Metamemory monitoring in mild cognitive impairment: Evidence of a less accurate episodic...
16
Neuropsychologia 45 (2007) 2811–2826 Metamemory monitoring in mild cognitive impairment: Evidence of a less accurate episodic feeling-of-knowing Audrey Perrotin a,∗ , Sylvie Belleville b , Michel Isingrini a a UMR-CNRS 6215 “Langage, M´ emoire et D´ eveloppement Cognitif ”, Universit´ e de Tours, France b Institut Universitaire de G´ eriatrie de Montr´ eal and Universit´ e de Montr´ eal, Qu´ ebec, Canada Received 9 November 2006; received in revised form 30 April 2007; accepted 3 May 2007 Available online 17 May 2007 Abstract This study aimed at exploring metamemory and specifically the accuracy of memory monitoring in mild cognitive impairment (MCI) using an episodic memory feeling-of-knowing (FOK) procedure. To this end, 20 people with MCI and 20 matched control participants were compared on the episodic FOK task. Results showed that the MCI group made less accurate FOK predictions than the control group by overestimating their memory performance on a recognition task. The MCI overestimation behavior was found to be critically related to the severity of their cognitive decline. In the light of recent neuroanatomical models showing the involvement of a temporal-frontal network underlying accurate FOK predictions, the role of memory and executive processes was evaluated. Thus, participants were also administered memory and executive neuropsychological tests. Correlation analysis revealed a between-group differential pattern indicating that FOK accuracy was primarily related to memory abilities in people with MCI, whereas it was specifically related to executive functioning in control participants. The lesser ability of people with MCI to assess their memory status accurately on an episodic FOK task is discussed in relation to both their subjective memory complaints and to their actual memory deficits which might be mediated by the brain vulnerability of their hippocampus and medial temporal system. It is suggested that their memory weakness may lead people with MCI to use other less reliable forms of memory monitoring. © 2007 Elsevier Ltd. All rights reserved. Keywords: Mild cognitive impairment (MCI); Metamemory monitoring; Feeling-of-knowing (FOK); Episodic memory; Executive functioning 1. Introduction Mild cognitive impairment (MCI; Flicker, Ferris, & Reisberg, 1991) is the term used to define a transitional zone between nor- mal aging and dementia. This intermediate stage of cognition has been characterized in many ways, but the most frequently endorsed criteria are those described by Petersen et al. (1999), involving a subjective as well as objective memory impairment, against a background of preserved general cognitive and func- tional abilities. The cognitive deficit must not be severe enough to meet dementia criteria. MCI is of considerable clinical rel- evance and is becoming a central focus of research as it helps identify people at high risk of developing dementia. Alzheimer’s Disease (AD) appears to be the most common cause of this mild ∗ Corresponding author at: D´ epartement de Psychologie, Universit´ e Franc ¸ois Rabelais, 3, rue des Tanneurs-BP 4103, 37041 Tours Cedex 1, France. Tel.: +33 6 19 18 78 01. E-mail address: [email protected] (A. Perrotin). cognitive decline, particularly in the amnestic subtype of MCI, but MCI may also be prodromal in other dementia disorders (Petersen et al., 2001). In some cases, the cognitive impair- ment may either improve or remain stable over time (Palmer, Wang, Backman, Winblad, & Fratiglioni, 2002; Ritchie, Artero, & Touchon, 2001). This inherent etiological heterogeneity and blurred boundaries of MCI as currently conceptualized has been widely criticized in the literature. To optimize its clini- cal significance, the validity of diagnosis criteria needs to be verified and the cognitive deficits better defined, notably with regard to the memory dysfunction profile. The aspect which undoubtedly raises the most controversy is the relevance of sub- jective memory complaints (SMC) in diagnosing MCI, and there has been a long-running debate about the predictive validity of memory complaints for memory impairment and dementia. Numerous cross-sectional studies relating SMC to memory per- formance have resulted in inconsistent outcomes, some authors finding an association (Bassett & Folstein, 1993; Jonker, Launer, Hooijer, & Lindeboom, 1996), others finding none (O’Connor, 0028-3932/$ – see front matter © 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.neuropsychologia.2007.05.003
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Metamemory monitoring in mild cognitive impairment: Evidence of a less accurate episodic...

A
eepIrCwmdw©
K
1
1mheiatteiD
RT
0d
Neuropsychologia 45 (2007) 2811–2826
Metamemory monitoring in mild cognitive impairment:Evidence of a less accurate episodic feeling-of-knowing
Audrey Perrotin a,∗, Sylvie Belleville b, Michel Isingrini a
a UMR-CNRS 6215 “Langage, Memoire et Developpement Cognitif”, Universite de Tours, Franceb Institut Universitaire de Geriatrie de Montreal and Universite de Montreal, Quebec, Canada
Received 9 November 2006; received in revised form 30 April 2007; accepted 3 May 2007Available online 17 May 2007
bstract
This study aimed at exploring metamemory and specifically the accuracy of memory monitoring in mild cognitive impairment (MCI) using anpisodic memory feeling-of-knowing (FOK) procedure. To this end, 20 people with MCI and 20 matched control participants were compared on thepisodic FOK task. Results showed that the MCI group made less accurate FOK predictions than the control group by overestimating their memoryerformance on a recognition task. The MCI overestimation behavior was found to be critically related to the severity of their cognitive decline.n the light of recent neuroanatomical models showing the involvement of a temporal-frontal network underlying accurate FOK predictions, theole of memory and executive processes was evaluated. Thus, participants were also administered memory and executive neuropsychological tests.orrelation analysis revealed a between-group differential pattern indicating that FOK accuracy was primarily related to memory abilities in peopleith MCI, whereas it was specifically related to executive functioning in control participants. The lesser ability of people with MCI to assess their
emory status accurately on an episodic FOK task is discussed in relation to both their subjective memory complaints and to their actual memoryeficits which might be mediated by the brain vulnerability of their hippocampus and medial temporal system. It is suggested that their memoryeakness may lead people with MCI to use other less reliable forms of memory monitoring.2007 Elsevier Ltd. All rights reserved.
g-of-
cb(mW&bbcvr
eywords: Mild cognitive impairment (MCI); Metamemory monitoring; Feelin
. Introduction
Mild cognitive impairment (MCI; Flicker, Ferris, & Reisberg,991) is the term used to define a transitional zone between nor-al aging and dementia. This intermediate stage of cognition
as been characterized in many ways, but the most frequentlyndorsed criteria are those described by Petersen et al. (1999),nvolving a subjective as well as objective memory impairment,gainst a background of preserved general cognitive and func-ional abilities. The cognitive deficit must not be severe enougho meet dementia criteria. MCI is of considerable clinical rel-
vance and is becoming a central focus of research as it helpsdentify people at high risk of developing dementia. Alzheimer’sisease (AD) appears to be the most common cause of this mild∗ Corresponding author at: Departement de Psychologie, Universite Francoisabelais, 3, rue des Tanneurs-BP 4103, 37041 Tours Cedex 1, France.el.: +33 6 19 18 78 01.
E-mail address: [email protected] (A. Perrotin).
ujhoNffiH
028-3932/$ – see front matter © 2007 Elsevier Ltd. All rights reserved.oi:10.1016/j.neuropsychologia.2007.05.003
knowing (FOK); Episodic memory; Executive functioning
ognitive decline, particularly in the amnestic subtype of MCI,ut MCI may also be prodromal in other dementia disordersPetersen et al., 2001). In some cases, the cognitive impair-ent may either improve or remain stable over time (Palmer,ang, Backman, Winblad, & Fratiglioni, 2002; Ritchie, Artero,Touchon, 2001). This inherent etiological heterogeneity and
lurred boundaries of MCI as currently conceptualized haseen widely criticized in the literature. To optimize its clini-al significance, the validity of diagnosis criteria needs to beerified and the cognitive deficits better defined, notably withegard to the memory dysfunction profile. The aspect whichndoubtedly raises the most controversy is the relevance of sub-ective memory complaints (SMC) in diagnosing MCI, and thereas been a long-running debate about the predictive validityf memory complaints for memory impairment and dementia.
umerous cross-sectional studies relating SMC to memory per-ormance have resulted in inconsistent outcomes, some authorsnding an association (Bassett & Folstein, 1993; Jonker, Launer,ooijer, & Lindeboom, 1996), others finding none (O’Connor,

2 ycholo
P2taLZmhdpGanpcfc
ijNbr1ppmihpiihrmooc2obpmpmteegiMrtiaSC
eOivatstaoutls&iMeaia
ctococtpkttcekswrtom1ttpttp
fo&
812 A. Perrotin et al. / Neurops
ollitt, Roth, Brook, & Reiss, 1990; Schmidt, Berg, & Deelman,001; Sunderland, Watts, Baddeley, & Harris, 1986). Subjec-ive complaints may be more closely associated with depressionnd anxiety disorders than actual memory impairment (Bolla,indgren, Bonaccorsy, & Bleecker, 1991; Hanninen et al., 1994;imprich, Martin, & Kliegel, 2003). On the other hand, theajority of data from community-based longitudinal studies
ave shown that subjective complaints of cognitive loss are pre-ictive of future cognitive impairment and dementia in elderlyeople with mild cognitive decline (see for a review Jonker,eerlings, & Schmand, 2000; for contradictory results, Jorm et
l., 1997), and even in older people with normal baseline cog-itive functions (Reisberg et al., 2005). These findings provideowerful legitimacy to the notion of SMC as part of the MCIoncept. However, while SMC as a criterion for MCI are theocus of much attention, the mechanisms by which such memoryomplaints are made have been under- or mis-exploited.
SMC are the product of a memory monitoring process whichs a metamemory component consisting of the individual’s sub-ective assessment of his or her own memory ability (Nelson &arens, 1990). The central role of this metamemory process isased on the idea that accurate monitoring allows optimal self-egulation of memory behavior (Koriat, 2000; Nelson & Narens,990, 1994) and should therefore lead to higher levels of memoryerformance (Metcalfe, 1993). Thus, the study of metamemoryrovides qualitative clues about the mechanisms of the humanemory system and how it changes. Examining metamemory
n people with MCI is of both clinical and theoretical interest,elping to characterize their cognitive deficits, while providingowerful knowledge about episodic memory functioning, whichs particularly vulnerable in these people. Furthermore, insightnto the possible impairment of metamemory processes couldelp draw up targeted rehabilitation programs. The few cur-ently available data likely to provide information on the memoryonitoring capacities of people with MCI come from studies
n the accuracy of the link between SMC and actual mem-ry impairment in MCI based on methodological approachesommonly used to assess deficits in cognitive awareness (Clare,004; Clare, Markova, Verhey, & Kenny, 2005). These meth-ds consist of comparing the perceived difficulties reportedy the subject with either those reported by an informant onarallel measures or the subject’s performance on objectiveemory tests. In general, it seems that people with MCI lack
recision in their own reports of cognitive impairment. Theseisjudgments mainly involve an underestimation of dysfunc-
ion (Albert et al., 1999; Collie, Maruff, & Currie, 2002; Vogelt al., 2004), but as well in the sense of an overestimation (Kalbet al., 2005). These cross-sectional studies have produced diver-ent results and are far from being in agreement about thedea of diminished self-awareness of cognitive impairment in
CI. An important factor that may account for variance in theesults concerns differences in patient sampling, particularly inerms of severity of overall cognitive impairment. Many stud-
es have documented significant relationships between impairedwareness and severity of cognitive decline in AD (Harwood,ultzer, & Wheatley, 2000; McDaniel, Edland, Heyman, & theERAD clinical investigators, 1995; Migliorelli et al., 1995; OttGpm(
gia 45 (2007) 2811–2826
t al., 1996; Sevush, 1999; Wagner, Spangenberg, Bachman, &’Connell, 1997). A similar association has also been reported
n MCI, suggesting that people with MCI may have a criticaliew of their performance in the earliest phase of impairmentnd then show a decrease of this insight with the progression ofhe disease (Kalbe et al., 2005). Results of longitudinal studiesuggest that lack of insight into their deficits in the cogni-ive area of memory (Tierney, Szalai, Snow, & Fisher, 1996)nd functional abilities (Tabert et al., 2002) can be predictivef dementia in people with MCI. However, both these studiesse questionnaires or self-report measures for operationaliza-ion of memory self-awareness or metamemory and contain aarge number of methodological limitations (for more detailsee Hertzog, Hultsch, & Dixon, 1989; Hertzog, Park, Morrell,
Martin, 2000; Trosset & Kaszniak, 1996). Despite their lim-tations, these earlier studies indicate that when people with
CI have to make global judgments of memory, they experi-nce certain difficulties in monitoring their memory functioningccurately. Moreover, they highlight the importance of look-ng at the severity of cognitive impairment when investigatingwareness-related processes.
