
Intelligence tests used to make Bob Sternberg a little
452
11 CHAPTER 425 Intelligence Intelligence tests used to make Bob Sternberg a little sick. “The school psychologist would come into the room and give us these group IQ tests. And I would freeze up, especially when I heard other kids turning the page and I was still on the first or second problem.” As a result, Sternberg routinely bombed his IQ tests. But his fourth-grade teacher didn’t believe the numbers, and she con- vinced Sternberg not to believe them either. His teacher was right. Sternberg grew up to be an insightful, influential researcher and—ironically—a world-renowned expert on intelligence, first as a psy- chology professor at Yale University and now as the dean of arts and sciences at Tufts University. Throughout his career, he has explored the question of what intelli- gence is, where it comes from, and how people can get more of it. But Sternberg’s own trajectory reminds us that the correlation between IQ scores and life success is far from 1.00. IQ tests are designed to measure intelligence, but do they? For that matter, what is intelligence? More than a decade ago, 52 experts offered a multifaceted definition of this term: “the ability to reason, plan, solve problems, think abstractly, compre- hend complex ideas, learn quickly and learn from experience” (Gottfredson, 1997a, p. 13). This is a complex definition, but we may need further complications, because, in this chapter, we’ll consider proposals that would expand this definition by taking into account important talents excluded from the experts’ conceptualization. We’ll also look at proposals that would subdivide the definition, so that we end up speak- ing about different types, and different aspects, of intelligence.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Intelligence tests used to make Bob Sternberg a little
11C
HA
PT
ER
425
Intelligence
Intelligence tests used to make Bob Sternberg a little
sick. “The school psychologist would come into the room and give us these group IQ
tests. And I would freeze up, especially when I heard other kids turning the page and
I was still on the first or second problem.” As a result, Sternberg routinely bombed
his IQ tests. But his fourth-grade teacher didn’t believe the numbers, and she con-
vinced Sternberg not to believe them either.
His teacher was right. Sternberg grew up to be an insightful, influential
researcher and—ironically—a world-renowned expert on intelligence, first as a psy-
chology professor at Yale University and now as the dean of arts and sciences at
Tufts University. Throughout his career, he has explored the question of what intelli-
gence is, where it comes from, and how people can get more of it. But Sternberg’s
own trajectory reminds us that the correlation between IQ scores and life success is
far from 1.00.
IQ tests are designed to measure intelligence, but do they? For that matter, what
is intelligence? More than a decade ago, 52 experts offered a multifaceted definition
of this term: “the ability to reason, plan, solve problems, think abstractly, compre-
hend complex ideas, learn quickly and learn from experience” (Gottfredson, 1997a,
p. 13). This is a complex definition, but we may need further complications, because,
in this chapter, we’ll consider proposals that would expand this definition by taking
into account important talents excluded from the experts’ conceptualization. We’ll
also look at proposals that would subdivide the definition, so that we end up speak-
ing about different types, and different aspects, of intelligence.
426 chapter 11 PINTELLIGENCEO
These points should make it clear that, after a century of research in this domain,there’s still room for debate about what intelligence is and how it should be defined.Despite these complications, we’ll see that in the last century, researchers have madeenormous progress in identifying the intellectual and motivational components thatcontribute to IQ scores, and also have learned an enormous amount about the rootsof these components. To understand this progress, we need some historical context:Researchers first set out to measure intelligence 100 years ago, and much of whatwe’ve learned—and many of the questions that remain—can be traced directly tothese early efforts. Let’s begin our story, therefore, at the beginning, in France in theopening years of the 20th century.
INTELLIGENCE TESTING
In 1904, the French minister of public instruction appointed a committee with thespecific task of identifying children who were performing badly in school and wouldbenefit from remedial education. One member of this committee, Alfred Binet(1857–1911; Figure 11.1), played a pivotal role and had an extremely optimistic view of theproject. As Binet saw things, the committee’s goal was both to identify the weaker stu-dents and then—crucially—to improve the students’ performance through training.
Measuring IntelligenceFor their task, Binet and the other committee members needed an objective way toassess each child’s abilities, and in designing their test, they were guided by the beliefthat intelligence is a capacity that matters for many aspects of cognitive functioning.This view led them to construct a test that included a broad range of tasks varying incontent and difficulty: copying a drawing, repeating a string of digits, understanding astory, arithmetic reasoning, and so on. They realized that someone might do well onone or two of these tasks just by luck or due to some specific experience (perhaps theperson had encountered that story before), but they were convinced that only a trulyintelligent person would do well on all the tasks in the test. Therefore, intelligencecould be measured by a composite score that took all the tasks into account. Moreover,they believed that the diversity of the tasks ensured that the test was not measuring
some specialized talent but was instead a measure of ability in general.Indeed, Binet put a heavy emphasis on this diversity, and even claimedthat, “It matters very little what the tests are so long as they are numer-ous” (1911, p. 329).
In its original form, the intelligence test was intended only for chil-dren. The test score was computed as a ratio between the child’s “mentalage” (the level of development reflected in the test performance) and hischronological age; the ratio was then multiplied by 100 to get the finalscore (Figure 11.2). This ratio (or quotient) was the source of the test’sname: The test evaluated the child’s “intelligence quotient,” or IQ.
Other, more recent forms of the test no longer calculate a ratiobetween mental and chronological age, but they’re still called IQ tests.One commonly used test for assessing children is the WechslerIntelligence Scale for Children (WISC), released in its fourth revision
11.1 Alfred Binet (1857–1911) Binetsought to measure intelligence and toimprove it. As his work developed, he prescribed courses in “mental orthopedics”for students who were performing poorly:In one book, his chapter on the “training ofintelligence” began with the ambitiousphrase: “After the illness, the remedy.”
This calculation of IQ scores, first proposed by Germanpsychologist William Stern, was adopted as the routineprocedure for many years.
Imagine little Johnny, born 10 years ago; his chronological age,therefore, is 10.
Johnny is able to do mental tasks that, on average, most 11-year-olds can’t do, but most 12-year-olds can do. Mentally,Johnny seems quite advanced, and he therefore seems toresemble a normal 12-year-old.
IQ = (mental age ÷ ÷ chronological age) 100
His IQ = (12 ÷÷ 10) 100 = 120
11.2 Calculating IQ
PIntelligence TestingO 427
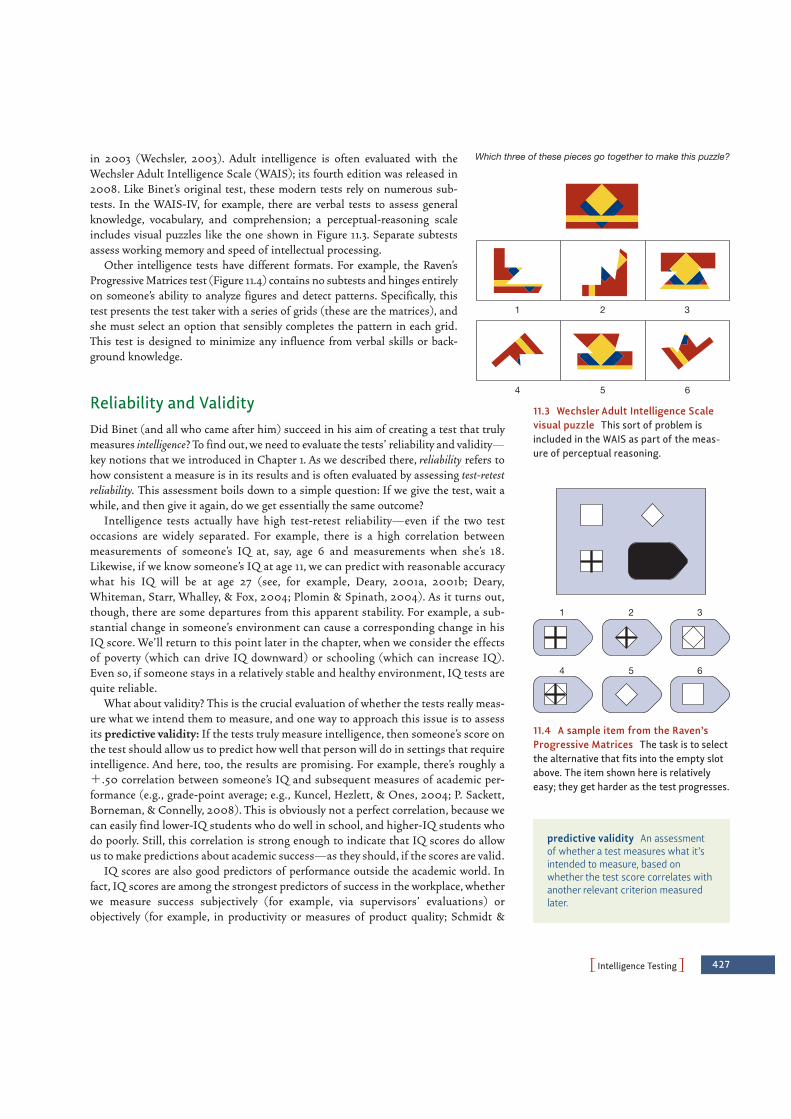
in 2003 (Wechsler, 2003). Adult intelligence is often evaluated with theWechsler Adult Intelligence Scale (WAIS); its fourth edition was released in2008. Like Binet’s original test, these modern tests rely on numerous sub-tests. In the WAIS-IV, for example, there are verbal tests to assess generalknowledge, vocabulary, and comprehension; a perceptual-reasoning scaleincludes visual puzzles like the one shown in Figure 11.3. Separate subtestsassess working memory and speed of intellectual processing.
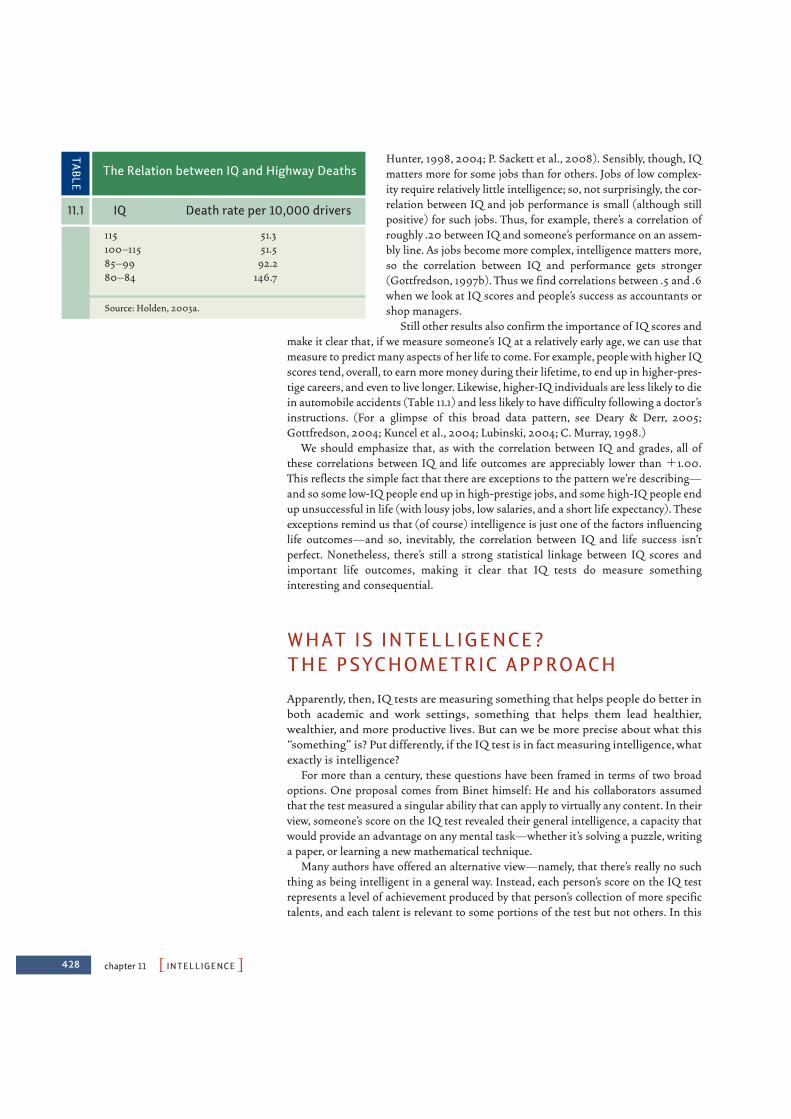
Other intelligence tests have different formats. For example, the Raven’sProgressive Matrices test (Figure 11.4) contains no subtests and hinges entirelyon someone’s ability to analyze figures and detect patterns. Specifically, thistest presents the test taker with a series of grids (these are the matrices), andshe must select an option that sensibly completes the pattern in each grid.This test is designed to minimize any influence from verbal skills or back-ground knowledge.
Reliability and ValidityDid Binet (and all who came after him) succeed in his aim of creating a test that trulymeasures intelligence? To find out, we need to evaluate the tests’ reliability and validity—key notions that we introduced in Chapter 1. As we described there, reliability refers tohow consistent a measure is in its results and is often evaluated by assessing test-retestreliability. This assessment boils down to a simple question: If we give the test, wait awhile, and then give it again, do we get essentially the same outcome?
Intelligence tests actually have high test-retest reliability—even if the two testoccasions are widely separated. For example, there is a high correlation betweenmeasurements of someone’s IQ at, say, age 6 and measurements when she’s 18.Likewise, if we know someone’s IQ at age 11, we can predict with reasonable accuracywhat his IQ will be at age 27 (see, for example, Deary, 2001a, 2001b; Deary,Whiteman, Starr, Whalley, & Fox, 2004; Plomin & Spinath, 2004). As it turns out,though, there are some departures from this apparent stability. For example, a sub-stantial change in someone’s environment can cause a corresponding change in hisIQ score. We’ll return to this point later in the chapter, when we consider the effectsof poverty (which can drive IQ downward) or schooling (which can increase IQ).Even so, if someone stays in a relatively stable and healthy environment, IQ tests arequite reliable.
What about validity? This is the crucial evaluation of whether the tests really meas-ure what we intend them to measure, and one way to approach this issue is to assessits predictive validity: If the tests truly measure intelligence, then someone’s score onthe test should allow us to predict how well that person will do in settings that requireintelligence. And here, too, the results are promising. For example, there’s roughly a!.50 correlation between someone’s IQ and subsequent measures of academic per-formance (e.g., grade-point average; e.g., Kuncel, Hezlett, & Ones, 2004; P. Sackett,Borneman, & Connelly, 2008). This is obviously not a perfect correlation, because wecan easily find lower-IQ students who do well in school, and higher-IQ students whodo poorly. Still, this correlation is strong enough to indicate that IQ scores do allowus to make predictions about academic success—as they should, if the scores are valid.
IQ scores are also good predictors of performance outside the academic world. Infact, IQ scores are among the strongest predictors of success in the workplace, whetherwe measure success subjectively (for example, via supervisors’ evaluations) orobjectively (for example, in productivity or measures of product quality; Schmidt &
Which three of these pieces go together to make this puzzle?
1 2 3
4 5 6
11.3 Wechsler Adult Intelligence Scalevisual puzzle This sort of problem isincluded in the WAIS as part of the meas-ure of perceptual reasoning.
predictive validity An assessmentof whether a test measures what it’sintended to measure, based onwhether the test score correlates withanother relevant criterion measuredlater.
1 2 3
4 5 6
11.4 A sample item from the Raven’sProgressive Matrices The task is to selectthe alternative that fits into the empty slotabove. The item shown here is relativelyeasy; they get harder as the test progresses.
428 chapter 11 PINTELLIGENCEO
Hunter, 1998, 2004; P. Sackett et al., 2008). Sensibly, though, IQmatters more for some jobs than for others. Jobs of low complex-ity require relatively little intelligence; so, not surprisingly, the cor-relation between IQ and job performance is small (although stillpositive) for such jobs. Thus, for example, there’s a correlation ofroughly .20 between IQ and someone’s performance on an assem-bly line. As jobs become more complex, intelligence matters more,so the correlation between IQ and performance gets stronger(Gottfredson, 1997b). Thus we find correlations between .5 and .6when we look at IQ scores and people’s success as accountants orshop managers.
Still other results also confirm the importance of IQ scores andmake it clear that, if we measure someone’s IQ at a relatively early age, we can use thatmeasure to predict many aspects of her life to come. For example, people with higher IQscores tend, overall, to earn more money during their lifetime, to end up in higher-pres-tige careers, and even to live longer. Likewise, higher-IQ individuals are less likely to diein automobile accidents (Table 11.1) and less likely to have difficulty following a doctor’sinstructions. (For a glimpse of this broad data pattern, see Deary & Derr, 2005;Gottfredson, 2004; Kuncel et al., 2004; Lubinski, 2004; C. Murray, 1998.)
We should emphasize that, as with the correlation between IQ and grades, all ofthese correlations between IQ and life outcomes are appreciably lower than !1.00.This reflects the simple fact that there are exceptions to the pattern we’re describing—and so some low-IQ people end up in high-prestige jobs, and some high-IQ people endup unsuccessful in life (with lousy jobs, low salaries, and a short life expectancy). Theseexceptions remind us that (of course) intelligence is just one of the factors influencinglife outcomes—and so, inevitably, the correlation between IQ and life success isn’tperfect. Nonetheless, there’s still a strong statistical linkage between IQ scores andimportant life outcomes, making it clear that IQ tests do measure somethinginteresting and consequential.
WHAT IS INTELLIGENCE? THE PSYCHOMETRIC APPROACH
Apparently, then, IQ tests are measuring something that helps people do better inboth academic and work settings, something that helps them lead healthier,wealthier, and more productive lives. But can we be more precise about what this“something” is? Put differently, if the IQ test is in fact measuring intelligence, whatexactly is intelligence?
For more than a century, these questions have been framed in terms of two broadoptions. One proposal comes from Binet himself: He and his collaborators assumedthat the test measured a singular ability that can apply to virtually any content. In theirview, someone’s score on the IQ test revealed their general intelligence, a capacity thatwould provide an advantage on any mental task—whether it’s solving a puzzle, writinga paper, or learning a new mathematical technique.
Many authors have offered an alternative view—namely, that there’s really no suchthing as being intelligent in a general way. Instead, each person’s score on the IQ testrepresents a level of achievement produced by that person’s collection of more specifictalents, and each talent is relevant to some portions of the test but not others. In this
115 51.3100–115 51.585–99 92.280–84 146.7
Source: Holden, 2003a.
The Relation between IQ and Highway Deaths
TABLE
11.1 IQ Death rate per 10,000 drivers

view, if we look closely at the test scores, we’re unlikely to find people who are success-ful in every aspect of the test or people who are inept in every mental task. Instead, eachperson will be strong on the tasks for which he has the relevant talents and somewhatweaker on the tasks that rely on talents he lacks. As a result, each person would have anindividualized profile of strengths and weaknesses. If we then represent that profilewith a single number—an IQ score—this is actually just a crude summary of the per-son’s abilities because it averages together the things a person is good at and the thingsthey’re not.
Which of these proposals is correct? Is the IQ score a reflection of intelligence ingeneral, so that it measures a capacity useful for all tasks? Or is the score just an aver-age created by summing together diverse components?
The Logic of PsychometricsWe have before us two hypotheses concerned with the nature of intelligence, and theway we’ve described the hypotheses points toward the means of deciding whichhypothesis is correct. What we need to do is take a closer look at the IQ tests them-selves and try to find patterns within the test scores. This kind of scrutiny reflects thepsychometric approach to intelligence—an approach that, at the start, deliberatelyholds theory and definitions to the side. Instead, it begins with the actual test resultsand proceeds on the belief that patterns within these results may be our best guidein deciding what the tests measure—and therefore what intelligence is. To see howthis works, let’s begin with a hypothetical example.
Imagine that we give a group of individuals three tests that seem at least initially dif-ferent from each other; let’s call the tests X, Y, and Z. One hypothesis is that all threetests measure the same underlying ability—and so, if a person has a lot of this ability,she has what she needs for all three tests and will do well on all of them. (This is, ofcourse, the idea that there’s a general ability used for many different tasks.) Based onthis hypothesis, a person’s score on one of these tests should be similar to her score onthe other tests because, whatever the level of ability happens to be, it’s the same abilitythat matters for all three tests. This hypothesis therefore leads to a prediction that therewill be a strong correlation between each person’s score on test X and his or her scoreon test Y, and the same goes for X and Z or for Y and Z.
A different hypothesis is that each of tests X, Y, and Z measures a different abil-ity. This is, of course, the idea that there’s no such thing as ability in general;instead, each person has their own collection of more specialized capacities. Basedon this view, it’s possible for a person to have the ability needed for X but not theabilities needed for Y or Z. It’s also possible for a person to have the abilities neededfor both Y and Z but not those needed for X. It’s possible for a person to have all ofthese abilities or none of them. In short, all combinations are possible becausewe’re talking about three separate abilities; thus, there is no reason to expect a cor-relation between someone’s X score and his Y score, or between his Y score and hisZ score, just as there’s no reason to expect a correlation between, say, someone’sability to knit well and the size of his vocabulary. Knitting and knowing a lot ofwords are simply independent capacities—so you can be good at one, or the other,or both, or neither.
We could also imagine intermediary hypotheses: Perhaps X and Y tap into the same,somewhat general ability, but Z taps into some other, more specialized ability. PerhapsY and Z overlap in the abilities relevant for each, but the overlap is only partial.Throughout, however, the logic is the same: If two tests overlap in the abilities they
PWhat Is Intelligence? The Psychometric ApproachO 429
psychometric approach to intelli-gence An attempt to understand thenature of intelligence by studying thepattern of results obtained on intelli-gence tests.

430 chapter 11 PINTELLIGENCEO
require, then they are to some extent measuring the same thing; so there should be a cor-relation between the scores on the two tests. If the overlap is slight, the correlation willbe weak; if the overlap is greater, the correlation will be correspondingly stronger. (For aslightly different—and somewhat whimsical—view of these points, see Figure 11.5.)
Factor Analysis and the Idea of General IntelligenceWhat do we find when we apply this logic to real test data? Both the WAIS and theWISC (the adult and child tests, respectively) rely, as we’ve said, on numerous subtests.This arrangement allows us to compare each person’s scores on one of the subtests totheir scores on all the other subtests. When we make these comparisons, we find animpressive level of consistency from one subtest to the next. People who do well on oneportion of the test tend to do well across the board; people who do poorly on one sub-test tend to do poorly on the other subtests as well. In other words, we find substantialcorrelations among all the subtests’ scores. The correlations aren’t perfect—and so weknow, by the logic we’ve developed, that the subtests don’t overlap completely in whatthey measure. Even so, the correlations are telling us that the subtests are far from inde-pendent of each other; instead, they all overlap in what they’re measuring.
To document and measure this overlap, psychologists rely on a statistical techniqueknown as factor analysis, developed by Charles Spearman (1863–1945). This techniquedistills from the pattern of correlations a broad summary of how all the scores arerelated to each other. Specifically, factor analysis (as its name implies) looks for com-mon factors—“ingredients” that are shared by several scores. The analysis detects theseshared factors by using the logic we’ve already developed: If the scores on two separatetasks are correlated with each other, this suggests the tasks are influenced by the samefactor. If scores on three tasks are all correlated with each other, then all the tasks, itseems, are influenced by the same factor. And so on.
Factor analyses confirm that there’s a common element shared by all the compo-nents of the IQ test; indeed, in children’s data, this single common element seems toaccount for roughly half of the overall data pattern (Watkins, Wilson, Kotz, Carbone, &Babula, 2006); a single common factor seems just as important in data drawn fromtesting of adults (e.g., Arnau & Thompson, 2000). The various subtests differ in howstrongly they rely on this common element, and so some subtests (e.g., someone’s com-prehension of a simple story) depend heavily on this general factor; other tests (e.g.,someone’s ability to recall a string of digits) depend less on the factor. Nonetheless, this
factor analysis A statistical methodfor studying the interrelations amongvarious tests. The goal is to discoverwhether the tests are all influenced bythe same factors, or by distinct factors.
11.5 The logic of psychometrics The analytic procedures used inpsychometrics are complex and mathematical, but the basic idea issimple. Imagine someone who observes these serpentine parts movingacross a lake. Is there one serpent here, or two? In other words, are thevisible pieces linked to each other (under the water)? This question issimilar to asking how different tests are linked to each other—the testscores themselves are visible, but the (potential) links—the overlap inthe capacities needed for each test—aren’t. To ask about the serpents,we’d want to know whether the visible bits rise and fall together. If therising and falling of, say, loop X are independent of the movements ofloop Y, this suggests that the loops aren’t linked, as shown in theobserver’s first hypothesis. But if loop Y always rises when loop X does,and vice versa, this suggests a link, as in the second hypothesis. We useroughly the same logic when we ask about test scores—using corre-spondence in the visible parts (the scores) to infer linkage in theunseen parts (the underlying capacities).
X Y
X Y X Y
Are X and Y not connected? Or are X and Y connected?

PWhat Is Intelligence? The Psychometric ApproachO 431
general factor seems to matter across the board, and that’s why all the subtests end upcorrelated with each other.
But what is this common element? If the subtests overlap in some way, what isthe nature of the overlap? More than 50 years ago, Charles Spearman offered theobvious hypothesis—namely, that the common element is general intelligence,usually abbreviated with the single letter g. Spearman proposed that g is a mentalattribute called on for virtually any intellectual task. It follows, therefore, that anyindividuals with a lot of g have an advantage in every intellectual endeavor; if g is inshort supply, the individual will do poorly on a wide range of tasks.
A Hierarchical Model of IntelligenceSpearman realized, however, that g is not the sole determinant of test performance(e.g., Spearman, 1927). Instead, he argued, each subtest depends both on g and onsome other abilities that are specific to that particular subtest. Thus, performance on anarithmetic subtest depends on how much g a person has and also on the strength ofthat person’s (more specialized) numerical skills; performance on vocabulary testsdepends on the combination of g and the person’s verbal skill; and so on. This patternwould explain both why the scores on all the subtests are correlated (because all thesubtests rely on g, and so all reflect whether the person has a lot of g or a little) and whythe correlations aren’t perfect (because performance on each subtest also depends onspecialized abilities).
More recent studies have supported Spearman’s claim and have also illuminatedwhat the more specialized abilities might be. One specialized ability involves verbaland linguistic skill, and so someone who has a lot of this ability will do well onalmost any task that hinges on language skills. A second specialized ability involvesquantitative or numerical ability; a third involves spatial or mechanical ability. Onthis basis, we can think of intellectual performance as having a hierarchical structureas shown in Figure 11.6. Researchers disagree about the details of this hierarchy; butby most accounts, g is at the top of the hierarchy and contributes to virtually all tasks.At the next level down are the abilities we just described—language, quantitative,and spatial—and, according to some authors, several more besides (including aspecialized ability for fast-paced mental tasks, a specialized ability to learn new mate-rials, and so on). Then at the next level are a large number of even more specificcapacities—at least 80 have been identified—each useful for a narrow and special-ized set of tasks (J. Carroll, 1993; W. Johnson, Nijenhuis, & Bouchard, 2007;McGrew, 2009; R. Snow, 1994, 1996).
This hierarchical conception leads to a number of predictions that have beenconfirmed by psychometric research. Specifically, if we choose tasks from two differentcategories—say, a verbal task and a task requiring arithmetic—we should expect to finda correlation in performance because, no matter how different these tasks seem, they dohave something in common: They both draw on g. If we choose tasks from the samecategory, though—say, two verbal tasks, or two quantitative tasks—we should expect tofind a higher correlation because these tasks have two things in common: They bothdraw on g, and they both draw on the more specialized capacity neededfor that category. The data confirm both of these predictions—moder-ately strong correlations among all of the IQ test’s subtests, and evenstronger correlations among subtests in the same category.
So where does this leave us regarding the two hypotheses we intro-duced earlier? One hypothesis, initially offered by Binet, is that intelli-gence is a general skill, useful for all endeavors. The other proposal is that
Linguistic ability Spatial abilityNumerical ability
General intelligence (g)
Specialized abilities
11.6 Hierarchical conception ofintelligence According to many moderntheories, intelligence has many compo-nents. At the highest level is g, a form ofintelligence that applies to virtually anymental task. Each person also has a num-ber of more specialized talents—so thatperformance on a verbal task dependsboth on g and on linguistic ability; perform-ance on a mathematical task depends bothon g and on numerical ability. Finally, eachperson also has a much larger number ofeven more specialized abilities—and soperformance on a particular verbal task isalso influenced by skills directly applicableto just that task; performance on a particu-lar mechanical task is also influenced byskills applicable to just that sort of task,and so on.
general intelligence (g) A mental attribute that is hypothesized as contributing to the performance of virtually any intellectual task.

432 chapter 11 PINTELLIGENCEO
there are multiple forms of intelligence, each useful for a particular type of task. We nowsee that both suggestions are correct. Each person has some amount of g, and he draws onthat capacity in virtually everything he does. As a result, there is consistency in someone’sperformance—an overall level of achievement shaped by the person’s g. But the consis-tency isn’t perfect, because mental tasks also require more specialized abilities—and eachperson has each of these to some extent. This is why, in addition to the overall level of con-sistency, each person has his own profile of strengths and weaknesses, things he doesrelatively well and things he does less well.
Fluid and Crystallized GPsychometric analyses of intelligence also draw our attention to another distinction.Alongside of verbal, quantitative, and spatial skills, we can also distinguish two moreforms of intelligence: fluid intelligence and crystallized intelligence, often abbreviated Gfand Gc. These forms of intelligence therefore take their place at the middle level ofthe hierarchy shown in Figure 11.6 (J. Carroll, 2005; Horn, 1985; Horn & Blankson,2005).
Fluid intelligence refers to the ability to deal with new and unusual problems. Itinvolves the deliberate and controlled use of mental operations and is the form of intel-ligence you need when you have no well-practiced routines you can bring to bear on aproblem. Crystallized intelligence, on the other hand, refers to your acquired knowl-edge. This includes your verbal knowledge and your broad repertoire of skills—skillsuseful for dealing with problems similar to those already encountered.
Fluid and crystallized intelligence are linked in an obvious way: Someone with ahigh level of fluid intelligence is likely to be a fast learner and so will easily acquire theskills and knowledge that crystallized intelligence comprises. As a result, someone witha lot of fluid intelligence will end up with a lot of crystallized intelligence. Even so, thereare several reasons to distinguish these types of intelligence. For example, crystallizedintelligence seems to increase with age—as long as the individual remains in anintellectually stimulating environment (see Chapter 14). Fluid intelligence, on the otherhand, generally reaches its height in early adulthood and then, for most people, declinessteadily with age (Horn, 1985; Horn & Noll, 1994; Salthouse, 2004). Similarly, manyfactors—including alcohol consumption, fatigue, depression, and some forms of braindamage—cause more impairment in tasks requiring fluid intelligence than in thosedependent on crystallized intelligence (J. Duncan, 1994; E. Hunt, 1995). Thus, to putthis concretely, someone who is tired (or drunk, or depressed) will probably performadequately on tests involving familiar routines and familiar facts because these testsdraw heavily on crystallized intelligence. That same individual, however, may bemarkedly impaired if the test requires quick thinking or a novel approach—both earmarks of fluid intelligence.
THE BUILDING BLO CKS OF INTELLIGENCE
Let’s pause to take stock. We’ve now seen that IQ scores are reliable predictors of manyimportant life outcomes; critically, the outcomes most closely linked to IQ—success inschool, for example, or success in complex jobs—are exactly the sorts of things thatshould be correlated with IQ if the IQ test is measuring what it’s intended to measure:intelligence.
fluid intelligence The ability to dealwith new and unusual problems.
crystallized intelligence Acquiredknowledge, including the person’srepertoire of verbal knowledge andcognitive skills.

PThe Building Blocks of IntelligenceO 433
These points prompted us to take a closer look at the IQ scores, and that’s what ledus to separate general intelligence (g) from more specialized forms of mental ability. Butcan we take our analysis further? What is it, inside a person, that gives them more g, orless? Do smart people have certain skills that the rest of us don’t have? Do smart peo-ple have bigger brains, or brains with a different structure? Let’s look at the evidencerelevant to these points.
Mental SpeedIntelligence tests require complex mental processes: The test taker has to detect compli-cated patterns, work her way through multiple-step plans, and so on. Each of theseprocesses takes some time, and this invites the proposal that the people we considerintelligent may just be those who are especially fast in these processes. This speedwould allow them to perform intellectual tasks more quickly; it also would give themtime for more steps in comparison with those of us who aren’t so quick.
One version of this hypothesis proposes that high-IQ people are faster in all mentalsteps, no matter what the steps involve (Eysenck, 1986; Nettelbeck, 2003; Vernon,1987). A related hypothesis proposes that high-IQ people are faster not in all mentalprocesses, but in just those needed for key mental operations such as memory retrieval(E. Hunt, 1976, 1985b). In either case, what could be the basis for this speed? Onepossibility is a greater degree of myelination of the neurons in the brains of high-IQpeople (E. Miller, 1994; bear in mind that it’s the myelin wrappers around axons thatallow fast transmission of the neural impulse; axons without these wrappers transmitthe action potential much more slowly; for details, see Chapter 3). Alternatively, high-IQ people may have a greater availability of metabolic “fuel” for the neurons (Rae,Digney, McEwan, & Bates, 2003). But, no matter what the neural mechanism might be,what is the evidence linking intelligence scores to measures of speed?
A number of studies have measured simple reaction time, in which the participantmerely responds as quickly as he can when a stimulus appears. Others have measuredchoice reaction time, in which the participant must again respond as quickly aspossible but now has to choose among several responses, depending on the stimuluspresented. In such tasks, reaction times are in fact correlated with intelligence scores(note, though, that the correlation is negative, and that lower times—indicating greaterspeed—are correlated with higher IQ; see, for example, Jensen, 1987).
Other studies have focused on measures of inspection time—the time someoneneeds to make a simple discrimination between two stimuli (which of two lines islonger, or which of two tones is higher). These measures correlate around ".50 withintelligence scores (see, for example, T. Bates & Shieles, 2003; Dantiir, Roberts, Schulze,& Wilhelm, 2005; Deary & Derr, 2005; Grudnik & Kranzler, 2001; Lohman, 2000;Petrill, Luo, Thompson, & Detterman, 2001; again, the correlation is negative becauselower response times go with higher scores on intelligence tests).
The suggestion, then, is that intelligent people may literally have brains that operatemore swiftly and more efficiently than the brains of less intelligent people. This idea findsfurther support in a classic study that examined the relationship between brain activityand someone’s ability to perform well on the Raven’s Matrices, often used as a measure ofg (see Figure 11.4). PET scans showed robust negative correlations between scores on theRaven’s test and glucose metabolism in many areas distributed around the cortex (Haieret al., 1988). In other words, the data showed less energy consumption by the brains ofpeople with higher IQs. This is certainly consistent with the idea that high g is somehowthe product of more efficient brain function—as if smarter people were simultaneouslygetting more “horsepower” as well as better “fuel economy” out of their mental engine!
simple reaction time A measure-ment of how quickly someone canrespond to a stimulus.
choice reaction time A measure ofthe speed of mental processing thattakes place when someone mustchoose between several responses,depending on which stimulus ispresented.
inspection time The time someoneneeds to make a simple discriminationbetween two stimuli.

434 chapter 11 PINTELLIGENCEO
Working Memory and AttentionMental speed is likely to be one contributor to intelligence, but there are other elements aswell—including a central role for working memory capacity. To understand the point here,bear in mind that many mental tasks involve multiple bits of information, and you needto keep track of them as you proceed. In addition, many tasks involve multiple steps, andthey demand that you shift your focus from one moment to the next—thinking aboutyour overall goal for a second, to figure out what to do next; then focusing on that nextstep, to deal with its specific demands; then focusing once again on your goal, to choosethe next step; and so on .
On this basis, perhaps the people we call “intelligent” are those who have particu-larly good working memories, so that they can hold onto the information they need forcomplex tasks. They may also have especially good control of their attention—sothey’re able to coordinate their goals and priorities in an appropriate way, first byfocusing here and then there, without getting lured off track by distraction.
To test this broad proposal, researchers have relied on measures that assesssomeone’s working memory capacity (WMC; e.g., Engle, Tuholski, Laughlin, &Conway, 1999; also see Chapter 8). There are several varieties of these measures; but inone common procedure, the participant is asked to read aloud a brief series ofsentences, such as
Due to his gross inadequacies, his position as director was terminated abruptly.It is possible, of course, that life did not arise on the Earth at all.
Immediately after reading the sentences, the participant is asked to recall thefinal word in each one—in this case, abruptly and all. Participants are tested in thisway with pairs of sentences (as in our example) and also with larger groups ofsentences—as many as 6 or 7. The aim, of course, is to find each participant’s limit:What’s the largest group of sentences for which the participant can do this read-and-recall task?
This seemingly peculiar task provides a good measure of WMC because it involvesstoring some material (the final words of sentences) for later use in the recall test, whilethe person is simultaneously thinking about other material (the full sentences, whichhave to be read out loud). This juggling of processes, as we move from one part of thetask to the next, is exactly how we use working memory and attention in everyday life.Thus, performance on this test is likely to reflect how efficiently a person’s workingmemory will operate in more natural settings. And if, as hypothesized, this efficiency isessential for intelligent performance, then these measurements of WMC should be cor-related with intelligence.
The data confirm this prediction. People with a larger WMC, measured as we’vedescribed, do have an advantage on many other tests. For example, people with a largerWMC do better on the verbal SAT, on tests of reasoning, on measures of reading com-prehension, and on tests specifically designed to measure g (A. Conway et al., 2005;Gathercole & Pickering, 2000a, 2000b; Daneman & Carpenter, 1980; Kane, Poole,Tuholski, & Engle, 2006; Lépine, Barrouillet, & Camos, 2005; Salthouse & Pink, 2008).
Executive ControlHow exactly does a larger WMC improve intellectual performance? A number ofinterrelated proposals have been offered; one proposal focuses on the construction andmaintenance of the task model needed to perform a task. This model provides the
working memory capacity (WMC)A measure of how efficiently a personcan manage multiple mental processesat once.
PThe Building Blocks of IntelligenceO 435
“mental agenda” that a person needs to carry out the task; the model is based on theperson’s understanding of the task’s goals, rules, and requirements as well as theirknowledge of the relevant facts. Once constructed, the model governs the person’smental steps as he works his way through the task.
Tasks differ in the complexity of the model they require. The model will have to bemore complicated (for example) if task performance involves either multiple goals ora sharp change in goals as certain cues come into view. Evidence suggests that theability to handle this complexity is strongly linked to measures of g—so that higher-gindividuals are able to maintain more complex task models, allowing them to out-perform lower-g people whenever such models are required (J. Duncan et al., 2008).
A different (but related) proposal is that measures of WMC are actually measures ofeach person’s executive control over her own thoughts. This term—which we first met inChapter 3—refers to the processes people use to launch mental actions, redirect theirattention, or shift their strategies. From this perspective, the link between intelligenceand WMC implies that smart people are literally in better control of their own thoughtsthan less intelligent people are.
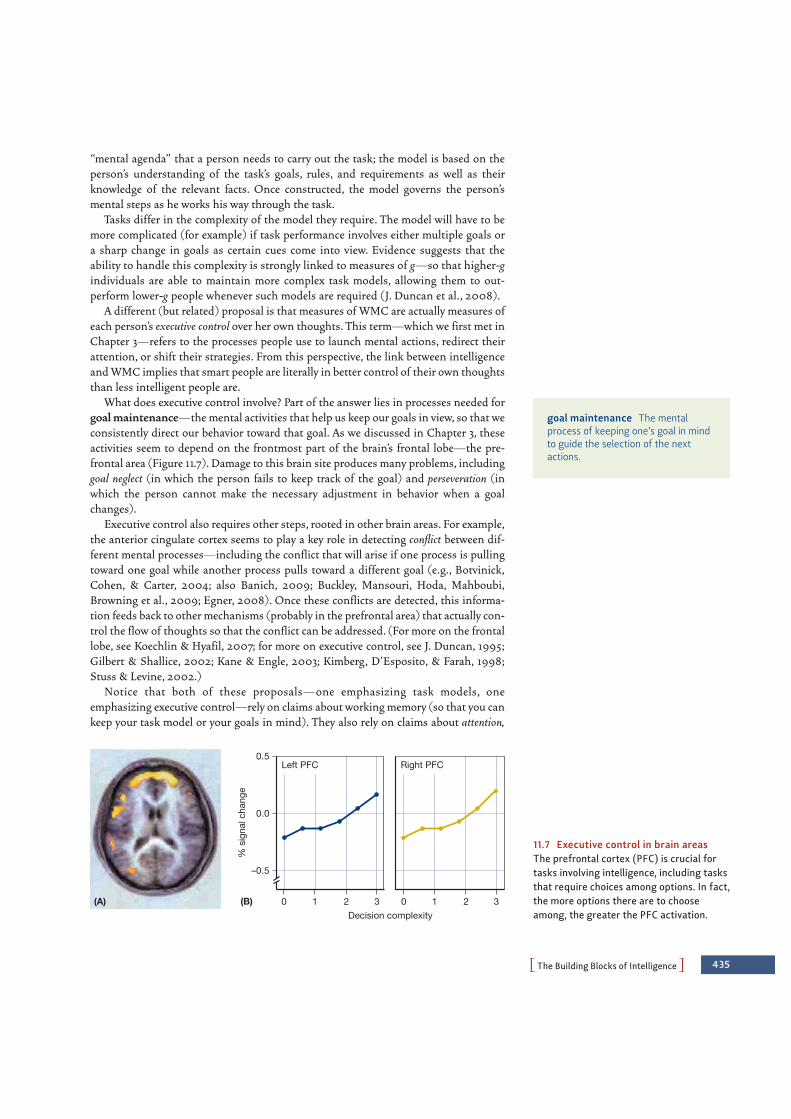
What does executive control involve? Part of the answer lies in processes needed forgoal maintenance—the mental activities that help us keep our goals in view, so that weconsistently direct our behavior toward that goal. As we discussed in Chapter 3, theseactivities seem to depend on the frontmost part of the brain’s frontal lobe—the pre-frontal area (Figure 11.7). Damage to this brain site produces many problems, includinggoal neglect (in which the person fails to keep track of the goal) and perseveration (inwhich the person cannot make the necessary adjustment in behavior when a goalchanges).
Executive control also requires other steps, rooted in other brain areas. For example,the anterior cingulate cortex seems to play a key role in detecting conflict between dif-ferent mental processes—including the conflict that will arise if one process is pullingtoward one goal while another process pulls toward a different goal (e.g., Botvinick,Cohen, & Carter, 2004; also Banich, 2009; Buckley, Mansouri, Hoda, Mahboubi,Browning et al., 2009; Egner, 2008). Once these conflicts are detected, this informa-tion feeds back to other mechanisms (probably in the prefrontal area) that actually con-trol the flow of thoughts so that the conflict can be addressed. (For more on the frontallobe, see Koechlin & Hyafil, 2007; for more on executive control, see J. Duncan, 1995;Gilbert & Shallice, 2002; Kane & Engle, 2003; Kimberg, D’Esposito, & Farah, 1998;Stuss & Levine, 2002.)
Notice that both of these proposals—one emphasizing task models, oneemphasizing executive control—rely on claims about working memory (so that you cankeep your task model or your goals in mind). They also rely on claims about attention,
(A) (B)
–0.5
0.0
0.5
0 1 2 3 0 1 2 3
% s
igna
l cha
nge
Decision complexity
Left PFC Right PFC
11.7 Executive control in brain areasThe prefrontal cortex (PFC) is crucial fortasks involving intelligence, including tasksthat require choices among options. In fact,the more options there are to chooseamong, the greater the PFC activation.
goal maintenance The mentalprocess of keeping one’s goal in mindto guide the selection of the nextactions.
436 chapter 11 PINTELLIGENCEO
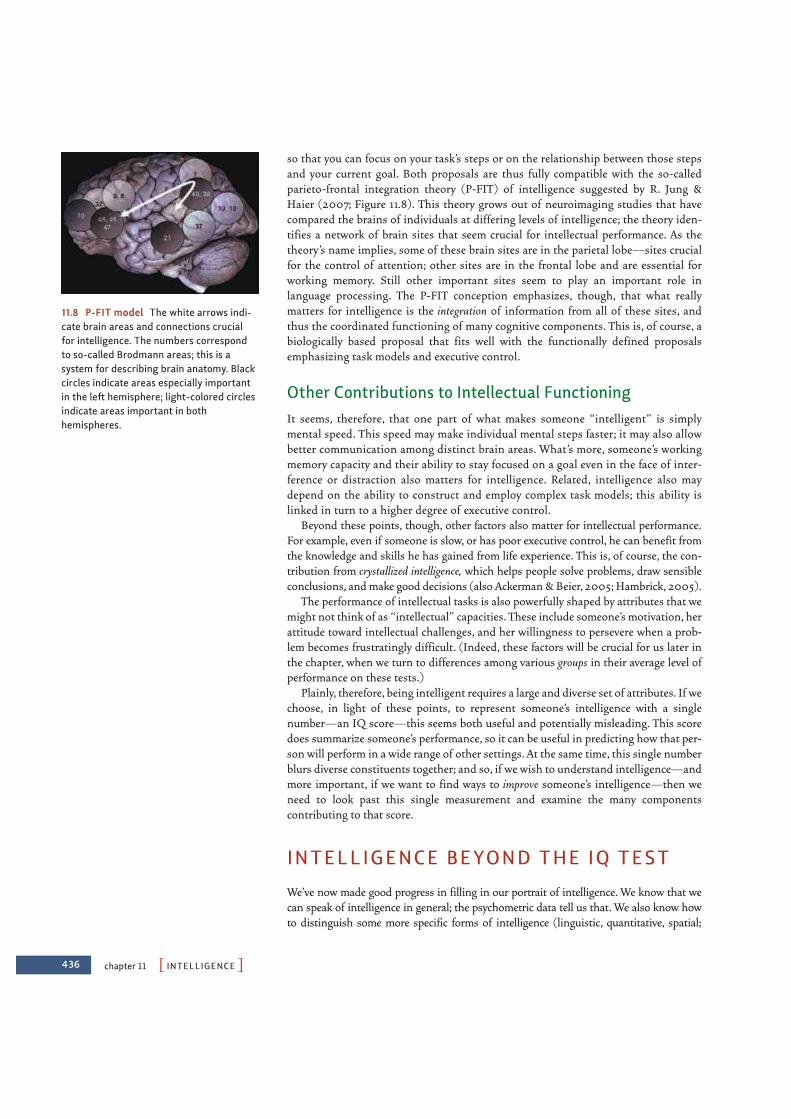
so that you can focus on your task’s steps or on the relationship between those stepsand your current goal. Both proposals are thus fully compatible with the so-calledparieto-frontal integration theory (P-FIT) of intelligence suggested by R. Jung &Haier (2007; Figure 11.8). This theory grows out of neuroimaging studies that havecompared the brains of individuals at differing levels of intelligence; the theory iden-tifies a network of brain sites that seem crucial for intellectual performance. As thetheory’s name implies, some of these brain sites are in the parietal lobe—sites crucialfor the control of attention; other sites are in the frontal lobe and are essential forworking memory. Still other important sites seem to play an important role inlanguage processing. The P-FIT conception emphasizes, though, that what reallymatters for intelligence is the integration of information from all of these sites, andthus the coordinated functioning of many cognitive components. This is, of course, abiologically based proposal that fits well with the functionally defined proposalsemphasizing task models and executive control.
Other Contributions to Intellectual FunctioningIt seems, therefore, that one part of what makes someone “intelligent” is simplymental speed. This speed may make individual mental steps faster; it may also allowbetter communication among distinct brain areas. What’s more, someone’s workingmemory capacity and their ability to stay focused on a goal even in the face of inter-ference or distraction also matters for intelligence. Related, intelligence also maydepend on the ability to construct and employ complex task models; this ability islinked in turn to a higher degree of executive control.
Beyond these points, though, other factors also matter for intellectual performance.For example, even if someone is slow, or has poor executive control, he can benefit fromthe knowledge and skills he has gained from life experience. This is, of course, the con-tribution from crystallized intelligence, which helps people solve problems, draw sensibleconclusions, and make good decisions (also Ackerman & Beier, 2005; Hambrick, 2005).
The performance of intellectual tasks is also powerfully shaped by attributes that wemight not think of as “intellectual” capacities. These include someone’s motivation, herattitude toward intellectual challenges, and her willingness to persevere when a prob-lem becomes frustratingly difficult. (Indeed, these factors will be crucial for us later inthe chapter, when we turn to differences among various groups in their average level ofperformance on these tests.)
Plainly, therefore, being intelligent requires a large and diverse set of attributes. If wechoose, in light of these points, to represent someone’s intelligence with a singlenumber—an IQ score—this seems both useful and potentially misleading. This scoredoes summarize someone’s performance, so it can be useful in predicting how that per-son will perform in a wide range of other settings. At the same time, this single numberblurs diverse constituents together; and so, if we wish to understand intelligence—andmore important, if we want to find ways to improve someone’s intelligence—then weneed to look past this single measurement and examine the many componentscontributing to that score.
INTELLIGENCE BEYOND THE IQ TEST
We’ve now made good progress in filling in our portrait of intelligence. We know that wecan speak of intelligence in general; the psychometric data tell us that. We also know howto distinguish some more specific forms of intelligence (linguistic, quantitative, spatial;
11.8 P-FIT model The white arrows indi-cate brain areas and connections crucialfor intelligence. The numbers correspondto so-called Brodmann areas; this is a system for describing brain anatomy. Blackcircles indicate areas especially importantin the left hemisphere; light-colored circlesindicate areas important in both hemispheres.

PIntelligence Beyond the IQ TestO 437
analytic intelligence The abilitytypically measured by intelligencetests and crucial for academic success.
practical intelligence The ability tosolve everyday problems throughskilled reasoning that relies on tacitknowledge.
11.9 Practical intelligence Bettors at a racetrack rely on sophisticated and complexstrategies in deciding which horses will win, but these strategies seem to depend on a formof intelligence separate from that which is assessed by the IQ test. Likewise, business exec-utives may depend more on “practical” intelligence than on “analytic” intelligence.
fluid, crystallized). And, finally, we know some of the elements that give someone a higheror lower g—namely, mental speed, working memory capacity, and executive control.
We might still ask, though, whether there are aspects of intelligence not included inthis portrait—aspects that are somehow separate from the capacities we measure withour conventional intelligence tests. For example, you probably know people who are“street-smart” or “savvy,” but not “school-smart.” Such people may lack the sort of ana-lytic skill required for strong performance in the classroom, but they’re sophisticated andastute in dealing with the practical world. Likewise, what about social competence—theability to persuade others and to judge their moods and desires? Shrewd salespeoplehave this ability, as do successful politicians, quite independent of whether they havehigh or low IQ scores.
A number of studies have explored these other nonacademic forms of intelligence.For example, one study focused on gamblers who had enormous experience in bettingon horse races and asked them to predict the outcomes and payoffs in several upcom-ing races. This is a tricky mental task that involves highly complex reasoning. Factorslike track records, jockeys, and track conditions all have to be remembered and weighedagainst one another. On the face of it, the ability to perform such mental calculationsseems to be part of what intelligence tests should measure. But the results provedotherwise; the gamblers’ success turned out to be completely unrelated to their IQs(Ceci & Liker, 1986). These findings and others have persuaded researchers that weneed to broaden our conception of intelligence and consider forms of intelligence thataren’t measured by the IQ test.
Practical IntelligenceOne prominent investigator, Robert Sternberg, has argued that we need to distinguishseveral types of intelligence. One type, analytic intelligence, is measured by standardintelligence tests. A different type is practical intelligence, needed for skilled reasoningin the day-to-day world (Sternberg, 1985; also see Henry, Sternberg, & Grigorenko,2005; Sternberg & Kaufman, 1998; Sternberg, R. Wagner, Williams, & Horvath, 1995;R. Wagner, 2000; Figure 11.9).
In one of Sternberg’s studies, business executives read descriptions of scenariosinvolving problems similar to those they faced in their professional work. The

438 chapter 11 PINTELLIGENCEO
executives also considered various solutions for each problem and rated them on a scalefrom 1 (poor solution) to 7 (excellent solution). These ratings were then used to assesshow much tacit knowledge each of the executives had—that is, practical know-howgleaned from their everyday experience. The data showed that this measure of tacitknowledge was predictive of job performance (and so was correlated with on-the-jobperformance ratings as well as salary). Crucially, though, measures of tacit knowledgeweren’t correlated with IQ—and so are plainly assessing something separate from thesorts of “intelligence” relevant to the IQ test (Sternberg & Wagner, 1993; R. Wagner,1987; R. Wagner & Sternberg, 1987).
Other research, however, has challenged the claim that practical intelligence isindependent of analytic intelligence. In one study, for example, measures of practical intel-ligence were correlated with measures of g (Cianciolo et al., 2006; also see N. Brody, 2003;Gottfredson, 2003a, 2003b; Sternberg, 2003). Even so, many researchers believe that prac-tical intelligence is different enough from analytic intelligence to justify separating them inour overall theorizing about people’s different levels and types of intellectual ability.
Emotional IntelligenceA different effort toward broadening the concept of intelligence involves claims aboutemotional intelligence—the ability to understand one’s own emotions and others’,and also the ability to control one’s emotions when appropriate. The term emotionalintelligence might seem an oxymoron, based on the widely held view that emotions oftenundermine our ability to think clearly and so work against our ability to reason intelli-gently. Many psychologists, however, reject this claim. They argue that emotion plays animportant role in guiding our problem solving and decision making (see, for example,Bechara, H. Damasio, & A. Damasio, 2000; A. Damasio, 1994); emotion also plays arole in guiding our attention and shaping what we remember (Reisberg & Hertel,2004). In these ways, emotion and cognition interact and enrich each other in impor-tant ways. (For more on emotion, see Chapter 12.)
One theory suggests that emotional intelligence actually has four parts. First, there’san ability to perceive emotions accurately—so that, for example, you can tell when afriend is tense or when someone is becoming angry. Second, there’s an ability to useemotions to facilitate thinking and reasoning, including a capacity to rely on your “gutfeelings” in guiding your own decisions. Third, there’s an ability to understand emo-tions, including the use of language to describe emotions, so that you’re alert to how afriend will act when she’s sad or to how fear can alter someone’s perspective; alsoincluded here is the ability to talk about emotions—to convey to others how you’re feel-ing and to understand what they tell you about their feelings. Finally, there’s an abilityto manage emotions in oneself and others; this includes the ability to abide by your cul-ture’s rules for “displaying” emotions as well as the ability to regulate your own emo-tions (Mayer, Roberts, & Barsade, 2008a; Mayer, Salovey, & Caruso, 2008b; Salovey &Mayer, 1990; also Brackett, Rivers, Shiffman, Lerner, & Salovey, 2006; for more on“emotion management,” see Chapter 12).
Researchers have developed various measures of emotional intelligence, includingthe Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT; Bracket & Mayer,2003; Mayer, Salovey, Caruso, & Sitarenios, 2003; Figure 11.10). This measure appearsto have predictive validity so that, for example, people who score higher on theMSCEIT seem to be more successful in social settings. They have fewer conflicts withtheir peers, are judged to create a more positive atmosphere in the workplace, are moretolerant of stress, and are judged to have more leadership potential (Lopes, Salovey,Côté, & Beers, 2005; Grewal & Salovey, 2005). Likewise, college students with higher
11.10 The Mayer-Salovey-CarusoEmotional Intelligence Test Shown hereare two items similar to those used on theMSCEIT.
tacit knowledge Practical “how-to”knowledge accumulated from every-day experience.
emotional intelligence The abilityto understand your own and others’emotions and to control your emotionsappropriately.

PIntelligence Beyond the IQ TestO 439
MSCEIT scores are rated by their friends as more caring and more supportive. Theyare also less likely to experience conflict with their peers (Brackett & Mayer, 2003;Mayer et al., 2008a).
The idea of emotional intelligence has received much attention in the media andpopular literature; as a result, various claims have been offered in the media that are notsupported by evidence. (For a glimpse of the relationship between the science and themythology here, and some concerns about the idea of emotional intelligence, seeMatthews, Zeidner, & Roberts, 2003, 2005.) Still, emotional intelligence does seem tomatter for many aspects of everyday functioning, it can be measured, and it is one moreway that people differ from one another in their broad intellectual competence.
The Theory of Multiple IntelligencesIt seems that our measures of g—so-called general intelligence—may not provide ascomplete a measurement as we thought. The capacities measured by g are surelyimportant, but so are other aspects of intelligence—including practical intelligence,emotional intelligence, and, according to some authors, social intelligence (see, for exam-ple, Kihlstrom & Cantor, 2000). Other authors would make this list even longer: In histheory of multiple intelligences, Howard Gardner argued for several further types ofintelligence (Gardner, 1983, 1998): Three of these are incorporated in most standardintelligence tests: linguistic intelligence, logical-mathematical intelligence, and spatialintelligence. But Gardner also argued that we should acknowledge musical intelligence,bodily-kinesthetic intelligence (the ability to learn and create complex patterns of move-ment), interpersonal intelligence (the ability to understand other people), intrapersonalintelligence (the ability to understand ourselves), and naturalistic intelligence (the abilityto understand patterns in nature).
Gardner based his argument on several lines of evidence, including studies ofpatients with brain lesions that devastate some abilities while sparing others. Thus,certain lesions will make a person unable to recognize drawings (a disruption of spatialintelligence), while others will make him unable to perform a sequence of movements(bodily-kinesthetic intelligence) or will devastate musical ability (musical intelligence).Gardner concluded from these cases that each of these capacities is served by a separatepart of the brain (and so is disrupted when that part of the brain is damaged), andtherefore each is distinct from the others.
Another argument for Gardner’s theory comes from the study of people withso-called savant syndrome. These individuals have a single extraordinary talent,even though they’re otherwise developmentally disabled (either autistic or mentallyretarded) to a profound degree. Some display unusual artistic talent. Others are “cal-endar calculators,” able to answer immediately (and correctly!) when askedquestions such as “What day of the week was March 17 in the year 1682?”. Still oth-ers have unusual mechanical talents or remarkable musical skills—for example, theycan effortlessly memorize lengthy and complex musical works (A. Hill, 1978; L. K.Miller, 1999).
Gardner’s claims have been controversial, partly because some of the data he cites areopen to other interpretations (see, for example, Cowan & Carney, 2006; L. K. Miller,1999; Nettelbeck & Young, 1996; Thioux, Stark, Klaiman, & Schultz, 2006). In addition,evidence indicates that several of the forms of “intelligence” Gardner describes are inter-correlated—and so if someone has what Gardner calls linguistic intelligence, they’re alsolikely to have logical-mathematical, spatial, interpersonal, and naturalistic intelligence.This obviously challenges Gardner’s assertion that these are separate and independentcapacities (Visser, Ashton & Vernon, 2006).
multiple intelligences In HowardGardner’s theory, the six essential, independent mental capacities (lin-guistic, logical-mathematical, spatial,musical, bodily-kinesthetic, and per-sonal intelligence).
savant syndrome A syndrome in adevelopmentally disabled person whohas some remarkable talent that con-trasts with his low level of generalintelligence.

440 chapter 11 PINTELLIGENCEO
There’s also room for disagreement about Gardner’s basic conceptualization. Withoutquestion, some individuals—whether savants or otherwise—have special talents; andthese talents are impressive (Figure 11.11). But is it appropriate to think of these talents asforms of intelligence? Or might we be better served by a distinction between intelligenceand talent? It does seem peculiar to use the same term, intelligence, to describe both thecapacity that Albert Einstein displayed in developing his theories and the capacity thatPeyton Manning displays on the football field. Similarly, we might celebrate the vocal tal-ent of Beyoncé Knowles; but is hers the same type of talent—and therefore sensiblydescribed by the same term, intelligence—that a skilled debater relies on in rapidly think-ing through the implications of an argument?
Whatever the ultimate verdict on Gardner’s theory, he has undoubtedly done us a valu-able service by drawing our attention to a set of abilities that are often ignored and under-valued. Gardner is surely correct in noting that we tend to focus too much on the skills andcapacities that help people succeed in school, and do too little to celebrate the talents dis-played by an artist at her canvas, a skilled dancer in the ballet, or an empathetic clergymanin a hospital room. Whether these other abilities should be counted as forms of intelli-gence or not, they’re surely talents to be highly esteemed and, as much as possible, nur-tured and developed.
The Cultural Context of IntelligenceYet another—and perhaps deeper—challenge to our intelligence tests, and a powerfulreason to think beyond the IQ scores, comes from a different source: the question ofwhether our tests truly measure intelligence, or whether they merely measure what’scalled intelligence in our culture.
Different cultures certainly have different ideas about what intelligence is. For exam-ple, some parts of the intelligence test put a premium on quick and decisive responses,but not all cultures share our Western preoccupation with speed. Indians (of southernAsia) and Native Americans, for example, place a higher value on being deliberate; ineffect, they’d rather be right than quick. They also prefer to qualify, or to say “I don’tknow” or “I’m not sure,” unless they’re absolutely certain of their answer. Such delib-eration and hedging would hurt their test scores on many intelligence tests because it’soften a good idea to guess whenever you’re not sure about the answer (Sinha, 1983;Triandis, 1989). Similarly, Taiwanese Chinese place a high priority on how they relateto others; this will, in some circumstances, lead them not to show their intelligence,thus undermining our standardized assessment (Yang & Sternberg, 1997; also Nisbett,2003; for other cultural differences in how intelligence is defined, see Serpell, 2000;Sternberg, 2004).
These cultural differences guarantee that an intelligence test that seems appropriatein one cultural setting may be inappropriate in other cultural settings (Figure 11.12).Moreover, the specific procedure we need for measuring intelligence also depends onthe cultural setting. This is because people in many countries fail to solve problems thatare presented abstractly or that lack a familiar context, but they do perfectly well withidentical problems presented in more meaningful ways. For example, consider theresponse of an unschooled Russian peasant who was asked, “From Shakhimardan toVuadil it takes three hours on foot, while to Fergana it is six hours. How much time doesit take to go on foot from Vuadil to Fergana?” The reply was “No, it’s six hours fromVuadil to Shakhimardan. You’re wrong. . . . It’s far and you wouldn’t get there in threehours” (Luria, 1976, p. 229). If this had been a question on a standard intelligence test,the peasant would have scored poorly—not because he was unintelligent, but becausehe did not regard the question as a test of arithmetical reasoning. It turned out that he
11.11 The original “Rain Man” Kim Peek(1951–2009) was a remarkable man withremarkable talents. He could read anentire book in an hour (scanning two pagesat a time) and remembered everythinghe’d read; by one estimate, he memorizedover 12,000 books. But, with an IQ of 73, hewas retarded; Peek’s story was told (in fic-tionalized form) in the 1988 film Rain Man.
11.12 Intelligence in context
“You can’t build a hut, you don’t know howto find edible roots and you know nothing
about predicting the weather. In other words,you do terribly on our I.Q. test.”
PThe Roots of IntelligenceO 441
was quite able to perform the relevant calculation but could not accept the form inwhich the question was presented.
In light of these concerns, we might well ask whether it’s possible to measure intel-ligence in a way that’s fair to all cultures and biased against none. The Raven’sProgressive Matrices (Figure 11.4) are often claimed to be fair to all groups because thetest is nonverbal and doesn’t rely on any sort of specific prior knowledge. But the veryidea of organizing items in rows and columns—an idea that’s essential for this test—isunfamiliar in some settings, and this puts test takers in those settings at a disadvantagewith this form of testing.
To put this worry somewhat differently, we could (if we wished) use a standard intel-ligence test to assess people living in, say, rural Zambia, and the test results probablywould allow us to predict whether the Zambians will do well in Western schools or in aWestern-style workplace. But this form of testing would tell us nothing about whetherthese Zambians have the intellectual skills they need to flourish in their own culturalsetting. Just as bad, our test would probably give us an absurd understatement of theZambians’ intellectual competence because our test is simply in the wrong form toreveal that competence.
Against this backdrop, it’s important to emphasize that some mental capacities canbe found in all cultures—including (as just one example) the core knowledge needed tounderstand some aspects of mathematics (see, for example, Dehaene, Izard, Pica, &Spelke, 2006). But it’s also clear that cultures differ not only in the skills they need andvalue but also in how they respond to our Westernized test procedures. As a result, weneed to be extremely careful in how we interpret or use our measures of intelligence.Intelligence tests do capture important aspects of intellectual functioning, but theydon’t capture all aspects or all abilities, and the meaning and utility of the tests has tobe understood in the appropriate cultural context. (For further discussion, seeGreenfield, 1997; Serpell, 2000; Sternberg, 2004.)
THE RO OTS OF INTELLIGENCE
We are, it seems, moving toward a mixed assessment of intelligence tests. On the one side,these tests do measure something important; but on the other side, there are important tal-ents and skills not tapped by these tests. Even so, the fact remains that these tests are widelyused—by educators deciding which students to admit to a program and by employersdeciding which applicants to hire. These are important matters, because these decisionsobviously can have large-scale, long-term consequences for all involved. It’s not surprising,therefore, that the test scores have been the focus of fierce debate regarding whether thetests are valid and fair. A large part of this debate has focused on why someone scores theway they do—and more specifically, the role of genetics in shaping intelligence.
The Politics of IQ TestingIntelligence testing has been mired in political controversy from the very beginning.Recall that Binet intended his test as a means of identifying schoolchildren who wouldbenefit from extra training. In the early years of the 20th century, however, somepeople—scientists and politicians—put the test to a different use. They noted the fact(still true today) that there was a correlation between IQ and socioeconomic status(SES): People with lower IQ scores usually end up with lower-paid, lower-status jobs;they’re also more likely to end up as criminals than are people with higher IQs. Thepoliticians therefore asked, why should we try to educate these low-IQ individuals? If

442 chapter 11 PINTELLIGENCEO
we know from the start that those with low intelligence scores are unlikely ever to getfar in life, then why waste educational resources on them?
In sharp contrast, advocates for the disadvantaged took a different view. To beginwith, they often disparaged the tests themselves, arguing that bias built into the testsfavored some groups over others. In addition, they argued that the connection betweenIQ and SES was far from inevitable. Good education, they suggested, can lift the statusof almost anyone—and perhaps lift their IQ scores as well. Therefore, spendingeducational resources on the poor was an important priority, especially since it mightbe the poor who need and benefit from these resources the most. (For reviews of thishistory, see S. J. Gould, 1981; Kamin, 1974.)
These contrasting views obviously lead to different prescriptions for social policy,and for many years, those who viewed low scorers as a waste of resources dominated thedebate. An example is the rationale behind the U.S. immigration policy between the twoWorld Wars. The immigration act of 1924 (the National Origins Act) set rigid quotas tominimize the influx of what were thought to be biologically “weaker stocks”—specifically, immigrants from southern and eastern Europe, Asia, and Africa. To “prove”the genetic intellectual inferiority of these immigrants, a congressional committeepointed to the scores by members of these groups on the U.S. Army’s intelligence test;the scores were indeed substantially below those attained by Americans of northernEuropean ancestry (Figure 11.13).
As it turns out, we now know that these differences among groups, observed in theearly 20th century, were due to the simple fact that the immigrants had been in theUnited States for only a short time. Because of their recent arrival, the immigrantslacked fluency in English and had little knowledge of certain cultural facts importantfor doing well on the tests. It’s no surprise, then, that their test scores were low. Afterliving in the United States for a while, the immigrants’ U.S. cultural knowledge andEnglish skills improved—and their scores became indistinguishable from those ofnative-born Americans. This observation plainly undermined the hypothesis of ahereditary difference in intelligence between, say, northern and eastern Europeans,but the proponents of immigration quotas didn’t analyze the results so closely. Theyhad their own reasons for restricting immigration, such as fears of competition fromcheap labor. The theory that the excluded groups were innately inferior provided aconvenient justification for their policies (Bronfenbrenner, McClelland, Wethington,Moen, & Ceci, 1996; Kamin, 1974; W. Williams & Ceci, 1997).
A more recent example of how intelligence testing can become intertwined withpolitical and social debate grew out of a highly controversial book—The Bell Curve, byRichard J. Herrnstein and Charles Murray (1994). This book, and the debate it set off,showcased the differences among racial groups in their test scores: Whites in theUnited States (i.e., Americans of European ancestry) had scores that averaged roughly10 points higher than the average score for blacks (Americans of African ancestry).Herrnstein and Murray argued that these differences had important policy implica-tions, and urged (among other things) reevaluation of programs that in their viewencouraged low-IQ people to have more babies.
Herrnstein and Murray’s claims were criticized on many counts (e.g., Devlin et al.,1997; S. Fraser, 1995; R. Jacoby & Glauberman, 1995; R. Lynn, 1999; Montagu, 1999;Neisser et al., 1996; and many more). There has been considerable debate, for example,about their interpretation of the test scores as well as about whether “race,” a key con-cept in their argument, is a meaningful biological category. We’ll return to these pointslater in the chapter; for now, it’s enough to note that these questions have profoundpolitical importance, so it’s imperative that we ensure policy debates are informed bygood science.
11.13 Anti-immigration sentiment in theUnited States “Immigration Restriction.Prop Wanted.” This cartoon, whichappeared in the January 23, 1903, issue ofthe Philadelphia Inquirer, called for morerestrictive immigration laws.

PThe Roots of IntelligenceO 443
The Problems with “Nature vs. Nurture”Plainly, people differ from one another in their intelligence and their talents. But whatcauses these differences? This question is often framed in terms of two alternatives—the notion that what matters is genetics and heredity, or the notion that what mattersis environment (and so learning and experience). The options, in other words, areboiled down to the dichotomy of “nature vs. nurture.”
As we discussed in Chapter 2, however, this framing of the issue makes no sense,because the influences of genes and environment are inevitably intertwined.Specifically, someone’s genetic heritage merely establishes his genotype; the traits heends up with (his phenotype) depend on how the process of development, guided by thatgenotype, unfolds. That developmental process is, of course, heavily shaped by geneticfactors. But it is also powerfully influenced by the person’s environment—what nutri-ents he’s exposed to, or what toxins; and, crucially, what experiences he has. In short:There’s no such thing as genetic influences independent of environment.
Likewise, how someone benefits from experience depends on her capacity to per-ceive, to understand, and to form memories. And these capacities depend on thebiological equipment that each person has—her eyes, for example, and her brain. Thisbiological equipment, in turn, is heavily shaped by the person’s genotype. As a result,there’s no way for experience to influence us independent of genetics.
Even with these points acknowledged, it’s clear that some traits are more directlyshaped by genetic influences than others. For example, the color of someone’s eyes(assuming he’s not wearing tinted contact lenses) depends almost entirely on thegenetic pattern he has inherited. Conversely, the language that someone speaks(French or Italian, Walbiri or Bantu) depends on where (and with whom) she grows up.As it turns out, to the fact that someone can learn language at all is heavily guided bygenetics (see Chapter 10). But the choice of language depends on the environment, noton genes.
Where does intelligence fall in this range from heavily influenced by genes (like eyecolor is) to less influenced (like choice of language)? We took some steps towardanswering this question in Chapter 2—and, as we saw there, the answer is complicated:In some circumstances, genetic factors play a large role; in others, genes count for less.And, as we’ll see, the role for genetic influences depends on whether we’re asking whyvarious individuals perform differently on intelligence tests, or whether we’re askingwhy various groups (racial groups in particular) perform differently on these tests. Let’sstart by asking why various individuals seem to have different levels of intelligence.
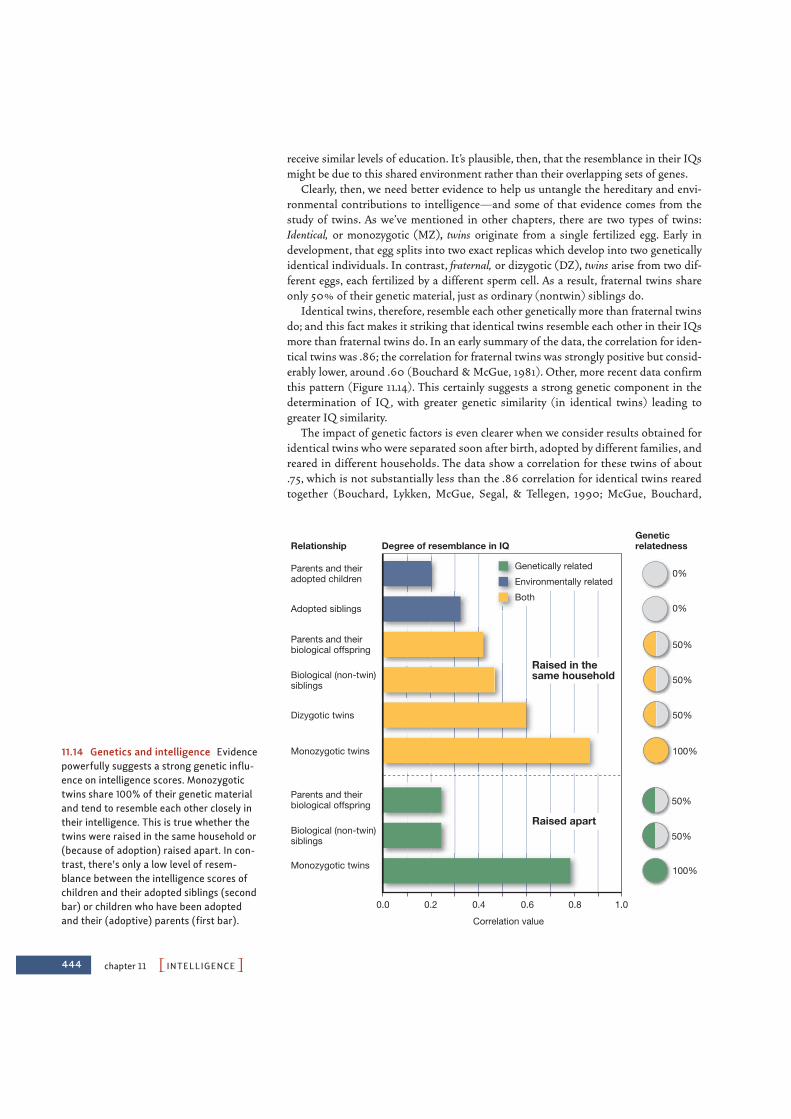
Genetics and Individual IQAs we first saw in Chapter 2, there are several ways to evaluate how strongly a given trait(eye color, height, career choice) is influenced by genetics. One of our main methods,though, begins with an examination of relatives, asking in particular whether peoplewho resemble each other genetically also resemble each other in terms of the target trait.For measures of intelligence, it turns out that the correlation between the IQs of childrenand the IQs of their biological parents is about !.40; the correlation between the IQsof biological siblings is roughly the same. These correlations indicate a relatively strongresemblance, but these correlations, on their own, are ambiguous. On the one side, bio-logically related family members resemble each other genetically, and this might be thesource of the resemblance in IQ scores. But on the other side, the members of a familyusually also resemble each other in their experiences: They live in similar social andfinancial circumstances; they all receive similar levels of health care and are likely to
444 chapter 11 PINTELLIGENCEO
receive similar levels of education. It’s plausible, then, that the resemblance in their IQsmight be due to this shared environment rather than their overlapping sets of genes.
Clearly, then, we need better evidence to help us untangle the hereditary and envi-ronmental contributions to intelligence—and some of that evidence comes from thestudy of twins. As we’ve mentioned in other chapters, there are two types of twins:Identical, or monozygotic (MZ), twins originate from a single fertilized egg. Early indevelopment, that egg splits into two exact replicas which develop into two geneticallyidentical individuals. In contrast, fraternal, or dizygotic (DZ), twins arise from two dif-ferent eggs, each fertilized by a different sperm cell. As a result, fraternal twins shareonly 50% of their genetic material, just as ordinary (nontwin) siblings do.
Identical twins, therefore, resemble each other genetically more than fraternal twinsdo; and this fact makes it striking that identical twins resemble each other in their IQsmore than fraternal twins do. In an early summary of the data, the correlation for iden-tical twins was .86; the correlation for fraternal twins was strongly positive but consid-erably lower, around .60 (Bouchard & McGue, 1981). Other, more recent data confirmthis pattern (Figure 11.14). This certainly suggests a strong genetic component in thedetermination of IQ , with greater genetic similarity (in identical twins) leading togreater IQ similarity.
The impact of genetic factors is even clearer when we consider results obtained foridentical twins who were separated soon after birth, adopted by different families, andreared in different households. The data show a correlation for these twins of about.75, which is not substantially less than the .86 correlation for identical twins rearedtogether (Bouchard, Lykken, McGue, Segal, & Tellegen, 1990; McGue, Bouchard,
Genetically related
Environmentally related
Both
Monozygotic twins
Raised apart
Raised in thesame household
Biological (non-twin)siblings
Parents and theirbiological offspring
Biological (non-twin)siblings
Parents and theirbiological offspring
Adopted siblings
Parents and theiradopted children
Relationship
0%
0%
100%
50%
50%
50%
50%
50%
100%
Geneticrelatedness
Monozygotic twins
Dizygotic twins
0.2
Correlation value
0.4
Degree of resemblance in IQ
0.6 0.8 1.00.0
11.14 Genetics and intelligence Evidencepowerfully suggests a strong genetic influ-ence on intelligence scores. Monozygotictwins share 100% of their genetic materialand tend to resemble each other closely intheir intelligence. This is true whether thetwins were raised in the same household or(because of adoption) raised apart. In con-trast, there’s only a low level of resem-blance between the intelligence scores ofchildren and their adopted siblings (secondbar) or children who have been adoptedand their (adoptive) parents (first bar).
PThe Roots of IntelligenceO 445
Iacono, & Lykken, 1993; Plomin & Spinath, 2004). It appears,then, that identical genotypes lead to highly similar IQs evenwhen the individuals grow up in different environments.
Similar conclusions derive from a study that drew its data fromthe Colorado Adoption Project (CAP). The CAP has been tracking245 adopted children for roughly 20 years, testing them periodi-cally on several different measures (Plomin, Fulker, Corley, &DeFries, 1997). Thus, we have intelligence scores for the childrenthemselves at various ages; we also have scores for the children’sbiological parents, who each share 50% of their genetic materialwith the children but who are not the adults who raised the chil-dren. Third, we have scores for the adoptive parents—the adultswho did raise the children and shared (and largely created) theenvironment in which the children grew up.
These scores allow us to compute the resemblance between thechildren and their biological parents, as an indicator of how much shared genes matter.The scores also allow us to compute the resemblance between the children and theiradoptive parents, as an indicator of how much a shared environment matters. The dataindicate a much greater resemblance in the first comparison—children and their bio-logical parents—even though we’re comparing individuals who (though biologicallyrelated) have never even met. This indicates a powerful role for genetic factors in shap-ing intellectual ability (Figure 11.15).
What’s especially striking about the CAP data, though, is that the resemblancebetween children and their biological parents increases as the years go by. When thechildren are 4 years old, for example, there’s roughly a .10 correlation between the chil-dren’s intelligence scores and their biological parents’ scores. By the time the childrenare 12, this correlation is almost .20. By the time the children are 16 years old, this cor-relation is almost .40—despite the fact that, by that point, it has been more than adozen years since the children and their biological parents have seen each other!
How should we think about this result? One possibility is that what’s inherited viathe genes is a learning capacity—and so, in early childhood, a child’s potential mightresemble that of her biological parents, but the potential hasn’t yet grown into skillswe can measure. To detect the resemblance, we must wait until the child has hadsome experience in the world—and thus opportunity to use her learning capacity andto gain from the potential she inherited. Only then, when the potential has bornefruit, can we detect the full resemblance between parents and their biological off-spring (cf. Plomin & DeFries, 1985; Plomin & Spinath, 2004; Figure 11.16).
Environment and Individual IQUndeniably, genetic influences play a powerful role in shaping someone’s intellectualcapacities. Indeed, researchers have begun to explore exactly how these genetic influ-ences unfold—including an effort to specify which genes, on which chromosomes, arethe ones that shape intelligence. (For glimpses of the modest progress so far, seePosthuma & deGeus, 2006; Zimmer, 2008.)
As we’ve repeatedly noted, though, genetic effects always unfold within an environ-mental context. So—inevitably—environmental factors also shape the development ofour intellect. Evidence for this point comes from many sources; and thus, as we’ll see,the IQ score someone ends up with depends on both her genes and the surroundingsin which she grew up.
BiologicalAdoptive
0
0.1
0.2
0.3
0.4
–0.12 4 6 8 10 12 14 16 180
Ave
rage
par
ent-
offs
prin
g co
rrel
atio
n
Age of child
11.15 Colorado Adoption Project Theintelligence scores for children in this studyresembled those of their biological parents,and not those of their adopted parents.Notice that the correlation between chil-dren and their biological parents increasedas the child grew, even though the childrenhad no contact with their biologicalparents.
11.16 Genetic pattern potential Thanksto genetic influences, there will eventuallybe a close resemblance between themother and her offspring. However, thatresemblance will be visible only after thepuppy has had a chance to develop herpotential. As a result, the genetically basedresemblance between biological kin willgrow stronger and stronger as the youngdog develops.

446 chapter 11 PINTELLIGENCEO
E F F E CTS O F C H A N G I N G T H E E N V I RO N M E N T
The effect of the environment on IQ scores is evident in many facts. For example, oneNorwegian study examined a huge data set that included intelligence scores for334,000 pairs of brothers. The researchers found that the correlation between thebrothers’ intelligence scores was smaller for brothers who were more widely separatedin age (Sundet, Eriksen, & Tambs, 2008). This result is difficult to explain genetically,because the genetic resemblance is the same for two brothers born, say, one year apartas it is for two brothers born five years apart. In both cases, the brothers share 50% oftheir genetic material. However, this result makes sense on environmental grounds. Thegreater the age difference between the brothers, the more likely it is that the family cir-cumstances have changed between the years of one brother’s childhood and the yearsof the other’s. Thus, a greater age difference would increase the probability that thebrothers grew up in different environments, and to the degree that these environmentsshape intelligence, we would expect the more widely spaced brothers to resemble eachother less than the closely spaced siblings.
We’ve also known for many years that impoverished environments can impede intel-lectual development. For example, researchers studied children who worked on canalboats in England during the 1920s and rarely attended school; they also studied chil-dren who lived in rural mountainous Kentucky, where little or no schooling was avail-able. These certainly seem like poor conditions for the development of intellectualskills, and it seems likely that exposure to these conditions would have a cumulativeeffect: The longer the child remains in such an environment, the lower his IQ should be(Figure 11.17). This is precisely what the data show—a negative correlation between IQand age. That is, the older the child (the longer she had been in the impoverished envi-ronment), the lower her IQ (Asher, 1935; H. Gordon, 1923; also see Heckman, 2006).Related results come from communities where schools have closed. These closingstypically lead to a decline in intelligence-test scores—in one study, a drop of about6 points for every year of school missed (R. L. Green, Hoffman, Morse, Hayes, &Morgan, 1964; see also Ceci & Williams, 1997; Neisser et al., 1996).
More optimistically, we also know that improving the environment can to some extentincrease IQ. For example, in a study in France, researchers focused on cases in which thegovernment had removed children from their biological parents because of abuse or neg-lect (Duyme, Dumaret, & Tomkiewicz, 1999) The researchers were thus able to comparethe children’s “pre-adoption IQ” (i.e., when the children were still living in a high-riskenvironment) with their IQ in adolescence—after years of living with their adoptive fam-ilies. The data (Figure 11.18) showed substantial improvements in the children’s scores,thanks to this environmental change.
A similar conclusion flows from the effects of explicit training. TheVenezuelan “Project Intelligence,” for example, gave underprivileged ado-lescents in Venezuela extensive training in various thinking skills(Herrnstein, Nickerson, de Sanchez, & Swets, 1986). Assessments aftertraining showed substantial benefits on a wide range of tests. A similarbenefit was observed for American preschool children in the CarolinaAbecedarian Project (F. A. Campbell & Ramey, 1994). These programs leaveno doubt that suitable enrichment and education can provide substantialimprovement in intelligence-test scores. (For still other evidence thatschooling lifts intelligence scores, see Ceci & Williams, 1997; Grotzer &Perkins, 2000; M. Martinez, 2000; Perkins & Grotzer, 1997.)
We should note in passing that there’s no conflict between theseresults and the results we mentioned earlier in the chapter when docu-
11.17 IQ and poverty IQ is clearly influenced by both genes and environment.The longer a child lives under conditions ofpoverty, the lower her IQ generally tends to be.
High-SES rearing
Mid-SES rearing
Low-SES rearing
80
70
90
100
Pre-adoption In adolescence
IQ
11.18 IQ improvement due to environmen-tal change Researchers examined the IQscores of children who were adopted out ofhorrible environments in which the childrenhad been abused or neglected. After theadoption (when the children were in betterenvironments), the children’s IQ scores weremarkedly higher—and all the more so if thechildren were adopted into a family withhigher socioeconomic status (SES).
PThe Roots of IntelligenceO 447
menting the reliability of the IQ test. There we noted that IQ scores are usually quitestable across the life span, so that (for example) if we know someone’s IQ at, say, age10, we can accurately predict what her IQ will be a decade or more later. This stabil-ity in scores is easily observed if a person lives in a consistent environment. As we nowsee, though, changes in the environment can produce substantial shifts in IQ—by adozen or more points. Thus the IQ test is reliable, but this doesn’t mean that IQscores can’t change.
W O R L D W I D E I M P RO V E M E N T I N I Q SCO R E S
The impact of environmental factors on IQ scores is also undeniablein another fact. Around the globe, scores on intelligence tests havebeen gradually increasing over the last few decades, at a rate ofapproximately 3 points per decade. This pattern is known as theFlynn effect, after James R. Flynn (1984, 1987, 1999, 2009; see alsoDaley, Whaley, Sigman, Espinosa, & Neumann, 2003; Kanaya,Scullin, & Ceci, 2003), one of the first researchers to document thiseffect systematically. This improvement has been documented inmany countries, including many developed (and relatively affluent)nations and also relatively impoverished third world nations (Figure11.19). (There’s also some suggestion that the improvement has nowleveled off in some countries—Britain, for example—and may evenbe reversing; but it’s too soon to make a judgment on this point; Flynn, 2009.)
Could it be that people in the modern world are simply accumulating more and moreinformation? If so, then the Flynn effect would be most visible in measures of crystal-lized intelligence. However, that’s not what the evidence shows. Instead, the effect isstronger in measures of fluid intelligence—such as the Raven’s Matrices—so it seemsto be a genuine change in how quickly and flexibly people can think.
Some scholars suggest that this broad increase in scores is attributable to wide-spread improvement in nutrition and health care, and these factors surely do contributeto the Flynn effect in some parts of the world (for a study in Kenya, for example, seeDaley et al., 2003). But we need some other explanation for why the effect is also evi-dent in middle-class populations in relatively wealthy countries (Flynn, 2009). Oneproposal is that this worldwide improvement is the result of the increasing complexityand sophistication of our shared culture: Each of us is exposed to more informationand a wider set of perspectives than were our grandparents, and this exposure may leadto a sharpening of skills that show up in our data as an improvement in IQ (for a broaddiscussion, see Dickens & Flynn, 2001; Greenfield, 2009; Neisser, 1997, 1998).
Whatever the explanation, though, one point is clear: The Flynn effect cannot beexplained genetically. While the human genome does change (a prerequisite, ofcourse, for human evolution), it doesn’t change at a pace commensurate with thiseffect. Therefore, this worldwide improvement becomes part of the larger package ofevidence documenting that intelligence can indeed be improved by suitable environ-mental conditions.
T H E I N T E R ACT I O N A M O N G G E N E T I C FACTO RS , S E S , A N D I Q
Let’s return, though, to the effects of poverty on IQ , because these effects are informa-tive in two ways. First, these effects help us understand exactly how the environmentshapes intelligence. Second, these effects also illuminate the interaction between envi-ronmental and genetic factors in shaping IQ.
Flynn effect A worldwide increase inIQ scores over the last severaldecades, at a rate of about 3 pointsper decade.
BelgiumNorwayNetherlands
BritainIsrael
85
90
95
100
80
75
701950 1960 1970 1980 19901940
IQ s
core
s
11.19 The Flynn effect IQ scores havebeen increasing across the last fewdecades, and this pattern has been docu-mented in many different countries.

448 chapter 11 PINTELLIGENCEO
The overall effects of poverty on IQ are easily documented, and in fact there’s a correlation of .40 between a child’s intelligence scores and the socioeconomic status ofthe family in which the child is raised (Lubinski, 2004). Looking beyond these broadeffects, though, we can ask what aspects of intelligence are especially affected as well ashow poverty shapes intelligence. We know, for example, that the impact of poverty isespecially salient in tests of language skills and also in tasks hinging on executivecontrol (Hackman & Farah, 2009). In addition, children who live in poverty in theirpreschool years seem more at risk than children who live in poverty in middle or latechildhood (G. Duncan, Yeung, Brooks-Gunn, & Smith, 1998; Farah et al., 2006).Apparently, then, many of the harmful effects of poverty aren’t due to inferior educa-tion. Instead, the effects derive from a mix of other factors, including exposure to vari-ous toxins found in lower-quality housing, lack of stimulation, poor nutrition, andinferior health care—and probably also the chronic stress that goes with poverty. All ofthese factors can interfere with the normal development of the brain, and they haveimportant (and deeply unfortunate) consequences for intellectual functioning. (Formore on the neurocognitive effects of poverty, see Hackman & Farah, 2009.)
These various problems, all associated with poverty, have a direct effect on braindevelopment and also interact with genetic influences on development (Turkheimer,Haley, Waldron, D’Onofrio, & Gottesman, 2003). Specifically, when researchers focuson higher-SES families, they find the pattern we’ve already described—an appreciablystronger resemblance between identical twins’ IQ scores than there is betweenfraternal twins’ scores. This tells us (as we’ve discussed) that genetic factors are playingan important role here, so that people who resemble each other genetically are likely toresemble each other in their test scores. Among lower-SES families, though, the patternis different. In this group, the degree of IQ resemblance is the same for identical andfraternal twins—which tells us that in this setting, genetic factors seem to matter muchless for shaping a person’s intelligence.
What’s going on here? We suggested one explanation in Chapter 2 and echoed thatproposal earlier in this chapter. Specifically, it may be best to think about our genes asproviding our potential—a capacity to grow and develop if we’re suitably nurtured. If,therefore, a child receives good schooling, health care, and adequate nutrition, he’ll beable to develop this potential; and as the years go by, he’ll be able to make the most ofthe genetically defined predisposition he was born with. But if a child grows up in animpoverished environment with poor schooling, minimal health care, and inadequatenutrition, it matters much less whether he has a fine potential—because the environ-ment doesn’t allow the potential to emerge. Hence, in impoverished environments,genetic factors—the source of the potential—count for relatively little.
Heritability RatiosClearly, then, the role of genetic factors in shaping intelligence depends on the circum-stances. In some settings, genes play a large role; in other settings, they do not. This invites anew question: Is there some way to measure the contribution of genetics so that we can ask,in a particular setting, how much of the data pattern can be understood in genetic terms?
To address this question, investigators often rely on a measure we first met inChapter 2: the heritability ratio (H ). For any trait, this measure involves a comparisonof two numbers. First, what is the total phenotypic variability—that is, how much doindividuals differ from each other in their actual characteristics? Second, how much ofthis variability can be understood in genetic terms? Heritability is then calculated as theratio between these two numbers—and so tells us, roughly, what percentage of the totalvariation can be attributed to genetics.
heritability ratio (H) A measurethat describes, for a given populationin a given environment, what propor-tion of the variance of a trait is due togenetic factors.

PThe Roots of IntelligenceO 449
Let’s be clear, though, that heritability is a measure that describes a group, because tocalculate heritability, we need to ask how much variation occurs within that group, fromone individual to the next. Thus, it makes no sense to apply measures of heritability tosingle individuals, and it would be a mistake (for example) to read a heritability esti-mate as implying that a certain percentage of a person’s IQ (say) came from her genes,and the remainder from her environment. Instead, as we’ve emphasized throughout,the influence of genes and environment is, for any individual, fully intertwined—withboth factors shaping all aspects of whatever the person becomes.
Overall, researchers estimate that the heritability for IQ is, in most environments,between .40 and .70; often, a figure of .50 or .60 is quoted (Neisser et al., 1996). Thiscan be understood as the assertion that, of the variability we observe in IQ , half or a lit-tle more is attributable to variations in genetic material. (And, since the other 50% isattributable to factors other than genetics, this means that genes and environment haveroughly equal weight in determining IQ.)
Let’s be very clear, though, that these estimates are always calculated with referenceto a particular group—and, in fact, we’ve already seen an example of how this matters:If we draw our data from low-SES groups, we find that the heritability of IQ is muchlower—and may even be zero (Turkheimer et al., 2003). Likewise, we mentionedearlier that the genetic influence on IQ becomes more visible as people move fromchildhood into adulthood; this, too, is reflected in heritability estimates: Overall, theheritability for IQ in middle-class children is estimated as around .50; the heritabilityof middle-class adults, in contrast, may be as high as .80 (Plomin & Spinath, 2004).
The linkage between heritability and a particular set of circumstances was alsoevident in Chapter 2 when we discussed the medical condition known phenyl-ketonuria, or PKU (Widaman, 2009). This condition is caused by a problem with asingle gene that ordinarily governs the production of an enzyme needed to digestphenylalanine, an amino acid that’s commonly part of our diet. A defect in this genederails production of the required enzyme, with the result that phenylalanine isinstead converted into a toxic agent. If an infant is born with PKU, the toxin accu-mulates in her bloodstream and damages her developing nervous system, leading toprofound mental retardation.
PKU is unmistakably of genetic origin; and for many years, we had no way toremedy this condition. As a result, the heritability was extremely high. The pheno-typic variation (whether someone did or did not have this type of retardation) wasalmost entirely attributable to whether or not he had the relevant genetic pattern.But we now know that a simple environmental manipulation can minimize theimpact of PKU: All we need to do is ensure that the infant (and, later, the child) getsa special diet that contains very little phenylalanine (Figure 11.20). If this diet isintroduced at an early enough age, retardation can be minimized or—far better—avoided altogether. As a result, the heritability estimate for PKU is, in most countries,currently quite low. Whether retardation is observed depends largely on the individ-ual’s diet, and so most of the phenotypic variation we observe is due to this environ-mental factor, not to genes.
Notice that the case of PKU offers us many lessons. First, the case reminds us onceagain that genetic effects don’t unfold in a vacuum; instead, genetic effects interact withenvironmental influences—sometimes with good effect, sometimes with bad. Second(and related), the example of PKU makes it clear that patterns that are powerfullyshaped by genes can still be dramatically altered. Indeed, PKU is a case in which havinga particular genotype can (with a carefully controlled diet) end up having no impact atall on the phenotype! Be aware, therefore, that genetic factors are important but do notset someone’s destiny (Figure 11.21).
11.20 Phenylalanine Many diet sodascontain the warning shown here. The warn-ing is irrelevant to most of the population,but it’s crucial for anyone suffering fromphenylketonuria.

450 chapter 11 PINTELLIGENCEO
Third, keeping the case of PKU in mind will be helpful when you think aboutheritability ratios. These ratios are a powerful—and often useful—data summary thatallows us to capture complex patterns in a single number. But the case of PKU remindsus that this number reflects only a particular set of circumstances for a particular groupof individuals, and the heritability ratio can change if the circumstances change. Inaddition, heritability ratios tell us nothing about the future. Even if a trait’s heritabilityratio is near 1.00 (as it used to be, for PKU), we may be able to alter the trait enormouslyonce a suitable intervention is found.
Group Differences in IQSo far, we’ve focused on the intelligence scores of specific individuals—for example,we’ve compared the IQ scores of particular twins and compared a specific child’s IQwith the IQs of her biological parents. But these person-by-person comparisons aren’tthe focus of the controversy over the roots of intelligence. The real fury is over anotherissue: the differences in average IQ , and the differences in academic achievement, thatare found between groups. In particular, debate has focused on two comparisons: thepossible difference between men and women in their intellectual skills, and the differ-ence between American whites and American blacks.
Before examining these comparisons, we need to emphasize that what’s at stake hereare the differences between averages—the average test score (for example) for men andthe average for women. This point is crucial, because—of course—men differ from eachother in their intellectual prowess, and so do women. Likewise, the scores of EuropeanAmerican test takers vary enormously, as do the scores of African American test takers.Indeed, this variation within each group (within each sex, or within a racially definedgroup) is much, much larger than any between-group variations researchers havedetected. We therefore learn little about any individual’s abilities simply by knowing hisor her group membership, and so it would be wrong (and in most settings, illegal) touse group membership as a basis for making decisions about that individual.Nonetheless, the differences between the averages remain, so let’s take a closer look atthe research scrutinizing these differences.
B E T W E E N - G RO U P A N D W I T H I N - G RO U P D I F F E R E N C E S
The differences in intellectual performance between men and women, and also betweenwhites and blacks, are relatively small. But the debate over these differences has been
(A) (B)
11.21 Heritability of hair color and height(A) The heritability of hair color regularlyrises and falls as a function of changes infashion. The genetic contribution to haircolor doesn’t change, of course; but the rel-ative importance of the genes—and so theheritability—drops whenever dying one’shair is in style (because then the phenotypemay bear little resemblance to the colorspecified in the genotype). (B) Our bestestimate for the heritability of height isabout .80. Still, the average height in mostnations has increased markedly in the lastcentury—probably because of improve-ments in nutrition and health care (seeRutter, 2006). This is one more reminderthat high levels of heritability in no wayimply that a trait cannot be modified.
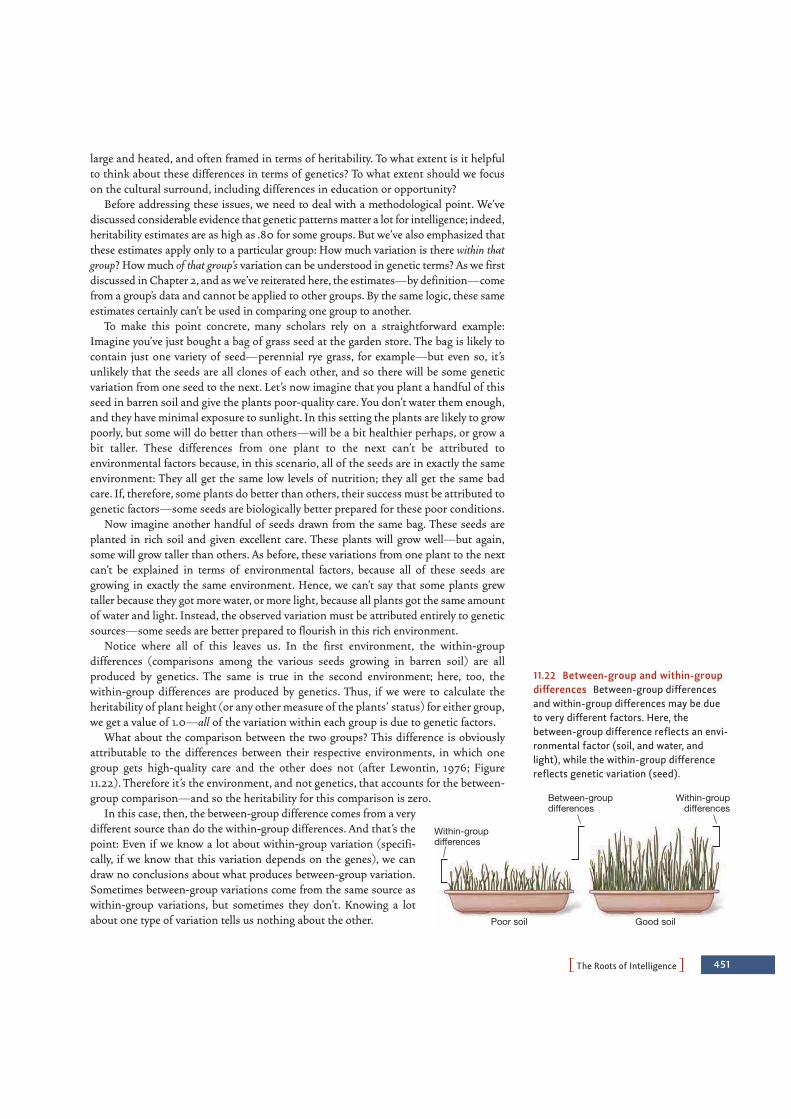
Poor soil Good soil
Within-groupdifferences
Within-groupdifferences
Between-groupdifferences
PThe Roots of IntelligenceO 451
large and heated, and often framed in terms of heritability. To what extent is it helpfulto think about these differences in terms of genetics? To what extent should we focuson the cultural surround, including differences in education or opportunity?
Before addressing these issues, we need to deal with a methodological point. We’vediscussed considerable evidence that genetic patterns matter a lot for intelligence; indeed,heritability estimates are as high as .80 for some groups. But we’ve also emphasized thatthese estimates apply only to a particular group: How much variation is there within thatgroup? How much of that group’s variation can be understood in genetic terms? As we firstdiscussed in Chapter 2, and as we’ve reiterated here, the estimates—by definition—comefrom a group’s data and cannot be applied to other groups. By the same logic, these sameestimates certainly can’t be used in comparing one group to another.
To make this point concrete, many scholars rely on a straightforward example:Imagine you’ve just bought a bag of grass seed at the garden store. The bag is likely tocontain just one variety of seed—perennial rye grass, for example—but even so, it’sunlikely that the seeds are all clones of each other, and so there will be some geneticvariation from one seed to the next. Let’s now imagine that you plant a handful of thisseed in barren soil and give the plants poor-quality care. You don’t water them enough,and they have minimal exposure to sunlight. In this setting the plants are likely to growpoorly, but some will do better than others—will be a bit healthier perhaps, or grow abit taller. These differences from one plant to the next can’t be attributed toenvironmental factors because, in this scenario, all of the seeds are in exactly the sameenvironment: They all get the same low levels of nutrition; they all get the same badcare. If, therefore, some plants do better than others, their success must be attributed togenetic factors—some seeds are biologically better prepared for these poor conditions.
Now imagine another handful of seeds drawn from the same bag. These seeds areplanted in rich soil and given excellent care. These plants will grow well—but again,some will grow taller than others. As before, these variations from one plant to the nextcan’t be explained in terms of environmental factors, because all of these seeds aregrowing in exactly the same environment. Hence, we can’t say that some plants grewtaller because they got more water, or more light, because all plants got the same amountof water and light. Instead, the observed variation must be attributed entirely to geneticsources—some seeds are better prepared to flourish in this rich environment.
Notice where all of this leaves us. In the first environment, the within-groupdifferences (comparisons among the various seeds growing in barren soil) are allproduced by genetics. The same is true in the second environment; here, too, thewithin-group differences are produced by genetics. Thus, if we were to calculate theheritability of plant height (or any other measure of the plants’ status) for either group,we get a value of 1.0—all of the variation within each group is due to genetic factors.
What about the comparison between the two groups? This difference is obviouslyattributable to the differences between their respective environments, in which onegroup gets high-quality care and the other does not (after Lewontin, 1976; Figure11.22). Therefore it’s the environment, and not genetics, that accounts for the between-group comparison—and so the heritability for this comparison is zero.
In this case, then, the between-group difference comes from a verydifferent source than do the within-group differences. And that’s thepoint: Even if we know a lot about within-group variation (specifi-cally, if we know that this variation depends on the genes), we candraw no conclusions about what produces between-group variation.Sometimes between-group variations come from the same source aswithin-group variations, but sometimes they don’t. Knowing a lotabout one type of variation tells us nothing about the other.
11.22 Between-group and within-groupdifferences Between-group differencesand within-group differences may be dueto very different factors. Here, thebetween-group difference reflects an envi-ronmental factor (soil, and water, andlight), while the within-group differencereflects genetic variation (seed).

452 chapter 11 PINTELLIGENCEO
CO M PA R I SO N S B E T W E E N M E N A N D W O M E N
With these preliminary points now established, we’re ready for the data—starting withthe difference between men and women. Of course, men and women do differ in someways. For example, men tend to be more physically aggressive than women; women, incontrast, rely on social aggression (gossiping, or ostracizing) more than men do(Chapters 1 and 14). But men and women are also alike in many ways—and so, as justone illustration, evidence makes it clear that there’s virtually no difference between menand women in their effectiveness as leaders or their competitiveness as negotiators(J. Hyde & Linn, 2006).
What about intellectual abilities? Overall, neither sex is more intelligent than theother; and there’s no reliable difference between men and women in their IQ scores(e.g., Held, Alderton, Foley, & Segall, 1993; R. Lynn, 1994; although see N. Brody, 1992).We do detect differences, though, when we consider more specialized abilities. Onaverage, men do better on certain tests designed to measure visuospatial abilities, suchas tests requiring mental rotation (Figure 11.23). Men also do better on tasks thatrequire them to navigate through a virtual (computerized) three-dimensional environ-ment (like the fictional worlds one must “travel through” in many computer games;Halpern, Benbow, Geary, Gur, Hyde et al., 2007). Women, for their part, on average dobetter on certain verbal tasks—especially tasks that require clear and fluent writing(Halpern, 1992, 2000; Halpern et al., 2007; L. Levine et al., 1999).
These differences are easily documented in the laboratory; but men and womenalso differ in their intellectual achievement outside of the lab, and the interpretationof this point has been a matter of controversy. To understand the debate, let’s startwith the fact that many studies have documented differences between men andwomen in educational achievement—a so-called gender gap. One study examined thetest scores for 15-year-olds in 41 different countries (Machin & Pekkarinen, 2008). Inevery country, girls outscored boys in tests of reading; in most countries, boysoutscored girls in tests of mathematics. The data also showed that in both reading andmathematics, scores for boys were more variable than scores for girls; more boys thangirls were likely to achieve scores rather distant from (above or below) the average fortheir sex (W. Johnson, Carothers, & Deary, 2008).
Another study compared the SAT scores of 40,000 American high-school students.The study showed that men (on average) did better than women on the math portionof the test, even when the investigators limited their comparison to men and womenwho had taken exactly the same high-school math courses and had expressed the samedegree of interest in mathematics (Benbow, 1988; Benbow, Lubinski, Shea, &Eftekhari-Sanjani, 2000; for related data, see Halpern et al., 2007).
Other considerations, however, complicate the comparison between the sexes. Asone concern, we probably shouldn’t be comparing men and women in terms of mathperformance overall, because the gender comparison may depend on what type of mathwe’re considering. For example, the advantage for men seems clearer for tests thatshowcase spatial relations or geometry (Crawford & Chaffin, 1997; Halpern et al., 2007;J. Hyde, 2005); for tests emphasizing computation, the advantage goes to women(J. Hyde & Linn, 2006).
In addition, some measures don’t show women falling behind in mathematics. Forexample, National Science Foundation data indicate that men and women areequally likely to take calculus in high school, and it’s the women who get bettergrades (A. Gallagher & Kaufman, 2005). Similarly, America’s No Child Left Behind(NCLB) legislation requires states to assess student progress annually. A 2008report on these assessments finds no difference between male and female high-
11.23 Mental rotation In the mental rotation task, participants have to judgewhether two stimuli are different shapes,or the same but merely viewed from different perspectives. Men tend to have anadvantage on this visuospatial task—andso they’re faster and more accurate in theirjudgments.

PThe Roots of IntelligenceO 453
school students in their average level of math achievement, although the scores formales continue to be somewhat more variable than the scores for females—so thatmales are more likely than females to obtain scores well below or well above the mean(J. Hyde, Lindberg, Linn, Ellis, & Williams, 2008; W. Johnson et al., 2008).
What about performance beyond high school? In college, men and women get equalmath grades (Bridgeman & Lewis, 1996), even when we match their math classes fordifficulty. Assessments of understanding of mathematical concepts in college courseslikewise show no difference between the sexes (J. Hyde & Linn, 2006).
What lies behind all of these findings? For those studies that do detect sexdifferences in educational performance, what’s the cause? And why is it that, in thelaboratory, men consistently have an advantage in visuospatial reasoning? Someauthors have suggested biological explanations for these facts, often pointing to apossible link between spatial abilities and the male sex hormone testosterone. In onestudy, for example, males who produced abnormally low levels of testosterone showedimpairments in spatial reasoning (Hier & Crowley, 1982); in another study, oldermales (aged 60–75) showed dramatic improvements in spatial reasoning after receiv-ing testosterone supplements (Cherrier et al., 2001; Janowsky, Oviatt, & Orwoll, 1994;also see Van Goozen, Cohen-Kettenis, Gooren, Frijda, & Can de Poll, 1995). But onthe other hand, several studies have failed to confirm these hormonal effects on visu-ospatial performance, so any conclusions about this point must be tentative (e.g.,Halari et al., 2005; Hines et al., 2003; Moffat & Hampson, 1996; also see Halpern,2000; N. Newcombe, 2007; Spelke, 2005).
A different hypothesis focuses on cultural influences—including the importantobservation that in most Western cultures, young boys receive much more supportand encouragement than young girls do for work in mathematics (Figure 11.24).Indeed, many people (including parents and teachers) seem to believe that womenare ill suited for math and expect women not to do well in this domain (Halpern,1992). Thus, parents expect their sons to do better in math courses than theirdaughters do (Frome & Eccles, 1998) and often attribute their sons’ success inmath to ability while attributing their daughter’s success in math to hard work(Parsons, Adler, & Kaczala, 1982). Even young children endorse these stereotypes(C. Steele, 2003) and, by middle adolescence, girls seem to receive less supportfrom their peers for science- and math-related activities than boys do (Stake &Nickens, 2005) .
Do these social factors influence how children behave and what they achieve?Studies show that women perform less well on some math tests if they’re asked, atthe start of the test, simply to record their gender on the test form. Presumably, thisserves to prime the relevant stereotype, and this undermines performance (Ambady,Shih, Kim, & Pittinsky, 2001; we’ll go into greater detail about “stereotype threat”shortly). Similarly, sex differences in test scores are powerfully influenced by factorsin the context that shape the test takers’ expectations. In one study, male and femalecollege students all took a math test. Half of the students were told that this test hadshown sex differences in the past; in this group, male students outperformed thefemales. The other half of the students were told that the test had been shown in thepast to be gender fair; in this group, there was no sex difference in performance(R. Brown & Josephs, 1999; Crawford & Chaffin, 1997; Halpern et al., 2007).
Hypotheses emphasizing the role of experience and encouragement find furthersupport in the fact that visuospatial skills can be markedly improved throughpractice—a point that has been documented in a wide range of studies (Halpern etal., 2007). In one experiment, male and female college students practiced playing anaction video game (Medal of Honor: Pacific Assault) for a total of 10 hours. This
(A) (B)
11.24 Gender stereotypes In a widerange of cultures (including Tibet, wherephoto A was taken), boys are encouragedto be tough and strong—and they’re oftenexpected to be good in math. In contrast,girls (including this young girl in Japan) areexpected to be soft and feminine—andpoor in math.

454 chapter 11 PINTELLIGENCEO
practice improved the spatial skills of all participants, but the improvement wasgreater in women and led to a clear reduction in the difference between the sexes(Feng, Spence, & Pratt, 2007).
Indeed, in light of the studies showing the positive influence of instruction, experi-ence, and encouragement, we may want to put less emphasis on the ultimate causes ofthe apparent sex differences in achievement. We might instead put our emphasis onefforts toward eradicating these differences, to make sure that all of us—male andfemale—reach our full potential. Otherwise, as one author put it, we may “waste a mostvaluable resource: the abilities and efforts of more than half the world’s population”(Shaffer, 2004, p. 237).
CO M PA R I SO N S B E T W E E N A M E R I CA N W H I T E S A N D A M E R I CA N B L AC KS
Controversy has also swirled around another comparison—that between the IQ scoresof American (and European) whites and those of African Americans. Many studieshave indicated a difference between these scores, with the average score of the Americanwhite population higher by 10 to 15 IQ points (Jencks & Phillips, 1998; Jensen, 1985;Loehlin, Lindzey, & Spuhler, 1975; Reynolds, Chastain, Kaufman, & McLean, 1987).There has been energetic debate over whether this gap between the racial groups hasbeen shrinking in recent years (e.g., Dickens & Flynn, 2006a, 2006b; Rushton &Jensen, 2006), and also debate over whether it’s “important or proper” to study theseracial differences at all (e.g., E. Hunt & Carlson, 2007a, 2007b; then N. Brody, 2007;Gottfredson, 2007; Sternberg & Grigorenko, 2007). Still, the difference in averagescores between blacks and whites is well documented—making it important for us toask what the difference is, and what it might or might not tell us about race differencesand about intelligence itself.
Let’s start with the hypothesis that has been most controversial, one that high-lights genetic factors. Could it be that genes of African ancestry somehow lead tolower IQ scores than do genes of European ancestry? This hypothesis is actuallyproblematic from the very start, because it assumes the groups we’re comparing(modern American whites and modern African Americans) really are distinct genet-ically. This assumption is questionable, because the genetic overlap between thesetwo groups is enormous (e.g., Cavalli-Sforza, Menozzi, & Piazza, 1994). More pow-erfully, though, researchers have used various methods to determine what propor-tion of someone’s ancestors were black Africans and what proportion wereEuropeans. (In early studies, this determination was done by carefully collectingfamily histories; in later studies, this was done by means of biochemical markers inthe blood.) If genetic factors are the cause of racial differences in IQ. then higherproportions of black African ancestry should be associated with lower IQ. They arenot, and the evidence indicates no link between IQ scores and ancestry (Scarr &Carter-Saltzman, 1983).
How, therefore, should we explain the race difference in test scores? One hypothe-sis focuses on the intelligence tests themselves and proposes that the race differenceis artificial—a result of bias built into the tests. This would surely be a problem if thetest relied on vocabulary that was more familiar to the community of white test takersthan to the community of black test takers. Likewise, the test might be biased if it werealways administered by someone white—someone who might be warmer and moreencouraging to white test takers than to blacks. These are real concerns that mustbe controlled if the racial comparison is to have any meaning at all. As it turns out,though, we can easily deal with these concerns—for example, by using nonverbal

PThe Roots of IntelligenceO 455
forms of testing (such as the Ravens’ Matrices), having whites tested by someonewhite, and having blacks tested by someone black. With these precautions in place, thedifference between blacks’ and whites’ scores (on average) remains. (For more on thispoint, see P. Sackett et al., 2008.)
A more promising hypothesis begins with the fact that—as we’ve noted—IQ scoresare undeniably influenced by poverty and poor schooling. Let’s now add that, sadly,blacks in the United States tend (on average) to have lower incomes than whites do,and blacks are also more likely to live in poverty. As a result, a higher proportion ofblacks than whites are exposed to poor nutrition, lower-quality educational resources,and poorer health care (Neisser et al., 1996). Could these socioeconomic factors be thesource of the race difference in IQ scores?
To address this question, let’s focus our comparison just on blacks and whites with sim-ilar backgrounds. For example, we’ll compare working-class blacks with working-classwhites, or educated black professionals with educated white professionals. In this way, wecan ask if race matters when we remove socioeconomic differences from the picture. And,in fact, studies using this logic find a reduced racial difference (see, for example, Jencks &Phillips, 1998). Clearly, then, factors associated with poverty do play a role here, and theymake a substantial contribution to the observed race difference.
A different line of evidence makes a similar point: Rather than trying to match testtakers based on their environments, we can ask what happens to test scores when theenvironment is changed. A widely cited example is a study of black children who wereadopted at an early age by white middle-class parents, most of whom were collegeeducated (Scarr & Weinberg, 1976). After adoption, these children had a mean IQ of110—a value exceeding the national average for black children by about 25 points. (Forfurther discussion, see Scarr & Carter-Saltzman, 1982; Scarr & Weinberg, 1983.)
We need to emphasize, though, that equalizing the socioeconomic variables dimin-ishes the black-white difference, but doesn’t erase it. Thus, it’s clear that the manyhardships associated with poverty are part of the explanation for the difference, butnot the whole story. So we still need to ask what other factors contribute to the con-trast between the races.
ST E R E OT Y P E T H R E AT
In the previous section, we asked whether blacks’ and whites’ IQ scores would be thesame if we could match their environments. If the answer is yes, then this obviouslypoints toward an environmental explanation of the race difference. But to tackle thisquestion in a thorough way, it may not be enough to match factors like parental educa-tion, income, and occupational level. Even if we succeed in matching for these aspectsof life, black and white children still grow up in different environments. This is because,after all, black children grow up knowing they are black and knowing a lot about whatlife paths are easily open to them and what life paths are likely. White children corre-spondingly grow up knowing they are white, and they too have a sense of what lifepaths are open or likely. Moreover, each group, because of the color of their skin, istreated differently by the people in their social environment. In these ways, their envi-ronments and experiences are not matched—even if the parents have similar jobs andsimilar income levels, and even if the children have similar educational experiences.
Do these social experiences matter for intelligence scores? As one indication thatthey do, consider studies of stereotype threat, a term used to describe the negativeimpact that social stereotypes, once activated, can have on task performance. Here’san example: Imagine an African American is taking an intelligence test. She mightwell become anxious because she believes this is a test on which she is expected to do
stereotype threat A mechanismthrough which a person’s perform-ance is influenced by her perceptionthat her score may confirm stereo-types about her group.
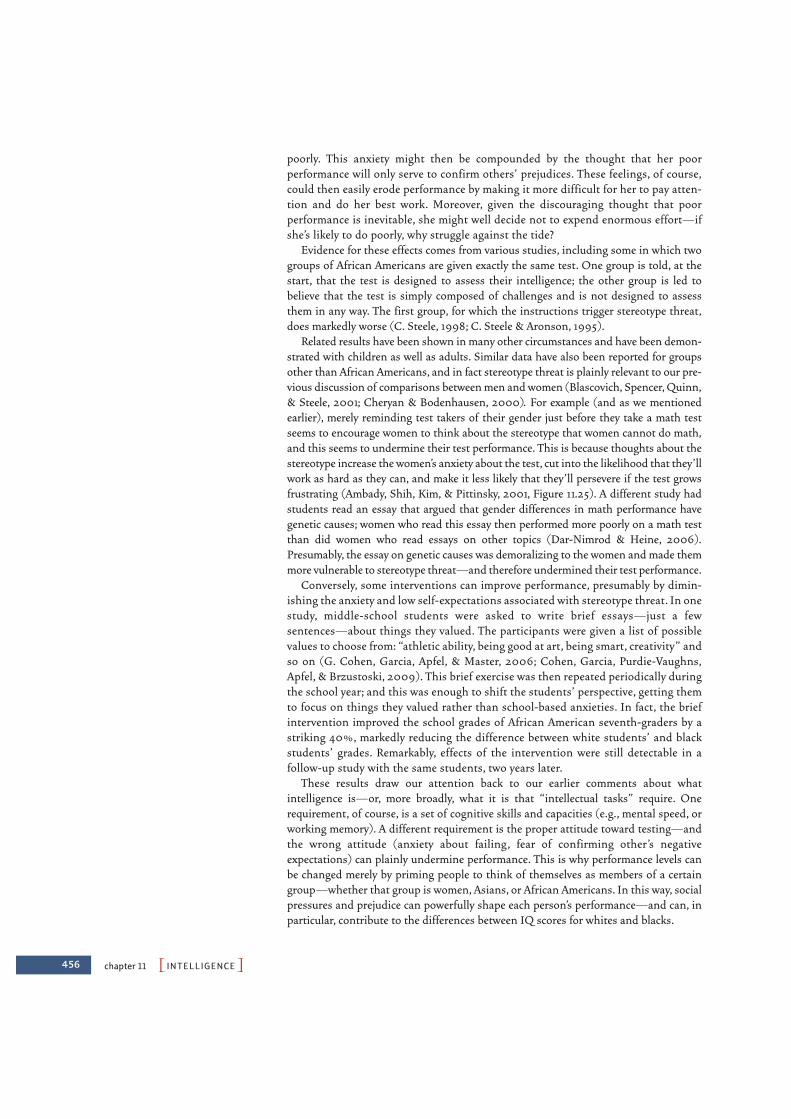
456 chapter 11 PINTELLIGENCEO
poorly. This anxiety might then be compounded by the thought that her poor performance will only serve to confirm others’ prejudices. These feelings, of course,could then easily erode performance by making it more difficult for her to pay atten-tion and do her best work. Moreover, given the discouraging thought that poor performance is inevitable, she might well decide not to expend enormous effort—ifshe’s likely to do poorly, why struggle against the tide?
Evidence for these effects comes from various studies, including some in which twogroups of African Americans are given exactly the same test. One group is told, at thestart, that the test is designed to assess their intelligence; the other group is led tobelieve that the test is simply composed of challenges and is not designed to assessthem in any way. The first group, for which the instructions trigger stereotype threat,does markedly worse (C. Steele, 1998; C. Steele & Aronson, 1995).
Related results have been shown in many other circumstances and have been demon-strated with children as well as adults. Similar data have also been reported for groupsother than African Americans, and in fact stereotype threat is plainly relevant to our pre-vious discussion of comparisons between men and women (Blascovich, Spencer, Quinn,& Steele, 2001; Cheryan & Bodenhausen, 2000). For example (and as we mentionedearlier), merely reminding test takers of their gender just before they take a math testseems to encourage women to think about the stereotype that women cannot do math,and this seems to undermine their test performance. This is because thoughts about thestereotype increase the women’s anxiety about the test, cut into the likelihood that they’llwork as hard as they can, and make it less likely that they’ll persevere if the test growsfrustrating (Ambady, Shih, Kim, & Pittinsky, 2001, Figure 11.25). A different study hadstudents read an essay that argued that gender differences in math performance havegenetic causes; women who read this essay then performed more poorly on a math testthan did women who read essays on other topics (Dar-Nimrod & Heine, 2006).Presumably, the essay on genetic causes was demoralizing to the women and made themmore vulnerable to stereotype threat—and therefore undermined their test performance.
Conversely, some interventions can improve performance, presumably by dimin-ishing the anxiety and low self-expectations associated with stereotype threat. In onestudy, middle-school students were asked to write brief essays—just a fewsentences—about things they valued. The participants were given a list of possiblevalues to choose from: “athletic ability, being good at art, being smart, creativity” andso on (G. Cohen, Garcia, Apfel, & Master, 2006; Cohen, Garcia, Purdie-Vaughns,Apfel, & Brzustoski, 2009). This brief exercise was then repeated periodically duringthe school year; and this was enough to shift the students’ perspective, getting themto focus on things they valued rather than school-based anxieties. In fact, the briefintervention improved the school grades of African American seventh-graders by astriking 40%, markedly reducing the difference between white students’ and blackstudents’ grades. Remarkably, effects of the intervention were still detectable in afollow-up study with the same students, two years later.
These results draw our attention back to our earlier comments about whatintelligence is—or, more broadly, what it is that “intellectual tasks” require. Onerequirement, of course, is a set of cognitive skills and capacities (e.g., mental speed, orworking memory). A different requirement is the proper attitude toward testing—andthe wrong attitude (anxiety about failing, fear of confirming other’s negativeexpectations) can plainly undermine performance. This is why performance levels canbe changed merely by priming people to think of themselves as members of a certaingroup—whether that group is women, Asians, or African Americans. In this way, socialpressures and prejudice can powerfully shape each person’s performance—and can, inparticular, contribute to the differences between IQ scores for whites and blacks.

PSome Final Thoughts: Scientific Evidence and Democratic ValuesO 457
SOME FINAL THOUGHTS: SCIENTIFICEVIDENCE AND DEMO CRATIC VALUESUndeniably, individuals differ in their intellectual capacities, and in many circum-stances genetic factors play a large role in shaping these capacities. But, as we’ve repeat-edly noted, these genetic influences don’t mean that intelligence is immutable, fixed foreach of us by our genetic heritage. The example of PKU serves as a powerful reminderthat patterns that are unambiguously rooted in the genome can be changed entirely bysuitable environmental intervention. And in the case of intelligence itself, we haveample evidence that environmental changes (most prominently, schooling) canincrease IQ scores and thus markedly improve life circumstances.
Perhaps, therefore, it does not matter what the origins are for the differences in IQscores—whether we’re comparing one individual to the next, or one group to another.In either case, whether the differences are produced primarily by genetic or environ-mental factors, the data tell us that training and enriched, supportive environments canimprove IQ—and the implications for our policy goals seem clear.
11.25 SCIENTIFIC METHOD: How do stereotypes influencetest performance?
Method1. One third of a group of Asian American girls were primed to remind them they were Asian Americans. One third of the children were primed to remind them of their gender. One third were not primed.
ResultsThe youngest and oldest children were influenced by the prime. If remindedof their identity as Asian Americans (a group often expected to do well in math), the children performed better. If reminded of their identity as females (a group expected to do less well), the children scored lower. (It’s not clear why this effect was not observed in the upper elementary school age group.)
2. They all took a standardized math test.
3. For each age group, researchers analyzedhow priming affected test scores.
CONCLUSION: Stereotypes relevant to test performance can significantly affecttest scores.
SOURCE STUDY: Ambady, Shih, Kim, & Pittinsky, 2001
Mat
h te
st a
ccur
acy
0.6
0.7
0.8
0.9
Lower elementary Upper elementary Middle school
Asianprime
Genderprime
No prime(control)

INTELLIGENCE TESTING
• Alfred Binet, the originator of intelligence tests, sought toidentify children who would benefit from remedial educa-tion. Binet understood intelligence to be a general attribute,applicable to a very wide range of mental tasks. He measuredintelligence by means of a comparison between a child’s men-tal age and her chronological age.
• Intelligence tests have been developed for various uses,including the WAIS. This test has high test-retest reliability,even with gaps of many decades between the first test andsubsequent tests. The test also seems valid, as indicated bycorrelations between IQ and academic performance, job per-formance, and other measurements.
WHAT IS INTELLIGENCE? THE PSYCHOMETRIC APPROACH
• The psychometric approach to intelligence seeks to understandintelligence by scrutinizing patterns among the test scores.One aspect of this approach is an examination of how differ-ent elements within the test are intercorrelated. These inter-correlations are readily observed, suggesting that all of thediverse subtests within the IQ test overlap in the abilitiesthey are assessing. This finding is confirmed by factor analy-sis, which isolates the common element in all the subtests.That element is often referred to as general intelligence, or g.
• A hierarchical notion of intelligence places g at the top of thehierarchy; at the next level are verbal ability, quantitative abil-
chapter 11 PINTELLIGENCEO458
S U M M A R Y C H A P T E R 1 1
Notice the irony here: More than a century ago, Binet designed the intelligence test inorder to identify weaker students who would benefit from special training. Binet’s concep-tion, in other words, was that each individual’s level of intelligence was pliable and certainlycould be lifted through education. On this point, it seems, Binet was exactly right.
As scientists, though, we still seek to explain how people differ from each other; andhere the data provide a relatively clear message: The differences in IQ from one individ-ual to the next seem influenced both by genetic and environmental factors. For the dif-ference between men and women, in contrast—or the difference between whites andblacks—the main source of group differences does appear to be environmental. Thus,women’s performance (especially in mathematics) is surely shaped by widespreadexpectations that “girls can’t do math.” Academic performance by African Americans isundercut by various societal and individual-level factors, ranging from the availabilityof role models to expectations that are manifest in stereotype threat.
These group differences make Binet’s optimistic goals all the more important. LowIQ scores are, as we’ve seen, statistically linked to a number of undesirable outcomes—ranging from poor school performance to lower levels of success in the workplace.Indeed, we mentioned earlier that low IQ scores are associated with shorter lifeexpectancy. Points like these obviously motivate us to seek ways to close the “achieve-ment gaps” between various groups, although this will require efforts on many fronts—including moves toward improving nutrition, health care, and education as well ascombating the destructive effects of stereotypes.
Finally, what about the IQ tests themselves? These tests surely have their limits; evenso, many researchers consider the enterprise of intelligence testing to be one of psychol-ogy’s great success stories. As we’ve seen in this chapter, there’s reason to believe ourintelligence measurements are valid. We understand many of the mental processes thathelp make someone intelligent. And we understand some of the neural bases for theseprocesses. It might seem overenthusiastic to declare this research—as one investigatordid—“one of the most successful undertakings” of modern psychology (K. Lamb, 1994,p. 386). Still, the broad enterprise launched by Binet has clearly flourished.
PSummaryO 459
ity, and spatial ability. Correlations between these abilitiesprovide evidence for g. The stronger correlations within thesemore specific categories tell us there are also more specializedforms of intelligence.
• Fluid g is the ability to deal with new and unusual problems;crystallized g refers to someone’s accumulated knowledge andskills. These two forms of intelligence are correlated, butthey’re also distinguishable in several ways. Fatigue andaging, for example, have a much greater impact on fluid intel-ligence than on crystallized intelligence.
THE BUILDING BLOCKS OF INTELLIGENCE
• One mechanism that contributes to intelligence is simply men-tal speed: Higher-IQ individuals show faster response times inmany tasks, including tasks measuring inspection time.
• Another contribution to intelligence is working memorycapacity—an ability to keep multiple goals in mind, and alsoan ability to control one’s own attention. This capacity mayallow the construction of more complex task models; it mayalso allow greater executive control over one’s own thoughts.These points fit well with the P-FIT theory of intelligence,which suggests that intelligence depends on the integratedfunctioning of many brain sites including those in the parietaland frontal lobes.
INTELLIGENCE BEYOND THE IQ TEST
• Some investigators have concerned themselves with certainaspects of the term intelligence that go beyond IQ, such aspractical intelligence. A related approach has led to measures ofemotional intelligence; people with this sort of intelligence havefewer conflicts with their peers and are more tolerant ofstress.
• A different proposal rests on the notion of multiple intelli-gences, which is buttressed by evidence from studies of brainlesions and people with savant syndrome.
• Our understanding of intelligence may also need to take intoaccount the cultural context. People in different cultures havedifferent abilities as well as a different understanding of thetest-taking situation.
THE ROOTS OF INTELLIGENCE
• Intelligence-test performance is determined by both environ-mental and genetic factors. Evidence for the role of genetic fac-tors includes the fact that the correlation between the IQs ofidentical (monozygotic) twins is higher than that for fraternaltwins, and also the observation that the correlation betweentheir IQ scores is remarkably high even when identical twinsare reared apart. Further evidence for a hereditary contribution
comes from adopted children, whose IQs correlate morehighly with the IQs of their biological parents than with theIQs of their adoptive parents. At the same time, however, evi-dence for environmental effects is provided by increases anddecreases in the mean IQ of populations whose cultural oreducational level has risen or fallen. Environmental effects arealso clearly implicated by the worldwide improvement in IQscores observed over the last few decades.
• The relative weight of genetic and environmental factors indetermining the variation of a given characteristic is given bythe heritability ratio, or H. The value of H depends in parton the given population, for H describes only the degree towhich the variability within that particular population can beattributed to genetic variance.
• In recent years, much interest (and debate) has focused onIQ differences among different groups of individuals—including a comparison between men and women, and acomparison between American whites and American blacks.Men and women do not differ in overall IQ, but men onaverage seem to have a small advantage in some tasksrequiring visuospatial reasoning; women on average have asmall advantage in some verbal tasks. These differences arecertainly fostered by a cultural environment in which boysand girls have different types of experiences and receivetypes of encouragement.
• Several studies have documented a 10- to 15-point differencebetween average scores of American whites and blacks. Thisdifference does not seem attributable to genetic factors. Partof the difference derives from the poverty and disadvantagedcircumstances in which many American blacks live; part canbe attributed to the effects of stereotype threat.
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
Motivational States 462
Thermoregulation 464
Hunger, Eating, and Obesity 466
Threat and Aggression 473
Sexual Behavior 478
Motives Beyond Drives 485
The Diversity of Motives 487
Emotion and Emotion Regulation 490
Some Final Thoughts: The “Why” of Behavior 500
Summary 501
CH
AP
TE
R
12
461
Motivation and Emotion
Northerners definitely took some getting used to,”
laughs Clint McCabe, a native of Mobile, Alabama, who recently graduated from a
university in the northeastern United States. Before winning a baseball scholarship
that took him 1,000 miles away from his home, Clint had sojourned north of the
Mason-Dixon Line only three times. “My family warned me that Yankees would be,
well, different. And they were right.”
The most obvious difference, he says, is that people in the North were simply less
polite. “I know it sounds like a stereotype, but it’s true. You go into the city, and cars
are honkin’ at each other. Kids are mouthin’ off at their mothers. Grown men are
hollerin’ and cursin’. If someone acted like that in Mobile, I’d be obliged to jerk a
knot in his head.”
Indeed, for his first two years of college, McCabe often found his hands curling into
fists and the back of his neck beading with cold sweat. After a while, though, he realized
that he was alone in his readiness to tussle. “My friends didn’t understand,” he says.
“They’d say, ‘Hey, they don’t mean anything by it. They’re just blowing off some steam.’”
As you will discover in this chapter, McCabe was caught in a centuries-old culture
clash. Back home in Alabama, Southern culture encouraged him to protect his honor
and to be careful of insulting anyone else’s. As a result, McCabe and his fellow
Southerners tend to be chivalrous and respectful. Once offended or provoked,
however, Southerners may explode—hence the saying, “Southerners will be polite
until they are angry enough to kill you.”
462 chapter 12 PMOTIVATION AND EMOTIONO
Northerners, on the other hand, are more likely to express anger early and often.That way, their thinking goes, the anger doesn’t build up and lead to a blowout.In fact, the North has long enjoyed lower rates of murder and other violent crimesthan has the South. Meanwhile, reflecting their willingness to use violence to protectpeople’s honor, Southerners execute more felons, mete out more corporal punishmentin their schools, and pass more lenient laws regarding gun ownership, child abuse,and spousal abuse.
After a few years up North, McCabe became more or less bicultural. While atschool, he lost his tendencies to greet strangers with whom he made eye contact andto couch pointed remarks in euphemism. He came to ignore low-level incivilities. Butonce he stepped off the plane back home, “I was all ‘Yes ma’am,’ ‘No sir,’ and ‘Thankyou kindly.’”
People everywhere feel anger and other emotions such as fear and happiness,shame and disgust—psychological experiences that affect our actions, ourfeelings, and our bodies. People everywhere also have deep-seated biologicalurges such as feeding, fighting, fleeing, affiliating, and mating—as well as morerecently evolved needs like achievement and self-actualization. Many of thesemotives reveal our basic mammalian core; like any other animal, we humans spendlarge portions of our lives finding food, seeking shelter, fending off rivals, tend-ing to our allies, and seeking sex—in short, pursuing pleasure and avoiding pain.
Yet as McCabe’s experiences in the North and South show, how we express theseimpulses is strongly shaped by the people and cultures around us. And our emo-tional responses are far from the only impulses that are jointly determined by ourbiological heritage and our cultural context. Take eating. All people eat. But culturesvary vastly in what, how, where, when, and with whom their members repast.Compared to French people, for example, Americans have more conflicting feelingsabout food and focus less on its taste and more on its contents—alternately worry-ing about fats, carbohydrates, protein, and cholesterol. French people, in contrast,largely view food as a path to pleasure, and so indulge in a wider variety of fare—chocolates and cheeses, tripe and truffles, champagnes and champignons. Byamusing their mouths with smaller amounts of more foods, French people wind up eating a healthier diet—and have the slimmer figures to show it, arguespsychologist Paul Rozin.
In this chapter, we will consider some of the major motivational states that shapeour behavior, as well as emotional states such as anger, happiness, fear, and sadness.For each, we will see how physiological, cultural, and cognitive factors interact toshape the ways the motive or emotion is expressed.
MOTIVATIONAL STATES
Questions about why we act in a certain way, or why we feel as we do, can be answeredin various ways. Some answers emphasize what we referred to in Chapter 2 as ultimatecauses, including the powerful influence, over thousands and thousands of years,of natural selection. This reflects the key fact that, as we saw in that earlier chapter, evo-lutionary forces have shaped not only our physical features but also our psychologicalfeatures.
Other answers about why we act or feel as we do focus on causes that are specific tothe individual, but are nonetheless fairly remote from the present situation. For exam-ple, why do some people prefer to take psychology courses, while others prefer astro-physics? Here, the cause may be rooted in the person’s childhood. Perhaps the personhappened to experience unusual events, and this triggered a lifelong interest in humanbehavior and mental processes. Or perhaps the person is seeking to distance herselffrom her parents, and her parents have always been skeptical about psychology.In either case, these decades-past circumstances are now shaping the person’s behavior.
Important as these remote causes are, they do not tell us everything we need toknow. After all, we do not eat because we think, “Natural selection requires that I eat.”Likewise, we usually do not choose courses by reasoning through “Will this selectionhelp me to be different from my mother?” We need to ask, therefore, what the bridge isbetween remote causes, on the one side, and actual behaviors, on the other. What arethe more immediate causes of our behavior?
The answer to this question can take many forms, because, quite simply, we are moti-vated by different forces in different circumstances. Early theorists emphasized the bio-logical roots of our motivation, describing our diverse motivational states as all arisingfrom genetically endowed instincts. Early theorists such as William James (1890)thought humans were impelled by innate motives that were activated by features of theenvironment, much as spiders spin webs and birds build nests (Figure 12.1). FollowingJames’s lead, early psychologists drew up lists of instincts that they believed governedhuman behavior. Thus, for example, William McDougal (1923) asserted that humanshave 13 instincts, including parenting, food seeking, repulsion, curiosity, and gregari-ousness (i.e., a tendency to seek out social contact).
Unfortunately, different theorists came up with quite different lists of instincts,and in 1924, sociologist Luther Bernard counted over 5,000 instincts that had beenproposed by one scholar or another. This meant that instinct theory was—at best—inelegant, but, worse, commentators increasingly wondered what work the theory wasactually doing. What did it mean to “explain” the impulse to parent one’s children bypostulating a “parenting instinct”? We could, on this model, “explain” why people voteby asserting that there is a “self-governance instinct,” and explain why they go shop-ping by asserting a “shopping instinct.” In each case, our “explanation” merely providesa new bit of jargon that offers us no new information.
A different conception of motivation turns out to be more productive. More thana century ago, the French physiologist Claude Bernard (1813–1878) noted that everyorganism has both an external environment and an internal one. The external
PMotivational StatesO 463
(A) (B)
12.1 Instinctual actions Early theoristssuggested that humans’ motivations arisefrom instincts like those that lead (A) spi-ders to spin webs or (B) birds to buildnests.
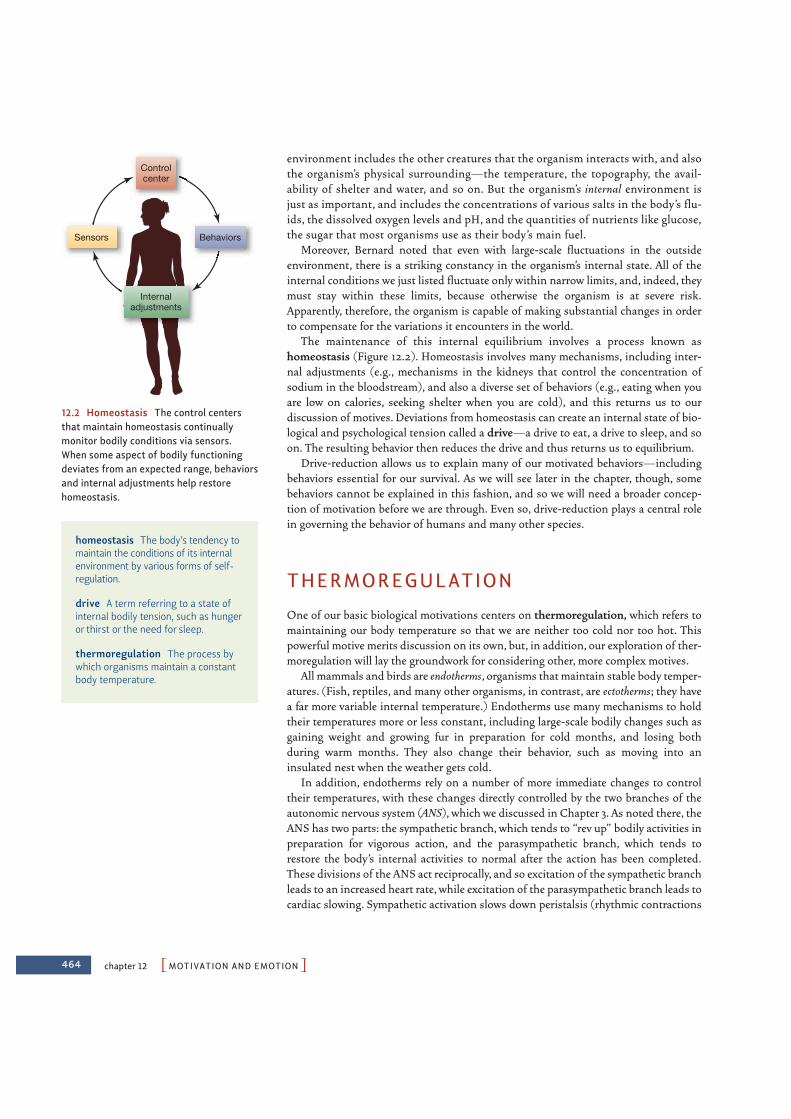
464 chapter 12 PMOTIVATION AND EMOTIONO
environment includes the other creatures that the organism interacts with, and alsothe organism’s physical surrounding—the temperature, the topography, the avail-ability of shelter and water, and so on. But the organism’s internal environment isjust as important, and includes the concentrations of various salts in the body’s flu-ids, the dissolved oxygen levels and pH, and the quantities of nutrients like glucose,the sugar that most organisms use as their body’s main fuel.
Moreover, Bernard noted that even with large-scale fluctuations in the outsideenvironment, there is a striking constancy in the organism’s internal state. All of theinternal conditions we just listed fluctuate only within narrow limits, and, indeed, theymust stay within these limits, because otherwise the organism is at severe risk.Apparently, therefore, the organism is capable of making substantial changes in orderto compensate for the variations it encounters in the world.
The maintenance of this internal equilibrium involves a process known as homeostasis (Figure 12.2). Homeostasis involves many mechanisms, including inter-nal adjustments (e.g., mechanisms in the kidneys that control the concentration ofsodium in the bloodstream), and also a diverse set of behaviors (e.g., eating when youare low on calories, seeking shelter when you are cold), and this returns us to ourdiscussion of motives. Deviations from homeostasis can create an internal state of bio-logical and psychological tension called a drive—a drive to eat, a drive to sleep, and soon. The resulting behavior then reduces the drive and thus returns us to equilibrium.
Drive-reduction allows us to explain many of our motivated behaviors—includingbehaviors essential for our survival. As we will see later in the chapter, though, somebehaviors cannot be explained in this fashion, and so we will need a broader concep-tion of motivation before we are through. Even so, drive-reduction plays a central rolein governing the behavior of humans and many other species.
THERMOREGULATION
One of our basic biological motivations centers on thermoregulation, which refers tomaintaining our body temperature so that we are neither too cold nor too hot. Thispowerful motive merits discussion on its own, but, in addition, our exploration of ther-moregulation will lay the groundwork for considering other, more complex motives.
All mammals and birds are endotherms, organisms that maintain stable body temper-atures. (Fish, reptiles, and many other organisms, in contrast, are ectotherms; they havea far more variable internal temperature.) Endotherms use many mechanisms to holdtheir temperatures more or less constant, including large-scale bodily changes such asgaining weight and growing fur in preparation for cold months, and losing both during warm months. They also change their behavior, such as moving into aninsulated nest when the weather gets cold.
In addition, endotherms rely on a number of more immediate changes to controltheir temperatures, with these changes directly controlled by the two branches of theautonomic nervous system (ANS), which we discussed in Chapter 3. As noted there, theANS has two parts: the sympathetic branch, which tends to “rev up” bodily activities inpreparation for vigorous action, and the parasympathetic branch, which tends torestore the body’s internal activities to normal after the action has been completed.These divisions of the ANS act reciprocally, and so excitation of the sympathetic branchleads to an increased heart rate, while excitation of the parasympathetic branch leads tocardiac slowing. Sympathetic activation slows down peristalsis (rhythmic contractions
homeostasis The body’s tendency tomaintain the conditions of its internalenvironment by various forms of self-regulation.
drive A term referring to a state ofinternal bodily tension, such as hungeror thirst or the need for sleep.
thermoregulation The process bywhich organisms maintain a constantbody temperature.
Controlcenter
Behaviors
Internaladjustments
Sensors
12.2 Homeostasis The control centersthat maintain homeostasis continuallymonitor bodily conditions via sensors.When some aspect of bodily functioningdeviates from an expected range, behaviorsand internal adjustments help restorehomeostasis.
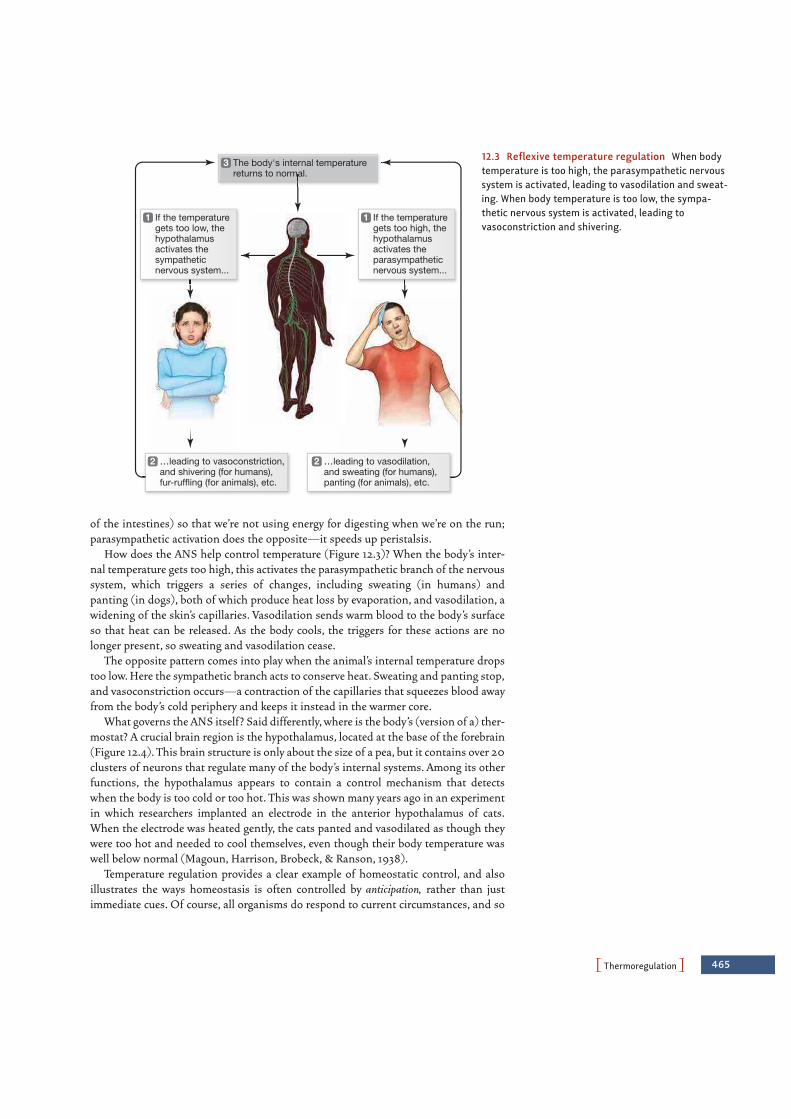
of the intestines) so that we’re not using energy for digesting when we’re on the run;parasympathetic activation does the opposite—it speeds up peristalsis.
How does the ANS help control temperature (Figure 12.3)? When the body’s inter-nal temperature gets too high, this activates the parasympathetic branch of the nervoussystem, which triggers a series of changes, including sweating (in humans) and panting (in dogs), both of which produce heat loss by evaporation, and vasodilation, awidening of the skin’s capillaries. Vasodilation sends warm blood to the body’s surfaceso that heat can be released. As the body cools, the triggers for these actions are nolonger present, so sweating and vasodilation cease.
The opposite pattern comes into play when the animal’s internal temperature dropstoo low. Here the sympathetic branch acts to conserve heat. Sweating and panting stop,and vasoconstriction occurs—a contraction of the capillaries that squeezes blood awayfrom the body’s cold periphery and keeps it instead in the warmer core.
What governs the ANS itself? Said differently, where is the body’s (version of a) ther-mostat? A crucial brain region is the hypothalamus, located at the base of the forebrain(Figure 12.4). This brain structure is only about the size of a pea, but it contains over 20clusters of neurons that regulate many of the body’s internal systems. Among its otherfunctions, the hypothalamus appears to contain a control mechanism that detectswhen the body is too cold or too hot. This was shown many years ago in an experimentin which researchers implanted an electrode in the anterior hypothalamus of cats.When the electrode was heated gently, the cats panted and vasodilated as though theywere too hot and needed to cool themselves, even though their body temperature waswell below normal (Magoun, Harrison, Brobeck, & Ranson, 1938).
Temperature regulation provides a clear example of homeostatic control, and alsoillustrates the ways homeostasis is often controlled by anticipation, rather than justimmediate cues. Of course, all organisms do respond to current circumstances, and so
PThermoregulationO 465
The body's internal temperaturereturns to normal.
3
If the temperaturegets too low, thehypothalamusactivates thesympatheticnervous system...
1
…leading to vasoconstriction,and shivering (for humans),fur-ruffling (for animals), etc.
2
If the temperaturegets too high, thehypothalamusactivates theparasympatheticnervous system...
1
…leading to vasodilation,and sweating (for humans),panting (for animals), etc.
2
12.3 Reflexive temperature regulation When bodytemperature is too high, the parasympathetic nervoussystem is activated, leading to vasodilation and sweat-ing. When body temperature is too low, the sympa-thetic nervous system is activated, leading tovasoconstriction and shivering.
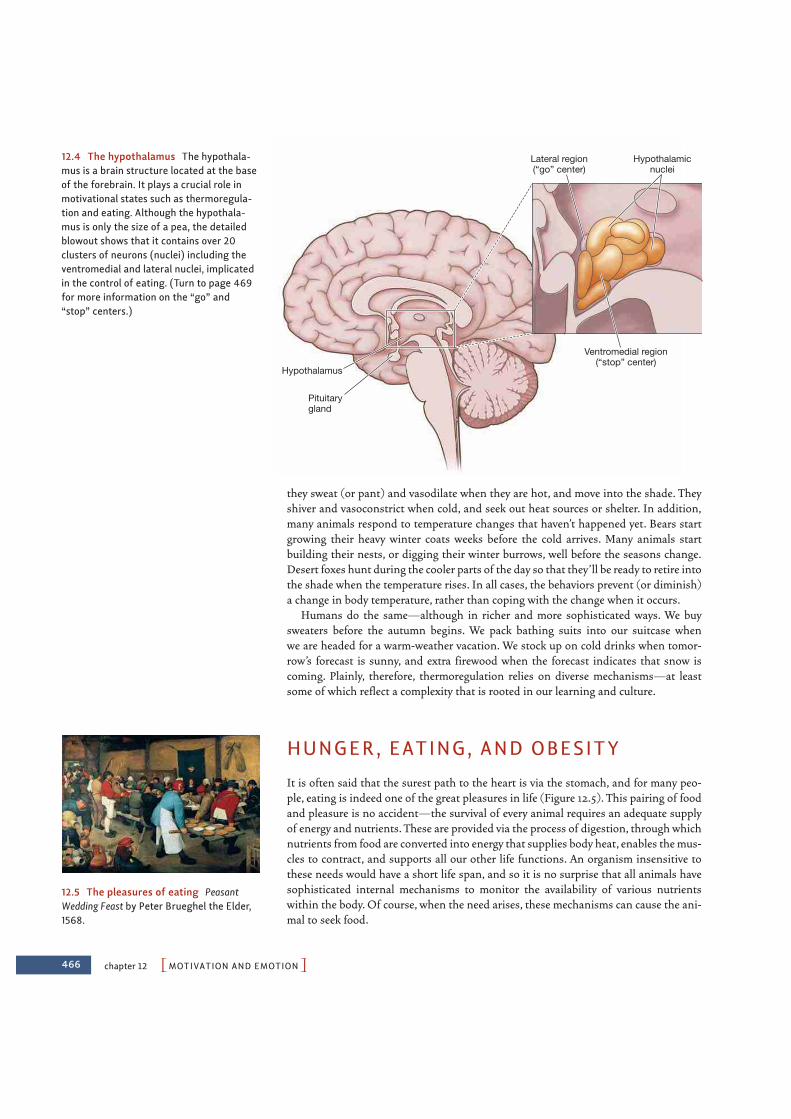
466 chapter 12 PMOTIVATION AND EMOTIONO
they sweat (or pant) and vasodilate when they are hot, and move into the shade. Theyshiver and vasoconstrict when cold, and seek out heat sources or shelter. In addition,many animals respond to temperature changes that haven’t happened yet. Bears startgrowing their heavy winter coats weeks before the cold arrives. Many animals startbuilding their nests, or digging their winter burrows, well before the seasons change.Desert foxes hunt during the cooler parts of the day so that they’ll be ready to retire intothe shade when the temperature rises. In all cases, the behaviors prevent (or diminish)a change in body temperature, rather than coping with the change when it occurs.
Humans do the same—although in richer and more sophisticated ways. We buysweaters before the autumn begins. We pack bathing suits into our suitcase when we are headed for a warm-weather vacation. We stock up on cold drinks when tomor-row’s forecast is sunny, and extra firewood when the forecast indicates that snow iscoming. Plainly, therefore, thermoregulation relies on diverse mechanisms—at leastsome of which reflect a complexity that is rooted in our learning and culture.
HUNGER, EATING, AND OBESITY
It is often said that the surest path to the heart is via the stomach, and for many peo-ple, eating is indeed one of the great pleasures in life (Figure 12.5). This pairing of foodand pleasure is no accident—the survival of every animal requires an adequate supplyof energy and nutrients. These are provided via the process of digestion, through whichnutrients from food are converted into energy that supplies body heat, enables the mus-cles to contract, and supports all our other life functions. An organism insensitive tothese needs would have a short life span, and so it is no surprise that all animals havesophisticated internal mechanisms to monitor the availability of various nutrientswithin the body. Of course, when the need arises, these mechanisms can cause the ani-mal to seek food.
Hypothalamicnuclei
Pituitarygland
Hypothalamus
Lateral region(“go” center)
Ventromedial region(“stop” center)
12.4 The hypothalamus The hypothala-mus is a brain structure located at the baseof the forebrain. It plays a crucial role inmotivational states such as thermoregula-tion and eating. Although the hypothala-mus is only the size of a pea, the detailedblowout shows that it contains over 20clusters of neurons (nuclei) including theventromedial and lateral nuclei, implicatedin the control of eating. (Turn to page 469for more information on the “go” and“stop” centers.)
12.5 The pleasures of eating PeasantWedding Feast by Peter Brueghel the Elder,1568.

How does the organism manage this feat of self-regulation? Is there an “appestat”that controls appetite and the behaviors that govern the intake of nutrients, the sameway a thermostat controls the body’s temperature? The answer turns out to be yes, butonly within the context of a complicated, multipart control system. To understand thiscontrol system, we must consider its physiological, cultural, and cognitive aspects.
Physiological Aspects of Hunger and Eating If animals are temporarily deprived of food, they usually eat more later, to return theirbodies to the original weight. If they are force-fed extra food, they later eat less. Theseobservations suggest that the animals have a caloric or body-weight set point that theyseek to maintain. In other words, animals do act as if they have an internal “appestat,”maintaining a relatively steady weight, just as the hypothalamus, acting as the body’sthermostat, maintains a relatively constant inner temperature.
Evidence for some sort of internal set point also comes from the fact that when foodis freely available, animals usually eat just about the right amount to satisfy their needs,while keeping their weight roughly constant. The “right amount” here refers not to thevolume of food, but to the number of calories in the food—and hence, the metabolicenergy it can provide. This was demonstrated in a study many years ago in whichresearchers decreased the caloric levels of rats’ food by adding nonnutritive cellulose.The more diluted the food, the more the rats ate, in a quantity that kept their totalcaloric intake roughly constant (Adolph, 1947). Similar claims apply to humans, withthe data indicating that each of us seems to have a target weight that our bodies workhomeostatically to maintain. However, this set point is to some extent adjustable, andgradual changes in one’s weight appear to alter the weight that is defended (Levitsky,2002; Pinel, Assanand, & Lehman, 2000; Ruderman, 1986).
Evidence for set points in humans comes from many sources, including the factthat crash dieters usually return to their starting weight soon after they go off theirdiets. Moreover, dieters do not lose nearly as much weight as we might expect basedon their reduced caloric intake. This is probably because the body compensates forthe caloric loss by reducing its metabolic rate (Guesbeck et al., 2001). In otherwords, when the body gets less food, it responds by burning fewer calories, defend-ing the set point weight. The consequence, of course, is that eating less does not leadto weight loss.
T H E RO L E O F T H E L I V E R
What mechanisms maintain someone’s body weight at its set point? The answerinvolves a number of internal signals, including signals that reflect the availability ofglucose (the sugar that serves as the body’s main fuel) in the blood.
Immediately after a meal, glucose is plentiful. Some is used right away, but much isconverted to glycogen and various fatty acids, which are stored for later use. When thisstored energy is needed, the process is reversed, and the glycogen and fatty acids areturned back into usable glucose. This conversion process is managed by the liver, andthe liver keeps other organs informed about the direction in which the metabolic trans-action is going, from glucose to glycogen or vice versa. If the supply of glucose exceedsthe body’s demand, so that the excess can be converted into glycogen and stored, theliver sends a satiety signal and the animal stops eating. If the body’s demand for glu-cose exceeds the supply, so that energy reserves are being used, the liver sends a hungersignal and the animal eats (M. I. Friedman & Stricker, 1976; Russek, 1971).
PHunger, Eating, and ObesityO 467
set point A general term for the levelat which negative feedback tries tomaintain stability.

468 chapter 12 PMOTIVATION AND EMOTIONO
Notice, though, that this regulatory system must—like the thermoregulatorysystem—anticipate the animal’s needs. Imagine that the liver only signaled the animalto eat when glucose supplies were already low. Since it often takes time to locate food,eat it, and then digest it, hours might elapse between the moment at which the liversends a “Need glucose!” signal and the time that the glucose finally arrives. Nutrientsupplies would be exhausted, and the animal could die. It’s not surprising, therefore,that organisms have a well-defined mechanism for avoiding this catastrophe. When anorganism has not eaten for a while, the level of glucose in the blood begins to drop.Before the level drops too far, the liver takes action, drawing some glycogen out ofstorage and converting it to glucose. As a result, the blood glucose level bounces back tonormal. The result of this sequence of events is an easily identifiable pattern—a grad-ual drop in blood glucose, usually lasting many minutes, followed by a quick rise, result-ing from the liver’s compensatory action.
This slow-drop/quick-rise pattern means that the organism is drawing on itsreserves, which signals the need for more glucose. When this blood glucose patternoccurs in rats, the animals start to eat (Campfield & Smith, 1990a, b). When it occursin humans, they say they are hungry (Campfield & Rosenbaum, 1992).
OT H E R CO N T RO L S I G N A LS FO R F E E D I N G
The liver is only one part of the body’s system for regulating food intake. The hypothal-amus also contains cells that are sensitive to glucose levels in the blood, and if theseglucoreceptors are damaged or disrupted, the result is ravenous eating (Miselis &Epstein, 1970).
Other signals come from other parts of the body. The stomach walls, for example, con-tain receptors sensitive to the nutrients dissolved in the digestive juices. When thesereceptors signal to the brain that nutrient supplies are on the way, the organism stopseating (Deutsch, Puerto, & Wang, 1978). Still other signals come from the fatty tissuesthemselves. To understand the importance of these signals, bear in mind that animalsdon’t eat just for the moment. After all, they can’t be sure that food will be available thenext time they need energy, and so they must eat enough both to satisfy their currentneeds and to store nutrients for later. This long-term store is provided by the fat, or adi-pose cells, distributed throughout their body. These cells absorb the fatty acids created bythe liver and swell in the process. The longer-term reserves then stand ready in case theanimal’s glycogen supplies are exhausted. If this happens, fatty acids drain from the adi-
pose cells into the bloodstream and are converted into glucose.Adipose tissue used to be regarded only as a kind of inert storage,
but we now know that it plays a major role in governing hunger. Fatcells, when full, secrete the chemical leptin into the bloodstream,where it is sensed by receptors in several places in the brain, includ-ing the hypothalamus (Bouret, Draper, & Simerly, 2004; Maffei etal., 1995; McGregor et al., 1996; Pinto et al., 2004). Leptin seems tosignal that there is plenty of fat in storage and no need to add more,and it may be one of the most important factors in governing anorganism’s food intake over the long term (Figure 12.6). Leptinappears to work by inhibiting the actions of several other neuro-chemicals, such as neuropeptide Y (NPY), manufactured in thehypothalamus and the gut. NPY itself turns out to be a powerfulappetite stimulant (Gibbs, 1996; B. G. Stanley, Magdalin, &
glucoreceptors Receptors in thebrain (in the area of the hypothala-mus) that detect the amount of glu-cose in the bloodstream.
leptin A chemical produced by theadipose cells that seems to signal thatplenty of fat is stored and that nomore fat is needed. This signal maydiminish eating.
neuropeptide Y (NPY) A chemicalfound widely in the brain and periph-ery. In the brain, it acts as a neuro-transmitter; when administered atsites in and near the hypothalamus, itis a potent elicitor of eating.
(A) (B)
12.6 Leptin deficiency The chemical lep-tin plays an important role in eating. A boywith total leptin deficiency (A) beforereceiving regular leptin injections, and (B)after receiving regular leptin injections.

PHunger, Eating, and ObesityO 469
Leibowitz, 1989), so leptin secretion from fat cells seems to provide the negative feed-back that holds NPY levels in check.
H Y P OT H A L A M I C CO N T RO L C E N T E RS
We have now talked about many cues that signal an organism’s nutritional needs, butwhat mechanism detects, and responds to, these cues? For years, the best candidate wasthe hypothalamus. We have already mentioned that the hypothalamus monitors bloodsugar levels, but in addition, the hypothalamus has been proposed as the receiving stationfor the body’s other eating-related cues, so that the hypothalamus becomes, in effect, themain control center for feeding. The dual-center theory proposed that one part of thehypothalamus—the lateral region—served as the “go” center for eating, while a differentpart—the ventromedial region—served as the “stop” center (Figure 12.4 on page 466).
Consistent with this claim, damage to the lateral region of the hypothalamus seemsto disrupt the initiation of feeding. If this region is lesioned, animals do not eat and willstarve to death unless force-fed. Conversely, damage to the ventromedial region dis-rupts circuits that would ordinarily tell the animal when to stop feeding. Surgicallyinduced lesions here cause rats to eat voraciously, until they finally reach a weight threetimes as great as before surgery (Figure 12.7). In humans, tumors in this hypothalamicregion have the same effect—leading to extreme obesity (Hoebel & Teitelbaum, 1976;N. E. Miller, Bailey, & Stevenson, 1950; Teitelbaum & Epstein, 1962).
Subsequent research has shown, however, that the mechanisms described in thistheory are only part of the story of how feeding is controlled. For example, lesions of theventromedial hypothalamus (the supposed “stop” center) have been found not just toincrease appetite (because the “stop” center is no longer functioning), but also toincrease the rate of fat storage (Stricker & Zigmond, 1976). In addition, the lateralhypothalamus appears to be only one of the “go” centers for feeding. This is indicatedby the fact that the appetite stimulant NPY exerts its strongest effects outside the lateralhypothalamus (Leibowitz, 1991). These and other results indicate that even though thehypothalamus is critical for the control of eating, other mechanisms are also crucial,some specialized for short-term energy needs, others for long-term storage.
W H Y SO M A N Y S I G N A LS ?
We have acknowledged a broad set of signals controlling when an organism startseating and when it stops, signals from the liver and from glucoreceptors in the brain,signals from the stomach and from the adipose tissue. In truth, other signals shouldbe added to this list, including, of course, the sensory qualities of the food itself.Thus, when we see a delicious-looking pastry or smell hot, fresh popcorn, these sen-sory cues can make us feel hungry and cause us to eat even if we are experiencing nocaloric need.
Why do we need so many cues? Part of the answer lies in the safety provided bybackup systems—so that if one system fails, the organism can still self-regulate. Andpart of the answer is that different signals monitor different aspects of our nutritionalneeds—some (such as leptin) keeping tabs on our longer-term needs, and others (likecues from the stomach) signaling our more immediate status and allowing us to dealwith hour-by-hour variations in our energy requirements.
The various cues also play different roles within the overall control of feeding.Some cues, like the sensory information from the food itself, directly signal the avail-ability of food in the environment. Other, less direct cues play their main role in
12.7 Rat with ventromedial hypothala-mus lesion
dual-center theory The hypothesisthat one area in the lateral hypothala-mus is the “on” center, the initiator ofeating, while another area in the ven-tromedial hypothalamus is the “off”center, the terminator of eating.Current evidence indicates thatalthough these brain regions are cru-cial for eating, the regulation of eatingalso involves other circuits.

470 chapter 12 PMOTIVATION AND EMOTIONO
creating a motivational state for the organism so that, broadly put, these cues lead theorganism to feel hungry so it is motivated to seek food. Finally, some cues potentiateother cues—that is, they make the other cues more salient and more persuasive. Inone study, for example, researchers recorded activity levels in cells in a waking mon-key’s hypothalamus (Mora, Rolls, & Burton, 1976; also Rolls, 1978). Those cells wereactivated when the animal was shown a peanut or banana, but only when the animalwas hungry. In this fashion, the cues reflecting the animal’s internal state did notdirectly influence its behavior. Instead, these cues potentiated the sensory cues, sothat the animal would be more likely to detect (and respond to) the immediate avail-ability of food when it needed nutrients.
Cultural and Cognitive Aspects of Hunger and EatingThe hypothalamus and other biological structures play a crucial role in deciding whenand how much we eat. But other factors are also critical, including the culture in whichwe live.
CU LT U R E A N D E AT I N G
Why do many Europeans feel hungry for their main meal of the day in the early after-noon, while others on the continent—the French, for example—hunger for their mainmeal only in the evening? Why is it that most Americans grow hungry for dinner at6:00 p.m. or so, while the British are likely to seek food a couple of hours earlier, at tea-time? These questions surely cannot be answered in terms of differences among French,American, or British livers, or geographical variation in how the hypothalamus is wired.Instead these points remind us that our feeding patterns are shaped by our culturalenvironment.
Culture also governs how much we eat. Many of us put considerable effort into con-trolling our food intake, usually with the aim of achieving a particular appearance. Butwhat defines the ideal toward which people are striving? The answer lies in the culturalsetting, and cultures set quite different standards. The women painted by Rubens,Matisse, and Renoir, for example, were considered the feminine ideal in their day, andall three artists (two of them living just a century ago) would probably judge today’ssupermodels to be undernourished and quite unappealing (Figure 12.8).
Cultural factors provide a constant backdrop for our thinking, expectations, and per-ceptions. But we are also influenced by specific situations. As one example, let’s note
that there are direct social influences on feeding, so that we are morelikely to eat when we are surrounded by others who are eating. Theclassic demonstration of this comes from an experiment done yearsago; it showed that a hen who has had her fill of grain will eagerlyresume her meal if joined by other hens that are still hungry (Bayer,1929). Similar effects can easily be observed with humans.
Social influences are also tied to people’s aspirations (and some-times unhealthy aspirations) toward thinness. In ways we will discussin Chapter 13, each of us is powerfully influenced by the peoplearound us, so that how we act and, indeed, what we think about our-selves are shaped by how they perceive us and what they expect fromus. The simple fact is that how people perceive us, and what theyexpect, are shaped by our bodily form—in particular, how heavy orthin we are.(A) (B)
12.8 Changing feminine ideals Culturalideals regarding body shape change overtime, as reflected by (A) Rubens’s Venusbefore a Mirror (1614–1615) and (B) modernmedia portrayals.
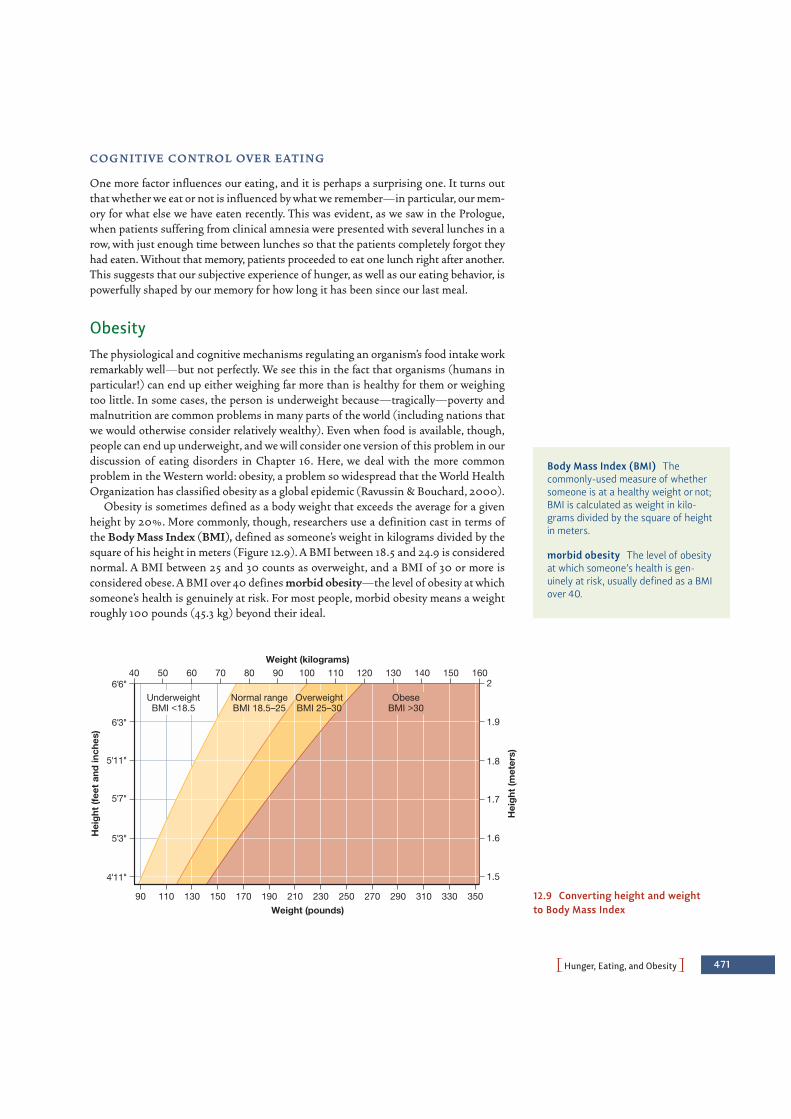
PHunger, Eating, and ObesityO 471
CO G N I T I V E CO N T RO L O V E R E AT I N G
One more factor influences our eating, and it is perhaps a surprising one. It turns outthat whether we eat or not is influenced by what we remember—in particular, our mem-ory for what else we have eaten recently. This was evident, as we saw in the Prologue,when patients suffering from clinical amnesia were presented with several lunches in arow, with just enough time between lunches so that the patients completely forgot theyhad eaten. Without that memory, patients proceeded to eat one lunch right after another.This suggests that our subjective experience of hunger, as well as our eating behavior, ispowerfully shaped by our memory for how long it has been since our last meal.
ObesityThe physiological and cognitive mechanisms regulating an organism’s food intake workremarkably well—but not perfectly. We see this in the fact that organisms (humans inparticular!) can end up either weighing far more than is healthy for them or weighingtoo little. In some cases, the person is underweight because—tragically—poverty andmalnutrition are common problems in many parts of the world (including nations thatwe would otherwise consider relatively wealthy). Even when food is available, though,people can end up underweight, and we will consider one version of this problem in ourdiscussion of eating disorders in Chapter 16. Here, we deal with the more commonproblem in the Western world: obesity, a problem so widespread that the World HealthOrganization has classified obesity as a global epidemic (Ravussin & Bouchard, 2000).
Obesity is sometimes defined as a body weight that exceeds the average for a givenheight by 20%. More commonly, though, researchers use a definition cast in terms ofthe Body Mass Index (BMI), defined as someone’s weight in kilograms divided by thesquare of his height in meters (Figure 12.9). A BMI between 18.5 and 24.9 is considerednormal. A BMI between 25 and 30 counts as overweight, and a BMI of 30 or more isconsidered obese. A BMI over 40 defines morbid obesity—the level of obesity at whichsomeone’s health is genuinely at risk. For most people, morbid obesity means a weightroughly 100 pounds (45.3 kg) beyond their ideal.
Body Mass Index (BMI) Thecommonly-used measure of whethersomeone is at a healthy weight or not;BMI is calculated as weight in kilo-grams divided by the square of heightin meters.
morbid obesity The level of obesityat which someone’s health is gen-uinely at risk, usually defined as a BMIover 40.
Hei
ght
(fee
t an
d in
ches
)
Hei
ght
(met
ers)
Weight (pounds)
Weight (kilograms)
210
40 50 60 70 80 90 100 110 120 130 140 150 160
1.5
1.6
1.7
1.8
1.9
2UnderweightBMI <18.5
Normal rangeBMI 18.5–25
OverweightBMI 25–30
ObeseBMI >30
310 330 350270 290190 230 25090 110 150130 170 12.9 Converting height and weight to Body Mass Index
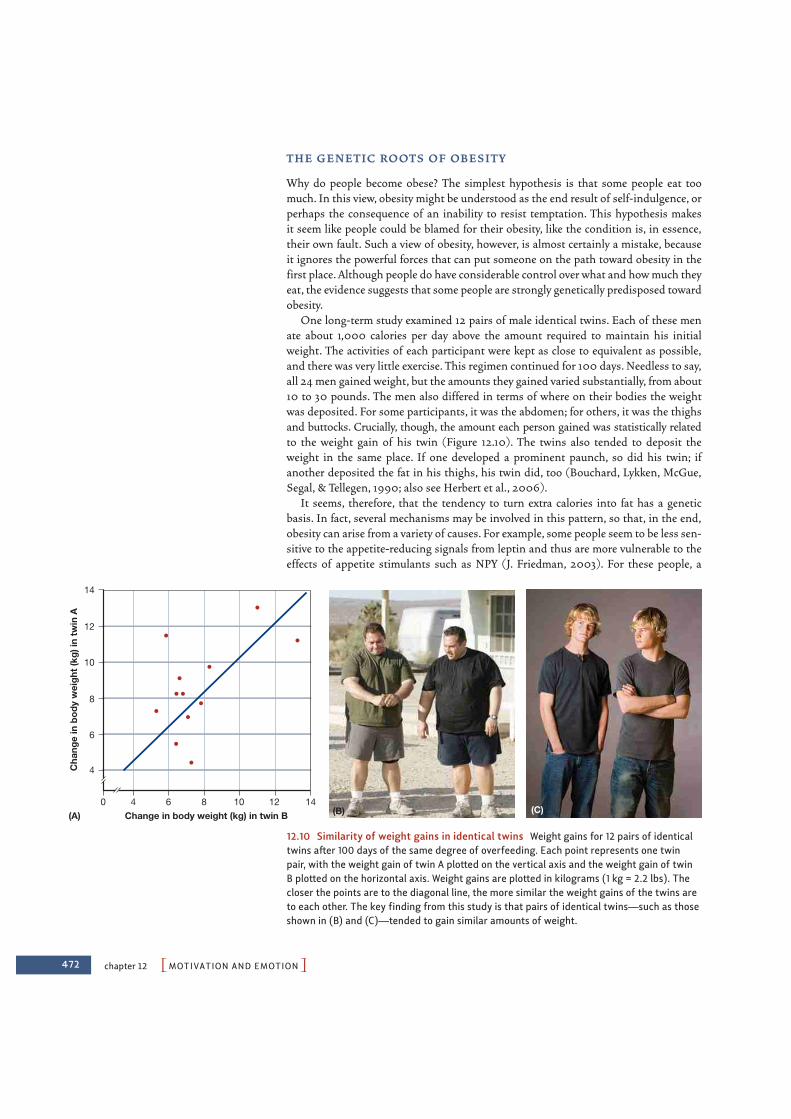
472 chapter 12 PMOTIVATION AND EMOTIONO
T H E G E N E T I C RO OTS O F OB E S I T Y
Why do people become obese? The simplest hypothesis is that some people eat toomuch. In this view, obesity might be understood as the end result of self-indulgence, orperhaps the consequence of an inability to resist temptation. This hypothesis makes it seem like people could be blamed for their obesity, like the condition is, in essence,their own fault. Such a view of obesity, however, is almost certainly a mistake, becauseit ignores the powerful forces that can put someone on the path toward obesity in thefirst place. Although people do have considerable control over what and how much theyeat, the evidence suggests that some people are strongly genetically predisposed towardobesity.
One long-term study examined 12 pairs of male identical twins. Each of these menate about 1,000 calories per day above the amount required to maintain his initialweight. The activities of each participant were kept as close to equivalent as possible,and there was very little exercise. This regimen continued for 100 days. Needless to say,all 24 men gained weight, but the amounts they gained varied substantially, from about10 to 30 pounds. The men also differed in terms of where on their bodies the weightwas deposited. For some participants, it was the abdomen; for others, it was the thighsand buttocks. Crucially, though, the amount each person gained was statistically relatedto the weight gain of his twin (Figure 12.10). The twins also tended to deposit theweight in the same place. If one developed a prominent paunch, so did his twin; ifanother deposited the fat in his thighs, his twin did, too (Bouchard, Lykken, McGue,Segal, & Tellegen, 1990; also see Herbert et al., 2006).
It seems, therefore, that the tendency to turn extra calories into fat has a geneticbasis. In fact, several mechanisms may be involved in this pattern, so that, in the end,obesity can arise from a variety of causes. For example, some people seem to be less sen-sitive to the appetite-reducing signals from leptin and thus are more vulnerable to theeffects of appetite stimulants such as NPY (J. Friedman, 2003). For these people, a
(A) (B) (C)
14
12
10
8
6
4
6 8 10 12 14Change in body weight (kg) in twin B
Cha
nge
in b
ody
wei
ght
(kg)
in t
win
A
0 4
12.10 Similarity of weight gains in identical twins Weight gains for 12 pairs of identicaltwins after 100 days of the same degree of overfeeding. Each point represents one twinpair, with the weight gain of twin A plotted on the vertical axis and the weight gain of twin B plotted on the horizontal axis. Weight gains are plotted in kilograms (1 kg = 2.2 lbs). Thecloser the points are to the diagonal line, the more similar the weight gains of the twins areto each other. The key finding from this study is that pairs of identical twins—such as thoseshown in (B) and (C)—tended to gain similar amounts of weight.
PThreat and AggressionO 473
tendency to overeat may be genetically rooted. In addition, people differ in the effi-ciency of their digestive apparatus, with some people simply extracting more caloriesfrom any given food. People also differ in their overall metabolic level; if, as a result,less nutrient fuel is burned up, then more is stored as fat (Astrup, 2000; also M. I.Friedman, 1990a, b; Sims, 1986).
Given these various mechanisms, should we perhaps think about obesity as somesort of genetic defect, a biologically rooted condition that leads to substantial healthrisk? Proponents of the “thrifty gene” hypothesis emphatically reject this suggestion.They note that our ancestors lived in times when food supplies were unpredictable andfood shortages were common, so natural selection may have favored individuals whohad especially inefficient metabolisms and, as a result, stored more fat. These individu-als would have been better prepared for lean times and thus may have had a survivaladvantage. As a result, the genes leading to this fat storage might have been assets, notdefects (J. Friedman, 2003; Fujimoto et al., 1995; Groop & Tuomi, 1997; Ravussin,1994).
E N V I RO N M E N TA L FACTO RS A N D OB E S I T Y
Clearly, then, “thrifty genes” might have helped our ancestors to maintain a healthybody weight, but our ancestors lived in a time in which food was scarce. The same geneswill have a different outcome in modern times—especially for people living in an afflu-ent culture in which a quick trip to the supermarket provides all the calories one wishes.In this modern context, the “thrifty genes” can lead to levels of obesity that create seri-ous health problems.
Whether for genetic reasons, though, or otherwise, the evidence is clear that obesityrates are climbing across the globe. In the United States, roughly 23% of the populationin 1991 was obese; more recent estimates of the rate—30%—are appreciably higher(J. Friedman, 2003). Similar patterns are evident in other countries. Over the last 10years, for example, the obesity rates in most European countries have increased by atleast 10%, and, in some countries, by as much as 40%. These shifts cannot reflectchanges in the human genome; genetic changes proceed at a much slower pace. Instead,the increase has to be understood in terms of changes in diet and activity level—withpeople consuming more calorically dense, high-fat foods and living a lifestyle thatcauses them to expend relatively few calories in their daily routines.
This increase in obesity rates is associated with increased rates of many healthproblems, including heart attack, stroke, Type 2 diabetes, and some types of cancer.The debate continues over the severity of these risks for people with moderate levels ofobesity—e.g., a BMI between 30 and 40 (Couzin, 2005; Yan et al., 2006). There is nodebate, however, about the health risks of so-called morbid obesity (a BMI of 40 orhigher), and this makes the worldwide statistics on obesity a serious concern for healthprofessionals.
THREAT AND AGGRESSION
Thermoregulation and hunger are primarily regulated by mechanisms that monitor andmaintain the organism’s internal environment (although, as we have seen, external cuesare also important). Other motives, in contrast, depend primarily on external triggers,and an example is our reaction to intense threat. In this case, the instigation is the lionabout to pounce, or the bully about to strike us down. Even so, our discussion of threat
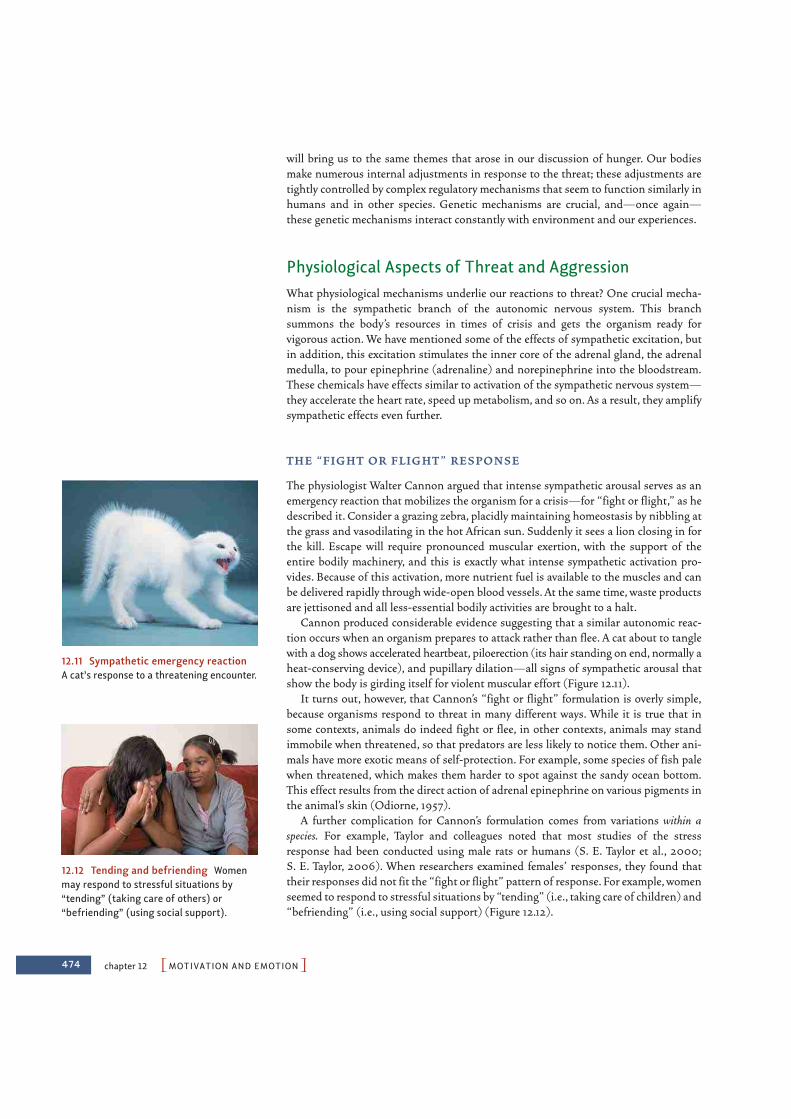
474 chapter 12 PMOTIVATION AND EMOTIONO
will bring us to the same themes that arose in our discussion of hunger. Our bodiesmake numerous internal adjustments in response to the threat; these adjustments aretightly controlled by complex regulatory mechanisms that seem to function similarly inhumans and in other species. Genetic mechanisms are crucial, and—once again—these genetic mechanisms interact constantly with environment and our experiences.
Physiological Aspects of Threat and AggressionWhat physiological mechanisms underlie our reactions to threat? One crucial mecha-nism is the sympathetic branch of the autonomic nervous system. This branchsummons the body’s resources in times of crisis and gets the organism ready forvigorous action. We have mentioned some of the effects of sympathetic excitation, butin addition, this excitation stimulates the inner core of the adrenal gland, the adrenalmedulla, to pour epinephrine (adrenaline) and norepinephrine into the bloodstream.These chemicals have effects similar to activation of the sympathetic nervous system—they accelerate the heart rate, speed up metabolism, and so on. As a result, they amplifysympathetic effects even further.
T H E “ F I G H T O R F L I G H T ” R E S P O N S E
The physiologist Walter Cannon argued that intense sympathetic arousal serves as anemergency reaction that mobilizes the organism for a crisis—for “fight or flight,” as hedescribed it. Consider a grazing zebra, placidly maintaining homeostasis by nibbling atthe grass and vasodilating in the hot African sun. Suddenly it sees a lion closing in forthe kill. Escape will require pronounced muscular exertion, with the support of theentire bodily machinery, and this is exactly what intense sympathetic activation pro-vides. Because of this activation, more nutrient fuel is available to the muscles and canbe delivered rapidly through wide-open blood vessels. At the same time, waste productsare jettisoned and all less-essential bodily activities are brought to a halt.
Cannon produced considerable evidence suggesting that a similar autonomic reac-tion occurs when an organism prepares to attack rather than flee. A cat about to tanglewith a dog shows accelerated heartbeat, piloerection (its hair standing on end, normally aheat-conserving device), and pupillary dilation—all signs of sympathetic arousal thatshow the body is girding itself for violent muscular effort (Figure 12.11).
It turns out, however, that Cannon’s “fight or flight” formulation is overly simple,because organisms respond to threat in many different ways. While it is true that insome contexts, animals do indeed fight or flee, in other contexts, animals may standimmobile when threatened, so that predators are less likely to notice them. Other ani-mals have more exotic means of self-protection. For example, some species of fish palewhen threatened, which makes them harder to spot against the sandy ocean bottom.This effect results from the direct action of adrenal epinephrine on various pigments inthe animal’s skin (Odiorne, 1957).
A further complication for Cannon’s formulation comes from variations within aspecies. For example, Taylor and colleagues noted that most studies of the stressresponse had been conducted using male rats or humans (S. E. Taylor et al., 2000;S. E. Taylor, 2006). When researchers examined females’ responses, they found thattheir responses did not fit the “fight or flight” pattern of response. For example, womenseemed to respond to stressful situations by “tending” (i.e., taking care of children) and“befriending” (i.e., using social support) (Figure 12.12).
12.11 Sympathetic emergency reactionA cat’s response to a threatening encounter.
12.12 Tending and befriending Womenmay respond to stressful situations by“tending” (taking care of others) or“befriending” (using social support).

