
Reproducibility of the incremental shuttle walk test for women with morbid obesity
Upload
independentCategory
view
2download
0
Author's Accepted Manuscript
Laparoscopic Roux-en-Y Gastric Bypass inAdolescents with Morbid Obesity- SurgicalAspects and Clinical Outcome
G. Göthberg, E. Gronowitz, C.-E. Flodmark, J.Dahlgren, K. Ekbom, S. Mårild, C. Marcus, T.Olbers
PII: S1055-8586(13)00067-XDOI: http://dx.doi.org/10.1053/j.sempedsurg.2013.10.015Reference: YSPSU50460
To appear in: Seminars in Pediatric Surgery
Cite this article as: G. Göthberg, E. Gronowitz, C.-E. Flodmark, J. Dahlgren, K.Ekbom, S. Mårild, C. Marcus, T. Olbers, Laparoscopic Roux-en-Y Gastric Bypassin Adolescents with Morbid Obesity- Surgical Aspects and Clinical Outcome,Seminars in Pediatric Surgery, http://dx.doi.org/10.1053/j.sempedsurg.2013.10.015
This is a PDF file of an unedited manuscript that has been accepted forpublication. As a service to our customers we are providing this early version ofthe manuscript. The manuscript will undergo copyediting, typesetting, andreview of the resulting galley proof before it is published in its final citable form.Please note that during the production process errors may be discovered whichcould affect the content, and all legal disclaimers that apply to the journalpertain.
www.elsevier.com/locate/semped-
surg
1
Laparoscopic Roux-en-Y Gastric Bypass in Adolescents with Morbid Obesity- Surgical Aspects and Clinical Outcome
G Göthberg1, E Gronowitz1, C-E Flodmark2, J Dahlgren1, K Ekbom3, S Mårild1, C Marcus3
and T Olbers1
1Sahlgrenska Academy at University of Gothenburg, Institute of Clinical Sciences, Dept. of Surgery, Medicine and Pediatrics and Centre of Obesity at the Queen Silvia Children’s Hospital, Gothenburg, Sweden 2 Childhood Obesity Unit, Skåne University Hospital, Malmö, Sweden
3Karolinska Institutet, Dept of Clinical Science, Intervention and Technology (CLINTEC) Division of Paediatrics, and National Childhood Obesity Centre, Children´s Hospital, Karolinska University Hospital, Stockholm, Sweden
Clinicaltrials.gov identifier: NCT00289705
Correspondence to: Dr Torsten Olbers, Dept for Gastrosurgical Research and Education,
Sahlgrenska University Hospital, 41345 Gothenburg, Sweden, [email protected]

2
Abstract
In this paper we address surgical aspects on bariatric surgery in adolescents from a nationwide
Swedish study
Eighty-one adolescents with morbid obesity (13–18 years) underwent laparoscopic gastric
bypass surgery while 81 adolescents with obesity matched by age, sex, and BMI received
conventional care. Another comparison group was adults undergoing gastric bypass at same
institution during the same time period. This report addresses the two-year clinical outcome
and five-year surgical adverse event rate.
Body-weight decreased form 133 kg (SD 22) at inclusion to 92 kg (SD 17) after one year and
89 (SD 18) after two years (p<0·001) representing a 32% (-35 to -30) weight loss after two
years, corresponding to 76% (-81 to -71) excess weight loss. Weight loss was similar in the
adult gastric bypass patients (-31%) while weight gain (+3%) was seen in the conventionally
treated obese adolescents. Significant improvement in cardiovascular and metabolic risk
factors and inflammation was seen after surgery. The treatment was generally well tolerated
and quality of life improved significantly. The surgical adverse events included
cholecystectomies (10%) and operations for internal hernia (9%) but no postoperative
mortality.
Adolescents undergoing laparoscopic gastric bypass surgery achieve similar weight loss to
adults. Improvements in risk factors and quality-of-life were substantial. There were surgical
complications similar to the adult group, which may be preventable.
Key words: Adolescent, bariatric, surgery, gastric bypass

