
LITERATURE REVIEW part 11
71
1 CORRELATING ANTIBIOTIC CONSUMPTION RATE WITH ANTIMICROBIAL RESISTANCE PATTERN OF UROPATHOGENS IN THE LAGOS UNIVERSITY TEACHING HOSPITAL. BY DR IFEANYI A. ONWUEZOBE FOR THE FULFILLMENT OF THE REQUIREMENT BY THE NATIONAL POSTGRADUATE MEDICAL COLLEGE FOR PART II EXAMINATION JULY, 2006.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of LITERATURE REVIEW part 11
1
CORRELATING ANTIBIOTIC CONSUMPTION RATE
WITH ANTIMICROBIAL RESISTANCE PATTERN OF
UROPATHOGENS IN THE
LAGOS UNIVERSITY TEACHING HOSPITAL.
BY
DR IFEANYI A. ONWUEZOBE
FOR THE FULFILLMENT OF THE REQUIREMENT BY THE
NATIONAL POSTGRADUATE MEDICAL COLLEGE
FOR PART II EXAMINATION
JULY, 2006.
2
CORRELATING ANTIBIOTIC CONSUMPTION RATE
WITH ANTIMICROBIAL RESISTANCE PATTERN OF
UROPATHOGENS IN THE
LAGOS UNIVERSITY TEACHING HOSPITAL.
SUBMITTED BY
DR IFEANYI A. ONWUEZOBE
FOR THE FULFILLMENT OF THE REQUIREMENT BY THE
NATIONAL POSTGRADUATE MEDICAL COLLEGE
FOR PART II EXAMINATION
SUPERVISOR- DR O. O. ODUYEBO
JULY, 2006.
i
3
CERTIFICATION
This is to certify that this work was carried out by Dr Ifeanyi A. Onwuezobe
of the Department of Medical Microbiology and Parasitology of the Lagos
University Teaching Hospital under my supervision.
………………..………………… Dr Ifeanyi A. Onwuezobe
……………….…………. Dr O. O Oduyebo SUPERVISOR
ii
4
DEDICATION
I dedicate this work to my family who stood by me especially during the
most difficult times of this project work, and to the Almighty God who made
all things possible.
iii
5
ACKNOWLEDGEMENTS
I wish to acknowledge the efforts of my supervisor Dr O. O. Oduyebo in
seeing to the progress of this work and Dr F. T. Ogunsola for her expert
advise and to Mr. Akintunde of the LUTH pharmacy Department for his
assistance and to the resident doctors in the Department of Medical
Microbiology and Parasitology LUTH for their moral support.
iv
6
TABLE OF CONTENTS
TITLE PAGE i
CERTIFICATION ii
DEDICATION iii
ACKNOWLEDGEMENT iv
TABLE OF CONTENT v
SUMMARY vii
CHAPTER ONE
INTRODUCTION 1
CHAPTER TWO
LITERATURE REVIEW 4
CHAPTER THREE
MATERIALS AND METHODS 32
CHAPTER FOUR
RESULTS 38
v
7
CHAPTER FIVE
DISCUSSION, CONCLUSION AND RECOMMENDATION
DISCUSSION 47
CONCLUSION 50
RECOMMENDATION 51
REFERENCES 52
APPENDIX I 60
APPENDIX II 61
APPENDIX III 62
vi
8
SUMMARY
The study on correlating antibiotic consumption rate with Antimicrobial
resistance pattern of uropathogens was carried out in the Lagos University
Teaching Hospital from January to June 2006. Midstream urine samples of
1520 patients with suspected urinary tract infections (UTI) which were sent
to the Microbiology Laboratory were processed. Cultured specimens with
growth of pathogen greater than 10,000 colony forming units per milliliter of
urine were biochemically identified using the Analytical profile index (API)
test kits. Antibiotic susceptibility testing was done on all identified
uropathogens and all Escherichia coli and Klebsiella pneumoniae resistant to
the third generation cephalosporins were tested for the production of
extended spectrum betalactamases (ESLBs). The antibiotic resistance
pattern of the isolated pathogens was correlated with the antibiotic
consumption pattern of patients in LUTH.
Two hundred and fifteen bacterial pathogens were isolated with Escherichia
coli being the most prevalent (57.2%). Twenty percent were Klebsiella
pneumoniae and 7.9% were Pseudomonas aeroginosa in that order of
prevalence. Other gram negative and gram positive bacteria isolates
constituted 14.9%. About 14% and 11.6% of Escherichia coli and Klebsiella
pneumoniae isolates respectively were found to be producing extended
spectrum betalactamase (ESBLs).
Majority of isolates were resistant to cotrimoxazole and amoxicillin-
clavulanate. There was high sensitivity of the pathogens isolated to
nitrofurantoin, ceftazidime, cefotaxime and cefoxithin.
vii
9
For all the antimicrobials, there was an increase in resistance which was
preceded by an increase in antimicrobial consumption. This increasing trend
of resistance of uropathogens to antimicrobials was more with the
Quinolones (ciprofloxacin and ofloxacin), cotrmoxazole (trimethoprim-
sulphamethoxazole) and amoxicillin-clavulanate in the face of increased
consumption of these drugs.
CHAPTER ONE
INTRODUCTION
Urinary tract infection (UTI) is a condition in which microorganisms are
established and multiplying in the bladder, prostate, collecting systems or
the kidneys and could present with symptoms like dysuria, frequency,
urgency and sometimes suprapubic tenderness when the lower tract is
involved and in an adult fever, loin pain and tenderness when the upper
urinary tract is involved (1).
These manifestations occur in cystitis, acute and chronic pyelonephritis and
papillary necrosis. Cystitis describes infection or inflammation of the bladder.
Whereas acute and chronic pyelonephritis are the descriptions used when
the infection involves the pelvis of the kidney, papillary necrosis is a
complication of pyelonephritis, which occur usually in the presence of
10
Diabetes mellitus, urinary tract obstruction, sickle cell disease or analgesic
abuse and can occur in the presence or absence of infection.
UTI is caused mainly by bacteria, the commonest agent being Escherichia
coli. Others include Klebsiella pneumoniae, Pseudomonas aeruginosa,
Proteus mirabilis, Acinetobacter baumanii and Enterococcus faecalis and
Staphylococcus sp. In nosocomial UTI the other bacteria like Pseudomonas,
Acinetobacter and Enterococcus play more important roles while E. coli
infection shows a decrease in incidence (2).
UTIs are treated with antibiotics which serve to eliminate the pathogens
causing it as well as preventing mortality and complications associated with
it. So it is necessary to be aware of trends in antibiotic sensitivity and
resistant patterns. Over the years antibiotic susceptibility pattern of the
isolates revealed that for outpatients, first generation cephalosporins,
nitrofurantoin, norfloxacin/ciprofloxacin are effective for treatment of urinary
tract infection but for inpatients, parenteral therapy with newer
aminoglycosides and third generation cephalosporins need to be advocated
as the organisms for nosocomial UTI exhibit a high degree of drug
resistance (3,4). Since patterns of antibiotic resistance in a wide variety of
pathogenic organisms vary even over short periods and depend on site of
11
isolation and on different environments, periodic evaluation of antibacterial
activity to update this information is always needed (5, 6, 7).
Recently, trimethoprim/sulphamethoxazole combination which has been a
frontline choice decides for UTI was found to be ineffective for the
treatment of urinary tract infections as all the uropathogens from inpatients
and outpatients showed high degree of resistance to it (8).
A study carried out in Kaduna on susceptibility pattern of uropathogens
showed that all isolates were poorly sensitive to the common first-line drugs
used in UTI isolates including, cotrimoxazole and ampicillin, but exhibited
good sensitivity to nalidixic acid, nitrofurantoin and ofloxacin (9).
Although multiple factors play a role in antimicrobial resistance, the selective
pressures of inappropriate and widespread use of antibiotics are considered
major contributors and rates of use of antibiotics usually correlate with the
level of antibiotic resistance (10, 11). Controlling antibiotic resistance
requires the monitoring of both susceptibility trends and antimicrobial usage
within specific areas of the hospital. Previous studies in Lagos and indeed in
Nigeria show high level resistance of antibiotics to uropathogens (9,12,13),
but these have never been correlated with rates of use of antibiotics.
The objectives of this study therefore are:
12
1. T o characterize the bacteria causing urinary tract infection in Lagos
University Teaching Hospital (LUTH).
2. To determine the sensitivity and resistance patterns of bacteria.
3. To correlate the resistance patterns of the bacteria with antibiotic
usage in the hospital.
CHAPTER TWO
LITERATURE REVIEW
DEFINITION
The urinary tract consists of the upper and lower parts. The upper part of
the urinary tract is made up of the kidneys, and the ureters, while the lower
part is made up of the bladder, and the urethra. Therefore, urinary tract
infections (UTI) are anatomically classified into lower tract infections and
upper tract infections (1).
The lower tract infections include cystitis, urethritis, prostatitis and
epididymitis while the upper urinary tract infections include pyelonephritis,
which is the most severe of the UTIs and can be acute or chronic. Acute
pyelonephritis is the inflammation of the renal parenchyma caused by either
13
bacteria or fungi. Chronic pyelonephritis refers to a diffuse, interstitial
inflammatory disease of the kidneys which could be caused by either an
infective agent or in some situations noninfective agents
UTIs are also classified as simple or complicated. Simple or uncomplicated
UTI refers to inflammation of the normal urinary tract in which case there is
no structural abnormalities in the urinary tract or associated conditions like
Diabetes mellitus, sickle cell disease or immunosuppression. UTI is said to
be complicated where there are either functional or structural abnormalities
in the diseased urinary tract. These abnormalities could be presence of
indwelling catheter or bladder or renal calculi. Simple UTI mainly refers to
acute cystitis, while pyelonephritis is the main example of complicated UTI.
All areas of the urinary tract above the urethra in a healthy person are
sterile. The transitional epithelium of the urethra is normally colonized by
resident flora which consist of coagulase negative staphylococci (with the
exception of S. saprophyticus), Viridans and nonhemolytic streptococci,
lactobacilli, diphtheriods, nonpathogenic Neisseria sp., anaerobic cocci,
Propionibacterium sp., anaerobic gram negative bacilli, commensal
Mycobacterium sp. and commensal Mycoplasma sp. Bacteriuria is
quantifiable. When the number in the voided urine exceeds the number that
can be expected from contamination from the anterior urethra (i.e.≥105
bacteria/mL), it becomes significant bacteriuria and this is an indication of
14
infection (1). Therefore, quantitative cultures popularized by Kass are used
to determine the presence of UTI and diagnosis is not made unless greater
than 105 colony forming units of bacteria per milliliter (CFU/ml) are present
in the urine. This is referred to as significant bacteriuria and is highly
indicative of infection in patients with acute cystitis, pyelonephritis, and
asymptomatic bacteriuria.
AETIOLOGICAL AGENTS
Urinary tract infections are mainly caused by bacteria; however a few fungi
can also cause UTI. The bacterial causes are; Escherichia coli,
Staphylococcus saprophyticus and epidermidis, Protus species,
Streptococcus faecalis, Klebseilla spp, Pseudomonas aerogenosa Serratia
marcescens and other coliforms. The fungal cause of urinary tract infection
is mainly Candida albicans which causes bladder infection predominantly in
diabetics and immunosuppressed patients. Other causes though rare are
Mycobacterium tuberculosis, Salmonella sp., Leptospira sp. and Mycoplasma
sp. Viruses are a very rare cause of UTI, however, genital herpes can cause
urethral syndrome which is sexually transmitted (28).
