
Alcoholic liver disease: A current molecular and clinical ...
Upload
khangminh22Category
view
4download
0
George et al. BMC Geriatrics (2022) 22:47 https://doi.org/10.1186/s12877-021-02721-w
RESEARCH
Is there an association between non-alcoholic fatty liver disease and cognitive function? A systematic reviewElena S. George*, Surbhi Sood, Robin M. Daly and Sze‑Yen Tan
Abstract
Background: Non‑alcoholic fatty liver disease (NAFLD) is represented as the most common liver disease worldwide. NAFLD is associated with metabolic risk factors underpinned by insulin resistance, inflammation and endothelial dysfunction, leading to extrahepatic changes in central nervous diseases such as cognitive impairment, Alzheimer’s disease and dementia. The aim of the review is to explore the association between NAFLD and cognitive function.
Methods: Using the PRISMA guidelines, a systematic electronic literature search was conducted in four databases: MEDLINE, PsychINFO, Embase and CINAHL from inception until March 2021. Neuropsychological tests utilised within each study were grouped into relevant cognitive domains including ‘general cognition’, ‘reasoning’, ‘mental speed, attention and psychomotor speed’, ‘memory and learning’, ‘language’, ‘visuospatial perception’ and ‘ideas, abstraction, figural creations and mental flexibility’.
Results: Eleven observational studies that involved 7978 participants with a mean age of 51 years were included. Those with NAFLD had poor cognitive performance in three cognitive domains, including ‘general cognition’, ‘mental speed, attention and psychomotor speed’, and ‘ideas, abstraction, figural creations and mental flexibility’.
Conclusion: The observed results from the 11 included studies showed that NAFLD was associated with lower cog‑nitive performance across several domains. However, studies conducted to date are limited to observational designs and are heterogeneous with varying diagnostic tools used to assess cognitive function.
Trial registration: PROSPERO Registration: CRD42 02016 1640.
Keywords: NAFLD, NAFLD, NASH, Cirrhosis, Cognition, Cognitive function, Cognitive impairment
© The Author(s) 2022. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
BackgroundNon-alcoholic fatty liver disease (NAFLD) is recog-nised as the most prevalent liver disease affecting approximately 30% of adults in Australia with simi-lar, high rates in the United States [1–4]. The burden of NAFLD continues to rise significantly in Australia with current estimates of 5.5 million cases in 2019, with expectations of seven million cases by 2030 [1, 5].
NAFLD is defined as a spectrum of diseases related to hepatic fat deposition, ranging from non-alcoholic fatty liver (NAFL) (simple steatosis) to non-alcoholic stea-tohepatitis (NASH), which can progress to increased fibrosis, cirrhosis and hepatocellular carcinoma [3, 6]. Progression from NAFLD to NASH is often described using the “two hit” hypothesis. The “first hit” consists of lipid accumulation of fatty acids, increasing susceptibil-ity of hepatocytes to secondary insults such as oxida-tive stress, insulin resistance and over production and release of pro-inflammatory cytokines. This can lead to the “second hit” which promotes steatohepatitis,
Open Access
*Correspondence: [email protected] of Exercise and Nutrition Sciences, Institute for Physical Activity and Nutrition (IPAN), Deakin University, Geelong, Victoria 3220, Australia

Page 2 of 19George et al. BMC Geriatrics (2022) 22:47
chronic inflammation and fibrosis [7]. NAFLD occurs in the absence of excessive alcohol consumption and is associated with a range of common chronic disease risk factors such as insulin resistance, hypertension, obesity and visceral fat accumulation, and dyslipidaemia [1, 6]. Such risk factors are known to be elucidated by inflam-mation and oxidative stress, which also play a role in extrahepatic diseases, including central nervous system diseases such as mild cognitive impairment, Alzhei-mer’s disease, and dementia [8–10].
The global number of individuals living with demen-tia is 50 million [11], with the prevalence of cogni-tive impairment and dementia rising and estimated to increase amongst older adults (60 years and above) to approximately 2 billion by 2050, accounting for 22% of the world’s population [12]. Cognitive function encom-passes multiple mental abilities and skills in reasoning, perception, memory, verbal and mathematical ability and problem solving [10, 13, 14]. Cognitive impair-ments have been associated with reduced ability to per-form complex tasks such as driving and work-related activities leading to impaired quality of life and in more serious cases, premature mortality [15]. Cardio-vascular disease (CVD), type 2 diabetes (T2DM) and metabolic syndrome (MetS) frequently co-exist with NAFLD and are also considered risk factors for cog-nitive decline [10] and dementia which are increased with ageing [16–18]. Individuals with NAFLD have high rates of metabolic syndrome components includ-ing dyslipidaemia, hypertension, abdominal obesity and insulin resistance, and there is also accumulating evi-dence that individuals with NAFLD have an increased risk of carotid atherosclerosis and carotid intima media thickness; all of which have been reported to contribute towards cognitive impairment [19, 20].
Previous cross-sectional and case-control studies have found that NAFLD is associated with poorer cog-nitive function across a number of cognitive domains as assessed using numerous common psychometric tests [21–23]. Studies in participants with NAFLD and hepatic encephalopathy have reported that they have lower brain volume [21], inflammation and hyperam-monemia [24], all of which are associated with cog-nitive impairment. Despite the known link between NAFLD and various cardiometabolic-related diseases and the underlying mechanisms which drive these chronic diseases as well as cognitive decline, to date there has been no published systematic review summa-rising the relationship between NAFLD and cognitive impairment. Thus, the aim of this review was to sys-tematically search the literature to explore the associa-tion between NAFLD and cognitive function.
MethodsAll methodology related to the analysis was specified prior to the literature search and detailed in a protocol registered with PROSPERO (CRD42020161640).
Search strategyThe review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [25], including independent execution of literature search and bias assessment, completed by author SS. MEDLINE, PsychINFO, Embase and CINAHL electronic databases were searched from inception until March 2021. The search terms were: (Cognit* or “Processing speed” or “mini mental state examination” or MMSE; Neuropsych* or Neurocog-nit* or Metacognit* or Recall or Memory or “Executive function” or “Verbal Fluency” or “Reaction time”) AND (“NAFLD” or “NASH” or “Cirrhosis” or “Non-alcoholic fatty liver” or “Nonalcoholic fatty liver” or “Non-alco-holic steatosis” or “Nonalcoholic steatosis”).
Eligibility criteriaStudies of all designs were included if they were in English language, conducted in humans, included adults aged 18 years and over with NAFLD or at risk of NAFLD (as deemed in each paper where NAFLD was an outcome) and assessed cognitive function in individ-uals with NAFLD. Studies were excluded if they were review articles, abstract only, or included participants with mental health and neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s Disease (PD) and PD-related disorders.
Selection processTitle and abstract screening was carried out by one researcher according to the predefined protocol, and duplicates and articles which did not meet the eligibil-ity criteria were excluded. Full text screening was con-ducted independently by two researchers (SS, SYT), and where there were any conflicts these were resolved by a third researcher (ESG). All articles included from the full-text screen were included in this systematic review. The search process is outlined in the PRISMA flowchart in Fig. 1.
Data extraction and groupingData was extracted from 11 studies by one researcher and then re-checked by a second researcher. Data extraction included the following: author, year pub-lished, study design, length, population characteristics, presence of co-morbidities, the measurement meth-ods for cognitive function and NAFLD, associations

Page 3 of 19George et al. BMC Geriatrics (2022) 22:47
between NAFLD and cognitive function, and any other relevant outcomes (e.g. body fat, visceral fat, CVD risk factors). These findings are shown in Table 1. Due to the wide range of cognitive tests available and identified across the 11 studies, the cognitive tests were grouped into the following seven categories (general cogni-tion, reasoning, mental speed and attention, memory and learning, language, visuospatial perception, ideas, abstraction, figural creations and mental flexibility) as
described by Goodwill et al. [26]. Grouping was carried out by two researchers.
Quality assessment and risk of biasThe quality of the included papers and risk of bias was assessed independently using The Academy of Nutrition and Dietetics Evidence Analysis Library Quality Criteria Checklist (Table 2) [34]. This checklist consists of an eval-uation of studies’ relevance (four questions) and validity
Fig. 1 PRISMA

