LASER PHYSICS LETTERS
11
www.lphys.org LASER PHYSICS LETTERS EDITORIAL BOARD W. Becker, Berlin D. Chorvat, Bratislava S. DeSilvestri, Milan M. V. Fedorov, Moscow A. Gaeta, Ithaca S. A. Gonchukov, Moscow M. Jelinek, Prague U. Keller, Zürich J. Lademann, Berlin J. T. Manassah, New York P. Meystre, Tucson R. B. Miles, Princeton P. P. Pashinin, Moscow G. Petite, Saclay L. P. Pitaevskii, Trento M. Pollnau, Enschede K. A. Prokhorov, Moscow M. Scalora, Huntsville V. M. Shalaev, West Lafayette J. E. Sipe, Toronto Ken-ichi Ueda, Tokyo I. A. Walmsley, Oxford E. Wintner, Vienna E. Yablonovitch, Los Angeles V. M. Yermachenko, Moscow I. V. Yevseyev, Moscow V. I. Yukalov, Dubna A. M. Zheltikov, Moscow REPRINT
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of LASER PHYSICS LETTERS
www.lphys.orgLASERPHYSICSLETTERS EDITORIAL BOARD
W. Becker, Berlin
D. Chorvat, Bratislava
S. DeSilvestri, Milan
M. V. Fedorov, Moscow
A. Gaeta, Ithaca
S. A. Gonchukov, Moscow
M. Jelinek, Prague
U. Keller, Zürich
J. Lademann, Berlin
J. T. Manassah, New York
P. Meystre, Tucson
R. B. Miles, Princeton
P. P. Pashinin, Moscow
G. Petite, Saclay
L. P. Pitaevskii, Trento
M. Pollnau, Enschede
K. A. Prokhorov, Moscow
M. Scalora, Huntsville
V. M. Shalaev, West Lafayette
J. E. Sipe, Toronto
Ken-ichi Ueda, Tokyo
I. A. Walmsley, Oxford
E. Wintner, Vienna
E. Yablonovitch, Los Angeles
V. M. Yermachenko, Moscow
I. V. Yevseyev, Moscow
V. I. Yukalov, Dubna
A. M. Zheltikov, Moscow
REPRINT

Laser Phys. Lett. 6, No. 2, 149–158 (2009) / DOI 10.1002/lapl.200810101 149
Abstract: The aim of this study was to evaluate the hypothesis
that low-level laser therapy (LLLT) 688 nm and 785 nm accel-
erate dentin barrier formation and repair process after traumatic
pulp exposure. The sample consisted of 45 premolars of capuchin
monkeys (Cebus apella) with pulp exposure Class V cavities. All
premolars were treated with calcium hydroxide (Ca(OH)2), di-
vided in groups of 15 teeth each, and analyzed on 7th, 25th, and
60th day. Group GI – only Ca(OH)2, GII – laser 688 nm, and
GIII – laser 785 nm. Laser beam was used in single and punc-
tual dose with the parameters: continuous, 688 nm and 785 nm
wavelength, tip’s area of 0.00785 cm2, power 50 mW, applica-
tion time 20 s, dose 255 J/cm2, energy 2 J. Teeth were capped
with Ca(OH)2, Ca(OH)2 cement and restored with amalgam. All
groups presented pulp repair. On 25th day the thickness of the
formed dentin barrier was different between the groups GI and
GII (p < 0.05) and between groups GI and GIII (p < 0.01). On
60th day there was difference between GI and GIII (p < 0.01).
It may be concluded that, LLLT 688 nm and 785 nm accelerated
dentin barrier formation and consequently pulp repair process,
with best results using infrared laser 785 nm.
200 μm
NN
7 days – Ca(OH)2 – Irregular layer of superficial coagulation
necrosis in the pulp exposure region (N) – H&E – 100×
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA
Evaluation of dental pulp repair using low level laser
therapy (688 nm and 785 nm) morphologic study in
capuchin monkeys
H. Pretel, 1,∗ J.A. Oliveira, 2 R.F.Z. Lizarelli, 3 and L.T.O. Ramalho 1
1 Dental School of Araraquara, Sao Paulo State University, Araraquara, SP, Brazil2 Dental School of Aracatuba, Sao Paulo State University, Aracatuba, SP, Brazil3 Physics Institute of Sao Carlos, University of Sao Paulo, Sao Carlos, SP, Brazil
Received: 15 September 2008, Revised: 18 September 2008, Accepted: 21 September 2008
Published online: 7 October 2008
Key words: Cebus; low-level laser therapy; pulp capping; atomic force microscopy; odontoblasts; calcium hydroxide
PACS: 47.54.Fj
1. Introduction
Pulp exposure treatments have been described in literature
since 1755, when Philips Pfaff sealed pulp exposures with
gold foils without the previously cauterization and devi-
talization of the pulp tissue apud [1]. Since then, different
techniques have been used for that purpose [1,2].
Hermann, who introduced the use of calcium hydrox-
ide as root canal filling curative in the middle of the twen-
ties, described in 1930 the technique of direct pulp capping
with the same material on pulp exposures [2].
Since then, calcium hydroxide has been the material of
choice for pulp capping because it stimulates healing, neu-
tralizes demineralized dentin layer acidity, promotes the
∗ Corresponding author: e-mail: [email protected]
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA

150 H. Pretel, J.A. Oliveira, et al.: Evaluation of dental pulp repair
remineralization and pulp vitality maintenance in cases of
exposure, besides its excellent bactericidal effect [3–7].
Different authors have described disadvantages of cal-
cium hydroxide application as capping material. These are
related to its high solubility in oral fluids, lack of adher-
ence to dentin tissues, low resistance and the tunnel de-
fect formation on the newly-formed dentin barrier [8–10].
Moreover, the superficial coagulation necrosis caused by
the high alkalinity of calcium hydroxide when in direct
contact with the pulp exposure allows designating this ma-
terial a as non-biocompatible [7,9].
Treatments aiming the pulp repair after traumatic in-
jury are complex and varied, and depend on several fac-
tors, such as the relationship of capping material and pulp
tissue, the extension of the exposure, the presence or ab-
sence of dentin chips, the presence of bacteria and the de-
gree of pulp inflammation should be taken in consideration
[7,9,11,12].
