find a taxi - what emotion do you feel? (Put this into the jug or pour some water representing the emotion into the other jug)You get to work, your boss is angry and has some strong words to use – what do you •
feel? (Put this into the jug or pour some water representing the emotion into the other jug)You are studying part time and receive an email from your lecturer telling you that •
you have not passed your last assignment – what do you feel? (Put this into the jug or pour some water representing the emotion into the other jug)Your mother phones to remind you that you have not sent the money you •
promised her to get your father some new glasses – what do you feel? (Put this into the jug or pour some water representing the emotion into the other jug)You race home remembering that your girlfriend wanted you to go and see a movie. •
When you get there, she is nowhere in sight. You wait two hours, try to get her on her cell phone – it is off. It is clearly too late now to go to a movie. There is nothing to eat at home and you have only eaten a sandwich at lunch – what do you feel? (Put this into the jug or pour some water representing the emotion into the other jug)She wanders in at about 8pm and says that she met a friend at the taxi rank who •
she has not seen for years so they had a drink together before she came home – this is the last straw. How do you feel? What do you say? What do you do? (If you are pouring water at this point it should overflow the jug and spill on the floor).
When our emotional jug or tank overflows things get pretty messy around us. Our feelings are out there on the floor for everyone to see. We do things and say things we may regret later. We hurt others (emotionally or physically). Uncontrolled anger is the cause of a lot of relationship problems and breakdowns, and it is not tolerated in most work places – we can be fired for losing control and shouting at or threatening colleagues or our boss. In this situation, many things happened to make us feel bad, and eventually angry. Who received the full brunt of our anger? Was she to blame? Was anyone to blame? What can we do alternatively? We talked in the previous session about taking a break, counting to 10 etc. But there are other things that can help us too. Let us write some of these down on the flipchart.

143National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• The first thing is to recognise when trouble is happening. Often when we have a bad day, we say we are stressed. Our stress can be felt in our bodies. Again, where do you experience your stress (stomach, shoulders, head, chest are typical places)?
• Physical exercise would be critical to have. Cardio vascular exercise – walking, running, swimming is important. But also any exercise that uses our big muscles (where the stress hormones are stored) like weight lifting, to help us physically release our stress.
• Talking to a friend. Women do this well – men often find it more difficult. Sometimes they just prefer to be with friends relaxing, playing sport, watching sport, laughing and talking about other things – sometimes at the bar. This is good, provided we don’t use the alcohol to drown the feelings we find unhelpful.
• Being in nature can help us release some of the negative emotions. • Water is soothing – a shower, a bath etc.• They may have many other suggestions. Ask for what helps them specifically.
ClosingDoing all these things helps us to “pour out” some of the negative emotions that are building up in our internal emotional jug. It is extremely important for all of us to learn to monitor our emotions and to know what to do to keep them in reasonable proportions so that we avoid emotional explosions and sometimes the violence that goes with them.
As men, it is important to reflect on how you react when someone has a different opinion than yours or when someone does something that makes you angry. It is not always easy, but it is important to take the time to think about your feelings BEFORE you react, especially when you are frustrated or angry. Sometimes, if you do not take the time to think about your feelings, you may react in a way that is hurtful or violent to another person or even yourself. Men need skills and support to talk with their wives and girlfriends about creating healthier relationships. There is little support for either men or women in making their relationships healthier. But gender rules for women allow them to ask each other for support and to talk about their feelings. The gender rules for men make it difficult for them to ask for support on personal matters or to show their emotions. The first step toward healthier relationships is to challenge these gender rules. Men need more opportunities and permission to ask for support. Men also need specific training on how to talk about their feelings and their relationships.

144 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 15: Reflection Sheet
What do I do when I am angry:
1. Think of a recent situation when you were angry. What happened? Write a short
description here of the incident (in one or two sentences).
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
2. Think about this incident and try to remember what you were thinking and feeling.
List one or two things that you felt in your body when you were angry:
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________

145National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
3. We often react with violence when we feel angry. This can even happen before we
realize we are angry. Some men react immediately, by shouting, throwing something
on the floor, or hitting something or someone. Sometimes, we can even become
depressed, silent and introspective. How did you demonstrate your anger during
this incident? How did you behave? (Write a sentence or a few words about how you
reacted and what you did when you were angry).
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
4. How could you have done things or behaved differently?
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________

146 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Taking Action
Section8

147National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Overview
Objectives• Increased knowledge on the legal provisions and services pertaining to GBV, SRH
and HIV&AIDS• Increased willingness to take part in community action teams aimed at challenging
the community with regards to GBV, SRH and HIV&AIDS• Enhanced skills in the development of community engagement activities targeted
towards creating greater awareness on GBV, SRH and HIV&AIDS.• Developing Action Plans
Total Time: 2-3 hours
Activity 8.1: The Legal Framework in Namibia
Objectives1. To briefly highlight important laws and policies that are pertinent to GBV, SRH and HIV/
AIDS and facilitate an understanding of how these laws protect both men and women’s
rights.
Time 40 minutes
Materials • Flipchart • Markers• Enough Brochures and Booklets from the relevant authorities containing applicable
Namibian laws for all the participants.
Facilitator’s notes Prior to the session, ensure that you have collected enough pamphlets of the laws and policies on GBV, SRH and HIV/AIDS. These can be sourced from the Legal Assistance Centre, the Ministry of health and Social Services, the Ministry of Gender Equality and Child Welfare, United Nations agencies, e.g. UNICEF, and local NGOs. Alternatively, you can download the relevant publications from the LAC or other website34 and print and copy them for the participants.

148 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps 1. Ask the group if they are aware of any of the Laws and Policies regarding what has
been discussed in the workshop thus far. List these on the flipchart.2. participants the Handout. You can go through them one by one, explaining what
they mean and answering any questions the group may have. If available, hand out the IEC material containing these laws.
3. Conclude the activity by emphasising that all these laws do not discriminate against men or women, and that all provisions contained within them apply to both sexes.

149National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 8.1: The Legal Framework in Namibia
There are laws and policies that directly or indirectly address the issues that are covered in this manual. These laws and their goals/objectives are outlined below:
National Gender Policy (2010 – 2020)This Policy envisions the creation of a society that is just, moral, tolerant and safe, and where legislative, socio-economic and political structures are in place to eliminate marginalisation, while ensuring peace, equality and equity between females and males in all spheres of life. It aims to achieve gender equality and the empowerment of women in the socio-economic, cultural and political development of Namibia.Combating of Domestic Violence Act (No. 4 of 2003)This legislation makes domestic violence a specific crime and has a broad definition of domestic violence which includes physical abuse, sexual abuse, economic abuse, intimidation, harassment and serious emotional-, verbal- or psychological abuse.
Maintenance Act (No. 9 of 2003)This law provides that both parents have a legal duty to provide for their children who are unable to support themselves, regardless of whether the children were born inside or outside of marriage, and whether or not parents are subject to any other system of customary law which might not recognise one or both parents’ liability to the child.
Combating of Rape Act (No. 8 of 2000).Even from an international perspective, this is one of the most progressive laws on rape. The Act gives greater protection to young girls and boys against rape. It provides for more stringent minimum sentences for rapists, and defines marital rape as an offence in the eyes of the law.
Married Persons Equality Act (No. 1 of 1996)This Act specifies equality of persons within civil marriage and does away with the legal definition of a man as head of the household. The Act also provides women who are married in community of property equal access to bank loans and equal power to administer joint property. It stipulates that immovable property may be registered in both spouses’ names.
Affirmative Action (Employment) Act (No. 29 of 1998)This Act identifies affirmative action as a set of measures to ensure that all Namibians have equal employment opportunities, and are equitably represented

150 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
in the workforce, focusing on previously disadvantaged groups such as women and the disabled.
Communal Land Reform Act (No. 5 of 2002)This legislation gives widows who reside in rural areas the right to remain on land allocated to their deceased husbands. It also provides that the right of a widow to remain on the land, is not affected by re-marriage.
Labour Act (No. 11 of 2007)This law provides for maternity leave (with the addition of maternity benefits under the Social Security Act No. 34 of 1994), and prohibits discrimination on the basis of pregnancy, as well as providing stronger protection against sexual harassment in the workplace.
The Children’s Status Act (No. 6 of 2006) This Act provides for equal treatment of children born out outside marriage in relation to those born in a marriage; especially on issues of inheritance. The Act also provides for equal guardianships and custody for unmarried parents.
National Policy on HIV/AIDSThe goal of this policy is to provide a supportive policy environment for the implementation of programmes to address HIV/AIDS that reduce new infections, improve care, treatment and support and mitigate the impact of HIV/AIDS – this in turn will assist with achieving vision 2030.
National Policy for Reproductive HealthThe long-term goal is to promote and protect the health of individuals and families through the provision of equitable, acceptable, accessible and affordable quality reproductive health services.
Abortion and Sterilization Act 2 of 1975The goal of this Act is to define the circumstances in which an abortion may be procured on a woman or in which a person who is incapable of consenting or incompetent to consent to sterilization, may be sterilized; and to provide for incidental matters.
These laws create a legal basis for gender equality and provide formal recourse to justice, access to services, and promoting health outcomes for men, women and children. However, inconsistent implementation and ineffective enforcement efforts continue to undermine the ability of these laws to achieve positive outcomes for all people.

