Latanoprost: A Review of its Pharmacological Properties, Clinical Efficacy and Tolerability in the...
16
Dnuo EvnluATIoN Drugs & Aging 1996 Nov; 9 (5): 363-378 1 | 7y2nxt96lm r'r -q363/508,m/0 O Adis ln?ernolionol Limiteo All rlghts reserved Latanoprost A Review of its Pharmacological Properties, Clinical Efficacy and Tolerability in the Management of Primary Open-Angle Glaucoma and Ocular Hypertension Sanjay S. Patel andCaroline M. Spancer Adis Intemational Limited, Auckland, New Zealand Various sections of the manuscript reviewed by: A. Alm, Department of Ophthalmology, University Hospital, Uppsala, Sweden; LZ. Bito, Department of Ophthalmology, College of Physicians and Sulgeons of Columbia University, New York, New York, USA; R.E Brubaket , Departmmt of Oph thalmology, The Mayo Clinic, Rodrester, Minnesota, US A; F,T. har"mfelilet Casey Eye lnstitute, Oregon Health Sciences University, Portland, Oregon, USA; B. Frisfiiim, Department of Ophthalmology, Link6ping University, Link(ping, Sweden; K.A. McClellaz, Department of Clinical Ophthalmology and Eye Health, Sydney Eye Hospitd, The University of Sydney, Sydney, New South Wales, Australia; H.K. Mishima, Department of Ophthalmology, Hiroshima University School of Medicine, Hiroshima, |apan; S.Nagasubtamanian, Glaucoma Unit, Moorfields Eye Hospital, London, England. Conlents Summory l. Overview of Gloucomo ond Oculor Hypertension 2. Phormocodynomic Properties 2.1 Mechonism of Action 2.2 Oculor Etfects 2,3 Generol Phormocology 3. Phormocokinetic Properties 3.1 Corneol Permeobility . . 3,2 Systemic Absorption 3.3 Metobolism ond Excretion . 4. Clinicol Evoluotion 4.1 Dose-Ronging Studies 4.2 Comporotive Studies . 4.3 Combinotion Theropy 5. Tolerobility 5.1 Conjunctivol Hyperoemio 5,2 lridiol Pigmentotion 5.3 Other Oculor Adverse Events 5.4 Systernic Adverse Events . Dosoge ond Administrotion . Ploce of Lotonoprost in the Monogement of Prirnory Open-Angle Gloucomo ond Oculor Hypertension ,3U , 365 . 366 . 366 . 366 . 368 . 368 368 . 368 . 368 . 369 . 370 , 370 . 371 . 37r . 371 . 373 . 373 . 373 , 373 . 374 6 7
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Latanoprost: A Review of its Pharmacological Properties, Clinical Efficacy and Tolerability in the...

Dnuo EvnluATIoN Drugs & Aging 1996 Nov; 9 (5): 363-3781 | 7y2nxt96lm r'r -q363/508,m/0
O Adis ln?ernolionol Limiteo All rlghts reserved
LatanoprostA Review of its Pharmacological Properties, Clinical Efficacyand Tolerability in the Management of Primary Open-AngleGlaucoma and Ocular Hypertension
Sanjay S. Patel andCaroline M. Spancer
Adis Intemational Limited, Auckland, New Zealand
Various sections of the manuscript reviewed by:A. Alm, Department of Ophthalmology, University Hospital, Uppsala, Sweden; LZ. Bito, Department ofOphthalmology, College of Physicians and Sulgeons of Columbia University, New York, New York, USA;R.E Brubaket , Departmmt of Oph thalmology, The Mayo Clinic, Rodrester, Minnesota, US A; F,T. har"mfeliletCasey Eye lnstitute, Oregon Health Sciences University, Portland, Oregon, USA; B. Frisfiiim, Departmentof Ophthalmology, Link6ping University, Link(ping, Sweden; K.A. McClellaz, Department of ClinicalOphthalmology and Eye Health, Sydney Eye Hospitd, The University of Sydney, Sydney, New South Wales,Australia; H.K. Mishima, Department of Ophthalmology, Hiroshima University School of Medicine,Hiroshima, |apan; S.Nagasubtamanian, Glaucoma Unit, Moorfields Eye Hospital, London, England.
Conlents
Summoryl. Overview of Gloucomo ond Oculor Hypertension2. Phormocodynomic Properties
2.1 Mechonism of Action2.2 Oculor Etfects2,3 Generol Phormocology
3. Phormocokinetic Properties3.1 Corneol Permeobility . .
3,2 Systemic Absorption3.3 Metobolism ond Excretion .
4. Clinicol Evoluotion4.1 Dose-Ronging Studies4.2 Comporotive Studies .
4.3 Combinotion Theropy5. Tolerobility
5.1 Conjunctivol Hyperoemio5,2 lridiol Pigmentotion5.3 Other Oculor Adverse Events5.4 Systernic Adverse Events .
Dosoge ond Administrotion .
Ploce of Lotonoprost in the Monogement of Prirnory Open-Angle Gloucomoond Oculor Hypertension
,3U, 365. 366. 366. 366. 368. 368
368. 368. 368. 369. 370, 370. 371
. 37r
. 371
. 373
. 373
. 373, 373
. 374
67

354 Patel €t Spencer
SurnmarySynopsis
PhormocodynomicProperlies
PhormqcokinelicProperties
Clinicol Evqluo?ion
Latanoprost is an ester prodrug analogue of prostaglandin Fzawhich effectivelyreduces intraocular pressure (lOP) by increasing uveoscleral outflow rather thanaltering conventiorul (trabeculo-canalicular) aqueous outflow. The lOP-loweringeffect of latanoprost lasts for 20 to 24 hours after a single dose, which allows a
single daily dosage regimen.Data from 4 randomised double-masked multicentre studies indicate that a
once daily dose of topical latanoprost 0.005Vo is as effective as timolol 0,5V0 twicedaily in the treatment of patients with primary open-angle glaucoma or ocularhypertension. A number of studies also demonstrate that latanoprost enhancesIOP-lowering effects when applied in combination with other antiglaucomaagents.
Latanoprost is well tolerated with flo, or barely detectable, conjunctivalhyperaemia, and, unlike timolol, is not associated with systemic adverse efficts.However 3 to l}Vo of patients treated with latanoprost 0.005V0 have shown in-creased iris pigmentation after 3 to 4.5 months'treatment.
In summary, the available data show that latanoprost is a potent loP-loweringagent with a number of positive features including a single daily dosage regimen,
a novel mechanism of action that enhances the lOP-lowering effict of contem-porary agents, and a lack of systemic adverse effects. These properties suitablypoise latanoprost for a prominent position in the management of patients withprimary open-angle glaucoma and ocular hypertension.
Latanoprost is an ester prodrug analogue of prostaglandin Fza with high selectivityfor the FP subtype of prostanoid receptors. Unlike contemporary antiglaucornaagents, latanoprost reduces intraocular pressure (IOP) by increasing uveoscleraloutflow, with linle or no alteration of conventional (trabeculo-canalicular) aqueous
outflow and no effects on retinal vasculature or perrneability of the blood-aqueousbarrier.
The reduction in IOP produced by latanoprost is dose-dependent. The IOP-lowering effects after a single dose of latanoprost 0.006Vo last for up to 20 to 24hours. Long term (6 months) application of latanoprost is not associated withmorphological alterations to the ciliary muscle or trabecular meshwork, according toanimal data. Furthermore, other body systems (brain, cardiovascular, respiratory)do not appear to be significantly affected by latanoprost at concentrations up tol0-fold greater than those used clinically for topical application.
Latanoprost is more Iipophilic than its parent prostaglandin and therefore betterable to penetrate the cornea. After uptake by the cornea, latanoprost is cornpletelyhydrolysed; the drug does not seem to be metabolised by other means in the eye.
In monkeys, the highest drug concentrations were observed in the cornea aftertopical administration, the acid of latanoprost was then released from the corneainto the anterior eye. The drug had an elimination half-life of 3 to 4 hours fromthe eye tissues.
Drug that is systemically absorbed has a short plasma elimination half-life.The major metabolic pathway is by p-oxidation and the metabolites are excretedprimarily via the kidneys. Recovery of radiolabelled drug appears to be complete.
Dose-ranging studies show that a once daily topical dose of latanoprost (optimal con-centration of 0.005 or 0.006Vo) effectively produces a decrease in IOP in patients
Gr Adis lnternotionol Limited. All rights reserved Drugs & Aging 1996 Nov; 9 (5)