Page 4 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
Extr
actio
n ta
ble
of in
clud
ed s
tudi
es a
sses
sing
the
asso
ciat
ion
betw
een
NA
FLD
and
cog
nitio
na
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Wei
nste
in e
t al.
(201
8) [2
7]U
nite
d St
ates
Cro
ss‑s
ectio
nal,
popu
latio
n‑ba
sed
sam
plin
g su
rvey
; N
HA
NES
Sur
vey
data
fro
m 2
011
to 2
014
1102
par
ticip
ants
239
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
68.6
year
sN
AFL
D ‑
BMI 3
5.0
kg/m
2O
besi
ty: 9
2.5%
Insu
lin re
sist
ance
: 62
.1%
HTN
: 76.
1%H
igh
chol
este
rol:
82.2
%M
etS:
58.
5%Co
ntro
l –BM
I 25.
00 kg
/m2
Obe
sity
: 19.
4%In
sulin
resi
stan
ce:
17.5
%H
TN: 6
1.2%
Hig
h ch
oles
tero
l: 74
.2%
Met
S: 1
1.1%
(1) T
he W
ord
Lear
n-in
g su
bset
‑ us
ed
to a
sses
s im
med
iate
an
d de
laye
d le
arni
ng
abili
ty(2
) The
Ani
mal
Flu
-en
cy T
est -
cat
egor
i‑ca
l ver
bal fl
uenc
y(3
) The
dig
it sy
m-
bol s
ubst
itutio
n - i
nvol
ves
proc
essi
ng
spee
d, s
usta
ined
and
w
orki
ng m
emor
y
Fatt
y liv
er in
dex
scor
e ≥
60
Span
ish.
(1) T
he W
ord
Lear
n-in
g su
bset
– Im
med
i‑at
e ve
rbal
mem
ory:
N
AFL
D o
nly
(SD
: 20
.5 ±
0.4
) vs
the
cont
rol g
roup
(SD
: 20
.0 ±
0.3
)D
elay
ed v
erba
l m
emor
y: N
AFL
D o
nly
grou
p (S
D: 6
.6 ±
0.2
) vs
the
cont
rol g
roup
(6
.4 ±
0.1
)(2
) AFT
–Ve
rbal
flue
ncy:
NA
FLD
on
ly (1
8.6 ±
0.3
) vs
con
trol
gro
up
(18.
3 ±
0.4
)(3
) DSS
T –
Proc
essi
ng s
peed
, su
stai
ned
atte
ntio
n,
wor
king
mem
ory:
N
AFL
D (5
5.9 ±
1.0
5)
vs c
ontr
ol g
roup
(5
3.6 ±
1.2
)

Page 5 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Celik
bile
k et
al.
(201
8) [2
2]Tu
rkey
Cro
ss‑s
ectio
nal
stud
y14
3 pa
rtic
ipan
ts70
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
46.9
year
s, F
(NA
FLD
): 41
, M (N
AFL
D):
29
NA
FLD
–T2
DM
: 30%
HTN
: 20%
Hyp
erlip
idae
mia
: 7.
1%M
etS:
48.
6%Co
ntro
l –T2
DM
: 4.1
%H
TN: 2
.7%
Hyp
erlip
idae
mia
: 1.
4%M
etS:
34.
3%
(1) M
ontr
eal C
ogni
-tiv
e A
sses
smen
t Tu
rkish
ver
sion.
(a)
visu
ospa
tial a
bilit
ies
‑ clo
ck‑d
raw
ing
task
an
d th
ree‑
dim
en‑
sion
al c
ube‑
copy
ing
task
, (b)
Mem
ory
‑ del
ayed
reca
ll (c
) Ex
ecut
ive
func
tion‑
ing
‑ Tra
il M
akin
g B
task
, a p
hone
mic
flu
ency
task
, and
a
two‑
item
ver
bal
abst
ract
ion
task
, (d)
A
tten
tion
‑ a s
eria
l su
btra
ctio
n ta
sk a
nd
digi
ts fo
rwar
d an
d ba
ckw
ard
task
s, (e
) La
ngua
ge ‑
thre
e‑ite
m c
onfro
ntat
ion
nam
ing
task
, rep
eti‑
tion
of tw
o sy
ntac
ti‑ca
lly c
ompl
ex s
en‑
tenc
es (f
) orie
ntat
ion
‑ orie
ntat
ion
to ti
me
and
plac
e is
als
o ev
alua
ted
Abd
omin
al u
ltra‑
sono
grap
hy(1
) MoC
A-T
R - s
core
s si
gnifi
cant
ly lo
wer
in
NA
FLD
gro
up in
co
mpa
rison
to c
ontr
ol
grou
p (P
< 0
.001
)(a
) Vis
uosp
atia
l abi
li‑tie
s: P
< 0
.05
(b) M
emor
y: P
= 0
.16
(c) E
xecu
tive
func
tion‑
ing:
P <
0.0
5(d
) Att
entio
n: P
= 0
.56
(e) L
angu
age:
P =
0.8
9(f
) Orie
ntat
ion:
P =
0.2
9
Taka
hash
i et a
l. (2
017)
[28]
Japa
nC
ross
‑sec
tiona
l st
udy
39 p
artic
ipan
ts24
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
54 ye
ars
NA
FLD
–T2
DM
: 41.
6%D
yslip
idae
mia
: 58
.3%
HTN
: 29.
2%Co
ntro
l –N
ot re
port
ed
(1) A
ver
bal fl
uenc
y ta
sk (V
FT)
Asi
a‑Pa
cific
Wor
king
Pa
rty
guid
elin
es fo
r th
e as
sess
men
t and
m
anag
emen
t of
NA
FLD
.U
ltras
onog
raph
y (in
th
e ab
senc
e of
oth
er
caus
es o
f chr
onic
liv
er d
isea
se e
.g.,
hepa
titis
C a
ntib
ody
nega
tive,
hep
atiti
s B
surf
ace
antig
en
nega
tive,
and
alc
o‑ho
l con
sum
ptio
n <
20
g/da
y)
(1) V
FT –
Num
ber o
f wor
ds
durin
g VF
T w
as
sign
ifica
ntly
hig
her i
n co
ntro
ls c
ompa
red
to
the
NA
FLD
: p <
0.0
32N
umbe
r of w
ords
dur
-in
g VF
T N
AFLD
: 12
Num
ber o
f wor
ds d
ur-
ing
VFT
cont
rols:
14

Page 6 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Filip
ovic
et a
l. (2
018)
[2
1]Se
rbia
Case
‑con
trol
stu
dy76
par
ticip
ants
40 N
AFL
D p
artic
i‑pa
nts
Mea
n N
AFL
D a
ge:
47.9
year
s,M
(NA
FLD
): 22
,F
(NA
FLD
): 18
NA
FLD
–T2
DM
: 30%
HTN
: 80%
Obe
se: 5
0%M
etS:
85%
Cont
rol –
T2D
M: 2
5%H
TN: 4
4%O
bese
: 11%
Met
S: 2
2%
(1) M
ontr
eal C
ogni
-tiv
e A
sses
smen
t te
st S
erbi
an v
ersio
n.(a
) alte
rnat
ing
con‑
nect
ions
, (b)
vas
o‑co
nstr
ictiv
e ab
ilitie
s ‑ d
raw
a c
ube
and
a cl
ock
in 1
1:10
pos
i‑tio
n of
clo
ck h
ands
, (c
) mem
ory
‑ num
‑be
rs re
peat
ed in
the
sam
e an
d re
vers
e or
der,
(d) a
tten
tion
‑ tap
whe
neve
r you
he
ar a
lett
er A
, ser
ial
subt
ract
ion
of 7
, st
artin
g w
ith a
hun
‑dr
ed (e
) sen
tenc
e re
peat
ing
and
verb
al
fluen
cy.
Abd
omin
al
ultr
ason
ogra
phy,
So
nogr
aphi
c ev
alu‑
atio
n (U
S) o
f hep
atic
st
eato
sis
(1) M
OCA
-SR
–Th
e co
gniti
ve s
tatu
s w
as lo
wer
in N
AFL
D
com
pare
d to
con
trol
:O
R 0.
096,
95%
CI
0.03
2–0.
289,
and
p
< 0
.001
Ellio
tt e
t al.
(201
3)
[23]
UK
(Eur
ope)
Coho
rt, P
rosp
ec‑
tive
follo
w‑u
p ov
er
3 ye
ars
431
part
icip
ants
224
NA
FLD
par
tici‑
pant
Mea
n N
AFL
D a
ge:
59 ye
ars,
F (N
AFL
D):
101,
M (N
AFL
D):
123
Not
repo
rted
(1) C
ogni
tive
Fail-
ures
Que
stio
nnai
re
(CFQ
) - m
easu
res
mem
ory,
att
en‑
tion,
con
cent
ratio
n,
forg
etfu
lnes
s, w
ord
findi
ng a
bilit
ies
and
conf
usio
n.
Live
r Ser
um B
io‑
chem
istr
y ‑ A
LT, A
LP,
ALB
, Bili
rubi
n.
(1) C
FQ –
Cogn
itive
sym
ptom
s C
FQ a
ssoc
iate
d w
ith
wor
se fu
nctio
nal
abili
ty in
NA
FLD
co
mpa
red
to c
ontr
ols:
r = 0
.4, p
< 0
.000
1

