
Does cognitive functioning predict chronic pain? Results from a prospective surgical cohort
Accepted Manuscript
Interoception, body awareness and chronic pain: results from a case-control study
Chiara Ribera d’Alcalà, Duncan G. Webster, Jorge E. Esteves
PII: S1746-0689(14)00067-4
DOI: 10.1016/j.ijosm.2014.08.003
Reference: IJOSM 341
To appear in: International Journal of Osteopathic Medicine
Received Date: 28 March 2014
Revised Date: 3 August 2014
Accepted Date: 5 August 2014
Please cite this article as: Ribera d’Alcalà C, Webster DG, Esteves JE, Interoception, body awarenessand chronic pain: results from a case-control study, International Journal of Osteopathic Medicine(2014), doi: 10.1016/j.ijosm.2014.08.003.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Interoception, body awareness and chronic pain: res ults from a case-control
study
Authors
Chiara Ribera d’Alcalà *
Research Center, The British School of Osteopathy 275 Borough High Street, London, United Kingdom, SE1 1JE
Duncan G. Webster
Research Center, The British School of Osteopathy 275 Borough High Street, London, United Kingdom, SE1 1JE
Jorge E. Esteves
Research Center, The British School of Osteopathy 275 Borough High Street, London, United Kingdom, SE1 1JE
*Corresponding Author Details:
Chiara Ribera d’Alcalà
The British School of Osteopathy
275 Borough High Street
London SE1 1JE
Tel + 44 (0)20 7089 5310 Email: [email protected]
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Title: 1
Interoception, body awareness and chronic pain: results from a case-control study 2
3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
1
Keywords: 2
3
Interoceptive awareness; chronic pain; body awareness, self-perception; 4
mindfulness; manual therapy. 5
6
Abstract: 7
8
Background 9
Chronic pain remains an unresolved issue in clinical practice despite the extensive 10
research investigating its behavioural and neural correlates. Evidence demonstrates 11
that chronic pain results in altered representation of the body in the brain. Arguably, 12
this impacts on the perception of the self and its associated processes; namely, 13
interoceptive awareness and body awareness. However, there is minimal research 14
investigating the links between interoceptive awareness, body awareness and 15
chronic pain. 16
Objectives and Method 17
This case-control study investigated the relationship between chronic pain and 18
interoceptive awareness; and the links between interoceptive awareness and body 19
awareness. A sample of 59 participants comprising of 22 patients with chronic pain 20
and 37 individuals without a history of chronic pain were assessed using a heartbeat 21
monitoring task (HBMT) and the Body Awareness Questionnaire (BAQ). The HBMT 22
was used to measure interoceptive awareness; and the BAQ to measure body 23
awareness. Data from variables regarded as potential confounders, were also 24
collected. 25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Results 1
The findings did not reveal a statistical significant difference in interoceptive 2
awareness and body awareness across the groups. Moreover, activities likely to 3
enhance proprioception or mindfulness based practice did not influence interoceptive 4
awareness. Notwithstanding this, a positive trend was identified between body 5
awareness and mindfulness based activities. 6
Conclusions 7
Several limitations of this study suggest scope for further research investigating 8
putative changes in interoceptive awareness in the presence of chronic pain and the 9
effect of osteopathic treatment on the perception of the self. The role of mindfulness 10
based activities in the management of chronic pain is also discussed. 11
12
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
Text: 1
2
1. INTRODUCTION 3
4
Chronic pain is a complex and at times debilitating phenomenon, the management of 5
which represents, to this day, a challenge in clinical practice. Consequently chronic 6
pain is the centre of burgeoning research which aims at a better understanding of this 7
phenomenon in order to achieve successful management according to the 8
individual’s context.1,2 Recent advances in neuroscience have enabled a clearer 9
understanding of the behavioural and neural correlates of pain and how these can 10
affect the individual. Pain is a sensory, cognitive and emotional experience.3 This 11
experience results from the complex integration and modulation of nociceptive and 12
non-nociceptive stimuli within a network of spinal pathways and central nervous 13
system (CNS) structures.4–7 This network, known as the ‘pain matrix’, includes, 14
mainly, the somatosensory cortices (S1, S2), the insular cortex, the anterior cingulate 15
cortex and the thalamus.1,8–10 However other cortical and subcortical regions such as 16
the hippocampus, amygdala, basal ganglia and the cerebellum are typically 17
implicated, depending upon the individual’s set of circumstances.11 This suggests 18
that the pain experience may differ in each individual according to their own 19
processing of pain.1,8,10 20
21
Research demonstrates that structural and functional changes are found in this 22
neural network in association with chronic pain, i.e. pain persisting beyond the time of 23
tissue healing. Although causality cannot be clearly established, the array of 24
chemical, functional and structural neural changes contributes to changes in the 25
individual’s behaviour, emotions and perception of the self.12,13 The perception of the 26
self is regarded as a superset of self-consciousness that includes the elements of 27

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
body schema, body image and body ownership and body awareness; the latter is 1
considered as the conscious awareness of all internal and external stimuli. Recently, 2
there has been an increasing interest in the understanding of the neural network 3
underlying the perception of the self within the context of psychopathologies and 4
disorders of body awareness, including those experienced by chronic pain 5
sufferers.14,15 Evidence demonstrates that the representation of the body in the brain 6
is associated with the result of the integration of multisensory stimuli across several 7
CNS structures.16–19 In particular, a growing body of evidence highlights the role of 8
the insular cortex, site of integration of interoceptive stimuli, in the perception of the 9
self.20–22 10
11
Interoception has been defined as the “sense of the physiological condition of the 12
body”, i.e. the perception of all internal bodily cues.20 Interoceptive awareness has 13
