
Medical Journal of Shree Birendra Hospital
55
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Medical Journal of Shree Birendra Hospital




1
1Dr Namrata Rawal, Consultant Neuropsychiatrist,2 Dr Praswas Thapa, Consultant Neuropsychiatrist,3Dr Yadav Bista, Head of Dept, Department of Neuropsychiatry, Shree Birendra Hospital, Kathmandu, Nepal
AbstractObjectives: Psychiatric consequences are very common following RTA. The study is sought to identify the prevalence of psychiatric morbidity (e.g. depressive symptoms, anxiety symptoms and symptoms related to PTSD(Post Traumatic Stress Disorder) following injury sustained
victims and psychiatric symptoms.Methods: The 102 (male=83,female=19) patients were interviewed using a questionnaire to collect the socio- demographic data, the Self Rating Questionnaire (SRQ) -Beck Depression Inventory(BDI),Beck Anxiety Inventory(BAI) and the Impact of Event Scale -Revised (IES-R). Patients were prospectively followed up for 1 month. Patients were aged between 20-69 years. The impact of injury was assessed by ISS (Injury Severity Scale) and ABI (Abbreviated injury Scale).Results:The mean age was 33.93 years (range 20-69). Overall, the prevalence rate o of Anxiety symptoms-19.6%, depressive symptoms-21.6% and PTSD symptoms-35.3%.Females had a higher rate of PTSD symptoms 52.6% (n = 10), compared to the males 31.3% (n=26). The majority of those with PTSD (47.2%) were young, 20 - 29 years.
symptoms 51% and then anxiety symptoms30.4%. The symptoms gradually reduced in the fourth week to PTSD - 35.3%, depression- 21.6% and anxiety-19.6%. The study also showed higher scales of psychiatric symptoms in major injuries in comparison to minor injuries showing direct correlation of psychiatric morbidity with severity of injury.Conclusion: Psychiatric symptoms are frequent and severe after major injuries and less severe after minor RTA. Psychopathology following injury is a frequent and persistent occurrence. Early information and advice might reduce psychological distress and symptoms.
Introduction
Motor vehicle accidents therefore are a
may occur even in those who have not suffered physical injuries. (1, 2)
on stress TS with only a
few maj and anxie ty. W l and pop
some of this vari in
this may also to the (3)
involving drivers, passengers, pedestrians or cyclist. The term ‘accident’ erroneously suggests that all collisions are random (unpredictable) and accidental (unpreventable). (4)
Injury is a disease resulting from an interaction of agent, host and environment. Once a person enters a health system for treatment of an injury, only then it is considered a health problem. (5) Injury now ranks among the leading causes of morbidity and mortality
as the primary cause of disease among children in the age group of 5 to 14 years, and the third leading cause among people between the ages of 15 to 29 years in 2000.
There is an increasing realization that trauma can have marked and sustained psychological effects. Up to 25% of severely injured patients experience
some patients these reactions can be long lasting and have profound adverse effects on quality of life. Those
effective treatment can be administered. (6)
In Nepal fall from a height accounting for the
Address for correspondence: [email protected]

2
accident is the commonest cause males are involved twice as the females which may be because males are being exposed to the risks of accidents. (7)
The motor vehicle accidents are the single
post traumatic stress disorder (PTSD).(8) Prevalence of PTSD following MVA, ranges from 10% (8) to 46% . (9)
In another study by (10) reported that most of
accidents in Nepal. However there are few studies related to accidents and injuries. But there are many studies in Western and European countries. In a study it is reported that in Nepal 61.5% of spinal injuries are due
to many factors like overcrowded roads, poor conditions of roads etc. (11) Thus the present study is an attempt to identify the prevalence psychiatric consequences
that some guidelines may be developed in future for the
with other departments.
Whiplash injuries commonly occur in road
somatic symptoms. (12) These somatic symptoms often accompanied by psychological symptoms such as initial ‘shock’ ‘dazed feeling, anxiety, anger. Depression,
libido altered appetite and weight, and in some cases, feeling of helplessness horror, despair and reliving experiences.(13) In severe cases where there has been an accompanying head injury with loss of consciousness, similar disorder may occur but post traumatic stress disorders appear to be less frequent. (14) Personality changes and cognitive impairment may occur following countercoup and penetrating head injuries. (15)
Patients with posttraumatic stress disorder experience disabling memories and anxiety related to
leading cause of post-traumatic stress disorder since Vietnam War. (16)
The primary psychosocial consequences of Motor Vehicle Accidents as beyond PTSD fall into the
emerging. First, mood disorders, especially new cases of major depression, are most common co-morbid problem: Second, study it was (17) found that 27.4% of survivors with PTSD had another current co-morbid anxiety disorder. Third, several studies MSE a measure
to constitute a psychiatric case .Finally there is travel
anxiety and driving reluctance: (18) found that 18.4% had travel anxiety at 1 year post MVA assessment; other (19) reported 18.2%.
Methods
Patients and Procedures;This prospective cross sectional study includes 102 patients, 83 men and 19 women, mean age 33.9 years (range: 20–69 years), who were admitted at orthopedic department after injury sustained due to RTA.
After obtaining informed consent, patients were
followed by other instrument to assess the symptoms of anxiety, depression and post traumatic stress disorder. Injury severity was assessed by administering ISS and ABI. Patients were again followed up after 4 weeks and the same scale used for the assessment. The questionnaires ask the patients to estimate their anxiety by using BAI (Beck Anxiety Inventory) (20) and depression by BDI (Beck Depression Inventory) (21) and HIES (Horowitz’s Impact of Event Scale) (22) to explore the psychological impact of a variety of traumas. The injury severity was assessed with use of ABI (Abbreviated Injury Score). (23)
Major injury caused the trauma in 55 patients and minor injury in 47 patients. Most patients had upper secondary
level education (n-53); third had primary education (n-19), fourth had lower secondary education (n-13) and some had a university education (n-2). To compare age groups, patients were divided into 5 groups as shown in table 2.
Data about the patients participating in the study were collected and analyzed using SPPS-10 for window.
InstrumentsSemi Structured Performa: Self-designed semi Structured Performa was prepared to obtain the socio-demographic characteristics of the patients. It is used to record patient’s name, age, sex address, education, marital status, occupation, religion, economic status and presenting complaints.
BDI (Beck Depression Inventory): This inventory assesses depression for patient’s subjective perception. The subject has to rate according to how he has been feeling during the past two weeks on a 4 point. Scale ranging from 0-3, maximum total score is 63. The total score is categorized into mild, moderate and severe depression. The inventory is considered as a standard scale for measuring severity of the symptoms of depression. The 21 item which are rated on a 4 point scales covers the wider Psychopathology of depression.
BAI (Beck Anxiety Inventory): BAI is a 21 item self

3
rated questionnaire that describes common symptoms of anxiety. This scale has a reliability value of 0-92 and a validity that ranges from 82-87 and inventory is considered as a standard instrument to measure anxiety symptoms. Scores have implication for both in measuring severity and assessing changes in symptoms due to intervention.
IES (Horowitz’s Impact of Event Scale): IES was originally developed in 1979, later it was used for exploring the psychological impact of a variety of traumas. Although many measures of PTSD symptoms have emerged (24), the IES remains widely used. The IES does not measure the hyper arousal symptoms of PTSD described in DSM-IV (25)
Injury Severity Score (ISS): ISS is used to assess
abbreviated injury scale which is assigned a value form 1 to 6, with: Minor injury (1) Moderate injury (2) Severe but not threatening (3) Life- threatening but survival likely (4) Critical with uncertain survival (5) Fatal (6) and its value correlates with the risk of mortality.
Results
102 patients (83 males and 19 females) were enrolled in study. The mean age was 33.93 years (range 20-69).The majority of RTA patients were male age group between 20-29(49.4% n=41) and female age group between 30-39 ( 38.8% n=7). Most of the participants were married (64.7% n = 66), Hindu by religion (88.8% n=90) and of secondary level educated (34.3% n=35). The majority of them were service holder (24.55 n=25) and from middle socio economic status (68.6% n=70).
Table 1: Above shows the prevalence of anxiety, depression and PTSD in 1 st and 4th week of patients of RTA. The anxiety symptoms in 1st and 4th st and 4th
DurationAnxiety symptoms
2
Yes (%) No (%)
1st week 31(30.4) 71(69.6)P=0.075
4th week 20(19.6) 82(80.4)
DurationDepressive Symptoms
2
Yes (%) No (%)
1st week 52(51.0) 50(49.0)
P=0.000014th week 22(21.6) 80(78.4)
DurationPTSD Symptoms
Yes (%) No (%) 2
1st week 95(93.1) 7(6.9)P=0.0000
4th week 36(35.3) 66(64.7)
4
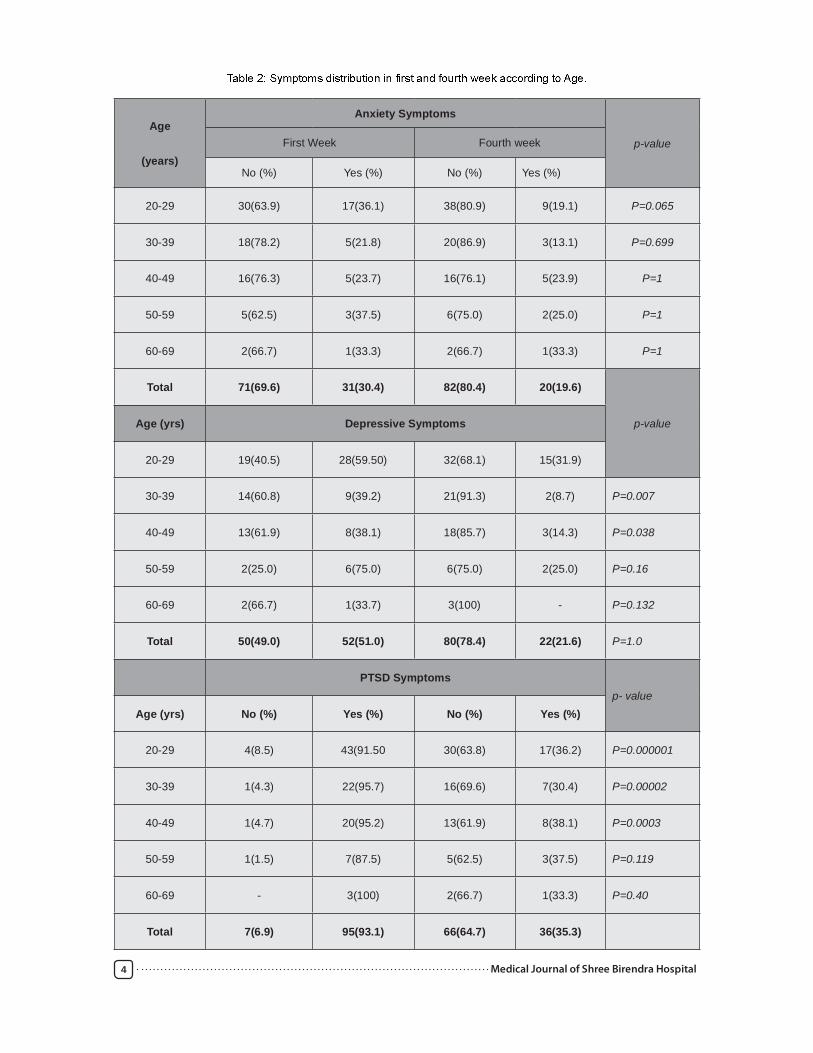
Age
(years)
Anxiety Symptoms
p-valueFirst Week Fourth week
No (%) Yes (%) No (%) Yes (%)
20-29 30(63.9) 17(36.1) 38(80.9) 9(19.1) P=0.065
30-39 18(78.2) 5(21.8) 20(86.9) 3(13.1) P=0.699
40-49 16(76.3) 5(23.7) 16(76.1) 5(23.9) P=1
50-59 5(62.5) 3(37.5) 6(75.0) 2(25.0) P=1
60-69 2(66.7) 1(33.3) 2(66.7) 1(33.3) P=1
Total 71(69.6) 31(30.4) 82(80.4) 20(19.6)
p-valueAge (yrs) Depressive Symptoms
20-29 19(40.5) 28(59.50) 32(68.1) 15(31.9)
30-39 14(60.8) 9(39.2) 21(91.3) 2(8.7) P=0.007
40-49 13(61.9) 8(38.1) 18(85.7) 3(14.3) P=0.038
50-59 2(25.0) 6(75.0) 6(75.0) 2(25.0) P=0.16
60-69 2(66.7) 1(33.7) 3(100) - P=0.132
Total 50(49.0) 52(51.0) 80(78.4) 22(21.6) P=1.0
PTSD Symptomsp- value
Age (yrs) No (%) Yes (%) No (%) Yes (%)
20-29 4(8.5) 43(91.50 30(63.8) 17(36.2) P=0.000001
30-39 1(4.3) 22(95.7) 16(69.6) 7(30.4) P=0.00002
40-49 1(4.7) 20(95.2) 13(61.9) 8(38.1) P=0.0003
50-59 1(1.5) 7(87.5) 5(62.5) 3(37.5) P=0.119
60-69 - 3(100) 2(66.7) 1(33.3) P=0.40
Total 7(6.9) 95(93.1) 66(64.7) 36(35.3)

5
Table 2: st
and 4th week. The PTSD symptoms in few of age group in 1st and 4th
20-29years (p=0.000001), 30-39years (p=0.00002) and 40-49years (p=0.0003).
Table 3
Table 3:
0.014 respectively) in 1st week but however in 4th
minor and major injury (p=0.018 and p=0.013 respectively). Using the ISS patients of minor injuries were 47(male=38, female=9) and major injuries were 55 (male=45, female=10).
Using BAI, the prevalence of anxiety in 4th week 20 (19.6%) was found among the patients enrolled in the study. The age of 20-29 years had maximum anxiety symptoms (19.1% n=9) and female (47.4% n=9) were affected more than male (26.5% n=22).According to severity of injury anxiety predominant in major injury patients (29% n=16) in comparison to minor injury patients (8.5% n=4). Likewise the prevalence for depression was found to be 22 (21.6%) in 4 th week. The age group affected more was 20-29 (31.9% n=15) and sex affected more was female (47.4% n=9) than male (51.8% n=43). Depression was found more with major injury (30.9% n=17) and less with minor injury (10.65 n=5).
An overall prevalence of 35.3% (n=36) PTSD was found in 4th week among the patients interviewed. The rate was higher among the females: 10 patients (52.6%) met the diagnostic criteria used compared to 26
more common among the middle aged patients. The majority, (38.1%) of the MVA survivors were in the age group 40 -49 years. The results regarding injury severity was like anxiety and depression, the major injury having higher rates of PTDS symptoms (41.8% n=23) than minor (27.75 n=13).
Discussion
general population in that they were mostly young. The predominance of males in the sample could be easily explained. Perhaps they were more likely to be motor vehicle drivers and hence more prone to injury compared to the females. There were greater
representation of married 64.7% and unmarried were 32.4%.The representation of unmarried were higher in males 36.1% than females 15.8% Marriage was identified as a possible risk factor especially females, 78.9% and for the males (64.7%) of RTA patients. Though these factors were associated with a greater risk and are similar to those of other studies on traumatic events other than motor vehicle accidents (26) they were not statistically
professionals and students had higher rates of a c c i d e n t s and developing psychological symptoms. An explanation for this could be that the groups more affected had greater understanding of the possible consequences of the accident and feared that their life goals and ambitions could be adversely affected.
The present study has several limitations. First, despite the fact that average number of patients
Symptoms distribution with Injury Score in First Week
SymptomsMinor Injury Major Injury
P valueNo. (%) No. (%)
Anxiety 7(14.9) 24(43.6) P=0.002
Depression 23(48.9) 29(52.7) P=0.703
PTSD 47(100) 48(87.3) P=0.014
Symptoms distribution with Injury Score in Fourth Week
SymptomsMinor Injury Major Injury
P valueNo. (%) No. (%)
Anxiety 4 (8.5) 16 (29.0) P=0.018
Depression 5(10.5) 17(30.9) P=0.013
PTSD 13(27.7) 23(41.8) P=0.136

6
participated in this study but there is no long-term follow-up, the decrease of post-traumatic stress during the study is a promising result. With regard to future research, it would be useful to investigate study population with a long time follow-up.
Anxiety symptoms The study showed that the anxiety symptoms seen higher in major than in minor injury and it was
that the anxiety symptoms were seen higher in females than in males. The anxiety symptoms in major injury
(p=0.012), this may be perhaps due to vulnerability of females to any stress.
Depressive Symptoms The study found depressive symptoms in 51.0%
20.5%. This study was similar to other Studies, O’ Donnell et al, 2004 showed the rates of depression following injury ranges from 5-23%. The present study found that depression was higher in age group 20-29 years and 30-39 years in 1st and 4th
The depressive symptoms in male and female differ
th week (p=1).
PTSD Symptoms In this y were
ogy in to
We did not use a interview on identifying xi
It is
their T be an
for the of PTSD this group.
Prevalence of PTSD (35.3%) is comparable to that found in the developed countries: range 7 - 39%. As in the other studies (27) the females were at a greater risk of developing PTSD. Among those who developed PTSD, 38.1% were in the age group 40-49 years. It appears therefore that the middle aged subjects are more prone to developing PTSD than the younger and older subjects. It is possible that the older subjects had learned coping mechanisms from past experience and younger has enhance their ability to cope with new traumas .(28)Not only has it been shown that higher age could imply a higher risk of developing post-traumatic stress symptoms,(29) but at the same time it also has been reported that no difference concerning post-traumatic stress measured with the instrument IES could be found between younger, older and middle-aged individuals.of patients with PTSD none had been previously diagnosed. All were attending the clinics purely for
their physical injuries. Other studies of post-traumatic stress among individuals in different age groups have shown different results.
In the present study, the IES was used to assess post- traumatic stress. This instrument has been used in previous studies of post-traumatic stress in vehicle related accidents mostly in whiplash injuries (31,32,33) The levels of post-traumatic stress with 102 patients suffering from moderate to severe stress symptoms in 4th week 35.3% which were clearly higher than previously reported early after injury (13%). (34)
Several workers (35, 36) have noted, in particular, that pre-existing major depressive disorder (MDD)
developing PTSD. In the present study since the pre-existing psychiatric illness were not excluded, so
which could be associated to be of greater risk of developing PTSD. In general those who had suffered psychiatric illness in the past had a greater risk of developing PTSD. Similarly those who had other physical illnesses were at a greater risk. Perhaps the accident acted as a further stressor to these individuals who were already overwhelmed.
Conclusion
The majority of MVA survivors do develop
to identify those at risk. A multidisciplinary approach is therefore essential in the management of the RTA survivors at the orthopedic and trauma clinics if their physical and psychological needs are to be adequately addressed. of all the y out-after vehicle in the
that will con- the of a very large public l
l
Despite these the high levels ology in the month following
that y and
Co-occur following a physical y
Health care systems targeted at have a sibility to
an ly and for early atric
v
accidents by implementing road safety measures such as safety belts, speed limit, improved road infrastructure and strict law enforcement measures on
MVA and therefore PTSD and other psychiatric problems.