A more reliable way of examining memory monitoring pro-esses is to use specific experimental metamemory paradigms. Inhe experimental literature on memory monitoring, a great dealf attention has been paid to ‘metamemory judgments’, whichonsist of evaluating the current state of one’s memory during anngoing memory task. This online monitoring of memory is typi-ally assessed by having people to predict item-by-item how wellhey will remember items during an upcoming memory test (i.e.,rospective monitoring judgments). In particular, the feeling-of-nowing (FOK) judgments consist in asking subjects to estimatehe likelihood that they will later recognize a piece of informa-ion they had just failed to recall with a cue. These predictionsoncern either semantic memory (Hart, 1965) or recently learnedpisodic memory information (Schacter, 1983). The feeling-of-nowing experience commonly occurs when one fails to retrievepecific information, and this feeling indicates the extent tohich the information seems available in memory for future
etrieval. In situations such as recall failure, the monitoring func-ion is therefore implemented to assess and infer from a varietyf clues (data or processes) the likelihood that the solicited infor-ation is retained in memory (Koriat, 1993; Nelson & Narens,
990). Accuracy of monitoring is thus deduced from the degreeo which a person’s judgment predicts memory performance. Athe present time and to our knowledge, the metamemory of peo-le with MCI has never been investigated experimentally withhese empirical monitoring measures. The aim of this paper iso undertake this type of investigation using an episodic FOKrocedure.
There is now a broad base of empirical observations using dif-erent versions of the FOK procedure confirming the accuracyf judgments which reliably predict performance (Gruneberg
Monks, 1974; see Metcalfe & Shimamura, 1994; Nelson,
erler, & Narens, 1984). Two theoretical views have been pro-osed to explain how FOK judgments are made to predict futureemory performance. One concerns the cue-familiarity accountMetcalfe, Schwartz, & Joaquim, 1993; Reder, 1987) suggesting

ycholo
tpFotoeiArfitbiuf(eatTd(1artTsdtatg&t(
tladmtaaielamtSsi(t
o(maiiBr1bcBScpf&2nlaia&cfiT
ophcAaa&dItitnmMafoMOot
A. Perrotin et al. / Neurops
hat the FOK is based on the overall familiarity or novelty of theresented cue. The other concerns the accessibility account ofOK (Koriat, 1993), proposing that FOK judgments are basedn the assessment of the overall accessibility of partial informa-ion retrieved about the solicited target item. Empirical studiesf FOK support both these views. The two views are not how-ver incompatible, and Koriat and Levy-Sadot (2001) suggestedntegrating the two within a two-step cascaded model of FOK.ccording to this model, a preliminary FOK is made on a
apid cue familiarity assessment, and if the cue evokes a suf-cient degree of familiarity, the search-and-retrieval process of
he solicited target is engaged and the accessibility of memoryy-products is assessed. The cognitive view of the accessibil-ty account of FOK has recently found support from a studysing functional neuroimaging in which a network of temporal-rontal activation was observed during accurate FOK predictionsSchnyer, Nicholls, & Verfaellie, 2005). This ‘accuracy system’ngages primarily the ventral medial part of the prefrontal cortexssumed to be critically involved in assessing partial informa-ion retrieved from the hippocampus and medial temporal lobe.his prefrontal region may thus serve a monitoring functionuring retrieval. The two distinctive processes—cue-familiarityMetcalfe et al., 1993; Reder, 1987) and accessibility (Koriat,993) both assumed to contribute to FOK, mirror the two dissoci-te systems of familiarity and recollection proposed in models ofetrieval memory and especially well theorized in the context ofhe recognition of past experience (Jacoby, 1996; Mandler, 1980;ulving, 1985). Familiarity is based on assessment of the globaltrength of the memory trace and pertains to a form of retrievalevoid of any recall of contextual information, whereas recollec-ion refers to a retrieval of qualitative and contextual informationbout the study event. Neuroanatomical studies have indicatedhat these two types of retrieval process rely on separate subre-ions of the prefrontal cortex (Henson, Rugg, Shallice, Josephs,
Dolan, 1999; Yonelinas, Otten, Shaw, & Rugg, 2005), andhat recollection requires additional hippocampus involvementAggleton & Brown, 1999).
In line with the above-mentioned FOK models, the cogni-ive processes that have been most analyzed in the metamemoryiterature for their potential contribution to FOK are memorynd executive functioning. Memory and metamemory are byefinition two intimately related processes. With regard to theonitoring process, Koriat’s accessibility model (1993) assumes
hat FOK judgments are based on the output of the search-nd-retrieval attempt for the target, and more precisely on themount of information retrieved surrounding the target. Accord-ng to this view, the accuracy of FOK judgments stems from theffectiveness of the memory processes themselves. This postu-ated link between memory and metamemory implies that FOKccuracy varies greatly with the many factors that affect theemory trace. Some findings have experimentally confirmed
his relationship (Carroll & Nelson, 1993; Nelson, Leonesio,himamura, Landwehr, & Narens, 1982). However, other results
uggest that memory loss is not consistently associated withmpaired FOK accuracy. For instance, Shimamura and Squire1986) found that people with anterograde amnesia predictedheir episodic memory performance as accurately as controls.ccfp
gia 45 (2007) 2811–2826 2813
Furthermore, several studies have emphasized the rolef executive functioning in memory monitoring in generalShallice, 2001) and in the production of accurate FOK judg-ents in particular (Shimamura, 1995). Executive functions areset of higher order cognitive processes including the monitor-
ng and control of behavior, planning, inhibition of irrelevantnformation, shifting, etc. (Lezak, 1995; Rabbitt, 1997; Stuss &enson, 1986). Executive processes are presumed to be closely
elated to the functioning of the prefrontal cortex (Duncan,995; Fuster, 1989; Shallice & Burgess, 1991). As proposedy some authors, executive functioning and metamemory pro-esses share many conceptual similarities (Fernandez-Duque,aird, & Posner, 2000; Shimamura, Janowsky, & Squire, 1991;tuss & Benson, 1986). This link is strongly supported by con-ordant results of studies using different methods. Studies ofatients with frontal lobe lesions have shown impaired per-ormance on an episodic FOK task (Janowsky, Shimamura,
Squire, 1989; Pinon, Allain, Zied Kefi, Dubas, & Le Gall,005; Schnyer et al., 2004). More generally, it appears thateurological patient groups characterized by signs of frontalobe pathology usually exhibit a decline in FOK accuracy (for
review see Pannu & Kaszniak, 2005). Recent fMRI stud-es have indicated that the prefrontal cortex is engaged duringccurate FOK judgments (Maril, Simons, Mitchell, Schwartz,
Schacter, 2003; Schnyer et al., 2005). Moreover, taking aorrelation approach, a specific association between executiveunctioning and episodic FOK accuracy has been demonstratedn healthy older adults (Perrotin, Isingrini, Souchay, Clarys, &aconnat, 2006; Souchay, Isingrini, & Espagnet, 2000).
Overall, previous work suggests that the accuracy of mem-ry monitoring on an episodic FOK task depends on memoryrocesses and/or executive functioning. According to thisypothesis, a disruption of either memory or executive abilitiesould produce episodic metamemory monitoring impairment. InD, patients who display substantial memory impairment and
lso some degree of executive deficit exhibit a clear decline in theccuracy of their episodic FOK judgments (Souchay, Isingrini,
Gil, 2002). Moreover, it has been observed that this FOKeficit is mediated by the poor memory performance of patients.n people with MCI, the episodic memory deficit is the main fea-ure of their clinical picture (Petersen et al., 1999). The memorympairment is shown at a neuroanatomical level by dysfunc-ions of the hippocampus and medial temporal regions. Theeuropathological phenotype of MCI has also been shown toatch that of AD (Jack et al., 2000; Markesbery et al., 2006;orris et al., 2001). Mild deficits in executive functions have
lso been reported in people with MCI whose executive per-ormance is lower than that of controls and greater than thatf people with AD (Crowell, Luis, Vanderploeg, Schinka, &ullan, 2002; Davie et al., 2004; Hanninen et al., 1997; Ready,tt, Grace, & Cahn-Weiner, 2003). Some neuroimaging studiesf people with MCI have indicated that alterations beginning inhe medial temporal regions subsequently spread to the frontal
ortical areas, with a greater metabolic decrease in the prefrontalortex of people developing AD (Drzezga et al., 2003). There-ore, it could be hypothesized that people with MCI exhibiting aattern of decline in episodic memory, and to a lesser extent
2 ychologia 45 (2007) 2811–2826
ia
omwgwtitsa
2
2
2Mvcatetawoppbtda(oiaofp
rr(vei
p1C
Ma(rtwwcsC
Table 1Characteristics of participants in the two study groups (means and standarddeviations)
MCI (n = 20) Controls (n = 20) p level
Mean S.D. Mean S.D.
Age 67.45 8.42 68.55 7.84 NSGender (M/F) 10/10 5/15 NSYears of education 14.65 3.70 14.40 3.28 NSMDRS (/144) 137.20 4.37 141.30 2.66 ***
MMSE (/30) 28.25 1.07 28.85 1.04 NSGDS (/5) 0.75 1.07 0.87 1.14 NS
Ni*
odBt1mCNS
2
2
d(sS(bwtwfsc
2
iTmc(pOs
sciF
cm
814 A. Perrotin et al. / Neurops
n executive functioning, are also impaired in episodic FOKccuracy.
The main goal of the present study was to explore mem-ry monitoring ability in MCI with a specific experimentaletamemory paradigm. The episodic memory FOK procedureas used to compare the accuracy of FOK judgments in an MCIroup with that of a healthy control group. Our second aimas to examine the relationship between FOK accuracy and
wo cognitive factors, episodic memory and executive function-ng, to determine which was associated most with FOK in thewo groups. For this purpose, all participants were administeredtandard neuropsychological tests measuring episodic memorynd executive functions.
. Method
.1. Participants
Two groups consisting of a total of 40 participants took part in the study:0 people with MCI and 20 control participants. People suspected of havingCI were referred by neurologists at the Research Center of the Institut Uni-
ersitaire de Geriatrie de Montreal. Control participants were recruited from theommunity through advertising or by word of mouth. All participants underwentcomplete clinical and neuropsychological battery of tests. On the basis of all
he information collected during testing, the diagnoses for research purposes ofither normal or MCI were made by clinicians. All MCI participants met the cri-eria for amnestic single- or multiple-domain form of MCI defined by Petersen etl. (2001), namely (1) complaint of memory loss, corroborated by an informanthen possible, (2) abnormal memory function, indicated by recall performancen standardized verbal memory tests at least 1.5 S.D. below the average level ofeople with similar age and education (for amnestic single domain MCI form),lus performance on a standardized neuropsychological test at least 1.5 S.D.elow the average level of people of a similar age and education (for amnes-ic multiple-domain MCI form), (3) normal general cognitive functioning, asetermined by the Mattis Dementia Rating Scale (MDRS; Mattis, 1976) (overdjusted age/education cut-off score), and the Mini-Mental State ExaminationMMSE; Folstein, Folstein, & McHugh, 1975) (over adjusted age/education cut-ff score), (4) minimal impairment in daily activities, as determined by clinicalnterview with the patient and an informant, and (5) not sufficiently cognitivelynd functionally impaired to meet the criteria for AD (McKhann et al., 1984)r other forms of dementia. Participants assigned to the control group did notulfill MCI or dementia criteria. These control participants were matched to theeople with MCI for sex, age and years of education.