been investigated in relation to psychopathologies such as anxiety and depression, 14
on the assumption that different attention to oneself would contribute to different 15
perception of external stimuli and therefore different behavioural responses to such 16
stimuli.23–26 For example Dunn and colleagues23 found that interoceptive accuracy is 17
positively linked with anxiety and that instead symptoms of depression weaken this 18
link. Similarly Pollatos and colleagues24 found that in healthy individuals symptoms of 19
anxiety are associated with high interoceptive awareness whereas reduced 20
interoceptive awareness is associated with depression. However, research exploring 21
the links between interoceptive awareness and chronic pain remains scarce. 22
23
The insula plays a role in both the ‘pain matrix’ and the neural network underlying the 24
representation of the body in the brain.7,10,22,27,28 Considering the CNS changes that 25
are associated with chronic pain,13,15,29–31 this crossover would suggest that a 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
disruption in the interoceptive pathway may contribute to changes in body awareness 1
experienced in long-term pain. The particular role of the insula has also been 2
highlighted by Tracey and Bushnell32 in their review of the most recent data from 3
neuroimaging studies on pain. Moreover Craig33 proposes a new view of pain as a 4
homeostatic emotion. Craig identifies a direct thalamocortical homeostatic afferent 5
pathway that projects to the posterior insula where it forms a representation of the 6
interoceptive information that subserve homeostasis. This cortical image is re-7
represented in the middle and anterior insula where it is associated with motivation, 8
affection and emotion; providing the “awareness of the material self as a feeling 9
entity”.33 In this view pain is processed in the insula as part of the interoceptive 10
feedback and as such it elicits a behavioural response. Here, we posited that chronic 11
pain sufferers would differ in interoceptive sensitivity from healthy individuals. 12
13
There is growing acceptance, amongst both healthcare practitioners and the patient 14
population, of manual therapy as a component of chronic pain management.34,35 15
Therefore, an increasing body of literature attempting to explain the mechanisms of 16
action of the ‘hands-on’ approach of manual therapy has emerged. Some of the 17
mechanisms that have been proposed involve direct or indirect stimulation of the 18
dorsal periacqueductal gray in the medulla, resulting in increased sympathetic activity 19
and hypoalgesia;36,37 influence on early sensory processing and somatosensory 20
integration within the CNS structures involved in these processes;38 reflex activity of 21
the segmental spinal cord level modulating nociceptive input. 39–41 However, the 22
putative effects of manual therapy on the perception of self in individuals affected by 23
long-term pain are under-researched. Moreover, the links between interoceptive 24
awareness, body awareness and chronic pain are largely unknown. To this end, we 25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
explored the links between interoceptive awareness and body awareness in adults 1
with chronic pain. 2
3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
2. METHODS 1
2
2.1. Design 3
4
We used a case-control design to compare measurements of interoceptive 5
awareness and body awareness in chronic pain sufferers and healthy individuals 6
without a history of chronic pain. 7
8
2.2. Participants 9
10
A sample of 59 individuals was recruited from the British School of Osteopathy 11
(BSO) patient and student populations. The cases (n = 22) were drawn from the 12
BSO outpatient clinic, with pain symptom duration of 3 months or longer. 13
Participants in the control group (n = 37) were healthy individuals, recruited from 14
the student and staff populations at the BSO and without a history of chronic pain 15
in the last 5 years. All participants were over 18 years of age, without a history of 16
diagnosed cardiovascular, rheumatological or respiratory conditions, 17
psychopathologies (e.g., depression, anxiety), white coat syndrome or eating 18
disorders; moreover they did not present to the clinic with an acute injury. This 19
was done to minimise participants’ distress and eliminate potential bias.24,26 20
Verbal and written consent was obtained from all participants. 21
22
2.3. Study measures 23
24
2.3.1 Heartbeat monitoring task 25
26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
A heartbeat monitoring task (HBMT) was used to obtain and compare 1
interoceptive awareness measures in the case and control groups. This HBMT is 2
an adaptation of the Mental Tracking Method42, a method widely used to measure 3
interoceptive awareness and with good test-retest reliability.24 In accordance with 4
previous studies43,44 the amount of time intervals for heartbeat counting differed 5
from the original. The HBMT consists in one short (15 s) training session and four 6
time intervals (100s, 45s, 35s and 25s) in which the actual experiment takes 7
place. 8
9
2.3.2 The Body Awareness Questionnaire 10
11
The Body Awareness Questionnaire (BAQ) was used to compare body 12
awareness in the case and control groups. The BAQ was developed with the aim 13
of creating a quantitative measure for the ability of an individual’s attentiveness to 14
normal physiological bodily processes without focusing on emotional states.45 It 15
has both good internal consistency (coefficient alpha = 0.82)45 and good reliability 16
compared to other measurements of body awareness.46 17
18
2.3.3 Demographic data and Body Mass Index 19
20
We developed a questionnaire to collect demographic data and confounding 21
variables considered to influence interoceptive awareness. Several studies have 22
reported that age, gender and Body Mass Index (BMI) influence the ability to 23
accurately perceive one’s heartbeat.24–26,43,47–49 BMI is a measure of individual’s 24
body weight relative to their height.50 Height and weight were obtained using a 25
scale with a measuring rod (Adam Equipment, MDW-250L, Milton Keynes) and 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
recorded directly on the laptop that was used for this study. In addition, it is 1
reasoned that interoceptive awareness is comprised of all the afferent information 2
arising within the body, including proprioceptive ones.46,51 There is evidence that 3
physical activity enhances proprioceptive awareness.52 For example, Jola and 4
