
Managing Chronic-Pain Patients in the New Millennium: Clinical Basis and Regulatory Viewpoint from...
25
© 2004 World Institute of Pain, 1530-7085/04/$15.00 Pain Practice, Volume 4, Issue 2, 2004 105–129 Blackwell Science, LtdOxford, UKPPRPain Practice1530-70852004 World Institute of Pain 42105129MiscellaneousManaging Chronic-Pain PatientsMEHENDALE et al. Address correspondence and reprint requests to: Anand W. Mehen- dale, Neurology, Addiction Medicine, Neurobiology Research Unit, Phoe- nix Medical Associates, 222 Sidney Baker South, Suite 500, Kerrville, TX 78028, U.S.A. E-mail: [email protected]. CLINICAL GUIDELINES Managing Chronic-Pain Patients in the New Millennium: Clinical Basis and Regulatory Viewpoint from Texas, U.S.A. Anand W. Mehendale, MD*; Donald Patrick, MD, JD † ; Mark Goldman, PhD ‡ *Neurology, Addiction Medicine, Neurobiology Research Unit, Phoenix Medical Associates, Kerrville, Texas; † Neurosurgery, Executive Director, Texas State Board of Medical Examiners, Austin, Texas; ‡ Neuropsychology, Neurobiology Research Unit, Phoenix Medical Associates, Kerrville, Texas, U.S.A. Abstract: Chronic pain is a very significant health care problem. It is estimated that 9% of the US adult population suffers from moderate to severe noncancer-related pain. It is very difficult to objectively and quantitatively measure a patient’s pain and response to treatment. This routinely results in under or overtreatment of pain in these patients. The authors’ goal is to provide physicians with practical rec- ommendations and guidelines for the treatment of the chronic-pain patient. This article also summarizes the neuro- biology of pain and contrasts acute vs. chronic pain, and it explores the complex interplay between the physical mani- festations of chronic pain and its emotional ramifications. In addition, this article offers clinician guidelines for the evalu- ation and treatment of chronic pain; treatment recommen- dations based on the current neurobiological understanding of pain; and numerous guidelines and position statements published by various physician associations, physician licens- ing boards, and local, state, and federal laws. A “Patient Pain Management Contract” and “Pain Treatment Functional Outcome Scale” are exhibited. Key Words: chronic pain, neurobiology, clinical guidelines MANAGING CHRONIC-PAIN PATIENTS IN THE NEW MILLENNIUM: A BALANCING ACT FOR PHYSICIANS Chronic pain is a very significant public health problem. Twenty-two percent primary care patients report pain. Eighty-three million adults in the United States state that pain affects their participation in some activities. A total of 4.5 million patients die in pain each year. Twenty-six percent of nursing home residents experience pain daily. One-third of chronic-pain patients reported that they received little or no relief from any past therapies. Twenty-eight percent believe that there is no solution to their pain. Less than half (42%) of pain patients believe that their physician completely understands how their pain makes them feel. 1–4 To complicate the matter further, chronic pain is a complex interaction between the individual and envi- ronment. As is the case in all chronic illnesses, it exerts a profound effect on the patient and their biological systems. The biological and psychological functions of the individual are intertwined and revealed through the patient’s quality of life. The concept of disease is more
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Managing Chronic-Pain Patients in the New Millennium: Clinical Basis and Regulatory Viewpoint from...
copy 2004 World Institute of Pain 1530-708504$1500Pain Practice Volume 4 Issue 2 2004 105ndash129
Blackwell Science LtdOxford UKPPRPain Practice1530-70852004 World Institute of Pain
4
2105129Miscellaneous
Managing Chronic-Pain PatientsMEHENDALE et al
Address correspondence and reprint requests to Anand W Mehen-dale Neurology Addiction Medicine Neurobiology Research Unit Phoe-nix Medical Associates 222 Sidney Baker South Suite 500 Kerrville TX78028 USA E-mail mehendaleneuroaolcom
CLINICAL GUIDELINES
Managing Chronic-Pain Patients in the New Millennium Clinical Basis
and Regulatory Viewpoint from
Texas USA
Anand W Mehendale MD Donald Patrick MD JD
dagger
Mark Goldman PhD
Dagger
Neurology Addiction Medicine Neurobiology Research Unit Phoenix Medical Associates Kerrville Texas
dagger
Neurosurgery Executive Director Texas State Board of Medical Examiners Austin Texas
Dagger
Neuropsychology Neurobiology Research Unit Phoenix Medical Associates Kerrville Texas USA
Abstract
Chronic pain is a very significant health careproblem It is estimated that 9 of the US adult populationsuffers from moderate to severe noncancer-related pain It isvery difficult to objectively and quantitatively measure apatientrsquos pain and response to treatment This routinelyresults in under or overtreatment of pain in these patientsThe authorsrsquo goal is to provide physicians with practical rec-ommendations and guidelines for the treatment of thechronic-pain patient This article also summarizes the neuro-biology of pain and contrasts acute vs chronic pain and itexplores the complex interplay between the physical mani-festations of chronic pain and its emotional ramifications Inaddition this article offers clinician guidelines for the evalu-ation and treatment of chronic pain treatment recommen-dations based on the current neurobiological understandingof pain and numerous guidelines and position statementspublished by various physician associations physician licens-ing boards and local state and federal laws A ldquoPatient PainManagement Contractrdquo and ldquoPain Treatment FunctionalOutcome Scalerdquo are exhibited
Key Words
chronic pain neurobiology clinicalguidelines
MANAGING CHRONIC-PAIN PATIENTS IN THE NEW MILLENNIUM A BALANCING ACT
FOR PHYSICIANS
Chronic pain is a very significant public health problemTwenty-two percent primary care patients report painEighty-three million adults in the United States state thatpain affects their participation in some activities A totalof 45 million patients die in pain each year Twenty-sixpercent of nursing home residents experience pain dailyOne-third of chronic-pain patients reported that theyreceived little or no relief from any past therapiesTwenty-eight percent believe that there is no solution totheir pain Less than half (42) of pain patients believethat their physician completely understands how theirpain makes them feel
1ndash4
To complicate the matter further chronic pain is acomplex interaction between the individual and envi-ronment As is the case in all chronic illnesses it exertsa profound effect on the patient and their biologicalsystems The biological and psychological functions ofthe individual are intertwined and revealed through thepatientrsquos quality of life The concept of disease is more
106 bull
mehendale et al
complex than it may seem Disease is both a naturalcategory and a social construction Medical anthropol-ogy distinguishes between three realities under thedifferent words defining ldquodiseaserdquo biological abnormal-ities (disease) subjective experience of altered physicalstate (illness) and the process of socialization of patho-logical episodes (sickness) The constructivist perspec-tive of the sociology of science shows that scientificknowledge reflects cultural beliefs and social values Adiagnosis is ldquoconstructedrdquo through the interactionbetween patients physicians and their respective repre-sentations of disease in a given scientific historical andsocial context
5
There is no better example of this thanin chronic painful conditions To complicate the matterfurther it is very difficult to objectively and quantita-tively measure a patientrsquos pain and response to treat-ment The physician must to a large extent rely on apatientrsquos report about the severity of pain A clever drug-addicted patient may wander from one physicianrsquos officeto the next complaining of pain It is only after thoroughassessment that a comprehensive treatment plan can beinitiated Recently a physician in Florida was convictedon manslaughter charges for prescribing long actingoxycodone (Oxycontin
reg
) At the same time an articleby Melanie R Margolis in the
New York Times
madea case against physicians that they are undertreatingchronic-pain patients The Joint Commission of Accred-itation of Healthcare Organizations (JCAHO) has sug-gested that pain should be considered as the fifth vitalsign and treated aggressively
While there are so-called ldquoOpiate Millsrdquo (wherepatients line up early in the morning to obtain prescrip-tions for opioids) operated by very few unscrupulousphysicians most physicians are highly ethical and areasking for a unified policy on how to treat pain patientsSuch unified guidelines will remove opiate-phobia andwould benefit both patients and physicians
The goal of our article is to review neurobiology painand offer practical recommendations and guidelines forthe treatment of the chronic-pain patients These recom-mendations flow from basic science research on painand incorporate guidelines and position statements pub-lished by various physician associations physicianlicensing boards local state and federal laws
NEUROBIOLOGY OF PAIN
Chronic pain is difficult to measure and precisely defineThere is no clear demarcation to indicate when acutepain becomes chronic However continuous pain3 months after there is no more healing of the patho-
logical process should be considered chronic pain Gen-erally acute pain is the nociceptive type except in veryrare circumstances when it is neuropathic (eg thalamicpain of DejerinendashRoussy Syndrome) chronic pain iseither purely neuropathic or mixed (see below)
Neuroanatomy of Pain Pathways
As outlined in Catalano et al
6
the spinothalamic tractis responsible for sending pain information to the brainThis process may occur at different rates of speed andresult in different sensations Large diameter A-betanerve fibers generally not involved in nociception arepresumed to transmit a sensation occasionally referredto as prepain Smaller diameter A-delta fiber and C-fibernerve transmission occurs at a slower rate of speed A-delta fiber pain is felt to be ldquosharp and stabbingrdquo whileC-fiber pain is ldquodull burning cramping and achingrdquo
Rapid pain travels along the neospinothalamic path-way to the thalamus and cortex Chronic pain proceedsalong the paleospinothalamic pathway finding its wayto the hypothalamus and limbic system The limbicstructures (ie amygdala and hippocampus) are inti-mately involved in the processing of the emotional com-ponent of chronic pain and establishing memories ofpain In addition an ldquoemotional signaturerdquo is assignedto the pain experience This results in significant anxietyandor depression as invariable accompaniments inchronic pain syndrome which must be treated aggres-sively to produce effective pain relief Under such con-ditions there is an increase in corticotrophin-releasingfactor (CRH) resulting in adrenocorticotrophic hor-mone (ACTH) secretion from the pituitary gland andcortisol from the adrenal gland These so-called ldquostresshormonesrdquo in chronic states have widespread deleteri-ous effects such as the suppression of the immune sys-tem and a decrease in brain-derived neurotrophic factor(BDNF) There is some evidence that this may result inatrophy of the neurons It is therefore very importantto treat aggressively these clinical accompaniments ofanxiety and depression
7
Types of Pain
Acute Pain (Nociceptive Somatic or Visceral)
Patients and their physicians are familiar with acutepain or pain caused by injury The term ldquonociceptivepainrdquo is applied when pain is perceived to be commen-surate with tissue damage associated with an identifiablesomatic or visceral lesion The pain is presumed to berelated to ongoing activation of primary afferentneurons responsive to noxious stimuli (nociceptors)
Managing Chronic-Pain Patients
bull 107
Researchers have long since appreciated that in thepresence of injury nociceptors may become hyperexcit-able A change in the expression of ion channels is onemechanism that may contribute to this hyperexcitabil-ity Data indicate that sodium channel expression indorsal root ganglion neurons is dynamic changingmarkedly after tissue or nerve injury
8
Importantly dif-ferent forms of injury induce different changes in theexpression of sodium channels For example nerveinjury in the form of axotomy results in a decrease inthe expression of tetrodotoxin (TTX)-resistant currentsand an increase in a rapidly reprinting TTX-sensitivesodium current In contrast inflammation results in anincrease in the expression of TTX-resistant sodium cur-rents and a decrease in the expression of a TTX-sensitivecurrent Utilizing a different nerve injury model in com-bination with antisense oligodeoxynucleotides researchindicates that a TTX-resistant sodium channel calledSNSPN3 is critical for the initiation and maintenanceof nerve injury-induced hyperalgesia and allodynia
9
Incontrast the recently identified NaN another TTX-resistant sodium channel does not appear to contributeto the maintenance of nerve injury-induced changes innociceptive thresholds
10
Research on the role of theTTX-resistant sodium currents in inflammation indi-cates that the currents are modulated by inflammatorymediators such as prostaglandin EZ 5-HT and adenos-ine consistent with their role in peripheral sensitiza-tion
11
There are additional data indicating that TTX-resistant channels are not only present and functionalin the peripheral terminals of nociceptors but that mod-ulation of these channels contributes to prostaglandin-induced mechanical hyperalgesia The role of otherchannels such as calcium-dependent potassium cur-rents in controlling the excitability of vagal afferents isbeing investigated
12
In the future it may be possible toassess the relative contribution of various sources ofcalcium responsible for the gating of the potassiumcurrents
Nociceptive pain that originates from somatic struc-tures (also known as somatic pain) is typically welllocalized and described as sharp aching throbbing orpressure-like Pain originating from viscera (visceralpain) is often more diffuse and described as gnawing orcramping when due to obstruction of a hollow viscusand aching sharp or throbbing when due to involve-ment of organ capsules or other mesentery Injury leadsto local inflammation Pain signals are sent to the brainThe brain in turn signals the muscles causing a reflexmuscle spasm The muscle spasm protects the injured
area The tightening of the muscles forms a natural castaround the injury and the negative sensation of painpromotes learning how to avoid similar injury in thefuture As tissues heal inflammation resolves and thecentral nervous system sends out fewer signals resultingin decreased pain and decreased muscle spasm Cellularneurobiology of this type of pain is better understoodalthough more work needs to be done on molecularneurobiology of acute pain
The injury is generally self-limiting and healingoccurs over a predictable time frame This pain respondsvery well to opioids and because there is a finite end-point to treatment most physicians are not concernedabout prescribing highly reinforcing opioids for a shortperiod of time
Chronic Pain (Neuropathic Pain Neuropathic CentralPain)
Compared to acute pain less is known about theneurobiology of chronic pain Chronic pain often occursin the absence of ongoing illness or after healing iscompleted A fundamental difference between inflam-matory pain with tissue hypersensitivity and neuro-pathic pain is that in the former the pain is relievedwhen inflammation has resolved while in the latter itmay persist after healing of the primary event Theepidemiology of central pain following stroke or spinalcord injurymdashor during the course of multiple sclerosisbrain injury or trauma to the central nervous systemmdashis much better understood than that following periph-eral nociceptive injury
13
Approximately 1 to 8 ofpatients with stroke have central pain whereas 10 to30 of patients with spinal cord injury are affected bypain during the course of their illness
14
There are nodata on the number of patients who have nociceptiveperipheral pain from small fiber neuropathies radi-culopathies brachial or lumbosacral plexopathiescomplex regional pain syndrome or inflammatoryperipheral conditions However because of the commonnature of the underlying causes there may be manypatients who have this problem
The major clinical features of neuropathic centralpain are
1 Hypersensitivity at the site of injury2 Mechanoallodynia3 Thermal hyperalgesia
15
4 Hyperpathia
16
5 Extraterritoriality (regional distribution of pain)in the case of complex regional pain syndromereflex sympathetic dystrophy
17
108 bull
mehendale et al
6 Associated neurogenic inflammation autonomicdysregulation and motor phenomena that areespecially found in complex regional pain syn-dromereflex sympathetic dystrophy
18
Central sensitization is the pivotal physiologic phe-nomenon underlying the clinical symptoms of neuro-pathic central pain following peripheral nerve injury
19
Central sensitization is primarily induced by the firingof unmyelinated nociceptive C-fibers that project tothe superficial layers of the dorsal horn (DH)
20
Thesefibers produce slow excitatory postsynaptic potentialsthat may last for up to 20 seconds Brief repetitiveafferent nociceptive fiber input causes temporal sum-mation of these slow potentials which induces theldquowinduprdquo phenomenon in central pain-projecting neu-rons (CPPNs) In this state subsequent C-fiber inputproduces a progressive increase in action potentialoutput of CPPNs The gain of this neuronal responseis controlled by an activity-dependent N-methyl-D-aspartate (NMDA) receptor
21
Additionally injury toaxons of C-fibers induces sprouting of A-beta termi-nals from Rexed laminae III and IV to lamina II Thisrewiring may be responsible for the allodynic stateseen in chronic neuropathic pain states
22
