Manufacturing and placing a bespoke support for the Marfan aortic root: description of the method...
6
ARTICLE IN PRESS www.icvts.org doi:10.1510/icvts.2009.220319 Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365 2010 Published by European Association for Cardio-Thoracic Surgery Institutional report - Vascular thoracic Manufacturing and placing a bespoke support for the Marfan aortic root: description of the method and technical results and status at one year for the first ten patients John Pepper, Tal Golesworthy, Martin Utley, John Chan, Skandadas Ganeshalingam, Michael Lamperth, Raad Mohiaddin, Tom Treasure* Royal Brompton Hospital, London SW3 6NP, UK Received 27 August 2009; received in revised form 18 November 2009; accepted 20 November 2009 Abstract Fatal aortic dissection commonly occurs in Marfan syndrome. Prevention currently relies on elective replacement of the aortic root. We are evaluating the placement of a manufactured, bespoke external support derived from a computer aided design in a prospective study. In the first ten patients, measurements were made consistently of the ascending aorta at the level of closure of the aortic valve cusps from magnetic resonance imaging (MRI) studies taken preoperatively and at fixed intervals thereafter. Before and after images were presented for measurement amongst duplicate images of 37 unoperated Marfan patients to permit assessment of intra-observer measurement reproducibility. All images were presented in random sequence to a radiologist unaware of the research question. The largest difference between the preoperative measurement and that made at least one year after surgery was determined. All patients had surgery as planned without complications and were alive at one year. In eight of the ten patients, the largest observed change was a marked reduction in aortic root diameter. The primary objective of this surgery was achieved in each case, reinforcing the ascending aorta whilst leaving the native aortic valve intact and conserving the bloodyendothelium interface. 2010 Published by European Association for Cardio-Thoracic Surgery. All rights reserved. Keywords: Marfan; Aorta; Aortic root; Computer aided design 1. Introduction Dissection of the ascending aorta is a characteristic man- ifestation of Marfan syndrome and is the commonest cause of death, killing as many as 70%, often in their twenties or thirties. The strongest predictors of likelihood of dissection are aortic root dimension and its rate of change w1–3x. Currently, prevention relies on replacing the ascending aorta before it dissects and ruptures. If a mechanical valve is incorporated the patient is committed to life-long anti- coagulation. Valve sparing operations have been devised and iteratively modified w4, 5x but these remain exacting to perform and prone to failure. Bioprosthetic replacement is a less technically exacting means of reducing thromboem- bolic risk but at the price of likely eventual valve failure with the need for reoperation. These options have recently been reviewed w6x. The development of a bespoke external aortic root support (EARS) using imaging and computer aided design to fit the individual patient’s ascending aorta has been achieved w7, 8x (Fig. 1), and here we report a prospective technical evaluation of the method and results at or beyond one year in the first ten patients. *Corresponding author. Clinical Operational Research Unit, UCL (Depart- ment of Mathematics), 4 Taviton Street, London WC1H 0BT, UK. Tel.: q44 79 57 16 87 54; fax q44 20 78 13 28 14. E-mail address: [email protected] (T. Treasure). 2. Materials and methods 2.1. Production of the bespoke external support Aortic root imaging: Magnetic resonance imaging (MRI) was used to avoid the radiation hazard of repeated com- puted tomography in the course of evaluation. In addition to standard views, images were collected to form the basis of the manufacturing process for the external support (EARS) using half Fourier single shot spin-echo sequence (typical imaging parameters, echo time: 1.3 ms, pixel size: 1.5 mm=2.0 mm, slice thickness 5–6 mm). A transaxial imaging plane was set up adjusted to a pseudo-transaxial position perpendicular to the patient’s ascending aorta. A set of contiguous image slices were then obtained from the left ventricular outflow to the aortic arch. A pseudo-sagittal imaging plane was set to lie parallel to the ascending aorta (Fig. 2). All images were ECG-gated to late diastole and acquired during a breath-hold. These images were obtained in a dedicated cardiovascular MRI unit at Royal Brompton Hospital by a single senior investigator (R.M.). EARS manufacture: For each patient, these images and the measurements illustrated in Fig. 2 were processed using a dedicated computer aided design routine to produce a 3D reconstruction of the patient’s aorta from the aorto ventricular junction to beyond the brachiocephalic artery using state of the art software further developed (M.L.)