151National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 8.2: Community Mapping35
Objectives1. To identify Resources and Organisations in the community that would support men and
boys with regard to GBV, SRH and HIV/AIDS.
Time 45 minutes
Materials • Flipchart • Markers• Enough copies of Handout : Community Mapping Worksheet
Facilitator’s notes If participants come from different communities, form groups with people from the same communities. If people are on their own, pair them up to work together to develop services maps of their own communities (each person will do their own service map but they can help each other brainstorm about the different type of services that might be available.)
Steps 1. Begin this session by asking the participants where they can go in their community if
they or a family member/friend were victims of violence, needed more information regarding reproductive health issues or wanted to access HIV/AIDS services. Ask them to think about resources available in their community.
2. Next, divide the participants into groups. Ideally, people living in the same community should be in the same group.
3. Ask each group to draw a physical map of their community. They should think carefully about specific resources that are available for survivors of violence. The second aspect should map out available resources for Sexual Reproductive Health. The third part should map out resources for HIV/AIDS. They should be creative and map out all resources that may apply.
4. Give each group about 15 - 20 minutes to map the resources, and then have each group share their maps.
5. Conclude this session with the following questions: How accessible are these resources? How does class or race or age affect one’s access to these resources? Are there any social networks (e.g., family, friends, faith communities, etc.) that

152 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
could also be of assistance? How can you be more a part of these services?
Closing It can be very difficult for individuals who suffer violence to speak out and seek help. For example, some women may fear that their partner might take revenge if they seek help or try to leave. Others may feel that they need to stay in an abusive relationship, especially if they are married and/or if there are children involved. For some, the economic consequences of leaving an intimate male partner might outweigh the emotional or physical suffering. There are various factors that can influence a woman’s response to violence. It is important to not judge individuals who do not leave relationships in which they are experiencing violence, but to try to think about how they can be supported to understand the consequences of violence and to seek the help they need. Additionally, it is equally important to think about ways of creating communities where women and men can live their lives free of violence, with good knowledge of accessible SRH and HIV/AIDS related service.
Training Option:The Facilitator can use the handout worksheet instead of getting the participants to draw their community maps. This can be done in groups as well.

153National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 8.2: Community Mapping Worksheet
Resources in the Community that can support men (and women) who are struggling with violence
Resources in the Community that support men with issues related to HIV
Resources in the Community who could assist men with Sexual and Reproductive Health
Resources in the Community who can help with counselling, communication, relationships, managing anger etc

154 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 8.3: Identifying Community Engagement Activities
Objectives1. To identify different types of community engagement activities that participants can
do as part of their action plansTime15 minutes
Materials• Flipchart paper and markers
Steps1. Ask participants to identify the various activities that can be implemented at the community level. Ask them to draw from their own experiences or from those of others in their communities. Write down all of the participants’ suggested activities on flipchart paper. If the following activities have not been mentioned after 10 minutes, add them to the list:• Street Drama/Theatre Performance• Media Campaigns• Choir• Murals• Talk Shows• Facilitated Group Discussions/Community Meetings/Mobile Seminars/Information
sessions• Door-to-Door Visits• Music Competitions• Sports Events• Marches
ClosingThe activities mentioned should form the basis for the participants Action Plans later in the training.

155National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 8.4: Developing Action Plans
ObjectivesTo have an opportunity to reflect on what participants have learned throughout the workshops and how that can help them make changes in their lives and in their communities
Time 60 minutes
Materials • Paper• Pens• Markers• Flipchart • Enough copies of Handout 8.4: Developing a Community Project and Handout 19: Community
Action Plan for all participants
Facilitator’s notes Part 2 of this activity involves the participants developing a community project to create awareness about an important social issue in their communities. It is up to the facilitator to decide if the group is ready to take on an activity of this kind, particularly in terms of time and resources. There might also be a need for other collaborators to help carry it out. Some organizations and facilitators are in a position to implement a community project, others are not. While it is important to engage the participants in this kind of exercise, it is also necessary to be realistic. A good starting point might be to collect examples of people who have mobilized themselves to promote awareness and change in their communities and discuss with participants the possibilities of doing something similar in their community.
In order to ensure that the project efforts are sustained over some period of time, it might be worth doing this activity at the onset of the group workshops so that the facilitator can provide support and follow up for at least the initial stages of the project. In that case, the last session can include Part 1 – Personal Reflections, as well as a discussion on how the project has progressed and how it can be sustained.

156 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps Part 1 – Personal Reflections (15 minutes)1. Ask participants to reflect individually on what they have learned throughout the
workshop and how it will help them to make positive changes in their lives and relationships.
2. Explain that they should create a collage, a short essay, a poem, or a drawing based on what they have learnt and how they will implement it in their own lives.
3. Allow 15 minutes for the participants to complete this task.4. Invite each participant to briefly present their reflections (in about two minutes) and
their medium of representation. 5. Open the discussion to the larger group with the following questions:
What will be some obstacles you might face in making these changes?•What will be some benefits?•How can you support each other to make these changes?•
Part 2 - Developing a Community Project (30 minutes)1. Explain to the participants that they are now going to think about the changes they
can try to make beyond their own lives and relationships. 2. Ask the participants to think of the most pressing social issues in their community
and how they are related to the topics they have discussed in the sessions. 3. As a group, ask them to select one of these issues to be the focus of their project. 4. Divide them into small groups to brainstorm what they can do with other men
and boys in their community or school about the social issue they have decided to address. Ask them to write down or sketch out their ideas on a flipchart paper. Tell them that the ideas do not need to be finished; they should simply list a number of first ideas, no matter how “raw” they may be. Allow about 30 minutes for the group work.
5. Invite each group to present its ideas.6. Ask the participants to help identify the main types of ideas presented, dividing them
into categories, for example: (1) political/advocacy action, (2) awareness campaigns in the community, (3) development of educational materials and information, and 4) implementation of a local plan in their schools and communities, etc.
7. Use the questions in the Handout to help the group focus and prioritize their ideas by asking them which ones they consider to be the most interesting and easiest to implement. Remember that it is important to leave the final decision to them.
8. Once the idea has been finalized, review Handout 15 and work with the group to answer the questions and determine an appropriate time to implement the plan. In other cases the group may wish to meet on their own to finalize the planning. The important thing for the facilitator is to assist the participants in developing a viable plan so that they have a sense of fulfilment and not frustration.
9. The groups should track their discussions in Handout 19.

157National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 8.4.1: Developing a Community Project
1. Description (in two or three phrases, describe your plan)2. Collaboration - Who do you need to work together with in order to put this plan into
operation? - How can you obtain this support and collaboration?3. Materials/Resources - What resources do you need to carry out your plan? - Where and how can you obtain such resources?4. Time Schedule - How long do you need to execute the plan? List in order the steps required to carry out the planning.5. Evaluation - How do you know if your plan is working? - What expectations do you have about the result of your activity?6. Risks - What things can go wrong? - How will these be addressed?

158 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout 8.4.2: Community Action Plan
Activity to be done
By Whom?Responsible
person
When?How long
will it take to complete?
What resources are needed to do this activity?
What challenges
may be met?
How will you know the
activity had an impact?

159National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Activity 8.5: Post-Test and Evaluation
Objective• To conduct an assessment of participants’ knowledge and attitudes regarding gender,
reproductive health, HIV/AIDS and GBV after the workshop• To evaluate the training week
Time30 – 40 minutes
Materials• Enough copies of the Post-test and Evaluation Form (see Appendices C and D) for all
participants• Pens and pencils
Steps1. First hand out the Evaluation form and allow for 10 minutes for the participants to
fill it in.2. After they finish and hand this in, explain to the participants that the purpose of the
pre-test and post-test is to help facilitators determine how well the objectives of the training were achieved.
3. Distribute the post-test to each participant. Ask them not to put their names on the test papers.
4. Allow 20 minutes for participants to complete the test.5. After 20 minutes, collect the post-tests for review later. If the participants have
questions about the answers, allow a few minutes to answer these.6. Mark the tests and compare the results with the pre-test in order to evaluate the
effectiveness of the training.

Optio
nal S
essio
nsAppendix
A:

161National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
1. Defining Abstinence
Objectives 1. To define abstinence and identify strategies for individuals who want to practice
abstinenceTime 45 minutes
Materials • Flipchart• Markers• Prestick
Advance preparation Prepare a flipchart of sexual and abstinence behaviours that includes the following:• Thinking about sexual behaviours• Dreaming about sexual behaviours• Talking about sexual behaviours• Flirting• Holding hands• Kissing• Deep kissing • Massage with clothes on• Massage with shirt/blouse off• Showering together• Rubbing bodies with clothes on• Rubbing bodies with clothes off• Hands on partner’s genitals• Masturbation • Mutual masturbation• Oral sexual intercourse• Anal sexual intercourse• Vaginal sexual intercourse• Reaching orgasm

162 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps 1. Introduce the activity by pointing out that failure to make good decisions about sex
is one reason individuals become infected with HIV or other STIs and/or experience an unintended pregnancy. Explain that one decision people can make about sex is to not have it—to abstain until a more appropriate time, especially for young people. Begin by writing the word abstinence on the flipchart.
2. Ask for ideas about what abstinence means. Be clear that you are talking about sexual abstinence.
3. Once two people have given answers, ask all the participants to write down their definitions of abstinence.
4. Give them two to three minutes to do so. When they are finished, ask them to share their answer with the person sitting next to them.
5. Once they have done this, have them form groups of five to six people and develop a common definition for the group. Give them five to eight minutes to prepare the group definition. [Note: This may prove difficult, given their various definitions, so push them to come up with one definition.]
6. Post the list of behaviours (the flipchart you prepared earlier) on the wall and ask the groups to use it to help them with their definitions. Give them five minutes or so to discuss what behaviours on the list would apply to their definitions and what behaviours would not.
7. Ask each group to share its definition—if any—and how it was arrived at.8. Follow up with these questions:
What was difficult about this exercise? Were you surprised by anything or by anyone’s response? Why is it hard to define abstinence? Do you think it is important to define abstinence? Is it harder for men or for women to abstain? Why? Why did we do this exercise? What can we do to help others abstain? Did you learn anything? What?
Closing Sexual abstinence means different things to different people. What is right for you may not be right for another. The decision to have sexual intercourse or to be sexually abstinent is a personal one that you make repeatedly in life. It is not a permanent, one-time decision, nor is it a decision that can be imposed on others. Like contraception, sexual abstinence is only effective when practiced correctly and consistently. It requires planning, commitment, and skill at being assertive. Knowledge of contraceptive options and how to protect oneself is extremely important, even for someone who is sexually abstinent and plans to remain so for the foreseeable future. It is also important to note

163National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
that even if someone chooses to abstain from sex, they may be pressured or forced into unwanted sexual activity. Therefore, an environment in which one’s sexual rights and choices—whatever they may be—are respected is the best environment to encourage sexual abstinence.
2. Learning about Condoms
Objectives 1. To discuss myths and truths about condoms and provide basic information about
correct condom use
Time 60 minutes
Materials • Small pieces of paper• Pens/pencils• Box or basket• Penis and Vagina models• Male and female condoms (if available)
Advance preparationThe following statements written on a separate piece of paper (one paper per statement):1. Talk about condom use.2. Buy or get condoms.3. Store the condoms in a cool, dry place.4. Check the expiration date.5. The man has an erection.6. Establish consent and readiness for sex.7. Open the condom package.8. Unroll the condom slightly to make sure it faces the correct direction over the
penis.9. Place the condom on the tip of the penis. Hint: If the condom is initially placed on
the penis backwards, do not turn the condom around; throw it away and start with a new one.
10. Squeeze the air out of the tip of the condom but still leave a bit of room.11. Roll the condom onto the base of the penis as you hold the tip of the condom.12. The man inserts his penis for intercourse.13. The man ejaculates.

