
MODULE 1. INTRODUCTION TO ERGONOMICS IN MIS ...
35
1 MODULE 1. INTRODUCTION TO ERGONOMICS IN MIS SURGERY SESSION 3. Ergonomics guidelines for orthopaedic surgery. This project has been funded with support from the European Commission. This publication reflects the views only of the author, and the Commission cannot be held responsible for any use which may be made of the information contained therein.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of MODULE 1. INTRODUCTION TO ERGONOMICS IN MIS ...
1
MODULE 1. INTRODUCTION TO ERGONOMICS IN MIS SURGERY
SESSION 3. Ergonomics guidelines for orthopaedic surgery.
This project has been funded with support from the European Commission. This publication reflects the views only of the author, and the Commission cannot be held responsible for any use which may be made of the information contained therein.

2
To begin
A general overview of the most important concepts exposed in this module is presented. Particularly this section is going to strengthen the student´s knowledge related to the upper-body ergonomics in Orthopaedic MIS Surgery. this session will bring together all general recommendations for surgeons as a summary of the present course. In addition, this session will contribute with more profound knowledge for the student regarding the ergonomics of the upper-body.

3
Objectives
The objectives of this session are:
To ensure the understanding of previous sessions of this module through simple and practical rules.
To review all important ergonomic aspects and concerns about upper-body joints and limbs.
To compile a catalogue of ergonomic recommendations for Orthopaedic MIS Surgeons.
To summarize the most important recommendations regarding ergonomics in the surgical practice.
To ensure the understanding of previous modules through the presentation of simple and practical ergonomic rules and principles.

4
1. Ergonomics body posture.
Concept
Any body posture can cause discomfort and fatigue if it is maintained for long periods of time.
(Canadian Centre for Occupational Health and Safety)
Body posture in MIS surgery is the most important factor influencing a risk of Work-related Musculoskeletal Disorders (WMSDs) for surgeons and scrub nurses. WRMSDs are a group of disorders that are caused by occupational risk factors. The physical and cognitive requirements during surgery pose substantial ergonomic stress (Dabholkar et al., 2015). It should be highlighted that the main factor that condributs to WMSDs is awkward body position. See in the Fig. 1 what kinds of aspects are important regarding awkward position.
Figure 1. The main aspects contributing WMSDs in MIS surgery Awkward postures determine static position which requires more force and increase the amount of recovery time that muscles usually need. Added force hastens the onset of fatigue and increases the likelihood of injury from overuse. According to the literature awkward postures include repeated or prolonged reaching, twisting, bending, kneeling, squatting, working overhead with the hands or arms, or holding fixed positions (Jaffar et al., 2011).
You can identify awkward posture when any joint of your body bends or twists excessively, outside a comfortable range of motion.

5
There are many negative consequenses of maitaining awkward and fixed position:
The joints and muscles must apply more effort to achieve the same force when the deviation
from neutral position is occured;
The further the deviation, the more force must be applied;
Working in awkward position increases the strain on tendons, ligaments and nerves and fatigue
of the body,
Awkward body posture increases the risk of disorders in the musculoskeletal system and injury,
Awkward postures require much recovery time that muscles need.
In general, awkward posture refers to a such position where the various parts of the body are not in their natural position. The body segments deviate significantly from their neutral positions. You can find the pattern specification of neutral position according to RULA method (McAtamney 1993) and scientific literature on ergonomics in the Fig. 2.
Examine the examples 1, 2, 3 presenting three typical awkward positions:
standing and sitting positions while performing hip (Fig. 3 and 4);
standing position while performing spine surgery (Fig. 5).
Figure 2. The specification of neutral body posture

6
Example 1
Figure 3. The example of awkward body posture of surgeon while performing hip replacement – standing position
Standing posture while performing hip replacement can force maintaining deeply bent and twisted position of trunk and neck. It results from the height of operating table and the necessity of visual accessing to operating field. Additionally, surgeons can maintain twisted body position or awkward arms position when reaching for surgical instrument. This is associated to operating room layout (position of instrument table and location of scrub nurse) and workflow including team cooperation and effectiveness of communication particularly in line surgeon – scrub nurse. In the same time the arms may be raised and abduct while using surgical tools when operating more dynamic and with repetitive movements e.g. during developing femur stem for prosthesis stem, doing bone cutters into the marrow cavity or sticking the prosthesis stem. Raised arms are the consequence of maintaining bending position of trunk. In addition, the difficult access to operating field in combination with the maladjusted tools’ design results the critical position of wrists.

7
Example 2
Figure 4. The example of awkward body posture of surgeon while performing spine surgery – seated position
According to biomechanical calculations performed with the use of Three Dimensional Static Strength Prediction Programme (3D SSPP, 2011), sitting position is slightly more stressed for musculoskeletal system in back than while standing. Taking into account the neutral positions of standing and sitting there is noted the low back compression for 50 percentile male at level 474 [N] and 635 [N] respectively. The movements of surgeon, that are dynamic and repetitive, additionally increase the static discomfort around low back, hips and arms. The static stress of musculoskeletal system increases also by less freedom of movements while sitting position as compared to upright position.

8
Example 3
Figure 5. The example of awkward body posture of surgeon while performing spine surgery
This example of postural pattern highlights tendency to maintain a vertical posture, with less back mobility and weight distribution. The twisted neck results from the monitor position which is located out of the horizontal plane and straight ahead of the surgeon. Additionally the limited mobility of arms’ movements cause the postural stress of upper limbs. Summarising all of the examples it can be concluded that they require investigation and changes immediately due to a high risk of WMSDs. According to RULA method they receive the worst score i.e. 7 in 7-points scale. Simultaneously, the examples show that both sitting and standing position as well as upper body and lower body position are non-ergonomic and cause postural stress.
The analysis performed in real environmental conditions with the use of observational methods revealed four essential groups of criteria influencing the surgeons’ postural deviation from neutral position as the sources of body postural risk in MIS:
1. The location of operating table and monitors.
2. Surgical instrument’s handle design.
3. Operating room layout including spatial arrangement of operating room as well as position of
table with instruments.
4. Workflow and surgical team cooperation.

