Moderating effects of empathic concern and personal distress on the emotional reactions of disaster...
14
1 Moderating effects of empathic concern and personal distress on the emotional reactions of disaster volunteers Ioana A. Cristea, Emanuele Legge, Marta Prosperi, Mario Guazzelli, Daniel David and Claudio Gentili 1 This study examines stress and mood outcomes in community volunteers who undertook one week’s worth of post-disaster relief work in L’Aquila, Italy, which had been hit by an earthquake four months earlier. The study team obtained pre- and post-relief work data from 130 volunteers involved in activities such as preparing food for the displaced, cleaning the camps and distributing clean linen. The Perceived Stress Scale, the State- Trait Anxiety Inventory and the Profile of Mood States were administered at the start and at the end of the aid activities. Psychopathological symptoms and empathy were assessed in the beginning, using the Symptom Checklist 90 Revised and the Interpersonal Reactivity Index, respectively. The results show that, following the assistance work, volunteers displayed decreases in perceived stress, general distress, anxiety and anger, as well as increases in positive emotions. The empathy facets empathic concern and personal distress showed different patterns in modulating the post-disaster relief work adaptation for some of the mood outcomes. Keywords: disaster relief, empathy, mood, stress, volunteers [A] Introduction [B] Facets of empathy and volunteer work Empathy has been defined as ‘an affective response that stems from the apprehension or comprehension of another’s emotional state or condition and is similar to what the other person is feeling or would be expected to feel’ (Eisenberg, 2000, p. 671). Differences in dispositional empathy were shown to be predictive of the willingness to encounter and assist people in need (Davis et al., 1999; Eisenberg and Fabes, 1990). Paradoxically, empathy is considered both a necessary quality for assistance work and a risk factor for secondary traumatisation and compassion fatigue in disaster responders (Figley, 2002). However, research has demonstrated that empathy is a multidimensional construct, encompassing distinct processes (Davis, 1983). In particular, two forms of empathy were found relevant in the context of helping behaviours: empathic concern and personal 1 Ioana A. Cristea is Research Fellow in the Department of Surgical, Medical, Molecular and Critical Pathology, University of Pisa, Pisa, Italy, and Assistant Professor at the Department of Clinical Psychology and Psychotherapy, Babes-Bolyai University, Cluj-Napoca, Romania; Emanuele Legge is Director of Staff Psychology in the Service of Psychology, Local Health District, L’Aquila, Italy; Marta Prosperi is Staff Psychologist in the Service of Psychology, Local Health District, L’Aquila, Italy; Daniel David is Professor in the Department of Clinical Psychology and Psychotherapy, Babes-Bolyai University, Cluj-Napoca, Romania, and Adjunct Professor in the Department of Oncological Sciences, Icahn School of Medicine at Mount Sinai, New York, United States; and Claudio Gentili is Assistant Professor in the Department of Surgical, Medical, Molecular and Critical Pathology, University of Pisa, Pisa, Italy. Mario Guazzelli (1948– 2012) was Full Professor of Clinical Psychology at the University of Pisa, Pisa, Italy; this paper is dedicated to his memory.
Transcript of Moderating effects of empathic concern and personal distress on the emotional reactions of disaster...

1
Moderating effects of empathic concern and personal distress on the emotional reactions of disaster volunteers Ioana A. Cristea, Emanuele Legge, Marta Prosperi, Mario Guazzelli, Daniel David and Claudio Gentili1 This study examines stress and mood outcomes in community volunteers who undertook one week’s worth of post-disaster relief work in L’Aquila, Italy, which had been hit by an earthquake four months earlier. The study team obtained pre- and post-relief work data from 130 volunteers involved in activities such as preparing food for the displaced, cleaning the camps and distributing clean linen. The Perceived Stress Scale, the State-Trait Anxiety Inventory and the Profile of Mood States were administered at the start and at the end of the aid activities. Psychopathological symptoms and empathy were assessed in the beginning, using the Symptom Checklist 90 Revised and the Interpersonal Reactivity Index, respectively. The results show that, following the assistance work, volunteers displayed decreases in perceived stress, general distress, anxiety and anger, as well as increases in positive emotions. The empathy facets empathic concern and personal distress showed different patterns in modulating the post-disaster relief work adaptation for some of the mood outcomes. Keywords: disaster relief, empathy, mood, stress, volunteers [A] Introduction [B] Facets of empathy and volunteer work Empathy has been defined as ‘an affective response that stems from the apprehension or comprehension of another’s emotional state or condition and is similar to what the other person is feeling or would be expected to feel’ (Eisenberg, 2000, p. 671). Differences in dispositional empathy were shown to be predictive of the willingness to encounter and assist people in need (Davis et al., 1999; Eisenberg and Fabes, 1990). Paradoxically, empathy is considered both a necessary quality for assistance work and a risk factor for secondary traumatisation and compassion fatigue in disaster responders (Figley, 2002).