Most urinary tracts infections are caused by E. coli but only a few
serogroups of E. coli, for example the 01 and 02 among others, cause a
high proportion of infections (3, 15, 29).
15
EPIDEMIOLOGY
UTI is one of the most common reasons adults seek medical consultation all
over the world, and it is also one of the most frequently occurring
nosocomial infections. The most common type of UTI is acute simple cystitis
in women (14, 15, 16). The most commonly isolated bacterial pathogen,
globally, both in children and adults is Escherichia coli. Some studies have
shown that this may not always be the case as the predominant isolate in
both inpatients and outpatients in a study done on patients with urinary
tract infection in Ibadan Nigeria in 1994 was Klebsiella species which
accounted for 52.8% of cases (4, 9). This unusual finding was due the fact
that most of the patients were inpatients and Klebsiella species are
frequently nosocomial. Also in Enugu (Eastern Nigeria), in 2005 the
predominant organisms were coliforms, Staphylococcus aureus and Proteus
spp. (13).
In Central African Republic, Escherichia coli was found to be the most
common cause of urinary tract infection in patients followed by Klebsiella
pneumoniae, Citrobacter diversus, Salmonella spp and other
Enterobactereceae in that order. Pseudomonas aeruginosa accounts for less
than 5%. The gram positive organisms isolated are Staphylococcus aureus,
Streptococcus agalactiae, and enterococcus feacalis (18).
16
In recurrent urinary tract infections (especially in the presence of structural
abnormalities of the urinary tract) although E. coli is still the commonest
pathogen relative frequency of infection caused by Proteus, Pseudomonas,
Klebsiella, and Enterobacter species and by enterococci and staphylococci
increases greatly. There is also the catheter-associated UTI and indeed it is
the most common nosocomial infection, accounting for greater than 1
million cases in hospitals and nursing homes (17). Coagulase-negative
staphylococci also cause urinary tract infection as reported in some parts of
the world (21). Staphylococcus saprophyticus cause infection in young
women of sexually active age and account for 5% to 15% of acute cystitis
episodes in the United States (1, 3).
Coagulase-positive staphylococcus most often invade the kidney from the
haematogenous route, resulting in intrarenal or perinephric abscesses.
Adenoviruses (particularly type II) have been implicated as causative agents
in haemorragic cystitis in children, especially boys, and in allogenic bone
marrow transplant recipients (22). Cell wall-deficient bacteria
(e.g.,Chlamydia spp) have been isolated in urine of patients with
pyelonephritis particularly in association with therapy using cell wall-active
antibiotics (22,23). Catheter-associated urinary tract infections account for
40 percent of all nosocomial infections and are the most common source of
gram-negative bacteremia in hospitalized patients (24).
17
Fungi (particularly candida species) occur in patients with indwelling
catheters who are receiving antimicrobial therapy (25). Mycobacterium
tuberculosis and anaerobes are known to cause urinary tract infection (26).
Candida species have been isolated as a cause of UTI in some patients.
Sex prevalence: Women are significantly more likely to experience UTI
than men due mainly to the anatomical difference in the length of the
urethra in which the female urethra is shorter and more proximal to the
anus than the male urethra. Nearly 1 in 3 women will have had at least one
episode of UTI requiring antimicrobial therapy by the age of 24 years.
Almost half of all women will experience one UTI during their lifetime (27).
Staphylococcus saprophyticus is the second most common cause in young
sexually active women after Escherichia coli.
Age prevalence: Specific age subpopulations are at increased risk of UTI.
The prevalence of UTI in the neonatal period is low and could result from
bacteremia which could lead to pyelonephritis. Infants of up to 3 months
especially boys experience urinary tract infection when they are not
circumcised. Urinary tract infection could also affect children in the
preschool and school age group (20).
18
PATHOGENESIS: The urinary tract is normally sterile. In cystitis the
bladder is invaded most often by enteric coliform bacteria (e.g., Escherichia
coli) that inhabit the periurethral vaginal introitus and ascend into the
bladder via the urethra.
Sexual intercourse may promote migration of microorganisms causing
infection to the bladder. This is because the coliform bacteria that colonize
the vaginal introitus could be displaced to the urethra and subsequently to
the bladder following sexual intercourse.
Urine is generally a good medium for growth of microorganism but there are
specific factors that are unfavorable to bacterial growth and these include a
low pH (5.5 or less), a high concentration of urea, and the presence of
organic acids derived from a diet that includes fruits and protein. Organic
acids enhance acidification of the urine leading to decreased pH and this
prevents the growth of bacteria.
Frequent and complete voiding has been associated with a reduction in the
incidence of UTI. Normally, a thin film of urine remains in the bladder after
emptying, and any bacteria present are removed by the mucosal cell
production of organic acids. UTI occurs when these mechanisms fail.
19
The gram negative rods not only thrive in urine, they are specially adapted
to cause infection by having fimbriae with terminal receptors for specific
glycolipids and glycoproteins in the urinary tract. The E. coli strains which
cause UTI’s typically have fimbriae with a terminal receptor for the “P”
antigen, a blood group marker present on the surface of cells lining the
perineum and urinary tract (4).
The P antigen is also found in vaginal and prostatic secretions: these
secreted P antigens are protective in that they bind to the bacterial receptor,
preventing binding of the organism to the surface epithelium. The
individuals most susceptible to UTI are those who express P antigen on their
cells and lack P antigen in their secretions.
Host defenses of the upper tract include local leukocyte phagocytosis and
renal production of antibodies that kill bacteria in the presence of complement
(3). When these fail pyelonephritis occurs.
Complicated UTI occurs in the setting of underlying structural, medical, or
neurologic disease. Patients with a neurogenic bladder or bladder
diverticulum and postmenopausal women with bladder or uterine prolapse
have an increased frequency of UTI due to incomplete bladder emptying.
This eventually allows residual bacteria to overwhelm local bladder mucosal
20
defenses. The high urine glucose content and the defective host immune
factors in patients with diabetes mellitus also predispose to infection (30).
Factors predisposing to UTI: Various risk factors predispose to UTI.
These are pregnancy, old age, spinal cord injuries catheters, diabetes
mellitus, multiple sclerosis, acquired immunodeficiency disease syndrome,
human immunodeficiency virus, and use of diaphragm and spermicides for
contraception in women (3, 17).
Other risk factors include abnormalities of the urinary tract that obstructs or
slows the flow of urine, making it easier for bacteria to grow. A stone in the
kidney or any part of the urinary tract can form such a blockage, creating
the conditions for a UTI. In men, an enlarged prostate gland can obstruct
urine flow and make infection difficult to treat.
CLINICAL MANIFESTATIONS
Cystitis – Infection of the bladder results in dysuria (painful urination),
urgency (the need to urinate without delay), increased frequency of
urination, suprapubic tenderness, small volume voiding, and pyuria. Pelvic
discomfort especially pre- and immediately postvoid which occurs in 20% of
women with uncomplicated UTI (31).
21
Hemorrhagic cystitis is characterized by large quantities of visible blood
in the urine as irritative voiding symptoms regardless of the origin which
may be infection or noninfection. When infectious in origin, signs and
symptoms of infection may also be encountered. Hemorrhagic cystitis is
differentiated from glomerulonephritis, by absence of hypertension (4, 22,
32).
ASYMPTOMATIC BACTERIURIA
This condition is due to bacterial presence of more than 100,000 CFU per ml
of voided urine in persons with no symptoms of urinary tract infection. This
is rarely seen in adult healthy men. However it occurs in young and elderly
women. In pregnancy asymptomatic bacteriuria occurs and could be a
danger to the developing fetus hence pregnant women are screened and
treated. The clinical guidelines for the prevention of the complications of
UTI in pregnancy include; the screening of all pregnant women for the
presence of bacteriuria on the first antenatal visit and at the twenty eight-
week, the treatment of asymptomatic bacteriuria with antimicrobials
considered safe in pregnancy and a follow-up cultures at 1 and 4 weeks
following therapy (1, 24).
LABORATORY DIAGNOSIS
22
The diagnosis of UTI is based on a quantitative urine culture yielding greater
than 100,000 colony-forming units (105CFU) per milliliter of urine, which is
termed "significant bacteriuria." This value is chosen because of its high
specificity for the diagnosis of true infection, even in asymptomatic persons
(33, 34).
23
Specimen collection and transport: There are various methods of
collecting urine from patients suspected of having UTI.
1. Clean catch midstream urine – Here, the patient should void the first
part of the urine stream which cleanses the anterior urethra, and then
the middle stream is collected in a sterile universal bottle making sure
that the external genitalia did not touch the specimen bottle.
2. Catheter specimen – This is a method of urine collection from
patients. Here, urine sample is collected from an indwelling catheter
using a syringe to collect urine sample from the junction between the
catheter tube and the bag after disinfecting the area.
3. Suprapubic aspiration involves collecting urine aseptically from the
suprapubic region for example, in bladder obstructions and in
children.
Urine samples should be transported immediately to the Laboratory for
processing within two hours following collection. Where delay is anticipated,
it should immediately be refrigerated at 4o or preserved with boric acid for
24 hours. A urine transport tube containing boric acid, glycerol and sodium
formate can preserve urine for 24 hours without refridgeration (29).
24
Microscopic examination of urine sample
1. Wet mount – this is done to detect the presence of white blood cells
(WBCs) and bacteria in urine sample. When there are more than 10
WBCs per high-power field in centrifuged urine, it is termed pyuria. If
bacteria (more than 20) is present in an unspurn urine, it is an
indication of UTI (28).
2. Gram stain – Here, a drop of uncentrifuged urine is placed to dry on a
microscope slide and then Gram stained. If greater than one
bacterium per oil immersion field is seen, the specimen has >105
bacteria/ml. If one bacterium is seen in 3-4 fields, the specimen has
<104 bacteria/ml (35). Also, centrifuged urine with a finding of 2-5
White Blood Cells (WBCs) or 15 or more bacteria per high power field
in the urine sediment is consistent with UTI (35).
Urine culture
Culture media – for primary isolation of uropathogens, most laboratories use
an enriched medium like 5% blood agar plate and a differential medium like
MacConkey agar (the contents are peptone, lactose, bile salts, sodium
chloride, neutral red, agar) MacConkey agar allows for the detection of
most gram-negative bacilli and some gram positive organisms.
25
Some laboratories prefer the use of cystein-lactose electrolyte deficient
(CLED) agar (contents are, peptone, tryptone, lactose, L-cystine,
bromothymol blue, to MacConkey agar because it supports the growth of
Gram negative and Gram positive pathogens (51). Special medium like the
Lowenstein Jensen medium could be used for the growth of mycobacterium
sp. Culture is done using different methods.
The growth of Enterococci spp. and other streptococci spp. may be
enhanced by using selective plates for gram-positive organisms such as
Columbia colistin-nalidixic acid agar (CNA) or phenylethyl alcohol agar.
These are rarely used because of their cost.
Two methods are employed to determine significant bacteriuria.
Quantitative loop method: Here, a calibrated platinum loops is used to
inoculate plates directly and count of bacterial colonies is done after
incubation to determine the number of microorganisms per ml (29).
Dip cultures: Here, special slides coated with media, are dipped in urine
specimen and incubated. Bacterial colony count is done directly (29).
Incubation is done at 350C to 370C for 18 -24 hours.

26
Rapid preliminary tests
Chemical tests using dip sticks coated with specific chemicals and/or
substrates – This involves a simple dipping of the sticks in urine and looking
for color changes in a few minutes. Some of the sticks used are; (a) Nitrate
(NO3) sticks in which the production of nitrite with colour change establishes
bacteriuria. Best results are gotten if used on first-void urine (first urination
in morning) specimens because at least 4 hours are required for coliforms to
convert nitrate to nitrite. (b) Leukocyte esterase sticks are used to establish
pyuria (20, 34).
