Injury care in low- and middle-income countries: identifying potential for change
Upload
khangminh22Category
view
3download
0
IVF and other ART in low- andmiddle-income countries a systematiclandscape analysisTendai M Chiware 12 Nathalie Vermeulen 3Karel Blondeel 24 Roy Farquharson3 James Kiarie2Kersti Lundin35 Thabo Christopher Matsaseng26Willem Ombelet78 and Igor Toskin 21Department of Obstetrics Gynecology amp Reproductive Sciences University of Vermont Medical Center Burlington VT USA2Department of Reproductive Health and Research UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of ResearchDevelopment and Research Training in Human Reproduction (HRP) World Health Organization Geneva Switzerland 3European Societyof Human Reproduction and Embryology Central Office Grimbergen Belgium 4Faculty of Medicine and Health Sciences GhentUniversity Ghent Belgium 5Reproductive Medicine Sahlgrenska University Hospital Gothenburg Sweden 6Reproductive Medicine UnitDepartment of Obstetrics amp Gynaecology Stellenbosch University Cape Town South Africa 7Faculty of Medicine and Life SciencesHasselt University Hasselt 3500 Belgium 8Genk Institute for Fertility Technology ZOL Hospitals Genk 3600 Belgium
Correspondence address Department of Reproductive Health and Research UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training in Human Reproduction (HRP) World Health Organization GenevaSwitzerland Tel thorn41-22-791-5096 E-mail toskiniwhoint (IT) University of Vermont Medical Center Department of ObstetricsGynecology amp Reproductive Sciences 111 Colchester Ave Smith 422 Mailstop 251 SM4 Burlington VT 05401 USATel thorn1-718-283-8600 E-mail tendaichiwarehotmailcom (TMC) httpsorcidorg0000-0001-6380-3597
Submitted on March 14 2018 resubmitted on August 6 2020 editorial decision on August 31 2020
TABLE OF CONTENTSbull Introductionbull Methods
Search strategy and selection criteriaRisk of bias and data analysis
bull ResultsART reports within regionsCost-limiting initiatives aiming at affordable ARTRisk of bias across studies
bull DiscussionLimitations
BACKGROUND Infertility affects 485 million couples worldwide with a prevalence estimated at 35ndash167 in low- and middle-incomecountries (LMIC) and as high as 30ndash40 in Sub-Saharan Africa ART services are not accessible to the majority of these infertile couplesdue to the high cost of treatments in addition to cultural religious and legal barriers Infertility and childlessness particularly in LMIChave devastating consequences which has resulted in considerable interest in developing affordable IVF procedures However there is apaucity of evidence on the safety efficiency and ability to replicate techniques under different field conditions and how to integrate moreaffordable ART options into existing infrastructures
OBJECTIVE AND RATIONALE This review was performed to investigate the current availability of IVF in LMIC and which other ARToptions are under development This work will unfold the landscape of available and potential ART services in LMIC and is a key elementin positioning infertility more broadly in the Global Public Health Agenda
VC The Author(s) 2020 Published by Oxford University Press on behalf of European Society of Human Reproduction and EmbryologyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc40) whichpermits non-commercial re-use distribution and reproduction in any medium provided the original work is properly cited For commercial re-use please contactjournalspermissionsoupcom
Human Reproduction Update Vol27 No2 pp 213ndash228 2021Advance Access Publication on November 25 2020 doi101093humupddmaa047
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
SEARCH METHODS A systematic literature search was performed of articles and gray literature on IVF and other ART options inLMIC published between January 2010 and January 2020 We selected studies on IVF and other ART treatments for infertile couples ofreproductive age (18ndash44 years) from LMIC The review was limited to articles published after 2010 based on the recent evolution in thefield of ART practices in LMIC over the last decade Citations from high-income countries including data prior to 2010 and focusing onspecialized ART procedures were excluded The literature search included PubMed Popline CINHAL EMBASE and Global IndexMedicus No restrictions were applied with regard to study design or language Two reviewers independently screened the titlesand abstracts and extracted data A search for gray literature was performed using the lsquoGooglersquo search engine and specific databases(worldcatorg greylitorg) In addition the reference lists of included studies were assessed
OUTCOMES The search of the electronic databases yielded 3769 citations After review of the titles and abstracts 283 studies were in-cluded The full texts were reviewed and a further 199 articles were excluded The gray literature search yielded 586 citations most ofwhich were excluded after screening the title and the remaining documents were excluded after full-text assessment due to duplicateentries not from LMIC not relevant or no access to the full document Eighty-four citations were included as part of the review andseparated into regions The majority of the studies were observational and qualitative studies In general ART services are available anddescribed in several LMIC ranging from advanced techniques in China to basic introduction of IVF in some African countries Efforts toprovide affordable ART treatments are described in feasibility studies and efficacy studies however most citations were of low to verylow quality We found no studies from LMIC reporting the implementation of low-cost ART that is effective accessible and affordable tomost of those in need of the services
WIDER IMPLICATIONS The World Health Organization is in a unique position to provide much needed guidance for infertility man-agement in LMIC This review provides insight into the landscape of ART in LMIC in various regions worldwide which will guide efforts toimprove the availability quality accessibility and acceptability of biomedical infertility care including ART in these countries
Key words infertility low- and middle-income countries IVF ART fertility care fertility coverage affordable ART accessible ART
IntroductionThe World Health Organization (WHO) defines health as lsquoa state ofcomplete physical mental and social well-being and not merely the ab-sence of disease or infirmityrsquo (World Health Organization 1948) In2010 an estimated 485 million couples worldwide were infertile de-fined at that time as an inability lsquoto have any live birth over a 5-year pe-riodrsquo (Mascarenhas et al 2012) The overall prevalence of infertility isestimated at 35ndash167 in low- and middle-income countries (LMIC)with the prevalence as high as 30ndash40 in some regions of Sub-SaharanAfrica (Ombelet 2009 Inhorn and Patrizio 2015) Infertility in LMICis more than a health problem it is a social issue and a public healthmatter that continues to be neglected (Bahamondes and Makuch2014)
Infertility is known to cause significant psychological and socialeffects such as fear guilt depression self-blame marital stress emo-tional abuse intimate partner violence divorce and abandonment ofthe partner social isolation economic deprivation loss of social statusand in some regions (eg Africa and Asia) even starvation diseaseviolence-induced suicide and loss of dignity in death (Ombelet et al2008 Hammarberg and Kirkman 2013 Stellar et al 2016)
The most common etiologies of infertility in LMIC are male factorand tubal disease secondary to sexually transmitted infections unsafeabortion and complications of childbirth (Ombelet 2009 van derPoel 2012) Tubal factor infertility is reported to be as high as 85 inSub-Saharan Africa compared with 33 worldwide (Ombelet 2009)The most effective treatment is ART (Sharma et al 2009Bahamondes and Makuch 2014)
Infertility and ART are not considered a priority in many LMICThe most often used arguments against the use of ART are overpopu-lation other health priorities (eg family planning vaccinations malariaHIV) limited government budgets and limited experience of providers
with inadequate facilities for performing sophisticated procedures(Ombelet and Campo 2007) Furthermore in some LMIC ART isconsidered to be expensive only moderately effective with risks ofcomplications and unknown effects on women and their offspring(Ombelet and Campo 2007) In 2008 ESHRE published a series ofmonographs by experts from around the world highlighting the impor-tance of infertility its prevalence access to treatment and outcomes indeveloping countries (ESHRE Special Task Force on lsquoDevelopingCountries and Infertilityrsquo 2008) Along with the WHO and ESHREother non-governmental organizations (NGOs) are involved in initia-tives aimed at improving access to ART in LMIC including theAmerican Society for Reproductive Medicine the InternationalFederation of Gynecology and Obstetrics the International Federationof Fertility Societies and the International Committee for MonitoringAssisted Reproductive Technologies
Providing ART services in an LMIC requires an understanding of thecountry-specific magnitude and character of the issue of infertility aswell as identification of pre-existing resources that may be utilized(Sharma et al 2009 Bahamondes and Makuch 2014) WHO is in aunique position with 194 member states worldwide to assist in evalu-ating the burden of disease by the systematic assessment of infertilityand resources available within various regions
There is complete absence of affordable and accessible ART serv-ices in some LMIC possibly due to high costs of IVF and underdevel-oped infrastructure in addition to cultural religious and legal barriersThis deficiency has led to considerable interest by NGOs policymakers and ART specialists in developing more affordable IVF proto-cols such as minimal ovarian stimulation However there is a paucityof evidence and systematic reviews on the safety and efficiency profileof low-cost ART on the ability to replicate various techniques in differ-ent laboratories and under various field conditions and on how to inte-grate ART into existing health systems and infrastructures
214 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
This review investigated the currently available IVF services in LMIC
and potential for future development This work will assist in unfoldingthe landscape of available services and the potential for ART servicesin LMIC This is a key element in positioning infertility more broadly inthe Global Public Health Agenda of WHO This work will also informfuture WHO guidelines concerning the provision of ART in LMIC
MethodsThis review was reported in accordance with the PRISMA andGATHER guidelines (Moher et al 2009 Stevens et al 2016) Theprotocol was registered on 24 April 2017 and published withPROSPERO International prospective register of systematic reviews(ID number CRD42017064413) There were no amendments to theprotocol after registration
Search strategy and selection criteriaThe electronic databases searched included PubMed PoplineCINAHL EMBASE and Global Index Medicus (regional WHO onlinedatabases) Citations were collected from inception until 1 January2020 An internet search was performed using lsquoGooglersquo search enginewith the terms lsquoinfertilityrsquo lsquolow- and middle-income countriesrsquo andlsquoin vitro fertilizationrsquo or lsquoassisted reproductive technologiesrsquo (limited toresults published after 2010) Similar search terms were used for grayliterature databases (worldcatorg greylitorg) In addition the refer-ence lists of included studies were checked Experts and professionalswithin the field of infertility and the members of the ESHRE SpecialInterest Group Global and Socio-cultural Aspects of Infertility(nfrac14 221) were contacted to provide information on any unpublishedpapers or data on the subject of lsquoART in low- and middle-incomecountriesrsquo
Search strategies were customized for each electronic databaseaccording to their individual subject headings and searching structureThe search strategy used for PUBMED is available in Supplementarydata In constructing the search terms accepted definitions of ARTand IVF were used (Zegers-Hochschild et al 2009 et al 2017) LMICwere defined according to the World Bank classification of countriesby Gross National Income per capita (low-income country (LIC) up to$995 lower-middle-income country (lower MIC) $996 to $3895 andupper-middle-income country (upper MIC) $3896 to $12 055)(World Bank Country and Lending Groups) Upper MIC which oftenhave ART services on par with high-income countries were labeled todistinguish them from LIC and lower MIC For this review no restric-tions were applied with regard to study design or language Reviewerswere able to read English French German Italian PortugueseSpanish and Russian studies Reports in other languages were includedand authors were asked to provide a translated version or some ofthe details of the study in English Endnote (Version X8) bibliographicsoftware was used to store the citations and remove duplicates
For inclusion in the review we selected citations on ART for adultwomen and men of reproductive age (18ndash44 years old) from LMIC(experiencing reproductive difficulties or infertility) All identified cita-tions irrespective of language published over the last decade from 1January 2010 to 1 January 2020 were assessed The review was limitedto articles published after 2010 based on the recent evolution in the
field of ART practices in LMIC over the last decade ART is defined asall interventions that include the in vitro handling of both humanoocytes and sperm or of embryos for the purpose of reproductionThis includes but is not limited to IVF and embryo transfer ICSI em-bryo biopsy preimplantation genetic testing assisted hatching gameteintrafallopian transfer zygote intrafallopian transfer gamete and em-bryo cryopreservation semen oocyte and embryo donation and ges-tational carrier cycles (Zegers-Hochschild et al 2017) This reviewfocused on IVF and embryo transfer procedures being performed inLMIC over the last decade Articles focusing solely on ICSI specializedART procedures and that did not discuss IVF were excluded Themain reason for this restriction was these advanced procedures not al-ways being accessible or affordable to the general population in anLMIC where the cost of ART is estimated to be up to 50 higherthan the gross national per capita income of many LMIC (Vayenaet al 2009)
Concerning outcomes articles were assessed for quantitative out-comes on the efficacy of the ART (mainly pregnancy rate or live birthrate (LBR)) or qualitative and quantitative outcomes on feasibility Wedefined feasibility as the process in which low-cost ART are deployedleading to their acceptability and usability All citations were evaluatedbased on the titles and abstracts by two independent reviewers(TMC and NV) In the absence of sufficient data in the abstract toassess relevance the full text was obtained A list of the excludedreports is available from the authors upon request The full-textreports were assessed for relevance and the data extracted by two in-dependent reviewers (TMC and NV) A third reviewer (IT) wasavailable to resolve queries and disagreements Attempts were madeto contact the authors to obtain missing information or clarificationwhenever necessary