3
Introduction
An increased risk of cardiovascular and endocrine disorders, metabolic syndrome, various
cancers and psychological problems in adolescents with severe obesity1-3 collectively results
in an increased risk of reduced quality of life and shorter life expectancy4. Yet behavioral
intervention constitutes the cornerstone of childhood and adolescent obesity treatment,3 the
results for adolescents are modest5. Among obese adolescents, the effect seems to be absent
and undoubtedly insufficient for long-term risk reduction6.
The most successful long-term treatment strategy for severely obese adults is bariatric
surgery, where long-term weight loss is associated with a decrease in mortality and morbidity
and improvements in quality of life7-9.
Few reports on bariatric surgery in adolescents exist in the literature, and surgery is not
generally endorsed under the age of 18 years except in extreme cases10. O’Brien and
colleagues published the only randomized trial between lifestyle intervention and
laparoscopic gastric banding surgery for morbid obesity demonstrating favorable weight loss
and improvements in cardiovascular risk factors as well as improved quality of life in the
surgically treated group11.
This paper, based on A Swedish nationwide study (AMOS)12, addresses the safety and
efficacy of using laparoscopic Roux-en-Y gastric bypass (gastric bypass) surgery in severely
obese adolescents which were followed for up to five years postoperatively regarding adverse
events. We are also reporting previously published data regarding weight changes up to two
years, in comparison to a conventionally treated adolescents group and an adult group
undergoing the same surgery as well as changes in metabolic risk factors and quality of life.

4
Material and Methods
Baseline characteristics and 1 and 2 year outcomes has previously been reported for three
groups of patients recruited between February 2006 and June 200912. The study is called
AMOS (Adolescent Morbid Obesity Surgery). In this paper we summarize results and expand
the presentation regarding surgical adverse events until Sept 2013.
Obese adolescents treated with gastric bypass
All adolescents referred to three specialist pediatric units in Sweden (Stockholm, Gothenburg
and Malmö) were offered assessment for gastric bypass surgery if they had been in a
comprehensive weight program and fulfilled the inclusion criteria of the study.
Inclusion criteria
- Consent to undergo surgical treatment
- Aged 13–18 years
- BMI≥40 or
- ≥35 kg/m2 with comorbidity (type 2 diabetes, sleep apnea, joint pain, high blood lipids).
- Pubertal Tanner stage >III and passed peak height growth velocity
Exclusion criteria
- Severe or insufficiently treated psychiatric disorder
- Ongoing drug abuse
- Obesity due to syndromes, monogenic disease or brain injury
- Reluctance to undergo long-term follow-up
Eighty-two adolescents were recruited. They had been in a comprehensive conventional
treatment program for at least one year and had passed the assessment for inclusion and
exclusion criteria after meeting a pediatrician, psychologist and dietician. Recruitment took

5
place between Feb 2006 and April 2009. One of the patients refused surgery on the day of the
operation; thus, 81 individuals (35% boys) underwent surgery (Table 1).
Controls
Obese adolescent receiving conventional treatment= controls
During the recruitment period, 81 adolescents (43% boys) were selected from the Childhood
Obesity Register in Sweden (BORIS) as conventional treatment controls (Table 1.)
Obese adults treated with gastric bypass
Eighty-one obese adults undergoing gastric bypass were matched by gender with the obese
adolescents obtaining surgery, ensuring that date of surgery coincided within ±1 month (table
1). The inclusion age was 35–45 years at surgery; all other inclusion and exclusion criteria
were the same as for the adolescents (Table 1).
Anthropometry, height and weight
Height was measured to the closest centimeter using a wall-mounted standard stadiometer
with the patient in standing position. Weight was measured with the subject in light clothing
to the nearest 0·1 kilogram on an electronic scale, which was calibrated at regular intervals.
In the adult group, weight was measured at inclusion and one year postoperatively, while two-
year weights were normally from measurement at their general practitioner. (Table 1.)
Surgery
Surgical patients were instructed to remain on a low calorie diet (LCD) for the three weeks
leading to surgery. The laparoscopic Roux-en-Y gastric bypass consisted of a small (<20 ml)
gastric pouch and an ante-colic, ante-gastric Roux-en-Y construction with a 80 cm long Roux