colleagues found that professional trained dancers (with at least two years of 5
training) displayed better proprioceptive skills than non-dancers.53 Therefore we 6
deemed appropriate to record each participant’s occupation and leisure activities 7
as well as the number of years that those activities had been practised for. 8
Moreover, activities that involve a mind-body approach such as meditation may 9
influence interoceptive awareness,46 thus we obtained similar information 10
regarding these types of activities. We classified as activities deemed to influence 11
the participant’s proprioceptive awareness, occupation and leisure activities, 12
involving balance training and body control skills such as, for example, dance, 13
swimming and martial arts. Activites such as Thai Chi, yoga, meditation, 14
Feldenkreis and Alexander Techniques54 were classified as involving a mind-body 15
approach. Activities likely to influence interoception, e.g. the practise of manual 16
therapy, were also included. Manual therapy requires skilled palpation to enable 17
clinicians to locate anatomical structures and identify changes in bodily tissues. 18
Proprioception has been considered to be a component of palpation, thus manual 19
therapy, if seen as practice of palpation skills, would potentially influence 20
interoception.55 This information was considered as possible confounding factor 21
as potentially influencing interoceptive awareness. Data concerning putative 22
confounding variables were included in the statistical analysis. One point was 23
assigned to each year of practice for each activity, up to ten years and eleven 24
points were assigned where the number of years of practise was greater than ten. 25
26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
1
2.4 Procedure 2
3
The study was approved by the BSO Research and Ethics Committee and all 4
participants gave their verbal and written informed consent. The setting for the 5
study was the BSO outpatient osteopathic clinic. All data collection was 6
conducted in a consultation room with constant temperature, light and noise 7
setting. The room was distant from the street side and the clock was removed to 8
create a neutral environment and to minimise disruption to participants’ 9
concentration. The study was first piloted with a total of six participants to test the 10
validity and repeatability of the procedures; data obtained were excluded from the 11
main study. Participants were drawn from the outpatient clinic as well as the staff 12
and student populations. They were recruited by a poster campaign; the BSO 13
internal email system was also used to help in the recruitment of participants 14
within the student and staff populations. Participants were taken individually to the 15
room by one of the researchers, and then asked to complete the BAQ and 16
demographic data questionnaires. Questionnaires were anonymised by reference 17
number allocation. Upon completion of the questionnaires, height and weight 18
measurements were recorded. 19
20
Participants were then briefed on the HBMT and asked to count their heartbeat 21
silently and without taking their own pulse for a training session of 15s. This was 22
followed by four different time intervals (100s, 45s, 35s and 25s), which were 23
signalled to participants by a bleep. The time intervals were defined by audio cues 24
and randomly presented using a MatLab programme designed for this purpose; 25
they were alternated with rest periods of 30s in between. Simultaneously, an ECG 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
machine (CamNtech Ltd., Cambridge) was used to record their actual 1
heartbeat.24,26,42 2
3
2.5 Data analysis 4
5
Interoceptive awareness was calculated from the results of the HBMT, using an 6
equation proposed in previous studies that made use of this method:43,44 7
8
¼ ∑ (1- (|recorded heartbeats – counted heartbeats|)/ recorded heartbeat) 9
10
Body awareness was calculated as the mean of the scores of the BAQ45. 11
Descriptive statistics were computed for demographic data HBMT and BAQ 12
scores, using SPSS statistics version 20.0. Using the Mann-Whitney U test we 13
tested the null hypotheses ‘there is no difference in interoceptive awareness 14
between chronic pain sufferers and healthy individuals in this sample’ and ‘there 15
is no difference in body awareness between chronic pain sufferers and healthy 16
individuals in this sample’. The null hypothesis ‘there is no association between 17
interoceptive awareness and body awareness’ was tested using the Spearman’s 18
rho correlation. The impact of age, BMI, occupation, activities enhancing 19
proprioceptive skills, mindfulness based activities, gender and pain on 20
interoceptive and body awareness was tested using t-tests and Mann-Whitney U 21
(for between-group differences) and Spearman’s rho and Pearson’s correlations 22
(for associations between variables). We also assessed for predictors of 23
interoceptive awareness using a backward stepwise linear regression model, 24
based on findings from previous studies43,49,51; we predicted that aside from pain, 25
other variables such as age, BMI, gender, physical activities and activities 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
involving a mind-body approach would influence interoceptive awareness. The 1
significance level for all analyses was set at p < 0.05. 2
3
3 RESULTS 4
5
3.1 Demographics and preliminary analyses 6
7
A sample of 59 individuals completed the study, with 22 participants in the chronic 8
pain group (n = 22; mean age = 48.3; SD = 15.1) and 37 in the control group (n = 9
37; mean age = 26.1; SD = 11.9). Interoceptive awareness was calculated for all 10
participants with the exception of one (n = 58) due to technical errors. All the 11
other variables were measured for all participants (n = 59). All variables were 12
tested for normality, based on skewness (-2 < z < 2), kurtosis (-2 < z < 2), and 13
Shapiro-Wilk (p > 0.05) values. On the basis of the distribution, t-tests and Mann-14
Whitney U were used to assess the differences between the two groups. Table 1 15
shows the individual values of the chronic pain and control groups for all variables 16
in this study. 17
18
--------------------------------------------- 19
Insert Table 1 about here 20
--------------------------------------------- 21
22
3.2 Interoceptive and body awareness and chronic pain 23
24
We predicted that a difference in interoceptive awareness, measured by the 25
