
Intuition, analysis and reflection: An experimental study into the decision-making processes and...
27
Accepted Manuscript Intuition, analysis and reflection: An experimental study into the decision-making processes and thinking dispositions of osteopathy students Jonathan Spadaccini, Jorge E. Esteves PII: S1746-0689(14)00029-7 DOI: 10.1016/j.ijosm.2014.04.004 Reference: IJOSM 329 To appear in: International Journal of Osteopathic Medicine Received Date: 17 February 2014 Revised Date: 9 April 2014 Accepted Date: 16 April 2014 Please cite this article as: Spadaccini J, Esteves JE, Intuition, analysis and reflection: An experimental study into the decision-making processes and thinking dispositions of osteopathy students, International Journal of Osteopathic Medicine (2014), doi: 10.1016/j.ijosm.2014.04.004. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Transcript of Intuition, analysis and reflection: An experimental study into the decision-making processes and...

Accepted Manuscript
Intuition, analysis and reflection: An experimental study into the decision-makingprocesses and thinking dispositions of osteopathy students
Jonathan Spadaccini, Jorge E. Esteves
PII: S1746-0689(14)00029-7
DOI: 10.1016/j.ijosm.2014.04.004
Reference: IJOSM 329
To appear in: International Journal of Osteopathic Medicine
Received Date: 17 February 2014
Revised Date: 9 April 2014
Accepted Date: 16 April 2014
Please cite this article as: Spadaccini J, Esteves JE, Intuition, analysis and reflection: An experimentalstudy into the decision-making processes and thinking dispositions of osteopathy students, InternationalJournal of Osteopathic Medicine (2014), doi: 10.1016/j.ijosm.2014.04.004.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Intuition, analysis and reflection: An experimental study into the decision-making
processes and thinking dispositions of osteopathy students
Authors
Jonathan Spadaccini
Research Center, The British School of Osteopathy 275 Borough High Street, London, United Kingdom, SE1 1JE
Jorge E. Esteves*
Research Center, The British School of Osteopathy 275 Borough High Street, London, United Kingdom, SE1 1JE
*Corresponding Author Details:
Dr Jorge E. Esteves
The British School of Osteopathy
275 Borough High Street
London SE1 1JE
Tel + 44 (0)20 7089 5310 Email: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTAbstract
Background
Decision-making and reflective thinking are fundamental aspects of clinical reasoning. How
osteopathy students think and make decisions will therefore have far-reaching implications
throughout their professional lives. Models of decision-making are firmly established in
cognitive science literature and their application is universal, yet the decision-making
processes and thinking dispositions of osteopathy students remain relatively unexplored.
Objectives and Method
Using the Cognitive Reflection Test (CRT)13 to measure decision-making preferences and
the 41-item Actively Open-minded Thinking disposition scale (AOT)29, this study set out to
explore how osteopathy students at the start (novice; n=44) and end (intermediate; n=32) of
their pre-professional training make decisions and how reflectively they think.
Results
Intermediate level practitioners demonstrate significantly more analytical decision-making
than their novice peers (p = 0.007; effect size = 0.31); however, reflective thinking
dispositions do not change as participants progress through their training (p = 0.07). No
significant association was found between analytical decision-making and reflective thinking
(p = 0.85).
Conclusions
The trend for intermediate level practitioners to demonstrate more analytical decision-making
than novices, without significant differences in reflective thinking processes, supports other
research that suggests osteopathic education promotes deductive over inductive reasoning
in its graduates and that reasoning and thinking dispositions may develop independently of
each other, given the skills and knowledge-based requirements of osteopathic education.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Intuition, analysis and reflection: An experimental study into the decision-making
processes and thinking dispositions of osteopathy students
1. Introduction
Clinical reasoning is the thinking and decision-making process that informs and underpins
autonomous clinical practice, involving the interrogation and application of both declarative
and procedural knowledge, reflection, and evaluation.1 Clinical reasoning in autonomous
health professions such as osteopathy is likely to make use of higher-order cognitive
processes associated with, for example, reasoning, problem-solving and decision-making.
Thinking and decision-making remain, however, an under-researched topic in osteopathy.
This is despite independent and responsible decision-making being the hallmarks of an
autonomous profession.2 The literature in the field of cognitive science is awash with
concepts and models of decision-making and during the last two decades, the Dual Process
theory has become widely accepted and established as a model of human reasoning and
decision-making.3 Dual Process theorists propose that everyday’s’ decision making is
underpinned by two distinct systems of judgment, which cluster at either end of a continuum
of cognitive effort.4-6 System 1 is an associative system, which uses basic cognitive
processes such as similarity, association, and memory retrieval; judgments are fast,
automatic, intuitive and largely unconscious. In contrast, System 2 is a rule-based system;
judgments are slow, deliberative and conscious.7, 8 The Dual Process theory illustrates the
two main forms of human reasoning: inductive and deductive.8 Whereas inductive reasoning
is primarily based on the rapid retrieval, and appraisal of world knowledge, i.e., System 1;
deductive reasoning depends on rule-based, formal procedures, i.e., System 2.