A series of biological events, that constitutes the in-
flammatory reaction, initiate immediately after a tissue in-
jury. Cellular events like alteration of membrane perme-
ability as well as vascular events, like vessel lumen en-
largement, induce increase blood and extracellular fluid in-
flux leading to pulp tissue swelling. The control of inflam-
matory reaction is of paramount importance as the lack of
extensibility of the dentin walls may cause a harmful com-
pression when pulp tissue suffers edema induced by the
inflammatory process [13].
The low level laser therapy (LLLT) stimuli promote
the inflammatory process modulation by stabilizing cell
membrane, altering the transmembrane electric potential,
activating Na+ and K+ ATPase pump, and increasing the
synthesis of adenosine triphosphate (ATP). These actions
prevent cell volume alteration although, its action mech-
anisms still need further investigations [14,15]. Besides,
there are leukocytes activity acceleration; interleukin (IL-
1) level reduction; angiogenesis capillary and lymphatic
increase, among several other factors that make LLLT an
efficient coadjutant tool on the modulation of inflamma-
tory process [14–24].
There are few studies described in the literature un-
til nowadays, on the effects of LLLT photo stimulation
associated with direct pulp capping on repair process of
pulp tissue after traumatic exposure. However, some stud-
ies related to reactionary dentinogenesis were carried out
utilizing LLLT [25,26]. Thus, it is necessary to conduct
further studies to evaluate the activity of pulp repair and
the formation of dentin barrier with different parameters
of LLLT.
The purpose of this work was to investigate the hy-
pothesis that in traumatic pulp exposure followed by di-
rect pulp capping with calcium hydroxide (Ca(OH)2) the
LLLT 688 nm and 785 nm, in a single dose, accelerates the
dentin barrier secretion and the pulp repair process.
Groups Treatment Period, day Total7th 25th 60th
GI Ca(OH)2 5 5 5 15 teeth
GII Ca(OH)2 5 5 5 15 teeth
+ Laser (688 nm)
GIII Ca(OH)2 5 5 5 15 teeth
+ Laser (785 nm)
Table 1 Distribution of the tooth number according to the peri-
ods and experimental groups
2. Materials and methods
Upper and lower premolars teeth of five eight-year-old
male tufted capuchin monkeys (Cebus apella), obtained
from the Tufted Capuchin Monkey Procreation Center
(Dental School of Aracatuba – UNESP – Brazil) were used
in the present study. The animals were kept in individual
metal cages under constant temperature and humidity con-
ditions. The experimental protocol was reviewed and ap-
proved by Ethics in Animal Research Committee of Dental
School of Araraquara, (process number 016/2003).
2.1. Pulp exposure
The initial procedure consisted of anesthesia with intra-
muscular injection of Ketamine Hydrochloride (Vetaset
Fort Dodge, Iowa, USA) at the dose of 15 mg/kg of body
weight, followed by application of intraperitoneal injec-
tion of sodium thiopenthal (Thionembutal – Abbot Lab-
oratories do Brasil Ltda., Rio de Janeiro, Brazil) at the
dose of 30 mg/kg of body weight and intramuscular in-
jection of benzodiazepine (Diazepan –Furp, Guarulhos,
Brazil) at dose of 0.12 mg/kg of body weight. Dental
cleaning, antisepsis and tooth complete isolation were car-
ried out and then, deep Class V cavity was prepared using
an inverted conical-shaped diamond burr (Diamond point
1033 – KG Sorensen, Sao Paulo, SP, Brazil) assembled
on a high-speed turbine under abundant refrigeration. The
pulps were intentionally exposed using a 56 exploratory
probe (Duflex – S.S. White, Rio de Janeiro, RJ, Brazil).
Abundant saline solution irrigation was used to remove
dentin chips and to wash the blood from the hemorrhage,
which was stopped by soft compressions with sterilized
paper towels cones (Tanari – Manacapuru, AM, Brazil).
2.2. Group assignment
The groups were distributed in such a way that every ani-
mal’s teeth were subjected to the three types of treatment
described below and resumed in Table 1. All the 45 teeth
were randomly assigned for each treatment. Experimental
groups were consisted of 15 teeth and the periods of as-
sessment were on the 7th, 25th, and 60th days after treat-
ments.
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA www.lphys.org

Laser Phys. Lett. 6, No. 2 (2009) 151
Characterization – pulp and inflammation (400×) ScoreComplete pulp disorganization and severe 4
inflammation (more than 25 inflammatory cells)
Moderate pulp disorganization and inflammation 3
(between 10 and 25 inflammatory cells)
Discrete pulp disorganization and mild 2
inflammation (less than 10 inflammatory cells)
Normal tissue and few inflammatory cells 1
Table 2 Scores attributed to histopathological events inflamma-
tion and organization of pulp tissue
In all groups the pulp exposures received direct appli-
cation of a layer of calcium hydroxide PA (Biodinamica
– Ibipora, PR, Brazil) in saline solution, and the lining
was made with application of calcium hydroxide cement
(Dycal – Dentsply, Rio de Janeiro, RJ, Brazil). Permanent
restorations were made with silver amalgam (Permite –
SDI, Bayswater, Victoria, Australian).
In experimental groups GII and GIII (Table 1) the
exposed pulps received applications of laser irradiation
688 nm and of 785 nm, respectively, before the direct ap-
plication of the calcium hydroxide.
The low-level laser source utilized in this experiment
was a Laser Beam Multi Laser DR 500 (Laser Beam,
Industria e Tecnologia Ltda., Niteroi, RJ, Brazil) with the
following parameters:
– GaAlAs semiconductor diode laser device, continuous,
λ = 688 nm, P = 50 mW, tip’s area of 0.00785 cm2,
t = 20 s, D = 255 J/cm2, E = 2.0 J;
– GaAlAs semiconductor diode laser device, continuous,
λ = 785 nm, P = 50 mW, tip’s area of 0.00785 cm2,
t = 20 s, D = 255 J/cm2, E = 2.0 J.
The animals were kept under observation until com-
plete recovering from anesthesia, when they received
0.3 mL of Paracetamol (Tylenol� 100 mg/ml – Janssen-
Cilag Farmaceutica Ltda., Sao Jose dos Campos, SP,
Brazil) given orally every 6 hours during 5 days.