Risk of bias and data analysisThe protocol for this review included assessment of risk of bias for allindividual articles The majority of included articles did not assess quan-titative outcomes (efficacy or others) related to a therapeutic or diag-nostic intervention but merely reported on feasibility (currentpractice) in a narrative fashion For studies assessing efficacy of inter-ventions the majority were either very small feasibility or pilot studies(assessed as high to very high risk of bias) or they were available onlyas an (conference) abstract For the remaining interventional studiesrisk of bias was assessed with the risk of bias in non-randomized stud-ies of interventions (ROBINs)-1 tool (Sterne et al 2016) Risk of biaswas only assessed when the full-text paper could be retrieved Thecollected data were as expected highly heterogeneous Statisticalcomparison of the data was not possible due to the variable studydesign and quantitative data in the included citations The resultsfrom included citations were collated in a descriptive fashion andmeta-analysis was not feasible
ResultsAn extensive search of the databases yielded 3769 citations afterremoval of duplicate entries After review of the titles and abstracts283 articles were included (Fig 1) The full texts of 283 articles werereviewed including case reports review papers commentaries gray
IVF in low- and middle-income countries 215
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
literature and abstracts from conference proceedings A further 199citations were excluded The gray literature search yielded 586 cita-tions of which 334 were excluded after screening of the title Furtherassessment of the remaining gray literature documents resulted in allcitations being excluded Exclusion of citations was based on duplicateentries from the database searches not LMIC not relevant or no ac-cess to the full document Of the 84 included articles 63 citationsmostly qualitative and observational studies described an overall pic-ture (efficacy feasibility and acceptability) of ART in LMIC Thesearticles were summarized into regions (Supplementary Tables SI-VIFig 2) Fourteen studies reported on the efficacy and feasibility ofcost-limiting initiatives aimed at affordable ART in LMIC (Table I) Asystematic review of literature was conducted however due to theheterogeneity of the included articles the results are collated and pre-sented here in a narrative fashion
ART reports within regionsEast Asia and PacificART in the region of East Asia and Pacific is described as a rapidlygrowing business (Wahlberg 2016) A survey reported that in thecountries within this region for which information was collected(China Indonesia Korea Malaysia Mongolia Myanmar PhilippinesSingapore Thailand and Vietnam) IVF is available for couples although
subsidized only in Singapore and Korea (Li et al 2018) Nine citationsreported mostly on the current practice in China and Thailand whichare upper MIC and may not be representative of the practice in LMICwithin this region (Supplementary Table SI) China is depicted as havinghigh standards of practice and technological developments are aggres-sively pursued (Ha 2013) Efficacy of ART in China was described assimilar to efficacy in developed high-income European countries suchas France and Spain (LBR per started cycle of 47 in womenlt35 years old from ART) (Audibert and Glass 2015) As expectedChina with a high population is also unique in the high number of IVFcycles and the term lsquoscaled up IVFrsquo has been used with 145 108 livebirths reported after ART in 2013 (Wahlberg 2016) Other countriesin this region report the use of ART to a lesser extent but there wereno articles describing the efficacy of treatments (Ye et al 2013)
With regards to the feasibility of ART a study from Indonesiareported barriers to access which included low confidence in infertilitytreatment high rates of switching between providers due to treatmentfailure the number and location of clinics the lack of a well-established referral system the cost of treatment and patients withfear of receiving the diagnosis of infertility fear of vaginal examinationsor embarrassment (Bennett et al 2012) In Thailand ART treatmentis considered out of reach for most average-income people In addi-tion three-quarters of infertility clinics are located in urban centerslimiting physical accessibility for rural populations (Whittaker 2016)
Records idenfied through database search
(n = 3868)
Screen
ing
Inclu
ded
Eligibility
Iden
ficao
n
Addional records idenfied through other sources
(n = 586)
Records aer duplicates removed (n = 3769)
Records screened (n = 3769)
Records excluded (n = 3486)
Full-text arcles assessed for eligibility
(n = 283)
Full-text arcles excluded with jusficaon
(n = 199)
Studies included in qualitave synthesis
(n = 84)
Studies included in quantave synthesis
(meta-analysis) (NA)
Figure 1 PRISMA flow diagram of included and excluded studies of the review
216 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
One report from China found lower cost with recombinant FSH com-pared to highly purified FSH with similar pregnancy outcomes and LBRbetween the groups (Ye et al 2013) Concerning acceptability it isreported that shame and stigma have decreased over time and ART isnow an accepted way to conceive (Whittaker 2016) Although ARTis well developed in China it is still out of reach for most infertile cou-ples due to an enormous demand for treatment resulting in long wait-ing times and costs estimated between US$5000 and US$16 000 perIVF cycle which is not covered by public or private insurance (Qiaoand Feng 2014 Audibert and Glass 2015)
Europe and Central AsiaART in Europe is widely studied and reported by the European IVFMonitoring Programme Six citations were included from LMIC whichwere all from upper MIC (Supplementary Table SII) Large differencesstill exist between the number of cycles per 1 million women (aged15ndash45 years) in these countries but overall there is reportedly goodaccess to ART services (European IVF monitoring Consortium (EIM)for the European Society of Human Reproduction and Embryologyet al 2017) Regarding efficacy of IVF the data reported from LMICare comparable to those in other higher income European countries(European IVF monitoring Consortium (EIM) for the European Societyof Human Reproduction and Embryology et al 2017) An LBR of172 per transfer was reported in Bosnia Herzegovina and 265 inSerbia both upper MIC (Balic 2011 Mitic et al 2012)
With regard to the feasibility and acceptability the costs of treat-ment are most often discussed along with legislative issues and regula-tions In Turkey government funding is reportedly provided (up to
two IVF cycles in women aged 23ndash39 years old) only if all otheroptions have been exhausted (Urman and Yakin 2010) Turkish ARTcenters are required to be licensed by the government (Aytoz 2012)In contrast other countries have reported very little regulation andART is influenced by market forces For example in Bulgaria whereminimal regulation of ART is described access and outcomes arepoor with 10 IVF clinics and low financial support for IVF treatments(Balabanova and Simonstein 2010) Within Europe a recent collabora-tive audit between ESHRE and the patient organization Fertility Europedemonstrated clear discrepancies in availability accessibility and fundingsupport within nine selected European Union countries (2017 FertilityEurope and European Society of Human Reproduction andEmbryology (ESHRE) 2017) Only one study reported on the attitudestoward ART a survey of 136 medical students nurses and doctors inRussia (upper MIC) reporting that 972 of respondents knew enoughabout ART and had a positive attitude toward it (Khamoshina et al2010)
Latin America and the CaribbeanData on the number of IVF clinics and treatment cycles are reportedin the Latin American Registry of Assisted Reproduction (REDLARA)(Zegers-Hochschild et al 2013 2014 2015 2016) The number ofcenters and countries in this region reporting data is increasing with13 citations included in the review (Supplementary Table SIII)Countries like Argentina and now Uruguay with a consistent policy to-ward recognizing the human right to start a family and ensuring accessto care demonstrated the highest number of ART cycles per popula-tion in contrast to countries where treatment depends on the
Figure 2 Results of studies from LMIC summarized within regions The numbers in parentheses represent the number of studies foundwithin regions and a summary of their themes is shown LMIC low- and middle-income countries Adapted from SDG Atlas 2018 The World ByRegion httpdatatopicsworldbankorgsdgatlasthe-world-by-regionhtml
IVF in low- and middle-income countries 217
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

SEARCH METHODS A systematic literature search was performed of articles and gray literature on IVF and other ART options inLMIC published between January 2010 and January 2020 We selected studies on IVF and other ART treatments for infertile couples ofreproductive age (18ndash44 years) from LMIC The review was limited to articles published after 2010 based on the recent evolution in thefield of ART practices in LMIC over the last decade Citations from high-income countries including data prior to 2010 and focusing onspecialized ART procedures were excluded The literature search included PubMed Popline CINHAL EMBASE and Global IndexMedicus No restrictions were applied with regard to study design or language Two reviewers independently screened the titlesand abstracts and extracted data A search for gray literature was performed using the lsquoGooglersquo search engine and specific databases(worldcatorg greylitorg) In addition the reference lists of included studies were assessed
OUTCOMES The search of the electronic databases yielded 3769 citations After review of the titles and abstracts 283 studies were in-cluded The full texts were reviewed and a further 199 articles were excluded The gray literature search yielded 586 citations most ofwhich were excluded after screening the title and the remaining documents were excluded after full-text assessment due to duplicateentries not from LMIC not relevant or no access to the full document Eighty-four citations were included as part of the review andseparated into regions The majority of the studies were observational and qualitative studies In general ART services are available anddescribed in several LMIC ranging from advanced techniques in China to basic introduction of IVF in some African countries Efforts toprovide affordable ART treatments are described in feasibility studies and efficacy studies however most citations were of low to verylow quality We found no studies from LMIC reporting the implementation of low-cost ART that is effective accessible and affordable tomost of those in need of the services
WIDER IMPLICATIONS The World Health Organization is in a unique position to provide much needed guidance for infertility man-agement in LMIC This review provides insight into the landscape of ART in LMIC in various regions worldwide which will guide efforts toimprove the availability quality accessibility and acceptability of biomedical infertility care including ART in these countries
Key words infertility low- and middle-income countries IVF ART fertility care fertility coverage affordable ART accessible ART
IntroductionThe World Health Organization (WHO) defines health as lsquoa state ofcomplete physical mental and social well-being and not merely the ab-sence of disease or infirmityrsquo (World Health Organization 1948) In2010 an estimated 485 million couples worldwide were infertile de-fined at that time as an inability lsquoto have any live birth over a 5-year pe-riodrsquo (Mascarenhas et al 2012) The overall prevalence of infertility isestimated at 35ndash167 in low- and middle-income countries (LMIC)with the prevalence as high as 30ndash40 in some regions of Sub-SaharanAfrica (Ombelet 2009 Inhorn and Patrizio 2015) Infertility in LMICis more than a health problem it is a social issue and a public healthmatter that continues to be neglected (Bahamondes and Makuch2014)
Infertility is known to cause significant psychological and socialeffects such as fear guilt depression self-blame marital stress emo-tional abuse intimate partner violence divorce and abandonment ofthe partner social isolation economic deprivation loss of social statusand in some regions (eg Africa and Asia) even starvation diseaseviolence-induced suicide and loss of dignity in death (Ombelet et al2008 Hammarberg and Kirkman 2013 Stellar et al 2016)
The most common etiologies of infertility in LMIC are male factorand tubal disease secondary to sexually transmitted infections unsafeabortion and complications of childbirth (Ombelet 2009 van derPoel 2012) Tubal factor infertility is reported to be as high as 85 inSub-Saharan Africa compared with 33 worldwide (Ombelet 2009)The most effective treatment is ART (Sharma et al 2009Bahamondes and Makuch 2014)
Infertility and ART are not considered a priority in many LMICThe most often used arguments against the use of ART are overpopu-lation other health priorities (eg family planning vaccinations malariaHIV) limited government budgets and limited experience of providers
with inadequate facilities for performing sophisticated procedures(Ombelet and Campo 2007) Furthermore in some LMIC ART isconsidered to be expensive only moderately effective with risks ofcomplications and unknown effects on women and their offspring(Ombelet and Campo 2007) In 2008 ESHRE published a series ofmonographs by experts from around the world highlighting the impor-tance of infertility its prevalence access to treatment and outcomes indeveloping countries (ESHRE Special Task Force on lsquoDevelopingCountries and Infertilityrsquo 2008) Along with the WHO and ESHREother non-governmental organizations (NGOs) are involved in initia-tives aimed at improving access to ART in LMIC including theAmerican Society for Reproductive Medicine the InternationalFederation of Gynecology and Obstetrics the International Federationof Fertility Societies and the International Committee for MonitoringAssisted Reproductive Technologies
Providing ART services in an LMIC requires an understanding of thecountry-specific magnitude and character of the issue of infertility aswell as identification of pre-existing resources that may be utilized(Sharma et al 2009 Bahamondes and Makuch 2014) WHO is in aunique position with 194 member states worldwide to assist in evalu-ating the burden of disease by the systematic assessment of infertilityand resources available within various regions
There is complete absence of affordable and accessible ART serv-ices in some LMIC possibly due to high costs of IVF and underdevel-oped infrastructure in addition to cultural religious and legal barriersThis deficiency has led to considerable interest by NGOs policymakers and ART specialists in developing more affordable IVF proto-cols such as minimal ovarian stimulation However there is a paucityof evidence and systematic reviews on the safety and efficiency profileof low-cost ART on the ability to replicate various techniques in differ-ent laboratories and under various field conditions and on how to inte-grate ART into existing health systems and infrastructures
214 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
This review investigated the currently available IVF services in LMIC
and potential for future development This work will assist in unfoldingthe landscape of available services and the potential for ART servicesin LMIC This is a key element in positioning infertility more broadly inthe Global Public Health Agenda of WHO This work will also informfuture WHO guidelines concerning the provision of ART in LMIC
