Molecular and traditional chemotherapy: A united front against prostate cancer
14
Mini-review Molecular and traditional chemotherapy: A united front against prostate cancer P. Singh c,1 , M. Yam a,b,1 , P.J. Russell a,b,d,e , A. Khatri a,b, * a Oncology Research Centre, Prince of Wales Hospital, Randwick, Sydney, NSW 2031, Australia b Faculty of Medicine, University of New South Wales, Kensington, NSW 2036, Australia c Centre for Medicine and Oral Health, Griffith University – Gold Coast GH1, High Street, Southport, Gold Coast, QLD 4215, Australia d Australian Prostate Cancer Research Centre – Queensland, Princess Alexandra Hospital, Woollangabba, QLD, Australia e Institute of Health and Biomedical Innovation, Queensland University of Technology, 60 Musk Avenue, Kelvin Grove, QLD 4059, Australia article info Article history: Received 29 October 2009 Received in revised form 23 November 2009 Accepted 27 November 2009 Keywords: Chemotherapy Docetaxel Molecular chemotherapy Purine nucleoside phosphorylase Gene directed pro-drug enzyme therapy Conditionally replicating adenovirus abstract Castrate resistant prostate cancer (CRPC) is essentially incurable. Recently though, chemo- therapy demonstrated a survival benefit (2 months) in the treatment of CRPC. While this was a landmark finding, suboptimal efficacy and systemic toxicities at the therapeutic doses warranted further development. Smart combination therapies, acting through multi- ple mechanisms to target the heterogeneous cell populations of PC and with potential for reduction in individual dosing, need to be developed. In that, targeted molecular chemo- therapy has generated significant interest with the potential for localized treatment to gen- erate systemic efficacy. This can be further enhanced through the use of oncolytic conditionally replicative adenoviruses (CRAds) to deliver molecular chemotherapy. The prospects of chemotherapy and molecular-chemotherapy as single and as components of combination therapies are discussed. Ó 2010 Elsevier Ireland Ltd. All rights reserved. 1. Prostate cancer: the current issues Despite high curative rates of localized prostate cancer (PC) with standard treatments, such as radical prostatecto- my and external beam radiation, one third of patients devel- op advanced PC [1] often with metastases. Initial androgen ablation therapy only provides short-term benefit (median treatment–response period of <30 months) with inadver- tent recurrence in a castrate-resistant state (CRPC), which is essentially incurable [2] (Fig. 1). Recently though, for the first time, chemotherapy showed activity against CRPC in a number of landmark trials; docetaxel treatment enhanced survival (by 2 months) in 40% of the patients [3,4]. How- ever, the issues of poor tissue-specificity and toxicity at clinical dosages remain significant hurdles. Currently, the best options to address this are through the development of PC-targeted biological therapies such as targeted gene therapies (via expression of therapeutic genes in transcrip- tionally and transductionally targeted vectors) and immu- notherapy (monoclonal antibodies, cytokines) [5]. However, given the complexity and the heterogeneity of CRPC (pathogenesis reviewed in [6]), there is no single all-encompassing therapeutic agent. Thus, a new paradigm whereby beneficial synergistic interactions of multimodal combined regimens can improve efficacy, patient manage- ment and quality of life, has emerged. Particularly for PC, combinations involving chemotherapy and molecular che- motherapy systems, e.g. gene-derived enzyme pro-drug therapy (GDEPT), have shown promise and are discussed in this review. 2. Chemotherapy and prostate cancer Prior to the 1980s, the use of chemotherapeutic agents for PC treatment was limited by the chemo-resistant 0304-3835/$ - see front matter Ó 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.canlet.2009.11.019 * Corresponding author. Address: Oncology Research Centre, Prince of Wales Hospital, Randwick, Sydney, NSW 2031, Australia. Fax: +61 02 93822629. E-mail address: [email protected] (A. Khatri). 1 Both authors have contributed equally to this manuscript. Cancer Letters 293 (2010) 1–14 Contents lists available at ScienceDirect Cancer Letters journal homepage: www.elsevier.com/locate/canlet
Transcript of Molecular and traditional chemotherapy: A united front against prostate cancer

Cancer Letters 293 (2010) 1–14
Contents lists available at ScienceDirect
Cancer Letters
journal homepage: www.elsevier .com/locate /canlet
Mini-review
Molecular and traditional chemotherapy: A united front againstprostate cancer
P. Singh c,1, M. Yam a,b,1, P.J. Russell a,b,d,e, A. Khatri a,b,*
a Oncology Research Centre, Prince of Wales Hospital, Randwick, Sydney, NSW 2031, Australiab Faculty of Medicine, University of New South Wales, Kensington, NSW 2036, Australiac Centre for Medicine and Oral Health, Griffith University – Gold Coast GH1, High Street, Southport, Gold Coast, QLD 4215, Australiad Australian Prostate Cancer Research Centre – Queensland, Princess Alexandra Hospital, Woollangabba, QLD, Australiae Institute of Health and Biomedical Innovation, Queensland University of Technology, 60 Musk Avenue, Kelvin Grove, QLD 4059, Australia
a r t i c l e i n f o a b s t r a c t
Article history:Received 29 October 2009Received in revised form 23 November 2009Accepted 27 November 2009
Keywords:ChemotherapyDocetaxelMolecular chemotherapyPurine nucleoside phosphorylaseGene directed pro-drug enzyme therapyConditionally replicating adenovirus
0304-3835/$ - see front matter � 2010 Elsevier Ireldoi:10.1016/j.canlet.2009.11.019
* Corresponding author. Address: Oncology ReseaWales Hospital, Randwick, Sydney, NSW 2031, Au93822629.
E-mail address: [email protected] (A. Khatri1 Both authors have contributed equally to this ma
Castrate resistant prostate cancer (CRPC) is essentially incurable. Recently though, chemo-therapy demonstrated a survival benefit (�2 months) in the treatment of CRPC. While thiswas a landmark finding, suboptimal efficacy and systemic toxicities at the therapeuticdoses warranted further development. Smart combination therapies, acting through multi-ple mechanisms to target the heterogeneous cell populations of PC and with potential forreduction in individual dosing, need to be developed. In that, targeted molecular chemo-therapy has generated significant interest with the potential for localized treatment to gen-erate systemic efficacy. This can be further enhanced through the use of oncolyticconditionally replicative adenoviruses (CRAds) to deliver molecular chemotherapy. Theprospects of chemotherapy and molecular-chemotherapy as single and as components ofcombination therapies are discussed.
� 2010 Elsevier Ireland Ltd. All rights reserved.
1. Prostate cancer: the current issues best options to address this are through the development
Despite high curative rates of localized prostate cancer(PC) with standard treatments, such as radical prostatecto-my and external beam radiation, one third of patients devel-op advanced PC [1] often with metastases. Initial androgenablation therapy only provides short-term benefit (mediantreatment–response period of <30 months) with inadver-tent recurrence in a castrate-resistant state (CRPC), whichis essentially incurable [2] (Fig. 1). Recently though, for thefirst time, chemotherapy showed activity against CRPC in anumber of landmark trials; docetaxel treatment enhancedsurvival (by �2 months) in 40% of the patients [3,4]. How-ever, the issues of poor tissue-specificity and toxicity atclinical dosages remain significant hurdles. Currently, the
and Ltd. All rights reserved.
rch Centre, Prince ofstralia. Fax: +61 02
).nuscript.
of PC-targeted biological therapies such as targeted genetherapies (via expression of therapeutic genes in transcrip-tionally and transductionally targeted vectors) and immu-notherapy (monoclonal antibodies, cytokines) [5].
However, given the complexity and the heterogeneityof CRPC (pathogenesis reviewed in [6]), there is no singleall-encompassing therapeutic agent. Thus, a new paradigmwhereby beneficial synergistic interactions of multimodalcombined regimens can improve efficacy, patient manage-ment and quality of life, has emerged. Particularly for PC,combinations involving chemotherapy and molecular che-motherapy systems, e.g. gene-derived enzyme pro-drugtherapy (GDEPT), have shown promise and are discussedin this review.
2. Chemotherapy and prostate cancer
Prior to the 1980s, the use of chemotherapeutic agentsfor PC treatment was limited by the chemo-resistant

Fig. 1. A flow schematic outlining the different treatments currently used at the various PC stages. Constructed using information sourced from [7–9].
2 P. Singh et al. / Cancer Letters 293 (2010) 1–14
nature of CRPC and the toxicities in aged patients. How-ever, new chemotherapeutic agents and novel combina-tion-regimens [10–12] have led to significant improvements.Following the success of a key clinical trial involving ad-vanced stage CRPC patients [13], the combination ofmitoxantrone with prednisone as a palliative standard forclinical care, was approved. Though not conferring any sur-vival advantage, it did establish that chemotherapy couldimprove clinical outcome in advanced stage CRPC. Sincethen, successful reduction of prostate specific antigen(PSA) levels and improved survival benefit establishedthe promise of docetaxel for treatment of CRPC [14].
2.1. Docetaxel as a monotherapy
In an early trial [14] involving 35 CRPC patients givendocetaxel (75 mg/m2 every 3 weeks), 46% displayed a de-cline in PSA greater than 50% with an objective responserate of 28% and median survival of 27 months. Subse-quently, another phase II trial [15] concluded that the low-er dose of docetaxel (36 mg/m2) following dexamethasoneinfusion did not compromise response rates, although tox-icity was decreased. Significantly though, a marginal sur-vival benefit in patients with CRPC was noted in TAX326[3] and SWOG9916 [4] trials, over a mitoxantrone plus ste-roids regimen. Since this was effective with no added tox-icity in patients >70 years [16], docetaxel and prednisone
as a first-line treatment for CRPC patients was approvedin 2004. A number of side effects including neutropenia, fa-tigue, dyspnoea, oncholysis and alopecia were reported,though, not requiring cessation of therapy or resulting indeath [14,17]. Whilst docetaxel-based drug regimens area significant milestone in systemic chemotherapy, themedian survival of these patients still remains at most18 months. Further, with the clinical heterogeneity of PC,therapeutic responses to docetaxel are also highly variable[18]. Thus, a clear need for improvement is recognized.
2.2. Docetaxel in combination with other therapies
Despite the success of docetaxel-therapy, significantroom for extending median survival and reducing side ef-fects exists. Consequently, its use in novel combinationswith other treatment modalities has been investigated.Strategically, agents with different cell-killing mechanismsto docetaxel are selected to maximize the potential forsynergy; an important consideration for PC, where variouscancer-cell subpopulations respond uniquely to differenttherapies. For example, molecular targeted therapeuticagents in combination with docetaxel have shown promis-ing results against different forms of PC; these includeangiogenesis [19,20] and EGFR inhibitors [21], vaccines[22] and anti-sense Bcl-2 oligodeoxynucleotides [23].Greatest clinical benefit, thus far, has been shown in com-

P. Singh et al. / Cancer Letters 293 (2010) 1–14 3
bination with the conventional chemotherapeutics, est-ramustine, prednisone and mitoxantrone [3,4] (TAX 327and SWOG 9916 trials). These were the first to demon-strate survival advantage in CRPC patients and hence, areexamined more closely below.
TAX327 compared docetaxel/prednisone (Table 1shows dosing schedule) with mitoxantrone/prednisone asa treatment for metastatic CRPC in an international, ran-domized phase III trial of 1006 patients [3]. A significant in-crease in median survival and 24% reduction in the hazardratio of death (p = 0.009) was demonstrated in the patientsfrom the 3-weekly docetaxel/prednisone treatment arm(18.9 months) compared with those given mitoxantrone/prednisone treatment (16.5 months). Correspondingly,clinically apparent improvements were also recorded inpatient pain response (35% vs. 22%; p = 0.01) and qualityof life (22% vs. 13%; p = 0.09).