9
ERGONOMICS GUIDELINES FOR GENERAL BODY POSTURE
The reccomended body posture pattern:
Neck: avoid flexion more than 10ᵒ as well as rotations and side-bending
Upper arm and shoulder: avoid abduction and raising
Elbow: maintain between 90ᵒ and 120ᵒ
Wrist: deviation less than 15ᵒ from the neutral position
Back: avoid flexion more than 20ᵒ as well as rotation and side-bending
Legs and Feet: should be well supported, do not stay on one leg
How you can overcome the postural ergonomic risk factors:
Adjust the high of the operating room table before or during surgery – it should be regulated to
a height of about 64-77cm from the ground, according to the surgeons’ stature
Adjust position of monitor. It should be more than one monitor and locate at eye level or
slightly lower
Select the handle of instrument with a maximum palm support and grip design avoiding wrist
hyperflexion, hyperextension or unnecessary twisting

10
2. Ergonomics of surgical instruments
Concept
The best tool would perform as an extension of the hand, rather
than as an object to be manipulated.
L. P. Mueller
Surgical instruments are helpful on the patient’s treatment, but often they can be the reason of medical
staff ailment (Zheng Li et al., 2016). The use of tools in combination with other limited conditions
forces unstated position, which may lead to discomfort within the musculoskeletal system (Intuitool).
Shape, size and functionality of surgical instruments are factors influencing on their ergonomics. They
determine how to use, the need for strength, muscle tone and hand position (fingers, wrist, elbow and
shoulders). The way of hold and manipulate have influence on comfort of work with the use of hand
instruments. These factors generate pressure points and ulnar deviation leading to a twist of wrist. The
hand position is ergonomics when the flexion of wrist is not more than 15 degrees from neutral hand
position (see Fig.2).
Figure 2. Ergonomic hand posture

11
Figure 3. The correct position of instrument relative of the lower arm
Important thing is that the instruments should be the extension of the lower arm so as to transfer the
turning movement directly to the effector (see Fig. 3). To maintain this principle handle tools are often
located at an angle of 70ᵒ – 90ᵒ to the shaft axis (Matern et al., 1999). A special case is the tool used by a
wide range of users. Users differ in terms of gender and specific anthropometric features, such as
spacing of the fingers or reach of limbs. The example 1 presents dimensions of the hand (a - the length
of the hand from the wrist to the end of the middle finger and b - the length of the middle finger) for
men.
Additionally, in the Fig. 4 you can see how wide are differences in anthropometric hands of men and
women in the 5 - 50 - 95 percentile.

12
Example 1
Figure 4. A range of dimensions of men hand of the 5-50-95 percentile (Anthropometric Atlas, 2001)
Dimension 5 C 50 C 95 C
a 10,0 [cm] 11,1 [cm] 12,3 [cm]
b 18,1 [cm] 19,6 [cm] 21,0 [cm]
Figure 5. The differences between hand anthropometry of man and woman in the 5-50-95 percentile
DIVERSITY OF SURGICAL INSTRUMENTS
In addition to standard tools used in surgery you can distinguish dedicated tools used in minimally
invasive surgery. The most characteristic hand instruments of minimally invasive orthoapedic surgery
are:
Retractors,
Curetters and osteotomes,
Graspers,
Forceps,
Bone Rongeurs.
From ergonomics point of view key aspect is the shape of grip. This is the basic feature of having a direct
impact on the feeling of comfort / discomfort by the user. There are the following forms of handles of
the tools (Example 2):
13
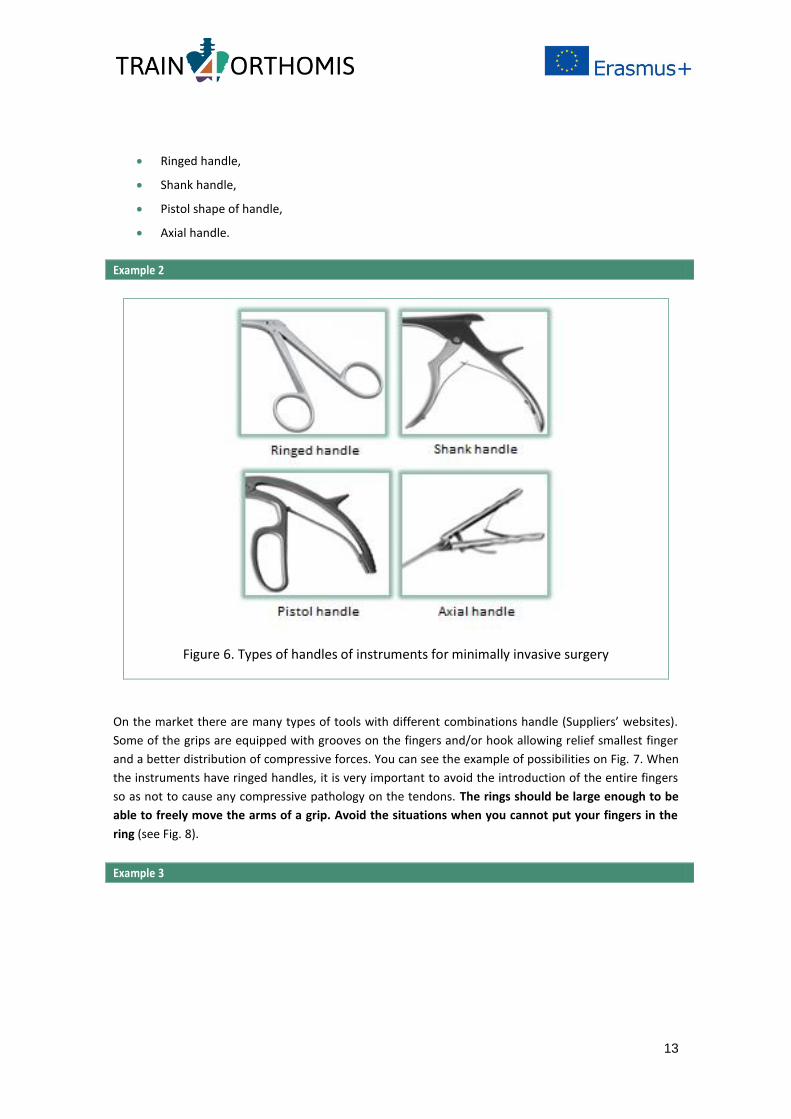
Ringed handle,
Shank handle,
Pistol shape of handle,
Axial handle.
Example 2
Figure 6. Types of handles of instruments for minimally invasive surgery
On the market there are many types of tools with different combinations handle (Suppliers’ websites).
Some of the grips are equipped with grooves on the fingers and/or hook allowing relief smallest finger
and a better distribution of compressive forces. You can see the example of possibilities on Fig. 7. When
the instruments have ringed handles, it is very important to avoid the introduction of the entire fingers
so as not to cause any compressive pathology on the tendons. The rings should be large enough to be
able to freely move the arms of a grip. Avoid the situations when you cannot put your fingers in the
ring (see Fig. 8).
Example 3