MethodsThis review was reported in accordance with the PRISMA andGATHER guidelines (Moher et al 2009 Stevens et al 2016) Theprotocol was registered on 24 April 2017 and published withPROSPERO International prospective register of systematic reviews(ID number CRD42017064413) There were no amendments to theprotocol after registration
Search strategy and selection criteriaThe electronic databases searched included PubMed PoplineCINAHL EMBASE and Global Index Medicus (regional WHO onlinedatabases) Citations were collected from inception until 1 January2020 An internet search was performed using lsquoGooglersquo search enginewith the terms lsquoinfertilityrsquo lsquolow- and middle-income countriesrsquo andlsquoin vitro fertilizationrsquo or lsquoassisted reproductive technologiesrsquo (limited toresults published after 2010) Similar search terms were used for grayliterature databases (worldcatorg greylitorg) In addition the refer-ence lists of included studies were checked Experts and professionalswithin the field of infertility and the members of the ESHRE SpecialInterest Group Global and Socio-cultural Aspects of Infertility(nfrac14 221) were contacted to provide information on any unpublishedpapers or data on the subject of lsquoART in low- and middle-incomecountriesrsquo
Search strategies were customized for each electronic databaseaccording to their individual subject headings and searching structureThe search strategy used for PUBMED is available in Supplementarydata In constructing the search terms accepted definitions of ARTand IVF were used (Zegers-Hochschild et al 2009 et al 2017) LMICwere defined according to the World Bank classification of countriesby Gross National Income per capita (low-income country (LIC) up to$995 lower-middle-income country (lower MIC) $996 to $3895 andupper-middle-income country (upper MIC) $3896 to $12 055)(World Bank Country and Lending Groups) Upper MIC which oftenhave ART services on par with high-income countries were labeled todistinguish them from LIC and lower MIC For this review no restric-tions were applied with regard to study design or language Reviewerswere able to read English French German Italian PortugueseSpanish and Russian studies Reports in other languages were includedand authors were asked to provide a translated version or some ofthe details of the study in English Endnote (Version X8) bibliographicsoftware was used to store the citations and remove duplicates
For inclusion in the review we selected citations on ART for adultwomen and men of reproductive age (18ndash44 years old) from LMIC(experiencing reproductive difficulties or infertility) All identified cita-tions irrespective of language published over the last decade from 1January 2010 to 1 January 2020 were assessed The review was limitedto articles published after 2010 based on the recent evolution in the
field of ART practices in LMIC over the last decade ART is defined asall interventions that include the in vitro handling of both humanoocytes and sperm or of embryos for the purpose of reproductionThis includes but is not limited to IVF and embryo transfer ICSI em-bryo biopsy preimplantation genetic testing assisted hatching gameteintrafallopian transfer zygote intrafallopian transfer gamete and em-bryo cryopreservation semen oocyte and embryo donation and ges-tational carrier cycles (Zegers-Hochschild et al 2017) This reviewfocused on IVF and embryo transfer procedures being performed inLMIC over the last decade Articles focusing solely on ICSI specializedART procedures and that did not discuss IVF were excluded Themain reason for this restriction was these advanced procedures not al-ways being accessible or affordable to the general population in anLMIC where the cost of ART is estimated to be up to 50 higherthan the gross national per capita income of many LMIC (Vayenaet al 2009)
Concerning outcomes articles were assessed for quantitative out-comes on the efficacy of the ART (mainly pregnancy rate or live birthrate (LBR)) or qualitative and quantitative outcomes on feasibility Wedefined feasibility as the process in which low-cost ART are deployedleading to their acceptability and usability All citations were evaluatedbased on the titles and abstracts by two independent reviewers(TMC and NV) In the absence of sufficient data in the abstract toassess relevance the full text was obtained A list of the excludedreports is available from the authors upon request The full-textreports were assessed for relevance and the data extracted by two in-dependent reviewers (TMC and NV) A third reviewer (IT) wasavailable to resolve queries and disagreements Attempts were madeto contact the authors to obtain missing information or clarificationwhenever necessary
Risk of bias and data analysisThe protocol for this review included assessment of risk of bias for allindividual articles The majority of included articles did not assess quan-titative outcomes (efficacy or others) related to a therapeutic or diag-nostic intervention but merely reported on feasibility (currentpractice) in a narrative fashion For studies assessing efficacy of inter-ventions the majority were either very small feasibility or pilot studies(assessed as high to very high risk of bias) or they were available onlyas an (conference) abstract For the remaining interventional studiesrisk of bias was assessed with the risk of bias in non-randomized stud-ies of interventions (ROBINs)-1 tool (Sterne et al 2016) Risk of biaswas only assessed when the full-text paper could be retrieved Thecollected data were as expected highly heterogeneous Statisticalcomparison of the data was not possible due to the variable studydesign and quantitative data in the included citations The resultsfrom included citations were collated in a descriptive fashion andmeta-analysis was not feasible
ResultsAn extensive search of the databases yielded 3769 citations afterremoval of duplicate entries After review of the titles and abstracts283 articles were included (Fig 1) The full texts of 283 articles werereviewed including case reports review papers commentaries gray
IVF in low- and middle-income countries 215
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
literature and abstracts from conference proceedings A further 199citations were excluded The gray literature search yielded 586 cita-tions of which 334 were excluded after screening of the title Furtherassessment of the remaining gray literature documents resulted in allcitations being excluded Exclusion of citations was based on duplicateentries from the database searches not LMIC not relevant or no ac-cess to the full document Of the 84 included articles 63 citationsmostly qualitative and observational studies described an overall pic-ture (efficacy feasibility and acceptability) of ART in LMIC Thesearticles were summarized into regions (Supplementary Tables SI-VIFig 2) Fourteen studies reported on the efficacy and feasibility ofcost-limiting initiatives aimed at affordable ART in LMIC (Table I) Asystematic review of literature was conducted however due to theheterogeneity of the included articles the results are collated and pre-sented here in a narrative fashion
ART reports within regionsEast Asia and PacificART in the region of East Asia and Pacific is described as a rapidlygrowing business (Wahlberg 2016) A survey reported that in thecountries within this region for which information was collected(China Indonesia Korea Malaysia Mongolia Myanmar PhilippinesSingapore Thailand and Vietnam) IVF is available for couples although
subsidized only in Singapore and Korea (Li et al 2018) Nine citationsreported mostly on the current practice in China and Thailand whichare upper MIC and may not be representative of the practice in LMICwithin this region (Supplementary Table SI) China is depicted as havinghigh standards of practice and technological developments are aggres-sively pursued (Ha 2013) Efficacy of ART in China was described assimilar to efficacy in developed high-income European countries suchas France and Spain (LBR per started cycle of 47 in womenlt35 years old from ART) (Audibert and Glass 2015) As expectedChina with a high population is also unique in the high number of IVFcycles and the term lsquoscaled up IVFrsquo has been used with 145 108 livebirths reported after ART in 2013 (Wahlberg 2016) Other countriesin this region report the use of ART to a lesser extent but there wereno articles describing the efficacy of treatments (Ye et al 2013)
With regards to the feasibility of ART a study from Indonesiareported barriers to access which included low confidence in infertilitytreatment high rates of switching between providers due to treatmentfailure the number and location of clinics the lack of a well-established referral system the cost of treatment and patients withfear of receiving the diagnosis of infertility fear of vaginal examinationsor embarrassment (Bennett et al 2012) In Thailand ART treatmentis considered out of reach for most average-income people In addi-tion three-quarters of infertility clinics are located in urban centerslimiting physical accessibility for rural populations (Whittaker 2016)
Records idenfied through database search
(n = 3868)
Screen
ing
Inclu
ded
Eligibility
Iden
ficao
n
Addional records idenfied through other sources
(n = 586)
Records aer duplicates removed (n = 3769)
Records screened (n = 3769)
Records excluded (n = 3486)
Full-text arcles assessed for eligibility
(n = 283)
Full-text arcles excluded with jusficaon
(n = 199)
Studies included in qualitave synthesis
(n = 84)
Studies included in quantave synthesis
(meta-analysis) (NA)
Figure 1 PRISMA flow diagram of included and excluded studies of the review
216 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
One report from China found lower cost with recombinant FSH com-pared to highly purified FSH with similar pregnancy outcomes and LBRbetween the groups (Ye et al 2013) Concerning acceptability it isreported that shame and stigma have decreased over time and ART isnow an accepted way to conceive (Whittaker 2016) Although ARTis well developed in China it is still out of reach for most infertile cou-ples due to an enormous demand for treatment resulting in long wait-ing times and costs estimated between US$5000 and US$16 000 perIVF cycle which is not covered by public or private insurance (Qiaoand Feng 2014 Audibert and Glass 2015)
Europe and Central AsiaART in Europe is widely studied and reported by the European IVFMonitoring Programme Six citations were included from LMIC whichwere all from upper MIC (Supplementary Table SII) Large differencesstill exist between the number of cycles per 1 million women (aged15ndash45 years) in these countries but overall there is reportedly goodaccess to ART services (European IVF monitoring Consortium (EIM)for the European Society of Human Reproduction and Embryologyet al 2017) Regarding efficacy of IVF the data reported from LMICare comparable to those in other higher income European countries(European IVF monitoring Consortium (EIM) for the European Societyof Human Reproduction and Embryology et al 2017) An LBR of172 per transfer was reported in Bosnia Herzegovina and 265 inSerbia both upper MIC (Balic 2011 Mitic et al 2012)
With regard to the feasibility and acceptability the costs of treat-ment are most often discussed along with legislative issues and regula-tions In Turkey government funding is reportedly provided (up to
two IVF cycles in women aged 23ndash39 years old) only if all otheroptions have been exhausted (Urman and Yakin 2010) Turkish ARTcenters are required to be licensed by the government (Aytoz 2012)In contrast other countries have reported very little regulation andART is influenced by market forces For example in Bulgaria whereminimal regulation of ART is described access and outcomes arepoor with 10 IVF clinics and low financial support for IVF treatments(Balabanova and Simonstein 2010) Within Europe a recent collabora-tive audit between ESHRE and the patient organization Fertility Europedemonstrated clear discrepancies in availability accessibility and fundingsupport within nine selected European Union countries (2017 FertilityEurope and European Society of Human Reproduction andEmbryology (ESHRE) 2017) Only one study reported on the attitudestoward ART a survey of 136 medical students nurses and doctors inRussia (upper MIC) reporting that 972 of respondents knew enoughabout ART and had a positive attitude toward it (Khamoshina et al2010)
Latin America and the CaribbeanData on the number of IVF clinics and treatment cycles are reportedin the Latin American Registry of Assisted Reproduction (REDLARA)(Zegers-Hochschild et al 2013 2014 2015 2016) The number ofcenters and countries in this region reporting data is increasing with13 citations included in the review (Supplementary Table SIII)Countries like Argentina and now Uruguay with a consistent policy to-ward recognizing the human right to start a family and ensuring accessto care demonstrated the highest number of ART cycles per popula-tion in contrast to countries where treatment depends on the
Figure 2 Results of studies from LMIC summarized within regions The numbers in parentheses represent the number of studies foundwithin regions and a summary of their themes is shown LMIC low- and middle-income countries Adapted from SDG Atlas 2018 The World ByRegion httpdatatopicsworldbankorgsdgatlasthe-world-by-regionhtml
IVF in low- and middle-income countries 217
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

This review investigated the currently available IVF services in LMIC
and potential for future development This work will assist in unfoldingthe landscape of available services and the potential for ART servicesin LMIC This is a key element in positioning infertility more broadly inthe Global Public Health Agenda of WHO This work will also informfuture WHO guidelines concerning the provision of ART in LMIC
MethodsThis review was reported in accordance with the PRISMA andGATHER guidelines (Moher et al 2009 Stevens et al 2016) Theprotocol was registered on 24 April 2017 and published withPROSPERO International prospective register of systematic reviews(ID number CRD42017064413) There were no amendments to theprotocol after registration
Search strategy and selection criteriaThe electronic databases searched included PubMed PoplineCINAHL EMBASE and Global Index Medicus (regional WHO onlinedatabases) Citations were collected from inception until 1 January2020 An internet search was performed using lsquoGooglersquo search enginewith the terms lsquoinfertilityrsquo lsquolow- and middle-income countriesrsquo andlsquoin vitro fertilizationrsquo or lsquoassisted reproductive technologiesrsquo (limited toresults published after 2010) Similar search terms were used for grayliterature databases (worldcatorg greylitorg) In addition the refer-ence lists of included studies were checked Experts and professionalswithin the field of infertility and the members of the ESHRE SpecialInterest Group Global and Socio-cultural Aspects of Infertility(nfrac14 221) were contacted to provide information on any unpublishedpapers or data on the subject of lsquoART in low- and middle-incomecountriesrsquo
Search strategies were customized for each electronic databaseaccording to their individual subject headings and searching structureThe search strategy used for PUBMED is available in Supplementarydata In constructing the search terms accepted definitions of ARTand IVF were used (Zegers-Hochschild et al 2009 et al 2017) LMICwere defined according to the World Bank classification of countriesby Gross National Income per capita (low-income country (LIC) up to$995 lower-middle-income country (lower MIC) $996 to $3895 andupper-middle-income country (upper MIC) $3896 to $12 055)(World Bank Country and Lending Groups) Upper MIC which oftenhave ART services on par with high-income countries were labeled todistinguish them from LIC and lower MIC For this review no restric-tions were applied with regard to study design or language Reviewerswere able to read English French German Italian PortugueseSpanish and Russian studies Reports in other languages were includedand authors were asked to provide a translated version or some ofthe details of the study in English Endnote (Version X8) bibliographicsoftware was used to store the citations and remove duplicates