Like 3-weekly docetaxel/prednisone treatment, thecombination of docetaxel with estramustine exhibited asurvival advantage over conventional mitoxantrone/pred-nisone regimen in the phase III SWOG 9916 study [4]. Pa-tients in the docetaxel/estramustine arm demonstrated anextension of median survival of 2 months, with a corre-sponding reduction in mortality risk of 20% (p = 0.01).However, these patients also exhibited higher rates ofnausea and vomiting, cardiovascular, neurologic and meta-bolic adverse events when compared with those from
Table 1Single agent and combination therapies involving docetaxel for the treatment of C
Type Docetaxel dose Other agent dose Stagstatu
Single agent (75 mg/m2q)b
every 3 wkscNAd Phas
II75 mg/m2qevery 3 wks
NA PhasII
36 mg/m2q/wkfor 6 of 8 wks
NA PhasII
36 mg/m2q/wkfor 6 of 8 wks
NA PhasII
35 mg/m2q/wkfor 6 of 8 wks
NA PhasII
Combinationtherapy
70 mg/m2qevery 3 wks
Estramustine 280 mg tdsf days 1–5 PhasII
70 mg/m2qevery 3 wks
Estramustine 280 mg tds days 1–5 + hydrocortisone 40 mg/day
PhasII
70 mg/m2qevery 3 wks
Estramustine 280 mg every 6 h � 5doses and Coumadin 2 mg daily
PhasII
TAX 327g 70 mg/m2qevery 3 wks
Prednisone 10 mg/day PhasIII
30 mg/m2q/wkfor 5 of 6 wks
Prednisone 10 mg/day
SWOGh 60 mg/m2qevery 3 wks
Estramustine 280 mg tds days 1–5 PhasIII
Information partially sourced from [47].a PSA response: decline in prostate specific antigen P 50%.b mg/m2q: milligram per meter square.c wks: weeks.d NA: not available.f tds: three times a day.g ASCO: American Society for Clinical Oncology.h SWOG: South West Oncology Group.
mitoxantrone/prednisone arm. Nevertheless, this combi-nation may be important in treatment of CRPC in diabeticpatients [24], who may not benefit from docetaxel/predni-sone treatment, or as a second line therapy in docetaxel-resistant CRPC patients [25]. However, due to their similarmechanisms of action, synergy with a third modality hasalso been explored, with improved cancer cell-killing, orrelief of pain and reduced bone fractures being the conclu-sions of many of these trials. The compounds studied in-clude hydrocortisone [26,27], prednisone [28,29],carboplatin [30,31], calcitriol [32], vinorelbine [33], cele-coxib [34], thalidomide [19], exisulind [35], enoxaparine[36] and zoledronic acid [37].
The success of these trials, has cemented docetaxel-based combination regimens as the standard of care forCRPC treatment. A combination of 3-weekly docetaxel plusprednisone has since been instigated as the standard treat-ment for CRPC patients [38].
Optimized drug scheduling to reduce the toxicity asso-ciated with higher doses of docetaxel has been the focus ofrecent preclinical research; for example an improvedunderstanding of the anti-angiogenic and cytotoxic prop-erties of metronomic docetaxel treatment [39] and itscombinations with 2-methoxyestradiol [40] and dexa-methasone [41] could aid these efforts tremendously.Further, treatments with greater tumour-specificity, thatspare host tissue, are needed to maximize the therapeutic
RPC patients.
e/s
Patients PSAresponse(%)a
Overallresponserate (%)
Mediansurvival(months)
Reference/year
e 35 46 24 27 1999 [14]
e 21 38 29 67% at15 months
1999 [42]
e 60 41 33 9.4 2001 [15]
e 25 46 40 9.7 2001 [43]
e 30 48 28 20 2003 [44]
e – 68 55 77% at 1 year 2000 [45]
e 47 68 50 20 2001 [26]
e 42 45 20 13.5 2002 [46]
e 1006 45 12 18.9 2004 [3]
48 8 17.3
e 770 50 17 18 2004 [4]

4 P. Singh et al. / Cancer Letters 293 (2010) 1–14
response. In this context, targeted gene therapy-based ap-proaches (alone and in combination) could play a signifi-cant role against PC (outlined in Fig. 2) [5]. Thesestrategies rely on the ability of vectors, usually given di-rectly into the primary tumour, to deliver the therapeuticgene. A number of viral and non-viral vectors have beenexplored in gene therapy; the advantages and disadvan-tages of which are outlined in Table 2.
3. Molecular-chemotherapy and prostate cancer
Given the recent success of chemotherapy against CRPC,molecular chemotherapy, engendered by GDEPT based ap-proaches has generated significant interest. Administeredlocally, GDEPT can potentially direct the toxicity of chemo-therapy specifically to the tumour cells, including those indistant locations. Prostate cancer is particularly suitable, asthe prostate is easily accessible for localized treatment andis not-essential for life.
Typically, a GDEPT system consists of two components:(1) a relatively non-toxic pro-drug (clinically relevant),administered systemically, and (2) the gene encoding anenzyme that converts the non-toxic pro-drug to its toxicmetabolites. The unique feature of these systems is the‘‘bystander effect” engendered by in situ spread of cytotox-icity beyond the transduced cell to surrounding and evendistant un-transduced cancer cells. The ‘‘bystander effect”is postulated to involve several mechanisms including dif-fusion of soluble toxic metabolites [48], dissemination of
Fig. 2. A schematic showing several gene therapy approaches explored for treAbbreviations: 1BRCA-1: breast cancer 1, early onset; 2Bcl-2: B-cell lymphoma 2;growth factor receptor 2; 5Bax: Bcl-2 associated X protein; 6HSV–tk/GVC: herpphosphorylase; 8CD/5FC: cytosine deaminase/5-fluorocytosine; 95FU:5-fluorou11NTR: nitroreductase; 12Ad: adenovirus; 13GM-CSF: granulocyte macrophage co16MHC-I: major histocompatibility complex-1; 17CTLA4: cytotoxic T-lymphocyte
apoptotic vesicles [49,50], transduction of endothelial cellsin tumour vessels [51] and stimulation of anti-tumour im-mune responses consisting of cytokines, natural-killer andT cells [52,53]. Thus, in contrast to most gene therapy ap-proaches, GDEPT systems can overcome the limitation oflow cell transduction efficiency and hence, have foundmore widespread applications in PC-targeted gene therapytrials.
For most pro-drug/enzyme combinations, the enzyme isof bacterial or viral origin to minimize the inadvertent hu-man enzyme mediated conversion of the pro-drug inuntargeted areas. This and other criteria defining the selec-tion of enzyme/pro-drug components have been examinedin a number of reviews [54,55].
Since the first successful trial in 1991 [56], severalGDEPT systems have been evaluated against cancers of co-lon, ovary, breast and liver, with varying degrees of suc-cess. By 2007, three of the 109 clinical trials evaluatingGDEPT that had been undertaken were at the phase IIIstage [57]. Unlike for traditional chemotherapy, these trialshave mainly been conducted in PC patients with newlydiagnosed or locally recurrent PC [58] with only a fewexceptions involving late stage PC patients [59]. Thus far,herpes simplex virus–thymidine kinase (HSV–tk) and cyto-sine deaminase (CD)-based GDEPT are the most exploredfor PC treatments and are discussed. The relatively newpurine nucleoside phosphorylase (PNP) GDEPT system pos-sesses a number of advantages that confer a greater futurepotential for its use against PC. Table 3 outlines the fea-
atment of PC and depicts potential combinations with other modalities.3KRAS: Kirsten rat sarcoma viral oncogene; 4Her-2 neu: human epidermales simplex virus-thymidine kinase/ganciclovir; 7PNP: purine nucleoside
racil; 10CDUPRT: cytosine deaminase uracil phosphoribosyl transferase;lony stimulating factor; 14TNF: tumour necrosis factor; 15IFN: interferon;antigen.

Table 2Advantages and disadvantages of different types of vectors used in gene therapy.
Type Advantages Disadvantages
Viral vectorsRetroviruses
(RNA virus)High transfection efficiency; stable integration leading tolong-term gene expression; infect hematopoietic andepithelial cells; absence of immunogenic viral proteins
Very unstable; low titer; integrate into the host cell genome soonly infect dividing cells; risk of malignant transformation inaffected cells due to integration into host genome; relativelysmall amount of genetic information (�9–12 kb)
Adenovirus (DNAvirus)
Well studied; high titer; stable and resistant to physical stress(e.g. freezing); non integrating, transient expression, sideeffects are less severe; infect epithelial cells at high frequency;higher packaging capacity; easy to engineer; infect dividingand non-dividing cells effectively, cellular proliferation notrequired
Immunogenic; potentially hepatotoxic; short term geneexpression as it does not integrate in host genome; virusneutralization with pre-existing antibodies
Adeno-associatedvirus
Stable; integrates into non-dividing cells at low frequency Small capacity for DNA; low titre; requires a helper virus
Herpes virus Infects a wide range of cell types; can achieve high titer; hasrelatively prolonged expression
No integration into genome of infected cells; cytotoxic;immunogenic; difficult to engineer/handle due to complexity;complex packaging system
Reovirus Infection limited to cells with activated ras pathway Not well characterized
Non-viral vectorsDNA cassettes Non-viral; easy to use and develop, can be used for sense and
anti-sense expressionLow efficiency of transfection in vivo; temporary expression,stability
Liposomes Non-viral, easy to develop Low frequency of modification, especially in vivo; cytotoxic tosome cell
Oligonucleotides Non-viral, small in size, potential use in RNA interference Low efficiency of transfection in vivo; temporary expression,stability
P. Singh et al. / Cancer Letters 293 (2010) 1–14 5
tures of the more widely tested non-mammalian enzyme/pro-drug combinations against PC (also reviewed in [60]).
3.1. Herpes simplex virus – thymidine kinase (HSV–tk) GDEPT
HSV–tk enzymatic conversion of the pro-drugs, ganciclo-vir (GCV), acyclovir (ACV) and valcyclovir (VCV), induces celldeath through apoptotic and non-apoptotic mechanisms(reviewed in [75]). Having shown its therapeutic effectsagainst PC in vitro and in vivo [61–64,76,77], the clinical effi-cacy and safety profile of the system has been assessed inseveral phase I and II trials. The toxicity of Adenovirus(Ad)-mediated HSV–tk/GCV was relatively low in patientswith clinically localized PC [64]; no grade 4 toxicities werereported and most other side effects resolved spontaneously.It was also deduced that tumour cell killing was mediated byanti-angiogenic effects, induction of local/systemic immuneresponses and stimulation of apoptosis. Other studies havedemonstrated that low host toxicity is maintained at higherAd-vector doses (up to 2 � 1012 viral particles) [58].
Overall though, clinical therapeutic effects of HSV–tkwere modest [78]. A phase I study in which an Ad-vectorwith osteocalcin promoter-driven HSV–tk was injected di-rectly into PC patient lymph nodes and bone metastases,resulted in limited efficacy due to suboptimal HSV–tkexpression and possibly due to the low tolerable doses ofGCV used (high doses cause bone marrow toxicity) [59].Thus, combination approaches have been explored to com-pensate for these shortfalls. Specifically, additional thera-peutic benefits have been achieved in preclinical andclinical studies when this therapy is combined with castra-tion [79], radiation therapy [80–82], immunotherapy [83–85] and virotherapy [83,86–89].
3.2. Cytosine deaminase (CD)–GDEPT
Similar success has been achieved using E. coli – oryeast-derived CD-based GDEPT, the second most widelyexploited GDEPT system. Here, tumour cell killing is fos-tered by CD-mediated conversion of 5-fluorocytosine (5-FC), into toxic 5-fluorouracil (5-FU), a potent inhibitor ofRNA and DNA synthesis. Both, 5-FC and 5-FU can passivelypenetrate tumour cells, thus propagating the local toxic ef-fects to non-transduced cells. This confers a significantadvantage over the cellular connexins (gap-junction)dependent HSV–tk system. Thus, when CD/5-FC GDEPTwas combined with HSV–tk GDEPT, greater therapeutic re-sponses were demonstrated, with tolerable, non-com-pounded toxicities [90]. In light of this, translation ofother novel combinations of suicide gene therapies to theclinic is a compelling idea. Particularly promising is thecombined use of CD and uracil phosphoribosyl transferase(UPRT), an enzyme which, unlike CD, converts 5-FC to 5-FUdirectly rather than through a series of intermediary stepsincluding the rate limiting production of 5-fluorouridinemonophosphate (5-FUMP) [66,67]. Used in conjunction,these two enzymes sensitize tumour cells to lower dosesof 5-FC. Thus, CDUPRT-GDEPT has been demonstrated tobe more effective than either GDEPT alone against DU145[68] and LNCaP human PC cells [91]. CDUPRT has also dem-onstrated efficacy and synergy with immuno-stimulatoryinterleukin (IL)-12 and IL-18 in RM1 mouse PC cells[66,92]. Enhanced efficacy of combinations involving othermodalities including irradiation have been translated tothe clinic, with success in using CD–GDEPT with irradia-tion, either alone or in combination with HSV–tk GDEPT[70,80].

Table 3GDEPT systems used in prostate cancer gene therapy.