There aregamma amino butyric acid (GABA)-A receptor ligand-gated chloride channels that hyperpolarize dorsal hornneurons and reduce neuronal responses to peripheralactivation This results in a decrease in the transmis-sion in the CPPNs This may be the basis of a salutaryeffect of GABAergic drugs in chronic pain Opioidreceptors are also found on the terminals of primaryafferent nociceptive fibers that enter the spinal cordOpioids block the potassium-evoked release of Sub-stance P and enhance the inhibition at dorsal rootganglia (DRG) Therefore opioids can have role intreatment of neuropathic pain
The major mechanisms that underlie nociceptive cen-tral pain are
1 Autosensitization of nociceptive receptors2 Ectopic firing of DRG cells3 Calcium-induced molecular cascades from excess
nociceptor glutamate4 Phenotypic change of afferent A-beta fibers and
DRG cells to the characteristics of those associ-ated with pain
5 Changes in gene expression of sodium channelsand neuropeptides both at nociceptive terminalsand at the DRG
6 Anatomic changes of the superficial layers of theDH This is a progressive but plastic process thatis clearly reversible in its early stages and requiresnociceptive input for its maintenance
Additionally mental stress may ldquoprimerdquo the centralnervous system for development of neural plasticity andwindup
23
In fact so-called ldquowinduprdquo and neural plas-ticity or central sensitization have distinct neurobiolog-ical substrates
24
Windup occurs when a peripheral nerveis stimulated at sufficient intensity to activate C-fibersrepetition of the fixed stimulus at low frequencies resultsin a progressive buildup in the amplitude of the responserecorded extracellularly as action potential discharge incat dorsal horn neurons
2526
Windup is very differentfrom another form of synaptic plasticity ie long-termpotentiation (LTP) in that windup requires a very lowfrequency input to elicit it and manifests only during thetrain of repetitive inputs LTP requires a brief high-frequency input and manifests as a potentiated responseto subsequent inputs for very prolonged periods UnlikeA-beta fibers which elicit a fast excitatory potentiallasting several milliseconds C-fibers generate a synapticpotential lasting up to 20 seconds a 1000-fold longerThis has both an NMDA receptor
27
and a tachykininreceptor-mediated component
28
indicating that it is theconsequence both of excitatory amino acid and neu-ropeptide release The very long duration of the synapticpotentials means that at low repetition rates markedtemporal summation will occur leading to depolariza-tion
29
This results in cumulative neural plasticityA more in-depth discussion of windup neural plas-
ticity the role of the immune system trophic factorscytokines nerve growth factor (NGF) receptor trans-duction and second messenger systems is beyond thescope of this article and the readers are referred toauthoritative publications by Coderre et al
30
ldquo
Neu-roimmunology and Mental Health
rdquo
31
Schwartzmanet al
32
and
Colloquium on Neurobiology of Pain
edited by Dubner and Gold
33
In addition in the samecolloquium Basbaum aptly stated the following ldquoPer-sistent pain should be considered a disease state of thenervous system not merely a prolonged acute painsymptom of some other disease conditionsrdquo Curiouslyso-called ldquoFunctional Somatic Syndromesrdquo championedby Barsky and Borus attribute many of the patientrsquossymptoms to be psychogenic in nature
34
These authorshowever ignore current neurobiological research inpain syndromes and espouse an outdated Cartesianduality of mind and body
Managing Chronic-Pain Patients
bull 109
Clinical Issues
Once again extensive discussion about specific painsyndromes is beyond the scope of this publication Wewill attempt to delineate some important issues that arevery common in pain practice and offer some guidanceto practicing physicians
Psychological Aspects
Depression anxiety and self-esteem all must be considered However as carefullydocumented in 1956 by Beecher
35
perception of theconsequences of pain significantly impacts the experi-ence of pain In this study soldiers with severe pain inbattlefield conditions complained significantly less thancivilians undergoing comparable surgical proceduresFor the soldiers the injury ended their time in battle andrequired a trip to the safety of a hospital However forthe civilians the surgery provoked significant feelings ofanxiety which in turn intensified their experience ofpain
Chronic pain often relegates the sufferer to the posi-tion of bystander as opposed to an active treatmentteam participant This helplessness may follow weeksmonths or years of conflicting diagnoses rounds ofvisits to a variety of treatment specialists (who may ormay not communicate with each other) perhaps numer-ous and differing medication regimes and in some casesmultiple surgeries with limited success Frustration andhopelessness ensue as the patient is wearied by thisprocess and perceives the exasperation and frustrationof well-intentioned treatment specialists who cannotprovide remediation for the condition
Vocational and family relationships are disruptedDisplaced anger may cause significant family conflictOccupational and household responsibilities are shiftedto other family members who in turn may also experi-ence anger guilt and despair The individual may expe-rience shame and loss of friendships Isolation andwithdrawal often promote further deterioration in bothbiological and emotional functioning Secondary gainwhether striven for consciously or as an unintendedconsequence reinforcing the maintenance of particularpatterns of behavior may develop and galvanize dys-functional beliefs and interactions A downward cyclebegins and the quality of life is compromised and grad-ually replaced by a mere day-to-day existence
Pharmacological Therapy
One of the most controver-sial issues is the use of opioids for chronic noncancerpain Chronic opioid therapy should be used as a last-resort therapy after the following pharmacologicalmodalities either alone or in combination (ldquorational
copharmacyrdquo) are tried These modalities normalize neu-rotransmitter perturbations encountered in chronic pain
1 Antiwindup medications include anticonvulsantssuch as phenytoin gabapentin topiramatezonisamide oxcarbazepine levetiracetam tiaga-bine and lamotrigine
36ndash38
They have been shownto be beneficial in neuropathic pain Some ofthem increase GABA in the central nervous sys-tem and others block various subtypes ofNMDA receptors Two or more anticonvulsantscan be combined due to different modes of action
2 Antidepressants are useful in treatment of chronicpain
39
Among antidepressants although tricy-clic antidepressants (TCAs) are superior to selec-tive serotonin reuptake inhibitors but theirusefulness is limited due to side effects
4041
TCAsrsquosuperior action is due to increase in norepineph-rine and serotonin In fact safer dual-action anti-depressant venlafaxine is found to be superior inefficacy to selective serotonin rc uptake inhibitors(SSRIs) and superior in safety to TCAs
41
3 Nonreinforcing (nonaddicting) muscle relaxantssuch as tizanidine which also reduce SubstanceP
42
is of significant value4 Tramadol which is a weak mu opiate agonist
with low addiction potential can produce desir-able pain relief
41
5 Botulinum toxin is very effective in some patientssuffering from chronic myofascial pain
4344
6 Although ldquorational copharmacyrdquo is commonlyused to correct neurochemical perturbations inchronic-pain patients care should be exercised toavoid a combination of medications that negateeach otherrsquos effects (such as psychostimulantsand sedativeshypnotics)
7 Fatigue either related to the disease or iatro-genic is best treated with an agent such asmodafinil which is nonaddicting rather thanamphetamines
Any prescribed medication including opioids shouldbe part of a multidisciplinary treatment plan thatincludes interventional anesthesia techniques physicaltherapy psychological counseling relaxation tech-niques and exercise routines
45
Opioids are very effec-tive for nociceptive pain but research is emerging thatthey also are effective in neuropathic pain
45
In 1990 Portenoy
46
proposed 11 guidelines forchronic opioid therapy for nonmalignant pain They arestill valid today
110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

106 bull
mehendale et al
complex than it may seem Disease is both a naturalcategory and a social construction Medical anthropol-ogy distinguishes between three realities under thedifferent words defining ldquodiseaserdquo biological abnormal-ities (disease) subjective experience of altered physicalstate (illness) and the process of socialization of patho-logical episodes (sickness) The constructivist perspec-tive of the sociology of science shows that scientificknowledge reflects cultural beliefs and social values Adiagnosis is ldquoconstructedrdquo through the interactionbetween patients physicians and their respective repre-sentations of disease in a given scientific historical andsocial context
5
There is no better example of this thanin chronic painful conditions To complicate the matterfurther it is very difficult to objectively and quantita-tively measure a patientrsquos pain and response to treat-ment The physician must to a large extent rely on apatientrsquos report about the severity of pain A clever drug-addicted patient may wander from one physicianrsquos officeto the next complaining of pain It is only after thoroughassessment that a comprehensive treatment plan can beinitiated Recently a physician in Florida was convictedon manslaughter charges for prescribing long actingoxycodone (Oxycontin
reg
) At the same time an articleby Melanie R Margolis in the
New York Times
madea case against physicians that they are undertreatingchronic-pain patients The Joint Commission of Accred-itation of Healthcare Organizations (JCAHO) has sug-gested that pain should be considered as the fifth vitalsign and treated aggressively
While there are so-called ldquoOpiate Millsrdquo (wherepatients line up early in the morning to obtain prescrip-tions for opioids) operated by very few unscrupulousphysicians most physicians are highly ethical and areasking for a unified policy on how to treat pain patientsSuch unified guidelines will remove opiate-phobia andwould benefit both patients and physicians
The goal of our article is to review neurobiology painand offer practical recommendations and guidelines forthe treatment of the chronic-pain patients These recom-mendations flow from basic science research on painand incorporate guidelines and position statements pub-lished by various physician associations physicianlicensing boards local state and federal laws
NEUROBIOLOGY OF PAIN
Chronic pain is difficult to measure and precisely defineThere is no clear demarcation to indicate when acutepain becomes chronic However continuous pain3 months after there is no more healing of the patho-
logical process should be considered chronic pain Gen-erally acute pain is the nociceptive type except in veryrare circumstances when it is neuropathic (eg thalamicpain of DejerinendashRoussy Syndrome) chronic pain iseither purely neuropathic or mixed (see below)
Neuroanatomy of Pain Pathways
As outlined in Catalano et al
6
the spinothalamic tractis responsible for sending pain information to the brainThis process may occur at different rates of speed andresult in different sensations Large diameter A-betanerve fibers generally not involved in nociception arepresumed to transmit a sensation occasionally referredto as prepain Smaller diameter A-delta fiber and C-fibernerve transmission occurs at a slower rate of speed A-delta fiber pain is felt to be ldquosharp and stabbingrdquo whileC-fiber pain is ldquodull burning cramping and achingrdquo
Rapid pain travels along the neospinothalamic path-way to the thalamus and cortex Chronic pain proceedsalong the paleospinothalamic pathway finding its wayto the hypothalamus and limbic system The limbicstructures (ie amygdala and hippocampus) are inti-mately involved in the processing of the emotional com-ponent of chronic pain and establishing memories ofpain In addition an ldquoemotional signaturerdquo is assignedto the pain experience This results in significant anxietyandor depression as invariable accompaniments inchronic pain syndrome which must be treated aggres-sively to produce effective pain relief Under such con-ditions there is an increase in corticotrophin-releasingfactor (CRH) resulting in adrenocorticotrophic hor-mone (ACTH) secretion from the pituitary gland andcortisol from the adrenal gland These so-called ldquostresshormonesrdquo in chronic states have widespread deleteri-ous effects such as the suppression of the immune sys-tem and a decrease in brain-derived neurotrophic factor(BDNF) There is some evidence that this may result inatrophy of the neurons It is therefore very importantto treat aggressively these clinical accompaniments ofanxiety and depression
7
Types of Pain
Acute Pain (Nociceptive Somatic or Visceral)
Patients and their physicians are familiar with acutepain or pain caused by injury The term ldquonociceptivepainrdquo is applied when pain is perceived to be commen-surate with tissue damage associated with an identifiablesomatic or visceral lesion The pain is presumed to berelated to ongoing activation of primary afferentneurons responsive to noxious stimuli (nociceptors)
Managing Chronic-Pain Patients
bull 107
Researchers have long since appreciated that in thepresence of injury nociceptors may become hyperexcit-able A change in the expression of ion channels is onemechanism that may contribute to this hyperexcitabil-ity Data indicate that sodium channel expression indorsal root ganglion neurons is dynamic changingmarkedly after tissue or nerve injury
8
Importantly dif-ferent forms of injury induce different changes in theexpression of sodium channels For example nerveinjury in the form of axotomy results in a decrease inthe expression of tetrodotoxin (TTX)-resistant currentsand an increase in a rapidly reprinting TTX-sensitivesodium current In contrast inflammation results in anincrease in the expression of TTX-resistant sodium cur-rents and a decrease in the expression of a TTX-sensitivecurrent Utilizing a different nerve injury model in com-bination with antisense oligodeoxynucleotides researchindicates that a TTX-resistant sodium channel calledSNSPN3 is critical for the initiation and maintenanceof nerve injury-induced hyperalgesia and allodynia
9
Incontrast the recently identified NaN another TTX-resistant sodium channel does not appear to contributeto the maintenance of nerve injury-induced changes innociceptive thresholds
10
Research on the role of theTTX-resistant sodium currents in inflammation indi-cates that the currents are modulated by inflammatorymediators such as prostaglandin EZ 5-HT and adenos-ine consistent with their role in peripheral sensitiza-tion
11
There are additional data indicating that TTX-resistant channels are not only present and functionalin the peripheral terminals of nociceptors but that mod-ulation of these channels contributes to prostaglandin-induced mechanical hyperalgesia The role of otherchannels such as calcium-dependent potassium cur-rents in controlling the excitability of vagal afferents isbeing investigated
12
In the future it may be possible toassess the relative contribution of various sources ofcalcium responsible for the gating of the potassiumcurrents
Nociceptive pain that originates from somatic struc-tures (also known as somatic pain) is typically welllocalized and described as sharp aching throbbing orpressure-like Pain originating from viscera (visceralpain) is often more diffuse and described as gnawing orcramping when due to obstruction of a hollow viscusand aching sharp or throbbing when due to involve-ment of organ capsules or other mesentery Injury leadsto local inflammation Pain signals are sent to the brainThe brain in turn signals the muscles causing a reflexmuscle spasm The muscle spasm protects the injured
area The tightening of the muscles forms a natural castaround the injury and the negative sensation of painpromotes learning how to avoid similar injury in thefuture As tissues heal inflammation resolves and thecentral nervous system sends out fewer signals resultingin decreased pain and decreased muscle spasm Cellularneurobiology of this type of pain is better understoodalthough more work needs to be done on molecularneurobiology of acute pain
The injury is generally self-limiting and healingoccurs over a predictable time frame This pain respondsvery well to opioids and because there is a finite end-point to treatment most physicians are not concernedabout prescribing highly reinforcing opioids for a shortperiod of time
Chronic Pain (Neuropathic Pain Neuropathic CentralPain)
Compared to acute pain less is known about theneurobiology of chronic pain Chronic pain often occursin the absence of ongoing illness or after healing iscompleted A fundamental difference between inflam-matory pain with tissue hypersensitivity and neuro-pathic pain is that in the former the pain is relievedwhen inflammation has resolved while in the latter itmay persist after healing of the primary event Theepidemiology of central pain following stroke or spinalcord injurymdashor during the course of multiple sclerosisbrain injury or trauma to the central nervous systemmdashis much better understood than that following periph-eral nociceptive injury
13
Approximately 1 to 8 ofpatients with stroke have central pain whereas 10 to30 of patients with spinal cord injury are affected bypain during the course of their illness
14
There are nodata on the number of patients who have nociceptiveperipheral pain from small fiber neuropathies radi-culopathies brachial or lumbosacral plexopathiescomplex regional pain syndrome or inflammatoryperipheral conditions However because of the commonnature of the underlying causes there may be manypatients who have this problem
The major clinical features of neuropathic centralpain are
1 Hypersensitivity at the site of injury2 Mechanoallodynia3 Thermal hyperalgesia
15
4 Hyperpathia
16
