Mapping and opportunities of human resource capacity ...
13
Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1 30 Introduction HIV/AIDS epidemic is in its third decade in India, significant challenges still remain. The complex nature of the HIV/AIDS epidemic, demands for a skilled technical and managerial human resource. Not only are existing human and material resources are facing constraints by the impact of the epidemic, the functions of such resources are changing, often in response to a broader and more urgent range of needs. [1,2] National Health Policy, 2002 and National Commission on Macroeconomics and Health clearly lay down that more than the availability of financial resources, a major barrier that limits India’s ability to achieve the MDGs, is inadequate supply of the required skills and competencies. [3,4] India produces a large number of personnel trained in discipline of medical, social, physical and management sciences, which are critical inputs for the AIDS control programme. However, the availability of a large manpower base does not translate into capacity for HIV control efforts due to lack of core public health and HIV/AIDS related knowledge and skills. [5] HIV medicine is not a part of the curriculum for most currently practicing health care professionals at the time of their medical training. Moreover, knowledge and practices in these fields are steadily changing and therefore require constant updating. Thus, human resource capacity building programs are most needed for sustainable response to HIV /AIDS problems in the country. As per the Comptroller and Auditor General of India (CAG) report (2004) out of 380367 health care workers in HIV/AIDS counseling only 163990 are trained amounting to 54% shortfall. [6] Whereas, out of 93882 sanctioned of doctors only 52707 (56%) are trained. Similarly out of 125303 nurses, 16323 technician and 147032 field officers Correspondence to: Dr. Syed Zahiruddin Quazi, Department of Community Medicine, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India. E-mail: [email protected] ORIGINAL ARTICLE Access this article online Quick Response Code: Website: www.atmph.org DOI: 10.4103/1755-6783.115176 Mapping and opportunities of human resource capacity building initiatives for HIV/AIDS in India Kavya Sharma 1 , Sanjay Zodpey 1 , Syed Zahiruddin Quazi 2 , Abhay Gaidhane 2 , Shailendra Sawleshwarkar 3 , Sunil Khaparde 4 1 Public Health Foundation of India, New Delhi, 2 Department of Community Medicine, Daa Meghe Institute of Medical Sciences, Wardha, Maharashtra, 3 Western Sydney Sexual Health Centre, Sydney Medical School, University of Sydney, Australia, 4 National AIDS Control Organization, New Delhi, India ABSTRACT Background: The complex nature of the HIV /AIDS epidemic in India demands for a skilled technical and managerial human resource. India’s response to the human resource capacity building initiatives for better response to HIV/AIDS seems to be impressive; however it faces some key challenges. Aim: The purpose of this paper is to identify and catalogue human resource capacity building initiatives and outline the challenges for better response to HIV/AIDS in India. Materials and Methods: We reviewed and analyzed published articles and reports, grey literature, including organizational websites, self-published tools and articles, non-academic reports and telephonic interview with some stakeholders. Snowballing approach was used to collect information. Results: We hope that this paper would provide an understanding of the current status of capacity building initiatives in India. We have identified certain challenges, particularly related to monitoring and evaluation that need to be addressed in capacity building programs at the planning stage. Conclusion: Moreover these challenges can be viewed as potential areas for operational research. Key words: Capacity Building, HIV/AIDS, NACO, training, workshop
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Mapping and opportunities of human resource capacity ...

30 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 130
Introduction
HIV/AIDS epidemic is in its third decade in India, significant challenges still remain. The complex nature of the HIV/AIDS epidemic, demands for a skilled technical and managerial human resource. Not only are existing human and material resources are facing constraints by the impact of the epidemic, the functions of such resources are changing, often in response to a broader and more urgent range of needs.[1,2]
National Health Policy, 2002 and National Commission on Macroeconomics and Health clearly lay down that more than the availability of financial resources, a major barrier that limits India’s ability to achieve the
MDGs, is inadequate supply of the required skills and competencies.[3,4]
India produces a large number of personnel trained in discipline of medical, social, physical and management sciences, which are critical inputs for the AIDS control programme. However, the availability of a large manpower base does not translate into capacity for HIV control efforts due to lack of core public health and HIV/AIDS related knowledge and skills.[5] HIV medicine is not a part of the curriculum for most currently practicing health care professionals at the time of their medical training. Moreover, knowledge and practices in these fields are steadily changing and therefore require constant updating.
Thus, human resource capacity building programs are most needed for sustainable response to HIV /AIDS problems in the country. As per the Comptroller and Auditor General of India (CAG) report (2004) out of 380367 health care workers in HIV/AIDS counseling only 163990 are trained amounting to 54% shortfall.[6] Whereas, out of 93882 sanctioned of doctors only 52707 (56%) are trained. Similarly out of 125303 nurses, 16323 technician and 147032 field officers
Correspondence to: Dr. Syed Zahiruddin Quazi, Department of Community Medicine, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India. E-mail: [email protected]
OR
IGIN
AL A
RTIC
LE
Access this article online
Quick Response Code: Website: www.atmph.org
DOI: 10.4103/1755-6783.115176
Mapping and opportunities of human resource capacity building initiatives for HIV/AIDS in IndiaKavya Sharma1, Sanjay Zodpey1, Syed Zahiruddin Quazi2, Abhay Gaidhane2, Shailendra Sawleshwarkar3, Sunil Khaparde4
1Public Health Foundation of India, New Delhi, 2Department of Community Medicine, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, 3Western Sydney Sexual Health Centre, Sydney Medical School, University of Sydney, Australia, 4National AIDS Control Organization, New Delhi, India
ABSTRACT
Background: The complex nature of the HIV /AIDS epidemic in India demands for a skilled technical and managerial human resource. India’s response to the human resource capacity building initiatives for better response to HIV/AIDS seems to be impressive; however it faces some key challenges. Aim: The purpose of this paper is to identify and catalogue human resource capacity building initiatives and outline the challenges for better response to HIV/AIDS in India. Materials and Methods: We reviewed and ana lyzed published articles and reports, grey litera ture, including organizational websites, self-published tools and articles, non-academic reports and telephonic interview with some stakeholders. Snowballing approach was used to collect information. Results: We hope that this paper would provide an understanding of the current status of capacity building initiatives in India. We have identified certain challenges, particularly related to monitoring and evaluation that need to be addressed in capacity building programs at the planning stage. Conclusion: Moreover these challenges can be viewed as potential areas for operational research.
