
Long-Term Efficacy and Safety of Fosamprenavir in Human Immunodeficiency Virus-Infected Pediatric...
18
BRIEF REPORTS POSTVACCINATION THROMBOCYTOPENIA IN CANADA Laura J. Sauve ´, MD, MPH,* Julie Bettinger, PhD,* David Scheifele, MD,* Scott Halperin, MD,† Wendy Vaudry, MD,‡ Barbara Law, MD,§ and the members of the Canadian Immunization Monitoring Program, and Active (IMPACT) Abstract: Active surveillance data from 12 Canadian tertiary-care hospi- tals on children hospitalized with postvaccination thrombocytopenia were analyzed. Since 1992, there have been 107 cases reported; while 96% of the children were symptomatic, only 2 had severe bleeding. With treat- ment, 28 children (26%) had normal platelet counts on discharge from hospital and 93% had documented recovery within 3 months. Key Words: adverse events following immunization, thrombocytopenia, measles vaccine Accepted for publication January 5, 2010. From the *Vaccine Evaluation Center, BC Children’s Hospital and the Univer- sity of British Columbia, Vancouver, British Columbia, Canada; †Canadian Center for Vaccinology, IWK Health Center and Dalhousie University, Halifax, Nova Scotia, Canada; ‡Division of Infectious Diseases, Depart- ment of Pediatrics, Stollery Children’s Hospital and University of Alberta, Edmonton, Alberta, Canada; and §Centre for Immunization and Respiratory Infectious Diseases Division, Surveillance and Outbreak Response Division, Public Health Agency of Canada, Ottawa, Ontario, Canada. The Canadian Immunization Monitoring Program, Active (IMPACT), is a national surveillance initiative funded by Public Health Agency of Canada, managed by the Canadian Pediatric Society and conducted by the IMPACT network of pediatric investigators. Address for correspondence: Laura Sauve ´, MD, MPH, Vaccine Evaluation Center, BC Children’s Hospital, 950 West 28th Avenue, Vancouver, British Columbia, Canada V5Z 4H4. E-mail: [email protected]. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.pidj.com). Copyright © 2010 by Lippincott Williams & Wilkins DOI: 10.1097/INF.0b013e3181d2bb45 T here is an increasing evidence to support a link between vacci- nations and thrombocytopenia, which occurs after approximately 1 in 25,000 to 1 in 40,000 doses of measles-mumps-rubella (MMR) vaccine 1–4 and less frequently after other vaccines. 4 Vaccine safety is important to ensure ongoing acceptance of vaccines. Active surveillance for adverse events following immu- nization is a significant part of assuring vaccine safety. A challenge with all surveillance for adverse events following immunization is determination of whether events are causally linked to a vaccine or are only temporally linked. In the case of postvaccination throm- bocytopenia, this is particularly difficult because possible cases often also have other risk factors for thrombocytopenia such as recent viral infection or use of certain medications. The purpose of this report is to review the clinical course and outcome of postvaccination thrombocytopenia in Canada since 1992 and to examine prevalence trends with the addition of new vaccines, such as varicella, to the childhood schedule. METHODS Since 1992, the Immunization Monitoring Program, Active (IMPACT) has collected active surveillance data on postvaccination thrombocytopenia. The 12 current participating centers account for more than 90% the nation’s tertiary care pediatric beds. The number of IMPACT centers has increased from 8 centers in 1992 to 10 in 1993–1995, 11 in 1996, and 12 since 1999. This review includes cases previously reported by Jadavji et al 5 from 1993 to 2002. Canada’s annual birth cohort is 350 to 400,000 live births. 6 Each province and territory sets its own publicly funded vaccination schedule. Nation- wide, the first dose of MMR vaccine is recommended after the first birthday, with a second dose either at 18 months or at 4 to 6 years. The estimated coverage of the first dose of MMR vaccine by the age of 2 is 97%, and is 79% for the second dose by age 7, 7 so approximately 700,000 doses are administered annually. Varicella vaccine was first licensed in Canada in 1998, and 1 dose is recommended after the first birthday. Uptake was low before it was funded as part of provincial public health vaccination programs between 2000 and 2005. 8 In the most recent national vaccine uptake survey, in 2004, only 32% of 2 year olds had received the vaccine. 7 Trained nurse monitors reviewed daily admissions and coded discharge diagnoses for children admitted with acute throm- bocytopenia with onset within 1 month of documented receipt of any vaccine. Each patient’s hospital record was abstracted using a standardized form that included demographics, vaccination his- tory, hematology laboratory data, underlying health conditions and information on the presentation, duration and management of the postvaccination thrombocytopenia. It also included information on other exposures potentially associated with thrombocytopenia such as recent acute viral infections and use of medications; cases were not excluded on the basis of such exposures. Follow-up data are collected up to 3 months later for children whose platelet counts had not normalized by the time of discharge based on data from either the medical record or the patient’s physician. The Brighton Collaboration, which sets standards for reporting adverse events following immunization, defines postvaccination thrombocytopenia as a platelet count of less than 150 10 9 /L. 9 IMPACT identifies the most severe cases, who are admitted to hospital with platelets 100 10 9 /L and no obvious other cause, such as cancer chemotherapy. The IMPACT project is approved by the research ethics board at each center. Information was entered into an Access database (Microsoft Corp., Redmond, WA) and analyzed using SAS 9.0 (SAS Corporation, Cary, NC). RESULTS We identified 107 hospitalized children with postvaccination thrombocytopenia, and the results are summarized in Table 1. There was a mean of 8.2 cases per year since 1996 (with the increase to 10 centers in the IMPACT network); this did not change after the introduction of varicella vaccine after 2002 (Fig., Supplemental Dig- ital Content 1, http://links.lww.com/INF/A377, which shows number of cases per year by vaccine group). The median age at presentation was 13 months (range, 9 weeks–15.6 years). Most children were previously healthy; underlying conditions included congenital heart disease, prematurity, and diabetes. Five children had had prior epi- sodes of thrombocytopenia, all unrelated to a vaccination; etiologies included prematurity with sepsis and congenital amegakaryocytic thrombocytopenia. Postvaccination thrombocytopenia was the pre- senting event for acute lymphocytic leukemia in one child. A preced- ing “viral” illness was reported in 76, or 71% of cases, and medication use that can be associated with thrombocytopenia was reported in 14 of those (no children had reported medication use without a preceding viral illness). There was no statistically significant difference between the proportions reporting a viral illness after MMR vaccine than other vaccines. A total of 77 cases followed administration of MMR vac- cine (Table 1); 25 of those 77 children had received one or more additional vaccines as well (Fig., Supplemental Digital Content 2, http://links.lww.com/INF/A378, which shows which vaccines were associated with thrombocytopenia). There were no substan- tive differences in demographics, presentation, or clinical course The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 www.pidj.com | 559
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Long-Term Efficacy and Safety of Fosamprenavir in Human Immunodeficiency Virus-Infected Pediatric...

BRIEF REPORTS
POSTVACCINATION THROMBOCYTOPENIA INCANADA
Laura J. Sauve, MD, MPH,* Julie Bettinger, PhD,*David Scheifele, MD,* Scott Halperin, MD,† Wendy Vaudry, MD,‡Barbara Law, MD,§ and the members of the CanadianImmunization Monitoring Program, and Active (IMPACT)
Abstract: Active surveillance data from 12 Canadian tertiary-care hospi-tals on children hospitalized with postvaccination thrombocytopenia wereanalyzed. Since 1992, there have been 107 cases reported; while 96% ofthe children were symptomatic, only 2 had severe bleeding. With treat-ment, 28 children (26%) had normal platelet counts on discharge fromhospital and 93% had documented recovery within 3 months.
Key Words: adverse events following immunization, thrombocytopenia,measles vaccine
Accepted for publication January 5, 2010.From the *Vaccine Evaluation Center, BC Children’s Hospital and the Univer-
sity of British Columbia, Vancouver, British Columbia, Canada; †CanadianCenter for Vaccinology, IWK Health Center and Dalhousie University,Halifax, Nova Scotia, Canada; ‡Division of Infectious Diseases, Depart-ment of Pediatrics, Stollery Children’s Hospital and University of Alberta,Edmonton, Alberta, Canada; and §Centre for Immunization and RespiratoryInfectious Diseases Division, Surveillance and Outbreak Response Division,Public Health Agency of Canada, Ottawa, Ontario, Canada.
The Canadian Immunization Monitoring Program, Active (IMPACT), is anational surveillance initiative funded by Public Health Agency ofCanada, managed by the Canadian Pediatric Society and conducted bythe IMPACT network of pediatric investigators.
Address for correspondence: Laura Sauve, MD, MPH, Vaccine EvaluationCenter, BC Children’s Hospital, 950 West 28th Avenue, Vancouver,British Columbia, Canada V5Z 4H4. E-mail: [email protected].
Supplemental digital content is available for this article. Direct URLcitations appear in the printed text and are provided in the HTML andPDF versions of this article on the journal’s Web site (www.pidj.com).
Copyright © 2010 by Lippincott Williams & WilkinsDOI: 10.1097/INF.0b013e3181d2bb45
There is an increasing evidence to support a link between vacci-nations and thrombocytopenia, which occurs after approximately
1 in 25,000 to 1 in 40,000 doses of measles-mumps-rubella (MMR)vaccine1–4 and less frequently after other vaccines.4
Vaccine safety is important to ensure ongoing acceptance ofvaccines. Active surveillance for adverse events following immu-nization is a significant part of assuring vaccine safety. A challengewith all surveillance for adverse events following immunization isdetermination of whether events are causally linked to a vaccine orare only temporally linked. In the case of postvaccination throm-bocytopenia, this is particularly difficult because possible casesoften also have other risk factors for thrombocytopenia such asrecent viral infection or use of certain medications.
The purpose of this report is to review the clinical courseand outcome of postvaccination thrombocytopenia in Canada since1992 and to examine prevalence trends with the addition of newvaccines, such as varicella, to the childhood schedule.
METHODSSince 1992, the Immunization Monitoring Program, Active
(IMPACT) has collected active surveillance data on postvaccinationthrombocytopenia. The 12 current participating centers account formore than 90% the nation’s tertiary care pediatric beds. The numberof IMPACT centers has increased from 8 centers in 1992 to 10 in1993–1995, 11 in 1996, and 12 since 1999. This review includes casespreviously reported by Jadavji et al5 from 1993 to 2002. Canada’s
annual birth cohort is 350 to 400,000 live births.6 Each province andterritory sets its own publicly funded vaccination schedule. Nation-wide, the first dose of MMR vaccine is recommended after the firstbirthday, with a second dose either at 18 months or at 4 to 6 years. Theestimated coverage of the first dose of MMR vaccine by the age of 2is 97%, and is 79% for the second dose by age 7,7 so approximately700,000 doses are administered annually. Varicella vaccine was firstlicensed in Canada in 1998, and 1 dose is recommended after the firstbirthday. Uptake was low before it was funded as part of provincialpublic health vaccination programs between 2000 and 2005.8 In themost recent national vaccine uptake survey, in 2004, only 32% of 2year olds had received the vaccine.7
Trained nurse monitors reviewed daily admissions andcoded discharge diagnoses for children admitted with acute throm-bocytopenia with onset within 1 month of documented receipt ofany vaccine. Each patient’s hospital record was abstracted using astandardized form that included demographics, vaccination his-tory, hematology laboratory data, underlying health conditions andinformation on the presentation, duration and management of thepostvaccination thrombocytopenia. It also included information onother exposures potentially associated with thrombocytopenia suchas recent acute viral infections and use of medications; cases werenot excluded on the basis of such exposures. Follow-up data arecollected up to 3 months later for children whose platelet countshad not normalized by the time of discharge based on data fromeither the medical record or the patient’s physician.
The Brighton Collaboration, which sets standards for reportingadverse events following immunization, defines postvaccinationthrombocytopenia as a platelet count of less than 150 � 109/L.9
IMPACT identifies the most severe cases, who are admitted tohospital with platelets �100 � 109/L and no obvious other cause,such as cancer chemotherapy.
The IMPACT project is approved by the research ethicsboard at each center. Information was entered into an Accessdatabase (Microsoft Corp., Redmond, WA) and analyzed usingSAS 9.0 (SAS Corporation, Cary, NC).
RESULTSWe identified 107 hospitalized children with postvaccination
thrombocytopenia, and the results are summarized in Table 1. Therewas a mean of 8.2 cases per year since 1996 (with the increase to 10centers in the IMPACT network); this did not change after theintroduction of varicella vaccine after 2002 (Fig., Supplemental Dig-ital Content 1, http://links.lww.com/INF/A377, which shows numberof cases per year by vaccine group). The median age at presentationwas 13 months (range, 9 weeks–15.6 years). Most children werepreviously healthy; underlying conditions included congenital heartdisease, prematurity, and diabetes. Five children had had prior epi-sodes of thrombocytopenia, all unrelated to a vaccination; etiologiesincluded prematurity with sepsis and congenital amegakaryocyticthrombocytopenia. Postvaccination thrombocytopenia was the pre-senting event for acute lymphocytic leukemia in one child. A preced-ing “viral” illness was reported in 76, or 71% of cases, and medicationuse that can be associated with thrombocytopenia was reported in 14of those (no children had reported medication use without a precedingviral illness). There was no statistically significant difference betweenthe proportions reporting a viral illness after MMR vaccine than othervaccines.
A total of 77 cases followed administration of MMR vac-cine (Table 1); 25 of those 77 children had received one or moreadditional vaccines as well (Fig., Supplemental Digital Content 2,http://links.lww.com/INF/A378, which shows which vaccineswere associated with thrombocytopenia). There were no substan-tive differences in demographics, presentation, or clinical course
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 www.pidj.com | 559