PThreat and AggressionO 475
These limitations notwithstanding, the mechanism Cannon highlighted—an emer-gency system rooted in the sympathetic nervous system—is essential for many individ-uals in many species. At the same time, however, arousal of the sympathetic branch ofthe ANS can be disruptive and even damaging. This is especially clear in humans. In ourday-to-day lives, we rarely encounter emergencies that call for violent physical effort,but our biological nature has not completely changed just because the modern worldcontains no threats from saber-toothed tigers. We are plagued instead by chronic stres-sors like traffic jams, ornery bosses, pressing deadlines, and agonizing world crises.Although we often feel impelled to defend ourselves against these threats of the mod-ern world, physical action is frequently inappropriate, ineffective, or illegal.Nonetheless, we are stuck with the same emergency reactions that our ancestors had,and so we keep ourselves armed physiologically against situations we cannot really con-trol. The resulting bodily wear and tear can take a serious toll (e.g., Sapolsky, 1998).
AG G R E SS I O N A N D P R E DAT I O N
It seems, then, that our biological reaction to threat may not always serve us well in ourmodern environment. Nonetheless, this reaction is well rooted in our biology, and it iscertainly similar to the reaction pattern easily observed in many other species. It is areaction pattern that has been shaped by natural selection and that has, over eachspecies’ history, contributed to survival by preparing the organism for whatever ener-getic activities it needs to escape the threat.
But what does the animal do once the emergency reaction is under way? Are thesubsequent steps also shared across species? To answer this question, it is helpful todraw on the comparative method, studying nonhumans as well as humans to see whatkinds of commonalities in our behavior reflect shared biological heritage.
As a first and crucial point, though, we need to distinguish two forms of violencethat organisms engage in—aggression and predation. Predators hunt and kill for food,but they do so quite dispassionately. A predator about to pounce on its prey shows noneof the signs of anger, and so a dog on the verge of catching a rabbit never growls, nordoes it have its ears laid back (K. Z. Lorenz, 1966). Predatory attack is instead moti-vated by hunger, and it is controlled by the same brain sites as eating (Hutchinson &Renfrew, 1966). In contrast, aggressive or self-defense behaviors are controlled by dis-tinct brain areas, are triggered by different situations, and certainly show differentbehavioral profiles. In our discussion of aggression, therefore, it will be best to holdpredatory attack to the side—as part of an animal’s food-gathering repertoire, and notpart of its response to threat.
M A L E AG G R E SS I O N A N D H O R M O N E S
Genuine combat is, in fact, widespread among animals, and there is probably nospecies that has forsworn aggression altogether (Figure 12.13). Fish chase and nipeach other; lizards lunge and push; birds attack with wing, beak, and claw; and onand on. In most cases, the individuals we identify as aggressive are male, because,among vertebrates, the male is by far the more physically aggressive sex. In somemammals, this sex difference in combativeness is apparent even in childhood play. Young male rhesus monkeys, for instance, engage in much more vigorousrough-and-tumble play than their sisters (Harlow, 1962). Among humans, boysworldwide are more physically aggressive than girls (Geary & Bjorklund, 2000),and as adults, male murderers outnumber females by a ratio of 10:1 (C. A. Anderson &Bushman, 2002).
12.13 Animal combat Animals in manyspecies often engage in ferocious combat,usually over some resource (such as food,territory, or a potential mate).
comparative method A researchmethod in which one makes system-atic comparisons among differentspecies in order to gain insights intothe function of a particular structureor behavior, or the evolutionary originsof that structure or behavior.

476 chapter 12 PMOTIVATION AND EMOTIONO
However, this gender difference holds only for physical aggression. Human femalesare also aggressive, but their aggression tends to rely on verbal or social assaults,not physical violence. Thus, females attack by means of insults or the spreading ofrumors; they take steps to isolate someone from friends and allies (Figure 12.14). If wefocus on these sorts of aggression, then it is women, not men, who are the aggressivesex (Oesterman et al., 1998).
Why is physical aggression so much more prevalent in men? Biological factors areclearly relevant, because aggression is partially influenced by hormones, particularly thesex hormone testosterone. High testosterone levels in the bloodstream are associatedwith increased physical aggressiveness in many different species, including fish, lizards,turtles, birds, rats, mice, and monkeys (D. E. Davis, 1964; A. Siegel & Demetrikopoulos,1993). However, the relationship between testosterone and physical aggression is com-plex. As one complication, at least some human aggression bears no relationship to testos-terone levels, so it must be shaped by other factors (e.g., Book, Starzyk, & Qunisey, 2001).In addition, high testosterone levels can be both a cause and an effect of aggressive behav-ior. Thus, testosterone administered externally can increase subsequent aggressiveness,but successful aggressive encounters can also cause increased secretion of testosterone(Dabbs, 1992; Rosenzweig, Leiman, & Breedlove, 1996; Sapolsky, 1998).
Cultural and Cognitive Aspects of Threat and AggressionIn many cases, humans (just like other animals) become aggressive in an effort tosecure or defend resources. This is evident in the wars that have grown out of nationaldisagreements about who owns a particular expanse of territory; on a smaller scale, it isevident when two drivers come to blows over a parking space. Humans also becomeaggressive for reasons that hinge on symbolic concerns, such as insults to honor orobjections to another person’s beliefs or behavior. The latter type of aggression is clearin many of the hateful acts associated with stereotyping. It is also a powerful contribu-tor to the conflict among ethnic groups or people of different religions.
I N D I V I D UA L D I F F E R E N C E S I N AG G R E SS I O N
Whatever the source of the aggression, it is obvious that people vary enormously in howaggressive they are (Figure 12.15). Some of us respond to provocation with violence.Some turn the other cheek. Some find nonviolent means of asserting themselves. Whatdetermines how someone responds?
For many years, investigators believed that aggression was more likely in people withrelatively low self-esteem, on the argument that such individuals wereparticularly vulnerable to insult and also likely to have few other meansof responding. More recent work, however, suggests that the opposite isthe case, that social provocations are more likely to inspire aggression ifthe person provoked has unrealistically high self-esteem (Baumeister,2001; Bushman & Baumeister, 2002). Such a person is particularlylikely to perceive the provocation as a grievous assault, challenging hisinflated self-image; in many cases, violence will be the result.
Other personality traits are also relevant to aggression, including afactor called sensation seeking, a tendency to seek out varied and novelexperiences in their daily lives. High levels of sensation seeking areassociated with aggressiveness, and so are high scores on tests that
12.14 Social aggression In males,aggression is often physical (pushing orpunching). In females, aggression usuallytakes a different form. They may attackeach other, for example, by spreading gos-sip or rumors; they take steps to isolatesomeone from friends and allies.
testosterone The principal male sexhormone in mammals.
(A) (B)
12.15 Variation in human aggressionHumans vary enormously in how aggressivethey are. (A) Some (like His Holiness theDalai Lama) develop a capacity for lovingcompassion that makes aggression almostunthinkable. (B) Others (like these gangmembers) participate in violent aggressionin almost every day of their lives.

PThreat and AggressionO 477
measure the trait of impulsivity, a tendency to act without reflecting on one’s actions(Anderson & Bushman, 2002; Joireman, Anderson, & Strathman, 2003).
In addition, whether someone turns to aggression or not is influenced heavily by theculture in which he was raised. Some cultures explicitly eschew violence; this is true, forexample, in communities of Quakers. But other cultures prescribe violence, often viarules of chivalry and honor that demand certain responses to certain insults. Gangviolence in many U.S. cities can be understood partly in this way, as can some of thefighting among the warlords of Somalia. Cultural differences are also evident when wecompare different regions within the United States; for example, the homicide rate inthe South is reliably higher than in the North, and statistical evidence suggests that thiscontrast is best attributed to social differences and not to factors like population den-sity, economic conditions, or climate (Nisbett & Cohen, 1996).
How exactly does culture encourage or discourage aggression? The answer in somecases involves explicit teaching—when, for example, our parents tell us not to beaggressive, or they punish us for some aggressive act. In other cases, the learninginvolves picking up subtle cues that tell us, for example, whether our friends think thataggression is acceptable, or repugnant, or cool. In still other cases, the learning is of adifferent sort and involves what we called observational learning in Chapter 7. This islearning in which the people around us model through their own actions how oneshould handle situations that might provoke aggression.
We noted in Chapter 7, though, that observational learning can also proceed on amuch larger scale, thanks to the societal influences that we are all exposed to. Considerthe violence portrayed on television and in movies. On some accounts, prime-time tel-evision programs contain an average of five violent acts per hour, as characters punch,shoot, and sometimes murder each other (Figure 12.16). Overall, investigators estimatethat the average American child observes more than 10,000 acts of TV violence everyyear (e.g., Anderson & Bushman, 2001).
Evidence that this media violence promotes violence in the viewer comes from studiesof violence levels within a community before and after television was introduced, or beforeand after the broadcast of particularly gruesome footage of murders or assassinations.These studies consistently show that assault and homicide rates increase after such expo-sures (Centerwall, 1989; Joy, Kimball, & Zabrack, 1986). Other studies indicate that chil-dren who are not particularly aggressive become more so after viewing TV violence (e.g.,Huesmann, Lagerspetz, & Eron, 1984; Huesmann & Miller, 1994; for related data show-ing the effects of playing violent video games, see Carnagey & Anderson, 2005).
These studies leave little doubt that there is a strong correlation, such that those whoview violence are more likely than other people to be violent themselves. But does thiscorrelation reveal a cause-and-effect relationship, in which the viewing can actuallycause someone to be more violent? Many investigators believe it can (Anderson &Bushman, 2001, 2002; Bushman & Anderson, 2009; Carnagey, Anderson, &Bartholow, 2007; Cassel & Bernstein, 2007). Indeed, the evidence persuaded six major professional societies (including the American Psychological Association, theAmerican Medical Association, and the American Psychiatric Association) to issue a joint statement noting that studies “point overwhelmingly to a causal connec-tion between media violence and aggressive behavior in some children” (JointStatement, 2000, p. 1).
L I M I T I N G AG G R E SS I O N
Whether motivated by a wish to defend a territory or a desire to repay an insult, aggres-sion is costly. If we focus just on the biological costs to the combatants, aggression is
12.16 Television violence Prime-timetelevision, on some estimates, displays anaverage of five violent acts per hour.Saturday-morning children’s programmingis far worse, as characters constantlypunch and shoot at and sometimes killeach other.
478 chapter 12 PMOTIVATION AND EMOTIONO
dangerous and can lead to injury or death. For some species, and for some forms of vio-lence, these costs are simply the price of certain advantages—for survival or for repro-duction (e.g., Pennisi, 2005). Even so, natural selection has consistently favored waysof limiting the damage done by aggression.
One way that natural selection seems to have done this is by ensuring that animalsare keenly sensitive to the strength of their enemies. If the enemy seems much stronger(or more agile or better armed or armored) than oneself, the best bet is to concededefeat quickly, or better yet, never to start the battle at all. Animals therefore use a vari-ety of strategies to proclaim their strength, with a goal of winning the battle before itstarts. They roar, they puff themselves up, and they offer all sorts of threats, all with theaim of appearing as powerful as they possibly can (Figure 12.17A). Conversely, once ananimal determines that it is the weaker one and likely to lose a battle, it uses a variety ofstrategies for avoiding a bloody defeat, usually involving specific conciliatory signals,such as crouching or exposing one’s belly (Figure 12.17B).
Similar mechanisms are evident in humans. For example, the participants in a barfight or a schoolyard tussle try to puff themselves up to intimidate their opponents, justas a moose or a mouse would. Likewise, we humans have a range of conciliatorygestures we use to avoid combat—body postures and words of appeasement.
All of these mechanisms, however, apply largely to face-to-face combat; sad to say,these biologically based controls have little effect on the long-distance, large-scaleaggression that our species often engages in. As a result, battles between nations willprobably not be avoided by political leaders roaring or thumping their chests; soldiersoperating a missile-launcher cannot see (much less respond to) their targets’ concilia-tory body posture. Our best hope for reducing human aggression, therefore, is that thehuman capacity for moral and intellectual reflection will pull us away from combat, andthat considering the cruelty and destruction of violence will lead us to reconcile ourdifferences by other means.
SEXUAL BEHAVIOR
We have now considered three powerful motives: thermoregulation, hunger, andresponses to threat. In each case, we have discussed mechanisms that we share with othercreatures (e.g., the autonomic responses associated with body temperature regulation,homeostatic regulation of blood sugar, the biological response to threat), and in each case,the adaptive function roots of these mechanisms are easy to discern. In addition, we have
(A) (B)
12.17 Threatening and conciliatorydisplays (A) Some species threaten byshouting at the top of their lungs, likehowler monkeys, who scream at each otherfor hours on end. (B) In most species, ani-mal combat ends before either animal suf-fers a mortal wound. As soon as one of thecombatants determines that its defeat islikely, it surrenders and explicitly signals thesurrender through a submissive display—such as exposing the belly or the throat.

PSexual BehaviorO 479
seen that these genetically rooted mechanisms are powerfully influenced by learning andculture (e.g., the fashions that dictate the clothes we wear, the implicit rules that determinewhat we eat, and the cultural practices that govern how we respond to provocation).
These motives are all very well and good, but you wouldn’t even exist without anothercrucial motive, namely, sex. This motive is unmistakably rooted in our physiology justas thermoregulation, hunger, and the response to threat are. In some ways, however, sexis different. Unlike the other biological motives, sex is inherently social, and in humansits pursuit is intertwined with all manner of cultural patterns and attitudes.
Let us start our discussion with the aspects of sexual behavior that are most obviouslybiological—mating itself and the role of hormones in controlling an organism’s behavior.We will then turn to aspects of sexual behavior for which the influence of biology, and ofevolution in particular, is still hotly debated, touching on some of the topics that we firstmet in Chapter 2, in our broader discussion of evolution. (We will consider love andromance in Chapter 13, when we focus on the ways people relate to each other.)
Physiological Aspects of SexualitySexual behavior in animals is ultimately about arranging for the union of sperm andova, but this can proceed only after male and female have met, courted, and determinedeach other to be a suitable mate. At that point, at least for terrestrial mammals andbirds, the male generally introduces his sperm cells into the genital tract of the female.The sperm then has to encounter a ready ovum, and finally, the fertilized egg can developif it is provided with the appropriate conditions. (In Chapter 14, we will consider howa fertilized egg grows into a child.) For now, we note that the sequence of eventsrequires a complex hormonal control system that links the brain, reproductive organs,and behavior.
H O R M O N A L C YC L E S
In sex, timing is everything. Most animals are sexually receptive, and both biologicallyand behaviorally prepared to mate, only at certain points in the year. In mammals, thisperiod of sexual receptivity is known as estrus, and how often it occurs depends on thespecies. Female rats, for example, go through a 15-hour estrus period every four days. Atall other times, they will resolutely reject any male’s advances. If a male nuzzles a femalewho is not in estrus or tries to mount, she will kick and bite him. But during estrus, thefemale responds quite differently to the male’s approach. She first retreats in small hops,then stops to look back and wiggles her ears (McClintock & Adler, 1978). Eventually, shestands still, her back arched, her tail held to the side—a willing sexual partner.
The mechanism that causes this change in the female’s behavior is an interlockingsystem of hormonal and neurological controls that involves the pituitary gland, thehypothalamus, and the ovaries. There are three phases (Figure 12.18). During the firstphase, follicles (ova-containing sacs) in the ovary mature under the influence of pitu-itary secretions. The follicles produce the sex hormone estrogen. As the concentrationof estrogen in the bloodstream rises, the hypothalamus responds by directing thepituitary to change its secretions. In consequence, follicle growth is accelerated until thefollicle ruptures and releases the mature ovum.
Release of the ovum triggers the second phase, during which the animal is in estrus.Estrogen production peaks and stimulates certain structures in the hypothalamus,which make the animal sexually receptive.
estrus In mammals, the period in thecycle when the female is sexuallyreceptive (in heat).
estrogen A female sex hormone thatdominates the first half of the femalecycle through ovulation.
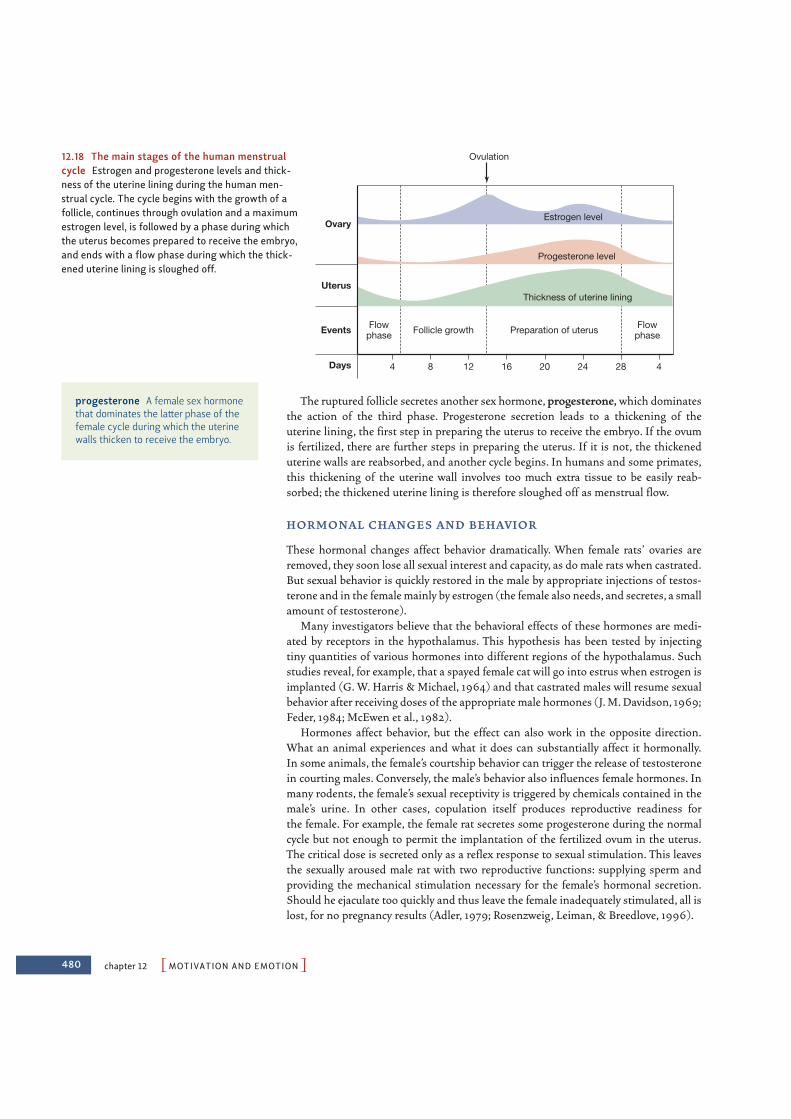
480 chapter 12 PMOTIVATION AND EMOTIONO
The ruptured follicle secretes another sex hormone, progesterone, which dominatesthe action of the third phase. Progesterone secretion leads to a thickening of the uterine lining, the first step in preparing the uterus to receive the embryo. If the ovumis fertilized, there are further steps in preparing the uterus. If it is not, the thickeneduterine walls are reabsorbed, and another cycle begins. In humans and some primates,this thickening of the uterine wall involves too much extra tissue to be easily reab-sorbed; the thickened uterine lining is therefore sloughed off as menstrual flow.
H O R M O N A L C H A N G E S A N D B E H AV I O R
These hormonal changes affect behavior dramatically. When female rats’ ovaries areremoved, they soon lose all sexual interest and capacity, as do male rats when castrated.But sexual behavior is quickly restored in the male by appropriate injections of testos-terone and in the female mainly by estrogen (the female also needs, and secretes, a smallamount of testosterone).
Many investigators believe that the behavioral effects of these hormones are medi-ated by receptors in the hypothalamus. This hypothesis has been tested by injectingtiny quantities of various hormones into different regions of the hypothalamus. Suchstudies reveal, for example, that a spayed female cat will go into estrus when estrogen isimplanted (G. W. Harris & Michael, 1964) and that castrated males will resume sexualbehavior after receiving doses of the appropriate male hormones (J. M. Davidson, 1969;Feder, 1984; McEwen et al., 1982).
Hormones affect behavior, but the effect can also work in the opposite direction.What an animal experiences and what it does can substantially affect it hormonally.In some animals, the female’s courtship behavior can trigger the release of testosteronein courting males. Conversely, the male’s behavior also influences female hormones. Inmany rodents, the female’s sexual receptivity is triggered by chemicals contained in themale’s urine. In other cases, copulation itself produces reproductive readiness for the female. For example, the female rat secretes some progesterone during the normalcycle but not enough to permit the implantation of the fertilized ovum in the uterus.The critical dose is secreted only as a reflex response to sexual stimulation. This leavesthe sexually aroused male rat with two reproductive functions: supplying sperm andproviding the mechanical stimulation necessary for the female’s hormonal secretion.Should he ejaculate too quickly and thus leave the female inadequately stimulated, all islost, for no pregnancy results (Adler, 1979; Rosenzweig, Leiman, & Breedlove, 1996).
Ovulation
Estrogen level
Preparation of uterusFollicle growthEvents
Uterus
Ovary
Days 4 8 12 16 20 24 28 4
Flowphase
Flowphase
Progesterone level
Thickness of uterine lining
12.18 The main stages of the human menstrualcycle Estrogen and progesterone levels and thick-ness of the uterine lining during the human men-strual cycle. The cycle begins with the growth of afollicle, continues through ovulation and a maximumestrogen level, is followed by a phase during whichthe uterus becomes prepared to receive the embryo,and ends with a flow phase during which the thick-ened uterine lining is sloughed off.
progesterone A female sex hormonethat dominates the latter phase of thefemale cycle during which the uterinewalls thicken to receive the embryo.
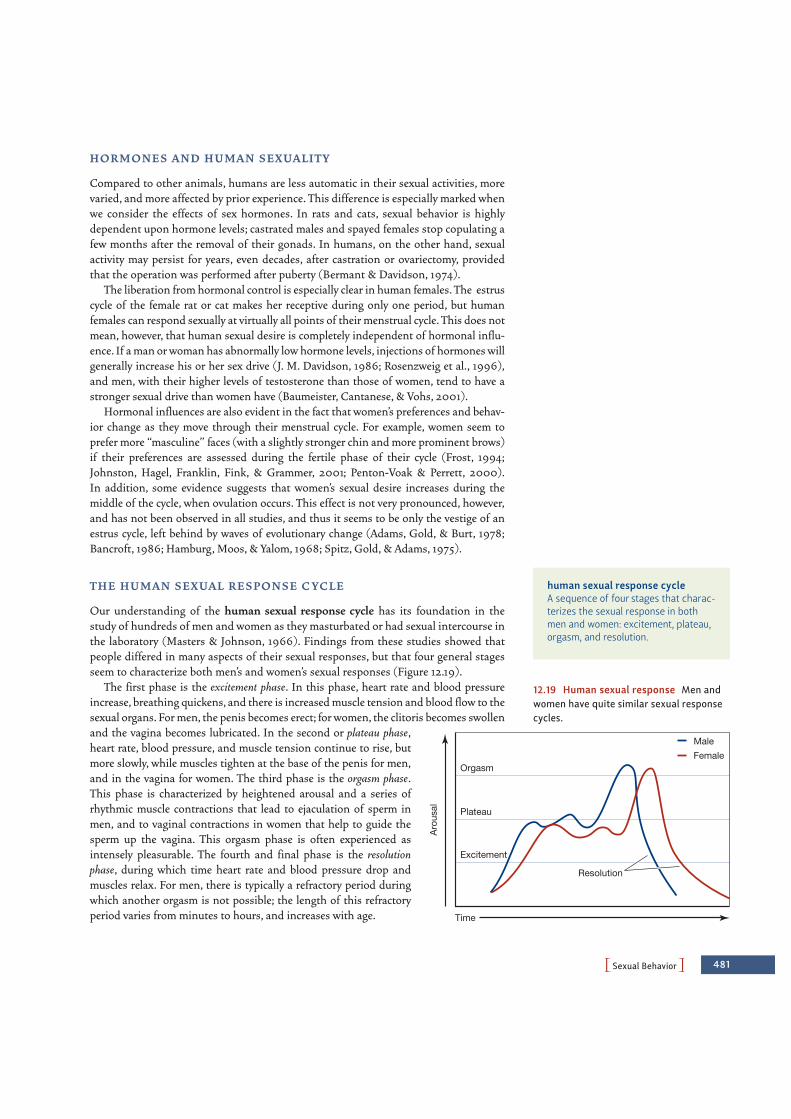
PSexual BehaviorO 481
H O R M O N E S A N D H U M A N S EX UA L I T Y
Compared to other animals, humans are less automatic in their sexual activities, morevaried, and more affected by prior experience. This difference is especially marked whenwe consider the effects of sex hormones. In rats and cats, sexual behavior is highlydependent upon hormone levels; castrated males and spayed females stop copulating afew months after the removal of their gonads. In humans, on the other hand, sexualactivity may persist for years, even decades, after castration or ovariectomy, providedthat the operation was performed after puberty (Bermant & Davidson, 1974).
The liberation from hormonal control is especially clear in human females. The estruscycle of the female rat or cat makes her receptive during only one period, but humanfemales can respond sexually at virtually all points of their menstrual cycle. This does notmean, however, that human sexual desire is completely independent of hormonal influ-ence. If a man or woman has abnormally low hormone levels, injections of hormones willgenerally increase his or her sex drive (J. M. Davidson, 1986; Rosenzweig et al., 1996),and men, with their higher levels of testosterone than those of women, tend to have astronger sexual drive than women have (Baumeister, Cantanese, & Vohs, 2001).
Hormonal influences are also evident in the fact that women’s preferences and behav-ior change as they move through their menstrual cycle. For example, women seem toprefer more “masculine” faces (with a slightly stronger chin and more prominent brows)if their preferences are assessed during the fertile phase of their cycle (Frost, 1994;Johnston, Hagel, Franklin, Fink, & Grammer, 2001; Penton-Voak & Perrett, 2000).In addition, some evidence suggests that women’s sexual desire increases during themiddle of the cycle, when ovulation occurs. This effect is not very pronounced, however,and has not been observed in all studies, and thus it seems to be only the vestige of anestrus cycle, left behind by waves of evolutionary change (Adams, Gold, & Burt, 1978;Bancroft, 1986; Hamburg, Moos, & Yalom, 1968; Spitz, Gold, & Adams, 1975).
T H E H U M A N S EX UA L R E S P O N S E C YC L E
Our understanding of the human sexual response cycle has its foundation in thestudy of hundreds of men and women as they masturbated or had sexual intercourse inthe laboratory (Masters & Johnson, 1966). Findings from these studies showed thatpeople differed in many aspects of their sexual responses, but that four general stagesseem to characterize both men’s and women’s sexual responses (Figure 12.19).
The first phase is the excitement phase. In this phase, heart rate and blood pressureincrease, breathing quickens, and there is increased muscle tension and blood flow to thesexual organs. For men, the penis becomes erect; for women, the clitoris becomes swollenand the vagina becomes lubricated. In the second or plateau phase,heart rate, blood pressure, and muscle tension continue to rise, butmore slowly, while muscles tighten at the base of the penis for men,and in the vagina for women. The third phase is the orgasm phase.This phase is characterized by heightened arousal and a series ofrhythmic muscle contractions that lead to ejaculation of sperm inmen, and to vaginal contractions in women that help to guide thesperm up the vagina. This orgasm phase is often experienced asintensely pleasurable. The fourth and final phase is the resolutionphase, during which time heart rate and blood pressure drop andmuscles relax. For men, there is typically a refractory period duringwhich another orgasm is not possible; the length of this refractoryperiod varies from minutes to hours, and increases with age.
Aro
usal
Time
Orgasm
Plateau
Excitement
Resolution
MaleFemale
12.19 Human sexual response Men andwomen have quite similar sexual responsecycles.
human sexual response cycleA sequence of four stages that charac-terizes the sexual response in bothmen and women: excitement, plateau,orgasm, and resolution.

482 chapter 12 PMOTIVATION AND EMOTIONO
Cultural and Cognitive Aspects of SexualityAs we have seen, our sexual behavior clearly has powerful physiological bases. At thesame time, it also has substantial cultural and cognitive components. In this section, weconsider proximal situational determinants of sexual behavior as well as more remoteevolutionary determinants of mate choice.
S I T UAT I O N A L D E T E R M I N A N TS O F S EX UA L B E H AV I O R
Sex is everywhere—in billboard advertisements, on television, in movies, and insupermarket tabloids (Figure 12.20). Do these sexually charged images encouragesexual feelings and behaviors? Or do they give vent to our sexual desires and therebydecrease our sexual behavior?
Laboratory studies find that men typically report greater sexual arousal in responseto sexually explicit materials than women do (Gardos & Mosher, 1999). However, thisfinding may in part reflect the fact that most sexually explicit materials are developed toappeal to men rather than to women. When researchers presented sexually explicitfilms that were chosen by women, there were no gender differences in response to thefilms (Janssen, Carpenter, & Graham, 2003).
Does this arousal actually encourage sexual behavior? Findings on this point havebeen mixed, but it appears that exposure to such material does, for at least a few hours,increase the likelihood of engaging in sexual behavior (Both, Spiering, Everaerd, &Laan, 2004). Much more concerning, however, have been findings from studies of theeffects of sexually explicit material on sexual attitudes. In one study, Zillmann andBryant (1988) found that viewing sexually explicit films made participants less satisfiedwith their partner’s appearance and sexual performance. Far more troubling, films ofwomen being sexually coerced increased male participants’ willingness to harm women(Zillman, 1989). In short, then, pornography may have a small effect in encouragingsexual behavior, but it may have a larger effect on perceptions, and, worst of all, violentpornography has a more powerful effect in encouraging sexual aggression.
M AT E C H O I C E
In most cultures in the modern world, both men and women are selective in choosingtheir sexual partners, and mating usually happens only when both partners consent.However, as we mentioned in Chapter 2, the sexes differ in the criteria they use inmaking their choices (Figure 12.21). According to a number of surveys, the physicalattractiveness of the partner seems more important to men than to women, while thesocial and financial status of the partner matters more to women than it does to men.It also appears that men generally prefer younger women, whereas women prefer oldermen. The data also indicate that all of these male-female differences are found inmany countries, including the United States, China, India, France, Nigeria, and Iran(D. M. Buss, 1989, 1992; D. M. Buss & Barnes, 1986).
How should we think about all of these points? In Chapter 2, we looked closely at theevolutionary account: An attractive woman is likely to be healthy and fertile, so a maleselecting an attractive partner would increase his chances of reproductive success.Likewise, a younger woman will have more reproductive years ahead of her, so a malechoosing a younger partner could plausibly look forward to more offspring. Any maleselecting his mates based on their youth and beauty would be more likely than othermales to have many healthy offspring to pass along his genes. Thus, through the
12.20 Sex in the media Many differentmedia use sexually laden images, often inorder to sell products.
12.21 Mating tendencies Ratherconsistently, women prefer mates some-what older than they are; men prefermates who are younger. For men, mateselection is often influenced by thewoman’s appearance; for women, mateselection is often influenced by the statusand resources of a potential partner.

PSexual BehaviorO 483
process of natural selection these preferences eventually would become widespreadamong the males of our species.
The female’s preferences are also sensible from an evolutionary perspective. Becauseof her high investment in each child (at the least, 9 months of carrying the baby in herwomb, and then months of nursing), she can maximize the chance of passing along her genes to future generations by having just a few offspring and doing all she can toensure the survival of each. A wealthy, high-status mate would help her reach this goal,because he would be able to provide the food and other resources their children need.Thus, there would be a reproductive advantage associated with a preference for such amale, and so a gradual evolution toward all females in the species having this preference(Bjorklund & Shackelford, 1999; Buss, 1992; Schmitt, 2005).
We also noted in Chapter 2 that cultural factors play an important role. For example,in many cultures human females only come to prefer wealthy, high-status males becausethe females have learned, across their lifetimes, the social and economic advantagesthey will gain from such a mate. In these cultures, women soon learn that their profes-sional and educational opportunities are limited, and so “marrying wealth” is their beststrategy for gathering resources for themselves and their young.
The importance of culture becomes clear when we consider cultures that providemore opportunities for women. In these cultures, “marrying wealth” is not a woman’sonly chance for economic and social security, so a potential husband’s resources becomecorrespondingly less important in mate selection. Various studies confirm this predic-tion and show that in cultures that afford women more opportunities, women attachless priority to a male’s social and economic status (Kasser & Sharma, 1999; also seeBaumeister & Vohs, 2004; Buller, 2005; Eagly & Wood, 1999; W. Wood & Eagly, 2002).
In short, there seems to be considerable consistency in mating preferences and acontrast between the criteria males and females typically use. This consistency has beendocumented in many cultures and across several generations. But there are also varia-tions in mate-selection preferences that are clearly attributable to the cultural context.These data clearly illustrate the interplay of biological and cultural factors that governsour motivational and emotional states.
Sexual OrientationSo far in this chapter, we have touched upon many different physiological and socialaspects of sexual behavior. However, up to this point, we have neglected one very impor-tant question: What determines our sexual orientation?
The roots of someone’s sexuality are established well before ado-lescence. As early as age 3 or 4, children start to have feelings of attrac-tion (Bell, Weinberg, & Hammersmith, 1981). The first real sexualattraction, however, usually begins by age 10 or so (Herdt &McClintock, 2000), and children of this age often imagine star-struck romances (R. Green, 1979; Zuger, 1984). These feelings sooncrystallize, and, by early adolescence, with the onset of puberty andan increased emphasis on social relations outside the family, sexualorientation becomes explicit, and actions based on the orientationbecome common (Figure 12.22).
How common is each of the sexual orientations—heterosexual,homosexual, or bisexual? Years ago, Alfred Kinsey and his associatesreported that more than 80% of American men describe themselvesas exclusively heterosexual and 4% as exclusively homosexual
12.22 Sexual orientation Differences insexual orientation are usually establishedearly on, often well before adolescence.
484 chapter 12 PMOTIVATION AND EMOTIONO
(Kinsey, Pomeroy, & Martin, 1948). The prevalence of exclusive homosexuality reportedby women was lower—about 2% (Kinsey, Pomeroy, Martin, & Gebhard, 1953). A sub-stantially larger group (13% of American men and 7% of women) described themselvesas predominantly homosexual but had also had some heterosexual experience. Morerecent surveys confirm Kinsey’s estimates, both in the United States and in otherWestern cultures (see, for example, ACSF Investigators, 1992; A. M. Johnson,Wadsworth, Wellings, Bradshaw, & Field, 1992; for some complications, though, seeSavin-Williams, 2006).
What makes a particular individual homosexual, heterosexual, or bisexual? There isclearly a genetic influence, because it turns out that if a man’s identical twin is gay, thenthe chances that he will also be gay are 52%; if the gay twin is fraternal, the chancesdrop to 22% (Bailey & Pillard, 1991). Likewise, a woman’s chance of having a homosex-ual orientation is 48% if she has a lesbian identical twin. If her gay twin is fraternal, thechances drop to 16% (Bailey, Pillard, Neale, & Agyei, 1993). Clearly, then, the greater thesimilarity in genetic makeup, the greater the likelihood of having the same sexual ori-entation, powerfully suggesting that one’s genotype carries a predisposition towardheterosexuality or homosexuality.
But how do genes influence sexual orientation? The mechanism probably involvesthe levels of prenatal hormones, especially the male hormone androgen. Part of theevidence on this point comes from androgenized females—those who were exposed inthe uterus to high androgen levels—who are far more likely than others to describethemselves as homosexual or bisexual (37%). In these women, the high androgen levels are produced by a specific genetic pattern, but the same hormonal patterns can beproduced by many other factors. In all cases, these shifts in hormone levels during pre-natal development seem to influence sexual orientation (Dittman, Kappes, & Kappes,1992; Ellis & Ames, 1987; Hines, 2004; Zucker, 2001).
If genes were the whole story, though, then identical twins (with 100% of the samegenes) would show 100% resemblance in their sexual orientation; instead, the concor-dance rate is just 52%. Obviously, therefore, factors other than the genes matter, but noone is yet sure what these other factors are. Many hypotheses have been offered, butmost of these are plainly wrong. For example, there is no evidence that especially strongfathers, or especially weak fathers, are more likely to have homosexual offspring. Thereis also no evidence that homosexuality derives from some sort of imitation; childrenwho grow up with gay or lesbian parents are no more likely to be homosexual them-selves (M. Bailey & Zucker, 1995; Golombok & Tasker, 1996).
What we do know is that the main predictor of adult homosexuality is the waypeople felt about sexuality when they were younger. As we mentioned earlier, sexualorientation can be detected in middle childhood—and certainly before the individ-ual experiences any sexual encounters, homosexual or heterosexual. Indeed, peopleof any sexual orientation might well identify with the sentiment voiced by manyhomosexuals when they report simply that “I’ve been that way all my life” (Saghir &Robins, 1973).
Overall, then, we still have much to learn about what makes someone homosexual,heterosexual, or bisexual. Genes are certainly relevant, but we are still figuring out whatthe rest of the story involves. Whatever the origins of sexual orientation, though, itbears emphasizing that a homosexual (or bisexual) orientation is not a psychologicaldisorder or defect. These orientations are “abnormal” only in the limited sense of beingdifferent from the majority. Many other traits are “abnormal” in exactly the samesense—being left-handed, for example. Gays, lesbians, and bisexuals are neither betternor worse than heterosexuals, and the factors that matter for their relationship qualityand stability seem to be exactly the same as those that matter for heterosexual couples
PMotives Beyond DrivesO 485
(Kurdek, 2005). Their number includes great painters (Leonardo da Vinci), athletes(Martina Navratilova), musicians (Aaron Copland), writers (Oscar Wilde, GertrudeStein), mathematicians and scientists (Alan Turing, Alfred Kinsey himself), philoso-phers (Wittgenstein), and warriors (Alexander the Great), but the great majority areordinary people with ordinary lives. The same no doubt holds for left-handers—and forheterosexuals.
MOTIVES BEYOND DRIVES
We can understand the motives we have considered so far principally in terms ofdrive-reduction. In each case, the motive involves some internal tension—feeling coldor hot, feeling hungry, feeling threatened, or feeling sexual needs—and the motivatedbehaviors help us reduce (or escape) the tension. But surely we are motivated not onlyto avoid negative experiences, but also to seek positive experiences. Consider the satisfac-tion of solving a difficult problem, the exhilaration of riding a roller coaster or dancing,or the ecstasy of fulfilled love. Plainly we value these kinds of experiences for their ownsake. Likewise, people will get out of bed and walk out into the cold simply to enjoy abeautiful sunrise. People will also spend money to see a play or attend a rock concert.All of these activities are difficult to understand in terms of drive-reduction.
In this section, we broaden our consideration of motivational states, and considermotives that go beyond tension-reduction, and are about more than survival. Theoristshave described many, many such motives (including motives that lead people to seek affil-iation, achievement, autonomy, control, competence, power, self-esteem, and differentia-tion, among others), and here we will consider two major motives that govern our dailyactivities, namely, our motive to belong to groups and our motive to achieve.
The Motive to BelongWe all want to belong, to have friends, and to fit in (Leary & Cox, 2008). Indeed, we goto great lengths to seek out and maintain friendships, and we are upset when our rela-tionships are severed. As we will see in Chapter 13, much of our mental lives are spentconsidering others’ thoughts and feelings toward us.
Abraham Maslow (1968, 1996) was one of the early theorists whoinsisted that to understand what is truly human, psychologists mustconsider all our motives, and he recognized in particular the motiveto belong as a powerful force in human behavior (Figure 12.23). Mostpsychologists agree. For example, Baumeister and Leary (1995) put itclearly when they said: “The need to belong is a powerful, fundamen-tal, and extremely pervasive motivation” (p. 497). Thus, people maygo without food to make themselves more attractive to others, andthey may risk life and limb to impress others around them.
At least part of the need to belong can be understood as yet anotherform of drive-reduction: We do not want to be alone, or rejected, andso we take steps to avoid these experiences (Schultheiss, 2008). Butit is crucial that the motive to belong also has a positive “approach-orientation,” as we seek out the many benefits of being with others.This latter, more positive aspect of affiliation is evident, for example,in the fact that social interaction is a powerful predictor of positiveemotion (Watson & Clark, 1994). In addition, a lack of meaningful
12.23 Motive to belong Other people arean important source of both pleasure andsupport, and the motive to belong power-fully shapes our interactions with others.

486 chapter 12 PMOTIVATION AND EMOTIONO
social interaction predicts a range of negative psychological and physical healthoutcomes.
Indeed, social contact provides many benefits. For example, other people can providetangible support, and, in fact, few of us would get by without practical help from manydifferent people—whether it’s borrowing money to do laundry or getting help proof-reading an assignment. Others also provide emotional support. Sometimes this sup-port is direct, as when a friend consoles us when we are sad or distracts us when we areangry; sometimes it is indirect, taking the form of the many emotional connections toothers that give our lives texture and meaning. A third reason we seek out others is thathow we feel about ourselves is powerfully shaped by how others view us. Indeed, someresearchers have argued that self-esteem is an internal readout of how one is faringsocially (Leary, Tambor, Terdal, & Downs, 1995).
The Motive to AchieveImagine that all of your social needs and all of your drive-based needs mentioned in thischapter were satisfied, and that you were warm, comfortable, safe, well-fed, and sur-rounded by people who love you. That probably sounds pretty wonderful indeed—but notperfect. What’s missing? For most of us, even this peaceful state of affairs wouldn’t beentirely fulfilling, because it wouldn’t satisfy the motive to create, accomplish, and achieve.
Like the motive to belong, the motive to achieve has a dual aspect—part avoidance,part approach. Half a century ago, McClelland and colleagues suggested that achieve-ment-related behavior can arise either from a fear of failure (avoidance) or from a desirefor success (approach) (D. C. McClelland, Atkinson, Clark, & Lowell, 1953). One mightthink that these two aspects of the achievement motive would be tightly correlated, butthey are in fact independent, and they operate differently. It is individuals with a desirefor success—rather than a fear of failure—who seek out challenges and excel when thegoing gets difficult (D. C. McClelland, 1989).
Achievement motivation matters, and in studies of high-school and college students,Duckworth and Seligman (2005) found that achievement motivation was a powerfulpredictor of school performance. A similar picture emerges from studies of scholars,artists, and athletes who were at the top of their respective fields (B. S. Bloom, 1995).Talent matters, but achievement motivation also matters a great deal (Figure 12.24).
What factors give rise to a fear of failure or a desire for success (Koestner &McClelland, 1990)? Early researchers focused on parenting style, and found someevidence that caregivers who punish failure but take success for granted can instill afear of failure. By contrast, caregivers can promote a more positive desire for successby rewarding achievement but not punishing failure. More recent research hasfocused on cognitive factors, such as whether a child adopts a mastery orientation,which is characterized by a focus on learning and improving, or a performance ori-entation, characterized by a focus on performing well in front of others in order tolook smart, or on avoiding failure to keep from looking stupid (Dweck, 1999; 2006).Two decades of research suggest that a mastery orientation is associated with highlevels of interest and a deep engagement with the material. When individuals with amastery orientation encounter adversity (such as a bad grade), they are likely toincrease their effort and seek out ways of benefiting from the experience. By contrast,when individuals with a performance orientation get negative feedback, they aremore likely to withdraw effort and shift their focus elsewhere (Senko, Durik, &Harackiewicz, 2008).
tangible support Social supportfocused on practical or material needs.
emotional support Social supportfocused on emotional needs.
mastery orientation A learning ori-entation characterized by a focus ongaining new knowledge or abilities andimproving.
performance orientation A learn-ing orientation characterized by afocus on presenting oneself well andappearing intelligent to others.
12.24 Motive to achieve The motive tocreate, accomplish, and achieve affectsboth the challenges we undertake, and thedegree to which we persist when difficul-ties arise.
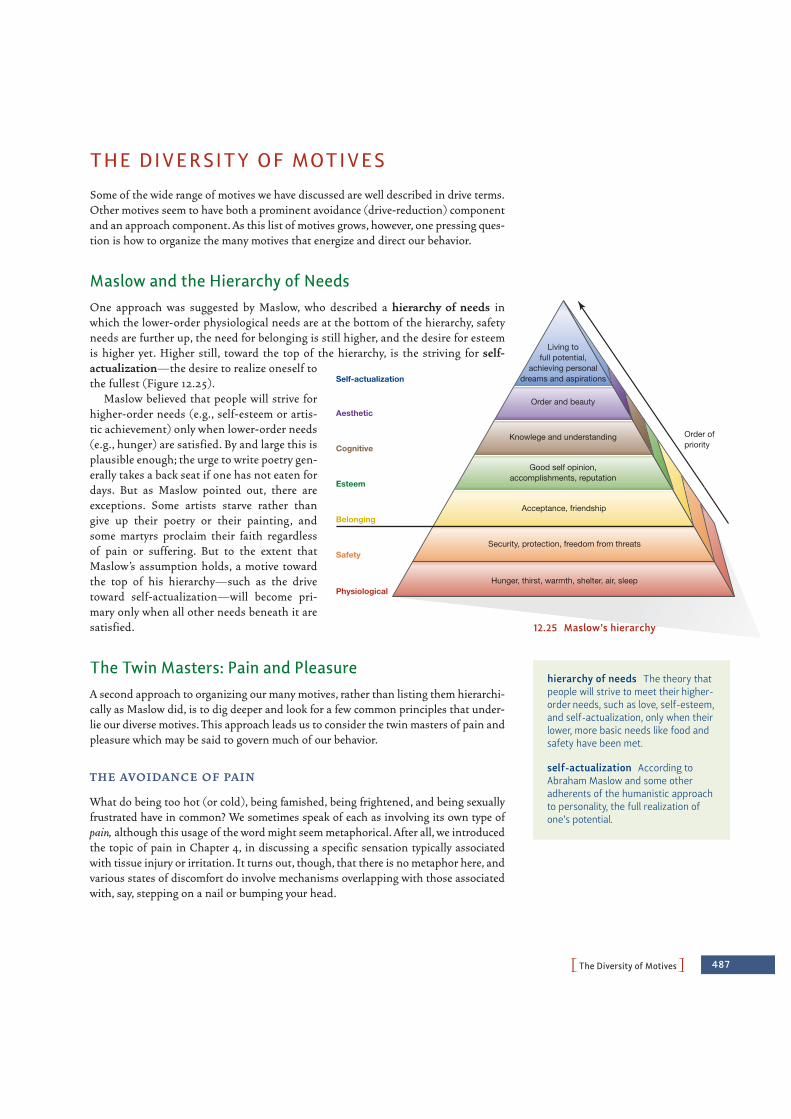
PThe Diversity of MotivesO 487
THE DIVERSITY OF MOTIVES
Some of the wide range of motives we have discussed are well described in drive terms.Other motives seem to have both a prominent avoidance (drive-reduction) componentand an approach component. As this list of motives grows, however, one pressing ques-tion is how to organize the many motives that energize and direct our behavior.
Maslow and the Hierarchy of Needs One approach was suggested by Maslow, who described a hierarchy of needs inwhich the lower-order physiological needs are at the bottom of the hierarchy, safetyneeds are further up, the need for belonging is still higher, and the desire for esteemis higher yet. Higher still, toward the top of the hierarchy, is the striving for self-actualization—the desire to realize oneself tothe fullest (Figure 12.25).
Maslow believed that people will strive forhigher-order needs (e.g., self-esteem or artis-tic achievement) only when lower-order needs(e.g., hunger) are satisfied. By and large this isplausible enough; the urge to write poetry gen-erally takes a back seat if one has not eaten fordays. But as Maslow pointed out, there areexceptions. Some artists starve rather thangive up their poetry or their painting, andsome martyrs proclaim their faith regardlessof pain or suffering. But to the extent thatMaslow’s assumption holds, a motive towardthe top of his hierarchy—such as the drivetoward self-actualization—will become pri-mary only when all other needs beneath it aresatisfied.
The Twin Masters: Pain and PleasureA second approach to organizing our many motives, rather than listing them hierarchi-cally as Maslow did, is to dig deeper and look for a few common principles that under-lie our diverse motives. This approach leads us to consider the twin masters of pain andpleasure which may be said to govern much of our behavior.
T H E AV O I DA N C E O F PA I N
What do being too hot (or cold), being famished, being frightened, and being sexuallyfrustrated have in common? We sometimes speak of each as involving its own type ofpain, although this usage of the word might seem metaphorical. After all, we introducedthe topic of pain in Chapter 4, in discussing a specific sensation typically associatedwith tissue injury or irritation. It turns out, though, that there is no metaphor here, andvarious states of discomfort do involve mechanisms overlapping with those associatedwith, say, stepping on a nail or bumping your head.
Living tofull potential,
achieving personaldreams and aspirations
Safety
Physiological
Good self opinion,accomplishments, reputation
Knowlege and understanding
Order and beauty
Order ofpriority
Acceptance, friendship
Security, protection, freedom from threats
Hunger, thirst, warmth, shelter, air, sleep
Belonging
Esteem
Self-actualization
Cognitive
Aesthetic
12.25 Maslow’s hierarchy
hierarchy of needs The theory thatpeople will strive to meet their higher-order needs, such as love, self-esteem,and self-actualization, only when theirlower, more basic needs like food andsafety have been met.
self-actualization According toAbraham Maslow and some otheradherents of the humanistic approachto personality, the full realization ofone’s potential.
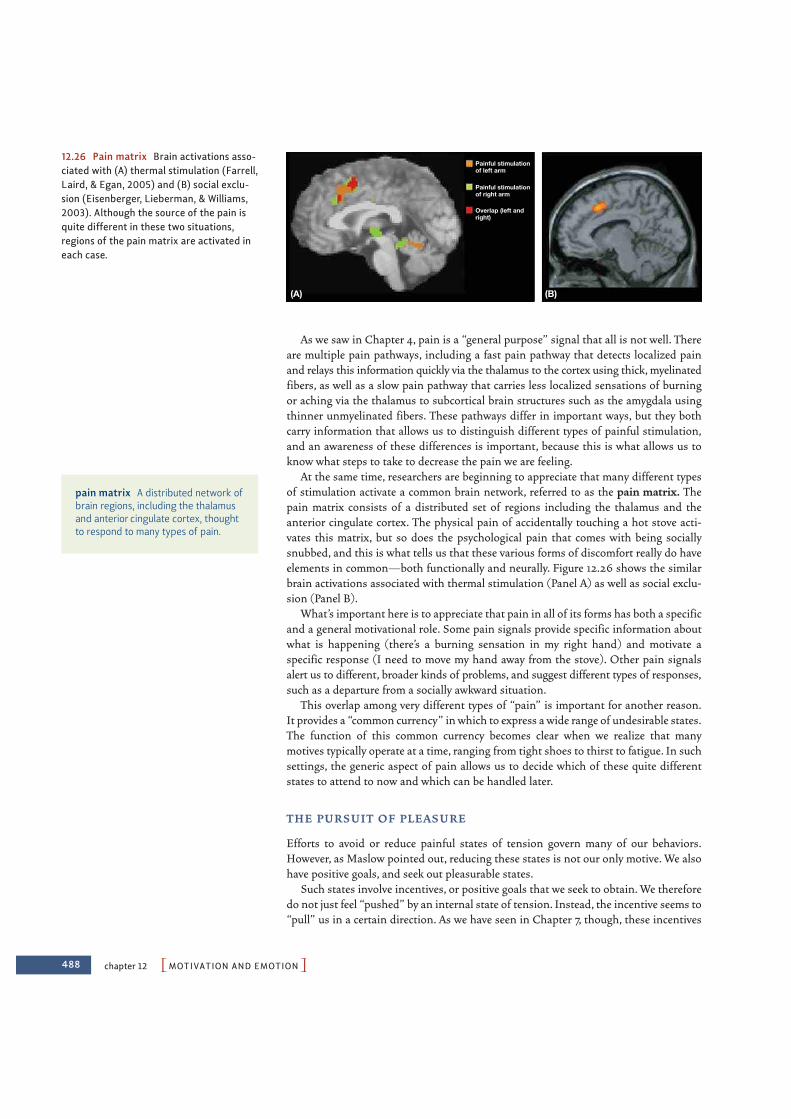
488 chapter 12 PMOTIVATION AND EMOTIONO
As we saw in Chapter 4, pain is a “general purpose” signal that all is not well. Thereare multiple pain pathways, including a fast pain pathway that detects localized painand relays this information quickly via the thalamus to the cortex using thick, myelinatedfibers, as well as a slow pain pathway that carries less localized sensations of burningor aching via the thalamus to subcortical brain structures such as the amygdala usingthinner unmyelinated fibers. These pathways differ in important ways, but they bothcarry information that allows us to distinguish different types of painful stimulation,and an awareness of these differences is important, because this is what allows us toknow what steps to take to decrease the pain we are feeling.
At the same time, researchers are beginning to appreciate that many different typesof stimulation activate a common brain network, referred to as the pain matrix. Thepain matrix consists of a distributed set of regions including the thalamus and theanterior cingulate cortex. The physical pain of accidentally touching a hot stove acti-vates this matrix, but so does the psychological pain that comes with being sociallysnubbed, and this is what tells us that these various forms of discomfort really do haveelements in common—both functionally and neurally. Figure 12.26 shows the similarbrain activations associated with thermal stimulation (Panel A) as well as social exclu-sion (Panel B).
What’s important here is to appreciate that pain in all of its forms has both a specificand a general motivational role. Some pain signals provide specific information aboutwhat is happening (there’s a burning sensation in my right hand) and motivate aspecific response (I need to move my hand away from the stove). Other pain signalsalert us to different, broader kinds of problems, and suggest different types of responses,such as a departure from a socially awkward situation.
This overlap among very different types of “pain” is important for another reason.It provides a “common currency” in which to express a wide range of undesirable states.The function of this common currency becomes clear when we realize that manymotives typically operate at a time, ranging from tight shoes to thirst to fatigue. In suchsettings, the generic aspect of pain allows us to decide which of these quite differentstates to attend to now and which can be handled later.
T H E P U RS U I T O F P L E AS U R E
Efforts to avoid or reduce painful states of tension govern many of our behaviors.However, as Maslow pointed out, reducing these states is not our only motive. We alsohave positive goals, and seek out pleasurable states.
Such states involve incentives, or positive goals that we seek to obtain. We thereforedo not just feel “pushed” by an internal state of tension. Instead, the incentive seems to“pull” us in a certain direction. As we have seen in Chapter 7, though, these incentives
Painful stimulationof left arm
Painful stimulationof right arm
Overlap (left andright)
(A) (B)
12.26 Pain matrix Brain activations asso-ciated with (A) thermal stimulation (Farrell,Laird, & Egan, 2005) and (B) social exclu-sion (Eisenberger, Lieberman, & Williams,2003). Although the source of the pain isquite different in these two situations,regions of the pain matrix are activated ineach case.
pain matrix A distributed network ofbrain regions, including the thalamusand anterior cingulate cortex, thoughtto respond to many types of pain.

PThe Diversity of MotivesO 489
come in different types. Some are an inherent part of the activity or object to which weare drawn (e.g., playing the guitar because the experience itself is fun). In such cases, theactivity or object is said to be intrinsically rewarding. Other incentives, by contrast, arenot an integral part of the activity or object to which we are drawn, but are instead arti-ficially associated with it (e.g., getting paid for painting a picture). In this case, we saythat the activity or object is extrinsically rewarding.
Historically, research on incentives has focused on external determinants of behavior—the specific rewards available to us and their influence on our behavior. It is becomingclear, however, that internal states of pleasure have a role in supporting incentives thatparallels the role of the internal states of pain in supporting drives. This realization hasdirected researchers’ attention to examining two different aspects of our responses torewarding stimuli, namely, wanting and liking.
Wanting refers to the organism’s motivation to obtain a reward and is measured bythe amount of effort the organism will exert to obtain it. Because wanting is definedbehaviorally, it can be assessed in any organism whose behavior we can measure. Withrats, we can ask how many times they will press the bar to dispense a food pellet. In asimilar fashion, we can see how hard people will work to obtain a reward: If you wantbrownies, do you want them badly enough to go through the trouble of making them?And if you don’t have the ingredients, do you want brownies badly enough to first goshopping and then make them?
In contrast to wanting, liking refers to the pleasure that follows receiving the reward,like the pleasure deriving from the luscious taste of the warm brownies. We all know thesensation of liking, but unlike wanting, liking is difficult to define behaviorally. However,we can explore the neural basis of this experience. Research on this point dates backmore than half a century to work by Olds and Milner, who electrically stimulated rats’brains in different regions. They found that stimulation in some regions led rats toengage in behaviors such as returning repeatedly to the location at which they were ini-tially stimulated, seemingly in an attempt to repeat the stimulation. To understand thisphenomenon, Olds and Milner made the brain stimulation contingent upon bar presses,and found that rats would bar press at very high rates for long periods of time, and to theexclusion of other activities, in order to obtain this stimulation (Figure 12.27). One par-ticularly important spot for this effect—in rats and humans—appears to be the medialforebrain bundle, a nerve tract consisting of neurons with cell bodies in the midbrainwhich synapse in the nucleus accumbens (in the striatum).
Apparently, stimulation in this brain area is strongly rewarding—but why? Is thisarea involved in wanting or in liking? Modern neuroimaging research suggests ananswer, and indicates that different brain regions are engaged by reward anticipation(wanting) and reward delivery (liking) (Schultz, Tremblay, & Hollerman, 2000). Inparticular, regions in the frontal cortex are activated by liking, whereas the nucleusaccumbens is especially sensitive to wanting. In one of the first studies to demonstratethis dissociation in humans, Knutson and colleagues used fMRI during a task in whichparticipants were shown various types of cues and were asked to respond to a target(Knutson, Fong, Adams, Varner, & Hommer, 2001). If participants responded quicklyenough, they were able to win one dollar, and target presentation was adjusted for eachindividual so that each participant succeeded approximately two-thirds of the time. Asshown in Figure 12.28, the period of anticipation and wanting was associated withgreater activation in the nucleus accumbens, whereas the period of liking the rewardwas associated with activation in the frontal cortex. These activation patterns suggestthat the processes of wanting and liking have separate bases in the brain.
Additional evidence that wanting and liking depend on separable brain systemscomes from studies of the neurotransmitters that underlie reward processing. When
12.27 Bar pressing for pleasure Whenrats receive brain stimulation for barpressing, they press at high rates for longperiods of time.
intrinsically rewarding An activityor object that is pursued for its ownsake.
extrinsically rewarding An activityor object that is pursued because ofrewards that are not an inherent partof the activity or object.
wanting An organism’s motivation toobtain a reward.
liking The pleasure that followsreceipt of a reward.
nucleus accumbens A dopamine-rich area in the forebrain that is criti-cal in the physiology of reward.
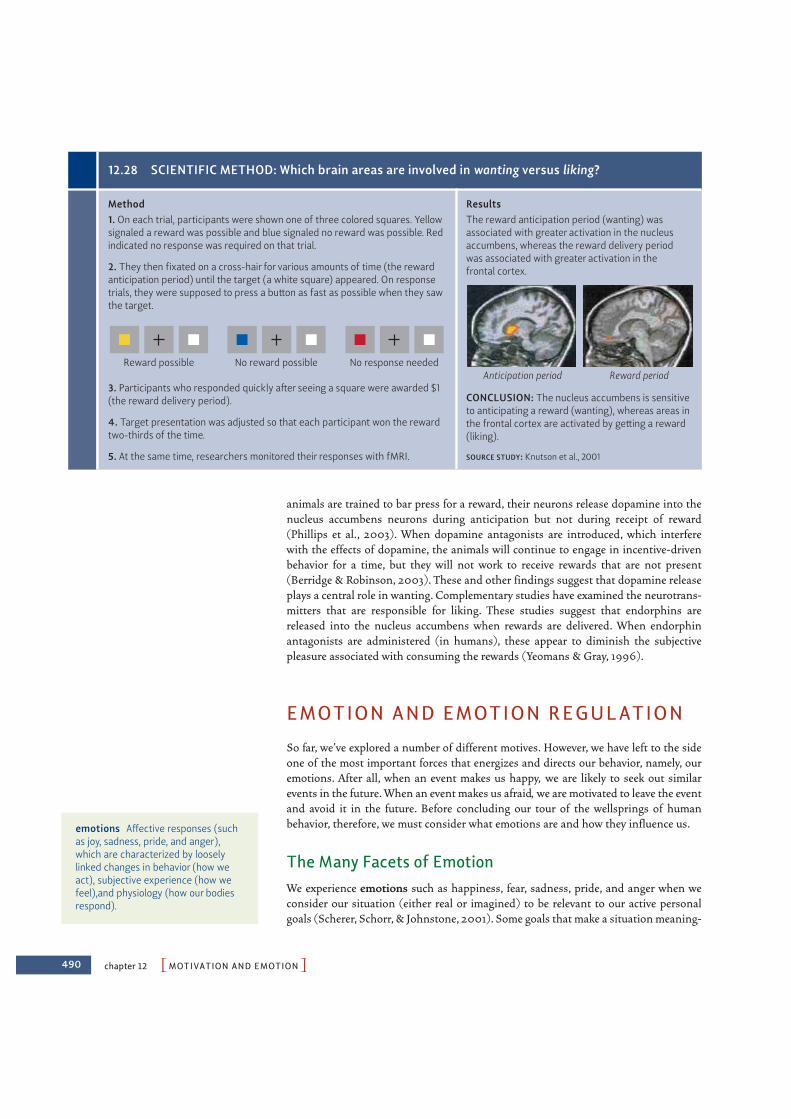
490 chapter 12 PMOTIVATION AND EMOTIONO
animals are trained to bar press for a reward, their neurons release dopamine into thenucleus accumbens neurons during anticipation but not during receipt of reward(Phillips et al., 2003). When dopamine antagonists are introduced, which interferewith the effects of dopamine, the animals will continue to engage in incentive-drivenbehavior for a time, but they will not work to receive rewards that are not present(Berridge & Robinson, 2003). These and other findings suggest that dopamine releaseplays a central role in wanting. Complementary studies have examined the neurotrans-mitters that are responsible for liking. These studies suggest that endorphins arereleased into the nucleus accumbens when rewards are delivered. When endorphinantagonists are administered (in humans), these appear to diminish the subjectivepleasure associated with consuming the rewards (Yeomans & Gray, 1996).
EMOTION AND EMOTION REGULATION
So far, we’ve explored a number of different motives. However, we have left to the sideone of the most important forces that energizes and directs our behavior, namely, ouremotions. After all, when an event makes us happy, we are likely to seek out similarevents in the future. When an event makes us afraid, we are motivated to leave the eventand avoid it in the future. Before concluding our tour of the wellsprings of humanbehavior, therefore, we must consider what emotions are and how they influence us.
The Many Facets of EmotionWe experience emotions such as happiness, fear, sadness, pride, and anger when weconsider our situation (either real or imagined) to be relevant to our active personalgoals (Scherer, Schorr, & Johnstone, 2001). Some goals that make a situation meaning-
12.28 SCIENTIFIC METHOD: Which brain areas are involved in wanting versus liking?
Method1. On each trial, participants were shown one of three colored squares. Yellowsignaled a reward was possible and blue signaled no reward was possible. Redindicated no response was required on that trial.
2. They then fixated on a cross-hair for various amounts of time (the rewardanticipation period) until the target (a white square) appeared. On responsetrials, they were supposed to press a button as fast as possible when they sawthe target.
3. Participants who responded quickly after seeing a square were awarded $1(the reward delivery period).
Reward possible No reward possible No response needed
ResultsThe reward anticipation period (wanting) wasassociated with greater activation in the nucleusaccumbens, whereas the reward delivery periodwas associated with greater activation in thefrontal cortex.
CONCLUSION: The nucleus accumbens is sensitiveto anticipating a reward (wanting), whereas areas inthe frontal cortex are activated by getting a reward(liking).
SOURCE STUDY: Knutson et al., 2001
4. Target presentation was adjusted so that each participant won the rewardtwo-thirds of the time.
5. At the same time, researchers monitored their responses with fMRI.
Anticipation period Reward period
emotions Affective responses (suchas joy, sadness, pride, and anger),which are characterized by looselylinked changes in behavior (how weact), subjective experience (how wefeel),and physiology (how our bodiesrespond).

PEmotion and Emotion RegulationO 491
ful are of long-term concern, such as wanting to be liked. Other goals may be more fleeting, such as hoping to get the last slice of cake, or rooting for the underdog in afootball match.
Whatever the goal may be, once we’ve evaluated a situation as being personally rele-vant, three types of changes are evident that, taken together, characterize emotion.These changes affect our behavior (how we act), our subjective experience (how wefeel), and our physiology (how various systems in the body are functioning) (Mauss,Levenson, McCarter, Wilhelm, & Gross, 2005). We can identify similar changes in thestates we call moods, but psychologists distinguish emotions from moods in severalways. For one, emotions typically have a clear object or target (e.g., we are happy aboutsomething, or mad at someone); moods do not. Emotions are also usually briefer thanmoods, lasting seconds or minutes rather than hours or days.
B E H AV I O R A L AS P E CTS O F E M OT I O N
Some of our bodily responses to emotion are quite general, such as a broad pattern ofapproaching with interest in response to emotionally positive stimuli, or a generalwithdrawal in response to emotionally negative stimuli. Perhaps the most prominentbehaviors associated with emotion, however, are our facial behaviors—our smiles,frowns, laughs, gapes, grimaces, and snarls.
Charles Darwin hypothesized that our facial expressions of emotion are actuallyvestiges of our ancestors’ basic adaptive patterns (1872b). He argued, for example, thatour “anger” face, often expressed by lowered brows, widened eyes, and open mouthwith exposed teeth, reflects the facial movements our ancestors would have madewhen biting an opponent. Similarly, our “disgust” face, often manifested as a wrinklednose and protruded lower lip and tongue, reflects the way our ancestors responded tofoul odors or spit out foods. (For elaborations, see Ekman, 1980, 1984; Izard, 1977;Tomkins, 1963.)
In support of this position, Darwin noted that our facial expressions resemble manyof the displays made by monkeys and apes, as we discussed in Chapter 2. Darwin alsobelieved that the expressions would be identical among humans worldwide, even“those who have associated but little with Europeans” (Darwin, 1872b, p. 15). Thispoint, too, can be confirmed—for example, in observations (also mentioned in Chapter2) of children born blind, who nonetheless express emotions using the typical, recog-nizable set of facial expressions despite the fact that they could not have learned theseexpressions through imitation (see, for example, Eibl-Eibesfeldt, 1970; Galati, Scherer,& Ricci-Bitti, 1997; Goodenough, 1932).
A different test of this universality claim involves comparisons between cultures(Russell, 1994; Tracy & Robins, 2008), but only a tiny number of studies have used theparticipants most crucial for this test: members of relatively isolated non-Western cul-tures (Ekman, 1973; Ekman & Oster, 1979; Fridlund, Ekman, & Oster, 1983; Izard,1971). Why is this group crucial? If research participants, no matter where they live,have been exposed to Western movies or television, their responses might indicate onlythe impact of these media and thus provide no proof of the universality claim.Therefore, we need participants who have not seen reruns of Western soap operas, orHollywood movies, or a slew of Western advertising.
In one of the few studies of this critical group, American actors were photographedshowing expressions that conveyed emotions such as happiness, sadness, anger, andfear. These photographs were then shown to members of various modern literate cultures(Swedes, Japanese, Kenyans) and to members of an isolated nonliterate New Guineatribe. All participants who saw the photos were asked to pick the emotion label that
moods Affective responses that aretypically longer-lasting than emotions,and less likely to have a specificobject.

492 chapter 12 PMOTIVATION AND EMOTIONO
matched each photograph. In other cases, the procedure was reversed. For example, theNew Guinea tribesmen were photographed portraying the facial expressions that theyconsidered appropriate to various situations, such as happiness at the return of a friend,grief at the death of a child, and anger at the start of a fight (Figure 12.29). Americancollege students then looked at the photographs and judged which situation thetribesmen in each photo had been asked to convey (Ekman & Friesen, 1975).
In these studies, all the participants, including those in relatively isolated cultures,did reasonably well. They were able to supply the appropriate emotion label for the pho-tographs, or to describe a situation that might have elicited the expression shown in thephotograph. But they were more successful at recognizing some expressions than atrecognizing others. In Chapter 2, we highlighted the biological roots of smiling, and, infact, these were, in this study, generally matched with “happy” terms and situations,with remarkable levels of consistency (Ekman, 1994; Izard, 1994; see also Russell,1994). Other emotions, such as disgust, were less well recognized, but still identified atlevels well above chance, suggesting that the meaning of emotional expressions tran-scends cultural and geographic boundaries.
Let us note, though, that even though the perception of emotions may be similar inall cultures, the display of emotions is surely not. A widely cited example comes fromresearch in which American and Japanese participants were presented with harrowingsurgical films (Figure 12.30). Participants first watched the films privately (i.e., with noone in the room with them), but their facial expressions were recorded by a hiddencamera. The facial reactions of Americans and Japanese were virtually identical. Butwhen the participants then watched one of the films again while being interviewed byan experimenter, the results were quite different. In this context, the Japanese showedmore positive emotion than the Americans showed (Ekman, 1972; Friesen, 1972). Thus,when in public, participants’ facial expressions were governed by the display rules setby their culture—deeply ingrained conventions, often obeyed without awareness, that
12.29 SCIENTIFIC METHOD: Are some emotional expressions universal?
Method1. American actors were photographedshowing expressions of happiness,sadness, suprise, disgust, anger, and fear.
ResultsAll participants, including thosein relatively isolated cultures,identified the expressions reasonablywell, but they accurately recognized some emotions (e.g., happiness)more consistently than others(e.g., fear).
2. These photographs were then shownto members of various modern culturesand members of an isolated nonliterateNew Guinea tribe.
CONCLUSION: The meaning ofthese basic emotional expressionstranscends cultural and geographicboundaries.
SOURCE STUDY: Ekman & Friesen, 1975
Happiness Disgust
4. The procedure was reversed.New Guinea tribesmen were photo-graphed portraying facial expressionsassociated with the same six emotions,and American college students wereasked to pick the emotion label foreach photograph.
3. All participants were asked to pickthe emotion label that matched eachphotograph.
12.30 Display rules Researchers foundthat when American and Japanese partici-pants watched surgical film clips privately,they displayed similar facial expressions.When they watched the clips in the presenceof the researcher, however, the Japaneseparticipants displayed more positive emo-tion than the Americans.
display rules Cultural rules that gov-ern the expression of emotion.
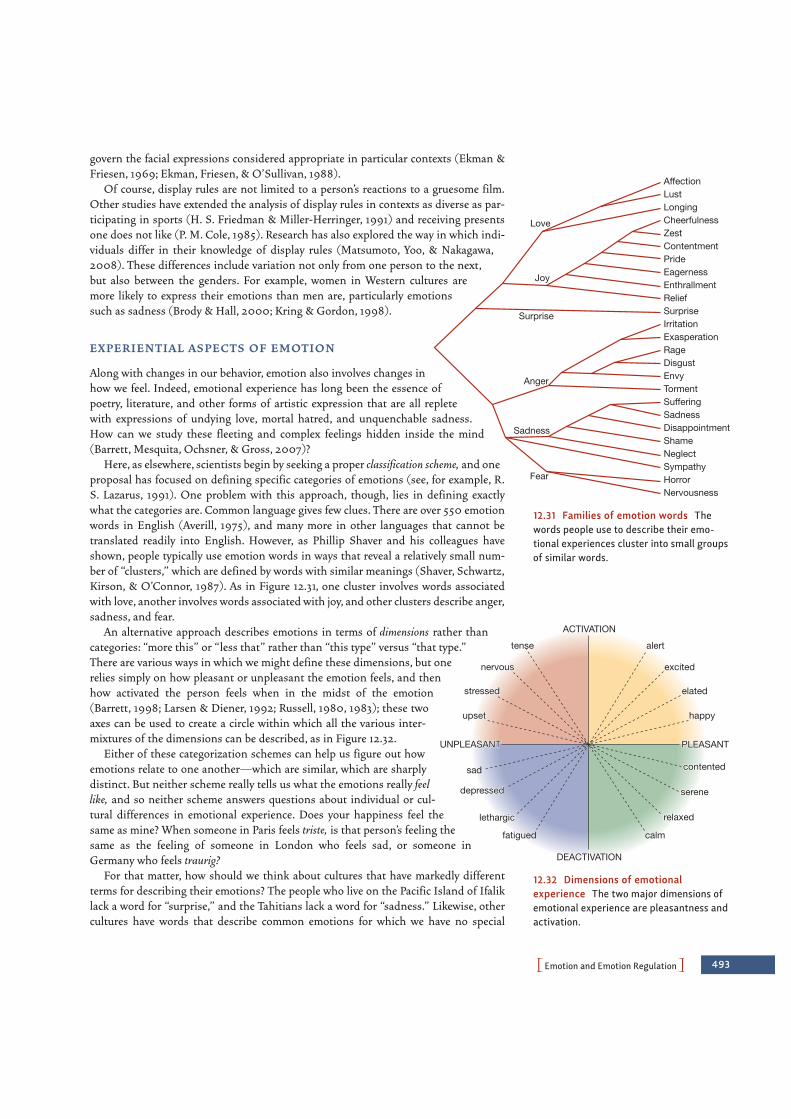
ACTIVATIONACTIVATION
DEACTIVATIONDEACTIVATION
UNPLEASANTUNPLEASANT
tense
nervousnervous
stressedstressed
upsetupset happy
contentedcontented
depresseddepressed
fatigued
lethargiclethargic
sereneserene
relaxedrelaxed
calm
elated
excited
alert
PLEASANTPLEASANT
ACTIVATION
DEACTIVATION
UNPLEASANT
tense
nervous
stressed
upset happy
contentedsad
depressed
fatigued
lethargic
serene
relaxed
calm
elated
excited
alert
PLEASANT
AffectionLustLongingCheerfulnessZestContentmentPrideEagernessEnthrallmentReliefSurpriseIrritationExasperationRageDisgustEnvyTormentSufferingSadnessDisappointmentShameNeglectSympathyHorrorNervousness
Love
Joy
Surprise
Anger
Sadness
Fear
PEmotion and Emotion RegulationO 493
govern the facial expressions considered appropriate in particular contexts (Ekman &Friesen, 1969; Ekman, Friesen, & O’Sullivan, 1988).
Of course, display rules are not limited to a person’s reactions to a gruesome film.Other studies have extended the analysis of display rules in contexts as diverse as par-ticipating in sports (H. S. Friedman & Miller-Herringer, 1991) and receiving presentsone does not like (P. M. Cole, 1985). Research has also explored the way in which indi-viduals differ in their knowledge of display rules (Matsumoto, Yoo, & Nakagawa,2008). These differences include variation not only from one person to the next,but also between the genders. For example, women in Western cultures aremore likely to express their emotions than men are, particularly emotionssuch as sadness (Brody & Hall, 2000; Kring & Gordon, 1998).
EX P E R I E N T I A L AS P E CTS O F E M OT I O N
Along with changes in our behavior, emotion also involves changes inhow we feel. Indeed, emotional experience has long been the essence ofpoetry, literature, and other forms of artistic expression that are all repletewith expressions of undying love, mortal hatred, and unquenchable sadness.How can we study these fleeting and complex feelings hidden inside the mind(Barrett, Mesquita, Ochsner, & Gross, 2007)?
Here, as elsewhere, scientists begin by seeking a proper classification scheme, and oneproposal has focused on defining specific categories of emotions (see, for example, R.S. Lazarus, 1991). One problem with this approach, though, lies in defining exactlywhat the categories are. Common language gives few clues. There are over 550 emotionwords in English (Averill, 1975), and many more in other languages that cannot betranslated readily into English. However, as Phillip Shaver and his colleagues haveshown, people typically use emotion words in ways that reveal a relatively small num-ber of “clusters,” which are defined by words with similar meanings (Shaver, Schwartz,Kirson, & O’Connor, 1987). As in Figure 12.31, one cluster involves words associatedwith love, another involves words associated with joy, and other clusters describe anger,sadness, and fear.
An alternative approach describes emotions in terms of dimensions rather thancategories: “more this” or “less that” rather than “this type” versus “that type.”There are various ways in which we might define these dimensions, but onerelies simply on how pleasant or unpleasant the emotion feels, and thenhow activated the person feels when in the midst of the emotion(Barrett, 1998; Larsen & Diener, 1992; Russell, 1980, 1983); these twoaxes can be used to create a circle within which all the various inter-mixtures of the dimensions can be described, as in Figure 12.32.
Either of these categorization schemes can help us figure out howemotions relate to one another—which are similar, which are sharplydistinct. But neither scheme really tells us what the emotions really feellike, and so neither scheme answers questions about individual or cul-tural differences in emotional experience. Does your happiness feel thesame as mine? When someone in Paris feels triste, is that person’s feeling thesame as the feeling of someone in London who feels sad, or someone inGermany who feels traurig?
For that matter, how should we think about cultures that have markedly differentterms for describing their emotions? The people who live on the Pacific Island of Ifaliklack a word for “surprise,” and the Tahitians lack a word for “sadness.” Likewise, othercultures have words that describe common emotions for which we have no special
12.31 Families of emotion words Thewords people use to describe their emo-tional experiences cluster into small groupsof similar words.
12.32 Dimensions of emotionalexperience The two major dimensions ofemotional experience are pleasantness andactivation.

494 chapter 12 PMOTIVATION AND EMOTIONO
terms. The Ifaluk sometimes feel an emotion they call fago, whichinvolves a complex mixture of compassion, love, and sadness experi-enced in relationships in which one person is dependent on the other(Lutz, 1986, 1988). And the Japanese report a common emotioncalled amae, which is a desire to be dependent and cared for (Doi,1973; Morsbach & Tyler, 1986). The German language reserves theword Schadenfreude for the special pleasure derived from another’smisfortune. Do people in these cultures experience emotions that wedo not (Figure 12.33)? Or are emotional experiences common acrosscultures, despite the variations in cultures’ labels for emotional expe-riences? On these difficult questions, the jury is still out.
P H YS I O LO G I CA L AS P E CTS O F E M OT I O N
When we respond emotionally, it is often a whole body affair, and the bodily reactionsassociated with different emotions certainly feel different from one another (Levenson,1994). That is, not only do the emotions differ in how they feel inside our “head,” butthey also seem to differ in how they feel in the rest of the body. The sick stomach andwrinkled nose of disgust, for example, feel decidedly different from the squared shoul-ders and puffed chest of pride. And anger’s hot head and coiled muscles seem oppositefear’s cold feet and faint heart.
From a common-sense perspective, it seems that emotions arise when weencounter a significant stimulus, and this encounter leads to bodily changes that dif-fer by emotion (Figure 12.34A). Interestingly, this sequence of events was turned onits head by one of the first emotion theories in the field, namely, William James’s the-ory that different emotions provoke different patterns of physiological response(James, 1884). According to the James-Lange theory of emotion (Carl Lange was aEuropean contemporary of James’s who offered a similar account), the reason emo-tions feel different from one another subjectively is that we sense the different phys-iological patterns produced by each emotion. Specifically, this view holds thatemotion begins when we perceive a situation of an appropriate sort—we see the bearor hear the insult. But our perception of these events is, as James put it, “purely cog-nitive in form, pale, colorless, destitute of emotional warmth” (1890, vol. 2, p. 450).What turns this perception into genuine emotion is our awareness of the bodilychanges produced by the arousing stimuli. These changes might consist of skeletalmovements (running) or visceral reactions (pounding heartbeat), but only when wedetect the biological changes do we move from cold appraisal to emotional feeling,from mere assessment to genuine affect (Figure 12.34B). Moreover, the claim is thatthe specific character of the biological changes is crucial—so that we feel fear becausewe are experiencing the pattern of bodily changes associated with fear; we feel hap-piness because of its pattern of changes in the body, and so on.
Subsequent theories, however, made quite different predictions about the degree ofphysiological patterning we should expect in emotion. For example, Walter Cannon,whom we met earlier in the chapter as a pioneer in the study of the “fight or flight”response, believed that our physiological responses are quite general (W. B. Cannon,1927). According to the Cannon-Bard theory of emotion (Philip Bard was a contem-porary of Cannon’s who espoused a similar view), it’s not easy to distinguish the bodilychanges associated with different emotions, so that the bodily changes associated withanger are actually rather similar to the changes associated with happy excitement(Figure 12.34C).
(A) (B)
12.33 Culturally defined emotions(A) The Japanese word amae refers to adesire to be dependent and cared for.(B) The German word Schadenfreude refersto the pleasure derived from another per-son’s misfortune.
James-Lange theory of emotionThe theory that the subjective experi-ence of emotion is the awareness ofone’s own bodily reactions in the pres-ence of certain arousing stimuli.
Cannon-Bard theory of emotionThe theory that a stimulus elicits anemotion by triggering a particularresponse in the brain (in the thala-mus) which then causes both thephysiological changes associated withthe emotion and the emotional experi-ence itself.
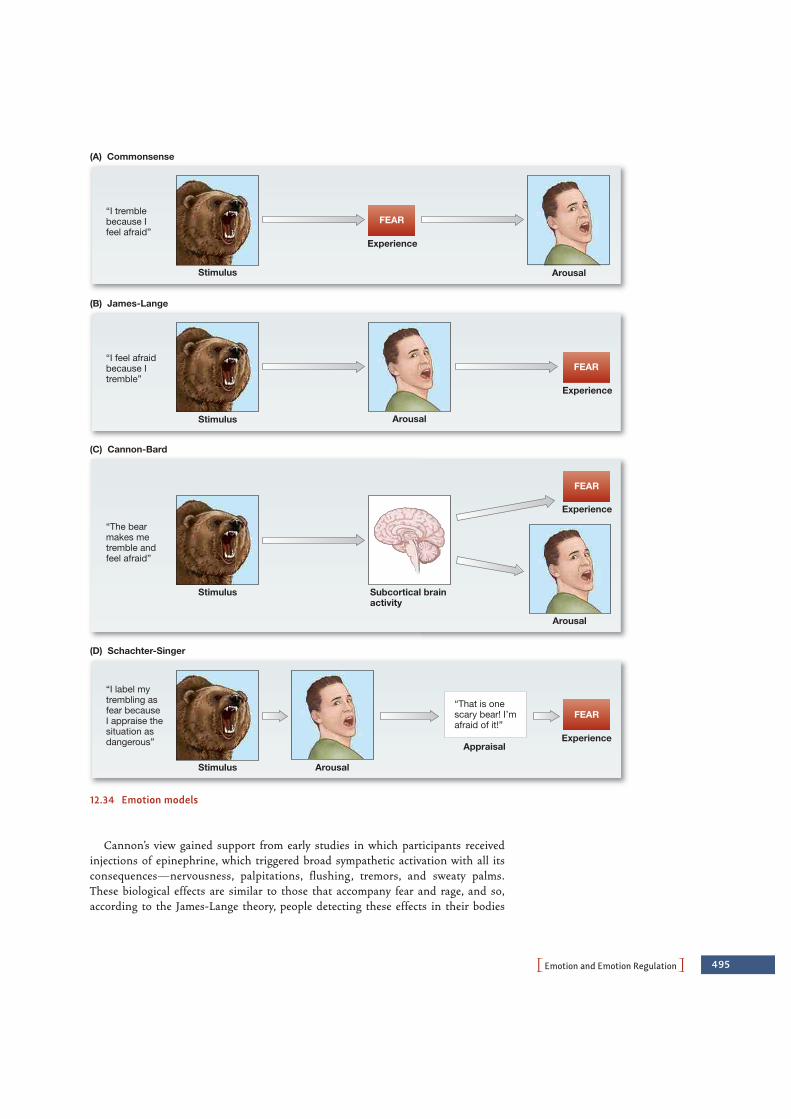
PEmotion and Emotion RegulationO 495
Cannon’s view gained support from early studies in which participants receivedinjections of epinephrine, which triggered broad sympathetic activation with all itsconsequences—nervousness, palpitations, flushing, tremors, and sweaty palms.These biological effects are similar to those that accompany fear and rage, and so,according to the James-Lange theory, people detecting these effects in their bodies
12.34 Emotion models
(B) James-Lange
FEAR
Arousal
Arousal
Experience
FEAR
Appraisal
“That is onescary bear! I’mafraid of it!”
“I label mytrembling asfear becauseI appraise thesituation asdangerous”
“The bearmakes metremble andfeel afraid”
“I feel afraidbecause Itremble”
(C) Cannon-Bard
Stimulus
Stimulus
Stimulus
Experience
Experience
Experience
Arousal
FEAR“I tremblebecause Ifeel afraid”
Stimulus
Subcortical brainactivity
Arousal
(D) Schachter-Singer
(A) Commonsense
FEAR

496 chapter 12 PMOTIVATION AND EMOTIONO
should experience these emotions. But that was not the case. Some of the participantswho received the injections simply reported the physical symptoms. Others said theyfelt “as if” they were angry or afraid, a kind of “cold emotion,” not the real thing(Landis & Hunt, 1932; Marañon, 1924). Apparently, the visceral reactions induced bythe stimulant were by themselves not sufficient to produce emotional experience.
Even so, there is an obvious challenge to the Cannon-Bard theory. If different emo-tions produce comparable physiological responses, then why do we have the subjectiveimpression that our bodies are doing quite different things in different emotional states?This question was addressed by the Schachter-Singer theory of emotion (Figure12.34D). According to this theory, behavior and physiology are (as James proposed) cru-cial for emotional experience. James was wrong, though, in claiming that the mere per-ception of these bodily changes is sufficient to produce emotional experience. That isbecause, in addition, emotion depends on a person’s judgments about why her body andphysiology have changed (Schachter & Singer, 1962).
In a classic study supporting this theory, participants were injected with a drug thatthey believed was a vitamin supplement but really was the stimulant epinephrine. Afterthe drug was administered, participants sat in the waiting room for what they thoughtwas to be a test of their vision. In the waiting room with them was a confederate of theexperimenter (someone who appeared to be another research participant but was actu-ally part of the research team). In one condition the confederate acted irritable, madeangry remarks, and eventually stormed out of the room. In another condition he actedexuberant, throwing paper planes out the window and playing basketball with balled-up paper. Of course, his behavior was all part of the experiment; the vision test that theparticipants were expecting never took place (Schachter & Singer, 1962). Participantsexposed to the euphoric confederate reported feeling happy, and, to a lesser degree, par-ticipants exposed to the angry confederate reported that they felt angry. Although thisstudy has come under criticism (G. D. Marshall & Zimbardo, 1979; Mezzacappa,Katkin, & Palmer, 1999; Reisenzein, 1983), it remains influential because it is areminder that bodily arousal only partially determines the emotion that is experienced.
Over the past 50 years, researchers have tried to clarify how the body responds dur-ing emotional experiences. One of the most interesting conclusions from this researchis that our perceptions of bodily differences among the emotions may in some cases beillusions, compelling experiences that are not well grounded in reality (Cacioppo,Berntson, & Klein, 1992). It seems, therefore, that the various emotions are surprisinglysimilar if we examine the body’s response “from the neck down.”
Even so, the emotions are distinguishable biologically—in the pattern of brainactivation associated with each emotion. Evidence on this point comes from studiesin the field of affective neuroscience (R. J. Davidson & Sutton, 1995; Panksepp, 1991,1998), whose proponents argue that emotions arise not in one, but in multiple neu-ral circuits. Some brain regions are activated in virtually all emotions (Murphy,Nimmo-Smith, & Lawrence, 2003; Phan, Wager, Taylor, & Liberzon, 2002)—forexample, the medial prefrontal cortex. One likely possibility is that this section of thebrain plays a general role in attention and meaning analysis related to emotion.Other brain regions, however, seem to be related to specific emotions. For example,fear is often associated with activation of the amygdala, and sadness is often associ-ated with activation of the cingulate cortex just below the corpus callosum (althoughactivation in these brain regions is not specific to these emotions; see Barrett &Wager, 2006). Many researchers are convinced that brain data like these will eventu-ally allow us to determine the extent to which different emotions have different phys-iological profiles.
Schachter-Singer theory of emotionThe theory that emotional experienceresults from the interpretation of bodilyresponses in the context of situationalcues.
confederate Someone who appearsto be a research participant but actu-ally is part of the research team.
affective neuroscience A field thatuses cognitive neuroscience researchmethods to study emotion and relatedprocesses.

PEmotion and Emotion RegulationO 497
The Functions of EmotionAs we have seen, emotions consist of coordinated changes in behavior, experience, andphysiology. Why is this? Is it possible that these interwoven effects were somehow use-ful to our ancestors, and so favored by evolution (Tooby & Cosmides, 1990)? One wayto pursue this issue is to look at the consequences of emotion and to ask whether theybenefit us.
Some aspects of our emotions plainly do help us—or, perhaps, helped our ancientancestors. Fear, for example, is associated with sympathetic nervous system activity thatprepares large muscles for fighting or fleeing (Frijda, 1986); these are exactly the bod-ily adjustments we would want for fending off (or escaping) a fearful encounter.Likewise, consider joy. In one study, participants had to prepare a speech that theybelieved would be videotaped and evaluated by judges (Fredrickson et al., 2000).Following this stressful task, the participants were randomly assigned to view a film clipthat elicited joy, a neutral film clip, or a film clip that elicited sadness. The data showedthat participants who had viewed the joy clip showed substantially greater cardiovascu-lar recovery from their speech than did participants who had watched either the neutralor the sad clip. This finding seems to suggest that joy (and other positive emotions) canhelp us recover from stress.
In addition to these physiological effects, emotions also involve a variety of changesin how we perceive and think about the environment around us. Perceptual effects offear include an increased intake of sensory information including widening of the eyesand greater nasal volume, while disgust involves a decreased sensory intake, includingnarrowing of the eyes and decreased nasal volume (Susskind et al., 2008; Figure 12.35).Emotions affect later information processing, too. Positive emotions like joy seem tolead us to greater cognitive flexibility and a broader focus, relying less on the details ofa situation and more on top-down, schematic processing (Fredrickson, 1998). Negativeemotions, in contrast, seem to focus our attention more narrowly—on specific aspectsof a situation. Why should this be? Anger, for example, may focus our attention on theobstacle preventing us from reaching our goal; this may be exactly the right focus if wewant to remove that obstacle in some way. Fear, in contrast, may focus our attentionon the likely outcomes of a situation; again, this may be the right focus if we wantto maximize our motivation to avoid this outcome (L. J. Levine & Pizarro, 2004;Phelps, 2006).
Emotions also have a powerful effect on memory, as we mentioned in thePrologue, and this brings its own benefits. Emotional events are likely to be conse-quential ones, involving great opportunities, for example, or powerful threats. Wewould be well served, therefore, by remembering these events well, and emotion
12.35 Perceptual effects of emotion (A) Fear involvesan increased intake of sensory information, whereas(B) disgust involves a decreased intake of sensory infor-mation (Susskind et al., 2008).

498 chapter 12 PMOTIVATION AND EMOTIONO
seems to promote this recollection. Several mechanisms probably contribute to thispoint, including the changes in our body chemistry that accompany emotion andactivation of the amygdala, a common feature of several emotions. These mecha-nisms may together promote the process of memory consolidation, the biologicalprocess through which memories are established in permanent storage (T. W.Buchanan & Adolphs, 2004; Dolcos, LaBar, & Cabeza, 2006; Kilpatrick & Cahill,2003; McGaugh, 2003; Reisberg & Hertel, 2004).
Emotions also serve interpersonal functions. One example is the way expressions ofemotion indicate social intent (Fridlund, 1994). When we smile, for example, we signalthat we are open to interacting with other people. When we scowl, we communicate“Back off!” When we burst into tears, we indicate that we need help (J. J. Gross,Fredrickson, & Levenson, 1994). Another example is the way emotion expressions facil-itate group functioning. When we show embarrassment, we indicate to others that weknow we have done something inappropriate (Keltner & Buswell, 1997). This signal hasthe effect of making amends for the gaffe. At the same time, embarrassment is a highlyaversive state, and feels in the moment like a real calamity. The function of embarrass-ment may therefore be not only to repair social damage, but also to motivate us to avoidthe same behavior in the future. Even expressions of pride—at least when they areappropriate to one’s performance—are associated with leadership in group problem-solving (L. A. Williams & DeSteno, 2008).
Emotion RegulationPlainly, then, emotions have many functions—preparing the body for action, directingour attention, facilitating social interactions, and more (Levenson, 1999). But emotionscan hurt us, too, if they happen at the wrong time or at the wrong intensity level.Indeed, inappropriate emotional responses are involved in many forms ofpsychopathology (Gross & Levenson, 1997; see also Chapter 16) and even many formsof physical illness (Baum & Posluszny, 1999).
For all these reasons, humans need to experience their emotions, but they also some-times need to regulate their emotions. Emotion regulation means influencing whichemotions we have, when we have them, and how we experience or express them(J. J. Gross, 1998b, 2007). Emotion regulation may involve decreasing, increasing, orsimply maintaining experiential, behavioral, or physiological aspects of emotion,depending on our goals. The most common forms of emotion regulation, though,involve efforts at decreasing the experience or behavior associated with anxiety,sadness, and anger (J. J. Gross, Richards, & John, 2006).
T W O FO R M S O F E M OT I O N R E G U L AT I O N
Two forms of emotion regulation have received the most attention (J. J. Gross, 2001).The first is called cognitive reappraisal, which occurs when someone tries to decreaseher emotional response by changing the meaning a situation has. For example, insteadof thinking of a job interview as a matter of life or death, a person might think aboutthe interview as a chance to learn more about the company, to see whether it would befun to work there. The second kind of emotion regulation is called suppression, whichoccurs when someone tries to decrease the emotion he shows on his face or in hisbehavior. For example, instead of bursting into tears upon receiving disappointingnews, a person might bite his lip and put on a brave face.
emotion regulation The ability toinfluence one’s emotions.
cognitive reappraisal A form ofemotion regulation in which an individ-ual changes her emotional response toa situation by altering her interpreta-tion of that situation.
suppression A form of emotionregulation that involves inhibitingemotion-expressive behavior.

PEmotion and Emotion RegulationO 499
While both strategies can decrease emotional behavior, reap-praisal seems to be a more effective way to regulate emotions. Inpart, this is because someone who suppresses an emotional reac-tion might block the display of emotion but does not make the feel-ings go away (J. J. Gross & Levenson, 1997). In fact, physiologically,suppression leads to even greater sympathetic nervous system acti-vation, presumably because the individual must exert herself tokeep her emotions from showing (J. J. Gross, 1998a). There is also acognitive cost to suppression. When participants in an experiment were asked aboutmaterial that had been presented while they were trying to suppress their emotions,they made more errors than they did when they had not been suppressing their emo-tions (Richards & Gross, 2000). Indeed, when asked to suppress their emotions, par-ticipants performed as badly on later memory tasks as participants who had beenencouraged not to pay attention at all to the material that was being presented(Richards & Gross, 2006).
In contrast, reappraisal can make one feel better, and it does not have cognitive orphysiological costs (J. J. Gross, 1998a). In one study, researchers showed participantsneutral or negative emotion-eliciting slides during an fMRI study (Ochsner et al., 2004;Figure 12.36). In the critical conditions, participants were asked either to view the nega-tive emotion-eliciting slides or to reappraise them by altering their meaning. For exam-ple, a participant might see a picture of women crying in front of a church. Instead ofthinking of a funeral scene, the participant might try to think of it as a wedding scenethat brought the woman to tears of joy. The reappraisal had many effects. Participantsreported feeling less negative emotion when reappraising than they did when just watch-ing the negative slides. Reappraisal also activated the prefrontal regions in the brain,which are associated with other kinds of self-regulation, and decreased activation in theamygdala and other brain regions associated with negative emotion.
The key message from these studies is that different forms of emotion regulationhave quite different consequences. This is not to say one should always reappraise ornever suppress. Both processes have their place. But it is becoming clear that comparedwith keeping a stiff upper lip by means of suppression, reappraisal is generally moreadaptive.
T H E D E V E LO P M E N T O F E M OT I O N R E G U L AT I O N
How do the emotion regulation skills that are so necessary in adulthood develop? Weknow that children respond emotionally from an early age. From birth, babies cry whenthey are distressed and cease crying when they are comforted. Newborns and younginfants also display facial responses when they are interested, distressed, disgusted, orcontented (Izard et al., 1995; Figure 12.37). Smiles appear—to parents’ delight—a bit
A
B
C
12.36 The neural bases of reappraisalResults from a functional magnetic reso-nance imaging study in which participantswere asked to use reappraisal to changetheir emotional responses to negativeemotion-eliciting slides. Findings indicatedthat reappraisal was associated withincreased activation in the (A) dorsolateraland (B) ventrolateral prefrontal cortex aswell as the (C) dorsomedial prefrontalcortex.
12.37 Facial displays of emotion Starting at an early age,infants produce facial expressions that resemble adultexpressions.

500 chapter 12 PMOTIVATION AND EMOTIONO
later. Fleeting smiles are visible in 1-month-old infants; smiles directed toward otherpeople appear when most infants are 2 or 3 months old. Fear arrives later still. Thefirst clear signs of fear typically emerge only when the child is 6 or 7 months old(Witherington, Campos, & Hertenstein, 2001).
Of course, very young infants show little ability to control their emotions, and so itis up to the caregiver to soothe, distract, or reassure them. Soon, though, infants startshowing the rudiments of regulation, so that 6-month-olds, for example, are likely toturn their bodies away from unpleasant stimuli (Mangelsdorf, Shapiro, & Marzolf,1995). By their first birthday, infants regulate their feelings by rocking themselves, orchewing on objects, or clinging tightly to some beloved toy or blanket.
Children also begin to use display rules—and so begin expressing their emotions ina socially acceptable way—at an early age, so that, for example, 11-month-old Americaninfants are more expressive of their feelings than Chinese babies (Freedman &Freedman, 1969). However, their self-control is limited at this early age, and clearadherence to display rules is usually not evident until the child is age 3 or so (Lewis,Stanger, & Sullivan, 1989)—and even then, children’s attempts at disguising their emo-tions are often unsuccessful. It is clear, though, that children learn relatively early thevalue of managing one’s expressions—sometimes to gain the response one wants fromothers, sometimes to protect others, and sometimes to deceive them (Vrij, 2002).
The real progress in emotion regulation, however, comes later, when the child is age4 or 5. By that age, children seem to understand, for example, that they can diminishtheir fear by fleeing from, or removing, the scary object; they learn that they can dimin-ish their sadness by seeking out an adult’s aid or by reassuring self-talk (Harris, Guz,Lipian, & Man-Shu, 1985; Lagattuta, Wellman, & Flavell, 1997). These early skills arelimited, but gradually grow and strengthen. Where do these skills come from?
Part of the answer lies in the child’s conversational experience, because children’sefforts in emotion regulation are influenced by the examples they have observed andthe instructions they have received (R. A. Thompson, 1994, 1998). In fact, these conver-sations convey a range of strategies to children, including distraction (“Try thinking ofsomething happy”), compensation (“Why don’t we get ice cream after the appointmentwith the doctor?”), and reappraisal (“Dumbledore didn’t really die; it’s just pretend”).Conversations with children about emotion also convey when emotions should orshould not be expressed, and the consequences of expressing or not expressing them(Eisenberg, Cumberland, & Spinrad, 1998).
SOME FINAL THOUGHTS: THE “WHY” OF BEHAVIOR
In this chapter, we have considered a number of crucial motives. However, there arecountless others besides these. For example, we sometimes feel an urge to drink a cupof coffee. Or feel like reading a book, texting a friend, meditating, or taking a nap.Over the decades, researchers have tried to categorize motives in different ways.Some have arranged them hierarchically. Others have sought to identify the biologi-cal bases of the pain and pleasure responses that form part of many differentmotives. Each approach has its merits, and in this chapter, we have drawn severalbroad distinctions among motivational states. For one, we have distinguished thedrive-based motives, such as thermoregulation, hunger, aggression, and sex, fromthe non-drive-based motives, such as the motive to belong and the motive to achieve.

MOTIVATIONAL STATES
• When explaining why people and other animals do what theydo, early theorists emphasized genetically endowed instincts.Other theorists have emphasized homeostatic mechanismsthat monitor the organism’s internal environment and workto maintain stability in that environment. Deviations fromhomeostasis create an internal state of biological and psycho-logical tension called a drive.
THERMOREGULATION
• Homeostatic control is evident in many settings, includingthermoregulation. When an endothermic organism is cold,thermoregulation activates the sympathetic branch of theautonomic nervous system, which leads to increased heartrate, vasodilation, a slowing down of digestion, and other
effects. When the organism is overheated, thermoregulationtriggers the parasympathetic branch of the autonomic nerv-ous system, which has the opposite effects.
HUNGER , EATING, AND OBESITY
• Homeostatic mechanisms also play a crucial role in the con-trol of eating. Each person seems to have a biologically deter-mined set point for his or her weight, and several mechanismswork to maintain that set point. Some of these mechanismsare in the liver; others depend on glucoreceptors in the hypo-thalamus; still others rely on signals from the adipose cells.When full of fat, these cells release leptin, a chemical thatcauses the organism to stop eating.
• This multiplicity of signals provides safety for the organism,because each signal provides a “backup” system in case the
PSummaryO 501
S U M M A R Y C H A P T E R 1 2
Whereas drives can be described in terms of restoring homeostasis and avoidingpainful states of tension, such concepts are less satisfactory descriptions of non-drive-based motives.
Emotions, though distinct from motives, share some of their important character-istics. Like other motivational states, emotions are biologically based responses thathave been shaped by a long evolutionary history, and given particular form both by anorganism’s learning history and by its present circumstances. Motives and emotionsalso both involve a change in the organism’s readiness to respond in particular ways, and this change in readiness often is felt as motives and emotions play them-selves out. One way that motives and emotions differ, however, is that motivationalstates are often tied more specifically to particular classes of stimuli than are emo-tions. Thus, one is typically hungry for food, and perhaps even food of a specific type.By contrast, one can feel anger about almost anything—the weather, the fact that onedoesn’t have a date this weekend, economic disparities among nations, or a room-mate’s goofy taste in music.
Whether we’re considering drive-based motives, non-drive-based motives, oremotions, what is important is that these motivational states are at play continually,and arise both because of external stimuli and by virtue of our thoughts. It is rarethat only one motive is active. Instead, many motives cooperate to shape ourthoughts, feelings, and behaviors. We must consider physiological, cultural, and cog-nitive factors to understand how even the most basic motives energize and direct ourbehavior. Even so, motives do not dictate our behavior. Instead, they make “sugges-tions” that carry varying degrees of weight. This means that we can regulate themotivational states that coordinate our responses to many kinds of situations. Thisregulation may take place in many different ways, and as we have seen—at least for the emotions—different approaches to self-regulation can have very differentconsequences.

502 chapter 12 PMOTIVATION AND EMOTIONO
other signals fail. In addition, the various signals play differ-ent roles, with some monitoring long-term needs, some pro-viding an index of immediate status, and some serving topotentiate other signals. Social signals also play an importantrole in governing eating.
• Some cases of obesity are produced by genetically rooted dif-ferences in a person’s set point; other cases involve changes inmetabolic efficiency. Obesity in some people may representthe operation of “thrifty genes” that code for slower metabo-lism. These genes were helpful in ancient times when foodwas scarce, but the same genes now promote unhealthyweights, thanks to the fact that we live in a world in whichfood is usually always available.
THREAT AND AGGRESSION
• Our response to threat is controlled by biological mechanismscentered on the operations of the autonomic nervous system.When we are threatened, the sympathetic branch activates thebody by (among other steps) increasing the available meta-bolic fuel and accelerating the fuel’s utilization by increasingheart rate and respiration. This emergency reaction was onceunderstood as preparing us for “fight or flight,” but actually itgets us ready for a number of different responses.
• Virtually every species shows some sort of aggression, and inmost species, physical aggression is more prevalent in males,perhaps because of the influence of the hormone testosterone.Human aggression is commonly triggered by complex beliefsand symbol systems, and, in this regard, it seems differentfrom aggression in other species. Humans vary in howaggressive they are, with some of the variation due to an indi-vidual’s personality, and some due to the social and culturalsetting.
SEXUAL BEHAVIOR
• Like all motivated behavior, sexual behavior is shaped by amix of biological factors and cultural influences. The timingof sexual behavior, for example, is heavily influenced in mostspecies by the estrus cycle, but the influence of this cycle ismuch less for humans than for other animals.
• The human sexual response cycle has four phases: excitement,plateau, orgasm, and resolution.
• A wide range of factors influence sexual behavior, and thereappear to be widespread differences between the genders inthe factors that govern mate preference. Men typically place
greater emphasis on youth and physical attractiveness,whereas women place greater emphasis on social and finan-cial status.
• Sexual preferences are rooted in childhood. One importantdeterminant of sexual preference is genetic makeup. Whileit is clear that other factors shape sexual preferences, it isnot clear what these nongenetic factors are or how theyoperate.
MOTIVES BEYOND DRIVES
• Whereas drives motivate us to reduce unpleasant tensionstates, other motives lead us to achieve positive goals.
• One nondrive motive is the motive to belong. Benefits ofsocial support include tangible and emotional support.Another important nondrive motive is the motive to achieve.
THE DIVERSITY OF MOTIVES
• According to Abraham Maslow’s hierarchy of needs, peoplestrive for higher-order needs only when lower-order needsare satisfied.
• Many different types of aversive stimulation activate a com-mon brain network called the pain matrix. Positive goals thatwe seek to obtain are called incentives. Two important incen-tive states are wanting and liking.
EMOTION AND EMOTION REGULATION
• Emotions involve changes in our behavior, including ourfacial behavior. The expression of emotion in the face may beuniversal (i.e., the same across cultures), although culturescertainly differ in their display rules.
• Emotions also involve changes in how we feel, and theoristshave offered various schemes for classifying these feelings.People in different cultures certainly describe emotions indifferent ways. Whether people in difficult cultures all feel thesame emotions, however, remains a matter for debate.
• Our bodily state changes when we are emotional.According to the James-Lange theory, emotions arise fromour bodily reactions. The Cannon-Bard theory proposes thatboth emotion and the bodily reaction are caused by brainactivity triggered by a suitable stimulus. According to theSchachter-Singer theory, emotion arises from the way weinterpret our bodily reactions. Current evidence suggests

PSummaryO 503
there may be fewer distinctions than we might expectamong emotions in the bodily changes produced. Thereare, however, changes in the brain that distinguish the var-ious emotions, and this is a topic scrutinized by affectiveneuroscience.
• Emotions serve many purposes. For example, joy can help usrecover from stress and can broaden our attentional focus.Negative emotions, in contrast, seem to focus attention.Emotion also promotes memory, perhaps because the bodilyarousal promotes memory consolidation. Emotions alsoserve a social function, helping to convey our feelings to otherpeople.
• It is often important to regulate our emotions—either bymeans of cognitive reappraisal or by means of suppression. Bothdecrease the emotional expression, but reappraisal seems todampen emotion without exacting a cognitive or physiologi-cal cost. The ability to regulate emotions develops over thecourse of childhood.
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
Social Cognition 506
Social Influence 519
Social Relations 531
Some Final Thoughts: The Social Animal? 540
Summary 541
13CH
AP
TE
R
505
CH
AP
TE
R
Social Psychology
Leaning over the corpse of Manadel al-Jamadi, U.S.
Army specialist Sabrina Harman flashes a thumbs-up and a smile. Were it not for
the dead body in the photograph, you might focus on how pretty she looks. But
blood dribbles from beneath Jamadi’s bandages, his bluish jaw is locked, and ice
surrounds his torso. Something very wrong has happened here.
A few months after this picture was taken at Iraq’s Abu Ghraib prison, the world
learned that indeed many wrongs had happened here. U.S. military police and CIA
interrogators killed Jamadi in November 2003 while interrogating him at the prison.
Other photographs revealed that U.S. soldiers and personnel routinely tortured,
humiliated, and sexually abused dozens of other prisoners—many of whom were
not guilty of any crime.
Following investigations, 12 soldiers, including Harman, were tried, convicted,
sentenced to federal prison, and dishonorably discharged from the military. Several
years have passed since the Abu Ghraib atrocities were revealed, but people are still
asking, Why did these seemingly normal soldiers behave so cruelly?
The easy answer is that these soldiers were just evil, or “bad apples,” as some
American leaders suggested. But despite their photographed smiles, many soldiers
were bewildered by their own behavior. “I can’t handle what’s going on. . . . What if
it was me in their shoes?” wrote Harman in a letter home, which was later
excerpted in an article in the New Yorker. Moreover, all the soldiers had passed the
Army’s psychiatric evaluation, suggesting that at least when they enlisted, they were
psychologically “normal.”
506 chapter 13 PSOCIAL PSYCHOLOGYO
And so we look to the situation: Working in a wartime prison, with substandardfood and water, they were members of a large group of similarly trained, youngsoldiers surrounded by enemies. Many were part-time reservists who joined themilitary to earn money for college. In their hasty training, many had not learnedabout the international laws protecting prisoners of war. In the ambiguous andoften frightening situation of Abu Ghraib, they looked to their leaders to showthem the way. And like good soldiers, they did what they were told. “I was just fol-lowing orders” was their common defense, echoing so many soldiers judged warcriminals in the past. As the New Yorker article points out, by taking pictures of theprisoners the Abu Ghraib guards “demonstrated two things: that they never fullyaccepted what was happening as normal, and that they assumed they had nothingto hide.”
In this chapter, you will learn about the many subtle reasons that ordinary peopleperform acts of extraordinary evil—as well as extraordinary good. As it turns out, thecommon thread that connects these explanations is that most human behavior is trig-gered in part by other people.
As you will also see, much of our everyday cognition resembles the work of social psy-chologists. We all try to figure out why people behave as they do—an activity called attri-bution. Like so much of our psychology, attribution is strongly shaped by culture. Just asAmerica’s leaders gave internal explanations for the Abu Ghraib guards’ actions,Americans and Western Europeans generally explain behavior in terms of internal, indi-vidual factors like personality, moral goodness, psychiatric status, and mental state.Meanwhile, much of the rest of the world tends to look outside the individual—to situa-tions, environments, relationships, and histories—for clues to account for people’sactions.
Perhaps because of our cultural tendency to look inside people to explain theiractions, Americans and Western Europeans are often wary of social influences. Yetthere is no such thing as an isolated individual, free of context and immune to others’influences. Humans are hardy, long-lived, and widespread precisely because we formsocial connections and cultural bonds that help us make sense of our environments.This social nature is not just a source of bias and wrongdoing, as it was at AbuGhraib; it is also the root of our strength, as individuals and as a species. To under-stand both our social vulnerabilities and our social prowess, we must consider howpeople think about, influence, and relate to one another. These topics will be our focusin this chapter.
SO CIAL CO GNITION
As members of a social species, we humans are exquisitely attuned to each other. Manyof our everyday behaviors—what we eat, how we dress, what kind of music we like, andhow we think about current events—are shaped by the people around us. Even whenwe are not directly mingling with other people, we are often thinking about them, mak-ing plans involving them, and maybe even fantasizing about them—not to mentionobeying (or breaking) their laws, using their products, reading their books, watchingtheir television shows, and speaking their languages. In other words, most of ourthoughts, feelings, and behaviors are shaped by the social world—often without useven noticing.

PSocial CognitionO 507
We don’t respond to all these influences in a mechanical or reflexive fashion, how-ever. Instead, our responses to the social world depend to an enormous extent on howwe interpret others’ behaviors and how others interpret ours. This is evident in the factthat if Mary smiles at you, your reaction will be quite different if you think she was flirt-ing as opposed to merely being polite. If the salesman recommends the Macintoshrather than the Dell, your purchase may depend on whether you believe the salesman issincere or, for that matter, knowledgeable. In these cases and most others, how werespond to other people depends on how we think about and interpret their actions.This crucial process of interpreting and thinking about the social world is referred to associal cognition.
AttributionPeople everywhere spend a lot of time and energy observing the people around themand asking, “Why did she (or he) do that?” Social psychologists call the process ofanswering this question causal attribution, and the study of how people form attri-butions is one of social psychology’s central concerns (see, for example, F. Heider,1958; E. E. Jones, & Nisbett, 1972; H. H. Kelley, 1967; H. H. Kelley & Michela, 1980).As we saw in Chapters 4, 5, 8, and 9, thinking about the world often requires us togo beyond the information we are actually given. We interpret the visual images onour retinas, for example, by using top-down knowledge to supplement what we see.We draw inferences from the observations we make, to reach broader conclusionsabout the world. As we will see, similar intellectual activity is essential in the socialdomain.
AT T R I B U T I O N AS L AY SC I E N C E
People make attributions in roughly the same way that scientists track down the causesof physical events (H. H. Kelley, 1967). For a scientist, an effect (such as an increase ingas pressure) is attributed to a particular condition (such as a rise in temperature) if theeffect occurs when the condition is present but does not occur when the condition isabsent. In other words, the scientist needs to know whether the cause and the effectcovary. According to social psychologist Harold Kelley, when people try to explain thebehavior of others, they use a similar covariation principle.
This means that, to answer the question “Why did Mary smile at me?” we have toconsider when Mary smiles. Does she smile consistently whenever you walk into theroom? Does she refrain from smiling when others arrive? If the answer to both of thesequestions is yes, then her smile does covary with your arrival, and so is probably bestunderstood as a result of her feelings about you. If it turns out, though, that Marysmiles just as broadly when greeting others, then we have to come up with a differentexplanation (F. Heider, 1958; H. H. Kelley, 1967).
Causal attributions can be divided into two broad types—those that focus on factorsexternal to the person (e.g., Mary smiled because the situation demanded that she bepolite) and those that focus on the person herself (e.g., Mary smiled because she isfriendly). Explanations of the first type are called situational attributions and involvefactors such as other people’s expectations, the presence of rewards or punishments, oreven the weather. Explanations of the second type, dispositional attributions, focuson factors that are internal to the person, such as traits, preferences, and other personalqualities (Figure 13.1).
causal attribution An inferenceabout what caused a person’sbehavior.
situational attributions Attributionsthat explain someone’s behavior interms of the circumstances ratherthan aspects of the person.
dispositional attributionsAttributions that explain someone’sbehavior in terms of factors internal tothe person, such as traits orpreferences.
508 chapter 13 PSOCIAL PSYCHOLOGYO
13.1 Challenges to attribution In decid-ing why someone is behaving as he is, weneed to decide whether his behavior isshaped primarily by the circumstances orprimarily by who he is. Did Al Franken playan outrageous character on Saturday NightLive because that is what he is really like orbecause that is the sort of behavior appro-priate for (and elicited by) a late-nightcomedy show? Does his behavior in thiscontext tell us anything about how he willact as an elected official?
CU LT U R E A N D AT T R I B U T I O N
How do people choose attributions for the behaviors they observe? Kelley’s proposalwas that people are sensitive to the evidence they encounter, just as a scientistwould be, and draw their conclusions according to this evidence. It turns out, how-ever, that this is not quite right, because people have strong biases in the way theyinterpret the behavior of others, biases that can sometimes lead them to overrulethe evidence. These biases come from many sources, including the culture in whichsomeone lives.
Every person is a part of many cultures—those defined by race, nationality, andethnicity, and also those defined by gender, socioeconomic status, sexual preference,urbanicity (e.g., city dwelling or rural dwelling), economy (e.g., agricultural orindustrial), and historical cohort (e.g., baby boomer or gen Xer). This diversitymeans that cultures differ on many dimensions, but there is reason to believe thatone dimension is especially important—whether a culture is more individualistic ormore collectivistic (Triandis, 1989, 1994).
As the name suggests, individualistic cultures cater to the rights, needs, andpreferences of the individual. The majority cultures (e.g., middle-class, of European her-itage) of the United States, western Europe, Canada, and Australia are individualistic(Figure 13.2). In these cultures, people tend to view themselves and others asindependent entities—that is, as fundamentally separate from others and their environ-ment. They also generally think that people behave according to their internal thoughts,feelings, needs, and preferences (A. P. Fiske, Kitayama, Markus, & Nisbett, 1998; Markus& Kitayama, 1991), and not according to outside influences, such as other people’s expec-tations or the demands of a situation. To emphasize their independence and distinctive-ness, people in individualistic cultures often strive to stand out by achieving personalgoals. They still feel obligated to their families and communities, but regularly overridethese social obligations in order to pursue their own paths.
Collectivistic cultures, on the other hand, stress the importance of maintainingthe norms, standards, and traditions of families and other social groups. Most of theworld’s cultures are collectivistic, including many of those of Latin America, Asia, andAfrica. In collectivistic cultures, people tend to view themselves and others asinterdependent—that is, as fundamentally connected to the people in their immedi-ate community and to their environment. They usually think that people behaveaccording to the demands of a situation or the expectations of others, and notaccording to their personal preferences or proclivities. People still have their owndreams, desires, and life plans, of course, but they are more likely to create thoseplans according to the wishes and expectations of others, and to change them whenthe situation demands.
individualistic cultures Cultures inwhich people are considered funda-mentally independent and which valuestanding out by achieving privategoals.
collectivistic cultures Cultures inwhich people are considered funda-mentally interdependent and whichemphasize obligations within one’sfamily and immediate community.

PSocial CognitionO 509
It bears emphasizing that not everyone in collectivistic cultures has aninterdependent notion of the person, just as not everyone in individualistic cultureshas an independent notion. Instead, these terms describe what is typical, as well aswhat each culture’s traditions, laws, religions, schools, and media encourage.
T H E F U N DA M E N TA L AT T R I B U T I O N E R RO R
These differences among cultures influence us in many ways—including theways we think about other people’s behavior. In particular, people from indi-vidualistic cultures routinely ascribe others’ behavior to dispositions and notto situations—even when there is ample reason to believe that situations areplaying a crucial role (Figure 13.3). Thus North Americans of European her-itage tend to see people on public assistance as lazy (a dispositional attri-bution), for example, rather than struggling in an economy with highunemployment and few entry-level positions (a situational attribu-tion). Likewise, members of these cultures tend to view poor per-formance on a test as a sign of low intelligence (disposition)rather than as a result of an overly difficult exam (situation). Thisbias is so pervasive that it is called the fundamental attributionerror (D. T. Gilbert & Malone, 1995; L. Ross, 1977; Sabini, Siepmann,& Stein, 2001).
To dramatize this error, one early study had American college students partici-pate in a simulated TV quiz show. Students were run in pairs and drew cards to decidewho would be the “quizmaster” and who the “contestant.” The quizmaster had to makeup questions, drawn from any area in which she had some expertise; the contestant hadto try to answer these questions. The game then proceeded, and, inevitably, some of thequizmasters’ questions were extremely difficult (e.g., “What do the initials W. H. standfor in the poet W. H. Auden’s name?”).* A student audience watched and subsequentlyrated how knowledgeable the two participants were.
The situation plainly favored the quizmasters, who could choose any question ortopic they wished. Hence, if a quizmaster had knowledge of just one obscure topic,he could focus all his questions on that topic, without revealing that he had littleknowledge in other domains. The contestants, on the other hand, were at the mercyof whatever questions their quizmaster posed. Any interpretation of the quizmasters’“superiority” should take this obvious situational advantage into account. But the
(A) (B)
13.2 Individualistic and collectivistic cul-tures Members of individualistic cultures (A) tend to view themselves and others asindependent and seek to stand out byachieving personal goals. Members of col-lectivistic cultures (B) tend to view them-selves and others as interdependent andseek to behave in accordance with situa-tional demands and the expectations ofothers.
fundamental attribution error Thetendency to attribute behaviors to aperson’s internal qualities whileunderestimating situational influences.
13.3 Fundamental attribution error
*The answer, by the way, is Wystan Hugh.

510 chapter 13 PSOCIAL PSYCHOLOGYO
observers consistently failed to do this. They knew that the roles in the setting—whowas quizmaster, who was contestant—had been determined by chance, for they hadwitnessed the entire procedure. Even so, they could not help regarding the quizmas-ters as more knowledgeable than the contestants—a tribute to the power of the fun-damental attribution error (L. Ross, Amabile, & Steinmetz, 1977).
The pattern of attributions is quite different, though, in collectivistic cultures. In onestudy, Hindu Indians and European Americans were asked to discuss vignettes aboutother people’s actions. Consistent with other research, the European Americans’comments included twice as many dispositional explanations as situational explana-tions. The Hindu Indians showed the opposite pattern. They gave twice as many situa-tional explanations as dispositional explanations. As an illustration, one of thevignettes used in the study described an accident in which the back wheel of a motor-cycle burst, throwing the passenger off the motorcycle, and the driver had done little tohelp the hurt passenger. Overall, the Americans typically described the driver as “obvi-ously irresponsible” or “in a state of shock,” whereas the Indians typically explainedthat it was the driver’s duty to be at work or that the other person’s injury must not havelooked serious (J. G. Miller, 1984; see also A. P. Fiske et al., 1998; Maass, Karasawa,Politi, & Suga, 2006; P. B. Smith & Bond, 1993).
Person PerceptionWhen we make causal attributions, we go beyond the information available to oursenses in order to make sense of a particular action—why someone smiled, or didwell on a test, or didn’t help more after an accident. The role of social cognition—and our tendency to supplement what we perceive—is just as important when we tryto make sense of another person—that is, whenever we ask ourselves, “What kind ofperson is she?”
I M P L I C I T T H E O R I E S O F P E RSO N A L I T Y
Imagine that a friend says her sister Marie is especially outgoing. Or say that you seeMarie at several parties, and each time she’s the center of attention. In either case, you’relikely to draw some inferences from what you hear about Marie or how you see herbehaving—but in the process, you may lose track of which bits of information are baseddirectly on what you’ve heard or seen and which bits are merely your interpretation.Thus, if you hear that Marie is outgoing, you may also remember (falsely) that yourfriend said she loves crowds, even though that was never mentioned (N. Cantor &Mischel, 1979; Dweck, Chiu, & Hong, 1995).
In this way, social cognition works much like other kinds of cognition. Our knowl-edge of the world is a blend of our own observations and the inferences we have madeusing our schematic knowledge—knowledge about the world in general. In the socialdomain, these schemas are called implicit theories of personality (Bruner & Tagiuri,1954; D. J. Schneider, 1973), and we use them to make inferences about what a personis really like and how she is likely to behave in the future. We all hold these informal the-ories, and they bring together a cluster of beliefs, linking one trait (such asextraversion) to others (such as loving crowds) but also linking these traits to specificbehaviors—so that we have expectations for what sort of husband the extravert will be,what sorts of sports he is likely to enjoy, and more.
These implicit theories are another point on which cultures differ (Church et al.,2006). People in individualistic cultures tend to understand the self as being stable
implicit theories of personalityBeliefs about what kinds of behaviorsare associated with particular traitsand which traits usually go together;used to develop expectations aboutpeople’s behavior.

PSocial CognitionO 511
across time and situations and so are more likely to go beyond the information givenand make global judgments about others’ personalities. People in collectivistic cul-tures, where the self is understood as changing according to relationships and situa-tions, tend to view personality as malleable. They therefore tend to make morecautious and more limited generalizations about other people’s personalities (Hong,Chiu, & Dweck, 1997).
ST E R E OT Y P E S
Implicit theories of personality—like schemas in any other domain—are enormouslyhelpful. Thanks to these schemas, we do not have to scrutinize every aspect of everysituation we encounter, because we can fill in any information we are missing by drawingon our schematic knowledge. Likewise, if our current information about a person is lim-ited (perhaps because we only met her briefly), we can still make reasonable assumptionsabout her based on what we know about people in general. Though these steps make oursocial perception quick and efficient and generally lead us to valid inferences, they do leaveus vulnerable to error, so that our perception (or recollection) of another person some-times ends up more in line with our preconceptions than with the facts. In many cases thisis a small price to pay for the benefits of using schemas, and for that matter, the errors pro-duced are often easily corrected. But schemas can also lead to more serious errors.
The hazard of schematic thinking is particularly clear in the case of social stereo-types, schemas about the characteristics of whole groups that lead us to talk aboutGreeks, Jews, or African Americans (or women, the elderly, or liberals andconservatives) as if we know all of them and they are all the same (Figure 13.4). Thesestereotypes are, on their own, worrisome enough, because they can lead us to makeserious errors of judgment about the different people we meet. Worse, stereotypes canlead to deeper problems, including (at the extreme) wars, genocides, and “ethniccleansings.” These larger calamities, however, are not fueled by stereotypes alone. Theyarise from prejudice, which can be defined as a negative attitude toward another per-son based on his group membership. Prejudice consists of three factors sometimesreferred to as the ABCs of prejudice: an affective (emotional) component, which leadsus to view the other group as “bad”; a behavioral component, which includes our ten-dencies to discriminate against other groups; and a cognitive component (the stereo-type itself). Prejudice can lead to extreme cruelties and injustices, making the study ofintergroup bias in general, and stereotypes and prejudice in particular, a topic of someurgency.
O R I G I N S A N D M E AS U R E M E N T O F ST E R E OT Y P E S
Whether stereotypes are negative or positive, they often have deep historical roots andare transmitted to each new generation both explicitly (“Never trust a . . .”) and implic-itly (via jokes, caricatures, portrayals in movies, and the like). Thus, in Western cul-tures, we hear over and over about athletic blacks, academic Asians, moody women,and lazy Latinos, and, like it or not, these associations eventually sink in and are likelyto affect our behavior—regardless of whether we believe that the association has anyfactual basis.
Other factors also foster the creation and maintenance of stereotypes. Consider, forexample, the fact that most of us have a lot of exposure to people in our own group, andas a result, we have ample opportunity to see that the group is diverse and made up ofunique individuals. We generally have less exposure to other groups, and so, with little
stereotypes Schemas that are oftennegative and are used to categorizecomplex groups of people.
prejudice A negative attitude towardanother person based on that person’sgroup membership.
13.4 Stereotypes Stereotypes areschemas about the characteristics of wholegroups. One example is the stereotypeabout older people, which holds that theycan’t read fine print as easily as youngeradults.

512 chapter 13 PSOCIAL PSYCHOLOGYO
opportunity for learning, we are likely to perceive the group as merely a mass of more orless similar people. This so-called out-group homogeneity effect is reflected in suchstatements as “All Asians are alike” or “All Germans are alike.” The first statement isalmost invariably made by a non-Asian; the second, by a non-German.
Just a few decades ago, many people did not hesitate to make derogatory commentsin public settings about blacks, or women, or Jews. This made studying stereotypesrelatively straightforward, in that researchers could use explicit measures, which involvesome form of self-report, to assess negative stereotypes about groups of individuals.
The times have changed, however, and stereotyping has become much less sociallyacceptable in most quarters of life. As a result, people are now much less likely to endorseexplicitly racist or sexist statements than they were in the recent past. Does this meanstereotypes no longer matter? Unfortunately not. Stereotypes still influence people’sbehavior, but the effects are quite subtle, often happening automatically, outside ourawareness (Bargh, Chen, & Burrows, 1996; but see also Cesario, Plaks, & Higgins, 2006).
To assess these less overt stereotypes, researchers have begun to use implicit measures.For example, some researchers have measured brain responses to stereotype-relevantstimuli (Ito, Willadsen-Jensen, & Correll, 2007) or response times to stereotype-relatedquestions (Fazio, 1995). These implicit measures allow us to detect biases that peoplemight prefer to keep hidden. They also allow us to observe biases that people don’t evenrealize they have—biases that, in fact, conflict with the person’s explicit (conscious)beliefs. Thus, people who explicitly hold egalitarian views may still have assumptionsabout various outgroup members, unconsciously believing, for example, that AfricanAmericans are more likely than whites to be criminals, or that Hispanics are more hot-tempered than non-Hispanics (Blair & Banaji, 1996; Chen & Bargh, 1997; Kawakami,Dion, & Dovidio, 1998; Wittenbrink, Judd, & Park, 1997). In fact, this conflict betweenconscious beliefs and unconscious assumptions and associations seems to occur rela-tively often, thanks to the fact that our implicit and explicit views are shaped by differ-ent influences, and so can sometimes contradict each other (e.g., Nosek, 2007; Rydell,McConnell, Mackie, & Strain, 2006).
Another commonly used means of detecting implicit assumptions and associationsis the Implicit Association Test (IAT; Greenwald et al., 2002; Greenwald, McGhee, &Schwartz, 1998; Grenwald, Nosek, & Banaji, 2003).* In the classic version of the IAT,people are asked to make two types of judgments: whether a face they see on the com-puter screen is that of a black person or a white person, and whether a word they see onthe screen is a “good” word (e.g., love, joy, honest, truth) or a “bad” word (e.g., poison,agony, detest, terrible). This seems simple enough, but the trick here is that the trials withfaces (black or white) are intermixed with the trials with words (good or bad), and par-ticipants must use the same two keys on the computer for both judgments. Thus, in onecondition, participants must use one key to indicate “black” if a black face is shown andthe same key to indicate “good” if a good word is shown; a different key is used for“white” (for face trials) and “bad” (for word trials). In another condition, things arearranged differently: Now participants use one key to indicate “black” and “bad” (forfaces and words, respectively) and the other key to indicate “white” and “good.”
This experiment assesses how easily the participants can manage each of these links.Do they have an easier time putting “white” and “good” together (and so using thesame key to indicate both) than putting “white” and “bad” together? It turns out thatthe first combination is easier for white research participants—and for many AfricanAmerican participants as well (Figure 13.5). This seems to suggest that the participantsarrive at the experiment already primed to associate each race with a certain evaluation
*To try the IAT yourself, see: https://implict.harvard.edu/implicit.
out-group homogeneity effectThe tendency for a member of a group(the in-group) to view members ofanother group (the out-group) as “allalike” or less varied than members ofhis or her own group.

PSocial CognitionO 513
and respond more slowly when the experiment requires them to break that association(see, for example, W. A. Cunningham, Preacher, & Banaji, 2001; Greenwald et al., 2002;Greenwald et al., 1998; B. K. Payne, 2001).
T H E E F F E CTS O F ST E R E OT Y P E S
Whether implicit or explicit, stereotypes have multiple effects. They influence what webelieve about other people and how we act toward them. Perhaps worst of all, stereo-types influence how the targets of our stereotypes act—so that, specifically, thestereotype leads members of the targeted group to behave in a way that confirms thestereotype. In this way, stereotypes create self-fulfilling prophecies.
In a classic demonstration, Rosenthal and Jacobson (1968) told a group of elementary-school teachers that some of their students were “bloomers” and could be expected toshow substantial increases in IQ in the year ahead. Although these “bloomers” were ran-domly chosen, they in fact showed substantial increases in their test scores over the courseof the next year, an effect apparently produced by the teachers’ expectations. Several fac-tors probably contributed to this effect, including the greater warmth and encouragementthe teachers offered, the individualized feedback they provided, and the increased numberof opportunities they gave the children they expected would do well (M. J. Harris &Rosenthal, 1985; for a cautionary note about the reliability of these effects, see Jussim &Harber, 2005; R. Rosenthal, 1991, 2002; H. H. Spitz, 1999).
How does this finding apply to stereotypes? Here, too, it turns out that people are heavily influenced by others’ expectations—even when we are consideringexpectations for a group, rather than expectations for an individual. As we saw in Chapter11, this influence is plainly visible in the way that stereotype threat influences performanceon tests designed to measure intellectual ability. In one study, for example, experimentersgave intelligence tests to African American students. Before taking the test, half of thestudents were led to think briefly about their race; the other half were not. The resultshowed—remarkably—that the students who thought about their race did less well on
Black primeWhite prime
13.5 SCIENTIFIC METHOD: Do people have implicit associations related to specific races?
Method
1. On each trial, non-black participants were briefly shown a picture of one oftwo kinds of faces (white or black) followed by a picture of one of two kinds ofobjects (tools or weapons).
Results
Participants identified guns quickly after seeinga black face, and they identified tools fasterafter seeing a white face.
2. Participants were instructed to ignore the face stimuli and to press one buttonif the stimulus was a weapon, and a different button if the stimulus was a tool.
Trial 1 Trial 2 Trial 3
CONCLUSION: Non-black participants have different implicit associations with blacks than with whites.
SOURCE STUDY: Payne, 2001
Ave
rage
resp
onse
tim
e (m
s)
400
425
450
475
Gun Tool
self-fulfilling prophecies Beliefsabout how a person will behave thatactually make the expected behaviormore likely.

514 chapter 13 PSOCIAL PSYCHOLOGYO
the test (Steele, 1998). In other studies, women have been given math tests, and justbefore the test, half have been led to think briefly about their gender. This reminder leadsthe women to do more poorly on the test (Shih, Pittinsky, & Ambady, 1999).
What’s going on in these studies? These reminders about group membership leadthe test takers to think about the stereotypes for their group—that African Americansare unintelligent, or that women can’t do math—and this makes the test takers anx-ious. They know that others expect them to do poorly, and they know that if they do notperform well, they will just confirm the stereotype. These fears distract the test takers,consume cognitive resources, and undermine their performance—so that the stereo-type ends up confirming itself (Johns, Inzlicht, & Schmader, 2008). In addition, thetest takers may fear that the stereotype is to some extent correct, and this fear may leadthe test takers to lower their expectations and not try as hard. This, too, would under-mine performance, which in turn would confirm the ugly stereotype.
AttitudesAs we have now seen, our relations with the people who surround us depend to a largeextent on our beliefs. These beliefs include our assumptions about how others’ behaviorshould be interpreted, and our beliefs about how the various attributes in someone’spersonality fit together, and also our beliefs about Jews, or African Americans, or theIrish. Moreover, these beliefs are not just “cold” cognitions—dispassionate assertions
about the world. Instead, they are often “hot,” in the sense that theyhave motivational components and can trigger (and be triggered by)various emotions. Psychologists refer to these beliefs as attitudes.
People have attitudes about topics as diverse as the death penalty,abortion, bilingual education, the importance of environmental pro-tection, and need for civility in everyday social interaction (Eagly &Chaiken, 1993). The belief that defines each attitude is almostinevitably associated with emotional feelings and a predisposition toact in accordance with the belief and feelings. Thus, people who dif-fer in their attitudes on abortion are certain to have different beliefsabout the moral status of this procedure, but also will have differentfeelings about the family planning clinic they pass every day, and dif-ferent levels of commitment to showing up at a rally protesting theirstate’s abortion laws (Figure 13.6).
AT T I T U D E FO R M AT I O N
How do attitudes arise? Some of our attitudes are based on our consideration of thefacts. We carefully weigh the pros and cons of an argument and make up our mindsabout whether we should endorse the argument’s conclusion or not. In many othercases, however, the sources of our attitudes are not quite so rational.
Sometimes we acquire our attitudes through one of the forms of learning we consid-ered in Chapter 7. In some cases, the learning is akin to classical conditioning. For exam-ple, we might repeatedly see a brand of cigarettes paired with an appealing person or acool cartoon character and wind up associating the two, leaving us with a positive atti-tude toward that brand of cigarettes (Figure 13.7; Cacioppo, Marshall-Goodell,Tassinary, & Petty, 1992). In other cases, attitudes can be formed via a process akin tooperant conditioning, when, for example, parents reward behavior they would like toencourage, such as hard work at school and good table manners. The end result of this
13.6 Attitudes Attitudes are beliefs thatare often highly emotionally charged.
attitude A fairly stable evaluation ofsomething as good or bad that makesa person think, feel, or behave posi-tively or negatively about some per-son, group, or social issue.
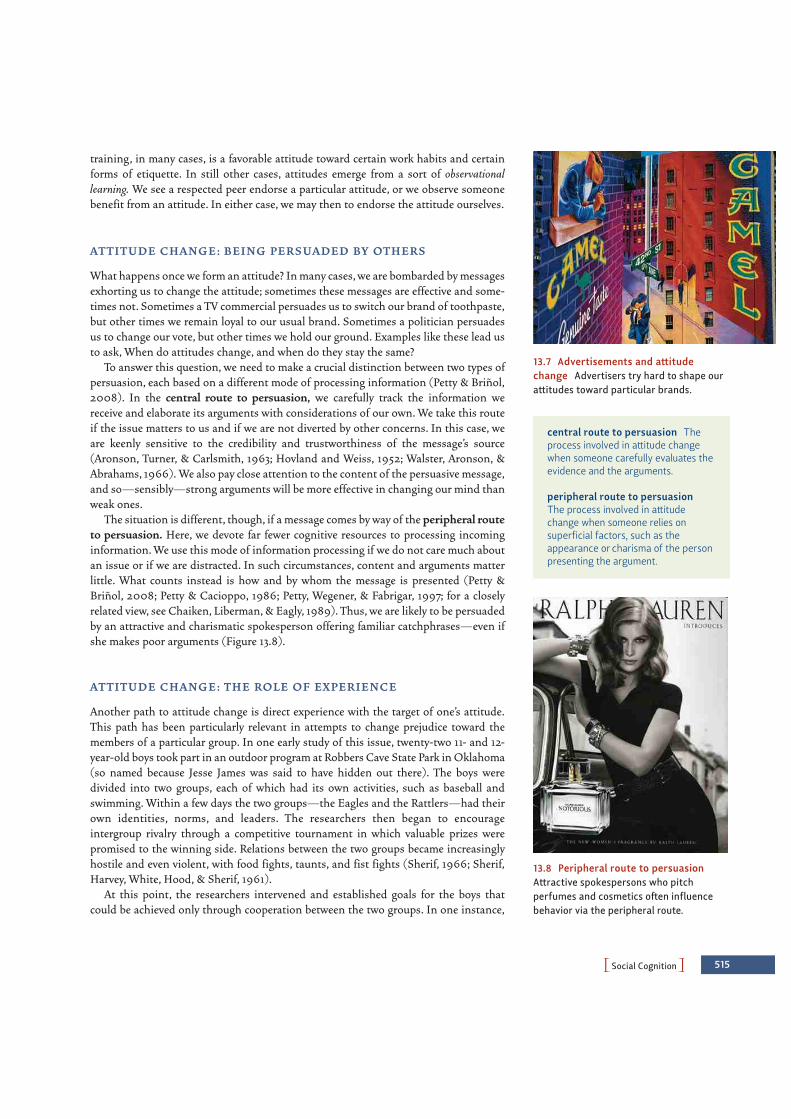
PSocial CognitionO 515
training, in many cases, is a favorable attitude toward certain work habits and certainforms of etiquette. In still other cases, attitudes emerge from a sort of observationallearning. We see a respected peer endorse a particular attitude, or we observe someonebenefit from an attitude. In either case, we may then to endorse the attitude ourselves.
AT T I T U D E C H A N G E : B E I N G P E RS UA D E D BY OT H E RS
What happens once we form an attitude? In many cases, we are bombarded by messagesexhorting us to change the attitude; sometimes these messages are effective and some-times not. Sometimes a TV commercial persuades us to switch our brand of toothpaste,but other times we remain loyal to our usual brand. Sometimes a politician persuadesus to change our vote, but other times we hold our ground. Examples like these lead usto ask, When do attitudes change, and when do they stay the same?
To answer this question, we need to make a crucial distinction between two types ofpersuasion, each based on a different mode of processing information (Petty & Briñol,2008). In the central route to persuasion, we carefully track the information wereceive and elaborate its arguments with considerations of our own. We take this routeif the issue matters to us and if we are not diverted by other concerns. In this case, weare keenly sensitive to the credibility and trustworthiness of the message’s source(Aronson, Turner, & Carlsmith, 1963; Hovland and Weiss, 1952; Walster, Aronson, &Abrahams, 1966). We also pay close attention to the content of the persuasive message,and so—sensibly—strong arguments will be more effective in changing our mind thanweak ones.
The situation is different, though, if a message comes by way of the peripheral routeto persuasion. Here, we devote far fewer cognitive resources to processing incominginformation. We use this mode of information processing if we do not care much aboutan issue or if we are distracted. In such circumstances, content and arguments matterlittle. What counts instead is how and by whom the message is presented (Petty &Briñol, 2008; Petty & Cacioppo, 1986; Petty, Wegener, & Fabrigar, 1997; for a closelyrelated view, see Chaiken, Liberman, & Eagly, 1989). Thus, we are likely to be persuadedby an attractive and charismatic spokesperson offering familiar catchphrases—even ifshe makes poor arguments (Figure 13.8).
AT T I T U D E C H A N G E : T H E RO L E O F EX P E R I E N C E
Another path to attitude change is direct experience with the target of one’s attitude.This path has been particularly relevant in attempts to change prejudice toward themembers of a particular group. In one early study of this issue, twenty-two 11- and 12-year-old boys took part in an outdoor program at Robbers Cave State Park in Oklahoma(so named because Jesse James was said to have hidden out there). The boys weredivided into two groups, each of which had its own activities, such as baseball andswimming. Within a few days the two groups—the Eagles and the Rattlers—had theirown identities, norms, and leaders. The researchers then began to encourageintergroup rivalry through a competitive tournament in which valuable prizes werepromised to the winning side. Relations between the two groups became increasinglyhostile and even violent, with food fights, taunts, and fist fights (Sherif, 1966; Sherif,Harvey, White, Hood, & Sherif, 1961).
At this point, the researchers intervened and established goals for the boys thatcould be achieved only through cooperation between the two groups. In one instance,
13.7 Advertisements and attitudechange Advertisers try hard to shape ourattitudes toward particular brands.
central route to persuasion Theprocess involved in attitude changewhen someone carefully evaluates theevidence and the arguments.
peripheral route to persuasionThe process involved in attitudechange when someone relies onsuperficial factors, such as theappearance or charisma of the personpresenting the argument.
13.8 Peripheral route to persuasionAttractive spokespersons who pitchperfumes and cosmetics often influencebehavior via the peripheral route.
516 chapter 13 PSOCIAL PSYCHOLOGYO
the researchers disrupted the camp’s water supply, and the boys had to pool theirresources in order to fix it. In another instance, the camp truck stalled, and the boys hadto team up to get it moving. By working together on goals they all cared about—butcould achieve only through collective effort—the boys broke down the divisions thathad previously dominated camp life and ended their stay on good terms.
More recent studies have confirmed the implication of this study—namely, thatintergroup contact can have a powerful effect on attitudes about the other group, espe-cially if the contact is sustained over a period of time, involves active cooperation inpursuit of a shared goal, and provides equal status for all participants (see, for example,Aronson & Patnoe, 1997; Henry & Hardin, 2006; Pettigrew, 1998; Pettigrew & Tropp,2006; Tropp & Pettigrew, 2005). We can also take steps to increase outgroup empathy(T. A. Cohen & Insko, 2008) and to encourage the prejudiced person to develop anindividualized perception of the other group and so lose the “they’re all alike” attitude(Dovidio & Gaertner, 1999).
AT T I T U D E C H A N G E : P E RS UA D I N G O U RS E LV E S
Yet another route to attitude change is through our own behavior. At first, this mayseem odd, because common sense argues that attitudes cause behavior, and not theother way around. But sometimes our own behaviors can cause us to change our viewsof the world.
In his classic work on this problem, Leon Festinger argued that people put a highvalue on being consistent, so that any perceived inconsistency among their beliefs,feelings, and behavior creates a very uncomfortable state of cognitive dissonance(Figure 13.9; J. Cooper, 2007; Festinger, 1957, 1962; Harmon-Jones & Mills, 1999). Howdo people escape this aversive state? In one study, Festinger and Carlsmith (1959)asked participants to perform several extremely boring tasks, such as packing spoolsinto a tray and then unpacking them, or turning one knob after another for a quarterturn. When they were finished, the participants were induced to tell the next partici-pant that the tasks were very interesting. Half the participants were paid reasonablywell for this lie (they were given $20); the others were given just $1. Later, when asked
cognitive dissonance An uncom-fortable inconsistency among one’sactions, beliefs, attitudes, or feelings.People attempt to reduce it by makingtheir actions, beliefs, attitudes or feel-ings more consistent with one another.
13.9 Cognitive dissonance

PSocial CognitionO 517
how much they enjoyed the tasks, the well-paid participants said that the tasks wereboring and that they understood that they had lied to the other participants. In con-trast, the poorly paid participants claimed that the monotonous tasks were fairly inter-esting, and that what they told the other participants was the truth.
What produces this odd pattern? According to Festinger, the well-paid liars knewwhy they had mouthed sentiments they did not endorse: $20 was reason enough. Thepoorly paid liars, however, had experienced cognitive dissonance, thanks to the fact thatthey had misled other people without good reason for doing so. They had, in otherwords, received insufficient justification for their action. Taken at face value, this madethem look like casual and unprincipled liars, a view that conflicted with how theywanted to see themselves. How could they reconcile their behavior with their self-concept? One solution was to reevaluate the boring tasks. If they could change theirmind about the tasks and decide they were not so awful, then there was no lie and henceno dissonance. Judging from the data, this is apparently the solution that the partici-pants selected—bringing their attitudes into line with their behavior.
These findings help make sense of why many organizations have difficult or aversiveentrance requirements (Figure 13.10). For example, many American college fraternitieshave hazing rituals that are unpleasant and in some cases humiliating or worse.Although these rituals may be objectionable, they do serve a function. They lead newfraternity members to place a higher value on their membership than they otherwisewould. They know what they have suffered to achieve membership, and it would createdissonance for them to believe that they have suffered for no purpose. They can avoidthis dissonance though, if they are convinced that their membership is really valuable.In that case, their suffering was “worth it.”
There is no question about the data patterns associated with cognitive dissonance, butmany researchers have disagreed with Festinger over why the pattern emerges. The mostimportant challenge to Festinger’s account is Daryl Bem’s self-perception theory (1967,1972). According to this conception, there is no need to postulate the emotional distressthat allegedly accompanies cognitive dissonance and, according to Festinger, propels atti-tude change. Instead, we can understand the data in terms of the information available tothe participants in these experiments. Specifically, the research participants are simply try-ing to make sense of their own behavior in much the same way that an outside observermight. Thus, in the knob-turning study, self-perception theory would hold that a partici-pant in the $1 condition would have known that $1 was insufficient justification for lyingand so would have concluded that he did not lie. On this basis, if he said the task was funand if he was not lying, then the task apparently was fun.
This line of interpretation makes sense of many other results as well. Consider stud-ies of the so-called foot-in-the-door technique originally devised by door-to-doorsalesmen. In one study, an experimenter asked suburban homeowners to comply withan innocuous request, to put a 3-inch-square sign advocating auto safety in a windowof their home. Two weeks later, a different experimenter came to visit the same home-owners and asked them to grant a much bigger request, to place on their front lawn anenormous billboard that proclaimed “Drive Carefully” in huge letters. The resultsshowed that whether people granted the larger request was heavily influenced bywhether they had earlier agreed to the smaller request. The homeowners who had com-plied with the small request were much more likely to give in to the greater one(Freedman & Fraser, 1966; although, for limits on this technique, see Burger &Guadagno, 2003; Chartrand, Pinckert, & Burger, 1999).
According to self-perception theory, the homeowners, having agreed to put up thesmall sign, now thought of themselves as active citizens involved in a public issue.“Why did I put up the sign? No one forced me to do it. I guess, therefore, that this is
13.10 Justification of effort Newlyaccepted members of a group tend to valuetheir group membership even more if theirinitiation was especially harsh, as in thecase of soldiers who have gone throughboot camp.
self-perception theory The theorythat we know our own attitudes andfeelings only by observing our ownbehaviors and deciding what probablycaused them, just as we do when try-ing to understand others.

518 chapter 13 PSOCIAL PSYCHOLOGYO
an issue that I care about.” Thus, they interpreted their actions as revealing a convic-tion that previously they did not know they had, and given that they now thought ofthemselves as active, convinced, and involved, they were ready to play the part on alarger scale. Fortunately for the neighbors, the billboards were never installed—afterall, this was an experiment. But in real life we may not be so easily let off the hook,and the foot-in-the-door approach is a common device for persuading the initiallyuncommitted.
AT T I T U D E STA B I L I T Y
We’ve now seen that attitudes can be changed in many ways—by certain forms ofpersuasion (if the source is credible and trustworthy and if the message is appropri-ate), by intergroup contact (in the case of prejudice), and by tendencies toward cog-nitive consistency (especially with regard to acts we have already performed). Giventhese points, and given all the many powerful forces aimed at changing our attitudes,it might seem that our attitudes would be in continual flux, changing from momentto moment and day to day. But on balance, the overall picture is one of attitude sta-bility rather than attitude change. Attitudes can be altered, but it takes some doing.By and large, we seem to have a tendency to hold on to the attitudes we already have(Figure 13.11).
Why should this be so? One reason for attitude stability is that people rarely makechanges in their social or economic environments. Their families, their friends and fellowworkers, their social and economic situations—all tend to remain much the same over theyears. All of this means that people will be exposed to many of the same influences year inand year out, and this sameness will obviously promote stability—in people’s beliefs,values, and inclinations. Moreover, most of us tend to be surrounded by people with atti-tudes not so different from our own. After all, top-level executives know other top execu-tives, college students know other college students, and trade union members know otherunion members. As a result, we are likely, day by day, to encounter few challenges to ourattitudes, few contrary opinions, and this, too, promotes stability.
Of course, some events may transform attitudes completely—not just our own, butthose of everyone around us. One example is the sneak attack on Pearl Harbor onDecember 7, 1941. Without a doubt, this led to an instant and radical change in Americans’attitudes toward Japan. A more recent example is the terrorist attacks of September 11,
13.11 Attitude stability One reason for attitude stability is that people often seek outothers who have similar backgrounds and interests.
PSocial InfluenceO 519
2001. These attacks dramatically increased Americans’ fear of terrorism and raised publicsupport for a number of actions (including two wars that would never have unfolded ifAmericans had been less concerned about the country’s security). But by their very nature,such events—and the extreme changes in attitudes they produce—are rare.
SO CIAL INFLUENCE
So far in this chapter, we have emphasized the perceptions and beliefs of the socialactor—how she interprets others’ behaviors; what she infers about people, in light oftheir behaviors; how she forms (and perhaps changes) her attitudes. These points arecrucial if we are going to understand how people act in groups, because—as we notedearly on—our actions in a social setting depend on how we understand what is goingon around us.
Let’s note, though, that all of this makes it sound like our behavior in social settingsis driven entirely “from within”—that is, shaped solely by our beliefs and perceptions.But, of course, our behavior is also powerfully shaped “from without”—that is, by var-ious influences from our social world. How do those influences guide us? In pursuingthis broad question, we need to distinguish three types of influence.
ConformityPeople often do what they see others do. Sometimes this is a good thing, such as whenpeople cross at the crosswalk, throw their trash in garbage cans, or drive on the side ofthe road they are supposed to. However, people’s propensity to do as others do can alsobe a bad thing, as when people litter or even steal when they see that others are failingto behave appropriately (Keizer, Lindenberg, & Steg, 2008). Confirmity occurs when-ever people change their behavior because of social pressure (either explicit or implicit).
One early demonstration of conformity comes from a classic study by Sherif (1937).In this study, participants seated in a dark room saw a point of light appear, move, andthen disappear. This happened a number of times, and the participants’ task was sim-ply to judge how far the light had moved on each trial. In reality, however, the lightnever moved, and the appearance of movement was the result of a perceptual illusionknown as the autokinetic effect.
When participants made their judgments alone, their responses differed substan-tially from one person to the next, ranging from an inch to more than a foot.Participants’ responses also varied considerably from trial to trial. When participantsviewed the light with one or two other people, however, their responses quickly beganto converge with those of the other members of their group. Different groups convergedupon different answers, but in each case the participants rarely strayed from the normthat had developed in their particular group.
Most telling, perhaps, was what Sherif found when he placed a confederate into thesituation, someone who appeared to be a participant, but who in reality was an accom-plice of the experimenters. When the confederate made responses that were much lowerthan those typically made by solitary participants, the other (real) participants quicklyfollowed suit, and a group norm emerged that was much lower than normal. Similarly,when the confederate made responses that were much higher than typical, the othersagain followed this lead, and the resulting group norm was much higher than usual.
Sherif’s findings are provocative because they suggest that others can influence evenour basic perceptions of the world. Note, though, that Sherif had concocted a highly
conformity A change in behaviordue to explicit or implicit socialpressure.

520 chapter 13 PSOCIAL PSYCHOLOGYO
ambiguous situation in which participants were literally groping in the dark for ananswer. Do people conform even when the correct answer is obvious?
Solomon Asch developed a procedure in which there could be no doubt as to the cor-rect response (Asch, 1951, 1952, 1955, 1956). In his experiments, Asch brought groupsof people into the laboratory and showed them pairs of cards, placed a few feet away(Figure 13.12). On one card was a black line, say, 8 inches long. On the other card werethree lines of varying lengths, say, 6, 8, and 7 inches. The participants were asked sim-ply to pick which of the three lines on the one card was equal in length to the single lineon the other card.
The three lines were clearly different, and one of them exactly matched the origi-nal line, so the task was absurdly simple. But there was a catch. There was actuallyonly one real participant. All of the others were confederates, with their seatsarranged so that most of them would call out their judgments before the real partici-pant had his turn.
In the first few trials, the confederates each called out the correct response and thereal participant did the same. After the initial trials, however, the confederates began tounanimously render false judgments on most of the trials—declaring, for example, thata 6-inch line equaled an 8-inch line, and so on (Figure 13.13). In this situation, the clearevidence of the participant’s senses was contradicted by everyone around him, so whatshould he do? Asch found that most participants wavered—sometimes offering thecorrect response but on many other trials yielding to the obviously mistaken suggestionoffered by the group. Indeed, the chances were less than one in four that the participantwould be fully independent and would stick to his guns on all trials on which the groupdisagreed with him (for an analysis that highlights the striking independence of someparticipants, see Friend, Rafferty, & Bramel, 1990).
T H E CAU S E S O F CO N FO R M I T Y
Why do people conform—in Asch’s studies, and in many other settings (Figure 13.14)?Two influences appear to be crucial (M. Deutsch & Gerard, 1955).
The first—known as informational influence—involves people’s desire to be right(Cialdini & Goldstein, 2004). Researchers have demonstrated the role of this sort ofinfluence by altering the Asch-type experiment to make discriminating among the linesegments very difficult. In this setting, we might expect people to be confused about thecorrect answer, and therefore more likely to seek out other cues for how they shouldrespond. Plausibly, they might listen more to what others say—leading to the predic-tion that with more difficult discriminations, more social conformity will occur. Thisprediction is correct (Crutchfield, 1955). Conversely, we can alter the situation so thatparticipants have less reason to listen to others (e.g., by convincing participants they aremore competent or knowledgeable than others in some domain). In this case, we wouldexpect the participants to rely less on the others’ views, and so we would predict lessconformity. This prediction also is correct (Campbell, Tesser, & Fairey, 1986;Wiesenthal, Endler, Coward, & Edwards, 1976).
This line of reasoning helps to explain why, in general, people seek the opinion ofothers when they encounter a situation that they do not fully understand. To evaluatethe situation, they need more information. If they cannot get it firsthand, they will askothers, and if that is not an option, then they can try to gain information by comparingtheir own reactions to those of others (Festinger, 1954; Suls & Miller, 1977). This pat-tern of relying on others in the face of uncertainty can also be observed in young chil-
1 2 3
13.12 The stimulus cards in Asch’s socialpressure experiment The cards aredrawn to scale.
13.13 The participant in a social pressureexperiment On hearing the unanimousverdict of the others, the true participantleans forward to look at the cards morecarefully.
informational influence A reasonfor conformity based on people’sdesire to be correct.

PSocial InfluenceO 521
dren, and even in infants. Infants who confront a scary situation and do not knowwhether to advance or retreat will glance toward their caretaker’s face. If she smiles, theinfant will tend to advance; if she frowns, he will tend to withdraw and return to her(we will come back to this point in Chapter 14). This early phenomenon of socialreferencing may be the prototype for what happens all our lives, a general process ofvalidating our reactions by checking on how others are behaving.
Another aspect of informational influence is that the decisions of other people canshape the information we receive, and this, too, can lead to conformity. Suppose you’retrying to decide what type of car to buy. If two of your neighbors have purchasedToyotas, you’ll have a chance to observe these cars closely and learn about their attrib-utes. In this way, your neighbors’ selection will bias the information available and maylead you to follow their lead when you choose your own car (Denrell, 2008).
A second reason for going along with the crowd—known as normative influence—revolves around people’s desire to be liked, or at least not to appear foolish (B. Hodges& Geyer, 2006). Consider the original Asch study in which a unanimous majority madean obviously incorrect judgment. In this context, the participant likely saw the worldmuch as it is, but he had every reason to believe that the others saw it differently. If henow said what he believed, he could not help but be embarrassed; the others wouldprobably think that he was a fool and might laugh at him. Under the circumstances, theparticipant would prefer to disguise what he really believed and go along, preferring tobe “normal” rather than correct.
Direct evidence for the role of embarrassment as a normative influence comes froma variant of the Asch experiment in which the participant entered the room while theexperiment was already in progress. The experimenter told her that since she arrivedlate, it would be simpler for her to write down her answers rather than to announcethem out loud. Under these circumstances, there was little conformity. The lines beingjudged were of the original unambiguous sort (e.g., 8 inches vs. 6 inches in height), sothat there was no informational pressure toward conformity. Since the judgments weremade in private (no one else knew what she had written down), there was no (or little)motivational pressure either. As a result, participants showed a great deal of independ-ence (Asch, 1952).
13.14 Conformity Within-group conform-ity is evident across generations in clothingstyles.
normative influence A reason forconformity based on people’s desire tobe liked (or not appear foolish).

522 chapter 13 PSOCIAL PSYCHOLOGYO
M I N O R I T Y I N F LU E N C E
Asch’s studies tell us that a unanimous majority exerts a powerful effect that makesit difficult for any individual to stray from the majority’s position. What happens,though, when the individual is no longer alone? In one variation of his experiment,Asch had one of the confederates act as the participant’s ally; all of the other con-federates gave wrong answers, while the ally’s judgments were correct. Under theseconditions, the pressure to conform largely evaporated, and the participant yieldedrarely and was not particularly upset by the odd judgment offered by (the majorityof ) the confederates.
Was the pressure to conform reduced because the ally shared the participant’s views?Or was it merely because the consensus was broken, so that the participant was nolonger alone in questioning the majority view? To find out, Asch conducted a variationof the study in which a confederate again deviated from the other confederates, but didnot do so by giving the correct answer. On the contrary, she gave an answer even farther
from the truth than the group’s. Thus, on a trial in which the correctanswer was 6 1/4 inches and the majority answer was 6 3/4 inches, theconfederate’s answer might be 8 inches. This response did not sup-port the participant’s perception (or reflect the truth!), but it helpedto liberate him even so. The participant now yielded much less thanwhen he was confronted by a unanimous majority. What evidentlymattered was the group’s unanimity; once this was broken, the par-ticipant felt that he could speak up without fear of embarrassment(Asch, 1952). Similar studies have been performed in other laborato-ries with similar results (V. L. Allen, 1975; V. L. Allen & Levine, 1971;Nemeth & Chiles, 1988). The power of even a lone dissident sug-gests that totalitarian systems have good reason to stifle dissent ofany kind. The moment one dissident voice is raised, unanimity isbroken, and then others may (and often do) find the courage toexpress their own dissent (Figure 13.15).
CU LT U R E A N D CO N FO R M I T Y
Asch’s studies of conformity and most others like it were conducted on participantsfrom an individualistic society, the United States. Many of these participants didconform but experienced enormous discomfort as a result, plainly suffering from thecontrast between their own perceptions and the perceptions of others. The pattern isdifferent in collectivistic cultures. Here individuals are less distressed about conform-ing even when it means being wrong. Over two dozen Asch-type conformity studieshave now been conducted in collectivistic cultures, and they support such a conclusion(Bond & Smith, 1996).
Members of collectivistic and individualistic societies tend to differ in other waystoo. Consider the group pressure that presumably led to conformity in Asch’s experi-ments. On the face of it, one might expect collectivists to be more sensitive to this pres-sure, and so to endorse the group’s judgments more often than do individualists. But itturns out that for collectivists, the likelihood of conformity depends on the nature ofthe group. Collectivists are more likely to conform with members of a group to whichthey are tied by traditional bonds—their family (including extended family), class-mates, close friends, and fellow workers. In contrast, they are less affected than are indi-vidualists by people with whom they do not share close interpersonal bonds(Moghaddam, 1998).
13.15 The effect of a consistent minorityA steadfast minority can gradually creategenuine changes in what people think andfeel, as in the case of the American civilrights movement. Martin Luther King Jr.and Coretta Scott King lead the 1965 marchfrom Selma to Montgomery.

PSocial InfluenceO 523
ObedienceConformity is one way that other people influence us. Another way is obedience, whenpeople change their behavior because someone tells them to. A certain degree of obedi-ence is a necessary ingredient of social life. After all, in any society some individualsneed to have authority over others, at least within a limited sphere. Someone needs todirect traffic; someone needs to tell people when they should put their garbage out atthe curb for collection; someone needs to instruct children and get them to do theirhomework (Figure 13.16). But obedience can also lead people to violate their own prin-ciples and do things they previously felt they should not do. The atrocities of the last100 years—the Nazi death camps, the Soviet “purges,” the Cambodian massacres, theRwandan and Sudanese genocides—give terrible proof that the disposition to obedi-ence can become a corrosive poison.
Why were people so obedient in these situations? Psychologists trying to answer thisquestion have adopted two different approaches. One is based on the intuitivelyappealing notion that some individuals who are more obedient than others are the pri-mary culprits. The other emphasizes the social situation in which the obedient personfinds herself.
P E RSO N A L I T Y A N D OB E D I E N C E
A half century ago, investigators proposed that it was people with authoritarian person-alities who were most likely to be highly obedient and to show a cluster of traits relatedto their obedience. They are prejudiced against various minority groups and hold cer-tain sentiments about authority, including a general belief that the world is best gov-erned by a system of power and dominance in which each of us must submit to thoseabove us and show harshness to those below. These authoritarian attitudes can berevealed (and measured) by a test in which people express how much they agree withstatements such as “Obedience and respect for authority are the most important virtueschildren should learn” and “People can be divided into two distinct classes: the weakand the strong” (Adorno et al., 1950).
Contemporary researchers have broadened the conception of the authoritarianpersonality by analyzing the motivational basis for conservative ideology (Jost,Nosek, & Gosling, 2008), building on the supposition that this ideology—like anybelief system—serves the psychological needs of the people who hold these beliefs.In particular, the motivated social cognition perspective maintains that peoplerespond to threat and uncertainty by expressing beliefs that help them to managetheir concerns. Evidence supporting this perspective has come from studies showingthat political conservatism is positively related to a concern with societal instabilityand death, a need for order and structure, and an intolerance of ambiguity (e.g., Jostet al., 2003).
S I T UAT I O N S A N D OB E D I E N C E
A very different approach to obedience is suggested by an often-quoted account of thetrial of Adolf Eichmann, the man who oversaw the execution of 6 million Jews andother minorities in the Nazi gas chambers. In describing Eichmann, historianHannah Arendt noted a certain “banality of evil”: “The trouble with Eichmann wasprecisely that so many were like him, and that the many were neither perverted norsadistic, that they were, and still are, terribly and terrifyingly normal” (Arendt, 1965,p. 276; Figure 13.17).
13.16 Obedience A certain degree of obe-dience is necessary for society to functionsmoothly. Think of the chaos that wouldensue if no one obeyed police officersdirecting traffic.
obedience A change in behavior inresponse to an instruction or com-mand from another person.
motivated social cognitionThinking about the social world inways that serve an emotional need,such as when people hold beliefs thathelp them feel less anxious.

