Metastatic melanoma positively influences pregnancy outcome in a mouse model: could a deadly tumor...
20
SUMMARY The incidence of melanoma is increasing worldwide. It is one of the leading cancers in pregnancy and the most common malignancy to metastasize to placenta and fetus. There are no publications about experimental models of melanoma and pregnancy. We propose a new experimental murine model to study the effects of melanoma on pregnancy and its metastatic process. We tested several doses of melanoma cells until we arrived at the optimal dose, which produced tumor growth and allowed animal survival to the end of pregnancy. Two control groups were used: control (C) and stress control (SC). and three different routes of inoculation: intravenous(IV), intraperitoneal (IP) and subcutaneous (SC). All the fetuses and placentas were examined macroscopically and microscopically. The results suggest that melanoma is a risk factor for intrauterine growth restriction but does not affect placental weight. When inoculated by the SC route, the tumor grew only in the site of implantation. The IP route produced peritoneal tumoral growth and also ovarian and uterine metastases in 60% of the cases. The IV route produced pulmonary tumors. No placental or fetal metastases were obtained, regardless of the inoculation route. The injection of melanoma cells by any route did not increase the rate of fetal resorptions. Surprisingly, animals in the IV groups had no resorptions and a significantly higher number of fetuses. This finding may indicate that tumoral factors released in the host organism to favor tumor survival may also have a pro-gestational action and consequently improve the reproductive performance of these animals. Title Metastatic melanoma positively influences pregnancy outcome in a mouse model: could a deadly tumor support embryo life? Authors Rubens H Bollos (Bollos, RH) a , Mary U Nakamura (Nakamura, MU) a , Valderez B V Lapchick (Lapchick, VBL) b , Estela M A F Bevilacqua (Bevilacqua, E) c , Mariangela Correa (Correa, M) d , Silvia Daher (Daher, S) a , Márcia M S Ishigai (Ishigai, MMS) e , Miriam G Jasiulionis (Jasiulionis, MG) d a Department of Obstetrics, Sao Paulo Federal University Medical School, Sao Paulo, Brazil
Transcript of Metastatic melanoma positively influences pregnancy outcome in a mouse model: could a deadly tumor...

SUMMARY
The incidence of melanoma is increasing worldwide. It is one of the leading cancers in pregnancy and
the most common malignancy to metastasize to placenta and fetus. There are no publications about
experimental models of melanoma and pregnancy. We propose a new experimental murine model to
study the effects of melanoma on pregnancy and its metastatic process. We tested several doses of
melanoma cells until we arrived at the optimal dose, which produced tumor growth and allowed
animal survival to the end of pregnancy. Two control groups were used: control (C) and stress control
(SC). and three different routes of inoculation: intravenous(IV), intraperitoneal (IP) and subcutaneous
(SC). All the fetuses and placentas were examined macroscopically and microscopically. The results
suggest that melanoma is a risk factor for intrauterine growth restriction but does not affect placental
weight. When inoculated by the SC route, the tumor grew only in the site of implantation. The IP route
produced peritoneal tumoral growth and also ovarian and uterine metastases in 60% of the cases.
The IV route produced pulmonary tumors. No placental or fetal metastases were obtained, regardless
of the inoculation route. The injection of melanoma cells by any route did not increase the rate of fetal
resorptions. Surprisingly, animals in the IV groups had no resorptions and a significantly higher
number of fetuses. This finding may indicate that tumoral factors released in the host organism to
favor tumor survival may also have a pro-gestational action and consequently improve the
reproductive performance of these animals.
Title
Metastatic melanoma positively influences pregnancy outcome in a mouse model: could a deadly
tumor support embryo life?
Authors
Rubens H Bollos (Bollos, RH)a, Mary U Nakamura (Nakamura, MU)a, Valderez B V Lapchick
(Lapchick, VBL)b, Estela M A F Bevilacqua (Bevilacqua, E)c, Mariangela Correa (Correa, M)d, Silvia
Daher (Daher, S)a, Márcia M S Ishigai (Ishigai, MMS)e, Miriam G Jasiulionis (Jasiulionis, MG)d
a Department of Obstetrics, Sao Paulo Federal University Medical School, Sao Paulo, Brazil

b Animal Experimental Laboratory, National Institute of Pharmacology, São Paulo Federal University
Medical school, Sao Paulo, Brazil
c Department of Cellular Biology and Development, Institute of Biomedical Sciences, São Paulo
University, Brazil
d Department of Immunology, Sao Paulo Federal University Medical School , Sao Paulo, Brazil
e Department of Pathology, Sao Paulo Federal University Medical School , Sao Paulo, Brazil
Text
Cancer is the second cause of death during reproductive years and complicates 0.1% of all
pregnancies.[1-4] The most common malignancies associated with pregnancy include melanoma,
lymphomas, leukemias and cervical, thyroid and breast cancer. Melanoma is the most lethal skin
cancer and its incidence is increasing dramatically over the last decade worldwide.[5-7] Furthermore,
malignant melanoma is the 6th most frequently diagnosed cancer in women, affecting 35% of them in
reproductive phase (15-44 years).[8;9] Consequently, melanoma is one of the leading malignancies
associated with pregnancy, accounting for about 8% of all cancers diagnosed during gestation with
an incidence rate of 2.8 per 1000 deliveries.[3]
Cutaneous melanomas originate from individual melanocytes in about two-thirds of the cases and
from pre-existing cutaneous nevi in one-third. This tumor is aggressive with an unpredictable biologic
behavior. If detected early, surgical resection is often curative, and long-term survival is excellent.
Unfortunately, diagnosis is often delayed in pregnant women because changes in color or size of nevi
may occur during normal pregnancy. Therefore the disease is often diagnosed in more advanced
stages in these patients [10]. Hence, the recommendation that any patient presenting a suspicious
lesion or skin hyperpigmentation should always be submitted to a biopsy and histologically examined
as soon as possible. [11-13]
Melanoma accounts for more than 50% of all tumors in pregnancy that metastasize to placenta and
fetus.[14-18] Thus in these patients, both placenta and fetus should be examined thouroughly.[19;20]
Since it would be impossible to conduct prospective randomized clinical trials on the treatment of