Key words: Capacity Building, HIV/AIDS, NACO, training, workshop

Sharma, et al.: HIV/AIDS capacity building in India
31Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
Colleges, Public Health Institutes and Universities of India and various organizations working for HIV/AIDS in India like – Family Health International (FHI), Pathfinder International, International Labour Organization (ILO), Project Concern International (PCI), AIDS prevention and Control Programs (APAC), Karnataka Health Promotion Trust (KHPT), Avery Society, Mumbai, Swasti Health International Karnataka, Society for promoting of youth and assess, Birds Karnataka etc was searched.
We reviewed and ana lyzed published articles and reports of the organization including the grey litera-ture like self-published tools, opinion/reviews and non academic reports.
Results
NACO’s capacity building initiatives briefly presented followed by initiatives from other organizations/ institutions in India. Information related to course/program/training, organization offering program, duration, key area of capacity building, probable participants/beneficiaries was presented in matrix, wherever available. Finally key challenges and opportunities for India’s HIV/AIDS capacity building initiatives in India were discussed.
Broadly two categories of capacity building initiatives, namely academic programs offered by institutions, university and some colleges and the programs that were aimed to build capacity of the staff of NGOs and implementing organizations.
NACO’s response to Human resource capacity building in HIVEmphasis on human resource capacity building in NACP I was minimal.[9] The training plan followed in NACP I was redesigned with the new standardized approach in NACP-II. An action plan was developed at the national level with clear operational guidelines and schedule of activities. The Working Groups constituted for NACP-III (2007-2012) planning have highlighted the lack of requisite capacity at all levels of the programme, in their respective focus areas. India’s NACP III has recognized that the availability of the critical mass of well trained human resources is the backbone to the elaborate organizational structures, institutional arrangements and strategies proposed under NACP-III.[2,10] Currently NACO is involved mostly in short term programs (STP) for building capacity of organizations implementing HIV/AIDS programs supported by NACO or SACS.
Other than the government initiatives, various other agencies (National, International, and/or donor
only 57403 (46%) nurses, 6150 (38%) technician and 44815 (30%) field officers are trained respectively.[7,8]
The purpose of this paper is to identify and catalogue human resource capacity building initiatives and outline the challenges for better response to HIV/AIDS in India.
Materials and Methods
This is a cross-sectional study to find out the capacity building initiatives for HIV/AIDS in India.
Data collection was done using two distinct approaches, used in parallel. Primarily data about capacity building for HIV/AIDS was abstracted through internet search, review of the published literature, desk review. Interviews and discussion were held with stakeholders to get the first hand information and their views regarding capacity building initiatives for HIV/AIDS in India.
Interview with stakeholders was held either in person or by email or telephonically, depending upon the feasibility. Snowballing approach was used to reach stakeholders like policy makers, program managers, program implementers and peers and people living with HIV/AIDS working in Public sector, universities, NGOs, CBOs development sector, international organizations etc. In all 126 persons were approached, however even after persistent follow-up, a relatively small number, that is 35 responded. The discussion was held on issues like, what current capacity building programs are being undertaken in their organizations and their views about the current capacity building programs, challenges faced by such programs and different opportunities for enhancing the capacity building initiatives for HIV/AIDS with focus on Indian context.
The internet search was conducted using the different internet search engines. Key words for HIV/AIDS capacity building initiatives in India were identified. Key words used were HIV/AIDS, capacity building, training, workshop, supportive supervision. Search was restricted to the HIV/AIDS programs offered in India. Search include all programs either short term or long term, in-service/induction training for staff working in HIV/AIDS program as well as academic programs in HIV/AIDS offered by universities or organizations. Website of National AIDS Control Organization (NACO), Ministry of Health and Family Welfare (MoHFW), Indira Gandhi National Open University (IGNOU), State AIDS Control Society (SACS), Public Health Foundation of India (PHFI), selected Medical

Sharma, et al.: HIV/AIDS capacity building in India
32 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 132
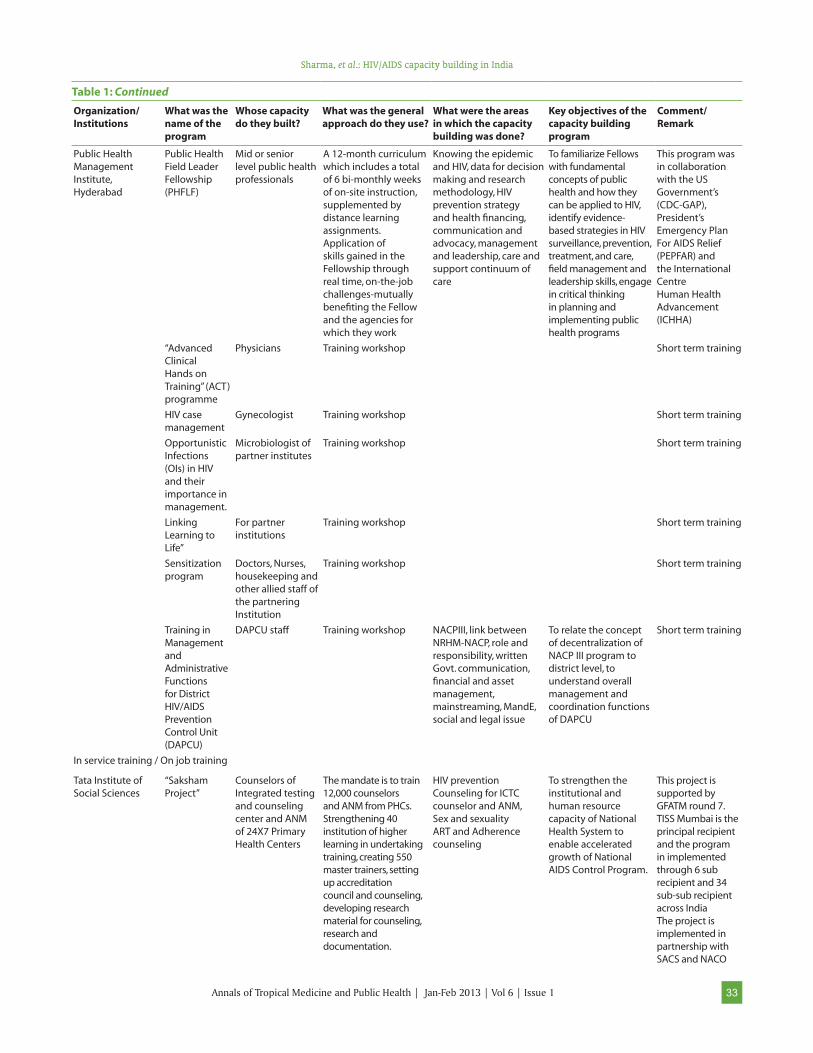
shown as a matrix [Table 1].