Page 7 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Wei
nste
in e
t al.
(201
9) [2
9]U
nite
d St
ates
Popu
latio
n‑ba
sed,
m
ulti‑
gene
ratio
nal
stud
y (T
he F
ram
ing‑
ham
Hea
rt S
tudy
) C
ross
‑sec
tiona
l st
udy
1287
par
ticip
ants
378
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
61.1
year
s, F
(NA
FLD
): 15
7, M
(NA
FLD
): 22
1
NA
FLD
–BM
I: 31
.0T2
DM
: 20.
5%H
TN (s
tage
1):
59.3
%Co
ntro
ls –
BMI:
26.8
T2D
M: 6
.9%
HTN
(sta
ge 1
): 38
.2%
(1) T
he W
echs
ler
Mem
ory
Scal
e ‑
verb
al a
nd v
isua
l m
emor
y(2
) Tim
e to
com
-pl
ete
trai
l-mak
ing
B m
inut
e tim
e to
co
mpl
ete
trai
l-m
akin
g A
test
(T
rB-T
rA) -
exe
cutiv
e fu
nctio
n(3
) The
sim
ilari
ties
test
(SIM
) - a
bstr
act
reas
onin
g sk
ills
(4) H
oope
r vis
ual
orga
niza
tion
test
(H
VOT)
- vi
sual
pe
rcep
tion.
Mul
ti‑de
tect
or
CT
with
8‑s
lice,
A
calib
ratio
n ph
anto
m
(Imag
e A
naly
sis,
Lexi
ngto
n, K
Y) w
ith
a w
ater
equ
ival
ent
com
poun
d ‑ t
hree
ar
eas
from
the
liver
an
d on
e fro
m a
n ex
tern
al p
hant
om
wer
e m
easu
red
(NA
FLD
was
de
fined
as
havi
ng
a liv
er/p
hant
om
ratio
≤ 0
.33)
.
(1) T
he W
echs
ler
Mem
ory
Scal
e -
p =
0.6
10(2
) TrB
-TrA
–
p =
0.4
18(3
) SIM
– p
= 0
.746
(4) H
VOT
– p =
0.5
28N
o sig
nific
ant a
sso-
ciat
ion
of N
AFLD
with
co
gniti
ve m
easu
res
iden
tified
.Pa
rtic
ipan
ts w
ith
NA
FLD
with
adv
ance
d fib
rosi
s w
as a
ssoc
iate
d w
ith p
oore
r per
for‑
man
ce o
n th
e Tr
B‑Tr
A
(P =
0.0
28) a
nd S
IM
test
(P =
0.0
09)

Page 8 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Tart
er e
t al.
(198
4)
[30]
Uni
ted
Stat
esCa
se‑c
ontr
ol s
tudy
40 p
artic
ipan
ts30
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
40.9
year
sN
ot re
port
ed(1
) Pea
body
pic
ture
in
telli
genc
e te
st –
ve
rbal
inte
llige
nce.
(2) R
aven
’s pr
ogre
s-si
ve m
atri
ces
‑ non
‑ve
rbal
inte
llige
nce.
(3) D
igit
span
fo
rwar
d.(4
) Dig
it sp
an
back
war
d.(5
) Wes
chle
r M
emor
y Sc
ale)
: (a)
Lo
gica
l mem
ory
(b)
Figu
ral m
emor
y, (c
) Pa
ired
asso
ciat
es, (
d)
Supr
asan
.(6
) Per
cept
ual-
Mot
or: (
a) F
inge
r ta
ppin
g, (b
) Pur
due
Pegb
oard
, (c)
Sta
ry
trac
ing,
(d) S
ymbo
l di
git m
odal
ities
.(7
) Spa
tial:
(a) B
lock
de
sign
, (b)
Tac
tual
pe
rfor
man
ce, (
c) T
rail
mak
ing.
(8) L
angu
age:
(a)
Flue
ncy,
(b) C
onfro
n‑ta
tion
nam
ing,
(c)
Resp
onsi
ve n
amin
g(9
) The
Tok
en T
est
‑com
preh
ensi
ve
capa
city
Hep
atic
dia
gnos
is
‑ clin
ical
, bio
‑ch
emic
al, s
erol
ogic
al
confi
rmed
by
liver
bi
opsy
(1) P
eabo
dy p
ictu
re
inte
llige
nce
test
– n
o di
ffere
nce
(2) R
aven
’s pr
ogre
s-si
ve m
atri
ces
– no
di
ffere
nce
(3) D
igit
span
for-
war
d –
no d
iffer
ence
(4) D
igit
span
bac
k-w
ard
– no
diff
eren
ce(5
) Wes
chle
r Mem
ory
Scal
e) –
no
diffe
renc
e(6
) Per
cept
ual-M
otor
– (a
) Fin
ger t
appi
ng: n
o di
ffere
nce
(b) P
urdu
e Pe
gboa
rd:
p <
0.0
1(c
) Sta
ry tr
acin
g: n
o di
ffere
nce
(d) S
ymbo
l dig
it m
odal
ities
: p <
0.0
1(7
) Spa
tial –
(a) B
lock
des
ign:
p
< 0
.06
(b) T
actu
al p
erfo
r‑m
ance
: p <
0.0
5(c
) Tra
il m
akin
g:
p <
0.0
5(8
) Lan
guag
e –
(a) F
luen
cy: n
o di
ffer‑
ence
(b) C
onfro
ntat
ion
nam
ing:
no
diffe
renc
e(c
) Res
pons
ive
nam
‑in
g: n
o di
ffere
nce
(9) T
he T
oken
Tes
t –
no d
iffer
ence

Page 9 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Tart
er e
t al.
(198
7)
[31]
Uni
ted
Stat
esCa
se‑c
ontr
ol s
tudy
46 p
artic
ipan
ts23
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D
age:
37.
2 ye
ars,
M (N
AFL
D):
11, F
(N
AFL
D):
12
Not
repo
rted
(1) D
igit
Span
Tes
t ‑
imm
edia
te m
emor
y(2
) Sup
rasp
an
Lear
ning
Tes
t - th
e nu
mbe
r of t
rials
re
quire
d ac
cura
tely
to
repe
at a
str
ing
of d
igits
that
is o
ne
digi
t lon
ger t
han
the
digi
ts fo
rwar
d sc
ore.
(3
) Ben
ton
Visu
al
Rete
ntio
n Te
st
(BVR
T) ‑
shor
t ter
m
visu
al(4
) Rey
-Ost
erre
ith
Com
plex
Fig
ure
Test
‑ in
cide
ntal
le
arni
ng a
bilit
y(5
) Bro
wn-
Pete
rson
Te
st ‑
mea
sure
s th
e ra
te o
f dec
ay o
f in
form
atio
n fro
m
shor
t‑te
rm m
emor
y.
Sero
logi
cal t
ests
, cl
inic
al h
isto
ry a
nd
phys
ical
exa
min
a‑tio
ns, a
nd w
as
confi
rmed
by
a pe
rcut
aneo
us li
ver
biop
sy.
(1) D
igit
Span
Tes
t –
no d
iffer
ence
(2) S
upra
span
Lea
rn-
ing
Test
– p
< 0
.05
(3) B
VRT
– p
< 0
.000
1(4
) Rey
-Ost
erre
ith
Com
plex
Fig
ure
Test
–
no d
iffer
ence
(5) B
row
n-Pe
ters
on
Test
– n
o di
ffere
nce
Seo
et a
l. (2
016)
[32]
Uni
ted
Stat
esC
ross
‑sec
tiona
l st
udy
(NH
AN
ES II
I ‑
surv
ey)
4472
par
ticip
ants
874
NA
FLD
par
tici‑
pant
Mea
n N
AFL
D a
ge:
40.9
year
sN
AFL
D –
T2D
M: 1
3.6%
HTN
: 36.
3%H
yper
chol
este
rola
e‑m
ia: 3
0.4%
Stro
ke: 1
.5%
Cont
rols
–T2
DM
: 5.2
%H
TN: 1
7.5%
Hyp
erch
oles
tero
‑le
stel
emia
: 22.
2%St
roke
: 0.5
%
(1) T
he S
impl
e Re
actio
n Ti
me
Test
(S
RTT)
- m
easu
res
resp
onse
tim
e,
visu
al‑m
otor
spe
ed(2
) The
Sym
bol
Dig
it Su
bstit
u-tio
n Te
st (S
DST
) - a
sses
ses
visu
al
atte
ntio
n an
d co
d‑in
g ab
ility
(3) T
he S
eria
l D
igit
Lear
ning
Te
st (S
DLT
) - te
st
lear
ning
, rec
all,
and
conc
entr
atio
n.
Gal
lbla
dder
exa
mi‑
natio
n by
ultr
asou
nd
with
a T
oshi
ba
SSA
‑90A
mac
hine
w
ith a
3.7
5 an
d 5.
0 M
Hz
tran
sduc
er.
Live
r enz
ymes
(ALT
, A
ST) w
ere
assa
yed
with
Hita
chi 7
37
auto
mat
ed m
ulti‑
chan
nel c
hem
istr
y an
alys
er. N
AFL
D w
as
defin
ed a
s m
oder
‑at
e/se
vere
ste
atos
is
as d
eter
‑ min
ed b
y ul
tras
ound
.
(1) S
RTT
– B =
7.8
27,
95%
CI 0
.975
to 1
4.67
9(2
) SD
ST –
B =
0.1
10,
95%
CI 0
.004
to 0
.216
(3) S
DLT
– B
= 0
.880
, 95
% C
I 0.3
17 to
1.4
43Pa
rtic
ipan
ts w
ith
NAF
LD h
ad lo
wer
pe
rfor
man
ces o
n SR
TT,
SDST
and
SD
LT