For both groups, the following exclusion criteria were adopted: past or cur-ent major psychiatric illness, neurological disease, drug or alcohol abuse, mentaletardation, traumatic brain injury, cerebrovascular disorders, Hachinski scoreHachinski et al., 1975) over the cut-off point of 4 (indicating that there may be aascular component to the cognition deficit), significant medical problems, gen-ral anesthesia within the previous 6 months, and significant manual mobilitympairment.
All participants were native French speakers. All gave their informed consentrior to inclusion in the study according to the ethical standards laid down in the964 Declaration of Helsinki. The study was approved by the Ethical Researchommittee of the Institut Universitaire de Geriatrie de Montreal.
Table 1 presents the participants’ characteristics and scores on the MDRS,MSE, and depression scale (Geriatric Depression Scale, GDS; Yesavage et
l., 1983). The two groups were comparable for sex, age and education (χ2 testχ2(1) = 2.67, p > .05); t-test (t(38) = −0.43, p > .05) and (t(38) = 0.23, p > .05),espectively). People with MCI did not differ from the control group with regardo the MMSE score (t(38) = −1.80, p = .080), but their performance on the MDRS
as significantly poorer (t(38) = −3.58, p < .001). No between-group differenceas noted on the GDS (t(38) = −0.33, p > .05). The two groups completed clini-al and neuropsychological tests, including standard tests such as the Hachinskicale, the Systeme de Mesure de l’Autonomie Fonctionnelle (SMAF; Hebert,arrier, & Bilodeau, 1988) measuring functional autonomy, a subjective mem-
sc(
p
ote. MDRS: Mattis Dementia Rating Scale, MMSE: Mini-Mental State Exam-nation, GDS: Geriatric Depression Scale. NS: non-significant.** p < .001.
ry questionnaire (Questionnaire d’Auto-evaluation de la Memoire, QAM; Vaner Linden, Wyns, Coyette, von Frenckell, & Seron, 1989) assessing SMC, theoston Naming Test (BNT; Kaplan, Goodglass, & Weintrub, 1983), the Ben-
on Judgment of Line Orientation (BJLO; Benton, Hamsher, Varney, & Spreen,983), the RL/RI-16 free and cued recall test (Van der Linden & the GREMEMembers, 2004), the Story Recall of the BEM-144 (Signoret, 1991), the Reyomplex Figure Test (Rey, 1960), the Victoria Stroop test (Regard, 1981), the-back test, and the Code subtest of the Revised Wechsler Adult Intelligencecale (WAIS-R; Wechsler, 1981).
.2. Material and procedure
.2.1. Subjective memory questionnaireMemory complaints in everyday life were assessed using the Questionnaire
’Auto-evaluation de la Memoire (QAM) developed by Van der Linden et al.1989). The questionnaire consists of 64 items grouped in 10 sections. The 10ections contain items relative to (1) Conversation, (2) Movies and Books, (3)lips of attention, (4) People, (5) Use of objects, (6) Political and social events,7) Places, (8) Actions to perform, (9) Personal events, (10) General. It shoulde noted that the inventory does not include items which could be associatedith a depressed mood (i.e., indecisiveness, slowed-down thinking, confusion of
houghts, etc.). Participants were asked to rate on a 6-point scale the frequencyith which they encountered difficulties in a particular situation. Rating ranged
rom ‘Never’ (0) to ‘Always’ (6). A mean score by subscale and a total meancore were calculated for each section. Higher test scores reflect greater memoryomplaints.
.2.2. Episodic feeling-of-knowing paradigmThe FOK procedure used here was similar to those conventionally used
n previous metamemory research (Schacter, 1983; Souchay et al., 2000).he stimulus list consisted of 40 critical cue-target pairs. These were low- tooderately-associated pairs of common French words. To determine the asso-
iation level between the cue and target words, we asked 76 adult participantsage range 18–89 years) (who did not take part in the critical experiment) toroduce the first word that came to mind when each target word was presented.nly low- to moderately-associated words (1 to 3 occurrences out of 76) were
elected to compose the 40 critical word pairs used in the FOK task.All participants were tested individually. Instructions and stimuli were pre-
ented on a computer screen. The procedure consisted of three phases: study,ued-recall and FOK judgment, and recognition. A training phase with threetems was carried out to familiarize participants with the different stages of theOK procedure.
Study. In the study phase, all participants were presented with the 40 criticalue-target word pairs (e.g., customs–CONTRABAND) and were told that theiremory of the target word would be tested later by presentation of the corre-
ponding cue from the list. The pairs were presented at a rate of 5 s per item. Theue word (e.g., customs) was written in lowercase letters with the target worde.g., CONTRABAND) in capital letters directly beside it.
Recall and feeling-of-knowing. Five minutes after the study phase, partici-ants were instructed to recall the target word that had been shown with a given

ycholo
cPmwttFdw
iwgEtla
2mss
2Nmgcrrttzr
22ttRT
daecstncwacitwr
Mlaao
fi3t
2bb&
SfltcuwgtIcp
mo1own
2
Ttm(Fol
3
3
mdhttrs(ppp
3
t
A. Perrotin et al. / Neurops
ue on the list (e.g., customs-. . .). Each cue was written in lowercase letters.articipants were given 15 s to recall each target, after which they were asked toake their feeling-of-knowing predictions. They indicated their FOK judgmentith a yes/no response: ‘yes’ if they thought they would be able to recognize a
arget among five alternatives in a subsequent recognition test, and ‘no’ if theyhought they would not be able to recognize it. They were given 5 s to respond.OK predictions were made on all items, both recalled and non-recalled. Imme-iately after completion of the 40 items for cued recall and FOK, the participantsere given the recognition test.
Recognition. A five-alternative, forced-choice recognition task was admin-stered for each of the 40 word pairs (recalled and non-recalled). Participantsere shown five alternative response words written in capital letters, the tar-et item plus four semantically similar distractors (e.g., FRAUD, TRAFFIC,XCHANGE, CONTRABAND, COUNTERFEITING), and were asked to say
he previously presented word. They performed this task at their own pace. Theist of alternative response-words was taken from Izaute, Larochelle, Morency,nd Tiberghien (1996).
.2.2.1. Episodic memory measures. The FOK task provided two episodicemory scores: one for cued recall and one for recognition. The cued recall
core was the number of correctly recalled target words, and the recognitioncore was the number of correctly recognized targets.
.2.2.2. Episodic metamemory measure. In the FOK paradigm (Hart, 1965;elson, 1984), FOK accuracy is generally assessed by comparing FOK judg-ents with recognition performance by calculating the Goodman-Kruskal
amma correlation (Nelson, 1984). The gamma index calculated represents theorrelation between the FOK judgment and recognition performance for non-ecalled items on cued recall. The gamma score is a continuous variable thatanges from −1 to +1. Gamma provides a measure of the association betweenwo ordered variables: large positive values correspond to a strong associa-ion between recognition performance and FOK judgments, values close toero correspond to no association, and negative values correspond to an inverseelationship.
.2.3. Neuropsychological tests
.2.3.1. Episodic memory measures. Three standardized neuropsychologicalests commonly used to measure episodic memory were selected. The memoryests assessed immediate and delayed recall, in the verbal modality (for theL/RI-16 and BEM-144 tests) and visual modality (for the Rey complex figure).hese tasks are known to be related to medial temporal functioning.
RL/RI-16 test. This task was an adaptation of Grober and Buschke’s proce-ure (Grober & Buschke, 1987) constructed and validated by Van der Lindennd the GREMEM members (2004). It consists of 16 words belonging to differ-nt semantic categories on four cards with four items per card. One four-itemard was presented at a time. First, the participant was asked to point to anday the relevant word (e.g., celery) when its semantic category was read byhe experimenter (e.g., vegetable). Once all four words had been correctlyamed, an immediate cued-recall task was given by providing each categoryue. Once all four words on the card had been recalled, the next set of itemsas presented. This 16-item learning phase was followed by three recall tri-
ls each consisting of: 20 s counting backwards, 2 min of free recall, andued recall of items not retrieved on free recall. The experimenter said thetems which had been missed on cued recall. After 20 min, a final retrievalrial was carried out with free recall, cued recall, and recognition. Scoresere the mean of the three immediate free-recall trials and the delayed free
ecall.Story recall task. This task was taken from the BEM (Batterie d’Efficience
nesique) 144 memory battery (Signoret, 1991). Participants were asked toisten to a story about a man whose car has broken down and who wants to buynother. The story is divided into 12 sections. Recall was tested immediately and
gain 20 min after presentation. Scores were the number of sections retrievedn immediate and delayed recall.Rey complex figure recall. Participants were asked to copy the Rey–Osterriethgure (Osterrieth, 1944; Rey, 1960) and then to reproduce it from memory afterand 20 min. The score was the number of accurately reproduced segments of
he diagram on immediate and delayed recall.
3
rmp
gia 45 (2007) 2811–2826 2815
.2.3.2. Executive functions measures. The following two tasks were chosenecause they are specifically designed to assess executive functioning and haveeen shown to be sensitive to prefrontal cortex dysfunction (Andres, 2003; Smith
Jonides, 1999).Victoria Stroop test. Based on the original Stroop Color-Word Test (SCWT;
troop, 1935), the Victoria version (Regard, 1981) is used to measure cognitiveexibility and mental set shifting to adapt to changing demands, and the ability
o inhibit an automatic response in favour of an unlikely one. It consists of threeolor-printed cards. Card 1 consists of colored dots. Card 2 is common wordsnrelated to the concept of color, and Card 3 (interference condition) is colorords. Each card contains six rows of four items. The colors used are blue,reen, red, and yellow. Participants are required to name the colors in whichhe stimuli are printed as quickly as possible, disregarding their verbal content.n our study, analysis was based on the number of errors in the interferenceondition (Card 3). These errors can be interpreted as inhibition errors or asroblems with conflict resolution.
N-back test. The n-back test assesses the executive component of workingemory and requires constant online monitoring, updating, and manipulation
f working memory representations (Jonides & Smith, 1997; Morris & Jones,990). The 2-back version of the n-back was used. The task consists of a stringf orally presented 30 letters. Participants had to identify whether the last letteras identical to the antepenultimate one, giving a ‘yes’/‘no’ response for eachew letter. The score was the number of correctly recognized letters.
.3. Data analysis
The STATISTICA 7.0 package (StatSoft, Inc.) was used for data analysis.he data were analyzed in two ways. First, analyses of variance (ANOVA) and t-
ests were used to compare performance across groups on the SMC, metamemoryonitoring FOK, memory and executive measures. Second, correlation analyses
Pearson correlations) were carried out to investigate the relationship betweenOK accuracy, SMC and GDS variables, and the contribution of episodic mem-ry and executive functioning to metamemory monitoring of FOK accuracy. Theevel of significance was set at alpha < .05.
. Results
.1. Subjective memory questionnaire
Data from QAM revealed whether people with MCI reportedore memory difficulties than control participants in every-
ay functioning. A t-test analysis showed that the MCI groupad a significantly higher overall SMC score than the con-rol group (M = 2.82, S.D. = 0.70 versus M = 2.33, S.D. = 0.53;(38) = 2.48, p < .05). For the QAM subscales, the MCI groupeported significantly more complaints on the Conversationection (t(38) = 2.07, p < .05), the Movies and Books sectiont(38) = 2.34, p < .05), the Slips of attention section (t(38) = 2.43,< .05), and on the General section (t(38) = 2.33, p < .05). Thus,eople with MCI expressed greater SMC than control partici-ants.
.2. Episodic feeling-of-knowing paradigm
The memory and metamemory data recorded on the FOKask are summarized in Table 2.
.2.1. Episodic memory measures
To investigate a possible group effect on cued recall andecognition performance, a t-test was carried out on the episodicemory measures. People with MCI had a significantly lower
erformance than control participants on cued recall and recog-

2816 A. Perrotin et al. / Neuropsychologia 45 (2007) 2811–2826
Table 2Means and standard deviations in percentage of scores for the feeling-of-knowing task for the two study groups
MCI (n = 20) Controls (n = 20) p level
Mean S.D. Mean S.D.