5 Extraterritoriality (regional distribution of pain)in the case of complex regional pain syndromereflex sympathetic dystrophy
17
108 bull
mehendale et al
6 Associated neurogenic inflammation autonomicdysregulation and motor phenomena that areespecially found in complex regional pain syn-dromereflex sympathetic dystrophy
18
Central sensitization is the pivotal physiologic phe-nomenon underlying the clinical symptoms of neuro-pathic central pain following peripheral nerve injury
19
Central sensitization is primarily induced by the firingof unmyelinated nociceptive C-fibers that project tothe superficial layers of the dorsal horn (DH)
20
Thesefibers produce slow excitatory postsynaptic potentialsthat may last for up to 20 seconds Brief repetitiveafferent nociceptive fiber input causes temporal sum-mation of these slow potentials which induces theldquowinduprdquo phenomenon in central pain-projecting neu-rons (CPPNs) In this state subsequent C-fiber inputproduces a progressive increase in action potentialoutput of CPPNs The gain of this neuronal responseis controlled by an activity-dependent N-methyl-D-aspartate (NMDA) receptor
21
Additionally injury toaxons of C-fibers induces sprouting of A-beta termi-nals from Rexed laminae III and IV to lamina II Thisrewiring may be responsible for the allodynic stateseen in chronic neuropathic pain states
22
There aregamma amino butyric acid (GABA)-A receptor ligand-gated chloride channels that hyperpolarize dorsal hornneurons and reduce neuronal responses to peripheralactivation This results in a decrease in the transmis-sion in the CPPNs This may be the basis of a salutaryeffect of GABAergic drugs in chronic pain Opioidreceptors are also found on the terminals of primaryafferent nociceptive fibers that enter the spinal cordOpioids block the potassium-evoked release of Sub-stance P and enhance the inhibition at dorsal rootganglia (DRG) Therefore opioids can have role intreatment of neuropathic pain
The major mechanisms that underlie nociceptive cen-tral pain are
1 Autosensitization of nociceptive receptors2 Ectopic firing of DRG cells3 Calcium-induced molecular cascades from excess
nociceptor glutamate4 Phenotypic change of afferent A-beta fibers and
DRG cells to the characteristics of those associ-ated with pain
5 Changes in gene expression of sodium channelsand neuropeptides both at nociceptive terminalsand at the DRG
6 Anatomic changes of the superficial layers of theDH This is a progressive but plastic process thatis clearly reversible in its early stages and requiresnociceptive input for its maintenance
Additionally mental stress may ldquoprimerdquo the centralnervous system for development of neural plasticity andwindup
23
In fact so-called ldquowinduprdquo and neural plas-ticity or central sensitization have distinct neurobiolog-ical substrates
24
Windup occurs when a peripheral nerveis stimulated at sufficient intensity to activate C-fibersrepetition of the fixed stimulus at low frequencies resultsin a progressive buildup in the amplitude of the responserecorded extracellularly as action potential discharge incat dorsal horn neurons
2526
Windup is very differentfrom another form of synaptic plasticity ie long-termpotentiation (LTP) in that windup requires a very lowfrequency input to elicit it and manifests only during thetrain of repetitive inputs LTP requires a brief high-frequency input and manifests as a potentiated responseto subsequent inputs for very prolonged periods UnlikeA-beta fibers which elicit a fast excitatory potentiallasting several milliseconds C-fibers generate a synapticpotential lasting up to 20 seconds a 1000-fold longerThis has both an NMDA receptor
27
and a tachykininreceptor-mediated component
28
indicating that it is theconsequence both of excitatory amino acid and neu-ropeptide release The very long duration of the synapticpotentials means that at low repetition rates markedtemporal summation will occur leading to depolariza-tion
29
This results in cumulative neural plasticityA more in-depth discussion of windup neural plas-
ticity the role of the immune system trophic factorscytokines nerve growth factor (NGF) receptor trans-duction and second messenger systems is beyond thescope of this article and the readers are referred toauthoritative publications by Coderre et al
30
ldquo
Neu-roimmunology and Mental Health
rdquo
31
Schwartzmanet al
32
and
Colloquium on Neurobiology of Pain
edited by Dubner and Gold
33
In addition in the samecolloquium Basbaum aptly stated the following ldquoPer-sistent pain should be considered a disease state of thenervous system not merely a prolonged acute painsymptom of some other disease conditionsrdquo Curiouslyso-called ldquoFunctional Somatic Syndromesrdquo championedby Barsky and Borus attribute many of the patientrsquossymptoms to be psychogenic in nature
34
These authorshowever ignore current neurobiological research inpain syndromes and espouse an outdated Cartesianduality of mind and body
Managing Chronic-Pain Patients
bull 109
Clinical Issues
Once again extensive discussion about specific painsyndromes is beyond the scope of this publication Wewill attempt to delineate some important issues that arevery common in pain practice and offer some guidanceto practicing physicians
Psychological Aspects
Depression anxiety and self-esteem all must be considered However as carefullydocumented in 1956 by Beecher
35
perception of theconsequences of pain significantly impacts the experi-ence of pain In this study soldiers with severe pain inbattlefield conditions complained significantly less thancivilians undergoing comparable surgical proceduresFor the soldiers the injury ended their time in battle andrequired a trip to the safety of a hospital However forthe civilians the surgery provoked significant feelings ofanxiety which in turn intensified their experience ofpain
Chronic pain often relegates the sufferer to the posi-tion of bystander as opposed to an active treatmentteam participant This helplessness may follow weeksmonths or years of conflicting diagnoses rounds ofvisits to a variety of treatment specialists (who may ormay not communicate with each other) perhaps numer-ous and differing medication regimes and in some casesmultiple surgeries with limited success Frustration andhopelessness ensue as the patient is wearied by thisprocess and perceives the exasperation and frustrationof well-intentioned treatment specialists who cannotprovide remediation for the condition
Vocational and family relationships are disruptedDisplaced anger may cause significant family conflictOccupational and household responsibilities are shiftedto other family members who in turn may also experi-ence anger guilt and despair The individual may expe-rience shame and loss of friendships Isolation andwithdrawal often promote further deterioration in bothbiological and emotional functioning Secondary gainwhether striven for consciously or as an unintendedconsequence reinforcing the maintenance of particularpatterns of behavior may develop and galvanize dys-functional beliefs and interactions A downward cyclebegins and the quality of life is compromised and grad-ually replaced by a mere day-to-day existence
Pharmacological Therapy
One of the most controver-sial issues is the use of opioids for chronic noncancerpain Chronic opioid therapy should be used as a last-resort therapy after the following pharmacologicalmodalities either alone or in combination (ldquorational
copharmacyrdquo) are tried These modalities normalize neu-rotransmitter perturbations encountered in chronic pain
1 Antiwindup medications include anticonvulsantssuch as phenytoin gabapentin topiramatezonisamide oxcarbazepine levetiracetam tiaga-bine and lamotrigine
36ndash38
They have been shownto be beneficial in neuropathic pain Some ofthem increase GABA in the central nervous sys-tem and others block various subtypes ofNMDA receptors Two or more anticonvulsantscan be combined due to different modes of action
2 Antidepressants are useful in treatment of chronicpain
39
Among antidepressants although tricy-clic antidepressants (TCAs) are superior to selec-tive serotonin reuptake inhibitors but theirusefulness is limited due to side effects
4041
TCAsrsquosuperior action is due to increase in norepineph-rine and serotonin In fact safer dual-action anti-depressant venlafaxine is found to be superior inefficacy to selective serotonin rc uptake inhibitors(SSRIs) and superior in safety to TCAs
41
3 Nonreinforcing (nonaddicting) muscle relaxantssuch as tizanidine which also reduce SubstanceP
42
is of significant value4 Tramadol which is a weak mu opiate agonist
with low addiction potential can produce desir-able pain relief
41
5 Botulinum toxin is very effective in some patientssuffering from chronic myofascial pain
4344
6 Although ldquorational copharmacyrdquo is commonlyused to correct neurochemical perturbations inchronic-pain patients care should be exercised toavoid a combination of medications that negateeach otherrsquos effects (such as psychostimulantsand sedativeshypnotics)
7 Fatigue either related to the disease or iatro-genic is best treated with an agent such asmodafinil which is nonaddicting rather thanamphetamines
Any prescribed medication including opioids shouldbe part of a multidisciplinary treatment plan thatincludes interventional anesthesia techniques physicaltherapy psychological counseling relaxation tech-niques and exercise routines
45
Opioids are very effec-tive for nociceptive pain but research is emerging thatthey also are effective in neuropathic pain
45
In 1990 Portenoy
46
proposed 11 guidelines forchronic opioid therapy for nonmalignant pain They arestill valid today
110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients
bull 107
Researchers have long since appreciated that in thepresence of injury nociceptors may become hyperexcit-able A change in the expression of ion channels is onemechanism that may contribute to this hyperexcitabil-ity Data indicate that sodium channel expression indorsal root ganglion neurons is dynamic changingmarkedly after tissue or nerve injury
8
Importantly dif-ferent forms of injury induce different changes in theexpression of sodium channels For example nerveinjury in the form of axotomy results in a decrease inthe expression of tetrodotoxin (TTX)-resistant currentsand an increase in a rapidly reprinting TTX-sensitivesodium current In contrast inflammation results in anincrease in the expression of TTX-resistant sodium cur-rents and a decrease in the expression of a TTX-sensitivecurrent Utilizing a different nerve injury model in com-bination with antisense oligodeoxynucleotides researchindicates that a TTX-resistant sodium channel calledSNSPN3 is critical for the initiation and maintenanceof nerve injury-induced hyperalgesia and allodynia
9
Incontrast the recently identified NaN another TTX-resistant sodium channel does not appear to contributeto the maintenance of nerve injury-induced changes innociceptive thresholds
10
Research on the role of theTTX-resistant sodium currents in inflammation indi-cates that the currents are modulated by inflammatorymediators such as prostaglandin EZ 5-HT and adenos-ine consistent with their role in peripheral sensitiza-tion
11
There are additional data indicating that TTX-resistant channels are not only present and functionalin the peripheral terminals of nociceptors but that mod-ulation of these channels contributes to prostaglandin-induced mechanical hyperalgesia The role of otherchannels such as calcium-dependent potassium cur-rents in controlling the excitability of vagal afferents isbeing investigated
12
In the future it may be possible toassess the relative contribution of various sources ofcalcium responsible for the gating of the potassiumcurrents
Nociceptive pain that originates from somatic struc-tures (also known as somatic pain) is typically welllocalized and described as sharp aching throbbing orpressure-like Pain originating from viscera (visceralpain) is often more diffuse and described as gnawing orcramping when due to obstruction of a hollow viscusand aching sharp or throbbing when due to involve-ment of organ capsules or other mesentery Injury leadsto local inflammation Pain signals are sent to the brainThe brain in turn signals the muscles causing a reflexmuscle spasm The muscle spasm protects the injured
area The tightening of the muscles forms a natural castaround the injury and the negative sensation of painpromotes learning how to avoid similar injury in thefuture As tissues heal inflammation resolves and thecentral nervous system sends out fewer signals resultingin decreased pain and decreased muscle spasm Cellularneurobiology of this type of pain is better understoodalthough more work needs to be done on molecularneurobiology of acute pain
The injury is generally self-limiting and healingoccurs over a predictable time frame This pain respondsvery well to opioids and because there is a finite end-point to treatment most physicians are not concernedabout prescribing highly reinforcing opioids for a shortperiod of time
Chronic Pain (Neuropathic Pain Neuropathic CentralPain)
Compared to acute pain less is known about theneurobiology of chronic pain Chronic pain often occursin the absence of ongoing illness or after healing iscompleted A fundamental difference between inflam-matory pain with tissue hypersensitivity and neuro-pathic pain is that in the former the pain is relievedwhen inflammation has resolved while in the latter itmay persist after healing of the primary event Theepidemiology of central pain following stroke or spinalcord injurymdashor during the course of multiple sclerosisbrain injury or trauma to the central nervous systemmdashis much better understood than that following periph-eral nociceptive injury
13
Approximately 1 to 8 ofpatients with stroke have central pain whereas 10 to30 of patients with spinal cord injury are affected bypain during the course of their illness
14
There are nodata on the number of patients who have nociceptiveperipheral pain from small fiber neuropathies radi-culopathies brachial or lumbosacral plexopathiescomplex regional pain syndrome or inflammatoryperipheral conditions However because of the commonnature of the underlying causes there may be manypatients who have this problem
The major clinical features of neuropathic centralpain are
1 Hypersensitivity at the site of injury2 Mechanoallodynia3 Thermal hyperalgesia
15
4 Hyperpathia
16
5 Extraterritoriality (regional distribution of pain)in the case of complex regional pain syndromereflex sympathetic dystrophy
17
108 bull
mehendale et al
6 Associated neurogenic inflammation autonomicdysregulation and motor phenomena that areespecially found in complex regional pain syn-dromereflex sympathetic dystrophy
18
Central sensitization is the pivotal physiologic phe-nomenon underlying the clinical symptoms of neuro-pathic central pain following peripheral nerve injury
19
Central sensitization is primarily induced by the firingof unmyelinated nociceptive C-fibers that project tothe superficial layers of the dorsal horn (DH)
20
Thesefibers produce slow excitatory postsynaptic potentialsthat may last for up to 20 seconds Brief repetitiveafferent nociceptive fiber input causes temporal sum-mation of these slow potentials which induces theldquowinduprdquo phenomenon in central pain-projecting neu-rons (CPPNs) In this state subsequent C-fiber inputproduces a progressive increase in action potentialoutput of CPPNs The gain of this neuronal responseis controlled by an activity-dependent N-methyl-D-aspartate (NMDA) receptor
21
Additionally injury toaxons of C-fibers induces sprouting of A-beta termi-nals from Rexed laminae III and IV to lamina II Thisrewiring may be responsible for the allodynic stateseen in chronic neuropathic pain states
22
There aregamma amino butyric acid (GABA)-A receptor ligand-gated chloride channels that hyperpolarize dorsal hornneurons and reduce neuronal responses to peripheralactivation This results in a decrease in the transmis-sion in the CPPNs This may be the basis of a salutaryeffect of GABAergic drugs in chronic pain Opioidreceptors are also found on the terminals of primaryafferent nociceptive fibers that enter the spinal cordOpioids block the potassium-evoked release of Sub-stance P and enhance the inhibition at dorsal rootganglia (DRG) Therefore opioids can have role intreatment of neuropathic pain
The major mechanisms that underlie nociceptive cen-tral pain are
1 Autosensitization of nociceptive receptors2 Ectopic firing of DRG cells3 Calcium-induced molecular cascades from excess
nociceptor glutamate4 Phenotypic change of afferent A-beta fibers and
DRG cells to the characteristics of those associ-ated with pain
5 Changes in gene expression of sodium channelsand neuropeptides both at nociceptive terminalsand at the DRG
6 Anatomic changes of the superficial layers of theDH This is a progressive but plastic process thatis clearly reversible in its early stages and requiresnociceptive input for its maintenance
Additionally mental stress may ldquoprimerdquo the centralnervous system for development of neural plasticity andwindup
23
In fact so-called ldquowinduprdquo and neural plas-ticity or central sensitization have distinct neurobiolog-ical substrates
24
Windup occurs when a peripheral nerveis stimulated at sufficient intensity to activate C-fibersrepetition of the fixed stimulus at low frequencies resultsin a progressive buildup in the amplitude of the responserecorded extracellularly as action potential discharge incat dorsal horn neurons
2526
Windup is very differentfrom another form of synaptic plasticity ie long-termpotentiation (LTP) in that windup requires a very lowfrequency input to elicit it and manifests only during thetrain of repetitive inputs LTP requires a brief high-frequency input and manifests as a potentiated responseto subsequent inputs for very prolonged periods UnlikeA-beta fibers which elicit a fast excitatory potentiallasting several milliseconds C-fibers generate a synapticpotential lasting up to 20 seconds a 1000-fold longerThis has both an NMDA receptor
27
and a tachykininreceptor-mediated component