Page 10 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 1
(con
tinue
d)
Aut
hor,
Year
Coun
try
Stud
y de
sign
; Le
ngth
Sam
ple
size
NA
FLD
mea
n ag
e,
sex
(n fe
mal
es, n
m
ales
)
Risk
fact
ors/
co-m
orbi
ditie
sCo
gniti
ve te
sts
NA
FLD
dia
gnos
isFi
ndin
gsb
Felip
o et
al.
(201
2)
[24]
Spai
n (E
urop
e)Ca
se c
ontr
ol s
tudy
179
part
icip
ants
29 N
AFL
D p
artic
i‑pa
nt
Mea
n N
AFL
D a
ge:
45 ye
ars,
F (N
AFL
D):
24, M
(NA
FLD
): 5
Not
repo
rted
(1) T
he D
igit
Sym
bol t
est (
DST
) –
men
tal s
peed
(2) T
he N
umbe
r Co
nnec
tion
Test
A
(NCT
-A) –
men
tal
spee
d(3
) The
Num
ber
Conn
ectio
n Te
st B
(N
CT-B
) – m
enta
l sp
eed
(4) T
he S
eria
l Dot
-tin
g Te
st –
men
tal
spee
d(5
) The
line
trac
ing
test
(LTT
) – v
isuo
s‑pa
tial
Live
r bio
psy
obta
ined
dur
ing
hist
olog
ical
stu
dy.
(1) D
ST –
no
dif‑
fere
nce
in N
AFL
D,
cirr
hosi
s or
NA
SH(2
) NCT
-A –
no
dif‑
fere
nce
in N
AFL
D,
impa
ired
in p
atie
nts
with
NA
SH a
nd c
ir‑rh
osis
(P <
0.0
01)
(3) N
CT-B
– n
o di
f‑fe
renc
e in
NA
FLD
, im
paire
d in
NA
SH a
nd
cirr
hosi
s (P
< 0
.001
)(4
) The
Ser
ial
Dot
ting
Test
– n
o di
ffere
nce
in N
AFL
D,
impa
ired
in c
irrho
sis
(P <
0.0
01) a
nd N
ASH
(P
< 0
.01)
(5) L
TT –
no
diffe
renc
e in
NA
FLD
, im
paire
d in
NA
SH a
nd c
irrho
sis
(P <
0.0
01)
Tutt
olom
ondo
et a
l. (2
018)
[33]
Italy
(Eur
ope)
Case
con
trol
stu
dy16
3 pa
rtic
ipan
ts80
NA
FLD
par
tici‑
pant
s
Mea
n N
AFL
D a
ge:
53.7
year
sN
AFL
D –
BMI:
28.7
HTN
: 35.
0%T2
DM
: 38.
8%D
yslip
idae
mia
: 18
.8%
Prev
ious
CVD
: 3.7
5%Co
ntro
ls –
BMI:
25.3
HTN
: 15.
7%T2
DM
: 8.4
%D
yslip
idae
mia
: 16
.9%
Prev
ious
CVD
: 0
(1) M
ini-m
enta
l st
ate
exam
inat
ion
(MM
SE)
Incr
ease
d se
rum
le
vels
of A
LT fo
r at
leas
t 6 m
onth
s an
d al
coho
l con
sum
p‑tio
n of
< 2
0 g/
day
in
the
prev
ious
yea
r. Li
ver u
ltras
ound
fin
ding
of s
teat
osis
an
d a
liver
stiff
ness
va
lue
> 6
kPa.
Liv
er
biop
sy fo
r NA
FLD
. H
epat
ic s
teat
osis
w
as d
efine
d by
de
tect
ion
of B
right
Li
ver E
cho
patt
ern.
(1) M
MSE
–N
AFL
D h
ad a
low
er
mea
n M
MSE
sco
re
whe
n co
mpa
red
to
cont
rols
(26.
9 ±
1.6
vs.
28.0
± 1
.36;
p =
0.0
05)
a Abb
revi
atio
ns: A
FT a
nim
al fl
uenc
y te
st, A
LT a
lani
ne a
min
otra
nsfe
rase
, ALP
alk
alin
e ph
osph
atas
e, A
ST a
spar
tate
am
inot
rans
fera
se, B
MI b
ody
mas
s in
dex,
BVR
T Be
nton
vis
ual r
eten
tion
test
, CFQ
Cog
nitiv
e Fa
ilure
s Q
uest
ionn
aire
, DSS
T Th
e di
git s
ymbo
l sub
stitu
tion
test
, DST
dig
it sy
mbo
l tes
t, H
VOT
hoop
er v
isua
l org
anis
atio
n te
st, H
TN h
yper
tens
ion,
LTT
line
trac
ing
test
, MoC
A-TR
Mon
trea
l cog
nitiv
e as
sess
men
t Tur
kish
ver
sion
, M
oCA-
SR M
ontr
eal c
ogni
tive
asse
ssm
ent S
erbi
an v
ersi
on, M
CI m
ild c
ogni
tive
impa
irmen
t, M
etS
met
abol
ic s
yndr
ome,
NAF
LD n
on-a
lcoh
olic
fatt
y liv
er d
isea
se, N
ASH
non
-alc
ohol
ic s
teat
osis
, NCT
A nu
mbe
r con
nect
ion
test
A,
NCT
B nu
mbe
r con
nect
ion
test
B, S
IM s
imila
ritie
s te
st, S
RRT
sim
ple
reac
tion
time
test
, SD
ST s
ymbo
l dig
it su
bstit
utio
n te
st, S
DT
seria
l dot
ting
test
, SD
LT s
eria
l dig
it le
arni
ng te
st, V
FT v
erba
l flue
ncy
task
b Sig
nific
ant e
ffect
(p <
0.0
5); n
o eff
ect (
p >
0.05
); CI
con
fiden
ce in
terv
al, O
R od
ds ra
tio, R
R re
lativ
e ris
k

Page 11 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 2
Crit
ical
app
rais
al o
f the
11
stud
ies
with
the
use
of Q
ualit
y C
riter
ia C
heck
lista
Celik
bile
k,
2018
[22]
Ellio
tt, 2
013
[23]
Felip
o, 2
012
[24]
Filip
ovic
, 20
18 [2
1]Se
o, 2
016
[32]
Taka
hash
i, 20
17 [2
8]Ta
rter
, 198
4 [3
0]Ta
rter
, 198
7 [3
1]Tu
ttol
omon
do,
2018
[33]
Wei
nste
in,
2018
[27]
Wei
nste
in,
2019
[29]
Rele
vanc
e Q
uest
ions
1.
Wou
ld
impl
emen
ting
the
stud
ied
inte
rven
tion
or p
roce
dure
(if
foun
d su
c‑ce
ssfu
l) re
sult
in im
prov
ed
outc
omes
for
the
patie
nts/
clie
nts/
popu
‑la
tion
grou
p?
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
NA
2.
Did
the
auth
ors
stud
y an
out
com
e (d
epen
dent
va
riabl
e) o
r to
pic
that
th
e pa
tient
s/cl
ient
s/po
pu‑
latio
n gr
oup
wou
ld c
are
abou
t?
YY
YY
YY
YY
YY
Y
3.
Is th
e fo
cus
of th
e in
terv
entio
n or
pro
cedu
re
(inde
pend
ent
varia
ble)
or
topi
c of
stu
dy
a co
mm
on
issu
e of
con
‑ce
rn to
die
tet‑
ics
prac
tice?
YY
YY
YY
YY
YY
Y
4.
Is th
e in
terv
entio
n or
pro
cedu
re
feas
ible
?
YY
YY
YY
YY
YY
Y
Valid
ity
Que
stio
ns
1. W
as th
e re
sear
ch q
ues‑
tion
clea
rly
stat
ed?
YY
YY
YY
YY
YY
Y