14
Figure 7. Examples available on the market handles in surgical instruments
Example 4
Figure 8. Non ergonomic hand position when using tool
Even distribution of pressure forces on all fingers and muscles of the hand reduces the occurrence of
feeling of discomfort in your hands. Handle that provides the maximum palm support and avoiding an
excessive deviation, hyperextension or unnecessary twisting is more ergonomic. Pistol grip requires the

15
use of a smaller muscle strength to grasp the tool. This type of grip strength can spread used on all the
fingers which reduces discomfort.
Good solution is instruments with rotary handle (see Fig. 9). It allows to minimize muscle fatigue and
lack of need for twisting wrists. When the instruments have ringed handles, it is very important to avoid
the introduction of the entire fingers so as not to cause any compressive pathology on the tendons.
Figure 9. A rotary handle
There is possibility to selecting tool with tip rotating - that has an adjustable ability to rotate the tip of
tool in the range of 360° and the ability to bend the tip, thereby maintaining the position of the wrist
without forced steering (Fig. 10).
Figure 10. Tool with rotary and flexibe tip
ERGONOMICS GUIDELINES FOR SELECTING THE SURGICAL TOOLS
THE SHAPE OF HANDLE
Select instruments with a handle made of material that minimizes slippage, coated silicone or
rubber inserts

16
ERGONOMICS GUIDELINES FOR SELECTING THE SURGICAL TOOLS
The edges of the handle should be smooth, rounded to minimize the feeling of the handle
indentation in hand
Recommended are the handles of the grooves on the fingers and hook allowing relief smallest
finger and a better distribution of compressive forces
If you are left-handed, choose the symmetric handle, becouse these can be used equally well by
both right and left hands
Functional elements should be easy to access
Select the instruments with handle allow to a maximum palm support and grip design avoiding
wrist hyperflexion, hyperextension or unnecessary twisting
SIZE
The handle must be adjustable for various hand sizes. (Matern et al., 1999)
The handle sholud be as small as it possible
The size of the grooves for fingers must allow the free positioning in the central part of the
groove
Distance between arms of grip should allow to free hold of the tool
Size and dimensions of the functional elements should allow easy manipulation
FUNCTIONALITY
The handle should allow several functions to be performer
The handle should allow to use all function only one hand
You can choose instruments with interchangeable tips. This solution allows to use of one good
matched and comfortable handle

17
3. Environmental conditions: operating table AND monitor Workspace is a determinant of how behaviour and taking positions in the performance of tasks. Surgical
team works in a special environment. This is an operating room, where team realize surgical procedures.
The general division of the operating theatre includes three zones: sterile, non-sterile and anesthetise
zone. (Albayrak, 2008)
Conditions in the operating theatre include a number of aspects related to both equipment, but also the
arrangement of working space, distribution of apparatus, equipment and tools.
The impact on working conditions in the operating theatre are: appropriately selected height of the
operating table, the correct positioning of monitors and the distribution and flow of surgical equipment.
Correct, unobstructed flow of resources allows for keeping comfort for work team, reducing the
duration of procedures and maintaining a high level of security.
Optimal height for operating table
The main piece of equipment in operating room is operating table. The table determines the distribution
of the whole room. It is located in the central part of the clean zone. Both, the team and flow of
materials are focused around the operating table.
The operating table height is a characteristic technical factor which operator can influence.
Appropriately selected height helps to reduce discomfort, and may neutralize the forced and awkward
positions which caused of other factors. Not optimal height of operating table can be the reason
ailments of neck and shoulders (Wauben et al., 2006).
In the literature you can find several methods for selecting the optimum height of the operating table.
These are:
Method based on the elbow distance from the ground;
Method based on the height of the surgeons;
Method based on the level of hand surgical instruments.
Method based on the elbow distance from the ground
The factor for selecting the optimal height of the operating table was set based on the static and
dynamic tests carried out on the group of volunteer surgeons (with different anthropometry
characteristics and experience). The study involved the analysis and (objective and subjective)
evaluation of comfort / discomfort. Evaluation based on the location of the upper limbs at six different
heights of the operating table (Van Veelen et al., 2002).
The basis for determining the table height was the distance elbow from the ground. It was determined
that the optimal (ergonomic) height of the operating table should be a factor of 0,7 to 0,8 height of the
elbow. At this height, it reported the smallest discomfort in backs, shoulders and wrists.
The example 1 shows the optimal height for the surgeons 5, 50 and 95 percentile.

