
ITTS Final Conference - Northern Periphery Programme
24
ITTS Final Conference Drumossie Hotel, Inverness 11-12 March 2014 www.transnational-telemedicine.eu
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ITTS Final Conference - Northern Periphery Programme
ITTS Final
Conference
Drumossie Hotel, Inverness
11-12 March 2014
www.transnational-telemedicine.eu
Welcome everyone to the final ITTS
conference! We have guests here
from Finland, Sweden, Norway,
Northern Ireland, the Republic of
Ireland, and the Netherlands, as well
as from Scotland.
It is hard to believe that this project is
drawing to a close, but we hope
that you will see over the next two
days that we have achieved much –
in total we have implemented or
extended 25 services across 40 sites
within the project. It has been a real
pleasure and privilege working on
this project. We would like to thank
our funders, the Northern Periphery
Programme. In our case funding was
supplemented by NHS Highland and
NHS Orkney and we would like to
thank them for their contribution to
the project. We would like to also
thank the clinicians and patients
across the participating countries who
took part in the demonstrator projects.
In the audience you will find clinicians,
patients, and a range of others
including health service planners,
technologists, academics and civil
servants. We hope you will find the
time to meet with many of these
people – knowledge exchange is a
vital ingredient. We have set the
conference up so that we won’t be
talking at you too much; there will be
plenty of opportunities for debate. This
begins with a showcase this morning,
and you are encouraged to visit the
ITTS project stands. We have also
asked other projects and organisations
to provide information, which we
hope you find relevant and useful, so
please visit during the allocated time,
or at some point later in the
proceedings.
We hope our international guests
enjoy their stay in the Highlands and
Islands. We will endeavour to give you
all a flavour of life here, and we hope
you will see a vibrant health sciences
community in spectacular
surroundings, no matter what the
weather may bring!
INSERT ITTS FACT
OR
QUOTE
XXXXX
Schedule of Events
Speakers About ITTS
ITTS Services ITTS Impact Delegate List
Contents
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 1
Welcome | ITTS Final Conference
Dr David Heaney, ITTS Project Director
2
4
6
7
16
14
10:45-11:00 Registration | Tea &Coffee
11:00-11:20 Welcome & Introduction| ITTS Briefing Alasdair Munro | David Heaney
11:20-12:30 ITTS Showcase Exhibition
13:30-15:00 ITTS Project Overviews | Questions
15:00-15:15 Break | Tea & Coffee
15:15-15:45 Project Evaluation Leila Eadie, ITTS Scotland
12:30-13:30 Lunch
15:45-16:30 eHealth: Scotland in Europe George Crooks, Scottish Centre for Telehealth and Telecare (SCTT) / NHS24
John Matheson, Scottish Government
Jim Millard, Scottish Government
16:30-17:00 Panel Discussion | Issues arising from Day 1
19:00-22:00 Conference Dinner | Ceilidh
17:00 Close of Day 1
Page 2 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
Schedule of Events | Day 1
Day 1: Tuesday 11 March
Notes
08:45-09:00 Registration | Tea &Coffee
09:00-09:15 Introduction to Day 2 David Heaney
09:15-10:30 Perspectives | Patient, clinician, health service, industry
11:00-11:15 Break | Tea & Coffee
11:15-11:45 Perspectives | International Telemedicine Advisory Service (ITAS)
11:45-12:45 Panel Discussion | The Future of Telemedicine: A European Perspective
10:30-11:00 Implications of ITTS David Heaney
12:45-13:45 Lunch | Conference Close*
13:45-14:45 Parallel Sessions:
ITAS Meeting | Citizen Panel Meeting
15:45-16:00 Break | Tea & Coffee
14:45-15:45 ISG Meeting
16:00 Conference Close
19:30-22:00 Partner Dinner
Day 2: Wednesday 12 March
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 3
*The conference programme will continue after lunch for project team only. Other delegates are free to depart after the morning
sessions. Lunch provided. Programme subject to change.
Schedule of Events | Day 2
Notes
Speakers
Prof. George Crooks
OBE, MBChB, FRCP, FRCGP
Medical Director NHS 24 (UK)
Professor George Crooks is
Medical Director for NHS 24 and
Director for the Scottish Centre
for Telehealth and Telecare
(SCTT).
George has a particular interest
in the field of unscheduled care,
including the development of
common assessment and triage
processes across the NHS and
the use of technology to
support the delivery of high
quality patient care to the
population of Scotland.
In 2011 George was elected
President of the European
Health Telematics Association
(EHTEL) and is also Chair of the
Scottish Assisted Living
Programme Board, leading on
the at scale delivery of
telehealth services.
John Matheson
Director of Health Finance, eHealth
and Pharmaceuticals, Scottish
Government
John has over 35 years' experience in
the public sector, including 25 as
Finance Director both at Health Board
level and, for the past 5 years, within
Central Government as Director of
Health Finance. His responsibilities also
include eHealth and Pharmacy.
Part of John's role is to oversee the
Scottish Government's eHealth
Programme with the strategic
objective to support improvements in
patient care and service
performance in line with Ministerial
objectives. The eHealth Programme
aims to improve patient care through
advances in technology, resulting in
better access to health information,
quicker test results for clinicians and
joined-up GP and hospital services.
The scope of eHealth includes all IT
systems, information and records
management, process change and
skills development required for
healthcare delivery, including
supporting infrastructure and business
systems.
Speakers
Page 4 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
Line Helen Linstad
Dept. Manager: Prevention & Self
Management, Norwegian Centre for
Integrated Care and Telemedicine
Line Linstad is the Manager of the
Advisory Department at the
Nowegian Centre for Integrated
Care and Telemedicine (NST).