Page 12 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 2
(con
tinue
d)
Celik
bile
k,
2018
[22]
Ellio
tt, 2
013
[23]
Felip
o, 2
012
[24]
Filip
ovic
, 20
18 [2
1]Se
o, 2
016
[32]
Taka
hash
i, 20
17 [2
8]Ta
rter
, 198
4 [3
0]Ta
rter
, 198
7 [3
1]Tu
ttol
omon
do,
2018
[33]
Wei
nste
in,
2018
[27]
Wei
nste
in,
2019
[29]
2.
Was
the
sele
ctio
n of
st
udy
sub‑
ject
s/pa
tient
s fre
e fro
m b
ias?
YY
YY
YY
NN
YY
Y
3.
Wer
e st
udy
grou
ps
com
para
ble
or
was
an
appr
o‑pr
iate
refe
r‑en
ce s
tand
ard
used
?
YN
Unc
lear
YY
YN
YY
YY
4.
Wer
e m
etho
ds
of h
andl
ing
loss
es fr
om
the
orig
inal
sa
mpl
e (w
ithdr
awal
s)
desc
ribed
?
YN
NA
YN
NN
NN
AN
AY
5.
Was
bl
indi
ng u
sed
to p
reve
nt
intr
oduc
tion
of b
ias?
YY
YY
YY
Unc
lear
YY
YY
6.
Was
the
inte
rven
tion/
trea
tmen
t re
gim
en/
expo
sure
fac‑
tor,
proc
edur
e,
proc
ess
or
prod
uct
of in
tere
st,
and
any
com
paris
on(s
) de
scrib
ed in
de
tail?
Wer
e in
terv
en‑
ing
fact
ors
desc
ribed
?
YY
YY
YY
YY
YY
Y

Page 13 of 19George et al. BMC Geriatrics (2022) 22:47
Tabl
e 2
(con
tinue
d)
Celik
bile
k,
2018
[22]
Ellio
tt, 2
013
[23]
Felip
o, 2
012
[24]
Filip
ovic
, 20
18 [2
1]Se
o, 2
016
[32]
Taka
hash
i, 20
17 [2
8]Ta
rter
, 198
4 [3
0]Ta
rter
, 198
7 [3
1]Tu
ttol
omon
do,
2018
[33]
Wei
nste
in,
2018
[27]
Wei
nste
in,
2019
[29]
7.
Wer
e ou
tcom
es
or c
ondi
tion
or s
tatu
s of
in
tere
st c
lear
ly
defin
ed a
nd
the
mea
sure
‑m
ents
val
id
and
relia
ble?
YY
YY
YY
YY
YY
Y
8.
Was
th
e st
atis
ti‑ca
l ana
lysi
s ap
prop
riate
fo
r the
stu
dy
desi
gn a
nd
type
of
outc
ome
indi
cato
rs?
YY
YY
YY
YU
ncle
arY
YY
9.
Are
co
nclu
sion
s su
ppor
ted
by
resu
lts w
ith
bias
es a
nd
limita
tions
ta
ken
into
co
nsid
erat
ion?
YY
NY
YY
NN
YY
Y
10
. Is
bias
du
e to
stu
dy’s
fund
ing
or
spon
sors
hip
unlik
ely?
YY
YY
YY
YN
YY
Y
Ove
rall
Ratin
gbPo
sitiv
e +
Posi
tive +
Posi
tive +
Posi
tive +
Posi
tive +
Posi
tive +
Posi
tive +
Neu
tral
ØN
eutr
al Ø
Posi
tive +
Posi
tive +
a The
Aca
dem
y of
Nut
ritio
n an
d D
iete
tics
Evid
ence
Ana
lysi
s Li
brar
y (E
AL)
and
Qua
lity
Crite
ria C
heck
list w
as u
sed
as th
e ap
prai
sal t
ools
b Abb
revi
atio
ns: N
A N
ot A
pplic
able
. Pos
itive
(+) =
mos
t of t
he a
nsw
ers
to th
e va
lidity
que
stio
ns a
re “Y
es” (
incl
udin
g cr
iteria
2, 3
, 6, a
nd 7
and
at l
east
one
add
ition
al “Y
es”)
. Neu
tral
(Ø) =
the
answ
ers
to th
e va
lidity
crit
eria
qu
estio
ns 2
, 3, 6
, and
7 d
o no
t ind
icat
e th
at s
tudy
is e
xcep
tiona
lly s
tron
g. N
egat
ive
(−) =
mos
t (si
x or
mor
e) o
f the
ans
wer
s to
the
valid
ity q
uest
ions
are
“No”

Page 14 of 19George et al. BMC Geriatrics (2022) 22:47
(ten questions). Based on these criteria, the researcher assigned each article a quality rating of positive, neutral or negative (+, Ø, −).
Data analysisQualitative analyses were carried out and results were presented narratively. For the qualitative analysis, differ-ence in measures between NAFLD and control groups or pre- and post- in prospective studies and change between groups where appropriate, were reported, depending on the analysis reported for individual studies. Data were considered statistically significant if the reported p-value was < 0.05. Due to the heterogeneity of interventions, and measured outcomes, a meta-analysis was not possible.
ResultsStudy selectionThe literature search process is shown in Fig. 1. The search strategy resulted in 1893 articles, of which 1229 remained after duplicates were removed. From this, 1135 articles were deemed ineligible as a result of title and abstract screening. Ninety-four studies were eligible for full-text screening and 84 were excluded for the following reasons: non-NAFLD population (n = 36), abstract only (n = 29), no cognitive outcome(s) (n = 15), duplicates (n = 2), and not available online (n = 2). One additional study was added through manual search of references (n = 1); there were no clinical trials found and thus, 11 observational studies were included in this systematic review.
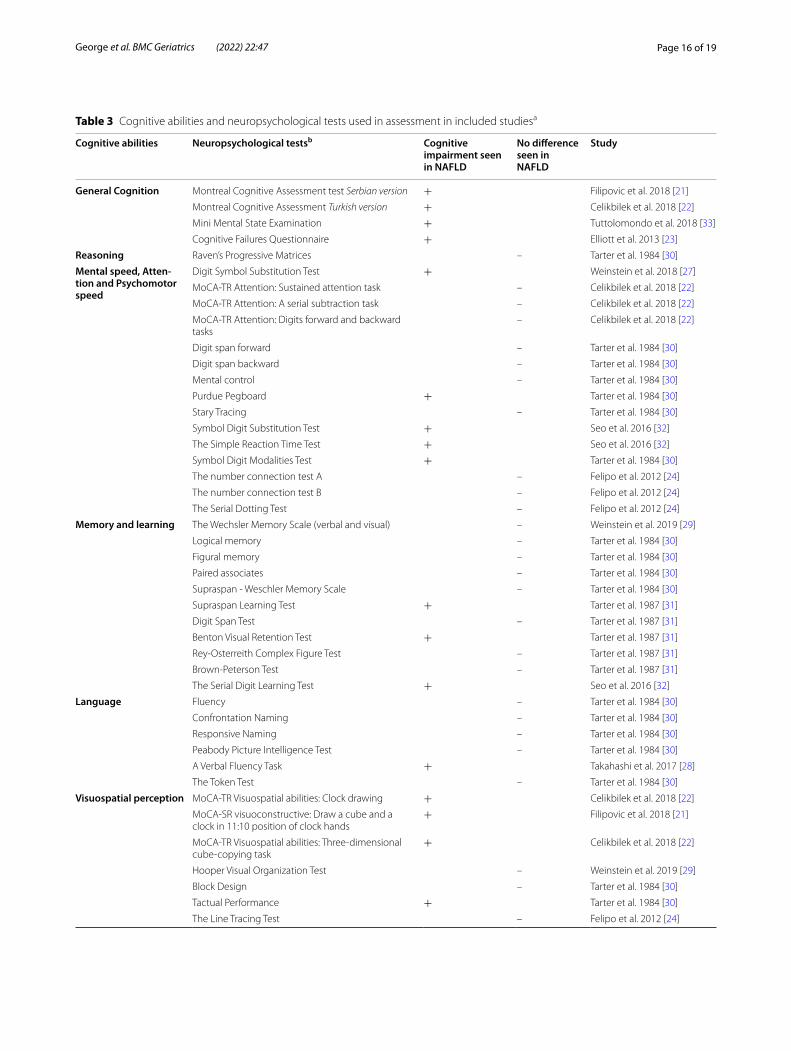
Study characteristicsThe data extracted from the included 11 studies are presented in Table 1. All studies were of observational design; five were case-control [21, 24, 30, 31, 33], five were cross-sectional [22, 27–29, 32], and one was a cohort study [23]. The articles were published between 1984 and 2019. The studies were conducted in the United States, Turkey, Japan, Serbia, United Kingdom, Italy and Spain, and included a total of 7978 participants aged between 37 and 70 years (mean 51 years). The risk of bias assessment for each study is reported in Table 2. Nine articles received a positive quality rating [21–24, 27–30, 32], and two articles received a neutral quality rating [31, 33]; indicating majority of the studies posed a low risk of bias. While the risk of bias tool applied does not assess publication bias there appears to be a combination of positive and negative results in the included studies. The cognitive abilities and associated neuropsychological tests measured in each study are summarised in Table 3.
Cognitive abilitiesGeneral cognitionFour studies including two case-control [21, 33], one cross-sectional [22] and one cohort study [23] inves-tigated the associations between general cognitive performance and NAFLD using multiple neuropsycho-logical tests. All four studies reported that individuals with NAFLD had significantly lower general cognitive function, measured with the Serbian [21] and the Turk-ish [22] MOCA (n = 76 and n = 213 respectively), MMSE (n = 163) [33], and the cognitive symptoms questionnaire (CFQ) (n = 431) [23].
ReasoningOne case-control study conducted in the US including 40 adults with a mean age of 41 years utilised the Raven’s Progressive Matrices to evaluate reasoning and found no significant difference between those with or without NAFLD [30].
Mental speed, attention and psychomotor speedFive studies including three cross-sectional [22, 27, 32] and two case-control studies [24, 30] reported on the mental speed, attention and psychomotor speed. Over-all, three studies indicated poorer performance in this cognitive domain in those with NAFLD [27, 30, 32], with one additional study indicating only those with the more progressed state of the disease, NASH, having poorer cognitive outcomes [24]. Two of these studies were cross-sectional studies conducted in the US and included 1102 and 4472 participants with mean ages of 69 and 41 years, respectively [27, 32]. Only one of the five included stud-ies in this domain indicated that NAFLD or NASH was not associated with cognitive performance. One study reported that individuals with NASH had evidence of cognitive decline [22, 24]. Collectively, it appears that mental speed, attention and psychomotor speed in the majority (three out of five studies) was negatively influ-enced in individuals with NAFLD.
Memory and learningFive studies including three case-control [22, 30, 31] and two cross-sectional studies [29, 32] utilised multiple neu-ropsychological tests to report on the memory and learn-ing domain. Two observational studies (one case-control and a cross-sectional study) reported lower memory and learning test scores (Supraspan Learning test and Ben-ton Visual Retention test and Serial Digit Learning test) in adults with NAFLD [31, 32]. Conversely, another three studies that used the Wechsler Memory Scale [27, 32] or the Delayed Recall Memory test (MoCA-TR) [22] did not observe significant difference in logical and figural