Approach Pro-drug Toxicmetabolite
Type Advantages/disadvantages
HSV–tk1 Ganciclovir Ganciclovirtriphosphate
Antimetabolites � In clinical trials� Associated with significant local and distant
‘bystander effects’� Activated drug is an S-phase specific cytotoxin and
hence, effective on fast dividing cells only� Dependence on cell to cell based gap junctions or
apoptosis vesicles for ‘bystander effects’
[50,51,61–64] Acyclovir Acyclovirtriphosphate
Valacyclovir Valacyclovirtriphosphate
E.coli CDUPRT 2[65,68] 5-Fluorocytosine 5-Fluorouracil Antimetabolite � In clinical trials� Kills dividing and non-dividing cells� Pro-drug activity depends on further metabolism of
enzyme� Development of 5-FU resistance in some cancer cells� Higher toxicity of activated end product (long half life)
HSV–tk and E. coli CDUPRT(double suicide genetherapy)
Ganciclovir Ganciclovirtriphosphate
Antimetabolites � Double suicide gene therapy leads to enhanced cancercell killing without enhancing toxicity to non-targetorgans
[69,70] 5-Fluorocytosine 5-FluorouracilE. coli PNP3(refer to
table IV)6-Methylpurine-2’-deoxyriboside(MeP-dR)
6-Methylpurine(6-MEP)
Antimetabolites � Currently in a phase I clinical trial� Associated with strong ‘bystander effect’ and results
in killing of dividing as well non-dividing cancer cells� 6-MeP exhibits prolonged retention in situ
[60] FludarabinePhosphate
2-Flouroadenine
E. coli Nitroreductase CB1954 (5-aziridin-1-yl)-2,4-dinitrobenzamide
Hydroxylamines Alkylator � Preclinical� Forms DNA cross-links in both cycling and non-cycling
cells� Local and distant ‘bystander effects’� Distant bystander effect may also involve induction of
stress proteins, HSP25 and HSP70[71,72] 2-Nitrobenzyl
carbamatesCytochrome P450
(CYP) [73,74]Cyclophosphamide Phosphoramide
mustardAlkylator � Preclinical
� Moderate local ‘bystander effect’� Cell-killing mechanisms independent of cell-cycle
1 HSV–tk: herpes simplex virus-thymidine kinase.2 CDUPRT: cytosine deaminase uracil phosphoribosyl transferase.3 PNP: purine nucleoside phosphorylase.
6 P. Singh et al. / Cancer Letters 293 (2010) 1–14
3.3. Purine nucleoside phosphorylase (PNP)–GDEPT
In preclinical studies, PNP–GDEPT has exhibited po-tency against a range of cancer types, including PC. Derivedfrom E. coli, this PNP differs from its mammalian counter-part structurally and functionally (reviewed in [93,94]),and uniquely cleaves the pro-drugs, fludarabine-phosphate(Fludara) and 6-methylpurine 2-deoxyriboside (6-MePDR),to toxic metabolites with minimal unwanted toxicityin vivo. Concerns regarding pro-drug conversion by endog-enous PNP, expressed by intestinal bacteria flora, have alsobeen addressed through methods including crystallo-graphic/computer remodeling of the PNP enzyme and con-comitant antibiotic therapy [60]. In comparison to HSV–tkGDEPT, PNP-GDEPT mediates greater cell-killing due to amore extensive ‘‘bystander effect” [95,96].
In-fact, expression of less than 1% expression of PNP ledto near-complete cell killing in a human colon cancer cellline [97], augmented through passive diffusion of toxinsindependent of cell–cell junctions. The cytotoxic purinesproduced after pro-drug conversion disrupt both DNAand RNA synthesis [97], making PNP-GDEPT independentof cell-cycle status. This is particularly relevant to slowgrowing PC where only 2% of cancer cells in a tumour are
dividing [98]. Finally, PNP-GDEPT mediated apoptosis isp53-independent; as demonstrated through its efficacyagainst PC cell lines lacking (PC-3) [99] and containing wildtype p53 (LNCaP) [100]. Given the significance of p53 genemutations in early and late stage PC pathogenesis [101],PNP-GDEPT may be particularly useful in patients whosePC exhibits aberrant p53 expression.
Direct comparisons of PNP with GDEPT other than HSV–tk have not been reported thus far. With respect to PC, itsefficacy has been demonstrated using an ovine atadenovirus(now approved for a phase I trial) in androgen-dependentand CRPC xenografts in nude and immunocompromisedmice (Table 4). Significantly, suppression of PC progressionand improved survival was reported in transgenic adenocar-cinoma of mouse prostate (TRAMP) models, which mimicthe development of human PC [102].
While, its anticipated beneficial effects regardingsafety and efficacy, in the clinical setting, remain unsub-stantiated, in the clinical setting, however, based on thepromising indications from the preclinical data (Table 3)the first two clinical trials evaluating PNP-GDEPT havebeen approved (one against CRPC) and data from thesewill be valuable in determining the potential of this sys-tem [103].
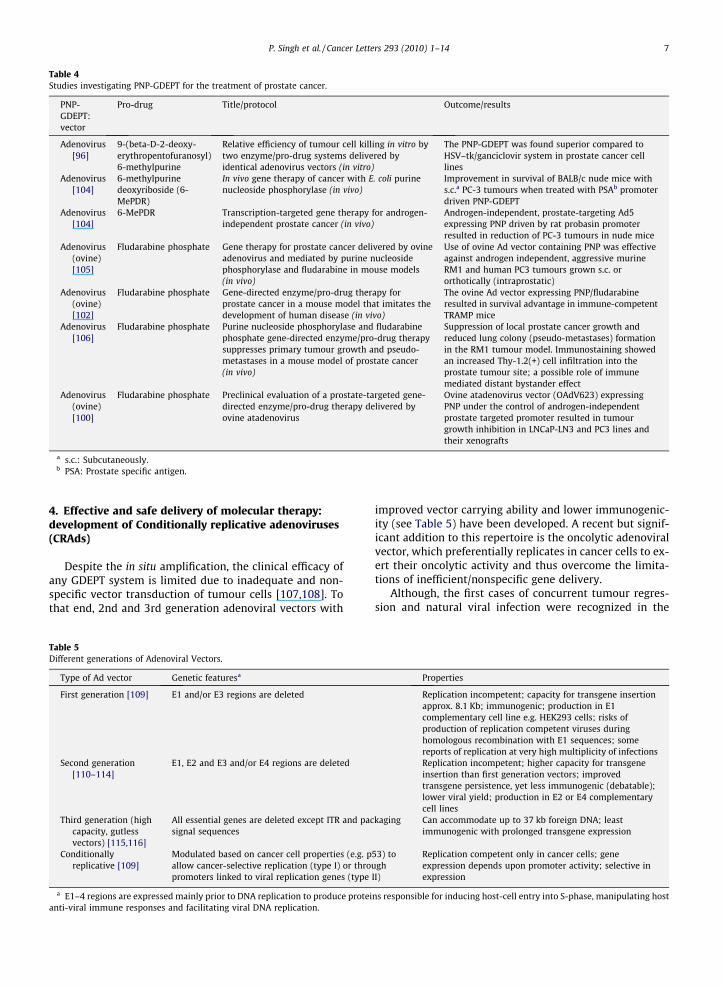
Table 4Studies investigating PNP-GDEPT for the treatment of prostate cancer.
PNP-GDEPT:vector
Pro-drug Title/protocol Outcome/results
Adenovirus[96]
9-(beta-D-2-deoxy-erythropentofuranosyl)6-methylpurine
Relative efficiency of tumour cell killing in vitro bytwo enzyme/pro-drug systems delivered byidentical adenovirus vectors (in vitro)
The PNP-GDEPT was found superior compared toHSV–tk/ganciclovir system in prostate cancer celllines
Adenovirus[104]
6-methylpurinedeoxyriboside (6-MePDR)
In vivo gene therapy of cancer with E. coli purinenucleoside phosphorylase (in vivo)
Improvement in survival of BALB/c nude mice withs.c.a PC-3 tumours when treated with PSAb promoterdriven PNP-GDEPT
Adenovirus[104]
6-MePDR Transcription-targeted gene therapy for androgen-independent prostate cancer (in vivo)
Androgen-independent, prostate-targeting Ad5expressing PNP driven by rat probasin promoterresulted in reduction of PC-3 tumours in nude mice
Adenovirus(ovine)[105]
Fludarabine phosphate Gene therapy for prostate cancer delivered by ovineadenovirus and mediated by purine nucleosidephosphorylase and fludarabine in mouse models(in vivo)
Use of ovine Ad vector containing PNP was effectiveagainst androgen independent, aggressive murineRM1 and human PC3 tumours grown s.c. ororthotically (intraprostatic)
Adenovirus(ovine)[102]
Fludarabine phosphate Gene-directed enzyme/pro-drug therapy forprostate cancer in a mouse model that imitates thedevelopment of human disease (in vivo)
The ovine Ad vector expressing PNP/fludarabineresulted in survival advantage in immune-competentTRAMP mice
Adenovirus[106]
Fludarabine phosphate Purine nucleoside phosphorylase and fludarabinephosphate gene-directed enzyme/pro-drug therapysuppresses primary tumour growth and pseudo-metastases in a mouse model of prostate cancer(in vivo)
Suppression of local prostate cancer growth andreduced lung colony (pseudo-metastases) formationin the RM1 tumour model. Immunostaining showedan increased Thy-1.2(+) cell infiltration into theprostate tumour site; a possible role of immunemediated distant bystander effect
Adenovirus(ovine)[100]
Fludarabine phosphate Preclinical evaluation of a prostate-targeted gene-directed enzyme/pro-drug therapy delivered byovine atadenovirus
Ovine atadenovirus vector (OAdV623) expressingPNP under the control of androgen-independentprostate targeted promoter resulted in tumourgrowth inhibition in LNCaP-LN3 and PC3 lines andtheir xenografts
a s.c.: Subcutaneously.b PSA: Prostate specific antigen.
P. Singh et al. / Cancer Letters 293 (2010) 1–14 7
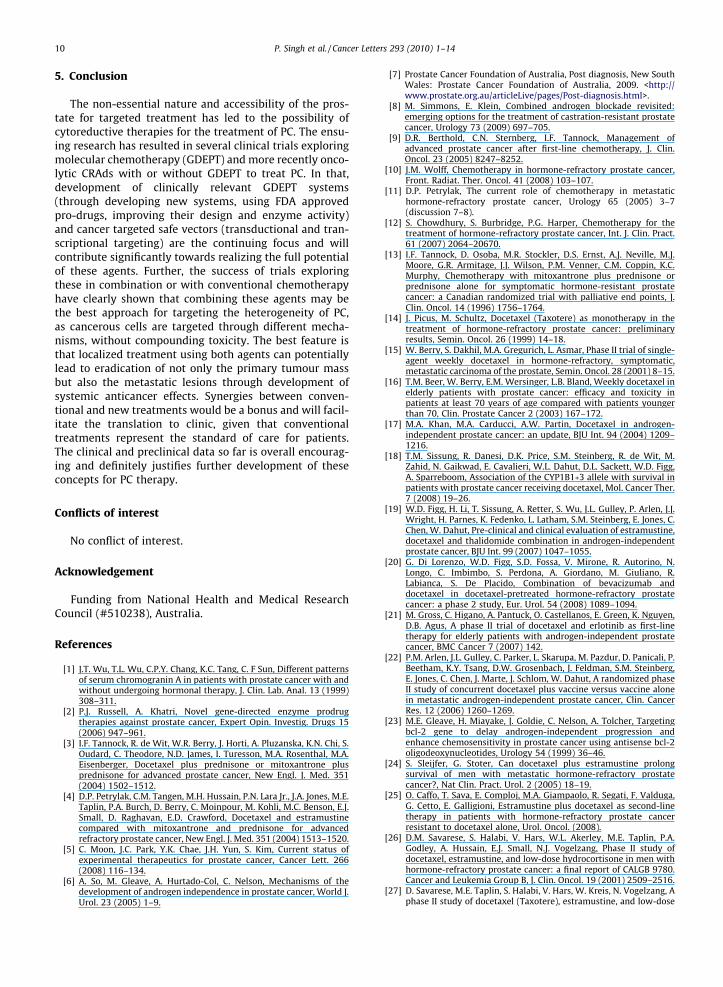
4. Effective and safe delivery of molecular therapy:development of Conditionally replicative adenoviruses(CRAds)
Despite the in situ amplification, the clinical efficacy ofany GDEPT system is limited due to inadequate and non-specific vector transduction of tumour cells [107,108]. Tothat end, 2nd and 3rd generation adenoviral vectors with
Table 5Different generations of Adenoviral Vectors.
Type of Ad vector Genetic featuresa
First generation [109] E1 and/or E3 regions are deleted
Second generation[110–114]
E1, E2 and E3 and/or E4 regions are deleted
Third generation (highcapacity, gutlessvectors) [115,116]
All essential genes are deleted except ITR and pacsignal sequences
Conditionallyreplicative [109]
Modulated based on cancer cell properties (e.g. pallow cancer-selective replication (type I) or throupromoters linked to viral replication genes (type
a E1–4 regions are expressed mainly prior to DNA replication to produce proteianti-viral immune responses and facilitating viral DNA replication.
improved vector carrying ability and lower immunogenic-ity (see Table 5) have been developed. A recent but signif-icant addition to this repertoire is the oncolytic adenoviralvector, which preferentially replicates in cancer cells to ex-ert their oncolytic activity and thus overcome the limita-tions of inefficient/nonspecific gene delivery.