2.3. Preparation and morphological analysis
After each experimental period, the animals were anes-
thetized and the teeth were surgically removed, and the
lower third of their root were cut and submitted to histo-
logical procedure fixed in 10% buffered Lillie’s formalin
solution, pH 7.2 during 96 hours. The pieces were soaked
in running water for 24 hours, and immersed in 10% EDTA
solution with changes every 3 days until the complete de-
calcification. The samples were neutralized in phosphate
buffer solution (pH 7.2) for 24 hours and washed in run-
ning water. Finally, the samples were gradually dehydrated
in alcohol solutions of increasing concentrations (70%,
90%, and absolute) and then submitted to xylol diafaniza-
tion. The specimens were embedded in paraffin and were
cut in 6 μm-thick semi-serial sections in the buccolingual
plane with a rotatory microtome (HM-325 – Microm –
Germany).
For the morphological analysis, the prepared micro-
scope slides were stained with hematoxylin and eosin
(H&E) and Masson’s trichrome (TM).
Morphological analyses were performed under a light
microscope (DM2000 – Leica – Reichert – Germany) and
the images were captured with digital camera (DFC-300
FX – Leica Microsystems – Germany). All histological
sections were independently evaluated by two previously
standard-trained examiners and the analyses conducted in
double-blind fashion type protocol. If the examiners dis-
agreed, each sample was reevaluated until a consensus be-
tween them could be established. Inflammatory response
and pulp tissue organization were graded (Table 2) accord-
ing to scores adapted from the literature [6,10,27,28]. The
images obtained from samples on the 25th and the 60th
day were analyzed using the software Image Tool 3.0 (Uni-
versity of Texas Health Science Center in San Antonio),
which made possible to measure in micrometers (μm) the
thickness of the newly-formed mineralized barrier. The fi-
nal measurement was obtained by calculating the average
of 5 different linear measurements enabling to perform a
comparative analysis and to measure with more discrim-
ination power the LLLT effects on the formation of the
mineralized barrier.
Atomic force microscopy analysis (AFM) (microscope
BioProbe, Park Scientific Instruments, Thermo Micro-
scopes – Veeco) was also performed to evaluate the to-
pographical organization of dentin barrier, with the device
operating in static contact mode. The barrier was bounded
in its upper surface by superficial coagulation necrosis and
in the lower portion by the subjacent trauma pulp tissue.
In this manner, the newly-formed tissue in dentin repair
was delimited by the analyzed area, observed on a scan-
ning frequency of 0.8 Hz per line, generating 256 lines
into an analysis field of 1×10−2 mm2, allowing a detailed
view of the topography of extracellular matrix located in
the dentin injured area. The software Image Processingand Data Analysis – Version 2.0.0 (TermoMicroscopes –
Veeco) was used to evaluate the general aspects of dentin
barrier surface considering the alignment and the homo-
geneity of collagen fiber distribution.
2.4. Statistical analysis
The data obtained in quantitative analysis of thickness lin-
ear measurement of the mineralized barrier were initially
examined by applying the normality test of Lilliefors.
Since data showed normal distribution, one-way ANOVA
test was used, being applied post hoc Student t test, consid-
ering (p < 0.05) as significant difference. The results from
histophatological analyses scores that evaluated inflamma-
tion degree and pulp tissue organization were submitted to
Kruskall-Wallis non-parametric test with significance level
of (p < 0.05). Both analyses were performed with the soft-
ware Bioestat 5.0.
www.lphys.orgc© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA
152 H. Pretel, J.A. Oliveira, et al.: Evaluation of dental pulp repair
Groups and periods of analyses Teeth – (n) Inflammation scores ∗ Mean (± standard deviation) of linear thickness, μm ∗∗
1 2 3 4
GI 7th day 5 – 3 1 1 –
Ca(OH)2 25th day 5 3 1 1 – 23.08(±6.96) a
60th day 5 5 – – – 88.78(±31.54) I
GII 7th day 5 – 4 – 1 –
Ca(OH)2 25th day 5 5 – – – 41.74(±14.73) b
+ Laser (688 nm) 60th day 5 4 1 – – 115.52(±29.73) I,II
GIII 7th day 5 – 4 1 – –
Ca(OH)2 25th day 5 4 1 – – 58.21(±15.86) b,c
+ Laser (785 nm) 60th day 5 5 – – – 153.95(±37.53) II
∗ Kruskal-Wallis test among the periods on the 7th, 25th, and 60th days (p > 0.05).∗∗ ANOVA test – Different letters represent significant statistic difference on the 25th day, and different roman numerals represent differences on the 60th day.
Table 3 Teeth distribution according to the scores attributed to histopathological events. Mean ± standard deviation of linear measure-
ment of the mineralized barrier in the different groups
200 μm
(a)(a)
100 μm
(b)(b)
200 μm
(c)(c)
100 μm
(f)(f)
200 μm
(e)(e)
100 μm
(d)(d)
NNNN
NN
NN
NN
NN
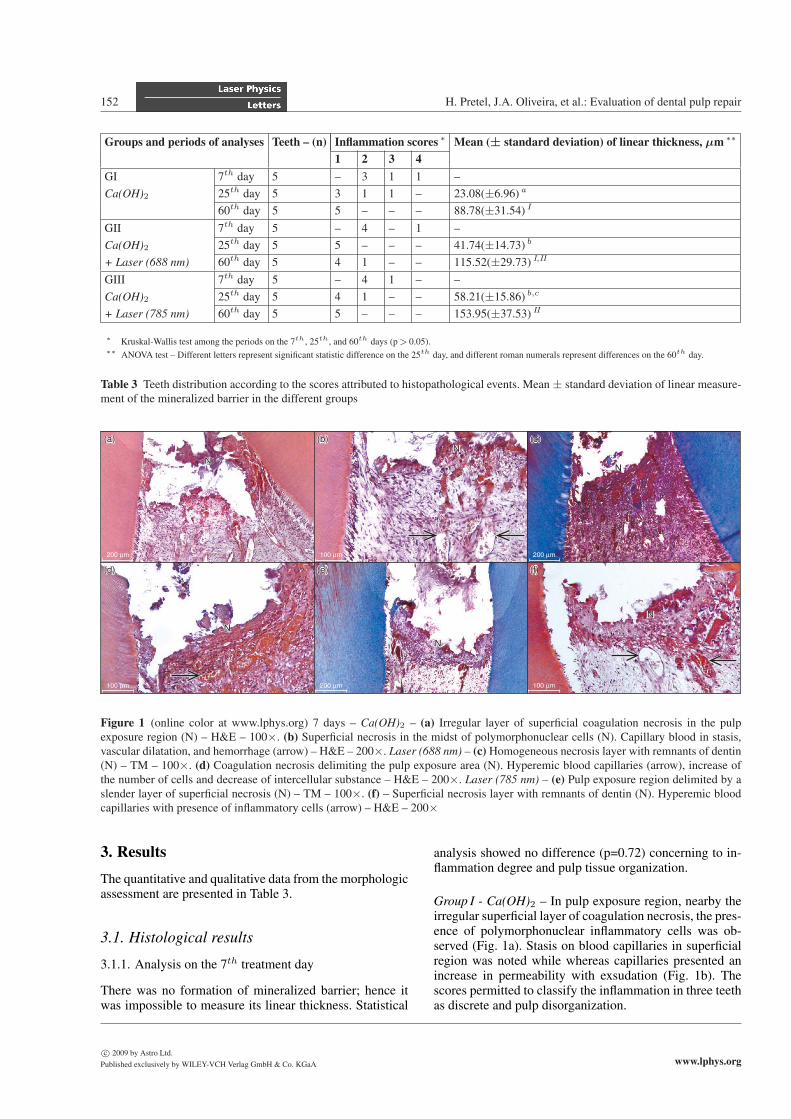
Figure 1 (online color at www.lphys.org) 7 days – Ca(OH)2 – (a) Irregular layer of superficial coagulation necrosis in the pulp