28
indicating that it is theconsequence both of excitatory amino acid and neu-ropeptide release The very long duration of the synapticpotentials means that at low repetition rates markedtemporal summation will occur leading to depolariza-tion
29
This results in cumulative neural plasticityA more in-depth discussion of windup neural plas-
ticity the role of the immune system trophic factorscytokines nerve growth factor (NGF) receptor trans-duction and second messenger systems is beyond thescope of this article and the readers are referred toauthoritative publications by Coderre et al
30
ldquo
Neu-roimmunology and Mental Health
rdquo
31
Schwartzmanet al
32
and
Colloquium on Neurobiology of Pain
edited by Dubner and Gold
33
In addition in the samecolloquium Basbaum aptly stated the following ldquoPer-sistent pain should be considered a disease state of thenervous system not merely a prolonged acute painsymptom of some other disease conditionsrdquo Curiouslyso-called ldquoFunctional Somatic Syndromesrdquo championedby Barsky and Borus attribute many of the patientrsquossymptoms to be psychogenic in nature
34
These authorshowever ignore current neurobiological research inpain syndromes and espouse an outdated Cartesianduality of mind and body
Managing Chronic-Pain Patients
bull 109
Clinical Issues
Once again extensive discussion about specific painsyndromes is beyond the scope of this publication Wewill attempt to delineate some important issues that arevery common in pain practice and offer some guidanceto practicing physicians
Psychological Aspects
Depression anxiety and self-esteem all must be considered However as carefullydocumented in 1956 by Beecher
35
perception of theconsequences of pain significantly impacts the experi-ence of pain In this study soldiers with severe pain inbattlefield conditions complained significantly less thancivilians undergoing comparable surgical proceduresFor the soldiers the injury ended their time in battle andrequired a trip to the safety of a hospital However forthe civilians the surgery provoked significant feelings ofanxiety which in turn intensified their experience ofpain
Chronic pain often relegates the sufferer to the posi-tion of bystander as opposed to an active treatmentteam participant This helplessness may follow weeksmonths or years of conflicting diagnoses rounds ofvisits to a variety of treatment specialists (who may ormay not communicate with each other) perhaps numer-ous and differing medication regimes and in some casesmultiple surgeries with limited success Frustration andhopelessness ensue as the patient is wearied by thisprocess and perceives the exasperation and frustrationof well-intentioned treatment specialists who cannotprovide remediation for the condition
Vocational and family relationships are disruptedDisplaced anger may cause significant family conflictOccupational and household responsibilities are shiftedto other family members who in turn may also experi-ence anger guilt and despair The individual may expe-rience shame and loss of friendships Isolation andwithdrawal often promote further deterioration in bothbiological and emotional functioning Secondary gainwhether striven for consciously or as an unintendedconsequence reinforcing the maintenance of particularpatterns of behavior may develop and galvanize dys-functional beliefs and interactions A downward cyclebegins and the quality of life is compromised and grad-ually replaced by a mere day-to-day existence
Pharmacological Therapy
One of the most controver-sial issues is the use of opioids for chronic noncancerpain Chronic opioid therapy should be used as a last-resort therapy after the following pharmacologicalmodalities either alone or in combination (ldquorational
copharmacyrdquo) are tried These modalities normalize neu-rotransmitter perturbations encountered in chronic pain
1 Antiwindup medications include anticonvulsantssuch as phenytoin gabapentin topiramatezonisamide oxcarbazepine levetiracetam tiaga-bine and lamotrigine
36ndash38
They have been shownto be beneficial in neuropathic pain Some ofthem increase GABA in the central nervous sys-tem and others block various subtypes ofNMDA receptors Two or more anticonvulsantscan be combined due to different modes of action
2 Antidepressants are useful in treatment of chronicpain
39
Among antidepressants although tricy-clic antidepressants (TCAs) are superior to selec-tive serotonin reuptake inhibitors but theirusefulness is limited due to side effects
4041
TCAsrsquosuperior action is due to increase in norepineph-rine and serotonin In fact safer dual-action anti-depressant venlafaxine is found to be superior inefficacy to selective serotonin rc uptake inhibitors(SSRIs) and superior in safety to TCAs
41
3 Nonreinforcing (nonaddicting) muscle relaxantssuch as tizanidine which also reduce SubstanceP
42
is of significant value4 Tramadol which is a weak mu opiate agonist
with low addiction potential can produce desir-able pain relief
41
5 Botulinum toxin is very effective in some patientssuffering from chronic myofascial pain
4344
6 Although ldquorational copharmacyrdquo is commonlyused to correct neurochemical perturbations inchronic-pain patients care should be exercised toavoid a combination of medications that negateeach otherrsquos effects (such as psychostimulantsand sedativeshypnotics)
7 Fatigue either related to the disease or iatro-genic is best treated with an agent such asmodafinil which is nonaddicting rather thanamphetamines
Any prescribed medication including opioids shouldbe part of a multidisciplinary treatment plan thatincludes interventional anesthesia techniques physicaltherapy psychological counseling relaxation tech-niques and exercise routines
45
Opioids are very effec-tive for nociceptive pain but research is emerging thatthey also are effective in neuropathic pain
45
In 1990 Portenoy
46
proposed 11 guidelines forchronic opioid therapy for nonmalignant pain They arestill valid today
110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

108 bull
mehendale et al
6 Associated neurogenic inflammation autonomicdysregulation and motor phenomena that areespecially found in complex regional pain syn-dromereflex sympathetic dystrophy
18
Central sensitization is the pivotal physiologic phe-nomenon underlying the clinical symptoms of neuro-pathic central pain following peripheral nerve injury
19
Central sensitization is primarily induced by the firingof unmyelinated nociceptive C-fibers that project tothe superficial layers of the dorsal horn (DH)
20
Thesefibers produce slow excitatory postsynaptic potentialsthat may last for up to 20 seconds Brief repetitiveafferent nociceptive fiber input causes temporal sum-mation of these slow potentials which induces theldquowinduprdquo phenomenon in central pain-projecting neu-rons (CPPNs) In this state subsequent C-fiber inputproduces a progressive increase in action potentialoutput of CPPNs The gain of this neuronal responseis controlled by an activity-dependent N-methyl-D-aspartate (NMDA) receptor
21
Additionally injury toaxons of C-fibers induces sprouting of A-beta termi-nals from Rexed laminae III and IV to lamina II Thisrewiring may be responsible for the allodynic stateseen in chronic neuropathic pain states
22
There aregamma amino butyric acid (GABA)-A receptor ligand-gated chloride channels that hyperpolarize dorsal hornneurons and reduce neuronal responses to peripheralactivation This results in a decrease in the transmis-sion in the CPPNs This may be the basis of a salutaryeffect of GABAergic drugs in chronic pain Opioidreceptors are also found on the terminals of primaryafferent nociceptive fibers that enter the spinal cordOpioids block the potassium-evoked release of Sub-stance P and enhance the inhibition at dorsal rootganglia (DRG) Therefore opioids can have role intreatment of neuropathic pain
The major mechanisms that underlie nociceptive cen-tral pain are
1 Autosensitization of nociceptive receptors2 Ectopic firing of DRG cells3 Calcium-induced molecular cascades from excess
nociceptor glutamate4 Phenotypic change of afferent A-beta fibers and
DRG cells to the characteristics of those associ-ated with pain
5 Changes in gene expression of sodium channelsand neuropeptides both at nociceptive terminalsand at the DRG
6 Anatomic changes of the superficial layers of theDH This is a progressive but plastic process thatis clearly reversible in its early stages and requiresnociceptive input for its maintenance
Additionally mental stress may ldquoprimerdquo the centralnervous system for development of neural plasticity andwindup
23
In fact so-called ldquowinduprdquo and neural plas-ticity or central sensitization have distinct neurobiolog-ical substrates
24
Windup occurs when a peripheral nerveis stimulated at sufficient intensity to activate C-fibersrepetition of the fixed stimulus at low frequencies resultsin a progressive buildup in the amplitude of the responserecorded extracellularly as action potential discharge incat dorsal horn neurons
2526
Windup is very differentfrom another form of synaptic plasticity ie long-termpotentiation (LTP) in that windup requires a very lowfrequency input to elicit it and manifests only during thetrain of repetitive inputs LTP requires a brief high-frequency input and manifests as a potentiated responseto subsequent inputs for very prolonged periods UnlikeA-beta fibers which elicit a fast excitatory potentiallasting several milliseconds C-fibers generate a synapticpotential lasting up to 20 seconds a 1000-fold longerThis has both an NMDA receptor
27
and a tachykininreceptor-mediated component
28
indicating that it is theconsequence both of excitatory amino acid and neu-ropeptide release The very long duration of the synapticpotentials means that at low repetition rates markedtemporal summation will occur leading to depolariza-tion
29
This results in cumulative neural plasticityA more in-depth discussion of windup neural plas-
ticity the role of the immune system trophic factorscytokines nerve growth factor (NGF) receptor trans-duction and second messenger systems is beyond thescope of this article and the readers are referred toauthoritative publications by Coderre et al
30
ldquo
Neu-roimmunology and Mental Health
rdquo
31
Schwartzmanet al
32
and
Colloquium on Neurobiology of Pain
edited by Dubner and Gold
33
In addition in the samecolloquium Basbaum aptly stated the following ldquoPer-sistent pain should be considered a disease state of thenervous system not merely a prolonged acute painsymptom of some other disease conditionsrdquo Curiouslyso-called ldquoFunctional Somatic Syndromesrdquo championedby Barsky and Borus attribute many of the patientrsquossymptoms to be psychogenic in nature
34
These authorshowever ignore current neurobiological research inpain syndromes and espouse an outdated Cartesianduality of mind and body
Managing Chronic-Pain Patients
bull 109
Clinical Issues
Once again extensive discussion about specific painsyndromes is beyond the scope of this publication Wewill attempt to delineate some important issues that arevery common in pain practice and offer some guidanceto practicing physicians
Psychological Aspects
Depression anxiety and self-esteem all must be considered However as carefullydocumented in 1956 by Beecher
35
perception of theconsequences of pain significantly impacts the experi-ence of pain In this study soldiers with severe pain inbattlefield conditions complained significantly less thancivilians undergoing comparable surgical proceduresFor the soldiers the injury ended their time in battle andrequired a trip to the safety of a hospital However forthe civilians the surgery provoked significant feelings ofanxiety which in turn intensified their experience ofpain
Chronic pain often relegates the sufferer to the posi-tion of bystander as opposed to an active treatmentteam participant This helplessness may follow weeksmonths or years of conflicting diagnoses rounds ofvisits to a variety of treatment specialists (who may ormay not communicate with each other) perhaps numer-ous and differing medication regimes and in some casesmultiple surgeries with limited success Frustration andhopelessness ensue as the patient is wearied by thisprocess and perceives the exasperation and frustrationof well-intentioned treatment specialists who cannotprovide remediation for the condition
Vocational and family relationships are disruptedDisplaced anger may cause significant family conflictOccupational and household responsibilities are shiftedto other family members who in turn may also experi-ence anger guilt and despair The individual may expe-rience shame and loss of friendships Isolation andwithdrawal often promote further deterioration in bothbiological and emotional functioning Secondary gainwhether striven for consciously or as an unintendedconsequence reinforcing the maintenance of particularpatterns of behavior may develop and galvanize dys-functional beliefs and interactions A downward cyclebegins and the quality of life is compromised and grad-ually replaced by a mere day-to-day existence
Pharmacological Therapy
One of the most controver-sial issues is the use of opioids for chronic noncancerpain Chronic opioid therapy should be used as a last-resort therapy after the following pharmacologicalmodalities either alone or in combination (ldquorational
copharmacyrdquo) are tried These modalities normalize neu-rotransmitter perturbations encountered in chronic pain
1 Antiwindup medications include anticonvulsantssuch as phenytoin gabapentin topiramatezonisamide oxcarbazepine levetiracetam tiaga-bine and lamotrigine
36ndash38
They have been shownto be beneficial in neuropathic pain Some ofthem increase GABA in the central nervous sys-tem and others block various subtypes ofNMDA receptors Two or more anticonvulsantscan be combined due to different modes of action
2 Antidepressants are useful in treatment of chronicpain
39
Among antidepressants although tricy-clic antidepressants (TCAs) are superior to selec-tive serotonin reuptake inhibitors but theirusefulness is limited due to side effects
4041
TCAsrsquosuperior action is due to increase in norepineph-rine and serotonin In fact safer dual-action anti-depressant venlafaxine is found to be superior inefficacy to selective serotonin rc uptake inhibitors(SSRIs) and superior in safety to TCAs
41
3 Nonreinforcing (nonaddicting) muscle relaxantssuch as tizanidine which also reduce SubstanceP
42
is of significant value4 Tramadol which is a weak mu opiate agonist
with low addiction potential can produce desir-able pain relief
41
5 Botulinum toxin is very effective in some patientssuffering from chronic myofascial pain
4344
6 Although ldquorational copharmacyrdquo is commonlyused to correct neurochemical perturbations inchronic-pain patients care should be exercised toavoid a combination of medications that negateeach otherrsquos effects (such as psychostimulantsand sedativeshypnotics)
7 Fatigue either related to the disease or iatro-genic is best treated with an agent such asmodafinil which is nonaddicting rather thanamphetamines
Any prescribed medication including opioids shouldbe part of a multidisciplinary treatment plan thatincludes interventional anesthesia techniques physicaltherapy psychological counseling relaxation tech-niques and exercise routines
45
Opioids are very effec-tive for nociceptive pain but research is emerging thatthey also are effective in neuropathic pain
45
In 1990 Portenoy
46
proposed 11 guidelines forchronic opioid therapy for nonmalignant pain They arestill valid today
110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients
bull 109
Clinical Issues
Once again extensive discussion about specific painsyndromes is beyond the scope of this publication Wewill attempt to delineate some important issues that arevery common in pain practice and offer some guidanceto practicing physicians
Psychological Aspects
Depression anxiety and self-esteem all must be considered However as carefullydocumented in 1956 by Beecher
35
perception of theconsequences of pain significantly impacts the experi-ence of pain In this study soldiers with severe pain inbattlefield conditions complained significantly less thancivilians undergoing comparable surgical proceduresFor the soldiers the injury ended their time in battle andrequired a trip to the safety of a hospital However forthe civilians the surgery provoked significant feelings ofanxiety which in turn intensified their experience ofpain
Chronic pain often relegates the sufferer to the posi-tion of bystander as opposed to an active treatmentteam participant This helplessness may follow weeksmonths or years of conflicting diagnoses rounds ofvisits to a variety of treatment specialists (who may ormay not communicate with each other) perhaps numer-ous and differing medication regimes and in some casesmultiple surgeries with limited success Frustration andhopelessness ensue as the patient is wearied by thisprocess and perceives the exasperation and frustrationof well-intentioned treatment specialists who cannotprovide remediation for the condition
Vocational and family relationships are disruptedDisplaced anger may cause significant family conflictOccupational and household responsibilities are shiftedto other family members who in turn may also experi-ence anger guilt and despair The individual may expe-rience shame and loss of friendships Isolation andwithdrawal often promote further deterioration in bothbiological and emotional functioning Secondary gainwhether striven for consciously or as an unintendedconsequence reinforcing the maintenance of particularpatterns of behavior may develop and galvanize dys-functional beliefs and interactions A downward cyclebegins and the quality of life is compromised and grad-ually replaced by a mere day-to-day existence
Pharmacological Therapy
One of the most controver-sial issues is the use of opioids for chronic noncancerpain Chronic opioid therapy should be used as a last-resort therapy after the following pharmacologicalmodalities either alone or in combination (ldquorational