524 chapter 13 PSOCIAL PSYCHOLOGYO
What could have led a “normal” man like Eichmann to commit such atrocities? Theanswer probably lies in the situation in which Eichmann found himself, one thatencouraged horrible deeds and powerfully discouraged more humane courses of action.But this simply demands a set of new questions: What makes a situation influential? Andhow coercive does a situation have to be in order to elicit monstrous acts? StanleyMilgram explored these questions in a series of experiments that are perhaps the best-known studies in all of social psychology (Milgram, 1963). In these studies, Milgramrecruited his participants from the local population surrounding Yale University inConnecticut via a newspaper advertisement offering $4.50 per hour to people willing toparticipate in a study of how punishment affected human learning.
Participants in this experiment were asked to serve as “teachers,” and their job was toread out the cue word for each trial, to record the “learner’s” spoken answer, and—mostimportant—to administer punishment—in the form of an electric shock—whenever alearner answered incorrectly (Figure 13.18). The first shock was slight. Each time thelearner made a mistake, though, the teacher was required to increase the voltage by onestep—proceeding through a series of switches on a “shock generator” with labels rang-ing from “Slight Shock” through “Danger: Severe Shock” to a final, undefined “XXX.”
In truth, there was no “learner.” Instead, a middle-aged actor who was a confederateof the experimenter pretended, at the experiment’s start, to be the learner and thenretreated into a separate room, with all subsequent communication between teacherand learner conducted over an intercom. And, in fact, the “shock generator” didn’tdeliver punishment. The point of the experiment was not to study punishment andlearning at all; that was just a cover story. It was actually to determine how far the par-ticipants would go in obeying the experimenter’s instructions.
13.17 The banality of evil Hannah Arendtfound Nazi war criminal Adolf Eichmann“terrifyingly normal.”
13.18 SCIENTIFIC METHOD: To what extent will people obey harmful instructions?
Method
1. The participant’s job was to be a “teacher” and administer shocks when the “learner”(a confederate) made mistakes on a purported memory test.
ResultsAbout 65% of Milgram’s subjects obeyed the experimenter in administering the highest level of voltage.
2. When the learner made a mistake, the experimenter (also a confederate) told theparticipant to increase the shock level by 15 volts, up to a maximum of 450 volts. (Thelearner was not actually shocked.)
3. As the voltage increased, so did the learner’s distress. At 150 volts, he demandedthat the experiment end; at 300 volts, he refused to answer more questions.
4. If the participant expressed reservations, the experimenter responded“The experiment requires that you continue,” “It is absolutely essential thatyou continue,” “You have no other choice, you must go on.”
CONCLUSION: In certain situations, most people will obey harmful instructions, despite their misgivings.
SOURCE STUDY: Milgram, 1963
The learner, strapped into his chair.
Milgram’s “shock box.”
PSocial InfluenceO 525
Within the procedure, the learner made a fair number of (scripted) errors, and so theshocks that the participant delivered kept getting stronger and stronger. By the time120 volts was reached, the learner shouted that the shocks were becoming too painful.At 150 volts, he demanded that he be let out of the experiment. At 180 volts, he criedout that he could no longer stand the pain, sometimes yelling, “My heart, my heart!” At300 volts, he screamed, “Get me out of here!” and said he would not answer anymore.At the next few shocks, there were agonized screams. After 330 volts, there was silence.
The learner’s responses were all predetermined, but the participants—theteachers—did not know that, so they had to decide what to do. When the learner criedout in pain or refused to go on, the participants usually turned to the experimenter forinstructions, a form of social referencing. In response, the experimenter told the partic-ipants that the experiment had to go on, indicated that he took full responsibility, andpointed out that “the shocks may be painful but there is no permanent tissue damage.”
How far did subjects go in obeying the experimenter? The results were astounding:About 65% of Milgram’s subjects—both males and females—obeyed the experimenterto the bitter end. Of course, many of the participants showed signs of being enormouslyupset by the procedure—they bit their lips, twisted their hands, sweated profusely, andin some cases, laughed nervously. Nonetheless, they did obey—and, in the process,apparently delivered lethal shocks to another human being. (See Burger, 2009, for acontemporary replication that showed obedience rates comparable to those in the initialMilgram reports. For similar data when the study was repeated in countries such asAustralia, Germany, and Jordan, see Kilham & Mann, 1974; Mantell & Panzarella, 1976;Shanab & Yahya, 1977.)
These are striking data—suggesting that it takes remarkably little within a situationto produce truly monstrous acts. But we should also note the profound ethical ques-tions raised by this study. Milgram’s participants were of course fully debriefed at thestudy’s end, and so they knew they had done no damage to the “learner” and hadinflicted no pain. But the participants also knew that they had obeyed the researcherand had (apparently) been willing to hurt someone—perhaps quite seriously. We there-fore need to ask whether the scientific gain from this study is worth the cost—includ-ing the horrible self-knowledge the study brought to the participants, or the stress theyexperienced. This question has been hotly debated, but this doesn’t take away from themain message of the data—namely, it takes very little to get people to obey extreme andinhuman commands.
Why were Milgram’s participants so obedient? Part of the answer may lie in how eachof us thinks about commands and authority. In essence, when we are following otherpeople’s orders, we feel that it is they, and not we, who are in control; they, and not we,who are responsible. The soldier following a general’s order and the employee followingthe boss’s command may see themselves merely as the agents who execute another’swill: the hammer that strikes the nail, not the carpenter who wields it. As such, they feelabsolved of responsibility—and, if the consequences are bad, absolved of guilt.
This feeling of being another person’s instrument, with little or no sense of personalresponsibility, can be promoted in various ways. One way is by increasing thepsychological distance between a person’s actions and their end result. To explore thispossibility, Milgram ran a variation of his procedure in which two “teachers” wereinvolved: one a confederate who administered the shocks, and the other—actually, thereal participant—who had to perform subsidiary tasks such as reading the words overa microphone and recording the learner’s responses. In this new role, the participantwas still an essential part of the experiment, because if he stopped, the learner wouldreceive no further shocks. In this variation, though, the participant was more removedfrom the impact of his actions, like a minor cog in a bureaucratic machine. After all, he

526 chapter 13 PSOCIAL PSYCHOLOGYO
did not do the actual shocking! Under these conditions, over 90% of the participantswent to the limit, continuing with the procedure even at the highest level of shock(Milgram, 1963, 1965; see also Kilham & Mann, 1974).
The obedient person also may reinterpret the situation to diminish any sense ofculpability. One common approach is to try to ignore the fact that the recipient ofone’s actions is a fellow human being. According to one of Milgram’s participants,“You really begin to forget that there’s a guy out there, even though you can hear him.For a long time I just concentrated on pressing the switches and reading the words”(Milgram, 1974, p. 38). This dehumanization of the victim allows the obedient per-son to think of the recipient of his actions as an object, not a person, reducing (andperhaps eliminating) any sense of guilt at harming another individual (Bernard,Ottenberg, & Redl, 1965; Goff, Eberhardt, Williams, & Jackson, 2008).
The dehumanization of the victim in Milgram’s study has a clear parallel outside thelaboratory. Enemies in war and victims of atrocities are rarely described as people, butinstead are referred to as bodies, objects, pests, and numbers (Figure 13.19). This dehu-manization is propped up by euphemistic jargon. The Nazis used terms such as finalsolution (for the mass murder of 6 million people) and special treatment (for death bygassing); the nuclear age contributed fallout problem and preemptive attack; the VietnamWar gave us free-fire zone and body count; other wars gave ethnic cleansing and collateraldamage—all dry, official phrases that keep the thoughts of blood and human sufferingat a psychologically safe distance.
Thus, people obeying morally questionable orders can rely on two different strategiesto let themselves off the moral hook—a cognitive reorientation aimed at holdinganother person responsible for one’s own actions, or a shift toward perceiving the vic-tim as an object, not a person. It is important to realize that neither of these intellectualadjustments happens in an instant. Instead, inculcation is gradual, making it impor-tant that the initial act of obedience be relatively mild and not seriously clash with theperson’s own moral outlook. But after that first step, each successive step can be slightlymore extreme. In Milgram’s study, this pattern created a slippery slope that participantsslid down unawares. A similar program of progressive escalation was used in the indoc-trination of death-camp guards in Nazi Germany and prison-camp guards in Somalia.The same is true for the training of soldiers everywhere. Draftees go through “basictraining,” in part to learn various military skills but much more importantly to acquirethe habit of instant obedience. Raw recruits are rarely asked to point their guns atanother person and shoot. It’s not only that they don’t know how; it’s that most of themprobably wouldn’t do it.
ComplianceWhen we conform or obey, we change our behaviors because of pressure from a groupor commands from authority. But we also alter our actions for a more mundane reason:Someone asks us to do so. Compliance is a third type of social influence. It occurswhen people change their behavior because someone merely asks them to.
According to Cialdini, we feel most compelled to comply with a request when therequester has done something for us in the past (Cialdini, 1993; Cialdini & Goldstein,2004). This is because of the norm of reciprocity—the notion that accepting a favorleads to a sense of indebtedness. Thus we feel that we must repay a donor, even if wedid not want his gift in the first place.
One example involves the Disabled American Veterans organization, which usesmail appeals for donations. For a regular appeal, the response rate is 18%. But when the
13.19 Dehumanizing the opponent Inwartime, propaganda posters routinelydehumanize the opponent, as in this WorldWar I poster that turns the German enemyinto a gorilla savaging an innocent maiden.This dehumanization helps motivate thepopulace in support of the war effort anddiminishes any sense of guilt about acts ofaggression conducted against the enemy.
dehumanization of the victimThinking about a potential victim inways that make him seem inhuman (asvermin, for example, or as a merenumber); this view makes aggressiontoward the victim more likely and lesstroubling to the aggressor.
compliance A change in behavior inresponse to a request.
norm of reciprocity The socialstandard that suggests that a favormust be repaid.
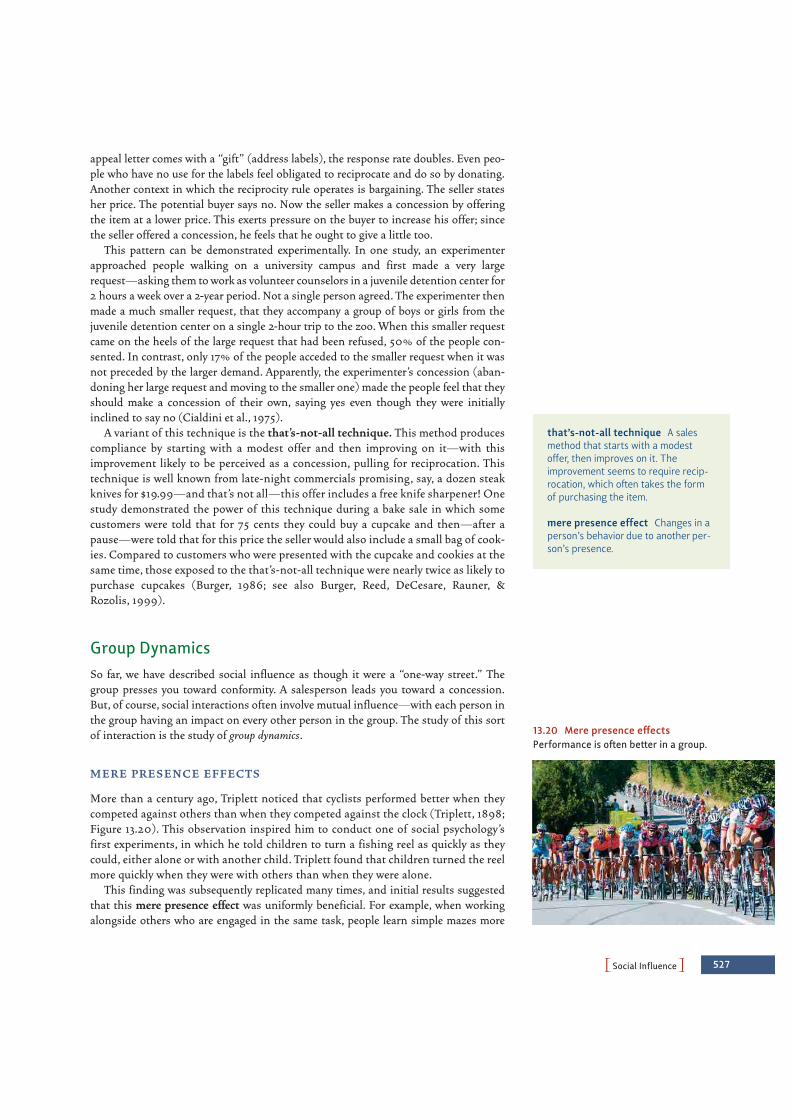
PSocial InfluenceO 527
appeal letter comes with a “gift” (address labels), the response rate doubles. Even peo-ple who have no use for the labels feel obligated to reciprocate and do so by donating.Another context in which the reciprocity rule operates is bargaining. The seller statesher price. The potential buyer says no. Now the seller makes a concession by offeringthe item at a lower price. This exerts pressure on the buyer to increase his offer; sincethe seller offered a concession, he feels that he ought to give a little too.
This pattern can be demonstrated experimentally. In one study, an experimenterapproached people walking on a university campus and first made a very largerequest—asking them to work as volunteer counselors in a juvenile detention center for2 hours a week over a 2-year period. Not a single person agreed. The experimenter thenmade a much smaller request, that they accompany a group of boys or girls from thejuvenile detention center on a single 2-hour trip to the zoo. When this smaller requestcame on the heels of the large request that had been refused, 50% of the people con-sented. In contrast, only 17% of the people acceded to the smaller request when it wasnot preceded by the larger demand. Apparently, the experimenter’s concession (aban-doning her large request and moving to the smaller one) made the people feel that theyshould make a concession of their own, saying yes even though they were initiallyinclined to say no (Cialdini et al., 1975).
A variant of this technique is the that’s-not-all technique. This method producescompliance by starting with a modest offer and then improving on it—with thisimprovement likely to be perceived as a concession, pulling for reciprocation. Thistechnique is well known from late-night commercials promising, say, a dozen steakknives for $19.99—and that’s not all—this offer includes a free knife sharpener! Onestudy demonstrated the power of this technique during a bake sale in which somecustomers were told that for 75 cents they could buy a cupcake and then—after apause—were told that for this price the seller would also include a small bag of cook-ies. Compared to customers who were presented with the cupcake and cookies at thesame time, those exposed to the that’s-not-all technique were nearly twice as likely topurchase cupcakes (Burger, 1986; see also Burger, Reed, DeCesare, Rauner, &Rozolis, 1999).
Group DynamicsSo far, we have described social influence as though it were a “one-way street.” Thegroup presses you toward conformity. A salesperson leads you toward a concession.But, of course, social interactions often involve mutual influence—with each person inthe group having an impact on every other person in the group. The study of this sortof interaction is the study of group dynamics.
M E R E P R E S E N C E E F F E CTS
More than a century ago, Triplett noticed that cyclists performed better when theycompeted against others than when they competed against the clock (Triplett, 1898;Figure 13.20). This observation inspired him to conduct one of social psychology’sfirst experiments, in which he told children to turn a fishing reel as quickly as theycould, either alone or with another child. Triplett found that children turned the reelmore quickly when they were with others than when they were alone.
This finding was subsequently replicated many times, and initial results suggestedthat this mere presence effect was uniformly beneficial. For example, when workingalongside others who are engaged in the same task, people learn simple mazes more
that’s-not-all technique A salesmethod that starts with a modestoffer, then improves on it. Theimprovement seems to require recip-rocation, which often takes the formof purchasing the item.
mere presence effect Changes in aperson’s behavior due to another per-son’s presence.
13.20 Mere presence effectsPerformance is often better in a group.

528 chapter 13 PSOCIAL PSYCHOLOGYO
quickly and perform more multiplication problems in the same period of time—illustrations of a pattern known as social facilitation (F. H. Allport, 1920). Other stud-ies, however, show that the presence of others can sometimes hinder rather thanhelp—an effect called social inhibition. While college students solve simple mazesmore quickly when working with others, they are considerably slower at solving morecomplex mazes when others are around (Hunt & Hillery, 1973; Zajonc, 1965, 1980).How can we reconcile such divergent results?
Zajonc (1965) argued that the presence of other people increases our level of bod-ily arousal, which strengthens the tendency to perform highly dominant responses—the ones that seem to come automatically. When the dominant response is also thecorrect one, as in performing simple motor skills or learning simple mazes, socialpresence should help. But when the task gets harder, as in the case of complex mazes,then the dominant response is often incorrect. As a result, performance gets worsewhen others watch, for in that case the dominant response (enhanced by increasedarousal) inhibits the less dominant but correct reaction.
Evidence supporting this view comes from a wide array of studies. In one study,researchers observed pool players in a college union building. When good playerscompeted in front of an audience of four others, their accuracy rose from 71 to 80%.But when poor players were observed, their accuracy dropped from 35 to 25%(Michaels, Bloomel, Brocato, Linkous, & Rowe, 1982). Similar effects can be observedeven in organisms very different from humans. In one study, cockroaches learned toescape from a bright light by running down a simple alley or by learning a maze. Someperformed alone; others ran in pairs. When in the alley, the cockroaches performedbetter in pairs than alone—for this simple task, the dominant response was appro-priate. In the maze, however, they performed better alone; for this more complex task,the dominant response was incorrect and inappropriate (Zajonc, Heingartner, &Herman, 1969).
SO C I A L LOA F I N G
The studies just described are concerned with people working independently of eachother or people working in the presence of an audience. But what about people work-ing together—such as a committee working on an administrative project, or a group ofstudents working on a class project? In cases like these, everyone is a performer and anaudience member, because every member of the group is contributing to the overallproduct. Likewise, everyone is able to see and perhaps evaluate others’ contributions.How do group members influence each other in this setting?
In this situation, we are likely to observe a phenomenon known as social loafing(Latané, 1981), a pattern in which individuals working together in a group generate lesstotal effort than they would if each worked alone. In one study, individual men wereasked to pull on a rope; the average force for these pulls was 139 pounds. When groupsof eight pulled together, the average was 546 pounds—only about 68 pounds per per-son. In another study, students were asked to clap and cheer as loudly as they could,sometimes alone, sometimes in groups of two, four, or six. Here, too, the results showedsocial loafing. Each person cheered and clapped less vigorously the greater the numberof others she was with (Latané, Williams, & Harkins, 1979). This general finding thatindividuals work less hard in groups has now been replicated many times in the UnitedStates, India, and China (Karau & Williams, 1993).
Why do individuals work less hard in groups? One reason is that they may feel lessaccountable and therefore are less motivated to try as hard as they can. Another reasonis that they may think that their contribution is not crucial to group success (Harkins
social facilitation The tendency toperform simple or well-practiced tasksbetter in the presence of others thanalone.
social inhibition The tendency toperform complex or difficult tasksmore poorly in the presence of others.
social loafing A pattern in whichpeople working together on a taskgenerate less total effort than theywould have if they had each workedalone.

PSocial InfluenceO 529
& Szymanski, 1989). There is an old adage: “Many hands make light work.” The trou-ble is that they do not always make it as light as they could.
D E I N D I V I D UAT I O N
Apparently, then, the presence of others can influence us in multiple ways—in somecircumstances facilitating our behavior, and in other circumstances inhibiting us. Butthe presence of others can also dramatically change how we act. In a riot or lynch mob,for example, people express aggression with a viciousness that would be inconceivableif they acted in isolation. A crowd that gathers to watch a disturbed person on a ledgeatop a tall building often taunts the would-be suicide, urging him to jump. What doesbeing in a crowd do to people to make them act so differently from their everydayselves?
One perspective on these questions describes crowd behavior as a kind of mass mad-ness. This view was first offered by Le Bon (1841–1931), a French social psychologistwho contended that people in crowds become wild, stupid, and irrational and give ventto primitive impulses. He believed their emotion spreads by a sort of contagion, risingto an ever-higher pitch as more and more crowd members become affected. Thus, fearbecomes terror, hostility turns into murderous rage, and each crowd member becomesa barbarian—“a grain of sand among other grains of sand, which the wind stirs up atwill” (Le Bon, 1895).
Many modern psychologists believe that although Le Bon may have overstated hiscase, his claims contain an important truth. To them, the key to crowd behavior is dein-dividuation, a state in which an individual in a group loses awareness of herself as aseparate individual (Figure 13.21). This state is more likely to occur when there is a highlevel of arousal and anonymity—just as would be the case in a large and angry crowd ora large and fearful gathering. Deindividuation tends to release impulsive actions thatare normally under restraint, and what the impulses are depends on the group and thesituation. In a carnival, the (masked) revelers may join in wild orgies; in a lynch mob,the group members may torture or kill (Diener, 1979; Festinger, Pepitone, & Newcomb,1952; Zimbardo, 1969).
To study deindividuation, one investigation had college students wear identicalrobes and hoods that made it impossible to identify them. Once in these hoods—which, not coincidentally, looked just like Ku Klux Klan robes—the students wereasked to deliver an electric shock to another person; they delivered twice as muchshock as those not wearing the robes (Zimbardo, 1970). In the robes, it seemed, thestudents felt free to “play the part”—and in this case the result was ugly. Other stud-ies, though, reveal the good that can be produced by deindividua-tion. In a different experiment, students were asked to wear nurses’uniforms rather than KKK costumes; dressed in this way, studentsdelivered less shock than a group without costumes (R. D. Johnson& Downing, 1979). Thus, deindividuation by itself is not bad—itsimply makes it easy for us to give in to the impulses cued by the sit-uation, and the nature of those impulses depends on the circum-stances.
Notice also that deindividuation can happen in several differentways. Being in a large crowd produces deindividuation; this is partof why mobs act as they do. Wearing a mask can also produce dein-dividuation, largely because of the anonymity it provides. But dein-dividuation can also result merely from someone’s wearing auniform and having an assigned role—in essence, he “becomes” the (A) (B)
13.21 Deindividuation (A) Some deindi-viduation effects are harmless. (B) Othersrepresent a menace to a humane,democratic society.
deindividuation A state in which anindividual in a group experiences aweakened sense of personal identityand diminished self-awareness.

530 chapter 13 PSOCIAL PSYCHOLOGYO
role. This third factor was plainly revealed in a classic study known as the StanfordPrison Experiment, in which Philip Zimbardo transformed the basement of StanfordUniversity’s psychology department into a mock prison and randomly assigned maleundergraduate participants to the role of either guards or prisoners (Figure 13.22;Haney, Banks, & Zimbardo, 1973; Zimbardo, 1973; see also Haney & Zimbardo, 1998).Guards and prisoners wore uniforms appropriate to their roles, and prisoners werecalled by assigned numbers instead of their names. The experimenter gave the partic-ipants few instructions, and placed few constraints on their behavior. What rapidlyevolved was a set of behaviors remarkably similar to those sometimes observed inactual prisons—with cruelty, inhumane treatment, and massive disrespect evident inall the participants. The behaviors observed were sufficiently awful that Zimbardoended his study after only 6 days, before things got really out of hand, rather than let-ting it run for 2 weeks, as was originally planned.
Sadly, the powerful effects of deindividuation and stepping into a role extend wellbeyond the confines of the laboratory setting. As we saw at the outset of this chapter,one now-infamous real-world example is the abusive behavior exhibited by militarypersonnel at Abu Ghraib prison. In the face of worldwide condemnation, Americans ofall stripes struggled to understand how their own countrymen and countrywomencould behave in such an unconscionable fashion. Mindful of the lessons of theStanford Prison Experiment, though, Zimbardo and other social psychologists haveargued that powerful social forces were at work here that included—among others—the power of deindividuation through reducing people to their roles (Zimbardo, 2007).As a result, the situation itself may have done far more to create these abuses than thepersonal qualities of any of the soldiers involved.
G RO U P P O L A R I ZAT I O N
Being in a group doesn’t just influence our behavior; it also influences our thoughts—and often for the worse. For example, consider the phenomenon of group polarization,a tendency for group decisions to be more extreme than the decisions that would havebeen made by any of the members on their own. This pattern arises in many differentgroup contexts, such as when juries decide how much money to award a plaintiff at theend of a lawsuit.
Often the polarization takes the form of a so-called risky shift, in which groupsappear more willing to take risks, or more willing to take an extreme stance, than thegroup members would be individually (Bennett, Lindskold, & Bennett, 1973; C. P.Morgan & Aram, 1975; Schroeder, 1973). However, group polarization can also take theopposite form. If the group members are slightly cautious to begin with or slightly con-servative in their choices, then these tendencies are magnified, and the group’s decisionwill end up appreciably more cautious than the decisions that would have been made bythe individuals alone (Levine & Moreland, 1998; Moscovici & Zavalloni, 1969).
What produces group polarization? One factor is the simple point that, during a dis-cussion, individuals often state, restate, and restate again what their views are, whichhelps to strengthen their commitment to these views (Brauer, Judd, & Gliner, 1995).Another factor involves the sort of confirmation bias that we discussed in Chapter 9—the fact that people tend to pay more attention to, and more readily accept, informationthat confirms their views, in comparison to their (relatively hostile) scrutiny ofinformation that challenges their views. How does this shape a group discussion? Inthe discussion, people are likely to hear sentiments on both sides of an issue. Owing toconfirmation bias, the arguments that support their view are likely to seem clear,
13.22 Stanford Prison Experiment InZimbardo’s classic study, students wererandomly assigned to act as either guardsor prisoners. The study had to be termi-nated early because of the inhumanebehavior shown by the guards.
Stanford Prison Experiment PhilipZimbardo’s study of the effect of roleson behavior. Participants were ran-domly assigned to play either prison-ers or guards in a mock prison. Thestudy was ended early because of the“guards’” role-induced cruelty.
group polarization A pattern ingroup discussions in which each mem-ber’s attitudes become more extreme,even though the discussion drawsattention to arguments that could havemoderated their views.
risky shift A pattern in which agroup appears more willing to takechances or to take an extreme stancethan any individual members wouldhave been on their own.

PSocial RelationsO 531
persuasive, and well informed. Opposing arguments, however, will seem weak andambiguous. This allows people to conclude that the arguments favoring their view arestrong, while the counterarguments are weak, which simply strengthens their commit-ment to their own prior opinion (for the classic example of this pattern, see C. G. Lord,Ross, & Lepper, 1979; also Kovera, 2002).
Another factor leading to group polarization hinges on two topics we have alreadymentioned. On the one hand, people generally try to conform with the other mem-bers of the group, both in their behavior and in the attitudes they express. But, inaddition, people in individualistic cultures want to stand out from the crowd and bejudged “better than average.” How can they achieve both of these goals—conform-ing and excelling? They can take a position at the group’s “leading edge”—similarenough to the group’s position so that they have honored the demands of conform-ity, but “out in front” of the group in a way that makes them seem distinctive. Ofcourse, the same logic applies to everyone in the group, so everyone will seek to takepositions and express sentiments at the group’s leading edge. As a result, this edgewill become the majority view! In this way, right at the start the group’s sentimentswill be sharpened and made a step or two more extreme—exactly the pattern ofgroup polarization.
G RO U P T H I N K
Group decision making also reveals a pattern dubbed groupthink (Janis, 1982). Thispattern is particularly likely when the group is highly cohesive—such as a group offriends or people who have worked together for many years—and when the group isfacing some external threat and is closed to outside information or opinions. Inthis setting, there is a strong tendency for group members to do what theycan to promote the sense of group cohesion. As a result, they downplaydoubts or disagreements, celebrate the “moral” or “superior” status ofthe group’s arguments, stereotype enemies (“our opponents are stupid”or “evil”), markedly overestimate the likelihood of success, and dis-count or ignore risks or challenges to the group (Figure 13.23).
Arguably, groupthink caused a number of disastrous decisions,including the U.S. government’s decision to invade Cuba in the early1960s (Janis, 1971) and the National Aeronautics and SpaceAdministration’s decision to launch the Challenger on a cold day in1986 despite the knowledge that one part of the space shuttle did notperform well at very cold temperatures (Moorhead, Ference, & Neck,1991). Social psychologists are still working to understand exactly whenthe groupthink pattern emerges and what steps can be taken to limit thenegative effects of groupthink on decision making (Kruglanski, Pierro,Mannetti, & De Grada, 2006; Packer, 2009).
SO CIAL RELATIONS
More than 2,000 years ago, the Greek philosopher Aristotle described humans as“social animals,” and, as we have seen, there are many facets to our social existence. Weperceive others’ actions, interpret those actions, and draw conclusions about whatother people are like. We are shaped by the people around us—conforming with them,obeying them, complying with their requests.
13.23 Groupthink
groupthink A pattern of thinkingthat occurs when a cohesive groupminimizes or ignores members’ differ-ences of opinion.

532 chapter 13 PSOCIAL PSYCHOLOGYO
Perhaps the most significant aspect of our social existence, though, concerns our socialrelationships—the way we interact with and feel about others and the way that they inter-act with and feel about us. These behaviors are social by definition, necessarily involvingother individuals, and include the aggressive ways that we hurt others, which we consid-ered in Chapter 12, as well as the positive things we do to help them, which we considerbelow. We also need to consider a central aspect of our social existence—the fact that wesometimes find ourselves attracted to others and even—at times—in love.
Helping and AltruismOne of our great sources of pride as a species is our ability to exhibit prosocial behav-iors, behaviors that help others—assisting them in their various activities, supportingand aiding them in their time of need. But, of course, we don’t always help. Sometimeswe ignore the homeless man as we walk by him; sometimes we throw away a charity’sfundraising plea; sometimes we scurry past the person who has just dropped hisgroceries. The question we need to ask, then, is why we sometimes help and sometimesdon’t. The answer, once again, involves a mix of factors—including our personalities(whether we tend to be helpful overall) and our social environment.
T H E BYSTA N D E R E F F E CT
Consider the case of Kitty Genovese, who was attacked and murdered one early morn-ing in 1964 on a street in Queens, New York (Figure 13.24). While the details of the caseare disputed (Manning, Levine, & Collins, 2007), it is clear that the assault lasted overhalf an hour, during which time Genovese screamed and struggled while her assailantstabbed her repeatedly. Many of her neighbors could see or hear her struggle but didnot come to her aid. Why not? Why, in general, do we often fail to help those who areobviously in need—perhaps even in extreme danger?
According to Latané and Darley, the failure to help is often produced by the way peo-ple understand the situation. It’s not that people don’t care. It’s that they don’t under-stand what should be done because the situation is ambiguous. In the Genovese case,witnesses later reported that they were not sure what was happening. Perhaps it was ajoke, a drunken argument, a lovers’ quarrel. If it were any of these, intervention mighthave been very embarrassing.
The situation is further complicated by the fact that the various witnesses to theGenovese murder realized that others were seeing or hearing what they did. Thiscircumstance created pluralistic ignorance. Each of the witnesses was uncertain whetherthere really was an emergency, and each looked to the others, trying to decide. Their rea-soning was simple: “If my neighbors don’t react, then apparently they’ve decided there’sno emergency, and, if there’s no emergency, there’s no reason for me to react.” The tragedy,of course, is that the neighbors were thinking roughly the same thoughts—with theconsequence that each took the inactivity of the others as a cue to do nothing.
Even when people are convinced that they are viewing an emergency, the presence ofmultiple bystanders still has an effect. It creates a diffusion of responsibility, with eachbystander persuaded that someone else will respond to the emergency, someone elsewill take the responsibility. This effect is illustrated by a study in which participantswere asked to join in what they thought was a group discussion about college life witheither one, three, or five other people. Participants sat in individual cubicles and tookturns talking to each other over an intercom system. In actuality, though, there was onlyone participant; all the other speakers were voices on a previously recorded tape. Thediscussion began as one of these other speakers described some of his personal prob-
13.24 Kitty Genovese
pluralistic ignorance A type of mis-understanding that occurs whenmembers of a group don’t realize thatthe other members share their per-ception (often, their uncertainty abouthow to react to a situation). As a result,each member wrongly interprets theothers’ inaction as reflecting their bet-ter understanding of the situation.
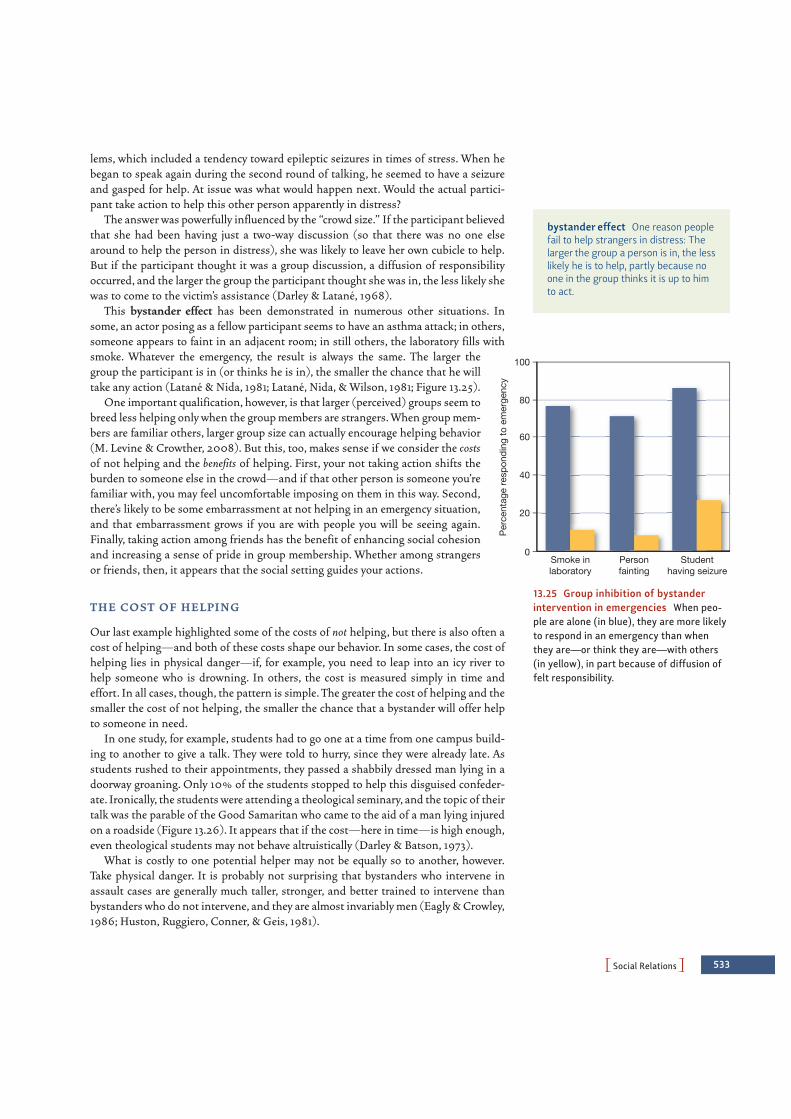
PSocial RelationsO 533
lems, which included a tendency toward epileptic seizures in times of stress. When hebegan to speak again during the second round of talking, he seemed to have a seizureand gasped for help. At issue was what would happen next. Would the actual partici-pant take action to help this other person apparently in distress?
The answer was powerfully influenced by the “crowd size.” If the participant believedthat she had been having just a two-way discussion (so that there was no one elsearound to help the person in distress), she was likely to leave her own cubicle to help.But if the participant thought it was a group discussion, a diffusion of responsibilityoccurred, and the larger the group the participant thought she was in, the less likely shewas to come to the victim’s assistance (Darley & Latané, 1968).
This bystander effect has been demonstrated in numerous other situations. Insome, an actor posing as a fellow participant seems to have an asthma attack; in others,someone appears to faint in an adjacent room; in still others, the laboratory fills withsmoke. Whatever the emergency, the result is always the same. The larger thegroup the participant is in (or thinks he is in), the smaller the chance that he willtake any action (Latané & Nida, 1981; Latané, Nida, & Wilson, 1981; Figure 13.25).
One important qualification, however, is that larger (perceived) groups seem tobreed less helping only when the group members are strangers. When group mem-bers are familiar others, larger group size can actually encourage helping behavior(M. Levine & Crowther, 2008). But this, too, makes sense if we consider the costsof not helping and the benefits of helping. First, your not taking action shifts theburden to someone else in the crowd—and if that other person is someone you’refamiliar with, you may feel uncomfortable imposing on them in this way. Second,there’s likely to be some embarrassment at not helping in an emergency situation,and that embarrassment grows if you are with people you will be seeing again.Finally, taking action among friends has the benefit of enhancing social cohesionand increasing a sense of pride in group membership. Whether among strangersor friends, then, it appears that the social setting guides your actions.
T H E CO ST O F H E L P I N G
Our last example highlighted some of the costs of not helping, but there is also often acost of helping—and both of these costs shape our behavior. In some cases, the cost ofhelping lies in physical danger—if, for example, you need to leap into an icy river tohelp someone who is drowning. In others, the cost is measured simply in time andeffort. In all cases, though, the pattern is simple. The greater the cost of helping and thesmaller the cost of not helping, the smaller the chance that a bystander will offer helpto someone in need.
In one study, for example, students had to go one at a time from one campus build-ing to another to give a talk. They were told to hurry, since they were already late. Asstudents rushed to their appointments, they passed a shabbily dressed man lying in adoorway groaning. Only 10% of the students stopped to help this disguised confeder-ate. Ironically, the students were attending a theological seminary, and the topic of theirtalk was the parable of the Good Samaritan who came to the aid of a man lying injuredon a roadside (Figure 13.26). It appears that if the cost—here in time—is high enough,even theological students may not behave altruistically (Darley & Batson, 1973).
What is costly to one potential helper may not be equally so to another, however.Take physical danger. It is probably not surprising that bystanders who intervene inassault cases are generally much taller, stronger, and better trained to intervene thanbystanders who do not intervene, and they are almost invariably men (Eagly & Crowley,1986; Huston, Ruggiero, Conner, & Geis, 1981).
bystander effect One reason peoplefail to help strangers in distress: Thelarger the group a person is in, the lesslikely he is to help, partly because noone in the group thinks it is up to himto act.
Smoke inlaboratory
Personfainting
Studenthaving seizure
Per
cent
age
resp
ondi
ng to
em
erge
ncy
20
40
60
80
100
0
13.25 Group inhibition of bystanderintervention in emergencies When peo-ple are alone (in blue), they are more likelyto respond in an emergency than whenthey are—or think they are—with others(in yellow), in part because of diffusion offelt responsibility.

534 chapter 13 PSOCIAL PSYCHOLOGYO
In addition, the costs of providing help are sometimes weighed against the benefitsof helping. Some of the benefits are various signs of social approval, as with a donor tocharity who is sure to make a lavish contribution so long as everyone knows. A differ-ent benefit is one we alluded to earlier—namely, the avoidance of shame or embarrass-ment. Many city dwellers give 50 or 75 cents to a homeless person, for example, notbecause they want to help but because it would be embarrassing just to say no.Occasionally, the benefits of giving involve sexual attraction. In one study, the investi-gators posed as motorists in distress trying to flag passing cars to provide help with aflat tire. The passing cars were much more likely to stop for a woman than for a man,and the cars that stopped were generally driven by young men alone. The best guess isthat the young men’s altruism was not entirely unalloyed by sexual interest (West,Whitney, & Schnedler, 1975).
One additional factor that shapes whether people help each other is their culturalcontext. Compared to Hindu Indians, for example, European Americans are less likelyto see that they have a moral imperative to help someone if they do not like that person(J. G. Miller & Bersoff, 1998). European Americans also see less of a moral imperativeto help someone who has helped them in the past (J. G. Miller, Bersoff, & Harwood,1990). And because of the cultural emphasis on taking care of “number one,”Americans will say that they are acting out of self-interest, even when they are not(D. T. Miller, 1999). Overall, these findings suggest that cultural emphasis on self-reliance and self-interest may cause Americans and other members of individualisticsocieties to think twice before helping, while the cultural emphasis on relationshipsand connection may cause members of collectivistic societies to offer aid more readily.
A LT RU I S M A N D S E L F - I N T E R E ST
The preceding discussion suggests a somewhat unflattering portrait of human nature,especially for those of us in individualistic cultures. It seems that we often fail to helpstrangers in need, and when we do, our help is rather grudging and calculated, based onsome expectation of later reciprocation. But that picture may be too one-sided. For whilepeople can be callous and indifferent, they are also capable of true generosity and even,at times, of altruism, or helping behavior that does not benefit the helper (Figure 13.27).People share food, give blood, contribute to charities, volunteer at AIDS hospices, andresuscitate accident victims. Even more impressive are the unselfish deeds of living,genetically unrelated donors who give one of their kidneys to a stranger who would oth-erwise die (Sadler, Davison, Carroll, & Kounts, 1971). Consider too those commemoratedby Jerusalem’s Avenue of the Righteous—the European Christians who sheltered Jewsduring the Holocaust, risking (and often sacrificing) their own lives to save those towhom they gave refuge (London, 1970).
Why do people engage in these activities? When asked, most report that such altruisticactions make them better people (Piliavin & Callero, 1991; M. Snyder & Omoto, 1992), andthe major texts of all major religions support this idea (Norenzayan & Shariff, 2008). Suchacts of altruism suggest that human behavior is not always selfish. To be sure, acts of altru-ism in which the giver gets no benefits at all—no gratitude, no public acclaim—are fairlyrare. The true miracle is that they occur at all.
AttractionActs of aggression or acts of helping often involve isolated incidents. Someone cuts youoff in traffic, and you angrily honk your horn; a stranger on a street corner asks you for afew coins, and you do (or perhaps don’t) give some. Other forms of social relationship
13.26 The Good Samaritan Painting byJacopo Bassano, 1517/18–1592.
© T
he N
atio
nal G
alle
ry, L
ondo
n
13.27 Helping The text describes many ofthe reasons why people often fail to helpeach other, but, happily, the fact remainsthat there are circumstances in which wedo help one another. One powerful examplecomes from the outpouring of assistancethat emerged following the attack on theWorld Trade Center. Many police officersand fire fighters performed heroically inimmediately helping the victims of theattack; in the days following, many peoplemade generous donations to help thevictims.
altruism Helping behavior that doesnot benefit the helper.

PSocial RelationsO 535
are more enduring—and can color your life for many years. These long-lasting relation-ships include friendship and the exciting, comforting, and sometimes vexing relation thatwe call love.
What initially draws people together as friends or lovers? How do we win someone’saffections? How do close relationships change over the long term? We first addressedthese questions in Chapter 2, when considering the biological roots of mate selection.We will now flesh out the story by considering these issues from the vantage point ofsocial psychology.
AT T R ACT I V E N E SS
Common sense tells us that physical appearance is an important determinant of attrac-tion, and formal evidence confirms that point. In one study, freshmen were randomlypaired at a dance and later asked how much they liked their partner and whether he orshe was someone they might want to date. After this brief encounter, what mainlydetermined each person’s desirability as a future date was his or her physical attractive-ness (Walster, Aronson, Abrahams, & Rottman, 1966). Similar results were foundamong clients of a commercial dating service who selected partners based on files thatincluded a photograph, background information, and details about interests, hobbies,and personal ideals. When it came down to the actual choice, the primary determinantwas the photograph (S. K. Green, Buchanan, & Heuer, 1984).
Physically attractive individuals also benefit from the common tendency to associatephysical attractiveness with a variety of other positive traits, including intelligence,happiness, and good mental health (e.g., Bessenoff & Sherman, 2000; Dion,Berscheid, & Walster, 1972; Eagly, Ashmore, Makhijani, & Longo, 1991; Feingold, 1992;Jackson, Hunter, & Hodge, 1995; Langlois et al., 2000). This is, in fact, part of a largerpattern sometimes referred to as the halo effect, a term that refers to our tendency toassume that people who have one good trait are likely to have others (and, conversely,that people with one bad trait are likely to be bad in other regards as well). In somecases, there may be a kernel of truth in this pattern of beliefs, but unmistakably the“halo” extends farther than it should (Anderson, Adams, & Plaut, 2008). For example,people seem to make judgments about how competent someone is based only on facialappearance, and so, remarkably, judgments about appearance turn out to be powerfulpredictors of whom people will vote for in U.S. congressional elections (Todorov,Mandisodza, Goren, & Hall, 2005).
P ROX I M I T Y
A second important factor in determining attraction is sheer proximity (Figure 13.28).By now, dozens of studies have shown that if you want to predict who will makefriends with whom, the first thing to ask is who is nearby. Students who live next toeach other in a dormitory or sit next to each other in classes develop stronger relationsthan those who live or sit only a bit farther away (Back, Schmukle, & Egloff, 2008).Similarly, members of a bomber crew became much friendlier with fellow crew mem-bers who worked right next to them than with others who worked only a few feet away(Berscheid, 1985).
In this case, what holds for friendship also holds for mate selection. The statisticsare rather impressive. For example, one classic study considered all the couples whotook out marriage licenses in Columbus, Ohio, during the summer of 1949. Amongthese couples, more than half were people who lived within 16 blocks of each otherwhen they went out on their first date (Clarke, 1952). Much the same holds for the
halo effect The tendency to assumethat people who have one good traitalso have other good traits.
“Do you really love me, Anthony, or is it justbecause I live on the thirty-eighth floor?”
13.28 Proximity
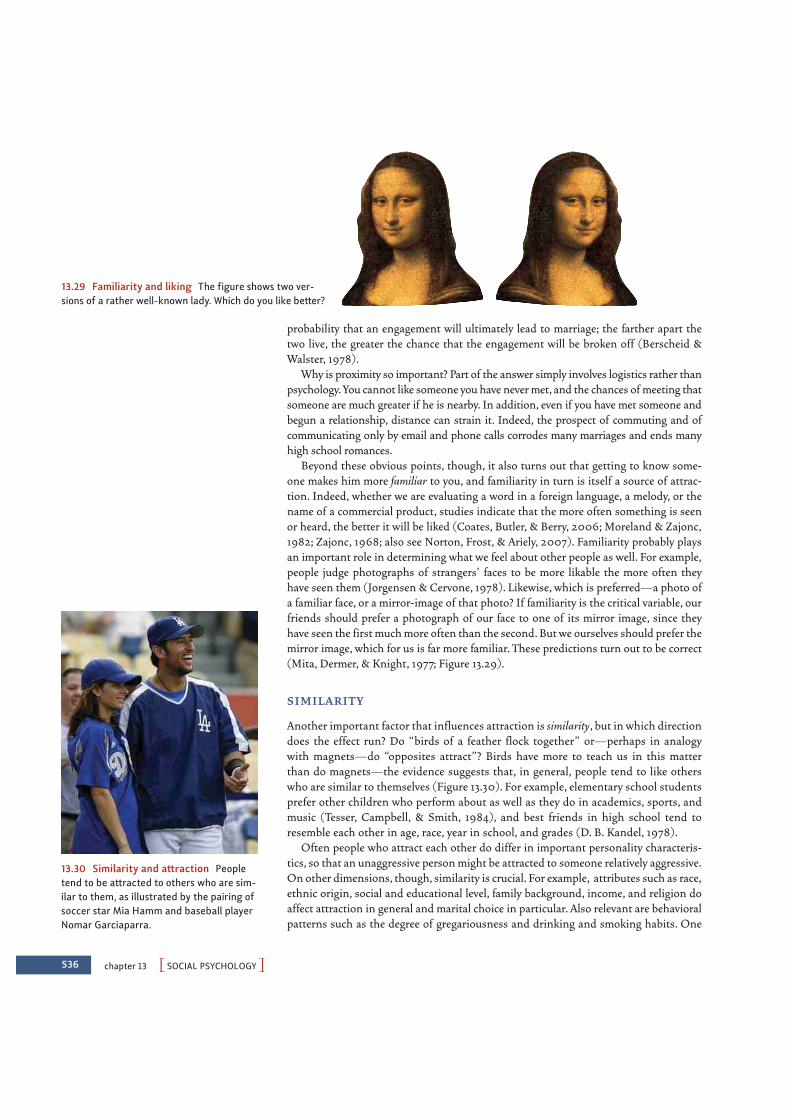
536 chapter 13 PSOCIAL PSYCHOLOGYO
13.29 Familiarity and liking The figure shows two ver-sions of a rather well-known lady. Which do you like better?
13.30 Similarity and attraction Peopletend to be attracted to others who are sim-ilar to them, as illustrated by the pairing ofsoccer star Mia Hamm and baseball playerNomar Garciaparra.
probability that an engagement will ultimately lead to marriage; the farther apart thetwo live, the greater the chance that the engagement will be broken off (Berscheid &Walster, 1978).
Why is proximity so important? Part of the answer simply involves logistics rather thanpsychology. You cannot like someone you have never met, and the chances of meeting thatsomeone are much greater if he is nearby. In addition, even if you have met someone andbegun a relationship, distance can strain it. Indeed, the prospect of commuting and ofcommunicating only by email and phone calls corrodes many marriages and ends manyhigh school romances.
Beyond these obvious points, though, it also turns out that getting to know some-one makes him more familiar to you, and familiarity in turn is itself a source of attrac-tion. Indeed, whether we are evaluating a word in a foreign language, a melody, or thename of a commercial product, studies indicate that the more often something is seenor heard, the better it will be liked (Coates, Butler, & Berry, 2006; Moreland & Zajonc,1982; Zajonc, 1968; also see Norton, Frost, & Ariely, 2007). Familiarity probably playsan important role in determining what we feel about other people as well. For example,people judge photographs of strangers’ faces to be more likable the more often theyhave seen them (Jorgensen & Cervone, 1978). Likewise, which is preferred—a photo ofa familiar face, or a mirror-image of that photo? If familiarity is the critical variable, ourfriends should prefer a photograph of our face to one of its mirror image, since theyhave seen the first much more often than the second. But we ourselves should prefer themirror image, which for us is far more familiar. These predictions turn out to be correct(Mita, Dermer, & Knight, 1977; Figure 13.29).
S I M I L A R I T Y
Another important factor that influences attraction is similarity, but in which directiondoes the effect run? Do “birds of a feather flock together” or—perhaps in analogywith magnets—do “opposites attract”? Birds have more to teach us in this matterthan do magnets—the evidence suggests that, in general, people tend to like otherswho are similar to themselves (Figure 13.30). For example, elementary school studentsprefer other children who perform about as well as they do in academics, sports, andmusic (Tesser, Campbell, & Smith, 1984), and best friends in high school tend toresemble each other in age, race, year in school, and grades (D. B. Kandel, 1978).
Often people who attract each other do differ in important personality characteris-tics, so that an unaggressive person might be attracted to someone relatively aggressive.On other dimensions, though, similarity is crucial. For example, attributes such as race,ethnic origin, social and educational level, family background, income, and religion doaffect attraction in general and marital choice in particular. Also relevant are behavioralpatterns such as the degree of gregariousness and drinking and smoking habits. One

widely cited study showed that engaged couples in the United States tend to be similaralong all of these dimensions (Burgess & Wallin, 1943), a pattern that provides evi-dence for homogamy—a powerful tendency for like to select like.
What produces the homogamy pattern? One possibility is that similarity really doeslead to mutual liking, so that homogamy can be taken at face value. A different possi-bility, though, is that similarity does not matter on its own; instead, the apparent effectsof similarity may be a by-product of proximity, of the fact that “few of us have anopportunity to meet, interact with, become attracted to, and marry a person markedlydissimilar from ourselves” (Berscheid & Walster, 1978, p. 87). The answer is uncertain,but in either case, the end result is the same. Like pairs with like, and heiresses rarelymarry the butler except in the movies. We are not really surprised when a princesskisses a frog and he turns into a prince. But we would be surprised to see the frog turninto a peasant and then see the princess marry him anyway.
LoveAttraction tends to bring people closer together. If they are close enough, theirrelationship may be more than friendship and become something we celebrate with theterm love. In fact, love involves many elements: a feeling, a physiological upheaval, adesire for sexual union, a set of living and parenting arrangements, a sharing ofresources (from bank accounts to friends), a mutual defense and caretaking pact, amerging of extended families, and more. So complex is human love that, according tosome authorities, psychologists might have been “wise to have abdicated responsibilityfor analysis of this term and left it to poets” (Reber, 1985, p. 409). Wise or not, psychol-ogists have tried to say some things about this strange state of mind that has puzzledboth sages and poets throughout the ages.
Psychologists distinguish among different kinds of love, and some of the resultingclassification systems are rather complex. One scheme tries to analyze love relation-ships according to the presence or absence of three main components: intimacy (feel-ings of being close), passion (sexual attraction), and commitment (a decision to stay withone’s partner) (Sternberg, 1986, 1988). Other psychologists propose that there are twobroad categories of love. One is romantic—or passionate—love, the kind of love thatone “falls into,” that one is “in.” The other is companionate love, a less turbulent statethat emphasizes companionship, mutual trust, and care (Hatfield, 1988).
RO M A N T I C LO V E
Romantic love has been described as essentially passionate: “a wildly emotional state[in which] tender and sexual feelings, elation and pain, anxiety and relief, altruism andjealousy coexist in a confusion of feelings” (Berscheid & Walster, 1978, p. 2). Lovers feelthat they are in the grip of an emotion they cannot control, which comes across in thevery language they use to describe their love. They “fall in love,” “are swept off theirfeet,” and “can’t stop themselves.” Perhaps surprisingly, men tend to fall in love moreoften and more quickly than women do, and women tend to fall out of love more easilythan men do (Hill, Rubin, & Peplau, 1976).
According to some authors, romantic love involves two distinguishable elements: astate of physiological arousal, and a set of beliefs and attitudes that leads the person tointerpret this arousal as passion. What leads to the arousal itself? One obvious sourceis erotic excitement, but other forms of stimulation may have the same effect. Fear,pain, and anxiety can all heighten general arousal and so can, in fact, lend fuel toromantic passion. One demonstration comes from a widely cited experiment in which
PSocial RelationsO 537
homogamy The tendency of like tomate with like.
romantic love An emotional statecharacterized by idealization of thebeloved, obsessive thoughts of thisperson, and turbulent feelings.
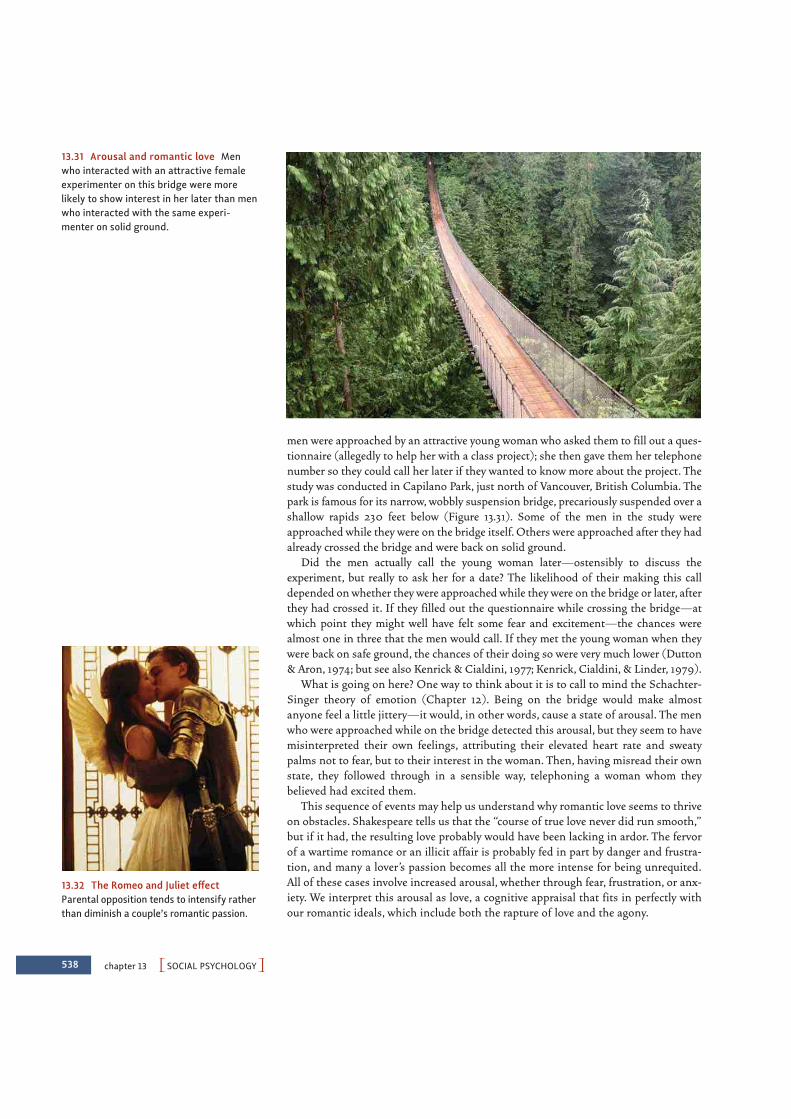
538 chapter 13 PSOCIAL PSYCHOLOGYO
13.31 Arousal and romantic love Menwho interacted with an attractive femaleexperimenter on this bridge were morelikely to show interest in her later than menwho interacted with the same experi-menter on solid ground.
13.32 The Romeo and Juliet effectParental opposition tends to intensify ratherthan diminish a couple’s romantic passion.
men were approached by an attractive young woman who asked them to fill out a ques-tionnaire (allegedly to help her with a class project); she then gave them her telephonenumber so they could call her later if they wanted to know more about the project. Thestudy was conducted in Capilano Park, just north of Vancouver, British Columbia. Thepark is famous for its narrow, wobbly suspension bridge, precariously suspended over ashallow rapids 230 feet below (Figure 13.31). Some of the men in the study wereapproached while they were on the bridge itself. Others were approached after they hadalready crossed the bridge and were back on solid ground.
Did the men actually call the young woman later—ostensibly to discuss theexperiment, but really to ask her for a date? The likelihood of their making this calldepended on whether they were approached while they were on the bridge or later, afterthey had crossed it. If they filled out the questionnaire while crossing the bridge—atwhich point they might well have felt some fear and excitement—the chances werealmost one in three that the men would call. If they met the young woman when theywere back on safe ground, the chances of their doing so were very much lower (Dutton& Aron, 1974; but see also Kenrick & Cialdini, 1977; Kenrick, Cialdini, & Linder, 1979).
What is going on here? One way to think about it is to call to mind the Schachter-Singer theory of emotion (Chapter 12). Being on the bridge would make almostanyone feel a little jittery—it would, in other words, cause a state of arousal. The menwho were approached while on the bridge detected this arousal, but they seem to havemisinterpreted their own feelings, attributing their elevated heart rate and sweatypalms not to fear, but to their interest in the woman. Then, having misread their ownstate, they followed through in a sensible way, telephoning a woman whom theybelieved had excited them.
This sequence of events may help us understand why romantic love seems to thriveon obstacles. Shakespeare tells us that the “course of true love never did run smooth,”but if it had, the resulting love probably would have been lacking in ardor. The fervorof a wartime romance or an illicit affair is probably fed in part by danger and frustra-tion, and many a lover’s passion becomes all the more intense for being unrequited.All of these cases involve increased arousal, whether through fear, frustration, or anx-iety. We interpret this arousal as love, a cognitive appraisal that fits in perfectly withour romantic ideals, which include both the rapture of love and the agony.

PSocial RelationsO 539
An interesting demonstration of this phenomenon is the so-called Romeo-and-Juliet effect (named after Shakespeare’s doomed couple, whose parents violentlyopposed their love; Figure 13.32). This term describes the fact that parental oppositiontends to intensify a couple’s romantic passion rather than to diminish it. In one study,couples were asked whether their parents interfered with their relationship. The greaterthis interference, the more deeply the couples fell in love (Driscoll, Davis, & Lipetz,1972). The moral is that if parents want to break up a romance, their best bet is toignore it. If the feuding Montagues and Capulets had simply looked the other way,Romeo and Juliet might well have become bored with each other by the end of thesecond act.
CO M PA N I O N AT E LO V E
Romantic love tends to be a short-lived bloom. That wild and tumultuous state, with itsintense emotional ups and downs, with its obsessions, fantasies, and idealizations,rarely, if ever, lasts forever. Eventually the adventure is over, and romantic love ebbs.Sometimes it turns into indifference or active dislike. Other times (and hopefully moreoften) it transforms into a related but gentler state of affairs—companionate love(Figure 13.33). This type of love is sometimes defined as the “affection we feel for thosewith whom our lives are deeply intertwined” (Berscheid & Hatfield, 1978, p. 176). Incompanionate love, the similarity of outlook, mutual caring, and trust that developthrough day-to-day living become more important than the fantasies and idealizationof romantic love, as the two partners try to live as happily ever after as it is possible todo in the real world. This is not to say that the earlier passion does not flare up occa-sionally. But it no longer has the obsessive quality that it once had, in which the loveris unable to think of anything but the beloved (Caspi & Herbener, 1990; Hatfield, 1988;Neimeyer, 1984).
CU LT U R E A N D LO V E
It will come as no surprise that concep-tions of love are—like the many otheraspects of our interactions with others—acultural product. Western cultural notionsof what love is and what falling in lovefeels like have been fashioned by a histori-cal heritage that goes back to Greek andRoman times (with tales of lovers hit byCupid’s arrows), was revived during theMiddle Ages (with knights in armor slay-ing dragons to win a lady’s favor), and wasfinally mass-produced by Hollywood (witha final fade-out in which the coupleembraces and lives happily ever after). Thiscomplex set of ideas about what love is,and who is an appropriate potential loveobject, constitutes the context that maylead us to interpret physiological arousalas love.
Romeo-and-Juliet effect The inten-sification of romantic love that canoccur when the couple’s parentsoppose relationship.
companionate love An emotionalstate characterized by affection forthose whose lives are deeply inter-twined with one’s own.
13.33 Companionate love This type oflove is based upon the affection we feel forthose with whom our lives are intertwined.

13.34 Culture and love Similar ideasabout romantic love are found in many dif-ferent cultural contexts.
540 chapter 13 PSOCIAL PSYCHOLOGYO
Similar ideas about romantic love are found in many other cultures (Figure 13.34).Hindu myths and Chinese love songs, for example, celebrate this form of love, and,indeed, a review of the anthropological research revealed that romantic love was pres-ent in 147 of 166 cultures (Jankowiak & Fischer, 1992). Even so, it seems unlikely thatany other culture has emphasized romantic love over companionate love to the extentthat Western culture does (e.g., De Rougemont, 1940; V. W. Grant, 1976). This isreflected in many ways, including the fact that popular American love songs are onlyhalf as likely as popular Chinese love songs to refer to loyalty, commitment, and endur-ing friendship, all features of companionate love (Rothbaum & Tsang, 1998).
Why do cultures differ in these ways? One proposal derives, again, from the contrastbetween individualistic and collectivistic cultures. Collectivistic cultures emphasizeconnection to one’s group, and this makes it unsurprising that (collectivistic) Chinawould prefer songs emphasizing loyalty—a focus on the relationship, rather than oneach individual’s feelings. To put this point differently, romantic love often places a highpremium on pursuing personal fulfillment, even, and perhaps especially, when it con-flicts with other duties. On this basis, members of individualistic cultures are morelikely than those in collectivistic cultures to consider romantic love important for mar-riage. (Dion & Dion, 1996).
SOME FINAL THOUGHTS: THE SO CIAL ANIM AL?
To what extent are we “social animals,” as Aristotle claimed? As we have seen, manyaspects of our thoughts, feelings, and behaviors are shaped by social forces. When welook out upon the world around us, the features of the landscape that register mostdeeply, and are most consequential for us, are often social features. We worry aboutwhat people think of us, whether they like us, and what intentions they harbor. We tryto make sense of what they want us to do (or not do) and decide whether or not to com-ply with their wishes. Indeed, much of what we think about—and the source of manyof our most intense emotions—is other people: strangers, friends, family, and roman-tic partners.

SOCIAL COGNITION
• How we understand someone’s behavior depends on theattribution we choose for the behavior. Situational attributionsinvolve factors external to the person we are observing; dispo-sitional attributions focus on factors internal to the person.
• People in collectivistic cultures emphasize the ways in whichpeople are interdependent and tend to make situational attri-butions. People in individualistic cultures view themselves andothers as independent and tend to make dispositional attri-butions; this tendency is so powerful that it is referred to asthe fundamental attribution error.
S U M M A R Y C H A P T E R 1 3
PSummaryO 541
One of the principal lessons of social psychology is that we are not the autonomousindividuals we might conceive ourselves to be. As we have seen, simply having anotherperson pay attention to us changes our behavior. Far more substantial changes in ourbehavior arise as we conform to others’ expectations, or when we are directly instructedor asked by others to act a certain way. We are intertwined within a complex web ofsocial and cultural influences that shapes how we perceive the world and how we feel,behave, and think.
But if our analysis were to stop here, we would have missed our mark. This is becauseeach of us is far from a passive and helpless player on the social stage. Instead, weactively try to make sense of the world, and so we work hard to understand what othersare doing and thinking, and through our interpretations we create the realities withwhich we contend. At the same time, we make frequent efforts to act directly on oursocial worlds. Sometimes these efforts have small effects, but at other times their impactcan be breathtaking.
A final lesson is that the social forces we have discussed can vary across time, place,and culture. Yet there is much commonality, too. Such diverse political theorists asAristotle, Hobbes, and Confucius are still read despite the fact that they lived manycenturies ago and under very different political systems than our own. They wroteabout human social behavior that we can recognize even today. History provides manyother examples of enduring social reactions. There are records of panics in Romanamphitheaters when the stands collapsed and of riots during sporting events inByzantium. The Great Wall of China, the pyramids of South and Central America, andthe cathedrals of Europe all testify to the ability of large groups of people to worktogether and to take direction from a leader. Some of the ancients even used familiartypes of propaganda. When the ancient Roman city of Pompeii was destroyed by a vol-cano in 79 C.E., the city was evidently in the midst of a municipal election. Modernarcheologists have found some of the election slogans on the excavated walls: “Votefor Vatius, all the whoremasters vote for him” and “Vote for Vatius, all the wife-beat-ers vote for him.” While the techniques of the anti-Vatius faction may be a bit crudefor our modern taste, they certainly prove that the psychology of the smear campaignhas a venerable history (Raven & Rubin, 1976). Phenomena of this sort suggest thatpeople’s social nature can produce similar practices, understandings, and products indifferent times and places.

542 chapter 13 PSOCIAL PSYCHOLOGYO
• We rely on implicit theories of personality when we think aboutor remember other individuals. These theories help usunderstand the situations we encounter but also leave us vul-nerable to error. These errors are obvious when we rely onsocial stereotypes, which are transmitted to each generationboth explicitly and implicitly.
• Stereotypes can influence people’s behavior implicitly. Bypriming a person’s stereotype, the person’s behavior can beinfluenced in an unconscious and automatic fashion.Stereotypes can also create self-fulfilling prophecies, leading theperson we are interacting with to behave in a fashion consis-tent with the stereotype. A related case involves stereotypethreat, in which anxiety about confirming the stereotypeundermines someone’s performance and in that fashion actu-ally confirms the stereotype.
• Attitudes are a combination of beliefs, feelings about the tar-get object or event, and some predisposition to act in accordwith those beliefs and feelings. Attitudes are learned, andthey can be changed in several ways. The central routeinvolves cases in which we care about the issue; what mattershere are arguments and evidence. If we do not care muchabout the issue or are distracted, we rely on the peripheralroute, in which we are influenced by how or by whom a per-suasive message is presented. Other paths to changing atti-tudes include intergroup contact (in the case of prejudice)and cognitive dissonance, which involves a person’s changingher attitudes to bring them into line with her behavior.
SOCIAL INFLUENCE
• Conformity, obedience, and compliance are often denigrated, butthese three forms of social influence are necessary for thesmooth functioning of any social group.
• In studies by Sherif and by Asch, people’s perceptions of theworld were shaped by the way others reported what theyperceived. One reason for this conformity was informationalinfluence—people’s desire to be right. Another reason wasnormative influence—people’s desire not to appear foolish.The informational influence is increased when the situationis genuinely ambiguous; this leads to increased socialreferencing.
• Conformity is much reduced if there is any break in thegroup’s unanimity. In collectivistic cultures, people appear tobe less distressed about conforming than people in individu-alistic cultures appear to be.
• Some researchers propose that people with authoritarian per-sonalities are more inclined to obedience. While there is somesupport for this claim, there is more powerful evidence for theinfluence of situations in producing obedience, as reflected inMilgram’s famous studies of obedience, in which participantsobeyed instructions even if these seemed to lead to injury toanother person.
• Obedience is more likely if the individual believes he is not ulti-mately responsible for the actions, and it is increased either bya sense of psychological distance between one’s actions and theresult of those actions or by dehumanizing the victim. Theseadjustments, however, are usually achieved gradually, as theperson slides down a slippery slope toward total obedience.
• Compliance with requests is often compelled by the norm ofreciprocity. This is evident in the success of the that’s-not-alltechnique.
• In mere presence effects, how people behave is influenced by thepresence of an audience, although the audience can produceeither social facilitation or social inhibition. This mixed data pat-tern is often explained by claiming that the audienceincreases an actor’s arousal, and this strengthens the ten-dency to perform highly dominant responses.
• When people work as a team, often the contributionproduced by each team member is less than the work shewould have done if she were on her own—an effect known associal loafing.
• The presence of other people can cause deindividuation, a statein which the individual gives in to the impulses suggested bythe situation. Deindividuation can lead to riotous behavior inlarge groups of people, but it can also lead to increased goodbehavior if the situation happens to produce impulsespromoting those behaviors. Deindividuation can be pro-duced by anonymity or by just having an assigned role, as wasshown in the Stanford Prison Experiment.
• Group polarization refers to a tendency for decisions made bygroups to be more extreme than the decisions that wouldhave been made by any of the group members working on hisown. This effect arises from several influences, including con-firmation bias operating during group discussion and fromeach member of the group trying to take a position at thegroup’s leading edge.
• Group decision making sometimes reveals groupthink, inwhich the group members do all they can to promote groupcohesion; as a result, they downplay any doubts or disagree-ments, and they overestimate the likelihood of success.

PSummaryO 543
SOCIAL RELATIONS
• People in groups of strangers are less likely to help othersthan are people who are alone or with friends, and severalmechanisms contribute to this bystander effect. One factor isambiguity in the situation, with many individuals convinc-ing themselves that help is not needed. Another factor ispluralistic ignorance, with each individual turning to the oth-ers to find out if help is needed; but, with all doing this,each is convinced by the others’ inaction that no help isneeded. Yet another factor is diffusion of responsibility, witheach group member able to think that others are the oneswho should help.
• People often choose not to help because they are concernedabout the time needed or the risks involved. The fact remains,however, that people sometimes do engage in altruistic acts ofhelping—even if doing so puts them in considerable danger.
• Many factors govern the ways people are drawn to oneanother, including physical attractiveness, proximity, andsimilarity. One reason physical attractiveness is emphasizedis because of the halo effect, which leads us to suppose thatpeople who have one good trait are likely to have others.
• The relationship of love involves many elements, including inti-macy, passion, and commitment. In addition, psychologistsoften distinguish two types of love—romantic love andcompanionate love. Romantic love is often tumultuous, and itinvolves a state of physiological arousal and a set of beliefsthat leads the person to interpret this arousal as passion.Companionate love involves a similarity of outlook, mutualcaring, and trust that develop through day-to-day livingtogether.
• Ideas about romantic love are found in many cultures, butromantic love plays a larger role in individualistic culturesthan in collectivistic cultures, plausibly because collectivistcultures emphasize connection and loyalty to one’s group,rather than the personal fulfillment often associated withromantic love.
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
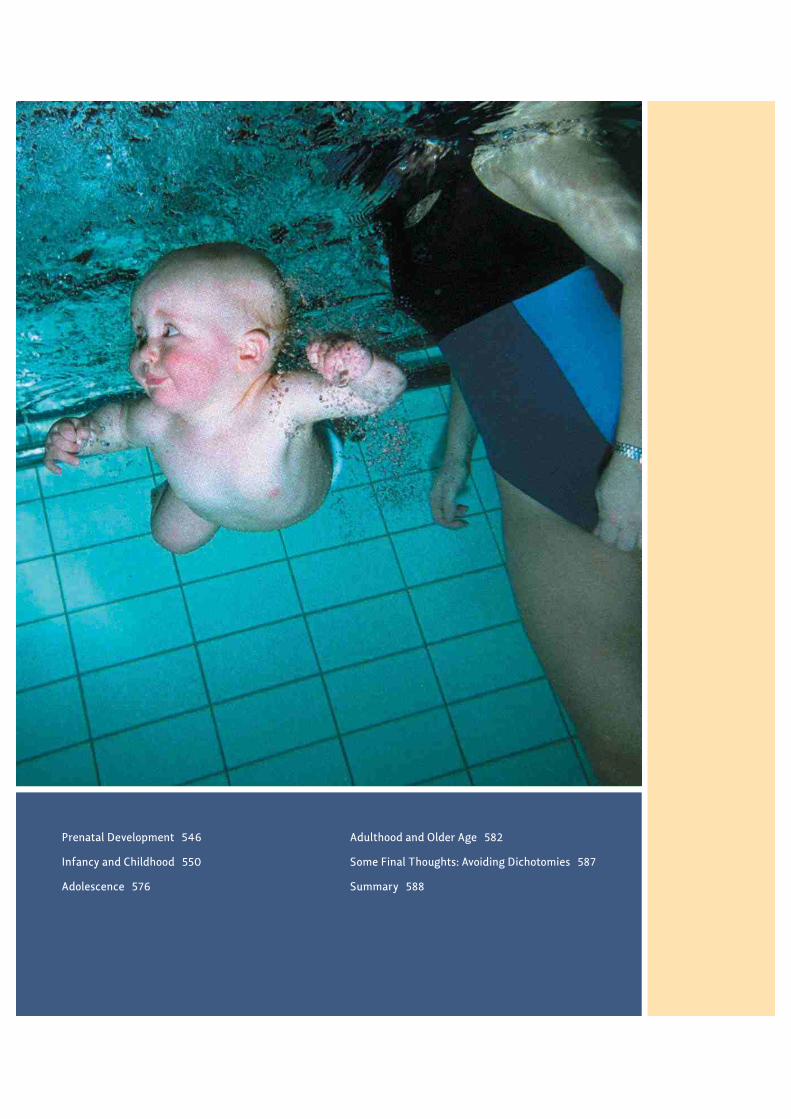
Prenatal Development 546
Infancy and Childhood 550
Adolescence 576
Adulthood and Older Age 582
Some Final Thoughts: Avoiding Dichotomies 587
Summary 588
14CH
AP
TE
R
545
Development
For their first few months, chimpanzee babies are much
better company than human infants. Chimps cry less, fuss less, and drool less.
They’re strong enough to support their heads and to ride, unassisted, on their moth-
ers’ bodies. When so inspired, they can even climb trees and swing from high
branches. Human infants, in contrast, can’t even hold up their heads, let alone cling
to mom. They usually need a whole year to master the art of walking, and even then
their gait resembles that of a slightly drunk person.
But as the weeks pass, we begin to see that lurking inside that chubby body is a
sophisticated physicist, a subtle psychologist, and a versatile linguist. As the infant
carefully watches the world, the world, in turn, is working on her psyche, teaching
her how things fit together and how they fall apart; whom to trust and whom to
avoid; what she can do with her building blocks and what to call the thing that
barks. She is not only beginning to master the functions of her mind and body and
the features of her environment, but also starting to understand the psyches of
others—a skill known as having a theory of mind. This skill will enable her to work
with fellow humans to imagine, plan, create, build, and do all the other things of
which her species is capable. And the rest, as they say, is history—the history of the
development of a single human being.
In this chapter, we’ll consider what developmental psychologists have learned by
studying all of these forms of development—physical and sensorimotor (changes in
the body and the ability to sense and move), cognitive (growth in knowledge and

546 chapter 14 PDEVELOPMENTO
intellectual skills), and socioemotional (growth in the skills needed to perceive, under-stand, and get along with others). And we’ll see how changes in each one of thesedomains affect all the others, as when physical changes in the brain enable new modesof thinking and self control, which in turn support new ways of interacting with others.
At the same time, people are not just empty vessels into which the world pours its wis-dom. To the contrary, a new generation of psychologists is showing that the mind comeswired with many ideas about the physical, social, and psychological worlds. As this chap-ter shows, those ideas continue to mature and change as development unfolds—throughthe social and cognitive flowering of childhood; to the risk-taking, back-talking tumult ofadolescence; to the application of our knowledge throughout adulthood into old age.
Of course, nature cannot unfold without nurture, genes require environments tobe expressed, and the individual needs other people to be fully realized. Accordingly,each of us provides part of the context in which others develop. As anyone who hasfetched a child’s thrown toy a dozen times can attest, children aren’t just hanging outand growing up—they actively shape their environments. At the other end of the lifespan, our grandparents aren’t just biding time in their rocking chairs. Rather, throughthe stories they tell, the examples they enact, and the things they create, they activelytransmit the cultures of which they have been a part.
In William Shakespeare’s As You Like It, the melancholy Jacques famously says, “Allthe world’s a stage / And all the men and women merely players; / They have theirexits and their entrances, / And one man in his time plays many parts / His acts beingseven ages.” Developmental psychologists might disagree about the stages of humandevelopment, but all agree that a person “plays many parts” across the lifespan. Thischapter will help you understand the parts you have played, the parts you are playing,and the parts you will play as you move through life.
PRENATAL DEVELOPMENT
The story of how we grow and change across the life span is one of the most interestingin all of psychology. But as with any story, we must begin at the beginning, with aconsideration of how genetic and environmental factors interact to shape us before weare even born.
From Conception to BirthThe voyage toward becoming a human being begins at conception, when a sperm and eggcell unite to form the fertilized egg or zygote (Figure 14.1). Within hours of this union ofsperm and egg, the nuclei of the two cells merge, creating a novel combination of23 pairs of chromosomes, half from the mother and half from the father. The zygote beginsa process of dividing and redividing, producing a blastocyst, a mass of identical cells.
About 10 to 14 days after fertilization, the blastocyst attaches itself to the wall of theuterus. Then, the embryonic stage begins (Figure 14.2). During this phase, criticalgenes turn on and produce chemical signals that induce a process of differentiationamong the proliferating cells. The mass of cells (now called an embryo) soon has threedistinct cell types—those that will become the nervous system and the outer skin; thosethat will form the skeletal system and voluntary muscles; and those that will form thegut and digestive organs.
14.1 Egg and sperm cells The voyagetoward becoming human begins at concep-tion, with the union of the egg and sperm.
zygote The fertilized egg, formed bythe union of sperm and egg.
embryonic stage The third througheighth week of prenatal development.
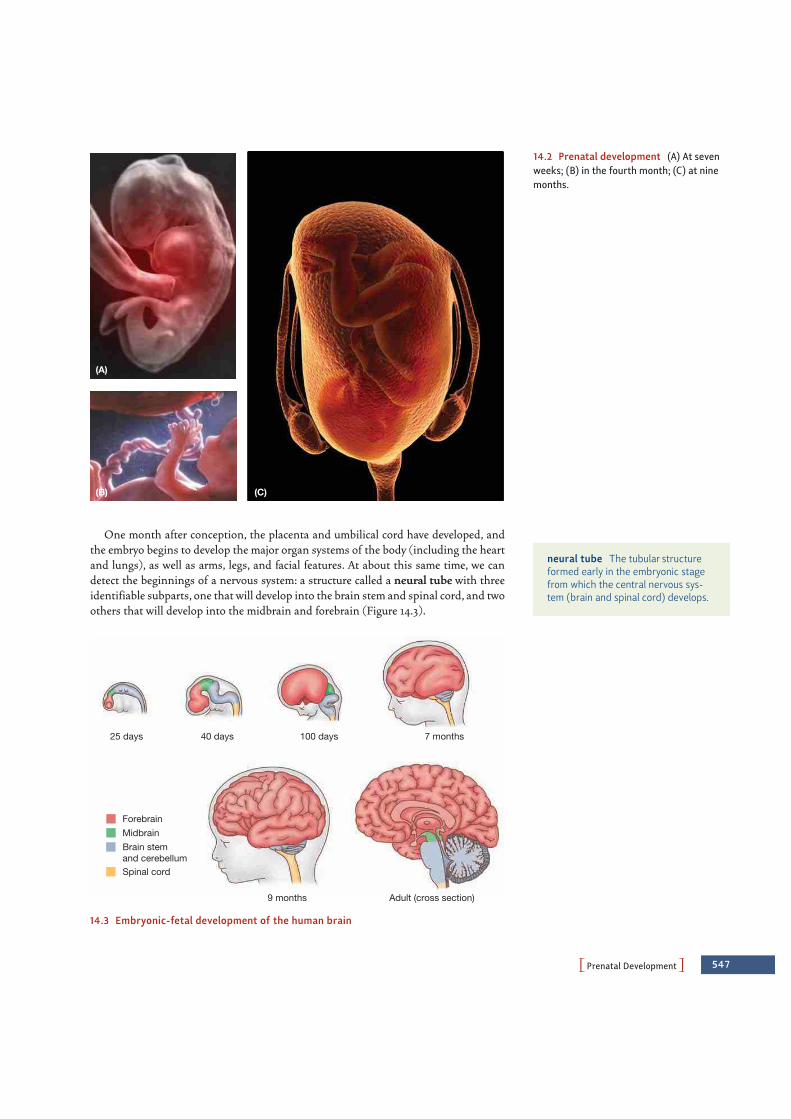
PPrenatal DevelopmentO 547
One month after conception, the placenta and umbilical cord have developed, andthe embryo begins to develop the major organ systems of the body (including the heartand lungs), as well as arms, legs, and facial features. At about this same time, we candetect the beginnings of a nervous system: a structure called a neural tube with threeidentifiable subparts, one that will develop into the brain stem and spinal cord, and twoothers that will develop into the midbrain and forebrain (Figure 14.3).
(A)
(B) (C)
14.2 Prenatal development (A) At sevenweeks; (B) in the fourth month; (C) at ninemonths.
neural tube The tubular structureformed early in the embryonic stagefrom which the central nervous sys-tem (brain and spinal cord) develops.
ForebrainMidbrainBrain stemand cerebellumSpinal cord
25 days 100 days 7 months
9 months Adult (cross section)
40 days
14.3 Embryonic-fetal development of the human brain

548 chapter 14 PDEVELOPMENTO
Two months after conception, the fetal stage begins. By this point, the mass of cells(now called a fetus) has grown to 1 inch in length and the heart has begun to beat. Thenervous system continues to grow at a remarkable pace. New nerve cells are generated ata rate that can approach 250,000 new cells per minute (Kolb & Whishaw, 2009;Mueller, 1996), and these cells start to form themselves into a network. Several mecha-nisms contribute to this networking, including specific genes that produce chemical sig-nals that serve as “beacons,” attracting connections that sprout from other nerve cells.
Even at this early stage, the fetus is capable of simple behaviors, and so will show asucking reflex if its lips are touched. It’s not long before other—more sophisticated—capacities come into view, including the capacity for learning. For example, in one now-classic study, DeCasper and Spence (1986) asked pregnant mothers to read aloud totheir unborn infants twice a day for the last 6 weeks of their pregnancy from one of twoDr. Seuss books. Once the children were born, researchers set up an apparatus that wascontrolled by the way the newborns sucked on a special pacifier; if they sucked in oneway, the apparatus played the story their mothers had read before they were born; ifthey sucked in another way, the apparatus played an unfamiliar story. The researchersfound that infants adjusted their sucking pattern so that they could listen to the storyto which they had been exposed in utero, indicating that the infants had “learned” onestory and preferred it to the story they did not know.
The Prenatal EnvironmentA great deal of prenatal development is powerfully guided by the genome.Environmental factors are just as important, however, as we have seen in the capacityof the fetus to learn from its experiences. But what in general does “environment” meanin this early stage of development?
Consider the earliest stages of embryonic growth. Some of the cells in the embryowill eventually become the brain; others will become the gall bladder or the bones of thefoot. But every cell in the embryo has the same genes, and so presumably all receive thesame genetic instructions. How does each cell manage to develop appropriately?
The answer seems to be that the fate of each cell is determined in part by its cellularneighbors—the cells that form its physical environment. Evidence comes from studiesof salamander embryos. Early in their development, salamanders have an outer layer oftissue that gradually differentiates, and cells in this layer will become teeth only if theymake contact with certain other cells in the embryo’s mouth region. Without this contact, cells in this layer become skin.
In humans, the cells that will become the brain initially show no distinction betweenneurons and glia. As the cells reproduce and differentiate, though, these two types becomedistinct, and the newly created neurons actually migrate toward their appropriate posi-tions. This migration process is guided by glia that act as guidewires. Various chemicalsalso guide the process by attracting some types of nerve cells and repelling other types(Hatten, 2002). In all cases, the migrating neurons approach the surface of the develop-ing cortex, but the first-arriving neurons stop short of the surface. Later-arriving neuronspass these now-stationary cells, and these late arrivals in turn are passed by even laterarrivals. As a result, the cortex literally develops from the inside out, with layers closer tothe surface established later than deeper layers.
Of course, it’s not enough that the nerve cells end up in the right places; they alsoneed to end up connected in the right way, so that each nerve cell sends its messages tothe right target. How does each developing nerve cell come to know its eventual target?The answer, of course, begins with the genes. Early in development, genetic specifica-
fetal stage The prenatal period fromthe ninth week until birth.

PPrenatal DevelopmentO 549
tions lead neurons to form protomaps, providing a rough “wiring diagram” for thebrain’s circuits. The areas mapped in this way seem to attract connections from theappropriate inputs, so that, for example, the protomap in the projection area for visionattracts afferent fibers from the thalamus, with the result that the visual cortex comesto receive the right input signals (e.g., Rakic, 1995; for some complexities, though, seeSur & Rubenstein, 2005).
Inevitably, there are some wiring errors, but there is a safeguard in place to deal withthese. Many more neurons are created than are needed, and each neuron tries to formfar more connections than are required. If a neuron’s connections prove either wrongor redundant, that neuron can withdraw its connections and find better targets, or itcan be given a message to die (Kuan, Roth, Flavell, & Rakic, 2000; Rubenstein & Rakic,1999). In fact, it is normal for between 20 and 80% of neurons to die as the braindevelops, depending upon the region of the brain. This decimation primarily occursearly in development—in humans, about 4 to 6 months after conception (Rosenzweig,Leiman, & Breedlove, 1996)—but according to some investigators, it continues at aslower rate for much longer, perhaps even a decade.
So far, we have focused on how the local environment surrounding each neuronguides its differentiation and migration. More global features of the environment alsoplay a major role, namely, the organism’s own bodily fluids, especially its blood. Thus,for example, hormones circulating in the fetus’s blood have a powerful influence on thedevelopment of the child’s external anatomy, the development of the nervous system,and even later sex-typical play (Auyeung et al., 2009). Moreover, the bloodstream ofmammalian embryos is intimately connected to the mother’s blood supply, and so herblood, too, becomes part of the embryo’s environment.
The maternal blood supplies oxygen and nutrition to the developing fetus, and thisis one of the reasons why normal development depends on the nutritional state of themother. But the mother’s blood supply also plays another role—it provides a conduitthrough which factors in the external environment can influence the fetus.Unfortunately, many of these external factors are teratogens—factors that can disruptdevelopment. The long list of teratogens includes environmental toxins such as leadand mercury, as well as alcohol, cigarette smoke, X-rays, and diseases such as rubella(German measles). Teratogens can have a number of negative effects, depending on thetype, timing, and amount of exposure. For example, when a pregnant woman drinksalcohol, the alcohol enters both her bloodstream and that of her fetus. Even light drink-ing can affect the brain of the developing fetus (Ikonomidou et al., 2000), and heavydrinking can lead to fetal alcohol syndrome, which is characterized by both psycholog-ical problems (learning disorders and behavior difficulties) and physical abnormalities(smaller stature and a characteristic pattern of facial abnormalities; Figure 14.4).
teratogens Environmental factorsthat can disrupt healthy neural devel-opment. These include lead, alcohol,and cigarette smoke.
fetal alcohol syndrome A develop-mental disorder that affects childrenwhose mothers consumed alcohol dur-ing pregnancy. Its effects include arange of psychological problems andphysical abnormalities.
(A) (B)
14.4 Fetal alcohol syndrome (A) Twochildren with fetal alcohol syndrome.(B) Clear differences are evident betweenthe brain of a normally developing child(left) and one with an extreme case of fetalalcohol syndrome (right).

550 chapter 14 PDEVELOPMENTO
INFANCY AND CHILDHO OD
Nine months after conception, the human fetus is ready to leave the uterus to enter theouter world. Ready, however, is a relative term. Most other animals can walk shortly afterbirth, and many can take care of themselves almost immediately. Humans, in contrast, areextraordinarily helpless at birth and remain utterly dependent on others for many years.
Why is human development so slow? Lions (as just one example) chase their male cubsaway from the pride by age 2 or 3. Human parents, in contrast, care for their offspring forthe better part of 2 decades (or more!). One might think that this would be a great disad-vantage for our species. It turns out, though, that this long period of dependency is ideal fora creature whose major specialization is its capacity for learning and whose basic inventionis culture—the ways of coping with the world that each generation hands on to the next.Human infants, in other words, have a huge capacity for learning and a great deal to learn.Under these circumstances, there is much to be gained by two decades or so of living athome—even if this arrangement is at times inconvenient for child and parent alike.
In the following sections, we will consider three major aspects of development,including the infant’s sensorimotor development, her cognitive development, and hersocioemotional development. We should be clear at the outset that the distinctionsamong these aspects of development are, to some extent, just a convenience forresearchers (and textbook writers), because the various aspects of development plainlyinteract with each other. The child’s intellectual development, for example, is shaped bywhat she perceives and how she interacts with the world. Similarly, the child’ssocioemotional development depends on her cognitive development, and vice-versa.
A similar point must be made regarding the interplay of genetic and environmentalfactors. These, too, constantly interact to codetermine a child’s developmentaltrajectory. For example, we mentioned in Chapters 2 and 11 that genetic factors are cru-cial for shaping a child’s intellectual functioning, but as we discussed in those chapters,the environment also plays a huge role. Some environmental factors are biochemical(nutrients, toxins), and one tragic reminder of this comes from studies of mental retar-dation. For years, many types of paint contained lead-based pigments, and as the paintdeteriorated, leaded dust would fall into the environment where it could be ingested orinhaled by children. Once inside the body, the lead interfered with the development ofthe nervous system, at large doses causing coma or even death, or at lower dosesproducing a litany of intellectual problems that often led to a diagnosis of mentalretardation. This is why lead paint was banned for use in U.S. residences in 1978; othercountries have similar (and older) bans in place.
Environmental influences also have other—and more positive—effects on thedeveloping nervous system. Stimulus information—including objects to explore ormanipulate, other organisms to interact with, and so on—seems by itself a spur to neuralgrowth. In addition, the specifics of the stimulation help to refine the nervous system’sfunctioning—so that the visual system, for example, becomes especially sensitive to thespecific shapes in the infant’s environment; circuits involved in language use are likewiseadjusted so that the neural apparatus for understanding and producing language is pre-cisely tuned to the language being spoken in the child’s surroundings (Chapter 10).
Physical and Sensorimotor Development in Infancy and ChildhoodThe immaturity of the human infant is apparent if we examine the brain itself. Figure14.5 shows sections of the human cortex in a newborn, a 3-month-old, and a 15-month-old child (Conel, 1939, 1947, 1955). Notice that the number of neural interconnections
(A) (B) (C)
14.5 Growth of neural interconnectionsSections of the human cortex in (A) a new-born, (B) a 3-month-old, and (C) a 15-month-old.

PInfancy and ChildhoodO 551
grows tremendously during this period. Indeed, by one estimate, new neural connec-tions are formed in the infant’s brain, and old ones removed, at an astonishing rate of100,000 per second (Rakic, 1995).
This growth in brain size and complexity, and, indeed, growth in all aspects of thechild’s body, continues for many years, coming in spurts that each last a few months.This pattern is obvious for growth of the body (Hermanussen, 1998) but is also true forthe child’s brain, with the spurts typically beginning around ages 2, 6, 10, and 14 (H. T.Epstein, 1978). Each of these spurts leaves the brain up to 10% heavier than it waswhen the spurt began (Kolb & Whishaw, 2009).
Even at birth, the infant’s immature brain is ready to support many activities. For exam-ple, infants’ senses function quite well from the start. Infants can discriminate betweentones of different pitch and loudness, and they show an early preference for their mother’svoice over that of a strange female (Aslin, 1987; DeCasper & Fifer, 1980). Newborns’ visionis not yet fully developed. Though quite near-sighted, newborns can see objects a foot or soaway (the distance to a nursing mother’s face) and readily discriminate brightness andcolor, and they can track a moving stimulus with their eyes (Aslin, 1987; Bornstein, 1985).
In contrast to newborns’ relatively advanced sensory capacities, infants initially havelittle ability to control their body movements. They thrash around awkwardly and can-not hold up their heads. But they do have a number of important reflexes (Figure 14.6),including the grasp reflex—when an object touches an infant’s palm, she closes her fisttightly around it. If the object is lifted up, the infant hangs on and is lifted along withit, supporting her whole weight for a minute or more.
Other infantile reflexes pertain to feeding. For example, the rooting reflex refers tothe fact that when a baby’s cheek is lightly touched, the baby’s head turns toward thesource of stimulation, his mouth opens, and his head continues to turn until the stim-ulus (usually a finger or nipple) is in his mouth. A related reflex, called the suckingreflex, then takes over and leads the child to suck automatically on whatever is placedin his mouth.
By her first birthday, the child will have gained vastly better control over her ownactions, and this increase in skill continues over the next decade. These skills emerge inan orderly progression, as shown in Figure 14.7 (see p. 552). Infants first learn to rollover (typically by 3 months), then to sit (usually by 6 months), then to creep and thento walk (usually by 12 months). However, the ages associated with these variousachievements must be understood as rough approximations, because there is variationfrom one infant to another and from one culture to another. For example, the Kipsigisof Kenya begin training their infants to stand and walk early on (Super, 1976), whereasthe Ache of Paraguay carry their children nearly everywhere, leading to delayed onset ofwalking (Kaplan & Dove, 1987).
(A) (B) (C)
14.6 Infant reflexes Infants have a num-ber of important reflexes, including (A) thegrasp reflex, (B) the rooting reflex, and(C) the sucking reflex.
grasp reflex An infantile reflex inwhich an infant closes her hand into afist when her palm is touched.
rooting reflex In an infant, the suck-ing elicited by stroking applied on oraround the lips; the reflex aids breast-feeding.
sucking reflex An infantile reflex inwhich an infant sucks on whatever isplaced in his mouth.
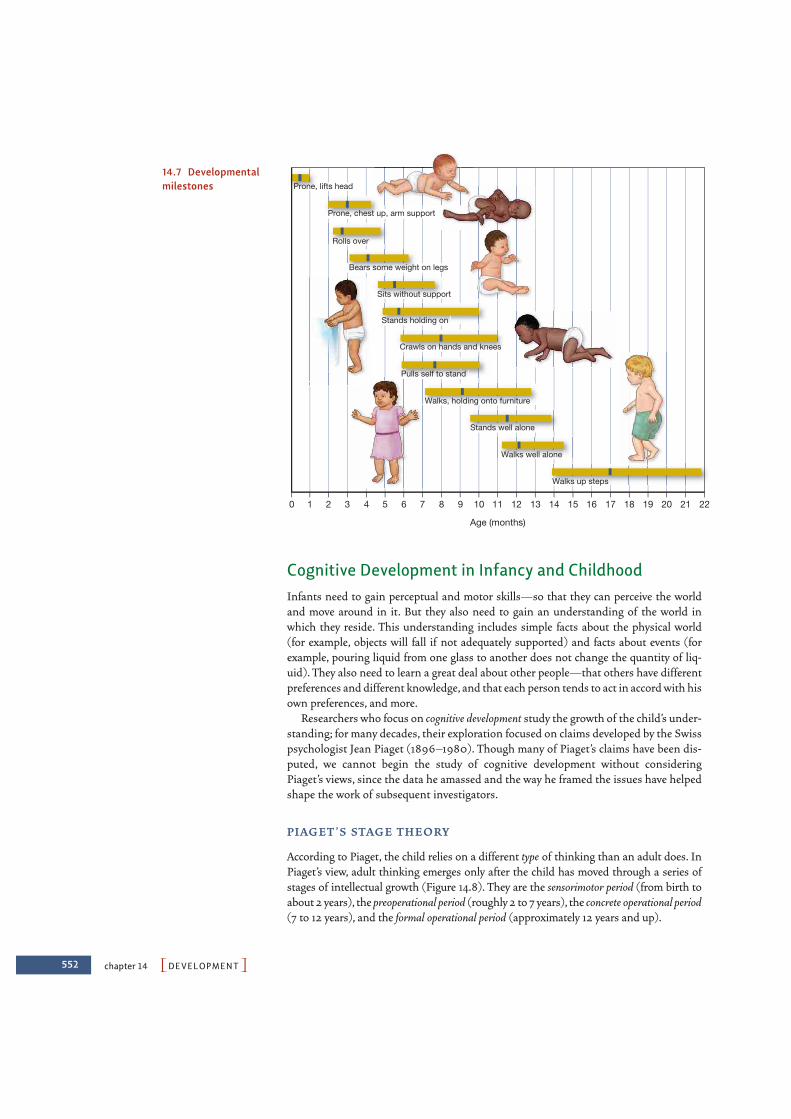
552 chapter 14 PDEVELOPMENTO
Cognitive Development in Infancy and ChildhoodInfants need to gain perceptual and motor skills—so that they can perceive the worldand move around in it. But they also need to gain an understanding of the world inwhich they reside. This understanding includes simple facts about the physical world(for example, objects will fall if not adequately supported) and facts about events (forexample, pouring liquid from one glass to another does not change the quantity of liq-uid). They also need to learn a great deal about other people—that others have differentpreferences and different knowledge, and that each person tends to act in accord with hisown preferences, and more.
Researchers who focus on cognitive development study the growth of the child’s under-standing; for many decades, their exploration focused on claims developed by the Swisspsychologist Jean Piaget (1896–1980). Though many of Piaget’s claims have been dis-puted, we cannot begin the study of cognitive development without consideringPiaget’s views, since the data he amassed and the way he framed the issues have helpedshape the work of subsequent investigators.
P I AG E T ’S STAG E T H E O RY
According to Piaget, the child relies on a different type of thinking than an adult does. InPiaget’s view, adult thinking emerges only after the child has moved through a series ofstages of intellectual growth (Figure 14.8). They are the sensorimotor period (from birth toabout 2 years), the preoperational period (roughly 2 to 7 years), the concrete operational period(7 to 12 years), and the formal operational period (approximately 12 years and up).
0
Prone, lifts head
Prone, chest up, arm support
Rolls over
Bears some weight on legs
Sits without support
Stands holding on
Crawls on hands and knees
Pulls self to stand
Walks, holding onto furniture
Stands well alone
Walks well alone
Walks up steps
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Age (months)
14.7 Developmentalmilestones
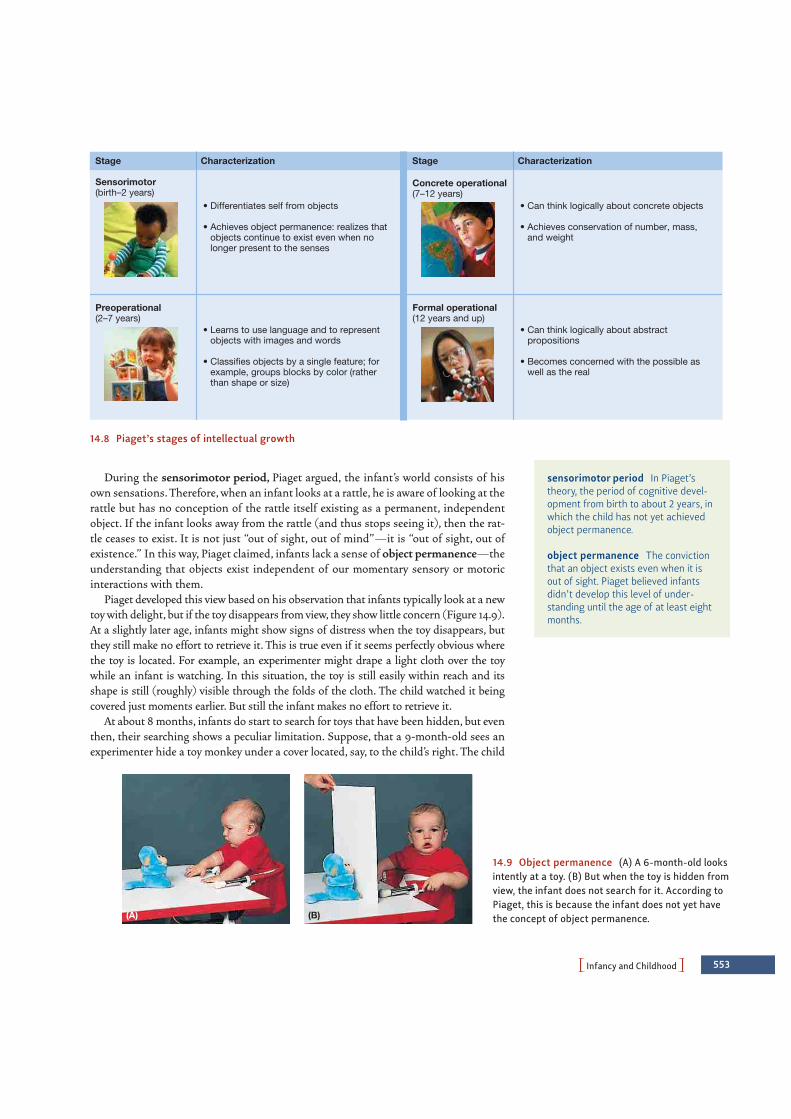
PInfancy and ChildhoodO 553
During the sensorimotor period, Piaget argued, the infant’s world consists of hisown sensations. Therefore, when an infant looks at a rattle, he is aware of looking at therattle but has no conception of the rattle itself existing as a permanent, independentobject. If the infant looks away from the rattle (and thus stops seeing it), then the rat-tle ceases to exist. It is not just “out of sight, out of mind”—it is “out of sight, out ofexistence.” In this way, Piaget claimed, infants lack a sense of object permanence—theunderstanding that objects exist independent of our momentary sensory or motoricinteractions with them.
Piaget developed this view based on his observation that infants typically look at a newtoy with delight, but if the toy disappears from view, they show little concern (Figure 14.9).At a slightly later age, infants might show signs of distress when the toy disappears, butthey still make no effort to retrieve it. This is true even if it seems perfectly obvious wherethe toy is located. For example, an experimenter might drape a light cloth over the toywhile an infant is watching. In this situation, the toy is still easily within reach and itsshape is still (roughly) visible through the folds of the cloth. The child watched it beingcovered just moments earlier. But still the infant makes no effort to retrieve it.
At about 8 months, infants do start to search for toys that have been hidden, but eventhen, their searching shows a peculiar limitation. Suppose, that a 9-month-old sees anexperimenter hide a toy monkey under a cover located, say, to the child’s right. The child
Stage Characterization
Sensorimotor(birth–2 years)
• Differentiates self from objects
• Achieves object permanence: realizes thatobjects continue to exist even when nolonger present to the senses
Preoperational(2–7 years)
• Learns to use language and to representobjects with images and words
• Classifies objects by a single feature; forexample, groups blocks by color (rather
than shape or size)
Concrete operational(7–12 years)
• Can think logically about concrete objects
• Achieves conservation of number, mass,and weight
Stage Characterization
Formal operational(12 years and up)
• Can think logically about abstractpropositions
• Becomes concerned with the possible as well as the real
14.8 Piaget’s stages of intellectual growth
sensorimotor period In Piaget’stheory, the period of cognitive devel-opment from birth to about 2 years, inwhich the child has not yet achievedobject permanence.
object permanence The convictionthat an object exists even when it isout of sight. Piaget believed infantsdidn’t develop this level of under-standing until the age of at least eightmonths.
(A) (B)
14.9 Object permanence (A) A 6-month-old looksintently at a toy. (B) But when the toy is hidden fromview, the infant does not search for it. According toPiaget, this is because the infant does not yet havethe concept of object permanence.

554 chapter 14 PDEVELOPMENTO
will happily push the cover off and snatch up the monkey. The experimenter now repeatsthe process a few times, always hiding the monkey under the same cover to the child’sright. Again and again the child pulls the cover off and retrieves the monkey. But now theexperimenter changes the procedure slightly. Very slowly and in full view of the child, shehides the toy in a different place, say, under a cover to the child’s left. The child closely watches her every movement—and then does exactly what he did before. Hesearches under the cover on the right, even though he saw the experimenter hide the toyin another place just a moment earlier.
This phenomenon is often called the A-not-B effect, where A designates the place wherethe object was first hidden and B the place where it was hidden last (Figure 14.10). Whydoes this peculiar error occur? Piaget (1952) argued that the 9-month-old still has notgrasped the fact that an object’s existence is independent of his own actions. Thus, the childbelieves that his reaching toward place A (where he found the toy previously) is as much apart of the monkey as the monkey’s tail is. In effect, then, the child is not really searchingfor a monkey; he is searching for the-monkey-that-I-find-on-the-right. No wonder, there-fore, that the child continues searching in the same place (Flavell, 1985; P. L. Harris, 1987).
According to Piaget, a major accomplishment of the sensorimotor period is comingto understand that objects exist on their own—even when they are not reached for,seen, heard, or felt. Piaget held that what makes this accomplishment possible is theinfant’s increasingly sophisticated schemas—ways of interacting with the world and (ata later stage of development) ways of interacting with ideas about the world.
Piaget believed that newborns start life with very few schemas, and these tend to involvethe infant’s built-in reactions,such as sucking or grasping.In Piaget’s view,these action pat-terns provide the infant’s only means of responding to the world, and thus they provide thefirst mental categories through which infants organize their world. Infants understand theworld, in other words, as consisting of the suckables, the graspables, and so on.
Across the first few months of life, though, the child refines and extends theseschemas and learns how to integrate them into more complex ways of dealing with theworld. This evolution, according to Piaget, depends on two processes that he claimedwere responsible for all cognitive development: assimilation and accommodation. Inthe process of assimilation, children use the mental schemas they have already formedto interpret (and act on) the environment; in other words, they assimilate objects in theenvironment into their existing schemas. In the process of accommodation, the child’sschemas change as a result of his experiences interacting with the world; that is, theschemas accommodate to the environment (Figure 14.11).
(A) (B) (C)
14.10 The A-not-B effect (A) A 7-month-old looks at a toy that has just been placed in B,one of the two wells. (B) He continues to look at well B after both wells are covered. (C)When finally allowed to reach for the toy, he uncovers well A, in which he found the toy on aprevious trial, rather than well B, in which he saw the toy being placed. In this particularsequence, he still looks at B while uncovering A, suggesting a dissociation between what theinfant knows and what he does.
A-not-B effect The tendency ofinfants to reach for a hidden objectwhere it was previously hidden(place A), rather than where it washidden most recently while the childwatched (place B).
assimilation In Piaget’s theory, thedeveloping child’s process of interpret-ing the environment in terms of theschemas he already has.
accommodation In Piaget’s theory,the developing child’s process ofchanging his schemas based on hisinteractions with the environment.
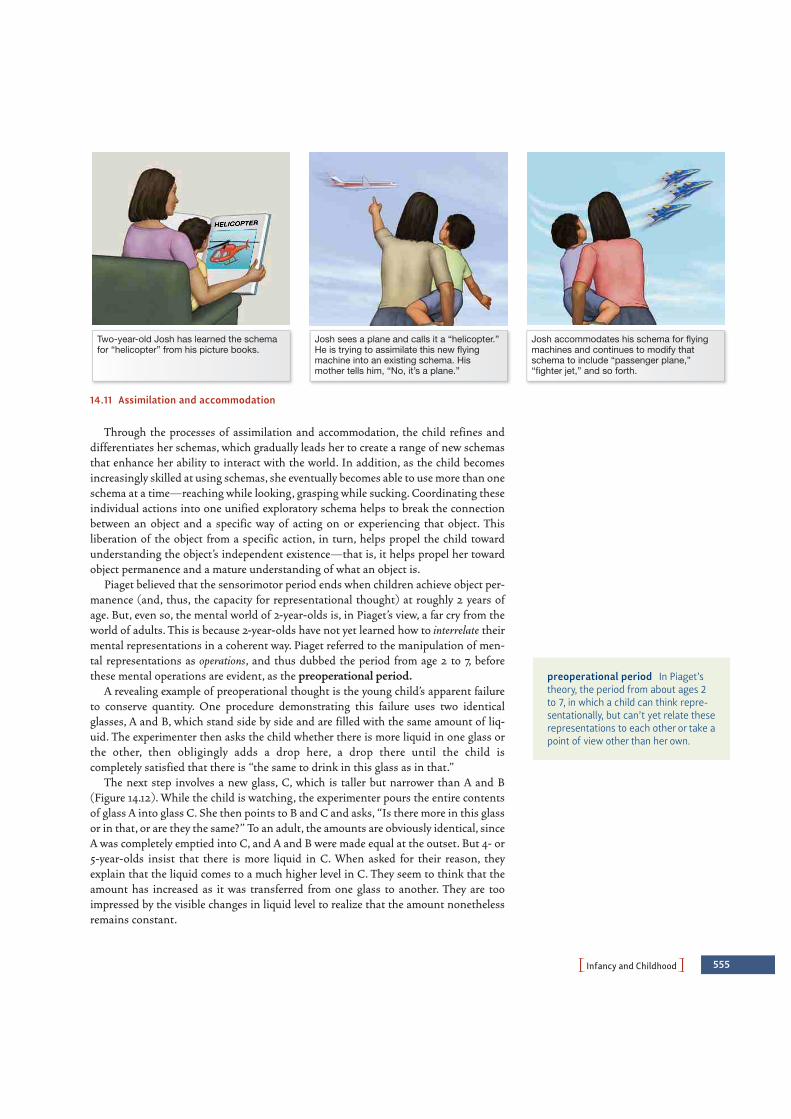
PInfancy and ChildhoodO 555
Through the processes of assimilation and accommodation, the child refines anddifferentiates her schemas, which gradually leads her to create a range of new schemasthat enhance her ability to interact with the world. In addition, as the child becomesincreasingly skilled at using schemas, she eventually becomes able to use more than oneschema at a time—reaching while looking, grasping while sucking. Coordinating theseindividual actions into one unified exploratory schema helps to break the connectionbetween an object and a specific way of acting on or experiencing that object. Thisliberation of the object from a specific action, in turn, helps propel the child towardunderstanding the object’s independent existence—that is, it helps propel her towardobject permanence and a mature understanding of what an object is.
Piaget believed that the sensorimotor period ends when children achieve object per-manence (and, thus, the capacity for representational thought) at roughly 2 years ofage. But, even so, the mental world of 2-year-olds is, in Piaget’s view, a far cry from theworld of adults. This is because 2-year-olds have not yet learned how to interrelate theirmental representations in a coherent way. Piaget referred to the manipulation of men-tal representations as operations, and thus dubbed the period from age 2 to 7, beforethese mental operations are evident, as the preoperational period.
A revealing example of preoperational thought is the young child’s apparent failureto conserve quantity. One procedure demonstrating this failure uses two identicalglasses, A and B, which stand side by side and are filled with the same amount of liq-uid. The experimenter then asks the child whether there is more liquid in one glass orthe other, then obligingly adds a drop here, a drop there until the child is completely satisfied that there is “the same to drink in this glass as in that.”
The next step involves a new glass, C, which is taller but narrower than A and B (Figure 14.12). While the child is watching, the experimenter pours the entire contentsof glass A into glass C. She then points to B and C and asks, “Is there more in this glassor in that, or are they the same?” To an adult, the amounts are obviously identical, sinceA was completely emptied into C, and A and B were made equal at the outset. But 4- or5-year-olds insist that there is more liquid in C. When asked for their reason, theyexplain that the liquid comes to a much higher level in C. They seem to think that theamount has increased as it was transferred from one glass to another. They are tooimpressed by the visible changes in liquid level to realize that the amount nonethelessremains constant.
Two-year-old Josh has learned the schemafor “helicopter” from his picture books.
Josh sees a plane and calls it a “helicopter.”He is trying to assimilate this new flyingmachine into an existing schema. Hismother tells him, “No, it’s a plane.”
Josh accommodates his schema for flyingmachines and continues to modify thatschema to include “passenger plane,”“fighter jet,” and so forth.
14.11 Assimilation and accommodation
preoperational period In Piaget’stheory, the period from about ages 2to 7, in which a child can think repre-sentationally, but can’t yet relate theserepresentations to each other or take apoint of view other than her own.

556 chapter 14 PDEVELOPMENTO
In the preoperational period, children also fail tests that depend on the conservationof number. In one such test, the experimenter first shows the child two rows of pennies,and the child agrees that both rows contain the same number of coins. The experimenterthen rearranges one row by spacing the pennies farther apart. Prior to age 5 or 6, chil-dren generally assert that there are now more coins in this row because “they’re morespread out.” But from about age 6 on, the child has no doubt that there are just as manycoins in the tightly spaced row as there are in the spread-out line.
Why do preschool children fail to conserve? According to Piaget, part of the problemis their inability to interrelate the different dimensions of a situation. To conserve liquid quantity, for example, the children must first comprehend that there are two relevant factors: the height of the liquid column, and the width of the glass. They mustthen appreciate that a decrease in the column’s height is accompanied by an increase in its width. Thus, the children must be able to attend to both dimensions simultaneously and relate the dimensions to each other. They lack this capacity, since itrequires using a higher-order schema to combine initially discrete aspects of a percep-tual experience into one conceptual unit.
By age 7 or so, once children have learned how to interrelate their mental represen-tations, they enter the concrete operational period. They now grasp the fact thatchanges in one aspect of a situation can be compensated for by changes in some otheraspect. They are also able to transform their own mental representations in a variety ofways and thus understand, for example, what would happen if the liquid were pouredback into its original glass. But according to Piaget, children’s intellectual capacities arestill limited in an important way: They can apply their mental operations only to con-crete objects or events (hence the term concrete operations). It is not until age 11 or 12that formal operations are possible, and we will consider this stage in the following sec-tion on adolescence.
B E Y O N D P I AG E T
Piaget’s theories have shaped the ways in which psychologists, educators, and evenparents conceptualize children’s intellectual growth. The striking phenomena Piagetdiscovered seem to provide key insights into children’s intellectual capacities andlimitations. At the same time, though, Piaget’s claims have not gone unchallenged. Inparticular, recent evidence has shown that Piaget underestimated the intellectualcapacities of infants. Their minds, it turns out, are not a mere jumble of sensoryimpressions and motor reactions. Instead, infants seem to have rudimentary con-
concrete operational period InPiaget’s theory, the period from aboutage 7 to about 12, in which the child isbeginning to understand abstractideas such as number and substance,but only as they apply to real, concreteevents.
This child understands that twoshort glasses (A and B) contain thesame amount of water.
She pours the water from one of theshort glasses (A) into a tall glass (C).
When asked which glass has morewater, she points to glass C, eventhough she poured the water fromthe equivalent shorter glass A.
A
A
ABB B
C C
14.12 Piaget’s conservation task
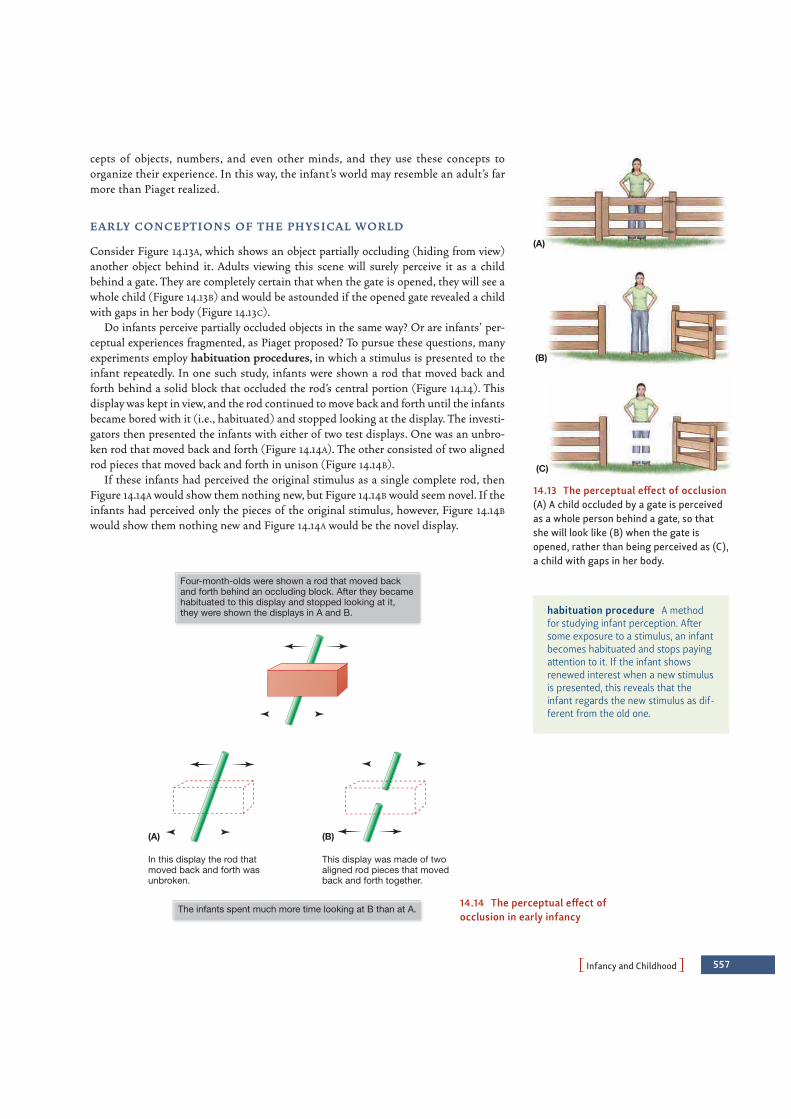
PInfancy and ChildhoodO 557
cepts of objects, numbers, and even other minds, and they use these concepts toorganize their experience. In this way, the infant’s world may resemble an adult’s farmore than Piaget realized.
E A R LY CO N C E P T I O N S O F T H E P H YS I CA L W O R L D
Consider Figure 14.13A, which shows an object partially occluding (hiding from view)another object behind it. Adults viewing this scene will surely perceive it as a childbehind a gate. They are completely certain that when the gate is opened, they will see awhole child (Figure 14.13B) and would be astounded if the opened gate revealed a childwith gaps in her body (Figure 14.13C).
Do infants perceive partially occluded objects in the same way? Or are infants’ per-ceptual experiences fragmented, as Piaget proposed? To pursue these questions, manyexperiments employ habituation procedures, in which a stimulus is presented to theinfant repeatedly. In one such study, infants were shown a rod that moved back andforth behind a solid block that occluded the rod’s central portion (Figure 14.14). Thisdisplay was kept in view, and the rod continued to move back and forth until the infantsbecame bored with it (i.e., habituated) and stopped looking at the display. The investi-gators then presented the infants with either of two test displays. One was an unbro-ken rod that moved back and forth (Figure 14.14A). The other consisted of two alignedrod pieces that moved back and forth in unison (Figure 14.14B).
If these infants had perceived the original stimulus as a single complete rod, thenFigure 14.14A would show them nothing new, but Figure 14.14B would seem novel. If theinfants had perceived only the pieces of the original stimulus, however, Figure 14.14B
would show them nothing new and Figure 14.14A would be the novel display.
(A)
(C)
(B)
14.13 The perceptual effect of occlusion(A) A child occluded by a gate is perceivedas a whole person behind a gate, so thatshe will look like (B) when the gate isopened, rather than being perceived as (C),a child with gaps in her body.
Four-month-olds were shown a rod that moved backand forth behind an occluding block. After they becamehabituated to this display and stopped looking at it,they were shown the displays in A and B.
The infants spent much more time looking at B than at A.
In this display the rod thatmoved back and forth wasunbroken.
This display was made of twoaligned rod pieces that movedback and forth together.
(A) (B)
14.14 The perceptual effect ofocclusion in early infancy
habituation procedure A methodfor studying infant perception. Aftersome exposure to a stimulus, an infantbecomes habituated and stops payingattention to it. If the infant showsrenewed interest when a new stimulusis presented, this reveals that theinfant regards the new stimulus as dif-ferent from the old one.

558 chapter 14 PDEVELOPMENTO
Since these infants had already habituated to the original stimulus, a novel stimulusshould attract their attention and hold it longer. Thus, by measuring how long theinfants looked at each test display, we can find out which of these displays the infantsconsidered novel—which reveals how they perceived the original display.
The evidence in this study is clear. The 4-month-old infants spent more time look-ing at the broken rod than at the complete rod. Apparently, they found the broken rodmore novel, which suggests that they had not perceived the original stimulus as broken.Instead, they had perceived the parts of the rod in the original stimulus as connected toeach other, just as an adult would (Kellman & Spelke, 1983; Kellman, Spelke, & Short,1986; also Johnson, 2004).
Researchers have extended this finding in many ways—using habituation proce-dures to ask what kinds of stimuli infants find novel, and therefore learning howinfants perceive the world in the first place. These studies make it clear that Piagetunderestimated the perceptual sophistication of the infant, and that infants do perceive objects as having certain properties (shapes, sizes, positions) independent ofthe infants’ momentary view of the objects. Put simply, Piaget seems to have beenwrong in asserting that infants lack (what he called) object permanence. But how,therefore, can we explain Piaget’s findings, which led him to conclude that infants lackobject permanence? Why does an 8- or 9-month-old consistently fail in retrievingobjects that are out of sight?
Most modern investigators suggest that—contrary to Piaget—infants do under-stand that objects continue to exist even when hidden from view, but they lack a fullunderstanding of how to deal with those objects. To illustrate this, let’s reconsider theA-not-B effect (Figure 14.10). If the infant has just reached toward A several times, thenthe reaching-toward-A response is well primed. To reach toward B, therefore, the infantmust override this newly acquired habit. The infant knows where the toy is, but she isunable to inhibit the momentarily potent reach-toward-A response.
Consistent with this idea, many infants look at B at the same time that they reach forA, as if they know where the object is but cannot tell their arms what they have learnedwith their eyes (Baillargeon & Graber, 1987). Some investigators believe that the ability to override a dominant action depends on the maturation of certain areas in theprefrontal cortex, a region just in front of the motor projection area. Evidence comesfrom studies on monkeys with lesions in this area; they show a pattern very similar tothe A-not-B error shown by human infants (A. Diamond, 1988, 1989; A. Diamond &Goldman-Rakic, 1989; also see Zelazo & Frye, 1998).
N U M B E R A N D M AT H E M AT I CA L R E ASO N I N G
Related points emerge when we scrutinize Piaget’s other claims, such as the idea thatchildren younger than 6 years do not conserve number, and so might say, for example,that a row of four buttons, all spread out, has more buttons in it than a row of fourbunched closely together. This certainly sounds like they have failed to grasp the con-cept of numbers, but experiments have shown that even very young children do havesome numerical ability. In one study, 6-month-olds were shown a series of slides thatdisplayed different sets of objects. The items shown varied from one slide to the next,but each slide contained exactly three objects. One slide, for example, might show acomb, a fork, and a sponge; another might show a bottle, a brush, and a toy drum; andso on. Each slide also differed in the spatial arrangement of the items. They might beset up with two on top and one below, or in a vertical column, or with one above andtwo below.

PInfancy and ChildhoodO 559
With all these variables, would the infants be able to detect the one property that theslides shared—the fact that all contained three items? To find out, the experimentersused the habituation technique. They presented these sets of three until the infantsbecame bored and stopped looking. Then they presented a series of new slides in whichsome of the slides showed two items, while others continued to show three. The infantsspent more time looking at the slides that displayed two items rather than three.Evidently, the infants were able to step back from all the particulars of the various slidesand detect the one property that all the slides had in common. In this regard, at least,the infants appear to have grasped the concept of “threeness” (Starkey, Spelke, &Gelman, 1983, 1990).
Toddlers, too, have more mathematical skill than Piaget realized and, even at thisearly age, grasp some aspects of what counting is all about. Thus, when asked to count,one 2-year-old counted “1, 2, 6,” and another said “1, 13, 19.” But what is important isthat they used these series consistently and realized that each of these number tags hasto be applied to just one object in the set to be counted. They also realized that the tagsmust always be used in the same order and that the last number applied is the numberof items in the set. Thus, the child who counted “1, 13, 19” confidently asserted thatthere were 13 items when she counted a two-item set, and 19 items when she counted athree-item set. This child is obviously not using the adult’s terms but does seem to havemastered some of the key ideas on which counting rests. (For more on the young child’sgrasp of mathematics, see Barth, Kanwisher, & Spelke, 2003; Brannon, 2003; Cordes &Brannon, 2008; Gallistel & Gelman, 2000; Gelman, 2006; Lipton & Spelke, 2006;McCrink & Wynn, 2004; N. S. Newcombe, 2002.)
Once again, though, we need to ask: If preschool children have a basic grasp ofcounting skills, why do they fail Piaget’s tests—for example, his test for conservation ofnumber? In part, the problem may lie in how the children were questioned in Piaget’sstudies. In these procedures, the child is typically questioned twice. First, the two rowsof items are presented in an evenly spaced manner, so that both rows are the samelength. When asked, “Which row has more, or do they both have the same?” the childquickly answers, “The same!” Now the experimenter changes the length of one of therows—perhaps spreading the items out a bit more or pushing them more closelytogether—and asks again, “Which row has more, or do they both have the same?”
Why is the same question being asked again? From the point of view of the child,this may imply that the experimenter did not like his first answer and so, as adults oftendo, is providing him the opportunity to try again. This would obviously suggest to thechild that his first answer must have been wrong, and so he changes it.
Of course, this misinterpretation is possible only because the child is not totally sureof his answer, and so he is easily swayed by what seems to be a hint from the experi-menter. In other words, Piaget was correct in noting the limits of the preschool child’sknowledge: The child’s grasp of numerical concepts is tentative enough so that even aslight miscue can draw him off track. But this does not mean the child has no under-standing of numbers or counting, and, in fact, if we question the child carefully, provideno misleading hints, and simplify the task just a little (by using smaller numbers ofitems), preschool children reliably succeed in the conservation task (Siegal, 1997).
SO C I A L CO G N I T I O N A N D T H E O RY O F M I N D
The social world provides yet another domain in which young children are surpris-ingly competent (Striano & Reid, 2006). For example, infants seem to have someunderstanding of other people’s intentions. Specifically, they understand the world

560 chapter 14 PDEVELOPMENTO
they observe in terms of others’ goals, and not just their movements. In one study,6-month-old infants saw an actor reach for a ball that was sitting just to the right ofa teddy bear. (The left–right position of the toys was reversed for half of the infantstested.) The infant watched this event over and over, until he became bored with it.At that point, the position of the toys was switched, so now the teddy bear was onthe right. Then the infant was shown one of two test events. In one, the actor againreached for the ball (although, given the switch in position, this was the first time theinfant had seen a reach toward the left). In the other condition, the actor againreached for the object on the right (although, given the switch, this was the first timethe infant had seen a reach toward the teddy bear).
If, in the initial observation, the infant was focusing on behavior (“reach right”), thenthe reach-for-ball test event involves a change, and so will be a surprise. If, however, theinfant was focusing on the goal (“reach for ball”), then it is the reach for the teddy bearthat involves a change, and will be a surprise. And, in fact, the latter is what the datashow: Six-month-olds are more surprised by the change in goal than by the change inbehavior (A. L. Woodward, 1998; Figure 14.15). Apparently, and contrary to Piaget, theyunderstand that the object reached for is separate from the reach itself, and they aresophisticated enough in their perceptions that they understand others’ actions in termsof intended goals (see also Brandone & Wellman, 2009; Luo & Baillargeon, 2005;Surian, Caldi, & Sperber, 2007; Woodward, 2009).
This emerging understanding of others’ intentions is important, because it allows theyoung child to make sense of, and in many cases predict, how others will behave.However, understanding intentions is just one aspect of the young child’s developingtheory of mind—the set of beliefs that someone employs whenever she tries to makesense of her own behavior or that of others (Leslie, 1992; D. Premack & Woodruff, 1978;
14.15 SCIENTIFIC METHOD: Can infants understand others’ intentions?
Method1. During training, 6-month-olds watched as an actor reached towarda ball on the right rather than a teddy bear on the left. The sameaction was repeated until the infants habituated to it.
Repetitionor
3. The researchers measured how long the infants looked ateach reach. (Longer looking would show that the infantsperceived the event as new and different from the training.
2. During the test, the toys’ positions were switched. In one condition,the actor again reached for the ball (same goal). In the othercondition, the actor reached for the object in the same right-sideposition (same reach).
Same goal Same reach
ResultsInfants looked longer at a reach toward a bear on the right (a new goal, but the same behavior); they looked only briefly at a reachtoward the ball on the left (same goal, but a new behavior).
CONCLUSION: Infants appear able to understand actions in terms of the actor’s goal.
SOURCE STUDY: A. L. Woodward, 1998
theory of mind The set of interre-lated concepts we use to make senseof our own thoughts, feelings, andbehaviors, as well as those of others.

PInfancy and ChildhoodO 561
H. M. Wellman, 1990). The theory of mind also involves preferences—and the youngchild must come to understand that people vary in their preferences and that people tendto make choices in accord with their preferences. Here, too, we see early competence: Inone study, 18-month-olds watched as experimenters made “yuck” faces after tasting onefood and smiled broadly after tasting another. The experimenters then made a generalrequest to these toddlers for food, and the children responded appropriately—offeringthe food that the experimenter preferred, even if the children themselves preferred theother food (Repacholi & Gopnik, 1997; Rieffe, Terwogt, Koops, Stegge, & Oomen, 2001;for more on the child’s theory of mind, see A. Gopnik & Meltzoff, 1997).
Yet another aspect of the theory of mind involves beliefs. Suppose you tell 3-year-oldSusie that Johnny wants to play with his puppy. You also tell her that Johnny thinks thepuppy is under the piano. If Susie is now asked where Johnny will look, she will sensi-bly say that he will look under the piano (H. M. Wellman & Bartsch, 1988). Like anadult, a 3-year-old understands that a person’s actions depend not just on what he seesand desires, but also on what he believes.
Let’s be careful, though, not to overstate young children’s competence. If asked, forexample, what color an object is, 3-year-olds claim that they can find out just as easilyby touching an object as they can by looking at it (O’Neill, Astington, & Flavell, 1992).Likewise, 4-year-olds will confidently assert that they have always known somethingeven if they first learned it from the experimenter just moments earlier (M. Taylor,Esbensen, & Bennett, 1994).
Another limitation concerns the child’s understanding of false beliefs. According tomany authors, a 3-year-old does not understand that beliefs can be true or false and thatdifferent people can have different beliefs. Evidence comes from studies using false-belief tests (Wimmer & Perner, 1983; also Lang & Perner, 2002). In a typical study ofthis kind, a child and a teddy bear sit in front of two boxes, one red and the other green.The experimenter opens the red box and puts a ball in it. He then opens the green boxand shows the child—and the bear—that this box is empty. The teddy bear is nowtaken out of the room (to play for a while), and the experimenter and the child movethe ball from the red box into the green one. Next comes the crucial step. The teddy bearis brought back into the room, and the child is asked, “Where will the teddy look for theball?” Virtually all 3-year-olds and some 4-year-olds will answer, “In the green box.” Ifyou ask them why, they will answer, “Because that’s where it is.” It would appear, then,that these children do not really understand the nature of belief. They seem to assumethat their beliefs are inevitably shared by others, and likewise, they seem not to under-stand that others might have beliefs that are false (Figure 14.16).
The child watches as theexperimenter makes the teddybear “hide” the ball in the red box.
While the teddy bear is gone, theexperimenter and the child movethe ball to the green box.
When the child is now asked, “Wheredoes the teddy bear think the ball is?”she points to the green box.
(A) (B) (C)
14.16 The false-belief test

562 chapter 14 PDEVELOPMENTO
However, by age 4-1/2 or so, children get the idea that not all knowledge is shared. Ifthey are asked, “Where will the teddy look for the candy?” they will answer, “He’ll lookin the red box because that’s where he thinks the candy is” (H. Wellman & Lagattuta,2000; H. Wellman, Cross, & Watson, 2001). The children now seem to have learnedthat different individuals have different beliefs, and that one’s beliefs depend on accessto the relevant information.
Socioemotional Development in Infancyand ChildhoodSo far, we have considered two major aspects of development—the child’s sensorimo-tor development and her cognitive development. We now turn to a third major aspectof development: the child’s emerging capacity to function as a social and emotional being.
Here, the growth from infancy to early childhood is immense. The newborn is keenlysensitive to (and quite vocal in expressing) her own needs but largely oblivious to theneeds of others. Likewise, the newborn has no clue what it means to be a “friend” orhow to behave differently at a birthday party than when sitting in church. Young chil-dren master these points—and many others—in a few short years.
As we turn to this third major aspect of development, recall that there are closeconnections among the various aspects of development. Thus the child’s ability to func-tion as a social being depends on her cognition and on her emerging theory of mind.Likewise, cognitive development is often spurred by learning from others—and so socialinteractions, which depend on newly developing social skills, can foster intellectualgrowth. With this important idea in mind, we take up the story of a child’s socioemo-tional development.
T H E E A R L I E ST I N T E R ACT I O N S
From the earliest days of life, infants seem predisposed to look at human faces, and evennewborns just a few minutes old look longer at schematic faces than at a scrambled face(Figure 14.17; Fantz, 1963; Goren, Sarty, & Wu, 1975; M. H. Johnson, 1993; but also seeTurati, 2004). Infants also tend to imitate faces. In one study, investigators sat face toface with infants less than 21 days old and made faces at them. The investigators stuckout their tongues at the infants or opened their mouths as wide as possible. Carefulscrutiny of the infants’ faces showed that when the investigators stuck out their tongues,the infants did too. When the investigators’ mouths gaped wide open, so did the babies’(Meltzoff, 2002; Figure 14.18).
As infants attend to—and respond to—the faces they see, they are gaining an under-standing of their social partners. For example, between 3 and 4months of age, infants begin to appreciate some rudimentary factsabout emotional expression and so respond more positively whentheir mother’s facial expression (happy or sad) matches the emotionaltone of the mother’s voice (Kahana-Kalman & Walker-Andrews, 2001;Montague & Walker-Andrews, 2002). Infants also learn early on thattheir caretakers are a source of relief in times of distress. By 6 monthsor so, they start to calm down, apparently anticipating an adult’s aid,as soon as they hear the sound of the adult’s approaching footsteps. Ifthe adult approaches and then does not pick up the distressed child,the infant is likely to protest loudly (Gekoski, Rovee-Collier, & Carulli-Rabinowitz, 1983; Lamb & Malkin, 1986).Face Scrambled Blank
14.17 Rudimentary face recognition innewborns Newborn babies look longer ata pattern showing a schematic face than ata scrambled or a blank pattern.

In these ways, even the very young child begins learning about social interactions—and,in particular, starts to develop expectations for others’ behavior. The opportunity for sociallearning broadens considerably when infants begin to crawl. This is because they soon endup in inappropriate or even dangerous situations: The infant wants to crawl toward thesteep staircase, or the mud puddle, or the broken glass, and the caretaker needs to thwartthese desires. Conflict is inevitable in these situations so it’s no wonder that parental pro-hibitions, including use of the word no, become much more common when the child beginsto move about (Zumbahlen & Crawley, 1997).
Locomotion also allows the infant to wander into strange or ambiguous situations, andthis is why infants at this age begin to rely on social partners for guidance about how theyshould respond to unfamiliar events (Campos et al., 2000). Specifically, infants engage insocial referencing—relying on the facial expression of their caregiver or some other adultas a source of information (Carver & Vaccaro, 2007). Is the cat dangerous? If Mom is look-ing at the cat and seems happy and unconcerned, then the infant relaxes. If Mom is look-ing at the cat and seems anxious, then the infant grows wary (Figure 14.19; Rosen,Adamson, & Bakeman, 1992; Striano & Rochat, 2000).
AT TAC H M E N T
As children start learning about the social world—developing expectations for how otherswill behave and learning to “read” the signals that others provide—they are also forming their first social relationship, with their primary caregiver, usually the mother. Thisis evident in the fact that,when they are between 6 and 8 months old, infants begin to showa pattern known as separation anxiety, in which they become visibly (and sometimes loudly)upset when their caregiver leaves the room. This is a powerful indication that the infant hasformed an attachment to the caregiver—a strong, enduring, emotional bond.
This bond seems to grow out of the psychological comfort the mother provides theinfant. Evidence for this claim comes from many sources, including a series of classicstudies by Harry Harlow (1905–1981). Harlow (e.g., 1958) raised rhesus monkeys with-out their mothers; each rhesus infant lived alone in a cage that contained two station-ary figures, one built of wire and the other of soft terry cloth. The wire figure wasequipped with a nipple that yielded milk, but the terry-cloth model had none. Whichfigure would the monkey infants prefer—the one that provided nutrition, or the onethat provided (what Harlow called) “contact comfort”? In fact, the infants spent much
PInfancy and ChildhoodO 563
14.18 Imitation in neonates In a remarkable study,investigators sat face-to-face with infants just a few daysold. When the investigators stuck out their tongues, theinfants did the same. When the investigators openedtheir mouths wide, or pursed their lips, the infants didtoo. The capacity for imitation, it seems, is in place evenfor very young babies!
14.19 Social referencing At an early age,children begin to rely on their social part-ners for guidance about how they shouldrespond to unfamiliar events. They do thisby examining an adult’s facial expression,and they use the expression as a signal forwhether a situation is dangerous or not.
social referencing A process ofusing others’ facial expressions as acue about the situation.
attachment The strong, enduring,emotional bond between a child andits caregivers that some psychologistsconsider the basis for relationshipslater in life.

564 chapter 14 PDEVELOPMENTO
more time on the terry-cloth “mother” than on the wire figure—especially when theywere frightened. When approached by a clanking mechanical toy, they invariablyrushed to the terry-cloth mother and clung tightly (Figure 14.20).
Is comfort (and not nutrition) also the key for human attachment? British psychia-trist John Bowlby argued forcefully that it is. In Bowlby’s view, children becomeattached to a caregiver because this adult provides a secure base for the child, a rela-tionship (and, for the young infant, a place) in which the child feels safe and protected(Figure 14.21). The child uses the secure base as a haven in times of threat, and, accord-ing to Bowlby, this provides the child with the sense of safety that allows her to explorethe environment. The child is able to venture into the unknown, and explore, and learn,because she knows that, if the going gets rough, she can always return to the securebase (Waters & Cummings, 2000).
Bowlby argued that this tendency to form attachments, and to rely on the psycho-logical comfort of a secure base, is rooted in our evolutionary past, and this is why wecan easily find parallels to human attachment in other species. For example, considerthe process of imprinting, a kind of learning that, in many species, provides the basisfor an infant’s attachment to its mother (e.g., Lorenz, 1935). To take a specific case, assoon as a duckling can walk (about 12 hours after hatching), it will approach and fol-low virtually any moving stimulus. If the duckling follows this moving object for about10 minutes, an attachment is formed, and the bird has now imprinted on this object.From this point forward, the duckling will continue to follow the attachment object,show distress if separated from it, and run to it in circumstances involving threat.
This simple kind of learning is usually quite effective, since the first moving stimu-lus a duckling sees is usually its mother. But imprinting can occur to other objects, byaccident or through an experimenter’s manipulations. In some studies, ducklings have
14.20 SCIENTIFIC METHOD: Is contact comfort or food more important for infant rhesus monkeys’ attachment?
Method1. Harlow and his team raised rhesus monkeysin sterile cages without their mothers.
2. Each cage contained two stationary“mothers.” One was built of wire, and the otherwas wrapped in soft terry-cloth.
4. Harlow measured the amount of time theinfant monkeys spent with each mother.
3. In one condition, the wire mother had anipple that provided milk, and the cloth motherdid not. In the other condition, only the clothmother provided milk.
Results: In both conditions, infants spent much more time on the terry-cloth motherthan on the wire mother.
CONCLUSION: Contact comfort, not the provision of food, seems to be a keyfeature of attachment for rhesus monkeys.
SOURCE STUDY: Harlow, 1958
14.21 Mother as “secure base”
secure base According to JohnBowlby, the relationship in which thechild feels safe and protected.
imprinting In many species, thelearned attachment that is formed at aparticular early period.

PInfancy and ChildhoodO 565
been exposed to a moving toy duck on wheels, or to a rectangle sliding back and forthbehind a glass window, or even to the researcher’s booted legs (Figure 14.22). In eachcase, the ducklings follow these objects as if following their mother, uttering plaintivedistress calls whenever the attachment object is not nearby (E. H. Hess, 1959, 1973).
Do human infants show a similar pattern of imprinting? Some studies have comparedthe attachment of infants who had after-birth contact with their mothers to those whodid not (usually due to medical complications in either mother or baby); the studiesfound little difference between the groups, and hence provided no evidence for a specific period during which human newborns form attachments (Eyer, 1992). Similarly,infants who must spend their initial days with a nurse or in an incubator do not form alasting attachment to either. Clearly, then, the pattern of imprint-to-object-of-first-exposure, common in many species, is not found in humans.
Even with these differences between humans and other animals, the fact remainsthat human infants form a strong attachment to a caregiver, usually the mother—presumably because young children in most cultures spend the vast majority of theirtime with their mothers (M. E. Lamb, 1987, 1997). What role does this leave for thefather? Infants do develop strong attachments to both parental figures (Pipp,Easterbrooks, & Brown, 1993), but mothers and fathers typically behave differentlywith their infant children, and there are corresponding differences in attachment.Fathers tend to be more physical and vigorous in their play, bouncing their children ortossing them in the air. In contrast, mothers generally play more quietly with their chil-dren, telling them stories or reciting nursery rhymes and providing hugs and caressesrather than tumbles and bounces. The children act accordingly, tending to run to themother for care and comfort but to the father for active play (Figure 14.23; Clarke-Stewart, 1978; M. E. Lamb, 1997; Parke, 1981).
D I F F E R E N C E S I N AT TAC H M E N T
Many aspects of the attachment process are similar for all children. But we also needto acknowledge that children differ in their patterns of attachment. To study thesedifferences, Mary Ainsworth and her colleagues developed a procedure for assessingattachment—the so-called strange situation (Figure 14.24; Ainsworth & Bell, 1970;Ainsworth, Blehar, Waters, & Wall, 1978). In this procedure, the 12-month-old child isbrought into an unfamiliar room that contains many toys and is allowed to exploreand play with the mother present. After a while, an unfamiliar woman enters, talks tothe mother, and then approaches the child. The next step is a brief separation—themother leaves the child alone with the stranger. After a few minutes, the motherreturns and the stranger leaves.
This setting is mildly stressful for most children, and by observing how the childhandles the stress, Ainsworth argued that we can determine the nature of the child’sattachment. Specifically, Ainsworth and subsequent researchers argued that children’sbehavior in this setting will fall into one of four categories. First, children who aresecurely attached will explore, play with the toys, and even make wary overtures to thestranger, so long as the mother is present. When the mother leaves, these infants willshow minor distress. When she returns, they greet her with great enthusiasm.
Other children show patterns that Ainsworth regarded as signs of insecureattachment. Some of these children are described as anxious/resistant. They do notexplore, even in the mother’s presence, and become quite upset when she leaves. Uponreunion, they act ambivalent, crying and running to her to be picked up, but then kick-ing or slapping her and struggling to get down. Still other children show the thirdpattern, called anxious/avoidant. They are distant and aloof while the mother is present,
14.22 Imprinted ducklings follow KonradLorenz.
14.23 Paternal bonding Mothers play amajor caregiving role across cultures.However, fathers also play an importantrole in caregiving.
strange situation An experimentalprocedure for assessing attachment, inwhich the child is allowed to explorean unfamiliar room with the motherpresent before the mother leaves for afew minutes, and then returns.

566 chapter 14 PDEVELOPMENTO
and, although they sometimes search for her in her absence, they typi-cally ignore her when she returns.
Children in the fourth category show an attachment pattern calleddisorganized (Main & Solomon, 1990). Children in this group seem tolack any organized way for dealing with the stress they experience. Inthe strange situation, they sometimes look dazed or confused. Theyshow inconsistent behaviors—for example, crying loudly while tryingto climb into their mothers’ laps. They seem distressed by their moth-ers’ absence, but sometimes move away from her when she returns.
In healthy, middle-class families, roughly 60% of the infantstested are categorized as “secure,” 10% as “anxious /resistant,” 15%as “anxious /avoidant,” and 15% as “disorganized” (van Ijzendoorn,Schuengel, & Bakermans-Kranenburg, 1999). The proportion of chil-dren showing “secure” attachment is lower in lower-income familiesand families in which there are psychological or medical problemsaffecting either the parents or the children. One study, for example,assessed children who were chronically undernourished; only 7% ofthese were “securely attached” (Valenzuela, 1990, 1997). Likewise,mothers who are depressed, neurotic, or anxious are less likely to havesecurely attached infants (NICHD Early Child Care ResearchNetwork, 1997).
Many theorists argue that a child’s attachment status shapes hissocial world in important ways. In part, this claim derives from thenotion of a secure base: A securely attached child feels safe, confident,
and willing to take initiative in a wide range of circumstances, and these traits will opena path to new experiences and new learning opportunities. Moreover, securely attachedchildren usually have a more harmonious relationship with their caregivers and aretherefore better able to learn from them; this, too, can lead to numerous advantages inmonths and years to come (cf. Bretherton, 1990).
In addition, Bowlby argued that the attachment relationship provides the child withan internal working model of the social world. This model includes a set of beliefsabout how people behave in social relationships, guidelines for interpreting others’actions, and habitual responses to make in social settings. This model grows out of thechild’s relationship with a caregiver, and according to Bowlby, it provides a templatethat sets the pattern for other relationships, including friendships and even romances.Thus, for example, if the child’s attachment figure is available and responsive, the childexpects future relationships to be similarly gratifying. If the child’s attachment figure isunavailable and insensitive, then the child develops low expectations for futurerelationships.
A number of studies have demonstrated that these working models of attachment doseem to have important consequences. For example, children who are securely attachedat 1 year of age are more attractive to other toddlers as playmates in comparison to chil-dren who were insecurely attached (B. Fagot, 1997; Vondra, Shaw, Swearingen, Cohen,& Owens, 2001; also B. Schneider, Atkinson, & Tardif, 2001; R. A. Thompson, 1998,1999). Likewise, children who were securely attached show more helping and concernfor peers (van IJzendoorn, 1997; also see DeMulder, Denham, Schmidt, & Mitchell,2000). Even more impressive, children who were securely attached as infants are morelikely, as teenagers, to have close friends (Englund, Levy, Hyson, & Sroufe, 2000;Feeney & Collins, 2001; Shulman, Elicker, & Sroufe, 1994) and are less likely to sufferfrom anxiety disorders in childhood and adolescence (Warren, Huston, Egeland, &Sroufe, 1997).
internal working model A set ofbeliefs and expectations about howpeople behave in social relationships,and also guidelines for interpretingothers’ actions, and habitualresponses to make in social settings.
A mother and child enteran unfamiliar room withmany interesting toys. Theinfant explores the roomand plays with the toys. Inthe meantime, a strangerenters the room and themother leaves.
When the mother returnsto the room, she picks upthe infant and comfortshim if he was upset thatshe had left the room.
The mother then putsdown the infant, who isfree to return to playingwith the toys.
14.24 The strange situation
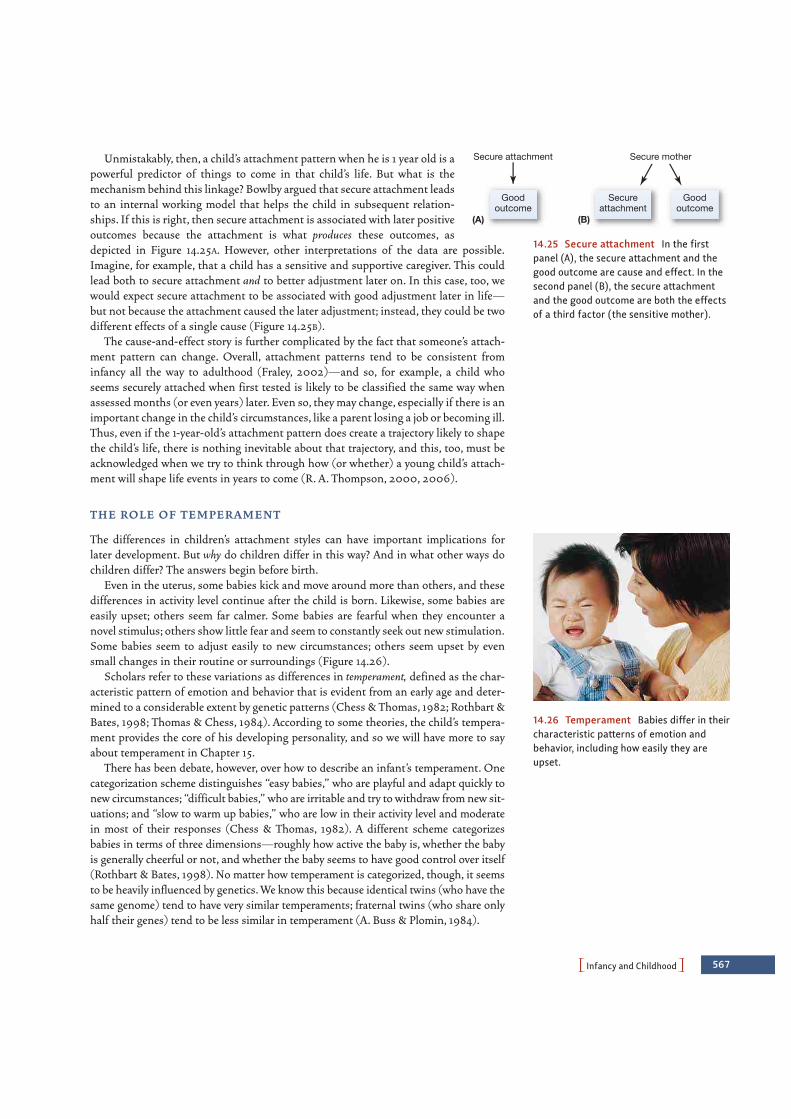
PInfancy and ChildhoodO 567
Unmistakably, then, a child’s attachment pattern when he is 1 year old is apowerful predictor of things to come in that child’s life. But what is themechanism behind this linkage? Bowlby argued that secure attachment leadsto an internal working model that helps the child in subsequent relation-ships. If this is right, then secure attachment is associated with later positiveoutcomes because the attachment is what produces these outcomes, asdepicted in Figure 14.25A. However, other interpretations of the data are possible.Imagine, for example, that a child has a sensitive and supportive caregiver. This couldlead both to secure attachment and to better adjustment later on. In this case, too, wewould expect secure attachment to be associated with good adjustment later in life—but not because the attachment caused the later adjustment; instead, they could be twodifferent effects of a single cause (Figure 14.25B).
The cause-and-effect story is further complicated by the fact that someone’s attach-ment pattern can change. Overall, attachment patterns tend to be consistent frominfancy all the way to adulthood (Fraley, 2002)—and so, for example, a child whoseems securely attached when first tested is likely to be classified the same way whenassessed months (or even years) later. Even so, they may change, especially if there is animportant change in the child’s circumstances, like a parent losing a job or becoming ill.Thus, even if the 1-year-old’s attachment pattern does create a trajectory likely to shapethe child’s life, there is nothing inevitable about that trajectory, and this, too, must beacknowledged when we try to think through how (or whether) a young child’s attach-ment will shape life events in years to come (R. A. Thompson, 2000, 2006).
T H E RO L E O F T E M P E R A M E N T
The differences in children’s attachment styles can have important implications forlater development. But why do children differ in this way? And in what other ways dochildren differ? The answers begin before birth.
Even in the uterus, some babies kick and move around more than others, and thesedifferences in activity level continue after the child is born. Likewise, some babies areeasily upset; others seem far calmer. Some babies are fearful when they encounter anovel stimulus; others show little fear and seem to constantly seek out new stimulation.Some babies seem to adjust easily to new circumstances; others seem upset by evensmall changes in their routine or surroundings (Figure 14.26).
Scholars refer to these variations as differences in temperament, defined as the char-acteristic pattern of emotion and behavior that is evident from an early age and deter-mined to a considerable extent by genetic patterns (Chess & Thomas, 1982; Rothbart &Bates, 1998; Thomas & Chess, 1984). According to some theories, the child’s tempera-ment provides the core of his developing personality, and so we will have more to sayabout temperament in Chapter 15.
There has been debate, however, over how to describe an infant’s temperament. Onecategorization scheme distinguishes “easy babies,” who are playful and adapt quickly tonew circumstances; “difficult babies,” who are irritable and try to withdraw from new sit-uations; and “slow to warm up babies,” who are low in their activity level and moderatein most of their responses (Chess & Thomas, 1982). A different scheme categorizesbabies in terms of three dimensions—roughly how active the baby is, whether the babyis generally cheerful or not, and whether the baby seems to have good control over itself(Rothbart & Bates, 1998). No matter how temperament is categorized, though, it seemsto be heavily influenced by genetics. We know this because identical twins (who have thesame genome) tend to have very similar temperaments; fraternal twins (who share onlyhalf their genes) tend to be less similar in temperament (A. Buss & Plomin, 1984).
Secure attachment
Goodoutcome
Secureattachment
Goodoutcome
(A)
Secure mother
(B)
14.25 Secure attachment In the firstpanel (A), the secure attachment and thegood outcome are cause and effect. In thesecond panel (B), the secure attachmentand the good outcome are both the effectsof a third factor (the sensitive mother).
14.26 Temperament Babies differ in theircharacteristic patterns of emotion andbehavior, including how easily they areupset.

568 chapter 14 PDEVELOPMENTO
T H E RO L E O F CU LT U R E
Another source of differences among children comes from the cultural context withinwhich the child develops. Some cultural influences on development are obvious. In
ancient Rome, for example, educated children learned to represent num-bers with Roman numerals; modern children in the West, in contrast,
learn to represent numbers with Arabic numerals. Modern children inthe Oksapmin culture (in New Guinea) learn yet a different system,counting using parts of the body rather than numbers (Figure 14.27;Saxe, 1981). In each case, this culturally provided tool guides (and in
some cases, limits) how the children think about and work withnumerical quantities.In addition,some social and cultural settings involve formal schooling,but
others do not, and schooling is a powerful influence on the child’s development(Christian, Bachman, & Morrison, 2000; Rogoff et al., 2003). Cultures also differ in whatactivities children are exposed to, how frequently these activities occur, and what the chil-dren’s role is in the activity. These factors play an important part in determining whatskills—intellectual and motor—the children will gain and the level of skill they will attain(M. Cole & Cole, 2001; Laboratory of Comparative Human Cognition, 1983; Rogoff, 1998,2000).
In understanding these various cultural influences, though, it is crucial to bear inmind that the child is not a passive recipient of social and cultural input. Instead, thechild plays a key role in selecting and shaping her social interactions in ways that, inturn, have a powerful effect on how and what she learns.
Part of the child’s role in selecting and shaping her social interactions is defined bywhat Lev Vygotsky (1978) called the zone of proximal development. This term refersto the range of accomplishments that are beyond what the child could do on her own,but that are possible if the child is given help or guidance. Attentive caregivers or teach-ers structure their input to keep the child’s performance within this zone—so that thechild is challenged, but not overwhelmed, by the task’s demands. Importantly, the childherself provides feedback to those around her that helps maintain this level of guid-ance. Thus, caregivers are able to monitor the child’s progress and, in some cases, thechild’s frustration level, as a project proceeds, and they can then adjust accordingly howmuch help they offer.
The child also plays an active role whenever the processes of learning or problemsolving involve the shared efforts of two or more people (after Rogoff, 1998). In suchcases, it is clear that we cannot understand development if we focus either on the childor on the social context; instead, we must understand the interaction of the two andhow each shapes the other.
One example of this interplay is seen in the child’s capacity for remembering lifeevents. This capacity might seem to depend entirely on processes and resources insidethe individual, with little room for social influence. Evidence suggests, however, that thecapacity for remembering events grows in part out of conversations in which adultshelp children to report on experiences. When the child is quite young, these conversa-tions tend to be one-sided. The parent does most of the work of describing the remem-bered event and gets little input from the child. (“Remember when we went to seeGrandma, and she gave you a teddy bear?”) As the child’s capacities grow, the parentretreats to a narrower role, first asking specific questions to guide the child’s report(“Did you see any elephants at the zoo?”), then, at a later age, asking only broaderquestions (“What happened in school today?”), and eventually listening as the childreports on some earlier episode. Over the course of this process, the parent’s specific
14.27 The role of culture in training chil-dren The Oksapmin used a 27-body-partcount system. Historically, the count beginswith the thumb on one hand and enumer-ates 27 places around the upper contour ofthe body, ending on the little finger of theopposite hand. To count past 27, reverse upthrough the wrist, forearm, and around thebody.
zone of proximal development Therange of accomplishments that arebeyond what the child can do on herown, but that she can achieve withhelp or guidance.

PInfancy and ChildhoodO 569
questions, the sequence of questions, and their level of detail all guide the child as hefigures out what is worth reporting in an event and, for that matter, what is worth pay-ing attention to while the event is unfolding (Fivush, 1998; Fivush & Nelson, 2004; K.Nelson & Fivush, 2000; Peterson & McCabe, 1994).
Of course, parents talk to their children in different ways. Some parents tend toelaborate on what their children have said; some simply repeat the child’s comments(Reese & Fivush, 1993). For example, Mexican Americans and Anglo-Americans differin how they converse with their children and in what they converse about, withMexican Americans’ emotion talk tending to be less explanatory than Anglo-Americans’. There are also differences in adult-child conversations if we compare work-ing-class and middle-class parents (see, for example, A. R. Eisenberg, 1999).
In each case, these differences in conversational pattern have an impact on how thechild structures his or her memory. As one example, evidence suggests that Americanmothers talk with their children about past events much more than Asian mothers do(Mullen & Yi, 1995). These conversations may help American children to start organiz-ing their autobiographical recall at an earlier age than Asian children. Consistent withthis suggestion, when Caucasian adults are asked to report their earliest childhoodmemories, they tend to remember events earlier in life than do Asian adults (Fivush &Haden, 2003; Mullen, 1994). The same logic may help explain why women tend toremember events from earlier in their lives than men do. This difference in memory mayresult from differences in the way parents converse with their sons and daughters(Fivush & Haden, 2003; Fivush & Nelson, 2004).
T H E RO L E O F PA R E N T I N G ST Y L E S
Other kinds of differences between parents also powerfully shape the developing child.Some parents are strict, others less so; some are anxious and others not; some explain theirinstructions (“Go to bed so that you will feel better tomorrow”) and others just assert theirauthority (“Go to bed!”). Across this diversity, though, researchers propose that parentingstyles can be largely described in terms of just two dimensions (Maccoby & Martin, 1983).First, parents differ in how accepting they are of their children, and, with that, how respon-sive they are to the child’s actions or needs. Second, parents differ in how demanding orcontrolling they are of their children’s behavior. Putting these two dimensions together, wecan think about parenting styles as being divided into four broad types.
Diana Baumrind (1967, 1971) described these four styles in detail. Authoritarianparents (high on demandingness but low on responsiveness) adhere to strict standardsabout how children should and should not speak and act, and attempt to mold their chil-dren’s behavior accordingly. Such parents set down firm rules and meet any infractionswith stern and sometimes severe punishment. Authoritarian parents do not believe it isnecessary to explain the rules to their children, but expect their children to submit tothem by virtue of parental authority: “It’s because I say so; that’s why.”
At the opposite extreme, permissive parents (low on demandingness but high onresponsiveness) set few explicit rules. These parents try not to assert their authority,impose few restrictions and controls, tend not to have set schedules (for, say, bedtimeor watching TV), and rarely use punishment. They also make few demands on theirchildren—such as putting toys away, doing schoolwork, or helping with chores.
Authoritarian parents brandish parental power; permissive parents abdicate it.A third approach lies between these extremes: Authoritative parents (high on bothresponsiveness and demandingness) exercise their power but also accept the reciprocalobligation to respond to their children’s opinions and reasonable requests. These

570 chapter 14 PDEVELOPMENTO
parents set down rules of conduct and enforce them, assign chores, and expect maturebehavior. But they also spend time teaching their children how to act appropriately,encourage independence, and allow a good deal of verbal give and take.
Finally, a fourth pattern is that of disengaged parents (low on both responsivenessand demandingness). These parents exhibit a lax and undemanding approach, possiblybecause they are so overwhelmed by their own concerns that they have little time forchild rearing. They provide few rules and demands and are relatively insensitive to theirchildren’s needs.
Why do parents adopt one parenting style over another? One factor is socioeconomic—poverty is associated with lower levels of involvement (Costello, Compton, Keeler, &Angold, 2003). A second factor is the characteristics of the child. Children who are dis-obedient and aggressive, for example, make it difficult for parents to use an authorita-tive style (Brody & Ge, 2001). Likewise, stubborn or impulsive children tend to elicitmore demanding forms of parenting (Stoolmiller, 2001). In addition, children matureat different speeds, and a child who learns to crawl, walk, speak, or read precociouslywill be treated differently from a child who does not. Likewise, a child who understandsand respects a logical reason (“Don’t touch that because you’ll get burned”) will bemore likely to elicit responsive parenting than a child who does not.
T H E I M PACT O F C H I L D CA R E
Families differ not only in their parenting but also in their childcare arrangements. Inthe United States, most children grow up in households in which both parents workoutside the home (National Research Council and Institute of Medicine, 2000); thesituation is the same in many other countries. As a result, children often stay longhours each day with babysitters or professional childcare providers; in most of thesecases, the child receives less one-on-one adult time and spends more time with otherchildren. How does this influence children’s development?
Reassuringly, research indicates that childcare centers do not harm children in anyway (NICHD Early Child Research Network, 2001, 2003, 2006); in fact, high-qualitychildcare seems in some cases to promote the child’s social competence (Figure 14.28).This optimistic assessment, however, must be tempered with concerns about variation inthe quality of the childcare. In high-quality settings, the caregivers have had some train-ing in child development and are usually warm, expressive, and responsive to the chil-dren’s needs. In these settings, there are usually no more than a half-dozen toddlers per
adult caregiver. In lower-quality settings, none of these conditions aremet, and the forecast is correspondingly less positive (Love et al.,2003; N. L. Marshall, 2004; NICHD Early Child Care ResearchNetwork, 2006). One study indicated that infants enrolled in poor-quality daycare centers end up inattentive and unsociable in pre-school, compared to children who spent the same amount of time ingood daycare centers (Howes, 1990). In a similar study, 4-year-oldswho attended higher-quality daycare centers showed better social andemotional development at age 8 than did children who attendedpoorer-quality centers, even when factors such as social class andincome were equated (Vandell, Henderson, & Wilson, 1988).
Even with lower-quality care, though, we may not need to sound thealarm. Whatever the quality of the childcare, the main predictor of thechild’s status seems to be the quality of home life, including the par-ents’ sensitivity to the child, the parents’ health, and so on. As onerecent report put it: “The primary conclusion is that parenting matters
14.28 Attachment and child care Whilesome contend that any early separationfrom the primary caregiver may adverselyaffect the child, others contend that it isnot the fact of child care that is importantso much as it is the quality of child care.
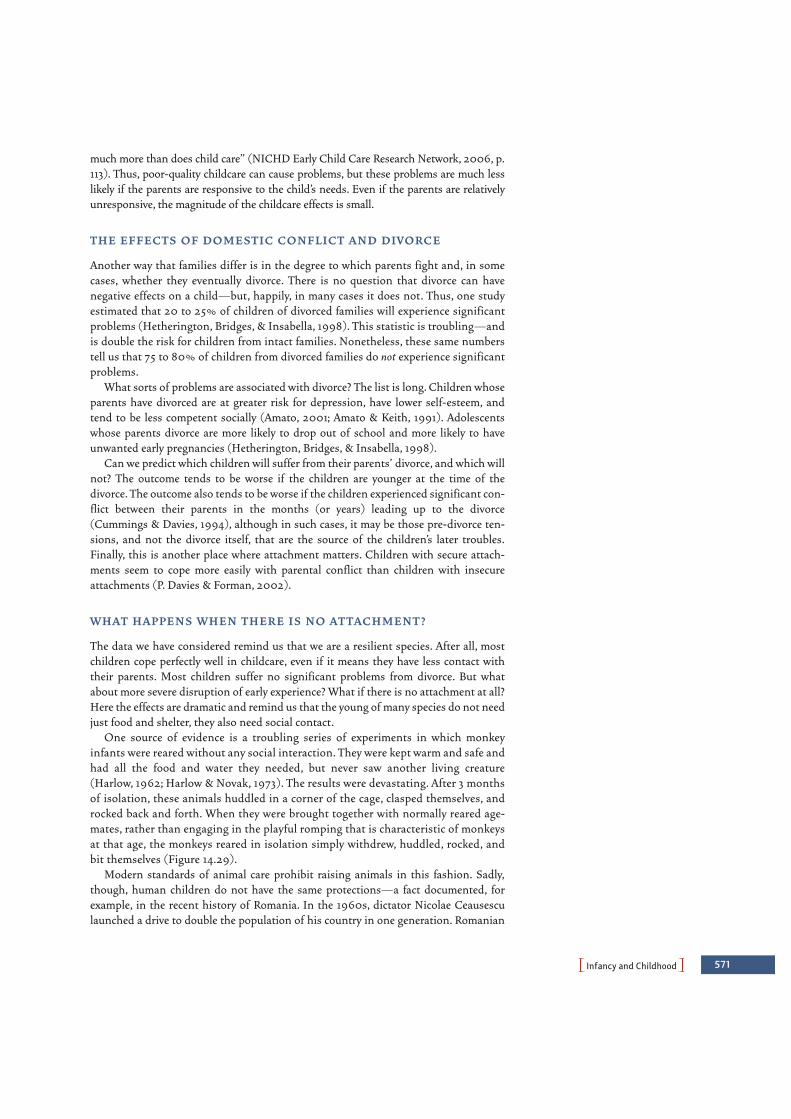
PInfancy and ChildhoodO 571
much more than does child care” (NICHD Early Child Care Research Network, 2006, p.113). Thus, poor-quality childcare can cause problems, but these problems are much lesslikely if the parents are responsive to the child’s needs. Even if the parents are relativelyunresponsive, the magnitude of the childcare effects is small.
T H E E F F E CTS O F D O M E ST I C CO N F L I CT A N D D I V O RC E
Another way that families differ is in the degree to which parents fight and, in somecases, whether they eventually divorce. There is no question that divorce can havenegative effects on a child—but, happily, in many cases it does not. Thus, one studyestimated that 20 to 25% of children of divorced families will experience significantproblems (Hetherington, Bridges, & Insabella, 1998). This statistic is troubling—andis double the risk for children from intact families. Nonetheless, these same numberstell us that 75 to 80% of children from divorced families do not experience significantproblems.
What sorts of problems are associated with divorce? The list is long. Children whoseparents have divorced are at greater risk for depression, have lower self-esteem, andtend to be less competent socially (Amato, 2001; Amato & Keith, 1991). Adolescentswhose parents divorce are more likely to drop out of school and more likely to haveunwanted early pregnancies (Hetherington, Bridges, & Insabella, 1998).
Can we predict which children will suffer from their parents’ divorce, and which willnot? The outcome tends to be worse if the children are younger at the time of thedivorce. The outcome also tends to be worse if the children experienced significant con-flict between their parents in the months (or years) leading up to the divorce(Cummings & Davies, 1994), although in such cases, it may be those pre-divorce ten-sions, and not the divorce itself, that are the source of the children’s later troubles.Finally, this is another place where attachment matters. Children with secure attach-ments seem to cope more easily with parental conflict than children with insecureattachments (P. Davies & Forman, 2002).
W H AT H A P P E N S W H E N T H E R E I S N O AT TAC H M E N T ?
The data we have considered remind us that we are a resilient species. After all, mostchildren cope perfectly well in childcare, even if it means they have less contact withtheir parents. Most children suffer no significant problems from divorce. But whatabout more severe disruption of early experience? What if there is no attachment at all?Here the effects are dramatic and remind us that the young of many species do not needjust food and shelter, they also need social contact.
One source of evidence is a troubling series of experiments in which monkeyinfants were reared without any social interaction. They were kept warm and safe andhad all the food and water they needed, but never saw another living creature(Harlow, 1962; Harlow & Novak, 1973). The results were devastating. After 3 monthsof isolation, these animals huddled in a corner of the cage, clasped themselves, androcked back and forth. When they were brought together with normally reared age-mates, rather than engaging in the playful romping that is characteristic of monkeysat that age, the monkeys reared in isolation simply withdrew, huddled, rocked, andbit themselves (Figure 14.29).
Modern standards of animal care prohibit raising animals in this fashion. Sadly,though, human children do not have the same protections—a fact documented, forexample, in the recent history of Romania. In the 1960s, dictator Nicolae Ceausesculaunched a drive to double the population of his country in one generation. Romanian
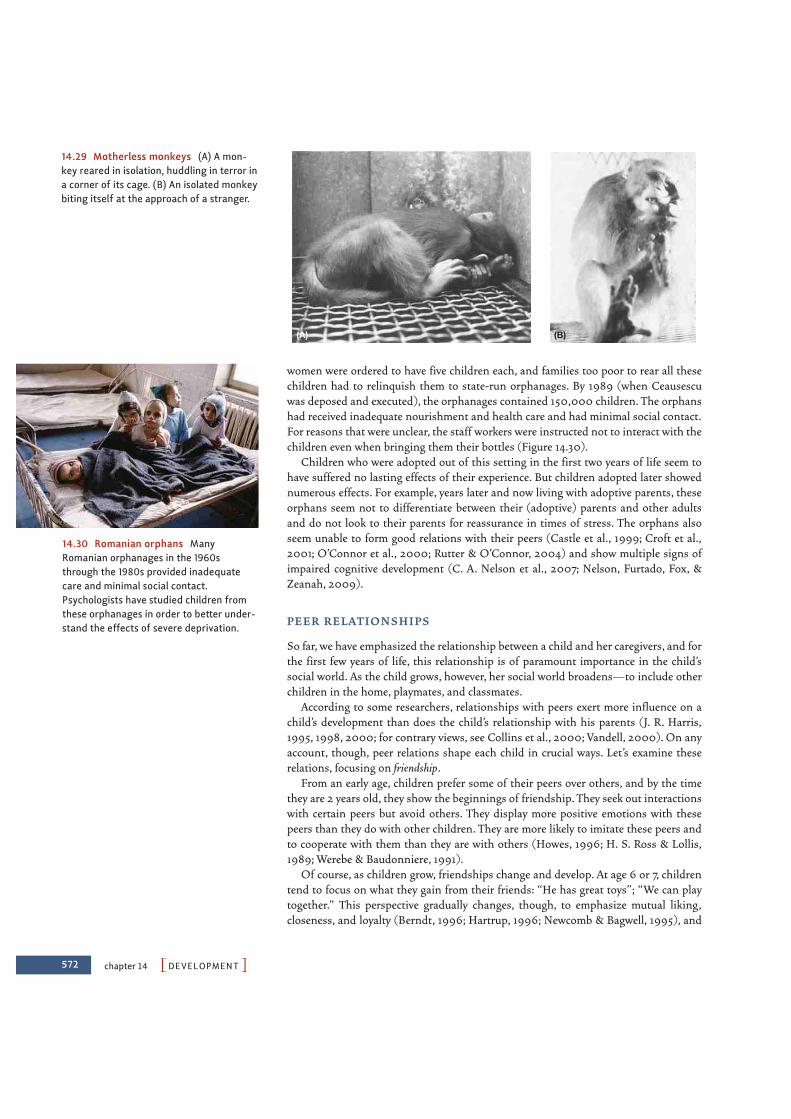
572 chapter 14 PDEVELOPMENTO
women were ordered to have five children each, and families too poor to rear all thesechildren had to relinquish them to state-run orphanages. By 1989 (when Ceausescuwas deposed and executed), the orphanages contained 150,000 children. The orphanshad received inadequate nourishment and health care and had minimal social contact.For reasons that were unclear, the staff workers were instructed not to interact with thechildren even when bringing them their bottles (Figure 14.30).
Children who were adopted out of this setting in the first two years of life seem tohave suffered no lasting effects of their experience. But children adopted later showednumerous effects. For example, years later and now living with adoptive parents, theseorphans seem not to differentiate between their (adoptive) parents and other adultsand do not look to their parents for reassurance in times of stress. The orphans alsoseem unable to form good relations with their peers (Castle et al., 1999; Croft et al.,2001; O’Connor et al., 2000; Rutter & O’Connor, 2004) and show multiple signs ofimpaired cognitive development (C. A. Nelson et al., 2007; Nelson, Furtado, Fox, &Zeanah, 2009).
P E E R R E L AT I O N S H I P S
So far, we have emphasized the relationship between a child and her caregivers, and forthe first few years of life, this relationship is of paramount importance in the child’ssocial world. As the child grows, however, her social world broadens—to include otherchildren in the home, playmates, and classmates.
According to some researchers, relationships with peers exert more influence on achild’s development than does the child’s relationship with his parents (J. R. Harris,1995, 1998, 2000; for contrary views, see Collins et al., 2000; Vandell, 2000). On anyaccount, though, peer relations shape each child in crucial ways. Let’s examine theserelations, focusing on friendship.
From an early age, children prefer some of their peers over others, and by the timethey are 2 years old, they show the beginnings of friendship. They seek out interactionswith certain peers but avoid others. They display more positive emotions with thesepeers than they do with other children. They are more likely to imitate these peers andto cooperate with them than they are with others (Howes, 1996; H. S. Ross & Lollis,1989; Werebe & Baudonniere, 1991).
Of course, as children grow, friendships change and develop. At age 6 or 7, childrentend to focus on what they gain from their friends: “He has great toys”; “We can playtogether.” This perspective gradually changes, though, to emphasize mutual liking,closeness, and loyalty (Berndt, 1996; Hartrup, 1996; Newcomb & Bagwell, 1995), and
(A) (B)
14.29 Motherless monkeys (A) A mon-key reared in isolation, huddling in terror ina corner of its cage. (B) An isolated monkeybiting itself at the approach of a stranger.
14.30 Romanian orphans ManyRomanian orphanages in the 1960sthrough the 1980s provided inadequatecare and minimal social contact.Psychologists have studied children fromthese orphanages in order to better under-stand the effects of severe deprivation.

PInfancy and ChildhoodO 573
by age 9 or so, children define friendship in terms of taking care of one another, help-ing each other, and sharing feelings.
Friendships are important for the child for many reasons. They provide the positiveexperiences of shared play and shared activity. They also provide support in times ofstress, information in times of uncertainty, and a training ground in which children cantry out, and master, a variety of social skills. For example, children need to learn to han-dle conflict, and much of this learning takes place with friends. Friends quarrel, maybeeven just as much as nonfriends (Fabes, Eisenberg, Smith, & Murphy, 1996). But theyfind ways to handle the conflict—through negotiation or cooperation—and are appre-ciably more likely than nonfriends to continue their interactions after the conflict isover. Having friends—and resolving conflicts with them—helps the child gain skills forsolving social problems (Rubin, Bukowski, & Parker, 1998).
Children also learn valuable lessons from the candor and intimacy that friendshipallows. All kinds of social interactions require interpreting others’ thoughts andemotional states, and one way for children to gain that skill is via friendship. Friends dis-cuss their thoughts and feelings in ways that nonfriends do not, and these conversationsprovide children with important insights into the minds of others (C. Hughes & Dunn,1998; Maguire & Dunn, 1997).
Given all these benefits, having friends is likely to help children both immediatelyand in the long term. In fact, having close friends as a child is associated with manypositive outcomes, including social success later in life and greater feelings of self-worth (Bagwell, Newcomb, & Bukowski, 1998; Hodges, Malone, & Perry, 1997;D. Schwartz, Dodge, Pettit, Bates, & the Conduct Problems Prevention Research Group,2000). Children who enter kindergarten along with friends seem to like school betterand have fewer adjustment problems, in comparison with children who enter kinder-garten without their friends’ company (Ladd, Kochenderfer, & Coleman, 1996; Ladd &Price, 1987). Children with friends are also less likely to become depressed (Bagwell,Newcomb, & Bukowski, 1998).
The effects of friendship can also be documented in another way—by looking atchildren who are rejected by their peers. Investigators have explored this point by firstgathering sociometric data—data that describe group interactions—to determinewhich children are popular (liked by many), which are rejected (disliked by many),and which are neglected by peers (neither liked nor disliked). Often this determina-tion is made simply by asking a group of children whom they like and whom they donot; a similar determination can be reached by asking teachers which of theirstudents are accepted and which are not (Cillessen & Bukowski, 2000; Terry & Coie,1991; Wu, Hart, Draper, & Olsen, 2001). No matter how this classification is carriedout, the picture is not bright for the rejected children. When interviewed, rejectedchildren report that they are lonely and, indeed, lonelier than the neglected children(Cassidy & Asher, 1992; N. R. Crick & Ladd, 1993). The rejected children are also theones who are at greater risk for developing antisocial behaviors or adjustment diffi-culties later in life (Coie & Dodge, 1983; Dodge & Pettit, 2003; Laird, Jordan, Dodge,Pettit, & Bates, 2001).
Why does a specific child end up being popular or neglected or rejected(Figure 14.31)? Many factors contribute, including the child’s attachment status (securechildren tend to be popular) and the parenting style in the child’s home (children withauthoritative parents are more likely to be popular). Temperament matters, as inhibitedor slow-to-warm-up children are more likely to be rejected (C. Hart, Newell, & Olsen,2003). Appearances also matter, making rejection less likely for children who haveattractive faces (Langlois et al., 2000) and attractive bodies (Sigelman, Miller, &Whitworth, 1986). For boys, maturing early tends to promote popularity (Duke et al.,
sociometric data Data that describehow individuals in a group interact.
14.31 Rejection Rejected children are atelevated risk for developing antisocialbehaviors and adjustment difficulties laterin life.

574 chapter 14 PDEVELOPMENTO
1982; Livson & Peskin, 1980); for girls, the opposite may be the case (Aro & Taipale,1987; Clausen, 1975).
Whatever the causes of acceptance or rejection, this dimension of social status surely does matter. We can debate which is the cause here and which is the effect, butthe data indicate that so-called aggressive-rejected children are more aggressive(Crick, 1996), less cooperative (Newcomb, Bukowski, & Pattee, 1993), and more likelyto become chronically hostile in adolescence and adulthood (J. Parker, Rubin, Price, &DeRosier, 1995; Rubin et al., 1998). Withdrawn-rejected children are likely to be anx-ious (Downey, Lebolt, Rincon, & Freitas, 1998; Zakriski & Coie, 1996) and are atincreased risk for depression (Hymel, Bowker, & Woody, 1993).
All of these results speak to the importance and benefits of friendship and tothe difficulties associated with being rejected. But we should also note that friendscan influence each other negatively. Aggressive and disruptive friends can teachthis kind of behavior (Berndt, 1999; Brendgen, Vitaro, & Bukowski, 2000).Likewise, as we will see in the next section, adolescents are often led into badhabits by their friends—including alcohol and substance abuse (Mounts &Steinberg, 1995; Urberg, Degirmenciogl & Pilgrim, 1997). Friendships are thus adouble-edged sword, capable of conferring both great benefit and lasting harm.
T H E D E V E LO P M E N T O F M O R A L T H I N K I N G
One last issue draws us back to the interplay between the child’s intellectual, social, andemotional development. This is the issue of morality—and the child’s growing sense ofright and wrong. For many years, researchers framed these issues in terms of claimsoffered by Lawrence Kohlberg. Kohlberg began with data gathered with a simplemethod. He presented boys with stories that posed moral dilemmas and questionedthem about the issues these stories raised. One often-quoted example is a story abouta man whose wife would die unless treated with a drug that cost far more money thanthe man had. The husband scraped together all the money he could, but it was notenough, so he promised the pharmacist that he would pay the balance later. The phar-macist still refused to give him the drug. In desperation, the husband broke into thepharmacy and stole the drug, and this led to the question for the research participants:They were asked whether the husband’s actions were right or wrong and why.
Kohlberg posed this question and similar ones to boys of various ages. Based ontheir answers, he concluded that moral reasoning develops through a series of threebroad levels; each level, in turn, is divided into an early stage and a late stage, so that theentire conception contains six distinct stages. The first pair of stages (and so the firstlevel) relies on what Kohlberg calls preconventional reasoning—moral judgmentsfocused on getting rewards and avoiding punishment. A child at this level might say, “Ifyou let your wife die, you’ll get in trouble.” The second pair of stages relies onconventional reasoning and is centered on social relationships, conventions, andduties. A response such as “Your family will think you’re bad if you don’t help your wife”would be indicative of this type of reasoning. The final pair of stages involvespostconventional reasoning and is concerned with ideals and broad moral principles:“It’s wrong to let somebody die” (Figure 14.32).
Kohlberg intended his conception to describe all people, no matter who they are orwhere they live, but a number of scholars have challenged this claim. One set of con-cerns was raised by Carol Gilligan (1982), who argued that Kohlberg’s test did a betterjob of reflecting males’ moral reasoning than females’. In her view, men tend to seemorality as a matter of justice, ultimately based on abstract, rational principles by which
aggressive-rejected The social sta-tus of children who are not respectedor liked by peers and become aggres-sive as a result.
withdrawn-rejected The social sta-tus of children who are not respectedor liked by peers and become anxiousas a result.
preconventional reasoningAccording to Kohlberg, the first andsecond stages of moral reasoning,which are focused on getting rewardsand avoiding punishments.
conventional reasoning Accordingto Kohlberg, the third and fourthstages of moral reasoning, which arefocused on social relationships, con-ventions, and duties.
postconventional reasoningAccording to Kohlberg, the fifth andsixth stages of moral reasoning, whichare focused on ideals and broad moralprinciples.
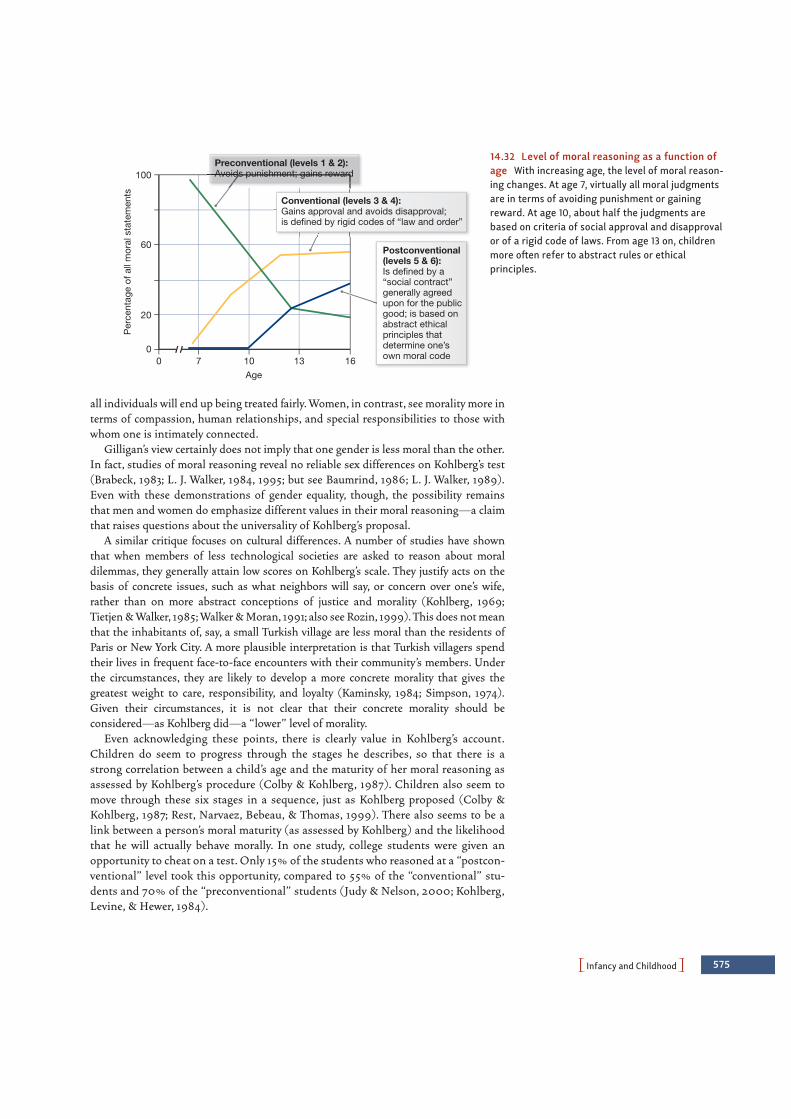
PInfancy and ChildhoodO 575
all individuals will end up being treated fairly. Women, in contrast, see morality more interms of compassion, human relationships, and special responsibilities to those withwhom one is intimately connected.
Gilligan’s view certainly does not imply that one gender is less moral than the other.In fact, studies of moral reasoning reveal no reliable sex differences on Kohlberg’s test(Brabeck, 1983; L. J. Walker, 1984, 1995; but see Baumrind, 1986; L. J. Walker, 1989).Even with these demonstrations of gender equality, though, the possibility remainsthat men and women do emphasize different values in their moral reasoning—a claimthat raises questions about the universality of Kohlberg’s proposal.
A similar critique focuses on cultural differences. A number of studies have shownthat when members of less technological societies are asked to reason about moraldilemmas, they generally attain low scores on Kohlberg’s scale. They justify acts on thebasis of concrete issues, such as what neighbors will say, or concern over one’s wife,rather than on more abstract conceptions of justice and morality (Kohlberg, 1969;Tietjen & Walker, 1985; Walker & Moran, 1991; also see Rozin, 1999). This does not meanthat the inhabitants of, say, a small Turkish village are less moral than the residents ofParis or New York City. A more plausible interpretation is that Turkish villagers spendtheir lives in frequent face-to-face encounters with their community’s members. Underthe circumstances, they are likely to develop a more concrete morality that gives thegreatest weight to care, responsibility, and loyalty (Kaminsky, 1984; Simpson, 1974).Given their circumstances, it is not clear that their concrete morality should beconsidered—as Kohlberg did—a “lower” level of morality.
Even acknowledging these points, there is clearly value in Kohlberg’s account.Children do seem to progress through the stages he describes, so that there is astrong correlation between a child’s age and the maturity of her moral reasoning asassessed by Kohlberg’s procedure (Colby & Kohlberg, 1987). Children also seem tomove through these six stages in a sequence, just as Kohlberg proposed (Colby &Kohlberg, 1987; Rest, Narvaez, Bebeau, & Thomas, 1999). There also seems to be alink between a person’s moral maturity (as assessed by Kohlberg) and the likelihoodthat he will actually behave morally. In one study, college students were given anopportunity to cheat on a test. Only 15% of the students who reasoned at a “postcon-ventional” level took this opportunity, compared to 55% of the “conventional” stu-dents and 70% of the “preconventional” students (Judy & Nelson, 2000; Kohlberg,Levine, & Hewer, 1984).
Preconventional (levels 1 & 2):Avoids punishment; gains reward
Conventional (levels 3 & 4):Gains approval and avoids disapproval;is defined by rigid codes of “law and order”
Postconventional(levels 5 & 6):Is defined by a“social contract”generally agreedupon for the publicgood; is based onabstract ethicalprinciples thatdetermine one’sown moral code
0
20
60
100
0 7 10 13 16
Per
cent
age
of a
ll m
oral
sta
tem
ents
Age
14.32 Level of moral reasoning as a function ofage With increasing age, the level of moral reason-ing changes. At age 7, virtually all moral judgmentsare in terms of avoiding punishment or gainingreward. At age 10, about half the judgments arebased on criteria of social approval and disapprovalor of a rigid code of laws. From age 13 on, childrenmore often refer to abstract rules or ethicalprinciples.