It has been claimed that osteopathy is distinguished from other health care professions by
the fact that it is practised according to an articulated philosophy.9 However, it can be argued
that the decision-making processes and thinking dispositions of osteopathic practitioners are

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
universal. Although firmly established as a model of reasoning and decision-making in the
field of cognitive science, the application of the Dual Process theory to medicine remains
uncommon10 and only limited attempts have been made to explore it in the context of
osteopathy.11, 12 In the UK, as primary contact practitioners, osteopaths have a statutory
obligation to demonstrate appropriate thinking skills in order to justify their clinical decision-
making, but also to regularly engage in reflective thinking to ensure their knowledge remains
relevant.13 The present study is especially timely as osteopathy’s inclusion in national
guidelines for the management of non-specific low back pain14 must make it more available
for scrutiny in the context of changing health care purchasing and provision.15
As a general psychological construct, System 1 processes can be adaptive and useful
strategies to reach reasonable, if not always considered, conclusions.16 Although there may
have been certain evolutionary advantages to fast intuitive thinking, it continues to exert
considerable control over human decision-making today.3 Frederick17 illustrates this well in
his extensive research involving over 3000 subjects across 35 separate studies. Despite
some methodological flaws, Frederick demonstrated an overwhelming tendency for subjects
to resort to System 1 processes to answer a simple three-item ‘Cognitive Reflection Test’
(CRT). Frederick17 argued that the items on the test are easily understood when the solutions
are explained, that high level mathematical skills are not needed, but that in order to reach
the correct answer, an erroneous, impulsive and intuitive response must be suppressed: “A
bat and ball cost $1.10 in total. The bat cost $1.00 more than the ball. How much does the
ball cost?” Although the correct answer is 5¢, the more common (and incorrect System 1)
answer given is 10¢. As a result of such examples, there is now considerable consensus in
the medical literature, often without criticism or investigation, on how faulty reasoning results
in diagnostic errors.18-22 On this point, Croskerry18 argues that whereas the majority of errors
occur with System 1 judgments and are to some extent expected, errors made with System 2
judgments are infrequent and unexpected.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
An additional feature of Frederick’s17 CRT may be its ability to implicate thinking dispositions,
especially those related to thinking reflectively. Performance on the CRT demands that a pre-
potent and incorrect response is overridden in favour of a more reflective (and therefore
correct) one. Baron23, p. 172 defines good thinking as a complex process that demonstrates the
“optimal search for possibilities, evidence and goals”. In contrast, poor thinking is
characterised by an inadequate search for evidence and the general tendency of people to
allow their own biases to affect their reasoning. The zenith of Baron’s23, p. 173 good thinking is
termed ‘actively open-minded thinking’, in which enhanced objectivity is ensured during the
search for, and review of, the evidence.
The existence of a dual process model of decision-making is well established. Indeed,
functional neuroimaging studies have demonstrated that depending on cognitive demand,
different cortical regions are recruited8 and that they differently affect human physiology.24
Notwithstanding this, the literature in the field of medical cognition is clearly divided over the
merits of one system over the other, and recent developments in cognitive science seem to
support combined approaches as a model of improved decision-making.25, 26 Despite this
growing evidence, however, research exploring decision-making and thinking dispositions in
osteopathy is scarce.
How osteopathy students think and make decisions will have potentially far-reaching
implications throughout their professional lives. In particular, given that the nature of
osteopathic intervention demands analysis and that as a profession, osteopathy has a
patient-centred responsibility to continue to reflect upon and evaluate its impact.27 It is also
assumed that throughout training, thinking and reasoning styles develop as clinical
experience and understanding grow. This study therefore set out to ask: what are the levels
of analytical decision-making and reflective open-minded thinking in osteopathy students at
different stages in their pre-registration education? In doing so, this study explores whether

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
osteopathy students favour System 1 or System 2 processes when making decisions; and
whether there is any relationship between students’ decision-making preferences and
thinking disposition. Finally, it also explored whether final year (intermediate practitioner)
students demonstrate more analytical decision-making and reflective thinking than their first
year (novice practitioner) colleagues, measured using the CRT and Actively Open-minded
Thinking Scale (AOT) scales respectively.