164 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
14. After ejaculation, hold the condom at the base of the penis while still erect. The man removes his penis from his partner carefully.
15. Take the condom off and tie it to prevent spills16. Throw the condom away. If available, try to bring a couple of male and female condoms to the session so that the men can see what they look and feel like. You may also provide the participants with information on where to get condoms in the community.
Steps Part 1 – Myths and Truths About Condoms (One hour) 1. Give the participants several pieces of paper and ask them to write one statement
(or phrase or idea) that comes to mind about condoms on each card. Encourage the participants to think of both positive and negative phrases.
2. Ask each participant to put his paper(s) in the box or basket, which should be placed in front of the group. Then, ask each participant to come forward, take a piece of paper from the box, read its statement out loud, and say if the statement is a myth or a truth.
3. Give the participants an opportunity to touch the male and female condoms, if available. Reinforce the importance of correct AND consistent condom use during sexual intercourse.
4. Open the discussion to the larger group with the following questions: Are condoms easily available in the community? Why or why not? What are the reasons that lead men, including those who know the importance
of using condoms, to not use them? What do you think about the female condom? Do you think men would be
interested in using it? Why or why not? How can you support the use of condoms in your community?
Part 2 – Correct Condom Use 1. Give one condom in its packet to each participant. Ask the participants to check that
the condom is not past its expiration date. Then ask them to open the packet and take out the condom. Encourage them to stretch and play with the condom.
2. Divide participants into pairs. Ask one member of each pair to place a condom over their hand. (Tell them to beware of sharp fingernails!) Next, tell them to close their eyes and to ask their partner to touch their fist with a finger. Ask the participants wearing the condoms: Can you feel the other person’s finger touching you? How much can you feel through the condom? How thick do you think the condom is now?

165National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
3. Have the participants stretch the condom as much as they can without breaking it. Ask if they can pull it over their arms or feet or blow it up. Ask the participants: How long did the condom get? How wide did it get? What happened to the condom when it was stretched? Did it break?
4. Ask participants to sum up what they learned from playing with the condoms. Emphasise two key points: The condom is extremely strong and yet sensitive to touch. This makes it a good form of protection from STIs (including HIV) without taking away the pleasure of sex.
5. Explain that you now want to talk about the correct steps in using a condom. Randomly distribute the “Condom Use Steps” cards. Then ask the participants to stand up and arrange themselves in the correct order of steps. Discuss these questions: What was challenging about this activity? Were you unsure of the order of any steps? Why? Could some of the steps have
gone in more than one place? Could some of the steps been switched? Do you think most people who use condoms follow these steps? Why or why
not?6. Give participants new condoms, and ask them to try putting it on the penis model
themselves. If you have time after the participants have finished, ask for a volunteer to demonstrate the correct use of a condom on the penis model. Once the volunteer is done, ask the participants to comment on whether or not the demonstration was done correctly.
7. Remind participants that condoms should always be stored in a cool, dry place. Using a water-based lubricant like K-Y jelly will decrease the chance of the condom breaking and may make intercourse more pleasurable. Oil-based lubricants like Vaseline, creams, or oils will cause the condom to break and should never be used.
Closing Simply knowing that condoms can help avoid pregnancy and STIs/HIV is not enough. It is important that you also know how to correctly use them and to understand the importance of consistent use. Moreover, you need to be able to engage your partners in discussions about the pros and cons of sexual intercourse, including the importance of abstaining before marriage. If you and a partner decide to have sexual intercourse, then you should discuss together how best to protect against unintended pregnancy or STI/HIV infection, including using a condom.

166 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
3. Male Circumcision as an HIV-Prevention Strategy
Objectives1. To assist in the understanding of the health benefits of male circumcision to a man
and his partner2. To discuss the means and messages to promote male circumcision
Time 45 minutes
Materials • Flipchart paper• Markers• Prestick
Advance preparation 1. Prepare a piece of flipchart paper with the following definition: The removal of the
foreskin that covers the head of the penis2. Cover the definition with a blank piece of flipchart paper.3. Write the following on sheets of flipchart paper: HIV/STI protective mechanisms:
• effect/keratinization (Skin on the head of the penis becomes less vulnerable to infection.)
• Reduced HIV target cells • Reduced genital ulcer disease
Other benefits: • Lower rates of urinary tract infections in male infants • Prevention of inflammation of the glans (balanitis) and the foreskin (posthitis) • Prevention of health problems associated with the foreskin, such as phimosis
(an inability to retract the foreskin) and paraphimosis (a swelling of the retracted foreskin, resulting in the inability of the foreskin to return it to its normal position)
• Circumcised men find it easier to maintain penile hygiene. • Two studies now suggest that female partners of circumcised men have a lower
risk of cancer of the cervix. • Circumcision is associated with a lower risk of penile cancer. • Circumcised men experience a lower incidence of certain sexually transmitted
infections, especially ulcerative diseases like chancroid and syphilis.

167National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Steps 1. Write the term “Male Circumcision” on the blank piece of flipchart paper and ask
the participants if they know what it means. After a few responses, remove the blank flipchart paper and reveal the definition underneath.
2. Explain that there is no age limit for male circumcision. Any male can be circumcised as an infant, a child, a young or older adult man. Use the flipchart you prepared in advance listing the protective mechanisms of circumcision.
3. Research also shows that removing the foreskin is associated with a variety of other health benefits, including: (Use the flipchart you prepared in advance listing the other benefits of circumcision :)
4. Explain that if a man is circumcised, he must wait six to eight weeks before he can resume sexual activity. If he does not, he might actually increase his risk of infection with STIs, including HIV, and more easily transmit HIV or STIs to a partner.
5. Reiterate that while male circumcision reduces the risk of female-to-male heterosexual HIV transmission, it does not eliminate that risk. (It is believed that circumcision offers only a 60% protective effect against HIV transmission.) Thus, circumcised men still need to use condoms.
6. In some communities, male circumcision is a part of a manhood ritual. It is often performed outside a clinical setting, during a period when boys are “becoming men.” In some of these communities, if a man is not circumcised in this ritual, he will never be considered a “man.” Sometimes, circumcisions are performed under unhygienic conditions. When possible, it is important to promote “medical circumcision.”
7. Conclude the activity by discussing the questions below: • Do you think it is important to promote male circumcision as an HIV-prevention
strategy—why or why not? • Do you think men will understand that even if they are circumcised, they still
need to use condoms? • Do you know where a man can go to get circumcised? • What have you learned from the exercise? • What can men do to encourage other men to think about circumcision?
Closing Male circumcision is an important strategy for HIV prevention. However, even though it does reduce the risk of female-to-male heterosexual HIV transmission, it does not eliminate that risk. Thus, circumcised men still need to use condoms.

168 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
4. The Facts: Understanding ARV’s
Objectives1. To understand how antiretroviral therapy (ART) delays the progression of HIV
infection 2. To consider the advantages and challenges of ART 3. To understand the implications of ART in combating the HIV and AIDS epidemic
Time 90 minutes
Materials • Flipchart • Markers • Enough copies of Handout: Antiretroviral Therapy for all participants• Flipchart on advantages/flipchart on challenges (see below)
Steps 1. Explain that the group will now talk more about how HIV-positive people can stay
healthy. Ask the group to brainstorm a list of behaviours that will help HIV-positive people live longer (e.g., eat well, take ARVs when appropriate, reduces stress, lower alcohol intake, stop smoking.)
2. Review the list and circle any of the comments that involve ART. Tell the participants that they are going to talk more about ART in this session. Before starting, stress the following points: • There are a lot of important things HIV-positive people can do, both before and
after they begin receiving ART. • Healthy behaviours such as a good diet, exercise, adequate rest, and abstaining
from drugs/smoking/alcohol are important habits to adopt before beginning ART and can help delay the need for taking ART medications.
• Just because a person is HIV-positive does not mean he needs ART immediately. However, over time, HIV diminishes a person’s ability to fight off infections. When this occurs, a person will need to start taking ART for the rest of his or her life.
3. Explain that you are going to help the participants understand ART by having a discussion using a series of handouts. Pass out both Handouts and discuss each page with participants
4. After the handouts have been discussed, divide the group into two teams. Explain that starting ART is a big decision and that the groups will be asked to think about the things a person should consider when making a decision about starting ART.

