Maternal and Child Health Services Title V Block Grant
121
Maternal and Child Health Services Title V Block Grant SUPPORTING DOCUMENT #3 Program Activities: Women/Maternal and Perinatal/Infant
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Maternal and Child Health Services Title V Block Grant

Maternal and Child Health Services Title V Block Grant SUPPORTING DOCUMENT #3
Program Activities:
Women/Maternal and Perinatal/Infant

SUPPORTING DOCUMENT #3: Program Activities – Women/Maternal and Perinatal/Infant
WOMEN/MATERNAL HEALTH Kansas Maternal Mortality Review Committee (KMMRC) ................................................3
Information pertaining to the KMMRC organizational structure, authority and objectives. Contents include:
· KMMRC Overview ................................................................................................... 4 · KMMRC Legislation ................................................................................................ 6 · KMMRC Member Roster ........................................................................................ 8 · KMMRC Action Alert ............................................................................................... 9
Family Planning Life Plan ..................................................................................................10 A workbook to assist women with family planning and identifying pregnancy intentions and desires.
PERINATAL/INFANT HEALTH Kansas Perinatal Quality Collaborative (KPQC) ................................................................39
Outlines the Neonatal Abstinence Syndrome (NAS) Initiative led by the KPQC. Contents include:
· Initiative Overview ................................................................................................... 40 · NAS Outcome Measure and Progress ................................................................... 42 · Centers of Excellence Designation Announcements ........................................... 47 · NAS Initiative Participants ...................................................................................... 48
Kansas Perinatal Community Collaboratives (KPCC) .......................................................49 Information regarding the KPCC and Becoming a Mom® efforts. Contents include:
· KPCC Infographics .................................................................................................. 50 · Becoming a Mom® 2018 State Aggregate Report ............................................... 52
Also available online at: https://www.kdheks.gov/c-f/perinatal_program_impact.htm
MATERNAL/PATERNAL BEHVAIORAL HEALTH Communities Supporting Perinatal Behavioral Health .....................................................102
Describes the Community Collaborative led by Title V to establish and implement the following MCH Leader recognitions related to perinatal mental health and substance use. Content includes;
· Project Overview & Components ........................................................................... 103 · Grantee Application ................................................................................................ 107
Paternal Postpartum Depression (PPD) ............................................................................110 Information for Kansas MCH programs related to PPD. Content includes:
· Paternal PPD Action Alert ....................................................................................... 111 · Information and Recommendations for Paternal PPD ......................................... 112

Kansas Maternal Mortality
Review Committee (KMMRC)
Information pertaining to the KMMRC organizational structure, authority and objectives.
SECTION CONTENTS
· KMMRC Overview ................................................................................................... 4 · KMMRC Legislation ................................................................................................ 6 · KMMRC Member Roster ........................................................................................ 8 · KMMRC Action Alert ............................................................................................... 9

Kansas Maternal Mortality Review Committee (KMMRC) http://www.kansasmch.org/mmr.asp
Purpose: The purpose of the review is to determine the factors contributing to maternal mortality in Kansas
and identify public health and clinical interventions to improve systems of care. Maternal Mortality includes
deaths occurring during pregnancy and up to one year after pregnancy.
Vision: The Maternal Mortality Review Committee’s vision is to eliminate preventable maternal deaths in
Kansas.
Mission: The mission is to increase awareness of the issues surrounding pregnancy-related death and to
promote change among individuals, communities, and healthcare systems in order to reduce the number of
deaths.
Goals: The goals of the Maternal Review Committee are to:
▪ Perform thorough record abstraction in order to obtain details of events and issues leading up to a mother’s death.
▪ Perform a multidisciplinary review of cases to gain a holistic understanding of the issues. ▪ Determine the annual number of maternal deaths related to pregnancy (pregnancy related mortality). ▪ Identify trends and risk factors among pregnancy related death in Kansas. ▪ Recommend improvements to care at the individual, provider, and system levels with the potential for
reducing or preventing future events. ▪ Prioritize findings and recommendations to guide development of effective preventive measures ▪ Recommend actionable strategies for prevention and intervention. ▪ Disseminate the findings and recommendations to a broad array of individuals and organizations. ▪ Promote the translation of findings and recommendations into quality improvement actions at all levels.
There are six (6) key decisions that maternal mortality review committees make for each death reviewed:
1) Was the death pregnancy related?
2) What was the cause of death?
3) Was the death preventable?
4) What were the critical contributing factors to the death?
5) What are the recommendations and actions that address those contributing factors?
6) What is the anticipated impact of those actions if implemented?
NOTE: While all six questions are essential, the last four questions highlight the unique and critical role of the review committees: preventability, contributing factors, recommendations for improvement and measurement of impact.
Authority & Protections:
K.S.A. 65-177 provides authority for the KDHE to conduct studies to reduce morbidity or mortality; all data shall be treated as confidential. Interviewing patients or family members must be done pursuant to K.S.A. 65-2422d. Provides authority for non-identifying aggregate statistical and narrative reports/publications.
K.S.A. 65-2422d authorizes the secretary to use birth, death and still birth certificates as identifiable data for purposes of maternal and child health surveillance and monitoring. The secretary or the secretary's designee may interview individuals for purposes of maternal and child health surveillance and monitoring only with an approval of the health and environmental institutional review board as provided in title 45, part 46 of the code of federal regulations

KANSAS MATERNAL MORTALITY REVIEW COMMITTEE (KMMRC) MEMBER ROSTER
Nola Ahlquist, APRN Prairie Band Potawatomie Nation Health Center
Karen Braman, RPh, MS Senior Vice President of Healthcare Strategy and Policy, KS Hospital Association
Katherine Campbell, BSN RN Nurture KC
Tara Chettiar, MD FACOG OB/GYN, Saint Luke's Women’s Health South
Mariah Chrans Director of Cradle Kansas City–an initiative of the Community Health Council of WY County
Deidre DeGrado, CPM Wichita Birth Assistance
Mary Sunshine-Delgado, MSN APRN Maternal Health Program Manager, United Health Care
Kim Dishman Clinical Education Specialist, Saint Luke’s Northland Hospital
Donna Eubanks SGT Topeka Police Department
Terrie Garrison, RN, BSN Deputy Director, Wyandotte County/KC KS Unified Government Public Health Department
Charles Gibbs, MD Assistant Professor, Maternal-Fetal Medicine, Center for Advanced Fetal Care, KUMC
Lisa Goins, RN WIC & Prenatal Class Instructor, Crawford County Health Department
Donna Gorman, MS LCMFT LCAC Clinical Coordinator, Women’s Recovery Center & Options Adult Services – DCCCA, Inc.
*Melissa Hague, MD Associate Clinical Professor, Asst. Program Director–Clinical, KU School of Medicine–Wichita; Heartland Women's Group
Jeri Harvey, MSN CNL Baker University School of Nursing / Stormont Vail Health
Renee Hulett, RN MSN MHA Director of Maternal Child Services & Behavioral Health Services, St. Catherine Hospital–Centura Health
Candace Johnson, LMSW Director of Reintegration, Saint Francis Ministries
Erin Johnson Overland Park Police Department, Criminal Investigations Division-Special Victims Unit
Alicia Johnson-Turner Special Assistant to the Secretary, Kansas Department for Children & Families
Michael Kennedy, MD McCann Professor & Associate Dean for Rural Health Education, Assistant Dean and Director of Major Academic Society,
Professor, Family Medicine – University of Kansas School of Medicine
Kelli Krase, MD OB/GYN, KU Medical Center
Melinda Lavon, PhD IBCLC Bloom Midwifery & Lactation Services
Lori Marshall, LSCSW Association of Community Mental Health Centers of Kansas, Inc.
Robert S. F. McKay, MD Professor & Chair, Department of Anesthesiology, KU School of Medicine—Wichita
**Randall Morgan, MD OB/GYN, Associates in Women’s Health, PA
Kathy Ray, MSW Director of Advocacy, Education & Rural Projects, KS Coalition Against Sexual & Domestic Violence
Heather Scruton, MBA MSN Assistant Director, Transport & EMS Relations–Critical Care Transport, Children’s Mercy Hospital
Sharla Smith, PhD MPH Assistant Professor KUMC Department of Preventative Medicine & Public Health
Terrah Stroda, CNM Flint Hills OB/GYN—Junction City
John Yeast, MD MSPH Professor, Maternal Fetal Medicine, Department of OB/GYN, University of Missouri Kansas City
Diana Zumbrunn Patient/Consumer
Kansas Department of Health and Environment (KDHE) Leadership & Staff
Farah Ahmed, MPH PhD Environmental Health Officer & State Epidemiologist, KDHE
Ashley Goss, MBA Deputy Secretary for Public Health, KDHE
Nadyne Hagmeier Abstractor for Maternal Mortality Review Committee, Kansas Foundation for Medical Care
Kay Haug Director, Office of Vital Statistics; Assistant State Registrar, KDHE
Jamie Kim, MPH MCH Epidemiologist, Bureau of Family Health, KDHE
Jennifer Marsh Women & Maternal Health Consultant, Bureau of Family Health, KDHE
Kasey Sorell, BSN, RN, CPC Health Planning Consultant/KMMRC Coordinator, Bureau of Family Health, KDHE
Rachel Sisson, MS Director, Bureau of Family Health, KDHE; Kansas Title V Maternal & Child Health Director
Stephanie Wolf, RN BSN Perinatal & Infant Consultant/Nurse, Bureau of Family Health, KDHE
*Chair **Co-Chair Rev. 8/13/2020

KANSAS MATERNAL MORTALITY ACTION ALERT Kansas Maternal Mortality Review Committee Findings
∗ Approximately 27% (10/37 deaths) were the result of a motor vehicle accident in 2016-2017. ∗ Frequently, the women were not wearing seat belts and were ejected from the vehicle.∗ Deaths occurred during pregnancy and the postpartum period.
What Providers Can Do ⇒ Talk with your patients about seat
belt use during pregnancy
⇒ Dispel myths around seat belts,airbags and pregnancy
Provide resources to patients to help them understand how to properly wear a seat belt around their growing belly
Remind pregnant and postpartum moms that their safety is just as important as the safety of their baby
What the State is Doing Partnering with Safe Kids Kansas to
create a campaign to remind moms, dads and kids about the importance of usingseat belts
Creating resources for maternal and child health providers and partners to share with their patients on the importance ofseat belt safety
Encouraging all those who interact with pregnant or postpartum women to discuss the importance of seat belt safety
A healthy pregnancy includes motor vehicle
safety for mom and baby.
For more information:Bureau of Family Health
Kansas Department of Health & Environment785-296-1205
https://kmmrc.org
Supported by the Kansas Department of Health and Environment
Issued December 2019

65-177. Study of diseases and deaths from maternal, perinatal and anesthetic causes; "data" defined;
medical records; confidentiality, use; liability, immunity; admissibility as evidence; reports, contents. (a) (1)
"Data," as used in K.S.A. 65-177 through 65-179, and amendments thereto, includes all facts, information, records of
interviews, written reports, statements, notes or memoranda secured in connection with an authorized medical
research study.
(2) "Maternal death" means the death of any woman from any cause while pregnant or within one calendar year
of the end of any pregnancy, regardless of the duration of the pregnancy or the site of the end of the pregnancy.
(b) (1) The secretary of health and environment shall have access to all law enforcement investigative
information regarding a maternal death in Kansas, any autopsy records and coroner's investigative records relating to
the death, any medical records of the mother and any records of the Kansas department for children and families or
any other state social service agency that has provided services to the mother.
(2) (A) The secretary may apply to the district court for the issuance of, and the district court may issue, a
subpoena to compel the production of any books, records or papers relevant to the cause of any maternal death being
investigated by the secretary. Any books, records or papers received by the secretary pursuant to the subpoena shall
be confidential and privileged information and not subject to disclosure.
(B) The provisions of this paragraph providing for confidentiality of records shall expire on July 1, 2023, unless
the legislature acts to reenact such provisions. The legislature shall review the provisions of this paragraph pursuant
to K.S.A. 45-229, and amendments thereto, prior to July 1, 2023.
(c) The secretary of health and environment shall:
(1) Identify maternal death cases;
(2) review medical records and other relevant data;
(3) contact family members and other affected or involved persons to collect additional relevant data;
(4) consult with relevant experts to evaluate the records and data collected;
(5) make determinations regarding the preventability of maternal deaths;
(6) develop recommendations and actionable strategies to prevent maternal deaths; and
(7) disseminate findings and recommendations to the legislature, healthcare providers, healthcare facilities and
the general public.
(d) (1) Healthcare providers licensed pursuant to chapters 65 and 74 of the Kansas Statutes Annotated, and
amendments thereto, medical care facilities licensed pursuant to article 4 of chapter 65 of the Kansas Statues
Annotated, and amendments thereto, maternity centers licensed pursuant to article 5 of chapter 65 of the Kansas
Statutes Annotated, and amendments thereto, and pharmacies licensed pursuant to article 16 of chapter 65 of the
Kansas Statutes Annotated, and amendments thereto, shall provide reasonable access to all relevant medical records
associated with a maternal death case under review by the secretary.
(2) A healthcare provider, medical care facility, maternity center or pharmacy providing access to medical
records pursuant to this section shall not be held liable for civil damages or be subject to criminal or disciplinary
administrative action for good faith efforts to provide such records.
(e) (1) Information, records, reports, statements, notes, memoranda or other data collected pursuant to this
section shall be privileged and confidential and shall not be admissible as evidence in any action of any kind in any
court or before another tribunal, board, agency or person. Such information, records, reports, statements, notes,
memoranda or other data shall not be exhibited nor their contents disclosed in any way, in whole or in part, by any
officer or representative of the department of health and environment or any other person, except as may be
necessary for the purpose of furthering the investigation of the case to which they relate. No person participating in
such investigation shall disclose, in any manner, the information so obtained.
(2) The provisions of this subsection providing for confidentiality of records shall expire on July 1, 2023, unless
the legislature acts to reenact such provisions. The legislature shall review the provisions of this subsection pursuant
to K.S.A. 45-229, and amendments thereto, prior to July 1, 2023.
(f) (1) All proceedings and activities of the secretary or representatives of the secretary under this section,
opinions of the secretary or representatives of the secretary formed as a result of such proceedings and activities and
records obtained, created or maintained pursuant to this section, including records of interviews, written reports and
statements procured by the secretary or any other person, agency or organization acting jointly or under contract with
the department of health and environment in connection with the requirements of this section, shall be confidential
and not subject to the provisions of the open records act or the open meetings act or subject to subpoena, discovery
or introduction into evidence in any civil or criminal proceeding. Nothing in this section shall be construed to limit

or otherwise restrict the right to discover or use in any civil or criminal proceeding any document or record that is
available and entirely independent of proceedings and activities of the secretary or representatives of the secretary
under this section.
(2) The secretary or representatives of the secretary shall not be questioned in any civil or criminal proceeding
regarding the information presented in or opinions formed as a result of an investigation. Nothing in this section
shall be construed to prevent the secretary or representatives of the secretary from testifying to information obtained
independently of this section or that is public information.
(3) The provisions of this subsection providing for confidentiality of records shall expire on July 1, 2023, unless
the legislature acts to reenact such provisions. The legislature shall review the provisions of this subsection pursuant
to K.S.A. 45-229, and amendments thereto, prior to July 1, 2023.
(g) Reports of aggregate non-individually identifiable data shall be compiled on a routine basis for distribution
in an effort to further study the causes and problems associated with maternal deaths. Reports shall be distributed to
healthcare providers and medical care facilities and other persons necessary to reduce the maternal death rate.
(h) The secretary of health and environment shall receive data secured in connection with medical research
studies conducted for the purpose of reducing morbidity or mortality from maternal, perinatal and anesthetic causes.
Such studies may be conducted by the secretary of health and environment and staff or with other qualified persons,
agencies or organizations. If such studies are conducted with any funding not provided by the state of Kansas, then
the source of such funding shall be clearly identified in such study. Where authorization to conduct such a study is
granted by the secretary of health and environment, all data voluntarily made available to the secretary of health and
environment in connection with such study shall be treated as confidential and shall be used solely for purposes of
medical research. Research files and opinions expressed upon the evidence found in such research shall not be
admissible as evidence in any action in any court or before any other tribunal, except that statistics or tables resulting
from such data shall be admissible and may be received as evidence. This section shall not affect the right of any
patient or such patient's guardians, representatives or heirs to require hospitals, physicians, sanatoriums, rest homes,
nursing homes or other persons or agencies to furnish such patient's hospital record to such patient's representatives
upon written authorization, or the admissibility in evidence thereof.
(i) No employee of the secretary of health and environment shall interview any patient named in any such report,
nor any relative of any such patient, unless otherwise provided in K.S.A. 65-2422d, and amendments thereto.
Nothing in this section shall prohibit the publication by the secretary of health and environment or a duly authorized
cooperating person, agency or organization, of final reports or statistical compilations derived from morbidity or
mortality studies, which reports or compilations do not identify individuals, associations, corporations or institutions
which were the subjects of such studies, or reveal sources of information.
History: L. 1961, ch. 289, § 1; L. 1974, ch. 352, § 46; L. 2010, ch. 143, § 1; L. 2018, ch. 66, § 2; July 1.

Family Planning Life Plan
A workbook to assist women with family planning and identifying pregnancy intentions and desires.

My Life, My GoalsFamily Planning Life Plan
A workbook to help youdecide if and when to havethe healthiest pregnancy
possible.


Making choices for your life is hard. We get it, we are right there with you. If you don’t know what your future plans are, that is OK. Things change, life happens, and we can’t plan for everything. But if we have an idea of what WE WANT it is so much easier to obtain those goals.
The goal of this booklet is to help you have a conversation about your plan for the next year. A plan that you want to make as a couple or just for yourself. Part of that plan, is about whether or not you want to get pregnant this year.

