
ST- segment elevation myocardial infarction - Postgraduate ...
Upload
independentCategory
view
0download
0
O
MwCEAE
ABrtflOpdoDdefPpttSamr
AiftvPUipPdlpM
DP4
A
©
RESEARCH
riginal Research
ajor Habitual Dietary Patterns Are Associatedith Acute Myocardial Infarction andardiovascular Risk Markers in a Southernuropean Population
NDREIA OLIVEIRA, PhD; FERNANDO RODRÍGUEZ-ARTALEJO, PhD; RITA GAIO, PhD; ANA CRISTINA SANTOS, PhD;
LISABETE RAMOS, PhD; CARLA LOPES, PhDojRpaia1wtp“f(pCCthdcvtvodJ
Tdtt
os(roppfcs
BSTRACTackground Most dietary pattern analyses in southern Eu-ope have relied on a priori food approaches using Medi-erranean-style diet indexes. These methods may not re-ect the current population’s food consumption.bjective To assess the association of a posteriori dietaryatterns with acute myocardial infarction (AMI) and car-iovascular risk markers in the general adult populationf Porto, Portugal.esign A population-based case-control study was con-ucted. Information was collected by trained interview-rs. Diet was assessed with a validated 82-item foodrequency questionnaire.articipants/setting Cases were patients consecutively hos-italized for an incident non-fatal AMI (n�820), and con-rols were individuals free of previous AMI selected fromhe hospitals’ catchment area (n�2,196).tatistical analyses Dietary patterns, representing mutu-lly exclusive clusters of individuals, were identified byultivariate finite mixture models among controls. Odds
atios (OR) and their 95% confidence intervals (CIs) were
. Oliveira is a nutritionist, research fellow, A. C. Santoss a nutritionist, professor, E. Ramos is a nutritionist, pro-essor, and C. Lopes is a nutritionist, professor, all withhe Department of Hygiene and Epidemiology and Cardio-ascular Research and Development Unit, University oforto Medical School, and the Public Health Institute,niversity of Porto, Porto, Portugal. F. Rodríguez-Artalejo
s a medical doctor, professor of preventive medicine andublic health, Department of Preventive Medicine andublic Health, School of Medicine, Universidad Autónomae Madrid/IdiPAZ, and CIBER of Epidemiology and Pub-
ic Health, Madrid, Spain. R. Gaio is a mathematician,rofessor, Public Health Institute, and Department ofathematics, University of Porto, Porto, Portugal.Address correspondence to: Andreia Oliveira, PhD,epartment of Hygiene and Epidemiology, University oforto Medical School, Alameda Prof. Hernâni Monteiro200-319 Porto, Portugal. E-mail: [email protected] accepted: August 24, 2010.Copyright © 2011 by the American Dietetic
ssociation.0002-8223/$36.00
bdoi: 10.1016/j.jada.2010.10.042
2011 by the American Dietetic Association
btained from unconditional logistic regression, with ad-ustment for main confounders.esults In comparison to women with a “healthy” dietaryattern, those with a “low fruit and vegetables” patternnd a “red meat and alcohol” (also characterized by lowerntake of dairy products and vegetables) pattern showedhigher risk of AMI (OR 1.85, 95% CI 1.01 to 3.39 and OR.91, 95% CI 1.17 to 3.12, respectively). Female controlsith the “red meat and alcohol” pattern also had a higher
otal to high-density lipoprotein cholesterol ratio. In com-arison to men with a “healthy” pattern, those with thered meat and alcohol” pattern, similar to the counterpartound in women, were more likely to experience an AMIOR 1.98, 95% CI 1.35 to 2.92); male controls with thisattern had higher diastolic and systolic blood pressure,-reactive protein, and uric acid levels.onclusions A dietary pattern with lower fruit and vege-able intakes in women, and a pattern characterized byigher consumption of red meat and alcohol (and lower ofairy products and vegetables) in both sexes, were asso-iated with an increased risk of AMI and adverse cardio-ascular risk profiles. These findings highlight the impor-ance of sustained recommendations for fruit andegetable intake and cautious guidance on consumptionf alcoholic beverages, which clusters with less healthyietary patterns of men and women.Am Diet Assoc. 2011;111:241-250.
he examination of relationships between diet andcoronary heart disease (CHD) has traditionally fo-cused on the effect of single foods and nutrients but,
ue to the conceptual and methodological limitations ofhis approach, dietary patterns have attracted great in-erest (1,2).
The mainstream dietary pattern analyses have reliedn a priori approaches; in southern Europe; these analy-es have often used Mediterranean-style diet indexes3,4). A main criticism of this approach is that it may noteflect the current population’s food consumption. More-ver, a priori methods are based on the assumption ofrotective or deleterious health effects of major food com-onents, but they do not acknowledge that clustering ofood components could vary across populations, reflectingultural traditions. For instance, moderate alcohol con-umption is usually considered a healthy behavior (5-7),
ut whereas some studies have reported positive associ-Journal of the AMERICAN DIETETIC ASSOCIATION 241

ahhlc
bdsrchlclr
e(a
MSAbiCCasb1twisawi
tsefsapfapdictcw
awcis
raayCpvust
tg
DAsfiHMcuh
f7aaoheswuEf
ar(mecstimnAfir
cwscmkcl
2
tions between alcohol and healthier foods (8,9), othersave found the opposite (10,11). It suggests that theealth effect of a single food can be confounded by popu-
ation-specific dietary behaviors. These caveats make thease for using dietary patterns defined a posteriori.
Though several studies have assessed the associationetween a posteriori dietary patterns and cardiovascularisease (12-16), only sparse information is available forouthern European populations. Portugal has a wideange of dietary exposures as well as a particularly highonsumption of wine and fish (17,18). Its singular foodabits, distinct from the Mediterranean-style diet fol-
owed by neighbor countries (19) and closer to the re-ently conceptualized Atlantic-style diet (20,21), couldead to unique food clusterings whose effect on coronaryisk is unknown.
This study assessed the association of a posteriori di-tary patterns with nonfatal acute myocardial infarctionAMI) and with some cardiovascular risk markers in thedult population of Porto, Portugal.
ETHODStudy Design and Participants
population-based case-control study was carried outetween 1999 and 2003 in Porto, an urban center locatedn northwest Portugal with almost 300,000 inhabitants.ases were selected after consecutive admission to theardiology Department of the four hospitals that providecute coronary care in Porto. Cases were included in thetudy if they had a first episode of AMI (22) and survivedeyond the fourth day post-AMI. During the study period,,248 patients with a first AMI were identified. Out ofhese, we excluded 37 who died before the interview, 65ho were unable to collaborate, 3 who refused to partic-
pate, 138 with cognitive impairment as indicated by acore �24 in the Mini-Mental State Examination (23,24),nd 164 with incomplete information. Further exclusionsere made for 21 who changed diet in the year before
nterview.Controls were individuals from the catchment area of
he participating hospitals, with no previous clinical orilent infarction according to self-reported data or/andlectrocardiographic evidence. Controls were selectedrom random digit dial of households, and then fromimple random sampling of Porto permanent residentsged �18 years. Of note is that during the recruitmenteriod, 97% of households had a telephone installed. Re-usals were not substituted within the same householdnd the participation rate was 70% (25). Out of 2,485articipants initially selected, 103 (4.1%) were excludedue to previous clinical or silent AMI, 51 with cognitivempairment, 60 with incomplete information, and 75 whohanged their food habits during the previous year. Forhe case-control analysis, the final sample included 820ases (194 women and 626 men) and 2,196 controls (1,362omen and 834 men).To examine the association between dietary patterns
nd cardiovascular risk markers, cross-sectional analysesere conducted among the controls only. Out of the 2,196
ontrols, we further excluded 328 individuals withoutnformation on at least one of the following outcomes:
ystolic and diastolic blood pressure, serum glucose, se- e42 February 2011 Volume 111 Number 2
um total to high-density lipoprotein cholesterol ratio,nd triglycerides. As a result, analyses with these vari-bles were conducted with 1,868 persons. Lastly, for anal-ses concerning high-sensitivity C-reactive protein (hs-RP), uric acid, and leukocyte count, a subsample of 925articipants was obtained, after exclusion of 1,209 indi-iduals without measurement of one of the biomarkersnder study, and 62 with hs-CRP above 10 mg/L, whichuggests the presence of a clinically relevant inflamma-ory condition (26).