169National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Provide each group with a sheet of flipchart paper. Ask Group One to identify the advantages of starting ART. Ask Group Two to identify the challenges of starting ART. Allow the groups 10 minutes to discuss and write down their answers. Bring the groups back together and review their responses. Ensure the following responses are included:
Advantages: • You can live longer and have a better quality of life. • You won’t get sick as often. • You will have more time to fulfil your dreams and goals. • If you have children, you will see them grow up and experience life. • You will have the opportunity to continue earning a living because you are well. • You will have more time to do things you enjoy.
Challenges: • ART is a lifelong treatment that must be taken every day at the same time and in the
same way. • In the beginning, ART seems complicated. • Sometimes you have to adjust what you eat and when you eat it, according to the
drugs you take. • Some types of ART require you take several pills each day. • Some types of ART may be harmful if taken with other drugs or during pregnancy. • ART can have side effects. Some will go away after a few weeks, while others will
need to be addressed by the health worker. • If you do not take your ART regularly, the medicine will not work anymore. This
means that you will have fewer options for ART in the future. • It is difficult to start taking ART when one has TB. • Only limited regimens are available in the government roll-out in some areas. • There is a lack of clarity about when to really start the ARV medication and whether
the doctor or the person taking it should make the decision.5. Conclude the session by asking the following discussion question:
We know that ART can prolong a person’s life and improve a person’s quality of life. •
What other benefits does ART bring to families and communities? 6. Raise the points listed in the closing, if they are not mentioned.
Closing ART can bring many benefits to individuals, families, and communities. These include:• Households can stay intact• Decreased number of orphans• Reduces mother-to-child transmission of HIV

170 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Increased number of people who accept HIV testing and counselling• Increased awareness in the community since more people get the test• Decreased stigma surrounding HIV infection, since treatment is now available• Less money spent to treat opportunistic infections and to provide palliative care• Increased motivation of health workers, since they feel they can do more for HIV-
positive people• Businesses can stay intact

171National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
155
Handout:AntiretroviralTreatment(ART)
Our body has an immune system that protects us from getting sick, just like a house
protectsusfromtherainandcold.Ifleftuntreatedovertime,theHIVviruswilltakeovera
body’s immunesystem, leavingaperson illwithopportunistic infections, just likeahouse
thatisleftuncaredfor.
Source:FamilyHealthInternational(FHI):ARTBasicsFlipChart
Handout: Antiretroviral Treatment (ART) 155
Handout:AntiretroviralTreatment(ART)
Our body has an immune system that protects us from getting sick, just like a house
protectsusfromtherainandcold.Ifleftuntreatedovertime,theHIVviruswilltakeovera
body’s immunesystem, leavingaperson illwithopportunistic infections, just likeahouse
thatisleftuncaredfor.
Source:FamilyHealthInternational(FHI):ARTBasicsFlipChart
Our body has an immune system that protects us from getting sick, just like a house protects us from the rain and cold. If left untreated over time, the HIV virus will take over a body’s immune system, leaving a person ill with opportunistic infections, just like a house that is left uncared for.
Source: Family Health International (FHI): ART Basics Flip Chart

172 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
If a person is sick from HIV, he or she can begin taking medicines called antiretroviral treatment. These medicines reduce the amount of HIV in the body. As a result, the body’s immune system can fight off disease and the person can become healthy again. Therefore, taking ART is like repairing a house. Based on several factors including the CD4 count, a doctor prescribes ART to such people. It is a choice, however, for individuals to decide if they want to take ART. There are many positive benefits; however, there can be side effects. It is important that individuals are given all the information.
156
If a person is sick from HIV, he or she can begin taking medicines called antiretroviral
treatment.ThesemedicinesreducetheamountofHIVinthebody.Asaresult,thebody’s
immunesystemcanfightoffdiseaseandthepersoncanbecomehealthyagain.Therefore,
taking ART is like repairing a house. Based on several factors including the CD4 count, a
doctor prescribesART to suchpeople. It is a choice, however, for individuals to decide if
theywanttotakeART.Therearemanypositivebenefits;however,therecanbesideeffects.
Itisimportantthatindividualsaregivenalltheinformation.
ABC
A.ARTisseveraldifferentmedications.Apersonmusttakeallofthem,everytime,every
dayfortherestofhisorherlifeforthetreatmenttobeeffective.
B.ARTdoesnotcureHIV.Therefore,thebodywillneedthemedicationseverydayinorder
tostayhealthy.Goingwithoutmedications,evenforashorttime,islikenotrepairingthe
house.
C.Ifapersondoesnottakehisorhermedicine,HIVwillmultiplyinthebodyandcontinue
todamagetheimmunesystem—andtakingARTinthefuturewillnotbeabletostopit.
A B C
A. ART is several different medications. A person must take all of them, every time, every day for the rest of his or her life for the treatment to be effective.
B. ART does not cure HIV. Therefore, the body will need the medications every day in order to stay healthy. Going without medications, even for a short time, is like not repairing the house.
C. If a person does not take his or her medicine, HIV will multiply in the body and continue to damage the immune system—and taking ART in the future will not be able to stop it.
5. Pleasure Brainstorm
Objectives 1. To identify ways to give and receive pleasure that do not involve sexual intercourse
Time 45 minutes

173National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Materials • Flipchart • Markers
Steps 1. Open the session by explaining that when people talk about sexual pleasure, they
often think immediately about vaginal, oral, or anal intercourse. While these can all be pleasurable experiences, they represent only a small number of ways people give and receive sensual pleasure. This activity will explore the other ways individuals can give and receive pleasure, often in a manner that carries much less risk for infection and pregnancy.
2. Divide the participants into three teams and provide each team with several sheets of flipchart paper and markers.
3. Explain that each team will be asked to make a list of as many ways they can think of to give pleasure, WITHOUT vaginal, oral, or anal intercourse. Remind the teams of the comprehensive definition of sensuality, which includes pleasure from all the five senses: touch, smell, sight, sound, and taste. Encourage the participants to be as creative as possible. Any method of providing pleasure of the senses counts. Feeding someone chocolate counts! Cooling off someone with a fan counts!
4. Explain that the teams will be competing against each other, and that they will have five minutes to write their lists. The team with the highest number of pleasurable activities wins.
5. Ask the teams to post their lists on a wall and to read the activities aloud. Allow participants from the other teams to ask any clarifying questions.
6. Count the total number of activities for each team and announce the winner. 7. Inform the group that a few additional awards will be given. Ask the group to make
nominations for the best responses. The categories for awards can include: • Most creative activity • Most romantic activity • Funniest activity • Most appropriate activity in a public place • Most inappropriate activity in a public place • Sexiest activity
8. Conclude the session with the questions below • How did it feel to do this activity? • Why do you think pleasure is often only associated with sexual intercourse,
rather than a wide variety of sensual activities?

174 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Is it easy to talk about pleasure? If not, are the challenges of talking about pleasure different for men and women? Why? What makes it hard for men to talk about this? What makes it hard for women?
• Do couples usually talk about pleasure? If not, why not?• How could a broader understanding of ways to give and receive pleasure
positively impact the HIV and AIDS epidemic?• What have you learned from this exercise? How can you apply this to your own
lives and relationships?
Closing There are many types of pleasure we can feel, sensual or otherwise. Sensual pleasure is not limited to sexual intercourse and, in fact, what gives pleasure can vary a lot from person to person and can include things we may not think of. Talking to your partner about what gives him or her pleasure and what gives you pleasure, as well as what does not, is an important part of communication in a relationship, though it may be difficult. At times, sexual intercourse is not desired or is not possible, and it is important to keep in mind that there are many other ways to give and receive pleasure.
6. STI Quiz
Objectives 1. To identify ways to give and receive pleasure that do not involve sexual intercourse
Time 45 minutes
Materials • Flipchart • Markers
Steps1. Divide the group into teams of about five or six members2. Tell the teams that you will read out some statements about STI’s. Ask each team a
question in turn. That team has to say whether the statement is “true” or “false”. Then they have to give a reason why they chose that answer. If they give the incorrect
answer, or are unable to answer, then one of the other teams gets a chance to answer that question. (See STI Quiz )
3. After each question, give the correct answer and reasons why. Give one point for each correct answer. Give another point if the team gives the correct reason for

175National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
their choice of answer. Continue until you have completed the list of statements. The winning team is the one with the most points at the end
4. If possible, have some small prizes that the teams can play for (e.g. sweets, pens, notebooks, etc.)
5. Correct any wrong answers and provide correct information about STI’s.
STI QUIZ (True or False?)
1. Anyone can get HIV if they have sex with someone infected with HIV2. Taking the contraceptive pill protects against STI’s3. A person can have an STI and not even know it4. You can get STI’s from toilet seats5. If you get an STI, you can get rid of it by giving it to someone6. You cannot get an STI if you only have sex with one person7. A discharge from the penis, vagina or anus can be a symptom of an STI8. Males are more likely than females to know they have an STI9. You can catch an STI the first time that you have sex10. Once you have had an STI, you cannot get it again
ANSWERS1. True It is possible to catch HIV if there is exchange of body fluids, such as blood, semen or
vaginal fluid as the HIV virus lives in body fluids2. False The contraceptive pill only prevents pregnancy. It does not protect against STI’s or
HIV/AIDS3. True Many STI’s show no signs or symptoms in either men or women4. False But public toilet seats can sometimes have other germs; it’s best to give them a
good wipe before use5. False STI’s don’t go away because you have sex with someone else; they just get spread
around. Both partners should have treatment at the same time6. False It’s always possible that one person has had sex with someone else. So always
practise safe sex7. True A discharge from the penis, vagina or anus may be a symptom of an STI; always have
it checked by a health worker or doctor

176 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
8. True This is because a man’s penis is on the outside of his body so the signs of most STI’s
are more easily seen9. True You can catch an STI any time that you have unprotected sexual intercourse (that is,
sex without using a condom)10. False Every time you have unprotected sexual intercourse you are at risk of catching an
STI
7. Community Action Teams
Objectives1. To develop the skills to identify and mobilize community action teams
Time60 minutes
Materials• Enough copies of Handout: A Way of Getting Started and Handout: Frequently Asked Questions about CATs for all participants
Facilitator NotesThis section is designed for individuals interested in helping to form a “community action team” or CAT. It is designed to help facilitators organize individuals to take action in their communities. Once a group of people has shown interest, the facilitator should call them together and begin the process of organizing a CAT. This can take time. The following sessions can help get the CAT off the ground
Steps1. Pass out Handout: A Way of Getting Started. Ask participants to read the case study
aloud.2. Discuss the following questions with the participants:
What do you think motivated the men in this story to join a community action team (CAT)?
What might motivate people in your community to join a CAT? In this story, the men discuss the tension between an inclusive, empowering
approach to planning a CAT, versus an approach that might be quicker. What are the pro’s and con’s of each approach? How would you handle this in your CAT?