latanoprost: A Review 355
Tolerobility
with primary open-angle glaucoma or ocular hypertension. Single daily applica-tion of latanoprost is at least as effective as a twice daily dose.
Three of 4long term (3 or 6 months) randomised, double-masked, multicentrestudies indicated that once daily latanoprost 0.005Vo was more effective than
timolol 0.57o twice daily in reducing IOP. A number of clinical studies have also
shown that latanoprost applied in combination with other antiglaucoma agents
produces enhanced IOP-lowering effects.
Data from phase trI clinical studies indicate that topical latanoprost 0.005 Vo onca
daily application is, overall, as well tolerated as timolol 0.5Vo twice daily. Atclinically effective doses, no or a barely detectable increase in conjunctivalhyperaemia was noted in at least gOVo of latanoprost or timolol recipients. Incontrast to timolol, latanoprost is not associated with systemic adverse effects.
On the other hand, increased iridial pigmentation has been noted in 3 to l0%o
of patients after 3 to 4.5 months'continuous treatrnent with latanoprost O.OOSVo.
It occurred only in patients with mixed colouririses (green-brown or bluelgrey-brown); freckles or naevi in the iris were not affected.
Once-daily topical instillation of latanoprost 0.005Vo is the recommended dosage
regimen for the treatment of patients with primary open-angle glaucoma or ocularhypertension. If used in combination with other topical antiglaucoma agents, the
drugs should be instilled at least 5 minutes apart.
Dosoge ondAdministrolion
Latanoprost (fig. 1) is one of a number of ration-ally designed ester prodrug analogues of prosta-
glandin Fzo eGF2q;lt-+l that have been investigated
as potential treatments for primary open-angleglaucoma (POAG) and ocular hypertension.ls-el
Latanoprost is the R component of an approxi-mately equimolar R/S epimeric mixture initiallyidentified as PhXA3 4.lr) The epimeric mixture was
originally evaluated for the treatment of POAG and
ocular hypertension,[10-l2l but later displaced in fa-
vour of latanoprosl.l I'l 3 I
This review describes the pharmacologicalproperties, clinical efficacy and tolerability of top-ically applied latanoprost for the treatment ofPOAG and ocular hypertension.
I. Overview of Gloucomoond Oculor Hyperlension
The terrn glaucorna encompasses a group ofdiseases that share all or some of the followingpathophysiological features: elevated intraocularpressure (IOP), excavation of the optic nerve head,
and loss of visual field (see Lesarl r4l). Glaucoma is
O Adis lnternotionol Limited. All rights reserved
a chronic disorder that, in the majority of patients,
results frorn an imbalance between aqueous humour
Latanoprost
Prostaglandin F.,.
Fig. 1. Structural formulae of prostaglandin F26 dnd latanoprost.
Drugs & Aging 1996 Nov; 9 (5)

Table l. Classification of glaucoma[l4]
Primary glaucoma
Open-angle
Angle closure
Secondary glaucoma
Open-angle
Angle closure
Congenital glaucoma
with pupillary blockwithout pupillary block
pretrabecular
trabecularpost-trElbecular
with pupillary blockwithout pupillary block
production and outflow from the anterior segrnent
of the eye (see Lesarll4l). Broadly, glaucoma can be
divided into open-angle, angle closure and primary,
secondary and congenital glaucoma (see table I fora detailed classificationl I 4l;.
Briefly, POAG, which is diagnosed in =90Vo ofpatients with primary glaucolrs, is bilateral and
insidious in onset (visual acuity remains normal
until the late stage of the disease).[14'ls] It is prob-
ably, at least partly, a consequence of inhibiteddrainage of aqueous humour because of chronic
low-grade partial obstruction of either the trabecu-
lar meshwork or Schlemm's canal (fig. 27.tt4l In
patients with POAG the IOP can rang€ from 25 to
45mm Hg, whereas in healthy eyes normal IOP
is maintained between l0 and 2lmm Hg.tl4'l6l IOP
is usually similar in both eyes but shows consider-
able circadian variation.[l4l Chronic elevation ofIOP may cause optic nerve ischaemia and conse-
quent progressive loss of vision.ll4l
Patients with ocular hypertension have elevated
IOP but normal visual fields and optic discs; this
contrasts with patients with normal-tension
glaucoma (present in > l5Vo of patients) in whom
IOP is normal (<21mm Hg) but there is loss ofvisual field and the optic disc is cupped.ll4'lsl
Ocular hypertension is often regarded as a pre-
glaucoma stage.llzl
Key factors that predispose individuals to
developing glaucoma (for review see Quiglerttsl;include high IOP, family history of glaucoffio,
age>40 yeirs, systemic vascular disease, high degree
of myopia, diabetes, long term topical or systemic
o Adis lnternotiorrol Umited. All rights reserved.
Patel I Spencu
corticosteroid use and ethnicity (particularlyAmericans of African heritage, Russians, Scandi-
navians and the Irish).114'lel
2. Pholmocodynomic ProPerlies
2.1 Mechonism of Action
Latanoprost is a highly selective agonist of the
FP subtype of prostanoid receptors;|201 its affinityfor this receptor is considerably higher than that
for other prostanoid receptors.[2t] Latanoprost, likeits congeners,[22-241lowers IOP by increasing uveo-
scleral outflow, with little or no effect on the con-
ventional aqueous outflow facility.lzst In the nor-
mal eye (fig, 2), outflow of aqueous humour occurs
by filtration through the trabecular meshwork toSchlemm's canal (i.e. conventional or trabeculo-canalicular route) and via uveoscleral outflowthrough the ciliary muscle, suprachoroidal space
and the scl era.176,271 The difference in the outflowrates between the 2 routes is marked: uveoscleral
outflow occurs at0.2 to 0.5 pl/min, compared with1.5 to 1.8 pl/min via the conventional route.[l4l
The process by which latanoprost produces an
IoP-lowering effect (i.e. increasing uveoscleraloutflow) is novel compared with that of existingnonprostaglandin agents used to treat glaucolrls,which act by increasing aqueous hurnour outflowvia the trabecular meshwork or by inhibitingaqueous humour production.[28] The basis forthe precise mechanism of action by which prosta-
glandins decrease IOP remains unclear at present
(see review by Camra5l2el; and the precise pro-
stanoid receptor(s) involved has not been fullyelucidated. Nevertheless, the FP subtype of pro-
stanoid receptors appears to be important as evi-dent from the IOP-lowering effect of latanoprost(section 4).
2.2 Oculor Effects
Most ocular effects of latanoprost in hurnans
parallel those seen with its congeners .1zsl As pre-
viously stated, latanoprost produces an increase
in uveoscleral outflow; an increase from 0.39 (at
baseline) to 0.87 pl/min (p < 0.05) occurred after 8
Drugs & Aging 1996 Nov; 9 (5)

Latanoprost: A Review
days of twice daily application with latanoprost0.006Vo in volunteers.t2sl Latanoprost 0.0O6Vo
twice daily for 5 days increased tonographic out-flow facility (by 24 to 30Vo) in I study (n = 20patients/20 volunteers)t30t but not in another studyof 22 volunteers adrninistered the same dosageregimep.[25] Latanoprost did not affect fluoro-photornetric outflow facility,lz5l which was repre-sented by the ratio of pharmacologically inducedchanges in aqueous flow : changes in IOP. At doses
that effectively reduced IOP, latanoprost also didnot affect retinal vasculature[31] or permeability ofthe blood-aqueous barrier - as indicated by rnini-mal effects on the rate of entry and polarisation offluorescein or aqueous flare intensity.t30l
Latanoprost, like PGFza- I -isopropyl esterls'81 and
PhXA3 4,u21lowered IOP without altering aqueous
flow in volunteers and patients.[2s'30] Placebo-
controlled (contralateral eye) studies in humanswith normotension or ocular hypertension haveshown significant decreases in IOP (by 22 to 25Vo)
after 5 to 8 days of treatment with latanoprost0.006Vo twice daily.l2s'301 Maximal decreases inIOP occurred within the first 2 days of initiatinglatanoprost treatment (as is also the case with pilo-carpinelzzll in patients with POAG or ocular hyper-tension .132'381 The IOP-lowering effect was inde-pendent of the time of application of the agent.[3e'401
Reductions in IOP with latanoprost can last for 20to 24 hours after a single dose '134'36,41I the reason
for this sustained effect is not adequately under-stood, although it can be explained, in part, by thehigh lipophilicity of the prodrug and consequentcorneal trapping of the de-esterified drug (see sec-tion 3. I ).
Anterior chamberCornea
Posterior chamberlris
Conjunctiva
Schlemm'scanal
IExtraocular
muscle
Optic stalk
Fig. 2- Anatomical features of the human eye under normal condiiions (a) and in primary open-angle glaucoma (b). ln the normaleye, aqueous humour (secreted into the posterior chambeo enters the anterior cfiamber through the pupil. ln the anterior chambe(it passes through the trabecular meshwork inlo Schlemm's canal and lrom there inlo the \renous system. ln primary open-angleglaucoma, lhe eye appears anatomically normal but the llow of aqueous humour is obstrucled at the trabeqJlar meshwork orSchlemm's canal, resulling in elevated inlraocular pressure.
cana! ,..-.r-i€ lris
humour flow ift=== Posterior
Ciliary Suspensorybody ligaments
Vitreous bodyOptic
@ Adis lnternotionol Limited. All rights reserved Drugs & Aging 1996 Nov; 9 (5)
367
b Trabecularmeshwork

