Medical conditions present during pregnancy and risk of perinatal death in Jamaica
20
Paediatric and Pcrinatal Epidemiology 1994,8, Suppl. 1,664s Medical conditions present during pregnancy and risk of perinatal death in Jamaica Deanna Ashle a,Rosemary Greenwoodb,Affette McCaw-Binnslc, Peter Thomasb#c and Jean Goldingb aMinisfry of Health, larnaica, bInsfifute of Child Health, University of Brisfol, UK and CUniversity of the West Indies, Jamaica Summary. In an attempt to identify causes of perinatal mortality and thence devise preventative strategies on the island of Jamaica,a study was made of the 1847 singleton perinatal deaths occumng over the 12-month period between 1 September 1986 and 31 August 1987. Complications of the pregnancy were elicited by questioning the mother as well as abstrad- ing data from the antenatal and clinical obstetricrecords. The deaths were classified using the Wigglesworth categorisation and the three largest groups were chosen for special study: antepartum fetal deaths, deaths of live births from immaturity and deaths from intrapartum asphyxia. The medical features of the pregnancieswere compared with data similarly obtained from 9919 women delivering singletons in the 2 months of September and October 1986 and who survived the first week of life. Unadjusted statistically significant associations were found with ma- ternal syphilis, vaginal infection or discharge, bleeding in the first two trimesters, bleeding in the third trimester, lowest haemoglobin, highest diastolic and first diastolic blood pressures, highest level of proteinuria, diabetes and antenatal eclampsia. Logistic regression taking account of social, environmental and health behaviour variables showed the follow- ing significant relationships. Antepartum fetal death was associated with adjusted odds ratio (AOR) for syphilis 2.88 [95% confidenceinterval (CI): 1.91, 4.321, bleeding in third trimester 3.86 [2.73, 5.441, highest diastolic blood pressure (P < 0.0001), highest level of proteinuria (P < O.OOOl), lowest Hb (P < 0.OOOl) and antenatal eclampticfits AOR 4.62 [1.47,14.501. Deaths from immaturity were independently associated with bleeding <28 weeks AOR 3.50 [2.39, 5.131, bleeding 28+ weeks AOR 1.93 [1.16, 3.221, highest diastolic blood pressure (P < 0.01) and highest level of proteinuria (P < 0.0o01). Infectionfeatured in deaths associated with intraparturn asphyxia, with syphilis AOR 2.17 [1.44,3.26] and vaginal infection/discharge (P < 0.01) Address for correspondence: Dr Deanna Ashley, Ministry of Health, 10 Caledonia Avenue, Kingston 5, Jamaica. 66
Transcript of Medical conditions present during pregnancy and risk of perinatal death in Jamaica

Paediatric and Pcrinatal Epidemiology 1994,8, Suppl. 1,664s
Medical conditions present during pregnancy and risk of perinatal death in Jamaica
Deanna Ashle a,Rosemary Greenwoodb, Affette McCaw-Binnslc, Peter Thomasb#c and Jean Goldingb aMinisfry of Health, larnaica, bInsfifute of Child Health, University of Brisfol, UK and CUniversity of the West Indies, Jamaica
Summary. In an attempt to identify causes of perinatal mortality and thence devise preventative strategies on the island of Jamaica, a study was made of the 1847 singleton perinatal deaths occumng over the 12-month period between 1 September 1986 and 31 August 1987. Complications of the pregnancy were elicited by questioning the mother as well as abstrad- ing data from the antenatal and clinical obstetric records. The deaths were classified using the Wigglesworth categorisation and the three largest groups were chosen for special study: antepartum fetal deaths, deaths of live births from immaturity and deaths from intrapartum asphyxia. The medical features of the pregnancieswere compared with data similarly obtained from 9919 women delivering singletons in the 2 months of September and October 1986 and who survived the first week of life.
Unadjusted statistically significant associations were found with ma- ternal syphilis, vaginal infection or discharge, bleeding in the first two trimesters, bleeding in the third trimester, lowest haemoglobin, highest diastolic and first diastolic blood pressures, highest level of proteinuria, diabetes and antenatal eclampsia. Logistic regression taking account of social, environmental and health behaviour variables showed the follow- ing significant relationships. Antepartum fetal death was associated with adjusted odds ratio (AOR) for syphilis 2.88 [95% confidence interval (CI): 1.91, 4.321, bleeding in third trimester 3.86 [2.73, 5.441, highest diastolic blood pressure (P < 0.0001), highest level of proteinuria (P < O.OOOl), lowest Hb (P < 0.OOOl) and antenatal eclamptic fits AOR 4.62 [1.47,14.501. Deaths from immaturity were independently associated with bleeding <28 weeks AOR 3.50 [2.39, 5.131, bleeding 28+ weeks AOR 1.93 [1.16, 3.221, highest diastolic blood pressure (P < 0.01) and highest level of proteinuria (P < 0.0o01).
Infection featured in deaths associated with intraparturn asphyxia, with syphilis AOR 2.17 [1.44,3.26] and vaginal infection/discharge (P < 0.01)
Address for correspondence: Dr Deanna Ashley, Ministry of Health, 10 Caledonia Avenue, Kingston 5, Jamaica.
66

Medical conditions and risk of perinatal death 67 independently associated; other strong associations were bleeding < 28 weeks AOR 2.10 11.57, 2.811, bleeding 28+ weeks AOR 2.32 11.62, 3.331, highest diastolic blood pressure (P < O.OOOl), first diastolic blood pressure (P < 0.OOOl) and antenatal eclampsia AOR 6.70 [2.63,17.13].
For all perinatal deaths combined, independent features were syphilis AOR 2.06 [1.49, 2.851, vaginal infection/discharge (P< 0.001), bleeding c 28 weeks AOR 2.01 11.60, 2.531, bleeding 28 + weeks AOR 2.65 12.02, 3.481, highest diastolic blood pressure (P < O.OOOl), first diastolic blood pressure (P < O.OOOl), proteinuria (P < 0.OOOl) and antenatal eclampsia AOR 4.22 [1.76,10.14]. The results help identify areas for monitoring and idenhfyq pregnancies at highest risk.
Introduction
Several medical conditions may arise de nova during the course of a pregnancy or be exacerbated by the pregnancy and contribute sigruficantly to the risk of maternal and perinatal mortality and morbidity. The relative importance of these conditions varies from country to country, and may be related to the treatment regimes, the socio-economic status and environment of the women. It has already been shown1e2 that the majority of maternal deaths in Jamaica can be attributed to three con- ditions: infection, hypertension and haemorrhage. The key question concerns how many pregnancies fail for the same reasons.
Infection In the past, infection has been a major cause of maternal and infant mortality in the developed world. Today antenatal infection is still thought to contribute to poor outcome of pregnancy, especially to preterm delivery. In the literature it has been reported that between 3 and 8% of pregnant women have asymptomatic bacteriu- ria; approximately 1% of these asymptomatic cases may progress to acute cystitis and pye l~nephr i t i s~~ and between 15 and 45% of them will develop symptomatic urinary tract infection if not treated.6 Many ~ tud ie s~-~* have postulated a relation- ship between asymptomatic bacteriuria in pregnancy with increased fetal mor- tality, preterm delivery, intrauterine growth retardation and Iow birthweight infants, but the evidence is inconclusive.
Syphilis during pregnancy, especially in the second trimester, may result in tragic sequelae: 20% preterm delivery, 20% miscarriage or perinatal death, 20% sub-clinical infection and 40% congenital infection with handicapping conditions have been reported.I2 Gonorrhoea is also a potentially serious infection of preg- nancy. Maternal infection rates have been reported to range from 1 to 5% in different studies,I3 but no studies have been published on perinatal mortality.