between those who received one vaccine and those who receivedmore than one vaccine. The interval between vaccination andpostvaccination thrombocytopenia presentation was slightly longerfor those who received a measles-containing vaccine (mean, 16.4days; 95% CI, 9.6–16.1) than for those who did not (mean, 12.8days; 95% CI, 14.7–18.1; P � 0.038), but in all other respects the2 groups were similar. The subjects who received MMR with nocoadministered vaccines presented a mean of 17 days (range, 6–31days) after immunization (Fig., Supplemental Digital Content 3,http://links.lww.com/INF/A379). No children received varicellavaccine without concomitant MMR vaccine.
The median platelet count on admission was 7 � 109/L,while the lowest platelet counts in hospital ranged from 1 to 82 �109/L (median, 6 � 109/L) (Table 1). Most (96%) of the childrenwere symptomatic: 100 (94%) had a petechial rash, 86 (80.4%)had bruising, and 39 (36.5%) had bleeding. One child had centralnervous system symptoms related to intracranial bleeding, 4 hadhematuria, and 8 had conjunctival hemorrhage. About 13 childrenwere anemic (5 with hemoglobin less than 80 g/L).
The average length of stay in hospital was 2.8 days (Table1). Most patients were treated with either intravenous immuno-globulin (78; 73%) or corticosteroids (21; 20%). Two children hadsevere bleeding-related complications, 1 had gastrointestinalbleeding requiring transfusion and intensive care admission, and 1had intracranial bleeding leading to death.5 On discharge, 28(26%) children had a platelet count approaching normal (�100 �109/L); in the remainder the platelet count was rising. Of theremaining 78 children, follow-up data were available for 71 (91%)and 6 (8%) still had abnormal platelet counts 3 months after
admission. Platelets increased to greater than 100 � 109/L by amedian of 2 weeks (mean, 3.6 weeks). About 55 children hadnormal platelets within 1 month of diagnosis.
There were no documented second episodes of postvacci-nation thrombocytopenia. Of 77 cases, 7 that occurred after mea-sles-containing vaccine followed a documented second dose ofMMR; none of these had a reported history of prior symptomaticthrombocytopenia. This group was not substantively differentfrom the group who had only one documented dose of MMRvaccine. They presented a median of 9 days after their vaccination,compared 17 days for with one documented dose (P � 0.31). Asimilar proportion had a preceding viral illness (71% comparedwith 76% (P � 0.8). The lowest mean platelet count was similar,20 � 109/L compared with 9 � 109/L (P � 0.26).
DISCUSSIONThis case series of postvaccination thrombocytopenia is one
of the largest reported to date. The demographic, clinical, treat-ment, and outcome information from this Canadian series issimilar to postvaccination thrombocytopenia reports from othercountries.1–3,10 Since the last report of IMPACT thrombocytope-nia data,5 12 of the 13 provinces and territories added varicellavaccination to the publicly funded schedule by 2005 and in 9provinces it is coadministered with MMR.7 To date, the number ofcases per year has not changed and the trends of clinical presen-tation and outcomes are similar.
Despite the severe nature of this adverse events followingimmunization, most of the children had a rapidly resolving, benigncourse and short hospital stays with contemporary management, witha median duration of thrombocytopenia of 2 weeks. However, thepotential for life-threatening complications was highlighted by the 2children with severe bleeding-related complications (including 1death).
Consistent with the Brighton Collaboration recommenda-tions, the IMPACT surveillance system does not exclude cases ofthrombocytopenia with alternative potential causes9; while all ofthe postvaccination thrombocytopenia cases reported here hap-pened within a month of vaccination, this does not provide proofthat vaccination caused all 107 cases. In fact, 77 (72%) of caseshad an alternate potential cause. There is no specific test to deter-mine the etiology of thrombocytopenia. Because chickenpox is some-times associated with thrombocytopenia, and transient aplastic anemiahas been described after varicella vaccination,11 it is plausible thatvaricella vaccine might also cause postvaccination thrombocytope-nia12; it was reassuring to note that despite the addition of varicellavaccine to the routine schedule with increased uptake since 2005,there was no increase in the number of cases per year.
Of the cases reported here, 30 (28%) occurred after avaccination that did not contain measles, mumps, rubella, orvaricella; there was no recognized difference between that groupand those who had a measles-containing vaccination. The Insti-tutes of Medicine report does not consider a causal link betweennon-MMR vaccines and thrombocytopenia to be well supported.13
It is not known how often postvaccination thrombocytope-nia recurs after repeat vaccination; there have been few reportedcases,14 but Oski et al15 demonstrated a drop in platelet countfollowing vaccine rechallenge in 1 patient. Stowe et al16 examinedthe risk of occurrence of idiopathic thrombocytopenic purpuraafter a second dose of MMR using linked hospital admissions dataand vaccine records in the United Kingdom and found no evidenceof increased risk, while France et al supported that finding; amongAmerican children with prior idiopathic thrombocytopenia, MMRvaccination did not precipitate a recurrence of thrombocytopenia.1
In our study, none of the 5 children with a prior history of
TABLE 1. Characteristics of 107 Children WithVaccine-Associated Thrombocytopenia
Characteristic Number (%)
Gender—male 65 (61)Age group
�12 mo 19 (18)12–23 mo 71 (66)24–59 mo 6 (6)�5 yr 11 (10)
Previously healthy 100 (94)No. vaccines administered
One only 67 (63)More than 1 40 (37)
No. patients who had one or more ofMMR 77 (72)DTP/DTaP 28 (26)Meningococcus C 14 (13)Varicella 10 (9)
Prior episode of thrombocytopenia 5 (5)Preceding “viral” illness 76 (71)*
Respiratory 50 (66)†
Diarrheal 9 (12)†
Fever and rash (unspecified) 11 (15)†
Fever only 4 (5)†
Other (acute otitis media, varicella) 2 (3)†
Recent use of thrombocytopenia-associated medicationsSulfonamides 4 (4)Beta-lactam antibiotic 9 (8)Phenobarbital 1 (1)
Platelet countsLowest platelet count documented—median � 109/L
(standard deviation)6 (�14)
Platelet count at admission—median � 109/L (SD) 7 (�25)Duration of hospitalization—mean days (SD) 2.8 (�1.7)
*Percentage of the total number (107) with postvaccination TP.†Percentage of the 76 with a reported viral illness.MMR indicates measles-mumps-rubella; DTP/DTaP, diphtheria/tetanus/pertussis
or diphtheria/tetanus/acellular pertussis; SD, standard deviation.
Sauve et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins560 | www.pidj.com

thrombocytopenia were known to have postvaccine thrombocyto-penia with the earlier episode and none of those with thrombocy-topenia after a confirmed second dose of MMR vaccine haddocumented prior vaccine associated thrombocytopenia.
There are some limitations to this data set. Although IMPACTcovers 90% of tertiary pediatric beds in Canada, some postvacci-nation thrombocytopenia cases may have been admitted to com-munity hospitals, precluding population-based calculation of inci-dence rates. In addition, mild episodes might not be admitted tohospital at all, so would not be captured by IMPACT.
A methodological challenge for postvaccination thrombo-cytopenia surveillance is that case detection requires documenta-tion of the administration of a vaccine in the previous month. Arecent American study1 found that treating physicians had askedparents of only 2 of 13 children with postvaccination thrombocy-topenia about recent vaccinations. The IMPACT system attemptsto avoid that challenge by reviewing most of the idiopathicthrombocytopenic purpura admissions and seeking vaccinationrecords from either public health or the primary care physician.However, while documentation of the vaccine in the month beforethe onset of thrombocytopenia was possible for all cases, completeprior vaccination records were available for 24 cases (22%).
ACKNOWLEDGMENTSThe authors acknowledge the IMPACT Monitors and staff
of the IMPACT data center. IMPACT members and coinvestiga-tors include the following: St. John’s: R. Morris; Halifax: S.Halperin; Quebec City: P. Dery; Montreal: M. Lebel, D. Moore;Ottawa: N. Le Saux; Toronto: D. Tran; Winnipeg: J. Embree;Saskatoon: B. Tan; Edmonton: W. Vaudry; Calgary: T. Jadavji;Vancouver: L. Sauve.
REFERENCES1. France EK, Glanz JM, Xu S, et al. Risk of immune thrombocytopenic
purpura after measles-mumps-rubella immunization in children. Pediatrics.2008;121:e687–e692.
2. Miller E, Waight P, Farrington CP, et al. Idiopathic thrombocytopenicpurpura and MMR vaccine. Arch Dis Child. 2001;84:227–229.
3. Black C, Kaye JA, Hershel J. MMR vaccine and idiopathic thrombocyto-paenic purpura. Br J Clin Pharmacol. 2003;55:107–111.
4. Rajantie J, Zeller B, Treutiger I, et al. Vaccination associated thrombocy-topenic purpura in children. Vaccine. 2007;25:1838–1840.
5. Jadavji T, Scheifele D, Halperin S, et al. Thrombocytopenia after immuni-zation of Canadian children, 1992 to 2001. Pediatr Infect Dis J. 2003;22:119–122.
6. Statistics Canada. Statistics Canada Website. Available at: http://www.statcan.gc.ca/start-debut-eng.html. Accessed October 26, 2009.
7. Public Health Agency of Canada. Canadian national report on immuniza-tion, 2006. Can Commun Dis Rep. 2006;32 S3:1–44.
8. Gustafson R, Skowronski DM. Disparities in varicella vaccine coverage inthe absence of public funding. Vaccine. 2005;23:3519–3525.
9. Wise RP, Bonhoeffer J, Beeler J, et al. Thrombocytopenia: case definitionand guidelines for collection, analysis, and presentation of immunizationsafety data. Vaccine. 2007;25:5717–5724.
10. Jonville-Bera AP, Autret EM, Galy-Eyraud CM, et al. Thrombocytopenicpurpura after measles, mumps and rubella vaccination: a retrospectivesurvey by the French regional pharmacovigilance centres and pasteur-merieux serums et vaccins. Pediatr Infect Dis J. 1996;15:44–48.
11. Angelini PM, Kavadas FM, Sharma NM, et al. Aplastic anemia followingvaricella vaccine. Pediatr Infect Dis J. 2009;28:746–748.
12. Rivest P, Bedard L, Valiquette L, et al. Severe complications associatedwith varicella: province of Quebec, April 1994 to March 1996. Can J InfectDis Med Microbiol. 2001;12:21–26.
13. Stratton KR, Howe CJ, Johnston SL Jr, eds. Adverse Events Associated withChildhood Vaccines: Evidence Bearing on Causality. Washington, DC:Institute of Medicine; 1994.
14. Beeler J, Varricchio F, Wise R. Thrombocytopenia after immunization withmeasles vaccines: review of the vaccine adverse events reporting system(1990 to 1994). Pediatr Infect Dis J. 1996;15:88–90.
15. Oski FA, Naiman JL. Effect of live measles vaccine on the platelet count.N Engl J Med. 1966;275:352–356.
16. Stowe J, Kafatos G, Andrews N, et al. Idiopathic thrombocytopenic purpuraand the second dose of MMR. Arch Dis Child. 2008;93:182–183.
HOSPITALIZATIONS FOR INVASIVEPNEUMOCOCCAL DISEASE AMONG HUMAN
IMMUNODEFICIENCY VIRUS-1 INFECTEDCHILDREN, ADOLESCENTS AND YOUNG ADULTSIN THE UNITED STATES IN THE ERA OF HIGHLYACTIVE ANTIRETROVIRAL THERAPY AND THE
CONJUGATE PNEUMOCOCCAL VACCINE
Athena P. Kourtis, MD, PhD,* Sascha Ellington, MSPH,*Pooja Bansil, MPH,† Denise J. Jamieson, MD, MPH,*and Samuel F. Posner, PhD*
Abstract: We describe hospitalization trends of invasive pneumococcaldisease (IPD) among human immunodeficiency virus-infected individuals�25 years of age since the introduction of highly active antiretroviraltherapy (HAART) and the 7-valent pneumococcal conjugate vaccine(PCV7) in the United States, using the Nationwide Inpatient Sample. Weestimated national trends of IPD hospitalizations during 3 periods: 1994 to1995 (pre-HAART and pre-PCV7 era); 1998 to 1999 (HAART andpre-PCV7 era); and 2004 to 2005 (HAART and early PCV7 era). Thenumber of IPD hospitalizations among human immunodeficiency virus-infected children and youth �25 years in the United States declined by78.7% between 1994/1995 and 2004/2005 (P � 0.03). This decrease wasmore pronounced among younger children.
Key Words: HIV-1, pneumococcus, invasive disease, hospitalization,vaccine, children, adolescentsAccepted for publication December 15, 2009.From the *Division of Reproductive Health, National Center for Chronic
Disease Prevention and Health Promotion, Centers for Disease Control andPrevention, Atlanta, GA; and †CONRAD, Atlanta, GA.
The findings and conclusions in this article are those of the authors and donot necessarily represent the views of the Centers for Disease Controland Prevention.
Address for correspondence: Athena P. Kourtis, MD, PhD, MPH, DRH/NCCDPHP/CDC, 4770 Buford Highway, MS-K34, Atlanta, GA30341. E-mail: [email protected].
DOI: 10.1097/INF.0b013e3181cfb65f
Invasive pneumococcal disease (IPD) represents a serious prob-lem for human immunodeficiency virus (HIV)-infected patients
globally, manifesting most commonly as pneumonia, but also asbacteremia, pericarditis, or meningitis.1 Introduced in 1996–1997,the wide implementation of highly active antiretroviral therapy(HAART) in the United States led to dramatic improvements in thelength and quality of life of HIV-infected patients, even though therisk of IPD has remained elevated compared with that of age-matched HIV-uninfected individuals.2
Rollout of the 7-valent conjugate pneumococcal vaccine(PCV7), which was recommended for all US children in 2000, hassignificantly reduced the rate of IPD among children.3 Data show-ing the effectiveness of PCV7 in HIV-infected children are limited.In a South African pediatric HIV-infected population with noaccess to HAART, a 9-valent PCV reduced the incidence ofvaccine-serotype IPD by 65% among vaccinated individuals.4
There has been only one article directly addressing theimpact of HAART and PCV7 on pediatric IPD in the UnitedStates. In a single center study of 256 children with HIV infection
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Pneumococcal Disease and HIV
© 2010 Lippincott Williams & Wilkins www.pidj.com | 561
followed from 1989 to 2006, Steenhoff et al5 reported a decreasein IPD after the introduction of HAART, but a nonsignificantincrease after introduction of PCV7. Currently, there are no datashowing the effect of HAART and PCV7 on the burden of IPDamong HIV-infected children and adolescents in the United States.The Nationwide Inpatient Sample (NIS) offers a nationally represen-tative sample to study this question among hospitalized individuals.
Our objective was to describe hospitalization trends amongHIV-infected children, adolescents, and young adults �25 years ofage with IPD in the United States during 3 periods: 1994 to 1995(baseline, pre-HAART, and pre-PCV7 era); 1998 to 1999(HAART and pre-PCV7 era); and 2004 to 2005 (HAART andPCV7 era). These trends were compared with the trends amongHIV-uninfected ones. In addition, we assessed trends for length ofhospital stay and hospital charges.
METHODSHospital discharge data were obtained from the NIS, the
largest all-payer inpatient care database in the United States. TheNIS is a stratified probability sample that approximates 20% of allUS community hospitals and has data on 7 million dischargedpatients from approximately 1000 community hospitals. The NISwas developed as part of the Healthcare Cost and UtilizationProject, sponsored by the Agency for Healthcare Research andQuality in partnership with state level data collection organiza-tions. Participating hospitals are sampled in 5 strata (ownership/control, bed size, teaching status, urban/rural, and US region), withsampling probabilities proportional to the number of US commu-nity hospitals in each stratum. The NIS collects data on allhospitalizations, and weighting and sampling variables are pro-vided for each year to calculate national estimates.
To account for changes in the sampling frame from 17 statesin 1994 to 37 states in 2004, we used an alternative set of dischargeand hospital weights as recommended and validated by the Agencyfor Healthcare Research and Quality. Our analysis included allhospital discharges except those for conditions related to preg-nancy and delivery (ie, discharge codes 630–677, 792.3, V22–V27, V15.7, V45.5, and V72.4). The International Classification ofDiseases, Ninth Revision, Clinical Modification discharge codes
were used to identify the following: (a) HIV infection (042.0–044.9, 079.53, 279.10, 279.19, 795.71, 795.8, V08); (b) IPD(038.2-pneumococcal septicemia, 041.2-pneumococcal infectionunclassified elsewhere, 320.1-pneumococcal meningitis, 420.99-pneumococcal pericarditis, 481-pneumococcal pneumonia). Thesediagnostic codes could be at any place in the discharge diagnosislist of 15 fields.
We analyzed data for patients �25 years of age from 1994to 1995 (pre-HAART, preconjugate pneumococcal vaccine era),1998 to 1999 (HAART, prevaccine era), and 2004 to 2005(HAART, conjugate vaccine era). Universal immunization of chil-dren in the United States with the PCV7 started in 2000, andcoverage with 3 or more doses among US children had risen to83% for children born during 2002 to 2004.6 Analytic methods thatadjusted for sampling weights were conducted using SUDAAN(Research Triangle Institute, Research Triangle Park, NC). Multi-variable logistic regression was used to investigate the trends inhospitalizations during the periods 1994 to 1995, 1998 to 1999, and2004 to 2005, by HIV status, while adjusting for sex, age, andexpected primary payer. The study was considered to be exempt fromreview by the Institutional Review Board of the Centers for DiseaseControl and Prevention, as it contained de-identified information.
RESULTSThere were an estimated total of 1275 hospitalizations with
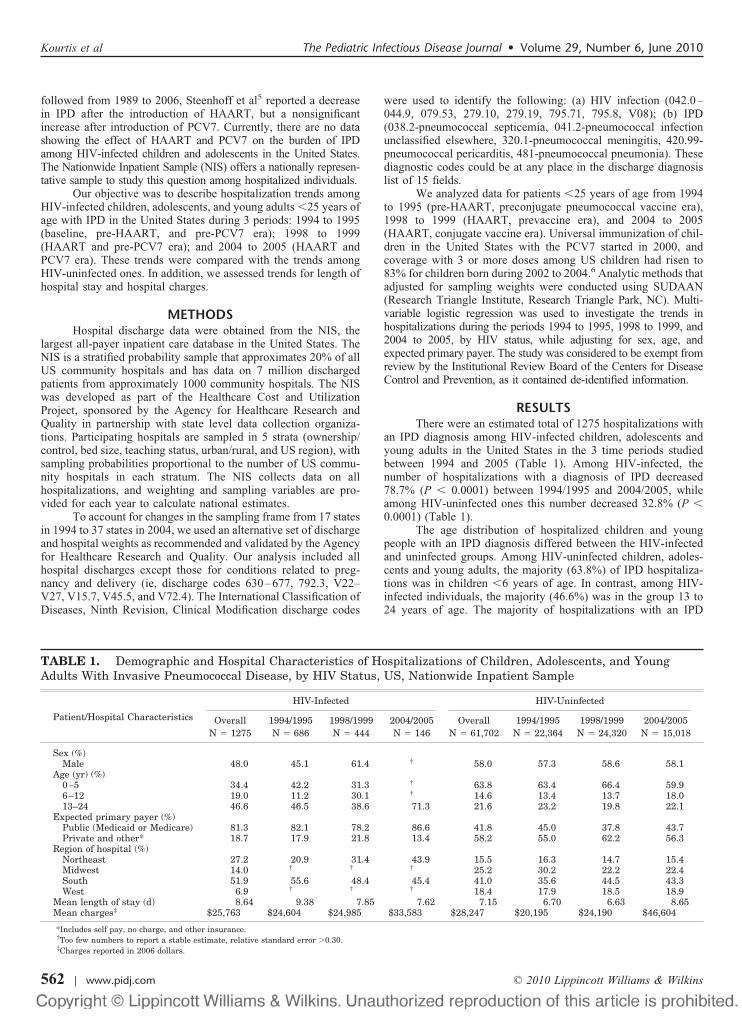
an IPD diagnosis among HIV-infected children, adolescents andyoung adults in the United States in the 3 time periods studiedbetween 1994 and 2005 (Table 1). Among HIV-infected, thenumber of hospitalizations with a diagnosis of IPD decreased78.7% (P � 0.0001) between 1994/1995 and 2004/2005, whileamong HIV-uninfected ones this number decreased 32.8% (P �0.0001) (Table 1).
The age distribution of hospitalized children and youngpeople with an IPD diagnosis differed between the HIV-infectedand uninfected groups. Among HIV-uninfected children, adoles-cents and young adults, the majority (63.8%) of IPD hospitaliza-tions was in children �6 years of age. In contrast, among HIV-infected individuals, the majority (46.6%) was in the group 13 to24 years of age. The majority of hospitalizations with an IPD
TABLE 1. Demographic and Hospital Characteristics of Hospitalizations of Children, Adolescents, and YoungAdults With Invasive Pneumococcal Disease, by HIV Status, US, Nationwide Inpatient Sample
Patient/Hospital Characteristics
HIV-Infected HIV-Uninfected
Overall 1994/1995 1998/1999 2004/2005 Overall 1994/1995 1998/1999 2004/2005N � 1275 N � 686 N � 444 N � 146 N � 61,702 N � 22,364 N � 24,320 N � 15,018
Sex (%)Male 48.0 45.1 61.4 † 58.0 57.3 58.6 58.1
Age (yr) (%)0–5 34.4 42.2 31.3 † 63.8 63.4 66.4 59.96–12 19.0 11.2 30.1 † 14.6 13.4 13.7 18.013–24 46.6 46.5 38.6 71.3 21.6 23.2 19.8 22.1
Expected primary payer (%)Public (Medicaid or Medicare) 81.3 82.1 78.2 86.6 41.8 45.0 37.8 43.7Private and other* 18.7 17.9 21.8 13.4 58.2 55.0 62.2 56.3
Region of hospital (%)Northeast 27.2 20.9 31.4 43.9 15.5 16.3 14.7 15.4Midwest 14.0 † † † 25.2 30.2 22.2 22.4South 51.9 55.6 48.4 45.4 41.0 35.6 44.5 43.3West 6.9 † † † 18.4 17.9 18.5 18.9
Mean length of stay (d) 8.64 9.38 7.85 7.62 7.15 6.70 6.63 8.65Mean charges‡ $25,763 $24,604 $24,985 $33,583 $28,247 $20,195 $24,190 $46,604
*Includes self pay, no charge, and other insurance.†Too few numbers to report a stable estimate, relative standard error �0.30.‡Charges reported in 2006 dollars.
Kourtis et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins562 | www.pidj.com