Although, the first cases of concurrent tumour regres-sion and natural viral infection were recognized in the
Properties
Replication incompetent; capacity for transgene insertionapprox. 8.1 Kb; immunogenic; production in E1complementary cell line e.g. HEK293 cells; risks ofproduction of replication competent viruses duringhomologous recombination with E1 sequences; somereports of replication at very high multiplicity of infectionsReplication incompetent; higher capacity for transgeneinsertion than first generation vectors; improvedtransgene persistence, yet less immunogenic (debatable);lower viral yield; production in E2 or E4 complementarycell lines
kaging Can accommodate up to 37 kb foreign DNA; leastimmunogenic with prolonged transgene expression
53) togh
II)
Replication competent only in cancer cells; geneexpression depends upon promoter activity; selective inexpression
ns responsible for inducing host-cell entry into S-phase, manipulating host

Table 6Some examples of transductional modifications incorporated into adenoviral vectors for gene therapy of prostate cancer.
Method of transductionalmodification
Transductional modification Vector Transgene Status Reference
Bispecific antibodies Conjugate of an anti-adenovirus fiber knob Fab-fragment and aPSMAa monoclonal antibody
Adenovirus eGFPb In vitro [120]
Conjugate of monoclonal anti-adenovirus knob and an anti-FGFc
antibodyAdenovirus LacZd In vitro [121]
Conjugate of monoclonal anti-adenovirus knob and an anti-alpha-323e
Adenovirus LacZ In vitro [121]
Genetic Retargeting Capsids modified to contain Ad serotype 3/5 chimeric knob Adenovirus Luc1f In vitro [122]Incorporation of recombinant RGDg fiber Adenovirus Delta-24h In vitro [123]
a PSMA: prostate specific membrane antigen.b eGFP: enhanced green fluorescent proteins.c FGF: fibroblast growth factor.d LacZ: beta-galactosidase.e anti-alpha-323: antibody against EpCAM (epithelial cell adhesion molecule).f Luc1: Luciferase1.g RGD: Arg-Gly-Asp sequence.h delta-24: CRAd with partial deletion of E1 region.
8 P. Singh et al. / Cancer Letters 293 (2010) 1–14
mid 19th century [117] interest in their use for cancertherapy was reignited in 1990s. Significant progress hasbeen made since then and several viruses are being evalu-ated in the clinic. The specificity and safety of these vectorsis achieved through: (1) capitalising on their biologicalfeatures that restrict replication to cancer cells only e.g.cancer cells that show aberrant expression of p53 will sup-port the replication of ONYX-015 virus [118,119] and/or,(2) through genetic modification to target these transduc-tionally (changed viral tropism) and/or transcriptionally(replication/gene-expression regulated by cancer specificpromoters) to the cancer cells e.g. conditionally replicatingAds (CRAds). (Table 6 outlines the specific transductionalmodifications and Table 7 lists promoters investigated forPC targeting.) The CRAd based approaches have been themost explored for PC in the clinic [109]. The concept is toutilize these either as an alternative or adjunct to GDEPTbased applications.
A phase I trial in twenty patients, of CV706, a CRAd withPSA selectivity reported significant reductions in PSA levels[160] with no significant adverse events. Similar levels ofsafety and efficacy were evident in phase I/II trials of CRAdCG7870 with different elements regulated by prostate-spe-cific, rat probasin and PSA promoters [160]. Promoters de-rived from the prostate specific membrane antigen (PSMA)gene specifically delivered suicide gene therapy to PC le-sions [161]. Unfortunately, these, like most other promot-ers, are active only in androgen-dependent PC. However,there has been progress with the use of osteocalcin pro-moter and the novel chimeric promoter, prostate specificenhancer sequence (PSES). Both of these demonstratedspecificity in androgen dependent and CRPC xenografts[38]. Though, limited spread of the CRAd, under PSES pro-moter control resulted in incomplete tumour eradication,thus, highlighting the need for improvement in these pro-moters/vectors.
4.1. CRAds in combination with other modalities
Use of oncolytic viral vectors may be particularly wellsuited in combination therapies as they are able to killapoptosis-resistant cancer cells [162]. Thus, if armed with
a cytotoxic gene these could further enhance the in situefficacy of treatment through enhanced vector penetrationwithin the tumour mass, which could be of particular sig-nificance against solid tumours such as PC. This factor to-gether with the modest outcomes of the clinical trials,has led to the investigation of CRAds in combination withother therapies. For PC, synergy has been demonstratedin clinical trials with radiation therapy and the CD andHSV–tk GDEPT systems [163,164]. Concurrent use of che-motherapy with oncolytic viruses for the treatment of PChas been the subject of several investigative studies. Onesuch animal study [165] analysed prostate specific CRAd(CV787) in combination with paclitaxel and docetaxeland demonstrated synergistic anti-tumour activity withno increase in toxicity. Indeed, a 1000-fold decrease invirus dose was effective in the combination compared withcontrols. Importantly, animals given the combinationtreatment displayed better health (body weight) comparedwith those given individual treatments. Similarly, tumour-targeted Ad OAS403 combined with doxorubicin in aLNCaP prostate tumour model significantly improved uponresponses recorded for either therapy alone [166].
As mentioned earlier, the concept of CRAds armed withGDEPT has generated great clinical interest with promisingresults from clinical trials evaluating CRAds armed withHSV–tk and CD genes. In patients with intermediate tohigh risk PC (phase I trial), use of CRAds equipped withboth CD and HSV–tk was efficacious and safe [80]. A five-year follow-up of patients given a similar regimen demon-strated an improvement in the PSA-doubling time, whichdelayed the need for salvage androgen suppression – oftenassociated with high morbidity [167]. This trial provides asignificant proof that combination CRAd and molecularchemotherapy has the potential to provide long-termbenefit to patients, with acceptable toxicity. Further tothat, recently, two phase I trials established the feasibilityand safety of a CRAd/radiation therapy combination in PCpatients [163], viral replication was not impaired. Giventhat CRPC patients usually receive radiation and/or chemo-therapy at the time of treatment, such synergistic interac-tions between CRAds and these standard therapies haveadded clinical relevance.

Table 7Promoters used for gene therapy of prostate cancer.
Promoter Vector Transgene Status Reference
Osteocalcin Adenovirus HSV–tk1 phase I/II [59,124]Adenovirus HSV–tk In vitro/in vivo [125,126]Adenovirus E1a (CRAd2) In vitro/in vivo [127]Plasmid (iNOS3) In vitro [128]
PSE-BC Lentivirus eGFP4/Luc5 In vitro/in vivo [129,130]PSMA6 Adenovirus eGFP/CD7 In vitro [131]
Adenovirus eGFP/CDUPRT 8 In vitro/in vivo [91]PSME9 Adenovirus Luc In vitro/in vivo [132]
Adenovirus E1A (CRAd) In vitro/in vivo [133]M6 Adenovirus HSV–tk In vitro/in vivo [134]Rat Probasin, PSA10 Adenovirus eGFP-CAT 11 In vitro [135]ARR(2)PB12 Adenovirus CAT/ Bax13 and Bad14 (pro-apoptotic) In vivo [136]
Lentivirus eGFP/HSV–tk In vitro [137]PSA Lentivirus eGFP/Diptheria Toxin A In vitro/in vivo [138]
Adenovirus HSV–tk In vivo (dogs) [139]Rat Probasin Adenovirus PNP15 In vitro/in vivo [140]Rat Probasin (Pb4) plus
PSME enhancerAdenovirus PNP In vitro/in vivo [100]
PEG-316 Adenovirus eGFP/p53/mda717/ IL-2418 In vitro/in vivo [141]COX-219 Plasmid/ poly-
ethylenimineGFP/Caspase-3 and 9 In vitro [142]
HTERT 20 Adenovirus E1A (CRAd) In vitro [143]Adenovirus E1A (CRAd) In vitro/in vivo [144]Adenovirus E1A (CRAd) and GFP under CMV
promoter in E3 regionIn vitro [145]
Adenovirus GFP/E1A (CRAd) In vitro/in vivo [146]Adenovirus HSV–tk In vivo [147]Retrovirus CXCR421 small hairpin RNA22 In vitro/in vivo [148]Plasmid NAT 23 In vitro [149]
VEGFR224 Adenovirus Caspase 9 In vitro [150]GDEP25 Plasmid In vitro [151]PC-126 Plasmid Luciferase In vitro [152]TARP27 Adenovirus Luciferase In vitro/in vivo [153]Synthetic beta-catenin-
dependent promoterAdenovirus LacZ28 Primary cultures (patient
samples)[154]
PSP9429 Plasmid LacZ In vivo [155]Uroplakin II Adenovirus E1 In vitro (LNCap) [156]Kallikrein 2 Adenovirus eGFP In vitro/in vivo [157]Caveolin-1 Adenovirus HSV–tk In vitro/in vivo [158]Survivin Plasmid GFP In vitro [159]
1 HSV–tk: herpes simplex virus–thymidine kinase.2 CRAd: conditionally replicative adenovirus.3 iNOS: nitric oxide synthase.4 eGFP: enhanced green fluorescent proteins.5 Luc: luciferase.6 PSMA: prostate specific membrane antigen.7 CD: cytosine deaminase.8 CDUPRT: cytosine deaminase uracil phosphoribosyl transferase.9 PSME: PSMA enhancer.
10 PSA: prostate specific antigen.11 CAT: chloramphenicol acetyltransferase.12 ARR(2)PB: androgen response region (2) probasin.13 Bax: Bcl-2 associated X promoter.14 Bad: Bcl-2 associated death promoter.15 PNP: purine nucleoside phosphorylase.16 PEG-3: progression-elevated gene-3.17 mda7: melanoma differentiation associated gene 7.18 IL-24: interleukin-24.19 COX-2: cyclooxygenase-2.20 HTERT: human telomerase reverse transcriptase.21 CXCR4: chemokine receptor 4.22 RNA: ribonucleic acid.23 NAT: nor-adrenaline transporter.24 VEGFR: vascular endothelial growth factor receptor-2.25 GDEP: gene differentially expressed in prostate cancer.26 PC-1: prostate and colon gene-1.27 TARP: T cell receptor gamma-chain alternate reading frame protein.28 LacZ: beta-galactosidase.29 PSP94: prostate secretory protein of 94 amino acids.
P. Singh et al. / Cancer Letters 293 (2010) 1–14 9
10 P. Singh et al. / Cancer Letters 293 (2010) 1–14
5. Conclusion
The non-essential nature and accessibility of the pros-tate for targeted treatment has led to the possibility ofcytoreductive therapies for the treatment of PC. The ensu-ing research has resulted in several clinical trials exploringmolecular chemotherapy (GDEPT) and more recently onco-lytic CRAds with or without GDEPT to treat PC. In that,development of clinically relevant GDEPT systems(through developing new systems, using FDA approvedpro-drugs, improving their design and enzyme activity)and cancer targeted safe vectors (transductional and tran-scriptional targeting) are the continuing focus and willcontribute significantly towards realizing the full potentialof these agents. Further, the success of trials exploringthese in combination or with conventional chemotherapyhave clearly shown that combining these agents may bethe best approach for targeting the heterogeneity of PC,as cancerous cells are targeted through different mecha-nisms, without compounding toxicity. The best feature isthat localized treatment using both agents can potentiallylead to eradication of not only the primary tumour massbut also the metastatic lesions through development ofsystemic anticancer effects. Synergies between conven-tional and new treatments would be a bonus and will facil-itate the translation to clinic, given that conventionaltreatments represent the standard of care for patients.The clinical and preclinical data so far is overall encourag-ing and definitely justifies further development of theseconcepts for PC therapy.
Conflicts of interest
No conflict of interest.
Acknowledgement
Funding from National Health and Medical ResearchCouncil (#510238), Australia.
References
[1] J.T. Wu, T.L. Wu, C.P.Y. Chang, K.C. Tang, C. F Sun, Different patternsof serum chromogranin A in patients with prostate cancer with andwithout undergoing hormonal therapy, J. Clin. Lab. Anal. 13 (1999)308–311.
[2] P.J. Russell, A. Khatri, Novel gene-directed enzyme prodrugtherapies against prostate cancer, Expert Opin. Investig. Drugs 15(2006) 947–961.
[3] I.F. Tannock, R. de Wit, W.R. Berry, J. Horti, A. Pluzanska, K.N. Chi, S.Oudard, C. Theodore, N.D. James, I. Turesson, M.A. Rosenthal, M.A.Eisenberger, Docetaxel plus prednisone or mitoxantrone plusprednisone for advanced prostate cancer, New Engl. J. Med. 351(2004) 1502–1512.
[4] D.P. Petrylak, C.M. Tangen, M.H. Hussain, P.N. Lara Jr., J.A. Jones, M.E.Taplin, P.A. Burch, D. Berry, C. Moinpour, M. Kohli, M.C. Benson, E.J.Small, D. Raghavan, E.D. Crawford, Docetaxel and estramustinecompared with mitoxantrone and prednisone for advancedrefractory prostate cancer, New Engl. J. Med. 351 (2004) 1513–1520.