Transcript of Manufacturing and placing a bespoke support for the Marfan aortic root: description of the method...

ARTICLE IN PRESS
www.icvts.org
doi:10.1510/icvts.2009.220319
Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
� 2010 Published by European Association for Cardio-Thoracic Surgery
Institutional report - Vascular thoracic
Manufacturing and placing a bespoke support for the Marfan aorticroot: description of the method and technical results and status at
one year for the first ten patientsJohn Pepper, Tal Golesworthy, Martin Utley, John Chan, Skandadas Ganeshalingam, Michael Lamperth,
Raad Mohiaddin, Tom Treasure*
Royal Brompton Hospital, London SW3 6NP, UK
Received 27 August 2009; received in revised form 18 November 2009; accepted 20 November 2009
Abstract
Fatal aortic dissection commonly occurs in Marfan syndrome. Prevention currently relies on elective replacement of the aortic root. Weare evaluating the placement of a manufactured, bespoke external support derived from a computer aided design in a prospective study.In the first ten patients, measurements were made consistently of the ascending aorta at the level of closure of the aortic valve cuspsfrom magnetic resonance imaging (MRI) studies taken preoperatively and at fixed intervals thereafter. Before and after images werepresented for measurement amongst duplicate images of 37 unoperated Marfan patients to permit assessment of intra-observer measurementreproducibility. All images were presented in random sequence to a radiologist unaware of the research question. The largest differencebetween the preoperative measurement and that made at least one year after surgery was determined. All patients had surgery as plannedwithout complications and were alive at one year. In eight of the ten patients, the largest observed change was a marked reduction inaortic root diameter. The primary objective of this surgery was achieved in each case, reinforcing the ascending aorta whilst leaving thenative aortic valve intact and conserving the bloodyendothelium interface.� 2010 Published by European Association for Cardio-Thoracic Surgery. All rights reserved.
Keywords: Marfan; Aorta; Aortic root; Computer aided design
1. Introduction
Dissection of the ascending aorta is a characteristic man-ifestation of Marfan syndrome and is the commonest causeof death, killing as many as 70%, often in their twenties orthirties. The strongest predictors of likelihood of dissectionare aortic root dimension and its rate of change w1–3x.Currently, prevention relies on replacing the ascendingaorta before it dissects and ruptures. If a mechanical valveis incorporated the patient is committed to life-long anti-coagulation. Valve sparing operations have been devisedand iteratively modified w4, 5x but these remain exactingto perform and prone to failure. Bioprosthetic replacementis a less technically exacting means of reducing thromboem-bolic risk but at the price of likely eventual valve failurewith the need for reoperation. These options have recentlybeen reviewed w6x. The development of a bespoke externalaortic root support (EARS) using imaging and computeraided design to fit the individual patient’s ascending aortahas been achieved w7, 8x (Fig. 1), and here we report aprospective technical evaluation of the method and resultsat or beyond one year in the first ten patients.
*Corresponding author. Clinical Operational Research Unit, UCL (Depart-ment of Mathematics), 4 Taviton Street, London WC1H 0BT, UK. Tel.: q4479 57 16 87 54; fax q44 20 78 13 28 14.
E-mail address: [email protected] (T. Treasure).
2. Materials and methods
2.1. Production of the bespoke external support
Aortic root imaging: Magnetic resonance imaging (MRI)was used to avoid the radiation hazard of repeated com-puted tomography in the course of evaluation. In additionto standard views, images were collected to form the basisof the manufacturing process for the external support(EARS) using half Fourier single shot spin-echo sequence(typical imaging parameters, echo time: 1.3 ms, pixel size:1.5 mm=2.0 mm, slice thickness 5–6 mm). A transaxialimaging plane was set up adjusted to a pseudo-transaxialposition perpendicular to the patient’s ascending aorta. Aset of contiguous image slices were then obtained from theleft ventricular outflow to the aortic arch. A pseudo-sagittalimaging plane was set to lie parallel to the ascending aorta(Fig. 2). All images were ECG-gated to late diastole andacquired during a breath-hold. These images were obtainedin a dedicated cardiovascular MRI unit at Royal BromptonHospital by a single senior investigator (R.M.).