For inclusion in the review we selected citations on ART for adultwomen and men of reproductive age (18ndash44 years old) from LMIC(experiencing reproductive difficulties or infertility) All identified cita-tions irrespective of language published over the last decade from 1January 2010 to 1 January 2020 were assessed The review was limitedto articles published after 2010 based on the recent evolution in the
field of ART practices in LMIC over the last decade ART is defined asall interventions that include the in vitro handling of both humanoocytes and sperm or of embryos for the purpose of reproductionThis includes but is not limited to IVF and embryo transfer ICSI em-bryo biopsy preimplantation genetic testing assisted hatching gameteintrafallopian transfer zygote intrafallopian transfer gamete and em-bryo cryopreservation semen oocyte and embryo donation and ges-tational carrier cycles (Zegers-Hochschild et al 2017) This reviewfocused on IVF and embryo transfer procedures being performed inLMIC over the last decade Articles focusing solely on ICSI specializedART procedures and that did not discuss IVF were excluded Themain reason for this restriction was these advanced procedures not al-ways being accessible or affordable to the general population in anLMIC where the cost of ART is estimated to be up to 50 higherthan the gross national per capita income of many LMIC (Vayenaet al 2009)
Concerning outcomes articles were assessed for quantitative out-comes on the efficacy of the ART (mainly pregnancy rate or live birthrate (LBR)) or qualitative and quantitative outcomes on feasibility Wedefined feasibility as the process in which low-cost ART are deployedleading to their acceptability and usability All citations were evaluatedbased on the titles and abstracts by two independent reviewers(TMC and NV) In the absence of sufficient data in the abstract toassess relevance the full text was obtained A list of the excludedreports is available from the authors upon request The full-textreports were assessed for relevance and the data extracted by two in-dependent reviewers (TMC and NV) A third reviewer (IT) wasavailable to resolve queries and disagreements Attempts were madeto contact the authors to obtain missing information or clarificationwhenever necessary
Risk of bias and data analysisThe protocol for this review included assessment of risk of bias for allindividual articles The majority of included articles did not assess quan-titative outcomes (efficacy or others) related to a therapeutic or diag-nostic intervention but merely reported on feasibility (currentpractice) in a narrative fashion For studies assessing efficacy of inter-ventions the majority were either very small feasibility or pilot studies(assessed as high to very high risk of bias) or they were available onlyas an (conference) abstract For the remaining interventional studiesrisk of bias was assessed with the risk of bias in non-randomized stud-ies of interventions (ROBINs)-1 tool (Sterne et al 2016) Risk of biaswas only assessed when the full-text paper could be retrieved Thecollected data were as expected highly heterogeneous Statisticalcomparison of the data was not possible due to the variable studydesign and quantitative data in the included citations The resultsfrom included citations were collated in a descriptive fashion andmeta-analysis was not feasible
ResultsAn extensive search of the databases yielded 3769 citations afterremoval of duplicate entries After review of the titles and abstracts283 articles were included (Fig 1) The full texts of 283 articles werereviewed including case reports review papers commentaries gray
IVF in low- and middle-income countries 215
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
literature and abstracts from conference proceedings A further 199citations were excluded The gray literature search yielded 586 cita-tions of which 334 were excluded after screening of the title Furtherassessment of the remaining gray literature documents resulted in allcitations being excluded Exclusion of citations was based on duplicateentries from the database searches not LMIC not relevant or no ac-cess to the full document Of the 84 included articles 63 citationsmostly qualitative and observational studies described an overall pic-ture (efficacy feasibility and acceptability) of ART in LMIC Thesearticles were summarized into regions (Supplementary Tables SI-VIFig 2) Fourteen studies reported on the efficacy and feasibility ofcost-limiting initiatives aimed at affordable ART in LMIC (Table I) Asystematic review of literature was conducted however due to theheterogeneity of the included articles the results are collated and pre-sented here in a narrative fashion
ART reports within regionsEast Asia and PacificART in the region of East Asia and Pacific is described as a rapidlygrowing business (Wahlberg 2016) A survey reported that in thecountries within this region for which information was collected(China Indonesia Korea Malaysia Mongolia Myanmar PhilippinesSingapore Thailand and Vietnam) IVF is available for couples although
subsidized only in Singapore and Korea (Li et al 2018) Nine citationsreported mostly on the current practice in China and Thailand whichare upper MIC and may not be representative of the practice in LMICwithin this region (Supplementary Table SI) China is depicted as havinghigh standards of practice and technological developments are aggres-sively pursued (Ha 2013) Efficacy of ART in China was described assimilar to efficacy in developed high-income European countries suchas France and Spain (LBR per started cycle of 47 in womenlt35 years old from ART) (Audibert and Glass 2015) As expectedChina with a high population is also unique in the high number of IVFcycles and the term lsquoscaled up IVFrsquo has been used with 145 108 livebirths reported after ART in 2013 (Wahlberg 2016) Other countriesin this region report the use of ART to a lesser extent but there wereno articles describing the efficacy of treatments (Ye et al 2013)
With regards to the feasibility of ART a study from Indonesiareported barriers to access which included low confidence in infertilitytreatment high rates of switching between providers due to treatmentfailure the number and location of clinics the lack of a well-established referral system the cost of treatment and patients withfear of receiving the diagnosis of infertility fear of vaginal examinationsor embarrassment (Bennett et al 2012) In Thailand ART treatmentis considered out of reach for most average-income people In addi-tion three-quarters of infertility clinics are located in urban centerslimiting physical accessibility for rural populations (Whittaker 2016)
Records idenfied through database search
(n = 3868)
Screen
ing
Inclu
ded
Eligibility
Iden
ficao
n
Addional records idenfied through other sources
(n = 586)
Records aer duplicates removed (n = 3769)
Records screened (n = 3769)
Records excluded (n = 3486)
Full-text arcles assessed for eligibility
(n = 283)
Full-text arcles excluded with jusficaon
(n = 199)
Studies included in qualitave synthesis
(n = 84)
Studies included in quantave synthesis
(meta-analysis) (NA)
Figure 1 PRISMA flow diagram of included and excluded studies of the review
216 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
One report from China found lower cost with recombinant FSH com-pared to highly purified FSH with similar pregnancy outcomes and LBRbetween the groups (Ye et al 2013) Concerning acceptability it isreported that shame and stigma have decreased over time and ART isnow an accepted way to conceive (Whittaker 2016) Although ARTis well developed in China it is still out of reach for most infertile cou-ples due to an enormous demand for treatment resulting in long wait-ing times and costs estimated between US$5000 and US$16 000 perIVF cycle which is not covered by public or private insurance (Qiaoand Feng 2014 Audibert and Glass 2015)
Europe and Central AsiaART in Europe is widely studied and reported by the European IVFMonitoring Programme Six citations were included from LMIC whichwere all from upper MIC (Supplementary Table SII) Large differencesstill exist between the number of cycles per 1 million women (aged15ndash45 years) in these countries but overall there is reportedly goodaccess to ART services (European IVF monitoring Consortium (EIM)for the European Society of Human Reproduction and Embryologyet al 2017) Regarding efficacy of IVF the data reported from LMICare comparable to those in other higher income European countries(European IVF monitoring Consortium (EIM) for the European Societyof Human Reproduction and Embryology et al 2017) An LBR of172 per transfer was reported in Bosnia Herzegovina and 265 inSerbia both upper MIC (Balic 2011 Mitic et al 2012)
With regard to the feasibility and acceptability the costs of treat-ment are most often discussed along with legislative issues and regula-tions In Turkey government funding is reportedly provided (up to
two IVF cycles in women aged 23ndash39 years old) only if all otheroptions have been exhausted (Urman and Yakin 2010) Turkish ARTcenters are required to be licensed by the government (Aytoz 2012)In contrast other countries have reported very little regulation andART is influenced by market forces For example in Bulgaria whereminimal regulation of ART is described access and outcomes arepoor with 10 IVF clinics and low financial support for IVF treatments(Balabanova and Simonstein 2010) Within Europe a recent collabora-tive audit between ESHRE and the patient organization Fertility Europedemonstrated clear discrepancies in availability accessibility and fundingsupport within nine selected European Union countries (2017 FertilityEurope and European Society of Human Reproduction andEmbryology (ESHRE) 2017) Only one study reported on the attitudestoward ART a survey of 136 medical students nurses and doctors inRussia (upper MIC) reporting that 972 of respondents knew enoughabout ART and had a positive attitude toward it (Khamoshina et al2010)
Latin America and the CaribbeanData on the number of IVF clinics and treatment cycles are reportedin the Latin American Registry of Assisted Reproduction (REDLARA)(Zegers-Hochschild et al 2013 2014 2015 2016) The number ofcenters and countries in this region reporting data is increasing with13 citations included in the review (Supplementary Table SIII)Countries like Argentina and now Uruguay with a consistent policy to-ward recognizing the human right to start a family and ensuring accessto care demonstrated the highest number of ART cycles per popula-tion in contrast to countries where treatment depends on the
Figure 2 Results of studies from LMIC summarized within regions The numbers in parentheses represent the number of studies foundwithin regions and a summary of their themes is shown LMIC low- and middle-income countries Adapted from SDG Atlas 2018 The World ByRegion httpdatatopicsworldbankorgsdgatlasthe-world-by-regionhtml
IVF in low- and middle-income countries 217
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
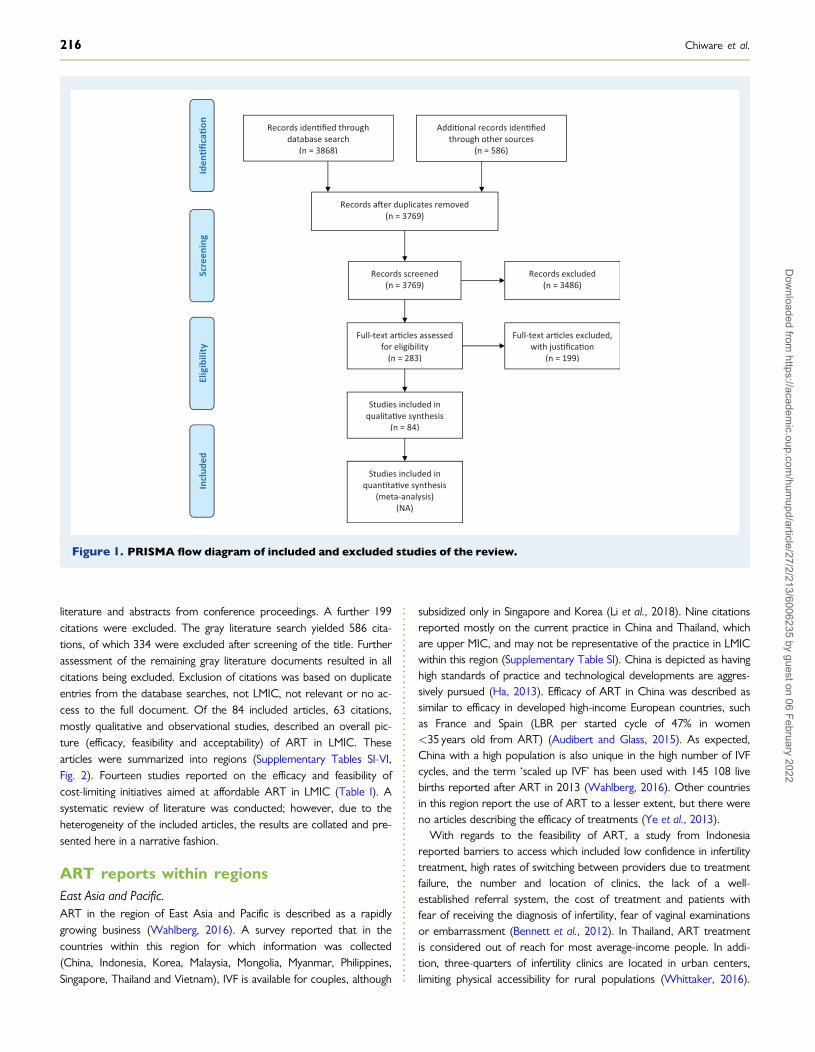
literature and abstracts from conference proceedings A further 199citations were excluded The gray literature search yielded 586 cita-tions of which 334 were excluded after screening of the title Furtherassessment of the remaining gray literature documents resulted in allcitations being excluded Exclusion of citations was based on duplicateentries from the database searches not LMIC not relevant or no ac-cess to the full document Of the 84 included articles 63 citationsmostly qualitative and observational studies described an overall pic-ture (efficacy feasibility and acceptability) of ART in LMIC Thesearticles were summarized into regions (Supplementary Tables SI-VIFig 2) Fourteen studies reported on the efficacy and feasibility ofcost-limiting initiatives aimed at affordable ART in LMIC (Table I) Asystematic review of literature was conducted however due to theheterogeneity of the included articles the results are collated and pre-sented here in a narrative fashion
ART reports within regionsEast Asia and PacificART in the region of East Asia and Pacific is described as a rapidlygrowing business (Wahlberg 2016) A survey reported that in thecountries within this region for which information was collected(China Indonesia Korea Malaysia Mongolia Myanmar PhilippinesSingapore Thailand and Vietnam) IVF is available for couples although
subsidized only in Singapore and Korea (Li et al 2018) Nine citationsreported mostly on the current practice in China and Thailand whichare upper MIC and may not be representative of the practice in LMICwithin this region (Supplementary Table SI) China is depicted as havinghigh standards of practice and technological developments are aggres-sively pursued (Ha 2013) Efficacy of ART in China was described assimilar to efficacy in developed high-income European countries suchas France and Spain (LBR per started cycle of 47 in womenlt35 years old from ART) (Audibert and Glass 2015) As expectedChina with a high population is also unique in the high number of IVFcycles and the term lsquoscaled up IVFrsquo has been used with 145 108 livebirths reported after ART in 2013 (Wahlberg 2016) Other countriesin this region report the use of ART to a lesser extent but there wereno articles describing the efficacy of treatments (Ye et al 2013)
With regards to the feasibility of ART a study from Indonesiareported barriers to access which included low confidence in infertilitytreatment high rates of switching between providers due to treatmentfailure the number and location of clinics the lack of a well-established referral system the cost of treatment and patients withfear of receiving the diagnosis of infertility fear of vaginal examinationsor embarrassment (Bennett et al 2012) In Thailand ART treatmentis considered out of reach for most average-income people In addi-tion three-quarters of infertility clinics are located in urban centerslimiting physical accessibility for rural populations (Whittaker 2016)
Records idenfied through database search
(n = 3868)
Screen
ing
Inclu
ded
Eligibility
Iden
ficao
n
Addional records idenfied through other sources
(n = 586)
Records aer duplicates removed (n = 3769)
Records screened (n = 3769)
Records excluded (n = 3486)
Full-text arcles assessed for eligibility
(n = 283)
Full-text arcles excluded with jusficaon
(n = 199)
Studies included in qualitave synthesis
(n = 84)
Studies included in quantave synthesis
(meta-analysis) (NA)
Figure 1 PRISMA flow diagram of included and excluded studies of the review
216 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
One report from China found lower cost with recombinant FSH com-pared to highly purified FSH with similar pregnancy outcomes and LBRbetween the groups (Ye et al 2013) Concerning acceptability it isreported that shame and stigma have decreased over time and ART isnow an accepted way to conceive (Whittaker 2016) Although ARTis well developed in China it is still out of reach for most infertile cou-ples due to an enormous demand for treatment resulting in long wait-ing times and costs estimated between US$5000 and US$16 000 perIVF cycle which is not covered by public or private insurance (Qiaoand Feng 2014 Audibert and Glass 2015)