Line is a political scientist from the
University of Oslo and has been with
NST since January 2002. At NST, Line
has extensive and long-standing
experience as an adviser to hospitals
on how to use telemedicine on a
strategic level, and as a project
manager of several eHealth and
telemedicine projects in Norway. She
has also been involved in numerous
European and international eHealth
and telemedicine projects.
Line is the National Lead for ITTS
Norway.
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 5
Speakers
Liam Glynn
Clinical Director of the Western
Research and Education Network
(WestREN) and Chairman of the
North Clare Primary Care Team,
Ireland.
Liam is the National Lead for ITTS
Ireland.
Thomas Molén
Strategist at Strategic Development
Office, Västerbotten County
Council
Thomas represents Sweden as a
member of the ITTS International
Telemedicine Advisory Service
(ITAS).
Eddie Ritson
Director, Centre for Connected
Health and Social Care (CCHSC),
Northern Ireland Public Health
Agency
Eddie is the National Lead for ITTS
Northern Ireland.
James Cameron
Head of Life Sciences,
Highlands and Islands Enterprise
XXXXXXXXXXXXXXXXXXXXXXXXXXX
XXXXXXXXXXXXXXXXXXXXXXXXXXX
XX
.
Jim Millard
Branch head / Senior Policy
Advisor, Scottish Government
XXXXXXXXXXXXXXXXXXXXXXXXXXX
XXXXXXXXXXXXXXXXXXXXXXXXXXX
XX
Seppo Heikkilä
Senior Consultant / EU Expert,
Deveplan Development Ltd
Seppo represents Finland as a
member of the ITTS International
Telemedicine Advisory Service
(ITAS).
A total of 25 new services have now
been implemented at more than 40
sites across the programme area.
Delivering healthcare to remote
and rural populations is a
significant challenge, requiring
innovative strategies to overcome
infrastructure deficits, travel
difficulties and staffing problems.
There is an urgent need to reduce
transport costs and carbon
footprint, plus a growing
acknowledgement that models of
long-term care will have to evolve
to cope with demographic
changes and the economic
downturn. Telemedicine may help
to provide equity of health service
regardless of distance from major
centres of care. Yet telemedicine is
not in common use; while there
have been numerous pilot studies,
on completion technology is often
withdrawn and the services have
not been sustained. The
disconnected nature of
developments has meant similar
problems are often encountered
during each new implementation
and knowledge is not shared
between sites. Implementing
Transnational Telemedicine
Solutions (ITTS) proposed
transnational knowledge
exchange about services already
proven to work in one country,
using this knowledge to implement
services in new settings.
Page 6 |www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
Background | About
ITTS has shown that
transnational knowledge
sharing can facilitate the
implementation of sustainable
telemedicine solutions.
Background | Telemedicine
The disconnected nature of
developments has meant similar
problems are often encountered
during each new implementation
and knowledge is not shared
between sites. Implementing
Transnational Telemedicine
Solutions (ITTS) proposed
transnational knowledge
exchange about services already
proven to work in one country,
using this knowledge to implement
services in new settings.
Delivering healthcare to remote
and rural populations is a
significant challenge, requiring
innovative strategies to overcome
infrastructure deficits, travel
difficulties and staffing problems.
There is an urgent need to reduce
transport costs and carbon
footprint, plus a growing
acknowledgement that models of
long-term care will have to evolve
to cope with demographic
changes and the economic
downturn. Telemedicine may help
to provide equity of health service
regardless of distance from major
centres of care. Yet telemedicine is
not in common use; while there
have been numerous pilot studies,
on completion technology is often
withdrawn and the services have
not been sustained.
About ITTS
ITTS was a project part-funded by the EU Northern Periphery
Programme (NPP), which aimed to implement transnational
telemedicine solutions at scale across Europe’s Northern
Periphery Programme area, introducing new telemedicine
applications to remote and rural areas in order to improve
healthcare delivery for rural communities. ITTS began in
September 2011 and built on previous work which mapped
telemedicine services available in remote and rural areas of
Northern Europe.
Six NPP area countries were actively involved and ten
demonstrator telemedicine projects were implemented.
The project teams were:
Scotland (Lead Partner): Centre for Rural Health,
University of Aberdeen
Finland: Oulu Arc Subregion
Ireland: National University of Ireland, Galway
Northern Ireland: Centre for Connected Health & Social
Care
Norway: Norwegian Centre for Integrated Care and
Telemedicine (NST)
Sweden: County Council of Västerbotten
[Teleconsultation] has led us to examine the
possibility of home VC for selected patients and
consider use by a wider range of health care
professionals in our discipline.
Prof Sandra MacRury, Consultant Diabetologist

Caption describing picture or graphic.
Follow us on twitter
@itts_telemed
#ITTSfinal
The ten demonstrator projects were classified into three themes:
ITTS Services
The major benefit of videoconferencing (VC) is to save travel time and costs, either for
the patient who can contact their doctor at a site nearer their home, or for the
healthcare staff, who need not travel large distances to visit patients. It also allows the
introduction of services to areas that have been previously deemed too remote to
allow cost-effective access. Because VC can use readily available, relatively
inexpensive technology with which many people and institutions now have
experience, it is a simple and economic introduction to telemedicine for clinics.