Paper strip test – A paper strip test known as the Griess test can be used to
detect the presence of nitrate-reducing enzymes produced by most
uropathogens.
URISCREEN – This is a manual screening system that measures the enzyme
catalase in urine. Hydrogen peroxide when added to the urine produces
bubbles which indicate the presence of aetiologic agents of UTI, as most of
them will produce catalase enzyme except streptococci (29).
Other test
Blood culture – In some patients with pyelonephritis and septicaemic
symptoms, blood culture is necessary for the detection of the aetiologic
agents.

27
PRINCIPLE OF ANTIBIOTIC THERAPY
The goal of treatment of a urinary tract infection is sterilization of the urine,
which should occur within hours of the first dose of an appropriately chosen
antimicrobial (31). To accomplish this, selection of a suitable drug is critical.
When choosing empiric therapy one must consider if the infection is
complicated or uncomplicated, the spectrum of activity of the drug against
the likely pathogen, potential untoward effects of the drug, patient
compliance, and cost. The duration of therapy should be guided by the
presumed extent of tissue involvement and concentration of antimicrobial in
the urine (32). It is desirable that the urine concentration of the drug
exceeds the minimum inhibitory concentration (MIC) of the infecting
pathogen by the highest amount for the longest period of time.
ANTIMICROBIALS
Trimethoprim-sulfamethoxazole, a combination that synergistically
interferes with folate metabolism of bacteria, is frequently used in the
treatment of uncomplicated urinary tract infections. With the notable
exceptions of Pseudomonas and Enterococcus species, it is effective against
a broad range of urinary pathogens (35). However, there have been reports
of an increased resistance to this drug (12, 13). The concentration in the
urinary tract is excellent and the effect on the fecal flora is minimal. The
28
drug is affordable in developing countries like Nigeria. However, skin rash
and gastrointestinal complaints are the main side effects. Use of this drug in
pregnancy and neonates under one month of age is contraindicated because
of the untoward effects in this age group.
Nitrofurantoin disrupts carbohydrate metabolism and inhibits bacterial cell
wall synthesis. It is effective against most uropathogens except
Pseudomonas and Proteus (34). Since nitrofurantoin reaches high levels in
the urine, but does not concentrate in tissue, it is ineffective in the
treatment of infection involving solid organs such as pyelonephritis or
prostatitis. There is limited interaction with the fecal reservoir resulting in
minimal problems with resistance. It is not used in patients with poor renal
function because of poor concentration ability (3).
Aminopenicillins (i.e. ampicillin and amoxicillin) are frequently used in the
treatment of a wide range of infectious processes including those in the
urinary tract. This frequent use has resulted in up to 30% resistance in
clinical isolates (36). Extended spectrum synthetic penicillins and those
combined with beta-lactamase inhibitors are occasionally used in parenteral
therapy for complicated pyelonephritis.
Aminoglycosides, which inhibit bacterial RNA synthesis, are a useful class
of drugs and, when combined with TMP-SMX or ampicillin, are parts of first
line therapy. They have largely maintained their spectrum of activity and,
29
with appropriate monitoring of levels, the danger of renal toxicity can be
minimized. Newer regimes of extended dose therapy which employ single
daily doses of up to 7 mg/kg are equally efficacious as standard dosing but
have a lower risk of nephrotoxicity (37).
Fluoroquinolones are inhibitors of DNA gyrase with a broad spectrum of
activity that is ideal for empiric treatment of urinary tract infection (38).
Coverage against Enterobacteriaceae and Pseudomonas species is high, with
high levels of activity against Staphylococcal species, though Streptococcal
coverage is marginal (39). Fluoroquinolones do have advantages in the
treatment of complicated UTIs, resistant organisms, or difficult-to-treat
pathogens such as Pseudomonas aeruginosa (40). Inappropriate use has
caused an increased incidence of resistant strains (41). Fluoroquinolones are
contraindicated in children because of theoretical danger in cartilage
formation, but side effects are rare in adults. Although as a class
fluoroquinolones are not nephrotoxic, their dosing must be adjusted in
patients with renal failure because of its metabolism in the kidneys.

30
MANAGEMENT OF URINARY TRACT INFECTION
In the treatment of UTIs, short-course antibiotic or long-course antibiotic
regimens has been considered
Short-course antibiotic regimens range from a single dose to 3 days
duration while long-course regimens range from 7 to 14 days. The short-
course regimens are used in the treatment of uncomplicated lower UTIs
especially in adults. They are effective, less expensive with fewer side
effects and may prevent reinfection with resistant organism (42). However
the efficacy and advantages of short-course antibiotic treatment of UTI in
adults are not seen in children. The reasons are that by the time UTIs is
identified in children, there is often upper tract involvement that cannot be
easily distinguished clinically from lower tract infection by signs and
symptoms and/or by laboratory tests (42). Also children are more likely to
have anatomic abnormalities predisposing them to pyelonephritis and so
would require longer treatment of up to 7 – 14 days; however, Randomized
Controlled Trials (RCTs) over the last 25 years have not provided evidence
supporting this practice (63). In fact, most of these studies have shown no
statistical significance difference in efficacy between short- and long-course
therapies (42).
31
In the past years (between 1970s and 1990s), the drugs mainly used for short-
course therapy are gentamicin, amikacin, cefotaxime, cephalexin and
pivmecillinam. Trimethoprim-sulphamethoxazole, nitrofurantion, sulphamethizole,
amoxicillin, ampicillin, nalidixic acid, sulfisoxazole and cefadroxil were used for
long-course therapy (42).
The use of these drugs over the years has been associated with treatment
failures manifesting as persistence of infection (when there is continued
positive urine culture 1 to 2 days of initiation of therapy) and relapse (when
there is symptoms and signs of infection with the same organism following a
bacteriologic cure) (42,43). None of them has demonstrated superiority over
the others in this respect.
One systematic review and two subsequent RCTs in women with acute
uncomplicated pyelonephritis found no consistent differences in
bacteriologic or clinical cure rates (43). However, there is evidence that
quinolones such as ciprofloxacin, levofloxacin, lomefloxacin and gatifloxacin
are more effective than narrow spectrum antibiotics such as amoxicillin and
trimethoprim-sulphamethoxazole in areas with high prevalence of resistance
(43,44).
Oral ciprofloxacin, levofloxacin, lomefloxacin and gatifloxacin are used for
the treatment of acute pyelonephritis (43).
32
CHALLENGES TO TREATMENT
Recurrent cystitis in women
Up to 20 percent of young women with acute cystitis develop recurrent
UTIs. During these recurrent episodes, the causative organism should be
identified by urine culture to help differentiate between relapse (infection
with the same organism) and recurrence (infection with different
organisms). Multiple infections caused by the same organism are, by
definition, complicated UTIs and this require longer courses of antibiotics for
up to 2 weeks (3). Fortunately, most recurrent UTIs in young women are
uncomplicated infections caused by different organisms (36, 45).
Women who have more than three UTI recurrences documented by urine
culture within one year can be managed using one of three preventive
strategies: Acute self-treatment with a three-day course of standard
therapy; Postcoital prophylaxis with trimethoprim-sulfamethoxazole given as
half the strength of a tablet (i.e. 40/200 mg) if the UTIs have been clearly
related to intercourse; and continuous daily prophylaxis with one of these
regimens for a period of six months: trimethoprim-sulfamethoxazole, one-
half tablet per day (40/200 mg); nitrofurantoin, 50 to 100 mg per day;
norfloxacin, 200 mg per day; cephalexin, 250 mg per day; or trimethoprim,
100 mg per day (3, 17, 29).
33
Each of these regimens has been shown to decrease the morbidity of
recurrent UTIs without a concomitant increase in antibiotic resistance and
long-term studies have shown antibiotic prophylaxis to be effective for up to
five years with trimethoprim, trimethoprim-sulfamethoxazole or
nitrofurantoin, without the emergence of drug resistance (29).
Unfortunately, antibiotic prophylaxis does not appear to alter the natural
history of recurrences because forty to sixty percent of these women were
observed to reestablish their pattern or frequency of infections within six
months of stopping prophylaxis (29).
Catheter-Associated UTI
Some patients who are hospitalized receive indwelling Foley catheter which
increase the risk of bacteriuria by approximately 5 percent per day. For
every patient on long-term catheterization, however bacteriuria is inevitable.
The diagnosis of catheter-associated urinary tract infection can be made
when the urine culture shows 100,000 or more CFU per mL of urine from a
catheterized patient.
Symptomatic bacteriuria in a patient with an indwelling Foleys catheter
should be treated with antibiotics that cover potential nosocomial
uropathogens such as E. coli and Proteus, Enterococcus, Pseudomonas,
Enterobacter, Serratia and Candida species. Patients with mild to moderate
34
infections may be treated with one of the oral quinolones, usually for 10 to
14 days. Parenteral antibiotic therapy may be necessary in patients with
severe infections or patients who are unable to tolerate oral medications.
The recommended duration of therapy for severe infections is 14 to 21 days.
Treatment is not recommended for catheterized patients who have
asymptomatic bacteriuria, with the following exceptions: patients who are
immunosuppressed after organ transplantation, patients at risk for bacterial
endocarditis and patients who are about to undergo urinary tract
instrumentation (24). In patients on long term catheterization, catheters
should be changed periodically to prevent the formation of concretions and
obstruction that can lead to infection. Although prophylactic systemic
antibiotics have been shown to delay the onset of bacteriuria in catheterized
patients, this strategy may lead to increased bacterial resistance (24).
Furthermore, antibiotic therapy has been successful in reducing the
frequency of bacteriuria only in patients who can be weaned from indwelling
catheters to intermittent catheterization.
35
Asymptomatic Bacteriuria
Asymptomatic bacteriuria is defined as the presence of more than 100,000
CFU per ml of voided urine in persons with no symptoms of urinary tract
infection. The largest patient population at risk for asymptomatic bacteriuria
is the elderly. Up to 40 percent of elderly men and women may have
bacteriuria without symptoms and should benefit from treatment (20). Other
groups of patients with asymptomatic bacteriuria have been shown to
benefit from treatment: patients with renal transplants, patients who are
about to undergo genitourinary tract procedures and pregnant women.
Between 2 and 10 percent of pregnancies are complicated by UTIs; if left
untreated, some of these women develop pyelonephritis (45, 46).
Pregnant women with asymptomatic bacteriuria should ideally be treated
with a three- to seven-day course of the antibiotics to which the cultured
isolate is sensitive to, and following treatment the urine should subsequently
be cultured to ensure cure and the avoidance of relapse (45). Although
amoxicillin has been the agent of choice, E. coli is now commonly resistant
to ampicillin, amoxicillin and cephalexin. Nitrofurantoin or trimethoprim-
sulfamethoxazole may also be used; however, caution should be exercised
in the third trimester because the sulfonamides compete with bilirubin
binding sites in the newborn (20). Thus, treatment should be based on the
results of susceptibility tests.
36
ANTIMICROBIAL RESISTANCE
Bacterial resistance to antibiotic
The antimicrobial agents traditionally used for treatment of UTI include
trimethoprim, trimethoprim-sulphamethoxazole, nitrofurantion, amoxicillin-
clavulanate, gentamicin and ciprofloxacin. However uropathogens are not
always fully sensitive to them as a report from 30 medical centers in the
United States of America and 10 medical centers from Canada shows an
overall resistance of uropathogens to ampicillin to be 37.7%, followed by
SMX/TMP (21.3%), nitrofurantoin (1.1%), ciprofloxacin (5.5%) and
levofloxacin (5.1%) (47).