Nothing about uswithout us, believe us,see us, hear us.
3

What is something about yourself you are proudof?
What type of work do you like to do?
What parts of your life bring you the most joy?
What parts of your life would you like to change?
What are some of your goals for this year?
All about you, the veryremarkable you
4

Choose three positive wordsthat describe you best
I am...___________________________________________________
&
___________________________________________________
5

“Proper spacing
between children
helps your body
rebuild sufficient
nutrients”
- Maude
“Proper planning
could offer a
healthier birth
outcome”- Emily
6

Making a plan fool-proofYou have already taken many steps to reach your goals. You have made many sacrifices, like taking an online class at night, or throwing away lighters to quit smoking.
We want you to think about your plan in three areas of your life: career goals, relationship health, and reproductive goals.
How fool-proof is your plan? The dictionary defines fool-proof as “incapable of going wrong.”
INSTRUCTIONS: Put an x on the line between 1 and 10, with ten being best.
Career goalsHow likely do you feel you will reach your career goals?
5 101
How much self love do you feel you practice?Your relationship with yourself
5 101
How healthy do you feel your current relationship is?Health of your relationship
5 101
Reproductive goalsHow likely will your current plan give you the results you want?
5 101
7

Let's reflect for a minuteWould becoming pregnant this year change
your plans or goals?
8

How not to have a baby
Here are the ones for someone who is great at keeping acalendar and will remember to take it everyday or have anappointment for shots every ____.
Use these choices every time to protect against STDs. Theyare the least effective to protect against pregnancy.
These methods are not as effective and often result in pregnancy: withdrawal, pulling out, and crossing fingers.
implant
IUD
pill shot
malecondom
femalecondom
Birth Control ChoicesHere are the ones that last a long time (3-10 years). They require the least amount of effort, don't require a lot of thought, and are reversible at any time.
Mos
t Effe
ctiv
eLe
ast E
ffect
ive
Least EffortM
ost Effort
9
To learn more about birth control options talk to your healthcare provider or visit https://www.hhs.gov/opa/pregnancy-prevention/birth-control-methods/index.html or
http://www.focusforwardok.org/bc101/

Let's focus on reproductive choices because that can be something within your control
Sexual positions don’t matter and attempts to pull out earlydon’t matter -- you can still get pregnant. Let’s work a bitmore on your plan, so you can be in charge of your future,your life!
8 out of 10couples whodon't have a planwill get pregnantwithin a year. *
*Statistics from the Centers for Disease Control, 2017**That means they were having sex one or more times a month.Some wanted to be pregnant, some didn’t.
10

Important Questions
Here's a space to jot down yourquestions and concerns.
11

Develop Your Plan
Yes, I plan to get pregnant within the next year so I will:
____________________________________________________________________________________________________
No, I do not plan to get pregnant within the next year so I will:____________________________________________________________________________________________________
I'm unsure if I want to get pregnant within the next year so I will:____________________________________________________________________________________________________
I'm okay either way so within the next year I will:____________________________________________________________________________________________________
Do I plan to become pregnant within thenext year?
12
To find a reproductive healthcare provider near you visit https://opa-fpclinicdb.hhs.gov/.

My Next Steps
Let's revisit your plan from page 7
After working through this booklet, would your plan stay thesame or would it change?
Your plan is unique to you. You can change it any time basedon how you feel, what you want, and when you want to reachyour goals.
For myself this month I will do:
__________________________________________________
For my health this month I will do:
__________________________________________________
For my relationship this month I will do:
__________________________________________________
And my plan to get pregnant or not pregnant is:
__________________________________________________
__________________________________________________
13

Notes
ReflectionsHere's a space to work on yourthoughts and concerns.
and
14

Loving YourselfLet's revisit your relationship with yourself.
How much self love do you feel you practice?Health of your relationships with yourself
5 101
What is a healthy choice you have made foryourself this month? How did it make you feel?
Think about the following questions:
How likely will your current plan give you the results you want?
5 101
Thinking about the past week, how stressed were you?
5 101
What would you like that number to be?What one thing could you do to lower that number
this week?
INSTRUCTIONS: Put an x on the line between 1 and 10, with10 being best, to indicate how you feel about each question.
15

Inner health is how you feel about yourself, your relationshipsand your purpose in life. It does not mean that you will never besad or angry. Everyone will have highs and lows in life. However,
when you feel good about yourself you will be able to bounceback from sad times faster.
Here are some ways to feel good about yourself.
Love Yourself
Value who you are and what you do:
Take care of your bodyThink positivelyMake time for activities that you enjoy and that are important to youFind your strength and what makes you feel special Learn about yourself and what makes you happy or sadDecide what you want from lifeSet goals and find ways to reach themRemember, it's okay to ask for help Learn positive ways to deal with stress, such as exercise and reading
Connect with OthersBe safe in relationships Spend time with people who respect and value youSpend time with people that care and support you Help others in needThink of others and how they feelBe open to others who are different than you
For free helpCrisis TextLine: Text HOME to 741741
National Suicide Prevention Hotline: 1-800-273-8255Teen Dating Violence Hotline: Text LOVE IS to 1-866-331-9474National Sexual Assualt Hotline: 1-800-656-4673 or rainn.org
16

Health of Your RelationshipINSTRUCTIONS: Put an x on the line between 1 and 10, with
10 being best, to indicate how you feel about each questions.
How healthy do you feel your current relationship is?Health of your relationship
5 101
Take a minute to reflect on your current relationshipList the three best things about your relationship:
1.2.3.How do these make you feel?
List the three hardest things about your relationship.
1.2.3.How do these make you feel?
What one thing could you do to change this?
What one thing could your partner change do to change this?
17

Staying healthy is an everyday habit.
Think about the questions below and ask yourself:
Do I...
Get 30 minutes of physical activity everyday?See a dentist once a year and brush/floss my teeth twice a day?Get a health check-up once a year?Know my family's medical history?Have a safe place to go to, or to stay at?Have a plan to stay tobacco free?Get 6-8 hours of sleep every night?Eat fresh fruits and vegetables every day?Take a vitamin with folic acid every day?Get tested for HIV/AIDS and other Sexually Transmitted Diseases (STDs)?
If you answered yes to most of these questions you are on theroad to a healthy lifestyle.
My Next StepsIf you are planning to become pregnant, or are OK either way,now is a great time to start taking a multivitamin with folic acidonce a day.
18

Whether or not you are planning on having a familysomeday, some habits can be harmful to your overall health.
Do I...Use tobacco products?Vape or use a hookah?Drink alcohol ?Binge drink (have 4 or more alcoholic drinks at one time?Use drugs?Use medications that aren't prescribed for you?Often eat too little or too much?Go more than a week without exercise?Go to bed hungry?Feel safe at home?Have sex with more than one partner?Have sex when I do not want to?
Now may be a good time to talk with a healthcare provider about how to make changes to be healthier and feel your best.
My Next StepsTalk to a healthcare provider to reduce your health risks. Smoking or using nicotine products (including vaping or hookah), drinking alcohol, and using drugs can be harmful to your body. These substances can be very risky for a pregnancy, too. These risks can include: birth defects, brain damage, low birth weight, and prematurity. If you are looking to quit visit kanquit.org for resources.
Think sbout the questions below and ask yourself:
19

Chronic diseases, like diabetes or obesity, can have serious effects on your health. You can help change that! If you have chronic health conditions, visit with a healthcare provider regularly and follow their guidance for managing your chronic condition. Ask your healthcare provider for referrals to specialists that can help like nutritionists or counselors.
If you have a chronic condition, such as those listed below, talk with your healthcare provider to manage them safely during pregnancy.
Do I have:High blood pressureSTDs (Sexually Transmitted Diseases such as genital wartsor herpes)DiabetesHIV/AIDSAsthma Obesity Thyroid conditions SeizuresDepression or anxiety
My Next StepsIt's important to continue your medications when you become pregnant. Discussing your reproductive life plans with a health care provider can ensure you are taking the right medication for you while you are pregnant. Never stop taking medication without talking with a healthcare provider first.
Stay on top of your health by visitinga healthcare provider regularly
20

Immunizations or vaccines can help you from getting certain diseases
Make sure your vaccinations are up-to-date. Some of the most common vaccinations are listed below.
VaccinesMeasles, Mumps, RubellaHepatitis BVaricella (chicken pox) TDaP (Tetanus, Diphtheria, and Pertussis) HPV (Human Papilloma Virus) if you are 27 or youngerMeningitisInfluenza (Flu)
My Next StepsAre your vaccines up to date? Do you have access to your vaccine record? If you are unsure, contact your primary care provider and ask for your vaccination record. If you are in school they may also have a record on file they can provide.
To find out what vaccinations are right for you, check out the Centers for Disease Control and Prevention (CDC) website then talk to a healthcare provider. www.cdc.gov/features/adultimmunizations/index.html
It is important to follow CDC guidelines for vaccinations. Some vaccines have multiple doses and must be given at specific times to be effective. You can find the CDC vaccine guidelines here www.cdc.gov/vaccines/schedules.
Did you know you can get vaccines at your local health department?
21

Here are a few steps you can take to ensure you arehealthy now and in the future:
I will exercise at least 30 minutes per day, 5 or more days a week (www.getupanddosomething.org has great tips to get you started)I will do my best to eat healthy (www.myplate.gov offers great ideas for healthy eating) I will take a multivitamin with folic acid every day I will talk to my healthcare provider about my reproductive life planI will talk to my healthcare provider about the health problems that could hurt me in the future - especially if I get pregnant - such as asthma, high blood pressure, diabetes, and infectionsI will ask my parents and other family members about their own health and what problems I could inherit from them. I will be especially sure to ask if there have been any babies born too small or too soon in my family. I will get help if I feel anxious, depressed or like hurting myself (Crisis TextLine: Text HOME to 741741 or ask your health care provider for help). I will make a promise to myself to be healthy because it will make me feel good about myself.
These will help me have the best chance of having ahealthy baby when I think the time is right.
22

Notes
Reflectionsand
2323

Notes
Reflectionsand
2324

Notes
Reflectionsand
2325

Notes
Reflectionsand
2326


Kansas Perinatal Quality Collaborative (KPQC)
Outlines the Neonatal Abstinence Syndrome (NAS) Initiative led by the KPQC.
SECTION CONTENTS
· Initiative Overview ................................................................................................... 40 · NAS Outcome Measure and Progress ................................................................... 42 · Centers of Excellence Designation Announcements ........................................... 47 · NAS Initiative Participants ...................................................................................... 48

Rev. 6/18
Vision: Kansas is the best place to be born and to be a mother Mission: To improve Kansas’ maternal and infant health outcomes by assuring quality perinatal care using data-driven, evidence-based practice, and quality improvement processes. Goals:
1. Establish and provide oversight for multiple state-wide quality improvement initiatives toimprove birth outcomes
2. Promote system changes by gathering data resources and increasing use of evidence-based practices for perinatal health
3. Bring personalized support to Kansas communities by providing education and resourcesfor perinatal health
Neonatal Abstinence Syndrome Kansas State Initiative Universal education for birthing hospitals in Kansas for standardization of care in
identification, evaluation, treatment and safe discharge of infants with NAS
IDENTIFICATION Partner with prenatal care providers to facilitate universal screening and early identification per ACOG guidelines Standardize protocol for infant drug screening Partner with treatment centers
EVALUATION Utilize one specific NAS scoring tool Standardize an NAS scoring education program assuring clinicians are trained upon hire with reliability checked yearly
TREATMENT Standardize protocol directed at avoiding separation of infant and mother outlining evaluation and non-pharmacologic treatment of the substance exposed infant Standardize education for families to engage in non-pharmacologic intervention Provide Vermont Oxford Network NAS Universal Education virtual classroom access to the interdisciplinary team and all involved in creating a culture of compassion and healing for the mother and infant. Standardize protocol outlining criteria for breastfeeding which promotes and supports breastfeeding in eligible mothers Standardize protocol for pharmacologic treatment of NAS
DISCHARGE Standardize a process to ensure safe discharge Establish appropriate follow-up for mother Liaison with child protective services to align expectations and assure that appropriate resources are available upon discharge Standardize a process for measuring and reporting NAS rates, data collection and outcome measures. Standardize a classification utilized to designate infants at risk for NAS and treated pharmacologically

Neonatal Abstinence Syndrome Kansas State Initiative SMART AIMS
AIM 1 By October 2020, 85% of all Kansas birth centers enrolled in VON NAS Universal Training Program will have achieved “Center of Excellence” designation
AIM 2 By October 2020, less than 50% of infants at risk for NAS will be directly admitted to the NICU
AIM 3 By October 2020, the number of infants at risk for NAS who require pharmacological treatment will decrease by 25%
AIM 4 By October 2020, the LOS of Kansas infants with NAS treated pharmacologically will decrease by 2 days
DEFINITIONS:
CENTER OF EXCELLENCE: Center of Excellence is awarded to a specific center when 85% of itsdesignated associates complete the VON NAS training modules
AT RISK FOR NAS: Infants are considered at risk if meeting one of the following criteria
1) Positive Maternal History of narcotic exposure (Methadone, Subutex, Suboxone, Heroin,Morphine, Codeine, Hydrocodone, Oxycodone, Tramadol, Benzodiazepines, Barbituratestaken ≥ 1/day, 3/week for 3 weeks prior to delivery)
2) Positive Maternal or Neonatal drug screen for opiates, benzodiazepines, or barbiturates.Indications for maternal and infant drug screening:
Maternal Indications: Absent, late, or inadequate prenatal care; previously documented or admitted history of drug abuse; a previous unexplained late fetal demise; unexplained hypertensive episodes; severe mood swings; cerebrovascular accidents; myocardial infarction; and repeated spontaneous abortions; precipitous labor; abruptio placentae -without underlying etiology (Hudak & Tan, 2012)
Infant Indications: Dysmorphic features consistent with Fetal Alcohol Syndrome; Atypical vascular incidents: cerebrovascular accidents, myocardial infarction and necrotizing enterocolitis in otherwise healthy full-term infant; Unexplained intrauterine growth restriction; Unexplained microcephaly; Infant which displays symptoms of Neonatal Abstinence Syndrome – tremors, excessive crying, poor feeding; monoclonic jerks, seizures, poor sleeping, gastrointestinal disturbances (Hudak & Tan, 2012). In infants presenting with NAS symptoms, drug screens will be inaccurate if the infant has voided or stools are no longer meconium.

KS PQC Website Informationhttps://kansaspqc.org/
NAS QI Initiative Monthly Outcome Measures
SMART AIM 1By October 2020, 85% of all Kansas birth centers enrolled in VON NAS Universal Training Program will have achieved “Center of Excellence” designation.
Progress Toward VON Completion These figures represent participating centers’ progress in completing the VON NAS Universal Training Program modules.
SMART AIM 2By October 2020, less than 50% of infants at risk for NAS will be directly admitted to the NICU.
Direct Admission to the NICU These figures represent the percentage of infants at risk for NAS directly admitted to the NICU where the numerator is admission to the NICU because of risk and the denominator is inborn infants identified as meeting the KPQC definition of “at risk for NAS” plus infants transferred in because of risk status.

SMART AIM 3By October 2020, the number of infants at risk for NAS who require pharmacological treatment will decrease by 25%.
At-risk Infants Treated Pharmacologically These figures represent the percentage of infants treated pharmacologically where the numerator is pharmacologic treatment and the denominator is inborn infants identified as meeting the KPQC definition of “at risk for NAS” plus infants transferred in because of risk status.

SMART AIM 4By October 2020, the LOS of Kansas infants with NAS treated pharmacologically will decreased by 2 days.
Average Length of Stay for Infants Treated Pharmacologically These figures represent the average length of stay of all infants treated across centers.
NAS Learning Forums – Archives/Recordings




1 | Kansas Perinatal Quality Collaborative
NAS Initiative Participants October 2018 to October 2020
BIRTH CENTER CITY ALLEN COUNTY REGIONAL HOSPITAL Iola
CITIZENS MEDICAL CENTER Colby
COMMUNITY HEALTHCARE SYSTEM OF NE KANSAS Onaga
COMMUNITY MEMORIAL HEALTHCARE INC Marysville
GEARY COMMUNITY HOSPITAL Junction City
HAYS MEDICAL CENTER Hays
HIAWATHA COMMUNITY HOSPITAL* Hiawatha
HUTCHINSON MEDICAL CENTER Hutchison
KANSAS MIDWIVES ALLIANCE Stafford
KEARNY COUNTY HOSPITAL Lakin
LABETTE HEALTH Parsons
LAWRENCE MEMORIAL Lawrence
MEMORIAL HOSPITAL Abilene
MENORAH MEDICAL CENTER* Overland Park
NEMAHA VALLEY COMMUNITY HOSPITAL Seneca
NEOSHO MEMORIAL REGIONAL MEDICAL CENTER Chanute
NEWMAN REGIONAL HEALTH* Emporia
OLATHE MEDICAL CENTER Olathe
OVERLAND PARK REGIONAL MEDICAL CENTER* Overland Park
RANSOM MEMORIAL HEALTH Ottawa
ROOKS COUNTY HOSPITAL Plainville
SHAWNEE MISSION MEDICAL CENTER* Merriam
SOUTH CENTRAL KANSAS REGIONAL MEDICAL CENTER* Arkansas City
SOUTHWEST MEDICAL CENTER Liberal
STORMONT VAIL HEALTH* Topeka
SUSAN B. ALLEN MEMORIAL HOSPITAL El Dorado
UNIVERSITY OF KANSAS HEALTH SYSTEM* Kansas City
UNIVERSITY OF KANSAS HEALTH SYSTEM, ST. FRANCIS Topeka
VIA CHRISTI HOSPITAL, MANHATTAN Manhattan
VIA CHRISTI HOSPITAL, ST. JOSEPH Wichita
WESLEY MEDICAL CENTER Wichita
WESTERN PLAINS MEDICAL CENTER Dodge City
*Spring Cohort: June 2018 to October 2020

Kansas Perinatal Community Collaboratives
(KPCC)
Information regarding the KPCC and Becoming a Mom® efforts.
SECTION CONTENTS
· KPCC Infographics .................................................................................................. 50 · Becoming a Mom® 2018 State Aggregate Report ............................................... 52
Also available online at: https://www.kdheks.gov/c-f/perinatal_program_impact.htm

PERINATAL COMMUNITY COLLABORATIVEUtilizing the Becoming a Mom® (BaM) CurriculumBecoming a Mom® (BaM)/Comenzando bien® (Cb) is a prenatal education curriculum (English and Spanish languages) for pregnant women created by the March of Dimes.
The prenatal curriculum and supplement materials provided by the Kansas Department of Health and Environment (KDHE) and Sunflower Health Plan are
designed to improve participants’ chances of having a healthy pregnancy and a healthy baby. The program has been implemented in a variety of settings including community-based organizations, hospitals, health departments,
clinical care settings, faith-based communities and worksites.
KANSAS
Three-Pronged Approach
+ +Perinatal
Care Perinatal
EducationPerinatal Support
DESIGNED TO PROMOTE HEALTHY PREGNANCIES THROUGH TWO CORE COMPONENTS:
COGNITIVEProvides accurate and timely information about:
PRENATAL CARE PREGNANCY POSTPARTUM INFANT CARE
BEHAVIORALPromotes changes in perinatal health behaviors, such as: Infant Care
SupportSeeking Prenatal
Care Taking Prenatal
Vitamins Eating Healthy
FoodsAvoiding Harmful
Substances
MOTHERS RECEIVING PRENATAL EDUCATION IN THE KANSAS BaM/Cb PROGRAM WERE:
More likely to be of racial/ethnic minorities
than all other Kansas mothers giving birth
More likely to have a lower education level than all other Kansas mothers giving birth
More likely to be younger than all other Kansas mothers giving
birth
More likely to be enrolled in WIC than
all other Kansas mothers
More likely to have non-private insurance than all other Kansas mothers giving birth
These are all indicators of the program reaching targeted high-risk populations.