melanoma in pregnancy, relevant data on therapy and management issues in pregnant women with
melanoma have been generated from case reports and matched historical cohort studies. Due to the
lack of sufficient data, it is difficult to draw firm conclusions about the effects of hormones and
pregnancy on melanoma, its prognosis and management in pregnant patients and also the safety of
prescribing oral contraceptives and hormone replacement therapy for patients with a history of
melanoma.[21;22] Most of the publications on the management and treatment of metastatic
melanoma in pregnancy have focused on the mother, with scarce analysis of placental and fetal
involvement.[23-25] Furthermore, the mechanism by which melanoma is able to overcome the
transplacental barrier is not well understood, and there are no well-established prognostic factors that
predict the increased probability of such fetal as placental metastasis.[26-28]
The objective of this study was to develop an experimental model for metastatic melanoma during
mice pregnancy. A second objective was to evaluate the effect of maternal melanoma on the fetus
and placenta, by morphological analysis.
METHODS
Cell line and culture
The murine melanocyte cell line melan-a[29] was cultured in RPMI pH 6.9 (Gibco, CA, USA),
supplemented with 5% fetal calf serum (Gibco) and garamicin (Invitrogen, CA, USA) at 37oC in a
humidified atmosphere of 5% CO2 and 95% air and 200 nM 12-o-tetradecanoyl PMA (Sigma, St.
Louis, MO). The murine melanomas cells lines Tm5[30;31] and B16F10 was cultured in the same
conditions, except for PMA. Cells were harvested after trypsin treatment of subconfluent monolayers
and counted, suspended in PBS in a concentration of 5.104cells in 100µl and injected as describe
below.
Animals
Sixty-eight female adult (8 weeks) virgin C57BL6 mice (Mus musculus domesticus), weighing
approximately 25 g, were included in the study. All animals were selected and maintained by the
Experimental Animal Laboratory of the Pharmacology Institute of São Paulo Federal University

(INFAR-UNIFESP). Animals were kept under 12h daylight cycles, with food and water ad libitum and
checked daily throughout the experiment. Females made estrous by induction, were caged overnight
with males (1:1) and successful mating was verified the following morning. The presence of a vaginal
plug indicated day “0” of pregnancy. All procedures were carried out in accordance with the
guidelines of the Brazilian College of Animal Experimentation and were authorized by the Committee
on Ethics in Animal Research - UNIFESP.
Groups and tumor cells inoculation
After mating, on day “0”, the 68 pregnant mice were randomly divided into 7 groups. Three groups
were inoculated with 5.104 Tm5 cells in 100µL PBS either subcutaneously (SC, n=10), intraperitonealy
(IP, n=10) and intravenously via tail vein (IVTm5, n=12). Two others groups were inoculated
intravenously with 5.104 B16F10(IVB16F10, n=8) and melan-a (IVmelan-a, n=8) cells. The control group
received no cells (C, n=10) and the stress control group received 100µL PBS intravenously (S, n=10).
Morphological assay
All animals were observed daily until the 19th day of gestation when they were euthanized by cervical
dislocation and submitted to a thoraco-abdominal laparotomy to expose internal organs. Various
maternal organs and tissues were carefully inspected to evaluate tumor dissemination. In each group,
fragments from different sites were collected for microscopic examination: the skin tumor from SC;
the peritoneum, uterus and ovaries from IP and the lungs from IV groups. The presence of tumor in
these organs meant successful cell implant. A uterine incision was then performed to extract the
fetuses and placentas. Resorptions were counted and weighed from each offspring. Maternal
organs and tissues as well as the fetal skin and placenta were examined under a stereoscopic
microscope in search of dark colored pigmented lesions. Placental tumoral involvement was defined
as gross or microscopic evidence of melanotic melanoma cells within any section of the placenta.
Similarly, fetal metastasis was defined as the presence of maternal neoplasic cells in the fetus, with
no evidence of a primary fetal tumor. Maternal organs, fetus, placenta and resorption tissues were
collected, analyzed, photographed and fixed n 10% para-formaldehyde in PBS 0.1 M, pH 7.2, for
morphological analysis.

