O efeito da prática de mindfulness na conectividade cerebral
Upload
independentCategory
view
1download
0
Mindfulness and Cognitive–Behavioral Interventions for Chronic Pain:Differential Effects on Daily Pain Reactivity and Stress Reactivity
Mary C. Davis, Alex J. Zautra, and Laurie D. WolfArizona State University
Howard TennenUniversity of Connecticut School of Medicine
Ellen W. YeungArizona State University
Objective: This study compared the impact of cognitive–behavioral therapy for pain (CBT-P), mindfulawareness and acceptance treatment (M), and arthritis education (E) on day-to-day pain- and stress-related changes in cognitions, symptoms, and affect among adults with rheumatoid arthritis (RA).Method: One hundred forty-three RA patients were randomized to 1 of the 3 treatment conditions.CBT-P targeted pain-coping skills; M targeted awareness and acceptance of current experience toenhance coping with a range of aversive experiences; E provided information regarding RA pain and itsmanagement. At pre- and posttreatment, participants completed 30 consecutive evening diaries assessingthat day’s pain, fatigue, pain-related catastrophizing and perceived control, morning disability, and sereneand anxious affects. Results: Multilevel models compared groups in the magnitude of within-personchange in daily pain and stress reactivity from pre- to posttreatment. M yielded greater reductions thandid CBT-P and E in daily pain-related catastrophizing, morning disability, and fatigue and greaterreductions in daily stress-related anxious affect. CBT-P yielded less pronounced declines in dailypain-related perceived control than did M and E. Conclusions: For individuals with RA, M produces thebroadest improvements in daily pain and stress reactivity relative to CBT-P and E. These findings alsohighlight the utility of a diary-based approach to evaluating the treatment-related changes in responsesto daily life.
Keywords: cognitive–behavioral, mindfulness, interventions, pain, reactivity, arthritis
Chronic pain is a prevalent health condition that requires indi-viduals to adapt to a daily life that can include episodes ofincreased pain, functional impairment, and affective disturbance(Banks & Kerns, 1996; Lawrence et al., 2008). Over the past 30years, a substantial body of empirical evidence has accrued estab-lishing the efficacy of psychosocial treatment of chronic painbeyond the effects of standard medical care (Astin, Beckner,Soeken, Hochberg, & Berman, 2002; Dixon, Keefe, Scipio, Perri,& Abernethy, 2007; Morley, Eccleston, & Williams, 1999). Inparticular, cognitive–behavioral therapy (CBT) has emerged asone of the most common and effective forms of psychosocialtreatment. From a cognitive–behavioral perspective, an individu-al’s beliefs regarding physical symptoms and the coping responses
that stem from those beliefs are central to adaptation to chronicpain. A key facet of CBT is training individuals to apply cognitivereappraisal strategies to address the faulty cognitions that contrib-ute to their poor adjustment. To that end, individuals are encour-aged to adopt a more detached or “decentered” view of thoughts,considering their thoughts are not facts but temporary mentalevents that can be evaluated to determine their veracity and/orutility and changed, if necessary. In addition to cognitive reap-praisal, CBT typically incorporates behavioral components, in-cluding training in relaxation techniques and activity pacing, withthe overarching goal of helping individuals respond to their painmore effectively. Over the long term, CBT aims to improve copingself-efficacy, psychological and physical symptoms, and func-tional health. A series of meta-analyses summarizing the benefitsof CBT has shown that it yields moderate to large effects forcognitive coping responses and small to moderate effects for painoutcomes relative to controls (Astin et al., 2002; Dixon et al.,2007).
More recently, alternative approaches have pointed to the valueof fostering both awareness and acceptance of pain and otheraversive experiences to help individuals with chronic pain effec-tively manage the physical and emotional demands of their illness(Hayes & Duckworth, 2006; Kabat-Zinn, 1990). Much like CBT,acceptance-based approaches foster the development of a decen-tered view that thoughts, emotions, and physical sensations aresimply temporary experiences. However, in contrast to the focus in
Mary C. Davis, Alex J. Zautra, and Laurie D. Wolf, Department ofPsychology, Arizona State University; Howard Tennen, Department ofCommunity Medicine and Health Care, University of Connecticut HealthCenter; Ellen W. Yeung, Department of Psychology, Arizona State Uni-versity.
This study was the National Institutes of Health Clinical TrialNCT00475111 and was supported by Grant R01 AR41687 from theNational Institute of Musculoskeletal, Immune, and Skin Disease.
Correspondence concerning this article should be addressed to Mary C.Davis, P.O. Box 1104, Department of Psychology, Arizona State Univer-sity, Tempe, AZ 85287-1104. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Journal of Consulting and Clinical Psychology © 2014 American Psychological Association2014, Vol. 82, No. 6, 000 0022-006X/14/$12.00 http://dx.doi.org/10.1037/a0038200
1
AQ: 1
AQ: au
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

CBT on promoting efforts to challenge and change faulty cogni-tions to control pain, the focus in acceptance-oriented treatments ison increasing individuals’ capacity to be both aware and nonjudg-mental of present moment experiences, including pain and theirreactions to pain. Acceptance-oriented treatments typically includeexercises designed to illustrate the principles of mindfulness; withnotable exceptions (e.g., Hayes & Duckworth, 2006), these exer-cises incorporate the regular practice of mindfulness meditation tobuild the capacity for increased awareness and acceptance. Mind-fulness training helps individuals attend to current experienceswithout suppressing or elaborating those experiences. Increasingthe capacity to sustain awareness without judgment when facedwith pain or stress may be key to decreasing automatic, maladap-tive responses, including hypervigilance to threats and catastroph-izing (Garland et al., 2012; Garland & Howard, 2013). One im-portant aim of an acceptance-oriented approach is to decreaseautomatic cognitive and emotional reactivity to aversive experi-ences, thereby increasing the ability to act more intentionally toresponse to pain and other stressors. A recent meta-analysis ofrandomized clinical trials of acceptance-based treatments forchronic pain indicated that they yield small improvements in painand depression, and small to moderate improvements in physicalwell-being relative to education controls or treatment-as-usual(Veehof, Oskam, Schreurs, & Bohlmeijer, 2011).
Taken together, the evidence to date suggests that both CBT andacceptance-based treatments for chronic pain improve physicaland psychological symptoms. Yet, most evaluations of the benefitsof these treatments have relied on global measures that ask indi-viduals to recall their symptoms, emotional experiences, and cop-ing responses over a period ranging from several days to severalweeks. Moreover, some assessments require individuals to recol-lect not simply the levels of their symptoms and/or coping re-sponses, but rather the covariation between the two (i.e., “when–then” relations). For example, a commonly used measure offunctional health, the 36-item Short-Form Health Survey (Ware &Sherbourne, 1992), asks individuals to estimate the extent to whichtheir physical or emotional problems have interfered with theirsocial activities or their performance of regular daily activities. Akey limitation of retrospective reports is that recall of past expe-rience can be heavily influenced by the enduring beliefs individ-uals hold about themselves, including how they typically feel orrespond, and their implicit theories about the relations betweenvariables (Robinson & Clore, 2002). Although this approach toassessment yields important information about general function-ing, it provides relatively little insight into whether treatmentsactually alter coping and adaptation on a daily basis among peoplewith chronic pain.
An approach that can complement the use of static retrospectivereports to evaluate intervention effects involves the intensive as-sessment of individuals over time and across contexts and has beentermed the daily process method, ecological momentary assess-ment, and experience sampling (Affleck, Zautra, Tennen, &Armeli, 1999; Csikszentmihalyi & Larson, 1987; Shiffman, Stone,& Hufford, 2008). In contrast to scales that require respondents torecall their symptoms and emotional experiences over periodsranging from days to weeks, daily process methods can focus diaryreports on a more limited timeframe, from the past few momentsto a single day, reducing the time between an experience and thereport of that experience and thus the error variance of the measure
(Epstein, 1979). The primary advantage, though, is that diary datahave the potential to shed light on intervention-related changes inthe dynamics of behavior in real-world contexts (Shiffman et al.,2008). Indeed, changes in relations among variables are often atthe heart of purported mechanisms of action, and the principalvalue of daily process data is that such changes can be capturedwith intensive within-person assessment. In the evaluation of treat-ments for chronic pain, pre- and postintervention assessment usingthe daily diary process method provides the opportunity to assesschange in the daily dynamics of responses to pain and other dailystressors as a function of treatment. That is, the covariation be-tween pain/stress and daily functioning can be estimated in thedata rather than based on respondents’ retrospective judgments ofthese covariations.
The use of diary methods to examine the covariation amongvariables has grown exponentially over the past 20 years. Yet,despite clear advantages for the evaluation of intervention effects,this particular application of daily process methods remains in itsinfancy. To our knowledge, in the arena of behavioral treatmentsfor chronic pain conditions in particular, only a single report hasexamined diary reports as a means of examining interventioneffects on real-time responses to pain (Gil et al., 2001). Gil andcolleagues (2001) evaluated postintervention daily diaries of chil-dren with sickle cell disease who had been randomized to briefcoping skills training (vs. usual care) to probe within-person rela-tions between daily pain, daily coping practice, and functioningduring the month following treatment. The findings were enlight-ening. On days of high pain, if children also reported higher use ofcoping practice, they were significantly less likely to have contactwith health care providers and to decrease school participation.These relations are intriguing, but interpretation of the findings isconstrained by the use of postintervention diary assessments onlyin the intervention group and not in a comparison condition. Thus,the extent to which the relations between pain, pain coping prac-tice, and daily functioning were the result of the interventioncannot be ascertained.
