Medicinal plant dynamics in indigenous medicines in farwest Nepal
10
Research Paper Medicinal plant dynamics in indigenous medicines in farwest Nepal Ripu M. Kunwar a,n , Ram P. Acharya b , Chhote L. Chowdhary c , Rainer W. Bussmann d a Department of Geosciences, Florida Atlantic University, United States b Practical Solution Consultancy, Kathmandu, Nepal c Food and Agriculture Organization, Kathmandu, Nepal d William L. Brown Center, Missouri Botanical Garden, United States article info Article history: Received 5 September 2014 Received in revised form 20 January 2015 Accepted 25 January 2015 Available online 2 February 2015 Keywords: Medicinal plants Secondary forests Non-indigenous species Traditional medicines Nepal abstract Ethnopharmacological relevance: Indigenous medicinal systems have evolved after the shock of original contact of traditional healers with the indigenous traditions because decreasing availability of indigenous medicinal plants and assimilation of new species are increasingly occurred. Materials and methods: In this study, we appraised the distribution and usage of indigenous and non- indigenous botanicals and their habitats and their uses in indigenous medicines of farwest Nepal following literature and herbarium specimens review, participatory field visits and ethnobotanical surveys. Results: Because farwest Nepal is least suitable for staple cereal crops, local people have always heavily relied on locally available wild plants. The extensive usage of medicinal plants in farwest Nepal indicates that the plant use is an integral part of culture. Indigenous plants are highly susceptible to overharvesting and their population and distributions have been impacted in response to the introduction of non- indigenous species. Sparse distribution of indigenous species and easy access to non-indigenous species and their habitats, compounded by the need to find for alternatives for species in decline and to treat new diseases, lead to the increment in use of non-indigenous species. Secondary and community forests are gaining importance for the harvest of non-indigenous medicinal plants as they are easily accessible and old-growth forests are overexploited. Besides easy access, ecological versatility and multiple- usefulness of secondary habitats and non-indigenous species also contribute to their increasing use in local pharmacopoeias. Conclusion: The acceptance of non-indigenous resources is analogous to the cultural evolution and dynamic indigenous knowledge systems, and considered as an adaptive asset. & 2015 Elsevier Ireland Ltd. All rights reserved. 1. Introduction At present, 6653 species of flowering plants have been reported from Nepal (Kunwar et al., 2010). About 50% of these can be classi- fied as useful (Kunwar and Bussmann, 2008). Various studies have recorded over 2100 indigenous and 300 non-indigenous plant species as ethnomedicinal (Ghimire, 2008; Rokaya et al., 2010), used by 125 different ethnic groups of the country (Government of Nepal, 2012). The high number of indigenous medicinal plants used, as well as the number of ailments treated, reflects the long history of contact of a community with nature (Prance, 1972; Thomas et al., 2008). Plant use in Nepal Himalaya, recorded in the 6500-year-old text of the Rigveda, ranks among the earliest uses of medicinal plants (Malla and Shakya, 1984). Another early account, the Saushrut Nighantu written in 878 AD recorded the uses of 278 Nepalese medicinal plants (Subedi and Tiwari, 2000). Later compendia of herbal phar- macopoeias such as Chandra Nighantu and Nepali Nighantu were published in 19th and 20th century (Ghimire, 2008). The Nepali Nighantu is an elaborated corpus with information on the traditional knowledge of 750 medicinal plant species published by the Royal Nepal Academy in 1969 (IUCN, 2004). It is widely reported that medicinal plants are inseparable from Nepal's livelihoods, and have long been collected, consumed, and conserved through indigenous knowledge (Singh et al., 1979). Current estimates suggest that in many developing countries about two third of the population relies heavily on traditional medicines and medicinal plants to meet primary health care (Farnsworth and Soejarto, 1991). Indigenous knowledge is often hailed for its versatility to recognize and respond to the livelihood changes (Turner and Clifton, 2009) but it has also been transformed by ecological and socio-cultural changes (Pirker et al., 2012). Palmer (2004) and Medeiros (2013) suggest that ethnomedicine has continued to evolve after the shock of orig- inal contact, with a decreasing availability of indigenous medicinal plants and the introduction of new species (Albuquerque, 2006; Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/jep Journal of Ethnopharmacology http://dx.doi.org/10.1016/j.jep.2015.01.035 0378-8741/& 2015 Elsevier Ireland Ltd. All rights reserved. n Corresponding author. E-mail address: [email protected] (R.M. Kunwar). Journal of Ethnopharmacology 163 (2015) 210–219
Transcript of Medicinal plant dynamics in indigenous medicines in farwest Nepal

Research Paper
Medicinal plant dynamics in indigenous medicines in farwest Nepal
Ripu M. Kunwar a,n, Ram P. Acharya b, Chhote L. Chowdhary c, Rainer W. Bussmann d
a Department of Geosciences, Florida Atlantic University, United Statesb Practical Solution Consultancy, Kathmandu, Nepalc Food and Agriculture Organization, Kathmandu, Nepald William L. Brown Center, Missouri Botanical Garden, United States
a r t i c l e i n f o
Article history:Received 5 September 2014Received in revised form20 January 2015Accepted 25 January 2015Available online 2 February 2015
Keywords:Medicinal plantsSecondary forestsNon-indigenous speciesTraditional medicinesNepal
a b s t r a c t
Ethnopharmacological relevance: Indigenous medicinal systems have evolved after the shock of originalcontact of traditional healers with the indigenous traditions because decreasing availability of indigenousmedicinal plants and assimilation of new species are increasingly occurred.Materials and methods: In this study, we appraised the distribution and usage of indigenous and non-indigenous botanicals and their habitats and their uses in indigenous medicines of farwest Nepalfollowing literature and herbarium specimens review, participatory field visits and ethnobotanicalsurveys.Results: Because farwest Nepal is least suitable for staple cereal crops, local people have always heavilyrelied on locally available wild plants. The extensive usage of medicinal plants in farwest Nepal indicatesthat the plant use is an integral part of culture. Indigenous plants are highly susceptible to overharvestingand their population and distributions have been impacted in response to the introduction of non-indigenous species. Sparse distribution of indigenous species and easy access to non-indigenous speciesand their habitats, compounded by the need to find for alternatives for species in decline and to treatnew diseases, lead to the increment in use of non-indigenous species. Secondary and community forestsare gaining importance for the harvest of non-indigenous medicinal plants as they are easily accessibleand old-growth forests are overexploited. Besides easy access, ecological versatility and multiple-usefulness of secondary habitats and non-indigenous species also contribute to their increasing use inlocal pharmacopoeias.Conclusion: The acceptance of non-indigenous resources is analogous to the cultural evolution anddynamic indigenous knowledge systems, and considered as an adaptive asset.
& 2015 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
At present, 6653 species of flowering plants have been reportedfrom Nepal (Kunwar et al., 2010). About 50% of these can be classi-fied as useful (Kunwar and Bussmann, 2008). Various studies haverecorded over 2100 indigenous and 300 non-indigenous plantspecies as ethnomedicinal (Ghimire, 2008; Rokaya et al., 2010), usedby 125 different ethnic groups of the country (Government of Nepal,2012). The high number of indigenous medicinal plants used, as wellas the number of ailments treated, reflects the long history of contactof a community with nature (Prance, 1972; Thomas et al., 2008).Plant use in Nepal Himalaya, recorded in the 6500-year-old text ofthe Rigveda, ranks among the earliest uses of medicinal plants (Mallaand Shakya, 1984). Another early account, the Saushrut Nighantuwritten in 878 AD recorded the uses of 278 Nepalese medicinal
plants (Subedi and Tiwari, 2000). Later compendia of herbal phar-macopoeias such as Chandra Nighantu and Nepali Nighantu werepublished in 19th and 20th century (Ghimire, 2008). The NepaliNighantu is an elaborated corpus with information on the traditionalknowledge of 750 medicinal plant species published by the RoyalNepal Academy in 1969 (IUCN, 2004). It is widely reported thatmedicinal plants are inseparable from Nepal's livelihoods, and havelong been collected, consumed, and conserved through indigenousknowledge (Singh et al., 1979). Current estimates suggest that inmany developing countries about two third of the population reliesheavily on traditional medicines and medicinal plants to meetprimary health care (Farnsworth and Soejarto, 1991).
Indigenous knowledge is often hailed for its versatility to recognizeand respond to the livelihood changes (Turner and Clifton, 2009) but ithas also been transformed by ecological and socio-cultural changes(Pirker et al., 2012). Palmer (2004) and Medeiros (2013) suggestthat ethnomedicine has continued to evolve after the shock of orig-inal contact, with a decreasing availability of indigenous medicinalplants and the introduction of new species (Albuquerque, 2006;
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jep
Journal of Ethnopharmacology
http://dx.doi.org/10.1016/j.jep.2015.01.0350378-8741/& 2015 Elsevier Ireland Ltd. All rights reserved.
n Corresponding author.E-mail address: [email protected] (R.M. Kunwar).