AFTER COMPLETING THE BaM/Cb PROGRAM, MOTHERS WERE MORE LIKELY TO REPORT THAT THEY WERE:
Very likely to talk with their healthcare provider if they experience depression or anxiety
Very knowledgeable about available resources in their community if they experience depression or anxiety
Very likely to breastfeed their baby
Very confident or confident in their ability to breastfeed their baby
Very likely to report talking to their provider about preventing pregnancy after the birth of their baby
Understanding there is great benefit in waiting 18-24 months between pregnancies
FOR BaM/Cb MOTHERS WITH AVAILABLE OUTCOMES DATA, THEY HAD A:
Significantly lower pre-term
birth rate
Similar, but slightly improved low birthweight
rate
Lower likelihood
of cesarean deliveries
Similar, but slightly higher rate of breastfeeding
initiation
4.9% 9.5%
BaM Births Kansas Births
6.9% 7.4%
BaM Births Kansas Births
BaM Births Kansas Births
27.4% 29.7% 90.9% 88.7%
BaM Births Kansas Births
These outcomes equate to healthier moms and babies and lower healthcare and other associated costs.
For more information, visit www.kdheks.gov/c-f/perinatal_community_collaboratives.
Source: Bureau of Epidemiology and Public Health Informatics analysis of Becoming a Mom program data, 2018 and Kansas Department of Health and Environment, Birth data, 2018
Impactful drop in infant mortality rates in the two longest running KPCC sites
1KDHE, Bureau of Epidemiology and Public Health Informatics
KPCCestablished July 2012
KPCCestablished Jan. 2010
11.9%
5.8%
9.0%
5.5%
2005-2009
2014-2018
2005-2009
2014-2018

Becoming a Mom® State Aggregate Report
January 2018-December 2018
Kansas Department of Health and Environment Bureau of Family Health
1000 SW Jackson Street, Suite 220 Topeka, KS 66612

Becoming a Mom® 2018 Evaluation Report Page 2
Kansas Department of Health and Environment Becoming a Mom® Program Evaluation
Report Covers January 2018 - December 2018 Program Data Report Published December 19, 2019
This report was prepared on behalf of: Lee A. Norman, M.D., Secretary
Kansas Perinatal Community Collaborative Program Coordinator
Stephanie Wolf, RN, BSN Kansas Department of Health and Environment
Bureau of Family Health [email protected]
785.296.1306
Maternal and Child Health Epidemiologist
Lawrence Panas, MPH, PhD Kansas Department of Health and Environment
Bureau of Epidemiology and Public Health Informatics [email protected]
785.296.8873
Reviewed by: Stephanie Wolf, RN, BSN Farah Ahmed, MPH, PhD
Acknowledgement
Special thanks go to all the program participants who completed the initial, completion and birth outcome surveys.

Becoming a Mom® 2018 Evaluation Report Page 3
Table of Contents Executive Summary ....................................................................................................................................... 4
Introduction .................................................................................................................................................. 7
Data/Methods ............................................................................................................................................... 8
Results/Analysis .......................................................................................................................................... 10
Recommendations ...................................................................................................................................... 34
References .................................................................................................................................................. 38
Appendix A: Program Background and History .......................................................................................... 39
Appendix B: Survey Questions .................................................................................................................... 45

Becoming a Mom® 2018 Evaluation Report Page 4
Executive Summary Improving prenatal education and support is key to improving the health of mom and baby. Kansas has been working to improve access to such services for all pregnant women in the state. The Kansas Department of Health and Environment has worked diligently with the March of Dimes to implement the Becoming a Mom®/Comenzando bien® (BaM/Cb) prenatal education curriculum across the state, in a consistent and reliable manner, since 2014. The Becoming a Mom® 2018 State Aggregate Report summarizes overall data for BaM sites based on single year data for the 2018 BaM calendar year and 2018 Kansas birth statistics. This report represents 15 sites aggregated together (two other existing sites, Thomas and Lincoln were excluded due to data considerations). In the initial phase of the program, BaM/Cb works to educate mothers about ways to improve their own health and steps to take to improve the health of their baby and to reduce preterm births. While the goal of the program is to improve health of mothers in the program in general, and will accept most all mothers who want to enroll in the program, the BaM/Cb program specifically aims to provide education to those mothers that are more likely to be at risk (low socioeconomic status, racial/ethnic minorities) to reduce disparities among those populations through time. The below data demonstrates success of the program in reaching these target populations. Mothers receiving prenatal education in the BaM/Cb program were
• More likely to be racial/ethnic minorities than mothers giving birth in the state, especially
Hispanics and non-Hispanic blacks.
o Non-Hispanic Black: BaM, 8.9%; Kansas Births, 6.9%
o Hispanic: BaM, 28.8%; Kansas Births, 16.5%
• More likely to be younger than Kansas mothers giving birth
o Under 17 years old: BaM, 3.2%; Kansas Births 1.3%
o 18-19 years old: BaM 8.8%; Kansas Births, 4.1%
o 20-24 years old: BaM 26.7%; Kansas Births, 21.6%
• More likely to have a lower education level than Kansas mothers giving birth in general
with about 43% of BaM/Cb moms having a high school education or less compared to
Kansas births where 36% of mothers had a high school education or less.
• More likely to be enrolled in WIC, with 47.6% of BaM/Cb moms reporting WIC enrollment
compared to 28.5% of mothers giving birth in the state.
• More likely to have non-private insurance than Kansas mothers giving birth in general
o Private Insurance: BaM, 37.6%; Kansas Births, 55.2%
o KanCare/Medcaid: BaM, 35.5%; Kansas Births, 31.2%
o None/Self Pay: BaM, 15.3%; Kansas Births, 7.0%
• More likely to initiate prenatal care in the first trimester than Kansas mothers giving birth
in general but also more likely to report not seeing a health care provider if not receiving
prenatal care in the first trimester
o First trimester: BaM, 85.7%; Kansas Births, 81.0%

Becoming a Mom® 2018 Evaluation Report Page 5
o Not Seeing A Provider: BaM, 6.0%; Kansas Births, 1.0%
• Almost two times less likely to be reporting smoking during pregnancy (5.5%) than Kansas
mothers giving birth (9.5%)
After completing the BaM/Cb program, mothers were more likely to report that they were
• Very likely to talk with their healthcare provider if they experience depression or anxiety
• Very knowledgeable about available resources in their community if they experience
depression or anxiety
• Very likely to breastfeed their baby
• Very confident or confident in their ability to breastfeed their baby
• Very likely to report talking to their provider about preventing pregnancy after the birth of
their baby
• Understanding there is great benefit in waiting 18-24 months between pregnancies
After completing the BaM/Cb program, BaM/Cb mothers showed a general significant improvement in their knowledge around signs of preterm labor, what to do in the case of preterm labor, postpartum symptoms of concern, the benefits of a full-term pregnancy, truths about breastfeeding, and safe sleep practices. While education of BaM/Cb mothers is a critical element of the program, it is also important to understand the impact of the education on pregnancy outcomes through time. For the BaM/Cb report, several measures are tracked to understand birth outcomes as well as the general health of both the mother and baby at the time of delivery. For the 2018 report, the first linkage of BaM records and vital records was attempted for key outcome measures including gestational age, low birth weight, induced deliveries, cesarean deliveries, and breastfeeding initiation to improve data reporting for mothers giving birth after participation in the BaM/Cb program. The linkage was largely successful and lead to an almost 50% increase in the possible records available for analysis of those measures. For BaM mothers with available outcomes data, they had a
• Significantly lower preterm birth rate (4.9%) than for Kansas births in general (9.5%)
• Similar, but slightly improved low birthweight rate (6.9%) compared to Kansas births in
general (7.4%)
• Lower likelihood of cesarean deliveries (27.4%) compared to Kansas births in general
(29.7%)
• Significantly higher rate of induced delivery (37.5%) compared to Kansas births in general
(33.6%)
o After linkage of birth record data to the BaM data, the induction rate significantly
reduced for BaM mothers (not shown), indicating potential overreporting or
misreporting in BaM records alone.
o Looking at only those mothers in the original BaM outcome survey who reported
a reason for induction (no reason is provided in the vital statistics record) and a
reported induction (after linkage), 100% of women reporting an elective induction
were for births with a gestational age of at least 39 weeks (not shown). This is in
line with ACOG recommendations for non-medically necessary inductions, and
other national education campaigns (i.e. Healthy Babies are Worth the Wait, by

Becoming a Mom® 2018 Evaluation Report Page 6
the March of Dimes; Is it Worth it, by the Eunice Kennedy Shriver National Institute
of Child Health and Human Development).
• Similar, but slightly higher rate of breastfeeding initiation (90.9%) as for Kansas births in
general (88.7%).
o After linkage of birth record data to the BaM data, the breastfeeding rate reduced
for BaM mothers (not shown). This may be related to differing assessment periods
or misreporting.
Other key findings worth noting
• BaM/Cb participants reported they had connected, or had planned to connect, to multiple services including breastfeeding support (75.1%), car seat (74.6%), WIC (68.6%), and Medicaid (62.9%)
• Over 70% of moms reported being referred from collaborative partners, reinforcing the significance of the KPCC model.
The above summary of findings suggests that while serving the most at risk populations in our state, the program is still highly successful in increasing knowledge, changing behaviors, and improving outcomes. This data demonstrates how outcomes are improved when education and support is gained through targeted interventions such as the Becoming a Mom®/Comenzando bien® (BaM/Cb) program and community partners are working together, as is demonstrated with the Kansas Perinatal Community Collaboratives (KPCC), to assure such resources are accessible in the community. This validates the importance of continuing, strengthening and expanding such initiatives in our state.

Becoming a Mom® 2018 Evaluation Report Page 7
Introduction This report is a summary of evaluation results for January 1, 2018 through December 31, 2018 for the
Becoming a Mom®/Comenzando bien® (BaM/Cb) program in Kansas. Specifically, this report summarizes
findings from the pre and post surveys and follow-up health outcome questionnaires and utilizes the
following forms: Initial Survey (Pre-Survey), Completion Survey (Post-Survey), Birth Outcome Card
(Outcomes), BaM Service Form, and KDHE Program Visit Form (Adult with Profile).
The BaM/Cb program (see Figure 1 for BaM program sites) analyses were conducted, and data were
reported for the following Kansas counties: Clay, Crawford, Dickinson, Finney, Geary, Kearny, Lyon,
Montgomery, Reno, Riley, Saline, Sedgwick, Seward, Shawnee, and Wyandotte. Lincoln County had
insufficient participation for analysis and Thomas County launched in the fourth quarter of 2018, therefore
excluded from analysis.
Figure 1. Location of Becoming a Mom® (BaM) Sites, Kansas 2018
BaM Sites included in 2018 report
New BaM Site in late 2018; not included in report
Insufficient participation for analysis; not included in report

Becoming a Mom® 2018 Evaluation Report Page 8
Data/Methods
This report includes the women who completed their post-survey (i.e., Completion Survey) in Data
Application and Integration Solutions for the Early Years (DAISEY) between January 1, 2018 and December
31, 2018. Two data sets were created: one for women completing their post-survey between January 1,
2018 and December 31, 2018 and another for those completing their outcome survey in the same time
frame.
Brief data descriptions of the primary datasets and the data cleaning methodology used for this report
are provided below. All datasets used for the analyses are derived from Kansas Department of Health and
Environment’s (KDHE) DAISEY system. Data operations including data cleaning, deduplication, recoding,
and transfer record creation, as well as the map of locations, were completed using R software (Version
3.5.2). For the final report, figures and tables were developed using SAS 9.4.
Pre-Survey
For the pre-survey, records were extracted from DAISEY for the year prior to the evaluation year, as well
as the current evaluation year (1/1/2017-12/31/2018). This allows for any mothers that may have started
the BaM program before the evaluation period, or left and returned to complete the program, to be
captured for analysis. Based on this data extract, there were 2,320 records for surveys completed during
the two-year period. After evaluation, cleaning, deduplication of records and inclusion of transfer records,
2,301 records were available for potential linkage with the post-survey. After removing Lincoln (N=3) (due
to small numbers) and Thomas (N=9) (due to launch in late 2018) pre-surveys, 2,289 potential pre-surveys
were available for linkage to the post-survey (2,288 records when transfers were removed.) Table 1 shows
those women who only took the pre-survey in the year 2018 to better represent who entered the program
that year.
Post-Survey
Records for the post-survey were extracted from DAISEY for the 2018 calendar year (1/1/2018-
12/31/2018). After evaluation, cleaning, deduplication of records and inclusion of transfer records, there
were 832 records available for the pre and post record linkage. This number decreased to 829 records
after removing records for Thomas County (N=3) and 827 records with transfers removed.
Pre-Post Linkage
Data for the pre- and post-survey were linked based on the participant’s ID in the DAISEY system. Some
participants may have multiple IDs in the system, so data exploration was also conducted to evaluate
mothers (based on Name and DOB) who had differing ID numbers. These ID numbers were then evaluated
between datasets, to establish transfer records (as noted above) or to correct erroneous records with
multiple IDs before linkage. Once the transfer (or duplicate) status of a participant was verified, records
were linked based on the final IDs available. There were 823 final records, including transfer cases, and
821 cases for statewide analysis when transfer cases were removed.

Becoming a Mom® 2018 Evaluation Report Page 9
Outcomes
For the outcomes records, data were extracted based on the 2018 calendar year (1/1/2018-12/31/2018).
There were 698 initial records extracted from the outcomes file, which was reduced to 695 records after
evaluation, cleaning, and deduplication of records, leaving 695 potential records for evaluation of infant
outcomes. After removing Thomas County records (N=3), 692 outcome records remained.
Surveys Collected by Site
Data presented throughout the report represent 827 unique mothers with a post-survey completed
between January 1, 2018 and December 31, 2018 (Table 1). The data in the outcome section represents
unique participants with a completed outcome survey in the same time frame (N=685).1
Table 1: Number of Becoming a Mom® Surveys Collected by Site Site Name Pre-Survey* Post-Survey* Outcome§
Clay County 7 7 5
Crawford County 47 35 31
Dickinson County 15† 12† 4
Finney 44 31 26
Geary County 91 68 59
Kearny 22 18 3
Lyon County 118 103 95
Montgomery County 24 13 15
Reno County 94 59 55
Riley County 101 84 78
Saline County 97† 74† 64
Sedgwick County 261 193 121
Seward 63 44 34
Shawnee County 43 32 32
Wyandotte County 89 56 63
Total 1,116 827 685
*The data represent participants who completed the respective form in 2018. §Note: This number reflects the number of unique mothers who completed the outcome survey (therefore does not reflect multiple births). †Transferred (counted only once in Total).
Outcomes Records
For the 2018 report, mothers from the BaM cohort were linked to the birth tables provided by the KDHE
Office of Vital Statistics to get a more complete picture of birth outcomes for moms in the BaM program.
Both pre-post records with no reported outcomes by the mothers and records with reported outcomes
were provided for linkage. For the pre-post records with no outcomes, this provided information about
available outcomes of interest and for the records with a reported outcome survey, it provided improved
information about outcomes. The available fields of interest that were returned from the linkage included
1 Note: All participants that completed an outcome form in 2018 were included for analysis. The date of completion for the form, however, does not necessarily represent a birth during the reporting period, only that the form was completed in the reporting period.

Becoming a Mom® 2018 Evaluation Report Page 10
birth weight, gestational age, induction, cesarean sections, plural births, breastfeeding initiation, and
deaths. Overall, the total outcome records for analyses were increased from 692 to 1,026 (1,024 when
removing transfer cases) outcomes records (1,013 unique moms) for the selected measures mentioned
above.
Results/Analysis Demographics
Sedgwick County had the greatest number of participant post-surveys (n=193), followed by Lyon County
(n=103) and Riley County (n=84). Six hundred and eighty-five mothers completed the outcome survey.
Births of multiples included a set of twins and a set of triplets in Geary County, a set of twins in Lyon
County, a set of twins in Saline County, and two sets of twins in Sedgwick County. One mother in Saline
County had two unique birth outcome surveys in 2018. Linkage with the vital records identified an
additional set of twins in the vital linked records. All together, 692 outcome surveys were included in the
analysis, representing the above described births.
The predominant racial/ethnic group was non-Hispanic white (55.2%), followed by Hispanic (28.8%), non-
Hispanic black (8.9%) and non-Hispanic others (7.1%) (Figure 2). The majority of participants (84.8%)
reported speaking English at home (Figure 3), which is a lower percentage than the state in general which
reports 88.7% speaking primarily English in the home.1 Age of participants ranged from less than 15 years
to 45 to 49 years, with the majority of participants being in their 20s and 30s (Figure 4). Overall, the
Becoming a Mom®/Comenzando bien® (BaM/Cb) participant demographics suggests the program is
reaching a more diverse population than is representative of the population of the state at large (based
on 2017 births), which is an aim of the program.

Becoming a Mom® 2018 Evaluation Report Page 11
Descriptive Characteristics
Employment status varied among participants, with the highest percentage being unemployed (Figure 5).
About 29% of the participants reported having a college degree, while 42.9% of the participants reported
having only a high school degree or less (Figure 6). About 47.6% of the participants were enrolled in
Women, Infants, and Children (WIC) (Figure 7), which is higher than the overall percentage of enrollment
among 2018 births (30.0%), indicating integration efforts between the two programs have been
successful. Thirty-five percent of the participants were insured by KanCare/Medicaid (higher percentage
than all Kansas births in 2018), 37.0% were insured by private insurance (lower percentage than all Kansas
births in 2018) and 15.1% did not have insurance (higher percentage than all Kansas births in 2018) (Figure
8). Nearly 60 %(58.2%) of the BaM/Cb participants were experiencing their first pregnancy (Figure 9). The
majority (85.7%) of participants initiated prenatal care in the first trimester (Figure 10), a higher
percentage than that of all Kansas births (81.2%). About 1 in 20 (5.5%) participants reported being a
smoker in the pre-survey (Figure 11). Roughly 1 in 8 (11.6%) participants were told they have a high-risk
pregnancy (Figure 12). While two-thirds of participants (65.8%) reported not having a health problem, the

Becoming a Mom® 2018 Evaluation Report Page 12
two most common health conditions were asthma (8.9%) and depression/anxiety (15.2%) (Figure 13).
About 40% of participants heard about BaM/Cb through a clinic and more than half (55.1%) of participants
started the program in their second trimester, which is a targeted entry point for the program (Figure 15).
Out of 598 participants with an Edinburgh score recorded, 13.4% required a referral based on their
Edinburgh score of 10 or greater (Figure 16). The majority (89.5%) of participants reported not having
anything keeping them from their prenatal appointments (Figure 17).

