
Motivational Interviewing With Parents for Obesity: An RCT
13
Motivational Interviewing Q:1 With Parents for Obesity: An RCT Q:2; 3 Amir H. Pakpour, PhD a , Paul Gellert b , Stephan U. Dombrowski c , Bengt Fridlund d abstract BACKGROUND AND OBJECTIVE: Motivational interviewing (MI) has Q:4 been shown to be an effective strategy for targeting obesity in adolescents, and parental involvement is associated with increased effectiveness. The aim of this study was to evaluate and compare the role of parental involvement in MI interventions for obese adolescents. METHODS: A total of 357 Iranian adolescents (aged 14–18 years) were randomized to receive an MI intervention or an MI intervention with parental involvement (MI + PI) or assessments only (passive control). Data regarding anthropometric, biochemical, psychosocial Q:5 , and behavioral measures were collected at baseline and 12 months later. A series of intention-to- treat, 2-way repeated-measures analysis of covariance were performed to examine group differences in change in outcomes measures over the 12-month follow-up period. RESULTS: Results revealed significant effects on most of the outcome parameters for MI + PI (eg, mean 6 SD BMI z score: 2.58 6 0.61) compared with the passive control group (2.76 6 0.70; post hoc test, P = .02), as well as an additional superiority of MI + PI compared with MI only (2.81 6 0.76; post hoc test, P = .05). This pattern was also shown for most of the anthropometric, biochemical, psychometric, and behavioral outcome variables. CONCLUSIONS: MI with parental involvement is an effective strategy in changing obesity-related outcomes and has additional effects beyond MI with adolescents only. These findings might be important when administering MI interventions in school settings. WHAT’S KNOWN ON THIS SUBJECT: Motivational Q:6 interviewing (MI) has been found to increase the effectiveness of weight loss programs in obese children and adolescents. Although parental involvement seems to be linked to its effectiveness, strong conclusions cannot be drawn. WHAT THIS STUDY ADDS: The present study found that MI with parental involvement is an effective strategy in changing obesity-related outcomes and has additional effects beyond MI with adolescents only. These findings are important when administering MI interventions in school settings. a Qazvin University of Medical Sciences, Qazvin, Iran; b Charité–Universitätsmedizin, Berlin, Germany; c University of Stirling, United Kingdom; and d Jönköping University, Jönköping, Sweden, Sweden Dr Pakpour conceptualized and designed the study, conducted the initial analyses, and drafted the initial manuscript; Dr Gellert analyzed and interpreted the data, drafted the initial manuscript, and reviewed and revised the manuscript critically; Drs Dombrowski and Fridlund interpreted the data and reviewed and revised the manuscript critically; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. This trial has been registered at www.clinicaltrials.gov (NCT0218080). www.pediatrics.org/cgi/doi/10.1542/peds.2014-1987 DOI: 10.1542/peds.2014-1987 Accepted for publication Dec 15, 2014 Address correspondence to Amir H. Pakpour, PhD, Department of Public Health, Qazvin University of Medical Sciences, Qazvin, Iran. E-mails: [email protected], [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. PEDIATRICS Volume 135, number 3, March 2015 ARTICLE
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Motivational Interviewing With Parents for Obesity: An RCT

Motivational InterviewingQ:1 With Parentsfor Obesity: An RCTQ:2; 3
Amir H. Pakpour, PhDa, Paul Gellertb, Stephan U. Dombrowskic, Bengt Fridlundd
abstractBACKGROUND AND OBJECTIVE: Motivational interviewing (MI) hasQ:4 been shown to be an effectivestrategy for targeting obesity in adolescents, and parental involvement is associated withincreased effectiveness. The aim of this study was to evaluate and compare the role of parentalinvolvement in MI interventions for obese adolescents.
METHODS: A total of 357 Iranian adolescents (aged 14–18 years) were randomized to receive anMI intervention or an MI intervention with parental involvement (MI + PI) or assessmentsonly (passive control). Data regarding anthropometric, biochemical, psychosocialQ:5 , andbehavioral measures were collected at baseline and 12 months later. A series of intention-to-treat, 2-way repeated-measures analysis of covariance were performed to examine groupdifferences in change in outcomes measures over the 12-month follow-up period.
RESULTS: Results revealed significant effects on most of the outcome parameters for MI + PI (eg,mean 6 SD BMI z score: 2.58 6 0.61) compared with the passive control group (2.76 6 0.70;post hoc test, P = .02), as well as an additional superiority of MI + PI compared with MI only(2.81 6 0.76; post hoc test, P = .05). This pattern was also shown for most of theanthropometric, biochemical, psychometric, and behavioral outcome variables.
CONCLUSIONS: MI with parental involvement is an effective strategy in changing obesity-relatedoutcomes and has additional effects beyond MI with adolescents only. These findings might beimportant when administering MI interventions in school settings.
WHAT’S KNOWN ON THIS SUBJECT: MotivationalQ:6
interviewing (MI) has been found to increase theeffectiveness of weight loss programs in obesechildren and adolescents. Although parentalinvolvement seems to be linked to itseffectiveness, strong conclusions cannot bedrawn.
WHAT THIS STUDY ADDS: The present studyfound that MI with parental involvement is aneffective strategy in changing obesity-relatedoutcomes and has additional effects beyond MIwith adolescents only. These findings areimportant when administering MI interventionsin school settings.
aQazvin University of Medical Sciences, Qazvin, Iran; bCharité–Universitätsmedizin, Berlin, Germany; cUniversity ofStirling, United Kingdom; and dJönköping University, Jönköping, Sweden, Sweden
Dr Pakpour conceptualized and designed the study, conducted the initial analyses, and drafted theinitial manuscript; Dr Gellert analyzed and interpreted the data, drafted the initial manuscript, andreviewed and revised the manuscript critically; Drs Dombrowski and Fridlund interpreted the dataand reviewed and revised the manuscript critically; and all authors approved the final manuscriptas submitted and agree to be accountable for all aspects of the work.
This trial has been registered at www.clinicaltrials.gov (NCT0218080).
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1987
DOI: 10.1542/peds.2014-1987
Accepted for publication Dec 15, 2014
Address correspondence to Amir H. Pakpour, PhD, Department of Public Health, Qazvin University ofMedical Sciences, Qazvin, Iran. E-mails: [email protected], [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant tothis article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts ofinterest to disclose.
PEDIATRICS Volume 135, number 3, March 2015 ARTICLE

ChildhoodQ:7 obesity is a global healthconcern, and many obese adults wereobese during childhood.1 Lifestylebehaviors are the main causes ofobesity in children and adolescents,and these behaviors present targetsfor intervention.2 Almost 10% ofschool-aged children worldwide areobese, and .60% of Europeanchildren are overweight.3,4 Indeveloping countries, childhoodobesity is also reaching criticallevels.5 In Iran, obesity amongchildren and adolescents ranges from7.1% to 12%.6,7 Childhood obesityincreases complications such asskeletal/joint problems, social andmental health issues due tostigmatization, and reduced self-esteem.8,9 Prediabetes,hyperglycemia, and sleep apnea areincreasingly prevalent among obesechildren.8,10 The prevention andtreatment of obesity in children arepriorities for public healthworldwide.