18
Example 1
Figure 1 The ranges of dimensions of optimal height of operating table for 5-50-95 percentile (Anthropometric Atlas, 2001)
Percentile Elbow distance
from the ground (x)
Optimal operating table
height
0,7 - 0,8x
5 96,0 67,2 - 76,8
50 107,8 75,46 - 86,24
95 119,0 83,3 - 95,2
Method based on the height of the surgeons
The second method of selecting optimal height of operating table takes into account surgeons all body
height. A study published by Kaur show a comparison of the level of comfort at the operating table in
relation to the height of the operator and table height. Experiment take into account the observation of
the operation surgeon at the operating table on six heights (65 to 90 cm) and assessment made during
the task items in respect of the position of the upper limbs (Kaur, 2008).
The basis for assessing the level of comfort were adopted angles in the shoulder joint (abduction and
adduction below 30 degrees), the elbow joint (flexion between 30 and 130 degrees) and wrist
(abduction and flexion less than 15 degrees).
When the operators had more freedom in movement and had less discomfort in the backs, shoulder and
wrists, then the comfort was considered at greatest. Results showed that ergonomic height of the
operational surface is in the 49% of the body height of the operator/assistant.
The example 2 shows the optimal height for the surgeons 5, 50 and 95 percentile.

19
Example 2
Figure 2. The ranges of dimensions of optimal height of operating table for 5-50-95 percentile (Anthropometric Atlas, 2001)
Percentile Surgeons height (x)
Optimal operating table
height
0.49x
5 153 [cm] 74,97[cm]
50 171,9[cm] 84,23[cm]
95 188,1[cm] 92,17 [cm]
METHOD BASED ON THE LEVEL OF HAND SURGICAL INSTRUMENTS
Because of limited operating field during minimally invasive surgical procedures surgeons use longer
instruments. This is the reason why the optimal height of the operating table is different as compared to
open surgery. Ergonomic study made by Berquer, Smith and Davis during MIS surgery showed that the
optimal height of operating table for this type of surgery should be related with position of surgical
instruments handles. Ergonomic position is on the elbow level or 10 cm lower. This is the factor
influencing on the correct position of operating table, which should be within the range from 64 to 77
cm (Berquer et al., 2002). This value is estimated for surgeons height 155 cm to 188 cm.
The Example 3 shows the dimensions of handles position related with table height.
Example 3
Percentile Height of surgeons
Elbow distance
from groud (x)
Level of handles position
x-10
5 153 [cm] 96,0 86,0 [cm]
50 171,9[cm] 107,8 97,8[cm]
95 188,1[cm] 119,0 109,0[cm]

20
Example 3
Figure 3. The ranges of dimensions of surgical instruments level (Anthropometric Atlas, 2001)
It is worth to note that the operating tables available on the market are height adjustable but also tilt
regulation and sectional structure. The sectional structure of the table allows to regulation different
parts of it.
Each of presented methods for selecting the height of the operating table gives a consistent value.
MONITOR
Minimally invasive orthopaedic surgical procedures are characterized by the limited operating field.
Therefore, for this type of treatment is used imaging system, for example arthroscope. In the operating
room there is additional equipment like monitors, on which the operating field is observed. The essence
of the functionality of the monitors is to reflect what would be visible to the surgeons in case of open
surgery.
The location of the monitors in relation to the surgeon is a key issue for the implementation of medical
procedures, but can cause adverse symptoms of the operator’ musculoskeletal system.
In addition to the deployment of monitors in the operating room, the other factors affecting ergonomics
are adjustability and image resolution (Sutton et al. 2012).
Good solution is to use ceiling or wall-mounted monitors with adjustment height and inclination (see
Fig. 4). This will allow adjust the monitor to an operator in such a way that the neck will be not twisted
and / or tilted or raised, what is not desirable situation.

21
Figure 4. Example of a) ceiling-mounted monitor (www.medicom.com.pl), b) range of adjustment inclination, c) wall-mounted arm for monitor (www.karlstorz.com)
The monitor should be in a horizontal plane of observer in such a way that the viewing angle facing
downward by 15 degrees. The optimal height of monitor position is about 160 cm from ground
(Zehetner et al. 2006). In the Fig. 5 you can see the recommendations for ergonomic monitor position.
Figure 5 Recommendation for ergonomic monitor position
Remember! To keep the ergonomic body position, you have to pay attention to the environment around you.
Take advantage of the possibilities offered by the equipment in the operating room - height adjustment of the operating table or monitor. Both the position of the operating table and the monitor should not cause excessive twist, bending or deviation of the neck, back, shoulders and wrists.