copharmacyrdquo) are tried These modalities normalize neu-rotransmitter perturbations encountered in chronic pain
1 Antiwindup medications include anticonvulsantssuch as phenytoin gabapentin topiramatezonisamide oxcarbazepine levetiracetam tiaga-bine and lamotrigine
36ndash38
They have been shownto be beneficial in neuropathic pain Some ofthem increase GABA in the central nervous sys-tem and others block various subtypes ofNMDA receptors Two or more anticonvulsantscan be combined due to different modes of action
2 Antidepressants are useful in treatment of chronicpain
39
Among antidepressants although tricy-clic antidepressants (TCAs) are superior to selec-tive serotonin reuptake inhibitors but theirusefulness is limited due to side effects
4041
TCAsrsquosuperior action is due to increase in norepineph-rine and serotonin In fact safer dual-action anti-depressant venlafaxine is found to be superior inefficacy to selective serotonin rc uptake inhibitors(SSRIs) and superior in safety to TCAs
41
3 Nonreinforcing (nonaddicting) muscle relaxantssuch as tizanidine which also reduce SubstanceP
42
is of significant value4 Tramadol which is a weak mu opiate agonist
with low addiction potential can produce desir-able pain relief
41
5 Botulinum toxin is very effective in some patientssuffering from chronic myofascial pain
4344
6 Although ldquorational copharmacyrdquo is commonlyused to correct neurochemical perturbations inchronic-pain patients care should be exercised toavoid a combination of medications that negateeach otherrsquos effects (such as psychostimulantsand sedativeshypnotics)
7 Fatigue either related to the disease or iatro-genic is best treated with an agent such asmodafinil which is nonaddicting rather thanamphetamines
Any prescribed medication including opioids shouldbe part of a multidisciplinary treatment plan thatincludes interventional anesthesia techniques physicaltherapy psychological counseling relaxation tech-niques and exercise routines
45
Opioids are very effec-tive for nociceptive pain but research is emerging thatthey also are effective in neuropathic pain
45
In 1990 Portenoy
46
proposed 11 guidelines forchronic opioid therapy for nonmalignant pain They arestill valid today
110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

110 bull
mehendale et al
1 Opioid maintenance therapy should be consid-ered only after all other reasonable attempts atanalgesia have failed
2 A history of substance abuse should be viewedas a relative contraindication
3 A single practitioner should take primaryresponsibility for treatment
4 Patients should provide informed consentbefore initiation of therapy
5 Medications should be administered on anaround-the-clock basis with the goal of main-taining an acceptable level of comfort
6 Failure to achieve at least partial analgesiaraises questions as to the propriety of continuedopioid treatment
7 Emphasis should be given to attempts to capi-talize on improved analgesia by gains in physi-cal and social function
8 Patients should be allowed to escalate drugdoses transiently when needed
9 Most patients should be seen and drugs pre-scribed at least monthly until their pain syn-dromes are stable Efficacy adverse effects andsigns of drug misuse should be monitored Theresults of careful assessments of drug use shouldbe documented in the medical record
10 Pain exacerbations not managed by small tran-sient increases in dose are best managed in thehospital where dose escalation can be observedclosely and where a return to the baseline dosecan be achieved in a controlled environment
11 Tapering and discontinuation of opioid mainte-nance therapy should follow evidence of drughoarding acquisition of drugs from other pre-scribers uncontrolled dose escalation or otheraberrant behavior To avoid drug diversion andemphasize patient responsibility it a good ideato have the patient sign a treatment agree-ment (see Appendix A for a sample treatmentagreement)
Guidelines for Clinicians
The evaluation and treatment of chronic pain must beperformed and documented
Complete History
A complete history should include(1) the nature and intensity of pain (including currentand past treatments for the pain) and (2) any underly-ing or comorbid conditions (including the effect of painon physical and psychological conditions and vice versa
history of substance abuse and the presence of one ormore recognized medical indications for the use of acontrolled substance)
Physical Examination
A complete physical examina-tion should ideally include (1) a mental statusexamination (2) a neurological examination (3) anexamination specific to areas of the body where the painis reported and (4) a Waddell nonorganic test if con-scious or subconscious deception or secondary gain(financial or otherwise) is suspected
47
Diagnostic Testing
Radiological studies such as mag-netic resonance imaging (MRI) scanning computedtomography (CT) myelogram and electrophysiologicalstudiesmdashsuch as needle electromyographynerve con-duction studies and electroencephalogramsmdashshould beordered if clinically warranted Disease-specific labora-tory or imaging studies should be generously ordered
Consultations with Other Health Professionals
Consultations should be obtained if the pain treatmentplan is going to be affected by coexisting medical con-ditions It may be wise to have a peer review consulta-tion if chronic opioid therapy for nonmalignant pain iscontemplated Full psychologicalpsychiatric assessmentof the patient should be undertaken especially if comor-bid substance abuse or psychiatric pathology wasuncovered in the medical history Interventional anes-thesia has made rapid advances in management of painand should be sought if conservative efforts fail Botu-linum toxin is found be effective in refractory myofas-cial pain syndromes including headaches and shouldbe considered before long-term opioid therapy is con-templated for nonmalignant pain syndromes
434448
Review of Past Medical Records
A review of pastmedical records is very important It prevents needlessretesting and provides the physician with valuable clin-ical information
Diagnosis
A specific diagnosis should be entered in therecord A provisional diagnosis can be entered whileawaiting testing and consultation reports The medicalrecord should also document the presence of one ormore recognized medical indications for the use of acontrolled substance if such therapy is planned
Initial treatment plan and periodic reviews designed toaddress these components
The complexity and inter-
Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients
bull 111
play of biopsychosocial factors in the diagnosis assess-ment and management of chronic pain requires aninterdisciplinary approach The medical and psycholog-ical factors must be carefully assessed and integrated inthe formulation of a treatment plan
The initial psychological examination generallyshould go beyond a mental status examination and care-fully address intellectual capacity concentration atten-tion immediate and delayed memory reasoning andexecutive functioning skills that are generally measuredby a neurocognitive examination The application of thetreatment plan relies upon the patientrsquos ability to par-ticipate in its development and to understand and carryout its directives Chronic pain often disrupts neurocog-nitive functioning Without careful scrutiny inaccurateassumptions may be made concerning the patientrsquos neu-rocognitive abilities resulting in suboptimal treatment
The psychological condition of the patient must beadequately assessed A careful clinical history is of vitalimportance especially as it provides detailed informa-tion about premorbid functioning However an ade-quate examination requires objective measures ofemotional functioning pain and perceived quality oflife These objective measures address the complex per-sonality dynamics at work that influence depressionanxiety hopelessness somatization anger perceptualinaccuracies secondary gain and the ability to adhereand respond to a treatment plan
Reevaluations
Adequate treatment necessitates an inte-grated individualized approach that periodically reeval-uates the patientrsquos progress and incorporates treatmentplan changes as clinically warranted One of the moreimportant criteria used by regulatory medical boards isthe outcome measure that documents the success orfailure of a treatment plan in general and the use ofopioid treatment in particular Follow-up visit progressnotes should carefully document the outcome of treat-ment It is a positive outcome that justifies the use ofopioids for nonmalignant pain syndromes and not thetype dose or quantity of opioids that are used Variousfunctional outcome scales are available and can be uti-lized (see Appendix B for an example)
Regulations and Position Statements
In its quest to stop the abuse of controlled substancesthe Drug Enforcement Administration (DEA) hasinstilled fear in the hearts of those physicians who pre-scribe such drugs Physicians who fear disciplinary
action or prosecution for overprescribing controlledsubstances may fail to relieve preventable pain inpatients The resulting undertreatment of pain in Amer-ica is well documented
4950
and many medical organiza-tions have produced practice guidelines and consensusstatements to meet this problem
5152
Fortunately mostof these position statements rules and regulationsemphasize balance and do not curb the appropriatemode of treatment of pain during the usual course ofmedical practice
The Controlled Substances Act of 1970 (CSA) is thesource of the DEAs authority to regulate controlledsubstances The CSA requires that physicians prescribecontrolled substances only for a ldquolegitimate medicalpurposerdquo While relieving legitimate pain is such a pur-pose uncertainty has interfered with the prescribing ofadequate medication for pain relief In an unprece-dented move although the DEA made it clear that itdoes not intend to restrict legitimate pain prescriptionsThe DEA along with 21 health organizations issuedits first-ever consensus statement on pain relief (seeAppendix C)
The Pain and Policy Group at the University of Wis-consin (supported by The Robert Wood Foundation)has done an excellent job of evaluating internationalfederal and state policies and has produced a 485-pagedocument entitled ldquoAchieving Balance in Federal andState Pain Policyrdquo Their conclusion is as follows
It is well understood that inadequate management ofpain is a serious public health problem in the UnitedStates Public and professional concern about painmanagement has never been higher Increasingly gov-ernment and nongovernment organizations withinterests in health care delivery professional educa-tion bioethics and end of life care are making painmanagement one of their priorities More organiza-tions are working to identify and address the barriersto pain management and to improve professionaltraining public awareness funding and provision ofpain relief In addition there is an unprecedentedtrend to revise governmental policies that regulateprofessional practice and controlled substances inparticular the opioid analgesics
This Evaluation Guide presents a framework that hasbeen developed by the Pain and Policy Studies Group(PPSG) to understand and to evaluate policies at thefederal and state level that relate to pain managementprimarily those policies that have the potential either toenhance or to inhibit professional medical practice and
112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

112 bull
mehendale et al
patient access to opioid analgesics The methodology toevaluate such policies is structured around a centralprinciple from which evaluation criteria are derived
The PPSG has named the central principle ldquoBalancerdquoldquoBalancerdquo refers to a fundamental principle that gov-ernment policies to prevent misuse of controlled sub-stances should not interfere in their essential uses for therelief of pain International and US federal policiesexpress a balanced policy while most states do notSome states have made changes to achieve more bal-anced policy some states have not and many continueto have policies that potentially interfere with pain man-agement and patient care
53
The Federation of State Medical Boards also has thewell-thought out ldquoModel Guideline for the Use ofControlled Substances for the Treatment of Painrdquo (seeAppendix D)
The State of Texas was the first state to pass anIntractable Pain Treatment Act (IPTA) in 1989 withsubsequent revisions in the 1990s Some other stateshave followed Texasrsquos lead but many have not Thesalient points of Texas IPTA include
Notwithstanding any other provision of law a phy-sician may prescribe or administer dangerous drugsor controlled substances to a person in the course ofthe physicianrsquos treatment of a person for intractablepain No hospital or health care facility may forbidor restrict the use of dangerous drugs or controlledsubstances when prescribed or administered by aphysician having staff privileges at that hospital orhealth care facility for a person diagnosed and treatedby a physician for intractable pain No physician maybe subject to disciplinary action by the board forprescribing or administering dangerous drugs or con-trolled substances in the course of treatment of aperson for intractable pain The provisions of this Actshall not apply to those persons being treated by thephysician for chemical dependency because of theiruse of dangerous drugs or controlled substances Theprovisions of this Act provide no authority to a phy-sician to prescribe or administer dangerous drugs orcontrolled substances to a person the physicianknows or should known to be using drugs for non-therapeutic purposes
54
Texas State Board of Medical Examiners is one of thefirst Boards to have a cogent rule (Board Rule 170) thatclearly defines authority of physician to prescribe for thetreatment of pain and has set the standard for the restof the medical Boards to follow (Appendix E)
Texas State Board of Medical Examinersrsquo (TSBME) Viewpoint on Prescribing Practices
Regulatory agencies look at physicians who prescribecontrolled substances for the management of chronicpain in a variety of ways Because these agencies learnof questionable prescribing practices through a systemof peer or patient complaints their focus is a snapshotof a physicianrsquos practice as seen through the lens of asingle patient chart
Generally the investigative process initiated by theagency on the basis of such a complaint takes severalsteps The first step begins with an interview of thecomplainant and then of the physician against whomthe complaint has been lodged These interviewsuncover valuable perspectives regarding personal inter-action office practices and origins of the incident orincidents leading to the complaint
Next investigators review the patientrsquos file andsearch for key elements in the physicianrsquos documenta-tion The thoroughness of the initial evaluation thecorrelation of symptoms with diagnostic tests and pre-vious treatment the relevance of the initial impressionand the logic of the plan of action should be easilydetected by an experienced investigator Documentationof discussions with the patient about informed consentissues regarding the risk of prescribing opioids shouldalso be included In complex cases where addiction andchronic painful states intersect it is wise for a painmanagement contract to be executed between physicianand patient The Federation of State Medical Boards(FSMB) gives some parameters for such a contract (seeAppendix D) and a sample contract is included inAppendix A
When the physicianrsquos documentation is compared tothe complainantrsquos narrative the two together shouldgive a snapshot of that doctorrsquos practice for that patientwith that condition If the records are thorough andshow a logical progression of thought leading to acoherent treatment program followed by follow-upevaluations at reasonable intervalsmdashalso well docu-mented and adhering to that programmdashthat is a bigplus Because many state medical boards and the FSMBmodel guidelines for the management of chronic painspecify that assessments of the patientrsquos quality of lifeshould be made at periodic intervals to indicate whetherthe controlled substance administration is having a sal-utary effect that fact should be included in mostprogress notes (see Appendix B for an example of onesuch functional scale)
Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients
bull 113
The investigatorrsquos next step is to compare the con-trolled substance prescriptions in the patientrsquos chart tothe pharmacy records to make certain that the physi-cianrsquos records reflect accurately the amount strengthand type of medication prescribed Any variations inthose facts will raise a skilled investigatorrsquos index ofsuspicion
Usually a consultant who practices in the same fieldas the physician under scrutiny is asked by the regula-tory agencies to review the patientrsquos record and thepharmacy printout Most of these agencies have rulesthat delineate the steps a physician should take whenprescribing controlled substances for patients withchronic pain These rules are considered by both theinvestigator and the consultant as a basis for the com-pleted investigationrsquos referral to the board for closure orfor corrective action
Medical boards know that controlled substance pre-scribing for chronic pain creates problems at both endsof the spectrum If patients need opioid administrationfor a long-standing painful condition they should beable to count on getting it If they are feigning a painfulcondition to get drugs for a hedonistic effect they shouldnot be entered into the same treatment program as thosewith a painful condition Everyone agrees to that prin-ciple The problem is that neither group comes with astamp on its forehead allowing easy distinction betweenthe two It takes care time finesse skill and experienceto dissect the two conditions from one another whichunfortunately sometimes blend into one another