Understanding the three main mechanisms by which uropathogenic
organisms manifest resistance to antimicrobials; natural resistance, selection
of resistant mutants, and transferable resistance, can help guide therapy.
Natural chromosomal resistance is exemplified by Proteus, which is never
sensitive to nitrofurantoin. Another examples, is Pseudomonas aeruginosa
which is inherently resistant to sulfonamides, trimethoprim, tetracycline and
chloramphenicol. These families of antibiotic are unable to accumulate in
Pseudomonas aeruginosa to a sufficient intracellular concentration due to
presence of efflux pumps (44, 48). These resistance patterns are predictable
and guide definitive therapy.
37
Selection of resistant mutants represents survival of a resistant strain that
was present prior to therapy but survives due to underdosing. In practice,
selection of resistant clones occurs in up to 10% of patients and can be
mitigated by ensuring the appropriate dosing of the antimicrobial.
Transferable resistance or R-factor resistance is caused by a plasmid-
mediated, transferable element that confers resistance, usually multi-drug
resistance. This manner of resistance is common and can be problematic
with improper use of antimicrobials in the hospital setting (26). The
transmission of R-factor occurs within the fecal reservoir of patients
receiving beta-lactams, trimethoprim-sulfamethoxazole (TMP-SMX),
aminoglycosides, and tetracyclines.
Such plasmids are responsible for β-lactamase-mediated ampicillin
resistance in Escherichia coli and Klebsiella spp. The bacteria undergo
simple point mutations that result in the production of extended-spectrum
β-lactamases (ESBLs) capable of hydrolyzing extended-spectrum
cephalosporins (e.g., cefotaxime, ceftriaxone, ceftizoxime, and ceftazidime)
and aztreonam, as well as older β-lactam drugs (49). Studies have shown
that ESBL-producing isolates are resistant to all extended-spectrum
penicillins, cephalosporins, and monobactams in vivo even if they are
susceptible to these agents invitro (50). The genes that codes for production
38
of ESBLs are often linked to other resistance genes, so that ESBL-producing
isolates are often resistant to many other antibiotic classes (e.g. resistant to
aminoglycosides and trimethoprim-sulfamethoxazole).
Antibiotic consumption and resistance
Resistance to antibiotics is a major public-health problem and antibiotic use
is being increasingly recognised as the main selective pressure driving this
resistance. Thus there have been studies world wide to demonstrate this
association and monitor drug use. In order to facilitate this, various
classification systems for drug consumed were developed. The European
Pharmaceutical Market Research Association (EPhMRA) classification system
was one such system. However due to the difficulties encountered in the
interpretation of results obtained by this system, it was not widely used
internationally. Another classification system, the Anatomical Therapeutic
Chemical (ATC) was developed which in combination with the Defined Daily
Dose (DDD) gained acceptance world wide (51). The ATC/DDD system is
used as a tool for presenting drug utilization statistics with the aim of
improving drug use. The ATC system groups drugs according to the organ
or system on which they act and their chemical, pharmacological and
therapeutic properties. It is especially suitable for evaluation for long term
trends in drug use. The (DDD) is a measurement of drug consumption and
39
is defined as the assumed average maintenance dose per day for a drug
used for its main indication in adults. It has been standardized for use in
hospital and community and data can be compared among hospitals and
regions, nationally and internationally. It can be used to identify possible
overuse, underuse or misuse of individual drugs. This information can then
be used to initiate specific studies or specific educational interventions.
Drug consumption is presented as numbers of DDDs/1000 inhabitants/day
or DDDs per 100 bed days in case of hospital use (51). Statistical packages
such as the Antibiotic Consumption Calculator (ABC CALC) have been
developed and successfully used for the calculations. The use of antibiotic
consumption data in DDDs in correlation to antibiotic resistance displayed by
microorganisms is not yet popular in developing countries like Nigeria,
however, it is widely used in Europe. For example, in an international
multicenter study of antimicrobials consumption and resistance in
Staphylococcus aureus isolated from 15 hospitals in 14 countries in Europe,
significant correlations were found between resistance and consumption of
antimicrobials in hospitals with MRSA prevalence of between 0% and 63%
(52). By calculating the DDDs of antibiotics, the trends of their usage over
time can be obtained and matched with the resistance of organisms to the
drugs. The use is not limited to drug resistance, but can be applied to
40
adverse drug reactions (53). For example in a Swedish study on adverse
drug reactions, the DDD was applied to the prescription data of drugs like
phenformin and metformin and this was used accurately in determining the
relative incidence in their adverse reactions by converting prescribed daily
doses of this drug consumed by the study population and the differences
between means were tested statistically (53).
41
CHAPTER THREE
MATERIALS AND METHODS
This study was carried out in the Medical Microbiology Laboratory of the
Lagos University Teaching Hospital for a period of six months (January to
June, 2006). All isolates obtained from the urine specimens of patients sent
to the Microbiology Laboratory were characterized and antimicrobial
susceptibility testing carried out on them. Antibiotic susceptibility data of
uropathogens isolated from LUTH laboratory for the periods January to
December 2005 was also reviewed. Data on antibiotic consumption pattern
for the periods January to December 2005 and January to June 2006 were
obtained from the in-patients Pharmacy department of the hospital and
correlated with the susceptibility patterns.
Ethical consideration
The study proposal was approved by the Ethics and Research committee of
the Lagos University Teaching Hospital.
Sampling Method
All urine specimen which grew cultures with greater than 100,000 colony
forming units (CFU) per milliliter of a single organism on MacConkey or
blood agar (significant bacteriuria) (54), were included in the study.
42
Procedure
All isolates cultured from consecutive specimens with significant bacteriuria
were analyzed. Isolates obtained were subcultured on MacConkey agar
(oxoid) and blood agar (45, 46). Incubation was done at 37oC for 18-24
hours. Subcultures were characterized by standard laboratory methods (55).
Gram negative bacilli
All isolate were stained by the Gram method. All gram negative bacilli were
tested for motility and oxidase (55). All gram negative bacilli that were
oxidase negative (whether motile or non motile) were further characterized
with API 20E (Biomerieux, France) to the specie level. The oxidase positive
gram negative bacilli were further characterized with API 20 NE
(Biomerieux) (56).
Gram positive cocci
All gram positive cocci were further identified by catalase test. Catalase
positive gram positive cocci were identified as Staphylococcus and further
characterized by coagulase test. Coagulase positive Staphylococcus was
identified as Staphylococcus aureus (56). Coagulase negative
Staphylococcus was further characterized by Urease, and Mannitol tests,
Bacitracin and Novobiocin disk test. Urease positive, mannitol negative,
Bacitracin variable and Novobiocin resistant coagulase negative
43
Staphylococus was identified as Staphylococcus saprophyticus. Novobiocin
sensitive, urease negative, Bacitracin negative and Mannitol variable
coagulase negative Staphylococcus was identified as coagulase negative
Staphylococcus (56).
The catalase negative gram positive cocci subculture on blood agar was
examined for hemolysis. The gamma or non hemolytic catalase negative,
gram positive cocci were identified as Enterococcus.
Other gram positive cocci and/or gram negative bacilli when isolated were
identified by standard methods to their specie levels (55).
Control organisms: ATCC 25922- E. coli and ATCC 27853- Pseudomonas
aerugenosa (for Gram negative controls), ATCC 460701- Staphylococcus
aureus (for Gram positive control) were used as standard controls for the
API systems and antibiotic sensitivity testings.
Antibiotic susceptibility testing
Sensitivity of the organisms was performed using the modified Kirby-Bauer
disk diffusion method on Mueller Hinton agar plates (56).
Plates were inoculated within 15 minutes of preparation of suspensions
using sterile cotton swab to streak on the entire surface.

44
Single antibiotic discs, six per plate were applied using forceps and
incubated for 18-24 hours at 370C.
The antibiotic discs and their concentrations per disk (µg) included:
Trimethoprim-sulfamethoxazole 25µg, nitrofurantoin 30µg, nalidixic acid
30µg gentamicin 10µg, ofloxacin 5µg, amoxicillin-clavulanic acid 30µg
ciprofloxacin 5µg, cefuroxime 30µg, ceftazidime 30µg, cefoxithin 30µg, and
cefotaxime 30µg.The diameters of the zones of inhibition were measured
using a milliliter rule. Organisms resistant to any of the third generation
cephalosporins (ceftazidime, cefotaxime) were tested for extended spectrum
beta-lactamases (ELBS) using the Double-Disk Synergy Test (DDST) method
(57, 58).
Interpretation of results
Each zone size was interpreted, by reference to an interpretive table of the
Clinical Standard for Laboratory Institute (CSLI) (formerly National
Committee for Clinical and Laboratory Standards (NCCLS) (19).
Detection of Extended spectrum beta-lactamase producers (ESBLs).
Isolates showing resistance to ceftazidime (≤22mm for 30µg disk) were
tested for the production of ESBLs by the DDST as described by Jarlire et al
(57) with the modifications suggested by Thompson and Sanders (58).
45
After inoculating Mueller-Hinton agar plates as for routine disk-difusion
method, 30µg, disks of cefoxithin, ceftazidime and cefotaxime were placed
20mm (34) center to center from an amoxicillin-clavulanate (20:10µg) disk
(Oxford UK). Accurate placement of each disk was expedited by melting
holes in the lid of a petri-dish plate and using the lid as a template to mark
the bottom of the agar plate (59). Inoculated media was incubated
overnight at 37oC. An enhanced zone of inhibition between any one of the
beta-lactam disks and the amoxicillin clavulanic acid disk was interpreted as
evidence of the presence of an extended spectrum beta-lactamase producer
(ESBL) (60).
Antimicrobial consumption data: Data on the antimicrobial usage was
obtained from the hospital in-patient pharmacy and analysed using ABC
CALC (10, 51).
Antimicrobial usage in LUTH in-patient wards from January to December
2005 were collected from the Pharmacy Department for parenteral and oral
drugs in grams and number of packages and doses or as defined daily doses
(DDD). These raw data were entered into a spreadsheet (ABC CALC) and
converted into DDD. The World Health Organisation (WHO) Anatomic
Therapeutic Classification (ATC) system to identify antibiotics and their DDD
46
was used (51). The DDD is based on the average daily doses used for the
main indication of the drug. The following ATC antibiotic subgroups were
used because the drugs were consumed in the hospital: Beta-lactam
combinations (amoxicillin + clavulanic acid, ampicillin-cloxacillin);
aminoglycosides ( gentamicin); fluoroquinolones (ciprofloxacin, ofloxacin,
perfloxacin, sparfloxacin, and levofloxacin); penicillins (benzylpenicillin);
second generation cephalosporins (cefuroxime, cefoxithin); third generation
cephalosporins (cefotaxime, ceftaxidime, and ceftriaxone); combinations
(sulfamethoxazole-trimethoprim).
Information on bed-days in LUTH in 2006 was obtained and entered into the
spread sheet and all antibiotic consumption data were calculated as number
of DDD/100 bed-days for each therapeutic subgroup.
Statistical analysis
Analysis was done using SPSS software. Association was determined with
Pearson’s correlation coefficient.