Becoming a Mom® 2018 Evaluation Report Page 13

Becoming a Mom® 2018 Evaluation Report Page 14

Becoming a Mom® 2018 Evaluation Report Page 15

Becoming a Mom® 2018 Evaluation Report Page 16
Change in Knowledge/Behavior
Post-intervention, participants report they were more likely to talk to a healthcare provider or access
available resources if she experienced depression and/or anxiety during or after pregnancy (Figure 18).
Participants also reported being more knowledgeable about available resources in the community related
to depression and/or anxiety (Figure 19). The majority of participants were already likely to discuss
medications with a healthcare provider before taking them, but the percent of participants reporting they
were very likely to discuss medications with a healthcare provider improved slightly post intervention.
(Figure 20). Furthermore, the majority of participants already knew alcohol, marijuana,
methamphetamine and narcotics should never be taken during pregnancy (Figure 21). There was
improvement in the number of cigarettes smoked per day from pre to post survey, but the change was
minimal. Over 9 in 10 participants were non-smokers during their time in BaM/Cb. Most of the women
who did smoke, reported smoking less than half a pack of cigarettes a day (Figure 22).

Becoming a Mom® 2018 Evaluation Report Page 17
There was an 8.8% increase (from 76.6% to 85.4%) in the number of women who reported being very
likely to breastfeed, post-intervention (Figure 23). Additionally, following program completion,
participants had gained confidence in their ability to breastfeed (Figure 24) and were more knowledgeable
about resources available to help with breastfeeding (Figure 25).
There was an increase in participants’ likelihood of discussing a plan for pregnancy prevention with their
provider during their prenatal care with a 14.9 % increase of participants saying they were very likely to
discuss with their provider post intervention (Figure 28). Post-program, more participants believe there is
great benefit (an increase of 14.2 percent) to waiting a minimum of 18 months between pregnancies
(Figure 29).
There was a slight improvement in participants’ intake of a prenatal or multivitamin containing folic acid
in the “Never” category and a related slight increase in taking a daily prenatal or multivitamin containing
folic acid was observed (Figure 30). Participants showed a slight overall increase in the number of days
per week they do 30 minutes of low-impact to moderate exercise (Figure31).

Becoming a Mom® 2018 Evaluation Report Page 18

Becoming a Mom® 2018 Evaluation Report Page 19

Becoming a Mom® 2018 Evaluation Report Page 20

Becoming a Mom® 2018 Evaluation Report Page 21

Becoming a Mom® 2018 Evaluation Report Page 22
All but one of the questions related to preterm labor signs had significant improvements from pre to post
surveys (Table 2). The question for contractions showed a significant change in the wrong direction. Two
questions related to what a woman should do if she is experiencing preterm labor symptoms showed
significant improvement, while participants showed a significant decrease for calling a health care
provider.
Questions related to postpartum symptoms all showed significant improvements in identifying
postpartum symptoms such as postpartum bleeding patterns, differences in bladder control, night sweats,
baby blues, postpartum panic, and needing a nap on the post survey.
Participants were able to demonstrate significantly increased knowledge about the benefits of full term
pregnancy and truths about breastfeeding. Participants also reported significantly greater knowledge
about “back to sleep”. They additionally demonstrated planned change in behavior, as there was an
increase pre to post intervention in those who reported planning to place their baby on his/her back to
sleep.
BaM/Cb participants also reported that they had connected, or had planned to connect, to multiple
services including breastfeeding support (75.1%), car seat (74.6%), WIC (68.6%), and Medicaid (62.9%)
(Table 3).

Becoming a Mom® 2018 Evaluation Report Page 23
Table 2: Pre/Post-Intervention Answers to Knowledge Questions (percentage answering correctly)
Question Pre-Survey (%) Post-Survey (%)
Signs of Preterm Labor
Color of discharge or bleeding 65.0 83.2*
Feeling that baby is pushing down 57.4 79.5*
Backache 49.7 78.7*
Belly cramps 40.8 72.5*
Cramps that feel like your period 53.8 77.7*
Should a pregnant woman do the following if she is experiencing preterm labor
Call her health care provider right away 88.4 85.1*
Stop what she is doing & rest on her left side for one hour 41.4 84.7*
Drink 2-3 glasses of water or juice (not coffee or soda) 36.2 74.7*
Do nothing, and wait for an hour or two to see if the symptoms go away 92.8 90.4
Postpartum Symptoms
After discharge from the hospital, bleeding more than a pad in an hour 75.3 86.5*
Fever 90.9 88.5
Difference in bladder control 51.2 62.0*
Night sweats 21.4 53.5*
Extreme fatigue 76.4 77.5
Baby blues 49.3 69.1*
Non-stop crying 82.5 85.5
Panic 79.8 83.7*
Needing a nap 64.9 80.1*
Lack of interest in baby 81.6 83.1
Benefits of Full Term Pregnancy
Full brain development 91.8 97.6*
Full lung development 90.5 93.7*
Less likely to be admitted to NICU 75.4 83.4*
Improved breastfeeding 69.3 76.6*
Truths about breastfeeding
My baby will be less likely to have diabetes later in life 54.7 77.7*
I will lower my risk of some types of cancer 51.3 77.2*
Frequency of breastfeeding within the first 48 hours after birth can have an effect on producing enough milk
68.0 80.8*
My breastfeeding experience should not be painful 42.1 66.6*
*The differences between pre- and post- survey results were statistically significant (P<0.05). The participant needs to have a response in both the pre and post survey to be included in the table.

Becoming a Mom® 2018 Evaluation Report Page 24
Table 3: Intent to Contact Community Services/ Programs (Post Survey)
Program Have Contacted/ Plan to Contact
Percent (N)
Total Respondents
Skipped Question (Number of
Respondents)
Breastfeeding 75.1% (605) 806 15
Car Seat 74.6% (598) 802 19
Childcare 41.9% (334) 798 23
Domestic Violence Prevention
5.5% (44) 795 26
Healthy Start 53.6% (430) 802 19
Housing 13.5% (107) 793 28
Medicaid 62.9% (509) 809 12
Mental Health 25.5% (202) 791 30
Parenting 61.1% (490) 802 19
SIDS Network 21.1% (166) 786 35
Substance Abuse 6.1% (48) 788 33
Tobacco Cessation 7.2% (57) 797 24
Transportation 13.7% (109) 797 24
WIC 68.6% (555) 809 12
Other Pregnancy Resource
38.6% (305) 791 30
Other Resource 25.3% (172) 680 141
N is number of respondents
Becoming a Mom® 2018 Evaluation Report Page 25
Outcomes
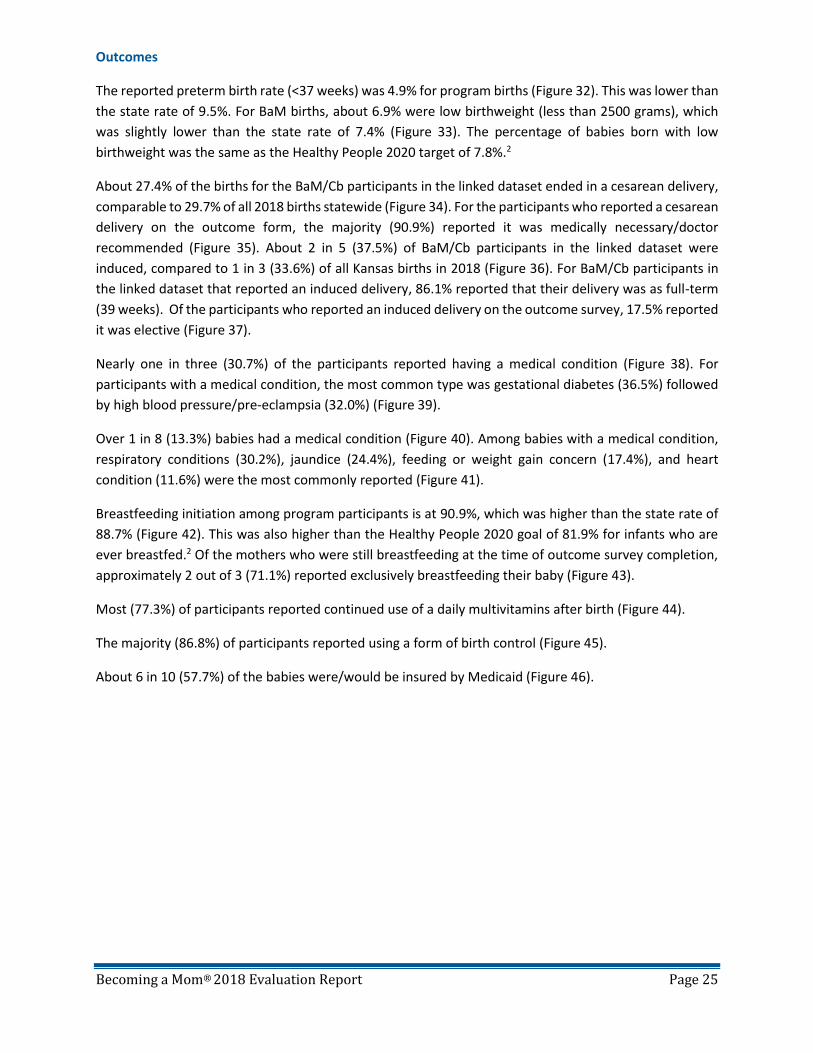
The reported preterm birth rate (<37 weeks) was 4.9% for program births (Figure 32). This was lower than
the state rate of 9.5%. For BaM births, about 6.9% were low birthweight (less than 2500 grams), which
was slightly lower than the state rate of 7.4% (Figure 33). The percentage of babies born with low
birthweight was the same as the Healthy People 2020 target of 7.8%.2
About 27.4% of the births for the BaM/Cb participants in the linked dataset ended in a cesarean delivery,
comparable to 29.7% of all 2018 births statewide (Figure 34). For the participants who reported a cesarean
delivery on the outcome form, the majority (90.9%) reported it was medically necessary/doctor
recommended (Figure 35). About 2 in 5 (37.5%) of BaM/Cb participants in the linked dataset were
induced, compared to 1 in 3 (33.6%) of all Kansas births in 2018 (Figure 36). For BaM/Cb participants in
the linked dataset that reported an induced delivery, 86.1% reported that their delivery was as full-term
(39 weeks). Of the participants who reported an induced delivery on the outcome survey, 17.5% reported
it was elective (Figure 37).
Nearly one in three (30.7%) of the participants reported having a medical condition (Figure 38). For
participants with a medical condition, the most common type was gestational diabetes (36.5%) followed
by high blood pressure/pre-eclampsia (32.0%) (Figure 39).
Over 1 in 8 (13.3%) babies had a medical condition (Figure 40). Among babies with a medical condition,
respiratory conditions (30.2%), jaundice (24.4%), feeding or weight gain concern (17.4%), and heart
condition (11.6%) were the most commonly reported (Figure 41).
Breastfeeding initiation among program participants is at 90.9%, which was higher than the state rate of
88.7% (Figure 42). This was also higher than the Healthy People 2020 goal of 81.9% for infants who are
ever breastfed.2 Of the mothers who were still breastfeeding at the time of outcome survey completion,
approximately 2 out of 3 (71.1%) reported exclusively breastfeeding their baby (Figure 43).
Most (77.3%) of participants reported continued use of a daily multivitamins after birth (Figure 44).
The majority (86.8%) of participants reported using a form of birth control (Figure 45).
About 6 in 10 (57.7%) of the babies were/would be insured by Medicaid (Figure 46).

Becoming a Mom® 2018 Evaluation Report Page 26

Becoming a Mom® 2018 Evaluation Report Page 27

Becoming a Mom® 2018 Evaluation Report Page 28

Becoming a Mom® 2018 Evaluation Report Page 29

Becoming a Mom® 2018 Evaluation Report Page 30

Becoming a Mom® 2018 Evaluation Report Page 31
Evaluation
Overall, the BaM/Cb participants rated their experience in the program positively, with 84.8% rating their
experience as excellent (Figure 47). Participants also favorably evaluated the social support component
(Figure 48 and Figure 49) and ease of understanding the material (Figure 50). Most participants reported
they had learned “a lot” (76.3%) from the program (Figure 51). All six sessions were helpful; every session
had more than 80% of the participants rate the session as “very” or “extremely” helpful (Table 4).

Becoming a Mom® 2018 Evaluation Report Page 32

Becoming a Mom® 2018 Evaluation Report Page 33
Table 4: Evaluation of the Becoming a Mom®/Comenzando bien® Sessions
Rating on the helpfulness of the session:
Not at all A little Somewhat Very Extremely
Did not attend session
Percent (N) Percent (N) Percent (N) Percent (N) Percent (N) Percent (N)
Prenatal Care 0.5% (4) 4.3% (35) 9.2% (75) 46.7% (380) 32.9% (268) 6.4% (52)
Pregnancy Health
1.0% (8) 5.1% (42) 9.4% (77) 42.6% (348) 37.0% (302) 4.9% (40)
Labor and Delivery
0.0% (0) 0.4% (3) 4.2% (34) 40.4% (331) 52.6% (431) 2.4% (20)
Infant Feeding 0.0% (0) 0.4% (3) 4.4% (36) 35.5% (290) 57.5% (469) 2.2% (18)
Infant Care 0.1% (1) 0.9% (7) 5.1% (42) 39.4% (322) 51.1% (418) 3.4% (28)
Postpartum Care
0.4% (3) 0.9% (7) 6.4% (52) 43.0% (349) 47.8% (388) 1.5% (12)
N is number of respondents

Becoming a Mom® 2018 Evaluation Report Page 34
Recommendations The data analysis and evaluation design provide important measures for the Becoming a
Mom®/Comenzando bien® (BaM/Cb) program and community collaborative model in Kansas. As with all
program evaluations, there are opportunities for improvement. The evaluation team from Kansas
Department of Health and Environment has provided the following recommendations based on the
results from 2018 data.
• Upon program intake, 15.2% of BaM/Cb participants reported depression/anxiety as a chronic
health condition, while 13.4% scored for referral upon screening with the Edinburgh Postnatal
Depression Scale (EPDS) during the program, and 25.5% report having contacted or planning to
contact mental health services upon program completion. Of note for the Edinburgh report is that
one of the larger sites (Sedgwick) does not administer the Edinburgh to moms. This leaves many
clients with an unknown EPDS score that may miss appropriate referral, creating a potential gap
in timely intervention.
• Evaluation also shows significant change in the beliefs or attitudes of BaM/Cb participants around
depression/anxiety during and after pregnancy. A significant increase in the number of
participants who report being very likely or likely to talk with their healthcare provider and/or
access available resources, as well as significantly increased participants' knowledge of mental
health resources in their community pre-to-post program, demonstrates the true benefit of
integration efforts that have been made by Kansas programs. Continue with integration efforts
around mental health, working with Wichita State University Community Engagement Institute to
promote and expand practices and interventions to improve outcomes in this targeted area. State
partners should continue to support local communities with expanded resources and increased
training opportunities. In communities where screening is taking place, local program staff should
be working with community partners to provide follow-up and assure women are not falling
through the cracks once screened and referred. In communities where screening is not yet taking
place, partners in the perinatal community collaboratives should be leading the way to
implementation, assuring an adequate system of care is being built to appropriately care for
women identified at risk.
• While 5.5% of participants reported being a smoker upon program intake, there were minimal
rates of cessation (1.4%) by program completion. Continue to build integration efforts and
partnerships around smoking cessation. Consider surveying current and former BaM/Cb
participants who are smokers, as to what kind of services, support, and incentives might better
encourage and support them in their cessation efforts. Expand locally provided cessation
programs such as Baby and Me Tobacco Free (BMTF) and Smoking Cessation Reduction in
Pregnancy Treatment (SCRIPT) with an emphasis on more direct targeting of pregnant women
who present as smoking. Strengthen partnerships with BaM/Cb participant prenatal care
providers and among other perinatal community collaborative partners to assure screening and
messaging around the importance of smoking cessation is consistent, strengthen referral and
follow-up systems, and support the use of Nicotine Replacement Therapy (NRT) when indicated.

Becoming a Mom® 2018 Evaluation Report Page 35
• Continue to support and monitor WIC participation rates. Consider follow-up integration training
as needed by program sites. Additionally, focus on Medicaid related integration efforts over the
next year. KDHE will continue to work with Managed Care Organizations (MCOs) to create a
streamlined direct referral process and consider coverage of transportation to BaM/Cb
educational sessions as well as other rewards as a part of their existing value-added services.
Local program staff should consider exporting DAISEY data to identify women who are potentially
income eligible for WIC and Medicaid who currently reported not utilizing these resources, to
assist in linkage with services. KDHE staff can provide additional TA support with these efforts if
needed.
• Attitudes about physical fitness and prenatal supplementation were largely unchanged in 2018, a
focus on curriculum delivery regarding the importance of exercising 30 minutes or more a day for
at least 4 times a week, as well as continued reinforcement of the need for daily folic acid intake,
including during the interconception period and throughout all potential childbearing years may
help to change attitudes about these behaviors. Continue to emphasize that participants review
the handout “Recommended exercises during pregnancy” that was incorporated in the 2017 and
also explore other approaches to educate moms. KDHE will seek program site feedback on
utilization of the “Pregnancy Exercise and Nutrition Program” (PEP) content and barriers to
implementation, in an effort to better identify needs and how KDHE can assist. Seeking participant
feedback in this topic area by local program staff is recommended to identify what it is that will
truly motivate women to make greater positive change in this area. Identifying useful/beneficial
resources for women is key in reducing complications and risk factors for developing diabetes and
high blood pressure later in life.
• Compared to the 2018 Kansas births, the 2018 BaM/Cb preterm birth was about half (4.8%) that
of the state (9.5%) (and significantly lower) but the low birthweight rate was about the same
(7.0%) as the state (7.4%) (and not statistically different). This is the first year where the report
has attempted BaM/Cb linkage with vital records for 2018 and presentation of data for the same
year as the report period. One limitation of this approach is that the release of vital statistics data
is variable and dependent on many factors outside of the control of KDHE’s Office of Vital
Statistics. More discussion is necessary to understand what data the Office of Vital Statistics can
release for reporting purposes to help facilitate access to the most up-to-date information in a
timelier manner. One potential solution could be a preliminary data cut for use before data is
returned from the federal government, but more discussion and strategizing is needed.
• The induction rate among BaM/Cb participants (37.5%) was significantly higher than the 2018
Kansas Births (33.6%) while the rates for cesarean deliveries was similar for BaM/Cb (27.4%) and
the State overall (29.7%). Of the BaM/Cb inductions reported in the outcome survey, 17.5% were
also reported as elective, compared to about 5.9% of the cesarean deliveries for the BaM/Cb
population. While linkage improved the overall rate by filling in missing or misreported
information, there still exists a gap between the State and BaM/Cb participants related to induced
deliveries. More work is needed to assess data quality and reporting, overall. Education may also
be needed to reduce misreporting by BaM mothers. KDHE will: identify sites with high elective
induction and elective cesarean delivery rates; further investigate data to compare with