However, research has demonstrated that empathy is a multidimensional construct, encompassing distinct processes (Davis, 1983). In particular, two forms of empathy were found relevant in the context of helping behaviours: empathic concern and personal
1 Ioana A. Cristea is Research Fellow in the Department of Surgical, Medical, Molecular and Critical Pathology, University of Pisa, Pisa, Italy, and Assistant Professor at the Department of Clinical Psychology and Psychotherapy, Babes-Bolyai University, Cluj-Napoca, Romania; Emanuele Legge is Director of Staff Psychology in the Service of Psychology, Local Health District, L’Aquila, Italy; Marta Prosperi is Staff Psychologist in the Service of Psychology, Local Health District, L’Aquila, Italy; Daniel David is Professor in the Department of Clinical Psychology and Psychotherapy, Babes-Bolyai University, Cluj-Napoca, Romania, and Adjunct Professor in the Department of Oncological Sciences, Icahn School of Medicine at Mount Sinai, New York, United States; and Claudio Gentili is Assistant Professor in the Department of Surgical, Medical, Molecular and Critical Pathology, University of Pisa, Pisa, Italy. Mario Guazzelli (1948–2012) was Full Professor of Clinical Psychology at the University of Pisa, Pisa, Italy; this paper is dedicated to his memory.

2
distress. Empathic concern—also labelled ‘sympathy’ (Eisenberg et al., 1994)—describes the observer’s experience of feelings of sympathy and compassion for a distressed target (Davis et al., 1999). Personal distress, while also referring to an affective reaction experienced by an observer in response to a distressed target, has to do with feelings of personal anxiety and discomfort. In this sense, one difference between these two facets of empathy is that while empathic concern is more markedly other-oriented than self-oriented, personal distress is self-oriented rather than other-oriented (Davis et al., 1999; Eisenberg and Fabes, 1990).
Evidence supports the idea that both empathic concern and personal distress are
associated with helping behaviours directed at somebody in need, but the theoretical mechanisms underlying these associations differ for the two constructs (Davis, 2004). Personal distress probably fosters helpful behaviour from an observer in order to relieve his or her own discomfort in the face of another’s plight. On the other hand, empathic concern seems to sustain a kind of help that is solely motivated by the concern for the welfare of another person, upholding the notion of ‘true altruism’ (Batson, Fultz, and Schoenrade, 1987; Batson, 1991). Moreover, empathic concern and personal distress are differentially affected by contextual factors in their influences on helping behaviours. While increased empathic concern can lead someone to help a needy target even when it is easy not to provide assistance, personal distress is not associated with helping someone in need when escape is easy (Batson, 1991).
The different associations of empathic concern and personal distress with
prosocial behaviours make it plausible that the their associated emotional experiences differ as well (Eisenberg, 2000). In fact, dispositional empathic concern and personal distress have been linked to differences in emotional response and regulation. While personal distress is related to heightened emotional intensity and low regulation, empathic concern is associated with moderately high emotional intensity and bears less of a link to emotional regulation (Eisenberg et al., 1994).
Finally, very few studies look at the effects of these forms of empathy in actual
community volunteers. Such volunteers are broadly defined as external individuals involved in local, national or international humanitarian organisations, which provide them with basic training in emergency response (Thormar et al., 2010). Omoto and Snyder (1995) show that a helping disposition—characterised not only by empathic concern, but also by nurturance and social responsibility—is associated with higher volunteer satisfaction and integration, even if it is not directly related to persistence in volunteering over time. In addition, Davis, Hall and Meyer (2003) demonstrate that in first-year volunteers, both dispositional empathic concern and personal distress were linked to feelings of sympathy. High empathic concern was strongly related to the accomplishment of altruistic aims over time, while personal distress displayed sporadic associations.
It is worth emphasising that while these two facets of empathy have been linked to
helping behaviours and corresponding emotional reactions, few relevant studies focus on

3
actual volunteers. Yet even among those that do,2 none concentrates on disaster relief activities. [B] Community volunteers in disaster relief In a review focused on the mental health impact of volunteering in disaster settings, Thormar et al. (2010) notice that while there is growing literature on the mental and physical health consequences of disaster survivors and of professional rescuers workers, there is a knowledge gap concerning consequences for community helpers. These volunteers are a heterogeneous group, usually coming from diverse demographic backgrounds and professions, with different levels of previous training in relief activities and varying degrees of experience. They are usually deployed upon need at disaster sites, where they may take on a number of roles, depending on the context, before returning to their communities, families and workplaces. While research is scarce, it appears to indicate that regardless of the disaster type, community volunteers are at increased risk for mental and physical health complaints (Thormar et al., 2010). Research has identified the length and severity of exposure to gruesome events during disaster work as predisposing factors (Fullerton, Ursano and Wang, 2004; Mitchell et al., 2004).
Post-disaster interventions have been categorised in four phases (Rao, 2006; Raphael, 1986). The first one—the rescue phase or heroic phase—covers roughly the first two weeks after the strike of the disaster; the initial intensive search and rescue efforts take place during this period. It is followed by a relief phase, also called the honeymoon phase, which lasts two to six months and is characterised by an outpour of relief supplies, both from the community and from external volunteer agencies. These two early phases of a disaster aftermath are followed by two later stages. During the rehabilitation phase, which is also known as the disillusionment stage and lasts for one to two years, the reality of the impact and of the associated difficulties sinks in. During the rebuilding or reconstruction phase, which can last for years, the individual and the community begin to return to the pre-disaster state.