7
References
1. O’Brien, L. S. Traumatic Events and Mental Health. University Press: Cambridge, 1998.
2. Blanchard EB, Hickling EJ, Taylor AE and Ross W R. Psychiatric morbidity associated with motor vehicle accidents. J. Nervous and Mental Disorder 1995; 183:495-504.
3. Central Bureau of Statistics. Statistical Abstract, Kenya Government Press: Nairobi, 1999.
4. Taylor S, Koch WJ, Fecteav, et al. Post traumatic
Patterns of response to cognitive behavior therapy. Journal of Consulting and Clinical Psychology, 2001; 69: 541-551.
Disorder. Geneva: World Health Organization, 1992.
6. Alexander DA. The psychiatric consequences of trauma. Hospital Medicine, 2002; 63:12-25.
7. Sharma K. Symposium of surgical and nursing management of patients with neurotrauma. Bir Hospital, Department of Anesthesia and Neurosurgery: Nepal, 1998; 44-56.
8. Malt UF. The long term psychiatric consequences of accidental injury. British Journal of Psychiatry.1988; 153:554-560.
9. Blanchard EB, Hickling EJ, Taylor AE, et al. Psychological morbidity associated with motor vehicle accidents. Behavior Research and Therapy, 1994; 32:283-290.
10. Shrestha M.L, Koirala B, Vaidya P.Pancreatic resection for trauma in children. International surgical conference of society of Surgeon of Nepal, 1998; 37.
11. Statistical Pocket Book 2002: His Majesty’s Government National Planning Commission Secretariat, Central Bureau of Statistics: Kathmandu, Nepal.
monograph of the Quebec task force on whiplash
management. Spine, 1995; 20:715-735.13. Mayou R and Radanov BP. Whiplash neck injury.
Journal of Psychosomatic medicine, 1996; 40: 461-474.
14. Mayou R, Bryant B. and Duthie R. Psychiatric
Medical Journal, 1993; 307:647-651.15. Lishman A. The Psychological Consequences of
Cerebral Disorder. Organic Psychiatry; 1987.16. Norris FH. Epidemiology of trauma: frequency
and impact of different potentially traumatic event on different demographic groups. Journal of Consulting and Clinical Psychology, 1992; 60:409-419.
17. Blanchard EB. Hickling EJ, Taylor AE, et al. Psychiatric morbidity associated with motor vehicle accidents. Journal of Nervous and Mental Disease, 1995; 183:495-504.
accidents. International Review of Psychiatry, 1992; 4: 45-54.
19. Kuch K, Cox BJ, and Evans RJ, et al. (1994)Phobia, panic and pain in SS survivors of road vehicle accidents. Journal of Anxiety Disorders, 1994; 8:181-187.
20. Beck A T, Brown G, Epstein N. and Steer RD. An inventory for measuring clinical anxiety. Journal of Consulting and Clinical Psychology, 1988; 56: (6), 893.
21. Beck A T, Ward C H, Mendenlson M, et al. An inventory for measuring depression. Archieves of General Psychiatry, 1961; 4: 561-571.
22. Horowitz M J, Wilner N, Kaltreider N and Alvarez W. Sigh and symptoms of post traumatic stress disorder. Archieves of General Psychiatry, 1980; 37: 85-92.
23. Greenspan L, McClellan BA. And Greig H. Abbreviated injury scale and injury severity score. A scoring chart. Journal of Trauma, 1985; 25:60-64.
24. Wilson AC. Assessing Psychological Traumas and PTSD. New York: Guilford Press; 1999.
25. American Psychiatric Association. Diagnostic and Statistical Manual 4th Edition (DSV-IV).Washington DC; 1994.
26. Kessler R C, Sonnega A, Bromet E J, Hughes M and Nelson C B. Posttraumatic stress disorder in the National co-morbidity survey. Arch. General Psych, 1995; 52:1048-1060.
27. Lyons J. Strategies for assessing the potential for positive adjustment following trauma. J Traumatic Stress, 1991; 4:93–111.
28. Lyons JM, McClendon OB. Changes in PTSD symptomatology as a function of aging. Nova-Psy Newsletter, 1990; 8:13–18.
29. Chung MC, Werrett J, Easthope Y, Farmer S. Coping with post- traumatic stress: young, middle-aged and elderly comparisons. Int J Geriatric Psychiatry, 2004; 19 :( 4) 333–343
30. Kongsted A, Bendix T, Qerama E, et al. Acute stress response and recovery after whiplash injuries. A one-year prospective study. Euro J Pain, 2008; 12: (4)455–463.Koopman C, Classen C, Cardena E, Spigel D. When disaster strikes, acute stress disorder may follow. J Trauma Stress, 1995; 829-46.
32. Harvey AG, Bryant RA: The relationship between acute stress disorder and posttraumatic stress disorder: a 2-year prospective evaluation. J Consult Clin Psychol, 1999; 67:985–988.
33. Shalev AY. Measuring Outcome in Posttraumatic Stress Disorder. J Clin Psychiatry, 2000; 61: (5) 33–42.
34. Breslau N, Davis G C, Andreski P. and Peterson E. Traumatic events and post traumatic stress disorder in an urban population of young adults. Arch. General Psych, 1991; 48:216-222. 20.
35. Baker SP, O’Neil B, Haddon WJ, Long WB. The Injury Severity Score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma, 1974; 14:187–196.
36. T l G, J B. Assessment of coma and impaired consciousness: a practical scale. Lancet, 1974; 2: 81–84.

8
Pande R
Rajib Pande, Consultant Physician, Shree Birendra Hospital, Kathmandu
Abstract
Introduction: Congestive cardiac failure is the failure of the heart to pump blood at a rate commensurate with the requirements of the metabolizing tissue and or its ability to do so requires an abnormally elevated pressure. CCF once sets in, pressure with malignant progression with one year mortality of 38% and 15% and six year mortality of 80% and 65% in men and women respectively. Acute rheumatic fever(ARF) and its sequel Rheumatic Heart Disease(RHD) may impair myocardial function to precipitate failure.
Aim: To study clinical features of Congestive Cardiac Failure in Rheumatic Heart Disease.
Methods: A prospective study with 50 patients admitted between August 2006 and September 2008 in Shree Birendra Hospital formed the subject of this study.
Patients of rheumatic valvular heart disease of both sexes in congestive cardiac failure at the time of admission or who developed failure during hospitalization were taken into the study. Detailed history was taken from all patients. Detailed examination was done in all patients with emphasis in cardiovascular
Results: A total of 50 patients with RHD in CCF were the subject of study. The average age was 33.78 years. The presenting clinical features of the patients were breathlessness on exertion and it was the commonest presenting complaint and was present in all patients. Palpitation was present 37 of 50 patients(74%). Basal crepitation was the commonest clinical sign present and 29 of 50 patients(58%)
other valves) and was seen in 94% (47) patients .
Key words: Congestive Cardiac Failure, Rheumatic Heart Disease
Address for Correspondence: [email protected]
Introduction
failure of the heart to pump blood at a rate commensurate with the requirements of the metabolizing tissue and or its ability to do so requires an abnormally elevated pressure1.
CCF once sets in, pressure with malignant progression with one year mortality of 38% and 15% and six year mortality of 80% and 65% in men and women respectively2,3. Pharmacotherapy only blunts the progression of CCF and increases the longevity, it does not eliminate the end point, so that patients with CCF despite optimum pharmacotherapy succumb to it after a lapse of months to years. Acute rheumatic fever(ARF) and its sequel Rheumatic Heart Disease(RHD) may
impair myocardial function to precipitate failure.
of rheumatic fever is to appropriately treat the previous episodes of streptococcal pharyngitis, as it is impossible to identify persons at risk for developing rheumatic fever after an episode of streptococcal pharyngitis4.
In a resource poor country like Nepal, where predisposing factors to rheumatic fever persists and prophylactic penicillin therapy is often inadequate, acute rheumatic carditis still frequently follows a fulminant course resulting in death or severe disability at an early age5.
A substantial number of patients of RHD presenting at hospital are failure and this remains the important cause of death in such patients6.

9
Methods
A total number of 50 patients admitted between August 2006 and September 2008 in Shree Birendra Hospital formed the subject of this study. Patients of rheumatic valvular heart disease of both sexes in congestive cardiac failure at the time of admission or who developed failure during hospitalization were taken into the study.
Detailed history was taken from all patients which included:
Past history of rheumatic fever, any recent changes in physical activity, details of drug intake including rheumatic prophylaxis and previous hospitalization. Detailed examination was done in all patients with emphasis in cardiovascular and relevant system. Precipitating factor was looked for in all patients.
All patients were subjected to:
1. Routine haematological examination to look for anaemia raised erythrocyte sedimentation rate (ESR) and evidence of infection.
2. Urine routine examination for evidence of infection, microscopic haematuria.
3. Chest X-ray to look for cardiomegaly, prominence of pulmonary arteries, dilatations of upper lobe pulmonary veins and infective focus.
4. Twelve lead electrocardiogram for evidence of chamber enlargement, axis, arrhythmia and to exclude other diagnosis.
5. Echocardiogram
6. Throat Swab Culture
7. ASO titre
8. C- Reactive protein
9. In suspected cases of infective endocarditis, blood culture was done by obtaining three samples at one hourly interval, under strict aseptic precaution
Diagnosis:
for the diagnosis of CCF. The presence of 3 or more of
these criteria was required to make diagnosis of CCF.
The severity of CCF was assessed by the New York Heart Association criteria (NYHA).
Assessment
Patient was considered to be anemic if Hb
dl as marked anemia. Chest infection was based on
Infective endocarditis as the precipitating factor was based on clinical features and vegetation seen on echocardiography.
The various parameters observed were noted, tabulated and statistically analyzed using SPSS version 10.0. and Chi Square test was applied to Correlating severity.
Results
A total of 50 patients with RHD in CCF were the subject of study.
Age distribution
Patients age ranged from 13 to 70 years. Most of the subjects of present study were between 21 and 30 years(30%). The average age was 33.78 years.
Sex distribution
The sex distribution of patients in the present study was1:1.27 (Male to female ratio)
Mode of Presentation (Table 1)
The presenting clinical features of the patients were breathlessness on exertion was the commonest presenting complaint and was present in all patients. Palpitation was present 37 of 50 patients(74%). Basal crepitation was the commonest clinical sign present and 29 of 50 patients(58%) had the raised jugular venous pressure.
of 27(54%) patients Class III, 22(44%) were in class II and only 1 patient was in class IV. Thirty four patients (68%) gave passed history suggestive of RF.

10
Table 1.Clinical features of 50 RHD patients in CCF
Clinical features Total No. Percentage
Symptoms
Breathlessness on exertion 50 100
Chest pain 21 42
Palpitation 37 74
Paroxysmal nocturnal dyspnoea 20 40
orthopnea 13 26
17 34
Signs
Raised jugular venous pressure 29 58
9 18
Basal crepitations 50 100
S3 gallop 11 22
Valvular Lesion
The various valvular lesions detected in patients studied are as depicted in table 2
Table 2: Valvular lesions
Valve involvement Male Female Total
Mitral 18 29 47(94)
Stenosis 06 11 17(34)
Regurgitation 01 01(02)
Both 02 06 08(16)
Aortic 10 04 14(28)
Stenosis - - -(-)
Regurgitation 03 - 03(06)
Both - - -(-)
Triscupid 03 07 10(20)
Stenosis - - -(-)
Regurgitation - - -(-)
Both - - -(-)
Pulmonary _ - -(-)

11
Mitral valve was the commonest valve involved
patients. Isolated mitral valve involvement was seen in 52% (26) patients. Of these isolated mitral stenosis was present in 34% (17) patients.
Isolated mitral regurgitation was seen in only one patient (2%) and combination of mitral stenosis and regurgitation in 08 patient (16%)
Aortic valve involvement was seen in 28% (14 patients) with isolated aortic regurgitation in 06% of cases while the other lesions were in combinations . Isolated aortic stenosis was not seen. Triscupid valve involvement was seen in 20% of cases, only in combination with mitral valve lesion. No pulmonary valve effection was noted. Mitral and Triscupid valvular lesion was seen more in females 58% and 14% respectively while aortic valve involvement was found more in female 20%
Electrocardiogram(ECG)
Most common abnormality in ECG in both NYHA class II patients were left atrial enlargement(LAE) seen in 77.3% and 70% of patients respectively. Atrial
P-R interval was not noticed in any of the patients.
Discussion
Congestive cardiac failure is major and growing public health problem. Its prevalence is 3 to 20 per 1000
after the onset of heart failure in Framingham study was 25% in men and 38% in women. The mortality rate of heart failure was 6 to 7 times that of general population7.
Inspite of pharmacological progress, end stage CHF is still associated with decrease in quality of life. Heart transplantation remains the last therapeutical option for these patients. While the one year survival rate has increased over the last few years upto 80%
donors8. In the present study, precipitating factor in rheumatic valvular heart disease as a cause of cardiac decompensation was studied.
Majorities of patients were in their third decade (30%). This is compatible with other studies where 33.8% and 36% of the cases fell in the same age group6,9. However in other studies, majority of patients have been noted in the second decade10,11,12,13.
The male to female ratio was 1:1:27 in the present study. This observation is in agreement with other studies where the male to female ratio was 1:1:7 respectively and 1:1:17 respectively10,14.
Breathlessness on exertion was the most common symptom that the patient presented with in this study(100%). The presenting symptom was breathlessness in more than 735 of patients6,12,15.
Past history of Rheumatic fever was obtained in 68%
observed by Roy SB et al15.However a lower incidence has been recorded by Subramaniyam et al (30%) and Raja Ram C et al (49.3%) respectively13,14.
Valvular lesions Mitral valve was the commonest valve involved (94%) with isolated mitral stenosis being the most common single
found to be 40%, 38% and 35% respectively5,13,15. However in
range of 43% to 98.4%6,10,11,12,14.
Isolated mitral regurgitation was found in only one patient in the present study(2%). This differs from the work of Marcus et al and Arora et al , where mitral regurgitation was found in 41% and 315 of patients respectively5,10. This difference could be due to a small sample size in the present study as compared to those of above Sanyal et al in their study observed, mitral regurgitation as the single most common valvular lesion comparing 91% of the cases16.
Combined mitral stenosis with regurgitation was seen in 16% of cases which is consistent with Arora et al and Raja Ram et al who found similar lesion in 22.7% and 14% respectively10,14
Marcus et al, Roy et al and Agrawal et al who observed the combination of mitral stenosiss and regurgitation in 31%, 63% and 26% respectively5,12,15. This difference in observation was
juvenile age group in the last study.
Aortic valve involvement was seen in285 of the patients out of which 22% were in combination with mitral valve which
and mitral involvement was found to be 15.8% and 24% respectively12,13.
None of the patient had aortic stenosis, isolated triscuspid and pulmonary valve involvement which is consistent
or involvement of pulmonary and triscupid valve16.

12
Conclusion
It was seen that there was no statistical
belonging to two NYHA. Classes were correlated on the basis of electrocardiogram, chest X-ray and echocardiogram. This indicates that the patient’s NYHA functional status was independent of the abnormalities recorded on relevant investigation. Hence it can be concluded that the severity can be probably related to
RHD is a disease of developing countries. While compliance with chemoprophylaxis can be upto 100% in closed or captive population, considerable variations are possible in compliance.
To avoid poor compliance with oral antibiotic regime, a single injection of Benzathine –penicilline G can be selected as the standard mode of therapy for all children with symptoms and signs suggestive of streptococcal pharyngitis4.
References
1. Eugene Braunwald. Harrisons principal of Internal Medicine 14th Ed.Vol.1.New York; McGraw Hills1998, International Edition:1287.
2. Kannel WB. Epidemiological Effect of heart failure. Cardiac Clinic 1989;7:1-9.
3. Kannel WB, Thomb TJ. Hurst’s The Heart. 8th Ed. Vol.1. New York; McGraw Hills1994, International Edition:185-97.
4. Rheumatic Heart Disease in Developing Countries. Editorial Ann.Int.Med 1994;120:243-245.
5. Marcus RH, Serali P, Pocock WA, Barlow JB. Spectrum of Severe Rheumatic Valve Disease in Developing Country. Ann.Int.Med 1994;120: 177-83.
6. Samani OT, Chandalia HB. Rheumatic Heart Disease in Bombay. IHJ 1965;17:283-292.
7. Delahaye F, de Gevigney G. Epidemiology and Natural History of Cardiac Failure. Rev Prat. 1997; 47(19): 2114-17.
8. Meiser BM, Von Scheidt W, Weis M et al. Heart Transplantation- State of art today. Herz. 1997;22(5):237-52.
9. Gr. A Streptococcal infection and ARF. Med Prog NEJM 1991; 325: 783-93.
10. Arora A, Subramaniyam G, Khalilullah, Gupta
Rheumatic Heart Disease.IHJ. 1981: 33: 264-69.
11. Datta BN, Nagrani B, Khatri HN et al. Rheumatic Heart Disease at autopsy. IHJ 1978; 30: 39-45.
12. Agrawal RK, Agrawal VK. Juvenile Rheumatic Heart Disease. IHJ 1969; 21: 166-73.
13. Subramaniyam G, Bjotra SP, Arora R et
Rheumatic Heart Disease.IHJ. 1979; 30: 359-60.
14. Rajaram C, Reddy M, Jagabandhu N. Rheumatic Heart Disease in Kurnool. IHJ 1968;2: 149-56.
15. Roy SB, Lazero EJ, Ramalingaswami V. Juvenile Mitral Stenosis in India. Lancet 1963; 2: 1193-95.
16. Sanyal SK, Berry AM, Duggal S et al. Sequel of initial attack of acute rheumatic fever in children from North India Circulation 1982; 65: 375-79.