Reproductive performance
The reproductive performance was assessed by fetal and placental weights and implantation and
resorption rates. Implantation rate was defined as the number of fetus/pregnant animal and resorption
rate as the number of resorption/pregnant animal.
Morphological analysis and histochemistry assay for identification of metastasis
All placentas, fetuses and resorbed embryos were sliced sagitally . Representative fragments from
maternal organ were embedded in paraffin and processed. The blocks were sliced using a microtome
adjusted at 3 µm. The slices were placed on glass slides previously lubricated with Mayer albumin.
The slides were left in an oven at 37ºC for 24 hours to dry and fix the material. All the slides
(maternal and fetal organs, placenta and resorptions) were then stained with hematoxylin-eosin (HE)
and Fontana-Masson[32] (which provides differential staining of melanotic cells). Two slides from
each blocks were examined by two observers using a conventional light photomicroscope (Olympus,
Optical Co. Ltd., Tokyo, Japan). All fields in each section were evaluated (x40, x100 and x400) for the
presence of pigmented areas and anaplasic cells. Representative microphotographs of the maternal,
fetal, placental and resorption tissues were obtained.
Statistical analysis
Numerical data, number of fetuses, resorbed embryos and the weights of placentas and fetuses were
expressed as means ± standard deviation, medians, minimum, maximum values. Differences among
the groups were analyzed and compared using the Kruskal–Wallis test (H). The Dunn’s test for
multiple comparisons was used when significant differences were observed. A 3.03 version of the
GraphPad TM software was used for this purpose. p < 0.05 was taken as statistically significant..
RESULTS
Maternal survival after tumor inoculation
Female mice were inoculated with different doses of melanoma cells via the subcutaneous route to
ascertain time to tumor progression and death (Figure 1). For gestational studies, 5.104 Tm5 cells

was chosen as the best inoculation dose for all inoculation routes, since mice injected with
subcutaneous tumors could carry a pregnancy to term (around 20 days). All inoculated pregnant
mice (100%) survived until the 19th gestational day, with no apparent fetal preterm death.
Tumor and metastasis presence versus routes of cell inoculation
To analyze the impact of different forms of tumor presentation on the pregnancy outcome, we chose
3 routes for tumor inoculation. The SC route, which most closely resembles the natural history of
melanoma, the IV route to simulate metastatic disease and the IP route to simulate pelvic organ
invasion. Microscopic analyses revealed viable melanoma cells in all pregnant mice (n=40),
regardless of the inoculation route. As shown in Figure 2A, 2B and 2C, all animals presented
subcutaneous tumors when inoculated via this route (n=10). Similarly, the injection of two tumor cells
intravenously (n=20) resulted in metastatic disease in all lungs study animals (Figure 2J,2K,2L,2M).
The injection of melan-a non-tumorigenic cell line intravenously (n=8) resulted in no tumor growth, as
expected (Figure 2N,2O). Locally invasive disease was found in the peritoneum surface (Figure
2D,2G,2H) in all mice injected via the intraperitoneal route (n=10). In this last group, ovarian and
uterine metastasis were identified in 80% and 20% of the animals, respectively (Figure 2E,2F, 2I).
Placental and fetal metastasis detection
A total of 800 slides from placentas and fetuses (C=78, IVTm5=170, IVB16F10=138, IVmelan-a=114, IP=82,
SC=114, S=104) were stained by hematoxylin-eosin (HE) and analyzed by conventional light
microscopy. Because throphoblast and melanoma cells share the expression of several antigens
used for melanoma immunological diagnosis (S100, Melan-A and HMB-45), the histochemical
method using the Fontana-Mason staining solution was chosen for melanoma and melanin pigment
detection to confirm HE findings. Although an extensive analysis was performed, no evidence of
metastatic disease to either the fetuses or placental tissues was observed (data not shown).
Implantation and resorption rates analysis
The number of implantations and resorptions was determined by direct visual examination of the
uterus. The implantation rate was significantly higher (p<0.001) in the IVTm5, IVB16F10 and IVmelan-a

groups and the resorption rate was significantly lower (p<0.005) just in the IV melanomas groups,
compared to all other groups, include IVmelan-a. In the IP and SC groups, 20% of pregnant mice had
only resorptions and no live fetuses (Table1, Figure 3).
Fetal and placental weight measurements
Fetal weight was negatively influenced by tumor cell injection by any route, and also by sham venous
puncture, suggesting that the stressful conditions of the experiment were responsible for this findings.
Unexpectedly, placental weight was not altered by any experimental conditions (Table 2, Figure 3).
DISCUSSION
Malignant melanoma accounts for more than 50% of all the tumors that metastasize to the fetus or
placenta. This tendency to metastasize to these structures is intriguing and poorly understood[33-35]
In combination with the fetal immune system, the placental barrier is remarkably efficient at
preventing the spread and allografting of the maternal tumor into the fetus and the transmission of
neoplastic and nonneoplastic maternal cells to the fetus that occurs during pregnancy involves only
aggressive and rapidly growing tumors such as melanomas and hematological malignancies.[36]
Alternatively the point in placental/fetal development at which they are exposed to maternal tumor
cells may be critical in terms of tumor tolerance or rejection.[37]Thus, once separation of the fetal and
maternal blood systems is breached and maternal intravascular tumor cells can pass through the
placenta, they commonly manifest initially as skin lesions or abdominal swelling and end up in the
fetal liver via the umbilical vein or in the fetal lungs via the ductus venosus or placental
implants.[38;39] In this experimental model we searched for metastatic cells in these fetal organs,
both macroscopically and microscopically. Due to its enormous blood supply, it can be difficult to
identify metastatic cells within the placenta, even using microscopy.[40;41] Because of this, in this
experiments we decided to examine not only tissue fragments but the entire placenta and fetus and
use both HE and a specific melanotic stain (Fontana-Masson). Despite all this, no melanoma cells
were identified in any of the fetuses or placentas in all groups.