Overview of the Current Study
The present study is based on diary data obtained from a clinicaltrial in which 144 individuals with rheumatoid arthritis (RA) wererandomized to either CBT for pain (CBT-P), mindful awarenessand acceptance therapy (M), or an arthritis education condition(E), which served as a placebo control (Zautra et al., 2008). InCBT-P, training in cognitive reappraisal, relaxation, and activitypacing were used to change faulty cognitions and coping responsesto pain episodes to responses that are more adaptive. In M, trainingin mindfulness skills was used to increase awareness and nonjudg-ment of aversive experiences, thereby decreasing reactivity andincreasing emotional regulation to not only pain, but also stressepisodes. An earlier report of findings from this trial detailedpre–post changes in overall daily levels of coping cognitions,emotions, and symptoms by aggregating scores across the 30 daysof pre- and 30 days of postintervention diaries. Results indicatedthat CBT-P and E yielded more improvement than did M in overalllevels of pain control in the sample as a whole. For the subgroupof individuals with a history of recurrent depression, however, Myielded more improvement than did CBT-P and E in overall levels
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM
of pain catastrophizing, coping efficacy, and positive and negativeaffect (Zautra et al., 2008).
In the current study, we reexamined the pre- and postinterven-tion diary data to evaluate the effects of the CBT-P, M, and Econditions on day-to-day pain and stress reactivity via the 30 dailydiary reports obtained at pre- and postintervention. We use theterm “reactivity” to refer to daily within-person changes in cogni-tions, fatigue and morning disability, and affect associated withdaily changes in pain and stress (Hamilton et al., 2008; Suls &Martin, 2005). Improvement in reactivity would be manifested byweakened relations between daily changes in pain or stress anddaily cognitions, symptoms, and affect from pre- to posttreatment.As a specific example, if individuals reacted to days of high painwith smaller increases in catastrophizing at posttreatment relativeto pretreatment, they would be demonstrating an enhanced abilityto limit the negative effects of pain flares (i.e., improved painreactivity). In line with its focus on teaching skills to manage andcontrol pain, we expected the CBT-P group to show improvementon pain-related changes in pain catastrophizing and control, fa-tigue, and morning disability compared with the E group, and onpain-related changes pain control compared with the M group. Incontrast, because M targets the development of broader emotionregulation skills to dampen the impact of pain and stress flares, weexpected the M group to show improvement in pain-relatedchanges in pain cognitions, fatigue, and morning disability relativeto the E group and in pain-related and stress-related changes inaffect relative to both the E and CBT-P groups.
Method
Participants
One hundred forty-four participants from the Phoenix, Arizona,metropolitan area were recruited from physician’s offices, referralsfrom Veterans Affairs hospital rheumatologists, senior citizen
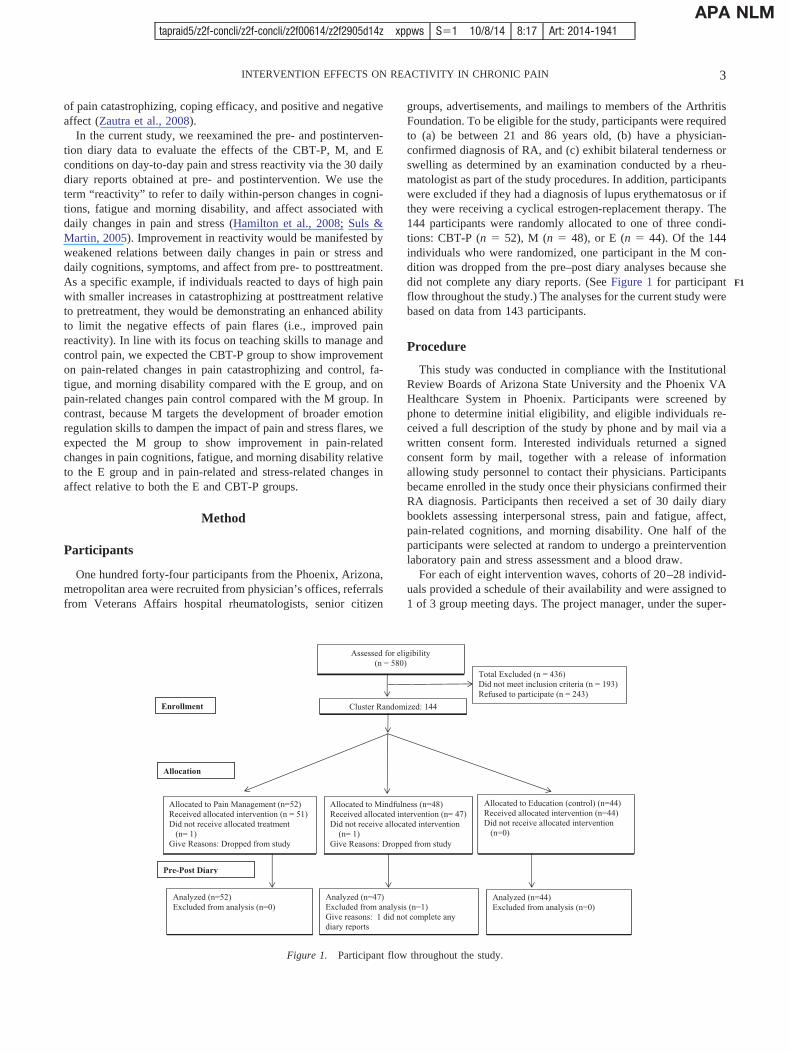
groups, advertisements, and mailings to members of the ArthritisFoundation. To be eligible for the study, participants were requiredto (a) be between 21 and 86 years old, (b) have a physician-confirmed diagnosis of RA, and (c) exhibit bilateral tenderness orswelling as determined by an examination conducted by a rheu-matologist as part of the study procedures. In addition, participantswere excluded if they had a diagnosis of lupus erythematosus or ifthey were receiving a cyclical estrogen-replacement therapy. The144 participants were randomly allocated to one of three condi-tions: CBT-P (n � 52), M (n � 48), or E (n � 44). Of the 144individuals who were randomized, one participant in the M con-dition was dropped from the pre–post diary analyses because shedid not complete any diary reports. (See Figure 1 for participantflow throughout the study.) The analyses for the current study werebased on data from 143 participants.
Procedure
This study was conducted in compliance with the InstitutionalReview Boards of Arizona State University and the Phoenix VAHealthcare System in Phoenix. Participants were screened byphone to determine initial eligibility, and eligible individuals re-ceived a full description of the study by phone and by mail via awritten consent form. Interested individuals returned a signedconsent form by mail, together with a release of informationallowing study personnel to contact their physicians. Participantsbecame enrolled in the study once their physicians confirmed theirRA diagnosis. Participants then received a set of 30 daily diarybooklets assessing interpersonal stress, pain and fatigue, affect,pain-related cognitions, and morning disability. One half of theparticipants were selected at random to undergo a preinterventionlaboratory pain and stress assessment and a blood draw.
For each of eight intervention waves, cohorts of 20–28 individ-uals provided a schedule of their availability and were assigned to1 of 3 group meeting days. The project manager, under the super-
Assessed for eligibility (n = 580)
Total Excluded (n = 436) Did not meet inclusion criteria (n = 193) Refused to participate (n = 243)
Enrollment Cluster Randomized: 144
Allocation
Allocated to Education (control) (n=44) Received allocated intervention (n=44) Did not receive allocated intervention (n=0)
Allocated to Pain Management (n=52) Received allocated intervention (n = 51) Did not receive allocated treatment (n= 1) Give Reasons: Dropped from study
Allocated to Mindfulness (n=48) Received allocated intervention (n= 47) Did not receive allocated intervention (n= 1) Give Reasons: Dropped from study
Pre-Post Diary
Analyzed (n=52) Excluded from analysis (n=0)
Analyzed (n=47) Excluded from analysis (n=1) Give reasons: 1 did not complete any diar
Analyzed (n=44) Excluded from analysis (n=0)
y reports
Figure 1. Participant flow throughout the study.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3INTERVENTION EFFECTS ON REACTIVITY IN CHRONIC PAIN
F1
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

vision of the study’s principal investigator, randomly assignedthese day clusters to one of three treatment conditions using arandom numbers table. A postintervention questionnaire, diaryassessment, and laboratory visit followed completion of the8-week intervention for all participants. Data collection beganJanuary 2003 and ended June 2005.
The current study draws on data from the pre- and postinter-vention diaries. An extensive description of all study componentsis available in Zautra et al. (2008).
Intervention plan. The CBT-P, M, and E groups followed aparallel format: Each treatment included eight modules that weredelivered in weekly 2-hr group meetings and addressed themesthat defined the content of that intervention. The CBT-P and Mtreatments included experiential activities designed to enhancetargeted skills, whereas the E group received information regard-ing pain and stress management but did not practice skills tomanage pain or emotional difficulties.
The CBT-P treatment focused explicitly on increasing painmanagement skills to enhance cognitive coping and functionalhealth and limit fatigue symptoms in response to pain, following astandard cognitive–behavioral format. Included among the topicscovered to provide cognitive and behavioral strategies to managedaily pain were (a) relaxation training, (b) autogenic training, (c)cognitive coping with pain, (d) activity pacing and managing dailyactivities, and (e) managing intense pain episodes. The M treat-ment focused on developing two distinct sets of skills: one toreduce the negative impact of pain and stress episodes on mood,symptoms, and functioning and the other to enhance positiveaffective engagement. The inclusion of training to boost positiveengagement, a focus not included in many mindfulness programs,is based on research pointing to the value of drawing on positiveresources to interrupt automatic responding to pain and otherstressors (e.g., Strand et al., 2006). The ultimate purpose of tar-geting emotion regulation was to position individuals to makemore intentional (vs. reflexive) choices both day-to-day and in thelong term. Specific targeted skills included (a) use of mindfultechniques (e.g., breathing meditation) to increase present-momentawareness and acceptance/nonjudgment of difficult experiencesand (b) identification of strategies (e.g., savoring positive events)to develop positive emotional resources, including more satisfyingsocial relations. The E group provided didactic information regard-ing the etiology, pathophysiology, and treatment of RA andhealthy lifestyles and physician–patient communication. The Econdition intentionally omitted information on coping practicesand did not engage participants in any experiential activities orskill rehearsal exercises.