Video-consultation
Mobile self-management
Home-based health services
Smartphones are becoming increasingly popular and can provide reminders, symptom
or activity tracking facilities, and of course, communication with health services, among
many other features, allowing an inexpensive method of interaction with large numbers
of patients. Similarly to websites, they can support self-management programmes,
providing an exchange of information for various health areas and the potential for
patients to participate in their health care more pro-actively, thereby reducing the
burden on existing services.
Finally, home-based care is of particular interest to people living in remote and rural areas,
especially those who suffer from multiple or complex health and social care needs, and
those who are restricted in their ability to travel by illness or mobility issues. Telemedicine
can reduce hospital visits and help keep patients in their own communities, bringing care
into their homes that they would otherwise not be able to, or have the opportunity to
access.
The ten demonstrator projects are detailed in the following pages.
Note: While most of the technology used in the demonstrator projects is in existence, the implementation
occurred in new sites, and in a co-ordinated fashion to promote sustainability.
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 7
Scotland | Norway | Sweden | Northern Ireland
Scotland | Sweden | Ireland | Northern Ireland
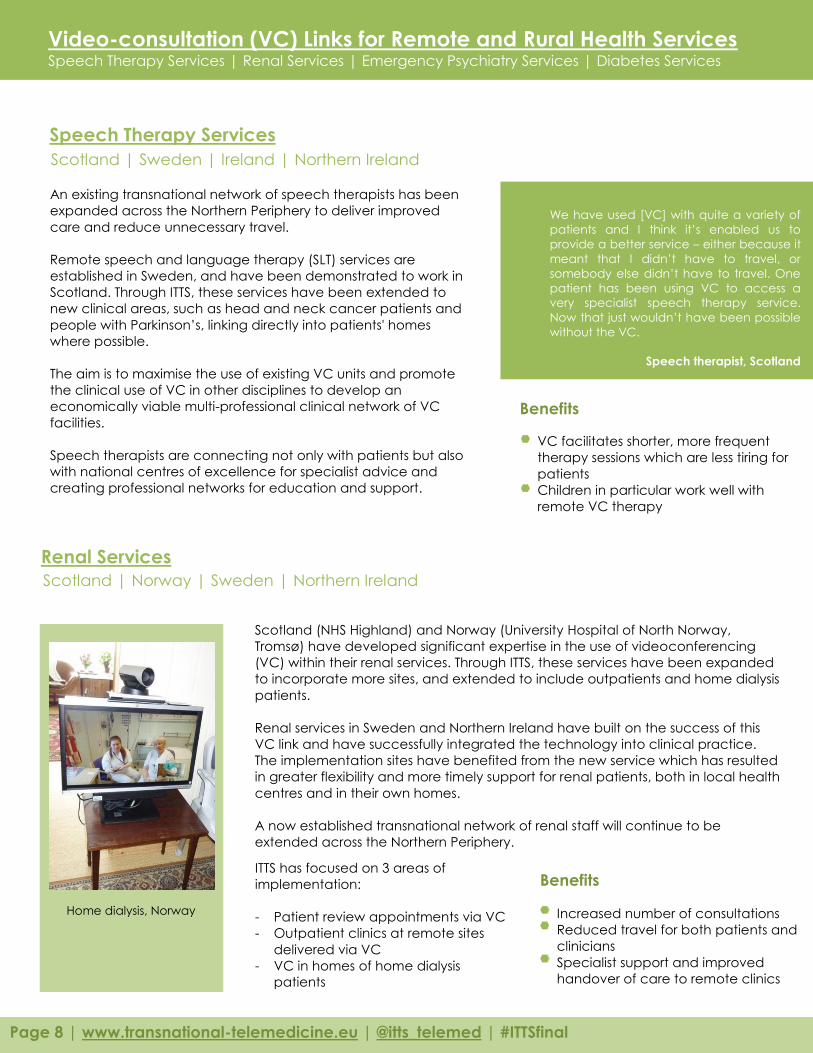
Scotland (NHS Highland) and Norway (University Hospital of North Norway,
Tromsø) have developed significant expertise in the use of videoconferencing
(VC) within their renal services. Through ITTS, these services have been expanded
to incorporate more sites, and extended to include outpatients and home dialysis
patients.
Renal services in Sweden and Northern Ireland have built on the success of this
VC link and have successfully integrated the technology into clinical practice.
The implementation sites have benefited from the new service which has resulted
in greater flexibility and more timely support for renal patients, both in local health
centres and in their own homes.
A now established transnational network of renal staff will continue to be
extended across the Northern Periphery.
ITTS has focused on 3 areas of
implementation:
- Patient review appointments via VC
- Outpatient clinics at remote sites
delivered via VC
- VC in homes of home dialysis
patients
We have used [VC] with quite a variety of
patients and I think it’s enabled us to
provide a better service – either because it
meant that I didn’t have to travel, or
somebody else didn’t have to travel. One
patient has been using VC to access a
very specialist speech therapy service.
Now that just wouldn’t have been possible
without the VC.
Speech therapist, Scotland
Video-consultation (VC) Links for Remote and Rural Health Services Speech Therapy Services | Renal Services | Emergency Psychiatry Services | Diabetes Services
Speech Therapy Services
Renal Services
Page 8 | www.transnational-telemedicine.eu | | #ITTSfinal @itts_telemed
An existing transnational network of speech therapists has been
expanded across the Northern Periphery to deliver improved
care and reduce unnecessary travel.
Remote speech and language therapy (SLT) services are
established in Sweden, and have been demonstrated to work in
Scotland. Through ITTS, these services have been extended to
new clinical areas, such as head and neck cancer patients and
people with Parkinson’s, linking directly into patients' homes
where possible.