diagnosis for HIV-infected individuals was in the southern regionof the United States and had a public expected primary payer(Table 1).
The greatest decrease in IPD hospitalizations between 1994/1995 and 2004/2005 was among the HIV-infected group �13years of age (88.6%), while in those 13 to 24 years the decreasewas 67.4%. Among the HIV-uninfected �13 years of age, thecorresponding decrease were 31.9% for those 0 to 12 years and36.2% for those 13 to 24 years.
While the mean length of stay for IPD hospitalizationssignificantly increased for HIV-uninfected children, adolescentsand young adults between 1994/1995 and 2004/2005 (P �0.0001), the mean length of stay for HIV-infected ones decreasedsignificantly during that time period (P � 0.0001). Accounting forinflation, the mean charges incurred significantly increased (P �0.0001) for both HIV-infected and uninfected hospitalized children,adolescents and young adults with an IPD diagnosis (Table 1).
When adjusting for age, sex, and payer, the odds ratio (OR)for an IPD hospitalization among HIV-infected children, adoles-cents and young adults in the United States was 0.71 (95%confidence interval �CI�, 0.42–1.20) in 2004/2005 compared with1994/1995 and 0.52 (95% CI, 0.32–0.86) in 2004/2005 comparedwith 1998/1999. There was also a significant decrease amongHIV-uninfected patients between 1994/1995 and 2004/2005 (ad-justed OR, 0.66; 95% CI, 0.59–0.73) and between 1998/1999 and2004/2005 (OR, 0.58; 95% CI, 0.52–0.64).
DISCUSSIONIn the pre-HAART era, the cumulative incidence of IPD
among HIV-infected children was 6.1 cases per 100 patient-yearsthrough age 7, a rate 100 to 300 times higher than that seen inHIV-uninfected children in the United States.7 Data have shownthat children receiving HAART remained at heightened suscepti-bility for IPD,8 highlighting the need for additional interventions.After the introduction of PCV7 in the United States in 2000, amulticenter Pediatric AIDS Clinical Trials Group report describeda greater than 75% reduction in overall bacteremia and bacterialpneumonia among HIV-infected children.9 While specific patho-gens were not examined in the Pediatric AIDS Clinical TrialsGroup report, pneumococcus causes a large proportion of bacte-remia and bacterial pneumonia in HIV-infected children.
We found a significant decrease in IPD hospitalizationsamong HIV-infected children, adolescents and young adults in theUnited States. This decrease became more pronounced after theintroduction of universal PCV7 vaccination of children and amongyounger children.
The benefits of PCV7 vaccination in HIV-infected childrenhave been demonstrated in clinical trials.10 One concern with theuse of PCV7 is the replacement of vaccine-contained serotypeswith nonvaccine serotypes causing disease. Continuous monitor-ing of changes in serotype distribution is necessary. Furthermore,there is recent evidence that HIV-infected vaccinees experience apartial loss of anamnestic responses to PCV7, which may suggestthe need for additional booster doses to optimize long-term pro-tection after vaccination in HIV-infected children.11
To our knowledge, this study is the first to explore on anational level the trends in hospitalizations among HIV-infectedchildren, adolescents and young adults in the United States afterthe introduction of HAART and PCV7. As such, the study’sstrengths are its larger sample size and its nationally representativeestimates. Our study also has limitations. Data on race were notavailable and we had no access to individual medical records orinformation, such as receipt of and response to antiretroviraltherapy among HIV-infected individuals or PCV7 vaccination
among individual children. We used calendar years as surrogatemarkers for HAART or PCV7 coverage in the population.Therefore, our conclusion that HAART and PCV7 are the mostlikely explanations for the decline in IPD hospitalization ratesis based on the coincidental timing of these events and consis-tency with biologic and clinical research. We cannot, however,exclude the effects of other changes in clinical or codingpractices during this time. In addition, information on pneumo-coccal serotype distribution or antimicrobial susceptibility ofthe bacterial isolates is not available in the NIS. Finally, theinclusion of only demonstrated pneumococcal pneumonia mighthave led to underestimation of IPD, as a specific cause is oftennot identified in children with pneumonia.
Results from this study concur with the evidence supportingthe overall, nationwide, beneficial effects of PCV7 on IPD amongHIV-infected individuals. In addition, this study’s results providereference data for future comparisons and trends. Monitoringfuture trends is warranted for 2 reasons: concerns for serotypereplacement disease; and disease in older children and adolescentspossibly pointing to a need for use of pneumococcal vaccineformulations in older HIV-infected children.
REFERENCES1. Klugman KP, Madhi SA, Feldman C. HIV and pneumococcal disease. Curr
Opin Infect Dis. 2007;20:11–15.
2. Heffernan RT, Barrett NL, Gallagher KM, et al. Declining incidence ofinvasive Streptococcus pneumoniae infections among persons withAIDS in an era of HAART, 1995–2000. J Infect Dis. 2005;191:2038 –2045.
3. Centers for Disease Control (CDC). Progress in introduction of pneumo-coccal conjugate vaccine-worldwide, 2000–2008. MMWR Morb MortalWkly Rep. 2008;57:1148–1151.
4. Klugman KP, Madhi SA, Huebner RE, et al. A trial of a 9-valent pneumo-coccal conjugate vaccine in children with and those without HIV infection.N Engl J Med. 2003;349:1341–1348.
5. Steenhoff AP, Wood SM, Rutstein R, et al. Invasive pneumococcal diseaseamong HIV-infected children, 1989–2006. Pediatr Infect Dis J. 2008;27:886–891.
6. Centers for Disease Control and Prevention. Vaccines and immunizations:coverage with individual vaccines and vaccination series. Available at:http://www.cdc.gov/nip/coverage/NIS/05/toc-05.htm. Accessed November1, 2008.
7. Mao C, Harper M, McIntosh K, et al. Invasive pneumococcal infections inHIV-infected children. J Infect Dis. 1996;173:870–876.
8. Kourtis AP, Bansil P, Posner SF, et al. Trends in hospitalizations ofHIV-infected children and adolescents in the United States: analysis of datafrom the 1994–2003 nationwide inpatient sample. Pediatrics. 2007;120:e236–e243.
9. Gona P, Van Dyke RB, Williams PL, et al. Incidence of opportunistic andother infections in HIV-infected children in the HAART era. JAMA.2006;296:292–300.
10. Abzug MJ, Pelton SI. Prevention of invasive pneumococcal disease inHIV-infected children: expanding the toolbox. J Infect Dis. 2009;199:1109–1111.
11. Madhi S, Klugman KP, Kuwanda L, et al. Quantitative and qualitativeanamnestic immune responses to pneumococcal conjugate vaccine in HIV-infected and HIV-uninfected children 5 years after vaccination. J Infect Dis.2009;199:1168–1176.
LONG-TERM EFFICACY AND SAFETYOF FOSAMPRENAVIR IN HUMAN
IMMUNODEFICIENCY VIRUS-INFECTEDPEDIATRIC PATIENTS
Claudia Palladino, PhD,* Veronica Briz, PhD,*Sergio Negre Policarpo, MD,† Laura Fernandez Silveira, MD,‡M Isabel de Jose, MD,§ M Isabel Gonzalez-Tome, MD,¶
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Fosamprenavir
© 2010 Lippincott Williams & Wilkins www.pidj.com | 563

David Moreno, MD,� Juan A. Leon Leal, MD,**M Jose Mellado, MD,†† Santiago J. de Ory, BSc,*Jose T. Ramos, MD,‡‡ and M Angeles Munoz-Fernandez, PhD, MD*
Abstract: Fosamprenavir (FPV) efficacy in human immunodeficiencyvirus (HIV)-infected pediatric patients is still being evaluated in ongoingclinical trials. The long-term efficacy and safety of FPV boosted withritonavir (FPV/r) was evaluated in 20 antiretroviral-naive and antiretrovi-ral-experienced HIV-vertically infected pediatric patients. Analyses ofCD4� T-cells, HIV-ribonucleic acid (RNA), and clinical status wereperformed during a median of 180 weeks. Initially, median HIV-RNA was4.6 log10 in naive and 4.4 log10 in pretreated patients. Median CD4� T-cellwas 17% and 31%, respectively. After FPV/r treatment, 18 of 20 patientsachieved undetectable HIV-RNA and 4 of 20 experienced adverse events.To date, FPV/r treatment has shown sustained antiviral response andimmunologic improvement in our 20 patients.
Key Words: HIV, fosamprenavir, HAART, children, adolescentsAccepted for publication December 11, 2009.From the *Laboratorio de Inmuno-Biología Molecular, Hospital General
Universitario “Gregorio Maranon,” Madrid, Spain; †Servicio de Enfer-medades Infecciosas, Hospital Universitari “La Fe,” Valencia, Spain;‡Servicio de Urgencias, Hospital de Sagunto, Valencia, Spain; §ServicioInfecciosas Infantil, Hospital Universitario “La Paz,” Madrid, Spain; ¶Ser-vicio de Infecciosas Pediatricas, Hospital Universitario “Doce de Oc-tubre,” Madrid, Spain; �Servicio de Pediatría, Unidad de Infectología eInmunodeciciencias, Hospital Regional Universitario “Carlos Haya,”Malaga, Spain; **Unidad de Infectología/Medicina Interna Pediatrica,Hospital Infantil Unversitario “Virgen del Rocío,” Sevilla, Spain; ††Ser-vicio de Pediatría, Hospital Universitario “Carlos III,” Madrid, Spain; and‡‡Servicio de Pediatría, Hospital Universitario de Getafe, Madrid, Spain.
Supported by grants from Fundacion para la Investigacion y Prevencion delSIDA en Espana, FIPSE (24632/07), Fundacion Caja Navarra, Red Tem-atica de Investigacion Cooperativa Sanitaria ISCIII (RD06–0006–0035),Fondo de Investigacion Sanitaria (FIS) of The Ministerio de Ciencia eInnovacion (PI052476, PI061479), Pediatric European network for treat-ment of AIDS (PENTA), and Task Force in Europe for Drug Developmentfor the Young (TEDDY). Supported by Fundacion Para la InvestigacionBiomedica del Hospital General Universitario “Gregorio Maranon” (to C.L.).Supported by Fondo de Investigacion Sanitaria (FI05/01046) (to V.B.).
The authors declare that they share no conflicts of interest.The first two authors contributed equally to the manuscript.Address for correspondence: Ma Angeles Munoz-Fernandez, PhD, MD,
Laboratorio Inmuno-Biología Molecular, Hospital General Universita-rio “Gregorio Maranon,” C/Doctor Esquerdo 46, 28007 Madrid, Spain.E-mail: [email protected].
Supplemental digital content is available for this article. Direct URLcitations appear in the printed text and are provided in the HTML andPDF versions of this article on the journal’s Web site (www.pidj.com).
DOI: 10.1097/INF.0b013e3181d285ac
T he immature immune system of human immunodeficiencyvirus (HIV)-infected children is unable to control HIV repli-
cation allowing higher plasma viral loads than adults. Virologicfailure and the emergence of HIV quasispecies resistant to anti-retroviral (ARV) drugs compromise the available treatment op-tions. To date, 25 compounds have been licensed for HIV infectionin adults1 and 17 in the pediatric population.2 The use of proteaseinhibitors (PIs) has led to a decrease in HIV-related morbidity andmortality. Fosamprenavir (FPV), approved in 2003 for adults and2007 for pediatric patients, is a potent PI that, boosted withritonavir (FPV/r), has shown potent ARV activity in ARV-naiveadults,3–5 ARV-naive and pretreated pediatric subjects aged 2 to18 years.6,7
Our aim was to assess the virologic, immunologic, andclinical response to a FPV/r-based regimen in combination withnucleoside reverse transcription inhibitors (NRTIs) and PIs and/ornon-nucleoside reverse transcription inhibitors (NNRTIs) in ARV-naive and ARV-experienced children and adolescents with previ-ous virologic failure and on highly active antiretroviral treatment(HAART). In addition, we addressed the safety and tolerability ofFPV/r in this cohort.
PATIENTS AND METHODSA multicenter retrospective study of vertically HIV-infected
children (2–12 years old) and adolescents (13–15 years old) of theHIV Spanish Pediatric Cohort (CoRISpe) receiving treatment withFPV/r followed up at least 1 year was carried out. Patients wereincluded in 1 of the 2 following categories: (i) ARV-naive and (ii)ARV-experienced individuals with at least one episode of viro-logic failure and on HAART. Baseline was considered FPV/rinitiation. A weight-adjusted dose of 30 mg/kg twice daily waschosen for naive patients from 4 to 18 years old and 18 mg/kgtwice daily for pretreated patients �6 years old. Visits werescheduled every 3 to 6 months. Demographics, clinical, andlaboratory parameters were recorded longitudinally. Clinical cat-egory was based on the Center for Disease Control and Preventionguidelines. Ethical approval for the survey was obtained from theEthical Committees of all hospitals and informed consent wasobtained from parents or guardians. Several biologic samples wereprovided by the Spanish HIV BioBank belonging to the SpanishAIDS Research Network (RIS).8 Plasma HIV-1 ribonucleic acid(RNA) was measured using the commercial quantitative AmplicorMonitor assay (Roche Diagnostic Systems) with a detection limitof 50 copies/mL while plasma HIV-2 RNA was measured usingthe commercial Nuclisens Easy Q (version 1.1) assay (EasyQ;bioMerieux) as previously described.9 CD4� T-lymphocytes werequantified by flow cytometry (Coulter, Madrid, Spain). Valueswere recorded as absolute numbers/percentage and medians werecalculated with their interquartile range. Mann-Whitney U test wasused to compare continuous variables. P-values were 2-tailed andstatistical significance was defined as P � 0.05. SPSS (v.12; SPSSInc., Chicago, IL) was used.
RESULTSTwenty vertically HIV-infected patients born from 1991 to
2004 fulfilling the inclusion criteria were enrolled from 2003 to2007 (Annex). Six (30%) were therapy-naive and 14 (70%) ther-apy-experienced. Median age was 6 (2–9) and 10 years, (6–13),respectively. The majority of patients were female (70%; n � 14)and Caucasian (85%; n � 17) (Table, Supplemental Digital Con-tent 1, http://links.lww.com/INF/A374). Only one child (fromEcuador) harbored HIV-2 subtype A.
At baseline, median HIV-1 RNA was 37,250 (4.6 log10)copies/mL (16,599–68,321) in naive and 21,990 (4.4 log10) cop-ies/mL (1920–78,283) in pretreated patients. Median CD4� T-cellcount was 376 (17%) cells/�L (180–862) and 722 (31%) cells/�L(502–1266), respectively. CD4� T-cell percentage was higher inpretreated patients compared with naive ones (P � 0.007). Three(50%) out of 6 naive patients presented a moderate immunologicsuppression (200–499 cells/�L) and 1 of 6 (17%) severe suppres-sion (�200 cells/�L) who harbored a resistant virus acquiredthrough vertical transmission. Two (14%) of 14 pretreatedpatients presented moderate immune suppression. Four (20%)out of 20 subjects (1 naive and 3 pretreated) were classified intoC clinical category (Table, Supplemental Digital Content 1,http://links.lww.com/INF/A374). The naive child harboring a re-sistant virus showed mutations to NRTIs (D67N, K70R, T215Y,
Palladino et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins564 | www.pidj.com