Fetal metastases require maternal tumor invasion and fetal inability to eliminate metastatic cells.
According to the literature, fetuses who develop melanoma metastases may have developed
immunologic tolerance because of exposure to tumor antigens at a time when the developing
immune system is not yet capable of responding.[42;43] One hypothesis is that the fetus rejects
maternal malignant cells as a homograft. Fetal T- and B-cell responses are thought to develop
around weeks 7 -10 and 14 -20, respectively, and most of the reported cases of fetal metastases
occurred in women who had metastatic disease before that period. Thus early fetal metastases,
before a critical phase of immunologic maturation of the fetus, might be the result of an inability to
recognize the tumor cells as foreign. Moreover the timing of maternal metastasis of melanoma does
not seem to differ in placental versus fetal metastasis.[44;45] In reviews, male infants seem to be at
higher risk than females for developing metastases of any maternal cancer. Males comprise 80% of
all infants with metastasis of melanoma and 75% with metastasis of all cancers indicating that gender
may influence survival.[46-50] A possible explanation is that female fetuses are more capable of
eliminating maternally derived melanoma or that male fetuses are more immunotolerant.[51;52] This
fact is very interesting since embryogenesis and consequently the genetic sex, is controlled by both
genetic and epigenetic mechanisms.[53-55]. Epigenetics and DNA methylation are being held
responsible for the appearance of cancer and cause strong and heritable transcriptional silencing of
genes subject to genomic imprinting or to X chromosome inactivation. Inactivation provides a unique
model for studying the establishment and maintenance of chromosome-wide gene silencing and
alterations in that mechanism could explain the high frequency of melanoma cell in male fetus.[56]
Since in our experiment there were no fetal metastasis we did not evaluate the gender of the fetuses.
The most likely way for dissemination of cancer by vertical transmission is through the hematogenous
route[57-59]. Because of this, we inoculated melanoma cell during mice pregnancy by three different
routes (IP, SC and IV) in order to produce vertical transmission or transplacental metastases. For
metastatic assay (IV) we inoculated two tumorigenic lineages (Tm5 and B16F10) and non-
tumorigenic cell line (melan-a). Despite the fact that all mothers developed melanoma and none of
them died, no tumoral cells implants were found in the fetuses or placentas. Ovarian (Figure 2E,2F)
and uterine (Figure 2I) metastases were identified in the IP group, demonstrating that this was an

adequate model for research in female intrapelvic organ metastases. Despite the lack of fetal or
placental metastasis, melanoma cells injected subcutaneously, intraperitoneally or intravenously
reduced fetal weight (Table 2, Figure 3). This suggests that metastatic maternal melanoma may have
a deleterious effect on embryo implantation and fetal development. The SC group mimics the natural
history of melanoma and in this group we found the highest resorption rates (Table 2, Figure 3). This
could perhaps indicate the presence of factors that inhibit trophoblast invasion and embryo
implantantion. Alternatively the poor reproductive performance could be the result of caquexy induced
by rapid tumoral growth, which eventually will lead to maternal death. It is possible that cytokines
involved in the process of caquexy (tumor necrosis factor alpha, interleukins 1, 2 and 6 and gama
interferon) could be implicated[60;61]. Melanomas release these cytokines recognizably involved in
the TH1 immunological response, which antagonizes trophoblast invasion and embryo
implantation.[62;63] These cytokines are also involved in missed abortions and placental diseases
such as gestational trophoblastic tumors, pre-eclampsia and intra-uterine growth retardation[64-66].
The high resorption rate could indicate the decline in maternal health due to disease spread with
consequent embryo death. In the IVTm5 and IVB16F10 groups lung metastases (Figure 2J,2K,2L,2M)
developed as expected in all mothers from the both melanomas groups. No metastasis or cell
developted in the lung of IVmelan-a group (Figure 2N,2O). As previously discussed, the complete
absence of resorptions and the elevated number of live fetuses were very significant (Table 1, Figure
3). These findings suggest that, contrary to the other groups, the intravenous inoculation of tumor
cells may actually favor trophoblast implantation and embryo development. Hence we hypothesize
that once melanoma metastatic cells reach the maternal blood stream produce a release of various
factors, as cytokine and growth factors and their receptors wich by autocrine and paracrine effect
enable them to grow autonomously and confer competence to metastasis. Autocrine growth factors
as basic fibroblast growth factor (bFGF), melanoma growth stimulatory activity (MGSA), platelet-
derived growth factor (PDGF)-A , stem cell growth factor, IL-8 and IL-10 are produced by melanocyte
and melanoma cells wich act on cell proliferation.[67;68] The growth factors produced by melanoma
cells as epidermal growth factor(EGF), transforming growth factor (TGF-β), (GM-CSF), insulin-like
growth factor-1 (IGF-1), nerve growth factor (NGF), hepatocyte growth (HGF), vascular endothelial
growth factor factor (VEGF) can have paracrine effects on other cells in the surrounding stroma while

