Measuring Case Management for Families with HIV
17
This article was downloaded by: [New York University] On: 06 December 2012, At: 08:23 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Social Work in Health Care Publication details, including instructions for authors and subscription information: http:// www.tandfonline.com loi/wshc20
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Measuring Case Management for Families with HIV

This article was downloaded by: [New YorkUniversity]On: 06 December 2012, At: 08:23Publisher: RoutledgeInforma Ltd Registered in England andWales Registered Number: 1072954Registered office: Mortimer House, 37-41Mortimer Street, London W1T 3JH, UK
SocialWork inHealthCarePublicationdetails,includinginstructions forauthors andsubscriptioninformation:http://www.tandfonline.com/loi/wshc20

MeasuringCaseManagementforFamilieswith HIVSusanAbramowitz PhDa , Nessa ObtenMSW a & HenryCohen MS ba Lower NewYork Consortiumfor Families withHIV, Departmentof Pediatrics,NB 811-E, NewYork UniversityMedical Center,550 FirstAvenue, NewYork, NY, 10016,USA
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

b Department ofEnvironmentalMedicine, NewYork UniversityMedical Center,USAVersion ofrecord firstpublished: 17Oct 2008.
To cite this article: Susan Abramowitz PhD, NessaObten MSW & Henry Cohen MS (1998): MeasuringCase Management for Families with HIV, SocialWork in Health Care, 27:3, 29-41
To link to this article: http://dx.doi.org/10.1300/J010v27n03_02
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research,teaching, and private study purposes. Any
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012
substantial or systematic reproduction,redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in anyform to anyone is expressly forbidden.
The publisher does not give anywarranty express or implied or make anyrepresentation that the contents will becomplete or accurate or up to date. Theaccuracy of any instructions, formulae, anddrug doses should be independently verifiedwith primary sources. The publisher shallnot be liable for any loss, actions, claims,proceedings, demand, or costs or damageswhatsoever or howsoever caused arisingdirectly or indirectly in connection with orarising out of the use of this material.
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

Measuring Case Management for Families with HIV
Susan Abramowitz, PhD Nessa Obten, MSW Henry Cohen, MS
ABSTRACT. Case management has been recognized as a major way for coordinating the multiple services needs for people with HIVIAIDS. Such coordination is required because of the progres- sively debilitating nature of this chronic disease and the fragmented health care and social services delivery system. One of the major problems with the study of case management is the difficulty in actually measuring it. Another major limitation has been the focus almost exclusively on adult models of HIVIAIDS case management. This study was undertaken to assess the efficacy of a time study methodology to measure differences in case management activities when case managers work with families and when they work with individuals. Ten case managers from two urban hospital pediatric and adult HIVIAIDS clinics and 10 case managers from 3 community organizations participated. Case management activity was sampled using a beeper carried by case managers which signaled randomly 8 times a day over 5 consecutive days. When the signal "beeped," case managers checked off on a I-page form the appropriate descrip- tor of their involvement concerning task initiation, interaction, loca- tion, type, function as well as information about client needs, HIV status, and family history. The results suggest that the Time Study methodology is a useful and valid way of measuring case manage- ment and of identifying differences in case mix, client need and background, and case management techniques when case managers
Susan Abramowitz is Co-Director and Nessa Obten is Case Management Coordinator, Lower New York Consortium for Families with HIV, Department of Pediatrics, NB 8 11-E, New York University Medical Center, 550 First Avenue, New York, NY 10016. Henry Cohen is Research Scientist, Department of Envi- ronmental Medicine, New York University Medical Center.
Social Work in Health Care, Vol. 27(3) 1998 O 1998 by The Haworth Press, Inc. All rights reserved. 29
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