6
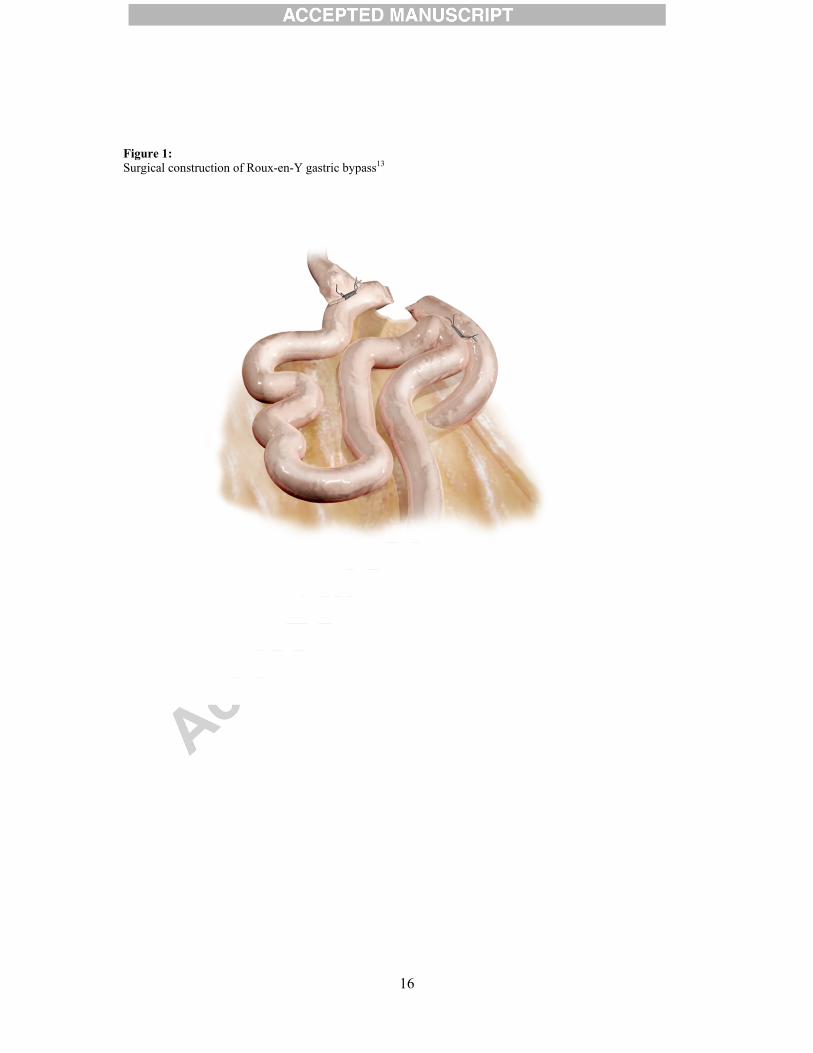
limb as described in detail elsewhere (Fig 1)13.
The technique is an original technique using a “double loop technique” which subsequently is
reconstructed to a true Roux-en-Y construction. The gastro-enteroanastomisis and entero-
entero anastomoses are created using a combined technique of linear stapling and hand
suturing.
Patient is placed in a supine position with the surgeon standing on the patient’s right side and
the assistant on the left. We recommend the use of four 12mm ports along with a Nathanson
liver retractor.
The Gothenburg technique to perform laparoscopic Roux-en-Y gastric bypass has been
established as the “gold standard” for bariatric surgery in the Scandinavian countries and
many surgeons all over the world. The technique was published as an original technique in
2003.13
We consider the main advantages to be:
a. The entire construction can be inspected during the whole procedure, thus limiting the risk
of technical errors
b. The gastro-enteroanastomosis in performed in a simplified way by using a combination of
linear stapling and hand suturing.
c. The technique is reasonably easily learnt, provided a good previous knowledge about
advanced laparoscopic techniques.
Initially was used a seven port technique but over the latest years we have reduced the number
of ports to four 12mm plus using the Nathanson liver retractor. The patient is placed in a
regular supine position with footrest and 30° anti Trendelenburg. Surgeon stands on the