68 D. Ashley et al.
Haemowhuge and anaemia Bleeding in the first two trimesters tends to be ignored by clinicians, yet the British Perinatal Mortality Survey showed that it was strongly predictive of excess risk of perinatal death.** In developing countries bleeding in the third trimester remains a major contributor to both maternal and perinatal death. The main causes of life- threatening antepartum bleeding are either placental abruption or placenta prae- via. However in about 50% of cases the antepartum haemorrhage is of uncertain 0rigir1.I~ Ascertainment rates are variable. Some episodes of bleeding are judged by the women to be trivial and therefore are not brought to the attention of the health worker. Nevertheless they may carry an increased risk.
In pregnancy the normal physiological changes result in a fall in haemoglobin concentration and an increase in transferring concentration mimicking an iron deficiency state. Free protoporphyrin in the red cell which is also increased in iron deficiency anaemia, rises during normal pregnancy. These facts have contributed to the difficulty in defining anaemia among pregnant women. The World Health Organisation16 after struggling with this problem set 11 g/dl as the level below which ‘anaemia or iron deficiency should be considered to exist’. Studies have shown, however, that black women have haemoglobin levels 1 g/dl below white women.16 This is the reason for setting the level of anaemia in black populations to below 10g/dl, but a more valid assessment may be to look at the point at which adverse outcome to both mother and fetus arises. This was a particular aim within the Jamaican study.
The hypertensive disorders of pregnancy The hypertensive disorders of pregnancy are associated with increased risk of perinatal mortality, particularly when the disorder is severe and occurs with proteinuria. In the UK in 1958 the main Wigglesworth categories of death associ- ated with hypertensive disorder were antepartum fetal deaths and conditions associated with premat~rity.’~ Preliminary analysis of the 2-month Jamaican co- hort has already shown that the hypertensive disorders of pregnancy in Jamaica were associated with increased perinatal mortality rates18 using just the perinatal deaths occurring in the 2 cohort months. Here the analyses are extended to include the full year of deaths.
Material and methods The Jamaican Perinatal Mortality Survey was designed to assess factors related to perinatal mortality, in order to devise preventative strategies. The study obtained information on 94% of all mothers delivering on the island in the 2 (cohort) months of September and October 1986 by interviewing the mother and abstracting infor- mation from the clinical records. Similar data were collected on all stillbirths

Medical conditions and risk of perinatal death 69
weighing 500g or more and all live births dying within 7 days of birth in the 12-month period from 1 September 1986 to 31 August 1987.19
Information collected on the pregnancies included the following data ab- stracted from the clinical antenatal records: the lowest Hb level measured, results of VDRL test, number of times blood pressure was measured, first reading (with date), reading with the highest diastolic pressure (with date), number of times urine tested, highest level of proteinuria found (with date), presence of oedema, whether mother had vaginal bleeding pre-28 weeks, vaginal bleeding post 28 weeks, diabetes, vaginal discharge or infection (with details of treatment given), urinary tract infection, gonorrhoea, syphilis or eclamptic fits.
In addition, and quite separately, the mother was asked whether she had had vaginal bleeding before or after 28 weeks gestation, and whether she had taken antibiotics.
The perinatal deaths were classified from information available from clinical and, where relevant, post-mortem records using the Wigglesworth classification to identlfy five groups - the antepartum fetal death (APFD), congenital malfor- mations, deaths of live births due to immaturity (IMMAT), deaths from intrapar- tum asphyxia (PA) and a small group of miscellaneous causes.Ig In this paper we present the data from the three largest groups (APFD, IMMAT and PA) as well as for all perinatal deaths combined. They are compared throughout with the pregnancies in the 2 cohort months which resulted in a baby who survived the first week of life (SURV). For the present analyses, singletons only are considered.
Statistical analyses
Initial comparison of survivors with deaths used chi-squared tests, with the Man- tel-Haenszel test for trend where appropriate, using the SPSS package. For 2 x 2 tables the continuity correction was employed, and where the expected number was less than 5, Fisher's Exact test was used.
Logistic regression models were built stepwise from all medical conditions with maternal age, regardless of whether they had been significantly associated with the outcome at the unadjusted stage. Subsequent models were derived after also taking account of the social, environmental and health behaviour variables shown elsewherGOJ1 to be related to the outcome.
Results
Unadjusted comparison of survivors with each group of deaths is shown in Appendix 1.

70 D. Ashley et al. lnfec tion Indirect evidence of infection is provided by the numbers of women who took antibiotics during pregnancy. In all, 13% of the mothers had taken these drugs, but there was no relationship with perinatal mortality. Jamaican women were not screened for urinary tract infection. Nevertheless 3.6% of women were reported as having had this infection during the antenatal period. This therefore is a reflection of the incidence of symptomatic infection. There was no increase in risk of any category of perinatal death among mothers with such infections.
Three-quarters of pregnant women were tested at least once for syphilis and of those tested, results were available for 85%. Of these, 4.9% had a positive VDRL test. In Appendix 1, the numbers with syphilis are those that have been identified in this way, but those in the 'no syphilis' group will include some that were not screened. The risks of perinatal mortality were significantly increased for both the APFD (P < 0.0001) and IPA (P < 0.01) groups and for all perinatal deaths (P < 0.0001) if the mother had had syphilis.
Gonorrhoea was much less frequently reported (0.5% of survivors, 1.0% deaths) and exhibited a statistically sigruficant increase in risk for all deaths combined (P<O.O5). One in five mothers was reported as having a vaginal infection or discharge. There was an increased risk of perinatal mortality in this group but only if the infection was not treated. This group included those who were reported as refusing treatment.
Bleeding and anaemia In the present study, 6.2 or 4.7% of mothers had a history of vaginal bleeding in the first two trimesters according to whether the information was obtained from the mother or from the antenatal records. In all, 6.6% of mothers of survivors had a bleeding episode recorded compared with 13.9% of perinatal deaths (P C 0.0001) with deaths from immaturity being the most at risk 24.9% (P < O.OOO1) (Appendix 1).
Mothers of survivors also reported slightly more bleeding in the third trimester (2.8%) than was recorded on the antenatal records (2.5%), with 3.4% of mothers altogether having bleeding recorded. Bleeding episodes were over three times more common in the perinatal death group than in the survivors (P<O.OOol) (Appendix 1). All the three groups of death were at increased risk ( P < 0.OOOl).
There is defdte evidence of a negative trend in overall perinatal mortality risk with increasing haemoglobin level (Appendix I), but this is mainly due to the association with antepartum fetal deaths. There is a high risk at very low haemo- globin levels, and a significant trend of decreasing risk with increasing haemo- globin levels. In all 50.5% of mothers of perinatal deaths and 59.0% of mothers of APFDs had a haemoglobin of under 11 g/dl compared with 40.4% of survivors (P < 0.OOOl).