2. Methods
2.1 Study design
A quasi-experimental design was used to explore links between year of pre-professional
training, decision-making and reflective thinking preferences. The independent variable was
expertise, with two levels (novice vs. intermediate), and dependent variables were decision-
making and reflective thinking preferences, measured using the Cognitive Reflection Test
(CRT) and the Actively Open-Minded Thinking Scale (AOT) respectively. This study draws
upon methodology commonly used in the field of cognitive science exploring decision-making
and thinking dispositions.17, 28-31
2.2 Participants
Seventy-six undergraduate students drawn from a convenience sample of students studying
at the British School of Osteopathy (BSO) and taken from years 1 (novices: n = 44) and final
year (intermediates: n = 32) of a four-year, pre-registration osteopathy course, initially
recruited through email invitation, participated in the study. Following the model of medical
expertise development initially proposed by Schmidt and colleagues32, students were
classified as novices or intermediates. Typically, in studies conducted by Schmidt and
colleagues33 in the domain of allopathic medicine, novices are students in their pre-clinical

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
training years whereas intermediates are students who have already completed a substantial
portion of their clinical training.
2.2.1 Inclusion criteria
All students from both years were contacted via their year forum intranet address. They
received written details of the study with an instruction to contact the researchers directly if
they wished to participate.
2.2.2 Exclusion criteria
In line with existing research in the field of cognitive science, English as second language
and familiarity with the tests were not regarded as exclusion criteria.28, 31 The items on the
CRT and AOT demonstrate sufficient internal reliability and validity that they may be easily
completed even with English as a second language. Moreover, Costa and colleagues.34 have
recently found that performance on the CRT is not affected by language; foreign language
does not reduce the impact of System 1 on participants’ decisions. Additionally, it was
assumed that students on the course possess competence in the English language, having
already fulfilled the entry requirements for the osteopathy pre-registration masters’ course.
With regard to familiarity with the CRT, it was reasoned that although some participants may
have already been familiar with items on the CRT, it is unlikely that they would have
memorised the correct answers. Therefore, even familiarity required participants to think
more analytically to score well. Finally, we did not screen participants for their cognitive
ability for two main reasons: firstly, we assumed they possessed the cognitive ability to study
at undergraduate level; and secondly, cognitive ability was not one of the study’s outcome
measures.
2.3 Equipment and procedure
2.3.1 Cognitive Reflection Test (CRT)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
The Cognitive Reflection Test introduced by Frederick17 is a brief 3-item test, which
differentiates between more impulsive and more reflective decision-makers.30 The CRT’s
three items are: “1) A bat and ball cost $1.10 in total. The bat cost $1.00 more than the ball.
How much does the ball cost?; 2) If it takes 5 machines 5 minutes to make 5 widgets, how
long would it take 100 machines to make 100 widgets?; 3) In a lake there is a patch of lily
pads. Every day, the patch doubles in size. If it takes 48 days for the patch to cover the entire
lake, how long would it take for the patch to cover half of the lake?” The CRT demonstrates
high levels of internal reliability (Cronbach’s Alpha = 0.83).28 It is scored in terms of accuracy,
thus subjects can score between 0 and 3 out of 3, with higher scores reflecting more
analytical and deliberative (System 2) decision-making.
2.3.2 Actively Open-Minded Thinking Scale (AOT)
The Actively Open-minded Thinking Scale35 is a 41-item thinking disposition scale in which
participants are asked to mark in the box which best describes their thoughts on each item,
from “Strongly Disagree” to “Strongly Agree” (with 4 other options between). Examples of
items include, “People should always take into consideration evidence that goes against their
beliefs”. Some of the items are reversed scored and a total score is achieved by summing
the responses. Higher scores implicate more open-minded thinking.36 The AOT also shows
high internal reliability and validity (Cronbach’s Alpha = 0.81)28 in assessing whether subjects
are able to separate prior beliefs and opinions from the evaluation of current evidence and
arguments.
Participants completed both the CRT and AOT individually during a single session, lasting on
average around ten minutes per person. Participants were able to complete the scales in any
order they preferred. They were advised verbally and in writing they could leave blank any of
the CRT questions they felt unable to answer, but to complete all 41 statements on the AOT.
Anonymity was assured verbally and in writing. All participants completed the scales in a

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
classroom setting with instruction to complete both measures without discussing their
answers with their peers, during or after completion. This study was approved by the BSO
Research Ethics Committee and conducted according to the 1964 Declaration of Helsinki.