13
Shakya N B1, Rajbhandari S L2, Sharma A3, Deo RK4 Jha SM5
1Dr. Nabin Bhakta Shakya,Dermato-venereologist,2Dr. Sudersan Lal Rajbhandari, Dermato-venereologist, Department of Dermatology and Venereology, 3Dr. Arun Sharma, Consultant Nephrologist, 3Dr Rajeeb Kumar Deo, Consultant Internal Medicine, Department of Medicine, 5Dr. Sagar Mani Jha, Dermato-venereologist and Head of the Department, Department of Dermatology and Venereology , Shree Birendra Hospital, Chhauni, Kathmandu, Nepal.
Abstract
Introduction: Chronic renal failure is a pathophysiologic process with multiple etiologies, resulting in the inexorable attrition of nephron number and function, and frequently leading to end stage renal disease. There are various cutaneous changes in chronic renal failure.
Objectives: in occurrence of cutaneous manifestation with modality of treatment of CRF.
Methods:
renal failure as control to facilitate comparison were considered in the Department of Dermatology and Venereology and the Department of Medicine, Shree Birendra Hospital, Chhauni from September 2008 to June 2010.
Results:pruritus followed by xerosis and pallor. Occurrence of pruritus was found to be more in HD patients (68%) than in IPD patients (38%). No correlation was found between ages, sex, and duration of dialysis with complaint of pruritus. Skin xerosis is considered an important factor contributing or initiating pruritus.
Conclusion: Pruritus is the commonest cutaneous manifestation of chronic renal failure.
Address for correspondence: [email protected]
Introduction
The skin is the most visible and easily accessible organ of the body. For an astute clinician, the skin may function as an important diagnostic window to disease affecting internal organ. This is especially true for the renal system1- 4.
Chronic renal failure is a pathophysiologic process with multiple etiologies, resulting in the inexorable attrition of nephron number and function, and frequently leading to end stage renal disease (ESRD) 5-
6.
ESRD represent a clinical state or condition in which there has been an irreversible loss of
render the patients permanently dependent upon renal replacement therapy (dialysis or transplantation) in order to avoid life threatening uremia7-10.
Uremia is the clinical and laboratory syndrome,
untreated acute or chronic renal failure.
For our study purpose cutaneous manifestations of chronic renal failure may be divided into 3 general categories including:
1. Cutaneous manifestations in patients on hemodialysis (HD).
2. Cutaneous manifestations in patients on intermittent peritoneal dialysis (IPD).
3. Cutaneous manifestations in patients on medical treatment.
Cutaneous Changes Associated With CRF:
Xerosis
Pallor
A sallow yellowish cast to the skin
Diffuse hyperpigmentation
Half and half nails
Eextensive eccymoes
Calcinosis cutis due to secondary hyperparathyroidism
Uremic frost
Lichen simplex chronicus
Prurigo nodularis
Xanthomas
Uremic Neuropathy
Cutaneous ischaemic ulceration7-13

14
Cutaneous Manifestations In Patients On Dialysis (Haemodialysis And Peritoneal Dialysis):
cannnula
Bullous disease of dialysis
Acquired perforating disease of hemodialysis
Priritus
Xerosis
Aalteration in skin pigmentation
Half and half nails
Calcinosis cutis
Calciphylaxis
Kyrle’s disease
Gynaecomeastia
Objectives
1. To observe the cutaneous manifestation in chronic renal failure.
2.
cutaneous manifestation with modality of treatment of CRF.
Methods
patients with chronic renal failure in the Department of Dermatology and Venereology and the Department of Medicine, Shree Birendra Hospital, Chhauni from September 2008 to June 2010.
admitted with other renal diseases but not suffering from chronic renal failure were considered as control to facilitate comparison.
Inclusion criteria:
1. Patients of both sexes with CRF receiving HD, IPD and medical treatment.
2. Patients with kidney diseases but not suffering from renal failure as control.
Exclusion criteria:
1. Patients who have recovered from CRF or who have received renal transplantation.
2. Patients with renal diseases with cutaneous manifestation as part of features of primary disease itself and not necessarily associated with CRF e.g. SLE, PSS, Amyloidosis etc.
3. Any previous history of pruritus or skin disease not relevant with the occurrence of CRF.
Observation and results
Table I: Distribution of The CRF And Non CRF Renal Patients By Age:
Table II: Distribution Of Patients By Sex:
Table III: Cutaneous Manifestations In Both (CRF And Non CRF) Groups Of Patients:
Table IV: Overall Cutaneous Manifestation in Patients Suffering From CRF:
Age group CRF (n=50) Non CRF (n=50)Freq Percent Freq Percent
1 < 20 year 8 16 8 16
2 21- 30 year 6 12 7 14
3 31- 40 year 16 12 7 14
4 41- 50 Year 8 16 16 32
5 > 50 Year 12 24 10 20
Total 50 100 50 100
Male FemaleCRF 26 (52%) 24 (48%)Non CRF 27 (54%) 23 (46%)Total 49 (49%) 51 (51%)
CRF (n=50) Non CRF (n= 50)
1. Pruritus 30 (60%) 06 (12%)
2. Xerosis 20 (40%) 02 (04%)
3. Pallor 20 (40%) 16 (32%)
4. Hyperpigmentation 04 (08%) Nil
5. Half and half nail 06 (12%) Nil
6.Other manifestation Nil Nil
S l No Manifestation HD (n=35) IPD (n=13)
CRF(No dialysis)
(n=02)1. Pruritus 24 (68.6%) 5 (38.5%) 1 (50%)
2. Xerosis 15 (42.8%) 5 (38.5%) 0
3. Pallor 14 (40%) 6 (46.2%) 0
4. Hyper pigmentation 03 (8.6%) 1 (7.7%) 0
5. Half & half nail 06 (17.1%) 0 0

15
Table V: Distribution of Pruritus:
Table VI: Distribution of Xerosis:
Table VII: Distribution of Pallor:
Table VIII: Distribution of Hyperpigmentation:
Table IX: Distribution of Half and half nail:
Discussion
Among the study cases of 50 patients, a total number of 80 cutaneous manifestations were noted.
pruritus, xerosis and pallor in CRF patients; the highest being pruritus followed by xerosis and pallor.
Pallor was noted in 30 patients (60%). Occurrence of pruritus was found to be more in HD patients (68%) than in IPD patients (38%). No correlation was found between ages, sex, and duration of dialysis with complaint of pruritus.
Skin xerosis is considered an important factor contributing or initiating pruritus. In our study it was found that, xerosis and pruritus co-existed in 17 patients (34%). Xerosis was noted in 20 patients (40%) out of
of CRF or type of dialysis.
Pallor was noted in 20 patients. All the cases were secondary to anaemia.
Hyperpigmentation was noted only in four (8%) patients. In two patients the pigmentation was generalized and in the other two it was more accentuated in exposed parts, especially on faces.
The study shows half and half nail in only six
nails not in toe nails.
made was noted in 23 cases out of 35 HD patients.
Conclusion
Pruritus is the commonest cutaneous manifestation of chronic renal failure.
References
1. Picó MR, Lugo-Somolinos A, Sánchez JL, Burgos-Calderón R. Cutaneous alterations in patients with chronic renal failure. Department of Dermatology, University of Puerto Rico School of Medicine, San Juan 00936-5067. Int J Dermatol.1992 Dec; 31(12):860-3.
2. Alain M, Particular cutaneous lesions and chronic renal failure, Hospital Georges Pompidou and Broussais, Paris, France July 18, 2008.
3. Julia R N, Dermatologic Manifestations of Renal Disease Department of Dermatology, Virginia Commonwealth University Medical Center Updated: Jan 22, 2009
4. Ponticelli C, Bencini P. The skin in chronic renal failure. In: Stewart Cameron, Alex M Davison, Jean-Pierre Grunfeld, eds. Oxford textbook of clinical nephrology. Oxford: Oxford Medical Publications: 1992:1390-4
5. Pico MR, Lugo-Somolinos A. Cutaneous alterations in patients with chronic renal failure. Int J Dermatol 1992; 31:860-3.
6. Morton CA, Lafferty M, Hau C, Henderson I, Jones M, Lowe JG. Pruritus and skin hydration during dialysis. Nephron Dial Transplant 1996; 11:2031-6.
7. Tawade N, Gokhale BB. Dermatologic manifestation of chronic renal failure. Indian J Dermatol Venereol Leprol 1996; 62:155-6.
8. Guptha AK, Guptha MA, Cardella CJ, Haberman HF. Cutaneous associations of chronic renal failure and dialysis. Int J Dermatol 1986; 25:498-504. Sweeney S, Cropley TG. Cutaneous changes in renal disorders. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick’s Dermatology in general medicine. 6th ed. Mc Graw-Hill: New York; 2003. p. 1622-4.
PruritusPresent Absent
CRF (n=50) 30 (60%) 20 (40%)Non CRF (n=50) 06 (12%) 44 (88%)Total 36 (36%) 64 (64%)
XerosisPresent Absent
CRF (n=50) 20 (40%) 30 (60%)Non CRF (n=50) 02 (4%) 48 (96%)Total 22(22%) 78 (78%)
Pallor
Present Absent
CRF (n=50) 20 (40%) 30 (60%)
Non CRF (n=50) 16 (32%) 34 (68%)
Total 36 (36%) 64 (64%)
HyperpigmentationPresent Absent
CRF (n=50) 04(08%) 46(92%)Non CRF (n=50) 0(0%) 50 (100%)Total 04 (04%) 96 (96%)
Half and half nailPresent Absent
CRF (n=50) 6(12%) 44(88%)
Non CRF (n=50) 0(0%) 50 (100%)
Total 6 (6%) 94 (94%)

16
9. Comaish JS. Ashcroft T, Kerr DN. The pigmentation of chronic renal failure. J Am Acad Dermatol 1975; 55:215-7.
10. Singh G, Singh SJ, Chakrabarthy N, Siddharaju KS, Prakash JC. Cutaneous manifestations of chronic renal failure. Indian J Dermatol Venereol Leprol 1989; 55:167-9.
11. Brenner BM, Lazarus JM. Chronic renal failure. In: Isselbacher KJ, Braunwald E, Wilson JD, Martin JB, Fauci AS, Kasper DL, editors. Harrison’s Principles of internal medicine. 13th ed. New York: McGraw-Hill; 1994. p. 1274-81.
12. Kint A, Bussels L, Fernandes M, Ringoir S. Skin and nail disorders in relation to chronic renal failure. Acta Derm Venereol 1974; 54:137-40.
13. Goh GL, Phay KL. Arterio- venous shunt dermatitis in chronic renal failure patients on haemodialysis. Clin Exp Dermatol 1988; 13:1038-40.

17
Khatri D1, Islam N2, Ali A3
1Dr. Devendra Khatri, Consultant cardiologist, Birendra Hospital, Chhauni. 2Prof. Nazrul Islam, Director, National Institute of Cardiovascular Diseases, Dhaka. 3Associate Prof. National Institute of Cardiovascular Diseases, Dhaka.
Abstract
Introduction:leucocytosis and relative neutrophilia. The elevation of white blood cell count (WBC) count usually develops within 2 hours after the onset of chest pain, reaches a peak 2-4 days after infarction, and returns
leucocyte count and the neutrophil percentage and the development of congestive heart failure in the patients with acute myocardial infarction (AMI).
Methods and result: The Prospective observational study was carried out over the period of 2 yrs where
discomfort, irrespective of age and sex were studied. Outcome measures included clinical episodes
evidence of contractile dysfunction. 54% patients had leucocytosis and 60.7% of patients had relative neutrophilia. Amongst heart failure patients 82.3% had leucocyte > 11.0x109
9
11.0x109 9
Conclusion:even relative neutrophilia on admission to the hospital and the subsequent development of congestive
interventions to prevent or reduce the risk of congestive heart failure.
Key words: leucocytosis, neutrophilia, myocardial infarction, congestive heart failure.
Address for correspondence: [email protected].
Introduction
Despite impressive improvement in diagnosis and management over the past decades, acute myocardial infarction is the major public health problem in the industrialized world and is becoming an increasingly important problem in developing countries. Of particular concern from a global perspective are projections from the World Heart Federation that the burden of disease in developing countries will become more closely
because of accelerated economic development and life style changes promoting atherosclerosis.
Almost all myocardial infarctions result from coronary atherosclerosis with superimposed coronary thrombosis. It has commonly been shown to occur as a result of the disruption of atherosclerotic plaque at a
thrombotic occlusion of a coronary artery with resulting downstream necrosis1. Atherosclerosis is not a single disease entity; rather it represents a common response of the artery to numerous potentially different forms
atherogenic lipoproteins in the arterial intima.2 Thus
and progression of atherosclerosis and systemic blood
emerged as a powerful predictor of coronary events.3
Acute myocardial infarction (AMI) is frequently associated with leucocytosis and an elevated peripheral neutrophil count. The elevation of white blood cell count (WBC) count usually develops within 2 hours after the onset of chest pain, reaches a peak 2-4 days after infarction, and returns to normal within 7 days; the peak white cell count usually ranges between 12,000 to 15,000
myocardial infarction. Often there is an increase in the percentage of polymorphonuclear leucocytes and a shift of the differential count to the band forms 4 .
Acute myocardial infarction is the leading cause of mortality & morbidity all over the world. Congestive heart failure (CHF) is one of the most common complications occurring after acute myocardial infarction. Rates of post infarction congestive heart failure ranging from 51% to 71% have been reported in elderly populations.5 Congestive heart failure is associated with 5 year mortality of about 50% and

18
the health care cost is reasonably high. Although the cause of contractile dysfunction in congestive heart failure may be multi-factorial, accumulating evidence suggests that oxidative stress and the release of pro-
probably contributes to its development.6
Methods
The Prospective observational study was carried out over the period of 2 yrs where a total of one hundred
with less than 12 hrs of chest discomfort, irrespective of age and sex were included. Patients with more than 12 hrs of onset of symptoms before hospital admission, acute myocardial infarction presenting with congestive heart failure requiring immediate treatment – Killip class II-IV, prior myocardial infarction, uncontrolled severe
acute or chronic infection, serious systemic disorders like chronic renal failure, patients using corticosteroids, patients suffering from malignant disorders and
gout, rheumatic fever etc. were not included in the study.
On admission ECG for the location of myocardial
differential count of White Blood Cell was obtained.
to total WBC count and neutrophil percentage. Total leucocytes count more than 11 x109
count >65% were considered as leucocytosis and neutrophilia respectively. All the patients selected for the study were followed up during hospital stay. Clinical evaluation for the presence of heart failure was done during follow-up. Features of congestive heart failure (CHF) were documented and echocardiographic evaluation was done for all the selected patients. Documented clinical symptoms and signs of heart
of left ventricular dysfunction i.e. ejection fraction (EF) <40% in echocardiography was taken into account.
Subsequent statistical analysis was done with emphasis particularly on neutrophilic leucocytosis, location of infarct and presence or absence of congestive heart failure. Compiled data were analyzed by using computer based package for Social science (SPSS) version 11.0 for windows. Mean ± standard deviation was calculated for continuous variables and absolute and relative frequencies were measured for discrete
between groups was analyzed by chi-square test in discrete variables. Student’s t-test was used to analyze the continuous variables. The p values less than 0.05
Observation and Results
Total 150 patients of acute myocardial infarction were studied out of which 137 were male and 13 were female. The mean age of the patients was a 53.4±9.2 year ranging from 36 to 75 years. The highest percentage of patients (35.8%) was in the age range of 50-59 years. The mean age of the heart failure patients was 56.4±9.6 years and the patient without heart failure was 51.2±8.2
(p<0.05) indicating the heart failure patients had higher age compared to without heart failure patients. In the study carried out by Emanuelsson et al5, they observed congestive heart failure in 51% of cases of myocardial infarction and patients with congestive heart failure
was found between male and female patients in regards to heart failure (p>0.05).
Among the important risk factors of coronary artery disease 46.7% were hypertensive, 46% were smoker, 20% were diabetics and 13.3% were dyslipidaemic and only 2.0% had family history of ischaemic heart disease. The mean number risk factor was 1.3±0.8 years ranging from 0 to 3. Among the male patients, the average number of risk factors was 1.3±0.8 and that of female patients was 1.2±0.9. There was no
and development of heart failure (p>0.05), although hypertension, smoking, diabetes and dyslipidaemia were higher amongst the patients who developed heart failure.
Present study showed that 41.3% patients developed heart failure during treatment and 58.7% did not. The mean day of onset of heart failure was 2.6±.2.The highest percentage of patients i.e.35.5% developed heart failure on 2nd day followed by 22.6% and 19.4% on 3rd day and 1st day respectively. Amongst the heart failure patients 35.4% had ejection fraction less than 40%. Cardiac enzyme (CK-MB) was higher among the patients with heart failure as compared to those without heart failure. Among the heart failure
by Kyne et al7 who reported heart failure in 43% of the post MI patients.
The mean number blood leucocyte count was 13.7x109
failure during the hospital stay and it was 11.3x109
the patients who did not develop heart failure and the
It was also found that among the patients with heart failure 82.3% had leucocyte more than 11.0x109
only 17.7% had less than 11.0x109
the patients who did not develop heart failure, total leucocyte count more than 11.0x109
cases and in 64.8% cases it was less than 11.0x109
The relative risk indicates, the total leucocyte count more than normal was 8.52 times higher among the patients with heart failure than the patients without
the reports made by Furman et al8the Global Registry of Acute Coronary Events (GRACE) where they reported that increasing leucocyte count is
failure for patients presenting with ACS. They also reported a 7% increase in odds of developing heart failure. In the study carried out by Menon et al9 they found that the patients with upper quintiles of WBC count (count >11.1x109
failure.
The mean percentage of neutrophil count was 77.9±6.2% among the patients with heart failure and in patients without heart failure it was 68.0±8.7%. The