Medical conditions and risk of perinatal death 71
Hypertension Appendix 1 shows that amongst all the categories of death, compared with the survivors, there was a much higher proportion of women whose highest diastolic blood pressure was 100 mmHg or more. This was true of 11.8% of aU deaths (16.7% of APFDs, 9.8% of IMMATs and 9.8% of IPAs) compared with 3.0% of survivors. Also statistically significant were the differences between the survivors and all deaths (and the three types of death) and the first diastolic blood pressure measured during pregnancy. For all categories of death there was an excess of women whose first blood pressure was 80mmHg or more: 15.7% of survivors; 27.5% of AF'FDs (P<O.OOOl), 19.8% of IMMATs (P<O.O5), 26.1% of IPAs (P < 0.0001) and 25.0% of all perinatal deaths (P < 0.0001).
Levels of proteinuria of 2 + or more were also much more common in the death groups than the groups of survivors: 3.2% of survivors; 14.3% of MFDs (P < 0.0001); 11.6% of IMMATs (P < 0.0001), 8.0% of IPAs (P C 0.OOOl) and 10.3% of all perinatal deaths (P < 0.0001) had this finding.
Oedema was present in 19.3% of survivors and 23.7% of all perinatal deaths (P < 0.001). The excess was apparent for the APFD group (P < 0.001) and the IPA group (P < O.Ol), but not for the deaths from immaturity.
Although the number of women who developed eclampsia in the antenatal period was small (0.3%), there were highly significant associations with antepar- turn fetal deaths (P < O.OOOl), and deaths from intrapartum asphyxia (P C 0.0001). For the group of 244 immaturity-associated deaths there were only three (1.2%) eclamptic cases but this was nevertheless .also significantly more than expected using Fishefs Exact Test.
Logistic regression analyses Information on some of the factors considered in this section was not known for a sizable proportion of the population. Such data are usually excluded on a case-wise basis for logistic regression analysis. Therefore in order to prevent the exclusion of a large proportion of women from the analyses, many of the variables considered include a category for 'missing data'.
Anteparturn fetal death The left hand column of Table 1 shows the results of the logistic regression of all the variables considered in this paper modelled together with maternal age for the outcome antepartum fetal death. The following variables failed to enter the model: antibiotics taken, urinary tract infection, gonorrhoea, vaginal discharge or in- fection, bleeding less than 28 weeks and oedema appearing during pregnancy. It can be seen that the following were strongly related: syphilis, bleeding in the third trimester, both the first diastolic blood pressure and the highest diastolic blood

72 D. Ashley et al. Table 1. Results of logistic regression analyses to predict antepartum fetal death using complications of pregnancy: (a) adjusting for one another and maternal age, (b) adjusting also for social, environmental and health behaviour variables
Variable Adjusted (a) OR 195% CII Adjusted (b) OR [95% CI]
syphilis No YeS X2 (I df)
No Yes X2 (1 df)
<8 8.0-9.9 10.0-10.9 11 .O-12.9 13 + Unknown X2 (5 df)
< 70 70-79 80-89 90-99 100-109 110+ Unknown X2 (6 df)
<60 60-69 70-79 80-89 90+ Unknown X2 (5 df)
None
Bleeding 28 weeks +
Lowest Hb (g/dl)
Highest diastolic (mm)
First diastolic (mm)
Highest proteinuria
+ ++ +++ Unknown X2 (4 df)
No Yes X2 (1 df)
Antenatal eclampsia
1 .00 reference 3.56 [2.50,5.061
39.9 ****
1 .OO reference 3.51 [2.55,4.841
47.4 ****
4.05 [2.03,8.061 2.63 [1.68,4.10] 2.18 [1.47,3.251 1 .OO reference 1.28 [0.71,2.291 2.13 [1.55,2.90
37.7 ****
1.29 [0.92, 1.821 1 .OO reference 0.76 [0.54,1.061 1.23 [0.80,1.89] 2.50 [1.47,4.26] 5.33 [2.92,9.74] 0.96 [0.52,1.751
45.9 ****
0.96 [0.61,1.531 1.00 reference 1.27 [0.94,1.70] 1.67 [1.12,2.49] 2.55 [1.53,4.231 1.59 [0.85,2.97]
15.7 *
1.00 reference 0.98 10.69, 1.391 2.04 [1.24,3.351 3.31 [1.88,5.831 1.78 [1.38,2.301
36.4 ****
1.00 reference 5.07 [2.08,12.31
10.6 **
1.00 reference 2.88 [1.91,4.321
21.7 ****
1.00 reference 3.86 [2.73,5.44]
48.3 ****
3.71 [1.74, 7.931 2.84 [1.72,4.681 2.03 [1.29,3.20] 1 .OO reference 1.31 10.69, 2.521 1.97 [ 1.38,2.83]
26.3 ***
1.06 [0.77,1.471 1.00 reference 0.87 [0.63,1.221 1.77 [1.15,2.72] 4.02 [2.35,6.86] 9.32 [5.03, 17.281 1.28 [OM, 1.831
66.8 ****
N.S.
1.00 reference 0.93 [0.62,1.391 1.65 [0.94,2.831 3.27 [1.71, 6.271 1.97 [1.48,2.621
32.3 ****
1 .OO reference 4.62 [1.47, 14.501 5.9 *