Most papers that examine rescue workers’ involvement in disaster areas are
focused on the time period and operations immediately after the event, or on the long-term consequences of this type of exposure to the immediate aftermath of a disaster. A review of the literature shows that few studies consider volunteer efforts in the subsequent stages, nor do they concentrate on the psychological needs and reactions of volunteers.
[B] Study objectives This study aims to address two gaps in the literature. First, hardly any research has focused on empathy and its two distinct facets in volunteers who undertake disaster relief activities. Second, there is a dearth of information on the emotional reactions of community volunteers in the relief phase of a disaster aftermath.
2See, for example, Davis, Hall and Meyer (2003) and Omoto and Snyder (1995).
4
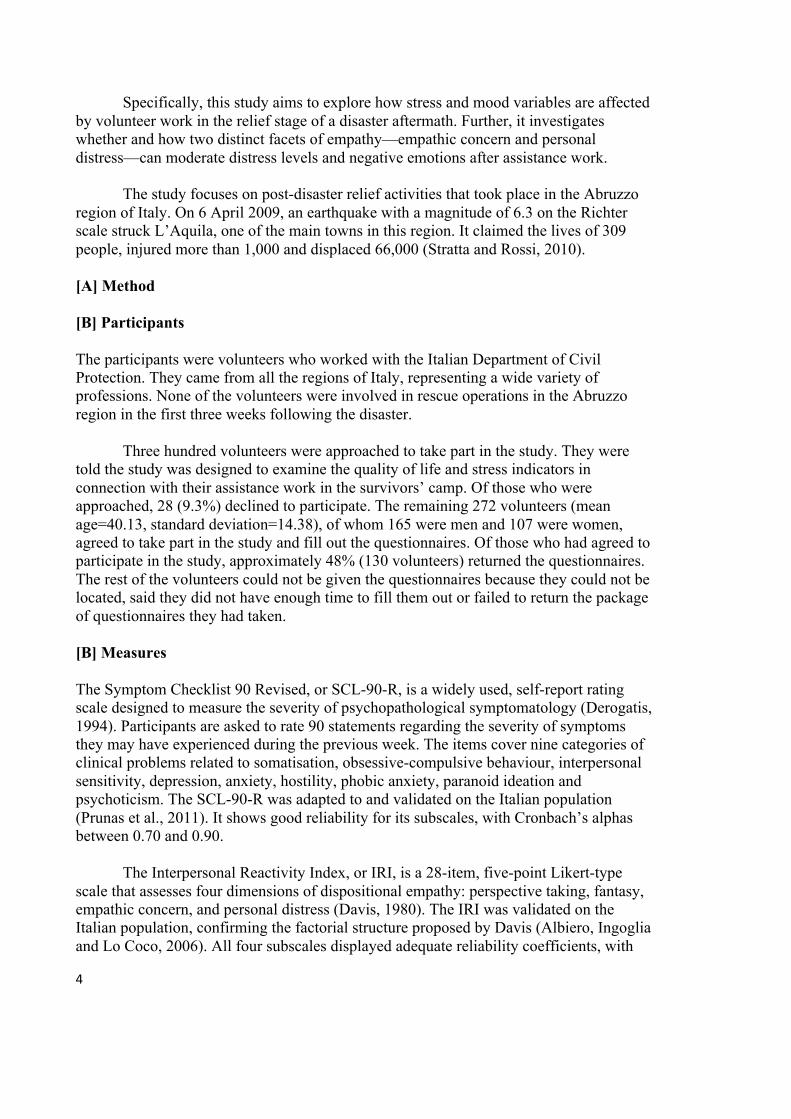
Specifically, this study aims to explore how stress and mood variables are affected by volunteer work in the relief stage of a disaster aftermath. Further, it investigates whether and how two distinct facets of empathy—empathic concern and personal distress—can moderate distress levels and negative emotions after assistance work.
The study focuses on post-disaster relief activities that took place in the Abruzzo
region of Italy. On 6 April 2009, an earthquake with a magnitude of 6.3 on the Richter scale struck L’Aquila, one of the main towns in this region. It claimed the lives of 309 people, injured more than 1,000 and displaced 66,000 (Stratta and Rossi, 2010).
[A] Method [B] Participants The participants were volunteers who worked with the Italian Department of Civil Protection. They came from all the regions of Italy, representing a wide variety of professions. None of the volunteers were involved in rescue operations in the Abruzzo region in the first three weeks following the disaster.
Three hundred volunteers were approached to take part in the study. They were told the study was designed to examine the quality of life and stress indicators in connection with their assistance work in the survivors’ camp. Of those who were approached, 28 (9.3%) declined to participate. The remaining 272 volunteers (mean age=40.13, standard deviation=14.38), of whom 165 were men and 107 were women, agreed to take part in the study and fill out the questionnaires. Of those who had agreed to participate in the study, approximately 48% (130 volunteers) returned the questionnaires. The rest of the volunteers could not be given the questionnaires because they could not be located, said they did not have enough time to fill them out or failed to return the package of questionnaires they had taken.
[B] Measures The Symptom Checklist 90 Revised, or SCL-90-R, is a widely used, self-report rating scale designed to measure the severity of psychopathological symptomatology (Derogatis, 1994). Participants are asked to rate 90 statements regarding the severity of symptoms they may have experienced during the previous week. The items cover nine categories of clinical problems related to somatisation, obsessive-compulsive behaviour, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism. The SCL-90-R was adapted to and validated on the Italian population (Prunas et al., 2011). It shows good reliability for its subscales, with Cronbach’s alphas between 0.70 and 0.90.