[5] C. Moon, J.C. Park, Y.K. Chae, J.H. Yun, S. Kim, Current status ofexperimental therapeutics for prostate cancer, Cancer Lett. 266(2008) 116–134.
[6] A. So, M. Gleave, A. Hurtado-Col, C. Nelson, Mechanisms of thedevelopment of androgen independence in prostate cancer, World J.Urol. 23 (2005) 1–9.
[7] Prostate Cancer Foundation of Australia, Post diagnosis, New SouthWales: Prostate Cancer Foundation of Australia, 2009. <http://www.prostate.org.au/articleLive/pages/Post-diagnosis.html>.
[8] M. Simmons, E. Klein, Combined androgen blockade revisited:emerging options for the treatment of castration-resistant prostatecancer, Urology 73 (2009) 697–705.
[9] D.R. Berthold, C.N. Sternberg, I.F. Tannock, Management ofadvanced prostate cancer after first-line chemotherapy, J. Clin.Oncol. 23 (2005) 8247–8252.
[10] J.M. Wolff, Chemotherapy in hormone-refractory prostate cancer,Front. Radiat. Ther. Oncol. 41 (2008) 103–107.
[11] D.P. Petrylak, The current role of chemotherapy in metastatichormone-refractory prostate cancer, Urology 65 (2005) 3–7(discussion 7–8).
[12] S. Chowdhury, S. Burbridge, P.G. Harper, Chemotherapy for thetreatment of hormone-refractory prostate cancer, Int. J. Clin. Pract.61 (2007) 2064–20670.
[13] I.F. Tannock, D. Osoba, M.R. Stockler, D.S. Ernst, A.J. Neville, M.J.Moore, G.R. Armitage, J.J. Wilson, P.M. Venner, C.M. Coppin, K.C.Murphy, Chemotherapy with mitoxantrone plus prednisone orprednisone alone for symptomatic hormone-resistant prostatecancer: a Canadian randomized trial with palliative end points, J.Clin. Oncol. 14 (1996) 1756–1764.
[14] J. Picus, M. Schultz, Docetaxel (Taxotere) as monotherapy in thetreatment of hormone-refractory prostate cancer: preliminaryresults, Semin. Oncol. 26 (1999) 14–18.
[15] W. Berry, S. Dakhil, M.A. Gregurich, L. Asmar, Phase II trial of single-agent weekly docetaxel in hormone-refractory, symptomatic,metastatic carcinoma of the prostate, Semin. Oncol. 28 (2001) 8–15.
[16] T.M. Beer, W. Berry, E.M. Wersinger, L.B. Bland, Weekly docetaxel inelderly patients with prostate cancer: efficacy and toxicity inpatients at least 70 years of age compared with patients youngerthan 70, Clin. Prostate Cancer 2 (2003) 167–172.
[17] M.A. Khan, M.A. Carducci, A.W. Partin, Docetaxel in androgen-independent prostate cancer: an update, BJU Int. 94 (2004) 1209–1216.
[18] T.M. Sissung, R. Danesi, D.K. Price, S.M. Steinberg, R. de Wit, M.Zahid, N. Gaikwad, E. Cavalieri, W.L. Dahut, D.L. Sackett, W.D. Figg,A. Sparreboom, Association of the CYP1B1�3 allele with survival inpatients with prostate cancer receiving docetaxel, Mol. Cancer Ther.7 (2008) 19–26.
[19] W.D. Figg, H. Li, T. Sissung, A. Retter, S. Wu, J.L. Gulley, P. Arlen, J.J.Wright, H. Parnes, K. Fedenko, L. Latham, S.M. Steinberg, E. Jones, C.Chen, W. Dahut, Pre-clinical and clinical evaluation of estramustine,docetaxel and thalidomide combination in androgen-independentprostate cancer, BJU Int. 99 (2007) 1047–1055.
[20] G. Di Lorenzo, W.D. Figg, S.D. Fossa, V. Mirone, R. Autorino, N.Longo, C. Imbimbo, S. Perdona, A. Giordano, M. Giuliano, R.Labianca, S. De Placido, Combination of bevacizumab anddocetaxel in docetaxel-pretreated hormone-refractory prostatecancer: a phase 2 study, Eur. Urol. 54 (2008) 1089–1094.
[21] M. Gross, C. Higano, A. Pantuck, O. Castellanos, E. Green, K. Nguyen,D.B. Agus, A phase II trial of docetaxel and erlotinib as first-linetherapy for elderly patients with androgen-independent prostatecancer, BMC Cancer 7 (2007) 142.
[22] P.M. Arlen, J.L. Gulley, C. Parker, L. Skarupa, M. Pazdur, D. Panicali, P.Beetham, K.Y. Tsang, D.W. Grosenbach, J. Feldman, S.M. Steinberg,E. Jones, C. Chen, J. Marte, J. Schlom, W. Dahut, A randomized phaseII study of concurrent docetaxel plus vaccine versus vaccine alonein metastatic androgen-independent prostate cancer, Clin. CancerRes. 12 (2006) 1260–1269.
[23] M.E. Gleave, H. Miayake, J. Goldie, C. Nelson, A. Tolcher, Targetingbcl-2 gene to delay androgen-independent progression andenhance chemosensitivity in prostate cancer using antisense bcl-2oligodeoxynucleotides, Urology 54 (1999) 36–46.
[24] S. Sleijfer, G. Stoter, Can docetaxel plus estramustine prolongsurvival of men with metastatic hormone-refractory prostatecancer?, Nat Clin. Pract. Urol. 2 (2005) 18–19.
[25] O. Caffo, T. Sava, E. Comploj, M.A. Giampaolo, R. Segati, F. Valduga,G. Cetto, E. Galligioni, Estramustine plus docetaxel as second-linetherapy in patients with hormone-refractory prostate cancerresistant to docetaxel alone, Urol. Oncol. (2008).
[26] D.M. Savarese, S. Halabi, V. Hars, W.L. Akerley, M.E. Taplin, P.A.Godley, A. Hussain, E.J. Small, N.J. Vogelzang, Phase II study ofdocetaxel, estramustine, and low-dose hydrocortisone in men withhormone-refractory prostate cancer: a final report of CALGB 9780.Cancer and Leukemia Group B, J. Clin. Oncol. 19 (2001) 2509–2516.
[27] D. Savarese, M.E. Taplin, S. Halabi, V. Hars, W. Kreis, N. Vogelzang, Aphase II study of docetaxel (Taxotere), estramustine, and low-dose

P. Singh et al. / Cancer Letters 293 (2010) 1–14 11
hydrocortisone in men with hormonerefractory prostate cancer:preliminary results of cancer and leukemia group B Trial 9780,Semin. Oncol. 26 (1999) 39–44.
[28] A. Boehmer, A.G. Anastasiadis, S. Feyerabend, U. Nagele, M. Kuczyk,D. Schilling, S. Corvin, A.S. Merseburger, A. Stenzl, Docetaxel,estramustine and prednisone for hormone-refractory prostatecancer: a single-center experience, Anticancer Res. 25 (2005)4481–4486.
[29] S. Oudard, E. Banu, P. Beuzeboc, E. Voog, L.M. Dourthe, A.C. Hardy-Bessard, C. Linassier, F. Scotte, A. Banu, Y. Coscas, F. Guinet, M.F.Poupon, J.M. Andrieu, Multicenter randomized phase II study oftwo schedules of docetaxel, estramustine, and prednisone versusmitoxantrone plus prednisone in patients with metastatichormonerefractory prostate cancer, J. Clin. Oncol. 23 (2005)3343–3351.
[30] N. Kikuno, S. Urakami, S. Nakamura, T. Hiraoka, T. Hyuga, N. Arichi,K. Wake, M. Sumura, T. Yoneda, H. Kishi, K. Shigeno, H. Shiina, M.Igawa, Phase-II study of docetaxel, estramustine phosphate, andcarboplatin in patients with hormone-refractory prostate cancer,Eur. Urol. 51 (2007) 1252–1258.
[31] W.K. Oh, S. Halabi, W.K. Kelly, C. Werner, P.A. Godley, N.J.Vogelzang, E.J. Small, A phase II study of estramustine, docetaxel,and carboplatin with granulocyte-colonystimulating factor supportin patients with hormone-refractory prostate carcinoma: Cancerand Leukemia Group B 99813, Cancer 98 (2003) 2592–2598.
[32] N.M. Tiffany, C.W. Ryan, M. Garzotto, E.M. Wersinger, T.M. Beer,High dose pulse calcitriol, docetaxel and estramustine for androgenindependent prostate cancer: a phase I/II study, J. Urol. 174 (2005)888–892.
[33] N.M. Hahn, S. Marsh, W. Fisher, R. Langdon, R. Zon, M. Browning, C.S.Johnson, T.J. Scott-Horton, L. Li, H.L. McLeod, C.J. Sweeney, HoosierOncology Group randomized phase II study of docetaxel, vinorelbine,and estramustine in combination in hormonerefractory prostatecancer with pharmacogenetic survival analysis, Clin. Cancer Res. 12(2006) 6094–6099.
[34] J. Carles, A. Font, B. Mellado, M. Domenech, E. Gallardo, J.L.Gonzalez-Larriba, G. Catalan, J. Alfaro, A. Gonzalez Del Alba, M.Nogue, P. Lianes, J.M. Tello, Weekly administration of docetaxel incombination with estramustine and celecoxib in patients withadvanced hormone-refractory prostate cancer: final results from aphase II study, Brit. J. Cancer 97 (2007) 1206–1210.
[35] N.A. Dawson, S. Halabi, S.S. Ou, D.D. Biggs, A. Kessinger, N.Vogelzang, G.H. Clamon, D.M. Nanus, W.K. Kelly, E.J. Small, Aphase II study of estramustine, docetaxel, and exisulind in patientswith hormone-refractory prostate cancer: results of cancer andleukemia group B trial 90004, Clin. Genitourin Cancer 6 (2008)110–116.
[36] A. Gonzalez-Martin, E. Fernandez, M.A. Vaz, J. Burgos, M. LopezGarcia, R. Rodriguez Patron, C. Guillen, T. Mayayo, A. Allona, F. Arias,A. Moyano, Long-term outcome of a phase II study of weeklydocetaxel with a short course of estramustine and enoxaparine inhormone-resistant prostate cancer patients, Clin. Transl. Oncol. 9(2007) 323–328.
[37] J.G. Kattan, F.S. Farhat, G.Y. Chahine, F.L. Nasr, W.T. Moukadem, F.C.Younes, N.J. Yazbeck, M.G. Ghosn, Weekly docetaxel, zoledronicacid and estramustine in hormonerefractory prostate cancer(HRPC), Invest. New Drugs 26 (2008) 75–79.
[38] L. Moser, M. Schostak, K. Miller, W. Hinkelbein, Controversies in thetreatment of prostate cancer, Front. Radiat. Ther. Oncol. 41 (2008)103–107.
[39] R. Benelli, S. Monteghirfo, C. Balbi, P. Barboro, N. Ferrari, Novelantivascular efficacy of metronomic docetaxel therapy in prostatecancer: hnRNP K as a player, Int. J. Cancer 124 (2009) 2989–2996.
[40] T. Reiner, A. de las Pozas, L.A. Gomez, C. Perez-Stable, Low dosecombinations of 2-methoxyestradiol and docetaxel block prostatecancer cells in mitosis and increase apoptosis, Cancer Lett. 276(2009) 21–31.
[41] C. Wilson, P. Scullin, J. Worthington, A. Seaton, P. Maxwell, D.O’Rourke, P.G. Johnston, S.R. McKeown, Dexamethasone potentiatesthe antiangiogenic activity of docetaxel in castration-resistantprostate cancer, Brit. J. Cancer 99 (2008) 2054–2064.
[42] D. Friedland, J. Cohen, R. Miller Jr., M. Voloshin, R. Gluckman, B.Lembersky, B. Zidar, M. Keating, N. Reilly, B. Dimitt, A phase II trialof docetaxel (Taxotere) in hormonerefractory prostate cancer:correlation of antitumor effect to phosphorylation of Bcl-2, Semin.Oncol. 26 (1999) 19–23.
[43] T.M. Beer, W.C. Pierce, B.A. Lowe, W.D. Henner, Phase II study ofweekly docetaxel in symptomatic androgen-independent prostatecancer, Ann. Oncol. 12 (2001) 1273–1279.
[44] G. Gravis, F. Bladou, N. Salem, G. Macquart-Moulin, G. Serment, J.Camerlo, D. Genre, V.J. Bardou, D. Maraninchi, P. Viens, Weeklyadministration of docetaxel for symptomatic metastatic hormone-refractory prostate carcinoma, Cancer 98 (2003) 1627–1634.