19
It was also found that among the patients with heart failure 93.5% had neutrophil count more than 65% and only 6.5% of cases had count less than or equal to 65%. Whereas amongst the patients without heart failure, percentage of
7 They reported development of heart failure after AMI in 92.5% of the cohort in whom neutrophil percentage was >65% compared to 45% of those in whom CHF did not develop. The relative risk indicates that the total neutrophil count was 24.16 times higher among the patients with heart failure than the patients without heart failure.
Table 1: Baseline characterstics of the study cohort
Total Patients 150 (male-137; female -13)
Age 36-75 ( mean 53.4±9.2)
Risk factors
Hypertension 73(46.7%)
Smoking 70(46.0%)
Diabetes Mellitus 34(20.0%)
Dyslipidaemia 24(13.3%)
Family history of CAD 7 (2.0%)
Laboratory test results
TLC >11×109 82 (54.7%)
TLC <11×109 68 (453%)
Neutrophil >65% 91 (607%)
Neutrophil <65% 59 (39.3%)
97 (64.7%)
Lymphocyte >25% 53 (353%)
CK-MB
Location of Infarct
Anterior 77 (51.3%)
Inferior 55 (36.7%)
NSTEMI 18 (12.0%)
Mean Hospital stay days 8.1±3.4
Outcome
Recovered 143 (95.3%)
Death 7 (47%)

20
Table 2: Distribution of the study patients by heart failure and total leucocyte count
Figure in parenthesis indicate percentage, n denotes number of patients. p value reached from chi -square test (p<0.001)
Table 3: Distribution of the study patients by congestive heart failure and neutrophil count
Neutrophil count
Heart Failure Total
N(%)p value
Present n (%) Absent n (%) >65% 58(93.5) 33(37.5) 91(60.7) 0.001
4(6.5) 55(62.5) 59(39.3)
Total 62(41.3) 88(58.7) 150(100.0)
Mean ±SD 77.9±6.2 68.0±8.7 72.1±9.1
Figure in parenthesis indicate percentage, n denotes number of patients. p value reached from chi- square test (p<0.001)
During this study it was also observed that among the patients with heart failure 82.3% of patients had neutrophilic leucocytosis, followed by neutrophilia without leucocytosis in11.3% and only 6.5% had normal range of leucocyte and neutrophil count. Whereas, in patients without heart failure, highest percentage (62.5%) had normal range of leucocyte and neutrophil count followed by neutrophilic leucocytosis in 35.2% and in 2.3% neutrophilia only without leucocytosis.
indicating that the patients with heart failure, neutrophilic
higher among the patients with heart failure compared to those without heart failure. To add to the fact that in those patients who had neutrophilia only, their leucocyte count was at the higher range of normal limit.
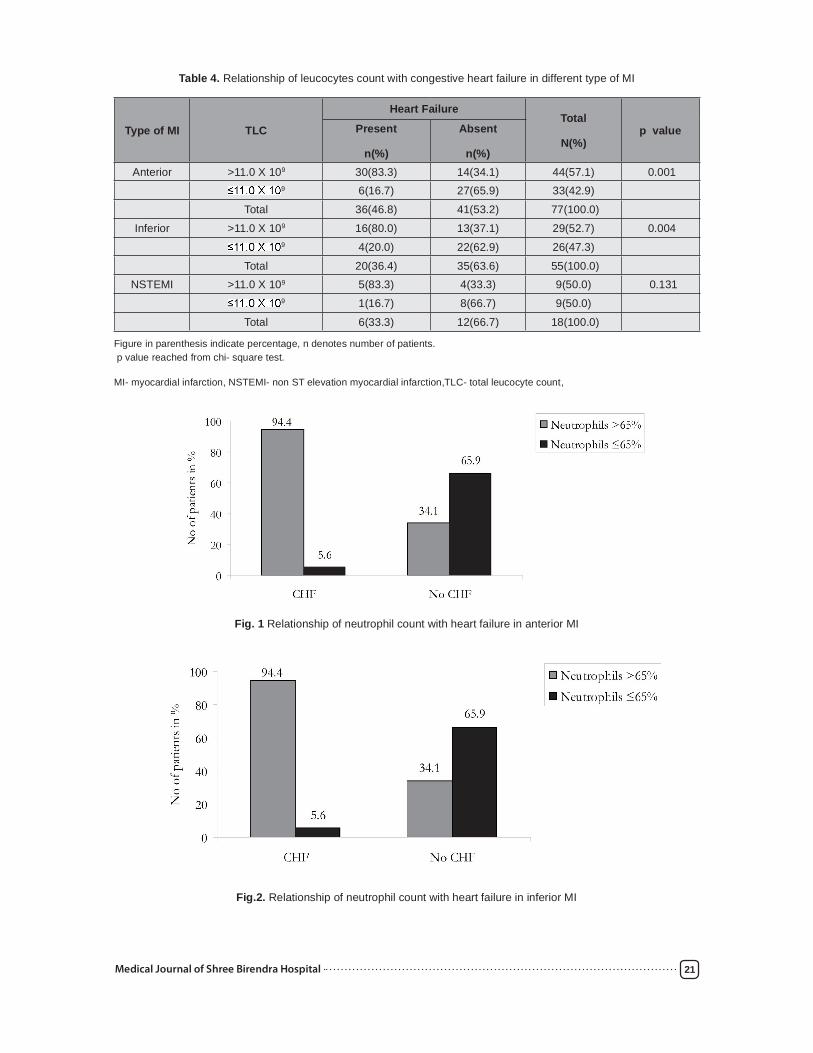
Analysis also revealed that amongst the patients who developed congestive heart failure, 58.1% had anterior myocardial infarction followed by inferior myocardial infarction in 32.3% and NSTEMI in 9.7%. Similar pattern of myocardial infarction was found among the patients without congestive heart failure with highest percentage of anterior myocardial infarction (46.6%) followed by inferior myocardial infarction (39.8%) and NSTEMI (13.6%).The proportion of anterior MI was higher among the patients who were found to have developed CHF and proportions of NSTEMI and inferior MI was higher among the patients without heart
was found between heart failure and type of myocardial infarction (p>0.05).
of congestive heart failure with leucocytes count and neutrophil count in different type of MI revealed that in anterior MI and inferior MI with heart failure, the
higher as compared to those without heart failure.
al7 who concluded neutrophilia >65% and leucocytosis >11x109
Furman et al8 who reported the association seen between increased leucocyte count and heart failure in patients with ST segment elevation AMI. But in case of NSTEMI with heart failure the difference was not
8 who showed positive association between leucocytosis and heart failure in NSTEMI also. This could be due to small number of patients included in this group; still incidence of heart failure was higher with increased leucocyte count and neutrophil count.
In hospital follow-up of the study patients total 7 (4.7%) patients succumbed to death and the proportion of death among the heart failure patients
10 They reported increased in-hospital case fatality rates mostly due to congestive heart failure and cardiogenic shock with increasing quintiles of leucocyte count.
Leucocyte count
Heart Failure Total
N(%)p valuePresent n (%) Absent n (%)
>11.0 x 109 51(82.3) 31(35.2) 82(54.7) 0.001
9 11(17.7) 57(64.8) 68(45.3)
Total 62(41.3) 88(58.7) 150(100.0)
Mean ±SD 13.7 x 109 11.3 x 109 12.3 x 109
21
Table 4. Relationship of leucocytes count with congestive heart failure in different type of MI
Type of MI TLC
Heart FailureTotal
N(%)p valuePresent
n(%)
Absent
n(%)Anterior >11.0 X 109 30(83.3) 14(34.1) 44(57.1) 0.001
9 6(16.7) 27(65.9) 33(42.9)
Total 36(46.8) 41(53.2) 77(100.0)
Inferior >11.0 X 109 16(80.0) 13(37.1) 29(52.7) 0.004
9 4(20.0) 22(62.9) 26(47.3)
Total 20(36.4) 35(63.6) 55(100.0)NSTEMI >11.0 X 109 5(83.3) 4(33.3) 9(50.0) 0.131
9 1(16.7) 8(66.7) 9(50.0)
Total 6(33.3) 12(66.7) 18(100.0)
Figure in parenthesis indicate percentage, n denotes number of patients. p value reached from chi- square test.
MI- myocardial infarction, NSTEMI- non ST elevation myocardial infarction,TLC- total leucocyte count,
Fig. 1 Relationship of neutrophil count with heart failure in anterior MI
Fig.2. Relationship of neutrophil count with heart failure in inferior MI

22
Fig.3. Relationship of neutrophil count with heart failure in NSTEMI
Discussion
the association between neutrophilic leucocytosis on admission and early development of congestive heart failure in patients with acute myocardial infarction. Heart failure is related to extent of myocardial damage. Heart failure after acute myocardial infarction occurs when 25% of the ventricular muscle is compromised11. The result of this study suggested that the presence of neutrophilic leucocytosis and relative neutrophilia is strongly associated with early development of CHF in patients with AMI. Barron et al12 has earlier demonstrated the prognostic importance of the neutrophil count for coronary events and made a remark that patients with elevated WBC count have higher risk of developing an acute myocardial infarction as well as development of complications like congestive heart failure. And in another study carried out by Thompson et al in patients admitted to the hospital with chest pain, relative lymphocytopaenia and relative neutrophilia were found to be accurate early markers of AMI.13 This study demonstrated that the presence of neutrophilic leucocytosis measured at the time of hospital admission in patients with AMI may be a
congestive heart failure independent of risk factors. This study is very much supported by the study of Furman et al10 who demonstrated a strong and consistent association between leucocyte count and all causes of mortality including congestive heart failure from AMI, independent of other therapeutic and prognostic factors. Furman et. al.8 in their multinational study also, demonstrated that, in patients with full spectrum of acute coronary syndrome, WBC count is independently associated with the development of congestive heart failure. Analysis also revealed that leucocyte count is positively correlated with neutrophil count, CHF, CK-MB and age but negatively correlated with lymphocyte
al.7 who stated that there was no association between the admission CPK activity level and leucocytosis, neutrophilia or CHF. But in the study carried out by Green et al.14 on 688 subjects of chest pain with non-diagnostic ECG found CK-MB level to be positively correlated with total WBC count following AMI. Present study is also supported by the study of Jones et al.15 who found WBC count >10x109
level.
The physiological basis for the association between neutrophilia and the risk of coronary events after acute myocardial infarction has been studied in several animal models. 16
ischaemic myocardium is an integral component of the
However, once activated neutrophils can change shape and adhere to the vascular endothelium, by increasing the vascular resistance and impairing dilatation of small coronary arterioles, they cause further myocardial ischaemia.17 Neutrophils thus mediates the vascular injury with subsequent ischaemia which compromises the activity of ventricular muscle.
Neutrophils also undergo cellular respiratory bursts and release O2 derived free radicals, which are
may occur, resulting in the release of lysosomal enzymes and arachidonic acid metabolites, which may increase coronary artery resistance, leading to the development of myocardial dysfunction.18 Neutrophilia also occur in response to myocardial necrosis, which is a potent acute phase stimulus that is associated
it is also a marker of the intensity of the peri-infarction 19
Neutrophilic leucocytosis may simply be a

23
marker of congestive heart failure or a causative agent. In this study it is not possible to establish whether there is causal relationship between neutrophilia and congestive heart failure. As the mechanism responsible for this association is unknown several hypotheses have been postulated, including leucocyte mediated
and indirect cytotoxicity mediated through pro-12
Conclusion
Commonest cause of morbidity and mortality after myocardial infarction is the development of congestive heart failure. This prospective observational
neutrophilic leucocytosis and early development of heart failure after acute myocardial infarction. The
neutrophilic leucocytosis and even relative neutrophilia on admission to the hospital and the subsequent development of congestive heart failure in patients with ST elevation myocardial infarction with good sensitivity,
that neutrophilic leucocytosis may serve as a simple non invasive marker to identify the patients at higher risk for the development of congestive heart failure after acute myocardial infarction. Monitoring neutrophilic leucocytosis may serve as a key to anticipating one of the dreadful complications of acute myocardial infarction and triage of patients may be possible to
can be very much helpful to identify the patients who may develop congestive heart failure and to take further decision at the periphery of the country where facilities for the investigation and management of patients are not adequate. Even at the centers with adequate intervention facilities, this simple investigation may help to be prepared for rescue procedures.
Study limitations
The present study dealt a relatively small number of cases. Selection bias may have occurred because sicker patients are often referred to this hospital. Cigarette smoking was not controlled in this study although previously it has been shown to be associated with leucocytosis and the risk of ischemic
protein were not measured. Another limitation of this study is that the neutrophil count was measured at only one point in time and this point was not consistent with all patients studied. Beside only short term in- hospital complications were observed among the study
subjects. As an observational investigation it can only identify association and not causality. Some drugs like B-blocker and aspirin may have altered the trend of WBC count.
References
1. Vanderwal, A.C., Becker, A.E., Vanderloos, C.M., Das, P.K. 1994, ‘Site of initial rupture or erosion of thrombosed coronary atherosclerosic plaque
irrespective of the dominant plaque morphology’, Circulation, vol.89, pp. 36-44.
2. Falk, E.& Fuster, V. 2001, ‘Atherogenesis and its determinants’, in Hurst’s The Heart, eds. V. Fuster, R.W. Alexender & R.A.O’Rourke, McGraw-Hill, New York, pp.1065- 1083.
3. Danesh, J., Collins, S., Appleby, P., Peto, R. 1998,
Albumin, and Leucocyte count with coronary heart disease; Meta-analysis of prospective studies’, JAMA, vol. 279, pp.1477-1482.
4. Antman, E.M., Braunwald, E. 2001. ‘Acute Myocardial Infarction’, in Heart Disease, eds Braunwald E., Zipes D.P.& Libby P.,W.B.Saunders Co. Philadelphia, pp. 1114-1231.
5. Emanuelsson, H., Karlson, B.W., Herlitz, J. 1994, ‘Characteristics and prognosis of patients with acute myocardial infarction in relation to occurrence of congestive heart failure’, E Heart J, vol.15, pp 761-768.
6. Dhalla, A.R., Hill, M.F., Singal, P. K. 1996, ‘Role of oxidative stress in transition of hypertrophy to heart failure’, J Am Coll of Cardiol, vol.28, pp 506-514.
7. Kyne, L., Hausdorff, J. M., Knight, E., Dukas,L., Azhar, G., Wei, J.Y. 2000, ‘Neutrophilia and congestive heart failure after myocardial infarction’, Am Heart J, vol. 139, pp. 94-100.
8. Furman, M.I., Anderson, F.A., Boudaz, A.,Goodman,S.G., Avezum, A., Sendon, L. A., Mukherjee, D., Dabbous, O.H, Goldberg R.J., Global, R.J.,GRACE, Investigators, 2004, ‘Elevated leucocyte count and adverse hospital events in patients with acute coronary
Acute Coronary Events’, Am Heart J, vol.147, pp.42-48.

24
9. Menon, V., Lessard, D., Yarzebski, J., furman, M., Gore, J.M., Goldberg, R.J. 2003, ‘Leucocytosis and adverse Hospital Outcomes after Acute Myocardial Infarction’, Am J Cardiol, vol.92, pp.368-372.
10. Furman,M.L.,Backer,R.C.,Yarzebski,J.,Savfegeau,J.,Gore,J.M.,Goldberg,R.J. 1996, ‘Effect of Elevated Leucocyte count on In-Hospital Mortality Following Acute Myocardial Infarction’, JACC,vol.78,pp945-948.
11. Alexander,RW.,Patt C.M., Ryan T.J., Roberts R 2001, ‘Diagnosis and management of patients with myocardial infarction’ in Hurst’s The Hear,eds. V. Fuster, R.W. Alexander & R.A O’Rourke, McGraw-Hill, Newyork, pp.1275-1360.
12. Barron, H.V., Cannon, C.P., Murphy, S.A., Braunwald, E., Gibson, C.M. 2000, ‘Association
myocardial perfusion, and clinical outcomes in the setting of acute myocardial infarction’, Circulation, vol.102, pp. 2329- 2334.
13. Thompson,S.P., Gibbons,R.J., Smars,P.A., Suman,V.J., Pierre,R.V., Santrach,P.J., Jiang,N.S. 1995, ‘Incremental value of the leucocyte differential count and the diagnosis of myocardial infarction’, Ann Intern Med., vol.122, pp.335-341.
14. Green, S.M., Vowels, J., Waterman, B., Rothrock, S.G., Kuniyoshi, G. 1996, Abstract
of ‘Leucocytosis: a new look at an old marker for acute myocardial infarction’, Academic Emergency Medicine, vol.3, pp.1034 -1041.
15. Jones,S.P., Weisley,G.G., Palazzo,A.J., Granger,D.N., Grisham,M.B., Huang,P.L. Lefer,D.J. 1999, ‘Myocardial reperfusion injury is exacerbated in the absence endothelial cells nitric oxide synthatase’, Am J physiol Heart circ. Physiol, vol.276, pp.1557-1573.
16. Dreyer, W.J., Michael, L.H., West, M.S.,Smith, C.W., Rothlein, R., Rossen, R.D., Anderson, D.C., Entman, M.L. 1991, ‘Neutrophil accumulation in ischaemic canine myocardium: insight into time course, distribution, and mechanism of localization during early reperfusion’, Circulation, vol.84, pp 400-411.
17. Weiss S.J. 1989, ‘Tissue destruction by neutrophil’, N Engl J Med, vol. 320, pp.1241-1251.
18. Mikelson, J.K., Simpson, P.J., Lucchesi, B.R. 1988, ‘Myocardial dysfunction induced by platelet activating factor in the post infracted rabbit isolated heart’, J Mol Cell Cardiol, vol.20, pp 547-561.
19. Entman, M.L., Micheal, L., Rossen, R.D., Dreyer, W.J., Anderson, D.C., Taylor, A., Smith,
early myocardial ischaemia’, FASEB J, vol. 5, pp.2529-37.