Medical condifions and risk of perinatal death 73 Table 1. contd.
Variable Adjusted (a) OR 195% CII Adjusted cb) OR [95% CII
Diabetes No 1.00 reference 1 .OO reference YeS 4.04 [2.24, 7.301 3.79 [1.92, 7.491 X2 (1 dD 16.8 *** 11.7 ***
No. in model: APFD 458 384 Survivors 9270 8334
N.S.: P > 0.05; *P < 0.05; **P < 0.01; ***P < 0.001; ****P < O.OOO1
pressure as well as the highest level of proteinuria and the presence of antenatal eclampsia. In addition there was a significant relationship with the lowest haemo- globin level, with mothers whose haemoglobin had fallen below 11.0 being at increased risk, and a strong trend such that the lower the lowest haemoglobin, the higher the risk of antepartum fetal death.
In the right hand column of Table 1, the results are shown after adjusting for the social, environmental and health variables shown elsewhere2°,21 to be associated with antepartum fetal death. Controlling for these variables made only one major difference to the model - the first diastolic blood pressure failed to reach statistical significance. Consequently it is clear that the major features that contribute towards antepartum fetal death are those that arise during pregnancy and comprise: syphi- lis, third trimester antepartum haemorrhage, highest diastolic blood pressure, highest level of proteinuria, lowest haemoglobin level and presence of eclampsia in the antenatal period. .
Deaths from immaturity
A similar procedure was undertaken for deaths from immaturity. In the presence of the terms in the final model and maternal age, the following terms failed to reach statistical significance: urinary tract infection, syphilis, taking of antibiotics, gonor- rhoea, vaginal discharge or infection, lowest haemoglobin and first diastolic blood pressure. The major and most significant factors to enter the model were bleeding in the first two trimesters of pregnancy (P < 0.0001) and the highest proteinuria level (P < 0.0001). Also statistically significant were bleeding in the third trimester (P C 0.011, highest diastolic blood pressure (with the lowest risk among mothers with a blood pressure between 90 and 99mm) and antenatal oedema (where the group of mothers with oedema had the lower risk). Controlling for social, environmental and health behaviour variables made little difference to these results (Table 2).

74 D. Ashley et al. Table 2. Results of logistic regression analyses to predict deaths from immaturity using complications of pregnancy: (a) adjusting for one another and maternal age, (b) adjusting also for social, environmental and health behaviour variables
Variable Adjusted (a) OR (95% CII Adjusted (b) OR [95% CII ~
Bleeding < 28 weeks No Yes X2 (1 df)
No YeS X2 (1 df)
< 70 70-79 80-89 90-99 100-109 100 + Unknown X2 (6 df)
None
Bleeding 28 weeks +
Highest diastolic (mm)
Highest proteinuria
+ ++ +++ unknown XZ (4 df)
No Yes Xz (1 df)
Antenatal oedema
1 .OO reference 3.70 [2.61,5.271 44.0 ****
1 .OO reference 2.06 [1.29,3.30] 8.1 **
1.01 [0.69, 1.501 1 .OO reference 0.95 [0.66,1.371 0.44 [0.19,1.031 2.54 [1.13,5.721 3.90 [1.64,9.271 1.05 [0.66,1.681 18.7 **
1 .OO reference 0.87 [0.51,1.481 3.41 [1.81,6.431 5.60 [2.44,12.91 2.43 [1.75,3.391
45.4 ****
1 .OO reference 0.57 [0.37,0.871 7.5 **
1.00 reference 3.50 [2.39,5.131 34.6 ****
1 .OO reference 1.93 [1.16,3.221 5.6 *
1.06 [0.71,1.601 1 .oO reference 0.89 [0.60,1.60] 0.37 [0.15,1.321 2.48 [1.05,0.951 3.41 [131,5.891 1.03 [ O H , 1.771 17.4 **
1 .OO reference 0.80 [0.46,1.421 3.57 [ 1 .a, 6.781 4.39 [1.68,11.51 2.18 [1.52,3.11] 33.8 ****
1 .OO reference 0.59 [0.38,0.91 I 6.3
No. in model: IMMAT SURV
216 8969
192 8829
*P < 0.05; **P < 0.01; ****P < O.OOO1
Intraparturn asphyxia
In contrast, features entering the model for deaths attributed to intrapartum asphyxia were more indicative of an effect of infection (Table 3). Thus, in the presence of one another and of maternal age, the variables antibiotic given, syphilis and vaginal discharge/infection entered the model, as did both bleeding in the first two trimesters, bleeding in the third trimester, the first diastolic blood pressure and the highest diastolic blood pressure and the antenatal eclampsia variable. Neither

Medical conditions and risk of perinatal death 75
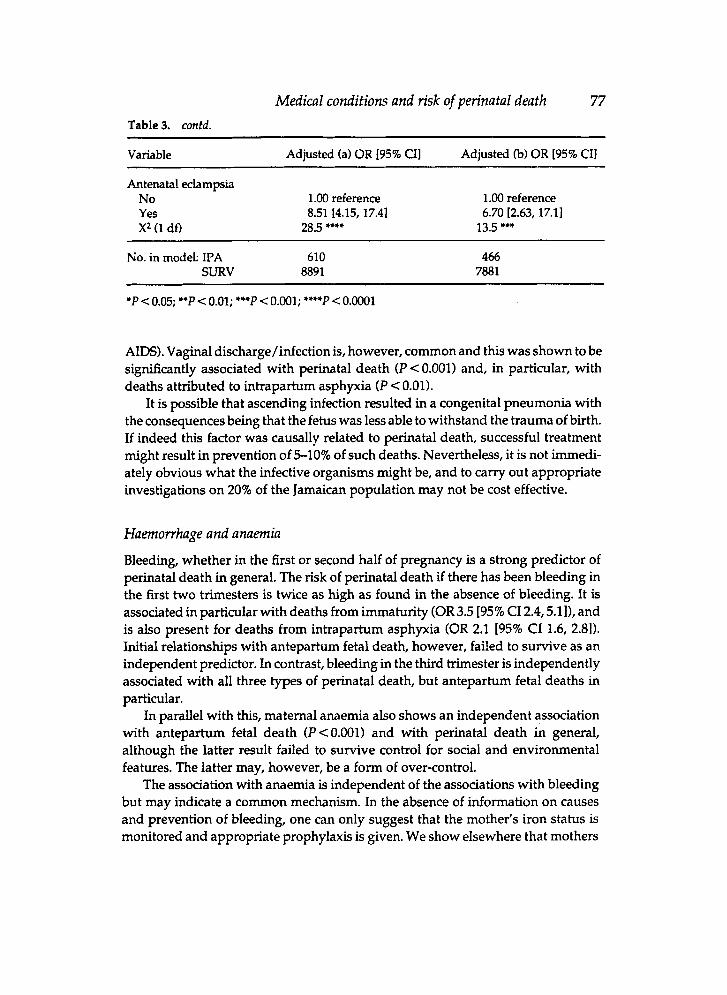
proteinuria nor oedema were statistically sigruficantly associated with intraparturn asphyxia once the blood pressure variables had been taken into account. There was no association with lowest haemoglobin level during pregnancy, but as might have been predicted the association between antenatal eclamptic fits and intrapartum asphyxia was very strong, with an odds ratio of 8.51 (95% CI 4.15,17.4).
When also allowing for the social, environmental and health behaviour vari- ables, only one factor - the giving of an antibiotic during pregnancy -dropped out of the logistic regression equation. This was no longer statistically sigruficant. Consequently one may conclude from Table 3 that those factors that put an infant at significantly increased risk of IPA relate to the presence of an infection such as syphilis or vaginal infection, bleeding episodes during the pregnancy and indi- cations of hypertension rather than proteinuria.
All perinatal deaths For all perinatal deaths, the model induded nine separate factors (Table 4). Ex- cluded were the antibiotics taken, urinary tract infection and gononhoea. All other factors entered the logistic regression equation and had a sipficance level of less than 0.0001. Allowing for social, environmental and health behaviour variables resulted in the lowest haemoglobin variable being dropped from the equation, but all other factors were retained in the model.
Discussion The striking feature about the logistic regression analyses lies in the robustness and consistency of the relationships found between many of the complications of pregnancy and the risk of different types of death. Very rarely did allowing for social and other features make any difference.
Infect ion The most common infections presenting in pregnancy in Jamaica are those of the genitourinary tract. Syphilis remained sigruficantly associated with all but one of the categories of death, and was particularly strongly related to antepartum fetal death. In a country where syphilis is common it is important to test and treat. McCaw-BinnsU has demonstrated that testing and treating those mothers who were found to be positive in early pregnancy results in a virtual abolition of risk of perinatal death. If testing were to be carried out on all women in early pregnancy (and results received promptly) then about 7% of all perinatal deaths might be prevented.
In contrast, there was little to suggest that detecting and treating urinary tract infection or gonorrhoea was important. The rate of HIV infection on the island was still low (1992 cumulative rate was 19 per 100000 population with recognised