358
Preliminary data from studies in animals in-dicated that long term apPlication of latanoprost(10 pgleye once daily for 6 months) was not asso-
ciated with morphological alterations in the ciliarymuscle or trabecular meshwork.l42l In contrast,previous studies with PGF2, (administered to
cynomolgus monkeys once or twice daily for <8
days) have indicated morphological changes to the
tissues involved with aqueous inflow/outflow (forreview see Ltitjen-Drecoll & Kaufmanta3l). Vitre-ous concentrations of latanoprost (up to l0 mg/L)did not affect the electroretinogram of rabbit eyes
in vitro,l44l and ocular blood flow wEIS unaffected
by intravenous doses of latanoprost in cynomolgusrnonkeys. t20;
2,3 Generol Phormocology
In cynomolgus monkeys, intravenous doses oflatanoprost (up to 1O-fold greater than those used
topically in clinical practice) did not produce sig-
nificant changes in cardiovascular parameters(blood pressure, cardiac output, heart rate, strokevolume, cardiac work and coronary blood flow) or
respiratory parameters (respiration rate and intra-thoracic inspiratory-expiratory pressure differ-ences).Jzol These doses also had no effect on bloodflow to the brain or splanchnic beds.l2ol
3. Phormocokinelic Properlies
Pharmacokinetic data pertaining to topical and
intravenous latanoprost have been generated using
tritium-labelled samples of the drug. Radioactivitywas determined by liquid scintillation countingand high performance liquid chrornatography withon-line radioactivity detection .145'461
3,1 Corneol Permeobility
Esterified prodrugs of prostaglandins, such as
latanoprost, are more lipophilic than the parent
drug and are therefore better able to penetrate
the cornea.l4T'481 After topical administration of[3H]latanoprost to the monkey eye, the drug was
shown to penetrate the cornea; the cornea showed
the highest concentration of radioactivity (0.6ng
,nol Limited. All rights reserved.
Patel €t Spencn
equivalents lmg tissue). The cornea then appeared
to release radioactivity to the anterior parts of the
eye. Peak concentrations of radioactivity in the
iris, anterior chamber and ciliary body were ob-
served t hour postdose with an elimination half-life from the eye tissues of 3 to 4 hours.l4el
3.2 Systemic Absorption
Drugs applied topically to the eye can enter the
systemic circulation via drainage through the
nasolacrimal duct and absorption from the naso-
pharyngeal mucosa.lsol In 4 healthy volunteerswho received [3H]latanoprost, maximum plasma
concentrations (Cr.*) of 0.6 and l2.51tg equiva-
lents/L were observed after topical (3pg) and intra-venous (2lOpg) administration, respectively.146l
Time to Cr.* (15 minutes) was independent of the
route of admi nistration.l46l
Latanoprost was 90Vo bound to plasma proteins
in the first few minutes after intravenous adminis-tration, although this decreased over time (60Vo 2
hours postdose).t+6t
3.3 Metobolism ond Excretion
Once partitioned into the cornea, latanoprostundergoes l00%o ester hydrolysis,t4s l probably
mostly in the corneal epithelium.l4el Latanoprost does
not appear to be subject to further ocular meta-
bolism, and, unlike other related phenyl analogues,
it is not a substrate for l5-hydroxyprostaglandindehydrogenase. t45l
Initial (tvrd and terrninal (tvril plasma elimina-tion half-lives of total radioactivity were 6.6 and
69 minutes, respectively, after 4 healthy volunteers
received a 2l01tg intravenous dose of [3H]-latanopys5l.la6l Radioactivity in plasma samples
was undetectable t hours after intravenous and 6hours after topical (3pg) doses .1461 In monkeys,
the main systemic metabolic pathway was by p-
oxidation in the liver.t2ol In humans, excretion oc-
curred primarily via the kidneys (88Vo and 97Vc
recovery of urinary radioactivity after topical and
intravenous doses, respectively), with some faecal
excretion (15 and l6Vo, respectively;.1+61
Drugs & Aging 1996 Nov; 9 (5)

Latanoprost: A Review 369
Table ll. Topical latanoprost (L) treatment in patients with primary open-angle glaucoma or ocular hyperlension: randomised double-masked
dose-ranging andor placebo-conttolled studies
Reference No. of Treatment Mean diumal intraocular pressure (mm Hg)
patients (duration; wk) [percentage change from baseline]
baseline time atter treatment initiation (wk)
24 12
Atm er at.l3sl 15 LO.OO350/" bid (4) 23.O 16.5" [J28] 17.9e11221 17.3" [J251
1 s L O.OO5% bid (4) 23.6 17 .Oa lJ28l 18.3a p22l 17 .8a [J2s]1 5 L 0.011 5olo bid (4) 23.0 16.4a lJ29l 17 .Oa tJ26l 17 .4a p24J
1s P (4) 23.4 n.8a f4 24.8a [16] 23.8a [t2lAtm er 61.1501 25 L 0.006% onb 1te; 24.8
2s L 0.006% bidb (12) 24.9
coakes et at.ts2l p L 0.00125"/o on (2) 23.4 20.4 tJ13l 19.4 [J17]'11 L O.OO25% on (2\ 24.1 18.3 [J24] 1e.1 [J21]'12 L O.OO5% on (2) 23.9 17.8 tJ26l 17.6 [JZe1't10 P (2) 23.e 21 .s tJsl 22s Il7)
Lusky s1 6;.tssl 50 totalc L 0.0015% bid (3) 23.8
L 0.00s% od (3) 25.7
L 0.005% od (3) 18.2e
after L 0.001 5% bid (3)
L 0.001s% bid (3) 17.2s
after L 0.005% od (3)
Nagasubramanian 20 L 0.006% od (2) 24.8 16.2 [J35]"' 1 5.9 [J36]"'et al.lsl
1 9 L 0.006% bid (2) 25.0 17.8 [J29].., 18.0 [J28]"',10 P (21 25.3 24.0 tJsl 23.6[J7]
Rdcz er at.l36l 9 L 0.006% on (5 days) 25.4 19h [J25J"6 P (5 days) 25.2 23.sh [u]
a Data rellect changes based on nlues al 8am and not mean diumal values.
b Topical timolol 0.5of twice daily and latanoprost treatmenl were applied concomitantly in all patients.
c Crossover study design.
d Measured value at swk after inithting treatmenl.
e Mean intraocular pressure betore latanoprost 0.0o5o/. administration.
I Measured value at 3wk afrercrossover.
g Mean intraocular pressure belore latanopost 0.0015% administration.
h Measured value at 5 days after initiating treatrnent.
Abbreviationsardsyrnbors.'bkl=twicedaily; od=oncedaily; on=oncedaityintheevening(night); P=placebo; T=timolol; J=decrease;1=increase;'p<O.O5vsplacebo;"p<0.01 rGcomparatorgroup(Almetal.lsl;6rbaselinevalue(R6czetal.tq); "'p<O.OO1 vsplacebo;t p = 0.045 tzs L 0.001250/o group.
4. Clinicol Evoluotion 4.1 Dose-Ronging Studies
A number of studies have evaluated topical la- Dose-ranging studies (n S 60 patients per study)
tanoprost for the treatment of patients with POAG generally showed that latanoprost, at concentrations
or ocular hypertension. The patient population in ranging from 0.00125 to 0.01157o, effectively pro-
these studies comprised a mix of those with either duced significant decreases in IOP compared withPOAG or ocular hypertension. Diurnal IOP was placebo (table II). The reduction in IOP was dose
defined as the mean IOP over the day based on dependent,tal'5r-s3l and the optimal IOP-loweringvalues obtained at 8 or 9am, l2 noon or lpm and 4 concentration was 0.005 or O.N6%.or 5pm. Goldmann applanation tonometry was used A once daily dose of latanoprost was at leastto measure IOP. as effective as a twice daily dose without any
16.8 [J32] 15.7 [J371"18.1 lJ27l 18.0 [J281
18.2d 1!Zt7n.2d tJffilfi st llzzl
19.1, IJ26I
o Adis lniernotionol Limited. Allrighh reserved, Drugs & Aging 1996 Nov; 9 (O