2.4 Data analysis
Descriptive statistics were computed for each group to establish the normality of the CRT
and AOT scores (Skewness and kurtosis; Shapiro-Wilk test and histogram inspections) and
to report measures of central tendency and spread of data. To examine the null hypothesis
“there is no difference in ‘intermediate’ and ‘novice’ students’ decision-making preferences
and reflective thinking skills”, we used a Mann-Whitney U test, an independent t test and
Spearman’s rank correlation. Cohen’s d and effect size correlations for CRT and AOT scores
were calculated if they reached statistical significance. The significance level for all analyses
was set at p < 0.05.
3. Results
3.1 Cognitive Reflection Test (CRT)
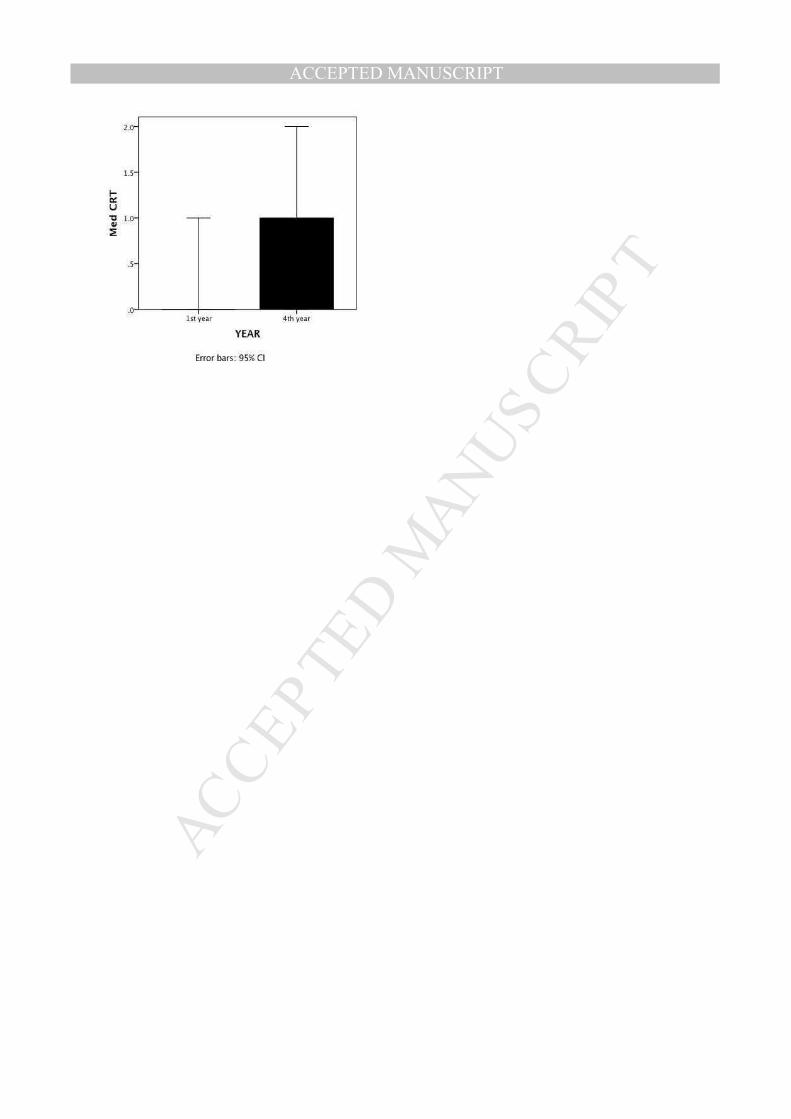
Figure 1 illustrates the CRT median scores (MDN) across the two levels of expertise (novice
and intermediate). For novices (n=44), 61% failed to answer any of the problems correctly,
with 4.5% solving all three items. For intermediates (n=32), 38% of participants did not solve
any of the problems, whilst 22% answered all 3 items correctly.
Differences in participants’ scores were examined using a Mann-Whitney U test. This
analysis revealed a statistically significant difference between intermediates and novices [U =
469.0; p = 0.007; effect size = 0.31] with intermediates scoring higher in the CRT (Mdn = 1)
than novices (Mdn = 0) with a medium effect size (r = 0.31).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
---------------------------------------------
Insert Figure 1 about here
---------------------------------------------
3.2 Actively Open-minded Thinking Scale (AOT)
The AOT scores in both groups were tested for normality based on skewness (-2 < Z < 2),
kurtosis (-2 < Z < 2) and Shapiro-Wilk (p > 0.05) values. All of the data were normally
distributed (novices, p = 0.955; intermediates, p = 0.352)
Table 1 shows the AOT mean scores (M) and standard deviations (SD). Differences in
participants’ reflective thinking dispositions were examined using an independent samples t
test. This analysis revealed no significant difference between novice and intermediate
reflective thinking scores [t (76) = 1.85, df = 73.2, p = 0.07].