[45] D.P. Petrylak, Docetaxel (Taxotere) in hormone-refractory prostatecancer, Semin. Oncol. 27 (2000) 24–29.
[46] V.J. Sinibaldi, M.A. Carducci, S. Moore-Cooper, M. Laufer, M.Zahurak, M.A. Eisenberger, Phase II evaluation of docetaxel plusone-day oral estramustine phosphate in the treatment of patientswith androgen independent prostate carcinoma, Cancer 94 (2002)1457–1465.
[47] A. Mancuso, S. Oudard, C.N. Sternberg, Effective chemotherapy forhormone-refractory prostate cancer (HRPC): present status andperspectives with taxane-based treatments, Crit. Rev. Oncol.Hematol. 61 (2007) 176–185.
[48] J.A. Bridgewater, R.J. Knox, J.D. Pitts, M.K. Collins, C.J. Springer, Thebystander effect of the nitroreductase/CB1954 enzyme/prodrugsystem is due to a cell-permeable metabolite, Hum. Gene Ther. 8(1997) 709–717.
[49] I. Kunishige, Y. Samejima, A. Moriyama, F. Saji, Y. Murata, cAMPstimulates the bystander effect in suicide gene therapy of humanchoriocarcinoma, Anticancer Res. 18 (1998) 3411–3419.
[50] S.M. Freeman, J.A. Zwiebel, Gene therapy of cancer, Cancer Invest.11 (1993) 676–688.
[51] Z. Ram, S. Walbridge, T. Shawker, K.W. Culver, R.M. Blaese, E.H.Oldfield, The effect of thymidine kinase transduction andganciclovir therapy on tumor vasculature and growth of 9Lgliomas in rats, J. Neurosurg. 81 (1994) 256–260.
[52] S.M. Freeman, R. Ramesh, M. Shastri, A. Munshi, A.K. Jensen,A.J. Marrogi, The role of cytokines in mediating the bystandereffect using HSV–tk xenogeneic cells, Cancer Lett. 92 (1995)167–174.
[53] S. Gagandeep, R. Brew, B. Green, S.E. Christmas, D. Klatzmann, G.J.Poston, A.R. Kinsella, Prodrug-activated gene therapy: involvementof an immunological component in the ‘‘bystander effect”, CancerGene Ther. 3 (1996) 83–88.
[54] I. Niculescu-Duvaz, C.J. Springer, Introduction to the background,principles, and state of the art in suicide gene therapy, Mol.Biotechnol. 30 (2005) 71–88.
[55] A.T. Silva, M.C. Chung, L.F. Castro, R.V. Guido, E.I. Ferreira, Advancesin prodrug design, Mini Rev. Med. Chem. 5 (2005) 893–914.
[56] K.W. Culver, W.R. Osborne, A.D. Miller, T.A. Fleisher, M. Berger, W.F.Anderson, R.M. Blaese, Correction of ADA deficiency in human Tlymphocytes using retroviral-mediated gene transfer, Transplant.Proc. 23 (1991) 170–171.
[57] John Wiley and Sons Ltd., Vectors Used in Gene Therapy ClinicalTrials, Wiley (2009), Retrieved sept.2009 from http://www.wiley.co.uk/genetherapy/clinical/.
[58] S.O. Freytag, H. Stricker, B. Movsas, J.H. Kim, Prostate cancer genetherapy clinical trials, Mol. Ther. 15 (2007) 1042–1052.
[59] H. Kubo, T.A. Gardner, Y. Wada, K.S. Koeneman, A. Gotoh, L. Yang, C.Kao, S.D. Lim, M.B. Amin, H. Yang, M.E. Black, S. Matsubara, M.Nakagawa, J.Y. Gillenwater, H.E. Zhau, L.W. Chung, Phase I doseescalation clinical trial of adenovirus vector carrying osteocalcinpromoter-driven herpes simplex virus thymidine kinase inlocalized and metastatic hormone-refractory prostate cancer,Hum. Gene Ther. 14 (2003) 227–241.
[60] D. Portsmouth, J. Hlavaty, M. Renner, Suicide genes for cancertherapy, Mol. Aspects Med. 28 (2007) 4–41.
[61] A. Hasenburg, X.W. Tong, A. Rojas-Martinez, C. Nyberg-Hoffman,C.C. Kieback, A.L. Kaplan, R.H. Kaufman, I. Ramzy, E. Aguilar-Cordova, D.G. Kieback, Thymidine kinase (TK) gene therapy of solidtumors: valacyclovir facilitates outpatient treatment, AnticancerRes. 19 (1999) 2163–2165.
[62] J. Cheon, H.K. Kim, D.G. Moon, D.K. Yoon, J.H. Cho, S.K. Koh,Adenovirus-mediated suicide-gene therapy using the herpessimplex virus thymidine kinase gene in cell and animal models ofhuman prostate cancer: changes in tumour cell proliferativeactivity, BJU Int. 85 (2000) 759–766.
[63] J.A. Eastham, S.H. Chen, I. Sehgal, G. Yang, T.L. Timme, S.J. Hall, S.L.Woo, T.C. Thompson, Prostate cancer gene therapy: herpes simplexvirus thymidine kinase gene transduction followed by ganciclovirin mouse and human prostate cancer models, Hum. Gene Ther. 7(1996) 515–523.
[64] G. Ayala, T. Satoh, R. Li, M. Shalev, Y. Gdor, E. Aguilar-Cordova, A.Frolov, T.M. Wheeler, B.J. Miles, K. Rauen, B.S. Teh, E.B. Butler, T.C.Thompson, D. Kadmon, Biological response determinants in HSV–tk + ganciclovir gene therapy for prostate cancer, Mol. Ther. 13(2006) 716–728.

12 P. Singh et al. / Cancer Letters 293 (2010) 1–14
[65] N.L. Brown, N.R. Lemoine, Clinical trials with GDEPT: cytosinedeaminase and 5-fluorocytosine, Meth. Mol. Med. 90 (2004) 451–457.
[66] A. Khatri, B. Zhang, E. Doherty, J. Chapman, K. Ow, H. Pwint, R.Martiniello-Wilks, P.J. Russell, Combination of cytosine deaminasewith uracil phosphoribosyl transferase leads to local and distantbystander effects against RM1 prostate cancer in mice, J. Gene Med.8 (2006) 1086–1096.
[67] P.J. Russell, A. Khatri, B. Zhang, E. Doherty, K. Ow, J. Chapman, R.Martiniello-Wilks, Gene directed enzyme prodrug therapy usingthe fusion gene, cytosine deaminase uracil phosphoribosyltransferase leads to a distant bystander effect in mouse models ofprostate cancer, Proc Amer Assoc Cancer Res. 46 (2005).
[68] T. Miyagi, K. Koshida, O. Hori, H. Konaka, H. Katoh, Y. Kitagawa, A.Mizokami, M. Egawa, S. Ogawa, H. Hamada, M. Namiki, Genetherapy for prostate cancer using the cytosine deaminase/uracilphosphoribosyltransferase suicide system, J. Gene Med. 5 (2003)30–37.
[69] Y. Xie, J.D. Gilbert, J.H. Kim, S.O. Freytag, Efficacy of adenovirus-mediated CD/5-FC and HSV-1 thymidine kinase/ganciclovir suicidegene therapies concomitant with p53 gene therapy, Clin. CancerRes. 5 (1999) 4224–4232.
[70] S.O. Freytag, M. Khil, H. Stricker, J. Peabody, M. Menon, M.DePeralta-Venturina, D. Nafziger, J. Pegg, D. Paielli, S. Brown, K.Barton, M. Lu, E. Aguilar-Cordova, J.H. Kim, Phase I study ofreplication-competent adenovirus-mediated double suicide genetherapy for the treatment of locally recurrent prostate cancer,Cancer Res. 62 (2002) 4968–4976.
[71] K.S. Lipinski, S. Pelech, A. Mountain, A.S. Irvine, R. Kraaij, C.H.Bangma, K.H. Mills, S.M. Todryk, Nitroreductase-based therapy ofprostate cancer, enhanced by raising expression of heat shockprotein 70, acts through increased anti-tumour immunity, CancerImmunol. Immunother. 55 (2006) 347–354.
[72] A.H. Djeha, T.A. Thomson, H. Leung, P.F. Searle, L.S. Young, D.J. Kerr,P.A. Harris, A. Mountain, C.J. Wrighton, Combined adenovirus-mediated nitroreductase gene delivery and CB1954 treatment: awell-tolerated therapy for established solid tumors, Mol. Ther. 3(2001) 233–240.
[73] D. Zhou, Y. Lu, M.S. Steiner, J.T. Dalton, Cytochrome P-450 2C9sensitizes human prostate tumor cells to cyclophosphamide via abystander effect, Antimicrob. Agents Chemother. 44 (2000) 2659–2663.
[74] Y. Jounaidi, D.J. Waxman, Use of replication-conditional adenovirusas a helper system to enhance delivery of P450 prodrug-activationgenes for cancer therapy, Cancer Res. 64 (2004) 292–303.
[75] M. Mesnil, H. Yamasaki, Bystander effect in herpes simplex virus-thymidine kinase/ganciclovir cancer gene therapy: role of gap-junctional intercellular communication, Cancer Res. 60 (2000)3989–3999.
[76] S. Ebara, S. Shimura, Y. Nasu, H. Kaku, H. Kumon, G. Yang, J. Wang,T.L. Timme, E. Aguilar-Cordova, T.C. Thompson, Gene therapy forprostate cancer: toxicological profile of four HSV–tk transducingadenoviral vectors regulated by different promoters, ProstateCancer Prostatic Dis. 5 (2002) 316–325.
[77] S.J. Hall, M.A. Sanford, G. Atkinson, S.H. Chen, Induction of potentantitumor natural killer cell activity by herpes simplex virus-thymidine kinase and ganciclovir therapy in an orthotopic mousemodel of prostate cancer, Cancer Res. 58 (1998) 3221–3225.
[78] G.U. Dachs, J. Tupper, G.M. Tozer, From bench to bedside for gene-directed enzyme prodrug therapy of cancer, Anticancer Drugs 16(2005) 349–359.
[79] S.J. Hall, S.E. Mutchnik, G. Yang, T.L. Timme, Y. Nasu, C.H. Bangma,S.L. Woo, M. Shaker, T.C. Thompson, Cooperative therapeuticeffects of androgen ablation and adenovirus-mediated herpessimplex virus thymidine kinase gene and ganciclovir therapyin experimental prostate cancer, Cancer Gene Ther. 6 (1999)54–63.
[80] S.O. Freytag, H. Stricker, J. Pegg, D. Paielli, D.G. Pradhan, J. Peabody,M. DePeralta-Venturina, X. Xia, S. Brown, M. Lu, J.H. Kim, Phase Istudy of replication-competent adenovirus-mediated double-suicide gene therapy in combination with conventional-dosethree-dimensional conformal radiation therapy for the treatmentof newly diagnosed, intermediate – to high-risk prostate cancer,Cancer Res. 63 (2003) 7497–7506.
[81] M. Chhikara, H. Huang, M.T. Vlachaki, X. Zhu, B. Teh, K.J. Chiu, S.Woo, B. Berner, E.O. Smith, K.C. Oberg, L.K. Aguilar, T.C. Thompson,E.B. Butler, E. Aguilar-Cordova, Enhanced therapeutic effect of HSV–tk + GCV gene therapy and ionizing radiation for prostate cancer,Mol. Ther. 3 (2001) 536–542.
[82] G. Atkinson, S.J. Hall, Prodrug activation gene therapy and externalbeam irradiation in the treatment of prostate cancer, Urology 54(1999) 1098–1104.
[83] S. Varghese, S.D. Rabkin, R. Liu, P.G. Nielsen, T. Ipe, R.L. Martuza,Enhanced therapeutic efficacy of IL-12, but not GM-CSF, expressingoncolytic herpes simplex virus for transgenic mouse derivedprostate cancers, Cancer Gene Ther. 13 (2006) 253–265.
[84] S.J. Hall, S.E. Canfield, Y. Yan, W. Hassen, W.A. Selleck, S.H. Chen, Anovel bystander effect involving tumor cell-derived Fas and FasLinteractions following Ad.HSV–tk and Ad.mIL-12 gene therapies inexperimental prostate cancer, Gene Ther. 9 (2002) 511–517.
[85] Y. Nasu, C.H. Bangma, G.W. Hull, G. Yang, J. Wang, S. Shimura, M.A.McCurdy, S. Ebara, H.M. Lee, T.L. Timme, T.C. Thompson,Combination gene therapy with adenoviral vector-mediated HSV–tk+GCV and IL-12 in an orthotopic mouse model for prostatecancer, Prostate Cancer Prostatic Dis. 4 (2001) 44–55.
[86] H. Fukuhara, R.L. Martuza, S.D. Rabkin, Y. Ito, T. Todo, Oncolyticherpes simplex virus vector g47delta in combination withandrogen ablation for the treatment of human prostateadenocarcinoma, Clin. Cancer Res. 11 (2005) 7886–7890.