Europe and Central AsiaART in Europe is widely studied and reported by the European IVFMonitoring Programme Six citations were included from LMIC whichwere all from upper MIC (Supplementary Table SII) Large differencesstill exist between the number of cycles per 1 million women (aged15ndash45 years) in these countries but overall there is reportedly goodaccess to ART services (European IVF monitoring Consortium (EIM)for the European Society of Human Reproduction and Embryologyet al 2017) Regarding efficacy of IVF the data reported from LMICare comparable to those in other higher income European countries(European IVF monitoring Consortium (EIM) for the European Societyof Human Reproduction and Embryology et al 2017) An LBR of172 per transfer was reported in Bosnia Herzegovina and 265 inSerbia both upper MIC (Balic 2011 Mitic et al 2012)
With regard to the feasibility and acceptability the costs of treat-ment are most often discussed along with legislative issues and regula-tions In Turkey government funding is reportedly provided (up to
two IVF cycles in women aged 23ndash39 years old) only if all otheroptions have been exhausted (Urman and Yakin 2010) Turkish ARTcenters are required to be licensed by the government (Aytoz 2012)In contrast other countries have reported very little regulation andART is influenced by market forces For example in Bulgaria whereminimal regulation of ART is described access and outcomes arepoor with 10 IVF clinics and low financial support for IVF treatments(Balabanova and Simonstein 2010) Within Europe a recent collabora-tive audit between ESHRE and the patient organization Fertility Europedemonstrated clear discrepancies in availability accessibility and fundingsupport within nine selected European Union countries (2017 FertilityEurope and European Society of Human Reproduction andEmbryology (ESHRE) 2017) Only one study reported on the attitudestoward ART a survey of 136 medical students nurses and doctors inRussia (upper MIC) reporting that 972 of respondents knew enoughabout ART and had a positive attitude toward it (Khamoshina et al2010)
Latin America and the CaribbeanData on the number of IVF clinics and treatment cycles are reportedin the Latin American Registry of Assisted Reproduction (REDLARA)(Zegers-Hochschild et al 2013 2014 2015 2016) The number ofcenters and countries in this region reporting data is increasing with13 citations included in the review (Supplementary Table SIII)Countries like Argentina and now Uruguay with a consistent policy to-ward recognizing the human right to start a family and ensuring accessto care demonstrated the highest number of ART cycles per popula-tion in contrast to countries where treatment depends on the
Figure 2 Results of studies from LMIC summarized within regions The numbers in parentheses represent the number of studies foundwithin regions and a summary of their themes is shown LMIC low- and middle-income countries Adapted from SDG Atlas 2018 The World ByRegion httpdatatopicsworldbankorgsdgatlasthe-world-by-regionhtml
IVF in low- and middle-income countries 217
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

One report from China found lower cost with recombinant FSH com-pared to highly purified FSH with similar pregnancy outcomes and LBRbetween the groups (Ye et al 2013) Concerning acceptability it isreported that shame and stigma have decreased over time and ART isnow an accepted way to conceive (Whittaker 2016) Although ARTis well developed in China it is still out of reach for most infertile cou-ples due to an enormous demand for treatment resulting in long wait-ing times and costs estimated between US$5000 and US$16 000 perIVF cycle which is not covered by public or private insurance (Qiaoand Feng 2014 Audibert and Glass 2015)
Europe and Central AsiaART in Europe is widely studied and reported by the European IVFMonitoring Programme Six citations were included from LMIC whichwere all from upper MIC (Supplementary Table SII) Large differencesstill exist between the number of cycles per 1 million women (aged15ndash45 years) in these countries but overall there is reportedly goodaccess to ART services (European IVF monitoring Consortium (EIM)for the European Society of Human Reproduction and Embryologyet al 2017) Regarding efficacy of IVF the data reported from LMICare comparable to those in other higher income European countries(European IVF monitoring Consortium (EIM) for the European Societyof Human Reproduction and Embryology et al 2017) An LBR of172 per transfer was reported in Bosnia Herzegovina and 265 inSerbia both upper MIC (Balic 2011 Mitic et al 2012)
With regard to the feasibility and acceptability the costs of treat-ment are most often discussed along with legislative issues and regula-tions In Turkey government funding is reportedly provided (up to
two IVF cycles in women aged 23ndash39 years old) only if all otheroptions have been exhausted (Urman and Yakin 2010) Turkish ARTcenters are required to be licensed by the government (Aytoz 2012)In contrast other countries have reported very little regulation andART is influenced by market forces For example in Bulgaria whereminimal regulation of ART is described access and outcomes arepoor with 10 IVF clinics and low financial support for IVF treatments(Balabanova and Simonstein 2010) Within Europe a recent collabora-tive audit between ESHRE and the patient organization Fertility Europedemonstrated clear discrepancies in availability accessibility and fundingsupport within nine selected European Union countries (2017 FertilityEurope and European Society of Human Reproduction andEmbryology (ESHRE) 2017) Only one study reported on the attitudestoward ART a survey of 136 medical students nurses and doctors inRussia (upper MIC) reporting that 972 of respondents knew enoughabout ART and had a positive attitude toward it (Khamoshina et al2010)
Latin America and the CaribbeanData on the number of IVF clinics and treatment cycles are reportedin the Latin American Registry of Assisted Reproduction (REDLARA)(Zegers-Hochschild et al 2013 2014 2015 2016) The number ofcenters and countries in this region reporting data is increasing with13 citations included in the review (Supplementary Table SIII)Countries like Argentina and now Uruguay with a consistent policy to-ward recognizing the human right to start a family and ensuring accessto care demonstrated the highest number of ART cycles per popula-tion in contrast to countries where treatment depends on the
Figure 2 Results of studies from LMIC summarized within regions The numbers in parentheses represent the number of studies foundwithin regions and a summary of their themes is shown LMIC low- and middle-income countries Adapted from SDG Atlas 2018 The World ByRegion httpdatatopicsworldbankorgsdgatlasthe-world-by-regionhtml
IVF in low- and middle-income countries 217
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
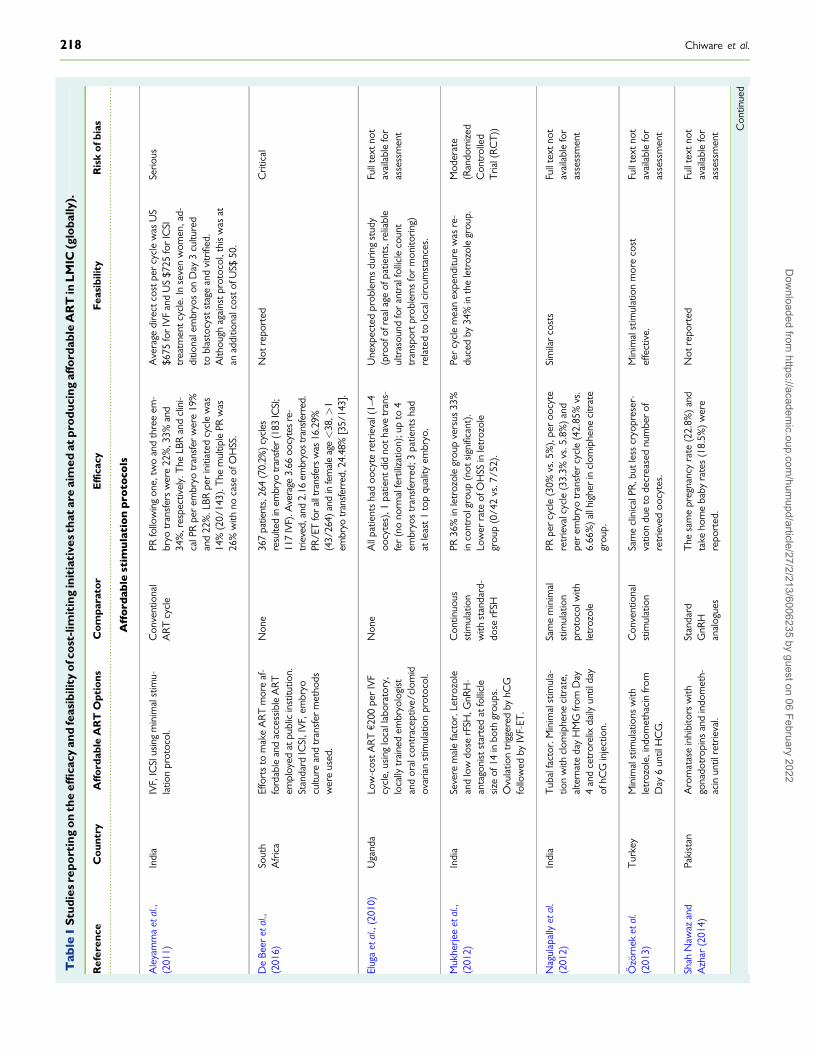
Tab
leI
Stu
dies
repo
rtin
gon
the
effi
cacy
and
feas
ibili
tyof
cost
-lim
itin
gin
itia
tive
sth
atar
eai
med
atpr
oduc
ing
affo
rdab
leA
RT
inL
MIC
(glo
bally
)
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Aff
ord
able
stim
ula
tio
np
roto
cols
Ale
yam
ma
etal
(2
011)
Indi
aIV
FIC
SIus
ing
min
imal
stim
u-la
tion
prot
ocol
C
onve
ntio
nal
AR
Tcy
cle
PRfo
llow
ing
one
two
and
thre
eem
-br
yotr
ansf
ers
wer
e22
3
3an
d34
r
espe
ctiv
ely
The
LBR
and
clin
i-ca
lPR
per
embr
yotr
ansf
erw
ere
19
and
22
LBR
per
initi
ated
cycl
ew
as14
(2
014
3)T
hem
ultip
lePR
was
26
with
noca
seof
OH
SS
Ave
rage
dire
ctco
stpe
rcy
cle
was
US
$675
for
IVF
and
US
$725
for
ICSI
trea
tmen
tcyc
leI
nse
ven
wom
ena
d-di
tiona
lem
bryo
son
Day
3cu
lture
dto
blas
tocy
stst
age
and
vitr
ified
A
lthou
ghag
ains
tpro
toco
lth
isw
asat
anad
ditio
nalc
osto
fUS$
50
Serio
us
De
Beer
etal
(2
016)
Sout
hA
fric
aEf
fort
sto
mak
eA
RT
mor
eaf
-fo
rdab
lean
dac
cess
ible
AR
Tem
ploy
edat
publ
icin
stitu
tion
Stan
dard
ICSI
IV
Fem
bryo
cultu
rean
dtr
ansf
erm
etho
dsw
ere
used
Non
e36
7pa
tient
s26
4(7
02
)cyc
les
resu
lted
inem
bryo
tran
sfer
(183
ICSI
11
7IV
F)A
vera
ge3
66oo
cyte
sre
-tr
ieve
dan
d2
16em
bryo
str
ansf
erre
dPR
ET
for
allt
rans
fers
was
162
9(4
326
4)an
din
fem
ale
agelt
38gt
1em
bryo
tran
sfer
red
244
8[3
514
3]
Not
repo
rted
Crit
ical
Elug
aet
al
(201
0)U
gand
aLo
w-c
ostA
RTe
200
per
IVF
cycl
eus
ing
loca
llab
orat
ory
loca
llytr
aine
dem
bryo
logi
stan
dor
alco
ntra
cept
ive
clom
idov
aria
nst
imul
atio
npr
otoc
ol
Non
eA
llpa
tient
sha
doo
cyte
retr
ieva
l(1ndash
4oo
cyte
s)1
patie
ntdi
dno
thav
etr
ans-
fer
(no
norm
alfe
rtili
zatio
n)u
pto
4em
bryo
str
ansf
erre
d3
patie
nts
had
atle
ast1
top
qual
ityem
bryo
Une
xpec
ted
prob
lem
sdu
ring
stud
y(p
roof
ofre
alag
eof
patie
nts
relia
ble
ultr
asou
ndfo
ran
tral
folli
cle
coun
ttr
ansp
ortp
robl
ems
for
mon
itorin
g)re
late
dto
loca
lcirc
umst
ance
s
Full
text
not
avai
labl
efo
ras
sess
men
t
Muk
herje
eet
al
(201
2)In
dia
Seve
rem
ale
fact
orL
etro
zole
and
low
dose
rFSH
GnR
H-
anta
goni
stst
arte
dat
folli
cle
size
of14
inbo
thgr
oups
O
vula
tion
trig
gere
dby
hCG
follo
wed
byIV
F-ET
Con
tinuo
usst
imul
atio
nw
ithst
anda
rd-
dose
rFSH
PR36
in
letr
ozol
egr
oup
vers
us33
in
cont
rolg
roup
(not
sign
ifica
nt)
Low
erra
teof
OH
SSin
letr
ozol
egr
oup
(04
2vs
75
2)
Per
cycl
em
ean
expe
nditu
rew
asre
-du
ced
by34
in
the
letr
ozol
egr
oup
Mod
erat
e(R
ando
miz
edC
ontr
olle
dT
rial(
RC
T))
Nag
ulap
ally
etal
(2
012)
Indi
aT
ubal
fact
orM
inim
alst
imul
a-tio
nw
ithcl
omip
hene
citr
ate
alte
rnat
eda
yH
MG
from
Day
4an
dce
tror
elix
daily
until
day
ofhC
Gin
ject
ion
Sam
em
inim
alst
imul
atio
npr
otoc
olw
ithle
troz
ole
PRpe
rcy
cle
(30
vs5
)
per
oocy
tere
trie
valc
ycle
(33
3vs
58
)a
ndpe
rem
bryo
tran
sfer
cycl
e(4
285
vs
6
66
)all
high
erin
clom
iphe
neci
trat
egr
oup
Sim
ilar
cost
sFu
llte
xtno
tav
aila
ble
for
asse
ssm
ent
Ozo
rnek
etal
(2
013)
Tur
key
Min
imal
stim
ulat
ions
with
letr
ozol
ein
dom
etha
cin
from
Day
6un
tilH
CG
Con
vent
iona
lst
imul
atio
nSa
me
clin
ical
PRb
utle
sscr
yopr
eser
-va
tion
due
tode
crea
sed
num
ber
ofre
trie
ved
oocy
tes
Min
imal
stim
ulat
ion
mor
eco
stef
fect
ive
Full
text
not
avai
labl
efo
ras
sess
men
t
Shah
Naw
azan
dA
zhar
(201
4)Pa
kist
anA
rom
atas
ein
hibi
tors
with
gona
dotr
opin
san
din
dom
eth-
acin
until
retr
ieva
l
Stan
dard
GnR
Han
alog
ues
The
sam
epr
egna
ncy
rate
(22
8)
and
take
hom
eba
byra
tes
(18
5)
wer
ere
port
ed
Not
repo
rted
Full
text
not
avai
labl
efo
ras
sess
men
t Con
tinue
d
218 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
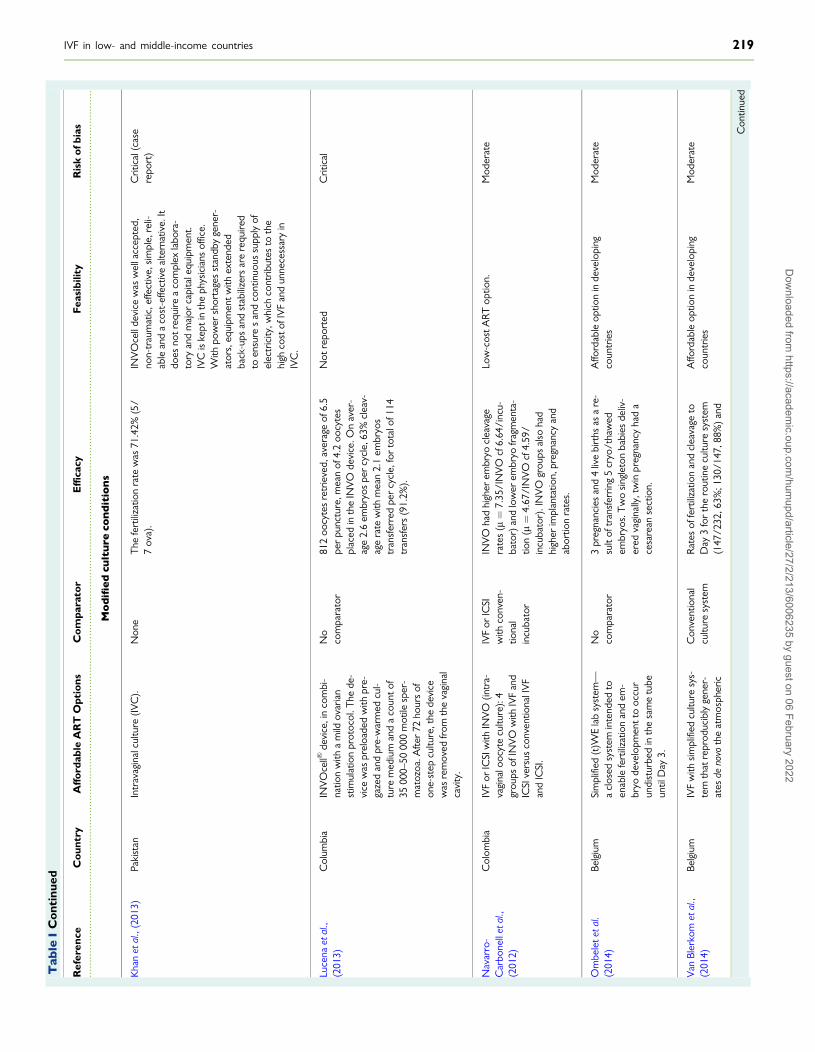
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
Mo
difi
ed
cult
ure
con
dit
ion
s
Kha
net
al
(201
3)Pa
kist
anIn
trav
agin
alcu
lture
(IVC
)N
one
The
fert
iliza
tion
rate
was
714
2(5
7
ova)
IN
VO
cell
devi
cew
asw
ella
ccep
ted
non-
trau
mat
ice
ffect
ive
sim
ple
reli-
able
and
aco
st-e
ffect
ive
alte
rnat
ive
Itdo
esno
treq
uire
aco
mpl
exla
bora
-to
ryan
dm
ajor
capi
tale
quip
men
tIV
Cis
kept
inth
eph
ysic
ians
offic
eW
ithpo
wer
shor
tage
sst
andb
yge
ner-
ator
seq
uipm
entw
ithex
tend
edba
ck-u
psan
dst
abili
zers
are
requ
ired
toen
sure
san
dco
ntin
uous
supp
lyof
elec
tric
ityw
hich
cont
ribut
esto
the
high
cost
ofIV
Fan
dun
nece
ssar
yin
IVC
Crit
ical
(cas
ere
port
)
Luce
naet
al
(201
3)C
olum
bia
INV
Oce
llVRde
vice
in
com
bi-
natio
nw
itha
mild
ovar
ian
stim
ulat
ion
prot
ocol
The
de-
vice
was
prel
oade
dw
ithpr
e-ga
zed
and
pre-
war
med
cul-
ture
med
ium
and
aco
unto
f35
000ndash
5000
0m
otile
sper
-m
atoz
oaA
fter
72ho
urs
ofon
e-st
epcu
lture
the
devi
cew
asre
mov
edfr
omth
eva
gina
lca
vity
No
com
para
tor
812
oocy
tes
retr
ieve
dav
erag
eof
65
per
punc
ture
mea
nof
42
oocy
tes
plac
edin
the
INV
Ode
vice
On
aver
-ag
e2
6em
bryo
spe
rcy
cle
63
clea
v-ag
era
tew
ithm
ean
21
embr
yos
tran
sfer
red
per
cycl
efo
rto
talo
f114
tran
sfer
s(9
12
)
Not
repo
rted
Crit
ical
Nav
arro
-C
arbo
nell
etal
(2
012)
Col
ombi
aIV
For
ICSI
with
INV
O(in
tra-
vagi
nalo
ocyt
ecu
lture
)4
grou
psof
INV
Ow
ithIV
Fan
dIC
SIve
rsus
conv
entio
nalI
VF
and
ICSI
IVF
orIC
SIw
ithco
nven
-tio
nal
incu
bato
r
INV
Oha
dhi
gher
embr
yocl
eava
gera
tes
(mfrac14
735
IN
VO
cf6
64i
ncu-
bato
r)an
dlo
wer
embr
yofr
agm
enta
-tio
n(mfrac14
467
IN
VO
cf4
59
incu
bato
r)I
NV
Ogr
oups
also
had
high
erim
plan
tatio
npr
egna
ncy
and
abor
tion
rate
s
Low
-cos
tAR
Top
tion
Mod
erat
e
Om
bele
teta
l(2
014)
Belg
ium
Sim
plifi
ed(t
)WE
lab
syst
emmdash
acl
osed
syst
emin
tend
edto
enab
lefe
rtili
zatio
nan
dem
-br
yode
velo
pmen
tto
occu
run
dist
urbe
din
the
sam
etu
beun
tilD
ay3
No
com
para
tor
3pr
egna
ncie
san
d4
live
birt
hsas
are
-su
ltof
tran
sfer
ring
5cr
yot
haw
edem
bryo
sT
wo
sing
leto
nba
bies
deliv
-er
edva
gina
llyt
win
preg
nanc
yha
da
cesa
rean
sect
ion
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Van
Bler
kom
etal
(2
014)
Belg
ium
IVF
with
sim
plifi
edcu
lture
sys-
tem
that
repr
oduc
ibly
gene
r-at
esde
novo
the
atm
osph
eric
Con
vent
iona
lcu
lture
syst
emR
ates
offe
rtili
zatio
nan
dcl
eava
geto
Day
3fo
rth
ero
utin
ecu
lture
syst
em(1
472
326
31
301
478
8)
and
Affo
rdab
leop
tion
inde
velo
ping
coun
trie
sM
oder
ate
Con
tinue
d
IVF in low- and middle-income countries 219
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

Tab
leI
Con
tinu
ed
Ref
eren
ceC
ount
ryA
fford
able
AR
TO
ptio
nsC
ompa
rato
rE
ffica
cyF
easi
bilit
yR
isk
ofbi
as
and
cultu
reco
nditi
ons
that
supp
ortn
orm
alfe
rtili
zatio
nan
dpr
eim
plan
tatio
nem
bryo
-ge
nesi
sto
the
hatc
hed
blas
to-
cyst
stag
ew
ithou
tthe
need
for
spec
ializ
edm
edic
al-g
rade
gase
sor
equi
pmen
t
sim
plifi
edcu
lture
syst
em(1
381
99
69
119
138
86
)w
ere
sim
ilar
With
the
sim
plifi
edcu
lture
syst
em8
23
embr
yos
impl
ante
don
em
isca
r-rie
dat
8w
eeks
ofge
stat
ion
and
seve
nhe
alth
yba
bies
have
been
born
Mo
difi
ed
clin
ico
rgan
izat
ion
Gno
thet
al
(201
3)
Eritr
eaPi
lotp
roje
ctim
plem
entin
gba
-si
cin
fert
ility
care
An
inte
nsiv
eco
urse
with
trai
ning
inhy
s-te
ro-c
ontr
ast-
sono
grap
hyan
don
e-st
epIU
Iwas
apo
ssib
leto
olto
intr
oduc
eba
sic
infe
rtil-
ityca
rein
toot
her
reso
urce
-po
orse
ttin
gs
Non
eN
otre
port
edT
heim
plem
enta
tion
and
inco
rpor
a-tio
nof
two
inte
nsiv
eco
urse
son
basi
cre
prod
uctiv
ean
din
fert
ility
care
into
anex
istin
gO
bG
ynre
siden
cypr
o-gr
amar
eno
tonl
yfe
asib
lebu
tpro
-vi
des
aso
lidfo
unda
tion
and
met
hod
ofsu
stai
nabi
lity
toad
dres
sth
isim
por-
tant
repr
oduc
tive
heal
this
sue
Crit
ical
Orh
ueet
al
(201
2)N
iger
iaT
hecy
cles
wer
eca
rrie
dou
tin
batc
hes
with
anav
erag
eof
30co
uple
spe
rba
tch
To
syn-
chro
nize
thei
rm
enst
rual
cycl
est
hew
omen
took
estr
a-di
olva
lera
tean
dno
reth
iste
r-on
eac
etat
e(s
eque
ntia
llyf
orva
ryin
gnu
mbe
rsof
days
over
1or
2m
onth
s)
Non
eC
linic
alpr
egna
ncy
occu
rred
in18
0(3
00
)of5
04w
omen
(84
0)
who
unde
rwen
tem
bryo
tran
sfer
Oft
he18
0pr
egna
ncie
s40
(66
)
ende
din
spon
tane
ous
abor
tion
and
4(0
6
)w
ere
ecto
pic
Of3
6m
ultip
lepr
eg-
nanc
ies
(60
)
8(1
3
)tr
iple
tsan
d28
(46
)
twin
soc
curr
edT
wo
(03
)
ofth
etr
iple
tpre
gnan
cies
ende
din
abor
tion
at16
and
20w
eeks
Oft
he28
twin
preg
nanc
ies
8(1
3
)en
ded
inab
ortio
n8
(13
)
wer
epr
eter
ma
nd12
(20
)
deliv
-er
edat
37w
eeks
OH
SSoc
curr
edin
6(1
0
)of
the
wom
en
The
cost
ofIV
For
ICSI
isab
outU
S$3
000
(for
good
resp
onde
rsp
oor
resp
onde
rsne
eded
mor
edr
ugs
and
ther
efor
epa
idm
ore)
com
pare
dan
aver
age
cost
ofU
S$4
000ndash
5000
for
conv
entio
nalm
etho
dsM
edia
was
used
for
only
1ba
tch
and
ther
ew
aslo
wst
affd
edic
atio
n
Serio
us
220 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