7
patient’s right side and the assistant on the left side.
Some technical issues:
1. The stomach pouch should be as small as technically feasible (<20 cc) aiming at leaving
only 1-2 cm of free stomach wall below the fatty pad of cardia on the anterior wall and avoid
including bulging back wall of the stomach.
2. A routine vertical split of the omentum enables a relatively easy pull up of the loop to the
pouch in almost all cases.
3. One should beware not to kinking the jejuno-jejunostomy if closure of the mesenteric
defect is used. This can lead to relative or total obstruction. However, mesenteric windows
were not routinely closed at the time of the study, but is today.
The technique includes no element in any way to limit the lumen of the GE thus leaving a
fully open passage for food to pass direct to the Roux limb. Our figures for postoperative
weight-loss match international standards (84% excess weight loss after 2 years), indicating
that a stoma size limitation is not an essential mechanism of action in the gastric bypass
construction.
One of two experienced gastric bypass surgeons performed all procedures, assisted by a
pediatric surgeon. All subjects, both adolescents and adults, were operated at Sahlgrenska
University Hospital, using the same surgical technique.
Follow-up after surgery
The adolescent surgical patients were assessed one month before surgery and 1, 3, 6, 12, and
24 months after surgery. Body weight and biochemical analyses were performed
preoperatively and at 12 and 24 months after surgery.

8
All subjects in the adolescent surgical group were prescribed daily multivitamin and mineral
supplements, vitamin B12 and Calcium–Vitamin D combination tablets. The girls were
prescribed iron tablets in addition.
Health-related quality of life
SF-36 v2 was used to measure generic health-related quality of life.14 SF-36 comprises eight
general health domains and scale scores range from 0 to 100, with higher scores indicating
better health status. Summary scores for physical and mental health are calculated using
norm-based scoring with a mean of 50.
Adverse events
Surgical adverse events have prospectively been assessed up to five years postoperatively in
surgical subjects. Adverse events were prospectively recorded in an e-CRF. A complementary
retrospective survey of medical records was conducted to capture missing data.
Statistical analysis
Descriptive statistics are given as means with standard deviations or medians with range.
Changes over time are expressed with 95% confidence intervals.
All p-values are two-tailed and p<0.05 was considered statistically significant. Statistical
analyses were carried out using the Stata statistical package 10.1 (Stata-Corp. 2007. Stata
Statistical Software: Release 10.1. College Station, TX; StataCorp LP.).
9
Results:
Baseline characteristics
Conventionally treated adolescents had a somewhat lower BMI than surgically treated
adolescents at baseline (BMI 42.0 vs. 45.5 respectively), and the corresponding values for
BMI standard deviation score were 3.9 vs. 4.1 (table 1). The proportion of males was 35% in
both surgical groups and 43% in conventionally treated adolescents. The mean body weight at
inclusion was 133 kg (SD 22 kg) in adolescents undergoing surgery, 124 kg (SD 21 kg) in
conventionally treated adolescents and 127 kg (SD 20 kg) in adults undergoing surgery. Mean
ages in the surgical groups were 16.5 years (SD 1.2) for adolescents undergoing surgery, 39.7
years (SD 2.9) for the adults and 15.8 years (SD 1.2) for the conventionally treated
adolescents.
In the adolescent surgical group twenty-five (31%) had neuropsychiatric diagnoses, 13 (16%)
had existing or previous self-destructive behavior and 33 (41%) had contacts with pediatric
psychiatric units. Poor school performance (truancy, leaving school without a diploma) was
frequently reported (>50%). Twenty-six adolescents (32%) had no recorded psychosocial
problems.
Primary hospitalization and postoperative complications
Median surgical time was 63 min (range 38–106) in the adolescent group. Median
postoperative inpatient stay was 4 days (range 2–11). None of the patients required treatment
in the intensive care unit. Two patients required blood transfusions for postoperative bleeding
and another was re-hospitalized with fever three days after being discharged and received
intravenous antibiotics due to an intra-abdominal infection confirmed by CT scan.

10
Weight changes
There was a 100% follow-up rate at one and two years for weight and height in both groups
undergoing surgery. In the conventionally treated adolescent group there was a 100% follow-
up for weight after one year, but this dropped to 73% (59 individuals) after two years.
As demonstrated in figure 2, there was a similar reduction in weight in the adolescent and
adult groups undergoing surgery, while conventionally treated adolescents had increased their
weight slightly. Weight change after two years was -32% (CI -35% to -30%) in surgically
treated adolescents, as compared to weight gain of +3% (CI 0–7%) in the conventionally
treated adolescents, and weight loss of -31% (CI -34% to -29%) in adults undergoing surgery.
Ninety-five per cent of operated adolescents achieved a weight loss exceeding 50% of excess
weight.
There were no significant differences in the weight loss between genders. Fifty-seven per cent
of the adolescents in the surgical group had a continuing weight loss while 43% increase in
weight during the second year after surgery (range -9.7 to +4.2 kg).
Changes in quality of life
In summary, one-year follow-up, significant improvements were observed in seven of the
eight SF-36 health domains and in the physical component summary score12. After two years,
significant improvements compared to baseline were evident in all four physical health
domains, in the physical component summary score, and in two of the four mental health
domains. Minor decreases in SF-36 scale scores between one- and two-year follow-up did not
reach significance.