[87] S. Varghese, S.D. Rabkin, Oncolytic herpes simplex virus vectors forcancer virotherapy, Cancer Gene Ther. 9 (2002) 967–978.
[88] S. Varghese, J.T. Newsome, S.D. Rabkin, K. McGeagh, D. Mahoney, P.Nielsen, T. Todo, R.L. Martuza, Preclinical safety evaluation of G207,a replication-competent herpes simplex virus type 1, inoculatedintraprostatically in mice and nonhuman primates, Hum. GeneTher. 12 (2001) 999–1010.
[89] T.J. Jorgensen, S. Katz, E.K. Wittmack, S. Varghese, T. Todo, S.D.Rabkin, R.L. Martuza, Ionizing radiation does not alter theantitumor activity of herpes simplex virus vector G207 insubcutaneous tumor models of human and murine prostatecancer, Neoplasia 3 (2001) 451–456.
[90] S.O. Freytag, H. Stricker, J. Pegg, D. Paielli, D.G. Pradhan, J. Peabody,M. DePeralta-Venturina, X. Xia, S. Brown, M. Lu, J.H. Kim, Phase Istudy of replication competent adenovirus-mediated double-suicide gene therapy in combination with conventional-dosethree-dimensional conformal radiation therapy for the treatmentof newly diagnosed, intermediate – to high-risk PC 63 (2003).
[91] P. Zhang, H. Zeng, Q. Wei, Y. Lu, X. Li, J. Wang, F. Zhao, H. Li,Improved effects of a double suicide gene system on prostatecancer cells by targeted regulation of prostatespecific membraneantigen promoter and enhancer, Int. J. Urol. 15 (2008) 442–448.
[92] A. Khatri, Y. Husaini, K. Ow, J. Chapman, P.J. Russell, cytosineDEAMINASE-uracil phosphoribosyltransferase and Interleukin (IL)-12 and IL-18: a multimodal anticancer interface marked by specificmodulation in serum cytokines, Clin. Cancer Res. 15 (2009) 2323–2334.
[93] A. Bzowskaa, E. Kulikowskaa, D. Shugar, Purine nucleosidephosphorylases: properties, functions and clinical aspects,Pharmacology and Therapeutics 88 (2000) 349–425.
[94] Y. Zhang, W.B. Parker, E.J. Sorscher, S.E. Ealick, PNP anticancer genetherapy, Curr. Top. Med. Chem. 5 (2005) 1259–1274.
[95] W.B. Parker, P.W. Allan, S.C. Shaddix, L.M. Rose, H.F. Speegle, G.Y.Gillespie, L.L. Bennett Jr., Metabolism and metabolic actions of 6-methylpurine and 2-fluoroadenine in human cells, Biochem.Pharmacol. 55 (1998) 1673–1681.
[96] L.J. Lockett, P.L. Molloy, P.J. Russell, G.W. Both, Relative efficiency oftumor cell killing in vitro by two enzyme-prodrug systemsdelivered by identical adenovirus vectors, Clin. Cancer Res. 3(1997) 2075–2080.
[97] E.J. Sorscher, S. Peng, Z. Bebok, P.W. Allan, L.L. Bennett Jr., W.B.Parker, Tumor cell bystander killing in colonic carcinoma utilizingthe Escherichia coli DeoD gene to generate toxic purines, Gene Ther1 (1994) 233–238.
[98] P. Patel, D. Ashdown, N. James, Is gene therapy the answer for prostatecancer?, Prostate Cancer Prostatic Dis. 7 (Suppl 1) (2004) S14–19.
[99] A.G. Carroll, H.J. Voeller, L. Sugars, E.P. Gelmann, p53 oncogenemutations in three human prostate cancer cell lines, Prostate 23(1993) 123–134.
[100] X.Y. Wang, R. Martiniello-Wilks, J.M. Shaw, T. Ho, N. Coulston, C.Cooke-Yarborough, P.L. Molloy, F. Cameron, M. Moghaddam, T.J.Lockett, L.K. Webster, I.K. Smith, G.W. Both, P.J. Russell, Preclinicalevaluation of a prostate-targeted gene-directed enzyme prodrugtherapy delivered by ovine atadenovirus, Gene Ther. 11 (2004)1559–1567.
[101] T.U. Krohne, S. Shankara, M. Geissler, B.L. Roberts, J.R. Wands, H.E.Blum, L. Mohr, Mechanisms of cell death induced by suicide genesencoding purine nucleoside phosphorylase and thymidine kinase in

P. Singh et al. / Cancer Letters 293 (2010) 1–14 13
human hepatocellular carcinoma cells in vitro, Hepatology 34(2001) 511–518.
[102] R. Martiniello-Wilks, A. Dane, D.J. Voeks, G. Jeyakumar, E.Mortensen, J.M. Shaw, X.Y. Wang, G.W. Both, P.J. Russell, Gene-directed enzyme prodrug therapy for prostate cancer in a mousemodel that imitates the development of human disease, J. GeneMed. 6 (2004) 43–54.
[103] NCT00625430: A Phase I Gene Therapy Study of FP253/Fludarabinefor Prostate Cancer FP253-, in, Biotech Equity Partners Pty Ltd. (Feb.2008) http://clinicaltrials.gov/ct2/show/NCT00625430.
[104] R. Martiniello-Wilks, J. Garcia-Aragon, M.M. Daja, P. Russell, G.W.Both, P.L. Molloy, L.J. Lockett, P.J. Russell, In vivo gene therapy forprostate cancer: preclinical evaluation of two different enzyme-directed prodrug therapy systems delivered by identicaladenovirus vectors, Hum. Gene Ther. 9 (1998) 1617–1626.
[105] D. Voeks, R. Martiniello-Wilks, V. Madden, K. Smith, E. Bennetts,G.W. Both, P.J. Russell, Gene therapy for prostate cancer deliveredby ovine adenovirus and mediated by purine nucleosidephosphorylase and fludarabine in mouse models, Gene Ther. 9(2002) 759–768.
[106] R. Martiniello-Wilks, X.Y. Wang, D.J. Voeks, A. Dane, J.M. Shaw, E.Mortensen, G.W. Both, P.J. Russell, Purine nucleosidephosphorylase and fludarabine phosphate gene directed enzymeprodrug therapy suppresses primary tumour growth andpseudometastases in a mouse model of prostate cancer, J. GeneMed. 6 (2004) 1343–1357.
[107] N.K. Green, L.W. Seymour, Adenoviral vectors: systemic deliveryand tumor targeting, Cancer Gene Ther. 9 (2002) 1036–1042.
[108] M. Morille, C. Passirani, A. Vonarbourg, A. Clavreul, J.P. Benoit,Progress in developing cationic vectors for non-viral systemic genetherapy against cancer, Biomaterials 29 (2008) 3477–3496.
[109] D. Majhen, A. Ambriovic-Ristov, Adenoviral vectors - how to usethem in cancer gene therapy? Virus Res. 119 (2006) 121–133.
[110] A. Amalfitano, M.A. Hauser, H. Hu, D. Serra, C.R. Begy, J.S.Chamberlain, Production and characterization of improvedadenovirus vectors with the E1, E2b, and E3 genes deleted, J.Virol. 72 (1998) 926–933.
[111] M. Lusky, M. Christ, K. Rittner, A. Dieterle, D. Dreyer, B. Mourot, H.Schultz, F. Stoeckel, A. Pavirani, M. Mehtali, In vitro and in vivobiology of recombinant adenovirus vectors with E1, E1/E2A, or E1/E4 deleted, J. Virol. 72 (1998) 2022–2032.
[112] M. Lusky, L. Grave, A. Dieterle, D. Dreyer, M. Christ, C. Ziller, P.Furstenberger, J. Kintz, D.A. Hadji, A. Pavirani, M. Mehtali,Regulation of adenovirus-mediated transgene expression by theviral E4 gene products: requirement for E4 ORF3, J. Virol. 73 (1999)8308–8319.
[113] J.W. Moorhead, G.H. Clayton, R.L. Smith, J. Schaack, A replication-incompetent adenovirus vector with the preterminal protein genedeleted efficiently transduces mouse ears, J. Virol. 73 (1999) 1046–1053.
[114] J.F. Engelhardt, X. Ye, B. Doranz, J.M. Wilson, Ablation of E2A inrecombinant adenoviruses improves transgene persistence anddecreases inflammatory response in mouse liver, Proc. Natl. Acad.Sci. USA 91 (1994) 6196–6200.
[115] A. Lieber, D.S. Steinwaerder, C.A. Carlson, M.A. Kay, Integratingadenovirus-adeno associated virus hybrid vectors devoid of all viralgenes, J. Virol. 73 (1999) 9314–9324.
[116] D.S. Steinwaerder, C.A. Carlson, A. Lieber, Generation of adenovirusvectors devoid of all viral genes by recombination betweeninverted repeats, J. Virol. 73 (1999) 9303–9313.
[117] E. Kelly, S.J. Russell, E. Kelly, S.J. Russell, History of oncolyticviruses: genesis to genetic engineering, Mol. Ther. 15 (2007)651–659.
[118] C. Heise, I. Ganly, Y.T. Kim, A. Sampson-Johannes, R. Brown, D. Kirn,Efficacy of a replication-selective adenovirus against ovariancarcinomatosis is dependent on tumor burden, viral replicationand p53 status, Gene Ther. 7 (2000) 1925–1929.
[119] J. Nemunaitis, C. Cunningham, A. Buchanan, A. Blackburn, G.Edelman, P. Maples, G. Netto, A. Tong, B. Randlev, S. Olson, D.Kirn, Intravenous infusion of a replication selective adenovirus(ONYX-015) in cancer patients: safety, feasibility and biologicalactivity, Gene Ther. 8 (2001) 746–759.
[120] R. Kraaij, A.L. van Rijswijk, M.H. Oomen, H.J. Haisma, C.H. Bangma,A.L.C.T. van Rijswijk, M.H.A. Oomen, Prostate specific membraneantigen (PSMA) is a tissue specific target for adenoviraltransduction of prostate cancer in vitro, Prostate 62 (2005) 253–259.
[121] C.H. Bangma, R. Kraaij, A. van Rijswijk, H.J. Haisma, V. vanBeusechem, W. Gerritsen, Transductional targeting of adenoviral
vectors to prostate cancer in vitro, Prostate Cancer Prostat. Dis. 2(1999) S5.
[122] M. Rajecki, A. Kanerva, U.-H. Stenman, M. Tenhunen, L.Kangasniemi, M. Sarkioja, M.Y. Ala-Opas, H. Alfthan, A. Sankila, E.Rintala, R.A. Desmond, T. Hakkarainen, A. Hemminki, Treatment ofprostate cancer with Ad5/3Delta24hCG allows non-invasivedetection of the magnitude and persistence of virus replicationin vivo, Mol. Cancer Ther. 6 (2007) 742–751.
[123] K. Suzuki, J. Fueyo, V. Krasnykh, P.N. Reynolds, D.T. Curiel, R.Alemany, A conditionally replicative adenovirus with enhancedinfectivity shows improved oncolytic potency, Clin. Cancer Res. 7(2001) 120–126.
[124] T. Shirakawa, S. Terao, N. Hinata, K. Tanaka, A. Takenaka, I. Hara, K.Sugimura, M. Matsuo, K. Hamada, K. Fuji, T. Okegawa, E.Higashihara, T.A. Gardner, C. Kao, L.W. Chung, S. Kamidono, M.Fujisawa, A. Gotoh, Long-term outcome of phase I/II clinical trial ofAd-OC-TK/VAL gene therapy for hormone-refractory metastaticprostate cancer, Hum. Gene Ther. 18 (2007) 1225–1232.
[125] K.S. Koeneman, C. Kao, S.C. Ko, L. Yang, Y. Wada, D.F. Kallmes, J.Y.Gillenwater, H.E. Zhau, L.W. Chung, T.A. Gardner, Osteocalcin-directed gene therapy for prostate-cancer bone metastasis, World J.Urol. 18 (2000) 102–110.
[126] C.L. Hsieh, T.A. Gardner, L. Miao, G. Balian, L.W. Chung, Cotargetingtumor and stroma in a novel chimeric tumor model involving thegrowth of both human prostate cancer and bone stromal cells,Cancer Gene Ther. 11 (2004) 148–155.
[127] S. Matsubara, Y. Wada, T.A. Gardner, M. Egawa, M.S. Park, C.L.Hsieh, H.E. Zhau, C. Kao, S. Kamidono, J.Y. Gillenwater, L.W. Chung,A conditional replication-competent adenoviral vector, Ad-OC-E1a,to cotarget prostate cancer and bone stroma in an experimentalmodel of androgen-independent prostate cancer bone metastasis,Cancer Res. 61 (2001) 6012–6019.