couplersquos capacity to pay (Zegers-Hochschild et al 2016) An IVF unitin Jamaica reported ART outcomes similar to high-income countries(LBR of 168 comparable to 213 in the UK) Furthermore the pa-per reports that establishment of this dedicated unit has contributedto educating the public about infertility and ART with increasing de-mand from infertile couples and also from less traditional families(Pottinger et al 2012)
More studies discussed feasibility and accessibility Health authoritiesin Brazil (upper MIC) have reported that lsquocomplex infertility treat-mentsrsquo referring to ART are unavailable to infertile couples (Makuchand Bahamondes 2012) Despite this a few public institutions arereported to offer infertility evaluation and IVF treatment with somepartially charging for the procedures Access to care is limited due tohigh costs long waiting times complex scheduling processes and lackof political initiatives to implement more affordable ART ART in Brazilis reportedly mostly offered in the private medical sector at high costand health care services are unable to meet the growing demand forinfertility treatment (Makuch and Bahamondes 2012 de Souza 2014Correa and Loyola 2015) It is reported there is no specific legislationregulating assisted conception Political economic and ethical chal-lenges exist for policy makers to decide on allocation of funds forART considering the universal access and free of charge nature of theBrazilian health care system (Garcia and Bellamy 2015) A recentstudy showed among the 4275 newborns enrolled in the Pelotas2015 Birth Cohort Study 18 births (04) were the result of ARTMost ART was IVF (706) and 90 women had double embryotransfer All cycles were performed in private clinics with directout-of-pocket payment In 2012 the right to start a family was em-braced by the Brazilian Unified Health System as a human rightSince then 12 clinics and hospitals received financial support fromthe Brazilian government to provide universal access to ART serv-ices Most of these clinics are situated in S~ao Paulo with no clinicsreported in Northern Brazil (Silva et al 2019) A study alsohighlighted that for people living with HIVAIDS who desire tohave a child face significant barriers to accessing ART treatmentand counseling (Rossi Ada et al 2011)
In some countries until recently laws existed prohibiting IVF InCosta Rica (upper MIC) the Inter-American Court of Human Rightsin 2012 ruled that the Supreme Court of Costa Ricarsquos judgment in2000 prohibiting IVF violated the human right to private and family lifethe human right to found and raise a family and the human right tonon-discrimination on grounds of disability financial means or gender(Zegers-Hochschild et al 2013) On the other hand in Brazil the gov-ernment launched a policy in 2012 establishing ART as a universal rightwithin the National Health System (Silva et al 2019)
REDLARA estimated that Mexico (upper MIC) had the thirdhighest number of reported ART cycles in 2013 (Zegers-Hochschild et al 2016) In 2015 52 ART centers were registeredwith the Federal Commission for the Protection of Sanitary Riskwho initiated a campaign of accreditation to verify that ART clinicsare working to appropriate standards Rather than generating ageneral comprehensive law assisted reproduction specialists inconjunction with representatives of government offices (egMinistry of Health) members of private and public hospitals andNGOs are developing standards of practice for assisted reproduc-tion services (Gonzalez-Santos 2016)
Middle East and North AfricaEight citations from this region were included in the review most fromIran and Egypt (Supplementary Table SIV) Iran (upper MIC) isreported as the only EMRO country in which gamete donation andsurrogacy are practiced The role of ART has become increasingly im-portant for the state which views the rise in voluntary childlessness asa national challenge and is facilitating infertility treatment for couples ofreproductive age (Tremayne and Akhondi 2016)
Over 60 infertility clinics operate in the capital Tehran as well asother major cities in Iran (Tremayne and Akhondi 2016) An ARTcenter in Iran quoted that 241 of IVFICSI cycles were successful(Abutorabi et al 2014) Infertility centers in Iran are reported to oper-ate outside of government-financed health facilities and services areonly provided to those who can afford it Although ART is limited bycosts in Iran the cost is relatively lower than neighboring countrieswhich encourages foreign infertile couples to travel to Iran to undergoART Lack of national auditing supervision and a registry are cited asthe major drawbacks of the quality of care of ART system in Iran(Sadeghi 2015 Abedini et al 2016)
Changes to the stimulation protocols to reduce costs were reportedfrom a single unit in Egypt which performed 3233 IVF and ICSI cyclesover 5 years using HMG-only protocols as a practical and more afford-able method of stimulation The authors describe similar clinical preg-nancy rates with a mean cost reduction of over US$600 in the HMG-only group (Sallam et al 2013) One report highlighted the need todevelop and implement strategies to improve the management of in-fertility and ART in Egypt Suggested strategies included continuousupdating of undergraduate and postgraduate education professionaldevelopment programs and in-service training (Gibreel et al 2015)
South AsiaA survey from this region reported that in the countries for which in-formation was available (Bangladesh India Nepal Pakistan and SriLanka) IVF is available for couples but is not subsidized by the gov-ernment Oocyte donation and surrogacy are available and regulatedin India Nepal and Sri Lanka Of these five countries only Indiareported having a national registry for IVF activities but it is not com-pulsory The typical cost per treatment cycle of IVF was US$2500 orabove in all responding countries and IUI varied widely among theresponding countries from less than US$200 to more than US$2500(Li et al 2018) Of the 11 citations included in the review from thisregion most were from India (Supplementary Table SV) IVFICSIgamete donation and surrogacy are established ART practices in Indiain both the public and private sectors allowing a maximum of threeembryos per transfer (Widge and Cleland 2011) The low cost easyaccess availability and economical prices of IVF drugs along with avail-ability of surrogates and gamete donors have fueled the growth of theART industry in this region Over the last decade there has been aprogressive increase in the number of ART clinics in India with thenumber of voluntary reporting IVF centers increasing However manycenters in India are still not registered with a regulating body and notreporting their ART cycles (Malhotra et al 2015)
Mishra (2013) described the drawback of the growing number ofcenters (now estimated to be over 500 clinics in India) and availabletreatments is that new ART therapies are often introduced directlyfrom the laboratory to clinical practice and (safety) data are collectedas patients are treated with new protocols The options for infertility
IVF in low- and middle-income countries 221
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

treatment in India vary from pharmacotherapy often clomiphene cit-rate as the initial approach for most women to more expensive ARToptions Often patients still turn to alternative systems of medicineand faith healing hoping for a quick and successful outcome (Palattyet al 2012)
Although considered the most important barrier for ART in mostcountries the financial burden was the commonest reason for drop-ping out of IVF cycles in India In spite of the financial constraints themajority of the couples consented to the first IVF cycle but they hadto stop treatment when repeated cycles of IVF were indicated Theauthors did not report on LBR (Kulkarni et al 2014) Efforts havebeen reported to reduce the costs of treatments (to one-third of thecost of conventional ART) by using minimal stimulation protocols andother cost-cutting measures in an attempt to provide more affordabletreatment (Aleyamma et al 2011 Olofsson et al 2013) Mild stimula-tion protocols in use in India have been noted to have a lower preg-nancy rate per cycle compared to conventional IVF protocols (176versus 286) although the cumulative LBR after 1 year of treatmentwas similar (434 versus 447) (Mahajan 2013) Quality manage-ment systems are being implemented in Indian ART clinics and it is ac-knowledged by practitioners that the critical determinants of a high-quality IVF laboratory are the people procedure equipment and thelaboratory design (Olofsson et al 2013)
In Bangladesh 10 tertiary level infertility centers reported 16 700new patients per year but only 5 proceeded to ART mainly due tofinancial constraints (Fatima et al 2015) Some centers in Pakistan of-fer minimal stimulation protocols ICSI at a reduced cost and even freeIVF in some cases to meet the demand (Shah Nawaz and Azhar2014) Infertility and its challenge and barriers to care can be deducedfrom evidence on IUI in a survey from Pakistan 90 of respondentsdeclined IUI because of religious and cultural taboos and if they re-ceived treatment they were not willing to disclose this to their family(Khalid and Qureshi 2012)
Sub-Saharan AfricaIt is reported that lt15 of the population of Africa has access toART (Ombelet and Onofre 2019) This review included 23 citationsfrom this region (Supplementary Table SVI) South Africa (upper MIC)is the most developed and experienced in provision of ART and waspreviously the only country with a published data registry (SouthAfrican registry for assisted reproductive techniques SARA) in this re-gion (SARA report 2014) More recently Dyer et al (2019) publisheddata from the newly developed African Network and Registry forAssisted Reproductive Technology with voluntary reporting from 40centers in 13 countries The Association for Fertility and ReproductiveHealth of Nigeria is active as a regulatory framework and provides eth-ical guidelines for ART (Okonta et al 2018) We found seven studiesexploring the efficacy of ART treatments (Eluga et al 2010 Olukoyaet al 2012 Orhue et al 2012 De Beer et al 2016)
One method to increase efficacy of treatment strongly practiced inSub-Saharan Africa is the transfer of multiple embryos justified as be-ing for economic reasons and the fear of failure (Onah and Okohue2010 Fadare and Adeniyi 2015) In Nigeria the LBR has beenreported as high as 76 but with high multiple pregnancy rates of upto 40 (Olukoya et al 2012) It is reported as common practice totransfer up to five embryos at once in Nigeria Ghana Mali andUganda (Fadare and Adeniyi 2015 Horbst 2016 Horbst and Gerrits
2016) Furthermore limited storage facilities and the quality thereof(power supply access to liquid nitrogen) costs associated with stor-age religious concerns about the fate of additional embryos and thepatientrsquos perspective on multiple pregnancies all support the justifica-tion for transfer of more than two embryos in these countries (Fadareand Adeniyi 2015) African women reportedly wish for and do notmind multiple gestations the complications notwithstanding particu-larly when they are over 35 years old with a long history of infertility(Onah and Okohue 2010) In contrast in South Africa (upper MIC)fewer embryos are transferred (up to three) as they have more expe-rience with ART better technical expertise and legal restrictions(Huyser and Boyd 2012 Fadare and Adeniyi 2015)
ART treatments in Sub-Saharan Africa are largely similar to practicesin high-income countries Owing to the lack of local knowledge guide-lines or legislation clinicians starting an ART clinic often refer toEuropeanAmerican guidelines organize collaborations and training inEuropean centers and even use second-hand equipment fromEuropean laboratories A recent case report showed the feasibility ofknowledge transfer from high- to low-income settings in the set-up ofa fertility clinic in Zimbabwe resulting in safe and affordable ART withsuccessful outcomes (Hammarberg et al 2018) Nevertheless localpractices are also implemented such as extended bed rest and hospi-talization in Ghana after embryo transfers (Gerrits 2016) and eggsharing to reduce costs for patients (Horbst 2016)
Regarding feasibility and accessibility most studies focused on costsaccessibility of clinicsservices public awareness and acceptability oftreatment There were no reports of state-funded ART treatments inthis region but affordable ART services have been introduced in somecountries (South Africa Uganda and Nigeria) (Eluga et al 2010Orhue et al 2012 De Beer et al 2016) Such affordable alternativesare reported to have an out-of-pocket cost of around US$200 per IVFcycle (Eluga et al 2010) while other studies quoted costs of up toUS$2700 per IVF cycle in Ghana up to US$4500 in Kenya and up toUS$10 000 in Nigeria (Fadare and Adeniyi 2015 Gerrits 2016Ndegwa 2016) These costs are to be seen in relation to the nationalmonthly minimum wage which is approximately US$110 in Nigeria(Fadare and Adeniyi 2015) One in five couples (22) in South Africa(upper MIC) incurred catastrophic expenditure defined as an out-of-pocket cost gt40 of annual non-food expenditure and reported cop-ing by reducing expenditure on clothing and food using of savings bor-rowing money and taking on extra work (Dyer et al 2013) Almost4 years after ART couples had not recovered financially from thetreatment (Dyer et al 2017) Costs are considered to be a factor inthe low utilization rates of ART services (Omokanye et al 2017Botha et al 2018 Dyer et al 2019 Ombelet and Onofre 2019)The accessibility of clinics is another barrier to ART treatment forpatients with only a few clinics reported in Kenya (Murage et al2011) Transnational ART is becoming common with people crossingborders to access treatment in South Africa and Ghana (Gerrits2016)
Public awareness and acceptability of ART treatments were studiedby surveys in Nigeria which reported several cultural concerns (eg le-gitimacy of children born patriarchy polygyny and value of children)and ethical issues (eg decision-making about the use of technologiesdiscrimination against children born psychological problems and lossof self-esteem side effects and costs) related to ART These issuesare largely dependent on the local context (urban and rural) and
222 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

religion (Catholic Muslim Anglican and traditional religions) (Fabamwoand Akinola 2013 Iliyasu et al 2013 Bello et al 2014 Menuba et al2014 Fadare and Adeniyi 2015 Omokanye et al 2017 Botha et al2018 Dyer et al 2019 Ombelet and Onofre 2019) We found nostudies exploring the acceptability of ART treatment in other Africancountries
Cost-limiting initiatives aiming at affordableARTSeveral options for lowering the cost of ART have been described in14 citations and compared to conventional ART although mostly insmall feasibility trials or pilot studies (Table I)
In India low-cost ART was evaluated in 143 carefully selectedpatients A mild stimulation protocol with several cost-cutting meas-ures (eg eliminating superfluous investigations) resulted in an LBR perstarted cycle of 14 at an average direct cost of US$675 for IVF(Aleyamma et al 2011) In South Africa a clinical pregnancy rate of163 per embryo transfer was reported with a low-cost protocol(mild ovarian stimulation optimum utilization of trained personnel andadapted laboratory procedures) (conference abstract) (De Beer et al2016) In another study low-cost ART using minimal ovarian stimula-tion the local laboratory and a locally trained embryologist wasassessed in 15 patients in Uganda All patients proceeded to oocyteretrieval but pregnancy outcomes were not reported (conference ab-stract) (Eluga et al 2010)