576 chapter 14 PDEVELOPMENTO
Even so, the relationship between someone’s capacity for moral reasoning and thelikelihood that he will behave morally is, at best, only moderate (Bruggeman & Hart,1996). This makes it clear that a number of other factors also influence moral behaviorin everyday life (Krebs & Denton, 2005).
CO N SC I E N C E A N D M O R A L F E E L I N G
One way to describe what’s missing from Kohlberg’s theory is any discussion of con-science—the desire to act in a moral manner, and a feeling of guilt when one does notact morally. A conscience can lead someone away from bad actions (Kochanska, 1993,2002) and toward good actions (Eisenberg, 1986, 2000), but how does a conscienceemerge? One proposal is that the child learns to feel guilty about bad acts by beingrewarded for good deeds and punished for bad ones.
This emphasis on reward and punishment would make sense according to the law ofeffect (Chapter 7). It would also make sense on other grounds. Freud argued, for exam-ple, that the threat of punishment creates anxiety in the child, and the anxiety thenbecomes a powerful source of “self-punishment” whenever the child approaches—oreven thinks about—a forbidden action (Chapter 15).
However, the data on the effects of physical punishment challenge these ideas. Ifpunishment leads a child to avoid bad actions, one might think that stronger, harsherpunishments would lead to more avoidance. This prediction turns out to be not onlyfalse but exactly backward. Evidence suggests that, in fact, a sense of conscience is lesslikely to emerge in children whose parents rely on severe or harsh discipline. For exam-ple, the children of power-asserting (authoritarian) parents are more likely to cheat fora prize when they think no one is looking, and less likely to feel guilt about their mis-deeds or to confess them when confronted (M. L. Hoffman, 1970).
Likewise, spanking (and other forms of physical punishment) seems to lead todecreased internalization of a moral code (Gershoff, 2002; Kazdin & Benjet, 2003), theopposite of what we would expect if physical punishments facilitate moral develop-ment. If severe physical punishment is not the key to developing a moral sense, what is?The answer lies in the child’s relationship with her parents. As we have seen, younginfants are intensely interested in social contact and interaction, and soon become verysensitive to an adult’s signs of approval or disapproval. For some children, the disap-proval itself serves as a punishment, and hence a source of anxiety.
For most children, though, the disapproval is upsetting because it undermines asocial relationship, and so the child tries to avoid the disapproval in order to preservethe relationship. To gain approval, the child also does what he can to imitate the par-ent’s behavior and motivations and to adopt the parent’s beliefs. Consistent with thisperspective, the better the quality of the parent-child relationship, the faster the child’sprogress in developing a conscience (Kochanska, 1997; Laible & Thompson, 2000).More specifically, conscience development seems to be fostered by a relationship inwhich the child and adult are each responsive to the other’s status and needs. By thesame logic, secure attachment is associated with conscience development (Kochanska,1995; Kochanska, Aksan, Knaack, & Rhines, 2004).
AD OLESCENCE
Adolescence is a time of transition during which children become adults. The bound-aries of this period are not precisely specified, but in Western society today, adolescencetypically is thought to span the period from puberty through the early twenties. It is

PAdolescenceO 577
important to note that the boundaries of adolescence have varied considerably acrosscultures and over time (Larson & Wilson, 2004). Indeed, even in our own culture, therehas been an expansion of adolescence over the past century or so.
By any measure, adolescence is a time of change. Adolescence involves physicalchanges, including a growth spurt, the attainment of sexual maturity, and importantchanges in the brain. There are also cognitive changes, including a developing capacityfor abstract thought, as well as socioemotional changes, including a growing sense ofself, romantic attachments, and increased independence from parents and other care-givers. Let’s look at each of these types of change in turn.
Physical Development in AdolescenceOne of the harbingers of adolescence is puberty, a several-year period of physical and sex-ual maturation during which time the body of a child morphs into its adult shape (Figure14.33). In boys, puberty usually begins at about age 12. It is accompanied by a growth spurtthat includes both primary sexual characteristics (bodily structures directly related toreproduction, such as penis, testes, and related internal organs) and secondary sexualcharacteristics (bodily structures that change with sexual maturity but are not themselvesdirectly related to reproduction, such as facial, pubic, and underarm hair, muscle growthin the upper torso, and a deepening of the voice). One milestone in early puberty is a boy’sfirst ejaculation, or spermarche, which typically occurs by about age 14.
In girls, puberty usually begins about age 10 and is accompanied by a growth spurtthat involves changes in both primary sexual characteristics (genitalia and reproductiveorgans) and secondary sexual characteristics (growth of breasts and hips, pubic andunderarm hair). One milestone in early puberty for girls is menarche, or the first men-strual period, which usually occurs about age 12.
As with all developmental phases, there are substantial individual differences in thetiming of the various steps in puberty—and these differences matter. For boys, early
Beginning ofejaculation
Growth of penisand testes
Pubic hairgrowth
Facial and underarmhair growth
Underarmhair growth
Enlargementof uterus
Beginning ofmenstruation
Pubic hairgrowth
Breastdevelopment
14.33 Body changes at puberty
puberty The period of physical andsexual maturation in which the child’sbody begins to develop into its adultform.
primary sexual characteristicsBodily structures directly related toreproduction.
secondary sexual characteristicsBodily structures that change withsexual maturity but are not directlyrelated to reproduction.
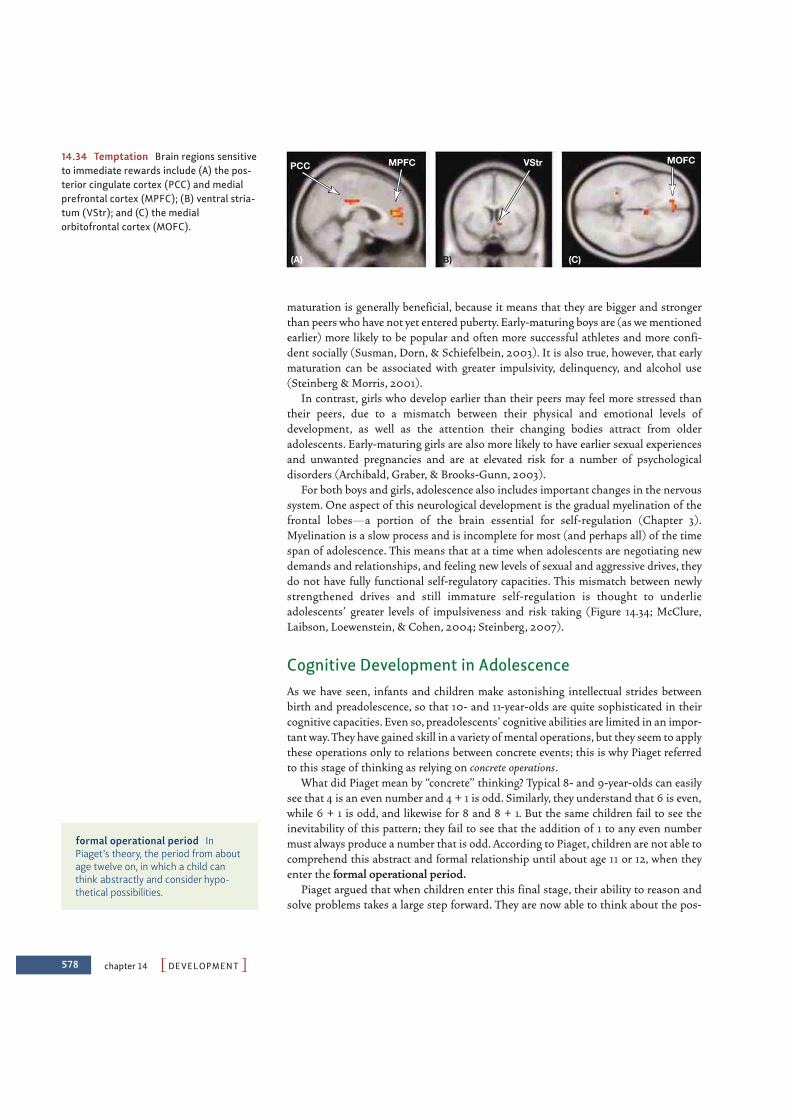
578 chapter 14 PDEVELOPMENTO
maturation is generally beneficial, because it means that they are bigger and strongerthan peers who have not yet entered puberty. Early-maturing boys are (as we mentionedearlier) more likely to be popular and often more successful athletes and more confi-dent socially (Susman, Dorn, & Schiefelbein, 2003). It is also true, however, that earlymaturation can be associated with greater impulsivity, delinquency, and alcohol use(Steinberg & Morris, 2001).
In contrast, girls who develop earlier than their peers may feel more stressed thantheir peers, due to a mismatch between their physical and emotional levels ofdevelopment, as well as the attention their changing bodies attract from olderadolescents. Early-maturing girls are also more likely to have earlier sexual experiencesand unwanted pregnancies and are at elevated risk for a number of psychologicaldisorders (Archibald, Graber, & Brooks-Gunn, 2003).
For both boys and girls, adolescence also includes important changes in the nervoussystem. One aspect of this neurological development is the gradual myelination of thefrontal lobes—a portion of the brain essential for self-regulation (Chapter 3).Myelination is a slow process and is incomplete for most (and perhaps all) of the timespan of adolescence. This means that at a time when adolescents are negotiating newdemands and relationships, and feeling new levels of sexual and aggressive drives, theydo not have fully functional self-regulatory capacities. This mismatch between newlystrengthened drives and still immature self-regulation is thought to underlieadolescents’ greater levels of impulsiveness and risk taking (Figure 14.34; McClure,Laibson, Loewenstein, & Cohen, 2004; Steinberg, 2007).
Cognitive Development in AdolescenceAs we have seen, infants and children make astonishing intellectual strides betweenbirth and preadolescence, so that 10- and 11-year-olds are quite sophisticated in theircognitive capacities. Even so, preadolescents’ cognitive abilities are limited in an impor-tant way. They have gained skill in a variety of mental operations, but they seem to applythese operations only to relations between concrete events; this is why Piaget referredto this stage of thinking as relying on concrete operations.
What did Piaget mean by “concrete” thinking? Typical 8- and 9-year-olds can easilysee that 4 is an even number and 4 + 1 is odd. Similarly, they understand that 6 is even,while 6 + 1 is odd, and likewise for 8 and 8 + 1. But the same children fail to see theinevitability of this pattern; they fail to see that the addition of 1 to any even numbermust always produce a number that is odd. According to Piaget, children are not able tocomprehend this abstract and formal relationship until about age 11 or 12, when theyenter the formal operational period.
Piaget argued that when children enter this final stage, their ability to reason andsolve problems takes a large step forward. They are now able to think about the pos-
PCC MPFC VStr MOFC
(B)(A) (C)
14.34 Temptation Brain regions sensitiveto immediate rewards include (A) the pos-terior cingulate cortex (PCC) and medialprefrontal cortex (MPFC); (B) ventral stria-tum (VStr); and (C) the medialorbitofrontal cortex (MOFC).
formal operational period InPiaget’s theory, the period from aboutage twelve on, in which a child canthink abstractly and consider hypo-thetical possibilities.

PAdolescenceO 579
sible as well as the real. This change is evident in an early study by Ward and Overton(1990), who asked children of various ages to perform tasks that required simplesteps of logical reasoning. Roughly 15% of the 4th graders they tested were able tomaster the tasks, in contrast to 25% of the 6th graders and roughly 50% of the 8thgraders. By the 12th grade, approximately 80% of the children showed evidence oflogical reasoning.
Children apply these new capacities in their schoolwork by thinking about scientifichypothesis testing or mathematical proofs in a way they could not before. They alsoapply these capacities to their own lives. They imagine new possibilities in their socialrelations, in politics, or in religion and may start to challenge beliefs and conventionsthat had seemed beyond question just a few years earlier.
There is room for debate, however, about whether we should think of these changes inthe terms Piaget described. Some theorists believe that adolescent cognition is not funda-mentally different from the thinking of middle childhood (e.g., Siegler, 1998). What, then,produces the advances in reasoning just described? The answer may lie in the fact thatolder children have acquired a set of more efficient strategies, and also have markedlygreater memory capacity, compared to younger children. This memory capacity (among itsother benefits) allows adolescents to relate different aspects of a task to one another inways they could not at an earlier age, and this is why their intellectual performance takesa large step forward.
No matter how we conceptualize these changes, though, one other point is crucial.Adolescents’ thinking is highly variable, using sophisticated logic in some cases, butrelying on much more concrete strategies in other settings. This is evident in thelaboratory, and also in adolescents’ day-to-day thinking (when, for example, they areexquisitely thoughtful in their challenges to political institutions but then remarkablyshort-sighted when thinking about the consequences of drinking and driving).
Similar variability is crucial when we compare adolescents (or adults) in differentcultures. Adults in many parts of the world fail Piaget’s tests of formal operations, invit-ing the notion that only a minority of the world’s people achieve formal thinking. Otherstudies, however, paint a different portrait—and suggest that cultural differences tell usmore about when and where people use logical thinking than about whether people canuse logical thinking.
Socioemotional Development in Adolescence The physical changes in adolescence are easily visible as young teens undergo a whole-sale remodeling of their bodies. Even more obvious are the changes in the adolescent’ssocial and emotional world as the adolescent asserts a new independence, his focusshifts from family to friends, and he copes with a wide range of new social, romantic,and sexual experiences.
The psychoanalyst Erik Erikson provided one influential framework for thinkingabout these and other major life changes in his “eight ages of man” (Figure 14.35).According to Erikson (1963), all human beings endure a series of crises as they gothrough the life cycle. At each stage, there is a critical confrontation between the self theindividual has achieved thus far and the various social and personal demands relevantto that phase of life (Erikson & Coles, 2000). The first few of these “crises” occur inearly childhood. However, a major new crisis arises in adolescence and lasts into earlyadulthood. This crisis concerns self-identity, and Erikson referred to this crisis asidentity versus role confusion.
identity versus role confusionAccording to Erikson, the major devel-opmental task of adolescence is devel-oping a stable ego identity, or sense ofwho one is. Failure results in develop-ing a negative identity or in roleconfusion.
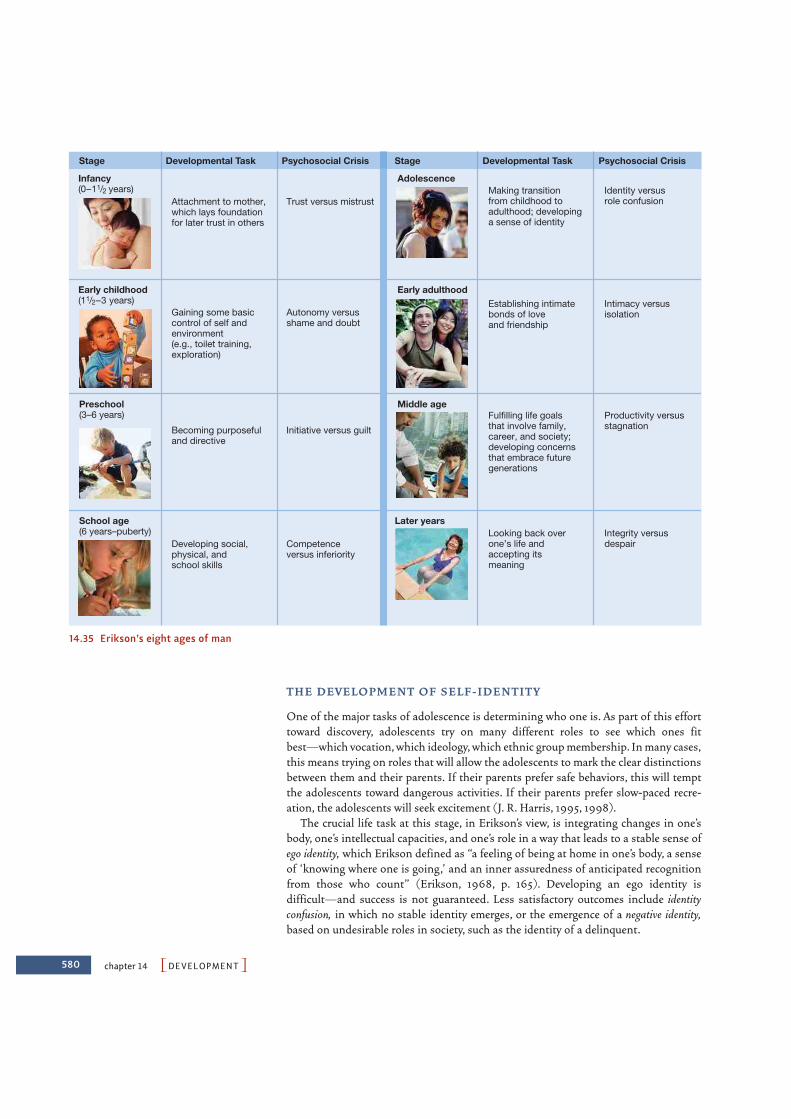
580 chapter 14 PDEVELOPMENTO
T H E D E V E LO P M E N T O F S E L F - I D E N T I T Y
One of the major tasks of adolescence is determining who one is. As part of this efforttoward discovery, adolescents try on many different roles to see which ones fit best—which vocation, which ideology, which ethnic group membership. In many cases,this means trying on roles that will allow the adolescents to mark the clear distinctionsbetween them and their parents. If their parents prefer safe behaviors, this will temptthe adolescents toward dangerous activities. If their parents prefer slow-paced recre-ation, the adolescents will seek excitement (J. R. Harris, 1995, 1998).
The crucial life task at this stage, in Erikson’s view, is integrating changes in one’sbody, one’s intellectual capacities, and one’s role in a way that leads to a stable sense ofego identity, which Erikson defined as “a feeling of being at home in one’s body, a senseof ‘knowing where one is going,’ and an inner assuredness of anticipated recognitionfrom those who count” (Erikson, 1968, p. 165). Developing an ego identity isdifficult—and success is not guaranteed. Less satisfactory outcomes include identityconfusion, in which no stable identity emerges, or the emergence of a negative identity,based on undesirable roles in society, such as the identity of a delinquent.
Stage Developmental Task Psychosocial Crisis
Infancy(0–11/2 years)
Gaining some basiccontrol of self andenvironment(e.g., toilet training,exploration)
Autonomy versusshame and doubt
Becoming purposefuland directive
Initiative versus guilt
Developing social,physical, andschool skills
Competenceversus inferiority
Attachment to mother,which lays foundationfor later trust in others
Trust versus mistrust
Preschool(3–6 years)
Early childhood(11/2–3 years)
School age(6 years–puberty)
Stage Developmental Task Psychosocial Crisis
Adolescence
Establishing intimatebonds of loveand friendship
Intimacy versusisolation
Fulfilling life goalsthat involve family,career, and society;developing concernsthat embrace futuregenerations
Productivity versusstagnation
Making transitionfrom childhood toadulthood; developinga sense of identity
Identity versusrole confusion
Middle age
Looking back overone’s life andaccepting itsmeaning
Integrity versusdespair
Later years
Early adulthood
14.35 Erikson’s eight ages of man

R E L AT I O N S W I T H PA R E N TS A N D P E E RS
Traditionally, adolescence has been considered a period of great emotional stress. Inadolescent years, children break away from parental control and seek to make their ownchoices about their activities, diet, schedule, and more. At the same time, adolescentsare shifting the focus of their social worlds, so that they spend more time with, and gainmuch more emotional support from, peers rather than family members (Figure 14.36).These shifts allow adolescents to explore a variety of newfound freedoms, includingparticipating in activities away from adult supervision—a prospect that is simultane-ously exciting and emotionally stressful.
With all of these changes, the stage seems to be set for tension between adolescentsand their parents, so it is no surprise that, across the centuries, literature (and, morerecently, film) has featured youths in desperate conflict with the adult world. Perhapssurprisingly, a number of studies suggest that emotional turbulence is by no means uni-versal among adolescents. There are conflicts, of course, and the nature of the conflictchanges over the course of adolescence (Laursen, Coy, & Collins, 1998). But many inves-tigators find that even though “storm and stress” is more likely during adolescence thanat other points (Arnett, 1999), for most adolescents “development . . . is slow, gradual,and unremarkable” (Josselson, 1980, p. 189).
What determines whether adolescence will be turbulent or not? Despite the grow-ing importance of peers during this period, parenting styles continue to make a cleardifference. Evidence suggests that the adolescent children of authoritative parents(who exercise their power, but respond to their children’s opinions and reasonablerequests) tend to be more cheerful, more responsible, and more cooperative—bothwith adults and peers (Baumrind, 1967). Teenagers raised by authoritative parentsalso seem more confident and socially skilled (Baumrind, 1991). This parental patternis also associated with better grades and better SAT scores as well as better socialadjustment (Dornbusch, Ritter, Liederman, Roberts, & Fraleigh, 1987; Steinberg,Elkman, & Mounts, 1989; L. H. Weiss & Schwarz, 1996). These are striking findingsand—impressively—are not limited to Western (individualistic) cultures.Authoritative parenting is also associated with better adolescent outcomes in collec-tivistic cultures (Sorkhabi, 2005; Steinberg, 2001).
No matter what the parents’ style, adolescence poses serious challenges as youngadults prepare to become autonomous individuals. Sometimes the process does not gowell. Some adolescents engage in highly risky forms of recreation. Some end up withunplanned (and undesired) pregnancies. Some commit crimes. Some become drugusers. Indeed, statistics show that all of these behaviors (including theft, murder, reck-less driving, unprotected sex, and use of illegal drugs) are more likely during adolescencethan at any other time of life (Arnett, 1995, 1999), although it bears emphasizing thatonly a minority of adolescents experience serious negative outcomes.
Why are risky and unhealthy behaviors more common among adolescents than amongother age groups? Several factors seem to contribute (Reyna & Farley, 2006). We havealready mentioned one—the absence of a fully mature forebrain may make it more difficultfor adolescents to rein in their impulses. As a further element, it seems in many settingsthat adolescents simply do not think about, or take seriously, the dangers and potentialconsequences of their behaviors, acting instead as if they are somehow invulnerable toharm or disease (Elkind, 1978). Moreover, other evidence suggests that adolescents areespecially motivated to seek out new and exciting experiences, and this sensation seekingregularly exposes them to risk (Arnett, 1995; Keating, 2004; Kuhn, 2006).
Hand in hand with this relative willingness to take risks, adolescents seek more andmore to identify with their own generation. As a result, their actions are increasinglyinfluenced by their friends—especially since, in adolescence, people care more and
PAdolescenceO 581
(A)
(B)
14.36 The shifting focus of adolescentsocial worlds Although family membersremain important to many adolescents,there is an increased focus on peerrelationships.

582 chapter 14 PDEVELOPMENTOchapter 14 PDEVELOPMENTO
more about being accepted by their friends (Bigelow & LaGaipa, 1975). They are alsoinfluenced by other peers, including the circle of individuals they interact with every dayand the “crowd” they identify with—the “brains” or the “jocks” or the “druggies” (B.Brown, Moray, & Kinney, 1994). And, of course, if their friends engage in risky activi-ties, it is more likely that they will, too (Berndt & Keefe, 1995; Reed & Roundtree, 1997).
We need to be careful, though, not to overstate the problems caused by peer influence.In fact, most teenagers report that their friends are more likely to discourage bad behav-iors than to encourage them (B. Brown, Clasen, & Eicher, 1986). More generally, mostpeer influence is aimed at neither good behaviors nor bad ones, but behaviors that aresimply different from those of the previous generation, like styles of clothing, hair styles,and slang that adolescents adopt (B. B. Brown, 1990; Dunphy, 1963). Of course, thesestyles change quickly. As they diffuse rapidly into the broader social world and in somecases become adult fashions, new trends spring up to maintain the differentiation.
ADULTHO OD AND OLDER AGEThe start of adolescence is typically defined by the onset of puberty. The end of adolescence,in contrast, and the entry into adulthood are not well marked. This is evident, for example,in the wide variety of ages that different countries (and different states) use for decidingwhen someone is eligible for “adult privileges” such as buying tobacco products or alcohol,voting,marrying,or serving in a nation’s armed forces.Many of these privileges arrive at dif-ferent ages, highlighting the uncertainty about when adulthood begins.
Even when young adults have cleared all these hurdles, though, development contin-ues. Young adults need to develop a capacity for closeness and intimacy through love.In many cases, they prepare for the commitments of marriage and then the joys andburdens of parenting. They learn how to manage the social and financial obligations ofadulthood and settle into their careers. They may have to cope with responsibilitiesboth for their children and for their aging parents. Eventually, as they age, they mustcome to terms with their own lives, accepting them with a sense of integrity rather thandespair. Erikson (1963) eloquently sums up this final reckoning: “It is the acceptance ofone’s own and only life cycle as something that had to be and that, by necessity, permit-ted of no substitutes” (p. 268).
Physical and Sensorimotor Changes in AdulthoodUnlike all prior developmental periods, which were characterized by increases in strengthand agility, changes in physical and sensorimotor abilities throughout adulthood arelargely a story of decline.Many of our physical and sensory abilities peak in our early to mid-twenties and then gradually deteriorate from this point forward. There are of course profes-sional athletes who manage to compete at the highest levels into their forties, and healthierlifestyles have made it possible for adults to run marathons and water ski into their eighties,but these individuals are the exceptions rather than the rule (Figure 14.37). The passingdecades still bring undeniable losses in physical and sensorimotor functioning.
Both sexes experience physical changes in middle age, including weight gain, loss ofmuscle mass, and hair thinning and graying. The age-related declines in physical andsensory capabilities accelerate in older age, and so, as people age, they become markedly weaker and slower. There are also significant declines in sight, smell, and hear-ing (see Figure 14.38). These various changes in turn cause other problems. For example,the risk of a fatal accident while driving (per mile driven) increases in later adulthoodand jumps markedly after age 70 (Coughlin, Mohyde, D’Ambrosio, & Gilbert, 2004).
14.37 Physical abilities in older agePhysical abilities peak in the early-to-mid-20s and decline from this point forward.There are, however, many people who con-tinue to remain physically fit and activewell into older age.
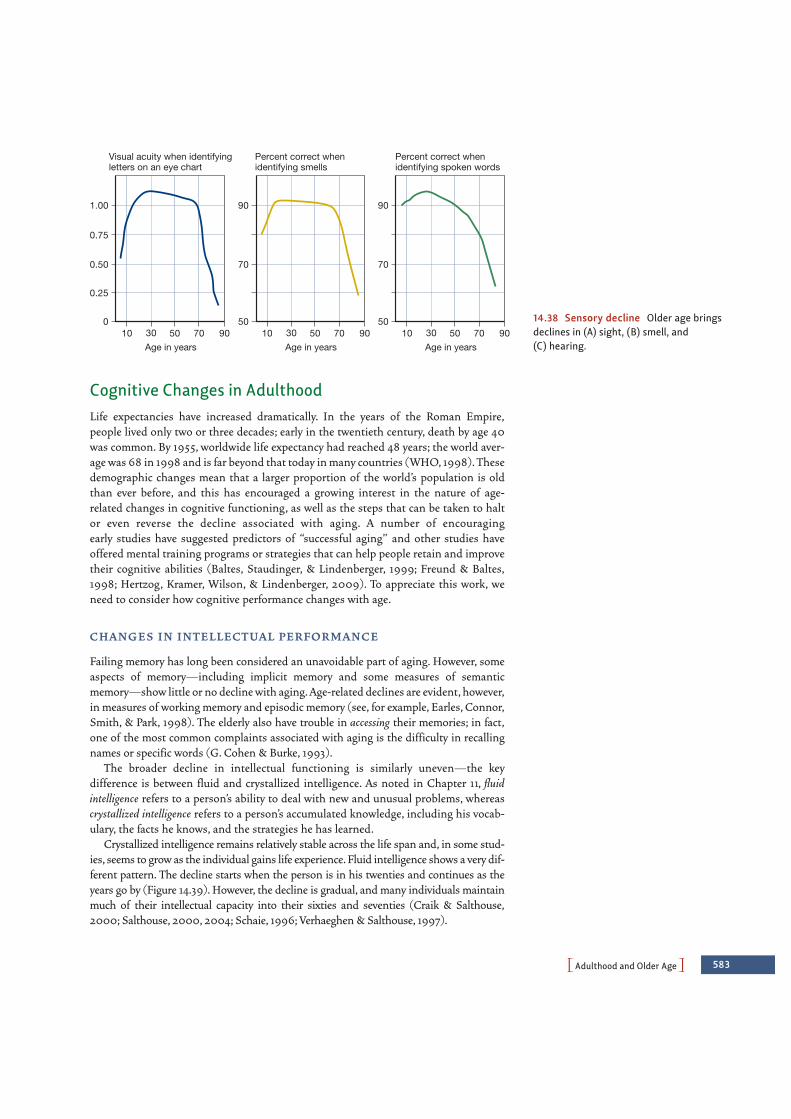
PAdulthood and Older AgeO 583
0
0.25
0.50
0.75
1.00
10 30 50 70 90Age in years
50
70
90
10 30 50 70 90Age in years
50
70
90
10 30 50 70 90Age in years
Visual acuity when identifyingletters on an eye chart
Percent correct whenidentifying smells
Percent correct whenidentifying spoken words
14.38 Sensory decline Older age bringsdeclines in (A) sight, (B) smell, and(C) hearing.
Cognitive Changes in AdulthoodLife expectancies have increased dramatically. In the years of the Roman Empire,people lived only two or three decades; early in the twentieth century, death by age 40was common. By 1955, worldwide life expectancy had reached 48 years; the world aver-age was 68 in 1998 and is far beyond that today in many countries (WHO, 1998). Thesedemographic changes mean that a larger proportion of the world’s population is oldthan ever before, and this has encouraged a growing interest in the nature of age-related changes in cognitive functioning, as well as the steps that can be taken to haltor even reverse the decline associated with aging. A number of encouraging early studies have suggested predictors of “successful aging” and other studies haveoffered mental training programs or strategies that can help people retain and improvetheir cognitive abilities (Baltes, Staudinger, & Lindenberger, 1999; Freund & Baltes,1998; Hertzog, Kramer, Wilson, & Lindenberger, 2009). To appreciate this work, weneed to consider how cognitive performance changes with age.
C H A N G E S I N I N T E L L E CT UA L P E R FO R M A N C E
Failing memory has long been considered an unavoidable part of aging. However, someaspects of memory—including implicit memory and some measures of semanticmemory—show little or no decline with aging. Age-related declines are evident, however,in measures of working memory and episodic memory (see, for example, Earles, Connor,Smith, & Park, 1998). The elderly also have trouble in accessing their memories; in fact,one of the most common complaints associated with aging is the difficulty in recallingnames or specific words (G. Cohen & Burke, 1993).
The broader decline in intellectual functioning is similarly uneven—the keydifference is between fluid and crystallized intelligence. As noted in Chapter 11, fluidintelligence refers to a person’s ability to deal with new and unusual problems, whereascrystallized intelligence refers to a person’s accumulated knowledge, including his vocab-ulary, the facts he knows, and the strategies he has learned.
Crystallized intelligence remains relatively stable across the life span and, in some stud-ies, seems to grow as the individual gains life experience. Fluid intelligence shows a very dif-ferent pattern. The decline starts when the person is in his twenties and continues as theyears go by (Figure 14.39). However, the decline is gradual, and many individuals maintainmuch of their intellectual capacity into their sixties and seventies (Craik & Salthouse,2000; Salthouse, 2000, 2004; Schaie, 1996; Verhaeghen & Salthouse, 1997).
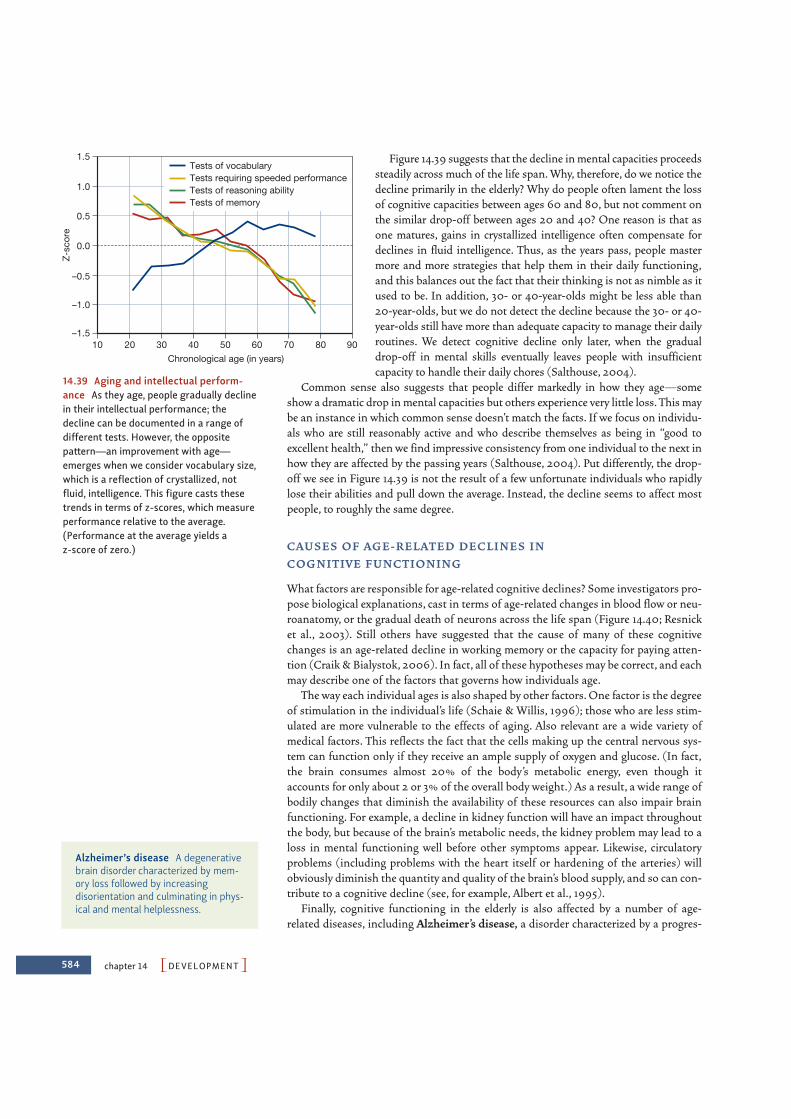
584 chapter 14 PDEVELOPMENTO
Figure 14.39 suggests that the decline in mental capacities proceedssteadily across much of the life span. Why, therefore, do we notice thedecline primarily in the elderly? Why do people often lament the lossof cognitive capacities between ages 60 and 80, but not comment onthe similar drop-off between ages 20 and 40? One reason is that asone matures, gains in crystallized intelligence often compensate fordeclines in fluid intelligence. Thus, as the years pass, people mastermore and more strategies that help them in their daily functioning,and this balances out the fact that their thinking is not as nimble as itused to be. In addition, 30- or 40-year-olds might be less able than20-year-olds, but we do not detect the decline because the 30- or 40-year-olds still have more than adequate capacity to manage their dailyroutines. We detect cognitive decline only later, when the gradualdrop-off in mental skills eventually leaves people with insufficientcapacity to handle their daily chores (Salthouse, 2004).
Common sense also suggests that people differ markedly in how they age—someshow a dramatic drop in mental capacities but others experience very little loss. This maybe an instance in which common sense doesn’t match the facts. If we focus on individu-als who are still reasonably active and who describe themselves as being in “good toexcellent health,” then we find impressive consistency from one individual to the next inhow they are affected by the passing years (Salthouse, 2004). Put differently, the drop-off we see in Figure 14.39 is not the result of a few unfortunate individuals who rapidlylose their abilities and pull down the average. Instead, the decline seems to affect mostpeople, to roughly the same degree.
CAU S E S O F AG E - R E L AT E D D E C L I N E S I N CO G N I T I V E F U N CT I O N I N G
What factors are responsible for age-related cognitive declines? Some investigators pro-pose biological explanations, cast in terms of age-related changes in blood flow or neu-roanatomy, or the gradual death of neurons across the life span (Figure 14.40; Resnicket al., 2003). Still others have suggested that the cause of many of these cognitivechanges is an age-related decline in working memory or the capacity for paying atten-tion (Craik & Bialystok, 2006). In fact, all of these hypotheses may be correct, and eachmay describe one of the factors that governs how individuals age.
The way each individual ages is also shaped by other factors. One factor is the degreeof stimulation in the individual’s life (Schaie & Willis, 1996); those who are less stim-ulated are more vulnerable to the effects of aging. Also relevant are a wide variety ofmedical factors. This reflects the fact that the cells making up the central nervous sys-tem can function only if they receive an ample supply of oxygen and glucose. (In fact,the brain consumes almost 20% of the body’s metabolic energy, even though itaccounts for only about 2 or 3% of the overall body weight.) As a result, a wide range ofbodily changes that diminish the availability of these resources can also impair brainfunctioning. For example, a decline in kidney function will have an impact throughoutthe body, but because of the brain’s metabolic needs, the kidney problem may lead to aloss in mental functioning well before other symptoms appear. Likewise, circulatoryproblems (including problems with the heart itself or hardening of the arteries) willobviously diminish the quantity and quality of the brain’s blood supply, and so can con-tribute to a cognitive decline (see, for example, Albert et al., 1995).
Finally, cognitive functioning in the elderly is also affected by a number of age-related diseases, including Alzheimer’s disease, a disorder characterized by a progres-
–1.5
–1.0
–0.5
0.0
0.5
1.0
1.5
20 30 40 50 60 70 80 9010Chronological age (in years)
Z-sc
ore
Tests of vocabularyTests requiring speeded performanceTests of reasoning abilityTests of memory
14.39 Aging and intellectual perform-ance As they age, people gradually declinein their intellectual performance; thedecline can be documented in a range ofdifferent tests. However, the oppositepattern—an improvement with age—emerges when we consider vocabulary size,which is a reflection of crystallized, notfluid, intelligence. This figure casts thesetrends in terms of z-scores, which measureperformance relative to the average.(Performance at the average yields az-score of zero.)
Alzheimer’s disease A degenerativebrain disorder characterized by mem-ory loss followed by increasingdisorientation and culminating in phys-ical and mental helplessness.
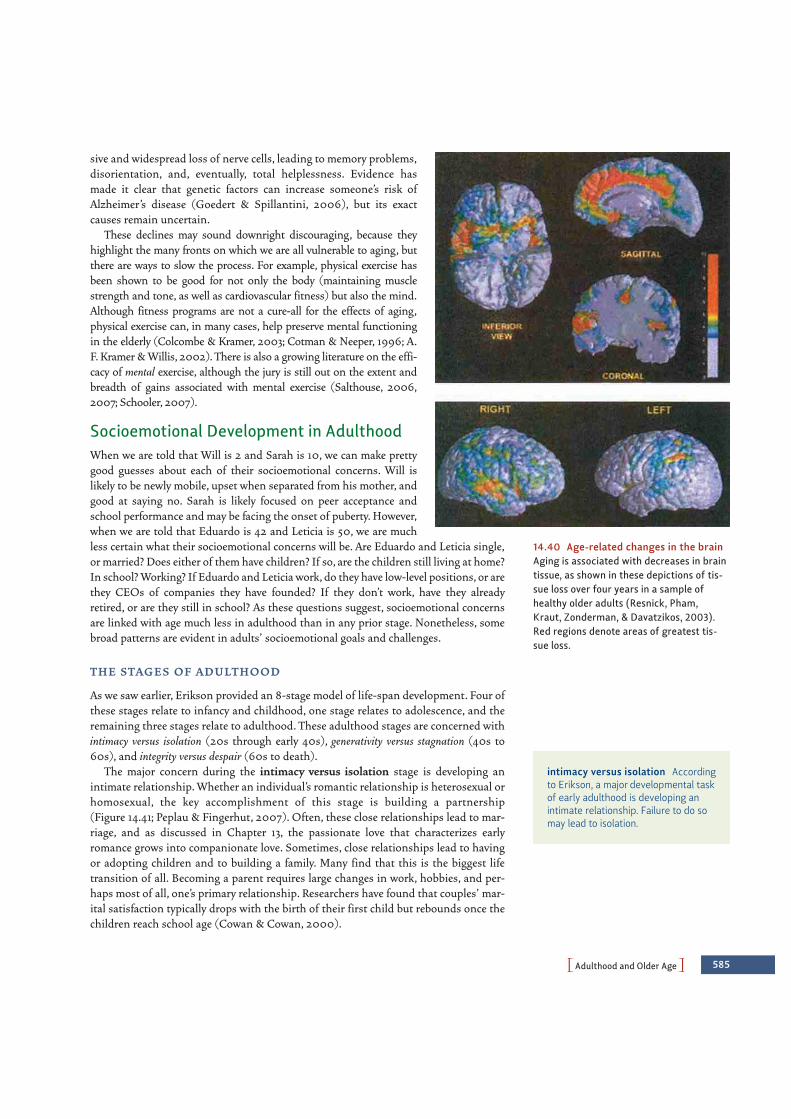
PAdulthood and Older AgeO 585
sive and widespread loss of nerve cells, leading to memory problems,disorientation, and, eventually, total helplessness. Evidence hasmade it clear that genetic factors can increase someone’s risk ofAlzheimer’s disease (Goedert & Spillantini, 2006), but its exactcauses remain uncertain.
These declines may sound downright discouraging, because theyhighlight the many fronts on which we are all vulnerable to aging, butthere are ways to slow the process. For example, physical exercise hasbeen shown to be good for not only the body (maintaining musclestrength and tone, as well as cardiovascular fitness) but also the mind.Although fitness programs are not a cure-all for the effects of aging,physical exercise can, in many cases, help preserve mental functioningin the elderly (Colcombe & Kramer, 2003; Cotman & Neeper, 1996; A.F. Kramer & Willis, 2002). There is also a growing literature on the effi-cacy of mental exercise, although the jury is still out on the extent andbreadth of gains associated with mental exercise (Salthouse, 2006,2007; Schooler, 2007).
Socioemotional Development in AdulthoodWhen we are told that Will is 2 and Sarah is 10, we can make prettygood guesses about each of their socioemotional concerns. Will islikely to be newly mobile, upset when separated from his mother, andgood at saying no. Sarah is likely focused on peer acceptance andschool performance and may be facing the onset of puberty. However,when we are told that Eduardo is 42 and Leticia is 50, we are muchless certain what their socioemotional concerns will be. Are Eduardo and Leticia single,or married? Does either of them have children? If so, are the children still living at home?In school? Working? If Eduardo and Leticia work, do they have low-level positions, or arethey CEOs of companies they have founded? If they don’t work, have they alreadyretired, or are they still in school? As these questions suggest, socioemotional concernsare linked with age much less in adulthood than in any prior stage. Nonetheless, somebroad patterns are evident in adults’ socioemotional goals and challenges.
T H E STAG E S O F A D U LT H O O D
As we saw earlier, Erikson provided an 8-stage model of life-span development. Four ofthese stages relate to infancy and childhood, one stage relates to adolescence, and theremaining three stages relate to adulthood. These adulthood stages are concerned withintimacy versus isolation (20s through early 40s), generativity versus stagnation (40s to60s), and integrity versus despair (60s to death).
The major concern during the intimacy versus isolation stage is developing anintimate relationship. Whether an individual’s romantic relationship is heterosexual or homosexual, the key accomplishment of this stage is building a partnership (Figure 14.41; Peplau & Fingerhut, 2007). Often, these close relationships lead to mar-riage, and as discussed in Chapter 13, the passionate love that characterizes earlyromance grows into companionate love. Sometimes, close relationships lead to havingor adopting children and to building a family. Many find that this is the biggest lifetransition of all. Becoming a parent requires large changes in work, hobbies, and per-haps most of all, one’s primary relationship. Researchers have found that couples’ mar-ital satisfaction typically drops with the birth of their first child but rebounds once thechildren reach school age (Cowan & Cowan, 2000).
14.40 Age-related changes in the brainAging is associated with decreases in braintissue, as shown in these depictions of tis-sue loss over four years in a sample ofhealthy older adults (Resnick, Pham,Kraut, Zonderman, & Davatzikos, 2003).Red regions denote areas of greatest tis-sue loss.
intimacy versus isolation Accordingto Erikson, a major developmental taskof early adulthood is developing anintimate relationship. Failure to do somay lead to isolation.

586 chapter 14 PDEVELOPMENTO
In contrast to the relationship goal of the intimacy versus isolation stage, the goal ofthe generativity versus stagnation stage concerns work, broadly defined. For some, thework that they do is merely a job—a means of earning a paycheck. For others, theircareer forms an important part of their self-identity. When asked who they are, theyrespond by saying what they do (“I am a doctor” or “I am a lawyer”). For others still,the work that they do is a calling—something they feel compelled to do and would doeven if they weren’t paid (Wrzesniewski, McCauley, Rozin, & Schwartz, 1997).
No matter what form their work takes, though, people are generative, in Erikson’sview, to the extent that they contribute to the next generation and, more generally, tocauses that will outlive them. Generativity can include teaching students, or training anew generation of executives. It may take the form of raising children, or of volunteeractivities, such as working in a soup kitchen, coaching a soccer team, or volunteering asa docent in a museum.
AG E - R E L AT E D C H A N G E S I N W E L L- B E I N G
Before we turn to the last of the crises Erikson describes, we need to deal with a sepa-rate issue, often mentioned in discussing the adult years. This is the so-called midlifetransition (or, sometimes, the midlife crisis), the point (according to conventional wis-dom) at which adults reappraise what they have done with their lives thus far and mayreevaluate their marriage and career (Wethington, 2000; Willis & Reid, 1999). It is aperiod when individuals begin to see physical changes that show that the summer oflife is over and its autumn has begun, a recognition that may occur earlier in womenthan in men (in part because of the psychological and physiological impact ofmenopause). There is a shift in the way one thinks about time, from “How long have Ilived?” to “How much time do I have left?” This is thought to prompt some people(especially men) to get hot new cars and seek younger playmates to reassure themselves(and the world) of their virility and power (Figure 14.42).
What do the data tell us about this period of apparent turmoil? Contrary to conven-tional accounts, depression, anxiety, and emotional instability do not appear to changethroughout the 40s (McCrae & Costa, 2003; Mroczek & Kolarz, 1998). People do, ofcourse, have emotional crises at various points, including their 40s. However, suchemotional crises do not appear to be particularly more likely in the 40s than at otherpoints in the life span.
It seems, then, that a midlife crisis is far from inevitable. One further crisis—and thethird in the series Erikson associated with adulthood—is, however, inevitable, because itis linked to the fact of eventual death. Erikson described this stage as revolving aroundthe polarity of integrity versus despair. In this stage, the individual looks back on his orher life and considers what it has all meant. If she is able to find meaning in the life shehas lived, she is said to have achieved integrity and may come to some sense of peace withher life. By contrast, if a person looks back on life with feelings of regret and disappoint-ment about missed opportunities, he is said to have fallen into despair.
A century ago in the United States, various support systems within the family, orwithin one’s neighborhood, made this transition appreciably easier. Different genera-tions often lived close together as an extended family, and there was much less segrega-tion by age. Nursing homes and retirement communities were unheard of. Older peoplecontributed to the family even when they were too old to work outside the home. Theycared for the children, helped with the housekeeping, and so on. Older people were alsosought out for advice on matters of child rearing and housekeeping. But today, it is lesscommon for the elderly to have such a recognized family role. They usually live apart fromtheir family, are effectively segregated from the rest of society, are excluded from theworkforce, and have lost their role as esteemed advisers. Given these changes, it follows
14.41 Intimacy versus isolation Buildinga partnership is a key accomplishment dur-ing early adulthood.
generativity versus stagnationAccording to Erikson, a major develop-mental task of later adulthood is find-ing meaning in one’s work, whichproduces a sense of generativity.Failure leads to a sense of stagnation.
integrity versus despair Accordingto Erikson, the major developmentaltask of older age is finding meaning inthe life that one has led. Success givesrise to a sense of integrity, whereasfailure leads to despair.

that the transition into senescence is quite different in the UnitedStates from what it was 100 years ago—the elderly now seem lessesteemed and are certainly more isolated.
These points seem to suggest that old age would be a sorrowfultime. Surprisingly, though, this hypothesis is wrong, and, in fact, pos-itive feelings seem to be greater in older age than in earlier periods(Mroczek, 2001). What produces this pattern? According to LauraCarstensen’s socioemotional-selectivity theory (2006), because of theirshrinking time horizon, older adults increasingly value emotionalgoals (feeling good rather than bad) over informational goals (learningnew things), and this leads to maintained or even increased levels ofpositive emotion. Older adults also report being able to better controltheir emotions than younger adults (Gross et al., 1998). These reportsare borne out by the finding that older adults attend to negativeaspects of their environments to a lesser degree than younger adults(Mather & Carstensen, 2003). Thus, despite the losses that olderadults face, these data tell us that they enjoy comparable—or even enhanced—levels ofwell-being, which is good news indeed for all of us who aspire to live to a ripe old age.
SOME FINAL THOUGHTS: AVOIDING DICHOTOMIES
In many domains, theorists are fond of dichotomies—either-or proposals, typically castin fairly stark terms. Over and over, though, we have seen that these dichotomies canmislead us. One prevalent dichotomy in the study of development is evident when weask, Does development proceed through distinct stages, or is it continuous? Theoristssuch as Piaget used the term stage in the same way that the term is used in embryology,to indicate distinct phases of an animal’s life with sharp discontinuities between them.As an example, the difference between a tadpole and a frog is not just a matter of “morethis” or “less that.” Instead, there is a qualitative difference between the two, with differ-ent anatomy (absence of tail, presence of legs), different breathing mechanisms (lungsvs. gills), different food needs, and more. To be sure, the change from one to the othertakes a while, but by the time the creature is a frog, its tadpole days are emphatically over.Is this stage conception a valid description of a child’s developmental trajectory, say, inthe domain of cognitive development? The answer turns out to be yes and no, becauseyoung children and older ones are plainly different but also have much in common.
The status of a stage theory is similarly unclear if we ask whether the intellectualabilities of older adults differ from those of younger adults. Sensory acuity and process-ing speed clearly change with age but crystallized intelligence remains largely intactthroughout adulthood. Even within a single domain—memory, for example—we findelements of change (e.g., a decline in working memory) and elements of stability (e.g.,in implicit memory). Over and over, we see that development involves change, but thereis much more continuity in development than a view emphasizing distinct stages wouldsuggest. In the end, the dichotomy between “stages” and “continuity” is unproductive,because each notion captures important aspects of the truth.
A second misleading dichotomy is evident when we ask, Should we understand develop-ment in terms of biological influences or experience? The “nature/nurture” distinction isjust as misleading here as it is in other domains, such as what determines a person’spersonality or IQ. Throughout development, we see a constant interplay between biological
PSome Final Thoughts: Avoiding DichotomiesO 587
14.42 Midlife transition

PRENATAL DEVELOPMENT
• Organisms grow as they change from a fertilized egg to anembryo, and then to a fetus. Prenatal development is guidedby the genome, but environmental factors are also crucial.
• Some environmental factors are local, such as those thatshape cell differentiation in the brain. Other environmentalfactors are global, such as the presence of teratogens, factorsthat disrupt development.
INFANC Y AND CHILDHOOD
• In humans, growth and brain maturation continue long afterbirth, but this lengthy period of development is advantageousfor a species whose major specialization is its capacity forlearning and whose basic invention is culture.
• Infants have a number of reflexes that help them throughtheir initial period of helplessness. Examples are the graspreflex, the rooting reflex, and the sucking reflex. Newborns alsohave reasonably mature sensory capacities.
• According to Jean Piaget, the first stage of cognitive develop-ment is the sensorimotor period (birth to to age 2). During thisperiod, the infant develops the concept of object permanence.In the preoperational period (age 2 to 7), children are capable ofrepresentational thought but lack the ability to organize thatthought. This is evident in their inability to conserve numberand quantity. Piaget believed that at about age 7, childrenbegin to manipulate mental representations. In his view, theyremain in the concrete operational period, which lacks an ele-ment of abstractness, until they are about age 12.
• Studies of visual perception using habituation procedures sug-gest that—despite Piaget’s claims—infants come equippedwith some built-in understanding of the physical world.Infants show appropriate reactions to perceptual occlusion
and have some concept of object permanence, although theyare rather inept in searching for hidden objects. One reasonis that the infant has difficulty in overriding the tendency toreach for an object at a place she had previously seen it, asshown by the A-not-B effect.
• Further studies show that infants can perceive numericalequivalence if the number of objects in the set is small enoughand that they have some rudiments of numerical reasoning.
• Piaget also underestimated infants’ capacity for social cogni-tion. Infants seem to understand others’ actions in terms oftheir goals, and not in terms of the specific movements them-selves. It also turns out that preschoolers have the rudimentsof a theory of mind, although their emerging competence sitsside by side with limitations, as can be seen in children’s poorperformance with false belief tasks.
• In the domain of socioemotional development, from a veryearly age, infants are keenly interested in face-to-face interac-tion. Between 7 and 9 months, infants begin to crawl, creat-ing the first conflicts between infants and caregivers (if theinfant crawls into a dangerous or inappropriate situation),and creating the need for social referencing.
• Infants begin to feel separation anxiety between 6 and 8months of age and have a need for contact comfort, which,according to Bowlby, provides the infant with a secure base.
• Infants differ in their beliefs about the social world—or inter-nal working models —and this is evident in different patternsof attachment. Attachment is usually assessed by observingthe behavior of children in the Strange Situation. In thissituation, some children are classified as securely attached,others show anxious/resistant or anxious/avoidant attachment,and others show a disorganized pattern of attachment. Stylesof attachment are relatively stable, but they can change if thechild’s circumstances change. The style of attachment is
S U M M A R Y C H A P T E R 1 4
588 chapter 14 PDEVELOPMENTO
influences and experience, with the biologically rooted maturational tendencies interactingwith (and sometimes dependent on) environmental factors that range from exposure to tox-ins, to educational opportunities, to patterns of physical and mental activity.
Finally, we also need to avoid either-or frameworks that imply clear distinctionsamong physical, cognitive, and socioemotional aspects of development. To take just oneexample, a child’s intellectual development depends on the physical maturation of hisbrain, as well as his social interactions with others. Intellectual development alsoincludes a growing ability to think about and understand others—the child’s theory ofmind. This interpenetration of physical, cognitive, and socioemotional aspects of func-tioning is also evident throughout adulthood: people seek to build on physical assets,and compensate for physical challenges, by using cognitive and emotional resources totheir fullest. Hence, just as the influences of nature and nurture are evident onlythrough their interaction, so physical, cognitive, and socioemotional development areinterwoven to constitute the whole person.

589
predictive of many subsequent events in the child’s social andemotional development, but there is debate over the mecha-nisms behind these correlational findings.
• Differences in attachment are in part due to differences intemperament, and in part due to differences in caregiverresponsiveness.
• Parents differ in their parenting styles, whether authoritarian,permissive, authoritative, or disengaged. Which style parentsadopt depends partly on the parents and partly on the child’sown characteristics. Evidence to date suggests that authorita-tive parenting is often preferable.
• Infants’ attachment does not seem to be disrupted by child-care, especially if the childcare is of high quality. However,social development may be disrupted by divorce or separationof the parents. Development is more severely disrupted ifthere is no attachment at all, as reflected in the tragic evidencefrom Romanian orphanages.
• Friendships are important for many reasons, including thesupport they provide for a child and the various skills andknowledge a child can gain from friendships. For example,children learn how to handle conflict by quarreling—andthen making up—with their friends.
• Children with friends seem better able to handle manystresses. Conversely, rejected children tend to be more aggres-sive and, in some cases, more anxious.
• The study of moral development has been strongly affected byKohlberg’s analysis of progressive stages in moral reasoning.There may, however, also be sex differences in moral orienta-tion and differences among cultural groups.
• A person’s moral reasoning is clearly tied to his moral behav-ior, but other factors also matter, including the person’s senseof conscience. The development of a conscience seems todepend on the child’s relationship with his parents and hiswish to preserve that relationship.
ADOLESCENCE
• Puberty is associated with the development of primary andsecondary sexual characteristics. For boys, early maturation isgenerally beneficial. For girls, early maturation appears to beless beneficial.
• Cognitive development in adolescence is characterized by theshift from concrete operations to formal operations around age 12.
• Erik Erikson charted socioemotional development duringadolescence. For Erikson, the key developmental focus duringadolescences is identity versus role confusion. A successful out-come of this stage is a stable sense of ego identity. Less satis-factory outcomes include identity confusion or the emergenceof a negative identity.
• While adolescence is sometimes turbulent, it is not usually so.Adolescence is also often characterized by risk-taking behav-iors; these are in turn the result of adolescents’ failing to take
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
dangers seriously and immaturity in the adolescents’ pre-frontal cortex. During this period, peer relationships assumean even greater importance than they have previously.
ADULTHOOD AND OLDER AGE
• Physical changes in adulthood include a general decline inphysical and sensory abilities.
• Cognitive changes are also evident during adulthood andolder age. Fluid intelligence refers to the efficiency and speed ofintellectual functioning, usually in areas that are new to theperson, and this aspect of intelligence declines across the lifespan. Crystallized intelligence refers to an individual’s accumu-lated knowledge, including his or her vocabulary, known facts,and learned strategies. This form of intelligence remains rela-tively stable over the life span and may even grow as the persongains more and more experience. Many hypotheses have beenoffered for what lies behind this decline. Some emphasize theindividual’s biological and/or medical status (includingAlzheimer’s disease). Others emphasize the individual’s men-tal life, so that people who are mentally more active preservetheir memory more fully as they age.
• According to Erikson, socioemotional development duringadulthood can be described using three stages: intimacy versusisolation, generativity versus stagnation, and integrity versus despair.
• One surprising finding concerning older age is that olderadults have relatively high levels of well-being. One explana-tion for these unexpectedly high levels of well-being is pro-vided by socioemotional-selectivity theory, which holds thatolder adults increasingly prioritize emotion regulation goals,which leads them to feel less negative emotion and more pos-itive emotion.
PSummaryO

The Trait Approach: Defining Our Differences 592
The Psychodynamic Approach: Probing the Depths 605
The Humanistic Approach: Appreciating Our Potential 615
The Social-Cognitive Approach: The Power of Beliefs 622
Some Final Thoughts: The Need for MultipleApproaches 631
Summary 632
591
CH
AP
TE
R
15 Personality
When Amanda Turner joined an Internet dating
service several years ago, she knew exactly what she wanted, and why.
“I was looking for someone who was somewhat extraverted and quite open to new
experiences, yet also very emotionally stable,” says Amanda. A researcher with a
marketing firm in New York City, Amanda studied personality psychology in graduate
school. As a result, she knew the lingo of the Big Five theory of personality, which
compresses the astounding range of human traits into five dimensions: openness to
experience, conscientiousness, extraversion, agreeableness, and neuroticism.
“I’m quite outgoing and adventurous myself, and so I wanted someone who shares
those qualities. He didn’t have to be super conscientious,” she continues, “because
I can run a tight ship all by myself. But he did need to be high in agreeableness. Trust,
after all, is the foundation of a good relationship.”
Amanda chose a Web site that offered personality tests with dimensions similar to
those of the Big Five. She then sorted through bachelors’ profiles until she found a
few who met her criteria. Within 3 years, she had met and married John Chu, a
New York stage actor.
John likewise consulted the site’s personality test results. “I was shy when I was a
kid—partly because my family had just immigrated, and so we were all a little cautious.
But I always liked the loud girls,” he laughs, “and so I knew I wanted to be with an
extravert.” Otherwise, though, John didn’t have strong preferences about the

592 chapter 15 PPERSONALITYO
personality traits of his partner. “I was more interested in people’s values andactivities,” he says. “After all, how people act so often depends on the situations theyfind themselves in, and how they view those situations.”
From choosing life partners, to describing our friends and enemies, to understanding ourselves, we appeal to the notion of personality. But are we really thesame person across situations, or do we act differently at different times? Amanda, forexample, chats with strangers on the subway, but finds herself subdued in museumsand places of worship. Likewise, John is often soft-spoken with his grandparents, butloud and commanding with his two younger brothers. “Those roughnecks need toknow who’s in charge,” he jokes.
But can we change our personalities entirely? Can others change us? John says thatmarriage has made him more conscientious, although he admits to carrying an electroniccalendar to compensate for his dispositional lateness. Amanda points out, though, thatJohn believes he can change more than she believes she can change. “I usually just try toaccept my personality quirks,” she says. “He tries to be a better person every day.”
Where do personalities come from, anyway—our genes, our experiences, or both?Amanda’s mother says that Amanda “was born early, and has been early to everythingever since.” Amanda notes, however, that her mother wouldn’t have tolerated anythingelse: “She’s done with her Christmas shopping by September, and expects herchildren to be, also.” And so Amanda’s experiences with her family enhanced herseemingly inborn inclination to be conscientious. Meanwhile, John notes that he wasan introverted child, but acting brought out his extraverted side.
People differ in many ways, including their desires, feelings, and behavior, theirviews of themselves and others, and their outlooks on the world. Some people are adelight; others are obnoxious. Some like to be with a crowd; others prefer to be alone.These distinctions and many others fall under the heading of personality, an area ofpsychology that describes how people differ and explores how the many aspects ofeach person come together. As it turns out, this is an undertaking so ambitious thatno one approach provides a completely satisfying account of all of personality. In thischapter, therefore, we describe four different approaches to personality and show howeach focuses on a different part of the puzzle of who we are.
THE TRAIT APPROACH: DEFINING OUR DIFFERENCES
The trait approach to the study of personality assumes that the differences among people can be captured by talking about what traits a person has—whether he is friendlyor not, helpful or not, formal or not. Unlike states, which are temporary (e.g., beingangry at this moment), traits are relatively enduring (e.g., being generally hot-headed),and, as a result, trait labels allow us to summarize what someone is like, often in a singleword, and serve as a basis for making predictions about what she is likely to do in thefuture. The trick, however, is to figure out which traits to use in forming a description ofa person that succinctly captures who he is but also is precise enough to predict hisactions.
Think about one of your close friends. How would you describe this person toothers? Shy? Confident? Bashful? Fun-loving? Upbeat? Notice how many words cometo mind. Indeed, if we want to describe how people differ from one another, we seem to
traits Relatively stable patterns ofthought, feeling, or behavior thatcharacterize an individual.
states Temporary patterns ofthought, feeling, or behavior.

PThe Trait Approach: Defining Our DifferencesO 593
have a nearly endless supply of terms to work with. But do we really need all of theseterms? Or can we reduce the list, perhaps by eliminating redundant or rarely usedterms, to reveal a (much smaller) set of basic personality traits?
The Big FiveAn unabridged English dictionary contains almost 18,000 personality-relevant terms(Allport & Odbert, 1936). To reduce this list to manageable size, early trait theorists putmany of these words to the side simply because they were synonyms, slang, or justuncommon words. Raymond Cattell, one of the pioneers in this arena, gave this kind ofshortened list of words to a panel of judges, asking them to use these words to rate agroup of people they knew well (Cattell, 1957). Their ratings were compared to find outwhich terms were redundant. This process allowed Cattell (1966) to eliminate theredundant terms, yielding what he thought were the 16 primary personality dimensions.
Subsequent investigators presented evidence from further analyses that severalof Cattell’s dimensions still overlapped, so they reduced the set still further. A fewinvestigators, such as Hans Eysenck (1967), argued that just two dimensions wereneeded to describe all the variations in personality, although he later added a third.Others argued that this was too severe a reduction, and, over time a consensus hasemerged around five major personality dimensions as the basis for describing allpersonalities; this has led to a personality system appropriately named the Big Five(D. W. Fiske, 1949; Norman, 1963; Tupes & Christal, 1961).
The Big Five dimensions are extraversion (sometimes called extroversion),neuroticism (sometimes labeled with its positive pole, emotional stability), agreeableness,conscientiousness, and openness to experience (L. R. Goldberg, 2001; John & Srivastava,1999; McCrae & Costa, 2003).* These dimensions seem useful for describing peoplefrom childhood through old age (Allik, Laidra, Realo, & Pullman, 2004; McCrae &Costa, 2003; Soto, John, Gosling, & Potter, 2008) in many different cultural settings(John & Srivastava, 1999; McCrae & Costa, 1997; McCrae & Terracciano, 2005;Yamagata et al., 2006). The Big Five traits even seem useful in describing the personal-ities of other species, including chimpanzees, dogs, cats, fish, and octopi (Gosling,2008; Gosling & John, 1999; Weiss, King, & Figueredo, 2000).
What do these dimension labels mean? Extraversion means having an energeticapproach toward the social and physical world. Extraverted people often feel positiveemotion and tend to agree with statements like “I see myself as someone who is outgo-ing, sociable,” while people who are introverted (low in extraversion) tend to disagreewith these statements. (This and the following items are from the Big Five Inventory:John, Donahue, & Kentle, 1991). Neuroticism means being prone to negative emotion,and its opposite is emotional stability. This dimension is assessed by finding outwhether people agree with statements like “I see myself as someone who is depressed,blue.” Agreeableness is a trusting and easygoing approach to others, as indicated byagreement with statements like “I see myself as someone who is generally trusting.”Conscientiousness means having an organized, efficient, and disciplined approach to life,as measured via agreement with statements like “I see myself as someone who doesthings efficiently.” Finally, openness to experience refers to unconventionality, intellectualcuriosity, and interest in new ideas, foods, and activities. Openness is indicated byagreement with statements like “I see myself as someone who is curious about manydifferent things.”
*To remember the Big Five, Oliver John (1990) suggests the mnemonic OCEAN.
Big Five Five crucial dimensions ofpersonality determined through factoranalyses of trait terms: extroversion,neuroticism (or emotional instability),agreeableness, conscientiousness, andopenness to experience.
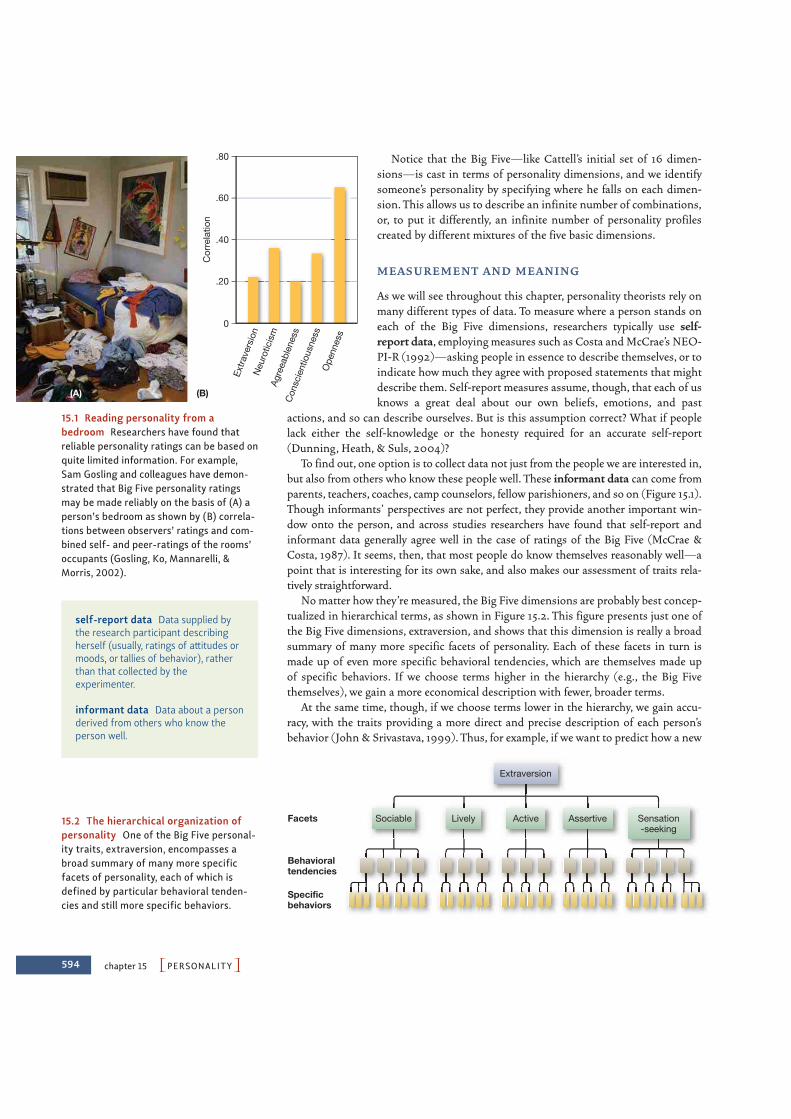
Notice that the Big Five—like Cattell’s initial set of 16 dimen-sions—is cast in terms of personality dimensions, and we identifysomeone’s personality by specifying where he falls on each dimen-sion. This allows us to describe an infinite number of combinations,or, to put it differently, an infinite number of personality profilescreated by different mixtures of the five basic dimensions.
M E AS U R E M E N T A N D M E A N I N G
As we will see throughout this chapter, personality theorists rely onmany different types of data. To measure where a person stands oneach of the Big Five dimensions, researchers typically use self-report data, employing measures such as Costa and McCrae’s NEO-PI-R (1992)—asking people in essence to describe themselves, or toindicate how much they agree with proposed statements that mightdescribe them. Self-report measures assume, though, that each of usknows a great deal about our own beliefs, emotions, and past
actions, and so can describe ourselves. But is this assumption correct? What if peoplelack either the self-knowledge or the honesty required for an accurate self-report(Dunning, Heath, & Suls, 2004)?
To find out, one option is to collect data not just from the people we are interested in,but also from others who know these people well. These informant data can come fromparents, teachers, coaches, camp counselors, fellow parishioners, and so on (Figure 15.1).Though informants’ perspectives are not perfect, they provide another important win-dow onto the person, and across studies researchers have found that self-report andinformant data generally agree well in the case of ratings of the Big Five (McCrae &Costa, 1987). It seems, then, that most people do know themselves reasonably well—apoint that is interesting for its own sake, and also makes our assessment of traits rela-tively straightforward.
No matter how they’re measured, the Big Five dimensions are probably best concep-tualized in hierarchical terms, as shown in Figure 15.2. This figure presents just one ofthe Big Five dimensions, extraversion, and shows that this dimension is really a broadsummary of many more specific facets of personality. Each of these facets in turn ismade up of even more specific behavioral tendencies, which are themselves made upof specific behaviors. If we choose terms higher in the hierarchy (e.g., the Big Fivethemselves), we gain a more economical description with fewer, broader terms.
At the same time, though, if we choose terms lower in the hierarchy, we gain accu-racy, with the traits providing a more direct and precise description of each person’sbehavior (John & Srivastava, 1999). Thus, for example, if we want to predict how a new
594 chapter 15 PPERSONALITYO
(A) (B)
Ope
nnes
s
Neu
rotic
ism
Con
scie
ntio
usne
ss
Agre
eabl
enes
s
Extra
vers
ion
Cor
rela
tion
.20
.40
.60
.80
0
15.1 Reading personality from abedroom Researchers have found thatreliable personality ratings can be based onquite limited information. For example,Sam Gosling and colleagues have demon-strated that Big Five personality ratingsmay be made reliably on the basis of (A) aperson’s bedroom as shown by (B) correla-tions between observers’ ratings and com-bined self- and peer-ratings of the rooms’occupants (Gosling, Ko, Mannarelli, &Morris, 2002).
Extraversion
ActiveLively Assertive Sensation-seeking
SociableFacets
Behavioraltendencies
Specificbehaviors
15.2 The hierarchical organization ofpersonality One of the Big Five personal-ity traits, extraversion, encompasses abroad summary of many more specificfacets of personality, each of which isdefined by particular behavioral tenden-cies and still more specific behaviors.
self-report data Data supplied bythe research participant describingherself (usually, ratings of attitudes ormoods, or tallies of behavior), ratherthan that collected by theexperimenter.
informant data Data about a personderived from others who know theperson well.

PThe Trait Approach: Defining Our DifferencesO 595
employee will perform on the job, or predict how well a nurse will perform under stress,we might want more than the overarching description provided by the Big Five itself;we might want to zoom in for a closer look at the way the Big Five traits can manifestthemselves in a particular individual. One way to do this is to use the Q-Sort, a set of100 brief descriptions that a rater sorts into a predetermined number of piles,corresponding to the degree to which they describe a person (Block, 2008). There arealso hundreds of more-specific measures available, each seeking to describe a particu-lar aspect of who someone is and how he or she behaves.
CU LT U R A L D I F F E R E N C E S
Cattell and the Big Five theorists developed their personality factors in English, andthey used mostly middle-class English-speaking subjects to validate their theories. Asdiscussed in Chapter 13, though, cultures differ in how they view human nature. Are theBig Five dimensions equally useful as we move from one culture to the next?
We have already alluded to the fact that the Big Five dimensions do seem todescribe personalities in a wide range of cultures. More precisely, as we move fromone culture to the next, we still find that the trait labels people use to describe eachother can be “boiled down” to the same five dimensions (McCrae & Costa, 1997;McCrae & Terracciano, 2005). There are, however, reasons to be cautious about thesefindings. As one concern, instead of allowing natives of a culture to generate andorganize personality terms themselves (Marsella, Dubanoski, Hamada, & Morse,2000), most researchers simply administer a test that was already developed usingEnglish-speaking subjects. This approach may not allow people’s natural or routineunderstandings to emerge (Greenfield, 1997), and so, even if these studies confirmthe existence of the Big Five dimensions in a population, they do not show uswhether these are the most frequently used categories in that culture, or whetherthey are useful in predicting the same behaviors from one culture to the next.
In fact, when participants have been allowed to generate personality terms on theirown, support for the cross-cultural generality of the Big Five has been mixed. Forexample, when researchers explored the personality traits used by Hong Kong andmainland Chinese samples, they found four factors that could be related to the BigFive, but one factor that seemed to be uniquely Chinese, which reflected interpersonalrelatedness and harmony (Cheung, 2004; Cheung & Leung, 1998; see Figure 15.3). InSpanish samples, seven factors seem best to describe personality (Benet-Martinez,1999), five of which map reasonably well onto the Big Five. Other researchers havefound three factors in Italian samples (Di Blas, Forzi, & Peabody, 2000), and nine fac-tors bearing little resemblance to the Big Five were used by students in Mexico (LaRosa & Diaz-Loving, 1991). Thus, although the Big Five seem to be well establishedamong many cultures, there is room for debate about whether these dimensions aretruly universal.
The Consistency ControversyWhether they endorse the Big Five dimensions or not, trait theorists agree that individ-uals’ personalities can be described in terms of stable and enduring traits. After all,when we say that someone is friendly and warm, we are doing more than describinghow he acted on a particular occasion. Instead, we are describing the person and, withthat, providing some expectations about how he will act on other occasions, in othersettings. But is this right? Is someone’s behavior stable in this way?
15.3 Culture and personality Interpersonalrelatedness and harmony are particularlyimportant in China.
596 chapter 15 PPERSONALITYO
H O W CO N S I ST E N T A R E P E O P L E ?
In one classic study, researchers examined the behavior of schoolchildren—and, in par-ticular, the likelihood that each child would be dishonest in one setting or another(Hartshorne & May, 1928). Quite remarkably, the researchers found little consistencyin children’s behavior: Children who were inclined to cheat on a school test were oftenquite honest in other settings (e.g., an athletic contest), and vice versa. Based on thesefindings, it would be misleading to describe these children with trait labels like“honest” or “dishonest”—sometimes they were one, and sometimes the other.
Some 40 years ago, Walter Mischel reviewed this and related studies, and concludedthat people behave much less consistently than a trait conception would predict, a stateof affairs which has been referred to as the personality paradox (Mischel, 1968). Thus,for example, the correlation between honesty measured in one setting and honestymeasured in another situation was .30, which Mischel argued was quite low. Mischelnoted that behaviors were similarly inconsistent for many other traits, such as aggres-sion, dependency, rigidity, and reactions to authority. Measures for any of these, takenin one situation, typically do not correlate more than .30 with measures of the sametraits taken in another situation. Indeed, in some studies, there is no detectable corre-lation at all (Mischel, 1968; Nisbett, 1980). These findings led Mischel to conclude thattrait conceptions of personality dramatically overstate the real consistency of a person’sbehavior.
W H Y A R E N ’ T P E O P L E M O R E CO N S I ST E N T ?
How should we think about these results? One option is to argue that our personalitiesare, in fact, relatively stable just as the trait approach suggests, but acknowledge thatsituations often do shape our behavior. Given a red light, most drivers stop; given agreen light, most go—regardless of whether they are friendly or unfriendly, stingy orgenerous, dominant or submissive. Social roles likewise often define what people doindependent of their personalities. To predict how someone will act in a courtroom, forexample, there is little point in asking whether he is sociable, careless with money, orgood to his mother. What we really want to know is the role that he will play—judge,prosecutor, defense attorney, or defendant.
In Chapter 13 we reviewed studies indicating that the influence of a situation can beincredibly powerful—leading ordinary college students to take on roles in which theyare vicious and hurtful to their peers. It’s no wonder, then, that there is sometimes lit-tle correspondence between our traits and our behavior and less consistency in ourbehavior than the trait perspective might imply. The reason, in brief, lies in what’s calledthe power of the situation. Because of that power, our behavior often depends more on thesetting we are in than on who we are.
Sometimes, though, our behavior does depend on who we are. Particularly in weaksituations—ones in which the environment provides few guides for our behavior—ourpersonalities shape our actions (Figure 15.4). Even in strong situations—ones in whichthe environment provides clear guides for our behavior—different people react to thesituation in somewhat different ways, so that their behavior in the end reflects the inter-action of the situation with their personality (Fleeson, 2004; Magnusson & Endler,1977). Moreover, it’s not a matter of chance how a particular person reacts to thissituation or that one; instead, people seem to be relatively consistent in how they act incertain types of situations. Thus, for example, someone might be punctual in profes-sional settings, but regularly late for social occasions; they might be shy in largergroups, but quite outgoing when they are with just a few friends.
personality paradox The idea thatpeople seem to behave much lessconsistently than a trait conceptionwould predict.

PThe Trait Approach: Defining Our DifferencesO 597
Evidence for these points comes from many sources, including a study in which chil-dren in a summer camp were observed in a variety of situations—settings, for example,in which they were teased or provoked by a peer, or settings in which they wereapproached in a friendly way by a peer, or settings in which they were scolded by an adult(Cervone & Shoda, 1999; Mischel, Shoda, & Mendoza-Denton, 2002). In this study, theresearchers relied on behavioral data—data based on observations of specific actions—and these data showed that each child’s behavior varied from one situation to the next.For example, one child was not at all aggressive when provoked by a friend, butresponded aggressively when scolded by an adult. Another child showed the reverse pat-tern. Thus, the trait label aggressive would not consistently fit either child—sometimesthey were aggressive and sometimes they were not.
There was, however, a clear pattern to the children’s behavior, but the pattern emergesonly when we consider both the person and the situation. As the investigators describedit, the data suggested that each of the children had a reliable “if . . . then . . .” profile: “If inthis setting, then act in this fashion; if in that setting, then act in that fashion” (Mischelet al., 2002). Because of these “if . . . then . . .” patterns, the children were, in fact, reason-ably consistent in how they acted, but their behaviors were “tuned” to the situations theyfound themselves in. Thus, we need to be careful when we describe any of these childrenas being “friendly” or “aggressive” or “helpful,” relying only on global trait labels. To givean accurate description, we need to be more specific, saying things like “tends to befriendly in this sort of setting,” “tends to be helpful in that sort of setting,” and so on.
A R E SO M E P E O P L E M O R E I N F LU E N C E D BY T H E S I T UAT I O N T H A N OT H E RS ?
There is one more complexity we must keep in mind as we consider how personalityand situations interact to shape behavior. Some individuals are more consistent thanothers across situations, or, turning this around, some individuals are more flexiblethan others. This difference among people is assessed by the Self-Monitoring Scale,developed by Mark Snyder and designed to assess the degree to which people are sen-sitive to their surroundings and likely to adjust their behaviors to fit in. The scaleincludes items such as “In different situations and with different people, I often act likevery different persons.”
High self-monitors care a great deal about how they appear to others, and so, at acocktail party, they are charming and sophisticated; in a street basketball game, they“trash talk.” In contrast, low self-monitors are less interested in how they appear to
(A) A weak situation (B) A strong situation
15.4 Weak and strong situations (A) Anexample of a weak situation is a casualparty where different people behave quitedifferently. (B) An example of a strong situ-ation is an examination, where very similarbehavior is seen across individuals.
behavioral data Data about a per-son based on direct observation ofthat person’s actions or behavior.
Self-Monitoring Scale A personalitymeasure that seeks to determine thedegree to which a person alters oradjusts their behavior in order to actappropriately in new circumstances.

598 chapter 15 PPERSONALITYO
others. They are who they are regardless of the momentary situation, making theirbehavior much more consistent across situations (Figure 15.5; Gangestad & Snyder,2000; M. Snyder, 1987, 1995). This suggests that the extent to which situations deter-mine an individual’s behavior varies by person, with situations being more importantdeterminants of high self-monitors’ behavior than of low self-monitors’ behavior.
How consistent individuals are also varies at the cultural level of analysis.Americans, for example, are relatively consistent in how they describe themselves, nomatter whether they happen at the time to be sitting alone, next to an authority figure,or in a large group (Kanagawa, Cross, & Markus, 2001). By contrast, Japanese partici-pants’ self-descriptions varied considerably across contexts, and they were far moreself-critical when sitting next to an authority figure than when they were by themselves.There also cultural differences in how consistent individuals want to be. In one study,researchers asked American and Polish participants how they would respond to arequest to take a survey about beverage preferences. When asked to imagine they hadpreviously agreed to such requests, American participants said they would again agreeto the request—apparently putting a high value on self-consistency. Polish partici-pants, by contrast, were much less concerned with self-consistency, and so were lessinfluenced by imagining that they had agreed to similar requests in the past (Cialdini,Wosinka, Barrett, Butner, & Gornik-Durose, 1999).
Traits and BiologyWhere does all of this leave us? Plainly, situations do matter in shaping how we act, and,as a result, we can easily document inconsistencies in how someone behaves: She mightbe honest in one setting but treacherous in another, friendly in one situation but hostileotherwise, with her behavior in each case governed as much by where she is as by whoshe is. At the same time, we can also document ways in which each of us is consistent inwho we are. We shouldn’t be surprised, therefore, that personality traits have been shownto predict important life outcomes (Ozer & Benet-Martinez, 2006; Roberts, Kuncel,Shiner, Caspi, & Goldberg, 2007). For example, the Big Five personality dimensions arerelated to outcomes ranging from career success (Barrick, Mount, & Gupta, 2003) to crim-inal activities (Wiebe, 2004) to health and mortality (Roberts, Walton, & Bogg, 2005).
Personality consistency thus seems to be alive and well, especially if we understandtrait labels to be descriptions of how a person tends to act in a certain sort of situation,rather than a description of what he is like at all times and in all places. However, thissimply leads to a new question: Given that people do differ in their personalities, howdo these differences arise?
(A) (B)
15.5 The extremes of the self-monitor-ing scale (A) Matt Damon as Tom Ripley inThe Talented Mr. Ripley: the high self-moni-tor, who can fit in with anybody, anywhere,anytime. (B) Heath Ledger as the Joker inThe Dark Knight: the ultimate low self-mon-itor, who stays true to himself regardless ofthe situation.
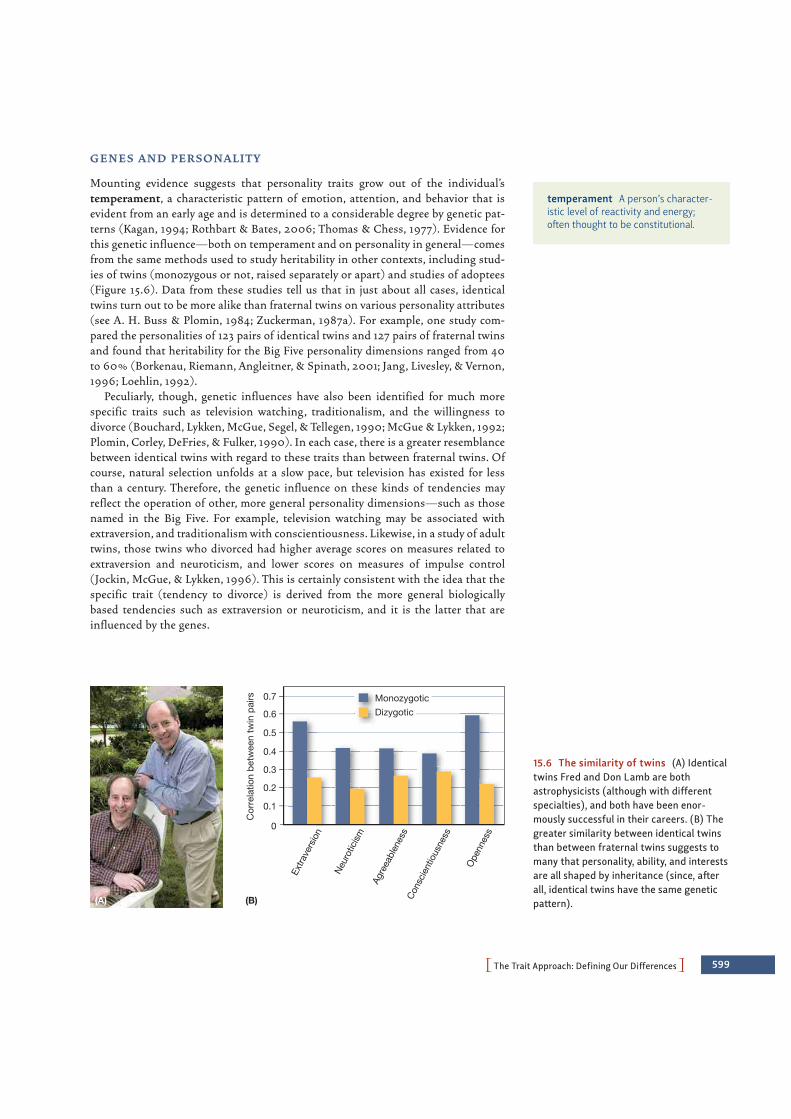
PThe Trait Approach: Defining Our DifferencesO 599
G E N E S A N D P E RSO N A L I T Y
Mounting evidence suggests that personality traits grow out of the individual’stemperament, a characteristic pattern of emotion, attention, and behavior that isevident from an early age and is determined to a considerable degree by genetic pat-terns (Kagan, 1994; Rothbart & Bates, 2006; Thomas & Chess, 1977). Evidence forthis genetic influence—both on temperament and on personality in general—comesfrom the same methods used to study heritability in other contexts, including stud-ies of twins (monozygous or not, raised separately or apart) and studies of adoptees(Figure 15.6). Data from these studies tell us that in just about all cases, identicaltwins turn out to be more alike than fraternal twins on various personality attributes(see A. H. Buss & Plomin, 1984; Zuckerman, 1987a). For example, one study com-pared the personalities of 123 pairs of identical twins and 127 pairs of fraternal twinsand found that heritability for the Big Five personality dimensions ranged from 40to 60% (Borkenau, Riemann, Angleitner, & Spinath, 2001; Jang, Livesley, & Vernon,1996; Loehlin, 1992).
Peculiarly, though, genetic influences have also been identified for much morespecific traits such as television watching, traditionalism, and the willingness todivorce (Bouchard, Lykken, McGue, Segel, & Tellegen, 1990; McGue & Lykken, 1992;Plomin, Corley, DeFries, & Fulker, 1990). In each case, there is a greater resemblancebetween identical twins with regard to these traits than between fraternal twins. Ofcourse, natural selection unfolds at a slow pace, but television has existed for lessthan a century. Therefore, the genetic influence on these kinds of tendencies mayreflect the operation of other, more general personality dimensions—such as thosenamed in the Big Five. For example, television watching may be associated withextraversion, and traditionalism with conscientiousness. Likewise, in a study of adulttwins, those twins who divorced had higher average scores on measures related toextraversion and neuroticism, and lower scores on measures of impulse control(Jockin, McGue, & Lykken, 1996). This is certainly consistent with the idea that thespecific trait (tendency to divorce) is derived from the more general biologicallybased tendencies such as extraversion or neuroticism, and it is the latter that areinfluenced by the genes.
temperament A person’s character-istic level of reactivity and energy;often thought to be constitutional.
MonozygoticDizygotic
(A) (B)
Cor
rela
tion
betw
een
twin
pai
rs
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Agre
eabl
enes
sC
onsc
ient
ious
ness
Neu
rotic
ism
Extra
vers
ion
Ope
nnes
s0
15.6 The similarity of twins (A) Identicaltwins Fred and Don Lamb are bothastrophysicists (although with differentspecialties), and both have been enor-mously successful in their careers. (B) Thegreater similarity between identical twinsthan between fraternal twins suggests tomany that personality, ability, and interestsare all shaped by inheritance (since, afterall, identical twins have the same geneticpattern).

600 chapter 15 PPERSONALITYO
P H YS I O LO GY A N D P E RSO N A L I T Y
If our personalities have a basis in our genes, what exactly do the genes code for? Usingphysiological data, psychologists are beginning to explore how people with differentpersonality traits differ in their biological functioning, with the hope that these datawill offer a glimpse into how our genes shape who we are.
One example of this work is inspired by Hans Eysenck’s theory of extraversion/introversion. Eysenck proposed that the observable difference in personality derivesfrom the fact that introverts react more strongly than extraverts to external stimuli(M. W. Eysenck, 1987). As a result, he argued, introverts often guard against stimula-tion from the outside, which to them feels like overstimulation. This is why, for exam-ple, introverts shy away from social settings—the stimulation in that setting would bemore than they are comfortable with. It also turns out that introverts have a lower tol-erance for pain (Bartol & Costello, 1976), and, when they are studying, they prefer lessnoise and fewer opportunities for socializing (J. B. Campbell & Hawley, 1982).
Can we confirm this proposal through studies of the brain? In one study, investiga-tors measured how people’s brain stems reacted when the people heard clicking noises.In line with Eysenck’s theory, introverts showed a quicker response than extraverts,indicating more reactive brain stems (Bullock & Gilliland, 1993; also see Kumari,Ffytche, Williams, & Gray, 2004).
Similar arguments may help us to understand a more specific trait, sensationseeking, which refers to the tendency to seek varied and novel experiences, to look forthrills and adventure, and to be highly susceptible to boredom (Zuckerman, 1979, 1994;Figure 15.7). People high in sensation-seeking are more likely to participate in riskysports; to get more restless in monotonous, confined situations; and to drive faster thanpeople with low sensation-seeking scores (Zuckerman, 1979, 1983).
What leads to this pattern of behavior? One suggestion is that sensation seekers arepeople whose neurotransmitter systems (especially those relying on norepinephrine anddopamine) are underreactive. As a result, these people are chronically underaroused, andthis makes them seek thrills and take risks to jog their sluggish neurotransmitter systemsinto greater activity (Zuckerman, 1987b, 1990, 1994). Consistent with this hypothesis,sensation seekers seem to be at greater risk for abusing drugs that influence dopamine lev-els. Researchers explain this finding by suggesting that in this case, the sensation seekersare using drugs, rather than activities such as sky diving or snake handling, to activatetheir underactive brain systems (Bardo, Donohew, & Harrington, 1996). These findingsare buttressed by those of researchers who have developed a “rat model” of drug use.
15.7 Sensation seeking Some people actively seek thrills and arousal; others seek quietactivities. This difference in personality may derive from the responsiveness of the person’snervous system.
physiological data Data about aperson derived from measurement ofbiological structures and processes.
sensation seeking A predispositionto seek novel experiences, look forthrills and adventure, and be highlysusceptible to boredom.

PThe Trait Approach: Defining Our DifferencesO 601
inhibited temperament A personal-ity style associated with introversionand neuroticism, and characterized bya fear of novelty that is evident early inlife.
Amy
15.8 SCIENTIFIC METHOD: Do inhibited individuals have lower thresholds for activation in theamygdala?
Method1. Adult participants had beenclassified either as inhibited oruninhibited at age two.
When viewing novel faces, adults previously classified as inhibited showed greater activations intheir amygdalae than those classified as uninhibited. This difference was markedly reducedwith familiar faces.
2. Participants first saw sixdifferent faces presentedrepeatedly in random orderso that these faces becamefamiliar.
3. During the test phase,fMRIs were taken as theparticipants viewed a seriesof faces that mixed familiarones with novel ones.
The most significant differencesin inhibited participants’ brain
responses centered in the amygdala.
Results
CONCLUSION: Inhibited people show stronger amygdalar responses to unfamiliar faces than uninhibited people do. These findings suggest that some patterns of brain activity relating to temperament are preserved from infancy into early adulthood.
SOURCE STUDY: Schwartz, Wright, Shin, Kagan, & Rauch, 2003
Am
ount
of a
myg
dala
act
ion
0.1
0.0
0.2
0.3
0.4
0.5
0.6
0.7
Novel facesviewed
Familiar facesviewed
InhibitedUninhibited
Using this model, researchers have shown that high levels of sensation seeking (measuredby animals’ activity levels in a novel environment) predict the animals’ propensity to givethemselves cocaine (Belin, Mar, Dalley, Robbins, & Everitt, 2008).
Sensation seeking is common among extraverts; a very different pattern—calledinhibited temperament—is associated with introversion and neuroticism (Fox,Henderson, Marshall, Nichols, & Ghera, 2005; Kagan, 1994, 2003; Kagan & Snidman,1991; Putnam & Stifter, 2005). As infants, people with inhibited temperaments tend toreact strongly when they are distressed, crying vigorously and showing high levels ofmotor activity. As young children, inhibited individuals are unwilling to approach novelstimuli or people, become anxious in new situations, and frequently seek reassurancefrom their caregivers. Adolescents and adults who were categorized as inhibited at anearly age are much less likely than others to be outgoing and socially spontaneous.
The explanation for inhibited temperament may mirror the account of sensationseeking, and in particular may be associated with an overreactive brain (and attemptsto compensate for this) just as sensation seeking is associated with an underreactivebrain. Specifically, Kagan and colleagues hypothesize that inhibited children have a lowthreshold for activity in the amygdala, a subcortical brain structure crucial for detectingimportant stimuli in the environment. This hypothesis was tested using an fMRI studyof young adults who had been classified when they were infants as either inhibited oruninhibited (Schwartz, Wright, Shin, Kagan, & Rauch, 2003; Figure 15.8). These participants viewed a series of familiar and unfamiliar faces. As predicted, when theinhibited participants viewed unfamiliar faces, their amygdalae showed higher levels ofactivation than did the amygdalae of uninhibited participants. The two groups did notdiffer, however, when they were viewing familiar faces, suggesting that it was the newnessof the faces that led the inhibited individuals’ amygdalae to respond more strongly.

602 chapter 15 PPERSONALITYO
Traits and the EnvironmentIt seems plausible, then, that genes influence personality in a variety of ways—by deter-mining the reactivity of neurotransmitter systems, the threshold for activation in theamygdala, and more. But, as we have repeatedly noted, genetic influence will emergeonly if certain environmental supports are in place. In addition, virtually any character-istic shaped by the genes is also likely to be shaped by environmental factors. What arethe environmental factors relevant to the development of someone’s personality? Threesources of influence have been widely discussed: cultures, families, and differencesamong members within the same family.
CU LT U R A L E F F E CTS
As we have seen, the evidence is mixed on whether the Big Five dimensions are as usefulfor describing personalities in Korea as they are in Kansas, as useful in Niger as they arein Newport. But no matter what we make of this point, we need to remember that the BigFive is simply a framework for describing how people differ; if the framework is in factuniversal, this simply tells us that we can describe personalities in different culturesusing the same (universal) measuring system, just as we can measure objects of differentsizes using the same ruler. This still leaves open, however, what the personalities are inany given culture—that is, what we will learn when we use our measuring system.
Scholars have long suggested that people in different cultures have differentpersonalities—so that we can speak of a “German personality,” or a “typical Italian,”and so on. One might fear that these suggestions amount to little beyond stereotyping,and indeed, some scholars have argued that these perceptions may be entirely illusory(McCrae & Terracciano, 2006). Mounting evidence suggests, however, that there is akernel of truth in some of these claims about national character. For example, onestudy has shown that there are differences from one country to the next in how consci-entious people seem to be. These differences are manifest in such diverse measures aspedestrians’ walking speed, postal workers’ efficiency, accuracy of public clocks, andeven longevity in each of these countries (Heine, Buchtel, & Norenzayan, 2008)!
Where might these cultural differences in personality come from? One long-standing hypothesis is that the key lies in how a group of people sustains itself, whetherthrough farming or hunting or trade (Barry, Child, & Bacon, 1959; Hofstede, 2001;Maccoby, 2000). More recent models, in contrast, take a more complex view, and sug-gest that cultural differences in personality—whether between nations or acrossregions within a single nation—arise via a combination of forces (Jokela, Elovainio,Kivimaki, & Keltikangas-Jarvinen, 2008; Rentfrow, Gosling, & Potter, 2008). Theseforces include historical migration patterns, social influence, and environmental factorsthat dynamically reinforce one another over time. To make this concrete, let’s considerimmigrants who first make their way to a new geographical region (whether fleeingpersecution or seeking prosperity). It seems unlikely that these trailblazers will be a ran-dom sample of the larger population. Instead, the mere fact that they decided to relo-cate suggests that they may be willing to take risks and more open to new experiencesin comparison to others who were not willing to emigrate. This initial difference mightthen be magnified via social influence—perhaps because the especially extraverted oropen individuals engaged in practices that shaped the thoughts, feelings, and behaviorsof those around them.
Arguments like these may help us understand why different regions within theUnited States often seem characterized by distinct personality types, with neuroticismespecially common in some of the mid-Atlantic states and openness to new experience
national character The idea thatpeople in different cultures have dif-ferent personalities.
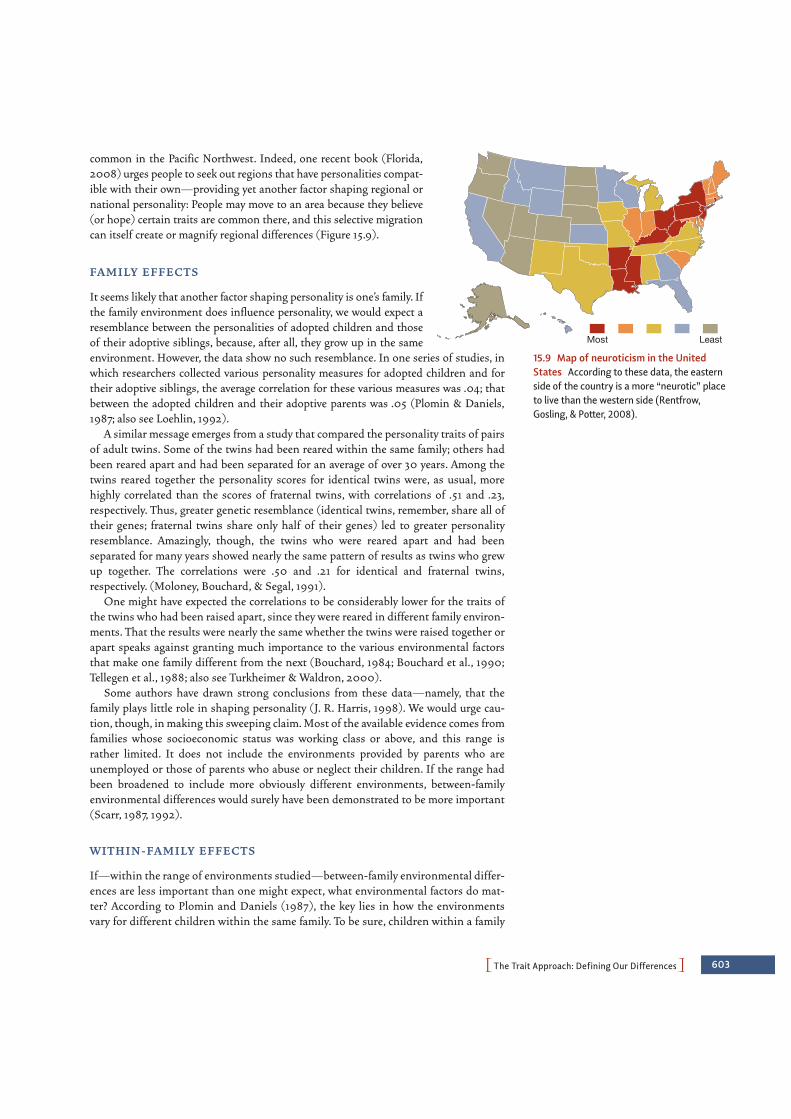
PThe Trait Approach: Defining Our DifferencesO 603
common in the Pacific Northwest. Indeed, one recent book (Florida,2008) urges people to seek out regions that have personalities compat-ible with their own—providing yet another factor shaping regional ornational personality: People may move to an area because they believe(or hope) certain traits are common there, and this selective migrationcan itself create or magnify regional differences (Figure 15.9).
FA M I LY E F F E CTS
It seems likely that another factor shaping personality is one’s family. Ifthe family environment does influence personality, we would expect aresemblance between the personalities of adopted children and thoseof their adoptive siblings, because, after all, they grow up in the sameenvironment. However, the data show no such resemblance. In one series of studies, inwhich researchers collected various personality measures for adopted children and fortheir adoptive siblings, the average correlation for these various measures was .04; thatbetween the adopted children and their adoptive parents was .05 (Plomin & Daniels,1987; also see Loehlin, 1992).
A similar message emerges from a study that compared the personality traits of pairsof adult twins. Some of the twins had been reared within the same family; others hadbeen reared apart and had been separated for an average of over 30 years. Among thetwins reared together the personality scores for identical twins were, as usual, morehighly correlated than the scores of fraternal twins, with correlations of .51 and .23,respectively. Thus, greater genetic resemblance (identical twins, remember, share all oftheir genes; fraternal twins share only half of their genes) led to greater personalityresemblance. Amazingly, though, the twins who were reared apart and had beenseparated for many years showed nearly the same pattern of results as twins who grewup together. The correlations were .50 and .21 for identical and fraternal twins,respectively. (Moloney, Bouchard, & Segal, 1991).
One might have expected the correlations to be considerably lower for the traits ofthe twins who had been raised apart, since they were reared in different family environ-ments. That the results were nearly the same whether the twins were raised together orapart speaks against granting much importance to the various environmental factorsthat make one family different from the next (Bouchard, 1984; Bouchard et al., 1990;Tellegen et al., 1988; also see Turkheimer & Waldron, 2000).
Some authors have drawn strong conclusions from these data—namely, that thefamily plays little role in shaping personality (J. R. Harris, 1998). We would urge cau-tion, though, in making this sweeping claim. Most of the available evidence comes fromfamilies whose socioeconomic status was working class or above, and this range israther limited. It does not include the environments provided by parents who areunemployed or those of parents who abuse or neglect their children. If the range hadbeen broadened to include more obviously different environments, between-familyenvironmental differences would surely have been demonstrated to be more important(Scarr, 1987, 1992).
W I T H I N - FA M I LY E F F E CTS
If—within the range of environments studied—between-family environmental differ-ences are less important than one might expect, what environmental factors do mat-ter? According to Plomin and Daniels (1987), the key lies in how the environmentsvary for different children within the same family. To be sure, children within a family
15.9 Map of neuroticism in the UnitedStates According to these data, the easternside of the country is a more “neurotic” placeto live than the western side (Rentfrow,Gosling, & Potter, 2008).
Most Least
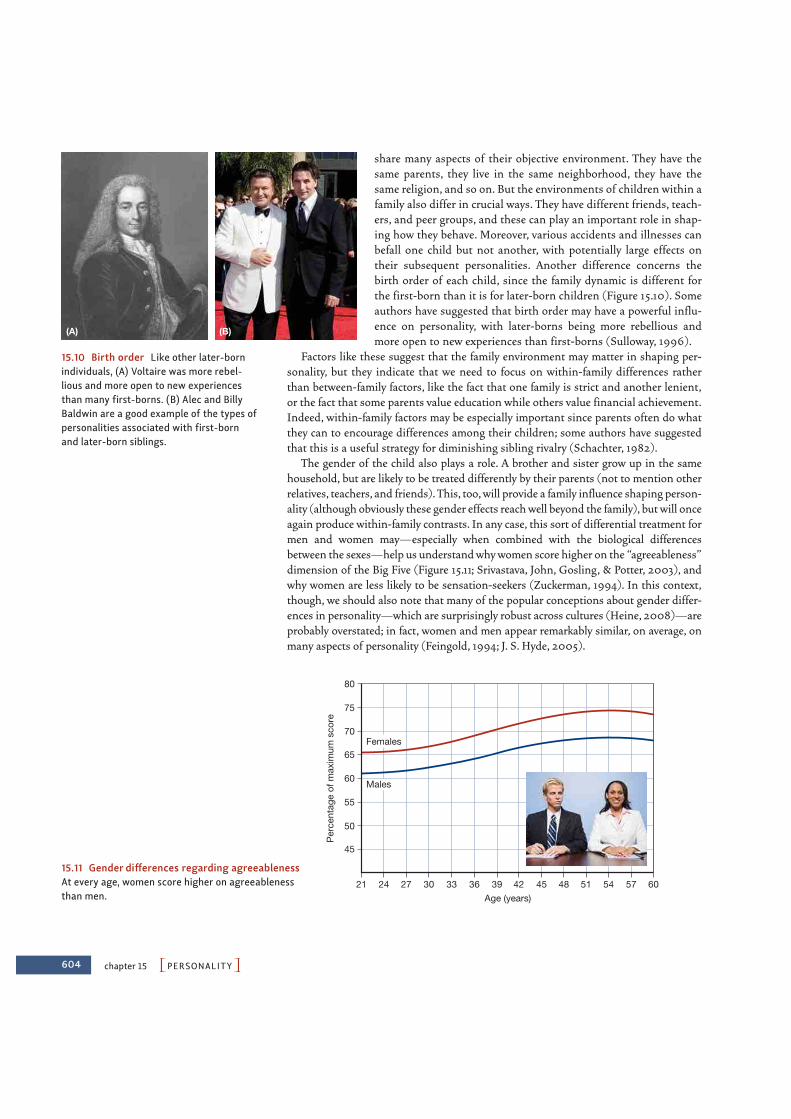
604 chapter 15 PPERSONALITYO
share many aspects of their objective environment. They have thesame parents, they live in the same neighborhood, they have thesame religion, and so on. But the environments of children within afamily also differ in crucial ways. They have different friends, teach-ers, and peer groups, and these can play an important role in shap-ing how they behave. Moreover, various accidents and illnesses canbefall one child but not another, with potentially large effects ontheir subsequent personalities. Another difference concerns thebirth order of each child, since the family dynamic is different forthe first-born than it is for later-born children (Figure 15.10). Someauthors have suggested that birth order may have a powerful influ-ence on personality, with later-borns being more rebellious andmore open to new experiences than first-borns (Sulloway, 1996).
Factors like these suggest that the family environment may matter in shaping per-sonality, but they indicate that we need to focus on within-family differences ratherthan between-family factors, like the fact that one family is strict and another lenient,or the fact that some parents value education while others value financial achievement.Indeed, within-family factors may be especially important since parents often do whatthey can to encourage differences among their children; some authors have suggestedthat this is a useful strategy for diminishing sibling rivalry (Schachter, 1982).
The gender of the child also plays a role. A brother and sister grow up in the samehousehold, but are likely to be treated differently by their parents (not to mention otherrelatives, teachers, and friends). This, too, will provide a family influence shaping person-ality (although obviously these gender effects reach well beyond the family), but will onceagain produce within-family contrasts. In any case, this sort of differential treatment formen and women may—especially when combined with the biological differencesbetween the sexes—help us understand why women score higher on the “agreeableness”dimension of the Big Five (Figure 15.11; Srivastava, John, Gosling, & Potter, 2003), andwhy women are less likely to be sensation-seekers (Zuckerman, 1994). In this context,though, we should also note that many of the popular conceptions about gender differ-ences in personality—which are surprisingly robust across cultures (Heine, 2008)—areprobably overstated; in fact, women and men appear remarkably similar, on average, onmany aspects of personality (Feingold, 1994; J. S. Hyde, 2005).
(A) (B)
15.10 Birth order Like other later-bornindividuals, (A) Voltaire was more rebel-lious and more open to new experiencesthan many first-borns. (B) Alec and BillyBaldwin are a good example of the types ofpersonalities associated with first-bornand later-born siblings.
Per
cent
age
of m
axim
um s
core
45
50
55
60
65
70
75
80
39 42 45 48 51 54 57 60363330272421Age (years)
Females
Males
15.11 Gender differences regarding agreeablenessAt every age, women score higher on agreeablenessthan men.

PThe Psychodynamic Approach: Probing the DepthsO 605
Contributions of the Trait ApproachPeople differ from one another in a huge number of ways, and one of the major contri-butions of the trait approach lies in its systematic description of these differences andits success in reducing the apparently large number of these differences to manageablesize. Moreover, the trait approach provides a set of continuous personality dimensionson which people can vary in almost infinite ways. This has certainly increased theprecision of our personality descriptions. The trait approach offers us a rich notion ofhow personality and situations jointly shape behavior—leaving us with a moresophisticated theory and appreciably better predictions about how people of variouspersonalities will behave in various settings.
The emergence of the broad Big Five framework has also enabled researchers work-ing within very different traditions to use agreed-upon measures and to share the datathey collect. As a result, progress on determining the genetic bases and brain corre-lates of personality differences has accelerated dramatically. Still, we must draw onother perspectives as well if we are to understand what a “personality” is, and how itcomes to be.
THE PSYCHODYNAMIC APPROACH:PROBING THE DEPTHS
The comic theater of the classical and Renaissance ages presented personality types asstable and well-defined. Once a character entered, the audience knew what to expect ofhim. If the actor wore the mask of the cowardly soldier, he would brag and run away; ifhe wore the mask of the miserly old man, he would jealously guard his money.
As we have seen, the trait approach has amended this view in important ways buthas still left one crucial claim: We are who we seem to be, and our various traits andmotivations are in plain view for all to see. Indeed, the trait approach often relies onself-report data—a reflection of the assumption that we can perceive ourselves withrelative accuracy.
According to the psychodynamic approach, however, we need to revise this under-standing both of personality and of self-knowledge—and shift to an understandingthat parallels a more modern approach to drama, in which nothing is quite what itseems. In this approach, actors playing a character must pay attention to the subtext,the unspoken thoughts that go through the character’s head while she speaks her lines.And many actors are interested in a still deeper subtext, the thoughts and wishes ofwhich the character is unaware. According to the psychodynamic approach, this deepersubtext is the wellspring of all human personality.
Adherents of the psychodynamic approach do not deny that some people are moresociable than others, or that some are more impulsive or emotionally unstable. But theycontend that it is superficial to explain such tendencies as either the expression of apersonality trait or the product of situational factors. In their view, what people do andsay—and even what they consciously think—is only the tip of the iceberg. As they seeit, human acts and thoughts are just the outer expression of a whole host of motivesand desires that are often derived from early childhood experiences, and that are for themost part unknown to the person himself. They believe that to understand a person isto understand these hidden psychological forces or dynamics.

606 chapter 15 PPERSONALITYO
Psychoanalysis: Theory and PracticeThe founder of psychoanalysis, Sigmund Freud (1856–1939; Figure 15.12), was a physi-cian by training. After a stint as a medical researcher, though, financial pressures ledFreud to open a neurology practice in which he found that many of his patients weresuffering from a disorder then called hysteria (now called conversion disorder). Thesymptoms of hysteria presented a helter-skelter catalog of physical and mental com-plaints—total or partial blindness or deafness, paralysis or anesthesia of various partsof the body, uncontrollable trembling or convulsive attacks, and gaps in memory. Wasthere any underlying cause that could make sense of this confusing array of symptoms?
F RO M H Y P N O S I S TO T H E TA L K I N G CU R E
Freud suspected that the hysterical symptoms were psychogenic symptoms—theresults of some unknown psychological cause—rather than the product of organicdamage to the nervous system. His hypothesis grew out of the work of Jean Charcot(1825–1893), a French neurologist who noticed that many of the bodily symptoms ofhysteria made no anatomical sense. For example, some patients who suffered fromanesthesia (i.e., lack of feeling) of the hand still had feeling above the wrist. This gloveanesthesia (so called because of the shape of the affected region) could not possibly becaused by any nerve injury, since an injury to any of the relevant nerve trunks wouldalso affect a portion of the arm above the wrist (Figure 15.13). This ruled out a simplephysical cause and suggested that glove anesthesia had some psychological basis.
In collaboration with another physician, Josef Breuer (1842–1925), Freud came tobelieve that these hysterical symptoms were a disguised way to keep certain emotionallycharged memories under mental lock and key (S. Freud & Breuer, 1895). The idea, inbrief, was that the patients carried some very troubling memory that they neededto express (because it held such a grip on their thoughts) but also to hide (becausethinking about it was so painful). The patients’ “compromise,” in Freud’s view, was toexpress the memory in a veiled form, and this was the source of their physical symptoms.
To support this hypothesis, Freud needed to find out both what a patient’s painfulmemory was and why she (almost all of Freud’s patients were women) found directlyexpressing her memory to be unacceptable. At first, Freud and Breuer tried to uncoverthese memories while the patients were in a hypnotic trance. Eventually, though, Freudabandoned this method, and came to the view that crucial memories could instead berecovered in the normal, waking state through the method of free association. In thismethod, his patients were told to say anything that entered their mind, no matter howtrivial it seemed, or how embarrassing or disagreeable. Since Freud assumed that allideas were linked by association, he believed that the emotionally charged “forgotten”memories would be mentioned sooner or later.
But a difficulty arose: Patients did not readily comply with Freud’s request. Instead,they avoided certain topics and carefully tuned what they said about others, showingresistance that the patients themselves were often unaware of. In Freud’s view, this resist-ance arose because target memories (and related acts, impulses, or thoughts) were espe-cially painful or anxiety-provoking. Years before, as an act of self-protection, the patientshad pushed these experiences out of consciousness, or, in Freud’s term, they hadrepressed the memories. The same self-protection was operating in free association,keeping the memories from the patients’ (or Freud’s) view. On this basis, Freud con-cluded that his patients would not, and perhaps could not, reveal their painful memoriesdirectly. He therefore set himself the task of developing indirect methods of analysis—as
15.12 Sigmund Freud (1856–1939) Thefounder of psychoanalysis.
(A) (B)
15.13 Glove anesthesia (A) Areas of thearm’s skin that send sensory information tothe brain by way of different nerves. (B) Atypical region of anesthesia in a patientwith hysteria. If there were a nerve injury(in the spinal cord), the anesthesia wouldextend over the length of the arm, followingthe nerve distribution shown in (A).
hysteria An older term for a group ofpresumably psychogenic disordersthat included a wide variety of physi-cal and mental symptoms.
psychogenic symptoms Symptomsbelieved to result from some psycho-logical cause rather than from tissuedamage.

PThe Psychodynamic Approach: Probing the DepthsO 607
he called it, psychoanalysis—that he thought would uncover these ideas and memoriesand the conflicts that gave rise to them.
I D, E G O, A N D S U P E R E G O
Much of Freud’s work, therefore, was aimed at uncovering his patients’ unconscious con-flicts. He was convinced that these conflicts were at the root of their various symptoms,and that, by revealing the conflicts, he could diminish the symptoms. But Freud alsobelieved that the same conflicts and mechanisms for dealing with them arise in normalpersons, so he viewed his proposals as contributions not only to psychopathology butalso to a general theory of personality.
But what sorts of conflict are we considering here? What are the warring factions,supposedly hidden deep inside each individual? According to Freud, the conflicts ham-pering each of us involve incompatible wishes and motives, such as a patient’s desire togo out with friends versus her guilt over leaving a sick father at home. Freud devised aconception of personality that encapsulated these conflicting forces within three dis-tinct subsystems: the id, the ego, and the superego (Figure 15.14). In some of his writings,Freud treated these three mental systems as if they were separate persons inhabitingthe mind. But this is only a metaphor that must not be taken literally; id, ego, andsuperego are just the names he gave to three sets of very different reaction patterns, andnot persons in their own right (S. Freud, 1923).
The id is the most primitive portion of the personality, the portion from which theother two emerge. It consists of all of the basic biological urges, and seeks constantly toreduce the tensions generated by these biological urges. The id abides entirely by thepleasure principle—satisfaction now and not later, regardless of the circumstances andwhatever the cost.
At birth, the infant’s mind is all id. But the id’s heated striving is soon met by coldreality, because some gratifications take time. Food and drink, for example, are notalways present; the infant or young child has to cry to get them. Over the course of earlychildhood, these confrontations between desire and reality lead to a whole set of newreactions that are meant to reconcile the two. Sometimes the result is appropriate
free association Method used inpsychoanalytic therapy in which thepatient is to say anything that comesto her mind, no matter how apparentlytrivial, unrelated, or embarrassing.
repression In psychoanalytic theory,a mechanism of defense by means ofwhich thoughts, impulses, or memoriesthat give rise to anxiety are pushedout of consciousness.
psychoanalysis A theory of humanpersonality development formulatedby Freud, based on assertions aboutunconscious conflict and earlypsychosexual development; also themethod of therapy that draws heavilyon this theory.
id In Freud’s theory, a term for themost primitive reactions of humanpersonality, consisting of blind strivingfor immediate biological satisfactionregardless of cost.
SuperegoInternalizedcode ofconduct
EgoReality principle
IdPleasure principle
UNCONSCIOUS
PRECONSCIOUS
CONSCIOUS
15.14 Models of mind Freud distinguished among threemental systems: the id, ego, and superego. He held thatthe id was unconscious, whereas the ego and superegowere partly unconscious, partly preconscious (easilybrought to consciousness), and partly conscious.

608 chapter 15 PPERSONALITYO
action (e.g., saying “please”), and sometimes the result is suppressing a forbiddenimpulse (e.g., not eating food from someone else’s plate). In all cases, though, theseefforts at reconciling desire and reality become organized into a new subsystem of thepersonality—the ego. The ego obeys a new principle, the reality principle. It tries to sat-isfy the id (i.e., to gain pleasure), but it does so pragmatically, finding strategies thatwork but also accord with the demands of the real world.
If, for a very young child, the ego inhibits some id-inspired action, it is for an imme-diate reason. Early in the child’s life, the reason is likely to be some physical obstacle(perhaps the food is present, but out of reach). For a slightly older child, the reason maybe social. Grabbing the food from your brother will result in punishment by a nearbyparent. As the child gets older still, though, a new factor enters the scene. Imagine thatthe child sees a piece of candy within reach but knows that eating the candy is forbid-den. By age 5 or so, the child may overrule the desire to eat the candy even when thereis no one around and so no chance of being caught and punished. This inhibition ofthe desired action occurs because the child has now internalized the rules and admoni-tions of the parents and so administers praise or scolding to himself, in a fashionappropriate to his actions. At this point, the child has developed a third aspect to hispersonality: a superego, an internalized code of conduct. If the ego lives up to thesuperego’s dictates, the child is rewarded with feelings of pride. But if one of the super-ego’s rules is broken, the superego metes out punishment—feelings of guilt or shame.
Psychological Defenses and DevelopmentFreud’s threefold division of the personality was just a way of saying that our thoughtsand actions are determined by the interplay of three major factors: our biological drives(the id), the commands and prohibitions of society (the superego), and the variousways we have learned to satisfy the former while respecting the latter (the ego).
Obviously, though, these three forces will sometimes pull us in differentdirections—for example, when we want to do something but know we cannot or shouldnot—and this guarantees conflict among the competing forces. Imagine that a childperforms some forbidden act and is then scolded or disciplined by his parents. Thechild feels threatened with the loss of his parents’ love and becomes anxious about this.This anxiety leaves its mark, and the next time the child is about to perform the sameact—say, touch his penis or pinch his baby brother—he will feel a twinge of anxiety, aninternal reminder that his parents may castigate him and the worry that he will beabandoned and alone.
P SY C H O LO G I CA L D E F E N S E S
Since anxiety is unpleasant, the child will do everything he can to ward it off. If thecause of the anxiety is a real-world event or object, the child can simply run away andremove himself from it. But how can he cope with a danger lurking within—a threat-ening fantasy, a forbidden wish? To quell this anxiety, the child must suppress thethoughts that triggered it, pushing the thoughts from conscious view. In short, thethought must be repressed.
According to Freud, repression serves as the primary defense mechanism that pro-tects the individual from anxiety. But repression is often incomplete. The thoughts andurges that were pushed underground may resurface along with the associated anxiety.As a result, various further mechanisms of defense are brought into play to reinforce theoriginal dam against the forbidden impulses.
ego In Freud’s theory, a set of reac-tions that try to reconcile the id’s blindpleasure strivings with the demands ofreality.
superego In Freud’s theory, reactionpatterns that emerge from within theego, represent the internalized rules ofsociety, and come to control the egoby punishment with guilt.
defense mechanism A collectiveterm for a number of reactions that tryto ward off or lessen anxiety by variousunconscious means.

PThe Psychodynamic Approach: Probing the DepthsO 609
One such mechanism is displacement—a process in which repressed urges findnew and often disguised outlets, outlets that are more acceptable to the ego and super-ego. An example is a child who is disciplined by her parents and who then vents heranger by punching or kicking her doll. A different defense is reaction formation, inwhich she guards against the repressed wish by turning to thoughts and behaviorswhich provide the diametrical opposite of the forbidden ideas. A young boy who hateshis sister and is punished for calling her names may protect himself by bombarding herwith exaggerated love and tenderness, a desperate bulwark against aggressive wishesthat he cannot accept.
In still other defense mechanisms, the repressed thoughts break through but are rein-terpreted or unacknowledged. One example of this is rationalization, in which the per-son interprets her own feelings or actions in more acceptable terms. The cruel fatherbeats his child mercilessly but is sure that he does so “for the child’s own good.” A relatedmechanism is projection. Here the forbidden urges well up and are recognized as such.But the person does not realize that these wishes are his own; instead, he attributes themto others. “I desire you” becomes “You desire me,” and “I hate you” becomes “You hateme”—desperate defenses against repressed sexual or hostile wishes that can no longerbe banished from consciousness (S. Freud, 1911; Schul & Vinokur, 2000).
STAG E S O F P SY C H O S EX UA L D E V E LO P M E N T
Why does one person develop one pattern of defenses, while the next develops anotherpattern? The answer for Freud lies in the events of early childhood, events that, inFreud’s view, were remarkably similar from person to person, and that give rise to a gen-eral set of stages through which we all pass (S. Freud, 1905). Freud called these thestages of psychosexual development, and, although he believed the stages wereuniversal, the way the conflicts at each stage were handled differed from person to per-son. It is these differences, Freud believed, that give rise both to observable variationsin personality and to psychopathology.
According to Freud, the child starts life as a bundle of instincts to seek pleasure, withthe pleasure readily found in the stimulation of certain sensitive zones of the body. Forthe youngest child, most of the pleasure seeking is through the mouth, a period of lifethat Freud termed the oral stage. As the infant attains bowel control, the emphasis shiftsto pleasures associated with the anus (the anal stage). Still later, the child showsincreased interest in pleasure from genital stimulation (the phallic stage). The culmina-tion of psychosexual development is attained in adult sexuality when pleasure involvesnot just one’s own gratification but also the social and bodily satisfaction brought toanother person (the genital stage).
Within this sequence, Freud held that the pivotal point in the child’s psychosexualdevelopment is the Oedipus complex, named after the Theban king of classical Greek liter-ature who unwittingly committed two awful crimes—killing his father and marrying hismother (Figure 15.15). Because Freud came to believe that the sequence of steps is some-what different in the two sexes (S. Freud, 1905), we will take them up separately.
At about the age of 3 or 4 years, the phallic stage begins for the young boy. At thistime, he becomes increasingly interested in his penis, and he seeks an external objectfor his sexual urges. The inevitable choice, in Freud’s view, is the most importantwoman in the boy’s young life—his mother. But there is an obstacle—the boy’s father.The little boy wants to have his mother all to himself, as a comforter as well as an eroticpartner, but this sexual utopia is out of the question. His father is a rival, and he is big-ger. The little boy therefore wants his father to go away and not come back—in short,to die.
displacement A redirection of animpulse from a channel that is blockedinto another, more available outlet.
reaction formation A mechanism ofdefense in which a forbidden impulseis turned into its opposite.
rationalization A mechanism ofdefense by means of which unaccept-able thoughts or impulses are reinter-preted in more acceptable and, thus,less anxiety-arousing terms.
projection A mechanism of defensein which various forbidden thoughtsand impulses are attributed to anotherperson rather than the self.
stages of psychosexual develop-ment The sequence of four develop-mental stages from infancy throughthe attainment of adult sexuality thatis considered universal in psychoana-lytic theory: the oral stage, the analstage, the phallic stage, and the geni-tal stage.
“Why can’t you be more like Oedipus?”
15.15 Oedipus complex

610 chapter 15 PPERSONALITYO
At this point, a new element enters into the family drama. The little boy begins tofear the father he is jealous of. According to Freud, this is because the boy is certain thatthe father knows of his son’s hostility and will surely answer hate with hate. With child-ish logic, the little boy becomes convinced the punishment his father will mete out willbe catastrophic. This leads to intolerable anxiety, and the anxiety escalates still furtheruntil the father is unconsciously viewed as an overwhelming ogre who threatens toannihilate his little son. As the little boy grows, so does his rivalry with his father andits accompanying terror. Eventually, though, he hits on a solution. He throws in thetowel, relinquishes his mother as an erotic object, identifies with his father, andrenounces genital pleasure until he is older.
What about girls? In Freud’s view, females go through essentially identical oraland anal phases as do males. In many ways, the development of the young girl’s phal-lic interests (Freud used the same term for both sexes) corresponds to the boy’s. Ashe focuses his erotic interests on the mother, so she focuses hers on the father. As heresents and eventually fears his father, so does she her mother. In short, there is afemale version of the Oedipus complex, sometimes called the Electra complex, afterthe Greek tragic heroine who goaded her brother into slaying their mother.
Of course, like young boys, young girls’ first attachment is to their mother. It is themother, after all, who nurses the infant (and so provides pleasure during the oralphase). It is likewise the mother who, for most infants, is the primary caregiver. So why,according to Freud, does a girl switch love objects and come to desire her father? Toanswer this question, Freud proposed that the shift of attachment begins as the littlegirl discovers that she does not have a penis. According to Freud, she regards this lackas a catastrophe, considers herself unworthy, and develops penis envy. One conse-quence is that she withdraws her love from the mother, whom she regards as equallyunworthy. Freud argued that, painfully, she turns to her father, who has the desirableorgan and who she believes can help her obtain a penis substitute—a child. From hereon, the rest of the process unfolds more or less like its counterpart in the boy: love offather, jealousy of mother, increasing fear of mother, eventual repression of the entirecomplex, and identification with the mother (S. Freud, 1925, 1933; LaFarge, 1993).
The Empirical Basis of Freud’s ClaimsMany people regard Freud’s claims—especially his account of the Electra complex—asincredibly far-fetched, but Freud believed firmly that his conception was demanded bythe evidence he collected. In the next section, we first consider why Freud believed hisclaims were justified. Then, in the following section, we consider contemporarycriticisms of Freud’s methods and inferences.
T H E N AT U R E O F F R E U D ’S E V I D E N C E
As we have seen, Freud believed that painful beliefs and ideas were repressed, but thatthe repression was never complete. Therefore, these anxiety-producing ideas would stillcome to the surface—but (thanks to other defense mechanisms) only in disguisedform. The evidence for Freud’s theory therefore had to come from a process of interpre-tation that allowed Freud to penetrate the disguise and thus to reveal the crucial under-lying psychological dynamics.
As one category of evidence, Freud continually drew attention to what he called the“psychopathology of everyday life.” For example, we might forget a name or suffer a slipof the tongue, and, for Freud, these incidents were important clues to the person’s
penis envy In psychoanalytic theory,the wish for a penis that is assumed toensue normally in females as part ofthe Electra complex.

(A) (B)
PThe Psychodynamic Approach: Probing the DepthsO 611
hidden thoughts: Perhaps the name reminded us of an embarrassingmoment, and perhaps the slip of the tongue allowed us to say some-thing that we wanted to say, but knew we shouldn’t (Figure 15.16).Freud argued that in some cases these slips were revealing, and, ifproperly interpreted in the context of other evidence, they could pro-vide important insights into an individual’s unconscious thoughtsand fears.
Freud also believed that we could learn much about an individualthrough the interpretation of dreams (S. Freud, 1900), because, inFreud’s view, all dreams are attempts at wish fulfillment. While oneis awake, a wish is usually not acted on right away, for there are con-siderations of both reality (the ego) and morality (the superego) thatmust be taken into account: Is it possible? Is it allowed? But duringsleep these restraining forces are drastically weakened, and the wishthen leads to immediate thoughts and images of gratification. Insome cases the wish fulfillment is simple and direct. Starving explor-ers dream of sumptuous meals; people stranded in the desert dream of cool mountainstreams. According to a Hungarian proverb quoted by Freud, “Pigs dream of acorns,and geese dream of maize.”
What about our more fantastic dreams, the ones with illogical plots, bizarre charac-ters, and opaque symbolism? These are also attempts at wish fulfillment, Freud believed,but with a key difference. They touch on forbidden, anxiety-laden ideas that cannot beentertained directly. As a result, various mechanisms of defense prohibit the literalexpression of the idea but allow it to slip through in disguised, symbolic form (e.g., apenis may be symbolized as a sword, a vagina as a cave). Because of this disguise, thedreamer may never experience the underlying latent content of the dream—the actualwishes and concerns that the dream is constructed to express. What he experiencesinstead is the carefully laundered version that emerges after the defense mechanismshave done their work—the dream’s manifest content. This self-protection takes mentaleffort, but, according to Freud, the alternative—facing our impulses unadulterated—would let very few of us sleep for long.
Yet another form of evidence that Freud pointed to are the myths, legends, and fairytales shared within a culture. He contended that just as dreams are a window intothe individual’s unconscious, these (often unwritten) forms of literature allow us aglimpse into the hidden concerns shared by whole cultural groups, if not all ofhumanity. Indeed, one of Freud’s earliest colleagues, the Swiss psychiatrist CarlJung (1875–1961), argued for a collective unconscious consisting of primordial sto-ries and images—he called these archetypes—that shape our perceptions and desiresjust as much as Freud’s psychodynamics (Jung, 1964; Figure 15.17). Psychoanalysts
“Good morning, beheaded—uh, I mean beloved.”
15.16 Freudian slip If this king wereHenry VIII, famous for executing severalwives, this would be a good example of aFreudian slip.
15.17 Jungian archetype and the collective unconsciousJung believed that humans have a collective or sharedunconscious, whose images are expressed in universalarchetypes such as this (A) Tibetan mandala and(B) Hebrew manuscript illustration.
collective unconscious A set ofprimordial stories and images,hypothesized by Carl Jung to beshared by all of humanity, and whichhe proposed underlie and shape ourperceptions and desires.
archetypes According to Carl Jung,the stories and images that constituteour collective unconscious.

612 chapter 15 PPERSONALITYO
who have delved into such tales have found, for example, an ample supply of Oedipalthemes. There are numerous ogres, dragons, and monsters to be slain before the prizecan be won. The villain is often a cruel stepparent—a fairly transparent symbol, intheir view, of Oedipal hostilities (see Figure 15.18).
CO N C E R N S A BO U T P SY C H O DY N A M I C E V I D E N C E
As we have just seen, Freud’s evidence generally involved his patients’ symptoms,actions, slips of the tongue, dreams, and so on. Freud was convinced, however, thatthese observations should not be taken at face value; instead, they needed to be inter-preted, in order to unmask the underlying dynamic that was being expressed. The diffi-culty, though, is that Freud allowed himself many options for this interpretation—andso, if someone said “I hate my father,” that might mean (via the defense of projection)that the person is convinced her father hates her or it might mean (via displacement)that the person hates her mother, or it might mean something else altogether. With thismuch flexibility, one might fear, there is no way to discover the correct interpretation ofthis utterance, and so no way to be certain our overall account is accurate. Indeed, it istelling that some of Freud’s followers were able to draw very different conclusions from
the same clinical cases that Freud himself studied—a powerful indi-cator that the interpretations Freud offered were in no sensedemanded by the evidence.
When we turn to more objective forms of evidence we often findfacts that do not fit well with Freudian theory. For example, one of thecornerstones of psychoanalytic thought is repression. Yet results ofempirical studies of repression have been mixed. Some results point inthe same direction as Freud’s claims about repression (M. C. Andersonet al., 2004; M. C. Anderson & Levy, 2006; Joslyn & Oakes, 2005), butother research yields no evidence for the mechanisms Freud proposed(Holmes, 1990), and at least some of the studies that allegedly showrepression have been roundly criticized by other researchers(Kihlstrom, 2002).
Psychodynamic Formulations after FreudPlainly, therefore, we need to be very careful about interpreting Freud’s claims—withpowerful challenges raised to both his central methods and his key concepts. Even so,many scholars are convinced that Freud’s body of work contains a number of important(some would say brilliant) insights, and so we might ask how we can preserve theseinsights without endorsing the entire Freudian conception. As it turns out, many schol-ars have tried to do this, producing a welter of schools and camps, each offering its ownextensions and elaborations of Freud’s thinking.
E G O P SY C H O LO GY A N D M E C H A N I S M S O F D E F E N S E
One major theme among those who carried forward the torch of psychoanalytic theorywas that Freud had not sufficiently emphasized the skills and adaptive capacities of theego. Writers of this persuasion, loosely grouped under the heading of ego psychology,sought to extend and complete Freud’s theorizing.
The various ego psychologists each have their own theoretical emphases, but allagree with Freud’s contention that unconscious conflict is found in the well adjusted as
15.18 Freud and mythology Many myths,legends, and stories can be interpreted inpsychoanalytic terms. According topsychoanalytic authors, this fairy tale is aveiled allegory of the Oedipal sequence(Bettelheim, 1975). The wicked queen is themother on whom the child projects her ownhate and sexual jealousy. The Electra com-plex is temporarily resolved as the child’serotic urges go underground and remaindormant for the seven years of the latencyperiod, symbolized both by the sevendwarfs and Snow White’s long sleep. At theend of this period, her sexuality is reawak-ened in adult form by the young prince.(The meaning of the sword is left as anexercise for the reader.)
ego psychology A school of psycho-dynamic thought that emphasizes theskills and adaptive capacities ofthe ego.

PThe Psychodynamic Approach: Probing the DepthsO 613
well as in people with disabling mental disorders. What is essential for these moremodern theorists, though, is how those conflicts can be resolved in a fashion that isappropriate, pragmatic, and, ultimately, healthy. Adherents of this position stress thepositive aspects of the self as it tries to cope with the world—to deal with reality as it israther than to distort it or hide from it. Seen in this light, the ego is not just an arbiterbetween id and superego, but a clever strategist with intrinsic competencies (A. Freud,1946; Hartmann, 1964).
Building on this perspective, investigators have explored how copingpatterns evolve over the course of the life span, and some of the dataderive from longitudinal studies covering a span of 20 to 30 years (J.Block & J. H. Block, 2006). An example is George Vaillant’s analysis ofthe case reports of 94 male Harvard College graduates studied at differ-ent points in their life span. They were extensively interviewed at age 19,then again at 31, and yet again at 47. Vaillant studied the predominantpatterns of defense—that is, ways of coping—each man used at thesethree ages. He classified the coping patterns according to their level ofpsychological maturity. At the bottom of the hierarchy were mecha-nisms that are often found in early childhood and during serious men-tal disorder, such as denial or gross distortions of external reality.Further up the ladder were patterns often seen in adolescence and indisturbed adults, such as projection, hypochondria, and irrational, emo-tional outbursts.Still higher were the mechanisms studied by Freud andseen in many adults—repression, reaction formation, and the like. At the top of the hierar-chy were coping patterns that Vaillant considered healthy—such as humor, suppression (aconscious effort to push anxiety-provoking thoughts out of mind, at least for the timebeing, as opposed to repression, which is an unconscious process), and altruism (in whichone tries to give to others what one might wish to receive oneself).
Vaillant’s findings indicated considerable continuity. Men with more adaptive copingpatterns at age 19 were more likely to have mature patterns in their forties, and thesepatterns in turn predicted the results on various objective indices that personality psy-chologists refer to as life data, such as satisfaction in marriage, rewarding friendships,gratifying jobs, and good physical health (Figure 15.19). As is often the case, it is unclearwhether the mature coping defenses produced success in marriage and career or vice versa,but it is worth knowing that the two tend to be correlated (Vaillant, 1974,1976,1977,1994).This correlation was also observed in a study of 131 inner-city males interviewed in juniorhigh school and then surveyed 30 years later (G. E. Vaillant, Bond, & Vaillant, 1986).
OBJ E CT R E L AT I O N S A N D AT TAC H M E N T T H E O RY
Yet another development of Freud’s thinking comes from scholars who broadly sup-ported Freud’s theorizing, but felt he had insufficiently emphasized the real (asopposed to fantasized) relations an individual had with others. Despite their manydifferences, these object relations theorists held that relationships with important oth-ers, whom they rather oddly referred to as “objects,” constitute a crucial and relativelyneglected motive underlying human behavior. Arguably, though, the object relationstheorist with the broadest and most enduring impact was John Bowlby (1907–1990).
As described in Chapter 14, Bowlby was a British psychiatrist who believed peoplewere motivated by the desire for connection and closeness with others. In particular,Bowlby believed that a child was powerfully shaped by her experiences with her primaryattachment figure (typically, but not always, her mother) and emerged from childhood
20%
0%Income
$20,000/yr(in 1967)
Satisfiedwith job
Marriagesatisfying
for 10+ yrs
Satisfyingfriendship
40%
60%
80%
100%
15.19 Maturity of defense mechanisms andlife adjustment Adult success at work andlove, as shown by men with predominantlymature (blue) and immature (yellow) adap-tive styles.
life data Data about a person con-cerning concrete, real-worldoutcomes.
object relations A school ofpsychodynamic thought that empha-sizes the real (as opposed to fanta-sized) relations an individual has withothers.

614 chapter 15 PPERSONALITYO
with a set of foundational beliefs about both herself (as essentiallygood and lovable or not) and others (as essentially good and lovingor not). These mental representations of self and other are referred toas internal working models.
Bowlby emphasized that different children develop different work-ing models, but it was Mary Ainsworth (1913–1999) who created anexperimental procedure designed to probe these differences, and,specifically, to assess what type of attachment a child had formed withhis caregiver (Ainsworth, Blehar, Waters, & Wall, 1978). As we dis-cussed in Chapter 14, this Strange Situation test can be used to cate-gorize children as securely attached, anxious/avoidant in theirattachment, anxious/resistant, or disorganized in their attachment.These attachment patterns, in turn, can then be used as predictors fora number of subsequent measures—including the child’s personalityin the next years, and the quality of the child’s social relations.
Atttachment theory has been a significant source of inspiration for researchers in per-sonality, who have found that the attachment patterns established in early childhoodseem to have considerable staying power (Bartholomew & Horowitz, 1991; Brennan,Clark, & Shaver, 1998; Mikulincer & Shaver, 2007). For example, Shaver and Clark(1994) found that compared to secure adults, anxious/avoidant adults are less interestedin romantic relationships and seem less upset when the relationships end. In contrast,anxious/resistant adults are highly focused on their relationships, and they fret and fumeabout them to a much greater extent than secure individuals (Figure 15.20).
Does all of this mean that one is simply out of luck if one has not developed the“right” working model in childhood? Happily, the answer appears to be no. Workingmodels of self and other seem to be at least somewhat malleable and context depend-ent, and new experiences (whether with friends, dating partners, or a therapist) seemto have the power to refashion a person’s early ideas about self and other. Even so,the ability to predict adult outcomes, based on childhood patterns, does support atleast one part of Freud’s perspective—namely, the claim that the early years play acritical role in shaping adult behaviors, expectations, and personality.
Contributions of the Psychodynamic ApproachIn the early part of the twentieth century, the public—especially in the United States—was fascinated by the bearded Viennese doctor who spoke so frankly about sex.Scholars in the social sciences, literature, and the arts flocked to read his writingsbecause they were so far-reaching in scope, so profound in their implications.
Since then, a number of criticisms have—as we have seen—been leveled against thepsychodynamic approach. Even with these criticisms, though, Freud’s contribution topsychology—and to Western thinking—is enormous (Figure 15.21). His work drawsour attention to a set of ideas whose relevance today belies the hundred plus years thathave passed since he started articulating his views (Westen, 1998). These ideas includethe notion that many important psychological processes—especially affective andmotivational processes—operate outside awareness, and the idea that our motives andimpulses are often at odds with one another. Contemporary psychologists would stillendorse Freud’s claim that people’s thoughts, feelings, and behaviors are strongly influ-enced by their mental representations of important people in their lives, as well as hisclaim that among other things, development revolves around finding socially accept-able ways of managing sexual and aggressive impulses. Admittedly, many of these ideashave their origins in theories predating Freud. It is also true that the modern conce-
(A) Secure attachment (B) Insecure attachment
15.20 Attachment styles (A) Securelyattached and (B) insecurely attachedpartners.
15.21 Reflecting on Freud Freud’s legacycontinues today.

PThe Humanistic Approach: Appreciating Our PotentialO 615
ption of these ideas is, in important ways, different from Freud’s specific proposals, andthat these ideas, in the modern era, have a less central position than they had in Freud’stheorizing. Nonetheless, Freud undeniably deserves credit for making these essentialideas prominent for many modern theories of personality.
THE HUM ANISTIC APPROACH:APPRECIATING OUR POTENTIAL
Half a century or so ago, a new approach to human motivation and personality—thehumanistic approach—gained prominence. According to its adherents, both trait theo-rists and psychodynamic theorists have lost sight of what is truly human about humanbeings. Healthy individuals, the humanists argue, want to feel free to choose and deter-mine their own lives rather than to exist as mere pawns pushed around by stimuli fromwithout or driven by demons from within. They seek more than food and sex, and strivefor more than mere adjustment—they want to grow and develop their potential.
Phenomenology and Self-actualizationAt the heart of the humanistic approach is a commitment to phenomenology, orunderstanding a person’s own unique first-person perspective on his life. Rather thandescribing how a person typically behaves (as in the trait perspective), or how a person’sunconscious dynamics operate (as in the psychodynamic perspective), a proponent ofthe humanistic perspective seeks to step into another person’s shoes and experience theworld as he does. The goal is to understand a person’s conscious experience by under-standing his construal, or interpretation, of the world around him.
A second defining feature of the humanistic approach is its conception of humanmotivation. As we have seen in Chapter 12, drive theories commonly view humans asbeing engaged in a never-ending struggle to remove some internal tension or make upfor some deficit. However, a release from anxiety and tension does not account foreverything we strive for. We sometimes seek things for their own sake, as positive goalsin themselves, and Maslow (1968, 1996) insisted that psychologists consider the fullrange of motives, not just those that arise from physical requirements such as food,water, and the like.
These concerns led Maslow to propose his hierarchy of needs (see Chapter 12), in which the lower-order physiological needs are at the bottom and the striving for self-actualization—realizing one’s potential to the fullest—is at the top. Butwhat exactly does self-actualization mean?
Maslow answered this question largely by presenting case historiesof people he and his collaborators regarded as self-actualized (Figure15.22). Some of them were individuals he had personally interviewed(the healthiest 1% of college students); others were historical figures(e.g., Thomas Jefferson and Eleanor Roosevelt) whose lives he stud-ied by means of historical documents. As Maslow (1968, 1970, 1996)saw it, these self-actualizers were all realistically oriented, acceptedthemselves and others, were spontaneous, cared more about the prob-lems they were working on than about themselves, had intimate rela-tionships with a few people rather than superficial relationships withmany, and had democratic values—all in all, an admirable list ofhuman qualities.
phenomenology The study ofindividuals’ own unique, first-person,conscious experience.
construal The way an individualmakes sense of the world around him.
15.22 Self-actualizers According toMaslow, Thomas Jefferson and EleanorRoosevelt are clear examples of peoplewho self-actualized.

616 chapter 15 PPERSONALITYO
These traits, and Maslow’s roll call of self-actualized individuals, might make self-actualization sound as though it were possible only for the few and the powerful. Not so.Even though self-actualization is rare, one of the major themes of humanistic psychol-ogy is that we each have within us the impulse to self-actualize. Indeed, one of the othermajor humanists—Carl Rogers (1902–1987)—regarded this as our one basic motive,and he argued that we often manage to self-actualize against extraordinary odds, muchas a plant improbably pushes through a crack in concrete. (C. R. Rogers, 1951, 1961).
The Self This discussion of self-actualization raises an important question: What exactly is the selfthat the humanists talked about, and where does it come from? More than a centuryago—well before the humanists such as Maslow and Rogers came onto the scene—William James (1890; Figure 15.23) distinguished two aspects of the self, which he calledthe “I” and the “me.” (This is the same William James whose emotion theory we consid-ered in Chapter 12.) The “I” is the self that thinks, acts, feels, and believes. The “me,” bycontrast, is the set of physical and psychological attributes and features that define whoyou are as a person. These include the kind of music you like, what you look like, and theactivities that currently give your life meaning.
Half a century after James first made this distinction, the humanist Carl Rogers usedsimilar language to talk about how the self-concept develops in early childhood andeventually comes to include one’s sense of oneself—the “I”—as an agent who takesactions and makes decisions. It also includes one’s sense of oneself as a kind of object—the “me”—that is seen and thought about, liked or disliked (C. R. Rogers, 1959, 1961).Indeed, the self-concept was such an important aspect of Rogers’ approach that hereferred to his theory as self theory, an approach that continues to inspire contempo-rary researchers who seek to explain the motives that activate and support humanbehavior (Deci & Ryan, 2000).
S E L F - SC H E M A
For each of us, our sense of self is a key aspect of our personality, and each of us has a setof beliefs about who we are and who we should be, and a body of knowledge about our val-ues and our past behaviors. This knowledge about ourselves constitutes, for each person, a
15.23 William James (1842–1910) Jameswas an important influence on the earlyfield of psychology—but no less of aninfluence on philosophy and religiousstudies!
Student
Self
Shy
Sister
Daughter
Type A
Movies
Soccer
Brunette
Clothing
Nice
15.24 Self-schema diagram The self-schemaconsists of interrelated descriptions of the self.Some descriptions are central to self (e.g.,daughter); other descriptions are relevant butless central (e.g., brunette); while others stillare not relevant to the self-schema (e.g., shy).
self theory Carl Rogers’s theory ofpersonality, which emphasizes theindividual’s active attempts to satisfyhis needs in a manner that is consis-tent with his self-concept.
self-schema An organized body ofknowledge about the self and thatshapes one’s behaviors, perceptions,and emotions.

Ideal self
Actual self
Ought self
PThe Humanistic Approach: Appreciating Our PotentialO 617
self-schema (Markus, 1977; Figure 15.24). This schema is not just a passive record of ourprior experiences; instead, the schema actively shapes our behaviors,perceptions,and emo-tions. For example, a person might have a schema of himself as a smart person who doeswell at school. This self-schema will make certain situations, such as academic tests, seemmore important and consequential. The self-schema will also guide many of his choices,such as opting to attend a more rigorous college rather than a “party school” or spendingthe extra hour polishing a term paper rather than heading off to get coffee with friends.
The self-schema is not just a random list of characteristics. Instead, it is a highlyorganized (although not always entirely consistent) narrative about who one is.McAdams and colleagues (McAdams, 1993, 2001; McAdams & Pals, 2006) refer to suchpersonal narratives as personal myths—in essence, “stories” that provide a sense ofdirection and meaning for our lives. Moreover, given this important role for these nar-ratives, it cannot be surprising that these narratives are resistant to change, and, in fact,studies have shown that even people with negative self-concepts tenaciously cling tothese views, and seek out others who will verify these views (Swann, Rentfrow, &Guinn, 2002).
Information relevant to our self-schema is also given a high priority. For example, in sev-eral studies, people have been shown a series of trait words and asked to make simple judg-ments regarding these words (e.g., Is the word in capital letters? Is it a positive word? Doesit describe me?). When asked later to remember the traits that they previously saw, partici-pants were more likely to recall words presented in the “Does it describe me?” conditionthan in the other conditions, suggesting that material encoded in relationship to the self isbetter remembered (T. B. Rogers, Kuiper, & Kirker, 1977). These findings are buttressed byneuroimaging studies that show the portions of the medial prefrontal cortex are particu-larly active when people are engaged in self-referential processes (as compared to when theyare making judgments about how the words are written,whether the words are good or bad,or even whether they are characteristic of a friend; Heatherton et al., 2006).
Interestingly, people seem to have schemas not only for who they are now, their actualselves, but also for who they may be in the future—mental representations ofpossible selves (Markus & Nurius, 1986; Figure 15.25). These include a sense ofthe ideal self that one would ideally like to be (e.g., someone who saves others’lives), and the ought self that one thinks one should be (e.g., someone who neverlies or deceives others) (E. T. Higgins, 1997). According to E. Tory Higgins, whenwe compare our actual self to our ideal self, we become motivated to narrow thedistance between the two, and we develop what he calls a promotion focus.When we have this sort of focus, we actively pursue valued goals—a pursuit thatresults in pleasure. In contrast, when we compare our actual self to our ought self,we become motivated to avoid doing harm, and we develop what Higgins calls aprevention focus. This kind of focus is associated with feelings of relief.
Notice, therefore, that schemas are not just dispassionate observations about our-selves; instead, they often have powerful emotions attached to them and can be acompelling source of motivation. This is why the schemas are typically thought of asan aspect of “hot” cognition (emotional and motivational) rather than “cold” cognition(dispassionate and analytical).
S E L F - E ST E E M A N D S E L F - E N H A N C E M E N T
The “hot” nature of self-schemas is also evident in the fact that these schemas play a pow-erful role in shaping a person’s self-esteem—a broad assessment that reflects the relativebalance of positive and negative judgments about oneself (Figure 15.26). Not surprisingly,self-esteem is not always based on objective self-appraisals. Indeed, people in Western
15.25 Possible selves People not onlyhave mental representations of their actualselves, or who they are now, but also possi-ble selves, including their ideal self andought self.
personal myths The personal narra-tives or stories that provide a personwith a sense of direction and meaning.
actual selves Self-schema for whomone is at the moment.
possible selves Self-schemas forwhom one may be in the future; theseinclude the ideal self and the oughtself.
promotion focus An orientation toactively pursue valued goals thoughtto arise when we compare our actualself to our ideal self.
prevention focus An orientation toavoid doing harm thought to arisewhen we compare our actual self toour ought self.
self-esteem The relative balance ofpositive and negative judgments aboutoneself.

618 chapter 15 PPERSONALITYO
cultures seem highly motivated to view themselves as different from andsuperior to other people—even in the face of evidence to the contrary(Sedikides & Gregg, 2008). This is manifest, for example, in the fact thatmost Americans judge themselves to be above average on a broad range ofcharacteristics (see Harter, 1990). Thus, in 1976–1977 the College Boardasked 1 million high-school students to rate themselves against their peerson leadership ability. In response, 70% said they were above average, andonly 2% thought they were below. Similar findings have been obtained inpeople’s judgments of talents ranging from managerial skills to drivingability (see Dunning, Meyerowitz, & Holzberg, 1989). And it is not justhigh-school students who show these effects. One study of university pro-fessors found that 94% believed they were better than their colleagues attheir jobs (Gilovich, 1991).
What is going on here? Part of the cause lies in the way we search ourmemories in order to decide whether we have been good leaders or bad, good drivers orpoor ones. Evidence suggests that this memory search is often selective, showcasing theoccasions in the past on which we have behaved well and neglecting the occasions onwhich we have done badly—leading, of course, to a self-flattering summary of thisbiased set of events (Kunda, 1990; Kunda, Fong, Sanitioso, & Reber, 1993).
In addition, people seem to capitalize on the fact that the meanings of these traits—effective leader, good at getting along with others—are often ambiguous. This ambigu-ity allows each of us to interpret a trait, and thus to interpret the evidence, in a fashionthat puts us in the best possible light. Take driving ability. Suppose Henry is a slow,careful driver. He will tend to think that he’s better than average precisely because he’sslow and careful. But suppose Jane, on the other hand, is a fast driver who prides her-self on her ability to whiz through traffic and hang tight on hairpin turns. She will alsothink that she’s better than average because of the way she’s defined driving skill. As aresult, both Henry and Jane (and, indeed, most drivers) end up considering themselvesabove average. By redefining success or excellence, we can each conclude that we aresuccessful (Dunning & Cohen, 1992; Dunning et al., 1989).
CU LT U R E A N D T H E S E L F
Although the self-schema is important for all of us, the content of the schema variesfrom individual to individual and, it seems, from one culture to the next. When theythink about themselves, Americans tend to think about their broad, stable traits, traitsthat apply in all settings, such as athletic, disorganized, and creative. Things are differ-ent for people living in interdependent, collectivist cultures. They also view themselvesas having certain traits, but only in specific situations, and so their self-descriptionstend to emphasize the role of the situation, such as quiet at parties, or gentle with theirparents (Ellemers, Spears, & Dossje, 2002; D. Hart, Lucca-Irizarry, & Damon, 1986;Heine, 2008). Similarly, people in interdependent cultures tend to have self-conceptsthat emphasize their social roles, and so, when asked to complete the statement “I am . . . ,” Japanese students are more likely to say things like “a sister” or “a student,”whereas American students are more likely to mention traits like “smart” or “athletic”(Cousins, 1989). Similar differences can show up within a single culture. Thus, asshown in Figure 15.27, Kenyans who were least westernized overwhelmingly describedthemselves in terms of roles and memberships and mentioned personal characteristicssuch as traits only 2% of the time. By contrast, Kenyans who were most westernizedused trait terms nearly 40% of the time, and only slightly less than American under-graduates (Ma & Schoeneman, 1997).
15.26 Canine self-esteem?
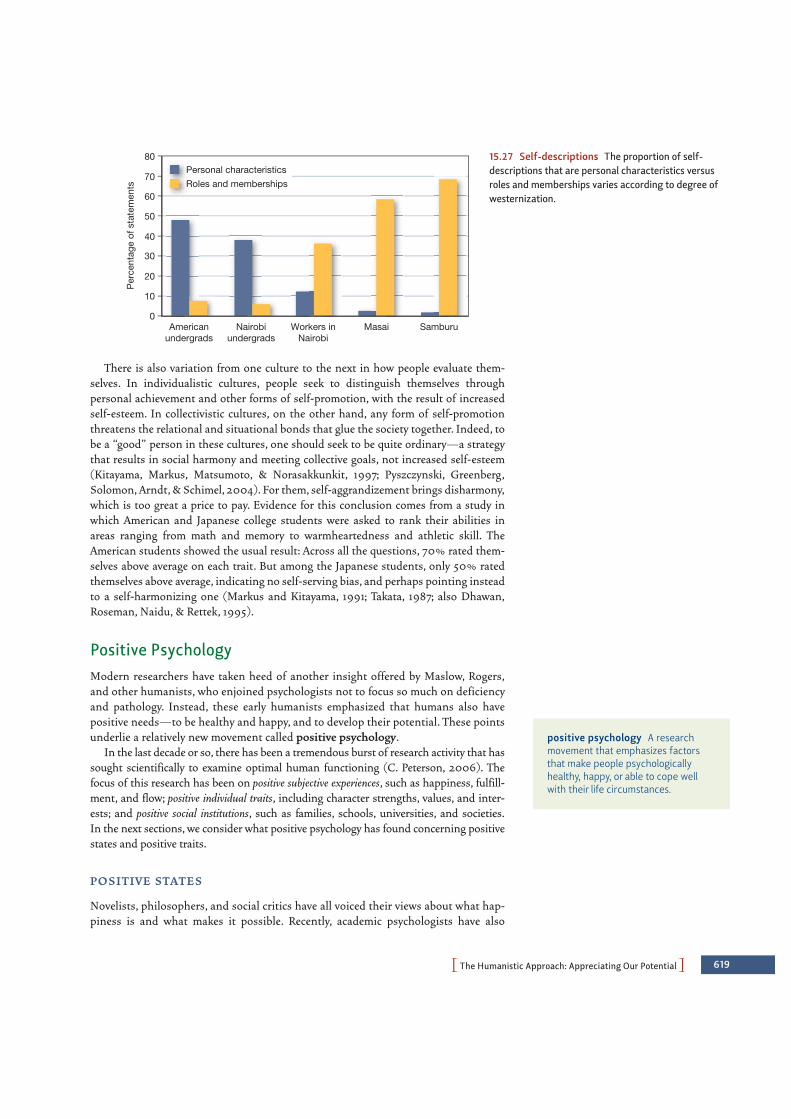
PThe Humanistic Approach: Appreciating Our PotentialO 619
There is also variation from one culture to the next in how people evaluate them-selves. In individualistic cultures, people seek to distinguish themselves throughpersonal achievement and other forms of self-promotion, with the result of increasedself-esteem. In collectivistic cultures, on the other hand, any form of self-promotionthreatens the relational and situational bonds that glue the society together. Indeed, tobe a “good” person in these cultures, one should seek to be quite ordinary—a strategythat results in social harmony and meeting collective goals, not increased self-esteem(Kitayama, Markus, Matsumoto, & Norasakkunkit, 1997; Pyszczynski, Greenberg,Solomon, Arndt, & Schimel, 2004). For them, self-aggrandizement brings disharmony,which is too great a price to pay. Evidence for this conclusion comes from a study inwhich American and Japanese college students were asked to rank their abilities inareas ranging from math and memory to warmheartedness and athletic skill. TheAmerican students showed the usual result: Across all the questions, 70% rated them-selves above average on each trait. But among the Japanese students, only 50% ratedthemselves above average, indicating no self-serving bias, and perhaps pointing insteadto a self-harmonizing one (Markus and Kitayama, 1991; Takata, 1987; also Dhawan,Roseman, Naidu, & Rettek, 1995).
Positive PsychologyModern researchers have taken heed of another insight offered by Maslow, Rogers,and other humanists, who enjoined psychologists not to focus so much on deficiencyand pathology. Instead, these early humanists emphasized that humans also havepositive needs—to be healthy and happy, and to develop their potential. These pointsunderlie a relatively new movement called positive psychology.
In the last decade or so, there has been a tremendous burst of research activity that hassought scientifically to examine optimal human functioning (C. Peterson, 2006). Thefocus of this research has been on positive subjective experiences, such as happiness, fulfill-ment, and flow; positive individual traits, including character strengths, values, and inter-ests; and positive social institutions, such as families, schools, universities, and societies.In the next sections, we consider what positive psychology has found concerning positivestates and positive traits.
P O S I T I V E STAT E S
Novelists, philosophers, and social critics have all voiced their views about what hap-piness is and what makes it possible. Recently, academic psychologists have also
Personal characteristicsRoles and memberships
Americanundergrads
Workers inNairobi
Masai SamburuNairobiundergrads
Per
cent
age
of s
tate
men
ts
10
20
30
40
50
60
70
80
0
15.27 Self-descriptions The proportion of self-descriptions that are personal characteristics versusroles and memberships varies according to degree ofwesternization.
positive psychology A researchmovement that emphasizes factorsthat make people psychologicallyhealthy, happy, or able to cope wellwith their life circumstances.
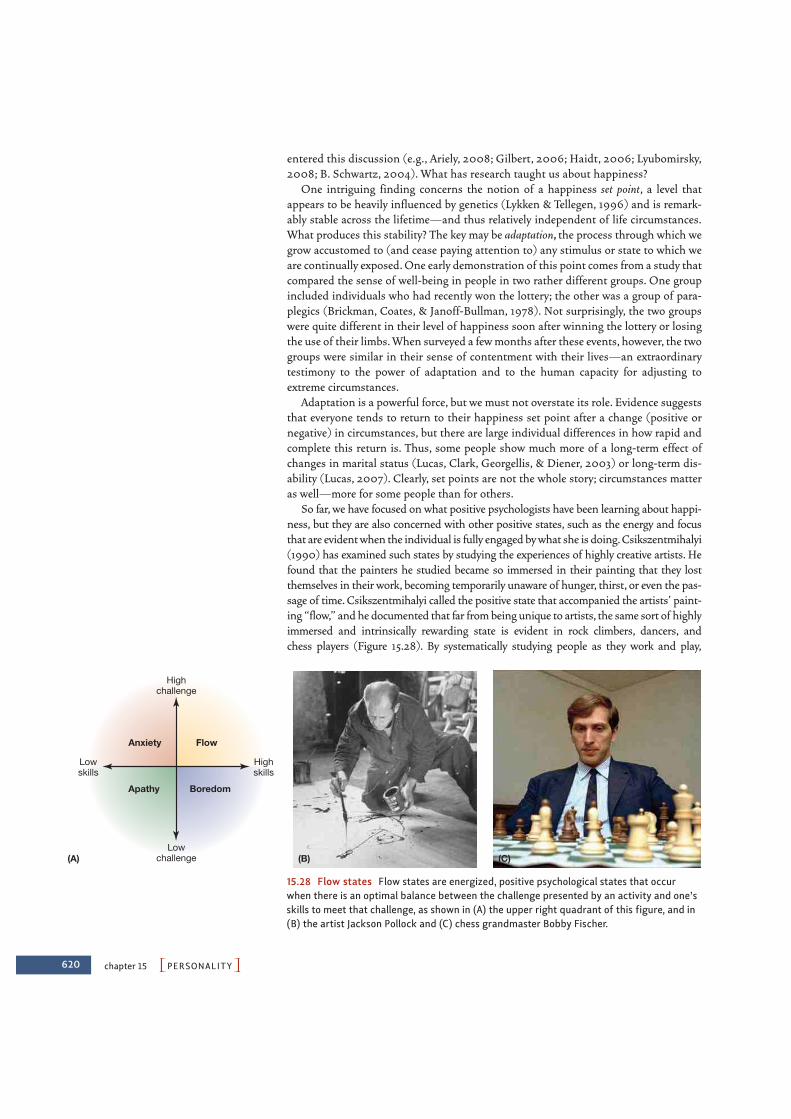
620 chapter 15 PPERSONALITYO
Anxiety Flow
Apathy Boredom
(C)(A)
Highchallenge
Lowskills
Highskills
Lowchallenge (B)
15.28 Flow states Flow states are energized, positive psychological states that occurwhen there is an optimal balance between the challenge presented by an activity and one’sskills to meet that challenge, as shown in (A) the upper right quadrant of this figure, and in(B) the artist Jackson Pollock and (C) chess grandmaster Bobby Fischer.
entered this discussion (e.g., Ariely, 2008; Gilbert, 2006; Haidt, 2006; Lyubomirsky,2008; B. Schwartz, 2004). What has research taught us about happiness?
One intriguing finding concerns the notion of a happiness set point, a level thatappears to be heavily influenced by genetics (Lykken & Tellegen, 1996) and is remark-ably stable across the lifetime—and thus relatively independent of life circumstances.What produces this stability? The key may be adaptation, the process through which wegrow accustomed to (and cease paying attention to) any stimulus or state to which weare continually exposed. One early demonstration of this point comes from a study thatcompared the sense of well-being in people in two rather different groups. One groupincluded individuals who had recently won the lottery; the other was a group of para-plegics (Brickman, Coates, & Janoff-Bullman, 1978). Not surprisingly, the two groupswere quite different in their level of happiness soon after winning the lottery or losingthe use of their limbs. When surveyed a few months after these events, however, the twogroups were similar in their sense of contentment with their lives—an extraordinarytestimony to the power of adaptation and to the human capacity for adjusting toextreme circumstances.
Adaptation is a powerful force, but we must not overstate its role. Evidence suggeststhat everyone tends to return to their happiness set point after a change (positive ornegative) in circumstances, but there are large individual differences in how rapid andcomplete this return is. Thus, some people show much more of a long-term effect ofchanges in marital status (Lucas, Clark, Georgellis, & Diener, 2003) or long-term dis-ability (Lucas, 2007). Clearly, set points are not the whole story; circumstances matteras well—more for some people than for others.
So far, we have focused on what positive psychologists have been learning about happi-ness, but they are also concerned with other positive states, such as the energy and focusthat are evident when the individual is fully engaged by what she is doing. Csikszentmihalyi(1990) has examined such states by studying the experiences of highly creative artists. Hefound that the painters he studied became so immersed in their painting that they lostthemselves in their work, becoming temporarily unaware of hunger, thirst, or even the pas-sage of time. Csikszentmihalyi called the positive state that accompanied the artists’ paint-ing “flow,” and he documented that far from being unique to artists, the same sort of highlyimmersed and intrinsically rewarding state is evident in rock climbers, dancers, and chess players (Figure 15.28). By systematically studying people as they work and play,

PThe Humanistic Approach: Appreciating Our PotentialO 621
Csikszentmihalyi has found that flow is most likely to be experienced when there is an opti-mal balance between the challenge presented by an activity and one’s skills to meet thatchallenge. If the level of challenge is too low for one’s ability, one feels bored. If the level ofchallenge is too high for one’s ability, one feels anxiety. But if the challenge is just right—and one feels that the activity is voluntarily chosen—one may experience flow.
P O S I T I V E T R A I TS
Positive psychologists have been concerned not just with positive states, like feelinghappy; they have also been concerned with positive traits—what we might think ofbroadly as being a good person (Peterson & Seligman, 2004). This interest has alignedthem to some degree with the trait approach, which we considered at the beginning ofthis chapter. However, positive psychologists emphasize delineating a set of narrowerand more specific traits, namely, the “positive” or “desirable” traits.
Defining and understanding these traits has been a central concern since the earli-est days of psychology (James, 1890), but the topic was set aside as too philosophicaland value-laden for many years. Only in the past decade has the systematic expositionof positive traits again come to the fore. One notable effort, led by Christopher Petersonand Martin Seligman, has focused on developing a classification of characterstrengths (Peterson and Seligman, 2004)—personal characteristics that (1) contributeto a person’s happiness without diminishing the happiness of others, (2) are valued intheir own right, rather than as a means to an end, (3) are trait-like and show variationacross people, (4) are measurable using reliable instruments, and (5) are evident acrosscultures, rather than specific to one or a few cultures (C. Peterson, 2006).
Peterson and Seligman have identified 24 character strengths with these attributes,organized into six clusters, as shown in Table 15.1. The first cluster of characterstrengths centers around wisdom and knowledge; the second cluster centers aroundcourage; the third cluster centers around humanitarian concerns; the fourth clustercenters around justice; the fifth cluster centers around temperance, defined by anabsence of excess; and the final cluster centers around transcendence.
This is a broad list—but may not be broad enough. For example, other researchers haveemphasized a role for optimism—a generalized expectation of desirable rather than unde-sirable outcomes (Scheier & Carver, 1985). Another important character strength isresilience, which refers to surviving and even thriving in the face of adversity—includingsuch extreme circumstances as serious illness, hostile divorce, bereavement, and even rape
character strengths Personalcharacteristics that contribute to aperson’s happiness without diminish-ing the happiness of others.
Creativity, curiosity, Authenticity, bravery, Kindness, love, Fairness, Mercy, modesty, Appreciationlove of learning, persistence, and zest and social leadership, and prudence of beauty or open-mindedness, (approaching life as intelligence team-orientation (not taking excellence, gratitude,and having an adventure) unreasonable hope, humor, and perspective risks), and self- spirituality
regulation
Peterson and Seligman’s 24 Character Strengths
TABLE
15.1CLUSTER 1 CLUSTER 2 CLUSTER 3 CLUSTER 4 CLUSTER 5 CLUSTER 6Wisdom and Courage Humanitarian Justice Temperance TranscendenceKnowledge Concerns

622 chapter 15 PPERSONALITYO
and the ravages of war. These positive tendencies appear to be associated with a numberof important life outcomes, such as greater success at work, with friends, and in marriage(Lyubomirsky, King, & Diener, 2005). The strengths also matter for one’s physiologicalfunctioning and health (Ryff et al., 2006; Salovey, Rothman, Detweiler, & Steward,2000). For example, people who are generally optimistic also have a better-functioningimmune system and so are more resistant to problems that range from the common coldto serious illness (Pressman & Cohen, 2005; Segerstrom, 2000).
Contributions of the Humanistic Approach How should we evaluate the humanistic approach to personality? We certainly need tobe cautious about the claims offered by Maslow, Rogers, and their contemporaries. Afterall, their key terms, like self-actualization or being yourself, are only vaguely defined, mak-ing it difficult to evaluate the humanists’ claims. In light of these (and related) concerns,some critics contend that the humanists’ concepts are too vague and their assertions toounproven (and maybe unprovable) to count as serious scientific accomplishments.
At the same time, the humanists have reminded us of several important points thatmore modern researchers have since developed in detail. These points include a crucialrole for each person’s sense of self—a sense that colors their perceptions, shapes theirbehavior, and in many ways defines their experience. The humanists also highlightedthe fact that people strive for more than food and sex and prestige; they read poetry, lis-ten to music, fall in love, and try to better themselves. Psychologists in the positive psy-chology movement are exploring these desires and tendencies using the tools of scienceto ask what makes us content with our lives and our relationships. Thus, among otherspecific issues, researchers are beginning to answer questions about how to stimulatecreativity, acquire wisdom, and nourish the intellect. Positive psychology is leadingresearchers in new directions, and it certainly carries on Maslow’s vision of a psychol-ogy concerned not only with what is basic about human nature, but also with what isgood and admirable about us.
THE SO CIAL-CO GNITIVE APPROACH:THE POWER OF BELIEFS Each of the perspectives we have considered has drawn our attention to a differentaspect of the personality puzzle. Trait theorists remind us that people do have stable,internal predispositions—that is, traits—and an emphasis on these traits allowed us toexplore a number of crucial issues, such as the biological underpinnings of personality.Psychodynamic theorists remind us of the importance of unconscious motivations andconflicts, and the need to dig beneath the surface in our understanding of who each ofus is. Humanistic theorists, in turn, remind us that humans have positive motivationsas well as negative ones—goals we hope to achieve, and not just hardships or tensionswe want to avoid or reduce.
The social-cognitive approach to personality endorses all of these claims, but notesthat we have still paid insufficient attention to one essential part of the puzzle—namely, the power of people’s beliefs in shaping their responses to others and to theworld around them. We saw the first inklings of this emphasis on beliefs in our discus-sion of the self, and the ways in which the self-schema influences our emotions andactions. However, in the social-cognitive approach, our beliefs about ourselves and ourworld take center stage.

PThe Social-Cognitive Approach: The Power of BeliefsO 623
Origins of the Social-Cognitive ApproachSocial-cognitive theories vary in their specifics, but all derive from two long-standingtraditions. The first is the behavioral tradition, set in the vocabulary of reward, punish-ment, instrumental responses, and observational learning (see Chapter 6). The second isthe cognitive view, which emphasizes the individual as a thinking being.
B E H AV I O R A L RO OTS O F SO C I A L- CO G N I T I V E T H E O R I E S
Central to the behavioral tradition is a worldview that, in its extreme form, asserts thatvirtually anyone can become anything given proper training. This American “can-do” viewwas distilled in a well-known pronouncement by the founder of American behaviorism,John B. Watson (Figure 15.29):
Give me a dozen healthy infants, well-formed, and my own specified world to bring themup in and I’ll guarantee to take any one at random and train him to become any type ofspecialist I might select—doctor, lawyer, artist, merchant-chief, and, yes, even beggar-man and thief, regardless of his talents, penchants, tendencies, abilities, vocations, andrace of his ancestors. (1925, p. 82)
Watson’s version of behaviorism was relatively primitive, but elements of his view are stillvisible in subsequent theorizing within the social-cognitive perspective. For example,Albert Bandura (like Watson) places a heavy emphasis on the role of experience and learn-ing, and the potential each of us has for developing in a variety of ways. But Bandura’s viewof personality goes considerably beyond Watson’s in its emphasis on the role we play asagents in fashioning our own lives. According to Bandura (2001), we observe relation-ships between certain actions (whether ours or others’) and their real-world consequences(rewards or punishments), and from this we develop a set of internalized outcomeexpectations, which then come to govern our actions.
In addition, we gradually become aware of ourselves as agents able to produce cer-tain outcomes, marking the emergence of a sense of self-efficacy, or a belief that onecan perform the behaviors that will lead to particular outcomes (Bandura, 2001,2006). When a person’s sense of self-efficacy is high, she believes that she canbehave in ways that will lead to rewarding outcomes. By contrast, when a person’ssense of self-efficacy is low, she believes herself incapable, and she may not even try.Researchers have found high self-efficacy beliefs to be associated with better socialrelationships, work, and health outcomes (Bandura, 1997; 2001; Maddux, 1995;Schwarzer, 1992). Likewise, self-efficacy beliefs about a particular task (“I’m sure Ican do this!”) are associated with success in that task. This attitude leads to morepersistence and a greater tolerance of frustration, both of which contribute to betterperformance (Schunk, 1984, 1985).
Once outcome expectations and beliefs about self-efficacy are in place, ouractions depend less on the immediate environment, and more on an internalizedsystem of self-rewards and self-punishments—our values and moral sensibilities.This reliance on internal standards makes our behavior more consistent than if wewere guided simply by the exigencies of the moment, and this consistency is whatwe know as personality. As seen from this view, personality is not just a reflection ofwho the individual is, with a substantial contribution from biology. Instead, inBandura’s perspective, personality is a reflection of the situations the person hasbeen exposed to in the past, and the expectations and beliefs that have been gleanedfrom those situations.
15.29 John B. Watson (1878–1958) Thefounder of American behaviorism.
outcome expectations A set ofbeliefs, drawn from experience, aboutwhat the consequences (rewards orpunishments) of certain actions arelikely to be.
self-efficacy The sense a person hasabout what things he can plausiblyaccomplish.