Episodic memory measuresCued recall
Correct 20.63 15.68 38.75 22.22 **
IncorrectOmission errors 70.25 19.68 54.88 20.56 *
Commission errors 9.13 8.00 6.38 6.56 NSRecognition 72.13 14.38 88.62 7.54 ***
Metamemory measuresFOK ratings
‘Yes’ judgment 88.11 18.64 92.21 18.01 NS‘No’ judgment 11.89 18.64 7.79 18.01 NS
FOK accuracyGamma index 29.42 25.98 53.03 31.07 *
‘Yes’ judgment and correct recognition 67.50 12.55 82.31 8.76 ***
‘Yes’ judgment and incorrect recognition 32.50 12.55 17.69 8.76 ***
‘No’ judgment and correct recognition 52.86 9.35 56.44 11.78 NS‘No’ judgment and incorrect recognition 47.14 9.35 43.56 11.78 NS
Note. FOK: feeling-of-knowing. NS: non-significant.* p < .05.
*
nrgtoRm
33fpnp(iMHncs
3FFrTfsaw
dptpFteeptatpmgoyptg3pgh
st
** p < .01.** p < .001.
ition tasks (t(38) = −3.01, p < .01; t(38) = −4.54, p < .001,espectively). Details of incorrect recall showed that the MCIroup made more omission responses on cued recall than con-rols (t(38) = 2.42, p < .05). However, the groups did not differn the number of commission responses (t(38) = 1.19, p > .05).esults on the FOK task confirm the existence of an episodicemory deficit in MCI.
.2.2. Episodic metamemory measures
.2.2.1. FOK ratings. To evaluate potential differences in therequency of FOK ratings made by the two groups, the pro-ortion of ‘yes’ and ‘no’ judgments as a function of the totalumber of items for which FOK judgments were made was com-ared using a 2 group (MCI versus controls) × 2 FOK ratings‘yes’ versus ‘no’ judgment) repeated measures ANOVA. Find-ngs showed a significant FOK ratings effect (F(1, 38) = 192.08,
SE = 0.07, p < .001), with more ‘yes’ than ‘no’ judgments.owever, the interaction between group and FOK ratings wasot significant (F(1, 38) = 0.50, MSE = 0.07, p > .05). MCI andontrol groups predicted their recognition performance with aimilar proportion of ‘yes’ and ‘no’ judgments.
.2.2.2. FOK accuracy. Memory monitoring accuracy in theOK procedure was determined by the relationship betweenOK judgment and recognition performance. The gamma cor-elation was computed to represent the FOK accuracy score.he FOK accuracy measure was reliably above the chance level
or both groups. Mean FOK values were analyzed with a one-ample t-test, and the FOK index was reliably non-zero withthreshold probability of p < .001. MCI and control groupsere compared on the gamma index with a t-test. A significant
tpgc
ifference was found between the two groups (t(38) = −2.61,< .05), indicating that people with MCI evaluated their ability
o recognize newly learned items less accurately than controlarticipants. To analyze the source of this lower accuracy onOK predictions and to determine whether MCI participants
ended to under- or over-estimate their recognition ability, wexamined the proportion of correct and incorrect predictions forach ‘yes’/‘no’ judgment. On the basis of incorrect metamemoryredictions, ‘yes’ judgments associated with incorrect recogni-ion represent an overestimation indicator, and ‘no’ judgmentsssociated with correct recognition represent an underestima-ion indicator. A 2 group (MCI versus controls) × 2 incorrectredictions (overestimation versus underestimation) repeatedeasures ANOVA was conducted to examine the effect of the
roup and its interaction with the sense of incorrect predictionsn the proportion of incorrect FOK predictions. The analysisielded a significant group effect (F(1, 38) = 6.11, MSE = 0.01,< .05) indicating that people with MCI made more predic-
ion errors than control subjects. The interaction between theroup and the sense of incorrect predictions was significant (F(1,8) = 13.31, MSE = 0.01, p < .001), revealing that although theroportion of underestimation responses did not differ betweenroups, the proportion of overestimation responses was reliablyigher in the MCI group than in the control group.
This overestimation appeared to be highly associated with theeverity of global cognitive impairment. Correlation analyses inhe MCI group showed a significant negative correlation between
he MDRS score and the overestimation indicator (r = −.61,< .01). No such significant correlation was found in the controlroup (r = −.33, p > .05). However, it should be noted that thisorrelation was not significantly lower than that of the MCI
ycholo
gdnTaarfcp
assoaspSg
retFs(rctpTcrc
3
sm
3
fOe(irsf1Mip
3
wcttpr
3
TM
E
N
*
A. Perrotin et al. / Neurops
roup (p > .05). The relationship between the severity of theisorder and the overestimation index is specific because no sig-ificant association was noted with the underestimation index.hus, people with MCI with more pronounced cognitive declinere more likely to overestimate their memory performance onrecognition task. Looking at the general gamma FOK accu-
acy index, the correlation with the MDRS score was significantor both groups (r = .48, p < .001) and tended towards signifi-ance within each group (r = .38, p = .096 for MCI group; r = .38,= .092 for control group).
The relationship between the SMC measure (QAM score)nd episodic metamemory measures were also assessed. Noignificant correlations were noted between the SMC overallcore and the various FOK indices: ratings, accuracy, and typesf prediction. As regards the QAM subscales, pooling MCInd control subjects, the FOK accuracy index was found to beignificantly related to the Slip of attention section (r = −.33,< .05) and to the Use of objects section (r = −.44, p < .01).ignificant correlations were not retrieved within each distinctroup.
As a growing body of research reports that SMC are robustlyelated to depressive symptoms (Bolla et al., 1991; Hanninent al., 1994; Zimprich et al., 2003), we looked at the rela-ion between the GDS score, performance on the QAM andOK. Pearson’s correlations showed that the overall QAMcore was not significantly associated with the GDS scorer = .10, p > .05 for both groups; r = .11, p > .05 for MCI group;= .16, p > .05 for control group). Similarly, no significantorrelation was found between the FOK accuracy index andhe GDS score (r = −.16, p > .05 for both groups; r = −.23,> .05 for MCI group; r = −.17, p > .05 for control group).
his lack of correlation enabled us to infer that subjectiveomplaints expressed by our participants and the lower accu-acy of their FOK judgments did not reflect a depressiveomponent.e
b
able 3eans and standard deviations of scores for memory and executive neuropsychologic
MCI (n = 20)
Mean S.D.
pisodic memory measuresRL/RI-16 recall test (/16)
Immediate free recall 9.07 2.90Delayed free recall 10.95 3.39
BEM-144 story recall test (/12)Immediate recall 6.89 2.20Delayed recall 6.39 1.82
Rey complex figure recall test (/36)3-minute recall 14.47 7.5220-minute recall 14.92 7.88
Executive functions measuresVictoria Stroop test (errors; /24) 1.70 1.84N-back test (correct responses; /28) 23.50 2.76
ote. RL/RI-16: Rappel Libre/Rappel Indice-16 items, BEM-144: Batterie d’Efficien* p < .05.
** p < .01.** p < .001.
gia 45 (2007) 2811–2826 2817
.3. Neuropsychological tests
Table 3 lists the results for each neuropsychological mea-ure for MCI and control groups. A t-test was applied on eacheasure to evaluate potential group differences.
.3.1. Episodic memory measuresAs a whole, we observed that people with MCI did not per-
orm as well as control participants on verbal memory tests.n immediate free-recall measures, the between-group differ-
nce tended towards significance for the RL/RI-16 recall testt(38) = −1.88, p = .068), and patients’ performance was signif-cantly worse than that of the controls on the BEM-144 storyecall test (t(38) = −3.78, p < .001). On delayed free-recall mea-ures, participants with MCI recalled fewer items than controlsor both the RL/RI-16 test (t(38) = −2.16, p < .05) and the BEM-44 test (t(38) = −3.17, p < .01). For the visual memory task,CI and control participants did not differ significantly on
mmediate (t(38) = −1.05, p > .05) and delayed (t(38) = −0.85,> .05) recall of the Rey complex figure.
.3.2. Executive functions measuresThe results for the Victoria Stroop test showed that people
ith MCI made more errors in the interference condition thanontrol participants (t(38) = 2.12, p < .05). For the N-back test,he MCI group made fewer correct responses than controls buthe between-group difference was not significant (t(38) = −1.08,> .05). Our findings suggest that people with MCI may expe-
ience a subtle decline in their executive functioning.
.4. Episodic feeling-of-knowing accuracy, memory and
xecutive functionsOur goal here was to explore the possible relationshipsetween FOK accuracy and memory and executive function-
al tests for the two study groups
Controls (n = 20) p level
Mean S.D.
10.48 1.73 NS12.90 2.17 *
9.20 1.58 ***
8.33 1.97 **
16.82 6.42 NS16.83 5.99 NS
0.70 1.03 *
24.32 1.83 NS
ce Mnesique-144. NS: non-significant.

2818 A. Perrotin et al. / Neuropsycholo
Table 4Pearson’s correlations between the feeling-of-knowing gamma index and thescores for memory and executive neuropsychological tests, for the two studygroups; and p level of the between-group correlation differences
FOK gamma index
MCI(n = 20)
Controls(n = 20)
p level
Episodic memory measuresRL/RI-16 recall test
Immediate free recall .46* .24 NSDelayed free recall .65** .27 NS
BEM-144 story recall testImmediate recall .23 .42† NSDelayed recall .26 .35 NS
Rey complex figure recall test3-minute recall .52* −.04 †20-minute recall .44† −.06 NS
Executive functions measuresVictoria Stroop test (errors) .17 −.49* *
N-back test (correct responses) .01 .53* †
Composite indicesImmediate memory index .49* .27 NSDelayed memory index .54* .27 NSExecutive functioning index −.13 .63** *
Note. FOK: feeling-of-knowing, RL/RI-16: Rappel Libre/Rappel Indice-16items, BEM-144: Batterie d’Efficience Mnesique-144. NS: non-significant.
*
imtbwipt
3n
efwmFatdFabicg
3n
tabmaatfpttcsccaufrsni(pp
rdaoagwioli
mcccmrgaFigi
p < .05.** p < .01.† p < .1.
ng. First, the FOK accuracy index was put in relation with eachemory and executive measure. Second, in order to summarize
he observed tendencies on the individual correlations, the linketween FOK accuracy and memory and executive functioningas evaluated after calculating memory and executive compos-
te indices. The results of these two correlation approaches areresented in Table 4. The table also indicates the reliability ofhe between-group correlation differences.
.4.1. Correlations between FOK accuracy and individualeuropsychological measures
Pearson’s correlations between the FOK accuracy index andach memory and executive measure were computed separatelyor the two groups. For the MCI group, significant correlationsere observed between the FOK accuracy index and episodicemory measures on the RL/RI-16 test and Rey complex figure.or the control group, the FOK index was significantly associ-ted with the memory functioning only at the immediate recall ofhe BEM-144 story. As a whole, there was no significant groupifference for the degree of relationship between memory andOK scores. However, concerning the link between the FOKccuracy index and the executive function measures, reliable
etween-group differences were observed. The FOK accuracyndex was highly correlated with the two executive scores in theontrol group while no correlations were observed in the MCIroup.aobr
gia 45 (2007) 2811–2826
.4.2. Correlations between FOK accuracy andeuropsychological composite indices
To obtain indices summarizing memory and executive func-ioning, composite z-scores were computed. Given that FOKccuracy may change as information decays (Koriat, 1993), andecause the memory deficit of people with MCI is typicallyore pronounced on delayed memory measures (Petersen et
l., 1999), we decided to differentiate performance on immedi-te memory and delayed recall tests to examine whether thesewo measures had a differential relationship with FOK per-ormance. Three composite indices were calculated for eacharticipant in the following way: first, performance on eachest was converted into standard units, and these z-scores werehen averaged. The composite immediate memory index wasalculated on the basis of the three immediate free-recall mea-ures acquired on the RL/RI-16 test, BEM-144 story and Reyomplex figure. The composite delayed memory index was cal-ulated on the basis of the three delayed free-recall measurescquired on the same three previous tests. The composite exec-tive functions index was calculated on the basis of the twoollowing measures: errors on the Victoria Stoop test and cor-ect responses on the N-back test. All composite indices werecaled so that high values reflected better performance. A sig-ificant group effect was reproduced on each composite index:mmediate memory (t(38) = −2.73, p < .01), delayed memoryt(38) = −2.55, p < .05) and executive functions (t(38) = −2.32,< .05), epitomizing MCI impairment in these three cognitiverocesses.