The Ethics Committees of the four participating hospi-als approved the study protocol, and every participantave written informed consent.
ata CollectionMI patients were interviewed during their in-hospitaltay after clinical stabilization, usually between theourth and eighth day after admission. Controls werenvited to a face-to-face interview at the Department ofygiene and Epidemiology of the University of Portoedical School. Data on cases and controls were collected
oncurrently by the same set of trained interviewers,sing the same questionnaire on sociodemographic, be-avioral, and clinical characteristics.Diet was collected with an 82-item semiquantitative food
requency questionnaire, previously validated against four-day food records (27,28). Each subject had to report theverage frequency of consumption for each food itemmong nine categories, ranging from “never or less thannce a month” to “six or more times a day”; subjects alsoad to choose the average portion consumed (lower,qual, or higher than the average portion size) and theeasonal variation of consumption. Food consumptionas converted into total energy intake and nutrientssing Food Processor Plus software (version 7.02, 1997,SHA Research, Salem, OR), adapted to Portuguese
oods and dishes.Age and education were recorded as completed years of
ge and years of schooling. Tobacco consumption wasegistered as daily (at least one cigarette/day), occasionalless than one cigarette/day), former (quit for at least 6onths), and never smoking. For analyses, only two cat-
gories were considered: current smoking (daily and oc-asional smokers) and nonsmoking (never and formermokers). Physical activity referred to the regular prac-ice (at least 30 minutes/week) of any leisure-time phys-cal activity with energy expenditure higher than 2.5
etabolic equivalents per hour, including walking, run-ing, and any sports activities, during the previous year.family history of AMI was considered when at least one
rst-degree relative had had an AMI or a sudden death,egardless of age at occurrence.Anthropometrics were performed with subjects in light
lothing and barefoot under standard procedures. Bodyeight was measured to the nearest 0.1 kg using a digital
cale (SECA, Columbia, SC), and height to the nearestentimeter with a wall stadiometer (SECA, Hamburg, Ger-any). Body mass index (BMI) was calculated as weight in
ilograms divided by the squared height in meters. Waistircumference was ascertained midway between the lowerimit of the rib cage and the iliac crest, and hip circumfer-
nce on the maximum circumference over the femoral tro-
cw
ssmma1thcdm2cpweILi
STasdewtaa
dsmi
iccawcozcw
mattfdta
wiTdwoctct
rieup
wSluac
a(lvatrhBitpb
Fnrc
hanters; both were measured to the nearest centimeterith a flexible and nondistensible tape.For the cross-sectional analyses, controls underwent
ome measurements. Systolic and diastolic blood pres-ure was measured on a single occasion using a standardercury sphygmomanometer after a 10-minute rest; theean of two blood pressure readings was used in the
nalyses. Also, a venous blood sample was drawn after a2-hour overnight fast, to measure glucose, total choles-erol, high-density lipoprotein cholesterol, triglycerides,s-CRP, uric acid, and blood leukocyte count. Serum glu-ose, cholesterol, triglycerides, and uric acid levels wereetermined using automatic standard routine enzymaticethods (coefficients of variation [CV] of 1.25%, 1.45%,
.80%, and 2.69%, respectively). High-density lipoproteinholesterol was measured after precipitation of apoli-oprotein B-containing lipoproteins (CV 1.92%). hs-CRPas determined with particle-enhanced immunoneph-lometry using an auto-analyzer (Behring, NephelometerI, BN II, Dade Behring, Marburg, Germany) (CV 7.6%).eukocyte count was determined from the whole blood,
mmediately after collection.
tatistical Analysishe food items of the food frequency questionnaire wereggregated into 14 food groups according to nutritionalimilarities (see the Figure). Given that there were sexifferences in the food groups distribution (P�0.001), di-tary patterns were identified separately for men andomen. Patterns were firstly identified among the con-
rols using multivariate finite mixture models, or equiv-lently, mixture of regressions with concomitant vari-
Food group Description
Red meat Beef, pork, lamb, viscera, fresh baconWhite meat Chicken, turkey, rabbitFish Fish (including canned), seafood, shellfish
and molluskVegetables Yellow and green vegetables, salads, beansFruits Fresh fruitsPasta/potatoes/rice Pasta, potatoes, riceDairy products Skimmed, semi-skimmed and whole milk,
yogurt, cheeseSoup Vegetable soupsCereals Bread and breakfast cereals (refined and
whole-grain cereals)Added fats Vegetable oils, butter, margarineSweets Biscuits, cookies, cakes, pastries, chocolate,
preserves, dairy desserts, ice creamFast foods Pizza, burgers, sausages, chorizos, meat
pies, chipsSoft drinks Carbonated and noncarbonated soft drinksAlcoholic beverages Wine, beer, spirits
igure. Description of the 14 food groups aggregated according toutritional similarities in a study assessing the association of a poste-iori dietary patterns with acute myocardial infarction and cardiovas-ular risk markers in the general adult population of Porto, Portugal.
bles as independent variables (29). The multivariate i
ependent variable represented the 14 food groups’ con-umption. This technique, like cluster analysis, definesutually exclusive groups of individuals (clusters) shar-
ng the same food pattern.Because high frequencies of zero consumption can orig-
nate problems in model fitting, food groups with a per-entage of nonconsumption �45% were dichotomized intoonsumption and nonconsumption. This was the case forlcohol in women and soft drinks in both men andomen; the remaining food groups did not present non-
onsumption �15%. The variables that were not dichot-mized were log-transformed, after adding 1 g to avoidero values. For the model structure, variances of theontinuous food group intakes were allowed to varyithin and between clusters.Screening of outliers was done by the sigma gapethod for right skewed distributions. Twenty-four men
nd 22 women were identified as outliers and removed forhe definition of patterns. Differences in food consump-ion with age as well as correlations between individualood-group consumption and total energy intake wereetected. Therefore, both age group and total energy in-ake were taken as independent and concomitant vari-bles.The final number of clusters (n�4 for both men andomen) was established by the cessation of the monoton-
cally decrease of the Bayesian Information Criterion.he mean of the individual posterior probabilities pre-icting the cluster membership were 89%�0.14% inomen and 92%�0.13% in men. Dietary characterization
f each cluster was based on results from tests of multipleomparisons of food group means. Dietary pattern iden-ification for AMI cases was done from the individualomponent membership probabilities of the model amonghe controls.
Categorical and continuous variables were summa-ized by percentages and means, respectively. Differencesn proportions were tested with the �2 test or the Fisher-xact test, as appropriate. The Mann-Whitney test wassed to compare continuous variables between two inde-endent samples.Because cardiovascular risk markers’ distributionsere highly skewed (normality was checked using thehapiro-Wilk criterion), generalized linear models with a
og link function and Gaussian error distribution weresed to estimate the point estimates (geometric means)nd their respective 95% confidence intervals (CIs) acrossategories of dietary patterns.The association between the identified dietary patterns
nd the risk of AMI was summarized with odds ratiosORs) and their 95% CI, calculated with unconditionalogistic regression. Both univariate (Model 1) and multi-ariate models were presented; multivariate models weredjusted for age, education, total energy intake (as con-inuous variables), smoking (current and nonsmoking),egular leisure-time physical activity (no, yes) and familyistory of AMI (no, yes) (Model 2). Further adjustment forMI (Model 3) and for self-reported hypertension, dyslip-
demia, and diabetes mellitus (Model 4) was done, al-hough we acknowledge that the latter variables mayartly act as intermediate variables in the relationshipetween diet and AMI. Lastly, we examined a possible
nteraction of BMI in the association between dietaryFebruary 2011 ● Journal of the AMERICAN DIETETIC ASSOCIATION 243
pa
w(pwt
RTswvldbfbad“ha(n
vtafi
phsasd
alecchvtlipephtthcialca
2
atterns and AMI, by using interaction terms constructeds the product of dietary pattern categories by BMI.Statistical analyses for dietary pattern identificationere conducted with the package flexmix from R software
version 2.7.1, 2008, R Foundation for Statistical Com-uting, Vienna, Austria). Other analyses were performedith Stata SE (version 10, 2007, Statacorp, College Sta-
ion, TX).