The aim is to maximise the use of existing VC units and promote
the clinical use of VC in other disciplines to develop an
economically viable multi-professional clinical network of VC
facilities.
Speech therapists are connecting not only with patients but also
with national centres of excellence for specialist advice and
creating professional networks for education and support.
VC facilitates shorter, more frequent
therapy sessions which are less tiring for
patients
Children in particular work well with
remote VC therapy
Benefits
Increased number of consultations
Reduced travel for both patients and
clinicians
Specialist support and improved
handover of care to remote clinics
Benefits
Home dialysis, Norway
Norway | Scotland
Videoconferencing (VC) is used
to deliver teleconsultations as
part of diabetes services where
there is considerable distance
between the consultant and
patient. Patients attending short
notice appointments, 6-monthly
or annual reviews can attend
clinics at a local site, remote
from the diabetes consultant
who is based in a central
location, saving either their travel
time and costs, or the
consultant’s. The patient is
escorted by a specialist diabetes
nurse at the remote site who
sends blood glucose data from
the patient’s meter via the
internet to the consultant. A
consultation can then take
place via VC in a similar way to
The pathway for the patient is shorter
because you are able to do the job more
efficiently and have more frequent
meetings with the patient.
Psychiatry nurse, Norway
Video-consultation (VC) Links for Remote and Rural Health Services Speech Therapy Services | Renal Services | Emergency Psychiatry Services | Diabetes Services
Emergency Psychiatry Services
Remote Diabetes Services
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 9
A videoconferencing (VC) solution provides patients in an acute
psychiatric state with access to specialist evaluation as close to
their home as possible. In addition, VC can enable a 24-hour
system where psychiatrists are available for patients who visit
emergency departments at district centres.
The rationale behind a VC solution includes difficulties in recruiting
specialists, minimising travel for patients and carers and the
provision of specialist services to remote locations. Studies in
Norway have shown that there are no differences between
telemedicine and conventional face-to-face methods with
regard to quality and satisfaction among patients and
professionals. Telepsychiatry has also proved to be cost effective.
It is important to develop a VC system where it is easy to involve a
specialist directly in a consultation, both when the patient is
admitted to 24-hour departments and when the patient is
consulted by an ambulatory team. In such a system the
specialists can be located in different local sites.
Locates patient assessment within
communities, preventing an automatic
transport for admission process
Provides local emergency care, saving
costs incurred in transporting patients
Prevents additional patient distress as a
result of relocation
Benefits
Scotland |Finland | Northern Ireland
a face-to-face consultation. After the
consultation, the doctor uses digital
dictation to make information
immediately available to the GP.
Incorporation of the specialities of
podiatry, dietetics and other relevant
specialties will also ensure a
comprehensive service is offered to
patients at remote sites.
ITTS has expanded the previous service
across the Scottish Highlands and into
the Orkney Islands, and started a new
service in Northern Ireland.
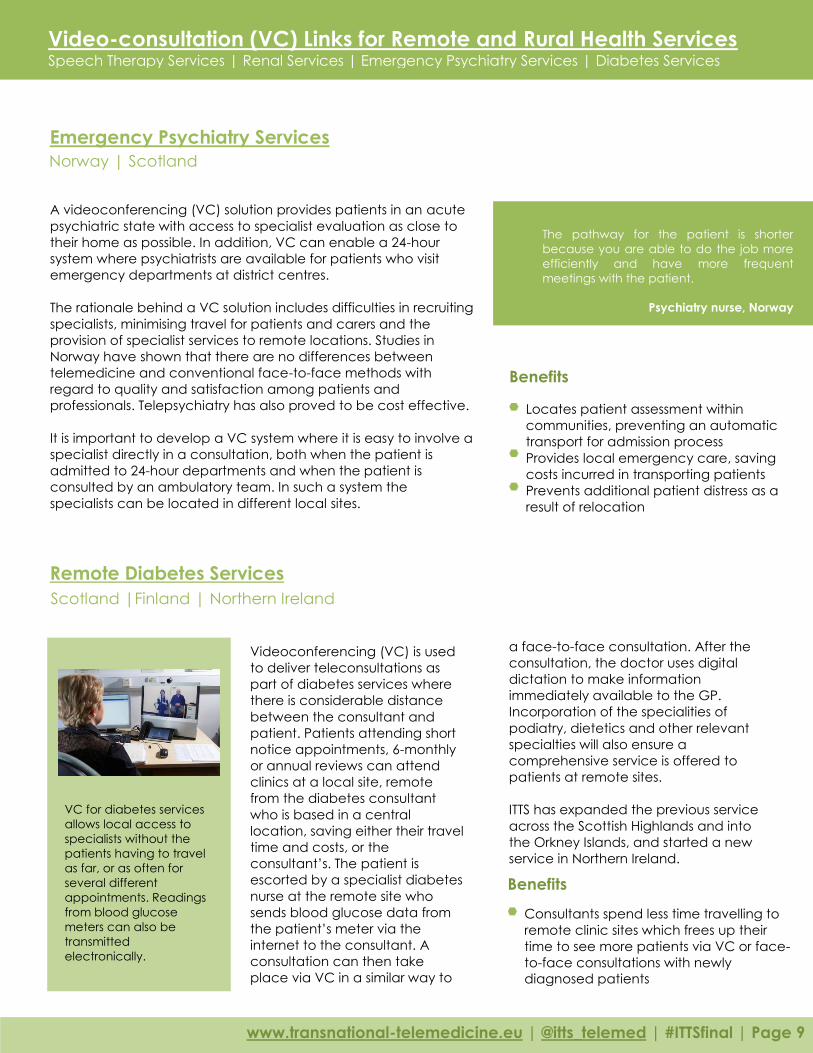
VC for diabetes services
allows local access to
specialists without the
patients having to travel
as far, or as often for
several different
appointments. Readings
from blood glucose
meters can also be
transmitted
electronically.