30 SOCIAL WORK IN HEALTH CARE
work with families and with individuals. [Arlicle copies available for a fee/rvtn The Hawor111 Document Delivety Setvice: 1-800-342-9678. E-ntail address: ge~it~o@~awor~I~pressinc.cont]
INTRODUCTION
Case management for children with chronic illness has been an essential part of health and social services delivery.' For children with HIVIAIDS, studies examining their needs and those of their families emphasize the importance of case management as a mecha- nism for insuring access to the multiple medical and psychosocial services they need.2 Women of childbearing age represent one of the groups with the fastest rising rate of infection? making the disease one that increasingly affects young families. Moreover, the virus disproportionately infects minority women in communities plagued by poverty, unemplo ment, bomelessness, poor education, 2 crime and substance abuse. These factors present special chal- lenges to case managers working with families, as the complexity of their HIV-related service needs is superimposed on an already existing set of stressors related to poverty and social isolation.
The methodology reported in the preceding paper was also used to examine family focussed case management activities, case mix, client needs and family history and to assess the methodology's ability to distinguish between case manager time spent with fami- lies and individuals with respect to these variables.
RESULTS
Case Mix
When working with family members, case managers are more likely to be working with clients with a history of physical abuse (27% vs. 13%), domestic violence (24% vs. 15%), and of crowded living conditions (32% vs. 23%). (See Table 1 .) On the other hand, when they are working with individuals, case managers are more likely to be working with clients with a history of substance abuse (72% vs. 61%) and of mental health problems (31% vs. 21%).
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

Abramowitz, Obten, and Cohen 3 1
Sewice Needs Beittg Addressed Case managers working with family members address a common
set of needs and those that are more specific to families. (See Table 2.) All case managers spend about the same amount of time addressing client needs for financial, basic, mental health, legal, and substance abuse services. However, case managers working with families are more likely to spend time addressing medical needs (54% vs. 41%) and needs for supportive (27% vs. 10%) and education/employment services (22% vs. 13%), as well as working with clients who have multiple service needs (37% vs. 27%).
TABLE 1. Number and Percentage Distribution of Time Points
Total CBOs
#of Tlme Points Percent 649 397 61%
Hospitals 252 Client-Related 409 Non-Client-Related 240 Family-Related (of client related) 225 Non-Family-Related (of client related) 184
TABLE 2. Case Manager Time Spent with Adults, Parents, and Children with Different HIV Status
Number of Time Percent of Time Points Points
HIV STAGE OF DISEASE Asymptomatic
Adult 87 21% Parent 60 15% Child 58 14%
Total 205 50%
Symptomatic Adult Parent Child
Total
Infected Adults 206 Infected Parents 142 Infected Children 99 Affected Family Members 82 Newly Diagnosed 51
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

32 SOCIAL WORK IN HEALTH CARE
Case Managetnent Activities
Case managers working with family members appear to spend more time involved in care plan formulation (16% vs. 8%), reas- sessment (13% vs. 7%), and in at least 2 or more case management functions (29% vs. 16%). (See Table 3.) They are also more likely to spend time case conferencing (1 6% vs. 9%) and providing family counseling (6% vs. 1%).
Task Type
There is no difference in the amount of time case managers spend with family members or individuals in scheduled or unscheduled appointments or in routine or non-routine tasks. (See Figure 1.) However, case managers working with families are more likely than those working with individuals to be involved in hard-to-resolve problems (30% vs. 16%). Moreover, when case managers are in- volved in hard-to-resolve issues, they are far more likely to be working with family members (70% vs. 3 1%) than with individu- als. Case managers are twice as likely to classify involvement with symptomatic parents as hard vs. easy-to-resolve (34% vs. 16%), while they report that working with symptomatic adults is, in more cases, easy rather than hard to resolve (32% vs. 21%). (See Table 4.)
The study results indicate that the nature of family-based case management is different than that of case management with individ- uals. (See Tables 5-7.) Several study findings suggest that working with children and families living with HIV presents case managers with a complexity of challenges that may not exist when working with individuals. This complexity is multifaceted. First, from the previous paper, we found that when case managers are working with an infected parent or an infected child, they are also likely to be addressing the needs of other infected or affected family mem- bers. Second, case managers are much more likely to report in- volvement in "hard to resolve" problems when working with an
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