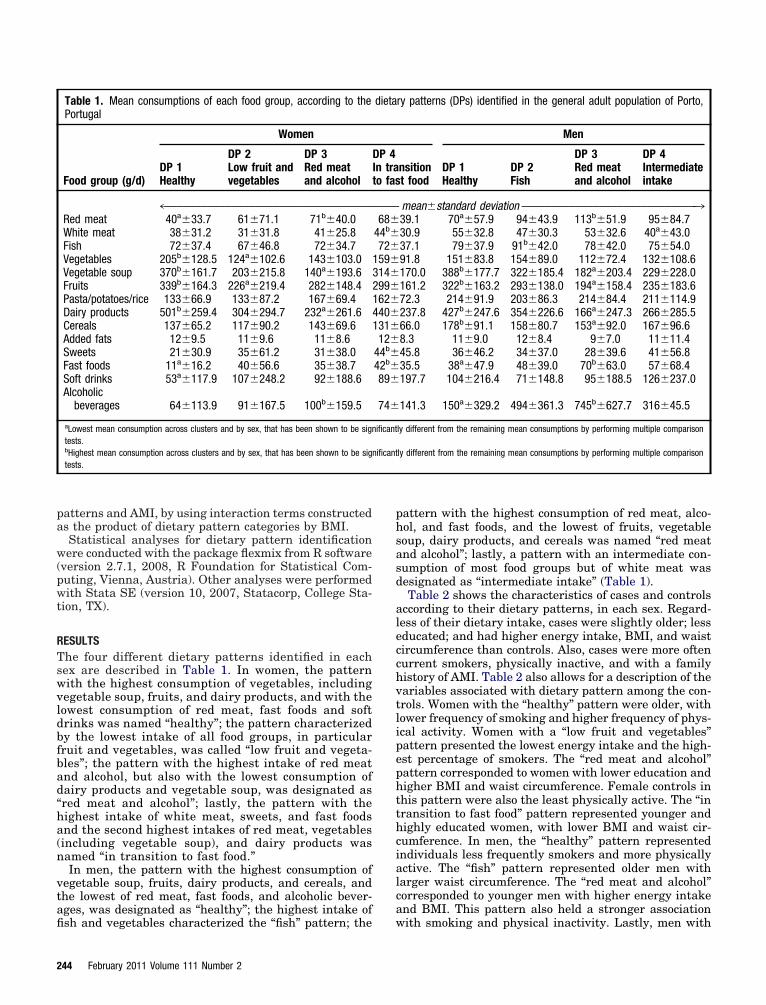
ESULTShe four different dietary patterns identified in eachex are described in Table 1. In women, the patternith the highest consumption of vegetables, includingegetable soup, fruits, and dairy products, and with theowest consumption of red meat, fast foods and softrinks was named “healthy”; the pattern characterizedy the lowest intake of all food groups, in particularruit and vegetables, was called “low fruit and vegeta-les”; the pattern with the highest intake of red meatnd alcohol, but also with the lowest consumption ofairy products and vegetable soup, was designated asred meat and alcohol”; lastly, the pattern with theighest intake of white meat, sweets, and fast foodsnd the second highest intakes of red meat, vegetablesincluding vegetable soup), and dairy products wasamed “in transition to fast food.”In men, the pattern with the highest consumption of
egetable soup, fruits, dairy products, and cereals, andhe lowest of red meat, fast foods, and alcoholic bever-ges, was designated as “healthy”; the highest intake of
Table 1. Mean consumptions of each food group, according to thePortugal
Food group (g/d)
Women
DP 1Healthy
DP 2Low fruit andvegetables
DP 3Red meatand alcohol
4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™Red meat 40a�33.7 61�71.1 71b�40.0White meat 38�31.2 31�31.8 41�25.8Fish 72�37.4 67�46.8 72�34.7Vegetables 205b�128.5 124a�102.6 143�103.0Vegetable soup 370b�161.7 203�215.8 140a�193.6Fruits 339b�164.3 226a�219.4 282�148.4Pasta/potatoes/rice 133�66.9 133�87.2 167�69.4Dairy products 501b�259.4 304�294.7 232a�261.6Cereals 137�65.2 117�90.2 143�69.6Added fats 12�9.5 11�9.6 11�8.6Sweets 21�30.9 35�61.2 31�38.0Fast foods 11a�16.2 40�56.6 35�38.7Soft drinks 53a�117.9 107�248.2 92�188.6Alcoholic
beverages 64�113.9 91�167.5 100b�159.5
aLowest mean consumption across clusters and by sex, that has been shown to be signtests.bHighest mean consumption across clusters and by sex, that has been shown to be signtests.
sh and vegetables characterized the “fish” pattern; the w
44 February 2011 Volume 111 Number 2
attern with the highest consumption of red meat, alco-ol, and fast foods, and the lowest of fruits, vegetableoup, dairy products, and cereals was named “red meatnd alcohol”; lastly, a pattern with an intermediate con-umption of most food groups but of white meat wasesignated as “intermediate intake” (Table 1).Table 2 shows the characteristics of cases and controls
ccording to their dietary patterns, in each sex. Regard-ess of their dietary intake, cases were slightly older; lessducated; and had higher energy intake, BMI, and waistircumference than controls. Also, cases were more oftenurrent smokers, physically inactive, and with a familyistory of AMI. Table 2 also allows for a description of theariables associated with dietary pattern among the con-rols. Women with the “healthy” pattern were older, withower frequency of smoking and higher frequency of phys-cal activity. Women with a “low fruit and vegetables”attern presented the lowest energy intake and the high-st percentage of smokers. The “red meat and alcohol”attern corresponded to women with lower education andigher BMI and waist circumference. Female controls inhis pattern were also the least physically active. The “inransition to fast food” pattern represented younger andighly educated women, with lower BMI and waist cir-umference. In men, the “healthy” pattern representedndividuals less frequently smokers and more physicallyctive. The “fish” pattern represented older men witharger waist circumference. The “red meat and alcohol”orresponded to younger men with higher energy intakend BMI. This pattern also held a stronger association
ry patterns (DPs) identified in the general adult population of Porto,
Men
nsitiont food
DP 1Healthy
DP 2Fish
DP 3Red meatand alcohol
DP 4Intermediateintake
mean�standard deviation ™™™™™™™™™™™™™™™™™™™™™™™™™™™™™339.1 70a�57.9 94�43.9 113b�51.9 95�84.730.9 55�32.8 47�30.3 53�32.6 40a�43.037.1 79�37.9 91b�42.0 78�42.0 75�54.091.8 151�83.8 154�89.0 112�72.4 132�108.6170.0 388b�177.7 322�185.4 182a�203.4 229�228.0161.2 322b�163.2 293�138.0 194a�158.4 235�183.672.3 214�91.9 203�86.3 214�84.4 211�114.9237.8 427b�247.6 354�226.6 166a�247.3 266�285.566.0 178b�91.1 158�80.7 153a�92.0 167�96.68.3 11�9.0 12�8.4 9�7.0 11�11.445.8 36�46.2 34�37.0 28�39.6 41�56.835.5 38a�47.9 48�39.0 70b�63.0 57�68.4197.7 104�216.4 71�148.8 95�188.5 126�237.0