There was insufficient, fragmented evidence of undertaking the comprehensive needs assessment
agencies) are also providing support for building India’s human resource capacity for response to HIV / AIDS in close collaboration with NACO. Organizations doing human capacity building for HIV/AIDS in India are
Table 1: Organization giving capacity building on HIV/AIDS
Organization/Institutions
What was the name of the program
Whose capacity do they built?
What was the general approach do they use?
What were the areas in which the capacity building was done?
Key objectives of the capacity building program
Comment/Remark
Academic Programs/Courses
Public Health Foundation of India
‘Short Intensive Professional Programme in HIV’
Mid-career level professionals
3 month, full time course
STI, HIV/AIDS, Sex and Sexuality
To provide a comprehensive overview of prevention and management of HIV infection
Till 2010 – one batch of10 fellows with support from ALFA and AusAID was intensively trained at University of Sydney
Indira Gandhi National Open University (IGNOU)
Diploma in HIV and Family Education (DAFE)
School teachers, NGO functionaries, para medicals and parents of adolescents and those interested in acquiring knowledge on the subject.
Duration – one to four years. Consists of seven courses and is of 32 credits of which the theory papers are of 4 credits each and the project work is of 8 credits
HIV/AIDS, sex and sexuality, family life education, alcohol and drug abuse and communication and counseling
The main objective of this programme is to enhance the knowledge and skills of functionaries involved in HIV/AIDS and related issues.
Eligibility: 10+2 or its equivalent or BPP from IGNOU OR Matriculation with higher qualification recognised by Central/State GovernmentCourse fees is Rs 2400/-
Indira Gandhi National Open University (IGNOU)
Certificate in HIV and Family Education (CAFE)
Target group - school teachers, NGO functionaries, para medicals and parents of adolescents and those interested in acquiring knowledge on the subject.
Duration – six month to two tear The programme has the following courses of 4 credits each. A learner has to choose 2 compulsory courses and any 2 optional from the 4 electives.
Issues involved in HIV/AIDS, family life education, alcohol and drug abuse and behaviour modification
To provide comprehensive knowledge about what, why and how of HIV/AIDS, family life education, facts of life and substance abuse.
Eligibility- 10+2 or equivalent or BPP from IGNOUORMatriculation with higher qualification recognized by Central / State Government
Christian Medical College Vellore and partner institutions (The School of Tropical Medicine, Kolkata and Maulana Azad Medical College, New Delhi, since 3 years)
Fellowship in HIV medicine
MBBS Doctors from both non-governmentaland governmental organizations are eligible.
COURSE DURATION: 12 monthsDistance course – 13 modules over 5 monthsContact courses – 6 weeks over one year andProject work – 6 months at the candidates’ work place.
(i) to enable the participants to improve their knowledge and skills in HIV care.(ii) To enable the practical development of accessible and high quality HIV clinical services in their hospitals.
So far, 107 students have successfully completed the course over the past six years of the course from CMC, Vellore.7th batch will complete training in Feb. 2010. 91 fellows have graduated from these two regional training centres.
Govt. Hospital of Thoracic Medicine Tambaram Sanatorium, Chennai
HIV/AIDS Clinical Fellowship
MBBS recognized by MCIPostgraduate degree/diploma in any disciplinePreferable.A commitment to a career in HIV medical careand/or programme management in India
The one-year hands-on trainingProgramme. Independent thesis projects at the hospital2-week Exposure Visit to an HIV NGOClassroom and bedside teaching experience atNACO trainingsClinical case studies
Clinical and Laboratory, including Infection ControlManagement and LeadershipEpidemiology and ResearchPublic Health SystemsPsychosocial and Behavioral IssuesTraining and Presentation Skills
Prepares physicians to be leaders in HIV care and support, training and management in India.
Started since 2005. Jointly sponsoredby the Govt. of Tamil Nadu and Global AIDS program of US Centers for Disease Control. Fellow (private) get a remuneration of Rs. 18,000/ per month
Sharma, et al.: HIV/AIDS capacity building in India
33Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
Public Health Management Institute, Hyderabad
Public Health Field Leader Fellowship (PHFLF)
Mid or senior level public health professionals
A 12-month curriculum which includes a total of 6 bi-monthly weeks of on-site instruction, supplemented by distance learning assignments. Application of skills gained in the Fellowship through real time, on-the-job challenges-mutually benefiting the Fellow and the agencies for which they work
Knowing the epidemic and HIV, data for decision making and research methodology, HIV prevention strategy and health financing, communication and advocacy, management and leadership, care and support continuum of care
To familiarize Fellows with fundamental concepts of public health and how they can be applied to HIV, identify evidence-based strategies in HIV surveillance, prevention, treatment, and care, field management and leadership skills, engage in critical thinking in planning and implementing public health programs
This program was in collaboration with the US Government’s (CDC-GAP), President’s Emergency Plan For AIDS Relief (PEPFAR) and the International Centre Human Health Advancement (ICHHA)
“Advanced Clinical Hands on Training” (ACT) programme
Physicians Training workshop Short term training
HIV case management
Gynecologist Training workshop Short term training
Opportunistic Infections(OIs) in HIV and their importance in management.
Microbiologist of partner institutes
Training workshop Short term training
Linking Learning to Life”
For partner institutions
Training workshop Short term training
Sensitization program
Doctors, Nurses, housekeeping and other allied staff of the partneringInstitution
Training workshop Short term training
Training in Management and Administrative Functions for District HIV/AIDS Prevention Control Unit (DAPCU)
DAPCU staff Training workshop NACPIII, link between NRHM-NACP, role and responsibility, written Govt. communication, financial and asset management, mainstreaming, MandE, social and legal issue
To relate the concept of decentralization of NACP III program to district level, to understand overall management and coordination functions of DAPCU
Short term training
In service training / On job training
Tata Institute of Social Sciences
“Saksham Project”
Counselors of Integrated testing and counseling center and ANM of 24X7 Primary Health Centers
The mandate is to train 12,000 counselors and ANM from PHCs. Strengthening 40 institution of higher learning in undertaking training, creating 550 master trainers, setting up accreditation council and counseling, developing research material for counseling, research and documentation.