Groups were cofacilitated by a doctoral-level clinical healthpsychologist and an advanced doctoral student in clinical psychol-ogy. Clinicians had prior training in CBT and mindfulness meth-ods, particularly with regard to the treatment of chronic pain. Eachintervention was manualized; manuals included information re-garding the rationale for the intervention and material regardingspecific objectives, didactic instructions, learning activities, andhomework assignments for each session. Prior to delivering theinterventions, clinicians reviewed the treatment manuals with thetreatment team to maximize treatment fidelity across the eightwaves of groups. During treatment waves, the treatment supervisorconducted weekly review sessions to foster adherence and addressclinical issues arising in treatment groups.
Diary assessment. After enrollment and completion of theinitial clinical interview, participants received 30 paper diaries andpreaddressed stamped envelopes by mail and were contacted by astaff member who provided diary instructions by phone. Partici-pants were asked to complete a diary each night approximately 30min prior to going to bed and to place the completed diary in themail the next day. Postmark verification was monitored to sub-stantiate compliance with instructions. Participants were compen-sated up to $90 for their completion of the diaries: $2/day for eachcompleted diary and a bonus of $1/day if they completed morethan 25 diaries. Immediately following the 8-week intervention,participants received and completed a second set of 30 diaries andreceived compensation according to the same criteria. Aggregatingacross participants, 95% of the pre diaries and 92.5% of the postdiaries were completed, and of those completed diaries, 97.3%were received with a verified postmark. Of the diaries with averified postmark, 80% were postmarked within 2 days of diarycompletion (allowing for weekend and holiday constraints on mailservice). Among other questions, the daily diary assessed thefollowing variables targeted in the current study: pain and inter-personal stress, fatigue, morning disability, pain-related cogni-tions, and serene and anxious affects.
Measures
Pain and fatigue. Daily pain and daily fatigue were assessedeach day with the standard instruction for a numerical rating scale(Jensen, Karoly, & Braver, 1986): “Please choose a number be-tween 0 and 100 that best describes the average level of pain(fatigue) you have experienced today due to your RA. A zero (0)would mean ‘no pain (fatigue)’ and a one hundred (100) wouldmean ‘pain (fatigue) as bad as it can be’” (Jensen et al., 1986). Theestimated intraclass correlations in the current sample were as-sessed for the diary reports by evaluating unconditional meansmodels (description follows). The intraclass correlation estimateswere .58 for pain and .54 for fatigue.
Morning disability. Morning disability was assessed with theitem, “After you woke up this morning, how long did it take youto reach your maximum physical ability for the day?” (Yazici,Pincus, Kautiainen, & Sokka, 2004). Ratings ranged from 1 (lessthan 15 min) to 5 (more than 1 hr). This assessment of morningstiffness is a widely used marker of functional disability in RA andreflects disease activity more than do traditional markers of in-flammation like joint counts (Westhoff, Buttgereit, Gromnica-Ihle,& Zink, 2008). The estimated intraclass correlation was .66 in thecurrent sample.
Interpersonal stress. Perceived interpersonal stress in so-cial relationships was assessed by asking participants to re-spond to four items regarding the stressfulness of their relationswithin four domains: spouse, friends, family, and work. Ratingsfor each item were made on a scale of 1 (not at all) to 4(extremely), and responses to the statements were averaged toyield a daily score for interpersonal stress (Watson, 1988). Theestimated intraclass correlation for interpersonal stress in thepresent sample was .25.
Pain-related cognitions. Two common pain-related cogni-tions were assessed in the diaries: pain catastrophizing and paincontrol. Existing evidence points to these particular pain cogni-tions as key mediators of treatment-related improvements in func-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

tional and psychological health among individuals in chronic pain(e.g., Smeets, Vlaeyen, Kester, & Knottnerus, 2006; Spinhoven etal., 2004; Turner, Holtzman, & Mancl, 2007). Pain catastrophizingwas assessed with two statements: “I worried about whether mypain would ever end” and “I felt my pain was so bad I couldn’tstand it anymore,” derived from the Coping Strategies Question-naire (Rosenstiel & Keefe, 1983). Ratings for each statement weremade on a scale of 1 (strongly disagree) to 5 (strongly agree), andresponses to the statements were averaged within day to yield adaily score for catastrophizing. Pain control was assessed with thestatement “What number between 0 and 10 best describes howmuch personal control you were able to exert over the amount ofpain you experienced today?”, with anchors of 0 (no control at all)and 10 (complete control). This item was a modified version of anitem drawn from the Arthritis Self-Efficacy Scale (Lorig, Chastain,Ung, Shoor, & Holman, 1989). Estimated intraclass correlationswere .53 for catastrophizing and .56 for pain control in the currentsample.
Serene and anxious affects. Serene and anxious affects wereassessed via items drawn from lower order subscales of the Pos-itive and Negative Affect Scale–Expanded Form (Watson & Clark,1994). Participants rated three adjectives describing serene affect(i.e., relaxed, at ease, calm) and four items describing anxiousaffect (i.e., nervous, afraid, scared, jittery) on a 5-point scaleranging from 1 (very slightly or not at all) to 5 (extremely). Thelower-order, empirically derived subscales of the Positive andNegative Affect Scale–Expanded Form reflect specific dimensionsof positive and negative affect, consistent with existing models ofemotion, and show good psychometric properties (Watson &Clark, 1994). Limiting the impact of pain on serenity and anxietywas a target of CBT-P and M, and decreased pain-related anxietyhas been linked to improved outcomes among individuals withchronic pain (McCracken & Gross, 1998). Mean serenity andanxiety scores were calculated for each day by averaging acrossitems. Within-person reliabilities were .61 for serenity and .42 foranxiety.
Analytic Approach
To examine the proportion of total variance in daily outcomesthat was between-person, unconditional means models werecomputed for each outcome, yielding estimates of the intraclasscorrelations (Singer, 1998). Multilevel analyses were then con-ducted to evaluate intervention group differences in daily painand stress reactivity, modeling up to 60 daily measurementoccasions (30 pre- and 30 postintervention diaries) nestedwithin each of the 143 participants. Thus, multilevel modelingpartitions the variance into two components: daily reports(Level 1) are clustered within individuals (Level 2). For eachperson within each set of diaries (pre and post), we first com-puted an average score across the 30 days for pain and stressmeasures. We then subtracted each person’s average score fromeach of his or her daily scores within a diary set, resulting in aset of up to 60 deviation scores for pain and stress (30 pre and30 post; Singer, 1998). These deviation scores, also termedperson-centered scores, index day-to-day within-person changerelative to an individual’s average level on the variable ofinterest. Deviation scores are denoted in this article by theGreek letter �. A day of positive deviation indicates a pain or
stress episode for that individual. The Level 2 variable in thecurrent analyses was group assignment (CBT-P, M, or E).
Pain reactivity was assessed for all outcomes whereas stressreactivity was assessed for affective outcomes. We first deter-mined whether groups were comparable prior to the interventionby examining group differences at pretreatment in pain- and/orstress-related changes (i.e., reactivity); these models includedGroup, �Pain/�Stress, and Group � �Pain/�Stress interactions aspredictors of each outcome. We next asked whether pain- and/orstress reactivity changed significantly from pre to post for eachintervention group separately by including Time, �Pain/�Stress,and Time � �Pain/Stress interactions as predictors in each model.Finally, we compared groups in the magnitude of change from preto post by including Group main effects and interaction terms inthe models. To illustrate this final set of analyses, the basicequation evaluating differences between interventions in their ef-fects on pain- and/or stress-related changes in anxious affect wasas follows:
Anxious affect � b0 � b1(Group) � b2(�Pain) � b3(�Stress)
� b4(Group � �Pain) � b5(Group � �Stress)
� b6(Time: Pre vs. Post) � b7(Group � Time)
� b8(Time � �Pain) � b9(Time � �Stress)
� b10(Group � Time � �Pain)
� b11(Group � Time � �Stress) � r.
b0 yields an estimate of the intercept for anxiety. Coefficientsb1–11 provide slope estimates of predictor variables, with slopesb10 and b11 testing for differences between groups in prepostchanges in pain and stress reactivity, respectively. The r standsfor the within-person residual. This approach mirrors the onetaken by Geschwind and colleagues (2011) to evaluate groupdifferences in pre- to posttreatment effects on affective reactiv-ity in recurrent depression. Repeating the analyses using athree-level approach (i.e., diary days, prepost assessment, andindividuals as levels) retained the pattern of findings for painand stress reactivity.
All multilevel analyses were conducted using the SAS (version9.3) PROC MIXED software, which furnished parameters in theform of unstandardized restricted maximum likelihood estimates(� coefficients). These are partial correlations, adjusted forbetween-unit differences, which serve as useful effect size estima-tions of magnitude and direction of changes in dependent variablesassociated with changes in independent variables. For all analyses,we allowed intercepts to vary randomly, thus enabling us togeneralize the findings to the population of persons from which thesample was drawn and the populations of observations from whichtheir daily reports were sampled. We also allowed the slopesreflecting changes in pain to vary randomly because doing soimproved the fit of the models. Autocorrelated residuals are acommon consequence of equally spaced observations and can biasstandard errors and significance levels; thus, a first order autore-gressive term (that is, AR[1]) was included in all models. Toillustrate significant Time � Group � �Pain/Stress interactioneffects, which were derived from continuous �Pain and �Stressvariables, we followed the guidelines of Aiken and West (1991) to
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5INTERVENTION EFFECTS ON REACTIVITY IN CHRONIC PAIN
AQ: 2
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM
plot the interactions. Specifically, we used values for �Pain/�Stress that were one standard deviation above the mean (i.e., highpain/stress days) and one standard deviation below the mean (i.e.,low pain/stress days) to generate plots of the average within-person pre- and postintervention slopes for each interventiongroup.