Journal of Ethnopharmacology 163 (2015) 210–219

Cadena-Gonzalez et al., 2013). Following Webb (1985), we consideredmedicinal plants which evolve naturally or have long been cultured,but are entirely independent to the human activity as indigenous. On aglobal scale, whether a species is native or non-native, is generallydetermined by one (or both) of two concepts: (i) presence in an areabefore an arbitrary cut-off date imparts native status and (ii) human-mediated movement of individuals results in nonnative status(Trudgen et al., 2012). The term native is synonymous to indigenousand more common in colloquial language (Schwartz, 1997). Thepresent study assesses the patterns of distribution and usage ofindigenous and non-indigenous medicinal plants, their habitats, andthe status of local traditional healers and healing traditions in farwestNepal. The dynamics of healing traditions and the species and habitatsutilized by them are discussed and the scope of secondary forests andnon-indigenous species is analyzed.
2. Study methods
2.1. Study area
Bajhang, Baitadi, Dadeldhura and Darchula districts (291010N to301150N/801030E to 811340E) represent the westernmost area ofNepal, with elevation ranges from 257 to 7132 m, and harborbioclimates from subtropical forests to alpine Betula-Rhododen-dron scrub (Elliott, 2012) within a varied topography (Devkota andKarmacharya, 2003; Pant and Panta, 2004). Dadeldhura andBaitadi districts represent the mid-elevational hills while Darchulaand Bajhang are mountainous districts (Lilleso et al., 2005). Mostof the area is arid, and access is difficult (Kunwar et al., 2012),resulting in isolation with a few government amenities andfrequent food deficiency (UNWFP, 2006). The local developmentindices are low, with frequent food and nutritional deficiencies,and shortage of supplies for basic needs (Chaudhary et al., 2010).Arable land is scarce (7–21%) and the cultivation of cereal cropsis least feasible (Jha et al., 1996). Due to variations in altitude,topography and bio-climate, the diversity of forest types andmedicinal plants and knowledge of their utilization varies widely.As mountainous districts, Bajhang and Darchula respectively haveonly 27% and 25% forests whereas the mid-elevational hill districtsBaitadi and Dadeldhura have 47% and 68%, respectively. Thestudied districts contain six forest ownership and managementtypes (national, protected, community, leasehold, religious, andprivate) but their extent varies. The largest cover of communityforest (69%) is found in Baitadi district, followed by 34% inDarchula, 20% in Dadeldhura and only 12% in Bajhang. Communityforests are restored and protected from exploitations since thesecond-growth vegetation developed and conserved by localforest users (Kunwar and Sharma, 2004). Community forests andtheir users of Sigas, Rameswor, Madhu, Bhumiraj and Trishuli ofBaitadi district; Shivsundari, Trishuli, Parshuram, and Siddhanathof Dadeldhura district; Dumling, Namjung, Tham and Brahmalekof Darchula district; and Hemantabada, Binayak and Lahare ofBajhang district were consulted. National forests were assessed atJogbudha and Deurali (Dadeldhura), Pancheswor and Melauli(Baitadi), Gokuleswor and Khar (Darchula) and Lataun and Deu-lekh (Bajhang). Local markets at Amargadhi and Bagarkot ofDadeldhura, Khalanga and Dumling of Darchula, Khodpe andPatan of Baitadi and Chainpur and Deura of Bajhang were assessed.
Upper Darchula district has much in common with Amaranth(Balick and Cox, 1996) and relict hemp cultures (Clarke, 2007) inother regions of Asia. A few remote villages of Dadeldhura districtare occupied by the Raute tribal group, who lives in and travelsbetween the Siwalik hills in the south and mountainous highlandsin the north and maintain livelihood by nomadic hunting andplant gathering (Manandhar, 1998; Fortier 2009). The major ethnic
groups of study area are Kshetri (450%), Brahmin (20%), Thakuri(7%), Kami (10%) and Sarki (8%). The first two groups are relativelyprivileged (Bennet, 2005), while the latter two are categorized asDalits in the socio-cultural class system of Nepal (Folmar, 2007).This allows Dalits a special access to opportunities provided by thegovernment (Daniel et al., 2012). Animal husbandry, seasonal cropproduction, collection and trade of medicinal plants and transhu-mance are the major livelihood strategies of these communities(Bhandari, 2013). Collection, usage and trade of medicinal plantsand their products are most important (Burlakoti and Kunwar,2008); however, medicinal plant collection is mostly carried out byDalits, which are also artisans (Cameron, 2009). The privilegedgroups engage in agriculture, animal husbandry and medicinal andaromatic plant cultivation and production.
2.2. Sampling, data collection and analysis
Before start of the fieldwork prior informed consent wasobtained at district, village, community and individual level, andplant collection permits were obtained from the respective autho-rities. After establishing consent with the participating entities,participant observations, discussions, walk-in-the-woods, inter-views and informal meetings were conducted during consecutiveannual field visits from May 2006 through June 2014. Sacredgrooves (Devisthans) were sparsely accessed. The field visits from2011 to 2014 focused especially on the dynamics of indigenousmedicines, use of indigenous and non-indigenous species, and theapplication of secondary habitats. Altogether 32 sites ranging from600 m (lowland) to an elevation of 3400 m were visited (Fig. 1)and 312 respondents were interviewed with the help of localassistants, using Nepali language questionnaires. The respondentsrepresented medicinal plant collectors, cultivators, traders, tradi-tional healers and the oldest persons of the villages.
After obtaining oral prior informed consent from the partici-pants, discussions were begun based on the checklists/inventorymethod (Mutchnick and McCarthy, 1997) employing visual cues(Alcorn, 1984). All species encountered during walk-in-the-woodswere free-listed (Quinlan et al., 2002), and the vouchers ofmedicinal plant species collected during the day were displayedin the evenings as discussion prompts. Informal meetings were heldduring the evening while staying with local communities, and at teavendors in the morning for information about ethnomedicinal plantspecies in decline or recently introduced in local pharmacopoeias.Plant species were collected, and the material was identified in theNational Herbarium and Plant Laboratories (KATH), Godawari,Lalitpur, Nepal as well as using voucher materials from MissouriBotanical garden (MO). Some of the material was lost while beingreturned to KATH. For the material stored in KATH the originalvoucher numbers are given in Supplementary Table 1. For all otherspecies the numbers of the MO vouchers used for identification aregiven. The plant species were collected following Cunningham(2001), and identified using ethnotaxonomic information andsecondary literature (Stainton and Polunin, 1984; Stainton, 1988).Local vernacular names were recorded (Singh, 2008). The housedherbarium specimens of 17 important medicinal plants (Kunwar etal., 2013, 2014) were reviewed to assess the distribution of speciesover time.
nowball sampling was employed for selecting healers, and villagecensus data and village secretaries were consulted to identify the fiveoldest people (Voeks, 2007) in the 12 villages for semi-structuredinterviews for cross-checking. The age range of the interviewee was70–85 years. The average Nepalese life expectancy is 65.8 years(WHO, 2010). Collaborators were asked about indigenous and non-indigenous botanicals, species decline, and species role in localpharmacopoeias. The use-value (UV) index was used to calculatethe citation of plants during interviews as proposed by Phillips and
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219 211

Gentry (1993) and adapted by Albuquerque et al. (2007). It iscalculated as follows:
UVc¼X
U=ns ð1Þ
where U is the sum of the total number of use citations by allinformants for a given species, divided by the total number ofinformants (ns). This method evaluates the relative importance (RI)of each medicinal plants based on its relative use among informants.
3. Results and discussion
3.1. Medicinal plants
We found a total of 258 plant species of 229 genera and 103families, of which 192 species were regarded as most useful(Supplementary Table 1). Fabaceae, Asteraceae and Rosaceae werethe dominant families, contributing 20, 15 and 11 species, respec-tively. A total of 66 ailments were treated by indigenous medicine,with dysentery, diarrhea, and skin problems receiving most atten-tion, with 24, 22, and 22 species used for treatment, respectively.Diarrhea and measles were the most common ailments in the studyarea (Government of Nepal, 2012). Among 192 useful species, 43%were herbs, 30% trees, 17% shrubs and 10% others. The highernumbers of herbs were recorded because they were more abundantand complementary to local vegetables, similar to the findings ofKosaka et al. (2013). A high presence of alkaloids, phenolic glycosides,and cyanogenic glycosides in herbs (Coley et al., 1985) makes themable to satisfy therapeutic treatments (Lyon and Hardesty, 2012).