HIV prevention Counseling for ICTC counselor and ANM,Sex and sexualityART and Adherence counseling
To strengthen the institutional and human resource capacity of National Health System to enable accelerated growth of National AIDS Control Program.
This project is supported by GFATM round 7. TISS Mumbai is the principal recipient and the program in implemented through 6 sub recipient and 34 sub-sub recipient across IndiaThe project is implemented in partnership with SACS and NACO
Table 1: Continued
Organization/ Institutions
What was the name of the program
Whose capacity do they built?
What was the general approach do they use?
What were the areas in which the capacity building was done?
Key objectives of the capacity building program
Comment/ Remark

Sharma, et al.: HIV/AIDS capacity building in India
34 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 134
Family Health International
Network of people living with HIV/AIDS
Build capacity of six state-level and 20 district-level networks in the most HIV-affected states in India.
Provides technical assistance to strengthen the capacity of Indian Network for People Living with HIV/AIDS (INP + ) in the national response to the epidemic.
Program was implemented with support from by Bill and Melinda Gates Foundation in 2004 (grant of up to $1.5 million over five)
Aastha Project Outreach workers Developed manuals and resources and conducted trainings
Aastha Project, sponsored by the Bill and Melinda Gates Foundation
Karnataka Health Promotion Trust (KHPT)
Capacity building of NGOs to support their outreach and peer-education programs.Also supports sex worker collectives.
NGO staff implanting HIV prevention projects supported by KHPT.Also supports sex worker collectives.
In-service training for the organizations implementing the HIV/AIDS project – Targeted Intervention project and Care and support project (SAMASTHA project – Karnataka, SPRUHA project Maharashtra)
Components of TI, care and support, ART, infection prevention, stigma and discrimination
To ensure a high standard of information and services to all end users throughout the KHPT Districts as well as to ensure efficiency and accountability
KHPT conducts some capacity building program in collaboration with other organization like - Engender Health
Knowledge management unit
Assist in capacity building of individuals and organizations
The unit has established a system to facilitate learning among various organizations working in HIV/AIDS in Karnataka, India
Development of learning sites, documentation and dissemination has been identified as three core functions of KMU.
To equipped individual and organizations to deliver high quality services and programs related to HIV/AIDS.
Training of CCC Medical Officer _ Maharashtra and Karnataka
ORW, doctors, LT, nurses (PPTCT)
Engender Health Reducing Stigma and Discrimination Related to HIV and AIDS: Training for Health Care Workers
Health Care Workers working in the field of HIV/AIDS
Training workshop Stigma and Discrimination Related to HIV and AIDS
Investigation of the root causes of stigma and discrimination. Review of clients’ rights in receiving health care services, Information about the use of standard precautions and proper infection prevention techniques to help minimize the risk of occupational exposure to HIV
Initially they are training of trainers (ToT) who will train health workers who are working in the field of care and support
Pathfinder Capacity building of NGO implementing Mukta Project (Sex Worker Project) in Maharashtra
All staff of Mukta Project
First basic training followed by refresher. The Technical Manager from Pathfinder give onsite training (supportive supervision) every month depending upon their needs
Training for Advocacy Officer Training for Peer educator Project management for Field officer/ Project Manager Training of Doctors in STI Diagnosis, and ManagementTraining of ANM in STITraining of CounselorTraining in Sex and Sexuality for all project staff Training in CMIS – Project Manager, MandE and accountant
To enhance capacity of project staff for better implementation of project activities
Currently the Mukta Project is in transition phase - from Pathfinder to Maharashtra State AIDS Control Society
Table 1: Continued
Organization/ Institutions
What was the name of the program
Whose capacity do they built?
What was the general approach do they use?
What were the areas in which the capacity building was done?
Key objectives of the capacity building program
Comment/ Remark

Sharma, et al.: HIV/AIDS capacity building in India
35Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
International Labor Organization (ILO DWT for South Asia and Country Office for India) (http://www.ilo.org/newdelhi/lang—en/WCMS_123290/index.htm)
Capacity building on HIV/AIDS in India
MOLandE, Workers’ Organizations, Employers’ Organizations, NACO/SACS, Enterprises and People Living with HIV
development of need-based training manuals, programmes and communications materials.
Strengthening the technical capacity of partners to effectively respond to HIV/AIDS
Work in collaboration with: Ministry of Labour and Employment (MoLE) workers’ organizations employers’ organizations NACO/SACS Collaboration with corporate groups Indian network of people living with HIV/AIDS (INP+)
Project Concern International (PCI)http://www.pciindia.org/html/Prog_HIVAIDS.php
“PATHWAY +” Project (Com-prehensive Community and Home-Based Care and Support for People Living with HIV/AIDS)
Home based care team at project site (medical staff, counselors, social workers, community health workers, and peer educators), CBOs, NGOs and other institutions
Training To assess the magnitude of epidemic at the community level, identifies probable beneficiaries, conducts a needs assessment, and develops linkages with service providers.Continuum of care, ART, Counseling, TB/DOTS, Home based care
Swasti Health Resource Centre, Karnataka India(http://www.impactalliance. org/ev_en.php? ID=49308_201 and ID2=DO_TOPIC)
Supportive Supervision System (SST): Building Local Capacity Towards Effectiveness and Efficiency of Local Organizations
Staff of CSOs working on HIV prevention and care programmes within the Province of Karnataka
Trainings at three levels – central (provincial level), regional (cluster of districts) and local (project site). Learning system was introduced through regular learning and sharing workshops, thematic workshops, newsletter etc
Supportive supervision
Society for promotion of youth and masses (http://www.spym.org/resourceprojects.htm)
Capacity building of NGOs on HIV and drug related issues
Staff of NGO and CSO
Preparation of training and education materials
IT, counseling, documentation, etcSTIs/HIV/AIDS, sex and sexuality, harm reduction
AIDS Prevention and Control Program (APAC) – Voluntary Health Services http://www.apacvhs.com (APAC is also managing the TSU of Kerala and Pondicherry)
Project staff and peer educators, Care Training for nurses, Peer Educators training,
Induction training for new staff, supportive supervision and refresher training
Induction training, NACP-III guidelines, Introduction to the Project, Basics on HIV/AIDS, Sex and sexuality, High risk group intervention (outreach planning, etc.) Counseling, CMIS and Data Quality Assurance, Accounting Procedures, Dialogue based interpersonal communication
APAC in also implementing TSU of Kerala and Pondicherry
Capacity building programs for nine DLNs
District level networks
Training, workshop CBO management, finance management, governance, leadership and documentation
Capacity building of NGOs, Health Care Providers, industrial establishments
Table 1: Continued
Organization/ Institutions
What was the name of the program
Whose capacity do they built?