177National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
3. Explain that when participants start engaging and reaching out to community members—including men—on issues related to male engagement and HIV, many express an interest in getting more involved. One way of getting people involved is through community action teams. Ask participants the following questions: What might be some of the benefits of pursuing a CAT strategy? What can a CAT do?
4. Pass out Handout: Frequently Asked Questions about CATs.

178 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout: A Way of Getting Started
Thabo and Sam ran into their friends John and Hitji at the Men As Partners (MAP) celebration of International Women’s Day. Sitting outside the Community Centre at the lunch break, the four of them started to talk about one of the speakers, who described inadequacies in the police and legal system response to sexual violence.
Sam: “She really gave it to the police, didn’t she?”John: “Oh yes, she did. The police really have to do more than pay lip service to
the new laws about rape. There was a girl in my neighbourhood who was raped by three men, and the police did nothing more than write down her complaint. No investigation, no assistance in reaching a clinic, nothing. They just listened like she was saying someone stole her radio, like, ‘What do you expect me to do about it?”
Hitji: “What I want to know is, what can we do about it? Couldn’t we have a march of men to the police station or something?”
Thabo: “Actually, Sam and I are starting a Community Action Team, like what you are saying. You both have been to a MAP Workshop right? We want to organise some men to do something about rape and sexual assault. You know, we have these new laws now that the Parliament has passed, but as far as I can see, not much has changed in the townships.”
Hitji: “That is too true, my friend. My sister tells me that many of her friends have been raped. They are afraid to go out even to community dances and things like that, unless there are many girls together who can look out for one another.”
John: “You know, we are now the vanguard. We have the training. We should just get some other young men together and tell them, we are going to do a march to the Police Station.”
Hitji: “Yes! We could put it together very quickly. We need some learners from the school to make flyers and hand them out for us. And the police would be very surprised to see a big march of men coming up the street, talking about gender and rape and that kind of thing!”
Sam: “I like what you are saying, but I think we need to go about organizing the CAT a little differently. The CAT is not about us telling other people what they need to do, even though that might get quick results. The CAT is about a group of people deciding together how to respond to the situation.”
John: “Maybe so—but the situation is very urgent. I don’t know that we can wait for a lot of people to plan it together. Wouldn’t it be faster if we just told

179National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
people what we want them to do? I think we can reach a lot more people that way, rather than inviting people to a lot of meetings.”
Thabo: “And what if they don’t agree? Or what if they do agree, but then it doesn’t turn out like we thought? Then they would blame us. No, it may take more time, but I think it is important to bring the CAT members along with us in our thinking. Maybe together we will even have more ideas—just like the four of us now have more ideas than just Sam and I had when we were talking.”
Hitji: “Okay, my friend. When do we get together to meet? Who should we invite?”

180 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Handout: Frequently Asked Questions about CATs
1. What is a CAT?A Community Action Team or CAT is a group of volunteers who join together to do something in their community about an issue of concern to them. For example, a CAT might form a hip-hop group to educate youth in schools about HIV and AIDS and gender based violence (GBV), or organizes a march on a university campus against rape, or pressure for lighting on a street in a neighbourhood.
A CAT may stay together for a long time and carry out a series of activities or campaigns, or it may come together for just a single action. Usually, someone from an organisation trained in male engagement gets the group started. Once a group of volunteers joins together in a CAT, they decide on a specific project or problem they want to address.Then, they plan out a strategy toward achieving their goals.
2. Why Pursue a Community Action Teams (CATs) Strategy?• CATs can reach more people.CATs can help organizations reach large number of people with messages about gender, male engagement, and HIV and AIDS. CATs take their message to the streets and to places where people gather, including bars, sports clubs, hostels, and faith-based organizations.
• CATs can provide ways to sustain involvement and behaviour change over time.
Once people understand how existing gender roles contribute to the HIV epidemic and other issues, many men and women are eager to challenge the gender roles. At the same time, changes in attitude and practice can be quickly eroded once people return to their day-to-day lives and the environment that socialized them in the first place. Involvement in CATs helps people to internalize the values associated with promoting gender equality and increases the probability of sustained involvement and behaviour change over the long term.• CATs can involve residents in creating and owning community change.People often feel disconnected from decision-making and even services in their communities. Yet we know that community change is best promoted by those who live and work in those communities. CATs create a sense that “this is our community and we can be a part of creating positive solutions.”

181National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• CATs can support CAT members to serve as role models to others.By acting in their communities, CAT members can create a new positive image of men—that of “gender equitable men”—who support gender equality, community development, children’s and family issues, and other positive social values. These role models reinforce the idea that women respect and like men who work for gender equality, and that these men are successful in society.
• CATs can promote changes in social norms and institutional practices at a local level
Through CATs, people will be more likely to support condom use, home- and community-based care, voluntary counselling and testing, prevention of mother to child transmission of HIV, gender equality, and non-violent relationships. Research suggests that health services are better used and health outcomes improve when communities are involved in demanding and shaping services and policies affecting them.
3. Who are members of a CAT?Many times, a CAT starts with 5 to 10 community volunteers who form the core of the CAT. The CAT may grow in size over time, or include some members who support the core group by attending occasionally. The core members of CATs meet regularly (sometimes every week, sometimes once a month) to plan activities. Sometimes, as many as 50 people may participate in a CAT activity or event. The great thing about CAT activities is that they provide regular people the chance to do something positive in their community, even if it’s just a one-day event.
4. What Are a CAT’s Goals?Before a CAT can decide on an area of interest or plan an active campaign, it needs to establish its primary goals. Goals should be activism-oriented and give a focus to the CAT’s work. Goals are vital to guiding the decision-making process within the CAT and helping to determine its direction. Here are some examples of possible strategic goals for a CAT:• Educate men and women to understand how they have been socialized into
gender roles that limit their full potential as human beings.• Provide education about HIV and AIDS, especially to those who may not be
getting this information anywhere else.• Encourage community institutions, such as clinics, schools and religious
institutions, to speak out about HIV and AIDS and male involvement on a regular basis.

182 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
5. Should a CAT be mixed gender groups?You may decide to have a CAT of all men, all women, or where men and women work together, side by side, to plan and do activities in the community. If your CAT is mixed gender, you may decide to have some times when the male CAT members and the female CAT members meet separately in order to discuss issues in a safe peer group.
In any case, it will be important to talk about gender dynamics in your CAT. Are women and men given equal opportunity to speak and take leadership? Is every CAT member valued, regardless of his or her gender? How do you address sexist behaviors when they arise? How are tasks divided up? If your CAT is made up of only men or only women, how do CAT members talk about the opposite sex? How are male and female CAT members perceived by your community?
6. Who leads a CAT?CAT facilitators are those who take on the responsibility of organizing the CAT, arranging for a location for CAT members to meet, and planning any CAT training activities—at least at the beginning. They can also provide advice and leadership so that the CAT can expand, carry out community campaigns, develop allies, and eventually function independently. Later, as new leaders emerge from within the CAT, the initial facilitators can take a step back and allow others to take on more responsibility.
Ideally, CAT facilitators are people who live in the community the CAT is serving.
CAT facilitators serve as catalysts—they “spark” people’s interest in an issue, get key community leaders to become allies, support new leaders, and generate enthusiasm and action.
Anyone who is interested in starting a CAT, listens well, gets along with other people, and understands HIV and AIDS and gender-based violence can learn how to be a CAT facilitator. The challenge for the facilitator is to balance the group’s focus on carrying out activities (tasks) and the group’s need to bond and learn as a group (relationships).
A CAT…• …is a task team with a defined focus and goals, formed by community members
who want to raise awareness/take action on issues that affect them.

183National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• …brings people together regularly to learn about, discuss, and solve community problems.
• …carries out campaigns (a series of actions and strategies to achieve the CAT’s goals).
• …is active in creating community change on two levels: 1) individuals’ knowledge, attitudes, and behaviours; and 2) institutional policies and practices.
• …can be short-term or long-term.
7. What Does a CAT Do?Throughout this Action Kit, you will find examples of what a CAT can do to increase male involvement in prevention of and response to HIV and AIDS and gender-based violence.Here are a few ideas:
Outreach:• Put up flyers and do one-on-one outreach in a school about the connection
between sexual harassment, sexual abuse, and HIV and AIDS.• Use the media—such as TV, radio, or newspaper interviews
Education:• Use a sports event—such as a tournament showcasing both male and female
residents in the community—to educate and inspire people.• Produce an “edutainment” theatre show in community gathering places, such
as taxi stands or mining hostels.
Alliance Building:• Call an informal meeting with tea and biscuits for all women’s or youth groups
in the community to talk and build trust.• Invite pastors from several Christian churches to a prayer breakfast to discuss
HIV and AIDS and gender-based violence from a faith perspective.
Advocacy to the Community for Behaviour Change:• Identify a place where women are at increased risk of rape or assault and then
organize men to pass out flyers there.
Advocacy for Institutional Change:• Convince the taxi associations to put up posters in the taxi ranks and on the
side of the taxis.