HBMT, would be found between the two groups. A Mann-Whitney U did not 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
reveal a statistically significant difference in HBMT scores between the chronic 1
pain and the control group U(56) = 370, Z = -0.30, p = 0.77. Therefore, the null 2
hypothesis ‘there is no difference in interoceptive awareness between chronic 3
pain sufferers and healthy individuals’ could not be rejected. 4
5
Similarly, we predicted that significant between-group differences in body 6
awareness, measured using the BAQ, would be found. A Mann-Whitney U did not 7
reveal statistically significant differences in BAQ scores between the chronic pain 8
and the control group U(57) = 401, Z = -0.09, p = 0.93. Therefore, the null 9
hypothesis ‘there is no difference in body awareness between chronic pain 10
sufferers and healthy individuals’ could not be rejected. 11
12
To explore the putative association between interoceptive awareness and body 13
awareness we used a Spearman’s rho correlation test. The analysis did not 14
reveal a statistically significant association between variables [r(56) = -0.04, p = 15
0.38]. In addition, we conducted a within-group analysis, which did not reveal a 16
significant association between interoceptive awareness and body awareness in 17
both chronic pain [r(19) = -0.11, p = 0.32], and control group [r(35) = -0.001, p = 18
0.50]. Based on these findings, we could not reject the null hypothesis ‘there is no 19
association between interoceptive awareness and body awareness’. 20
21
3.3 Supplementary analyses 22
23
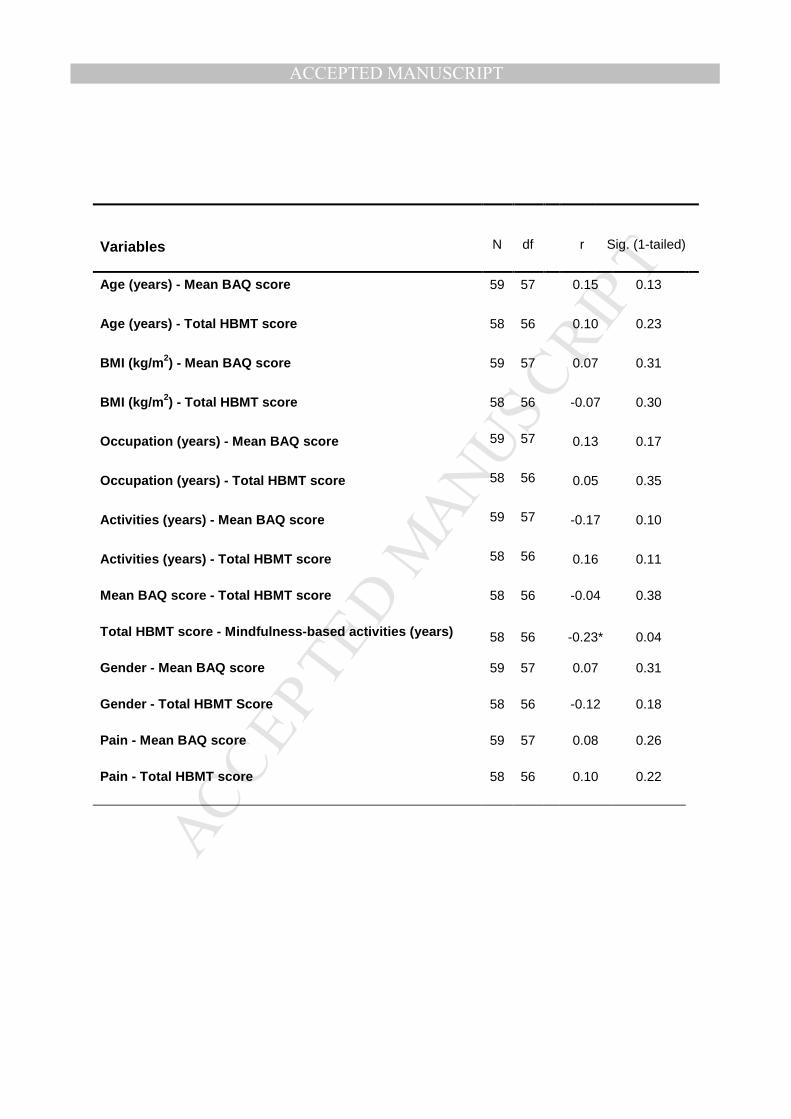
Supplementary analyses were conducted to assess the impact of age, BMI, 24
occupation, activities enhancing proprioceptive skills, mindfulness based 25
activities, gender and pain on interoceptive and body awareness (see table 2). 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
Statistical significant differences between the chronic pain and the control group 1
were only found for age t(57) = 7.91, p < 0.001; BMI U(57) = 231, Z = -2.76, p = 2
0.01; and years of occupation involving activities enhancing proprioception U(57) 3
= 231, Z= -3.53, p = 0.00. To examine the links between interoceptive awareness 4
(HBMT scores), body awareness (BAQ scores) and all other variables, we used 5
Spearman’s rho and Pearson’s correlations. A statistical significant association 6
was found only between interoceptive awareness and years of mindful activities 7
[r(56) =-.23, p =0.04]. 8
9
--------------------------------------------- 10
Insert Table 2 about here 11
--------------------------------------------- 12
13
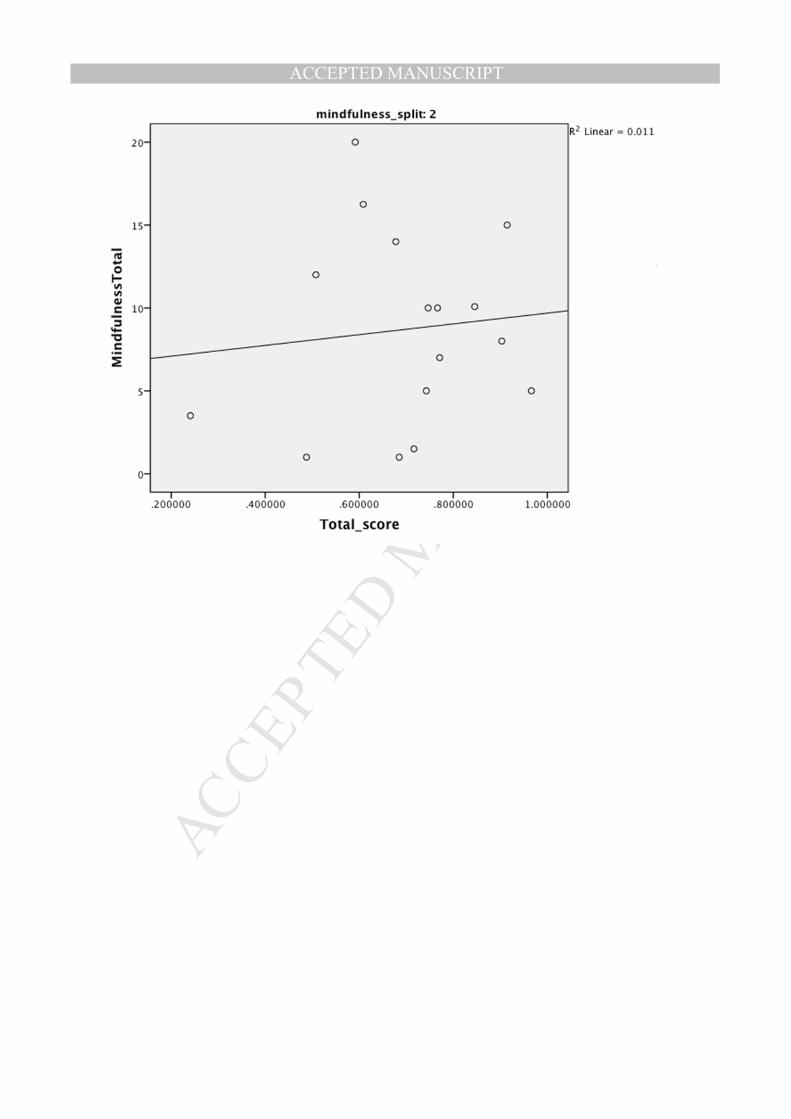
Considering the use of mind-body approach activities and therapies to improve a 14
‘mindful’ non-judgmental body awareness in the therapeutic context,54 it was 15
hypothesised that perception of physiological bodily processes would be 16
enhanced by mindfulness related activities. However, the practise of activities 17
involving a mind-body approach was mainly reported by chronic pain sufferers. 18
The negative correlation was therefore further investigated removing the outliers 19
and a positive trend, although not significant, was found between HBMT score 20
and years of activities with a focus on the mind-body connection (see Fig. 1). 21
22
--------------------------------------------- 23
Insert Figure 1 about here 24
--------------------------------------------- 25
26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
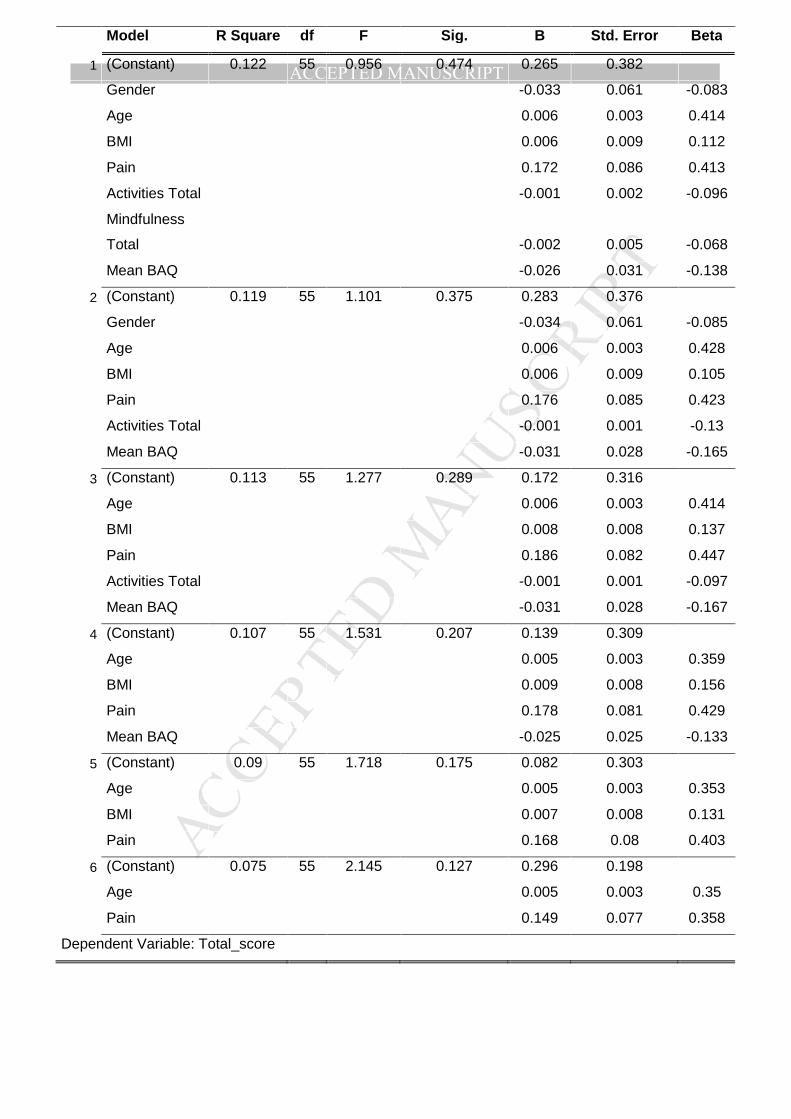
To investigate the relation between the variables that were hypothesised to 1
influence interoceptive awareness (age, gender, BMI, chronic pain, body 2
awareness, proprioception and mindfulness related activities) a backward 3
stepwise linear regression was used. This analysis did not identify any significant 4
predictors for interoceptive awareness (see Table 3). On the basis of the 5
assumptions for linear regression, residuals were also tested for normality and 6
they resulted normally distributed. 7
8
--------------------------------------------- 9
Insert Table 3 about here 10
--------------------------------------------- 11
12
4. DISCUSSION 13
14
The aim of this case-control study was two-fold: firstly, to investigate the 15
relationship between chronic pain and interoceptive awareness; and secondly, to 16
investigate links between interoceptive awareness and body awareness. 17
Supplementary analyses were performed to investigate links between 18
interoception and putative confounding variables such as activities involving a 19
mind-body approach, activities enhancing proprioceptive skills, age, gender and 20
BMI. To the best of our knowledge, this is the first study investigating the role of 21
interoceptive awareness in individuals affected by chronic pain. We predicted that 22
the interoceptive aspect of self-perception, as measured via the HBMT, would 23
differ between chronic pain sufferers and healthy individuals. We also predicted 24
that changes in interoceptive awareness would be positively correlated with 25
changes in body awareness, as measured by the BAQ. In addition we posited 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
that other factors (age, gender, BMI, activities enhancing proprioceptive skills and 1
activities involving a mind-body approach) would influence interoceptive accuracy. 2
Based on the results of our analyses we identified a positive trend between body 3
awareness and mindfulness related activities; however, we could not reject the 4
study’s main two null hypotheses. The main limitations of the study are discussed 5
to highlight possibilities for further research. Moreover, the observed positive 6
trend is considered within the context of a developing interest in mind-body 7
therapies and mindfulness training as part of chronic pain management. 8
9
Clear limitations of the study included a small sample size, which was further 10
reduced by equipment failure with one participant, and difficulties in recruiting 11
homogeneous groups of participants. On this point, there is evidence that age 12
and BMI affect interoceptive awareness,49,51 therefore differences between cases 13
and controls could have influenced the results. 14
15
The employed methodology also included certain limitations. Some confusion 16
amongst participants could have been caused by not using the suggested 17
standard instructions for the HBMT.56 Moreover, despite evidence supporting the 18
HBMT as a reliable method for measuring interoceptive awareness,24,43 19