What was the general approach do they use?
What were the areas in which the capacity building was done?
Key objectives of the capacity building program
Comment/ Remark

Sharma, et al.: HIV/AIDS capacity building in India
36 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 136
Birds, Karnataka Staff of partner NGOs and Community Group
Every eight week in house training
In Belgaum DistrictIndo Canadian collaboration
Training of counselor
Counselor 18 months training of counselor
Counseling In collaboration with South India Action- Programme and Netherlands Gestalt Institute. 40 counsellors successfully completed the course and have been certified by the Netherlands Gestalt Institute
Training of Trainers for Peer Education
Staff of 29 NGO partner of Avert Society Implementing TI in Maharashtra
Training / workshop – 11 month course
Peer educator 93 NGO staff and more than 400 peers have been trained and supervised in this program
Table 1: Continued
Organization/ Institutions
What was the name of the program
Whose capacity do they built?
What was the general approach do they use?
What were the areas in which the capacity building was done?
Key objectives of the capacity building program
Comment/ Remark
process before the launch of HIV/AIDS capacity building programs. Academic programs offer mostly certificate courses, diplomas or fellowship, and are administered as full time program, distance learning program with contact courses.
Training modules and resource material are standardized and mostly are in English language. The learning objectives mostly focused on cognitive, and in some cases, psychomotor domain.
With regards to scheduling, most of the training program were clustering in last three months of the year.[11] It was general apprehension that major time of the program implementers is spent for training.
The capacity building programs for staff working in HIV/AIDS program mostly undertake basic trainings initially, followed by onsite supportive supervision and refresher training.
Almost all the capacity building programs were doing the routine quantitative structured reporting, but detail narrative reports were infrequently documented. A very significant gap was observed with regards comprehensive evaluation of capacity building programs, for those who were undertaking it was mostly the process evaluation. Operational research and documentation of best practices and success stories for Indian context are hardly undertaken by the implementing organizations as well as by funders.
The organizations implementing capacity building programs are mostly working solitarily. It was observed that organizations which were linked with each other were implementing similar type of programs. Organizations undertaking training related to targeted interventions are poorly networked with organizations undertaking capacity building programs for care and support or counseling for ICTC counselor. Furthermore, the institutions offering academic programs have poor linkages with organizations implementing capacity building initiatives from programmatic context.
Almost all, excluding some academic program, the capacity building initiatives were program oriented and funder driven. The effort towards the sustainability seems to be completely lacking. Stakeholders interviewed were grossly unaware of the concept of sustainability of capacity building initiatives.
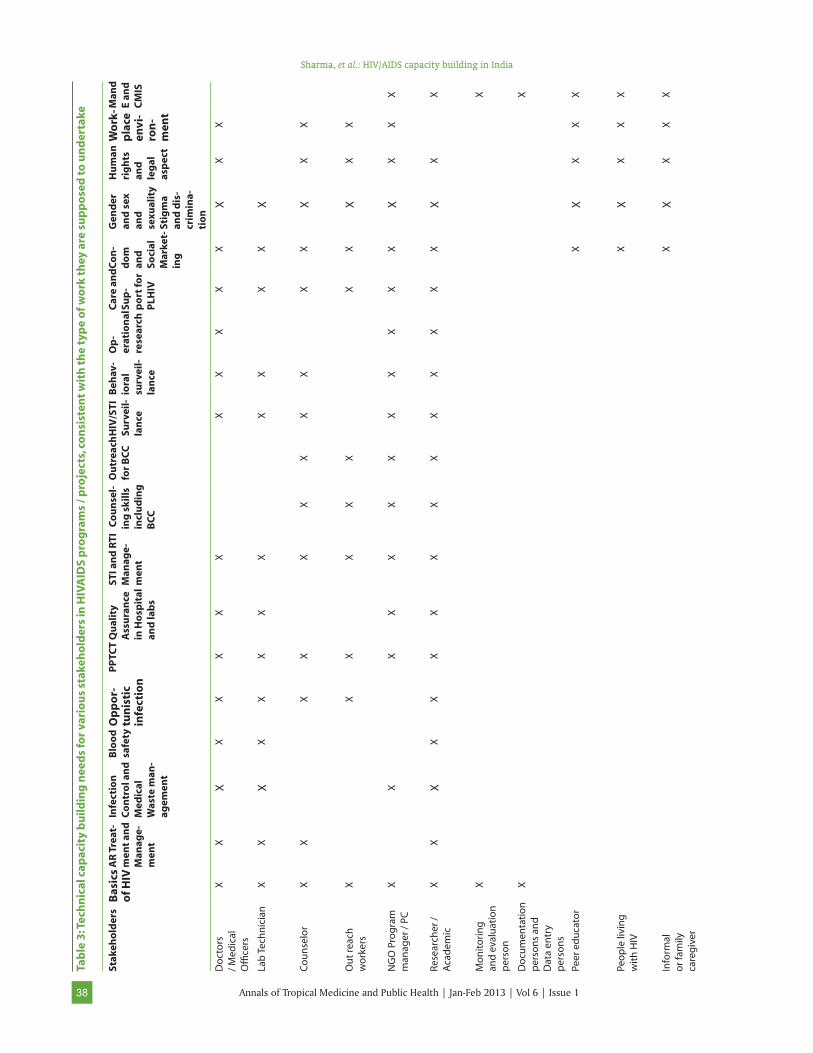
We undertook the opinion of the various stakeholders about the most appropriate area of capacity building for various categories of staff working for HIV/AIDS programs. The overall capacity building efforts of HIV/ AIDS programs were categorized as technical and managerial capacity building. The matrix presented in Table 2 highlights managerial capacity building and Table 3 highlights technical capacity building needs for various stakeholders in HIV/AIDS programs/projects, consistent with the type of work they are supposed to undertake.