47
CHAPTER FOUR
RESULTS
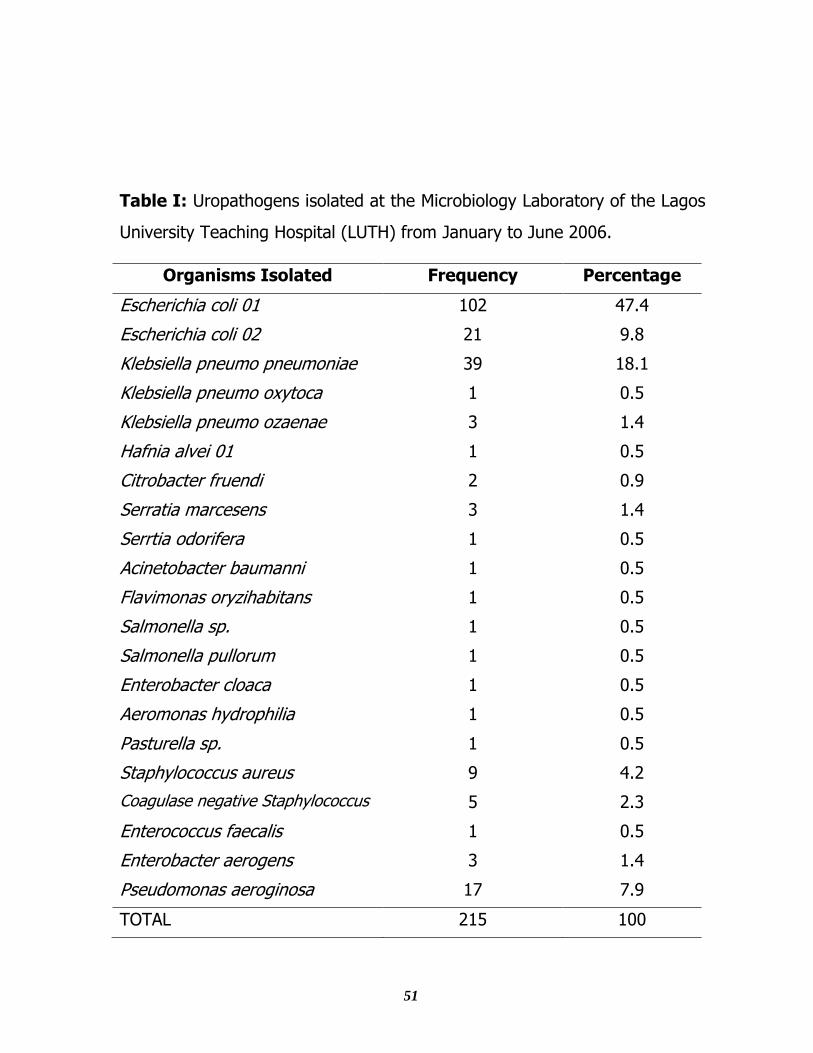
During the six months period of the study, 215 bacteria were isolated from
1520 urine samples sent to the Microbiology Laboratory in LUTH
corresponding to a rate of isolation of 14.4%. Urine samples of the in-
patients were 913 with significant bacterial isolates of 174, while that of out-
patients were 607 with significant bacterial isolates of 41. As shown in Table
I, Escherichia coli was most prevalent making up 57.2% (123 isolates) of
the total. Klebsiella pneumoniae (subspecies pneumoniae, oxytoca and
ozoanae) was the second most prevalent (43 isolates, 20%) followed by
Pseudomonas aeruginosa (17 isolates, 7.9%). Many other gram negative
bacteria were isolated. The gram positive bacteria isolated were
Staphylococcus aureus (9 isolates, 4.2%), coagulase negative
Staphylococcus (5 isolates, 2.3%), Enterococcus faecalis (1 isolate, 0.5%),
and Enterobacter aerogens (3 isolates, 1.4%).
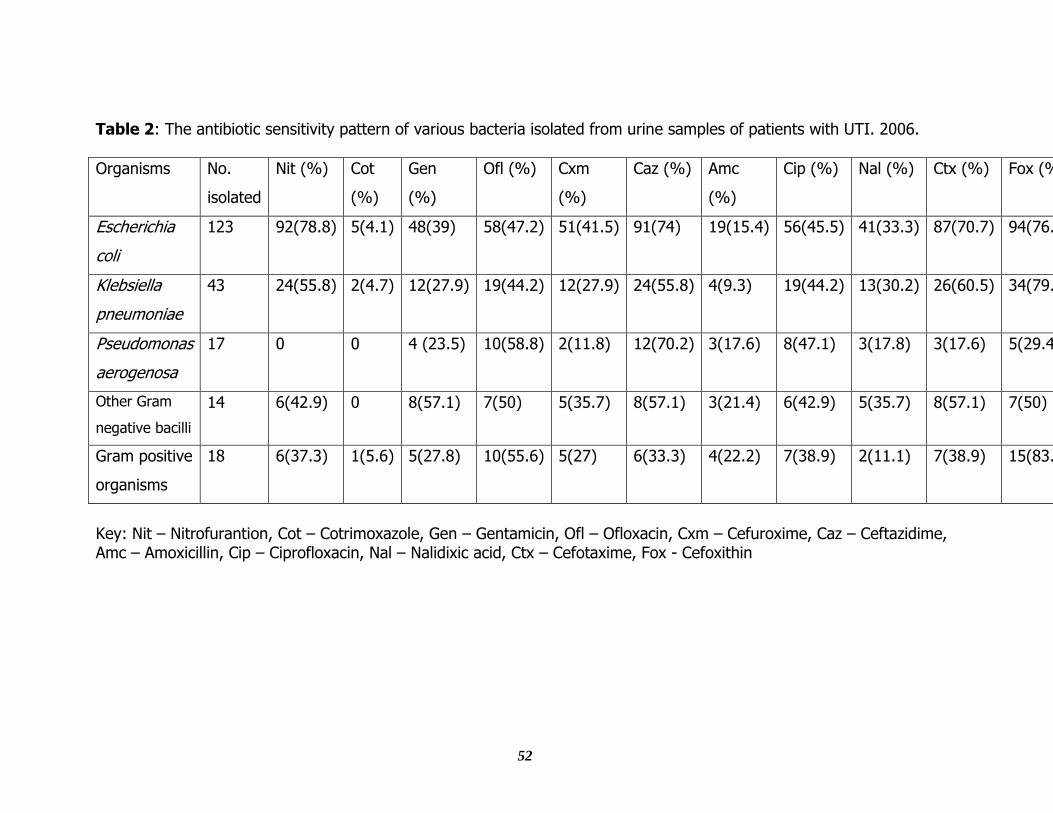
Many isolates of Escherichia coli were sensitive to nitrofurantion (74.8%),
ceftazidime (74%), cefotaxime (70.7%) and cefoxitin (76.4%) while many
were resistant to cotrimoxazole (95.9%), amoxicillin-clavulanate (84.4%),
gentamicin (61%), ofloxacin (52.8%), cefuroxime (58.5%), ciprofloxacin
48
(54.5%) and nalidixic acid (66.7%). The overall resistance rate ranged from
23.6% (cefoxitin) to 95.9% (cotrimoxazole), (Table 2).
As shown in Table 2, the sensitivity rates of Klebsiella pneumoniae to the
various antimicrobials were nitrofurantoin (55.8%), ceftazidime (55.8%),
cefotaxime (60.5%) and cefoxitin (79.1%), while the resistance rates of the
other antimicrobials were ofloxacin (55.8 %), ciprofloxacin (55.8%),
cotrimoxazole (95.3%), gentamicin (72.1%), cefuroxime (72.1%),
amoxicillin clavulanate (90.7%) and nalidixic acid (69.8%).
Pseudomonas aeruginosa isolates were mainly sensitive to ceftazidime
(70.2%) and ofloxacin (58.8%). Resistance to ciprofloxacin was 52.9%. The
isolates were resistant to nitrofurantoin (100%) and cotrimoxazole (100%),
cefuroxime (88.2%), gentamicin (76.5%), amoxicillin-clavulanate, nalidixic
acid, and cefotaxime (82.4% respectively) and cefoxitin (70.6%), (Table 2).
The sensitivity rates of other gram negative bacilli were nitrofurantion
(42.9%), gentamicin (57.1%), ceftazidime (57.1%), cefotaxime (57.1%),
ofloxacin (50%), ciprofloxacin (42.9%) and cefoxitin (50%). Many of them
were resistant to cotrimoxazole (100%), amoxicillin-clavulanate (78.6%),
and nalidixic acid (64.2%), (Table 2).
49
The gram positive cocci isolated showed a high rate of resistance of 80%
and above to Cotrimoxazole, Nalidixic acid, Cloxacillin and Cefoxithin, (Table
2).
The resistance rates of the isolates from urine of patients sent to the
Microbiology Laboratory in LUTH in 2005 from January to June and July to
December (124 and 198 isolates respectively) are shown in Table 3, with
the organisms being more resistant to Clotrimoxazole and Amoxicillin –
clavulanate.
Also shown are the drugs that were dispensed by the LUTH pharmacy and
consumed by patients diagnosed of having infection including UTI included
cotrimoxazole, gentamicin, ofloxacin, cefuroxime, ceftazidime, ciprofloxacin
and amoxicillin-clavulanate.
Overall amoxicillin-clavulanate was the most consumed while ceftazidime
was the least consumed; (Table 3). Co-trimoxazole showed the highest
resistance rates (96 – 98%), followed by amoxicillin clavulanic acid.
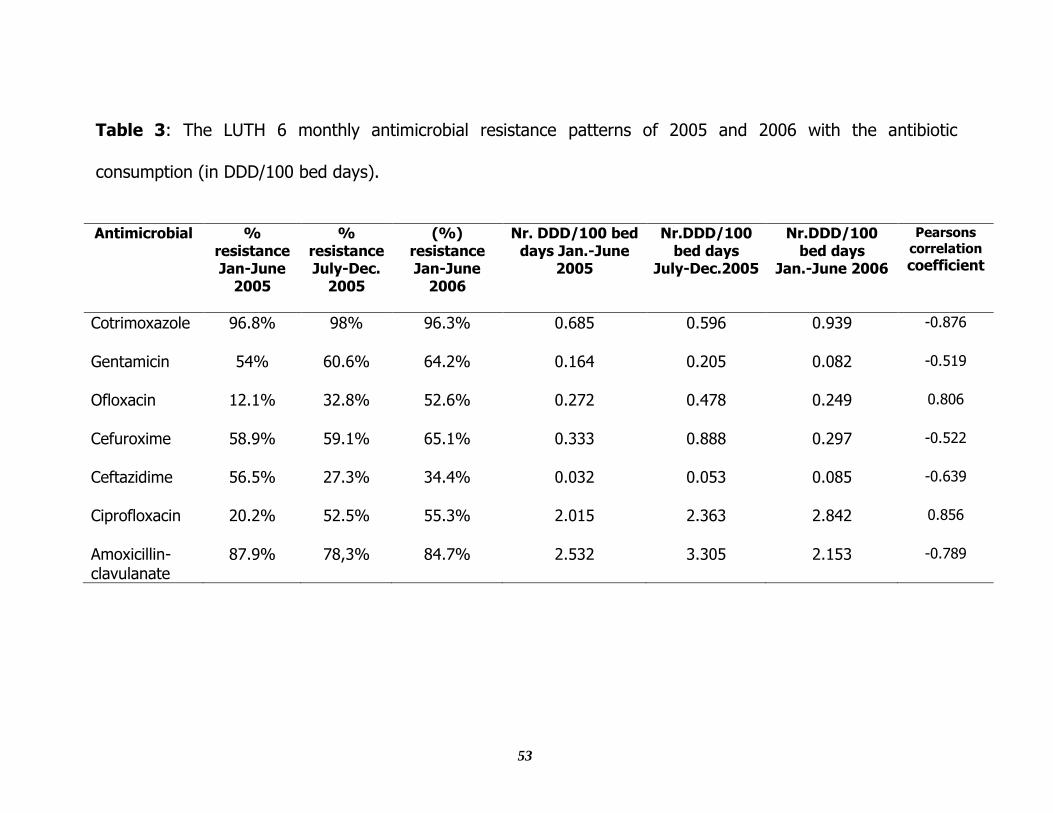
Generally, the resistance rates to the antibiotics were high. For all the
antimicrobials except cotrimoxazole, there was an increase in the rates of
consumption from the first and second periods which were accompanied by
an increase in the resistance from the second to the third period. These
50
associations were statistically significant. The rate of consumption of
ciprofloxacin increased steadily over the three 6 monthly periods and this
was significantly associated with a steady increase in resistance. Also
associated with a steady increase in resistance is the increase in the
consumption of ofloxacin in the first two periods.