neuroimaging methods such as functional magnetic resonance imaging (fMRI) or 20
positron emission tomography (PET) utilised in recent studies in this field 20,21,27 21
may be more appropriate. Furthermore we recorded activities that would 22
potentially influence participants’ proprioception and interoception. However, 23
despite recording the number of years that each activity was practiced for, we 24
failed to obtain information related to the frequency of practise. To measure body 25
awareness we used the BAQ, which at the outset of the study, was regarded as 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
one of the most reliable body awareness questionnaires46. However, new insights 1
into self-perception suggest that body awareness is the sum of more complex 2
cognitive, sensorimotor and emotional processes22,57,58, and as such, a more 3
complete measurement is needed. Recently, Mehling and colleagues59 have 4
developed a questionnaire for the assessment of self-perception which 5
encompasses several dimensions of self-awareness and we suggest its use in 6
future studies. 7
8
We consider that particular attention should be given to the population from where 9
the study sample was drawn. All chronic pain sufferers were drawn from the BSO 10
outpatient clinic; therefore, they all received osteopathic manipulative treatment 11
(OMT) on a regular basis. It has been hypothesised that, osteopathy greatly relies 12
on touch to affect multimodal receptors present in the skin, fascia and joints, 13
through a series of manipulative and myofascial techniques, and thus elicit 14
changes in the function of bodily tissues.40,41,60–62 Within the interplay of 15
multisensory stimuli that together result in an online representation of the body in 16
the brain, touch is undoubtedly of great importance.16,63,64 Considering the role 17
played by tactile stimuli in an individual’s body schema, it is plausible to argue 18
that OMT, or manual therapy in general, should be considered as a confounding 19
factor in any study into body’s representation. Further investigation is therefore 20
suggested into the effects of OMT on body schema controlling for the use of 21
OMT. This would enable us to assess possible effects of osteopathic treatment on 22
individuals’ interoceptive and body awareness and consequent applications in 23
clinical practice. For this purpose and to further reduce sampling bias we also 24
suggest that further studies should use consecutive sampling of chronic pain 25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
sufferers, including new patients who would have not previously been exposed to 1
OMT. 2
3
In addition, patients suffering from psychopathologies such as anxiety or 4
depression were excluded from the study to minimise participants’ distress. 5
However, there is robust evidence demonstrating that the affective and emotional 6
component of chronic pain are intrinsic factors of the pain experience.7,13,65–67 To 7
this end the emotional components of the pain experience cannot be dismissed. 8
Depression and anxiety are associated with long-term pain, as well as negative 9
emotions such as fear, frustration and anger.68,69 Several studies have shown 10
changes in interoceptive awareness in relation to depression, anxiety and panic 11
disorders.23–26,56 Furthermore, the insula, considered to play a key role in 12
interoceptive awareness, has been shown to play a fundamental role in emotional 13
response and behaviour.10,28 However in this study the emotional response part of 14
the individual’s pain experience was not reported. We therefore suggest that to 15
explore the true implication of interoceptive awareness in chronic pain, research 16
should be conducted in a population of chronic pain sufferers that includes a 17
record of the emotional experience associated with the individual’s pain 18
processing, as this association would provide a more thorough analysis of the 19
potential differences in interoceptive accuracy. 20
21
To conclude, we would like to draw attention to the positive trend identified 22
between activities involving a mind-body approach and interoceptive awareness. 23
Osborn and Smith70 found that in the presence of chronic pain, the parts of the 24
body that ache are rejected from the ‘self’ and are not considered as part of one’s 25
body. It has also been shown that higher acceptance of one’s body in pain allows 26

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
for a better quality of life and is associated with lower negative emotional 1
response to pain.71,72 Mindfulness is a non-judgmental awareness of the self and 2
the surrounding stimuli.54,73 The link between mindfulness and ‘adaptive’ body 3
awareness46 has been considered beneficial in the management of chronic pain. 4
Indeed, there is an increasing use of body awareness therapies and mindfulness 5
based interventions in the care of chronic pain sufferers.74,75 We therefore argue 6
that further research should be carried out to investigate the links between 7
interoceptive awareness and activities involving a mind-body approach. This 8
would provide a better understanding of the use of body-mind therapies and 9
mindfulness practice as components of chronic pain management and further 10
support it. 11
12
5. CONCLUSION 13
14
Further investigation is suggested into the role of interoceptive awareness and its 15
role in chronic pain. This would enable clinicians and researchers to have a better 16
understanding of this complex phenomenon and potential implications in the 17
therapeutic approach to chronic pain. Particular attention should be given to the 18
possible effects of osteopathic treatment and other forms of manual therapy on 19
body schema through tactile and proprioceptive stimulation; this could further 20
support the use of manual therapy in the management of chronic pain. Moreover 21
further investigation should be carried into the use of mindfulness practise in the 22
management of chronic pain as well as its effects onto body awareness and 23
interoceptive awareness. 24
25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
Statement of Competing Interests: 1
Jorge E Esteves is an Associate Editor of the Int J Osteopath Med but was not 2
involved in review or editorial decisions regarding this manuscript. 3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
References:
1 Wand BM, Parkitny L, O’Connell NE, Luomajoki H, McAuley JH, Thacker M, et
al. Cortical changes in chronic low back pain: current state of the art and
implications for clinical practice. Man Ther 2011; 16: 15–20.