141.3 150a�329.2 494�361.3 745b�627.7 316�45.5
ly different from the remaining mean consumptions by performing multiple comparison
ly different from the remaining mean consumptions by performing multiple comparison
dieta
DP 4In trato fas
™™™™68�
44b�72�
159�314�299�162�440�131�12�
44b�42b�89�
74�
ificant
ificant
ith smoking and physical inactivity. Lastly, men with
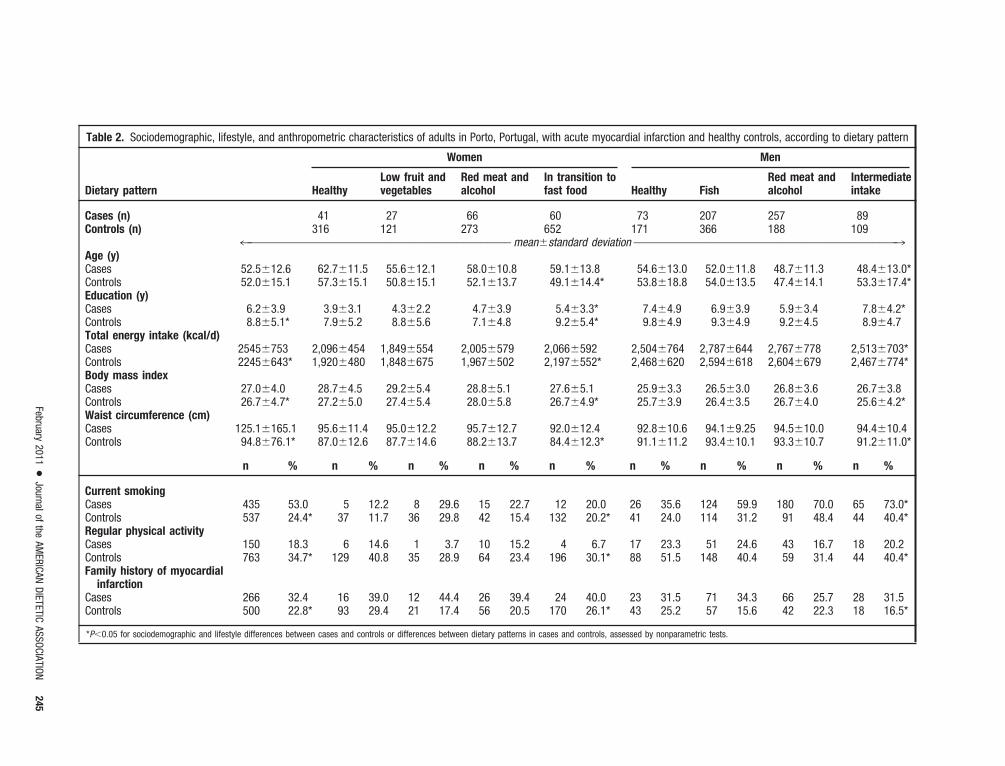
Table 2. Sociodemographic, lifestyle, and anthropometric characteristics of adults in Porto, Portugal, with acute myocardial infarction and healthy controls, according to dietary pattern
Dietary pattern
Women Men
HealthyLow fruit andvegetables
Red meat andalcohol
In transition tofast food Healthy Fish
Red meat andalcohol
Intermediateintake
Cases (n) 41 27 66 60 73 207 257 89Controls (n) 316 121 273 652 171 366 188 109
4™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™ mean�standard deviation ™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™3Age (y)Cases 52.5�12.6 62.7�11.5 55.6�12.1 58.0�10.8 59.1�13.8 54.6�13.0 52.0�11.8 48.7�11.3 48.4�13.0*Controls 52.0�15.1 57.3�15.1 50.8�15.1 52.1�13.7 49.1�14.4* 53.8�18.8 54.0�13.5 47.4�14.1 53.3�17.4*Education (y)Cases 6.2�3.9 3.9�3.1 4.3�2.2 4.7�3.9 5.4�3.3* 7.4�4.9 6.9�3.9 5.9�3.4 7.8�4.2*Controls 8.8�5.1* 7.9�5.2 8.8�5.6 7.1�4.8 9.2�5.4* 9.8�4.9 9.3�4.9 9.2�4.5 8.9�4.7Total energy intake (kcal/d)Cases 2545�753 2,096�454 1,849�554 2,005�579 2,066�592 2,504�764 2,787�644 2,767�778 2,513�703*Controls 2245�643* 1,920�480 1,848�675 1,967�502 2,197�552* 2,468�620 2,594�618 2,604�679 2,467�774*Body mass indexCases 27.0�4.0 28.7�4.5 29.2�5.4 28.8�5.1 27.6�5.1 25.9�3.3 26.5�3.0 26.8�3.6 26.7�3.8Controls 26.7�4.7* 27.2�5.0 27.4�5.4 28.0�5.8 26.7�4.9* 25.7�3.9 26.4�3.5 26.7�4.0 25.6�4.2*Waist circumference (cm)Cases 125.1�165.1 95.6�11.4 95.0�12.2 95.7�12.7 92.0�12.4 92.8�10.6 94.1�9.25 94.5�10.0 94.4�10.4Controls 94.8�76.1* 87.0�12.6 87.7�14.6 88.2�13.7 84.4�12.3* 91.1�11.2 93.4�10.1 93.3�10.7 91.2�11.0*
n % n % n % n % n % n % n % n % n %
Current smokingCasesControls
435537
53.024.4*
537
12.211.7
836
29.629.8
1542
22.715.4
12132
20.020.2*
2641
35.624.0
124114
59.931.2
18091
70.048.4
6544
73.0*40.4*
Regular physical activityCasesControls
150763
18.334.7*
6129
14.640.8
135
3.728.9
1064
15.223.4
4196
6.730.1*
1788
23.351.5
51148
24.640.4
4359
16.731.4
1844
20.240.4*
Family history of myocardialinfarction
CasesControls
266500
32.422.8*
1693
39.029.4
1221
44.417.4
2656
39.420.5
24170
40.026.1*
2343
31.525.2
7157
34.315.6
6642
25.722.3
2818
31.516.5*
*P�0.05 for sociodemographic and lifestyle differences between cases and controls or differences between dietary patterns in cases and controls, assessed by nonparametric tests.
February2011
●Journalof
theAM
ERICANDIETETIC
ASSOCIATION245
ai
p“car9tm(f4s3mtyta(B
tAWscPaPhPpah(Fnm
DIapwpAtbhwtwwfdip
ttfrtobpptewh
wmabet
2
n “intermediate intake” pattern had both lower energyntake and BMI (Table 2).
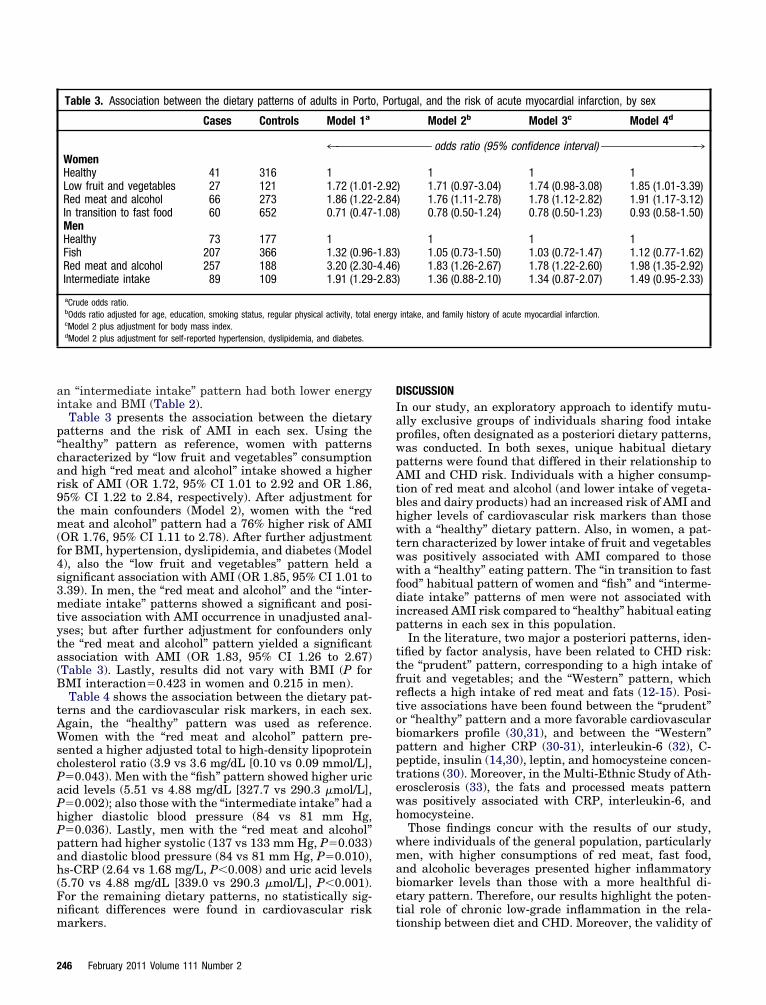
Table 3 presents the association between the dietaryatterns and the risk of AMI in each sex. Using thehealthy” pattern as reference, women with patternsharacterized by “low fruit and vegetables” consumptionnd high “red meat and alcohol” intake showed a higherisk of AMI (OR 1.72, 95% CI 1.01 to 2.92 and OR 1.86,5% CI 1.22 to 2.84, respectively). After adjustment forhe main confounders (Model 2), women with the “redeat and alcohol” pattern had a 76% higher risk of AMI
OR 1.76, 95% CI 1.11 to 2.78). After further adjustmentor BMI, hypertension, dyslipidemia, and diabetes (Model), also the “low fruit and vegetables” pattern held aignificant association with AMI (OR 1.85, 95% CI 1.01 to.39). In men, the “red meat and alcohol” and the “inter-ediate intake” patterns showed a significant and posi-
ive association with AMI occurrence in unadjusted anal-ses; but after further adjustment for confounders onlyhe “red meat and alcohol” pattern yielded a significantssociation with AMI (OR 1.83, 95% CI 1.26 to 2.67)Table 3). Lastly, results did not vary with BMI (P forMI interaction�0.423 in women and 0.215 in men).Table 4 shows the association between the dietary pat-