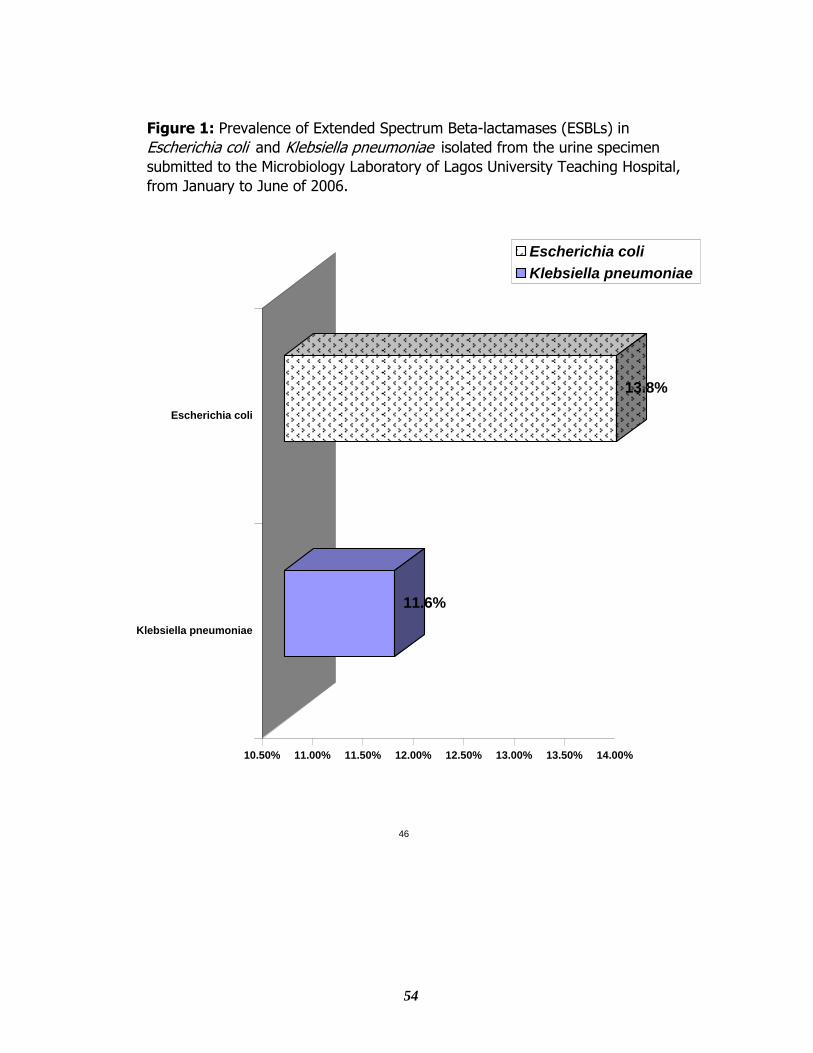
Seventeen of the 123 isolates of Escherichia coli (13.8%) that were resistant
to Ceftazidime and Cefotaxime were found to produce extended spectrum
beta lactamases (ESBLs), while all the 5 Klebsiella spp. (11.6%) that were
resistant to Ceftazidime and Cefotaxime were found to produce ESBLs
(figure 1).
51
Table I: Uropathogens isolated at the Microbiology Laboratory of the Lagos
University Teaching Hospital (LUTH) from January to June 2006.
Organisms Isolated Frequency Percentage
Escherichia coli 01 102 47.4
Escherichia coli 02 21 9.8
Klebsiella pneumo pneumoniae 39 18.1
Klebsiella pneumo oxytoca 1 0.5
Klebsiella pneumo ozaenae 3 1.4
Hafnia alvei 01 1 0.5
Citrobacter fruendi 2 0.9
Serratia marcesens 3 1.4
Serrtia odorifera 1 0.5
Acinetobacter baumanni 1 0.5
Flavimonas oryzihabitans 1 0.5
Salmonella sp. 1 0.5
Salmonella pullorum 1 0.5
Enterobacter cloaca 1 0.5
Aeromonas hydrophilia 1 0.5
Pasturella sp. 1 0.5
Staphylococcus aureus 9 4.2
Coagulase negative Staphylococcus 5 2.3
Enterococcus faecalis 1 0.5
Enterobacter aerogens 3 1.4
Pseudomonas aeroginosa 17 7.9
TOTAL 215 100
52
Table 2: The antibiotic sensitivity pattern of various bacteria isolated from urine samples of patients with UTI. 2006.
Organisms No.
isolated
Nit (%) Cot
(%)
Gen
(%)
Ofl (%) Cxm
(%)
Caz (%) Amc
(%)
Cip (%) Nal (%) Ctx (%) Fox (%) Cxc
(%)
Escherichia
coli
123 92(78.8) 5(4.1) 48(39) 58(47.2) 51(41.5) 91(74) 19(15.4) 56(45.5) 41(33.3) 87(70.7) 94(76.4) 0
Klebsiella
pneumoniae
43 24(55.8) 2(4.7) 12(27.9) 19(44.2) 12(27.9) 24(55.8) 4(9.3) 19(44.2) 13(30.2) 26(60.5) 34(79.1) 0
Pseudomonas
aerogenosa
17 0 0 4 (23.5) 10(58.8) 2(11.8) 12(70.2) 3(17.6) 8(47.1) 3(17.8) 3(17.6) 5(29.4) 0
Other Gram
negative bacilli
14 6(42.9) 0 8(57.1) 7(50) 5(35.7) 8(57.1) 3(21.4) 6(42.9) 5(35.7) 8(57.1) 7(50) 0
Gram positive
organisms
18 6(37.3) 1(5.6) 5(27.8) 10(55.6) 5(27) 6(33.3) 4(22.2) 7(38.9) 2(11.1) 7(38.9) 15(83.3) 2(11.1)
Key: Nit – Nitrofurantion, Cot – Cotrimoxazole, Gen – Gentamicin, Ofl – Ofloxacin, Cxm – Cefuroxime, Caz – Ceftazidime, Amc – Amoxicillin, Cip – Ciprofloxacin, Nal – Nalidixic acid, Ctx – Cefotaxime, Fox - Cefoxithin
53
Table 3: The LUTH 6 monthly antimicrobial resistance patterns of 2005 and 2006 with the antibiotic
consumption (in DDD/100 bed days).
Antimicrobial %
resistance Jan-June
2005
% resistance July-Dec.
2005
(%) resistance Jan-June
2006
Nr. DDD/100 bed days Jan.-June
2005
Nr.DDD/100 bed days
July-Dec.2005
Nr.DDD/100 bed days
Jan.-June 2006
Pearsons
correlation
coefficient
Cotrimoxazole 96.8% 98% 96.3% 0.685 0.596 0.939 -0.876
Gentamicin 54% 60.6% 64.2% 0.164 0.205 0.082 -0.519
Ofloxacin 12.1% 32.8% 52.6% 0.272 0.478 0.249 0.806
Cefuroxime 58.9% 59.1% 65.1% 0.333 0.888 0.297 -0.522
Ceftazidime 56.5% 27.3% 34.4% 0.032 0.053 0.085 -0.639
Ciprofloxacin 20.2% 52.5% 55.3% 2.015 2.363 2.842 0.856
Amoxicillin-clavulanate
87.9% 78,3% 84.7% 2.532 3.305 2.153 -0.789
54
11.6%
13.8%
10.50% 11.00% 11.50% 12.00% 12.50% 13.00% 13.50% 14.00%
Klebsiella pneumoniae
Escherichia coli
Escherichia coli
Klebsiella pneumoniae
Figure 1: Prevalence of Extended Spectrum Beta-lactamases (ESBLs) in
Escherichia coli and Klebsiella pneumoniae isolated from the urine specimen
submitted to the Microbiology Laboratory of Lagos University Teaching Hospital,
from January to June of 2006.
46
55
CHAPTER FIVE
DISCUSSION
In this study, over 80% of the uropathogens isolated were from in-patients,
and Escherichia coli was the most prevalent making up 57.2% while the
other pathogens made up 43.8%. This pattern fits the trend observed in
hospital based patients. Although the prevalence of Escherichia coli in
community acquired UTI is higher, and could be as high as 85%, it is
relatively lower in hospitalized patients in which case the other pathogens
play a more significant role compared with community acquired infection (4,
61). Klebsiella pneumoniae was found to be the second and Pseudomonas
aeruginosa the third most prevalent. This pattern has been well documented
(12, 21).
Other isolates which are Hafnia alvei, Citrobacter fruendii, Serratia
marcescens, Serratia odorifera, Acinetobacter baumanni, Flavimonas
oryzihabitans, Salmonella sp., Salmonella pullorum, Enterobacter cloaca,
Aeromonas hydrophylia, Pastuerella sp., and Enterococcus aerogens are not
frequently reported in our environment due to the fact that Analytical Profile
Index (API) kits used for their identification in this study are not always
used. It is noteworthy that these organisms could cause septicaemia
associated with high rate of mortality in improperly treated patient, (1, 55).
56
The sensitivity pattern of Escherichia coli which was the most prevalent
uropathogen in this study suggests that antibiotics like ceftazidime,
cefotaxime and nitrofurantion would be useful for empiric therapy of in-
patients because over 70% of isolates were sensitive. Cotrimoxazole,
amoxicillin-clavulanate and gentamicin which were traditionally the first line
drugs for UTI are no longer useful as such because only 39-45% of isolates
were sensitive to them. Studies carried out in the past recommended that
the quinolones which were quite active then, be kept in reserve to combat
resistance problems, but as found in this study, and various others, overuse
has led to increase in resistance (9, 12, 13).
Fourteen percent and 11.6% respectively of cephalosporin resistant E. coli
and K. pneumoniae produce ESBLs. Such isolates cannot be treated with
cefotaxime, ceftriazone and ceftazidime. ESBLs are associated with
overuse. ESBLs producers spread easily and can cause outbreaks in
hospitals especially because the transferable resistance conferred is plasmid
mediated (3).
As found in this study, the treatment of UTI caused by the other gram
negative bacilli and the gram positive cocci should be based on the result of
57
sensitivity patterns because they showed high rates of resistance to all the
antibiotics tested.
For all antibiotics consumed in this study except cotrimoxazole, increased
consumption correlated with increased resistance and on the hand, the
uropathogens were highly sensitive to nitrofurantoin and cefoxitin which
were not consumed during the study period. Studies around the world have
correlated drug overuse with increased antimicrobial resistance and a much
clearer picture of this would be painted in the hospital of study if this trend
is allowed to continue (62). To discontinue this trend, the hospital needs to
stop the use of the relevant antibiotics especially cotrimoxazole and
amoxicillin clavulanate for the treatment of UTI in hospitalized patients. An
antibiotic policy should be developed to reduce or restrict the use of other
antibiotics. There is also need to continue to monitor resistance of the
relevant antibiotics in order to demonstrate a reduction in response to
reduced consumption. The classical case of upward trend in the resistance
of pathogens due to upward trend in the consumption of ciprofloxacin was
seen in this study. And if the consumption is discontinued, the resistance
rate will be reduced in response as shown by a study (63).