2 Gallagher R. The pain medicine and primary care community rehabilitation
model: monitored care for pain disorders in multiple settings. Clin J Pain 1999;
15: 1–3.
3 Simons LE, Elman I, Borsook D. Psychological processing in chronic pain: a
neural systems approach. Neurosci Biobehav Rev 2014; 39: 61–78.
4 Shacklock MO. Central pain mechanisms: A new horizon in manual therapy.
Aust J Physiother 1999; 45: 83–92.
5 Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science. , McGraw-
Hill Medical, 2000.
6 Todd AJ. Neuronal circuitry for pain processing in the dorsal horn. Nat Rev
Neurosci 2010; 11: 823–36.
7 Bingel U, Tracey I. Imaging CNS modulation of pain in humans. Physiology
(Bethesda) 2008; 23: 371–80.
8 Moseley GL. A pain neuromatrix approach to patients with chronic pain. Man
Ther 2003; 8: 130–40.
9 Apkarian VA, Bushnell MC, Treede R-D, Zubieta J-K. Human brain
mechanisms of pain perception and regulation in health and disease. Eur J
Pain 2005; 9: 463–84.
10 Tracey I, Mantyh PW. The cerebral signature for pain perception and its
modulation. Neuron 2007; 55: 377–91.
11 Tracey I. Imaging pain. Br J Anaesth 2008; 101: 32–9.
12 Moseley GL, Flor H. Targeting cortical representations in the treatment of
chronic pain: a review. Neurorehabil Neural Repair 2012; 26: 646–52.
13 Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its
disruption in chronic pain. Nat Rev Neurosci 2013; 14: 502–11.
14 Giummarra MJ, Gibson SJ, Georgiou-Karistianis N, Bradshaw JL. Mechanisms
underlying embodiment, disembodiment and loss of embodiment. Neurosci
Biobehav Rev 2008; 32: 143–60.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
15 Moseley GL. I can’t find it! Distorted body image and tactile dysfunction in
patients with chronic back pain. Pain 2008; 140: 239–43.
16 Maravita A, Spence C, Driver J. Multisensory integration and the body schema:
close to hand and within reach. Curr Biol 2003; 13: R531–R539.
17 Tsakiris M, Haggard P. The rubber hand illusion revisited: visuotactile
integration and self-attribution. J Exp Psychol Hum Percept Perform 2005; 31:
80–91.
18 Walsh LD, Moseley GL. Proprioceptive signals contribute to the sense of body
ownership. J Physiol 2011; 589: 3009–21.
19 Suzuki K, Garfinkel SN, Critchley HD, Seth AK. Multisensory integration across
exteroceptive and interoceptive domains modulates self-experience in the
rubber-hand illusion. Neuropsychologia 2013; 51: 2909–17.
20 Craig A. Interoception: the sense of the physiological condition of the body.
Curr Opin Neurobiol 2003; 13: 500–5.
21 Critchley HD, Wiens S, Rotshtein P, Ohman A, Dolan RJ. Neural systems
supporting interoceptive awareness. Nat Neurosci 2004; 7: 189–95.
22 Berlucchi G, Aglioti SM. The body in the brain revisited. Exp Brain Res 2010;
200: 25–35.
23 Dunn BD, Stefanovitch I, Evans D, Oliver C, Hawkins A, Dalgleish T. Can you
feel the beat? Interoceptive awareness is an interactive function of anxiety- and
depression-specific symptom dimensions. Behav Res Ther 2010; 48: 1133–8.
24 Pollatos O, Traut-Mattausch E, Schandry R. Differential effects of anxiety and
depression on interoceptive accuracy. Depress Anxiety 2009; 26: 167–73.
25 Dunn BD, Dalgleish T, Ogilvie AD, Lawrence AD. Heartbeat perception in
depression. Behav Res Ther 2007; 45: 1921–30.
26 Zoellner L a, Craske MG. Interoceptive accuracy and panic. Behav Res Ther
1999; 37: 1141–58.
27 Craig A. How do you feel--now? The anterior insula and human awareness.
Nat Rev Neurosci 2009; 10: 59–70.
28 Craig A. Interoception and emotion: a neuroanatomical perspective. In: Lewis
M, Haviland-Jones JM, Barrett LF, editors. Handbook of emotion, Third.
London, The Guilford Press, 2008: 272–88.
29 Schweinhardt P, Bushnell MC. Pain imaging in health and disease--how far
have we come? J Clin Invest 2010; 120: 3788–97.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
24
30 Baliki MN, Schnitzer TJ, Bauer WR, Apkarian VA. Brain Morphological
Signatures for Chronic Pain. PLoS One 2011; 6: e26010.
31 Bray H, Moseley GL. Disrupted working body schema of the trunk in people
with back pain. Br J Sport Med 2011; 45: 168–73.
32 Tracey I, Bushnell MC. How neuroimaging studies have challenged us to
rethink: is chronic pain a disease? J Pain 2009; 10: 1113–20.
33 Craig A. A new view of pain as a homeostatic emotion. Trends Neurosci 2003;
26: 303–7.
34 Artus M, Croft P, Lewis M. The use of CAM and conventional treatments
among primary care consulters with chronic musculoskeletal pain. BMC Fam
Pract 2007; 8: 26.
35 Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among
primary care patients using opioid therapy for chronic pain. BMC Complement
Altern Med 2007; 7: 15.
36 Kingston L, Claydon L, Tumilty S. The Effects Of Spinal Mobilizations On The
Sympathetic Nervous System: A Systematic Review. Man Ther 2014; 19: 281–
7.
37 Schmid A, Brunner F, Wright A, Bachmann LM. Paradigm shift in manual
therapy? Evidence for a central nervous system component in the response to
passive cervical joint mobilisation. Man Ther 2008; 13: 387–96.
38 Haavik H, Murphy B. The role of spinal manipulation in addressing disordered
sensorimotor integration and altered motor control. J Electromyogr Kinesiol
2012; 22: 768–76.