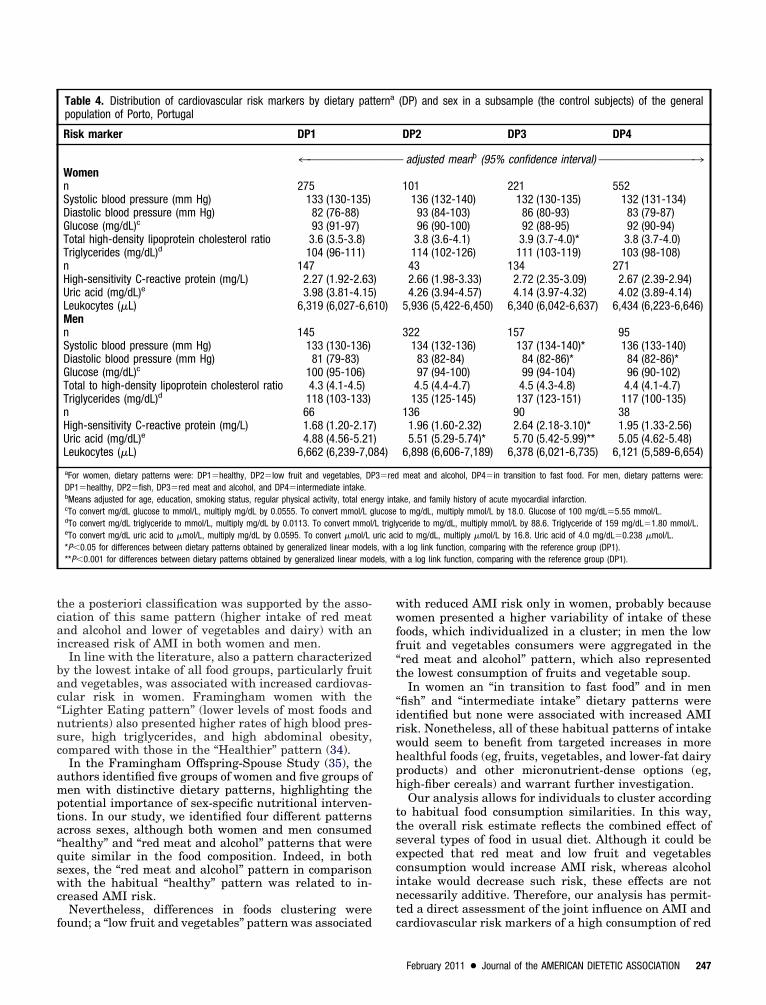
erns and the cardiovascular risk markers, in each sex.gain, the “healthy” pattern was used as reference.omen with the “red meat and alcohol” pattern pre-
ented a higher adjusted total to high-density lipoproteinholesterol ratio (3.9 vs 3.6 mg/dL [0.10 vs 0.09 mmol/L],�0.043). Men with the “fish” pattern showed higher uriccid levels (5.51 vs 4.88 mg/dL [327.7 vs 290.3 �mol/L],�0.002); also those with the “intermediate intake” had aigher diastolic blood pressure (84 vs 81 mm Hg,�0.036). Lastly, men with the “red meat and alcohol”attern had higher systolic (137 vs 133 mm Hg, P�0.033)nd diastolic blood pressure (84 vs 81 mm Hg, P�0.010),s-CRP (2.64 vs 1.68 mg/L, P�0.008) and uric acid levels5.70 vs 4.88 mg/dL [339.0 vs 290.3 �mol/L], P�0.001).or the remaining dietary patterns, no statistically sig-ificant differences were found in cardiovascular risk
Table 3. Association between the dietary patterns of adults in Porto
Cases Controls Model 1a
4™™™™™™™WomenHealthy 41 316 1Low fruit and vegetables 27 121 1.72 (1.01Red meat and alcohol 66 273 1.86 (1.22In transition to fast food 60 652 0.71 (0.47MenHealthy 73 177 1Fish 207 366 1.32 (0.96Red meat and alcohol 257 188 3.20 (2.30Intermediate intake 89 109 1.91 (1.29
aCrude odds ratio.bOdds ratio adjusted for age, education, smoking status, regular physical activity, totalcModel 2 plus adjustment for body mass index.dModel 2 plus adjustment for self-reported hypertension, dyslipidemia, and diabetes.
arkers. t
46 February 2011 Volume 111 Number 2
ISCUSSIONn our study, an exploratory approach to identify mutu-lly exclusive groups of individuals sharing food intakerofiles, often designated as a posteriori dietary patterns,as conducted. In both sexes, unique habitual dietaryatterns were found that differed in their relationship toMI and CHD risk. Individuals with a higher consump-
ion of red meat and alcohol (and lower intake of vegeta-les and dairy products) had an increased risk of AMI andigher levels of cardiovascular risk markers than thoseith a “healthy” dietary pattern. Also, in women, a pat-
ern characterized by lower intake of fruit and vegetablesas positively associated with AMI compared to thoseith a “healthy” eating pattern. The “in transition to fast
ood” habitual pattern of women and “fish” and “interme-iate intake” patterns of men were not associated withncreased AMI risk compared to “healthy” habitual eatingatterns in each sex in this population.In the literature, two major a posteriori patterns, iden-
ified by factor analysis, have been related to CHD risk:he “prudent” pattern, corresponding to a high intake ofruit and vegetables; and the “Western” pattern, whicheflects a high intake of red meat and fats (12-15). Posi-ive associations have been found between the “prudent”r “healthy” pattern and a more favorable cardiovasculariomarkers profile (30,31), and between the “Western”attern and higher CRP (30-31), interleukin-6 (32), C-eptide, insulin (14,30), leptin, and homocysteine concen-rations (30). Moreover, in the Multi-Ethnic Study of Ath-rosclerosis (33), the fats and processed meats patternas positively associated with CRP, interleukin-6, andomocysteine.Those findings concur with the results of our study,here individuals of the general population, particularlyen, with higher consumptions of red meat, fast food,
nd alcoholic beverages presented higher inflammatoryiomarker levels than those with a more healthful di-tary pattern. Therefore, our results highlight the poten-ial role of chronic low-grade inflammation in the rela-
tugal, and the risk of acute myocardial infarction, by sex
Model 2b Model 3c Model 4d
™™™™™ odds ratio (95% confidence interval) ™™™™™™™™™™™™™™™™3
1 1 1) 1.71 (0.97-3.04) 1.74 (0.98-3.08) 1.85 (1.01-3.39)) 1.76 (1.11-2.78) 1.78 (1.12-2.82) 1.91 (1.17-3.12)) 0.78 (0.50-1.24) 0.78 (0.50-1.23) 0.93 (0.58-1.50)
1 1 1) 1.05 (0.73-1.50) 1.03 (0.72-1.47) 1.12 (0.77-1.62)) 1.83 (1.26-2.67) 1.78 (1.22-2.60) 1.98 (1.35-2.92)) 1.36 (0.88-2.10) 1.34 (0.87-2.07) 1.49 (0.95-2.33)
intake, and family history of acute myocardial infarction.