11
Adverse events in surgically treated adolescents
During the two-year follow-up, twelve adolescents (15%) underwent additional surgical
interventions, five (6.2%) needed an operation for internal hernia; six (7.4%) underwent
cholecystectomy due to symptomatic gallstone and one was laparoscopically operated with
finding of adhesions. Four patients visited an emergency intake due to non-specific abdominal
pain. Additional incomplete follow up until five years postoperatively revealed four others
operated for ileus, two for internal hernias and two more were cholecystectomized. All
remedial surgeries were performed by laparoscopy.
We identified poor compliance in the intake of prescribed vitamin and mineral supplements in
two thirds of patients.
Excess skin
Most adolescents having undergone surgery experienced problems with excessive skin
following weight loss; this aspect was not formally addressed in the current study.
Discussion
In this study we could demonstrate a substantial weight loss over two years (32%) following
gastric bypass surgery for severely obese adolescents, which was similar to the weight loss in
an adult comparison group (31%). Ninety-five per cent of operated adolescents achieved more
than 50% excess weight loss. Minor weight gain (3%) was seen in conventionally treated
adolescents. Cardiovascular risk factors were ameliorated, mirrored by lowering of insulin
and serum lipids levels, and a reduction of inflammatory activity12. Furthermore, we have
shown improvement in quality of life after surgery, although psychological and surgical
adverse events occurred.
RYGB has established as the “gold standard” in Scandinavian bariatric surgery and

12
constitutes currently more than 90% of bariatric procedures. One previous study has
demonstrated that laparoscopic gastric banding is feasible and effective in adolescents
recruited directly from the community when compared to the best conventional therapy11. In
contrast, other studies have not been successful with gastric banding in adolescents15. A
previous gastric banding study for adolescents in Sweden was abandoned due to poor results
and, together with the fact that gastric bypass has compared favorably with gastric banding in
most studies, we considered gastric bypass to offer the best trade-off between weight loss and
initial risks with surgery.
We currently recommend closure of mesenteric defects as also proposed by others16. At the
time of surgery in this study we hadn’t established a safe technique for closure of defects and
therefore didn’t want to insert an element of learning curve in this series. A medical
prophylaxis for gallstone formation was not used in this series but obviously even adolescent
develop gallstones as a result of rapid weight and a prophylaxis with ursodeoxycholic acid
should be considered17.
We offered surgery to a consecutive group of adolescents demonstrating a high prevalence of
psychiatric and psychosocial morbidity and refractory to conventional treatment in tertiary
medical centers involved in this study. Despite having a fourth of outpatient visits compared
to the study by O’Brien et al11, the weight loss among adolescents in this study was similar to
an adult comparison group undergoing gastric bypass surgery. This indicates that
physiological mechanisms are strong determinants of weight loss after gastric bypass surgery
rather than learned lifestyle changes. Until recently, the success of gastric bypass was
attributed to mechanical restriction through gastric volume reduction and calorie
malabsorption as a consequence of the bypass of the duodenum and proximal jejunum. Other

13
mechanisms contributing to weight loss after gastric bypass include: reduced hunger18,
augmented satiety19-21, increased energy expenditure22 , and altered taste perception, all of
which may be at least partly mediated by alterations in gastrointestinal and central neuro-
endocrine signaling.
We observed a substantial amelioration in cardiovascular risk factors with significantly better
glucose and lipid control, as previously demonstrated in adults12. A theoretical advantage of
early intervention would be a shorter exposure to metabolic risk factors and thereby reduced
risk for developing structural and functional cardiovascular impairment. Furthermore, fasting
insulin levels decreased to one fourth of preoperative levels. We also found a major decrease
in inflammatory activity postoperatively, as previously demonstrated in adults after bariatric
surgery23 .
A possible disadvantage of intervention in adolescents could be their physical and
psychological immaturity. Therefore, the poor compliance in vitamin and mineral
supplementation requires careful attention for a long time. Another issue that needs
consideration in adolescents is the development of excessive skin as a result of weight loss,
which we will address in a separate paper from this study.
There were broad improvements in quality of life in adolescents after surgery from a group
perspective, supporting the findings of a previous study24. We consciously did not exclude
patients with psychiatric and psychosocial problems in this study possibly leading to more
psychosocial issues in the cohort. When treating this group of patients the multidisciplinary
team must offer an extended postoperative support role, as recommended previously25.