22
ERGONOMICS GUIDELINES FOR SELECTING THE OPTIMAL POSITION OF OPERATING TABLE AND MONITOR
How you can adjust work environment to be an ergonomic and comfortable:
There are three methods of selecting optimal height of operating table. Each of them gives
consistent value. You can count the ergonomic height with use the following factors: factor of
elbow distance (70 - 80% height of elbow level from the ground), factor of surgeons' height
(49% of this value) or factor of the level of surgical instruments handles (should be on elbow
level or maximum 10 cm below)
The table should have sectional structure and maximally wide range of adjust.
The monitor should have adjustable of height and inclination
The monitor should be placed in front of the surgeon at eye level or slightly below, avoiding
the rotating or tilting of the neck, as well as excessive flexion or extension of the cervical
vertebrae
The height of the monitor should be lower than height of the surgeon’ body. This should be
enough to reduce discomfort from neck pain which is the result of bent or twist

23
4. Operating room layout
Concept
A good layout of the service facility […] can improve the overall service efficiency and quality.
(Lee, 2012)
Operating room layout represents a spacial arrangement including surgical team members, surgical tools and auxiliary equipment. There are three essential elements determining ergonomically correct working conditions while performing surgical procedures:
Location of instruments table and scrub nurse in regards to surgeon operator;
The number and location of monitors;
Organization of auxiliary surgical equipment.
The problem of the organization of work in the operating room within MIS surgery is associated inter alia with previously unforeseen and totally different manner of work when compared to traditional open surgery. Changing the manner of performing surgeries from the open to minimally invasive has not led to remarkable changes in the organization of the work space in operating rooms. The advances in the field of surgical procedures, such as development of optics video with higher resolution and improved operational instruments on the one hand allowed doctors to perform more advanced ohopaedical surgeries; on the other hand, this progress has not been accompanied by changes in the design of operating rooms. Hence, incorrectly organized work space in operating room can lead to work burden of surgical staff, particularly by determining postural stress. Location of instruments table and scrub nurse in regards to surgeon operator Study the examples of correct (Fig. 1) and incorrect (Fig. 2) location of instruments table and scrub nurse in regard to surgeon operator. The red circles on the pictures suggest the ranges of passing the instruments by scrub nurse.

24
Example 1
Figure 1. Correctly organized space of instruments table and scrub nurse
The scrub nurse and instrument table are placed on the side of the dominant hand of surgeon operator. A scrub nurse has in range: surgeon operator, surgeon assistant and main instrument table and can give or take surgical tools without excessive postural stress and effort from the musculoskeletal system.
Example 2
Figure 2. Incorrectly organized space of instruments table and scrub nurse
Scrub nurse and the instrument table is placed in opposite to the dominant hand of surgeon operator. The operator is reaching for the tool by right hand what determines axial rotation of his back and neck.

25
Because the scrub nurse has to have in range: surgeon operator, surgeon assistant and main instrument table, she handles or takes surgical tools with excessive stress of body posture and effort from the musculoskeletal system. The scrub nurse’s back and neck are flexed and rotated. The red circle indicates a large range of passing the instruments by scrub nurse. Find two propositions improving the questioned layout. Regarding proposition a) the instrument table is relocated whereby a scrub nurse have directly access to surgeons. Surgeon operator reaches a tool without excessive twisting. Proposition b) shows a moment of handling tool to right hand of surgeon operator. This solution eliminates back twisting of surgeons. However scrub nurse should be more mobile in order to service the surgical assistant.
Example 3
a) b)
Figure 3. Propositions improving the layout of instruments table and scrub nurse
Laying out the instruments and equipment on table and around
Another problem of space organization in operating room is laying out the necessary instruments and equipment on table and around. The key aspects of it is to handle instrument in timely manner. There are two different methods for organizing instrument arrangement:
1. Dynamic arrangement.
2. Static arrangement.
In most cases it is not possible to have all the instruments laid out on one table. A scrub nurse usually re-configures the organization of instruments taking into account a certain phase of surgical procedure. The most relevant instruments at given moment or most frequently used instruments should be laid out in front of her, in particular order and nearest to a surgeon. In the same time scrub nurse removes the unused tool and places on main table next tools. Such a way of organizing instrument table requires anticipating next step performed by surgeon. The dynamic arrangement of surgical tools may not only designed to support a nurses’ own contributing so that she can pass the next instrument in a timely manner (Swenson et al. 2007). The static arrangements means the same place of instruments regardless the phase of a surgical procedure. However the essential aspect of such behavior is to order instrument set according to a frequency of their use. In addition and regardless of the method, it is recommended to leave a gaps between tools in order to support the visibility of certain instrument and support grasping and taking a tool from table. The orientation and direction of the instruments also can facilitate how the scrub nurse transfers a tool from the table directly into the hand of the surgeon (Swenson et al. 2007).

26
ERGONOMICS GUIDELINES FOR LOCATION OF INSTRUMENTS TABLE AND SCRUB NURSE
Scrub nurse should have directly hand contact with surgeon operator
Instrument table should be placed slightly to the side of a nurse and in range of the operator’s
hand
If possible, the instrument table and scrub nurse should be placed on a side of the dominant
hand of surgeon operator
The most relevant instruments at given moment or most frequently used instruments should
be laid out in front of scrub nurse, in particular order and nearest to a surgeon
If using the same tools they should be laid out at the same place
The number and location of monitors There are three problematic areas connected with monitor location:
1. The monitor is located too high the neck/head is bent to top.
2. The monitor is located behind operator the neck/head and back is twisted.
3. The monitor is located too far from operator the upper body is bent to forward or/and
twisted.
ERGONOMICS GUIDELINES FOR THE MONITOR LOCATION
Find important recommendations for monitor placement (Van Det et al., 2009; Xiao et al., 2012):
1. In the horizontal plane, the monitor should be straight ahead of each person in line with the
forearm–instrument motor axis, avoiding axial rotation of the spine.
2. In the sagittal plain, the monitor should be positioned lower than eye level to avoid neck
extension. The most comfortable viewing direction is approximately 15° downward. The most
efficient monitor position is with an additional monitor near the operative field, implicating a
more inclined viewing direction.
3. Viewing distance is highly dependent on monitor size. It should be far enough to avoid
extensive accommodation of the eyes and conversion by the extraocular musculature, and it
should be close enough to avoid staring and loss of detail.
However, the location of the monitor presented above in the table, is associated with two problematic consequences: Firstly, each additional monitor increases the cost of purchasing equipment. Secondly the layout of the monitors in a specific position, especially below the line of sight causes huge changes in the organization of the whole workplace. Traditionally, the monitor is located above the equipment due to the concentration of people and devices at the operating table.