Minimal stimulation compared to conventional stimulation wasassessed in Turkey (upper MIC) and showed that minimal stimulationresulted in similar clinical pregnancy rates while being more cost effec-tive (Ozornek et al 2013) A study comparing two minimal stimula-tion protocols in normal responders with tubal factor infertilityreported improved outcomes with clomiphene citrate as compared toletrozole and concluded that such stimulation is feasible in the Indiancontext (Nagulapally et al 2012) Other studies evaluated minorchanges to the stimulation drugs to reduce costs In India women un-dergoing treatment for severe male factor infertility with letrozole re-duced the total dose of GnRH agonist required and reduced the costby 34 while pregnancy rates were comparable with conventionalGnRH agonist protocols (Mukherjee et al 2012) A randomized con-trolled trial from Pakistan only accessible as an abstract comparedstimulation with aromatase inhibitors gonadotrophins and indometha-cin to standard stimulation with GnRH analogs and reported similarpregnancy and LBR (Shah Nawaz and Azhar 2014)
In addition to minimal stimulation protocols and changes in stimula-tion drugs novel simplified culture systems have been tested A studyfrom Colombia assessed the INVOcellVR device for intravaginal cultureA mean of 42 oocytes was inseminated and cultured in theINVOcellVR device resulting in on average 26 embryos and a clinicalpregnancy rate of 40 per cycle (Lucena et al 2013) In another studyfrom the same research group good quality embryos higher implanta-tion and pregnancy rates were obtained using INVOcellVR compared toconventional IVFICSI (Navarro-Carbonell et al 2012 Lucena et al2013) A case report from Pakistan reported that using intravaginal cul-ture with the INVOcellVR device was successful and accep to the pa-tient (Khan et al 2013)
International initiatives have been focusing on bringing ART to low-resource settings The Walking Egg project aims to reach the goal of
lsquoglobal access to infertility carersquo (Dhont 2011) As part of the projectfeasibility and pilot studies on low-cost ART have been published In aprospective non-inferiority study IVF with the simplified culture sys-tem without the need for specialized medical-grade gases or equip-ment was evaluated against the routine culture system in 40 patientsof whom 35 reached embryo transfer (Day 3) Fertilization ratescleavage rates and clinical pregnancy rates (812 with simplified versus212 with standard culture) were similar (Van Blerkom et al 2014)In a next step a feasibility study of the simplified (t)WE lab system aclosed [same tube] system for fertilization and development until Day3 resulted in three pregnancies and four live births (Ombelet et al2014) All these studies were performed in Belgium Recently thesame research group published a study on how to implement thesesystems in low-resource settings (Ombelet and Goossens 2016) andthey reported the birth of the first baby in Ghana (Ombelet andOnofre 2019)
Other studies have assessed the efficacy and feasibility of improve-ments to the ART clinic organization Batching treatment cycles isused in Nigeria as a method of reducing the costs with a clinical preg-nancy rate of 30 per embryo transfer (Orhue et al 2012) An inten-sive course with training in hystero-contrast-sonography and one-stepIUI was a possible tool as a first step to introduce basic infertility careinto resource-poor settings like Eritrea before advancing to ART(Gnoth et al 2013) Despite these studies and efforts most of the ini-tiatives come from high-income countries and are still not immediatelytransferable to all LMIC settings (Bahamondes and Makuch 2014)
Risk of bias across studiesRisk of bias of individual studies is recorded in I We found 14 studiesfocusing on efficacy feasibility and acceptability of more affordableART options of which two provided indirect evidence (moderate riskof bias) as they were conducted as pilot studies in high-income coun-tries (Ombelet et al 2014 Van Blerkom et al 2014) Of the remain-ing 12 studies five could be accessed as a (conference) abstract only(Eluga et al 2010 Nagulapally et al 2012 Ozornek et al 2013 ShahNawaz and Azhar 2014 De Beer et al 2016) three were scored asat critical risk of bias (Gnoth et al 2013 Khan et al 2013 Lucenaet al 2013) two at serious risk (Aleyamma et al 2011 Orhue et al2012) and two at moderate risk of bias (Mukherjee et al 2012Navarro-Carbonell et al 2012)
DiscussionThe primary aim of this review was to establish the availability of IVFand other ART services in LMIC focusing on accessibility efficacy fea-sibility and acceptability In addition we summarized citations on thecurrently available affordable ART services or cost-reducing interven-tions While performing the review it was evident from many studiesthat high-cost ART treatments are being offered in LMIC often in pri-vate clinics and with the aim of providing ART access to the moreeconomically affluent population Such ART treatments are not acces-sible to the low- and middle-income people living in urban areas asthe cost is estimated to be up to 50 higher than the gross nationalper capita income in many LMIC (Vayena et al 2009) Affordable
IVF in low- and middle-income countries 223
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

ART was considered to be ART that is not cost prohibitive and is ac-cessible to the general population of an LMIC
There were recurring themes among the citations reviewedReports included national data with regard to number of clinics suc-cess rates costs and drawbacks being faced Several of the includedstudies discussed suggestions for increasing access availability and ac-ceptability of ART within a country Finally studies also reported onattitudes toward infertility and ART and a shift in perception that canbe made through education of health care providers patients andcommunities (Vayena et al 2009)
Very few papers were found specifically discussing low-cost ARToptions and most were small feasibility studies or pilot studies per-formed in developed countries rather than large-scale evaluations ofthe efficacy safety and feasibility of these treatments in LMICAffordable ART initiatives include the Walking Egg project and theINVOcellVR device These projects are integral in bringing adapted ARTservices to LMIC but they should be evaluated through robust re-search for efficacy and safety and further adapted to the local infra-structure Recommendations on how to establish an ART center in alow-resource setting have been published to improve access (Cookeet al 2008)
When bringing ART to LMIC the variation in the etiology of infertil-ity should be taken into consideration Male infertility is more commonin some regions and is managed using various ART (for instance spermextraction along with ICSI) or IUI However local culture and stigmain some regions prevents the man of the infertile couple undergoingfertility testing which significantly affects the female partner but mayalso influence availability and research on treatments for male factor in-fertility (Agarwal et al 2015) Secondary infertility often followingunsafe abortions and complications at childbirth is also frequentlyreported in some LMIC and infertility management should include pre-ventative measures in addition to implementing more affordable ARTstrategies
In addition to the varying composition of infertile populations inLMIC the differences in settings between countries and regions aresignificant LMIC is too wide a category to assess and summarize fertil-ity treatments appropriately There was a vast difference betweenART offered in low-income countries and lower MIC compared toupper MIC The upper MIC such as China implement new cuttingedge treatments and technologies aggressively without technicalrestrictions (Ha 2013) while at the other end of the spectrum low-income countries struggle to introduce fertility assessment and low-cost options (Gnoth et al 2013) The need for ART regulating bodieswithin countries and regions was universally reported by the studies
Another aspect of ART in LMIC that raises concern is cross-borderreproductive care where possibly as a consequence of the lack ofART legislation private clinics offer high-quality ART procedures toforeign infertile couples at a high cost (Abedini et al 2016) Cross-border reproductive care could be beneficial to local residents as itboosts the economy as well as bringing resources technologies andtreatments to their country (Sadeghi 2015) However the local inhab-itants are generally not able to afford the same treatments and arerarely offered cost-saving opportunities such as egg sharing Youngwomen have the potential to be exploited as egg donors or surrogatesfor wealthy foreigners
While performing the review it was noted that there is basic sci-ence and clinical research occurring in LMIC which is helping to inform
and improve outcomes in ART worldwide In addition national andregional registries are attempting to collect data on ART treatmentswith some success in Latin America and Africa (Zegers-Hochschildet al 2013 SARA report 2014 Zegers-Hochschild et al 2014 et al2015 et al 2016) More rigorous data reporting collection and verifi-cation are needed from LMIC to enable a meta-analysis in the future(Kushnir et al 2017)
In conclusion the results of this review demonstrate some degreeof availability of IVF and other ART services in LMIC but highlight aneed for the development of more affordable and accessible ARToverall Infertility continues to be a global health problem that is stillnot being adequately addressed worldwide This review was per-formed to inform the WHO guidelines and to consider ART servicesas an important strategy in the management of men and women withinfertility in LMIC These guidelines will hopefully assist policy makersin including the management of infertility including IVF and other ARTservices in the reproductive health agenda and hence to improveoverall access to reproductive care in LMIC
LimitationsHealth care systems and populations largely vary among differentcountries even within the same geographic region and information onthese variations is not readily available In addition to this regional vari-ation the availability heterogeneity and quality of studies largely influ-enced the conclusions to be drawn for the different regions Theheterogeneity of studies and reports can also be attributed to the lessrestrictive inclusion criteria for outcomes which were set as such toincrease the sensitivity of the search strategy
Regarding the options for affordable ART in LMIC the most signifi-cant limitation was the lack of high-quality studies Of the 14 studiesincluded in the section lsquoCost limiting initiatives aiming at affordableARTrsquo only four were of moderate risk of bias of which two providedindirect evidence Although attempts were made to contact authorsand to find the published trials of references included as an abstractwe may have missed valuable data from studies not available in the in-cluded databases or retrievable through the English search terms andunpublished data
Supplementary dataSupplementary data are available at Human Reproduction Updateonline
AcknowledgementsWe would like to thank Tomas Allen (WHO) and Nancy Bianchi(University of Vermont) for their advice and assistance with the searchstrategies
Authorsrsquo rolesIT was responsible for the concept of this protocol TMC and KBwrote the protocol and designed the search strategy IT RF and KLreviewed and edited the protocol KB performed the final literature
224 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

search TMC and NV extracted the data performed the analysis ofthe articles and wrote the manuscript All the authors contributed tothe design interpretation of the results and critical revision of themanuscript
The authors JK and IT are staff members of the World HealthOrganization The authors alone are responsible for the viewsexpressed in this publication and they do not necessarily represent theviews decisions or policies of the World Health Organization
FundingThis study was supported by the World Health OrganizationDepartment of Reproductive Health and Research This work was alsofunded by the UNDP-UNFPA-UNICEF-WHO-World Bank SpecialProgramme of Research Development and Research Training inHuman Reproduction (HRP) a cosponsored program executed by theWorld Health Organization
Conflict of interestNone declared
ReferencesAbedini M Ghaheri A Omani Samani R Assisted reproductive tech-
nology in Iran the first national report on centers 2011 Int J FertilSteril 201610283ndash289
Abutorabi R Razavi V Baghazade S Sharegh L Mostafavi FSEvaluation of the success rate of assisted reproductive techniques(ART) in Shahid Beheshti infertility center Isfahan Iran J IsfahanMed School 2014321767ndash1781
Agarwal A Mulgund A Hamada A Chyatte MR A unique view onmale infertility around the globe Reprod Biol Endocrinol 20151337
Aleyamma TK Kamath MS Muthukumar K Mangalaraj AM GeorgeK Affordable ART a different perspective Hum Reprod 2011263312ndash3318
Audibert C Glass D A global perspective on assisted reproductivetechnology fertility treatment an 8-country fertility specialist sur-vey Reprod Biol Endocrinol 201513133
Aytoz A Female health care professionals in fertility services inTurkey Hum Reprod 201227 ii18
Bahamondes L Makuch MY Infertility care and the introduction ofnew reproductive technologies in poor resource settings ReprodBiol Endocrinol 20141287
Balabanova E Simonstein F Assisted reproduction a comparative re-view of IVF policies in two pro-natalist countries Health Care Anal201018188ndash202
Balic D How to make assisted reproductive technologies (ART) af-fordable in Bosnia and Herzegovina experience after the first 105cycles Med Arh 201165119ndash121
Banerjee K Singla BAcceptance of donor eggs donor sperms ordonor embryos in Indian infertile couples J Hum Reprod Sci 201811169ndash171
Bello FA Akinajo OR Olayemi O In-vitro fertilization gamete dona-tion and surrogacy perceptions of women attending an infertilityclinic in Ibadan Nigeria Afr J Reprod Health 201418127ndash133
Bennett LR Wiweko B Hinting A Adnyana IB Pangestu MIndonesian infertility patientsrsquo health seeking behaviour and pat-terns of access to biomedical infertility care an interviewer admin-istered survey conducted in three clinics Reprod Health 2012924
Botha B Shamley D Dyer S Availability effectiveness and safety ofART in sub-Saharan Africa a systematic review Hum Reprod Open20182018hoy003
Cooke I Gianaroli L Hovatta O Trounson A Affordable ART andthe Third World difficulties to overcome Hum Reprod 2008200893ndash96
Correa MCDV Loyola MA Tecnologias de reproduc~ao assistida noBrasil opc~oes para ampliar o acesso Physis (Rio J) 201525753ndash777
De Beer MW Matsaseng TC Erasmus EL Nel NA Pillay DNosarka S Affordable ART outcomes at the Tygerberg FertilityClinic Tygerberg Academic Hospital (TBAH) South Africa-specialreference to tubal factor infertility Reprod Biomed Online 201632S3
MdCB de Souza Latin America and access to assisted reproductivetechniques a Brazilian perspective JBRA Assist Reprod 20141847ndash51
Dhont N The Walking Egg non-profit organisation Facts Views VisObgyn 20113253ndash255
Dyer S Archary P de Mouzon J Fiadjoe M Ashiru O Assisted re-productive technologies in Africa first results from the AfricanNetwork and Registry for Assisted Reproductive Technology2013 Reprod Biomed Online 201938216ndash224
Dyer SJ Sherwood K McIntyre D Ataguba JE Catastrophic paymentfor assisted reproduction techniques with conventional ovarianstimulation in the public health sector of South Africa frequencyand coping strategies Hum Reprod 2013282755ndash2764