184 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
• Join in national campaigns to expand access to treatment, through marches, meetings with clinics, or media interviews.
Service:• Involve a CAT in providing care to people living with AIDS and providing respite
to other caretakers.• Sponsor a day of service where men carry out tasks traditionally seen as women’s
work.CATs choose different actions depending on their interest, purpose, resources, and community. Sometimes a CAT’s actions are carefully chosen and sequenced in light of long-term goals. Other times, a CAT starts out with a simple action that doesn’t require a lot of planning, and that action can build energy and momentum for the group.
8. Who do you invite to a CAT?A CAT may be open to all community members, or it may have a specific profile of members that the facilitator/s seeks to involve. For example, some CATs may involve only young men or only young women. Some CATs might specifically seek the involvement of religious leaders. Some CATs might seek the membership of people living with HIV and AIDS. Some CATs may want to target young men returning to the community after incarceration, and therefore need to recruit men who share that experience.
CAT facilitators and the first CAT members have the task of recruiting new members.Some CATs decide to recruit periodically throughout the life of the CAT, to keep the membership lively and full.
Inviting People to Join the CATConversations with community residents are a key part of building your CAT. Relationship building is a vital component of social-change work, and much of that happens in one on one conversations. It’s been said that people don’t join causes, they join people.
Therefore, your skill in listening to community members and engaging their interest will make a big difference in how many people join with you to prevent HIV and AIDS and gender-based violence.

185National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Following are some ideas for how to contact, meet with, and invite people into the CAT:• Male Engagement Workshops: Have there been any participants in recent
workshops who were particularly interested in the issue? How can you contact them?
• Personal Networks: Think about your networks of friends, relatives, or co-workers: Who do you know who might be interested in joining your CAT?
• One-on-One Conversations: Go to where potential CAT members hang out or work.
Have some one-on-one conversations explaining the CAT and ask people to come to a meeting or event. Follow up with a personal visit.• Flyers: Develop a flyer and put it up around the community. Make sure to put a
phone number or address where people can get more information. Better yet, list dates of the first CAT meetings.
• Outreach to Religious Institutions: Ask a religious leader to make an announcement or to allow you to make a presentation at your church, mosque, or other institution about the CAT—either to the entire congregation or perhaps to the youth group. Invite people to join you after the service for a brief conversation about the CAT. Make sure to have a sign-up sheet with their names and ways to contact them.
• Health Clinic Outreach: Post flyers at the local health clinic. Ask the clinic director if you can make a presentation to the staff or to the HIV support group at the clinic.
• Open Houses/Educational Event: Arrange an open house at the local MAP organization with presentations about the CAT. You may want to show a video about HIV and AIDS and gender that might inspire people to join the CAT. Be sure to have a sign-up sheet!
• Local Media Publicity: Local radio may allow you to be interviewed on the air—or a newspaper may let you write a short article or interview you for an article.
• Street Theatre: Gather your CAT members to perform street theatre, music, or dance performances in public spaces, such as at markets, taxi ranks, celebrations, or other places people gather. Do performances that dramatize the issues—“edutainment”—and invite people to join the CAT.
• Text Messaging (SMS): Use text messaging (sms) on cell phones to send reminders about when and where the CAT meetings are held. Ask new or existing CAT members to forward the text message to one or two friends, inviting them to the CAT meeting.

Wor
ksho
p Ene
rgize
rsAppendix
B:

187National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
It is very effective to use warm ups and energizers throughout the program to keep the sessions
lively and fun. Warm ups serve two basic purposes:
1. They can serve as a metaphorical introduction to the topic of the session.
You can choose a warm up that evokes some of the issues you will be exploring in the day’s
session.
2. They can simply be lively exercises to bring the energy back into the group when they are
feeling tired or too serious.
There are fun warm-ups, games, and energizers in every culture, so spend some time adding
local favourites to the ones listed below, and do not use those that do not seem appropriate for
your community. After the first few sessions, consider having the participants lead the warm ups
and come up with creative new ones on their own!
Introductory games
Remember the circle
Ask the group to sit in a circle. Someone introduces themselves and saying one thing they enjoy
for example, ‘Hello! My name is Nicola and I love to eat chocolate’. The person next to the
facilitator goes next. They introduce themselves and say something that they enjoy or like doing.
They then introduce themselves for example, ‘Hello! My name is Nambili and I love singing, this
is Nicola and she loves chocolate’. The game continues until each person is introduced. This game
can be adapted to fit the theme of your workshop for example participants could introduce their
name and a fact that they know about an issue/hope to change and so on. Good to encourage
people to listen.
Human Bingo
Ask each participant to draw a grid with nine boxes. Ask them to write down (in any box they
choose) a statement such as ‘has brown eyes’, ‘has grandchildren’, ‘lives in a city’. Once everyone
has finished writing their nine statements, ask the group to move around the room asking
people questions to see if they match the statements on their grid. Each participant must get the
signature of the person who matches the criteria for each square. The person who gets all nine
boxes signed first wins. This game can be used as an introductory session and or fit the theme
of your workshop if you suggest a theme for the statements, i.e., about people’s cultures or
hobbies, or an issue you are working on.
Geo-exercise
To gauge where people are from (i.e.: A region, town or village in Namibia) and warm the group
up, ask a person where they are from and invite them to place themselves in a position in the
room, or as facilitator you can place yourself and call it the place you are all meeting, or the place
where you are from. Outline an imaginary map of Namibia, keeping in mind where internationals

188 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
might be placed and orient people – i.e. Either by identifying north-south-east-west or by saying
Okahandja is here, Keetmanshoop there, etc. Then invite the group to place themselves where
they feel is relatively appropriate, a place in the room they feel represents where they are from.
Get people to talk to others around them to work out where they might be in relation to each
other. The facilitator can then invite each person to introduce themselves to the group, where
they are from and an image that they see i.e., when they walk outside of their home or other
prompts about expectations or their heritage. Close the exercise by inviting the group to bring
themselves into the workshop space, carry with them the comfort of their home but leave
aside the stresses or worries of their other life so they can be fully present and focus on the
workshop.
Paired Interviews
Members of the group pair up with someone they don’t know so well. They go to some part of
the room for about 5 minutes to find out 5 pieces of information about each other that they will
be happy to share with the whole group. They return to the group to share all the information
they have learnt from each other, each person introducing their partner.
Hand Prints – an alternative to paired interviews
In pairs describe something about yourselves using the palms of your hands.
• Palm = what relationships and values do you consider as being very important to you?
• Thumb = what activities are most important to you?
• Fingers = what ‘things’ are you interested in but are perhaps less important
• Wrist = what group/organization would you describe yourself as being most associated with?
• Introduce each other to the rest of the small group
This may work best with smaller groups who are wishing to get to each other a little better. Of
course other questions can be asked that relate to expectations of the workshop or evaluation.
Check-in activities
By check-in, we refer to ‘how people are feeling’.
Grab a hat/find an object from inside or outside (i.e.: rock, feather, leaf, sand) that •matches your mood. Equipment: different hats or place to collect things from.
Collect an object that matches your mood and explain to group why you chose this •object. You can use this to get people to introduce themselves and provide a pile of hats
or objects in the middle of the space for people to pick and choose
Say good morning/hello in different languages and then how you are feeling or what you •are looking forward to.
Choose a color that matches your mood and explain to group why you chose this color. •Each person does a movement, makes a sound or a combination of both that matches •their mood. The group then copies all together.

189National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Invite people to identify an animal that speaks to their mood or feeling about something •specific, their expectations for the workshop or meeting or just how they’re feeling and
describe to the group.
5 for Fun
Prepare a flipchart before the ice breaker with these 5 questions:
• I've always wondered about...
• If I could stay at any age, I'd like to be...
• If I had the day off tomorrow, I would...
• The most fun thing I did this year is...
I've always wanted to (but never had the courage) ....
Give participants 3 minutes to prepare their answers and have each person give their answers in
the large group. Be mindful of the time!
Energizers
Have you ever…
Form a circle of chairs (one for each person) and then take one away. One person stands in the
middle and calls a question beginning with "Have you ever …….", for example “Have you ever
eaten watermelon”. Everyone who has eaten watermelon then jumps up and moves to a place
vacated by someone else who has moved. The last person who is left without a seat remains in
middle to call out something else beginning with “Have you ever………..?”
What are you doing?
Participants stand in a circle. One person moves to the centre and begins acting an activity, such
as building a sandcastle. It is important that the people really do the activity. A second person
enters the circle and asks, “What are you doing?” The first person then responds, while still
doing the original activity: “Brushing my hair.” The second person then begins brushing their hair,
and the first person leaves the centre. Another person enters and asks, “What are you doing?”
The person in the centre, while still doing her activity, replies: “Climbing a tree” (or any other
activity whatsoever), etc. etc.
It can be suggested that actions relate to workshop content to consolidate/have fun with learning
if you want to. Good to use once people at least slightly know each other. As the game grows
there are lots of laughs. It is good to encourage people not to think of ‘what to do’ and just say/
do anything. You can also play it and have everyone stay in the circle until everyone is in.
Hand beat
Get the group to kneel on the floor on their knees with their hands out, palms down in front of
them, and close together if possible. One person lifts and slaps their left palm and then right
palm down one at a time and then the beat rolls around the circle as each person repeats.

190 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Variations are infinite such as everyone raises their right hand and places it to the right of the left
hand of the people beside them. You can add that someone slaps a hand down twice then the
beat is reversed. Can be useful in diverse groups.
Train smash
Standing in a circle holding hands 3 or so people are nominated as ‘train stations’ (TS) and 2 as
‘junctions’ (J) depending on the size of the group. Facilitator squeezes the hand of a person next
to them and sends a ‘pulse’ which is the train around the circle. When the train reaches a TS they
make a sound e.g.: “toot toot” and when it reaches a J it can change direction if the J chooses.
Then a person has to go into the middle of the circle (train spotter) to guess where the train is at
by touching the person they think has it. When they are correct they swap with that person and
the game continues.
Zip Zap Zop
Standing in a circle people place their palms together in front of them, explain that inside their
palms is a ball of energy. The facilitator explains to the group that Zip Zap Zop all refer to different
directions that they will point their hands. Zip: left; Zap: right and Zop: across the circle (or
whatever you like). Whoever starts chooses one of Zip, Zap or Zop says it out loud for example
“Zip” an passes/points their hands to the person on their left, it carries on (domino effect) with
each person turning to the left with their hands and saying “Zip” until someone says something
different such as “Zap” and then the direction changes to the right. It can just get faster or people
who slip up sit down. And you can add different sounds like ‘boing’ that bounce the energy back
to the person who sent it to you.
I’m talking to you
Standing in a circle people one at a time say “I’m talking to you” in different ways. Each person
clearly says “I’m talking to you” to a particular person and as they say it they walk towards them.
Before they reach that person they have spoken to that person needs to say it someone else
and start walking to the person they spoke to. The person who says “I’m talking to you” take the
place of the person they spoke to. Great to reinforce clear communication.
Do what I do
Invite people to do a physical stretch or dance and the rest of the group copies.
Balloon in the middle
Throw a balloon into the middle of the group and everyone has to keep it from touching the
ground, you can add rules like people cannot touch it more than once in a row. You can also do
this by having everyone lay on the ground with their feet or heads touching in the centre of a
circle and then throw the balloon in the middle.