---------------------------------------------
Insert Table 1 about here
---------------------------------------------
3.3 Supplementary Analysis
Supplementary analyses were conducted to examine the association between decision-
making preferences (CRT) predicting thinking dispositions (AOT). A Spearman’s rho
correlation did not reveal a statistically significant association between analytical decision-
making (CRT) and reflective thinking (AOT) [rs (74) = -0.022, p = 0.85] (see Figure 2).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
---------------------------------------------
Insert Figure 2 about here
---------------------------------------------
4. Discussion
This study explored how pre-registration osteopathy students at different levels of expertise
think and make decisions. It also examined whether any relationship exists between their
reasoning preferences and thinking dispositions. The results show that students nearing the
end of their education demonstrate significantly more analytical decision-making than their
novice peers; however, there was no evidence to suggest that reflective thinking dispositions
change as students progress through their training. Moreover, there was no significant
association between analytical decision-making and reflective thinking. Taken together, the
results from this study provide preliminary empirical evidence suggesting that in contrast to
novices, students at point of graduation resort to analytical (System 2) decision-making
strategies. However, they do not engage in significantly more open-minded or reflective
thinking, despite their lengthier exposure to osteopathic education. The lack of association
between reasoning and reflection suggests that one may not be a predictor of the other.
Therefore, intermediate practitioners who are not yet separating their beliefs and biases to
think openly and reflectively across a range of domains, may nevertheless have begun to
develop strategies to override cognitive shortcuts when making decisions.
Despite the significant difference between the reasoning preferences of each group, overall
median scores suggest that System 1 decision-making strategies may still prevail. This is
consistent with much of the literature in the field of cognitive science, which supports the
notion of a ‘cognitive miser’, predisposing people to resort to heuristics or short-cuts in their
decision-making.17, 37, The term ‘cognitive miser’ was initially proposed by Fiske and Taylor38

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
to illustrate the fact that individuals commonly evaluate information and make decisions using
cognitive shortcuts. In the field of clinical reasoning, Kassirer39 argued that the analytical
reasoning approach fails to take into consideration the fact that humans are human, not
computer processors. As a consequence, they tend to jump to conclusions, using intuitive
heuristics. According to Stanovich6, the cognitive system tends to default to the state
requiring minimal cognitive effort, i.e., the ‘cognitive miser’ function. Importantly, much of the
medical cognition literature supports this tendency in otherwise thoughtful and educated
individuals (medics) when making clinical decisions.18-22, 40 Notwithstanding this tendency,
there is a significant move away from this in subjects nearing the end of their osteopathic
education. That is to say, intermediate practitioners are starting to reason more analytically
and this analytical reasoning may be consistent with the ‘technical rationality’, or the reliance
on factual knowledge and skills applied in predictable ways that Thomson et al 27 argue
current osteopathic education promotes, and which is generally attributed to novice
healthcare practitioners.41 Intriguingly, the ‘professional artistry’ associated with more
experienced practitioners, comfortable with the ambiguities of clinical practice, implicates a
much greater predisposition towards the intuitive, pattern recognition approach inherent in
System 1. If, as it is widely acknowledged within osteopathic literature, that “evaluation within
osteopathic practice is a complex thing” 42, p. 280, then what emerges from the literature is
curious, as it seems to suggest that with expertise comes pattern recognition and therefore
System 1 reasoning. In contrast, System 2 approaches, encouraged by osteopathic
education and endorsed by the profession’s governing body13, may overload the system and
exceed the decision-making capacities of the individual.43 For novices, this then presents
something of a dilemma, as they are more likely to consider the problem as complex and
possess insufficient knowledge, yet may benefit from advice to use their intuition and
experience to solve it.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
This combination of reasoning approaches and reflective thinking required of practitioners
may be regarded as ‘metacognition’44, or the ability of the practitioner to reflect in action.19
This ‘thinking about thinking’ encourages practitioners to constantly monitor and adjust their
thoughts and reasoning processes from both deductive (System 2) and inductive (System 1)
approaches. Certainly, when subjects solve complex everyday problems45 or clinical
problems25 with specific instruction to use both reasoning strategies, there are fewer
cognitive or reasoning errors. Arguably, metacognition may provide the link between
analytical and non-analytical processing in clinical decision-making in osteopathic
medicine.12 However, it would appear that for osteopathy students in this study at least, a
metacognitive disparity exists if, as the results suggest, components such as reflective
thinking and analytical reasoning develop at different rates and that one may not predict the
other.