Becoming a Mom® 2018 Evaluation Report Page 36
gestational age, complications, etc. to look for any trends or explanations; continue to monitor
rates in the next year; consider assisting with possible local focus groups in identified locations.
Local program staff should continue to focus on curriculum delivery to discourage elective
inductions prior to 39 weeks and elective cesarean delivery; assure showing of brief video clip “Is
It Worth It” that was imbedded in the session 3 PowerPoint during the 2017 relaunch; discuss
trends with perinatal community collaborative partners; consider participating in above
mentioned focus groups.
• Although demographics of BaM/Cb participants shows an improved reach across disparity groups,
state technical assistance and integration efforts as well as local collaborative and recruitment
efforts should continue to focus on recruitment of the Medicaid and uninsured populations,
minority groups, and lower education populations, to better reach the targeted “disparity”
population the program is aimed at, further driving the rate of improvement in outcomes.
• As of 2020, revisions for BaM forms will occur based on calendar year, and not fiscal year, moving
changes in BaM forms to January 1 of each year. Minor changes to the DAISEY evaluation tool are
recommended for January 2020 revisions. Money, work and insurance were all areas of concern
reported for other reasons that moms were prevented from prenatal care; however, these
options are already present as main options. Clarifying language or examples may help to prevent
moms from indicating areas of concern as other when they are already listed. For moms that
presented other reasons for babies being admitted to the neonatal intensive care unit (N=31), low
blood sugar was a commonly reported condition (19.4%). This concern should be evaluated to
determine if this option should be included for future BaM participants.
• While BaM/Cb outcome data demonstrates sites are highly successful in educating, encouraging
and supporting participants to initiate breastfeeding and breastfeed exclusively, more can be
done to support exclusivity and duration rates. Timing of completion of the outcome survey
varies. Moms can report an outcome at any given time when they return to the participant
location and complete the form. A question does exist about the age of the baby, but it is not an
exact date of birth. It is recommended that the age of the baby question be changed to get the
exact date of birth which will help improve evaluation. Additionally, it is suggested that fields be
added to the BaM Service Form to capture follow-up contact made with participants who are
breastfeeding following the birth of their baby, at targeted time frames when rates of early
weaning increase statistically, in an effort to improve breastfeeding duration throughout these
difficult times in the early postpartum period.
• The question related to breastfeeding exclusivity does not have a set timeframe and therefore
cannot be compared to Healthy People 2020 targets or other data sources. Sites currently do not
collect information from BaM/Cb participants regarding breastfeeding duration at the 6 month
and 1 year mark or breastfeeding exclusivity at 3 or 6 months, which are Healthy People 2020
measures. Recommendations would include the development of a tool to be used by BaM/Cb
program staff or partner agencies to provide follow-up at targeted time frames throughout the
first year when statistics show women are most likely to begin supplementation or discontinue

Becoming a Mom® 2018 Evaluation Report Page 37
breastfeeding. This allows the opportunity to provide greater support and resources to BaM/Cb
participants, as well as collect data regarding continuation and exclusivity rates.
• As mentioned above, timing of completion of the outcome survey varies and obtaining the
outcome data has been challenging. A recommendation is to collaborate with the Office of Vital
Statistics Data Analysis to develop and utilize linked BaM/Cb participant data to vital records:
birth, stillbirth, infant death. While initial linkage of live births has occurred for the first time for
the 2018 population, more work can be done. Conversations will continue to explore other areas
of linkage.
• About one-quarter (23.1%) of BaM/Cb participants enter the program in their third trimester,
while first thru second trimester are recommended points of entry. Target recruitment efforts
across BaM/Cb sites to encourage earlier provider referral and entry of pregnant women into the
program.
• Program sites are encouraged to assess and consider recommendations made by program
participants via the “additional feedback” portion of the Completion Survey. Most of these appear
to be site specific and therefore will not be presented in this aggregate report but could bring
value to individual programs. Additionally, KDHE will assess for any common themes across
program sites that could be addressed at a higher state level.
• Sites are encouraged to continue focusing on “family/consumer engagement” in SFY2020-2021,
including BaM/Cb participant/alumni representation on advisory boards, maternal and child
health councils, perinatal collaboratives, etc. to gather feedback and input on the program from
the consumers themselves. Remember the saying “nothing about us, without us”.
• Overall the BaM/Cb program was rated very highly and the information was reported as easy to
understand. Continue effective delivery of program materials with improvements incorporated
as described and recommended above. Curriculum standardization and enhancement efforts that
involve the development of supplemental curriculum handouts, PowerPoints, lesson plans,
activity plans have been completed. Sites are encouraged to communicate suggested edits to
KDHE for incorporation in the January 2020 updates.
• Several data points are currently compiled for sites in a BaM participant risk report, which
provides easy access to the data identifying their most at risk participants. Discuss pulling
additional data fields into this report that might also identify a high-risk infant following birth
(BaM data indicates one in eight (13.3%) babies had a medical condition that required NICU
admission), as well as identifying risk factors for the mother that should be followed during the
postpartum period. BaM data shows the most commonly reported pregnancy complication is
gestational diabetes (36.5%) followed by high blood pressure/pre-eclampsia (32.0%). This data
validates recommendations by the Kansas Maternal Mortality Review Committee, where findings
indicate chronic health conditions and complications of pregnancy are among the top three
causes of maternal mortality in our state. In support of this, the AWHONN Post-Birth Warning

Becoming a Mom® 2018 Evaluation Report Page 38
Signs Toolkit is also recommended for integration into the BaM program and at a state-wide MCH
programming level.
• Attitudes about alcohol and illegal substance use has consistently been unchanged pre to post
program since the 2015 inclusion of these questions on the evaluation tools. It is recommended
to remove these fields and replace with the SBIRT screening questions to be implementing across
other MCH programs in July 2020.
• While participants continue to show significant decrease in identifying “call health care provider
right away” as a correct response to “I should do the following if I’m experiencing preterm labor”,
the number of correct responses has improved over previous years following changing of
educational components on this topic in 2018. Education efforts should continue to be improved
by seeking input from sites on recommended changes. A deep dive into this data is recommended
as well, to determine any trends among incorrect responses.
• As 5% of participants report they plan to or have contacted domestic violence services, and 6%
report the same for substance abuse services, it is recommended to incorporate screening tools
in these two areas. This should be done in a fashion consistent with integration of these
screenings in other MCH programs supported by KDHE.
References 1. U.S. Census Bureau, 2013-2017 American Community Survey 5-Year Estimates. Language spoken
at home. Table S1601. Available at:
https://data.census.gov/cedsci/table?q=s1601&hidePreview=false&table=S1601&tid=ACSST1Y2
017.S1601&lastDisplayedRow=12&g=0400000US20 [accessed August 22, 2019].
2. US Department of Health and Human Services. Office of Disease Prevention and Health
Promotion. Healthy People 2020. Available at: https://www.healthypeople.gov/2020/data-
search/Search-the-Data#topic-area=3492 [accessed January 25, 2017].

Becoming a Mom® 2018 Evaluation Report Page 39
Appendix A: Program Background and History Introduction In Kansas, and across the United States, the primary causes for infant mortality following congenital
anomalies is premature birth and low birthweight, Sudden Unexplained Infant Death (SUID), and maternal
factors and complications.1 These rates continue to be significantly affected by racial, ethnic,
socioeconomic, and geographic disparities. In response, the Kansas Maternal and Child Health Council
(KMCHC) supports the original recommendations by the Kansas Blue Ribbon Panel on Infant Mortality
(est. 2009) to include the March of Dimes Becoming a Mom® (BaM)/Comenzando bien® (Cb) Birth
Disparities program as an initiative to help address these issues. Implementation of the BaM/Cb bilingual
prenatal curriculum in other states has shown an increase in adequate prenatal care and prenatal health
knowledge improving health behaviors and birth outcomes (March of Dimes California Chapter,
Evaluation of Becoming a Mom, Sept. 2013). To date, Kansas has found similar outcomes among program
participants across our state.
Kansas’ Perinatal Community Collaborative Model
In 2010, following the release of the Kansas Blue Ribbon Panel recommendations, coupled with cuts in
state and local funding, the March of Dimes (MOD) Greater Kansas Chapter partnered with state and local
public health partners to create an innovative concept. This concept included a perinatal community
collaborative education model utilizing the Becoming a Mom®/Comenzando bien® curriculum to address
birth disparities primarily among low-income, minority women who are eligible for Medicaid. Starting with
a pilot program in Salina, Kansas (Saline County), the model has a two-fold focus of clinical services and
prenatal education that is driven by private and public partnerships across the state and local level
including: Title V Maternal & Child Health (MCH), Medicaid, local public health departments, federally
qualified health centers, clinical providers, hospitals, and health foundations. The community
collaborative model brings permanent MCH infrastructure, leveraged and shared resources, change in the
prenatal care delivery services paradigm, a vehicle to identify community needs, a standardized
evaluation system, and new funding opportunities for community collective impact, and improved birth
outcomes.
Statewide Expansion
This innovative model was first replicated in Junction City (Geary County), Kansas in 2012 with the similar
preliminary successes of the pilot program. With two effective sites implementing the model, program
evaluation tools were refined and standardized in 2013 in partnership with evaluators from the University
of Kansas School of Medicine-Wichita and Wichita State University. Preliminary data reports showed
improvements in participant’s knowledge, behaviors, and growth of community partnerships and shared
resources.
In 2014, the Kansas Department of Health and Environment (KDHE) committed to partner with the March
of Dimes for further expansion of the model across the state, as well as securing long-term sustainability
of the program by integrating it into Title V MCH services. This model has become known as the Kansas
Perinatal Community Collaboratives (KPCC) utilizing the March of Dimes Becoming a Mom® curriculum,
and has since been being replicated across the state. Three additional sites were brought on in 2014,

Becoming a Mom® 2018 Evaluation Report Page 40
including: Crawford County in southeast Kansas and Wyandotte County and Riley County, both in
northeast Kansas. Amerigroup (WellPoint), one of Kansas’ three Medicaid (KanCare) managed care
organizations, joined as a partner and investor in 2014. In January of 2015, two new sites were launched.
These two sites included Reno County and Newman Regional Health Center (in Lyon County), located in
central Kansas. In late 2015 (November), three additional sites launched between north and south central
Kansas. These sites included: Clay County, Dickinson County, and Sedgwick County (led by KU School of
Medicine in Wichita). In October 2016, the eleventh program site was launched in Montgomery County
in the southeast corner of the state. This site was launched with support and partnership from a
neighboring program in Crawford County. In October 2017, the twelfth program site was launched in
Shawnee County, home of our state capital in northeast Kansas. In 2018, four more sites were launched,
including Kearny County Hospital (January), Finney County Health Department (February), Seward County
Health Department (May), and Thomas County (October 2018). These counties are all located in the
western part of the state and were established as the state’s first Regional launch. Ford County, in
southwest Kansas, has continued to partner regionally with other lead sites in the region while working
to launch their own local program site in 2019. Additionally, in 2018, following the piloting of a virtual
implementation model between Saline County and Lincoln County, Lincoln County launched as a lead site.
Although this site is extremely small, they expressed the capacity and desire to host live sessions locally,
which provides a great resource in this rural area. Expansion work included hosting two implementation
trainings in southwest Kansas in July 2016, where work began to develop and launch the first regional
KPCC model in the state, as mentioned above. This regional approach in the southwestern part of the
state includes 16 counties. Lead program sites are located in the four counties with the region’s largest
birthing hospitals (per reported birth numbers), in partnership with outlying counties referring into these
lead sites. Additional opportunity is available for such counties to provide the program locally via virtual
connection with one of the lead sites, if the need exists and capacity is available. Pilot of this virtual
approach occurred in north central Kansas, as mentioned above, and a toolkit on Virtual Implementation
has since been developed and made available. Other expansion efforts include utilizing the Title V MCH
Aid-to-Local application as an opportunity for inquiring about the applicant’s interest in implementation
of the KPCC model / BaM/Cb program. As interest is voiced in the application or by other means, KDHE
staff reach out to the interested parties and provide linkage to the KPCC website. Via the website,
communities can begin self-exploration of the model and criteria, and navigation through convening of
collaborative partners, building of the collaborative structure, and implementation of the BaM/Cb
prenatal education component. Current expansion planning also involves prioritizing locations for
program implementation based on birth disparities, interest by the community and will to collaborate,
and lack of MCH services of this nature in the area.
Program Enhancements
Training and Support
Technical assistance, training, evaluation support, and infrastructure development has continued to be
enhanced through the March of Dimes and Kansas Department of Health and Environment partnership.
Through August 2015, March of Dimes led state coordination efforts including program implementation
trainings and technical assistance support. In April 2015, the Kansas Department of Health and
Environment increased their investment by hiring a Maternal Child Health (MCH) Consultant to support
these efforts and take on the role of state coordination in-house, with the intention of expanding and

Becoming a Mom® 2018 Evaluation Report Page 41
building long-term sustainability of the Becoming a Mom® (BaM)/Comenzando bien® (Cb) program and
the Kansas Perinatal Community Collaborative (KPCC) model. Part of such long-term sustainability efforts
have included the development of two websites. One website is a public website housing resources on
Collective Impact and the KPCC model. The other website is a private website for committed BaM/Cb
programs, housing training and other implementation resources.
Integration of state and local resources has been another focused enhancement to the program since
2015. Led by the March of Dimes investment in the Saline County program as a pilot site, along with the
support of KDHE staff, 2015 was spent developing and piloting an integration plan for all BaM/Cb program
sites in Kansas. This plan specifically targeted the integration of state entities such as Kansas Tobacco
Quitline, WIC, Kansas Breastfeeding Coalition, and the Kansas Infant Death and SIDS (KIDS) Network. This
integration included redesign of the infant feeding session (session 4), including the incorporation of an
evidence-based, breastfeeding-focused curriculum. Along with this, a BaM/WIC integration plan
streamlined enrollment in both programs from the other program, while incentivizing dual participation
in programs. It included the development of a toolkit focused on the integration of tobacco cessation
services, that includes standardized screening, referral, resources, and follow-up. Additionally, all sites
were trained in implementing the nationally recognized, evidence-based “Baby and Me Tobacco Free”
program. Following a year-long pilot of the program in the state, an additional intervention was
implemented utilizing another nationally recognized evidence-based program known as SCRIPT®.
Updating and standardization of the safe sleep/SIDS risk reduction message as a part of the infant care
session (session 5) was another focus area, as well as the development of a standardized process for
screening, resources, referral, and follow-up related to mental health. Training of all ten sites (at the time)
on these integration components began in November 2015 and was completed in February 2016. In July
2017 training was again provided to all program sites, providing updates on previously integrated
components, as well as providing training on new integration components including oral health (in
partnership with Oral Health Kansas) and a pregnancy exercise and nutrition program (PEP - in
collaboration with KU School of Medicine, Wichita). With launch of the private website, training on all
integration components has been made available to all program sites on an ongoing basis via recorded
webinars. Work on the integration of services has continued throughout the years and will continue
throughout the life of the program due to KDHE’s commitment to these efforts. Integration components
currently on our radar for development include: Pre and Early Term Birth (focus on appropriate utilization
of progesterone and low-dose aspirin); Screening, Brief Intervention, and Referral to Treatment (SBIRT)
and Neonatal Abstinence Syndrome (NAS); Reproductive Life Plan including the One Key Question
initiative. Through enhanced outreach, health education, public awareness and increased referral services
available to the program’s participants, we aim to continually drive the improvement of birth outcomes
in our state.
Curriculum Standardization
In addition to the integration efforts outlined above, extensive work was done in late 2016 and early 2017
to enhance the original Becoming a Mom® curriculum developed and owned by MOD. This enhancement
work included the addition of standardized supplemental handouts identified as needed topic content to
fill gaps in education around a number of key priority areas. This work was led by KDHE, in partnership
with a curriculum review committee initiated by the KU School of Medicine - Wichita (Sedgwick County
program) and input from multiple local BaM/Cb programs. Support by MOD has provided guidance around

Becoming a Mom® 2018 Evaluation Report Page 42
this work in adherence to copyright laws protecting the original curriculum and Becoming a Mom® logo.
Printing of the curriculum for all Kansas program participants in 2017 and again in 2018 was provided
thanks to partnership and financial investment from Sunflower Health Plan, another one of Kansas’ three
managed care organizations. Additional infrastructure support occurred throughout 2017 with the
development of standardized PowerPoints, lesson and activity plans, and recommended resource
documents, to be used during BaM/Cb sessions across all Kansas program sites in an effort to improve
program fidelity. These materials are the product of a partnership between KU School of Medicine –
Wichita (Sedgwick County) and KDHE. Additional infrastructure support continues with the ongoing
buildout and enhancement of a KDHE sponsored public website for Kansas Perinatal Community
Collaboratives (KPCC) and a private website for BaM/Cb implementation, as mentioned above.
Program Evaluation
Another area of focused enhancement over the past years has been the evaluation component of the
program. In the early years of program existence, there had been concern related to the value of results
from program evaluation tools. It had appeared that perhaps the way some questions had been asked
was either confusing to participants, or leading. As well, there had been a number of questions where
there was not a statistically significant difference between pre and post survey results. In May 2015, KDHE
contracted with the University of Kansas Center for Public Partnerships and Research (KU-CPPR) to
conduct analysis on the pre- and post-program survey instruments. A brief discussion of the statistical
analysis methodology and results is included in the next section of this appendix, for a historical
perspective on this process. As a result, evaluation tools were redesigned by the joint effort of KU-CPPR,
KDHE, and MOD. These evaluation tools were built into the new data system “DAISEY”, utilized by KDHE
for data collection of Bureau of Family Health – Aid-to-Local programs, and is supported and maintained
by KU-CPPR staff. DAISEY provides a single secure place for KDHE funded Family Health programs to enter
all data required for state and federal reporting. DAISEY is a shared measurement system designed by
social scientists to help communities see the difference they are making in the lives of at-risk children,
youth, and families. It has been exciting to have the opportunity we have had to be included in the use of
this new system as a part of our evaluation efforts for the BaM/Cb program. This system gives confidence
in the sustainability of the program long term. BaM/Cb programs began as the first pilot sites for DAISEY,
with the input of program data from new program participants as of November 1, 2015. Now well into
utilization of the new evaluation tools and data system, program staff are seeing the benefit of data
collection in real time via this web-based system. The “BaM/Cb Report” was developed by KDHE and KU-
CPPR teams and made available to sites through the DAISEY live environment in August 2016. The report’s
intention is to allow BaM/Cb program staff to track and evaluate participants’ enrollment, session
completion, form completion, program completion and identified risk factors and referrals, in an easy-to-
use and meaningful way. The KDHE and KU-CPPR teams continue to collaborate with local BaM/Cb sites
to support continuous data quality improvement efforts. In 2019 KDHE created the BaM-DAISEY
Dashboard, which displays data trends of key program measures on a quarterly basis, promoting real-time
analysis and response. Ultimately, the high quality BaM/Cb data is being used in Title V MCH operations,
decision making and planning, as well as by KPCCs for service planning and development at the local level
across partnerships.