TABLE 3. Case Manager Time Spent Exclusively with lnfected Children, Parents, and Adults
No. Time Points % No. Time Points % Infected Child 50 12 With Affected Families 13 26 Infected Parent 93 23 With Affected Families 27 29 Infected Parent-Child Dyad 46 12 With Affected Families 10 22
Total Infected 189 50 Infected Adults 210 53 30 14 Total 399 80
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

34 SOCIAL WORK IN HEALTH CARE
FIGURE 1. Task Type and Family-Related vs. Non Family-Related Case Manager Activity
I Related F? @ 225 I Family-Related
Non
infected parent, child, or family member. This may be explained by the significant amount of time case managers spend with clients reporting a family history of domestic violence, physical abuse, and overcrowded living conditions, all risk factors for serious social and family disruption which present potentially "hard to resolve" is- sues. This also may reflect the complex feelings that arise when dealing with children who are ill. The issues parents face concern- ing disclosure of HIV to their child, for example, are complex and not easily resolved.
Third, there appears to be a difference between the needs of and services required by families on one hand, and individuals on the other. Case managers focus more on addressing medical needs, the
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

TABLE 4. Time Spent with Clients with Different Risk Factors: All Time Points, Time Points for Those Involved with Families. and Those Involved with Individuals
Total # Tlme Points
FAMILY HISTORY Substance Abuse 263 Financial 186 Homelessness 122 Mental Health 101 Physical Violence 57 Domestic Violence 57 Overcrowded 111 Incarceration 59 Other 46 Family History of 1 Risk Factor 109 Family History of 2 Risk Factors 90 Family History of 3 Risk Factors 78 Family History of 4 + Risk Factors 98
Family #Time Polnts %
lndivldual #Time Polnts % Chi Square
71% 'chi-square = 3.58 p > .06 46% 34% 31% 'chi square = 4.38 p > .04 13% 'chi square = 12.49 p > .OO 15% 'chi square = 4.82 p > .03 23% 'chi sauare = 4.57 D > .03 16% 7% 'chi square = 6.87 p > ,008 26%
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012
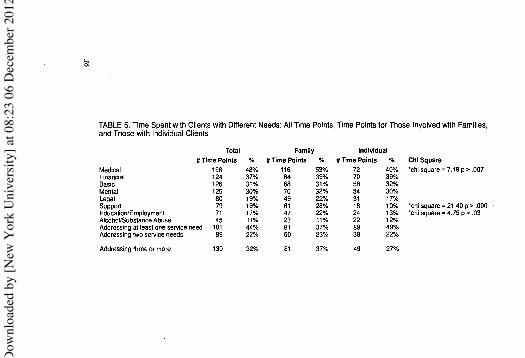
TABLE 5. Time Spent with Clients with Different Needs: All Tme Points, Time Points for Those Involved with Families, and Those with Individual Clients
Total #Time Points %
Medical 198 48% Financial 124 37% Basic 126 31% Mental 125 30% Legal 80 19% Support 79 19% EducationlEmployment 71 17% AlwhoVSubstance Abuse 45 11% Addressing at least one sewice need 181 44% Addressing two service needs 89 22%
Famlly #Time Points Oh
lndivldual #Time Points % Chi Square
72 40% 'chi square = 7.19 p > ,007 70 39% 58 32% 54 30% 31 17% 18 10% 'chi square = 21.40 p > ,000 ,
24 13% 'chi square = 4.75 p > .03 22 12%
Addressing three or more 130 32% 81 37% 49 27Oh
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

TABLE 6. Time on Case Management Functions for All Time Points, Time Points for Those Involved with Families, and Those Involved with Individual Clients
Intake Initial Assessment Care Plan Reassessment One or two CM functions Making a referral Following up on a referral Making or following up
on a referral or both Chart documentation Case conferencing Individual counseling Family counseling Group counseling Bereavement counseling One or two counseling interventior Crisis intervention Other Involvement in All CM activities
None One CM activity Two or more CM Activities
Total #Time Points
Famlly #Time Points %
0 0%
lndivid #Time Points
5 7
15 12 34 36 26
54 40 16 28
1 2 4
32 9
21
25 124 33
ual % 3% 4% 8% 7%
19% 20% 14%
30% 22% 9%
15% 1 % 1 O h
2% 18% 5%
12%
1 4% 69% 18%
Chi Square 'chi square = 7.98 p > ,005
'chi square = 5.62 p > .02 'chi square = 4.38 p > .04
'chi square = 4.75 p > .03
'chi square - 9.29 p > ,002
'chi square = 7.13 p > .008
'chi sauare = 7 recode
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