As a general rule self-destructive behavior by thepatient is a fairly reliable sign of primary substanceabuse Examples include an insistence on extensive sur-gical procedures not indicated social withdrawal aban-doning home and workplace responsibilities doctor andpharmacy hopping demanding a wide variety of psy-choactive drugs and bingeing on prescribed drugs Inessence these patients become less and less able to copedespite huge doses of opioids and related pharmaceuti-cals rather than reaching and maintaining a comfortlevel with one or two opioid compounds as is typical ofthose with painful states
To some degree much of this behavior is also seenin patients with chronic nonmalignant pain It is a mat-ter of degree and frequency that distinguishes betweenthe individuals seeking medication solely for self-grati-fication and those who genuinely wish to control onlytheir painful symptoms
The extremes of the spectrum created by metastaticcancer on one end and illegal drug trafficking on the
other are relatively easy to spot A doctor withldquochronic-pain patientsrdquo lined up at his door and snak-ing out into the parking lotmdashwith whom he spends oneminute and enters cryptic notes on their trumped-upchartsmdashis a disgrace to the profession and essentiallyis daring the regulatory world to snatch away his illegallivelihood
On the other hand patients with chronic pain con-ditions that are not easily anatomically discernible andwho are on high doses of opioids and a variety ofsupplemental drugs are the ones who require the high-est possible cognitive skill to manage Sometimes thereis a fine line between a narcotic abuser and a chronicpain sufferer and at times the two conditions overlapHow then does a practitioner proceed under thesecircumstances
Indecipherable interactions between addiction andillness the addition of benzodiazapines amphetaminesmuscle relaxants hypnotics other opioids and othercontrolled substances and comorbid psychological andsocial factors can create a near-impossible therapeuticchallenge As a general rule the more complexityinvolved in the case the more coherent the documenta-tion required A few scribbled notes or alternatively acomputer-driven one-size-fits-all program are sure signsto an investigator that little thought and cognitive skillhas been injected into the doctorndashpatient relationshipUnder this scrutiny the physician could be perceived aslittle more than a codependent facilitator A rule ofthumb if physicians feel that these challenges are toooverwhelming they should refer the patient to someonewith more experience and training
If the patient does not have the mobility or financialbacking to go to a distant specialist on a regular basisa one-time consultation must be arranged The plan ofaction devised by the specialist can then be implementedby the local practitioner A consistent phenomenon seenby regulators is the unwillingness of physicians to admitthat a very complex illness is better managed by some-one else with more expertise This is especially true inpain management which is a mistake that can haveunpleasant consequences to the patient physician andthe community he or she serves
In summary chronic-pain patients are a growingpopulation in our country and the public demands thatthey be treated actively humanely and accurately Alarge proportion of these are single opioid users with ademonstrable anatomic or physiologic basis for theirmedication need A smaller but unfortunately increas-ingly higher percentage of patients with poor correla-
114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

114 bull
mehendale et al
tion between few physical manifestations of chronicpain and demands for multiple high-dose controlledsubstances are creating a huge challenge to the healthcare delivery system Because the drug-seeking behaviorof both groups can be identical the distinctions can beblurred The more skillful the practitioners are at usingtheir entire armamentarium of clinical diagnosis indexof suspicion documentation thoughtful prescribingand appropriate referral the less likely they will comeafoul of professional regulatory agencies
Texas State Board of Medical Examinersrsquo (TSBME) Looks at Physicians Who Take Opioids
for Chronic Pain
Another important sensitive and controversial issue iswhat to do about physicians in chronic pain who areactively practicing medicine In Texas for example phy-sicians that were prescribed opioids for chronic pain bytheir attending physician rarely if ever reached Boardof Medical Examinerrsquos attention
It is easy to investigate and discipline physicians whouse drugs on a daily basis or who are self-prescribingprescribing to fictitious patients prescribing to familymembers or have found other illegal methods of obtain-ing their drug or drugs of choice A far more difficultquestion is can physicians practice medicine and takelegitimately prescribed daily opioids Can truck driverstake daily opioids and drive Can judges take dailyopioids and sit on the bench More to the point sincea direct parallel has been drawn between the profes-sions can airline pilots perform their duties while takingdaily opioids There seem to be more questions thananswers to these issues
55
If any of those questions can be answered withldquo5berdquo is it then a matter of degree Can Doctor X take80 mg of oxycontin per day and still do broncho-scopies Intracranial surgery Emergency medicineOccupational medicine Dermatology What if it is40 mg From what we know about opioids the effectivedosage for pain relief may increase with the passage oftime So Doctor X is allowed to practice radiology on40 mg oxycontin per day but when it goes to 60 mgwill he be automatically impaired We donrsquot know forsure for each case is individual However those that areimpaired are impaired because their judgment is affectedby the opiate causing the impairment
56
Are the physicians prescribing the medicine requiredto report the physician he is treating with opioids to theregulatory agency in his state Yes if they feel their
physician-patient is impaired Otherwise the answer isldquonordquo Anecdotally a report of this nature has been sentto our agency (Texas State Board of Medical Examiners)only once
Patients if given an option may skirt a wide patharound a physician taking daily opioids Regulatoryagencies should act decisively against an attending phy-sician supplying prescription of opioids to an impairedcolleague in active practice who does not report thatfact to the regulatory agency The regulatory agencyshould also act decisively against the actively practicinglicensee who takes daily opioids that are causing impair-ment This action could range from a reprimand torevocation of license to practice medicine
So what is the solution Does every physician whorequires daily opioids to control his chronic pain haveto retire Does every physician who requires daily opi-oids to control his chronic pain have to suffer in orderto practice Does every physician who requires dailyopioids to control his chronic pain have to try and beatthe system so he can earn a living Can we order abattery of tests for cognitive ability while getting bloodlevels for opioids to see how impaired a physician mightbe when taking a particular dose What happens whenthe dosage is increased due to the tachyphylactic effectWhat about tramadol and propoxyphene and othercontrolled substances that are not opioids Are thereany drugs an actively practicing physician can take dailyfor chronic pain Once again there is room for debateSmall doses may not produce the same degree of impair-ment as opioids do but where do we draw the lineIs it all right for dermatologists to take such drugs ona daily basis but not all right for cardiovascularsurgeons
This is a problem with inadequate solutions
51
Per-haps the best recommendation is to encourage allactively practicing physicians with chronic pain to useevery noncontrolled substance technique possible tocontrol their pain If opioids or other controlled sub-stance analgesics are inevitably the only method for painrelief the actively practicing physicians find effective andnecessary they will be in an ethical dilemma and so willtheir treating physician
This is not the first time this subject has come upnor will it be the last Our contention is that physicianswith chronic pain have the same rights as other patientsto take medications that give them relief But becausethe practice of medicine in this country is a privilegenot a right a different set of issues emerge when opioidmaintained physicians practice medicine
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
Managing Chronic-Pain Patients
bull 115
REFERENCES
1 Gureje O et al Persistent pain and well being
JAMA
1998280147ndash1512 Gallup Inc
Pain in America
Available at httpwwwarthritisorgconditionsspeakingofpainfactsheetaspAccessed April 17 2003
3 Foley K Dismantling the barriers providing pallia-tive and pain care
JAMA
20002831154 Won A Lapane K Gambassi G Bernabei R Mor V
Lipsitz LA Correlates and management of nonmalignant painin the nursing home
J Am Geriatr Soc
199947 936ndash9425 Thomas E Ginies P Blotman F Fibromyalgia as a
national issue the French example
Baillieres Best Pract ResClin Rheumatol
199913525ndash5296 Catalano EM Hardin KN
The Chronic Pain Con-trol Workbook A Step-by-Step Guide for Coping with andOvercoming Pain
2nd edn Oakland CA New HarbingerPublications 1996
7 Garcia R Stress metaplasticity and antidepressants
Curr Mol Medical
20022629ndash6458 Waxman SG Dib-Hajj S Cummins TR Black JA
Sodium channels and pain
Proc Natl Acad Sci USA
1999967649ndash7651
9 Porreca F Lai J Bian D et al A comparison of thepotential role of the tetrodotoxin-insensitive sodium channelsPN3SNS and NaNSNS2 in rat models of chronic pain
ProcNatl Acad Sci USA
1999967647ndash765210 Dib-Hajj SD Tyrell L Black JA Waxman SG NaN
a novel voltage-gated Na channel is expressed preferentiallyin peripheral sensory neurons and down-regulated after axo-tomy
Proc Natl Acad Sci USA
1998958963ndash896811 Gold MS Tetrodotoxin-resistant Na
+
currents andinflammatory hyperalgesia
Proc Natl Acad Sci USA
1999967645ndash7649
12 Cordoba-Rodriguez R Moore KA Kao JPY Wein-reich D Calcium regulation of a slow post-spike hyperpolar-ization in vagal afferent neurons
Proc Natl Acad Sci USA
1999967650ndash765713 Bonica JJ Introduction semantic epidemiologic
and educational issues In Casey KL ed
Pain and CentralNervous System Disease
New York NY RavenPress 199913ndash29
14 Gildenberg PL Stereotactic treatment of head andneck pain
Bes Clin Stud Headache
19785102ndash12115 Hua XY Chen P Marsala M Yaksh TL Intrathecal
Substance P-induced thermal hyperalgesia and spinal releaseof prostaglandin E2 and amino acids
Neuroscience
199989525ndash548
16 Campbell JN Raja SN Meyer RA Painful sequellaeof nerve injury In Dubner R Gebhart GF Bond MR eds
Pain Research and Clinical Management
Amsterdam theNetherlands Elsevier 1998
17 Tal M Bennett GJ Extra-territorial pain in rats witha peripheral mononeuropathy mechano-hyperalgesia and
mechano-allodynia in the territory of an uninjured nerve
Pain
199457525ndash45218 Schwartzman RJ Explaining reflex sympathetic dys-
trophy
Arch Neurol
199956521ndash52219 Woolf CJ A new strategy for the treatment of inflam-
matory pain prevention or elimination of central sensitiza-tion Drugs 199447(suppl 5)1ndash9
20 Thompson SWN King AE Woolf CJ Activitydependent changes in rat ventral horn neurones in vitro sum-mation of prolonged afferent evoked post-synaptic depolariza-tion produce a D-APV sensitive windup Cur J Neumsci 19902645ndash649
21 Sivilotti LG Thompson SW Woolf CJ Rate of riseof the cumulative depolarization evoked by repetitive stimu-lation of small-caliber afferents is a predictor of action poten-tial windup in rat spinal neurons in vitro J Neurophysiol1993691621ndash1652
22 Woolf CJ Shortland P Coggeshall RE Peripheralnerve injury triggers central sprouting of myelinated afferentsNature 199235575ndash78
23 Mehendale AW Goldman MP Fibromyalgia Syn-drome idiopathic widespread persistent pain or syndrome ofmyalgic encephalopathy (SME) what is its nature Pain Prac2002236ndash46
24 Woolf CJ Windup and central sensitization are notequivalent Pain 199666105ndash108
25 Mendell LM Physiological properties of non-myelinated fibre projection to the spinal cord Exp Neurol196616316ndash332
26 Mendell LM Wall PD Responses of dorsal cord cellsto peripheral cutaneous unmyelinated fibres Nature196520697ndash99
27 Thompson SWN King AE Woolf CJ Activity-dependent changes in rat ventral horn neurones in vitrosummation of prolonged afferent evoked postsynapticdepolarizations produce a D APV sensitive windup Eur JNeurosci 19902645ndash649
28 Nagy I Maggi CA Dray A Woolf CJ Urban L Therole of neurokinin and N-methyl-D-aspartate receptors in syn-aptic transmission from capsaicin sensitive primary afferentsin the rat spinal cord in vitro Neuroscience 1993521029ndash1052
29 Sivilotti LG Thompson SWN Woolf CJ The rate ofrise of the cumulative depolarization evoked by repetitivestimulation of small-calibre afferents is a predictor of actionpotential windup in rat spinal neurones in vitro J Neurophys-iol 1993691621ndash1652
30 Coderre TJ Katz J Vaccarino AL Melzack RContribution of neural plasticity to pathological pain reviewof clinical and experimental evidence Pain 199352259ndash285
31 Vitkovic L Koslow SH Neuroimmunology andmental health a report on neuroimmunology research NIHPublication September 199494ndash5274
116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

116 bull mehendale et al
32 Schwartman RJ Grothusen J Kiefer TR Rohr PNeuropathic central pain epidemiology etiology and treat-ment options Arch Neurol 2001581547ndash1550
33 Dubner R Gold M National Academy of SciencesrsquoColloquium On The Neurobiology of Pain 1999
34 Barsky AJ Borus JF Functional somatic syndromesAnn Intern Med 1999130910ndash921
35 Beecher 1956 in Catalano EM Hardin KN TheChronic Pain Control Workbook A Step-by-Step Guide forCoping with and Overcoming Chronic Pain 2nd edn Oak-land CA New Harbinger Publications 1996
36 Chadda VS Mathur MS Double blind study of theeffects of diphenylhydantoin sodium on diabetic neuropathyJ Assoc Physicians India 197826403ndash406
37 Backonja M Beydoun A Edwards KR et al Gaba-pentin for the symptomatic treatment of painful neuropathyin patients with diabetes mellitus a randomized controlledtrial JAMA 19982801831ndash1836
38 McQuay H Carroll D Jadad AR Wiffen P MooreA Anticonvulsant drugs for management of pain a systematicreview BMJ 19953111047ndash1052
39 McQuay H Moore RA An Evidence-Based Resourcefor Pain Relief London Oxford University Press 1998
40 Max MB Lynch SA Muir J Shoaf SE Smoller BDubner R Effects of desipramine amitriptyline and fluoxet-ine on pain in diabetic neuropathy N Engl J Med 19923261250ndash1256
41 Kiayias JA Vlachou ED Lakka-Papadodima E Ven-lafaxine HCl in the treatment of painful peripheral diabeticneuropathy Diabetes Care 200023699
42 Ono H Mishima A Ono S Fukuda H Vasko MRInhibitory effects of clonidine and tizanidine on release ofSubstance P from slices of rat spinal cord and antagonism byalpha-adrenergic receptor antagonists Neuropharmacology199130585ndash589
43 Childers MK Use of Botulinum Toxin Type a in PainManagement A Clinicianrsquos Guide New York Demos MedicalPublishing 1999
44 Relja MA Botulinum toxin type A in the treatmentof tension-type headache International Conference Basic andTherapeutic Aspects of Botulinum and Tetanus Toxins199967
45 Lipman AG Jackson IIKC Use of Opioids inChronic Noncancer Pain A Multidisciplinary ContinuingEducation Program Developed by PowerPak CE April 12000
46 Portenoy RK Chronic opioid therapy in nonmalig-nant pain J Pain Symptom Manage 19905S46ndashS62
47 Waddell G McCulloch JA Kummel E Venner RMNonorganic physical signs in low-back pain Spine 19805117ndash125
48 Cheshire WP Abashian SW Mann JD Botulinumtoxin in the treatment of myofascial pain syndrome Pain19945965ndash69
49 Discipline of Oregon Physician for UndertreatingPain is an Appropriate Response to a Serious ProblemAvailable at httpwwwlawuheduhealthlawperspectivesBioethics990921Disciplinehtml Accessed March 1 2003
50 Physician Disciplined for Undertreating Pain Avail-able at httpwwwlawuheduhealthlawperspectivesBioethics990913Physicianhtml Accessed March 1 2003
51 A Report by the American Society of Anesthesiolo-gists Task Force on Pain Management Chronic Pain SectionAvailable at httpwwwasahqorgpublicationsAndServiceschronic_painhtml Accessed March 1 2003
52 The Use of Opioids for the Treatment of ChronicPain Available at httpwwwpainmedorgproductpubstatementsopioidstmthtml Accessed March 1 2003
53 Pain and Policy Studies Group Available at httpwwwmedschwiscedupainpolicy Accessed March 1 2003
54 Texas Civil Statutes Title 71 Health Public Art4495c Intractable Pain Treatment Act
55 Chapman SL Byas-Smith MG Reed BA Effects ofintermediate- and long-term use of opioids on cognition inpatients with chronic pain Clin J Pain Aug 200218(suppl4)S83ndashS90
56 Sjogren P Thomsen AB Olsen AK Impaired neu-ropsychological performance in chronic nonmalignant painpatients receiving long-term oral opioid therapy J Pain Symp-tom Manage 200019100ndash108
57 Gibson AM Joranson DE Controlled substancesand pain management changes in knowledge and attitudesof state medical regulators J Pain Symptom Manage20011227ndash223
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
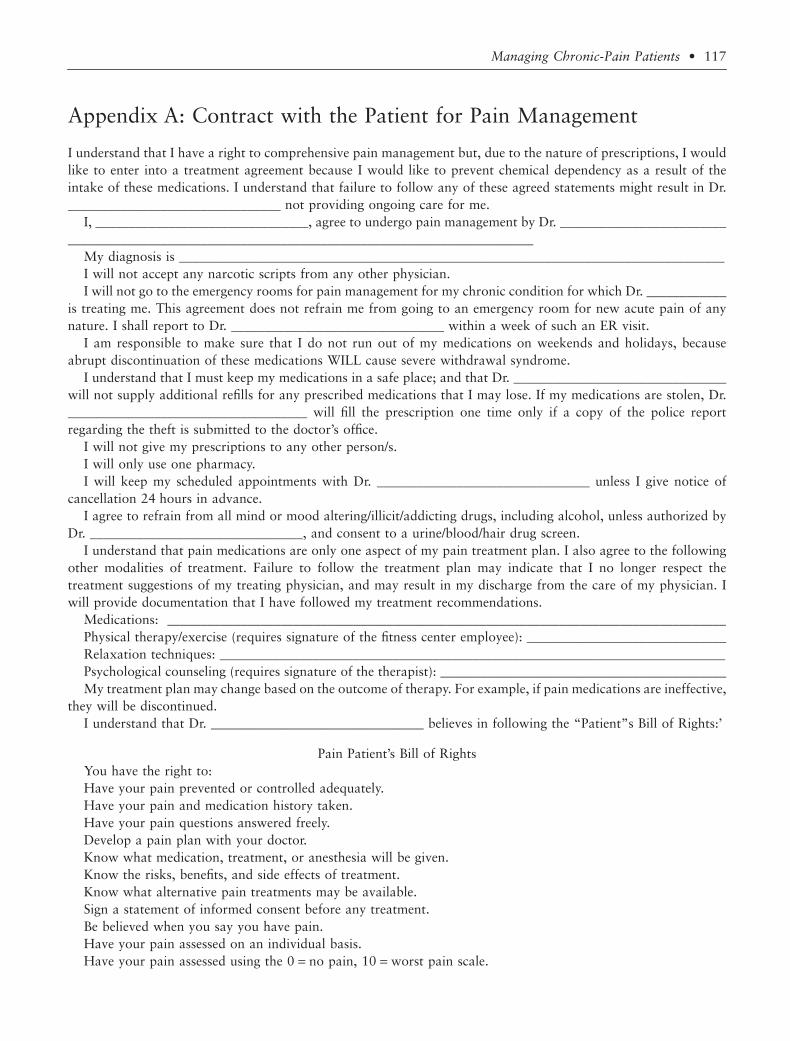
Managing Chronic-Pain Patients bull 117
Appendix A Contract with the Patient for Pain Management
I understand that I have a right to comprehensive pain management but due to the nature of prescriptions I wouldlike to enter into a treatment agreement because I would like to prevent chemical dependency as a result of theintake of these medications I understand that failure to follow any of these agreed statements might result in Dr________________________________ not providing ongoing care for me
I ________________________________ agree to undergo pain management by Dr _______________________________________________________________________________________________
My diagnosis is __________________________________________________________________________________I will not accept any narcotic scripts from any other physicianI will not go to the emergency rooms for pain management for my chronic condition for which Dr ____________