The Interpersonal Reactivity Index, or IRI, is a 28-item, five-point Likert-type scale that assesses four dimensions of dispositional empathy: perspective taking, fantasy, empathic concern, and personal distress (Davis, 1980). The IRI was validated on the Italian population, confirming the factorial structure proposed by Davis (Albiero, Ingoglia and Lo Coco, 2006). All four subscales displayed adequate reliability coefficients, with

5
Cronbach’s alphas ranging from 0.63 to 0.75. For purposes of this study, the empathic concern and the personal distress scales were used. Empathic concern is reflected by statements such as the following:
• ‘I often have tender, concerned feelings for people less fortunate than me.’ • ‘When I see someone being taken advantage of, I feel kind of protective towards
them.’ Personal distress is indicated by assertions such as:
• ‘I sometimes feel helpless when I am in the middle of a very emotional situation.’ • ‘When I see someone who badly needs help in an emergency, I go to pieces.’
The Profile of Mood States, or POMS, is a 58-item questionnaire that measures six
affective states: tension–anxiety, fatigue, anger–hostility, depression, confusion–bewilderment and vigour (McNair, Lorr and Droppleman, 1981). The POMS was adapted to the Italian population (Farne et al., 1991). Cronbach’s alphas for the Italian version of the scale and its subscales ranged from 0.84 to 0.95. The present study uses a total distress score—constructed by summarising the five scales that measure negative emotions—as a distress measure. The score on the vigour scale is used as an index of positive emotions.
The State-Trait Anxiety Inventory Y, or STAI Y1-State, asks participants to
evaluate how they feel ‘right now’ by rating 20 statements regarding anxious mood in terms of perceived intensity (Spielberger et al., 1983). The STAI Y was adapted and validated on the Italian population (Pedrabissi and Santinello, 1989). Cronbach’s alpha for the Italian version of the scale is over 0.90.
The Perceived Stress Scale is a ten-item self-report questionnaire that measures a
person’s evaluation of the degree to which the situations in the previous week were stressful, meaning unpredictable, uncontrollable or the like (Cohen and Williamson, 1988). It has been shown to be a reliable and valid instrument for measuring perceived stress (Roberti, Harrington and Storch, 2006). For this sample, the reliability for the scale was satisfactory, with Cronbach’s alphas of 0.72 and 0.78 as pre- and post-test measures, respectively.
[B] Procedure Volunteers were deployed in the survivors’ camp in L’Aquila for one week. They took part in aid activities, such as preparing food for the refugees, cleaning the camp and the survivors’ tents, and distributing clean linen. Since they conducted their work around the survivors’ tents and lived in the same camp—albeit in a separate part—interaction with the survivors was unavoidable although it was not specifically required. The whole operation lasted six weeks, starting in August 2009 (four months after the earthquake); new groups of 50 volunteers were deployed each week.
Before each group began work, coordinators of the survivors’ camp organised an orientation meeting and explained how the volunteers should go about their tasks. At the

6
same meeting, a team of psychologists informed the volunteers that they could choose to participate in this study. Interested volunteers were assigned a number, which was given to them on a sheet of paper, together with a set of questionnaires to fill out. They were instructed to write this number on all questionnaires. After they had completed their assistance work, individual volunteers were approached and asked whether they wished to continue participating in the study; if they agreed, they were given the questionnaires and again instructed to label them with their number. In an effort to ensure confidentiality, the psychologists responsible for the data collection were not involved in entering the data in the database.
All potential participants were screened for clinical problems prior to their
involvement. Only volunteers who presented no evidence of clinical problems on any of the nine subscales of the SCL-90-R were included in the study, meaning that their scores had to be under the cut-off point of 65. As a result, two volunteers were excluded form the study. Stress and mood measures were administered both before the volunteer work began, as a baseline measure, and after the one-week volunteering period. Empathy was assessed before the relief work began.
[A] Results Table 1 presents the correlations between the two selected dimensions of empathy—empathic concern and personal distress—and the selected stress and mood outcomes. Empathic concern bore small and, for the most part, non-significant correlations with the emotional outcomes. Personal distress had significant medium-size correlations with the emotional outcomes, indicating that they refer to distinct, albeit related, constructs. Table 1 Correlations between empathy dimensions and emotional variables at baseline (n=272) 1 2 3 4 5 6 7 8 9 10 11
1. Empathic concern
Empathy dimensions
2. Personal distress
0.07
3. Perceived stress
0.10 0.51
4. General distress
0.17 0.43 0.57
5. Anxiety 0.16 0.41 0.51 0.52 6. Anxiety–tension
0.12 0.39 0.50 0.83 0.47
7. Depression 0.14 0.37 0.52 0.89 0.47 0.66 8. Anger–hostility
0.07 0.31 0.46 0.90 0.41 0.70 0.79
9. Fatigue 0.22 0.44 0.51 0.81 0.47 0.66 0.64 0.61 10. Confusion–bewilderment
0.22 0.35 0.45 0.76 0.43 0.55 0.59 0.59 0.63
Emotional variables
11. Vigour– positive emotions
-0.03 -0.37 -0.42 -0.25 -0.48 -0.15 -0.31 -0.19 -0.27 -0.14

7
Notes: Shaded cells indicate p<0.05 Holm–Bonferroni corrected for multiple comparisons. 1–2: Interpersonal Reactivity Index; 3: Perceived Stress Scale; 4, 6–11: Profile of Mood States; 5: State-Trait Anxiety Inventory, Form Y1-State. Source: authors.