K219Q), NNRTIs (K103N, G190A), and PIs (L90M, I54V). ARV-experienced patients had a median duration of HAART exposureof 94.6 months (59.8–131.1) and 6 of 14 (43%) developed muta-tions to NRTIs (M41L, D67N, K70R, L74V, M184V, L210W,T215Y, K219Q), NNRTIs (K103N, Y181C, G190A, P225H), andto PIs (M46I/L, V82A, L90M).
The median time of follow-up with FPV/r was 180 weeks(134.5–229.1), with 17 of 20 (85%) patients exposed �129 weeks.Only one patient received unboosted (without ritonavir) FPV.Backbone ARV treatment was 2 NRTI being the most commondrugs lamivudine and abacavir. Eighteen (90%) out of 20 patients(6 naive and 12 pretreated) reached undetectable HIV-1 RNA: 15(75%) within the first 4 months and 3 at the fifth, sixth, andeleventh month, respectively. Seventy-eight percent of patients (4naive and 10 pretreated) maintained undetectable HIV-1 RNA.Three of them were enrolled in the HIV-infected adults SpanishCohort (CoRIS) at the end of the study and a simplificationregimen was performed replacing FPV-based regimen by Atripla.In 2 pretreated children with insufficient viral response, FPVtherapy was replaced by etravirine, darunavir, and maraviroc.Nevertheless, a decrease in HIV-1 RNA �2 log10 was detectedduring follow-up.
At the end of the study, median increase from baseline inCD4� T-cell counts was observed in 5 of 6 naive and 8 of 14ARV-experienced patients (�217 cells/�L and �251 cells/�L,respectively). Among the 7 patients experiencing a decrease inT-cells, one naive child had 492 cells/�L, while the restmaintained a CD4� T-cell value �500 cells/�L. Laboratoryabnormalities, ARV adherence, and ARV-related adverseevents are summarized in Table, Supplemental Digital Content1, http://links.lww.com/INF/A374. The child who developed asevere skin rash, initially considered an abacavir reaction, wasnegative for HLA-B*5701 genetic variation. Four (20%) subjectspermanently interrupted FPV-based therapy (Table, SupplementalDigital Content 1, http://links.lww.com/INF/A374), but only onebecause of high-resistance to FPV: the emergence of the I54Lmutation after 197 weeks conferred, along with baseline resistancemutations (M46L, V82A, L90M), complete resistance to the drug.One patient received unboosted FPV and showed a long (197weeks) virologic and immunologic response as observed inpatients having boosted FPV.
DISCUSSIONAn increasing number of HIV-infected children and adoles-
cents are failing the available treatment options. Currently, therecently approved PIs FPV (Lexiva), tipranavir (Aptivus), anddarunavir (Prezista) for the pediatric population are still beingevaluated in ongoing clinical trials, representing potential newdrug alternatives to HIV-1 infection treatment in children andadolescents.7,10,11 The rather limited studies published so far inpediatric population on FPV-based regimen correspond to theAPV20003 and APV29005 (interim data) clinical trials6,7 and noinformation on FPV/r use in routine clinical practice has beenpublished to date. Notably, the present study represents the firstepidemiologic survey characterizing the clinical, virologic, andimmunologic response to a combined FPV/r therapy in naive andARV-experienced HIV-infected pediatric patients followed up formore than a median of 180 weeks in a clinical set-up. Evidencessupport that FPV/r exerts its effect in both naive and ARV-experienced children according to recent trials.6,7 The study pop-ulation was comparable in terms of age, gender, ethnicity, baselineviral load with the APV29005 (interim data) group. Concerningimmunologic status, no data are available in the APV29005 (in-terim data) trial to perform a comparison between the 2 groups
(estimated study completion date: December 2012). The virologicresponse achieved mainly during the first 4 months of follow-upwas potent and durable, with a proportion of responders higherthan previously reported.7 However, as early evidenced, pooradherence and initial resistance mutations might compromise theeffectiveness of FPV-based therapy. A long-term sustained immu-nologic improvement was observed, as highlighted by others.4
Nevertheless, a considerable proportion of HIV-infected subjectsentered the study with a minimally compromised immune system.The low rate of adverse events related to FPV/r regimen confirmedits safe profile as previously reported.7 The emergence of resis-tance mutations to FPV/r occurred late during follow-up, in agree-ment with observations described in HIV-1 infected adults,4 sug-gesting high genetic barrier to this drug. Further analyses involvinglarger cohorts remain necessary.
Although the limited size of the study population representsthe main shortcoming, our results are supported by clinical trials inadults,3–5 children, and adolescents,6,7 being our study the longestcarried out to date evaluating FPV/r efficacy. Moreover, 2 inter-esting cases never described earlier are presented. The first case isrepresented by a severely immunocompromised naive child whoharbored a HIV-1 resistant virus at enrolment. FPV/r was associ-ated with long-term clinical benefit, although a viral load reboundwas observed at 120 weeks. The second case is an HIV-2 infectedpatient who showed good response to FPV/r therapy.
ACKNOWLEDGMENTSThe authors thank the patients in this study for their partic-
ipation and the HIV BioBank belonging to the Spanish AIDSResearch Network (RIS) and collaborating centers for the clinicalsamples provided.
REFERENCES1. De Clercq E. Anti-HIV drugs: 25 compounds approved within 25 years
after the discovery of HIV. Int J Antimicrob Agents. 2009;33:307–320.
2. Working Group on Antiretroviral Therapy and Medical Management ofHIV-Infected Children. Guidelines for the Use of Antiretroviral Agents inPediatric HIV Infection. February 23, 2009. pp. 113–139. Available at:http://aidsinfo.nih.gov/ContentFiles/PediatricGuidelines.pdf. Accessed June 5,2009.
3. Rodriguez-French A, Boghossian J, Gray GE, et al. The NEAT study: a48-week open-label study to compare the antiviral efficacy and safety ofGW433908 versus nelfinavir in antiretroviral therapy-naive HIV-1-infectedpatients. J Acquir Immune Defic Syndr. 2004;35:22–32.
4. Gathe JC Jr, Wood R, Sanne I, et al. Long-term (120-week) antiviralefficacy and tolerability of fosamprenavir/ritonavir once daily in therapy-naive patients with HIV-1 infection: an uncontrolled, open-label, single-armfollow-on study. Clin Ther. 2006;28:745–754.
5. Eron J Jr, Yeni P, Gathe J Jr, et al. The KLEAN study of fosamprenavir-ritonavir versus lopinavir-ritonavir, each in combination with abacavir-lamivudine, for initial treatment of HIV infection over 48 weeks: a ran-domised non-inferiority trial. Lancet. 2006;368:476–482.
6. Chadwick E, Borkowsky W, Fortuny C, et al. Safety and antiviral activityof fosamprenavir/ritonavir once daily regimens in HIV-infected pediatricsubjects ages 2 to 18 years (48-week interim data, study APV20003). In:14th Conference on Retroviruses and Opportunistic Infections; February25–28, 2007; Los Angeles, CA. Abstract 719.
7. Cunningham C, Freedman A, Read S, et al. Safety and antiviral activity offosamprenavir-containing regmens in HIV-infected 2- to 18-year-old pedi-atric subjects (Interim Data, Study APV29005). In: 14th Conference onRetroviruses and Opportunistic Infections; February 25–28, 2007; LosAngeles, CA. Abstract 718.
8. Garcia-Merino I, de Las Cuevas N, Jimenez JL, et al. The Spanish HIVBioBank: a model of cooperative HIV research. Retrovirology. 2009;6:27.
9. Rodes B, Sheldon J, Toro C, et al. Quantitative detection of plasma humanimmunodeficiency virus type 2 subtype A RNA by the Nuclisens EasyQAssay (version 1.1). J Clin Microbiol. 2007;45:88–92.
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Fosamprenavir
© 2010 Lippincott Williams & Wilkins www.pidj.com | 565

10. Salazar JC, Cahn P, Yogev R, et al. Efficacy, safety and tolerability oftipranavir coadministered with ritonavir in HIV-1-infected children andadolescents. AIDS. 2008;22:1789–1798.
11. Bologna R, Rugina S, Cahn P, et al. Safety and efficacy of darunavirco-administered with low-dose ritonavir in treatment-experienced childrenand adolescents at week 24. In: 15th Conference on Retroviruses andOpportunistic Infections; February 3–6, 2008; Boston, MA. Abstract 78LB.
ANNEXHospital Universitari “La Fe,” Valencia (7 patients), HospitalUniversitario “La Paz,” Madrid (4 patients), Hospital Universitario“Doce de Octubre,” Madrid (3 patients), Hospital Regional Uni-versitario “Carlos Haya,” Malaga (2 patients), Hospital “Virgendel Rocio,” Sevilla (2 patients), Hospital Universitario “CarlosIII,” Madrid (1 patient), Hospital Universitario de Getafe, Madrid(1 patient).
Spanish Group of Pediatric HIV Infection:Participating Hospitals and Personnel Staff in ThisPaper
Hospital General Universitario “Gregorio Maranon,” C.Palladino; V. Briz; S. J. de Ory; D. García Alonso; M. D.Gurbindo; M. L. Navarro; and M. A. Munoz-Fernandez. HospitalUniversitari “La Fe,” S. Negre Policarpo; Laura Fernandez Sil-veira. Hospital Universitario “La Paz,” M. I. de Jose. HospitalUniversitario “Doce de Octubre,” M. I. Gonzalez-Tome. HospitalRegional Universitario “Carlos Haya,” D. Moreno. Hospital Infan-til Unversitario “Virgen del Rocío,” J. A. Leon Leal. HospitalUniversitario de Getafe, J. T. Ramos. Hospital Universitario “Car-los III,” M. J. Mellado.
SPATIOTEMPORAL DYNAMICS OF ROTAVIRUSDISEASE IN EUROPE
CAN CLIMATE OR DEMOGRAPHIC VARIABILITYEXPLAIN THE PATTERNS OBSERVED
Christina Atchison, MB BChir,* Miren Iturriza-Gomara, PhD,†Clarence Tam, PhD,* and Ben Lopman, PhD*†
Abstract: We found a south to north movement of rotavirus activity acrossEurope. Lower birth rates, higher winter temperatures, and higher winterrainfall were associated with variations in timing of rotavirus activitybetween European countries but not with temporal variations withincountries. Patterns of rotavirus activity are likely to be driven by a complexinteraction of population, virus, and environmental factors.
Key Words: rotavirus, Europe, timing, births, weatherAccepted for publication December 15, 2009.From the *London School of Hygiene and Tropical Medicine, Epidemiology
and Population Health, London, United Kingdom; and †Centre for Infec-tions, Health Protection Agency, London, United Kingdom.
Supported by a PhD studentship grant from the Medical Research Council(to C.J.A.).
The funding body had no role in the design, conduct, analysis or reportingof the study. The views and opinions expressed in this paper do notnecessarily reflect those of the funding body.
Address for Correspondence: Christina J. Atchison, Infectious Diseases Epi-demiology Unit, Department of Epidemiology and Population Health,London School of Hygiene and Tropical Medicine, London WC1E 7HT,United Kingdom. E-mail: [email protected].
Supplemental digital content is available for this article. Direct URLcitations appear in the printed text and are provided in the HTML andPDF versions of this article on the journal’s Web site (www.pidj.com).
DOI: 10.1097/INF.0b013e3181d06fcd
I n the United States, rotavirus activity crosses the US states fromsouth-west to north-east in a repetitive yearly pattern with a delay
in peak activity observed in recent years.1 Pitzer et al2 haveexplained these patterns to largely be due to variation in birth ratesacross states and declining birth rates over time. In Europe,Koopmans and Brown3 observed a similar geographical pattern ofrotavirus activity. Their analysis, based on data from 5 Europeancountries in the late 80s and early 90s, suggested a south-west tonorth movement of rotavirus activity across Europe.3 Our studyextends this work by examining seasonality data from 17 Europeancountries between 1999 and 2009. We examined the association ofbirth rates (as identified in the United States) and weather factorswith timing of rotavirus activity across Europe.
METHODSWeekly counts of laboratory-confirmed rotavirus infec-
tions between 1999 and 2009 were extracted from the EuropeanRotavirus Network (EuroRotaNet) database. EuroRotaNet is aEuropean collaborative network of sentinel surveillance labo-ratories for rotavirus that has been established to gather stan-dardized, comprehensive information on the rotavirus typescocirculating throughout Europe.4 Crude birth rates (live birthsper 1000 estimated population per year) for European countrieswere obtained from the European Commission statistical data-base Eurostat.5 Data on weather variables were obtained fromthe MIDAS Land Surface Observation database.6 For eachEuropean country, we constructed population-weighted meanweekly series for ambient temperature, relative humidity, andtotal rainfall as previously described by Atchison et al.7 Weused population-weighted weather series to better representweather conditions in populated areas and improve our abilityto detect the influence of weather factors on timing of rotavirusactivity. Subsequently, we collapsed these weather series toobtain average weather series for the winter (December, Janu-ary, and February) each year from 1999 to 2009.
Using methods similar to those described by Pitzer et al,2
we conducted univariable and multivariable regression analysesto explore the contribution of birth rates and weather factors onthe spatiotemporal timing of rotavirus epidemics across Europe.For each country (c), timing of rotavirus activity was defined asthe mean week (T) of the rotavirus season (r), where each weekin the season was weighted by the number of rotavirus reportsas follows:
Tc,r �
w�1,52�
w � casesc,r,w
w�1,52�
casesc,r,w
where w is week of the rotavirus season running from 1 to52, where week 1 starts July 1st and week 52 ends June 30th, andcasesc,r,w is the number of reported rotavirus infections in countryc in rotavirus season r and week w. We used the Bonferronicorrection to adjust for multiple testing during the exploratoryanalysis with 4 explanatory variables (birth rates, ambient temper-
Atchison et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins566 | www.pidj.com
ature, relative humidity and rainfall). Only explanatory variables inunivariable analysis with a P value below 0.05/4 � 0.0125 wereincluded in the multivariable regression model.
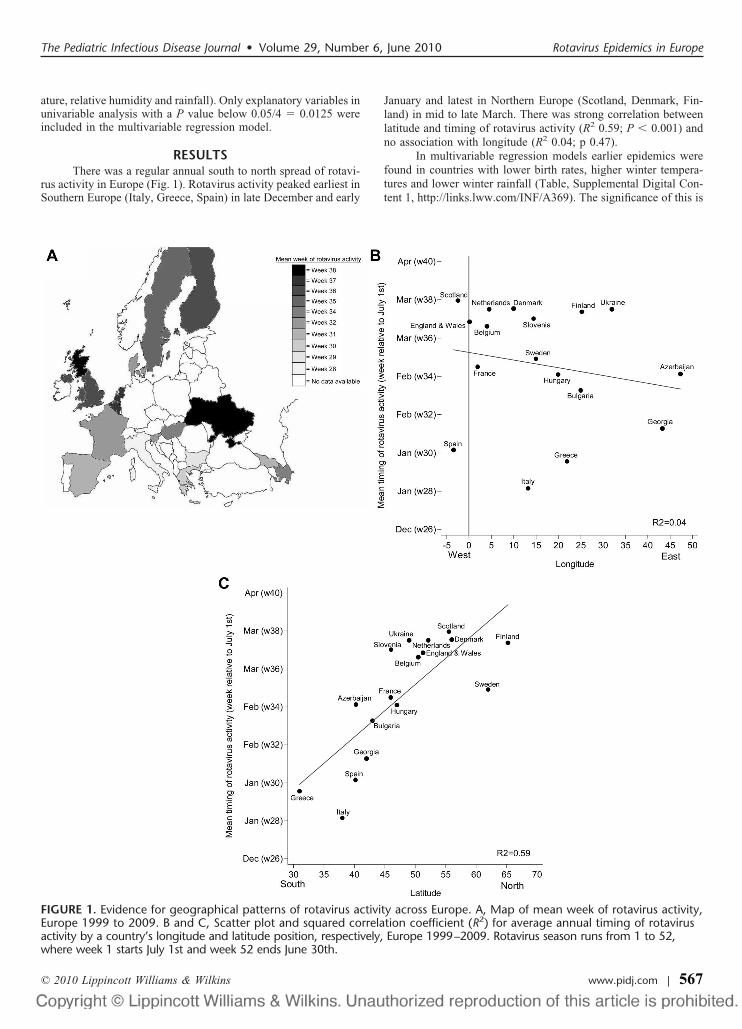
RESULTSThere was a regular annual south to north spread of rotavi-
rus activity in Europe (Fig. 1). Rotavirus activity peaked earliest inSouthern Europe (Italy, Greece, Spain) in late December and early
January and latest in Northern Europe (Scotland, Denmark, Fin-land) in mid to late March. There was strong correlation betweenlatitude and timing of rotavirus activity (R2 0.59; P � 0.001) andno association with longitude (R2 0.04; p 0.47).
In multivariable regression models earlier epidemics werefound in countries with lower birth rates, higher winter tempera-tures and lower winter rainfall (Table, Supplemental Digital Con-tent 1, http://links.lww.com/INF/A369). The significance of this is
FIGURE 1. Evidence for geographical patterns of rotavirus activity across Europe. A, Map of mean week of rotavirus activity,Europe 1999 to 2009. B and C, Scatter plot and squared correlation coefficient (R2) for average annual timing of rotavirusactivity by a country’s longitude and latitude position, respectively, Europe 1999–2009. Rotavirus season runs from 1 to 52,where week 1 starts July 1st and week 52 ends June 30th.
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Rotavirus Epidemics in Europe
© 2010 Lippincott Williams & Wilkins www.pidj.com | 567