191National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Ozone and sun
Before the game begins each person chooses someone who is their sun (S) and ozone (O) and
keeps this to themselves. People start to move around the space and make sure that for the
entire time the O is between them and the S.
‘Mother’ duck
As everyone has their eyes closed for the whole game. At the start the facilitator chooses one
person to be the ‘mother duck’ that stays quiet throughout the entire game, the rest of the
people are ducklings. Facilitator says “go ducklings” and every ‘duckling’ walks around quacking
looking for their mum/parent (etc). Each duckling knows when they have found their ‘mum’
because they are the only quiet one. They then stay quiet close to their ‘mum’ and eventually all
of the ducks are huddled together quietly.
Rain
A facilitator talks the group through this energiser. Get everyone to stand up. Start tapping your
head lightly with your fingers imagining soft rain. Let it slowly get heavier the further you move
your hands down your body. Let the rain turn into a thunderstorm on your calves. Clap them
hard with your hands. Then move your hands back up your body, ending with soft rain on your
head. Everyone copies.
Touch blue
Have everyone touch something blue on someone else, something yellow, a knee, some glasses,
etc. Call the next thing as soon as people touch whatever has been named.
Waking up in the Jungle
Ask people to think of their favourite animal and its noise, and to pretend that they are that
animal waking up. As they wake up, the noises should get louder and louder. This is a good quick
game for sleepy groups.
Clapping game
This game mixes the logical and creative sides of the brain. It is a good preparation for tackling
complex issues that require both logical analysis and creative solutions. Sit in a circle on the floor
or around a table. Everybody then places their hands flat on the surface, the arms crossing over
with those of the neighbours. Start the game by clapping one hand on the surface. Let the clap
run around the circle, so that always the hand claps that is next to the one that clapped last.
After practicing this for a couple of rounds, introduce a complication. If a hand claps twice, the
direction of the clap changes direction. Again, practice. When everyone has understood the
rules, start the game proper. Any hand that claps out of turn or doesn't clap should be put behind
the person's back. When somebody has both hands out of the game, then they have to drop out

192 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
of the game. Increase the speed of the game as you go along. The more people there are in the
group, the less exciting it is for the individual player. It is a good idea to form two or more groups
for the game if there are more than twelve people.
What're You Worth
Form participants into teams of 3, grouping people who have not worked together so far. Use
a creative way to do this, such as by their months of birth, number of pets they have, etc....Ask
them all to dig into their pockets or handbags, and pull out their coins (no paper money). Ask
them to quickly add up the money in their group. The group with the most money wins.
Right hand, left hand
Write on the flipchart in advance or pre-prepare a slide with this graphic:
173
aroundatable.Everybodythenplacestheirhandsflatonthesurface,thearmscrossingoverwith
those of the neighbours. Start the game by clapping one hand on the surface. Let the clap run
aroundthecircle,sothatalwaysthehandclapsthatisnexttotheonethatclappedlast.
After practicing this for a couple of rounds, introduce a complication. If a hand claps twice, the
directionof theclapchangesdirection.Again,practice.Wheneveryonehasunderstood the rules,
start the gameproper.Anyhand that clapsout of turnor doesn't clap shouldbeput behind the
person'sback.Whensomebodyhasbothhandsoutofthegame,thentheyhavetodropoutofthe
game.Increasethespeedofthegameasyougoalong.Themorepeoplethereareinthegroup,the
lessexcitingitisfortheindividualplayer.Itisagoodideatoformtwoormoregroupsforthegame
iftherearemorethantwelvepeople.
What'reYouWorth
Form participants into teams of 3, grouping peoplewho have notworked together so far. Use a
creativewaytodothis,suchasbytheirmonthsofbirth,numberofpetstheyhave,etc....Askthem
all todig into their pocketsorhandbags, andpull out their coins (nopapermoney).Ask them to
quicklyaddupthemoneyintheirgroup.Thegroupwiththemostmoneywins.
Righthand,lefthand
Writeontheflipchartinadvanceorpre‐prepareaslidewith thisgraphic:
Nextexplaintoeveryonewhattheyhavetodo.Asyouallreadthroughthealphabet,they'retoput
theirhandupaccordingtotheinstructionbelowtheletter.R=rightarm,L=leftarmandB=both
arms. Finish the alphabet slowly. This is fairly easy so do it again in half the time. Next do it
backwards.Finishbyaskingwhethereveryoneiswarmedupandhowdotheirarmsfeel.
Funwaystogetpeopleintogroups
‘Numbering’off
Using numbers, fruits, emotions or any theme it could be ‘role play’ characters related to the
workshopcontent, ifyouwant5groupsusefivethingsandhavepeopleyelloutaroundthecircle
1,2,3,4,5orwhatever.
Next explain to everyone what they have to do. As you all read through the alphabet, they're to
put their hand up according to the instruction below the letter. R = right arm, L = left arm and B =
both arms. Finish the alphabet slowly. This is fairly easy so do it again in half the time. Next do it
backwards. Finish by asking whether everyone is warmed up and how do their arms feel.
Fun way s to get people into groups
‘Numbering’ off
Using numbers, fruits, emotions or any theme it could be ‘role play’ characters related to the
workshop content, if you want 5 groups use five things and have people yell out around the circle
1,2,3,4,5 or whatever.
Fruit salad
Ask everyone to sit on a chair in a circle. Ask one volunteer to stand in the middle of the circle.
Remove their chair from the circle to the side of the room. Go around the circle and name

193National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
everyone ‘apple’, ‘banana’ or ‘orange’. Remember to give the volunteer in the middle a name
too! When you shout out ‘Apple’ everybody who is named apple must jump up out of their place
and try to sit on an empty chair. The person standing in the middle must also try and sit down on
an empty chair. The person left without a seat must stand in the middle. People named ‘banana’
and ‘orange’ must do the same if their fruit is shouted out. If you shout ‘fruit salad’, everybody
in the circle must jump up and rush to find an empty seat! After the game people can go into the
groups/categories that they were in initially.
Fire on the Mountain
Have the group run around in the room. While doing so, the facilitator shouts ‘there’s a fire on
the mountain’. The group responds by saying ‘run, run, run’. Facilitator then calls out numbers
that they clump into. Repeat with different numbers. Whatever number you want in each group
call out that number for the final clump.
Body parts and number/Body bump
(Very similar to clumps) Have the group walking around the space and then call out a number
and body part, for example 5 elbows. So people get into groups of 5 and touch elbows. Repeat
with different numbers and body parts. Whatever number you want in each group call out that
number for the final clump.
Dots
Equipment: Sticky dots in a range of colours.
Dots encourage non-verbal communication. Fix a coloured dot onto the cheek of each participant.
You can give some thought to how you want to mix the groups. Ask the participants to stand up
and move around the room in silence. Participants must find out what colour their dot is without
talking. Once they know what colour their dot is, they find others with the same colour and that
will be their group.
Jigsaws/photos/pictures
Equipment: A set of jigsaw pieces, one for each group, from a range of jigsaws. It could also be
a photo or picture cut up. Give a jigsaw/photos/picture piece to each participant. Ask them to
walk around the room and try to find people with pieces that would go with theirs. Eventually
the various members of the small groups find themselves together joining up their pieces to
make the picture, and they become a group. If you want to look at a particular theme: condom
use; gender; community relations; this can determine the pictures you will use.
Peruvian Ball
Everyone in the room has an imaginary ball. Each ball has its own special movement pattern,
and its own sound. The participants practice "throwing" or "bouncing" the invisible balls by
themselves, while simultaneously making the sounds ("boi-oi-oing," "zip-zap," "wheeeee," ..)
After everyone has the movements and sounds decided, the participants start walking around

194 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
the space. The facilitator calls "freeze," and then instructs everyone to trade balls with someone.
There is no talking allowed, only demonstrating the sounds and movements of the balls. Once
everyone has traded, everyone starts walking around the space again, this time with their new
balls. The facilitator calls "freeze" again, and instructs everyone to trade with another person.
After four to six trades have been made (depending on the size of the group), the facilitator
instructs everyone to find their original balls. Everyone must then move about, demonstrating
the balls they are holding, while searching for the ball they originally created. If a participant
finds his ball, they trade with the person who has it, and then takes their ball to the side out of
the playing space. It is rare for everyone to find their original balls in this game.