Becoming a Mom® 2018 Evaluation Report Page 43
Factor Analysis of Pre- and Post-Program Survey Instruments
To examine the properties of the surveys and the characteristics of the items, item analysis and reliability
analysis were performed by the University of Kansas Center for Public Partnerships and Research (KU-
CPPR). Also, in order to explore the dimensions of knowledge about pregnancy, principle component
analysis (PCA) was conducted. The efficacy of the program was evaluated by comparing participants’
performance on pre- and post-program surveys using repeated measures multivariate analysis of variance
(MANOVA). Before performing all planned analyses, items were scored dichotomously based on
participants’ responses, with “1” representing a correct answer and “0” representing an incorrect answer
or response of “I don’t know”.
Item analysis was conducted to examine the difficulty and discrimination of items. Operationally, item
difficulty was defined as the proportion of participants who answered a given item correctly, and
discrimination as the point-biserial correlation between participants’ scores on a given item and the total
scores on the survey. A negative discrimination score suggests participants who answered the item
incorrectly obtained a high total score. A low discrimination score (item-total correlation less than .20)
indicates participants’ performance on the item did not significantly impact their overall performance on
the survey. Items that met either of these criteria were removed from further analyses. After item
analyses, 13 items were removed due to either negative or low discrimination scores.
The internal consistency among the remaining 26 items was examined by calculating Cronbach’s α
coefficient. A Cronbach’s α coefficient of .834 indicated a good internal consistency of the pre-program
survey scores.
Principle component analysis (PCA) was chosen over exploratory factor analysis for two reasons. First,
knowledge on pregnancy was considered a domain of study rather than an unobserved theoretical
construct. Therefore, the primary focuses were on information summary and item/dimension reduction.
Second, after reducing a pool of items into a small number of components, the components could be used
as core domains to further evaluate the efficacy of the program in improving participants’ knowledge.
Kaiser-Myer-Olkin test (KMO) and Bartlett’s test of sphericity were run in order to determine the
appropriateness of using PCA. Items were retained based on the magnitude of their “factor loadings” and
if they theoretically made sense. Items with a factor loading of 0.40 or greater were retained. Since the
survey was designed to assess participants’ knowledge within six domains: healthy living during
pregnancy, pregnancy, labor and pain management, infant feeding, infant care, and postpartum care; in
PCA, the number of components to yield was fixed to six.
The six components that emerged from pre-program survey responses were named as: Pregnancy health,
Post-pregnancy health, Pre-term labor, Pre-term labor response, Normal post-partum, and Abnormal
post-partum. While these were not the original hypothesized “factors”, they did make sense in accordance
with topics covered in the BaM program. To examine the consistency and stability of the obtained
component structure, a PCA was also run on the post-program survey data. PCA failed to confirm the
component structure of the survey. Therefore, the validity of the survey construct is suspect and fails to
measure accurate post-intervention results.

Becoming a Mom® 2018 Evaluation Report Page 44
McNemar Test
For the change in knowledge questions in Figures 18-29 and Table 2, a McNemar test was used to test the
change in proportions.
Outcomes Worth Noting
In review of outcome findings noted in the Outcomes section of the report, please call attention to the
improvements in outcomes over state level data and Healthy People 2020 goals, particularly related to
breastfeeding initiation rates (Figure 40). We would also like to make special note of the improvement in
Infant Mortality Rate (IMR) per 1,000 live births (5-year average) from pre-implementation to post
implementation in the counties of our two longest running Becoming a Mom® sites. IMR in these two
counties has significantly decreased since the inception of local perinatal community collaboratives. The
Saline County IMR decreased significantly from 10.1 (95% CI 7.2-13.7) in 2004-2008 to 4.3 (95% CI 2.5-7.1)
in 2012-2016. The Geary County IMR decreased significantly from 11.9 (95% CI 8.6-16.0) in 2005-2009 to
5.4 (95% CI 3.6-7.7) in 2012-2016.
Inception January 2010
Saline County 2004-2008 2005-2009 2010-2014 2011-2015 2012-2016
IMR (5-year average) (95% CI)
10.1 (7.2-13.7) 9.0 (6.3-12.3) 5.5 (3.4-8.3) 4.2 (2.4-6.9) 4.3 (2.5-7.1)
Inception
July 2012
Geary County 2004-2008 2005-2009 2006-2010 2007-2011 2012-2016
IMR (5-year average) (95% CI)
10.5 (7.3-14.7) 11.9 (8.6-16.0) 10.4 (7.5-14.0) 9.9 (7.2-13.3) 5.4 (3.6-7.7)
95% CI: Confidence Interval Source: Bureau of Epidemiology and Public Health Informatics

Becoming a Mom® 2018 Evaluation Report Page 45
Appendix B: Survey Questions
Pre/Post Questions
Before the launch of DAISEY, the program utilized de-identified pre and post-survey instruments to
evaluate participant responses to the educational intervention. The curriculum and questions were
designed to assess knowledge of risks of pregnancy and current and future behaviors. Pregnant women
indicated their response to 5-point Likert scales, yes/no, multiple choice, single choice, and fill-in-the-
blank questions based on their current understanding (unassisted). The survey was comprised of thirty-
seven main items with multiple sub-questions. Three (3) questions were demographic questions used to
describe the population. The post-survey also included questions on the woman’s experience in the
program.
With the launch of DAISEY in November 2015, pre and post-survey instruments, as well as the outcome
survey, were revised. In addition, demographic data fields were pulled out of the original surveys and
placed on a separate program visit form in DAISEY, which collects demographic data consistently across
KDHE MCH programs. The newly revised evaluation tools consist of the following questions and response
types, as displayed below.
Visit Form
The DAISEY KDHE Program Visit Form with Profile collects the following demographic data:
Question Type*
Primary Healthcare Coverage SC
Secondary Healthcare Coverage SC
Has the client had a well visit during the last 12 months? SC
Does the client have a special health care need or disability? Y/N
Does the client care for any children who have special health care needs or disabilities? Y/N
Household Size FB
Annual Household Income FB
Education Level SC
Current Student SC
Employment SC
Marital Status SC
Date of Birth FB
Sex SC
Race MC
Ethnicity SC
Primary Language SC
Limited English Proficiency Y/N
*Type of Answer Choices: FB: Fill-in-Blank MC: Multiple Choice SC: Single Choice Y/N: Yes and No (and Don’t Know)

Becoming a Mom® 2018 Evaluation Report Page 46
Pre Survey
The pre-survey in DAISEY includes the following knowledge and behavior questions and response types:
Question Type*
How did you first hear about Becoming a Mom/Comenzando bien? SC
Is this your first pregnancy? Y/N
If no, have you had a premature birth (gestational age of baby less than 37 weeks)? Y/N
If yes, was the premature birth spontaneous, meaning you went into labor on your own? Y/N
How many babies have you had weighing less than 5 lbs. 8 oz.? FB
How many miscarriages have you had? FB
Have you had a baby that was not born alive? Y/N
Have you had a baby that died within the 1st year? Y/N
Do you have any other children living in the home? Y/N
If yes, Indicate the number of children in the home less than 1 yr old FB
If yes, Indicate the number of children in the home age 1 to 11 yrs old FB
If yes, Indicate the number of children in the home age 12 to 22 yrs old FB
Number of these children who have Special Health Care Needs: FB
How pregnant are you now? SC
When is your due date? FB
Have you had your first prenatal appointment? Y/N
If no, is your appointment scheduled? Y/N
If no, what is the reason for no prenatal appointment? SC
What trimester did you begin seeing a health care provider for this pregnancy? SC
What is the name of your healthcare provider/clinic? FB
Do you have any of the following health problems? MC
If you have a health problem not listed, please explain: FB
Has your healthcare provider told you that you have a “high risk” pregnancy? Y/N
If yes, please indicate the reason(s). FB
Are you enrolled in the WIC Program? Y/N
I attend scheduled prenatal care visits with my healthcare provider (Doctor or Nurse Midwife): SC
The following sometimes prevents me from attending my prenatal appointments: MC
Please specify “other” barrier(s) to attending prenatal appointments: FB
I currently take prenatal or multi-vitamins containing folic acid: SC
Which of the following are signs of preterm labor/labor? MC
I should do the following if I’m experiencing preterm labor (before 37 weeks): MC
The following postpartum symptoms are normal for a mother to experience after delivery: MC
If I experience depression and/or anxiety during or after my pregnancy, I am ___ about available resources in my community.
SC
If I experience depression and/or anxiety during or after my pregnancy, I am ___ to talk with my healthcare provider and/or access available resources:
SC
I have talked to my healthcare provider about medications that I’m taking (prescription and/or over the counter, herbal, etc.):
SC
If I am considering taking medications (prescription and/or over the counter, herbal, etc.), I am _____to talk to my healthcare provider before taking them.
SC
I walk or do at least 30 minutes of moderate, low-impact physical activity _____ days per week.
SC
I currently smoke _____ cigarettes per day. SC
I believe I can use alcohol _____ without harming my baby. SC
I believe I can use narcotics _____ without harming my baby. SC
I believe I can use marijuana _____ without harming my baby. SC
I believe I can use methamphetamines or amphetamines _____ without harming my baby. SC

Becoming a Mom® 2018 Evaluation Report Page 47
I am _____ to develop a birth plan and talk to my healthcare provider about it. SC
A pregnancy is full-term when it reaches _____ weeks. SC
The following are benefits of a full-term pregnancy: MC
The following is true about breastfeeding: (check all that apply) MC
I am _____ to breastfeed my baby. SC
If I am having difficulty breastfeeding my baby or if I have questions about breastfeeding, I know about _____ available resources in my community.
SC
I feel _____ about my ability to breastfeed. SC
After delivery, I plan to take prenatal vitamins or multi-vitamins containing folic acid: SC
I will put my baby to sleep on his/her: MC
At home, my baby will sleep: MC
I am ___ to talk about Safe Sleep with my child's other care providers (family members, childcare providers, etc).
SC
I am _____ to talk to my healthcare provider during my prenatal care about methods for preventing pregnancy after the birth of my baby.
SC
What method are you planning to use/talk to your healthcare provider about? MC
I believe there is _____ to my health and the health of my next baby if I wait a minimum of 18 months before my next pregnancy.
SC
*Type of Answer Choices: FB: Fill-in-Blank MC: Multiple Choice SC: Single Choice Y/N: Yes and No (and Don’t Know)
Post Survey
The post-survey in DAISEY includes the same knowledge and behavior questions plus the following
evaluation fields:
Question Type*
Please indicate whether you have contacted or plan to contact the following community resources:
• Heathy Start
• Childcare Services
• Substance Abuse Treatment Services
• Medicaid/KanCare
• Tobacco Cessation
• Domestic Violence Prevention Services
• Mental Health Services
• Kansas Infant Death and SIDS Network
• WIC Services
• Breastfeeding Support Services
• Car Seat Installation
• Parenting/Early Childhood Services
• Transportation
• Housing
• Other Pregnancy Resources (i.e. Text-4-Baby, other local pregnancy services or childbirth classes, etc.)
• Other (i.e. local food program, cloth diapering resources, etc.)
SC
How was your overall experience with the Becoming a Mom/Comenzando bien program? SC
I felt a connection to and supported by other pregnant women in the classes. Likert
I felt a connection to and supported by my class teacher or group leader. Likert
How hard was the information in the Becoming a Mom/Comenzando bien session to understand? SC
How much new information did you learn from the Becoming a Mom/Comenzando bien program? SC

Becoming a Mom® 2018 Evaluation Report Page 48
The Becoming a Mom/Comenzando bien teacher/instructor: MC
How helpful/valuable was Session 1, the Prenatal Care session (common discomforts, prenatal care, conditions/complications, preterm labor, etc.)?
SC
How helpful/valuable was Session 2, the Pregnancy Health session (medications, avoiding alcohol, smoking, weight gain, healthy diet and exercise, effects of: stress, certain foods, infections, environmental exposures, etc.)?
SC
How helpful/valuable was Session 3, the Labor and Delivery session (preterm labor, labor and birth, coping mechanisms, birth plan, etc.)?
SC
How helpful/valuable was Session 4, the Infant Feeding session (breastfeeding, bottle feeding, hunger cues, etc.)?
SC
How helpful/valuable was Session 5, the Infant Care session (Period of Purple Crying, infant calming techniques, safe swaddling, SIDS Risk Reduction/Safe Sleep, infant car seat installation and other infant safety topics)?
SC
How helpful/valuable was Session 6, the Postpartum Care session (physical changes, emotional changes, keeping healthy after baby, birth spacing, family planning options, etc.)?
SC
Please provide below any additional feedback you may have regarding the Becoming a Mom/Comenzando bien program:
Narrative
*Type of Answer Choices: FB: Fill-in-Blank Likert: 5-point Likert Scale from Strongly Disagree to Strongly Agree MC: Multiple Choice SC: Single Choice Y/N: Yes and No (and Don’t Know)
Outcome Questions
The program utilized different methods at each program site to gather birth outcome data. Most data was
self-reported by participants and some was extracted from accessible medical records by those involved
in usual maternity care/services and reported to the program (as described in participant consent form).
The questions in DAISEY include the following:
Question Type*
What is the name of the hospital where you gave birth? FB
Name of child: FB
At what gestational age was your baby born? SC
What was your baby's weight at birth? SC
Were you induced? Y/N
If you were induced, what was the reason? SC
If “other”, please explain: Narrative
How was your baby delivered? SC
If by Cesarean delivery, what was the reason? SC
If “other”, please explain: Narrative
Did you develop any medical conditions during your pregnancy? Y/N
If yes, please indicate the medical conditions you developed: MC
Other medical condition: Narrative
Are you currently breastfeeding your baby? Y/N
If yes, how old is your baby currently? SC
If no, did you nurse at all? Y/N
If yes, how long did you nurse? SC
Are you using: SC
Did any information that you learned in class change your mind about: MC

Becoming a Mom® 2018 Evaluation Report Page 49
How old is your baby? FB
Have you had/scheduled your first postpartum check-up? SC
Where are you going/planning to go for postpartum care? MC
Are you enrolled in the WIC Program? Y/N
Please indicate whether you have or plan to contact the following community resources:
• Healthy Start
• Childcare Services
• Substance Abuse Services
• Medicaid/KanCare
• Tobacco Cessation
• Domestic Violence Prevention Services
• Mental Health Services
• Kansas Infant Death and SIDS Network
• WIC Services
• Breastfeeding Support Services
• Car Seat Installation
• Parenting/Early Childhood Services
• Transportation
• Housing
• Other Pregnancy Resources (i.e. Text-4-Baby, other local pregnancy services or childbirth classes, etc.)
• If “other pregnancy resources”, please specify:
• Other (i.e. local food program/resources other than WIC, cloth diapering resources, etc.)
• If “other”, community resource, please specify:
SC
Have you scheduled or attended your baby’s first check up? Y/N
Do you have a doctor for your baby? Y/N
What type of insurance do you have for your child? SC
At birth, did your baby have any medical conditions/ concerns which required NICU admission?
Y/N
If yes, please indicate the conditions/concerns: MC
Are you taking multivitamins/prenatal vitamins? SC
I currently smoke ___cigarettes per day. SC
Have you talked to your doctor about options for preventing pregnancy? Y/N
Are you using or do you plan to use any method to prevent pregnancy? Y/N
What method are you using/planning to use? MC
Would you like to become pregnancy within the next year? Y/N
*Type of Answer Choices: FB: Fill-in-Blank MC: Multiple Choice SC: Single Choice Y/N: Yes and No (and Don’t Know)
Outcome Record Linkage
In 2019, the first linkage between BaM participant records and the Office of Vital Statistics Birth Tables
was conducted. Records for BaM participants were linked to the birth records based on 1) exact match on
provided last name with married name in vital, 2) exact match on provided last name with maiden name
in vital, and 3) SPEDIS (spelling distance) approximate matching in SAS, which matches based on how close
the recorded last name in BaM matches (based on character placement) to the recorded names in the
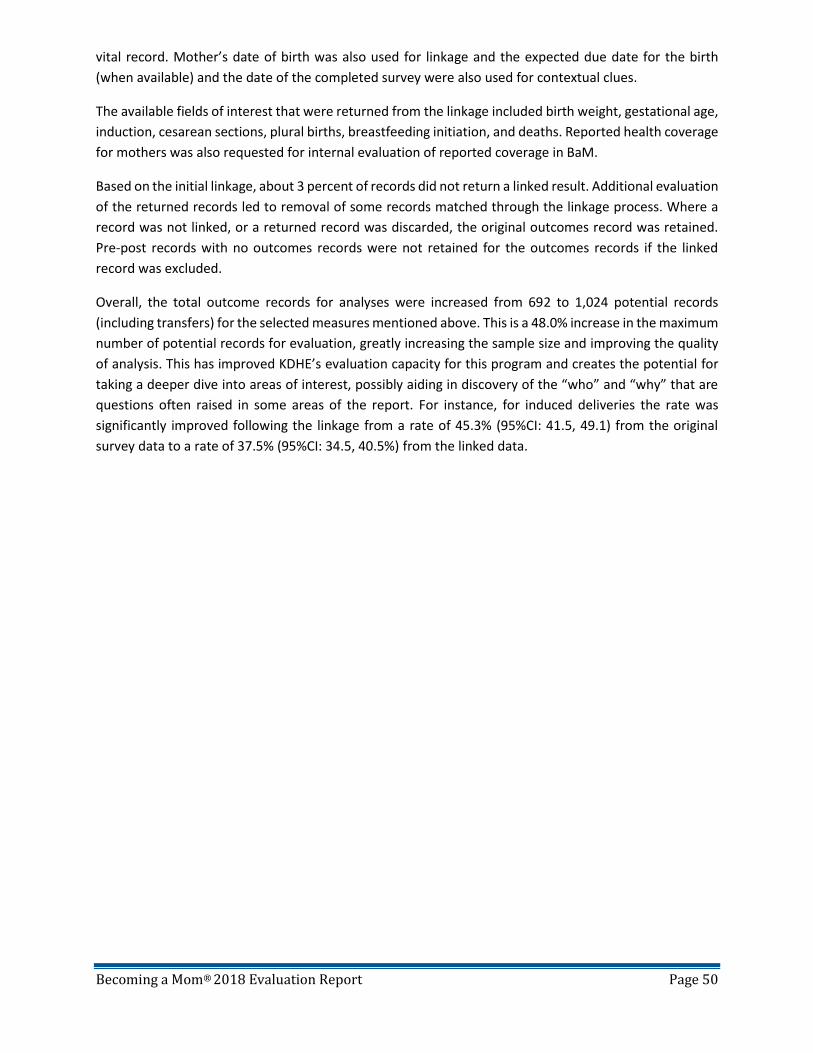
Becoming a Mom® 2018 Evaluation Report Page 50
vital record. Mother’s date of birth was also used for linkage and the expected due date for the birth
(when available) and the date of the completed survey were also used for contextual clues.
The available fields of interest that were returned from the linkage included birth weight, gestational age,
induction, cesarean sections, plural births, breastfeeding initiation, and deaths. Reported health coverage
for mothers was also requested for internal evaluation of reported coverage in BaM.
Based on the initial linkage, about 3 percent of records did not return a linked result. Additional evaluation
of the returned records led to removal of some records matched through the linkage process. Where a
record was not linked, or a returned record was discarded, the original outcomes record was retained.
Pre-post records with no outcomes records were not retained for the outcomes records if the linked
record was excluded.
Overall, the total outcome records for analyses were increased from 692 to 1,024 potential records
(including transfers) for the selected measures mentioned above. This is a 48.0% increase in the maximum
number of potential records for evaluation, greatly increasing the sample size and improving the quality
of analysis. This has improved KDHE’s evaluation capacity for this program and creates the potential for
taking a deeper dive into areas of interest, possibly aiding in discovery of the “who” and “why” that are
questions often raised in some areas of the report. For instance, for induced deliveries the rate was
significantly improved following the linkage from a rate of 45.3% (95%CI: 41.5, 49.1) from the original
survey data to a rate of 37.5% (95%CI: 34.5, 40.5%) from the linked data.