Results
Participants
The sample was primarily female (68.5%) and White (85%),with an average age of 54.28 years (SD � 13.80, range 21 to 81).Although some participants did not complete high school (6%), thevast majority of participants graduated from high school (10%),attended trade school (13%), or college (29%), or graduated fromcollege (42%). The average annual family income of the samplewas between $30,000 and $39,000. The three interventiongroups were comparable in age, income, and education, Fs �1.58, ps � .21, and in proportions of females and Whites,�2(2) � 3.32, ps � .19.
Pretreatment Group Comparisons of Diary Reports
The first sets of models tested whether daily increases in painand/or stress above an individual’s average were related to same-day changes in cognitive, symptom, and affective outcomes in thepretreatment diaries within each treatment group, and then whethergroups differed in their pretreatment reactivity to daily pain and/or
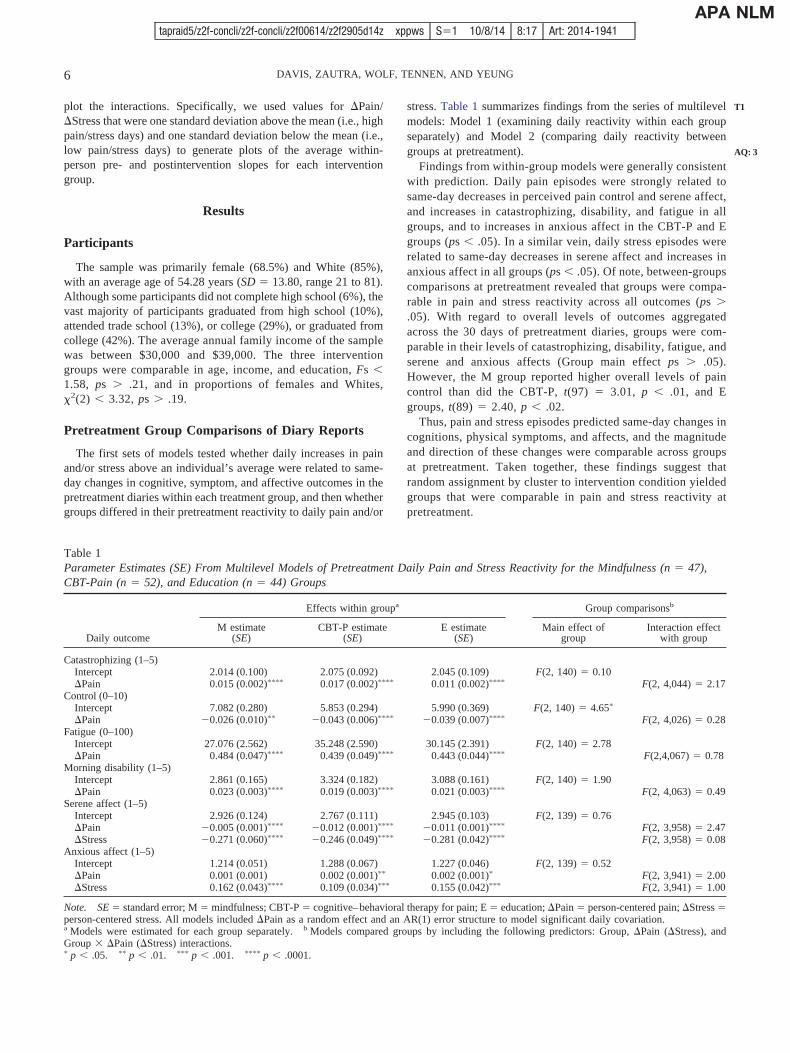
stress. Table 1 summarizes findings from the series of multilevelmodels: Model 1 (examining daily reactivity within each groupseparately) and Model 2 (comparing daily reactivity betweengroups at pretreatment).
Findings from within-group models were generally consistentwith prediction. Daily pain episodes were strongly related tosame-day decreases in perceived pain control and serene affect,and increases in catastrophizing, disability, and fatigue in allgroups, and to increases in anxious affect in the CBT-P and Egroups (ps � .05). In a similar vein, daily stress episodes wererelated to same-day decreases in serene affect and increases inanxious affect in all groups (ps � .05). Of note, between-groupscomparisons at pretreatment revealed that groups were compa-rable in pain and stress reactivity across all outcomes (ps �.05). With regard to overall levels of outcomes aggregatedacross the 30 days of pretreatment diaries, groups were com-parable in their levels of catastrophizing, disability, fatigue, andserene and anxious affects (Group main effect ps � .05).However, the M group reported higher overall levels of paincontrol than did the CBT-P, t(97) � 3.01, p � .01, and Egroups, t(89) � 2.40, p � .02.
Thus, pain and stress episodes predicted same-day changes incognitions, physical symptoms, and affects, and the magnitudeand direction of these changes were comparable across groupsat pretreatment. Taken together, these findings suggest thatrandom assignment by cluster to intervention condition yieldedgroups that were comparable in pain and stress reactivity atpretreatment.
Table 1Parameter Estimates (SE) From Multilevel Models of Pretreatment Daily Pain and Stress Reactivity for the Mindfulness (n � 47),CBT-Pain (n � 52), and Education (n � 44) Groups
Daily outcome
Effects within groupa Group comparisonsb
M estimate(SE)
CBT-P estimate(SE)
E estimate(SE)
Main effect ofgroup
Interaction effectwith group
Catastrophizing (1–5)Intercept 2.014 (0.100) 2.075 (0.092) 2.045 (0.109) F(2, 140) � 0.10�Pain 0.015 (0.002)���� 0.017 (0.002)���� 0.011 (0.002)���� F(2, 4,044) � 2.17
Control (0–10)Intercept 7.082 (0.280) 5.853 (0.294) 5.990 (0.369) F(2, 140) � 4.65�
�Pain 0.026 (0.010)�� 0.043 (0.006)���� 0.039 (0.007)���� F(2, 4,026) � 0.28Fatigue (0–100)
Intercept 27.076 (2.562) 35.248 (2.590) 30.145 (2.391) F(2, 140) � 2.78�Pain 0.484 (0.047)���� 0.439 (0.049)���� 0.443 (0.044)���� F(2,4,067) � 0.78
Morning disability (1–5)Intercept 2.861 (0.165) 3.324 (0.182) 3.088 (0.161) F(2, 140) � 1.90�Pain 0.023 (0.003)���� 0.019 (0.003)���� 0.021 (0.003)���� F(2, 4,063) � 0.49
Serene affect (1–5)Intercept 2.926 (0.124) 2.767 (0.111) 2.945 (0.103) F(2, 139) � 0.76�Pain 0.005 (0.001)���� 0.012 (0.001)���� 0.011 (0.001)���� F(2, 3,958) � 2.47�Stress 0.271 (0.060)���� 0.246 (0.049)���� 0.281 (0.042)���� F(2, 3,958) � 0.08
Anxious affect (1–5)Intercept 1.214 (0.051) 1.288 (0.067) 1.227 (0.046) F(2, 139) � 0.52�Pain 0.001 (0.001) 0.002 (0.001)�� 0.002 (0.001)� F(2, 3,941) � 2.00�Stress 0.162 (0.043)���� 0.109 (0.034)��� 0.155 (0.042)��� F(2, 3,941) � 1.00
Note. SE � standard error; M � mindfulness; CBT-P � cognitive–behavioral therapy for pain; E � education; �Pain � person-centered pain; �Stress �person-centered stress. All models included �Pain as a random effect and an AR(1) error structure to model significant daily covariation.a Models were estimated for each group separately. b Models compared groups by including the following predictors: Group, �Pain (�Stress), andGroup � �Pain (�Stress) interactions.� p � .05. �� p � .01. ��� p � .001. ���� p � .0001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
T1
AQ: 3
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM
Intervention Effects on Pain and Stress Reactivity forE, P, and M Groups
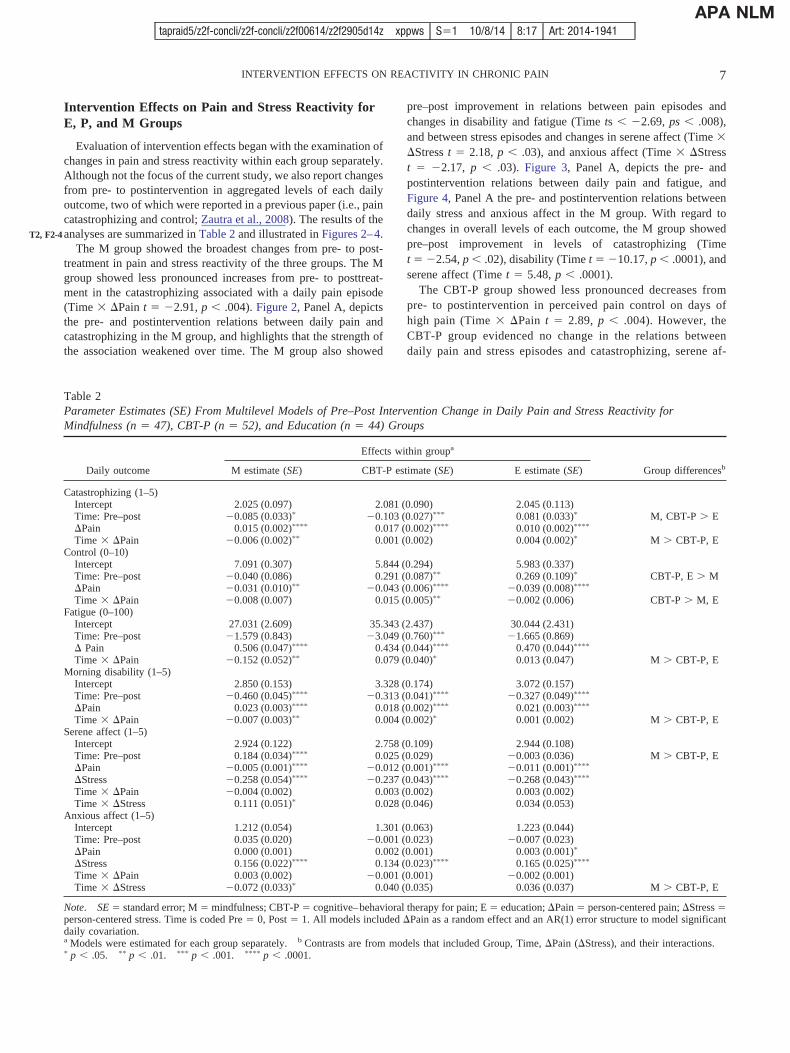
Evaluation of intervention effects began with the examination ofchanges in pain and stress reactivity within each group separately.Although not the focus of the current study, we also report changesfrom pre- to postintervention in aggregated levels of each dailyoutcome, two of which were reported in a previous paper (i.e., paincatastrophizing and control; Zautra et al., 2008). The results of theanalyses are summarized in Table 2 and illustrated in Figures 2–4.