14
In summary, we have demonstrated that RYGB surgery results in similar weight loss in
adolescents as in adults over two years. We found substantial improvements in risk factors for
co-morbidities and improvements in quality of life. Nonetheless, the surgical and psychiatric
adverse events that appeared in this psychosocially vulnerable cohort require careful attention.
It appears so far that RYGB is a viable option for future interventional studies in severely
obese adolescents.
Acknowledgements:
Primary funding source: Research council, Västra Götalandsregionen, Sweden,
http://www.vgregion.se/sv/Vastra-Gotalandsregionen/startsida/
Additional funding source:
Fru Mary von Sydow’s foundation, Gothenburg, Sweden

15
Legends to figures Figure 1: Surgical construction of Roux-en-Y gastric bypass13
Figure 2 Weight change over two years in adolescents and adults undergoing gastric bypass surgery (n=81+81) and adolescents in conventional treatment (n=81). Mean (95% CI). Table 1: Baseline anthropometric characteristics Table 2. Surgical adverse events up to 5years postoperatively in 81 adolescents who have undergone Laparoscopic gastric bypass
16
Figure 1: Surgical construction of Roux-en-Y gastric bypass13

17
Figure 2 Weight change over two years in adolescents and adults undergoing gastric bypass surgery (n=81+81) and adolescents in conventional treatment (n=81). Mean (95% CI).