This apparent discrepancy in metacognition, reflected in the lack of association between
CRT and AOT scores, is consistent with cognitive science research. This research suggests
that cognitive ability (of any level) is independent of that individual’s ability to decouple their
prior beliefs and opinions from their evaluation of the evidence and arguments before
them.29, 36 It is therefore possible that pre-registration professional osteopathic education
encourages analytical or deductive reasoning (System 2) as rules, procedures and facts that
must be learned and understood at a high level before they are applied clinically. Therefore,
the move towards more analytical reasoning, as demonstrated by the intermediate level
practitioners, is a reflection of this. Consequently, the requirement to demonstrate inductive,
or actively open-minded thinking, may develop post-graduation if, as Thomson et al 27, p. 6
argue; “an undergraduate curriculum which is excessively skill-based may not promote
critical evaluation”. It is widely acknowledged that metacognition plays an important role in
the development of diagnostic expertise and professional autonomy.46 For example, Rivett
and Jones47, p.406 have argued that expert clinicians are able to effectively use metacognitive

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
strategies to self-monitor and self-evaluate their cognitive processes. Consequently, in the
absence of metacognition, clinicians are unable to effectively use their clinical reasoning to
manage clinical complexity.47 Although the concept of ‘professional artistry’ may imply a
greater predisposing towards System 1 processing, we argue that the development of
metacognitive proficiency is a critical component of an osteopath’s clinical competence
profile. During their professional journey from novice to expert, clinicians should develop their
skills of criticality and their ability to reflect on, and analyse their practice experiences in and
on action.11, 12
Investigating the cognitive aspects of clinical reasoning, such as thinking and decision-
making, inevitably means removing them from the larger context of clinical relevance, as
ultimately subjects were not called upon to make clinical decisions. One of the major flaws of
this study is a lack of osteopathic context, particularly, as Croskerry20 argues, decision-
making relies heavily on contextual cues, both to provide meaning but also to minimise
cognitive effort. This is especially important for System 1 reasoning, which, as has been
shown, may be more prone to error. Future research investigating students’ reasoning and
thinking dispositions may therefore need to consider using clinically relevant scenarios that
require decisions to be made, or even a more qualitative approach, consistent with previous
clinical reasoning research in physiotherapy 2 and occupational therapy.48 We also propose
that in future research, consideration should be given to the inclusion of a group of
experienced osteopaths in the study design. This may prove to be a useful benchmark for
the two student groups, as it would enable researchers to investigate reasoning strategies
and reflective thinking dispositions along the continuum from novice to expert.
Other methodological flaws may also limit the validity of these findings beyond pilot study
status, namely the recruitment of peers and the number of subjects ultimately recruited. The
very nature of convenience sampling prevents the significance of these findings being

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
applied to a population beyond the institution from where the sample was drawn. Arguably,
those interested in research and willing to participate already demonstrate levels of reflective
thinking and reasoning processes at odds with the rest of the student population. Despite a
medium effect size observed with the CRT outcome, participant numbers may have been
insufficient to identify differences in reflective thinking dispositions, if, as previously
acknowledged, trends are more subtle and preferences may develop differently over time.
A final area worth scrutiny concerns the tools used to measure the dependent variables.
Although both the CRT and AOT demonstrate consistent levels of internal validity and
reliability, the CRT relies on numerical calculation, however basic, and may therefore be a
measure of intelligence and not reasoning, ultimately correlating with measures of
mathematical ability and predicting bias in tasks of calculation and IQ only. Moreover,
familiarity with the CRT test items and awareness that deliberative decision making
processes might be required before an answer is given, may have skewed the results.
Similarly, the length of the AOT and some of the less culturally relevant items, for example, ‘I
believe the “new morality” of permissiveness is no morality at all’, may limit its relevance in
assessing the true reflective thinking dispositions of current undergraduate students.