TABLE 7. Case Manager Time Spent with Asymptomatic and Symptomatic Children, Parents, and Adults Working on Easy vs. Hard-to-Resolve Tasks
Variable Hard-to-Resolve Easy-to-Resolve #Time Pts. % Total Time Pts. #Time Pts. % Total Time Pts. Chi Square
Asymptomatic Child 15 15% 98 43 14% 311 Symptomatic Child 12 12% 98 29 9% 311 Asymptomatic Parent 18 18% 98 42 14% 311 Symptomatic Parent 33 34Oh 98 49 16% 311 8.096 p < .0001 Asymptomatic Adult 10 10% 98 77 25% 311 Symptomatic Adult 21 21% 98 98 32% 311 9.94 p < .OOOO
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012

Abramowirz, Obten, and Cohet~ 39
need for supportive services, and for education/employment ser- vices when working with families as opposed to working with individuals. The large amount of time family-focussed case manag- ers spend addressing medical needs can be explained by the repre- sentation of case managers from hospital pediatric/family HIV clin- ics in the sample. On the other hand, regardless of setting, case managers working with families spend a large amount of time ad- dressing supportive and educational service needs. Supportive ser- vices include service needs typical of families with children-child care, parenting, recreation, and transportation. Additionally, there are manv school-related service needs for children with HIV and their siblings. These may include arranging for special educational or early intervention programs, or they may relate to frequent ab- sences from school (sometimes unexplained because of the secrecy surrounding the diagnosis), academic and behavior problems which may result from family disruption andlor illness progression, or the need for school-based supportive services for infected and affected children, or home-based educational services for children too sick to attend school. These findings confirm reports in the literature describing the complexity of needs of families affected by pediatric HIV.~
The case managers working with families appear to spend more time on case conferencing, care plan formulation, and reassessment than those working with individuals. These results may be ex- plained by the fact that almost half of the case managers studied work in clinical settings and function as part of a provider team where case conferencing, care plan formulation, and reassessment are routine aspects of patient care. Case managers working with families also spend more time doing family counseling, a finding that is not surprising considering the demands the illness places on the family system.6 Whether infected or affected, family members are dealing with shame and fear of disclosure, issues of abandon- ment and bereavement (for both parent and child), custody deci- sions, parentification of children as their parents become ill, and a myriad of other stressors that threaten the equilibrium of the family. Additionally, Mellins and Ehrhardt's study of stress and coping in families affected by pediatric HIV concluded that among inner city families, the diagnosis of HIV and the attendant threat of multiple
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012
40 SOCIAL WORK IN HEALTH CARE
losses, places burdens on families unlike that of any disease pre- viously s t ~ d i e d . ~
The complexity of the case management function for case man- agers working with families and children living with HIVIAIDS was successfi~lly identified using the time study methodology. Moreover, the results have face validity, given their consistency with descrip- tions of family case management found in the l i terat~re.~
Accepted for Publication: 11/07/97
REFERENCES
I. Davis B.D., & Steele S. (January-February, 1991). Case management for young children with special health care needs. Pediatric Nursing, Vol. 17, No. 1.