370 Patel & Spencu
diminution in the IOP-lowering effect for up to 3
months (table II). The reason for this paradoxical
but consistent and beneficial observation is unclear
at present.
4,2 Comporotive Studies
Four long term (3 or 6 months) randomised,
double-masked, multicentre studies (total n = 1013
patients) have compared the efficacy of latanoprost(0.005Vo single daily application) versus tirnolol(0.5Vo twice daily) in patients with IOP >20mm
Hg.ts6-sel Three trials measured diurnal IOP.l57-5el
the remaining trial measured IOP at garn only.ts6t
Both agents reduced IOPfrom baseline by 27 to35Vo
(latanoprost) and l9 to 33Vo (timolol) throughoutthe treatment periods (fig. 3).t56-5el In 3 of these
studies, Iatanoprost produced a greater decrease in
mean IOP than timolol at 3 or 6 months (p <
0.001).t56'sz'5el Although the fourth study did not
find the difference between the treatments sig-
nificant at 6 months, latanoprost was significantlymore effective than timolol at 12 and l8 weeks
(fig. 4).ts8l Latanoprost applied in the eveningproduced a significantly better response than
morning application (p < 0.0011.ts21
Whereas the IOP-lowering effect of latano-prost was unaffected by variables such as gender,
age, race or diagnosis (POAG vs ocular hyper-
Alm et al.tszl Watson et al.[sa] Camras et a!.lsel Mishima et al.tsel
\o,s\,t\,sn\ o"^t',d s,$l,tto \,.,s\--$o\
E 10
ooECL
(u ,-.EEEe7=_=E 20kxoltrE;eooE0)cE 30
tr Latanoprost om
I Latanoprost on x 3mothen om x 3mo
I Latanoprost om x 3mothen on x 3mo
I Latanoprost on
E Timolol bid
Fig. 3. Comparative efficacy ol latanoprost and timolol. Data {rom 4 randomised double-masked multicentre studies showingpercentage reductions in intraocular pressure 6tt97 $tsol or 6ls7-ssl months'treatmenl wiih eiiher latanoplost 0.005% once dailyor timolol 0.5% twice daily in evaluable patients with primary open-angle glaucoma or ocular hypertension. All reduciions were
significant ys baseline. Abfevhtions: bid = twice daily; om = once daily in lhe morning; on = once daily in the evening; ' p < 0.001
vs timolol.
(l Adis lnternotionol Limited All rights reserved Drugs & Aging 1996 Nov; 9 (5)

Latanoprost: A Review 377
tension;,t57-5el Watson et al.t581 noted that timololproduced greater reductions in IOP in men (9.0vs 7.lmm Hg in women; p < 0.01) and in patients
with POAG (9.4 v.r 7.lmm Hg in patients withocular hypertension; p < 0.01). Iris colour did notaffect the IoP-lowering effect of timolol or oflatanoprost in 2 studies,[s7'5el whereas a thirdstudy noted that patients with hazel eyes had abetter response than those with blue- or green-grey
eyes (9.3 v.r 8.0mm Hg reduction in IOP withlatanoprost; p = 0.006).t581
4.3 Combinotion Theropy
Six clinical studies (n S 50 patients per study)have examined the effects of topical latanoprostapplied in cornbination with other topical or oralantiglaucoma agents (table III). Monotherapywas administered for about 1 or 2 weeks and was
followed by combination therapy for the same re-spective time frames (table III). At the end of themonotherapy period, there was a trend towards a
greater reduction of IOP with latanoprost than withdipivefrine, pilocarpine or timolol (although thestatistical significance of this was not stated). Atthe end of the combination therapy period, IOP had
decreased even further (relative to baseline) thanafter monotherapy (table III). Thus, these datashow that latanoprost can be administered in com-bination with other antiglaucoma agents to pro-duce enhanced lowering of IOP.
5. Tolerobility
Previous investigations of topical prostaglandin
analogues have identified agents with unaccept-able adverse effects .l't,e,22,63-6sl The prototypicalagent, PGF2q- I -isopropyl ester, was associatedwith initial increases in IOP, photophobia, ocularirritation and conjunctival hyperaemia.l5'61 Al-though latanoprost, which is also an isopropyl ester(fig. 1), has been associated with some of these
adverse effects, it is better tolerated than its analo-gous predecessors. Overall, latanoprost was welltolerated in 4 pivotal phase III clinical studies com-paring latanoprost with timolol.ls6-sel
nol Limiled. All rights reserved
25
212 18 26
Duration of treatment (wk)
Fig. 4. lntraocular pressure response profiles with latanoprostand timolol. Comparative profiles of intraocular pressure re-sponse (9am measurements) to latanoprost 0.005% (oncedaily) and timolol 0.5% (twice daily) over 6 months'treatment inpatients with primary open-angle glaucoma or ocular hyper-tension (n = 268).ts8l Symbols: ',p .0.05; " p .0.02 vstimolol.
5. I Conjunctivol Hyperoemio
Barely detectable, or no, conjunctival hyperaemiawas noted among patients treated with topical la-
tanOprOSt adminiStered alOnel I 3'30'32-36,38,41,5 1,55.57-591
or in combination with dipivefrinel6ol or timo-161.1331 Hyperaemia was graded using visual ana-
logue scales or by comparisons with standard
baseline photographs; scores were defined by an
arbitrary scale ranging from 0 to 3 with 0 corre-
sponding to no hyperaemia and 3 to severe hyper-
aemla.
The mean hyperaemia score with latanoprost
treatment, based on maximal hyperaemia observed
during the day,was predominantly <0.5.ts7-5el
The incidence of conjunctival hyperaemia was
most pronounced within the first 2 days of initiat-ing latanoprost therapy, and diminished withtime (after 2 to 4 weeks).134'lsl Although the inci-dence of hyperaemia was greater with latanoprost
than with timolol (p < 0.001),1581 the degree ofhyperaemia was mild. A comparison of maximumhyperaemia scores at baseline and at 6 months in 2studies showed that, in at least 90Vo of patients,
6-E20E
o
E lsoct(U
3 10o(U
s5
Drugs & Aging ]996 Nov; 9 (5)
372 Patel E Spencer
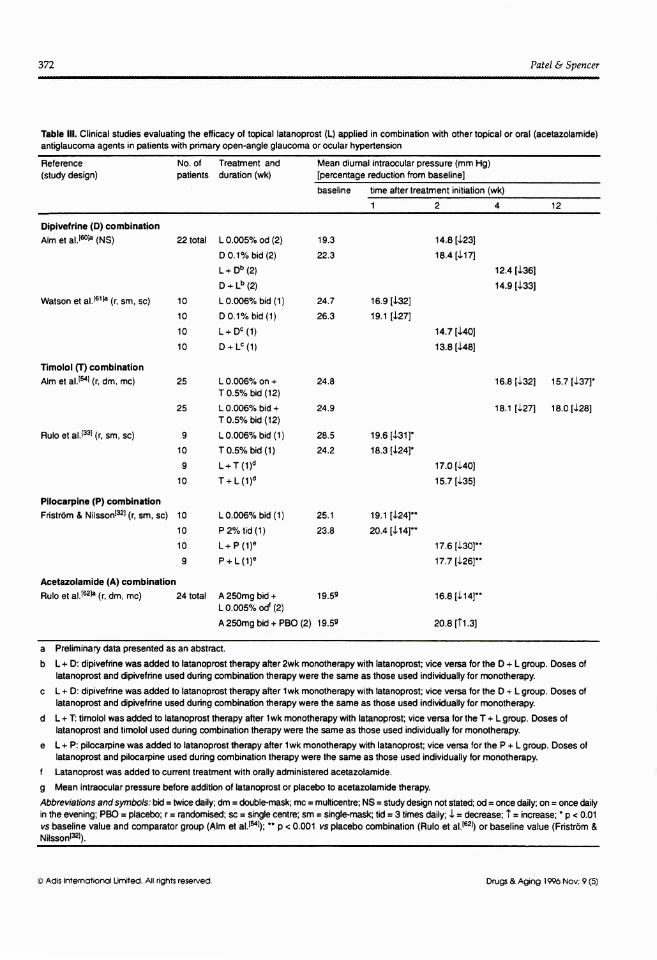
Table lll. Clinical studies evaluating the efficacy of topical latanoprost (L) applied in combination with oihertopical or oral (acehzolamide)antiglaucoma agenls in patients with primary open-angle glaucoma or ocular hypertension
Reference No. o, Treaunent and Mean diumal intraocular pressure (mm Hg)(study design) palients duration (wk) [percentage reduction lrom baseline]
baseline time after treatment initiation (wk)
2412
Dipivefrine (D) combinationAtm er 31.te0F (NS) 22 totat L 0.005o/o od (2) 19.3
D 0.1 y. bad (2) 22.3
t+ Db (e)
o+tb(z)Watson et at.l61F (r, sm, sc; 10 L 0.0060/o bid (1) 24.7 16.9 [J32]
10 D 0.1% bid (1) 26.3 1e.1 lL27)
10 L+ Dc (1)
10 D+Lc(1)
Timolol (T) combinationAlm et 31.t5ol (r, dm, mc) 25 L 0.0060/. on + 24.8
T O.5% b.d (12)
25 L 0.0060/o bid + 24.9
T O.5o/o bid (12)
Rulo et al.lsl (r, sm, sc) I L 0.006o/o bid (1) 28.5 19.6 [J31]'10 T o.s% bid (1 ) 24.2 18.3 [J24]'
9 L+T(l)d10 T+L(1)d
Pilocarpine (P) combination
Fristrom & Nilssonlsz) (r sm, sc) 10 L 0.0O60/o bid (1) 25.1 19.1 [J24J"10 P 2Yo rid (1) 23.8 20.4 [J14J"10 L+ P (1)e
9 P + L (1)e
Acetazolamide (A) combinationRulo
"1 ";.t62la (r, dm, mc) 24 total A250mg bid + 1g.Se
L 0.005o/o oot (e)
A 250m9 bid + PBO (2) 19.5s
14.8 [J23]
18.4 tJ14
14.7 tJ40l
13.8 [J48]
17.0 [J4o]
15.7 tJ3sl
17.6 [J3Ol.,
17.7 lL26l"
16.9 tJ 14J"
20.8 tTl.3I
12.4 [J361
14.s [J33l
16.8 [J32] 1 s.7 [J371',
18.1 ll27l 18.0 lJ28I
a Preliminary data presented as an abstract.
b L + D: dipivelrine was added to latanopK,st therapy after 2wk monotherapy with latranoprost; vice v€rsa lor the D + L group. Doses ofhtanopost and dipivefrine used during combination therapy were the same as those used indivilually lor rmnotherapy.
c L + D: dipivefrine was added to latanoprost lh€rapy after lwk monotherapy with htanoprost; vice \rersa lor the D + L group. DosBs oflatanoprost and dipivetrine used during combination therapy were the same as lhose used indivi.Jually lor nonotherapy.
d L + T timolol was added to latanopiost therapy after l wk monotherapy with latanoprost; vice versa for the T + L grcup. Doses ollatanoprosl and timolol used dudng combinalion therapy were the same as those used individually lor monotherapy.
e L + P: pilocarpine was added to latanoprost therapy after l wk monotherapy whh latanoprost; vice versa lor the P + L group. Doses ollatanoprosl and pilocarpine used during combinalion lherapy were the same as those used individually lor rnonotherapy.
f Latanopost was added lo curent treatment with orally administered acetazolamide.
g Mean intraocular pressure betore addition of latianoprost or placebo to acelazolamide therapy.
Abbreiations andsynbols: bil = twice daily; dm = double-mask; mc = multicentre; NS = study design not stat€d; od = once daily; on = once daiyintheevening; PBO=placebo; r=randomised;sc=singlecentre; sm=singlemask;lid=3timesdaily; J=decrease; 1=increase;'p<0.01vs baseline value and compaEtor gKrup (Alm et al.lgl;; " p < O.OOI r4s placebo combinalion (Rulo et al.l62f or baseline value (Fdstr6m &Nilssonlsl).
@ Adis lnternotionol Limited. All rights reserued Dru$ & Aging 1996 Nov; 9 (5)