Sharma, et al.: HIV/AIDS capacity building in India
37Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
Discussion
India’s response to the human resource capacity building initiatives for better response to HIV/AIDS seems to be impressive; however it faces some key challenges. Based on the information collected for the paper by various approaches, we identified some potential challenges and opportunities for the India’s human resource capacity building initiatives for HIV/AIDS programs.
The key area of capacity building must go with the needs of stakeholders or implementers. Most of the stakeholders commented that capacity building programs were matched with the job that staff working in HIV/AIDS programs has to perform; however, there was not enough evidence to suggest that the comprehensive needs assessment was done before the launch of the programs.
The academic programs for capacity building in HIV/AIDS must also address the country’s capacity building need for better response to HIV/AIDS, however; its implementation, assessment or evaluation may be different, so as to suit the academic requirement for award of certificate. The specific areas/thematic issues on which these academic programs are developed should address the gaps identified in needs assessment and national priority for prevention and control of HIV/AIDS.
Capacity building resource material must clearly articulate the specific learning objectives. Objective must clearly spell out cognitive domain (to achieve progressive complex learning and thinking); psychomotor domain (to demonstrate the enhanced skills in complex thinking and its application to creative problem solving); and affective domain (to achieve progressive skill building and behaviours in
Table 2: Managerial capacity building needs for various stakeholders in HIVAIDS programs / projects, consistent with the type of work they are supposed to undertake
Stakeholders Policy Leader-ship and strategic Manage-
ment
Program management
Commu-nication /
BCC
NGO man-agement
Planning and Man-agement
of TI
Mand E and Impact As-sessment
Strategic MIS and
CMIS
Procure-ment,
Logistics, Supply and Equipment
Manage-ment
Finance Manage-ment and
Accounting
Community Mobili-zation,
Conver-gence and
Partnership
Policy Makers X X
Senior technical program Managers* (National, State and District Level)
X X X X X X X X X X
Mid Professionals** (National, State and District Level)
X X X X X X X X X X
NGO Directors X X X X X X X X X X
NGO Program managers / Project coordinators
X X X X X X X X X X
Finance Managers and Accountants
X X X
Monitoring, Evaluation and Documentation Managers
X X
Counselor X X
Outreach workers
X X
Peers / peer educators
X X
People living with HIV (GIPA)
Sharma, et al.: HIV/AIDS capacity building in India
38 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 138
Tab
le 3
: Tec
hn
ical
cap
acit
y b
uild
ing
nee
ds
for
vari
ou
s st
akeh
old
ers
in H
IVA
IDS
pro
gra
ms
/ pro
ject
s, c
on
sist
ent
wit
h t
he
typ
e o
f wo
rk t
hey
are
su
pp
ose
d t
o u
nd
erta
ke
Stak
eho
lder
sB
asic
s o
f HIV
AR
Tre
at-
men
t an
d
Man
age-
men
t
Infe
ctio
n
Co
ntr
ol a
nd
M
edic
al
Was
te m
an-
agem
ent
Blo
od
sa
fety
Op
po
r-tu
nis
tic
infe
ctio
n
PP
TCT
Qu
alit
y A
ssu
ran
ce
in H
osp
ital
an
d la
bs
STI a
nd
RTI
M
anag
e-m
ent
Co
un
sel-
ing
sk
ills
incl
ud
ing
B
CC
Ou
trea
ch
for
BC
CH
IV/S
TI
Surv
eil-
lan
ce
Beh
av-
iora
l su
rvei
l-la
nce
Op
-er
atio
nal
re
sear
ch
Car
e an
d
Sup
-p
ort
for
PLH
IV
Co
n-
do
m
and
So
cial
M
arke
t-in
g
Gen
der
an
d s
ex
and
se
xual
ity
Stig
ma
and
dis
-cr
imin
a-ti
on
Hu
man
ri
gh
ts
and
le
gal
as
pec
t
Wo
rk-
pla
ce
envi
-ro
n-
men
t
Man
d
E an
d
CM
IS
Do
cto
rs
/ M
edic
al
Offi
cers
XX
XX
XX
XX
XX
XX
XX
XX
Lab
Tec
hn
icia
nX
XX
XX
XX
XX
XX
XX
Co
un
selo
rX
XX
XX
XX
XX
XX
XX
X
Ou
t re
ach
w
ork
ers
XX
XX
XX
XX
XX
X
NG
O P
rog
ram
m
anag
er /
PC
XX
XX
XX
XX
XX
XX
XX
XX
Res
earc
her
/
Aca
dem
ic
XX
XX
XX
XX
XX
XX
XX
XX
XX
Mo
nit
ori
ng
an
d e
valu
atio
n
per
son
XX
Do
cum
enta
tio
n
per
son
s an
d
Dat
a en
try
per
son
s
XX
Peer
ed
uca
tor
XX
XX
X
Peo
ple
livi
ng
w
ith
HIV
XX
XX
X
Info
rmal
o
r fam
ily
care
giv
er
XX
XX
X

Sharma, et al.: HIV/AIDS capacity building in India
39Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
completing a task and develop positive attitude and feelings in addition to knowledge and skills). Currently most training programmes focus on cognitive and at the most psychomotor domain, but not necessarily the affective domain.
Currently, in many programs the resource manual used is in English and needs to be translated in the local language. Moreover, even though the curriculum and modules are standardized, there is a need to recognize the effect of socio-cultural and religious influences while developing resource material/module or tools. This issue has repeatedly come up throughout the process of evaluation of STRC of many states.[12] Stakeholders, specially the program implementers also identified the need to update the modules periodically with latest information and relevant case studies and illustration which are currently not happening.
Identification of resource person to deliver trainings is critical problem faced by many organizations implementing trainings. Even if the qualified persons are identified, the implementers are finding it difficult to avail their services as per the training calendar, as many capacity building trainings happens simultaneously, and moreover many of them are also full time employed in some other organization. The cost-opportunity paid to trainer as per the NACO guidelines is not competitive; hence resource persons prefer engaging in other work.[13]
Regular updating of trainers’ skills and knowledge is important for ensuring the effectiveness of capacity building programs. However, due to busy schedule, often trainers do not attain the training of trainers for update, which may affect quality of the training conducted by them. Recently there is an effort by SACS and NACO to engage the community members as trainers, especially for training of peer educators as they can better understand the issues or ground realities while implementing programs. However, before utilizing services of community members, it must be endured that they are properly trained in content as well as in the delivery of training. The training conducted by community members must be rigorously monitored and appropriately documented to measure its impact.