exposure region (N) – H&E – 100×. (b) Superficial necrosis in the midst of polymorphonuclear cells (N). Capillary blood in stasis,
vascular dilatation, and hemorrhage (arrow) – H&E – 200×. Laser (688 nm) – (c) Homogeneous necrosis layer with remnants of dentin
(N) – TM – 100×. (d) Coagulation necrosis delimiting the pulp exposure area (N). Hyperemic blood capillaries (arrow), increase of
the number of cells and decrease of intercellular substance – H&E – 200×. Laser (785 nm) – (e) Pulp exposure region delimited by a
slender layer of superficial necrosis (N) – TM – 100×. (f) – Superficial necrosis layer with remnants of dentin (N). Hyperemic blood
capillaries with presence of inflammatory cells (arrow) – H&E – 200×
3. Results
The quantitative and qualitative data from the morphologic
assessment are presented in Table 3.
3.1. Histological results
3.1.1. Analysis on the 7th treatment day
There was no formation of mineralized barrier; hence it
was impossible to measure its linear thickness. Statistical
analysis showed no difference (p=0.72) concerning to in-
flammation degree and pulp tissue organization.
Group I - Ca(OH)2 – In pulp exposure region, nearby the
irregular superficial layer of coagulation necrosis, the pres-
ence of polymorphonuclear inflammatory cells was ob-
served (Fig. 1a). Stasis on blood capillaries in superficial
region was noted while whereas capillaries presented an
increase in permeability with exsudation (Fig. 1b). The
scores permitted to classify the inflammation in three teeth
as discrete and pulp disorganization.
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA www.lphys.org

Laser Phys. Lett. 6, No. 2 (2009) 153
50 μm
(a)(a)
10 μm
(b)(b)
50 μm
(c)(c)
10 μm
(f)(f)
50 μm
(e)(e)
10 μm
(d)(d)
NN
PP
DBDB
PP
DBDB
PP
DB
DB
PP
DBDB
PP
DB
DB PP
DBDB
Figure 2 (online color at www.lphys.org) 25 days – Ca(OH)2 – (a) Incomplete formation of mineralized barrier (DB) under the
coagulation necrosis (N). At center, pulp tissue is found with normality characteristics (P) – TM – 400×. (b) Dentin barrier (DB) with
odontoblastic cells in intense metabolic activity (arrow). At the center of pulp tissue newly-formed blood capillaries (P) – TM – 1000×.
Laser (688 nm) – (c) Complete mineralized bridge formation with presence of cellular inclusions (DB). At the center of the pulp, tissue
with normality characteristics with presence of capillaries vessels and nerve endings (P) – TM – 400×. (d) Formed dentin barrier (DB)
with presence of odontoblastic cells with reduced metabolism (arrow). Characteristic of normality of the pulp tissue (P) – TM – 1000×.
Laser (785 nm) – (e) Dentin bridge (DB) in contact with dentin lateral wall. Pulp tissue with several blood capillaries (P) – TM – 400×.
(f) Mineralized bridge (DB) with presence of cells with clear nucleus and nucleolus in intense metabolic activity (arrow). Center of the
pulp tissue with several newly-formed capillaries (P) – H&E – 1000×
Group II - Laser (688 nm) – It could be observed a slender
necrosis surface layer with delimitation between the pulp
exposure and the dentin lateral walls (Fig. 1c). Presence
of severe vascular hyperemia, reduction of blood flow, in-
crease in number of cells, and consequently, intercellu-
lar substance reduction were noted. The presence of dis-
crete disorganization and sparse inflammatory cells was
observed in pulp tissue of three teeth (Fig. 1d).
Group III - Laser (785 nm) – The mechanically exposed
region presented itself covered with coagulation necro-
sis in which sparse cellular inclusions could be seen
(Fig. 1e). Within the pulp there was the presence of vas-
cular hyperemia and inflammatory cells located isolated
near dentin residues (Fig. 1f). The pulp connective tissue
presented discrete disorganization when compared to the
other groups.
3.1.2. Analysis on the 25th treatment day
At this intermediary period, statistical analysis allowed
to identify significant difference between groups GI and
GII (p < 0.05) as well as between groups GI and GIII
(p < 0.01) concerning the thickness linear measurement of
formed dentin barrier. There was no statistical difference
(p=0.29) on inflammation degree and pulp tissue organi-
zation.
Group I - Ca(OH)2 – In this period there was incomplete
formation of mineralized bridge under the coagulation
necrosis region (Fig. 2a). The barrier presented trapped
cells in the midst and differentiated cells undergoing in-
tense extracellular matrix synthesis (Fig. 2b). The remain-
ing connective pulp tissue presented normality character-
istics in three teeth.
Group II - Laser (688 nm) – Presence of mineralized bar-
rier showing greater thickness next to dentin side walls
with cellular inclusions was seen. The pulp center had
normal appearance with presence of cells, capillaries and
nerve endings (Fig. 2c). Highly stained odontoblastic cells
were seen, presenting elongated cell nucleus with dark
and acidophil cytoplasm evidencing decrease of secretion.