, Por
™™™™
-2.92-2.84-1.08
-1.83-4.46-2.83
energy
ionship between diet and CHD. Moreover, the validity of
tcai
bac“nsc
ampta“qswc
f
wwff“t
“irwhph
ttsecint
els, wi
he a posteriori classification was supported by the asso-iation of this same pattern (higher intake of red meatnd alcohol and lower of vegetables and dairy) with anncreased risk of AMI in both women and men.
In line with the literature, also a pattern characterizedy the lowest intake of all food groups, particularly fruitnd vegetables, was associated with increased cardiovas-ular risk in women. Framingham women with theLighter Eating pattern” (lower levels of most foods andutrients) also presented higher rates of high blood pres-ure, high triglycerides, and high abdominal obesity,ompared with those in the “Healthier” pattern (34).In the Framingham Offspring-Spouse Study (35), the
uthors identified five groups of women and five groups ofen with distinctive dietary patterns, highlighting the
otential importance of sex-specific nutritional interven-ions. In our study, we identified four different patternscross sexes, although both women and men consumedhealthy” and “red meat and alcohol” patterns that wereuite similar in the food composition. Indeed, in bothexes, the “red meat and alcohol” pattern in comparisonith the habitual “healthy” pattern was related to in-
reased AMI risk.Nevertheless, differences in foods clustering were
Table 4. Distribution of cardiovascular risk markers by dietary patpopulation of Porto, Portugal
Risk marker DP1
4™™™™™™™™™™™Womenn 275Systolic blood pressure (mm Hg) 133 (130-135)Diastolic blood pressure (mm Hg) 82 (76-88)Glucose (mg/dL)c 93 (91-97)Total high-density lipoprotein cholesterol ratio 3.6 (3.5-3.8)Triglycerides (mg/dL)d 104 (96-111)n 147High-sensitivity C-reactive protein (mg/L) 2.27 (1.92-2.63Uric acid (mg/dL)e 3.98 (3.81-4.15Leukocytes (�L) 6,319 (6,027-6,6Menn 145Systolic blood pressure (mm Hg) 133 (130-136)Diastolic blood pressure (mm Hg) 81 (79-83)Glucose (mg/dL)c 100 (95-106)Total to high-density lipoprotein cholesterol ratio 4.3 (4.1-4.5)Triglycerides (mg/dL)d 118 (103-133)n 66High-sensitivity C-reactive protein (mg/L) 1.68 (1.20-2.17Uric acid (mg/dL)e 4.88 (4.56-5.21Leukocytes (�L) 6,662 (6,239-7,0
aFor women, dietary patterns were: DP1�healthy, DP2�low fruit and vegetables, DPDP1�healthy, DP2�fish, DP3�red meat and alcohol, and DP4�intermediate intake.bMeans adjusted for age, education, smoking status, regular physical activity, total enecTo convert mg/dL glucose to mmol/L, multiply mg/dL by 0.0555. To convert mmol/L gdTo convert mg/dL triglyceride to mmol/L, multiply mg/dL by 0.0113. To convert mmol/eTo convert mg/dL uric acid to �mol/L, multiply mg/dL by 0.0595. To convert �mol/L*P�0.05 for differences between dietary patterns obtained by generalized linear model**P�0.001 for differences between dietary patterns obtained by generalized linear mod
ound; a “low fruit and vegetables” pattern was associated c
ith reduced AMI risk only in women, probably becauseomen presented a higher variability of intake of these
oods, which individualized in a cluster; in men the lowruit and vegetables consumers were aggregated in thered meat and alcohol” pattern, which also representedhe lowest consumption of fruits and vegetable soup.
In women an “in transition to fast food” and in menfish” and “intermediate intake” dietary patterns weredentified but none were associated with increased AMIisk. Nonetheless, all of these habitual patterns of intakeould seem to benefit from targeted increases in moreealthful foods (eg, fruits, vegetables, and lower-fat dairyroducts) and other micronutrient-dense options (eg,igh-fiber cereals) and warrant further investigation.Our analysis allows for individuals to cluster according
o habitual food consumption similarities. In this way,he overall risk estimate reflects the combined effect ofeveral types of food in usual diet. Although it could bexpected that red meat and low fruit and vegetablesonsumption would increase AMI risk, whereas alcoholntake would decrease such risk, these effects are notecessarily additive. Therefore, our analysis has permit-ed a direct assessment of the joint influence on AMI and
(DP) and sex in a subsample (the control subjects) of the general
DP2 DP3 DP4
™ adjusted meanb (95% confidence interval) ™™™™™™™™™™™™™™™™3
101 221 552136 (132-140) 132 (130-135) 132 (131-134)93 (84-103) 86 (80-93) 83 (79-87)96 (90-100) 92 (88-95) 92 (90-94)3.8 (3.6-4.1) 3.9 (3.7-4.0)* 3.8 (3.7-4.0)
114 (102-126) 111 (103-119) 103 (98-108)43 134 2712.66 (1.98-3.33) 2.72 (2.35-3.09) 2.67 (2.39-2.94)4.26 (3.94-4.57) 4.14 (3.97-4.32) 4.02 (3.89-4.14)
5,936 (5,422-6,450) 6,340 (6,042-6,637) 6,434 (6,223-6,646)
322 157 95134 (132-136) 137 (134-140)* 136 (133-140)83 (82-84) 84 (82-86)* 84 (82-86)*97 (94-100) 99 (94-104) 96 (90-102)4.5 (4.4-4.7) 4.5 (4.3-4.8) 4.4 (4.1-4.7)
135 (125-145) 137 (123-151) 117 (100-135)136 90 38
1.96 (1.60-2.32) 2.64 (2.18-3.10)* 1.95 (1.33-2.56)5.51 (5.29-5.74)* 5.70 (5.42-5.99)** 5.05 (4.62-5.48)
6,898 (6,606-7,189) 6,378 (6,021-6,735) 6,121 (5,589-6,654)
meat and alcohol, DP4�in transition to fast food. For men, dietary patterns were:
ke, and family history of acute myocardial infarction.to mg/dL, multiply mmol/L by 18.0. Glucose of 100 mg/dL�5.55 mmol/L.ceride to mg/dL, multiply mmol/L by 88.6. Triglyceride of 159 mg/dL�1.80 mmol/L.id to mg/dL, multiply �mol/L by 16.8. Uric acid of 4.0 mg/dL�0.238 �mol/L.a log link function, comparing with the reference group (DP1).th a log link function, comparing with the reference group (DP1).
terna
™™™™
))10)
))84)
3�red
rgy intalucoseL triglyuric acs, with
ardiovascular risk markers of a high consumption of red
February 2011 ● Journal of the AMERICAN DIETETIC ASSOCIATION 247

mv
ieiptetslichwA“sagFbiferpst
lriwacwdrtthMbii5
mshptpatnomrBc
iba
ts(Aogiteha“btA
MTttbsilwaorl
cmbsod(dtc
paetmptambfpsracf
2
eat and alcohol accompanied by a low consumption ofegetables and dairy products.Of note is that alcohol consumption has seldom been
dentified as a main component of most a posteriori di-tary patterns in the literature. One reason might be thensufficient variation in alcohol intake in North Americanopulations, where most studies have been conducted. Onhe other hand, the European region has one of the high-st alcohol intakes in the world and, in particular, Por-ugal presents a high level and a large variation in con-umption of alcohol from wine sources in men (36,37). Inine with our results, in the ATTICA Study in Greece (16),n which 15 dietary patterns were extracted by principalomponent analysis, the pattern characterized by theigh intake of red meat, alcohol, sweets, and hard cheeseas prospectively associated with cardiovascular disease.lso, in the Moli-sani project conducted in Italy (38), the
Pasta and Meat” pattern (high intake of pasta, tomatoauce, red meat, animal fats, and alcohol) was positivelyssociated with some cardiovascular risk markers (ie,lucose, lipids, and hs-CRP). Moreover, women of theramingham Offspring-Spouse study (34) characterizedy the “wine and moderate eating” pattern (ie, higherntakes of alcohol, particularly wine, cholesterol-richoods, high-fat dairy, and snack foods) had higher rates oflevated blood pressure, as found in our study. Previousesults have already suggested that women with thisattern may be at somewhat higher risk of carotid steno-is (39), which is in line with our findings on the effect ofhe “red meat and alcohol” pattern on AMI occurrence.