Behavioral interventions targetingchanges in physical activity and dietare effective for weight loss.11,12
Nearly 80% of pediatricians reportfrustration with modifying children’sobesity, however.13 Patientmotivation is associated withprogram adherence and predictsweight reduction.14 Including briefmotivational techniques such asmotivational interviewing (MI) inweight control interventionsincreases effectiveness.15,16
MI is a client-centered clinical methodto facilitate behavioral change.17
Originally developed as anintervention for addictive behaviors,MI is applied to a multitude ofbehavior change contexts.18 As part ofMI, the participants’ readiness tochange is assessed and guides thediscussions. The core principles of MIareQ:8 : expressing empathy, developinga discrepancy, rolling with resistance,and supporting self-efficacy.18,19 MIinvites participants to indicate theirfeelings, thoughts, and ambivalenceabout change, and it helps reaching
decisional balance.17,20 Comparedwith other approaches such aseducation and nonspecific counseling,MI has been found to improve healthbehaviors and outcomes.19
Parental involvement in MIinterventions21 can improve theeffectiveness of school-based healthprograms. In a recent meta-analysisof MI interventions for healthbehavior change in adolescents, theoverall effect size (Hedges’ g)compared with other active treatmentor no treatment was 0.28 (37studies). Obesity interventions hada smaller effect size (g = 0.15; 12studies). Regarding the interventiontarget/recipient,22 MI studiestargeting both the adolescent andparent yielded the largest effect sizes(g = 0.59) and were more effectivethan conducting MI with eitherparent (g = 0.27) or child (g = 0.26)individually.23
Although parental involvement islinked to effectiveness, conclusionsabout the appropriate intensitycannot be drawn due to the smallnumber of studies and inconsistentresults.24,25 Parenting skills (genericand specific to lifestyle behavior)were frequently present in effectiveweight control interventions,24 andindirect methods to engage parentswere commonly used, although directapproaches were more likely to resultin positive outcomes.24,26
Parental involvement requires furtherinvestigation with the use ofrandomized controlled trial (RCT)designs.23 Although meta-analyticaldifferences in effect sizes favorparental involvement, no existing RCTstudies compare .2 of the 3 targetgroups (eg, MI, MI + PI, control) in thesame trial experimentally.23,27–29
The goal of the present RCT was toevaluate the effectiveness of an MIweight loss intervention for obeseadolescents including parentalinvolvement (MI + PI) versus MIwithout parental involvement (MIonly) and a passive control group
over a period of 12 months. Wehypothesized that MI + PI would beeffective in changing BMI and otherrelevant outcomes compared witha control condition. We furtherhypothesized that MI + PI would besuperior in changing weight lossoutcomes compared with MI only.
METHODS
Participants and Recruitment
Obese adolescents (ie, BMI $95thpercentile for age and gender30)between 13 and 18 years of age wererecruited from a local outpatientpediatric clinic in Qazvin, Iran.Exclusion criteria were taking weight-related medication, havinga diagnosis of an eating disorder,being pregnant, and having clinicalmental health conditions orpsychosis. Eligible adolescents livedwith a parent or adult caregiver whowas prepared to be involved intreatment.
Study Design
The present study includeda prospective RCT design in whichpatients were randomly assigned toa control group, MI with parentalinvolvement, or MI without parentalinvolvement (Fig 1). Anthropometric,biochemical, psychosocial, andbehavioral measures were obtainedat baseline and 12 months later.
All participants provided writteninformed consent; parental assentwas also requested for adolescentsaged ,16 years. The ethicscommittee Q:9of the [BLINDED]approved the study. A total of 409adolescents were recruited betweenFebruary 2011 and April 2013.
Power Analysis and RandomizationProcedure
The sample size was calculated basedon previous studies considering aneffect size of 0.47, a power of 95%,and an a level of .05.31 Assuminga dropout rate of 15%, a sample size
2 PAKPOUR et al

of 136 participants per condition wasestimated.
To ensure adequate concealment ofallocation, a research coordinatorperformed the randomizationprocedure by using a computer-generated randomization schedule/sequence (SPSS version 17.0, IBMSPSS Statistics, IBM Corporation,Armonk, NY). After recruitment andconsenting procedures werecompleted, baseline data werecollected, and a research coordinatorassigned adolescents randomly to the3 groups: control (n = 119), MI (n =119), and MI + PI (n = 119).Adolescents could not be blinded tointervention allocation.Anthropometric measures at baselineand 12 months after randomizationwere taken by 2 assessors blinded togroup allocation.
Intervention Groups
The MI intervention componenttargeted improved eating and
physical activity behavior. Theadolescents were encouraged to eata variety of foods from each of the 4major food groups and low-fatalternatives.32 They were alsoencouraged to achieve at least 60minutes of moderate to vigorousintensity physical activity daily asrecommended by the World HealthOrganization33 (SupplementalAppendix).
MI Group With Parental Involvement
All sessions were delivered by 2trained interventionists at the sametime; each interventionist haddifferent expertise (ie, registereddietitian and exercise specialist). Allparticipants in the interventionalgroups attended pediatric clinics andreceived the weekly sessions lastingfor 40 minutes. Both interventiongroups received identical MI sessions(Supplemental Appendix). However,parents or guardians of participantsfrom the MI + PI group (n = 119)
received 1 additional session with.60 minutes in the clinic deliveredby the same 2 interventionists at theend of the 6 sessions. An identical MIstyle Q:10was used for parents, focusingon the adolescents’ weight, parentattitudes and behaviors regardingchildren’s physical activity anddietary habits, parent monitoring, andsupervision; the goal was to promoteprogress toward the child’sintervention goals and attitudes bythe parents.
MI Integrity
All MI sessions were audiotaped andquality checked by using theMotivational Interviewing TreatmentIntegrity (MITI) instrument.34
Twenty-five percent of the interviewswere selected randomly and assessedby 2 trained evaluators. The MITI has2 components: global scores andbehavior counts. Five globaldimensions are rated on a 5-pointLikert scale ranging from 1 (low) to 5(high): evocation, collaboration,autonomy/support, direction, andempathy. A behavior count requiresthe coder to tally instances ofparticular interviewer behaviors,including providing information, MI-adherent behavior, MI-nonadherentbehavior, simple reflections, complexreflections, and open and closedquestions. In addition to theaforementioned scores, summaryscores were computed as thefollowing; global spirit rating(evocation + collaboration +autonomy/support)/3, percentcomplex reflections (number ofcomplex reflections/number of totalreflections ) 3 100, percent openquestions (number of openquestions/number of total questions)3 100, reflection-to-question ratio(number of total reflections/numberof total questions) 3 100, andpercent MI-adherent (number of MI-adherent statements/number of MI-adherent and MI-nonadherentstatements) 3 100. As recommendedaccording to the MITI, summaryscores have applications for therapy
FIGURE 1Flow chart of participants according to the Consolidated Standards of Reporting Trials.
PEDIATRICS Volume 135, number 3, March 2015 3
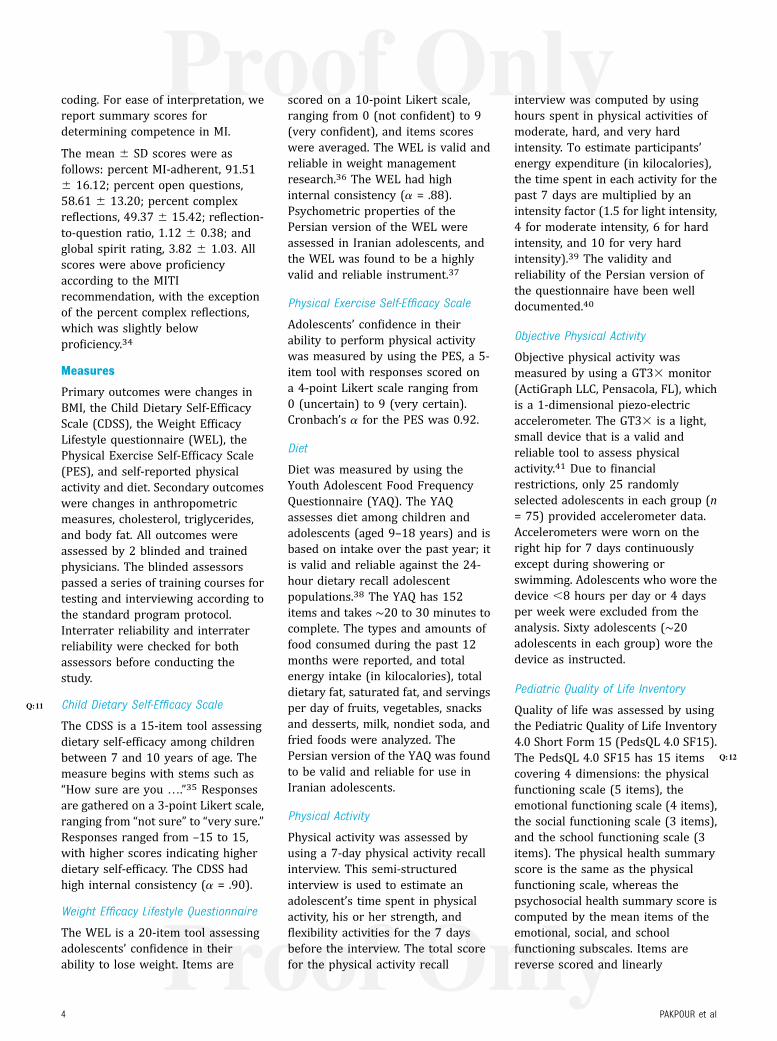
coding. For ease of interpretation, wereport summary scores fordetermining competence in MI.