Latanoprost: A Review 373
there was no or a barely detectable increase inhyperaemia with both latanoprost and timolol(fie s).
5.2 lridiol Pigmentotion
Topical latanoprost therapy (0.005Vo appliedonce daily) was associated with increased iridialpigmentation in 3 to l}Vo of patients after 3 to 4.5
months' continuous treatment in randomiseddouble-masked rnulticentre stud1.t.l57-sel The
increase in iridial pigmentation occurred onlyin patients whose eyes were already of mixed col-ours (i.e. green-brown or blue/grey-brownl.[57'581However, freckles and naevi in the iris were unaf-fected; i.e. they did not change shape or colourduring treatment. [ 57-5e]
No other pharmacological agent has been re-
ported to produce changes in iris pigmentation.lssl
The precise mechanisrn of this effect with latano-prost is not adequately understood, althoughstimulation of melanin synthesis rather than pro-
liferation of melanocytes is thought to be a keycomponent.t5T-5el Long term follow-up studies are
required to establish whether or not this increasedpigmentation is an irreversible effect.
5.3 Other Oculor Adverse Events
Latanoprost 0.0O5Vo once daily was as welltolerated as timolol 0.5 Vo twice daily with respectto other ocular adverse events: of the 3 phase IIIstudies to perform a statistical analysis, none re-ported a significant difference in the ocular ad-
verse events between the 2 groups throughout the 6
months of treatment.lsT'sel These events includedpunctate keratopathy, dry eye sensation, blurredvision, excessive tearing, ocular or eyelid discom-fort, burning, stinging, itching and foreign bodysensations.l5T-5el
Although a few cells in the anterior chamberand slight flare were detected rarely,l35's+'s6'581
neither latanoprost nor timolol caused significantinfiltration of cells into the anterior charnber orsignificant changes in aqueous flare intensity orpupillary diametsl.[57-5el Changes in aqueous hu-mour protein concentrations after either Ia-
nol Limited. All rights reserved.
tanoprostll3'30's3l or timolslts3l ffeatment were notsignificantly different from those at baseline. Visualacuity or refraction were not affected by latano-prost or timolsl.tsT-sel Worsening of the visual fieldor significant changes in laboratory tests (haema-
tology, clinical chemistry or urinalysis) after la-
tanoprost therapy have not been reported either.Latanoprost, like PhXA34, has not been associatedwith elevation of IOP.
5.4 Systemic Adverse Events
Topical latanoprost had little effect on heart rate
or systemic blood pressure in patients.[33-35'56-5el
In contrast, topically applied timolol resulted inreduced mean heart rate (by 3 to 4 beats/min; p <
0.05 vr pretreatment)l'7'sel and mean systolicblood pressure in one study (by 3mm Hg; p < 0.05vs baseline at 3 monthslsell but not in another.ts7l
A number of other systemic adverse events such as
upper respiratory tract infection, musculoskeletalpain, eczemalallergy were reported with both treat-ments, but these effects did not appear to be relatedto the drugs.
Respiratory function, heart rate and systolic and
diastolic blood pressures were not adversely af-fected in patients with asthma who received 2 to20ttg (total doses) of latanoprost.l66)
6. Dosoge ond Administrolion
Latanoprost 0.O05Vo is the recommended con-centration for once daily topical (eye) instillationin patients with POAG or ocular hypertension. Itcan be used in combination with other topicalophthalmic agents to reduce IOB although the drugs
must be instilled at least 5 minutes apart.
7. Plqce of Lolonoprosl in theMonogement of Pdmory Open-AngleGlqucomo ond Oculor Hyperlension
Although glaucoma can develop at any age,l67'6al
it is most common in the elderly population (up
to lU%o of persons aged >75 years).[l6.6el It is
estimated that glaucoma may remain undetected inup to 507o of individuals.lT0l Once the diagnosis of
Drugs & Aging 1996 Nov; 9 (5)