18
Table 1: Baseline anthropometric characteristics BMI values were related to Swedish standards for age and gender with standard deviation score (BMI SDS). Mean (SD).
Adolescents -surgery
Adolescents-control with obesity
Adults- surgery
number total 81 81 81
male/ female 28/53 35/46 28/53 Age (yrs)
total 16.5 (1.2) 15.8 (1.2) 39.7 (2.9) male 16.6 (1.3) 15.9 (1.2) 40.2 (3.5)
female 16.5 (1.1) 15.7 (1.3) 39.5 (2.6) Height (m)
total 1.71 (9.3) 1.71 (9.3) 1.71 (0.1) male 1.78 (10.4) 1.78 (7.9) 1.82 (0.1)
female 1.67 (6.4) 1.66 (7.7) 1.66 (0.1) Weight (kg)
total 133 (22) 124 (21) 127 (20) male 147 (23) 135 (20) 142 (17)
female 125 (17) 115 (17) 120 (17) BMI (kg/m2)
Total 45.5 (6) 42.0 (5) 43.5 (5) male 47.0 (6) 43.0 (5) 43.0 (6)
female 45.0 (6) 42.0 (5) 44.0 (5) BMI (SDS)
total 4.1 (0.45) 3.9 (0.39) nd male 4.4 (0.45) 4.0 (0.39) nd
female 4.1 (0.43) 3.9 (0.39) nd
19
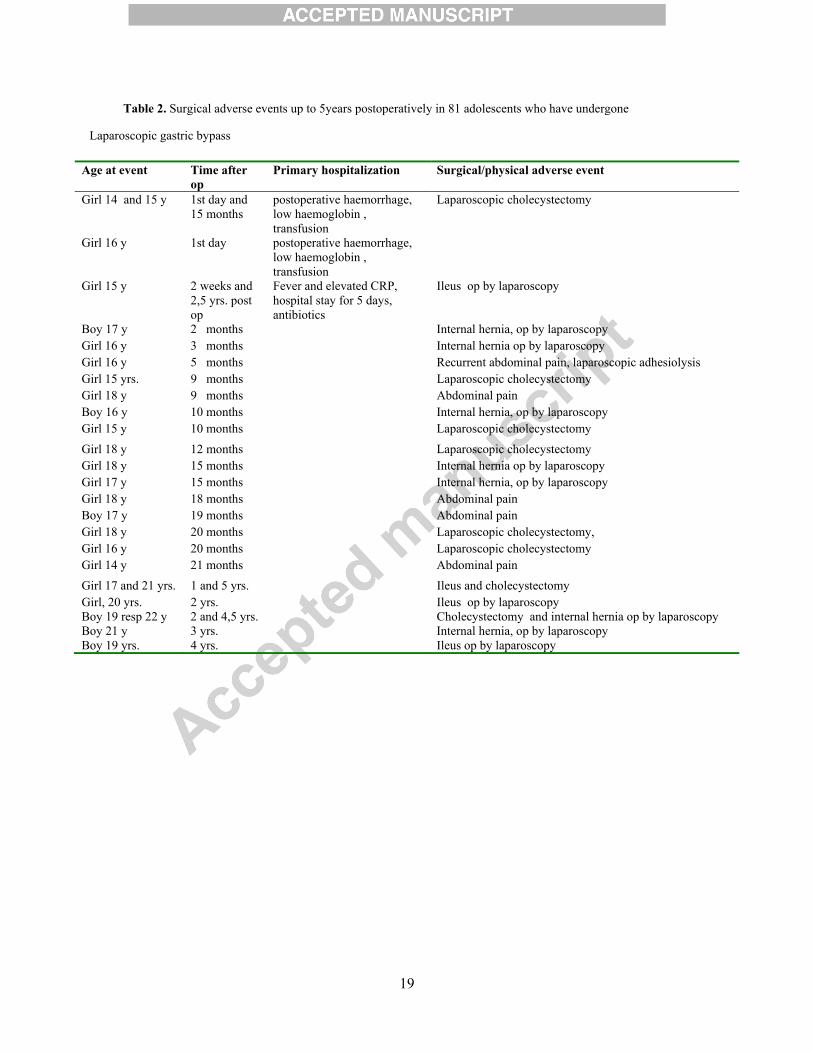
Table 2. Surgical adverse events up to 5years postoperatively in 81 adolescents who have undergone
Laparoscopic gastric bypass
Age at event Time after op
Primary hospitalization Surgical/physical adverse event
Girl 14 and 15 y 1st day and 15 months
postoperative haemorrhage, low haemoglobin , transfusion
Laparoscopic cholecystectomy
Girl 16 y 1st day postoperative haemorrhage, low haemoglobin , transfusion
Girl 15 y 2 weeks and 2,5 yrs. post op
Fever and elevated CRP, hospital stay for 5 days, antibiotics
Ileus op by laparoscopy
Boy 17 y 2 months Internal hernia, op by laparoscopy Girl 16 y 3 months Internal hernia op by laparoscopy Girl 16 y 5 months Recurrent abdominal pain, laparoscopic adhesiolysis Girl 15 yrs. 9 months Laparoscopic cholecystectomy Girl 18 y 9 months Abdominal pain Boy 16 y 10 months Internal hernia, op by laparoscopy Girl 15 y 10 months Laparoscopic cholecystectomy Girl 18 y 12 months Laparoscopic cholecystectomy Girl 18 y 15 months Internal hernia op by laparoscopy Girl 17 y 15 months Internal hernia, op by laparoscopy Girl 18 y 18 months Abdominal pain Boy 17 y 19 months Abdominal pain Girl 18 y 20 months Laparoscopic cholecystectomy, Girl 16 y 20 months Laparoscopic cholecystectomy Girl 14 y 21 months Abdominal pain Girl 17 and 21 yrs. 1 and 5 yrs. Ileus and cholecystectomy Girl, 20 yrs. 2 yrs. Ileus op by laparoscopy Boy 19 resp 22 y 2 and 4,5 yrs. Cholecystectomy and internal hernia op by laparoscopy Boy 21 y 3 yrs. Internal hernia, op by laparoscopy Boy 19 yrs. 4 yrs. Ileus op by laparoscopy