uncertain as neither birth rates nor weather factors were associatedwith temporal variation in rotavirus timing within countries.
DISCUSSIONWe found a general south to north movement of rotavirus
activity across Europe. This pattern of rotavirus activity is similarto the geographical pattern observed in the United States.2 Pitzer et alrecently demonstrated that earlier epidemics were associated withhigher birth rates, whereas weather factors could not explain theobserved variability in timing of rotavirus epidemics either acrossstates or over time in the United States.2 In contrast to what wasobserved in the United States, birth rates in Southern Europe tendto be lower than in Northern Europe, where epidemics occur later.We found that neither birth rates nor weather factors were asso-ciated with both spatial and temporal patterns in rotavirus timingacross Europe. Spatiotemporal variations in birth rate in Europerange from 8 to13 live births per 1000 population per year and arelower (United States: 11 to 20 live births per 1000 population peryear) and changing less than those in US states. This could explain,in part, why, unlike in the United States, varying birth rates are notimportant in determining the timing of rotavirus epidemics inEurope.
The use of rotavirus surveillance data and crude birth ratesaggregated at a national level, as well as national weather series asan aggregate weather series for the whole of a country may dilutethe weather and birth effects seen on timing of rotavirus activitywithin and across European countries. More detailed region orcity-specific analysis would address this problem albeit at the lossof statistical power because some countries reported only smallnumbers of laboratory-confirmed rotavirus infections to the Euro-RotaNet database. The Health Protection Agency has reliablycollected reports of laboratory-confirmed rotavirus infections fromlaboratories across England and Wales since the early nineties andthe data can be readily broken down by region.8 A survey ofclinical laboratory practices found that most laboratories in En-gland and Wales test for rotavirus all year round in all cases ofgastroenteritis of those 5 years of age or younger and that thedegree of under-reporting and the testing criteria for rotavirus hasnot varied significantly over time.8 Therefore, these data are verylikely to be representative of patterns of rotavirus disease in thepopulation. We explored the association between birth rates andweather factors and the timing of rotavirus activity in each regionof England and Wales between 1993 and 2009. There was noevidence of any association (Table, Supplemental Digital Content2, http://links.lww.com/INF/A370). This adds further support toour findings from our European analysis.
In summary, higher birth rates are associated with earliertiming of rotavirus activity in the United States,2 but not acrossEurope. Rotavirus transmission is likely to be driven by a complexinteraction of population demographics, environmental factors andcirculation of rotavirus strains. Under different epidemiologicconditions, different factors may be responsible for variation inlocal patterns.
ACKNOWLEDGMENTSThe authors thank the members of EuroRotaNet and all
collaborating institutes for contributing data from participatingsurveillance sites.
REFERENCES1. Turcios RM, Curns AT, Holman RC, et al. Temporal and geographic trends
of rotavirus activity in the United States, 1997–2004. Pediatr Infect Dis J.2006;25:451–454.
2. Pitzer VE, Viboud C, Simonsen L, et al. Demographic variability, vaccina-tion, and the spatiotemporal dynamics of rotavirus epidemics. Science.2009;325:290–294.
3. Koopmans M, Brown D. Seasonality and diversity of group A rotaviruses inEurope. Acta Paediatr Suppl. 1999;88:14–19.
4. Iturriza-Gomara M, Dallman T, Banyai K, et al. Rotavirus surveillance inEurope, 2005–2008: web-enabled reporting and real-time analysis of geno-typing and epidemiological data. J Infect Dis. 2009;200(suppl 1):S215–S221.
5. Eurostat: population and social conditions. Available at: www.ec.europa.eu/eurostat. Accessed September 27, 2009.
6. The British Atmospheric Data Centre. Met Office—MIDAS Land SurfaceObservation Stations Data. Available at: http://badc.nerc.ac.uk/data/ukmo-midas/. Accessed September 24, 2009.
7. Atchison CJ, Tam CC, Hajat S, et al. Temperature-dependent transmission ofrotavirus in Great Britain and The Netherlands. Proc Biol Sci. 2009 Nov 25.�Epub ahead of print.�
8. Atchison CJ, Lopman BA, Harris CJ, et al. Clinical laboratory practices forthe detection of rotavirus in England and Wales: can surveillance based onroutine laboratory testing data be used to evaluate the impact of vaccination?Euro Surveill. 2009;14.
LONG-TERM IMMUNITY AFTER TWO DOSES OFINACTIVATED HEPATITIS A VACCINE, IN
ARGENTINEAN CHILDREN
Eduardo L. Lopez, MD,* María M. Contrini, MD,*Alicia Mistchenko, MD,† and Roberto Debbag, MD‡
Abstract: We examined long-term anti-hepatitis A virus antibody persis-tence in Argentinean children 10 years after the initial study in which theyreceived 2 doses of inactivated hepatitis A vaccine (Avaxim 80U). Of the111 children, 48 from the initial trial were enrolled. Of 48, 47 (97.9%)participants had serum anti-hepatitis A virus antibody titers �20 mIU/mL,with the geometric mean concentration of 390.91 (�370.14) mIU/mL;(95% confidence interval, 282.2–499.5 mIU/mL), range, 36 to 1860.
Key Words: hepatitis A, immunization, pediatric, ArgentinaAccepted for publication January 13, 2010.From the *Infectious Diseases Program, Hospital de Ninos “Dr. Ricardo Gutierrez,”
Buenos Aires, Argentina; †Laboratory of Virology, Hospital de Ninos “Dr.Ricardo Gutierrez,” Buenos Aires, Argentina; and ‡Sanofi Pasteur, BuenosAires, Argentina.
Reprints: Eduardo L. Lopez, MD, Guido 2676, Piso 10, 1425 BuenosAires, Argentina. E-mail: [email protected].
DOI: 10.1097/INF.0b013e3181d57a85
From 2002 through 2005, the Argentinean Health Departmentwas notified of �120,000 hepatitis A (HA) cases, mainly in 5
to 9 year olds. Children provide a reservoir for hepatitis A virus(HAV) in communities.1 Effective and well-tolerated HA vaccinesfor children exist1 including a pediatric formulation of the inacti-vated HA vaccine, Avaxim (Avaxim 80U Pediatric, Sanofi Pas-teur, Lyon, France). A 2-dose Avaxim 80U schedule has demon-strated good immunogenicity and safety profiles in children 1 to 15years of age.2 In one clinical trial in Buenos Aires, Argentina, 2doses of Avaxim 80U were administered 6 months apart tochildren aged between 1 and 15 years. In 111 children, those agedbetween 12 and 47 months were seronegative at inclusion, HAVantibody titers (anti-HAV) geometric mean concentration (GMC)at baseline and weeks 2, 24 (prebooster), and 27 (postbooster) ofthe initial schedule were respectively 6.25, 98.5, 190, and 6743mIU/mL.2 Although Dagan et al3 have demonstrated the persis-tence of anti-HAV antibodies in children after 2 Avaxim 80Udoses after 3 years, no longer term immunogenicity data inchildren have yet been published. We describe the evaluation oflong-term anti-HAV antibody persistence 10 years after 2 doses ofAvaxim 80U.2
Lopez et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins568 | www.pidj.com

MATERIALS AND METHODS
Trial Design and Study PopulationHealthy children who were 12 to 47 months of age at the
time of primary vaccination, when they received 2 doses ofAvaxim 80U 6 months apart were invited for serum anti-HAVmeasurements 10 years later. Participants were excluded if theyhad received an additional dose of HA vaccine after the firstbooster or if they had moderate or severe illness, immunodefi-ciency, or ongoing immunosuppressive therapy, if they had previ-ous treatment with growth hormone or human immunoglobulins orif they had received whole blood cells or blood product transfusionduring the last 6 months. The protocol was approved by theinternal review board and the ethics committee of the Hospital deNinos “Dr. Ricardo Gutierrez.” Informed, written consent fromparents/guardians and the children’s agreement was obtained fol-lowing explanation of the purpose of the trial, before inclusion(specific questions asked at the time of recontact, to determineeligibility were as follows:
1. Did your child receive HA vaccine during participationin the initial trial vaccine 10 years ago?
2. Were blood samples taken from your child to measureHAV antibodies before and after the vaccination 10years ago?
3. In the last 10 years, has your child received any extradose of HA vaccine in addition to the 2 doses adminis-tered in the trial 10 years ago?
4. Has your child received blood or blood products in thelast 6 months?
Vaccine and VaccinationsInactivated HA vaccine Avaxim 80U Pediatric (Sanofi Pas-
teur, Lyon, France) was used in the initial study. It is preparedfrom cultured purified formaldehyde-inactivated GBM strain ofHAV and contains 80 HAV antigen units per 0.5 mL dose andreduced aluminum hydroxide content (0.15 mg). Each dose con-tains 2-phenoxyethanol (2.5 �L), formaldehyde (12.5 �g), andMedium 199, water for injection up to 0.5 mL. It was administeredintramuscularly into the deltoid muscle. An additional dose wasoffered to participants whose anti-HAV titer was less than or equalto the lower limit of detection of the serology assay (�20 mIU/mL) when measured 10 years after the 2-dose vaccination course.This value is known to protect against HA infection.4
Laboratory TestsSerum anti-HAV antibody titers were measured by VIDAS
Anti-HAV Total (HAVT, BioMerieux, France). The assay com-bines a 2-step enzyme immunoassay competition method withfluorescent detection (ELFA).5 Results are calculated automati-cally and the samples’ relative fluorescent value is interpreted bythe VIDAS system. Results are expressed in mIU/mL (WHOreference standard first Reference Preparation Hepatitis A Immu-noglobulin �100 mIU/mL�). Sera with anti-HAV �20 mIU/mLwere considered seropositive. The test used in the initial study wasnot available (antibody titers had been assessed using commercialradioimmunoassay �HAVAB, Abbot Laboratories, North Chicago�modified to increase the sensitivity).5
Statistical AnalysisThe study was descriptive. GMC with 95% confidence
intervals were calculated. �2 and Mann-Whitney tests were usedwhen appropriate using STATA software (Version 8.0; StataCorporation, College Station, TX). Participants also completed aquestionnaire about potential exposure to natural HAV infectionsince the initial immunization.
RESULTSBetween May and November 2007, 48 of the 111 children
who had been included in the initial trial were enrolled in this10-year follow-up study; of the 63 children who were not includedin this follow-up trial, 30 children had moved to a differentneighborhood or city, 26 children could not be contacted since thetelephone number had changed, 1 child’s family was contacted butdid not consent to the child’s participation in the follow-up trial,and 6 children were excluded due to being seropositive in theinitial trial. Of the 48 children included in the follow-up trial, 26(54.2%) were female, mean age was 156.06 (�11.7) months; nosignificant age difference was observed between sexes (P � 0.64).All participants had had anti-HAV titers �20 mIU/mL at inclusion10 years previously. Fourteen days after the first vaccination,100% had had anti-HAV �20 mIU/mL. GMC increased during the6 months after the first vaccine dose and all participants hadanti-HAV �20 mIU/mL at week 24. A strong anamnestic responseto the second dose was seen at week 27.2 There was no significantdifference between anti-HAV titers of the 48 participants enrolledin the follow-up study and the whole population at week 27(postbooster) in the initial study (P � 0.25). Ten year persistenceof anti-HAV �20 mIU/mL was observed in 47/48 (97.9%) par-ticipants, with GMC 390.91 (�370.14) mIU/mL; (95% confidenceinterval, 282.2–499.5 mIU/mL), range, 36–1860 (Table 1). Therewas no significant difference in titers between sexes (P � 0.18).
Regarding potential exposure to natural HAV infection,17/48 (35.4%) had had known close contact with an acute HA casesince immunization. Contacts were as follows: household, 4/48(8.33%); school, 11/48 (22.9%); close neighbors, 7/48 (14.6%).Four of 17 (23.5%) had had more than one contact. There was nosignificant difference between anti-HAV titers in children report-ing exposure (445.6 ��464.4 mIU/mL, range: 108–1860 mIU/mL�) and those reporting no contact with HA patients during thelast 10 years (359.9 ��309.2 mIU/mL, range: 36–1460 mIU/mL�).Moreover, previous titers at postbooster (week 27) in the initialstudy for these 2 groups were 7564 (�7004 mIU/mL, range:902–31,424 mIU/mL) reporting contact versus 7484 (�4942 mIU/mL, range: 1200 – 20,592 mIU/mL) for those reporting no contact(P � 0.78). The one participant with anti-HAV �20 mIU/mL atyear 10 was revaccinated and his titer reached 1400 mIU/mL, evenhigher than after the first booster dose (1200 mIU/mL at week 27).
DISCUSSIONInactivated HA vaccines are highly immunogenic although
an absolute protective anti-HAV antibody titer threshold has notbeen defined. Serum antibody concentrations after passive transfer
TABLE 1. Anti-HAV Titers in Subjects* Enrolled in10-yr Follow-Up Study
Time PointGMC
†,
mIU/mL (�SD),(n � 48)
95% CI Range(mIU/mL)
Baseline (week 0) 7.12 (3.9) 5.9–8.2 5.0–18.0Post-first dose
(week 2)100.02 (60.6) 82–118 25–349
Pre-booster dose(week 24)
266.75 (234.1) 196.4–337.1 35–939
Post-booster dose(week 27)
7513.63 (6328) 5718.6–9245.7 902–31424
10-yr follow-up 390.91 (370.14) 282.2–499.5 36–1860
*One participant with anti-HAV �20 mIU/mL at 10-yr time point excluded.†GMC, geometric mean concentration.
HAV indicates hepatitis A virus; SD, standard deviation; CI, confidence interval.
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Long-Term Immunity After HA Vaccine in Children
© 2010 Lippincott Williams & Wilkins www.pidj.com | 569