The mean 6 SD scores were asfollows: percent MI-adherent, 91.516 16.12; percent open questions,58.61 6 13.20; percent complexreflections, 49.37 6 15.42; reflection-to-question ratio, 1.12 6 0.38; andglobal spirit rating, 3.82 6 1.03. Allscores were above proficiencyaccording to the MITIrecommendation, with the exceptionof the percent complex reflections,which was slightly belowproficiency.34
Measures
Primary outcomes were changes inBMI, the Child Dietary Self-EfficacyScale (CDSS), the Weight EfficacyLifestyle questionnaire (WEL), thePhysical Exercise Self-Efficacy Scale(PES), and self-reported physicalactivity and diet. Secondary outcomeswere changes in anthropometricmeasures, cholesterol, triglycerides,and body fat. All outcomes wereassessed by 2 blinded and trainedphysicians. The blinded assessorspassed a series of training courses fortesting and interviewing according tothe standard program protocol.Interrater reliability and interraterreliability were checked for bothassessors before conducting thestudy.
Child Dietary Self-Efficacy ScaleQ:11
The CDSS is a 15-item tool assessingdietary self-efficacy among childrenbetween 7 and 10 years of age. Themeasure begins with stems such as“How sure are you ….”35 Responsesare gathered on a 3-point Likert scale,ranging from “not sure” to “very sure.”Responses ranged from –15 to 15,with higher scores indicating higherdietary self-efficacy. The CDSS hadhigh internal consistency (a = .90).
Weight Efficacy Lifestyle Questionnaire
The WEL is a 20-item tool assessingadolescents’ confidence in theirability to lose weight. Items are
scored on a 10-point Likert scale,ranging from 0 (not confident) to 9(very confident), and items scoreswere averaged. The WEL is valid andreliable in weight managementresearch.36 The WEL had highinternal consistency (a = .88).Psychometric properties of thePersian version of the WEL wereassessed in Iranian adolescents, andthe WEL was found to be a highlyvalid and reliable instrument.37
Physical Exercise Self-Efficacy Scale
Adolescents’ confidence in theirability to perform physical activitywas measured by using the PES, a 5-item tool with responses scored ona 4-point Likert scale ranging from0 (uncertain) to 9 (very certain).Cronbach’s a for the PES was 0.92.
Diet
Diet was measured by using theYouth Adolescent Food FrequencyQuestionnaire (YAQ). The YAQassesses diet among children andadolescents (aged 9–18 years) and isbased on intake over the past year; itis valid and reliable against the 24-hour dietary recall adolescentpopulations.38 The YAQ has 152items and takes ∼20 to 30 minutes tocomplete. The types and amounts offood consumed during the past 12months were reported, and totalenergy intake (in kilocalories), totaldietary fat, saturated fat, and servingsper day of fruits, vegetables, snacksand desserts, milk, nondiet soda, andfried foods were analyzed. ThePersian version Q:12of the YAQ was foundto be valid and reliable for use inIranian adolescents.
Physical Activity
Physical activity was assessed byusing a 7-day physical activity recallinterview. This semi-structuredinterview is used to estimate anadolescent’s time spent in physicalactivity, his or her strength, andflexibility activities for the 7 daysbefore the interview. The total scorefor the physical activity recall
interview was computed by usinghours spent in physical activities ofmoderate, hard, and very hardintensity. To estimate participants’energy expenditure (in kilocalories),the time spent in each activity for thepast 7 days are multiplied by anintensity factor (1.5 for light intensity,4 for moderate intensity, 6 for hardintensity, and 10 for very hardintensity).39 The validity andreliability of the Persian version ofthe questionnaire have been welldocumented.40
Objective Physical Activity
Objective physical activity wasmeasured by using a GT33 monitor(ActiGraph LLC, Pensacola, FL), whichis a 1-dimensional piezo-electricaccelerometer. The GT33 is a light,small device that is a valid andreliable tool to assess physicalactivity.41 Due to financialrestrictions, only 25 randomlyselected adolescents in each group (n= 75) provided accelerometer data.Accelerometers were worn on theright hip for 7 days continuouslyexcept during showering orswimming. Adolescents who wore thedevice ,8 hours per day or 4 daysper week were excluded from theanalysis. Sixty adolescents (∼20adolescents in each group) wore thedevice as instructed.
Pediatric Quality of Life Inventory
Quality of life was assessed by usingthe Pediatric Quality of Life Inventory4.0 Short Form 15 (PedsQL 4.0 SF15).The PedsQL 4.0 SF15 has 15 itemscovering 4 dimensions: the physicalfunctioning scale (5 items), theemotional functioning scale (4 items),the social functioning scale (3 items),and the school functioning scale (3items). The physical health summaryscore is the same as the physicalfunctioning scale, whereas thepsychosocial health summary score iscomputed by the mean items of theemotional, social, and schoolfunctioning subscales. Items arereverse scored and linearly
4 PAKPOUR et al
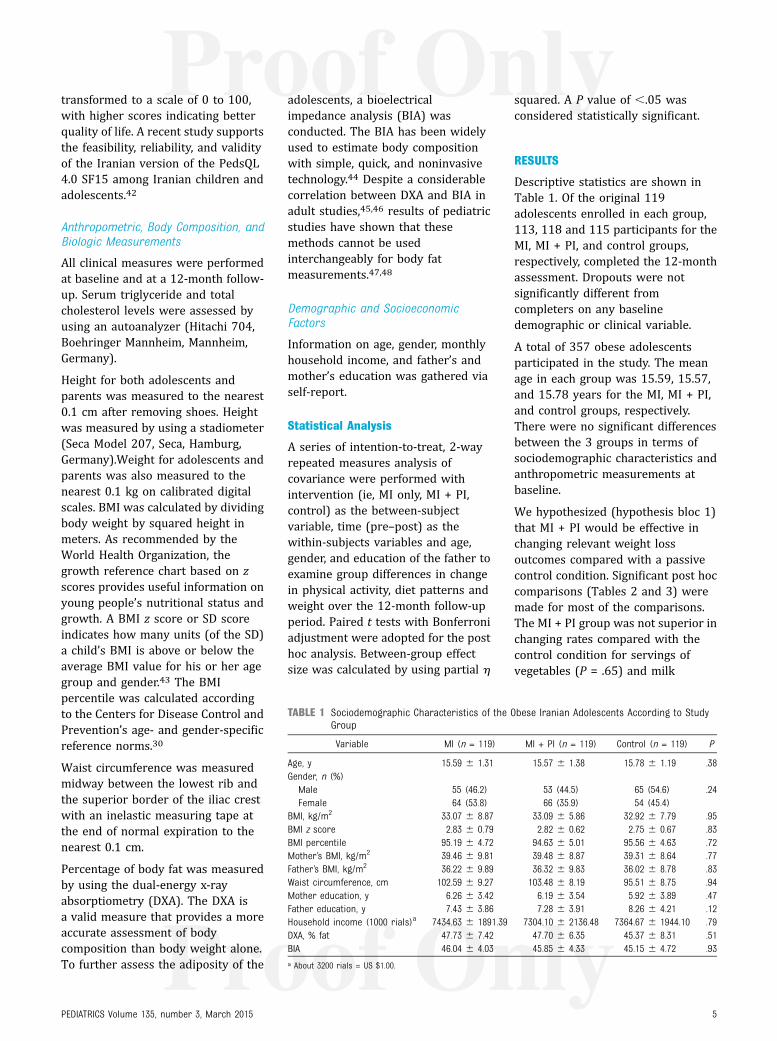
transformed to a scale of 0 to 100,with higher scores indicating betterquality of life. A recent study supportsthe feasibility, reliability, and validityof the Iranian version of the PedsQL4.0 SF15 among Iranian children andadolescents.42
Anthropometric, Body Composition, andBiologic Measurements
All clinical measures were performedat baseline and at a 12-month follow-up. Serum triglyceride and totalcholesterol levels were assessed byusing an autoanalyzer (Hitachi 704,Boehringer Mannheim, Mannheim,Germany).