The levels of perceived stress, distress, negative emotions and positive ones before the volunteer work were compared with those measured after the intervention. To measure the changes from pre- to post-assistance levels, paired comparisons were employed for each of the variables of interest, taking into account the number of volunteers who had completed the questionnaires both before and after the relief work (‘completers’). Prior to this, in an effort to ensure that completers and non-completers did not differ on the variables of interest, independent sample t tests were conducted to compare participants who had completed both the pre- and post-assistance work evaluations with the ones who had completed solely the baseline evaluations. No differences were found on any of the stress and mood outcome variables (perceived stress, general distress, anxiety, negative emotions, positive emotions) or on the two empathy components (empathic concern and personal distress).
Table 2 presents the means (M) and standard deviations (SD) for the target
outcome variables, as well as the results of paired sample t tests for completers. Observed p values were adjusted for multiple testing using the false discovery rate (FDR) correction (Benjamini and Hochberg, 1995), with a rate of 0.05. Table 2 Stress and mood outcomes at the baseline and after relief work
Baseline
Post-relief work
M SD M SD
df
t
p (FDR corrected)
Perceived stress* 11.47 5.65 10.43 5.75 124 2.45 0.036 General distress** 20.90 17.30 18.20 14.58 121 2.06 0.061 Anxiety*** 34.31 8.58 31.13 7.71 111 4.03 0.000 Anxiety–tension** 5.19 3.26 4.47 2.48 126 2.59 0.033 Depression** 2.98 4.85 2.36 3.62 132 1.74 0.094 Anger–hostility** 3.56 5.44 2.60 4.67 130 2.09 0.061 Fatigue** 3.24 3.45 3.44 3.31 130 -0.83 0.406 Confusion–bewilderment** 5.94 3.58 5.43 3.09 130 1.74 0.094 Vigour–positive emotions** 20.49 5.93 21.62 5.41 129 -2.63 0.033 Notes: *Perceived Stress Scale; **Profile of Mood States; ***State-Trait Anxiety Inventory, Form Y1-State. M=means; SD=standard deviation. The p-values are corrected using a false discovery rate (FDR) of 0.05. Significant differences are shaded. Source: authors.
The results of the t tests indicated that after having finished relief activities, volunteers displayed significantly lower levels of perceived stress (t(124)=2.45, p=0.036, Cohen’s d=0.18), with a trend in the same direction for general distress (t(121)=2.06,

8
p=0.061). Regarding negative emotions after the assistance period, participants showed lower levels of anxiety as measured by both the STAI Y1 (t(111)=4.03, p<0.001, Cohen’s d=0.39) and the anxiety–tension subscale of the POMS (t(126)=2.59, p=0.033, Cohen’s d=0.25), with a trend in the same direction for anger (t(130)=2.09, p=0.06). Volunteers also reported a significantly higher level of positive emotions after the relief work (t(129)=-2.63, p=0.033, Cohen’s d=0.20). There were no significant differences from the baseline to post-assistance levels regarding depression, fatigue or confusion–bewilderment.
Moderation analyses were conducted to assess whether the evolution from pre- to
post-assistance levels was influenced by the two aspects of empathy—empathic concern and personal distress—using each of these two trait variables as moderators. Baseline values served as predictors, while values at the completion of the relief activities were used as outcome measures. The approach recommended by Hayes (2005) was used to test for moderation; according to Hayes, a moderation effect reveals itself statistically as an interaction between the predictor and the moderator, in a regression model of the outcome variable. In this approach, the moderator is kept as a continuous variable.
For empathic concern, the analysis revealed evidence of moderation for
depression, Finterac(3,125)= 36.83, p<0.001, confusion–bewilderment, Finterac(3,123)= 4.22, p=0.042, and general distress, Finterac(3,115)= 4.58, p=0.034. For personal distress, it found evidence of moderation for depression, Finterac(3,120)= 4.15, p=0.044, anger, Finterac(3,118)= 5.15, p=0.025, fatigue, Finterac(3,118)= 11.67, p=0.0009, and general distress, Finterac(3,110)= 5.37, p=0.022. There was no evidence of moderation for the other outcome variables (perceived stress, state anxiety or the other specific emotions measured by the POMS).
Significant moderating effects were explored further using the pick-a-point
approach, which involves probing at different moderator values. A graphical representation is displayed in Figure 1. Moderation was probed at mean values of the trait variables and respectively, one standard deviation under and over the mean.