25
Piya E1, Panth R1, Singh S1
1Consultant pathologists,Pathology Department, Shree Birendra Hospital Chhauni
Abstract
Introduction:palpable lesions done in Shree Birendra Hospital, Chhauni, over a period of one year from 14 th April 2008 to 13th April 2009.
Aim: sites.
Methods: A total of 323 cytological diagnoses of palpable lumps performed in one year by pathologists were retrieved. Sites of FNA and diagnoses were analyzed and correlated with age and sex of the patients.
Results:This study has included 323 FNACs. Lymph node was the most common site for FNAC (32%), followed by breast (29%), thyroid (22%), and salivary gland (2%). Other site comprised 15% of cases. In lymph node, reactive lymphadenitis was the most common benign lesion (42.7%) and metastatic squamous cell carcinoma was the commonest malignant lesion(12.62%). In breast, benign proliferative breast disease was the most common(84.1%) and ductal carcinoma was commonest among malignant lesions(8.5%). Among thyroid lesions, benign proliferative thyroid disease was the commonest one (47.9%)followed by papillary carcinoma among malignant lesions(11.3%).Among salivary gland lesions,
among benign lesions(25%) and carcinoma comprised 25%. Lipoma was the commonest lesion ( 63%) from other sites.
Conclusion: Wide range of lesions, both benign and malignant, can be diagnosed by FNAC thus restricting surgery to cases only requiring further histopathological evaluation.
Address for correspondence: [email protected]
Introduction
Fine needle aspiration cytology (FNAC) is a diagnostic procedure used to investigate easily papable
breast, lymph nodes, and salivary glands . Modern imaging techniques mainly ultrasonography(USG) and computed tomography (CT) guided FNA are carried out on those lesions not easily palpable and located in deeper areas and organs such as lungs, mediastinum and abdominal, retroperitoneal and pelvic regions 1,2. FNAC is safer and less traumatic, relatively painless with speedy result and cheap. Major complications are usually rare 3. Common complications include bruising and soreness. Its accuracy in many situations, when applied by experienced and well trained pathologists, can approach that of histopathology in providing workable diagnosis. However, aspiration cytology is not a substitute for surgical histopathology. Instead it
pretreatment investigation. False negative results may sometimes be obtained because of low cell yield or
be possible in conditions with haemorrahge, infarction and reparative changes which at times mimic neoplastic features1. Therefore information obtained by FNAC must always be correlated with clinical features and relevant investigations.
Aim
The main aim of this study is to analyze different
FNAC.
Material And Method
A total of 323 cytological diagnoses of palpable lumps performed in one year by pathologists were retrieved. Sites of FNA and diagnoses were analyzed and correlated with age and sex of the patients.
and organs such as lungs, mediastinum and abdominal, retroperitoneal and pelvic organs and tissues were excluded from this study.
Results
A total of 323 FNA were done from various sites. The various sites and their and percentages are shown in the pie chart.

26
There were a total 268 (83%) benign and 55 malignant cases (17%) as depicted in the pie chart.
Lymph Nodes
103 FNAC were done from enlarged lymph nodes, 44 of which were reported as reactive lymphadenitis, 26 as granulomatous lymphadenitis. 33 cases were diagnosed to have malignancy. Metastatic malignancy was more common than lymphoma (2.9%) Cervical lymph was the most common site (85%).
FNAC Diagnosis Number Percentage(%)
Reactive Lymphadenitis 44 42.72
Granulomatous Lymphadenitis 26 25.25
Metastatic Squamous Cell Carcinoma 13 12.60
Lymphoma 3 2.92
Metastatic Adenocarcioma 4 3.90
Metastatic Malignant melanoma 4 3.90
Metastatic Small Cell Carcinoma 3 2.90
Positive for malignant Cells 3 2.90
Metastatic Hepatocellular Carcinoma 1 0.97
MetastaticPapillary Carcinoma 1 0.97
Metastatic Clear cell carcinoma 1 0.97
Total 103 100
Reactive and granulomatous lymphadenitis were seen relatively in younger age group (mean age 23years) whereas mean age was 46 years for malignant cases. Male -to -female ratio was 3:1 in malignant cases.

27
Breast
A total of 94 FNAs were done from breast. Various lesions diagnosed on FNA are tabulated as follows.
Breast was the second common site for FNAC. Benign proliferative breast disease was the commonest lesion in the age group of 20 to 45years. Among malignant lesions, which favoured patients above 50years of age ductal carcinoma was the commonest (88%). Male - to- female ratio was 1:8 in case of malignant lesions.
FNAC Diagnosis Number Percentage(%)
Benign Proliferative Breast Disease 79 84..1
Gynaecomastia 4 4.2
Ganulomatous Lesion 2 2.1
Ductal Carcinoma 8 8.5
Lobular carcinoma 1 1.1
Total 94 100
Thyroid Gland
Out of 71 thyroid lesions, 63 were benign and 8 were malignant. cases. Benign proliferative thyroid disease was the commonest (54.9%) lesion followed by colloid goitre (23.2%). Papillary carcinoma was the most common malignant lesion (11.3%). Male to female ratio was 1:8 in case of malignant lesions and the mean age was 26years.
Salivary Gland
Various salivary gland lesions diagnosed on FNAC are listed below. The most common site for FNAC was parotid gland. 25% of total cases was found to be malignant. Male-to-female ratio in case of malignancy was 1:1.
FNA Diagnosis Number Percentage (%)
Benign Proliferative Thyroid Disease 34 47.9
Colloid Goitre 17 23.2
Subacute Thyroiditis 4 5.7
Lymphocytic Thyroiditis 3 4.2
Hashimoto Thyroiditis 3 4.2
Thyroglossal Cyst 1 1.4
Follicular adenoma 1 1.4
Papillary Carcinoma 8 11.3
Total 71 100
FNA Diagnosis Number Percentage(%)
Chronic Sialoadenitis 3 37.5
Pleomorphic Adenoma 2 25
Benign salivary Lesion 1 12.5
Mucoepidemoid Carcinoma 1 12.5
Hyalinizing Clear Cell Carcinoma 1 12.5
Total 8 100

28
FNA Diagnosis Number Percentage(%)
Lipoma 30 63.7
Haemangioma 4 8.6
Keratinous Cyst 4 8.6
3 6.3
Paraganglioma 3 6.4
Malignant Melanoma 2 4.3
Fibromyxoid Sarcoma 1 2.1
Total 47 100
Other Sites
Out of 47 FNA done from other palpable lumps, lipoma was the commonest benign lesion, with malignant melanoma being the commonest of two malignant cases.
Discussion
investigations in patients with palpable lumps. Its importance in detecting cancer is widely recognized 2
. Out of 323 FNACs, 83% of lesions were benign and 17% were malignant.
The most common site of FNAC was lymph node (32%). Reactive lymphadenitis was the most common lesion(42.72%) followed by granulomatous lymphadenitis (25.25%). This is similar to the study done by Haque MA et al in which cervical lymph node was the commonest site (87%). 4. This matched with our experience (85%). In his study, reactive lymphadenitis comprised 27.1% and granulomatous lesions 40% which in contrast with 42.72% and 25.25% respectively. Prasoon D reported 27.2% as granulomatous lymphadenitis which matches to our study (25.25%)5. In the study done by Ahmad S et al, 53.6% of cases were diagnosed as reactive hyperplasia and 32.8% as tubercular lymphadenitis. In his study, 46.4% of cases were AFB positive6 whereas in our study 19.2% of cases were AFB positive. On the other hand, Haque M.A et al found 3.5%AFB positive cases.
Haque MA et al reported squamous cell carcinoma as the most common metastatic malignancy (16.6%) 4, this very well correlates with our study(12.62%). We report 2.9% lymphoma where as Tilak et al and Egea et al reported 5.6% and 9.5% cases of lymphoma respectively in their studies7,8.
Breast was the second common site for FNAC. Benign proliferative breast disease was the commonest lesion (84.1%) in the age group of 20 to 45yrs. Among malignant lesions, ductal carcinoma was the most common and affected patients above 50 years. Niazi S. et al found that benign breast disease is common (65%) in younger age group followed by malignancy (29%) in 5th to 6th decade 9 . This is comparable to our study.
Third common site for FNAC was thyroid gland.
Benign proliferative thyroid disease was the commonest (47.9%) which is similar to the result obtained by Matos L.G et al. In his study, benign thyroid lesion comprised 55% and neoplasm comprised 15% 11. Papillary carcinoma was the most common tumor in our study( 11.3%) which is also the most common malignant neoplasm in other studies.
Pleomorphic adenoma was the commonest tumor of all primary salivary tumors and parotid gland was the commonest site (80%). This tallies with the study conducted by S. Ahamed et al (70%) .In his study pleomorphic adenoma was the commonest benign tumor(73%) of all primary salivary gland tumor (73%). Adenoid cystic carcinoma was the most common malignancy (35.7%)12 Whereas mucoepidermoid carcinoma and hyalinizing clear cell carcinoma comprised 12.2% each in our study. The highest incidence for benign lesions was in the 3rd and 4th decade and malignant lesions in 4th to 5th decades of life. S. Ahmad et al observed benign tumors in age group of 30 to 70 years while pick incidence of malignant tumors was 6th to 7th decades.
Conclusion
Wide range of lesions, both benign and malignant, can be diagnosed by FNAC thus restricting surgery to cases only requiring further histopathological evaluation.
References
1. Svante R O,Gregory F.S, Walters M N, Whitaker
cytology,3rd edition, Churchill Livingstone 2002: 3-6.
2 . Winifred G, Mckee GT, diagnostic Cytopathology, 2nd edition, Churchill Livingstone 2003, 281-283.
3. Fine needle aspiration in cancer diagnosis, Ian D Buley, BMJ, 2004, July 31;329(7460):244-245.

29
needle aspiration cytology (FNAC) of lymph node in Mymensingh, Mymensingh Med J, 2003 Jan; 12 (1): 33-35.
5. Prasoon D. Acid fast bacilli in FNA smears from tuberculous lymph nodes. Acta
cytologica;2000:44:297-300.
needle aspiration cytology in lymphadenopathy with special reference tobacid fast in case of tuberculosis. JK Science Vol 7, No. 1; Jan-March 2005.
7. Tilak V, Dhadel AV, Jain R. Fine needle aspiration cytology of head and neck masses.
Ind J Path Microbiol 2002;45(1): 23-30 Aspiration biopsy. Acta Cytologica 2002: 46:368-39.
8. Egea AS, Gonzalez NAM et al. Usefulness of
aspiration.
9. Shahida Niazi, Farukh Kamal: Fine needle aspiration cytology (FNAC); Role in parable breast lesions. The Professionals Vol 7, No. 04, Oct, Nov, Dec. 2004.
10. Godinho M L, Kocjan G., Kurtz A. Contribution of
management of thyroid disease. Clin pathol. 1992, May; 45(5): 391-395.
11. S. Ahmad, M. Lateef; R. Ahamd. Clinopathlogical Study of Primary Salivary Gland Tumors in Kashmir. JK practitioner 2002;9(4)231-233.

30
Rajkarnikar S1, Gurung A2, Bist RR3 Shrestha R4, Shrestha SM5
1Dr Sagar Rajkarnikar, Ophthalmologist, 2Dr Anu Gurung, Ophthalmologist and Head of the Department, 3Dr Ramesh Raj Bist, Senior Consultant Ophthalmologist, 4Dr Ram Shrestha, Ophthalmologist, Department of Ophthalmology, Shree Birendra Hospital, Chhauni, 5Mr Susan Man Shrestha, Statistician, Mother and Infant Research Activities
Abstract
Introduction: Blindness is one of the most tragic yet often avoidable disabilities in the developing world. The pattern of ocular diseases varies in different parts of Nepal due to differences in socioeconomic and
Valley.
Aim: To assess the patterns of ocular disease in the patients attending the outpatient department of Ophthalmology from 14th April 2009 to 13th April 2010 at the Army Hospital.
Methods: This is a retrospective study and all the new cases which attended the department of Ophthalmology of Shree Birendra Hospital in the year 2066 were included. The diseases were divided into 11 groups i.e. lid & adenexal disorder, disease of conjunctiva & sclera, corneal diseases, lens associated disorders, diseases of uveal tract, refractive error, glaucoma & its associations, posterior segment diseases, ocular & systemic neoplastic disorders, Nekebadi (annual medical check up) and others.
Result: The total number of patients recorded in the department of Ophthalmology is 16709. Among them 4473 were regular serving army personnel and 12236 were ex-army and army families.
Conclusion: The pattern of eye disease varies in different age groups. In younger age group conjunctival, scleral disease and refractive error were commonly seen whereas in elder age group lens disorder was frequently seen. The number of blind patients was more in females than in male patients.
Key words: Conjunctivitis, Cataract, Blindness.
Address for correspondence: [email protected]
Introduction Blindness is one of the most tragic yet often avoidable disabilities in the developing world1. The pattern of Eye diseases vary in different parts of Nepal due to differences in socioeconomic and geographic factors. The army hospital in Kathmandu not only treats army personnel but also their family and ex- servicemen who comprise almost 60% of the population. This retrospective study is helpful for the study of pattern of ocular diseases among army personnel and their families.
Aim To study and assess the different patterns of ocular diseases in the patients attending the outpatient department from 14th April 2009 to 13th April 2010 in the Army Hospital.
Methods This is a retrospective study and all the new cases which were diagnosed in the department of Ophthalmology, Shree Birendra Hospital from 14th April 2009 to 13th April 2010 were included. In this study the patients were divided into army personnel, their families and ex-army. The ocular diseases were divided into different 11 groups. Data was tabulated and interpreted in terms of percentage using SPSS version 18.0.
Results
The total number of cases recorded was 16709. Among them 4473 were serving army personnel and 12236 were ex-army and army families.
In total 16709 patients there are 29923 cases. Some patients have one problem in one eye and some had more than one problem in one or both eyes.
Among the patients, the youngest patient is of 18 days and eldest is of 96 year with mean age 46.59 years.
(i.e. 5080 and 7156). Among the number of serving army personnel, male (4101) is more than female (372) and
45.1%).
The patients are divided into 11 different groups according to ocular diseases. Group I (Lid & Adenexa):Chronic Dacryocystitis, Dacryoadenitis, Entropion,
Surgery, Ethmoidocele, Ptosis, Pre-septal Cellulitis, Cellulitis, Caranculitis, Trichiasis, Lid Edema, Epiphora, Concretion, Meibominitis, Wart, Canthal Cyst etc.

31
Group II (Conjunctiva & Sclera): Conjunctivitis, Trachoma, Pinguecula, Pterygium, Episcleritis, Scleritis, Sub
Group III (Cornea): Keratitis, laceration, dystrophies, degeneration, opacity, ulcer, foreign body, Microcornea, Bullous Keratopathy, Penetrating Keratoplasty etc.
Group IV (Lens)
Group V (Uveal Tract): Uveitis, Endophthalmitis, panophthalmitis etc.
Group VI: Refractive errors, presbyopia, asthenopia, amblyopia, headache etc.
Group VII (Posterior Segment)choroidal detachment etc.
Group VIII (Glaucoma): Primary and secondary glaucoma, glaucoma suspect etc.
Group IX (Tumours): consists of any neoplasm effecting eye include Ca Maxilla, melanoma, cerebro-pontine angle tumor, glioma, angioma etc.
Group X (Others): Systemic diseases affecting eye (HTN, DM, Thyroid Disease, Henson’s Disease, Chicken Pox, Meningitis, Myasthenia Gravis, Seizure Disorder, Gilbert syndrome, Aplastic Anemia, Hepatitis, Vertigo, Xanthelesma,
Diplopia, Post Lightening, Retrobulbar Neuritis, Trauma, Squint, Computer Vision Syndrome, Cranial Nerve Palsies (3rd, 4th,5th, 6th, 7th) etc.
Group XI: Nekebadi (Annual Medical Check Up) of army personnel.
The number and percentages of the eye diseases are given in Table 1.