Dyer SJ Vinoos L Ataguba JE Poor recovery of households fromout-of-pocket payment for assisted reproductive technology HumReprod 2017322431ndash2436
Eluga M Tamale Sali E Desmet B Albano C Devroey P OmbeletW Platteau P Controlled ovarian stimulation for in vitro fertiliza-tion in a low resource setting a pilot study in Kampala-UgandaHum Reprod 201025i21ndashi22
ESHRE special task force on lsquodeveloping countries and infertilityrsquoESHRE Monographs 200820081ndash117
European IVF monitoring Consortium (EIM) for the EuropeanSociety of Human Reproduction and Embryology Calhaz-Jorge CDe Geyter C Kupka MS de Mouzon J Erb K Mocanu EMotrenko T Scaravelli G Wyns C Goossens V et al Assisted re-productive technology in Europe 2013 results generated fromEuropean registers by ESHRE Hum Reprod 2017321957ndash1973
European Policy Audit on Fertility (EPAF) 2017Fabamwo AO Akinola OI The understanding and acceptability of
assisted reproductive technology (ART) among infertile women inurban Lagos Nigeria J Obstet Gynaecol 20133371ndash74
Fadare JO Adeniyi AA Ethical issues in newer assisted reproductivetechnologies a view from Nigeria Niger J Clin Pract 201518 SupplS57ndashS61
IVF in low- and middle-income countries 225
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Fatima P Ishrat S Rahman D Banu J Deeba F Begum N AnwarySA Hossain HB Quality and quantity of infertility care inBangladesh Mymensingh Med J 20152470ndash73
Fertility Europe European Society of Human Reproduction andEmbryology (ESHRE) A Policy Audit on Fertility Analysis of 9 EUCountries 2017 httpwwwfertilityeuropeeuour-projectspolicy-audit (5 October 2020 date last accessed)
Garcia S Bellamy M Assisted conception services and regulationwithin the Brazilian context JBRA Assist Reprod 201519198ndash203
Gerrits T Assisted reproductive technologies in Ghana transnationalundertakings local practices and lsquomore affordablersquo IVF ReprodBiomed Soc Online 2016232ndash38
Gibreel A Eladawi N El-Gilany AH Allakkany N Shams M How doEgyptian gynecologists manage infertility Cross-sectional study JObstet Gynaecol Res 2015411067ndash1073
Gnoth C Kaulhausen H Marzolf S First steps into gynaecological en-docrinology and reproductive medicine in resource-poor countriesan eritrean experience J Reprod Med Endokrinol 20131044ndash48
Gonzalez-Santos SP From esterilologıa to reproductive biology thestory of the Mexican assisted reproduction business ReprodBiomed Soc Online 20162116ndash127
Ha JO Risk disparities in the globalisation of assisted reproductivetechnology the case of Asia Glob Public Health 20138904ndash925
Hammarberg K Kirkman M Infertility in resource-constrained set-tings moving towards amelioration Reprod Biomed Online 201326189ndash195
Hammarberg K Trounson A McBain J Matthews P Robertson TRobertson F Magli C Mhlanga T Makurumure T Marechera FImproving access to ART in low-income settings through knowl-edge transfer a case study from Zimbabwe Hum Reprod Open20182018hoy017
Horbst V lsquoYou cannot do IVF in Africa as in Europersquo the making ofIVF in Mali and Uganda Reprod Biomed Soc Online 20162108ndash115
Horbst V Gerrits T Transnational connections of health professio-nals medicoscapes and assisted reproduction in Ghana andUganda Ethn Health 201621357ndash374
Huyser C Boyd L Assisted reproduction laboratory cost-drivers inSouth Africa value virtue and validity Obstet Gynaecol Forum20122215ndash21
Iliyasu Z Galadanci HS Abubakar IS Bashir FM Salihu HM AliyuMH Perception of infertility and acceptability of assisted reproduc-tion technology in northern Nigeria Niger J Med 201322341ndash347
Inhorn MC Patrizio P Infertility around the globe new thinking ongender reproductive technologies and global movements in the21st century Hum Reprod Update 201521411ndash426
Khalid SN Qureshi IZ Perceptions of infertile couples regarding in-fertility and intrauterine insemination (IUI) in a rural populationand services at government hospitals in Punjab Pakistan HumReprod 201227 ii7-8
Khamoshina MB Arkhipova MP Rudneva OD Vostrikova TVRadzinskaya EV The level of awareness of ART and the attitudeto it of medical students and workers without work experience inIVF clinics Reprod Biomed Online 201020S89
Khan M Zafar S Syed S Successful intravaginal culture of human em-bryos for the first time in Pakistanmdashan experience at the Sindh
Institute of Reproductive Medicine Karachi J Pak Med Assoc 201363630ndash632
Kulkarni G Mohanty NC Mohanty IR Jadhav P Boricha BG Surveyof reasons for discontinuation from in vitro fertilization treatmentamong couples attending infertility clinic J Hum Reprod Sci 20147249ndash254
Kushnir VA Barad DH Albertini DF Darmon SK Gleicher NSystematic review of worldwide trends in assisted reproductivetechnology 2004-2013 Reprod Biol Endocrinol 2017156
Kwek LK Saffari SE Tan HH Chan JK Nada SComparison betweensingle and double cleavage-stage embryo transfers single and dou-ble blastocyst transfers in a South East Asian In Vitro FertilisationCentre Ann Acad Med Singapore 201847451
Li HWR Tank J Haththotuwa R Asia and Oceania Federation ofObstetrics and Gynaecology Updated status of assisted reproduc-tive technology activities in the Asia-Oceania region J ObstetGynaecol Res 2018441667ndash1672
Lucena EE Moran AA Saa AA Pulido CC Lombana OO BonillaEE Invovagina complex replaces conventional incubators FertilSteril 2013100S527
Mahajan N Should mild stimulation be the order of the day J HumReprod Sci 20136220ndash226
Makuch MY Bahamondes L Barriers to access to infertility care andassisted reproductive technology within the public health sector inBrazil Facts Views Vis Obgyn 20124221ndash226
Malhotra J Malhotra N Pai HD Goswami D Retrospective six yearanalysis of ART directory of India Hum Reprod 201530i442ndashi443
Mascarenhas MN Flaxman SR Boerma T Vanderpoel S StevensGA National regional and global trends in infertility prevalencesince 1990 a systematic analysis of 277 health surveys PLoS Med20129e1001356
Menuba IE Ugwu EO Obi SN Lawani LO Onwuka CI Clinicalmanagement and therapeutic outcome of infertile couples insoutheast Nigeria Ther Clin Risk Manag 201410763ndash768
Mishra V IVF scenario in India Int J Fertil Steril 2013720ndash21Mitic D Kopitovic V Popovic J Milatovic S Basic M Milojevic M
[Results of in vitro fertilization cycles at the Clinic for Gynecologyand Obstetrics Clinical Center of Nis] Med Pregl 201265315ndash318
Moher D Liberati A Tetzlaff J Altman DG Group P Preferredreporting items for systematic reviews and meta-analyses thePRISMA statement BMJ 2009339b2535
Mukherjee S Sharma S Chakravarty BN Letrozole in a low-costin vitro fertilization protocol in intracytoplasmic sperm injectioncycles for male factor infertility a randomized controlled trial JHum Reprod Sci 20125170ndash174
Murage A Muteshi MC Githae F Assisted reproduction servicesprovision in a developing country time to act Fertil Steril 201196966ndash968
Nagulapally S Mittal S Malhotra N A randomized controlled studyof minimal stimulation IVF with two different protocols in normalresponders Hum Reprod 201227 ii7-8
Navarro-Carbonell DE Lucena-Quevedo E Saa-Madri~nan AMComparacion de la calidad embrionaria entre fertilizacion in vitro(FIV) y cultivo intravaginal de ovocitos (INVO) en el CentroColombiano de Fertilidad y EsterilidadmdashCECOLFES BogotaColombia Rev Colomb Obstet Ginecol 201263227ndash233
226 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Ndegwa SW Affordable ART in Kenya the only hope for involun-tary childlessness Facts Views Vis Obgyn 20168128ndash130
Nigam M Nigam R Chaturvedi R Jain A Ethical and legal aspects ofartificial reproductive techniques including surrogacy AnilAggrawalrsquos Internet J Forensic Med Toxicol 2011121ndash21
Okafor NI Joe-Ikechebelu NN Ikechebelu JIPerceptions of infertilityandin vitro fertilization treatment among married couples inAnambra State Nigeria Afr J Reprod Health 20172155
Okonta PI Ajayi R Bamgbopa K Ogbeche R Okeke CCOnwuzurigbo K Ethical issues in the practice of assisted reproduc-tive technologies in Nigeria empirical data from fertility practi-tioners Afr J Reprod Health 20182251ndash58
Olofsson JI Banker MR Sjoblom LP Quality management systemsfor your in vitro fertilization clinicrsquos laboratory why bother J HumReprod Sci 201363ndash8
Olukoya OY Okeke CC Kemi AI Ogbeche RO Adewusi AJAshiru OA Multiple gestationspregnancies from IVF process in afertility center in Nigeria 2009-2011 implementing policy towardsfewer (double and single) embryo transfer Nig Q J Hosp Med20122280ndash84
Ombelet W Reproductive healthcare systems should includeaccessible infertility diagnosis and treatment an important chal-lenge for resource-poor countries Int J Gynaecol Obstet 2009106168ndash171
Ombelet W Campo R Affordable IVF for developing countriesReprod Biomed Online 200715257ndash265
Ombelet W Cooke I Dyer S Serour G Devroey P Infertility andthe provision of infertility medical services in developing countriesHum Reprod Update 200814605ndash621
Ombelet W Goossens J The Walking Egg Project how to start aTWE centre Facts Views Vis Obgyn 20168119ndash124
Ombelet W Onofre J IVF in Africa what is it all about Facts ViewsVis Obgyn 20191165ndash76
Ombelet W Van Blerkom J Klerkx E Janssen M Dhont NMestdagh G Nargund G Campo R The (t)WE lab simplified IVFprocedure first births after freezingthawing Facts Views Vis Obgyn2014645ndash49
Omokanye L Olatinwo A Durowade K Raji H Raji S Biliaminu SGaniyu S Determinants of utilization of assisted reproductive tech-nology services in Ilorin Nigeria J Med Soc 201731109
Onah HE Okohue J Case against single embryo transfer in AfricanIVF clinics Middle East Fertil Soc J 201015296ndash297
Orhue AA Aziken ME Osemwenkha AP Ibadin KO Odoma G Invitro fertilization at a public hospital in Nigeria Int J GynaecolObstet 201211856ndash60
Ozornek H Ozay A Oztel Z Atasever E Turan E Ergin E Minimalstimulation is as effective as classical stimulation in a single embryotransfer program in Turkey Fertil Steril 2013100S277
Palatty PL Kamble PS Shirke M Kamble S Revankar M RevankarVM A clinical round up of the female infertility therapy amongstIndians J Clin Diagn Res 201261343ndash1349
Pottinger AM Everett-Keane D McKenzie C Evolution of in vitrofertilization at the University of the West Indies Jamaica West IndMed J 201261460ndash462
Qiao J Feng HL Assisted reproductive technology in China compli-ance and non-compliance Transl Pediatr 2014391ndash97
Rossi Ada S Amaral E Makuch MY Access of people living with HIVto infertility services perspective of Brazilian healthcare professio-nals AIDS Care 2011231329ndash1335
Sadeghi MR Access to infertility services in middle east J ReprodInfertil 201516179
Sallam H Ezzeldin F Sallam N Agameya A Sallam S Farrag AHMG-only protocol for IVF a practical and more affordable optionfor developing countries Hum Reprod 201328i138
SARA report South African Registry for assisted reproductive techni-ques 2014 report (6th ANNUAL SARA report) 2014 httpanara-africacomwp-contentuploads201709SARA-2014-22052017pdf (5 October 2020 date last accessed)
Shah Nawaz S Azhar A Amazing low cost IVFICSI inductionprotocol in developing countries Hum Reprod 201429 Suppl 1i1ndashi389
Sharma S Mittal S Aggarwal P Management of infertility in low re-source countries BJOG 2009116 Suppl77ndash83
Silva SGD Bertoldi AD Silveira MFD Domingues MR Evenson KRSantos ISD Assisted reproductive technology prevalence and as-sociated factors in Southern Brazil Rev Saude Publica 20195313
Stellar C Garcia-Moreno C Temmerman M van der Poel S A sys-tematic review and narrative report of the relationship between in-fertility subfertility and intimate partner violence Int J GynaecolObstet 20161333ndash8
Sterne JA Hernan MA Reeves BC Savovic J Berkman NDViswanathan M Henry D Altman DG Ansari MT Boutron I et alROBINS-I a tool for assessing risk of bias in non-randomised stud-ies of interventions BMJ 2016355i4919
Stevens GA Alkema L Black RE Boerma JT Collins GS Ezzati MGrove JT Hogan DR Hogan MC Horton R et al Guidelines foraccurate and transparent health estimates reporting the GATHERstatement Lancet 2016388e19ndashe23
Tremayne S Akhondi MM Conceiving IVF in Iran Reprod Biomed SocOnline 2016262ndash70
Urman B Yakin K New Turkish legislation on assisted reproductivetechniques and centres a step in the right direction ReprodBiomed Online 201021729ndash731
Van Blerkom J Ombelet W Klerkx E Janssen M Dhont N NargundG Campo R First births with a simplified culture system for clini-cal IVF and embryo transfer Reprod Biomed Online 201428310ndash320
van der Poel SZ Historical walk the HRP Special Programme and in-fertility Gynecol Obstet Invest 201274218ndash227
Vayena E Peterson HB Adamson D Nygren K-G Assisted repro-ductive technologies in developing countries are we caring yetFertil Steril 200992413ndash416
Wahlberg A The birth and routinization of IVF in China ReprodBiomed Soc Online 2016297ndash107
Whittaker A From lsquoMung Mingrsquo to lsquoBaby Gammyrsquo a local history ofassisted reproduction in Thailand Reprod Biomed Soc Online 2016271ndash78
Widge A Cleland J Negotiating boundaries accessing donor game-tes in India Facts Views Vis Obgyn 2011353ndash60
World Bank Country and Lending Groups httpsdatahelpdeskworldbankorgknowledgebasearticles906519-world-bank-country-and-lending-groups (30 January 2020 date last accessed)
IVF in low- and middle-income countries 227
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022

World Health Organization Preamble to the Constitution of the
World Health Organization as adopted by the International HealthConference New York 19-22 June 1946 signed on 22 July 1946by the representatives of 61 States (Official Records of the WorldHealth Organization no 2 p 100) and entered into force on 7April 1948 httpwww who intgovernanceebwho_constitution_en pdf 1948 (5 October 2020 date last accessed)
Ye H Huang GN Cao YX Zhong Y Huang YH Zhu GJ Zhou LMChen ZJ Shi JZ Zeng Y et al [Effect of domestic highly purifiedurinary follicle stimulating hormone on outcomes of in vitrofertilization-embryo transfer in controlled ovarian stimulation]Zhonghua Fu Chan Ke Za Zhi 201348838ndash842
Zegers-Hochschild F Adamson GD de Mouzon J Ishihara OMansour R Nygren K Sullivan E Van der Poel S The internationalcommittee for monitoring assisted reproductive technology(ICMART) and the world health organization (WHO) revised glos-sary on ART terminology 2009 Hum Reprod 2009242683ndash2687Simultaneously Published in Fertil Steril 200926921520ndash2684
Zegers-Hochschild F Adamson GD Dyer S Racowsky C deMouzon J Sokol R Rienzi L Sunde A Schmidt L Cooke ID et alThe international glossary on infertility and fertility care 2017
Hum Reprod 2017321786ndash1801 Simultaneous Publication in FertilSteril 201711081393ndash1406
Zegers-Hochschild F Dickens BM Dughman-Manzur S Human rightsto in vitro fertilization Int J Gynaecol Obstet 201312386ndash89
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2011 J Brasil Reprod Assist 201317216ndash221
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies in Latin America theLatin American Registry 2012 Reprod Biomed Online 20153043ndash51
Zegers-Hochschild F Schwarze JE Crosby JA Musri C de SouzaMdCB Assisted reproductive technologies (ART) in Latin Americathe Latin American Registry 2012 JBRA Assist Reprod 201418127ndash135
Zegers-Hochschild F Schwarze JE Crosby JA Musri C UrbinaMT Latin American Network of Assisted ReproductionAssisted reproductive techniques in Latin America the LatinAmerican Registry 2013 Reprod Biomed Online 201632614ndash625
228 Chiware et al
Dow
nloaded from httpsacadem
icoupcomhum
updarticle2722136006235 by guest on 06 February 2022
Copyright © 2022 FDOKUMEN