Consultants spend less time travelling to
remote clinic sites which frees up their
time to see more patients via VC or face-
to-face consultations with newly
diagnosed patients
Benefits

There are numerous technological
options available to help support
and streamline diabetes care, but
information about optimum
clinical solutions is often scarce.
Many institutions resort to creating
their own tools and would benefit
from a forum for knowledge and
expertise sharing.
Self-help tools on a mobile
platform enable diabetic patients
(and other patient groups) to self-
monitor their disease. Functionality
can cover food intake, physical
activity and blood glucose
measures as well as a personal
goal-setting module for following
up on own achievements.
ITTS partners have experience in a
variety of self-care platforms and
the challenges connected to the
ITTS has created an international
network of expertise to advise on
how to improve diabetes care
using technology to support
patients and clinicians and also
integrate care systems.
We believe knowledge sharing can
provide answers to common
questions and solutions to
upcoming challenges to assist
everyone involved or interested in
diabetes care.
Ireland | Scotland | Norway | Sweden
Northern Ireland | Ireland | Scotland | Norway
Through the ITTS project we have learnt
the benefits of transnational knowledge
exchange and we hope to produce
tangible results from the investment of
bringing these people together.
David Heaney, ITTS Project Director
Smartphones and Internet Support for Remote and Rural Health Services Tracking & Promoting Physical Activity | Diabetes Services | Inflammatory Bowel Disease (IBD) Support
Tracking & Promoting Physical Activity
Diabetes Services
Page 10 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
An increase in obesity, COPD and
diabetes, to name a few health
concerns, has prompted
governments to endorse regular
physical activity as an essential tool in
promoting an individual's health. The
aim of this project was to harness
smartphone software technology to
monitor and promote physical
activity and improve associated
health outcomes.
Using smartphones to monitor
physical activity was run as a pilot
project in Ireland and revealed
impressive results: over the course of
the pilot, the average daily step
count in a control group had
decreased by 156 steps per day with
the step count in the intervention
group increasing by 2,359 steps per
day.
Following the success of this pilot,
the app was ‘prescribed’ by GPs in
Ireland, and Scotland; a diabetes
consultant in Northern Ireland; and
weight loss groups in Norway.
Weekly step counts are
sent to the practice nurses
who then monitor the
data and set new targets,
gradually increasing
patients' activity levels.
Patients who own smartphones
generally tend to carry these with
them all the time and so no
additional equipment is required.
All that’s needed is the will to walk!
Benefits
implementation of such tools
and services. ITTS enables the
partner countries to engage in
knowledge exchange, to learn
from each other and to better
understand the barriers to
implementation and how these
can be avoided.
Key points

Ireland | Scotland | Norway | Sweden
Smartphones and Internet Support for Remote and Rural Health Services Tracking & Promoting Physical Activity | Diabetes Services | Inflammatory Bowel Disease (IBD) Support
Support for Patients with Inflammatory Bowel Disease (IBD)
There’s a sense we’re at the crest
of a wave of how smartphone
technology will be used in the
future to improve people’s
health, but also to capacity build
around them managing their own
health which I think is the goal of
all primary healthcare systems
around the world. Prevention is
better than cure…
General Practitioner, Ireland
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 11
There is a wide spectrum of disease
among patients with Crohn’s and
ulcerative colitis, including patients
whose disease is well controlled
and those who need more
intensive management. In addition
to the geographic challenge of
delivering high quality health in
rural areas, there is a professional
challenge to general practitioners
who may only have one patient
with Crohn’s or colitis in his/her
practice.
This project was launched to help
patients manage their own disease
through the use of smartphones,
whilst giving them access to the
best specialist advice. A
smartphone application (app) was
designed to enable patients to
record their symptoms; this
information is then monitored by a
specialist IBD nurse who calls the
patient for a consultation should
any symptoms deviate from
normal. The IBD nurse can then
direct the patient’s care
appropriately.
Since September 2013, following
successful implementation
in Scotland, ITTS Ireland have
trialled a service with Galway
University Hospital, clinical research
facility and IBD patients in the
associated referral area.
The app facilitates close
monitoring and a prompt response
which should help reduce
admissions and catch problems
before they worsen, or alternatively
reassure patients that all is well and
they can avoid unnecessary
outpatient appointments.
Each patient has a range of symptoms
that can be displayed graphically, and if
any of the symptoms deviate from a
normal level, this will alert both the
patient (via the smartphone) and the IBD
nurse.
The app was developed and trialled in a
collaboration between Angus Watson, a
surgeon at Raigmore Hospital, Inverness,
and OpenBrolly, a Scottish technology
developer company, to help monitor
inflammatory bowel disease.
Scotland | Ireland | Sweden | Finland
Scotland | Northern Ireland | Finland
Home-based Support for Remote and Rural Health Services Medical & Social Care Emergencies | Exercise Classes for Rehabilitation | Patients with Multimorbidity
Medical & Social Care Emergencies
Exercise Classes for Rehabilitation
Page 12 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
I think the service definitely needs to be
sustained. Our population is getting
much older so they’re going to be less
likely to be able to come into the
surgery; if we can reach out to them
with the technology it could be
beneficial for the future.