EARS manufacture: For each patient, these images andthe measurements illustrated in Fig. 2 were processed usinga dedicated computer aided design routine to produce a3D reconstruction of the patient’s aorta from the aortoventricular junction to beyond the brachiocephalic arteryusing state of the art software further developed (M.L.)

ARTICLE IN PRESS
361J. Pepper et al. / Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
New
IdeasInstitutional
ReportW
orkin
ProgressReport
ESCVSArticle
NegativeResults
State-of-the-artBest
EvidenceTopic
BriefCom
munication
CaseReport
Follow-up
PaperEditorial
ProtocolProposalfor
Bail-out
ProcedureN
omenclature
HistoricalPages
Fig. 1. Magnetic resonance images of the ascending aorta before and afterplacement of a bespoke external aortic root support (EARS) in the firstpatient w7x.
Fig. 3. The aortic model covered with the external aortic root support (EARS)made of a medical grade polymer mesh.
Fig. 2. An example of the imaging, some of the measurements, and the aorticmodel made by computer aided design and rapid prototyping.
for this purpose (Fig. 2 inset). The X, Y and Z coordinatesof the reconstructed aorta were exported to a rapid pro-totyping machine and a model of the patient’s aorta madein thermoplastic. This model was the former upon whichthe external support was manufactured from a medicalgrade polymer mesh (Fig. 3). The finished support, still onits manufacturing former, was then sterilised, packagedand sent to the surgeon with a vertical seam that can beopened by the surgeon to place the support around theaorta (Fig. 3).
2.2. Surgical methods
The study was approved by and conducted in accordancewith the requirements of the Royal Brompton HospitalResearch Ethics Committee. All patients were fullyinformed that this was innovative surgery and had adetailed discussion of the risks and benefits with theoperating surgeon (J.P.). Patients with aortic sinus diame-ters of 4–5 cm were considered; in our institution thethreshold diameter for advising root replacement is 5 cm.
The chest was opened through median sternotomy. Theaorta was completely dissected from the aorto-ventricularjunction to the origin of the brachiocephalic artery. Cardio-pulmonary bypass was available but only used in the firstoperation. The EARS was brought to the operating table onthe former, a model of the patient’s own aorta (Fig. 3).The longitudinal seam at the front was opened (Video 1)and the support placed around the aorta (Video 2). Notethat the material extends proximal to the coronary arteriesto the aorto-ventricular junction. It is engineered to havehigh hoop strength preventing ‘annular’ dilatation.
2.3. Assessment of change in aortic dimensions
Based on MRI studies, we sought to assess differences overtime in the dimensions of the aorta of each EARS patient.Additionally, we sought to put any differences observed inthe context of the intra-observer reproducibility of meas-urements made from similar MRI studies.
MRI studies were conducted on each EARS patient priorto operation and wherever possible at six months, 12months, and annually thereafter. In addition, we collateda set of MRI studies of other Marfan patients, undertakenat the Royal Brompton Hospital since 2004; we selected atrandom 40 patients and an MRI study of each.
An experienced reader (J.C.) selected from each MRIstudy an image that showed a cross-section of the aorta atthe level of closure of the aortic valve cusps. This ensuredthat the levels were comparable within each patient and

ARTICLE IN PRESS
362 J. Pepper et al. / Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
Video 1. The support has been removed from its former and as can be seenthe material is soft and porous. It is, however, very strong. The surgeon ispreparing the openings to allow it to surround the origin of the coronaryarteries.
Video 2. The support is in place and fits closely to the aorta and moveswith it.
Fig. 4. An MRI image at the level of the aortic valve closure with aortic diameters measured by the radiologist superposed along with the traced outline (left).Removal of the MRI image leaves the three diameters and the outline depiction of the image (centre). The image is reversed (right) to convert the orientationfrom the cross-sectional imaging convention (view from below) to the anatomical view (from above) w9x. MRI, magnetic resonance imaging.
at the same point in the cardiac cycle (diastole). An imagewas also selected of the aortic arch to show a maximumtransverse diameter at diastole because a frequent ques-tion is whether supporting the ascending aorta shifts thepoint of maximal stress to beyond the supported segment.Each image relating to a non-EARS patient was duplicatedto provide a means of assessing the reproducibility of themeasurements obtained from such images.