76 D. Ashley et al. Table 3. Results of logistic regression analyses to predict deaths associated with intrapartum asphyxia using complications of pregnancy: (a) adjusting for one another and maternal age, (b) adjusting also for social, environmental and health behaviour variables
-~ ~ ~ ~ ~
Variable Adjusted (a) OR 195% CII Adjusted (b) OR 195% CIl
Antibiotic given No Yes X2 (1 dfl
Syphilis No Yes X2 (1 dD
None Treated Untreated Treatment unknown X2 (3 dO
No Yes X2 (1 dfl
No YeS X2 (1 dD
< 70 70-79 80-89 90-99 100-109 110+ Unknown X2 (6 dD
< 60 60-69 70-79 80-89 90+ Unknown Xz (5 dD
Vaginal discharge/infection
Bleeding < 28 weeks
Bleeding 28 weeks +
Highest diastolic (mm)
First diastolic (mm)
1.00 reference 0.75 [0.58,0.98] 4.6 *
1-00 reference 2.06 [1.41,3.01] 11.9 ***
1 .OO reference 1.23 [0.96,1.59] 2.23 [1.57,3.18] 1.22 [OM, 1.781 18.7 ***
1 .OO reference 2.03 [1.57,2.631 25.8 ****
1 .M) reference 2.09 [1.51,2.88] 17.6 ****
1.25 [0.93,1.671 1.00 reference 0.83 [0.64,1.09] 1.04 [0.71,1.521 1.96 [1.19,3.221 3.55 [2.08,6.051 0.78 [0.46,1.331 35.2 ****
1.22 I0.84,1.771 1 .OO reference 1.38 11.08, 1.7'71 2.05 [1.48,2.841 2.32 [ 1.39,3.861 1.84 [1.07,3.181 24.1 ***
N.S.
1.00 reference 2.17 [1.44,3.261
11.8 ***
1 .00 reference 1.17 [0.88,1.551 2.30 [1.54,3.443 1.09 [0.70,1.691 14.6 **
1 .OO reference 2.10 [1.57,2.811
22.0 ****
1 .OO reference 2.32 [1.62,3.331 18.3 ****
1.20 [0.85,1.681 1 .OO reference 0.76 [0.55, 1.041 0.91 [0.57,1.451 1.78 [l.OO,3.18] 3.79 [2.06,6.961 0.82 i0.45, 1.481 31.5 ****
1.00 [0.63,1.59] 1 .OO reference 1.40 [1.04,1.871 2.44 [1.67,3.561 2.94 [1.63,5.301 2.02 [1.09,3.721 28.6 ****
Medical conditions and risk of perinatal death 77 Table 3. contd.
~
Variable Adjusted (a) OR 195% CII Adjusted (b) OR 195% CII
Antenatal eclampsia No 1.00 reference 1.00 reference Yes 8.51 [4.15, 17.41 6.70 [2.63, 17.11 X2 (1 do 28.5 **** 13.5 ***
No. in model: IPA 610 466 SURV 8891 7881
*P < 0.05; **P c 0.01; ***P < 0.001; ****P < o.oO01
AIDS). Vaginal discharge/infection is, however, common and this was shown to be significantly associated with perinatal death (P < 0.001) and, in particular, with deaths attributed to intrapartum asphyxia (P < 0.01).
It is possible that ascending infection resulted in a congenital pneumonia with the consequences being that the fetus was less able to withstand the trauma of birth. If indeed this factor was causally related to perinatal death, successful treatment might result in prevention of 510% of such deaths. Nevertheless, it is not immedi- ately obvious what the infective organisms might be, and to carry out appropriate investigations on 20% of the Jamaican population may not be cost effective.
Haemowhage and anaemia Bleeding, whether in the first or second half of pregnancy is a strong predictor of perinatal death in general. The risk of perinatal death if there has been bleeding in the first two trimesters is twice as high as found in the absence of bleeding. It is associated in particular with deaths from immaturity (OR3.5 [95% CI 2.4,5.11), and is also present for deaths from intrapartum asphyxia (OR 2.1 195% CI 1.6, 2.81). Initial relationships with anteparturn fetal death, however, failed to survive as an independent predictor. In contrast, bleeding in the third trimester is independently associated with all three types of perinatal death, but anteparturn fetal deaths in particular.
In parallel with this, maternal anaemia also shows an independent association with antepartum fetal death (P<O.OOl) and with perinatal death in general, although the latter result failed to survive control for social and environmental features. The latter may, however, be a form of over-control.
The association with anaemia is independent of the associations with bleeding but may indicate a common mechanism. In the absence of information on causes and prevention of bleeding, one can only suggest that the mother’s iron status is monitored and appropriate prophylaxis is given. We show elsewhere that mothers