Physiotherapist, Ireland
Remote support in medical and social
care emergencies is facilitated through
the use of telecare. Telecare employs
the use of a range of monitoring and
alarm-based technologies in the home
setting. It is used primarily to support
individuals with a range of health
and/or social needs to live more
independently and remain at home
safely.
A basic telecare technology package
includes a base unit, body transmitter
and other sensors such as smoke
detectors. An enhanced telecare
package includes a wide range of
peripheral sensors, including epilepsy
sensors and DDA (Disability
Discrimination Act) pagers for people
with sensory impairments. These alarms
and devices trigger a response from
a call centre, alerting them to
problems and arranging to provide
any help required.
One of the key challenges in
dealing with medical and
social care emergencies is
the high incidence of false
and unnecessary alerts; this is
especially problematic given
the rural nature of northern
periphery areas of Europe.
Many patients who would benefit from
rehabilitation classes are not well
enough to travel; for these patients to
participate from home helps their
recovery and can allow them to get
well enough to potentially join
standard classes.
The use of VC widens access to these
classes, which are often
oversubscribed, with long waiting lists.
Key points
Remote exercise classes can be used in the rehabilitation of a
number of long-term conditions such as COPD, stroke and pain
conditions. Patients who live far from clinics or have travel difficulties
may be unable to attend rehabilitation groups.
A home-based solution, or one available closer to home (e.g. in a
local healthcare centre), offers these patients the opportunity to take
part in classes, ensuring they are offered the same clinical, social and
educational benefits as those living closer to larger clinics.
A technology solution using internet-based VC enables patients to
view their physiotherapist and other class members at the same time
from the comfort and convenience of their home.
The exercise programmes are designed in a similar format to those
run in regular exercise classes, but using equipment readily available
in or near the home. The physiotherapist is able to monitor the
patients by seeing and speaking to them and also by remote
monitoring using equipment appropriate to the particular condition.
The alarm system allows both
patients and staff to call for help
It also warns staff when patients
unexpectedly leave the building
Benefits
Patients have peace of mind
that their condition is being
monitored
Patients gain greater
understanding of their condition
and how to manage it
Less risk of unplanned admissions
to hospital
Reduced anxiety for carers and
family
Scotland | Northern Ireland | Sweden | Finland
Home-based Support for Remote and Rural Health Services Medical & Social Care Emergencies | Exercise Classes for Rehabilitation | Patients with Multimorbidity
www.transnational-telemedicine.eu | | #ITTSfinal | Page 13 @itts_telemed
Patients with Multimorbidity
Based on previous experience of
home-based services for patients
with complex care requirements,
this project takes different forms in
different countries:
In Ireland, a self-monitoring station
is based within a GP clinic where
patients can check their blood
pressure and weight and use
exercise equipment.
In Sweden, clinic-based blood
pressure self-monitoring services
were implemented, in addition to a
second service: a “check-up bag”
that nurses use on home visits to
evaluate blood pressure and
calculate the INR blood clotting
measure.
In Finland’s Oulu Arc Subregion,
patients use a web portal to
access laboratory results, monitor
their health and contact
healthcare staff with any questions,
plus housebound patients with
social and health care needs were
offered a VC care option.
In northern Sweden, a drop-in service
for self-measuring of blood pressure
and INR values is now available at
healthcare centres in Malå (since
November 2012), Sorsele (since
January 2013) and Storuman. To date,
over 500 patients have used this new
service.
Benefits
Options for self-care can help patients learn more
about their health and take responsibility, with support and encouragement from clinicians.
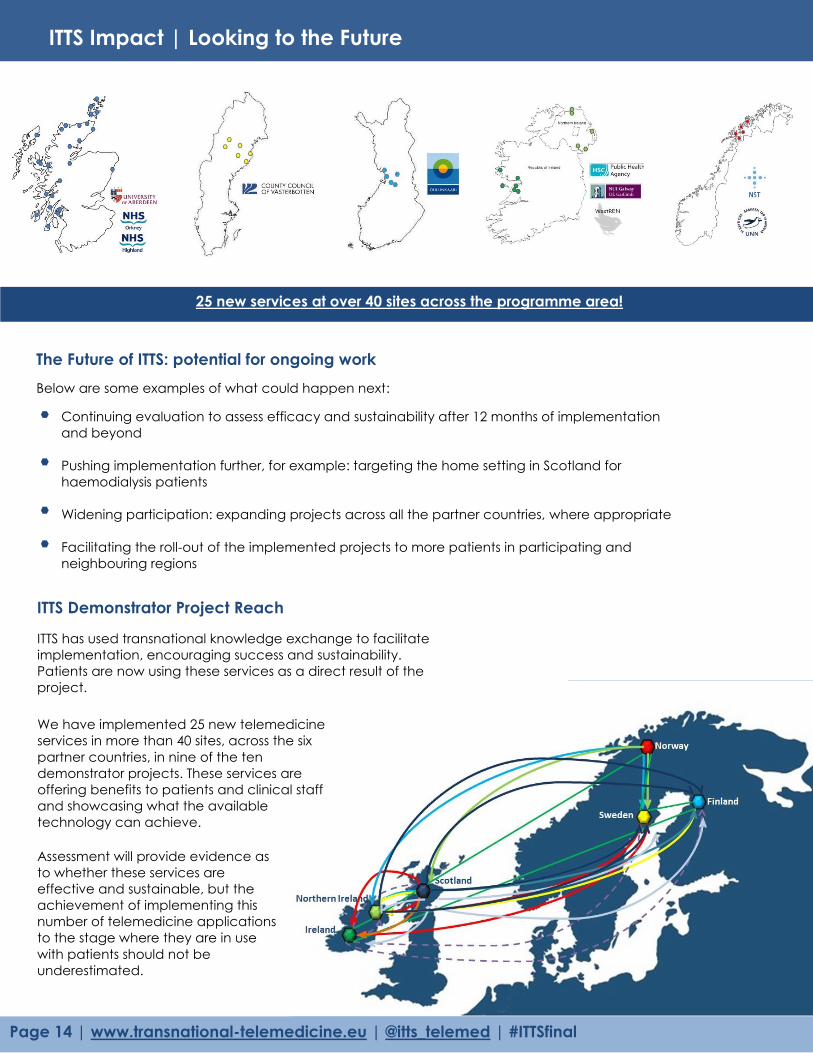
ITTS Impact | Looking to the Future
ITTS Demonstrator Project Reach
Page 14 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
25 new services at over 40 sites across the programme area!