Communities Supporting
Perinatal Behavioral Health
Describes the Community Collaborative led by Title V to establish and implement the following MCH Leader recognitions related to perinatal mental
health and substance use.
SECTION CONTENTS
· Project Overview & Components ........................................................................... 103 · Grantee Application ................................................................................................ 107

Kansas Maternal and Child Health
Communities Supporting Perinatal Behavioral Health Community Collaborative Becoming an MCH Leader in Perinatal Behavioral Health
Request for Applications
COMMUNITY COLLABORATIVE OVERVIEW The Communities Supporting Perinatal Behavioral Health Community Collaborative is a partnership between five MCH Aid-To-Local Grantees and the Bureau of Family Health’s MCH Program. Oversight of the learning collaborative will be provided by the Bureau’s Behavioral Health Consultant. Participants are expected to actively work towards obtaining the MCH leader recognitions outlined below. Participants can work towards the leader commitment recognition activities while participating in the learning collaborative, if they are also working toward the other MCH leader recognitions. Each organization participating in the Community Collaborative (maximum allowed is five), will receive an $8,000 stipend to be used for administrative costs associated with implementation of project activities. See the Community Collaborative Project Overview for more information.
What are the MCH leader recognitions?
Communities Supporting Perinatal Behavioral Health Community Collaborative Timeline: • May 15, 2020 – Announcement of the Collaborative; now accepting applications• May 30, 2020 – Deadline to submit applications• June 1-5, 2020 – Application reviews (KDHE staff)• June 8, 2020 – Announcement of the selected applicants• July 1, 2020 – Community Collaborative Kickoff• August 2020 (est.) - First Quarter Community Collaborative Webinar• November 2020 (est.) - Second Quarter Community Collaborative Webinar• February 2021 (est.) - Third Quarter Community Collaborative Webinar• May 2021 (est.) - Fourth Quarter Community Collaborative Webinar• June 30, 2021 – Conclusion of the Community Collaborative• TBD – Community Collaborative Celebration

Communities Supporting Perinatal Behavioral Health Community Collaborative APPLICATION
Applicant Contact Information
Applicant/Organization:
Contact Person’s Name and Title:
Phone Number:
Email Address:
Benchmark #1 – MCH Benchmark Leader in Perinatal Mental Health
The questions below reference activities required as part of the MCH Benchmark Leader in Perinatal Mental Health recognition award. There is not a right or wrong response to the questions. The Bureau of Family Health’s MCH Program wants to gain a better understanding of the applicant’s current efforts, successes, and challenges related to perinatal mental health. Responses will be used to guide training, technical assistance, and other support activities throughout the duration of the Community Collaborative.
Question 1: Describe current Perinatal Mood and Anxiety Disorder (PMAD) screening practices. Is there a universal PMAD screening policy? What screening tool is used? What is the screening frequency? Who facilitates the screening?
Question 2: Describe current procedures following a positive PMAD screening. Include information about any brief interventions that occur, referrals to treatment, response to crisis situations, etc. Include any online referral systems used (i.e., IRIS).
Question 3: What activities has the organization led to increase awareness, decrease bias, and provide more information to perinatal women and their families about PMADs? Describe ideas for future activities.
Question 4: Describe the organization’s partnerships with mental health treatment providers/organizations, if any.

Question 5: Describe process for measuring compliance and adherence to organizational policy (e.g., how do you know policies are being followed, brief interventions are occurring, referrals to treatment are being made, etc.). How are DAISEY reports to guide quality improvement projects? Response should be specific to PMADs.
Question 6: Describe any perinatal mental health support groups, or efforts made to start a perinatal support group, in the applicant’s community. Is the support group led by staff or by individuals with lived experience?
Question 7: What do you anticipate being the biggest challenge in becoming an MCH Leader in Perinatal Mental Health?
Benchmark #2 – MCH Benchmark Leader in Perinatal Substance Use
The questions below reference activities required as part of the MCH Benchmark Leader in Perinatal Substance Use recognition award. There is not a right or wrong response to the questions. The Bureau of Family Health’s MCH Program wants to gain a better understanding of the applicant’s current efforts, successes, and challenges related to perinatal substance use. Responses will be used to guide training, technical assistance, and other support activities throughout the duration of the Community Collaborative.
Question 8: Describe current perinatal substance use screening practices. Is there a universal screening policy? What screening tool is used? What is the screening frequency? Who facilitates the screening?
Question 9: Describe current procedures following a positive substance use screening. Include information about any brief interventions that occur, referrals for further assessment, response to crisis situations, etc. Include any online referral systems used (i.e., IRIS).

Question 10: What activities has the organization led to increase awareness, decrease bias, and provide more information to perinatal women and their families about substance use? Describe ideas for future activities.
Question 11: Describe the organization’s partnerships with substance use treatment providers/organizations, if any.
Question 12: Describe process for measuring compliance and adherence to organizational policy (e.g., how do you know policies are being followed, brief interventions are occurring, referrals to treatment are being made, etc.). How are DAISEY reports to guide quality improvement projects? Response should be specific to perinatal substance use.
Question 13: Describe any perinatal substance use support groups, or efforts made to start a perinatal support group, in the applicant’s community. Is the support group led by staff or by individuals with lived experience?
Question 14: What do you anticipate being the biggest challenge in becoming an MCH Leader in Perinatal Substance Use?
Submit application to Kelsee Torrez, Behavioral Health [email protected]
Maternal and Child Health (MCH) Programs - Community Collaborative Opportunity
Communities Supporting Perinatal Behavioral Health: Becoming an MCH Leader in Perinatal Behavioral Health
PROJECT COMPONENTS
GOAL: Implement perinatal behavioral health screenings, brief interventions, and referrals to treatment into clinical practice that meets both benchmark standards. Once a participant completes both benchmarks, they will be recognized as an MCH Leader in Perinatal Behavioral Health for communities supporting perinatal behavioral health.
Benchmark #1 – MCH Benchmark Leader in Perinatal Mental Health: Implement perinatal mood and anxiety disorders (PMADs) screenings, brief interventions, and referrals to treatment into clinical practice. To meet this benchmark, participants will need to complete all required activities. The activities are divided into two phases, referred to as “level one components” and “level two components.” Participants are encouraged to complete the “level one components” before focusing on “level two components,” but progress can be started on “level two components” while “level one components” are in progress. Once a participant completes all components, they will be recognized as an MCH Benchmark Leader in Perinatal Mental Health. Benchmark #2 – MCH Benchmark Leader in Perinatal Substance Use: Implement perinatal substance use screenings, brief interventions, and referrals to treatment into clinical practice. To meet this benchmark, participants will need to complete all required activities. The activities are divided into two phases, referred to as “level one components” and “level two components.” Participants are encouraged to complete the “level one components” before focusing on “level two components,” but progress can be started on “level two components” while “level one components” are in progress. Once a participant completes all components, they will be recognized as an MCH Benchmark Leader in Perinatal Substance Use. MCH Leaders Committed to Improving Perinatal Behavioral Health: These activities are above and beyond the MCH Leader in Behavioral Health standards. These optional activities are not included in the requirements for becoming an MCH Benchmark Leader in Perinatal Mental Health, MCH Benchmark Leader in Perinatal Substance Use, or MCH Leader in Behavioral Health. Completion of any of these activities will result in additional recognition as a MCH leader committed to improving perinatal behavioral health. Each activity is a standalone achievement; completion of all activities is not required for the commitment recognition.
• Community Committed to Supporting Quality Mental Health Care for Perinatal Women: Recognition occurs when an MCH program has a recognized partnership with a local community mental health services provider who has completed the Postpartum Support International’s 2-Day PMAD Training. A “recognized partnership” can be demonstrated with an active Memorandum of Agreement/Understanding (MOA/MOU).
• Community Committed to Supporting Perinatal Women’s Mental Health: Recognition occurs when an MCH program staff complete the Postpartum Support International’s Frontline Provider Training.
• Community Committed to Supporting Moms Who Support Moms: Recognition occurs when an MCH program establishes a referral partnership with a perinatal women’s peer support group that has completed the Group Peer Support (GPS) for Parents training.
The Communities Supporting Perinatal Behavioral Health Learning Collaborative is an opportunity for five local MCH agencies to partner with KDHE’s Bureau of Family Health to receive targeted technical assistance and one on one guidance to obtain recognition as a Community Supporting Perinatal Behavioral Health. Participants will also have the opportunity to actively work towards obtaining the MCH leader recognitions outlined below. Each organization participating in the Community Collaborative (maximum allowed is five), will receive an $8,000 stipend to be used for administrative costs associated with implementation of project activities. If a second cohort of Communities Supporting Perinatal Behavioral Health Learning Collaborative is established, participants from the first cohort might be asked to serve in a mentor/coach capacity for participants in the second cohort.

To become an MCH Benchmark Leader in Perinatal Mental Health, participants must complete the following: MCH Benchmark Leader in Perinatal Mental Health: Implement perinatal mood and anxiety disorders (PMADs) screenings, brief interventions, and referrals to treatment into clinical practice that includes both level one and level two components.
Level 1 Components: • Create, inform staff, and adhere to a universal PMAD screening policy for pregnant and postpartum women.
The policy should include a response protocol for positive screens and crisis intervention. Individual(s) with lived experience of PMADs should be engaged in this process.
• Adopt the Edinburgh Postnatal Depression Scale (EPDS) as the validated PMAD screening tool used in practice.
• Determine screening frequency. • Conduct validated PMAD screening during the established timed patient encounters. Provide brief
interventions and referrals to treatment, when indicated. Screenings, brief interventions, and referrals to treatment should meet compliance with the adopted policy.
• 100% of all screens and action plans are entered into DAISEY. • Utilization of the Perinatal Provider Behavioral Health Consultation Line, as needed. • Establish at least one organization-level educational initiative (e.g., class, brochures/handouts, posters, etc.)
aimed at increasing awareness, decreasing bias, and providing information to perinatal women and their families about PMADs.
Level 2 Components: • Establish a Memorandum of Agreement/Understanding (MOA/MOU) with a local community mental health
treatment provider and/or with a mental health treatment provider who will provide services using telehealth.
• Follow the established IRIS Community Standards for making referrals and “closing the loop” communication practices. For non-IRIS communities, make referrals for treatment, when indicated, and follow up to ensure patient was able to access treatment services.
• Participate in a training focused on brief intervention skills-building. • Establish local standards for recognition and response to measure compliance, understand individual
performance, and track outcomes. Use DAISEY reports to guide quality improvement projects. • Establish and/or promote a community perinatal support group. The group should be registered on
http://SupportGroupsInKansas.org. • Establish at least one community-level educational initiative (e.g., social media campaign, multi-media
advertisements, etc.) aimed at increasing awareness, decreasing bias, and providing information to perinatal women and their families about PMADs.
• Establish a local system of care for perinatal women and their families, which should include (where available), but is not limited to, MCH programs, an obstetrician/gynecologist, a pediatrician/family physician, a mental health treatment provider, and a person with lived experience of PMADs. Members of the local system of care should establish community standards that include building and maintaining a non-judgmental culture of safety and care.

To become an MCH Benchmark Leader in Perinatal Mental Health, participants must complete the following: MCH Benchmark Leader in Perinatal Substance Use: Implement perinatal substance use screenings, brief interventions, and referrals to treatment into clinical practice that includes both level one and level two components.
Level 1 Components: • Create, inform staff, and adhere to a universal substance use screening policy for pregnant and postpartum
women. The policy should include a response protocol for positive screens and crisis intervention. Individual(s) with lived experience of perinatal substance use should be engaged in this process.
• Adopt the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) as the validated substance use screening tool used in practice.
• Determine screening frequency. • Complete the Kansas Department for Aging and Disability Services’ (KDADS) Screening. Brief Intervention,
and Referral to Treatment training, as established in KDADS policy BHS/MCO 503. • Conduct validated substance use screening during the established timed patient encounters. Provide brief
interventions and referrals to treatment, when indicated. Screenings, brief interventions, and referrals to treatment should meet compliance with the adopted policy.
• 100% of all screens and action plans are entered into DAISEY. • Utilization of the Perinatal Provider Behavioral Health Consultation Line, as needed. • Establish at least one organization-level educational initiative (e.g., class, brochures/handouts, posters, etc.)
aimed at increasing awareness, decreasing bias, and providing information to perinatal women and their families about perinatal substance use.
Level 2 Components: • Establish a Memorandum of Agreement/Understanding (MOA/MOU) with a local substance use treatment
provider for substance use assessments and/or with a substance use treatment provider who will conduct assessments using telehealth.
• Follow the established IRIS Community Standards for making referrals and “closing the loop” communication practices. For non-IRIS communities, make referrals for treatment, when indicated, and follow up to ensure patient was able to access treatment services.
• Participate in a training focused on brief intervention skills-building. • Establish local standards for recognition and response to measure compliance, understand individual
performance, and track outcomes. Use DAISEY reports to guide quality improvement projects. • Establish and/or promote a community perinatal support group. The group should be registered on
http://SupportGroupsInKansas.org. • Establish at least one community-level educational initiative (e.g., social media campaign, multi-media
advertisements, etc.) aimed at increasing awareness, decreasing bias, and providing information to perinatal women and their families about perinatal substance use.
• Establish a local system of care for perinatal women and their families, which should include (where available), but is not limited to, MCH programs, an obstetrician/gynecologist, a pediatrician/family physician, a substance use treatment provider, and a person with lived experience of perinatal substance use. Members of the local system of care should establish community standards that include building and maintaining a non-judgmental culture of safety and care.

Paternal Postpartum
Depression (PPD)
Information for Kansas MCH programs related to PPD.
SECTION CONTENTS
· Paternal PPD Action Alert ....................................................................................... 111 · Information and Recommendations for Paternal PPD ......................................... 112

50%
10%
14%
0% 10% 20% 30% 40% 50% 60%
Paternal PPD when MotherExperiences Perinatal Depression
Paternal Postpartum Depression
Perinatal Depression
Prevalence of Depression in ParentsNearly one in ten fathers experience postpartum depression.
The prevalence increases to 50% when the mother is also experiencing perinatal depression.
Prevalence*
Impact on Child Development
How to Support Fathers’ Mental Health
Nurturing parent-child relationships and environments are vital for healthy development.
When the family’s social needs are met, it is more likely that children will succeed in school and work as well as experience lower rates of chronic disease.**
Early identification, intervention, and treatment of paternal depression helps reduce adverse emotional and behavioral outcomes in children, as well as improve the quality of life for the father and family.***
Screen for paternal depression. The Edinburgh Postnatal Depression Scale (EPDS) is validated for use with fathers but requires 2-point lower cutoff score than screenings for mothers. KDHE recommends use of EPDS for paternal depression screening with a cutoff score for referral at 8.
Connect fathers with treatment, support, and educational resources. More information about this connection options can be found in theKDHE Paternal PPD Information and Recommendations guide.
*Earls MF, Yogman MW, Mattson G, Rafferty J, Committee On Psychosocial Aspects Of C, Family H: Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics. 2019;143. Available here.**National Institute for Children’s Health Quality. Maternal Depression: First Steps families and Advocates Can Take to Help Mothers and Babies Thrive.2018. Available here. ***Ramchandani P, Stein A, Evans J, O’Connor TG, ALSPAC study team (June 25-July 1, 2005). Paternal depression in the postnatal period and child development: a prospective population study. Available here.
PATERNALPOSTPARTUMDEPRESSION

June 2020 – Page 1
Paternal Postpartum Depression (Paternal PPD) Information and Recommendations for Kansas MCH Programs
Mental health conditions and substance use disorders affect men and women of all ages, races, and socioeconomic groups. These conditions can cause changes in thinking, feeling, mood, and behavior, as well as affect someone’s ability to relate to others and function each day. While common, recurrent, and sometimes serious, these mental health conditions and substance use disorders are treatable, and people do recover. Perinatal depression is a mental health condition that includes major and minor depressive episodes that occur during pregnancy or in the first twelve months after delivery. Perinatal depression is one of the most common medical complications of pregnancy, affecting one in seven women. While there is an increase in awareness, identification, and treatment of perinatal depression, many are surprised to learn that fathers can also experience postpartum depression!
Paternal PPD The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) defines depression “with peripartum onset” as a major depressive episode during pregnancy or within four weeks after parturition.1 Numerous research studies have reviewed onset of PPD in men and findings suggest the DSM-5 definition is not adequate for diagnosis of the condition:
• PPD develops more slowly and gradually over the more protracted course of a full year postpartum among men; longitudinal studies suggest that the rate of depression during the prenatal period decreases shortly after childbirth but increases over the course of the first year. 2
• A 1996 study found that 4.8% of first-time fathers in Portugal met criteria for depression during pregnancy and 4.8% of fathers were depressed at three months postpartum, but 23.8% of fathers were depressed at 12 months postnatal.3
• Additionally, a 2010 study found that prenatal and PPD was evident in about 10% of men and was relatively higher in the three- to six-month postpartum period.4
Therefore, PPD is often defined as an episode of major depressive disorder occurring soon after the birth of a child; it is more frequently reported in mothers but can also occur in fathers.5 See Figure 1 for an overview of paternal postpartum depression, including risk factors and outcomes. PPD is a treatable condition and people do recover. Clinicians are encouraged to screen for depression in fathers, particularly during the first year postpartum, as early identification, intervention, and treatment can improve the quality of life for the father and family, as well as decrease the risk for emotional and behavioral problems in his children.6
1 American Psychiatric Association. In: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association; 2013. Depressive Disorders; pp. 153–188. Available here. 2 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 3 Areias, M., Kumar, R., Barros, H., & Figueiredo, E. (1996). Correlates of Postnatal Depression in Mothers and Fathers. British Journal of Psychiatry, 169(1), 36-41. doi:10.1192/bjp.169.1.36. Available here. 4 Paulson JF and Bazemore SD (May 19, 2010). Prenatal and postpartum depression in fathers and its association with maternal depression: a meta-analysis. Available here. 5 Scarff J (May 1, 2019). Postpartum Depression in Men. Available here. 6 Scarff J (May 1, 2019). Postpartum Depression in Men. Available here.