Height for both adolescents andparents was measured to the nearest0.1 cm after removing shoes. Heightwas measured by using a stadiometer(Seca Model 207, Seca, Hamburg,Germany).Weight for adolescents andparents was also measured to thenearest 0.1 kg on calibrated digitalscales. BMI was calculated by dividingbody weight by squared height inmeters. As recommended by theWorld Health Organization, thegrowth reference chart based on zscores provides useful information onyoung people’s nutritional status andgrowth. A BMI z score or SD scoreindicates how many units (of the SD)a child’s BMI is above or below theaverage BMI value for his or her agegroup and gender.43 The BMIpercentile was calculated accordingto the Centers for Disease Control andPrevention’s age- and gender-specificreference norms.30
Waist circumference was measuredmidway between the lowest rib andthe superior border of the iliac crestwith an inelastic measuring tape atthe end of normal expiration to thenearest 0.1 cm.
Percentage of body fat was measuredby using the dual-energy x-rayabsorptiometry (DXA). The DXA isa valid measure that provides a moreaccurate assessment of bodycomposition than body weight alone.To further assess the adiposity of the
adolescents, a bioelectricalimpedance analysis (BIA) wasconducted. The BIA has been widelyused to estimate body compositionwith simple, quick, and noninvasivetechnology.44 Despite a considerablecorrelation between DXA and BIA inadult studies,45,46 results of pediatricstudies have shown that thesemethods cannot be usedinterchangeably for body fatmeasurements.47,48
Demographic and SocioeconomicFactors
Information on age, gender, monthlyhousehold income, and father’s andmother’s education was gathered viaself-report.
Statistical Analysis
A series of intention-to-treat, 2-wayrepeated measures analysis ofcovariance were performed withintervention (ie, MI only, MI + PI,control) as the between-subjectvariable, time (pre–post) as thewithin-subjects variables and age,gender, and education of the father toexamine group differences in changein physical activity, diet patterns andweight over the 12-month follow-upperiod. Paired t tests with Bonferroniadjustment were adopted for the posthoc analysis. Between-group effectsize was calculated by using partial h
squared. A P value of ,.05 wasconsidered statistically significant.
RESULTS
Descriptive statistics are shown inTable 1. Of the original 119adolescents enrolled in each group,113, 118 and 115 participants for theMI, MI + PI, and control groups,respectively, completed the 12-monthassessment. Dropouts were notsignificantly different fromcompleters on any baselinedemographic or clinical variable.
A total of 357 obese adolescentsparticipated in the study. The meanage in each group was 15.59, 15.57,and 15.78 years for the MI, MI + PI,and control groups, respectively.There were no significant differencesbetween the 3 groups in terms ofsociodemographic characteristics andanthropometric measurements atbaseline.
We hypothesized (hypothesis bloc 1)that MI + PI would be effective inchanging relevant weight lossoutcomes compared with a passivecontrol condition. Significant post hoccomparisons (Tables 2 and 3) weremade for most of the comparisons.The MI + PI group was not superior inchanging rates compared with thecontrol condition for servings ofvegetables (P = .65) and milk
TABLE 1 Sociodemographic Characteristics of the Obese Iranian Adolescents According to StudyGroup
Variable MI (n = 119) MI + PI (n = 119) Control (n = 119) P
Age, y 15.59 6 1.31 15.57 6 1.38 15.78 6 1.19 .38Gender, n (%)Male 55 (46.2) 53 (44.5) 65 (54.6) .24Female 64 (53.8) 66 (35.9) 54 (45.4)
BMI, kg/m2 33.07 6 8.87 33.09 6 5.86 32.92 6 7.79 .95BMI z score 2.83 6 0.79 2.82 6 0.62 2.75 6 0.67 .83BMI percentile 95.19 6 4.72 94.63 6 5.01 95.56 6 4.63 .72Mother’s BMI, kg/m2 39.46 6 9.81 39.48 6 8.87 39.31 6 8.64 .77Father’s BMI, kg/m2 36.22 6 9.89 36.32 6 9.83 36.02 6 8.78 .83Waist circumference, cm 102.59 6 9.27 103.48 6 8.19 95.51 6 8.75 .94Mother education, y 6.26 6 3.42 6.19 6 3.54 5.92 6 3.89 .47Father education, y 7.43 6 3.86 7.28 6 3.91 8.26 6 4.21 .12Household income (1000 rials)a 7434.63 6 1891.39 7304.10 6 2136.48 7364.67 6 1944.10 .79DXA, % fat 47.73 6 7.42 47.70 6 6.35 45.37 6 8.31 .51BIA 46.04 6 4.03 45.85 6 4.33 45.15 6 4.72 .93a About 3200 rials = US $1.00.
PEDIATRICS Volume 135, number 3, March 2015 5

products (P = .27) per day, waistcircumference (P = .51), and socialfunctioning (P = .12). For all otherpsychometric variables (eg, schoolfunctioning [P = .03], physical [P =.01] and psychosocial [P = .01] health,exercise [P = .003], dietary self-efficacy [P , .001]), dietary factors(eg, fat intake [P = .01], servings ofsnacks [P , .001] and fried food [P =.01], total calories [P = .002]), andanthropometric measures (eg,physical activity [P = .001], energyexpenditure [P = .001], BMI [P =.001], cholesterol [P = .02],triglycerides [P = .02], DXA [P = .01],BIA [P = .001]), the comparison of MI+ PI versus the control group yieldedsignificant differences in favor of theintervention.
We further hypothesized (hypothesisbloc 2) that MI + PI would besuperior in changing weight lossoutcomes compared with MI only. Thepattern of results was similar, albeitslightly weaker differences werefound. For many outcome variables,significant post hoc differencesemerged (Tables 2 and 3). The MI +PI group was not significantlysuperior compared with MI foradolescents only for servings of fruits(P = .17), vegetables (P = .77), andmilk products (P = .34) per day; waistcircumference (P = .71); DXA (P =.38); BIA (P = .38); and social (P =.10) and psychosocial (P = .35)functioning. For the otherpsychometric variables (eg, schoolfunctioning [P = .02], physical [P =.04], exercise [P = .003], dietary self-efficacy [P , .001]), dietary habits(eg, fat intake [P = .04], servings ofsnacks [P = .04] and fried food [P =.04], total calories [P = .03]), andanthropometric measures (eg,physical activity [P = .01], energyexpenditure [P = .003], BMI [P =.048], cholesterol [P = .049],triglycerides [P = .031]), thecomparison of MI + PI with MI onlyfor adolescents exhibited significantdifferences.