The Future of ITTS: potential for ongoing work
Continuing evaluation to assess efficacy and sustainability after 12 months of implementation
and beyond
Pushing implementation further, for example: targeting the home setting in Scotland for
haemodialysis patients
Widening participation: expanding projects across all the partner countries, where appropriate
Facilitating the roll-out of the implemented projects to more patients in participating and
neighbouring regions
Assessment will provide evidence as
to whether these services are
effective and sustainable, but the
achievement of implementing this
number of telemedicine applications
to the stage where they are in use
with patients should not be
underestimated.
ITTS has used transnational knowledge exchange to facilitate
implementation, encouraging success and sustainability.
Patients are now using these services as a direct result of the
project. We have implemented 25 new telemedicine
services in more than 40 sites, across the six
partner countries, in nine of the ten
demonstrator projects. These services are
offering benefits to patients and clinical staff
and showcasing what the available
technology can achieve.
Below are some examples of what could happen next:
On the back of your family’s newsletter, you
may want to add a simple greeting, poem, or
an example of your children’s artwork. This is
the first part of the newsletter that your loved
ones will see, so make sure that it is festive and
eye-catching.
You can add your own artwork to the back of
a family newsletter by scanning in a drawing
or a photograph.
Hats off to all those who helped us
make ITTS such a great project. We
think we have made a difference
to people living in the Northern
Periphery.
We also think we have unleashed
the potential for future
developments, as technology
advances, and as clinicians,
patients and service planners get
used to telemedicine being part of
everyday practice.
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 15
Follow us on Twitter | @ITTS_telemed
Like us on Facebook | ITTSProject
Find out more…
For further information about the work of ITTS
please visit our website:
www.transnational-telemedicine.eu
You can also keep up to date with all our latest
activity via social media:
Learning from the project will be used to inform the
following publications:
A Case for Telemedicine
Telemedicine into Everyday Practice
Background and contextual information: a portfolio
of the ten individual business cases, the business case
for the sustainability of ITAS, the collective, and the
international evaluation plan.
A guide with an interactive checklist for use by
policymakers and service planners.
These publications will be available to
download from the ITTS website in the
coming months, together with a number of
other project materials including
newsletters, promotional films and peer
reviewed papers.

David Heaney (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Lee Dowie (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Leila Eadie (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Gerry King (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Emma Coats (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Steph Kelly (ITTS) Centre for Rural Health, University of Aberdeen [email protected]
Frances Mair (ITAS) University of Glasgow [email protected]
George Crooks SCTT | NHS24 [email protected]
Donna Henderson SCTT | NHS24 [email protected]
Cathy Dorrian SCTT | NHS24 [email protected]
Linda Kirkland NHS Highland [email protected]
Angus Watson NHS Highland [email protected]
Grace Fergusson NHS Highland [email protected]
Lesley Patience NHS Highland [email protected]
Margaret Moss NHS Highland [email protected]
Michael Flavell NHS Highland [email protected]
Rob Peel NHS Highland [email protected]
Sandra MacRury NHS Highland [email protected]
Beatrice Wood NHS Highland [email protected]
Andrew Evennett NHS Highland [email protected]
Maimie Thompson NHS Highland [email protected]
Robert Scully NHS Lothian [email protected]
Jim Millard Scottish Government [email protected]
Frances Elliot Scottish Government [email protected]
John Matheson Scottish Government [email protected]
Caroline Coleman Scotland Europa [email protected]
Jeff Foot Highlands and Islands Enterprise (HIE) [email protected]
Denise Pirie Highlands and Islands Enterprise (HIE) [email protected]
James Cameron Highlands and Islands Enterprise (HIE) [email protected]
Stephanie Andrew Highlands and Islands Enterprise (HIE) [email protected]
Graham Scott Highlands and Islands Enterprise (HIE) [email protected]
Jacqueline McGuigan Highlands and Islands Enterprise (HIE) [email protected]
Sue Scotland Digital Health Institute (DHI) [email protected]
Elizabeth Brooks Digital Health Institute (DHI) [email protected]
Alasdair Munro Centre for Health Science Company [email protected]
Lindsey Moodie Centre for Health Science Company [email protected]
Barbara Isaacs Centre for Rural Health, University of Aberdeen [email protected]
Phil Wilson Centre for Rural Health, University of Aberdeen [email protected]
Alasdair Mort Centre for Rural Health, University of Aberdeen [email protected]
Pam Sherriff Centre for Rural Health, University of Aberdeen [email protected]
Steve Dodsworth D Health [email protected]
David Sim OpenBrolly [email protected]
Geoff Wilcock OpenBrolly [email protected]