All the images were put in random order and presentedto a radiologist (S.G.) independent of the EARS researchteam and not informed of the research question. Fromeach cross-sectional image of the aorta, the distancebetween each of the three commissures and the furthestpoint in the opposite sinus of Valsalva was measured andrecorded, the marked image being saved. These aorticdiameters were identified separately by the named sinus:left, right, or non-coronary (Fig. 4). From each selectedimage of the aortic arch, a measurement was recorded ofthe diameter at its midpoint.
From each available MRI study of each EARS patient, adepiction of the anatomical view of the aorta at the level
of closure of the aortic valve cusps was produced, basedon the marked MRI images, by a non-clinically trainedmember of the research team (Fig. 4) (M.U.).
2.4. Analysis
A prospective plan for the analysis of MRI images wasadhered to. For each pair of duplicated images of theaortic root of non-EARS patients, we calculated the threedifferences between the paired measurements of the non-coronary, left-coronary, and the right-coronary diameters.We then plotted the difference of largest magnitude versusthe mean of the pair giving rise to this difference (Blandand Altman method w10, 11x).
Similarly, for each EARS patient we calculated the threedifferences between diameter measurements from themost recent MRI study and the corresponding measurementsfrom the preoperative study. We plotted the difference oflargest magnitude against the mean of the measurementsgiving rise to this difference, superposing these data pointsonto the Bland–Altman plot (Fig. 5). We prospectivelychose to present the largest difference to ensure that ourmethod was as sensitive as possible to aortic dilation,which would signify a technical failure of the externalsupport. An analogous plot was constructed using the aorticarch diameters measured.
A chart was constructed showing for each EARS patient adepiction of the cross-sectional image and measurementsfrom all MRI scans available for that patient.
3. Results
3.1. Surgical outcomes and operative details
The first ten patients underwent EARS between May 2004and March 2007; the operation was completed as plannedin all ten patients. Aortic valve function and coronary ostialflow were confirmed in each case by intraoperative echo-cardiography. Operative data on the first ten EARS patientsare presented in the Table 1. In none was there a need toabort the operation or convert to root replacement. All tenpatients have completed at least one-year follow-up; therehave been no deaths, late events or detected changes inaortic valve function.

ARTICLE IN PRESS
363J. Pepper et al. / Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
New
IdeasInstitutional
ReportW
orkin
ProgressReport
ESCVSArticle
NegativeResults
State-of-the-artBest
EvidenceTopic
BriefCom
munication
CaseReport
Follow-up
PaperEditorial
ProtocolProposalfor
Bail-out
ProcedureN
omenclature
HistoricalPages
Fig. 5. Open circles represent un-operated Marfan patients. From duplicatedMRI images of the aortic root diameter (see text for details) the largestdifference in an aortic root diameter is plotted against the mean of thepaired measurements to provide a backdrop of the intra-observer reproduc-ibility of such measurements (Bland and Altman w10, 11x). The solid red cir-cles represent the ten EARS patients. The largest difference between anaortic root diameter measured from the most recent MRI study and thatmeasured from the preoperative study is plotted against the mean of thetwo measurements. EARS, external aortic root support; MRI, magnetic res-onance imaging.
Fig. 6. Open circles represent un-operated Marfan patients. From duplicatedMRI images of their aortic arch, the difference between measurements ofthe arch diameter is plotted against the mean of the pair to provide someinformation on reproducibility. The solid red circles represent the ten EARSpatients. The difference between the diameter of the aortic arch measuredfrom the most recent MRI study and that measured from the preoperativestudy for is plotted against the mean of the two measurements. EARS, exter-nal aortic root support; MRI, magnetic resonance imaging.
Table 1Demographic and operative data for the first ten consecutive patients havingexternal aortic root support (EARS) surgery
Patient and operativecharacteristics
n 10Male:Female 6:4Median age (range) 31 (18–58)Median operation time in minutes (range) 150 (91–200)Bypass time in minutes (range) 0 (0–20*)Cross-clamp time in minutes (range) 0Deaths in-hospital 0Arrhythmia (transient atrial fibrillation) 2Median postoperative days in-hospital (range) 7 (4–16)
*First patient only.