While designing and implementing capacity building initiatives, planners must consider the implementing partners’ and training organization /institutes time lines. Conducting majority of programs towards the end of financial year may adversely affect the quality of trainings and may hamper the performance of the implementing organizations. Such practice needs to be avoided by preparing the training calendar in
advance and judiciously following it. Very often the core thematic areas also overlap in different training programs, the capacity building program planners must take these issues into consideration while planning and scheduling to avoid repetition. The follow-up training programs or refresher training should be appropriately placed and the schedule or curriculum should be need based.
With regards to documentation of capacity building process, other than routine quantitative output reporting, organizations undertaking such program should maintain process documentation of entire program. This will be useful in evaluation of the program, particularly evaluating the long term impact of the program.[13-15] At SACS level, management information system should be able to maintain and analyze data on the status of trainings provided and the training needs of all staff in state. Respective SACS as well as at NACO level there should be comprehensive database of trainers, resources, number trained, number needs to be trained. Currently this information is available in piecemeal and moreover, information of capacity building programs or trainings undertaken by organizations other than NACO, are very difficult to retrieve.
The capacity building programs must be an ongoing process to ensure the effective transfer of learning and application of the knowledge and skills acquired at their workplaces and also to explore new areas / issues at workplace that needs to be addressed in future programs. The organizers implementing the capacity building programs were trying to ensure this by following the typical process of basic training, refresher and supportive supervision. The general comment was that the capacity building initiatives actually enhance the performance of staff in HIV/AIDS program, however there no evidence to document that training were responsible for better outcome.[16,17] Monitoring and evaluation of capacity building initiatives/training programs was a very weak link in India’s HIV/AIDS capacity building initiatives. What is needed is to undertake a comprehensive assessment of impact of capacity building over the short, medium and long terms as discussed in Logic Model for M and E of Human Resource Capacity Building Initiatives in Table 4. Furthermore, to rigorously monitor and evaluate capacity building programs there is a need for common standardized outcome indicators. Currently most of the human resource capacity building programs for HIV/AIDS in India undertakes assessment of immediate reaction of participants about program and learning that occurred in trainings.[18] However the medium term and short term impact and its cost effectiveness of capacity building program are scarcely studied.

Sharma, et al.: HIV/AIDS capacity building in India
40 Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 140
Efforts for operational research, dissemination and documentation of success stories are infrequently undertaken, and if done, they are not easily available in public domain. Even if they are available, they are not comprehensive, and tend to focus on the work of a single proj ect, organization, or donor. There is a scope for developing virtual or physical libraries for this purpose. This impedes the establishment of best practices and presents a particular challenge to establishing capacity building as a proven means of improving outcome of health organizations and sys tems. Conducting system-atic research and publishing the findings will provide evidences to donors, local implementing organiza-tions, and capacity building providers for better implementation of capacity build ing programs.[19] Less priority on the agenda of donor / funder for monitoring and evaluation or research related to capacity building could be the reason for this.
Whatever research evidence related to capacity building is available; the implementing institutions/organizations must utilize these findings in the planning and developing new initiatives along with the findings of the needs assessment, as discussed above. Bridging this gap between research and practice requires a commitment to evidence-based decision-mak ing and systematic incorporation of promising practices. Evidence-based decision-making is also essential in higher level decisions such as funding, strategic planning, and policy therefore; implementing organizations should facilitate the pro cess by providing data or evidence.
A knowledge exchange network is clearly needed to maximize the impact of capacity building program at the country level. Identification, setting up and networking of training institutions and master trainers is essential at the state as well as national level for sharing best practices and learning from others
experiences. To facilitate experience sharing, review meetings are successfully tried by some organizations. NACO and SACS need to develop a district or national-level database of regional resources and consultants to facilitate this process. NACO should have a comprehensive list of the resources, TOT, trainers and trained staff. SACS can also maintain the directory at their respective states.
Innovations in capacity building initiatives are rare. Traditionally the programs are offered in workshop or classroom training mode with a component of site visit or supportive supervision. NACO or academic institutes running capacity building programs should develop interactive website (web based learning or e-learning). Online courses can also be offered through such website. Material and resources (books, journal articles, case studies, success stories etc) should be periodically added to the web after validation by technical experts. Training institutions or organizations must have basic infrastructure that can help individuals to communicate and network.
Sustainability of capacity building programs is a key component of all HIV/AIDS programs. Increasing sustainability in capac ity building can be viewed as a process for sustaining desired changes brought about even after the end of the project. This can be ensured by enhancing the implementing institute’s or organizations’ ability to use skills to evaluate their own performance and generate innovation and using them over time in capacity building programs. Therefore, to create the lasting impact, strategies for long term sustainability are critical aspect of any capacity building program.[19] However, the currently capacity building programs do not address this issues adequately. Capacity building program implementers and organizations must advocate and develop efforts for sustaining change after capacity building ends.
Table 4: Logic Model for M & E of Human Resource Capacity Building Initiatives
Strategy Output Outcome Medium term outcome
Long term outcome / Impact
Technical knowledge and skill building - Prevention (for TI NGOs, Palliative care, Counseling, OVC, Clinical care, PPTCT, STI, Laboratory (PPTCT)
Training program conductedIndividuals / stakeholders trained
Improved technical and management skills
Improved technical and management effectiveness Improve capacity to plan and implement the program
Increased reach of program/ more access to services
Improve service delivery and quality of care
Management and leadership skill building – leadership, supply chain management, Policy (HIV), financing
Improved HIV education, knowledge, skills
Overall impact -Better response to HIV/AIDS in India
Approach Implementation evaluation, process evaluation includes – input analysis and output analysis
Outcome monitoring, outcome evaluation
Summative evaluationIndicator assessment (against set quantitative indicators)Cost effectiveness assessment Cost benefit assessment

Sharma, et al.: HIV/AIDS capacity building in India
41Annals of Tropical Medicine and Public Health | Jan-Feb 2013 | Vol 6 | Issue 1
The limitation of this paper is that it only talks about human resource capacity building initiatives and do not address organizational and programmatic capacity building initiatives. The other two aspects of capacity building are equally important for sustainable response to HIV/AIDS epidemic in the country. Leadership at national, state and local level; finances; commitment and infrastructure of organizations delivering capacity building programs are critical to deliver the quality. Further studies are needed to understand these concerns in India’s HIV/AIDS capacity building initiatives.