The M group showed the broadest changes from pre- to post-treatment in pain and stress reactivity of the three groups. The Mgroup showed less pronounced increases from pre- to posttreat-ment in the catastrophizing associated with a daily pain episode(Time � �Pain t � 2.91, p � .004). Figure 2, Panel A, depictsthe pre- and postintervention relations between daily pain andcatastrophizing in the M group, and highlights that the strength ofthe association weakened over time. The M group also showed
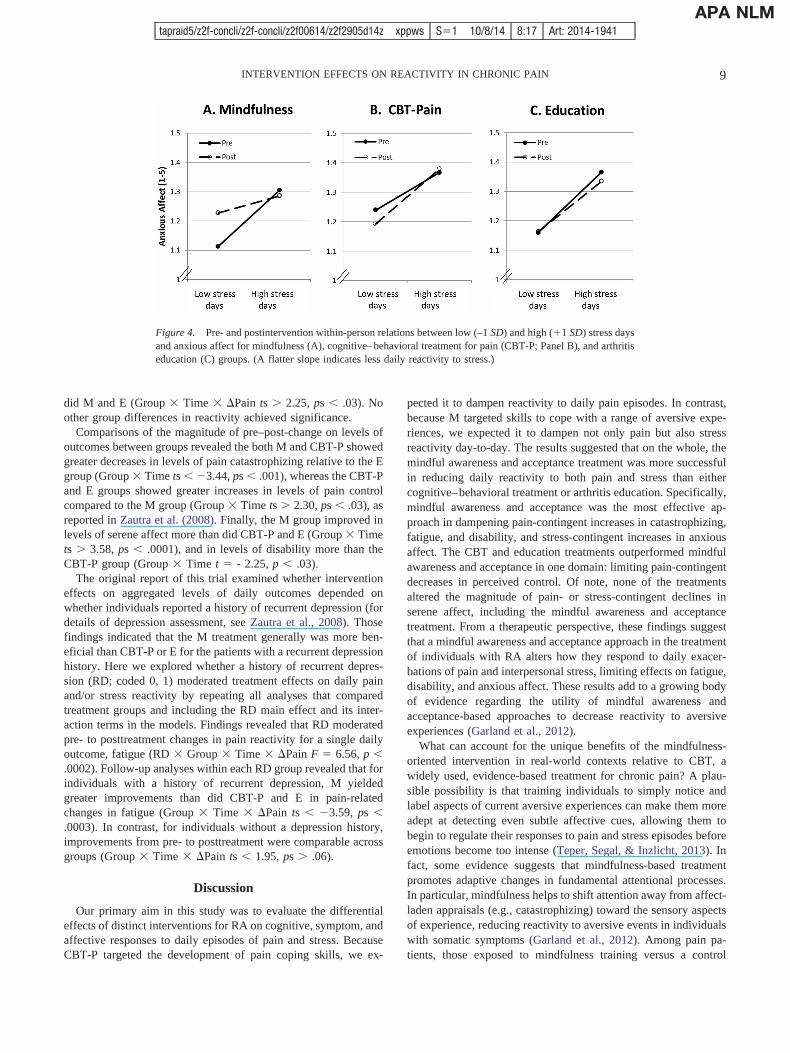
pre–post improvement in relations between pain episodes andchanges in disability and fatigue (Time ts � 2.69, ps � .008),and between stress episodes and changes in serene affect (Time ��Stress t � 2.18, p � .03), and anxious affect (Time � �Stresst � 2.17, p � .03). Figure 3, Panel A, depicts the pre- andpostintervention relations between daily pain and fatigue, andFigure 4, Panel A the pre- and postintervention relations betweendaily stress and anxious affect in the M group. With regard tochanges in overall levels of each outcome, the M group showedpre–post improvement in levels of catastrophizing (Timet � 2.54, p � .02), disability (Time t � 10.17, p � .0001), andserene affect (Time t � 5.48, p � .0001).
The CBT-P group showed less pronounced decreases frompre- to postintervention in perceived pain control on days ofhigh pain (Time � �Pain t � 2.89, p � .004). However, theCBT-P group evidenced no change in the relations betweendaily pain and stress episodes and catastrophizing, serene af-
Table 2Parameter Estimates (SE) From Multilevel Models of Pre–Post Intervention Change in Daily Pain and Stress Reactivity forMindfulness (n � 47), CBT-P (n � 52), and Education (n � 44) Groups
Daily outcome
Effects within groupa
Group differencesbM estimate (SE) CBT-P estimate (SE) E estimate (SE)
Catastrophizing (1–5)Intercept 2.025 (0.097) 2.081 (0.090) 2.045 (0.113)Time: Pre–post 0.085 (0.033)� 0.103 (0.027)��� 0.081 (0.033)� M, CBT-P � E�Pain 0.015 (0.002)���� 0.017 (0.002)���� 0.010 (0.002)����
Time � �Pain 0.006 (0.002)�� 0.001 (0.002) 0.004 (0.002)� M � CBT-P, EControl (0–10)
Intercept 7.091 (0.307) 5.844 (0.294) 5.983 (0.337)Time: Pre–post 0.040 (0.086) 0.291 (0.087)�� 0.269 (0.109)� CBT-P, E � M�Pain 0.031 (0.010)�� 0.043 (0.006)���� 0.039 (0.008)����
Time � �Pain 0.008 (0.007) 0.015 (0.005)�� 0.002 (0.006) CBT-P � M, EFatigue (0–100)
Intercept 27.031 (2.609) 35.343 (2.437) 30.044 (2.431)Time: Pre–post 1.579 (0.843) 3.049 (0.760)��� 1.665 (0.869)� Pain 0.506 (0.047)���� 0.434 (0.044)���� 0.470 (0.044)����
Time � �Pain 0.152 (0.052)�� 0.079 (0.040)� 0.013 (0.047) M � CBT-P, EMorning disability (1–5)
Intercept 2.850 (0.153) 3.328 (0.174) 3.072 (0.157)Time: Pre–post 0.460 (0.045)���� 0.313 (0.041)���� 0.327 (0.049)����
�Pain 0.023 (0.003)���� 0.018 (0.002)���� 0.021 (0.003)����
Time � �Pain 0.007 (0.003)�� 0.004 (0.002)� 0.001 (0.002) M � CBT-P, ESerene affect (1–5)
Intercept 2.924 (0.122) 2.758 (0.109) 2.944 (0.108)Time: Pre–post 0.184 (0.034)���� 0.025 (0.029) 0.003 (0.036) M � CBT-P, E�Pain 0.005 (0.001)���� 0.012 (0.001)���� 0.011 (0.001)����
�Stress 0.258 (0.054)���� 0.237 (0.043)���� 0.268 (0.043)����
Time � �Pain 0.004 (0.002) 0.003 (0.002) 0.003 (0.002)Time � �Stress 0.111 (0.051)� 0.028 (0.046) 0.034 (0.053)
Anxious affect (1–5)Intercept 1.212 (0.054) 1.301 (0.063) 1.223 (0.044)Time: Pre–post 0.035 (0.020) 0.001 (0.023) 0.007 (0.023)�Pain 0.000 (0.001) 0.002 (0.001) 0.003 (0.001)�
�Stress 0.156 (0.022)���� 0.134 (0.023)���� 0.165 (0.025)����
Time � �Pain 0.003 (0.002) 0.001 (0.001) 0.002 (0.001)Time � �Stress 0.072 (0.033)� 0.040 (0.035) 0.036 (0.037) M � CBT-P, E
Note. SE � standard error; M � mindfulness; CBT-P � cognitive–behavioral therapy for pain; E � education; �Pain � person-centered pain; �Stress �person-centered stress. Time is coded Pre � 0, Post � 1. All models included �Pain as a random effect and an AR(1) error structure to model significantdaily covariation.a Models were estimated for each group separately. b Contrasts are from models that included Group, Time, �Pain (�Stress), and their interactions.� p � .05. �� p � .01. ��� p � .001. ���� p � .0001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7INTERVENTION EFFECTS ON REACTIVITY IN CHRONIC PAIN
T2, F2-4
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

fect, or anxious affect (Figures 2– 4, Panel B). Moreover, theCBT-P group actually showed greater pain-reactivity from pre-to posttreatment, reflected in strengthened associations betweendaily pain episodes and same-day fatigue and disability(Time � �Pain ts � 1.97, ps � .05; see Figure 3, Panel B).With regard to changes in overall levels of each outcome, theCBT-P group showed improvement from pre- to posttreatmentin levels of catastrophizing (Time t � 3.85, p � .0003), aswell as pain control (Time t � 3.35, p � .002), disability (Timet � 7.55, p � .0001), and fatigue (Time t � 4.01, p �.0002).