TABLE2
DietaryandAnthropometricOutcom
esAccordingto
InterventionGroupfor
Q:18
BaselineandFollow-up
Variable
Baseline
12-moFollow-up
TimeEffects
Post
HocTesta
MI(n=119)
MI+PI
(n=119)
Control(n
=119)
MI(n=113)
MI+
PI(n
=118)
Control(n
=115)
TimeEffect
Time3
Group
Effect
MI+
PIVersus
Control
MI+PI
Versus
MI
Mean6
SDMean6
SDMean6
SDMean6
SDMean6
SDMean6
SDF
Php2
FP
hp2
PP
Diet/foodintake
Totalcalories,kcal
3022.226
1442.70
3000.526
1449.14
2930.366
1342.81
2785.216
1240.31
2256.086
1351.46
2919.956
1471.92
58.09
,.001
0.14
25.03
,.001
0.12
.002
.032
Totaldietaryfat,g
105.55
663.50
102.80
660.85
95.236
40.16
98.426
49.83
74.406
42.39
95.736
40.10
28.74
,.001
0.75
15.77
,.001
0.09
.012
.041
Saturatedfat,g
36.526
23.70
36.296
24.57
36.496
23.75
32.546
22.86
35.526
21.48
30.036
20.84
300.43
,.001
0.46
50.60
,.001
0.22
,.001
.029
Fruits
andjuice,
servings/d
1.27
60.98
1.27
60.97
1.21
60.97
1.31
60.96
1.33
60.93
1.23
60.97
2.85
.09
0.01
0.26
.77
0.00
.030
.17
Vegetables,servings/d
1.64
60.76
1.66
60.75
1.66
60.73
1.71
60.80
1.77
60.76
1.64
60.80
4.61
.03
0.01
2.24
.10
0.01
.65
.77
Snacks/desserts,
servings/d
4.43
61.52
4.33
61.82
4.49
61.63
4.12
61.43
3.89
61.65
4.55
61.71
41.28
,.001
0.10
17.65
,.001
0.09
,.001
.04
Nondietsoda,servings/d
0.87
60.66
0.85
60.53
0.89
60.42
0.77
60.38
0.48
60.35
0.95
60.33
33.23
,.001
0.09
5.46
,.001
0.14
.001
.01
Milk,servings/
d0.94
60.49
0.95
60.38
0.98
60.48
0.95
60.29
0.96
60.43
0.97
60.37
0.02
.89
0.00
0.08
.92
0.00
.27
.34
Friedfoods,servings/d
0.81
60.38
0.82
60.33
0.84
60.45
0.82
60.30
0.63
60.33
0.90
60.44
6.45
.10
0.01
14.76
,.001
0.08
.01
.042
Anthropometry
andbody
composition
Totalcholesterol,mmol/L
4.42
60.73
4.40
60.82
4.18
60.96
4.41
60.72
4.27
60.78
4.20
60.97
4.26
.04
0.01
4.70
.010
0.03
.021
.049
Triglycerides,mmol/L
1.01
60.78
1.02
60.77
1.05
60.68
1.01
60.77
0.86
60.78
1.09
60.72)
5.68
.018
0.02
10.55
.001
0.06
.001
.031
BMI,kg/m
233.076
8.87
33.096
5.86
32.926
7.79
32.446
7.45
31.046
6.46
32.956
8.78
25.51
,.001
0.07
14.76
.001
0.08
.01
.032
BMIz
score
2.83
60.79
2.82
60.62
2.75
60.67
2.81
60.76
2.58
60.61
2.76
60.70
12.73
,.001
0.04
12.13
,.001
0.06
.02
.048
DXA,%
fat
47.736
7.42
47.706
6.35
45.376
8.31
46.616
7.91
45.966
6.34
45.406
7.45
44.49
,.001
0.11
13.47
,.001
0.07
.012
.38
BIA
46.046
4.03
45.856
4.33
45.156
4.72
45.626
4.32
42.326
3.56
45.336
4.86
13.45
,.001
0.04
11.77
,.001
0.06
.001
.38
Waist
circum
ference,cm
102.59
69.27
103.48
68.19
95.516
8.75
101.97
69.11
101.70
69.21
99.906
8.26
2.67
.10
0.00
2.36
.09
0.01
.512
.717
Unless
otherw
iseindicated,
data
arepresentedas
mean6
SD.h
p2=partialhsquared(m
easure
ofeffect
size).
aBonferroni
adjustment.
6 PAKPOUR et al

DISCUSSION
To evaluate the role of parentalinvolvement in MI weight lossinterventions for obese adolescents,a prospective RCT was performedcomparing 3 intervention groups: MIfor adolescents only, MI foradolescents with parentalinvolvement, and a passive controlgroup. Anthropometric, biochemical,psychosocial, and behavioral datawere collected at baseline and 12months later. Results revealedsignificant effects for MI withparental involvement compared withthe control group (hypothesis bloc 1)and compared with MI foradolescents only (hypothesis bloc 2).This pattern could be shown for mostof the anthropometric, biochemical,psychosocial, and behavioral outcomevariables supporting the hypotheses.
The present results are in line withfindings of a recent meta-analysisregarding MI interventions fordifferent types of health behaviors, aswell as interventions targeting theobese adolescent populationdirectly.23 The additionaleffectiveness of parental involvementsupport the associations found in themeta-analysis. According to Gayeset al,23 studies that assessed MI withboth adolescent and parental inputreported the largest effects,demonstrating that conducting MIwith both parent and adolescent ismore effective than conducting MIwith either parent or adolescent only.Previous behavioral interventions forobese adolescents were inconclusiveregarding the role of parentalinvolvement.24–26 The present studycan strengthen the evidence forparental involvement in the context ofan MI intervention.
Some study limitations must beacknowledged. Despite theappropriate sample size and the lowdropout rate in an understudiedpopulation, the results might belimited to Persian culture. Thus,generalizability to other studycontexts should be made withTA
BLE3
Energy
Expenditure
andQuality
ofLife
Outcom
esAccordingto
InterventionGroupforBaselineandFollow-up
Variable
Baseline
12-moFollow-up
TimeEffects
Post
HocTesta
MI(n
=119)
MI+
PI(n
=119)
Control(n
=119)
MI(n=113)
MI+PI
(n=118)
Control(n
=115)
TimeEffect
Time3
GroupEffect
MI+
PIVersus
Control
MI+PI
Versus
MI
Mean6
SDMean6
SDMean6
SDMean6
SDMean6
SDMean6
SDF
Php2
FP
hp2
PP
Measure
CDSS
6.16
62.46
6.14
62.51
6.02
62.32
6.88
62.72
7.11
62.62
5.71
62.82
34.56
,.001
0.09
23.59
,.001
0.12
,.001
.01
WEL
87.106
27.37
87.296
28.94
93.616
29.14
101.27
627.23)
108.05
624.28)
93.216
29.60
45.01
,.001
0.11
12.51
,.001
0.07
.002
.04
PES
5.61
61.74
5.59
61.87
5.69
61.82
6.75
61.15
6.68
61.97
5.39
62.18
70.12
,.001
0.16
38.01
,.001
0.17
.003
.01
Self-reported
PAlength
0.84
60.49
0.86
60.45)
0.70
60.35
1.12
60.61
1.30
60.66)
0.66
60.32)
35.16
,.001
0.09
13.43
,.001
0.07
.004
.01
Self-reported
energy
expenditure
247.73
6160.36
220.50
6106.63
271.87
6127.99
434.07
6128.98
509.07
6128.15
268.14
6109.08
115.08
,.001
0.54
31.92
,.001
0.39
.002
.02
ObjectivePA
length
0.67
60.38
0.68
60.28
0.65
60.39)
0.98
60.37
0.59
60.40
1.34
60.42
36.26
,.001
0.09
17.06
,.001
0.09
.001
.01
Objectiveenergy
expenditure
280.17
682.83
274.90
685.32
293.95
681.83)
500.02
694.94
680.08
688.14
262.92
699.22
82.65
,.001
0.59
33.67
,.001
0.54
.001
.003
Measure
Totalscore
63.196
20.58
62.466
20.18
64.746
19.91
64.346
21.11
65.146
18.88
63.736
17.16
3.05
.08
0.01
4.081
.01
0.02
.21
.31
Physical
health
66.716
19.35
66.176
19.28
65.126
24.53
70.136
19.20
71.846
20.88
62.936
25.85
8.55
,.001
0.02
8.97
,.001
0.05
.01
.04
Psychosocial
health
67.696
17.19
67.046
18.49
67.546
19.3
69.086
21.62
70.166
15.09
66.306
16.83
4.26
.04
0.01
5.85
,.001
0.04
.01
.35
Emotionalfunctioning
68.976
19.34
68.356
20.42
69.596
19.92
71.646
19.99
71.816
21.79
68.276
21.82
7.15
.008
0.02
6.20
.002
0.03
.03
.24
Social
functioning
69.846
18.41
69.126
19.74
70.126
17.42
70.846
19.08
69.126
19.47
70.016
17.98
3.49
.06
0.01
3.48
.03
0.02
.12
.10
School
functioning
65.016
15.79
64.186
16.78
68.836
20.63
66.806
17.62
71.266
18.20
65.736
23.77
5.40
.02
0.01
12.70
,.001
0.07
.03
.02
hp2
=partialhsquared(m
easure
ofeffect
size);PA
=physical
activity.