the endothelial cell, fibroblasts, monocytes, lymphocytes wich are involved in tumor growth and
invasion.[69] Autocrine and paracrine effects could explain the beneficial effects on embryo and
placental development by melanoma cells observed in IVTm5 and IVB16F10 groups (Table 1). Also in
IVmelan-a group we observed this benefit effect by elevated number of fetuses once melanocytes cell
can express many of these factors during their development by autocrine regulation. Oppositely, the
number of resorptions was elevated in this group (Table 1), revealing that just malignant cells
produce excessive levels of autocrine and paracrine grow factors and proliferate autonomoysly and
infinitevely[70].
As part of the metastatic model recently proposed[71] metastatic cells must alter the expression of
numerous genes, including expression or repression of specific cell adhesion molecules, elaboration
of matrix-digesting enzymes, expression of proto-oncogene products, activation of telomerase and
the acquisition of a rich blood supply before they are able to invade and establish themselves in an
alternative tissue environment. Under this model many similarities exist between metastatic cancer
cells implantation and embryo implantation. The trophoblast cells of the placenta proliferate, migrate
and invade the pregnant uterus and its vasculature in order to nourish the developing fetus in a way
that is imitated by malignant tumors.[72;73] The placenta is an exceptionally vascular organ and
produces several growth factors (placental growth factor, HGF, VEGF and tissue factor). These
placental angiogenic factors also have been reported to be released by and influence the growth of
melanoma cells in culture.[74;75] Also expression of endothelial intercellular adhesion molecules
(ICAM), in particular ICAM-1 and the upperegulation of N-cadherin, α5β3 integrin and
downregulation of E-cadherin and α6β1 integrin, encourage adhesion, survival and invasion of
melanoma cells and metastatic spreading to distant sites. However, the precise mechanism by which
these growth factors contribute to these processes has yet to be defined and more research is
needed. Furthermore, some studies have shown that the thickness of melanomas diagnosed during
pregnancy is significantly greater than that of site matched melanomas in non-pregnant women in the
same age range.[76-79] This may be due to growth factors released during normal pregnancy which
may offer a selective growth advantage to the developing malignant melanocytes. This could also

justify the relative affinity of melanomas for placental and fetal metastasis once the risk of vertical
transmission in mothers with placental metastasis involvement is 25%.[80;81]
The similarities between trophoblast invasion and metastatic cells bring to mind the phenomenon of
multiple or simultaneous cancers. In humans and a few animals, a second tumor may sometimes
arise at another location, within a short time after the appearance of the first malignancy. In such
cases, studies have reported hat the first cancer immunologically enhances the growth of other
cancers from premalignant cells.[82-84] This led us to wonder if the development of one tumor
(melanoma) could facilitate the outgrowth of another “tumor” (trophoblasts). The higher rate of
implantation and absence of resorptions in the IV groups seem to indicate this could have occurred
in those animals. However, the other groups, which received the same melanoma cells by other
routes had a poor reproductive performance (Table 1). This may suggest that perhaps pregnancy
outcome may be influenced not only by the presence of tumor cells but also by the route of
inoculation. These findings are very intriguing and further questions have been formulated.
In summary, an experimental model for the study of metastatic melanoma during mice pregnancy
was developed. Surprisingly, the intravascular inoculation of melanoma cells in pregnancy seems to
favor trophoblast and embryo development. These findings may contribute to our understanding of
the mechanisms involved in trophoblast invasion and embryo implantation. Furthermore, these
findings may also be potentially useful in the development of new therapies for immunological
miscarriages, placental diseases and assisted reproduction.
Acknowledgements
This work was supported by grants from FAPESP (Fundação de Amparo à Pesquisa do Estado de
São Paulo) and CAPES. We thank Drs. Gilberto Costa Freitas and Maria Regina Torloni for reviewing
the manuscript and offering helpful comments.
Reference List

1. Borden EC (2000) Melanoma and pregnancy. Semin Oncol 27: 654-656
2. Oduncu FS, Kimmig R, Hepp H, Emmerich B (2003) Cancer in pregnancy: maternal-fetal conflict. J Cancer Res Clin Oncol 129: 133-146
3. Pavlidis NA (2002) Coexistence of pregnancy and malignancy. Oncologist 7: 279-287
4. Weisz B, Schiff E, Lishner M (2001) Cancer in pregnancy: maternal and fetal implications. Hum Reprod Update 7: 384-393
5. Cohn-Cedermark G, Mansson-Brahme E, Rutqvist LE, Larsson O, Johansson H, Ringborg U (2000) Trends in mortality from malignant melanoma in Sweden, 1970-1996. Cancer 89: 348-355
6. Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, Thun MJ (2006) Cancer statistics, 2006. CA Cancer J Clin 56: 106-130
7. Marrett LD, Nguyen HL, Armstrong BK (2001) Trends in the incidence of cutaneous malignant melanoma in New South Wales, 1983-1996. Int J Cancer 92: 457-462
8. O'Meara AT, Cress R, Xing G, Danielsen B, Smith LH (2005) Malignant melanoma in pregnancy. A population-based evaluation. Cancer 103: 1217-1226
9. Weisz B, Schiff E, Lishner M (2001) Cancer in pregnancy: maternal and fetal implications. Hum Reprod Update 7: 384-393
10. Katz VL, Farmer RM, Dotters D (2002) Focus on primary care: from nevus to neoplasm: myths of melanoma in pregnancy. Obstet Gynecol Surv 57: 112-119
11. Saenz-Badillos J, Brady MS (2000) Pregnancy-associated melanoma occurring in two generations. J Surg Oncol 73: 231-233
12. Katz VL, Farmer RM, Dotters D (2002) Focus on primary care: from nevus to neoplasm: myths of melanoma in pregnancy. Obstet Gynecol Surv 57: 112-119
13. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
14. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
15. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
16. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
17. Trumble ER, Smith RM, Pearl G, Wall J (2005) Transplacental transmission of metastatic melanoma to the posterior fossa. Case report. J Neurosurg 103: 191-193
18. Oduncu FS, Kimmig R, Hepp H, Emmerich B (2003) Cancer in pregnancy: maternal-fetal conflict. J Cancer Res Clin Oncol 129: 133-146
19. Alexander A, Harris RM, Grossman D, Bruggers CS, Leachman SA (2004) Vulvar melanoma: diffuse melanosis and metastasis to the placenta. J Am Acad Dermatol 50: 293-298
20. Oduncu FS, Kimmig R, Hepp H, Emmerich B (2003) Cancer in pregnancy: maternal-fetal conflict. J Cancer Res Clin Oncol 129: 133-146