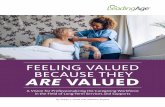
The correlation pattern obtained between the FOK accu-acy index and the three composite indices (immediate memory,elayed memory and executive functions) is shown in Table 4nd by scatter plots in Fig. 1. The results indicate that mem-ry and executive processes contribute differentially to FOKccuracy as a function of the diagnosed group. In the MCIroup, the FOK accuracy index was significantly correlatedith the two memory indices, but not with the executive
ndex, whereas in the control group the reverse pattern wasbserved: the FOK accuracy index was significantly corre-ated with the executive index, but not with the two memoryndices.
To isolate any specific relationships between each of theemory and executive indices and FOK accuracy, partial
orrelations were calculated. Results indicated an unchangedorrelation pattern: after controlling for the executive index,orrelations between FOK accuracy and immediate and delayedemory stayed significant in the MCI group (r = .54, p < .05 and= .56, p < .05, respectively) and not significant in the controlroup (r = −.03, p > .05 and r = −.08, p > .05, respectively), andfter controlling for both memory indices, correlations betweenOK accuracy and the executive index were again not significant
n the MCI group (r = −.16, p > .05) and significant in the controlroup (r = .59, p < .05). The FOK did not appear to be related tonformation decay as it was associated similarly to immediatend delayed memory. The issue of immediate and delayed mem-
ry indices will therefore be raised later without distinguishingetween them as a single memory index. On the whole, cor-elation analyses suggest that the accuracy of FOK predictions
A. Perrotin et al. / Neuropsychologia 45 (2007) 2811–2826 2819
F a indea
ca
4
mmmaOniada
4
imafpatwi
ig. 1. Scatter plots with regression line between the feeling-of-knowing gammnd (c) executive functions, for the two study groups.
ould depend on two distinct functional profiles between MCInd control participants.
. Discussion
The central purpose of this study was to investigate theemory monitoring ability in MCI via a specific experimentaletamemory paradigm. Using an FOK task for episodic infor-ation, we found that people with MCI did not have the same
bility as controls to assess their memory system accurately.ur second objective was to explore the cognitive determi-ants supporting the production of accurate FOK judgments by
nvestigating memory and executive processes. This revealeddifferential pattern highlighting certain cognitive functioningifferences between MCI and control participants influencingccurate FOK.aiat
x and the three composite indices: (a) immediate memory, (b) delayed memory
.1. Episodic feeling-of-knowing accuracy and MCI
The task of FOK in episodic memory is a metamemory mon-toring procedure that allows participants to monitor their own
emory functioning directly during an episodic memory testnd make judgments on their ability to recognize items theyailed to recall. Monitoring accuracy is assessed by comparingredictions with effective recognition performance. When MCInd control participants were compared on this episodic FOKask, results show a significantly lower accuracy index in peopleith MCI. This outcome constitutes one of the major new find-
ngs of this study and suggests that people with MCI may not be
ble to predict their recognition performance for newly learnednformation as accurately as control participants. More detailednalyses indicated that people with MCI judged more frequentlyhan controls that they would recognize an item that in fact they
2 ycholo
dmiiT
swpdppmbrmmpicebodtceAteamtcrwnSporaeisitspmodttttw
tAbhmgtfoaaaftcdeapsmotc
4m
dFrtTmicsgp
aKiomcprtftn
820 A. Perrotin et al. / Neurops
id not recognize. Observation in people with MCI of misjudg-ents in the sense of an overestimation of their performance
s in accordance with previous studies comparing patient andnformant reports of cognitive functioning (Albert et al., 1999;abert et al., 2002; Vogel et al., 2004).
These FOK task findings appear at first sight to be incon-istent with our own data on SMC which showed that peopleith MCI expressed more memory difficulties than controlarticipants on a subjective memory questionnaire about every-ay life (regardless of the accuracy of these self-reports inredicting actual memory functioning). Thus, our MCI groupresented greater SMC than controls, but overestimated theiremory performance on an episodic memory task. As suggested
y McGlynn and Kaszniak (1991), these apparently divergentesults between SMC and experimental metamemory perfor-ance arise from the fact that the two approaches differ inany respects. At a conceptual level, although both methods
urport to measure the same underlying metamemory monitor-ng construct, they each tap one singular aspect of this broadoncept. SMC involve global memory judgments assessing gen-ral ‘metacognitive knowledge’ (i.e., general knowledge andeliefs that people have about memory and their own mem-ry functioning; Flavell, 1979) encompassing various memoryomains, such as episodic, semantic or procedural. In addition,hese judgments are retrospective. Whereas FOK involves spe-ific judgments of memory generated during the course of anpisodic memory activity, and these judgments are prospective.t a methodological level, when people are asked to assess
heir memory through a questionnaire, direct questions aboutpisodes and examples of memory problems are given, andnswers are often provided by explicitly suggesting potentialemory difficulties. By contrast, FOK tasks require participants
o initiate the online monitoring of their own present memoryontents or processes (Pannu & Kaszniak, 2005). Thus, clinicaleports and experimental metamemory tasks should be equatedith caution because they differ fundamentally in the metacog-itive processes involved. In the light of these considerations, ourMC and FOK results should not be viewed as opposing, but asroviding two kinds of informative record regarding metamem-ry monitoring abilities in MCI. People with MCI may have aelative awareness of their memory decline (in contrast to thenosognosia profile in AD) in addition to certain difficultiesvaluating online their memory functioning. Furthermore, annteraction between these two metamemory components can beeen with reference to the basic work of Flavell (1979) suggest-ng that the online monitoring of cognitive activities pertainso general ‘metacognitive knowledge’. An intuitive suggestioneems to ensue from this view to account for the FOK profile ofeople with MCI. In spite of an intact ability to recognize theiremory difficulties, it is probable that people with MCI may
verestimate their memory performance on a task because theyo not use their metacognitive knowledge spontaneously andhen integrate relevant information about factors that may affect
heir memory (such as information about their memory decline)o update their memory predictions. An alternative hypothesiso account for the overestimation behavior could be that peopleith MCI have not estimated properly the recognition test ofarAm
gia 45 (2007) 2811–2826
he FOK paradigm and the processes that its execution needed.s suggested by the SMC result, people with MCI may haveeen aware of their memory recollective failures, and they couldave relied on their perceived efficiency of their familiarity judg-ents to guess perform well at the recognition task. However,
iven the semantic relatedness of the distractors to the target,he recognition task may have required more recollection thanamiliarity-based retrieval processes. Thus, the particular formatf the task could have deceived the MCI judgments. To directlyddress this possibility, future studies are necessary to assess theccuracy of FOK judgments with an FOK paradigm includingless recollection-dependent recognition task. For instance, a
orced-choice recognition test with three rather than four dis-ractors sharing a lesser degree of relatedness with the targetould be employed. To keep a forced-choice design may indeedemand more familiarity processes and thus would be more ben-ficial in MCI than a yes/no recognition design (Westerberg etl., 2006). The MCI overestimation behavior could also reflectrocesses pertaining for instance to the general attitude of theubjects towards the task, as a response bias and self-defenseechanism when faced with their memory weakness. However,
ur findings showed that the MCI group predicted recognition ofhe target item in the same proportion of yes/no judgments as theontrol group, which may not support the previous hypothesis.
.2. Episodic feeling-of-knowing accuracy determinants:emory and executive functions
To understand better the nature of the MCI deficit to pre-ict with accuracy their memory performance on an episodicOK task, the second purpose of this study was to explore theespective contribution of memory and executive processes tohe accuracy of FOK judgments in MCI and control groups.he correlation approach emphasizes that FOK accuracy isainly associated with the executive index in control partic-
pants and with memory indices in people with MCI. Thisontrasted correlation pattern emerging as a group effect con-titutes an interesting finding and highlights that the ability toenerate accurate FOK predictions is based on distinct cognitiverocesses according the diagnosed group.
With regard to the mechanisms underlying episodic FOKccuracy, the theoretical cognitive models of FOK (Koriat, 1993;oriat & Levy-Sadot, 2001) and recent neuroanatomical find-
ngs (Schnyer et al., 2005) suggest that the FOK decision consistsf implementing the memory search or retrieval process andonitoring the by-products of the retrieval attempt. More pre-
isely, Schnyer et al. (2004, 2005) have demonstrated that therefrontal region is significantly engaged in monitoring theetrieval process during accurate FOK judgments. Given thathe executive control is commonly associated with frontal lobeunctioning, executive processes may be critically involved inhe monitoring function of FOK. Furthermore, the functionaleuroimaging study (Schnyer et al., 2005) has also shown that
ccurate FOK implies the hippocampus and the lateral tempo-al cortex, although at a lesser extend than prefrontal cortex.s usually suggested, the medial temporal cortex may underlieemory storage and retrieval. Thus, memory may contribute to
ycholo
FesAtacfmpnFttoanpattrivlfdo2
miaoMboeo(cglostcdbeartaccM
dmaaa2Fmpag(p1eghdKiFrtpconfitmFeboetrHtdscybnMakthmtf
A. Perrotin et al. / Neurops
OK process in that it provides the basis on which the monitoringxerts its action to produce FOK judgments. This claim has beenupported at a cognitive level by the Koriat’s (1993) FOK model.dditionally, neuropathological studies have underlined a con-
rasted degree of memory and executive involvement in FOKccuracy, in which the executive part may be greater. Researchonducted with patients with lesions restricted to frontal lobeound that they exhibited impairment in episodic FOK judg-ents (Schnyer et al., 2004). On the other hand, amnesic
atients with damage restricted to medial temporal lobe, witho frontal lobe deficit, have been found to have intact episodicOK accuracy (Shimamura & Squire, 1986). One explanation
o the metamemory profile exhibited by amnesics could be thatheir efficient executive functioning compensates their mem-ry decline to generate accurate FOK judgments (Janowsky etl., 1989; Shimamura & Squire, 1986). As a whole, whethereuroimaging and neuropathological data both emphasized therefrontal cortex role in FOK accuracy, contrary to cognitivend neuroimaging results, the amnesic patient case indicateshat medial temporal lobe and memory function are not impor-ant for FOK. In fact, the memory contribution to FOK could beeal but secondary, and memory impairment could be a worsen-ng factor only faced with frontal dysfunction. In line with thisiew, a growing metamemory literature on neurological popu-ations support that “patients with memory loss in addition torontal lobe dysfunction, typical of the syndromes that occur inementia and Korsakoff’s syndrome, perform the most poorlyn [monitoring] metamemory tasks” (p. 122, Pannu & Kaszniak,005).