32
Tab 1. Visual Acuity and Diagnosis
Percentage of Total Cases
Disease-wise Percentage
Percentage of Total Cases
Disease-wise Percentage
Percentage of Total Cases
Percentage of Total Cases
Disease-wise Percentage
Percentage of Total Cases
Disease-wise Percentage
No. of cases
No. of cases
Disease-wise Percentage
No. of cases
No. of cases
No. of cases
Percentage of total blind cases

33
Among 29923 cases, total blind cases are 3562,
the maximum number of blind cases (1472) is due to lens and its disorders which account 18.8% of lens problem and 4.9% among the total cases that attended in OPD and 41.3% of whole blind cases. Similarly 18.8% (240) of corneal disorder cases are blind i.e. 6.7% of whole blind cases and 0.8% cases are blind due to corneal disorder. Blindness due to posterior segment and glaucoma accounts for 0.7 & 0.3% (224 & 119) respectively.
Tab 2. Diagnosis and Age Group
Diagnosis 0-14 Yrs (%) 15-40 Yrs (%) 41-60 Yrs (%) > 60 Yrs (%) Total (%)
Normal 30 (2.0) 120 (2.1) 45 (1.2) 9 (0.2) 204 (1.3)
Lid & Adenexa 185 (12.5) 480 (8.5) 159 (4.3) 134 (3.2) 958 (6.4)
Conjunctiva & Sclera 585 (39.7) 1560 (27.9) 943 (25.6) 425 (10.4) 3515 (23.7)
Cornea 46 (3.1) 474 (8.4) 172 (4.6) 110 (2.6) 802 (5.4)
Lens 22 (1.4) 170 (3.0) 918 (24.9) 2693 (66.0) 3803 (25.6)
Uveal Tract 8 (0.5) 71 (1.2) 22 (0.5) 23 (0.5) 124 (0.8)
Refractive Error 541 (36.8) 1281 (22.9) 752 (20.4) 222 (5.4) 2796 (18.8)
Posterior Segment 8 (0.5) 149 (2.6) 113 (3.0) 175 (4.2) 445 (1.4)
Glaucoma 2 (0.1) 78 (1.3) 59 (1.6) 71 (1.7) 210 (1.4)
Tumors 3 (0.2) 4 (0.2) 8 (0.2) 9 (0.2) 24 (0.1)
Others 30 (2.0) 275 (4.9) 176 (4.7) 207 (5.0) 698 (4.7)
Nekebadi 910 (16.3) 311 (8.4) 1221 (8.2)
Total 1470 (9.9) 5582 (37.6) 3678 (24.8) 4078 (27.5) 14808 (100.0)
Table 2 shows the diagnosis and age group of patients. In all age group, except > 60 years, the most common ocular disease is conjunctival & scleral disorders 3515 (23.7%) followed by refractive error 2796 (18.8%). In the group >60 years, the maximum no. of patients are of lens disorder 2693 (66%) and 2nd most common disease is conjunctiva & scleral problem 425 (10.4%) followed by refractive error 222 (5.4%), others 207 (5.0%) and posterior segment problem accounts 175 (4.2%).
In age group 41-60 yrs, 2nd most common disease is lens disorder 918 (24.9%) followed by refractive error 752 (20.4%). Similarly in age group 15-40 yrs & 0-14 yrs also conjunctival & scleral disorder is the most common problem 1560 & 585 (27.9 & 39.7%) respectively. In these group second most common problem is refractive error 1281 & 541 (22.9 & 36.8%).

34
Tab 3. Age and Visual Acuity
Percentage of total patients
Total
(%)
Blind (< 3/60)
(%)
Severe Visual
Impairment
(< 6/60- 3/60)
(%)
Visual Impairment
(< 6/18- 6/60)
(%)
Normal (6/6- 6/18)
(%)
Percentage of total
patients
Total
(%)
Blind (< 3/60)
(%)
Severe Visual
Impairment
(< 6/60- 3/60)
(%)
Visual Impairment
(< 6/18- 6/60)
(%)
Normal (6/6- 6/18)
(%)

35
Table 3 shows the age, sex and visual acuity of patients. In the age group 0-14 yrs, 72.3% had normal vision, 9.8% had visual impairment (VI), 2.0% had severe visual impairment (SVI) and 15.6% were blind. In 15-40 yr age group 5.0% were blind. Similarly 10.7 & 20.0% patients were blind in 41-60 yrs & > 60 yrs respectively.
The percentage of blind patient is the highest in the eldest age group (>60 yrs) i.e. 4.2 % of whole attending OPD patients. Among the age group 41-60 yrs about 2% patients are blind and that of age group 15-40 yrs is 1.6% and in youngest group is 1.25% of whole attending OPD patients.
53.8% patients were male and 46.05 % were female patients. Among male patients 17.8% were blind, 2.45% had SVI, 13.1% had VI and 66.4% had normal vision. Similarly among females, 57.35% had normal vision, 16.35% had VI, 2.9% had SVI and 23.15% were blind. Thus this OPD data showed there is larger number of blind patients in female than male.
Tab 4. Nekebadi
Diseases Number PercentNormal 1025 83.9%Lid & Adenexa 5 0.4%Conjunctiva & Sclera 99 8.1%Cornea 5 0.4%Refractive Error 78 6.4%Glaucoma 7 0.6%Others 2 0.2%Total 1221 100.0%
Table 4 shows the number of regular army personnel who attended OPD for Nekebadi (routine medical check up). Among 1221, 1025 (83.9%) were normal but rest 196 (16.1%) had different problems. Among these 8.1% (99) had conjunctival & scleral problem, 6.4% (78) refractive errors, 0.6% (7) glaucoma, 0.4% (5) cases with lid & adenexal and corneal problem. 0.2% (2) had other problems.
Discussion
In 1988, the world population was approximately 5.1 billion. Over the last 20 years, it has increased by approximately 30%, reaching 6.7 billion in 2008. During the same period, the world population has also become proportionally older, as the number of people aged 65 years and over has increased by approximately 55%, from 320 million in 1988 to 500 million in 2008. Since the prevalence of visual impairment becomes higher as people age, this combination of an increasing population and an ageing population is expected to
people2. In 1988, the number of people who were blind was estimated to be 37 million worldwide. By 2002–04, the latest period for which, it was estimated to be 45 million: 8 million blind due to uncorrected refractive error and 37 million blind due to other causes.3,4 It is thought that at least 60% of blind people are women2,5,6,7.
Globally, based on the 2002 world population, more than 161 million people were visually impaired, of whom 124 million had low vision and 37 million were blind, including 1.4 million under the age of 15 years.8
Using the World Health Organization (WHO)
less, it is estimated that currently there are 45 million individuals worldwide who are bilaterally blind and another 135 million that have severely impaired vision in both eyes. The fact that there are 180 million people in the world today who are in some way severely visually disabled is a tragic, unacceptable situation in both social and economic terms, but this number does not even begin to address the additional hundreds of millions who are disabled by monocular visual loss9.
According to the World Health Organization worldwide there are an estimated 45 million people that are blind with an additional 135 million individuals visually impaired.10 Globally it is known that cataract is the leading cause of blindness, with some 16–20 million people suffering from blinding cataract.11,12 In
highest number of blind people (over 9 million) with the most prevalent cause of blindness and low vision being unoperated cataract, as indicated by several population based studies over the past two decades.13-15
In many parts of the country, lack of awareness and ignorance about any eye disease is still widespread where people take it as a curse of god or sin of previous birth, and very often, they turn to local shamans and spiritual healers for cure in such a situation instead of getting timely medical treatment in the hospital17.
Causes of blindness
Over the last twenty years, the causes of blindness have changed in proportion and actual number. Cataract has remained the major cause of blindness globally. It is particularly important in Asia. The numbers of people blinded by trachoma,
to decrease over the last twenty years18.
In our study, the major cause of blindness is due to lens and its disorder which accounts 41.3% of whole blind cases. Second major cause of blindness is due to conjunctiva and scleral disorder (19.0%), then lid and adexenal disorder (8.3%) followed by others (7.8%), corneal cause (6.7%) and posterior segment disorder (6.2%) are the cause of blindness in our study.

36
In worldwide the major cause of blindness is cataract5,9,17-20. Besides cataract the cause of blindness vary in different parts of world. The two most common causes of blindness in Asian studies are cataract and under corrected refractive errors. This contrasts with Western populations, in which the leading cause of blindness (accounting for more than 50% of cases) is age related macular degeneration (AMD) in white people, and cataract and glaucoma in black people However, in Singapore and Mongolia, glaucoma was the principal cause of both unilateral and bilateral blindness while in the Shihpai Eye Study in Taiwan, retinal diseases as a group, including AMD and myopic degeneration, were the leading cause There is an increasing body of epidemiological data on the major age related eye diseases in Asian populations. The epidemiology of glaucoma and refractive errors, in particular appears to be well characterized. In contrast, there remains paucity of well conducted population based studies on the prevalence of DR and AMD in Asia7,8,18.
Cataract causes 41.8% of global blindness (15
probable cause of the vast majority7. Senile cataract and anterior segment eye infection were the two eye diseases most frequently seen in Giwa community. The results of this study showed that preventable and curable eye diseases were most common19.
In recent years the epidemiology of blindness has changed, shifting away from traditional infectious causes, such as trachoma, onchocerciasis, and leprosy, to other important causes, such as cataract. Indeed, so much emphasis has been placed on managing the backlog of cataract surgery in many developing countries that programmes dealing with other causes of blindness have in some cases been neglected9.
Ocular disease and Age group In our study, the most frequent ocular disease is conjunctival and scleral disorder in all age groups except the eldest age group, followed by refractive error. However, an increasing number of people are at risk of visual impairment as populations grow and people live longer. Developing countries are already aging much faster than those in the developed world. In 2000 more than 248 million (59%), of the roughly 418 million persons aged 65 and over, lived in developing countries. By the year 2020 this is projected to rise to 67%. The UN estimates that by 2020 there will be a global elderly population of 698 million21.
In the youngest age group (0-14 yrs), the most common problem is of conjunctival and scleral disease followed by refractive error, corneal disorders which were similar with other studies.20,22,23,29
Blindness prevalence surveys have been conducted in Nepal nationally and in one region of Pakistan that yielded all age blindness prevalence rates of 0.8% and 1.0% respectively.24,25A subsequent
a blindness prevalence of 3.0% in people 45 years and older5,26.
The proportion of subjects with normal vision
was found to be greater with increased age5.
In our study also as the increased age, the pattern of disease also varies. Lens disorder is seen as the most common problem in eldest age group (66%) followed by conjunctival and scleral problem, refractive error and then posterior segment problem.
A study done in school eye health screening in Kaduna, Northern Nigeria by A.V. Kehinde et al found the commonest causes of eye disorders were allergic conjunctivitis, refractive error, and infective conjunctivitis in school studying students29.
Ocular disease and Sex There was a marked difference in presenting visual acuity between women and men. There was a higher prevalence of blindness in women (1.72%) than men (1.06%) in the study conducted in Bangladeshi adults. In our study the number of female blind patients was
seen in other studies 5,6,24,26,27,28.
Conclusion As we age, we should be aware of the most common eye diseases which can rob our vision. If we understand some of the symptoms, some of which seem of only minor importance on their own, we are more likely to take them seriously and act on them30.
To decrease morbidity from vision loss and blindness, public health professionals must increase public awareness about Age Related Eye Diseases; integrate and coordinate timely screening, diagnosis, and treatment to prevent or correct vision loss31.
There is a general feeling among people; Blindness is punishment of the God due to ignorance and superstition and lack of information about its pathology. Usually the blind is regarded as a helpless and unproductive human. Attention to the needs of the Blind and Partially Sighted (BPS) persons has never been a national priority in Nepal. The blind has always been neglected in all aspect of development.
Neglect of timely and proper medical cure for a sensitive body part like eye is contributing to a rise in the number of cases of blindness in Nepal17.
References1. Resnikoff S. Global data on visual impairment
in the year 2002: Bull World Health Organ 2004;82: 844–851.
2. Allen Foster, Clare Gilbert, Gordon Johnson. Changing patterns in global blindness: 1988–2008. Community Eye Health J 2008;21(67): 37-39.
3. J Hubley and C Gilbert. Eye health promotion and the prevention of blindness in developing countries: critical issues: Br J Ophthalmol. 2006 March; 90(3): 279–284.
4. Resnikoff S et al. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004: Bull World Health Organ 2008;86: 63–70.

37
5. SapkotaYD, Pokharel GP, Nirmalan PK, Dulal S, Maharjan IM, Prakash K. Prevalence of blindness and cataract surgery in Gandaki Zone, Nepal: Br J Ophthalmol 2006;90:411-416.
6. Dineen BP, Bourne RRA, Ali SM, Noorul Huq DM and Johnson GJ. Prevalence and causes of blindness and visual impairment in Bangladeshi adults: results of the National Blindness and Low Vision Survey of Bangladesh: Br J Ophthalmol. 2003 July; 87(7): 820–828.
7. B. Thylefors. Global data on blindness: Bulletin of the World Health Organization, 1995, 73 (1): 115-121.
8. Dr Ivo Kocur. Global pattern of blindness changes with success in tackling infectious disease and as population ages: Bulletin of the World Health Organization. DECEMBER 2004.
9. Whitcher JP, Upadhyay MP, Srinivasan M. Corneal blindness: a global perspective. Bull World Health Organ vol.79 no.3 Genebra 2001.
10. World Health Organization. Programme for the Prevention of Blindness and Deafness. Global initiative for the elimination of avoidable blindness. Geneva: WHO, 1997:1–7.
11. Thylefors B, Négrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness Bull World Health Organ 1995;73:115–21.
12. Arnold J. Global cataract blindness: the unmet challenge. Br J Ophthalmol 1998;82:593–6.
13. Limburg H, Vaidyathan K. Cataract blindness on the rise? Results of a door-to-door examination in Mohadi. Indian J Ophthalmol 1996;44:241–4.
14. Gupta SK. Prevalence and risk factors of cataract in India: a review. Dev Ophthalmol 1997;27:1–5.
15. Dandona L, Dandona R, Naduvilath TJ. Is current eye-care policy focus almost exclusively on cataract adequate to deal with blindness in India? Lancet 1998;351:1312–16.
16. Murthy GVS, Gupta S, Ellwein LB. A population-based eye survey of older adults in a rural district of Rajasthan. I. Central vision impairment, blindness, and cataract surgery. Ophthalmology 2001;108:679–85.
17. Self-reliant in eye treatment. Blind World Magazine January 16,2006.
18. Allen Foster, Clare Gilbert Gordon Johnson. Changing patterns in global blindness: 1988–2008. Community Eye Health J 2008;21(67): 37-39.
19. Wong T Y, Loon SC, Saw SM. The epidemiology of age related eye diseases in Asia: Br J Ophthalmol 2006;90:506–511.
20. Ogwurike S, Pam V. Pattern of Eye Diseases in Kaduna State – A rural community outreach experience: Nigerian Journal of Ophthalmology ; Vol 12, No 1 (2004).
21. Ivo Kocur. Global data on visual impairment in the year 2002. Bulletin of the World Health Organization; DECEMBER 2004.
22. Ajaiyeoba AI, Isawumi MA. Prevalence and Causes of Eye Diseases amongst Students in South-Western Nigeria. Annals of African Medicine: Vol. 5, No 4; 2006: 197-203.
23. Ajaiyeoba AI, Isawumi MA. Pattern of eye diseases and visual impairment among students in southwestern Nigeria. Int Ophthalmol (2007) 27: 287–292.
24. Brilliant GE, Pokharel RP. The epidemiology of blindness in Nepal: report of the 1981 Nepal Blindness Survey. Chelsea, Michigan: The Seva Foundation, 1988.
25. Khan MA, Gulab A, Khan MD. Prevalence of blindness and low vision in North West Frontier Province of Pakistan. Pakistan J Ophthalmol 1994;10: 39–42.
26. Pokharel GP, Regmi G. Prevalence of blindness and cataract surgery in Nepal. Br J Ophthalmol 1998;82:600–5.
27. Dandona L, Dandona R. Is current eye-care policy focus almost exclusively on cataract adequate to deal with blindness in India? Lancet 1998; 351: 1312–16.
28. Murthy GVS, Gupta S. A population-based eye survey of older adults in a rural district of Rajasthan. I. Central vision impairment, blindness, and cataract surgery. Ophthalmology 2001;108:679–85.
29. Kehinde AV, Ogwurike SC, Eruchalu UV, Pam V and Samaila E. School eye health screening in Kaduna -Northern Nigeria. Nigerian journal of surgical research Vol 7, No1-2,2005: 191 – 194.
30. Hitesh K Patel. Leading causes of Visual Impairment and Blindness in America according to Edison Eye Surgeon. Edison, New Brunswick, Central New Jersey, August 2010.
31. Dorothy MG, Appathurai B, Barbara AL, Christopher M. Age-related Eye Diseases: An Emerging Challenge for Public Health Professionals. Prev Chronic Dis 2005 Jul, Volume 2: NO. 3: 1-6.