624 chapter 15 PPERSONALITYO
CO G N I T I V E RO OTS O F SO C I A L- CO G N I T I V E T H E O R I E S
A related tradition underlying social-cognitive theories of personality is the cognitiveview, first detailed by George Kelly (1955). Like many other psychologists, Kellyacknowledged that people’s behavior depends heavily on the situation. Crucially,though, he emphasized that much depends on their interpretations of the situation,which Kelly called their personal constructs, or the dimensions they use to organizetheir experience.
From Kelly’s perspective, each person seeks to make sense of the world and findmeaning in it. To explain how people do this, Kelly used the metaphor of a scientist whoobtains data about the world and then develops theories to explain what he hasobserved. These theories concern specific situations, but, when taken together, consti-tute each individual’s personal construct system. To assess these personal constructs,Kelly used the Role Construct Repertory Test. This test asks people to list three key indi-viduals in their life, and then to say how two of these three were different from a third.By repeating this process with different groups of three ideas, traits, or objects, Kellywas able to elicit the dimensions each person used (such as intelligence, strength, orgoodness) to make sense of the world.
Kelly’s work is important in its own right, but his influence is especially visible in thework of his former student, Walter Mischel. For Mischel (whom we met earlier), thestudy of personality must consider neither fixed traits nor static situations, but shouldfocus instead on how people dynamically process various aspects of their ever-changingworld. Like Kelly, Mischel contends that the qualities that form personality are essentiallycognitive: different ways of seeing the world, thinking about it, and interacting with it,all acquired over the course of an individual’s life. But how should we conceptualize thiscognition, and, with it, the interaction between the individual and the setting?
Mischel’s answer to this broad question is framed in terms of each individual’scognitive-affective personality system (CAPS), which consists of five key qualities onwhich people can differ. The first is the individual’s encodings, the set of construals bywhich the person interprets inner and outer experiences. Second, individuals developexpectancies and beliefs about the world, which include the outcome expectations andsense of self-efficacy stressed by Bandura. Third, people differ in their affects—that is,their emotional responses to situations. Fourth, they differ in their goals and values, theset of outcomes that are considered desirable. Finally, CAPS includes the individual’scompetencies and self-regulatory plans, the way an individual regulates her own behaviorby various self-imposed goals and strategies (Mischel, 1973, 1984, 2004; Mischel &Shoda, 1995, 1998, 2000).
Other researchers have filled in many details about what these various beliefsinvolve. For example, as we saw in Chapter 12, Carol Dweck and her colleagues haveargued that people differ in their fundamental assumptions about their own abilities(Dweck, 1999, 2006; Dweck & Leggett, 1988; Molden & Dweck, 2006). Some peopleassume their abilities are relatively fixed and unlikely to change in the future. In con-trast to this entity view, others hold an incremental view—assuming their abilities canchange and grow in response to new experience or learning (Figure 15.30). Theseassumptions turn out to be rather important, because people with the incremental vieware more willing to confront challenges and better able to bounce back from frustration(Dweck, 2009). Evidence comes from many sources, including studies that have triedto shift people’s thinking from the entity view to the incremental view. In one study,Blackwell, Trzesniewski, and Dweck (2007) randomly assigned junior high school stu-dents either to a regular study skills group or to an experimental condition that taughtstudents that the brain is like a muscle and can get stronger with use. Compared to
personal constructs The dimen-sions used by a person to organize hisor her experience.

PThe Social-Cognitive Approach: The Power of BeliefsO 625
those in the study skills group, those in the experimental group showed increased moti-vation and better grades.
These differences in belief are another point in which cultures differ. Evidence sug-gests, for example, that Americans tend toward the entity view, while the Japanese tendtoward an incremental view. This is reflected in the belief among many students in theUnited States that the major influence on intelligence is genetics; Japanese students, incontrast, estimate that the majority of intelligence is due to one’s efforts (Heine et al.,2001). This result is likely related to another finding we mentioned earlier in thechapter: Americans tend to perceive themselves as consistent in their behaviors as theymove from one situation to the next, a view similar to the entity view of intelligence,which emphasizes the stability of one’s abilities. Some other cultures put less emphasison personal consistency, leaving them ready to embrace the potential for growth andchange at the heart of the incremental view.
Key Social-Cognitive ConceptsSocial-cognitive theorists differ in focus and emphasis, but across theorists, three con-cepts play a crucial role. These are control, attributional style (which refers to how wetypically explain the things that happen in our lives), and self-control. We take up eachof these in turn.
CO N T RO L
There is a great deal of evidence that people desire control over the circumstances oftheir life and benefit from feeling that they have such control (C. Peterson, 1999; Rodin,1990; also see Chapter 6).
A widely cited illustration involves elderly people in a nursing home. Patients on onefloor of the nursing home were given small houseplants to care for, and they were alsoasked to choose the time at which they wanted to participate in some of the nursing-homeactivities (e.g., visiting friends, watching television, planning social events). Patients onanother floor were also given plants but with the understanding that the plants would betended by the staff. They participated in the same activities as the first group of patients,but at times chosen by the staff. The results were clear-cut. According to both nurses’ andthe patients’ own reports, the patients who tended their own houseplants and scheduledtheir own activities were more active and felt better than the patients who lacked this con-trol, a difference that was still apparent a year later (Langer & Rodin, 1976; Rodin &Langer, 1977; Figure 15.31).
(A) (B)
15.30 Beliefs about intelligence(A) Children with incremental views regard-ing intelligence believe their intelligencecan grow, and respond positively to chal-lenging feedback. (B) Children with entityviews regarding intelligence believe theirintelligence is fixed, and respond negativelyto challenging feedback.

626 chapter 15 PPERSONALITYO
Having control means being able to make choices, and so, if having control is a goodthing, then having choices would seem to be a good thing too, and the more the better.This line of reasoning is certainly consistent with the way various goods and services aremarketed—with both retail stores and large corporations offering us dozens of optionswhenever we order a latte, buy a new cell phone, select an insurance plan, or go on a vaca-tion. However, in a series of studies, Sheena Iyengar and Mark Lepper (2000) found thatthere is such a thing as too much choice. One of these studies was conducted in a gour-met food store, where the researchers created displays featuring fancy jams thatcustomers could taste. Some displays had 6 kinds of jam to taste. Other displays had24 kinds of jam to taste. Although people flocked to the larger display, it turned out thatpeople were actually 10 times as likely to purchase a jam they had tasted if they had seenthe smaller display as compared to the larger display. Reviewing this and related studies,Barry Schwartz (2004) concluded that although having some choice (and hence con-trol) is extremely important, having too much choice leads to greater stress and anxietyrather than greater pleasure. These findings indicate there can be too much of an appar-ently good thing, and suggest that other considerations (such as managing the anxietyoccasioned by having too many choices) may under some circumstances lead us to prefer lesser rather than greater control (see also Shah & Wolford, 2007).
AT T R I B U T I O N A L ST Y L E
Control beliefs are usually forward looking: Which jam will I buy? When will I visitmy friends? A different category of beliefs, in contrast, is oriented toward the pastand—more specifically—concerns people’s explanations for the events they haveexperienced.
In general, people tend to offer dispositional attributions for their own successes(“I did well on the test because I’m smart”), but situational attributions for their fail-ures (“My company is losing money because of the downturn in the economy”; “I lostthe match because the sun was in my eyes”). This pattern is obviously self-serving, andhas been documented in many Western cultures (Bradley, 1978). In most studies, par-ticipants perform various tasks—ranging from alleged measures of motor skills to testsof social sensitivity—and then receive fake feedback on whether they had achievedsome criterion of success (see, for example, Luginbuhl, Crowe, & Kahan, 1975;D. T. Miller, 1976; Sicoly & Ross, 1977; M. L. Snyder, Stephan, & Rosenfield, 1976;Stevens & Jones, 1976). The overall pattern of results is always the same: By and large,the participants attribute their successes to internal factors (they were pretty good at
(A) Too little control? (B) Just the right amount of control?
15.31 Control A person’s well-being as sheages may be strongly influenced by whethershe has (A) a high degree or (B) a lowdegree of control over her routine and herenvironment.

PThe Social-Cognitive Approach: The Power of BeliefsO 627
such tasks, and they worked hard) and their failures to external factors (the task wastoo difficult, and they were unlucky).
The same pattern is evident outside the laboratory. One study analyzed the com-ments of football and baseball players following important games, as published innewspapers. Of the statements made by the winners, 80% were internal attributions:“Our team was great,” “Our star player did it all,” and so on. In contrast, only 53% ofthe losers gave internal attributions, and they often explained the outcomes by referringto external, situational factors: “I think we hit the ball all right. But I think we’reunlucky” (Lau & Russell, 1980, p. 32).
These attributions are offered, of course, after an event—after the team has wonor lost, or after the business has succeeded or failed. But a related pattern arisesbefore an event, allowing people to protect themselves against failure and disappoint-ment. One such strategy is known as self-handicapping, in which one arranges anobstacle to one’s own performance. This way, if failure occurs, it will be attributed tothe obstacle and not to one’s own limitations (Higgins, Snyder, & Berglas, 1990;Jones & Berglas, 1978). Thus, if Julie is afraid of failing next week’s biology exam, shemight spend more time than usual watching television. Then, if she fails the exam,the obvious interpretation will be that she did not study hard enough, rather thanthat she is stupid.
Not surprisingly, all these forms of self-protection are less likely in collectivisticcultures—that is, among people who are not motivated to view themselves as differ-ent from and better than others. But there is some subtlety to the cultural patterning.A recent analysis of the self-serving bias found that the Japanese and Pacific Islandersshowed no self-serving biases, Indians displayed a moderate bias, and Chinese andKoreans showed large self-serving biases. It is not clear why these differences arose,and explaining this point is a fruitful area for future research. In the meantime,though, this analysis reminds us of the important point that there is a great deal ofvariation within collectivistic, interdependent cultures.
Even within a given culture, there are notable differences in attributional style, theway a person typically explains the things that happen in his or her life (Figure 15.32).This style can be measured by a specially constructed attributional-style questionnaire(ASQ) in which a participant is asked to imagine himself in a number of situations(e.g., failing a test) and to indicate what would have caused those events if they hadhappened to him (Dykema, Bergbower, Doctora, & Peterson, 1996; C. Peterson & Park,1998; C. Peterson et al., 1982). His responses on the ASQ reveal how he explains hisfailure. He may think he did not study enough (an internal cause) or that the teacher
self-handicapping A self-protectivestrategy of arranges for an obstacle toone’s own performance, so that failurecan be attributed to the obstacleinstead of one’s own limitations.
attributional style The way a per-son typically explains the things thathappen in his or her life.
(A) Negative attributional style (B) Positive attributional style
15.32 Attributional style (A) A. A. Milne’sEeyore personifies a negative attributionalstyle. (B) Cheerful SpongeBob SquarePantshas a positive attributional style.
628 chapter 15 PPERSONALITYO
misled him about what to study (an external cause). He may think he is generally stu-pid (a global explanation) or is stupid on just that test material (a specific explanation).Finally, he may believe he is always bound to fail (a stable explanation) or that with alittle extra studying he can recover nicely (an unstable explanation).
Differences in attributional style matter (Peterson & Park, 2007). More specifically,greater use of external, specific, and unstable attributions for failure predicts importantoutcomes ranging from performance in insurance sales (Seligman & Schulman, 1986) tosuccess in competitive sports (Seligman, Nolen-Hoeksema, Thornton, & Thornton,1990). Importantly, variation in attributional style has also been shown to predict theonset of some forms of psychopathology, such as whether a person is likely to suffer fromdepression (see Chapter 16). Specifically, being prone to depression is correlated with aparticular attributional style—a tendency to attribute unfortunate events to causes thatare internal, global, and stable. Thus, a person who is prone to depression is likely toattribute life events to causes related to something within her that applies tomanyother situations and will continue indefinitely (G. M. Buchanan & Seligman, 1995;C. Peterson & Seligman, 1984; C. Peterson & Vaidya, 2001; Seligman & Gillham, 2000).
S E L F - CO N T RO L
So far we have emphasized each person’s control over his life circumstances, but just asimportant for the social-cognitive theorists is the degree of control each person hasover himself and his own actions. Surely people differ in this regard, and these differ-ences in self-control are visible in various ways (Figure 15.33). People differ in theirability to do what they know they should—whether the issue is being polite to anobnoxious supervisor at work, or keeping focused despite the distraction of a talkativeroommate. They also differ in whether they can avoid doing what they want to do butshould not—for example, not joining friends for a movie the night before an exam.People also differ from each other in their capacity to do things they dislike in order toget what they want eventually—for example, studying extra hard now in order to dowell later in job or graduate school applications.
Examples of self-control (and lack thereof) abound in everyday life. Self-control ismanifested whenever we get out of bed in the morning, because we know we should,even though we are still quite sleepy. It is also evident when we eat an extra helping ofdessert when we’re dieting (or don’t), or quit smoking (or don’t). In each case, the abil-ity to control oneself is tied to what people often call willpower, and, according to popu-lar wisdom, some people have more willpower than others. But do they really? That is, is“having a lot of willpower” a trait that is consistent over time and across situations?
Walter Mischel (1974, 1984) and his associates (Mischel, Shoda, & Rodriguez, 1992)studied this issue in children. The participants in his studies were between four and fiveyears of age and were shown two snacks, one preferable to the other (e.g., twomarshmallows or pretzels versus one). To obtain the snack they preferred, they had towait about 15 minutes. If they did not want to wait, or grew tired of waiting, they imme-diately received the less desirable treat but had to forgo the more desirable one.
Whether the children could manage the wait was powerfully influenced by whatthe children did and thought about while they waited. If they looked at the marsh-mallow, or worse, thought about eating it, they usually succumbed and grabbed thelesser reward. But they were able to wait for the preferred snack if they found (or wereshown) some way of distracting their attention from it, for example, by thinking ofsomething fun, such as Mommy pushing them on a swing. They could also wait forthe preferred snack if they thought about the snack in some way other than eating it,for example, by focusing on the pretzels’ shape and color rather than on their15.33 Self-control?
self-control The ability to pursue agoal while adequately managing inter-nal conflicts about it, or to delay pur-suing a goal because of otherconsiderations or constraints.
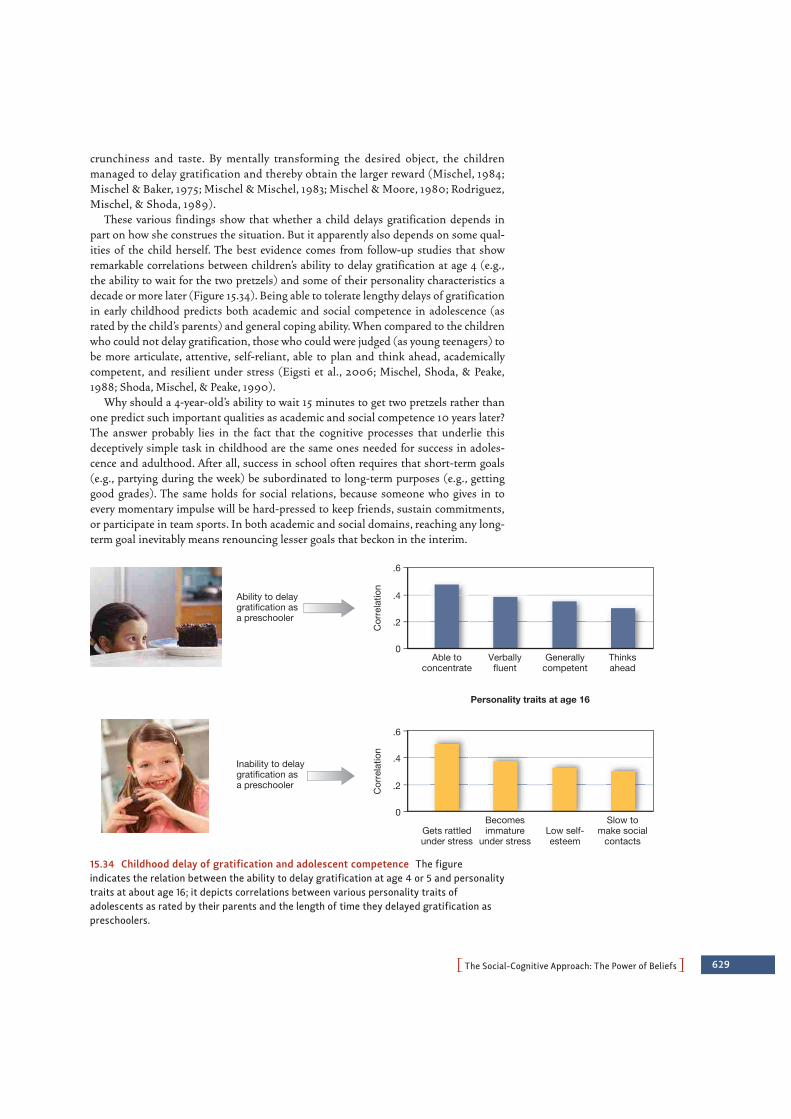
PThe Social-Cognitive Approach: The Power of BeliefsO 629
crunchiness and taste. By mentally transforming the desired object, the childrenmanaged to delay gratification and thereby obtain the larger reward (Mischel, 1984;Mischel & Baker, 1975; Mischel & Mischel, 1983; Mischel & Moore, 1980; Rodriguez,Mischel, & Shoda, 1989).
These various findings show that whether a child delays gratification depends inpart on how she construes the situation. But it apparently also depends on some qual-ities of the child herself. The best evidence comes from follow-up studies that showremarkable correlations between children’s ability to delay gratification at age 4 (e.g.,the ability to wait for the two pretzels) and some of their personality characteristics adecade or more later (Figure 15.34). Being able to tolerate lengthy delays of gratificationin early childhood predicts both academic and social competence in adolescence (asrated by the child’s parents) and general coping ability. When compared to the childrenwho could not delay gratification, those who could were judged (as young teenagers) tobe more articulate, attentive, self-reliant, able to plan and think ahead, academicallycompetent, and resilient under stress (Eigsti et al., 2006; Mischel, Shoda, & Peake,1988; Shoda, Mischel, & Peake, 1990).
Why should a 4-year-old’s ability to wait 15 minutes to get two pretzels rather thanone predict such important qualities as academic and social competence 10 years later?The answer probably lies in the fact that the cognitive processes that underlie thisdeceptively simple task in childhood are the same ones needed for success in adoles-cence and adulthood. After all, success in school often requires that short-term goals(e.g., partying during the week) be subordinated to long-term purposes (e.g., gettinggood grades). The same holds for social relations, because someone who gives in toevery momentary impulse will be hard-pressed to keep friends, sustain commitments,or participate in team sports. In both academic and social domains, reaching any long-term goal inevitably means renouncing lesser goals that beckon in the interim.
Ability to delaygratification asa preschooler
Inability to delaygratification asa preschooler
Cor
rela
tion
Cor
rela
tion
.2
.4
.6
Able toconcentrate
Verballyfluent
Personality traits at age 16
Generallycompetent
Thinksahead
Gets rattledunder stress
Becomesimmature
under stressLow self-esteem
Slow tomake social
contacts
.2
0
0
.4
.6
15.34 Childhood delay of gratification and adolescent competence The figureindicates the relation between the ability to delay gratification at age 4 or 5 and personalitytraits at about age 16; it depicts correlations between various personality traits ofadolescents as rated by their parents and the length of time they delayed gratification aspreschoolers.
630 chapter 15 PPERSONALITYO
If there is some general capacity for delaying gratification, useful for child and adultalike, where does it originate? As we saw in Chapter 11, intelligence has a heritablecomponent, and the executive control processes that support delaying gratification alsomay have a heritable component. It seems likely, however, that there is also a largelearned component. Children may acquire certain cognitive skills (e.g., self-distraction,reevaluating rewards, and sustaining attention to distant goals) that they continue toapply and improve upon as they get older. However they originate, though, these atten-tion-diverting strategies appear to emerge in the first two years of life and can be seenin the child’s attachment behavior with the mother. In one study, toddlers wereobserved during a brief separation from their mothers, using a variant of the StrangeSituation task already discussed. Some of the toddlers showed immediate distress,while others distracted themselves with other activities. Those who engaged in self-distraction as toddlers were able to delay gratification longer when they reached the ageof 5 (Sethi, Mischel, Aber, Shoda, & Rodriguez, 2000).
But what if one didn’t develop these valuable self-regulatory capacities and skills byearly childhood? Is one simply out of luck? Proponents of a social cognitive perspectivewould argue not, pointing to studies in which self-regulatory ability was enhanced bysimple changes in how individuals construed the situation in which they foundthemselves. In one study, for example, Magen and Gross (2007) asked participants tosolve simple math problems. What made this task difficult was that a hilarious comedyroutine was playing loudly on a television just beside the monitor on which the mathproblems were being presented. Participants were instructed to do their best, and theyunderstood that they could win a prize if they had a particularly good math score. Eventhough they were motivated to do well, participants peeked at the television show eventhough this hurt their performance on the test. Then, halfway through the math test,one group of test-takers was simply reminded to do as well as they could on the secondhalf of the math test. The second group got the same reminder, but in addition, theywere told that they might find it helpful to think of the math test as a test of theirwillpower. Because these participants highly valued their willpower, this provided anextra incentive for them to stay focused on their task. This simple reconstrual of themath test context as a test of their willpower led them to peek less often during the sec-ond half of the math test than did the participants in the other instructional group.
Contributions of the Social-Cognitive ApproachLike the trait approach theorists, social-cognitive theorists have taken a considerableinterest in relatively stable personality traits, as revealed by studies of attributional styleand delay of gratification. How, then, do social-cognitive theorists differ from trait theo-rists? There are two answers. One has to do with the role of the situation. By now, theo-rists from all perspectives agree that both traits and situations matter, but even so,social-cognitive theorists are more likely than trait theorists to stress the role of the sit-uation and how the individual understands and deals with it. Thus, Mischel found thatdelay of gratification is an index of a surprisingly stable personal attribute, but he wasquick to point out that this index is strongly affected by the way the situation was set up(was the reward visible?) and how it was construed (did the child think about eating thereward?). The second answer concerns the origins of personality. Unlike trait theorists,who tend to emphasize the genetic basis of personality, social-cognitive theorists typi-cally place greater emphasis on the role played by learning in shaping personality.
Like the psychodynamic theorists, social-cognitive theorists want to dig deeper thanthe surface of personality in order to understand the psychological processes that sup-

PSome Final Thoughts: The Need for Multiple ApproachesO 631
port behavior and mental processes. In doing so, social-cognitive theorists are oftenaddressing problems such as delay of gratification that come straight out of Freud’splaybook, and the psychological processes that these two types of theorists are inter-ested in overlap considerably, particularly if we include the ego psychologists, with theiremphasis on an adaptive, active ego, and the object relations theorists with theiremphasis on social reinforcement. Note, however, the differences. Theorists from thesocial-cognitive and psychodynamic approaches go about their work using starklydifferent languages and methods and holding up quite different views of the role ofconscious processes. Social-cognitive theorists emphasize cognitive processes such asconstrual and beliefs, and prioritize tightly controlled experiments. In contrast, psycho-dynamic theorists emphasize unconscious impulses and defenses, and rely on insightsdrawn from clinical work with patients.
The parallels between the social-cognitive approach and the humanistic approachare similarly instructive. The positive outlook of the humanistic psychologist CarlRogers resonates with social-cognitive theorists such as Bandura. Both are optimisticabout the individual’s capacity to overcome difficult circumstances and to show extraor-dinary resilience in the face of trying times. This optimism hinges for both schools ofthought on the conviction that we are not just passively shaped by the swirl of lifearound us, but also actively seek to shape our world. Despite this shared optimismabout the human capacity for growth and change, the traditions differ. The humanistictheorist describes the growth in terms of a self that is actualized to varying degrees,while the social-cognitive theorist draws attention to a malleable set of processes thatguide how the individual acts and, ultimately, who he is.
SOME FINAL THOUGHTS: THE NEEDFOR MULTIPLE APPROACHES
As our tour of the major approaches to studying personality draws to a close, we can seethat each of these approaches focuses on a different part of the puzzle of who we are,and each privileges a somewhat different combination of the various types of data usedby personality psychologists, including self-report data, informant data, behavioraldata, physiological data, and life data.
Today, relatively few theorists would espouse any of these approaches in their mostextreme form, or would claim that none of the other approaches has any merit in under-standing personality. Most adherents of the trait perspective, for example, appreciatethe power of situations that are construed in different ways by different people. Mostpsychodynamic theorists see unconscious defenses and conscious coping mechanismsas parts of a continuum, and they recognize the extent to which each individual is richlyembedded in a social network. Most humanistically oriented theorists grant that whatpeople do depends on both traits and situations, as well as the motive to self-actualize.
Even so, some important differences in approach clearly remain. Some aspects ofpersonality have clear temperamental origins (trait theory); others are learned, and theyderive from how we think about ourselves and the world (social-cognitive theory).Some reflect conflicts of which we are not aware (psychodynamic theory); still othersreveal the need for self-actualization (the humanistic approach). We cannot envisionwhat a complete theory of personality will ultimately look like, but it will surely have todescribe all of these aspects of human functioning.

THE TRAIT APPROACH:DEFINING OUR DIFFERENCES
• Traits define a person’s predominant thoughts, feelings, andbehaviors. Five personality dimensions have been identified—extraversion, neuroticism, agreeableness, conscientiousness,and openness to experience—the so-called Big Five. There hasbeen debate, however, about how useful the Big Five dimen-sions are for describing personalities across cultures.
• One challenge to trait theories is the personality paradox:people often behave less consistently than might be expected.Part of the explanation for this paradox is the power of thesituation. Most theorists now believe that both personalityand situations matter, usually in interaction, and sometheorists describe personalities in terms of an if . . . then . . .pattern: “If in this setting, then act in this fashion; if in thatsetting, then act in that fashion.” Some people are more con-sistent in their behaviors than others; this complexity isassessed by the Self-Monitoring Scale.
• Traits grow to some extent out of the individual’s tempera-ment, or characteristic emotional or behavioral pattern. Twinstudies of the Big Five dimensions confirm a high heritability.In the case of extraversion, genetic influences may depend oneach individual’s level of central nervous system reactivity,with introverts more reactive than extraverts. A similar logichas been used to explain sensation seeking and inhibitedtemperament.
• Studies of national character underline the importance ofcultural differences in personality. Family effects are alsoimportant, but they reflect differences within families (e.g.,contrasts between first-borns and second-borns) rather thandifferences between families. The correlation between thepersonality traits of adopted children and their adoptive sib-lings is essentially zero, and the correlations between thetraits of identical twins reared together are comparable tothose of identical twins reared apart.
THE PSYCHODYNAMIC APPROACH:PROBING THE DEPTHS
• The psychodynamic approach to personality is derived fromSigmund Freud’s theory of psychoanalysis. Freud distin-guished three subsystems of personality: the id, a blind striv-
ing toward biological satisfaction that follows the pleasureprinciple; the ego, a system that tries to reconcile id-derivedneeds with the actualities of the world; and the superego,which represents the internalized rules of the parents andpunishes deviations through feelings of guilt.
• According to Freud, internal conflict gives rise to anxiety, whichleads a child to push the forbidden thoughts out of conscious-ness. Repression is the primary vehicle for this, but the repressedmaterials may surface again, demanding the use of other defensemechanisms, including displacement, reaction formation, rationali-zation, and projection.
• According to Freud, the child passes through specific stages ofpsychosexual development, with each stage characterized by theerogenous zones through which gratification is obtained.Freud proposed that during the phallic stage, the boysdevelop the Oedipus complex and girls develop the Electracomplex.
• Freud drew evidence from several sources, including theerrors that people make in everyday life. He also felt thatdreams hold important clues about the unconscious mind,although it was crucial to understand a dream’s latent contentand not just its manifest content. Another source of informa-tion about the unconscious comes from the study of mythsand legends, which may give insights into our collectiveunconscious.
• After Freud, psychodynamic theorists, called ego psychologists,focused on the skills and adaptive capacities of the ego. Theyemphasized coping patterns, which show considerable consis-tency over an individual’s lifetime. Other psychodynamictheorists, called object relations theorists, focused on the rela-tions an individual has with others.
THE HUMANISTIC APPROACH:APPRECIATING OUR POTENTIAL
• The humanistic approach maintains that what is mostimportant about people is how they achieve their own self-hood and actualize their potential. This approachemphasizes phenomenology, or each person’s own uniqueperspective based on that person’s construal, or interpreta-tion of the world around him.
• This perspective emphasizes positive human motives, such asself-actualization, rather than what it calls deficiency needs.
632 chapter 15 PPERSONALITYO
S U M M A R Y C H A P T E R 1 5

According to Carl Rogers’ self theory, children only achieve asolid sense of personal self-worth if they have experienceda sense of unconditional positive regard.
• Self-schemas play a powerful role in determining a person’s self-esteem. The content of self-schema vary by culture.
• Many themes stressed by humanistic psychologists underlie amore recent movement called positive psychology, which hasled to a number of empirical investigations regarding positivesubjective experiences, positive individual traits, and positivesocial institutions.
THE SOCIAL-COGNITIVE APPROACH:THE POWER OF BELIEFS
• Social-cognitive theorists focus on the various cognitive char-acteristics along which personalities may differ. Albert Banduraemphasizes the role of experience, through which individualsdevelop outcome expectations that govern their actions; individ-uals also develop a sense of self-efficacy. Walter Mischel hasemphasized the way people interpret the world around them,and also their competencies and self-regulatory plans.
• Social-cognitive theorists emphasize the notion of control—a person’s ability to do what he wants to do.
• They also emphasize attributional style, the way a person typi-cally explains the things that happen in his or her life.
• A third crucial construct is self-control, which refers to anindividual’s ability to refrain from doing what he wants to doin order to get something he wants even more. The impor-tance of self-control is reflected in evidence that 4-year-oldswho are able to tolerate delay of gratification show moresocial and academic competence in adolescence.
PSummaryO 633
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
Conceptions of Mental Disorders 636
Defining, Assessing, and Diagnosing Mental Disorders 639
Anxiety Disorders 644
Mood Disorders 652
Schizophrenia 658
Other Axis I and Axis II Disorders 666
Some Final Thoughts: Syndromes Without Stigma? 672
Summary 674
CH
AP
TE
R
635
CH
AP
TE
R
16Psychopathology
British singer/songwriter Amy Winehouse shot to the
top of the charts in 2006 with such international hits as “Rehab,” “Love Is a Losing
Game,” and “You Know I’m No Good.” Awards quickly followed, including a record
number of Grammys and several big prizes in Great Britain. Meanwhile, Winehouse’s
beehive hairdo, dramatic eye makeup, vintage dresses, and elaborate tattoos caught
the imagination of the public and fashion designers alike.
But as her career took off, Winehouse’s life spun out of control. Her
hospitalizations for overdoses of heroin, ecstasy, cocaine, and alcohol; arrests for
possessing drugs and assaulting fans; no-shows at concerts; and bizarre public
behavior filled the tabloids. Her increasingly skimpy clothes revealed dramatic weight
loss and self-inflicted wounds.
The media has focused on Winehouse’s drug and alcohol problems, but is substance
abuse her only woe? She has talked about struggling with depression, as well as eating
disorders and self-harm. Some observers suggest that she may have bipolar disorder,
an illness that causes people to cycle between deep depressions and extreme manias,
often with intermittent stretches of relative calm. Many creative people throughout
history—from composer Ludwig van Beethoven, to artist Vincent van Gogh, to writer
Virginia Woolf, to scientist Isaac Newton, to politician Winston Churchill—have
shown symptoms of bipolar disorder, and Winehouse’s eccentric flair and haunting
lyrics may bear the marks of this condition. Her substance abuse may be another sign,
as nearly 60% of people with this illness abuse alcohol or drugs.
636 chapter 16 PPSYCHOPATHOLOGYO
Winehouse’s behaviors are also consistent with borderline personality disorder, adiagnosis that shares many symptoms with bipolar disorder, including mood swingsand impulsivity. Unique to borderline personality disorder, however, is a profoundfear of abandonment, which Winehouse has expressed in songs such as “Rehab.”Cutting, which Winehouse admits to, is also a symptom of borderline personalitydisorder.
As we scan the list of possible explanations for Amy Winehouse’s behavior—a listthat could also include attention-deficit/hyperactivity disorder (ADHD), anorexianervosa, an eccentric personality, or some combination of all these—you may wonderwhy it matters which disorders she (or anyone else) may have. One reason is that thecorrect diagnosis of mental illness can lead to correct treatment, while an incorrectdiagnosis can exacerbate mental problems. The antidepressants that ease depression,for example, can fuel a manic phase in a person with bipolar disorder. Diagnosis alsogives us clues about the origins of mental disorders. As you will learn in this chapter,most mental disorders arise from a complex interplay of nature and nurture, biologiesand environments, diatheses (vulnerabilities) and stressors. Understanding thesemany interacting factors can help us not only to treat mental illnesses more effectivelybut also to try to prevent them.
But there is one other reason to care about Amy Winehouse’s struggles. In her wesense the familiar: most of us know someone with psychiatric problems and perhapshave a few of our own. Almost half of Americans will have at least one mentaldisorder during their lifetimes. The information about psychopathology that you areabout to encounter may hit close to home and may, we hope, instill a deepcompassion for people living with mental disorders.
CONCEPTIONS OF MENTAL DISORDERS
We have seen over the past two chapters that people differ from one another in manyways, both in their desirable qualities, like being intelligent or helpful, and in theirundesirable ones, like being selfish or aggressive. Even so, the attributes we haveconsidered all fall within the range that most people consider acceptable or normal. Inthis chapter, we consider differences that are outside the normal range of variation—differences that carry us into the realm of mental disorders such as depression, anxiety,
and schizophrenia. These are conditions that cause considerable suffer-ing and profoundly disrupt people’s lives—both the lives of the peopleafflicted with the disorders and, often, the lives of others around them.
The study of mental disorders is the province of psychopathology,or, as it is sometimes called, abnormal psychology. Like many corners ofpsychology, this domain has been studied scientifically only in the lastcentury. Concerns about mental illness, however, have a much longerhistory. One of the earliest-known medical documents, the Eberspapyrus (written about 1550 C.E.), refers to the disorder we now knowas depression (Okasha & Okasha, 2000). Other ancient cases includeKing Saul of Judaea, who alternated between bouts of homicidal frenzyand suicidal depression, and the Babylonian king Nebuchadnezzar,who walked on all fours in the belief that he was a wolf (Figure 16.1).Across the millennia, though, people have had very different concep-tions of what causes these disorders.
16.1 An early example of mental disorderKing Nebuchadnezzar as depicted byWilliam Blake (1795).

Early Conceptions of Mental DisordersThe earliest theories held that a person afflicted by a mental disorder was possessed byevil spirits. As we will see in Chapter 17, people tried various extreme remedies to deal withthis problem, such as flogging and starving, with the aim of driving the evil spirits away.
In recent centuries, a more sophisticated conception of mental disorders began todevelop—namely, that they are a type of disease, to be understood in the same wayas other illnesses. Proponents of this somatogenic hypothesis (from the Greeksoma, meaning “body”) argued that mental disorders, like other forms of illness,could be traced to an injury or infection. This position gained considerable credibil-ity in the late nineteenth century, thanks to discoveries about general paresis.
General paresis is a disorder characterized by a broad decline in physical and psy-chological functions, culminating in marked personality aberrations that may includegrandiose delusions (“I am the king of England”) or profound hypochondriacaldepressions (“My heart has stopped beating”). Without treatment, the deteriorationprogresses to the point of paralysis, and death occurs within a few years. The break-through in understanding paresis came in 1897, when the Viennese physician Richardvon Krafft-Ebing (1840–1902) discovered that it was actually a consequence of infec-tion with syphilis. This discovery paved the way for the development of antibiotics thatcould cure the infection, and, if the drugs were given early enough, the symptoms ofparesis could be avoided altogether.
It seems, then, that general paresis can be understood and treated like any othermedical problem. Should other forms of mental disorder be understood in the samefashion—as the result of an infection or perhaps an injury? This view gained manysupporters in the late 1800s, including Emil Kraepelin (Figure 16.2), whose textbook,Lehrbuch der Psychiatrie, emphasized the importance of brain pathology in producingmental disorders.
However, a somatogenic approach cannot explain all mental disorders. Forexample, more than a hundred years ago, scholars realized that this approach was notappropriate for the disorder then known as hysteria, which we encountered in ourdiscussion of psychoanalysis (see Chapter 15). Patients with hysteria typically showedodd symptoms that seemed to be neurological, but with other indications that madeit plain there was no neurological damage. Some patients reported that their limbswere paralyzed, but under hypnosis they could move their arms and legs perfectly well,indicating that the nerves and muscles were fully functional. Their symptoms,therefore, were not the result of a bodily injury; instead, they had to be understoodin terms of a psychogenic hypothesis, which holds that the symptoms arise viapsychological processes.
Across much of the late 19th and early 20th centuries, the most prominent version ofthis hypothesis was Sigmund Freud’s, which described mental illness as resulting frominner conflicts and defensive maneuvers aimed at dealing with those conflicts. Early inthe 20th century, other theorists offered alternative conceptions of mental illness—but,like Freud, argued that the illness arose from psychological processes, and not from bod-ily injury. For example, the early behaviorists offered learning models of mental illness,building on the mechanisms we discussed in Chapter 7. In this view, many mental disor-ders result from maladaptive learning and are best corrected with remedial learning.
Modern Conceptions of Mental DisordersHistorically, the somatogenic and psychogenic approaches were offered as sharply dis-tinct proposals, and scholars debated the merits of one over the other. We now know
PConceptions of Mental DisordersO 637
16.2 Emil Kraepelin (1856–1926) Themajor figure in psychiatric classification,Kraepelin distinguished two groups ofsevere mental disorders, schizophrenia andmanic-depressive psychosis (now calledbipolar disorder).
psychopathology The study of men-tal disorders, or a term for the mentaldisorder itself.
somatogenic hypothesis Thehypothesis that mental disorders resultfrom organic (bodily) causes.
psychogenic hypothesis Thehypothesis that mental disorders resultfrom psychological causes.
learning model The hypothesis thatmental disorders result from someform of faulty learning.
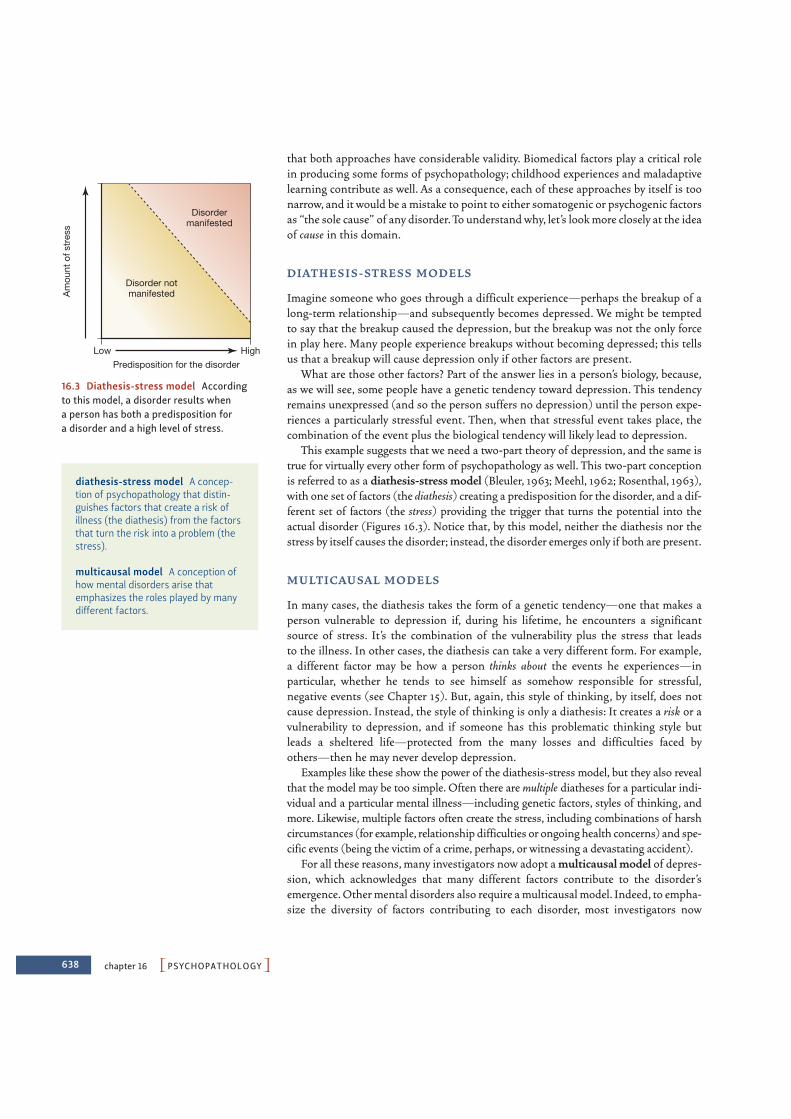
638 chapter 16 PPSYCHOPATHOLOGYO
that both approaches have considerable validity. Biomedical factors play a critical rolein producing some forms of psychopathology; childhood experiences and maladaptivelearning contribute as well. As a consequence, each of these approaches by itself is toonarrow, and it would be a mistake to point to either somatogenic or psychogenic factorsas “the sole cause” of any disorder. To understand why, let’s look more closely at the ideaof cause in this domain.
D I AT H E S I S - ST R E SS M O D E LS
Imagine someone who goes through a difficult experience—perhaps the breakup of along-term relationship—and subsequently becomes depressed. We might be temptedto say that the breakup caused the depression, but the breakup was not the only forcein play here. Many people experience breakups without becoming depressed; this tellsus that a breakup will cause depression only if other factors are present.
What are those other factors? Part of the answer lies in a person’s biology, because,as we will see, some people have a genetic tendency toward depression. This tendencyremains unexpressed (and so the person suffers no depression) until the person expe-riences a particularly stressful event. Then, when that stressful event takes place, thecombination of the event plus the biological tendency will likely lead to depression.
This example suggests that we need a two-part theory of depression, and the same istrue for virtually every other form of psychopathology as well. This two-part conceptionis referred to as a diathesis-stress model (Bleuler, 1963; Meehl, 1962; Rosenthal, 1963),with one set of factors (the diathesis) creating a predisposition for the disorder, and a dif-ferent set of factors (the stress) providing the trigger that turns the potential into theactual disorder (Figures 16.3). Notice that, by this model, neither the diathesis nor thestress by itself causes the disorder; instead, the disorder emerges only if both are present.
M U LT I CAU SA L M O D E LS
In many cases, the diathesis takes the form of a genetic tendency—one that makes aperson vulnerable to depression if, during his lifetime, he encounters a significantsource of stress. It’s the combination of the vulnerability plus the stress that leadsto the illness. In other cases, the diathesis can take a very different form. For example,a different factor may be how a person thinks about the events he experiences—inparticular, whether he tends to see himself as somehow responsible for stressful,negative events (see Chapter 15). But, again, this style of thinking, by itself, does notcause depression. Instead, the style of thinking is only a diathesis: It creates a risk or avulnerability to depression, and if someone has this problematic thinking style butleads a sheltered life—protected from the many losses and difficulties faced byothers—then he may never develop depression.
Examples like these show the power of the diathesis-stress model, but they also revealthat the model may be too simple. Often there are multiple diatheses for a particular indi-vidual and a particular mental illness—including genetic factors, styles of thinking, andmore. Likewise, multiple factors often create the stress, including combinations of harshcircumstances (for example, relationship difficulties or ongoing health concerns) and spe-cific events (being the victim of a crime, perhaps, or witnessing a devastating accident).
For all these reasons, many investigators now adopt a multicausal model of depres-sion, which acknowledges that many different factors contribute to the disorder’semergence. Other mental disorders also require a multicausal model. Indeed, to empha-size the diversity of factors contributing to each disorder, most investigators now
Am
ount
of s
tres
s
Low High
Disordermanifested
Disorder notmanifested
Predisposition for the disorder
16.3 Diathesis-stress model Accordingto this model, a disorder results when a person has both a predisposition for a disorder and a high level of stress.
diathesis-stress model A concep-tion of psychopathology that distin-guishes factors that create a risk ofillness (the diathesis) from the factorsthat turn the risk into a problem (thestress).
multicausal model A conception ofhow mental disorders arise thatemphasizes the roles played by manydifferent factors.

urge that we take a biopsychosocial perspective, which considers biological factors(like genetics), psychological factors (like a style of thinking), and social factors (likethe absence of social support; Figure 16.4).
DEFINING, ASSESSING, ANDDIAGNOSING MENTAL DISORDERS
What exactly are mental disorders? And how can a clinician learn whether someonehas one?
Defining Mental DisordersPhrases such as “mental disorder” and “abnormal psychology” suggest that whendefining mental disorders, we should start with some conception of normalcy and thendefine disorders as variations that are not normal. Thus, taking depression as anexample, we might acknowledge that everyone is occasionally sad, but we might worryabout (and try to treat) someone whose sadness is deeper and lasts longer than normalsadness.
However, this perspective invites difficulties, because even something normal can beproblematic. For example, almost everyone gets cavities, which makes them normal, butthis does not change the fact that cavities are a problem. Likewise, many things are“abnormal” without necessarily being symptoms of disorders. Pink is not a normal haircolor, but this does not mean that someone who dyes his hair pink is sick. It seemsclear, therefore, that we cannot equate being “abnormal” with being “ill.”
How, then, should we define mental disorders? The most commonly accepted defi-nition is the one provided by the American Psychiatric Association (2000) in theDiagnostic and Statistical Manual of Mental Disorders (now in the text revisionof its fourth edition, and hence known as the DSM-IV-TR; for the sake of simplicity,we’ll refer to this work as DSM from this point forward). The DSM states that each ofthe mental disorders is a
Behavioral or psychological syndrome or pattern that occurs in a person and that is asso-ciated with present distress (e.g., a painful symptom) or disability (i.e., impairment inone or more important areas of functioning) or with a significantly increased risk ofsuffering death, pain, disability, or an important loss of freedom. In addition, thissyndrome or pattern must not be merely an expectable and culturally sanctionedresponse to a particular event, for example, the death of a loved one. Whatever its origi-nal cause, it must currently be considered a manifestation of a behavioral, psychological,or biological dysfunction in the individual. (p. xxxi)
Notice that this is a functional definition—it focuses on distress and disability—rather than one that specifies the causes or origins of the problem. Notice too therequirement that the behaviors in question be not “expectable and culturally sanc-tioned.” This aspect of the definition is important, because what is expectable variesacross cultures and over time, and so it’s valuable to remind ourselves that we need totake social context into account when assessing an individual’s thoughts, feelings, andbehaviors.
PDefining, Assessing, and Diagnosing Mental DisordersO 639
16.4 Social support
Diagnostic and Statistical Manualfor Mental Disorders (DSM) Themanual that provides specific guid-ance on how to diagnose each of thenearly 200 psychological disorders;currently in its fourth edition, textrevision (DSM-IV-TR).
biopsychosocial perspective A per-spective on psychopathology thatemphasizes the biological, psychologi-cal, and social factors that contributeto mental illness.
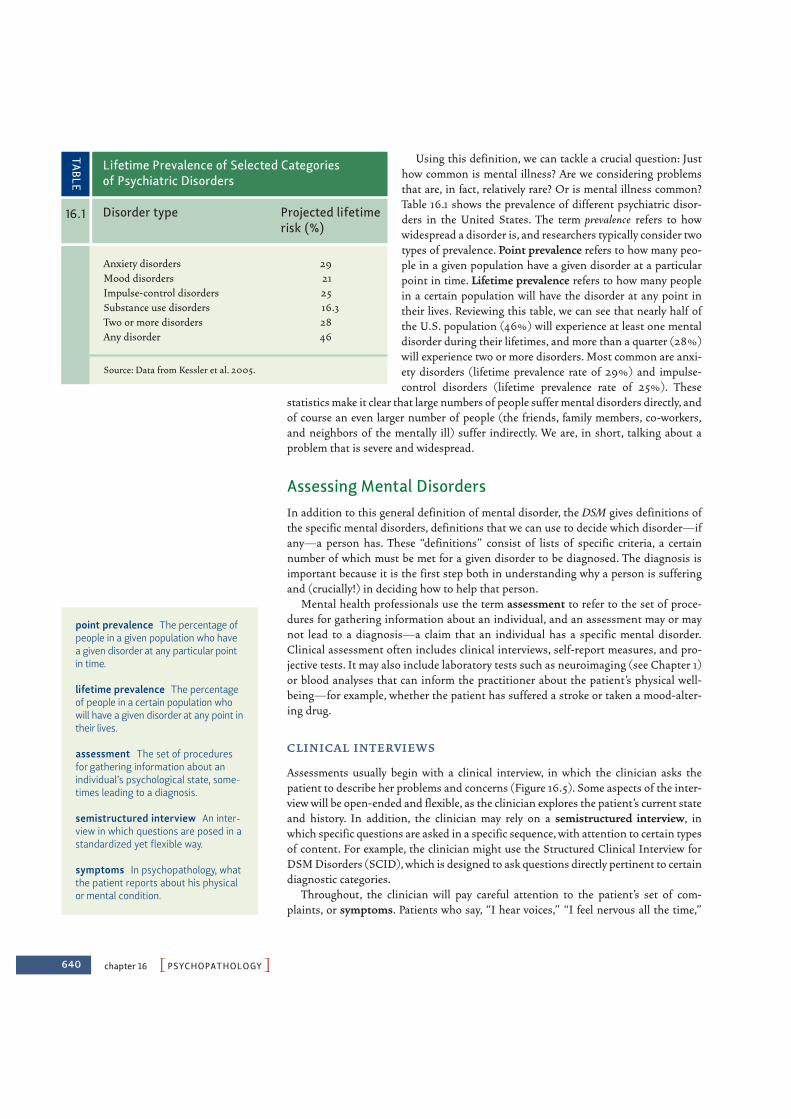
640 chapter 16 PPSYCHOPATHOLOGYO
Using this definition, we can tackle a crucial question: Justhow common is mental illness? Are we considering problemsthat are, in fact, relatively rare? Or is mental illness common?Table 16.1 shows the prevalence of different psychiatric disor-ders in the United States. The term prevalence refers to howwidespread a disorder is, and researchers typically consider twotypes of prevalence. Point prevalence refers to how many peo-ple in a given population have a given disorder at a particularpoint in time. Lifetime prevalence refers to how many peoplein a certain population will have the disorder at any point intheir lives. Reviewing this table, we can see that nearly half ofthe U.S. population (46%) will experience at least one mentaldisorder during their lifetimes, and more than a quarter (28%)will experience two or more disorders. Most common are anxi-ety disorders (lifetime prevalence rate of 29%) and impulse-control disorders (lifetime prevalence rate of 25%). These
statistics make it clear that large numbers of people suffer mental disorders directly, andof course an even larger number of people (the friends, family members, co-workers,and neighbors of the mentally ill) suffer indirectly. We are, in short, talking about aproblem that is severe and widespread.
Assessing Mental DisordersIn addition to this general definition of mental disorder, the DSM gives definitions ofthe specific mental disorders, definitions that we can use to decide which disorder—ifany—a person has. These “definitions” consist of lists of specific criteria, a certainnumber of which must be met for a given disorder to be diagnosed. The diagnosis isimportant because it is the first step both in understanding why a person is sufferingand (crucially!) in deciding how to help that person.
Mental health professionals use the term assessment to refer to the set of proce-dures for gathering information about an individual, and an assessment may or maynot lead to a diagnosis—a claim that an individual has a specific mental disorder.Clinical assessment often includes clinical interviews, self-report measures, and pro-jective tests. It may also include laboratory tests such as neuroimaging (see Chapter 1)or blood analyses that can inform the practitioner about the patient’s physical well-being—for example, whether the patient has suffered a stroke or taken a mood-alter-ing drug.
C L I N I CA L I N T E R V I E W S
Assessments usually begin with a clinical interview, in which the clinician asks thepatient to describe her problems and concerns (Figure 16.5). Some aspects of the inter-view will be open-ended and flexible, as the clinician explores the patient’s current stateand history. In addition, the clinician may rely on a semistructured interview, inwhich specific questions are asked in a specific sequence, with attention to certain typesof content. For example, the clinician might use the Structured Clinical Interview forDSM Disorders (SCID), which is designed to ask questions directly pertinent to certaindiagnostic categories.
Throughout, the clinician will pay careful attention to the patient’s set of com-plaints, or symptoms. Patients who say, “I hear voices,” “I feel nervous all the time,”
Anxiety disorders 29Mood disorders 21Impulse-control disorders 25Substance use disorders 16.3Two or more disorders 28Any disorder 46
Source: Data from Kessler et al. 2005.
Lifetime Prevalence of Selected Categories of Psychiatric Disorders
TABLE
16.1 Disorder type Projected lifetimerisk (%)
point prevalence The percentage ofpeople in a given population who havea given disorder at any particular pointin time.
lifetime prevalence The percentageof people in a certain population whowill have a given disorder at any point intheir lives.
assessment The set of proceduresfor gathering information about anindividual’s psychological state, some-times leading to a diagnosis.
semistructured interview An inter-view in which questions are posed in astandardized yet flexible way.
symptoms In psychopathology, whatthe patient reports about his physicalor mental condition.

1. Sadness0 I do not feel sad.1 I feel sad much of the time.2 I am sad all the time.3 I am so sad or unhappy that I can’t
stand it.
4. Loss of Pleasure0 I get as much pleasure as I ever did from
the things I enjoy.1 I don’t enjoy things as much as I used to.2 I get very little pleasure from the things I
used to enjoy.3 I can’t get any pleasure from the things I
used to enjoy.
PDefining, Assessing, and Diagnosing Mental DisordersO 641
and “I feel hopeless” are reporting symptoms. The clinician also looks for any objectivesigns that might accompany these symptoms. If the same patients, respectively, turntoward a stapler as though it were speaking, shake visibly, and look teary-eyed, thesewould be signs that parallel the patients’ symptoms. Sometimes, though, symptoms donot correspond to signs, and such discrepancies are also important. For example, apatient might state, “My head hurts so bad it’s like there’s a buzz saw running throughmy brain,” even thought the patient seems to be calm and unconcerned, and thisdiscrepancy, too, is informative.
The full pattern of the patient’s symptoms and signs, taken together with theironset and course, will usually allow the clinician to form an opinion as to the specificdisorder(s). This diagnosis is not set in stone, but serves as the practitioner’s bestjudgment about the patient’s current state. The diagnosis may well be revised as theclinician gains new information, including information about how the patientresponds to a particular form of treatment.
S E L F - R E P O RT M E AS U R E S
In some clinical assessments, a clinician will also seek information about a patient byadministering self-report measures. Some of these measures are relatively brief and target acertain set of symptoms. These include measures such as the Beck Depression Inventory(Beck, Steer, & Brown, 1996); sample items from this inventory are shown in Figure 16.6.Other self-report measures are much broader (and longer), such as the MinnesotaMultiphasic Personality Inventory, or MMPI. This test was developed in 1940 and wasredesigned in 1989; the current version, the MMPI-2, includes an imposing 567 items(Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 2001; Butcher et al., 1992).
To construct the MMPI, its authors began with a large pool of test questions andadministered them to patients known to have a variety of different mental disorders, aswell as to a group of nonpatients. Next, they compared the patients’ responses to thoseof the nonpatients. If all groups tended to respond to a particular question in the sameway, that question was deemed uninformative and was removed from the test. Aquestion was kept on the test only if one of the patient groups tended to answer itdifferently from how the nonpatient group answered it. The result was a test specifically
16.5 The clinical interview The clinicalinterview involves an open-ended andflexible exploration of a patient’s currentconcerns. During the interview, theclinician observes the patient’s grooming,mannerisms, style and content of speech,and overall mood, and may ask the patientto engage in brief tasks to assess attention,memory, and judgment.
16.6 Sample items from the BeckDepression Inventory This inventoryconsists of 21 items such as these. For eachitem the patient picks one statement ineach group that best describes the way heor she has been feeling during the past twoweeks, including today.
signs In psychopathology, what theclinician observes about a patient’sphysical or mental condition.
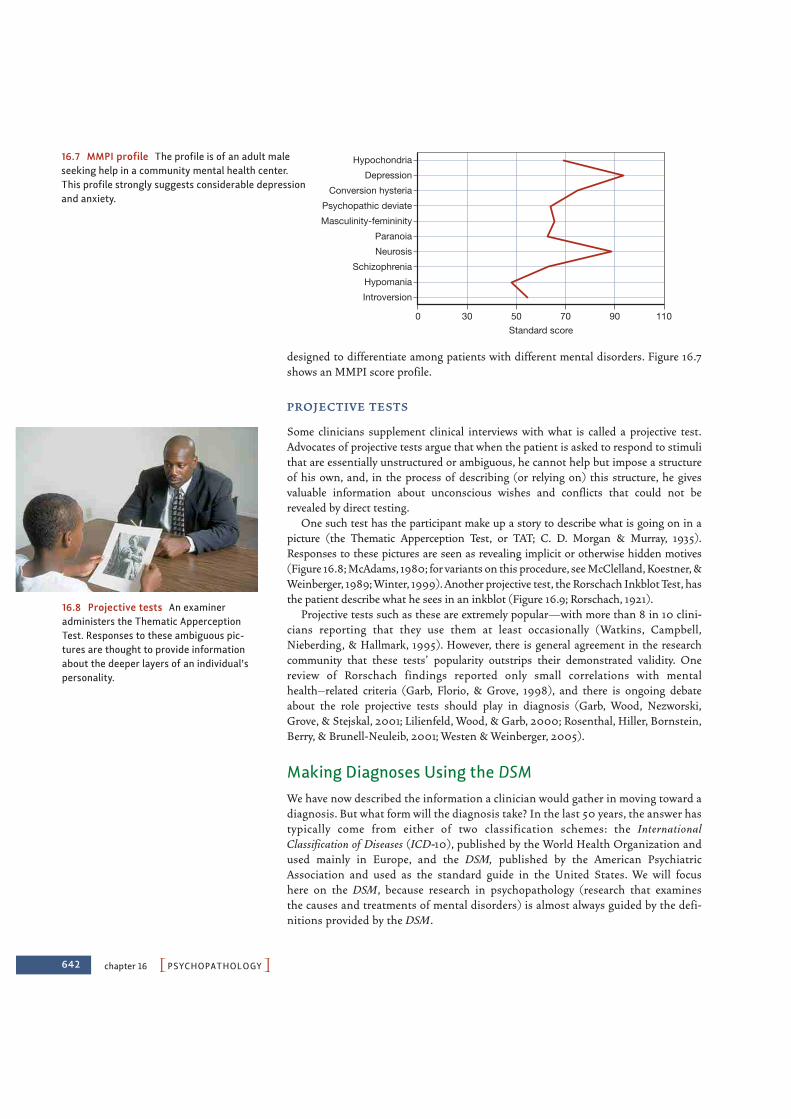
642 chapter 16 PPSYCHOPATHOLOGYO
designed to differentiate among patients with different mental disorders. Figure 16.7shows an MMPI score profile.
P ROJ E CT I V E T E STS
Some clinicians supplement clinical interviews with what is called a projective test.Advocates of projective tests argue that when the patient is asked to respond to stimulithat are essentially unstructured or ambiguous, he cannot help but impose a structureof his own, and, in the process of describing (or relying on) this structure, he givesvaluable information about unconscious wishes and conflicts that could not berevealed by direct testing.
One such test has the participant make up a story to describe what is going on in apicture (the Thematic Apperception Test, or TAT; C. D. Morgan & Murray, 1935).Responses to these pictures are seen as revealing implicit or otherwise hidden motives(Figure 16.8; McAdams, 1980; for variants on this procedure, see McClelland, Koestner, &Weinberger, 1989; Winter, 1999). Another projective test, the Rorschach Inkblot Test, hasthe patient describe what he sees in an inkblot (Figure 16.9; Rorschach, 1921).
Projective tests such as these are extremely popular—with more than 8 in 10 clini-cians reporting that they use them at least occasionally (Watkins, Campbell,Nieberding, & Hallmark, 1995). However, there is general agreement in the researchcommunity that these tests’ popularity outstrips their demonstrated validity. Onereview of Rorschach findings reported only small correlations with mentalhealth–related criteria (Garb, Florio, & Grove, 1998), and there is ongoing debateabout the role projective tests should play in diagnosis (Garb, Wood, Nezworski,Grove, & Stejskal, 2001; Lilienfeld, Wood, & Garb, 2000; Rosenthal, Hiller, Bornstein,Berry, & Brunell-Neuleib, 2001; Westen & Weinberger, 2005).
Making Diagnoses Using the DSMWe have now described the information a clinician would gather in moving toward adiagnosis. But what form will the diagnosis take? In the last 50 years, the answer hastypically come from either of two classification schemes: the InternationalClassification of Diseases (ICD-10), published by the World Health Organization andused mainly in Europe, and the DSM, published by the American PsychiatricAssociation and used as the standard guide in the United States. We will focushere on the DSM, because research in psychopathology (research that examinesthe causes and treatments of mental disorders) is almost always guided by the defi-nitions provided by the DSM.
30 50 70 90 1100Standard score
Hypochondria
Depression
Conversion hysteria
Psychopathic deviate
Masculinity-femininity
Paranoia
Neurosis
Schizophrenia
Hypomania
Introversion
16.7 MMPI profile The profile is of an adult maleseeking help in a community mental health center.This profile strongly suggests considerable depressionand anxiety.
16.8 Projective tests An examineradministers the Thematic ApperceptionTest. Responses to these ambiguous pic-tures are thought to provide informationabout the deeper layers of an individual’spersonality.

PDefining, Assessing, and Diagnosing Mental DisordersO 643
The first edition of the Diagnostic and Statistical Manual of Mental Disorders(DSM-I) was published in 1952; since then, the manual has been reviewed andrevised several times. In particular, the DSM-III, published in 1980, was heavilyrevamped to emphasize the specific signs and symptoms required for each diagnosis,holding theory to the side as much as possible. Subsequent revisions (including themost recent, DSM-IV-TR, published in 2000) have continued this trend, as will thenext edition (DSM-V), which is due out in 2012. In addition, some terms(“neurosis”) have been dropped as not meaningful, and some diagnostic labels(“hysteria”) have been largely abandoned. Moreover, some disorders have beeneliminated altogether—with the most prominent example being homosexuality.Until DSM-III, homosexuality was counted as a “disorder” to be “diagnosed.” Forthe last 30 years, though, the successive editions of DSM have abandoned thisposition as indefensible, and modern psychologists no longer count homosexualityas a “disorder” in any sense.
Across all of its editions, the DSM has tackled a crucial clinical question—namely,how severe does a set of symptoms have to be before it merits a diagnosis? After all,every one of us sometimes feels sad; how long must the sadness last and what othersymptoms must be present for this to count as depression? Every one of us sometimesfeels fearful; under what circumstances should feelings of fear be counted as a phobia?As we will see in the following sections, the DSM-IV-TR addresses these issues bysetting out specific criteria for each disorder—often in terms of a particular durationfor the symptoms, or a certain frequency.
Using the DSM, a clinician evaluates an individual with reference to five axes, ordimensions of functioning. The first two axes are designed to describe an individual’scurrent psychological condition: Axis I describes clinical syndromes such as depres-sion, eating disorders, and drug dependence. Axis II describes two broad sets of diffi-culties: mental retardation and personality disorders (such as antisocial personalitydisorder). Axis III is concerned with general medical conditions that may contribute toa person’s psychological functioning (such as constant pain from a continuing medicalproblem). Axis IV assesses social or environmental problems (including family or legaldifficulties), and Axis V provides a global assessment of functioning—that is, how wella person is coping with her overall situation.
The current version of the DSM also includes, as an appendix, disorders thatseem to appear in only some cultures. These culture-specific disorders include dhat,a term used in India to refer to severe anxiety about the discharge of semen; shenjingshauiro, a diagnosis in China characterized by fatigue, dizziness, and headaches;and ghost sickness, a powerful preoccupation with death found among some NativeAmerican tribes. Despite this nod toward cultural context, even some of the disor-ders listed in the main section of the DSM may be culture-bound—for example,bulimia nervosa, an eating disorder that we will consider later in this chapter, seemsto appear only in Western cultures or in cultures that have been heavily exposed tothe West (Smith, Spillane, & Annus, 2006). It may well be that all of the DSM’sdiagnostic categories are best understood in terms of their cultural setting—a pointthat’s certainly in line with the DSM’s broad definition of what a “mental disorder”actually is.
Our discussion in this chapter will focus largely on the Axis I classifications,although we will also say a little about Axis II. We will emphasize just a handful of thediagnostic categories. Nonetheless, the mental disorders we will discuss are persistentand prominent sources of human suffering. Studying how psychologists think aboutand try to explain them will help us to understand how they approach the other 200 orso disorders included in the DSM.
16.9 An inkblot of the type used in theRorschach test The Rorschach InkblotTest consists of 10 cards which are pre-sented one at a time, with each card show-ing a symmetrical inkblot, some coloredand some black and white. For each card,the examinee is asked what he sees.Responses are scored according to variouscategories, such as portion of the blot usedin the response (e.g., the whole blot, a largedetail, a small detail), attributes of thestimulus that are the basis of the response(e.g., form, shading, color), and content ofthe response (e.g., human figures, parts ofhuman figures, animals or parts of animals,inanimate objects, blood).
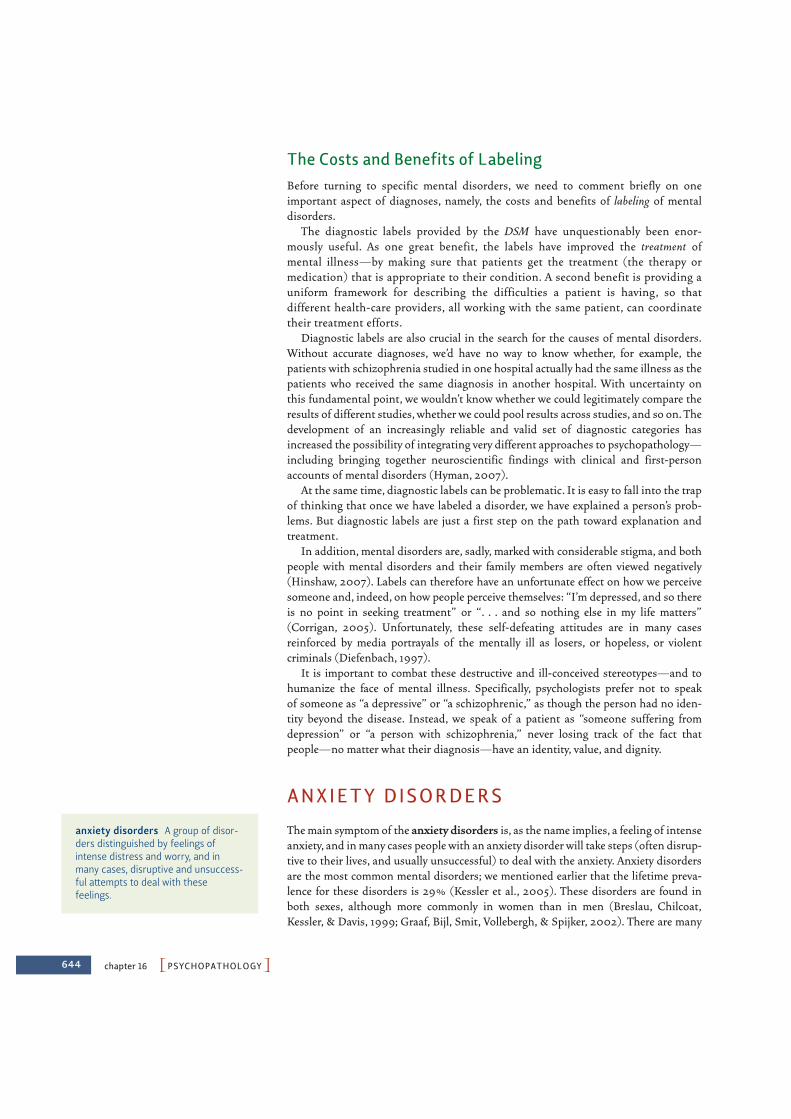
644 chapter 16 PPSYCHOPATHOLOGYO
The Costs and Benefits of LabelingBefore turning to specific mental disorders, we need to comment briefly on oneimportant aspect of diagnoses, namely, the costs and benefits of labeling of mentaldisorders.
The diagnostic labels provided by the DSM have unquestionably been enor-mously useful. As one great benefit, the labels have improved the treatment ofmental illness—by making sure that patients get the treatment (the therapy ormedication) that is appropriate to their condition. A second benefit is providing auniform framework for describing the difficulties a patient is having, so thatdifferent health-care providers, all working with the same patient, can coordinatetheir treatment efforts.
Diagnostic labels are also crucial in the search for the causes of mental disorders.Without accurate diagnoses, we’d have no way to know whether, for example, thepatients with schizophrenia studied in one hospital actually had the same illness as thepatients who received the same diagnosis in another hospital. With uncertainty onthis fundamental point, we wouldn’t know whether we could legitimately compare theresults of different studies, whether we could pool results across studies, and so on. Thedevelopment of an increasingly reliable and valid set of diagnostic categories hasincreased the possibility of integrating very different approaches to psychopathology—including bringing together neuroscientific findings with clinical and first-personaccounts of mental disorders (Hyman, 2007).
At the same time, diagnostic labels can be problematic. It is easy to fall into the trapof thinking that once we have labeled a disorder, we have explained a person’s prob-lems. But diagnostic labels are just a first step on the path toward explanation andtreatment.
In addition, mental disorders are, sadly, marked with considerable stigma, and bothpeople with mental disorders and their family members are often viewed negatively(Hinshaw, 2007). Labels can therefore have an unfortunate effect on how we perceivesomeone and, indeed, on how people perceive themselves: “I’m depressed, and so thereis no point in seeking treatment” or “. . . and so nothing else in my life matters”(Corrigan, 2005). Unfortunately, these self-defeating attitudes are in many casesreinforced by media portrayals of the mentally ill as losers, or hopeless, or violentcriminals (Diefenbach, 1997).
It is important to combat these destructive and ill-conceived stereotypes—and tohumanize the face of mental illness. Specifically, psychologists prefer not to speakof someone as “a depressive” or “a schizophrenic,” as though the person had no iden-tity beyond the disease. Instead, we speak of a patient as “someone suffering fromdepression” or “a person with schizophrenia,” never losing track of the fact thatpeople—no matter what their diagnosis—have an identity, value, and dignity.
ANXIETY DISORDERS
The main symptom of the anxiety disorders is, as the name implies, a feeling of intenseanxiety, and in many cases people with an anxiety disorder will take steps (often disrup-tive to their lives, and usually unsuccessful) to deal with the anxiety. Anxiety disordersare the most common mental disorders; we mentioned earlier that the lifetime preva-lence for these disorders is 29% (Kessler et al., 2005). These disorders are found inboth sexes, although more commonly in women than in men (Breslau, Chilcoat,Kessler, & Davis, 1999; Graaf, Bijl, Smit, Vollebergh, & Spijker, 2002). There are many
anxiety disorders A group of disor-ders distinguished by feelings ofintense distress and worry, and inmany cases, disruptive and unsuccess-ful attempts to deal with thesefeelings.
PAnxiety DisordersO 645
types of anxiety disorders, and in the following sections, we discuss each of the majortypes in turn before considering the roots of these disorders.
PhobiasA phobia is characterized by intense and irrational fear coupled with great efforts toavoid the feared object or situation (Figure 16.10). The word irrational is importanthere. Someone living in the middle of a swamp and constantly worried about snakesis not manifesting a phobia; her fear is perfectly reasonable. But someone living ina San Francisco apartment and incapacitated by the same fear probably does havea phobia. And it does not help that the person with the phobia knows that the fear isgroundless; for someone with a phobia, this knowledge does not in any way diminishthe fear.
S P E C I F I C P H OB I AS
There are several types of phobias, including specific phobias, that are directed at a par-ticular object, like snakes or blood (Figure 16.11). During the nineteenth century, manyof these irrational fears were cataloged and assigned exotic-sounding Greek or Latinnames. Examples are fear of high places (acrophobia), enclosed places (claustropho-bia), crowds (ochlophobia), germs (mysophobia), cats (ailurophobia), and even thenumber 13 (triskaidekaphobia)—the list is long. However, these phobias are not equallycommon; some are quite frequent (fear of heights, fear of snakes); others are extremelyrare (fear of specific numbers). Overall, though, the lifetime prevalence for any kind ofspecific phobia is estimated at 13% (Kessler et al., 2005), and women are about twice aslikely as men to have specific phobias (Bourdon et al., 1988).
Some of these phobias seem relatively harmless, but others can be life changing,because the person suffering from a phobia almost always develops strategies(sometimes elaborate ones) for avoiding the phobic object. Thus, people with claustro-phobia may climb many flights of stairs rather than step into an elevator. Likewise, anexecutive with a fear of heights may choose to quit his job rather than accept a promo-tion that gives him an office with a glorious view from a 20th-story window. These pho-bias will often expand in scope, so that a fear of spiders, say, can grow to become a fearof insects—and a fear of being outdoors where the spiders or insects might lurk, or afear of anything brushing across the person’s face, because it might be a spiderweb.
How do these fears feel to the person experiencing the phobia? One person describesthe fear of flying this way:
I used to start dreading a plane trip a month before I was due to leave. It was an awfulfeeling when that airplane door closed and I felt trapped. My heart would pound, andI would sweat bullets. When the airplane would start to ascend, it just reinforced thefeeling that I couldn’t get out. When I think about flying, I picture myself losing control,freaking out, and climbing the walls, but of course I never did that. I’m not afraid ofcrashing or hitting turbulence. It’s just that feeling of being trapped. . . . These days I onlygo places where I can drive or take a train. My friends always point out that I couldn’t getoff a train traveling at high speeds either, so why don’t trains bother me? I just tell themit isn’t a rational fear. (NIMH, 2009, p. 11)
Similar accounts can be offered for most of the other specific phobias, but, even so,one of the phobias is unique: the blood-injection-injury phobia. This phobia often isexperienced as a feeling of disgust rather than fear, and is also distinctive in how people
16.10 Phobias Fear of flying is one of themost widespread phobias.
16.11 Specific phobias Phobias relatingto spiders and snakes are very common,even though other objects in our worldpose a much greater threat. Falls in bath-tubs, for example, are more frequent thansnakebites, but this fact seems not to giverise to bathtub phobias.
phobia An anxiety disorder charac-terized by an intense and, at least onthe surface, irrational fear.
specific phobias Any of the disor-ders characterized by extreme andirrational fear of a particular object orsituation.

646 chapter 16 PPSYCHOPATHOLOGYO
react to the feared object. For most phobias, an encounter with the phobic stimulusproduces panic responses: quick pulse, elevated blood pressure, sweating, and tremor.These are all emergency reactions produced by the sympathetic branch of the auto-nomic nervous system (Lang, Davis, & Öhman, 2000; see Chapter 3). For the blood-injection-injury phobia, the reaction is essentially the opposite. The pulse slows, theblood pressure drops, the muscles go slack, and the person can fall to the ground in afaint. In addition, the treatment for blood-injection-injury phobia runs exactlyopposite of that for other phobias. For most phobias, the treatment involves teachingthe phobic person to relax. For the blood-injection-injury phobia, the sufferer mustkeep up her blood pressure, and so must learn, on cue, to become tense (Hellstrom,Fellenius, & Ost, 1996).
SO C I A L P H OB I A
Unlike the object-specific fears seen in specific phobias, individuals with social phobia(also referred to as social anxiety disorder) are intensely afraid of being watched andjudged by others (Figure 16.12). Typically, these concerns center around negative evalu-ations (“He’ll think I’m an idiot”), but there is increasing evidence that even positiveevaluations can be threatening (Weeks, Heimberg, Rodebaugh, & Norton, 2008). Thelifetime prevalence for social phobia is 13% (Kessler et al., 2005), and women and menare equally affected by this disorder.
Social phobia typically emerges in childhood or adolescence (Robins & Regier, 1991)and may be accompanied by other anxiety disorders or depression (Regier et al., 1998).Sometimes a person’s fears are limited to one type of situation (e.g., speaking in frontof others, writing in front of others, or eating in front of others). For others, manydifferent situations trigger the anxiety; in this case, social phobia is described as being“generalized.”
People with social phobia will desperately try to avoid situations in which they mustexpose themselves to public scrutiny. They will avoid public speaking or performingbecause they think others will think they are stupid, they will not eat in restaurants forfear that they will choke on their food, and they will not go to parties or meetingsbecause they may stutter and stammer when trying to talk. As one person with socialanxiety disorder put it, “In school I was always afraid of being called on, even when Iknew the answers. When I got a job, I hated to meet with my boss. I couldn’t eat lunchwith my co-workers. I worried about being stared at or judged, and worried that I wouldmake a fool of myself. My heart would pound, and I would start to sweat when Ithought about meetings. The feelings got worse as the time of the event got closer.Sometimes I couldn’t sleep or eat for days before a staff meeting” (NIMH, 2007a, p. 7).When forced into situations of this sort, they may try to “fortify” themselves withalcohol or drugs, making substance abuse or dependence a real risk (Pollack, 2001).
Panic Disorder and AgoraphobiaA different type of anxiety disorder is panic disorder, characterized by the occurrenceof unexpected panic attacks—sudden episodes of terrifying bodily symptoms, such aslabored breathing, choking, dizziness, tingling hands and feet, sweating, trembling,heart palpitations, and chest pain. In many cases, the person becomes convinced thatshe is having a heart attack and is near death. It is no surprise that panic attacks usu-ally include feelings of intense terror and a sense of impending doom (Figure 16.13).
Panic attacks occur in almost all anxiety disorders, so that, for example, a snake-phobiasufferer may have one at the sight of a snake. But the hallmark of panic disorder is that the
16.12 Social phobia Interacting withothers can make people with social phobiaintensely anxious.
panic disorder An anxiety disordercharacterized by repeated or disablingpanic attacks.
panic attack A sudden episode ofterrifying bodily symptoms such aslabored breathing, choking, dizziness,tingling hands and feet, sweating,trembling, heart palpitations, andchest pain.
PAnxiety DisordersO 647
panic attacks seem to come out of the blue. As a result, the patient often has an intenseexperience of unreality and fears that he is losing control or going insane. Panic disorderis diagnosed when there are recurrent unexpected attacks and when either behavioral orpsychological troubles follow the attacks. Based on those criteria, panic disorder is foundin about 5% of women and 2% of men (see, for example, Barlow, 2002).
One person with panic attacks describes her first attack this way:
When I had my first panic attack I literally thought I was going crazy. I was 17 years oldand I was the passenger in a car when suddenly I felt my heart racing. I was terrified butI did not really know why. I just had very strong feelings of dread and fear. Almostimmediately I felt I needed to escape. . . . The problem was that . . . we were on a windingnarrow road leading up [a] mountain. It was very dark and lightly raining.
I began to feel as though I could not breathe. I was trying my best to hide my anguishfrom my boyfriend. I did not want him to think I was crazy. . . . Although my symptomswere basic textbook panic attack symptoms, at the time this was happening I did notknow what panic attacks were. . . . I asked my boyfriend if we could stop the car for aminute but of course he wanted to know why and . . . explained that there really was notanyplace to stop. I truly was trapped in the vehicle.
There was no way that I could explain to him how I was feeling. . . . I remember having flashes of opening my car door and jumping out. I was glad it was dark becauseI was sure that my fear was obviously showing on my face. My hands were shaking andI felt dizzy. I was not thinking straight; I only knew that I needed to get away from thesituation as quickly as possible. (Allen, 2009)
Panic attacks are frightening enough, but even the mere anticipation of the attackscan be awful. Indeed, people with panic disorder sometimes develop a profound fear ofhaving an attack, especially in public places, where an attack might be embarrassing, orin circumstances such as driving, where the attack could be dangerous. As a result,people with panic disorder often develop a powerful tendency not to venture outsidetheir designated “safe” places—their houses or even just their bedrooms. This is whypanic disorder is often accompanied by agoraphobia, a fear of being in situations inwhich help might not be available or escape might be difficult or embarrassing.Agoraphobia can be quite paralyzing, and someone with this disorder might refuse toleave her home for days or weeks at a time (Robins & Regier, 1991).
Generalized Anxiety DisorderBoth phobias and panic attacks are a source of enormous suffering and can be horriblydisruptive to someone’s life. But both are limited in an important sense: In the absenceof the phobic stimulus, someone with phobias feels all right. Between attacks, someonewith panic disorder can function more or less normally. These limits are not in place,however, for someone who suffers from generalized anxiety disorder (GAD). For thisperson, the anxiety is not related to anything in particular; instead, it is continuous,pervasive, and very difficult to control.
GAD is relatively common, with a lifetime prevalence of 6% (Kessler et al., 2005),and it is seen twice as frequently in women as in men. Patients with this disorder arevisibly worried almost all the time. One form this may take is worry about family mem-bers: as one patient put it, “I worry all the time about whether my husband is safe so Itelephone him half a dozen times a day to see if he’s okay” (White, 1999, p. 72). Anotherform it may take is worry about work: as another patient put it, “I’m so nervous aboutmaking a mistake at work I take all my reports home to rewrite them the night before
16.13 Panic attacks The Scream (1893) by Edvard Munch vividly illustrates theoverwhelming anxiety associated withpanic attacks. Munch himself is thought tohave suffered from bipolar disorder.
agoraphobia A fear of being insituations in which help might not beavailable or escape might be difficultor embarrassing.
generalized anxiety disorder (GAD)A disorder characterized by pervasive, free-floating anxiety.

648 chapter 16 PPSYCHOPATHOLOGYO
I’m supposed to hand them in” (White, 1999, p. 72). In fact, people with GAD worryabout anything and everything. As still another patient put it, “I was worried all thetime about everything. It didn’t matter that there were no signs of problems, I just gotupset. I was having trouble falling asleep at night, and I couldn’t keep my mind focusedat work. I felt angry at my family all the time” (NIMH, 2007b, p. 7).
People with GAD feel inadequate, are oversensitive, cannot concentrate, and maysuffer from insomnia. They have enormous difficulty making decisions and worryafterward about whether each decision was a mistake. This state of affairs is oftenaccompanied by bodily symptoms: rapid heart rate, irregular breathing, excessivesweating, and chronic diarrhea (Rickels & Rynn, 2001).
Obsessive-Compulsive DisorderIn obsessive-compulsive disorder (OCD), the main symptoms are, as the name implies,obsessions (recurrent unwanted and disturbing thoughts) and compulsions (ritualisticbehaviors that serve in some way to deal with the obsessions). OCD afflicts about 2% ofthe population sometime in their lives (Kessler et al., 2005; March, Leonard, & Swedo,1995). It affects both sexes equally and is quite serious: If untreated, most cases worsenover time and are accompanied by recurrent bouts of depression (Barlow, 1988).
One striking feature of OCD is how early it often starts. One-third of adults withOCD developed their symptoms in childhood, often before age 10. As one person withOCD describes it:
When I was six years old I started picking up things with my elbows because I thoughtI would get my hands dirty if I picked things up with my hands. By the time I was sevenI was washing my hands 35 times a day. . . . When I swallowed saliva I had to crouch downand touch the ground. I didn’t want to lose any saliva—for a bit I had to sweep theground with my hand—and later I had to blink my eyes if I swallowed. I was frustratedbecause I couldn’t stop the compulsions. Each time I swallowed I had to do something.For a while I had to touch my shoulders to my chin. I don’t know why. I had no reason.I was afraid. It was just so unpleasant if I didn’t. (Rapoport, 1989, pp. 43–44)
The obsessions come in many varieties, but common ones involve concerns aboutdirt and contamination (Figure 16.14), fears of harming someone, and an extraordinaryneed for balance and symmetry. A salesperson, for example, might worry constantlyabout infection and so refuse to shake hands with his customers; an otherwise lovingparent may have recurrent thoughts of strangling her children; and a seemingly normalbusinessman may spend hours each night straightening the paintings hanging in hisapartment.
Obsessive thoughts can produce considerable anxiety, and many compulsions maybe understood as attempts to counteract this anxiety. An obsession with dirt may leadto compulsions like ritualistic cleaning or continual hand washing; in severe cases,someone with OCD will wash her hands so often to ward off germs that she will endup with open and bleeding sores on her skin. An obsession with forgetting thingsmight lead to checking and rechecking—to make sure that the alarm clock is reallyturned on, or that the door is really locked. Here, too, the compulsion can becomecrippling: Someone with OCD may check and recheck the stove so many times, makingcertain it is really turned off, that he needs hours to leave the house for even thesimplest errand. And, in most cases, the sufferers know that their behavior is irrationaland that they are washing or checking far more than they need to. However, they areunable to stop their thoughts and urges, and so are all the more tormented by them.
obsessive-compulsive disorder(OCD) A disorder whose symptomsare obsessions and compulsions, whichseem to serve as defenses againstanxiety.
obsessions Recurrent unwanted ordisturbing thoughts.
compulsions Repetitive or ritualisticacts that, in OCD, serve in some way todeal with the obsessions.
16.14 Symptoms of OCD One commonobsession involves a concern with dirtand contamination. This is typicallyaccompanied by a compulsion to washone’s hands.
PAnxiety DisordersO 649
The Stress DisordersOne final category of anxiety disorders includes the two stressdisorders, both of which are triggered abruptly by an identifiable andhorrific event (Figure 16.15). For women, the most common suchevent is rape or physical assault; for men, it is military combat. Othercalamities can also trigger the stress disorders—being in a seriousautomobile accident, witnessing a homicide, or encountering thedevastation following a natural disaster or terrorist attack(Andreasen & Black, 1996; Wolf & Mosnaim, 1990).
Regardless of what the traumatic event is, the psychologicaleffects are usually the same. Immediately after the trauma, there isgenerally a period of numbness, during which the sufferer feels wholly estranged,socially unresponsive, and oddly unaffected by the event, a reaction technically knownas dissociation. With this acute stress disorder, there are often recurrent nightmaresand waking flashbacks of the traumatic event. These can be so intense and intrusivethat the sufferer may momentarily believe that she is back in the situation, reliving thebattle, or being attacked once again by the rapist. For some people, the reactions to suchtraumas are enduring, and if they persist for 1 month after the stressor, the diagnosisbecomes post-traumatic stress disorder (PTSD).
The lifetime prevalence of PTSD is 7% (Kessler et al., 2005), and women are more likelyto develop PTSD than men, even when controlling for differences in the number of poten-tially traumatic events to which women and men are exposed (Olff, Langeland, Draijer, &Gersons, 2007; Tolin & Foa, 2006; for some complications in diagnosing PTSD, andtherefore some complexity in estimating the prevalence of PTSD, see Dobbs, 2009).
One patient describes her experience with PTSD as follows:
I was raped when I was 25 years old. For a long time, I spoke about the rape as though itwas something that happened to someone else. I was very aware that it had happened tome, but there was just no feeling. Then I started having flashbacks. They kind of cameover me like a splash of water. I would be terrified. Suddenly I was reliving the rape. Everyinstant was startling. I wasn’t aware of anything around me, I was in a bubble, just kindof floating. And it was scary. Having a flashback can wring you out. The rape happenedthe week before Thanksgiving, and I can’t believe the anxiety and fear I feel every yeararound the anniversary date. It’s as though I’ve seen a werewolf. I can’t relax, can’t sleep,don’t want to be with anyone. I wonder whether I’ll ever be free of this terrible problem.(NIMH, 2009, p. 7)
Symptoms of PTSD fall into three major clusters. Re-experiencing symptoms includenightmares about the event and recalling the traumatic event, often in the form offlashbacks that seize the person’s thoughts. The flashbacks are often an accurate reflec-tion of the event but may sometimes be a composite of different events or of differentperspectives on the event. In other cases, the flashbacks may include images of what theperson thought might happen as part of the trauma. Arousal symptoms include difficul-ties in concentration, problems falling asleep, and extreme responses to being startled.Avoidance symptoms include an active avoidance of people, places, or objects that arelinked to the trauma (Friedman, Keane, & Resick, 2007). Other common symptomsinclude emotional numbness, a loss of interest in things that once were pleasurable,and outbursts of anger. Still another symptom may be “survivor guilt”—that is, thefeeling that one has done something wrong by surviving a traumatic event when friendsor relatives were harmed or killed (M. J. Friedman & Marsella, 1996).
acute stress disorder A reactionsometimes observed in individualswho have experienced a trauma, char-acterized by flashbacks and recurrentnightmares.
post-traumatic stress disorder(PTSD) A chronic, sometimes lifelongdisorder that may follow a traumaticexperience. Symptoms include dissoci-ation, recurrent nightmares, flash-backs, and sleep disturbances.
16.15 Stress disorders Post-traumaticstress disorders are triggered by identifi-able traumas such as those associated withmilitary combat.

650 chapter 16 PPSYCHOPATHOLOGYO
Roots of the Anxiety DisordersAs we have now seen, the DSM distinguishes among a number of different anxiety dis-orders. However, there is considerable comorbidity among these disorders, meaningthat having one of these anxiety disorders makes it more likely that one will haveanother anxiety disorder. Indeed, more than half the people with one anxiety disorderwill at some point also have some other anxiety disorder (T. Brown et al., 2001). Thissuggests that there are risk factors shared by the various anxiety disorders (factors thatmake a person vulnerable to more than one of these disorders) as well as specificrisk factors (factors that make someone vulnerable to one of the disorders but notthe others).
G E N E T I C R I S K FACTO RS
One cluster of risk factors involves the person’s genetic pattern, because twin studies clearlyshow a heritable basis for the anxiety disorders. Thus, the probability that one member of atwin pair will have an anxiety disorder if the other does (the concordance rate) is muchhigher for identical twins than for fraternal twins (or ordinary siblings) (Hettema, Neale, &Kendler, 2001).
A number of different genes are thought to contribute to the anxiety disorders(Binder et al., 2008; Kendler, Karkowski, & Prescott, 1999; Lesch et al., 1996; Noyes etal., 1992), and genetic factors may be particularly important in OCD (Black & Noyes,1990; S. A. Rasmussen, 1993). In fact, different aspects of OCD seem to have separateinheritance paths so that, for example, someone may inherit a specific tendency towardhoarding, or a specific tendency toward excessive cleaning (Leckman, Zhang,Alsobrook, & Pauls, 2001; but see Holden, 2008b). However, here as elsewhere, it isimportant to emphasize that these genetic factors do not directly “cause” the anxietydisorders. Instead, the genetic factors provide part of the diathesis for these disorders,and the disorder itself will emerge only if the person with the genetic vulnerability isexposed to some sort of stressor (Binder et al., 2008; Stein, Schork, & Gelernter, 2008).
B R A I N BAS E S
Genetic factors clearly play a role in anxiety disorders, but what is this role? How doesa person’s biology contribute to the problems we have discussed? We still have muchto learn about the biological underpinnings of these disorders, but some intriguingfindings recently have begun to emerge.
For example, functional neuroimaging studies show that the anxiety disorders,despite all they have in common, are quite different from each other in their biologicalunderpinnings. Thus, the brain regions implicated in fear learning (including theamygdala and insula) seem to be especially active in people suffering from the specificphobias and social phobia (Etkin & Wager, 2007; Goldin et al., 2009). The pattern isdifferent, though, in PTSD; here studies show that people with this disorder have lessbrain activation in prefrontal regions associated with emotion regulation. Yet adifferent pattern of brain activity is associated with panic disorder—one that involvesapparent instability in the autonomic nervous system (Andreasen & Black, 1996;Wilhelm, Trabert, & Roth, 2001). OCD in turn may be linked to overactivity in threeother brain areas—the orbitofrontal cortex, the caudate nucleus, and the anteriorcingulate—although it is unclear whether this activity is the cause of the disease or oneof its consequences (Micallef & Blin, 2001).
comorbidity The tendency for differ-ent mental disorders to occur togetherin the same person.
concordance rate The probabilitythat a person with a particular familialrelationship to a patient (e.g., an iden-tical twin) has the same disorder asthe patient.

PAnxiety DisordersO 651
P SY C H O LO G I CA L R I S K FACTO RS
So far, we have focused on genetic and biological risk factors. Other risk factors are psy-chological. Some of these, such as psychological maltreatment in childhood, seem toconfer a general risk for several different anxiety disorders (Scher & Stein, 2003). Otherpsychological risk factors play a role in specific anxiety disorders, especially specificphobias and PTSD.
Many have proposed that specific phobias are the result of experiences that createda mental association between the phobic stimulus and a fearful idea, and often thisproposal is cast in the language of Pavlovian conditioning (Chapter 7). The broadnotion is that, at some point in the past, the person who suffers from the phobiaexperienced a painful, frightening, or embarrassing event; this is the unconditionedstimulus, leading to the unconditioned response of fear. The conditioned stimulus, inturn, was an object or cue linked to the event. Perhaps, for example, the person was ina closed space when something frightening happened. As a result, he now associatesthe closed space with fear, in much the same way that the ringing of a bell that isfollowed by food delivery becomes a signal that the food will soon arrive. In this way,claustrophobia (fear of closed spaces) might be produced (Wolpe, 1958).
In fact, the onset of many phobias can be traced to a traumatic experience, just as theconditioning account requires (see, for example, Hackmann, Clark, & McManus,2000). But we need more theory than this if we are to account for all the facts aboutphobias. For example, phobias sometimes emerge without a history of conditioning—so that, for example, someone can develop a snake phobia even if he has never had afrightening experience with a snake. In addition, a simple conditioning account doesnot explain why some phobias are rare while others are common. For example, cars,bathtubs, and hammers are all (statistically) dangerous; painful accidents involvingthem are not uncommon. In contrast, few people have been bitten by a snake or aspider. If associations with pain or trauma produce phobias, we would expect to seemany hammer or bathtub phobias but relatively few snake or spider phobias. But theopposite is the case.
These puzzles are easily solved. A century ago, Ivan Pavlov argued that classical con-ditioning was necessarily rooted in an organism’s own experiences, but more recentstudies have demonstrated vicarious conditioning, in which a person (or, in some stud-ies, a monkey) can acquire a conditioned response merely by observing someone else’sfear (e.g., Mineka & Ben Hamida, 1998). In addition, in Chapter 7 we discussed the factthat organisms seem “prepared” for some associations (and so learn them quickly) but“unprepared” for other associations (and so learn them more slowly if at all), and, ineach case, the degree of preparedness is usually understandable in evolutionary terms.
How does this apply to phobias? Snakes and spiders were common dangers for ourprimate ancestors; natural selection may therefore have favored animals that wereinnately predisposed (i.e., prepared) to learn to fear snakes and spiders very quickly,after just one or two experiences with them (Öhman & Mineka, 2001; Seligman, 1971).If this was the case, limited but painful experience with these stimuli might still beenough to create and sustain a substantial number of phobias. With these relativelysmall modifications, then, we can preserve the claim that, in many cases, phobias arethe product of learning—and, in particular, the product of classical conditioning(Mineka & Zinbarg, 2006).
With PTSD, the stress that precipitated the disorder is often obvious—a rape, a ter-rorist attack, a battlefield experience. But even when the trauma is easily identified, weneed to consider more than just this immediate stress as the “cause” of the disorder.Not everyone who experiences a trauma develops PTSD. Indeed, according to one
652 chapter 16 PPSYCHOPATHOLOGYO
estimate, more than 90% of the U.S. population have experienced a trauma at somepoint, but only 5 to 12% develop PTSD (Lee & Young, 2001). Among Vietnam War vet-erans, many of whom were exposed to horrific violence, only one in ten developedPTSD (Dohrenwend et al., 2006).
Why is this? Part of the answer lies in the severity of the trauma; more severe trauma ismore likely to produce the disorder (McNally, 2006; Sutker, Allain, & Winstead, 1993;E. Jones & Wessely, 2001). The individual’s level of social support is also relevant, withmore and better support after a trauma associated with a decreased likelihood of laterdeveloping PTSD (Ozer & Weiss, 2004). Yet another factor is the diathesis inherent in theperson’s genetic pattern. The odds of developing PTSD increase fivefold if a parent has hadit (Radant, Tsuang, Peskind, McFall, & Raskind, 2001); identical twins who served inVietnam were found to be far more similar to one another than fraternal twins in the like-lihood of developing PTSD, and,for those who did develop PTSD, in the type of symptomsthey experienced (True et al., 1993).
MO OD DISORDERS
In the anxiety disorders, the primary symptoms involve heightened levels ofanxiety. In the mood disorders, the predominant disturbances lie in positive andnegative mood. Specifically, the DSM distinguishes depression (also called majordepressive disorder or unipolar depression) and bipolar disorder (formerly calledmanic-depressive illness). These disorders (sometimes called affective disorders)are characterized by emotional and energetic extremes—the despair of depression,the maelstrom of mania, or both.
DepressionDepression involves feelings of sadness, hopelessness, and broad apathy about life; thedepressed person loses interest in eating, hobbies, sex, and, for that matter, almosteverything else. Of course, everyone has these feelings at one point or another, espe-cially after some difficult event, such as sickness or the death of a friend, the end of arelationship, a significant career failure, and so on. But diagnosable depression is dif-ferent, distinguished by both its severity and duration. In fact, the DSM suggests a diag-nosis of depression only if the feelings of sadness have lasted at least 2 weeks and areaccompanied by other symptoms such as insomnia and feelings of worthlessness.
Depression is one of the most common mental disorders, with a lifetime prevalence of7 to 12% in men and 20 to 25% in women (Kessler et al., 2005; Figure 16.16). It is not clearwhy women are more likely to become depressed than men, but one crucial factor seemsto be women’s greater use of maladaptive forms of rumination—which involve repetitivelyturning emotional difficulties over and over in their mind (Nolen-Hoeksema, Wisco, &Lyubomirsky, 2008; Treynor, Gonzalez, & Nolen-Hoeksema, 2003).
In his memoir Darkness Visible (1990), the novelist William Styron (1925–2006)provided a portrait of depression:
All sense of hope vanished, along with the idea of a futurity; my brain, in thrall to itsoutlaw hormones, had become less an organ of thought than an instrument registering,minute by minute, varying degrees of its own suffering. The mornings themselves werebecoming bad now as I wandered about lethargic . . . but afternoons were still the worst,when I’d feel the horror, like some poisonous fogbank, roll in upon my mind, forcing me
16.16 Depression Woman Sitting on a Quilt(1993) by Helen J. Vaughn.
mood disorders A group of disor-ders distinguished primarily bychanges in positive and negativeaffective state.
depression A mood disorder charac-terized by disabling sadness, hope-lessness, and apathy; a loss of energy,pleasure, and motivation; and distur-bances of sleep, diet, and other bodilyfunctions.

PMood DisordersO 653
into bed. There I would lie for as long as six hours, stuporous and virtually paralyzed,gazing at the ceiling and waiting for that moment of evening when, mysteriously, thecrucifixion would ease up just enough to allow me to force down some food and then, likean automaton, seek an hour or two of sleep again. (1990, pp. 58–59)
Many people with depression experience considerable anxiety, and about 20% suf-fer from psychotic delusions—unshakable false beliefs. Some are variations on thetheme of worthlessness: “It would be better if I had not been born. . . . I am the mostinferior person in the world” (Beck, 1967, p. 38). Other delusions concern guilt aboutan unspeakable, unpardonable sin, and some patients report hearing the devil tell themthat they will burn in hell for eternity (Andreasen & Black, 1996). Whatever the mani-festation, depressions with psychotic features are more severe, less responsive to treat-ment, and more likely to recur (Coryell, 1996).
Specific cognitive deficits, including disrupted attention and working memory, alsoaccompany severe depression. Moreover, depressed patients often exhibit physicalmanifestations that can include a loss of appetite and weight, weakness, fatigue, poorbowel functioning, sleep disorders, and lack of interest in sex. It is as if both bodily andpsychic batteries have run down completely.
Depression is not tied to any particular age or life stage. It is most common in ado-lescence through middle adulthood, but depression can also emerge in children and inthe elderly (Garber & Horowitz, 2002; Kessler, Keller, & Wittchen, 2001). Depressedadolescents show most of the symptoms we have described, but some of their symp-toms may come in distinctly teenage form. Their despair often leads them to substanceabuse; their apathy about life shows up in the number of classes they miss; theirirritability emerges as belligerence and defiance. To be sure, all these behaviors canoccur without depression, but any or all of them, together with other symptoms ofdepression, can indicate profound emotional problems.
Bipolar Disorder Unlike depression, which is characterized by depressed mood and/or a loss of pleasure,bipolar disorder is characterized by manic and depressive episodes (with normalperiods interspersed) (Figure 16.17). These episodes may be as short as a few hours oras long as several months, and they need not alternate. Some patients with bipolardisorder rarely have manic episodes; others have a large number. Moreover, althoughdepression and mania were once regarded as opposite and mutually exclusive, they arenow known to co-occur. In such mixed states, patients exhibit signs of both (e.g.,tearfulness and pessimism combined with grandiosity and racing thoughts).
In their milder form, manic states are often hard to distinguish from buoyant spir-its. At this point the person is said to show hypomania. She seems to have shifted intohigh gear. She is infectiously happy, utterly self-confident, and inde-fatigable. It is hard to see that something is amiss unless one noticesthat she jumps from one plan to another, seems unable to sit still fora moment, and quickly shifts from unbounded elation to brittle irri-tation if she meets even the smallest frustration. Kay RedfieldJamison, an expert on bipolar disorder—and a sufferer of it aswell—provided a lyrical and frank account of the ecstatic allure ofhypomania:
When you’re high it’s tremendous. The ideas and feelings are fastand frequent like shooting stars, and you follow them until you
bipolar disorder A mood disorder inwhich the patient swings betweenemotional extremes, experiencingboth manic and depressive episodes.
mixed states A pattern sometimesobserved with bipolar disorder inwhich the person displays a combina-tion of manic and depressivesymptoms.
hypomania A mild manic state inwhich the individual seems infec-tiously merry, extremely talkative,charming, and tireless.
16.17 Bipolar disorder Actress and writerCarrie Fisher (at left, as Princess Leia inStar Wars) is frank about her struggles withbipolar disorder and chronicles her ups anddowns in the autobiographical one-womanshow Wishful Drinking (right).

654 chapter 16 PPSYCHOPATHOLOGYO
find better and brighter ones. Shyness goes, the right words and gestures are suddenlythere, the power to captivate others a felt certainty. There are interests found in unin-teresting people. Sensuality is pervasive and the desire to seduce and be seduced irre-sistible. Feelings of ease, intensity, power, well-being, financial omnipotence, andeuphoria pervade one’s marrow. (1995, p. 67)
Hypomania feels good, but it may breed overconfidence and the relentless pursuitof overly ambitious goals (Johnson, 2005). Even more serious problems arise whenhypomania develops into full-blown mania. Now the motor is racing and all brakes areoff, and in her perceived invincibility the sufferer will likely stop taking her mood-stabilizing medication. She may begin to stay up all night or engage in an endlessstream of talk that runs from one topic to another and knows no inhibitions of socialor personal propriety.
These feelings of omnipotence are short-lived, however. They recede as acute orpsychotic mania sets in, and feelings of invincibility are replaced by terror as the per-son loses her grip on reality. People in the acute manic state may burst into shouts ofsong, smash furniture, exercise endlessly, sleep only rarely, engage in reckless sexualescapades, spend all their money on gambling, conceive grandiose plans for redirectingthe nation’s foreign policy or making millions in the stock market, and go on drinkingor drug binges (nearly 60% of people with bipolar disorder are alcohol or drug abusers;Feinman & Dunner, 1996). Jamison described this chaotic state:
I kept on with my life at a frightening pace. I worked ridiculously long hours and sleptnext to not at all. When I went home at night it was a place of increasing chaos: Books,many of them newly purchased, were strewn everywhere. . . . There were hundreds ofscraps of paper as well. . . . One scrap contained an incoherent and rambling poem;I found it weeks later, apparently triggered by my spice collection, which, needless to say,had grown by leaps and bounds during my mania. I had titled it, for reasons that I amsure made sense at the time, “God is an Herbivore.” (1995, p. 79)
Bipolar disorder—which has a lifetime prevalence rate of 4% (Kessler et al.,2005)—is a recurrent disorder: nearly everyone with bipolar disorder has recurrences,and between episodes, most experience mild-to-moderate symptoms (Miklowitz &Johnson, 2006). Although we have focused only on adults, children can also have bipo-lar disorder. Indeed, there has been a 40-fold increase in the past decade or so in thenumber of people under 20 who have received a diagnosis of bipolar disorder (Morenoet al., 2007). It is not clear, however, whether this dramatic increase reflects a changein the way diagnostic labels are used or whether there is really an increase in theprevalence of childhood onset bipolar disorder (Holden, 2008a).
Both those with depression and those in a depressive phase of bipolar disorder canbecome suicidal. Some actually attempt suicide, and more than a few succeed. Here isKay Jamison’s description of an episode of depression:
Each day I awoke deeply tired, a feeling as foreign to my natural self as being bored orindifferent to life. Those were next. Then a gray, bleak preoccupation with death, dying,decaying, that everything was born but to die, best to die now and save the pain whilewaiting. (1995, p. 38)
The risk of suicide is greater among those with bipolar disorder than among thosewith any other psychiatric disorder, even depression. In fact, up to 20% of individualswith bipolar disorder commit suicide. As might be expected, people with bipolar disor-
mania A state characterized by rac-ing thoughts, pressured speech, irri-tability or euphoria, and impairedjudgment.

PMood DisordersO 655
der rarely commit suicide during manic episodes (Andreasen & Black, 1996), but sur-prisingly, suicide risk is also relatively low for those in the depths of depression. At thatpoint, gloom is deepest, but so is inertia, and although the patient may have decided tokill herself, she will have neither the energy nor the tenacity to complete the act. She ismore likely to follow through on her resolution as she begins to recover from depres-sion and emerges from closely supervised care. Times of greatest risk, therefore, includeweekend leaves from a hospital and the period immediately after discharge.
In general, women are three times as likely to attempt suicide as men, but when menmake the attempt, they are much more likely to succeed; in fact, four times as many menas women kill themselves (Arias et al., 2003). One reason for the difference is thechoice of methods. Women are more likely than men to cut their wrists or swallow abottle of sleeping pills, methods for which there is some chance of rescue. Men tend touse methods that are irreversible, such as shooting themselves or jumping off a rooftop(Fremouw, Perczel, & Ellis, 1990).
The Roots of Mood DisordersWhat produces the mood disorders? Depression and bipolar disorder are thought toresult from multiple contributing factors, factors that include genetic, neurochemical,and psychological influences.
G E N E T I C FACTO RS
The mood disorders have important genetic components. This is reflected in the factthat the concordance rate is roughly two times higher in identical twins than in frater-nal twins (Sullivan, Neale, & Kendler, 2000). The pattern is even clearer for bipolar dis-order: If someone’s identical twin has the disorder, there is a 60% chance that he, too,will have the disorder; the concordance rate for fraternal twins is much lower, 12%(Kelsoe, 1997).
Adoption studies point to the same conclusion, and the biological relatives ofadopted children with depression are themselves at high risk for depression (Wender,Kety, Rosenthal, Schulsinger, & Ortmann, 1986). Likewise, the risk of suicide is muchhigher among the biological relatives of depressed adoptees than it is in the biologicalkin of nondepressed adoptees (Wallace, Schneider, & McGuffin, 2002).
Importantly, though, the genetic evidence indicates a clear distinction betweendepression and bipolar disorder. The two disorders overlap in their symptoms (i.e.,clinical depression resembles the depressed phase of bipolar disorder), but they proba-bly arise from different sources. This is evident, for example, in the fact that people withone of these disorders tend to have relatives with the same condition but not the other.Apparently, then, there are separate inheritance pathways for each, making it likely thatthey are largely separate disorders (Gershon, Nurnberger, Berrettini, & Goldin 1985;Moffitt, Caspi, & Rutter, 2006; Torgersen, 1986; Wender et al., 1986).
B R A I N BAS E S
Drugs that influence the effects of various neurotransmitters can often relieve symp-toms of mood disorders, and this suggests that these mood disorders arose in the firstplace because of a disorder in neurotransmission. Three neurotransmitters seem criti-cal for mood disorders: norepinephrine, dopamine, and serotonin. Many of the anti-depressant and mood-stabilizing medications work by altering the availability of thesechemicals at the synapse (Miklowitz & Johnson, 2006; Schildkraut, 1965).
656 chapter 16 PPSYCHOPATHOLOGYO
How these neurochemical abnormalities lead to mood disorders is uncertain, but itis clear that these disorders involve more than a simple neurotransmitter shortage orexcess. In the case of depression, this is evident in the fact that antidepressant drugswork almost immediately to increase the availability of neurotransmitters, but theirclinical effects usually do not appear until a few weeks later. Thus, neurotransmitterproblems are involved in depression (otherwise the drugs would not work at all), butthe exact nature of those problems remains unclear.
In the case of bipolar disorder, the mystery lies in the cycling between manic anddepressive episodes, especially since, in some patients, this cycling is quite rapid andseemingly divorced from external circumstances. Some believe the cycling is relatedto dysfunction in neuronal membranes, with the consequence that the membranesmismanage fluctuations in the levels of various neurotransmitters (Hirschfeld &Goodwin, 1988; Meltzer, 1986).
To better understand the underlying brain bases of these mood disorders, researchershave used both structural and functional brain imaging. Studies using positron emissiontomography (PET) show that severe depression is associated with heightened brain acti-vation in a limbic system region known as the subgenual cingulate cortex (Drevets,1998). This finding makes sense, given that inducing sadness in healthy participantsleads to increased activation in this brain region (Mayberg et al., 1999), as well as the evi-dence that when depression is successfully treated, brain activity in this region returnsto normal levels (Mayberg et al., 1997). (We will return to this point in Chapter 17.)
In the case of bipolar disorder, imaging studies suggest that adults with bipolar dis-order have greater amygdala volumes than age-matched healthy controls (Brambrillaet al., 2003). Functional-imaging studies parallel these structural studies, showinggreater brain activity in subcortical emotion-generative brain regions such as the amyg-dala (Phillips, Ladouceur, & Drevets, 2008).
P SY C H O LO G I CA L R I S K FACTO RS
Our account of the mood disorders also needs to take account of life experiences. Forexample, depression and bipolar disorder are often precipitated by an identifiable lifecrisis, whether that crisis involves marital or professional difficulties, serious physicalillness, or a death in the family (S. L. Johnson, 2005a; Monroe & Hadjiyannakis, 2002;Neria et al., 2008). Broader contextual factors, such as whether someone lives in a goodor bad neighborhood, may also influence whether a person develops depression, evenwhen controlling for risk factors associated with the person’s age, ethnicity, income,education, and employment status (Cutrona, Wallace, & Wesner, 2006). The impor-tance of psychological factors is also evident in the fact that individuals with mood dis-orders are at much greater risk for relapse if they return after hospitalization to familieswho show high levels of criticism and hostility (Hooley, Gruber, Scott, Hiller, &Yurgelin-Todd, 2005; Miklowitz, 2007; Segal, Pearson, & Thase, 2003).
As we mentioned earlier, though, personal and environmental stresses do not, bythemselves, cause mood disorders. What we need to ask is why some people are unableto bounce back after a hard blow and why, instead of recovering, they spiral downwardinto depression.
Part of the explanation may be genetic, and some researchers are focusing on a genethat regulates how much serotonin is available at the synapse. As discussed in Chapter 2,the gene itself is not the source of depression; instead, the gene seems to create a vulner-ability to depression. The illness itself will emerge only if the vulnerable person alsoexperiences some significant life stress (Caspi et al., 2003). However, this finding has

PMood DisordersO 657
been controversial, and research in this area is ongoing (e.g., Munafo, Durrant, Lewis, &Flint, 2009; Risch et al., 2009).
Another part of the explanation for why stress puts some people at greater risk fordepression than others turns out to be social: severe stress is less likely to lead to amood disorder if a person has supportive family and friends (Brown & Harris, 1978;Johnson et al., 1999; Joiner, 1997). Still another crucial factor is how a person thinksabout stressful events when they occur.
Many depressed individuals—whether they are experiencing unipolar depressionor are in the depressive phase of bipolar disorder—believe that both they and theworld are hopeless and wretched. It seems plausible that these beliefs are produced bythe patient’s mood, but, according to the psychiatrist Aaron Beck, the opposite is true,at least in the case of depression: The beliefs come first; they produce the depression(see, for example, Beck, 1967, 1976). Beck argues that depression stems from a set ofintensely negative and irrational beliefs: the beliefs some people hold that they areworthless, that their future is bleak, and that whatever happens around them is sureto turn out for the worst. These beliefs form the core of a negative cognitive schemaby which a person interprets whatever happens to her, leaving her mood nowhere togo but down.
A related account of depression also focuses on how people think about whathappens to them. As we saw in Chapter 15, people differ in how they explain bad events.Do we think that a bad event happened because of something we did, so that, in somedirect way, we caused the event? Do we believe that similar bad events will arise in otheraspects of our lives? And do we think that bad events will continue to happen to us,perhaps for the rest of our lives? Peterson and Seligman propose that much depends onhow we answer these questions, and, moreover, they suggest that each of us has aconsistent style for how we tend to answer such questions—which they call anexplanatory style. In their view, a person is vulnerable to depression if her explanatorystyle tends to be internal (“I, and not some external factor, caused the event”), global(“This sort of event will also happen in other areas of my life”), and stable (“This isgoing to keep happening”). This explanatory style is not by itself the source of depres-sion; once again, we need to separate diathesis and stress. But if someone has thisexplanatory style and then experiences a bad event, that person is at considerablyelevated risk for depression (Peterson & Seligman, 1984). In addition, it appears thatthe explanatory style usually predates the depression, with the clear implication thatthis way of interpreting the world is not caused by depression but is instead a factorpredisposing an individual toward depression (Abramson et al., 2002; Alloy,Abramson, & Francis, 1999; Peterson & Park, 2007).
SO C I A L A N D CU LT U R A L R I S K FACTO RS
Clearly, there are both biochemical and cognitive contributors to mood disorders. As wementioned earlier, though, mood disorders are also influenced by social settings. Thisis evident, for example, in the fact that depression is less likely among people with astrong social netowork of friends or family. The importance of social surroundings isalso visible in another way: the role of culture in shaping the likelihood that depressionwill emerge, or the form that the disorder takes.
Depression occurs in all cultures, and, in fact, the World Health Organizationranked depression fourth among all causes of disability worldwide (Miller, 2006b).However, its prevalence varies widely from one country to the next. For example,depression is—not surprisingly— more common in countries such as Afghanistan that
negative cognitive schemaAccording to Aaron Beck, the corecognitive component of depression,consisting of an individual’s automaticnegative interpretations concerninghimself, his future, and the world.
explanatory style A person’s char-acteristic way of explaining his experi-ences. Consistently attributing badexperiences to internal, global, andstable causes may increase vulnerabil-ity to depression.
658 chapter 16 PPSYCHOPATHOLOGYO
have been torn apart by war (Bolton & Betancourt, 2004; Figure 16.18); the difficulties insuch countries also lead to other disorders, including post-traumatic stress disorder. Incontrast, depression is much less commonly diagnosed in China, Taiwan, and Japan thanin the West. When the disorder is detected in these Asian countries, the symptoms are lessoften psychological (such as sadness or apathy) and more often bodily (such as sleep dis-turbance, weight loss, or, in China, heart pain; Kleinman, 1986; G. Miller, 2006a; Tsai &Chentsova-Dutton, 2002). Why is this? There are several possibilities, starting with thefact that cultures differ in their display rules for emotion (see Chapter 12), which will obvi-ously influence the presentation and diagnosis of almost any mental disorder. In addition,people in these Asian countries may differ in how they understand and perhaps even expe-rience their own symptoms, and this, too, can influence diagnosis.
Even within a single country, the risk of mood disorders varies. Depression, forexample, is more common among lower socioeconomic groups (Dohrenwend, 2000;Monroe & Hadjiyannakis, 2002), perhaps because these groups are exposed to morestress. In contrast, bipolar disorder is more common among higher socioeconomicgroups (Goodwin & Jamison, 1990), conceivably because the behaviors producedduring a person’s hypomanic phases may lead to increased accomplishment.
SCHIZOPHRENIA
So far, we have considered two of the most common types of mental disorders, theanxiety disorders and the mood disorders. We now turn to schizophrenia, whose namewas coined by the Swiss psychiatrist Eugen Bleuler from the Greek schizo, “split,” andphren, “mind,” to designate what he regarded as an abnormal disintegration of mentalfunctions (1911).*
The lifetime prevalence of schizophrenia is about 1% (roughly the same prevalenceas epilepsy). This overall estimate may be misleading, however, because the rates ofschizophrenia are especially high in some nations and in some regions—including, forexample, Croatia and the western half of Ireland; conversely, the schizophrenia rate isquite low in Papua New Guinea. These geographic variations are not well understood.
*The Greek roots of this term are probably the source of the widespread confusion between schizophrenia and whatused to be called a split personality (now called dissociative identity disorder). Schizophrenia does not involve “mul-tiple personalities.”
16.18 Depression around the world War has many horrideffects—including an increase in the rate of mental disease.Depression rates are, for example, high in countries likeAfghanistan that have been torn apart by war, with manypeople displaced from their homes and living in poverty inrefugee camps like this one.
schizophrenia A group of severemental disorders characterized by atleast some of the following: markeddisturbance of thought, withdrawal,inappropriate or flat emotions, delu-sions, and hallucinations.
prognosis The forecast of how asituation (including an illness) willimprove or fail to improve in thefuture.
psychosis Loss of contact with real-ity, most often evidenced as delusionsor hallucinations.

PSchizophreniaO 659
Schizophrenia is typically diagnosed in late adolescence or early adulthood andtends to begin earlier in men than in women (Jablensky & Cole, 1997). Men also seemto develop a more severe form of the disorder (Nopoulos, Flaum, & Andreasen, 1997).
Unfortunately, the prognosis (the prospect for recovery) for people with this disor-der is discouraging. One study tracked down 200 people in the United States who hadbeen diagnosed with schizophrenia some 30 years previously. Of these patients,20% were doing well at the time of the follow-up, while 45% were incapacitated. Two-thirds had never married, and 58% had never worked (Andreasen & Black, 1996;Cutting, 1986).
Signs and SymptomsPeople with schizophrenia experience many different types of symptoms (Hyman,2007). Positive symptoms are behaviors that are not evident in healthy people. Negative(deficit) symptoms reflect an absence of behaviors that are usually evident in healthypeople. Cognitive symptoms reflect impairments in executive functions such as workingmemory and attentional control and can include the state of psychosis, or loss ofcontact with reality, so that the beliefs and perceptions of someone withschizophrenia are often extremely bizarre (Figure 16.19). Here is one account of whatit feels like to have schizophrenia:
When my first episode of schizophrenia occurred, I was 21, a senior in college in Atlanta,Georgia. I was making good grades, assistant vice president of my chapter in my sorority, president of the Spanish club, and very popular. Everything in my life was justperfect. . . .
All of a sudden things weren’t going so well. I began to lose control of my life and,most of all, myself. I couldn’t concentrate on my school-work, I couldn’t sleep, and whenI did sleep, I had dreams about dying. I was afraid to go to class, imagined that peoplewere talking about me, and on top of that I heard voices. I called my mother in Pittsburghand asked for her advice. She told me to move off campus into an apartment with mysister.
After I moved in with my sister, things got worse. I was afraid to go outside and whenI looked out of the window, it seemed that everyone outside was yelling “kill her, kill her.”My sister forced me to go to school. I would go out of the house until I knew she hadgone to work; then I would return home. Things continued to get worse. I imagined thatI had a foul body odor and I sometimes took up to six showers a day. I recall going to thegrocery store one day, and I imagined that the people in the store were saying “Get saved,Jesus is the answer.” Things worsened—I couldn’t remember a thing. I had a notebookfull of reminders telling me what to do on that particular day. I couldn’t remember myschoolwork, and I would study from 6:00 p.m. until 4:00 a.m., but never had thecourage to go to class on the following day. I tried to tell my sister about it, but she did-n’t understand. She suggested that I see a psychiatrist, but I was afraid to go out of thehouse to see him. (O’Neal, 1984, pp. 109–110)
P O S I T I V E SY M P TO M S
Positive symptoms—behaviors that are not evident in healthy people—can take several forms. People with schizophrenia typically suffer from delusions—incorrectbeliefs that are rigidly maintained despite the absence of any evidence for the belief,and, in many cases, despite contradictory evidence. By one estimate, 90% of all
16.19 Paintings by sufferers ofschizophrenia Paintings by people withschizophrenia often have an odd, eeriequality. In many cases the usual artisticconventions are disregarded, and thepictures include written comments, digits,and other idiosyncratic material.(top) Saint-Adolf-Grand-Grand-God-Father(1915), a painting by Adolf W., who wasinstitutionalized in early adulthood andelaborated a fantastic autobiography inwhich he featured himself as Saint Adolf II,a young god who travels through space andhas many adventures. (bottom) GuardianAngels by Else B., an institutionalizedwoman with schizophrenia. In all her worksthe legs of angels are painted as thoughthey had fused at the top, to make surethat “nothing happens there.”
delusions Systematized false beliefs,often of grandeur or persecution.

660 chapter 16 PPSYCHOPATHOLOGYO
patients with schizophrenia suffer from delusions (Cutting, 1995). Thus a patientwith schizophrenia might be convinced he is Moses, or the king of England, or aspecial messenger from God. Likewise, people with schizophrenia often believe thattheir thoughts or actions are being controlled by someone else (by space aliens, forexample, or by the CIA; Figure 16.20). Sometimes they believe their thoughts arebeing broadcast (and so are fully audible) to other people. Delusions of reference arealso common, in which the patient is convinced that some neutral environmentalevent is somehow directed at her. For example, a patient might observe two strangerstalking and be certain they are talking about him; she sees some people walk by anddecides they are following her; he sees a television commercial and is sure it containsa secret message aimed only at him.
A second type of positive symptom is hallucinations—sensory experiences in theabsence of any actual input. Most common in schizophrenia are auditory hallucina-tions, and, in particular, voices. Thus, the patient might “hear” the voice of God, or thedevil, or a neighbor. If the patient can make out what the voices are saying, she willoften report that they are talking about her, shouting obscenities at her, threateningher, or telling her what to do. Researchers have explored these hallucinations via func-tional brain imaging and have documented increased brain activation, during thehallucinations, in primary auditory regions in the temporal lobe (Lennox, Park, Medley,Morris, & Jones, 2000). This finding suggests that when people with schizophreniahave auditory hallucinations, they are hearing voices that sound every bit as vivid andreal to them as actual voices.
Positive symptoms also may take the form of unusual behaviors. People withschizophrenia sometimes dress peculiarly (wearing layers of warm clothing on a hotday) and show disorganized behavior, becoming frenzied, running haphazardly, shoutingnonsensically, and acting violently (Figure 16.21). In many ways, the disorganizedbehavior associated with schizophrenia is the closest match to the popular stereotypeof madness: A person who has schizophrenia may have speech that is bizarre andbabbling, and while he is talking, he may giggle, make silly smiles or odd grimaces,assume odd postures, and have sudden fits of laughing and crying.
N E G AT I V E SY M P TO M S
In addition to positive symptoms, people with schizophrenia may show several types ofnegative symptoms. One negative symptom is a flattening or cessation of behavioralresponses. For example, someone with schizophrenia may express little emotion, maysay relatively little, and may be unable to persist in many activities. People who havebeen ill for a long time will often stare vacantly into space, their faces expressionless,and, if they answer questions at all, they do so in a monotone. At the extreme, individ-uals with schizophrenia may show catatonic behavior, standing or sitting “frozen” forhours on end, sometimes in unusual postures (Figure 16.22).
A second type of negative symptom is anhedonia, the loss of interest in activitiesthat we would ordinarily expect to be pleasurable. People with schizophrenia also seemnot to anticipate pleasure in the way that healthy people do, a finding that correspondswith lower levels of goal-oriented behavior (Gard et al., 2007).
A third negative symptom—which may be related to the failure to anticipate pleasure—is withdrawal from other people (Tarbox & Pogue-Geile,2008).In some patients, this with-drawal begins quite early, with a history of few childhood friends and limited adolescentsocial contact. In others, the individual gradually develops an inner world that becomesmore and more private and less and less involved with the social world. As a result, thethoughts of this person become ever more idiosyncratic, until she may have trouble com-
hallucinations Perceived experi-ences that occur in the absence ofactual sensory stimulation.
16.20 Delusions In A Beautiful Mind,Russell Crowe depicted John Nash’sstruggle with schizophrenia, includingelaborate delusions.
16.21 Odd attire Unusual dressing can beone positive symptom of schizophrenia.

PSchizophreniaO 661
municating with others even if she wants to. This situation makes it even more likely thatothers will rebuff her because they cannot understand her and think she is “weird.” Thevicious cycle of rejections can lead to further withdrawal and idiosyncrasy.
CO G N I T I V E SY M P TO M S
People with schizophrenia often display marked cognitive difficulties. They seem unableto maintain a coherent train of thought, but rather skip from one idea to the next, and thistypically shows up in their speech. An example is a fragment of a letter written by one ofBleuler’s patients. The writing starts out normally enough, but then deteriorates:
I am writing on paper. The pen I am using is from a factory called “Perry & Co.” Thisfactory is in England. I assume this. Behind the name of Perry Co., the city of London isinscribed; but not the city. The city of London is in England. I know this from my school-days. Then, I always liked geography. My last teacher in that subject was ProfessorAugust A. He was a man with black eyes. I also like black eyes. There are also blue andgray eyes and other sorts too. I have heard it said that snakes have green eyes. All peoplehave eyes. There are some, too, who are blind. These blind people are led about by a boy.(1911, p. 17)
It is also common for people with schizophrenia to have significant impairments start-ing with the earliest stages of sensory processing (Walker, Kestler, Bollini, & Hochman,2004) and extending through episodic memory and cognitive control (Reichenberg &Harvey, 2007). Other perceptual and motor abnormalities are evident in people who havenot been diagnosed with schizophrenia but who are at elevated risk for the disease; theseabnormalities include deficits in two-point discrimination (distinguishing between 1 and2 points touching the skin) and simple line drawing (Lenzenweger, 2006). These (andother) cognitive problems may all contribute to the broad pattern of symptoms that aretypical of schizophrenia. An inability to inhibit thoughts and actions, for example, con-tributes to disrupted speech and behavior, while difficulties in executive function interferewith the ability to reason and so foster the delusions.
The Roots of SchizophreniaWhat leads to these symptoms? Like the other causes of disorders we have discussed,the causes of schizophrenia are complex, involving genetic, prenatal, neural, social, andpsychological factors.
G E N E T I C A N D P R E N ATA L FACTO RS
It has long been known that schizophrenia runs in families (Figure 16.23). For example, if a person has a sibling with schizophrenia, the likelihood that he has (or will get) the disease himself is four times greater than the likelihood of schizophre-nia in the general population—8%, compared with 1 or 2% in the broad population(Andreasen & Black, 1996; D. Rosenthal, 1970). But this fact, by itself, does not provea genetic contribution. (After all, the increased risk among siblings might reflect afactor in the home or family environment.) Better evidence comes from concordancerates between twins, which are between 41 and 65% if twins are identical, and between0 and 28% if they are fraternal (Cardno & Gottesman, 2000).
Separate evidence comes from adoption studies. Consider a child who is born to amother with schizophrenia and placed in a foster home (with foster parents who are
16.22 Catatonic schizophrenia Thispatient, who was diagnosed with catatonicschizophrenia, spent virtually all his wakinghours in a crouched position.
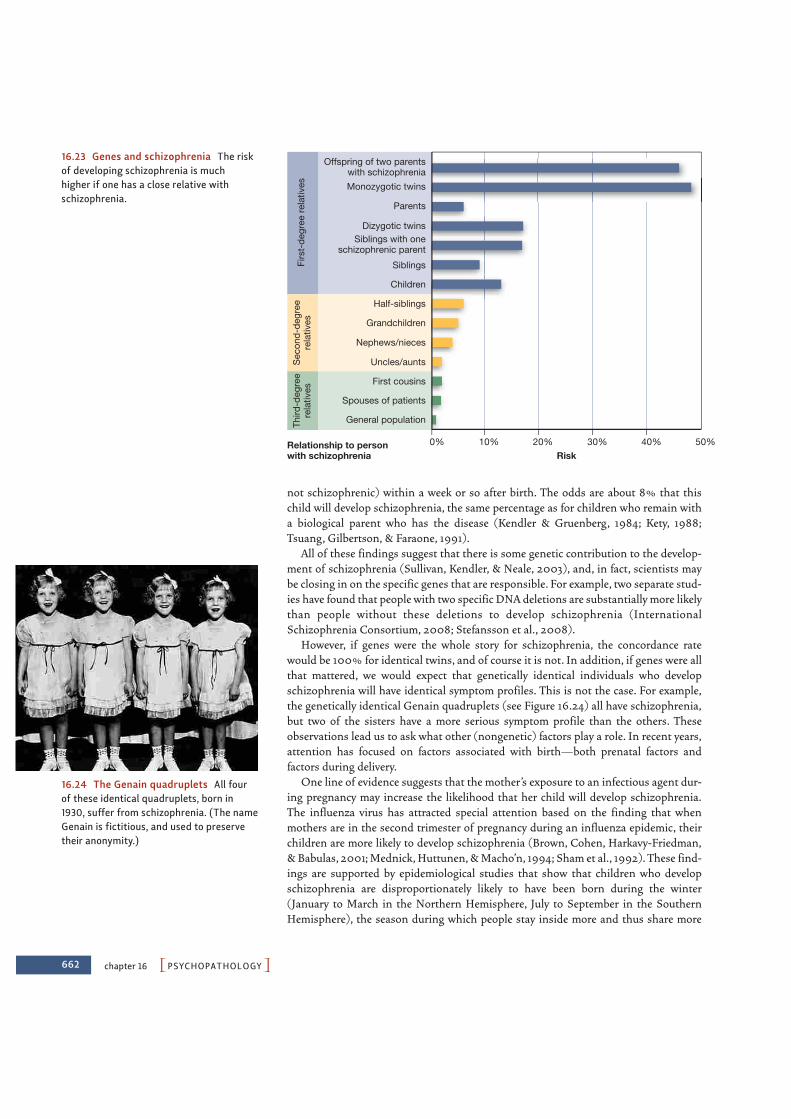
662 chapter 16 PPSYCHOPATHOLOGYO
not schizophrenic) within a week or so after birth. The odds are about 8% that thischild will develop schizophrenia, the same percentage as for children who remain witha biological parent who has the disease (Kendler & Gruenberg, 1984; Kety, 1988;Tsuang, Gilbertson, & Faraone, 1991).
All of these findings suggest that there is some genetic contribution to the develop-ment of schizophrenia (Sullivan, Kendler, & Neale, 2003), and, in fact, scientists maybe closing in on the specific genes that are responsible. For example, two separate stud-ies have found that people with two specific DNA deletions are substantially more likelythan people without these deletions to develop schizophrenia (InternationalSchizophrenia Consortium, 2008; Stefansson et al., 2008).
However, if genes were the whole story for schizophrenia, the concordance ratewould be 100% for identical twins, and of course it is not. In addition, if genes were allthat mattered, we would expect that genetically identical individuals who developschizophrenia will have identical symptom profiles. This is not the case. For example,the genetically identical Genain quadruplets (see Figure 16.24) all have schizophrenia,but two of the sisters have a more serious symptom profile than the others. Theseobservations lead us to ask what other (nongenetic) factors play a role. In recent years,attention has focused on factors associated with birth—both prenatal factors andfactors during delivery.
One line of evidence suggests that the mother’s exposure to an infectious agent dur-ing pregnancy may increase the likelihood that her child will develop schizophrenia.The influenza virus has attracted special attention based on the finding that whenmothers are in the second trimester of pregnancy during an influenza epidemic, theirchildren are more likely to develop schizophrenia (Brown, Cohen, Harkavy-Friedman,& Babulas, 2001; Mednick, Huttunen, & Macho’n, 1994; Sham et al., 1992). These find-ings are supported by epidemiological studies that show that children who developschizophrenia are disproportionately likely to have been born during the winter(January to March in the Northern Hemisphere, July to September in the SouthernHemisphere), the season during which people stay inside more and thus share more
Relationship to personwith schizophrenia
Firs
t-de
gree
rela
tives
Sec
ond-
degr
eere
lativ
esTh
ird-d
egre
ere
lativ
es
General population
Spouses of patients
First cousins
Uncles/aunts
Nephews/nieces
Grandchildren
Half-siblings
Children
Siblings
Dizygotic twins
Parents
Monozygotic twins
Siblings with oneschizophrenic parent
Offspring of two parentswith schizophrenia
0% 10% 20% 30% 40% 50%Risk
16.23 Genes and schizophrenia The riskof developing schizophrenia is much higher if one has a close relative withschizophrenia.
16.24 The Genain quadruplets All fourof these identical quadruplets, born in1930, suffer from schizophrenia. (The nameGenain is fictitious, and used to preservetheir anonymity.)
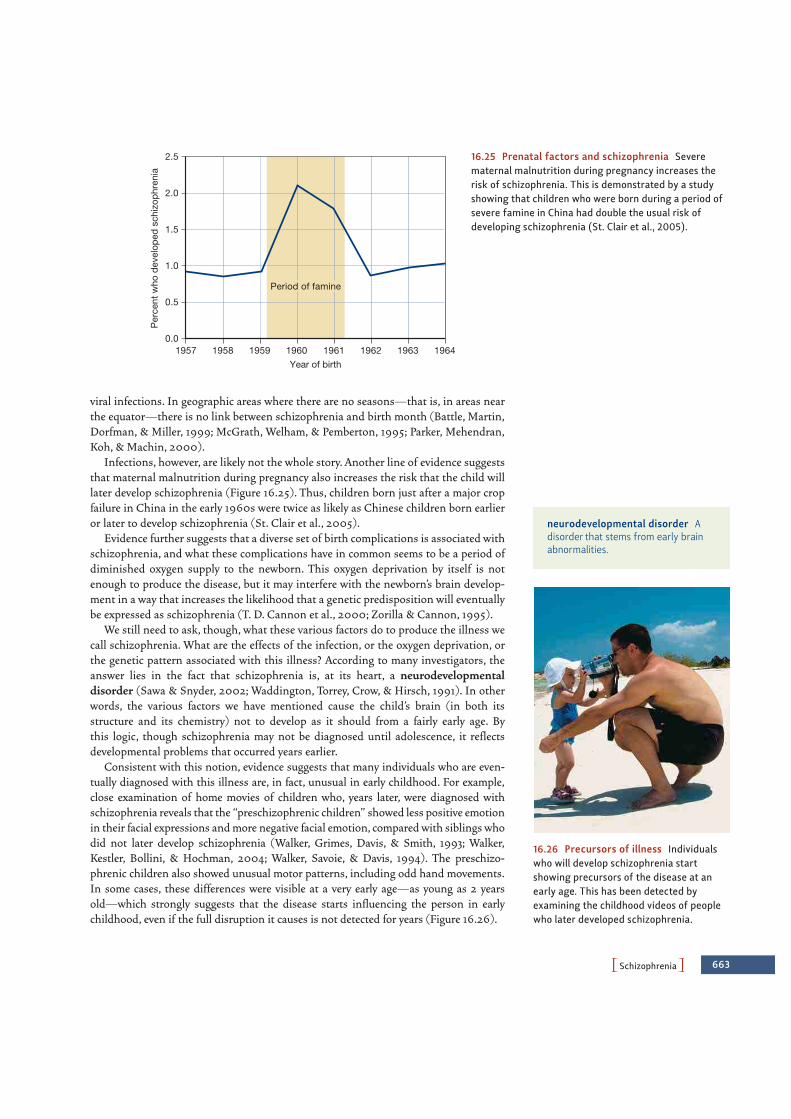
PSchizophreniaO 663
viral infections. In geographic areas where there are no seasons—that is, in areas nearthe equator—there is no link between schizophrenia and birth month (Battle, Martin,Dorfman, & Miller, 1999; McGrath, Welham, & Pemberton, 1995; Parker, Mehendran,Koh, & Machin, 2000).
Infections, however, are likely not the whole story. Another line of evidence suggeststhat maternal malnutrition during pregnancy also increases the risk that the child willlater develop schizophrenia (Figure 16.25). Thus, children born just after a major cropfailure in China in the early 1960s were twice as likely as Chinese children born earlieror later to develop schizophrenia (St. Clair et al., 2005).
Evidence further suggests that a diverse set of birth complications is associated withschizophrenia, and what these complications have in common seems to be a period ofdiminished oxygen supply to the newborn. This oxygen deprivation by itself is notenough to produce the disease, but it may interfere with the newborn’s brain develop-ment in a way that increases the likelihood that a genetic predisposition will eventuallybe expressed as schizophrenia (T. D. Cannon et al., 2000; Zorilla & Cannon, 1995).
We still need to ask, though, what these various factors do to produce the illness wecall schizophrenia. What are the effects of the infection, or the oxygen deprivation, orthe genetic pattern associated with this illness? According to many investigators, theanswer lies in the fact that schizophrenia is, at its heart, a neurodevelopmentaldisorder (Sawa & Snyder, 2002; Waddington, Torrey, Crow, & Hirsch, 1991). In otherwords, the various factors we have mentioned cause the child’s brain (in both itsstructure and its chemistry) not to develop as it should from a fairly early age. Bythis logic, though schizophrenia may not be diagnosed until adolescence, it reflectsdevelopmental problems that occurred years earlier.
Consistent with this notion, evidence suggests that many individuals who are even-tually diagnosed with this illness are, in fact, unusual in early childhood. For example,close examination of home movies of children who, years later, were diagnosed withschizophrenia reveals that the “preschizophrenic children” showed less positive emotionin their facial expressions and more negative facial emotion, compared with siblings whodid not later develop schizophrenia (Walker, Grimes, Davis, & Smith, 1993; Walker,Kestler, Bollini, & Hochman, 2004; Walker, Savoie, & Davis, 1994). The preschizo-phrenic children also showed unusual motor patterns, including odd hand movements.In some cases, these differences were visible at a very early age—as young as 2 yearsold—which strongly suggests that the disease starts influencing the person in earlychildhood, even if the full disruption it causes is not detected for years (Figure 16.26).
0.0
0.5
1.0
1.5
2.0
2.5
1957 1958 1959 1960 1961 1962 1963 1964
Per
cent
who
dev
elop
ed s
chiz
ophr
enia
Year of birth
Period of famine
16.25 Prenatal factors and schizophrenia Severematernal malnutrition during pregnancy increases therisk of schizophrenia. This is demonstrated by a studyshowing that children who were born during a period ofsevere famine in China had double the usual risk ofdeveloping schizophrenia (St. Clair et al., 2005).
neurodevelopmental disorder Adisorder that stems from early brainabnormalities.
16.26 Precursors of illness Individualswho will develop schizophrenia startshowing precursors of the disease at anearly age. This has been detected byexamining the childhood videos of peoplewho later developed schizophrenia.
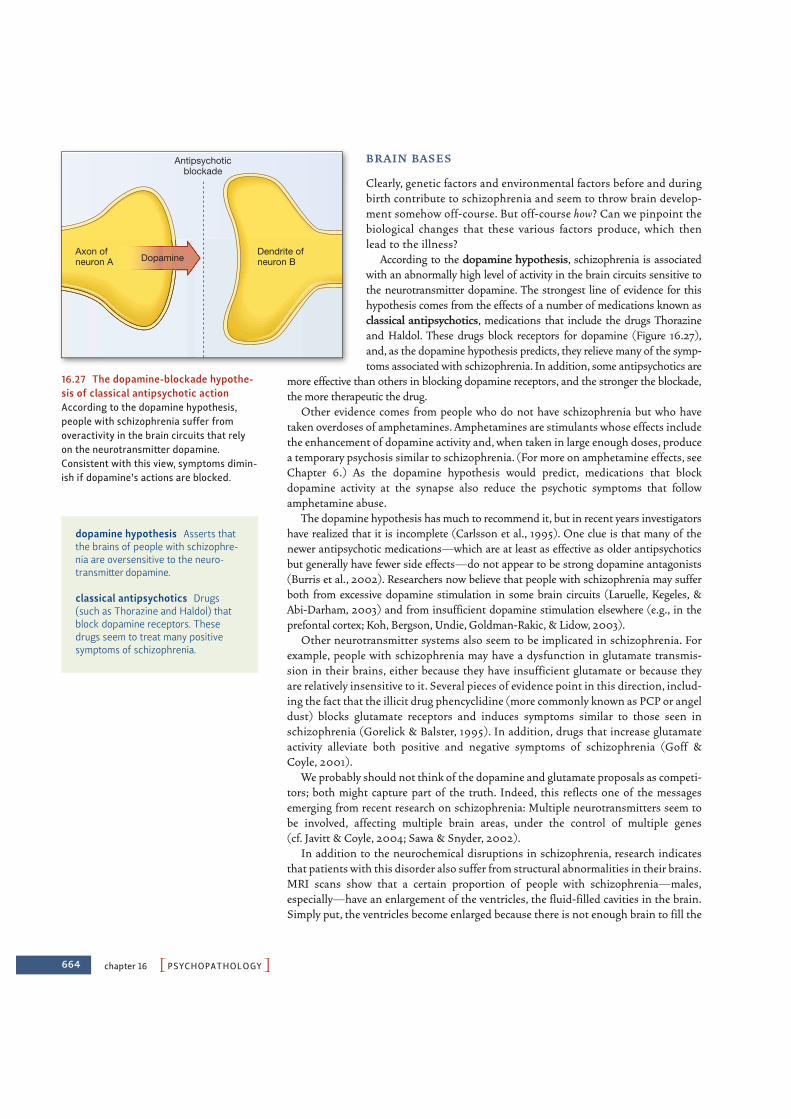
664 chapter 16 PPSYCHOPATHOLOGYO
B R A I N BAS E S
Clearly, genetic factors and environmental factors before and duringbirth contribute to schizophrenia and seem to throw brain develop-ment somehow off-course. But off-course how? Can we pinpoint thebiological changes that these various factors produce, which thenlead to the illness?
According to the dopamine hypothesis, schizophrenia is associatedwith an abnormally high level of activity in the brain circuits sensitive tothe neurotransmitter dopamine. The strongest line of evidence for thishypothesis comes from the effects of a number of medications known asclassical antipsychotics, medications that include the drugs Thorazineand Haldol. These drugs block receptors for dopamine (Figure 16.27),and, as the dopamine hypothesis predicts, they relieve many of the symp-toms associated with schizophrenia. In addition, some antipsychotics are
more effective than others in blocking dopamine receptors, and the stronger the blockade,the more therapeutic the drug.
Other evidence comes from people who do not have schizophrenia but who havetaken overdoses of amphetamines. Amphetamines are stimulants whose effects includethe enhancement of dopamine activity and, when taken in large enough doses, producea temporary psychosis similar to schizophrenia. (For more on amphetamine effects, seeChapter 6.) As the dopamine hypothesis would predict, medications that blockdopamine activity at the synapse also reduce the psychotic symptoms that followamphetamine abuse.
The dopamine hypothesis has much to recommend it, but in recent years investigatorshave realized that it is incomplete (Carlsson et al., 1995). One clue is that many of thenewer antipsychotic medications—which are at least as effective as older antipsychoticsbut generally have fewer side effects—do not appear to be strong dopamine antagonists(Burris et al., 2002). Researchers now believe that people with schizophrenia may sufferboth from excessive dopamine stimulation in some brain circuits (Laruelle, Kegeles, &Abi-Darham, 2003) and from insufficient dopamine stimulation elsewhere (e.g., in theprefontal cortex; Koh, Bergson, Undie, Goldman-Rakic, & Lidow, 2003).
Other neurotransmitter systems also seem to be implicated in schizophrenia. Forexample, people with schizophrenia may have a dysfunction in glutamate transmis-sion in their brains, either because they have insufficient glutamate or because theyare relatively insensitive to it. Several pieces of evidence point in this direction, includ-ing the fact that the illicit drug phencyclidine (more commonly known as PCP or angeldust) blocks glutamate receptors and induces symptoms similar to those seen inschizophrenia (Gorelick & Balster, 1995). In addition, drugs that increase glutamateactivity alleviate both positive and negative symptoms of schizophrenia (Goff &Coyle, 2001).
We probably should not think of the dopamine and glutamate proposals as competi-tors; both might capture part of the truth. Indeed, this reflects one of the messagesemerging from recent research on schizophrenia: Multiple neurotransmitters seem tobe involved, affecting multiple brain areas, under the control of multiple genes (cf. Javitt & Coyle, 2004; Sawa & Snyder, 2002).
In addition to the neurochemical disruptions in schizophrenia, research indicatesthat patients with this disorder also suffer from structural abnormalities in their brains.MRI scans show that a certain proportion of people with schizophrenia—males,especially—have an enlargement of the ventricles, the fluid-filled cavities in the brain.Simply put, the ventricles become enlarged because there is not enough brain to fill the
Antipsychoticblockade
Axon ofneuron A Dopamine
Dendrite ofneuron B
16.27 The dopamine-blockade hypothe-sis of classical antipsychotic actionAccording to the dopamine hypothesis,people with schizophrenia suffer fromoveractivity in the brain circuits that relyon the neurotransmitter dopamine.Consistent with this view, symptoms dimin-ish if dopamine’s actions are blocked.
dopamine hypothesis Asserts thatthe brains of people with schizophre-nia are oversensitive to the neuro-transmitter dopamine.
classical antipsychotics Drugs(such as Thorazine and Haldol) thatblock dopamine receptors. Thesedrugs seem to treat many positivesymptoms of schizophrenia.

PSchizophreniaO 665
skull (Figure 16.28). This finding indicates that in many cases ofschizophrenia, there is either a dramatic loss of brain tissue or a defi-ciency that existed from the start (Andreasen et al., 1986; Chua &McKenna, 1995; Lawrie & Abukmeil, 1998; Nopoulos, Flaum, &Andreasen, 1997).
Abnormalities associated with schizophrenia have also beenreported in other areas of the brain (Heckers, 1997; L. K. Jacobsenet al., 1997), but the most persuasive findings involve the frontal andtemporal lobes (Black & Andreasen, 1994; Martin & Albers, 1995).Studies of brain structure have documented a loss of gray matter inprefrontal regions that support working memory, and the degree of tis-sue loss seems to be correlated with symptom severity (Cannon et al., 2002). When these areas are examined during autopsy,individuals with schizophrenia also show various irregularities,including missing or abnormally sized neurons. These neuronaldefects—not surprisingly—affect overall brain function: neuroimag-ing studies of patients with schizophrenia indicate atypical function-ing in the areas where neuronal defects are common (Barch et al., 2001; Tan et al., 2006).
SO C I A L A N D P SY C H O LO G I CA L R I S K FACTO RS
Almost a century ago, epidemiological studies revealed a link between schizophrenia andsocioeconomic status, or SES (Faris & Dunham, 1939). In fact, one study suggested thatlow-SES individuals are nine times more likely to develop schizophrenia than are high-SES individuals (Hollingshead & Redlich, 1958). The same point can be madegeographically, since the prevalence of schizophrenia is highest in the poorest and mostdilapidated areas of a city and diminishes as one moves toward higher-income regions(Figure 16.29; M. L. Kohn, 1968).
What produces this relationship? Part of the answer is, sadly, daily stress—poverty,inferior status, and low occupational rank are all stressful, and so can help trigger schiz-ophrenia in someone who is (for biological reasons) already vulnerable (Goldberg &Morrison, 1963). But there is another reason why schizophreniais associated with poverty: Someone who suffers fromschizophrenia is less likely to do well in schooland less likely to get or hold a good job. As aresult, people with schizophrenia sufferfrom downward drift. Their disease pro-duces problems that, in turn, put theminto a lower social class (Dohrenwend etal., 1992; Jones et al., 1993). Notice, then,that cause and effect run in both directionshere: Poverty is a risk factor for schizophrenia,making the disease more likely, but schizophre-nia is itself a risk factor that makes povertymore likely.
What about someone’s immediateenvironment—for example, her family?Some investigators have looked to the per-sonality of a person’s parents as a potentialsource of schizophrenia. Others have focused oncommunication patterns in the family (Bateson,
16.28 MRI scans of the brains of twinsMRI scans of the brains of 28-year-oldidentical twins. One (right) is hospitalizedfor schizophrenia; the other (left) is well.The twin with schizophrenia has enlargedcerebral ventricles. The fact that just onetwin has schizophrenia shows that heredityis not the only factor in producing this dis-order; the slightly different prenatal envi-ronments of the twins, as well as birthcomplications, may be involved.
Schizophreniarate per 10,000
100+60–9940–5930–3920–2910–19
16.29 The prevalence of schizophreniain different regions of a city A map ofChicago (1922–1934) is represented by aseries of concentric zones. The center zoneis the business and amusement area, whichis without residents except for sometransients and vagabonds. Surroundingthis center is a slum region inhabitedlargely by unskilled laborers. Farther outare more stable regions: a zone largelypopulated by skilled workers, followed byzones of middle- and upper-middle-classapartment dwellers, and, farthest out, theupper-middle-class commuters. The mapshows clearly that the incidence ofschizophrenia increases the closer one getsto the city’s center.
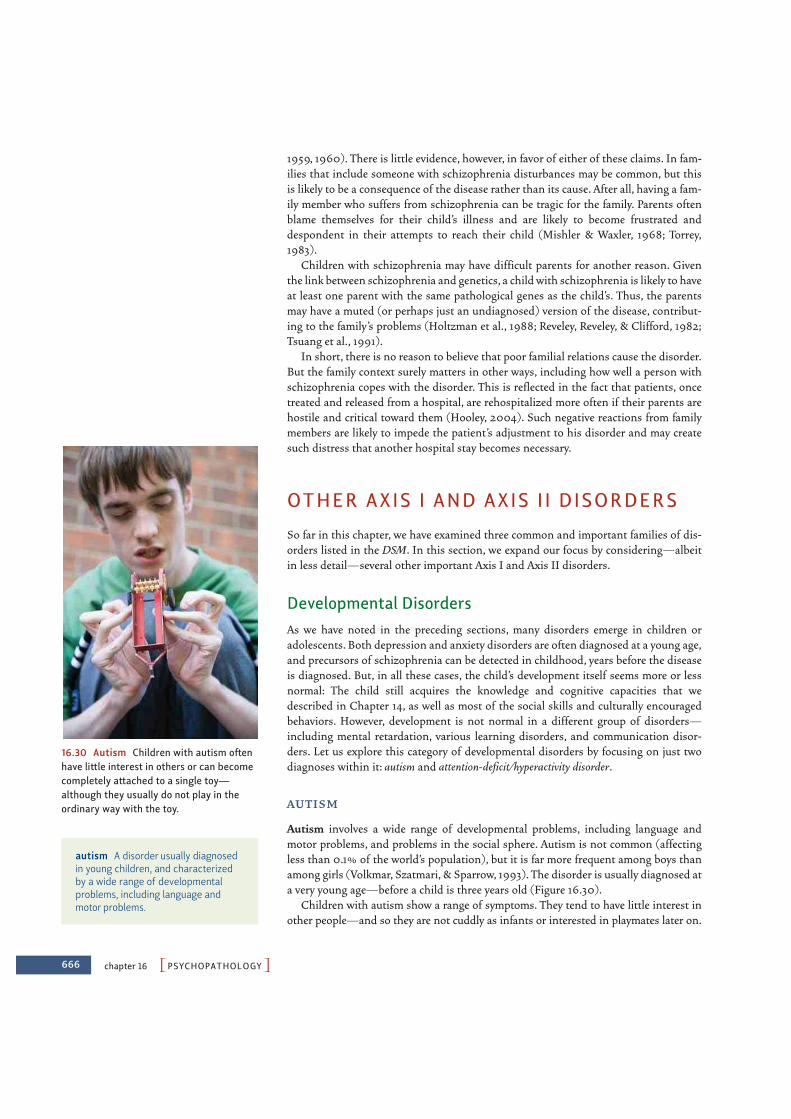
666 chapter 16 PPSYCHOPATHOLOGYO
1959, 1960). There is little evidence, however, in favor of either of these claims. In fam-ilies that include someone with schizophrenia disturbances may be common, but thisis likely to be a consequence of the disease rather than its cause. After all, having a fam-ily member who suffers from schizophrenia can be tragic for the family. Parents oftenblame themselves for their child’s illness and are likely to become frustrated anddespondent in their attempts to reach their child (Mishler & Waxler, 1968; Torrey,1983).
Children with schizophrenia may have difficult parents for another reason. Giventhe link between schizophrenia and genetics, a child with schizophrenia is likely to haveat least one parent with the same pathological genes as the child’s. Thus, the parentsmay have a muted (or perhaps just an undiagnosed) version of the disease, contribut-ing to the family’s problems (Holtzman et al., 1988; Reveley, Reveley, & Clifford, 1982;Tsuang et al., 1991).
In short, there is no reason to believe that poor familial relations cause the disorder.But the family context surely matters in other ways, including how well a person withschizophrenia copes with the disorder. This is reflected in the fact that patients, oncetreated and released from a hospital, are rehospitalized more often if their parents arehostile and critical toward them (Hooley, 2004). Such negative reactions from familymembers are likely to impede the patient’s adjustment to his disorder and may createsuch distress that another hospital stay becomes necessary.
OTHER AXIS I AND AXIS II DISORDERS
So far in this chapter, we have examined three common and important families of dis-orders listed in the DSM. In this section, we expand our focus by considering—albeitin less detail—several other important Axis I and Axis II disorders.
Developmental DisordersAs we have noted in the preceding sections, many disorders emerge in children oradolescents. Both depression and anxiety disorders are often diagnosed at a young age,and precursors of schizophrenia can be detected in childhood, years before the diseaseis diagnosed. But, in all these cases, the child’s development itself seems more or lessnormal: The child still acquires the knowledge and cognitive capacities that wedescribed in Chapter 14, as well as most of the social skills and culturally encouragedbehaviors. However, development is not normal in a different group of disorders—including mental retardation, various learning disorders, and communication disor-ders. Let us explore this category of developmental disorders by focusing on just twodiagnoses within it: autism and attention-deficit/hyperactivity disorder.
AU T I S M
Autism involves a wide range of developmental problems, including language andmotor problems, and problems in the social sphere. Autism is not common (affectingless than 0.1% of the world’s population), but it is far more frequent among boys thanamong girls (Volkmar, Szatmari, & Sparrow, 1993). The disorder is usually diagnosed ata very young age—before a child is three years old (Figure 16.30).
Children with autism show a range of symptoms. They tend to have little interest inother people—and so they are not cuddly as infants or interested in playmates later on.
autism A disorder usually diagnosedin young children, and characterizedby a wide range of developmentalproblems, including language andmotor problems.
16.30 Autism Children with autism oftenhave little interest in others or can becomecompletely attached to a single toy—although they usually do not play in theordinary way with the toy.

POther Axis I and Axis II DisordersO 667
When they do interact with others, they seem to have little understanding of the others’intentions, beliefs, or goals and show little or no empathy (Oberman & Ramachandran,2007). It is not surprising, then, that children with autism often seem unable to joincooperative activities or form friendships. They also seem to lack emotional intelligence(Chapter 11), and so seem unable to understand others’ expressions of emotions or howto use their own faces and gestures to convey emotion (Charman et al., 1998).
Children with autism also show marked deficits in language—often not speaking, andtypically showing neither skill nor interest in communicating with others. In many cases,they produce high-pitched, birdlike noises instead of speech, or show a pattern of simplyechoing speech they have heard—perhaps just a moment ago, or perhaps a few daysearlier. Often, they have trouble with pronouns—reversing I and you and referring tothemselves by name, rather than saying “I” (Lee, Hobson, & Chiat, 1994).
Autistic children also show peculiar repetitive movement patterns—spinningaround for long periods of time, or rocking back and forth for hours. They also seeminsistent on sameness, and so become deeply upset—and may throw severetantrums—if the furniture in the house is rearranged, or their parents vary the house-hold routine in some small way. They may become completely attached to one singletoy, carrying it around constantly, but often not playing with it in the ordinary manner.
Finally, children with autism are often mentally retarded, but here there is an oddtwist. In a minority of cases, they show islands of preserved (indeed, enhanced) skill,so that a child with autism might turn out to be an extraordinary musician or unbeliev-ably fast in arithmetic calculations.
What produces this broad range of symptoms? There is compelling evidence thatautism has a substantial genetic component (Sutcliffe, 2008), and most accounts ofautism emphasize some form of biological dysfunction, but there are a variety of pro-posals about what we should count as the “core problem.” One hypothesis is that indi-viduals with autism have some problem in the functioning of their amygdala, a brainstructure that plays an essential role in emotion and motivation (Waterhouse, Fein, &Modahl, 1996). A different hypothesis focuses on abnormalities in the cerebellum(Courchesne, Townsend, & Saitoh, 1994). Another hypothesis is that the problem liesin a brain structure that specifically helps the child learn about and understand otherpeople’s thoughts and intentions (Scott & Baron-Cohen, 1996).
Whatever the causes of autism, treatment typically focuses on modifying the behav-ior of the person with autism. Various medications for autism have been tried, but noneseem particularly effective. Instead, therapists have had more success with behavior-modification techniques—building on the principles of shaping and reinforcementthat we described in Chapter 7. These efforts seem to improve both social and intellec-tual functioning and can produce appreciable long-term benefits.
AT T E N T I O N - D E F I C I T/ H Y P E R ACT I V I T Y D I SO R D E R
Children with attention-deficit/hyperactivity disorder (ADHD) are impulsive, doingor saying the first thing that occurs to them, often blurting out answers in class with-out raising their hands. They also fidget, getting out of their seats at school and tappingpencils, fingers, or feet (Figure 16.31). They have difficulty keeping their attentionfocused on a task and have trouble organizing or completing projects. Their school per-formance tends to be poor, and they usually are perceived by others as intrusive andimmature.
ADHD is common: It is estimated 8% of children are diagnosed with ADHD, with agreater prevalence in boys than in girls (CDC, 2005). Symptoms are most common inyoung children (e.g., before age 8) and frequently persist into adulthood. ADHD is
16.31 ADHD ADHD is a real disorder,but there is concern that it is beingoverdiagnosed and may be a label given toany child who is just particularly active.
attention-deficit/hyperactivitydisorder (ADHD) A disorder usuallydiagnosed in young children, andcharacterized by impulsivity, difficultystaying focused on a task, and a rangeof behavioral problems.

668 chapter 16 PPSYCHOPATHOLOGYO
often treated using the stimulant methylphenidate, which is sold under tradenamessuch as Ritalin and Concerta. There is no question that these medications can be effec-tive, and global spending on ADHD medications rose threefold from 1993 through2003 (Jensen et al., 2007; Scheffler, Hinshaw, Modrek, & Levine, 2007). Given thesymptoms of ADHD, it may seem odd that a stimulant would be prescribed to treat it,but methylphenidate enhances the release of dopamine and norepinephrine, which inturn activates inhibitory circuits that guard against impulses that might be triggered bythe person’s environment.
The ADHD diagnosis has been a source of great controversy because many worrythat this “diagnosis” is sometimes just a handy label for children who are particularlyactive or children who don’t easily adjust to a school routine or a crowded classroom(Livingstone, 1997; Panksepp, 1998). Critics point out that the number of peoplediagnosed as having ADHD has dramatically increased over the past few decades. Eventoday, prevalence rates differ dramatically by country, as well as by region within theUnited States (LeFever, Arcona, & Antonuccio, 2003). The potential for overdiagnosisis troubling for many reasons, ranging from the stigma associated with receiving anydiagnosis of a mental disorder to the fact that (especially in the United States) manychildren who are diagnosed with ADHD take stimulants for years (Diller, 1999), eventhough these drugs are known to have clear addictive potential.
Despite this controversy, most now agree that ADHD is a genuine mental disorder(Hinshaw, 2008; World Federation for Mental Health, 2005), and that genetic factorsplaying a large role in producing the symptoms (Burt, Krueger, McGue, & Iacono, 2001;Rutter, 2006; Tannock, 1998). One key biological feature of ADHD appears to be a defi-ciency in prefrontal brain circuits (Barkley, 1997). When these circuits are working nor-mally, they protect us from distractions and momentary impulses; when these circuitsare dysfunctional, the result is the pattern of scattered thoughts and actions that char-acterize ADHD.
Eating DisordersTwo different eating disorders are identified by the DSM. The first—anorexia nervosa—is defined by a refusal to maintain a minimally appropriate body weight. The second—bulimia nervosa—is defined by an alternating sequence of “binges” and “purges”—rapidfood intake followed by maladaptive (and often extreme) attempts to keep from gain-ing weight.
A N O R EX I A N E R V O SA
Individuals with anorexia nervosa are preoccupied with food and eating and havean intense fear of gaining weight. This fear is nurtured by a disturbance in how thesepeople perceive their own bodies—they genuinely believe themselves to be fat,despite the fact that in many cases they are extremely, even dangerously, thin(Figure 16.32). They spend enormous amounts of time measuring various parts oftheir bodies and critically examining themselves in the mirror. Any slight change inweight is momentous to them, with tiny decreases celebrated and minute gainslamented (Figure 16.33). It’s not surprising, therefore, that individuals with anorexianervosa relentlessly pursue thinness and usually achieve unhealthy reductions in bodyweight through a regimen of incredibly strict dieting. They may also exercise excessivelyor purge (self-induce vomiting or misuse laxatives or diuretics).
16.32 Eating disorders Women withanorexia nervosa often have severely dis-turbed perceptions of their own bodies.
anorexia nervosa An eating disordercharacterized by an extreme concernwith being overweight and by compul-sive dieting, sometimes to the point ofself-starvation.
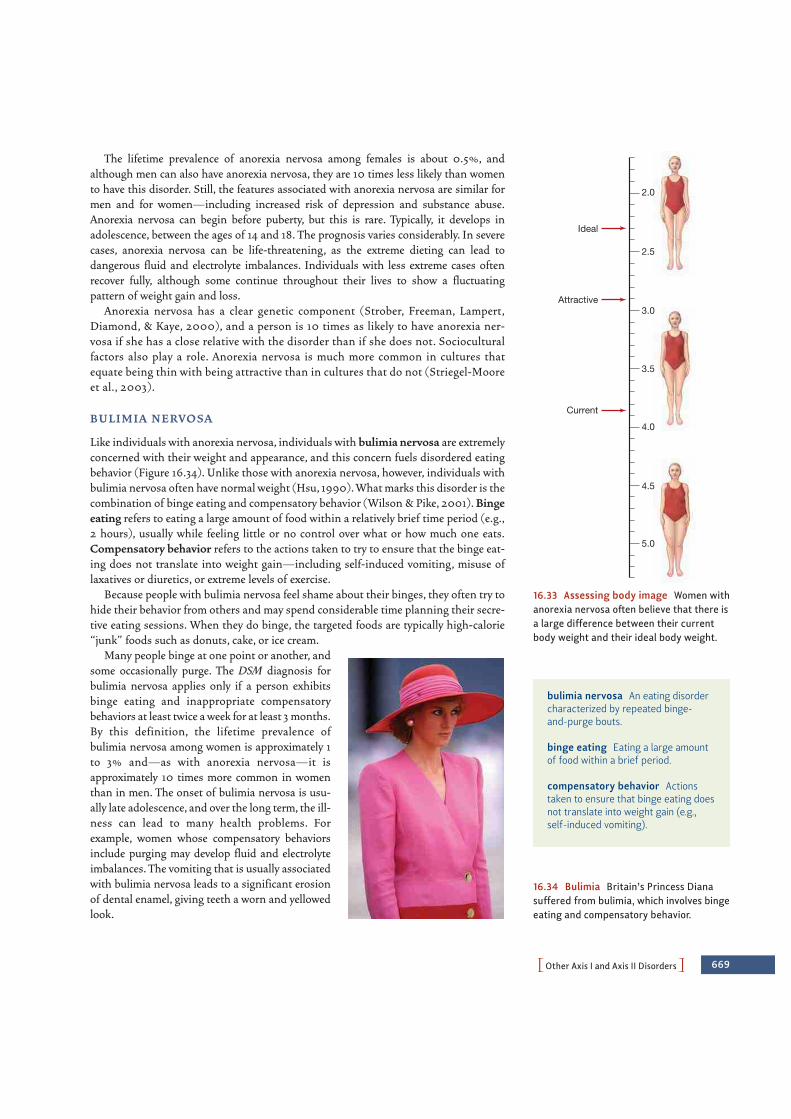
POther Axis I and Axis II DisordersO 669
The lifetime prevalence of anorexia nervosa among females is about 0.5%, andalthough men can also have anorexia nervosa, they are 10 times less likely than womento have this disorder. Still, the features associated with anorexia nervosa are similar formen and for women—including increased risk of depression and substance abuse.Anorexia nervosa can begin before puberty, but this is rare. Typically, it develops inadolescence, between the ages of 14 and 18. The prognosis varies considerably. In severecases, anorexia nervosa can be life-threatening, as the extreme dieting can lead todangerous fluid and electrolyte imbalances. Individuals with less extreme cases oftenrecover fully, although some continue throughout their lives to show a fluctuatingpattern of weight gain and loss.
Anorexia nervosa has a clear genetic component (Strober, Freeman, Lampert,Diamond, & Kaye, 2000), and a person is 10 times as likely to have anorexia ner-vosa if she has a close relative with the disorder than if she does not. Socioculturalfactors also play a role. Anorexia nervosa is much more common in cultures thatequate being thin with being attractive than in cultures that do not (Striegel-Mooreet al., 2003).
B U L I M I A N E R V O SA
Like individuals with anorexia nervosa, individuals with bulimia nervosa are extremelyconcerned with their weight and appearance, and this concern fuels disordered eatingbehavior (Figure 16.34). Unlike those with anorexia nervosa, however, individuals withbulimia nervosa often have normal weight (Hsu, 1990). What marks this disorder is thecombination of binge eating and compensatory behavior (Wilson & Pike, 2001). Bingeeating refers to eating a large amount of food within a relatively brief time period (e.g.,2 hours), usually while feeling little or no control over what or how much one eats.Compensatory behavior refers to the actions taken to try to ensure that the binge eat-ing does not translate into weight gain—including self-induced vomiting, misuse oflaxatives or diuretics, or extreme levels of exercise.
Because people with bulimia nervosa feel shame about their binges, they often try tohide their behavior from others and may spend considerable time planning their secre-tive eating sessions. When they do binge, the targeted foods are typically high-calorie“junk” foods such as donuts, cake, or ice cream.
Many people binge at one point or another, andsome occasionally purge. The DSM diagnosis forbulimia nervosa applies only if a person exhibitsbinge eating and inappropriate compensatorybehaviors at least twice a week for at least 3 months.By this definition, the lifetime prevalence ofbulimia nervosa among women is approximately 1to 3% and—as with anorexia nervosa—it isapproximately 10 times more common in womenthan in men. The onset of bulimia nervosa is usu-ally late adolescence, and over the long term, the ill-ness can lead to many health problems. Forexample, women whose compensatory behaviorsinclude purging may develop fluid and electrolyteimbalances. The vomiting that is usually associatedwith bulimia nervosa leads to a significant erosionof dental enamel, giving teeth a worn and yellowedlook.
Current
Attractive
Ideal
3.5
3.0
2.5
2.0
4.0
4.5
5.0
16.33 Assessing body image Women withanorexia nervosa often believe that there isa large difference between their currentbody weight and their ideal body weight.
bulimia nervosa An eating disordercharacterized by repeated binge-and-purge bouts.
binge eating Eating a large amountof food within a brief period.
compensatory behavior Actionstaken to ensure that binge eating doesnot translate into weight gain (e.g.,self-induced vomiting).
16.34 Bulimia Britain’s Princess Dianasuffered from bulimia, which involves bingeeating and compensatory behavior.

670 chapter 16 PPSYCHOPATHOLOGYO
Both genetic and sociocultural factors contribute to the onset and maintenance ofbulimia nervosa. Women who have close relatives with bulimia nervosa are four timesmore likely to have this disorder than are women who do not (Strober et al., 2000). Inaddition, research suggests that bulimia nervosa may be confined to westernized cul-tural contexts (Keel & Klump, 2003); as cultures become more westernized, rates ofbulimia nervosa increase (Nasser, 1997).
Dissociative DisordersThere is no question that many disorders—and, indeed, many life experiences—involve considerable pain or distress. To protect themselves against this discomfort,people engage in a variety of defensive strategies. One of these strategies, which wehave mentioned in other contexts, is dissociation—a term that covers the various waysin which people try to distance themselves psychologically from ongoing events. Theyestablish this distance by saying things like “This can’t be happening” or “This is all adream” or “This isn’t happening to me.” With these defenses in place, people may,during a calamity, even experience themselves as eerily calm, floating outside their ownbodies as they watch themselves react.
These adjustments are often adaptive, a way of coping with horrific events. Butsuch adjustments can go too far and, in their extreme form, are the defining feature ofthe dissociative disorders. In some cases, for example, a person develops dissociativeamnesia and is suddenly unable to remember some period of his life, or even hisentire past, including his own identity. Such episodes usually last less than 1 week(Kihlstrom & Schacter, 2000; Maldonado, Butler, & Spiegel, 2002). In other cases,the dissociation produces dissociative fugue, in which the person wanders away fromhome and then, days or even months later, suddenly realizes that she is in a strangeplace, does not know how she got there, and has total amnesia for the entire period.
Far more controversial is the diagnosis of dissociative identity disorder (DID), acondition formerly known as multiple personality disorder. Here the dissociation issaid to be so massive that it results in two or more distinct personalities, each with itsown style, habits, and beliefs. The personalities often differ in their interests, their age,their sexual orientation, and their morals.
In one case, a patient named Julie mentioned, during therapy, that she wanted tointroduce someone to the therapist. She closed her eyes, frowned, and then opened hereyes slowly, asserting that she was Jerrie, not Julie. Roughly 1 hour later, in the sameway, she introduced Jenny, a third personality in the same body. These three womenwere different in many ways: Julie and Jenny were heterosexuals; Jerrie was a lesbian.Jenny was frightened and insecure; Julie was a sophisticated and caring mother. Jerriewas accomplished and proficient in the business world and hated the fact that Julie wasa heavy smoker (Davis & Osherson, 1977).
Until several decades ago, cases like this were rare, with fewer than 200 reportedbefore 1975. Now cases number in the thousands; the large majority are women (Kluft,1987; C. A. Ross, 1999). The number of personalities reported in each case has alsoincreased dramatically: A review of the early cases indicated that most people with DIDhad only 2 or 3 separate identities (Taylor & Martin, 1944); a more recent surveyindicates that the average number of identities reported by patients is 15, with somecases reporting far more than this (C. A. Ross, 1997).
These massive increases are one of the reasons this disorder has been a focus of somuch debate, with some critics arguing that the flood of diagnoses may reflect a fadamong therapists who inadvertently lead suggestible patients to develop the signs and
dissociative amnesia The inabilityof an individual to remember someperiod of her life, or even her entirepast, including her identity; oftenunderstood as a way of coping withextremely painful events.
dissociative fugue A state in whichsomeone leaves home, then, days ormonths later, suddenly realizes he is ina strange place and doesn’t know howhe got there; often understood as ameans of coping with (and escapingfrom) extremely painful events.
dissociative identity disorder (DID)A disorder that results in a persondeveloping two or more distinctpersonalities.

POther Axis I and Axis II DisordersO 671
symptoms of the syndrome (Lalonde, Hudson, Gigante, & Pope, 2001; Lilienfeld et al.,1999; Spanos, 1996; for a very different view, see Lewis, Yeager, Swica, Pincus, & Lewis,1997). Contributing to this trend, the critics claim, are the books and movies aboutDID, including Sybil and The Three Faces of Eve (Figure 16.35).
What should we make of this debate? It seems likely that at least some cases ofDID are in fact faked or inadvertently created by therapists. But it also seems likelythat many cases are genuine, and debate continues about the nature of this disorder,its causes, and the best way to treat it (Lilienfeld et al., 1999; C. A. Ross, 1999).
Stepping away from the controversy over DID, and returning to the broader categoryof dissociative disorders, we can ask: What factors or events lead to these disorders? Here,too, some investigators propose a genetic basis, but research has yielded mixed results(Jang, Paris, Zweig-Frank, & Livesley, 1998; Waller & Ross, 1997). One thing we do knowis that people naturally seem to differ in how much, and under what circumstances, theydissociate. Some of the relevant evidence comes from a measure known as the DissociativeExperiences Scale, which asks people directly how often they have experienced variousperceptions or behaviors characteristic of dissociation (Carlson & Putnam, 1993). Otherevidence comes from work on hypnosis, which some investigators regard as a form ofguided dissociation (Hilgard, 1986; for more on hypnosis, see Chapter 6). People differenormously in how readily or how deeply they can be hypnotized (Ganaway, 1989), andthis opens an interesting possibility: Perhaps some people were, as children, particularlyadept at self-hypnosis and learned to use this skill as a defense—putting themselves intoa self-induced hypnotic trance to escape from the stresses (or perhaps traumas) in theirlives (Bliss, 1980). This skill may then create a readiness to dissociate in everyday life, per-haps predisposing these individuals to develop a dissociative disorder.
Thus, a skill in (or habit of) dissociation may create the diathesis for a dissociative dis-order. To precipitate the full-fledged disorder, however, there also has to be some unusualstress, and, in fact, most cases of dissociative amnesia occur after the same kinds of cata-clysmic events that lead to post-traumatic stress disorder. The same holds for dissociativefugues, which can also develop suddenly after personal misfortunes or financial pressures(Andreasen & Black, 1996). The same may be true as well for dissociative identity disor-der: In a large percentage of DID case histories, there are terrifying stories of brutal phys-ical or sexual abuse in childhood, often including incest (Putnam, Guroff, Silberman,Barban, & Post, 1986). However, these reports—like the diagnosis of DID itself—havebeen controversial, inasmuch as they often rely on the person’s recall of the abuse, and, aswe discussed in Chapter 8, there has been debate over how to interpret this recall.
Personality DisordersAll of the disorders we have considered so far are included on Axis I of the DSM.Each involves a specific syndrome with a well-defined set of signs and symptoms.DSM’s Axis II diagnoses, in contrast, are characterized by much broader patterns ofbehaviors and problems that are much more consistent across the lifespan (Clark,2009). These diagnoses are concerned with traits or habits that characterize almosteverything a person does, and so are disorders, in essence, in someone’s personality.
Of course, people differ widely in their personalities (see Chapter 15), and, becauseof these variations, some people are easier to be with than others, and some have asmoother path through life than others. In some cases, though, a person’s personalityis so maladaptive that it creates considerable distress both for that person and for thosearound her and impairs the person’s day-to-day functioning. Someone with these dif-ficulties may well be diagnosed as having one or another of the personality disorders.
16.35 Dissociative identity disorderAccording to some critics, the hugeincrease in DID diagnoses is the result ofa diagnostic fad among therapists, orperhaps a result of people imitatingfamous cases of DID—including the casedepicted in the 1958 movie The Three Facesof Eve.
personality disorders Relativelystable, pervasive patterns of behaviorand inner experience that are cultur-ally discrepant and lead to distress orimpairment; noted on Axis II of theDSM.

672 chapter 16 PPSYCHOPATHOLOGYO
The DSM recognizes 10 personality disorders. These are paranoid personality disorder(in which a person shows widespread suspiciousness and mistrust of others); schizoidpersonality disorder (in which a person shows a striking detachment from others); schizo-typal personality disorder (in which a person shows a discomfort with close relationships,cognitive or perceptual distortions, and odd behavior); antisocial personality disorder(in which a person shows consistent disregard for—and violation of—others’ rights);borderline personality disorder (in which a person shows impulsive behavior and markedinstability in relationships, self-concept, and affect); histrionic personality disorder(in which a person shows an unusual degree of attention seeking and emotionality);narcissistic personality disorder (in which a person is grandiose, lacks empathy, and needsthe attention and admiration of others); avoidant personality disorder (in which a personshows social inhibition and social insecurity); dependent personality disorder (in which aperson shows an excessive need to be taken care of by others); and obsessive-compulsivepersonality disorder (in which a person is preoccupied with orderliness, perfection, andcontrol). Each of these disorders, and indeed all of the Axis II personality disorders, aredifficult to diagnose, and disagreements about diagnosis are common (L. A. Clark &Harrison, 2001; Livesley, 2001).
Part of the difficulty is that the definitions of these disorders tell us what a clear-cutand “pure” case of the disorder might look like. In reality, though, an individual’s traitsare likely only to approximate this prototype, and many people have traits that leavethem resembling more than one of the prototypes (Shea, 1995). This obviously makesdiagnosis complicated. In addition, each of these disorders can be thought of as merelythe extreme of some ordinary pattern (Livesley, 2001; Widiger & Sanderson, 1995).Many people, for example, are vain, and it is therefore a judgment call whether some-one’s vanity is so powerful that it signals a narcissistic personality disorder. Likewise,many people are shy, and it is sometimes difficult to decide whether someone’s shynessis consistent with avoidant personality disorder. Clinicians often disagree in thesejudgments, increasing the uncertainty of the Axis II diagnoses.
These diagnostic problems have in turn been difficult for researchers, because it isobviously hard to study a group that cannot be accurately identified (Clark, 2007).Despite this limitation, investigators have made impressive progress in understandingseveral of the personality disorders. For example, the diagnosis of antisocial personal-ity disorder (and the closely related diagnosis of psychopathy) is a powerful predictorof whether someone will slide into crime again after a period of imprisonment (Hare,Cooke, & Hart, 1999; Hemphill, Hare, & Wong, 1998) and so can be an importantsource of information in making parole decisions about a prisoner. Similarly, the diag-nosis of borderline personality disorder predicts compromised social cognition, as evi-denced in neuroimaging findings that show that people with borderline personalitydisorder fail to discriminate between situations in which another person signaled thatthey trusted the diagnosed individual and situations in which the other person signaledno trust (King-Casas, Sharp, Lomax-Bream, Lohrenz, Fonagy, & Montague, 2008;Meyer-Lindenberg, 2008).
SOME FINAL THOUGHTS: SYNDROMES WITHOUT STIG M A?
Throughout this chapter, we have described the diagnostic criteria for each mentalillness—and, in particular, the diagnostic criteria identified by the DSM. These criteriahave allowed clinicians to achieve impressive reliability and validity in their diagnoses,

PSome Final Thoughts: Syndromes Without Stigma?O 673
and, as we have mentioned, this has been a boon for both therapists and researchers.At the same time, we should acknowledge that the boundaries associated with many
diagnoses—the lines that separate “mentally ill” from “not ill”—are actually quiteporous. Thus, someone who “has” a disorder may differ by only a single symptom fromsomeone who “does not have” a disorder, and the mental disorders themselves oftenappear to be related as points on a continuum rather than as discrete and distinctcategories (Krueger & Markon, 2006; Widiger & Trull, 2007).
The “fuzziness” in these diagnostic categories is not often a problem, because withmany patients, the diagnosis is clear-cut. In these cases, there is no question that theperson is experiencing both considerable disruption in his life and significant emo-tional distress—whether it is the paralyzing fears associated with the phobias, the sad-ness of depression, or the emotional flattening common in schizophrenia. In situationslike these, it seems fully appropriate to offer a diagnosis and to seek treatment for theafflicted person, trying to bring him back to a normal life.
But what about people who have a subsyndromal case of a disorder—people who doshow symptoms, but not at the level that would justify a formal diagnosis? This wouldinclude people who worry about whether they really did turn off the gas and so checkand recheck the stove so often that it becomes an inconvenience—but not oftenenough to justify a diagnosis of OCD. It would also include people who are sad and notsleeping well but not quite at the level of severity or for the duration required for a diag-nosis of depression. Should these people be diagnosed and treated?
If we do not offer a formal diagnosis for these cases, we risk ignoring people who doneed help, even if their condition does not quite reach the level specified by our diag-nostic manual. But if we diagnose them, we risk creating a situation in which more andmore people with less and less extreme symptoms are defined as having mental disor-ders. In the end, the term mental disorder might be stretched so far that it loses mean-ing and is applied to virtually any form of human behavior that causes social harm orpersonal unhappiness. We need to broaden our diagnostic categories enough to includeeveryone who could benefit from help, without expanding them so far that they losemeaning. Where this balance point lies is a matter of debate. The one certainty is thatour categories will continue to change as our knowledge grows.
One other issue that deserves attention is what attitude we should take towardmental disorders. Historically, mental disorders have been a source of severe stigma,both for the person with the disorder and for the person’s family (Hinshaw, 2007).Today, the stigma associated with mental disorders may be easing. It’s now been adecade since U.S. president Bill Clinton held the first White House conference onmental health and the surgeon general of the United States wrote thefirst report on mental disorders, in which he described stigma as thegreatest obstacle to progress. Official attention to mental disorderscontinued with the President’s New Freedom Commission onMental Health (2003), and many celebrities have now come forth todescribe their experiences with mental disorders, including depres-sion (Mike Wallace, Sheryl Crow), anxiety (Kim Basinger, JohnMadden), bipolar disorder (Jane Pauley), and ADHD (MichaelPhelps) (Figure 16.36).
At the same time, the stigma of having a mental disorder persists,delaying people from seeking treatment and multiplying the distressassociated with these disorders. These issues are all the more trou-bling in light of the enormous number of people they affect:Statistics indicate that nearly half of us will develop a mental disor-der in our lifetimes, and this means that virtually every one of us
16.36 Celebrities with mental disordersIn recent years, many celebrities havecourageously shared their struggles withmental disorders including Kim Basingerand Michael Phelps.