is treating me This agreement does not refrain me from going to an emergency room for new acute pain of anynature I shall report to Dr ________________________________ within a week of such an ER visit
I am responsible to make sure that I do not run out of my medications on weekends and holidays becauseabrupt discontinuation of these medications WILL cause severe withdrawal syndrome
I understand that I must keep my medications in a safe place and that Dr ________________________________will not supply additional refills for any prescribed medications that I may lose If my medications are stolen Dr____________________________________ will fill the prescription one time only if a copy of the police reportregarding the theft is submitted to the doctorrsquos office
I will not give my prescriptions to any other personsI will only use one pharmacyI will keep my scheduled appointments with Dr ________________________________ unless I give notice of
cancellation 24 hours in advanceI agree to refrain from all mind or mood alteringillicitaddicting drugs including alcohol unless authorized by
Dr ________________________________ and consent to a urinebloodhair drug screenI understand that pain medications are only one aspect of my pain treatment plan I also agree to the following
other modalities of treatment Failure to follow the treatment plan may indicate that I no longer respect thetreatment suggestions of my treating physician and may result in my discharge from the care of my physician Iwill provide documentation that I have followed my treatment recommendations
Medications ____________________________________________________________________________________Physical therapyexercise (requires signature of the fitness center employee) ______________________________Relaxation techniques ____________________________________________________________________________Psychological counseling (requires signature of the therapist) ___________________________________________My treatment plan may change based on the outcome of therapy For example if pain medications are ineffective
they will be discontinuedI understand that Dr ________________________________ believes in following the ldquoPatientrdquos Bill of Rightsrsquo
Pain Patientrsquos Bill of RightsYou have the right toHave your pain prevented or controlled adequatelyHave your pain and medication history takenHave your pain questions answered freelyDevelop a pain plan with your doctorKnow what medication treatment or anesthesia will be givenKnow the risks benefits and side effects of treatmentKnow what alternative pain treatments may be availableSign a statement of informed consent before any treatmentBe believed when you say you have painHave your pain assessed on an individual basisHave your pain assessed using the 0 = no pain 10 = worst pain scale
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
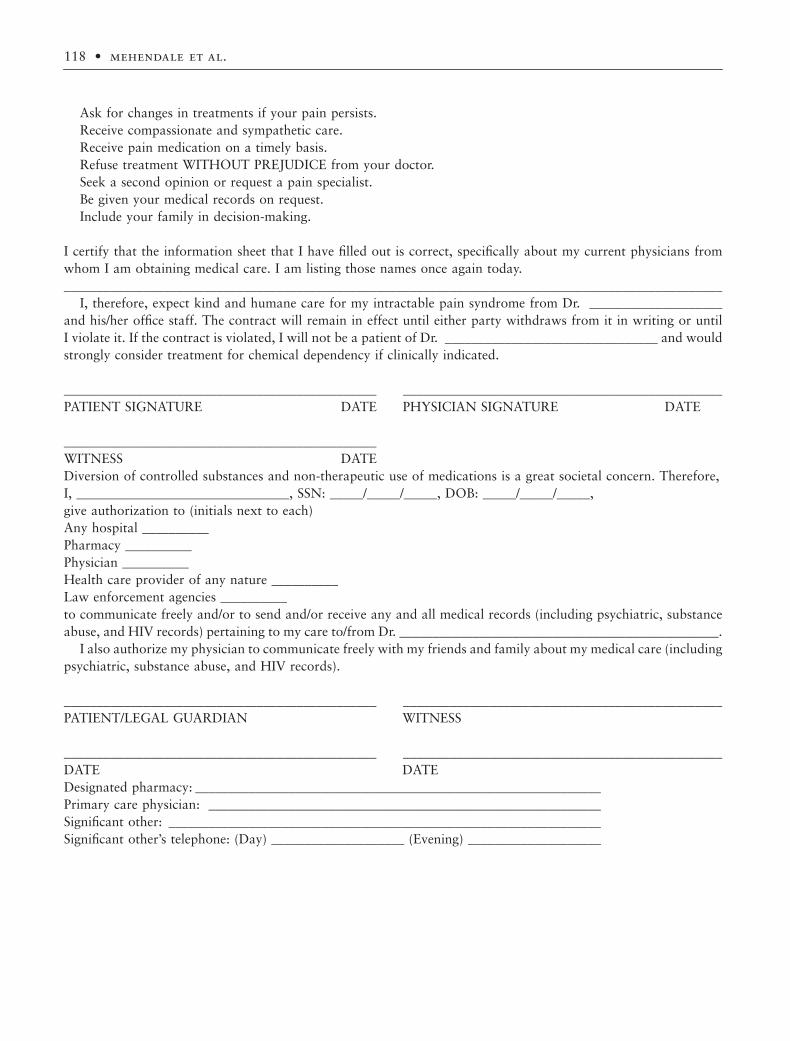
118 bull mehendale et al
Ask for changes in treatments if your pain persistsReceive compassionate and sympathetic careReceive pain medication on a timely basisRefuse treatment WITHOUT PREJUDICE from your doctorSeek a second opinion or request a pain specialistBe given your medical records on requestInclude your family in decision-making
I certify that the information sheet that I have filled out is correct specifically about my current physicians fromwhom I am obtaining medical care I am listing those names once again today___________________________________________________________________________________________________
I therefore expect kind and humane care for my intractable pain syndrome from Dr ____________________and hisher office staff The contract will remain in effect until either party withdraws from it in writing or untilI violate it If the contract is violated I will not be a patient of Dr ________________________________ and wouldstrongly consider treatment for chemical dependency if clinically indicated
_______________________________________________ ________________________________________________PATIENT SIGNATURE DATE PHYSICIAN SIGNATURE DATE
_______________________________________________WITNESS DATEDiversion of controlled substances and non-therapeutic use of medications is a great societal concern ThereforeI ________________________________ SSN _______________ DOB _______________give authorization to (initials next to each)Any hospital __________Pharmacy __________Physician __________Health care provider of any nature __________Law enforcement agencies __________to communicate freely andor to send andor receive any and all medical records (including psychiatric substanceabuse and HIV records) pertaining to my care tofrom Dr ________________________________________________
I also authorize my physician to communicate freely with my friends and family about my medical care (includingpsychiatric substance abuse and HIV records)
_______________________________________________ ________________________________________________PATIENTLEGAL GUARDIAN WITNESS
_______________________________________________ ________________________________________________DATE DATEDesignated pharmacy _____________________________________________________________Primary care physician ___________________________________________________________Significant other _________________________________________________________________Significant otherrsquos telephone (Day) ____________________ (Evening) ____________________
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
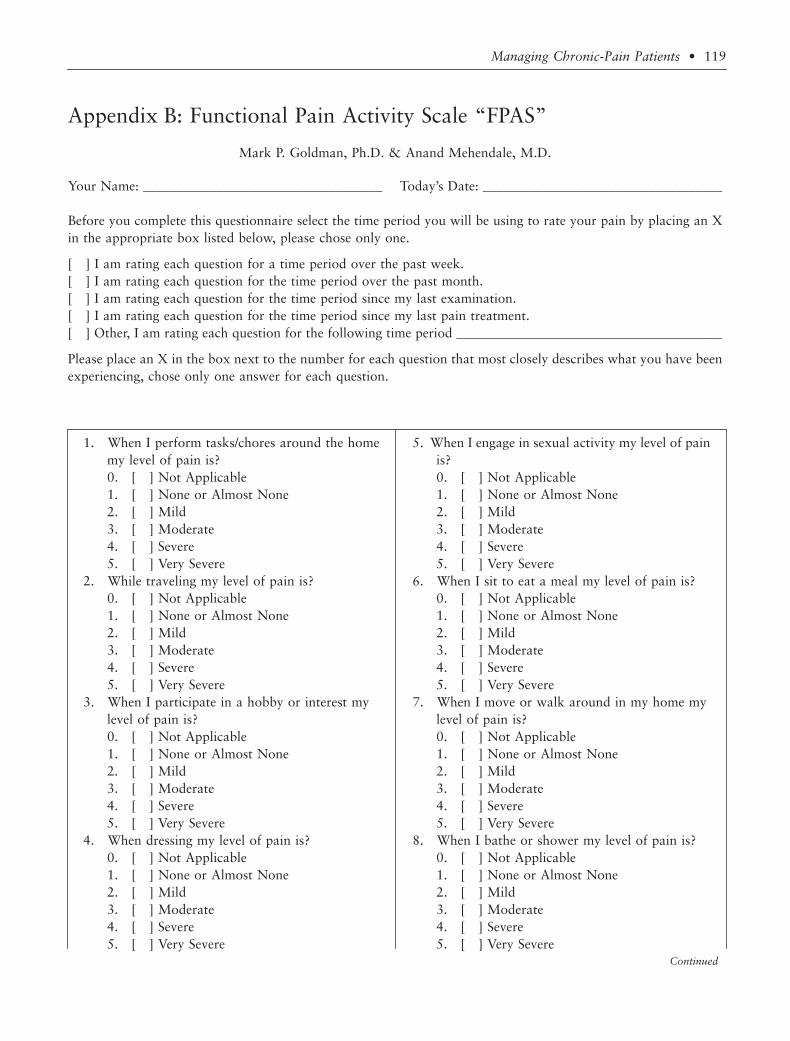
Managing Chronic-Pain Patients bull 119
Appendix B Functional Pain Activity Scale ldquoFPASrdquo
Mark P Goldman PhD amp Anand Mehendale MD
Your Name ____________________________________ Todayrsquos Date ____________________________________
Before you complete this questionnaire select the time period you will be using to rate your pain by placing an Xin the appropriate box listed below please chose only one
[ ] I am rating each question for a time period over the past week[ ] I am rating each question for the time period over the past month[ ] I am rating each question for the time period since my last examination[ ] I am rating each question for the time period since my last pain treatment[ ] Other I am rating each question for the following time period ________________________________________
Please place an X in the box next to the number for each question that most closely describes what you have beenexperiencing chose only one answer for each question
1 When I perform taskschores around the home 5 When I engage in sexual activity my level of painmy level of pain is is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
2 While traveling my level of pain is 6 When I sit to eat a meal my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
3 When I participate in a hobby or interest my 7 When I move or walk around in my home mylevel of pain is level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
4 When dressing my level of pain is 8 When I bathe or shower my level of pain is0 [ ] Not Applicable 0 [ ] Not Applicable1 [ ] None or Almost None 1 [ ] None or Almost None2 [ ] Mild 2 [ ] Mild3 [ ] Moderate 3 [ ] Moderate4 [ ] Severe 4 [ ] Severe5 [ ] Very Severe 5 [ ] Very Severe
Continued
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
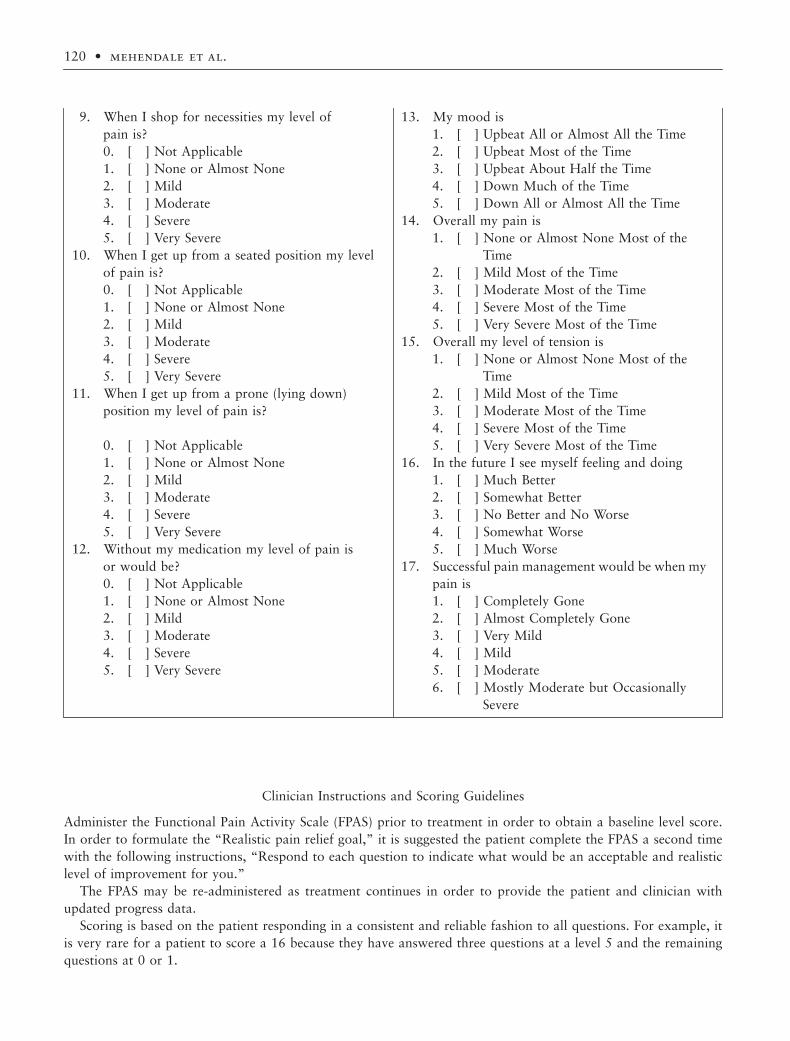
120 bull mehendale et al
Clinician Instructions and Scoring Guidelines
Administer the Functional Pain Activity Scale (FPAS) prior to treatment in order to obtain a baseline level scoreIn order to formulate the ldquoRealistic pain relief goalrdquo it is suggested the patient complete the FPAS a second timewith the following instructions ldquoRespond to each question to indicate what would be an acceptable and realisticlevel of improvement for yourdquo
The FPAS may be re-administered as treatment continues in order to provide the patient and clinician withupdated progress data
Scoring is based on the patient responding in a consistent and reliable fashion to all questions For example itis very rare for a patient to score a 16 because they have answered three questions at a level 5 and the remainingquestions at 0 or 1
9 When I shop for necessities my level of 13 My mood ispain is 1 [ ] Upbeat All or Almost All the Time0 [ ] Not Applicable 2 [ ] Upbeat Most of the Time1 [ ] None or Almost None 3 [ ] Upbeat About Half the Time2 [ ] Mild 4 [ ] Down Much of the Time3 [ ] Moderate 5 [ ] Down All or Almost All the Time4 [ ] Severe 14 Overall my pain is5 [ ] Very Severe 1 [ ] None or Almost None Most of the
10 When I get up from a seated position my level Timeof pain is 2 [ ] Mild Most of the Time0 [ ] Not Applicable 3 [ ] Moderate Most of the Time1 [ ] None or Almost None 4 [ ] Severe Most of the Time2 [ ] Mild 5 [ ] Very Severe Most of the Time3 [ ] Moderate 15 Overall my level of tension is4 [ ] Severe 1 [ ] None or Almost None Most of the5 [ ] Very Severe Time
11 When I get up from a prone (lying down) 2 [ ] Mild Most of the Timeposition my level of pain is 3 [ ] Moderate Most of the Time
4 [ ] Severe Most of the Time0 [ ] Not Applicable 5 [ ] Very Severe Most of the Time1 [ ] None or Almost None 16 In the future I see myself feeling and doing2 [ ] Mild 1 [ ] Much Better3 [ ] Moderate 2 [ ] Somewhat Better4 [ ] Severe 3 [ ] No Better and No Worse5 [ ] Very Severe 4 [ ] Somewhat Worse
12 Without my medication my level of pain is 5 [ ] Much Worseor would be 17 Successful pain management would be when my0 [ ] Not Applicable pain is1 [ ] None or Almost None 1 [ ] Completely Gone2 [ ] Mild 2 [ ] Almost Completely Gone3 [ ] Moderate 3 [ ] Very Mild4 [ ] Severe 4 [ ] Mild5 [ ] Very Severe 5 [ ] Moderate
6 [ ] Mostly Moderate but Occasionally Severe
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
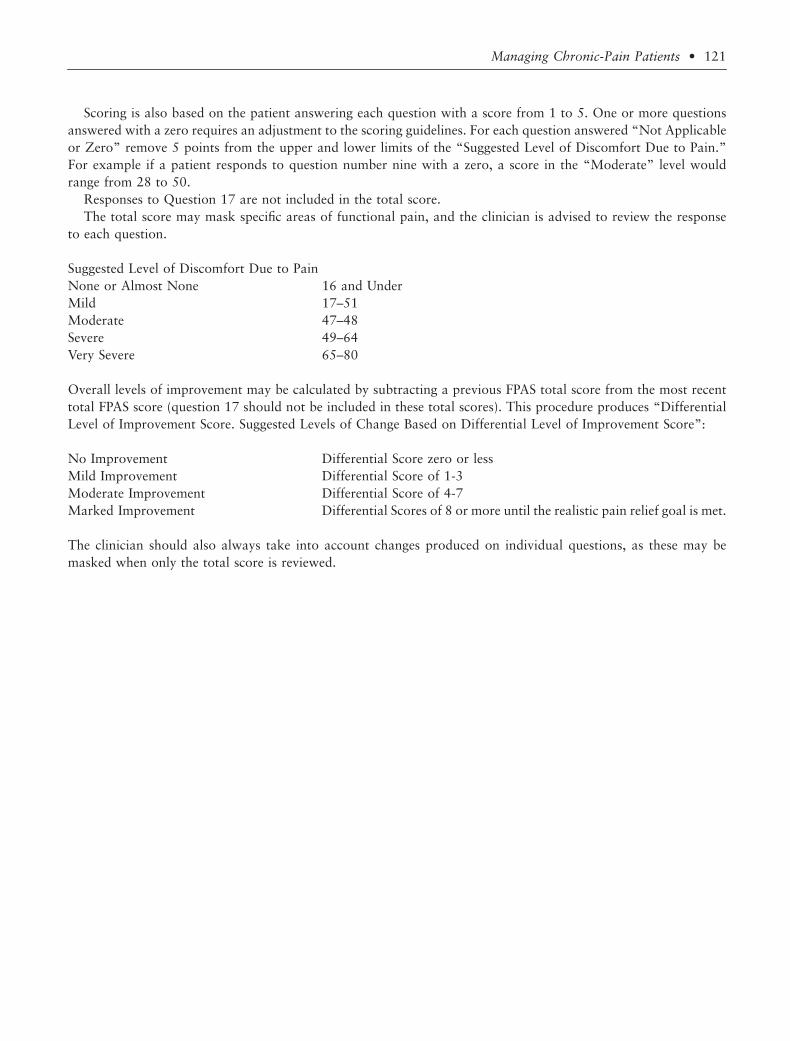
Managing Chronic-Pain Patients bull 121
Scoring is also based on the patient answering each question with a score from 1 to 5 One or more questionsanswered with a zero requires an adjustment to the scoring guidelines For each question answered ldquoNot Applicableor Zerordquo remove 5 points from the upper and lower limits of the ldquoSuggested Level of Discomfort Due to PainrdquoFor example if a patient responds to question number nine with a zero a score in the ldquoModeraterdquo level wouldrange from 28 to 50
Responses to Question 17 are not included in the total scoreThe total score may mask specific areas of functional pain and the clinician is advised to review the response
to each question
Suggested Level of Discomfort Due to PainNone or Almost None 16 and UnderMild 17ndash51Moderate 47ndash48Severe 49ndash64Very Severe 65ndash80
Overall levels of improvement may be calculated by subtracting a previous FPAS total score from the most recenttotal FPAS score (question 17 should not be included in these total scores) This procedure produces ldquoDifferentialLevel of Improvement Score Suggested Levels of Change Based on Differential Level of Improvement Scorerdquo
No Improvement Differential Score zero or lessMild Improvement Differential Score of 1-3Moderate Improvement Differential Score of 4-7Marked Improvement Differential Scores of 8 or more until the realistic pain relief goal is met
The clinician should also always take into account changes produced on individual questions as these may bemasked when only the total score is reviewed
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
122 bull mehendale et al
Appendix C Promoting Pain Relief and Preventing Abuse of Pain Medications A Critical Balancing Act
A Joint Statement of the DEA and 21 Health OrganizationsAmerican Academy of Family Physicians
American Academy of Hospice and Palliative MedicineAmerican Academy of Pain Medicine
American Alliance of Cancer Pain InitiativesAmerican Cancer Society
American Medical AssociationAmerican Pain Foundation
American Pain SocietyAmerican Pharmaceutical AssociationAmerican Society of Anesthesiologists
American Society of Law Medicine and EthicsAmerican Society of Pain Management Nurses
American Society of Regional Anesthesia and Pain MedicineCommunity-State Partnerships to Improve End-of-Life Care
Drug Enforcement AdministrationLast Acts
Midwest Bioethics CenterNational Academy of Elder Law Attorneys
National Hospice and Palliative Care OrganizationPartnership for Caring Inc
University of Wisconsin Pain and Policy Studies Group
As representatives of the health care community and law enforcement we are working together to prevent abuseof prescription pain medications while ensuring that they remain available for patients in need Both health careprofessionals and law enforcement and regulatory personnel share a responsibility for ensuring that prescriptionpain medications are available to the patients who need them and for preventing these drugs from becoming asource of harm or abuse We all must ensure that accurate information about both the legitimate use and the abuseof prescription pain medications is made available The roles of both health professionals and law enforcementpersonnel in maintaining this essential balance between patient care and diversion prevention are critical Preventingdrug abuse is an important societal goal but there is consensus by law enforcement agencies health carepractitioners and patient advocates alike that it should not hinder patientsrsquo ability to receive the care they needand deserve This consensus statement is necessary based on the following facts Under-treatment of pain is a seriousproblem in the United States including pain among patients with chronic conditions and those who are criticallyill or near death Effective pain management is an integral and important aspect of quality medical care and painshould be treated aggressively For many patients opioid analgesicsmdashwhen used as recommended by establishedpain management guidelinesmdashare the most effective way to treat their pain and often the only treatment optionthat provides significant relief Because opioids are one of several types of controlled substances that have potentialfor abuse they are carefully regulated by the DEA and other state agencies For example a physician must belicensed by state medical authorities and registered with the DEA before prescribing a controlled substance In spiteof regulatory controls drug abusers obtain these and other prescription medications by diverting them fromlegitimate channels in several ways including fraud theft forged prescriptions and via unscrupulous healthprofessionals Drug abuse is a serious problem Those who legally manufacture distribute prescribe and dispensecontrolled substances must be mindful of and have respect for their inherent abuse potential Focusing only on theabuse potential of a drug however could erroneously lead to the conclusion that these medications should be
Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients bull 123
avoided when medically indicated generating a sense of fear rather than respect for their legitimate propertiesHelping doctors nurses pharmacists other health care professionals law enforcement personnel and the generalpublic become more aware of both the use and abuse of pain medications will enable all of us to make proper andwise decisions regarding the treatment of pain
124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

124 bull mehendale et al
Appendix D Federation of State Medical Boards
Model Guidelines for the Use of Controlled Substances for the Treatment of PainPain Management and State Regulatory Policy Workgroup
JE West G Aronoff JL Dahl et al
Section I Preamble
The (name of board) recognizes that principles of quality medical practice dictate that the people of the State of(name of state) have access to appropriate and effective pain relief The appropriate application of up-to-dateknowledge and treatment modalities can serve to improve the quality of life for those patients who suffer frompain as well as to reduce the morbidity and costs associated with untreated or inappropriately treated pain TheBoard encourages physicians to view effective pain management as a part of quality medical practice for all patientswith pain acute or chronic and it is especially important for patients who experience pain as a result of terminalillness All physicians should become knowledgeable about effective methods of pain treatment as well as statutoryrequirements for prescribing controlled substances
Inadequate pain control may result from physiciansrsquo lack of knowledge about pain management or an inadequateunderstanding of addiction Fears of investigation or sanction by federal state and local regulatory agencies mayalso result in inappropriate or inadequate treatment of chronic-pain patients Accordingly these guidelines havebeen developed to clarify the Boardrsquos position on pain controlmdashspecifically as related to the use of controlledsubstancesmdashto alleviate physician uncertainty and to encourage better pain management The Board recognizesthat controlled substances including opioid analgesics may be essential in the treatment of acute pain (due totrauma or surgery) and chronic pain whether due to cancer or non-cancer origins Physicians are referred to theUS Agency for Health Care and Research Clinical Practice Guidelines for a sound approach to the managementof acute and cancer-related pain The medical management of pain should be based upon current knowledge andresearch and includes the use of both pharmacological and non-pharmacological modalities Pain should be assessedand treated promptly and the quantity and frequency of doses should be adjusted according to the intensity andduration of the pain Physicians should recognize that tolerance and physical dependence are normal consequencesof sustained use of opioid analgesics and are not synonymous with addiction The (name of board) is obligatedunder the laws of the State of (name of state) to protect the public health and safety