38
Bhandari BB1, Hamal BK2
1Dr. Bharat Bhandari, Consultant Urologist ,2Dr. Bhairab kumar Hamal, Professor and Consultant Urologist,Shree Birendra Hospital
Address for correspondence: [email protected]
Abstract
AIMS : A retrospective evaluation and statistical analysis of outcome in patients who underwent bulbar end to end anastomosis for stricture of bulbar urethra in Army Hospital.
Methodology: 50 patients with average age of 35 years who underwent bulbar end to end anastomosis between 2005 and 2009 at Army Hospital were analyzed. Mean follow up was 24 months. Stricture etiology was catheter induced 40%, perineal trauma 30%, infection 13%, instrumentation 10% and unknown in 7%. Stricture length was 1cm (59%), 1 to 2 cm (37%) and above 2cm (4%). 30% of the patients were previously subjected to multiple dilatations and internal urethrotomy and clinical outcome was considered failure if postoperative instrumentation was required. Postoperative sexual dysfunction was judged using nonvalidated questionnaire.
Results: Of the 50 cases, 80% were successful and treatment failure was 20 %. Failed cases are
there sexual function out of which 5 had ejaculatory dissatisfaction, 3 with compromised erection and 2 had decreased glans sensitivity.
Conclusion: Bulbar end to end anastomosis has success rate of 80%, with better outcome in fresh cases than in previously intervened cases. Sexual outcome is successful in 80%.
Key words: bulbar urethra, stricture, anastomosis, outcome
Introduction
The anterior urethra is subject to blunt and penetrating injuries, of which blunt trauma predominates.1 Of these injuries, straddle injury, in which the immobile bulbar urethra is crushed against the under surface pubic symphysis, is most common.2 The primary morbidity is urethral stricture formation.3 When a patient presents acutely after injury, one should obtain a history of the mechanism of injury and of the post injury voiding pattern. Suspicious clinical signs include blood at the meatus, gross hematuria, perineal hematoma, urinary retention and frank urethral extrusion through the skin.4
Surgical treatment of urethral strictures includes numerous options such as dilation, vision internal urethrotomy, stent and reconstructive surgical techniques.5 The etiology, site, length and density
management. The surgical technique used in the repair of the bulbar urethral stricture is selected according to stricture length.6 Contusions are generally managed by temporary urethral catheterization.7 Short uncomplicated strictures are generally amenable to complete excision with primary anastomosis. Longer strictures are managed using augmented roof strip anastomosis or substitution only graft urethroplasty. For patients with strictures associated with local adverse conditions, 2-stage urethroplasty might be suggested. End-to-end anastomosis is the most successful treatment for bulbar urethral strictures with a reported high success rate and low postoperative morbidity.8 - 11
Materials and Methods
Shree Birendra Army Hospital caters the Nepal Army personnel and their families. In the past 15 years, the hospital had to manage most of the casualties
Urethral stricture, mostly iatrogenic, was one of the most common complications encountered. Urethral stricture cases were managed depending upon stricture types with dilatation, optical internal urethrotomy and reconstructive surgical techniques. A retrospective analysis of 50 patients who underwent bulbar end to end anastomosis from 2005 January to 2009 December for post traumatic stricture was done.
All the 50 cases were performed by the same surgeon following the standard technique. Catheter was kept for a week and removed. Micturating cystourethrogram was performed after 2 weeks along with urine culture. Patients were told to review immediately in OPD if they experienced decrease in
follow up after four months. If any instrumentation including dilatation was required, outcome of the urethroplasty was considered a failure. Failed cases were managed with OIU and buccal mucosal graft and are being followed up.
Our aim was primarily to assess the outcome of urethroplasty in terms of urinary function and sexual function, which were recorded on the basis of patients’ post operative complaints and indirect questions including penile erection, ejaculation and sensation, which were recorded on a Performa.

39
Results
From 2005 to 2009 a total of 50 patients with average age of 35 (Figure 1) years underwent bulbar end to end anastomosis. Stricture etiology was catheter induced in 40% cases, perineal injury in 30% cases, Infection 13%, instrumentation 10% and unknown in 7% (Figure 2). Stricture length was less than 1cm (59%), 1 to 3 cm (37%) and above 3 cm (4%) (Figure 3). 30% of the patients were previously subjected to multiple dilatations and internal urethrotomy.
All the 50 patients were managed with end to end bulbar urethroplasty and followed up. If any instrumentation including dilatation was required, outcome of the urethroplasty was considered a failure. Of 50 cases, 40 were successful and 10 were considered failure. Analysis of the stricture etiology
revealed 98% success in infective pathology, 90% in urethral instrumentation, 90 % in unknown etiology, 85% in catheter induced and only 70% in trauma induced (Figure 4). In the age distribution, 2 patients each from the age group less than 19, 30 – 39, 40 – 49 and 50 or more failed while 3 patients from age group 20 – 29 were considered failure. 5 of the patients had stricture length less than 1 cm, 4 had 1 – 3 cm and 1 had more than 3 cm.
80 % of the patients had satisfactory sexual
with their sexual function, out of which 5 had ejaculatory dissatisfaction, 3 with compromised erection and 2 had decreased glans sensitivity. 2 patients each were from 50 years or more, 30 – 39 years and 20 – 29 years, 4 patients were 40 – 49 years.
Figure 1 : Age distribution of the patients
12
18
7
10
3
02468
101214161820
Less than 19years
20 - 29 years 30 - 39 years 40 - 49 years 50 or more
Figure 2 : Etiology of Stricture of Bulbar Urethra
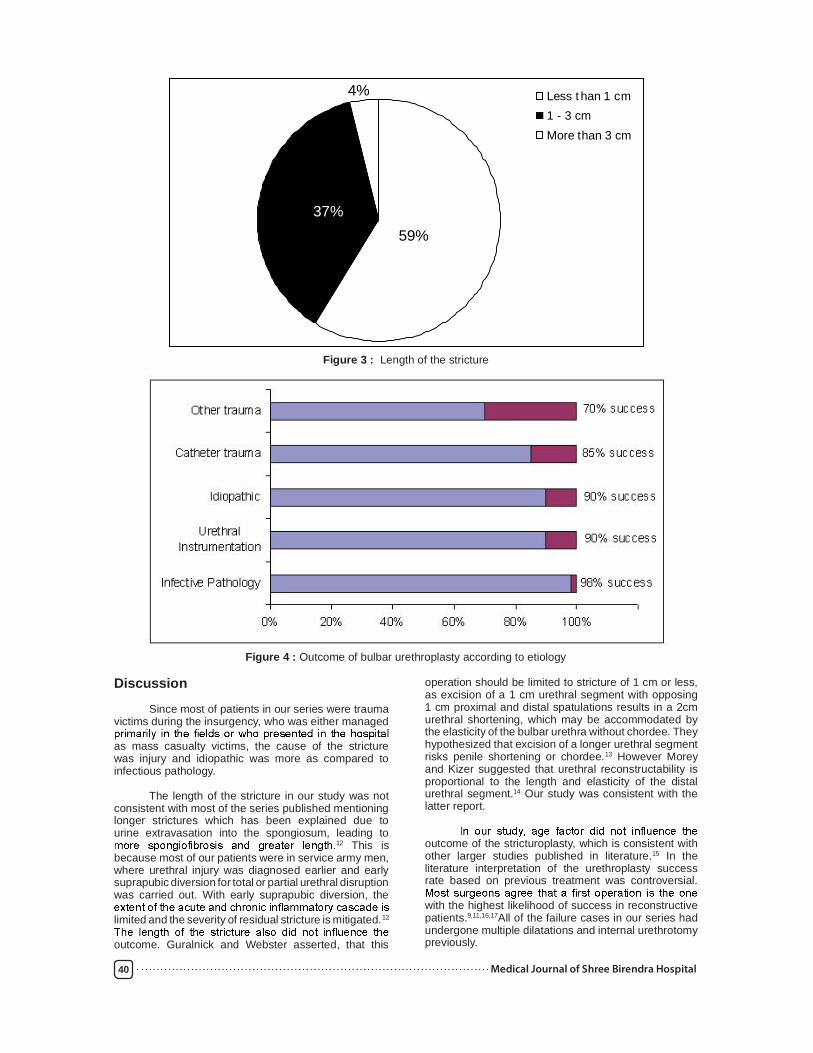
40
Figure 3 : Length of the stricture
37%59%
4% Less t han 1 cm 1 - 3 cm More than 3 cm
Figure 4 : Outcome of bulbar urethroplasty according to etiology
Discussion
Since most of patients in our series were trauma victims during the insurgency, who was either managed
as mass casualty victims, the cause of the stricture was injury and idiopathic was more as compared to infectious pathology.
The length of the stricture in our study was not consistent with most of the series published mentioning longer strictures which has been explained due to urine extravasation into the spongiosum, leading to
12 This is because most of our patients were in service army men, where urethral injury was diagnosed earlier and early suprapubic diversion for total or partial urethral disruption was carried out. With early suprapubic diversion, the
limited and the severity of residual stricture is mitigated.12
outcome. Guralnick and Webster asserted, that this
operation should be limited to stricture of 1 cm or less, as excision of a 1 cm urethral segment with opposing 1 cm proximal and distal spatulations results in a 2cm urethral shortening, which may be accommodated by the elasticity of the bulbar urethra without chordee. They hypothesized that excision of a longer urethral segment risks penile shortening or chordee.13 However Morey and Kizer suggested that urethral reconstructability is proportional to the length and elasticity of the distal urethral segment.14 Our study was consistent with the latter report.
outcome of the stricturoplasty, which is consistent with other larger studies published in literature.15 In the literature interpretation of the urethroplasty success rate based on previous treatment was controversial.
with the highest likelihood of success in reconstructive patients.9,11,16,17All of the failure cases in our series had undergone multiple dilatations and internal urethrotomy previously.

41
Sexual satisfaction was found to be unsatisfactory in elderly age group in our series. This probably was due to other physiological and psychological factors apart from the operative etiology. The cause of sexual dissatisfaction has been explained as due to surgical damage to the branches of the perineal nerves or bulbospongiosum muscles which has a
urine.18
Conclusions
End-to-end anastomosis of the bulbar urethra is an effective surgical option for patients with bulbar stricture. Age should not be a factor from withholding a patient from bulbar end to end anastomosis. Multiple previous manipulations to the urethra decrease the possibility of success of urethroplasty.
References
1. Monga M, Moreno T, Hellstorm WJ. Gunshot wounds ot the male genitalia. J Trauma 1995; 38: 855.
2. Lim PH, Chng HC. Initial management of acute urethral injuries. Br. J Urol 1989; 64: 165.
3. Trifa M, Njeh M, Bahloul A, Jemal S, Mhiri MN. Traumatic rupture of the anterior urethra. Ann Urol 1997; 31 : 313.
4. Witherington R, Mc Kinney JE. An unusual case of anterior urethral injury. J Urol 1983; 130:564.
5. Peterson AC and Webster GD: Management of urethral stricture disease: developing options for surgical intervention. BJU Int 2004; 94: 971.
6. Barbagli G, Palminteri E, Lazzeri M and Guazzoni G: Anterior urethral strictures. BJU Int 2003; 92: 497.
7. Armenakas NA, McAninch JW. Acute anterior urethral injuries: diagnosis and initial management. Traumatic and Reconstructive Urology. Ed. JW McAninch, Philadelhia: WB Saunders Cp. Chapt 45, pp 543 – 550, 1996.
8. MacDonald MF, Al-Qudah HS and Santucci RA: Minimal impact urethroplasty allows same-day surgery in most patients. Urology 2005; 66: 850.
9. Santucci RA, Mario LA and McAninch JW: Anastomotic urethroplasty for bulbar urethral stricture: analysis of 168 patients. J Urol 2002; 167: 1715.
10. Santucci RA, McAninch JW, Mario LA, Rajpurkar A, Chopra AK, Miller KS et al: Urethroplasty in patients older than 65 years: indications, results, outcomes and suggested
11. Eltahawy EA, Virasoro R, Schlosemberg SM, McCammon KA and Jordan GH: Long-term followup for excision and primary anastomosis for anterior urethral strictures. J Urol 2007; 177: 1803
12. Park S, Mc Aninch JW. Straddle injuries to the bulbar urethra : Management and outcomes in 78 patients. The Journal of Urology 2004; 171: 722- 725.
13. Guralnick ML and Webster GD: The augmented anastomotic urethroplasty: indications and outcome in 29 patients. J Urol 2001; 165: 1496.
14. Morey AF and Kizer WS: Proximal bulbar urethroplasty via extended anastomotic approach what are the limits? J Urol 2006; 175: 2145.
15. Santucci RA, McAninch JW, Mario LA, Rajpurkar A, Chopra AK, Miller K Setal: Urethroplasty in patients older than 65 years: indications, results, outcomes and suggested
16. Barbagli G, Palminteri E, Lazzeri M, Guazzoni G and Turini D: Long-term outcome of urethroplasty after failed urethrotomy versus primary repair. J Urol 2001; 165: 1918.
17. Culty T and Boccon-Gibod L: Anastomotic urethroplasty for posttraumatic urethral stricture: previous urethral manipulation has a
2007; 177: 1374.
18. Yucel S and Baskin LS: Neuroanatomy of the male urethra and perineum. BJU Int 2003; 92: 624.

42
Giri NK1, Rawal SB2, Malla 3, Rayamajhi J4
1Dr Naresh Kumar Giri, Consultant Surgeon and Head of the Department, 2Dr Sushil Bahadur Rawal, Consultant Surgeon, 3Dr Srijan Malla, 4Dr Jyoti Rayamajhi, Surgeon Shree Birendra Hospital ,Kathmandu
Abstract
Pancreatic tuberculosis is an extremely rare condition, even in an endemic region like Nepal, and
In this case report, we present a young male who was diagnosed with pancreatic tuberculosis and inadvertent surgery avoided following proper workup of the patient.
Key words: tuberculosis, pancreas, ascites
Address for correspondence: [email protected]
A 22 year-old gentle man presented with abdominal pain for 1 year and abdominal distention for 1 month. Pain was in the epigastric region, it was dull in nature and radiating to right upper quadrant and decreased after taking analgesics. Pain was associated with nausea.
Distension of abdomen used to increase after taking food but distension and discomfort continued since 1 month and was gradually increasing. There was history of weight loss. He had good health in the past and did not have any history of pulmonary tuberculosis in the past.
Physical examination showed ascites, but was
dl; white blood cell count 7.9 × 109L; liver enzymes and renal function tests normal; and erythrocyte
red blood cell and white blood cell and 10% neutrophils and 90% lymphocytes and no atypical cells. On gram staining no micro organism was seen. No acid fast bacilli (AFB) was seen. Protein was 5.8g%, LDH was
Ultrasonography of abdomen showed encysted
of pancreas and ascites. A computed tonography scan of the abdomen showed a hetetogeneous mass measuring 43.6 × 23.3 mm and demonstrating central cystic area measuring 22.6× 23.6 mm in head of the pancreas with moderate amount of ascites. There was lymphadenopathy in the hepatoduodenal ligament. A computed tomography scan of his lungs showed
needle aspiration (FNAC) yieded few scattered epithelial
and negative for malignant cells.
On Peritoneoscopic examination there was multiple peritoneal adhesion and peritoneal cavity was stucked with nodules. The biopsy taken revealed multiple necrotizing epithelial cells, granulomas and multinucleated langhans gaint cells which was consistent with tuberculosis. A ZN stain did not show acid fast bacilli.
A diagnosis of tuberculous infection of the pancreas was made and he is being treated with ethambutol. Pyrezinamide, Isoniazid and rifampicin.
Discussion
Tuberculosis is common in developing countries, but tuberculosis affecting intraabdominal organs is relatively uncommon. Even though Tuberculosis can involve any part of the gastrointestinal tract and is the sixth most frequent site of extra pulmonary involvement. Abdominal tuberculosis mainly involves abdominal lymph nodes and the ileocecal junction, other organs that are uncommonly involved the rest of gastrointestinal tract, peritoneum, liver spleen12. Tuberculosis bacteria reach the gastrointestinal tract via haematogenous spread, ingestion of infected sputum, or direct spread form infected contiguous lymph nodes and fallopian tubes.
Peritoneal tuberculosis occurs in three forms:
type with omental thickening and loculated ascites. The most common site of involvement of the gastrointestinal tuberculosis is the ileocaecal region. Tuberculosis (TB) can involve any part of the gastrointestinal tract form mouth to anus, the peritoneum and pancreatobiliary system.
The postulated mechanisms by which the tubercle bacilli reach the gastrointestinal tract are: (i) haematogenous spread form the primary lung focus in childhood, with later reactivation; (ii) ingestion of bacilli in sputum form active pulmonary focus; (iii) direct spread form adjacent organs; and (iv)and through lymph channels form infected nodes.
The pancreas is biologically protected form infection by Mycobacterium tuberculosis, probably because of the presence of pancreatic enzymes that interfere with the seeding of M tuberculosis. However, when pathogens are able to overcome the resistance, they can have diverse presentations, such as pancreatic masses that can mimic carcinoma, obstructive jaundice, pancreatitis, and gastrointestinal bleeding.
Pancreatic involvement of TB is extremely rare.