674 chapter 16 PPSYCHOPATHOLOGYO
anxiety disorder is characterized by continuous and all-pervasive feelings of anxiety. Obsessive-compulsive disorderinvolves both obsessions (disturbing thoughts) and compulsions(ritualistic behaviors). The stress disorders result from identifi-able and horrific events such as rape or military combat.
• A number of different genes are thought to contribute to theanxiety disorders, and neuroimaging studies reveal that dif-ferent anxiety disorders have quite different biological bases.Conditioning accounts of the anxiety disorders emphasizethe role played by learning.
MOOD DISORDERS
• Mood disorders—also known as affective disorders—involvedisturbances of positive and negative mood. In major depres-sion, patients suffer periods of sadness, apathy, and lack ofenergy. In bipolar disorder, patients endure manic episodesand episodes of deep depression. Both disorders are associ-ated with a considerable suicide risk.
• Mood disorders have important hereditary components.A disruption of neurotransmission is also implicated, withnorepinephrine, dopamine, and serotonin systems involved.
• Life crises often trigger depression, although the crises bythemselves do not cause the disorder. According to AaronBeck, depression is more likely to occur if a person interpretslife events through a negative cognitive schema rather than apositive one. A related account focuses on explanatory style, orhow people explain what happens to them. Individuals whoexplain bad things that happen to them as the result ofinternal, global, and stable factors are at elevated risk ofdepression.
SCHIZOPHRENIA
• Someone suffering from schizophrenia is likely to suffer frompositive symptoms (e.g., delusions, hallucinations, disorganizedbehavior), negative symptoms (e.g., an absence of emotionalexpression), and cognitive symptoms (e.g., impairments inworking memory and attentional control).
CONCEPTIONS OF MENTAL DISORDERS
• Early views of mental disorders held to the somatogenichypothesis, which perceives the disorders as the result of aspecific injury or infection. Sigmund Freud, in contrast,argued for the psychogenic hypothesis, which considers mentaldisorders to be rooted in psychological processes.
• Modern theorists describe mental disorders using a diathesis-stress model, with the diathesis creating the predispositiontoward mental disorder, and the stress providing a trigger thatturns the risk into the actual disorder. However, the fact thatmultiple factors often give rise to both diathesis and stresshas led theorists to propose a multicausal model guided by abiopsychosocial viewpoint.
DEFINING, ASSESSING, AND DIAGNOSING MENTAL DISORDERS
• A diagnosis is generally made with reference to the categoriesidentified in the Diagnostic and Statistical Manual for MentalDisorders (DSM). The prevalence of a disorder refers to howwidespread it is. The Axis I classifications in the DSM includethe more familiar categories of mental disorders; Axis II clas-sifications describe various personality disorders.
• Assessment of any individual may include a semi-structuredinterview, which is one way in which a clinician evaluates thepatient’s symptoms and signs. The assessment may also includeself-report measures (such as the Beck Depression Inventory)or projective measures (such as the Thematic ApperceptionTest).
• Diagnostic labels have evolved over time and psychiatriclabeling has both costs and benefits.
ANXIETY DISORDERS
• Anxiety disorders are the most common mental disorder. Thephobias are characterized by intense and irrational fear, as wellas efforts to avoid the feared object or situation. Panic disorderis characterized by the occurrence of panic attacks. Generalized
S U M M A R Y C H A P T E R 1 6
either has been or will be touched—at least indirectly—by mental disorder. In thischapter, we have avoided reducing people to their disorders, and we have providedmany case vignettes both to humanize the face of mental disorders and to bring closerthe time when all of us will respond with informed compassion to those with mentaldisorders.

• Evidence suggests that genetic predisposition, a period ofdiminished oxygen supply to the newborn, and a variety ofprenatal viral infections contribute to schizophrenia. Thesefactors suggest that schizophrenia is a neurodevelopmentaldisorder, and, consistent with this view, precursors ofschizophrenia may be detected in early childhood.
• Schizophrenia involves problems with neurotransmission,with evidence coming from the efficacy of the classical antipsy-chotics. There is debate about whether the problem lies indopamine systems, glutamate systems, or both. People withschizophrenia also have defects in the structure of many areasof the brain.
• Stress also contributes to schizophrenia, and this factor isone reason schizophrenia is especially prevalent amongpeople with a low socioeconomic status.
OTHER AXIS I AND AXIS II DISORDERS
• Developmental disorders include autism and attention-deficit/hyperactivity disorder. Children with autism show arange of symptoms, including little interest in other people,marked defects in language, and peculiar movement patterns;they are often mentally retarded. Children with attention-deficit/hyperactivity disorder are impulsive, fidget constantly,and have difficulty keeping their attention focused
• Eating disorders include anorexia nervosa and bulimia nervosa.Individuals with anorexia nervosa are preoccupied with foodand eating, have an intense fear of gaining weight, and areoften severely underweight. Individuals with bulimia nervosaare also very concerned with their weight and appearance, buttypically have normal weight, and engage in binge eating fol-lowed by compensatory behaviors that include vomiting, laxa-tive use, or extreme levels of exercise.
• Dissociative disorders involve extreme responses to horrificevents. In dissociative amnesia, the person is unable to remem-ber some period of her life; in dissociative fugue, the personwanders away from home, loses track of who he is, and then,months later, realizes that he is in a strange place and doesnot know how he got there. The diagnosis of dissociativeidentity disorder—in which a person develops more than onepersonality—remains highly controversial.
• Personality disorders involve traits or habits that characterizealmost everything a person does. These disorders are difficultto diagnose, in part because the diagnostic manual describes“pure” cases and in part because the same behavior patternsoften emerge in less extreme, less disruptive forms in ordi-nary personalities.
PSummaryO 675
Go to StudySpace, wwnorton.com/studyspace, to accessadditional review and enrichment materials, including the fol-lowing resources for each chapter:
Organize• Study Plan• Chapter Outline• Quiz+ Assessment
Learn• Ebook• Chapter Review• Vocabulary Flashcards• Drag-and-Drop Labeling
Exercises• Audio Podcast Chapter
Overview
Connect• Critical Thinking Activity• Studying the Mind Video
Podcasts• Video Exercises• Animations• ZAPS Psychology Labs
O N L I N E S T U D Y T O O L S
Treatments Past and Present 678
Psychological Treatments 683
Biomedical Treatments 694
Common Factors and Combined Treatments 703
Evaluating Treatments 705
Some Final Thoughts: Far, but Not Yet Far Enough 713
Summary 714
17CH
AP
TE
R
677
CH
AP
TE
R
Treatment of Mental Disorders
We figured out it wasn’t depression after I had been
taking Prozac for about three months,” recalls Chris Clark, a restaurant owner living
in Memphis, Tennessee. Clark was a junior in college when he was diagnosed with
depression and prescribed the antidepressant Prozac. “I had spent a semester locked
in my dorm room, thinking about killing myself and feeling horribly guilty about it.”
But after taking the Prozac: “Next thing I know, I’m in Mexico, trying to open a
chain of drive-thru gourmet French restaurants with some woman I met at a club in
New Orleans.
“It seemed like a great idea at the time,” Clark muses, “despite the fact that
turning gourmet French cuisine into fast food is pretty much impossible.” After he
charged about $20,000 worth of restaurant equipment to his father’s credit card,
Clark reports, “my dad flew down, scooped me up, and deposited me directly in the
psych ward.” There, the doctors changed his diagnosis to bipolar disorder—the
mood disorder that makes people cycle between depression, mania, and normalcy—
and prescribed lithium, a mood stabilizer.
Unlike antidepressants, which can trigger a manic episode in people with bipolar
disorder, mood stabilizers regulate both the highs and the lows of the condition.
“But man, I hated that lithium,” Clark recalls. “I felt totally out of it.” Nevertheless,
he took lithium through college, eventually graduating with honors.
Once on his own, though, Clark stopped taking his meds and within a year his
mood plummeted. He reached out to a psychologist but did not disclose his

678 chapter 17 PTREATMENT OF MENTAL DISORDERSO
diagnosis of bipolar disorder. “I think I was in denial.” he says. “Somehow, depressionwas more acceptable to me than bipolar.” He also refused to take medications, optinginstead to try just talk therapy and exercise.
Two marathons and one year of therapy later, Clark was feeling good—and thentoo good. He stopped seeing his therapist, explaining that he was “cured.” He tookover a friend’s struggling restaurant and, suddenly needing only three hours of sleepper night, threw all his energy into rescuing the business. Just as the restaurant beganto rebound, though, Clark took off for a month of partying in Greece.
When he followed the trip by splurging on a vintage Camaro, Clark’s friendsconfronted him about his irresponsibility, but he didn’t listen. The restaurantfoundered. His girlfriend left him. He overdrew his bank account. Then came thecrash. “One morning, I just couldn’t get out of bed. After sleeping for 30 hours, andthen hating myself for another 10, I had to confront the truth: I have bipolar disorder,and I have to treat it, all the time, with everything I’ve got.”
Clark enlisted the help of a psychiatrist, who prescribed Lamictal, a medicationthat for many people has fewer side effects than lithium. He returned to his therapist,who helped him with his feelings of hopelessness. Through the Depression andBipolar Support Alliance he met people who understood his problems. And hesupplemented his running with adequate sleep, good nutrition, and meditation toreduce stress.
Although Clark has since opened a successful restaurant, he says, “My main jobwill always be managing my mind.” The same is true for millions who struggle withpsychological disorders. As this chapter shows, people now have more and betteroptions for doing this job than ever before. Just as Clark relies on medication, talktherapy, social support, and a healthy lifestyle to manage his bipolar disorder, so domany people combine treatments to suit their individual needs. The mind, after all, isa biological, psychological, and social achievement, so mental health requiresbiological, psychological, and social balance.
The previous chapter described a number of mental disorders that can causeextreme suffering and disrupt people’s lives, making it hard to hold a job, sustain arelationship, or, in some cases, manage the basics of day-to-day life. Because manyfactors give rise to these disorders, the different approaches to treatment each have adistinct focus. Practitioners who rely on psychological approaches employ variouskinds of psychotherapy. Others favor biomedical interventions such as medications.Still others use an amalgam of psychological and biomedical treatments. Do thesetreatments help? Are some better than others? This chapter will examine the optionsfor treatment and look at the evidence that the right treatments often can genuinelyimprove the lives of people with mental disorders.
TREATMENTS PAST AND PRESENT
Mental disorders have been with us since the dawn of recorded history. So too haveefforts to alleviate the suffering—as well as the problematic behaviors—associatedwith these disorders. Early treatments stemmed from the view that mental disorderswere caused by evil spirits, and these treatments were often harsh and rarely effective.As our understanding of mental disorders grew, other (often more humane) treatmentsdeveloped. In this chapter, we will examine two major types of treatments—

PTreatments Past and PresentO 679
psychological and biomedical—and assess whether these treatments work as intended.Before doing so, we first set the stage by considering historical trends as well ascontemporary practices.
Early Treatments for Mental Disorders The early idea that mental disorders were caused by evil spirits suggested a number ofstrategies for treatment. In some cases, large holes were cut in a person’s skull, so thatthe demons could be driven out through this “exit.” Other treatments sought tocalm the demons with music, to chase them away with prayers, or to purge them withpotions that induced vomiting. Another approach was to make the evil spirits souncomfortable in the patient’s body that they would be induced to flee. Accordingly,patients were starved, flogged, or immersed in boiling water. Not surprisingly, thesetreatments did not work and often made patients worse.
As we saw in Chapter 16, recent centuries have seen the rise of a very different con-ception of mental illness, one that treats mental disorders as physical diseases like anyother. Unfortunately, this conception has not always lead to more humane treatmentof the afflicted. In the Middle Ages, diseased “madmen” were given little sympathy,and the interests of society were deemed best served by “putting them away.”Beginning in the 16th century, a number of special hospitals for the insane were estab-lished throughout Europe (Figure 17.1). But most of these institutions were hospitalsin name only. Their real function was to confine all kinds of social “undesirables”and isolate them from the rest of humanity. Criminals, beggars, epileptics, and“incurables” of all sorts were institutionalized and treated along with the mentallydisturbed. And the treatments were barbaric. One author described conditions in themajor mental hospital for Parisian women at the end of the 1700s: “Madwomenseized by fits of violence are chained like dogs at their cell doors, and separated fromkeepers and visitors alike by a long corridor protected by an iron grille; through thisgrille is passed their food and the straw on which they sleep; by means of rakes, partof the filth that surrounds them is cleaned out” (Foucault, 1965, p. 72).
Gradually, reformers succeeded in eliminating the worst of these practices. TheFrench physician Philippe Pinel (1745–1826), for example, was put in charge of theParisian hospital system in 1793, at the height of the French Revolution. Pinel wantedto remove the inmates’ shackles and chains and give them exercise and fresh air; thegovernment permitted these changes—although only grudgingly. A half century later,in the United States, a retired schoolteacher named Dorothea Dix became a passionate
17.1 Early mental institutions The tarotcard (left) shows a 16th-century depictionof a madhouse. The painting (right) showsLondon’s Bethlehem Hospital (known asBedlam, as it sounds when pronouncedwith a Cockney accent), where patientswere exhibited as though they were zooanimals to anyone curious enough to paythe required penny per visit. In 1814, therewere 96,000 such visits. (William Hogarth,The Rake’s Progress: The Rake in Bedlam[1735])

680 chapter 17 PTREATMENT OF MENTAL DISORDERSO
advocate for appropriate treatment for the mentally ill. In her report to theMassachusetts legislature in 1843, Dix said: “I come as the advocate of helpless, forgot-ten, insane, and idiotic men and women; of beings, sunk to a condition from which themost unconcerned would start with a real horror. . . . I proceed, Gentlemen, briefly tocall your attention to the present state of Insane Persons confined within thisCommonwealth, in cages, closets, cellars, stalls, pens! Chained, naked, beaten with rods, andlashed into obedience” (Shannonhouse, 2000, pp. 8–11). Dix’s report is, of course, apowerful indictment of the treatment of the mentally ill in 19th-century America, andfortunately the indictment had an effect. Dix’s tireless work on behalf of the mentally illwas an important impetus to the dramatic growth of state-supported institutions formental care during the latter part of the 19th century.
Amid calls for reform, other developments in the 19th century profoundly shaped howpeople thought about, and tried to treat, mental illness. One triumph was the treatmentof paresis (see Chapter 16). This was important for its own sake, but it can also be under-stood as the leading edge of a much larger trend, and, across the next decades, it becamemore and more common to take a medical perspective on mental illness—in many cases,this meant treatment via medications of one sort or another. Another major develop-ment, also at the end of the 19th century, was the advent of Freud’s “talking cure.” Thistreatment proved to be the first in a long line of psychological therapies, whichcollectively drew attention to the environmental and social dimensions of mental illnessand provided many powerful tools for treating mental disorders.
Current Treatments for Mental Disorders As we saw in Chapter 16, mental disorders typically involve many factors, some biolog-ical and some rooted in a person’s circumstances. Different treatments target differentaspects of this network of interrelated causes. Psychological treatments aim to alterpsychological and environmental processes via “talk therapy.” Biomedical treatmentsseek to alter underlying biological processes directly, often through medication orneurosurgery.
For convenience, we will use this distinction between psychological and biomedicaltreatments in this chapter. However, this shorthand does risk introducing someconfusion. If we focus narrowly on the overt steps in treatment, we can distinguishpsychological approaches (talking to a patient, perhaps leading her to new insights or newbeliefs) from biomedical approaches (perhaps prescribing a pill for the patient to taketwice a day). However, if we broaden our focus, the distinction between the psychologicaland the biological becomes less clear-cut. After all, psychological processes are the prod-ucts of functioning brains—and so changes in people’s psychology necessarily involvechanges in their brain. Hence psychological treatments have biological effects. Conversely,biomedical treatments may in many cases work by altering a person’s thought processes orshifting a person’s mood; for this reason, the biological treatments often need to be under-stood in “psychological” terms. In either direction, therefore, a distinction between “psy-chological” and “biological” treatments is somewhat artificial (Kumari, 2006). Inaddition, as we will see, contemporary treatments often combine talk therapy with med-ication, further blurring the line between psychological and biological treatment.
That said, it is still useful to distinguish between treatments that emphasize psycho-logical approaches and those that emphasize biological approaches, and this leads us toask: How does a practitioner decide which emphasis is best in a given case? The answerdepends on the illness and our understanding of its causes. If the illness seems shapedprimarily by environmental causes (such as a hostile family environment) or by theperson’s perceptions and beliefs, then a psychological intervention may be best—

PTreatments Past and PresentO 681
helping the person to find ways to cope with (or change) the environment, or persuad-ing the person to adopt new beliefs. If the illness seems shaped primarily by somebiological dysfunction (perhaps an overreactive stress response, for example, or a short-age of some neurotransmitter), then a biomedical intervention may be preferable.
However, these points are at best rough rules of thumb. In many cases, there may beno direct correspondence between what triggers a disorder (a specific biologicaldysfunction or some life problem) and the nature of the treatment. Some problemsarising from a difficult situation are best treated medically; some problems arising froma biological dysfunction are best treated with psychotherapy. In choosing a form oftherapy, practitioners must focus on what works, rather than focusing exclusively onhow the disorder arose.
T R E AT M E N T P RO V I D E RS
We will have a great deal to say in this chapter about these two broad emphases intreatment—the psychological and the biological—and the specific ways that treatmentunfolds. Before we turn to these details, let’s consider the providers and recipients ofthese treatments.
An extraordinarily wide range of professionals and non-professionals provide treat-ments for mental disorders. Individuals licensed to provide psychological treatmentsinclude clinical psychologists; psychiatrists; psychiatric nurses; marriage, family, andchild counselors; school and vocational counselors; mental health counselors; andclinical social workers. Psychological interventions are also administered by individu-als with varying degrees of psychological training including pastoral counselors, reli-gious leaders, and paraprofessionals. A description of each of these treatment providersis given in Table 17.1.
Clinical psychologist Assessment and psychological Private practice, medical centers, agencies,treatment clinics, schools
Psychiatrist Assessment and psychological Private practice, medical centers, clinicsand biological treatment
Neurologist Assessment and treatment, with a Private practice, medical centers, clinicsfocus on the brain and nerves
Psychiatric nurse Assessment and psychological and Medical centers, clinicsbiological treatment
Marriage, family, and child Psychological treatment, with a focus Private practice, clinicsCounselor on couples, families, and children
School and vocational counselor Assessment and counseling, with a Schoolsfocus on vocation and adjustment
Mental health counselor Assessment and counseling Private practice, medical centers, agencies,clinics
Clinical social worker Psychological treatment and assistance Private practice, medical centers, agencies,with housing, health care, and treatment clinics
Pastoral counselor Counseling and support, with a focus Religious institutions, medical centerson spiritual well-being
Treatment Providers
TABLE
17.1 Occupation Duties Setting

682 chapter 17 PTREATMENT OF MENTAL DISORDERSO
Surprisingly, more experienced providers are not always more effective than lessexperienced providers (McFall, 2006), and even professional credentials are not neces-sarily a good predictor of therapeutic success (Blatt, Sanislow, Zuroff, & Pilkonis,1996). These findings suggest that who the therapist is, what he or she does, and howwell this matches the patient’s needs may be far more important than the therapist’slevel of experience or the degrees he has earned. Also crucial is the quality of the rapportthe therapist establishes with the patient—whether the patient respects and trusts thetherapist and feels comfortable in the therapeutic setting. This rapport, too, is oftenmore important than the therapist’s credentials or type and degree of training.
Psychological treatments can be administered either with or without a license (withthe license usually given by the state in which the therapist is practicing). In clear con-trast, the administration of biomedical treatments does require a license. Here too,however, there are many different providers, including psychiatrists, neurologists, andpsychiatric nurses. In fact, this list has been growing, with some jurisdictions now per-mitting “prescription privileges” for clinical psychologists—that is, allowing peoplewith Ph.D.s to write prescriptions, a privilege that used to be reserved for people withmedical degrees.
T R E AT M E N T R E C I P I E N TS
People seek treatment for a wide variety of reasons. Some seek relief from the pain anddysfunction associated with a diagnosable mental disorder. Others suffer with subsyn-dromal disorders—versions of mental disorders that don’t meet the criteria for diag-nosis but that may nonetheless cause significant problems (Ratey & Johnson, 1997).Others have neither a full-fledged nor a sybsyndromal disorder but instead seek helpwith feelings of loss, grief, or anxiety, with relationship difficulties, or with confusionabout a major life decision. Still others seek therapy in order to live happier and morefulfilled lives.
Just as important is a listing of people who might benefit from therapy but don’t seekit. Surveys reveal that in the United States, only about 40% of those with clinicallysignificant disorders (such as depression, anxiety, or substance use disorders) hadreceived treatment in the past year (Wang, Bergulund, et al., 2005). Women are more likely than men to seek treatment (Addis & Mahalik, 2003; Wang, Berglund, etal., 2005), and European Americans are more likely to seek treatment than AsianAmericans and Hispanic Americans (Sue & Lam, 2002; Wang, Berglund, et al., 2005).
There is yet another (and very large) group of people who might benefit from therapy but cannot get it. According to the World Health Organization, roughly 450 million people worldwide suffer from various mental disorders, and the clearmajority live in developing countries—90% of these people have no access to treat-ment (Miller, 2006b). Access is also an issue in developed countries. Many forms ofmental illness are more common among the poor, but the poor are less likely to haveinsurance coverage that will make the treatment possible (Wang, Lane, et al., 2005).
CU LT U R A L CO N S I D E R AT I O N S
Some of the problems just described could—in theory—easily be solved. We couldtrain more therapists and open more clinics so that treatment would be available tomore people. We could improve insurance coverage or arrange for alternative forms offinancing. These steps, however, would not be sufficient, because there is still anotherfactor that limits the number of people who can benefit from therapy: the limitedavailability of culturally appropriate therapy and culturally competent therapists.
subsyndromal disorder An instanceof a mental disorder in which someonedoes show symptoms, but not at alevel of intensity, frequency, or dura-tion that would justify a formaldiagnosis.
PPsychological TreatmentsO 683
A therapist shows cultural competence by understanding how a patient’s beliefs,values, and expectations for therapy are shaped by his cultural background (Sue, 1998).A therapist with this understanding can modify the goals of therapy to conform to thepatient’s values (Hwang, 2006). For example, many Asian cultures emphasize formal-ity in all their affairs. Social roles within these cultures are often clearly defined andtend to be structured largely by age and sex, such that a father’s authority is rarely chal-lenged within the family. Growing up in such a culture may play an important part inshaping the values a patient brings to therapy. A therapist insensitive to these valuesrisks offending the patient and endangering the therapy. Similarly, a therapy thatemphasizes individual autonomy over family loyalties might inadvertently violate thepatient’s cultural traditions and so be counterproductive.
Cultural sensitivity also includes other issues. For example, therapists who expecttheir patients to take responsibility for making changes in their lives may be ineffectivewith patients whose cultural worldview stipulates that important events are caused byfactors such as fate, chance, or powerful others. Likewise, practitioners who considerpsychotherapy a secular endeavor would do well to remember that in many cultures, anykind of healing must acknowledge the patient’s spirituality.
Attention to such cultural differences may also be valuable for another reason: it’spossible that the Western world can learn something about the treatment of mentaldisorders from the cultures in developing countries. For example, the long-term prog-nosis for schizophrenia is considerably better in developing countries than it is in theUnited States (Thara, 2004). Patients with schizophrenia in India, as one illustration,show far more remission of symptoms and fewer relapses than patients with schizo-phrenia in the United States and often recover enough to hold a full-time job, marry,and otherwise lead reasonably normal lives.
Why is this? Some suggest that physicians in the United States rely too much onmedication in treating schizophrenia and too little on interventions that emphasize jobtraining and a supportive social network. The opposite is the case in India, where med-ication is often not available and institutionalization is usually not an option. Indeed,it is estimated that roughly 99% of individuals with schizophrenia live with their fam-ilies in India, compared with 15 to 25% in the United States (Thara, 2004). Of course,the style of treatment in the United States is encouraged by many factors, includingfamilies that may want to distance themselves from the patient and insurance compa-nies that will reimburse patients for psychotropic drugs but hesitate to pay for socialprograms.
It seems, then, that cultural competence needs to be broadly understood. It includesthe need for Western-style practitioners to be alert to the cultural background (and soto the assumptions, beliefs, and values) of their patients. But it also includes an open-ness to the possibility that the style of treating mental illness in other cultures may, forsome disorders, be preferable to the methods used in the developed countries. We needto keep these points in mind as we turn to a consideration of what the various forms oftreatment involve.
PSYCHOLO GICAL TREATMENTS
Psychological treatments involve systematic efforts to change a patient’s thinking andbehavior, usually by means of some form of discussion, instruction, or training. In theminds of many people, psychotherapy involves a patient lying on a couch, talking abouthis distant childhood, and a therapist quietly drawing conclusions about unconscious
cultural competence An under-standing of how a patient’s culturalbackground shapes his beliefs, values,and expectations for therapy.

684 chapter 17 PTREATMENT OF MENTAL DISORDERSO
fears or desires (Figure 17.2). This image fails to do justice to the fact that psychother-apy comes in over 500 forms (Eisner, 2000). Indeed, the form of therapy implied bythis common image is actually quite rare.
Some forms of psychotherapy are based on psychoanalysis; these are the closest tothe popular image of therapy, emphasizing unconscious conflicts and encouragingintrospection and insight. Other modes of therapy grow out of the humanistic tradi-tion and focus on questions of growth and realizing one’s potential. Still others rely onbehavioral findings from human and nonhuman experimentation; these seek to iden-tify maladaptive responses and then teach new responses. Others take a cognitiveapproach, focusing on the disabling role of faulty thinking while teaching more rationalthought. In what follows, we will discuss some of the more common modes of psy-chotherapy that have grown out of each of these various approaches.
Psychodynamic ApproachesPsychodynamic approaches to therapy have their origins in the psychoanalytic methodthat Sigmund Freud developed at the beginning of the twentieth century. Freud’s basicassumption was that a patient’s ills (in Freud’s terms, her neuroses) stemmed fromunconscious conflicts that developed early in childhood (see Chapter 15). By adulthood,the patient had developed a range of defenses to deal with these conflicts, but thesedefenses also shielded her from seeing clearly both the outer world and her own innerworld. This led to a range of problems that manifested as psychological symptoms.
Freud believed that for a patient to overcome her neuroses, she must gain insightinto her own buried thoughts and wishes. Importantly, though, this insight cannot bejust an intellectual matter. Freud argued that the person must “work through” theconflict, in order to gain control over her passions and not just intellectualize them. Ifthis working through is successful, the person will integrate her thoughts and memo-ries in a coherent way, and will at last overcome the maladaptive patterns that grew outof the unresolved conflicts.
What does it mean to “work through” a conflict? For Freud, the process involvedmany elements, but one crucial aspect is transference, the patient’s tendency torespond to the analyst in ways that re-create her responses to the major figures in herown life. Thus, the patient ends up loving or hating the analyst just as she loved orhated her mother, father, siblings, and, more recently, her lovers or friends. All of thesefeelings are “transferred” to the analyst, as a kind of repetition of the unresolved prob-lems of the patient’s childhood.
Freud argued that the transference-charged relationship with the analyst could be apowerful therapeutic tool. It lets the analyst hold up a mirror to the patient to show herhow she really feels and acts toward the important people in her life. For example, takea person who expresses violent anger toward his psychoanalyst and then is immediatelyanxious. How would his analyst interpret this? Perhaps the patient is reacting to theanalyst much as he would respond to his tyrannical father, and having acted with dis-respect, is now expecting some horrible retribution. Needless to say, the analyst will notact like Daddy, but instead might say something mildly reassuring, such as “That washard to get out, wasn’t it?” The analyst might then point out how the patient’s trau-matic memories of Daddy (and, more generally, the pattern of the patient’s past rela-tionships) are distorting his current relationships.
Through many such experiences, the patient’s symptoms lessen. By maintaining herneutrality, the analyst allows herself temporarily to stand in for the significant charac-ters in the patient’s early family drama but does not let herself be drawn into the play.
17.2 Psychologist as comic book hero?Popular portrayals of psychotherapy have along history in the media; this comic bookseries appeared in 1955.
psychodynamic approachesApproaches to therapy that arederived from psychoanalytic theory,which asserts that clinical symptomsarise from unconscious conflictsrooted in childhood.
transference A patient’s tendency torespond to the analyst or therapist inways that re-create her responses tomajor figures in her life.

PPsychological TreatmentsO 685
She lets the patient say the same old lines and go through the sameold motions, but she does not respond to them as the cast of charac-ters from the patient’s childhood did. Her job is to let the patient seewhat she is really doing and to help the patient see that old patternsneed not be repeated. The result of all this emotional reeducation isthe creation of a new life script with better lines and more acceptableoutcomes.
Many present-day psychotherapists use techniques that bearFreud’s imprint, but they have modified the treatment in variousways. Most have stepped away from the intensity of Freud’s regimen(he insisted on at least three sessions per week) and abandoned thefamiliar icon of Freud’s practice—the analyst’s couch (which, inFreud’s office, allowed the patient to relax while Freud sat in a posi-tion out of the patient’s sight; Figure 17.3). These more modern prac-titioners endorse many of Freud’s claims, they tend to emphasizecurrent interpersonal and cultural factors rather than the psycholog-ical traumas of early childhood. If they discuss early development with their patients, itis strictly to identify how the patterns of interaction established in childhood influencecurrent choices. In these more modern therapies, conscious thoughts receive as muchscrutiny as unconscious conflicts, and therapist and patient work together to help thepatient develop a coherent and complete sense of self, and to find ways of relating to oth-ers that are undistorted by past conflicts or maladaptive defense mechanisms.
In Chapter 15, we discussed the fact that many of the neo-Freudian traditionsemphasize an individual’s social relationships. These more modern approaches have ledto several forms of therapy, including interpersonal therapy (IPT), a brief (12- to16-session) treatment that builds on the claim that mental disorders are often createdby a social isolation that cuts a person off from the emotional sustenance provided byhealthy relationships (Klerman & Weissman, 1993; Weissman & Markowitz, 1994).
IPT is often used as a treatment for depression, and so a course of IPT might startwith an assessment of what factors changed in the person’s life at the time the depres-sion began. For example, one class of factors involves interpersonal role transitions,such as graduation from college, beginning a love affair, or getting married. The thera-pist can help a person having trouble with these transitions learn to act the new partand fill the expectations of the other people involved in the new social setting. (Thus,for example, a recently married man must learn what it means to be a husband.) Thetherapist will also help the patient understand the advantages and disadvantages ofboth the old and the new roles. In these ways, the therapy helps the patient gain anunderstanding of how he interacts with others and then helps him learn new and morebeneficial ways of interacting and communicating.
Humanistic ApproachesWe have seen that Freud played a pivotal role in launching the treatment that we now callpsychotherapy; indeed, the idea of a “talking cure” that could help someone deal withmental distress through conversation or instruction was essentially unknown beforeFreud. Nonetheless, most modern psychotherapists employ methods very different fromFreud’s and base their therapies on conceptions that explicitly reject many of Freud’s ideas.
As we discussed in Chapter 15, psychologists who take a humanistic approach haveregarded psychoanalysis as being too concerned with basic urges (like sex and aggres-sion) and not concerned enough with the search for meaning. This orientation led
17.3 Extensions of psychotherapy Evenpets can benefit from a good therapist.
interpersonal therapy (IPT) A formof therapy focused on helping thepatient understand how she interactswith others and then learn better waysof interacting and communicating.
humanistic approach An approachto therapy centered around the ideathat people must take responsibilityfor their lives and actions.

686 chapter 17 PTREATMENT OF MENTAL DISORDERSO
them to propose several different types of therapy, which have in common theidea that people must take responsibility for their lives and their actions and livefully in the present.
Carl Rogers’s client-centered therapy seeks to help a person accept himself as heis and to be himself with no pretense or self-imposed limits. In this therapy, the ther-apist listens attentively and acceptingly to the patient (Figure 17.4). The therapist isnot there to question or to direct, but to create an atmosphere in which the patientfeels valued and understood (Rogers, 1951, 1959). Based on his analysis of his ownand others’ therapeutic attempts, Rogers concluded that three factors were crucial toa therapist’s success: genuineness, or sharing authentic reactions with the patient;unconditional positive regard, which refers to a nonjudgmental and accepting stance;
and empathic understanding, which refers to sensing what it must be like to be in the patient’sshoes (Rogers, 1980).
Rogers’s therapeutic stance is evident in the following interaction with a patient:
PATIENT: I cannot be the kind of person I want to be. I guess maybe I haven’t the guts orthe strength to kill myself, and if someone else would relieve me of the responsi-bility or I would be in an accident, I—just don’t want to live.
ROGERS: At the present time things look so black that you can’t see much point in living.PATIENT: Yes, I wish I’d never started this therapy. I was happy when I was living in my
dream world. There I could be the kind of person I wanted to be. But now thereis such a wide, wide gap between my idea and what I am . . .
ROGERS: It’s really tough digging into this like you are, and at times the shelter of yourdream world looks more attractive and comfortable.
PATIENT: My dream world or suicide . . . So I don’t see why I should waste your time coming in twice a week—I’m not worth it—what do you think?
ROGERS: It’s up to you. . . . It isn’t wasting my time. I’d be glad to see you whenever youcome, but it’s how you feel about it.
PATIENT: You’re not going to suggest that I come in oftener? You’re not alarmed and thinkI ought to come in every day until I get out of this?
ROGERS: I believe you’re able to make your own decision. I’ll see you whenever you want to come.
PATIENT: I don’t believe you are alarmed about—I see—I may be afraid of myself but youaren’t afraid for me.
ROGERS: You say you may be afraid of yourself and are wondering why I don’t seem to beafraid for you.
PATIENT: You have more confidence in me than I have. I’ll see you next week, maybe.
[The patient did not attempt suicide.] (Rogers, 1951, p. 49)
Rogers’s client-centered therapy has, in turn, inspired a number of other forms ofintervention, one of which is motivational-enhancement therapy (Miller & Rollnick,2002). This is a brief, nonconfrontational, client-centered intervention designed tochange problematic behavior (such as alcohol and other drug use) by reducing ambiva-lence and clarifying discrepancies between how individuals are actually living and howthey say they would like to live (Ball et al., 2007).
A second humanistic therapy is Fritz Perls’s Gestalt therapy. Perls was a highlycharismatic and original clinician who was trained psychodynamically but drew inspi-ration from the gestalt theory of perception (Chapter 5). Perls believed that psycho-logical difficulties stemmed from a failure to integrate mutually inconsistent aspectsof self into an integrated whole or gestalt. His techniques were aimed at helping
17.4 Active listening Carl Rogers (right)empathizes with a client during this grouptherapy session.
client-centered therapy A form ofhumanistic therapy associated withCarl Rogers, in which the therapist’sgenuineness, unconditional positiveregard, and empathic understandingare crucial to therapeutic success.
motivational-enhancement therapyA brief, nonconfrontational, client-centered therapy designed to changespecific problematic behaviors such asalcohol or drug use.
Gestalt therapy A form of humanis-tic therapy associated with Fritz Perlsthat aims to help the patient integrateinconsistent aspects of herself into acoherent whole by increasing self-awareness and self-acceptance.

PPsychological TreatmentsO 687
patients become aware of and then integrate disparate aspects of self by increasingself-awareness and self-acceptance (Perls, 1967, 1969).
For example, Perls was famous for asking his patients about what they were feelingin the moment, and for pointing out apparent discrepancies between what they saidthey felt and how they appeared to be feeling. Perls also used the empty chair technique,in which a patient imagines that he is seated across from another person, such as hisparent or his partner, and tells him honestly what he feels. Using such strategies, Perlshelped his patients acknowledge and confront their feelings.
In more modern versions of humanistic therapies—collectively referred to as theexperiential therapies—these approaches are integrated, seeking to create a genuinelyempathic and accepting atmosphere but also to challenge the patient in a more activefashion with the aim of deepening his experience (Elliott, Greenberg, & Lietaer, 2004;Follette & Greenberg, 2005). This approach views the patient and, indeed, all humansas oriented toward growth and full development of their potential, and the therapistuses a number of techniques to encourage these tendencies.
Although these challenges to live more actively and deeply can be disconcerting,experiential therapies involve genuine concern and respect for the person, with anemphasis on all her qualities, and not just those symptoms that led to a particulardiagnosis. The person’s subjective experience is also a primary focus, and the thera-pist tries to be as empathic as possible, in order to understand that experience.Moreover, experiential therapists reject Freud’s notion of transference; in their view,the relationship between patient and therapist is a genuine connection between two people, one that provides the patient with an opportunity for a new, emotionallyvalidating experience.
Behavioral Approaches Like the humanistic therapies, behavior therapies emerged in part asa reaction to the Freudian tradition of psychoanalysis (Figure 17.5).But while the humanists regarded psychoanalysis as too mechanis-tic, the behavior theorists, ironically, offered exactly the opposite crit-icism; they regarded psychoanalysis as too loose and unscientific.
Behavior therapists focus on overt behavior rather than uncon-scious thoughts and wishes, which they regard as hard to define andimpossible to observe. The patient’s behaviors, in other words, arenot regarded as “symptoms” through which one can identify andthen cure an underlying illness. Instead, these therapists view themaladaptive behaviors themselves as the problem to be solved. Thesebehaviors, in turn, are, from a behaviorist’s perspective, simply theresults of learning—albeit learning that led the person to undesiredor undesirable behaviors.
The remedy, therefore, involves new learning, in order to replace old habits withmore effective or adaptive ones. For this purpose, the therapeutic procedures draw onthe principles of behavior change that have been well documented in the laboratory—classical conditioning, operant conditioning, and modeling, as discussed in Chapter 7.
C L ASS I CA L CO N D I T I O N I N G T E C H N I Q U E S
To see how behavior therapy proceeds, consider the treatment for specific phobias(Emmelkamp, 2004; Wolpe & Plaud, 1997). According to behavior therapists, the irra-tional fears that characterize these phobias are simply classically conditioned
experiential therapies A family oftherapies that seek to create anempathic and accepting therapeuticatmosphere, while challenging thepatient to deepen his experience.
17.5 Therapeutic approaches

688 chapter 17 PTREATMENT OF MENTAL DISORDERSO
responses, evoked by stimuli that have become associated with a truly fearful stimulus(see Chapters 7 and 16). The way to treat these phobias, therefore, is to break the con-nection between the phobic stimuli and the associated fears, using a technique akin tothe extinction procedures that are effective in diminishing conditioned responses in thelaboratory.
One early version of this procedure is the technique originally known as systematicdesensitization, now referred to as exposure therapy. Here, the therapist seeks notonly to break the connection between the phobic stimulus and the fear response butalso to create a new connection between this stimulus and a different response, onethat is incompatible with fear and will therefore displace it (Figure 17.6). The newresponse is usually deep muscular relaxation, and the patient is taught a relaxationtechnique, typically through meditation-like exercises, before the formal therapybegins. Then, once the patient has learned to relax deeply on cue, the goal is to condi-tion this relaxation response to the stimuli that have been evoking fear.
To begin the therapy, the patient constructs an anxiety hierarchy, in which feared sit-uations are identified and then ranked from least to most anxiety provoking. This hier-archy is then used to set the sequence for therapy. The patient starts out by imaginingthe first scene in the hierarchy (e.g., being on the first floor of a tall building) while ina state of deep relaxation. He will stay with this scene—imagining and relaxing—untilhe no longer feels any anxieties. After this, he imagines the next scene (perhaps look-ing out a fourth-floor window in the building), and this scene, too, is thoroughly “counter-conditioned,” meaning that the old link between the scene and an anxiety response isbroken, and a new link between the scene and a relaxation response is forged. Theprocess continues, climbing up the anxiety hierarchy until the patient finally can imag-ine the most frightening scene of all (leaning over the railing of the building’s observa-tion tower, more than 100 floors above the ground) and still be able to relax.
Sometimes this imagined exposure is sufficient to treat the phobia, but oftenpatients need to extend the graduated exposure to the real world—for example, actu-ally visiting a tall building rather than merely thinking about one. This process, calledin vivo desensitization, may take place with the therapist present or may use guidedhomework assignments (Figure 17.7; Craske, 1999; Goldfried & Davison, 1994). Inaddition, interactive computer graphics now provide yet another option: exposing thepatient to a virtual-reality version of the frightening stimulus, which seems to beanother way to extend and strengthen the desensitization procedure (Figure 17.8;see, for example, Emmelkamp et al., 2002). However the feared stimulus or situation ispresented, exposure is a key ingredient in therapeutic success.
17.6 Exposure therapy Exposure therapy begins with the construction of an anxiety hier-archy, in which feared objects or situations are ranked from least to most anxiety-producing. While maintaining a state of relaxation, the patient then calls to mind eachobject or situation in turn, and process which often culminates in actually encountering thefeared object or situation.
17.7 In vivo desensitization
String Worm Handling aworm Snake
Handling asnake
1 2 3 4 5 6
exposure therapy A behavior ther-apy that aims to remove the anxietyconnected to a feared stimulus bygradually conditioning relaxedresponses to the stimulus.
in vivo desensitization One keystep in the behavioral treatment of aphobia in which the patient is gradu-ally exposed to the phobic stimulus.

PPsychological TreatmentsO 689
O P E R A N T CO N D I T I O N I N G T E C H N I Q U E S
A second set of behavioral techniques is based on the principles of instrumental oroperant conditioning. These techniques aim to change behavior through reinforcementby emphasizing the relationship between acts and consequences.
An example of this approach is the use of token economies in hospital psychiatricwards. In these settings, patients earn the tokens through various helpful or healthybehaviors such as making the bed, being neatly dressed, or performing ward chores.They can then exchange tokens for desirable items, such as snacks or the chance towatch TV. In this fashion, the patient is systematically rewarded for producing desirablebehaviors and is not rewarded for producing undesirable ones.
As in the learning laboratory, the reinforcement contingencies can then be gradu-ally adjusted, using the process known as shaping. Early on, the patient might be rein-forced merely for getting out of bed; later, tokens might be awarded only for gettingout of bed and walking to the dining hall. In this fashion, the patient can be led, step-by-step, to a higher level of functioning. The overall effects of this technique are thatthe patients become less apathetic and the general ward atmosphere is muchimproved (Higgins, Williams, & McLaughlin, 2001).
Other reinforcement procedures can be useful in individual behavior therapy as partof contingency management. In this procedure, the person learns that certain behav-iors will be followed by strict consequences (Craighead, Craighead, Kazdin, &Mahoney, 1994). For example, a child who is oppositional and defiant can be presentedwith a menu of “good behaviors” and “bad behaviors,” with an associated reward andpenalty for each. Being a “good listener” can earn the child the chance to watch a video,cleaning up her room every day can get her a dessert after dinner, and so forth, whereastalking back to Mom or making a mess may result in an early bedtime or a time-out inher room. The idea is not to bribe or coerce the child but to show her that her actionscan change the way people react to her. Ideally, her changed behavior will result in amore positive social environment that will eventually make explicit rewards and pun-ishments unnecessary.
These operant techniques have been applied to a number of mental disorders. In onestudy, parents spent 40 hours a week attempting to shape the behavior of their uncom-municative 3-year-olds who had autism (Lovaas, 1987). By first grade, more than half ofthe children were functioning successfully in school, and these treatment gains were stillevident four years later (McEachin, Smith, & Lovaas, 1993). In a group of 40 compara-ble children who did not receive this intervention, only one child showed comparableimprovement by first grade. Others have applied this technique to other serious mentaldisorders such as mental retardation, with positive results (Reid, Wilson, & Faw, 1991).
17.8 High-tech therapy A common way to treat anxietyis to expose patients gradually to the anxiety-provokingstimulus. Psychologists sometimes use virtual-reality dis-plays, like this combat scene, to make the exposuresmore and more realistic as the therapy progresses.
token economy A behavioral ther-apy technique based on operant con-ditioning in which patients’ positivebehaviors are reinforced with tokensthat they can exchange for desirableitems.
contingency management A formof behavior therapy in which certainbehaviors are reliably followed bywell-defined consequences.
690 chapter 17 PTREATMENT OF MENTAL DISORDERSO
M O D E L I N G T E C H N I Q U E S
One last (and powerful) technique for the behavior therapist is modeling, in whichsomeone learns new skills or changes his behavior by imitating another person (Figure17.9). Sometimes, the therapist serves as the model, but this need not be the case.Therapy with children, for example, may draw on young “assistants” (children roughlythe same age as the child in therapy) who work with the therapist and model the desiredbehaviors or skills.
Modeling is not limited to overt behaviors; a therapist can also model a thoughtprocess or a decision-making strategy. In some forms of therapy, the therapist “thinksout loud” about commonplace decisions or situations, in this way providing a model forhow the patient should consider similar settings (Kendall, 1990; Kendall & Braswell,1985). Likewise, modeling can be used for emotional responses, so that, for example, thetherapist can model fearlessness in the presence of some phobic stimulus and in thisfashion diminish the phobia (Bandura, 1969, 2001).
Modeling can also be supported by vicarious reinforcement, a procedure in whichthe patient sees the model experience some good outcome after exhibiting the desiredbehavior or emotional reaction. Like other forms of reinforcement (Chapter 7), vicari-ous reinforcement seems to increase the likelihood that the person in therapy will laterproduce the desired behavior or reaction.
Cognitive-Behavioral ApproachesIn its early versions, behavior therapy focused on overt behaviors and regarded a per-son’s inner thoughts and feelings as unimportant, and, in any case, not somethingthat could be studied or influenced directly. Several decades ago, however, behaviortherapists started to broaden their view, realizing both that thoughts and perceptionsdo matter and that some of the techniques they had already developed could beapplied to these mental events in much the same way they are applied to behaviors.This is obvious in the case of modeling, for example, in which the target for change isoften how someone thinks or feels. However, the same is true for operant techniques,which also can be used to encourage more positive self-evaluations and various adap-tive strategies.
In the 1950s, Albert Ellis began to focus on the role cognitions play in causing psy-chological difficulties (Ellis, 1962). He expounded an approach that is now known asrational emotive behavioral therapy. In Ellis’s view, people typically believe that thethings that happen to them (such as being ignored at a party by a roommate) directlylead them to feel or behave in certain ways (such as feeling angry). One way of puttingthis idea is that people believe that an activating event, which we can call A, leads to aconsequence, which we can call C.
Ellis made the point that if this were true—that A directly caused C—then everyoneshould respond the same way to activating event A each time A occurs. It’s obvious,however, that neither of these things is true. Why not? According to Ellis, what peoplefail to notice is the hidden element tucked between the A and the C, namely, a belief, orB. That is, Ellis argued that the A never has the power to cause us to feel or behaveunless there’s also a belief that translates A into C, leading to an A : B : C sequence.Different people can react to A in different ways because they have their own distinctbeliefs. Individuals’ beliefs can also change, leading to new consequences the next timethey encounter the activating event.
Ellis claimed that these beliefs, linking activating events to consequences, are oftenthe cause of the problems that lead people to seek therapy. In particular, Ellis suggested
17.9 Modeling By watching another per-son’s behavior, a patient learns new skillsand behavior patterns.
rational emotive behavioraltherapy A form of cognitive therapyassociated with Albert Ellis, in whichthe therapist actively challenges thepatient’s irrational beliefs.

PPsychological TreatmentsO 691
that some people have highly irrational beliefs, such as “Everything I do must be per-fect” or “I must be in complete control at all times.” Ellis viewed these beliefs as thesource of a person’s problems and targeted them with his clinical intervention.
To the A : B : C sequence Ellis added D (disputing the irrational beliefs) and E (substituting more effective beliefs). Ellis sought to effect change in a directfashion—by means of argument and instruction. He would explicitly discuss and liter-ally dispute (D) the patient’s beliefs and would offer specific—and more effective (E)—substitutes. His manner was teacherlike, and he frequently lectured his patients andexhorted them to modify their irrational ideas about themselves and the world.
In a similar vein, Aaron Beck—who was initially trained as a psychoanalyst—developed cognitive therapy (Beck, 1976; Beck, Rush, Shaw, & Emery, 1979). Beck’s coreinsight—like Ellis’s—is that dysfunctional cognitions play a key role in the developmentof mental disorders. For example, Beck held that depressed people have negative beliefsabout themselves (“I am unlovable”), the world (“It’s a cruel world out there”), and thefuture (“Things are only going to get worse”). These beliefs are supported by distortedthought processes, such as all-or-nothing thinking (“Now that I’ve lost the election,I’m worthless”), overgeneralization (“I lost my car keys—that’s just like me, I lose every-thing!”), disqualifying the positive (“My doing well on the test today was just a fluke”),and emotional reasoning (“I feel it, therefore I know it’s true”) (Burns, 1980).
To challenge these thought processes, Beck used cognitive restructuring, a set oftechniques for changing a person’s beliefs or habits of interpreting the world. Thesetechniques include outright persuasion and, in some cases, confronting the patientwith her maladaptive beliefs. In other cases, patients are taught strategies for keepingcertain thoughts readily available, to be applied instead of more destructive or distress-ing interpretations of life’s events. In short, there is no single list of techniques that areused in cognitive therapy, but the effort is always toward changing both a person’sbehaviors and how she thinks about the world.
To get a feel for how Beck interacts with his patients, consider the followinginterview with a 26-year-old graduate student who sought treatment for depression:
PATIENT: I agree with the descriptions of me, but I guess I don’t agree that the way I thinkmakes me depressed.
BECK: How do you understand it?PATIENT: I get depressed when things go wrong. Like when I fail a test.BECK: How can failing a test make you depressed?PATIENT: Well, if I fail I’ll never get into law school.BECK: So failing the test means a lot to you. But if failing a test could drive people into
clinical depression, wouldn’t you expect everyone who failed the test to havea depression? . . . Did everyone who failed get depressed enough to requiretreatment?
PATIENT: No, but it depends on how important the test was to the person.BECK: Right, and who decides the importance?PATIENT: I do.BECK: And so, what we have to examine is your way of viewing the test (or the way that
you think about the test) and how it affects your chances of getting into lawschool. Do you agree?
PATIENT: Right.BECK: Do you agree that the way you interpret the results of the test will affect you? You
might feel depressed, you might have trouble sleeping, not feel like eating, andyou might even wonder if you should drop out of the course.
PATIENT: I have been thinking that I wasn’t going to make it. Yes, I agree.
cognitive therapy An approach totherapy that tries to change some ofthe patient’s habitual modes of think-ing about herself, her situation, andher future.
cognitive restructuring A set of cog-nitive therapy techniques for changinga person’s maladaptive beliefs or inter-pretations through persuasion andconfrontation.
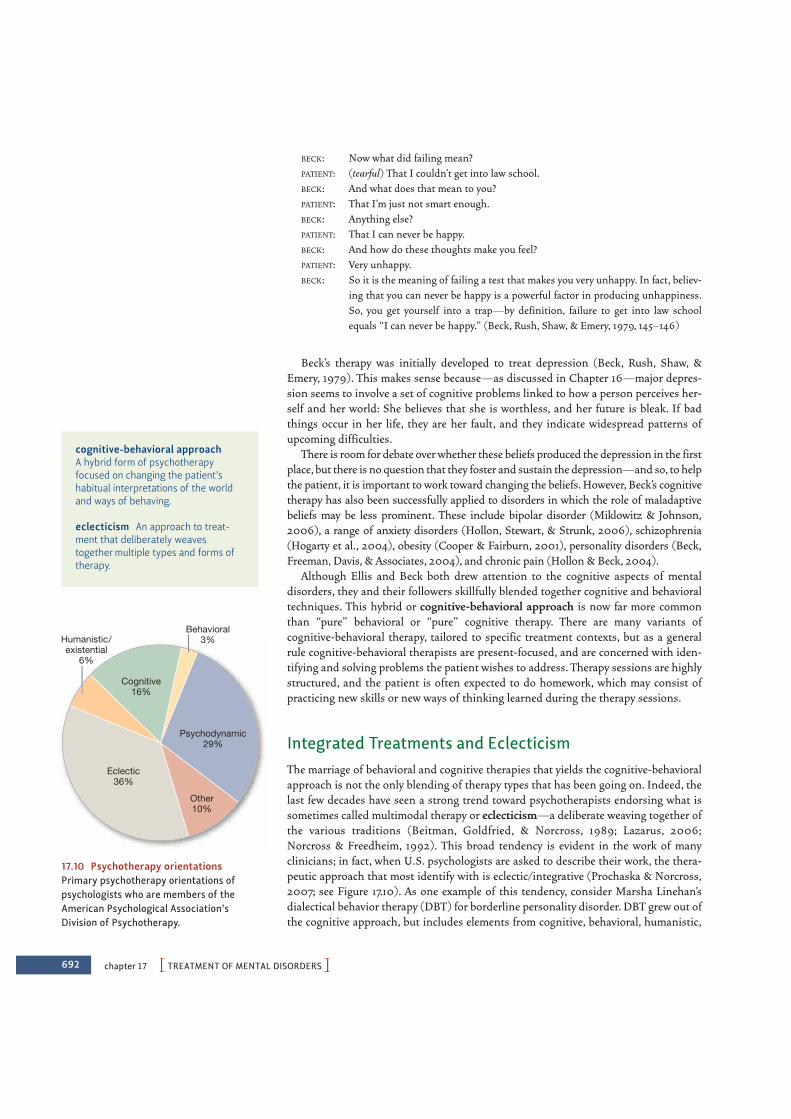
692 chapter 17 PTREATMENT OF MENTAL DISORDERSO
BECK: Now what did failing mean?PATIENT: (tearful) That I couldn’t get into law school.BECK: And what does that mean to you?PATIENT: That I’m just not smart enough.BECK: Anything else?PATIENT: That I can never be happy.BECK: And how do these thoughts make you feel?PATIENT: Very unhappy.BECK: So it is the meaning of failing a test that makes you very unhappy. In fact, believ-
ing that you can never be happy is a powerful factor in producing unhappiness.So, you get yourself into a trap—by definition, failure to get into law schoolequals “I can never be happy.” (Beck, Rush, Shaw, & Emery, 1979, 145–146)
Beck’s therapy was initially developed to treat depression (Beck, Rush, Shaw, &Emery, 1979). This makes sense because—as discussed in Chapter 16—major depres-sion seems to involve a set of cognitive problems linked to how a person perceives her-self and her world: She believes that she is worthless, and her future is bleak. If badthings occur in her life, they are her fault, and they indicate widespread patterns ofupcoming difficulties.
There is room for debate over whether these beliefs produced the depression in the firstplace, but there is no question that they foster and sustain the depression—and so, to helpthe patient, it is important to work toward changing the beliefs. However, Beck’s cognitivetherapy has also been successfully applied to disorders in which the role of maladaptivebeliefs may be less prominent. These include bipolar disorder (Miklowitz & Johnson,2006), a range of anxiety disorders (Hollon, Stewart, & Strunk, 2006), schizophrenia(Hogarty et al., 2004), obesity (Cooper & Fairburn, 2001), personality disorders (Beck,Freeman, Davis, & Associates, 2004), and chronic pain (Hollon & Beck, 2004).
Although Ellis and Beck both drew attention to the cognitive aspects of mentaldisorders, they and their followers skillfully blended together cognitive and behavioraltechniques. This hybrid or cognitive-behavioral approach is now far more commonthan “pure” behavioral or “pure” cognitive therapy. There are many variants ofcognitive-behavioral therapy, tailored to specific treatment contexts, but as a generalrule cognitive-behavioral therapists are present-focused, and are concerned with iden-tifying and solving problems the patient wishes to address. Therapy sessions are highlystructured, and the patient is often expected to do homework, which may consist ofpracticing new skills or new ways of thinking learned during the therapy sessions.
Integrated Treatments and EclecticismThe marriage of behavioral and cognitive therapies that yields the cognitive-behavioralapproach is not the only blending of therapy types that has been going on. Indeed, thelast few decades have seen a strong trend toward psychotherapists endorsing what issometimes called multimodal therapy or eclecticism—a deliberate weaving together ofthe various traditions (Beitman, Goldfried, & Norcross, 1989; Lazarus, 2006;Norcross & Freedheim, 1992). This broad tendency is evident in the work of manyclinicians; in fact, when U.S. psychologists are asked to describe their work, the thera-peutic approach that most identify with is eclectic/integrative (Prochaska & Norcross,2007; see Figure 17.10). As one example of this tendency, consider Marsha Linehan’sdialectical behavior therapy (DBT) for borderline personality disorder. DBT grew out ofthe cognitive approach, but includes elements from cognitive, behavioral, humanistic,
Eclectic36%
Psychodynamic29%
Cognitive16%
Behavioral3%Humanistic/
existential6%
Other10%
17.10 Psychotherapy orientationsPrimary psychotherapy orientations ofpsychologists who are members of theAmerican Psychological Association’sDivision of Psychotherapy.
cognitive-behavioral approachA hybrid form of psychotherapyfocused on changing the patient’shabitual interpretations of the worldand ways of behaving.
eclecticism An approach to treat-ment that deliberately weavestogether multiple types and forms oftherapy.

“When Jud accuses Zack, here, of hostility towards his daughter,like he seems to every session, why, it’s plain to me he’s only
rationalizing his own lack of gunption in standing up to astepson who’s upsurping the loyalty of his second wife.”
PPsychological TreatmentsO 693
and psychodynamic therapies to address the profound emotion dysregulation associ-ated with borderline personality disorder (Linehan, Bohus, & Lynch, 2007).
This eclecticism obviously allows the therapist flexibility to tailor his approach to thespecific needs and symptoms of each patient. And over the course of treatment, itallows the therapist to pursue lines of discussion or specific interventions that areworking and to back off from interventions that are ineffective. In addition, multimodaltherapy makes sense theoretically. In Chapter 16, we saw that mental disorders rarelyhave a single cause; instead, they emerge from a complex set of factors creating thediathesis as well as factors creating the more immediate stressors. It seems sensible,therefore, that treatment might need to work on multiple fronts, which is precisely whatmultimodal therapy is designed to do.
Beyond One-on-One TherapySo far, we have considered various approaches to one-on-one therapy—that is, onetherapist working with one patient. Over the past few decades, therapists have alsobeen exploring various modes of group therapy that feature all conceivable permuta-tions: one therapist and several patients, several therapists and several patients, severalpatients and no therapist, and so on. Treating patients in groups has an obvious advan-tage: more patients can be accommodated by a limited number of therapists. But grouptreatment is appealing for other reasons as well, including the fact that it allows thera-pists to observe and work with problems that emerge more readily in group settings.
S H A R E D P ROB L E M G RO U P S
One approach to group therapy is to gather people who have the same problem.They may all be alcoholics, or abuse victims, or ex-convicts. The membersmeet, share relevant advice and information, help newcomers along, andexhort and support one another in their resolve to overcome their difficul-ties (Figure 17.11). The classic example is Alcoholics Anonymous (AA),which gives the recovering alcoholic the knowledge that she is not alone,helps her weather crises without suffering a relapse, and assists her in get-ting back on her feet if relapses do occur. Another is Toastmasters, a socialclub for people with public-speaking phobias. In these “we are all in thesame boat” groups, the primary aim is to manage the problem that all themembers share. Relatively little attention is paid to any one individual’sunique emotional problems.
T H E R A P Y G RO U P S
The rules of the game are very different in groups explicitly organized forgroup therapy. Here, a number of selected patients, usually around 8 to 10, aretreated together under the guidance of a trained therapist. Within this format, the tech-niques used by the therapist vary considerably. In some groups, the therapist encour-ages psychodynamically oriented insights; in others, the therapist may use behavioralor cognitive procedures. No matter the technique, the treatment of each group memberreally begins as he realizes that he is not all that different from the others. He learnsthat there are other people who are painfully afraid of rejection, are desperately lonely,have hostile fantasies about their parents, and so on. Additional benefits come from asense of group belongingness, support, and encouragement. Most importantly, thegroup provides a ready-made laboratory in interpersonal relations. The patient can
17.11 Group therapy

694 chapter 17 PTREATMENT OF MENTAL DISORDERSO
discover just what he does that rubs others the wrong way, how he can relate to certainkinds of people more effectively, and the like.
CO U P L E T H E R A P Y A N D FA M I LY T H E R A P Y
In the therapy groups we have considered so far, the members are almost alwaysstrangers before the sessions begin. This contrasts markedly with couple and familytherapy. Here, the people seeking help know one another very well (sometimes all toowell) before they enter therapy.
Couple therapy (including marriage counseling) and family therapy have becomemajor therapeutic movements (Figure 17.12; Kerr & Bowen, 1988; Minuchin, 1974; Satir,1967; Snyder, Castellani, & Whisman, 2006). It is probably no coincidence that thisgrowth has occurred during a time of turmoil in American families, evidenced by spiral-ing divorce rates and reports of child and spousal abuse and by the increasing numberof single-parent households.
Family and couple therapists generally regard the family as an emotional system,with the feelings and functioning of each individual heavily influenced by interactionswithin the system. Thus, one person in the family may be depressed, or one member ofa couple may be aggressive, but the difficulty does not lie in that person alone. Instead,she is merely the “identified patient” within the system, and her symptoms may reflectsome broader problem within the family or the couple (Dadds, 1995). Likewise, whenone person in the couple or family has a problem, its effects can ricochet through thefamily and affect all its members.
For example, let’s imagine that one family member suffers from bipolar disorder.This will lead to behaviors that may be destructive to the whole family—disruptingtheir routines, causing them to worry, draining their finances. This may lead tohostility, or perhaps overprotection, toward the patient with the initial disorder, andthis, in turn, can cause further problems for the patient, aggravating the disorder andproducing new difficulties. As a result, the treatment may have to include medicationfor the bipolar disorder and steps to repair the dynamic within the family. In fact,there is now good evidence that patients with bipolar disorder are less likelyto relapse if their treatment plan includes family-level interventions as well asmedication (Miklowitz, 2007).
BIOMEDICAL TREATMENTS
The psychological treatments described so far are widely used and, as we will discusslater, are often quite effective. However, as we mentioned at the outset of this chapter,there is a second major class of treatments—the biomedical treatments—which aredesigned to alter the brain’s functioning more directly.
Biomedical treatments for mental illness have a long history. As mentioned earlier,the first known biomedical treatment is a prehistoric surgical procedure called trephi-nation, in which pieces of the skull were removed to provide an escape path for the spir-its or demons thought to be causing the affliction (Figure 17.13). Other early proceduresinvolved bloodlettings or purgatives, both intended somehow to restore mental equilib-rium. Later developments were hardly milder. For example, Benjamin Rush(1745–1813), one of the signers of the Declaration of Independence and the acknowl-edged father of American psychiatry, submerged patients in hot or cold water until theywere just short of drowning or twirled them on special devices at speeds that rendered
17.12 Couple therapy In couple therapy, atherapist works with both members of acouple, sometimes together and sometimesseparately.
17.13 Trephination The ancient practiceof trephination involved the cutting ofholes in the skull, through which demonscould be driven out. This photo shows atrephined prehistoric skull found in Peru.The patient apparently survived the opera-tion for a while, for there is some evidenceof bone healing.

PBiomedical TreatmentsO 695
them unconscious (Figure 17.14). Such methods were said to reestablish balancebetween bodily and mental functions. They almost certainly had no such positiveeffects, although hospital attendants probably welcomed them, since they undoubtedlyterrified the inmates and so helped to “keep order” (Mora, 1975).
More recent biomedical treatments have been more humane, have had more secureempirical foundations, and have certainly been more effective than these early treat-ments. Some of these are pharmacological and consist of medications that alter infor-mation flow at the synapse, thereby influencing thoughts, feelings, and behaviors.Others are nonpharmacological and involve the direct manipulation of the nervoussystem via surgery or electrical or magnetic pulses.
Pharmacological TreatmentsThe past half century or so has seen the development of a number of psychotropicdrugs, medications that control, or at least moderate, the manifestations of mentaldisorders. These medications have had an enormous impact on mental-health care andhave allowed patients with many different disorders to be treated successfully, oftenwithout hospitalization. The development of psychotropic drugs has gone hand inhand with advances in our understanding of mental illness. As we have learned moreabout the causes of each disorder, better understanding has often pointed the waytoward new drug treatments, and—conversely—new drug treatments have oftenallowed us to test claims about what the causes might be. At the same time, many ofthese treatments have important limitations, which we will also consider.
A N T I P SY C H OT I C M E D I CAT I O N S
As we discussed in Chapter 16, schizophrenia involves many elements, including a spe-cific chemical abnormality involving the neurotransmitter dopamine. A major source ofevidence for this neurochemical abnormality was the effectiveness of certain drugscalled antipsychotics. The classical antipsychotics, most of which were developed in the1950s, reduce the major positive symptoms of schizophrenia, such as thought disorderand hallucination (see Chapter 16), apparently by blocking dopamine receptors in key
17.14 Early methods for treating mentaldisorders (A) A centrifugal-force bed; (B) a crib for violent patients; (C) a swing-ing device.
(A)
(B) (C)
psychotropic drugs Medicationsthat control, or at least moderate, themanifestations of some mentaldisorders.

696 chapter 17 PTREATMENT OF MENTAL DISORDERSO
brain pathways; the most common versions of these antipsychotics include Thorazine,Haldol, and Stelazine.
Unfortunately, these drugs are less effective in treating negative symptoms, such asflat affect and the inability to feel pleasure. This shortcoming has been addressed by anewer set of medications, the so-called atypical antipsychotics, such as Risperdal,Clozaril, and Seroquel (Glick, Murray, Vasudevan, Marder, & Hu, 2001). Like the clas-sical antipsychotics, the atypical antipsychotics block the neurotransmission ofdopamine, but their enhanced benefits, especially with negative symptoms, are proba-bly caused by other mechanisms. These may include alterations in serotonin neuro-transmission or a more selective effect on particular subsets of dopamine neurons(Bantick, Deakin, & Grasby, 2001; Kapur & Remington, 2001; Tandon & Kane, 1993;Wirshing, Marder, Van Putten, & Ames, 1995).
These medications have provided enormous advances in our treatment of schizo-phrenia; however, the benefits have not come without problems. In the United States,the development of the first antipsychotic medications in the 1950s spurred a move-ment called deinstitutionalization, intended to allow for better and less expensive carefor patients in their own communities, at local community mental-health centers ratherthan at large, centralized hospitals. To some extent, this movement worked. In the1950s, mental hospitals housed about 600,000 patients; the current figure is a mere10% of that figure (Lamberg, 2004). Medications have also made it possible todischarge patients with schizophrenia more quickly than ever. Prior to the introductionof the antipsychotic medications, two out of three patients with schizophrenia spentmost of their lives in mental hospitals. In the 1980s, the average stay was about twomonths (J. M. Davis, 1985a; Lamb, 1984; Lamb & Bachrach, 2001).
But deinstitutionalization was at best a partial success. Many individuals withserious mental illness have not found appropriate care in community settings, norhave they been integrated into the community, in terms of employment, or socialrelations, or support services. As a result, some 200,000 mentally ill individuals arehomeless in the United States, and an equal number are in jail, often for minorcrimes (Fleishman, 2004; Lamberg, 2004; Figure 17.15). Thousands more exist inmarginal living situations, and although it is true that fewer patients with schizo-phrenia remain in psychiatric hospitals, the number of times they are readmitted forshort stays has increased by 80% since the 1960s (Rosenstein, Milazzo-Sayre, &Manderscheid, 1989). The current inadequacy—and, in many cases, the completelack—of appropriate community services for mental illness may be linked tothe point, raised earlier, that the outlook for a patient with schizophrenia is appre-ciably worse in the United States than it is in countries where such support is moreavailable.
A N T I D E P R E SSA N T A N D M O O D - STA B I L I Z I N G M E D I CAT I O N S
Even with all their complications, the antipsychotic medications have provided enor-mous advances in the treatment of schizophrenia. Medications have been just asimportant in the treatment of other mental disorders. Shortly after the introductionof antipsychotics as a treatment for schizophrenia, drugs were found that seemedto act specifically on depression. These early antidepressants fell into two majorclasses, the monoamine oxidase (MAO) inhibitors, such as Nardil, and the tricyclicantidepressants (so called because of their chemical structure), such as Tofranil.Of these, the tricyclics became the more widely used, mostly because patients tak-ing MAO inhibitors must conform to difficult dietary restrictions (Burke &Preskhorn, 1995).
17.15 Adverse effects of deinstitutiona-lization Some of the homeless inAmerican cities are people who have beendischarged from mental hospitals and areunable to adjust to the world outside.
deinstitutionalization A movement that began in the 1950s that aimed toprovide better, less expensive care forchronically mentally ill patients in theirown communities rather than at large,centralized hospitals.
antidepressants Medicationsdesigned to counteract depression.
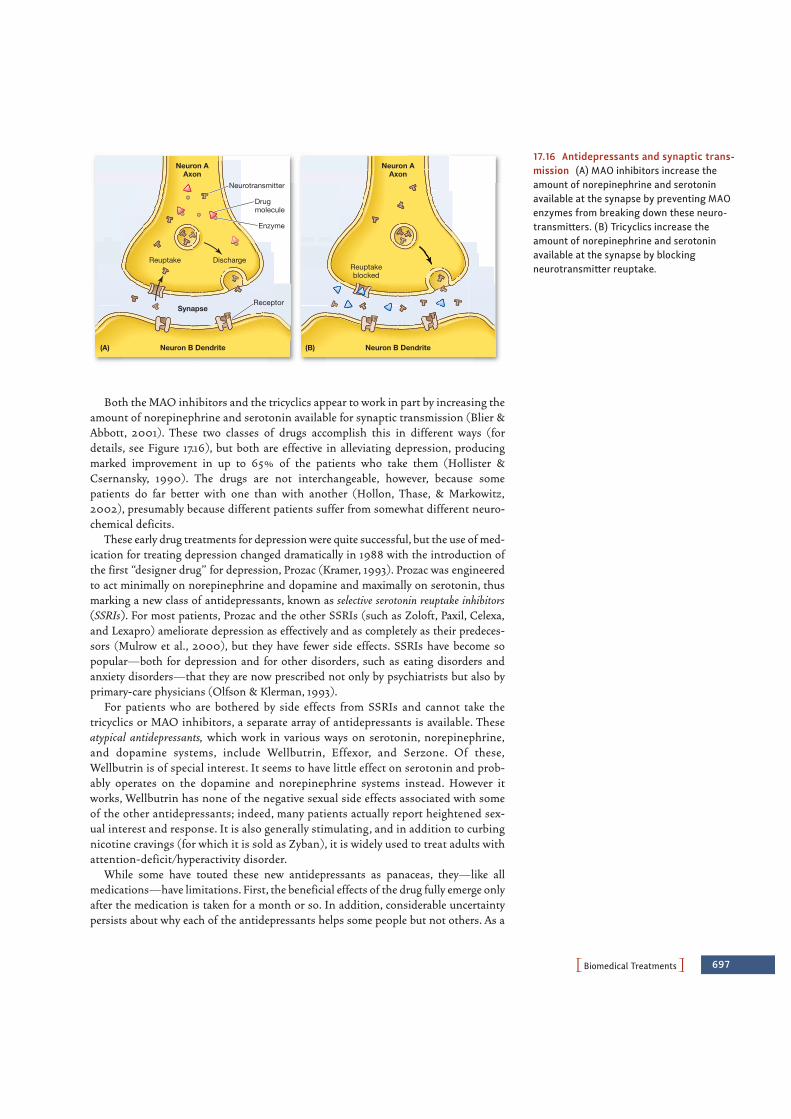
PBiomedical TreatmentsO 697
Both the MAO inhibitors and the tricyclics appear to work in part by increasing theamount of norepinephrine and serotonin available for synaptic transmission (Blier &Abbott, 2001). These two classes of drugs accomplish this in different ways (fordetails, see Figure 17.16), but both are effective in alleviating depression, producingmarked improvement in up to 65% of the patients who take them (Hollister &Csernansky, 1990). The drugs are not interchangeable, however, because somepatients do far better with one than with another (Hollon, Thase, & Markowitz,2002), presumably because different patients suffer from somewhat different neuro-chemical deficits.
These early drug treatments for depression were quite successful, but the use of med-ication for treating depression changed dramatically in 1988 with the introduction ofthe first “designer drug” for depression, Prozac (Kramer, 1993). Prozac was engineeredto act minimally on norepinephrine and dopamine and maximally on serotonin, thusmarking a new class of antidepressants, known as selective serotonin reuptake inhibitors(SSRIs). For most patients, Prozac and the other SSRIs (such as Zoloft, Paxil, Celexa,and Lexapro) ameliorate depression as effectively and as completely as their predeces-sors (Mulrow et al., 2000), but they have fewer side effects. SSRIs have become sopopular—both for depression and for other disorders, such as eating disorders andanxiety disorders—that they are now prescribed not only by psychiatrists but also byprimary-care physicians (Olfson & Klerman, 1993).
For patients who are bothered by side effects from SSRIs and cannot take thetricyclics or MAO inhibitors, a separate array of antidepressants is available. Theseatypical antidepressants, which work in various ways on serotonin, norepinephrine,and dopamine systems, include Wellbutrin, Effexor, and Serzone. Of these,Wellbutrin is of special interest. It seems to have little effect on serotonin and prob-ably operates on the dopamine and norepinephrine systems instead. However itworks, Wellbutrin has none of the negative sexual side effects associated with someof the other antidepressants; indeed, many patients actually report heightened sex-ual interest and response. It is also generally stimulating, and in addition to curbingnicotine cravings (for which it is sold as Zyban), it is widely used to treat adults withattention-deficit/hyperactivity disorder.
While some have touted these new antidepressants as panaceas, they—like allmedications—have limitations. First, the beneficial effects of the drug fully emerge onlyafter the medication is taken for a month or so. In addition, considerable uncertaintypersists about why each of the antidepressants helps some people but not others. As a
17.16 Antidepressants and synaptic trans-mission (A) MAO inhibitors increase theamount of norepinephrine and serotoninavailable at the synapse by preventing MAOenzymes from breaking down these neuro-transmitters. (B) Tricyclics increase theamount of norepinephrine and serotoninavailable at the synapse by blockingneurotransmitter reuptake.
Neurotransmitter
Drugmolecule
Enzyme
Receptor
Neuron AAxon
Neuron B Dendrite
Neuron AAxon
Neuron B Dendrite
DischargeReuptake
Synapse
Reuptakeblocked
(A) (B)
698 chapter 17 PTREATMENT OF MENTAL DISORDERSO
result, therapists often resort to a process of trial and error, prescribing a variety ofdrugs, one at a time, until they find one that helps the particular patient. This trial anderror can take quite some time since, as we have said, the drugs often take effect onlyafter a month or so.
In addition, all of these drugs do have side effects, which vary by drug and by personbut which, overall, include weight gain, nausea, diarrhea, and—in upward of 30% ofpatients—insomnia, as well as a loss of sexual desire or response (Clayton, 2001;Ferguson, 2001; Gursky & Krahn, 2000; E. Hollander & McCarley, 1992; Jacobsen,1992; Montgomery, 1995). There has also been some concern that these drugs may beaddictive, although many regard the evidence supporting this claim as unpersuasive(Haddad, 1999).
Medications to treat bipolar disorder are called mood stabilizers (so called becausethey treat or prevent manic, mixed, or depressive states). The first medication usedspecifically for its mood stabilizing action was lithium carbonate. Patients who begintaking lithium can generally expect that their manic episodes will subside within 5 to10 days. Because of this delay, antipsychotic medications are sometimes also prescribedto reduce agitation until the lithium takes effect. In addition, antidepressants are oftenprescribed along with lithium because lithium is more effective in reducing manic thanin reducing depressive symptoms (Sachs & Thase, 2000).
Unfortunately, lithium works in only 60 to 70% of patients with bipolar disorder(Miklowitz & Johnson, 2007). Taking it also causes unpleasant side effects for manypatients, such as weight gain, sedation, dry mouth, and tremors. Moreover, the fact thatlithium is toxic at higher doses means that patients must have their blood tested fre-quently and makes it a risky treatment for patients who are potentially suicidal andmight overdose. Nor can lithium be taken during pregnancy or when a patient has kid-ney disease. In addition, many patients with bipolar disorder choose not to take theirmedication because they do not want to give up either the pleasures or the productivityoften associated with the manic state; they may decide that these elements outweigh the(sometimes enormous) disruption and distress that the disorder also produces.
A N T I A N X I E T Y M E D I CAT I O N S
Patients suffering from disabling anxiety are often treated with medications that arepopularly called tranquilizers and technically known as anxiolytics. Most anxiolyticsapparently work by increasing neurotransmission at synapses containing theneurotransmitter gamma-aminobutric acid (GABA; Brailowsky & Garcia, 1999;Shader & Greenblatt, 1995). Probably the most commonly used anxiolytic, though, isself-administered and not prescribed by a therapist: alcohol. Many people, patients orotherwise, medicate themselves for their anxiety as part of their lifestyle, inviting therisk of alcohol abuse.
Physicians also sometimes treat the anxiety disorders by prescribing a beta-blocker, amedication intended to control autonomic arousal. In addition, for the uncomfortablefeelings associated with anxiety, they often prescribe one of the benzodiazepines. Someof these medications, such as Valium Xanax, or Klonopin are prescribed so often thattheir names have become household words. They are useful as short-term treatments(usually taking effect in 30 or 40 minutes) for generalized anxiety disorder, panic dis-order, post-traumatic stress disorder, alcohol withdrawal, insomnia, muscle spasms,tension headaches, and various other stress-related disorders.
Benzodiazepines are rarely used for long-term treatment, however, because they arehighly addictive, interact dangerously with alcohol, and like alcohol, can causeprofound fetal damage if a patient is pregnant. There are also concerns that the benzo-
mood stabilizers Medications thattreat bipolar disorder, such as lithium.
anxiolytics Drugs that alleviate thesymptoms of anxiety.

PBiomedical TreatmentsO 699
diazepines can produce a “rebound” effect, so that a person who stops taking the med-ication may end up more anxious than she was prior to taking the drug (Chouinard,2004). These are, of course, major concerns, and so researchers continue to seek newanxiolytics. Happily, some of the newer drugs, such as BuSpar, are not addictive and arebecoming popular substitutes for the older medications, especially for patients who areprone to alcohol or drug abuse or have to take the medication over a long period of time(Lydiard, Brawman-Mintzer, & Ballenger, 1996; Schweitzer, Rickels, & Uhlenhuth,1995). Anxiety is also commonly treated using tricyclic antidepressants and SSRIs.
CO STS A N D B E N E F I TS O F M E D I CAT I O N
Overall, drug therapies effectively reduce symptoms for people with a wide range ofmental disorders. Indeed, these drugs have lifted many people out of misery anddistress and help them resume a reasonably normal life. These drugs have also allowedmany patients to remain in a family or community setting when they would otherwisehave been relegated to the hospital. These are, by any measure, enormous gains.
At the same time, drug therapy for mental disorders is not an unqualified success.Drugs do not cure the disorder; instead, they help to control it, and in many cases, if theperson stops taking his pills, he quickly relapses into his full set of symptoms. It is alsooften tricky to get the doses correct for many of these drugs, because individuals differboth in their drug reactions and in how rapidly they metabolize the medication. Thereare also some group differences—for example, many African Americans metabolizeantidepressant medications more slowly than whites (U.S. Department of Health andHuman Services, 2001). This aggravates a concern that we have already raised—namely, that a clinician prescribing one of these medications often needs some amountof trial and error to find the right drug at the right dose.
We have also highlighted the fact that many of these drugs have unpleasant(or even dangerous) side effects. These include increases as well asdecreases in sleepiness and agitation, decreased sexual performance,and facial tics. These side effects are bad enough on their own, but, inaddition, they often lead people to stop taking their medication, inwhich case (obviously) the drugs can bring no benefit. Thus, a col-lege student might refuse to take her antidepressant because she isconcerned about the associated weight gain, even though, withoutthe drug, her bulimia nervosa may cause long-term health prob-lems. Likewise, someone might refuse to take medication because ofa fear that it will disrupt sexual functioning, even though, without it,depression is disrupting his life to the point where a relationship isnot possible.
A more general concern about these psychoactive drugs is that theymay be overprescribed (Figure 17.17). This worry is magnified by the fact thatthese drugs are increasingly used to treat a wide variety of conditions in childrenand adolescents, even though we know less about their side effects in children than inadults. Two flashpoints for this particular controversy are the use of SSRIs for depres-sion and the use of stimulants for ADHD.
Some researchers have raised questions about whether the SSRIs may increase therisk of suicide in some young people. But others claim the opposite is the case, and thatby alleviating depression, SSRIs decrease suicide risk (Bachtold, 2003; Couzin, 2004).In view of the potential for risks, however, the U.S. Food and Drug Administration(FDA) now requires “black box” warnings on SSRIs (literally, a black box around thelabel) regarding possible increased risk of suicide (Figure 17.18).
17.17 Overprescribing
700 chapter 17 PTREATMENT OF MENTAL DISORDERSO
As we have seen, controversy also swirls around the number of prescriptions now beingwritten for ADHD, which has increased fourfold since the early 1990s. Critics claim thatactive children are being medicated so that they will behave themselves in crowded andunderstimulating classrooms where they are expected to perform well on standardizedtests. Others reply that medications are an important treatment tool as long as children arethoroughly assessed by appropriate professionals.
Nonpharmacological Treatments Nonpharmacological treatments for mental illness include psychosurgery and electro-convulsive therapy as well as a number of promising newer treatments. These treat-ments conjure up disturbing images for many people, in part because of the portrayalsof these techniques in the popular media (see Figure 17.19). However, as we will seebelow, there is a place for each of these treatments in contemporary practice.
P SY C H O S U RG E RY
Psychosurgery, or brain surgery, aims to alter thinking or behavior by removing brainareas or disconnecting them from each other. In a prefrontal lobotomy, for example,the surgeon severs the neurological connections between the thalamus and the frontallobes, in whole or in part. This operation was originally meant to liberate a patient’sthoughts from the pathological influence of her emotions, on the ill-informedassumption that thought and emotion were localized in the frontal lobes and thethalamus, respectively. In the 1940s and 1950s, tens of thousands of patients weresubjected to lobotomies, and early reports on the procedure were quite enthusiastic.It soon became clear, however, that the surgery had powerful side effects, including a disruption of many higher cognitive functions such as memory and the ability to plan and self-regulate, and so the procedure is now rarely used (Tierney, 2000;Valenstein, 1986).
Recently, psychosurgery has reemerged as a useful technique, but it has beenrefined considerably, both in the procedures used and in the patients judged suitablefor them (Hurley, Black, Stip, & Taber, 2000). Neurosurgeons still manipulate thenervous system directly, but they do so by creating very precise lesions in specificbrain areas instead of disconnecting or destroying whole lobes or regions(see Figure 17.20). In these cases, the surgery is reserved for patients who are severely
17.18 Antidepressant “black box” label The FDA requires warning labels on SSRIsthat alert patients to a possible increase in the risk of suicide.
17.20 Neurosurgery Neurosurgeons canuse a computer-controlled robot arm tolocate and remove small brain tumors withminimal damage to surrounding areas. Thecomputer screen shows virtual realityimages of the device using CT and 3-D MRI.
17.19 Negative media portrayals ofnonpharmacological treatmentsMcMurphy’s electroshock treatments inOne Flew Over the Cuckoo’s Nest (1975).Negative portrayals have given this type of treatment a bad name. However,electroconvulsive therapy as currentlyadministered is an important tool formanaging severe depression.
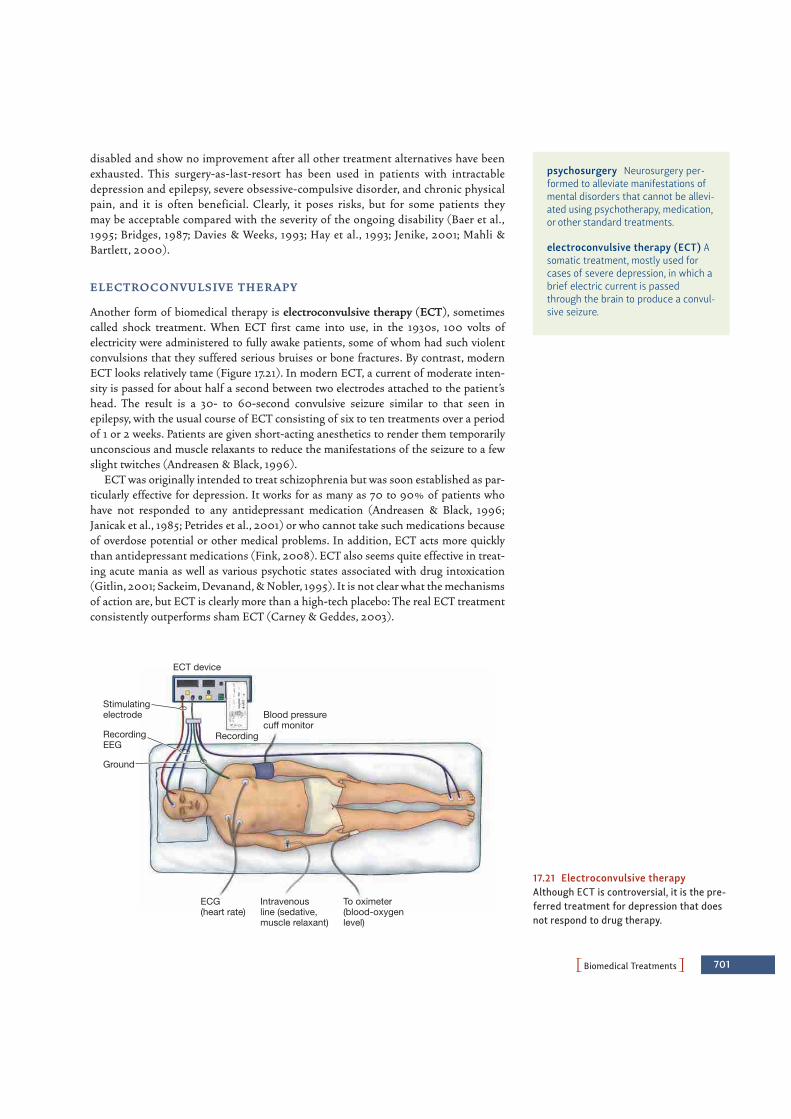
PBiomedical TreatmentsO 701
disabled and show no improvement after all other treatment alternatives have beenexhausted. This surgery-as-last-resort has been used in patients with intractabledepression and epilepsy, severe obsessive-compulsive disorder, and chronic physicalpain, and it is often beneficial. Clearly, it poses risks, but for some patients theymay be acceptable compared with the severity of the ongoing disability (Baer et al.,1995; Bridges, 1987; Davies & Weeks, 1993; Hay et al., 1993; Jenike, 2001; Mahli &Bartlett, 2000).
E L E CT RO CO N V U LS I V E T H E R A P Y
Another form of biomedical therapy is electroconvulsive therapy (ECT), sometimescalled shock treatment. When ECT first came into use, in the 1930s, 100 volts ofelectricity were administered to fully awake patients, some of whom had such violentconvulsions that they suffered serious bruises or bone fractures. By contrast, modernECT looks relatively tame (Figure 17.21). In modern ECT, a current of moderate inten-sity is passed for about half a second between two electrodes attached to the patient’shead. The result is a 30- to 60-second convulsive seizure similar to that seen inepilepsy, with the usual course of ECT consisting of six to ten treatments over a periodof 1 or 2 weeks. Patients are given short-acting anesthetics to render them temporarilyunconscious and muscle relaxants to reduce the manifestations of the seizure to a fewslight twitches (Andreasen & Black, 1996).
ECT was originally intended to treat schizophrenia but was soon established as par-ticularly effective for depression. It works for as many as 70 to 90% of patients whohave not responded to any antidepressant medication (Andreasen & Black, 1996;Janicak et al., 1985; Petrides et al., 2001) or who cannot take such medications becauseof overdose potential or other medical problems. In addition, ECT acts more quicklythan antidepressant medications (Fink, 2008). ECT also seems quite effective in treat-ing acute mania as well as various psychotic states associated with drug intoxication(Gitlin, 2001; Sackeim, Devanand, & Nobler, 1995). It is not clear what the mechanismsof action are, but ECT is clearly more than a high-tech placebo: The real ECT treatmentconsistently outperforms sham ECT (Carney & Geddes, 2003).
psychosurgery Neurosurgery per-formed to alleviate manifestations ofmental disorders that cannot be allevi-ated using psychotherapy, medication,or other standard treatments.
electroconvulsive therapy (ECT) Asomatic treatment, mostly used forcases of severe depression, in which abrief electric current is passedthrough the brain to produce a convul-sive seizure.
ECT device
Recording
Blood pressurecuff monitor
To oximeter(blood-oxygenlevel)
Intravenousline (sedative,muscle relaxant)
ECG(heart rate)
Stimulatingelectrode
RecordingEEG
Ground
17.21 Electroconvulsive therapyAlthough ECT is controversial, it is the pre-ferred treatment for depression that doesnot respond to drug therapy.

702 chapter 17 PTREATMENT OF MENTAL DISORDERSO
Despite these advantages, ECT remains controversial, partly because in many casesit produces memory impairment (Rami-Gonzalez et al., 2001). These cognitive sideeffects are diminished if the ECT is delivered to just one side of the brain during ther-apy, as is now commonly done (Sackeim et al., 2000). In any case, ECT is generally usedonly after medication has failed or when there seems to be a serious chance of suicide.In such contexts, there is now a clear consensus that modern ECT represents one of themost effective treatments for depression (Glass, 2001).
E M E RG I N G B I O M E D I CA L T R E AT M E N TS
A number of emerging biomedical treatments have also attracted attention. Here we’llhighlight three treatments that are in varying stages of development and testing.The first—vagal nerve stimulation—involves implanting a battery-poweredstimulator in the chest just underneath the skin. This stimulator delivers carefully cali-brated electrical pulses to the vagus nerve. Although this treatment has FDA approvalfor use with treatment-resistant depression, information about its short- and long-term efficacy is still being gathered.
A second promising treatment is deep brain stimulation (DBS). This treatment isbased on the finding that severe forms of psychopathology are often associated withabnormalities in the activation levels of certain brain systems, as described inChapter 16. For example, depression is associated with heightened brain activation in alimbic system region known as the subgenual cingulate cortex. On the basis of thesefindings, Mayberg and her colleagues implanted electrodes in these brain areas inpatients whose severe depression had not responded to conventional interventions.
17.22 SCIENTIFIC METHOD: Does deep brain stimulation relieve depressive symptoms?
Method1. The six patients selected had severe depression that could not be treatedby conventional methods.
ResultsIn an initial study, four of the six patients who received deep brain stimulation showed clear decreases in depressive symptoms.
CONCLUSION: Deep brain stimulation may provide some relief for some patients with otherwise intractable depression.
SOURCE STUDY: Mayberg et al., 2005
2. Two holes were drilled in each patient’s headand electrodes were implanted deep in thebrain, underneath the anterior portion of thecorpus callosum on both sides of the brain.
3. A battery pack and pulse generatorwere implanted in the chest wall,beneath the skin, to stimulate theelectrodes implanted in the brain.
4. After surgery, the patient’s medical team determined the magnitudeand frequency of the electrical pulses that the patient received.
Electrode
Pulsegenerator
One patient who has received deep brain stimulation of the sort described by Mayberg is shown to the right. The X-ray shows her electrodes and the wires that connect her electrodes to the pulse generator in her chest.
vagal nerve stimulation An emerg-ing biomedical treatment for depres-sion that involves electricallystimulating the vagus nerve with asmall battery-powered implant.
deep brain stimulation (DBS)An emerging biomedical treatment fordepression and OCD that involvesstimulating specific parts of the brainwith implanted electrodes.

PCommon Factors and Combined TreatmentsO 703
They then used DBS to disrupt abnormal patterns of activity, thereby normalizing theactivity of this portion of the brain (Mayberg et al., 2005; Figure 17.22). In initial find-ings, four of six patients showed clear benefits from this treatment, a finding that hasprovoked considerable interest and spurred research efforts to better understand thebrain bases of depression (Lozano et al., 2008; Ressler & Mayberg, 2007; for more onDBS, see Miller, 2009). This treatment is currently being evaluated by other groups,both for depression and for other disorders, such as medication-resistant obsessive-compulsive disorder (Abelson et al., 2005; Mallet et al., 2008).
A third type of treatment is called repetitive transcranial magnetic stimulation(rTMS). In this treatment, rapid pulses of magnetic stimulation from a hand-heldcoil placed close to the scalp are used to alter neuronal activity in fully awakeparticipants (Figure 17.23). Treatments last 20 to 30 minutes for several weeks, andthe procedure is painless and not associated with any cognitive side effects. Whenused to treat medication-resistant depression, rTMS has been shown to be as effec-tive as ECT (Janicak et al., 2002). These are exciting findings because, unlike ECT,rTMS does not require anesthetic and doesn’t appear to have cognitive side effects(Janicak, 2005).
COMMON FACTORS AND COMBINED TREATMENTS
We have now described the major modes of psychological and biomedical treatment,emphasizing how each of these forms of therapy is distinct from the others—both inits conceptual grounding and in its practice. With respect to the psychologicaltreatments, some modes of therapy focus on behaviors; some focus on thoughts andpatterns of interpretation that the patient can see within himself; others focus onunconscious beliefs or memories. In some modes of therapy, the therapist actively gives
repetitive transcranial magneticstimulation (rTMS) An emergingbiomedical treatment for depressionthat involves applying rapid pulses ofmagnetic stimulation to the brain froma coil held near the scalp.
Wire coilMaximumfield depth
Pulsed magneticfield
Positioningframe
17.23 Magnets for the mind Repetitivetranscranial magnetic stimulation (rTMS)sends a painless magnetic field through theskull to the cortical surface, where pulsescan be used to stimulate or dampen activ-ity in various areas.

704 chapter 17 PTREATMENT OF MENTAL DISORDERSO
instructions or directions; in others, the therapist merely asks questions; in still others,the therapist is a quiet listener. With respect to the biomedical therapies, in pharmaco-logical treatments, newer generations of drugs are constantly being developed with the aim of targeting increasingly specific neurotransmitter systems. At the same time,nonpharmacological treatments are focusing on increasingly specific regions in thenervous system.
Common FactorsEven within this diversity of treatments—particularly psychological treatments—theforms of therapy have elements in common. These include establishing a strong rela-tionship with the patient, instilling hope, and offering new ways of thinking, feeling,and behaving (Frank & Frank, 1991; Miller, Duncan, & Hubbel, 2005). These sharedelements must be considered when we ask how—or whether—therapy helps peoplewith their problems.
R E L AT I O N S H I P E F F E CTS
Several benefits of therapy are not the direct result of any specific therapeutic tech-niques; instead, these benefits grow out of the relationship that the patient estab-lishes with the therapist (Figure 17.24). One of these benefits is simply that thepatient gains an ally against his problems; this therapeutic alliance helps mostpatients believe that they really can conquer their difficulties and achieve better lives(Barber, Connolly, Crits-Christoph, Gladis, & Siqueland, 2000). In fact, someresearchers believe that the therapeutic alliance is the most important ingredient ineffective psychotherapy and is indispensable even when medication is the primarytreatment.
Why is the relationship so important? Among other considerations, it provides thepatient with an intimate, confiding connection with another person, reassuring thepatient that there is at least one other person in the world whom he can trust and whowill help him. This connection also allows the patient to safely say things that otherwisemight never be said, and in this fashion provides what some people think of as a kindof secular confessional.
H O P E
People who seek help often feel discouraged and hopeless. They worry that their prob-lems are weird or shameful and either too trivial to warrant therapy or so severe that notreatment will work. They may yearn for, yet dread, the chance to reveal things they havekept secret, often for years.
All psychotherapists, regardless of their approach, spend a great deal of time hear-ing these concerns and secrets and responding to them in an accepting and nonjudg-mental manner. With some reassurance and a little education, patients often let goof their anxieties as they learn that their problems are understandable, rather com-mon, not shameful, and quite treatable. As the therapist confidently describes therationale for treatment, and what benefits might be expected, the patient begins tofeel hope for recovery, often for the first time. This hope is a crucial common factoracross therapies.
17.24 Relationship effects Films such asGood Will Hunting (1997) portray a positive(if somewhat dramatic) relationshipbetween therapist and client.
therapeutic alliance The relation-ship between therapist and patientthat helps many patients feel hopefuland supported.

PEvaluating TreatmentsO 705
The fostering of hope is also a feature of the biomedical therapies. When a patientspeaks with a medical professional about his problems and finally hears a name givento what previously seemed a mass of unconnected symptoms, the patient often feelsgreat relief. Hearing that a medication may help him, the patient may feel that at lastthere’s hope he may get better, which may amplify the drug’s effects. Indeed, as we willshortly see, placebo effects—which may arise because of an expectation that symptomswill improve—are so powerful that they need to be controlled whenever we try to testthe effectiveness of a biomedical therapy.
N E W WAYS O F T H I N K I N G , F E E L I N G , A N D B E H AV I N G
People who seek treatment often feel “stuck” and unsure how to proceed with one ormore aspects of their lives. Psychological or biomedical treatments can address thesefeelings by exposing the patient to new ways of thinking about their problems. Inpsychodynamic therapies, a patient may for the first time understand her role in inter-personal conflicts that seem to repeat themselves. In humanistic-experiential therapies,a patient may begin to appreciate her conflicting goals and see a path toward reconcil-ing them. In behavioral therapies, a patient may gain understanding of the triggers forhis anxiety and develop confidence that he can interact with the feared objectdespite his anxiety. In cognitive-behavioral therapies, a new way of viewing the worldmay open up as the patient for the first time sees the powerful role of automaticthoughts that can make relatively innocuous events seem like life-or-death situations.Even in the biomedical therapies, a patient may gain an appreciation of the biologicalprocesses that underlie his mental disorder and come to view this disorder as just astreatable as other medical problems. In each case, new ways of thinking provide thebasis for healthier and more adaptive ways of feeling and behaving.
Combined TreatmentsIn light of these common factors, it seems likely that the various forms of therapy allcontain some of the same “active ingredients.” Of course, the trend toward multimodaltherapy, in which therapists from each tradition borrow ideas and techniques fromother traditions, also leads to increasing overlap among their approaches.
Another development that makes the distinctions between therapy types less clear-cut is that many therapists join a multimodal approach to psychotherapy with medica-tion. Indeed, one survey indicates that more than half the patients being treated formental disorders receive both drugs and psychotherapy (Pincus et al., 1999). Thus, forexample, patients suffering from depression are often treated with antidepressants andcognitive-behavioral therapy, with the aim that the drugs will ease the patients’ distressin the short term and the therapy will provide longer-lasting effects (DeRubeis, Siegle, &Hollon, 2008; Hollon & Fawcett, 1995). By a similar logic, patients suffering from anxi-ety disorders often receive medication as well as psychotherapy (Walkup et al., 2008).
EVALUATING TREATMENTS
Now that we have considered some important differences between therapy types, weneed to ask: How do we know whether any of these therapies actually help people feelbetter and function better?
706 chapter 17 PTREATMENT OF MENTAL DISORDERSO
The Importance of Empirically Supported TreatmentsPractitioners of any form of therapy obviously want to be sure that they are providingbenefits and doing no harm, and this has led many clinicians and researchers to seekways of validating their therapy—making certain it works (Figure 17.25). In addition,validation has become more urgent in the last few years, fueled by a worldwide move-ment toward identifying empirically supported treatments (EST)—that is, treat-ments that are based on solid research. This movement was initially aimed at the broadpractice of medicine (Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000; Sox &Woolf, 1993) but has led to a similar movement within education, social work, and psy-chology (American Psychological Association Presidential Task Force on Evidence-Based Practice, 2006; Chambless & Ollendick, 2001; de los Reyes & Kazdin, 2008).
Many factors have contributed to this movement toward EST in psychology. Oneconsideration lies in a number of prominent critiques of psychotherapy. An early attacklaunched by the British psychologist Hans Eysenck was particularly concerned with theefficacy of psychoanalysis and similar “insight” therapies (Eysenck, 1952). Althoughmore recent studies have challenged Eysenck’s conclusion that psychotherapy has nocurative effects, his criticisms and concerns fed into the broader movement demandingthat psychotherapy be validated empirically.
A second factor that has contributed to the EST movement has been the develop-ment of pharmacological treatments. These medications, as we have seen, can beextremely helpful, but they can also have unfortunate side effects, making it crucial thatwe use them only for the patients and the disorders for which they are clearly effective.In addition, the availability of these medications invites questions about the value ofnonmedical treatment—namely, psychotherapy. Is it possible that hours of therapymight be replaced by simply taking a pill? This notion obviously demands a carefulevaluation of whether psychotherapy works or not.
One last factor fueling the EST movement involves the cost of therapy.Psychotherapy requires hours with a trained professional, and many of the medicationsfor mental disorders are quite expensive, too. In many cases, the expenses are coveredby insurance, but as health expenses have risen, insurance companies have grown moreconcerned about making certain that the treatments they are paying for are worthwhile(Zarkin, Grabowski, Mauskopf, Bannerman, & Weisler, 1995).
The Logic of Outcome ResearchHow can we find out whether a psychological or biomedical treatment truly providesrelief for someone with a particular mental disorder? As a way of tackling this issue, letus suppose that we want to find out whether a given drug—say, Wellbutrin—reducesthe symptoms of depression. For a first step, we could administer Wellbutrin to a groupof patients diagnosed with depression, and assess the patients’ status before and after
17.25 Efficacy
empirically supported treatments(EST) Clinical methods that researchhas shown to be effective for treatinga given disorder.

PEvaluating TreatmentsO 707
receiving the medication. This assessment would provide useful information, but a lit-tle reflection shows that relying only on this procedure would be a mistake.
One problem with the before-and-after assessment is that it ignores the possibility ofspontaneous improvement. With some disorders, many patients get better on their own,whether they receive treatment or not. Therefore, if patients are indeed better off aftertaking Wellbutrin than they were before, their improvement might simply reflectspontaneous improvement and have nothing to do with the medication. In addition, evenwithout spontaneous improvement, most disorders fluctuate in their severity, and itseems likely that patients will seek treatment when they are feeling particularly bad. If so,the odds are good that the normal ups and downs of the disorder will make the patientslook better a few weeks (or months) later. If they have been taking medication duringthose weeks, we might be inclined to assume that the drugs had caused the improvement.
To control for these factors, we need to compare two groups of patients, with onegroup taking Wellbutrin for, say, 6 weeks, while the other group receives no treatment.We also need to make certain that these two groups are matched at the start of thestudy—with similar symptoms, similar backgrounds, and so on. As we discussed inChapter 1, our best means of achieving this matching would be via random assignment—with a coin toss (or the equivalent) determining whether each participant in the studyends up in the treatment group or the no-treatment group. Then, if the participants inthe two groups differ at the end of the procedure, we can be reasonably sure that the dif-ference arose during the study—presumably as a result of the treatment.
In addition, we would want to ensure that the participants in our study are reason-ably uniform in their disorder. Thus, we would want to make certain that all of the par-ticipants were truly depressed, and that their depression was not complicated by otherproblems that might mask the effects of the treatment. Likewise, we would probablywant to make sure the participants were all similar to one another in the duration andseverity of their depression. Otherwise, variations from one participant to the nextmight prevent us from detecting the therapy’s effects.
Evaluating Psychological vs. Biomedical Treatments The elements we have described characterize what is usually termed a randomizedclinical trial (RCT), so called because of the random assignment of participants togroups. In most ways an RCT would be run in the same fashion for evaluating a newmedication or for evaluating a specific type of therapy. There are, however, a few differ-ences between RCTs for drugs and RCTs for therapy.
CO N T RO L L I N G FO R P L AC E BO E F F E CTS
In evaluating biomedical treatments, we need to be alert to the possibility ofplacebo effects—the influence of a patient’s beliefs and expectations in bringing abouta cure. We generally test for placebo effects by giving the patient a medically neutral sub-stance (the placebo); the placebo often diminishes symptoms, but because it has noactive ingredients, its effect has to be understood in terms of the patient’s beliefs: Thepatient believes in the pill’s powers, and it is his faith in the medication, not the med-ication itself, that brings the benefits.
In the broad practice of medicine, the evidence is mixed regarding how powerfulplacebos are. In some studies, placebos seem to produce real improvement (Benson &Friedman, 1996); in others, the placebo effect is weak or nonexistent (Hrobjartsson &Gotzsche, 2001). In the study of mental disorders, though, we need to take the placebo
randomized clinical trial (RCT) Aprocedure for evaluating the outcomeof therapy, usually involving randomassignment of participants to one or more treatment groups or a no-treatment control group.
placebo A chemically inert substancethat produces real medical benefitsbecause the patient believes it will help her.

708 chapter 17 PTREATMENT OF MENTAL DISORDERSO
effect seriously because it is surely plausible that a patient’s distress might be alleviatedby her belief in the cure rather than by the cure itself.
In studies of a medication, therefore, we give the medication we are interested in—Wellbutrin, in our example—to one group of patients, and a placebo to the other group.This second group will receive the same attention from the treatment staff as theWellbutrin group, and they will be told exactly the same things about their treatment.They will also be given the same number of pills as the patients in the true-drug group,and on the same schedule. In this fashion, we ensure that the two groups have the sameexpectations and the same beliefs about the treatment. If we find, therefore, that the groups differ at the end of the study, the difference must be attributed to the oneelement that distinguished the two groups—the fact that the patients in one groupactually took a medication, while those in the other took inert pills.
In principle, the same logic regarding a placebo control applies to the study of psy-chological treatments. In practice, however, it is not clear what the placebo would be inthis case. Would we want the placebo group to work with a therapist who listens, butwithout warmth? A therapist who expresses warmth, but provides no counsel? A thera-pist who offers counsel irrelevant to the patient’s problems? The choice between these(or other) options is not clear, making this one source of ambiguity in interpreting RCTdata for psychotherapy (Nathan et al., 2000). For this reason, many RCTs forpsychological treatments do not have special placebo control conditions. Instead, thetreatment of interest is compared either to other standard treatments or to a wait-listcontrol. The wait-list control is one in which participants are randomly assigned toreceive either immediate or delayed treatment, and the immediate treatmentparticipants’ responses to treatment are evaluated by comparing them to the delayedtreatment participants—who have not yet started therapy.
M A N UA L I Z E D T H E R A P Y
There is one other important way in which RCT procedures differ for psychological andbiomedical treatments. When we are testing a medicine, it is easy to ensure that eachpatient gets the same number of pills and that the chemical constituents of the pills arethe same for everyone in the study. But how can we ensure, in a study of therapy, thateach patient gets the same treatment and the same “dose”?
Investigators usually address this point by developing a treatment manual that tellsthe therapists exactly how to proceed during the study—what steps to take in therapy,what instructions to offer, and so on. This manualized therapy denies the therapist theoption of improvising or adjusting procedures midstream, which may sometimesundermine the quality of the therapy (Addis & Krasnow, 2000). However, this stan-dardization seems essential if we are to assess whether a particular therapy is effective.
Clearly, there are trade-offs associated with manualized therapy. On the positiveside, this procedure seems our best hope for learning whether a particular type oftreatment works. On the negative side, it may not accurately represent the waythat treatment would be used outside the study, since most clinicians adopt an eclecticapproach. Clinicians also often adjust their approach as the therapy proceeds and theylearn which steps seem promising for a particular individual and which do not.
Efficacy vs. UtilityRCT data are extremely useful for allowing us to identify certain therapies as “empiri-cally supported treatments.” But some authors are skeptical about the reliance on RCTdata (Nathan et al., 2000; Westen & Bradley, 2005; Westen, Novotny, & Thompson-
wait-list control In randomized clin-ical trials, a control condition in whichpatients receive delayed treatmentrather than no treatment. Before beingtreated, they are compared to patientstreated earlier.
manualized therapy A form of ther-apy, often used in research, in which amanual describes a set course of ther-apy, indicating what steps the thera-pist should take, what instructions tooffer, and so on.
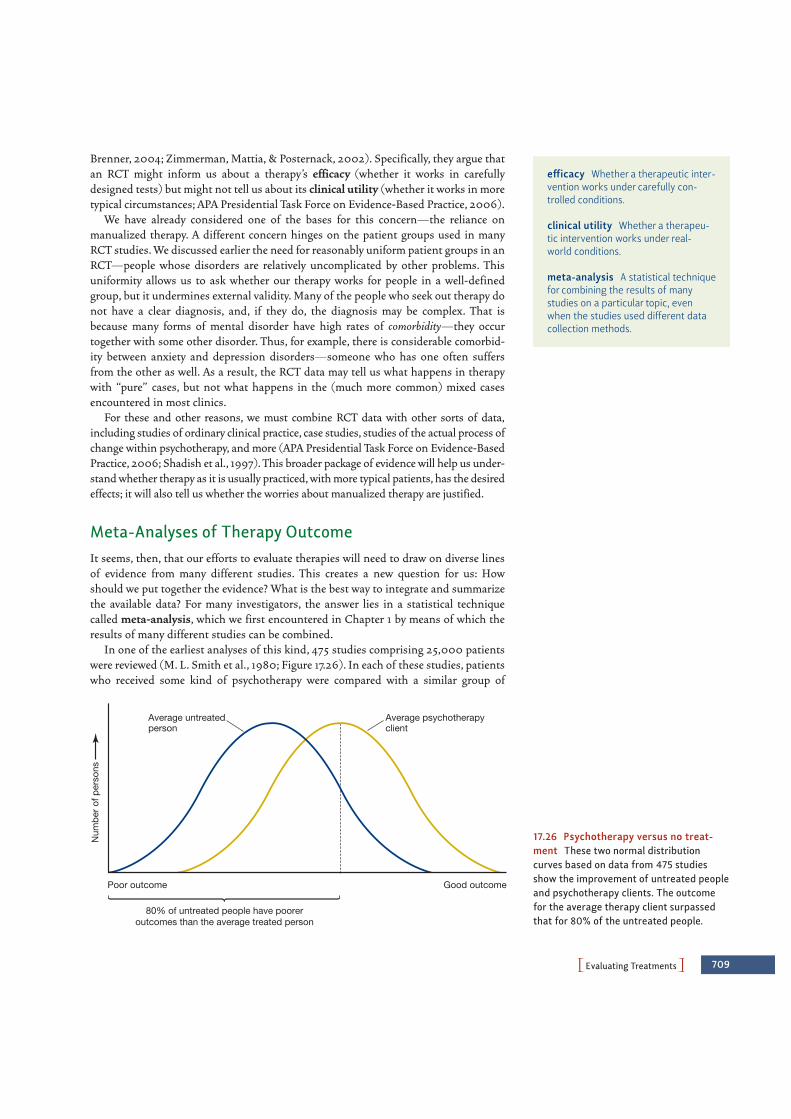
PEvaluating TreatmentsO 709
Brenner, 2004; Zimmerman, Mattia, & Posternack, 2002). Specifically, they argue thatan RCT might inform us about a therapy’s efficacy (whether it works in carefullydesigned tests) but might not tell us about its clinical utility (whether it works in moretypical circumstances; APA Presidential Task Force on Evidence-Based Practice, 2006).
We have already considered one of the bases for this concern—the reliance onmanualized therapy. A different concern hinges on the patient groups used in manyRCT studies. We discussed earlier the need for reasonably uniform patient groups in anRCT—people whose disorders are relatively uncomplicated by other problems. Thisuniformity allows us to ask whether our therapy works for people in a well-definedgroup, but it undermines external validity. Many of the people who seek out therapy donot have a clear diagnosis, and, if they do, the diagnosis may be complex. That isbecause many forms of mental disorder have high rates of comorbidity—they occurtogether with some other disorder. Thus, for example, there is considerable comorbid-ity between anxiety and depression disorders—someone who has one often suffersfrom the other as well. As a result, the RCT data may tell us what happens in therapywith “pure” cases, but not what happens in the (much more common) mixed casesencountered in most clinics.
For these and other reasons, we must combine RCT data with other sorts of data,including studies of ordinary clinical practice, case studies, studies of the actual process ofchange within psychotherapy, and more (APA Presidential Task Force on Evidence-BasedPractice, 2006; Shadish et al., 1997). This broader package of evidence will help us under-stand whether therapy as it is usually practiced, with more typical patients, has the desiredeffects; it will also tell us whether the worries about manualized therapy are justified.
Meta-Analyses of Therapy OutcomeIt seems, then, that our efforts to evaluate therapies will need to draw on diverse linesof evidence from many different studies. This creates a new question for us: Howshould we put together the evidence? What is the best way to integrate and summarizethe available data? For many investigators, the answer lies in a statistical techniquecalled meta-analysis, which we first encountered in Chapter 1 by means of which theresults of many different studies can be combined.
In one of the earliest analyses of this kind, 475 studies comprising 25,000 patientswere reviewed (M. L. Smith et al., 1980; Figure 17.26). In each of these studies, patientswho received some kind of psychotherapy were compared with a similar group of
efficacy Whether a therapeutic inter-vention works under carefully con-trolled conditions.
clinical utility Whether a therapeu-tic intervention works under real-world conditions.
meta-analysis A statistical techniquefor combining the results of manystudies on a particular topic, evenwhen the studies used different datacollection methods.
Num
ber o
f per
sons
Poor outcome
80% of untreated people have pooreroutcomes than the average treated person
Good outcome
Average untreatedperson
Average psychotherapyclient
17.26 Psychotherapy versus no treat-ment These two normal distributioncurves based on data from 475 studiesshow the improvement of untreated peopleand psychotherapy clients. The outcomefor the average therapy client surpassedthat for 80% of the untreated people.
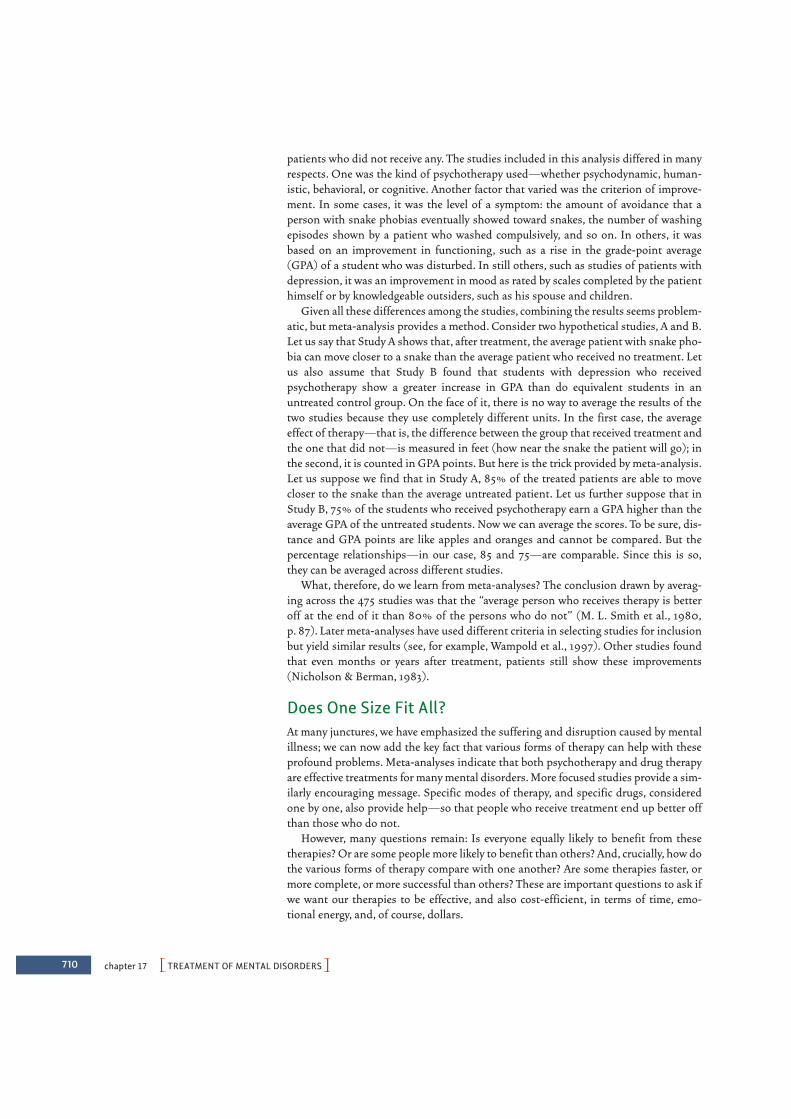
710 chapter 17 PTREATMENT OF MENTAL DISORDERSO
patients who did not receive any. The studies included in this analysis differed in manyrespects. One was the kind of psychotherapy used—whether psychodynamic, human-istic, behavioral, or cognitive. Another factor that varied was the criterion of improve-ment. In some cases, it was the level of a symptom: the amount of avoidance that aperson with snake phobias eventually showed toward snakes, the number of washingepisodes shown by a patient who washed compulsively, and so on. In others, it wasbased on an improvement in functioning, such as a rise in the grade-point average(GPA) of a student who was disturbed. In still others, such as studies of patients withdepression, it was an improvement in mood as rated by scales completed by the patienthimself or by knowledgeable outsiders, such as his spouse and children.
Given all these differences among the studies, combining the results seems problem-atic, but meta-analysis provides a method. Consider two hypothetical studies, A and B.Let us say that Study A shows that, after treatment, the average patient with snake pho-bia can move closer to a snake than the average patient who received no treatment. Letus also assume that Study B found that students with depression who receivedpsychotherapy show a greater increase in GPA than do equivalent students in anuntreated control group. On the face of it, there is no way to average the results of thetwo studies because they use completely different units. In the first case, the averageeffect of therapy—that is, the difference between the group that received treatment andthe one that did not—is measured in feet (how near the snake the patient will go); inthe second, it is counted in GPA points. But here is the trick provided by meta-analysis.Let us suppose we find that in Study A, 85% of the treated patients are able to movecloser to the snake than the average untreated patient. Let us further suppose that inStudy B, 75% of the students who received psychotherapy earn a GPA higher than theaverage GPA of the untreated students. Now we can average the scores. To be sure, dis-tance and GPA points are like apples and oranges and cannot be compared. But thepercentage relationships—in our case, 85 and 75—are comparable. Since this is so,they can be averaged across different studies.
What, therefore, do we learn from meta-analyses? The conclusion drawn by averag-ing across the 475 studies was that the “average person who receives therapy is betteroff at the end of it than 80% of the persons who do not” (M. L. Smith et al., 1980,p. 87). Later meta-analyses have used different criteria in selecting studies for inclusionbut yield similar results (see, for example, Wampold et al., 1997). Other studies foundthat even months or years after treatment, patients still show these improvements(Nicholson & Berman, 1983).
Does One Size Fit All? At many junctures, we have emphasized the suffering and disruption caused by mentalillness; we can now add the key fact that various forms of therapy can help with theseprofound problems. Meta-analyses indicate that both psychotherapy and drug therapyare effective treatments for many mental disorders. More focused studies provide a sim-ilarly encouraging message. Specific modes of therapy, and specific drugs, consideredone by one, also provide help—so that people who receive treatment end up better offthan those who do not.
However, many questions remain: Is everyone equally likely to benefit from thesetherapies? Or are some people more likely to benefit than others? And, crucially, how dothe various forms of therapy compare with one another? Are some therapies faster, ormore complete, or more successful than others? These are important questions to ask ifwe want our therapies to be effective, and also cost-efficient, in terms of time, emo-tional energy, and, of course, dollars.

PEvaluating TreatmentsO 711
FO R W H O M D O E S T H E R A P Y W O R K ?
Overall, therapy often improves the lives of adults who suffer from a range of psycho-logical, addictive, and health problems (see, for example, Barlow, 2004; Nathan &Gorman, 2002; Roth & Fonagy, 2004; Wampold et al., 1997). Therapy also helpschildren at various ages (Kazdin & Weisz, 2003; Weisz, Hawley, & Doss, 2004; Weisz,Doss, & Hawley, 2006).
Even so, therapy does not work for every individual, and, in fact, a certain proportionof patients—between 5 and 10%—actually get worse as a result of therapy (Lambert &Bergin, 1994; Lilienfeld, 2007; M. L. Smith, Glass, & Miller, 1980). What produces thisdeterioration? In many cases, the problem seems to be a bad therapist-patient relation-ship; in other cases, the problem may be outright incompetence in the therapist(Hadley & Strupp, 1976; M. L. Smith, Glass, & Miller, 1980). Still other cases of deteri-oration may have a subtler cause. Psychotherapy sometimes disrupts what is stable inthe patient’s life yet provides no substitute (Hadley & Strupp, 1976; Lambert & Bergin,1994). For example, the therapy may lead a patient to regard her marriage as unsatis-factory, but as she takes steps toward separation or divorce, she may become severelydepressed at the prospect of being alone. Good psychotherapists are alert to such dan-gers and attempt to avert such deterioration whenever possible.
For many years, researchers thought that therapy was most likely to succeed withpatients who were young, physically attractive, high in verbal ability, intelligent, andsuccessful in other domains; however, these turn out not to be the key factors (Nathan,Stuart, & Dolan, 2000). Instead, therapy seems to have roughly equal benefits forpeople from a wide range of socioeconomic backgrounds (Petry, Tennen, & Afflect,2000; Prochaska & Norcross, 2007). To put the point somewhat differently, whatmatters for the therapeutic benefit may not be who exactly the patient is, but (as wehighlighted earlier) whether the patient feels a strong sense of alliance with the thera-pist (J. P. Barber et al., 2000; Martin, Garske, & Davis, 2000). Also crucial is whetherthe patient is, at the start, fully motivated to participate in the therapy and optimisticabout the chances of recovery (Mussell et al., 2000). Improvement is also more likelywith more therapy sessions rather than fewer (Hansen, Lambert, & Forman, 2002;Seligman, 1995). And some disorders—for example, phobias—are more responsive topsychotherapy than others, such as schizophrenia.
One point, however, is less clear and remains the focus of debate: Should peoplewith subsyndromal conditions be treated? Some critics believe that they should andnote that evidence suggests that these syndromes are a genuine concern. For example,one study surveyed over 2,000 individuals for the presence of major depression. Basedon their signs and symptoms, these individuals were classified into three groups: nor-mal, diagnosable for major depression, or having subsyndromal depression—that is,they had some of the signs and symptoms of major depression but not enough to bediagnosed as having the disorder. On most measures, the people with subsyndromaland major depression were equally impaired (Judd, Paulus, Wells, & Rapaport, 1996;also Rapaport & Judd, 1998).
Others argue that treating all these individuals (and so offering similar therapies tothose diagnosed with depression and those who are not-quite-depressed) would be afirst step down a dangerous path, one in which people take pills or seek therapyto adjust their personalities just as they now seek nose jobs, liposuction, and face-liftsto adjust their body shapes. Indeed, this view might lead to a world in which nearly anyeccentricity is regarded as problematic and a candidate for treatment, with the termnormal reserved for the relatively few who are sufficiently bland to avoid labeling.Moreover, such indiscriminate diagnosis might lead people to use their subsyndromal
A2 appendix PSTATISTICS: THE DESCRIPTION, ORGANIZATION, AND INTERPRETATION OF DATAO
the difference in sex rather than to other factors (such as intellectual development,social class, and so on).
We discussed in Chapter 1 how investigators design studies and collect data. Sowe’ll start here with what investigators do once their data have been collected. Theirfirst task is to organize these data in a meaningful way. Suppose the study used twogroups of 50 boys and 50 girls, each observed on 10 separate occasions. This meansthat the investigators will end up with at least 1,000 separate numerical entries, 500for the boys and 500 for the girls. Something has to be done to reduce this mass ofnumbers into some manageable form. This is usually accomplished by some process ofaveraging scores.
The next step involves statistical interpretation. Suppose the investigators findthat the average score for physical aggression is greater for the boys than for the girls.(It probably will be.) How should this fact be interpreted? Should it be taken seri-ously, or might it just be a fluke, some sort of accident? For it is just about certain thatthe data contain variability: the children within each group will not perform identicallyto each other; furthermore, the same child may very well behave differently on oneoccasion than on another. Thus, the number of aggressive acts for the boys might be,say, 5.8 on average, but might vary from a low of 1.3 (the score from completely calmCalvin) to a high of 11.4 (the score from awfully aggressive Albert). The average num-ber of aggressive acts for the girls might be 3.9 (and so lower than the boys’ average),but this derives from a range of scores that include 0 (from serene Sarah) and 6.2(from aggressive Agnes).
Is it possible that this difference between boys and girls is just a matter of chance,an accidental by-product of this variability? For example, what if boys and girls are, infact, rather similar in their levels of aggression, but—just by chance—the study hap-pened to include four or five extremely aggressive boys and a comparable number ofextremely unaggressive girls? After all, we know that our results would have been differ-ent if Albert had been absent on the day of our testing; the boys’ average, without hiscontribution, would have been lower. Likewise, Agnes’s twin sister was not included inour test group because of the random process through which we selected our researchparticipants. If she had been included, and if she was as aggressive as her twin, thenthe girls’ average would have been higher. Is it possible that accidents like these are thereal source of the apparent difference between the groups? If so, then another study,without these same accidents, might yield a different result. One of the main reasonsfor using statistical methods is to deal with questions of this sort, to help us draw use-ful conclusions about behavior despite the unavoidable variability, and, specifically,allowing us to ask in a systematic way whether our data pattern is reliable (and sowould emerge in subsequent studies) or just the product of accidents.
DESCRIBING THE DATA
In the example above, we assumed that the investigators would be collecting numericaldata. We made this assumption because much of the power of statistics results from thefact that numbers can be manipulated using the rules of arithmetic, unlike open-endedresponses in an interview, videotapes of social interactions, or lists of words recalled ina memory experiment. (How could you average together one participant’s response of“Yes, I like them” with another’s response of “Only on weekends”?) As a result, scien-tists prefer to use numerical response measures whenever possible. Consider our hypo-

PDescribing the DataO A3
thetical study of physical aggression. The investigators who watched the research par-ticipants might rate their physical aggression in various situations from 1 to 5, with 1being “extremely docile” and 5 being “extremely aggressive,” or they might count thenumber of aggressive acts (say, hitting or kicking another child). This operation ofassigning numbers to observed events is called scaling.
There are several types of scales that will concern us. They differ by the arithmeticaloperations that can be performed on them.
Categorical and Ordinal ScalesSometimes the scores assigned to individuals are merely categorical (also called nominal).For example, when respondents to a poll are asked to name the television channel theywatch most frequently, they might respond “4,” “2,” or “13.” These numbers serve only togroup the responses into categories. They can obviously not be subjected to any arith-metic operations. (If a respondent watches channels 2 and 4 equally often, we can’t sum-marize this by claiming that, on average, she watches channel 3!)
Ordinal scales convey more information, in that the relative magnitude of each num-ber is meaningful—not arbitrary, as in the case of categorical scales. If individuals areasked to list the ten people they most admire, the number 1 can be assigned to the mostadmired person, 2 to the runner-up, and so on. The smaller the number assigned, themore the person is admired. Notice that no such statement can be made of televisionchannels: channel 4 is not more anything than channel 2, just different from it.
Scores that are ordinally scaled cannot, however, be added or subtracted. The firsttwo persons on the most-admired list differ in admirability by 1; so do the last two. Yetthe individual who has done the ranking may admire the first person far more than theother nine, all of whom might be very similar in admirability. Imagine, for example, achild who, given this task, lists his mother first, followed by the starting lineup of theChicago Cubs. In this case, the difference between rank 1 and rank 2 is enormous; thedifference between rank 2 and rank 3 (or any other pair of adjacent ranks) is apprecia-bly smaller. Or, to put it another way, the difference of eight between person 2 andperson 10 probably represents a smaller difference in judged admirability than the dif-ference of one obtained between persons 1 and 2 (at least so the mother hopes).
Interval ScalesScales in which equal differences between scores, or intervals, can be treated as equalunits are called interval scales. Response time is a common psychological variable that isusually treated as an interval scale. In some memory experiments, for example, the par-ticipant must respond as quickly as possible to each of several words, some of which shehas seen earlier in the experiment; the task is to indicate, by pressing the appropriatebutton, whether each word had appeared earlier or not.
Suppose that someone requires an average of 2 seconds to respond to nouns, 3 secondsto verbs, and 4 seconds to adjectives. The difference in decision time between verbs andnouns (3 " 2 = 1 second) is the same as the difference in decision time between adjectivesand verbs (4 " 3 = 1 second). We can make this statement—which in turn suggests vari-ous hypotheses about the factors that underlie such differences—precisely becauseresponse time can be regarded as an interval scale.
Ratio ScalesScores based on an interval scale allow subtraction and addition. But they do not allowmultiplication and division. Consider the Celsius scale of temperature. The difference
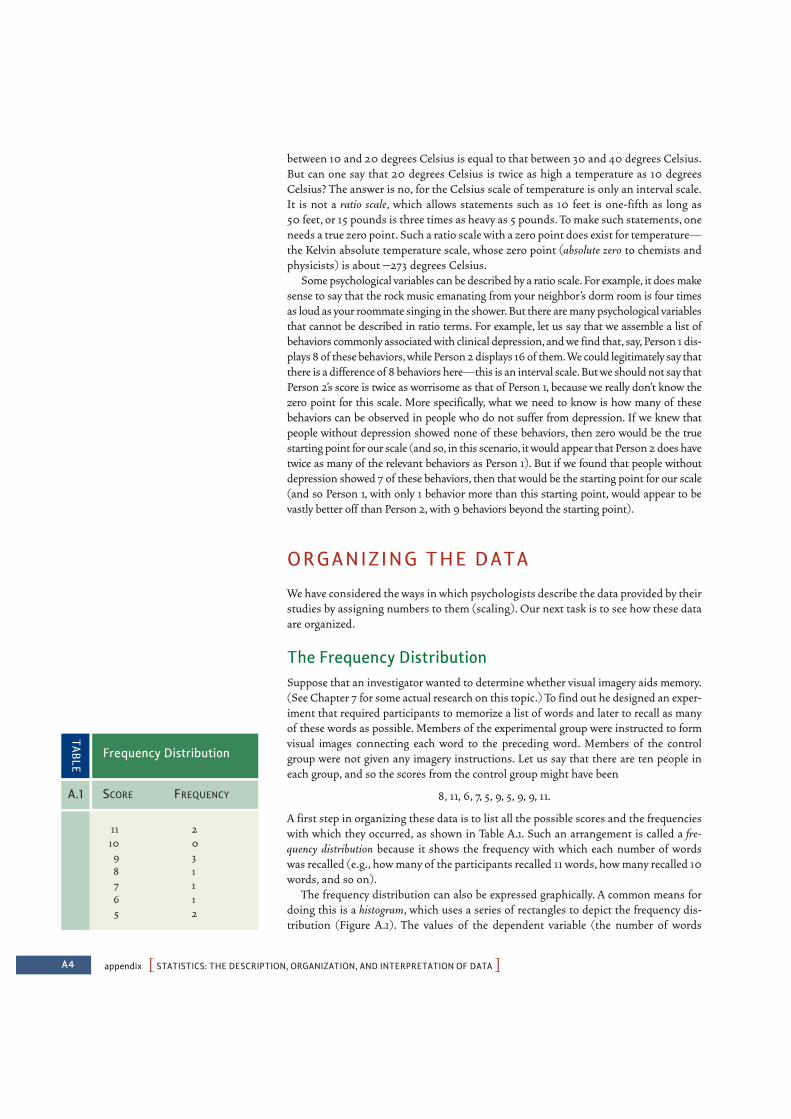
A4 appendix PSTATISTICS: THE DESCRIPTION, ORGANIZATION, AND INTERPRETATION OF DATAO
between 10 and 20 degrees Celsius is equal to that between 30 and 40 degrees Celsius.But can one say that 20 degrees Celsius is twice as high a temperature as 10 degreesCelsius? The answer is no, for the Celsius scale of temperature is only an interval scale.It is not a ratio scale, which allows statements such as 10 feet is one-fifth as long as 50 feet, or 15 pounds is three times as heavy as 5 pounds. To make such statements, oneneeds a true zero point. Such a ratio scale with a zero point does exist for temperature—the Kelvin absolute temperature scale, whose zero point (absolute zero to chemists andphysicists) is about "273 degrees Celsius.
Some psychological variables can be described by a ratio scale. For example, it does makesense to say that the rock music emanating from your neighbor’s dorm room is four timesas loud as your roommate singing in the shower. But there are many psychological variablesthat cannot be described in ratio terms. For example, let us say that we assemble a list ofbehaviors commonly associated with clinical depression, and we find that, say, Person 1 dis-plays 8 of these behaviors,while Person 2 displays 16 of them.We could legitimately say thatthere is a difference of 8 behaviors here—this is an interval scale.But we should not say thatPerson 2’s score is twice as worrisome as that of Person 1, because we really don’t know thezero point for this scale. More specifically, what we need to know is how many of thesebehaviors can be observed in people who do not suffer from depression. If we knew thatpeople without depression showed none of these behaviors, then zero would be the truestarting point for our scale (and so, in this scenario, it would appear that Person 2 does havetwice as many of the relevant behaviors as Person 1). But if we found that people withoutdepression showed 7 of these behaviors, then that would be the starting point for our scale(and so Person 1, with only 1 behavior more than this starting point, would appear to bevastly better off than Person 2, with 9 behaviors beyond the starting point).
ORGANIZING THE DATA
We have considered the ways in which psychologists describe the data provided by theirstudies by assigning numbers to them (scaling). Our next task is to see how these dataare organized.
The Frequency DistributionSuppose that an investigator wanted to determine whether visual imagery aids memory.(See Chapter 7 for some actual research on this topic.) To find out he designed an exper-iment that required participants to memorize a list of words and later to recall as manyof these words as possible. Members of the experimental group were instructed to formvisual images connecting each word to the preceding word. Members of the controlgroup were not given any imagery instructions. Let us say that there are ten people ineach group, and so the scores from the control group might have been
8, 11, 6, 7, 5, 9, 5, 9, 9, 11.
A first step in organizing these data is to list all the possible scores and the frequencieswith which they occurred, as shown in Table A.1. Such an arrangement is called a fre-quency distribution because it shows the frequency with which each number of wordswas recalled (e.g., how many of the participants recalled 11 words, how many recalled 10words, and so on).
The frequency distribution can also be expressed graphically. A common means fordoing this is a histogram, which uses a series of rectangles to depict the frequency dis-tribution (Figure A.1). The values of the dependent variable (the number of words
11 210 0
9 38 17 16 15 2
Frequency Distribution
TABLE
A.1 SCORE FREQUENCY
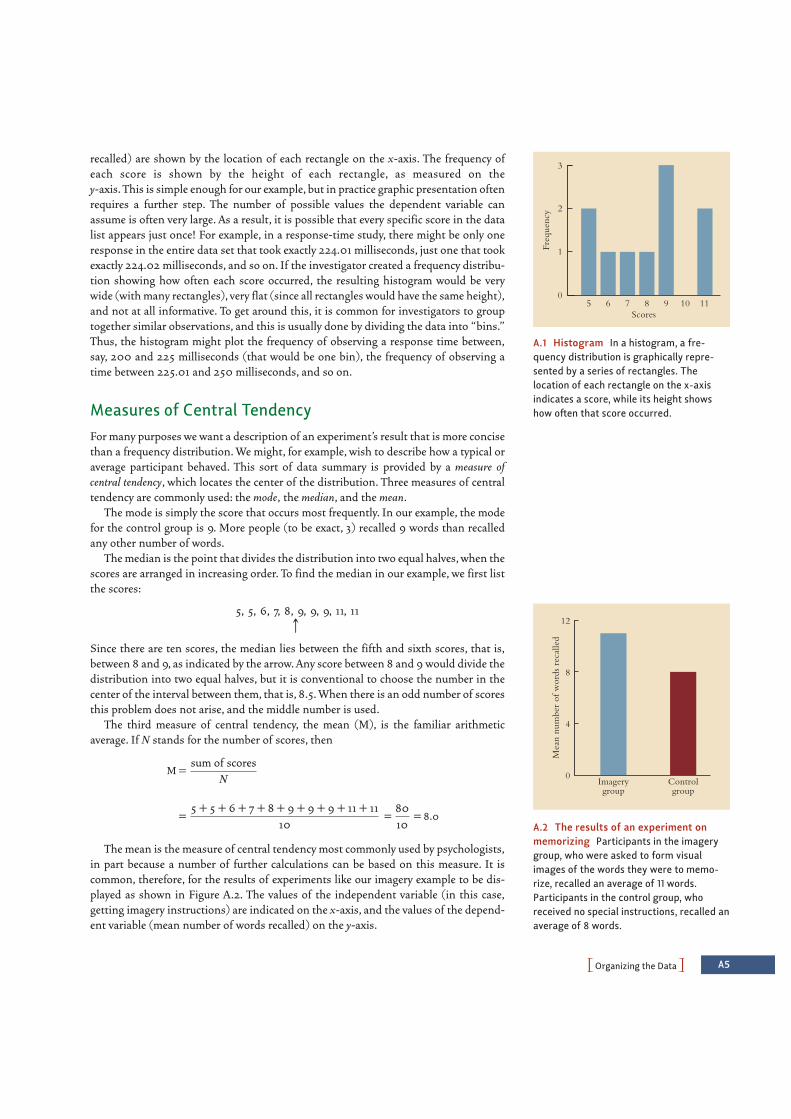
POrganizing the DataO A5
recalled) are shown by the location of each rectangle on the x-axis. The frequency ofeach score is shown by the height of each rectangle, as measured on the y-axis. This is simple enough for our example, but in practice graphic presentation oftenrequires a further step. The number of possible values the dependent variable canassume is often very large. As a result, it is possible that every specific score in the datalist appears just once! For example, in a response-time study, there might be only oneresponse in the entire data set that took exactly 224.01 milliseconds, just one that tookexactly 224.02 milliseconds, and so on. If the investigator created a frequency distribu-tion showing how often each score occurred, the resulting histogram would be verywide (with many rectangles), very flat (since all rectangles would have the same height),and not at all informative. To get around this, it is common for investigators to grouptogether similar observations, and this is usually done by dividing the data into “bins.”Thus, the histogram might plot the frequency of observing a response time between,say, 200 and 225 milliseconds (that would be one bin), the frequency of observing atime between 225.01 and 250 milliseconds, and so on.
Measures of Central TendencyFor many purposes we want a description of an experiment’s result that is more concisethan a frequency distribution. We might, for example, wish to describe how a typical oraverage participant behaved. This sort of data summary is provided by a measure ofcentral tendency, which locates the center of the distribution. Three measures of centraltendency are commonly used: the mode, the median, and the mean.
The mode is simply the score that occurs most frequently. In our example, the modefor the control group is 9. More people (to be exact, 3) recalled 9 words than recalledany other number of words.
The median is the point that divides the distribution into two equal halves, when thescores are arranged in increasing order. To find the median in our example, we first listthe scores:
5, 5, 6, 7, 8, 9, 9, 9, 11, 11c
Since there are ten scores, the median lies between the fifth and sixth scores, that is,between 8 and 9, as indicated by the arrow. Any score between 8 and 9 would divide thedistribution into two equal halves, but it is conventional to choose the number in thecenter of the interval between them, that is, 8.5. When there is an odd number of scoresthis problem does not arise, and the middle number is used.
The third measure of central tendency, the mean (M), is the familiar arithmeticaverage. If N stands for the number of scores, then
M =
= = = 8.0
The mean is the measure of central tendency most commonly used by psychologists,in part because a number of further calculations can be based on this measure. It iscommon, therefore, for the results of experiments like our imagery example to be dis-played as shown in Figure A.2. The values of the independent variable (in this case,getting imagery instructions) are indicated on the x-axis, and the values of the depend-ent variable (mean number of words recalled) on the y-axis.
8010
5 + 5 + 6 + 7 + 8 + 9 + 9 + 9 + 11 + 11 10
sum of scoresN
A.1 Histogram In a histogram, a fre-quency distribution is graphically repre-sented by a series of rectangles. Thelocation of each rectangle on the x-axisindicates a score, while its height showshow often that score occurred.
3
2
1
0
Scores
Freq
uenc
y
5 6 7 8 9 10 11
A.2 The results of an experiment onmemorizing Participants in the imagerygroup, who were asked to form visualimages of the words they were to memo-rize, recalled an average of 11 words.Participants in the control group, whoreceived no special instructions, recalled anaverage of 8 words.
12
8
4
0Imagerygroup
Controlgroup
Mea
n nu
mbe
r of
wor
ds r
ecal
led
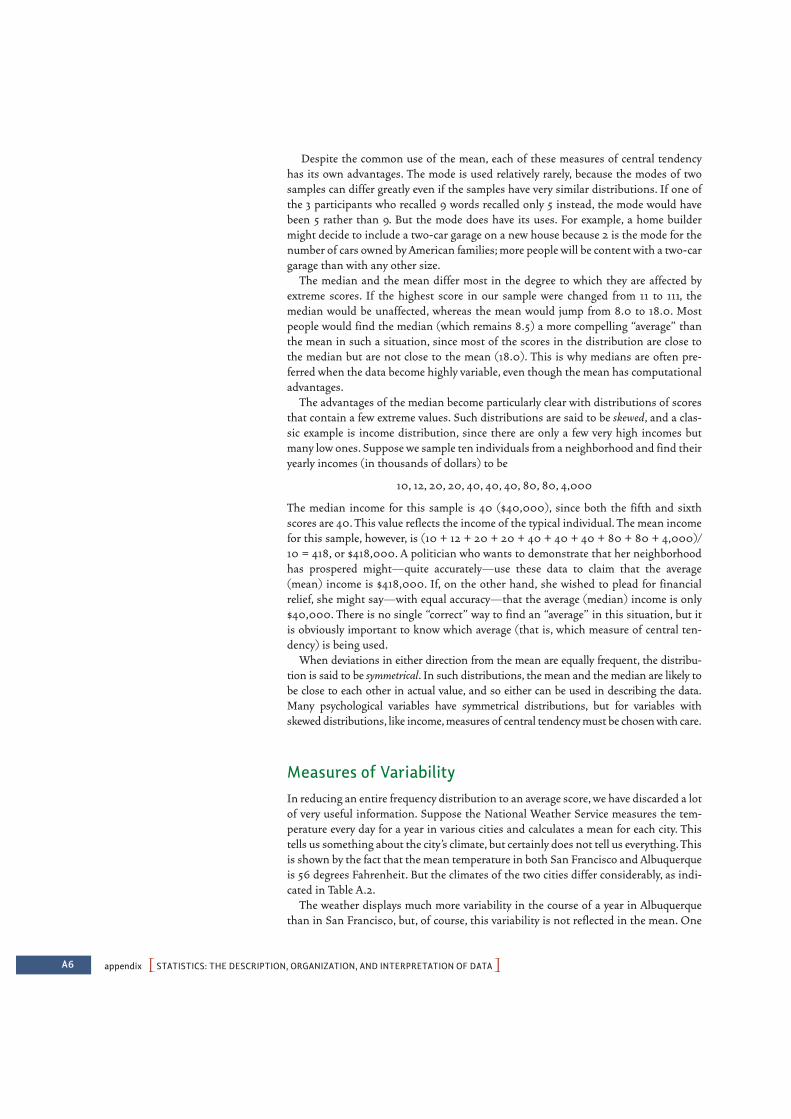
A6 appendix PSTATISTICS: THE DESCRIPTION, ORGANIZATION, AND INTERPRETATION OF DATAO
Despite the common use of the mean, each of these measures of central tendencyhas its own advantages. The mode is used relatively rarely, because the modes of twosamples can differ greatly even if the samples have very similar distributions. If one ofthe 3 participants who recalled 9 words recalled only 5 instead, the mode would havebeen 5 rather than 9. But the mode does have its uses. For example, a home buildermight decide to include a two-car garage on a new house because 2 is the mode for thenumber of cars owned by American families; more people will be content with a two-cargarage than with any other size.
The median and the mean differ most in the degree to which they are affected byextreme scores. If the highest score in our sample were changed from 11 to 111, themedian would be unaffected, whereas the mean would jump from 8.0 to 18.0. Mostpeople would find the median (which remains 8.5) a more compelling “average” thanthe mean in such a situation, since most of the scores in the distribution are close tothe median but are not close to the mean (18.0). This is why medians are often pre-ferred when the data become highly variable, even though the mean has computationaladvantages.
The advantages of the median become particularly clear with distributions of scoresthat contain a few extreme values. Such distributions are said to be skewed, and a clas-sic example is income distribution, since there are only a few very high incomes butmany low ones. Suppose we sample ten individuals from a neighborhood and find theiryearly incomes (in thousands of dollars) to be
10, 12, 20, 20, 40, 40, 40, 80, 80, 4,000
The median income for this sample is 40 ($40,000), since both the fifth and sixthscores are 40. This value reflects the income of the typical individual. The mean incomefor this sample, however, is (10 + 12 + 20 + 20 + 40 + 40 + 40 + 80 + 80 + 4,000)/10 = 418, or $418,000. A politician who wants to demonstrate that her neighborhoodhas prospered might—quite accurately—use these data to claim that the average(mean) income is $418,000. If, on the other hand, she wished to plead for financialrelief, she might say—with equal accuracy—that the average (median) income is only$40,000. There is no single “correct” way to find an “average” in this situation, but itis obviously important to know which average (that is, which measure of central ten-dency) is being used.
When deviations in either direction from the mean are equally frequent, the distribu-tion is said to be symmetrical. In such distributions, the mean and the median are likely tobe close to each other in actual value, and so either can be used in describing the data.Many psychological variables have symmetrical distributions, but for variables withskewed distributions, like income, measures of central tendency must be chosen with care.
Measures of VariabilityIn reducing an entire frequency distribution to an average score, we have discarded a lotof very useful information. Suppose the National Weather Service measures the tem-perature every day for a year in various cities and calculates a mean for each city. Thistells us something about the city’s climate, but certainly does not tell us everything. Thisis shown by the fact that the mean temperature in both San Francisco and Albuquerqueis 56 degrees Fahrenheit. But the climates of the two cities differ considerably, as indi-cated in Table A.2.
The weather displays much more variability in the course of a year in Albuquerquethan in San Francisco, but, of course, this variability is not reflected in the mean. One

POrganizing the DataO A7
way to measure this variability is the range, the highest score minus the lowest. Therange of temperatures in San Francisco is 15, while in Albuquerque it is 42.
A shortcoming of the range as a measure of variability is that it reflects the values ofonly two scores in the entire sample. As an example, consider the following distribu-tions of ages in two college classes:
Distribution A: 19, 19, 19, 19, 19, 20, 25Distribution B: 17, 17, 17, 20, 23, 23, 23
Intuitively, distribution A has less variability, since all scores but one are very close to themean. Yet the range of scores is the same (6) in both distributions. The problem arisesbecause the range is determined by only two of the seven scores in each distribution.
A better measure of variability would incorporate every score in the distribution ratherthan just two. One might think that the variability could be measured by asking how fareach individual score is away from the mean, and then taking the average of these dis-tances. This would give us a measure that we could interpret (roughly) as ìon average, allthe data points are only two units from the mean (or “. . . three units . . .” or whatever itturned out to be). The most straightforward way to measure this would be to find thearithmetic difference (by subtraction) between each score and the mean (that is, comput-ing [score " M] for each score), and then to take the average of these differences (that is,add up all of these differences, and divide by the number of observations):
This hypothetical measure is unworkable, however, because some of the scores aregreater than the mean and some are smaller, so that the numerator is a sum of both pos-itive and negative terms. (In fact, it turns out that the sum of the positive terms equalsthe sum of the negative terms, so that the expression shown above always equals zero.)The solution to this problem is simply to square all the terms in the numerator, thusmaking them all positive.* The resulting measure of variability is called the variance (V):
V = (1)sum of (score " M)2
N
sum of (score " M)N
Albuquerque, 35 56 77 42New Mexico
San Francisco, 48 56 63 15California
Temperature Data for Two Cities (Degrees Fahrenheit)
TABLE
A.2 CITY LOWEST MONTH MEAN HIGHEST MONTH RANGE
* An alternative solution would be to sum the absolute value of these differences, that is, to consider only the magni-tude of this difference for each score, not the sign. The resulting statistic, called the average deviation, is little used,however, primarily because absolute values are not easily dealt with in certain mathematical terms that underlie sta-tistical theory. As a result, statisticians prefer to transform negative into positive numbers by squaring them.
A8 appendix PSTATISTICS: THE DESCRIPTION, ORGANIZATION, AND INTERPRETATION OF DATAO
The calculation of the variance for the control group in the word-imagery experiment isshown in Table A.3. As the table shows, the variance is obtained by subtracting themean (M, which equals 8) from each score, squaring each result, adding all the squaredterms, and dividing the resulting sum by the total number of scores (N, which equals10), yielding a value of 4.4.
Because deviations from the mean are squared, the variance is expressed in units dif-ferent from the scores themselves. If our dependent variable were a distance, measuredin centimeters, the variance would be expressed in square centimeters. As we will see inthe next section, it is convenient to have a measure of variability that can be added toor subtracted from the mean; such a measure ought to be expressed in the same unitsas the original scores. To accomplish this end, we employ another measure of variabil-ity, the standard deviation, or SD. The standard deviation is derived from the variance bytaking the square root of the variance. Thus
SD = ! V–
In our example, the standard deviation is about 2.1, the square root of the variancewhich is 4.4.
Converting Scores to Compare ThemSuppose a person takes two tests. One measures his memory span—how many digitshe can remember after one presentation. The other test measures his reading speed—how quickly he can read a 200-word essay. It turns out that he can remember8 digits and needs 140 seconds for the essay. Is there any way to compare these twonumbers, to decide whether he can remember digits as well (or worse or equally well )as he can read? On the face of it, the question seems absurd; it seems like comparingapples and oranges. But for some purposes, we would want to compare these numbers.For example, a first step toward identifying people with dyslexia is documenting thattheir reading ability is markedly lower than we would expect, based on their intellectualperformance in other areas. For this purpose, a comparison much like the one just
8 8 – 8 = 0 02 = 011 11 – 8 = 3 32 = 96 6 – 8 = "2 ("2)2 = 47 7 – 8 = "1 ("1)2 = 15 5 – 8 = "3 ("3)2 = 99 9 – 8 = 1 12 = 15 5 – 8 = "3 ("3)2 = 99 9 – 8 = 1 12 = 19 9 – 8 = 1 12 = 111 11 – 8 = 3 32 = 9
sum = 44
V = = = 4.44410
sum of (score – mean)2
N
Calculating Variance
TABLE
A.3 SCORE SCORE " MEAN (SCORE " MEAN)2

POrganizing the DataO A9
sketched might be useful. But how do we compare digits-remembered to number-of-seconds-needed-for-reading?
In fact, there is a way to make this comparison, starting with an assessment of howeach of these two scores compares to the scores of other persons who have been giventhe same two tests.
P E RC E N T I L E R A N KS
One way of doing this is by transforming each of the two scores into a percentile rank. Thepercentile rank of a score indicates the percentage of all scores that lie below that givenscore. Let us assume that 8 digits is the 78th percentile. This means that 78 percent ofthe relevant comparison group remembers fewer digits. Let us further assume that ascore of 140 seconds in the reading task is the 53rd percentile of the same comparisongroup. We can now answer the question with which we started. This person can remem-ber digits more effectively than he can read. By converting into percentile ranks we haverendered incompatible scores compatible, allowing us to compare the two.
STA N DA R D SCO R E S
For many statistical purposes there is an even better method of comparing scores or ofinterpreting the meaning of individual scores. This is to express them by reference tothe mean and standard deviation of the frequency distribution of which they are a part.This is done by converting the individual scores into standard scores (often called z-scores). The formula for calculating a z-score is:
z = (2)
Suppose you take a test that measures aptitude for accounting and are told yourscore is 36. In itself, this number cannot help you decide whether to pursue or avoid acareer in accounting. To interpret your score you need to know both the average scoreand how variable the scores are. If the mean is 30, you know you are above average, buthow far above average is 6 points? This might be an extreme score or one attained bymany, depending on the variability of the distribution.
Let us suppose that the standard deviation of the distribution is 3. Your z-score onthe accounting test is (36 " 30)/3 = +2. That is, your score is 2 SDs above the mean.
But how to use this information? Let us say that you are still unsure whether tobecome an accountant, and so you take a screen test to help you decide whether tobecome an actor instead. Here, your score is 100. This is a larger number than the36 you scored on the earlier test, but it may not reveal much acting aptitude.Suppose the mean score on the screen test is 80, and the standard deviation is 20;then your z-score is (100 " 80)/20 = +1. In acting aptitude, you are 1 SD above themean (that is, z = +1)—above average but not by much. In accounting aptitude, youare 2 SDs above the mean (that is, z = +2), and so the use of z-scores makes yourrelative abilities clear.
Percentile rank and a z-score give similar information, but, to convert one into theother, we need a bit more information.
The Normal DistributionFrequency histograms can have a wide variety of shapes, but many variables that inter-est psychologists have a normal distribution (often called a normal curve), which is a
(score " M)SD
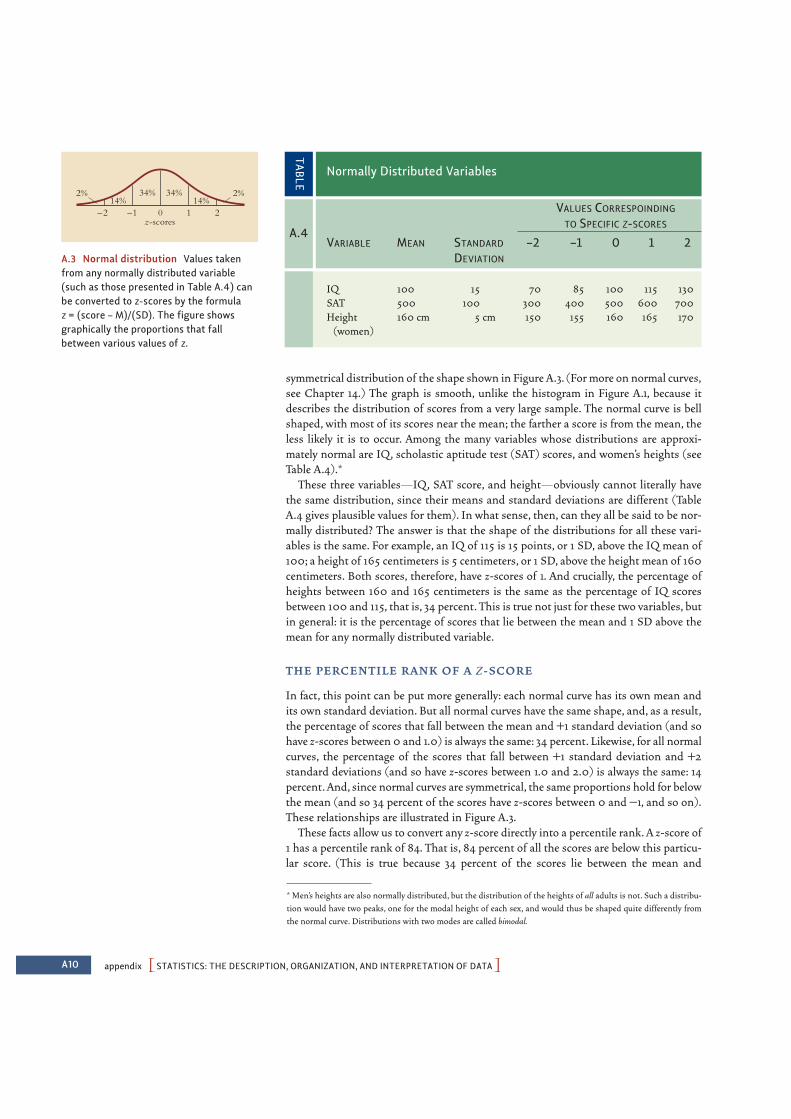
A10 appendix PSTATISTICS: THE DESCRIPTION, ORGANIZATION, AND INTERPRETATION OF DATAO
symmetrical distribution of the shape shown in Figure A.3. (For more on normal curves,see Chapter 14.) The graph is smooth, unlike the histogram in Figure A.1, because itdescribes the distribution of scores from a very large sample. The normal curve is bellshaped, with most of its scores near the mean; the farther a score is from the mean, theless likely it is to occur. Among the many variables whose distributions are approxi-mately normal are IQ, scholastic aptitude test (SAT) scores, and women’s heights (seeTable A.4).*
These three variables—IQ, SAT score, and height—obviously cannot literally havethe same distribution, since their means and standard deviations are different (TableA.4 gives plausible values for them). In what sense, then, can they all be said to be nor-mally distributed? The answer is that the shape of the distributions for all these vari-ables is the same. For example, an IQ of 115 is 15 points, or 1 SD, above the IQ mean of100; a height of 165 centimeters is 5 centimeters, or 1 SD, above the height mean of 160centimeters. Both scores, therefore, have z-scores of 1. And crucially, the percentage ofheights between 160 and 165 centimeters is the same as the percentage of IQ scoresbetween 100 and 115, that is, 34 percent. This is true not just for these two variables, butin general: it is the percentage of scores that lie between the mean and 1 SD above themean for any normally distributed variable.
T H E P E RC E N T I L E R A N K O F A Z- SCO R E
In fact, this point can be put more generally: each normal curve has its own mean andits own standard deviation. But all normal curves have the same shape, and, as a result,the percentage of scores that fall between the mean and +1 standard deviation (and sohave z-scores between 0 and 1.0) is always the same: 34 percent. Likewise, for all normalcurves, the percentage of the scores that fall between +1 standard deviation and +2standard deviations (and so have z-scores between 1.0 and 2.0) is always the same: 14percent. And, since normal curves are symmetrical, the same proportions hold for belowthe mean (and so 34 percent of the scores have z-scores between 0 and "1, and so on).These relationships are illustrated in Figure A.3.
These facts allow us to convert any z-score directly into a percentile rank. A z-score of1 has a percentile rank of 84. That is, 84 percent of all the scores are below this particu-lar score. (This is true because 34 percent of the scores lie between the mean and
IQ 100 15 70 85 100 115 130SAT 500 100 300 400 500 600 700Height 160 cm 5 cm 150 155 160 165 170
(women)
Normally Distributed Variables
TABLE
A.4
VALUES CORRESPOINDING
TO SPECIFIC Z-SCORES
VARIABLE MEAN STANDARD –2 –1 0 1 2DEVIATION
* Men’s heights are also normally distributed, but the distribution of the heights of all adults is not. Such a distribu-tion would have two peaks, one for the modal height of each sex, and would thus be shaped quite differently fromthe normal curve. Distributions with two modes are called bimodal.
A.3 Normal distribution Values takenfrom any normally distributed variable(such as those presented in Table A.4) canbe converted to z-scores by the formula z = (score – M)/(SD). The figure showsgraphically the proportions that fallbetween various values of z.
34% 34%14% 14%
2%2%
0 1 2–2 –1z-scores
POrganizing the DataO A11
z = 1, and 50 percent of the scores lie blow the mean). Likewise, a z-score of "1 (1 SDbelow the mean) corresponds, in a normal distribution, to a percentile rank of 16: only16 percent of the scores are lower. And so on.
H O W T H E N O R M A L CU R V E A R I S E S
Why should variables such as height or IQ (and many others) form distributions that havethis particular shape? Mathematicians have shown that whenever a given variable is thesum of many smaller variables, its distribution will be close to that of the normal curve.One example is lifetime earnings—obviously the sum of what one has earned on manyprior occasions. A different example is height. Height can be thought of as the sum of thecontributions of the many genes and the many environmental factors that influence thistrait; it, therefore, satisfies the general condition. The basic idea is that the many differentfactors that influence a given measure (such as the genes for height) operate independ-ently of the others, and, for each of these factors, it is a matter of chance whether the fac-tor applies to a particular individual or not. Thus, if someone’s father had a certainheight-promoting gene on one chromosome but not on the other chromosome in the pair,then it would literally be a matter of chance whether the person inherited this gene or not(and likewise for each of the other genes—and surely there are many—that determineheight). The person’s height would also depend on accidents in his experience—for exam-ple, whether, just by bad luck, he happened to catch the flu at an age that interrupted whatwould have otherwise been a strong growth spurt.
In essence, then, we can think of each person’s height as dependent on a successionof coin tosses, with each toss describing whether that person received the height-promoting factor or not—inherited the gene or not, got the flu at just the wrong timeor not, and so on. Of course, each factor contributes its own increment to the person’sheight, and so his ultimate height depends on how many of these factors fell the rightway. Thus, if we want to predict the person’s height, we need to explore the (relativelysimple) mathematics that describe how these chance events unfold.
Let us imagine that someone literally does toss a coin over and over, with each headcorresponding to a factor that tends to increase height and each tail to a factor that tendsto diminish it. Predicting the person’s height, therefore, would be equivalent to predict-ing how many heads, in total, the person will obtain after a certain number of tosses. Ifthe coin is tossed only once, then there will be either 0 heads or 1 head, and these areequally likely. The resulting distribution is shown in the top panel of Figure A.4.
If the number of tosses (which we will call N) is 2, then 0, 1, or 2 heads can arise.However, not all these outcomes are equally likely: 0 heads come up only if the sequencetail-tail (TT) occurs; 2 heads only if head-head (HH) occurs; but 1 head results fromeither HT or TH. The distribution of heads for N = 2 is shown in the second panel ofFigure A.4. The area above 1 head has been subdivided into two equal parts, one for eachpossible sequence containing a single head.*
As N increases, the distribution of the number of heads looks more and more like thenormal distribution,as the subsequent panels of Figure A.4 show.When N becomes as largeas the number of factors that determine height, the distribution of the number of heads isvirtually identical to the normal distribution, and this gives us just the claim we were after:as we have described, this logic of coin tossing corresponds reasonably well to the logic ofthe factors governing height, and so, just as the distribution of coin tosses will (withenough tosses) be normally distributed,so will height.The same logic applies to many other
A.4 Histograms showing expected num-ber of heads in tossing a fair coin N timesIn successive panels, N = 1, 2, 4, and 8. Thebottom panel illustrates the case when N = 100 and shows a smoothed curve.
.4
.3
.2
.1
T
1
H
0
N = 1
.5
0 1 2
N = 2
.5
.25THTT HH
Rel
ativ
e fr
eque
ncy
of h
eads
0 1 2 3 4
N = 4
.25
TTTT TTTH THHT HHHT HHHH
TTHT THTH HHTH
THTT TTHH HTHH
HTTT HTTH THHH
HTHT
HHTT
0 1 2 3 4 5 6 7 8
N = 8
.3
.2
.1
0
N = 100
10025 50 75Number of heads
T = TailH = Head
HT
* The distribution of the number of heads is called the binomial distribution, because of its relation to the binomialtheorem: the number of head-tail sequences that can lead to k heads is the (k + 1)st coefficient of (a + b)N.

PREFERENCESO R33
“executive attention.” Journal of Experimental Psychology:Learning, Memory & Cognition, 32, 749–777.
KAPLAN, H., & DOVE, H. (1987). Infant developmentamong the Ache of eastern Paraguay. DevelopmentalPsychology, 23, 190–198.
KAPUR, N. (1999). Syndromes of retrograde amnesia.Psychological Bulletin, 125, 800–825.
KAPUR, S., & REMINGTON, G. (1996). Serotonin-dopamine interaction and its relevance to schizophrenia.American Journal of Psychiatry, 153, 466–476.
KAPUR, S., & REMINGTON, G. (2001). Dopamine D(2)receptors and their role in atypical antipsychotic action:still necessary and may even be sufficient. BiologicalPsychiatry, 50(11), 873–883.
KARAU, S. J., & WILLIAMS, K. D. (1993). Social loafing: Ameta-analytic review and theoretical integration. Journalof Personality and Social Psychology, 65(4), 681–706.
KARCH, S. (Ed.). (2007). Drug abuse handbook (2nd ed.).New York: Taylor & Francis.
KASSER, T., & SHARMA, Y. S. (1999). Reproductive free-dom, educational equality, and females’ preference forresource-acquisition characteristics in mates.Psychological Science, 10(4), 374–377.
KASSIN, S. M., & GUDJONSSON, G. H. (2004). The psy-chology of confession evidence: A review of the literatureand issues. Psychological Science in the Public Interest, 5,35–69.
KATO, T., & KATO, N. (2000). Mitochondrial dysfunctionin bipolar disorder. Bipolar Disorders, 2(3, Pt. 1), 180–190.
KATZ, J. J., & FODOR, J. A. (1963). The structure of asemantic theory. Language, 39, 170–210.
KAUFFMAN, T., THEORET, H., & PASCUAL-LEONE, A. (2002).Braille character discrimination in blindfolded humansubjects. Neuroreport, 13, 571–574.
KAWAKAMI, K., DION, K. L., & DOVIDIO, J. F. (1998). Racialprejudice and stereotype activation. Personality and SocialPsychology Bulletin, 24(4), 407–416.
KAY, P. (1996). Intra-speaker relativity. In J. J. Gumperz &S. C. Levinson (Eds.), Rethinking linguistic relativity.Studies in the social and cultural foundations of language.Cambridge: Cambridge University Press.
KAY, P., & REGIER, T. (2006). Language, thought, andcolor: Recent developments. Trends in Cognitive Sciences,10(2), 51–54.
KAZDIN, A. E. (2003). Psychotherapy for children andadolescents. Annual Review of Psychology, 54, 253–276.
KAZDIN, A. E., & BENJET, C. (2003). Spanking children:Evidence and issues. Current Directions in PsychologicalScience, 12(3), 99–103.
KAZDIN, A. E., & WEISZ, J. R. (EDS.). (2003). Evidence-based psychotherapies for children and adolescents. NewYork: Guilford.
KEATING, D. (2004). Cognitive and brain development.In R. Lerner & L. Steinberg (Eds.), Handbook of adolescentpsychology (pp. 45–84). New York: Wiley.
KECK, P. E., JR., & MCELROY, S. L. (2002). Carbamazepineand valproate in the maintenance treatment of bipolardisorder. Journal of Clinical Psychiatry, 63(Suppl. 10),13–17.
KEEL, P. K., & KLUMP, K. L. (2003). Are eating disordersculture-bound syndromes? Implications for conceptual-izing their etiology. Psychological Bulletin, 129(5),747–769.
KEGL, J., SENGHAS, A., & COPPOLA, M. (1999). Creationthrough contact: Sign language emergence and sign lan-guage change in Nicaragua. In M. Degraff (Ed.),Language creation and language change: Creolization,diachrony, and development (pp. 179–237). Cambridge,MA: MIT Press.
KEIL, F. L. (1989). Concepts, kinds, and cognitive develop-ment. Cambridge, MA: MIT Press.
KEIZER, K., LINDENBERG, S., & STEG, L. (2008). Thespreading of disorder. Science, 322, 1681–1685.
KELLEY, H. H. (1967). Attribution theory in social psy-chology. In D. Levine (Ed.), Nebraska Symposium onMotivation (pp. 192–238). Lincoln: University ofNebraska Press.
KELLEY, H. H., & MICHELA, J. L. (1980). Attribution theoryand research. Annual Review of Psychology, 31, 457–501.
KELLEY, S., & MIRER, T. W. (1974). The simple act of vot-ing. American Political Science Review, 68, 572–591.
KELLMAN, P. J., GARRIGAN, P., & SHIPLEY, T. F. (2005).Object interpolation in three dimensions. PsychologicalReview, 112, 586–609.
KELLMAN, P. J., & SHIPLEY, T. F. (1991). A theory of visualinterpolation in object perception. Cognitive Psychology,23, 141–221.
KELLMAN, P. J., & SPELKE, E. S. (1983). Perception of par-tially occluded objects in infancy. Cognitive Psychology, 15,483–524.
KELLMAN, P. J., SPELKE, E. S., & SHORT, K. R. (1986). Infantperception of object unity from translatory motion indepth and vertical translation. Child Development, 57,72–86.
KELLY, G. A. (1955). The psychology of personal constructs.New York: Norton.
KELLY, M. H., & MARTIN, S. (1994). Domain-general abil-ities applied to domain-specific tasks: Sensitivity toprobabilities in perception, cognition, and language. InL. R. Gleitman & B. Landau (Eds.), Lexical acquisition[Special issue]. Lingua, 92, 108–140.
KELSOE, J. R. (1997). The genetics of bipolar disorder.Psychiatric Annals, 27, 285–292.
KELTNER, D., & BUSWELL, B. N. (1997). Embarrassment:Its distinct form and appeasement functions.Psychological Bulletin, 122, 250–270.
KELTNER, D., GRUENFELD, D. H., & ANDERSON, C. (2003).Power, approach, and inhibition. Psychological Review, 110,265–284.
KENDALL, P. C. (1990). Cognitive processes and proce-dures in behavior therapy. In C. M. Franks, G. T. Wilson,P. C. Kendall, & J. P. Foreyt (Eds.), Review of behavior ther-apy: Theory and practice (pp. 103–137). New York:Guilford.
KENDALL, P. C., & BRASWELL, L. (1985). Cognitive-behav-ioral therapy for impulsive children. New York: Guilford.
KENDALL-TACKETT, K. A., WILLIAMS, L. M., & FINKELHOR,D. (1993). Impact of sexual abuse on children: A review
and synthesis of recent empirical studies. PsychologicalBulletin, 113, 164–180.
KENDLER, K. S., & BAKER, J. H. (2007). Genetic influenceson measures of the environment: A systematic review.Psychological Medicine, 37, 615–626.
KENDLER, K. S., & GRUENBERG, A. M. (1984). An inde-pendent analysis of the Danish adoption study of schiz-ophrenia: VI. The relationship between psychiatricdisorders as defined by DSM-III in the relatives andadoptees. Archives of General Psychiatry, 41, 555–564.
KENDLER, K. S., KARKOWSKI, L. M., & PRESCOTT, C. A.(1999). Fears and phobias: Reliability and heritability.Psychological Medicine, 29, 539–553.
KENNY, D., & ZACCARO, S. J. (1983). An estimate of vari-ance due to traits in leadership. Journal of AppliedPsychology, 68, 678–685.
KENRICK, D. T., & CIALDINI, R. B. (1977). Romantic attrac-tion: Misattribution versus reinforcement explanations.Journal of Personality and Social Psychology, 35, 381–391.
KENRICK, D. T., CIALDINI, R. B., & LINDER, D. E. (1979).Misattribution under fear-producing circumstances:Four failures to replicate. Personality and Social PsychologyBulletin, 5, 329–334.
KENSINGER, E. (2007). Negative emotion enhances mem-ory accuracy. Current Directions in Psychological Science, 16,213–218.
KEREN, G. (2007). Framing, intentions, and trust-choiceincompatibility. Organizational Behavior and HumanDecision Processes, 103, 238–255.
KERR, M. E., & BOWEN, M. (1988). Family evaluation. NewYork: Norton.
KERR, N., & BRAY, R. (2005). Simulation, realism, and thestudy of the jury. In N. Brewer & K. Williams (Eds.),Psychology and law: An empirical perspective(pp. 322–364).New York: Guilford.
KERR, N. L., & TINDALE, R. S. (2004). Group performanceand decision making. Annual Review of Psychology, 55,623–655.
KESSLER, R. C., AVENEVOLI, S., & RIES MERIKANGAS, K.(2001). Mood disorders in children and adolescents: Anepidemiologic perspective. Biological Psychiatry, 49,1002–1014.
KESSLER, R. C., BERGLUND, P., DEMLER, O., JIN, R.,MERIKANGAS, K. R., & WALTERS, E. E. (2005). Lifetimeprevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity SurveyReplication. Archives of General Psychiatry, 62, 593–602.
KESSLER, R. C., HEERINGA, S., LAKOMA, M. D., PETUKHOVA,M., RUPP, A. E., SCHOENBAUM, M., ET AL. (2008).Individual and societal effects of mental disorders onearnings in the United States: Results from the NationalComorbidity Survey Replication. American Journal ofPsychiatry, 165, 703–711.
KESSLER, R. C., KELLER, M. B., & WITTCHEN, H.-U. (2001).The epidemiology of generalized anxiety disorder.Psychiatric Clinics of North America, 24, 19–39.
KESSLER, R. C., MCGONAGLE, K. A., ZHAO, S., NELSON, C.B., HUGHES, M., ESHLEMAN, S., ET AL. (1994). Lifetime and12-month prevalence of DSM-III-R psychiatric disordersin the United States: Results from the National

R34 PREFERENCESO
Comorbidity Survey. Archives of General Psychiatry, 51,8–19.
KETY, S. S. (1988). Schizophrenic illness in the families ofschizophrenic adoptees: Findings from the DanishNational Sample. Schizophrenia Bulletin, 14, 217–222.
KHAN, R., LUK, C.-H., FLINKER, A., AGGARWAL, A., LAPID,H., HADDAD, R., ET AL. (2007). Predicting odor pleasant-ness from odorant structure: Pleasantness as a reflectionof the physical world. Journal of Neurosicence, 27,10015–10023.
KHANNA, S. M., & LEONARD, D. G. B. (1982). Basilar mem-brane tuning in the cat cochlea. Science, 215, 305–306.
KIHLSTROM, J. F. (1993). The recovery of memory in thelaboratory and the clinic. Paper presented at the 1993conventions of the Rocky Mountain and the WesternPsychological Associations, Phoenix, AZ.
KIHLSTROM, J. F. (1987). The cognitive unconscious.Science, 238, 1638.
KIHLSTROM, J. F. (1997). Suffering from reminiscences:Exhumed memory, implicit memory, and the return ofthe repressed. In M. Conway (Ed.), Recovered memoriesand false memories (pp. 100–117). New York: OxfordUniversity Press.
KIHLSTROM, J. F. (2002). No need for repression. Trends inCognitive Sciences, 6(12), 502.
KIHLSTROM, J. F., & CANTOR, N. (2000). Social intelli-gence. In R. J. Sternberg (Ed.), Handbook of intelligence(2nd ed., pp. 359–379). Cambridge, England: CambridgeUniversity Press.
KIHLSTROM, J. F., & MCCONKEY, K. M. (1990). WilliamJames and hypnosis: A centennial reflection. PsychologicalScience, 1 (3), 174–178.
KIHLSTROM, J. F., & SCHACTER, D. L. (2000). Functionalamnesia. In F. Boller & J. Grafman (Eds.), Handbook ofneuropsychology (2nd ed., Vol. 2, pp. 409–427).Amsterdam: Elsevier.
KILHAM, W., & MANN, L. (1974). Level of destructive obe-dience as a function of transmitter and executant roles inthe Milgram obedience paradigm. Journal of Personalityand Social Psychology, 29, 696–702.
KILLEEN, P. R., & NASH, M. R. (2003). The four causes ofhypnosis. International Journal of Clinical and ExperimentalHypnosis, 51, 195–231.
KILPATRICK, L., & CAHILL, L. (2003). Amygdala modula-tion of parahippocampal and frontal regions duringemotionally influenced memory storage. Neuroimage, 20,2091–2099.
KIM, C.-Y., & BLAKE, R. (2005). Psychophysical magic:Rendering the visible “invisible.” Trends in CognitiveSciences, 9, 381–388.
KIM, H., & MARKUS, H. R. (1999). Deviance or unique-ness, harmony or conformity? A cultural analysis. Journalof Personality and Social Psychology, 77(4), 785–800.
KIM, J. Y., & NAM, S. H. (1998). The concept and dynam-ics of face: Implications for organizational behavior inAsia. Organization Science, 9(4), 522–534.
KIM, W.-Y., & SNIDER, W. (2008). Overcoming inhibi-tions. Science, 322, 869–872.
KIMBERG, D. Y., D’ESPOSITO, M., & FARAH, M. J. (1998).Cognitive functions in the prefrontal cortex—working
memory and executive control. Current Directions inPsychological Science, 6, 185–192.
KIMBLE, G. A. (1961). Hilgard and Marquis’ conditioningand learning. New York: Appleton-Century-Crofts.
KIMURA, D., & WATSON, N. (1989). The relation betweenoral movement and speech. Brain and Language, 37,565–590.
KING-CASAS, B., SHARP, C., LOMAX-BREAM, L., LOHRENZ, T.,FONAGY, P., & MONTAGUE, P. (2008). The rupture andrepair of cooperation in borderline personality disorder.Science, 321(5890), 806–810.
KINGSTONE, A., FRIESEN, C., & GAZZANIGA, M. (2000).Reflexive joint attention depends on lateralized corticalconnections. Psychological Science, 11, 159–166.
KINOSHITA, S. (2001). The role of involuntary awarememory in the implicit stem and fragment completiontasks: A selective review. Psychonomic Bulletin & Review, 8,58–69.
KINSBOURNE, M. (2000). How is consciousnessexpressed in the cerebral activation manifold? Brain andMind, 2, 265–274.
KINSEY, A., POMEROY, W. B., & MARTIN, C. E. (1948).Sexual behavior in the human male. Philadelphia: Saunders.
KINSEY, A., POMEROY, W., MARTIN, C., & GEBHARD, P.(1953). Sexual behavior in the human female. Philadelphia:Saunders.
KINZLER, K. D., DUPOUX, E., & SPELKE, E. S. (2007). Thenative language of social cognition. Proceedings of theNational Academy of Sciences, 104, 12577–12580.
KINZLER, K. D., SHUTTS, K., DEJESUS, J., & SPELKE, E. S. (inpress). Accent trumps race in guiding children’s socialpreferences. Social Cognition.
KIRSCH, I. (2001). The response set theory of hypnosis:Expectancy and physiology. American Journal of ClinicalHypnosis, 44, 69–73.
KIRSCH. I., & BRAFFMAN, W. (2001). Imaginative sug-gestibility and hypnotizability. Current Directions inPsychological Science, 10(2), 57–61.
KITANO, J., & BOLNICK, D. I. (2008). Reverse evolution ofarmor plates in the threespine stickleback. CurrentBiology, 18, 769–774.
KITAYAMA, S., MARKUS, H. R., MATSUMOTO, H., &NORASAKKUNKIT, V. (1997). Individual and collectiveprocesses in the construction of the self: Self-enhance-ment in the United States and self-criticism in Japan.Journal of Personality and Social Psychology, 72, 1245–1267.
KITAYAMA, S., SNIBBE, A. C., MARKUS, H. R., & SUZUKI, T.(2004). Is there any “free” choice? Self and dissonancein two cultures. Psychological Science, 15, 527–533.
KITZINGER, C. (2001). Sexualities. In R. K. Unger (Ed.),Handbook of the psychology of women and gender(pp. 272–285). New York: Wiley.
KLAHR, D., & SIMON, H. A. (2001). What have psycholo-gists (and others) discovered about the process of scien-tific discovery? Current Directions in Psychological Science,10, 75–79.
KLAUER, K. C., MUSCH, J., & NAUMER, B. (2000). Onbelief bias in syllogistic reasoning. Psychological Review,107, 852–884.
KLAUS, M. H., & KENNELL, J. H. (1976). Maternal-infantbonding: The impact of early separation or loss on familydevelopment. St. Louis, MO: Mosby.
KLAUS, M. H., KENNELL, J. H., PLUMB, N., & ZUEHLKE, S.(1970). Human maternal behavior at the first contactwith her young. Pediatrics, 46, 187.
KLEINMAN, A. (1986). Social origins of distress and disease:Neurasthenia, depression, and pain in modern China. NewHaven, CT: Yale University Press.
KLERMAN, G., & WEISSMAN, M. (1993). Interpersonal psy-chotherapy for depression: Background and concepts. InNew applications of interpersonal therapy. Washington, DC:American Psychological Association Press.
KLIMA, E., & BELLUGI, U., WITH BATTISON, R., BOYES-BRAEM, P., FISCHER, S., FRISHBERG, N., ET AL. (1979). Thesigns of language. Cambridge, MA: Harvard UniversityPress.
KLINE, P. (1995). A critical review of the measurement ofpersonality and intelligence. In D. H. Saklofske & M.Zeidner (Eds.), International handbook of personality andintelligence (pp. 505–524). New York: Plenum.
KLOPFER, B., AINSWORTH, M., KLOPFER, W. G., & HOLT, R.R. (1954). Developments in the Rorschach technique.Yonkers, NY: World Book.
KLUFT, R. P. (1987). An update on multiple-personalitydisorder. Journal of Hospital and Community Psychiatry, 38,363–373.
KNUTSON, B. (2004). Sweet revenge? Science, 305,1246–1247.
KNUTSON, B., FONG, G. W., ADAMS, C. M., VARNER, J. L., &HOMMER, D. (2001). Dissociation of reward anticipationand outcome with event-related fMRI. Neuroreport,12(17), 3683–3687.
KOCH, C. (2008). The neuroscience of consciousness. InL. R. Squire, F. E. Bloom, N. C., Spitzer, S. du Lac, A.Ghosh & D. Berg (Eds.), Fundamental Neuroscience, 3rdEd. (pp. 1223–1236). Burlington, MA: Academic Press.
KOCHANSKA, G. (1993). Toward a synthesis of parentalsocialization and child temperament in early develop-ment of conscience. Child Development, 64, 325–347.
KOCHANSKA, G. (1995). Children’s temperament,mother’s discipline, and security of attachment: Multiplepathways to emerging internalization. Child Development,66, 597–615.
KOCHANSKA, G. (1997). Multiple pathways to consciencefor children with different temperaments: From toddler-hood to age 5. Developmental Psychology, 33, 228–240.
KOCHANSKA, G. (2001). Emotional development in chil-dren with different attachment histories: The first threeyears. Child Development, 72(2), 474–490.
KOCHANSKA, G. (2002). Mutually responsive orientationbetween mothers and their young children: A context forthe early development of conscience. Current Directions inPsychological Science, 11(6), 191–195.
KOCHANSKA, G., AKSAN, N., KNAACK, A., & RHINES, H.(2004). Maternal parenting and children’s conscience:Early security as a moderator. Child Development, 75,1229–1242.