Pre &
Post
Test
Appendix C:

196 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Pre/Post QuestionnaireCode:____________
Instructions: All of your answers are
confidential. The results of this survey will be
used to adapt the training content and evaluate
the overall effectiveness of the training. Answer
all of the questions to the best of your ability.
Do not leave any questions blank. There are
no correct answers. We would appreciate your
honest responses to the questions. If you have
any questions about the questionnaire please
consult the facilitator.
Demographic Questions
Sex 1.
Male_______ Female_______
Age _______2.
In which region do you currently live? 3.
______________________________
What type of relationship are you 4.
currently involved in?
Married_____1-
Long term relationship ( a 2-
relationship lasting longer than 6
months)____
Casual Relationship (a short term 3-
relationship with no long term
commitments) _____
Not in a relationship______4-
Employment Status 5.
Unemployed_______ 1-
Part Time______ 2-
Full-time_______ 3-
Highest level of Education 6.
Primary______ 1-
Secondary_______ 2-
Tertiary _______3-
Section 1: Understanding Gender
What is the difference between sex 1.1
and gender? ____________________
_______________________________
_______________________________
_______________________________
_______________________________
__________________________
1.2 How are Sexual Reproductive Health,
Gender Based Violence and HIV and AIDS
related? Give examples. _________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
____________________
Section 2: HIV risks and Prevention
2.1 Describe the difference between HIV and
AIDS? _______________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
2.2 Which of the following activities do
not place men and women and children at
risk for contracting HIV? (Circle the correct
statements)
1- Kissing a person who is infected

197National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
with HIV
Having unprotected sex with 1-
more than one sexual partner at
the same time
Touching and/or hugging a person 2-
who is infected with HIV
A mother infected with HIV 3-
breastfeeding her new born baby
Sharing cups, plates, spoons etc 4-
with a person who is infected with
HIV
Having protected (consistent and 5-
correct usage of condoms) sexual
intercourse with a person who is
infected with HIV
Section 3: Gender and Power
3.1 If a woman betrays a man, he can hit her.
1- I agree_____
2- I slightly agree_____ 3- I
disagree______
3.2 A man must make all the decisions in the
household since he’s the head of the house.
1- I agree _____
2- I slightly agree_____
3- I disagree______
Section 4: Violence
4.1 If someone insults me, I will defend my
reputation, even if it means using violence.
1- I agree _____
2- I slightly agree _____
3- I disagree______
4.2 It’s ok for a man to hit his partner if she
refuses to have sex with him.
1- I agree _____
2- I slightly agree _____
3- I disagree______
4.3 If I insult or yell at someone for doing
something wrong that is not a form of
violence.
1- I agree_____
2- I slightly agree_____
3- I disagree_____
Section 5: Sexual Reproductive Health
5.1 Can you think of 3 Sexual Reproductive
Health issues that men face in Namibia? ____
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_________________________________
5.2 If a woman is pregnant, preventing her
unborn baby from being infected with HIV is
the mother’s responsibility since she is the
one who is carrying the child.
1- I agree______
2- I slightly agree_____
3- I disagree______
5.3 All people have the right to decide how,
with whom and when to have sex.
1- I agree ______
2- I slightly agree _____
3- I disagree_____
5.4 List at least 3 sexually transmitted infections
that you are aware of. ___________________
_____________________________________
_____________________________________
_____________________________________
__________________
5.5 List 3 methods generally used as
contraceptives. ________________________
_____________________________________
_____________________________________
_____________________________________
_____________

198 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Section 6: Gender Norms and Violence
Real men do not cry.6.1
1- I agree _____
2- I slightly agree _____
3- I disagree______
It is a real man’s duty to always protect 6.2
others despite the circumstances.
1- I agree _____
2- I slightly agree_____
3- I disagree______
Section 7: Alternatives to Violence
List possible ways of reacting to 1.1
circumstances that do not involve using
violence. _______________________
_______________________________
______________________________
______________________________
______________________________
__________________________
Section 8: Taking Action
8.1 How would you react in a situation where
you walk past a couple arguing across the
street in your neighbourhood? ___________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
__________________________
8.2 How would you react in situation where
you hear your neighbours fighting next door?
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
8.3 How would you react in a situation where
you notice a group of men sexually harassing a
woman down in a street corner? __________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
___________________________
8.4 What laws are you aware of that are geared
towards action for sexual and reproductive
health, HIV & AIDS and gender based violence?
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
8.5 What is the importance of getting tested
for HIV? ______________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_____________________________________
_______
Thank you for completing the test!

Trai
ning
Eval
uatio
n
Appendix D:

200 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Please fill in this form to provide the training team with feedback about the course:
Location: ___________________________________________________________
Date: ___________________________________________________________
Please note that all data is collected anonymously and there is no link to your identity, organisation
or location.
Rating
Poor
Fair
Average
Good
Very Good
Excellent
Comments
Overall Content of Course
Presentation of Material by Trainers
Participant / Group Activities
Facilitation of Activities by Trainers
Facilities
Workshop Evaluation

201National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Do the examples or illustrations help you learn, give reasons for your answer?
_____________________________________________________________________________
_____________________________________________________________________________
Do the practice exercises help you learn, give reasons for your answer?
_____________________________________________________________________________
_____________________________________________________________________________
Do you feel you gained valuable knowledge from the course, give reasons for your answer?
_____________________________________________________________________________
_____________________________________________________________________________
Suggestion for Improvement and general comments
_____________________________________________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
Thank you for completing this evaluation!

Reso
urce
sAppendix
E:

203National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Publications:
These publications are useful for training purposes:
Legal Assistance Centre, • Guide to the Combating of Rape Act, 2001 (English, Afrikaans, Oshiwambo, Otjiherero, Khoekhoegowab, Silozi)Legal Assistance Centre, • Guide to the Combating of Domestic Violence Act, 2005 (English, Afrikaans, Oshiwambo, Otjiherero, Khoekhoegowab)Legal Assistance Centre, • Namibia Domestic Violence and Sexual Abuse Service Directory, 2005 – a directory of services available for victims of domestic violence and sexual abuse.Legal Assistance Centre, • Guidelines for Service Providers on the Combating of Rape Act, 2005 – aimed at police, prosecutors, magistrates, medical professionals, social workers and counsellors.Legal Assistance Centre, • Guidelines for Service Providers on the Combating of Domestic Violence Act, 2005 – aimed at police, prosecutors, magistrates, medical professionals, social workers and counsellors.
These publications are useful if you want to read more about the issues discussed in this manual:
Ministry of Gender Equality and Child Welfare (MGECW) 2010: • National Gender Policy 2010-2020.Ministry of Gender Equality and Child Welfare (MGECW) 2008: • Knowledge, Attitudes and Practices Study on Factors and Traditional Practices that may Perpetuate or Protect Namibians from Gender Based Violence and Discrimination. SIAPACMinistry of Health and Social Services (MoHSS) 2001: • National Policy for Reproductive Health.Ministry of Health and Social Services (MoHSS) 2007: • National Policy for HIV & AIDS.Ministry of Health and Social Services (MoHSS) 2004: • An assessment of the nature and consequences of intimate male-partner violence in Windhoek, Namibia: A Sub study of the WHO Multi-Country Study on Women’s Health and Domestic Violence.Ministry of Health and Social Services (MoHSS) [Namibia] and Macro International •Inc. (Macro). 2008. Namibia Demographic and Health Survey 2006-07. Windhoek, Namibia and Calverton, Maryland, USA: MoHSS and Macro.LaFont, S. And Hubbard, D. 2007: • Unravelling Taboos: Gender and Sexuality in Namibia. Legal Assistance Centre, Windhoek.Debie LeBeau, “The Changing Status of Women in Namibia and its Impact on Violence •against Women”, in Ingolf Diener and Olivier Graefe (eds), Contemporary Namibia: The first landmarks of a Post-apartheid Society, Gamsberg MacMillan, Windhoek, 2001.

204 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
Videos:These videos are useful for training sessions, as ways to spark discussion and debate.
Multi-Media Campaign on Violence against Women and Children, • A Trust Betrayed (2000). A Namibian video in English dealing with rape and incest. (60 minutes) Legal Assistance Centre, • Love and Respect (2001). A drama about rape and domestic violence available in English, Afrikaans, Otjiherero, Oshiwambo and Khoekhoegowab, particularly suitable for rural audiences. (approximately 1 hour) Legal Assistance Centre, • Whispers in the Wind (2002). A drama about domestic violence in Namibia, dealing with child abuse and HIV/AIDS, available in English only. (74 minutes)Soul City Institute, Untold Stories in a time of HIV & AIDS (2008). A series of short •films from Southern Africa, dealing with HIV & AIDS, available in English only. (2 hours)
Key organisations:
Ministry of Gender Equality and Child Welfare • has offices in all regions. Staff can provide advice and training.
Building, Independence Avenue Private Bag 13359, Windhoek Tel: 061 283 3111 Fax: 061 238 941 E-mail: [email protected]
Women & Child Protection Units (WACPU) • were established by NAMPOL to provide sensitised and integrated services to victims of violence and abuse. There is a WACPU in every region. The local police will have details of the nearest WACPU.
Legal Assistance Centre • can provide advice and training. 4 Korner Street, Windhoek P.O Box 604, Windhoek Tel: 061 223 356 Fax: 061 234 953 E-mail: [email protected] Website: www.lac.org.na
LifeLine/ChildLine Namibia • provides a confidential telephone counselling service, face-to-face counselling by appointment and a number of training and awareness programmes on topical issues. LL/CL also has an outreach centre in Rundu (Tel: 066 255 354) and offices in Ondangwa (Tel: 0652 46252) and Eenhana (Tel: 081 127 8272) and in Rehoboth (062 524254)

205National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS
45 Bismarck Street, Windhoek P.O Box 5477, Windhoek Tel: 061 22 6889 (office) Tel: 061 23 2221 (crisis) Child Helpline: 116 (Toll free from all networks) Fax: 061 22 6894
The PEACE Centre • (People’s Education, Assistance and Counselling for Empowerment Centre) provides counselling for traumatised victims of violence.
26 Rhino Street PO Box 50617 Bachbrecht Windhoek Tel: 061 37 1550 Fax: 061 37 1555 E-mail: [email protected]
Philippi Trust • provides counselling based on Christian principles, and training in counselling.
Ara Street, Dorado Valley PO Box 4447 Windhoek Tel: 051 259 291 Fax: 061 259 210 E-mail: [email protected]
Namibia Planned Parenthood Association (NAPPA)• 23 Simpson Street, Windhoek West Tel: 061 230 250 Email: [email protected] Website: www.nappa.com.na

206 National Training Manual and Training Plan for Men and Boys on GBV, SRH and HIV/AIDS