3.2. Change in aortic dimensions
A suitable image at the level of closure of the aortic valvecusps could not be obtained in three of the 40 MRI studiesof non-EARS Marfan patients. The open circles in Fig. 5show the differences between measurements made of theremaining 37 pairs of identical images and give an indica-tion of the measurement error of the process by whichaortic diameters were measured; we estimate the accuracyof this measurement process as being "2 mm. Superposedfor each EARS patient is the largest difference betweenaortic diameter measurements made of the most recentMRI study and of the preoperative study (closed red cir-cles). For eight of the ten EARS patients, the largestobserved difference is a marked reduction in the diameterof the aortic root (Fig. 5).
Fig. 6 shows the corresponding data from MRI images ofthe aortic arch.
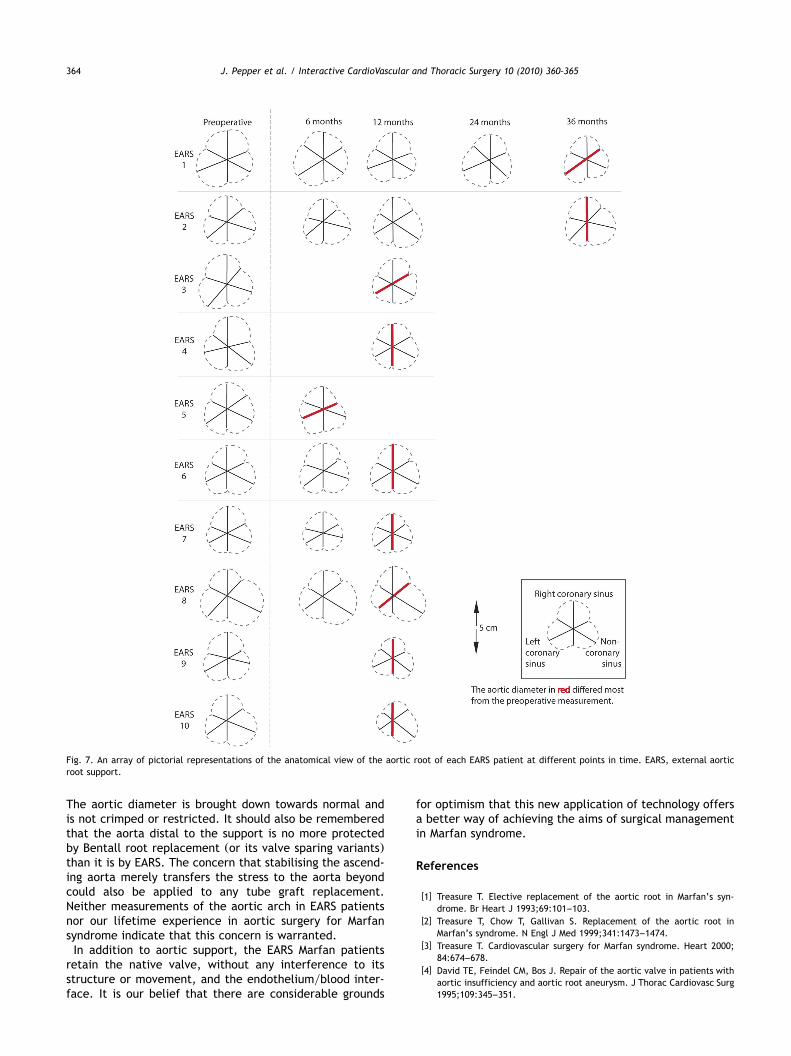
Fig. 7 shows the graphical depiction in anatomical viewof the cross-section of the aortic valve sinuses for MRIstudies of the first ten EARS patients.
4. Discussion
The purpose of aortic root surgery in Marfan syndrome isto pre-empt the risk of aortic dilatation and dissection thussaving the patient from aortic regurgitation and death dueto aortic dissection. A one-year technical study does notpermit us to comment on long-term effects and whetherthe objective of preventing dissection will be achieved.However, the technical objective of precise positioning ofa non-expansible external support has been consistentlyachieved in this prospective study. The material is of provendurability and far stronger than required to resist anybiological forces.