Conclusion
Human resource capacity building plays a central role in the effective implementation of HIV/AIDS programs and therefore better response to prevention and control of HIV/AIDS in India. NACP III program guidelines of India have done well by recognizing capacity building as an important objective, rather than just a process. This paper would provide an understanding of the current status of capacity building initiatives in India. We have identified certain challenges, particularly related monitoring and evaluation that need to be addressed. Moreover these challenges can be viewed as potential areas for operational research.
References
1. Annual report 2009-10. Department of AIDS control. Ministry of Health and family Welfare. Available from: http://www.nacoonline.org/upload/AR%202009-10/NACO_AR_English%20corrected.pdf
2. To halt and reverse the HIV epidemic in India. NACP III. NACO, New Delhi. Available from: http://www.nacoonline.org/upload/Publication/IEC%20and%20Mainstreaming/NACP%20III%20-%20To%20Halt%20and%20Reverse%20the%20HIV%20Epidemic%20in%20India.pdf [Last accessed on 2012 May 8].
3. Summation. National Health Policy, 2002. Available from: http://mohfw.nic.in/np2002.htm. [Last accessed on 2012 May 8].
4. Human Resource Development: Building Capacity. Chapter 12. Avaliable from: http://www.ngogateway.org/.../12%20Human%20Resource%20Development.doc. [Last accessed on 2012 May 8].
5. HIV/AIDS Capacity Building Survey. An analysis of 72 capacity building initiatives world-wide. Community Reach Program, Washington Nov 2009. USAID and PACT. Available from: http://www.pactworld.org/galleries/resource-center/FINAL%20Report%20-%20Community%20Reach%20Survey.pdf. [Last accessed on 2012 May 8].
6. Training of healthcare workers in HIV/AIDS counselling. Annex-XIX. Comptroller and Auditor General of India. http://www.cag.gov.in/html/reports/reports/civil/2004_3/annex19.htm and http://www.cag.gov.in/html/reports/reports/civil/2004_3/annex21.htm [Last accessed on 2012 May 8].
7. Training of doctors/nurses/technicians/field officers. Annex-XXI. Available from: http://www.cag.gov.in/html/reports/reports/civil/2004_3/annex21.htm). [Last accessed on 2012 May 8].
8. Prassana Kumar N. The National AIDS Control Program. Info Change News and Features, March 2008. Available from: http://www.hivaidsonline.in/index.php/Response/the-national-aids-control-programme-1-2-3.html and www.nacoonline.org [Last accessed on 2012 May 8]
9. Draft report on Independent Evaluation of National AIDS Control Programme. Available from: http://www.nacoonline.org/upload/Finance/Draft%20Report%20on%20Independent%20Evaluation%20of%20NACP.pdf [Last accessed on 2012 May 8]
10. Building a training program. Availablew from: http://www.go2itech.org/HTML/TT06/toolkit/curricula/print/BuildingaTraining%20Program.pdf [Last accessed on 2012 May 8].
11. STRC evaluation Reports 2009-10. Availbale from: http://www.nacoonline.org/Divisions/NGO__Targeted_Interventions2/CapacityBuilding/State_Training_Resource_Centre/STRC_Evaluation_Reports_2009-10/ [Last accessed on 2012 May 8].
12. STRC CORT Evaluation Report. Conducted by PRAXIS, New Delhi. Available from: http://nacoonline.org/upload/NGO%20and%20Targeted/Capacity%20Building/Evaluation%20Reports%202009-10/STRC%20Gujarat%20and%20DandD.pdf. [Last accessed on 2012 May 8].
13. NACO evaluation of STRC Kerala and Lakshadweep 2009. Conducted by PRAXIS, New Delhi. Available from: http://nacoonline.org/upload/NGO%20and%20Targeted/Capacity%20Building/Evaluation%20Reports%202009-10/STRC%20KL%20and%20LD%20.pdf [Last accessed on 2012 May 8].
14. STRC Gandhigram evaluation report 2009. Conducted by PRAXIS, New Delhi. Available from: http://nacoonline.org/upload/NGO%20and%20Targeted/Capacity%20Building/Evaluation%20Reports%202009-10/STRC%20Tamil%20Nadu.pdf [Last accessed on 2012 May 8].
15. STRC Birds Evaluation report 2009. Conducted by PRAXIS, New Delhi. Available from: http://nacoonline.org/upload/NGO%20and%20Targeted/Capacity%20Building/Evaluation%20Reports%202009-10/STRC%20Karnataka.pdf [Last accessed on 2012 May 8].
16. Calderon RM, Amon J, Kotellos K, Benazerga WG, Markowicz ML. The HIV/AIDS Prevention and Control SYNOPSIS Series. Published by the Latin America and Caribbean Regional Office of The AIDS Control and Prevention (AIDSCAP) Project, Family Health International. Available from: http://www.fhi.org/NR/Shared/enFHI/PrinterFriendly.asp. [Last accessed on 1997 Dec].
17. Framework for training. Available from: http://www.go2itech.org/what-we-do/health-workforce-development/framework-for-training/i-techs-framework-for-training [Last accessed on 2012 May 8].
18. Report of evaluation of STRC 2009. Conducted by PRAXIS, New Delhi. Available from: http://www.nacoonline.org/Divisions/NGO__Targeted_Interventions2/CapacityBuilding/State_Training_Resource_Centre/STRC_Evaluation_Reports_2009-10/. [Last accessed on 2010 Dec 10].
19. Challenges Encountered in Capacity Building: Review of Literature and Selected Tools. Position paper – Management Sciences for Health No 10 April 2010. Available from: http://www.reliefweb.int/rw/lib.nsf/db900sid/MINE86XSPR/$file/msh_apr2010.pdf?openelement [Last accessed on 2012 May 8].
Cite this article as: Sharma K, Zodpey S, Quazi SZ, Gaidhane A, Sawleshwarkar S, Khaparde S. Mapping and opportunities of human resource capacity building initiatives for HIV/AIDS in India. Ann Trop Med Public Health 2013;6:30-41.
Source of Support: Nil, Conflict of Interest: Nil.
Copyright of Annals of Tropical Medicine & Public Health is the property of MedknowPublications & Media Pvt. Ltd. and its content may not be copied or emailed to multiple sitesor posted to a listserv without the copyright holder's express written permission. However,users may print, download, or email articles for individual use.