Because the area is least suitable for staple cereal crops, localpeople have always heavily relied on locally available wild plants.Many not domesticated wild plants are important for local liveli-hoods (Cunningham, 2001), and are inseparable from indigenousfood and therapeutic systems (Etkin and Ross, 1982; Gessler et al.,1998). Dependence on the collection and trade of wild medicinalplants is high inwest Nepal (Bhattarai, 1992; Manandhar, 1998; Olsenand Larsen, 2003; Kunwar et al., 2013). Of about 1265 plant speciesfound inwestern Nepal (Rokaya et al., 2012), about 50% are subject totraditional use, often for medicine (Kunwar and Bussmann, 2008).The extensive usage of plants for indigenous medicines indicates thatthis is clearly an important part of culture.
Between 125 and 178 medicinal plants and products arecommercially sold in the country (Bhattarai and Ghimire, 2006;Srivastava, 2009), 51 species are traded from Humla district(Chaudhary et al., 2010), and 45 species are commonly found inmedicinal plant trade in study area. Sapindus mukorossi Gaertn.and Zanthoxylum armatum DC., both indigenous medicinals to thestudy area, are traded in the largest volume in both the study areaand Nepal. The estimated volume of annual medicinal plantcollection and trade for Nepal ranged from 480 to 2500 t before2003 (Olsen and Larsen, 2003), and was about 2700 t per annumin the last decade (Government of Nepal, 2013). Farwest Nepalcontributes about one third of the volume, and our study areaalone contributes about 20% of the national medicinal plant trade.Therefore the study area is important for medicinal plants, theirtrade and indigenous uses and management.
We found that the increase of collections of botanical materialswas clearly tied to increasing commerce. The medicinal plants
Fig. 1. Study area.
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219212

collected with highest preference for markets and local use wereOphiocordyceps sinensis (Berk) G.H.Sung, J.M.Sung, Hywel-Jones &Spatafor, Zanthoxylum armatum, Valeriana jatamansi Jones, Swertiachirayita H. Karst., Bergenia ciliata A. Br. ex Engl., all are indigenous.The households involved in Ophiocordyceps sinensis collection inDarchula district gathered 140 kg in 1998 to 1440 kg in 2004(Chhetri and Lodhiyal, 2008), and 4500 kg in 2008 (Pal, 2009)indicating the steady growth in commercial collection for gettingquick economic return. Yet the commercial collection of medi-cinal plants at lower part of study area (Baitadi and Dadeldhuradistricts) was dated back to a couple of decades (Bista and Webb,2006), the pursuit was historic to Bajhang and Darchula districts(Manzardo, 1977). Our results show that about 67% of the collec-tions were sold, and only about one third was domesticallyconsumed. The market and price differentials between wild andcultivated products, placing a premium on wild crafted species,encourage the premature collection, overexploitation and market-ing of indigenous medicinal plants. Overexploitation of wild andindigenous species resulting in threatened population was alreadyinto account (Kunwar et al., 2013; Shrestha et al., 2014). Multi-purpose species Abies spectabilis Mirb., Bergenia ciliata, Parispolyphylla Hand.-Mazz., Zanthoxylum armatum were in particulardemand. Abies leaf needles are sniffed for cough and cold and treesare logged for furniture and agricultural implements. The survivalof species with multiple uses as spices, condiments, medicines,tonic, etc. is clearly compromised because they fetch highermarket prices.
3.1.1. Botanical dynamicsFive indigenous species Cuscuta reflexa Roxb. (useful for asthma),
Angelica glauca Edgew. (for indigestion), Nigella sativa L. (for coughand cold), Euphorbia royleana Boiss. (for inflammations and eyecomplaints) and Nephrolepis cordifolia (L.) C. Presl. (as galactogogueand tonic) were reported as in fast decline. The UV was highest with43% for Nigella sativa for usage of cough and cold and 25% for Angelicaglauca for usage for indigestion. The older respondents indicated thatover lifetime some species like Aloe vera (L.) Burm. f., Ageratumconyzoides L., Ageratina adenophora (Spreng.) R.M. King & H. Rob.,Jatropha curcas L., Lantana camara L., Melia azedarach L. wereintroduced and incorporated in indigenous medicines. Principal usesfor non-indigenous species include animal forage, medicine, food,timber, and others similar to the findings of other ethnobotanicalsurveys (Blanckaert et al., 2007; Ayantunde et al., 2008). Previouslythere were tendencies to either overlook non-indigenous species infavor of indigenous ones or else not recognize them as important(Harris, 2010). Now they are gaining importance for local andindigenous traditions (Hu, 1990; Bennett and Prance, 2000). Wefound that the local population used 24 (12%) non-indigenous plantsin their indigenous medicines, of which Jatropha curcas, Ageratinaadenophora, Plumeria rubra L., Aloe vera, Ricinus communis L. wereused for multiple purposes. Similar studies elsewhere reported theuse of 15–44% of non-indigenous plants in traditional medicines(Hutchen, 1992; Parrotta, 2001; Geissler et al., 2002). Of 24 species, 14belong to four families (Asteraceae, Fabaceae, Euphorbiaceae andApocynaceae). The prevalence of Asteraceae and Fabaceae, especiallycommon in lower elevations, in local pharmacopoeias was alsopreviously reported (Prance and Plana, 1998; Bennett and Prance,2000; Janni and Bastien, 2004), and the high number of species ofAsteraceae with pharmacological and organoleptic properties isespecially noteworthy (Gottlieb et al., 1995; Milliken and Albert,1997). Moerman (1998) suggested that Asteraceae dominate tradi-tional pharmacopoeias as medicinal resources because their ten-dency to grow in secondary habitats near residential areas makes iteasier to collect them. Our findings supported the ecological appear-ance theory that states the most common and accessible species and
habitats are more valued (Phillips and Gentry, 1993; Thomas et al.,2009). It is believed that the more abundant a plant is, the moremedicinal virtues it may possess (Coe and Anderson, 1996). Sparsedistribution of indigenous species and easy access to non-indigenousones, compounded by the need to find for alternatives for species indecline and to treat new diseases, e.g. malaria due to the upwardsspread of mosquitoes, or more frequent food borne illnesses due tofailure of traditional storage methods under warmer conditions, leadto the increment in use of non-indigenous species (Humphreys,2014). Use of non-indigenous species is also consistent with theutilitarian redundancy hypothesis, which states that the use offunctionally similar species can be part of a strategy to maintainthe resilience of local knowledge (Albuquerque, 2006; Albuquerqueand Oliveira, 2007). Palmer (2004) anticipated a decrease of indi-genous plants in pharmacopoeias would lead to an accelera-ted capacity of indigenous peoples to integrate new and introducedplants in their pharmacopoeias (Diamond, 1997; Bennett and Prance,2000).
3.1.2. Species incorporationRichness of non-indigenous species and their introductions in
local pharmacopoeias were highest at lower elevations of studyarea, and the use of indigenous species was more common in highaltitude areas where wild crafting was often employed. Looking atnon-medicinal uses of plants provided first insights into thereason for introductions. Crosby (1972) noted that by 1600 AD,all of the important Old World food crops had been introduced tothe Americas, making them as of now available for secondary usesas medicines for nearly four centuries. This is also an analogy tothe fact that the therapeutic uses of plants were often character-ized with secondary value, showing their versatility. Many non-indigenous species were introduced for other reasons (Blanckaertet al., 2007) and the medicinal properties were discovered later.Non-indigenous species Jatropha curcas was introduced as a plantfor biofencing, and Ageratina adenophora, Plumeria rubra andLantana camara as ornamentals (Chapman and Le Maitre, 2001).Jatropha curcas (locally called Inna) seed oil is applied for arthritisand boils and bark is useful in skin problems. Flowers of Plumeriarubra (locally called Galaincha phool) are folkloric for indigestionand cholera. However, some non-indigenous species were intro-duced as medicine, especially Aloe vera (locally called Ghiukumari)and Ocimum gratissimum L. (locally called Bantulasi). Other non-indigenous species like Ageratum conyzoides, Acmella calva (DC.)R.K. Jansen, Cirsium verutum (D. Don.) Spreng., Cissampelos pareiraL., Datura stramonium L., Eclipta prostrata (L.) L., Elephantopusscaber L., Holarrhena pubescens Wall. ex G. Don., Ipomoea carneaJacq., Ricinus communis, and Xanthium strumarium L. were inad-vertently introduced and colonized in secondary sites (Kunwar,2003), and introduced as indigenous medicines over time. The useof non-indigenous species in traditional medicines in Darchulawas first reported by Joshi (2008). Besides their easy access (Voeks,1996; Pochettino et al., 2008), palatability (Albuquerque, 2006),reliability (Medeiros, 2013), ecological versatility (Van den Berg,1982; Stepp and Moerman, 2001), multiple usefulness of non-indigenous species explains their increasing incorporations else-where. The use of non-indigenous species is aided due to theireasy availability attributed to the growing abundance of anthro-pogenic and secondary habitats (Molares and Ladio, 2009). Thetotal richness of indigenous and non-indigenous species in phar-macopoeia reveals the dynamism of indigenous knowledge and anability to adjust the requirements. We observed that the accep-tance of non-indigenous plants was complementary to diversifythe stock of available plants (Alencar et al., 2010) and sometimesto fill the need to find alternatives for species in decline, and toheal new diseases that could not be treated using indigenous
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219 213

plants. The acceptance of non-indigenous species indicates cul-tural evolution and dynamic traditional knowledge systems andwas considered as an adaptive asset.