There is a limitation in the accuracy with which we canmeasure differences between any individual’s pre- andpostoperative aortic dimensions, using the MRI protocol inplace in 2004 for rapid as possible data collection duringfew breath holds. It is, however, adequate for a largestructure such as the ascending aorta. Furthermore, itshould be noted that the rigour and the completeness ofthe measurement protocol exceeds any comparable studyof which we are aware.
The external support surgery reported by Robicsek andThubrikar w12–14x is not technically comparable; operativephotographs show stiff graft material failing to match theaortic contours in contrast to the bespoke, intimatelyfitting, flexible support involved in the EARS operation.Furthermore, the material used in the EARS operation doesnot need to contain the blood and can be very flexible andhave macroscopic porosity (Fig. 3 and Video 1). We envisagethat this mesh will become intimately incorporated in theaortic adventitia, facilitating support and, potentially, theability to contain a limited dissection. We have not as yetbeen required to confirm this hypothesis at re-operation orautopsy but we cannot envisage the EARS presenting anobstacle to subsequent surgery; it may indeed facilitatesurgery.
In eight of ten patients, the aortic root dimension ismarkedly reduced from the preoperative measurement.
ARTICLE IN PRESS
364 J. Pepper et al. / Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
Fig. 7. An array of pictorial representations of the anatomical view of the aortic root of each EARS patient at different points in time. EARS, external aorticroot support.
The aortic diameter is brought down towards normal andis not crimped or restricted. It should also be rememberedthat the aorta distal to the support is no more protectedby Bentall root replacement (or its valve sparing variants)than it is by EARS. The concern that stabilising the ascend-ing aorta merely transfers the stress to the aorta beyondcould also be applied to any tube graft replacement.Neither measurements of the aortic arch in EARS patientsnor our lifetime experience in aortic surgery for Marfansyndrome indicate that this concern is warranted.
In addition to aortic support, the EARS Marfan patientsretain the native valve, without any interference to itsstructure or movement, and the endotheliumyblood inter-face. It is our belief that there are considerable grounds
for optimism that this new application of technology offersa better way of achieving the aims of surgical managementin Marfan syndrome.
References
w1x Treasure T. Elective replacement of the aortic root in Marfan’s syn-drome. Br Heart J 1993;69:101–103.
w2x Treasure T, Chow T, Gallivan S. Replacement of the aortic root inMarfan’s syndrome. N Engl J Med 1999;341:1473–1474.
w3x Treasure T. Cardiovascular surgery for Marfan syndrome. Heart 2000;84:674–678.
w4x David TE, Feindel CM, Bos J. Repair of the aortic valve in patients withaortic insufficiency and aortic root aneurysm. J Thorac Cardiovasc Surg1995;109:345–351.

ARTICLE IN PRESS
365J. Pepper et al. / Interactive CardioVascular and Thoracic Surgery 10 (2010) 360–365
New
IdeasInstitutional
ReportW
orkin
ProgressReport
ESCVSArticle
NegativeResults
State-of-the-artBest
EvidenceTopic
BriefCom
munication
CaseReport
Follow-up
PaperEditorial
ProtocolProposalfor
Bail-out
ProcedureN
omenclature
HistoricalPages
w5x Yacoub MH, Gehle P, Chandrasekaran V, Birks EJ, Child A, Radley-SmithR. Late results of a valve-preserving operation in patients with aneu-rysms of the ascending aorta and root. J Thorac Cardiovasc Surg 1998;115:1080–1090.
w6x Kirsch ME, Ooka T, Zannis K, Deux JF, Loisance DY. Bioprostheticreplacement of the ascending thoracic aorta: what are the options? EurJ Cardiothorac Surg 2009;35:77–82.
w7x Golesworthy T, Lamperth M, Mohiaddin R, Pepper J, Thornton W,Treasure T. The tailor of Gloucester: a jacket for the Marfan’s aorta.Lancet 2004;364:1582.
w8x Golesworthy T, Treasure T, Lamperth M, Pepper J. Reducing fear andthe risk of death in Marfan syndrome: a Chaucerian pilgrimage. Br JCardiol 2006;13:267–272.