The E group showed no pre- to postintervention change in therelations between pain and stress episodes and any outcome(see Figures 2– 4, Panel C). Moreover, the E group showedgreater pain-reactivity from pre to post, reflected in strength-ened associations between daily pain episodes and same-daycatastrophizing from pre–post treatment (Time � �Pain t �2.15, p � .05; see Figure 3, Panel C). With regard to changesin overall levels of outcomes, the E group showed improvementin levels of perceived pain control (Time t � 2.47, p � .02) and
disability (Time t � 6.73, p � .0001), but worsening in levelsof catastrophizing (Time t � 2.49, p � .02).
Group Differences in Magnitude ofPre–Post Changes in Reactivity
Findings of analyses comparing the magnitude of change indaily pain and stress reactivity from pre- to posttreatment acrossgroups indicated that groups showed pronounced differences inresponse to treatment. On the whole, the M group yielded moresubstantial benefits than the other two groups. M yielded greaterimprovements than did CBT-P and E in pain-related changes incatastrophizing (Group � Time � �Pain ts � 2.68, ps � .006;see Figure 2), morning disability (Group � Time � �Paints � 2.37, ps � .02), and fatigue (Group � Time � �Paints � 2.35, ps � .02; see Figure 3). The M group also showedgreater improvement in stress-related changes in anxious affectthan did CBT-P and E (Group � Time � �Pain ts � 2.07, ps �.04; see Figure 4). In contrast, CBT-P exhibited greater pre–postimprovements in pain-related changes in perceived control than
Figure 2. Pre- and postintervention within-person relations between low (–1 SD) and high (1 SD) pain daysand catastrophizing for mindfulness (A), cognitive–behavioral treatment for pain (CBT-P; Panel B), and arthritiseducation (C) groups. (A flatter slope indicates less daily reactivity to pain.)
Figure 3. Pre- and postintervention within-person relations between low (–1 SD) and high (1 SD) pain daysand fatigue for mindfulness (A), cognitive–behavioral treatment for pain (CBT-P; Panel B), and arthritiseducation (C) groups. (A flatter slope indicates less daily reactivity to pain.)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
AQ: 4
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM
did M and E (Group � Time � �Pain ts � 2.25, ps � .03). Noother group differences in reactivity achieved significance.
Comparisons of the magnitude of pre–post-change on levels ofoutcomes between groups revealed the both M and CBT-P showedgreater decreases in levels of pain catastrophizing relative to the Egroup (Group � Time ts � 3.44, ps � .001), whereas the CBT-Pand E groups showed greater increases in levels of pain controlcompared to the M group (Group � Time ts � 2.30, ps � .03), asreported in Zautra et al. (2008). Finally, the M group improved inlevels of serene affect more than did CBT-P and E (Group � Timets � 3.58, ps � .0001), and in levels of disability more than theCBT-P group (Group � Time t � - 2.25, p � .03).
The original report of this trial examined whether interventioneffects on aggregated levels of daily outcomes depended onwhether individuals reported a history of recurrent depression (fordetails of depression assessment, see Zautra et al., 2008). Thosefindings indicated that the M treatment generally was more ben-eficial than CBT-P or E for the patients with a recurrent depressionhistory. Here we explored whether a history of recurrent depres-sion (RD; coded 0, 1) moderated treatment effects on daily painand/or stress reactivity by repeating all analyses that comparedtreatment groups and including the RD main effect and its inter-action terms in the models. Findings revealed that RD moderatedpre- to posttreatment changes in pain reactivity for a single dailyoutcome, fatigue (RD � Group � Time � �Pain F � 6.56, p �.0002). Follow-up analyses within each RD group revealed that forindividuals with a history of recurrent depression, M yieldedgreater improvements than did CBT-P and E in pain-relatedchanges in fatigue (Group � Time � �Pain ts � 3.59, ps �.0003). In contrast, for individuals without a depression history,improvements from pre- to posttreatment were comparable acrossgroups (Group � Time � �Pain ts � 1.95, ps � .06).
Discussion
Our primary aim in this study was to evaluate the differentialeffects of distinct interventions for RA on cognitive, symptom, andaffective responses to daily episodes of pain and stress. BecauseCBT-P targeted the development of pain coping skills, we ex-
pected it to dampen reactivity to daily pain episodes. In contrast,because M targeted skills to cope with a range of aversive expe-riences, we expected it to dampen not only pain but also stressreactivity day-to-day. The results suggested that on the whole, themindful awareness and acceptance treatment was more successfulin reducing daily reactivity to both pain and stress than eithercognitive–behavioral treatment or arthritis education. Specifically,mindful awareness and acceptance was the most effective ap-proach in dampening pain-contingent increases in catastrophizing,fatigue, and disability, and stress-contingent increases in anxiousaffect. The CBT and education treatments outperformed mindfulawareness and acceptance in one domain: limiting pain-contingentdecreases in perceived control. Of note, none of the treatmentsaltered the magnitude of pain- or stress-contingent declines inserene affect, including the mindful awareness and acceptancetreatment. From a therapeutic perspective, these findings suggestthat a mindful awareness and acceptance approach in the treatmentof individuals with RA alters how they respond to daily exacer-bations of pain and interpersonal stress, limiting effects on fatigue,disability, and anxious affect. These results add to a growing bodyof evidence regarding the utility of mindful awareness andacceptance-based approaches to decrease reactivity to aversiveexperiences (Garland et al., 2012).
What can account for the unique benefits of the mindfulness-oriented intervention in real-world contexts relative to CBT, awidely used, evidence-based treatment for chronic pain? A plau-sible possibility is that training individuals to simply notice andlabel aspects of current aversive experiences can make them moreadept at detecting even subtle affective cues, allowing them tobegin to regulate their responses to pain and stress episodes beforeemotions become too intense (Teper, Segal, & Inzlicht, 2013). Infact, some evidence suggests that mindfulness-based treatmentpromotes adaptive changes in fundamental attentional processes.In particular, mindfulness helps to shift attention away from affect-laden appraisals (e.g., catastrophizing) toward the sensory aspectsof experience, reducing reactivity to aversive events in individualswith somatic symptoms (Garland et al., 2012). Among pain pa-tients, those exposed to mindfulness training versus a control
Figure 4. Pre- and postintervention within-person relations between low (–1 SD) and high (1 SD) stress daysand anxious affect for mindfulness (A), cognitive–behavioral treatment for pain (CBT-P; Panel B), and arthritiseducation (C) groups. (A flatter slope indicates less daily reactivity to stress.)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9INTERVENTION EFFECTS ON REACTIVITY IN CHRONIC PAIN
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

condition showed decreases in attentional bias to and increases indisengagement from pain-related cues, assessed through use of thedot probe technique (Garland & Howard, 2013; Vago & Naka-mura, 2011). A similar pattern of findings is evident in compari-sons of long-term meditators and nonmeditators; for example,experienced meditators and nonmeditators are similar in thethreshold of stimulation required to induce pain, but meditatorsshow less neural activation in anticipation of the painful stimulusand a less negative appraisal of their pain compared to nonmedi-tators (Brown & Jones, 2010). Thus, mindfulness-based treatmentmay yield benefits in part because it refocuses attention, therebydiminishing hypervigilance toward and cognitive elaboration ofthreatening experiences.
CBT, on the other hand, involves reinterpreting the meaning ofan experience to change one’s emotional response to it. Althoughcognitive reappraisal is effective, it is often deployed after emo-tions have intensified, and thus its success hinges on the availabil-ity of sufficient cognitive resources to implement it. Yet, existingevidence suggests that the demands imposed by intense pain andstress may deplete the reservoir of self-regulatory resourcesneeded to cope effectively (Baumeister & Heatherton, 1996). Infact, individuals choose to engage in reappraisal to regulate theiremotions only when negative emotional intensity is low, but preferto use distraction when negative emotional intensity is high (Shep-pes, Scheibe, Suri, & Gross, 2011). Moreover, even when individ-uals are well-trained in the use of cognitive reappraisal strategiesto manage fear responses to an aversive stimulus, they use thosestrategies effectively only in low but not high stress conditions(Raio, Orederu, Palazzolo, Shurick, & Phelps, 2013).
Nevertheless, acceptance is not always more effective thanreappraisal in reducing reactivity to provocation. Investigationsemploying brief laboratory inductions of acceptance versus reap-praisal strategies to regulate responses to aversive experiences inthe immediate term have yielded mixed results. Some findingshave favored reappraisal (Hofmann, Heering, Sawyer, & Asnaani,2009; Szasz, Szentagotai, & Hofmann, 2011), others acceptance(Gutiérrez, Luciano, Rodríguez, & Fink, 2004), and still others,neither approach (Low, Stanton, & Bower, 2008; Wolgast, Lundh,& Viborg, 2011). In their meta-analysis of experiments that com-pared brief inductions of acceptance with other emotion regulationstrategies, Kohl, Rief, and Glombiewski (2012) found some areasof superiority for acceptance. Acceptance was more effective inincreasing pain tolerance across samples, and in limiting acutedistress in clinical but not healthy samples. Thus, the relativebenefits of acceptance, reappraisal, or other strategies are likely tohinge on a host of factors, including the nature of the stressor, thecharacteristics of the individual (e.g., health status), and the time-frames of both the intervention and the outcome assessment.