2. See, for example: Mawn, B., Karthas, N., Burke, K., Foster, S., Calvin, R., Hale, A., Mclntosh, K., & Melchiono, M. Case management of the HIV positive child and family. AIDS Patient Care. April, 1994, 76-78; Boland, M.G., Czar- niecki, L., & Haiken, H. Coordinated Care for Children with HIV Infection, pp. 165-181. In Cliildren and AIDS, (ed.) Margaret L. Stuber, American Psychiat- ric Press, Washington, DC, 1992; and Indyk, D., Belville, R., Lachapelle, S., Gordon, G., & Dewart, T.A. Community-based approach to HIV case management: Sys- tematizing the unmanageable. Social Work. Volume 38, Number 4, July 1993, 380-387.
3. Families in Crisis, The Working Committee on HIV, Children, and Families, June 1996.
4. See for example: Gillies, P., Tolley, K., & Wolstenholme, J. Is AIDS a dis- ease of poverty? AIDS Care, Vol. 8, No. 3, pp. 351-363. 1996; Ward, M.C.A. Dif- ferent Disease: HIVIAIDS and Health Care for Women in Poverty. Culture, Medi- cirle and Psyclziatry, 17, 413-430, 1993; Quinn, S.C. AlDS and the African American Woman: The Triple Burden of Race, Class and Gender. Health Educa- ti011 Quarterly, Vol. 20(3): 305-320, Fall 1993; Walker, G. and Small, S. AIDS, Crack, Poverty, and Race in the African-American Community: The Need for an Ecosystemic Approach. Family System Application to Social Work. The Haworth Press, Inc. 1991; Walton, R.A. HIV Infection and AIDS: Another Layer to Con- sider in Addressing Indigent Health Care in the United States, Journal of Health & Social Policy, Vol. 2(1), 1990; Havens, J.F., Mellins, C.A. & Pilowski, K. Men- tal health issues in HIV-affected women and children. It~tetnational Review of Psy- chiatry, 8, pp. 21 7-225, 1996.
5. See for example: Wiener, L., Moss, H., Davidson, R., & Fair, C. Pediatric AIDS: The Emerging Psychosocial Challenges of thc AlDS Epidemic. Cliild and Adolescent Social Work Journal, Volume 9, Number 5, October 1992; Mellins, C.A., & Ehrhardt, A.A. Families Affected by Pediatric Acquired Immunodefi- ciency Syndrome: Sources of Stress and Coping. Developmet~tal and Behavioral
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012
Abramowifz, Oblen, and Cohen 41
Pediatrics. Vol. 15, No. 3, June 1994; Havens, J.F., op. cit.; Wiener, L., Theut, S., Steinberg, S. et al. The HIV-Infected Child: Parental Responses and Psychosocial Implications. American Journal of Orthopsychiatry 64(3). July 1994.
6. See for example: Mellins, C.A., op. cit.; Reidy, M., Taggart, M. E., Asselin, L. Psychosocial needs expressed by the natural caregivers o f HIV infected chil- dren, AlDS Care, Vol. 3, No. 3, 199 l; Wiener, L., 1992, op. cit.; Lippmann, S.B., James, W.A., & Frierson, R.L. AlDS and the family: Implications for counseling. AIDS Care, Vol. 3, No. I, 1993.
7. Mellons, C.A., op. cit. 8. See Maw, B., Indyk, D., & Mangos, J.A., op. cit.
HAWORTH JOURNALS ARE AVAILABLE ON MICROFORM
Ail Haworth journals are available In either mlcroflche or microfilm from The Haworth Press. lnc.
Microfiche and microfilms are available to hardcopy subscribers at the lower "individual" subscription rate. Other microform subscribers may purchase microfiche or microform at the "library" subscrlption rate.
Microfilm specifications: 35mm: diazo or silver. Microfiche specificatlonr: 105mm x 184mm (4' x 6'): reduction ratio: 24X;
nonsiiver (diazo) positive polarity. Microform are mailed upon completion of each volume.
For further information. contact Janette Hall. Microform Contact. The Haworth Press. Inc.. 10 Alice Street. Blnghamton. NY 13904-1580; Tel: (800) 342-9678 (ext. 328); Fax: (607) 722-1424; E-Mall: getinfoOhaworthpressinc.com
Orders for microform may also be placed with University Mlcrofilms International. 300 North Zeeb Road. Ann Arbor. MI 48106; Tel: (303) 761-4700.
Dow
nloa
ded
by [N
ew Y
ork
Uni
vers
ity] a
t 08:
23 0
6 D
ecem
ber 2
012