5. Conclusion
Using a three-item cognitive reflection test and a 41-item thinking disposition scale, this study
set out to explore the reasoning strategies and reflective thinking dispositions of osteopathy
students. Furthermore, it examined whether exposure to osteopathy education results in
more analytical and reflective thinking. The results demonstrate that students nearing the
end of their undergraduate education display significantly more analytical decision-making
than their novice peers. However, reflective thinking dispositions do not change with
increased exposure to osteopathic education and nor does analytical reasoning predict
reflective thinking preferences. Results from the CRT are consistent with cognitive science

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
research that supports a Dual Process Model of decision-making. However, the trend for
intermediate level practitioners to demonstrate significantly more analytical reasoning lends
support to recent osteopathic research that suggests osteopathic education promotes the
development of deductive (System 2) reasoning in its graduates. This suggested emphasis
on ‘technical rationality’ might ultimately be at the expense of students developing reflective
thinking styles, which arguably develop alongside reasoning post-graduation to become
‘metacognition’. The development of metacognitive proficiency is, in our opinion, a critical
component of an osteopath’s clinical competence profile. The lack of association between
analytical decision-making and reflective thinking in this study supports both this notion and
previous research that suggests cognitive ability is separate from thinking bias and
preference.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
Statement of Competing Interests
JEE is an Associate Editor of the Int J Osteopath Med but was not involved in review or
editorial decisions regarding this manuscript.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
References
1 Higgs J, Jones MA. Clinical decision making and multiple problem spaces. In: Higgs J, Jones MA, Loftus S, Christensen N, editors. Clinical reasoning in the health professions: 3rd edn Edition. Philadelphia: Elsevier; 2008; 3-18.
2 Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen G. Clinical reasoning strategies in physical therapy. Phys Ther 2004; 84:312-335.
3 Evans JS. Dual-processing accounts of reasoning, judgment, and social cognition. Annu Rev Psychol 2008; 59:255-78.
4 Kahneman D. A perspective on judgment and choice: mapping bounded rationality. Am Psychol 2003; 58:697-720.
5 Stanovich KE, West RF. Individual differences in reasoning: implications for the rationality debate? Behav Brain Sci 2000; 23:645-65; discussion 665-726.
6 Stanovich KE. The robot's rebellion. Finding meaning in the age of Darwin. Chicago, Illinois: University of Chicago Press; 2004.
7 Schwartz A, Elstein AS. Clinical reasoning in medicine. In: Higgs J, Jones MA, Loftus S, Christensen N, editors. Clinical reasoning in the health professions: 3rd edn Edition. Philadelphia: Elsevier; 2008; 223-34.
8 Barbey AK, Barsalou LW. Reasoning and problem solving: Models. In: Squire LR, editor. Encyclopedia of Neuroscience. Oxford: Academic Press; 2009; 35-43.
9 Seffinger MA. Osteopathic philosophy. In: Ward RC, editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins; 1997; 3-12.
10 Pelaccia T, Tardif J, Triby E, Charlin B. An analysis of clinical reasoning through a recent and comprehensive approach: the dual-process theory. Med Educ Online 2011; 16:5890.
11 Esteves JE, Spence C. Developing competence in diagnostic palpation: Perspectives from neuroscience and education. Int J Osteopath Med 2014; 17:52-60.
12 Esteves JE. Diagnostic Palpation in Osteopathic Medicine: A Putative Neurocognitive Model of Expertise. Oxford: Oxford Brookes University; 2011.
13 GOsC. Osteopathic Practice Standards. London: General Osteopathic Council, 2012. Available from http://www.osteopathy.org.uk/uploads/osteopathic_practice_standards_public.pdf. accessed on 2 December 2012

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
14 NICE. Low back pain: early management of persistent non-specific low back pain (Clinical guideline 88): National Institute for Health and Clinical Excellence, 2009
15 NHS. Any qualified provider (AQP): National Health Service, 2012
16 Kahneman D, Tversky A. Judgement under uncertainty: Heuristics and Biases. New York: Cambridge University Press; 1982.
17 Frederick S. Cognitive reflection and decision making. Journal of Economic Perspectives 2005; 19:25-42.
18 Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimise them. Acad Med 2003; 78:775-780.
19 Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv Health Sci Educ Theory Pract 2009; 14 Suppl 1:27-35.
20 Croskerry P. Context is everything or how could I have been that stupid? Healthcare Quarterly 2009; 12:e171-6.
21 Elstein AS, Schwarz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ 2002; 324:729-32.
22 Klein J. Five pitfalls in decisions about diagnosis and prescribing. BMJ 2005; 330:781-784.
23 Baron J. Beliefs about thinking. In: Voss JF, Perkins DN, Segal JW, editors. Informal reasoning and education. Hillsdale, N. J.: Erlbaum; 1991; 169-186.
24 Masicampo E, Baumeister R. Towards a physiology of dual-process reasoning and judgement. Psychological Science 2008; 19:255-260.
25 Ark T, Brooks L, Eva K. The benefits of flexibility: the pedagogical value of instructions to adopt multifaceted diagnostic reasoning strategies. Med Educ 2007; 41:281-287.