by immune globulin or active induction by vaccination are 10- to100-fold lower than those produced by natural infection. Concen-trations of 10 to 20 mIU/mL, 1 to 2 months after immunoglobulinadministration protect against HA infection.1 In vitro studies usingcell culture-derived HAV show antibody concentrations �20mIU/mL can be neutralizing.4 The lower limit of detection of aparticular assay is considered as protective. After vaccination,persons who are anti-HAV seronegative by standard assays mightnevertheless have protective concentrations of antibody.6
This study presents a 10-year follow-up of an Avaxim 80UPediatric clinical trial. In the initial study, 99.1% of vaccinees hadanti-HAV titers �20 mIU/mL 2 weeks after the first vaccine dose,and 100% at week 24 (prebooster) and at week 27 (postbooster).
Serum anti-HAV persistence has been studied in childrenand in adults1,3,6–10 but, to our knowledge, only 3-year follow-updata in children have been published for Avaxim 80U vaccine andno longer term data are available. This is the first long-termevaluation of humoral immunity showing 10-year persistence ofanti-HAV antibodies in 97.9% of healthy children after 2-doses ofAvaxim 80U Pediatric. Similar long-term data were previouslyshown for other inactivated HA vaccines in different age popula-tions11,12 while mathematical models predict that in childrenanti-HAV will persist for 14 to 30 years.11,13
The results of this study support “The International Con-sensus Group on Hepatitis A Virus Immunity,” which concludedthat after a full vaccination course, protective antibody amountspersist beyond 10 years in healthy individuals, and underlyingimmune memory provides protection far beyond the duration ofanti-HAV antibodies.11 Even in the small population, in our study,no differences were observed related to sex as also was shown inchildren and adults in other studies.8,13 No difference in anti-HAVtiters was observed in children who recorded having had closecontact with HA patients versus those with no known potentialexposure, although it is known that the natural exposure to HAVproduces high anti-HAV titers.11
In 2006, the Argentinean Department of Health, introducedHA vaccine into the national immunization program because of theepidemiologic situation of the preceding 4 years. Only one dosewas indicated based on the assumption that natural exposure toHAV would act as a natural booster and provide good protectionagainst disease. Although the number of participants in this studyis limited, potentially HAV exposed children did not have higheranti-HAV titers than those reporting no contact. Because all hadreceived a complete 2-dose schedule, it is not known whethernatural exposure to HAV acts as a natural booster after only onedose of inactivated HA vaccine.
This study show that Avaxim 80U Pediatric induces hightiters of anti-HAV, which persist for over 10 years following 2doses in children demonstrating long-term protection. Our datasupport the International Consensus Statement that today nodata support the need for booster doses of HA vaccine inimmunocompetent individuals who have received a full vacci-nation course.11
ACKNOWLEDGMENTSThe authors thank Simon M. Jones and Anvar Rasuli for
their constructive review of the study report and of this manuscript.
REFERENCES1. Bell B, Feinstone S. Hepatitis A vaccines. In: Plotkin S, Orenstein W, eds.
Vaccines. Philadelphia, PA: WB Saunders; 2004:269–297.
2. Lopez EL, Del C, X, Torrado LE, et al. Safety and immunogenicity of apediatric formulation of inactivated hepatitis A vaccine in Argentineanchildren. Pediatr Infect Dis J. 2001;20:48–52.
3. Dagan R, Greenberg D, Weber F. Immunogenicity of an inactivatedhepatitis A pediatric vaccine: three-year post-booster follow-up. Vaccine.2005;23:5144–5148.
4. Lemon SM, Murphy PC, Provost PJ, et al. Immunoprecipitation andvirus neutralization assays demonstrate qualitative differences betweenprotective antibody responses to inactivated hepatitis A vaccine andpassive immunization with immune globulin. J Infect Dis. 1997;176:9 –19.
5. Miller WJ, Clark W, Hurni W, et al. Sensitive assays for hepatitis Aantibodies. J Med Virol. 1993;41:201–204.
6. Fiore AE, Wasley A, Bell BP. Prevention of hepatitis A through activeor passive immunization: recommendations of the Advisory Committeeon Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55:1–23.
7. Lolekha S, Pratuangtham S, Punpanich W, et al. Immunogenicity andsafety of two doses of a paediatric hepatitis A vaccine in Thai children:comparison of three vaccination schedules. J Trop Pediatr. 2003;49:333–339.
8. Rendi-Wagner P, Korinek M, Winkler B, et al. Persistence of seroprotection10 years after primary hepatitis A vaccination in an unselected studypopulation. Vaccine. 2007;25:927–931.
9. Van Herck K, Van Damme P. Inactivated hepatitis A vaccine-inducedantibodies: follow-up and estimates of long-term persistence. J Med Virol.2001;63:1–7.
10. Van Herck K, Van Damme P, Lievens M, et al. Hepatitis A vaccine:indirect evidence of immune memory 12 years after the primary course.J Med Virol. 2004;72:194–196.
11. Van Damme P, Banatvala J, Fay O, et al. Hepatitis A booster vaccination:is there a need? Lancet. 2003;362:1065–1071.
12. Hammitt LL, Bulkow L, Hennessy TW, et al. Persistence of antibody tohepatitis A virus 10 years after vaccination among children and adults.J Infect Dis. 2008;198:1776–1782.
13. Fan PC, Chang MH, Lee PI, et al. Follow-up immunogenicity of aninactivated hepatitis A virus vaccine in healthy children: results after 5years. Vaccine. 1998;16:232–235.
ADOLESCENT WITH NEUROPSYCHIATRICSYMPTOMS ASSOCIATED WITH NOVELINFLUENZA A (H1N1) VIRUS INFECTION
Marta German-Diaz, MD, Rosa Pavo-Garcia, MD,Judit Diaz-Diaz, MD, Elisa Giangaspro-Corradi, MD,and Sagrario Negreira-Cepeda, PhD
Abstract: Neurologic complications have been described previously inassociation with seasonal influenza A or B viruses, but the frequency withwhich these occur with novel influenza A (H1N1) virus infection isunknown. We describe a case of an adolescent with a bizarre neuropsy-chiatric picture associated with novel influenza A (H1N1) virus infection.
Key Words: encephalopathy, neurologic complications, altered mentalstatus, neuropsychiatric manifestations, novel influenza A, swineinfluenzaAccepted for publication December 29, 2009.From the Department of Pediatrics Infectious Diseases, Hospital 12 de Octubre,
Madrid, Spain.Address for correspondence: Marta German-Diaz, MD, Avda de Cordoba
s/n, Madrid 28041, Spain. E-mail: [email protected]: 10.1097/INF.0b013e3181d411a9
Neurologic complications, including seizures, encephalitis orencephalopathy have been described previously in associa-
tion with respiratory tract infection with seasonal influenza A or Bviruses,1,2 but the frequency with which these occur with novelinfluenza A (H1N1) virus infection is unknown. We describe acase of encephalopathy associated with novel influenza A (H1N1)virus infection in a Spanish adolescent.
German-Diaz et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins570 | www.pidj.com

CASE REPORTA previously healthy white male aged 13 years presented to the
emergency department because of altered mental status, with confu-sion and markedly slow and intermittent responsiveness to questions.This occurred after 2 days of persistent cough and several episodes ofvomiting. He had no fever. At presentation, the patient was confused,with inattentiveness and slow speech. The rest of the physical andneurologic examination was normal. Blood tests, including ammoniaand liver enzymes, and cerebrospinal fluid (CSF) were normal. Acomputed tomography head scan showed 2 small low density lesions,suggestive of a choroidal fissure cyst. Urine toxicology screen wasnegative. Empiric treatment with acyclovir was initiated. During thefirst day of his stay in hospital, his mental status fluctuated, with aprogressive deterioration and incidents of aggression, so the patientwas transferred to a reference Hospital intensive-care unit.
Physical examination in our hospital revealed a normal mentalstatus and no fever or seizures. A diagnosis of influenza A infectionwas made by the detection of the virus by real time reverse tran-scriptase-polymerase chain reaction in a nasopharyngeal swab spec-imen collected from the patient. Oseltamivir was initiated. During theensuing days he began showing signs of delirious behavior, whichwas controlled with risperidone. Lumbar puncture was repeated andCSF values were again normal; CSF cultures were sterile and reversetranscriptase-polymerase chain reaction for enteroviruses and herpes-virus were negative. Acyclovir therapy was stopped. An electroen-cephalogram was consistent with encephalopathy, without epilepto-genic focus. He completed a 5-day course of oseltamivir and wasdischarged on day 10 without apparent sequelae. He will continue tobe evaluated by the Child Neurology and Psychiatry departments.
DISCUSSIONNeurologic complications associated with influenza have
been reported for more than century. Most recently, an epidemic ofinfluenza in Japan in the late 1990s was associated with hundredsof cases of encephalopathy among children.1 Small numbers ofchildren with neurologic complications have been reported spo-radically in Europe and Canada. Nevertheless, the frequency ofneurologic disease associated with novel influenza A (H1N1) virusinfection is unknown.
Our patient had a bizarre neuropsychiatric picture associ-ated with an influenza illness. Neurologic complications associatedwith pandemic influenza A H1N1 have been described,3 but, to ourknowledge, our patient is the first case with predominant neuro-psychiatric manifestations associated with this virus.
Neurologic manifestations associated with influenza virusinfection (A and B) include alterations in mental status rangingfrom confusion and lethargy to coma, acute inflammatory demy-elinating polyneuropathy (Guillain-Barre syndrome), acute dis-seminated encephalomyelitis, transverse myelitis, abnormal move-ments, acute psychosis, frontal lobe syndromes, mutism, andvisual hallucinations.2,4,5 Some patients develop encephalopathywith severe complications and even death.1
Influenza A virus strains with certain hemagglutinin (H) andneuraminidase (N) profiles are more often associated with centralnervous system (CNS) complications. In particular, influenza A(H3N2) virus infections have been found in the majority of enceph-alopathy cases reported in Japan and Europe, although occasionallyinfluenza A (H1N1) viruses have been isolated as well.2
In Japan, approximately 80% of influenza-associated en-cephalopathy cases occur in children aged �5 years, and neuro-logic signs typically develop within 1 to 2 days of influenzasymptom onset.1,6
The pathogenic mechanism of influenza virus infection onthe nervous system remains to be elucidated. Only occasionally are
viral antigens detected in CNS tissue at autopsy and isolation ofthe virus from CSF is equally rare, suggesting that neurologicmanifestations might result from an immunologic effect more thana direct invasion of CNS.2,7 Neuroimaging studies are usuallynormal, but in severe cases, abnormalities can include diffusecerebral edema and bilateral thalamic lesions. Electroencephalo-gram can show diffuse abnormalities.1,2,8
Antiviral drugs reduce the symptoms, signs and duration ofacute uncomplicated influenza respiratory disease,9 but there areno studies about the impact of antiviral treatment on influenza-associated CNS manifestations; however, there are some reports ofchildren with influenza and neurologic complications treated withoseltamivir.5,10 It seems reasonable to recommend initial antiviraltreatment for any hospitalized patient with neurologic symptomsand suspected seasonal influenza or novel influenza A (H1N1)virus infection. However, the effectiveness of antiviral treatment toprevent influenza-associated encephalopathy sequelae is unknown,and additional studies are needed to evaluate its role in thetreatment of influenza-related encephalopathy.
To our knowledge, these kind of manifestations associ-ated with novel influenza A (H1N1) infection have been mainlyreported in children. In addition, it has been reported thatchildren are infected by influenza A more frequently thanadults. Thus, we recommend considering influenza-associatedencephalopathy in the differential diagnosis for children whopresent with new-onset seizures or mental status changes,during the influenza season.
REFERENCES1. Morishima T, Togashi T, Yokota S, et al. Encephalitis and encephalopathy
associated with an influenza epidemic in Japan. Clin Infect Dis. 2002;35:512–517.
2. Maricich SM, Neul JL, Lotze TE, et al. Neurologic complications associ-ated with influenza A in children during the 2003–2004 influenza season inHouston, Texas. Pediatrics. 2004;114:e626–e633.
3. Centers for Disease Control and Prevention. Neurologic complications associ-ated with novel influenza A (H1N1) virus infection in children-Dallas, Texas,May 2009. MMWR Morb Mortal Wkly Rep. 2009;58:773–778.
4. Huang YC, Lin TY, Wu SL, et al. Influenza A-associated central nervoussystem dysfunction in children presenting as transient visual hallucination.Pediatr Infect Dis J. 2003;22:366–368.
5. Newland J, Romero J, Varman M, et al. Encephalitis associated withinfluenza B virus infection in 2 children and a review of the literature. ClinInfect Dis. 2003;36:e87–e95.
6. Wada T, Morishima T, Okumura A, et al. Differences in clinical manifes-tations of influenza-associated encephalopathy by age. Microbiol Immunol.2009;53:83–88.
7. Ito Y, Ichiyama T, Kimura H, et al. Detection of influenza virus RNA byreverse transcription-PCR and proinflammatory cytokines in influenza-virus-associated encephalopathy. J Med Virol. 1999;58:420–425.
8. Amin R, Ford-Jones E, Richardson SE, et al. Acute childhood encephalitisand encephalopathy associated with influenza: a prospective 11-year re-view. Pediatr Infect Dis J. 2008;27:390–395.
9. Kaiser L, Wat C, Mills T, et al. Impact of oseltamivir treatment oninfluenza-related lower respiratory tract complications and hospitalizations.Arch Intern Med. 2003;163:1667–1672.
10. Straumanis J, Tapia M, King J. Influenza B infection associated withencephalitis: treatment with oseltamivir. Pediatr Infect Dis J. 2002;21:173–175.
COMMON BILE DUCT STENOSIS ANDPANCREATITIS IN KAWASAKI DISEASE
TWO CASES AND A REVIEW OF THE LITERATURE
Rebecca Cherry, MD, MPH,* Hillel Naon, MD,†Hartley Cohen, MD,† Masato Takahashi, MD,‡Cornelia Kaminsky, MD,§ and Wilbert Mason, MD¶
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 KD and Pancreatitis
© 2010 Lippincott Williams & Wilkins www.pidj.com | 571