27
Organization of auxiliary surgical equipment
Auxiliary equipment such as tubes, cables, wires can cause dangerous of tripping of medical staff. This equipment should be grouped, tapped to the floor and run off from operating field in order to not impede or limit surgeon’s movements.
ERGONOMICS GUIDELINES FOR THE ORGANIZATION OF AUXILIARY EQUIPMENT
Remember:
Tubes, cables or wires should not impede surgical work. They should be ordered, grouped and removed from operating field.
Study how to support workplace organization with the use of method 5S The method 5S supports workplace organization for efficiency and effectiveness by identifying and storing the items used, maintaining the area and items, and sustaining the new order according to a list of five stages: seiri, seiton, seiso, seiketsu, and shitsuke (from Japanise) what means respectively: sort, straighten, shine, standarize, sustain. This method can be used for improvement and support organization in operating room (Gapp 2008). Despite the fact that the origin of 5S method is menufacturing, it can be particularly beneficial in health care because a frantic search for supplies to treat an in-trouble patient (a chronic problem in health care) can have dire consequences (Graban 2012).
ERGONOMICS GUIDELINES FOR THE ORGANIZATION OF OPERATING ROOM LAYOUT WITH THE USE OF 5S METHOD
Sort:
Remove from directly operating area unnecessary items like unused equipment or tools
Eliminate obstacles and remove waste, like utilized or empty containers
Segregate unwanted materials from the operating area or operating room
Straighten:
Arrange all necessary items so that they can be easily selected for use, make and use a checklist
for surgical tools, materials and auxiliary equipment. Keep in ready spare tools and materials
Prevent loss and waste of time by arranging work space in such a way that all
tooling/equipment is in close proximity especially in operating area of scrub nurse
Make it easy to find and pick up necessary items like surgical tools and medical materials
All of the above work should be done on regular basis
Shine:
Clean a workspace from unused tools and materials
Prevent medical equipment deterioration
Standardize:
Standardize the best practices in the work area
Maintain high standards in workplace organization at all times

28
ERGONOMICS GUIDELINES FOR THE ORGANIZATION OF OPERATING ROOM LAYOUT WITH THE USE OF 5S METHOD
Maintain orderliness. Maintain everything in order and according to its standard
Everything in its right place
Every process has a standard
Sustain:
To keep in proper working order
Also translates as "do without being told"
Perform regular audits
Training and discipline
Training is goal-oriented process. Its resulting feedback is necessary monthly
In some quarters, 5S has become 6S, the sixth element being safety (Gapp 2008).

29
5. Workflow and surgical team cooperation
Concept
The background of teamwork is workflow which means possessing proper information by proper team member in proper time in order to do tasks in best possible way in all stages of surgical procedures.
Efficient and effective surgical teamwork is characterized by an interrelated set of team member thoughts, behaviour, feelings and communication (Salas et al. 2008).
In general, surgical workflow is the sequence of surgical steps and actions that are accomplished to perform a treatment. Surgical workflow is a subject of many studies. However, there are found in the literature different approaches to the workflow research in surgery. The differences are mostly connected to the recipient and subject of using workflow and to the method of workflow process modelling. For instance, in (Franke et al. 2015) the objective of the workflow improvements was dedicated directly to surgeons and operating room staff, and particularly the aim was to unburden the surgeon and other staff from manual maintenance and information seeking tasks by implementation of an intelligent systems behaviour thanks to automatic adaptation of assistance functions to the contextual situation in the theatre. In turn the research presented in (Elfering et al. 2015) is focused on workflow interruptions and its importance in the prediction of errors in surgery and generally failures in health care. The survey conducted among nurses and physician indicated that the reasons of interruptions are malfunctions and organizational constraints. Hence, the recommended solution is to redesign work processes. The way of predict medical errors is to design appropriate expert decision-making system. That idea in the context of clinical workflow in minimal invasive surgery is proposed in (Jalote-Parmar et al. 2010). There was established a prototype version for guiding minimally invasive procedures based on intra-operative image-guidance for clinical procedures. Hence, the important component of expert systems is information visualization. Additionally, a component of workflow and simultaneously one of the key roles within surgical team cooperation play the communication (Carthey et al. 2001; de Levalet al. 2000; Kenyon 2001; Lingard 2004; Moorthy 2006; Gawande 2003) and information/knowledge transfer. You can study the example of workflow analysis. Workflow is represented graphically. The basis for developing workflow was registration of real surgeries in range of hip replacement. In the Fig. 1 you can see two general sections in the graphical representation of workflow:
1. Specification of job elements, inter alia: procedure stages, tolls handling, operational activities,
disruptions, deficiencies,
2. The processing of job elements showed by use of charts.
All job elements are synchronized with video materials what allows for identification of problems in range of work organization and communication within surgical team as well as their causes and consequences.