78 D. Ashley et al. Table 4. Results of logistic regression analyses to predict deaths associated with perinatal death using complications of pregnancy: (a) adjusting for one another and maternal age, (b) adjusting also for social, environmental and health behaviour variables
Variable Adjusted (a) OR [95% CIl Adjusted cb) OR [95% CII
syphilis No Yes X2 (1 dfl
None Treated Untreated Treatment unknown F (3 dfl
No YeS
F(1 dfl
No Yes X2 (1 dfl
<8 8.0-9.9 10.0-10.9 11.0-12.9 13.0 + Unknown X2 (5 dfl
< 70 70-79 80-89 90-99 100-109 110+ Unknown X2 (6 dfl
<a 60-69 70-79 80-89 90+ Unknown X2 (5 do
Vaginal discharge
Bleeding < 28 weeks
Bleeding 28 weeks +
Lowest Hb (g/dl)
Highest diastolic (mm)
First diastolic (mm)
1 .OO reference 2.29 [1.76,2.981 34.1 ****
1.00 reference 1.11 [0.93,1.331 1.84 [1.40,2.411 1.18 [0.91,1.54] 19.2 ***
1 .OO reference 1.92 [ 1.59,2.321 42.0 **I*
1 .OO reference 2.48 [1.98,3.12] 56.5 ****
2.05 [1.28,3.291 1.47 [1.11,1.95] 1.46 [1.16,1.83] 1.00 reference 1.06 [0.77,1.481 1.49 [1.26, 1.761 29.5 ****
1.22 [l.OO, 1.501 1 .OO reference 0.84 [0.70,1.021 1.01 [0.76,1.33] 1.87 [1.29,2.711 3.82 [2.48,5.88] 0.75 [0.51,1.091
63.1 ****
1.18 [0.91,1.541 1.00 reference 1.37 I1.15, 1.631 1.80 [1.42,2.28] 2.50 [1.74,3.59] 1.86 [1.26,2.761 41.6 ****
1 .OO reference 2.06 [1.49,2.851 17.4 ****
1 .OO reference 1.00 [0.80,1.251 2.13 [1.54,2.94] 1.18 [0.85, 1.631 19.6 w*
1 .OO reference 2.01 [1.60,2.531 33.2 ****
1 .OO reference 2.65 [2.02,3.481 45.2 ****
N.S.
1.15 [0.90,1.481 1.00 reference 0.80 [0.64,1.011 1.05 [0.75,1.501 1.55 I0.98,2.441 3.23 [1.90,5.491 0.94 [0.60,1.491 31.8 ****
1.11 [0.79,1.561 1.00 reference 1.40 [1.14,1.741 1.80 ]1.35,2.401 3.08 [1.99,4.781 1.57 [0.97,2.54] 32.9 ****

Medical condifions and risk of perinafal deafh 79 Table 4. contd.
Variable Adjusted (a) OR [95% CIl Adjusted 6) OR [95% CI1
Highest proteinuria None + ++ +++ Unknown X2 (4 dfl
No YeS
X2 (1 dfl Diabetes
No YeS X2 (1 dfl
Antenatal eclampsia
1 .OO reference 0.94 [0.76,1.161 1.67 [1.18,2.351 3.02 [1.99,4.571 2.10 [1.81,2.441
11 8 *+**
1 .OO reference 5.99 [3.15,11.41
27.9 *+**
1.00 reference 2.39 11.50, 3.801
12.0 +*+
1 .00 reference 0.98 10.76, 1.271 1.50 [0.98,2.28] 3.13 [1.88,5.21] 2.28 [1.90,2.73]
91.0 ****
1 .OO reference 4.22 [1.76,10.141 9.4 ++
1 .OO reference 2.01 [1.13,3.58] 5.1 +
~~ -
No. in model: Deaths 1380 Survivors 8891
949 7230
N.S.: P > 0.05; *P < 0.05; **P < 0.01; **+P < 0.001; ****P < 0.0001
taking iron during their pregnancies have a significant reduction in risk of perinatal death.=
Hypertension Of all the conditions discussed, the hypertensive disorders are the largest contribu- tors to maternal and perinatal deaths. The highest diastolic blood pressure remained associated with all causes of perinatal death, particularly for blood pressures of 100 mmHg or more. The fmt blood pressure during pregnancy proved not to be independently associated with antepartum fetal death or immaturity- related deaths but remained associated with intrapartum asphyxia-related deaths and all perinatal deaths even in the presence of the highest blood pressure. The highest level of proteinuria also remained statistically significant for all categories of death, with the exception of inbapartum asphyxia, where hypertension was clearly found to be the strongest factor. In the models for antepartum fetal death, intraparturn asphyxia, and all perinatal deaths, antenatal eclampsia remained sighcant. Oedema however carried no independent excess risk of death and indeed was negatively associated with deaths from immaturity.
The need for intervention in hypertensive pregnancies in Jamaica has been