Abstract: We report 2 children with Kawasaki disease, who developedpancreatitis and common bile duct abnormalities. After reviewing theliterature, we conclude that Kawasaki disease may lead to such changes asa result of the underlying vasculitis characterizing this disease, or of directinflammation of the biliary tree.
Key Words: Kawasaki disease, pancreatitis, bile duct stenosisAccepted for publication January 5, 2010.From the *Division of Gastroenterology, Rady Children’s Hospital, University
of California, San Diego, CA; and Divisions of †Gastroenterology, ‡Car-diology, §Radiology, and ¶Infectious Diseases, Childrens Hospital, KeckSchool of Medicine, University of Southern California, Los Angeles, CA.
Address for correspondence: Rebecca Cherry, MD, 3020 Children’s Way,MC 5030, San Diego, CA 92123. E-mail: [email protected].
DOI: 10.1097/INF.0b013e3181d2bb0b
Kawasaki disease (KD), one of the most common childhoodvasculitides, is frequently associated with gallbladder hy-
drops. There are few reports of other clinically apparent pan-creaticobiliary changes in KD. Here, we describe 2 patientswith common bile duct (CBD) changes in the setting of KD andsymptomatic pancreatitis.
CASE 1A 6-year-old boy presented to an outside hospital with 4
days of fever, maculopapular rash, conjunctivitis, strawberrytongue, nausea, and scrotal edema. C-reactive protein (CRP) was12.6 mg/dL (normal: �1.0 mg/dL), and a blood culture andMonospot test were both negative. On day 5 of his illness,echocardiogram showed a mild proximal saccular aneurysm of theright coronary. The patient was treated for KD with intravenousimmunoglobulins (IVIG), 2 g/kg, and high-dose aspirin. A secondinfusion of IVIG was required because of persistent fever. Labo-ratory studies on admission included aspartate aminotransferase(AST) 65 �/L, alanine aminotransferase (ALT) 190 �/L, andalkaline phosphatase 360 �/L. He had no abdominal pain orjaundice. The patient was discharged home on day 7 from initialonset of fever, with a CRP of 8 mg/dL. Discharge regimenincluded aspirin at 486 mg q6 hours (100 mg/kg/d) for 5 days,followed by a dose of 81 mg daily (4.25 mg/kg/d) for an antici-pated 2 to 3 months.
On day 30, the patient developed abdominal and back painwith emesis. In a local emergency department, laboratory testingrevealed AST 687 �/L, ALT 724 �/L, and alkaline phosphatase502 �/L. Amylase was 193 �/L (normal: 35–140 �/L) and lipase420 �/L (normal: 15–55 �/L). Total bilirubin was 1.1 mg/dL. Hewas diagnosed with pancreatitis and had symptomatic improve-ment after 3 days of nil per os status.
One week later, on day 37, he presented to our hospital withrecurrent abdominal pain, jaundice, and persistent elevation of histransaminases. The AST was 727 �/L, ALT 601 �/L, and gammaglutamyl-transferase (GGT) 364 �/L. Total bilirubin was elevated,peaking at 8.7 mg/dL with conjugated bilirubin of 6.3 mg/dL. Atthat point, his biochemical pancreatitis had resolved, with a normalamylase of 31 �/L (normal: 30–100 �/L) and lipase of 81 �/L(normal: 23–300 �/L). Abdominal ultrasound showed dilatation ofthe intrahepatic central biliary tree and CBD. Abdominal com-puted tomography the following day confirmed CBD stenosis atthe level of the pancreatic head, with dilatation of the CBD toat least 9 mm and diffuse intrahepatic biliary duct dilatation. Hehad endoscopic retrograde cholangiopancreatography (ERCP)performed for CBD stent placement. He also had subtle nar-rowing of his pancreatic duct on ERCP.
The patient subsequently did well with rapid improvementof his jaundice and biochemical abnormalities. The CBD stent was
removed endoscopically 2 months after placement. He has had nofurther pancreatic or hepatobiliary symptoms more than 1 yearafter discharge. His coronary artery aneurysm has resolved.
CASE 2A 3-year-old boy presented to our hospital with a 4-day
history of fever, rash, and swelling of his left anterior neck. He hadinjected sclera, cracked bleeding lips, palmar erythema, and a 2-cmleft submandibular lymph node on examination. He was treatedpresumptively for both KD and streptococcal illness, with IVIG 2g/kg, aspirin 90 mg/kg/d, ampicillin, and clindamycin. ASO titerwas less than 25 IU/mL. IVIG dose was repeated twice during theadmission because of persistence of fever. On day 12 of illness, thepatient received methylprednisolone in a dosage of 30 mg/kg.Echocardiogram was normal on admission, but on day 8 of hisillness, there was dilatation of the right, left main, and left anteriordescending coronary arteries.
The patient had elevated transaminase values and hyperbi-lirubinemia on admission, with hepatosplenomegaly on examina-tion. Abdominal ultrasound was normal. Over the course of ad-mission, total bilirubin rose to a peak of 6.0 mg/dL, withconjugated bilirubin of 3.8 mg/dL, AST 156 �/L, ALT 165 �/L,and GGT 240 �/L. On day 11 of illness, he was found to haveelevated serum lipase, which peaked on day 15 at 3224 �/L, withserum amylase of 465 �/L. Abdominal pain consistent with pan-creatitis began at that time. His pancreatitis was initially thoughtdue to the recent use of high-dose steroids for treatment ofrefractory KD. However, because of persistent biochemical andclinical pancreatitis, magnetic resonance cholangiopancreatogra-phy was performed on day 21. Magnetic resonance cholangiopan-creatography revealed a mild dilatation of the CBD with taperingnear the ampulla of Vater, consistent with a stenosis. Ductaldilation extended into the proximal intrahepatic ducts. No furtherintervention was performed and his pancreatitis resolved after 1month of nil per os status and total parenteral nutrition. He has hadno further pancreatic or hepatobiliary symptoms more than 1 yearafter discharge. His coronary artery abnormalities have resolved.
REVIEW OF THE LITERATURE AND DISCUSSIONOur cases show similarities with others that have been
reported in individual case reports. Additionally, in a series of 6KD patients, Karthik and Harrington1 presented 2 with ALTelevated to 99 and 386 �/L, and with hyperbilirubinemia of 1.3and 5.2 mg/dL. In regard to CBD changes, our cases are similar toa 10-year-old described by Petersen et al2 in 1994, who developedpainless jaundice and elevated amylase values, with biliary dila-tation, hydrops of the gallbladder, and enlargement of the pan-creas. On ERCP, she had a string-like stenosis in the prepapillaryCBD. Zulian et al described 10 patients with KD presenting withacute surgical abdomen, 6 of whom were greater than 5 years old.In that series, 5 patients had a postoperative diagnosis of gallblad-der hydrops with cholestasis, and 3 required percutaneous trans-hepatic biliary drainage.3
Autopsy studies provide some information on the biliarytree and pancreas in KD. In 1980, Amano et al4 reported autopsiesof 37 patients with KD and coronary artery involvement, with amedian age of 11 months. Pancreatitis was identified in 22% ofsubjects overall, and 53% had inflammation of the pancreatic duct.The incidence of pancreatitis varied with duration of illness asfollows: patients who died within 30 days of the onset of illnesshad a 40% incidence of pancreatitis, and those who died 31 to 60days from onset had a 17% incidence. Pancreatitis was not seen inthose with disease duration of 61 days or longer.
Cherry et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins572 | www.pidj.com

Rowley et al5 studied tissue from 14 KD patients who diedof cardiac complications between 1970 and 1999. Median age was7.5 months, and 3 patients were treated with IVIG. One-third ofpatients had vasculitis of small branches of the pancreatic artery. Inall 14 patients, IgA plasma cells infiltrated the pancreas in aperiductular distribution. IgA plasma cells were present aroundsmall bile ducts in 7 of 12 patients for whom this tissue wasavailable, but were not found in liver parenchyma. A similarfinding, of selective biliary ductular epithelial cell destruction, wasseen on liver biopsy in an 8-month-old with severe KD reported byEdwards et al.6 Biliary inflammation in the absence of vasculitis ina 16-year-old KD patient was also reported by Suddleson et al.7
Amano’s and Rowley’s series suggest that in fatal KD,histological pancreatitis is relatively common, being seen in 22%to 36% of cases. Inflammation of the pancreatic and small bileducts has also been seen. Case reports of clinical pancreatitis,however, are few, and to our knowledge, there is only one previouscase report of CBD stenosis or stricture in KD. There are severalpossible explanations for this discordance.Severity of Disease. As all the patients in these series died of KDcomplications, greater disease severity may explain the frequentobservation of pancreatitis in those cases. The few case reports ofpancreatitis in KD may similarly be among patients with severeillness. Deaths from KD have decreased in frequency since 1988,when the American Academy of Pediatrics and the AmericanHeart Association endorsed IVIG as the recommended treatment,with recent mortality rates of 0.08% in Japan8 and 0.17% in theUnited States.9 The rate of pancreatic involvement may be simi-larly low, occurring in severe and potentially fatal cases. Both ofour cases, described above, failed to respond to an initial dose ofIVIG, suggesting relative disease severity.Age. While most of the patients in the autopsy series were infants,those with symptomatic pancreatitis have all been 3 years of age orolder. Older children may be more prone to pancreatic or hepato-biliary complications of the disease. Alternatively, pancreatitismay be undetected in younger KD patients due to their inability todescribe symptoms.Duration of Illness. In Amano’s study, the highest frequency ofpancreatitis and inflammation of the pancreatic duct was seenwithin 30 days of illness. However, it is unknown at which pointpancreatitis might peak. Patients may receive IVIG as specifictherapy for KD before these pathological changes have developed.
In conclusion, both pancreatitis and CBD stenosis with orwithout obstructive jaundice can be seen in patients with KD whoare relatively older and have more severe disease. Pancreatic andbiliary changes may be self-limited; interventions such as chole-cystectomy and CBD or pancreatic duct stenting should be con-sidered carefully before undertaken. KD should be included as adifferential diagnosis in children with pancreatitis or jaundice inthe presence of systemic illness. Children with KD who either haveabdominal pain or are preverbal should be evaluated for thepresence of pancreatitis so that appropriate treatment measures canbe taken.
REFERENCES1. Karthik SV, Harrington B. Hepatocellular dysfunction in children with
Kawasaki’s Disease—a possible marker of severity. Am J Gastroenterol.2004;99:S173.
2. Petersen C, Mildenberger H, Jablonski M. Painless cholestasis in Kawasakisyndrome associated with pancreatitis. Pediatr Surg Int. 1994;9:118–119.
3. Zulian F, Falcini F, Zancan L, et al. Acute surgical abdomen as presentingmanifestation of Kawasaki disease. J Pediatr. 2003;142:731–735.
4. Amano S, Hazama F, Kubagawa H, et al. General pathology of Kawasakidisease. On the morphological alterations corresponding to the clinicalmanifestations. Acta Pathol Jpn. 1980;30:681–694.
5. Rowley AH, Shulman ST, Mask CA, et al. IgA plasma cell infiltration ofproximal respiratory tract, pancreas, kidney, and coronary artery in acuteKawasaki disease. J Infect Dis. 2000;182:1183–1191.
6. Edwards KM, Glick AD, Greene HL. Intrahepatic cholangitis associatedwith mucocutaneous lymph node syndrome. J Pediatr Gastroenterol Nutr.1985;4:140–142.
7. Suddleson EA, Reid B, Woolley, et al. Hydrops of the gallbladder associatedwith Kawasaki syndrome. J Pediatr Surg. 1987;22:956–959.
8. Yanagawa H, Nakamura Y, Yashiro M, et al. Results of the nationwideepidemiologic survey of Kawasaki disease in 1995 and 1996 in Japan.Pediatrics. 1998;102:E65.
9. Chang RK. Hospitalizations for Kawasaki disease among children in theUnited States, 1988–1997. Pediatrics. 2002;109:e87.
ACUTE LIVER FAILURE ASSOCIATED WITHRUBELLA VIRUS IN A CHILD
Cristina Adelaide Figueiredo, MSc,*Nancy Therezinha Barbagallo Cordovani, MD,†Silvana Beres Castrignano, PhD,*Venancio Avancini Ferreira Alves, PhD,‡Cristina Takami Kanamura, MSc,§ Maria Isabel de Oliveira, PhD,*Flora Maria de Campos Fernandes, PhD,¶Giselle Burlamaqui Klautau, MSc,� and Edison Luiz Durigon, PhD**
Abstract: Acute liver failure is a syndrome with a wide range of etiologicpossibilities in children, but in up to 50% of the cases in the literature nodiagnosis is established. This case report adds rubella virus to the list ofpossible causes of acute liver failure. This association was made by serologic,cell culture, molecular, histopathologic, and immunohistochemical methods.
Key Words: rubella virus, acute liver failure, virus isolation, genotype,giant cell hepatitisAccepted for publication January 4, 2010.From the *Setor de Virologia, Instituto Adolfo Lutz, Sao Paulo, Brazil; †Departa-
mento de Pediatria, Santa Casa de Sao Paulo, Sao Paulo, Brazil; ‡Divisão deAnatomia Patológica do Hospital das Clinicas da Faculdade de Medicina da,Universidade de Sao Paulo, Sao Paulo, Brazil; §Divisão de Patologia, InstitutoAdolfo Lutz, São Paulo, Brazil; ¶Centro de Pesquisas Gonçalo Moniz, Funda-cao Oswaldo Cruz, Salvador, Bahia, Brazil; �2° Unidade de Internação, Institutode Infectologia Emílio Ribas, Sao Paulo, Brazil; and **Departamento deMicrobiologia, Universidade de São Paulo, Brazil.
Address for correspondence: Cristina A. Figueiredo, MSc, Servico deVirologia do Instituto Adolfo Lutz, Av. Dr. Arnaldo, 355, Sao Paulo,SP, Brazil, 01246–902. E-mail: [email protected].
Supplemental digital content is available for this article. Direct URLcitations appear in the printed text and are provided in the HTML andPDF versions of this article on the journal’s Web site (www.pidj.com).
DOI: 10.1097/INF.0b013e3181d3ce4c
Acute liver failure (ALF) in children is defined as a multisystemdisease process in a patient with severe liver dysfunction
without a previous history of liver disease.1 Its etiology in childrenolder than 1 year comprises viral hepatitis, drug exposure, immunedysregulation, metabolic or infectious diseases; but in approxi-mately half of the patients the cause is not established.1,2 Our caselinks ALF with acquired rubella virus infection, a heretoforeundocumented association.
CASEA 2.5-year-old boy with ALF necessitated a liver transplant
25 days after the onset of symptoms. The first reported alterationswere fever, abdominal pain, diarrhea, vomiting, and, afterward,jaundice, dark urine, and clay-colored stools were noticed. Therewas no history of cutaneous rash. Worsening of his clinical statusand diagnosis of encephalopathy grade II led to his transference toa pediatric liver transplant service. The boy’s socioeconomic status
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Rubella Virus and Acute Liver Failure
© 2010 Lippincott Williams & Wilkins www.pidj.com | 573

is low. There was no previous history of severe, opportunistic, orrepeated infections. It was said that he had received all therecommended vaccines, including against rubella, without proofby a vaccination certificate. The physical examination on thearrival at this last service showed a boy in regular general state,icteric, pale, height: 25th percentile, weight: 75th percentile, arte-rial pressure: 112/72 mm Hg, afebrile, alternating periods ofsomnolence and agitation. Liver was palpable 3-cm below thecostal margin. No exanthem, ecchymoses, petechiae, edema, orascites were present. Laboratory evaluation revealed hemoglobin:8.4 g/100mL, reticulocytes: 4.8%, leukocytes: 15.3 � 103/mm3,platelets: 631 � 103/ mm3, alanine and aspartate aminotransferase:571 and 552 U/L, respectively, total and direct bilirubin: 21.8 and 4.6mg/100mL, respectively, gamma glutamyl transpeptidase: 42 U/L,alkaline phosphatase: 541 U/L, total protein and albumin: 7.3 and 3.1g/100mL, respectively, prothrombin time: 42 seconds, internationalnormalized prothrombin ratio: 11.4, activated partial thromboplastintime: 62 seconds, factor V: 10%, fibrinogen: 109mg/100mL, glice-mia: 17mg/100mL, lactic dehydrogenase: 1048 U/L, ammonia: 550�g/100mL, urea: 9mg/100mL, creatinine: 0.2 mg/100mL.
Investigations focusing metabolic, autoimmune, and drug-induced hepatitis were negative. The investigations for infectiousdiseases included serologic tests for hepatitis A, B, and C viruses,cytomegalovirus, parvovirus B19, measles virus (MV), and rubellavirus. The only positive results were IgG antibodies against MV,and IgG and IgM antibodies against rubella virus. PCR analysis fordetection of MV, human herpesvirus 6, and parvovirus B19 werenegative.
The patient underwent orthotopic liver transplantation ofcadaveric donor and has been in good health since then.
To further investigate the etiologic agent of ALF, peripheralblood mononuclear cells collected before transplantation werespread on Vero cell line. Cells showed cytopathic effects charac-teristic of rubella virus after 7 days. This isolated virus as well assamples of the explanted liver were used for RNA extraction andamplification of rubella virus genome, using primers previouslydescribed.3 Sequence analysis of the E1 gene segment from bothsamples showed identical sequences (GenBank accession no.DQ458965; strain Brazil/994), phylogenetically aligned with ge-notype 1a rubella virus, confirming the recent circulation of thisgenotype in Brazil.5 Histologic diagnosis of the resected liver wasacute giant cell hepatitis with submassive hepatic necrosis (Fig.,Supplemental Digital Content 1, http://links.lww.com/INF/A382).Immunohistochemistry enabled identification of E1 rubella vi-rus antigen as intracytoplasmic deposits in hepatocytes,Kupffer, and endothelial cells (Fig., Supplemental Digital Con-tent 1, http://links.lww.com/INF/A382).
Rubella virus has been reported to cause hepatitis in thecongenital6,7 and acquired acute infection in children8 and adults,9
but severe hepatitis have been definitely reported only in neonatalrubella.6,7 A study of neurologic diseases associated with postnatalrubella infection described a case of carotid artery thrombosis inwhich an extensive hepatic necrosis was found at postmortemexamination. Rubella virus antigen could not be demonstrated inliver tissue of that patient.10
In the present case of ALF, it was possible to detect rubellavirus genome in liver fragments and also to find rubella virusantigen in the cytoplasm of hepatic cells, suggesting that rubellavirus was actively replicating in liver tissue.
Since rubella cases continue to occur in many countries inspite of being a vaccine-preventable disease, this case report alertsthe physicians about the fact that rubella virus, a previouslyunrecognized cause of ALF, should be remembered in patientswith this syndrome even if there is no recent history of exanthem.
ACKNOWLEDGMENTSThe authors thank Instituto Adolfo Lutz for their support.
REFERENCES1. Cochran JB, Losek JD. Acute liver failure in children. Pediatr Emerg Care.
2007;23:129–135.
2. Squires RH Jr. Acute liver failure in children. Semin Liver Dis. 2008;28:153–166.
3. Frey TK, Abernathy ES. Identification of strain-specific nucleotidesequences in the RA 27/3 rubella virus vaccine. J Infect Dis. 1993;168:854 – 864.
4. Reef SE, Frey TK, Theall K, et al. The changing epidemiology of rubellain the 1990s: on the verge of elimination and new challenges for control andprevention. JAMA. 2002;287:464–472.
5. Figueiredo CA, Klautau GB, Afonso AM, et al. Isolation and genotypeanalysis of rubella virus from a case of Guillain-Barre syndrome. J ClinVirol. 2008;43:343–345.
6. Stern H, Williams BM. Isolation of rubella virus in a case of neonatalgiant-cell hepatitis. Lancet. 1966;1:293–295.
7. Esterly JR, Slussner RJ, Ruebner BH. Hepatic lesions in the congenitalrubella syndrome. J Pediatr. 1967;71:676–685.
8. Sugaya N, Nirasawa M, Mitamura K, et al. Hepatitis in acquired rubellainfection in children. Am J Dis Child. 1988;142:817–818.
9. Tameda Y, Kosaka Y, Shiraki K, et al. Hepatitis in an adult with rubella.Intern Med. 1993;32:580–583.
10. Connolly JH, Hutchinson WM, Allen IV, et al. Carotid artery thrombosis,encephalitis, myelitis and optic neuritis associated with rubella virus infec-tions. Brain. 1975;98:583–594.
HERPES ZOSTER IN HEALTHY INFANTS ANDTODDLERS AFTER PERINATAL EXPOSURE TO
VARICELLA-ZOSTER VIRUS
A CASE SERIES AND REVIEW OF THE LITERATURE
Xavier Rodríguez-Fanjul, MD,* Antoni Noguera, MD, PhD,*Asuncion Vicente, MD,† Maria Antonia Gonzalez-Ensenat, MD,†Rafael Jimenez, MD, PhD,* and Claudia Fortuny, MD, PhD*
Abstract: Exposure to varicella-zoster virus in utero or during the first monthsof life is the main risk factor for the development of herpes zoster (HZ) inhealthy children. We report a case series of 16 infants and toddlers whopresented with HZ after early exposure to varicella-zoster virus. Two patientshad recurrences. Despite the severity of the rash in some cases, the benigncourse and the long-term good prognosis of HZ in healthy children isnoteworthy.
Key Words: acyclovir, healthy infant, herpes zoster, varicella-zoster virusAccepted for publication December 8, 2009.From the *Pediatric Infectious Diseases Unit, Department of Pediatrics, and
†Department of Dermatology, Hospital Sant Joan de Deu, Universitat deBarcelona, Barcelona, Spain.
Address for Correspondence: Antoni Noguera, MD, PhD, Infectious DiseasesUnit, Pediatrics Department—Hospital Sant Joan de Deu; Passeig Sant Joande Deu 2, 08950 Esplugues, Barcelona, Spain. E-mail: [email protected].
Supplemental digital content is available for this article. Direct URLcitations appear in the printed text and are provided in the HTML andPDF versions of this article on the journal’s Web site (www.pidj.com).
DOI: 10.1097/INF.0b013e3181d76f7f
Herpes zoster (HZ), also named shingles, is caused by thereactivation of latent varicella-zoster virus (VZV) infection
within dorsal root and cranial nerve ganglia. While chickenpoxusually occurs in the first years of life, HZ is uncommon inchildhood and its incidence increases with age and with othercauses of decreased cellular immunity.1 Children infected with
Rodríguez-Fanjul et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins574 | www.pidj.com