Each pattern described in this study points to certainess healthful food choices, which could guide nutritionecommendations and help reduce CHD risk. Therefore,n our particular population and probably also in othersith similar drinking and eating patterns, guidance onlcohol intake must be extremely prudent, since alcohollustered with red meat intake was inversely associatedith other, healthier foods, such as fruit, vegetables, andairy products, resulting in an overall increase of AMIisk in both sexes. Also of note is that the magnitude ofhe association between the “red meat and alcohol” pat-ern and AMI was similar in each sex, despite the muchigher alcohol intake observed in men than in women.oreover, recommendations to increase fruit and vegeta-
les consumption might serve to reduce coronary morbid-ty even in our population, which already has a highntake of such foods (mean consumption of approximately00 g/day of fruit and vegetables).The association between dietary patterns and sociode-ographic, lifestyle, and anthropometric characteristics
uggest that food choices are a part of a larger pattern ofealth behaviors. Individuals with the “healthy” dietaryattern were more often nonsmokers and physically ac-ive; in contrast, men with the “red meat and alcohol”attern had higher BMI, and were less physically active,nd were the most frequently smokers. Therefore, al-hough analyses have adjusted for these factors, it doesot rule out an interaction between dietary patterns andther cardiovascular risk factors. For instance, BMI couldodify the relation between dietary patterns and CHD
isk (15), but we found no significant interaction betweenMI and diet on AMI risk. Including BMI or waist cir-
umference as covariates in multivariate models resulted v
48 February 2011 Volume 111 Number 2
n a small attenuating effect, suggesting that the relationetween diet and AMI could be independent of body fat,s reported elsewhere (12,13).Also noteworthy are the similarities between some of
he identified patterns and the concept of an Atlantic-tyle diet (20,21) rooted in regions on the Atlantic shoreparticularly Northern Portugal and Galiza, Spain). Thetlantic-style diet is characterized by a high consumptionf fresh fish, cod fish, red meat and pork products, le-umes, vegetables, and potatoes, as well as by a moderatentake of wine (40). In our study, it seems that a transi-ion from a traditional Atlantic-style diet to a more West-rn-type pattern is ongoing, since women in this patternave already adopted products such as fast foods, sweets,nd white meats as main food consumptions. In men, thefish” pattern, characterized by the highest intake of fish,ut also higher intakes of red meat and vegetables, par-icularly vegetable soup, holds important features of thetlantic-style diet.
ethodologic Aspectshis is a population-based case-control study, whose con-rols were selected from the catchment area of the hospi-als where cases were recruited. A previous comparisonetween community participants and refusals in ourtudy (25) showed that nonparticipation had little or nompact on risk estimates of AMI, which suggests a lowikelihood of nonresponse bias. Recruitment of AMI casesas done consecutively, which minimizes selection biast this level. Moreover, participating hospitals are thenes providing acute coronary care in Porto, so that aepresentative sample of all nonfatal AMI patients wasikely obtained.
To minimize survival and recall bias, only incident AMIases were included. Also, data collection was done im-ediately after diagnosis, to avoid bias resulting from
ehavior change after the coronary event. Previous re-earch has shown that dietary patterns are fairly stablever time (30,41), which supports a single assessment ofietary intake. Moreover, we also excluded individuals21 cases and 75 controls) who reported dietary changesuring the preceding year. However, as in any case-con-rol study, some recall bias may have occurred given thatases tend to recall past diet differently than controls.Most studies have used factor analysis, principal com-
onent analysis, or combinatorial algorithms of clusternalysis to derive a posteriori dietary patterns (42). How-ver, recent research suggests that the use of finite mix-ure models for the identification of dietary patternsight entail some advantages over the previous ap-
roaches (29). This method allows that problems of de-ermining the number of clusters and of choosing anppropriate clustering method to be recast as statisticalodel choice problems. It also produces posterior cluster
elonging probabilities for each subject, given individualood intakes and any other relevant variables, thereforeroviding measures of uncertainty of the associated clas-ification (in this study we found high individual poste-ior probabilities: 89% in women and 94% in men). Inddition, it allows for the adjustment of food consumptionovariates simultaneously with the fitting process, andor the size of pattern to depend on a set of (concomitant)
ariables. Moreover, in our study food nonconsumption
wit
CDwarwp(batetraah
SNt
F(a
hhHG
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
as not treated as a continuous variable; our solutionncluded dichotomizing food groups whose nonconsump-ion was, roughly, �50%.
ONCLUSIONSietary patterns identified in the population of Portoere characterized by differing levels of more-healthfulnd less-healthful foods and varying levels of diseaseisk. Compared to a healthy dietary pattern, a patternith lower fruit and vegetable intakes in women, and aattern with higher consumption of red meat and alcoholand lower intake of dairy products and vegetables) inoth sexes, were associated with an increased risk of AMInd adverse cardiovascular risk profiles. Nonetheless,hese findings suggest that all dietary patterns may ben-fit from targeted and sex-specific nutrition interventionso reduce coronary risk and to achieve current expertecommendations for improving nutritional status, suchs increase fruit and vegetable consumption, and limitnimal fats and alcohol intake, which clusters with lessealthy dietary patterns of men and women.
TATEMENT OF POTENTIAL CONFLICT OF INTEREST:o potential conflict of interest was reported by the au-
hors.FUNDING/SUPPORT: This study was funded by
undação para a Ciência e a Tecnologia, Portugal.POCTI/ESP/42361/2001, POCTI/SAU-ESP/61160/2004,nd SFRH/BD/31131/2006).ACKNOWLEDGEMENTS: The authors thank the
ead and staff of the Cardiology Departments of the fourospitals collaborating in this study: Hospital São João,ospital Pedro Hispano, Centro Hospitalar Vila Nova deaia, and Hospital Geral Santo António.
eferences1. Hu FB. Dietary pattern analysis: A new direction in nutritional epi-
demiology. Curr Opin Lipidol. 2002;13:3-9.2. Hu FB, Willett WC. Optimal diets for prevention of coronary heart
disease. JAMA. 2002;288:2569-2578.3. Bach A, Serra-Majem L, Carrasco JL, Roman B, Ngo J, Bertomeu I,
Obrador B. The use of indexes evaluating the adherence to the Med-iterranean diet in epidemiological studies: A review. Public HealthNutr. 2006;9:132-146.
4. Kant AK. Dietary patterns and health outcomes. J Am Diet Assoc.2004;104:615-635.
5. Alberti-Fidanza A, Fidanza F. Mediterranean Adequacy Index of Ital-ian diets. Public Health Nutr. 2004;7:937-941.
6. Panagiotakos DB, Pitsavos C, Arvaniti F, Stefanadis C. Adherence tothe Mediterranean food pattern predicts the prevalence of hyperten-sion, hypercholesterolemia, diabetes and obesity, among healthyadults; the accuracy of the MedDietScore. Prev Med. 2007;44:335-340.
7. Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence toa Mediterranean diet and survival in a Greek population. N EnglJ Med. 2003;348:2599-2608.
8. Ruidavets JB, Bataille V, Dallongeville J, Simon C, Bingham A,Amouyel P, Arveiler D, Ducimetière P, Ferrières J. Alcohol intake anddiet in France, the prominent role of lifestyle. Eur Heart J. 2004;25:1153-1162.
9. Sieri S, Agudo A, Kesse E, Klipstein-Grobusch K, San-José B, WelchAA, Krogh V, Luben R, Allen N, Overvad K, Tjønneland A, Clavel-Chapelon F, Thiébaut A, Miller AB, Boeing H, Kolyva M, Saieva C,Celentano E, Ocké MC, Peeters PH, Brustad M, Kumle M, DorronsoroM, Fernandez Feito A, Mattisson I, Weinehall L, Riboli E, Slimani N.Patterns of alcohol consumption in 10 European countries participat-ing in the European Prospective Investigation into Cancer and Nu-
trition (EPIC) project. Public Health Nutr. 2002;5:1287-1296.0. Breslow RA, Guenther PM, Smothers BA. Alcohol drinking patterns3
and diet quality: The 1999-2000 National Health and Nutrition Ex-amination Survey. Am J Epidemiol. 2006;163:359-366.