39 Pickar JG. Neurophysiological effects of spinal manipulation. Spine J 2002; 2:
357–71.
40 Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The
mechanisms of manual therapy in the treatment of musculoskeletal pain: a
comprehensive model. Man Ther 2009; 14: 531–8.
41 Pickar JG, Bolton PS. Spinal manipulative therapy and somatosensory
activation. J Electromyogr Kinesiol 2012; 22: 785–94.
42 Schandry R. Heart beat perception and emotional experience.
Psychophysiology 1981; 18: 483–8.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
25
43 Tsakiris M, Tajadura-Jiménez A, Costantini M. Just a heartbeat away from
one’s body: interoceptive sensitivity predicts malleability of body-
representations. Proc R Soc B Biol Sci 2011; 278: 2470–6.
44 Pollatos O, Kurz A-L, Albrecht J, Schreder T, Kleemann AM, Schöpf V, et al.
Reduced perception of bodily signals in anorexia nervosa. Eat Behav 2008; 9:
381–8.
45 Shields S, Mallory M. The body awareness questionnaire: Reliability and
validity. J Pers 1989; 53: 802–15.
46 Mehling WE, Gopisetty V, Daubenmier J, Price CJ, Hecht FM, Stewart A. Body
awareness: construct and self-report measures. PLoS One 2009; 4: e5614.
47 Brener J, Michael Jones J. Interoceptive discrimination in intact humans:
Detection of cardiac activity. Physiol Behav 1974; 13: 763–7.
48 Jones GE, Jones KR, Rouse CH, Scott DM, Caldwell J a. The effect of body
position on the perception of cardiac sensations: an experiment and theoretical
implications. Psychophysiology 1987; 24: 300–11.
49 Khalsa SS, Rudrauf D, Tranel D. Interoceptive awareness declines with age.
Psychophysiology 2009; 46: 1130–6.
50 Samaras TT, Bartke A, Rollo CD. Human body size and the laws of scaling:
physiological, performance, growth, longevity and ecological ramifications. ,
Nova Publishers, 2007.
51 Cameron OG. Interoception: the inside story--a model for psychosomatic
processes. Psychosom Med 2001; 63: 697–710.
52 Ribeiro F, Oliveira J. Aging effects on joint proprioception: the role of physical
activity in proprioception preservation. Eur Rev Aging Phys Act 2007; 4: 71–6.
53 Jola C, Davis A, Haggard P. Proprioceptive integration and body
representation: insights into dancers’ expertise. Exp Brain Res 2011; 213: 257–
65.
54 Mehling WE, Wrubel J, Daubenmier JJ, Price CJ, Kerr CE, Silow T, et al. Body
Awareness: a phenomenological inquiry into the common ground of mind-body
therapies. Philos Ethics Humanit Med 2011; 6: 6.
55 Esteves, JE. Diagnostic palpation in osteopathic medicine: a putative
neurocognitive model of expertise. In: Faculty of humanities and social
sciences. Oxford Brookes University, Oxford; 2011.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
26
56 Ehlers a, Breuer P. Increased cardiac awareness in panic disorder. J Abnorm
Psychol 1992; 101: 371–82.
57 Longo MR, Schüür F, Kammers MPM, Tsakiris M, Haggard P. What is
embodiment? A psychometric approach. Cognition 2008; 107: 978–98.
58 Ferri F, Frassinetti F, Ardizzi M, Costantini M, Gallese V. A sensorimotor
network for the bodily self. J Cogn Neurosci 2012; 24: 1584–95.
59 Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, Stewart A. The
Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS One
2012; 7: e48230.
60 Di Giovanna EL, Schiowitz S, Dowling DJ, Spinaris T, Scariati P, Crow WT, et
al. Section II: Osteopathic Manipulation. In: Di Giovanna EL, Schiowitz S,
Dowling DJ, editors. An osteopathic approach to diagnosis and treatment, 3rd
ed. Philadelphia, Lippincott Williams & Wilkins, 2005: 75 – 122.
61 Boal RW, Gillette RG. Central neuronal plasticity, low back pain and spinal
manipulative therapy. J Manip Physiol Ther 2004; 27: 314–26.
62 Simmonds N, Miller P, Gemmell H. A theoretical framework for the role of
fascia in manual therapy. J Bodyw Mov Ther 2012; 16: 83–93.
63 Serino A, Haggard P. Touch and the body. Neurosci Biobehav Rev 2010; 34:
224–36.
64 Press C, Taylor-Clarke M, Kennett S, Haggard P. Visual enhancement of touch
in spatial body representation. Exp Brain Res 2004; 154: 238–45.
65 Apkarian VA, Sosa Y, Krauss BR, Thomas SP, Fredrickson BE, Levy RE, et al.
Chronic pain patients are impaired on an emotional decision-making task. Pain
2004; 108: 129–36.
66 Gallagher RM. Biopsychosocial pain medicine and mind-brain-body science.
Phys Med Rehabil Clin N Am 2004; 15: 855–82, vii.
67 Lynch M, Craig KD, Peng PWH. The challenge of pain: a multidimensional
phenomenon. In: Lynch ME, Craig KD, Peng PWH, editors. Clinical Pain
Management: A Practical Guide. , Blackwell Publishing Ltd., 2011: 3–5.
68 Rainville P, Bao QVH, Chrétien P. Pain-related emotions modulate
experimental pain perception and autonomic responses. Pain 2005; 118: 306–
18.
69 Linton SJ, Shaw WS. Impact of psychological factors in the experience of pain.
Phys Ther 2011; 91: 700–11.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
27
70 Osborn M, Smith JA. Living with a body separate from the self. The experience
of the body in chronic benign low back pain: an interpretative
phenomenological analysis. Scand J Caring Sci 2006; 20: 216–22.
71 Afrell M, Biguet G, Rudebeck CE. Living with a body in pain - between
acceptance and denial. Scand J Caring Sci 2007; 21: 291–6.
72 McCracken LM, Vowles KE. Acceptance of chronic pain. Curr Pain Headache
Rep 2006; 10: 90–4.
73 Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al.
Meditation experience is associated with increased cortical thickness.
Neuroreport 2005; 16: 1893–7.
74 Mars TS, Abbey H. Mindfulness meditation practise as a healthcare
intervention: A systematic review. IJOM 2010; 13: 56–66.