w9x Treasure T, Gallivan S, Golesworthy T, Thornton W, Lamperth M,Mohiaddin R, Pepper J, Anderson RH. Unknown unknowns: the aortathrough the looking glass. Eur J Cardiothorac Surg 2009;35:925–926.
w10x Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986;1:307–310.
w11x Bland JM, Altman DG. Comparing methods of measurement: whyplotting difference against standard method is misleading. Lancet 1995;346:1085–1087.
w12x Robicsek F, Thubrikar MJ. Conservative operation in the managementof annular dilatation and ascending aortic aneurysm. Ann Thorac Surg1994;57:1672–1674.
w13x Robicsek F, Thubrikar MJ. Hemodynamic considerations regarding themechanism and prevention of aortic dissection. Ann Thorac Surg 1994;58:1247–1253.
w14x Robicsek F, Thubrikar M. The mechanism and prevention of aorticdissection in Marfan syndrome. In: Hetzer R, Gehke P, Ennker J, editors.Cardiovascular Aspects of Marfan Syndrome, Darmstadt: Steinkopff,1995.
eComment: Internal versus external aortic support
Author: Stefano Nazari, Fondazione Alexis Carrel, Via Marconi, Res Parco152, 20080 Basiglio, MI, Italy
doi:10.1510/icvts.2009.220319AThis paper w1x is very important as it finally provides the old, simple and
theoretically incontestable w2x principle of the aneurysm external wrappingwith a thorough and reproducible surgical solution, thus opening the way towider and systematic clinical application in the appropriate patients.
An important aspect of this paper, at least in my opinion, is the fact thatthe described technique is in line with the concept of aortic wall strength-ening, implicit in the mesh structure of the prosthesis used as well as in thename given to the repair (EARS – external aortic root support), rather thanfull prosthetic substitution, which is still the final aim of the standardtreatment for aneurysm.
Appreciation that strengthening rather than substitution is the repairtheoretically proportionate to the primary lesion to be treated (weakeningof the aortic wall) may offer new perspectives not only in external, as inthis Brompton Hospital and University College London report, but also andprobably mainly, in endovascular repair. Net prosthesis w3x, bespoke to theaortic tract to be reinforced, with a larger mesh (G5 mm w3x) and a structureideally shaped to be kept in contact with the aortic wall by the bloodstream itself, within 2–4 weeks is totally incorporated into the intima layerw3x, thus providing enough endovascular aortic wall strengthening to arrestaneurysm progression, without interferring with collateral branches circula-tion (see video and paper at: http://www.fondazionecarrel.org/carrel/vasc/files/aortic/aortic.htm). This will be obviously particularly useful in thoseaortic tracts where standard repair is mostly dangerous because of the verylow ischemic tolerance of tissues perfused by collateral branches (i.e. aorticarch and thoraco-abdominal tract of the aorta).
Marfan patients moreover may represent, for their very frequent aorticaneurysm development and progression, an ideal, first group of patientsthat could take advantage of early, prophylactic, endovascular net prosthesisreinforcement. Obviously, the expected advantage of endovascular netprosthesis repair cannot be extended ipso facto to the aortic valve, whichis efficiently provided, at least at one year w1x, by the whole ascendingaorta external wrapping described by the authors w1x.
References
w1x Pepper J, Golesworthy T, Utley M, Chan J, Ganeshalingam S, LamperthM, Mohiaddin R, Treasure T. Manufactoring and placing a bespokesupport for the Marfan aortic root: description of the method andtechnical results and status at one year for the first ten patients.Interact CardioVasc Thorac Surg 2010;10:360–365.
w2x Robicsek F, Thubrikar MJ. Hemodynamic considerations regarding themechanism and prevention of aortic dissection. Ann Thorac Surg 1994;58:1247–1253.
w3x Nazari S, Luzzana F, Carli F, Mourad Z, Salvi S, Guagliano A, Banfi C,Cinquini C. Aortic wall structural strenghtening by intraluminal netprosthesis to arrest aneurysm progression and to prevent dissection andrupture. Eur J Cardiothorac Surg 1996;10:264–272.