Figure 1 Significant moderating effects of empathic concern (IRI–EC) and personal distress (IRI–PD) before and after volunteering

9
Source: authors. [A] Discussion While most research regarding volunteer workers focuses on the immediate phase of a disaster aftermath—the rescue stage—this study considers workers involved in the relief phase. It argues that an essential distinction between the two phases is that while the
10
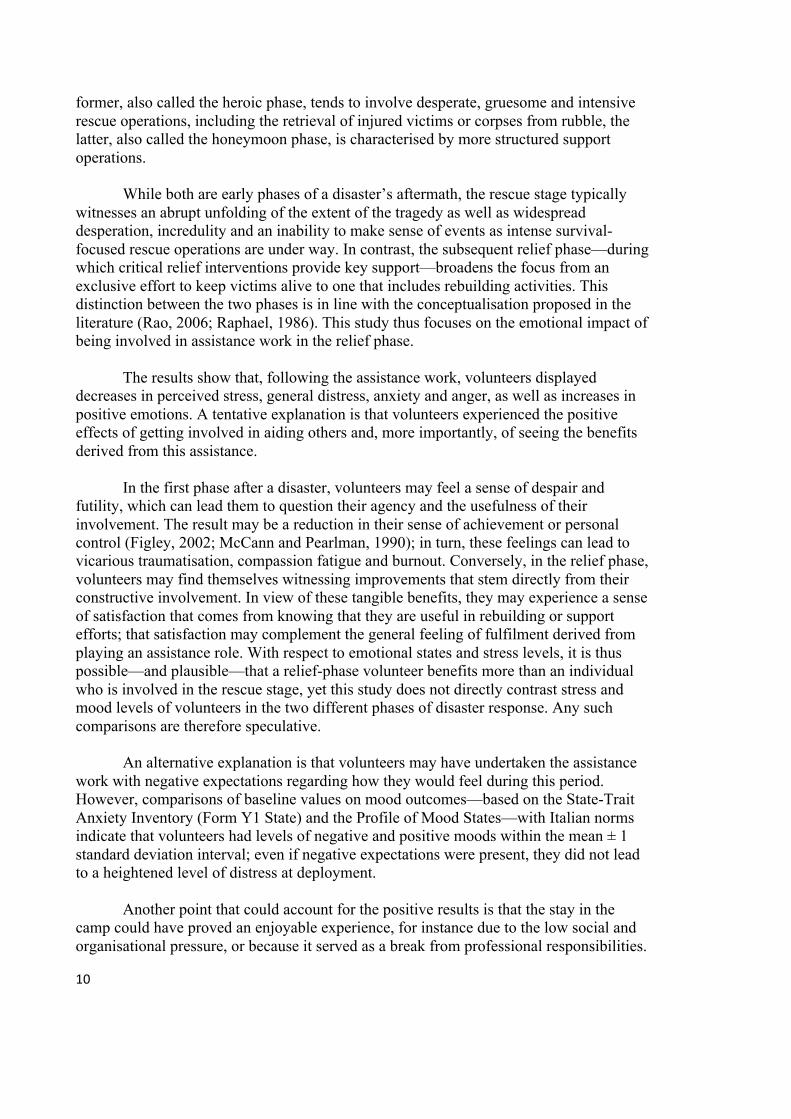
former, also called the heroic phase, tends to involve desperate, gruesome and intensive rescue operations, including the retrieval of injured victims or corpses from rubble, the latter, also called the honeymoon phase, is characterised by more structured support operations.
While both are early phases of a disaster’s aftermath, the rescue stage typically witnesses an abrupt unfolding of the extent of the tragedy as well as widespread desperation, incredulity and an inability to make sense of events as intense survival-focused rescue operations are under way. In contrast, the subsequent relief phase—during which critical relief interventions provide key support—broadens the focus from an exclusive effort to keep victims alive to one that includes rebuilding activities. This distinction between the two phases is in line with the conceptualisation proposed in the literature (Rao, 2006; Raphael, 1986). This study thus focuses on the emotional impact of being involved in assistance work in the relief phase.
The results show that, following the assistance work, volunteers displayed decreases in perceived stress, general distress, anxiety and anger, as well as increases in positive emotions. A tentative explanation is that volunteers experienced the positive effects of getting involved in aiding others and, more importantly, of seeing the benefits derived from this assistance.
In the first phase after a disaster, volunteers may feel a sense of despair and
futility, which can lead them to question their agency and the usefulness of their involvement. The result may be a reduction in their sense of achievement or personal control (Figley, 2002; McCann and Pearlman, 1990); in turn, these feelings can lead to vicarious traumatisation, compassion fatigue and burnout. Conversely, in the relief phase, volunteers may find themselves witnessing improvements that stem directly from their constructive involvement. In view of these tangible benefits, they may experience a sense of satisfaction that comes from knowing that they are useful in rebuilding or support efforts; that satisfaction may complement the general feeling of fulfilment derived from playing an assistance role. With respect to emotional states and stress levels, it is thus possible—and plausible—that a relief-phase volunteer benefits more than an individual who is involved in the rescue stage, yet this study does not directly contrast stress and mood levels of volunteers in the two different phases of disaster response. Any such comparisons are therefore speculative.
An alternative explanation is that volunteers may have undertaken the assistance
work with negative expectations regarding how they would feel during this period. However, comparisons of baseline values on mood outcomes—based on the State-Trait Anxiety Inventory (Form Y1 State) and the Profile of Mood States—with Italian norms indicate that volunteers had levels of negative and positive moods within the mean ± 1 standard deviation interval; even if negative expectations were present, they did not lead to a heightened level of distress at deployment.
Another point that could account for the positive results is that the stay in the
camp could have proved an enjoyable experience, for instance due to the low social and organisational pressure, or because it served as a break from professional responsibilities.