PREFERENCESO R35
KOECHLIN, E., & HYAFIL, A. (2007). Anterior prefrontalfunction and the limits of human decision-making.Science, 318, 594–598.
KOEKOEK, S., HULSCHER, H., DORTLAND, B., HENBROEK, R.,ELGERSMA, Y., RUIGROK, T., ET AL. (2003). Cerebellar LTDand learning-dependent timing of conditioned eyelineresponses. Science, 301, 1736–1739.
KOESTNER, R., & MCCLELLAND, D. C. (1990). Perspectiveson competence motivation. In L. A. Pervin (Ed.),Handbook of personality theory and research (pp. 527–548).New York: Guilford.
KOH, P. O., BERGSON, C., UNDIE, A. S., GOLDMAN-RAKIC, P.S., & LIDOW, M. S. (2003). Up-regulation of the D1dopamine receptor-interacting protein, calcyon, inpatients with schizophrenia. Archives of GeneralPsychiatry, 60, 311–319.
KOHLBERG, L. (1969). Stage and sequence: The cognitivedevelopmental approach to socialization. In D. A. Goslin(Ed.), Handbook of socialization theory of research (pp.347–480). Chicago: Rand McNally.
KOHLBERG, L., LEVINE, C., & HEWER, A. (1984). Synopsesand detailed replies to critics. In L. Kohlberg (Ed.), Thepsychology of moral development: The nature and validity ofmoral stages (pp. 320–386). San Francisco: Harper &Row.
KOHN, A. (1993). Punished by rewards. New York:Houghton Mifflin.
KOHN, M. L. (1968). Social class and schizophrenia: Acritical review. In D. Rosenthal & S. S. Kety (Eds.), Thetransmission of schizophrenia (pp. 155–174). London:Pergamon.
KOLB, B., GIBB, R., & ROBINSON, T. E. (2003). Brain plas-ticity and behavior. Current Directions in PsychologicalScience, 12, 1–5.
KOLB, B., & WHISHAW, I. Q. (2009). Fundamentals ofhuman neuropsychology (6th ed.). New York: Worth.
KOLB, I., & WHISHAW, I. Q. (2009). An introduction tobrain and behavior. 6th ed. New York: Worth.
KOLERS, P., & ROEDIGER, H. (1984). Procedures of mind.Journal of Verbal Learning and Verbal Behavior, 23,425–449.
KONDZIOLKA, D., WECHSLER, L., GOLDSTEIN, S., MELTZER,C., THULBORN, K. R., GEBEL, J., ET AL. (2000).Transplantation of cultured human neuronal cells forpatients with stroke. Neurology, 55(4), 565–569.
KORN, J. H. (1997). Illusions of reality: A history of deceptionin social psychology. Albany: State University of New YorkPress.
KOSSLYN, S. M., BALL, T. M., & REISSER, B. J. (1978). Visualimages preserve metric spatial information: Evidencefrom studies of image scanning. Journal of ExperimentalPsychology: Human Perception and Performance, 4, 1–20.
KOSSLYN, S. M., PASCUAL-LEONE, A., FELICIAN, O.,CAMPOSANO, S., KEENAN, J. P., THOMPSON, W. L., ET AL.(1999). The role of area 17 in visual imagery: Convergentevidence from PET and rTMS. Science, 284, 167–170.
KOTTER, R., & MEYER, N. (1992). The limbic system: Areview of its empirical foundation. Behavioural BrainResearch, 52, 105–127.
KOVACS, A., & MEHLER, J. (2009). Cognitive gains in 7-month-old bilingual infants. Proceedings of the NationalAcademy of Sciences, 106(16), 6556–6560.
KOVELMAN, I., SHALINSKY, M. H., BERENS, M. S., & PETITTO,L. (2008). Shining new light on the brain’s “bilingualsignature”: A functional Near Infrared Spectroscopyinvestigation of semantic processing. NeuroImage, 39(3),1457–1471.
KOVERA, M. B. (2002). The effects of general pretrialpublicity on juror decisions: An examination of modera-tors and mediating mechanisms. Law and HumanBehavior, 26(1), 43–72.
KRAMER, A. F., & WILLIS, S. L. (2002). Enhancing the cog-nitive vitality of older adults. Current Directions inPsychological Science, 11, 173–177.
KRAMER, P. D. (1993). Listening to Prozac. New York:Viking.
KRASNE, F. B., & GLANZMAN, D. L. (1995). What we canlearn from invertebrate learning. Annual Review ofPsychology, 45, 585–624.
KRAUS, S. J. (1995). Attitudes and the prediction ofbehavior: A meta analysis of the empirical literature.Personality and Social Psychology Bulletin, 21(1), 58–75.
KREBS, D. L., & DENTON, K. (2005). Toward a more prag-matic approach to morality: A critical evaluation ofKohlberg’s model. Psychological Review, 112(3), 629–649.
KREBS, J. R. (1982). Territorial defence in the great tit(Parus Major L.). Ecology, 52, 2–22.
KRING, A. M., & GORDON, A. H. (1998). Sex differences inemotion: Expression, experience, and physiology. Journalof Personality and Social Psychology, 74, 686–703.
KRUEGER, R. F., & MARKON, K. E. (2006). Understandingpsychopathology: Melding behavior genetics, personal-ity, and quantitative psychology to develop an empiricallybased model. Current Directions in Psychological Science, 15,113–117.
KRUGLANSKI, A. W., PIERRO, A., MANNETTI, L., & GRADA, E.D. (2006). Groups as epistemic providers: Need for clo-sure and the unfolding of group-centrism. PsychologicalReview, 113(1), 84–100.
KRUPNICK, J. L., SOTSKY, S. M., SIMMENS, S., MOYER, J.,ELKIN, I., WATKINS, J., ET AL. (1996). The role of the ther-apeutic alliance in psychotherapy and pharmacotherapyoutcome: Findings in the National Institute of MentalHealth Treatment of Depression Collaborative ResearchProgram. Journal of Consulting and Clinical Psychology, 64,532–539.
KRUSCHKE, J. K., & BLAIR, N. J. (2000). Blocking andbackward blocking involve learned inattention.Psychonomics Bulletin and Review, 7, 636–645.
KUAN, D. Y., ROTH, K. A., FLAVELL, R. A., & RAKIC, P.(2000). Mechanisms of programmed cell death in thedeveloping brain. Trends in Neuroscience, 23, 291–297.
KUHL, P., WILLIAMS, K., LACERDA, F., STEVENS, K., &LINDBLOM, B. (1992). Linguistic experience alters pho-netic perception in infants by six months of age. Science,255, 606–608.
KUHN, D. (2006). Do cognitive changes accompanydevelopments in the adolescent brain? Perspectives onPsychological Science, 1, 59–67.
KUHN, D., NASH, S., & BRUCKEN, L. (1978). Sex-role con-cepts of two- and three-year-olds. Child Development, 49,445–451.
KUMARI, V. (2006). Do psychotherapies produce neuro-biological effects? Acta Neuropsychiatrica, 18, 61–70.
KUMARI, V., FFYTCHE, D. H., WILLIAMS, S. C., & GRAY, J. A.(2004). Personality predicts brain responses to cognitivedemands. Journal of Neuroscience, 24, 10636–10641.
KUNCEL, N. R., HEZLETT, S. A., & ONES, D. S. (2004).Academic performance, career potential, creativity, andjob performance: Can one construct predict them all?Journal of Personality and Social Psychology, 86, 148–161.
KUNDA, Z. (1990). The case for motivated reasoning.Psychological Bulletin, 108, 480–498.
KUNDA, Z., FONG, G. T., SANITIOSO, R., & REBER, E. (1993).Directional questions direct self conceptions. Journal ofExperimental Social Psychology, 29(1), 63–86.
KUNDA, Z., & NISBETT, R. E. (1986). The psychometrics ofeveryday life. Cognitive Psychology, 18, 195–224.
KURDEK, L. A. (2005a). Gender and marital satisfactionearly in marriage: A growth curve approach. Journal ofMarriage and Family, 67(1), 68–84.
KURDEK, L. A. (2005b). What do we know about gay andlesbian couples? Current Directions in Psychological Science,14, 251–254.
KURIHARA, K., & KASHIWAYANAGI, M. (1998). Introductoryremarks on umami taste. Annals of the New York Academyof Sciences, 855, 393–397.
KURTZ, S. N. (1991). Polysexualization: A new approachto Oedipus in the Trobriands. Ethos, 19, 68–101.
KURZBAN, R., & LEARY, M. R. (2001). Evolutionary originsof stigmatization: The functions of social exclusion.Psychological Bulletin, 127, 187–208.
KYLLONEN, P. C., & CHRISTAL, R. E. (1990). Reasoningability is (little more than) working memory capacity?Intelligence, 14(4), 389–433.
LABAR, K. (2007). Beyond fear: Emotional memorymechanisms in the human brain. Current Directions inPsychological Science, 16, 173–177.
LABAR, K. S., & CABEZA, R. (2006). Cognitive neuro-science of emotional memory. Nature ReviewsNeuroscience, 7, 54–64.
LABORATORY OF COMPARATIVE HUMAN COGNITION. (1983).Culture and cognitive development. In P. Mussen (Ed.),Handbook of child psychology: Vol. 1. History, theory andmethods (4th ed.). New York: Wiley.
LABOV, W. (1972). Language in the inner city: Studies in theBlack English vernacular. Philadelphia: University ofPennsylvania Press.
LABOV, W. (2007). Transmission and diffusion. Language,83(2), 344–387.
LADD, G., KOCHENDERFER, B., & COLEMAN, C. (1996).Friendship quality as a predictor of young children’s earlyschool adjustment. Child Development, 67, 1103–1118.
LADD, G., & PRICE, J. (1987). Predicting children’s socialand school adjustment following the transition from pre-school to kindergarten. Child Development, 58, 1168–1189.

R36 PREFERENCESO
LADEFOGED, P. (1975). A course in phonetics. New York:Harcourt Brace Jovanovich.
LADEFOGED, P., & MADDIESON, I. (1996). The sounds of theworld’s languages. Cambridge, MA: Blackwell.
LAFARGE, L. (1993). The early determinants of penis envy.In R. A. Glick & S. P. Roose (Eds.), Rage, power, andaggression. The role of affect in motivation, development, andadaptation: Vol. 2 (pp. 80–101). New Haven, CT: YaleUniversity Press.
LAGATTUTA, K., WELLMAN, H., & FLAVELL, J. (1997).Preschoolers’ understanding of the link between think-ing and feeling: Cognitive cuing and emotional change.Child Development, 68, 1081–1104.
LAIBLE, D. (2004). Mother-child discourse surrounding achild’s past behavior at 30 months: Links to emotionalunderstanding and early conscience development at 36months. Merrill-Palmer Quarterly, 50, 159–180.
LAIBLE, D., & THOMPSON, R. A. (1998). Attachment andemotional understanding in preschool children.Developmental Psychology, 34, 1038–1045.
LAIBLE, D., & THOMPSON, R. A. (2000). Mother-child dis-course, attachment security, shared positive affect, andearly conscience development. Child Development, 71,1424–1440.
LAIBLE, D., & THOMPSON, R. A. (2002). Mother-childconflict in the toddler years: Lessons in emotion, moral-ity, and relationships. Child Development, 73, 1187–1203.
LAIRD, R., JORDAN, K., DODGE, K., PETTIT, G., & BATES, J.(2001). Peer rejection in childhood, involvement withantisocial peers in early adolescence, and the develop-ment of externalizing problems. Development andPsychopathology, 13, 337–354.
LALONDE, J. K., HUDSON, J. I., GIGANTE, R. A., & POPE, H.G., JR. (2001). Canadian and American psychiatrists’attitudes toward dissociative disorders diagnoses.Canadian Journal of Psychiatry, 46, 407–412.
LALUMIERE, M., BLANCHARD, R., & ZUCKER, K. (2000).Sexual orientation and handedness in men and women:A meta-analysis. Psychological Bulletin, 126, 575–592.
LAMARINE, R. (1995). Child and adolescent depression.Journal of School Health, 65, 390–394.
LAMB, H. R. (1984). Deinstitutionalization and thehomeless mentally ill. Hospital Community Psychiatry, 35,899–907.
LAMB, H. R. (1998). Deinstitutionalization at the begin-ning of the new millennium. Harvard Review of Psychiatry,6, 1–10.
LAMB, H. R., & BACHRACH, L. L. (2001). Some perspec-tives on deinstitutionalization. Psychiatric Services, 52,1039–1045.
LAMB, K. (1994). Genetics and Spearman’s “g” factor.Mankind Quarterly, 34, 379–391.
LAMB, M., & MALKIN, C. (1986). The development ofsocial expectations in distress-relief sequences: A longi-tudinal study. International Journal of BehavioralDevelopment, 9, 235–249.
LAMB, M. E. (ED.). (1987). The father’s role: Cross-culturalperspectives. Hillsdale, NJ: Erlbaum.
LAMB, M. E. (ED.). (1997). The role of the father in childdevelopment (3rd ed.). New York: Wiley.
LAMBERG, L. (2004). Efforts to keep mentally ill out ofjails. Journal of the American Medical Association, 292(5),555–556.
LAMBERT, M. J., & BERGIN, A. E. (1994). The effectivenessof psychotherapy. In A. E. Bergin & S. L. Garfield (Eds.),Handbook of psychotherapy and behavior change (4th ed.,pp. 143–189). New York: Wiley.
LANDAU, B. (1982). Will the real grandmother pleasestand up? The psychological reality of dual meaning rep-resentations. Journal of Psycholinguistic Research, 11,47–62.
LANDAU, B., & GLEITMAN, L. R. (1985). Language and expe-rience: Evidence from the blind child. Cambridge, MA:Harvard University Press.
LANDAU, B., & MUNNICH, E. (1998). The representation ofspace of spatial language: Challenges for cognitive sci-ence. In P. Olivier & K. Gapp (Eds.), Representation andprocessing of spatial expressions (pp. 263–272). Mahwah,NJ: Erlbaum.
LANDAU, B., SMITH, L., & JONES, S. (1988). The impor-tance of shape in early lexical learning. CognitiveDevelopment, 3, 299–321.
LANDAU, B., & STECKER, D. (1990). Objects and places:Geometric and syntactic representations in early lexicallearning. Cognitive Development, 5, 287–312.
LANDAU, B., & ZUKOWSKI, A. (2002). Objects, motions,and paths: Spatial language of children with WilliamsSyndrome. Developmental Neuropsychology [Special issue,C. B. Mervis (Ed.)].
LANDIS, C., & HUNT, W. A. (1932). Adrenalin and emo-tion. Psychological Review, 39, 467–485.
LANE, S. D., CHEREK, D. R., TCHEREMISSINE, O. V., LIEVING,L. M., & PIETRAS, C. J. (2005). Acute Marijuana Effects onHuman Risk Taking. Neuropsychopharmacology, 30,800–809.
LANEY, C., MORRIS, E. K., BERNSTEIN, D. M., WAKEFIELD, B.M., & LOFTUS, E. F. (2008). Asparagus, a love story:Healthier eating could be just a false memory away.Experimental Psychology, 55, 291–300.
LANG, B., & PERNER, J. (2002). Understanding of inten-tion and false belief and the development of self-control.British Journal of Developmental Psychology, 20(1), 67–76.
LANG, P. J., DAVIS, M., & OHMAN, A. (2000). Fear andanxiety: Animal models and human cognitive psy-chophysiology. Journal of Affective Disorders, 61, 137–159.
LANGER, E. J., & RODIN, J. (1976). The effects of choice andenhanced personal responsibility for the aged: A fieldexperiment in an institutional setting. Journal ofPersonality and Social Psychology, 34, 191–198.
LANGLOIS, J. H., & DOWNS, A. C. (1980). Mothers, fathers,and peers as socialization agents of sex-typed play behav-iors in young children. Child Development, 51, 1237–1347.
LANGLOIS, J. H., KALAKANIS, L., RUBENSTEIN, A. J., LARSON,A., HALLAM, M., & SMOOT, M. (2000). Maxims or mythsof beauty? A meta-analytic and theoretical review.Psychological Bulletin, 126(3), 390–423.
LANGLOIS, J. H., ROGGMAN, L. A., CASEY, R. J., RITTER, J. M.,RIESER-DANNER, L. A., & JENKINS, V. Y. (1987). Infant pref-erences for attractive faces: Rudiments of a stereotype.Developmental Psychobiology, 23, 363–369.
LANYON, R. I., & GOLDSTEIN, L. D. (1971). Personalityassessment. New York: Wiley.
LAPIERE, R. (1934). Attitudes versus actions. Social Forces,13, 230–237.
LARSEN, R. J., & DIENER, E. (1992). Promises and prob-lems with the circumplex model of emotion. In M. S.Clark (Ed.), Emotion: Review of personality and social psy-chology (Vol. 13, pp. 25–59). Newbury Park, CA: Sage.
LARSON, R., & WILSON, S. (2004). Adolescence acrossplace and time: Globalization and the changing pathwaysto adulthood. In R. M. Lerner & L. Steinberg (Eds.),Handbook of adolescent psychology (pp. 299–330). NewYork: Wiley.
LA ROSA, J., & DIAZ-LOVING, R. (1991). Evaluation of theself-concept: A multidimensional inventory/Evaluaciondel autoconcepto: una escala multidimensional. RevistaLatinoamericana de Psicologia. Special Personality, 23,15–33.
LARSEN, R. J., KASIMATIS, M., & FREY, K. (1992).Facilitating the furrowed brow: An unobtrusive test ofthe facial feedback hypothesis applied to unpleasantaffect. Cognition and Emotion, 6, 321–338.
LARUELLE, M., KEGELES, L. S., & ABI-DARHAM, A. (2003).Glutamate, dopamine, and schizophrenia: From patho-physiology to treatment. Annals of the New York Academy ofSciences, 1003, 138–158.
LASSITER, G. D. (2000). The relative contributions ofrecognition and search-evaluation processes to high-level chess performance: Comment on Gobet and Simon.Psychological Science, 11(2), 172–173.
LATANÉ, B. (1981). The psychology of social impact.American Psychologist, 36, 343–356.
LATANÉ, B., & NIDA, S. (1981). Group size and helping.Psychological Bulletin, 89, 308–324.
LATANÉ, B., NIDA, S. A., & WILSON, D. W. (1981). Theeffects of group size on helping behavior. In J. P. Rushton& R. M. Sorrentino (Eds.), Altruism and helping behavior:Social, personality, and developmental perspectives. Hillsdale,NJ: Erlbaum.
LATANÉ, B., WILLIAMS, K., & HARKINS, S. (1979). Manyhands make light the work: The causes and consequencesof social loafing. Journal of Personality and SocialPsychology, 37, 822–832.
LATTAL, K. M., HONARVAR, S., & ABEL, T. (2004). Effects ofpost-session injections of anisomycin on the extinctionof a spatial preference and on the acquisition of a spatialreversal preference. Behavioural Brain Research, 153,327–339.
LAU, R. R., & RUSSELL, D. (1980). Attributions in thesports pages. Journal of Personality and Social Psychology,39, 29–38.
LAU, H. C., ROGERS, R. D., HAGGARD, P., & PASSINGHAM, R.E. (2004). Attention to intention. Science, 303 (5661),1208–1210.
LAURSEN, B., COY, K., & COLLINS, W. (1998).Reconsidering changes in parent-child conflict acrossadolescence: A meta-analysis. Child Development, 69,817–832.
LAUREYS, S. (2005). The neural correlate of (un)aware-ness: Lessons from the vegetative state. Trends in CognitiveSciences, 9 (12), 556–559.

PREFERENCESO R37
LAWRIE, S. M., & ABUKMEIL, S. S. (1998). Brain abnormal-ity in schizophrenia: A systematic and quantitativereview of volumetric magnetic resonance imaging stud-ies. British Journal of Psychiatry, 172, 110–120.
LAYZER, D. (1972). Science or superstition: A physical sci-entist looks at the I.Q. controversy. Cognition, 1,265–300.
LAZAREVA, O. F., FREIBURGER, K. L., & WASSERMAN, E. A.(2004). Pigeons concurrently categorize photographs atboth basic and superordinate levels. Psychonomic Bulletin& Review, 11(6), 1111–1117.
LAZARUS, A. A. (1971). Behavior therapy and beyond. NewYork: McGraw-Hill.
LAZARUS, A. A. (1981). The practice of multi-modal therapy.New York: McGraw-Hill.
LAZARUS, A. A. (2006). Brief but comprehensive psychother-apy: The multimodal way. New York: Springer.
LAZARUS. R. S. (1991). Emotion and adaptation. Oxford,England: Oxford University Press.
LE BON, G. (1895). The crowd. New York: Viking Press,1960.
LEA, S. E. G., & RYAN, C. M. E. (1990). Unnatural con-cepts and the theory of concept discrimination in birds.In M. L. Commons, R. J. Herrnstein, S. Kosslyn, & D.Mumford (Eds.), Quantitative analysis of behavior, Vol. 8:Behavioral approaches to pattern recognition and concept for-mation (pp. 165–185). Hillsdale, NJ: Erlbaum.
LEAPER, C., ANDERSON, K. J., & SANDERS, P. (1998).Moderators of gender effects on parents’ talk to theirchildren: A meta-analysis. Developmental Psychology,34(1), 3–27.
LEARY, M. R., & COX, C. B. (2008). Belongingness moti-vation: A mainspring of social action. In J. Y. Shah & W.L. Gardner (Eds.), Handbook of motivation science(pp. 27–40). New York: Guilford.
LEARY, M. R., TAMBOR, E. S., TERDAL, S. K., & DOWNS, D. L.(1995). Self-esteem as an interpersonal monitor: Thesociometer hypothesis. Journal of Personality and SocialPsychology, 68, 518–530.
LEBEDEV, M., & NICOLELIS, M. (2006). Brain-machineinterfaces: Past, present and future. Trends in Neuro-sciences, 29, 536–546.
LECKMAN, J. F., ZHANG, H., ALSOBROOK, J. P., & PAULS, D. L.(2001). Symptom dimensions in obsessive-compulsivedisorder: Toward quantitative phenotypes. AmericanJournal of Medical Genetics, 105, 28–30.
LEDOUX, J. E. (1995). Emotion: Clues from the brain.Annual Review of Psychology, 46, 209–235.
LEDOUX, J. E. (1996). The emotional brain: The mysteri-ous underpinnings of emotional life. New York: Simon &Schuster.
LEE, A., HOBSON, R. P., & CHIAT, S. (1994). I, you, me, andautism: An experimental study. Journal of Autism andDevelopmental Disorders, 24, 155–176.
LEE, D., & YOUNG, K. (2001). Post-traumatic stress disor-der: Diagnostic issues and epidemiology in adult sur-vivors of traumatic events. International Review ofPsychiatry, 13, 150–158.
LEE, P., & BROWN, N. (2004). Delay related changes inpersonal memories for September 11, 2001. AppliedCognitive Psychology, 14, 1007–1015.
LEFEVER, G. B., ARCONA, A. P., & ANTONUCCIO, D. O.(2003). ADHD among American schoolchildren:Evidence of overdiagnosis and overuse of medication.Scientific Review of Mental Health Practice, 2, 49–60.
LEHMAN, D., LEMPERT, R. O., & NISBETT, R. E. (1988). Theeffects of graduate training on reasoning: Formal disci-pline and thinking about everyday-life events. AmericanPsychologist, 43, 431–442.
LEHMAN, D., & NISBETT, R. (1990). A longitudinal study ofthe effects of undergraduate education on reasoning.Developmental Psychology, 26, 952–960.
LEIBOWITZ, S. F. (1991). Brain neuropeptide Y: An integra-tor of endocrine, metabolic and behavioral processes.Brain Research Bulletin, 27, 333–337.
LEICHSENRING, F., & RABUNG, S. (2008). Effectiveness oflong-term psychodynamic psychotherapy: A meta-analy-sis. Journal of the American Medical Association, 300,1551–1565.
LENNEBERG, E. H. (1967). Biological foundations of lan-guage. New York: Wiley.
LENNOX, B. R., PARK, B. G., MEDLEY, F., MORRIS, P. G., &JONES, P. B. (2000). The functional anatomy of auditoryhallucinations in schizophrenia. Psychiatry Research:Neuroimaging, 100, 13–20.
LENZENWEGER, M. F. (2006). Schizotypy: An organizingframework for schizophrenia research. Current Directionsin Psychological Science, 15(4), 162–166.
LÉPINE, R., BARROUILLET, P., & CAMOS, V. (2005). Whatmakes working memory spans so predictive of high-levelcognition? Psychonomic Bulletin and Review, 12, 165–170.
LEPPER, M. R., GREENE, D., & NISBETT, R. E. (1973).Undermining children’s intrinsic interest with extrinsicrewards: A test of the “overjustification” hypothesis.Journal of Personality and Social Psychology, 28, 129–137.
LEROITH, D., SHILOACH, J., & ROTH, J. (1982). Is there anearlier phylogenetic precursor that is common to boththe nervous and endocrine systems? Peptides, 3, 211–215.
LESCH, K. P., BENGEL, D., HEILS, A., SABOL, S. Z.,GREENBERG, B. D., PETRI, S., ET AL. (1996). Association ofanxiety-related traits with a polymorphism in the sero-tonin transporter gene regulatory region. Science,274(5292), 1527–1531.
LESLIE, A. M. (1992). Pretense, autism, and the theory ofmind module. Current Directions in Psychological Science, 1,18–21.
LETTVIN, J. Y., MATURAN, H. R., MCCULLOCH, W. S., &PITTS, W. H. (1959). What the frog’s eye tells the frog’sbrain. Proceedings of the Institute of Radio Engineers, 47,1940–1951.
LEVAY, S. (1991). A difference in hypothalamic sctructurebetween heterosexual and homosexual men. Science, 253,1034–1037.
LEVELT, W. (1970). A scaling approach to the study of syn-tactic relations. In G. Flores d’Arcais & W. Levelt (Eds.),Advances in psycholinguistics (pp. 109–121). Amsterdam:North-Holland.
LEVELT, W. J. M. (1989). Speaking: From intention to articu-lation. Cambridge, MA: MIT Press.
LEVENSON, R. W. (1992). Autonomic nervous system dif-ferences among emotions. Psychological Science, 3, 23–27.
LEVENSON, R. W. (1994). The search for autonomic speci-ficity. In P. Ekman & R. J. Davidson (Eds.), Human emo-tions: A functional view (pp. 252–257). New York: OxfordUniversity Press.
LEVENSON, R. W. (1999). The intrapersonal functions ofemotion. Cognition and Emotion, 13, 481–504.
LEVENSON, R. W. (2003). Autonomic specificity and emo-tion. In R. J. Davidson, K. R. Scherer, & H. H. Goldsmith(Eds.), Handbook of affective sciences (pp. 212–224). NewYork: Oxford University Press.
LEVENSON, R. W., EKMAN, P., HEIDER, K., & FRIESEN, W. V.(1992). Emotion and autonomic nervous system activityin the Minangkabau of West Sumatra. Journal ofPersonality and Social Psychology, 62, 972–988.
LEVEY, D. J., DUNCAN, R. S., & LEVINS, C. F. (2004). Animalbehaviour: Use of dung as a tool by burrowing owls.Nature, 431, 39.
LEVIN, I., & GAETH, G. (1988). How consumers areaffected by the framing of attribute information beforeand after consuming the product. Journal of ConsumerResearch, 15, 374–378.
LEVIN, I. P., GAETH, G. J., EVANGELISTA, F., ALBAUM, G., &SCHREIBER, J. (2001). How positive and negative framesinfluence the decisions of persons in America andAustralia. Asia-Pacific Journal of Marketing and Logistics, 13,64–71.
LEVINE, J. M., & MORELAND, R. L. (1998). Small groups. InD. Gilbert, S. Fiske, & G. Lindzey (Eds.), The handbook ofsocial psychology (4th ed., pp. 415–469). Boston:McGraw-Hill.
LEVINE, L. J., & PIZARRO, D. A. (2004). Emotion and mem-ory research: A grumpy overview. Social Cognition, 22(5),530–554.
LEVINE, L. J., STEIN, N. L., & LIWAG, M. D. (1999).Remembering children’s emotions: Sources of concor-dant and discordant accounts between parents and chil-dren. Developmental Psychology, 35, 790–801.
LEVINE, M., & CROWTHER, S. (2008). The responsivebystander: How social group membership and group sizecan encourage as well as inhibit bystander intervention.Journal of Personality and Social Psychology, 95, 1429–1439.
LEVINE, S. C., HUTTENLOCHER, J., TAYLOR, A., & LANGROCK,A. (1999). Early sex differences in spatial skill.Developmental Psychology, 35, 940–949.
LEVINSON, S. (2003). Space in language and cognition:Explorations in linguistic diversity. Cambridge:Cambridge University Press.
LEVITSKY, D. A. (2002). Putting behavior back into feed-ing behavior: A tribute to George Collier. Appetite, 38,143–148.
LEVY, G. D., TAYLOR, M. G., & GELMAN, S. A. (1995).Traditional and evaluative aspects of flexibility in genderroles, social conventions, moral rules, and physical laws.Child Development, 66(2), 515–531.
LEVY, J. (1985). Right brain, left brain: Facts and fiction.Psychology Today, 19, 38–44.

R38 PREFERENCESO
LEVY, W. B., & STEWARD, O. (1979). Synapses as associa-tive memory elements in the hippocampal formation.Brain Research, 175, 233–245.
LEWIN, K. (1939). Field theory and experiment in socialpsychology: Concepts and methods. American Journal ofSociology, 44, 868–897.
LEWINSOHN, P. M., JOINER, T., & ROHDE, P. (2001).Evaluation of cognitive diathesis-stress models in pre-dicting major depressive disorder in adolescents. Journalof Abnormal Psychology, 110, 203–215.
LEWIS, C., & KEREN, G. (1999). On the difficulties under-lying Bayesian reasoning: A comment on Gigerenzer andHoffrage. Psychological Review, 106, 411–416.
LEWIS, D. O., YEAGER, C. A., SWICA, Y., PINCUS, J. H., &LEWIS, M. (1997). Objective documentation of childabuse and dissociation in 12 murderers with dissociativeidentity disorder. American Journal of Psychiatry, 154,1703–1710.
LEWIS, J. R., BATES, B. C., & LAWRENCE, S. (1994).Empirical studies of projection: A critical review. HumanRelations, 47(11), 1295–1319.
LEWIS, M., ALESSANDRI, S., & SULLIVAN, M. (1990).Violation of expectancy, loss of control, and angerexpressions in young infants. Developmental Psychology,26, 745–751.
LEWIS, M., STANGER, C., & SULLIVAN, M. W. (1989).Deception in 3-year-olds. Developmental Psychology, 25(3),439–443.
LEWIS, M. D., & GRANIC, I. (2000). Emotion, development,and self-organization: Dynamic systems approaches to emo-tional development. New York: Cambridge UniversityPress.
LEWONTIN, R. C. (1976). Race and intelligence. In N. J.Block & G. Dworkin (Eds.), The IQ controversy (pp.78–92). New York: Pantheon.
LI, P., ABARBINELL, L., PAPAFRAGOU, A., & GLEITMAN, L.. (Inpress). Spatial reasoning skills in Tenejapan Mayans.Ms., University of Pennsylvania (under review,Cognition).
LI, P., & GLEITMAN, L. R. (2002). Turning the tables:Language and spatial reasoning. Cognition, 83, 265–294.
LIBERMAN, A. M., COOPER, F. S., SHANKWEILER, D. P., &STUDDERT-KENNEDY, M. (1967). Perception of the speechcode. Psychological Review, 74, 431–461.
LIBET, B., GLEASON, C. A., WRIGHT, E. W., & PEARL, D. K.(1983). Time of conscious intention to act in relation toonset of cerebral activity (readiness-potential). Theunconscious initiation of a freely voluntary act. Brain,106, 623–642.
LICHTER, D. G., & CUMMINGS, J. L. (Eds.). (2001). Frontal-subcortical circuits in psychiatric and neurological disorders.New York: Guilford.
LIDZ, J., GLEITMAN, H., & GLEITMAN, L. (2003). Under-standing how input matters: Verb learning and the foot-print of universal grammar. Cognition, 87(3), 151–178.
LIEBERMAN, J. A. (1995). Signs and symptoms.Commentary. Archives of General Psychiatry, 52, 361–363.
LIEBERMAN, M. D., OCHSNER, K. N., GILBERT, D. T., &SCHACTER, D. L. (2001). Attitude change in amnesia andunder cognitive load. Psychological Science, 12, 135–140.
LIFF, Z. A. (1992). Psychoanalysis and dynamic tech-niques. In D. K. Freedheim (Ed.), History of psychotherapy.Washington, DC: American Psychological Association.
LILIENFELD, S. O. (2007). Psychological treatments thatcan cause harm. Perspectives on Psychological Science, 2,53–70.
LILIENFELD, S. O., KIRSCH, I., SARBIN, T. R., LYNN, S. J.,CHAVES, J. F., GANAWAY, G. K., ET AL. (1999). Dissociativeidentity disorder and the sociocognitive model: Recallingthe lessons of the past. Psychological Bulletin, 125,507–523.
LILIENFELD, S. O., LYNN, S. J., NAMY, L. L., & WOOLF , N. J.(2008). Psychology: From inquiry to understanding. Boston:Allyn & Bacon.
LILIENFELD, S. O., WOOD, J. M., & GARB, H. N. (2000).The scientific status of projective techniques.Psychological Science in the Public Interest, 1, 27–66.
LILLARD, A. (1998). Enthnopsychologies: Cultural varia-tions in theories of mind. Psychological Bulletin, 123, 3–32.
LILLARD, A. S. (1997). Other folks’ theories of mind andbehavior. Psychological Science, 8, 268–274.
LINEHAN, M. M., BOHUS, M., & LYNCH, T. R. (2007).Dialectical behavior therapy for pervasive emotion dys-regulation: Theoretical and practical underpinnings. In J.J. Gross (Ed.), Handbook of emotion regulation (pp.581–605). New York: Guilford.
LINTON, M. (1978). Real world memory after six years: Anin vivo study of very long term memory. In M. M.Gruneberg, P. E. Morris, & R. N. Sykes (Eds.), Practicalaspects of memory (pp. 69–76). London: Academic Press.
LIPTON, J. S., & SPELKE, E. S. (2006). Preschool childrenmaster the logic of number word meanings. Cognition,98, B57–B66.
LISMAN, J. (2003). Long-term potentiation: Outstandingquestions and attempted synthesis. PhilosophicalTransactions of the Royal Society London: B. BiologicalScience, 348, 829–842.
LIVESLEY, W. J. (ED.). (2001). Handbook of personality dis-orders: Theory, research, and treatment. New York: Guilford.
LIVINGSTONE, K. (1997, Spring). Ritalin: Miracle drug orcop-out? Public Interest, 127, 3–18.
LIVSON, N., & PESKIN, H. (1980). Perspectives on adoles-cence from longitudinal research. In J. Adelsen (Ed.),Handbook of adolescent psychology. New York: Wiley.
LOCKE, J. (1690). An essay concerning human understanding.A. D. Woozley (Ed.). Cleveland: Meridian Books, 1964.
LOCKRIDGE, C., & BRENNAN, S. (2002). Addressees’ needsinfluence speakers’ early syntactic choices. PsychonomicBulletin and Review, 9, 550–557.
LOEHLIN, J. C. (1992). Genes and environment in personalitydevelopment. Newbury Park, CA: Sage.
LOEHLIN, J. C., LINDZEY, G., & SPUHLER, J. N. (1975). Racedifference in intelligence. San Francisco: Freeman.
LOFTUS, E. F. (1993). The reality of repressed memories.American Psychologist, 48, 518–537.
LOFTUS, E. F. (1997). Creating false memories. ScientificAmerican, 277(3), 70–75.
LOFTUS, E. F. (2003). Make-believe memories. AmericanPsychologist, 58(11), 867–873.
LOFTUS, E. F. (2004). Memories of things unseen.Current Directions in Psychological Science, 13, 145–147.
LOFTUS, E. (2005). Planting misinformation in thehuman mind: A 30-year investigation of the malleabilityof memory. Learning and Memory, 12, 361–366.
LOFTUS, E. F., & GUYER, M. J. (2002). Who abused JaneDoe? The hazards of the single case history. SkepticalInquirer, 26, 24–32.
LOGOTHETIS, N. K. (1998). Single units and consciousvision. Philosophical Transactions of the Royal Society ofLondon Series B-Biological Sciences, 353, 1801–1818.
LOGUE, A. W. (1986). The psychology of eating and drinking.New York: Freeman.
LOHMAN, D. (2000). Complex information processingand intelligence. In R. J. Sternberg (Ed.), Handbook ofhuman intelligence (2nd ed., pp. 285–340). Cambridge,MA: Cambridge University Press.
LONDON, P. (1970). The rescuers: Motivational hypothe-ses about Christians who saved Jews from the Nazis. In J.Macaulay & L. Berkowitz (Eds.), Altruism and helpingbehavior (pp. 241–250). New York: Academic Press.
LOPES, P. N., SALOVEY, P., CÔTÉ, S., & BEERS, M. (2005).Emotion regulation ability and the quality of social inter-action. Emotion, 5, 113–118.
LORD, C. G., ROSS, L., & LEPPER, M. R. (1979). Biasedassimilation and attitude polarization: The effects ofprior theories on subsequently considered evidence.Journal of Personality and Social Psychology, 37(11),2098–2109.
LORD, R. G., DEVADER, C. L., & ALLIGER, G. M. (1986). Ameta-analysis of the relationship between personalitytraits and leadership perceptions: An application ofvalidity generalization procedures. Journal of AppliedPsychology, 7, 401–410.
LORENZ, K. (1935). Der Kumpan in der Umwelt desVogels. Der Artgenosse als auslösendes Moment sozialerVerhaltensweisen. Journal für Ornithologie, 83, 137–215,289–413.
LORENZ, K. Z. (1966). On aggression. London: Methuen.
LOVAAS, O. I. (1987). Behavioral treatment and normaleducational and intellectual functioning in young autis-tic children. Journal of Consulting and Clinical Psychology,55(1), 3–9.
LOVE, J., HARRISON, L., SAGI-SCHWARTZ, A., ET AL. (2003).Child care quality matters: How conclusions may varywith context. Child Development, 74, 1021–1033.
LOZANO, A. M., MAYBERG, H. S., GIACOBBE, P., HAMANI, C.,CRADDOCK, R. C., & KENNEDY, S. H. (2008). Subcallosalcingulate gyrus deep brain stimulation for treatment-resistant depression. Biological Psychiatry, 64, 461–467.
LUBINSKI, D. (2004). Introduction to the special sectionon cognitive abilities: 100 years after Spearman’s (1904)“‘General intelligence,’ objectively determined and meas-ured.” Journal of Personality and Social Psychology, 86,96–111.
LUBINSKI, D., & BENBOW, C. P. (2000). States of excel-lence. American Psychologist, 55(1), 137–150.
LUBORSKY, L. I., SINGER, B., & LUBORSKY, L. (1975).Comparative studies of psychotherapies. Archives ofGeneral Psychiatry, 20, 84–88.

PREFERENCESO R39
LUCAS, R. E. (2007). Long-term disability is associatedwith lasting changes in subjective well-being: Evidencefrom two nationally representative longitudinal studies.Journal of Personality and Social Psychology, 92, 717–730.
LUCAS, R. E., CLARK, A. E., GEORGELLIS, Y., & DIENER, E.(2003). Reexamining adaptation and the set point modelof happiness: Reactions to changes in marital status.Journal of Personality and Social Psychology, 84, 527–539.
LUCHINS, A. S. (1942). Mechanization in problem-solv-ing: The effect of Einstellung. Psychological Monographs,54(entire no. 248).
LUGINBUHL, J. E. R., CROWE, D. H., & KAHAN, J. P. (1975).Causal attributions for success and failure. Journal ofPersonality and Social Psychology, 31, 86–93.
LUMINET, O., & CURCI, A. (EDS.). (2009). Flashbulb mem-ories: New issues and new perspectives. New York:Psychology Press.
LUO, Y., & BAILLARGEON, R. (2005). Can a self-propelledbox have a goal? Psychological reasoning in 5-month-oldinfants. Psychological Science, 16, 601–608.
LURIA, A. R. (1966). Higher cortical functions in man. NewYork: Basic Books.
LURIA, A. R. (1976). Cognitive development: Its culturaland social foundations. Cambridge, MA: HarvardUniversity Press.
LUTZ, A., BREFCZYNSKI-LEWIS, J., JOHNSTONE, T., &DAVIDSON, R. J. (2008). Regulation of the neural circuitryof emotion by compassion meditation: Effects of medita-tive expertise. PLoS ONE 3 (3).
LUTZ, A., GREISCHAR, L. L., RAWLINGS, N. B., RICARD, M., &DAVIDSON, R. J., (2004). Long-term meditators self-induce high-amplitude gamma synchrony during mentalpractice. Proceedings of the National Academy of Sciences,101 (46), 16369–16373.
LUTZ, C. (1986). The domain of emotion words on Ifaluk.In R. Harr (Ed.), The social construction of emotions(pp. 267–288). Oxford, England: Blackwell.
LUTZ, C. (1988). Unnatural emotions. Chicago: Universityof Chicago Press.
LUZZATTI, C., RAGGI, R., ZONCA, G., PISTARINI C., CONTARDI
A., & PINNA G. (2001). Verb-noun double dissociation inaphasic lexical impairments: The role of word frequencyand imageability. Brain and Language, 1–13.
LYDIARD, R. B., BRAWMAN-MINTZER, O., & BALLENGER, J. C.(1996). Recent developments in the psychopharmacol-ogy of anxiety disorders. Journal of Consulting and ClinicalPsychology, 64, 660–668.
LYKKEN, D. T., & TELLEGEN, A. (1996). Happiness is a sto-chastic phenomenon. Psychological Science, 7, 186–189.
LYNN, R. (1994). Sex differences in intelligence and brainsize: A paradox resolved. Personality and IndividualDifferences, 17(2), 257–271.
LYNN, R. (1999). The attack on The Bell Curve. Personalityand Individual Differences, 26, 761–765.
LYNN, S. J., LOCK, T. G., MYERS, B., & PAYNE, D. G. (1997).Recalling the unrecallable: Should hypnosis be used torecover memories in psychotherapy? Current Directions inPsychological Science, 6, 79–83.
LYUBOMIRSKY, S. (2008). The how of happiness: A scientificapproach to getting the life you want. New York: Penguin.
LYUBOMIRSKY, S., KING, L. A., & DIENER, G. (2008). Thebenefits of frequent positive affect: Does happiness leadto success? Psychological Bulletin, 131, 803–855.
MA, V., & SCHOENEMAN, T. J. (1997). Individualism versuscollectivism: A comparison of Kenyan and American self-concepts. Basic and Applied Social Psychology, 19, 261–273.
MAASS, A., KARASAWA, M., POLITI, F., & SUGA, S. (2006).Do verbs and adjectives play different roles in differentcultures? A cross-linguistic analysis of person represen-tation. Journal of Personality and Social Psychology, 90,734–750.
MACCOBY, E. E. (2000). Parenting and its effects on chil-dren: On reading and misreading behavior genetics.Annual Review of Psychology, 51, 1–27.
MACCOBY, E. E., & JACKLIN, C. N. (1974). The psychology ofsex differences. Stanford, CA: Stanford University Press.
MACCOBY, E. E., & JACKLIN, C. N. (1980). Sex differencesin aggression: A rejoinder and reprise. Child Development,51, 964–980.
MACCOBY, E. E., & MARTIN, J. A. (1983). Socialization inthe context of the family: Parent-child interaction. In P.H. Mussen (Ed.) & M. E. Hetherington (Vol. Ed.),Carmichael’s manual of child psychology: Vol. 4. Socialization,personality and social development (pp. 1–102). New York:Wiley.
MACDONALD, A. W., III, COHEN, J. D., STENGER, V. A., &CARTER, C. S. (2000). Dissociating the role of dorso-lat-eral prefrontal cortex and anterior cingulated cortex incognitive control. Science, 288, 1835–1837.
MACDONALD, M. C., PEARLMUTTER, N. J., & SEIDENBERG,M. S. (1994). The lexical nature of syntactic ambiguityresolution. Psychological Review, 101(4), 676–703.
MACDONALD, T. K., ZANNA, M. P, & FONG, G. T.(1996).Why common sense goes out the window: Effectsof alcohol on intentions to use condoms. Personality andSocial Psychology Bulletin, 22, 763–775.
MACFARLANE, A. (1975). Olfaction in the development ofsocial preferences in the human neonate. Parent-infantinteraction. Amsterdam: CIBA Foundation Symposium.
MACGUIRE, E. A., GADIAN, D. G., JOHNSRUDE, I. S., GOOD,C. D., ASHBURNER, J., FRACKOWIAK, R. S., & FRITH, C. D.(2000). Navigation-related structural change in the hip-pocampi of taxi drivers. Proceedings of the NationalAcademy of Sciences, 97, 4398–4403.
MACHIN, S., & PEKKARINEN, T. (2008). Global sex differ-ences in test score variability. Science, 322, 1331–1332.
MACK, A. (2003). Inattentional blindness: Looking with-out seeing. Current Directions in Psychological Science, 12,180–184.
MACK, A., & ROCK, I. (1998). Inattentional blindness.Cambridge, MA: MIT Press.
MACLEAN, P. (1949). Psychosomatic disease and the “vis-ceral” brain: Recent developments bearing on the Papeztheory of emotion. Psychosomatic Medicine, 11, 338–353.
MACLEAN, P. (1952). Some psychiatric implications ofphysiological studies on frontotemporal portion of lim-bic system (visceral brain). Electroencephalography &Clinical Neurophysiology, 4, 407–418.
MACNAMARA, J. (1982). Names for things. Cambridge, MA:MIT Press.
MACNICHOL, E. F., JR. (1986). A unifying presentation ofphotopigment spectra. Vision Research, 29, 543–546.
MACPHAIL, E. M. (1996). Cognitive function in mam-mals: The evolutionary perspective. Cognitive BrainResearch, 3, 279–290.
MADDUX, J. E. (1995). Self-efficacy, adaptation, and adjust-ment: Theory, research, and application. Englewood Cliffs,NJ: Prentice-Hall.
MAFFEI, M., HALAAS, J., RAVUSSIN, E., PRATLEY, R. E., LEE,G. H., ZHANG, Y., ET AL. (1995). Leptin levels in humanand rodent: Measurement of plasma leptin and ob RNAin obese and weight-reduced subjects. Nature Medicine, 1,1155–1161.
MAGEN, E., & GROSS, J. J. (2007). Harnessing the need forimmediate gratification: Cognitive reconstrual modu-lates the reward value of temptations. Emotion, 7,415–428.
MAGNUSSON, D., & ENDLER, N. S. (1977). Interactionalpsychology: Present status and future prospects. In D.Magnusson & N. S. Endler (Eds.), Personality at the cross-roads (pp. 3–31). New York: Wiley.
MAGOUN, H. W., HARRISON, F., BROBECK, J. R., & RANSON,S. W. (1938). Activation of heat loss mechanisms by localheating of the brain. Journal of Neurophysiology, 1,101–114.
MAGUIRE, M. C., & DUNN, J. (1997). Friendships in earlychildhood, and social understanding. InternationalJournal of Behavioral Development, 21(4), 669–686.
MAGUIRE, E. A., GADIAN, D. G., JOHNSRUDE, I. S., GOOD, C.D., ASHBURNER, J., FRACKOWIAK, R. S. J., ET AL. (2000).Navigation-related structural change in the hippocampiof taxi drivers. Proceedings of the National Academy ofSciences of the United States of America, 97(8), 4398–4403.
MAHER, B. A. (1966). Principles of psychopathology. NewYork: McGraw-Hill.
MAHON, B. Z., & CARAMAZZA, A. (2009). Concepts andcategories: A cognitive neuropsychological perspective.Annual Review of Psychology, 60, 27–51.
MAHEU, M. M., & GORDON, B. L. (2000). Counseling andtherapy on the Internet. Professional Psychology: Researchand Practice, 31, 484–489.
MAIA, T. V., & CLEEREMANS, A. (2005). Consciousness:Converging insights from connectionist modeling andneuroscience. Trends in Cognitive Sciences, 9, 397–404.
MAIN, M., & SOLOMON, J. (1990). Procedures for identify-ing infants as disorganized/disoriented during theAinsworth Strange Situation. In M. T. Greenberg, D.Cicchetti, & E. M. Cummings (Eds.), Attachment in thepreschool years: Theory, research, and intervention (pp.121–160). Chicago: University of Chicago Press.
MALDONADO, J. R., BUTLER, L. D., & SPIEGEL, D. (2002).Treatments for dissociative disorders. In P. Nathan and J.M. Gorman (Eds.), A guide to treatments that work (2nded., pp. 463–496). New York: Oxford University Press.
MALHI, G. S., & BARTLETT, J. R. (2000). Depression: A rolefor neurosurgery? British Journal of Neurosurgery, 14,415–422.

R40 PREFERENCESO
MALINOWSKI, B. (1926). Crime and custom in savage society.London: Paul, Trench, and Trubner.
MALINOWSKI, B. (1927). Sex and repression in savage society.New York: Meridian, 1955.
MALLET, L., POLOSAN, M., JAAFARI, N., BAUP, N., WELTER,M.-L., FONTAINE, D., ET AL. (2008). Subthalamic nucleusstimulation in severe obsessive-compulsive disorder. NewEngland Journal of Medicine, 359, 2121–2134.
MANDLER, J. M. (2000). Perceptual and conceptualprocesses in infancy. Journal of Cognition and Development,1, 3–36.
MANGELSDORF, S. C., SHAPIRO, J. R., & MARZOLF, D.(1995). Developmental and temperamental differences inemotional regulation in infancy. Child Development,66(6), 1817–1828.
MANNING, R., LEVINE, M., & COLLINS, A. (2007). The KittyGenovese murder and the social psychology of helping:The parable of the 38 witnesses. American Psychologist,62(6), 555–562.
MANTELL, D. M., & PANZARELLA, R. (1976). Obedience andresponsibility. British Journal of Social and ChildPsychology, 15, 239–245.
MARAÑON, G. (1924). Review of Fr. Endocrinology, 2, 301.
MARCH, J. S., LEONARD, H. L., & SWEDO, S. E. (1995).Obsessive-compulsive disorder. In J. S. March (Ed.),Anxiety disorders in children and adolescents (pp. 251–275).New York: Guilford.
MARCUS, D. E., & OVERTON, W. F. (1978). The develop-ment of cognitive gender constancy and sex-role prefer-ences. Child Development, 49, 434–444.
MARCUS, G. F. (2001). The algebraic mind: Integrating con-nectionism and cognitive science. Cambridge, MA: MITPress.
MARCUS, G. F. (2004). The birth of the mind: How a tinynumber of genes creates the complexity of the human mind.New York: Basic Books.
MARCUS, G. F., PINKER, S., ULLMAN, M., HOLLANDER, M.,ROSEN, T. J., & XU, F. (1992). Overregularization in lan-guage acquisition. Monographs of the Society for Research inChild Development, 57(4, Serial No. 228).
MARCUS, G. F., VIJAYAN, S., BANDI RAO, S., & VISHTON, P. M.(1999). Rule learning by seven-month-old infants.Science, 283, 77–80.
MARCUS, J., HANS, S. L., AUERBACH, J. G., & AUERBACH, A.G. (1993). Children at risk for schizophrenia: TheJerusalem Infant Development Study. II. Neuro behav-ioral deficits at school age. Archives of General Psychiatry,50, 797–809.
MARESCHAL, D. (2000). Object knowledge in infancy:Current controversies and approaches. Trends in CognitiveScience, 4, 408–416.
MARKMAN, E. (1989). Categorization and naming in chil-dren: Problems of induction. Cambridge, MA: MIT Press.
MARKMAN, E. M. (1994). Constraints children place onword meanings. In P. Bloom (Ed.), Language acquisition:Core readings. Cambridge, MA: MIT Press.
MARKMAN, E. M., & HUTCHINSON, J. E. (1984). Children’ssensitivity to constraints on word meaning: Taxonomicvs. thematic relations. Cognitive Psychology, 16, 1–27.
MARKMAN, E. M., & WACHTEL, G. A. (1988). Children’suse of mutual exclusivity to constrain the meaning ofwords. Cognitive Psychology, 20, 121–157.
MARKSON, I., & BLOOM, P. (1997). Evidence against a ded-icated system for word learning in children. Nature, 385,813–815.
MARKUS, H. R. (1977). Self-schemata and processinginformation about the self. Journal of Personality andSocial Psychology, 35, 63–78.
MARKUS, H. R., & KITAYAMA, S. (1991). Culture and theself: Implications for cognition, emotion, and motiva-tion. Psychological Review, 98, 224–253.
MARKUS, H. R., & NURIUS, P. (1986). Possible selves.American Psychologist, 41, 954–969.
MARLER, P. R. (1970). A comparative approach to vocallearning: Song development in white-crowned sparrows.Journal of Comparative and Physiological PsychologyMonographs, 71 (No. 2, Part 2), 1–25.
MARLOWE, F., & WETSMAN, A. (2001). Preferred waist-to-hip ratio and ecology. Personality and IndividualDifferences, 30, 481–489.
MARR, D. (1982). Vision. San Francisco: Freeman.
MARSELLA, A. J., DUBANOSKI, J., HAMADA, W. C., & MORSE,H. (2000). The measurement of personality across cul-tures: Historical conceptual, and methodological issuesand considerations. American Behavioral Scientist, 44,41–62.
MARSHALL, G. D., & ZIMBARDO, P. G. (1979). Affective con-sequences of inadequately explained physiologicalarousal. Journal of Personality and Social Psychology, 37,970–988.
MARSHALL, N. L. (2004). The quality of early child careand children’s development. Current Directions inPsychological Science, 13, 165–168.
MARSLEN-WILSON, W. (1975). Sentence perception as aninteractive parallel process. Science, 189, 226–228.
MARSLEN-WILSON, W. D., & TEUBER, H. L. (1975). Memoryfor remote events in anterograde amnesia: Recognition ofpublic figures from news photographs. Neurobiologia, 13,353–364.
MARTIN, D. J., GARSKE, J. P., & DAVIS, M. K. (2000).Relation of the therapeutic alliance with outcome andother variables: A meta-analytic review. Journal ofConsulting and Clinical Psychology, 68, 438–450.
MARTIN, M., & JONES, G. V. (2006). Visual sharpnesscontingency in recognition memory for orientation:Mnemonic illusion suppressed by sensory signature.Journal of Experimental Psychology: General, 135, 542–552.
MARTIN, J. A., KING, D. R., MACCOBY, E. E., & JACKLIN, C.N. (1984). Secular trends and individual differences intoilet-training progress. Journal of Pediatric Psychology, 9,457–467.
MARTIN, L. (1986). “Eskimo words for snow”: A casestudy in the genesis and decay of an anthropologicalexample. American Anthropologist, 88, 418–423.
MARTIN, P., & ALBERS, P. (1995). Cerebellum and schizo-phrenia: A review. Schizophrenia Bulletin, 21, 241–251.
MARTINEZ, J. L., & DERRICK, B. E. (1996). Long-termpotentiation and learning. Annual Review of Psychology,47, 173–203.
MARTINEZ, M. E. (2000). Education as the cultivation ofintelligence. Mahwah, NJ: Erlbaum.
MARX, J. (2003). Cellular warriors at the battle of thebulge. Science, 299, 846–849.
MASLACH, C. (1979). Negative emotional biasing of unex-plained physiological arousal. Journal of Personality andSocial Psychology, 37, 953–969.
MASLOW, A. H. (1968). Toward a psychology of being (2nded.). Princeton, NJ: Van Nostrand.
MASLOW, A. H. (1970). Motivation and personality (2nded.). New York: Harper.
MASLOW, A. H. (1996). Future visions: The unpublishedpapers of Abraham Maslow (E. Hoffman, Ed.). ThousandOaks, CA: Sage.
MASSIMINI, M., FERRARELLI, F., HUBER, R., ESSER, S. K.,SINGH, H., & TONONI, G. (2005). Breakdown of corticaleffective connectivity during sleep. Science, 309,2228–2232.
MASTERS, M. S., & SANDERS, B. (1993). Is the gender dif-ference in mental rotation disappearing? BehaviorGenetics, 23, 337–341.
MASTERS, W. H., & JOHNSON, V. E. (1966). Human sexualresponses. Boston: Little, Brown.
MATARAZZO, J. D. (1983). The reliability of psychiatric andpsychological diagnosis. Clinical Psychology Review, 3,103–145.
MATHER, M., & CARSTENSEN, L. L. (2003). Aging andattentional biases for emotional faces. PsychologicalScience, 14, 409–415.
MATIN, L., PICOULT, E., STEVENS, J., EDWARDS, M., &MACARTHUR, R. (1982). Ocuparalytic illusion: Visual-field dependent spatial mislocations by humans partiallyparalyzed with curare. Science, 216, 198–180.
MATSON, J. L., & SEVIN, J. A. (1994). Issues in the use ofaversives: Factors associated with behavior modificationfor autistic and other developmentally disabled people.In E. Schopler & G. B. Mesibov (Eds.), Behavioral issues inautism (pp. 211–225). New York: Plenum.
MATSUMOTO, D., & WILLINGHAM, B. (2009). Spontaneousfacial expressions of emotion of congenitally and non-congenitally blind individuals. Journal of Personality andSocial Psychology, 96, 1–10.
MATSUMOTO, D., YOO, S. H., HIRAYAMA, S., & PETROVA, G.(2005). Development and validation of a measure of dis-play rule knowledge: The Display Rule AssessmentInventory. Emotion, 5, 23–40.
MATSUMOTO, D., YOO, S. H., & NAKAGAWA, S. (2008).Culture, emotion regulation, and adjustment. Journal ofPersonality and Social Psychology, 94(6), 925–937.
MATTHEWS, G., ZEIDNER, M., & ROBERTS, R. D. (2003).Emotional intelligence: Science and Myth. Cambridge, MA:MIT Press.
MATTHEWS, G., ZEIDNER, M., & ROBERTS, R. D. (2005).Emotional intelligence: An elusive ability? In O. Wilhelm& R. Engle (Eds.), Handbook of understanding and measur-ing intelligence (pp. 79–99). Thousand Oaks, CA: Sage.
MATTHEWS, K. A., BATSON, C. D., HORN, J., & ROSENMAN,R. H. (1981). “Principles in his nature which interest himin the fortune of others . . .”: The heritability of empathicconcern for others. Journal of Personality, 49(3), 237–247.

PREFERENCESO R41
MATTISON, A., & MCWHIRTER, D. (1987). Male couples:The beginning years. Intimate Relationships: SomeSocial Work Perspectives on Love [Special issue]. Journalof Social Work and Human Sexuality, 5, 67–78.
MAUSS, I. B., LEVENSON, R. W., MCCARTER, L., WILHELM, F.H., & GROSS, J. J. (2005). The tie that binds? Coherenceamong emotional experience, behavior, and autonomicphysiology. Emotion, 5, 175–190.
MAY, C. P., & HASHER, L. (1998). Synchrony effects ininhibitory control over thought and action. Journal ofExperimental Psychology: Human Perception andPerformance, 24, 363–379.
MAYBERG, H. S., BRANNAN. S. K., MAHURIN, R. K., JERABEK,P. A., BRICKMAN, J. S., TEKELL, J. L., ET AL. (1997).Cingulate function in depression: A potential predictorof treatment response. Neuroreport, 8, 1057–1061.
MAYBERG, H. S., LIOTTI, M., BRANNAN, S. K., MCGINNIS, S.,MAHURIN, R. K., JERABEK, P. A., ET AL. (1999). Reciprocallimbic-cortical function and negative mood: ConvergingPET findings in depression and normal sadness.American Journal of Psychiatry, 156, 675–682.
MAYBERG, H. S., LOZANO, A. M., VOON, V., MCNEELY, H. E.,SEMINOWICZ, D., HAMANI, C., ET AL. (2005). Deep brainstimulation for treatment-resistant depression. Neuron,45(5), 651–660.
MAYER, J. D., ROBERTS, R. D., & BARSADE, S. G. (2008a).Human abilities: Emotional intelligence. Annual Review ofPsychology, 59, 507–536.
MAYER, J. D., SALOVEY, P., & CARUSO, D. R. (2008b).Emotional intelligence: New ability or eclectic traits?American Psychologist, 63, 503–517.
MAYER, J. D., SALOVEY, P., CARUSO, D. R., & SITARENIOS, G.(2003). Measuring emotional intelligence with theMSCEIT V2.0. Emotion, 3, 97–105.
MAYES, A. R. (1988). Human organic memory disorders.New York: Cambridge University Press.
MAYHAN, W. G. (2001). Regulation of blood-brain barrierpermeability. Microcirculation, 8, 89–104.
MCADAMS, D. P. (1980). A thematic coding system for theintimacy motive. Journal of Research in Personality, 14,413–432.
MCADAMS, D. P. (1993). The stories we live by: Personalmyths and the making of the self. New York: Morrow.
MCADAMS, D. P. (2001). The psychology of life stories.Review of General Psychology, 5, 100–122.
MCADAMS, D. P., & PALS, J. L. (2006). A new Big Five:Fundamental principles for an integrative science of per-sonality. American Psychologist, 61, 204–217.
MCCLEARN, G. E., & DEFRIES, J. C. (1973). Introduction tobehavioral genetics. San Francisco: Freeman.
MCCLEARN, G. E., JOHANSSON, B., GERG, S., PEDERSEN, N.,AHEM, F., PETRILL, S., ET AL. (1997). Substantial geneticinfluence on cognitive abilities in twins 80 or more yearsold. Science, 276, 1560–1563.
MCCLELLAND, D. C. (1989). Human motivation. New York:Cambridge University Press.
MCCLELLAND, D. C., ATKINSON, J. W., CLARK, R. A., &LOWELL, E. L. (1953). The achievement motive. New York:Appleton-Century-Crofts.
MCCLELLAND, D. C., KOESTNER, R., & WEINBERGER, J.(1989). How do self-attributed and implicit motives dif-fer? Psychological Review, 96, 690–702.
MCCLELLAND, J. L., & PATTERSON, K. (2002). Rules or con-nections in past-tense inflections: What does the evi-dence rule out? Trends in Cognitive Science, 6(11), 465–472.
MCCLELLAND, J. L., & RUMELHART, D. E. (EDS.). (1986).Parallel distributed processing: Explorations in themicrostructure of cognition: Vol. 2. Psychological and biologi-cal models. Cambridge, MA: MIT Press.
MCCLELLAND, J. L., RUMELHART, D. E., & HINTON, G. E.(1986). The appeal of parallel distributed processing. InD. E. Rumelhart, J. L. McClelland, and the PDP ResearchGroup (Eds.), Parallel distributed processing: Vol. 1.Foundations (pp. 3–44). Cambridge, MA: MIT Press.
MCCLELLAND, J. L., & SEIDENBERG, M. S. (2000). Why dokids say goed and brang? Science, 287, 47–48.
MCCLINTOCK, M. K. (1971). Menstrual synchrony andsuppression. Nature, 229, 244–245.
MCCLINTOCK, M. K., & ADLER, N. T. (1978). The role ofthe female during copulation in wild and domesticNorway rats (Rattus Norvegicus). Behaviour, 67, 67–96.
MCCLOSKEY, M., WIBLE, C. G., & COHEN, N. J. (1988). Isthere a special flashbulb-memory mechanism? Journal ofExperimental Psychology: General, 117, 171–181.
MCCLURE, S. M., LAIBSON, D. I., LOEWENSTEIN, G., &COHEN, J. D. (2004). Separate neural systems valueimmediate and delayed monetary rewards. Science, 306,503–507.
MCCONNELL, A. R., & LEIBOLD, J. M. (2001). Relationsamong the Implicit Association Test, discriminatorybehavior, and explicit measures of racial attitudes. Journalof Experimental Social Psychology, 37(5), 435–442.
MCCRAE, R. R., & COSTA, P. T. (1987). Validation of thefive-factor model of personality across instruments andobservers. Journal of Personality and Social Psychology, 52,81–90.
MCCRAE, R. R., & COSTA, P. T., JR. (1990). Personality inadulthood. New York: Guilford.
MCCRAE, R. R., & COSTA, P. T., JR. (2003). Personality inadulthood: A five-factor theory perspective (2nd ed.). NewYork: Guilford.
MCCRAE, R. R., & TERRACCIANO, A. (2005). Universal fea-tures of personality traits from the observer’s perspective:Data from 50 cultures. Journal of Personality and SocialPsychology, 88, 547–561.
MCCRAE, R. R., & TERRACCIANO, A. (2006). Nationalcharacter and personality. Current Directions inPsychological Science, 15, 156–161.
MCCRANIE, E. W., HYER, L. A., BOUDEWYNS, P. A., &WOODS, M. G. (1992). Negative parenting behavior, com-bat exposure and PTSD symptom severity. Test of a per-son-event interaction model. Journal of Nervous andMental Disease, 180, 431–438.
MCCREARY, D. R. (1994). The male role and avoiding fem-ininity. Sex Roles, 31, 517–531.
MCCRINK, K., & WYNN, K. (2004). Large-number addi-tion and subtraction by 9-month-old infants.Psychological Science, 15, 776–781.
MCDANIEL, M. A., MAIER, S. F., & EINSTEIN, G. O. (2002).“Brain-specific” nutrients: A memory cure? PsychologicalScience in the Public Interest, 3, 12–38.
MCDOUGAL, W. (1923). Outline of psychology. New York:Scribner.
MCEACHIN, J. J., SMITH, T., & LOVAAS, O. I. (1993). Long-term outcome for children with autism who received earlyintensive behavioral treatment. American Journal onMental Retardation, 97, 359–372.
MCEWEN, B. S., BIEGON, A., DAVIS, P. G., KREY, L. C.,LUINE, V. N., MCGINNIS, M., ET AL. (1982). Steroid hor-mones: Humoral signals which alter brain cell propertiesand functions. Recent Progress in Brain Research, 38,41–83.
MCFALL, R. M. (2006). Doctoral training in clinical psy-chology. Annual Review of Clinical Psychology, 2, 21–49.
MCFALL, R. M., & TREAT, T. A. (1999). Quantifying theinformation value of clinical assessments with signaldetection theory. Annual Review of Psychology, 50,215–242.
MCGAUGH, J. L. (2000). Memory—a century of consoli-dation. Science, 287, 248–251.
MCGAUGH, J. (2003). Memory and emotion. New York:Columbia University Press.
MCGEE, A. W., YANG, Y., FISCHER, Q. S., DAW, N. W., &STRITTMATTER, S. M. (2005). Experience-driven plasticityof visual cortex limited by myelin and Nogo receptor.Science, 5744, 2222–2226.
MCGEOCH, J. A., & IRION, A. L. (1952). The psychology ofhuman learning (2nd ed.). New York: Longmans, Green.
MCGHIE, A., & CHAPMAN, J. (1961). Disorders of attentionand perception in early schizophrenia. British Journal ofMedical Psychology, 34, 103–116.
MCGRATH, J., WELHAM, J., & PEMBERTON, M. (1995).Month of birth, hemisphere of birth, and schizophrenia.British Journal of Psychiatry, 167, 783–785.
MCGREGOR, G. P., DESAGA, J. F., EHLENZ, K., FISCHER, A.,HEESE, F., HEGELE, A., ET AL. (1996). Radiommunologicalmeasurement of leptin in plasma of obese and diabetichuman subjects. Endocrinology, 137, 1501–1504.
MCGREW, K. (2009). CHC theory and the human cogni-tive abilities project: Standing on the shoulders of thegiants of psychometric intelligence research. Intelligence,37, 1–10.
MCGUE, M., BOUCHARD, T. J., JR., IACONO, W. G., &LYKKEN, D. T. (1993). Behavioral genetics of cognitiveability: A life span perspective. In R. Plomin & G. E.McClearn (Eds.), Nature, nurture and psychology(pp. 59–76). Washington, DC: American PsychologicalAssociation.
MCGUE, M., & LYKKEN, D. T. (1992). Genetic influence onrisk of divorce. Psychological Science, 3, 368–372.
MCGUIRE, W. J. (1985). The nature of attitude and atti-tude change. In G. Lindzey & E. Aronson (Eds.),Handbook of social psychology: Vol. 2 (3rd ed.). New York:Random House.
MCINTOSH, A. R., RAJAH, M. N., & LOBAUGH, N. J. (1999).Interactions of prefrontal cortex in relation to awarenessin sensory learning. Science, 284, 1531–1533.

R42 PREFERENCESO
MCNALLY, R. J. (2003a). Progress and controversy in thestudy of posttraumatic stress disorder. Annual Review ofPsychology, 54, 229–252.
MCNALLY, R. J. (2003b). Remembering trauma.Cambridge, MA: Harvard University Press.
MCNALLY, R. J. (2006). Psychiatric casualties of war.Science, 313, 923–924.
MCNALLY, R., & GERAERTS, E. (2009). A new solution tothe recovered memory debate. Perspectives on PsychologicalScience, 4, 126–134.
MCNAUGHTON, B. L., DOUGLAS, R. M., & GODDARD, G. V.(1978). Synaptic enhancement in fascia dentata:Cooperativity among coactive afferents. Brain Research,157, 277–293.
MEAD, G. H. (1934). Mind, self, and society from the stand-point of a social behaviorist (C. W. Morris, Ed.). Chicago:University of Chicago Press.
MEAD, M. (1928). Coming of age in Samoa. New York:William Morrow.
MEALEY, L., BRIDGSTOCK, R., & TOWNSEND, G. C. (1999).Symmetry and perceived facial attractiveness: A monozy-gotic co-twin comparison. Journal of Personality and SocialPsychology, 76, 151–158.
MEDIN, D. I., ATRAN, S., COX, D., COLEY, J., & PROFFITT, J. S.(2006). Folkbiology of freshwater fish, Cognition, 99(3),237–273.
MEDIN, D. L., & BAZERMAN, M. H. (1999). Broadeningbehavioral decision research: Multiple levels of cognitiveprocessing. Psychonomic Bulletin & Review, 6, 533–546.
MEDIN, D. L., GOLDSTONE, R. L., & GENTNER, D. (1993).Respects for similarity. Psychological Review, 100(2),254–278.
MEDIN, D. L., SCHWARTZ, H., BLOK, S. V., & BIRNBAUM, L.A. (1999). The semantic side of decision making.Psychonomics Bulletin and Review, 6, 562–569.
MEDINA, T. N., TRUESWELL, J., SNEDEKER, J., & GLEITMAN,L. (2008, November 2). When the shoe fits: Cross-situa-tional word learning in realistic learning environments. Talkpresented at the Boston University Conference onLanguage Development (BUCLD), Boston, MA.
MEDNICK, S. A., HUTTUNEN, M. O., & MACHO’N, R. A.(1994). Prenatal influenza infections and adult schizo-phrenia. Schizophrenia Bulletin, 20, 263–267.
MEDNICK, S., NAKAYAMA, K, & STICKGOLD, R. (2003).Sleep-dependent learning: A nap is as good as a night.Nature Neuroscience, 6, 697–698.
MEEHL, P. E. (1962). Schizotaxia, schizotypy, schizophre-nia. American Psychologist, 17, 827–838.
MEETER, M., & MURRE, J. M. J. (2004). Consolidation oflong-term memory: Evidence and alternatives.Psychological Bulletin, 130, 843–857.
MEHLER, J., ET AL. (1996). Coping with linguistic diver-sity: The infant’s viewpoint. In J. L. Morgan & K. Demuth(Eds.), Signal to syntax: Bootstrapping from speech to gram-mar in early acquisition (pp. 101–116). Hillsdale, NJ:Erlbaum.
MEHLER, J., JUSCZYK, P., LAMBERTZ, G., HALSTED, N.,BERTONCINI, J., & AMIEL-TISON, C. (1988). A precursor tolanguage acquisition in young infants. Cognition, 29,143–178.
MEHLER, J., & NESPOR, M. (2004). Linguistic rhythm andthe development of language. In A. Belletti & L. Rizzi(Eds.), Structures and beyond: The cartography of syntacticstructures. Oxford, England: Oxford University Press.
MEICHENBAUM, D. (1985). Stress inoculation training. NewYork: Pergamon.
MEICHENBAUM, D. (1993). Changing conceptions of cog-nitive behavior modification: Retrospect and prospect.Journal of Consulting and Clinical Psychology, 61, 202–204.
MEICHENBAUM, D. (1996). Stress inoculation training forcoping with stressors. Clinical Psychologist, 49, 4–7.
MELLERS, B., CHANG, S.-J., BIRNBAUM, M., & ORDÓÑEZ, L.(1992). Preferences, prices, and ratings in risky decisionmaking. Journal of Experimental Psychology: HumanPerception and Performance, 18, 347–361.
MELLERS, B., HERTWIG, R., & KAHNEMAN, D. (2001). Dofrequency representations eliminate conjunction effects?An exercise in advance collaboration. PsychologicalScience, 12, 269–275.
MELLERS, B. A., & MCGRAW, A. P. (1999). How to improveBayesian reasoning: Comment on Gigerenzer andHoffrage. Psychological Review, 106, 417–424.
MELNYK, L., Crossman, A. M., & Scullin, M. H. (2007).The suggestibility of children’s memory. In M. P. Toglia, J.D. Read, D. F. Ross, & R. C. L. Lindsay (Eds.), Handbookof eyewitness psychology, Vol. 1: Memory for events (pp.401–427). Mahwah, NJ: Erlbaum.
MELTZER, H. Y. (1986). Lithium mechanisms in bipolarillness and altered intracellular calcium functions.Biological Psychiatry, 21, 492–510.
MELTZER, H. Y. (1987). Biological studies in schizophre-nia. Schizophrenia Bulletin, 13, 77–111.
MELTZOFF, A. N. (1995). Understanding the intentions ofothers: Re-enactment of intended acts by 18-month-oldchildren. Developmental Psychology, 31(5), 838–850.
MELTZOFF, A. N. (2002). Elements of a developmentaltheory of imitations. In A. N. Meltzoff, N. Andrew, & W.Prinz (Eds.), The imitative mind: Development, evolution,and brain bases (pp. 19–41). Cambridge studies in cogni-tive perceptual development. New York: CambridgeUniversity Press.
MELTZOFF, A. N., GOPNIK, A., & REPACHOLI, B. M. (1999).Toddlers’ understanding of intentions, desires and emo-tions: Explorations of the dark ages. In P. D. Zelazo & J.W. Astington (Eds.), Developing theories of intention: Socialunderstanding and self-control (pp. 17–41). Mahwah, NJ:Erlbaum.
MELTZOFF, A. N., & MOORE, M. K. (1977). Imitation offacial and manual gestures by human neonates. Science,198, 75–78.
MELTZOFF, A. N., & MOORE, M. K. (1998). Infant inter-subjectivity: Broadening the dialogue to include imita-tion, identity and intention. In S. Braten (Ed.),Intersubjective communication and emotion in early ontogeny.Cambridge: Cambridge University Press.
MELZACK, R., & CASEY, K. (1968). Sensory, motivationaland central control determinants of pain. In D. Kenshalo,(Ed.), The skin senses (pp. 423–443). Springfield, IL:Thomas.
MELZACK, R., & WALL, P. (1982). The challenge of pain. NewYork: Basic Books.
MENNELLA, J. A., PEPINO, M. Y., & REED, D. R. (2005).Genetic and environmental determinants of bitter per-ception and sweet preferences. Pediatrics, 115, 216–222.
MENYUK, P. (1977). Language and maturation. Cambridge,MA: MIT Press.
MENZEL, E. W. (1973). Chimpanzee spatial memoryorganization. Science, 182, 943–945.
MENZEL, E. W. (1978). Cognitive maps in chimpanzees.In S. H. Hulse, H. Fowler, & W. K. Honig (Eds.), Cognitiveprocesses in animal behavior (pp. 375–422). Hillsdale, NJ:Erlbaum.
MERVIS, C. B., & CRISAFI, M. (1978). Order acquisition ofsubordinate, basic, and superordinate level categories.Child Development, 49, 988–998.
METCALFE, J. (1986). Premonitions of insight predictimpending error. Journal of Experimental Psychology:Learning, Memory and Cognition, 12, 623–634.
METCALFE, J., & WEIBE, D. (1987). Intuition in insight andnoninsight problem solving. Memory and Cognition, 15,238–246.
MEYER, D. E., & SCHVANEVELDT, R. W. (1971). Facilitationin recognizing pairs of words: Evidence of a dependencebetween retrieval operations. Journal of ExperimentalPsychology, 90, 227–234.
MEYER-BAHLBURG, H. F. L., GRUEN, R. S., NEW, M. I., BELL,J. J., MORISHIMA, A., SHIMSHI, M., ET AL. (1996). Genderchange from female to male in classical congenital adre-nal hyperplasia. Hormones and Behavior, 30, 319–332.
MEYER-LINDENBERG, A. (2008). Trust me on this. Science,321, 778–780.
MEZZACAPPA, E. S., KATKIN, E. S., & PALMER, S. N. (1999).Epinephrine, arousal, and emotion: A new look at two-factor theory. Cognition and Emotion, 13, 181–199.
MICALLEF, J., & BLIN, O. (2001). Neurobiology and clini-cal pharmacology of obsessive-compulsive disorder.Clinical Neuropharmacology, 24, 191–207.
MICHAEL, R. P., & KEVERNE, E. B. (1968). Pheromones inthe communication of sexual status in primates. Nature,218, 746–749.
MICHAELS, J. W., BLOOMEL, J. M., BROCATO, R. M.,LINKOUS, R. A., & ROWE, J. S. (1982). Social facilitationand inhibition in a natural setting. Replications in SocialPsychology, 2, 21–24.
MIKLOWITZ, D. J. (2007). The role of the family in thecourse and treatment of bipolar disorder. CurrentDirections in Psychological Science, 16(4), 192–196.
MIKLOWITZ, D. J., & JOHNSON, S. L. (2006). The psy-chopathology and treatment of bipolar disorder. AnnualReview of Clinical Psychology, 2, 199–235.
MIKULINCER, M., & SHAVER, P. R. (2005). Attachment the-ory and emotions in close relationships: Exploring theattachment-related dynamics of emotional reactions torelational events. Personal Relationships, 12, 149–168.
MIKULINCER, M., & SHAVER, P. R. (2007). Attachment inadulthood: Structure, dynamics, and change. New York:Guilford.
MILAM, J. E., RICHARDSON, J. L., MARKS, G., KEMPER, C. A.,& MCCUTCHAN, A. J. (2004). The roles of dispositionaloptimism and pessimism in HIV disease progression.Psychology & Health, 19, 167–181.

PREFERENCESO R43
MILGRAM, S. (1963). Behavioral study of obedience.Journal of Abnormal and Social Psychology, 67, 371–378.
MILGRAM, S. (1965). Some conditions of obedience anddisobedience to authority. Human Relations, 18, 57–76.
MILGRAM, S. (1974). Obedience to authority. New York:Harper & Row.
MILGRAM, S., & MURRAY, T. H. (1992). Can deception inresearch be justified? In B. Slife & J. Rubenstein (Eds.),Taking sides: Clashing views on controversial psychologicalissues (7th ed.). Guilford, CT: Dushkin Publishing Group.
MILLER, (2007).
MILLER, A. G. (1986). The obedience experiments: A casestudy of controversy in social science. New York: Praeger.
MILLER, D. T. (1976). Ego involvement and attribution forsuccess and failure. Journal of Personality and SocialPsychology, 34, 901–906.
MILLER, D. T. (1999). The norm of self-interest. AmericanPsychologist, 54(12), 1053–1060.
MILLER, E. M. (1994). Intelligence and brain myelination:A hypothesis. Personality and Individual Differences, 17,803–832.
MILLER, G. (2005a). The dark side of glia. Science, 308,778–781.
MILLER, G. (2005b). Mutant mice reveal secrets of thebrain’s impressionable youth. Science, 309, 2145.
MILLER, G. (2006a). China: Healing the metaphoricalheart. Science, 311, 462–463.
MILLER, G. (2006b). The unseen: Mental illness’s globaltoll. Science, 311, 458–460.
MILLER, G. (2007). Hunting for meaning after midnight.Science, 315 (5817) 1360–1363.
MILLER, G. (2009). Rewiring faulty circuits in the brain.Science, 323(5921), 1554–1556.
MILLER, G. A. (1956). The magical number seven plus orminus two: Some limits in our capacity for processinginformation. Psychological Review, 63, 81–97.
MILLER, J., SCOTT, E., & OKAMOTO, S. (2006). Publicacceptance of evolution. Science, 313, 765–766.
MILLER, J. G. (1984). Culture and the development ofeveryday social explanation. Journal of Personality andSocial Psychology, 46, 961–978.
MILLER, J. G., & BERSOFF, D. M. (1998). The role of likingin perceptions of the moral responsibility to help: A cul-tural perspective. Journal of Experimental Social Psychology,34(5), 443–469.
MILLER, J. G., BERSOFF, D. M., & HARWOOD, R. L. (1990).Perceptions of social responsibilities in India and in theUnited States: Moral imperatives or personal decisions?Journal of Personality and Social Psychology, 58(1), 33–47.
MILLER, L. C., PUTCHA-BHAGAVATULA, A. D., & PEDERSEN,W. C. (2002). Men’s and women’s mating preferences:Distinct evolutionary mechanisms? Current Directions inPsychological Science, 11, 88–93.
MILLER, L. K. (1999). The savant syndrome: Intellectualimpairment and exceptional skill. Psychological Bulletin,125, 31–46.
MILLER, N. E., BAILEY, C. J., & STEVENSON, J. A. F. (1950).Decreased “hunger” but increased food intake resultingfrom hypothalamic lesions. Science, 112, 256–259.
MILLER, P. A., EISENBERG, N., FABES, R. A., & SHELL, R.(1989). Mothers’ emotional arousal as a moderator inthe socialization of children’s empathy. New Directions forChild Development, 44.
MILLER, R. R., BARNET, R. C., & GRAHAME, N. J. (1995).Assessment of the Rescorla-Wagner model. PsychologicalBulletin, 117, 363–387.
MILLER, S. D., DUNCAN, B. L., & HUBBLE, M. A. (2005).Outcome-informed clinical work. In J. C. Norcross & M.R. Goldfried (Eds.), Handbook of psychotherapy integration(2nd ed., pp. 84–102). New York: Oxford UniversityPress.
MILLER, W. R., & ROLLNICK, S. (2002). Motivational inter-viewing: Preparing people to change. New York: Guilford.
MILLS, J., & CLARK, M. S. (1994). Communal andexchange relationships: Controversies and research. InR. Erber & R. Gilmour (Eds.), Theoretical frameworks forpersonal relationships (pp. 29–42). Hillsdale, NJ: Erlbaum.
MILNER, B. (1966). Amnesia following operation on thetemporal lobes. In C. W. M. Whitty & O. L. Zangwill(Eds.), Amnesia (pp. 109–133). London: Butterworth.
MILNER, B., CORKIN, S., & TEUBER, H.-L. (1968). Furtheranalysis of the hippocampal syndrome: 14-year follow-upstudy of H. M. Neuropsychologia, 6, 215–234.
MILNER, B., & PETRIDES, M. (1984). Behavioural effects offrontal-lobe lesions in man. Trends in Neurosciences, 7,403–407.
MINEKA, S., & BEN HAMIDA, S. (1998). Observational andnonconscious learning. In W. O’Donohue (Ed.), Learningand behavior therapy (pp. 421–439). Needham Heights,MA: Allyn & Bacon.
MINEKA, S., & ÖHMAN, A. (2002). Phobias and prepared-ness: The selective, automatic, and encapsulated natureof fear. Biological Psychiatry, 52, 927–937.
MINEKA, S., & ZINBARG, R. (2006). A contemporarylearning theory perspective on the etiology of anxiety dis-orders: It’s not what you thought it was. AmericanPsychologist, 61(1), 10–26.
MINSKY, M. (1986). The society of mind. New York: Simon& Schuster.
MINUCHIN, S. (1974). Families and family therapy.Cambridge, MA: Harvard University Press.
MISCHEL, W. (1968). Personality and assessment. NewYork: Wiley.
MISCHEL, W. (1973). Towards a cognitive social learningreconceptualization of personality. Psychological Review,80, 252–283.
MISCHEL, W. (1974). Processes in delay of gratification. InL. Berkowitz (Ed.), Advances in experimental social psychol-ogy: Vol. 7. New York: Academic Press.
MISCHEL, W. (1984). Convergences and challenges in thesearch for consistency. American Psychologist, 39, 351–364.
MISCHEL, W. (2004). Toward an integrative science of theperson. Annual Review of Psychology, 55, 1–22.
MISCHEL, W., & BAKER, N. (1975). Cognitive appraisalsand transformations in delay behavior. Journal ofPersonality and Social Psychology, 31, 254–261.
MISCHEL, W., & MISCHEL, H. N. (1983). Development ofchildren’s knowledge of self-control strategies. ChildDevelopment, 54, 603–619.
MISCHEL, W., & MOORE, B. (1980). The role of ideation involuntary delay for symbolically presented awards.Cognitive Therapy and Research, 4, 211–221.
MISCHEL, W., & SHODA, Y. (1995). A cognitive-affectivesystem theory of personality: Reconceptualizing situa-tions, dispositions, dynamics, and invariance in person-ality structure. Psychological Review, 102, 246–268.
MISCHEL, W., & SHODA, Y. (1998). Reconciling processingdynamics and personality dispositions. Annual Review ofPsychology, 49, 229–258.
MISCHEL, W., & SHODA, Y. (2000). A cognitive-affectivesystem theory of personality: Reconceptualizing situa-tions, dispositions, dynamics, and invariance in person-ality structure. In E. T. Higgins & A. W. Kruglanski(Eds.), Motivational science: Social and personality perspec-tives (pp. 150–176). Philadelphia: Psychology Press/Taylor & Francis.
MISCHEL, W., SHODA, Y., & MENDOZA-DENTON, R. (2002).Situation-behavior profiles as a locus of consistency inpersonality. Current Directions in Psychological Science, 11,50–54.
MISCHEL, W., SHODA, Y., & PEAKE, P. K. (1988). The natureof adolescent competencies predicted by preschool delayof gratification. Journal of Personality and SocialPsychology, 54, 687–696.
MISCHEL, W., SHODA, Y., & RODRIGUEZ, M. L. (1992).Delay of gratification in children. In G. Loewenstein & J.Elster (Eds.), Choice over time (pp. 147–164). New York:Russell Sage Foundation.
MISELIS, R. R., & EPSTEIN, A. N. (1970). Feeding inducedby 2-deoxy-D-glucose injections into the lateral ventricalof the rat. Physiologist, 13, 262.
MISHLER, E. G., & WAXLER, N. E. (1968). Family interac-tion and schizophrenia: Alternative frameworks of inter-pretation. In D. Rosenthal & S. S. Kety (Eds.), Thetransmission of schizophrenia (pp. 213–222). New York:Pergamon.
MISTLBERGER, R. E. (2005). Circadian regulation ofmammalian sleep: Role of the suprachiasmatic nucleus.Brain Research Reviews, 49, 429–454.
MITA, T. H., DERMER, M., & KNIGHT, J. (1977). Reversedfacial images and the mere exposure hypothesis. Journalof Personality and Social Psychology, 35, 597–601.
MIYASHITA, Y. (1995). How the brain creates imagery:Projection to primary visual cortex. Science, 268,1719–1720.
MOFFAT, S., & HAMPSON, E. (1996). A curvilinear relation-ship between testosterone and spatial cognition inhumans: Possible influence of hand preference.Psychoendocrinology, 21, 323–337.
MOFFITT, T. E., CASPI, A., HARKNESS, A. R., & SILVA, P. A.(1993). The natural history of change in intellectual per-formance: Who changes? How much? Is it meaningful?Journal of Child Psychology and Psychiatry and AlliedDisciplines, 34(4), 455–506.
MOFFITT, T. E., CASPI, A., & RUTTER, M. (2006). Measuredgene-environment interactions in psychopathology:Concepts, research strategies, and implications forresearch, intervention, and public understanding ofgenetics. Perspectives on Psychological Sciences, 1, 5–27.

R44 PREFERENCESO
MOGHADDAM, F. (1998). Social psychology: Exploring uni-versals across cultures. New York: Freeman.
MOLDEN, D. C., & DWECK, C. S. (2006). Finding “mean-ing” in psychology: A lay theories approach to self-regu-lation, social perception, and social development.American Psychologist, 61, 192–203.
MOLONEY, D. P., BOUCHARD, T. J., JR., & SEGAL, N. L.(1991). A genetic and environmental analysis of thevocational interests of monozygotic and dizygotic twinsreared apart. Journal of Vocational Behavior, 39, 76–109.
MONEY, J. (1980). Love and love sickness. Baltimore: JohnsHopkins University Press.
MONEY, J., & EHRHARDT, A. A. (1972). Man and woman, boyand girl. Baltimore: Johns Hopkins University Press.
MONROE, S. M., & HADJIYANNAKIS, K. (2002). The socialenvironment and depression: Focusing on severe lifestress. In I. H. Gotlib and C. L. Hammen (Eds.),Handbook of depression (pp. 314–340). New York:Guilford.
MONTAGU, A. (ED.). (1999). Race & IQ. New York: OxfordUniversity Press.
MONTAGUE, D., & WALKER-ANDREWS, A. (2002). Mothers,fathers, and infants: The role of person familiarity andparental involvement in infants’ perception of emotionalexpressions. Child Development, 73, 1339–1352.
MONTE, C. F., & SOLLOD, R. N. (2003). Beneath the mask:An introduction to theories of personality (7th ed.). Danvers,MA: Wiley.
MONTGOMERY, S. A. (1995). Selective serotonin reuptakeinhibitors in the acute treatment of depression. In F. E.Bloom & D. Kupfer (Eds.), Psychopharmacology: The fourthgeneration of progress (pp. 1043–1051). New York: Raven.
MOONEY, C. (2005). The Republican war on science. NewYork: Basic Books.
MOORE, C., & DUNHAM, P. (EDS.). (2004). Joint attention:Its origin and role in development. Hillsdale, NJ: Erlbaum.
MOORHEAD, G., FERENCE, R., & NECK, C. P. (1991). Groupdecision fiascoes continue: Space shuttle Challenger anda revised groupthink framework. Human Relations, 44(6),539–550.
MORA, F., ROLLS, E. T., & BURTON, M. J. (1976).Modulation during learning of the responses of neuronsin the lateral hypothalamus to the sight of food.Experimental Neurology, 53, 508–519.
MORA, G. (1975). Historical and theoretical trends inpsychiatry. In A. M. Freedman, H. I. Kaplan, & B. J.Sadock (Eds.), Comprehensive textbook of psychiatry: Vol. 1(pp. 1–75). Baltimore: Williams & Wilkins.
MORAY, N. (1959). Attention in dichotic listening:Affective cues and the influence of instructions. QuarterlyJournal of Experimental Psychology, 11, 56–60.
MORELAND, R. L., & ZAJONC, R. B. (1982). Exposureeffects in person perception: Familiarity, similarity, andattraction. Journal of Experimental Social Psychology, 18,395–415.
MORELLI, G., ROGOFF, B., OPPENHEIM, D., & GOLDSMITH,D. (1992). Cultural variation in infants sleeping arrange-ments: Questions of independence. DevelopmentalPsychology, 28, 604–613.
MORENO, C., LAJE, G., BLANCO, C., JIANG, H., SCHMIDT, A.B., & OLFSON, M. (2007). National trends in the outpa-tient diagnosis and treatment of bipolar disorder inyouth. Archives of General Psychiatry, 64, 1032–1039.
MOREWEDGE, C., & NORTON, M. I. (2005). When dream-ing is believing: The (motivated) interpretation ofdreams. Journal of Personality and Social Psychology, 96,249–254.
MORGAN, M. J. (2000). Ecstasy (MDMA): A review of itspossible persistent psychological effects. Psycho-pharmacology, 152, 230–248.
MORGAN, C. D., & MURRAY, H. A. (1935). A method forinvestigating fantasies: The Thematic Apperception Test.Archives of Neurological Psychiatry, 34, 289–306.
MORGAN, C. P., & ARAM, J. D. (1975). The preponderanceof arguments in the risky shift phenomenon. Journal ofExperimental Social Psychology, 11(1), 25–34.
MORGAN, J. L. (1996). A rhythmic bias in preverbalspeech segmentation. Journal of Memory and Language, 35,666–688.
MORRIS, M. W., & PENG, K. (1994). Culture and cause:American and Chinese attributions for social and physi-cal events. Journal of Personality and Social Psychology, 67,949–971.
MORSBACH, H., & TYLER, W. J. (1986). In R. Harr (Ed.),The social construction of emotions (pp. 289–307). Oxford,England: Blackwell.
MORSELLA, E. (2005). The function of phenomenalstates: Supramodular interaction theory. PsychologicalReview, 112, 1000–1021.
MORSELLA, E., LEVINE, L. R., & BARGH, J. A. (2004).Nonconscious activation of action plans: A cascademodel of automatic social behavior. Unpublished manu-script, Yale University.
MOSCOVICI, S., & ZAVALLONI, M. (1969). The group as apolarizer of attitudes. Journal of Personality and SocialPsychology, 12(2), 125–135.
MOSER, M. B. (1999). Making more synapses: A way tostore information? Cellular and Molecular Life Sciences, 55,593–600.
MOTOHASHI, K., & UMINO, M. (2001). Heterotopicpainful stimulation decreases the late component ofsomatosensory evoked potentials induced by electricaltooth stimulation. Brain Research, 11, 39–46.
MOUNTS, N. S., & STEINBERG, L. (1995). An ecologicalanalysis of peer influence on adolescent grade point aver-age and drug use. Developmental Psychology, 31(6),915–922.
MOZEL, M., SMITH, B., SMITH, P., SULLIVAN, R., &SWENDER, P. (1969). Nasal chemoreception in flavoridentification. Archives of Otolaryngology, 90, 131–137.
MROCZEK, D. K. (2001). Age and emotion in adulthood.Current Directions in Psychological Science, 10, 87–90.
MROCZEK, D. K., & KOLARZ, C. M. (1998). The effect ofage on positive and negative affect: A developmental per-spective on happiness. Journal of Personality and SocialPsychology, 75(5), 1333–1349.
MUELLER, W. A. (1996). Developmental biology. New York:Springer-Verlag.
MULFORD, R. (1986). First words of the blind child. In M.Smith & J. Locke (Eds.), The emergent lexicon: The child’sdevelopment of a linguistic vocabulary. New York: AcademicPress.
MULICK, J. A. (1990). The ideology and science of punish-ment in mental retardation. American Journal on MentalRetardation, 95, 142–156.
MULLEN, M. K. (1994). Earliest recollections of child-hood: A demographic analysis. Cognition, 52(1), 55–79.
MULLEN, M. K., & YI, S. (1995). The cultural context oftalk about the past: Implications for the development ofautobiographical memory. Cognitive Development, 10(3),407–419.
MULROW, C. D., WILLIAMS, J. W., JR., CHIQUETTE, E.,AGUILAR, C., HITCHCOCK-NOEL, P., LEE, S., ET AL. (2000).Efficacy of newer medications for treating depression inprimary care patients. American Journal of Medicine, 108,54–64.
MUNAFO, M. R., DURRANT, C., LEWIS, G., & FLINT, J.(2009). Gene X environment interactions at the sero-tonin transporter locus. Biological Psychiatry, 65, 211–219.
MUNNICH, E., LANDAU, B., & DOSHER, B. (2001) Spatiallanguage and spatial representation: A cross-linguisticcomparison. Cognition, 81(3), 171–208.
MURPHY, F. C., NIMMO-SMITH, I., & LAWRENCE, A. D.(2003). Functional neuroanatomy of emotion: A meta-analysis. Cognitive, Affective, and Behavioral Neuroscience, 3,207–233.
MURPHY, G. L. (2002). The big book of concepts.Cambridge, MA: MIT Press.
MURRAY, C. (1998). Income inequality and IQ.Washington, DC: American Enterprise Institute.
MURRAY, L., & TREVARTHEN, C. (1985). Social perception ininfants. New York: Ablex.
MUSOLINO, J., CHUNYO, G., & LANDAU, B. (In press).Uncovering knowledge of core syntactic and semanticprinciples in individuals with Williams syndrome.Language Learning and Development.
MUSSELL, M., MITCHELL, J., CROSBY, R., FULKERSON, J.,HOBERMAN, H., & ROMANO, J. (2000). Commitment totreatment goals in prediction of group cognitive-behav-ioral therapy treatment outcome for women with bulimianervosa. Journal of Consulting and Clinical Psychology, 68,432–437.
NADEL, L., & JACOBS, W. J. (1998). Traumatic memory isspecial. Current Directions in Psychological Science, 7,154–157.
NADEL, L., & MOSCOVITCH, M. (2001). The hippocampalcomplex and long-term memory revisited. Trends inCognitive Science, 5, 228–230.
NAGEL, T. (1974). What is it like to be a bat? PhilosophicalReview, 83, 435–450.
NAIGLES, L. G. (1990). Children use syntax to learn verbmeanings. Journal of Child Language, 17, 357–374.
NAKAMURA, J., & CSIKSZENTMIHALYI, M. (2001). Catalyticcreativity: The case of Linus Pauling. AmericanPsychologist, 56(4), 337–341.
NAPPA, R., WESSEL, A., MCELDOON, K. L., GLEITMAN, L. R.,& TRUESWELL, J. C. (2009). Use of speaker’s gaze and syn-

PREFERENCESO R45
tax in verb learning. Language Learning and Development,5(4), 203–234.
NARROW, W. REGIER, D., RAE, D., MANDERSCHEID, R., &LOCKE, B. (1993). Use of services by persons with mentaland addictive disorders: Findings from the NationalInstitute of Mental Health Epidemiologic CatchmentArea Program. Archives of General Psychiatry, 50, 95–107.
NASH, M. R. (2001). The truth and hype of hypnosis.Scientific American, 285, 36–43.
NASSER, M. (1997). Culture and weight consciousness.London: Routledge.
NATHAN, P. E., & GORMAN, J. M. (EDS.). (2002). A guide totreatments that work (2nd ed.). New York: OxfordUniversity Press.
NATHAN, P. E., STUART, S. P., & DOLAN, S. L. (2000).Research on psychotherapy efficacy and effectiveness:Between Scylla and Charybdis? Psychological Bulletin, 126,964–981.
NATIONAL INSTITUTE OF MENTAL HEALTH (NIMH).(2000). NIMH Research on Treatment for AttentionDeficit Hyperactivity Disorder (ADHD): Questions andAnswers about the Multimodal Treatment Study.Retrieved from http://www.nimh.nih.gov/health/trials/nimh-research-treatment-adhd-study.shtml
NATIONAL INSTITUTE OF MENTAL HEALTH (NIMH).(2007a). Always embarrassed: Social phobia (social anx-iety disorder). NIH Publication No. 07-4678. Bethesda,MD: National Institutes of Health.
NATIONAL INSTITUTE OF MENTAL HEALTH (NIMH).(2007b). When worry gets out of control: Generalizedanxiety disorder. NIH Publication No. 07-4677.Bethesda, MD: National Institutes of Health.
NATIONAL INSTITUTE OF MENTAL HEALTH (NIMH).(2009). Anxiety disorders. NIH Publication No. 09-3879. Bethesda, MD: National Institutes of Health.
NATIONAL RESEARCH COUNCIL AND INSTITUTE OF MEDICINE
(2000). From neurons to neighborhoods: The science of earlychildhood development. Committee on Integrating theScience of Early Childhood Development. J. Shonkoff &D. Phillips (Eds.), Board on Children, Youth, andFamilies, Commission on Behavioral and Social Sciencesand Education. Washington, DC: National AcademyPress.
NAUTA, W. J. H., & FEIRTAG, M. (1986). Fundamental neu-roanatomy. New York: Freeman.
NAVARRA, P., DELLO RUSSO, C., MANCUSO, C., PREZIOSI, P.,& GROSSMAN, A. (2000). Gaseous neuromodulators inthe control of neuroendocrine stress axis. Annals of theNew York Academy of Sciences, 917, 638–646.
NAZZI, T., BERTONCINI, J., & MEHLER, J. (1998). Languagediscrimination by newborns: Toward an understandingof the role of rhythm. Journal of Experimental Psychology:Human Perception and Performance, 24(3), 756–766.
NEEDHAM, D., & BEGG, I. (1991). Problem-oriented train-ing promotes spontaneous analogical transfer: Memory-oriented training promotes memory for training. Memoryand Cognition, 19, 543–557.
NEIMEYER, G. J. (1984). Cognitive complexity and maritalsatisfaction. Journal of Social and Clinical Psychology, 2,258–263.
NEISSER, U. (1982a). Memory observed. San Francisco:Freeman.
NEISSER, U. (1982b, January). On the trail of the tape-recorder fallacy. Paper presented at a symposium on “Theinfluence of hypnosis and related states on memory:Forensic implications” at the meetings of the AmericanAssociation for the Advancement of Science,Washington, DC.
NEISSER, U. (1986). Remembering Pearl Harbor: Reply toThompson and Cowan. Cognition, 23, 285–286.
NEISSER, U. (1997). Rising scores on intelligence tests.American Scientist, 85, 440–447.
NEISSER, U. (ED.). (1998). The rising curve: Long-term gainsin IQ and related measures. Washington, DC:AmericanPsychological Association.
NEISSER, U., & BECKLEN, R. (1975). Selective looking:Attending to visually specified events. CognitivePsychology, 7(4), 480–494.
NEISSER, U., BOODOO, G., BOUCHARD, T. J., JR., BOYKIN, A.W., BRODY, N., CECI, S. J., ET AL. (1996). Intelligence:Knowns and unknowns. American Psychologist, 51(2),77–101.
NEISSER, U., & HARSCH, N. (1992). Phantom flashbulbs:False recollections of hearing the news about Challenger.In E. Winograd & U. Neisser (Eds.), Affect and accuracy inrecall: Studies of “flashbulb” memories (pp. 9–31).Cambridge: Cambridge University Press.
NELSON, C. A., III, FURTADO, E., FOX, N., & ZEANAH, C.(2009). The deprived human brain. American Scientist, 97,222–229.
NELSON, C. A., III, ZEANAH, C. H., FOX, N. A., MARSHALL,P. J., SMYKE, A. T., & GUTHRIE, D. (2007). Cognitive recov-ery in socially deprived young children: The BucharestEarly Intervention Project. Science, 318, 1937–1940.
NELSON, K., & FIVUSH, R. (2000). Socialization of mem-ory. In E. Tulving & F. I. M. Craik (Eds.), The Oxford hand-book of memory (pp. 283–295). London: OxfordUniversity Press.
NEMETH, C., & CHILES, C. (1988). Modeling courage: Therole of dissent in fostering independence. EuropeanJournal of Social Psychology, 18, 275–280.
NERIA, Y., OLFSON, M., GAMEROFF, M. J., WICKRAMARATNE,P., PILOWSKY, D., VERDELI, H., ET AL. (2008). Trauma expo-sure and posttraumatic stress disorder among primarycare patients with bipolar spectrum disorder. BipolarDisorder, 10, 503–510.
NESPOR, M., PEÑA, M., & MEHLER, J. (2003). On the dif-ferent roles of vowels and consonants in speech process-ing and language acquisition. Lingue e Linguaggio, 2,221–240.
NETTELBECK, T. (2003). Inspection time and g. In H.Nyborg (Ed.), The scientific study of General intelligence: Atribute to Arthur Jensen (pp. 77–92). New York: Elsevier.
NETTELBECK, T., & YOUNG, R. (1996). Intelligence and thesavant syndrome: Is the whole greater than the sum ofthe fragments? Intelligence, 22, 49–68.
NEUGEBAUER, R. (1979). Medieval and early modern the-ories of mental illness. Archives of General Psychiatry, 36,477–484.
NEWCOMB, A. F., & BAGWELL, C. L. (1995). Children’sfriendship relations: A meta-analytic review. PsychologicalBulletin, 117(2), 306–347.
NEWCOMB, A. F., BUKOWSKI, W. M., & PATTEE, L. (1993).Children’s peer relations: A meta-analytic review of pop-ular, rejected, neglected, controversial, and average socio-metric status. Psychological Bulletin, 113(1), 99–128.
NEWCOMBE, F., RATCLIFF, G., & DAMASIO, H. (1987).Dissociable visual and spatial impairments followingright posterior cerebral lesions: Clinical, neuropsycho-logical, and anatomical evidence. Neuropsychologia, 25(1B), 149–161.
NEWCOMBE, N. S. (2002). The nativist-empiricst contro-versy in the context of recent research on spatial andquantitative development. Psychological Science, 13,395–401.
NEWCOMBE, N. S. (2007). Taking science seriously:Straight thinking about spatial sex differences. In S. Ceci& W. Williams (Eds.), Why aren’t more women in science?(pp. 69–77). Washington, DC: American PsychologicalAssociation.
NEWELL, A., & SIMON, H. A. (1972). Human problem solv-ing. Englewood Cliffs, NJ: Prentice-Hall.
NEWMAN, E. A., & ZAHS, K. R. (1998). Modulation of neu-ronal activity by glial cells in the retina. Journal ofNeuroscience, 18, 4022–4028.
NEWPORT, E. L. (1990). Maturational constraints on lan-guage learning. Cognitive Science, 14, 11–28.
NEWPORT, E. L. (1999). Reduced input in the acquisitionof signed languages: Contributions to the study of cre-olization. In M. DeGraff (Ed.), Language creation and lan-guage change: Creolization, diachrony, and development.Cambridge, MA: MIT Press.
NEWPORT, E. L., & ASHBROOK, E. F. (1977). The emergenceof semantic relations in American Sign Language. Papersand Reports in Child Language Development, 13, 16–21.
NICHD EARLY CHILD CARE RESEARCH NETWORK. (1997).The effects of infant child care on infant-mother attach-ment security: Results of the NICHD study of early childcare. Child Development, 68, 860–879.
NICHD EARLY CHILD CARE RESEARCH NETWORK. (2001).Child-care and family predictors of preschool attach-ment and stability from infancy. DevelopmentalPsychology, 37, 847–862.
NICHD EARLY CHILD CARE RESEARCH NETWORK.(2003).Does quality of child care affect child outcomes atage 4 1/2? Developmental Psychology, 39, 451–469.
NICHD EARLY CHILD CARE RESEARCH NETWORK. (2006).Child-care effect sizes for the NICHD Study of EarlyChild Care and Youth Development. AmericanPsychologist, 61, 99–116.
NICHOLSON, R. A., & BERMAN, J. S. (1983). Is follow-upnecessary in evaluating psychotherapy? PsychologicalBulletin, 93, 261–278.
NICKERSON, R. A., & ADAMS, M. J. (1979). Long-termmemory for a common object. Cognitive Psychology, 11,287–307.
NISBETT, R. E. (1980). The trait construct in lay and pro-fessional psychology. In L. Festinger (Ed.), Retrospectionson social psychology (pp. 109–130). New York: OxfordUniversity Press.

R46 PREFERENCESO
NISBETT, R. E. (2003). The geography of thought: Why wethink the way we do. New York: Free Press.
NISBETT, R. E., & COHEN, D. (1996). Culture of honor: Thepsychology of violence in the South. Boulder, CO: WestviewPress.
NISBETT, R. E., KRANTZ, D. H., JEPSON, C., & KUNDA, Z.(1983). The use of statistical heuristics in everyday induc-tive reasoning. Psychological Review, 90, 339–363.
NISBETT, R. E., & MIYAMOTO, Y. (2005). The influence ofculture: Holistic versus analytic perception. Trends inCognitive Science, 9, 467–473.
NISBETT, R. E., PENG, K., CHOI, I., & NORENZAYAN, A.(2001). Culture and systems of thought: Holistic versusanalytic cognition. Psychological Review, 108(2), 291–310.
NISBETT, R. E., & ROSS, L. (1980). Human inference:Strategies and shortcomings of social judgment. EnglewoodCliffs, NJ: Prentice-Hall.
NISBETT, R. E., & SCHACHTER, S. (1966). Cognitive manip-ulation of pain. Journal of Experimental Social Psychology,2, 277–236.
NISBETT, R. E., & WILSON, T. D. (1977). Telling more thanwe can know: Verbal reports on mental processes.Psychological Review, 84, 231–259.
NOLEN-HOEKSMA, S. (1987). Sex differences in unipolardepression: Evidence and theory. Psychological Bulletin,101, 259–282.
NOLEN-HOEKSEMA, S., WISCO, B. E., & LYUBOMIRSKY, S.(2008). Rethinking rumination. Perspectives on Psycho-logical Science, 3, 400–424.
NOPOULOS, P., FLAUM, M., & ANDREASEN, N. C. (1997). Sexdifferences and brain morphology in schizophrenia.American Journal of Psychiatry, 154, 1648–1654.
NORBURY, H. M., WAXMAN, S. R., & SONG, H. (2008).Tight and loose are not created equal: An asymmetryunderlying the representation of fit in English- andKorean-speakers. Cognition. 109(3), 316–325.
NORCROSS, J. C., & FREEDHEIM, D. K. (1992). Into thefuture: Retrospect and prospect in psychotherapy. In D.K. Freedheim (Ed.), History of psychotherapy. Washington,DC: American Psychological Association.
NORENZAYAN, A., & SHARIFF, A. F. (2008). The origin andevolution of religious prosociality. Science, 322(5898),58–62.
NORMAN, W. T. (1963). Toward an adequate taxonomy ofpersonality attributes: Replicated factor structure in peernomination personality ratings. Journal of Abnormal andSocial Psychology, 66, 574–583.
NORTON, M. I., FROST, J. H., & ARIELY, D. (2007). Less ismore: The lure of ambiguity, or why familiarity breedscontempt. Journal of Personality and Social Psychology, 92,97–105.
NOSEK, B. A. (2007). Implicit-explicit relations. CurrentDirections in Psychological Science, 16(2), 65–69.
NOVECK, J., & SPERBER, D. (2005). Experimental pragmat-ics. Oxford: Oxford University Press.
NOVICK, J. M., THOMPSON-SCHILL, S., & TRUESWELL, J. C.(2008). Putting lexical constraints in context into thewvisual-world paradigm. Cognition, 107(3), 850–903.
NOVICK, J. M., TRUESWELL, J. C., & THOMPSON-SCHILL, S. L.(2005). Cognitive control and parsing: Re-examiningthe role of Broca’s area in sentence comprehension.
Journal of Cognitive, Affective, and Behavioral Neuroscience,5(3), 263–281.
NOYES, R., WOODMAN, C., GARVEY, M. J., COOK, B. L.,SUELZER, M., CLANCY, J. ET AL. (1992). Generalized anxietydisorder vs. panic disorder: Distinguishing characteris-tics and patterns of comorbidity. Journal of Nervous &Mental Disease, 180(6), 369–379.
NUTT, D. J. (2001). Neurobiological mechanisms in gen-eralized anxiety disorder [Suppl.]. Journal of ClinicalPsychiatry, 62(11), 22–27.
NYITI, R. M. (1976). The development of conservation inthe Meru children of Tanzania. Child Development, 47(4),1122–1129.
OAKES, P. J., & TURNER, J. C. (1980). Social categorizationand intergroup behavior: Does minimal intergroup dis-crimination make social identity more positive? EuropeanJournal of Social Psychology, 10, 295–301.
OBERMAN, L. M., & RAMACHANDRAN, V. S. (2007). Thesimulating social mind: The role of the mirror neuronsystem and simulation in the social and communicativedeficits of autism spectrum disorders. PsychologicalBulletin, 133(2), 310–327.
OBERAUER, K., SCHULZE, R., WILHELM, O., & SÜSS, H.-M.(2005). Working memory and intelligence: Their correla-tion and their relation: Comment on Ackerman, Beier,and Boyle (2005). Psychological Bulletin, 131, 61–65.
OBHI, S., PLANETTA, P., & SCANTLEBURY, J. (2009). On thesignals underlying conscious awareness of action.Cognition, 110, 65–73.
OCHSNER, K. N., KNIERIM, K., LUDLOW, D. H., HANELIN, J.,RAMACHANDRAN, T., GLOVER, G., ET AL. (2004). Reflectingupon feelings: An fMRI study of neural systems support-ing the attribution of emotion to self and other. Journal ofCognitive Neuroscience, 16, 1746–1772.
O’CONNOR, T. G., RUTTER, M., BECKETT, C., KEAVENEY, L.,KREPPNER, J. M., & ENGLISH AND ROMANIAN ADOPTION
STUDY TEAM. (2000). The effects of global severe priva-tion on cognitive competence: Extension and longitudi-nal follow-up. Child Development, 71(2), 376–390.
ODIORNE, J. M. (1957). Color changes. In M. E. Brown(Ed.), The physiology of fishes: Vol. 2. New York: AcademicPress.
OESTERMAN, K., BJOERKQVIST, K., LAGERSPETZ, K. M. J.,KAUKIAINEN, A., LANDAU, S. F., FRACZEK, A., ET AL. (1998).Cross-cultural evidence of female indirect aggression.Aggressive Behavior, 24(1), 1–8.
OFSHE, R. (1992). Inadvertent hypnosis during interro-gation: False confession due to dissociative state; mis-identified multiple personality and the Satanic CultHypothesis. International Journal of Clinical andExperimental Hypnosis, 40, 125–136.
OGDEN, J. A. (2005). Fractured minds: A case-studyapproach to clinical neuropsychology. New York: OxfordUniversity Press.
ÖHMAN, A. (2005). The role of the amygdala in humanfear: Automatic detection of threat. Psychoneuro-endocrinology, 30, 953–958.
ÖHMAN, A., & MINEKA, S. (2001). Fears, phobias, andpreparedness: Toward an evolved module of fear and fearlearning. Psychological Review, 108, 483–522.
ÖHMAN, A., & MINEKA, S. (2003). The malicious serpent:Snakes as a prototypical stimulus for an evolved moduleof fear. Current Directions in Psychological Science, 12, 5–9.
ÖHMAN, A., & SOARES, J. J. (1993). On the automaticnature of phobic fear: Conditioned electrodermalresponses to masked fear-relevant stimuli. Journal ofAbnormal Psychology, 102(1), 121–132.
ÖHMAN, A., & SOARES, J. J. F. (1994). “Unconscious anxi-ety”: Phobic responses to masked stimuli. Journal ofAbnormal Psychology, 103, 231–240.
O’KANE, G., KENSINGER, E. A., & CORKIN, S. (2004).Evidence for semantic learning in profound amnesia: Aninvestigation with patient H.M. Hippocampus, 14(4),417–425.
OKASHA, A., & OKASHA, T. (2000). Mental health inCairo (Al-Qahira). International Journal of Mental Health,28, 62–68.
OLFF, M., LANGELAND, W., DRAIJER, N., & GERSONS, B.P.R.(2007). Gender differences in posttraumatic stress dis-order. Psychological Bulletin, 133(2), 183–204.
OLFSON, M., & KLERMAN, G. L. (1993). Trends in the pre-scription of psychotropic medications. The role of physi-cian specialty. Medical Care, 31, 559–564.
OLLENDICK, T., & KING, N. (EDS.). (1994). Internationalhandbook of phobic and anxiety disorders in children andadolescents: Issues in clinical child psychology. New York:Plenum.
OLSON, D. J. (1991). Species differences in spatial mem-ory among Clark’s nutcrackers, scrub jays, and pigeons.Journal of Experimental Psychology: Animal BehaviorProcesses, 17(4), 363–376.
OLSON, W. K. (1997). The excuse factory: How employmentlaw is paralyzing the American workplace. New York: FreePress.
O’NEAL, J. (1984). First person account: Finding myselfand loving it. Schizophrenia Bulletin, 10, 109–110.
O’NEILL, D. K., ASTINGTON, J. W., & FLAVELL, J. H. (1992).Young children’s understanding of the role that sensoryexperiences play in knowledge acquisition. ChildDevelopment, 63(2), 474–490.
ONISHI, K., & BAILLARGEON, R. (2005). Do 15-month-oldinfants understand false belief? Science, 308, 255–258.
OPPENHEIM, D., SAGI, A., & LAMB, M. (1988). Infant-adultattachments on the kibbutz and their relation to socioe-motional development 4 years later. DevelopmentalPsychology, 24, 427–433.
ORLANSKY, H. (1949). Infant care and personality.Psychological Bulletin, 46, 1–48.
ORNE, M. T. (1951). The mechanisms of hypnotic ageregression: An experimental study. Journal of Abnormaland Social Psychology, 58, 277–299.
ORNE, M. T., & EVANS, F. J. (1965). Social control in thepsychological experiment: Antisocial behavior and hyp-nosis. Journal of Personality and Social Psychology, 1,189–200.
ORNSTEIN, P. A., BAKER-WARD, L., MYERS, J., PRINCIPE, G.F., & GORDON, B. N. (1995). Young children’s long-termretention of medical experiences: Implications for testi-mony. In F. E. Weinert & W. Schneider (Eds.), Memoryperformance and competencies: Issues in growth and develop-ment (pp. 347–371). Mahwah, NJ: Erlbaum.

PREFERENCESO R47
ORTONY, A., CLORE, G. L., & COLLINS, A. (1988). The cog-nitive structure of emotions. New York: CambridgeUniversity Press.
OZER, E. J., & WEISS, D. S. (2004). Who develops post-traumatic stress disorder? Current Directions inPsychological Science, 13, 169–172.
OZER, D. J., & Benet-Martínez, V. (2006). Personalityand the prediction of consequential outcomes. AnnualReview of Psychology, 57, 401–421.
PACIFICI R., ZUCCAROA, P., FARRÉB, M., PICHINIA,S., DI
CARLOA, S., ROSETB, P. N., ORTUÑOB, J., PUJADASB, M.,BACOSIA, A., MENOYOB, E., SEGURAB, J., & DE LA TORREB, R.(2001). Effects of repeated doses of MDMA (“Ecstasy”)on cell-mediated immune response in humans. LifeSciences, 69, 2931–2941.
PACKER, D. J. (2009). Avoiding groupthink: Whereasweakly identified members remain silent, strongly identi-fied members dissent about collective problems.Psychological Science, 20, 546–548.
PALLIER, C., CHRISTOPHE, A., & MEHLER, J. (1997).Language-specific listening. Trends in Cognitive Science,1(4).
PALMER, S. E. (2002). Perceptual grouping: It’s later thanyou think. Current Directions in Psychological Science, 11(3),101–106.
PANKSEPP, J. (1991). Affective neuroscience: A conceptualframework for the neurobiological study of emotions.International Review of Studies on Emotion, 1, 59–99.
PANKSEPP, J. (1998). Affective neuroscience: The foundationsof human and animal emotions. Oxford, England: OxfordUniversity Press.
PANKSEPP, J. (1998). Attention deficit/hyperactivity disor-ders, psychostimulants, and intolerance of childhoodplayfulness: A tragedy in the making? Current Directionsin Psychological Science, 7, 91–98.
PAPAFRAGOU, A.; CASSIDY, K., & GLEITMAN, L. R. (2007).When we think about thinking: The acquisition of beliefverbs. Cognition, 105(1), 125-165.
PAPAFRAGOU, A., MASSEY, C., & GLEITMAN, L. R. (2006).When English proposes what Greek presupposes.Cognition, 98(3), B75–B86.
PARKE, R. D. (1981). Fathers. Cambridge, MA: HarvardUniversity Press.
PARKER, G., MAHENDRAN, R., KOH, E. S., & MACHIN, D.(2000). Season of birth in schizophrenia: No latitude atthe equator. British Journal of Psychiatry, 176, 68–71.
PARKER, J., RUBIN, K., PRICE, J., & DEROSIER, M. (1995).Peer relationships, child development and adjustment: Adevelopmental psychopathology. In D. Cicchetti & D.Cohen (Eds.), Developmental Psychopathology. New York:Wiley.
PARNAS, J., & JORGENSEN, A. (1989). Premorbid psy-chopathology in schizophrenia spectrum. British Journalof Psychiatry, 155, 623–627.
PARSONS, J. E., ADLER, T. F., & KACZALA, C. M. (1982).Socialization of achievement attitudes and beliefs:Parental influences. Child Development, 53(2), 310–321.
PASHLER, H., JOHNSTON, J. C., & RUTHRUFF, E. (2000).Attention and performance. Annual Review of Psychology,52, 629–651.
PATTERSON, B. W. (2004). The “tyranny of the eyewit-ness.” Law & Psychology Review, 28, 195–203.
PATTERSON, D., & JENSEN, M. (2003). Hypnosis and clini-cal pain. Psychological Bulletin, 129 (4), 495–521.
PAVLOV, I. (1927). Conditioned reflexes. Oxford, England:Oxford University Press.
PAYNE, B. K. (2001). Prejudice and perception: The role ofautomatic and controlled processes in misperceiving aweapon. Journal of Personality and Social Psychology, 81,181–192.
PAYNE, J. D., NADEL, L., BRITTON, W. B., & JACOBS, W. J.(2004). The biopsychology of trauma and memory. In D.Reisberg & P. Hertel (Eds.), Memory and emotion(pp. 76–128). New York: Oxford University Press.
PEARCE, J. M., & BOUTON, M. E. (2001). Theories of asso-ciative learning in animals. Annual Review of Psychology,52, 111–139.
PEDERSEN, P. B., FUKUYAMA, M., & HEATH, A. (1989).Client, counselor, and contextual variables in multicul-tural counseling. In P. B. Pedersen, J. G. Draguns, W. J.Lonner, & J. E. Trimble (Eds.), Counseling across cultures(pp. 23–52). Honolulu: University of Hawaii.
PEDERSEN, W. C., MILLER, L. C., PUTCHA-BHAGAVATULA, A.D., & YANG, Y. (2002). Evolved sex differences in thenumber of partners desired? The long and the short of it.Psychological Science, 13, 157–161.
PEDERSON, E., DANZIGER, E., WILKINS, D., LEVINSON, S.,KITA, S., & SENFT, G. (1998). Semantic typology and spa-tial conceptualization. Language 74(3), 557–589.
PEÑA, M., BONATTI, L., NESPOR, M., & MEHLER, J. (2002).Signal driven computations in speech processing. Science,298, 604–607.
PEÑA, M., MAKI, A. , KOVA, D., DEHAENE-LAMBERTZ, G.,KOIZUMI, H., BOUQUET, F., ET AL. (2003). Sounds andsilence: An optical topography study of language recogni-tion at birth. Proceedings of the National Academy ofSciences, 100(20), 11702–11705.
PENDERGAST, M. (1995). Victims of memory: Sex abuse accu-sations and shattered lives. Hinesburg, VT: Upper Access.
PENFIELD, W., & RASMUSSEN, T. (1950). The cerebral cortexof man. New York: Macmillan.
PENNEBAKER, J. W. (2004). Writing to heal: A guided jour-nal for recovering from trauma and emotional upheaval.Oakland, CA: New Harbinger Press.
PENNISI, E. (2005). Strong personalities can pose prob-lems in the mating game. Science, 309, 694–695.
PENTON-VOAK, I. S., & PERRETT, D. I. (2000). Female pref-erence for male faces changes cyclically: Further evidence.Evolution and Human Behavior, 21(1), 39–48.
PEPLAU, L. A. (2003). Human sexuality: How do men andwomen differ? Current Directions in Psychological Science,12, 37–40.
PEPLAU, L. A., & FINGERHUT, A. W. (2007). The close rela-tionships of lesbians and gay men. Annual Review ofPsychology, 58, 405–424.
PEPPERBERG, I. (1999). Rethinking syntax: A commentaryon E. Kako’s “Elements of syntax in the systems of three
language-trained animals.” Animal Learning & Behavior,27, 15–17.
PERANI, D., PAULESCU, E., SEBASTIAN-GALLES, N., DUPOUX,E., DEHAENE, S., BETTINARDI, V., CAPPA, S., FAZIO, F., &MEHLER, J. (1998) The bilingual brain: Proficiency andage of acquisition of the second language. Brain, 121,1841–1852.
PERDUE, C. W., DOVIDIO, J. F., GURTMAN, M. B., & TYLER, R.B. (1990). Us and them: Social categorization and theprocess of intergroup bias. Journal of Personality and SocialPsychology, 59, 475–486.
PERKINS, D. N., & GROTZER, T. A. (1997). Teaching intelli-gence. American Psychologist, 52, 1125–1133.
PERLS, F. S. (1967). Group vs. individual therapy. ETC, 24,306–312.
PERLS, F. S. (1969). Gestalt therapy verbatim. Moab, UT:Real People Press.
PERNER, J., & LANG, B. (1999). Development of theory ofmind and executive control. Trends in Cognitive Science, 6,337–344.
PERNER, J., & RUFFMAN, T. (2005). Infants’ insight intothe mind: How deep? Science, 308, 214–216.
PERROTT, D. A., GENTNER, D., & BODENHAUSEN, G. V.(2005). Resistance is futile: The unwitting insertion ofanalogical inferences in memory. Psychonomics Bulletin &Review, 12, 696–702.
PETERSON, C. (1999). Personal control and well-being. InD. Kahneman, E. Diener, & N. Schwarz (Eds.), Well-being:The foundations of hedonic psychology (pp. 288–301). NewYork: Russell Sage Foundation.
PETERSON, C. (2006). A primer in positive psychology. NewYork: Oxford University Press.
PETERSON, C., & MCCABE, A. (1994). A social interaction-ist account of developing decontextualized narrativeskill. Developmental Psychology, 30(6), 937–948.
PETERSON, C., & PARK, C. (1998). Learned helplessnessand explanatory style. In D. F. Barone, M. Hersen, & V.Van Hasselt (Eds.), Advanced personality (pp. 287–310).New York: Plenum.
PETERSON, C., & PARK, N. (2007). Explanatory style andemotion regulation. In J. Gross, Handbook of emotion reg-ulation (pp. 159–179). New York: Guilford.
PETERSON, C., & SELIGMAN, M. E. P. (1984). Causal expla-nations as a risk factor for depression: Theory and evi-dence. Psychological Review, 91, 341–374.
PETERSON, C. T., & SELIGMAN, M. E. P. (2004). Characterstrengths and virtues: A handbook and classification.Washington, DC: APA Press and Oxford UniversityPress.
PETERSON, C., SEMMEL, A., VON BAEYER, C., ABRAMSON, L.Y., METALSKY, G. I., & SELIGMAN, M. E. P. (1982). TheAttributional Style Questionnaire. Cognitive Therapy andResearch, 6, 287–299.
PETERSON, C., & VAIDYA, R. S. (2001). Explanatory style,expectations, and depressive symptoms. Personality andIndividual Differences, 31, 1217–1223.
PETERSON, M. A., & ENNS, J. T. (2005). The edge complex:Implicit memory for figure assignment in shape percep-tion. Perception & Psychophysics, 67, 727–740.

R48 PREFERENCESO
PETERSON, R. S., & BEHFAR, K. J. (2005). Leadership asgroup regulation. In D. M. Messick & R. M. Kramer(Eds.), The psychology of leadership: New perspectives andresearch (pp. 143–162). Mahwah, NJ: Erlbaum.
PETERSON, S. E., FOX, P. T., POSNER, M. I., MINTUN, M., &RAICHLE, M. E. (1988). Positron emission tomographicstudies of the processing of single words. Journal ofCognitive Neuroscience, 1, 153–170.
PETRIDES, G., FINK, M., HUSAIN, M. M., KNAPP, R. G.,RUSH, A. J., MUELLER, M., ET AL. (2001). ECT remissionrates in psychotic versus nonpsychotic depressedpatients: A report from CORE. Journal of ECT, 17(4),244–253.
PETRILL, S. A., LUO, D., THOMPSON, L. A., & DETTERMAN, D.K. (2001). Inspection time and the relationship amongelementary cognitive tasks, general intelligence, and spe-cific cognitive abilities. Intelligence, 29, 487–496.
PETRY, N. M., TENNEN, H., & AFFLECK, G. (2000). Stalkingthe elusive client variable in psychotherapy research. InC. R. Snyder & R. Ingram (Eds.), Handbook of psychologi-cal change: Psychotherapy processes and practices for the 21stcentury (pp. 88–108). New York: Wiley.
PETTIGREW, T. F. (1998). Intergroup contact theory.Annual Review of Psychology, 49.
PETTIGREW, T. F., & TROPP, L. R. (2006). A meta-analytictest of intergroup contact theory. Journal of Personalityand Social Psychology, 90, 751–783.
PETTITO, L. (1988). “Language” in the prelinguistic child.In F. S. Kessel (Ed.), The development of language and lan-guage researchers: Essays in honor of Roger Brown(pp. 187–222). Hillsdale, NJ: Erlbaum.
PETTY, R. E., & BRIÑOL, P. (2008). Persuasion: From sin-gle to multiple to metacognitive processes. Perspectives onPsychological Science, 3(2), 137–147.
PETTY, R. E., & CACIOPPO, J. T. (1985). The elaborationlikelihood model of persuasion. In L. Berkowitz (Ed.),Advances in experimental social psychology: Vol. 19. NewYork: Academic Press.
PETTY, R. E., & CACIOPPO, J. T. (1986). Communicationand persuasion: Central and peripheral routes to attitudechange. New York: Springer-Verlag.
PETTY, R. E., WEGENER, D. T., & FABRIGAR, L. R. (1997).Attitudes and attitude change. Annual Review ofPsychology, 48, 609–647.
PEZDEK, K. (2004). Event memory and autobiographicalmemory for the events of September 11, 2001. AppliedCognitive Psychology, 14, 1033–1045.
PEZDEK, K., BLANDON-GITLIN, I., & GABBAY, P. (2006).Imagination and memory: Does imagining implausibleevents lead to false autobiographical memories,Psychonomic Bulletin & Review, 13, 764–769.
PHAN, K. L., WAGER, T. D., TAYLOR, S. F., & LIBERZON, I.(2002). Functional neuroanatomy of emotion: A meta-analysis of emotion activation studies in PET and fMRI.Neuroimage, 16, 331–348.
PHELPS, E. A. (2006). Emotion and cognition: Insightsfrom studies of the human amygdala. Annual Review ofPsychology, 57, 27–53.
PHILIPS, M. F., MATTIASSON, G., WIELOCH, T., BJÖRKLAND,A., JOHANSSON, B. B., & TOMASEVIC, G. (2001).Neuroprotective and behavioral efficacy of nerve growth
factor-transfected hippocampal progenitor cell trans-plants after experimental traumatic brain injury. Journalof Neurosurgery, 94, 765–774.
PHILLIPS, A. T., WELLMAN, H. M., & SPELKE, E. S. (2002).Infants’ ability to connect gaze and emotional expressionto intentional action. Cognition, 85, 53–78.
PHILLIPS, M. L., LADOUCEUR, C. D., & DREVETS, W. C.(2008). A neural model of voluntary and automatic emo-tion regulation: Implications for understanding thepathophysiology and neurodevelopment of bipolar dis-order. Molecular Psychiatry, 13, 833–857.
PHILLIPS, P.E.M., STUBER, G. D., HEIEN, M. L.A.V.,WIGHTMAN, R. M., & CARELLI, R. M. (2003). Subseconddopamine release promotes cocaine seeking. Nature, 422,614–618.
PIAGET, J. (1952). The origins of intelligence in children. NewYork: International University Press.
PICCINELLI, M., PINI, S., BELLANTUONO, C., & WILKINSON,G. (1995). Efficacy of drug treatment in obsessive-com-pulsive disorder: A meta-analytic review. British Journal ofPsychiatry, 166, 424–443.
PILIAVIN, J. A., & CALLERO, P. L. (1991). Giving blood: Thedevelopment of an altruistic identity. Baltimore, MD:Johns Hopkins University Press.
PINCUS, H., ZARIN, D., TANIELIAN, T., JOHNSON, J., WEST, J.,PETTIT, A., ET AL. (1999). Psychiatric patients and treat-ments in 1997: Findings from the American PsychiatricAssociation Practice Research Network. Archives ofGeneral Psychiatry, 56, 441–449.
PINEL, J.P.J., ASSANAND, S., & LEHMAN, D. R. (2000).Hunger, eating, and ill health. American Psychologist, 55,1105–1116.
PINKER, S. (1984). Language learnability and language devel-opment. Cambridge, MA: Harvard University Press.
PINKER, S. (1994). The language instinct: How the mind cre-ates language. New York: HarperPerennial.
PINKER, S. (1995). Why the child holded the baby rabbits:A case study in language acquisition. In L. R. Gleitman &M. Liberman (Eds.), Language: An invitation to cognitivescience: Vol. 1 (2nd ed., pp. 107–133). Cambridge, MA: MITPress.
PINKER, S. (1997). How the mind works. New York: Norton
PINKER, S. (1999a). How the mind works. New York:Norton.
PINKER, S. (1999b). Words and rules: The ingredients of lan-guage. New York: Basic Books.
PINKER, S. (2002). The blank slate. New York: Viking.
PINKER, S. (2003). The blank slate: The modern denial ofhuman nature. Skeptical Inquirer, 27, 37–41.
PINKER, S., & ULLMAN, M. T. (2002). The past and futureof the past tense. Trends in Cognitive Sciences, 6(11),456–463.
PINTO, S., ROSEBERRY, A., LIU, H., DIANO, S.,SHANABROUGH, M., CAI, X., ET AL. (2004). Rapid rewiringof arcuate nucleus feeding circuits by leptin. Science, 304,110–115.
PIPE, M.-E., GOODMAN, G. S., QUAS, J., BIDROSE, S., ABLIN,D., & CRAW, S. (1997). Remembering early experiencesduring childhood: Are traumatic events special? In J. D.Read & D. S. Lindsay (Eds.), Recollections of trauma:
Scientific evidence and clinical practice (pp. 417–423). NewYork: Plenum.
PIPE, M.-E., LAMB, M., ORBACH, Y., & CEDERBORK, A.-C.(EDS). (2007). Child sexual abuse: Disclosure, delay, anddenial. Mahwah, NJ: Erlbaum.
PIPP, S., EASTERBROOKS, M. A., & BROWN, S. R. (1993).Attachment status and complexity of infants’ self- andother-knowledge when tested with mother and father.Social Development, 2, 1–14.
PITTENGER, C., & KANDEL, E. R. (2003). In search of gen-eral mechanisms for long-lasting plasticity: Aplysia andthe hippocampus. Philosophical Transactions of the RoyalSociety London: B. Biological Science, 358, 757–763.
PLATEK, S. M., BURCH, R. L., PANYAVIN, I. S., WASSERMAN,B. H., & GALLUP, JR., G. G. (2002). Reactions to children’sfaces: Resemblance affects males more than females.Evolution and Human Behavior, 23, 159–166.
PLATEK, S. M., RAINES, D., GALLUP, JR., G., MOHAMED, F.,THOMSON, J., MYERS, T. ET AL. (2004). Reactions to chil-dren’s faces: Males are more affected by resemblance thanfemales are, and so are their brains. Evolution and HumanBehavior, 25, 394–405.
PLOMIN, R., CORLEY, R., DEFRIES, J. C., & FULKER, D. W.(1990). Individual differences in television viewing inearly childhood: Nature as well as nurture. PsychologicalScience, 1, 371–377.
PLOMIN, R., & DANIELS, D. (1987). Why are children fromthe same family so different from one another? Behavioraland Brain Sciences, 10, 1–16.
PLOMIN, R., & DEFRIES, J. C. (1985). A parent-offspringadoption study of cognitive abilities in early childhood.Intelligence, 9, 341–356.
PLOMIN, R., FULKER, D. W., CORLEY, R., & DEFRIES, J. C.(1997). Nature, nurture, and cognitive development from1 to 16 years: A parent-offspring adoption study.Psychological Science, 8, 442–447.
PLOMIN, R., & MCGUFFIN, P. (2003). Psychopathology inthe postgenomic era. Annual Review of Psychology, 54,205–228.
PLOMIN, R., & SPINATH, F. M. (2004). Intelligence:Genetics, genes, and genomics. Journal of Personality andSocial Psychology, 86, 112–129.
POEPPEL, D., & HACKL, M. (2007). The architecture ofspeech perception. In J. Pomerantz (Ed.),Topics in integra-tive neuroscience: From cells to cognition. Cambridge,England: Cambridge University Press.
POLDRACK, A., & WAGNER, A. (2004). What can neu-roimaging tell us about the mind? Insights from pre-frontal cortex. Current Directions in Psychological Science,13, 177–181.
POLEY, W. (1974). Dimensionality in the measurement ofauthoritarian and political attitudes. Canadian Journal ofBehavioral Science, 6, 83–94.
POLLACK, M. H. (2001). Comorbidity, neurobiology, andpharmacotherapy of social anxiety disorder [Suppl.].Journal of Clinical Psychiatry, 62(12), 24–29.
POPE, H. G., GRUBER, A. J., & YURGELUN-TODD, D. (2001).Residual neuropsychologic effects of cannabis. CurrentPsychiatry Report, 3, 507–512.

PREFERENCESO R49
POPE, H. G., HUDSON, J. I., BODKIN, J. A., & OLIVA, P.(1998). Questionable validity of “dissociative amnesia”in trauma victims. British Journal of Psychiatry, 172,210–215.
PORSOLT, R. D., LEPICHON, M., & JALFRE, M. (1977).Depression: A new animal model sensitive to antidepres-sant treatments. Nature, 266, 730–732.
PORTER, R., & SCHAAL, B. (1995). Olfaction and develop-ment of social preferences in neonatal organisms. In R.L. Doty (Ed.), Handbook of olfaction and gustation(pp. 229–321). New York: Marcel Dekker.
PORTER, S., BIRT, A. R., YUILLE, J. C., & LEHMAN, D. R.(2000). Negotiating false memories: Interviewer andrememberer characteristics relate to memory distortion.Psychological Science, 11, 507–510.
PORTER, S., & PEACE, K. A. (2007). The scars of memory:A prospective, longitudinal investigation of the consis-tency of traumatic and positive emotional memories inadulthood. Psychological Science, 18, 435–441.
POSNER, M. I., & ROTHBART, M. K. (2007). Research onattention networks as a model for the integration of psy-chological science Annual Review of Psychology, 58, 1–23.
POSNER, M., SNYDER, C., & DAVIDSON, B. (1980).Attention and the detection of signals. Journal ofExperimental Psychology: General, 109, 160–174.
POSTHUMA, D., & DEGEUS, E. (2006). Progress in themolecular-genetic study of intelligence, CurrentDirections in Psychological Science, 15, 151–155.
POULOS, C. X., & CAPPELL, H. (1991). Homeostatic theoryof drug tolerance: A general model of physiological adap-tation. Psychological Review, 98, 390–408.
POVINELLI, D. J. (2000). Folk physics for apes: Tthe chim-panzee’s theory of how the world works. Oxford, England:Oxford University Press.
POVINELLI, D. J., BERING, J. M., & GIAMBRONE S. (2000).Toward a science of other minds: Escaping the argumentby analogy. Cognitive Science, 24, 509–542.
POWDERLY, W. G., LANDAY, A., & LEDERMAN, M. M. (1998).Recovery of the immune system with antiretroviral ther-apy: The end of opportunism? Journal of the AmericanMedical Association, 280, 72–77.
POWELL, H. A. (1969). Genealogy, residence, and kinshipin Kiriwina. Man, 4, 177–202.
PRASADA, S., & PINKER, S. (1993a). Generalizations of reg-ular and irregular morphology. Language and CognitiveProcesses, 8, 1–56.
PRASADA, S., & PINKER, S. (1993b). Similarity-based andrule-based generalizations in inflectional morphology.Language and Cognitive Processes, 8, 1–56.
PREMACK, A., & PREMACK, D. (1983). The mind of an ape.New York: Norton.
PREMACK, D. (1965). Reinforcement theory. In D. Levine(Ed.), Nebraska Symposium on motivation. Lincoln:University of Nebraska Press.
PREMACK, D. (1976). Intelligence in ape and man. Hillsdale,NJ: Erlbaum.
PREMACK, D. (1978). On the abstractness of human con-cepts: Why it would be difficult to talk to a pigeon. In S.H. Hulse, H. Fowler, & W. K. Honig (Eds.), Cognitiveprocesses in animal behavior. Hillsdale, NJ: Erlbaum.
PREMACK, D., & WOODRUFF, G. (1978). Does the chim-panzee have a theory of mind? Behavioral and BrainSciences, 4, 515–526.
PRENTICE, D. A., & MILLER, D. T. (1993). Pluralistic igno-rance and alcohol use on campus: Some consequences ofmisperceiving the social norm. Journal of Personality andSocial Psychology, 64, 243–256.
PRESSMAN, S. D., & COHEN, S. (2005). Does positive affectinfluence health? Psychological Bulletin, 131, 925–971.
PRINCIPE, G., KANAYA, T., CECI, S., & SINGH, M. (2006).How rumors can engender false memories in preschool-ers. Psychological Science, 17, 243–248.
PRINZ, J. J. (2002). Furnishing the mind: Concepts and theirperceptual basis. Cambridge, MA: MIT Press.
PROCHASKA, J. O., & NORCROSS, J. C. (2007). Systems ofpsychotherapy: A transtheoretical approach (6th ed.). PacificGrove, CA: Brooks/Cole.
PROVINE, W. B. (1971). The origins of theoretical populationgenetics. Chicago: University of Chicago Press.
PULLUM, G. K. (1991). The great Eskimo vocabulary hoaxand other irreverent essays on the study of language. Chicago:University of Chicago Press.
PUTNAM, F. W., GUROFF, J. J., SILBERMAN, E. K., BARBAN, L.,& POST, R. M. (1986). The clinical phenomenology ofmultiple personality disorder: Review of 100 recentcases. Journal of Clinical Psychiatry, 47, 285–293.
PUTNAM, K. E. (1979). Hypnosis and distortions in eyewitness memory. International Journal of Clinical andExperimental Hypnosis, 27, 437–448.
PUTNAM, S. P., & Stifter, C. A. (2005). Behavioralapproach-inhibition in toddlers: Prediction from infancy,positive and negative affective components, and relationswith behavior problems. Child Development, 76, 212–226.
PYSZCZYNSKI, T., GREENBERG, J., SOLOMON, S., ARNDT, J., &SCHIMEL, J. (2004). Why do people need self-esteem? Atheoretical and empirical review. Psychological Bulletin,130, 435–468.
QUINE, W. (1960). Word and object. New York: Wiley.
QUINLAN, P. T. (2003). Visual feature integration theory:Past, present and future. Psychological Bulletin, 129,643–673.
RADANT, A., TSUANG, D., PESKIND, E. R., MCFALL, M., &RASKIND, W. (2001). Biological markers and diagnosticaccuracy in the genetics of posttraumatic stress disorder.Psychiatry Research, 102, 203–215.
RAE, C., DIGNEY, A. L., MCEWAN, S. R., & BATES, T. C.(2003). Oral creatine monohydrate supplementationimproves brain performance: A double-blind, placebo-controlled, cross-over trial. Proceedings of the Royal Societyof London, Series B: Biological Sciences, 270, 2147–2150.
RAFAL, R., & ROBERTSON, L. (1995). The neurology ofvisual attention. In M. Gazzaniga (Ed.), The cognitive neu-rosciences (pp. 625–648). Cambridge, MA: MIT Press.
RAINVILLE, P, DUNCAN, G., PRICE, D., CARRIER, B., &BUSHNELL, M. (1997). Pain affect encoded in humananterior cingulated but not somatosensory cortex.Science, 277, 968–971.
RAJARAM, S. (1993). Remembering and knowing: Twomeans of access to the personal past. Memory &Cognition, 21, 89–102.
RAKIC, P. (1995). Corticogenesis in human and nonhu-man primates. In M. Gazzaniga (Ed.), The cognitive neuro-sciences (pp. 127–145). Cambridge, MA: MIT Press.
RAKIC, P. (2006). No more cortical neurons for you.Science, 313, 928–929.
RAMI-GONZALEZ, L., BERNARDO, M., BOGET, T., SALAMERO,M., GIL-VERONA, J. A., & JUNQUE, C. (2001). Subtypesof memory dysfunction associated with ECT:Characteristics and neurobiological bases. Journal of ECT,17, 129–135.
RAMÓN Y CAJAL, S. (1913). Degeneration and regeneration ofthe nervous system (R. M. Day, Trans., 1928). London:Oxford University Press.
RAMÓN Y CAJAL, S. (1937). Recollections of my life(E. Horne-Craigie, Trans.). Philadelphia: AmericanPhilosophical Society.
RAMUS, F., NESPOR, M., & MEHLER, J. (1999). Correlates oflinguistic rhythm in the speech signal. Cognition, 73,265–292.
RANGANATH, C. , YONELINAS, A. P., COHEN, M. X., DY, C. J.,TOM, S., & D’ESPOSITO, M. (2003). Dissociable correlatesfor familiarity and recollection within the medial tempo-ral lobes. Neuropsychologia, 42, 2–13.
RAPAPORT, M. H., & JUDD, L. L. (1998). Minor depressivedisorder and subsyndromal depressive symptoms:Functional impairment and response to treatment.Journal of Affective Disorders, 48, 227–232.
RAPAPORT, M. H., PANICCIA, G., & JUDD, L. L. (1995). Areview of social phobia. Psychopharmacology Bulletin, 31,125–129.
RAPOPORT, J. L. (1989). The boy who couldn’t stop washing:The experience and treatment of obsessive-compulsive disor-der. New York: New American Library.
RAPPAPORT, Z. H. (1992). Psychosurgery in the modernera: Therapeutic and ethical aspects. Medicine and Law, 11,449–453.
RASCH, B., & BORN, J. (2008). Reactivation and consoli-dation of memory during sleep. Current Directions inPsychological Science, 17 (3), 188–192.
RASMUSSEN, S. A. (1993). Genetic studies of obsessive-compulsive disorder. Annals of Clinical Psychiatry, 5,241–247.
RATEY, J., & JOHNSON, C. (1997). Shadow syndromes. NewYork: Pantheon.
RAUCH, S. L., & SAVAGE, C. R. (2000). Investigating cor-tico-striatal pathophysiology in obsessive-compulsivedisorders: Procedural learning and imaging probes. In W.K. Goodman, M. J. Rudorfer, & J. D. Maser (Eds.),Obsessive-compulsive disorder: Contemporary issues in treat-ment. Personality and clinical psychology series (pp.133–154). Mahwah, NJ: Erlbaum.
RAVEN, B. H., & RUBIN, J. Z. (1976). Social psychology:People in groups. New York: Wiley.
RAVUSSIN, E. (1994). Effects of a traditional lifestyle onobesity in Pima Indians. Diabetes Care, 17, 1067–1074.

R50 PREFERENCESO
RAVUSSIN, E., & BOUCHARD, C. (2000). Human genomicsand obesity: Finding appropriate drug targets. EuropeanJournal of Pharmacology, 410, 131–145.
RAYNER, K., CARLSON, M., & FRAZIER, L. (1983). The inter-action of syntax and semantics during sentence process-ing: Eye movements in the analysis of semanticallybiased sentences. Journal of Verbal Learning and VerbalBehavior, 22, 358–374.
RAYNER, K., SMITH, T. J., MALCOLM, G. L., & HENDERSON, J.M. (2009). Eye movements and visual encoding duringscene perception. Psychological Science, 20, 6–10.
REBER, A. S. (1985). The Penguin dictionary of psychology.New York: Viking Penguin.
REBERG, D., & BLACK, A. H. (1969). Compound testing ofindividually conditioned stimuli as an index of excitatoryand inhibitory properties. Psychonomic Science, 17, 3031.
RECANZONE, G., SCHREINER, C., & MERZENICH, M. (1993).Plasticity in the frequency representation of primaryauditory cortex following discrimination training inadult owl monkeys. Journal of Neuroscience, 13, 87–103.
RECHT, D. R., & LESLIE, L. (1988). Effect of prior knowl-edge on good and poor readers’ memory of text. Journalof Educational Psychology, 80(1), 16–20.
REDELMEIER, D. A., & SHAFIR, E. (1995). Medical decisionmaking in situations that offer multiple alternatives.Journal of the American Medical Association, 273, 302–305.
REED, M., & ROUNDTREE, P. (1997). Peer pressure and ado-lescent substance abuse. Journal of QuantitativeCriminology, 13, 143–180.
REESE, E., & FIVUSH, R. (1993). Parental styles of talkingabout the past. Developmental Psychology, 29(3),596–606.
REES, G. & FRITH, C. (2007). Methodologies for identify-ing the neural correlates of consciousness. In M.Velmans. & S. Schneider (Eds.), The Blackwell companionto consciousness (pp. 553–566). Oxford, England:Blackwell.
REES, G., KREIMAN, G., & KOCH, C. (2002). Neural corre-lates of consciousness in humans. Nature ReviewsNeuroscience, 3(4), 261–270.
REEVES, L., & WEISBERG, R. W. (1994). The role of contentand abstract information in analogical transfer.Psychological Bulletin, 115(3), 381–400.
REGAN, P. C., & BERSCHEID, E. (1999). Lust: What we knowabout human sexual desire. Thousand Oaks, CA: Sage.
REGIER, D. A., RAE, D. S., NARROW, W. E., KAELBER, C. T., &SCHATZBERG, A. F. (1998). Prevalence of anxiety disordersand their comorbidity with mood and addictive disor-ders. British Journal of Psychiatry, 34(Suppl.), 24–28.
REGIER, T., KAY, P., & COOK, R. S. (2005). Focal colors areuniversal after all. Proceedings of the National Academy ofSciences, 102(23), 8386–8391.
REICHENBERG, A., & HARVEY, P. D. (2007).Neuropsychological impairments in schizophrenia:Integration of performance-based and brain imagingfindings. Psychological Bulletin, 133(5), 833–858.
REID, D. H., WILSON, P. G., & FAW, G. D. (1991). Teachingself-help skills. In J. L. Matson & J. A. Mulick (Eds.),Handbook of mental retardation (pp. 436–450). New York:Pergamon.
REINER, W. (2004). Psychosexual development in geneticmales assigned female: The cloacal exstrophy experience.Child and Adolescent Psychiatric Clinics of North America, 13,657–674.
REISBERG, D. (2010). Cognition: Exploring the science of themind (4th ed.). New York: Norton.
REISBERG, D., & HERTEL, P. (EDS.). (2004). Memory andemotion. New York: Oxford University Press.
REISBERG, D., & HEUER, F. (2004). Memory for emotionalevents. In D. Reisberg & P. Hertel (Eds.), Memory andemotion (pp. 3–41). New York: Oxford University Press.
REISBERG, D., & HEUER, F. (2005). Visuospatial images. InP. Shah & A. Miyake (Eds.), The Cambridge Handbook ofVisuospatial Thinking (pp. 35–80). New York: CambridgeUniversity Press.
REISBERG, D., SMITH, J. D., BAXTER, D. A., & SONENSHINE,M. (1989). “Enacted” auditory images are ambiguous;“Pure” auditory images are not. Quarterly Journal ofExperimental Psychology, 41A, 619–641.
REISENZEIN, R. (1983). The Schachter theory of emotions:Two decades later. Psychological Bulletin, 94, 239–264.
REISS, D., & MARINO, L. (2001). Mirror self-recognitionin the bottlenose dolphin: A case of cognitive conver-gence. Proceedings of the National Academy of Science,98(10), 5937–5942.
REISS, D., MCCOWAN, B., & MARINO L. (1997).Communicative and other cognitive characteristics ofbottlenose dolphins. Trends in Cognitive Science, 1(2),140–145.
RENSINK, R. A. (2002). Change detection. Annual Reviewof Psychology, 53, 245–277.
RENTFROW, P. J., GOSLING, S. D., & POTTER, J. (2008). Atheory of the emergence, persistence, and expression ofregional variation in psychological characteristics.Perspectives on Psychological Science, 3, 339–369.
REPACHOLI, B. M., & GOPNIK, A. (1997). Early reasoningabout desires: Evidence from 14- and 18-month-olds.Developmental Psychology, 33(1), 12–21.
RESNICK, S. M., PHAM, D. L., KRAUT, M. A., ZONDERMAN, A.B., & DAVATZIKOS, C. (2003). Longitudinal magnetic res-onance imaging studies of older adults: A shrinkingbrain. Journal of Neuroscience, 23(8), 3295–3301.
RESCORLA, R. A. (1967). Pavlovian conditioning and itsproper control procedures. Psychological Review, 74,71–80.
RESCORLA, R. A. (1988). Behavioral studies of Pavlovianconditioning. Annual Review of Neuroscience, 11, 329–352.
RESCORLA, R. A. (1991). Associative relations in instru-mental learning: The eighteenth Bartlett Memorial lec-ture. Quarterly Journal of Experimental Psychology, 43b,1–23.
RESCORLA, R. A. (1993a). Inhibitory associations betweenS and R extinction. Animal Learning and Behavior, 21,327–336.
RESCORLA, R. A. (1993b). Preservation of response-out-come associations through extinction. Animal Learningand Behavior, 21, 238–245.
RESCORLA, R. A., & WAGNER, A. R. (1972). A theory ofPavlovian conditioning: Variations in the effectiveness ofreinforcement and non-reinforcement. In A. H. Black &
W. F. Prokasy (Eds.), Classical conditioning II. New York:Appleton-Century-Crofts.
RESSLER, K. J., & MAYBERG, H. S. (2007). Targeting abnor-mal neural circuits in mood and anxiety disorders: Fromthe laboratory to the clinic. Nature Neuroscience, 10,1116–1124.
REST, J., NARVAEZ, D., BEBEAU, M., & THOMAS, J. (1999).Postconventional moral thinking: A neo-Kohlbergianapproach. Mahwah, NJ: Erlbaum.
REUTER-LORENZ, P. A. (2002). New visions of the agingmind and brain. Trends in Cognitive Science, 6, 394–400.
REVELEY, A. M., REVELEY, M. A., CLIFFORD, C. A., ET AL.(1982). Cerebral ventricular size in twins discordant forschizophrenia. Lancet, 1, 540–541.
REY, G. (1996). Concepts and stereotypes. In E. Margolis& S. Laurence (Eds.), Concepts: Core readings(pp. 278–299). Cambridge, MA: MIT Press.
REYNA, V., & FARLEY, F. (2006). Risk and rationality inadolescent decision-making: Implications for theory,practice, and public policy. Psychological Science in thePublic Interest, 7, 1–44.
REYNOLDS, C. R., CHASTAIN, R. L., KAUFMAN, A. S., &MCLEAN, J. E. (1987). Demographic characteristics andIQ among adults: Analysis of the WAIS-R standardiza-tion sample as a function of the stratification variables.Journal of School Psychology, 25(4), 323–342.
RHODES, G. (2006). The evolutionary psychology offacial beauty. Annual Review of Psychology, 57, 199–226.
RHODES, G., PROFFITT, F., GRADY, J. M., & SUMICH, A.(1998). Facial symmetry and the perception of beauty.Psychonomics Bulletin and Review, 5, 659–669.
RHODES, G., SUMICH, A., & BYATT, G. (1999). Are averagefacial configurations attractive only because of their sym-metry? Psychological Science, 10, 52–59.
RIBOT, T. (1882). Diseases of memory. New York: Appleton.
RICHARDS, J. M., & GROSS, J. J. (2000). Emotion regula-tion and memory: The cognitive costs of keeping one’scool. Journal of Personality and Social Psychology, 79,410–424.
RICHARDS, J. M., & GROSS, J. J. (2006). Personality andemotional memory: How regulating emotion impairsmemory for emotional events. Journal of Research inPersonality, 79(3), 410–424.
RICKARD, T. C., CAI, D. J., RIETH, C. A., JONES, J., & ARD, M.C. (2008). Sleep does not enhance motor sequencelearning. Journal of Experimental Psychology: Learning,Memory, and Cognition, 34 (4), 834–842.
RICKELS, K., & RYNN, M. A. (2001). What is generalizedanxiety disorder? [Suppl.] Journal of Clinical Psychiatry,62(11), 4–12.
RIEFFE, C., TERWOGT, M. M., KOOPS, W., STEGGE, H., &OOMEN, A. (2001). Preschoolers’ appreciation of uncom-mon desires and subsequent emotions. British Journal ofDevelopmental Psychology, 19, 259–274.
RIGGIO, R. E., & MURPHY, S. E. (EDS.). (2002). Multipleintelligences and leadership. Mahwah, NJ: Erlbaum.
RINCK, M. (1999). Memory for everyday objects: Whereare the digits on numerical keypads? Applied CognitivePsychology, 13, 329–350.

PREFERENCESO R51
RINCÓN-LIMAS, D. E., LU, C. H., CANAL, I., CALLEJA, M.,RODRÍGUEZ-ESTEBAN, C., IZPISÚA-BELMONTE, J. C. ET AL.(1999). Conservation of the expression and function ofapterous orthologs in Drosophila and mammals.Proceedings of the National Academy of Sciences, 96,2165–2170.
RINGELMANN, M. (1913). Recherches sur les moteurs ani-més: Travail de l’homme. Annales de l’institut NationalAgronomique (Series 2), 12, 1–40.
RIPS, L. (1990). Reasoning. Annual Review of Psychology,41, 321–353.
RISCH, N., HERRELL, R., LEHNER, T., LIANG, K.-Y., EAVES, L.,HOH, J., ET AL. (2009). Interaction between the serotonintransporter gene (5-HTTLPR), stressful life events, andrisk of depression: A meta-analysis. Journal of AmericanMedical Association, 301, 2462–2471.
RIZZOLATTI, G., & CRAIGHERO, L. (2004). The mirror-neu-ron system. Annual Review of Neuroscience, 27, 169–192.
ROBBIN, A. A. (1958). A controlled study of the effects ofleucotomy. Journal of Neurology, Neurosurgery andPsychiatry, 21, 262–269.
ROBBINS, S. J. (1990). Mechanisms underlying sponta-neous recovery in autoshaping. Journal of ExperimentalPsychology: Animal Behavior Processes, 16, 235–249.
ROBERSON, D., ET AL. (2005). Color categories: Evidencefor the cultural relativity hypothesis. Cognitive Psychology,50, 378–411.
ROBERTS, B. W., KUNCEL, N., SHINER, R., N., CASPI, A., &GOLDBERG, L. R. (2007). The power of personality: Thecomparative validity of personality traits, socio-economicstatus, and cognitive ability for predicting important lifeoutcomes. Perspectives on Psychological Science, 2, 313–345.
ROBERTS, B. W., WALTON, K., & BOGG, T. (2005).Conscientiousness and health across the life course.Review of General Psychology, 9, 156–168.
ROBERTSON, I. H., & MANLY, T. (1999). Sustained atten-tion deficits in time and space. In G. W. Humphreys & J.Duncan (Eds.), Attention, space, and action: Studies in cog-nitive neuroscience (pp. 297–310). New York: OxfordUniversity Press.
ROBERTSON, L., TREISMAN, A., FRIEDMAN-HILL, S., &GRABOWECKY, M. (1997). The interaction of spatial andobject pathways: Evidence from Balint’s syndrome.Journal of Cognitive Neuroscience, 9(3), 295–317.
ROBINS, L. N., & REGIER, D. A. (Eds.). (1991). Psychiatricdisorders in America: The epidemiologic catchment area study.New York: Free Press.
ROBINSON & BERRIDGE, 2003
ROBINSON, L. A., BERMAN, J. S., & NEIMEYER, R. A. (1990).Psychotherapy for the treatment of depression: A com-prehensive review of controlled outcome research.Psychological Bulletin, 108, 30–49.
RODIN, J. (1990). Control by any other name:Definitions, concepts, and processes. In J. Rodin, C.Schooler, & K. W. Schaie (Eds.), Self-directedness: Causeand effects throughout the life course (pp. 1–17). Hillsdale,NJ: Erlbaum.
RODIN, J., & LANGER, E. J. (1977). Long-term effects of acontrol-relevant intervention with the institutionalizedaged. Journal of Personality and Social Psychology, 35,897–902.
RODMAN, H. R., GROSS, C. G., & ALBRIGHT, T. D. (1989).Afferent basis of visual response properties in area MT ofthe macaque: I. Effects of striate cortex removal. Journal ofNeuroscience, 9, 2033–2050.
RODRIGUEZ, M. L., MISCHEL, W., & SHODA, Y. (1989).Cognitive person variables in the delay of gratification ofolder children at risk. Journal of Personality and SocialPsychology, 57, 358–367.
ROEDIGER, H. L., III. (1980). Memory metaphors in cog-nitive psychology. Memory and Cognition, 8, 231–246.
ROEDIGER, H., & MCDERMOTT, K. (1995). Creating falsememories: Remembering words not presented in lists.Journal of Experimental Psychology: Learning, Memory &Cognition, 21, 803–814.
ROEDIGER, H., & MCDERMOTT, K. B. (2000). Tricks ofmemory. Current Directions in Psychological Science, 9,123–127.
ROFFWARG, MUZIO, & DEMENT, 1966
ROGERS, C. R. (1951). Client-centered therapy: Its currentpractice, implications, and theory (2nd ed.). Boston:Houghton Mifflin.
ROGERS, C. R. (1959). A theory of therapy, personality,and interpersonal relationships as developed in theclient-centered framework. In S. Koch (Ed.), Psychology: Astudy of a science: Vol. 3. New York: McGraw-Hill.
ROGERS, C. R. (1961). On becoming a person: A therapist’sview of psychotherapy. Boston: Houghton Mifflin.
ROGERS, C. R. (1980). A way of being. Boston: HoughtonMifflin.
ROGERS, T. B., KUIPER, N. A., & KIRKER, W. S. (1977). Self-reference and the encoding of personal information.Journal of Personality and Social Psychology, 35, 677–688.
ROGOFF, B. (1990). Apprenticeship in thinking. New York:Oxford University Press.
ROGOFF, B. (1998). Cognition as a collaborative process.In W. Damon (Ed.), Handbook of child psychology, Vol. 2(5th ed., pp. 679–744). New York: Wiley.
ROGOFF, B. (2000). Culture and development. New York:Oxford University Press.
ROGOFF, B., PARADISE, R., ARAUZ, R. M., CORREA-CHÁVEZ,M., & ANGELILLO, C. (2003). Firsthand learning throughintent participation. Annual Review of Psychology, 54,175–203.
ROLAND, P. E., LARSEN, B., LASSEN, N. A., & SKINHØJ, E.(1980). Supplementary motor area and other corticalareas in organization of voluntary movements in man.Journal of Neurophysiology, 43, 539–560.
ROLLS, E. J. (1978). Neurophysiology of feeding. Trends inNeurosciences, 1, 1–3.
ROMANES, G. J. (1882). Animal intelligence. London: KeganPaul.
ROOPNARINE, J. L., JOHNSON, J. E., & HOOPER, F. H. (1994).Children’s play in diverse cultures. Albany, NY: SUNY Press.
ROPER, T. J. (1983). Learning as a biological phenome-non. In T. R. Halliday & P. J. B. Slater (Eds.), Genes, devel-opment and behavior: Vol. 3. Animal Behavior (pp. 178–212).Oxford, England: Blackwell.
RORSCHACH, H. (1921). Psychodiagnostik. Berne: Bircher.
ROSCH, E. H. (1973a). Natural categories. CognitivePsychology, 4, 328–350.
ROSCH, E. H. (1973b). On the internal structure of per-ceptual and semantic categories. In T. E. Moore (Ed.),Cognitive development and the acquisition of language. NewYork: Academic Press.
ROSCH, E. H. (1978). Principles of categorization. In E.Rosch & B. Lloyd (Eds.), Cognition and categorization.Hillsdale, NJ: Erlbaum.
ROSCH, E. H., & MERVIS, C. B. (1975). Family resem-blances: Studies in the internal structure of categories.Cognitive Psychology, 7, 573–605.
ROSEN, G. (1966). Madness in society. Chicago: Universityof Chicago Press.
ROSEN, W. D., ADAMSON, L. B., & BAKEMAN, R. (1992). Anexperimental investigation of infant social referencing:Mothers’ messages and gender differences.Developmental Psychology, 28(6), 1172–1178.
ROSENFELD, P., GIACALONE, R. A., & TEDESCHI, J. T. (1984).Cognitive dissonance and impression managementexplanations for effort justification. Personality and SocialPsychology Bulletin, 10, 394–401.
ROSENSTEIN, M. J., MILAZZO-SAYRE, L. J., & MANDER-SCHEID, R. W. (1989). Care of persons with schizophre-nia: A statistical profile. Schizophrenia Bulletin, 15, 45–58.
ROSENTHAL, A. M. (1964). Thirty-eight witnesses. NewYork: McGraw-Hill.
ROSENTHAL, D. (1963). A suggested conceptual frame-work. In D. Rosenthal (Ed.), The Genain quadruplets (pp.505–516). New York: Basic Books.
ROSENTHAL, D. (1970). Genetic theory and abnormal behav-ior. New York: McGraw-Hill.
ROSENTHAL, R. (1991). Teacher expectancy effects: A briefupdate 25 years after the Pygmalion experiment. Journalof Research in Education, 1, 3–12.
ROSENTHAL, R. (2002). Covert communication in class-rooms, clinics, courtrooms, and cubicles. AmericanPsychologist, 57, 839–849.
ROSENTHAL, R., HILLER, J. B., BORNSTEIN, R. F., BERRY,D.T.R., & BRUNELL-NEULEIB, S. (2001). Meta-analyticmethods, the Rorschach, and the MMPI. PsychologicalAssessment, 13(4), 449–451.
ROSENTHAL, R., & JACOBSON, L. (1968). Pygmalion in theclassroom: Teacher expectation and pupils’ intellectualdevelopment. New York: Holt, Rinehart & Winston.
ROSENZWEIG, M. R., LEIMAN, A. K., & BREEDLOVE, S. M.(1996). Biological psychology. Sunderland, MA: Sinauer.
ROSENZWEIG ET AL., 1999
ROSER, M., & GAZZANIGA, M. S. (2004). Automaticbrains—interpretive minds. Current Directions inPsychological Science, 13, 56–59.
ROSS, C. A. (1997). Dissociative identity disorder: Diagnosis,clinical features, and treatment of multiple personality. NewYork: Wiley.
ROSS, C. A. (1999). Subpersonalities and multiple per-sonalities: A dissociative continuum? In J. Rowan and M.Cooper (Eds.), The plural self: Multiplicity in everyday life(pp. 183–197). London: Sage.

R52 PREFERENCESO
ROSS, D. F., READ, J. D., & TOGLIA, M. P. (EDS). (1994).Adult eyewitness testimony: Current trends and developments.New York: Cambridge University Press.
ROSS, H. S., & LOLLIS, S. P. (1989). A social relationsanalysis of toddler peer relationships. Child Development,60(5), 1082–1091.
ROSS, J., & LAWRENCE, K. Q. (1968). Some observationson memory artifice. Psychonomic Science, 13, 107–108.
ROSS, L. (1977). The intuitive psychologist and his short-comings: Distortions in the attribution process. In L.Berkowitz (Ed.), Advances in experimental social psychology:Vol. 10. New York: Academic Press.
ROSS, L., AMABILE, T. M., & STEINMETZ, J. L. (1977). Socialroles, social control, and biases in social perceptionprocesses. Journal of Experimental Social Psychology, 35,817–829.
ROSS, M., & SICOLY, F. (1979). Egocentric biases in avail-ability and attribution. Journal of Personality and SocialPsychology, 37, 322–336.
ROTH, A., & FONAGY, P. (2004). What works for whom? Acritical review of psychotherapy research (2nd ed.). NewYork: Guilford.
ROTHBART, M. K., & AHADI, S. A. (1994). Temperamentand the development of personality. Journal of AbnormalPsychology, 103, 55–66.
ROTHBART, M., & BATES, J. (1998). Temperament. In W.Damon & N. Eisenberg (Eds.), Handbook of child psychol-ogy (5th ed.): Vol. 3. Social, emotional and personality devel-opment (pp. 105–176). New York: Wiley.
ROTHBART, M. K., & BATES, J. E. (2006). Temperament inchildren’s development. In W. Damon, R. Lerner, & N.Eisenberg (Eds.), Handbook of child psychology, Vol. 3:Social, emotional, and personality development (5th ed.,pp. 99–166). New York: Wiley.
ROTHBAUM, F., & TSANG, B. Y. P. (1998). Lovesongs in theUnited States and China: On the nature of romanticlove. Journal of Cross-Cultural Psychology, 29, 306–319.
ROTHBAUM, F., WEISZ, J., POTT, M., MIYAKE, K., & MORELLI,G. (2000). Attachment and culture: Security in theUnited States and Japan. American Psychologist, 55,1093–1104.
ROTHCHILD, E. (1997). E-mail therapy. American Journal ofPsychiatry, 154, 1476–1477.
ROUACH, N. KOULAKOFF, A. ABUDARA, V., WILLECKE, K, &GIAUME, C. (2008). Astroglial metabolic networks sus-tain hippocampal synaptic transmission. Science, 322,1551–1555.
ROVEE-COLLIER, C. (1999). The development of infantmemory. Current Directions in Psychological Science, 8(3),80–85.
ROVEE-COLLIER, C. K. (1990). The “memory system” ofprelinguistic infants. In A. Diamond (Ed.), The develop-ment and neural bases of higher cognitive functions. NewYork: New York Academy of Sciences.
ROVEE-COLLIER, C., & GERHARDSTEIN, P. (1997). Thedevelopment of infant memory. In N. Cowan (Ed.), Thedevelopment of memory in childhood: Studies in developmen-tal psychology. Hove, England: Psychology Press.
ROVEE-COLLIER, C. K., & HAYNE, H. (1987). Reactivationof infant memory: Implications for cognitive develop-
ment. In H. W. Reese (Ed.), Advances in child developmentand behavior: Vol. 20. New York: Academic Press.
ROWE, A. D., BULLOCK, P. R., POLKEY, C. E., & MORRIS, R.G. (2001). “Theory of mind” impairments and their rela-tionship to executive functioning following frontal lobeexcisions. Brain, 124, 600–616.
ROZIN, E. (1973). The flavor principle. New York: HawthornBooks.
ROZIN, P. (1999). The process of moralization.Psychological Science, 10, 218–221.
ROZIN, P., DOW, S., MOSCOVITCH, M., & RAJARAM, S.(1998). What causes humans to begin and end a meal? Arole for memory for what has been eaten, as evidenced bya study of multiple meal eating in amnesic patients.Psychological Science, 9, 392–396.
ROZIN, P., & KALAT, J. W. (1971). Specific hungers and poi-son avoidance as adaptive specializations of learning.Psychological Review, 78, 459–486.
ROZIN, P., & KALAT, J. W. (1972). Learning as a situation-specific adaptation. In M. E. P. Seligman & J. L. Hager(Eds.), Biological boundaries of learning (pp. 66–96). NewYork: Appleton-Century-Crofts.
ROZIN, P., MARKWITH, M., & STOESS, C. (1997).Moralization and becoming a vegetarian: The transfor-mation of preferences into values and the recruitment ofdisgust. Psychological Science, 8, 67–73.
ROZIN, P., & SCHULL, J. (1988). The adaptive-evolutionarypoint of view in experimental psychology. In R. C.Atkinson, R. J. Herrnstein, G. Lindzey, & R. D. Luce(Eds.), Steven’s handbook of experimental psychology: Vol. 1.Perception and motivation (2nd ed., pp. 503–546). NewYork: Wiley.
RUBENSTEIN, J. L., & RAKIC, P. (1999). Genetic control ofcortical development. Cerebral Cortex, 9, 521–523.
RUBIN, H., BUKOWSKI, W., & PARKER, J. (1998). Peer inter-actions, relationships and groups. In W. Damon & N.Eisenberg (Eds.), Handbook of child psychology (5th ed.):Vol. 3. Social, emotional and personality development (pp.619–700). New York: Wiley.
RUDERMAN, A. J. (1986). Dietary restraint: A theoreticaland empirical review. Psychological Bulletin, 99, 247–262.
RUFFMAN, T., PERNER, J., & PARKIN, L. (1999). How parent-ing style affects false belief understanding. SocialDevelopment, 8, 395–411.
RUGG, M., & CURRAN, T. (2007). Event-related potentialsand recognition memory. Trends in Cognitive Sciences, 11,251–257.
RUMELHART, D. E. (1997). The architecture of mind: Aconnectionist approach. In J. Haugeland (Ed.), Minddesign 2: Philosophy, psychology, artificial intelligence (2nded.). Cambridge, MA: MIT Press.
RUMELHART, D. E., & MCCLELLAND, J. L. (1986). On learn-ing past tenses of English verbs. In J. L. McClelland & D.E. Rumelhart (Eds.), Parallel distributed processing: Vol. 2(pp. 216–271). Cambridge, MA: MIT Press.
RUSHTON, J. P., & JENSEN, A. R. (2006). The totality ofavailable evidence shows the race IQ gap still remains.Psychological Science, 17, 921–922.
RUSSEK, M. (1971). Hepatic receptors and the neurophys-iological mechanisms controlling feeding behavior. In S.
Ehrenpreis (Ed.), Neurosciences research: Vol. 4. New York:Academic Press.
RUSSELL, J. A. (1980). A circumplex model of affect.Journal of Personality and Social Psychology, 39, 1161–1178.
RUSSELL, J. A. (1983). Pan-cultural aspects of human con-ceptual organization of emotions. Journal of Personalityand Social Psychology, 45, 1281–1288.
RUSSELL, J. A. (1994). Is there universal recognition ofemotion from facial expressions? A review of the cross-cultural studies. Psychological Bulletin, 115, 102–141.
RUTTER, M. (2006). Genes and behavior: Nature-nurtureinterplay explained. Malden, MA: Blackwell.
RUTTER, M., & O’CONNOR, T. G. (2004). Are there biolog-ical programming effects for psychological development?Findings from a study of Romanian adoptees.Developmental Psychology, 40, 81–94.
RYDELL, R. J., MCCONNELL, A. R., MACKIE, D. M., & STRAIN,L. M. (2006). Of two minds: Forming and changingvalence-inconsistent implicit and explicit attitudes.Psychological Science, 17, 954–958.
RYFF, C. D., DIENBERG, L. G., URRY, H. L., MULLER, D.,ROSENKRANZ, M. A., FRIEDMANN, E. M., ET AL. (2006):Psychological well-being and ill-being: Do they have dis-tinct or mirrored biological correlates? Psychotherapy andPsychosomatics, 75, 85–95.
RYFF, C. D., & SINGER, B. (1998). The contours of positivehuman health. Psychological Inquiry, 9, 1–28.
SABINI, J., SIEPMANN, M., & STEIN, J. (2001). The reallyfundamental attribution error in social psychologicalresearch. Psychological Inquiry, 12, 1–15.
SACHS, G. S., & THASE, M. E. (2000). Bipolar disordertherapeutics: maintenance treatment. BiologicalPsychiatry, 48(6), 573–581.
SACKEIM, H. A., DEVANAND, D. P., & NOBLER, M. S. (1995).Electroconvulsive therapy. In F. E. Bloom & D. Kupfer(Eds.), Psychopharmacology: The fourth generation ofprogress (pp. 1123–1141). New York: Raven.
SACKEIM, H. A., PRUDIC, J., DEVANAND, D. P., KIERSKY, J. E.,FITZSIMONS, L., MOODY, B. J., ET AL. (1993). Effects ofstimulus intensity and electrode placement on the effi-cacy and cognitive effects of electroconvulsive therapy.New England Journal of Medicine, 328, 839–846.
SACKEIM, H. A., PRUDIC, J., DEVANAND, D. P., NOBLER, M.S., LISANBY, S. H., PEYSER, S., ET AL. (2000). A prospective,randomized, double-blind comparison of bilateral andright unilateral electroconvulsive therapy at differentstimulus intensities. Archives of General Psychiatry, 57,425–434.
SACKETT, D. L., STRAUS, S. E., RICHARDSON, W. S.,ROSENBERG, W., & HAYNES, R. B. (2000). Evidence-basedmedicine: How to practice and teach EBM (2nd ed.).London: Churchill Livingstone.
SACKETT, P., BORNEMAN, M., & CONNELLY, B. (2008).High-stakes testing in higher education and employ-ment: Appraising the evidence for validity and fairness.American Psychologist, 63, 215–227.
SACKS, O. (1985). The man who mistook his wife for a hat.Simon & Schuster.