80 D. Ashley et al. recognised since the study of Thomas17 pointed to a number of deficiencies in the treatment of hypertension once it was identified: reliance on sedatives (e.g. pheno- barbitone) rather than antihypertensives, and a reluctance to induce and deliver a mother with severe disease. In consequence, a series of guidelines for detection and care of women with hypertension are currently being augmented in one area of the country. If shown to be successful then they will be developed further and in- troduced across the island.
Other disorders
In a review of pregnant diabetic women attending hospitals in the 1940s Peal and OakleyZ4 found that perinatal mortality was high. Over the past 40 years the situation has changed significantly and data now indicate that at the present time, perinatal mortality in diabetic women in the developed world is only slightly higher than the rate in the general Diabetes is recognised to be associated with an increased risk of congenital abnormalities (especially skeletal and cardiac abnormalities and neural tube defects), miscamage, preterm delivery (mainly because of the widespread policy of elective Caesarean section before term) and macrosomia (and associated birth trauma). Little is known as to perinatal mortality risks in the third world.
Less than 1% of the Jamaican mothers were reported as having diabetes, but 2.5% of perinatal deaths were to women who were diabetic (P < 0.0001). The risk of mortality from intraparturn asphyxia was not significantly higher but antepartum fetal deaths showed a five-fold increase. Only two deaths to diabetic women had a major malformation.
This pattern is different from that in the developed world and indicates that the policy of induction of labour at 38 weeks gestation may well save some children that would otherwise become antepartum fetal deaths.
No other disorders were recognised as contributing substantially to the burden of perinatal death. Other features were in contrast to studies of perinatal death in Europe at a time when the mortality rate was similar to that found in Jamaica currently. At that time Rhesus iSoimmunisation was responsible for 3% of perinatal deaths,I4 among a population where 17% of mothers were Rhesus negative. In Jamaica 10% of mothers are Rhesus negative, but perinatal death from this cause was only identified in two cases (i.e. 0.1% of deaths). This is unlikely to be due to misclassification as the mortality rate showed no sign of being higher in preg- nancies of Rhesus negative women in this survey.
Conclusion
Two studies of maternal mortality in Jamaica in the 1980s have shown the major causes to be related to the hypertensive disorders, haemorrhage and infection.'?
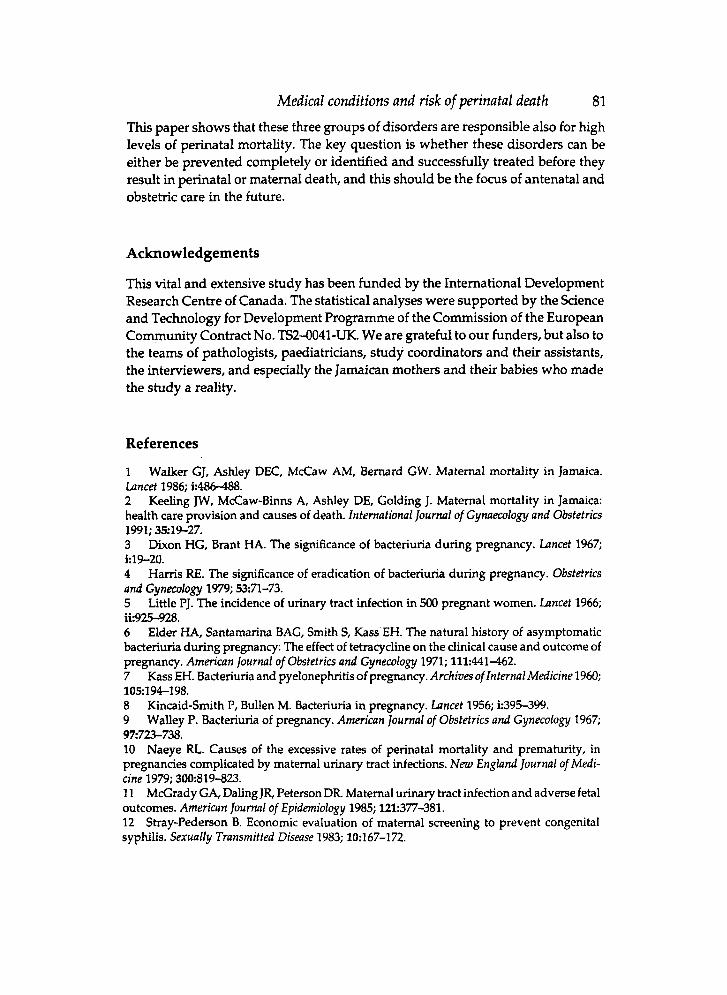
Medical conditions and risk of perinatal death 81 This paper shows that these three groups of disorders are responsible also for high levels of perinatal mortality. The key question is whether these disorders can be either be prevented completely or identified and successfully treated before they result in perinatal or maternal death, and this should be the focus of antenatal and obstehic care in the future.
Acknowledgements
This vital and extensive study has been funded by the International Development Research Centre of Canada. The statistical analyses were supported by the Science and Technology for Development Programme of the Commission of the European Community Contract No. TS2-0041-UK. We are grateful to our funders, but also to the teams of pathologists, paediatricians, study coordinators and their assistants, the interviewers, and especially the Jamaican mothers and their babies who made the study a reality.
References
1 Lancet 1986; k486488.
Walker GJ, Ashley DEC, McCaw A Bernard GW. Maternal mortality in Jamaica.
2 Keeling JW, McCaw-Binns A, Ashley DE, Golding J. Maternal mortality in Jamaica: health care provision and causes of death. International j o u m l of Gynuecology and Obstetrics 1991; 35:19-27. 3 Dixon HG, Brant HA. The significance of bacteriuria during pregnancy. Lancet 1967; k19-20. 4 Hams RE. The significance of eradication of bacteriuria during pregnancy. Obstetrics and Gynecology 1979; %71-73. 5 Little PJ. The incidence of urinary tract infection in 500 pregnant women. Lancet 1966; ik925-928. 6 Elder HA, Santamarina BAG, Smith S, Kass EH. The natural history of asymptomatic bacteriuria during pregnancy: The effect of tetracycline on the clinical cause and outcome of pregnancy. Amm'can journal of Obstetrics and Gynecology 1971; 111:441-462. 7 Kass EH. Bacteriuria and pyelonephritis of pregnancy. Archives of Internal Medicine 1960; 105:194-198. 8 Kincaid-Smith P, Bullen M. Bacteriuria in pregnancy. Lancet 1956; k395-399. 9 Walley P. Bacteriuria of pregnancy. Americnn Journal of Obsfetrics and Gynecology 1967; 9E723-738. 10 Naeye RL. Causes of the excessive rates of perinatal mortality and prematurity, in pregnancies complicated by maternal urinary tract infections. Nezu England Iournal of Medi- cine 1979; 3W819-823. 11 McGrady GA, Daling JR, Peterson DR. Maternal urinary tract infection and adverse fetal outcomes. American Journal of Epidemiology 1985; 121:377-381. 12 Stray-Pederson 8. Economic evaluation of maternal screening to prevent congenital syphilis. Sexually Transmitted Disease 1983; 10167-1 72.

82 D. AshZey et al. 13 Alexander ER. Maternal and infant sexually transmitted diseases. Urologic Clinics of North America 1984; 11:131-139. 14 Butler NR, Bonham DG. Perinatul Mortality: the First Report of the 1958 British Perinatal Mortality Survey. Edinburgh: E & S Livingstone, 1963. 15 Watson R. Anteparturn haemorrhage of uncertain origin. British Journal of Clinical Practice 1982; 36222-226. 16 World Health Organisation. The Prevalenceof Nutritional Anaemia in Women in Developing Countries. Geneva: World Health Organisation, 1979. 17 Thomas PW. Hypertensive disorders of pregnancy: Classification, prediction and out- come. University of Bristol, UK: PhD thesis, 1990. 18 Thomas PW, Ashley D, Bernard GW. Incidence, risk factors and outcome of the hypertensive disorders of pregnancy in Jamaica. Clinical and Expen’mental Hypertension Part 8: Hypertension in Pregnancy B 1990; 9:169-198. 19 Ashley D, McCaw-Binns A, Golding J, Keeling J, Escoffery C, Coard K et al. Perinatal Mortality Survey in Jamaica: aims and methodology. Paediatric and Perinatal Epidemiology 1994; 8 Supp1.1:6-16. 20 Golding J, Greenwood R, McCaw-Binns A, Thomas P. Associations between social and environmental factors and perinatal mortality in Jamaica. Paediatric and Perinatul Epidemi-
21 Greenwood R, McCaw-Binns A. Does maternal behaviour influence the risk of perinatal death in Jamaica? Paediatric and Perinatal Epidemiology 1994; 8 Suppl.l:54-65. 22 McCaw-Binns A. Does antenatal care make a difference? An examination of antenatal care in Jamaica and its relationship to pregnancy outcome. University of Bristol, UK PhD thesis, 1993. 23 McCaw-Binns A, Greenwood R, Ashley D, Golding J. Antenatal and perinatal care in Jamaica: do they reduce perinatal death rates? Paediutric and Perinatal Epidemiology 1994; 8 Suppl.l:86-97. 24 Peel J, Oakley W. The management of diabetes in pregnancy. In: Transactions ofthe 12th Congress of Obstetrics 6 Gynaecology, London Royal College of Obstetricians and Gynaecolo- gists 1949; p.161. 25 Macfarlane A., Mugford M. Birth counts. Statistics of pregnancy and childbirth. London: Her Majesty’s Stationery Office, 1984; p. 10. 26 Oloffson P, Liedhold H, Sartor G, et al. Diabetes and pregnancy. A 21-yr Swedish material. Acta Obstetriciu Gynecologica Scandinauica 1984; Suppl. 127-62 .
ology 1994; 8 S~ppl.l:17-39.