Patel €t Spencer
BD
Alm et al. tszl
glaucoma has been confirmed, topical drug ther-apy is usually the first-line option; the aim of thistreatment is preservation of visual function bymanaged control of IOP.I l6'2E,71 I At present, topicalp-adrenergic antagonists (e.g. timolol, carteolol) are
the agents of first choice for the management ofPOAG and ocular hypertension,l l6'28'721 with topi-cal adrenergic agonists [e.g. epinephrine (adrenaline)
and dipivefrinel and parasympathomimetic agents(e.g. pilocarpine, carbachol) as second-line agent5.l72l
Oral carbonic anhydrase inhibitors (e.g. acetazol-amide) and systernic hyperosmolar agents (e.g.
O Adis lnternotionol Limited. All rights reserved.
I Latanoprost
Timolol
BD MiId
Watson et al. tssl
mannitol) are also used for the treatment of glau-coma, though the latter type are used only for acute
treatment.l | 6'2E,721 Recently, topically active uno-prostonel65.73l (a PGFza derivative) and dorzol-amidett4l (a topical carbonic anhydrase inhibitor)have been approved for clinical use .1721
Patients refractory to topical drug therapy orwho are persistently poorly compliant require la-ser therapy (trabeculoplasty) or surgical interven-tion (trabeculectomy).f 16'71'721 In most patientswith POAG or ocular hypertension, the prognosisis good; progression to blindness is rare with early
Flg. 5. Degree of increase in conjunctival hyperaemia with topical latanoprost or limolol treatment in palienis with primary open-angleglaucoma or ocular hypertension. Percentage of patients with an increase in maximum conjunctival hyperaemia versus baselineexamination after 6 months'treatment wilh latanoprost 0.005% once daily (n = 175Js7) n = 138t$l) or timolol 0.5% iwice daily (n =821sz1n = 131l5El). Abbteviations: BD = barely detec{able increase; MM = mild to moderale increase; Nl = no inciease.
Drugs & Aging 1996 Nov; 9 (5)
374
A60soC.o(uCL
ociz
40

Latanoprost: A Review 375
diagnosis, adequate and closely monitored drugtreatment, and good patient compliance.llal
In recent years, this traditional approach to the
management of glaucoma has been re-examined
because conventional treatment addresses justone (elevated IOP) of the several risk factors, al-
though it is the only risk factor amenable to treat-
ment.lte'7s'761 More importantly, adequate controlof IOP may not necessarily confer a protectiveeffect against underlying pathological processes,
since there is no long term proof of a cause and
effect relationship. t72'7sl Preliminary data indicatethat glaucoma may also be associated with elevated
levels of excitatory amino acids (such as gluta-rnate) in the eye.lle)
Latanoprost is an effective IOP-lowering agentwith a clinical profile that compares favourablywith that of other antiglaucoma agents (section 4).
The beneficial effect of latanoprost is evident at
considerably lower concentrations (0.005 or0.006Vo) than those required with other topicalagents (e.g . 0.25 to ZVo for p-adrenergic antago-
nists, 0.5 to ZVo for adrenergic agonists, and 0.03to 4Vo for parasympathomimetic agents). Althoughcomparative clinical data are limited at present,
further (long term) studies comparing latanoprostmonotherapy with other established and more re-cently introduced antiglaucoma agents should en-
able consolidation of its place among these agents.
Four large multicentre studies (n > 180 per study)have already shown that latanoprost comparesfavourably with timolol.
A major advantage of latanoprost is its longduration of action, which means that it can be ad-
ministered as a single daily dose. In contrast, mostestablished topical antiglaucoma agents requireat least twice daily application, although a newforrnulation of timolol has been developed thatcan be administered once daily. Another advantage
of latanoprost is its novel mechanism of action(section 2) which means that combination therapyallows more effective control of IOP. Neverthe-less, studies of latanoprost administered in combi-nation with other new agents (e.9. dorzolamide) are
awaited.
O Adis lnternotionol Limited All rights reserved,
Despite the pharmacological advantages and
favourable clinical profile of latanoprost, some un-certainty has been expressed about the long term
effects of topi c al pros tagl and i ns . l7 s'1 7 ) S pec i fi c al I y,
these are the long term effects of chronic increases
in uveoscleral outflow, effects on chorioretinal cir-culation or episcleral venous pressure and, moreimportantly, the overall effect on the glaucomatousproces s.I7s,77l Comparative long term studiesshould help address some of these concerns.
The selectivity of latanoprost has resulted ina marked improvement in tolerability over that ofits antecedents (see AlmtT8l and otherstle-9t I for an
overview of the historical development of prosta-glandins as IoP-lowering agents). It is as well tol-erated as tirnolol, despite its unusual and uncom-mon effect of increasing iris pigmentation inselected populations during long term (6 months)studies (section 5.2). Although latanoprost, likeall other topically applied ophthalmic drugs, isabsorbed into the systemic circulation (section 3),even long term application of this agent has not
been associated with adverse systemic effects. Thismay be due, in part, to the extremely small arnountof active agent applied to the eye and to its very
effective renal excretion. This profile sharplycontrasts with that of topical p-adrenergic antago-nists (which can precipitate respiratory and/orcardiovascular complications and cause mentaland physical lethargy and erectile dysfunction), ad-
renergic agonists (which can induce tachycardiaand allergic reactions, mydriasis and pigmented
corneal and conjunctival deposits), parasympatho-
mimetic agents (which can cause pupillary miosis,reduced vision and myopia) or carbonic anhydraseinhibitors (which can cause paraesthesia, uretero-lithiasis, mental and physical lethargy and erectiled Ysfuncti on ) .l
t 6'28'7 2' 8 2'83 I
In conclusion, latanoprost is a potent IOP-lowering agent with key favourable features: a
single daily dosage regimen that produces a highlyeffective IOP reduction around-the-clock; a novelmechanisrn of action that facilitates enhanced IOP-lowering effects in combination with other agents;
and a tolerability profile that is likely to be superior
Drugs & Aging .l996
Nov; 9 (5)