75 Taylor AG, Goehler LE, Galper DI, Innes KE, Bourguignon C. Top-down and
bottom-up mechanisms in mind-body medicine: development of an integrative
framework for psychophysiological research. Explore (NY) 2010; 6: 29–41.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
28
Figures:
Fig. 1: Positive trend between interoceptive awareness and mindfulness
based activities
Tables:
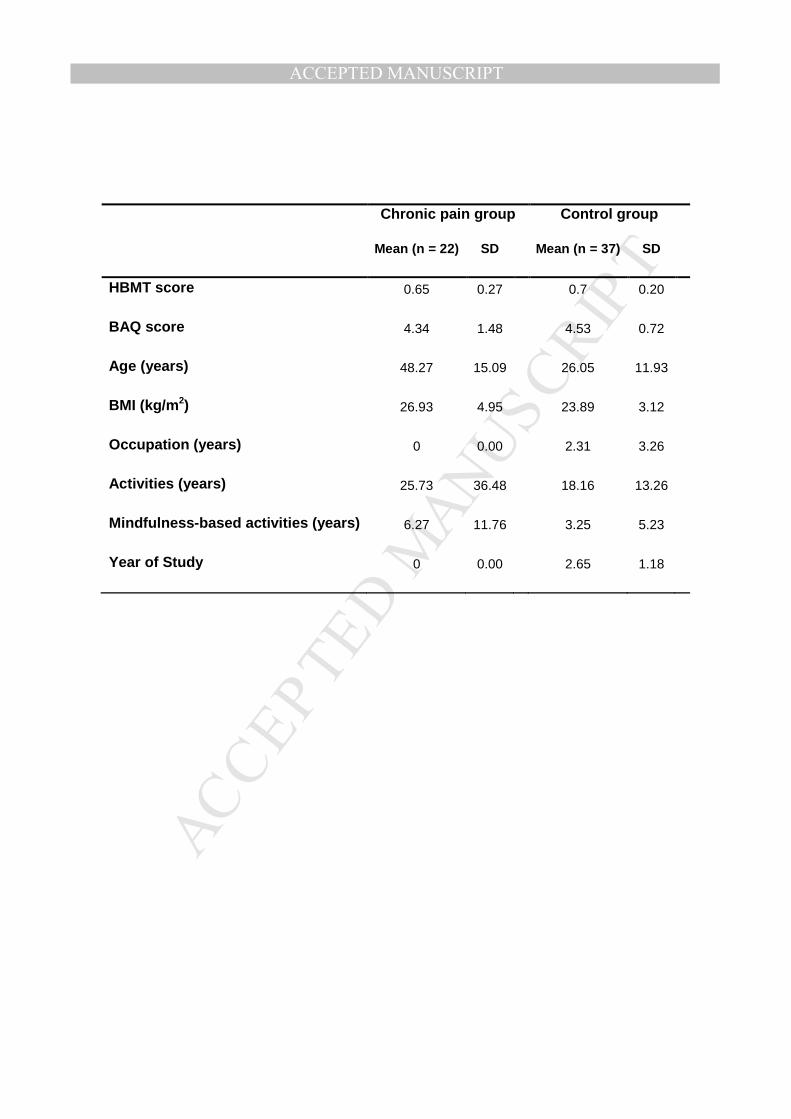
Table 1: Mean scores and standard deviations (SD) per group
Table 2: Correlations between variables. * indicates a significant correlation
p < 0.05
Table 3: Backward stepwise linear regression model

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Acknowledgements
We would like to thank Kevin Brownhill for his support in software development and
implementation of the experimental task; and Michael Ford for his support in the
statistical analysis of the data.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Chronic pain group Control group
Mean (n = 22) SD Mean (n = 37) SD
HBMT score 0.65 0.27 0.7 0.20
BAQ score 4.34 1.48 4.53 0.72
Age (years) 48.27 15.09 26.05 11.93
BMI (kg/m2) 26.93 4.95 23.89 3.12
Occupation (years) 0 0.00 2.31 3.26
Activities (years) 25.73 36.48 18.16 13.26
Mindfulness-based activities (years) 6.27 11.76 3.25 5.23
Year of Study 0 0.00 2.65 1.18
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Variables
N
df
r
Sig. (1-tailed)
Age (years) - Mean BAQ score 59 57 0.15 0.13
Age (years) - Total HBMT score 58 56 0.10 0.23
BMI (kg/m2) - Mean BAQ score 59 57 0.07 0.31
BMI (kg/m2) - Total HBMT score 58 56 -0.07 0.30
Occupation (years) - Mean BAQ score 59 57 0.13 0.17
Occupation (years) - Total HBMT score 58 56 0.05 0.35
Activities (years) - Mean BAQ score 59 57 -0.17 0.10
Activities (years) - Total HBMT score 58 56 0.16 0.11
Mean BAQ score - Total HBMT score 58 56 -0.04 0.38
Total HBMT score - Mindfulness-based activities (years) 58 56 -0.23* 0.04
Gender - Mean BAQ score 59 57 0.07 0.31
Gender - Total HBMT Score 58 56 -0.12 0.18
Pain - Mean BAQ score 59 57 0.08 0.26
Pain - Total HBMT score 58 56 0.10 0.22
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Model R Square df F Sig. B Std. Error Beta
1 (Constant) 0.122 55 0.956 0.474 0.265 0.382
Gender -0.033 0.061 -0.083
Age 0.006 0.003 0.414
BMI 0.006 0.009 0.112
Pain 0.172 0.086 0.413
Activities Total -0.001 0.002 -0.096
Mindfulness
Total -0.002 0.005 -0.068
Mean BAQ -0.026 0.031 -0.138
2 (Constant) 0.119 55 1.101 0.375 0.283 0.376
Gender -0.034 0.061 -0.085
Age 0.006 0.003 0.428
BMI 0.006 0.009 0.105
Pain 0.176 0.085 0.423
Activities Total -0.001 0.001 -0.13
Mean BAQ -0.031 0.028 -0.165
3 (Constant) 0.113 55 1.277 0.289 0.172 0.316
Age 0.006 0.003 0.414
BMI 0.008 0.008 0.137
Pain 0.186 0.082 0.447
Activities Total -0.001 0.001 -0.097
Mean BAQ -0.031 0.028 -0.167
4 (Constant) 0.107 55 1.531 0.207 0.139 0.309
Age 0.005 0.003 0.359
BMI 0.009 0.008 0.156
Pain 0.178 0.081 0.429
Mean BAQ -0.025 0.025 -0.133
5 (Constant) 0.09 55 1.718 0.175 0.082 0.303
Age 0.005 0.003 0.353
BMI 0.007 0.008 0.131
Pain 0.168 0.08 0.403
6 (Constant) 0.075 55 2.145 0.127 0.296 0.198
Age 0.005 0.003 0.35
Pain 0.149 0.077 0.358
Dependent Variable: Total_score
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Author Contributions
This article is based on Chiara Ribera d’Alcalà masters dissertation, which was
supervised by Jorge E. Esteves and realised with the collaboration of Duncan G.
Webster for its conception and design, data collection and data analysis and
interpretation. Chiara Ribera d’Alcalà and Jorge E. Esteves drafted the article; all
authors approved the final version.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Implications for practice
- Chronic pain remains an unresolved issue in clinical practice. Further
research should investigate the putative links between interoceptive
awareness and chronic pain and the effect of osteopathic treatment on the
perception of the self.
- Mindfulness-based practice is effective in the management of chronic
pain; however, its effects onto body awareness and interoceptive
awareness are largely unknown and further research is therefore
warranted.
Copyright © 2022 FDOKUMEN




