Dentin barrier with tertiary reparative dentin characteris-
tics was observed (Fig. 2d). All the five teeth presented
normal pulp characteristics.
Group III - Laser (785 nm) – Homogeneous mineral-
ized barrier was visualized covering the entire pulp expo-
sure region (Fig. 2e). The odontoblasts presented clear nu-
cleolus, large and voluminous nucleus in the midst of in-
tense cytoplasm undergoing extracellular matrix synthesis
activity (Fig. 2f). The pulp connective tissue had normal
characteristics in four teeth with many newly-formed cap-
illaries.
www.lphys.orgc© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA
154 H. Pretel, J.A. Oliveira, et al.: Evaluation of dental pulp repair
50 μm
(a)(a)
10 μm
(b)(b)
50 μm
(c)(c)
10 μm
(f)(f)
50 μm
(e)(e)
10 μm
(d)(d)
PP
DBDB
TDTD
DBDB TDTD
PP
PP RD
RD
PP
CC
RD
RD
PP
LDLD
DBDB
DB
DB PP
PDPD
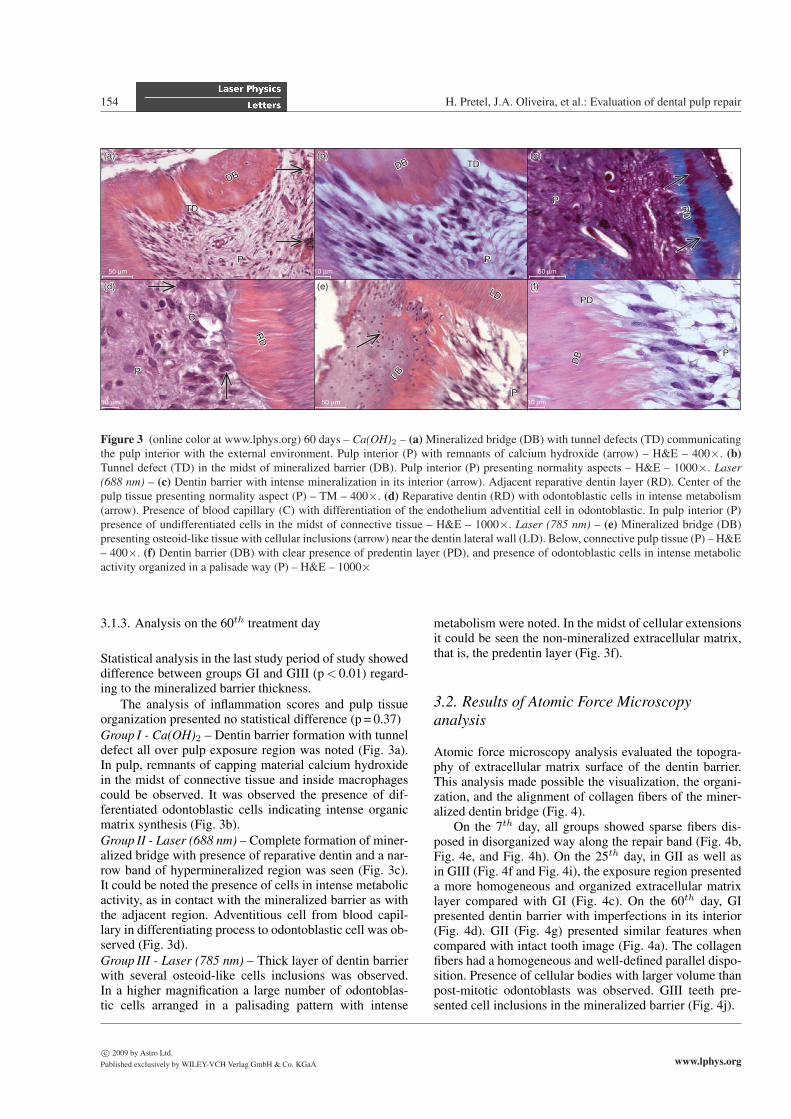
Figure 3 (online color at www.lphys.org) 60 days – Ca(OH)2 – (a) Mineralized bridge (DB) with tunnel defects (TD) communicating
the pulp interior with the external environment. Pulp interior (P) with remnants of calcium hydroxide (arrow) – H&E – 400×. (b)Tunnel defect (TD) in the midst of mineralized barrier (DB). Pulp interior (P) presenting normality aspects – H&E – 1000×. Laser(688 nm) – (c) Dentin barrier with intense mineralization in its interior (arrow). Adjacent reparative dentin layer (RD). Center of the
pulp tissue presenting normality aspect (P) – TM – 400×. (d) Reparative dentin (RD) with odontoblastic cells in intense metabolism
(arrow). Presence of blood capillary (C) with differentiation of the endothelium adventitial cell in odontoblastic. In pulp interior (P)
presence of undifferentiated cells in the midst of connective tissue – H&E – 1000×. Laser (785 nm) – (e) Mineralized bridge (DB)
presenting osteoid-like tissue with cellular inclusions (arrow) near the dentin lateral wall (LD). Below, connective pulp tissue (P) – H&E
– 400×. (f) Dentin barrier (DB) with clear presence of predentin layer (PD), and presence of odontoblastic cells in intense metabolic
activity organized in a palisade way (P) – H&E – 1000×
3.1.3. Analysis on the 60th treatment day
Statistical analysis in the last study period of study showed
difference between groups GI and GIII (p < 0.01) regard-
ing to the mineralized barrier thickness.
The analysis of inflammation scores and pulp tissue
organization presented no statistical difference (p = 0.37)
Group I - Ca(OH)2 – Dentin barrier formation with tunnel
defect all over pulp exposure region was noted (Fig. 3a).
In pulp, remnants of capping material calcium hydroxide
in the midst of connective tissue and inside macrophages
could be observed. It was observed the presence of dif-
ferentiated odontoblastic cells indicating intense organic
matrix synthesis (Fig. 3b).
Group II - Laser (688 nm) – Complete formation of miner-
alized bridge with presence of reparative dentin and a nar-
row band of hypermineralized region was seen (Fig. 3c).