43
lack of high index suspicion always misled by pancreatic neoplasm’s. Similarly the wide spectrum of presentation
recognize3. Therefore, pancreatic tuberculosis should be kept in mind among the differential diagnosis of solitary masses in the pancreas, especially in young people in developing countries. The development of abdominal tuberculosis is independent of pulmonary disease in most patients. Auerbach reported in 1944 that 4.7% of 297 autopsy cases of miliary tuberculosis involved the pancreas4. Paraf et al in 1966 reviewed autopsy studies of miliary tuberculosis between 1891 and 1961 and
or peripancreatic involvment. In 1977, Bhansali did not report a single case involvement of the pancreas in 300 patients with abdominal tuberculosis from India6.
Tuberculosis although rare, should be considered as a differential diagnosis in patients with a pancreatic cystic lesion, especially in those with constitutional symptoms7. Several factors have made doctors overlook the diagnosis of pancreatic tuberculosis: (1) the disease is rare; (2) tuberculosis is a stigma of the poor; (3) and abdominal tuberculosis may not always be associated with active pulmonary tuberculosis.
A diagnosis of tuberculosis that can be suggested
tuberculosis, pleural effusion, enlarged celiac lymph nodes, lesions in other solid viscera, ascites, mural thickening in the ileocecal region or positive tuberculin test8, .9,10.
and presence of neutrophils and monocytes. Adenosine deaminase (ADA) an enzyme found in many cells types-macrophages, lymphocytes and erythrocytes. It is a marker host immune response in case of abdominal tuberculosis. Serum ADA activity values of more than 42
11. Serum lactate
patients with intestinal tuberculosis12.
Abdominal CT and US may show an enlarged pancreas with focal hypodense or hypoechoic lesion, usually in the head region, sometimes with irregular multilobular cyst arising form pancreas. However, these
pancreatic neoplasms. US or CT-guided percutaneous FNAC of tumor and to obtain proof of the bacilli by the Ziehl-Neelsen stain or by culture is one diagnostic option, however, the aspiration of material form
even if acid-fast stain for exact sampling, it showed to be positive only in 33-41% of cases of abdominal tuberculosis13,14. The polymerase chain reaction (PCR) of ascites was reported sometimes useful for those the bacterial cultures were negative15. Another diagnostic option involves initiating treatment with antituberculous drugs and evaluating the response of a tumor to this treatment.
Conclusion Pancreatic tuberculosis should be kept in mind among the differential diagnosis of solitary masses in the pancreas, especially in young people in developing
reliable biochemical test. Diagnostic laparoscopic
examination and biopsy are useful for conformation of diagnosis and avoids unnecessary surgery.
References
1. Hulnick DH, Megibow AJ, Naidich DP, Hilfon S, Cho KC, Balthazar EJ: Abdominal tuberculosis: CT evaluation. Radiology 1985, 157:199-204
2. Bhansali SK: Abdominal tuberculosis. Experience with 300 cases. Am J Gastroenterology 1977, 67:324-337
3. Ismail Y, Mihamad A, Surg M. protein manifestation of gastrointestinal tuberculosis. Med L Malasiya, 2003;58:XX-XX.
4. Auerbach O: Acute generalized military tuberculosis. Am J Pathol 1944, 20:121-136.
5. Quanda Liu, Zhenping he and Pain Bie; Solitary pancreatic tuberculous abscess mimicking pancreatic cystadenocarcioma: a cases report, BMC Gastroenterology 2003, 3:1
6. Bhansali SK: Abdominal tuberculosis. Experience with 300 cases. Am J Gastroenterol 1977, 67:324-337.
7. S.F.Lo, A.K. Ahchong, C.N. Tang and A. W. C. Yap;Pancreatic tuberculosis: case report and review of the literature, R.Coll. Surg.Edinb.,43,Febeuary 1998.65-69,
8. Pombo F, Diaz Candamio MJ, Rodroguez E,
Abdom Imaging 1998, 23:394-397.
9. Takhtai D, Gupta S, Suman K, Kakkat N, challa S, Wig JD, Suri S: Radioligy of pancreatic tuberculosis: a report of three cases. Am J Gastroenterol 1996, 91:1832-1834
10. Akhan O, Pringot J: Imging of abdominal tuberculsis. Eur Radiol 2002, 12:312-23.
11. Petroianni A, Mugnaini I, Laurendi G et al , AbDominal tuberculosis mimicking Crohn’s
2002; 44: 155-158.
12. Rangaabashyam N, Ananda BS, Om Prakash R,. Abdominal tuberculosis, oxford text book of surgery, vol 3, 2nd edn. Oxford: OUP, 2000; 3237-3249.
13. Kqduri VG, Janardhanan R, Hagan P, Brodmerkel GJ: Pancreatic TB: diagnosis by needle aspiration.
Am J Gastroenterol 1992, 87:1206-1209
14. Lo SF, Ahchong AK, Tang CN, Yip A WC: Pancreatic tuberculosis: case reports and review of the literature. J R Coll Surg Edinb 1998, 43:65-69
15. Hashimoto M, Koyama H, Noie T, Shibayama K, Katamura N: Abdominal tuberculoma mimciking a pancreatic neoplasm: report of a case. Surg Today 1995, 25:365-368.

44
Khatri R1, Manandhar R2, Pradhan N3, Manandhar B4, Rawal S5
1Dr Ratna Khatri, 2Dr Rita Manandhar, 3Dr Neelam Pradhan,4Dr Bekeha Manandhar, 5Dr Sunuti Rawal, Obstetrician and Gynecologist, Department of Obstertics and Gynaecology, TUTH, Kathmandu Nepal
Abstract We report a case of Chrioangima of placenta resulting to hydropsfetalis. A 24 yrs old primigravida with polyhydramnios and large placental chorioangioma at 24 wks of gestation expelled a nonimmune hydropic male baby weighing 900gms. The baby expired after 5 minutes of expulsion.
Keywords: Placental chorioangioma, Hydropsfetalis, Polyhydraamnios
Address for correspondence: [email protected]
Introduction
Placental chorioangioma is the most common benign tumor of placenta. The incidence being 1% of pregnancies. The relationship of vascularised chorioangiomas to adverse pregnancy outcome is well recognized. 50% of all cases will lead to maternal and fetal complications. Ultrasonography and Doppler ultrasonography are useful in establishing the prenatal diagnosis and the prognosis.
Case Report
A 24 yrs old primi- gravida, resident of Kathmandu was admitted in the female surgical ward on 11 chaitra 062 for observation with the diagnosis of 27 +3 weeks of gestation with chorioangioma by USG. She had 2 ante-natal visit,1st at 18 wks, 2nd at 26+5 weeks of gestation. at TUTH.
She attained menarche at 14 yrs. and had
Her LMP was on18.06.062 and EDD calculated to be on 25.03.063.
No family history suggestive of chorioangioma.
She was non smoker, non alcoholic. In her last ante-natal visit, at 26 weeks of gestation on examination perabdominally she was found to have uterus of 30 weeks size, it was tense in consistency with foetal parts not palpable and FHS was present. Since uterine height was more than the period of gestation urgent USG was advised keeping in mind she might have polyhydramnios, abruptio placentae, multiple pregnancy. USG revealed single live foetus of 24 week gestation with adequate liquor. And a separate placental mass measuring 8.8 x 9 cm size was also noted, giving the impression of chorioangioma of placenta. So she was advised admission for observation. Next day she went into premature labour and expelled an alive male
Baby was cyanosed, had generalized oedema, and ascitis. There was no gross congenital anomaly.
The liver and spleen were not palpable.
Grossly umbilical cord was 23cm Placenta measured 13x 14 x 5 cm size and was friable. There were two separate pieces of smooth brown coloured mass measuring 9x10x3 cm & 10 x 60 x 2 cm size, which was lobulated on the outer surface.

45
On microscopic examination section from umbilical cord showed 2 arteries & 1 vein. Placental section showed multiple chorionic villi lined by trophoblasts with increased vascularity in the mesenchymal cone. The separate tumour mass composed mainly of small blood capillaries along with
Her intranatal and post natal period was uneventful and she was discharged on 3rd post natal day.
Discussion
Chorioangima is the most frequent non trophoblastic tumour of the placenta with a incidence ranging from 0.01 - 1.3% of pregnancies. This term is used to describe abnormal proliferation of vessels arising from chorionic tissue (1). It is the most common benign tumour of the placenta (2). Small placental chorioangiomas are found in 1% of
Large chorioangiomas larger than 5 cm are much less common with an estimated incidence of 1 in 2000-3500 births, but are associated with high perinatal mortality of 40% (3). It is usually single but occasionally multiple. This case also had two placental chorioangiomas with size measuring more than 5 cms. Hpoxia and genetic factors are predisposing factors (4). The majority are small not visible on external surface are asymptomatic.
most commonly protrudes from the foetal surface of the placenta near the insertion of cord. The size more than 5 cm is associated with complications (5).
There are multiple risk factors for chorioangioma. It is divided into moderate and high risks. Moderate risk factors include age of the patient >35 years, increased BP during second trimester, new paternity and dietetic factor: famine, anorexia. Environmental factors like high altitude, smoking, controlled diabetes mellitus, genetic factor.
BMI more than 25, primiparous, past family
to premature placental release, cocaine, tobacco or caffeine use, molar pregnancy, uncontrolled diabetes mellitus, scleroderma, chronic hypertension, anti-phospholipid syndrome, past history of deep vein thromosis, thrombophilia, past history of placental vascular pathology, IUFD, abruptio placentae, IUGR, repeated foetal loss, hyperhomocystinaemia are the high risk factors for chorioangioma of placenta (6). In this case clinically and by history she was not suggestive of any of the risk factors mentioned above except she was primigravida.
Maternal complications includes
Polyhydroamnios, Precipitate labour, Pre-eclampsia, maternal thrombocytopenia, maternal coagulopathy, Hypertonic uterus,PROM, Haemorrhage- both APH &PPH (6). This case had polyhydramnios, pre term premature rupture of membrane and precipitate labour.
Foetal Complication includes: Abortion due to hypoxia, IUGR, and IUD because the considerable proportion foetal blood passes through the tumour rather than the functional placental tissue. So foetus is supplied by deoxygenated blood and nutrient poor state.
There can be foetal cardiomegaly due to peripheral AV shunts leading to increased foetal cardiac output. The cause of neonatal oedema can be cardia failure or
hypoalbuminaemia – because of trasudation of protein from the surface vessels of the tumour or from chorionic foetomaternal bleeding from haemangioma.
Neonatal thrombocytopaenia is due to injury within the tumour vessels.
DIC may occur due to release of thromboplastic substance from the haemangioma. Neonatal anaemia is due to sequestration of foetal erythrocytes within the tumour, or
massive foetomaternal bleed from the haemangioma or microangiopathic haemolytic anaemia induced by injury
Ultrasonogram, maternal serum AFP- increased prenatally , Colour doppler imaging- to differentiate placental chorioangima from other placental lesions.
but clear foetal waveforms in its periphery can be demonstrated (7). 3D power doppler angiography- clearly shows highly vascularized placental mass including its feeding vessels& drainage at the foetal surface of the tumour (5).
This case was diagnosed ultrasonographically
The most effective way of diagnosing chorioangioma

46
is doppler ultrasonography but we could not apply it in this case, it was planned but same night she went into preterm labour.
Various modalities of treatment of chorioangioma of placenta have been reported in different case reports.1. Treating the cause is by occluding the vascular
supply like
a. Foetoscopic devascularization by ablating the feeding vessels (8).
b. Microcoil embolization by ultrasound guided laser therapy which leads to tissue coagulation causing complete cessation of tumor blood
c. Intravascular injection of absolute alcohol in the feeding vessels of large tumour – this may be one of the best choices due to its high
(10).d. Ligation of tumor vessels.
2. Treating the foetal complications produced by chorioangioma prenatally by intrauterine transfusion. It is necessary if foetal anaemia is diagnosed by cordocentesis in early pregnancy. There is risk of repeated transfusion, pre-term labour and iron overload, so some form of embolization or tumour devascularization is necessary(8).
3. Symptomatic treatment like amniodrainage:
pocket 12 cm and excessive maternal symptoms.
Prognosis is poor for large tumor. It largely depends on foetal haemodynamic tolerance with large placental chorioangioma. 50% lead to maternal & foetal complication (11).
References
1. Sepulveda W, Alcade JL, Schnapp C, Bravo M. Perinatal outcome after prenatal diagnosis of placental chorioangioma. JACOG 2003;102:1028-33.
2. Napolitano R, Maruotti GM, Mazzarelli LL, Quaglia F, Tessitore G, Pecorare M et al. Prenatal diagnosis of placental chorioangioma: our experience. Minerva Ginecol. 2005; 57(6): 649-54.
3. Lau TK, Leung TY, Yu SCH, To KF, Leung TN. Prenatal treatment of chorioangioma by microcoil embolization. A case reort. BJOG 2003;110:70-73.
4. Noack F, Sotlar k, Thorns C, Smreek J, Diedrich K, Feller AC et al. VEGF-KIT protein and
chorioangioma? Placenta 2003; 24(7):758-66.
5. Hata T, Inubashiri E, Kanenishi K, Akiyama M, Tanaka H, Yaagihara T. Three dimensional power doppler angiographic features of placental chorioangioma. J Ultrasound Med 2004; 23:1517-20.
6. Foidart JM, Seak-San S, Emonts P, Schaaps JP. Vascular placental pathology in high-risk groups:
154(5): 332-9.
7. Maymon R, Hermann G, Reish A, Strauss S, Sherman D, Heyman E. Chorioangioma and its severe infantile sequelae: case report. Prenat Diagn 2003;15(12); 976-80.
8. Witters I, Van Damme M, Racemakers P, Van Assche F, Fryns JP. Benign multiple diffuse neonatal haemangimatsis after a pregnancy complicated by polyhydramnios and a placental chorioangioma. European Journal of Obstetrics& Gynaecology and Reproductive Biology 2003; 106:83-85.
9. Bhide A, Perfumo F, Sairam S, Carvelho J, Thilaganathan B. Ultrasound guided interstitial laser therapy for the treatment o placental chorioangioma. Obstet Gynecol 2003;102: 1189-91.
10. Wanpirak C. Tongsong T, Sirichotiyakul S, Chanprapaph P. Alcoholization: the choice of intrautrine treatment for chorioangioma. J Obstet Gynaecol Res. 2002;28 (2):71-5.
11. Wehrens XH, Offermans JP, Snijders M, Peeters LL. Foetal cardiovascular response to large placental chorioangiomas. J Perinat Med. 2004; 32(2): 107-12.

47
Rajbhandary GL
Dr Gambhir Lal Rajbhandary, Prof. of CTVS (NAMS), Shree Birendra Hospital
Address for correspondence: [email protected]
Introduction Like in many agriculture farming countries Cystic Echinococcal disease is Endemic in Nepal also1,2. Incidence of liver & pulmonary hydatid cysts are common among adult population in Nepal, but there are few literature published on surgical experience with pulmonary hydatid cyst in pediatric age group in Nepal3.
Material During last 14 years since 1994 to 2008, 18 cases of pulmonary hydatid cyst were operated at Cardio-thoracic surgery unit of Birendra Hospital. There were 14 male & 4 female. Their age range from 7 years to 70 years. There were 2 patients between 7 years to 14 years. Recently there were more presentation of hydatid cyst in young age group.
Case no 1 (Operated 2008 )
Pediatric case No 1 A 14 years old boy presented with Rt sided chest pain, cough & fever one month, X-ray chest showed huge round Radio Opaque shadow over Rt lung. CT scan of chest reveled Cystic homogenous opacity - Rt lung Lung Cyst on Rt. lower lobe size – 12cm x 10cmPt had Pre-Operative, Tab. Albendazole 400 mg BD for 4 weeks 4,5 .Operation:- Rt Thoracotomy & enucleation of hydatid cyst from Rt lower lobe 6,7 .The bronchi at opening were closed with Proline suture . The cavity is closed with Vicryl suture Post operation period was smooth. Patient had unilocator hydatid cyst & on
Echinococcal pathology.
Case no 2. Operated 2008 AD
Pediatric case No. 2 A 7 years old boy presented with cough, fever, Hemoptysis – 2 months on x-ray chest there were two large rounds opacities over Rt lung one Upper lobe & one is Rt lower lobe lung. CT scan of chest revealed Cyst Size – 10 cm x 8 cm on Rt Lung Lower lobe . Cyst Size – 8cm x 6cm on Rt lung upper lobe. On USG abdomen there was no hepatic cyst. Blood agglutinate test for Ecchinococcus was Negative. Ptatient was operated after 4 weeks of Albendazole 400 mg daily. During surgery there was large unilocator cyst over Rt lower lobe lung Cyst of Rt. Lobe was enucleated, Cavity closed multiple layers. Another lung cyst on Rt upper lobe was also enucleated & cavity obliterated, Pt had smooth post overactive recovery. Fig 1,2,3,4 shows the patient during and post operation.
Fig. 1
Fig. 2
Fig. 3

48
Fig. 4
Discussion
Cystic hydatid cyst of lung & liver are common in adult age group in Nepal.There were not many cases presented with hydatid cyst in Pediatric age group in Nepal.Recently we have noticed increase in pulmonary hydatid cyst in young age group in Nepal.Most of the cyst in our country present as Unilocator Cysts but size were large 7,8 .- Both the Pediatric pulmonary hydatid cysts fall in WHO group 1 larger than 2 cm. & active9 .
- All the patients had smooth post operative recovery & there was no reporting of recurrence in 14 years of follow up10 . - VATS surgery was not used due to large size of Pulmonary Cyst & to avoid rupture & recurrence11 .
Conclusion
Pulmonary hydatid cyst is still common in Nepal.Now we see more in younger age group. Prognosis of surgery in younger age group is good. In our Study most of the Pulmonary Hydatid Cysts were large but unilocator.
References
1 Schantz PM : Epidemiology of Cystic Echinococosis Global distribution & Pattern of
Transmission, Proceeding of National Seminar on Echinococosis, Kathmandu, Nepal 1996
2 Joshi AB, Joshi DD, Schantz PM etal, Epidemiological Assessment of Echinococosis in Nepal Proceedings of National Seminar on Echinococosis Kathmandu, Nepal 1996
3 Robert W. Tohan, Echinococcosis E-Medicine. Jan 22, 2009
4 Harton, Chemotherapy of Echinococcus infection in Man with Albendazole, Pharmacopia Martin Dale 1993
5 Rajbhandary G.L., Hydatid Cysts complete resolution following Albendazole J.Nep. Med. Assoc. 1995.33,131-132
6 Gizzberg E. Pulmonary Hydatid Cyst. Robs Smith’s Operative Surgery Thoracic Surgery Jackson JW, Cooper DKC, Butter Worth, London 1986, 194 - 203
7 Rajbhandary G.L. Surgical Experience with Hydatid Cysts of Lung & Liver. J.Society of Surgeons of Nepal 1998 – Vol 1, 13 - 15
8 Ayten A. Yten Kayi Cangir Srugical Treatment of Pulmonary Hydatid Cysts in Children Journal of Pead. Surgery. 2001, Vol 36 Issue 6 Page (917 – 920) .
9 WHO Informal working group on Echinococosis 2003. 3 grouping of Echinocococus Cyst.
10 Keramidas DC, Passalides AG, Soutis M. Hydatidosis Management in Children: Depend on Anatomical location for Treatment International Association of Hydatology. News letter of Hydatidosis 1997 is. 15
11 WUM, Jhag LW 2 Hutt, Qian Z-X Surgical Treatment of Thoracic Hydatidosis Review of 1230 Cases. Chinese Medical Journal 2005: 118, 1665.

1st
Brig. Gen. Dr. Gambhir Lal Rajbhandari
Commandant

nd
Editor in ChiefBrig Gen. Prof. Dr. Bachhu Ram. K.C.

Synthetic Absorbable Suture Non Absorbable Suture
For Business- Contact In NepalLife Guard Surgical Pvt. Ltd.
Near - Sarbang Nursing HomeKupondol, LalitputPh: +977-1-6202678
Email: [email protected]
R

-
- -




