Page 15 of 19George et al. BMC Geriatrics (2022) 22:47
memory among those with NAFLD. Collectively, the limited data available assessing memory and learning in those with NAFLD is conflicting and inconclusive.
LanguageTwo studies including one cross-sectional [28] and one case-control [30] examined the effects of NAFLD on the language domain of cognitive performance. One cross-sectional study in Japan (n = 39) reported significantly lower scores in the Verbal Fluency Task (VFL) among individuals with NAFLD [28]. On the other hand, another study in the US (n = 40) did not find significant group differences using the VFT, the Confrontation Naming task, and the Peabody Picture Intelligence test and Token test [30]. However, this latter study used a Crohn’s Dis-ease control group. It is also difficult to compare the findings between studies due to the different cognitive function tests used. Overall, the number of studies and participants included in this cognitive domain is limited, include small sample sizes, and the findings are conflict-ing and thus inconclusive.
Visuospatial perceptionFive studies including two cross-sectional [22, 29] and three case-control studies [21, 24, 30] reported on the visuospatial perception cognitive domain. Three of the five studies found poorer visuospatial perception scores, measured with MOCA [21, 22] or Tactual Performance task [30], in individuals with NAFLD. Conversely, no sig-nificant group differences were found in three studies for visuospatial perception as assessed using the Hooper Visual Organisation test [29], Block Design task [30] and Line Tracing test were used [24]. Together, these observa-tions indicate that NAFLD may be associated with lower visuospatial perception and cognitive impairment.
Ideas, abstraction, figural creations and mental flexibilityFour studies including three cross-sectional [22, 27, 29] and one case-control [30] observed differences in the Ideas, Abstraction, Figural creations and Mental flex-ibility domain. Three studies (one case-control and two cross-sectional) reported significantly higher scores in the Trail Making task, indicating cognitive impairment, in individuals with NAFLD [22, 29, 30]. Another cross-sectional study that used the Animal Fluency test also observed cognitive decline (lower scores) in those with NAFLD [27]. Individuals with NAFLD also had poorer abstract reasoning skills in two studies, as measured by the Phenomic Fluency, Two-item Verbal Abstraction and Similarities test [22, 29]. In total, all available studies consistently reported that NAFLD was associated with poorer ideas, abstraction, figural creations and mental flexibility.
DiscussionThis systematic review, which is the first to examine the association between NAFLD and cognitive function, included 11 observational studies with 7978 participants across five countries. Based on the current literature available, the findings indicate that NAFLD is likely asso-ciated with poorer cognitive function across a number of domains. Specifically, three out of seven domains assessed in this review indicated there was evidence of poor cognitive performance in participants with NAFLD, including ‘general cognition’, ‘mental speed, attention and psychomotor speed’, and ‘ideas, abstraction, figural creations and mental flexibility’. The remaining cogni-tive domains (reasoning, memory and learning, language, visuospatial perception) produced conflicting and thus inconclusive findings potentially due to the limited num-ber of studies and heterogenous designs and methodolo-gies (e.g. study populations and cognitive tests).
The findings from this review indicating that NAFLD, the ‘hepatic manifestation’ of the metabolic syndrome, was associated with cognitive decline is in line with other literature indicating that metabolic syndrome and its components are strongly implicated in cognitive decline [35]. The reason why only three of the seven cog-nitive domains explored in this review were more likely to be impacted by NAFLD may relate to differences in the characteristics of the studies included. As all studies included the assessment of multiple cognitive domains, it is unlikely results showing cognitive decline with NAFLD were due to study design or sample size in the respective studies. Studies that investigate cognitive decline typi-cally focus on older adults as this is when cognition is most sensitive to change [36, 37]. What was noted how-ever was that only one of the 11 studies in this review included older adults with a mean age above 65 years and the overall mean age of participants in this review was middle aged [27]. Therefore, there was heterogeneity in the timing and rate of cognitive decline in different cog-nitive measures based on age and this may explain the mixed findings in terms of the link with only three of the seven cognitive domains assessed in this review. There are known disparate effects on cognition with numerous cognitive domains exhibiting decline such as memory and fluid cognition, while others are preserved with age such as language or vocabulary [38]. Declines in ‘general cognition’, ‘mental speed, attention and psychomotor speed’, and ‘ideas, abstraction, figural creations and men-tal flexibility’ may be explained by the fact that cognitive tasks requiring verbal fluency, processing or transform-ing information to make a decision, working memory and executive functioning are particularly sensitive to changes with age [35]. This decline is worsened with age, but the fact that this review demonstrated a decline in
Page 16 of 19George et al. BMC Geriatrics (2022) 22:47
Table 3 Cognitive abilities and neuropsychological tests used in assessment in included studiesa
Cognitive abilities Neuropsychological testsb Cognitive impairment seen in NAFLD
No difference seen in NAFLD
Study
General Cognition Montreal Cognitive Assessment test Serbian version + Filipovic et al. 2018 [21]
Montreal Cognitive Assessment Turkish version + Celikbilek et al. 2018 [22]
Mini Mental State Examination + Tuttolomondo et al. 2018 [33]
Cognitive Failures Questionnaire + Elliott et al. 2013 [23]
Reasoning Raven’s Progressive Matrices – Tarter et al. 1984 [30]
Mental speed, Atten-tion and Psychomotor speed
Digit Symbol Substitution Test + Weinstein et al. 2018 [27]
MoCA‑TR Attention: Sustained attention task – Celikbilek et al. 2018 [22]
MoCA‑TR Attention: A serial subtraction task – Celikbilek et al. 2018 [22]
MoCA‑TR Attention: Digits forward and backward tasks
– Celikbilek et al. 2018 [22]
Digit span forward – Tarter et al. 1984 [30]
Digit span backward – Tarter et al. 1984 [30]
Mental control – Tarter et al. 1984 [30]
Purdue Pegboard + Tarter et al. 1984 [30]
Stary Tracing – Tarter et al. 1984 [30]
Symbol Digit Substitution Test + Seo et al. 2016 [32]
The Simple Reaction Time Test + Seo et al. 2016 [32]
Symbol Digit Modalities Test + Tarter et al. 1984 [30]
The number connection test A – Felipo et al. 2012 [24]
The number connection test B – Felipo et al. 2012 [24]
The Serial Dotting Test – Felipo et al. 2012 [24]
Memory and learning The Wechsler Memory Scale (verbal and visual) – Weinstein et al. 2019 [29]
Logical memory – Tarter et al. 1984 [30]
Figural memory – Tarter et al. 1984 [30]
Paired associates – Tarter et al. 1984 [30]
Supraspan ‑ Weschler Memory Scale – Tarter et al. 1984 [30]
Supraspan Learning Test + Tarter et al. 1987 [31]
Digit Span Test – Tarter et al. 1987 [31]
Benton Visual Retention Test + Tarter et al. 1987 [31]
Rey‑Osterreith Complex Figure Test – Tarter et al. 1987 [31]
Brown‑Peterson Test – Tarter et al. 1987 [31]
The Serial Digit Learning Test + Seo et al. 2016 [32]
Language Fluency – Tarter et al. 1984 [30]
Confrontation Naming – Tarter et al. 1984 [30]
Responsive Naming – Tarter et al. 1984 [30]
Peabody Picture Intelligence Test – Tarter et al. 1984 [30]
A Verbal Fluency Task + Takahashi et al. 2017 [28]
The Token Test – Tarter et al. 1984 [30]
Visuospatial perception MoCA‑TR Visuospatial abilities: Clock drawing + Celikbilek et al. 2018 [22]
MoCA‑SR visuoconstructive: Draw a cube and a clock in 11:10 position of clock hands
+ Filipovic et al. 2018 [21]
MoCA‑TR Visuospatial abilities: Three‑dimensional cube‑copying task
+ Celikbilek et al. 2018 [22]
Hooper Visual Organization Test – Weinstein et al. 2019 [29]
Block Design – Tarter et al. 1984 [30]
Tactual Performance + Tarter et al. 1984 [30]
The Line Tracing Test – Felipo et al. 2012 [24]