3.2. Habitats
We recorded 49.5% collections of medicinal plants from com-munity forests and 18.5% from government-managed forests.Community forests were thus the main sources of medicinal plantsand their products. Forests regenerating occurred largely throughnatural processes after human interferences are known as sec-ondary forests (Chokkalingam et al., 2000). In case of Nepal mostof the forests outside protected areas are secondary forests (Kaneland Shrestha, 2001). Community forests are anthropogenicallymanaged and characterized with a large variety of secondaryhabitats suitable for a number of species. Most of the speciesfound in community forests are introduced, non-indigenous(MoFSC, 2013) and managed or selectively relegated (Mikkola,2002), and nurtured for commercial purposes (Shrestha et al.,2010). High species collection from community forests can beattributed to the accessibility and species diversity due to thephysiography and elevational gradients. Community forests arelargely distributed in the mid-hills and temperate zone (1500–2500 m) (Adhikari et al., 2004), an elevation range known for apeak in plant species richness (Grytness and Vetaas, 2002) andhigh accessibility. We computed the database of indigenousmedicinal plants of West Nepal (Rokaya et al., 2012) and foundthat the distribution resembled the mid-elevation peak model at2000–2500 m as observed by Grytness and Vetaas (2002) (Fig. 2).
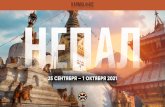
Secondary forests are gaining importance for medicinal plantcollection over time as old growth forests become overexploited(Fig. 3) (Salick et al., 1995; Chazdon and Coe, 1999). They are likelyto be increasingly used for ethnobotany and ethnomedicine asthey are easily accessible and pharmacologically rich (Kohn, 1992;Stepp and Moerman, 2001). Ethnobotanical studies in the Neo-tropics confirm that the second-growth habitats are rich inmedicinal plants and may be utilized more intensively by tradi-tional peoples (Toledo et al., 1995). Toledo et al. (1992) found thatprimary forests are tended to be concentrated for food and timberand the secondary forests for medicinal and other non-timberproducts. Our result however partially repudiated these findingsand indicated in farwest Nepal that the secondary forests were lessforaged by healers, despite their easy access. Primary forests andwild habitats, the use of indigenous species, and self-collectionswere priorities for healers, while laypeople rather favored acces-sible areas, secondary forests and non-indigenous species. It isfound that the accessible areas are primary considerations forgeneralists because they often start to collecting plants from easierand common sites and resort to less accessible and specific areas ifthe first attempts do not achieve the expected effects. It is there-fore validated that the indigenous communities use more primaryforests and indigenous species than do non-indigenous commu-nities (Prance, 1972), which show greater use of accessible areas,secondary vegetation, cultivated plants, and weed species (Voeks,1996). Yet there was no significant difference between districts,about three fourth of non-indigenous species were found to beintroduced at lower elevations (Dadeldhura and Baitadi districts).We hypothesized that the greater number of introductions of non-indigenous species at lower elevation could be the result ofpopulation migration (Maren et al., 2013) and preferences to thecommon species. Population density per square km was increasedfrom 117 to 165 in Baitadi, 56 to 92 in Dadeldhura, 38 to 57 inDarchula and 36 to 57 in Bajhang (Government of Nepal, 2012) sowe can deduce that the more heterogeneous the population, thehigher the non-indigenous species introductions.
Indigenous species are expected to be highly susceptible to achange in environmental conditions, and they are shifting upalong the altitudinal gradient as a response to climate changeand intrusion of non-indigenous species. Alterations of the dis-tribution range of indigenous medicinal plants (Abies spectabilis,Rhododendron arboreum Sm.) were already reported (Suwal, 2010;Gaire and Bhuju, 2010; Kunwar et al., 2014). The biogeographicinformation of plants showed an increase in altitude for collec-tions over time. The distribution records of species from loweraltitudes in earlier days and the subsequent records from thesuccessive higher altitudes were corroborated with distributionupshift; however the adjustment was species and plant typesspecific. We found the weakest upshift of distribution of semi-domesticated medicinal plants (Sapindus mukorossi (r2¼0.008),Zanthoxylum armatum (r2¼0.08), Swertia chirayita (r2¼0.02), etc.)than that of wild ones (Fritillaria cirrhosa D. Don. (r2¼0.29) andHippophae salicifolia D. Don. (r2¼0.28)) (Fig. 4). The upshift of wildspecies was the lowest for Betula utilis D. Don. (r2¼0.01) possiblybecause the species has restricted distribution (Shrestha et al.,2007). In our study area, Zanthoxylum armatum, Swertia chirayita,Sapindus mukorossi, Valeriana jatamansi, etc. are both in-situconserved and cultivated medicinal.
Because of the adjustments in distribution, some of the tradi-tional collecting sites of medicinal plants were found to no longercoincide with species distribution and the abilities of the harvest-ers to collect and use those plants was already limited. The growthsites of medicinal plants, particularly for collection of wild speciesand especially in high altitude areas were greatly diminishing.Early bud burst and changes in flowering in contrast to traditionalindigenous knowledge regarding climate change impacts werealso reported elsewhere (Salick and Byg, 2007; Cavaliere, 2009;Chaudhary and Bawa, 2011). These changes increased the impor-tance of the use of secondary resources and the collections fromsecondary and community forests. Since about half of the collec-tions were made from community forests, it is clear that the
R² = 0.63
0
60
120
180
240
300
360
420
480
540
600
0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000
No
of sp
ecie
s
Elevation (m asl)
Fig. 2. Distribution of medicinal plants resembled mid-elevation peak model.
Fig. 3. Degradation and over-exploitation of primary forest (Bajhang district).
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219214

community forests are important for local livelihoods, in particularfor the supply of indigenous medicines in farwest Nepal.
3.3. Healers
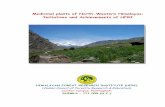
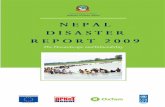
We found a 15% increase in medicinal plant collectors, produ-cers and traders in Darchula, Baitadi and Dadeldhura districtsduring the two study years. There were on average 1700 medicinalplant collectors, producers and traders in these districts in 2006and 2000 at the end of 2007. This increment in collection could beattributed to the lucrative business of high value medicinal plantsand supports from SAHAKARYA project of Canadian center ofInternational studies and Cooperation (CECI). The generalist orcommon collectors of medicinal plants were all family members oflocal farmers and traditional healers. However, the collectionswere varied across the sites, gender, age groups, species, productsand ethnic groups. Children (aged between 7 and 12) and oldpeople were involved in collection of low value medicinal plantsand products and from nearby and accessible areas. They didcollection while herding cattle and foraging (Figs. 5 and 6). Elderlypeople were very specific in collecting particular products atspecific locations. Most household heads that had been collectingplants/products since infancy used their children for support. Wefound that about 20% of the collectors were children, but theirinvolvement was limited, particularly to the private forests andfarmlands, lower elevations, and community forests. This indicatesthat accessible areas particularly the secondary sites are importantin supply of complementary medicinal plant products. Collectionfrom private forests has increased in Dadeldhura district(Maharjan and Joshi, 2007). Foraging high value medicinal plantsfrom wild forests and high altitude areas is however still persist-ing, and commonly practiced by experts.