Tara French Glasgow School of Art [email protected]
John Bruce John Bruce Associates [email protected]
Paul McNamee Health Economics Research Unit, University of Aberdeen
Nelson Norman Institute of Remote Healthcare [email protected]
Graham Page Institute of Remote Healthcare [email protected]
Pam Nicol NHS Education for Scotland
William McKerrow NHS Education for Scotland [email protected]
Chris Robinson General Practitioner: Glen Mor Surgery, Fort William
Joe Tangney General Practitioner: Glen Mor Surgery, Fort William [email protected]
Chris Evans Citizen Panel, ITTS Scotland
Margaret MacKechnie Citizen Panel, ITTS Scotland Val Moffat Citizen Panel, ITTS Scotland Joanne McCoy Citizen Panel, ITTS Scotland
Line Linstad (ITTS) Norwegian Centre for Integrated Care and Telemedicine
(NST) [email protected]
Siri Bjørvig (ITTS) Norwegian Centre for Integrated Care and Telemedicine
(NST) [email protected]
Undine Knarvik (ITTS) Norwegian Centre for Integrated Care and Telemedicine
(NST) [email protected]
Delegate List
Page 16 | www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal

Frank Larsen (ITTS) Norwegian Centre for Integrated Care and Telemedicine
(NST) [email protected]
Trine Bergmo (ITAS) Norwegian Centre for Integrated Care and Telemedicine
(NST) [email protected]
Eli Arild Norwegian Centre for Integrated Care and Telemedicine [email protected]
Merja. H. Mourujarvi University Hospital of North Norway (UNN) [email protected]
Rita I. Johansen University Hospital of North Norway (UNN) [email protected]
Morten Borgen University Hospital of North Norway (UNN) [email protected]
Didrik Klivær University Hospital of North Norway (UNN) [email protected]
Käte Alrutz (ITTS) Västerbotten County Council [email protected]
Brith Granström (ITTS) Västerbotten County Council [email protected]
Annika Olsson (ITTS) Västerbotten County Council [email protected]
Thomas Molen (ITAS) Västerbotten County Council [email protected]
Maria Jermolin Västerbotten County Council [email protected]
Erik Nordhall Västerbotten County Council [email protected]
Seija Dahlgren Citizen Panel, ITTS Sweden
Karin Sandtröm
Karin Sandström Citizen Panel, ITTS Sweden Sören Sandström Citizen Panel, ITTS Sweden
Matti Matero (ITTS) Oulu Arc
Tiina Vuononvirta (ITTS) Oulu Arc [email protected]
Seppo Heikkila (ITAS) Deveplan Management Consulting [email protected]
H. Tapio Hanhela Oulu Arc [email protected]
Liam Glynn (ITTS) National University of Ireland, Galway [email protected]
Pat Hayes (ITTS) National University of Ireland, Galway [email protected]
Monica Casey (ITTS) National University of Ireland, Galway [email protected]
Breda Kelleher (ITTS) National University of Ireland, Galway [email protected]
Fergus Glynn (ITAS) General Practitioner: Corofin Medical Centre, Co. Clare [email protected]
Stephen Bradish Health Service Executive [email protected]
Idé Ni Chonghaile Health Service Executive [email protected]
Lorraine Dillane Health Service Executive [email protected]
Eddie Ritson (ITTS) Centre for Connected Health & Social Care (CCHSC) [email protected]
Soo Hun (ITTS) Centre for Connected Health & Social Care (CCHSC) [email protected]
Roy Harper South Eastern Health and Social Care Trust [email protected]
Fionae Paterson Southern Health and Social Care Trust [email protected]
Shane McNamee Western Health and Social Care Trust [email protected]
Sean Donaghy Health and Social Care Board [email protected]
Dawn Braden Northern Health and Social Care Trust [email protected]
Julie-Ann Augusto South Eastern Health and Social Care Trust [email protected]
Jonathan Wallace University of Ulster [email protected]
Gloria Mills Belfast Health and Social Care Trust [email protected]
John Farrell Department of Health, Social Services and Public Safety [email protected]
Bronagh Mooney Northern Health and Social Care Trust [email protected]
Patrick Black Northern Health and Social Care Trust [email protected]
Pamela Armstrong Northern Health and Social Care Trust [email protected]
Christine Breen Health and Social Care Board [email protected]
Brian Dunn Health and Social Care Board [email protected] Paraig O’Brien Northern Ireland Housing Executive / DHSSPS [email protected]
Christopher Parker Northern Periphery Programme (NPP) [email protected]
Arend Roos NV Economische Impuls Zeeland [email protected]
Wim Renders Brainport Development NV [email protected]
Tom Daly Cooperation and Working Together (CAWT) [email protected]
Bernie McCrory Cooperation and Working Together (CAWT) [email protected]
Wesley Henderson Cooperation and Working Together (CAWT) [email protected]
Aigars Miezitis National Health Service, Latvia [email protected]
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal | Page 17
Delegate List

Notes…
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal

Notes…
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal
Notes…
www.transnational-telemedicine.eu | @itts_telemed | #ITTSfinal

Project Partnership
SCOTLAND | LEAD PARTNER
NORWAY
SWEDEN
FINLAND
IRELAND
NORTHERN IRELAND
This project was part-funded by the
Northern Periphery Programme (NPP) 2007-2013
Centre for Rural Health (CRH),
University of Aberdeen
Norwegian Centre for Integrated
Care and Telemedicine (NST)
County Council of Västerbotten
Oulu Arc Subregion
National University of Ireland,
Galway (NUIG)
Centre for Connected Health
and Social Care (CCHSC)