1. Kesse E, Clavel-Chapelon F, Slimani N, van Liere M. Do eating habitsdiffer according to alcohol consumption? Results of a study of theFrench cohort of the European Prospective Investigation into Cancerand Nutrition (E3N-EPIC). Am J Clin Nutr. 2001;74:322-327.
2. Fung TT, Willett WC, Stampfer MJ, Manson JE, Hu FB. Dietarypatterns and the risk of coronary heart disease in women. Arch InternMed. 2001;161:1857-1862.
3. Hu FB, Rimm EB, Stampfer MJ, Ascherio A, Spiegelman D, WillettWC. Prospective study of major dietary patterns and risk of coronaryheart disease in men. Am J Clin Nutr. 2000;72:912-921.
4. Kerver JM, Yang EJ, Bianchi L, Song WO. Dietary patterns associ-ated with risk factors for cardiovascular disease in healthy US adults.Am J Clin Nutr. 2003;78:1103-1110.
5. Osler M, Helms Andreasen A, Heitmann B, Hoidrup S, Gerdes U,Morch Jorgensen L. Food intake patterns and risk of coronary heartdisease: A prospective cohort study examining the use of traditionalscoring techniques. Eur J Clin Nutr. 2002;56:568-574.
6. Panagiotakos D, Pitsavos C, Chrysohoou C, Palliou K, Lentzas I,Skoumas I, Stefanadis C. Dietary patterns and 5-year incidence ofcardiovascular disease: A multivariate analysis of the ATTICA study.Nutr Metab Cardiovasc Dis. 2009;19:253-263.
7. Marques-Vidal P, Ravasco P, Dias CM, Camilo ME. Trends of foodintake in Portugal, 1987-1999: Results from the National HealthSurveys. Eur J Clin Nutr. 2006;60:1414-1422.
8. Robertson A, Tirado C, Lobstein T, Jermini M, Knai C, Jensen J. Foodand health in Europe: A new basis for action. Copenhagen, Denmark:WHO Regional Publications; 2004. European Series No. 96.
9. Rodrigues SS, Caraher M, Trichopoulou A, de Almeida MD. Portu-guese households’ diet quality (adherence to Mediterranean food pat-tern and compliance with WHO population dietary goals): Trends,regional disparities and socioeconomic determinants. Eur J ClinNutr. 2008;62:1263-1272.
0. IV International Meeting of Diet and Nutrition in the XXI century—Atlantic Diet. Obesity as a Public Health problem [in Spanish]. Ma-drid, Spain: Fundación Española de la Nutrición; 2008.
1. Varela G, Moreiras O, Ansón R, Ávila JM, Cuadrado C, Estalrich P.Food Consumption in Galicia—the Atlantic Diet [in Spanish]. Madrid,Spain: Fundación Española de la Nutrición; 2004.
2. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarctionredefined—A consensus document of The Joint European Society ofCardiology/American College of Cardiology Committee for the redef-inition of myocardial infarction. J Am Coll Cardiol. 2000;36:959-969.
3. Folstein M, Folstein S, McHush R. ‘Mini-mental state’. A practicalmethod for grading the cognitive state of patients for the clinician.J Psychiatr Res. 1975;12:189-198.
4. Anthony JC, LeResche L, Niaz U, von Korff MR, Folstein MF. Limitsof the ‘Mini-Mental State’ as a screening test for dementia and delir-ium among hospital patients. Psychol Med. 1982;12:397-408.
5. Ramos E, Lopes C, Barros H. Investigating the effect of nonpartici-pation using a population-based case-control study on myocardialinfarction. Ann Epidemiol. 2004;14:437-441.
6. Yeh ET, Willerson JT. Coming of age of C-reactive protein: Usinginflammation markers in cardiology. Circulation. 2003;107:370-371.
7. Lopes C. Reproducibility and validity of a semi-quantitative food-frequency questionnaire. In: Diet and Acute Myocardial Infarction: APopulation-Based Case-Control Study [in Portuguese]. Porto, Portu-gal: University of Porto; 2000:79-115.
8. Lopes C, Aro A, Azevedo A, Ramos E, Barros H. Intake and adiposetissue composition of fatty acids and risk of myocardial infarction in amale Portuguese community sample. J Am Diet Assoc. 2007;107:276-286.
9. Fahey MT, Thane CW, Bramwell GD, Coward WA. ConditionalGaussian mixture modelling for dietary pattern analysis. J Royal StatSoc Series A. 2007;170(Part 1):149-166.
0. Fung TT, Rimm EB, Spiegelman D, Rifai N, Tofler GH, Willett WC,Hu FB. Association between dietary patterns and plasma biomarkersof obesity and cardiovascular disease risk. Am J Clin Nutr. 2001;73:61-67.
1. Lopez-Garcia E, Schulze MB, Fung TT, Meigs JB, Rifai N, MansonJE, Hu FB. Major dietary patterns are related to plasma concentra-tions of markers of inflammation and endothelial dysfunction. Am JClin Nutr. 2004;80:1029-1035.
2. Esmaillzadeh A, Kimiagar M, Mehrabi Y, Azadbakht L, Hu FB,Willett WC. Dietary patterns and markers of systemic inflammationamong Iranian women. J Nutr. 2007;137:992-998.
3. Nettleton JA, Steffen LM, Mayer-Davis EJ, Jenny NS, Jiang R, Her-rington DM. Dietary patterns are associated with biochemical mark-
February 2011 ● Journal of the AMERICAN DIETETIC ASSOCIATION 249

3
3
3
3
3
3
4
4
2
ers of inflammation and endothelial activation in the Multi-EthnicStudy of Atherosclerosis (MESA). Am J Clin Nutr. 2006;83:1369-1379.
4. Sonnenberg L, Pencina M, Kimokoti R, Quatromoni P, Nam BH,D’Agostino R. Dietary patterns and the metabolic syndrome in obeseand non-obese Framingham women. Obes Res. 2005;13:153-162.
5. Millen BE, Quatromoni PA, Gagnon DR, Cupples LA, Franz MM,D’Agostino RB. Dietary patterns of men and women suggest targetsfor health promotion: The Framingham Nutrition Studies. Am JHealth Promot. 1996;11:42-52.
6. Rehn N, Room R, Edwards G. Alcohol in the European region—Consumption, harm and policies. World Health Organization, Re-gional Office for Europe Web site. 2001. http://www.euro.who.int/document/E76240.pdf. Accessed March 8, 2010.
7. Marques-Vidal P, Dias CM. Trends and determinants of alcoholconsumption in Portugal: Results from the national health sur-
veys 1995 to 1996 and 1998 to 1999. Alcohol Clin Exp Res. 2005;29:89-97.4
50 February 2011 Volume 111 Number 2
8. Centritto F, Iacoviello L, di Giuseppe R, De Curtis A, Costanzo S, ZitoF, Grioni S, Sieri S, Donati MB, de Gaetano G, Di Castelnuovo A.Dietary patterns, cardiovascular risk factors and C-reactive protein ina healthy Italian population. Nutr Metab Cardiovasc Dis. 2009;19:697-706.
9. Millen BE, Quatromoni PA, Nam BH, O’Horo CE, Polak JF,D’Agostino RB. Dietary patterns and the odds of carotid atheroscle-rosis in women: The Framingham Nutrition Studies. Prev Med. 2002;35:540-547.
0. Oliveira A, Lopes C, Rodríguez-Artalejo F. Adherence to the South-ern-European Atlantic diet and occurrence of non-fatal acute myocar-dial infarction. J Am Clin Nutr. 2010;92:1-7.
1. Mikkila V, Rasanen L, Raitakari OT, Pietinen P, Viikari J. Consistentdietary patterns identified from childhood to adulthood: The cardio-vascular risk in Young Finns Study. Br J Nutr. 2005;93:923-931.
2. Newby PK, Tucker KL. Empirically derived eating patterns usingfactor or cluster analysis: A review. Nutr Rev. 2004;62:177-203.
Copyright © 2022 FDOKUMEN




