At the light of these processes sustaining accurate FOK judg-ents, how can we interpret the finding that FOK accuracy
s related differentially to memory and executive functioningccording to the group, and by what mechanisms can mem-ry impairment account for episodic FOK accuracy decline inCI? In the normal aging framework, the relationship observed
etween FOK and executive index indicates that the accuracyf FOK predictions in older people is primarily determined byxecutive functioning. This specific association within a healthylder adult group is in line with the findings of Souchay et al.2000) and Perrotin et al. (2006). Regarding the non-significantorrelation between FOK and memory index noted in the controlroup, this result is keeping with data from neurological popu-ations (Shimamura & Squire, 1986). Therefore, our findings onlder control participants may be in accordance with proposalsupporting the role of executive-frontal processes in the produc-ion of accurate FOK judgments. However, in contrast to theontrol group, the ability of people diagnosed with MCI to pre-ict with accuracy their recognition performance was shown toe related primarily to their memory abilities rather than to theirxecutive functioning. The role of memory functioning in FOKccuracy seems coherent with cognitive (Koriat, 1993) and neu-oanatomical findings of FOK (Schnyer et al., 2005). However,his result appears surprising in comparison with the data from
mnesic patients and with the important role of executive pro-esses in FOK. We will try to explain these inconsistencies all inonsidering the relation between memory and FOK accuracy inCI. Episodic memory impairment is the hallmark of MCI, asttad
gia 45 (2007) 2811–2826 2821
emonstrated by neuropsychological data showing poor perfor-ance on different memory measures (Petersen et al., 1999), and
lso found in our study, and by neuropathological data reportingbnormalities in the hippocampus region and medial temporalreas (Jack et al., 2000; Markesbery et al., 2006; Morris et al.,001). In view of the positive association described betweenOK accuracy and memory abilities in people with MCI, theemory impairment probably associated with the medial tem-
oral lobe functioning may be a central factor of the diminishedccuracy of FOK in MCI. This result observed in our MCIroup corroborates directly previous reports of people with ADSouchay et al., 2002). These observations are in line with theosition of Prevey and colleagues (Prevey, Delaney, & Mattson,988; Prevey, Delaney, Mattson, & Tice, 1991) suggesting thatarly damage within a particular domain of memory leads toreater metamemory deficits in that domain. The question isow to understand the memory mediation of the FOK accuracyecline. With reference to the accessibility account of FOK,oriat (1993, 1995) has suggested that the amount of partial
nformation retrieved from memory about the target gives rise toOK judgments or ratings. According to this claim, an expectedesult is that the lower amount of information retrieved about thearget because of a memory deficit induces a reduction of the pro-ortion of positive FOK judgments for recognition performance,ompared to subjects without memory impairment. However,ur results showed that the frequency of FOK judgments doesot differ significantly between MCI and control groups. Thus atrst sight, the less accurate FOK judgments in MCI may be due
o a memory monitoring deficit. By contrast, amnesic patientsay predict their memory performance accurately in an episodicOK task (Shimamura & Squire, 1986) because they may havefficient memory monitoring. The executive functioning coulde the cognitive ability that essentially distinguishes the profilef pure amnesia from that of MCI. Indeed, besides deficits inpisodic memory tasks, a mild impairment in executive func-ion tests was observed in our MCI group and has also beeneported in other studies (Crowell et al., 2002; Davie et al., 2004;anninen et al., 1997; Ready et al., 2003). These subtle execu-
ive limitations in MCI might therefore mediate the monitoringecline. However, with respect to the large body of evidencehowing that the memory monitoring function is a prefrontalortex-related executive process, and insofar as correlation anal-sis of the MCI group did not reveal any significant relationshipetween executive processes and FOK accuracy, our results doot support the hypothesis of a memory monitoring deficit in ourCI group. An alternative hypothesis to account for the FOK
ccuracy decline could be proposed which distinguishes twoinds of monitoring, one based on the familiarity assessment andhe other based on the recollection assessment. This distinctionas been highlighted by two approaches, first, by metamemoryodels like that of Koriat and Levy-Sadot (2001) which assumes
hat FOK judgments result from the combined influence of cue-amiliarity and the accessibility of partial information about the
arget, and second, by more general models of retrieval memoryhat dissociate familiarity and recollection-based retrieval mech-nisms (Jacoby, 1996; Mandler, 1980). Recent findings haveemonstrated that MCI memory decline may be more precisely
2 ycholo
cbhamfiwfbTftcooaiemlovmlMmadpactiatpstfbifcmfeutsosAtrAa
tTFpa
oeucvrairmM
4
tntrtamvanbotmwoAimmaaspdietbmjb
822 A. Perrotin et al. / Neurops
haracterized by a deficit in recollection rather than familiarity-ased retrieval (Westerberg et al., 2006). The idea suggestedere is that because of a smaller amount of partial informationccessed, people with MCI might primarily rely on the assess-ent of the familiarity of the cue item presented and on the
amiliarity of the partial information retrieved, rather than bas-ng their FOK judgments on the quantitatively and qualitativelyeak memory contents. However, FOK judgments based on a
amiliarity system may critically be less accurate than judgmentsased on qualitative and detailed information about the target.hus, the memory impairment in MCI and more precisely the
ailure of these patients to recollect the details pertaining to thearget (probably associated with additional discrete control pro-ess impairment) may lead them to adopt a monitoring relyingn other bases which may be less effective in predicting mem-ry performance accurately. Further work is needed to test thisssumption more thoroughly. The increased reliance on famil-arity of people with MCI to produce their FOK judgments mightxplain their tendency to overestimate their recognition perfor-ance insofar as they are not able to appreciate completely the
ower validity of partial information retrieved when they usether bases than recollection for FOK judgments. Spurious acti-ation or irrelevant information about the target might inflateemory contents and consequently misguide FOK judgments,
eading patients to overestimate their recognition performance.oreover, this interpretation whereby people with MCI, due toemory impairment, may fulfil the FOK metamemory task indistinctively different way than their counterparts, involving
ifferent cognitive processes, could account for the dissociateattern of correlation between executive functioning and FOKccuracy within the two groups. Indeed, the monitoring processarried out by healthy older adults may involve executive func-ions such as those tapped by the executive tasks used here (i.e.,nhibition (Victoria Stroop test), on-line monitoring, updating,nd manipulation of working memory representations (N-backest)). On the other hand, the monitoring process carried out byeople with MCI may entail lesser executive control. In thisense, Schnyer et al. (2004) found in an episodic FOK taskhat frontal patients displayed an intact ability to monitor theamiliarity of the cue item, but they failed when monitoring wasased on retrieved information. Furthermore, in the light of find-ngs from neuroimaging studies showing that recollection- andamiliarity-based retrieval processes involve distinct prefrontalortex subregions (Henson et al., 1999; Yonelinas et al., 2005),onitoring based on familiarity could require other executive
unctions than those tapped by our executive tasks. This couldxplain the lack of correlation between FOK accuracy and exec-tive processes in MCI, and also reduce inconsistency noted inhe case of amnesic patients. Indeed, executive function mea-ures used in this study reflect only specific and limited aspectsf executive functioning. One critical limitation of the currenttudy was to not have more fully exploited executive functioning.ccordingly, future research should investigate executive func-
ioning in a more extensive and comprehensive way to specifyeliably how executive control is related to the FOK accuracy.n alternative way to assess the executive contribution to FOK
ccuracy in MCI could be to compare pure amnestic and amnes-
m
ci
gia 45 (2007) 2811–2826
ic multiple-domain MCI subgroups on an episodic FOK task.he underlying hypothesis would be that if the MCI decline inOK accuracy is related to executive functioning, people withure amnesic MCI may exhibit intact ability to predict withccuracy their recognition performance.
Overall, the data reported here also add to the metamem-ry literature with regard to the cognitive processes underlyingpisodic FOK accuracy. They suggest that memory and exec-tive functioning may be two crucial factors entering into theomputation of FOK, consistent with the multiply determinediew of FOK (Koriat & Levy-Sadot, 2001). Furthermore, ouresults provide new cognitive evidence adding to an increasingnd convergent set of patient and neuroimaging studies suggest-ng that FOK involves a frontal-temporal network with prefrontalegions monitoring and coordinating the recollection of episodicemories stored in the medial temporal lobe (Conway, 2005;oscovitch & Winocur, 1992, 2002).
.3. Theoretical and clinical contributions to MCI
Findings described in this paper provide new knowledge onhe cognitive profile of people in a transitional state betweenormal aging and dementia. The experiment highlights thathere is a decline in the metamemory FOK accuracy in MCI,aising questions about the implications and consequences inheoretical and practical terms of this dysfunction. First, from
theoretical viewpoint, the role of metamemory processes inemory functioning must be considered. Metamemory plays a
ital role in the efficient operation of the basic memory system,nd monitoring is seen as an essential component of metacog-itive processes (Metcalfe, 1993). Optimal control of memoryehavior is achieved by accurate monitoring of the current statef memory. Therefore, the lower efficiency of people with MCIo evaluate accurately their memory status, related to their actual
emory decline, may misguide the memory control processith an ill-adapted regulation of memory behavior (e.g., mem-ry strategies), which in turn may lead to memory disturbance.n eloquent example regarding feeling-of-knowing experience
s that when people with MCI carry out a memory activity, theyay have a strong FOK that erroneously signals that some infor-ation is available in their memory store, and as a result they
re likely to stop their learning prematurely – if this feeling isssociated with an encoding process, or to make great effortsearching in vain for the information – if the feeling accom-anies a retrieval process. The idea outlined here and whicheserves to be explored is that a deficit in memory monitor-ng FOK accuracy could be an exacerbating factor in the poorpisodic memory performance in MCI. Regarding the core fea-ure of memory impairment in MCI and the strong interrelationetween memory and metamemory, memory monitoring and,ore generally, metamemory processes should form the sub-
ect of careful attention in MCI. Metamemory in MCI shoulde further investigated through procedures assessing memory
onitoring as well as the memory control function.From a clinical point of view, the role of the severity ofognitive impairment has to be considered. A recurrent reportn research on dementia is that anosognosia tends to increase

ycholo
aVdai(twgolwtaFsrzpIctfpiommqtpFdiMealufomfsfta
4
idcjmm
mpeltatssapme
A
lI(tta
R
A
A
A
A
B
B
B
C
C
C
C
C
A. Perrotin et al. / Neurops
s the disease progresses (Aalten, Van Valen, Clare, Kenny, &erhey, 2005; Harwood et al., 2000). In the present work, weemonstrated that the severity of cognitive decline is also founds an associate factor in lower accuracy of memory monitor-ng. Our results showed that the overall cognitive functioningMDRS score) of people with MCI was negatively correlatedo the overestimation index of the FOK task. This correlationas both specific to the group and to the FOK response cate-ory. Thus, the most severely impaired people may significantlyverestimate their recognition performance compared to thoseess affected. Moreover, Souchay et al. (2002) have observedith a similar episodic FOK procedure to ours that people in
he early stages of AD were impaired in their monitoring FOKccuracy compared to older control adults. While the accuracy ofOK predictions of our MCI group was better than chance level,uggesting some memory monitoring capacity, the FOK accu-acy index of the AD group was not significantly different fromero, indicating an inability of people with AD to accuratelyredict their recognition performance (Souchay et al., 2002).n the light of these data, we can hypothesize that there is aontinuum of decline in the memory monitoring FOK accuracyhat follows cognitive impairment, first within MCI and thenrom MCI to AD. Furthermore, although stronger in nature, theattern of FOK accuracy impairment in AD appears very sim-lar to that noted in MCI. Similarities in the FOK performancef people with MCI and AD concern the tendency to overesti-ate recognition and the specific positive relationship betweenemory abilities and accurate FOK judgments. Thus, despite
uantitative variations that may correlate with the severity ofhe overall cognitive decline, at a qualitative level it seems thateople with MCI and AD process information on an episodicOK task according to a similar functional profile, significantlyistinct from that of healthy older people. In view of these mean-ngful similarities and given that a high proportion of people with
CI may progress to AD (Petersen et al., 1999), it would be rel-vant to analyze whether people with poor memory monitoringccuracy on an FOK task are more likely to develop AD. Theimited perspective of a cross-sectional study does not enables to establish the predictive value of the monitoring FOK dys-unction in MCI for AD, but results from longitudinal studiesn clinic-based samples could provide more conclusive infor-ation. Indeed, it has been postulated that overestimation of
unctional abilities in people with MCI is predictive of progres-ion to AD (Tabert et al., 2002). It would be valuable therefore toollow-up an MCI patient cohort with an episodic FOK measureo determine whether impaired memory monitoring accuracy isn early sign of AD.