June 2020 – Page 2
Figure 1: Model of paternal postpartum depression7
Prevalence of Paternal PPD Research shows that nearly one in ten fathers experience postpartum depression (PPD). The prevalence increases to 50% when the mother is also experiencing perinatal depression.8 Up to 18% of these dads develop a clinically significant anxiety disorder, such as generalized anxiety disorder, obsessive-compulsive disorder, and post-traumatic stress disorder at some point during the perinatal period.9 Figure 2: Parental depression prevalence comparison chart
Impact on Child Development During the child’s early years – the most active period for establishing neural connections – “serve and return” interactions between parent and child are vital for healthy development. In the absence of responsive caregiving, or if
7 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 8 Earls MF, Yogman MW, Mattson G, Rafferty J, Committee On Psychosocial Aspects Of C, Family H: Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics. 2019;143. Available here. 9 Postpartum Support International. (2019). Dad’s Mental Health. Available here.
50%
10%
14%
0% 10% 20% 30% 40% 50% 60%
Paternal PPD when MotherExperiences Perinatal Depression
Paternal Postpartum Depression
Perinatal Depression
Prevalence of Depression in Parents
June 2020 – Page 3
responses are unreliable or inappropriate, the brain’s architecture does not form as expected, which can lead to disparities in learning and behavior.10 Studies show that nurturing parent-child relationships and environments where the family’s social needs are met, make it more likely that children will succeed in school and the workforce, and experience lower rates of chronic disease.11 A 2005 study found that depression in fathers during the postnatal period was associated with adverse emotional and behavioral outcomes in children aged 3.5 years, and an increased risk of conduct problems in boys; these effects remained even after controlling for maternal and paternal depression.12 While more research is needed to determine the full impact of paternal depression on child development, it is reasonable to conclude there is an adverse impact. As such, paternal depression screening, intervention, and treatment are critical preventive care tools.
Paternal Postpartum Depression Risk Factors Maternal depression has consistently been found to be the most important risk factor for depression in fathers, both prenatally and postnatally.13 One study found that fathers whose partners were depressed had nearly two-and-a-half times the normal risk for depression.14 Other factors that can contribute to depression in fathers include15:
• Personal or family history of depression • Worries about being a parent and/or low parental self-efficacy • Feeling overwhelmed with expectations in your role at work and your role as a father • Financial problems • Lack of social and/or emotional support • Stress in relationship with family or spouse • Missing attention and/or sex from your partner • Stressful birthing experience • Lack of sleep after the baby is born • Feeling excluded from the bond between mom and baby
Depression Symptoms in Men When men experience depression, their symptoms can look different than women’s depression symptoms. Women experienced four symptoms at significantly greater rates than men: stress, crying, sleep problems, and loss of interest or pleasure in things they usually enjoy.16 The same study found that men experienced the following symptoms at significantly higher rates than women: anger attacks/aggression, substance use, and risk-taking behavior. The American Academy of Pediatrics (AAP) also reports men are more likely to present with symptoms of substance use, domestic violence, and undermining breastfeeding instead of sadness.17 Figure 3 outlines the difference in “typical” depressive symptoms and those experienced by men.
10 Harvard University, Center on the Developing Child. Brain Architecture. Available here. 11 National Institute for Children’s Health Quality. Maternal Depression: First Steps families and Advocates Can Take to Help Mothers and Babies Thrive. 2018. Available here. 12 Ramchandani P, Stein A, Evans J, O’Connor TG, ALSPAC study team (June 25-July 1, 2005). Paternal depression in the postnatal period and child development: a prospective population study. Available here. 13 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 14 National Institute for Health Care Management (NIHCM) (June 2010). Identifying and Treating Maternal Depression: Strategies and Considerations for Health Plans. Available here. 15 Pacific Postpartum Support Society (2020). Signs of Postpartum Depression and Anxiety in Men. Available here. 16 Martin L, Neighbors H, and Griffith D (October 2013). The Experience of Symptoms of Depression in Men vs. Women: Analysis of the National Comorbidity Survey Replication. Available here. 17 Earls MF, Yogman MW, Mattson G, Rafferty J, Committee On Psychosocial Aspects Of C, Family H: Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics. 2019;143. Available here.

June 2020 – Page 4
Figure 3: Symptoms of Depression18,19 Classic Symptoms of Depression Symptoms of Men’s Depression
• Depressed, sad mood • Loss of interest or pleasure • Significant weight loss or gain • Trouble sleeping or over-sleeping • Restless feelings and inability to sit still or slow down • Fatigue, loss of energy, or tired all the time • Worthless or guilty feelings • Impaired concentration and difficulty making
decisions • Recurrent thoughts of death or suicide
• Increased anger and conflict with others • Increased use of alcohol or other drugs • Frustration or irritability • Violent behavior • Losing weight without trying • Isolation from family and friends • Being easily stressed • Impulsiveness and taking risks (i.e., reckless driving
and extramarital sex) • Feeling discouraged • Increase in complaints about physical problems (i.e.,
headaches, digestion problems or pain) • Problems with concentration and motivation • Loss of interest in work, hobbies, and sex • Working constantly • Increased concerns about productivity and functioning
at school or work • Fatigue • Experiencing conflict between how you think you
should be as a man and how you actually are • Thoughts of suicide
As the symptoms experienced by men differ from those experienced by women, paternal PPD often goes unidentified. Other contributing factors to the underreporting of paternal depression is stigma of mental illness and gender expectations. A 2019 University of Nevada Las Vegas study20 focused on first-hand accounts from new fathers found online; researchers identified six themes:
1. Needing education. Fathers did not know men could suffer from PPD. Mothers who noticed mood changes with their partner were not sure what to call it. Men complained about experiencing pushback or not receiving information from doctors. Men were also frustrated that the resources they did find focused solely on how to help their female partner.
2. Adhering to gender expectations. Many fathers felt pressure to adhere to traditional “tough guy” stereotypes. In fact, one man told another father to “suck it up.” He admitted knowing this was bad advice but explained that is what is expected of men.
3. Repressing feelings. Men are reluctant to share their feelings in fear of sounding ridiculous or looking weak to their partners, who were the primary caregivers.
4. Overwhelmed. Many of the new fathers found it difficult to express their emotions of confusion, exhaustion, helplessness, loneliness, and feeling trapped.
5. Resentment of baby. While many fathers expressed joy and excitement for the arrival of their child, others resented their baby’s constant needs and attention. Like women who experience a perinatal mood and anxiety disorder (PMAD), a few of the men talked about suppressing urges to hurt the baby or themselves.
18 PostpartumMen (2008-2020). Men’s Depression. Available here. 19 Pacific Postpartum Support Society (2020). Signs of Postpartum Depression and Anxiety in Men. Available here. 20 University of Nevada Las Vegas (March 7, 2019). Forgotten fathers: New dads also at risk for postpartum depression. Available here.

June 2020 – Page 5
6. Experience of neglect. The fathers felt lost, forgotten, and neglected – by their partners, the health care system, and society. One father described “uncomfortably laughing” while reading PPD screening questions typically asked of women during routine checkups: “I began to feel like someone should be asking me the same questions.”
Results from the October 2013 study suggests that relying only on men’s disclosure of symptoms could lead to an under-diagnosis of depression in men. 21 Health care providers should consider other clues and behavioral changes when screening or assessing depression in men.
Screening The Edinburgh Postnatal Depression Scale (EPDS) has been validated and used extensively in screening for depression in new mothers, both in English speaking and non-English speaking communities. A May 2001 research study determined the EPDS to be a reliable and valid measure of mood in fathers.22 Other recommendations on the EPDS as a screening tool for paternal PPD include:
• AAP encourages pediatricians to consider screening the mother’s partner at the 6-month infant well-visit using the EPDS.23 AAP suggests completing the screen either in person, if the partner is present, or by having the partner fill out the screen at home and mail it back.
• Postpartum Support International (PSI) emphasizes that the EPDS is a reliable and valid measure of mood in fathers. PSI recommends using a two-point lower cut-off score than used with mothers for screening fathers.24 More information about cut-off scores is included in the following section.
• Additionally, the EPDS-Partner Version (EPDS-P), a screening tool for paternal depression through maternal report, to be a reliable and valid measure of paternal PPD when compared to other well-validated measures of depression.25 The EPDS-P has clinical utility in the maternal child health care system by making it possible to screen for paternal depression without the father being present.26
Alternatively, the Patient Health Questionnaire (PHQ-9) demonstrated validation when screening for paternal PPD.27 A comparison study was conducted in 2017, and results suggest the PHQ-9 and EPDS have similar accuracy in screening for major depressive episodes.28 Of note, this study was based on major depression and did not measure accuracy between the two tools for mild or moderate depression nor was it specific to maternal and paternal depression. As a reminder, guidelines for screening practices are as follows, “Screening must exist in an adequate system of care that includes educated providers, social support for families, and a protocol to follow up with those who have screened above the cut-off score on an evidence-based screening tool.”29 Additionally, screening tools are designed to measure
21 Martin L, Neighbors H, and Griffith D (October 2013). The Experience of Symptoms of Depression in Men vs. Women: Analysis of the National Comorbidity Survey Replication. Available here. 22 Matthey S, Barnett B, Kavanagh DJ, and Howie P (May 2001). Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. Available here. 23 Earls MF, Yogman MW, Mattson G, Rafferty J, Committee On Psychosocial Aspects Of C, Family H: Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics. 2019;143. Available here. 24 Postpartum Support International (2020). Screening Recommendations. Available here. 25 Moran TE, O’Hara MW (July 2006). A partner-rating scale of postpartum depression: the Edinburgh Postnatal Depression Scale – Partner (EPDS-P). Available here. 26 Fisher SD, Koperlman R, and O’Hara MW (August 2012). Partner report of paternal depression using the Edinburgh Postnatal Depression Scale-Partner. Available here. 27 Scarff J (May 1, 2019). Postpartum Depression in Men. Available here. 28 Santos IS, Tavares B, Munhoz, T, Manzolli P, de Avila G, Jannke E, and Matijasevich A (2017). Patient Health Questionnaire-9 versus Edinburgh Postnatal Depression Scale in screening for major depressive episode: a cross-sectional population-based study. Available here. 29 Postpartum Support International (2020). Screening Recommendations. Available here.

June 2020 – Page 6
risk of experiencing depression and should not be used as a diagnostic tool. It is also important to recognize the onset of paternal PPD is more prevalent in the late-postpartum period. This should be taken into consideration when establishing universal screening protocols.
EPDS Scoring for Paternal PPD The EPDS validation study suggests that screening for depression or anxiety disorders in fathers requires a two-point lower cut-off score than screening for depression or anxiety in mothers. The recommended cut-off score was determined to be 5/6 for a positive screen, which was two points lower than the cut-off score for mothers.30 Several other studies have been conducted to determine the score cut-off for men, with results ranging from 5/6 to 10; the cut-off scores for men still need to be validated for different measures.31 This variation of research findings is based on cultural norms, timing of the screen, and the differences in symptoms experienced by men, which are not all included on the EPDS. For example, question 9 on the EPDS is, “I have been so unhappy that I have been crying.” While crying could be a symptom experienced by fathers, they are not as likely to cry as to become aggressive. Additionally, men may be less expressive about their feelings than women, thus, fathers are likely to score lower in the self-reported screening.32 Figure 4: Apparent prevalence of depression in the study sample at different EPDS cutoffs based on the literature33
The development of measures and validation of cut-off scores for paternal PPD are important for more sensitive and accurate diagnosis, intervention, and treatment.34 While additional research is necessary, a consistent finding thus far is that screening for PPD in fathers requires a two-point lower cut-off score than screening for mothers. The Kansas Department of Health and Environment (KDHE) Bureau of Family Health (BFH) promotes the use of the EPDS across Maternal and Child Health (MCH) services in the state for mothers with a cutoff score for referral at 10.35
→ Recommendation: KDHE BFH is recommending the use of the EPDS across MCH services for fathers with a cutoff score for referral at 8.
30 Matthey S, Barnett B, Kavanagh DJ, and Howie P (May 2001). Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. Available here. 31 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 32 Matthey S, Barnett B, Kavanagh DJ, and Howie P (May 2001). Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. Available here. 33 Shaheen N, AlAtiq Y, MPhil, Thomas A. (February 18, 2019). Paternal Postnatal Depression Among Fathers of Newborn in Saudi Arabia. Available here. 34 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 35 KDHE BFH (May 2019). Mental Health Integration Toolkit. Available here.

June 2020 – Page 7
Programs, Supports, and Treatment Programming With such a strong correlation between prevalence for maternal depression and paternal depression, educational programs for all parents experiencing PPD could be more effective than gender specific programming.36
→ Recommendation: Consider integrating fathers into existing programs typically offered only to perinatal women. Social Supports Increasing natural support system for anyone experiencing symptoms of mental illness is a protective factor. This is especially important during life transitions, such as the birth of a child. Proper supports from society that focus on the active roles of fathers would help new fathers ease their stress in the early postpartum period; for instance, encouraging fathers to seek help from health professionals for complete assessments and consideration of psychotherapy or antidepressants might significantly improve their family health.37
→ Recommendation: Explore options for starting PPD support groups for all parents in your community. Paternal Depression Treatment Prevention and early treatment of depression in fathers may benefit not only themselves but also their partner and their children.38
→ Recommendation: Encouraging fathers to seek support from health care professionals can improve the family’s health. Fathers should talk to a health care professional about what treatment options might be best for them. Options include:
• Psychotherapy – There are many types of therapy available, but all have the same goal: to teach skills
and insight to feel better as well as prevent future depressive episodes. Therapy can be a very effective treatment option for this reason. To find a treatment provider in your community, use the Behavioral Health Treatment Services Locator or call your local Community Mental Health Center (CMHC).
• Medication – Antidepressants may help relieve some of the symptoms (i.e., sleep, appetite, and concentration problems) of moderate and severe depression, but they can take several weeks to be effective.39 To learn more about medication options, contact a prescribing physician (i.e., family doctor, primary care provider, etc.) or local CMHC for a psychiatric assessment. Health care providers can also call the Perinatal Provider Consultation Line for assistance with perinatal behavioral health questions, including case consultation and best prescribing practices. A licensed mental health clinician is available to answer calls Monday-Friday from 8:00am – 5:00pm. Call 833-765-2004 or submit an inquiry online.
KDHE BFH Recommendations for MCH services In addition to the programs, supports, and treatment recommendations outlined above, KDHE BFH recommends MCH programs screen for depression in fathers, particularly during the first year postpartum, as early identification, intervention, and treatment can improve the quality of life for the father and family. The EPDS should be used across all MCH services for fathers with a cutoff score for referral at 8. Screening should occur universally and at the same time as PMAD screening occurs for women, when possible. KDHE BFH’s Mental Health Integration Toolkit includes resources to help MCH programs implement screenings into their practice. Resources include algorithms, templates for local use, provider resources, and patient resources. See Figure 5 for more information on supporting fathers’ mental health.
36 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 37 Kim P and Swain J (February 2007). Sad Dads: Paternal Postpartum Depression. Available here. 38 Areias, M., Kumar, R., Barros, H., & Figueiredo, E. (1996). Correlates of Postnatal Depression in Mothers and Fathers. British Journal of Psychiatry, 169(1), 36-41. doi:10.1192/bjp.169.1.36. Available here. 39 National Institute of Mental Health (2020). Men and Depression. Available here.

June 2020 – Page 8
Figure 5: Supporting Fathers’ Mental Health Infographic40
40 National Institute for Children’s Health Quality (2020). Supporting Fathers’ Mental Health. Available here.

June 2020 – Page 9
Resources for Fathers
Mental Health Treatment Resources Behavioral Health Treatment Services Locator can help find local treatment providers by a simple ZIP code search. https://findtreatment.samhsa.gov/ Kansas Community Mental Health Centers (CMHCs) serve as the community-based public mental health services safety net. This means services can be provided regardless of an individual’s ability to pay. CMHCs can provide evaluation and diagnostic, medication management, psychotherapy, case management, and 24-hour emergency (crisis) support services. There are 26 CMHCs across the state; view the CMHC Map to find the CMHC in your area. http://www.acmhck.org/wp-content/uploads/2018/01/CommunityMentalHealthCentersofKS-Revised-1-10-18.pdf If you are feeling overwhelmed, not sure where to start, or are nervous about your first appointment, dedicate some time to reviewing A Roadmap to Behavioral Health: A Guide to Using Mental Health and Substance Use Disorder Services. While intended for individuals with health insurance, there is helpful information for anyone seeking behavioral health services and supports. https://www.cms.gov/files/document/roadmap-behavioral-health-updated-2019pdf
Support Resources Bootcamp for New Dads is a best practice workshop to help fathers gain the tools and confidence they need during their fatherhood journey. The online workshops are for men expecting their first child. https://www.bootcampfornewdads.org/ The Center for Men’s Excellence, a social network that also offers advice and videos for fathers. https://www.menexcel.com/advice-for-new-dads/ Life of Dad offers fatherhood support groups for all dads, single dads, geek dads, and expectant dads. https://www.LifeOfDad.com Padre Cadre is a “just for dads” social support network dedicated to connecting fathers with fathers and other resources to help make the most out of the fatherhood journey. https://www.padrecadre.com Postpartum Men provides information for fathers hosts an online forum for fathers to connect with each other. http://postpartummen.com/
Postpartum Support International (PSI) aims to promote awareness, prevention, and treatment of mental health issues related to childbearing in every country worldwide. PSI offers several support services, including the following for dads:
• Helpline: You are not alone, and you are not to blame. PSI is here to help. You will get better. Call 1-800-944-4773 or Text 503-894-9453 https://www.postpartum.net/get-help/help-for-moms/
• Chat with an Expert: “Chat for Dads” is available for fathers, partners, other support people, and professionals to find answers and support from an expert – and from other men. You’ll find honest and compassionate talk about the adjustment to parenthood, information about how fatherhood can affect you, and some helpful advice. To participate, call 1-800-944-8766 and use code 73162# at 7:00pm on the first Monday of every month. https://www.postpartum.net/get-help/resources-for-fathers/chat-with-an-expert-for-dads/

June 2020 – Page 10
• Support Coordinators are available in all fifty states and in forty other countries. The PSI Kansas SupportCoordinators can help guide you through the process of finding a professional near you with expertise andexperience in treating perinatal mood disorders, including paternal depression.https://psichapters.com/ks/#get-help
• Tips for taking care of your stress and emotions.https://www.postpartum.net/get-help/family/tips-for-postpartum-dads-and-partners/
• Video testimonials from dads who have experienced postpartum anxiety and depression.https://www.postpartum.net/news-and-blog/ifmhd/
Educational Resources National Institute of Mental Health (NIMH) offers information about mental health, including a publication on Men and Depression. https://www.nimh.nih.gov/health/publications/men-and-depression/mendepression-508_142046.pdf
Pacific Postpartum Support Society offers Tips to Help Dads Deal with Postpartum Depression and Anxiety. http://postpartum.org/services/dads/tips-help-dads-deal-ppda/