11
While studies have identified two components of empathy—empathic concern and personal distress—with different mechanisms that foster helping behaviour, the potential moderating effects of these components on the emotional reactions and adaptive abilities of volunteers have barely been studied. This paper examines how empathic concern and personal distress intervened in the prediction of emotional reactions following assistance work. It finds that while their moderating effects had an impact on common as well as specific emotional outcomes, the directions of these effects were dissimilar.
Empathic concern acted as a moderator in the relationship between baseline and post-assistance scores for depression, confusion–bewilderment and general distress. Results show that higher levels of empathic concern acted as a kind of buffer in the evolution of these outcomes, in the sense that even high baseline scores on these variables were conducive of much lower post-intervention scores for subjects with an increased degree of empathic concern. The pattern was reversed for personal distress, which appears to have acted as a moderator for depression, fatigue, anger and general distress. In this case, lower levels were protective, so that even high baseline values of these emotional outcomes were conducive to lower post-assistance scores—strikingly lower in some cases, such as for anger or fatigue—for subjects with a low degree of personal distress. In fact, for values of personal distress one standard deviation lower than the mean, baseline levels on the variables did not predict post-assistance ones (all bs non-significant at p<0.05). Again, this suggests a protective effect of low levels of personal distress on negative emotions. In the literature, both empathic concern and personal distress are shown to be related to involvement in helping behaviours, although they are assumed to act according to distinct mechanisms (Batson, 1991; Davis, 2004). Empathic concern was thought to be a marker of ‘true altruism’, indicating an involvement in helping behaviours motivated exclusively by a concern for the welfare of others. Conversely, personal distress, albeit also related to taking part in helping behaviours, was thought linked to a mechanism designed to relieve the helper’s own distress in the face of the suffering of a fellow human being. This paper contributes to this literature by showing that for community volunteers who were involved in a circumscribed relief activity in the aftermath of a disaster, these two facets of empathy differentially affect the development of emotional reactions. The findings suggest that a personality profile characterised by high empathic concern and low personal distress would be most favourable with respect to the emotional impact of disaster interventions on community volunteers. This research has clear limitations. A large part of the volunteer sample was not available for the study. While enough participants completed the pre- and post-assistance evaluations, the imposed subject selection may have influenced the results. The reasons for the loss of participants were diverse—ranging from direct refusal to a failure to return the questionnaires—yet it is possible that other reasons, such as elevated distress, may have deterred a significant number of volunteers from taking part in the study. This limitation was partially addressed through testing that revealed that completers and non-

12
completers did not differ at the baseline with respect to dispositional empathy or the outcome measures of stress or mood.
Given the nature of the sample and the fact participants were involved in a demanding aid activity, this study is restricted to a few measures of mood and stress. A more extensive evaluation of personality variables could identify other possible factors that might have an effect on the relationships between dispositional empathy and mood outcomes. For instance, Wilhelm and Bekkers (2010) show that the association between empathic concern and prosocial behaviours is mediated by a variable entitled the ‘principle of care’, defined as the moral obligation to help those in need. This factor could also influence the ways in which the different sides of empathy affect emotional outcomes, perhaps even clarifying their underlying mechanisms.
Furthermore, it might be relevant to look at whether some emotion regulation
difficulties, as well as the habitual use of different adaptive or maladaptive strategies of regulation, could relate differently to empathic concern and personal distress, and to the ways in which each moderates the evolution of mood outcomes. In support of this idea, Eisenberg et al. (1994) provide evidence that empathic concern and personal distress, as distinct modes of dispositional empathy, display different patterns of association with the intensity of negative emotions and their successful regulation. By examining these aspects in active community volunteers who are involved in disaster relief work, future studies could contribute to our understanding of these relationships.
[A] Acknowledgements The authors would like to thank Elisabetta Balsamo, Olivia Bernini, Carmen Berrocal, Francesco Blengini, Francesca Bonci, Valentina Centi, Virginia Equizi, Irene Ghicopulos, Tiziana Pennato, Silvia Pratali, Giuseppina Rota, Myriam Santilli, Donatella Tarquini, Francesco Tramonti and Stefania Vincenzi for their help in the camp and in collecting the data. [A] Correspondence Claudio Gentili, University of Pisa, Via Roma 67, Pisa 56126, Italy. Telephone: +39 050992658. E-mail: [email protected].[A] Endnotes Rick: please place the endnotes here. [A] References Albiero, P., S. Ingoglia and A. Lo Coco (2006) ‘Contributo all’adattamento italiano
dell’Interpersonal Reactivity Index’ [Contribution to the Italian Validation of the Interpersonal Reactivity Index]. Testing Psicometria Metodologia. 13, pp. 107–25.

13
Batson, C.D. (1991) The Altruism Question: Toward a Social-psychological Answer. Hillsdale, NJ: Lawrence Erlbaum.
Batson, C.D., J. Fultz and P.A. Schoenrade (1987) ‘Distress and Empathy: Two Qualitatively Distinct Vicarious Emotions with Different Motivational Consequences’. Journal of Personality. 55(1), pp. 19–39.
Benjamini, Y. and Y. Hochberg (1995) ‘Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing’. Journal of the Royal Statistical Society—Series B (Methodological). 57(1), pp. 289–300.