The increase in collectors and traders may indicate an increas-ing market of herbal medicine. However, the number of profes-sional healers was decreasing fast (about 7% per annum). This wasconfirmed by the participating healers. There were on average 16traditional healers in each studied village in 2013 and 15 in 2014who all had learned the knowledge of healing during apprentice-ship. We found that about 16% of the healers had learned fromAyurvedic Baidhyas and more than 50% were descendants ofAyurvedic Baidhyas. About 30% of the healers were both descen-dants and apprentices of Ayurvedic Baidhyas. Ayurvedic Baidhyasare Ayurveda practitioners particularly of the western mid-hills ofNepal (Bhattarai, 1992). The declining number of healers might bethe consequence of Ayurvedic Baidhyas emigrating to the cities aswell as increasing access to modern medicine, and socio-acculturation. Only about 5% of the healers interviewed had learnthealing outside their native village. The number of people residingin rural areas changed from 95% in 1951 to 90% in 1981 (Goldsteinet al., 1983), and 80% in 2011 (Government of Nepal, 2012).Although farwest Nepal is less affected by migration, a continuousoutmigration for menial work in India (Maharjan, 2003; Poertner
et al., 2011) clearly accelerates a decline in the number of healersand associated indigenous knowledge, which in turn can giveincentive to use easily recognizable introduced species (Reiter,2001). The effects of outmigration are multi-fold: agriculturalfields are left fallow, lack of labor (Maren et al., 2013) anddecreased productivity (Bhandari, 2013). All these factors areinherent to the spread of non-indigenous species. Local healers,however, still favored indigenous species and showed higher
R² = 0.29
3000
3300
3600
3900
4200
4500
1965 1970 1975 1980 1985 1990 1995 2000
Alti
tude
(m a
sl)
R² = 0.28
2000
2500
3000
3500
4000
1970 1975 1980 1985 1990 1995 2000 2005
Alti
tude
(m a
sl)
Fig. 4. Herbarium collection records of Fritillaria cirrhosa and Hippophae salicifolia.
Fig. 5. Local women are on their way to collect medicinal plants (Bajhang district).
Fig. 6. Collection of non-indigenous medicinal plants from secondary habitats(along the trail and roadsides) (Bajhang district).
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219 215

preferences for wild habitats, self-crafted materials and self-processing to assure that they had the right materials, compositionand procedure. Laypeople mostly focused on secondary habitatsand easily recognizable introduced species (Figs. 5–7). If healerswere unable to collect their own plants, they relied on relatives orapprentices to collect for them, similar to the findings of Coe andAnderson (1996).
3.4. Healing traditions
Medicinal knowledge in the study area is made available viadifferent healing traditions such as tribal lore, home herbalremedies, and Baidhya, Ayurveda and Amchi systems. The formeris restricted to the Raute tribal group in study area (Manandhar,1998). Baidhya and home herbal remedies are indigenous tofarwest Nepal (Bhattarai, 1992; Kunwar et al., 2009) and are partlyinfluenced by the Ayurveda (Kunwar and Bussmann, 2008). Thetribal lore and home herbal remedies are considered folklore andshared orally and or informally among family members andsometimes among community members. In folklore, communitiesbelieve that illness reflects not only physical, but also psychologi-cal problems of an individual and consult for difficulties in therelationships with their families, communities, environment,crops, animals and universe. A total of 55% of the older partici-pants had learnt about the folklore from their predecessors andthe rest acquired the knowledge from both local healers and theirpredecessors in informal apprenticeships. Pant et al. (2005) statedthat there was huge knowledge gap between older and youngergeneration in Darchula district. Treatment of illnesses by homeherbal and Baidhya traditions is based on a holistic approach tocuring, addressing both the spiritual and physical needs of thepatient and its surroundings. Healers employ materials of biolo-gical and mineral origin but the plant materials predominate (Rautand Khanal, 2011). The wide use of Baidhya and home herbalremedies in farwest Nepal is also due to relatively homogenousresource users and less encroachment from immigrants.
The Baidhya healing tradition originated in the mid-hills offarwest Nepal (Bhattarai, 1992; Burlakoti and Kunwar, 2008), andadjoining areas of India (Kala, 2005). Although knowledge transferis manuscript based, it is informal and decreasing. The Baidhyahealing tradition relies on local medicinal plants and resources.Water and fire are extensively used (Mahat, 2013) as bothprincipal and secondary ingredients and catalysts. Water is usedas a solvent, and sometimes as a coolant. Fire is used to burn themedicines so that patients can inhale the smoke, and sometimesfor keeping the patients warm. In Baidhya tradition, the mainknowledge of healing is kept with some secrecy and is confined to
a few healers. It is generally believed among healers that themedicines would lose their efficacy if too many people know abouttheir use. Ayurveda and Amchi in contrast are scholarly systems(Gewali, 2008) following recorded theories, scripts and knowledgetransfer. There is one Ayurveda hospital in each district and oneAyurveda dispensary in between five villages providing Ayurvedicservices to the communities (Gewali, 2008). Amchi, the traditionalhealing system native to remote mountainous areas, is widelyaccepted and practiced throughout high altitude areas of Nepal(Lama et al., 2001), and also important in higher parts of Darchuladistrict. The Himalayan Amchi Association, an institution aimed atsafeguarding traditional health care knowledge, is devoted toprotect and strengthen the knowledge of Amchi healers (Craigand Bista, 2005). We found that most healing traditions wereincreasingly incorporating non-indigenous species and indicated ahigh level of constant experimentation whereas the Amchi tradi-tion was rather less flexible in application of non-indigenousspecies. The knowledge base for these traditions was stemmedfrom spirituality, customs, livelihood strategies, experimentation,and nearby resources. These traditions were less expensive andmore culturally integrated within trans-cultural environment andethnic traditions. Because of their ancient existence and use andcultural integrity, all these healing traditions are inseparable fromlocal culture (Singh et al., 1979; Bhattarai, 1992).
4. Conclusions
In far-western Nepal the use of introduced and secondaryresources as medicinals is gaining ground, as old growth forestbecome over-exploited and indigenous species decline. A total of24 non-indigenous plant species were found introduced in theindigenous medicinal system. Sparse distribution of indigenousspecies and easy access to non-indigenous ones, compounded bythe need to find for alternatives for species in decline, lead toincreasing use of non-indigenous species. Continuous outmigra-tion foments a decline in the number of healers and associatedindigenous knowledge. The decreasing knowledge of indigenousspecies again leads in turn to the application of easily availablenon-indigenous species. Secondary and community forests aregaining importance for medicinal plants collection, because oldgrowth forests become over-exploited. Their easy accessibility andhigh species diversity due to the physiography and elevationalgradients make them preferred collection sites. The application ofnon-indigenous species and secondary resources represents astrategy to diversify the indigenous medicinal repertoire, increas-ing the availability of complementary medicines, improving liveli-hoods and the environment, and offsetting the pressures onindigenous resources. The acceptance of introduced species isanalogous to cultural evolution and dynamic indigenous knowl-edge systems, and considered an adaptive asset.
Conflict of interests
Authors declare that there is no conflict of interest regardingthe publication of this paper.
Acknowledgments
The authors are grateful to all communities who participated inthe field works and dedicated a lot of time and efforts. GokarnaThapa and Madan Suwal are acknowledged for editing GPS geo-coordinates and preparing study area map and Narad Rijal forlanguage editing. Authors express thanks to anonymous reviewers
Fig. 7. Local level processing of medicinal plants by a Baidhya for indigenousmedicines (Baitadi district).
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219216

for their critical remarks on the paper. Author RMK is thankful toWLBC, Missouri Botanical Garden, Garden Club of America, andAnne S. Chatham Fellowship, USA, for providing supports for fieldworks. Authors RMK, RPA and CLC are also thankful to ICIMOD andCECI, Nepal for providing various supports for field visits.
Appendix A. Supporting information
Supplementary data associated with this article can be found inthe online version at http://dx.doi.org/10.1016/j.jep.2015.01.035.
References
Adhikari, B., Di Falco, S., Lovett, J.C., 2004. Household characteristics and forestdependency: evidence from common property forest management in Nepal.Ecological Economics 48, 245–257.
Albuquerque, U.P., 2006. Re-examining hypotheses concerning the use and knowl-edge of medicinal plants: a study in Caatinga vegetation of NE Brazil. Journal ofEthnobiology and Ethnomedicine 2, 30.
Albuquerque, U.P., Oliveira, R.F., 2007. Is the use-impact on native Caatinga speciesin Brazil reduced by the high species richness of medicinal plants? Journal ofEthnopharmacology 113, 156–170.
Albuquerque, U.P., Medeiros, P.M., Almeida, A.L., Monteiro, J.M., Linsneto, E.M.F.,Melo, J.G., Santos, J.P., 2007. Medicinal plants of the Caatinga semi-aridvegetation of NE Brazil: a quantitative approach. Journal of Ethnopharmacology114, 325–354.
Alcorn, J.B., 1984. Huastec Mayan Ethnobotany. University of Texas Press, Austin,Texas.