375
to that of timolol with regard to systemic adverse
effects. Thus, although the long term effects oflatanoprost are unknown, the available data forthis drug point towards its prominence in the man-
agement of patients with POAG and ocular hyper-
tenston.
Referencesl. Stjernschantz J, Resul B. Phenyl substituted prostaglandin
analogs for glaucoma treatment. Drugs Future 1992 Aug; 17:
69t-7042. Resul B, Stjernschantz J. Structure-activity relationships of
prostaglandin analogues as ocular hypotensive agents. CurrOpin Ther Pat I 993;3 (6): 781'95
3. Resul B, Stjernschantz J, No K, et al. Phenyl-substituted prosta-
glandins: potent and selective antiglaucoma agents. J Med
Chem 1993 Jan; 36 (\:2a3-84. Liljebris C, Sel6n G, Resul B, et al. Derivatives of l7-phenyl-
18,1g,2Q-trinorprostaglandin Fzcr isopropyl ester: potential
antiglaucoma agents. J Med Chem t995; 38:289'3045. Villumsen J, Alm A. Prostaglandin F2s'isopropylester eye
drops: effects in normal human eyes. Br J Ophthalmol 1989;
73:419-266. Villumsen J, Alm A, S6derstr6m M. Prostaglandin F2s'
isopropylester eye drops: effects on intraocular pre.ssure in
open angle glaucoma. Br J Ophthalmol 1989; 73:975'97. Camras CB, Siebold EC, Lustgarten JS, et al. Maintained re-
duction of intraocular pressure by prostaglandin Fz61- l -isopro-pyl ester applied in multiple doses in ocular hypertensive and
glaucoma patients. Ophthalmology 1989; 96: 1329-36
8. Kerstetter JR, Brubaker RF, Wilson SE, et al. ProstaglandinFtl-isopmpylester lowers intraocular pressure without de-
creasing aqueous humor flow. Am J Ophthalmol 1988: 105:
30-49. Lee P-Y, Shao H, Xu L, et al. The effect of prostaglandin F2c
on intraocular pressure in normotensive human subjects.
Invest Ophthalmol Vi.s Sci 1988 Oct; 29 (10): A7a-710. Camras CB, Schumer RA, Marsk A, et al. Intraocular pressure
reduction with PhXA34, a new prostaglandin analogue, inpatients with ocular hypertension. Arch Ophthalmol 1992
Dec; I l0: 1733-8
I l. Villumsen J, Alrn A. PhXA34 ' a prostaglandin F2 alpha
analogue. Effect on intraocular pressure in patients withocular hyperten.sion. Br J Ophthalmol 1992 Apr: 76: 214-7
12. Alm A, Villumsen J. PhXA34, a new Potent ocular hypotensive
drug. A study on dose-response relationship and on aqueous
hurnor dynamics in healthy volunteers. Arch OphthalmolI 99 I Nov; 109: I 564-8
13. Hotehama Y Mishima HK. Clinical efficacy of PhXA34 and
PhXA4l, two novel prostaglandin Fza:isopropyl ester ana-
logues for glaucorna treatment. Jpn J Ophthalmol 1993:37(3):259-69
14. Lesar TS. Glaucoma. In: DiPiro JT, Talbert RL. Hayes PE, et
al., editors. Pharmacotherapy: a pathophysiologic approach.
Znd ed. Norwalk, CT: Appleton & Lange, 1993: 1363-76
15. Tucker JB. Screening for open-angle glaucoma. Am Fam Phy-
sician 1993 Jul; 48: 75-8016. Capino DG, Leibowitz HM. Glaucoma: screening. diagnosis,
and therapy. Hosp Pract 1990 May; 25:73'9117. lay JL. The management of patients with glaucoma. Prescr J
1989 Aug; 29: 124-31
@ Adis lnternofionol Limited. All rights reserued.
Patel & Spencer
18. Quigley HA. Open-angle glaucoma. N Engl J Med 1993 Apr;328 (15): 1097-106
19. Dreyer EB. Preserving eyesight with foresight. Harvard Health
Lett 1994 Oct; 19: 4'620. Stjernschantz J, Sel6n G, Sjtiquist B, et al. Preclinical pharma-
cology of latanoprost, a phenyl-substituted PGFza analogue.
In: Samuelsson B et al., editors. Advances in prostaglandin,
thromboxane, and leukotriene research. v.23. New York: Ra-
ven Press Ltd, 1995:513-821. Karlsson M, Sel6n G, Stjernschantz J, et al. Receptor profile of
PhXA4l, a new phenyl substituted prostaglandin ester [ab-stract no. I lJ. Proceedings of the lOth International Congress
of Eye Research; 1992 Sep; Stresa, Itdy, 155.
22. Giuffrd G. The effects of prostaglandin Fzc in the human eye.
Graefes Arch Clin Exp Ophthalmol 1985; 222 (3):1394123. GabeltBT, Kaufman PL. Prostaglandin F2q, increases uveoscle-
ral outflow in the cynomolgus monkey. Exp Eye Res [989;49:389-402
24. Nilsson SFE, Samuelson M, Bill A, et al. Increised uveoscleral
outflow as a possible mechanism of ocular hypotension
caused by prostaglandin Fzo-l-isopropylester in the cyno'molgus monkey. Exp Eye Res 1989; 48:7O7-16
25. Toris CB, Camras CB, Yablonski ME. Effects of PhXA4l. a
new prostaglandin F2 analog, on aqueous humor dynamicsin human eyes. Ophthalmology 1993 Sep; 100: 1297'304
26. Bill A. Conventional and uveo-scleral drainage of aqueous
humour in the cynornolgus monkey (Macaca irus) at normaland high intraocular pressures. Exp Eye Res 1966; 5:45-54
27. BillA. Uveoscleral drainage of aqueous humor: physiology and
pharmacology. In: Bito LZ, Stjernschantz J, editors. The oc-
ular effects of prostaglandins and other eicosanoids. v.312.New York: Alan R Liss Inc., 1989: 417'27
28. McClellan K. Topical eye preparation.s: optimum use. CurrTherI995 Jan; 36: 6l-6
29. Ctmras CB. Mechanism of the prostaglandin-induced reductionof intraocular pressure in humans. In: Samuelsson B et al.,
editors. Advances in prostaglandin, thromboxane, and leuko-
triene research. v. 23. New York: Raven Press Ltd, 1995:
5t9-2530. Ziai N, Dolan JW, Kacere RD, et al. The effects on aqueous
dynamics of PhXA 41, irnew prostaglandin Fza analogue, after
topical application in normat and ocular hypenensive human
eyes. Arch Ophthalmol 1993 Oct; I I l: l35l-83 I . Rulo A, Greve E, Hoyng P, et al. A study of the effect of latano-
prost on the intraocular pressure and retinal vruculature inpseudophakic patients [abstract no. 1059]. Proceedings of the
Association for Research in Vision and Ophthalmology, 1994
May l-6; Sarasota, Florida, USA.
32. FristrOID B, Nilsson SEG. Interaction of PhXA41, a new pros'taglandin analogue, with pilocarpine. A study on patients withelevated intraocular pressure. Arch Ophthalmol 1993 May;lll: 662-5
33. Rulo AH, Greve EL, Hoyng PF. Additive effect of latanoprost,a prostaglandin F-2q analogue, and timolol in patients withelevated intraocular pressure. Br J Ophthalmol 1994 Dec: 78:
899-90234. Nagasubramanian S, Sheth GP, Hitchings RA, et al. Intraocular
pressure-reducing effect of PhXA4l in ocular hypertension:
comparison of dose regimens-. Ophthalmology 1993 Sep; 100:
1305-ll35. Alm A, Villum.sen J, Tdrnquist P, et al. Intraocular pressure-re-
ducing effect of PhXA4l in patients with increa"sed eye pres-
sure: a one-month study. Ophthalmology 1993 Sep; 100:
t3t2-1
Drugs & Aging 1996 Nov; 9 (5)