CONCLUSION
58
(1). Escherichia coli was the pathogen most commonly isolated from the
urine of hospitalized patients in Lagos University Teaching Hospital.
(2). Majority of isolates were resistant to cotrimoxazole and amoxicillin-
clavulanate and this resistance appear to be endemic. They also
showed high sensitivity nitrofurantoin, ceftazidime, cefotaxime and
cefoxithin
(3). Fourteen percent of Escherichia coli and 11.6% of Klebsiella
pneumoniae were found to be ESBLs producers.
(4). For all the antimicrobials, there was an increase in resistance which
was preceded by increased antimicrobial consumption.
(5). There was a trend of increased resistance of uropathogens to
antimicrobials especially to the Quinolones (ciprofloxacin and
ofloxacin), gentamicin, cefuroxime, ceftazidime and amoxicillin-
clavulanate in the face of increased consumption of these drugs.
There is urgent need for intervention to stop this trend.
RECOMMENDATION
59
(1). The medical personnel prescribing antibiotics in LUTH should be
educated on the current trend and the need for intervention.
(2). The use of co-trimoxazole and amoxicillin-clavulanate should be
stopped. They should be replaced by the more sensitive antimicrobials.
(3). The hospital needs to have an antibiotic policy to ensure rational use
and restrict the use of antibiotics to combat future resistance problems.
(4). That further research should be conducted on the resistance of
uropathogens to antibiotics in relation to the consumption of such drugs in
LUTH over time to monitor the intervention instituted.
60
REFERENCES
1. Richard ER, Robert FB. Practical approach to infectious diseases. 3rd
ed. London: Little Brown Books. 1991.
2. Ashkenazi S, Even TS, Samra Z, Dinari G. Uropathogens of various
populations and their antibiotic susceptibility. Paediatr Infect Dis.
1991; 10:742-46.
3. Jack DS, Donald K. Urinary tract infections. In: Mandel GL, Bennett
JE, Dolin R. Principles and Practice of Infectious Diseases. London:
Elsevier Churchill Livingstone, 2005. pp 875-878.
4. Wammanda RD, Ewa BO. Urinary tract pathogens and their
antimicrobial sensitivity patterns in children. Annals of Tropical Paed.
2002; 22: 197-198.
5. Jones RN, Thornsberry C. A review of in vitro antimicrobial properties
and spectrum of activity. Rev Inf Dis 1982; 4: 5300-5315.
6. Fu KP, Neu HC. Betalactamase stability of HR 756 a novel
cephalosporin, compared to that of cefuroxime and cefotaxime.
Antimicrob Agents chemother 1978; 14:322-326.
7. Nokashino SS, Nakamuro M. In vitro activity of cefotaxime against
clinically significant pathogens. Drugs 1988; 35: (2) 14-21.
61
8. Gupta V, Yadav A, Joshi RM. Antibiotic resistance pattern in
uropathogens. Indian J Med Microbiol 2002; 20 :96-98.
9. Adeyemo AA, Gbadegesin RA, Onyemenem TN, Ekweozor CC.
Urinary tract pathogens and antimicrobial sensitivity patterns in
children in Ibadan, Nigeria. Ann Trop Paediatr. 1994; 14: (4) 271-274.
10. McGowan JE. Antimicrobial resistance in hospital organisms and its
relation to antibiotic use. Rev Infect Dis 1983; 5:1033 48.
11. Harbarth S, Anthony D H, Yehuda C, Matthew H S. Parallel Analysis of
Individual and Aggregated Data on Antibiotic Exposure and Resistance
in Gram-Negative Bacilli. Clinical Infectious Diseases. 2001; 33:1462-
1468
12. Odutola A, Ogunsola FT, Odugbemi T, Mabedeje FB. A study on the
prevalence of urinary tract infection in hypertensive patients attending
an urban hospital in Lagos, Nigeria. Nig Qt J Hosp Med. 1998; 8: (3)
190-192.
13. Ozumba UC. Increasing incidence of bacterial resistance to antibiotic
by isolates from urinary tract. Niger J Clin Pract 2005; 8 (2): 107 – 9.
14. Gruneberg RN. Changes in urinary pathogens and their antibiotic
sensitivities, 1971 – 1992. J. Antimicrob. Chemother. 1994; 33
(Suppl. A): 1–8.
62
15. MacGowan AP, Brown NM, Holt HA, McCulloch SY, Reeves D.S. An
eight-year survey of the antimicrobial susceptibility patterns of 85 971
bacteria isolated from patients in a district general hospital and the
local community. J. Antimicrob. Chemother. 1993; 31: 543–57.
16. Gastmeier P, Kampf G, Wischnewski N. Prevalence of nosocomial
infections in representative German hospitals. J. Hosp. Infect. 1998;
38: 37–49.
17. Larcombe J. Clinical evidence of urinary tract infection in children.
BMJ. 1996; 319(7218): 1173-1175.
18. Hadiza HL, Didier M Antoine T. Antimicrobial resistance among
uropathogens that cause community-acquired urinary tract infections
in Bangui, Central Afican Republic: 2003:51:192-194.
19. Evan BC, Anthony JS. Urinary tract Infections in Adult. Digital Urology
journal; 2006:3
20. Robert Orenstein DO, Edward SW. Urinary tract Infections in Adult.
Amer Fam Phy 1999; 59 (5)1-3
21. Peal R, Crump J, Maskell R. Staphylococci as urinary pathogen. J Clin
Pathol. 1977;30:427-431.
22. Numazaki Y, Kumasaka T, Yano N. Further Study on acute
haemorrhagic cystitis due to adenovirus . N Eng J. Med. 1973;
289:344-347.
63
23. Sharma S. Current understanding of Pathogenic mechanisms in UTIs.
Ann Natl Acad Med Sci 1997; 33(1):31-8.
24. Hooton TM. A prospective study of risk factors for symptomatic
urinary tract infection in young women. New England Journal of
Medicine. 1996; 335:(7): 468-74.
25. Jacobs LG. Fungal urinary tract infection in the elderly: Treatment
guidelines. Drugs Aging.1996; 8: 89-96.
26. Shanson DC. Microbiology in Clinical Practice. 3rd ed. London:
Butterworth Heinemann Books. 1999.
27. Foxman B. Epidemiology of urinary tract infection: incidence, morbity
and economic cost. Dis Mon 2003; 49(2):53-70.
28. Baron EJ, Peterson LR, Finegold SM. Bailey & Scotts Diagnostic
Microbiology. 9th ed. Boston: Mosby Books. 1990.
29. Johnson JR, Stamm W E. Diagnosis and treatment of acute urinary
tract infections. Infectious Disease Clinics of North America. 1987;
1:(4) 773.
30. David SH, Shelise MH. Urinary tract infection male, female. eMedicine
2006 [cited 2005 April 25]; 2: 1-8. Available from
http://www.medline.com
31. Stamey TA. Pathogenesis and Treatment of Urinary Tract Infections.
1st ed. Baltimore: Williams & Wilkins Company Books. 1980.
64
32. Stamey TA, Fair WR, Timothy MM. Serum versus urinary antimicrobial
concentrations in cure of urinary tract infections. New England Journal
of Medicine. 1974; 291: 1159.
33. Brun-Buisson C, Legrand P, Philippon A. Transferable enzymatic
resistance to third-generation cephalosporins during nosicomial
outbreak of multiresistant Klebsiella pneumonia. Lancet. 1987; 2:
302-6.
34. Iravani A. Advances in the understanding and treatment of urinary
tract infections in young women. Urology. 1991; 37: 503.
35. Stamm WE, Hooton TM. Management of urinary tract infections in
adults. N Engl J Med 1993; 329:1328-34.
36. Hooton TM, Stamm WE. Management of acute uncomplicated urinary
tract infections in adults. Medical Clinics of North America. 1991; 75:
339.
37. Barza M. Single or multiple daily doses of aminoglycosides: A meta-
analysis British Medical Journal. 1996; 312: (7027) 338-45.
38. Hooper DC, Wolfson JD. Fluoroquinolone antimicrobial agents. New
England Journal of Medicine. 1991; 324: (6) 384.
39. Dalkin BL, Schaeffer AJ. Fluoroquinolone antimicrobial agents: Use in
the treatment of urinary tract infections and clinical urologic practice.
Problems in Urology. 1988; 2: 476.
65
40. Wright AJ, Walker RC, Barrett DM. The fluoroquinolones and their
appropriate use in treatment of genitourinary tract infections. AUA
Update Series American Urologic Association. 1993; 50-55.
41. Johnson JR, Lyons MF, Pearce W. Therapy for women hospitalized
with acute pyelonephritis: A randomized trial of ampicillin versus
trimethoprim-sulfamethoxazole for 14 days. Journal of Infectious
Diseases. 1991; 163: 325.
42. Keren R, Chan E. A meta-analysis of Randomized, Controlled Trials
comparing short and long-course antibiotic therapy for urinary tract
infections in children. American Academy of Paed., 2002; 109:(5) 1-8.
43. Neumann I, Rojas MF, Moore P. Pyelonephritis in Non-pregnant
women. 2006 BMJ Clinical evidence (cited Dec 2006) 1: 1 – 2.
Available from http://www. BMJ Clinical evidence.com
44. Kohler T, Kok M, Michea-Hamzehpour M, Plesiat P, Gotoh N, Nishino
T. Multidrug efflux in intrinsic resistance to trimethoprim and
sulfamethoxazole in Pseudomonas aeruginosa. Antimicrob Agents
Chemother 1996; 40(10):2288-2290.
45. Raz R, Stamm WE. A controlled trial of intravaginal estriol in
postmenopausal women with recurrent urinary tract infections. New
England Journal of Medicine. 1993; 329: 753-756.
66
46. Wong ES, McKevitt RC, Running K. Management of recurrent urinary
tract infections with patient-administered single-dose therapy. Annals
of Internal Medicine. 1985; 102: 302-307.
47. Karlowsky JA, Clyde T, Jones ME. Susceptibility of Antimicrobial-
Resistant Urinary Escherichia coli Isolates to Flouoroquinolones and
Nitrofurantion. 2006; 1-2
48. Lee A, Mao W, Warren MS, Mistry A, Hoshino K, Okumura R. Interplay
between efflux pumps may provide either additive or multiplicative
effects on drug resistance. J Bacteriol 2000; 182(11):3142-3150.
49. Bush K. New β-lactamases in gram-negative bacteria: diversity and
impact on the selection of antimicrobial therapy. Clin. Infect. Dis.
2001;32:1085-1089.
50. Paterson DL. Recommendation for treatment of severe infections
caused by Enterobactericeae producing extended-spectrum β-
lactamases (ESBLs). Clin. microbiol Infect. 2000; 6: 460-463.
51. WHO. ATC/DDD system. [cited 2006 Sep 22]. Available from:
http://www.whocc.no/atcddd/.
52. Henrik W, Zinn CS, Rosdahl VT. An Iternational Multicenter Study of
Antimicrobial Consumption and Resistance in Staphylococcal aureus
67
Isolates from 15 Hospitals in 14 Countries. Microbial Drug Resistance.
2004; 10: (2) 169-175.
53. Bergman U, Boman G, Wiholm BE. Epidemiology of adverse drug
reactions to phenformin and metformin. Br Med J. i978; 2: (6) 464 –
466.