Alencar, N.L., Araújo, T.A.S.A., Amorim, E.L.C., Albuquerque, U.P., 2010. The inclusionand selection of medicinal plants in traditional pharmacopoeias – evidence insupport of the diversification hypothesis. Economic Botany 64, 68–79.
Ayantunde, A., Briejer, M., Hiernaux, P., Udo, H., Tabo, R., 2008. Botanical knowledgeand its differentiation by age, gender and ethnicity in Southwestern Niger.Human Ecology 36, 881–889.
Balick, M.J., Cox, P.A., 1996. Plants, People and Culture: The Science of Ethnobotany.Scientific American Library, New York (229 p.).
Bennet, L., 2005. Gender, caste and ethnic exclusion in Nepal: following the policyprocess from analysis to action. In: Proceedings of the Paper Presented at NewFrontiers of Social Policy: Development in a Globalizing World Conference,Arusha, Tanzania. ⟨http://siteresources.worldbank.org/INTRANETSOCIALDEVELOPMENT/Resources/Bennett.rev.pdf⟩.
Bennett, B.C., Prance, G.T., 2000. Introduced plants in the indigenous pharmaco-poeia of Northern South America. Economic Botany 54, 90–102.
Bhandari, G., 2013. Effect of rainfall on the yield of major cereals in Darchula districtof Nepal. International Journal of Environment 3 (1), 205–213.
Bhattarai, K.R., Ghimire, M., 2006. Commercially important medicinal and aromaticplants of Nepal and their distribution pattern and conservation measure alongthe elevation gradient in Himalayas. Banko Janakari 16 (1), 3–13.
Bhattarai, N.K., 1992. Medical ethnobotany in Karnali zone, Nepal. Economic Botany46 (3), 257–261.
Bista, S., Webb, E.L., 2006. Collection and marketing of non-timber forest productsin farwestern hills of Nepal. Environmental Conservation 33 (3), 244–255.
Blanckaert, I., Vancraeynest, K., Swennen, R.L., Espinosa–García, F.J., Piñero, D., Lira–Saade, R., 2007. Non-crop resources and the role of indigenous knowledge insemi-arid production of Mexico. Agriculture, Ecosystems and Environment 119,39–48.
Burlakoti, C., Kunwar, R.M., 2008. Folk herbal medicines of Mahakali watershed,Nepal. In: Jha, P.K., Karmacharya, S.B., Chettri, M.K., Thapa, C.B., Shrestha, B.B.(Eds.), Medicinal Plants in Nepal: An Anthology of Contemporary Research.Ecological Society, Nepal, pp. 187–193.
Cadena-Gonzalez, A.L., Sorensen, M., Theilade, I., 2013. Use and valuation of nativeand introduced medicinal plant species in Campo Hermosa and Zetaquira,Colombia. Journal of Ethnobiology and Ethnomedicine 9, 23.
Cameron, M.M., 2009. Untouchable healing: a dalit Ayurvedic doctor from Nepalsuffers his country's ills. Medical Anthropology: Cross-Cultural Studies inHealth and Illness 28, 235–267. http://dx.doi.org/10.1080/01459740903070865.
Cavaliere, C., 2009. The effects of climate change on medicinal and aromatic plants.Herbalgram 81, 44–57.
Chapman, R.A., Le Maitre, D.C., 2001. Scenarios for Alien Invading Woody Plants(Research Report No. 907/1/01). Water Research Commission, Pretoria.
Chaudhary, P., Bawa, K.S., 2011. Local perceptions of climate change validated byscientific evidence in the Himalayas. Biology Letters 7 (5), 767–770.
Chaudhary, R.P., Shrestha, K.K., Jha, P.K., Bhatta, K., 2010. Kailash Sacred LandscapeConservation Initiative Feasibility Assessment Report. ICIMOD and CentralDepartment of Botany, Tribhuvan University, Kathmandu, Nepal.
Chazdon, R.L., Coe, F.G., 1999. Ethnobotany of woody species in second-growth, old-growth and selectively logged forests of Northeastern Costa Rica. ConservationBiology 13 (6), 1312–1322.
Chhetri, R., Lodhiyal, L.S., 2008. Collection of Ophiocordyceps sinensis and itsimplication to rural livelihood and biodiversity conservation: a case of
Darchula, Nepal. In: Jha, P.K., Karmacharya, S.B., Chettri, M.K., Thapa, C.B.,Shrestha,B.B. (Eds.), Medicinal Plants in Nepal: An Anthology of Contemporary Research.Ecological Society, Nepal, pp. 214–223.
Chokkalingam, U., De Jong, W., Smith, J., Sabogal, C., 2000. Tropical secondaryforests in Asia: introduction and synthesis. In : Proceedings of the PaperPrepared for “Tropical Secondary Forests in Asia: Reality and PerspectivesWorkshop”, CIFOR, Indonesia, April 10–14, 2000.
Clarke, R.C., 2007. Traditional cannabis cultivation in Darchula district, Nepal –
seed, resin and textiles. Journal of Industrial Hemp 12 (2), 19–42. http://dx.doi.org/10.1300/J237v12n02_03.
Coe, F.G., Anderson, G.J., 1996. Ethnobotany of the garifuna of Eastern Nicaragua.Economic Botany 50 (1), 71–107.
Coley, P.D., Bryant, J.P., Chapin III, F.S., 1985. Resource availability and plantherbivore defense. Science 230, 895–899.
Craig, S., Bista, G., 2005. Himalayan healers in transition: professionalization,identity and conservation among practitioners of gso rig pa in Nepal. In:Thomas, Y.A., Karki, M., Gurung K., Parajuli, D., (Eds.), Proceeding of WisePractices and Experimental Learning in Conservation and Management ofHimalayan Medicinal Plants, Kathmandu, pp. 411–433.
Crosby Jr., A., 1972. The Colombian Exchange: Biological and Cultural Consequencesof 1492. Greenwood Press, Westport, CT.
Cunningham, A.B., 2001. Applied Ethnobotany, People, Wild Plant Use andConservation. Earthscan Publishing Limited, London p. 300.
Daniel T., Hasham, N., Lanning, K., Shintani, M., Yadav, V., 2012. Health is Wealth:Health Care Access for Dalit Communities in Saptari, Nepal, SAMATA Founda-tion ⟨https://sipa.columbia.edu/sites/default/files⟩.
Devkota, R., Karmacharya, S.B., 2003. Documentation in Indigenous knowledge ofmedicinal plants in Gwallek VDC, Baitadi, Nepal. Botanica Orientalis 3, 135–143.
Diamond, J., 1997. Guns, Germs, and Steel: The Fate of Human Societies. WWNorton and Co., New York.
Elliott, A., 2012. Botanical Exploration of Darchula District, Farwest Nepal. ScottishRock Garden Club, Royal Botanic Garden Edinburgh, The University of Edin-burgh, Edinburgh, UK.
Etkin, N.L., Ross, P.J., 1982. Food as medicine and medicine as food: an adaptiveframework for interpretation of plant utilization among Hausa of NorthernNigeria. Social Science and Medicine 16, 1559–1573.
Farnsworth, N.R., Soejarto, D.D., 1991. Global importance of medicinal plants. In:Akerele, O., Heywood, V., Synge, H. (Eds.), The Conservation of Medicinal Plants.Cambridge University Press, Cambridge, UK, pp. 25–51.
Folmar, S., 2007. Identity politics among Dalits in Nepal. Himalaya 27, 41–53.Fortier, J. (Ed). 2009. Kings of the forests, the cultural resilience of Himalayan
hunter- gatherers. University of Hawaii Press, Honolulu, USA, p. 215.Gaire, N.P., Bhuju, D.R., 2010. Tree Line Dynamics With Climate Change: a Study in
Manaslu Region, Nepal Himalaya. Report. Nepal Academy of Science andTechnology, Nepal.
Gessler, M., Hodel, U., Eyzaguirre, P.B., 1998. Home Gardens and Agro-biodiversity:Current State of Knowledge with Reference to Relevant Literature (IPGRI HomeGardens Project Document). IPGRI, Rome, Italy.
Geissler, P.W., et al., 2002. Medicinal plants used by Luo mothers and children inBondo district, Kenya. Journal of Ethnopharmacology 83, 39–54.
Gewali, M.B., 2008. Aspects of Traditional Medicine in Nepal. Institute of NaturalMedicine, University of Toyama, Japan (175 p.).
Ghimire, S.K., 2008. Medicinal plants in Nepal Himalaya: current issues,sustainable harvesting, knowledge gaps and research priorities. In: Jha, P.K.,Karmacharya, S.B., Chettri, M.K., Thapa, C.B., Shrestha, B.B. (Eds.), MedicinalPlants in Nepal: An Anthology of Contemporary Research. Ecological Society,Nepal, pp. 25–42.