30
Example 1
Figure 1. Graphical representation of workflow while performing hip replacement
The characteristic elements describing surgical workflow and influencing ergonomics as well as effectiveness of procedure are:
Disruptions like: improper lighting of the operative field and the need for its corrections;
viability of a pump suction and flushing, which consequently can lead to replace with a new
one;
Passive action of surgeon operator results from such causes like: waiting for surgical
instruments, waiting for materials etc.
Deficiencies like: lack of materials, devices etc.
Cases, where surgeon operator covers activities normally performed by an assistant,
Cases, where surgeon operator must correct activities performed by an assistant.
Most of these elements are assosiated to misunderstanding and poor information or knowledge
transfer. There is a high degree of knowledge diversity and interactions between variety staff from
different units involved in surgical procedures. The problem is that particular member of surgical team
does not cooperate in frame of the same team neither during surgeries in operating rooms nor working
in wards.
Additionally, it is significant that surgical team consists of variety types of medical specialists who
possess different kind of knowledge, motivations, personalities or abilities and that they can have
different patterns of behaviour as well as different educational paths. In addition, the multiplicity of tasks within hospital processes and surgical team requires multidisciplinary knowledge recourses. However, it can be recognized several problem areas related to the knowledge management in surgical team:

31
There are technical knowledge gaps among surgical team member. In particular technical
knowledge is related to proper using and maintaining surgical tools and devices. The ways of
acquiring such knowledge are usually: instructions, surgical techniques manuals, observations,
less often trainings. As a result the staff participating in surgery use different degree of
knowledge - this concerns even a tool names. The problem is particularly important by
frequently staff rotation.
There are different degrees of knowledge absorption abilities among surgical team members.
To a small extent staff use the manual or manuals of surgical techniques, although they are a
necessary basis for the proper use and maintenance of equipment and surgical expertise. This is
due to the lack of fit forms of presentation of the contents of technical capacity issues.
Simultaneously, medical staff mainly have no necessary back-substantive technical
competencies.
There is no open access to certain type of knowledge recourses. The manuals and instructions
are usually stored in one office (e.g. only in the ward nurse's office), which may cause
significant aggravations with access by more people.
Surgical team requires multidisciplinary knowledge recourses which require unified and common knowledge management principles. This improves communication process.
There are two main ways of communication:
Direct way with the participation of speakers (with immediate feedback) does not require
additional communication devices.
Indirect way with use of additional devices like: paper, phone, messaging, social networks,
webmail etc.
Additionally, two main forms of direct communication are used:
Verbal form – spoken messages.
Nonverbal form in the shape of gestures and facial expression.
The communication is reflected in a large informal dimension concerning the specifics of organizational culture in the hospital, not only in operating room. This on the one hand is significant and indicates the strong relations between the hospital staff and the so-called non-technical-interpersonal skills, very important from the point of view of the integration of activities and teamwork. On the other hand, spoken messages, which are not formal communications but spontaneous expressions, carry a number of risks related to misunderstanding and not meeting the expectations. In addition, the strong ties between workers are found but only within a given department or within a particular group of workers in the operation room. Such relationships are not observed among employees from different departments or hospital units, in spite the fact that they are often linked to a patient's medical history. Such a situation, in the absence of other effective forms of communication, creates the problems of repetition of the same tasks, generating the same information, and therefore lengthening surgical procedures or exposing patient to a risk.
Because the team communication breakdowns are associated with degraded team performance (Parush et al., 2011) it is necessary to solve the problem by using different kind of methods.

32
There are many of methods improving knowledge transfer and communication as well workflow in operating room:
briefings and debriefing sessions,
simulation plays,
interactive seminars,
workshops,
virtual games.
Particularly, trainings improve the operating room staff’s familiarity with and performance of new MIS techniques can be beneficial to both surgeons and perioperative nurses and technicians (Sang, 2012).
GUIDELINES FOR WORKFLOW AND SURGICAL TEAM COOPERATION
The best way of well communication are clear and repetitive messages and the same abilities
of different team members to absorption of knowledge.
You can learn these skills based on common and regularly trainings e.g. with use of simulation
and staging techniques.
You can also improve surgical workflow by trainings that can take different forms like briefings
and debriefing sessions, simulation plays, interactive seminars, workshops, virtual games etc.
It is essential to design specially team of perioperative nurses and physicians because they can
accomplish tasks more quickly and efficiently than a random group of circulating surgical team
members (Reddy et al. 2011; Lafreniere et al. 2003; Franson et al. 2011).
References
3D Static Strength Prediction Program. User Manual, 2011. The University of Michigan Center for Ergonomics.
Anthropometric Atlas. Data for the ergonomic design and evaluation. (2001) Central Institute for Labour Protection, Warsaw (Atlas miar człowieka. Dane do projektowania i oceny ergonomicznej (2001) Centralny Instytut Ochrony Pracy, Warszawa)
Armaĝan Albayrak , (2008) Ergonomics in the operating room transition from
open to image-based surgery, uuid:ab713973-b6bb-40e7-8567-bc8a92219bd2
Berguer R, Smith WD, Davis S (2002) An ergonomic study of the optimum operating table height for laparoscopic surgery. Surgical Endoscopy 16(3): 416–421.
Carthey J.,de Leval, MR,Reason JT (2001) The human factor in cardiac surgery: errors and near misses in a high technology medical domain. Ann. Thorac. Surg. 72:300-305.