The Board recognizes that inappropriate prescribing of controlled substances including opioid analgesics maylead to drug diversion and abuse by individuals who seek them for other than legitimate medical use Physiciansshould be diligent in preventing the diversion of drugs for illegitimate purposes Physicians should not feardisciplinary action by the Board or other state regulatory or enforcement agency for prescribing dispensing oradministering controlled substances including opioid analgesics for a legitimate medical purpose and in the usualcourse of professional practice The Board will consider prescribing ordering administering or dispensing con-trolled substances for pain to be for a legitimate medical purpose if based on accepted scientific knowledge of thetreatment of pain or if based on sound clinical grounds All such prescribing must be based on clear documentationof unrelieved pain and in compliance with applicable state or federal law Each case of prescribing for pain willbe evaluated on an individual basis The Board will not take disciplinary action against a physician for failing toadhere strictly to the provisions of these guidelines if good cause is shown for such deviation The physicianrsquosconduct will be evaluated to a great extent by the treatment outcome taking into account whether the drug usedis medically andor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individualneedsmdashincluding any improvement in functioningmdashand the recognition that some types of pain cannot be com-pletely relieved The Board will judge the validity of prescribing based on the physicianrsquos treatment of the patientand on available documentation rather than on the quantity and chronicity of prescribing The goal is to controlthe patientrsquos pain for its duration while effectively addressing other aspects of the patientrsquos functioning includingphysical psychological social and work-related factors The following guidelines are not intended to definecomplete or best practice but rather to communicate what the Board considers to be within the boundaries ofprofessional practice
Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

Managing Chronic-Pain Patients bull 125
Section II Guidelines
The Board has adopted the following guidelines when evaluating the use of controlled substances for paincontrol
Evaluation of the PatientA complete medical history and physical examination must be conducted and documented in the medical recordThe medical record should document the nature and intensity of the pain current and past treatments for painunderlying or coexisting diseases or conditions the effect of the pain on physical and psychological function andhistory of substance abuse The medical record should also document the presence of one or more recognizedmedical indications for the use of a controlled substance
Treatment PlanThe written treatment plan should state objectives that will be used to determine treatment success such as painrelief and improved physical and psychosocial function and should indicate if any further diagnostic evaluationsor other treatments are planned After treatment begins the physician should adjust drug therapy to the individualmedical needs of each patient Other treatment modalities or a rehabilitation program may be necessary dependingon the etiology of the pain and the extent to which the pain is associated with physical and psychosocial impairment
Informed Consent and Agreement for TreatmentThe physician should discuss the risks and benefits of the use of controlled substances with the patient personsdesignated by the patient or with the patientrsquos surrogate or guardian if the patient is incompetent The patientshould receive prescriptions from only one physician and one pharmacy where possible If the patient is determinedto be at high risk for medication abuse or to have a history of substance abuse the physician may employ the useof a written agreement between physician and patient outlining patient responsibilities including (a) urineserummedication levels screening when requested (b) the number and frequency of all prescription refills and (c) reasonsfor which drug therapy may be discontinued (ie violation of agreement)
Periodic ReviewAt reasonable intervals based upon the individual circumstances of the patient the physician should review thecourse of treatment and any new information about the etiology of the pain Continuation or modification oftherapy should depend on the physicianrsquos evaluation of progress toward stated treatment objectives such as animprovement in the patientrsquos pain intensity and improved physical andor psychosocial function (such as ability towork need of healthcare resources activities of daily living and quality of social life) If treatment goals are notbeing achieved despite medication adjustments the physician should re-evaluate the appropriateness of continuedtreatment The physician should monitor the patientrsquos compliance with medication usage and related treatmentplans
ConsultationThe physician should be willing to refer the patient as necessary for additional evaluation and treatment in orderto achieve treatment objectives Special attention should be given to those pain patients who are at risk for misusingtheir medications and those whose living arrangement pose a risk for medication misuse or diversion Themanagement of pain in patients with a history of substance abuse or with a co-morbid and psychiatric disordermay require extra care monitoring documentation and consultation with or referral to an expert in the manage-ment of such patients
Medical RecordsThe physician should keep accurate and complete records including (a) a medical history and physical examina-tion (b) diagnostic therapeutic and laboratory results (c) evaluations and consultations (d) treatment objectives(e) a discussion of risks and benefits (f) treatments (g) medications (including date type dosage and quantityprescribed)] (h) instructions and agreements and (i) periodic reviews Records should remain current and bemaintained in an accessible manner and readily available for review
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
126 bull mehendale et al
Compliance with Controlled Substances Laws and RegulationsTo prescribe dispense or administer controlled substances the physician must be licensed in the state and mustcomply with applicable federal and state regulations Physicians are referred to the Physicians Manual of the USDrug Enforcement Administration and (any relevant documents issued by the state medical board) for specific rulesgoverning controlled substances as well as applicable state regulations
Section III Definitions
For the purposes of these guidelines the following terms are defined as follows
Acute pain Acute pain is the normal predicted physiological response to an adverse chemical thermal ormechanical stimulus and is associated with surgery trauma and acute illness Acute pain is generally time limitedand is responsive to opioid and other therapies
Addiction Addiction is a neurobehavioral syndrome with genetic and environmental influences that results inpsychological dependence on the use of a substance for its psychic effects and is characterized by compulsive usedespite harm Addiction may also be referred to by terms such as ldquodrug dependencerdquo and ldquopsychological depen-dencerdquo Physical dependence and tolerance are normal physiological consequences of extended opioid therapy forpain and should not be considered addiction
Analgesic tolerance Analgesic tolerance is the need to increase the dose of opioid to achieve the same level ofanalgesia Analgesic tolerance may or may not be evident during opioid treatment and does not equate withaddiction
Chronic pain Chronic pain is a pain state that is persistent and in which the cause of the pain cannot be removedor otherwise treated Chronic pain may be associated with a long-term incurable or intractable medical conditionor disease
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damageor described in terms of such damage
Physical Dependence Physical dependence on a controlled substance is a physiologic state of neuroadaptationthat is characterized by the emergence of a withdrawal syndrome if drug use is stopped or decreased abruptly orif an antagonist is administered Physical dependence is an expected result of opioid use Physical dependence byitself does not equate with addiction
Pseudoaddiction Pseudoaddiction is a pattern of drug-seeking behavior of pain patients who are receivinginadequate pain management that can be mistaken for addiction
Substance Abuse Substance abuse is the use of any substance(s) for nontherapeutic purposes or the use ofmedication for purposes other than those for which it is prescribed
Tolerance Tolerance is a physiologic state resulting from regular use of a drug in which an increased dosage isneeded to produce the same effect or in which a reduced effect is observed with a constant dose
Gibson-Joranson Review of Current State of Knowledge of the Regulators
Despite very unambiguous language in the Federation of State Medical Boardsrsquo ldquoModel Guidelines for the Use ofControlled Substances for the Treatment of Painrdquo Gibson and Joranson57 found that policy awareness legalityand clinical knowledge of situations in which to prescribe opioids (especially in non-cancer conditions) amongstboard members was low although it had improved in 1997 compared with 1991 (see Table D1 below) To rectifythis Gibson and Joranson suggest that improving pain management in the US will depend in part on a three-partprogram that includes (a) more intensive educational programs for state medical board members and staff (b) anaccelerated policy development by state medical boards to encourage pain management and address concerns aboutregulatory scrutiny and (c) increased communication between clinicians and their regulators
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
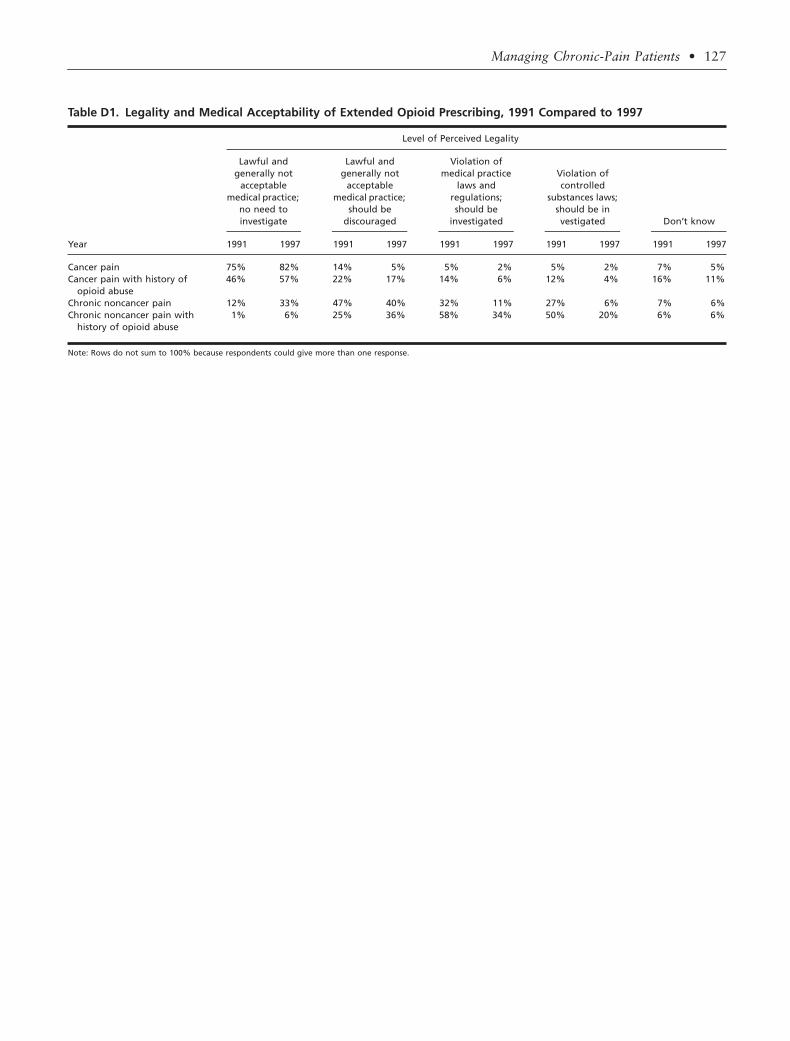
Managing Chronic-Pain Patients bull 127
Table D1 Legality and Medical Acceptability of Extended Opioid Prescribing 1991 Compared to 1997
Year
Level of Perceived Legality
Lawful and generally not
acceptable medical practice
no need to investigate
Lawful and generally not
acceptable medical practice
should be discouraged
Violation of medical practice
laws and regulations should be
investigated
Violation of controlled
substances laws should be in vestigated Donrsquot know
1991 1997 1991 1997 1991 1997 1991 1997 1991 1997
Cancer pain 75 82 14 5 5 2 5 2 7 5Cancer pain with history of
opioid abuse46 57 22 17 14 6 12 4 16 11
Chronic noncancer pain 12 33 47 40 32 11 27 6 7 6Chronic noncancer pain with
history of opioid abuse1 6 25 36 58 34 50 20 6 6
Note Rows do not sum to 100 because respondents could give more than one response
128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000

128 bull mehendale et al
Appendix E Texas State Board of Medical Examiners
Authority of Physician to Prescribe for the Treatment of PainChapter 170
Authority of Physician to Prescribe for the Treatment of Pain1701-1703
1701 Purpose The purpose of this chapter is to recognize that some dangerous drugs and controlled substanceslisted in Chapter 481 and 483 of the Texas Health and Safety Code are indispensable for the treatment of painand are useful for relieving and controlling many other related symptoms that patients may suffer It is the positionof the board that these drugs may be prescribed for the treatment of pain and other related symptoms after areasonably based medical diagnosis has been made in adequate doses and for appropriate lengths of time whichin some cases may be as long as the pain or related symptoms persist The board recognizes that pain includingintractable pain and many other related symptoms are subjective complaints and that the appropriateness and theadequacy of drug and dose will vary from individual to individual The practitioner is expected to exercise soundmedical judgment in treating pain and related symptoms with dangerous drugs and controlled substances
1702 Definitions The following words and terms as used in the Medical Practice Act Article 4495b Section308 shall have the following meanings in the context of providing medications for pain and related symptoms
(1) Abuser of narcotic drugs controlled substances and dangerous drugsmdashA person who takes a drug or drugsfor other than legitimate medical purposes
(2) Intractable painmdashA pain state in which the cause of the pain cannot be removed or otherwise treated andwhich in the generally accepted course of medical practice no relief or cure of the cause of the pain ispossible or none has been found after reasonable efforts
(3) Non-therapeutic in nature or mannermdashA medical use or purpose that is not legitimate(4) Prescribing pharmaceuticals or practicing consistent with the public health and welfaremdashPrescribing phar-
maceuticals and practicing medicine for a legitimate medical purpose in the usual course of professionalpractice
1703 Guidelines The Texas State Board of Medical Examiners will use the following guidelines to determinewhether a physicianrsquos conduct violates the Medical Practice Act Sections 308(4)(E) 308(4)(F) and 308(18) inregard to the prescribing administering ordering or dispensing of pain medications and other drugs necessary toaddress their side effects
(1) The treatment of pain including intractable pain with dangerous drugs and controlled substances is alegitimate medical purpose when done in the usual course of professional practice
(2) A physician or surgeon duly authorized to practice medicine in Texas and to prescribe controlled substancesand dangerous drugs in this state shall not be subject to disciplinary action by the board for prescribingordering administering or dispensing dangerous drugs or controlled substances for the treatment and reliefof pain including intractable pain in the usual course of professional practice for a legitimate medicalpurpose in compliance with applicable state and federal law
(3) Prescribing ordering administering or dispensing dangerous drugs or controlled substances for pain willbe considered to be for a legitimate medical purpose if based upon accepted scientific knowledge of thetreatment of pain including intractable pain not in contravention of applicable state or federal law andif prescribed ordered administered or dispensed in compliance with the following guidelines whereappropriate and as is necessary to meet the individual needs of the patient(A) After a documented medical history which may be provided orally or in writing by the patient and
physical examination by the physician providing the medication including an assessment and con-
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000
Managing Chronic-Pain Patients bull 129
sideration of the pain physical and psychological function any history and potential for substanceabuse coexisting diseases and conditions and the presence of a recognized medical indication forthe use of a dangerous drug or controlled substance
(B) Pursuant to a written treatment plan tailored for the individual needs of the patient by whichtreatment progress and success can be evaluated with stated objectives such as pain relief andorimproved physical and psychosocial function Such a written treatment plan shall consider pertinentmedical history and physical examination as well as the need for further testing consultationsreferrals or use of other treatment modalities
(C) The physician should discuss the risks and benefits of the use of controlled substances with the patientor guardian
(D) Subject to documented periodic review of the care by the physician at reasonable intervals in viewof the individual circumstances of the patient in regard to progress toward reaching treatmentobjectives which takes into consideration the course of medications prescribed ordered adminis-tered or dispensed as well as any new information about the etiology of the pain
(E) Complete and accurate records of the care provided as set forth in subparagraphs (A)-(D) of thisparagraph should be kept When controlled substances are prescribed names quantities prescribeddosages and number of authorized refills of the drugs should be recorded keeping in mind that painpatients with a history of substance abuse or who live in an environment posing a risk for medicationmisuse or diversion require special consideration Management of these patients may require closermonitoring by the physician managing the pain and consultation with appropriate health careprofessionals
(4) A decision by a physician not to strictly adhere to the provisions of paragraph (3) of this section will forgood cause shown be grounds for the board to take no disciplinary action in regard to the physician Eachcase of prescribing for pain will be evaluated on an individual basis The physicianrsquos conduct will beevaluated to a great extent by the treatment outcome taking into account whether the drug used is medicallyandor pharmacologically recognized to be appropriate for the diagnosis the patientrsquos individual needsincluding any improvement in functioning and recognizing that some types of pain cannot be completelyrelieved
(5) If the provisions as set out in paragraphs (1)-(4) of this section are met and if all drug treatment is properlydocumented the board will consider such practices as prescribing in a therapeutic manner and prescribingand practicing medicine in a manner consistent with public health and welfare
(6) Quantity of pharmaceutical and chronicity of prescribing will be evaluated on the basis of the documentedappropriate diagnosis and treatment of the recognized medical indication documented persistence of therecognized medical indication and properly documented follow-up evaluation with appropriate continuingcare as set out in this chapter
(7) A physician may use any number of treatment modalities for the treatment of pain including intractablepain which are consistent with legitimate medical purposes
(8) These rules shall not be construed so as to apply to the treatment of acute pain with dangerous drugs orcontrolled substances for purposes of short-term care
Effective November 19 2000




