21. MacKie RM, Bray CA (2004) Hormone replacement therapy after surgery for stage 1 or 2 cutaneous melanoma. Br J Cancer 90: 770-772
22. MacKie RM (1999) Pregnancy and exogenous hormones in patients with cutaneous malignant melanoma. Curr Opin Oncol 11: 129-131
23. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
24. O'Meara AT, Cress R, Xing G, Danielsen B, Smith LH (2005) Malignant melanoma in pregnancy. A population-based evaluation. Cancer 103: 1217-1226
25. Weisz B, Schiff E, Lishner M (2001) Cancer in pregnancy: maternal and fetal implications. Hum Reprod Update 7: 384-393
26. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
27. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
28. Trumble ER, Smith RM, Pearl G, Wall J (2005) Transplacental transmission of metastatic melanoma to the posterior fossa. Case report. J Neurosurg 103: 191-193
29. Bennett DC, Cooper PJ, Hart IR (1987) A line of non-tumorigenic mouse melanocytes, syngeneic with the B16 melanoma and requiring a tumour promoter for growth. Int J Cancer 39: 414-418
30. Oba-Shinjo SM, Correa M, Ricca TI, Molognoni F, Pinhal MA, Neves IA, Marie SK, Sampaio LO, Nader HB, Chammas R, Jasiulionis MG (2006) Melanocyte transformation associated with substrate adhesion impediment. Neoplasia 8: 231-241
31. Correa M, Machado J, Jr., Carneiro CR, Pesquero JB, Bader M, Travassos LR, Chammas R, Jasiulionis MG (2005) Transient inflammatory response induced by apoptotic cells is an important mediator of melanoma cell engraftment and growth. Int J Cancer 114: 356-363
32. Sakaki M, Shek TW, Hirokawa M, Kashima K, Daa T, Gamachi A, Sano T (2004) Melanotic oncocytic metaplasia of the nasopharynx: a report of seven cases and review of the literature. Virchows Arch 444: 345-349
33. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
34. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
35. Trumble ER, Smith RM, Pearl G, Wall J (2005) Transplacental transmission of metastatic melanoma to the posterior fossa. Case report. J Neurosurg 103: 191-193
36. Gourley C, Monaghan H, Beattie G, Court S, Love C, Gabra H (2002) Intra-uterine death resulting from placental metastases in adenocarcinoma of unknown primary. Clin Oncol (R Coll Radiol ) 14: 213-216
37. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434

38. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
39. Dildy GA, III, Moise KJ, Jr., Carpenter RJ, Jr., Klima T (1989) Maternal malignancy metastatic to the products of conception: a review. Obstet Gynecol Surv 44: 535-540
40. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
41. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
42. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
43. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
44. Altman JF, Lowe L, Redman B, Esper P, Schwartz JL, Johnson TM, Haefner HK (2003) Placental metastasis of maternal melanoma. J Am Acad Dermatol 49: 1150-1154
45. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
46. Dodge JE, Ramsahoye BH, Wo ZG, Okano M, Li E (2002) De novo methylation of MMLV provirus in embryonic stem cells: CpG versus non-CpG methylation. Gene 289: 41-48
47. Haines TR, Rodenhiser DI, Ainsworth PJ (2001) Allele-specific non-CpG methylation of the Nf1 gene during early mouse development. Dev Biol 240: 585-598
48. Jones PA, Baylin SB (2002) The fundamental role of epigenetic events in cancer. Nat Rev Genet 3: 415-428
49. Li E (2002) Chromatin modification and epigenetic reprogramming in mammalian development. Nat Rev Genet 3: 662-673
50. Srinivas S (2000) Development: nature and nurture. J Cell Sci 113 (Pt 20): 3549-3550
51. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
52. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
53. Baylin S, Bestor TH (2002) Altered methylation patterns in cancer cell genomes: cause or consequence? Cancer Cell 1: 299-305
54. Jirtle RL, Sander M, Barrett JC (2000) Genomic imprinting and environmental disease susceptibility. Environ Health Perspect 108: 271-278
55. Mintz A, Debinski W (2000) Cancer genetics/epigenetics and the X chromosome: possible new links for malignant glioma pathogenesis and immune-based therapies. Crit Rev Oncog 11: 77-95