It could be noted the presence of cells in intense metabolic
activity, as in contact with the mineralized barrier as with
the adjacent region. Adventitious cell from blood capil-
lary in differentiating process to odontoblastic cell was ob-
served (Fig. 3d).
Group III - Laser (785 nm) – Thick layer of dentin barrier
with several osteoid-like cells inclusions was observed.
In a higher magnification a large number of odontoblas-
tic cells arranged in a palisading pattern with intense
metabolism were noted. In the midst of cellular extensions
it could be seen the non-mineralized extracellular matrix,
that is, the predentin layer (Fig. 3f).
3.2. Results of Atomic Force Microscopyanalysis
Atomic force microscopy analysis evaluated the topogra-
phy of extracellular matrix surface of the dentin barrier.
This analysis made possible the visualization, the organi-
zation, and the alignment of collagen fibers of the miner-
alized dentin bridge (Fig. 4).
On the 7th day, all groups showed sparse fibers dis-
posed in disorganized way along the repair band (Fig. 4b,
Fig. 4e, and Fig. 4h). On the 25th day, in GII as well as
in GIII (Fig. 4f and Fig. 4i), the exposure region presented
a more homogeneous and organized extracellular matrix
layer compared with GI (Fig. 4c). On the 60th day, GI
presented dentin barrier with imperfections in its interior
(Fig. 4d). GII (Fig. 4g) presented similar features when
compared with intact tooth image (Fig. 4a). The collagen
fibers had a homogeneous and well-defined parallel dispo-
sition. Presence of cellular bodies with larger volume than
post-mitotic odontoblasts was observed. GIII teeth pre-
sented cell inclusions in the mineralized barrier (Fig. 4j).
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA www.lphys.org

Laser Phys. Lett. 6, No. 2 (2009) 155
(I)
Groups
7 days
(b)
2.00
μm
/div
80.00 μm40.000
(a)
1.00
μm
/div
80.00 μm40.000
(II) 7 days
(e)
1.00
μm
/div
80.00 μm40.000
(III) 7 days
(h)
2.00
μm
/div
80.00 μm40.000
60 days
(d)
2.00
μm
/div
80.00 μm40.000
60 days
(g)
1.00
μm
/div
80.00 μm40.000
60 days
(j)
1.00
μm
/div
80.00 μm40.000
25 days
(c)
1.00
μm
/div
80.00 μm40.000
25 days
(f)
1.00
μm
/div
80.00 μm40.000
25 days
(i)
2.00
μm
/div
80.00 μm40.000
DD
PDPD
DBDB
DBDB
PDPD
DBDB
Figure 4 (online color at www.lphys.org) Representative photomicrography of atomic force of the groups and periods analyzed. (a)(illustrative photomicrography) represents a healthy tooth with dentin layer (D), the predentin layer (PD), below, odontoblastic cells
in the midst of the pulp cells. (b), (e), and (h) show the different groups on the 7th day, with the initial formation of disorganized
extracellular matrix in the midst of coagulation necrosis. (c), (f), and (i) on the 25th day, identify a more homogeneous topography of
the extracellular matrix, but with disruption of collagen fibers. (d) on the 60th day, illustrates the mineralized barrier (DB) with internal
defects (arrow) detected by the topographic difference. (g) evidences the formation of dentin barrier (DB) presenting a topographically
higher band in its interior (arrow), and a slender layer of predentin (PD). Note the orientation and organization of collagen fibers in the
midst of extracellular matrix. (j) illustrates an extensive homogeneous layer of dentin barrier (DB) with cellular inclusions evidenced
by holes in the matrix interior (arrow)
www.lphys.orgc© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA

156 H. Pretel, J.A. Oliveira, et al.: Evaluation of dental pulp repair
4. Discussion
The laser both high-and low-power has been a tool very
employed in many specialties of dentistry [25,29–33].
More studies showing the real application at clinical prac-
tice are welcome to allow an improvement of curative pro-
cedures. One of these important studies is about pulp tissue
reaction after low level laser therapy.
The LLLT application prior to direct pulp capping
stimulated a greater formation of dentin bridge in the pulp
exposure region. These data support other studies about
pulp tissue repair [25,26,29]. Utsunomiya showed 1998
[29] that LLLT accelerated lectins and collagen type I and
type III expressions in dentin barrier, fact that could ex-
plain the best results in pulp repair in the irradiated groups.
The initial effects of calcium hydroxide on pulp ex-
posure were described by Schroder [4], who highlights
the formation of the necrosis layer at first, followed by
vascular alterations, cellular migration and proliferation,
and finally collagen synthesis and mineralization. This se-
quence of events, which was also been described by other
authors [34,35], corresponds to ours findings in capuchin
monkeys’ teeth. However, the obtained results from LLLT
irradiated groups confirm that there is an anticipation of
the events involving pulp repair, culminating in advanced
formation of mineralized barrier.
The area of coagulation necrosis, also described as firm
necrosis layer by Shroder [4] or as mummified zone by
Stanley [36], corresponds to the slender layer composed
by cells and denatured plasmatic proteins produced by
the corrosive action of calcium hydroxide on the exposed
pulp. The area of coagulation necrosis is essential to trig-
ger the repair process of tissue [3–5,25–37], as the depo-
sition of extracellular matrix and fibronectin begins subja-
cent to this layer [38]. Fibronectin is an adhesion glycopro-
tein with high molecular weight and is directly involved in
pulp tissue repairing and odontogenesis by promoting the
link between the extracellular matrix and undifferentiated
cells during the cytological changes and through differen-
tiation in odontoblastic cells [38,39]. Nevertheless, during
pulpal healing process, unlike odontogenesis, undifferen-
tiated mesenchymal cells neither have the support nor the
basal membrane signaling to induce adhesion and differen-
tiation in order to establish the pulp repair process, since it
occurs subjacent to the coagulation necrosis layer [38,40].
When compared to control group, in both LLLT irradi-
ated groups teeth at the 7th day after pulp exposure, it was
already possible to observe a layer of homogeneous and
organized necrosis (Fig. 1). This apparently better organi-
zation of the necrosis layer may have occurred because of
the acceleration of cellular metabolism induced by photo-
chemical interaction of LLLT. It is believed that photons
interact directly with the respiratory chain by increasing
the electrons flow at mitochondrial crest promoting an in-
crease in energetic cellular metabolism, and consequently
an increase in the extracellular matrix synthesis [18,41].