aBonferroni
adjustment.
PEDIATRICS Volume 135, number 3, March 2015 7

caution, although the present findingsare in line with evidence obtained inWestern samples.21 However, morestudies are needed to directlycompare the effects of parentalinvolvement and MI among samplesfrom different cultures. In addition,we did not use objective outcomephysical activity measures for thewhole sample. Furthermore,intervention was delivered by trainedinterventionists; consecutive studiesare needed to validate thereplicability of our findings withother interventionists but also withother nonspecialist interventionistssuch as trained teachers (coachedaccording to the MI training manual).Finally, the present study wasconducted by using a 12-monthfollow-up. A subsequent next stepwould be to investigate the longerterm effects of the intervention (ie,after several years).
CONCLUSIONS
Because our study was a clinicalassessment, future studies shouldreplicate our findings in real-worldsettings, such as integrating MI asa brief strategy into the daily routinesof a school, particularly for obeseadolescents, but for nonobeseadolescents as a prevention tool aswell. Effects of parental involvementshould be tested via invitation letterssent by the school and brief trainingsessions, in which adolescents andtheir parents could be motivated tochange their dietary and physicalactivity habits.
Future studies might extend theinvestigation to different types of thedelivery mode, not only involvinga parent but also varying the intensitylevel of parental involvement becausethis dose–response relation has beenexamined by previous meta-analyses.Beyond that, examination of subgroupeffects would provide further insightsinto the topic; for example, the effectsof parental involvement might varyaccording to the gender, age, qualityof the relationship between
adolescent and parent, or the family’scooking habits.49
The present study evaluated andcompared the role of parentalinvolvement in MI interventions forobese adolescents compared with MIfor adolescents only and controlsubjects. The results show that MIwith parental involvement is aneffective strategy in changing obesity-related outcomes and has additionaleffects beyond MI with adolescentsonly, which is important whenadministering MI interventions inschool settings.
REFERENCES
1. Schmidt Morgen C, Rokholm B, SjöbergBrixval C, et al. Trends in prevalence ofoverweight and obesity in Danish infants,children and adolescents—are we stillon a plateau? PLoS One. 2013;8(7):e69860
2. Moraes AC, Falcão MC. Lifestyle factorsand socioeconomic variables associatedwith abdominal obesity in Brazilianadolescents. Ann Hum Biol. 2013;40(1):1–8
3. Lobstein T, Baur L, Uauy R; IASOInternational Obesity Task Force. Obesityin children and young people: a crisis inpublic health. Obes Rev. 2004;5(suppl 1):4–104
4. World Q:13Health Organization. TheChallenge of Obesity—Quick Statistics.2012 ed. Geneva, Switzerland: WorldHealth Organization; 2012
5. Raj M, Kumar RK. Obesity in children &adolescents. Indian J Med Res. 2010;132:598–607
6. Moayeri H, Bidad K, Aghamohammadi A,et al. Overweight and obesity and theirassociated factors in adolescents inTehran, Iran, 2004-2005. Eur J Pediatr.2006;165(7):489–493
7. Behzadnia S, Vahidshahi K, HamzehHosseini S, Anvari S, Ehteshami S.Obesity and related factors in 7-12 year-old elementary school students during2009-2010 in Sari, Iran. Med Glas(Zenica). 2012;9(1):86–90
8. Centers Q:14for Diseases Control andPrevention. Childhood Obesity Facts.Atlanta, GA: Centers for Diseases Controland Prevention; 2012
9. Puhl R, Brownell KD. Bias, discrimination,and obesity. Obes Res. 2001;9(12):788–805
10. Ebbeling CB, Pawlak DB, Ludwig DS.Childhood obesity: public-health crisis,common sense cure. Lancet. 2002;360(9331):473–482
11. Budd GM, Hayman LL, Crump E, et al.Weight loss in obese African Americanand Caucasian adolescents: secondaryanalysis of a randomized clinical trial ofbehavioral therapy plus sibutramine. JCardiovasc Nurs. 2007;22(4):288–296
12. Pimenta F, Leal I, Maroco J, Ramos C.Brief cognitive-behavioral therapy forweight loss in midlife women:a controlled study with follow-up. Int JWomens Health. 2012;4:559–567
13. Jelalian E, Boergers J, Alday CS, Frank R.Survey of physician attitudes andpractices related to pediatric obesity.Clin Pediatr (Phila). 2003;42(3):235–245
14. Befort CA, Nollen N, Ellerbeck EF, SullivanDK, Thomas JL, Ahluwalia JS.Motivational interviewing fails toimprove outcomes of a behavioralweight loss program for obese AfricanAmerican women: a pilot randomizedtrial. J Behav Med. 2008;31(5):367–377
15. Hardcastle SJ, Taylor AH, Bailey MP,Harley RA, Hagger MS. Effectiveness ofa motivational interviewing interventionon weight loss, physical activity andcardiovascular disease risk factors:a randomised controlled trial with a 12-month post-intervention follow-up. Int JBehav Nutr Phys Act. 2013;10:40
16. Wong EM, Cheng MM. Effects ofmotivational interviewing to promoteweight loss in obese children. J ClinNurs. 2013;22(17–18):2519–2530
17. Martins RK, McNeil DW. Review ofmotivational interviewing in promotinghealth behaviors. Clin Psychol Rev. 2009;29(4):283–293
18. Miller WR, Rollnick S. MotivationalInterviewing: Preparing People forChange. 2nd ed. New York, NY: GuilfordPress; 2002
19. Levensky ER, Forcehimes A, O’DonohueWT, Beitz K. Motivational interviewing: anevidence-based approach to counselinghelps patients follow treatmentrecommendations. Am J Nurs. 2007;107(10):50–58, quiz 58–59
8 PAKPOUR et al

20. Rollnick S, Butler CC, McCambridge J,Kinnersley P, Elwyn G, Resnicow K.Consultations about changing behaviour.BMJ. 2005;331(7522):961–963
21. Sormunen M, Tossavainen K, Turunen H.Finnish parental involvement ethos,health support, health educationknowledge and participation: resultsfrom a 2-year school health intervention.Health Educ Res. 2013;28(2):179–191
22. Davidson KW, Goldstein M, Kaplan RM,et al. Evidence-based behavioralmedicine: what is it and how do weachieve it? Ann Behav Med. 2003;26(3):161–171
23. Gayes LA, Steele RG. A meta-analysis ofmotivational interviewing interventionsfor pediatric health behavior change. JConsult Clin Psychol. 2014;82(3):521–535
24. van der Kruk JJ, Kortekaas F, Lucas C,Jager-Wittenaar H. Obesity: a systematicreview on parental involvement in long-term European childhood weight controlinterventions with a nutritional focus[published online ahead of print JuneQ:15 4,2013]. Obes Rev. doi: 10.1111/obr.12046