[128] H.O. McCarthy, J.A. Coulter, J. Worthington, T. Robson, D.G. Hirst,Human osteocalcin: a strong promoter for nitric oxide synthasegene therapy, with specificity for hormone refractory prostatecancer, J. Gene Med. 9 (2007) 511–520.
[129] N. Pariente, K. Morizono, M.S. Virk, F.A. Petrigliano, R.E. Reiter, J.R.Lieberman, I.S. Chen, A novel dual-targeted lentiviral vectorleads to specific transduction of prostate cancer bone metastasesin vivo after systemic administration, Mol. Ther. 15 (2007) 1973–1981.
[130] J.Y. Adams, M. Johnson, M. Sato, F. Berger, S.S. Gambhir, M. Carey,M.L. Iruela-Arispe, L. Wu, Visualization of advanced humanprostate cancer lesions in living mice by a targeted gene transfervector and optical imaging, Nat. Med. 8 (2002) 891–897.
[131] H. Zeng, Q. Wei, R. Huang, N. Chen, Q. Dong, Y. Yang, Q. Zhou,Recombinant adenovirus mediated prostate-specific enzyme pro-drug gene therapy regulated by prostate-specific membraneantigen (PSMA) enhancer/promoter, J. Androl. 28 (2007) 827–835.
[132] S.J. Lee, H.S. Kim, R. Yu, K. Lee, T.A. Gardner, C. Jung, M.H. Jeng, F.Yeung, L. Cheng, C. Kao, Novel prostate-specific promoter derivedfrom PSA and PSMA enhancers, Mol. Ther. 6 (2002) 415–421.
[133] S.J. Lee, Y. Zhang, S.D. Lee, C. Jung, X. Li, H.S. Kim, K.H. Bae, M.H.Jeng, C. Kao, T. Gardner, Targeting prostate cancer withconditionally replicative adenovirus using PSMA enhancer, Mol.Ther. 10 (2004) 1051–1058.
[134] M. Ahn, S.J. Lee, X. Li, J.A. Jimenez, Y.P. Zhang, K.H. Bae, Y.Mohammadi, C. Kao, T.A. Gardner, Enhanced combined tumor-specific oncolysis and suicide gene therapy for prostate cancerusing M6 promoter, Cancer Gene Ther. 16 (2009) 73–82.
[135] R. Kraaij, L. van der Weel, C.M. de Ridder, H.A. van der Korput, J.L.Zweistra, A.L. van Rijswijk, C.H. Bangma, J. Trapman, A smallchimeric promoter for high prostate-specific transgene expressionfrom adenoviral vectors, Prostate 67 (2007) 829–839.
[136] Y. Zhang, J. Yu, E. Unni, T.C. Shao, B. Nan, T. Snabboon, S. Kasper, F.Andriani, L. Denner, M. Marcelli, Monogene and polygene therapyfor the treatment of experimental prostate cancers by use ofapoptotic genes bax and bad driven by the prostate-specificpromoter ARR(2)PB, Hum. Gene Ther. 13 (2002) 2051–2064.
[137] D. Yu, C. Scott, W.W. Jia, A. De Benedetti, B.J. Williams, L. Fazli, Y.Wen, M. Gleave, C. Nelson, P.S. Rennie, Targeting and killing ofprostate cancer cells using lentiviral constructs containing asequence recognized by translation factor eIF4E and aprostatespecific promoter, Cancer Gene Ther. 13 (2006) 32–43.
[138] D. Yu, D. Chen, C. Chiu, B. Razmazma, Y.H. Chow, S. Pang, Prostate-specific targeting using PSA promoter-based lentiviral vectors,Cancer Gene Ther. 8 (2001) 628–635.
[139] H.S. Park, J. Cheon, H.Y. Cho, Y.H. Ko, J.H. Bae, D.G. Moon, J.J. Kim, Invivo characterization of a prostate-specific antigen promoter-based

14 P. Singh et al. / Cancer Letters 293 (2010) 1–14
suicide gene therapy for the treatment of benign prostatichyperplasia, Gene Ther. 10 (2003) 1129–1134.
[140] R. Martiniello-Wilks, T. Tsatralis, P. Russell, D.E. Brookes, D.Zandvliet, L.J. Lockett, G.W. Both, P.L. Molloy, P.J. Russell,Transcription-targeted gene therapy for androgenin dependentprostate cancer, Cancer Gene Ther. 9 (2002) 443–452.
[141] D. Sarkar, I.V. Lebedeva, Z.Z. Su, E.S. Park, L. Chatman, N. Vozhilla, P.Dent, D.T. Curiel, P.B. Fisher, Eradication of therapy-resistanthuman prostate tumors using a cancer terminator virus, CancerRes. 67 (2007) 5434–5442.
[142] W.T. Godbey, A. Atala, Directed apoptosis in Cox-2-overexpressingcancer cells through expression-targeted gene delivery, Gene Ther.10 (2003) 1519–1527.
[143] N.A. Lanson Jr., P.L. Friedlander, P. Schwarzenberger, J.K. Kolls, G.Wang, Replication of an adenoviral vector controlled by the humantelomerase reverse transcriptase promoter causes tumor-selectivetumor lysis, Cancer Res. 63 (2003) 7936–7941.
[144] J. Irving, Z. Wang, S. Powell, C. O’Sullivan, M. Mok, B. Murphy, L.Cardoza, J.S. Lebkowski, A.S. Majumdar, Conditionally replicativeadenovirus driven by the human telomerase promoter providesbroad-spectrum antitumor activity without liver toxicity, CancerGene Ther. 11 (2004) 174–185.
[145] T. Fujiwara, S. Kagawa, H. Kishimoto, Y. Endo, M. Hioki, Y. Ikeda, R.Sakai, Y. Urata, N. Tanaka, T. Fujiwara, Enhanced antitumourefficacy of telomerase-selective oncolytic adenoviral agent OBP-401 with docetaxel: preclinical evaluation of chemovirotherapy,Int. J. Cancer 119 (2006).
[146] P. Huang, M. Watanabe, H. Kaku, Y. Kashiwakura, J. Chen, T. Saika,Y. Nasu, T. Fujiwara, Y. Urata, H. Kumon, Direct and distantantitumor effects of a telomeraseselective oncolytic adenoviralagent, OBP-301, in a mouse prostate cancer model, Cancer GeneTher. 15 (2008) 315–322.
[147] Y. Zhang, J.C. Qi, W.F. Lian, W.Q. Cai, W. Li, K.L. Liu, The animalresearch of recombinant adenovirus controlled by humantelomerase reverse transcriptase promoter in the treatment ofhuman prostate cancer, Zhonghua Wai Ke Za Zhi 44 (2006) 1252–1255.
[148] Y. Xing, M. Liu, Y. Du, F. Qu, Y. Li, Y. Xiao, J. Zhao, F. Zeng, C. Xiao,Tumor cellspecific blockade of CXCR4/SDF-1 interactions inprostate cancer cells by hTERT promoter induced CXCR4knockdown: a possible metastasis preventing and minimizingApproach, Cancer Biol. Ther. 7 (2008).
[149] N.E. Fullerton, M. Boyd, R.J. Mairs, W.N. Keith, O. Alderwish, M.M.Brown, A. Livingstone, D. Kirk, Combining a targeted radiotherapyand gene therapy approach for adenocarcinoma of prostate,Prostate Cancer Prostatic Dis. 7 (2004) 355–363.
[150] W. Song, Z. Dong, T. Jin, M.G. Mantellini, G. Nunez, J.E. Nor, Cancergene therapy with iCaspase-9 transcriptionally targeted to tumorendothelial cells, Cancer Gene Ther. 15 (2008) 667–675.
[151] D.S. Cross, J.K. Burmester, Functional characterization of the GDEPpromoter and three enhancer elements in retinoblastoma andprostate cell lines, Med. Oncol. 25 (2008) 40–49.
[152] J. Wang, H. Zhang, R.X. Liang, B. Pang, Q.G. Shi, P.T. Huang, C.F.Huang, J.G. Zhou, Identification and characterization of the novelhuman prostate cancer-specific PC-1 gene promoter, Biochem.Biophys. Res. Commun. 357 (2007) 8–13.
[153] H. Dzojic, W.S. Cheng, M. Essand, Two-step amplification of thehuman PPT sequence provides specific gene expression in animmunocompetent murine prostate cancer model, Cancer GeneTher. 14 (2007) 233–240.
[154] K.S. Lipinski, H.A. Djeha, J. Gawn, S. Cliffe, N.J. Maitland, D.H.Palmer, A. Mountain, A.S. Irvine, C.J. Wrighton, Optimization of asynthetic beta-catenin-dependent promoter for tumor-specificcancer gene therapy, Mol. Ther. 10 (2004) 150–161.
[155] M.Y. Gabril, T. Onita, P.G. Ji, H. Sakai, F.L. Chan, J. Koropatnick, J.L.Chin, M. Moussa, J.W. Xuan, Prostate targeting: PSP94 genepromoter/enhancer region directed prostate tissue-specificexpression in a transgenic mouse prostate cancer model, GeneTher. 9 (2002) 1589–1599.
[156] J. Zhang, N. Ramesh, Y. Chen, Y. Li, J. Dilley, P. Working, D.C. Yu,Identification of human uroplakin II promoter and its use in theconstruction of CG8840, a urotheliumspecific adenovirus variantthat eliminates established bladder tumors in combination withdocetaxel, Cancer Res. 62 (2002) 3743–3750.
[157] X. Xie, X. Zhao, Y. Liu, C.Y. Young, D.J. Tindall, K.M. Slawin, D.M.Spencer, Robust prostate-specific expression for targeted genetherapy based on the human kallikrein 2 promoter, Hum. GeneTher. 12 (2001) 549–561.
[158] C. Pramudji, S. Shimura, S. Ebara, G. Yang, J. Wang, C. Ren, Y. Yuan,S.A. Tahir, T.L. Timme, T.C. Thompson, In situ prostate cancer genetherapy using a novel adenoviral vector regulated by the caveolin-1promoter, Clin. Cancer Res. 7 (2001) 4272–4279.
[159] X.M. Luo, J.Y. Liu, M.Q. Su, X.K. Hao, Detection of transcriptionalactivities of tumorspecific survivin promoter in human prostaticcarcinoma, Zhonghua Nan Ke Xue 13 (2007) 502–506.
[160] M.L. Figueiredo, C. Kao, L. Wu, Advances in preclinicalinvestigation of prostate cancer GENE therapy, Mol. Ther. 15(2007) 1053–1064.
[161] A. Uchida, D.S. O’Keefe, D.J. Bacich, P.L. Molloy, W.D. Heston, In vivosuicide gene therapy model using a newly discovered prostate-specific membrane antigen promoter/enhancer: a potentialalternative approach to androgen deprivation therapy, Urology 58(2001) 132–139.
[162] T.C. Liu, D. Kirn, Gene therapy progress and prospects cancer:oncolytic viruses, Gene Ther. 15 (2008) 877–884.
[163] S.O. Freytag, B. Movsas, I. Aref, H. Stricker, J. Peabody, J. Pegg, Y.Zhang, K.N. Barton, S.L. Brown, M. Lu, A. Savera, J.H. Kim, Phase Itrial of replication-competent adenovirus-mediated suicide genetherapy combined with IMRT for prostate cancer, Mol. Ther. 15(2007) 1016–1023.
[164] S.J. Advani, J.J. Mezhir, B. Roizman, R.R. Weichselbaum, ReVOLT:radiation-enhanced viral oncolytic therapy, Int. J. Radiat. Oncol.Biol. Phys. 66 (2006) 637–646.
[165] D.C. Yu, Y. Chen, J. Dilley, Y. Li, M. Embry, H. Zhang, N. Nguyen, P.Amin, J. Oh, D.R. Henderson, Antitumor synergy of CV787, aprostate cancer-specific adenovirus, and paclitaxel and docetaxel,Cancer Res. 61 (2001) 517–525.
[166] P.C. Ryan, J.L. Jakubczak, D.A. Stewart, L.K. Hawkins, C. Cheng,L.M. Clarke, S. Ganesh, C. Hay, Y. Huang, M. Kaloss, A. Marinov,S.S. Phipps, P.S. Reddy, P.S. Shirley, Y. Skripchenko, L. Xu, J.Yang, S. Forry-Schaudies, P.L. Hallenbeck, Antitumor efficacy andtumor-selective replication with a single intravenous injection ofOAS403, an oncolytic adenovirus dependent on two prevalentalterations in human cancer, Cancer Gene Ther. 11 (2004) 555–569.
[167] S.O. Freytag, H. Stricker, J. Peabody, J. Pegg, D. Paielli, B. Movsas,K.N. Barton, S.L. Brown, M. Lu, J.H. Kim, Five-year follow-up of trialof replication-competent adenovirus-mediated suicide genetherapy for treatment of prostate cancer, Mol. Ther. 15 (2007)636–642.