54. Thomas GM, Jr, Madeline MJ. Antibiotic Resistance Patterns of
Uropathogens in Pediatric Emergency Department Patients. Acad Emerg
Med. 2003; 10:(4) 347-351.
55. Murray PR, Baron EJ, Jorgensen JH, Pfaller MA, Yolken RH. Manual of
Clinical Microbiology. American Society for Microbiology, Washington
D.C. 8th Edition 2003:1183-1185.
56. Uehling DT. Vaginal mucosal immunization for recurrent urinary tract
infection: Phase II clinical trial. Journal of Urology. 1997; 157: (6)
2049-52.
57. Jarlier V, Nicolas MH, Fournier G, Philippon A. Extended broad-
spectrum beta-lactamases conferring transferable resistance to newer
beta-lactamases agents in Enterobacteriacea: hospital prevalence and
susceptibility patterns. Rev. Infect Dis. 1988;10: 867-878.
58. Thompson KS, Sanders CC. Detection of extended-spectrum beta-
lactamases in members of the family Enterobacteriacea: comparison
68
of the double-disk and three-dimensional test. Antimicrob. Agents
Chemother. 1992; 36: 1877 – 1882.
59. Coudron PE, Moland ES, Sanders CC. Occurrence and detection of
extended-spectrum beta-lactamases in members of the family
Enterobatericeae at a Veterans Medical Center: seek and you may
find. J. Clin. Microbiol. 1997; 35:2593-2597.
60. Ibukun A, Odugbemi T, Brian JM. Extended-spectrum beta-lactamases
in isolates of Klebsialla spp and Escherichia coli from Lagos, Nigeria.
Nigerian Journal of Health and Biomedical Sciences. 2003;2:(2)53-70.
61. Odugbemi T, Anandan N, Olivia FL. Urinary tract pathogens with a
special reference to muciod Pseudomonas aerogenosa at Aflaj General
Hospital. Annals of Saudi Medicine. 1992; 12: (6) 581-582.
62. Hooper DC. Mechanism of quinolone resistance. In: Hooper DC,
Rubinstein E, editors. Quinolone Antimicrobial Agents. d. Washington
DC: ASM Press, 2003. pp 41-47.
63. Cook PP, Catrou P, Gooch M, Holbert D. Effect of reduction in
ciprofloxacin use on prevalence of methicillin resistant staphylococcus
aureus rate with individual units of a tertiary care hospital. J hosp
infect, 2006; 64: (4) 384.
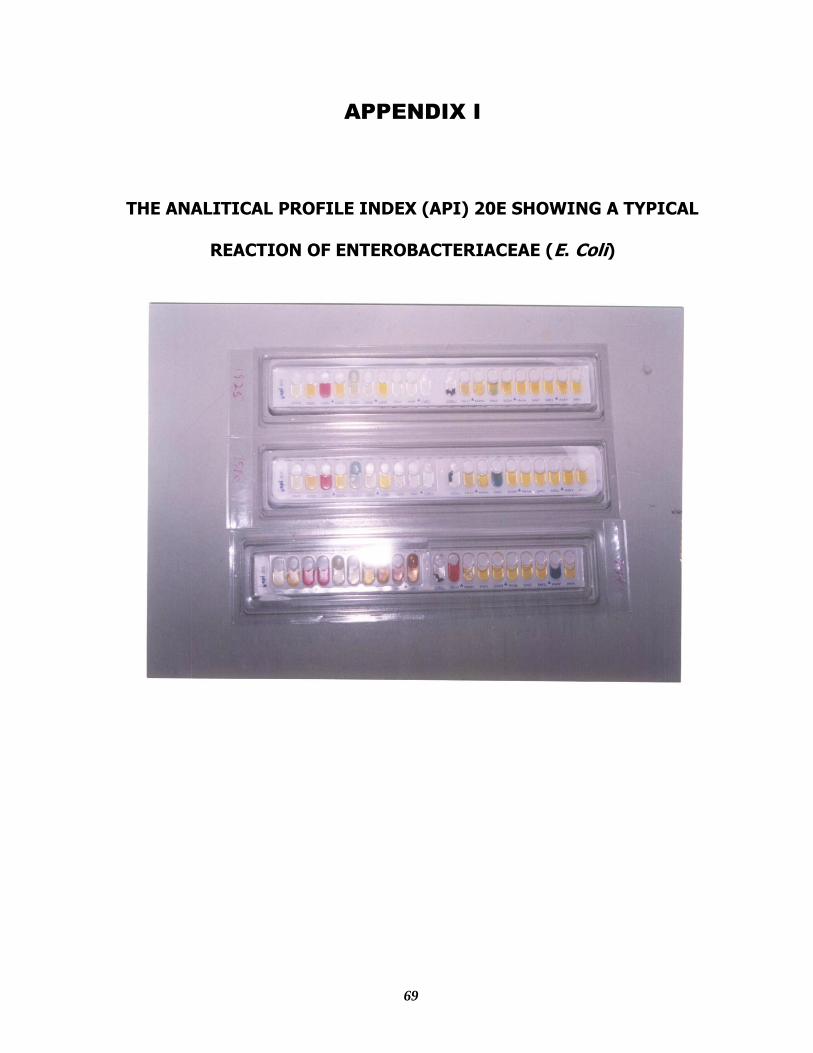
69
APPENDIX I
THE ANALITICAL PROFILE INDEX (API) 20E SHOWING A TYPICAL
REACTION OF ENTEROBACTERIACEAE (E. Coli)
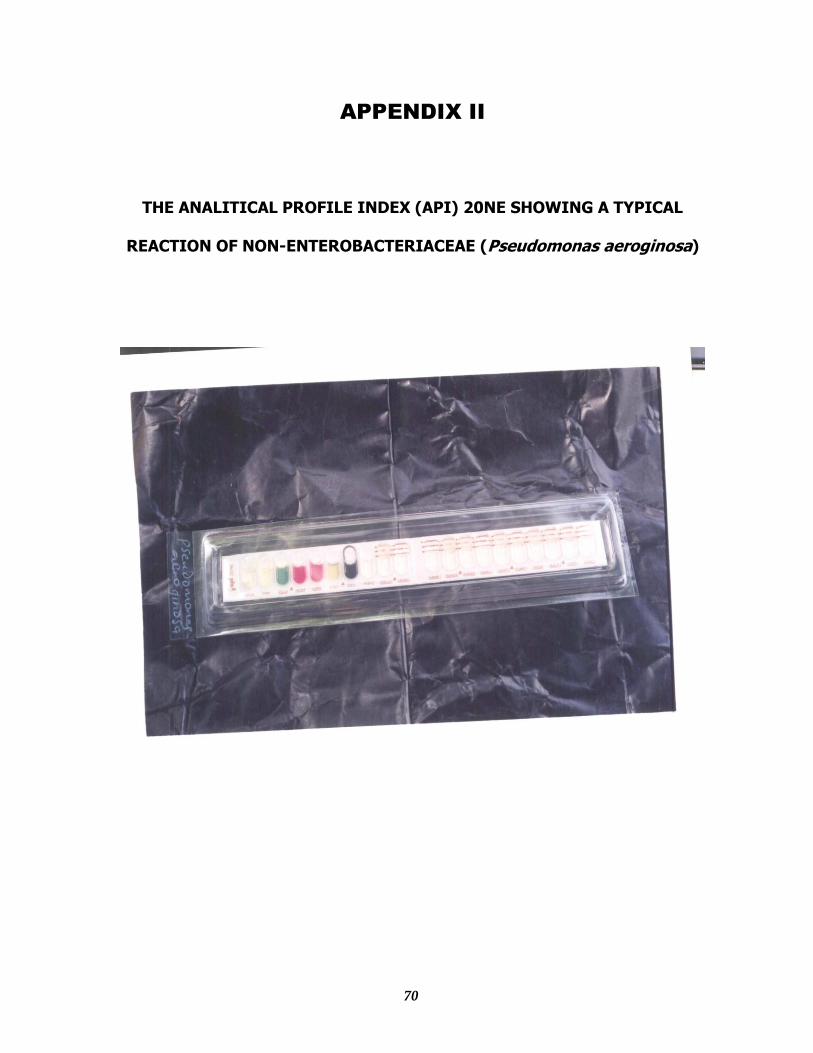
70
APPENDIX II
THE ANALITICAL PROFILE INDEX (API) 20NE SHOWING A TYPICAL
REACTION OF NON-ENTEROBACTERIACEAE (Pseudomonas aeroginosa)
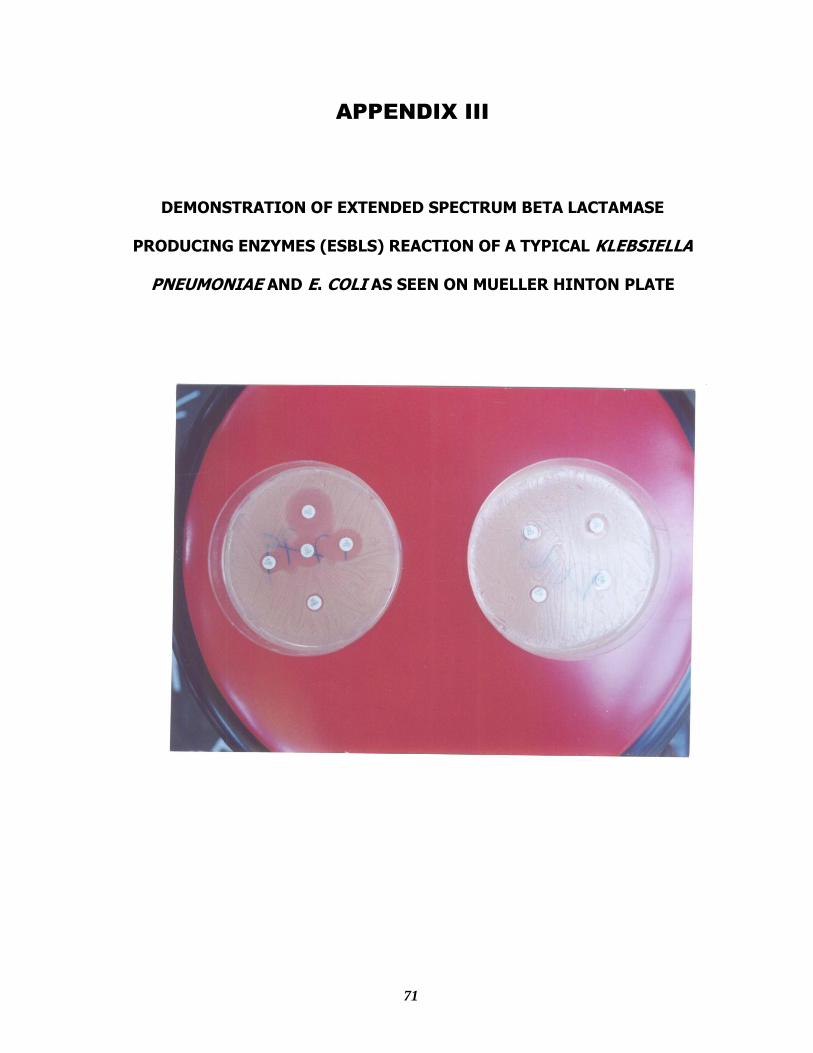
71
APPENDIX III
DEMONSTRATION OF EXTENDED SPECTRUM BETA LACTAMASE
PRODUCING ENZYMES (ESBLS) REACTION OF A TYPICAL KLEBSIELLA
PNEUMONIAE AND E. COLI AS SEEN ON MUELLER HINTON PLATE




