Interventions for chronic pain strive to build both coping re-sources and the skill needed to apply those resources when cir-cumstances require it. To what extent do they succeed? One meansof addressing this question is to consider the findings regardingintervention effects on daily pain reactivity side-by-side with thosefor pre–post changes in overall levels for pain cognitions. Withregard to catastrophizing, although both the mindfulness and CBTconditions improved overall levels, only mindfulness also im-proved individuals’ ability to limit catastrophizing when confront-ing periods of high daily pain. For pain control, CBT improved notonly overall levels of perceived control, but also individuals’
capacity to sustain a sense of control during pain episodes to agreater extent than did mindfulness. Taken together, this pattern ofresults underscores the fact that bolstering coping resources ingeneral does not necessarily enhance the capacity of individuals todraw on those resources when they are most needed. Maximizingintervention effects, then, is likely to entail ensuring that individ-uals are developing not only a repertoire of coping strategies, butalso the proficiency to use them effectively.
The study has a number of noteworthy strengths. To our knowl-edge, this is the first study to capitalize on the richness of pre- andpostintervention diary data to examine changes in the dynamics ofdaily coping with pain and stress in a large randomized clinicaltrial. The design compared two distinct treatments (i.e., mindful-ness and CBT) with an active control condition (i.e., arthritiseducation), providing the opportunity to test for differential inter-vention effects on daily pain and stress reactivity beyond theeffects of group support, therapist contact, the passage of time, andother nonspecific factors. Finally, the low level of attrition fromintervention groups and of missing diary data strengthens confi-dence in the validity of the findings.
The study also has several limitations that deserve comment.First, the sample was comprised primarily of White women withRA, constraining generalizability of the findings to individualswith a similar background and pain condition. Second, althoughour treatments were manualized and clinicians supervised through-out treatment delivery, the clinicians’ training regarding treatmentdelivery did not include extensive opportunities for role-playing,rehearsal, or booster sessions. Moreover, we did not include obtainand evaluate recordings of sessions to verify clinicians’ compe-tence and compliance with the treatment manuals, verification thatis strongly recommended and would enhance the internal validityof the trial (Perepletchikova, Treat, & Kazdin, 2007). Third, thedaily assessment involved paper-and-pencil diaries. Although di-aries were mailed back to the research team on a daily basis, andevaluation of postmarks assured compliance with mailing instruc-tions, we cannot assure that the diaries were completed in theevening. Fourth, the differences we observed were statisticallysignificant but very small in magnitude. For example, a 30-pointincrease in daily pain above a person’s average daily pain pre-dicted an increase in same-day fatigue at pre- and postinterventionfor the M group of 15.2 and 10.6 points, respectively; for theCBT-P group of 13.0 and 15.4 points, respectively; and for the Egroup of 14.1 and 14.5 points, respectively. The clinical impact ofchanges of this magnitude remains to be determined. Fifth, themodels we evaluated tested same-day relations between pain andstress and study outcomes, but did not test for carryover effectsfrom one day to the next. Future investigations that include within-day assessments may be better positioned to capture the temporalordering of the processes of interest, which likely occur during atimeframe ranging from minutes to hours. Sixth, the study dem-onstrated that CBT and mindfulness-based treatment impacteddaily reactivity, but it did not address how these reductions wereaccomplished. Although from a theoretical perspective, reappraisaland acceptance are central components of CBT and M approaches,respectively, we did not explicitly measure changes in the capacityfor decentering, awareness, reappraisal, or acceptance from pre- toposttreatment. As a result, we cannot be certain that either reap-praisal or acceptance were the “active” ingredients driving thechanges we observed in reactivity. Moreover, because the inter-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
10 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

ventions were complex, it is possible that differences betweengroups are due to different “doses” of the active ingredientsdelivered in each treatment. For example, the less robust effects ofCBT versus M may have been due to the inclusion of componentsthat may be less effective in reducing reactivity than is reappraisal,such as relaxation. As a result, the “doses” of training in reap-praisal offered in the CBT condition may have been smaller thanthe doses of training in awareness and acceptance offered in the Mcondition and may account for the relative inferiority of CBT incomparison with M.
In summary, the present study suggests that mindful awarenessand acceptance treatment targeting regulation of emotion yieldsbenefits in the management of daily pain and stress that arebroader than those offered by a cognitive–behavioral approach orarthritis education. Mindfulness limited the effects of pain flareson catastrophizing, fatigue, and disability, and of stress on anxiousaffect. However, despite its emphasis on boosting positive engage-ment, it did not help individuals sustain serene affect in the face ofpain and stress episodes. On the other hand, CBT limited theeffects of pain flares on perceived control. Although small inmagnitude, the effects demonstrated here reflect changes in day-to-day processes, and the benefits to overall functioning mayincrease as small daily changes are compounded over time. Thesefindings serve as a reminder that therapeutic change can be ef-fected in subtler ways than can be assessed by static measurementof primary outcomes. Indeed, psychological treatments in generalattempt to help people change their habitual responses to ongoingchallenges, and success of therapies over the long term depends onthe application of skills learned in treatment to problems in dailylife. Even with the advent of technological advances, diary assess-ments impose a larger burden on research participants than domore global types of assessment. Yet, when they can shed light onimportant aspects of how treatments work, diary reports can beworth the additional burden. A daily process approach is onepromising avenue toward identifying specific, dynamic mecha-nisms of change and refining interventions.
References
Affleck, G., Zautra, A., Tennen, H., & Armeli, S. (1999). Multilevel dailyprocess designs for consulting and clinical psychology: A preface for theperplexed. Journal of Consulting and Clinical Psychology, 67, 746–754.http://dx.doi.org/10.1037/0022-006X.67.5.746
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing andinterpreting interactions. Thousand Oaks, CA: Sage.
Astin, J. A., Beckner, W., Soeken, K., Hochberg, M. C., & Berman, B.(2002). Psychological interventions for rheumatoid arthritis: A meta-analysis of randomized controlled trials. Arthritis & Rheumatism: Ar-thritis Care and Research, 47, 291–302. http://dx.doi.org/10.1002/art.10416
Banks, S. M., & Kerns, R. D. (1996). Explaining high rates of depressionin chronic pain: A diathesis-stress framework. Psychological Bulletin,119, 95–110. http://dx.doi.org/10.1037/0033-2909.119.1.95
Baumeister, R. F., & Heatherton, T. F. (1996). Self-regulation failure: Anoverview. Psychological Inquiry, 7, 1–15. http://dx.doi.org/10.1207/s15327965pli0701_1
Brown, C. A., & Jones, A. K. P. (2010). Meditation experience predictsless negative appraisal of pain: Electrophysiological evidence for theinvolvement of anticipatory neural responses. Pain, 150, 428–438.http://dx.doi.org/10.1016/j.pain.2010.04.017
Csikszentmihalyi, M., & Larson, R. (1987). Validity and reliability of theexperience sampling method. Journal of Nervous and Mental Disease,175, 526–536. http://dx.doi.org/10.1097/00005053-198709000-00004
Dixon, K. E., Keefe, F. J., Scipio, C. D., Perri, L. M., & Abernethy, A. P.(2007). Psychological interventions for arthritis pain management inadults: A meta-analysis. Health Psychology, 26, 241–250. http://dx.doi.org/10.1037/0278-6133.26.3.241
Epstein, S. (1979). The stability of behavior: I. On predicting most of thepeople much of the time. Journal of Personality and Social Psychology,37, 1097–1126. http://dx.doi.org/10.1037/0022-3514.37.7.1097
Garland, E. L., Gaylord, S. A., Palsson, O., Faurot, K., Douglas Mann, J.,& Whitehead, W. E. (2012). Therapeutic mechanisms of a mindfulness-based treatment for IBS: Effects on visceral sensitivity, catastrophizing,and affective processing of pain sensations. Journal of Behavioral Med-icine, 35, 591–602. http://dx.doi.org/10.1007/s10865-011-9391-z
Garland, E. L., & Howard, M. O. (2013). Mindfulness-oriented recoveryenhancement reduces pain attentional bias in chronic pain patients.Psychotherapy and Psychosomatics, 82, 311–318. http://dx.doi.org/10.1159/000348868
Geschwind, N., Peeters, F., Drukker, M., van Os, J., & Wichers, M. (2011).Mindfulness training increases momentary positive emotions and rewardexperience in adults vulnerable to depression: A randomized controlledtrial. Journal of Consulting and Clinical Psychology, 79, 618–628.http://dx.doi.org/10.1037/a0024595
Gil, K. M., Anthony, K. K., Carson, J. W., Redding-Lallinger, R., Dae-schner, C. W., & Ware, R. E. (2001). Daily coping practice predictstreatment effects in children with sickle cell disease. Journal of PediatricPsychology, 26, 163–173. http://dx.doi.org/10.1093/jpepsy/26.3.163
Gutiérrez, O., Luciano, C., Rodríguez, M., & Fink, B. C. (2004). Compar-ison between an acceptance-based and a cognitive-control-based proto-col for coping with pain. Behavior Therapy, 35, 767–783. http://dx.doi.org/10.1016/S0005-7894(04)80019-4
Hamilton, N. A., Affleck, G., Tennen, H., Karlson, C., Luxton, D.,Preacher, K. J., & Templin, J. L. (2008). Fibromyalgia: The role of sleepin affect and in negative event reactivity and recovery. Health Psychol-ogy, 27, 490–497. http://dx.doi.org/10.1037/0278-6133.27.4.490
Hayes, S. C., & Duckworth, M. P. (2006). Acceptance and commitmenttherapy and traditional cognitive behavior therapy approaches to pain.Cognitive and Behavioral Practice, 13, 185–187. http://dx.doi.org/10.1016/j.cbpra.2006.04.002
Hofmann, S. G., Heering, S., Sawyer, A. T., & Asnaani, A. (2009). Howto handle anxiety: The effects of reappraisal, acceptance, and suppres-sion strategies on anxious arousal. Behaviour Research and Therapy, 47,389–394. http://dx.doi.org/10.1016/j.brat.2009.02.010
Jensen, M. P., Karoly, P., & Braver, S. (1986). The measurement of clinicalpain intensity: A comparison of six methods. Pain, 27, 117–126. http://dx.doi.org/10.1016/0304-3959(86)90228-9
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of yourbody and mind to face stress, pain, and illness. New York, NY: Dela-corte.