56. Li E (2002) Chromatin modification and epigenetic reprogramming in mammalian development. Nat Rev Genet 3: 662-673
57. Tolar J, Neglia JP (2003) Transplacental and other routes of cancer transmission between individuals. J Pediatr Hematol Oncol 25: 430-434
58. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
59. Daryanani D, Plukker JT, De Hullu JA, Kuiper H, Nap RE, Hoekstra HJ (2003) Pregnancy and early-stage melanoma. Cancer 97: 2248-2253
60. Soundararajan R, Rao AJ (2004) Trophoblast 'pseudo-tumorigenesis': significance and contributory factors. Reprod Biol Endocrinol 2: 15
61. Rodriguez-Cuesta J, Vidal-Vanaclocha F, Mendoza L, Valcarcel M, Gallot N, Martinez de TG (2005) Effect of asymptomatic natural infections due to common mouse pathogens on the metastatic progression of B16 murine melanoma in C57BL/6 mice. Clin Exp Metastasis 22: 549-558
62. Chaouat G, Zourbas S, Ostojic S, Lappree-Delage G, Dubanchet S, Ledee N, Martal J (2002) A brief review of recent data on some cytokine expressions at the materno-foetal interface which might challenge the classical Th1/Th2 dichotomy. J Reprod Immunol 53: 241-256
63. Saito S (2000) Cytokine network at the feto-maternal interface. J Reprod Immunol 47: 87-103
64. Saito S (2000) Cytokine network at the feto-maternal interface. J Reprod Immunol 47: 87-103
65. Raghupathy R (1997) Th1-type immunity is incompatible with successful pregnancy. Immunol Today 18: 478-482
66. Soundararajan R, Rao AJ (2004) Trophoblast 'pseudo-tumorigenesis': significance and contributory factors. Reprod Biol Endocrinol 2: 15
67. Shih IM, Herlyn M (1993) Role of growth factors and their receptors in the development and progression of melanoma 7. J Invest Dermatol 100: 196S-203S
68. Lazar-Molnar E, Hegyesi H, Toth S, Falus A (2000) Autocrine and paracrine regulation by cytokines and growth factors in melanoma 1. Cytokine 12: 547-554
69. Lazar-Molnar E, Hegyesi H, Toth S, Falus A (2000) Autocrine and paracrine regulation by cytokines and growth factors in melanoma 1. Cytokine 12: 547-554
70. Lazar-Molnar E, Hegyesi H, Toth S, Falus A (2000) Autocrine and paracrine regulation by cytokines and growth factors in melanoma 1. Cytokine 12: 547-554
71. Hanahan D, Weinberg RA (2000) The hallmarks of cancer. Cell 100: 57-70
72. Soundararajan R, Rao AJ (2004) Trophoblast 'pseudo-tumorigenesis': significance and contributory factors. Reprod Biol Endocrinol 2: 15
73. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186

74. Lacal PM, Failla CM, Pagani E, Odorisio T, Schietroma C, Falcinelli S, Zambruno G, D'Atri S (2000) Human melanoma cells secrete and respond to placenta growth factor and vascular endothelial growth factor. J Invest Dermatol 115: 1000-1007
75. Graeven U, Rodeck U, Karpinski S, Jost M, Andre N, Schmiegel W (2000) Expression patterns of placenta growth factor in human melanocytic cell lines. J Invest Dermatol 115: 118-123
76. Slingluff CL, Jr., Reintgen DS, Vollmer RT, Seigler HF (1990) Malignant melanoma arising during pregnancy. A study of 100 patients. Ann Surg 211: 552-557
77. Schwartz JL, Wang TS, Hamilton TA, Lowe L, Sondak VK, Johnson TM (2002) Thin primary cutaneous melanomas: associated detection patterns, lesion characteristics, and patient characteristics. Cancer 95: 1562-1568
78. Pennoyer JW, Grin CM, Driscoll MS, Dry SM, Walsh SJ, Gelineau JP, Grant-Kels JM (1997) Changes in size of melanocytic nevi during pregnancy. J Am Acad Dermatol 36: 378-382
79. MacKie RM, Bufalino R, Morabito A, Sutherland C, Cascinelli N (1991) Lack of effect of pregnancy on outcome of melanoma. For The World Health Organisation Melanoma Programme. Lancet 337: 653-655
80. Alexander A, Samlowski WE, Grossman D, Bruggers CS, Harris RM, Zone JJ, Noyes RD, Bowen GM, Leachman SA (2003) Metastatic melanoma in pregnancy: risk of transplacental metastases in the infant. J Clin Oncol 21: 2179-2186
81. Baergen RN, Johnson D, Moore T, Benirschke K (1997) Maternal melanoma metastatic to the placenta: a case report and review of the literature. Arch Pathol Lab Med 121: 508-511
82. Peros-Golubicic T, Smojver-Jezek S, Gorecan M, Gredelj N, Tekavec-Trkanjec J, Alilovic M (2005) Multiple primary intrathoracic neoplasms: case report and a review of the literature. Mt Sinai J Med 72: 274-278
83. Mullen CA, Urban JL, Van WC, Rowley DA, Schreiber H (1985) Multiple cancers. Tumor burden permits the outgrowth of other cancers. J Exp Med 162: 1665-1682
84. Koutsopoulos AV, Dambaki KI, Datseris G, Giannikaki E, Froudarakis M, Stathopoulos E (2005) A novel combination of multiple primary carcinomas: urinary bladder transitional cell carcinoma, prostate adenocarcinoma and small cell lung carcinoma--report of a case and review of the literature. World J Surg Oncol 3: 51
Competing interests statement: The authors declare no competing financial interests.
Table 1.
Table 1 - Implantation and resorption rates analysis
group implantation
rate resorption
rate
control (C)
n = 10
3,9 ± 1,37 3,5
2 / 6
1,5 ± 0,71 1,5
1 / 2
stress (S)
n = 10
5,2 ± 1,48 5,5
3 / 7
2 ± 1 2
1 / 3