Goldstein, M., Ross, J., Schuler, S., 1983. From a mountain/rural to a plains/urbansociety: implications of the 1981 Nepalese consensus. Mountain Research andDevelopment 3, 61–64.
Government of Nepal, 2012. National Population and Housing Census 2011(National Report). Vol. 1. Central Bureau of Statistics, Government of Nepal,Kathmandu.
Government of Nepal, 2013. Hamro Ban (Our Forests). Annual Publication. Depart-ment of Forests, Government of Nepal, Kathmandu.
Gottlieb, O.R., Borin, D.R., Bosisio, B.M., 1995. Chemosystematic clues for the choiceof medicinal and food plants in Amazonia. Biotropica 27 (3), 401–406.
Grytness, J.A., Vetaas, O.R., 2002. Species richness and altitude: a comparisonbetween null models and interpolated plant species richness along theHimalayan altitudinal gradient, Nepal. The American Naturalist 159 (3),294–304.
Harris, S., 2010. Non-native plants and their medicinal uses. In: Hsu, E., Harris,S. (Eds.), Plants, Health and Healing on the Interface of Ethnobotany andMedical Anthropology. Berghan Book, NY, pp. 53–82.
Hu, S.Y., 1990. History of the introduction of exotic elements into traditionalChinese medicine. Journal of the Arnold Arboretum 71, 487–526.
Humphreys, G., 2014. Reframing climate change as a health issue. Bulletin of theWorld Health Organization 92, 551–552.
Hutchen, A.R., 1992. A Handbook of Native American Herbs. Shambala, London.IUCN, 2004. National Register of Medicinal and Aromatic Plants. IUCN, Nepal,
Kathmandu (161 p.).Janni, K.D., Bastien, J.W., 2004. Exotic botanicals in the Kallawaya pharmacopoeia.
Economic Botany 58 (Suppl.), S274–S279.
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219 217

Jha, P.K., Shrestha, K.K., Upadhyay, M.P., Stimart, D.P., Spooner, D.M., 1996. Plantgenetic resources of Nepal: a guide for plant breeders of agriculture, horticul-ture and forestry crops. Euphytica 87 (3), 189–210.
Joshi, K.R., 2008. Ethnomedicinal uses of plants: a case study of Sharmoli VDC,Darchula, Nepal. In: Jha, P.K., Karmacharya, S.B., Chettri, M.K., Thapa, C.B.,Shrestha, B.B. (Eds.), Medicinal Plants in Nepal: An Anthology of ContemporaryResearch. Ecological Society, Nepal, pp. 178–187.
Kala, C.P., 2005. Current status of medicinal plants used by traditional Baidhya inUttaranchal state of India. Journal of Ethnobotany Research & Applications 3,267–278.
Kanel, K.R., Shrestha, K., 2001. Tropical secondary forests in Nepal and theirimportance to local people. Journal of Tropical Forest Science 13 (4),691–704.
Kohn, E.O., 1992. Some observations on use of medicinal plants from primary andsecondary growth by the Runa of eastern Ecuador. Journal of Ethnobiology 12,141–152.
Kosaka, Y., Xayvongsa, L., Vilayphone, A., Chanthavong, H., Takeda, S., Kato, M., 2013.Wild edible herbs in paddy fields and their sale in a mixture in HouaphanProvince, the Lao People's Democratic Republic. Economic Botany 67,335–349.
Kunwar, R.M., 2003. Invasive alien plants and Eupatorium: Biodiversity andlivelihood. Himalayan Journal of Sciences 1 (2), 129–133.
Kunwar, R.M., Bussmann, R.W., 2008. Ethnobotany in the Nepal Himalaya. Journalof Ethnobiology and Ethnomedicine 4, 24.
Kunwar, R.M., Sharma, S., 2004. Quantitative analysis of tree species in twocommunity forests of Dolpa district, Nepal. Himalayan Journal of Sciences 2(3), 23–28.
Kunwar, R.M., Shrestha, K, Dhungana, S.K., Shrestha, P.R., Shrestha, K.K., 2010. Floralbiodiversity of Nepal: an update. Journal of Natural History Museum 25,295–311.
Kunwar, R.M., Mahat, L., Sharma, L.N., Shrestha, K.P., Kominee, H., Bussmann, R.W.,2012. Underutilized plant species in farwest Nepal. Journal of Mountain Science9, 589–600 (DOI: 10.1007/s11629-012-2315-8).
Kunwar, R.M., Mahat, L., Acharya, R.P., Bussmann, R.W., 2013. Medicinal plants,traditional medicine, markets and management in far-west Nepal. Journal ofEthnobiology and Ethnomedicine 9, 24.
Kunwar, R.M., Pandey, M.L., Mahat Kunwar, L., Bhandari, A., 2014. Medicinal plantsand ethnomedicine in Peril: a case study from Nepal Himalaya. Evidence-BasedComplementary and Alternative Medicine 7, 10.1155/2014/792789.
Kunwar, R.M., Uprety, Y., Burlakoti, C., Chowdhary, C.L., Bussmann, R.W., 2009.Indigenous use and ethnopharmacology of medicinal plants in farwest Nepal.Journal of Ethnobotany Research & Applications 7, 5–28.
Lama, Y.C., Ghimire, S.K., Thomas, Y.A., 2001. Medicinal Plants of Dolpo: Amchis'Knowledge and Conservation. People and Plants Program and WWF Nepal,Kathmandu (150 p.).
Lilleso, J.B., Shrestha, T.B., Dhakal, L.P., Nayaju, R.P., Shrestha, R., 2005. The map ofpotential vegetation of Nepal: a forestry/agroecological/biodiversity classifica-tion system. Forest & Landscape Development and Environment Series 2 andCFC-TIS Document Series 110.
Lyon, L., Hardesty, L., 2012. Quantifying medicinal plant knowledge among non-specialist Antanosy villagers in southern Madagascar. Economic Botany 66,1–12.
Maharjan, K.L., 2003. Peasantry in Nepal: A Study on Subsistence Farmers and TheirActivities Pertaining to Food Security. Research Center for Regional Geography,Hiroshima, Japan.
Maharjan, K.L., Joshi, N.P., 2007. A Poverty Analysis in Baitadi District, RuralFarwestern Hills of Nepal: An Inequality Decomposition Analysis. GraduateSchool for International Development, Hiroshima University.
Mahat, L., 2013. Dalits and Their Traditional Medicinal Practices in Bhanu VDCof Tanahun District, Western Nepal (Dissertation). Tribhuvan University,Kathmandu.
Malla, S.B., Shakya, S.R., 1984. Medicinal plants of Nepal. In: Majupuria, T.C. (Ed.),Nepal Natures' Paradise. White Lotus Ltd., Bangkok, Thailand, pp. 261–297.
Manandhar, N.P., 1998. Native phytotherapy among the Raute tribe of Dadeldhuradistrict, Farwest Nepal. Journal of Ethnopharmacology 60, 199–206.
Manzardo, A.E., 1977. Ecological constraints on trans-Himalayan trade in Nepal.Contributions to Nepalese Studies 4, 63–81.
Maren, I., Bhattarai, K.R., Chaudhary, R.P., 2013. Forest ecosystem services andbiodiversity: the resource flux from forests to farms in the Himalayas. TechnicalReport, Kathmandu, Nepal.
Medeiros, P.M., 2013. Why is change feared? Exotic species in traditional pharma-copoeias. Ethnobiology and Conservation 2, 3.
Mikkola, K., 2002. Community Forestry's Impacts on Biodiversity Conservation inNepal (M.Sc. thesis). Imperial College at Wye, University of London, UK.
Milliken, W., Albert, B., 1997. The use of medicinal plants by the Yanomami Indiansof Brazil. Economic Botany 51 (3), 264–278.
Moerman, D.E., 1998. Native North American food and medicinal plants: episte-mological considerations. In: Etkin, N.L., Harris, D.R., Houghton, P.J., Prender-gast, H.D.V. (Eds.), Plants for Food and Medicine. Royal Botanical Gardens, UK,pp. 69–74.
MoFSC, 2013. Invasion and colonization of alien species: a threat or benefits inNepal. In: Nepal Policy Brief, REDD-Forestry and Climate Change Cell, Ministryof Forest and Soil Conservation, www.mofsc-redd.gov.np.
Molares, A.L.S., Ladio, A., 2009. Ethnobotanical review of the Mapuche medicinalflora: use patterns on a regional scale. Journal of Ethnopharmacology 122,251–260.