20
References 1. Baker JL, Olsen LW, Sorensen TI. Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med 2007; 357(23): 2329-37. 2. Biro FM, Wien M. Childhood obesity and adult morbidities. The American journal of clinical nutrition 2010; 91(5): 1499S-505S. 3. Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA : the journal of the American Medical Association 2003; 289(2): 187-93. 4. Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet 2010; 375(9727): 1737-48. 5. Oude Luttikhuis H, Baur L, Jansen H, et al. Interventions for treating obesity in children. Cochrane Database Syst Rev 2009; (1): CD001872. 6. Danielsson P SV, Kowalski J, Nyberg G, Ekblom Ö and Marcus C. Importance of Age for Three-year Continuous Behavioral Obesity Treatment Success and Dropout Rate. Obesity Facts 2011; 5(2012:1): 34-44. 7. Karlsson J, Taft C, Ryden A, Sjostrom L, Sullivan M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. International journal of obesity (2005) 2007; 31(8): 1248-61. 8. Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004; 351(26): 2683-93. 9. Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007; 357(8): 741-52. 10. Inge TH, Xanthakos SA, Zeller MH. Bariatric surgery for pediatric extreme obesity: now or later? International journal of obesity (2005) 2007; 31(1): 1-14. 11. O'Brien PE, Sawyer SM, Laurie C, et al. Laparoscopic adjustable gastric banding in severely obese adolescents: a randomized trial. JAMA : the journal of the American Medical Association 2010; 303(6): 519-26. 12. Olbers T, Gronowitz E, Werling M, et al. Two-year outcome of laparoscopic Roux-en-Y gastric bypass in adolescents with severe obesity: results from a Swedish Nationwide Study (AMOS). International journal of obesity (2005) 2012; 36(11): 1388-95. 13. Olbers T, Lonroth H, Fagevik-Olsen M, Lundell L. Laparoscopic gastric bypass: development of technique, respiratory function, and long-term outcome. Obesity surgery 2003; 13(3): 364-70. 14. Taft C, Karlsson J, Sullivan M. Performance of the Swedish SF-36 version 2.0. Qual Life Res 2004; 13(1): 251-6. 15. Widhalm K, Dietrich S, Prager G, Silberhummer G, Orth D, Kispal ZF. Bariatric surgery in morbidly obese adolescents: a 4-year follow-up of ten patients. Int J Pediatr Obes 2008; 3 Suppl 1: 78-82. 16. Rodriguez A, Mosti M, Sierra M, et al. Small bowel obstruction after antecolic and antegastric laparoscopic Roux-en-Y gastric bypass: could the incidence be reduced? Obesity surgery 2010; 20(10): 1380-4. 17. Miller K, Hell E, Lang B, Lengauer E. Gallstone formation prophylaxis after gastric restrictive procedures for weight loss: a randomized double-blind placebo-controlled trial. Annals of surgery 2003; 238(5): 697-702. 18. Schultes B, Ernst B, Wilms B, Thurnheer M, Hallschmid M. Hedonic hunger is increased in severely obese patients and is reduced after gastric bypass surgery. The American journal of clinical nutrition 2010; 92(2): 277-83.

21
19. Korner J, Bessler M, Cirilo LJ, et al. Effects of Roux-en-Y gastric bypass surgery on fasting and postprandial concentrations of plasma ghrelin, peptide YY, and insulin. J Clin Endocrinol Metab 2005; 90(1): 359-65. 20. Laferrere B, Teixeira J, McGinty J, et al. Effect of weight loss by gastric bypass surgery versus hypocaloric diet on glucose and incretin levels in patients with type 2 diabetes. J Clin Endocrinol Metab 2008; 93(7): 2479-85. 21. le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Annals of surgery 2006; 243(1): 108-14. 22. Bueter M, Lowenstein C, Olbers T, et al. Gastric bypass increases energy expenditure in rats. Gastroenterology 2010; 138(5): 1845-53. 23. Sovik TT, Aasheim ET, Taha O, et al. Weight loss, cardiovascular risk factors, and quality of life after gastric bypass and duodenal switch: a randomized trial. Ann Intern Med 2011; 155(5): 281-91. 24. Zeller MH, Reiter-Purtill J, Ratcliff MB, Inge TH, Noll JG. Two-year trends in psychosocial functioning after adolescent Roux-en-Y gastric bypass. Surg Obes Relat Dis 2011. 25. Jarvholm K, Olbers T, Marcus C, et al. Short-term psychological outcomes in severely obese adolescents after bariatric surgery. Obesity (Silver Spring); 20(2): 318-23.
Copyright © 2022 FDOKUMEN




