Another LLLT action in tissue repair is due to the in-
crease in vascularization [42,43]. LLLT is able to promote
relaxation of diaphragm of capillaries endings thereby in-
creasing local circulation [17]. It also promotes capil-
lary angiogenesis with the increase in the endothelial cell
trophism [43,44]. The effects on microcirculation activa-
tion raise the oxygenation levels and tissue nutrition con-
siderably increasing the metabolism and tissue regenera-
tion [42,44].
LLLT control of inflammatory process is widely de-
scribed in literature [14,15,17,19,20,29,43]. However, no
significant statistic difference in pulp inflammation degree
between irradiated groups and control was found. This ob-
servation may be explained by the fact that calcium hy-
droxide, in addition to causing coagulation necrosis on the
pulpal surface, can also cause a chronic irritation in the
inner portion of the pulp when in contact, due to its high
alkalinity. This reaction allows qualifying calcium hydrox-
ide as non compatible biomaterial. In Figure 3A it is pos-
sible to see remnants of calcium hydroxide in the midst of
pulp tissue and macrophages after 60 days.
The statistical analysis showed no difference between
both irradiated groups (GII and GIII) in different periods
concerning the linear measurement of the newly-formed
barrier. However, both groups presented difference for this
parameter with respect to control group at the 25th day,
but only group GIII (785 nm) showed difference to con-
trol group, at the 60th day. The best results with infrared
laser may be explained by the greater penetration power
of this wavelength when compared to the red laser. This
characteristic provided a benefit to a larger area by elec-
tromagnetic radiation, since laser application was in single
and punctual dose in pulp exposure tissue.
Different authors suggest that the use of electromag-
netic radiation with wavelength ranging from 524 nm to
904 nm are appropriated to stimulate tissue repair, increase
collagen synthesis, stimulate cellular mitosis and capillary
angiogenesis [43,45].
The laser therapy effects are dose-dependent, which
means, wavelength, power, frequency, fluency and energy
parameters are of utmost importance to achieve good tis-
sue responses [43,46]. The use of fixed parameters for
LLLT application, varying only the wavelengths, had the
purpose to compare its effects on pulp, since in previous
work good results concerning repair of tissue and bone
with the use of the same parameters were obtained in pre-
vious study [43]. Our aim with the single-dose application
on pulp exposure was to prove its efficiency and provide
scientific evidences to the dentistry officer develop clini-
cal protocols using LLLT in conjunction with direct pulp
capping by calcium hydroxide.
Atomic force microscopy analyses allowed the obser-
vation of the organization and topography of the injured
region, characterized by the alignment and the arrange-
ment of collagen fibers of the extracellular matrix. The
region indicated by the arrow in the Fig. 4g represents a
newly synthesized slender band of sclerotic or mineralized
dentin. Through AFM analysis this region appears topo-
graphically higher, which characterizes a thicker and more
voluminous collagen fibers set. This information was con-
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA www.lphys.org

Laser Phys. Lett. 6, No. 2 (2009) 157
firmed by histopathological analyses. Fig. 3c represents
the same region in which this same band is noted with a
more evident staining than the rest of the dentin.
In order to achieve success in the procedure of direct
pulp capping is necessary the bleeding control, the direct
contact of calcium hydroxide with all the injured area,
the absence of dentin chips and the non formation of em-
bolism in blood capillaries due to calcium hydroxide par-
ticles [36]. Calcium hydroxide causes a delay in the pro-
cess of pulp repair, as it does not present mechanical seal
properties, its water solubility is high and causes a long-
lasting pulp irritation. For these reasons there is a tendency
nowadays to work with materials that provide better seal-
ing properties as, for example, the mineral trioxide aggre-
gate (MTA) [10]. Although the results found in this study
might be considered good, the search for new materials
and/or less aggressive techniques of formation of superfi-
cial necrosis that promote the process of pulpal repair and
formation of mineral bridge should to be encouraged.
5. Conclusion
All teeth of the evaluated groups presented pulp tissue re-
pair to a certain degree. However, LLLT stimulated groups
688 nm and 785 nm in single dose, evidenced an acceler-
ation on dentin barrier secretion and consequently on the
pulp repair process. The best results were obtained with
infrared laser 785 nm.
Acknowledgements The authors gratefully thank CAPES
(Coordenacao de Aperfeicoamento de Pessoal de Nıvel Supe-
rior) for supporting this investigation, Tufted Capuchin Monkey
Procreation Center of the UNESP Sao Paulo State University,
Dental School of Aracatuba for providing the animals, and
NUPEN (Nucleo de Pesquisa e Ensino em Fototerapia nas
Ciencias da Saude) for supporting and calibrating the laser
equipment. We also thank Claudia Misue Kanno and Isabela
Mascia Silveira for the review of English language.
References
[1] M.E. Ring, Dentistry: An Illustrated History (Harry N.
Abrams Inc., New York, 1985), p. 320.
[2] T. Dammaschke, J. Hist. Dent. 56, 9–23 (2008).
[3] G. Bergenholtz, Oral Surg. Oral Med. Oral Pathol. Oral Ra-
diol. Endod. 100, S102–S108 (2005).
[4] U. Schroder, J. Dent. Res. 64, Spec. No., 541–548 (1985).
[5] D.R. Heys, R.J. Heys, C.F. Cox, and J.K. Avery, J. Oral
Pathol. Med. 9, 372–379 (1980).
[6] R.K. Subay and S. Asci, Oral Surg. Oral Med. Oral Pathol.
76, 485–492 (1993).
[7] K. Yoshiba, N. Yoshiba, and M. Iwaku, J. Endod. 21, 16–20
(1995).
[8] C.F. Cox, C.L. Keall, H.J. Keall, E. Ostro, and G. Bergen-
holtz, J. Prosthet. Dent. 57, 1–8 (1987).
[9] C.F. Cox, R.K. Subay, E. Ostro, S. Suzuki, and S.H. Suzuki,
Oper. Dent. 21, 4–11 (1996).
[10] M.D. Accorinte, R. Holland, A. Reis, M.C. Bortoluzzi, S.S.
Murata, E. Dezan, V. Souza, and L.D. Alessandro, J. Endod.
34, 1–6 (2008).
[11] Y. Kitasako, P.E. Murray, J. Tagami, and A.J. Smith,
Quintessence Int. 33, 600–608 (2002).