Mutchnick, P.A., McCarthy, B.C., 1997. An ethnobotanical analysis of the tree speciescommon to the subtropical moist forest of the Peten, Guatemala. EconomicBotany 51, 158–183.
Olsen, C.S., Larsen, H.O., 2003. Alpine medicinal plant trade and Himalayanmountain livelihood strategies. The Geographical Journal 169, 243–254.
Pal, T.B., 2009. A Study on Ophiocordyceps sinensis (Yarsagumba) Collection inDarchula District of Nepal (MSc thesis). Central Department of Economics,Tribhuvan University, Kathmandu.
Palmer, C., 2004. The inclusion of recently introduced plants in the Hawaiianethnopharmacopoeia. Economic Botany 58 (Suppl.), S280–S293.
Pant, S.R., Panta, I.R., 2004. Indigenous knowledge on medicinal plants in BhagawatiVDC, Darchula, Nepal. Botanica Orientalis 4, 79–81.
Pant, S.R., Dhami, N.R., Panta, I.R., 2005. Wild edible plants of Lekham area,Darchula, Farwestern Nepal. Scientific World 3, 73–77.
Parrotta, J.A., 2001. Healing Plants of Peninsular India. CABI Publishing, Wallingford.Phillips, O., Gentry, A.H., 1993. The useful plants of Tambopata, Peru: II. Additional
hypothesis testing in quantitative ethnobotany. Economic Botany 47 (1),33–43.
Pirker, H., Haselmair, R., Kuhn, E., Schunko, C., Vogl, C.R., 2012. Transformation oftraditional knowledge of medicinal plants: the case of Tyroleans (Austria) whomigrated to Australia, Brazil and Peru. Journal of Ethnobiology and Ethnome-dicine 8, 44.
Pochettino, M.L., Arenas, P., Sanchez, D., Correa, R., 2008. Conocimiento botanicotradicional, circulacion comercialy consumo de plantas medicinales en un areaurbana de Argentina. Boletin Latinoamericano y del Caribe de Plantas Medici-nalesy Aromaticas 7 (3), 141–148.
Poertner, E., Junginger, M., Muller-Boker, U., 2011. Migration in farwest Nepal.Critical Asian Studies 43, 23–47.
Prance, G.T., Plana, V., 1998. The use of alien plants in tropical South American folkmedicines. In: Etkin, N.L., Harris, D.R., Houghton, P.J., Prendergast, H.D.V. (Eds.),Plants for Food and Medicine. Royal Botanical Gardens, UK, pp. 185–200.
Prance, G.T., 1972. An ethnobotanical comparison of four tribes of AmazonianIndians. Acta Amazonica 2 (2), 7–27.
Quinlan, M.B., Quinlan, R.J., Nolan, J.M., 2002. Ethnophysiology and herbal treat-ments of intestinal worms in Dominica, West Indies. Journal of Ethnopharma-cology 80, 75–83.
Raut, B., Khanal, D.P., 2011. Present status of traditional healthcare system in Nepal.International Journal of Recent advances in Physics 2 (3), 876–882.
Reiter, P., 2001. Climate change and mosquito-borne disease. Environmental HealthPerspectives. 109 (Suppl. 1), S141–S161.
Rokaya, M.B, Munzbergova, Z., Timsina, B., 2010. Ethnobotanical study of medicinalplants from the Humla district of western Nepal. Journal of Ethnopharmacology130 (3), 485–504.
Rokaya, M.B., Munzbergova, Z., Shrestha, M.R., Timsina, B., 2012. Distributionpatterns of medicinal plants along an elevational gradient in central Himalaya,Nepal. Journal of Mountain Science 9, 201–213.
Salick, J., Byg, A., 2007. Indigenous Peoples and Climate Change. Tyndall Centre,Oxford, UK..
Salick, J., Mejia, A, Anderson, T., 1995. Non-timber forest products integrated withnatural forest management, Rio San Juan, Nicaragua. Ecological Applications 5,878–895.
Schwartz, M.W., 1997. Defining indigenous species: an introduction. In: Luken, J.O.,Thieret, J.W. (Eds.), Assessment and Management of Plant Invasion. Springer-Verlag, New York, pp. 7–16.
Shrestha, U.B., Shrestha, B.B., Shrestha, S., 2010. Biodiversity conservation incommunity forests of Nepal: rhetoric and reality. International Journal ofBiodiversity and Conservation 2 (5), 98–104.
Shrestha, N., Prasai, D., Shrestha, K.K., Shrestha, S., Zhang, Z.C., 2014. Ethnomedic-inal practices in the highlands of central Nepal: a case study of Syaphru andLangtang village in Rasuwa district. Journal of Ethnopharmacology 155,1204–1213.
Shrestha, B.B., Ghimire, B., Lekhak, H.D., Jha, P.K., 2007. Regeneration of treelinebirch (Betula utilis) forest in a trans-Himalayan dry valley in central Nepal.Mountain Research and Development 27 (3), 259–267.
Singh, H., 2008. Importance of local names of some useful plants in ethnobotanicalstudy. Indian Journal of Traditional Knowledge 7 (2), 365–370.
Singh, M.P., Malla, S.B., Rajbhandari, S.B., Manandhar, A., 1979. Medicinal plants ofNepal – retrospects and prospects. Economic Botany 33 (2), 185–198.
Srivastava, D., 2009. Resources of Nepalese medicinal and aromatic plants: statusand development. Plant Resources 31, 127–131.
Stainton, A., 1988. Flowers of the Himalaya: A Supplement. Oxford University Press,New Delhi, India (86 p.).
Stainton, A., Polunin, O., 1984. Flowers of the Himalaya. Oxford University Press,New Delhi, India (580 p.).
Stepp, J.R., Moerman, D.E., 2001. The importance of weeds in ethnopharmacology.Journal of Ethnopharmacology 75, 19–23.
Subedi, K.R., Tiwari, N.N., 2000. Shausruta Nighantu (in Sanskrit). MahendraSanskrit University, Nepal.
Suwal, M.K., 2010. Tree species line advance of Abies spectabilis in ManasluConservation Area, Nepal Himalaya (M.S. thesis). Central Department of Botany,Tribhuvan University, Kathmandu, Nepal.
Thomas, E., Vandebroek, I., Goetghebeur, P., Sanca, S., Arrazola, S., Van Damme, P.,2008. The relationship between plant use and plant diversity in the BolivianAndes, with special reference to medicinal plant use. Human Ecology 36 (6),861–879.
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219218

Thomas, E., Vandebroek, I., Van Damme, P., Goetghebeur, P., Douterlungne, D.,Sanca, S., Arrazola, S., 2009. The relation between accessibility, diversity andindigenous valuation of vegetation in the Bolivian Andes. Journal of AridEnvironment 73, 854–861.
Toledo, V.M., Batis, A.I., Bacerra, R., Martinez, E., Ramos, C.H., 1995. La silva util:ethnobotanica cuantitativa de los grupos indigenas del tropico humido deMexico. Interciencia 20, 177–187.
Toledo, V.M., Batis, A.I., Becerra, R., Martínez, R., 1992. Products from the tropicalrain forests of Mexico: an ethnoecological approach. In: Plotkin, M., Famolare, L.(Eds.), Sustainable Harvest and Marketing of Rainforest Products. Island Press,Covelo, California, pp. 99–109.
Trudgen, M.S., Webber, B.L., Scott, J.K., 2012. Human-mediated introduction ofLivistona palms into central Australia, conservation and management implica-tions. Proceedings of the Royal Society B 279 (1745), 4115–4117.
Turner, N.J., Clifton, H., 2009. It's so different today: climate change and indigenouslife ways in British Columbia, Canada. Global Environmental Change 19 (2),180–190.
UNWFP, 2006. Food Security Bulletin: No. 15. UNWFP, Nepal (October 2006).Van den Berg, M.E., 1982. Plantas medicinais na Amazonica: Contdbuiq�o ao seu
conhecimento sistemitico. Conselho Nacional de Desenvolvimento Cientffico eTecnol6gico, PTU/MPEG, Bel6m.
Voeks, R.A., 1996. Tropical forest healers and habitat preference. Economic Botany50, 381–400.
Voeks, R.A., 2007. Are women reservoirs of traditional plant knowledge? Gender,ethnobotany and globalization in northeast Brazil. Singapore Journal of TropicalGeography 28, 7–20.
Webb, D.A., 1985. What are the criteria for presuming native status? Watsonia 15,231–236.
WHO, 2010. Nepal Health Profile World Health Organization data. ⟨http://www.Worldlifeexpectancy.com⟩ (accessed 26.06.14.).
R.M. Kunwar et al. / Journal of Ethnopharmacology 163 (2015) 210–219 219