.4. Conclusion
In summary, the present work aimed at probing metamemoryn MCI by assessing the accuracy of the memory monitoringuring an episodic memory FOK procedure. The results indi-
ate that people with MCI are less accurate in their recognitionudgments than healthy matched control subjects, by overesti-ating their future memory performance. In the MCI group, theetamemory impairment is correlated with deficits in episodic
C
gia 45 (2007) 2811–2826 2823
emory, and not with executive functioning, while the oppositeattern is noted for the control group. This between-group differ-ntial profile suggests that people with MCI may take other andess effective ways than controls to monitor their memory func-ioning, probably because of their recollective limitations. Inddition to bring some cues on the cognitive functioning in MCI,he data reported here could make contribution to research onubjective memory complaints in early dementia and also raiseome theoretical and clinical questions. As well, the findingsdd to the metamemory literature with regard to the cognitiverocesses underlying episodic FOK accuracy, suggesting thatemory and executive functioning may be two important factors
ntering into the computation of FOK.
cknowledgments
This study was supported by grants from the GIS Institut dea longevite et du vieillissement to Audrey Perrotin and Michelsingrini, and from the Canadian Institutes of Health ResearchCIHR) and Fonds de la Recherche en Sante du Quebec (FRSQ)o Sylvie Belleville. We thank Caroline Proulx for her assis-ance with the testing of participants. We wish also to thank thenonymous referees for their helpful comments.
eferences
alten, P., Van Valen, E., Clare, L., Kenny, G., & Verhey, F. (2005). Awarenessin dementia: A review of clinical correlates. Aging and Mental Health, 9,414–422.
ggleton, J. P., & Brown, M. W. (1999). Episodic memory, amnesia, and thehippocampal-anterior thalamic axis. The Behavioral and Brain Sciences,22(3), 425–490.
lbert, S. M., Michaels, K., Padilla, M., Pelton, G., Bell, K., Marder, K., etal. (1999). Functional significance of mild cognitive impairment in elderlypatients without a dementia diagnosis. American Journal of Geriatric Psy-chiatry, 7, 213–220.
ndres, P. (2003). Frontal cortex as the central executive of working memory:Time to revise our view. Cortex, 39, 871–895.
assett, S. S., & Folstein, M. F. (1993). Memory complaint, memory perfor-mance, and psychiatric diagnosis: A community study. Journal of GeriatricPsychiatry and Neurology, 6, 105–111.
enton, A. L., Hamsher, K., Varney, N. R., & Spreen, O. (1983). Contributionsto neuropsychological assessment. Oxford University Press: New York.
olla, K. I., Lindgren, K. N., Bonaccorsy, C., & Bleecker, M. L. (1991). Memorycomplaints in older adults. Archives of Neurology, 48, 61–64.
arroll, M., & Nelson, T. O. (1993). Effect of overlearning on the feelingof knowing is more detectable in within-subjects than in between-subjectdesigns. American Journal of Psychology, 106, 227–235.
lare, L. (2004). Awareness in early-stage Alzheimer’s disease: A review ofmethods and evidence. British Journal of Clinical Psychology, 43, 177–196.
lare, L., Markova, I., Verhey, F., & Kenny, G. (2005). Awareness in dementia:A review of assessment methods and measures. Aging and Mental Health,9, 394–413.
ollie, A., Maruff, P., & Currie, J. (2002). Behavioral characterization of mildcognitive impairment. Journal of Clinical Experimental Psychology, 24,720–733.
onway, M. A. (2005). Memory and the self. Journal of Memory and Language,
53, 594–628.rowell, T. A., Luis, C. A., Vanderploeg, R. D., Schinka, J. A., & Mullan, M.(2002). Memory patterns and executive functioning in mild cognitive impair-ment and Alzheimer’s disease. Aging, Neuropsychology, and Cognition, 9,288–297.

2 ycholo
D
D
D
F
F
F
F
FG
G
H
H
H
H
H
H
H
H
H
I
J
J
J
J
J
J
J
K
K
K
K
K
K
L
M
M
M
M
M
M
M
M
M
M
M
M
824 A. Perrotin et al. / Neurops
avie, J. E., Azuma, T., Goldinger, S. D., Connor, D. J., Sabbagh, M. N., &Silverberg, N. B. (2004). Sensitivity to expectancy violations in healthyaging and mild cognitive impairment. Neuropsychology, 18, 269–275.
rzezga, A., Lautenschlager, N., Siebner, H., Riemenschneider, M., Willoch,F., Minoshima, S., et al. (2003). Cerebral metabolic changes accompanyingconversion of mild cognitive impairment into Alzheimer disease: A PETfollow-up study. European Journal of Nuclear Medicine and MolecularImaging, 30, 1104–1113.
uncan, J. (1995). Attention, intelligence, and the frontal lobes. In M. S. Gaz-zaniga (Ed.), The cognitive neurosciences (pp. 721–733). Cambridge, MA:MIT Press.
ernandez-Duque, D., Baird, J., & Posner, M. (2000). Executive attention andmetacognitive regulation. Consciousness and Cognition, 9, 288–307.
lavell, J. H. (1979). Metacognition and cognitive monitoring: A new area ofcognitive-developmental inquiry. American Psychologist, 34, 906–911.
licker, C., Ferris, S. H., & Reisberg, B. (1991). Mild cognitive impairment inthe elderly: Predictors of dementia. Neurology, 41, 1006–1009.
olstein, N., Folstein, S., & McHugh, P. (1975). “Mini-Mental State”: A practicalmethod for grading the cognition state of patients for the clinician. Journalof Psychiatry Research, 12, 189–198.
uster, J. M. (1989). The prefrontal cortex (2nd ed.). New York: Raven Press.rober, E., & Buschke, H. (1987). Genuine memory deficits in dementia. Devel-
opmental Neuropsychology, 3, 13–36.runeberg, M., & Monks, J. (1974). Feeling-of-knowing and cued recall. Acta
Psychologica, 38, 257–265.achinski, V. C., Iliff, L. D., Zilhka, E., Du Boulay, G. H., McAllister, V. L.,
Marshall, J., et al. (1975). Cerebral blood flow in dementia. Archives ofNeurology, 32(9), 632–637.
anninen, T., Hallikainen, M., Koivisto, K., Partanen, K., Laakso, M. P., Riekki-nen, P. J., et al. (1997). Decline of frontal lobe functions in subjects withage-associated memory impairment. Neurology, 48, 148–153.
anninen, T., Reinkainen, K. J., Helkala, E., Koivisto, K., Mykkanen, L., Laakso,M., et al. (1994). Subjective memory complaints and personality traits innormal elderly subjects. Journal of the American Geriatrics Society, 42,1–4.
art, J. T. (1965). Memory and the feeling-of-knowing experiments. Journal ofEducational Psychology, 56, 208–216.
arwood, D. G., Sultzer, D. L., & Wheatley, M. V. (2000). Impaired insight inAlzheimer disease: Association with cognitive deficits, psychiatric symp-toms, and behavioral disturbances. Neuropsychiatry, Neuropsychology andBehavioral Neurology, 13, 83–88.
ebert, R., Carrier, R., & Bilodeau, A. (1988). Le Systeme de Mesure del’Autonornie Fonctionnelle (SMAF) [The functional autonomy measure-ment system]. Revue de Geriatrie, 13, 161–167.
enson, R. N., Rugg, M. D., Shallice, T., Josephs, O., & Dolan, R. J. (1999). Rec-ollection and familiarity in recognition memory: An event-related functionalmagnetic resonance imaging study. The Journal of Neuroscience, 19(10),3962–3972.
ertzog, C., Hultsch, D. F., & Dixon, R. A. (1989). Evidence for the conver-gent validity of two self-report metamemory questionnaires. DevelopmentalPsychology, 25, 687–700.
ertzog, C., Park, D. C., Morrell, R. W., & Martin, M. (2000). Ask and yeshall receive: Behavioral specificity in the accuracy of subjective memorycomplaints. Applied Cognitive Psychology, 14, 257–275.
zaute, M., Larochelle, S., Morency, J., & Tiberghien, G. (1996). La validite dusentiment de savoir au rappel et a la reconnaissance. Revue Canadienne dePsychologie Experimentale, 50, 136–180.
ack, C. R., Petersen, R. C., Xu, Y. C., O’Brien, P. C., Smith, G. E., Ivnik, R. J.,et al. (2000). Rates of hippocampal atrophy correlate with change in clinicalstatus in aging and AD. Neurology, 55, 484–489.
acoby, L. L. (1996). Dissociating automatic and consciously controlled effectsof study/test compatibility. Journal of Memory and Language, 35(1), 32–52.
anowsky, J. S., Shimamura, A. P., & Squire, L. R. (1989). Memory and
metamemory: Comparisons between patients with frontal lobe lesions andamnesic patients. Psychobiology, 17, 3–11.onides, J., & Smith, E. E. (1997). The architecture of working memory. In M. D.Rugg (Ed.), Cognitive neuroscience (pp. 243–276). Cambridge, MA: MITPress.
M
M
gia 45 (2007) 2811–2826
onker, C., Geerlings, M. I., & Schmand, B. (2000). Are memory complaintspredictive for dementia? A review of clinical and population-based studies.International Journal of Geriatric Psychiatry, 15, 983–991.
onker, C., Launer, L. J., Hooijer, C., & Lindeboom, J. (1996). Memory com-plaints and memory impairment in older individuals. Journal AmericanGeriatrics Society, 44, 44–49.
orm, A. F., Christensen, H., Korten, A. E., Henderson, A. S., Jacomb, P. A., &Mackinnon, A. (1997). Do cognitive complaints either predict future cog-nitive decline or reflect past cognitive decline? A longitudinal study of anelderly community sample. Psychological Medicine, 27, 91–98.
albe, E., Salmon, E., Perani, D., Holthoff, V., Sorbi, S., Elsner, A., et al. (2005).Anosognosia in very mild Alzheimer’s disease but not in mild cognitiveimpairment. Dementia and Geriatric Cognitive Disorders, 19, 349–356.
aplan, E., Goodglass, H., & Weintrub, S. (1983). Boston Naming Test. Philadel-phia: Lea & Febiger.
oriat, A. (1993). How do we know that we know? The accessibility model ofthe feeling-of-knowing. Psychological Review, 100, 609–639.
oriat, A. (1995). Dissociating knowing and the feeling of knowing: Furtherevidence for the accessibility model. Journal of Experimental Psychology:General, 124(3), 311–333.
oriat, A. (2000). The feeling of knowing: Some metatheoretical implicationsfor consciousness and control. Consciousness and Cognition, 9, 149–171.
oriat, A., & Levy-Sadot, R. (2001). The combined contributions of the cue-familiarity and accessibility heuristics to feelings-of-knowing. Journal ofExperimental Psychology: Learning, Memory, and Cognition, 27, 34–53.
ezak, M. D. (1995). Neuropsychological assessment. New York: Oxford Uni-versity Press.
andler, G. (1980). Recognizing: The judgement of previous occurrence. Psy-chological Review, 87, 252–271.
aril, A., Simons, J. S., Mitchell, J. P., Schwartz, B. L., & Schacter, D. L.(2003). Feeling-of-knowing in episodic memory: An event-related fMRIstudy. Neuroimage, 18, 827–836.
arkesbery, W. R., Schmitt, F. A., Kryscio, R. J., Davis, D. G., Smith, C.D., & Wekstein, D. R. (2006). Neuropathologic substrate of mild cognitiveimpairment. Archives of Neurology, 63, 38–46.
attis, S. (1976). Mental status examination for organic mental syndrome inthe elderly patient. In L. Bellak & T. B. Karasu (Eds.), Geriatric psychiatry(pp. 77–121). New York: Grune & Stratton.
cDaniel, K. D., Edland, S. D., Heyman, A., & the CERAD clinical investiga-tors. (1995). Relationship between level of insight and severity of dementiain Alzheimer disease. Alzheimer Disease and Associated Disorders, 9,101–104.
cGlynn, S. M., & Kaszniak, A. W. (1991). When metacognition fails: Impairedawareness of deficit in Alzheimer’s disease. Journal of Cognitive Neuro-sciences, 3, 183–189.
cKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stad-lan, E. M. (1984). Clinical diagnosis of Alzheimer’s disease: Report of theNINCDS-ADRDA Work Group under the auspices of Department of Healthand Human Services Task Force on Alzheimer’s Disease. Neurology, 34,939–944.
etcalfe, J. (1993). Novelty monitoring, metacognition, and control in a com-posite holographic associative recall model: Implications for Korsakoffamnesia. Psychological Review, 100, 3–22.
etcalfe, J., Schwartz, B. L., & Joaquim, S. G. (1993). The cue-familiarityheuristic in metacognition. Journal of Experimental Psychology: Learning,Memory, and Cognition, 19, 851–864.
etcalfe, J., & Shimamura, A. P. (1994). Metacognition: Knowing about know-ing. Cambridge: MIT Press.
igliorelli, R., Teson, A., Sabe, L., Petracca, G., Petracchi, M., Leiguarda, R.,et al. (1995). Anosognosia in Alzheimer’s disease: A study of associatedfactors. Journal of Neuropsychiatry and Clinical Neuroscience, 7, 338–344.