25. Van Lippevelde W, Verloigne M, DeBourdeaudhuij I, et al. Does parentalinvolvement make a difference in school-based nutrition and physical activityinterventions? A systematic review ofrandomized controlled trials. Int J PublicHealth. 2012;57(4):673–678
26. Hingle MD, O’Connor TM, Dave JM,Baranowski T. Parental involvement ininterventions to improve child dietaryintake: a systematic review. Prev Med.2010;51(2):103–111
27. Gourlan M, Sarrazin P, Trouilloud D.Motivational interviewing as a way topromote physical activity in obeseadolescents: a randomised-controlledtrial using self-determination theory asan explanatory framework. PsycholHealth. 2013;28(11):1265–1286
28. Lloyd-Richardson EE, Jelalian E, Sato AF,Hart CN, Mehlenbeck R, Wing RR. Two-year follow-up of an adolescentbehavioral weight control intervention.Pediatrics. 2012;130(2). Available at:www.pediatrics.org/cgi/content/full/130/2/e281
29. Walpole B, Dettmer E, Morrongiello BA,McCrindle BW, Hamilton J. Motivationalinterviewing to enhance self-efficacy andpromote weight loss in overweight and
obese adolescents: a randomizedcontrolled trial. J Pediatr Psychol. 2013;38(9):944–953
30. Kuczmarski RJ, Ogden CL, Guo SS,Grummer-Strawn LM, Flegal KM, Mei Z,et al. 2000 CDC growth charts for theUnited States: methods anddevelopment. Vital Health Stat. 2002(246):1–190
31. Burke BL, Arkowitz H, Menchola M. Theefficacy of motivational interviewing:a meta-analysis of controlled clinicaltrials. J Consult Clin Psychol. 2003;71(5):843–861
32. National Health and Medical ResearchCouncil. Food for Health: DietaryGuidelines for Children and Adolescentsin Australia. Canberra, Australia:Commonwealth Department of Healthand Ageing; 2003
33. World Q:16Health Organization. GlobalRecommendations on Physical Activityfor Health. Geneva, Switzerland: WorldHealth Organization; 2010
34. Moyers TB, Martin T, Manuel JK, MillerWR, Ernst D. Motivational InterviewingTreatment Integrity 3.1.1: Revised GlobalScales. Albuquerque, NM: University ofNew Mexico; 2010
35. Parcel GS, Edmundson E, Perry CL, et al.Measurement of self-efficacy for diet-related behaviors among elementaryschool children. J Sch Health. 1995;65(1):23–27
36. Clark MM, Abrams DB, Niaura RS, EatonCA, Rossi JS. Self-efficacy in weightmanagement. J Consult Clin Psychol.1991;59(5):739–744
37. Navidian A, Abedi M, Baghban I,Fatehizadeh M. Reliability and Q:17validity ofthe Weight Efficacy Lifestylequestionnaire in overweight and obeseindividuals. JBS. 2009;3:217–222
38. Rockett HR, Breitenbach M, Frazier AL,et al. Validation of a youth/adolescentfood frequency questionnaire. Prev Med.1997;26(6):808–816
39. Gross LD, Sallis JF, Buono MJ, Roby JJ,Nelson JA. Reliability of interviewersusing the seven-day physical activityrecall. Res Q Exerc Sport. 1990;61(4):321–325
40. Vasheghani-Farahani A, Tahmasbi M,Asheri H, Ashraf H, Nedjat S, Kordi R. ThePersian, last 7-day, long form of the
International Physical ActivityQuestionnaire: translation and validationstudy. Asian J Sports Med. 2011;2(2):106–116
41. Crouter SE, Horton M, Bassett DR Jr. Useof a two-regression model for estimatingenergy expenditure in children. Med SciSports Exerc. 2012;44(6):1177–1185
42. Pakpour AH. Psychometric properties ofthe Iranian version of the PediatricQuality of Life Inventory� Short Form 15Generic Core Scales. Singapore Med J.2013;54(6):309–314
43. Chen H-J, Wang Y. Use of percentiles andz -scores in anthropometry. In: Preedy V,ed. Handbook of Anthropometry: PhysicalMeasures of Human Form in Health andDisease. London, UK: Springer; 2012:29–48
44. Houtkooper LB, Lohman TG, Going SB,Howell WH. Why bioelectrical impedanceanalysis should be used for estimatingadiposity. Am J Clin Nutr. 1996;64(suppl3):436S–448S
45. Malavolti M, Mussi C, Poli M, et al. Cross-calibration of eight-polar bioelectricalimpedance analysis versus dual-energyx-ray absorptiometry for the assessmentof total and appendicular bodycomposition in healthy subjects aged 21-82 years. Ann Hum Biol. 2003;30(4):380–391
46. Demura S, Sato S, Kitabayashi T.Percentage of total body fat as estimatedby three automatic bioelectricalimpedance analyzers. J PhysiolAnthropol Appl Human Sci. 2004;23(3):93–99
47. Eisenmann JC, Heelan KA, Welk GJ.Assessing body composition among 3- to8-year-old children: anthropometry, BIA,and DXA. Obes Res. 2004;12(10):1633–1640
48. Ellis KJ. Measuring body fatness inchildren and young adults: comparisonof bioelectric impedance analysis, totalbody electrical conductivity, and dual-energy x-ray absorptiometry. Int J ObesRelat Metab Disord. 1996;20(9):866–873
49. Bauer KW, Neumark-Sztainer D, HannanPJ, Fulkerson JA, Story M. Relationshipsbetween the family environment andschool-based obesity prevention efforts:can school programs help adolescentswho are most in need? Health Educ Res.2011;26(4):675–688
PEDIATRICS Volume 135, number 3, March 2015 9

1—Please verify author names and provide academic degrees for each author.
2—Please expand/revise each affiliation so complete location is given (name of institution, city, country). Also,if pertinent, add relevant department/division name.
3—Please verify correspondence information is correct/complete as given.
4—Please confirm whether funding for this research was provided by the National Institutes of Health. If so,please provide any relevant grant information if it has not already been noted.
5—Per journal style, all abstracts must have fewer than 250 words. If your abstract extends beyond this limit,please edit as necessary (if changes are extensive, include or e-mail an electronic text file with the newabstract).
6—Per journal style, the text for “What’s known on this subject” and “What this study adds” may not exceed40 words each. Please amend as necessary to meet this requirement.
7—Please review the edited text carefully. At spots, it appeared that some text was repeated or text wasmissing. Please revise further as needed.
8—See statement beginning "The core principles of MI....";is "developing a discrepancy" clear/correct?
9—Please revise for clarity the statement beginning "The ethics committee..."
10—See statement beginning "An identical MI style..."; please confirm meaning of "attitudes by parents"(expand so this is clear).
11—Please see paragraph entitled "Child Dietary Self-Efficacy Scale." Please confirm wording here; it appearssome text was missing.
12—Is reference needed for the statement beginning "The Persian version of the YAQ...."?