[12] Y. Kitasako, S. Inokoshi, and J. Tagami, J. Dent. 27, 257–
263 (1999).
[13] A.R. Ten Cate, Histologia Bucal, Desenvolvimento, Estru-
tura e Funcao (Guanabara-Koogan, Rio de Janeiro, 2001),
p. 438.
[14] A. Amat, J. Rigau, R.W. Waynant, I.K. Ilev, and J.J. Anders,
J. Photochem. Photobiol. B 82, 152–160 (2006).
[15] S. Passarella, E. Casamassima, S. Molinari, D. Pastore, E.
Quagliariello, I.M. Catalano, and A. Cingolani, FEBS Lett.
175, 95–99 (1984).
[16] M. Schaffer, H. Bonel, R. Sroka, P.M. Schaffer, M. Busch,
M. Reiser, and E. Duhmke, J. Photochem. Photobiol. B 54,
55–60 (2000).
[17] E. Mester, A.F. Mester, and A. Mester, Lasers Surg. Med. 5,
31–39 (1985).
[18] T. Karu, Health Phys. 56, 691–704 (1989).
[19] J.S. Kana, G. Hutschenreiter, D. Haina, and W. Waidelich,
Arch. Surg. 116, 293–296 (1981).
[20] W. Posten, D.A. Wrone, J.S. Dover, K.A. Arndt, S. Silapunt,
and M. Alam, Dermatol. Surg. 31, 334–340 (2005).
[21] G.K. Reddy, L. Stehno-Bittel, and C.S. Enwemeka, Wound
Repair Regen. 9, 248–255 (2001).
[22] Y.-D. Kim, S.-S. Kim, D.-S. Hwang, G.-C. Kim, S.-H. Shin,
U.-K. Kim, J.-R. Kim, and I.-K. Chung, Laser Phys. Lett. 4,
681–685 (2007).
[23] Y.-D. Kim, S.-S. Kim, T.-G. Kim, G.-C. Kim, S.-B. Park,
and W.-S. Son, Laser Phys. Lett. 4, 616–623 (2007).
[24] C.F. Oliveira, J. Hebling, P.P.C. Souza, N.T. Sacono, F.R.
Lessa, R.F.Z. Lizarelli, and C.A.S. Costa, Laser Phys. Lett.
5, 680–685 (2008).
[25] A.N.S. Ferreira, L. Silveira, Jr., W.J. Genovese, V.C. de
Araujo, L. Frigo, R.A. de Mesquita, and E. Guedes, Pho-
tomed. Laser Surg. 24, 358–365 (2006).
[26] G.E.P. Villa, A.B.C.E.B. Catirse, R.C.C. Lia, and R.F.Z.
Lizarelli, Laser Phys. Lett. 4, 690–695 (2007).
[27] C.F. Cox, G. Bergenholtz, M. Fitzgerald, D.R. Heys, R.J.
Heys, J.K. Avery, and J.A. Baker, J. Oral. Pathol. 11, 327–
339 (1982).
[28] C.A.S. Costa, M.F. Oliveira, E.M.A. Giro, and J. Hebling,
Int. Endod. J. 36, 831–839 (2003).
[29] T. Utsunomiya, J. Endod. 24, 187–193 (1998).
[30] R.F.Z. Lizarelli, M.M. Costa, E. Carvalho-Filho, F.D.
Nunes, and V.S. Bagnato, Laser Phys. Lett. 5, 63–69 (2008).
[31] D.A.M.P. Malta, M.M. Costa, J.E.P. Pelino, M.F. de An-
drade, and R.F.Z. Lizarelli, Laser Phys. Lett. 5, 144–150
(2008).
[32] D.A.M.P. Malta, M.A.M. Kreidler, G.E. Villa, M.F. de An-
drade, C.R. Fontana, and R.F.Z. Lizarelli, Laser Phys. Lett.
4, 153–156 (2007).
[33] L.M.G. Sierpinsky, D.M. Lima, M.S.M. Candido, V.S. Bag-
nato, and S.T. Porto-Neto, Laser Phys. Lett. 5, 547–551
(2008).
[34] A.J. Smith, N. Cassidy, H. Perry, C. Begue-Kirn, J.V. Ruch,
and H. Lesot, Int. J. Dev. Biol. 39, 273–280 (1995).
[35] D. Tziafas, Int. J. Dev. Biol. 39, 281–290 (1995).
www.lphys.orgc© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA
158 H. Pretel, J.A. Oliveira, et al.: Evaluation of dental pulp repair
[36] H.R. Stanley, Oral. Surg. Oral. Med. Oral. Pathol. 68, 628-
639 (1989).
[37] R.L. Glass and H.A. Zander, J. Dent. Res. 28, 97–107
(1949).
[38] E. Piva, S.B.C. Tarquınio, F.F. Demarco, A.F. Silva, and V.C.
de Araujo, Oral Surg. Oral Med. Oral Pathol. Oral Radiol.
Endod. 102(4), e66–e71 (2006).
[39] D. Tziafas, N. Panagiotakopoulos, and A. Komnenou, Arch.
Oral. Biol. 40, 23–31 (1995).
[40] Y. Kitasako, S. Shibata, C.F. Cox, and J. Tagami, Int. Endod.
J. 35, 996–1004 (2002).
[41] T. Karu, L. Pyatibrat, and G. Kalendo, J. Photochem. Pho-
tobiol. B 27, 219–223 (1995).
[42] M.A. Trelles and E. Mayayo, Lasers Surg. Med. 7, 36–45
(1987).
[43] H. Pretel, R.F.Z. Lizarelli, and L.T.O. Ramalho, Lasers Surg.
Med. 39, 788–796 (2007).
[44] A. Benedicenti, M. Verrando, F. Cherlone, and O. Brunetti,
Parodontol. Stomatol. (Nuova) 23, 167–178 (1984).
[45] P. Moore, T.D. Ridgway, R.G. Higbee, E.W. Howard, and
M.D. Lucroy, Lasers Surg. Med. 36, 8–12 (2005).
[46] R. Bortoletto, N.S. Silva, R.A. Zangaro, M.T.T. Pacheco,
R.A. Matta and C. Pacheco-Soares, Lasers Med. Sci. 18,
204–206 (2004).
c© 2009 by Astro Ltd.
Published exclusively by WILEY-VCH Verlag GmbH & Co. KGaA www.lphys.org