Latanoprost: A Review 377
36. Rdcz P, Ruzsonyi MR, Nagy ZT,, et al. Maintained intraocularprqssure reduction with once-a-day application of a new pros-
taglandin F2 analogue (PhXA4l). An in-hospital, placebo-
controlled .study. Arch Ophthalmol 1993 Muy; I I l: 657-61
37. Alm A, Villumsen J, Ttirnquist P, et al, lntraocular pressure
reducing effect of PhXA4l in ocular hypertensive patients -
a placebo controlled double musked dose finding study [ab-stract no.27731. Proceedings of the Association for Research
in Vision and Ophthalmology Meeting; 1992 May 3'8;Sua.sota, Florida, USA.
38. Kjellgren D, Douglru D. Mikelberg FS, et al. The short-timeeffect of latanoprost on the intraocular pressure in normalpressure glaucoma. Acta Ophthalmol Scand 1995; 73:233-6
39. Kiuchi Y Takamusu M, Mishima HK. PhXA4l, a prostaglan-
din Fzo analogue reduced the intraocular pressure (lOP) inhuman volunteers during day and night [abstract no.4273431.Proceedings of the Association for Research in Vision and
Ophthalmology; 1994 May l-6; Sarasota, Florida, USA.40. Rdcz P, Ruzsonyi MR, Nagy Tl, et al. Around+he-clock in-
traocular pressure reduction with once-daily application oflatanopro.st by itself or in combination with timolol. Arch
Ophthalmol 1996 Mar; ll4:268-7341. Hotehama Y, Mishima HK, Kitazawa Y, et al. Ocular hypoten-
sive effect of phXA4l in patients with ocular hypertension orprimary open-angle glaucoma. Jpn J Ophthalmol 1993: 37(3):270-a
42. Svedbergh B. Forsberg I. A morphological study on the effectsof chronic administration of latanoprost (LP) on the ciliarymuscle and trabecular meshwork in monkeys [abstrirct no.
I 152-681. Proceedings of the Association for Research in Vi-sion and Ophthalmology; 1993 May 2-7; Sarasota, Florida,USA.
43. Liiden-Drecoll E, Kaufman PL. Morphological changes in pri-mate aqueous humor formation and drainage tissues afterlong-term treatment with antiglaucomatous drugs. J Glau-coma 1993:2:316-28
44. Brugad6ttir R, Jarkman S. Effects of PhXA4L, aprostaglandinanalogue, and PGFza on the corneal and intruetinal d.c. elec-troretinogram (ERG) of the albino rabbit eye. Curr Eye Res
1995; l4: 1073-8045. Basu S, Sj6quist B, Stjernschantz J, et al. Corneal permeability
to and ocular metabolism of phenyl substituted prostaglandinesters in vitro. Prostaglandins Leukot Essent Fatty Acids 1994
APt; 50: 16l -846. Sj0quist B, Byding P, Resul B, et al. The systemic pharmacoki-
netics of latanoprost in man after intravenous and topical ad-
ministration [abstract no. 4481-331. Proceedings of TheAssociation for Research in Vision and Ophthalmology: 1994
May l-6; Sarasota, Florida, USA.47. Bito LZ, Baroody RA. The ocular pharmacokinetics of
eicosanoids and their derivatives. l. Comparison of oculareicosanoid penetration and distribution following topical ap-plication of PGFzo PGFzr I -methyl ester, and PGFa- l -iso-propyl ester. Exp Eye Res 1987; 44:217 -26
48. Camber O, Edman P, Olsson L-8. Permeability of prostaglandinF2a and prostaglandin F2a esters across cornea in vitro. IntJ Pharm 1986; 29: 259-66
49. Sj0quist B. Johasson A. The ocular pharmacokinetics oflatanoprost, a new antiglaucoma drug,studied by autoradiog-raphy [abstract no. 3809]. Invest Ophthalmol Vis Sci 1995
Mar l5; 36 (a): 582350. Alvan G. Calissendorff B, Seideman P et al. Absorption of
ocular timolol. Clin Pharmacokinet 1980: 5: 95
O Adis lnternotionol Limited. All rigfrts reserved.
5 l. Hoyng PFJ, Rulo AH. Greve EL. The ocular hypotensive effectof latanoprost in normal pressure glaucoma patients [abstractno 14.241. Proceedings of the lOth Congress European Soci-ety of Ophthalmology: 1995 lun25-29; Milan, Italy.
52. Coakes RL, O'Neill E, Potts MJ, et al. Dose-finding study withPhXA4l (latanoprost) in patients with elevated intraocularpressure [abstractl. Proceedings of the Annual Congress of theCollege of Ophthalmologisus; 1993 May I l -14; Birmingham,England.
53. Diestelhorst M, Roters S, Krieglstein GK. The effect oflatanoprost (PhXA4l ) on the intraocular pre.ssure and aque-ous humor protein concentration: a randomized, doublemasked comparison of 50 pglml vs 15 pg/ml with timolol0.5?o as control [abstract no. 3810J. Invest Ophthalmol VisSci 1995 Mar; 36 (4) Suppl.: 5823
54. Alm A, Widengerd I. Kjellgrer D, et al. Latanoprost adminis-tered once daily caused a maintained reduction of intraocularpressure in glaucoma patients treated concomitantly withtimolol. Br J Ophthalmol 1995 lm;79: 12-6
55. Lusky M, Glovinsky J, Melamed S, et al. Comparison of twodose regimens of latanoprost in patients with open angle glau-coma or ocular hypertension [abstract no. SP576]. Proceed-ings of the 27th International Congress of Ophthalmology:1994 lun 26-30: Toronto, Canada.
56. Mishima H, Masuda K, Kitazawa Y et al. A comparison oflatanoprost and timolol in primary open-angle glaucoma andocular hypenension: a l2-week study. Arch Ophthalmol 1996Aug; ll4:929-32
57. Alm A, Stjernschantz J, the Scandinavian Latanoprost StudyGroup. Effects on intraocular pressure and side effects of0.N57o latanoprost applied once daily, evening or morning.Ophthalmology 1995 Dec; 102 (12): 1743-52
58. Watson P, Stjernsch'antz J, the Latanoprost Study Group. A six-month, randomized, double-masked study comparinglatanoprost with timolol in open-angle glaucoma and ocularhypertension. Ophthalmology 1996 Jzrn; 103 (l): 126-37
59. Camras CB, the United States Latanoprost Study Group. Com-parison of latanoprost and timolol in patients with ocular hy-pertension and glaucoma. Ophthalmology 1996 Jan; 103 ( I ):138-47
60. Alm A, Widengfird I. Mlpea O. Combination of latanoprostwith dipivefrin in patients with open angle glaucoma or ocularhypertension [abstract no. 56T-04], Proceedings of the 27thInternational Congress of Ophthalmology; 1994 Jun 26-30;Toronto, Canada.
6 [. Watson PG, Barnett F, Parker V. The additive effect of PhXA4land propine in patients with primary open angle glaucoma
[abstract no.6a]. 1992 Jul; Oxford, England,3262. Rulo AH, Greve EL. Hoyng PFJ. Additive ocular hypotensive
effect of latanoprost 'and acetazolamide in glaucoma patients
[abstract no. I 4. I 6]. Proceedi ngs of the I Oth Congress EuropeanSociety of Ophthalmology; 1995 lun 25-29; Milan, Italy.
63. Villumsen J, Alm A. Ocular effects of two different prostaglan-din F2 esters: a doublema.sked cross-over study on normo-tensive eyes. Acta Ophtharlmol I990: 68: 341-3
64. Nakajima M, Goh Y. Azuma I, et al. Effects of pro.staglandin D2
and its analogue, BW245C, on intruocular pressure in hu-mans. Graefes Arch Clin Exp Ophthalmol l99l:229:41l-3
65. Sekurai M, Araie M, OshikaT, et al. Effects of topical applica-tion of UF-021, a novel prostaglandin derivative. on agueoushumor dynamics in normal human eyes. Jpn J Ophthalmoll99l: 35 (2): 156-65
66. Hedner J, Lunde H, Svedmyr N. et al. Respiratory and cardio-vir"scular effects of PhXA4l [abs^tract no. MT-05]. Proceed-
Drugs & Aging 1996 Nov; 9 (O

378 Patel I Spencer
ings of the 4th Congress of the European Glaucoma Society:1992 May 20-24; Amsterdam, Holland. 169
67. Bengtsson B. The prevalence of glaucoma. Br J Ophthalmoll98l ; 65: 46-9
68. Bengtsson B. The incidence of manifest glaucoma. Br J Op-hthalmol 1989; 73: 483-7
69. Klein BEK. Klein R, Sponsel WE, et al. Prevalence of glau-coma: the Beaver Dam Eye Study. Ophthalmology 1992 Oct;99 ( l0): 1499-504
70. Tuck M, Crick R. Testing and referral for chronic glaucoma.
Health Trend 1989: 2l: l3l-471. Coyle D, Drummond M. The econornic burden of glaucoma in
the UK. The need for a far-sighted policy. PharmacoEconom-ics 1995; 7 (6):484-9
72. Rosenberg LF. Glaucoma: early detection and therapy for pre-vention of vision loss. Am Fam Physician 1995 Dec;52 (8):2289-98
73. Fujisawa launches unoprostone eye drops in Japan. Scrip Mag1994 Oct I 8 (1967): 2l
74. Higginbotham EI. Dorzolamide: a brief overview. Chibret Int J
Ophthalmol 1994; l0 (3): 50-375. Lichter PR. Another blockbuster glaucoma drug? [editorial].
Ophthalmology 1993 S.p; 100: l28l-276. Van Buskirk EM, Cioffi GA. Predicted outcomes from hypo-
tensive therapy for glaucomatous optic neuropathy [commen-taryJ. Am J Ophthalmol 1993 Nov; I l6: 636-40
77. Nagasubramanian S. Latanoprost: a prornising new glaucornadrug [commentary]. Br J Ophthalmol 1995 lan;79:3-4
78. Alm A. The potential of prostaglandin derivates in glaucomatherapy. Curr Opin Ophthalmol 1993 Apr; 4:44-50
79. Bito LZ, Stjernschantz J. Resul B. et al. The ocular effects ofprostaglandins and the therapeutic potential of a new PGFzq
analog, PhXA4l (latanopro.st), for glaucoma management. J
Lipid Mediat 1993 Mar-Apr; 6: 535-4380. Alm A, Villumsen J. Effects of topically applied PGFza and its
isopropylester on normal and glaucomatous human eyes. Prog
Clin Biol Res 1989; 312:447-5881. Stjernschantz J. Prostaglandins as ocular hypotensive agents;
development of an analogue for glaucoma treatment. In:Sarnuelsson B et al., editors. Advances in prostaglandin.thromboxane, and leukotriene research. v. 23. New York: Ra-
ven Press Ltd, 1995: 63-882. Fraunfelder FT, Meyer SM. Sexual dysfunction secondary to
topical ophthalmic timolol [etter]. JAMA 1985 Jun: 253 (21):
3092-383. Epstein RJ, Allen RC. Lunde MW. Organic impotence associ-
ated with carbonic anhydrase inhibitor therapy for glaucoma.Ann Ophthalmol 1987 Feb; l9 (2):48-50
Correspondence: &roline M. Spmcer, Adis InternationalLimited, 41 Centorian Drive, Private Bag 65901, MairangiBay, Auckland 10, New Zealand.
O Adis lnternotionol Limited. All rrghh reserved. Drugs & Aging 1996 Nov; 9 (5)