26 Hogarth R. Deciding analytically or trusting your intuition? The advantages and disadvantages of analytic and intuitive thought. In: Betsch T, Haberstroh S, editors. Routines of Decision Making. Mahwah: Erlbaum; 2005; 67-82
27 Thomson OP, Petty NJ, Moore AP. A qualitative grounded theory study of the conceptions of clinical practice in osteopathy - A continuum from technical rationality to professional artistry. Man Ther 2013:http://dx.doi.org/10.1016/j.math.2013.06.005.
28 Toplak M, West R, Stanovich K. The Cognitive Reflection Test as a predictor of performance on heuristics-and-biases tasks. Memory and Cognition 2011; 39:1275-1289.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
29 West R, Meserve R, Stanovich K. Cognitive sophistication does not attenuate the blind spot. Journal of Personality and Social Psychology 2012: http://dx.doi.org/10.1037/a0028857.
30 Oechssler J, Roider A, Schmidt PW. Cognitive abilities and behavioral biases. Journal of Economic Behavior & Organization 2009; 72:147-152.
31 Cokely ET, Feltz A. Individual differences, judgment biases, and theory-of-mind: Deconstructing the intentional action side effect asymmetry. Journal of Research in Personality 2009; 43:18-24.
32 Schmidt HG, Norman GR, Boshuizen HP. A cognitive perspective on medical expertise: theory and implication. Acad Med 1990; 65:611-21.
33 Boshuizen HP, Schmidt HG. On the role of biomedical knowledge in clinical reasoning by experts, intermediates and novices. Cognitive Science 1992; 16:185-204.
34 Costa A, Foucart A, Arnon I, Aparici M, Apesteguia J. "Piensa" twice: On the foreign language effect in decision making. Cognition 2014; 130:236-254.
35 Sa W, Kelley C, Ho C, Stanovich K. Thinking about personal theories: Individual differences in the coordination of theory and evidence. Personality and Individual Differences 2005; 38:1149-1161
36 Stanovich K, West R. Natural myside bias is independent of cognitive ability. Thinking and reasoning 2007; 13:225-247.
37 Krueger J, Funder DC. Towards a balanced social psychology: consequences and cures for the problem-seeking approach to social cognition and behaviour. Behavioural and Brain Sciences 2004; 27:313-327.
38 Fiske ST, Taylor SE. Social cognition. Reading, Mass: Addison-Wesley Pub. Co; 1984.
39 Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med 2010; 85:1118-24.
40 Graber M, Franklin N, Gordon R. Diagnostic error in internal medicine. Archives of Internal Medicine 2005; 165:1493-1499.
41 Smith M, Joy H, Ellis E. Effect of experience on clinical decision-making by cardio-respiratory physiotherapists in acute care settings. Physiotherapy Theory and Practice 2010; 26:89-99.
42 Stone C. Science in the art of osteopathy: Osteopathic principles and practice. Cheltenham: Stanley Thornes; 1999.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
43 Norman G, Eva K. Diagnostic error and clinical reasoning. Med Educ 2010; 44:94-100.
44 Flavell JH. Metacognition and cognitive monitoring. A new area of cognitive-developmental inquiry. American Psychologist 1979; 34:906-911.
45 Pretz J. Intuition versus Analysis: strategy and experience in complex everyday problem solving. Memory and Cognition 2008; 36:554-566.
46 Jones M, Jensen G, Edwards I. Clinical Reasoning in Physiotherapy. In: Higgs J, Jones MA, editors. Clinical Reasoning in the Health Professions. Oxford: Butterworth-Heinemann; 2000; pp 117-127.
47 Rivett DA, Jones MA. Improving clinical reasoning in manual therapy. In: Jones MA, Rivett DA, editors. Clinical Reasoning for Manual Therapists. Oxford: Butterworth-Heinemann; 2004; 403-419.
48 Mattingly C. Clinical reasoning: Forms of inquiry in a therapeutic practice. Philadelphia: F.A. Davis; 1994.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
Tables
Table 1: AOT Results
Figures
Figure 1: Median outcomes for novice (1st yr) and intermediate (4th Yr) groups
Figure 2: Scatter plot for AOT and CRT scores

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Subjects n M SD
Novices 44 125.2 14.6
Intermediates 32 119.6 11.7
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Implications for practice
• Graduating students display significantly more analytical decision-making
than their novice peers; however, reflective thinking dispositions do not
change with increased exposure to osteopathic education.
• Analytical reasoning does not predict reflective thinking preferences in
osteopathy students.
• The emphasis on ‘technical rationality’ in osteopathic education might
prevent students from developing reflective thinking styles, which are
central role to the development of metacognitive proficiency, a critical
component of an osteopath’s clinical competence profile.




