Kohl, A., Rief, W., & Glombiewski, J. A. (2012). How effective areacceptance strategies? A meta-analytic review of experimental results.Journal of Behavior Therapy and Experimental Psychiatry, 43, 988–1001. http://dx.doi.org/10.1016/j.jbtep.2012.03.004
Lawrence, R. C., Felson, D. T., Helmick, C. G., Arnold, L. M., Choi, H.,Deyo, R. A., . . . National Arthritis Data Workgroup. (2008). Estimatesof the prevalence of arthritis and other rheumatic conditions in theUnited States. Part II. Arthritis and Rheumatism, 58, 26–35. http://dx.doi.org/10.1002/art.23176
Lorig, K., Chastain, R. L., Ung, E., Shoor, S., & Holman, H. R. (1989).Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis and Rheumatism, 32, 37–44.http://dx.doi.org/10.1002/anr.1780320107
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
11INTERVENTION EFFECTS ON REACTIVITY IN CHRONIC PAIN
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

Low, C. A., Stanton, A. L., & Bower, J. E. (2008). Effects of acceptance-oriented versus evaluative emotional processing on heart rate recoveryand habituation. Emotion, 8, 419–424. http://dx.doi.org/10.1037/1528-3542.8.3.419
McCracken, L. M., & Gross, R. T. (1998). The role of pain-related anxietyreduction in the outcome of multidisciplinary treatment for chronic lowback pain: Preliminary results. Journal of Occupational Rehabilitation,8, 179–189. http://dx.doi.org/10.1023/A:1021374322673
Morley, S., Eccleston, C., & Williams, A. (1999). Systematic review andmeta-analysis of randomized controlled trials of cognitive behaviourtherapy and behaviour therapy for chronic pain in adults, excludingheadache. Pain, 80, 1–13. http://dx.doi.org/10.1016/S0304-3959(98)00255-3
Perepletchikova, F., Treat, T. A., & Kazdin, A. E. (2007). Treatmentintegrity in psychotherapy research: Analysis of the studies and exam-ination of the associated factors. Journal of Consulting and ClinicalPsychology, 75, 829–841. http://dx.doi.org/10.1037/0022-006X.75.6.829
Raio, C. M., Orederu, T. A., Palazzolo, L., Shurick, A. A., & Phelps, E. A.(2013). Cognitive emotion regulation fails the stress test. PNAS Pro-ceedings of the National Academy of Sciences of the United States ofAmerica, 110, 15139 –15144. http://dx.doi.org/10.1073/pnas.1305706110
Robinson, M. D., & Clore, G. L. (2002). Belief and feeling: Evidence foran accessibility model of emotional self-report. Psychological Bulletin,128, 934–960. http://dx.doi.org/10.1037/0033-2909.128.6.934
Rosenstiel, A. K., & Keefe, F. J. (1983). The use of coping strategies inchronic low back pain patients: Relationship to patient characteristicsand current adjustment. Pain, 17, 33–44. http://dx.doi.org/10.1016/0304-3959(83)90125-2
Sheppes, G., Scheibe, S., Suri, G., & Gross, J. J. (2011). Emotion-regulation choice. Psychological Science, 22, 1391–1396. http://dx.doi.org/10.1177/0956797611418350
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momen-tary assessment. Annual Review of Clinical Psychology, 4, 1–32. http://dx.doi.org/10.1146/annurev.clinpsy.3.022806.091415
Singer, J. D. (1998). Using SAS PROC MIXED to fit multilevel models,hierarchical models and individual growth models. Journal of Educa-tional and Behavioral Statistics, 24, 323–355. http://dx.doi.org/10.2307/1165280
Smeets, R. J. E. M., Vlaeyen, J. W. S., Kester, A. D. M., & Knottnerus,J. A. (2006). Reduction of pain catastrophizing mediates the outcome ofboth physical and cognitive-behavioral treatment in chronic low backpain. The Journal of Pain, 7, 261–271. http://dx.doi.org/10.1016/j.jpain.2005.10.011
Spinhoven, P., Ter Kuile, M., Kole-Snijders, A. M., Hutten Mansfeld, M.,Den Ouden, D.-J., & Vlaeyen, J. W. (2004). Catastrophizing and internalpain control as mediators of outcome in the multidisciplinary treatmentof chronic low back pain. European Journal of Pain, 8, 211–219.http://dx.doi.org/10.1016/j.ejpain.2003.08.003
Strand, E. B., Zautra, A. J., Thoresen, M., Ødegård, S., Uhlig, T., & Finset,A. (2006). Positive affect as a factor of resilience in the pain-negativeaffect relationship in patients with rheumatoid arthritis. Journal of Psy-chosomatic Research, 60, 477– 484. http://dx.doi.org/10.1016/j.jpsychores.2005.08.010
Suls, J., & Martin, R. (2005). The daily life of the garden-variety neurotic:Reactivity, stressor exposure, mood spillover, and maladaptive coping.Journal of Personality, 73, 1485–1510. http://dx.doi.org/10.1111/j.1467-6494.2005.00356.x
Szasz, P. L., Szentagotai, A., & Hofmann, S. G. (2011). The effect ofemotion regulation strategies on anger. Behaviour Research and Ther-apy, 49, 114–119. http://dx.doi.org/10.1016/j.brat.2010.11.011
Teper, R., Segal, Z. V., & Inzlicht, M. (2013). Inside the mindful mind:How mindfulness enhances emotion regulation through improvements inexecutive control. Current Directions in Psychological Science, 22,449–454. http://dx.doi.org/10.1177/0963721413495869
Turner, J. A., Holtzman, S., & Mancl, L. (2007). Mediators, moderators,and predictors of therapeutic change in cognitive-behavioral therapy forchronic pain. Pain, 127, 276–286. http://dx.doi.org/10.1016/j.pain.2006.09.005
Vago, D. R., & Nakamura, Y. (2011). Selective attentional bias towardspain-related threat in fibromyalgia: Preliminary evidence for effects ofmindfulness meditation training. Cognitive Therapy and Research, 35,581–594. http://dx.doi.org/10.1007/s10608-011-9391-x
Veehof, M. M., Oskam, M.-J., Schreurs, K. M., & Bohlmeijer, E. T.(2011). Acceptance-based interventions for the treatment of chronicpain: A systematic review and meta-analysis. Pain, 152, 533–542.http://dx.doi.org/10.1016/j.pain.2010.11.002
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item Short-FormHealth Survey (SF-36). I. Conceptual framework and item selection.Medical Care, 30, 473– 483. http://dx.doi.org/10.1097/00005650-199206000-00002
Watson, D. (1988). Intraindividual and interindividual analyses of positiveand negative affect: Their relation to health complaints, perceived stress,and daily activities. Journal of Personality and Social Psychology, 54,1020–1030. http://dx.doi.org/10.1037/0022-3514.54.6.1020
Watson, D., & Clark, L. A. (1994). Manual for the Positive and NegativeAffect Schedule - Expanded Form. University of Iowa. Retrieved fromhttp://ir.uiowa.edu/psychology_pubs/11
Westhoff, G., Buttgereit, F., Gromnica-Ihle, E., & Zink, A. (2008). Morn-ing stiffness and its influence on early retirement in patients with recentonset rheumatoid arthritis. Rheumatology, 47, 980–984. http://dx.doi.org/10.1093/rheumatology/ken137
Wolgast, M., Lundh, L.-G., & Viborg, G. (2011). Cognitive reappraisal andacceptance: An experimental comparison of two emotion regulationstrategies. Behaviour Research and Therapy, 49, 858–866. http://dx.doi.org/10.1016/j.brat.2011.09.011
Yazici, Y., Pincus, T., Kautiainen, H., & Sokka, T. (2004). Morningstiffness in patients with early rheumatoid arthritis is associated morestrongly with functional disability than with joint swelling and erythro-cyte sedimentation rate. The Journal of Rheumatology, 31, 1723–1726.
Zautra, A. J., Davis, M. C., Reich, J. W., Nicassario, P., Tennen, H., Finan,P., . . . Irwin, M. R. (2008). Comparison of cognitive behavioral andmindfulness meditation interventions on adaptation to rheumatoid ar-thritis for patients with and without history of recurrent depression.Journal of Consulting and Clinical Psychology, 76, 408–421. http://dx.doi.org/10.1037/0022-006X.76.3.408
Received January 23, 2014Revision received August 28, 2014
Accepted September 15, 2014 �
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
12 DAVIS, ZAUTRA, WOLF, TENNEN, AND YEUNG
tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z xppws S�1 10/8/14 8:17 Art: 2014-1941APA NLM

JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 1 OUTPUT: Wed Oct 8 08:17:52 2014/tapraid5/z2f-concli/z2f-concli/z2f00614/z2f2905d14z
AQau—Please confirm the given-names and surnames are identified properly by the colors.� Given-Name, � Surname
The colors are for proofing purposes only. The colors will not appear online or in print.
AQ1—Author: Running head must be 50 characters or fewer (including spaces). Please reviewchanges.
AQ2—Author: Should this be “Anxious effect”?
AQ3—Author: Sentence okay as edited?
AQ4—Author: Please note that “pre-to-post” was changed to “pre–post” for consistency.
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES 1
Copyright © 2022 FDOKUMEN