Cohen, S. and G. Williamson (1988) ‘Perceived Stress in a Probability Sample of the United States’. In S. Spacapan and S. Oskamp (eds.). The Social Psychology of Health: Claremont Symposium on Applied Social Psychology. Newbury Park, CA: Sage.
Davis, M.H. (1980) ‘A Multidimensional Approach to Individual Differences in Empathy’. JSAS Catalog of Selected Documents in Psychology. 10, p. 85.
Davis, M.H. (1983) ‘Measuring Individual Differences in Empathy: Evidence for a Multidimensional Approach’. Journal of Personality and Social Psychology. 44, pp. 113–26.
Davis, M.H. (2004) ‘Empathy: Negotiating the Border between Self and Other’. In L.Z. Tiedens and C.W. Leach (eds.). The Social Life of Emotions. Cambridge: Cambridge University Press, pp. 19–42.
Davis, M.H., J.A. Hall and M. Meyer (2003) ‘The First Year: Influences on the Satisfaction, Involvement, and Persistence of New Community Volunteers’. Personality & Social Psychology Bulletin. 29(2), pp. 248–60.
Davis, M.H. et al. (1999) ‘Empathy, Expectations, and Situational Preferences: Personality Influences on the Decision to Participate in Volunteer Helping Behaviors’. Journal of Personality. 67(3), pp. 469–503.
Derogatis, L.R. (1994) Symptom Checklist-90-R: Administration, Scoring and Procedures Manual, 3rd edn. Minneapolis: National Computer Systems.
Eisenberg, N. (2000) ‘Emotion, Regulation, and Moral Development’. Annual Review of Psychology. 51, pp. 665–97.
Eisenberg, N. and R.A. Fabes (1990) ‘Empathy: Conceptualization, Measurement, and Relation to Prosocial Behavior’. Motivation and Emotion. 14(2), pp. 131–49.
Eisenberg, N. et al. (1994) ‘The Relations of Emotionality and Regulation to Dispositional and Situational Empathy-related Responding’. Journal of Personality and Social Psychology. 66(4), pp. 776–97.
Farne, M. et al. (1991) Adattamento italiano del POMS [Profile of Mood States Manual]. Florence: Organizzazioni Speciali.
Figley, C.R. (2002) ‘Compassion Fatigue: Psychotherapists' Chronic Lack of Self Care’. Journal of Clinical Psychology. 58(11), pp. 1433–41.
Fullerton, C.S., R.J. Ursano and L. Wang (2004) ‘Acute Stress Disorder, Posttraumatic Stress Disorder, and Depression in Disaster or Rescue Workers’. American Journal of Psychiatry. 161(8), pp. 1370–76.
Hayes, A.F. (2005) Statistical Methods for Communication Science. Hillsdale, NJ: Lawrence Erlbaum Associates.
McCann, I.L. and L.A. Pearlman (1990) ‘Vicarious Traumatization: A Framework for Understanding the Psychological Effects of Working with Victims’. Journal of Traumatic Stress. 3(1), pp. 131–49.

14
McNair, D.M., M. Lorr and L.F. Droppleman (1981) Manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Services.
Mitchell, T.L., et al. (2004) ‘“We Will Never Ever Forget”: The Swissair Flight 111 Disaster and Its Impact on Volunteers and Communities’. Journal of Health Psychology. 9(2), pp. 245–62.
Omoto, A.M. and M. Snyder (1995) ‘Sustained Helping without Obligation: Motivation, Longevity of Service, and Perceived Attitude Change among AIDS Volunteers’. Journal of Personality and Social Psychology. 68(4), pp. 671–86.
Pedrabissi, L. and M. Santinello (1989) Inventario per l’ansia di stato e di tratto, forma Y. [State-Trait Anxiety Inventory, Y Form Manual]. Florence: Organizzazioni Speciali.
Prunas, A. et al. (2011) ‘Psychometric Properties of the Italian Version of the SCL-90-R: A Study on a Large Community Sample’. European Psychiatry: The Journal of the Association of European Psychiatrists. 27(8), pp. 591–97.
Rao, K. (2006) ‘Psychosocial Support in Disaster-affected Communities’. International Review of Psychiatry. 18(6), pp. 501–05.
Raphael, B. (1986) When Disaster Strikes: How Individuals and Communities Cope with Catastrophe. New York: Basic Books.
Roberti, J.W., L.N. Harrington and E.A. Storch (2006) ‘Further Psychometric Support for the 10-Item Version of the Perceived Stress Scale’. Journal of College Counseling. 9(2), p. 135.
Spielberger, C.D. et al.(1983) Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
Stratta, P. and A. Rossi (2010) ‘Subjective Adjustment of Individuals with Psychiatric Disorders in the Aftermath of the L'Aquila Earthquake’. American Journal of Psychiatry. 167(3), pp. 352–53.
Thormar, S.B. et al. (2010) ‘The Mental Health Impact of Volunteering in a Disaster Setting: A Review’. Journal of Nervous and Mental Disease. 198(8), pp. 529–38.
Wilhelm, M.O. and R. Bekkers (2010) ‘Helping Behavior, Dispositional Empathic Concern, and the Principle of Care’. Social Psychology Quarterly. 73(1), pp. 11–32.