VZV in utero or before one year of age have an increased risk ofdeveloping HZ.2,3 We report a case series of 16 previously healthychildren who developed HZ after exposure to VZV during gesta-tion or early infancy and who were referred to and followed up ina tertiary-care pediatric hospital in Barcelona (Spain) from 1993 to2008.
CASE REPORTSThe main clinical characteristics of the patients are summa-
rized in Table 1. In brief, most patients were male (12 of 16) andthe median age at presentation was 22 months (range: 5 to 60months). Five children had been exposed to VZV in utero, 6patients developed mild chickenpox by the age of 4 months (noneof them received acyclovir at that time), and the parents reportedcontact during the first months of life with siblings or otherrelatives affected with chickenpox for 3 children; VZV exposuresource and age was unknown for 2 patients. None of the patientsin our series had received the Oka vaccine strain of VZV. Apartfrom these data, the medical history was unremarkable in all cases.
All children presented with a 2- to 7-day history of progressivevesicular rash consistent with HZ in different regions (Fig., Supple-mental Digital Content 1, http://links.lww.com/INF/A410; and Fig.,Supplemental Digital Content 2, http://links.lww.com/INF/A411 ): incranial nerve (9 of 16), in lumbosacral (5 of 16), and in cervical andthoracic dermatomes (one each); involvement of 2 adjacent der-matomes occurred in 6 children. Other complaints at presentationwere irritability and/or pruritus (16 patients) and fever (6 patients;rectal temperature ranging from 38°C to 39.4°C); enlarged locallymph nodes were noted in 2 children. Clinical diagnosis was con-firmed in all cases, by means of identification of multinucleated giantcells with eosinophilic intranuclear inclusion bodies on Tzancksmears and, most recently, by means of VZV-specific polymerasechain reaction assays in vesicular fluid in 9 children.
Patients with moderate-to-severe rash or irritability (n � 5) andthose in whom ocular involvement could not be ruled out (n � 7)were admitted for intravenous administration of acyclovir (30 mg perkg of body weight per day, divided every 8 hours) and/or painmanagement; the rest of the children received oral acyclovir (80 mgper kg of body weight per day, divided every 6 hours). Patients 4, 12,13, and 16 were not treated because the HZ lesions were healing bythe time the children were first seen. All treated patients completed a
sequential intravenous-oral 7- to 10-day course of acyclovir. Com-plete recovery after 1 to 3 weeks was observed in all cases.
The 8 patients with HZ affecting the ophthalmic division of thetrigeminal nerve (V1) were referred to the ophthalmologist for eval-uation. Only patient 10 showed ocular involvement. He showedneither discomfort nor decrease in vision, but examination of the lefteye showed marginal keratitis (dendriform lesions) and mild anterioruveitis. The patient completed a 7-day regimen of intravenous acy-clovir and a 2-week treatment with atropine and prednisone eye drops,with complete recovery.
No cases of post-HZ neuralgia occurred, but 4 children re-ported hypopigmentation in the affected area, that recovered withinsome months. HZ recurred in patients 14 and 15, 12 years and 3months after the first episode, respectively, affecting the same der-matomes and healing completely within one week; again, ocularinvolvement was ruled out in both cases. Only patient 15, aged 8months, received one week of oral acyclovir for the second episode.An immunologic work-up was undertaken in 10 children (includingthose with recurrent HZ) which consisted of a complete blood count,lymphocyte subset count and percentage, mitogen stimulation tests,serum immunoglobulin (IgG, IgA, and IgM) and IgG subclass values,humoral response to tetanus and rubella antigens, and human immu-nodeficiency virus antibodies. A primary or secondary immunodefi-ciency was not identified in any of the patients. After a medianfollow-up of 5 years (only one patient was lost to follow-up) allpatients have remained well.
DISCUSSIONHZ is uncommon among children. In classic studies, its
incidence in the pediatric age ranged from 0.2 to 0.74 cases per1000 person-years.2,3 A large population-based study from Icelandin the early 90s reported a higher incidence rate, up to 1.6 cases per1000 person-years.4 It is possible that the disease occurs morefrequently than it is thought in children, but remains under reportedbecause of its benign course, as many patients would not seekmedical care.
In the largest published case series of HZ in children to date,only 10% of the patients were apparently healthy at inclusion.5
Because that study was organized around a hospital-based surveil-lance system, the inclusion criteria probably biased these results.Despite this, and in the absence of updated population-based
TABLE 1. Main Clinical Characteristics of the 16 Healthy Patients With HZ AfterPerinatal Exposure to VZV
CaseNumber Gender and Age (mo) Evolution at
Presentation (d) Exposure Dermatome
1 M 60 3 24 wk of gestation Right CN V12 M 9 4 26 wk of gestation Left C2–C33 F 28 3 36 wk of gestation Left CN V14 M 8 7 38 wk of gestation Right T55 F 21 3 39 wk of gestation Right CN V1–V26 M 57 2 PVI at 6 wk of age Left CN V17 M 48 2 PVI at 6 wk of age Left L28 M 14 4 PVI at 8 wk of age Left L4–L59 M 14 3 PVI at 8 wk of age Left L2
10 M 48 2 PVI at 9 wk of age Left CN V111 M 36 3 PVI at 13 wk of age Right CN V112 F 18 5 At 8 wk of age, sibling with PVI Left S2–S313 M 16 6 At 16 wk of age, sibling with PVI Left L4–L514 M 25 2 At 15 wk of age, father with PVI Right CN V115 F 5 3 Unknown Right CN V1–V216 M 23 5 Unknown Right C5
M indicates male; F, female; PVI, primary VZV infection; CN, cranial nerve.
The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010 Zoster in Healthy Infants
© 2010 Lippincott Williams & Wilkins www.pidj.com | 575

studies, most experts agree that HZ is more common amongimmunocompromised children,1,3,6,7 especially in patients affectedwith acute leukemia.8
Among healthy children, primary VZV infection during ges-tation or the first year of life is the major risk factor for childhoodonset HZ (incidence rate: 4.1 cases per 1000 person-years).2,3 In ourseries, VZV primary infection had occurred in most patients by theage of 4 months. At this early age, the infant is protected bytransplacentally transferred maternal VZV-specific antibodies9 but isunable to develop adequate cellular and humoral immunity toVZV.10,11 Not surprisingly, the age at onset of HZ has been reportedto be lower after early primary VZV infection,7 reflecting the bluntingof VZV-specific immune memory in these patients. The median ageat onset of HZ in our series was 22 months, clearly lower than themean age in other large series of pediatric HZ.3–5,7
The diagnosis of HZ is based on clinical judgment.12 Sev-eral sensitive microbiologic methods performed on blister fluid/scrapings are available in case of doubt, including viral cultures,polymerase chain reaction, and direct fluorescent antibody testing.Rashes that may resemble HZ are contact dermatitis, herpes simplexskin infection, and staphylococcal impetigo.12 HZ in healthy childrenis mildly symptomatic and usually shows a benign and self-limitedcourse in 1 to 3 weeks; its more common complications are bacterialsecondary infection, depigmentation, and scarring. Thoracic der-matomes are involved in 65% to 75% of cases.3,4 Ocular involvement,which is very frequent in the adult patient, must be always ruled outwhen the ophthalmic branch of the trigeminal nerve (V1) is aff-ected.13 Disseminated cutaneous HZ, neurologic complications,visceral dissemination, post-HZ neuralgia, and other sequelae havebeen very rarely reported in immunocompetent children.5,7,14 Twoof the patients in our series had a second episode of HZ in the samedermatome, which recovered uneventfully. Recurrences have notbeen previously reported in early childhood HZ and are alsoinfrequent in the immunocompetent adult patient. Junker andTilley15 hypothesized that a failure to maintain or evoke a second-ary VZV-specific immune response could explain recurrent chick-enpox in a series of 23 healthy and apparently immunocompetentchildren.
Antiviral therapy and hospital admission are rarely needed.4
In fact, acyclovir in the healthy child is only recommended whenophthalmic HZ or moderate-to-severe symptomatic rash occur; anal-gesics and appropriate skin care are more often required. In our series,a referral bias probably explains both the predominance of cranialnerve dermatome involvement and the high rates of hospital admis-sion and acyclovir treatment. Despite the severity of the cases wereport, a benign course and lack of sequelae ensued in all cases,reflecting the excellent prognosis of pediatric HZ.4
Although HIV infection and pediatric malignancies are com-monly associated with HZ, childhood HZ has not been found to be theharbinger of an underlying immunodeficiency or malignancy.4 Be-cause of this, an immunologic work-up should not be routinelyperformed in previously healthy children affected with a first episodeof HZ and would only be justified when recurrences occur.6 Finally,several cases of mild and uncomplicated HZ caused by the Okavaccine strain of VZV have been reported, 65% of them in children
�5 years of age.16 The incidence of HZ in children is higher afternatural varicella infection than after varicella vaccination, in healthyand immunocompromised children.17 Currently, varicella immuniza-tion with the Oka attenuated VZV strain is not publicly funded inCatalonia, despite the recommendation by the Asociacion Espanolade Pediatría.18 Universal vaccination programs will probably impactHZ epidemiology in the future, as has happened with varicella.19
REFERENCES1. Dworkin RH, Johnson RW, Breuer J, et al. Recommendations for the
management of herpes zoster. Clin Infect Dis. 2007;44:S1–S26.
2. Baba K, Yabuuchi H, Takahashi M, et al. Increased incidence of herpeszoster in normal children infected with varicella zoster virus duringinfancy: community-based follow-up study. J Pediatr. 1986;108:372–377.
3. Guess HA, Broughton DD, Melton LJ III, et al. Epidemiology of herpeszoster in children and adolescents: a population-based study. Pediatrics.1985;76:512–517.
4. Petursson G, Helgason S, Gudmundsson S, et al. Herpes zoster in childrenand adolescents. Pediatr Infect Dis J. 1998;17:905–908.
5. Wootton SH, Law B, Tan B, et al. The epidemiology of childrenhospitalized with herpes zoster in Canada: Immunization MonitoringProgram, Active (IMPACT), 1991–2005. Pediatr Infect Dis J. 2008;27:112–118.
6. Donahue JG, Choo PW, Manson JE, et al. The incidence of herpes zoster.Arch Intern Med. 1995;155:1605–1609.
7. Takayama N, Yamada H, Kaku H, et al. Herpes zoster in immunocom-petent and immunocompromised Japanese children. Pediatr Int. 2000;42:275–279.
8. Novelli VM, Brunell PA, Geiser CF, et al. Herpes zoster in children withacute lymphocytic leukemia. Am J Dis Child. 1988;142:71–72.
9. Heininger U, Desgrandchamps D, Schaad UB. Seroprevalence of varicellazoster virus IgG antibodies in Swiss children during the first 16 months ofage. Vaccine. 2006;24:3258–3260.
10. Grose C. Congenital varicella-zoster virus infection and the failure toestablish virus-specific cell-mediated immunity. Mol Biol Med. 1989;6:453–462.
11. Terada K, Kawano S, Yoshihiro K, et al. Varicella-zoster virus (VZV)reactivation is related to the low response of VZV-specific immunity afterchickenpox in infancy. J Infect Dis. 1994;169:650–652.
12. Feder HM Jr, Hoss DM. Herpes zoster in otherwise healthy children.Pediatr Infect Dis J. 2004;23:451–457.
13. Pavan-Langston D. Herpes zoster ophthalmicus. Neurology. 1995;45:S50–S51.
14. Chiang CP, Chiu CH, Huang YC, et al. Two cases of disseminatedcutaneous herpes zoster in infants after intrauterine exposure to varicellazoster virus. Pediatr Infect Dis J. 1995;14:395–397.
15. Junker AK, Tilley P. Varicella-zoster virus antibody avidity and IgG-subclass patterns in children with recurrent chickenpox. J Med Virol.1994;43:119–124.
16. Galea SA, Sweet A, Beninger P, et al. The safety profile of varicellavaccine: a 10-year review. J Infect Dis. 2008;197:S165–S169.
17. Hardy I, Gershon AA, Steinberg SP, et al. The incidence of zoster afterimmunization with live attenuated varicella vaccine. A study in childrenwith leukemia. Varicella Vaccine Collaborative Study Group. N EnglJ Med. 1991;325:1545–1550.
18. Bernaola Iturbe E, Gimenez Sanchez F, Baca Cots M, et al. Vaccinationschedule of the Spanish association of pediatrics: recommendations 2009�in Spanish�. An Pediatr (Barc). 2009;70:72–82.
19. Nguyen HQ, Jumaan AO, Seward JF. Decline in mortality due to varicellaafter implementation of varicella vaccination in the United States. N EnglJ Med. 2005;352:450–458.
Rodríguez-Fanjul et al The Pediatric Infectious Disease Journal • Volume 29, Number 6, June 2010
© 2010 Lippincott Williams & Wilkins576 | www.pidj.com




