Medical conditions and risk of perinatal death 83
Appendix 1. Distribution of medical conditions in pregnancy among suMvors, anteparturn fetal deaths, deaths from immaturity, deaths from intrapartum asphyxia and all perinatal deaths.
Variable SURV APFD IMMAT IPA AllPND
Antibiotics taken YeS No
12.8% 14.3% 14.9% 11.9% 13.4% 87.2% 85.7% 85.1% 68.1% 86.6%
(n) = 100% (1847)
Chi-squared 1 df 0.9 0.9 0.5 0.3 N.S. N.S. N.S. N.S.
Urinary tract infection YeS 3.6% 4.3% 4.2% 3.2% 3.7% No 96.4% 95.7% 95.8% %A% 96.3%
(n) = 100% (9919) (558) (309) (813) (1847)
Chi-squared I df 0.5 0.1 0.3 0.0 N.S. N.S. N.S. N.S.
Syphilis YeS No
2.8% 8.2% 3.2% 4.6% 5.2% 97.2% 91.8% 96.8% 95.4% 94.0%
Chi-squared 1 df 49.7 0. I 7.2 28.8 ** **** N.S. **.*
Diabetes YeS No
0.7% 3.0% 1.6% 1.1% 1.8% 99.3% 97.0% 98.4% 98.9% 98.2%
( n ) = 100% (9919) (558) (309) (813) (1847)
Chi-squared I df 33.8 3.2 I .5 21.7 *... N.S. N.S. *... Gonorrhoea
YeS 0.5% 1.1% I .3% 1.0% 1.0% No 99.5% 98.9% 98.7% 99.0% 99.0%
(n) = 100% (9919) (558) (309) (813) (1847)
Chi-squared 1 df 1.8 1.8 F.E. 5.2 N.S. N.S. N.S.

84 D. Ashley et al. Appendix 1. contd.
Variable SURV APFD IMMAT IPA ALLPND
Vaginal discharge or infection No Yes (treated) Yes (not treated) Yes (treatment not known)
79.9% 75.2% 73.5% 73.4% 74.6% 12.190 13.5% 13.7% 13.7% 13.4% 3.1% 4.6% 7.7% 6.7% 5.9% 4.9% 6.7% 5.1% 6.2% 6.1%
Chi-squared 3 df 7.3 16.7 30.0 38.2 ... .-* ..** N.S.
Bleeding < 28 weeks (data from antenatal records and mother) Yes 6.6% 10.0% 24.9% 13.5% 13.9% No 93.4% 90.0% 75.1% 86.5% 86.1%
(n) = 100% (991 9) (558) (309) (813) (1847)
Chi-squared 1 df 9.4 149 53.7 116 ** .... .*.. ....
Bleeding 28 + weeks YeS 3.490 11.6% 11,7% 9.5% 10.7% No 96.6% 88.4% 88.3% 90.5% 89.3%
(n) = 100% (9919) (558) (309) (813) (1847)
Chi-squared 1 df 93.9 54.9 71.9 186 ..*. *I* .... .... Lowest Hb (g/dl)
€ 8 8.0-9.9 10.0-10.9 11.0-12.9 13+
2.6% 6.9% 5.6% 3.5% 4.9% 12.1% 20.7% 16.9% 14.8% 16.2% 25.7% 31.4% 20.2% 30.0% 29.4% 48.8% 31.4% 44.9% 41.7% 39.8% 10.8% 9.6% 12.4% 9.9% 9.7%
Chi-squared 4 df
Trend 1 df
Deviation from trend 3 df
36.4 6.0 7.3 28.9 N.S. N.S.
28.0 1.3 5.5 23.5 N.S.
0.4 4.7 1.8 5.4 N.S. N.S. N.S.
**.. ****
.... .***
Highest diastolic blood pressure € 69 70-79 80-89 90-99 100-109 110+
21.5% 21.4% 22.0% 20.7% 20.9% 40.7% 32.0% 39.5% 34.9% 35.3% 27.8% 19.4% 25.9% 25.1% 23.4% 7.1% 10.4% 2.9% 9.1% 8.5% 2.0% 7.0% 3.9% 4.6% 5.2% 1.0% 9.7% 5.9% 5.6% 6.6%
Chi-squared 5 df 286 53.0 I 2 3 280 .... **.. I).** ....

Medical conditions and risk of perinatal death 85
Appendix 1. contd.
Variable SURV APFD lMMAT IPA ALLPND
First (or only) diastolic blood pressure s 59 6.7% 6.0% 6.3% 6.2% 6.2% 60-69 41.5% 34.2% 33.3% 33.190 33.8% 70-79 36.1% 32.3% 40.6% 34.7% 35.1% 80-89 13.3% 15.8% 15.0% 20.0% 17.5% 90+ 2.4% 11.7% 4.8% 6.1% 7.5%
Chi-squared 4 df 130 9.7 57.5 129 H1. *- ....
Highest level of protein in urine None/ trace 85.0% 75.9% 80.9% 81.8% 79.7% + 11.7% 9.8% 7.4% 10.2% 10.0% ++ 2.3% 5.9% 6.0% 3.7% 4.6% +++ or more 0.9% 8.4% 5.6% 4.3% 5.7%
(n) = 100% (8611) (4271 (215) (600) (1362)
Chi-squared 3 df 230 84.7 79.0 245 WI. 8.W ..U ....
Antenatal oedema No YeS
W.7% 73.1% 83.390 75.390 76.3% 19.3% 26.9% 16.7% 24.7% 23.7%
Chi-squared 1 df 14.8 0.8 10.7 14.7 H ... N.S. *W
Antenatal eclampsia No YeS
99.8% 97.8% 98.8% 96.790 97.7% 0.2% 2.2% 1.2% 3.390 2.3%
(n) = 100% (9270) (458) (244) (670) (1519)
Chi-squared 1 df 105 **..
F.E. F.E. F.E. w. ..**
N.S.: P > 0.05; *P < 0.05; -P < 0.01; *-P < 0.001; *-*P < O.ooO1 F.E. =Fisher's Exact Test