13—Is ref. 4 correct/complete as expanded?
14—Please revise ref. 8 further for accuracy/completeness.
15—If possible, please update status of ref. 24.
16—Is ref. 33 correct/complete as expanded?
17—Ref. 37 could not be confirmed. Please revise and provide issue number, as needed.
18—Tables 3 and 4: boldface is not allowed in tables and has been removed. If you would like to differentiatethese data, please do so with a footnote symbol.
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES

Supplemental Information
APPENDIX
MI Intervention
All MI sessions were held in a quiet,private, and comfortable setting insidethe clinic. The sessions were deliveredby a trained and registered dietitian(female, .8 years of experienceworking in pediatric nutrition, and hadreceived 51 hours of MI training) anda trained sport and exercise specialist(male, 11 years of experience workingin exercise education, and had received48 hours of MI training). The dietitianand exercise specialist both deliveredthe session at the same time. Thefacilitators completed 20 hours of MItraining by a certified and experiencedMI trainer. Participants in both in-tervention groups received 6 individualcounseling sessions on diet and exer-cise with an extra session for parentsin the MI1 PI group. All sessions weredelivered weekly, and each sessionlasted ∼40 minutes.The intervention was initiated based onthe underlying “spirit of the MI.” Alladolescents were encouraged to ex-press their personal motivation tochange their physical activity and di-etary behavior. The goal of the MI ses-sion was to assist the adolescents withreducing resistance and overcomingambivalence about behavior change.The role of the facilitator was to informthe participants about negative effectsof unhealthy eating behavior and beingphysically inactive. MI techniques suchas reflective listening, open-ended ques-tions, rolling with resistance, agendasetting, and eliciting self-motivationalstatements, change talk, and affirma-tions were used as the core motiva-tional interviewing techniques.
All 6MI sessionsusedasemi-structuredformat and were each organized into 4component parts that lasted for ∼10minutes.
In the first phase, the facilitators in-troduced themselves to theadolescentsand assured them that the conser-vations would be kept private. Thepurpose of the meeting was describedto the participants. The facilitators in-vited participants to broach topics thatthey wanted to discuss. Moreover,facilitators asked some questions typ-ically important in an adolescent’s lifesuch as what they do after school.These questions helped the counselorsto foster a confident relationship withthe adolescents. Furthermore, thecounselors tried to elicit adolescents’concerns on their current situations byasking open-ended questions (eg,“What concerns you about your currentsituation?”, “What are some reasonsyou might see for making a change?”,“How do you feel about your weight?”).The counselors also Q:1facilitated weigh-ing up of the perceived costs and ben-efits of the adolescent’s current weightstatus. Some questions were used toaddress the positive and negativeeffects of obesity and relevant behav-iors (eg, “What do you see as the pos-itive and negative consequences ofyour current situation?” and “What aresome of the good and bad things abouta possible healthy diet and being moreactive?”). This session was aimed atincreasing the adolescents’ awarenessof their current weight status. Thecounselors tried to develop discrep-ancies between the current situationand possible future states (eg, “If youmake changes, how would your life bedifferent from what it is today”). The
adolescents were encouraged to ex-press their concerns and to exploreand resolve ambivalence. The counse-lors tried to raise awareness of risks inrelation to their current weight situa-tion in a nonconfrontational manner.
In the second phase Q:2(ie, once the ado-lescents had expressed the risks andbenefits of their current weight status),alternative courses of action weretaken into account by the counselors(eg, not going to restaurants, limittelevision watching, making differ-ent snacking choices). The costs andbenefits of the alternative behaviorswere subsequently discussed, and ado-lescents’ readiness to change thesebehaviors was rated on a scale from 1(I am not willing to change) to 10 (I willdo anything that I need to change). Theimportance of exercise and a healthydiet were also raised by the counselorsand were rated by the obese adoles-cents on a scale from 0 (least impor-tant) to 10 (most important). Scalingquestions were followed by open-ended questions that invited adoles-cents to further elaborate on theirchoices (eg, “Why did you choosea [current number] instead of a [lowernumber]?”, “What would need to hap-pen to make it a [higher number]?”). Inaddition to importance, counselorsalso considered confidence in ability tochange by asking similar questions(eg, “On a scale from 0 to 10 where 10 isthe most confident and 0 is the least,what number would you give for howconfident you are that you could exer-cise and eat a healthy diet?”, “So youfeel it at least a little bit confident(1–3)/somewhat confident (4–7)/veryconfident (8–10)”, “Why are you at[stated number] and not [lower
PEDIATRICS Volume 135, Number 3, March 2015 SI1
ARTICLE

number]?”). The adolescents werealso encouraged to think about what itwould be like to make the change inimagining a possible future. For ex-ample, the counselors asked adoles-cents to imagine future situations (eg,“Suppose you continue as you havebeen, without changing, without en-gaging in regular physical activity/healthy diet, what do you imaginewould happen to your ability to live out?”,“If you were successful in engaging inregular physical activity/healthy diet,how would things be different?”, or“What would be the impact on yourability to live out?”). Furthermore, theadolescents were asked to think aboutwhat they would be able to do in termsof the kinds of activities or diets.
In the third phase, adolescents wereinvited to engage in goal setting andplanning for change. The formulatedgoals had to fulfill the criteria of beingmeasurable, realistic, behavioral, anddesirable. Asking some questionshelped the participants to make ac-ceptable goals (eg, “I hear you aremostinterested in losing weight right nowand at the same time I am very con-cerned about your physical activity anddiet; whatmight be the first step to lookat both of those goals?”). Worksheetswere given to the participants to re-view and complete. In the worksheets,the adolescents identified some of the
things they would need to do to achievea given goal. Furthermore, the coun-selors encouraged the adolescents tocreate an action plan by specifyingwhere, when, how, for how long, andwith whom they were planning to en-gage in the selected physical activity/healthy eating behavior. Becausesome barriers might interfere withenacting the selected action plan,adolescents were also asked toanticipate situations in which thebehavior to be changed may not bemaintained and were encouraged toidentify those strategies that helpedto overcome these barriers (copingplanning).
Parental MI Session
During 1 in-person session, reduc-tions in parents’ ambivalence andincreases in readiness to providehelp for their children were targeted.The same facilitators contacted theparents (for MI 1 PI group only) bytelephone and invited them to attenda single session. At the beginning ofthe session, the parents were en-couraged to express their feelingsand motivations regarding healthylifestyle behaviors (ie, nutrition andphysical activity) for their child orchildren. Moreover, the role of parent-ing in preparing healthy foods for theirchild and encouraging/monitoring them
for being physically active were dis-cussed. At this stage, the aim was toexplore and resolve the parent’s am-bivalence. The key techniques wereopen-ended questioning, applying re-flection, rolling with resistance, andproviding summery. Barriers and facil-itators for behavior change in theirchild or children were also explored.Current child behaviors were discussedwith parents and desired healthbehaviors for them addressed. Parentswere also helped to encourage in-dicating the pros and cons of engagingtheir children in healthy behaviorchanges. The level of commitment andlikelihood of success were ratedby parents on a scale of 0 to 10. Theinterventionist then provided infor-mation by sharing facts on propernutrition, healthy snacking, and beingphysically active at recommendedlevels. Parents were then encouragedto imagine their children in the futurewith and without change. In the end,parents were told that their childrenset goals and made a plan for changingtheir behavior. The parents were alsoinstructed to set a target for theirchildren’s behavior change. It wasemphasized that parents should helptheir children by providing them withan alarm on their telephone or a stickynote that would remind them to adhereto their plans.
SI2 PAKPOUR et al
1—In the statement beginning “The counselors also...,” what does “weighing up” mean?
2—Please confirm that the questions as given in the paragraph beginning “In the second phase....” are clearlywritten.
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES




