33
Dabholkar T, Yardi S, Dabholkar YG, Khanvilkar A (2015) Work Related Musculoskeletal Disorders in Surgeons Performing Minimal Invasive Procedures in Mumbai & Navi Mumbai India. International Journal of Health Sciences and Research 5 (8): 347-355.
deLeval MR,Carthey J,Wright DJ et al. (2000) Human factors and cardiac surgery: a multicenter study. J. ThoracCardiovasc Surg. 119:661-672.
Elfering A, Nützi M, Koch P, Baur H (2015) Workflow Interruptions and Failed Action Regulation in Surgery Personnel Workflow interruptions during surgery may cause a threat to patient’s safety Safety and Health at Work 5:1-6.
Franke S, Meixensberger J, Neumuth T (2015) Multi-perspective workflow modeling for online surgical situation models. Journal of Biomedical Informatics 54:158–166.
Franson R, Khabbaz FH, Kapoor A, Patriciu A (2011) A system for laparoscopic surgery ergonomics and skills evaluation. Journal of Endourology 25(7):1111–1114.
Gapp R, Fisher R, Kobayashi K (2008) Implementing 5S within a Japanese context: an integrated managament approach. Management Decision”. 46 (4):565-579
Gawande AA,Zinner, M.J.,Studdert, DM et al. (2003) Analysis of errors reported
by surgeons at three teaching hospitals.Surgery.133:614-421
Graban M (2012) Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement. Boca Raton, Fl: CRC Press.
Gurvinder Kaur (2008) Role of OT Table Height on the Task Performance of Minimal Access Surgery, World Journal of Laparoscopic Surgery 1 (1): 49-55
Jaffar N, Abdul-Tharim AH, Mohd-Kamar IF, Lop NS (2011) A Literature Review of Ergonomics Risk Factors in Construction Industry. Procedia Engineering 20: 89–97.
Jalote-Parmar A, Badke-Schaub P, Ali W, Samset E (2010) Cognitive processes as integrative component for developing expert decision-making systems: A workflow centered framework, Journal of Biomedical Informatics 43:60–74.
Kenyon, T.A.,Urbach, D.R.,Speer, J.B. et al., 2001.Dedicated minimally invasive surgery suites increase operating room efficiency. Surg, Endosc. 15, 1140-1143
Koradecka D (2008) Bezpieczeństwo i higiena pracy. Centralny Instytut Ochrony Pracy - Państwowy Instytut Badawczy, Warszawa.
Lafreniere R, Berguer R, Seifert P, Belkin M, Roth S, Williams K, Maria E, Napolitano L (2003) Preparation of the operating room. ACS Surgery: Principles and Practice. 2003:1–14.

34
Lee, H Y (2012) Integrating simulation and ant colony optimization to improve the service facility layout in a station. Journal of Computing in Civil Engineering, 26 (2): 259–269.
Lingard, L.,Espin, S.,Whyte, S. et al., 2004. Communication failures in the operating room: an observational classification of recurrent types and effects. Qual. Saf. Health Care.13, 330-334
Matern U., Waller P., (1999) Instruments for minimally invasive surgery. Principles of ergonomic handles, Surgical Endoscopy. Ultrasound and Interventional Techniques 13: 174–182
McAtamney, L, Corlett, EN (1993) RULA: a survey method for the investigation of work-related upper limb disorders. Applied Ergonomics 24, 91-99.
Moorthy, K.,Munz, Y.,Forrest, D. et al., 2006.Surgical crisis management skills training and assessment: a simulation[corrected]-based approach to enhancing operating room performance. Ann. Surg.224, 139-147
Mueller L. P., (1993) Laparoscopic instrument grips, Surgical Endoscopy 7:465-466
Parush A, Kramer C, Foster-Hunt T, Momtahan K, Hunter A, Sohmer B (2011) Communication and Team Situation Awareness in the OR: Implications for augmentative information display. Journal of Biomedical Informatics, 44:477-
485.
Reddy, PP, Reddy TP, Roig-Francoli J, Cone L, Sivan B, DeFoor WR, Gaitonde K, Noh PH (2011) The Impact of the Alexander technique on improving posture and surgical ergonomics during minimally invasive surgery: pilot study. The Journal of Urology 186(4):1658–1662.
Salas, E., Diaz Granados, D., Weaver, S.J., King, H., 2008. Does team training work? Principles for health care. Acad. Emerg. Med. 15: 1002-1009.
Sang D (2012) A Review of the Ergonomic Issues in the Laparoscopic Operating Room. Journal of Healthcare Engineering 3(4): 587-603.
Sutton E. R. H., Park A., (2012) Ergonomics in Operating Room Design in: Soper N. J., Scott-Conner C. E.H.(edit.) (2012) The SAGES Manual. Volume 1. Basic
Laparoscopy and Endoscopy, Springer
Swenson MS, Heath Ch, Luff P (2007) Instrumental action: the timely exchange of implements during surgocal operations. In: Bannon L. Wagner I, Gutwin C, Harper R, Schmidt K (eds.) ECSCW 2007: Proceedings of the 10th European Conference on Computer Supported Cooperative Work, 24-28 September, Limerick, Ireland 41-60.
The Intuitool: A Comfortable Laparoscopic Grasper, http://www.unemed.com/wp-content/uploads/2013/11/UNEMED-intuitool-supplement.pdf

35
Van Det MJ, Meijerink WJHJ, Hoff C, Totté ER, Pierie JPEN (2009) Optimal ergonomics for laparoscopic surgery in minimally invasive surgery suites: a review and guidelines. Surg Endosc 23:1279-85.
Wauben LSGL, van Veelen MA, Gossot D, Goossens RHM (2006) Application of ergonomic guidelines during minimally invasive surgery: a questionnaire survey of 284 surgeons. Surg Endosc 20(8):1268–74.
Xiao DJ, Jakimowicz JJ, Albayrak A, Goossens RHM (2012) Ergonomic factors on task performance in laparoscopic surgery training. Applied Ergonomics 43:548-53.
Zehetner J., Kaltenbacher A., Wayand W.,Shamiyeh A., (2006) Screen height as an ergonomic factor in laparoscopic surgery, Surgical Endoscopy and Other Interventional Techniques 20: 139–141
Zheng Li, Guohui Wang, Juan Tan , Xulong Sun, Hao Lin, Shaihong Zhu, (2016) Building a framework for ergonomic research on laparoscopic instrument handles, International Journal of Surgery 30: 74-82
Suppliers’ websites:
http://www.medicalexpo.com/prod/micromed-medizintechnik/product-74784-
463808.html;
https://www.spinecenter.com/miss-instruments---equipment.html;
http://advanceeurope.com.pl;
http://www.innomed.net;
http://medi-portal.pl;
http://www.arthrex.com;
http://www.rudolf-med.com




