Page 17 of 19George et al. BMC Geriatrics (2022) 22:47
cognition which was more pronounced in NAFLD in individuals aged 37-61 years suggests that this condition may contribute to early onset cognitive decline particu-larly in certain domains.
There are numerous potential underlying mechanisms that may explain the possible early onset of cognitive decline with NAFLD. These include insulin resistance and progressive lipid deposition in the liver in NAFLD, comorbidities which are highly prevalent in middle aged populations and have been shown to increase periph-eral hyperinsulinemia, lipid peroxidation, and system-atic inflammatory damage to brain cells [38]. Obesity, T2DM and the MetS co-exist with NAFLD and are all driven by inflammation and oxidation, which contribute to impaired vascular function, and subsequently poorer cognitive function [39]. Furthermore, emerging evi-dence suggests that NAFLD poses an additional risk for dysbiosis by disrupting the gut brain axis and thus may also deteriorate cognition in individuals with this disease [40]. Liver diseases especially NAFLD and its more pro-gressed form, NASH, can lead to elevated ammonia lev-els (also known as hyperammonemia) [41, 42], and when combined with inflammation this can lead to cognitive impairment [24]. This is supported by the only study in this review that assessed NAFLD severity and demon-strated that participants with NASH showed significant cognitive impairment compared to those with only sim-ple steatosis (NAFLD) [24]. Therefore, NAFLD co-exist-ing with multiple co-morbidities (e.g. chronic diseases, hyperinsulinemia, systemic inflammation and extrahe-patic change to the central nervous system) and/or more progressed NAFLD, namely NASH, theoretically will
exacerbate cognitive impairment. In part support of this notion, there is evidence in middle-aged adults showing that cognitive decline is associated with the presence of other comorbidities such as adiposity [40]. The findings from this review shows some early evidence that this may be the case for NAFLD and cognition, although more research is needed to confirm this relationship.
This review contains several strengths including a com-prehensive and systematic search in multiple databases and achieving an overall positive Risk of Bias assessment score (Table 2). Furthermore, this review provides early evidence on the possible association between NAFLD and cognition across various domains. All of the studies included measured cognitive function using validated diagnostic criteria, including a variety of standardised neuropsychological tests such as MoCA, MMSE and CFQ. This review was also robust in that we pooled and discussed studies based on cognitive domains using a previously established method [26]. However, the review had several limitations such as the small number of stud-ies and participant numbers included and an absence of clinical trials to demonstrate causation. All studies were observational in design and predominantly case-control and cross-sectional. A further limitation was the hetero-geneous diagnostic tools, with unknown cross-compa-rability used to measure cognitive function, making the comparison of research findings difficult. This limitation has also been raised in previous reviews, where there is an urgent need for consensus on using standard cogni-tive assessments [44, 45]. In addition, due to the hetero-geneity of populations, with regard to co-morbidities and severity of NAFLD and tools to assess cognition amongst
Table 3 (continued)
Cognitive abilities Neuropsychological testsb Cognitive impairment seen in NAFLD
No difference seen in NAFLD
Study
Ideas, abstraction, figural creations and mental flexibility
The Animal Fluency Test + Weinstein et al. 2018 [27]
Trail Making + Tarter et al. 1984 [30]
MoCA‑TR Executive functioning abilities: Trail Making B task
+ Celikbilek et al. 2018 [22]
MoCA‑TR Executive functioning abilities: Phonemic fluency task
+ Celikbilek et al. 2018 [22]
MoCA‑TR Executive functioning abilities: Two‑item verbal abstraction task
+ Celikbilek et al. 2018 [22]
Time to complete trail‑making B minus time to complete trail‑making A test
+ Weinstein et al. 2019 [29]
The Similarities Test + Weinstein et al. 2019 [29]a Abbreviations: MOCA-TR Montreal Cognitive Assessment Turkish, MOCA-SR Montreal Cognitive Assessment Serbian, NAFLD Non-alcoholic fatty liver disease, NASH Non-alcoholic steatohepatitis, MMSE Mini mental state examination, T2DM Type 2 diabetes mellitus, CFQ Cognitive failures questionnaire, VFT Verbal fluency taskb Plus (+) = impaired cognitive function observed in NAFLD for specific cognitive test. Negative (−) = no association or similar association observed in NAFLD for specific cognitive test

Page 18 of 19George et al. BMC Geriatrics (2022) 22:47
studies and the scarcity of literature reporting on the relationship between NAFLD and cognitive function, a meta-analysis could not be conducted. Finally, there is a known association between cognition and other chronic conditions such as diabetes and cardiovascular disease and therefore without well designed studies that can con-trol for these cardiometabolic conditions it is difficult to deduce what the role of NAFLD is specifically, outside of the cluster of metabolic conditions.
ConclusionIn conclusion, this review of 11 studies indicates that there is an association between NAFLD and lower cog-nitive performance. Particularly, that young and middle-aged adults with NAFLD had poorer cognitive function across several domains, including ‘general cognition’, ‘mental speed, attention and psychomotor speed’, and ‘ideas, abstraction, figural creations and mental flexibil-ity’. This suggests that NAFLD in mid-life may accelerate cognitive decline in certain domains, particularly those that aren’t preserved with older age. However, prospec-tive, adequately powered longitudinal studies that used valid and sensitive tools are needed to confirm the asso-ciation between NAFLD and cognition in the future. Future studies should also consider standard tools to enable comparison of results between studies, in order to promote a better understanding of the relationship between NAFLD and cognition, and as practical tools to identify those at risk of cognitive decline.
AbbreviationsALD: Alcoholic liver disease; AFT: Animal fluency test; ALT: Alanine aminotrans‑ferase; ALP: Alkaline phosphatase; AST: Aspartate aminotransferase; BMI: Body mass index; BVRT: Benton visual retention test; CFQ: Cognitive Failures Questionnaire; CVD: Cardiovascular disease; DSST: The digit symbol substitu‑tion test; DST: Digit symbol test; HVOT: Hooper visual organisation test; HTN: Hypertension; LTT: Line tracing test; MoCA‑TR: Montreal cognitive assessment Turkish version; MoCA‑SR: Montreal cognitive assessment Serbian version; MCI: Mild cognitive impairment; MetS: Metabolic syndrome; NAFLD: Non‑alcoholic fatty liver disease; NASH: Non‑alcoholic steatosis; NCTA : Number connection test A; NCTB: Number connection test B; PRISMA: Preferred reporting items for systematic reviews and meta‑analysis; SIM: Similarities test; SRRT : Simple reaction time test; SDST: Symbol digit substitution test; SDT: Serial dotting test; SDLT: Serial digit learning test; T2DM: Type 2 diabetes mellitus; VFT: Verbal fluency task.
AcknowledgementsWe would like to thank Annie Curtis for her help as a second reviewer for the full text screening of papers included in this systematic review.
Authors’ contributionsESG, RMD and SYT conceptualised and designed this review. ESG, SS and SYT conducted the systematic literature review and analyzed and interpreted the results. All authors read and approved the final manuscript.
FundingThe authors have no funding to declare.
Availability of data and materialsDetailed findings of the selection process of included and excluded articles are available upon request.
Declarations
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Received: 28 May 2021 Accepted: 14 December 2021
References 1. Adams LA, Roberts SK, Strasser SI, Mahady SE, Powell E, Estes C, et al.
Nonalcoholic fatty liver disease burden: Australia, 2019–2030. J Gastro‑enterol Hepatol. 2020;35:1628.
2. Trovato FM, Castrogiovanni P, Malatino L, Musumeci G. Nonalcoholic fatty liver disease (NAFLD) prevention: role of Mediterranean diet and physical activity. Hepatobiliary Surg Nutr. 2019;8(2):167.
3. Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40(6):1387–95.
4. Kim D, Cholankeril G, Loomba R, Ahmed A. Prevalence of fatty liver disease and fibrosis detected by fibroscan in adults in the United States, 2017‑2018. Clin Gastroenterol Hepatol. 2020;19(7):1499–501.
5. GESA. Economic cost and health burden of liver disease in Australia: Gas‑troenterological Society of Australia. 2013. Available from: https:// www. gesa. org. au/ resou rces/ econo mic‑ cost‑ and‑ health‑ burden‑ of‑ liver‑ disea se‑ in‑ austr alia/.
6. Mirmiran P, Amirhamidi Z, Ejtahed H‑S, Bahadoran Z, Azizi F. Relationship between diet and non‑alcoholic fatty liver disease: a review article. Iran J Public Health. 2017;46(8):1007.
7. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple‑hit pathogenesis of non‑alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–48.
8. Bertolotti M, Lonardo A, Mussi C, Baldelli E, Pellegrini E, Ballestri S, et al. Nonalcoholic fatty liver disease and aging: epidemiology to manage‑ment. World J Gastroenterol: WJG. 2014;20(39):14185.
9. Yilmaz Y, Ozdogan O. Liver disease as a risk factor for cognitive decline and dementia: an under‑recognized issue. Hepatology. 2009;49(2):698.
10. Colognesi M, Gabbia D, De Martin S. Depression and cognitive impair‑ment—extrahepatic manifestations of NAFLD and NASH. Biomedicines. 2020;8(7):229.
11. Nichols E, Szoeke CE, Vollset SE, Abbasi N, Abd‑Allah F, Abdela J, et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(1):88–106.
12. Mavrodaris L, Powell J, Thorogood M. Prevalences of dementia and cogni‑tive impairment among older people in sub‑Saharan Africa: a systematic review. Bull World Health Organ. 2013;91:773–83.
13. Collie A. Cognition in liver disease. Liver Int. 2005;25(1):1–8. 14. Brodersen C, Koen E, Ponte A, Sánchez S, Segal E, Chiapella A, et al. Cogni‑
tive function in patients with alcoholic and nonalcoholic chronic liver disease. J Neuropsychiatry Clin Neurosci. 2014;26(3):241–8.
15. Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50(6):2014–21.
16. Raffaitin C, Gin H, Empana J‑P, Helmer C, Berr C, Tzourio C, et al. Metabolic syndrome and risk for incident Alzheimer’s disease or vascular dementia: the Three‑City study. Diabetes Care. 2009;32(1):169–74.