orris, J. C., Storandt, M., Miller, J. P., McKeel, D. W., Price, J. L., Rubin, E. H.,et al. (2001). Mild cognitive impairment represents early-stage Alzheimer’s
disease. Archives of Neurology, 58, 397–405.orris, N., & Jones, D. M. (1990). Memory updating in working memory: Therole of the central executive. British Journal of Psychology, 81, 111–121.
oscovitch, M., & Winocur, G. (1992). The neuropsychology of memory andaging. In F. I. M. Craik & T. A. Salthouse (Eds.), The handbook of aging

ycholo
M
N
N
N
N
N
O
O
O
P
P
P
P
P
P
P
P
R
R
R
R
R
R
R
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
SS
T
T
T
T
A. Perrotin et al. / Neurops
and cognition (pp. 315–372). Hillsdale, NJ: Lawrence Erlbaum Associates,Publishers.
oscovitch, M., & Winocur, G. (2002). The frontal cortex and working withmemory. In D. T. Stuss & R. T. Knight (Eds.), Principles of frontal lobefunction (pp. 188–209). New York: Oxford University Press.
elson, T. O. (1984). A comparison of current measures of the accuracy offeeling-of-knowing predictions. Psychological Bulletin, 95, 109–133.
elson, T. O., Gerler, D., & Narens, L. (1984). Accuracy of feeling-of-knowingjudgments for predicting perceptual identification and relearning. Journal ofExperimental Psychology: General, 113(2), 282–300.
elson, T. O., Leonesio, R. J., Shimamura, A. P., Landwehr, R. F., & Narens, L.(1982). Overlearning and the feeling of knowing. Journal of ExperimentalPsychology: Learning, Memory, and Cognition, 8, 279–288.
elson, T. O., & Narens, L. (1990). Metamemory: A theoretical frameworkand new findings. In G. H. Bower (Ed.), The psychology of learning andmotivation: Advances in research and theory (pp. 125–173). San Diego:Academic Press.
elson, T. O., & Narens, L. (1994). Why investigate metacognition? In J. Met-calfe & A. Shimamura (Eds.), Metacognition: Knowing about knowing (pp.1–25). Cambridge, MA: Bradford Books.
’Connor, D. W., Pollitt, P. A., Roth, M., Brook, P. B., & Reiss, B. B. (1990).Memory complaints and impairment in normal, depressed, and dementedelderly persons identified in a community survey. Archives of General Psy-chiatry, 47, 224–227.
sterrieth, P. A. (1944). Le test de copie d’une figure complexe [Thetest of copying a complex figure]. Archives de Psychologie, 30, 206–356.
tt, B. R., Lafleche, G., Whelihan, W. M., Buongiorno, G. W., Albert, M. S.,& Fogel, B. S. (1996). Impaired awareness of deficits in Alzheimer disease.Alzheimer Disease and Associated Disorders, 10, 68–76.
almer, K., Wang, H. X., Backman, L., Winblad, B., & Fratiglioni, L. (2002). Dif-ferential evolution of cognitive impairment in nondemented older persons:Results from the Kungsholmen Project. American Journal of Psychiatry,159, 436–442.
annu, J. K., & Kaszniak, A. W. (2005). Metamemory experiments in neurolog-ical populations: A review. Neuropsychology Review, 15, 105–130.
errotin, A., Isingrini, M., Souchay, C., Clarys, D., & Taconnat, L. (2006).Episodic feeling-of-knowing accuracy and cued recall in the elderly: Evi-dence for double dissociation involving executive functioning and processingspeed. Acta Psychologica, 122, 58–73.
etersen, R. C., Doody, R., Kurz, A., Mohs, R. C., Morris, J. C., Rabins, P. V.,et al. (2001). Current concepts in mild cognitive impairment. Archives ofNeurology, 58, 1985–1992.
etersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J., Tangalus, E. G., &Kokmen, E. (1999). Mild cognitive impairment. Archives of Neurology, 56,303–308.
inon, K., Allain, P., Zied Kefi, M., Dubas, F., & Le Gall, D. (2005). Moni-toring processes and metamemory experience in patients with dysexecutivesyndrome. Brain and Cognition, 57, 185–188.
revey, M. L., Delaney, R. C., & Mattson, R. H. (1988). Metamemory in temporalepilepsy: Self-monitoring of memory functions. Brain and Cognition, 24,298–311.
revey, M. L., Delaney, R. C., Mattson, R. H., & Tice, D. M. (1991). Feeling ofknowing in temporal lobe epilepsy: Monitoring knowledge inaccessible toconscious recall. Cortex, 27, 81–92.
abbitt, P. (1997). Introduction: Methodologies and models in the study of exec-utive function. In P. Rabbitt (Ed.), Methodology of frontal and executivefunction (pp. 1–38). Hove, England: Psychology Press.
eady, R. E., Ott, B. R., Grace, J., & Cahn-Weiner, D. A. (2003). Apathy andexecutive dysfunction in mild cognitive impairment and Alzheimer disease.American Journal of Geriatric Psychiatry, 11, 222–228.
eder, L. M. (1987). Strategy selection in question answering. Cognitive Psy-chology, 19, 90–138.
egard, M. (1981). Cognitive rigidity and flexibility: A neuropsychologi-cal study. Unpublished Ph.D. dissertation. University of Victoria, BritishColumbia.
eisberg, B., Ferris, S., de Leon, M. J., Torossian, C., Kadiyala, S., & Zhu, W.(2005). Subjective cognitive impairment: The pre-mild cognitive impairment
V
V
gia 45 (2007) 2811–2826 2825
stage of brain degeneration: Longitudinal outcome after a mean of 7 yearsfollow-up. Neuropsychoplarmacology, 30(Suppl. 1), S81.
ey, A. (1960). Test de la figure complexe de Rey [The Rey complex figure test].Paris: Les Editions du Centre de Psychologie Appliquee.
itchie, K., Artero, S., & Touchon, J. (2001). Classification criteria for mildcognitive impairment. Neurology, 56, 37–41.
chacter, D. L. (1983). Feeling-of-knowing in episodic memory. Journal ofExperimental Psychology: Learning, Memory and Cognition, 9, 39–54.
chmidt, I. W., Berg, I. J., & Deelman, B. G. (2001). Relations between subjec-tive evaluations of memory and objective memory performance. Perceptualand Motor Skills, 93, 761–776.
chnyer, D. M., Nicholls, L., & Verfaellie, M. (2005). The role of VMPCin metamemorial judgments of content retrievability. Journal of CognitiveNeurosciences, 17, 832–846.
chnyer, D. M., Verfaellie, M., Alexander, M. P., LaFleche, G., Nicholls, L., &Kaszniak, A. W. (2004). A role of right medial prefrontal cortex in accu-rate feeling-of-knowing judgments: Evidence from patients with lesions tofrontal cortex. Neuropsychologia, 42, 957–966.
evush, S. (1999). Relationship between denial of memory deficit and demen-tia severity in Alzheimer disease. Neuropsychiatry, Neuropsychology andBehavioral Neurology, 12, 88–94.
hallice, T. (2001). Deconstructing retrieval mode. In M. Naveh-Benjamin, M.Moscovitch, & H. L. Roediger III (Eds.), Perspectives on human memoryand cognitive aging: Essays in Honour of Fergus Craik (pp. 124–134). AnnArbor: Edwards Brothers.
hallice, T., & Burgess, P. (1991). Higher-order cognitive impairments andfrontal lobe lesions in man. In H. S. Levin, H. M. Eisenberg, & A. L. Ben-ton (Eds.), Frontal lobe function and dysfunction (pp. 125–137). New York:Oxford University Press.
himamura, A. P. (1995). Memory and frontal lobe function. In M. S. Gazzaniga(Ed.), The cognitive neurosciences. Cambridge, MA: MIT Press.
himamura, A., & Squire, L. (1986). Memory and metamemory: A study of thefeeling of knowing phenomenon in amnesic patients. Journal of Experimen-tal Psychology: Learning, Memory and Cognition, 12, 452–460.
himamura, A. P., Janowsky, J. S., & Squire, L. R. (1991). What is the roleof prefrontal lobe damage in memory disorders? In H. S. Levin, H. M.Eisenberg, & A. L. Benton (Eds.), Frontal lobe function and dysfunction(pp. 173–195). New York: Oxford University Press.
ignoret, J. L. (1991). Batterie d’Efficience Mnesique: BEM 144 [The memoryefficiency battery]. Paris: Elsevier.
mith, E. E., & Jonides, J. (1999). Storage and executive processes in the frontallobes. Science, 283, 1657–1661.
ouchay, C., Isingrini, M., & Espagnet, L. (2000). Aging, episodic memoryfeeling-of-knowing, and frontal functioning. Neuropsychology, 2, 299–309.
ouchay, C., Isingrini, M., & Gil, R. (2002). Alzheimer’s disease and feeling-of-knowing in episodic memory. Neuropsychologia, 40, 2386–2396.
troop, J. R. (1935). Studies of interference in serial verbal reactions. Journalof Experimental Psychology, 18, 643–662.
tuss, D. T., & Benson, D. F. (1986). The frontal lobes. New York: Raven Press.underland, A., Watts, K., Baddeley, A. D., & Harris, J. E. (1986). Subjec-
tive memory assessment and test performance in elderly adults. Journal ofGerontology, 41, 376–384.
abert, M. H., Albert, S. M., Borukhova-Milov, L., Camacho, Y., Pelton, G.,Liu, X., et al. (2002). Functional deficits in patients with mild cognitiveimpairment: Prediction of AD. Neurology, 58, 758–764.
ierney, M. C., Szalai, J. P., Snow, W. G., & Fisher, R. H. (1996). The predic-tion of Alzheimer disease. The role of patient and informant perceptions ofcognitive deficits. Archives of Neurology, 53, 423–427.
rosset, M. W., & Kaszniak, A. W. (1996). Measures of deficit unawareness forpredicted performance experiments. Journal of the International Neuropsy-chological Society, 2, 315–322.
ulving, E. (1985). Memory and consciousness. Canadian Psychology, 26(1),1–12.
an der Linden, M., & the GREMEM members. (2004). L’evaluation des trou-bles de la memoire: Presentation de quatre tests de memoire episodique(avec leur etalonnage). Marseille: Solal.
an der Linden, M., Wyns, C., Coyette, F., von Frenckell, R., & Seron, X. (1989).Questionnaire d’Auto-evaluation de la Memoire. Bruxelles: Editest.

2 ycholo
V
W
W
W
Y
Y
826 A. Perrotin et al. / Neurops
ogel, A., Stokholm, J., Gade, A., Andersen, B. B., Hejl, A. M., & Waldemar, G.(2004). Awareness of deficits in mild cognitive impairment and Alzheimer’sdisease: Do MCI patients have impaired insight? Dementia and GeriatricCognitive Disorders, 17, 181–187.
agner, M. T., Spangenberg, K. B., Bachman, D. L., & O’Connell, P.(1997). Unawareness of cognitive deficit in Alzheimer disease andrelated dementias. Alzheimer Disease and Associated Disorders, 11, 125–
131.echsler, D. (1981). Wechsler Adult Intelligence Scale-Revised. WAIS-R. NewYork: Psychological Corporation.
esterberg, C. E., Paller, K. A., Weintraub, S., Mesulam, M. M., Holdstock,J. S., Mayes, A. R., et al. (2006). When memory does not fail: Familiarity-
Z
gia 45 (2007) 2811–2826
based recognition in mild cognitive impairment and Alzheimer’s disease.Neuropsychology, 20, 193–205.
esavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M. B., etal. (1983). Development and validation of a geriatric depression screeningscale: A preliminary report. Journal of Psychiatric Research, 17, 37–49.
onelinas, A. P., Otten, L. J., Shaw, K. N., & Rugg, M. D. (2005). Separating thebrain regions involved in recollection and familiarity in recognition memory.
The Journal of Neuroscience, 25(11), 3002–3008.imprich, D., Martin, M., & Kliegel, M. (2003). Subjective cognitive complaints,memory performance, and depressive affect in old age: A change-orientedapproach. International Journal of Aging and Human Development, 57,339–366.