subcutaneous (SC)
n = 10
5,7 ± 2,91 6
0 / 10
3,5 ± 1,87 3,5
1 / 6
intraperitoneum (IP)
n = 10
4,1 ± 2,89 5
0 / 8
2,5 ± 1,29 2,5
1 / 4
intravenous (IVTm5) n = 12
7,08 ± 1,38
7*
5 / 10
0 ± 0
0*
0 / 0
intravenous (IVB16F10)
n = 8
8,6 ± 0,91
9*
7 / 10
0 ± 0
0*
0 / 0
intravenous (IVmelan-a)
n = 8
7,1 ± 1,12
7* 6 / 9
2,5 ± 1 2
1 / 4
datas are :
mean ± s.d. median
min./ max
* Kruskal–Wallis test showed significant differences among the groups p<0,001
Table 2.
Table 2 - Fetal and placental weight measurements
group placenta weight
fetus weight
control (C)
n = 10
0,12 ± 0,02 0,13
0,08 / 0,15
1,06 ± 0,04
1,08* 0,99 / 1,11
stress (S)
n = 10
0,13 ± 0,007 0,13
0,12 / 0,14
0,99 ± 0,03 0,99
0,95 / 1,03
subcutaneous (SC)
n = 10
0,13 ± 0,005 0,13
0,12 / 0,14
0,99 ± 0,02 0,99
0,96 / 1,03
intraperitoneum (IP)
n = 10
0,13 ± 0,01 0,12
0,11 / 0,16
0,99 ± 0,02 0,99
0,94 / 1,03
intravenous (IVTm5) n = 12
0,12 ± 0,01 0,12
0,11 / 0,14
0,99 ± 0,01 0,99
0,97 / 1,01
intravenous (IVB16F10)
n = 8
0,13 ± 0,01 0,13
0,12 / 0,14
0,99 ± 0,02 0,98
0,97 / 1,02
intravenous (IVmelan-a)
n = 8
0,12 ± 0,01 0,13
0,11 / 0,14
0,95 ± 0,04 0,98
0,94 / 1,01
datas are :
mean ± s.d. median
min./ max
* Kruskal–Wallis test showed significant differences among the groups, p<0,005

0 2 4 6 8 10 12 14 16 18 200
20
40
60
80
1002.105 NG
2.105 G
105 G
5.104 G
p<0,05
days after inoculation
% t
um
or-
free a
nim
als
A
0 2 4 6 8 10 12 14 16 18 20 22 240
20
40
60
80
100
2.105 NG
2.105 G
105 G
5.104 G
p<0,05
days of inoculation
% s
urv
ival
B
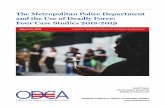
Figure 1 legend. Tumoral doses versus tumoral growth and maternal survival after tumor
implant: the figure (A) displays the time needed for tumoral growth after the inoculation of melanoma
cells. The subcutaneous route was used for inoculation in the first studies for this model. Females
were inoculated on day “0” of pregnancy (vaginal plug). The 5.104 dose produced palpable tumoral
growth (>20mm3) in all mice within 16 days and allowed maternal survival in good conditions beyond
the end of pregnancy (20th day), showing be the best dose as figure (B) depicts.

Figure 2 legend. Morphology assay: (A) skin tumor (arrow) in pregnant mouse of SC group, (D)
melanoma implants in epiploon (arrow) after IP inoculation of melanoma. (G) Resorption (black
arrow) in IP group and melanoma metastasis on the epiploon (white arrows). (J) Black dots (arrow)
represent lung metastases after IV inoculation of melanoma cells. Uterus and fetuses exposed.
Photomicrograph of histological analysis of tissue sections from the skin (B,C) in SC group; ovaries
(E,F), epiploon (H) and uterus (I) metastasis of mouse from IP group and lung metastasis (K,L,M)
and lung after IV inoculation of melanocyte cell stained by Fontana-Mason histochemistry
(E,H,I=x40);(C,K,O=x100);(F,M=x400) and Hematoxylin-Eosin (B,L,N=x100).
D A G J
K E B
H
L C F I
M
N
O

C S SC IP IVTm5 IVB16F10 IVmelan-a0
2
4
6
8
10
12increase of implantation rate in IV group
* **
*p<0,0001
nu
mb
er
of
fetu
s
A
____C S SC IP IV
Tm5IV
B16F10IV
melan-a0
1
2
3
4
5
6
7
*p<0,005
absence of reabsortion in IV melanoma groups
**
nu
mb
er
of
rea
bs
ort
ion
B
C S SC IP IVTm5 IVB16F10 IVmelan-a
0.95
0.97
1.00
1.02
1.05
1.07
1.10
1.12
*fetal under weight by melanoma and stress
*p<0,005C
we
igh
/g
C S SC IP IVTm5
IVB16F10
IVmelan-a
0.07
0.09
0.11
0.13
0.15
0.17placental weight was not change by tumor
p=ns
we
igh
t/g
D
Figure 3 legend. Boxplots of reproductive maternal performance in experimental model of
metastasis in mice pregnancy by inoculation of Tm5 melanoma cells via intraperitoneum (IP),
subcutaneous (SC) and inoculation of Tm5, B16F10 and non-tumorigenic melan-a cell intravenous
(IV) routes. Two control groups were used: stress group for puncture (S) and pregnant control (C). In
the IV groups there was an increased number of fetuses (A) and no resorptions (B) just in
melanomas groups, suggesting that intravenous injection of tumoral cells could support trophoblast
implantation and fetal development. Tumor and stress produced reduction of fetal weight (C) but did
not affect placental weight (D). * P-values were computed using the Kruskal-Wallis test.