Page 19 of 19George et al. BMC Geriatrics (2022) 22:47
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
17. Vieira JR, Elkind MS, Moon YP, Rundek T, Boden‑Albala B, Paik MC, et al. The metabolic syndrome and cognitive performance: the northern Manhat‑tan study. Neuroepidemiology. 2011;37(3‑4):153–9.
18. Yates KF, Sweat V, Yau PL, Turchiano MM, Convit A. Impact of metabolic syndrome on cognition and brain: a selected review of the literature. Arterioscler Thromb Vasc Biol. 2012;32(9):2060–7.
19. Peila R, Rodriguez BL, Launer LJ. Type 2 diabetes, APOE gene, and the risk for dementia and related pathologies: the Honolulu‑Asia aging study. Diabetes. 2002;51(4):1256–62.
20. Brea A, Mosquera D, Martín E, Arizti A, Cordero JL, Ros E. Nonalcoholic fatty liver disease is associated with carotid atherosclerosis: a case–con‑trol study. Arterioscler Thromb Vasc Biol. 2005;25(5):1045–50.
21. Filipovic B, Markovic O, Duric V, Filipovic B. Cognitive changes and brain volume reduction in patients with nonalcoholic fatty liver disease. Can J Gastroenterol Hepatol. 2018;2018:9638797.
22. Celikbilek A, Celikbilek M, Bozkurt G. Cognitive assessment of patients with nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol. 2018;30(8):944–50.
23. Elliott C, Frith J, Day CP, Jones DE, Newton JL. Functional impairment in alcoholic liver disease and non‑alcoholic fatty liver disease is significant and persists over 3 years of follow‑up. Dig Dis Sci. 2013;58(8):2383–91.
24. Felipo V, Urios A, Montesinos E, Molina I, Garcia‑Torres ML, Civera M, et al. Contribution of hyperammonemia and inflammatory factors to cogni‑tive impairment in minimal hepatic encephalopathy. Metab Brain Dis. 2012;27(1):51–8.
25. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta‑analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41.
26. Goodwill AM, Szoeke C. A systematic review and meta‑analysis of the effect of low vitamin D on cognition. J Am Geriatr Soc. 2017;65(10):2161–8.
27. Weinstein AA, de Avila L, Paik J, Golabi P, Escheik C, Gerber L, et al. Cogni‑tive performance in individuals with non‑alcoholic fatty liver disease and/or type 2 diabetes mellitus. Psychosomatics. 2018;59(6):567–74.
28. Takahashi A, Kono S, Wada A, Oshima S, Abe K, Imaizumi H, et al. Reduced brain activity in female patients with non‑alcoholic fatty liver disease as measured by near‑infrared spectroscopy. PLoS One. 2017;12(4):e0174169.
29. Weinstein G, Davis‑Plourde K, Himali JJ, Zelber‑Sagi S, Beiser AS, Seshadri S. Non‑alcoholic fatty liver disease, liver fibrosis score and cognitive function in middle‑aged adults: the Framingham study. Liver Int. 2019;39(9):1713–21.
30. Tarter RE, Hegedus AM, Van Thiel DH, Schade RR, Gavaler JS, Starzl TE. Nonalcoholic cirrhosis associated with neuropsychological dysfunction in the absence of overt evidence of hepatic encephalopathy. Gastroenterol‑ogy. 1984;86(6):1421–7.
31. Tarter RE, Arria AM, Carra J, Van Thiel DH. Memory impairments concomi‑tant with nonalcoholic cirrhosis. Int J Neurosci. 1987;32(3‑4):853–9.
32. Seo SW, Gottesman RF, Clark JM, Hernaez R, Chang Y, Kim C, et al. Nonal‑coholic fatty liver disease is associated with cognitive function in adults. Neurology. 2016;86(12):1136–42.
33. Tuttolomondo A, Petta S, Casuccio A, Maida C, Corte VD, Daidone M, et al. Reactive hyperemia index (RHI) and cognitive performance indexes are associated with histologic markers of liver disease in subjects with non‑alcoholic fatty liver disease (NAFLD): a case control study. Cardiovasc Diabetol. 2018;17(1):28.
34. Evidence analysis manual: steps in the academy evidence analysis pro‑cess. Chicago: Academy of Nutrition and Dietetics; 2020. Available from: https:// www. andeal. org/ evide nce‑ analy sis‑ manual. Accesssed 14 Jan 2021.
35. Feinkohl I, Janke J, Hadzidiakos D, Slooter A, Winterer G, Spies C, et al. Associations of the metabolic syndrome and its components with cogni‑tive impairment in older adults. BMC Geriatr. 2019;19(1):1–11.
36. Zaninotto P, Batty GD, Allerhand M, Deary IJ. Cognitive function trajecto‑ries and their determinants in older people: 8 years of follow‑up in the English longitudinal study of ageing. J Epidemiol Community Health. 2018;72(8):685–94.
37. Parikh NS, Kumar S, Rosenblatt R, Zhao C, Cohen DE, Iadecola C, et al. Association between liver fibrosis and cognition in a nationally repre‑sentative sample of older adults. Eur J Neurol. 2020;27(10):1895–903.
38. Salthouse TA. Selective review of cognitive aging. J Int Neuropsychol Soc. 2010;16(5):754.
39. Godoy‑Matos AF, Júnior WSS, Valerio CM. NAFLD as a continuum: from obesity to metabolic syndrome and diabetes. Diabetol Metab Syndr. 2020;12(1):1–20.
40. Takeda S, Sato N, Morishita R. Systemic inflammation, blood‑brain bar‑rier vulnerability and cognitive/non‑cognitive symptoms in Alzheimer disease: relevance to pathogenesis and therapy. Front Aging Neurosci. 2014;6:171.
41. Shawcross DL, Davies NA, Williams R, Jalan R. Systemic inflammatory response exacerbates the neuropsychological effects of induced hyper‑ammonemia in cirrhosis. J Hepatol. 2004;40(2):247–54.
42. Montoliu C, Piedrafita B, Serra MA, Del Olmo JA, Urios A, Rodrigo JM, et al. IL‑6 and IL‑18 in blood may discriminate cirrhotic patients with and without minimal hepatic encephalopathy. J Clin Gastroenterol. 2009;43(3):272–9.
43. Morys F, Dadar M, Dagher A. Association between mid‑life obesity, its metabolic consequences, cerebrovascular disease and cognitive decline. J Clin Endocrinol Metab. 2021;106(10):e4260–74.
44. Strachan M, Frier B, Deary I. Cognitive assessment in diabetes: the need for consensus. Diabet Med. 1997;14(6):421–2.
45. Torres DS, Abrantes J, Brandão‑Mello CE. Cognitive and neurophysiologi‑cal assessment of patients with minimal hepatic encephalopathy in Brazil. Sci Rep. 2020;10(1):1–13.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub‑lished maps and institutional affiliations.
Copyright © 2022 FDOKUMEN




