PREFERENCESO R53
SADATO N., PASCUAL-LEONE, A., GRAFMAN, J., IBANEZ, V.,DEIBER, M., DOLD, G., ET AL. (1996). Activation of the pri-mary visual cortex by Braille reading in blind subjects.Nature, 380, 526–528.
SADLER, H., DAVISON, L., CARROLL, C., & KOUNTS, S. L.(1971). The living, genetically unrelated, kidney donor.Seminars in Psychiatry, 3, 86–101.
SAFFRAN, J. R. (2003). Statistical language learning:Mechanisms and constraints. Current Directions inPsychological Science, 12, 110–114.
SAFFRAN, J. R., ASLIN, R. N., & NEWPORT, E. L. (1996).Statistical learning by 8-month-old infants. Science,274(5294), 1926–1928.
SAFFRAN, J. R., SENGHAS, A., & TRUESWELL, J. C. (2001).The acquisition of language by children. PNAS, 98(23),12874–12875.
SAGHIR, M. T., & ROBINS, E. (1973). Male and female homo-sexuality. Baltimore: Williams & Wilkins.
SAGI, A., & HOFFMAN, M. L. (1976). Empathic distress inthe newborn. Developmental Psychology, 12, 175–176.
ST. CLAIR, D., XU, M., WANG, P., YU, Y., FANG, Y., ZHANG, F.,ET AL. (2005). Rates of adult schizophrenia followingprenatal exposure to the Chinese famine of 1959–1961.Journal of the American Medical Association, 294, 557–562.
SALOVEY, P., & MAYER, J. D. (1990). Emotional intelli-gence. Imagination, Cognition, and Personality, 9, 185–211.
SALOVEY, P., ROTHMAN, A. J., DETWEILER, J. B., & STEWARD,W. T. (2000). Emotional states and physical health.American Psychologist, 55(1), 110–121.
SALTHOUSE, T. A. (1991). Theoretical perspectives on cogni-tive aging. Hillsdale, NJ: Erlbaum.
SALTHOUSE, T. A. (2000). Steps toward the explanationof adult age differences in cognition. In T. J. Perfect & E.A. Maylor (Eds.), Models of cognitive aging. New York:Oxford University Press.
SALTHOUSE, T. A. (2004). What and when of cognitiveaging. Current Directions in Psychological Science, 13,140–144.
SALTHOUSE, T. A. (2006). Mental exercise and mentalaging: Evaluating the validity of the “use it or lose it”hypothesis. Perspectives on Psychological Science, 1(1),68–87.
SALTHOUSE, T. A. (2007). Reply to Schooler: Consistent isnot conclusive. Perspectives on Psychological Science, 2(1),30–32.
SALTHOUSE, T. A., & PINK, J. (2008). Why is workingmemory related to fluid intelligence? PsychonomicsBulletin & Review, 15, 364–371.
SANFEY, A. G., RILLING, J. K., ARONSON, J. A., NYSTROM, L.E., & COHEN, J. D. (2003). The neural basis of economicdecision-making in the Ultimatum Game. Science, 300,1755–1758.
SANTARELLI, L., SAXE, M., GROSS, C., SURGET, A.,BATTAGLIA, F., DULAWA, S., ET AL. (2003). Requirement ofhippocampal neurogenesis for the behavioral effects ofantidepressants. Science, 301, 805–809.
SANTINI, E., GE, H., REN, K., DEORTIZ, S., & QUIRK, G.(2004). Consolidation of fear extinction requires proteinsynthesis in the medial prefrontal cortex. Journal ofNeuroscience, 24, 5704–5710.
SAPOLSKY, R. M. (1998). The trouble with testosterone. NewYork: Simon & Schuster.
SATIR, V. (1967). Conjoint family therapy (rev. ed.). PaloAlto, CA: Science and Behavior Books.
SAVAGE-RUMBAUGH, E. S., & FIELDS, W. (2000).Linguistic, cultural and cognitive capacities of bonobos(Pan paniscus). Culture & Psychology, 6, 131–153.
SAVIN, H. B. (1973). Professors and psychologicalresearchers: Conflicting values in conflicting roles.Cognition, 2, 147–149.
SAVIN-WILLIAMS, R. C. (2006). Who’s gay? Does it mat-ter? Current Directions in Psychological Science, 15(1),40–44.
SAVOVA, V., ROY, D., SCHMIDT, L., & TENENBAUM, J. B.(2007). Discovering syntactic hierarchies. Proceedings ofthe Twenty-Ninth Annual Conference of the Cognitive ScienceSociety, Nashville, TN.
SAWA, A., & SNYDER, S. H. (2002). Schizophrenia:Diverse approaches to a complex disease. Science, 296,692–695.
SAWAMOTO, K., NAKAO, N., KAKISHITA, K., OGAWA, Y.,TOYAMA, Y., YAMAMOTO, A., ET AL. (2001). Generation ofdopaminergic neurons in the adult brain from mesen-cephalic precursor cells labeled with a nestin-GFP trans-gene. Journal of Neuroscience, 21, 3895–3903.
SAWYER, K. (2006). Explaining creativity: The science ofhuman innovation. New York: Oxford University Press.
SAXE, G. (1981). Body parts as numerals: A developmen-tal analysis of numeration among the Oksapmin inPapua, New Guinea. Child Development, 52, 306–316.
SAXE, R., CAREY, S., & KANWISHER, N. (2004).Understanding other minds: Linking developmental psy-chology and functional neuroimaging. Annual Review ofPsychology, 55, 87–124.
SAXENA, S., BRODY, A. L., MAIDMENT, K. M., DUNKIN, J. J.,COLGAN, M., ALBORZIAN, S., ET AL. (1999). Localizedorbitofrontal and subcortical metabolic changes and pre-dictors of response to paroxetine treatment in obsessive-compulsive disorder Neuropsychopharmacology, 21,683–693.
SAYWITZ, K. J., & GEISELMAN, E. (1998). Interviewing thechild witness: Maximizing completeness and minimizingerror. In S. Lynn & K. McConkey (Eds.), Truth in memory(pp. 190–223). New York: Guilford Press.
SCAIFE, M., & BRUNER, J. S. (1975). The capacity for jointvisual attention in the infant. Nature, 253(5489),265–266.
SCARR, S. (1987). Distinctive environments depend upongenotypes. Behavioral and Brain Sciences, 10, 38–39.
SCARR, S. (1992). Developmental theories for the 1990s:Development and individual differences. ChildDevelopment, 63, 1–19.
SCARR, S. (1997). Why child care has little impact onmost children’s development. Current Directions inPsychological Science, 6, 143–148.
SCARR, S., & CARTER-SALTZMAN, L. (1982). Genetics andintelligence. In R. J. Sternberg (Ed.), Handbook of humanintelligence (pp. 792–896). New York: CambridgeUniversity Press.
SCARR, S., & WEINBERG, R. A. (1976). IQ test performanceof black children adopted by white families. AmericanPsychologist, 31, 726–739.
SCARR, S., & WEINBERG, R. A. (1983). The Minnesotaadoption studies genetic differences and malleability.Child Development, 54, 260–267.
SCERIF, G., & KARMILOFF-SMITH, A. (2005). The dawn ofcognitive genetics: Crucial developmental caveats. Trendsin Cognitive Science, 9, 126–135.
SCHACTER, D. L. (1996). Searching for memory: The brain,the mind and the past. New York: Basic Books.
SCHACHTER, F. (1982). Sibling deidentification and split-parent identification: A family tetrad. In M. Lamb and B.Sutton-Smith (Eds.), Sibling relationships: Their nature andsignificance over the lifespan. Hillsdale, NJ: Erlbaum.
SCHACHTER, S., & SINGER, J. (1962). Cognitive, social andphysiological determinants of emotional state.Psychological Review, 69, 379–399.
SCHACHTER, S., & SINGER, J. E. (1979). Comments on theMaslach and Marshall-Zimbardo experiments. Journal ofPersonality and Social Psychology, 37, 989–995.
SCHAFE, G., NADER, K., BLAIR, H., & LEDOUX, J. (2001).Memory consolidation of Pavlovian fear conditioning: Acellular and molecular perspective. Trends in Neuroscience,24, 540–546.
SCHAIE, K. W. (1996). Intellectual development in adulthood:The Seattle Longitudinal study. New York: CambridgeUniversity Press.
SCHAIE, K. W., & WILLIS, S. L. (1996). Psychometric intel-ligence and aging. In F. Blanchard Fields & T. M. Hess(Eds.), Perspectives on cognitive change in adulthood andaging (pp. 293–322). New York: McGraw-Hill.
SCHARFMAN, H., & HEN, R. (2007). Is more neurogenesisalways better? Science, 315, 336–338.
SCHEFFLER, R. M., HINSHAW, S. P., MODREK, S., & LEVINE,P. (2007). The global market for ADHD medications.Health Affairs, 26(2), 450–457.
SCHER, C. D., & STEIN, M. B. (2003). Developmentalantecedents of anxiety sensitivity. Journal of AnxietyDisorders, 17, 253–269.
SCHERER, K. R., SCHORR, A., & JOHNSTONE, T. (EDS.).(2001). Appraisal processes in emotion: Theory, methods,research. New York: Oxford University Press.
SCHILDKRAUT, J. J. (1965). The catecholamine hypothesisof affective disorders: A review of supporting evidence.American Journal of Psychiatry, 122, 509–522.
SCHEIER, M. F., & CARVER, C. S. (1985). Optimism, cop-ing, and health: Assessment and implications of general-ized outcome expectancies. Health Psychology, 4, 219–247.
SCHMIDT, C., COLLETTE, F., LECLERCQ, Y., STERPENICH, V.,VANDEWALLE, G., BERTHOMIER, P., ET AL. (2009).Homeostatic sleep pressure and responses to sustainedattention in the suprachiasmiatic area. Science, 324,516–519.
SCHMIDT, F. L., & HUNTER, J. E. (1998). The validity andutility of selection methods in personnel psychology:Practical and theoretical implications of 85 years ofresearch findings. Psychological Bulletin, 124(2), 262–274.
SCHMIDT, F. L., & HUNTER, J. E. (2004). General mentalability in the world of work: Occupational attainment

R54 PREFERENCESO
and job performance. Journal of Personality and SocialPsychology, 86, 162–173.
SCHMIDT, V., & GÖSELE, U. (2007). How nanowires grow.Science, 316(5825), 698–699.
SCHMITT, D. P. (2005). Fundamentals of human matingstrategies. In D. M. Buss (Ed.), The handbook of evolution-ary psychology (pp. 258–291). New York: Wiley.
SCHMITT, D. P., & BUSS, D. M. (2001). Human matepoaching: Tactics and temptations for infiltrating exist-ing mateships. Journal of Personality & Social Psychology,80(6), 894–917.
SCHNEIDER, B., ATKINSON, L., & TARDIF, C. (2001). Child-parent attachment and children’s peer relations: A quan-titative review. Developmental Psychology, 37, 86–100.
SCHNEIDER, B., & STEVENSON, D. (1999). The ambitiousgeneration: America’s teenagers, motivated but directionless.New Haven: Yale University Press.
SCHNEIDER, D. J. (1973). Implicit personality theory: Areview. Psychological Bulletin, 79, 294–309.
SCHNEIDER, W., GRUBER, H., GOLD, A., & OPWIS, K.(1993). Chess expertise and memory for chess positionsin children and adults. Journal of Experimental ChildPsychology, 56(3), 328–349.
SCHOFIELD, W. (1964). Psychotherapy: The purchase offriendship. Englewood Cliffs, NJ: Prentice-Hall.
SCHOOLER, C. (2007). Use it—and keep it, longer, prob-ably: A reply to Salthouse (2006). Perspectives onPsychological Science, 2(1), 24–29.
SCHOOLER, J. (2001). Discovering memories of abuse inthe light of meta-awareness. Journal of Aggression,Maltreatment & Trauma, 4, 105–136.
SCHOOLER, J., OHLSSON, S., & BROOKS, K. (1993).Thoughts beyond words: When language overshadowsinsight. Journal of Experimental Psychology: General, 122,166–183.
SCHRAW, G., DUNKLE, M., & BENDIXEN, L. (1995).Cognitive processes in well-defined and ill-defined prob-lem solving. Applied Cognitive Psychology, 9, 523–538.
SCHROEDER, H. E. (1973). The risky shift as a generalchoice shift. Journal of Personality and Social Psychology,27(2), 297–300.
SCHUL, Y., & VINOKUR, A. D. (2000). Projection in personperception among spouses as a function of the similarityin their shared experiences. Personality and SocialPsychology Bulletin, 26(8), 987–1001.
SCHULTHEISS, O. C. (2008). Implicit motives. In O. P.John, R. W. Robins, & L. A. Pervin (Eds.), Handbook ofpersonality: Theory and research (3rd ed., pp. 603–633).New York: Guilford.
SCHULTZ, W., TREMBLAY, L., & HOLLERMAN, J. R. (2000).Reward processing in primate orbitofrontal cortex andbasal ganglia. Cerebral cortex, 10(3), 272–284.
SCHULZ-HARDT, S., FREY, D., LÜTHGENS, C., & MOSCOVICI,S. (2000). Biased information search in group decisionmaking. Journal of Personality and Social Psychology, 78,655–669.
SCHUNK, D. H. (1984). Self-efficacy perspective onachievement behavior. Educational Psychologist, 19(1),48–58.
SCHUNK, D. H. (1985). Self-efficacy and classroom learn-ing. Psychology in the Schools, 22(2), 208–223.
SCHWARTZ, S., & MAQUET, P. (2002). Sleep imaging andthe neuropsychological assessment of dreams. Trends inCognitive Sciences, 6, 23–30.
SCHWARTZ, B. (2004). The paradox of choice: Why less ismore. New York: HarperCollins.
SCHWARTZ, B., WASSERMAN, E. A., & ROBBINS, S. (2002).Psychology of learning and behavior (5th ed.). New York:Norton.
SCHWARTZ, B. L. (1999). Sparkling at the end of thetongue: The etiology of tip-of-the-tongue phenomenol-ogy. Psychonomics Bulletin & Review, 5, 379–393.
SCHWARTZ, C. E., WRIGHT, C. I., SHIN, L. M., KAGAN, J., &RAUCH, S. L. (2003). Inhibited and uninhibited infants“grown up”: Adult amygdalar response to novelty. Science,300, 1952–1953.
SCHWARTZ, D., DODGE, K., PETTIT, G., BATES, J., & THE
CONDUCT PROBLEMS PREVENTION RESEARCH GROUP.(2000). Friendship as a moderating factor in the path-way between early harsh home environment and latervictimization in the peer group. Developmental Psychology,36, 646–662.
SCHWARZ, N. (1999). Self-reports: How the questionsshape the answers. American Psychologist, 54, 93–105.
SCHWARZER, R. (ED.). (1992). Self-efficacy: Thought controlof action. Washington, DC: Hemisphere.
SCHWEDER, R. A. (1994). “You’re not sick, you’re just inlove”: Emotion as an interpretive system. In P. Ekman &R. J. Davidson (Eds.), The nature of emotion (pp. 32–47).New York: Oxford University Press.
SCHWEITZER, E., RICKELS, K., & UHLENHUTH, E. H. (1995).Issues in the long-term treatment of anxiety disorders. InF. E. Bloom & D. Kupfer (Eds.), Psychopharmacology: Thefourth generation of progress (pp. 1349–1359). New York:Raven.
SCOTT, F. J., & BARON-COHEN, S. (1996). Imagining realand unreal things: Evidence of a dissociation in autism.Journal of Cognitive Neuroscience, 8, 371–382.
SCRIBNER, S. (1975). Recall of classical syllogisms: Across-cultural investigation of error on logical problems.In R. J. Falmagne (Ed.), Reasoning, representation andprocess in children and adults (pp. 153–174). Hillsdale, NJ:Erlbaum.
SEDIKIDES, C., & GREGG, P. A. (2008). Self-enhancement:Food for thought. Perspectives on Psychological Science, 3,102–116.
SEDIVY, J. C., TANENHAUS, M. K., CHAMBERS, C. G., &CARLSON, G. N. (1999). Achieving incremental sentenceinterpretation through contextual representation.Cognition, 71(2), 109–147
SEEMAN, M. V. (1997). Psychopathology in women andmen: Focus on female hormones. American Journal ofPsychiatry, 154, 1641–1647.
SEGAL, Z., PEARSON, J., & THASE, M. (2003). Challenges inpreventing relapse in major depression: Report of aNational Institute of Mental Health Workshop on stateof the science of relapse prevention in major depression.Journal of Affective Disorders, 77, 97–108.
SEGALL, M. H., DASEN, P. R., BERRY, J. W., & POORTINGA, Y.H. (1999). Human behavior in global perspective: An intro-duction to cross-cultural psychology (2nd ed.). New York:Pergamon Press.
SEGERSTROM, S. C. (2000). Personality and the immunesystem: Models, methods, and mechanisms. Annals ofBehavioral Medicine, 22, 180–190.
SEIDENBERG, M. (2005). Connectionist models of wordreading. Current Directions in Psychological Science, 14,238–242.
SEIDENBERG, M. S., & ZEVIN, J. D. (2006). Connectionistmodels in developmental cognitive neuroscience: Criticalperiods and the paradox of success. In Y. Munakata & M.Johnson (Eds.), Processes of change in brain and cognitivedevelopment. Attention and Performance XXI. Oxford, UK:Oxford University Press.
SELFRIDGE, O. G. (1959). Pandemonium: A paradigm forlearning. In D. V. Blake & A. M. Uttley (Eds.), Proceedingsof the Symposium on the Mechanisation of Thought Processes.London: HM Stationery Office.
SELIGMAN, M. E. P. (1970). On the generality of the lawsof learning. Psychological Review, 77, 406–418.
SELIGMAN, M. E. P. (1971). Phobias and preparedness.Behavior Therapy, 2, 307–320.
SELIGMAN, M. E. P. (1975). Helplessness: On depression,development, and death. San Francisco: Freeman.
SELIGMAN, M. E. P. (1995). The effectiveness of psy-chotherapy: The Consumer Reports study. AmericanPsychologist, 50, 965–974.
SELIGMAN, M. E. P., & CSIKSZENTMIHALYI, M. (2000).Positive psychology: An introduction. AmericanPsychologist, 55(1), 5–14.
SELIGMAN, M. E. P., & GILLHAM, J. (2000). The science ofoptimism and hope: Research essays in honor of Martin E. P.Seligman. Philadelphia: Templeton Foundation Press.
SELIGMAN, M. E. P., & HAGER, J. L. (EDS.). (1972).Biological boundaries of learning. New York: Appleton-Century-Crofts.
SELIGMAN, M. E. P., KLEIN, D. C., & MILLER, W. R. (1976).Depression. In H. Leitenberg (Ed.), Handbook of behaviormodification and behavior therapy. Englewood Cliffs, NJ:Prentice-Hall.
SELIGMAN, M. E. P., & MAIER, S. F. (1967). Failure toescape traumatic shock. Journal of ExperimentalPsychology, 74, 1–9.
SELIGMAN, M. E. P., MAIER, S. F., & SOLOMON, R. L. (1971).Unpredictable and uncontrollable aversive events. In F.R. Brush (Ed.), Aversive conditioning and learning. NewYork: Academic Press.
SELIGMAN, M. E. P., NOLEN-HOEKSEMA, S., THORNTON, N.,& THORNTON, K. M. (1990). Explanatory style as a mech-anism of disappointing athletic performance.Psychological Science, 1, 143–146.
SELIGMAN, M. E. P., STEEN, T., PARK, N., & PETERSON, C.(2005). Positive psychology progress: Empirical valida-tion of interventions. American Psychologist, 60, 410–421.
SELIGMAN, M. E., & SCHULMAN, P. (1986). Explanatorystyle as a predictor of productivity and quitting amonglife insurance sales agents. Journal of Personality & SocialPsychology, 50, 832–838.

PREFERENCESO R55
SEMMLER, C., & BREWER, N. (2006). Postidentificationfeedback effects on face recognition confidence: Evidencefor metacognitive influences. Applied Cognitive Psychology,20, 895–916.
SENGHAS, A. (1995a). Conventionalization in the firstgeneration: A community acquires a language. Journal ofContemporary Legal Issues, 6, 501–519.
SENGHAS, A. (1995b). The development of NicaraguanSign Language via the language acquisition process. In D.MacLaughlin & S. McEwen (Eds.), Proceedings of theBoston University Conference on Language Development, 19,543–552.
SENGHAS, A., KITA, S., & ÖZYÜREK, A. (2004). Childrencreating core properties of language: Evidence from anemerging sign language in Nicaragua. Science,305(5691), 1779–1782.
SENGHAS, A., ROMÁN, D., & MAVILLAPALLI, S. (2006).Simply unique. London: Leonard Cheshire International.
SENKO, C., DURIK, A. M., & HARACKIEWICZ, J. M. (2008).Historical perspectives and new directions in achieve-ment goal theory: Understanding the effects of masteryand performance-approach goals. In J. Y. Shah and W. L.Gardner (Eds.), Handbook of motivation science(pp. 100–113). New York: Guilford.
SERENO, A. B., & MAUNSELL, J. H. R. (1998). Shape selec-tivity in primate lateral intraparietal cortex. Nature, 395,500–503.
SERPELL, R. (2000). Intelligence and culture. In R. J.Sternberg (Ed.), Handbook of intelligence (2nd ed., pp.549–580). New York: Cambridge University Press.
SERVIN, A., NORDENSTROM, A., LARSSON, A., & BOHLIN, G.(2003). Prenatal androgens and gender-typed behavior:A study of girls with mild and severe forms of congenitaladrenal hyperplasia. Developmental Psychology, 39(3),440–450.
SETHI, A., MISCHEL, W., ABER, J. L., SHODA, Y., &RODRIGUEZ, M. L. (2000). The role of strategic attentiondeployment in development of self-regulation: Predictingpreschoolers’ delay of gratification from mother-toddlerinteractions. Developmental Psychology, 36, 767–777.
SHADER, R. I., & GREENBLATT, D. J. (1995). The pharma-cotherapy of acute anxiety. In F. E. Bloom & D. Kupfer(Eds.), Psychopharmacology: The fourth generation ofprogress (pp. 1341–1348). New York: Raven.
SHADISH, W. R., MATT, G. E., NAVARRO, A. M., SIEGLE, G.,CRITS-CHRISTOPH, P., HAZELRIGG, M., ET AL. (1997).Evidence that therapy works in clinically representativeconditions. Journal of Consulting and Clinical Psychology,65, 355–365.
SHAFFER, D. (2004). Social and personality development(5th ed.). New York: Wadsworth.
SHAFIR, E., SIMONSON, I., & TVERSKY, A. (1993). Reason-based choice. Cognition, 49, 11–36.
SHAH, A. M., & WOLFORD, G. (2007). Buying behavior asa function of parametric variation of number of choices.Psychological Science, 18, 369–370.
SHAM, P. V. C., O’CALLAGHAN, E., TAKEI, N., MURRAY, G. K.,HARE, E. H., & MURRAY, R. M. (1992). Schizophrenia fol-lowing pre-natal exposure to influenza epidemicsbetween 1939 and 1960. British Journal of Psychiatry, 160,461–466.
SHANAB, M. E., & YAHYA, K. A. (1977). A behavioral studyof obedience in children. Journal of Personality and SocialPsychology, 35, 530–536.
SHANNONHOUSE, R. (Ed). (2000). Out of her mind: Womenwriting on madness. New York: Modern Library.
SHAPIRO, C. M., BORTZ, R., MITCHELL, D., BARTELL, P., &JOOSTE, P. (1981). Slow wave sleep: A recovery period afterexercise. Science, 214, 1253–1254.
SHAVER, P., & CLARK, C. (1994). The psychodynamics ofadult romantic attachment. In J. Masling & R. Bornstein(Eds.), Empirical perspectives on object relations theory.Empirical studies of psychoanalytic theories: Vol. 5 (pp.105–156). Washington, DC: American PsychologicalAssociation.
SHAVER, P., SCHWARTZ, J., KIRSON, D., & O’CONNOR, C.(1987). Emotion knowledge: Further exploration of aprototype approach. Journal of Personality and SocialPsychology, 52, 1061–1086.
SHAVITT, S., SWAN, S., LOWREY, T. M., & WANKE, M. (1994).The interaction of endorser attractiveness and involve-ment in persuasion depends on the goal that guides mes-sage processing. Journal of Consumer Psychology, 3(2),137–162.
SHEA, M. (1995). Interrelationships among categories ofpersonality disorders. In W. J. Livesley (Ed.), The DSM-IVpersonality disorders (pp. 397–406). New York: Guilford.
SHEAR, M. K., PILKONIS, P. A., CLOITRE, M., & LEON, A. C.(1994). Cognitive behavioral treatment compared withnonprescriptive treatment of panic disorder. Archives ofGeneral Psychiatry, 51, 395–401.
SHEEHAN, P. W., GREEN, V., TRUESDALE, P. (1992).Influence of rapport on hypnotically inducedpseudomemory. Journal of Abnormal Psychology, 101 (4),690–700.
SHELLEY, P. B. (1821). To a skylark. As published in A. T.Quiller-Couch (Ed.), The Oxford book of English verse(1900). Oxford, England: Clarendon.
SHEPARD, R. N., & COOPER, L. A. (1982). Mental imagesand their transformations. Cambridge, MA: MIT Press.
SHEPHERD, G. M. (1994). Discrimination of molecularsignals by the olfactory receptor neuron. Neuron, 13,771–790.
SHERIF, M. (1937). An experimental approach to the studyof attitudes. Sociometry, 1, 90–98.
SHERIF, M. (1966). The common predicament: Social psy-chology of intergroup conflict and cooperation. Boston:Houghton Mifflin.
SHERIF, M., HARVEY, O. J., WHITE, B. J., HOOD, W. R., &SHERIF, C. W. (1961). Intergroup conflict and competition:The Robbers Cave experiment. Norman: University ofOklahoma Book Exchange.
SHERRINGTON, C. (1906). The integrative action of the nerv-ous system. New Haven, CT: Yale University Press.
SHETTLEWORTH, S. J. (1972). Constraints on learning. InD. S. Lehrman, R. A. Hinde, & E. Shaw (Eds.), Advances inthe study of behavior: Vol. 4. New York: Academic Press.
SHETTLEWORTH, S. J. (1983). Memory in food-hoardingbirds. Scientific American, 248, 102–110.
SHETTLEWORTH, S. J. (1984). Learning and behavioralecology. In J. R. Krebs & N. B. Davies (Eds.), Behavioral
ecology (2nd ed., pp. 170–194). Oxford, England:Blackwell.
SHETTLEWORTH, S. J. (1990). Spatial memory in food-storing birds. Philosophical Transactions of the RoyalSociety, Series B, 329, 143–151.
SHI, R., MORGAN, J. L., & ALLOPENNA, P. (1998).Phonological and acoustic bases for earliest grammaticalcategory assignment: A cross-linguistic perspective.Journal of Child Language, 25, 169–201.
SHIAH, I. S., & YATHAM, L. N. (2000). Serotonin in maniaand in the mechanism of action of mood stabilizers: Areview of clinical studies. Bipolar Disorders, 2, 77–92.
SHIH, M., PITTINSKY, T. L., & AMBADY, N. (1999).Stereotype susceptibility: Identity salience and shifts inquantitative performance. Psychological Science, 10,80–83.
SHIPLEY, E. F., KUHN, I. F., & MADDEN, E. C. (1983).Mothers’ use of superordinate category terms. Journal ofChild Language, 10, 571–588.
SHOBE, K. K., & KIHLSTROM, J. F. (1997). Is traumaticmemory special? Current Directions in Psychological Science,6, 70–74.
SHODA, Y., MISCHEL, W., & PEAKE, P. K. (1990). Predictingadolescent cognitive and self-regulatory competenciesfrom preschool delay of gratification: Identifying diag-nostic conditions. Developmental Psychology, 26,978–986.
SHORS, T. (2009). Saving new brain cells. ScientificAmerican, 300, 47–54.
SHULMAN, S., ELICKER, J., & SROUFE, L. A. (1994). Stages offriendship growth in preadolescence as related to attach-ment history. Journal of Social and Personal Relationships,11(3), 341–361.
SICOLY, F., & ROSS, M. (1977). Facilitation of ego-biasedattributions by means of self-serving observer feedback.Journal of Personality and Social Psychology, 35, 734–741.
SIEGAL, M. (1997). Knowing children: Experiments in conver-sation and cognition (2nd ed.). New York: PsychologyPress.
SIEGEL, A., & DEMETRIKOPOULOS, M. K. (1993).Hormones and aggression. In J. Schulkin (Ed.),Hormonally induced changes in mind and brain(pp. 99–127). San Diego, CA: Academic Press.
SIEGEL, J. M. (2003). Why we sleep. Scientific American,289, 92–97.
SIEGEL, S. (1977). Morphine tolerance acquisition as anassociative process. Journal of Experimental Psychology:Animal Behavior Processes, 3, 1–13.
SIEGEL, S. (1983). Classical conditioning, drug tolerance,and drug dependence. In Y. Israel, F. B. Slower, H. Kalant,R. E. Popham, W. Schmidt, & R. G. Smart (Eds.), Researchadvances in alcohol and drug abuse: Vol. 7 (pp. 207–246).New York: Plenum.
SIEGEL, S., & ALLAN, L. G. (1998). Learning and home-ostasis: Drug addiction and the McCollough effect.Pyschological Bulletin, 124, 230–239.
SIEGEL, S., KIM, J. A., & SOKOLOWSKA, M. (2003).Situational-specificity of caffeine tolerance. Circulation,108, E38.

R56 PREFERENCESO
SIEGLER, R. S. (1996). Emerging minds: The process ofchange in children’s thinking. New York: Oxford UniversityPress.
SIEGLER, R. S. (1998). Children’s thinking (3rd ed.). UpperSaddle River, NJ: Prentice Hall.
SIGELMAN, C. K., MILLER, T. E., & WHITWORTH, L. A.(1986). The early development of stigmatizing reactionsto physical differences. Journal of Applied DevelopmentalPsychology, 7(1), 17–32.
SILK, J. B. (1986). Social behavior in evolutionary per-spective. In B. B. Smuts, D. L. Cheney, R. M. Seyfarth, R.W. Wrangham, & T. T. Struhsaker (Eds.), Primate societies.Chicago: University of Chicago Press.
SILVERMAN, P., & RETZLAFF, P. (1986). Cognitive stateregression through hypnosis: Are earlier cognitive statesretrievable? International Journal of Clinical andExperimental Hypnosis, 34, 192–204.
SIMCOCK, G., & HAYNE, H. (2002). Breaking the barrier?Children fail to translate their preverbal memories in lan-guage. Psychological Science, 13, 225–231.
SIMNER, M. L. (1971). Newborn’s response to the cry ofanother infant. Developmental Psychology, 5, 136–150.
SIMON, H. A. (1983). Reason in human affairs. Stanford,CA: Stanford University Press.
SIMONS, D. J. (2000). Attentional capture and inatten-tional blindness. Trends in Cognitive Science, 4, 147–155.
SIMONS, D. J., & CHABRIS, C. F. (1999). Gorillas in ourmidst: Sustained inattentional blindness for dynamicevents. Perception, 28(9), 1059–1074.
SIMONTON, D. K. (2000). Creativity: Cognitive, personal,developmental, and social aspects. American Psychologist,55(1), 151–158.
SIMONTON, D. K. (2003). Scientific creativity as con-strained stochastic behavior: The integration of product,person, and process perspectives. Psychological Bulletin,129, 475–494.
SIMPSON, E. L. (1974). Moral development research: Acase of scientific cultural bias. Human Development, 17,81–106.
SIMS, E. A. (1986). Energy balance in human beings: Theproblems of plentitude. Vitamins and Hormones: Researchand Applications, 43, 1–101.
SINGER, W. (1996). Neuronal synchronization: A solu-tion to the binding problem? In R. R. Llinas & P. S.Churchland (Eds.), The mind-brain continuum: Sensoryprocesses (pp. 101–130). Cambridge, MA: MIT Press.
SINGH, D. (1993). Adaptive significance of female physi-cal attractiveness: Role of waist-to-hip ratio. Journal ofPersonality and Social Psychology, 65, 293–307.
SINGH, D. (1994). Waist-to-hip ratio and judgment ofattractiveness and healthiness of female figures by maleand female physicians. International Journal of Obesity andRelated Metabolic Disorders, 18, 731–737.
SINGH, D., & LUIS, S. (1995). Ethnic and gender consen-sus for the effect of waist-to-hip ratio on judgment ofwomen’s attractiveness. Human Nature, 6, 51–65.
SINGLETON, J. L., & NEWPORT, E. L. (2004). When learn-ers surpass their models: The acquisition of AmericanSign Language from inconsistent input. CognitivePsychology, 49, 370–407.
SINHA, D. (1983). Human assessment in the Indian con-text. In S. H. Irvine & J. W. Berry (Eds.), Human assess-ment and cultural factors (pp. 17–34). New York: Plenum.
SIO, U. N., & ORMEROD, T. C. (2009). Does incubationenhance problem solving? A meta-analytic review.Psychological Bulletin, 135, 94–120.
SKINNER, B. F. (1938). The behavior of organisms. New York:Appleton-Century-Crofts.
SKOTKO, B. G., KENSINGER, E. A., LOCASCIO, J. J., EINSTEIN,G., RUBIN, D. C., TUPLER, L. A., ET AL. (2004). Puzzlingthoughts for H. M.: Can new semantic information beanchored to old semantic memories? Neuropsychology,18(4), 756–769.
SLOANE, R. B., STAPLES, F. R., CRISTOL, A. H., YORKSTON, N.J., & WHIPPLE, K. (1975). Psychotherapy vs. behavior therapy.Cambridge, MA: Harvard University Press.
SLOBIN, D. I. (1978) A case study of early language aware-ness. In A. Sinclair, R. Jarvella, & W.J.M. Levelt (Eds.),The child’s conception of language (pp. 45–54). Heidelberg:Springer-Verlag.
SLOMAN, S. A. (1996). The empirical case for two systemsof reasoning. Psychological Bulletin, 119, 3–22.
SLOVIC, P., FISCHOFF, B., & LICHTENSTEIN, S. (1982). Factsversus fears: Understanding perceived risk. In D.Kahneman, P. Slovic, & A. Tversky (Eds.), Judgment underuncertainty: Heuristics and biases. New York: CambridgeUniversity Press.
SMITH, C. (1996). Women, weight and body image. In J.C. Chrisler, C. Golden, & P. D. Rozee (Eds.), Lectures onthe psychology of women. New York: McGraw-Hill.
SMITH, C., & LLOYD, B. (1978). Maternal behavior andperceived sex of infant: Revisited. Child Development, 49,1263–1265.
SMITH, E. E., & MEDIN, D. L. (1981). Categories and con-cepts. Cambridge, MA: Harvard University Press.
SMITH, E. E., OSHERSON, D. N., RIPS, L. J., & KEANE, M.(1988). Combining prototypes: A selective modificationmodel. Cognitive Science, 12, 485–527.
SMITH, G. T., SPILLANE, N. S., & ANNUS, A. M. (2006).Implications of an emerging integration of universal andculturally specific psychologies. Perspectives onPsychological Science, 1(3), 211–233.
SMITH, L. (2005). Psychotherapy, classism, and the poor:Conspicuous by their absence. American Psychologist, 60,687–696.
SMITH, L. B., & THELEN, D. (1993). A dynamic systemsapproach to development: Applications. Cambridge, MA:MIT Press.
SMITH, L. B., & THELEN, E. (2003). Development as adynamic system. Trends in Cognitive Science, 7, 343–348.
SMITH, L. B., THELEN, E., TITZER, R., & MCLIN, D. (1999).Knowing in the context of acting: The task dynamics ofthe A-not-B error. Psychological Review, 106, 235–260.
SMITH, L. B., & YU, C. (2008). Infants rapidly learn word-referent mappings via cross-situational statistics.Cognition, 106, 333–338.
SMITH, M. (1983). Hypnotic memory enhancement ofwitnesses: Does it work? Psychological Bulletin, 94,387–407.
SMITH, M. B. (1950). The phenomenological approach inpersonality theory: Some critical remarks. Journal ofAbnormal and Social Psychology, 45, 516–522.
SMITH, M. L., GLASS, G. V., & MILLER, R. L. (1980). Thebenefits of psychotherapy. Baltimore: Johns Hopkins Press.
SMITH, P., & DALISH, L. (1977). Sex differences in parentand infant behavior in the home. Child Development, 48,1250–1254.
SMITH, P. B., & BOND, M. B. (1993). Social psychology acrosscultures. New York: Harvester Wheatsheaf.
SMITH, P. B., MISUMI, J., TAYEB, M., PETERSON, M., & BOND,M. (1989). On the generality of leadership style meas-ures across cultures. Journal of Occupational Psychology,62(2), 97–109.
SMITH, S. M. (1979). Remembering in and out of context.Journal of Experimental Psychology: Human Learning andMemory, 5, 460–471.
SMITH, S. M., & BLANKENSHIP, S. E. (1989). Incubationeffects. Bulletin of the Psychonomic Society, 27(4), 311–314.
SMITH, S. M., & VELA, E. (2001). Environmental context-dependent memory: A review and meta-analysis.Psychonomics Bulletin and Review, 8, 203–220.
SMOLENSKY, P. (1999). Grammar-based connectionistapproaches to language. Cognitive Science, 23, 589–613.
SNEDEKER, J., GEREN, J., & SHAFTO, C. (2007). Startingover: International adoption as a natural experiment inlanguage development. Psychological Science, 18(1),79–86.
SNEDEKER, J., & GLEITMAN, L. (2004). Why it is hard tolabel our concepts. G. Hall & S. Waxman (Eds.), Weavinga lexicon (pp. 207–294). New York: Cambridge UniversityPress.
SNEDEKER, J., & TRUESWELL, J. (2003). Using prosody toavoid ambiguity: Effects of speaker awareness and refer-ential context. Journal of Memory and Language, 48,103–130.
SNIBBE, A., & MARKUS, H. R. (2005). You can’t always getwhat you want: Social class, agency, and choice. Journal ofPersonality and Social Psychology, 88, 703–720.
SNOW, C., & HOEFNAGEL-HOHLE, M. (1978). The criticalperiod for language acquisition: Evidence from secondlanguage learning. Child Development, 49, 1114–1128.
SNOW, R. E. (1994). Abilities in academic tasks. In R. J.Sternberg & R. K. Wagner (Eds.), Mind in context:Interactionist perspectives on human intelligence (pp. 3–37).Cambridge, England: Cambridge University Press.
SNOW, R. E. (1996). Aptitude development and educa-tion. Psychology, Public Policy, and Law, 2, 536–560.
SNYDER, D. K., CASTELLANI, A. M., & WHISMAN, M. A.(2006). Current status and future directions in coupletherapy. Annual Review of Psychology, 57, 317–344.
SNYDER, M. (1987). Public appearances/private realities.New York: Freeman.
SNYDER, M. (1995). Self-monitoring: Public appearancesversus private realities. In G. G. Brannigan & M. R.Merrens (Eds.), The social psychologists: Research adven-tures (pp. 35–50). New York: McGraw-Hill.
SNYDER, M., & OMOTO, A. M. (1992). Who helps andwhy? The psychology of aids volunteerism. In S.Spacapan & S. Oskamp (Eds.), Helping and being helped:

PREFERENCESO R57
Naturalistic studies (pp. 213–239). Thousand Oaks, CA:Sage.
SNYDER, M., TANKE, E. D., & BERSCHEID, E. (1977). Socialperception and interpersonal behavior: On the self-ful-filling nature of social stereotypes. Journal of Personalityand Social Psychology, 44, 510–517.
SNYDER, M. L., STEPHAN, W. G., & ROSENFIELD, D. (1976).Egotism and attribution. Journal of Personality and SocialPsychology, 33, 435–441.
SNYDER, S. H. (1976). The dopamine hypothesis of schiz-ophrenia. American Journal of Psychiatry, 133, 197–202.
SOJA, N. N., CAREY, S., & SPELKE, E. S. (1991). Ontologicalcategories guide young children’s inductions of wordmeaning: Object terms and substance terms. Cognition,38, 179–211.
SOKOLOWSKA, M., SIEGEL, S., & KIM, J. A. (2002).Intraadministration associations: Conditional hyperal-gesia elicited by morphine onset cues. Journal ofExperimental Psychology: Animal Behavior Processes, 28(3),309–320.
SORKHABI, N. (2005). Applicability of Baumrind’s parenttypology to collective cultures: Analysis of cultural expla-nation of parent socialization effects. InternationalJournal of Behavioral Development, 29, 552–563.
SOTO, C. J., JOHN, O. P., GOSLING, S. D., & POTTER, J.(2008). The developmental psychometrics of Big Fiveself-reports: Acquiescence, factor structure, coherence,and differentiation from ages 10 to 20. Journal ofPersonality and Social Psychology, 94, 718–737.
SOX, H. C., JR., & WOOLF, S. H. (1993). Evidence-basedpractice guidelines from the U.S. Preventive Services TaskForce. Journal of the American Medical Association, 269,2678.
SPANOS, N. P. (1986). Hypnotic behavior: A social-psy-chological interpretation of amnesia, analgesia, and“trance logic.” Behavioral & Brain Sciences, 9 (3),449–467.
SPANOS, N. P. (1996). Multiple identities and false memories:A sociocognitive perspective. Washington, DC: AmericanPsychological Association.
SPANOS, N. P., BURGESS, C. A., BURGESS, M. F., SAMUELS,C., & BLOIS, W. O. (1999). Creating false memories ofinfancy with hypnotic and nonhypnotic procedures.Applied Cognitive Psychology, 13, 201–218.
SPANOS, N. P., & COE, W. C. (1992).A social-psychologicalapproach to hypnosis. In E. Fromm & M. Nash (Eds.),Contemporary hypnosis research (pp. 102–130). New York:Guilford Press.
SPEAR, L. P. (2000). The adolescent brain and age-relatedbehavioral manifestations. Neuroscience and BiobehavioralReviews, 24, 417–463.
SPEARMAN, C. (1927). The abilities of man. London:Macmillan.
SPIEGEL, K., SHERIDAN, J. F., & VAN CAUTER, E. (2002).Reduced immune response to influenza virus vaccinationin a state of sleep debt. Journal of the American MedicalAssociation, 288(12), 1471–1472.
SPELKE, E. (2003). Core knowledge. In N. Kanwisher & J.Duncan (Eds.), Attention and performance: Vol. 20.Functional neuroimaging of visual cognition. New York:Oxford University Press.
SPELKE, E. S. (1994). Initial knowledge: Six suggestions.Cognition, 50(1–3), 431–445.
SPELKE, E. S. (2005). Sex differences in intrinsic aptitudefor mathematics and science? A critical review. AmericanPsychologist, 60(9), 950–958.
SPELKE, E. S., & NEWPORT, E. (1998). Nativism, empiri-cism, and the development of knowledge. In R. Lerner(Ed.), Handbook of child psychology: Vol. 1. Theoretical mod-els of human development (5th ed.). New York: Wiley.
SPEMANN, H. (1967). Embryonic development and induction.New York: Hafner.
SPERBER, D., & WILSON, D. (1986). Relevance: Commu-nication and cognition. Oxford, England: Blackwell.
SPERLING, G. (1960). The information available in briefvisual presentations. Psychological Monographs, 74(WholeNo. 11).
SPIRO, M. (1982). Oedipus in the Trobriands. Chicago:University of Chicago Press.
SPIRO, M. E. (1992). Oedipus redux. Ethos, 20, 358–376.
SPITZ, C. J., GOLD, A. R., & ADAMS, D. B. (1975). Cognitiveand hormonal factors affecting coital frequency. Archivesof Sexual Behavior, 4, 249–264.
SPITZ, H. H. (1999). Beleaguered Pygmalion: A history ofthe controversy over claims that teacher expectancy raisesintelligence. Intelligence, 27, 199–234.
SPRINGER, S. P., & DEUTSCH, G. (1998). Left brain, rightbrain: Perspectives from cognitive neuroscience (5th ed.).New York: Freeman.
SQUIRE, L. R. (1977). ECT and memory loss. AmericanJournal of Psychiatry, 134, 997–1001.
SQUIRE, L. R. (1986). Mechanisms of memory. Science,232, 1612–1619.
SQUIRE, L. R. (1987). Memory and brain. New York:Oxford University.
SQUIRE, L. R., & COHEN, N. J. (1979). Memory and amne-sia: Resistance to disruption develops for years afterlearning. Behavioral Biology and Neurology, 25, 115–125.
SQUIRE, L. R., & COHEN, N. J. (1982). Remote memory,retrograde amnesia, and the neuropsychology of mem-ory. In L. S. Cermak (Ed.), Human memory and amnesia(pp. 275–304). Hillsdale, NJ: Erlbaum.
SQUIRE, L. R., & COHEN, N. J. (1984). Human memoryand amnesia. In J. McGaugh, G. Lynch, & N. Weinberger(Eds.), Neurobiology of learning and memory. New York:Guilford.
SRIVASTAVA, S., & BEER, J. S. (2005). How self-evaluationsrelate to being liked by others: Integrating sociometerand attachment perspectives. Journal of Personality andSocial Psychology, 89, 966–977.
SRIVASTAVA, S., JOHN, O. P., GOSLING, S. D., & POTTER, J.(2003). Development of personality in early and middleadulthood: Set like plaster or persistent change? Journalof Personality and Social Psychology, 84, 1041–1053.
SROUFE, L. A., EGELAND, B., CARLSON, E., & COLLINS, W. A.(2005). The Development of the person: The Minnesota Studyof Risk and Adaptation from Birth to Adulthood. New York:Guilford.
STAKE, J., & NICKENS. S. (2005). Adolescent girls’ andboys’ science peer relationships and perceptions of thepossible self as scientist. Sex Roles, 52, 1–11.
STANLEY, B. G., MAGDALIN, W., & LEIBOWITZ, S. F. (1989).A critical site for neuropeptide Y-induced eating lies inthe caudolateral paraventricular/perifornical region ofthe hypothalamus. Society for Neuroscience Abstracts, 15,894.
STANLEY, J. (1993). Boys and girls who reason well math-ematically. In G. R. Beck & K. Ackrill (Eds.), The originsand development of high ability. Chichester, England:Wiley.
STANOVICH, K. E., & WEST, R. F. (1998). Who uses baserates and P(D|~H)? An analysis of individual differences.Memory & Cognition, 26, 161–179.
STANOVICH, K. E., & WEST, R. F. (2000). Individual differ-ences in reasoning: Implications for the rationalitydebate. Behavioral and Brain Sciences, 23, 645–665.
STARKEY, P., SPELKE, E. S., & GELMAN, R. (1983). Detectionof intermodal numerical correspondences by humaninfants. Science, 222, 179–181.
STARKEY, P., SPELKE, E. S., & GELMAN, R. (1990).Numerical abstraction by human infants. Cognition, 36,97–127.
STEELE, C. M. (1998). Stereotyping and its threat are real.American Psychologist, 53, 680–681.
STEELE, C. M., & ARONSON, J. (1995). Stereotype threatand the intellectual test performance of AfricanAmericans. Journal of Personality and Social Psychology,69(5), 797–811.
STEELE, C. M., & JOSEPHS, R. A. (1990). Alcohol myopia:Its prized and dangerous effects. American Psychologist,45, 921–933.
STEELE, J. (2003). Children’s gender stereotypes aboutmath: The role of stereotype stratification. Journal ofApplied Social Psychology, 33, 2587–2606.
STEFANSSON, H., RUJESCU, D., CICHON, S., PIETILÄINEN, O.P., INGASON, A., STEINBERG. S., ET AL. (2008). Large recur-rent microdeletions associated with schizophrenia.Nature, 455(7210), 232–236.
STEIN, M. B., SCHORK, N. J., & GELERNTER, J. (2008).Interaction for anxiety sensitivity, an intermediate phe-notype for anxiety disorders. Neuropsychopharmacology,33, 312–319.
STEINBERG, L. (2001). We know some things: Adolescent-parent relationships in retrospect and prospect. Journalof Research in Adolescence, 11, 1–20.
STEINBERG, L. (2007). Risk taking in adolescence: Newperspectives from brain and behavioral science. CurrentDirections in Psychological Science, 16(2), 55–59.
STEINBERG, L., ELKMAN, J. D., & MOUNTS, N. S. (1989).Authoritative parenting, psychosocial maturity, and aca-demic success among adolescents. Child Development,60(6), 1424–1436.
STEINBERG, L., & MORRIS, A. S. (2001). Adolescent devel-opment. Annual Review of Psychology, 52, 83–110.
STERN, J. A., BROWN, M., ULETT, G. A., & SLETTEN, I.(1977). A comparison of hypnosis, acupuncture, mor-phine, valium, aspirin, and placebo in the management ofexperimentally induced pain. In W. E. Edmonston (Ed.),

R58 PREFERENCESO
Conceptual and investigative approaches to hypnosis and hyp-notic phenomena (Vol. 296, pp. 175–193). New York:Annals of the New York Academy of Sciences.
STERN, K., & MCCLINTOCK, M. (1998). Regulation of ovu-lation by human pheromones. Nature, 392, 177–179.
STERN, P. C., & CARSTENSEN, L. L. (2000). The aging mind.Washington, DC: National Academy Press.
STERNBERG, R. J. (1977). Intelligence, information processing,and analogical reasoning: The componential analysis ofhuman abilities. Hillsdale, NJ: Erlbaum.
STERNBERG, R. J. (1985). General intellectual ability. In R.Sternberg (Ed.), Human abilities: An information processingapproach. New York: Freeman.
STERNBERG, R. J. (1986). A triangular theory of love.Psychological Review, 93, 119–135.
STERNBERG, R. J. (1988). Triangulating love. In R. J.Sternberg & M. L. Barnes (Eds.), The psychology of love(pp. 119–138). New Haven, CT: Yale University Press.
STERNBERG, R. J. (1990). Metaphors of mind. New York:Cambridge University Press.
STERNBERG, R. J. (2000). The holey grail of general intel-ligence. Science, 289, 399–401.
STERNBERG, R. J. (2003). Our research program validatingthe triarchic theory of successful intelligence: Reply toGottfredson. Intelligence, 31, 399–413.
STERNBERG, R. J. (2004). Culture and intelligence.American Psychologist, 59, 325–338.
STERNBERG, R. J., & DAVIDSON, J. E. (1983). Insight in thegifted. Educational Psychologist, 18, 51–57.
STERNBERG, R. J., & DESS, N. K. (Eds.). (2001). Creativityfor the new millenium. American Psychologist, 56(4),332–362.
STERNBERG, R., & GRIGORENKO, E. L. (2007). The diffi-culty of escaping preconceptions in writing an articleabout the difficult of escaping preconceptions:Commentary on Hunt & Carlson (2007). Perspective onPsychological Science, 2, 221–223.
STERNBERG, R. J., & KAUFMAN, J. C. (1998). Human abili-ties. Annual Review of Psychology, 49, 479–502.
STERNBERG, R. J., & WAGNER, R. K. (1993). The egocentricview of intelligence and job performance is wrong.Current Directions in Psychological Science, 2, 1–5.
STERNBERG, R. J., WAGNER, R. K., WILLIAMS, W. M., &HORVATH, J. A. (1995). Testing common sense. AmericanPsychologist, 50, 912–927.
STEVENS, A., & COUPE, P. (1978). Distortions in judgedspatial relations. Cognitive Psychology, 10, 422–437.
STEVENS, L., & JONES, E. E. (1976). Defensive attributionsand the Kelley cube. Journal of Personality and SocialPsychology, 34, 809–820.
STEVENS, S. S. (1955). The measurement of loudness.Journal of the Acoustical Society of America, 27, 815–819.
STEWART, T. D. (1957). Stone age surgery: A generalreview, with emphasis on the New World. Annual Reviewof the Smithsonian Institution. Washington, DC:Smithsonian Institution.
STICKGOLD, R. (2005). Why we dream. In M. H. Kryger, T.Roth, & W. C. Dement (Eds.), Principles and practice ofsleep medicine. Philadelphia: Elsevier Saunders.
STICKGOLD, R., WHIDBEE, D., SCHIRMER, B., PATEL, V., &HOBSON J. A. (2000). Visual discrimination taskimprovement: A multi-step process occurring duringsleep. Journal of Cognitive Neuroscience, 12, 246–254.
STOKOE, W. C., JR. (1960). Sign language structure: Anoutline of the visual communication systems. Studies inLinguistics, Occasional Papers 8.
STOLZ, J. A., & BESNER, D. (1999). On the myth of auto-matic semantic activation in reading. Current Directions inPsychological Science, 8(2), 61–65.
STOOLMILLER, M. (2001). Synergistic interaction of childmanageability problems and parent-discipline tactics inpredicting future growth in externalizing behavior forboys. Developmental Psychology, 37(6), 814–825.
STORMS, M. D. (1973). Videotape and the attributionprocess: Reversing actors’ and observers’ points of view.Journal of Personality and Social Psychology, 27, 165–175.
STOWE, L. (1987). Thematic structures and sentence com-prehension. In G. Carlson & M. Tanenhaus (Eds.),Linguistic structure in language processing. Dordrecht:Reidel.
STRACK, F., MARTIN, L. L., & STEPPER, S. (1988). Inhibitingand facilitating conditions of the human smile: A nonob-trusive test of the facial feedback hypothesis. Journal ofPersonality and Social Psychology, 54, 768–777.
STRIANO T., & REID, V. M. (2006). Social cognition in thefirst year. Trends in Cognitive Sciences, 10(10), 471–476.
STRIANO, T., & ROCHAT, P. (2000). Emergence of selectivesocial referencing in infancy. Infancy, 1(2), 253–264.
STRICKER, E. M., & ZIGMOND, M. J. (1976). Recovery offunction after damage to catecholamine-containing neu-rons: A neurochemical model for the lateral hypothalamicsyndrome. In J. M. Sprague & A. N. Epstein (Eds.),Progress in psychobiology and physiological psychology: Vol. 6(pp. 121–188). New York: Academic Press.
STRIEGEL-MOORE, R. H., DOHM, F. A., KRAEMER, H. C.,TAYLOR, C. B., DANIELS, S., CRAWFORD, P. B., ET AL. (2003).Eating disorders in White and Black women. AmericanJournal of Psychiatry, 160, 1326–1331.
STROBER, M., FREEMAN, R., LAMPERT, C., DIAMOND, J., &KAYE, W. (2000). A controlled family study of anorexianervosa and bulimia nervosa: Evidence of shared liabilityand transmission of partial syndromes. American Journalof Psychiatry, 157, 393–401.
STROOP, J. R. (1935). Studies of interference in serial ver-bal reactions. Journal of Experimental Psychology, 18,643–662.
STUMPF, H., & STANLEY, J. C. (1998). Stability and changein gender-related differences on the College BoardAdvanced Placement and Achievement tests. CurrentDirections in Psychological Science, 7, 192–198.
STUSS, D. T., & LEVINE, B. (2002). Adult clinical neu-ropsychology: Lessons from studies of the frontal lobes.Annual Review of Psychology, 53, 401–433.
STYRON, W. (1990). Darkness visible: A memoir of madness.New York: Random House.
SUE S. (1998). In search of cultural competence in psy-chotherapy and counseling. American Psychologist, 53,440–448.
SUE, D. W., & KIRK, B. A. (1973). Psychological character-istics of Chinese-American college students. Journal ofCounseling Psychology, 19,142–148.
SUE, S., & LAM, A.G. (2002). Cultural and demographicdiversity. In J.C. Norcross (Ed.), Psychotherapy:Relationships that work (pp. 401–422). New York: OxfordUniversity Press.
SUGRUE, K., & HAYNE, H. (2006). False memories pro-duced by children and adults in the DRM paradigm.Applied Cognitive Psychology, 20, 625–631.
SULLIVAN, P. F., KENDLER, K. S., & NEALE, M. C. (2003).Schizophrenia as a complex trait: Evidence from a meta-analysis of twin studies. Archives of General Psychiatry, 60,1187–1192.
SULLIVAN, P. F., NEALE, M. C., & KENDLER, K. S. (2000).Genetic epidemiology of major depression: Review andmeta-analysis. American Journal of Psychiatry, 157,1552–1562.
SULLOWAY, F. (1996). Born to rebel. New York: PantheonBooks.
SULLOWAY, F. J. (1979). Freud, biologist of the mind: Beyondthe psychoanalytic legend. Cambridge, MA: HarvardUniversity Press.
SULS, J. M. (1972). A two-stage model for the appreciationof jokes and cartoons: An information processing analy-sis. In J. H. Goldstein & P. E. McGhee (Eds.), The psychol-ogy of humor (pp. 81–100). New York: Academic Press.
SULS, J. M. (1983). Cognitive processes in humor appreci-ation. In P. E. McGhee & J. H. Goldstein (Eds.), Handbookof humor research: Vol. 1 (pp. 39–58). New York: Springer.
SULS, J. M., & MILLER, R. L. (EDS.). (1977). Social compari-son processes: Theoretical and empirical perspectives. NewYork: Washington Hemisphere.
SUNDET, J., ERIKSEN, W., & TAMBS, K. (2008). Intelligencecorrelations between brothers decrease with increasingage difference: Evidence for shared environmental effectsin young adults. Psychological Science, 19, 843–847.
SUPALLA, I., & NEWPORT, E. L. (1978). How many seats ina chair? The derivation of nouns and verbs in AmericanSign Language. In P. Siple (Ed.), Understanding languagethrough sign language research. New York: Academic Press.
SUPER, C. M. (1976). Environmental effects on motordevelopment: A case of African infant precocity.Developmental Medicine and Child Neurology, 18, 561–567.
SUR, M., & RUBENSTEIN, J. L. R. (2005). Patterning andplasticity of the cerebral cortex. Science, 310, 805–810.
SURIAN, L., CALDI, S., & SPERBER, D. (2007). Attributionof beliefs by 13-month-old infants. Psychological Science,18(7), 580–586.
SUROWIECKI, J. (2004). The wisdom of crowds. New York:Doubleday.
SUSMAN, E. J., DORN, L. D., & SCHIEFELBEIN, V. L. (2003).Puberty, sexuality, and health. In R. M. Lerner, M. A.Easterbrooks, & J. Mistry (Eds.), Handbook of psychology,Vol 6: Developmental psychology. New York: Wiley.
SUSSKIND, J. M., LEE, D. H., CUSI, A., FEIMAN, R., GRABSKI,W., ANDERSON, A. K., ET AL. (2008). Expressing fearenhances sensory acquisition. Nature Neuroscience, 11,843–850.

PREFERENCESO R59
SUTCLIFFE, J. S. (2008). Insights into the pathogenesis ofautism. Science, 321(5886), 208–209.
SUTKER, P. B., ALLAIN, A. N., JR., & WINSTEAD, D. K. (1993).Psychopathology and psychiatric diagnoses of WorldWar II Pacific Theater prisoner of war survivors and com-bat veterans. American Journal of Psychiatry, 150, 240–245.
SWANN, W. B., JR., RENTFROW, P. J., & GUINN, J. (2002).Self-verification: The search for coherence. In M. Learyand J. Tagney (Eds.), Handbook of self and identity. NewYork: Guilford.
SWEDO, S. E., PIETRINI, P., LEONARD, H. L., SCHAPIRO, M.B., RETTEW, D. C., GOLDBERGER, E. L., ET AL. (1992).Cerebral glucose metabolism in childhood-onset obses-sive-compulsive disorder. Revisualization during phar-macotherapy. Archives of General Psychiatry, 49, 690–694.
SWETS, J. A., DAWES, R. M., & MONAHAN, J. (2000).Psychological Science can improve diagnostic decisions.Psychological Science in the Public Interest, 1, 1–26.
SWINGLEY, D., & FERNALD, A. (2002). Recognition ofwords referring to present and absent objects by 24-month-olds. Journal of Memory and Language, 46, 39–56.
SYMONS, D. (1979). The evolution of human sexuality. NewYork: Oxford University Press.
TAJFEL, H., & BILLIG, M. (1974). Familiarity and catego-rization in intergroup behavior. Journal of ExperimentalSocial Psychology, 10, 159–170.
TAJFEL, H., BILLIG, M., BUNDY, R., & FLAMENT, C. (1971).Social categorization and intergroup behaviour. EuropeanJournal of Social Psychology, 1, 149–178.
TAKAHASHI, K. (1986). Examining the Strange-Situationprocedure with Japanese mothers and 12-month-oldinfants. Developmental Psychology, 22, 265–270.
TAKATA, T. (1987). Self-deprecative tendencies in self-evaluation through social comparison. Japanese Journal ofExperimental Social Psychology, 27, 27–36.
TALMI, D. GRADY, C. L., GOSHEN-GOTTSTEIN, Y., &MOSCOVITCH, M. (2005). Neuroimaging the serial posi-tion curve: A test of single-store versus dual-store mod-els. Psychological Science, 16, 716–723.
TAN, H. Y., SUST, S., BUCKHOLTZ, J. W., MATAY, V. S., MEYER-LINDENBERG, A., EGAN, M. F., ET AL. (2006). Dysfunctionalprefrontal region specialization and compensation inschizophrenia. American Journal of Psychiatry, 163,1969–1977.
TANDON, R., & KANE, J. M. (1993). Neuropharmacologicbasis for clozapine’s unique profile [Letter]. Archives ofGeneral Psychiatry, 50, 158–159.
TANENHAUS, M. K., SPIVEY-KNOWLTON, M. J., EBERHARD, K.M., & SEDIVY, J. C. (1995). Integration of visual and lin-guistic information in spoken language comprehension.Science, 268(5217), 1632–1634.
TANENHAUS, M. K., & TRUESWELL, J. C. (2006). Eye move-ments and spoken language comprehension. In M. J.Traxler & M. A. Gernsbacher (Eds.), Handbook of psy-cholinguistics (2nd ed.). Amsterdam: Elsevier.
TANGNEY, J. P., BAUMEISTER, R. F., & BOONE, A. L. (2004).High self-control predicts good adjustment, less pathol-ogy, better grades, and interpersonal success. Journal ofPersonality, 72, 271–324.
TANNER, J. M. (1990). Fetus into man: Physical growth fromconception to maturity (rev. ed.). Cambridge, MA: HarvardUniversity Press.
TANNOCK, R. (1998). Attention deficit hyperactivity dis-order: Advances in cognitive, neurobiological and geneticresearch. Journal of Child Psychology and Psychiatry, 39,65–99.
TARBOX, S., & POGUE-GEILE, M. F. (2008). Developmentof social functioning in preschizophrenia children andadolescents: A systematic review. Psychological Bulletin,34(4), 561–583.
TARR, M. J. (1995). Rotating objects to recognize them: Acase study on the role of viewpoint dependency in therecognition of three-dimensional objects. PsychonomicBulletin & Review, 2, 55–82.
TAYLOR, M., ESBENSEN, B. M., & BENNETT, R. T. (1994).Children’s understanding of knowledge acquisition: Thetendency for children to report that they have alwaysknown what they have just learned. Child Development,65(6), 1581–1604.
TAYLOR, S. E. (2006). Tend and befriend: Biobehavioralbases of affiliation under stress. Current Directions inPsychological Science, 15(6), 273–277.
TAYLOR, S. E., & FISKE, S. T. (1975). Point of view and per-ceptions of causality. Journal of Personality and SocialPsychology, 32, 439–445.
TAYLOR, S. E., KLEIN, L. C., LEWIS, B. P., GRUENEWALD, T. L.,GURUNG, R.A.R., & UPDEGRAFF, J. A. (2000).Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107(3),411–429.
TAYLOR, W. S., & MARTIN, M. F. (1944). Multiple person-ality. Journal of Abnormal and Social Psychology, 39,281–300.
TEITELBAUM, P., & EPSTEIN, A. N. (1962). The lateral hypo-thalamic syndrome: Recovery of feeding and drinkingafter lateral hypothalamic lesions. Psychological Review,69, 74–90.
TELLEGEN, A. & ATKINSON, G. (1974). Openness toabsorbing and self-altering experiences (“absorption”), atrait related to hypnotic susceptibility. Journal ofAbnormal Psychology, 83, 268–277.
TELLEGEN, A., LYKKEN, D. T., BOUCHARD, T. J., WILCOX, K. J.,SEGAL, N. L., & RICH, S. (1988). Personality of twinsreared apart and together. Journal of Personality and SocialPsychology, 54, 1031–1039.
TERR, L. C. (1991). Acute responses to external events andposttraumatic stress disorders. In M. Lewis (Ed.), Childand adolescent psychiatry: A comprehensive textbook (pp.755–763). Baltimore: Williams & Wilkins.
TERR, L. C. (1994). Unchained memories: True stories oftraumatic memories, lost and found. New York: Basic.
TERRY, R., & COIE, J. D. (1991). A comparison of methodsfor defining sociometric status among children.Developmental Psychology, 27(5), 867–880.
TERVOORT, B. T. (1961). Esoteric symbolism in the com-munication behavior of young deaf children. AmericanAnnals of the Deaf, 106, 436–480.
TESSER, A., CAMPBELL, J., & SMITH, M. (1984). Friendshipchoice and performance: Self-evaluation maintenance in
children. Journal of Personality and Social Psychology, 46,561–574.
TETLOCK, P. E., PETERSON, R. S., MCGUIRE, C., CHANG, S.-J., ET AL. (1992). Assessing political group dynamics: Atest of the groupthink model. Journal of Personality andSocial Psychology, 63(3), 403–425.
THAPAR, A., & GREENE, R. (1994). Effects of level of pro-cessing on implicit and explicit tasks. Journal ofExperimental Psychology: Learning, Memory and Cognition,20, 671–679.
THARA, R. (2004). Twenty-year course of schizophrenia:The Madras Longitudinal Study. Canadian Journal ofPsychiatry, 49, 564–569.
THELEN, E., SCHÖNER, G., SCHIER, C., & SMITH, L. B.(2001). The dynamics of embodiment: A field theory ofinfant perseverative reaching. Behavioral & Brain Sciences,24, 34–86.
THEWISSEN, J.G.M., COOPER, L. N., CLEMENTS, M. T.,BAJPAI, S., & TIWARI, B. N. (2009). Hippopotamus andwhale phylogeny: Reply. Nature, 458, E5.
THIOUX, M., STARK, D. E., KLAIMAN, C., & SCHULTZ, R. T.(2006). The day of the week when you were born in 700ms: Calendar computation in an autistic savant. Journalof Experimental Psychology: Human Perception andPerformance, 32, 1155–1168.
THOMAS, A., & CHESS, S. (1977). Temperament and develop-ment. New York: Brunner/Mazel.
THOMAS, A., & CHESS, S. (1984). Genesis and evaluationof behavioral disorders: From infancy to early adult life.American Journal of Psychiatry, 141, 1–9.
THOMSEN, D. K., & BERNTSEN, D. (2009). The long-termimpact of emotionally stressful events on memory char-acteristics and life story. Applied Cognitive Psychology, 23,579–598.
THOMPSON, C. P., & COWAN, T. (1986). Flashbulb memo-ries: A nicer recollection of a Neisser recollection.Cognition, 22, 199–200.
THOMPSON, M. M., ZANNA, M. P., & GRIFFIN, D. W. (1995).Let’s not be indifferent about (attitudinal) ambivalence.In R. E. Petty & J. A. Krosnick (Eds.), Attitude strength:Antecedents and consequences: Vol. 4 (pp. 361–386).Mahwah, NJ: Erlbaum.
THOMPSON, R. A. (1994). Emotion regulation: A theme insearch of definition. In N. Fox (Ed.), The development ofemotion regulation and dysregulation: Biological and behav-ioral aspects. Monographs of the Society for Research in ChildDevelopment, 59(240), 25–52.
THOMPSON, R. A. (1998). Early sociopersonality develop-ment. In W. Damon (Ed.), Handbook of child psychology(5th ed.): Vol. 3. Social, emotional, and personality develop-ment (N. Eisenberg, Vol. Ed.; pp. 25–104). New York:Wiley.
THOMPSON, R. A. (1999). Early attachment and laterdevelopment. In J. Cassidy & P. Shaver (Eds.), Handbookof attachment (pp. 265–286). New York: Guilford.
THOMPSON, R. A. (2000). The legacy of early attach-ments. Child Development, 71, 145–152.
THOMPSON, R. A. (2006). The development of the per-son: Social understanding, relationships, self, con-science. In W. Damon & R. M. Lerner (Eds.), Handbook ofchild psychology (6th ed.): Vol. 3. Social, emotional, and

R60 PREFERENCESO
personality development (N. Eisenberg, Vol. Ed.). NewYork: Wiley.
THOMPSON, R. A., LAIBLE, D., & ONTAI, L. (2003). Earlyunderstanding of emotion, morality, and the self:Developing a working model. In R. Kail (Ed.), Advances inChild Development and Behavior: Vol. 31 (pp. 137–171). SanDiego: Academic.
THOMPSON, W. L., & KOSSLYN, S. M. (2000). Neural sys-tems activated during visual mental imagery: A reviewand meta-analyses. In J. Mazziotta & A. Toga (Eds.),Brain mapping II: The applications. New York: AcademicPress.
THORNHILL, R., & GANGESTAD, S. G. (1999). Facial attrac-tiveness. Trends in Cognitive Science, 3, 452–460.
TIERNEY, A. J. (2000). Egas Moniz and the origins of psy-chosurgery: A review commemorating the 50th anniver-sary of Moniz’s Nobel Prize. Journal of the History ofNeuroscience, 9, 22–36.
TIETJEN, A. M., & WALKER, L. J. (1985). Moral reasoningand leadership among men in a Papua New Guinea soci-ety. Developmental Psychology, 21, 982–989.
TIMBERLAKE, W. (1995). Reconceptualizing reinforce-ment: A causal system approach to reinforcement andbehavior change. In W. O’Donohue & L. Krasner (Eds.),Theories in behavior therapy (pp. 59–96). Washington,DC: APA Books.
TIMBERLAKE, W., & ALLISON, J. (1974). Response depriva-tion: An empirical approach to instrumental perform-ance. Psychological Review, 81, 146–164.
TODOROV, A., MANDISODZA, A., GOREN, A., & HALL, C.(2005). Inferences of competence from faces predictelection outcomes. Science, 308(5728), 1623–1626.
TOLIN, D. F., & FOA, E. B. (2006). Sex differences intrauma and posttraumatic stress disorder: A quantitativereview of 25 years of research. Psychological Bulletin,132(6), 959–992.
TOLMAN, E. C. (1932). Purposive behavior in animals andmen. New York: Appleton-Century-Crofts.
TOLMAN, E. C. (1948). Cognitive maps in rats and men.Psychological Review, 55, 189–208.
TOLMAN, E. C., & HONZIK, C. H. (1930). Introduction andremoval of reward, and maze performance in rats.University of California Publications in Psychology, 4,257–275.
TOLSTOY, L. (1868). War and peace (second epilogue). H.Gifford (Ed.), L. Maude & A. Maude (Trans.). New York:Oxford University Press, 1922.
TOMASELLO, M. (1994). Can an ape understand a sen-tence? A review of Language comprehension in ape and childby E. S. Savage-Rumbaugh et al. Language &Communication, 14, 377–390.
TOMASELLO, M. (2000). The cultural origins of human cog-nition. Cambridge, MA: Harvard University Press.
TOMASELLO, M. (2001). Perceiving intentions and learn-ing words in the second year of life. In M. Bowerman &S. Levinson (Eds.), Language acquisition and conceptualdevelopment. New York: Cambridge University Press.
TOMASELLO, M. (2002). The social bases of languageacquisition. Social Development, 1(1), 67–87.
TOMASELLO, M. (2003). Constructing a language.Cambridge, MA: Harvard University Press.
TOMASELLO, M. (2008). Origins of human communication.Cambridge, MA: MIT Press.
TOMASELLO, M., & FARRAR, M. J. (1986). Joint attentionand early language. Child Development, 57, 1454–1463.
TOMASELLO, M., KRUGER, A., & RATNER, H. (1993).Cultural learning. Behavioral and Brain Sciences, 16,495–552.
TOMASELLO, M., STROSBERG R., & AKHTAR, N. (1996).Eighteen month old children learn words in non-osten-sive contexts. Journal of Child Language, 23, 157–176.
TOMKINS, S. S. (1962). Affect, imagery, consciousness: Thepositive affects (Vol. 1). New York: Springer.
TOMKINS, S. S. (1963). Affect, imagery, consciousness: Vol. 2.The negative affects. New York: Springer.
TONG, F., NAKAYAMA, K., VAUGHAN, J. T., & KANWISHER, N.(1998). Binocular rivalry and visual awareness in humanextrastriate cortex. Neuron, 21, 753–759.
TONONI, G. (2004). An information integration theory ofconsciousness. BMC Neuroscience 5(42).
TOOBY, J., & COSMIDES, L. (1990). The past explains thepresent: Emotional adaptations and the structure ofancestral environments. Ethology and Sociobiology, 11,375–424.
TORGERSEN, S. (1986). Genetic factors in moderatelysevere and mild affective disorders. Archives of GeneralPsychiatry, 43, 222–226.
TORREY, E. F. (1983). Surviving schizophrenia: A family man-ual. New York: Harper & Row.
TORREY, E. F. (1992). Freudian fraud: The malignant effect ofFreud’s theory on American thought and culture. New York:HarperCollins.
TOURANGEAU, R., & ELLSWORTH, P. C. (1979). The role offacial response in the experience of emotion. Journal ofPersonality and Social Psychology, 37, 1519–1531.
TRACY, J. L., & ROBINS, R. W. (2008).The nonverbalexpression of pride: Evidence for cross-cultural recogni-tion. Journal of Personality and Social Psychology, 94(3),516–530.
TREISMAN, A. M. (1986a). Features and objects in visualprocessing. Scientific American, 255, 114–125.
TREISMAN, A. M. (1986b). Properties, parts, and objects.In K. R. Boff, L. Kaufman, & J. P. Thomas (Eds.),Handbook of perception and human performance: Vol. II(Chapter 35). New York: Wiley.
TREISMAN, A. M. (1988). Features and objects: TheFourteenth Barlett Memorial Lecture. Quarterly Journal ofExperimental Psychology, 40A, 201–237.
TREISMAN, A. M., & GELADE, G. (1980). A feature-integra-tion theory of attention. Cognitive Psychology, 12, 97–136.
TREISMAN, A. M., & SOUTHER, J. (1985). Search assymetry:A diagnostic for preattentive processing of separable fea-tures. Journal of Experimental Psychology: General, 114,285–310.
TREYNOR, W., GONZALEZ, R., & NOLEN-HOEKSEMA, S.(2003). Rumination reconsidered: A psychometric analy-sis. Cognitive Therapy and Research, 27(3), 247–259.
TRIANDIS, H. (1994). Major cultural syndromes and emo-tion. In S. Kitayama & H. R. Markus (Eds.), Emotion andculture (pp. 285–306). Washington, DC: AmericanPsychological Association.
TRIANDIS, H. C. (1989). Cross-cultural studies of individ-ualism and collectivism. Nebraska Symposium onMotivation, 37, 41–134. Lincoln: University of NebraskaPress.
TRIANDIS, H. C., & SUH, E. M. (2002). Cultural influenceson personality. Annual Review of Psychology, 53(1),133–160.
TRIMBLE, J. E. (1993). Cultural variations in the use ofalcohol and drugs. In W. Lonner & R. Malpass (Eds.),Readings in psychology and culture. Boston, MA: Allyn &Bacon.
TRIPLETT, N. (1898). The dynamogenic factors in pace-making and competition. American Journal of Psychology,9, 507–533.
TRIVERS, R. L. (1972). Parental investment and sexualselection. In B. Campbell (Ed.), Sexual selection and thedescent of man (pp. 139–179). Chicago: Aldine.
TROPP, L. R., & PETTIGREW, T. F. (2005). Relationshipsbetween intergroup contact and prejudice among minor-ity and majority status groups. Psychological Science, 16,951–957.
TRUE, W. R., RISE, J., EISEN, S., HEATH, A. C., GOLDBERG, J.,LYONS, M., ET AL. (1993). A twin study of genetic andenvironmental contributions to liability for posttrau-matic stress symptoms. Archives of General Psychiatry, 50,257–264.
TRUESWELL, J. C., SEKERINA, I., HILL, N. M., & LOGRIP, M. L.(1999). The kindergarten-path effect: Studying on-linesentence processing in young children. Cognition, 73(2),89–134.
TRUESWELL, J. C., & TANENHAUS, M. K. (1992). Consultingtemporal context during reading. In Proceedings of the 14thAnnual Conference of the Cognitive Science Society (pp.492–497). Hillsdale, NJ: Erlbaum.
TRUESWELL, J. C., & TANENHAUS, M. K. (1994). Toward alexicalist framework of constraint-based syntactic ambi-guity resolution. In C. Clifton, Jr., & L. Frazier (Eds.),Perspectives on sentence processing (pp. 155–179). Hillsdale,NJ: Erlbaum.
TRUESWELL, J. C., TANENHAUS, M. K., & GARNSEY, S. M.(1994). Semantic influences on parsing: Use of thematicrole information in syntactic ambiguity resolution.Journal of Memory and Language, 33, 285–318.
TSAI, J. L., & CHENTSOVA-DUTTON, Y. (2002). Differentmodels of cultural orientation in American- and over-seas-born Asian Americans. In K. Kurasaki, S. Okazaki, &S. Sue (Eds.), Asian American mental health: Assessment the-ories and methods (pp. 95–106). New York: KluwerAcademic/Plenum.
TSUANG, M. T., GILBERTSON, M. W., & FARAONE, S. V.(1991). The genetics of schizophrenia. SchizophreniaResearch, 4, 157–171.
TUCKER, M., & ELLIS, R. (2001). The potentiation of grasptypes during visual object categorization. VisualCognition, 8, 769–800.
TUCKER, M., & ELLIS, R. (2004). Action priming by brieflypresented objects. Acta Psychologica, 116, 185–203.

PREFERENCESO R61
TULVING, E. (1985). How many memory systems arethere? American Psychologist, 40, 385–398.
TULVING, E., & OSLER, S. (1968). Effectiveness ofretrieved cues in memory for words. Journal ofExperimental Psychology, 77, 593–606.
TULVING, E., SCHACTER, D. L., MCLACHLAN, D. R., &MOSCOVITCH, M. (1988). Priming of semantic autobio-graphical knowledge: A case study of retrograde amnesia.Brain and Cognition, 8, 3–20.
TULVING, E., SCHACTER, D. L., & STARK, H. A. (1982).Priming effects in word-fragment completion are inde-pendent of recognition memory. Journal of ExperimentalPsychology: Learning, Memory, and Cognition, 8, 336–342.
TULVING, E., & THOMSON, D. M. (1973). Encoding speci-ficity and retrieval processes in episodic memory.Psychological Review, 80, 352–373.
TUPES, E. C., & CHRISTAL, R. E. (1961, May). Recurrent per-sonality factors based on trait ratings (ASD-TR-61–97).Lackland Air Force Base, TX: Aeronautical SystemsDivision, Personnel Laboratory.
TURATI, C. (2004). Why faces are not special to new-borns: An alternative account of the face preference.Current Directions in Psychological Science, 13, 5–8.
TURKHEIMER, E., HALEY, A., WALDRON, M., D’ONOFRIO, B.,& GOTTESMAN, I. I. (2003). Socioeconomic status modi-fies heritability of IQ in young children. PsychologicalScience, 14, 623–628.
TURKHEIMER, E., & WALDRON, M. (2000). Nonsharedenvironment: A theoretical, methodological, and quanti-tative review. Psychological Bulletin, 126(1), 78–108.
TURNER, J., BROWN, R., & TAJFEL, H. (1979). Social com-parison and group interest in ingroup favouritism.European Journal of Social Psychology, 9, 187–204.
TVERSKY, A. (1977). Features of similarity. PsychologicalReview, 84(4), 327–352.
TVERSKY, A., & KAHNEMAN, D. (1973). Availability: Aheuristic for judging frequency and probability. CognitivePsychology, 5, 207–232.
TVERSKY, A., & KAHNEMAN, D. (1981). The framing of deci-sions and the psychology of choice. Science, 211, 453–458.
TWENEY, R. D., DOHERTY, M. E., & MYNATT, C. R. (1981).On scientific thinking. New York: Columbia UniversityPress.
TYACK, P. (2000). Functional aspects of cetacean com-munication. In J. Mann, R. C. Connor, P. L. Tyack, & H.Whitehead (Eds.), Cetacean societies (pp. 270–307).Chicago: University of Chicago Press.
TYLER, L. K., BRIGHT, P., FLETCHER, P., & STAMATAKIS, E. A.(2004). Neural processing of nouns and verbs: The roleof inflectional morphology. Neuropsychologia, 42(4),512–523.
UNGERLEIDER, L. G., & HAXBY, J. V. (1994). “What” and“where” in the human brain. Current Opinions inNeurobiology, 4, 157–165.
UNGERLEIDER, L. G., & MISHKIN, M. (1982). Two corticalvisual systems. In D. J. Ingle, M. A. Goodale, & R. J. W.Mansfield (Eds.), Analysis of visual behavior(pp. 549–586). Cambridge, MA: MIT Press.
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES.(1999). Mental health: A report of the surgeon general.Rockville, MD: Author.
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES.(2001). Mental health: Culture, race, and ethnicity—A sup-plement to mental health: A report of the Surgeon General.Rockville, MD: U.S. Department of Health and HumanServices, Public Health Service, Office of the SurgeonGeneral.
U.S. DEPARTMENT OF LABOR. (1995). Marital and familycharacteristics of the labor force from the March 1994 CurrentPopulation Survey. Washington, DC: Bureau of LaborStatistics.
URBERG, K. A., DEGIRMENCIOGLU, S. M., & PILGRIM, C.(1997). Close friend and group influence on adolescentcigarette smoking and alcohol use. DevelopmentalPsychology, 33(5), 834–844.
URWIN, C. (1983). Dialogue and cognitive functioning inthe early language development of three blind children.In A. E. Mills (Ed.), Language acquisition in the blind child.London: Croom Helm.
VAILLANT, G. E. (1974). Natural history of male psycho-logical health: II. Some antecedents of healthy adultadjustment. Archives of General Psychiatry, 31, 15–22.
VAILLANT, G. E. (1976). Natural history of male psycho-logical health: V: Relation of choice of ego mechanisms ofdefense to adult adjustment. Archives of GeneralPsychiatry, 33, 535–545.
VAILLANT, G. E. (1977). Adaptation to life. Boston: Little,Brown.
VAILLANT, G. E. (1994). “Successful aging” and psychoso-cial well-being: Evidence from a 45-year study. In E. H.Thompson (Ed.), Older men’s lives: Vol. 6. Research on menand masculinities (pp. 2–41). Thousand Oaks, CA: Sage.
VAILLANT, G. E., BOND, M., & VAILLANT, C. O. (1986). Anempirically validated hierarchy of defense mechanisms.Archives of General Psychiatry, 43, 786–794.
VALENSTEIN, E. S. (1986). Great and desperate cures. NewYork: Basic Books.
VALENZUELA, M. (1990). Attachment in chronicallyunderweight young children. Child Development, 61,1984–1996.
VALENZUELA, M. (1997). Maternal sensitivity in a develop-ing society: The context of urban poverty and infantchronic undernutrition. Developmental Psychology, 33,845–855.
VAN DE VLIERT, E. (2006). Autocratic leadership aroundthe globe: Do climate and wealth drive leadership cul-ture? Journal of Cross-Cultural Psychology, 37(1), 42–59.
VAN DER LELY, H. K., & CHRISTIAN, V. (2000). Lexical wordformation in Grammatical SLI children: A grammar-spe-cific or input processing deficit? Cognition, 75, 33–63.
VAN ESSEN, D. C., & DEYOE, E. A. (1995). Concurrent pro-cessing in the primate visual cortex. In M. S. Gazzaniga(Ed.), The cognitive neurosciences (pp. 383–400).Cambridge, MA: MIT Press.
VAN GEERT, P. (2002). Developmental dynamics, inten-tional action, and fuzzy sets. In N. Granott & J. Parziale
(Eds.), Microdevelopment: Transition processes in develop-ment and learning. New York: Cambridge University Press.
VAN GOOZEN, S., COHEN-KETTENIS, P., GOOREN, L., FRIJDA,N., & VAN DE POLL, N. (1995). Gender differences inbehavior: Activating cross-sex hormones. Psycho-neuroendocrinology, 20, 343–363.
VAN IJZENDOORN, M. (1997). Attachment, emergentmorality and aggression: Toward a developmental socioe-motional model of antisocial behaviour. InternationalJournal of Behavioral Development, 21, 703–727.
VAN IJZENDOORN, M., SCHUENGEL, C., & BAKERMANS-KRANENBURG, M. (1999). Disorganized attachment inearly childhood: Meta-analysis of precursors, concomi-tants, and sequelae. Development and Psychopathology, 11,225–249.
VAN SICKLE, M., DUNCAN, M., KINGSLEY, P., MOUIHATE, A.,URBANI, P., MACKIE, K., ET AL. (2005). Identification andfunctional characterization of brainstem cannabinoidCB2 receptors. Science, 310, 329–332.
VANDELL, D. L. (2000). Parents, peer groups, and othersocializing influences. Developmental Psychology, 36(6),699–710.
VANDELL, D. L., HENDERSON, V. K., & WILSON, K. S.(1988). A longitudinal study of children with day careexperiences of varying quality. Child Development, 59,1286–1292.
VAUGHN, B. E., EGELAND, B. R., SROUFE, L. A., & WATERS,E. (1979). Individual differences in infant-motherattachment at twelve and eighteen months: Stability andchange in families under stress. Child Development, 50,971–975.
VAULTIN, R. G., & BERKELEY, M. A. (1977). Responses ofsingle cells in cat visual cortex to prolonged stimulusmovement: Neural correlates of visual aftereffects. Journalof Neurophysiology, 40, 1051–1065.
VEIZOVIC, T., BEECH, J. S., STROEMER, R. P., WATSON, W. P.,& HODGES, H. (2001). Resolution of stroke deficits fol-lowing contralateral grafts of conditionally immortalneuroepithelial stem cells. Stroke, 32, 1012–1019.
VENTER, J. C., ADAMS, M. D., MYERS, E. W., LI, P. W.,MURAL, R. J., SUTTON, G. G., ET AL. (2001). The sequenceof the human genome. Science, 291, 1304–1351.
VERHAEGHEN, P., & SALTHOUSE, T. A. (1997). Meta-analy-ses of age-cognition relations in adulthood: Estimates oflinear and nonlinear age effects and structural models.Psychological Bulletin, 122(3), 231–249.
VERKHRATSKY, A. (1998). Calcium signalling in glial cells.Journal of Physiology, 506, 15.
VERNON, P. A. (ED.). (1987). Speed of information processingand intelligence. Canada: Ablex.
VICKERS, J. C., DICKSON, T. C., ADLARD, P. A., & SAUNDERS,H. L. (2000). The causes of neural degeneration inAlzheimer’s disease. Neurobiology, 60, 139–165.
VISSER, B., ASHTON, M., & VERNON, P. (2006). Beyond“g”: Putting multiple intelligences theory to the test.Intelligence, 34, 487–502.
VITEVITCH, M. S. (2003). Change deafness: The inabilityto detect changes between two voices. Journal ofExperimental Psychology: Human Perception andPerformance, 29, 333–342.

R62 PREFERENCESO
VOLKMAR, F. R., SZATMARI, P., & SPARROW, S. S. (1993). Sexdifferences in pervasive developmental disorders. Journalof Autism and Developmental Disorders, 23, 579–591.
VONDRA, J., SHAW, D., SWEARINGEN, L., COHEN, M., &OWENS, E. (2001). Attachment stability and emotionaland behavioral regulation from infancy to preschool age.Development and Psychopathology, 13, 13–33.
VRIJ, A. (2002). Deception in children: A literature reviewand implications for children’s testimony. In H. Westcott,G. Davies, & R. Bull (Eds.), Children’s testimony: A hand-book of psychological research and forensic practice (pp.175–194). New York: Wiley.
VUL, E., & PASHLER, H. (2007). Incubation benefits onlyafter people have been misdirected. Memory andCognition, 35, 701–710.
VUONG, Q. C., & TARR, M. J. (2004). Rotation directionaffects object recognition. Vision Research, 44, 1717–1730.
VYGOTSKY, L. S. (1978). Mind in society. Cambridge, MA:Harvard University Press.
WACHTEL, P. L. (1977). Psychoanalysis and behavior therapy:Toward an integration. New York: Basic Books.
WACHTEL, P. L. (1982). What can dynamic therapies con-tribute to behavior therapy? Behavior Therapy, 13,594–609.
WADDINGTON, J. L., TORREY, E. F., CROW, T. J., & HIRSCH, S.R. (1991). Schizophrenia, neurodevelopment, and dis-ease. Archives of General Psychiatry, 48, 271–273.
WAGNER, A. D., KOUTSTAAL, W., & SCHACTER, D. L. (1999).When encoding yields remembering: Insights fromevent-related neuroimaging. Philosophical Transactions ofthe Royal Society of London, Biology, 354, 1307–1324.
WAGNER, A. D., SCHACTER, D. L., ROTTE, M., KOUTSTAAL,W., MARIL, A., DALE, A., ET AL. (1998). Building memories:Remembering and forgetting of verbal experiences aspredicted by brain activity. Science, 281, 1188–1191.
WAGNER, A. D., SHANNON, B. J., KAHN, I., & BUCKNER, R.(2005). Parietal lobe contributions to episodic memoryretrieval. Trends in Cognitive Science, 9, 445–453.
WAGNER, R. K. (1987). Tacit knowledge in everyday intel-ligent behavior. Journal of Personality and Social Psychology,52, 1236–1247.
WAGNER, R. K. (2000). Practical intelligence. In R. J.Sternberg (Ed.), Handbook of human intelligence (pp.380–395). New York: Cambridge University Press.
WAGNER, R. K., & STERNBERG, R. J. (1987). Tacit knowl-edge in managerial success. Journal of Business andPsychology, 1, 301–312.
WAKEFIELD, J. C. (1992). The concept of mental disorder:On the boundary between biological facts and social val-ues. American Psychologist, 47(3), 373–388.
WALKER, E., GRIMES, K. E., DAVIS, D. M., & SMITH, A. J.(1993). Childhood precursors of schizophrenia: Facialexpressions of emotion. American Journal of Psychiatry,150, 1654–1660.
WALKER, E., KESTLER, L., BOLLINI, A., & HOCHMAN, K.(2004). Schizophrenia: Etiology and course. AnnualReview of Psychology, 55, 401–430.
WALKER, E., SAVOIE, T., & DAVIS, D. (1994). Neuromotorprecursors of schizophrenia. Schizophrenia Bulletin, 20,441–452.
WALKER, L. J. (1984). Sex differences in the developmentof moral reasoning: A critical review. Child Development,55, 677–691.
WALKER, L. J. (1989). Sex differences in the developmentof moral reasoning: A reply to Baumrind. ChildDevelopment, 57, 522–526.
WALKER, L. J. (1995). Sexism in Kohlberg’s moral psychol-ogy. In W. M. Kurtines & J. L. Gewirtz (Eds.), Moral devel-opment: An introduction. Boston: Allyn & Bacon.
WALKER, L. J., & MORAN, T. J. (1991). Moral reasoning ina communist Chinese society. Journal of Moral Education,20, 139–155.
WALKER, M. P., BRAKEFIELD, T., HOBSON, J. A., &STICKGOLD, R. (2003). Dissociable stages of humanmemory consolidation and reconsolidation. Nature, 425,616–620.
WALKUP, J. T., ALBANO, A., PIACENTINI, J., BIRMAHER, B.,COMPTON, S. N., SHERRILL, J. T., ET AL. (2008). Cognitivebehavioral therapy, sertraline, or a combination in child-hood anxiety. New England Journal of Medicine, 359,2753–2766.
WALLACE, J., SCHNEIDER, T., & MCGUFFIN, P. (2002).Genetics of depression. In I. Gotlib & C. Hammen(Eds.), Handbook of depression (pp. 169–191). New York:Guilford.
WALLACE, P. (1977). Individual discrimination of humansby odor. Physiology and Behavior, 19, 577–579.
WALLACE, R. L., GILBERT, J. J., & KING, C. E. (2001). Inmemoriam: WT Edmondson (1916–2000). Hydro-biologia, 446/447, xv–xxi.
WALLAS, G. (1926). The art of thought. New York:Harcourt, Brace.
WALLER, N. G., & ROSS, C. A. (1997). The prevalence andbiometric structure of pathological dissociation in thegeneral population: Taxometric and behavior geneticfindings. Journal of Abnormal Psychology, 106, 499–510.
WALSH, J. K., DEMENT, W. C., & DINGES, D. F. (2005).Sleep medicine, public policy, and public health. In M. H.Kryger, T. Roth, & W. C. Dement (Eds.), Principles andpractice of sleep medicine. Philadelphia: Elsevier Saunders.
WALSTER, E., ARONSON, E., & ABRAHAMS, D. (1966). Onincreasing the persuasiveness of a low prestige commu-nicator. Journal of Experimental Social Psychology, 2,325–342.
WALSTER, E., ARONSON, E., ABRAHAMS, D., & ROTTMAN, L.(1966). The importance of physical attractiveness in dat-ing behavior. Journal of Personality and Social Psychology, 4,508–516.
WAMPOLD, B. E., MONDIN, G. W., MOODY, M., STICH, F.,BENSON, K., & AHN, H. (1997). A meta-analysis of out-come studies comparing bona fide psychotherapies:Empirically, “all must have prizes.” Psychological Bulletin,122, 203–216.
WANG, P. S., BERGLUND, P., OLFSON, M., PINCUS, H. A.,WELLS, K. B., & KESSLER, R. C. (2005). Failure and delayin initial treatment contact after first onset of mental dis-orders in the National Comorbidity Survey Replication.Archives of General Psychiatry, 62(6): 603–613.
WANG, P. S., LANE, M., OLFSON, M., PINCUS, H. A., WELLS,K. B., & KESSLER, R. C. (2005). Twelve-month use ofmental health services in the United States: results fromthe National Comorbidity Survey Replication. Archives ofGeneral Psychiatry, 62(6): 629–640.
WAPNER, W. T., JUDD, T., & GARDNER, H. (1978). Visualagnosia in an artist. Cortex, 14, 343–364.
WARD, S. L., & OVERTON, W. F. (1990). Semantic familiar-ity, relevance, and the development of deductive reason-ing. Developmental Psychology, 26, 488–493.
WARREN, S. L., HUSTON, L., EGELAND, B., & SROUFE, L. A.(1997). Child and adolescent anxiety disorders and earlyattachment. Journal of the American Academy of Child &Adolescent Psychiatry, 36, 637–644.
WARRINGTON, E. K., & WEISKRANTZ, L. (1978). Furtheranalysis of the prior learning effect in amnesic patients.Neuropsychologia, 16, 169–176.
WASON, P. C. (1960). On the failure to eliminatehypotheses in a conceptual task. Quarterly Journal ofExperimental Psychology, 12, 129–140.
WASON, P. C. (1966). Reasoning. In B. Foss (Ed.), Newhorizons in psychology (pp. 135–151). Middlesex, England:Penguin.
WASON, P. C. (1968). On the failure to eliminate hypothe-ses—A second look. In P. C. Wason & P. N. Johnson-Laird (Eds.), Thinking and reasoning. Harmondsworth,England: Penguin.
WASSERMAN, E. A., HUGART, J. A., & KIRKPATRICK-STEGER,K. (1995). Pigeons show same-different conceptualiza-tion after training with complex visual stimuli. Journal ofExperimental Psychology: Animal Behavior Processes, 21,248–252.
WATERHOUSE, L., FEIN, D., & MODAHL, C. (1996).Neurofunctional mechanisms in autism. PsychologicalReview, 103, 457–489.
WATERS, E., & CUMMINGS, E. M. (2000). A secure basefrom which to explore close relationships. ChildDevelopment, 71(1), 164–172.
WATERS, E., MERRICK, S., TREBOUX, D., CROWELL, J., &ALBERSHEIM, L. (2000). Attachment security in infancyand early adulthood: A twenty-year longitudinal study.Child Development, 71, 684–689.
WATERS, E., WIPPMAN, J., & SROUFE, L. A. (1979).Attachment, positive affect, and competence in the peergroup: Two studies in construct validation. ChildDevelopment, 50, 821–829.
WATKINS, C. E., CAMPBELL, V. L., NIEBERDING, R., &HALLMARK, R. (1995). Contemporary practice of psycho-logical assessment by clinical psychologists. ProfessionalPsychology: Research and Practice, 26, 54–60.
WATKINS, M., WILSON, S., KOTZ, K., CARBONE, M., &BABULA, T. (2006). Factor structure of the WechslerIntelligence Scale for Children—Fourth edition amongreferred students. Educational and PsychologicalMeasurement, 66, 975–983.
WATSON, D., & CLARK, L. A. (1992). Affects separable andinseparable: On the hierarchical arrangement of the neg-ative affects. Journal of Personality and Social Psychology,62, 489–505.
WATSON, D., & CLARK, L. A. (1994). The vicissitudes ofmood: A schematic model. In P. Ekman and R. Davidson

PREFERENCESO R63
(Eds.), The nature of emotion: Fundamental questions(pp. 400–405). New York: Oxford University Press.
WATSON, J. B. (1925). Behaviorism. New York: Norton.
WATSON, J. B., & RAYNER, R. (1920). Conditioned emo-tional reactions. Journal of Experimental Psychology, 3,1–14.
WATSON, J. S. (1967). Memory and “contingency analy-sis” in infant learning. Merrill-Palmer Quarterly, 13,55–76.
WAUGH, N. C., & NORMAN, D. A. (1965). Primary memory.Psychological Review, 72, 89–104.
WEBB, W. B. (1972). Sleep deprivation: Total, partial, andselective. In M. H. Chase (Ed.), The sleeping brain(pp. 323–362). Los Angeles: Brain Information Service,Brain Research Institute.
WEBB, W. (1974). Sleep as an adaptive response.Perceptual and Motor Skills, 38 (3), 1023–1027.
WEBB, W. (1994). Sleep as a biological rhythm: A histori-cal review. Sleep, 17 (2), 188–194.
WECHSLER, D. (1958). The measurement and appraisal ofadult intelligence (4th ed.). Baltimore: Williams & Wilkins.
WECHSLER, D. (2003). Wechsler intelligence scale for chil-dren—Fourth edition. San Antonio, TX: PsychologicalCorporation.
WECHSLER, H., DAVENPORT, A., DOWDALL, G., MOEYKENS,B., & CASTILLO, S. (1994). Health and behavioral conse-quences of binge drinking in college: A national survey ofstudents at 140 campuses. Journal of the American MedicalAssociation, 272, 1672–1677.
WEEDEN, J., & SABINI, J. (2005). Physical attractivenessand health in Western societies: A review. PsychologicalBulletin, 131, 635–653.
WEEKS, J. W., HEIMBERG, R. G., RODEBAUGH, T. L., &NORTON, P. J. (2008). Exploring the relationship betweenfear of positive evaluation and social anxiety. Journal ofAnxiety Disorders, 22(3), 386–400.
WEGNER, D. M. (2002). The illusion of conscious will.Cambridge, MA: MIT Press.
WEINFIELD, N., SROUFE, L., & EGELAND, B. (2000).Attachment from infancy to early adulthood in a high-risk sample: Continuity, discontinuity, and their corre-lates. Child Development, 71, 695–702.
WEINGARTNER, H., & PARKER, E. S. (EDS.). (1984). Memoryconsolidation: Psychobiology of cognition. Hillsdale, NJ:Erlbaum.
WEISBERG, R. (1986). Creativity: Genius and other myths.New York: Freeman.
WEISKRANTZ, L. (1986). Blindsight: A case study and impli-cations. Oxford, England: Clarendon.
WEISKRANTZ, L. (1997). Consciousness lost and found. NewYork: Oxford University Press.
WEISKRANTZ, L., & WARRINGTON, E. K. (1979).Conditioning in amnesic patients. Neuropsychologia, 18,177–184.
WEISS, A., KING, J. E., & FIGUEREDO, A. J. (2000). The her-itability of personality factors in chimpanzees (Pantroglodytes). Behavior Genetics, 30, 213–221.
WEISS, L. H., & SCHWARZ, J. C. (1996). The relationshipbetween parenting types and older adolescents’ person-
ality, academic achievement, adjustment, and substanceuse. Child Development, 67, 2101–2114.
WEISS, Y., SIMONCELLI, E. P., & ADELSON, E. H. (2002).Motion illusions as optimal percepts. NatureNeuroscience, 5(6), 598–604.
WEISSMAN, M. M., & MARKOWITZ, J. C. (1994).Interpersonal psychotherapy: Current status. Archives ofGeneral Psychiatry, 51, 599–606.
WEISZ, J. R., DOSS, A., & HAWLEY, K. (2005). Youth psy-chotherapy outcome research: A review and critique ofthe evidence base. Annual Review of Psychology, 56,337–364.
WEISZ, J. R., DOSS, A. J., & HAWLEY, K. M. (2006).Evidence-based youth psychotherapies versus usual clin-ical care: A meta-analysis of direct comparisons. AmericanPsychologist, 61, 671–689.
WEISZ, J. R., HAWLEY, K., & DOSS, A. (2004). Empiricallytested psychotherapies for youth internalizing and exter-nalizing problems and disorders. Child and AdolescentPsychiatric Clinics of North America, 13, 729–815.
WELDON, M. S. (2001). Remembering as a social process.Psychology of Learning and Motivation, 40, 67–120.
WELLMAN, H., CROSS, D., & WATSON, J. (2001). Meta-analysis of theory-of-mind development: The truth aboutfalse belief. Child Development, 72, 655–684.
WELLMAN, H., & GELMAN, S. (1992). Cognitive develop-ment: Foundational theories of core domains. AnnualReview of Psychology, 43, 337–375.
WELLMAN, H., & LAGATUTTA, K. H. (2000). In S. Baron-Cohen, H. Tager-Flusberg, & D. J. Cohen (Eds.),Understanding other minds (pp. 21–49). New York: OxfordUniversity Press.
WELLMAN, H. M. (1990). The child’s theory of mind.Cambridge, MA: MIT Press.
WELLMAN, H. M., & BARTSCH, K. (1988). Young children’sreasoning about beliefs. Cognition, 30, 239–277.
WELLMAN, H. M., & WOOLEY, J. D. (1990). From simpledesires to ordinary beliefs: The early development ofeveryday psychology. Cognition, 35, 245–275.
WELLS, G., & OLSON, E. (2002). Eyewitness identifica-tion. Annual Review of Psychology, 54, 277–295.
WELLS, G. L., OLSON, E. A., & CHARMAN, S. D. (2002). Theconfidence of eyewitnesses in their identifications fromlineups. Current Directions in Psychological Science, 11,151–154.
WENDER, P. H., KETY, S. S., ROSENTHAL, D., SCHULSINGER,F., & ORTMANN, J. (1986). Psychiatric disorders in thebiological relatives of adopted individuals with affectivedisorders. Archives of General Psychiatry, 43, 923–929.
WEREBE, M. G., & BAUDONNIERE, P.-M. (1991). Social pre-tend play among friends and familiar preschoolers.International Journal of Behavioral Development, 14(4),411–428.
WERKER, J. (1991). The ontogeny of speech perception. InI. G. Mattingly & M. Studdert-Kennedy (Eds.),Modularity and the motor theory of speech perception:Proceedings of a conference to honor Alvin M. Liberman (pp.91–109). Hillsdale, NJ: Erlbaum.
WERKER, J. F. (1995). Exploring developmental changesin cross-language speech perception. In L. R. Gleitman &
M. Liberman (Eds.), An invitation to cognitive science: Vol. 1(pp. 87–106). Cambridge, MA: MIT Press.
WERKER, J. F., & TEES, R. C. (1984). Cross-languagespeech perception: Evidence for perceptual reorganiza-tion during the first year of life. Infant Behavior andDevelopment, 7, 49–63.
WERTHEIMER, M. (1912). Experimentelle Studien über dasGesehen von Bewegung. Zeitschrift frPsychologie, 61,161–265.
WERTHEIMER, M. (1923). Untersuchungen zur Lehre vonder Gestalt, II. Psychologische Forschung, 4, 301–350.
WEST, S. G., WHITNEY, G., & SCHNEDLER, R. (1975).Helping a motorist in distress: The effects of sex, race,and neighborhood. Journal of Personality and SocialPsychology, 31, 691–698.
WESTCOTT, H. L., DAVIES, G. M., & BULL, R. H. C. (Eds.).(2002). Children’s testimony: A handbook of psychologicalresearch and forensic practice. West Sussex, England:Wiley.
WESTEN, D. (1998). The scientific legacy of SigmundFreud: Toward a psychodynamically informed psycholog-ical science. Psychological Bulletin, 124, 333–371.
WESTEN, D., & BRADLEY, R. (2005). Empirically supportedcomplexity: Rethinking evidence-based practice in psy-chotherapy. Current Directions in Psychological Science, 14,266–271.
WESTEN, D., NOVOTNY, C., & THOMPSON-BRENNER, H.(2004). The empirical status of empirically supportedpsychotherapies: Assumptions, findings, and reportingin controlled clinical trials. Psychological Bulletin, 130,631–663.
WESTEN, D., & WEINBERGER, J. (2005). Clinical judgmentin science. American Psychologist, 60, 659–661.
WESTERMEYER, J. (1987). Public health and chronic men-tal illness. American Journal of Public Health, 77, 667–668.
WETHINGTON, E. (2000). Expecting stress: Americansand the “midlife crisis.” Motivation & Emotion, 24,85–103.
WHEELER, L. R. (1942). A comparative study of the intel-ligence of East Tennessee mountain children. Journal ofEducational Psychology, 33, 321–334.
WHITE, D. J., & GALEF, B. G. (1998). Social influence onavoidance of dangerous stimuli by rats. Animal Learningand Behavior, 26(4), 433–438.
WHITE, G. L. (1980). Physical attractiveness andcourtship progress. Journal of Personality and SocialPsychology, 39, 660–668.
WHITE, J. (1999). Overcoming generalized anxiety disor-der—client manual: A relaxation, cognitive restructuring, andexposure-based protocol for the treatment of GAD. Oakland,CA: New Harbinger.
WHORF, B. (1956). Language, thought, and reality: Selectedwritings of Benjamin Lee Whorf. New York: Wiley.
WICKELGREN, W. A. (1974). How to solve problems. SanFrancisco: Freeman.
WIDAMAN, K. F. (2009). Phenylketonuria in children andmothers: Genes, environments, behavior. CurrentDirections in Psychological Science, 18, 48–52.

R64 PREFERENCESO
WIDIGER, T. A., & CLARK, L. A. (2000). Toward DSM-Vand the classification of psychopathology. PsychologicalBulletin, 126, 946–963.
WIDIGER, T. A., & SANDERSON, C. J. (1995). Toward adimensional mode of personality disorders. In W. J.Livesley (Ed.), The DSM-IV personality disorders(pp. 433–458). New York: Guilford.
WIDIGER, T. A., & TRULL, T. J. (2007). Plate tectonics inthe classification of personality disorder: Shifting to adimensional model. American Psychologist, 62, 71–83.
WIEBE, R. P. (2004). Delinquent behavior and the FiveFactor model: Hiding in the adaptive landscape?Individual Differences Research, 2, 38–62.
WIENS, A. N., & MENUSTIK, C. E. (1983). Treatment out-come and patient characteristics in an aversion therapyprogram for alcoholism. American Psychologist, 38,1089–1096.
WIESENTHAL, D. L., ENDLER, N. S., COWARD, T. R., &EDWARDS, J. (1976). Reversibility of relative competenceas a determinant of conformity across different percep-tual tasks. Representative Research in Social Psychology, 7,319–342.
WILCOXIN, H. C., DRAGOIN, W. B., & KRAL, P. A. (1971).Illness-induced aversions in rat and quail: Relativesalience of visual and gustatory cues. Science, 171,826–828.
WILEY, J. L. (1999). Cannabis: Discrimination of “inter-nal bliss”? Pharmacology, Biochemistry, & Behavior, 64,257–260.
WILHELM, F. H., TRABERT, W., & ROTH, W. T. (2001).Physiologic instability in panic disorder and generalizedanxiety disorder. Biological Psychiatry, 49, 596–605.
WILLIAMS, G. C. (1966). Adaptation and natural selection.Princeton, NJ: Princeton University Press.
WILLIAMS, J. E., SATTERWHITE, R. C., & BEST, D. L. (1999).Pancultural gender stereotypes reivisited: The five factormodel. Sex Roles, 40(7–8), 513–525.
WILLIAMS, L. (1994). Recall of childhood trauma: Aprospective study of women’s memories of child sexualabuse. Journal of Consulting and Clinical Psychology, 62,1167–1176.
WILLIAMS, L. A., & DESTENO, D. (2009). Pride: Adaptivesocial emotion or seventh sin? Psychological Science, 20,284–288.
WILLIAMS, W. M., & CECI, S. J. (1997). Are Americansbecoming more or less alike? Trends in race, class, andability differences in intelligence. American Psychologist,52, 1226–1235.
WILLIAMS, H. L., TEPAS, D. I., & MORLOCK, J. H. C. (1962).Evoked responses to clicks and electroencephalographicstages of sleep in man. Science, 138, 685–686.
WILLIS, S. L., & REID, J. D. (EDS.). (1999). Life in the mid-dle: Psychological and social development in middle age. SanDiego: Academic Press.
WILSON, D. H., REEVES, A. G., GAZZANIGA, M. S., &CULVER, C. (1977). Cerebral commissurotomy for thecontrol of intractable seizures. Neurology, 27, 708–715.
WILSON, G. T. (1991). Chemical aversion conditioning inthe treatment of alcoholism: Further comments.Behaviour Research and Therapy, 29, 415–419.
WILSON, G. T. (1998). Manual-based treatment and clin-ical practice. Clinical Psychology: Science and Practice, 5,363–375.
WILSON, G. T., & FAIRBURN, C. G. (2002). Treatments foreating disorders. In P. E. Nathan & J. M. Gorman (Eds.),A guide to treatments that work (2nd ed., pp. 559–592).New York: Oxford University Press.
WILSON, G. T., & PIKE, K. M. (2001). Eating disorders. InD. H. Barlow (Ed.), Clinical handbook of psychological dis-orders (3rd ed., pp. 332–375). New York: Guilford.
WILSON, J. Q. (1997). Moral judgment: Does the abuseexcuse threaten our legal system? New York: Basic Books.
WILSON, T. D. (2002). Strangers to ourselves: Discoveringthe adaptive unconscious. Cambridge, MA: HarvardUniversity Press.
WILSON, T. D., & DUNN, E. (2004). Self-knowledge: Itslimits, value, and potential for improvement. AnnualReview of Psychology, 55, 493–518.
WILSON, T. D., WHEATLEY, T. P., MEYERS, J. M., GILBERT, D.T., & AXSOM, D. (2000). Focalism: A source of durabilitybias in affective forecasting. Journal of Personality andSocial Psychology, 78, 821–836.
WIMMER, H., & PERNER, J. (1983). Beliefs about beliefs:Representation and constraining function of wrongbeliefs in young children’s understanding of deception.Cognition, 13, 103–128.
WINNER, E. (2000). The origins and ends of giftedness.American Psychologist, 55(1), 159–169.
WINOGRAD, E., & NEISSER, U. (EDS.). (1993). Affect andaccuracy in recall: Studies of “flashbulb” memories. NewYork: Cambridge University Press.
WINTER, D. G. (1999). Linking personality and “scien-tific” psychology: The development of empirically derivedThematic Apperception Test measures. In L. Gieser & M.I. Stein (Eds.), Evocative images: The Thematic ApperceptionTest and the art of projection (pp. 107–124). Washington,DC: American Psychological Association.
WIRSHING, W. C., MARDER, S. R., VAN PUTTEN, T., & AMES,D. (1995). Acute treatment of schizophrenia. In F. E.Bloom & D. Kupfer (Eds.), Psychopharmacology: The fourthgeneration of progress (pp. 1259–1266). New York: Raven.
WITHERINGTON, D. C., CAMPOS, J. J., & HERTENSTEIN, M. J.(2001). Principles of emotion and its development ininfancy. In G. Bremner & A. Fogel (Eds.), Blackwell hand-book of infant development (pp. 427–464). Malden, MA:Blackwell Publishing.
WITTENBRINK, B., JUDD, C. M., & PARK, B. (1997).Evidence for racial prejudice at the implicit level and itsrelationship with questionnaire measures. Journal ofPersonality and Social Psychology, 72(2), 262–274.
WITTGENSTEIN, L. (1953). Philosophical investigations. G. E.M. Anscombe (Trans.). Oxford, England: Blackwell.
WIXTED, J. T. (2004). The psychology and neuroscience offorgetting. Annual Review of Psychology, 55, 235–269.
WOHL, J. (1989). Cross-cultural psychotherapy. In P. B.Pedersen, J. G. Draguns, W. J. Lonner, & J. E. Trimble(Eds.), Counseling across cultures (pp. 79–113). Honolulu:University of Hawaii.
WOICIECHOWSKY, C., VOGEL, S., MEYER, B. U., & LEHMANN,R. (1997). Neuropsychological and neurophysiological
consequences of partial callosotomy. Journal ofNeurosurgical Science, 41, 75–80.
WOLF, M. E., & MOSNAIM, A. D. (1990). Post-traumaticstress disorder: Etiology, phenomenology, and treatment.Washington, DC: American Psychiatric Press.
WOLFE, J. M. (2003). Moving towards solutions to someenduring controversies in visual search. Trends inCognitive Science, 7, 70–76.
WOLFE, J. M., & HOROWITZ, T. S. (2004). What attributesguide the deployment of visual attention and how dothey do it? Nature Reviews Neuroscience, 5, 1–7.
WOLFE, J., KLUENDER, K., & LEVI, D. (2006). Sensation andperception. Sunderland, MA: Sinauer Associates.
WOLLEN, K. A., WEBER, A., & LOWRY, D. (1972).Bizarreness versus interaction of mental images as deter-minants of learning. Cognitive Psychology, 3, 518–523.
WOLPE, J. (1958). Psychotherapy by reciprocal inhibition.Stanford, CA: Stanford University Press.
WOLPE, J. (1996). The practice of behavior therapy (4th ed.).New York: Pergamon Press.
WOLPE, J., & LAZARUS, A. A. (1966). Behavior therapy tech-niques: A guide to the treatment of neuroses. Elmsford, NY:Pergamon.
WOLPE, J., & PLAUD, J. J. (1997). Pavlov’s contributions tobehavior therapy: The obvious and the not so obvious.American Psychologist, 52, 966–972.
WOOD, A. J., & GOODWIN, G. M. (1987). A review of thebiochemical and neuropharmacological actions oflithium. Psychological Medicine, 17, 579–600.
WOOD, N., & COWAN, N. (1995). The cocktail party phe-nomenon revisited: How frequent are attention shifts toone’s name in an irrelevant auditory channel? Journal ofExperimental Psychology: Learning, Memory and Cognition,21, 255–260.
WOOD, W. (2000). Attitude change: Persuasion andsocial influence. Annual Review of Psychology, 51, 539–570.
WOOD, W., & EAGLY, A. H. (2002). A cross-cultural analy-sis of the behavior of women and men: Implications forthe origins of sex differences. Psychological Bulletin,128(5), 699–727.
WOODRUFF, P. W. R., WRIGHT, I. C., BULLMORE, E. T.,BRAMMER, M., HOWARD, R. J., WILLIAMS, S. C. R., ET AL.(1997). Auditory hallucinations and the temporal corticalresponse to speech in schizophrenia: A functional mag-netic resonance imaging study. American Journal ofPsychiatry, 154, 1676–1682.
WOODS, S. C., & RAMSAY, D. S. (2000). Pavlovian influ-ences over food and drug intake. Behavior and BrainResearch, 10, 175–182.
WOODWARD, A. L. (1998). Infants selectively encode thegoal object of an actor’s reach. Cognition, 69, 1–34.
WOODWARD, A. L. (2009). Infants’ grasp of others’intentions. Current Directions in Psychological Science, 18,53–57.
WOOLF, N. J. (1998). A structural basis for memory stor-age in mammals. Progress in Neurobiology, 55, 59–77.
WORLD FEDERATION FOR MENTAL HEALTH. (2005). Withoutboundaries—challenges and hopes for living with ADHD: Aninternational survey. Retrieved Aug. 19, 2009, fromLearning Disabilities Association of Alberta website,

PREFERENCESO R65
http://www.ldaa.ca/assets/pdfs/freeResources/ADHDWithoutBoundaries.pdf.
WORLD HEALTH ORGANIZATION (WHO). (1998). The worldhealth report 1998—Life in the 21st century: A vision for all.Geneva: Author.
WORLD HEALTH ORGANIZATION (WHO). (2001). Mentalhealth: New understanding, new hope. New York: Author.
WRIGHT, R. D., & WARD, L. M. (2008). Orienting of atten-tion. New York: Oxford University Press.
WRZESNIEWSKI, A., MCCAULEY, C. R., ROZIN, P., &SCHWARTZ, B. (1997). Jobs, careers, and callings: People’srelations to their work. Journal of Research in Personality,31, 21–33.
WU, X., HART, C., DRAPER, T., & OLSEN, J. (2001). Peer andteaching sociometrics for preschool children: Cross-informant concordance, temporal stability, and reliabil-ity. Merrill-Palmer Quarterly, 47, 416–443.
WYNN, K. (1992). Addition and subtraction by humaninfants. Nature, 358, 749–750.
WYNN, K. (1995). Infants possess a system of numericalknowledge. Current Directions in Psychological Science, 4,172–176.
XU, F. (2002). The role of language in acquiring objectconcepts in infancy. Cognition, 85, 223–250.
XU, F., & GARCIA, V. (2008). Intuitive statistics by 8-month-old infants. Proceedings of the National Academy ofSciences, 105, 5012–5015.
XU, F., & TENENBAUM, J. (2007). Word learning asBayesian inference. Psychological Review, 114(2), 245–272.
YAMAGATA, S., SUZUKI, A., ANDO, J., ONO, Y., KIJIMA, N.,YOSHIMURA, K., ET AL. (2006). Is the genetic structure ofhuman personality universal? A cross-cultural twin studyfrom North America, Europe, and Asia. Journal ofPersonality and Social Psychology, 80, 987–998.
YAN, L, DAVIGLUS, M., LIU, K., STAMLER, J., WANG, R.PIRZADA, A., ET AL. (2006). Midlife Body Mass Index andhospitalization and mortality in older age. Journal of theAmerican Medical Association, 295, 190–198.
YANG, S.-H., CHENG, P.-H., BANTA, H., PIOTROWSKA-NITSCHE, K., YANG, J.-J., CHENG, E. C. H., et al. (2008).Towards a transgenic model of Huntington's disease in anonhuman primate. Nature, 453, 921–924.
YANG, S.-Y., & STERNBERG, R. J. (1997). Taiwanese Chinesepeople’s conceptions of intelligence. Intelligence, 25,21–36.
YANIV, I., & MEYER, D. E. (1987). Activation and metacog-nition of inaccessible stored information: Potential basesfor incubation effects in problem solving. Journal ofExperimental Psychology: Learning, Memory, and Cognition,13, 187–205.
YARMEY, A. (1973). I recognize your face but I can’tremember your name: Further evidence on the tip-of-the-tongue phenomenon. Memory & Cognition, 1, 287–290.
YEHUDA, R. (1997). Sensitization of the hypothalamic-pituitary-adrenal axis in posttraumatic stress disorder. InR. Yehuda & A. C. McFarlane (Eds.), Psychobiology of
posttraumatic stress disorder. Annals of the New YorkAcademy of Sciences, 821, 57–75.
YEOMANS, M. R., & GRAY, R. (1996). Selective effects ofnaltrexone on food pleasantness and intake. Physiology &Behavior, 60, 439–446.
YONELINAS, A. (2002). The nature of recollection andfamiliarity: A review of 30 years of research. Journal ofMemory and Language, 46, 441–517.
YOUNGSTEDT, S. D., O’CONNOR, P. J., & DISHMAN, R. K.(1997). The effects of acute exercise on sleep: a quantita-tive synthesis. Sleep, 20, 203–214.
YU, D., & SHEPARD, G. (1998). Is beauty in the eye of thebeholder? Nature, 396, 321–322.
YUSSEN, S. R., & LEVY, V. M. (1975). Developmentalchanges in predicting one’s own span of memory. Journalof Experimental Child Psychology, 19, 502–508.
ZAIDEL, E. (1976). Auditory vocabulary of the right hemi-sphere following brain bisection or hemidecortication.Cortex, 12, 191–211.
ZAIDEL, E. (1983). A response to Gazzaniga. Language inthe right hemisphere, convergent perspectives. AmericanPsychologist, 38(5), 542–546.
ZAIDI, L. Y., & FOY, D. W. (1994). Childhood abuse expe-riences and combat-related PTSD. Journal of TraumaticStress, 7, 33–42.
ZAJONC, R. B. (1965). Social facilitation. Science, 149,269–274.
ZAJONC, R. B. (1968). Attitudinal effects of mere expo-sure. Journal of Personality and Social Psychology,9(Monograph suppl.), 1–27.
ZAJONC, R. B. (1980). Feeling and thinking: Preferencesneed no inferences. American Psychologist, 35, 151–175.
ZAJONC, R. B. (1984). On the primacy of affect. AmericanPsychologist, 39, 117–123.
ZAJONC, R. B., ADELMANN, P. K., MURPHY, S. T., &NIEDENTHAL, P. M. (1987). Convergence in the physicalappearance of spouses. Motivation and Emotion, 11,335–346.
ZAJONC, R. B., HEINGARTNER, A., & HERMAN, E. M. (1969).Social enhancement and impairment of performance inthe cockroach. Journal of Personality and Social Psychology,13, 83–92.
ZAJONC, R. B., & MCINTOSH, D. N. (1992). Emotionsresearch: Some promising questions and some question-able promises. Psychological Science, 3, 70–74.
ZAKRISKI, A., & COIE, J. (1996). A comparison of aggres-sive-rejected and non-aggressive-rejected children’sinterpretations of self-directed and other-directedaggression. Child Development, 67, 1048–1070.
ZARAGOZA, M. S., & MITCHELL, K. J. (1996). Repeatedexposure to suggestion and the creation of false memo-ries. Psychological Science, 7, 294–300.
ZARKIN, G. A., GRABOWSKI, H. G., MAUSKOPF, J.,BANNERMAN, H. A., & WEISLER, R. H. (1995). Economicevaluation of drug treatment for psychiatric disorders. InF. E. Bloom & D. Kupfer (Eds.), Psychopharmacology: Thefourth generation of progress (pp. 1897–1905). New York:Raven.
ZARZO, M., & STANTON, D. (2009). Understanding theunderlying dimensions in perfumers’ odor perceptionspace as a basis for developing meaningful odor maps.Attention, Perception & Psychophysics, 71, 225–247.
ZELAZO, P. D. (2006). The dimensional change card sort(DCCS): A method of assessing executive function inchildren. Nature Protocols, 1, 297–301.
ZELAZO, P. D., & FRYE, D. (1998). Cognitive complexityand control: II. The development of executive function inchildhood. Current Directions in Psychological Science, 7,121–125.
ZENTALL, T. R. (2000). Symbolic representation bypigeons. Current Directions in Psychological Science, 9,118–123.
ZENTALL, T. R. SUTTON, J., & SHERBURNE, L. (1996). Trueimitative learning in pigeons. Psychological Science, 7,343–346.
ZHDANOVA, I. V., & WURTMAN, R. J. (1997). Efficacy ofmelatonin as a sleep-promoting agent. Journal ofBiological Rhythms, 12(6), 644–650.
ZHONG, C., DIJKSTERHUIS, A., & GALINSKY, A. D. (2008).The merits of unconscious thought in creativity.Psycholological Science, 19, 912–918.
ZIGLER, E., & CHILD, I. L. (1969). Socialization. In G.Lindzey & E. Aronson (Eds.), The handbook of social psy-chology: Vol. 3 (pp. 450–589). Reading, MA: Addison-Wesley.
ZIGLER, E. F., & CHILD, I. L. (1973). Socialization and per-sonality development. Reading, MA: Addison-Wesley.
ZIHL, J., VON CRAMON, D., & MAI, N. (1983). Selective dis-turbance of movement vision after bilateral brain dam-age. Brain, 106, 313–340.
ZILBOORG, G., & HENRY, G. W. (1941). A history of medicalpsychology. New York: Norton.
ZILLMANN, D. (1989). Effects of prolonged consumptionof pornography. In D. Zillmann & J. Bryant (Eds.),Pornography: Research advances and policy considerations(pp. 127–157). Hillsdale, NJ: Erlbaum.
ZILLMANN, D., & BRYANT, J. (1988). Pornography’s impacton sexual satisfaction. Journal of Applied Social Psychology,18, 438–453.
ZIMBARDO, P. G. (1969). The human choice:Individuation, reason, and order versus deindividuation,impulse and chaos. In W. J. Arnold & E. Levine (Eds.),Nebraska Symposium on Motivation (pp. 237–308).Lincoln: University of Nebraska Press.
ZIMBARDO, P. G. (1970). The human choice:Individuation, reason and order versus deindividuation,impulse and chaos. In W. J. Arnold & D. Levine (Eds.),Nebraska Symposium on Motivation: Vol 18. Lincoln:University of Nebraska Press.
ZIMBARDO, P. G. (1973). On the ethics of intervention inhuman psychological research: With special reference tothe Stanford prison experiment. Cognition, 2(2),243–256.
ZIMBARDO, P. G. (2005). Abu Ghraib: The evil of inaction,and the heroes who acted. The Western Psychologist, 18(1),4–5.
ZIMBARDO, P. G. (2007). The Lucifer effect: Understandinghow good people turn evil. New York: Random House.

R66 PREFERENCESO
ZIMMER, C. (2008). The search for intelligence. ScientificAmerican, October, 68–75.
ZIMMERMAN, M., MATTIA, J. I., & POSTERNACK, M. A.(2002). Are subjects in pharmacological treatment trialsof depression representative of patients in routine clini-cal practice? American Journal of Psychiatry, 159, 469–473.
ZORILLA, L.T. E., & CANNON, T. D. (1995). Structural brainabnormalities in schizophrenia: Distribution, etiology,and implications. In S. A. Mednick (Ed.), Neuraldevelopment in schizophrenia: Theory and research. NewYork: Plenum Press.
ZUBIN, J., & SPRING, B. (1977). Vulnerability: A new viewof schizophrenia. Journal of Abnormal Psychology, 86,103–126.
ZUCKER, K. J. (2001). Biological influences on psychosex-ual differentiation. In R. K. Unger (Ed.), Handbook of thepsychology of women and gender. New York: Wiley.
ZUCKER, K. J., BRADLEY, S. J., OLIVER, G., BLAKE, J.,FLEMING, S., & HOOD, J. (1996). Psychosexual develop-ment of women with congenital adrenal hyperplasia.Hormones and Behavior, 30, 300–318.
ZUCKERMAN, M. (1979). Sensation seeking: Beyond the opti-mum level of arousal. Hillsdale, NJ: Erlbaum.
ZUCKERMAN, M. (1983). A biological theory of sensationseeking. In M. Zuckerman (Ed.), Biological bases of sensa-tion seeking, impulsivity, and anxiety. Hillsdale, NJ:Erlbaum.
ZUCKERMAN, M. (1987a). All parents are environmental-ists until they have their second child. Peer commentaryon Plomin, R., & Daniels, D. Why are children from thesame family so different from one another? Behavioraland Brain Sciences, 10, 38–39.
ZUCKERMAN, M. (1987b). A critical look at three arousalconstructs in personality theories: Optimal levels ofarousal, strength of the nervous system, and sensitivities
to signals of reward and punishment. In J. Strelau & H. J.Eysenck (Eds.), Personality dimensions and arousal:Perspectives on individual differences (pp. 217–230). NewYork: Plenum.
ZUCKERMAN, M. (1990). The psychophysiology of sensa-tion seeking [Special issue]. Biological foundations ofpersonality: Evolution, behavioral genetics, and psy-chophysiology. Journal of Personality, 58, 313–345.
ZUCKERMAN, M. (1994). Behavioral expressions and bioso-cial bases of sensation seeking. New York: CambridgeUniversity Press.
ZUGER, B. (1984). Early effeminate behavior in boys.Journal of Nervous and Mental Disease, 172, 90–96.
ZUMBAHLEN, M., & CRAWLEY, A. (1997). Infants’ early ref-erential behavior in prohibition contexts: The emergenceof social referencing. Infant Behavior and Development,19(1), 243–244.
G1
A-delta fibers One of the types of fibers crucial for perceiving pain. Thesefibers allow rapid transmission of pain signals. See also C fibers.
A-not-B effect The tendency of infants to reach for a hidden object where itwas previously hidden (place A), rather than where it was hidden mostrecently while the child watched (place B).
absolute threshold The smallest quantity of a stimulus that an individualcan detect.
accommodation In Piaget’s theory, the developing child’s process ofchanging his schemas based on his interactions with the environment.See assimilation.
achromatic colors Colors, such as black, white, and the neutral grays, that donot have the property of hue.
acquisition The processes of gaining new information and placing it inmemory.
action potential A brief change in the electrical charge of a neuronal mem-brane; the physical basis of the signal that travels the length of the neuron.
activation-synthesis hypothesis The hypothesis that dreams may be just abyproduct of the sleeping brain’s activities (activation), which are later assem-bled into a semicoherent narrative (synthesis).
activity dependence A property of neuronal plasticity such that changes in aneuron’s functioning will occur only if that neuron is active (i.e., firing) at thesame time as another neuron.
actual selves Self-schema for whom one is at the moment.
acuity The ability to distinguish between separate points projected on theretina. Acuity is greatest in the fovea, where the receptors are closely bunchedtogether.
acute stress disorder A reaction sometimes observed in individuals whohave experienced a trauma, characterized by flashbacks and recurrentnightmares.
ADHD See attention-deficit/hyperactivity disorder.
affective forecasting Predicting one’s own emotional response to upcomingevents.
affective neuroscience A field that uses cognitive neuroscience researchmethods to study emotion and related processes.
afferent neurons Nerves that carry messages inward toward the central nerv-ous system.
aggressive-rejected The social status of children who are not respected orliked by peers and become aggressive as a result.
agonists Drugs that enhance a neurotransmitter’s activity.
agoraphobia A fear of being in situations in which help might not be avail-able or escape might be difficult or embarrassing. See also phobia.
all-or-none law The law that all action potentials have the same strength andspeed regardless of the triggering stimulus.
allele An alternative form of a specific gene.
alpha rhythm A pattern of regular pulses, between 8 and 12 per second, vis-ible in the EEG of a person who is relaxed but awake and typically has her eyesclosed.
altruism Helping behavior that does not benefit the helper.
Alzheimer’s disease A degenerative brain disorder characterized by memoryloss followed by increasing disorientation and culminating in physical andmental helplessness.
American Sign Language (ASL) The manual-visual language used by mostdeaf persons in the United States.
amplitude The height of a wave crest, used (in the case of sound waves) as ameasure of sound intensity.
amygdala An almond-shaped, temporal lobe structure that plays a centralrole in emotion and evaluating stimuli.
anal stage In psychoanalytic theory, the stage of psychosexual developmentduring which the focus of pleasure is on activities related to elimination.
Glossary

G2 PGLOSSARYO
analogical representation An idea that shares some of the actualcharacteristics of the object it represents. See also symbolic representation.
analytic intelligence The ability typically measured by intelligence tests andcrucial for academic success.
anecdotal evidence Evidence (usually just a few cases) collected informally,as in stories told by one person to another.
anorexia nervosa An eating disorder characterized by an extreme concernwith being overweight and by compulsive dieting, sometimes to the point ofself-starvation. See also bulimia nervosa.
antagonists Drugs that impede the activity of a neurotransmitter.
anterograde amnesia A memory deficit suffered after some kinds of braindamage, in which the patient seems unable to form new explicit memories;however, memories acquired before the injury are spared. See also retrogradeamnesia.
antidepressants Medications designed to counteract depression.
ANS See autonomic nervous system.
antisocial personality disorder Also called psychopathy or sociopathy.The term describes persons who get into continual trouble with society, areindifferent to others, are impulsive, and have little concern for the future orremorse about the past.
anxiety disorders A group of disorders distinguished by feelings of intensedistress and worry, and in many cases, disruptive and unsuccessful attemptsto deal with these feelings.
anxiolytics Drugs that alleviate the symptoms of anxiety.
aphasia Any of a number of linguistic disorders caused by injury to or mal-formation of the brain. See also fluent aphasia, nonfluent aphasia.
apparent movement The perception of movement produced by stimuli thatare stationary but are presented first at one positions and then, at an appro-priate time interval, presented at a different position.
apraxia A serious disturbance in beginning or carrying out voluntarymovements.
archetypes According to Carl Jung, the stories and images that constituteour collective unconscious.
ASL See American Sign Language.
assessment The set of procedures for gathering information about an indi-vidual’s psychological state, sometimes leading to a diagnosis.
assimilation In Piaget’s theory, the developing child’s process of interpretingthe environment in terms of the schemas he already has. See accommodation.
association A linkage between two psychological processes or representa-tions as a result of past experience in which the two have occurred together.
associative links In network-based models of mental representation, con-nections between the symbols (or nodes) in the network.
attachment The strong, enduring, emotional bond between a child and itscaregivers that some psychologists consider the basis for relationships laterin life.
attention-deficit/hyperactivity disorder (ADHD) A disorder usually diag-nosed in young children, and characterized by impulsivity, difficulty stayingfocused on a task, and a range of behavioral problems.
attitude A fairly stable evaluation of something as good or bad that makes aperson think, feel, or behave positively or negatively about some person,group, or social issue.
attributional style The way a person typically explains the things thathappen in his or her life.
atypical antidepressants A recently developed group of medications thatwork in varied ways on serotonin, norepinephrine, and dopamine systems tocombat the symptoms of depression.
auditory canal The tube that carries sound from the outer ear to the eardrum.
auditory ossicles The three bones of the middle ear that transmit the vibra-tions of the eardrum to the oval window.
authoritarian parents One of the four types of parents; they adhere to strictstandards about how children should behave, and attempt to mold their chil-dren’s behavior accordingly.
authoritarian personality A cluster of personal attributes (e.g., submissionto persons above and harshness to those below) and social attitudes (e.g., prejudice against minority groups) that is sometimes held to constitutea distinct personality.
authoritative parents One of the four types of parents; they exercise powerover their children, but accept the reciprocal obligation to respond to theirchildren’s opinions and reasonable demands.
autism A disorder usually diagnosed in young children, and characterized bya wide range of developmental problems, including language and motorproblems.
automaticity The ability to do a task without paying attention to it.
autonomic nervous system (ANS) The division of the peripheral nervoussystem that receives information from and controls the internal organs.
availability heuristic A strategy for judging how frequently somethinghappens—or how common it is—based on how easily examples of it come tomind.
avoidant personality disorder A personality disorder characterized by socialinhibition and social insecurity.
axon The part of a neuron that transmits impulses to glands, muscles, orother neurons.
axon terminals The knoblike swellings on the ends of an axon. The termi-nals contain the synaptic vesicles that are filled with neurotransmitters.
basic level A concept at some accessible, middling degree of abstractness orinclusiveness (e.g., dog, spoon). See also subordinates, superordinates.
basilar membrane A membrane running the length of the cochlea; soundwaves cause a deformation of this membrane, bending the hair cells in thecochlea and thus stimulating the auditory receptors. See also cochlea.
behavioral contrast A response pattern in which an organism evaluates areward relative to other available rewards or those that have been availablerecently.
behavioral data Data about a person based on direct observation of thatperson’s actions or behavior.
belongingness in learning The fact that the ease of forming associationsdepends on the items to be associated. This holds for CS-US associations inclassical conditioning and response-reinforcer associations in instrumentalconditioning. See also biological constraints.
benzodiazepines A class of medications used to combat anxiety; the classincludes Valium, Xanax, and Klonopin.
beta-blocker A medication intended to control autonomic arousal, and oftenused in the treatment of anxiety disorders.
PGLOSSARYO G3
beta rhythm The rhythmic pattern in the brain’s electrical activity oftenobserved when a person is actively thinking about some specific topic.
between-subject comparisons Within a study, comparing one group ofindividuals to a different group.
Big Five Five crucial dimensions of personality determined through factoranalyses of trait terms: extroversion, neuroticism (or emotional instability),agreeableness, conscientiousness, and openness to experience.
binding problem The problem confronted by the brain of recombining theelements of a stimulus, given the fact that these elements are initially analyzedseparately by different neural systems.
binge eating Eating a large amount of food within a brief period.
binocular disparity A depth cue based on the differences between the twoeyes’ views of the world. This difference becomes less pronounced the fartheran object is from the observer.
binocular rivalry Either a perceptual phenomenon resulting from two sepa-rate images, one in front of each eye, or the procedure used to establish thisphenomenon. The visual system is unable to interpret both stimuli at once orto fuse the stimuli into a single perception. Instead, the visual system alter-nates between the stimuli, so that the person is aware of one for a while andthen the other.
biological constraints Principles governing what each species can learn eas-ily and what it cannot learn at all. See also belongingness in learning.
biopsychosocial perspective A perspective on psychopathology that empha-sizes the biological, psychological, and social factors that contribute to mentalillness.
bipolar cells The intermediate neural cells in the eye that are stimulated bythe receptors and excite the ganglion cells.
bipolar disorder A mood disorder in which the patient swings between emo-tional extremes, experiencing both manic and depressive episodes.
blind spot The region of the retina that contains no visual receptors andtherefore cannot produce visual sensations.
blindsight The ability of a person with a lesion in the visual cortex to reachtoward or correctly “guess” about objects in the visual field even though theperson reports seeing nothing.
blocking effect A result showing that an animal learns nothing about a stim-ulus if the stimulus provides no new information.
blood-brain barrier Specialized membranes that surround the blood vesselswithin the brain and filter harmful chemicals out of the brain’s blood supply.
Body Mass Index (BMI) The commonly-used measure of whether someoneis at a healthy weight or not; BMI is calculated as weight in kilograms dividedby the square of height in meters.
borderline personality disorder A personality disorder characterized by impul-sive behavior and marked instability in relationships, self-concept, and affect.
brain lesion Damage to the brain cells, caused by injury or disease.
brain plasticity The capacity for the brain to alter its structure and function.
brain stem The brain region at the top of the spinal cord that includes themedulla and the pons.
brightness A perceived dimension of visual stimuli—an indication of howlight or dark they appear.
brightness constancy The capacity to perceive an object as having anunchanging brightness, even though changes in illumination cause a changein how much light reflects off the object and reaches the eye.
brightness contrast The perceptual tendency to exaggerate the physical dif-ference in the light intensities of two adjacent regions. As a result, a gray patchlooks brighter on a black background and darker on a white background.
Broca’s area A brain area in the frontal lobe crucial for language production.See also aphasia, nonfluent aphasia.
bulimia nervosa An eating disorder characterized by repeated binge-and-purge bouts. See also anorexia nervosa.
bystander effect One reason people fail to help strangers in distress: Thelarger the group a person is in, the less likely he is to help, partly because noone in the group thinks it is up to him to act.
C fibers One of the types of fibers crucial for perceiving pain. These unmyeli-nated fibers provide slow transmission of pain signals. See also A-delta fibers.
Cannon-Bard theory of emotion The theory that a stimulus elicits an emo-tion by triggering a particular response in the brain (in the thalamus) whichthen causes both the physiological changes associated with the emotion andthe emotional experience itself.
case marker A word or affix that indicates the semantic role played bysome noun phrase in a sentence. English case marks pronouns (e.g., he ver-sus him) but usually marks semantic roles by word order, e.g., the first nounphrase in simple sentences usually plays the actor role. Many languages casemark all noun phrases and thus word order may be quite free in theselanguages.
case study An intensive study of one person.
causal attribution An inference about what caused a person’s behavior.
cell body The portion of the neuron containing the metabolic machinery thatkeeps the cell alive and functional.
central fissure The anatomical “valley” that divides the frontal lobes on eachside of the brain from the parietal lobes.
central nervous system (CNS) The brain and spinal cord.
central route to persuasion The process involved in attitude change whensomeone carefully evaluates the evidence and the arguments.
cerebellum The part of the brain that controls muscular coordination andequilibrium.
cerebral cortex The outermost layer of the forebrain.
cerebral hemisphere One-half (left or right) of the cerebrum, the topmostpart of the brain.
cerebrospinal fluid A clear body fluid that surrounds and helps protect thebrain.
character strengths Personal characteristics that contribute to a person’shappiness without diminishing the happiness of others.
choice reaction time A measure of the speed of mental processing that takesplace when someone must choose between several responses, depending onwhich stimulus is presented.
chromatic colors Colors that have a discernible hue. These are in contrast tothe achromatic colors, which include black, the various shades of gray,and white.
chromosomes Structures in the nucleus of each cell that contain the genes,the units of hereditary transmission. A human cell has 46 chromosomesarranged in 23 pairs. See also gene.
chunking A process of reorganizing (or recoding) materials in workingmemory by combining a number of items into a single, larger unit.

G4 PGLOSSARYO
classical antipsychotics Drugs (such as Thorazine and Haldol) that blockdopamine receptors. These drugs seem to treat many positive symptoms ofschizophrenia. See dopamine hypothesis.
classical conditioning A form of learning in which one stimulus is pairedwith another so that the organism learns a relationship between the stimuli.
client-centered therapy A form of humanistic therapy associated with CarlRogers, in which the therapist’s genuineness, unconditional positive regard,and empathic understanding are crucial to therapeutic success.
clinical utility Whether a therapeutic intervention works under real-worldconditions.
CNS See central nervous system.
cochlea The coiled structure in the inner ear that contains the basilarmembrane. See also basilar membrane.
cognitive-behavioral approach A hybrid form of psychotherapy focused onchanging the patient’s habitual interpretations of the world and ways ofbehaving.
cognitive dissonance An uncomfortable inconsistency among one’s actions,beliefs, attitudes, or feelings. People attempt to reduce it by making theiractions, beliefs, attitudes or feelings more consistent with one another.
cognitive reappraisal A form of emotion regulation in which an individualchanges her emotional response to a situation by altering her interpretation ofthat situation.
cognitive restructuring A set of cognitive therapy techniques for changing aperson’s maladaptive beliefs or interpretations through persuasion andconfrontation.
cognitive therapy An approach to therapy that tries to change some of thepatient’s habitual modes of thinking about herself, her situation, and herfuture.
cognitive unconscious The mental support processes outside our awarenessthat make our perception, memory, and thinking possible.
collective unconscious A set of primordial stories and images, hypothesizedby Carl Jung to be shared by all of humanity, and which he proposed underlieand shape our perceptions and desires.
collectivistic cultures Cultures in which people are considered fundamen-tally interdependent and which emphasize obligations within one’s family andimmediate community. See also individualistic cultures.
comorbidity The tendency for different mental disorders to occur together inthe same person.
companionate love An emotional state characterized by affection for thosewhose lives are deeply intertwined with one’s own. See also romantic love.
comparative method A research method in which one makes systematiccomparisons among different species in order to gain insights into the func-tion of a particular structure or behavior, or the evolutionary origins of thatstructure or behavior.
compensatory behavior Actions taken to ensure that binge eating does nottranslate into weight gain (e.g., self-induced vomiting).
compensatory response A response that offsets the effects of the upcomingunconditioned stimulus.
complementary colors Two colors that, when additively mixed in the rightproportions, produce the sensation of gray.
compliance A change in behavior in response to a request.
compulsions Repetitive or ritualistic acts that, in OCD, serve in some way todeal with the obsessions. See obsessions, obsessive-compulsive disorder.
computerized tomography scan See CT (computerized tomography) scan.
concept A mental category.
concordance rate The probability that a person with a particular familialrelationship to a patient (e.g., an identical twin) has the same disorder as thepatient.
concrete operational period In Piaget’s theory, the period from about age 7to about 12, in which the child is beginning to understand abstract ideas suchas number and substance, but only as they apply to real, concrete events.
conditioned reinforcer An initially neutral stimulus that acquires reinforc-ing properties by pairing with another stimulus that is already reinforcing.
conditioned response (CR) A response elicited by an initially neutralstimulus—the conditioned stimulus (CS)—after it has been paired repeatedlywith an unconditioned stimulus (US). See also conditioned stimulus (CS),unconditioned response (UR), unconditioned stimulus (US).
conditioned stimulus (CS) An initially neutral stimulus that comes to elicita new response due to pairings with the unconditioned stimulus. See alsoconditioned response (CR), unconditioned response (UR), unconditionedstimulus (US).
cones Visual receptors that respond to greater light intensities and give riseto chromatic (color) sensations. See also rods.
confederate Someone who appears to be a research participant but actuallyis part of the research team.
confirmation bias (1) The tendency to seek evidence to support one’shypothesis rather than looking for evidence that will undermine it. (2) Thetendency to take evidence that’s consistent with your beliefs more seriouslythan evidence that’s inconsistent with your beliefs.
confirmed hypothesis A hypothesis that has been tested many times andeach time has made successful predictions.
conformity A change in behavior due to explicit or implicit social pressure.
conjunction search A search in which the target is defined by a combinationof features.
consciousness Moment-by-moment awareness of ourselves, our thoughts,and our environment.
construal The way an individual makes sense of the world around him.
construct validity The attribute of truly reflecting the variable named in theresearcher’s hypothesis.
content morpheme A morpheme that carries the main semantic and referen-tial content of a sentence. In English content morphemes are usually nouns,verbs, adjectives, or adverbs. See also function morpheme.
context reinstatement A way of improving retrieval by re-creating the stateof mind that accompanied the initial learning.
contingency management A form of behavior therapy in which certainbehaviors are reliably followed by well-defined consequences.
contralateral control The typical pattern in vertebrates in which movementsof the right side of the body are controlled by the left hemisphere, while move-ments of the left side are controlled by the right hemisphere.
control group A group within an experiment that does not experience theexperimental manipulation.
conventional reasoning According to Kohlberg, the third and fourth stagesof moral reasoning, which are focused on social relationships, conventions,and duties.
PGLOSSARYO G5
convolutions The wrinkles visible in the cortex that allow the enormous surfacearea of the human cortex to be stuffed into the relatively small space of the skull.
cornea The eye’s transparent outer coating.
corpus callosum The thick bundle of fibers connecting the cerebralhemispheres.
correct negative One of the four possible outcomes in a detection task.A response correctly indicating that no signal is present. See also miss.
correlation The tendency of two variables to change together. If one goes upas the other goes up, the correlation is positive; if one goes up as the other goesdown, the correlation is negative.
correlation coefficient (r) A number that expresses both the size and thedirection of a correlation, varying from !1.00 (perfect positive correlation) to"1.00 (perfect negative correlation).
correlational studies Studies in which the investigator analyzes the relation-ships among variables that were in place before the study, without manipulat-ing those variables.
correspondence problem As your view changes, the perceptual task of deter-mining which aspects of the current view correspond to which aspects of theview seen a moment ago.
counterirritation The phenomenon in which painful sensations from onepart of the body trigger the gate neurons and so decrease the sensitivity topain elsewhere in the body. See also gate control theory.
CR See conditioned response.
crib bilingual A prelinguistic infant who is exposed to two or more languagesin the home environment.
crystallized intelligence Acquired knowledge, including the person’s reper-toire of verbal knowledge and cognitive skills. See also fluid intelligence.
CS See conditioned stimulus.
CT (computerized tomography) scan A technique for examining brainstructure by constructing a composite of X-ray images taken from many differ-ent angles.
cultural competence An understanding of how a patient’s cultural back-ground shapes his beliefs, values, and expectations for therapy.
DBS See deep brain stimulation.
debriefing A step at the end of an experiment in which the researcherexplains the study’s purpose and design to each participant and undoes anymanipulations to participants’ beliefs or state.
decibels The logarithmic units used to describe sound intensity (oramplitude).
decision criteria An organism’s rule for how much evidence it needs beforeresponding.
declarative knowledge Knowledge of information that can be expressed inwords.
deep brain stimulation (DBS) An emerging biomedical treatment fordepression and OCD that involves stimulating specific parts of the brain withimplanted electrodes.
deep processing An approach to memorization that involves focusing on themeaning of the stimulus.
defense mechanism A collective term for a number of reactions that try toward off or lessen anxiety by various unconscious means.
definitional theory of word meaning The theory that mental representa-tions of word meanings consist of a necessary and sufficient set of semanticfeatures. The representation of apple, for example, might be [round], [edible],[sweet], [red], [juicy].
dehumanization of the victim Thinking about a potential victim in waysthat make him seem inhuman (as vermin, for example, or as a mere number);this view makes aggression toward the victim more likely and less troubling tothe aggressor.
deindividuation A state in which an individual in a group experiences aweakened sense of personal identity and diminished self-awareness.
deinstitutionalization A movement that began in the 1950s that aimed toprovide better, less expensive care for chronically mentally ill patients in theirown communities rather than at large, centralized hospitals.
delta rhythm The rhythmic pattern in the brain’s electrical activity oftenobserved when a person is in slow-wave sleep.
delusions Systematized false beliefs, often of grandeur or persecution.
demand characteristics The cues in a study that might tell a research partic-ipant what behaviors are expected or desirable in that setting.
dendrites The branched part of a neuron that receives impulses and con-ducts them toward the cell body.
dendritic spines Little knobs attached to the surface of the dendrites andserving as the “receiving stations” for most synapses.
deoxyribonucleic acid See DNA.
dependent personality disorder A personality disorder characterized by anexcessive need to be taken care of by others.
dependent variable The variable that is measured or recorded in anexperiment.
depolarize In the nervous system, to lose the charge that normally existsacross the neuronal membrane.
depressants Drugs that diminish activity levels in the nervous system.
depression A mood disorder characterized by disabling sadness, hopeless-ness, and apathy; a loss of energy, pleasure, and motivation; and disturbancesof sleep, diet, and other bodily functions. Also called major depression orunipolar depression.
depth cues Sources of information that signal the distance from the observerto the distal stimulus.
descriptive statistics Mathematical procedures that allow a researcher tocharacterize a data pattern; these procedures include measures of central ten-dency and of variability.
desensitization See in vivo desensitization.
Diagnostic and Statistical Manual for Mental Disorders (DSM) Themanual that provides specific guidance on how to diagnose each of the nearly200 psychological disorders; currently in its fourth edition, text revision(DSM-IV-TR).
diathesis-stress model A conception of psychopathology that distinguishesfactors that create a risk of illness (the diathesis) from the factors that turn therisk into a problem (the stress).
DID See dissociative identity disorder.
difference threshold The smallest amount that a given stimulus must beincreased or decreased so that an individual can detect the difference.
diffusion of responsibility See bystander effect.
directed thinking Thinking aimed at a particular goal.

G6 PGLOSSARYO
disconfirmed hypothesis A hypothesis that has been tested but for whichthe data do not conform to the pattern it predicted.
discrimination An aspect of learning in which the organism learns torespond differently to stimuli that have been associated with a US (or rein-forcement), and stimuli that have not.
discriminative stimuli In instrumental conditioning, a stimulus that signalsa particular relationship between the instrumental response and the rein-forcer. For example, if a pigeon gets a reinforcer (food) for hopping on a plat-form only while a green light is on, the green light is a positive discriminativestimulus. If a red light signals that hopping on the platform will not lead to areinforcer, the red light is a negative discriminative stimulus.
disengaged parents One of the four types of parents; they provide few rulesand demands and are relatively insensitive to their children’s needs.
dishabituation An increase in responsiveness when something novel is pre-sented, following a series of presentations of something familiar.
displacement A redirection of an impulse from a channel that is blocked intoanother, more available outlet.
display rules Cultural rules that govern the expression of emotion.
dispositional attributions Explanations of someone’s behavior in terms offactors internal to the person, such as traits or preferences.
dissociation (1) A way of demonstrating that two brain functions canoperate independently, by documenting cases in which one of the functionsis impaired while the other is preserved. (2) In the stress disorders, theperiod of numbness immediately after the trauma in which the sufferer feelsestranged, socially unresponsive, and oddly unaffected by the traumaticevent. (3) A defense mechanism in which one seeks to create a sense ofphysical or psychological distance from a threatening event, person, orstimulus.
dissociative amnesia The inability of an individual to remember some periodof her life, or even her entire past, including her identity; often understood asa way of coping with extremely painful events.
dissociative disorders Disorders in which a whole set of mental eventsseems to be stored out of ordinary consciousness. These include dissocia-tive amnesia, fugue states, and, very rarely, cases of dissociative identitydisorder.
dissociative fugue A state in which someone leaves home, then, days ormonths later, suddenly realizes he is in a strange place and doesn’t know howhe got there; often understood as a means of coping with (and escaping from)extremely painful events.
dissociative identity disorder (DID) A disorder that results in a persondeveloping two or more distinct personalities.
distal stimulus An object or event in the outside world. See also proximalstimulus.
distance cues See depth cues.
dizygotic (DZ) twins Twins that develop from two different eggs that aresimultaneously fertilized by two sperm. Like ordinary siblings, they share 50%of their genes. Also called fraternal twins. See also monozygotic (MZ) twins.
DNA (deoxyribonucleic acid) The complex molecule that is the constituentof genes.
dodo bird verdict An expression often used to summarize the comparison ofthe effectiveness of different forms of psychotherapy. According to the dodobird in Alice in Wonderland, “Everyone has won and all must have prizes.”Regarding psychotherapy, this statement is understood to mean that all themajor forms of psychotherapy are equally effective.
dominant A term for a gene that directs the development of a particularcharacteristic even when the corresponding gene on the other chromosome isdifferent, i.e. some other allele.
dopamine hypothesis Asserts that the brains of people with schizophreniaare oversensitive to the neurotransmitter dopamine. See classicalantipsychotics.
double-blind design The technique of assigning participants to experimen-tal conditions while keeping both the participants and the researchersunaware of who is assigned to which group.
drive A term referring to a state of internal bodily tension, such as hunger orthirst or the need for sleep.
DRM paradigm A common procedure for studying memory, in which partic-ipants read and then immediately recall a list of related words, but the wordproviding the “theme” for the list is not included.
drug tolerance The diminished response to a drug that results fromextended use, so that over time the user requires larger doses to experience thedrug’s effects.
DSM See Diagnostic and Statistical Manual for Mental Disorders.
dual-center theory The hypothesis that one area in the lateral hypothalamusis the “on” center, the initiator of eating, while another area in the ventrome-dial hypothalamus is the “off” center, the terminator of eating. Current evi-dence indicates that although these brain regions are crucial for eating, theregulation of eating also involves other circuits.
dual-process theory The proposal that judgment involves two types ofthinking: a fast, efficient, but sometimes faulty set of strategies, and a slower,more laborious, but less risky set of strategies.
DZ twins See dizygotic (DZ) twins.
eardrum The taut membrane that transmits the vibrations caused by soundwaves from the auditory canal to the ossicles in the middle ear.
eclecticism An approach to treatment that deliberately weaves together mul-tiple types and forms of therapy. Also called multimodal therapy.
ECT See electroconvulsive therapy.
edge enhancement A process that relies on brightness contrast and allowsus to see the edges between objects more clearly.
EEA See environment of evolutionary adaptiveness.
EEG See electroencephalogram.
effect size The magnitude of the difference between groups in a study, oftencomputed by subtracting the mean of one group’s scores from mean the other’sscores.
efferent neurons Nerves that carry messages outward from the central nerv-ous system.
efficacy Whether a therapeutic intervention works under carefully controlledconditions.
ego In Freud’s theory, a set of reactions that try to reconcile the id’s blindpleasure strivings with the demands of reality. See also id, superego.
ego psychology A school of psychodynamic thought that emphasizes theskills and adaptive capacities of the ego.
Electra complex See Oedipus complex.
electroconvulsive therapy (ECT) A somatic treatment, mostly used for casesof severe depression, in which a brief electric current is passed through thebrain to produce a convulsive seizure.
PGLOSSARYO G7
electroencephalogram (EEG) A record of the brain’s electrical activityrecorded by placing electrodes on the scalp.
embryonic stage The third through eighth week of prenatal development.
emotion regulation The ability to influence one’s emotions.
emotional intelligence The ability to understand your own and others’ emo-tions and to control your emotions appropriately.
emotional support Social support focused on emotional needs.
emotions Affective responses (such as joy, sadness, pride, and anger), whichare characterized by loosely linked changes in behavior (how we act), subjec-tive experience (how we feel),and physiology (how our bodies respond).
empirical claims Claims that can be true or false depending on the facts.
empirically supported treatments (EST) Clinical methods that researchhas shown to be effective for treating a given disorder.
empiricism A school of thought holding that all knowledge comes by way ofthe senses.
empty chair technique A therapeutic technique associated with Gestalt ther-apy in which the patient imagines he is seated across from another person,and then tells her honestly what he feels.
encoding specificity The hypothesis that when information is stored inmemory, it is not recorded in its original form but translated (“encoded”) intoa form that includes the thoughts and understanding of the learner.
endocrine system The system of glands that release secretions directly intothe bloodstream and affect organs elsewhere in the body.
environment of evolutionary adaptiveness (EEA) The environment thatwas in place when a trait was evolving.
episodic memory Memory for specific events and experiences.
ERP See event-related potential.
EST See empirically supported treatments.
estrogen A female sex hormone that dominates the first half of the femalecycle through ovulation.
estrus In mammals, the period in the cycle when the female is sexually recep-tive (in heat).
event-related potential (ERP) Electrical changes in the brain that corre-spond to the brain’s response to a specific event; measured with EEG.
excitation threshold The voltage difference between a neuron’s interior andexterior that, if exceeded, causes the neuron to fire.
executive control Processes such as making plans or overriding habitualresponses that let the brain direct its own cognitive activities.
experiential therapies A family of therapies that seek to create an empathicand accepting therapeutic atmosphere, while challenging the patient todeepen his experience.
experiment A study of causal relationships in which the researcher manipu-lates an independent variable to examine its effect on a dependent variable.
experimental group The group within an experiment that experiences theresearcher’s manipulation of the independent variable.
experimental manipulation The deliberate alteration of the independent vari-able in an experiment in order to learn about its effects on the dependent variable.
explanatory style A person’s characteristic way of explaining his experiences.Consistently attributing bad experiences to internal, global, and stable causesmay increase vulnerability to depression.
explicit memory Conscious memories that can be described at will and canbe triggered by a direct question. See also implicit memory.
exposure therapy A behavior therapy that aims to remove the anxiety con-nected to a feared stimulus by gradually conditioning relaxed responses to thestimulus.
external validity The degree to which a study’s participants, stimuli, andprocedures adequately reflect the world as it actually is.
extinction The weakening of a learned response that is produced if a condi-tioned stimulus is now repeatedly presented without the unconditioned stim-ulus, or if a previously reinforced operant behavior is no longer reinforced.
extrinsically rewarding An activity or object that is pursued because ofrewards that are not an inherent part of the activity or object.
factor analysis A statistical method for studying the interrelations amongvarious tests. The goal is to discover whether the tests are all influenced by thesame factors.
false alarm One of the four possible outcomes in a detection task. A responseindicating that a signal is present when it actually is not. See also hit.
familiarity A general sense that a certain stimulus has been encounteredbefore.
family resemblance structure An overlapping set of semantic featuresshared by members of a category, such that no members of the category needto have all of the features but all members have at least one of them.
feature detectors Neurons in the retina or brain that respond to specificattributes of the stimulus, such as movement, orientation, and so on.
feature net A model of pattern recognition involving a network of detectorsand having feature detectors as the network’s starting point.
Fechner’s law The observation that the strength of a sensation is propor-tional to the logarithm of physical stimulus intensity.
fetal alcohol syndrome A developmental disorder that affects childrenwhose mothers consumed alcohol during pregnancy. Its effects include arange of psychological problems and physical abnormalities.
fetal stage The prenatal period from the ninth week until birth.
figure The object focused on; the rest of the stimulus input is consideredmerely as “background.” See also ground.
flashbulb memories Vivid, detailed memories said to be produced by unex-pected and emotionally important events.
fluent aphasia A syndrome, derived from a specific form of brain damage, inwhich the person seems able to produce speech but is unable to understandwhat is said to her. In most cases, the sentences she produces make littlesense, consisting instead of “word salad.”
fluid intelligence The ability to deal with new and unusual problems. See alsocrystallized intelligence.
Flynn effect A worldwide increase in IQ scores over the last several decades,at a rate of about 3 points per decade.
fMRI See functional MRI (fMRI) scan.
forebrain In mammals, the bulk of the brain. Its foremost region includes thecerebral hemispheres; its rear includes the thalamus and hypothalamus.
forgetting curve The graphic pattern representing the relationship betweenmeasures of learning and the length of the retention interval: As the retentioninterval gets longer, memory decreases.

G8 PGLOSSARYO
formal operational period In Piaget’s theory, the period from about age twelveon, in which a child can think abstractly and consider hypothetical possibilities.
fovea The area roughly at the retina’s center where cones are plentiful andvisual acuity is greatest.
fragment-completion task A procedure sometimes used for testing implicitmemory; the participant is given a fragment of a word (C_O_O_I_E)and has to fill in the missing letters to complete an actual word(CROCODILE).
framing The way a decision is phrased or the way options are described.Seemingly peripheral aspects of the framing can influence decisions by chang-ing the point of reference.
fraternal twins See dizygotic (DZ) twins.
free association Method used in psychoanalytic therapy in which the patientis to say anything that comes to her mind, no matter how apparently trivial,unrelated, or embarrassing.
free recall A test of memory that asks for as many items in a list as a researchparticipant can recall, regardless of order.
frequency The number of wave peaks per second. In sound, frequency gov-erns the perceived pitch of the sound.
frequency distribution An arrangement for tabulating data values based onhow often they occur in a data set.
frequency estimates A person’s estimates of how often he has encountered aparticular event or object.
frontal lobe The area at the front of each cerebral hemisphere; includes tis-sue crucial for many aspects of planning and controlling thoughts andbehavior.
function morpheme A morpheme that, while adding such content as time,mode, individuation, and evidentiality, also serves a grammatical purpose(e.g., the suffixes –s and –er, or the connecting words and or if). See also con-tent morpheme.
functional MRI (fMRI) scan A technique for examining brain function bymeasuring blood flow and oxygen use within the brain.
fundamental attribution error The tendency to attribute behaviors to a per-son’s internal qualities while underestimating situational influences.
g See general intelligence.
GAD See generalized anxiety disorder.
ganglion cells In the retina, one of the intermediate links between the recep-tor cells and the brain. The axons of the ganglion cells converge into a bundleof fibers that leave the eyeball as the optic nerve. See also bipolar cells.
garden path A premature, false syntactic analysis of a sentence as it is beingheard or read, which must be mentally revised when later information withinthe sentence falsifies the initial interpretation, as in, e.g., Put the ball on the floorinto the box.
gate control theory The proposal that pain sensations must pass through aneural “gate” in order to reach the brain and can be blocked at that gate byneurons that inhibit signals from the nociceptors.
gene A section of a DNA molecule that contains instructions for how and whento assemble a protein. Genes are located on chromosomes. See also chromosomes.
general intelligence (g) A mental attribute that is hypothesized as contribut-ing to the performance of virtually any intellectual task.
generalization gradient The curve showing the relationship between thetendency to respond to a new stimulus and its similarity to the original condi-tioned stimulus (CS).
generalized anxiety disorder (GAD) A disorder characterized by pervasive,free-floating anxiety.
generativity versus stagnation According to Erikson, a major developmentaltask of later adulthood is finding meaning in one’s work, which produces asense of generativity. Failure leads to a sense of stagnation.
generic memory See semantic memory.
geniculate nucleus See lateral geniculate nucleus.
genital stage In psychoanalytic theory, the stage of psychosexual develop-ment reached in adult sexuality in which sexual pleasure involves not onlyone’s own gratification but also the social and bodily satisfaction brought toanother person.
genome The complete set of a species’ genes.
genotype The complete set of an organism’s genes. See also phenotype.
geons (geometric ions) Simple geometric figures, such as cubes, cylinders,and pyramids, that can be combined to create all other shapes. An early (andcrucial) step in some models of object recognition is determining which geonsare present.
Gestalt psychology A theoretical approach that emphasizes the role oforganized wholes in perception and other psychological processes.
Gestalt therapy A form of humanistic therapy associated with Fritz Perlsthat aims to help the patient integrate inconsistent aspects of herself into acoherent whole by increasing self-awareness and self-acceptance.
glia A type of cell in the nervous system long believed to provide a “support”function for neurons; recent research indicates that glia provide many otherfunctions as well.
global workspace hypothesis A hypothesis about the neural basis of con-sciousness. It proposes that specialized neurons, called workspace neurons,give rise to consciousness by allowing us to link stimuli or ideas in dynamic,coherent representations.
glomeruli Sites in the brain’s olfactory bulb where signals from the smellreceptors converge.
glove anesthesia A loss of feeling in the entire hand that does not extendabove the wrist. This symptom makes no organic sense given the arrangementof the nerves, which indicates that it has a psychological basis.
glucoreceptors Receptors in the brain (in the area of the hypothalamus) thatdetect the amount of glucose in the bloodstream.
goal maintenance The mental process of keeping one’s goal in mind to guidethe selection of the next actions.
goal state The situation one is trying to reach when solving a problem.
good continuation A factor in visual grouping; we tend to perceive contoursin a way that alters their direction as little as possible.
grammar See rules of syntax (or grammar).
grasp reflex An infantile reflex in which an infant closes her hand into a fistwhen her palm is touched.
gray matter The tissue of the brain that appears gray. It consists of the cellbodies, dendrites, and unmyelinated axons that comprise the nervous system’smicrocircuitry.
ground The backdrop against which a figure is viewed. See also figure.
PGLOSSARYO G9
group polarization A pattern in group discussions in which each member’sattitudes become more extreme, even though the discussion draws attentionto arguments that could have moderated their views.
groupthink A pattern of thinking that occurs when a cohesive groupminimizes or ignores members’ differences of opinion.
H See heritability ratio.
habituation A decline in the response to a stimulus once the stimulus hasbecome familiar.
habituation procedure A method for studying infant perception. After someexposure to a stimulus, an infant becomes habituated and stops paying atten-tion to it. If the infant shows renewed interest when a new stimulus is pre-sented, this reveals that the infant regards the new stimulus as different fromthe old one.
hair cells The auditory receptors in the cochlea, lodged between the basilarmembrane and other membranes above.
hallucinations Perceived experiences that occur in the absence of actual sen-sory stimulation.
hallucinogens Drugs that powerfully change perception and can trigger sen-sory experiences in the absence of any inputs.
halo effect The tendency to assume that people who have one good trait alsohave other good traits.
heritability ratio (H) A measure that describes, for a given population in agiven environment, what proportion of the variance of a trait is due to geneticdifferences.
hertz (Hz) A measure of the frequency of a sound wave in number of cyclesper second.
heuristics A strategy for making judgments quickly, at the price of occasionalmistakes.
hierarchy of needs The theory that people will strive to meet their higher-order needs, such as love, self-esteem, and self-actualization, onlywhen their lower, more basic needs like food and safety have been met. See alsoself-actualization.
hippocampus A temporal lobe structure that plays a pivotal role in learningand forming new memories.
histrionic personality disorder A personality disorder characterized by anunusual degree of attention seeking and emotionality.
hit One of the four possible outcomes in a detection task. A response cor-rectly indicating that a signal is present. See false alarm.
homeostasis The body’s tendency to maintain the conditions of its internalenvironment by various forms of self-regulation.
homogamy The tendency of like to mate with like.
hormone A chemical released by a gland. Hormones travel through thebloodstream and influence functions such as metabolic rate, arousal level, andthe liver’s sugar output.
hue A perceived dimension of visual stimuli whose meaning is close to theterm color (e.g., red, blue).
human sexual response cycle A sequence of four stages that characterizesthe sexual response in both men and women: excitement, plateau, orgasm,and resolution.
humanistic approach An approach to therapy centered around the idea thatpeople must take responsibility for their lives and actions.
hypnosis A highly relaxed, suggestible state of mind in which a person islikely to feel that his actions and thoughts are happening to him rather thanbeing produced voluntarily.
hypnotic analgesia A reduction in pain produced through hypnotic suggestion.
hypomania A mild manic state in which the individual seems infectiouslymerry, extremely talkative, charming, and tireless.
hypothalamus A subcortical structure that plays a vital role in controllingmany motivated behaviors, like eating, drinking, and sexual activity.
hysteria An older term for a group of presumably psychogenic disorders thatincluded a wide variety of physical and mental symptoms.
Hz See hertz.
id In Freud’s theory, a term for the most primitive reactions of human per-sonality, consisting of blind striving for immediate biological satisfactionregardless of cost. See also ego, superego.
ideal self The concept that each person holds of the self that she would mostlike to be.
identical twins See monozygotic (MZ) twins.
identity versus role confusion According to Erikson, the major develop-mental task of adolescence is developing a stable ego identity, or sense of whoone is. Failure results in developing a negative identity or in role confusion.
ill-defined problem A problem for which the goal state is defined only ingeneral terms, so the steps toward a solution are unclear.
illumination The third of Wallas’s four stages of problem solving. In his the-ory, this is the stage in which new insights suddenly arrive. See also incubation,preparation, verification.
illusory conjunction A pattern of errors in which observers correctly perceivethe features present in a display, such as color and shape, but misperceive howthey were combined. For example, they might report seeing a green O and ared X when a green X and red O were presented.
implicit memory Memories that we may not recall consciously, but that arestill demonstrable through an indirect test. See also explicit memory.
implicit theories of personality Beliefs about what kinds of behaviors areassociated with particular traits and which traits usually go together; used todevelop expectations about people’s behavior.
imprinting In many species, the learned attachment that is formed at a par-ticular early period.
impulsivity A tendency to act without reflecting on one’s actions.
in vivo desensitization One key step in the behavioral treatment of a phobiain which the patient is gradually exposed to the phobic stimulus.
incidental learning Learning without trying to learn, and often withoutawareness that learning is occurring.
incubation The second of Wallas’s four stages of problem solving. In his the-ory, this is the stage in which new ideas emerge through unconscious thought.See also illumination, preparation, verification.
independent variable The variable that the experimenter manipulates as abasis for making predictions about the dependent variable.
individualistic cultures Cultures in which people are considered fundamen-tally independent and which value standing out by achieving private goals.See also collectivistic cultures.

G10 PGLOSSARYO
induced motion Perceived movement of a stationary stimulus, usuallycaused by movement of a surrounding framework or nearby objects.
induced motion of the self A pattern in which surrounding objects that are moving are misperceived as stationary, and the self is thereforemisperceived as moving. An example occurs in traffic, when a neighboringcar rolls forward but appears stationary, and one’s own car momentarilyseems to roll backward.
inferential statistics Mathematical procedures that allow a researcher todraw further claims from a data pattern, including claims about whether thepattern observed in the sample is likely to be observed in other samples.
informant data Data about a person derived from others who know theperson well.
informational influence A reason for conformity based on people’s desire tobe correct.
informed consent A research participant’s agreement to take part in thestudy, based on full information about what the experiment will involve.
inhibited temperament A personality style associated with introversion andneuroticism, and characterized by a fear of novelty that is evident early in life.
inhibitor A stimulus signaling that an event is not coming, which elicits aresponse opposite to the one that the event usually elicits.
initial state The status of a person at the start of her attempts to solve aproblem. See also goal state.
inner ear The internal portion of the ear in which the transduction of soundtakes place.
inspection time The time someone needs to make a simple discriminationbetween two stimuli.
instrumental conditioning A form of learning in which the participantreceives a reinforcer only after performing the desired response, and therebylearns a relationship between the response and the reinforcer. Also calledoperant conditioning.
integrity versus despair According to Erikson, the major developmental taskof older age is finding meaning in the life that one has led. Success gives riseto a sense of integrity, whereas failure leads to despair.
intentional learning Placing new information into memory in anticipationof being tested on it later.
inter-rater reliability A measure of the agreement among several independ-ent observers of an event or stimulus.
internal validity The characteristic of a study that allows us to conclude thatthe manipulation of the independent variable caused the observed changes inthe dependent variable.
internal working model A set of beliefs and expectations about how peoplebehave in social relationships, and also guidelines for interpreting others’actions, and habitual responses to make in social settings.
interneurons Neurons that are neither afferent nor efferent, but insteadcarry information from one neuron to another.
interpersonal therapy (IPT) A form of therapy focused on helping thepatient understand how she interacts with others and then learn better waysof interacting and communicating.
interposition A monocular cue to distance that relies on the fact that objectsfarther away are blocked from view by closer objects.
interval schedule A pattern of delivering reinforcements only after a certainamount of time has passed.
intimacy versus isolation According to Erikson, a major developmental taskof early adulthood is developing an intimate relationship. Failure to do so maylead to isolation.
intrinsically rewarding An activity or object that is pursued for its own sake.
introspection The process of “looking within” to observe one’s ownthoughts, beliefs, and feelings.
intrusion errors Memory mistakes in which elements that were not part ofthe original information get mixed into (“intrude” into) someone’s recall.
inverted spectrum The notion that if someone had inverted color vision,there would be no way to determine that his color perceptions differed fromthe norm. Philosophers use this hypothetical situation to convey the impossi-bility of knowing another person’s subjective experience.
ion channels Biochemical “windows” in a cell wall that allow ions to flow inor out of the cell.
ion pumps Biochemical mechanisms that use energy to move ions either intoor out of the cell.
IPT See interpersonal therapy.
iris The smooth circular muscle in the eye that surrounds the pupil and con-tracts or dilates under reflex control to govern the amount of light entering.
James-Lange theory of emotion The theory that the subjective experience ofemotion is the awareness of one’s own bodily reactions in the presence of cer-tain arousing stimuli.
jnd See just-noticeable difference.
judgment The process of extrapolating from evidence to draw conclusions.
just-noticeable difference (jnd) The smallest difference that an organismcan reliably detect between two stimuli.
kinesthesis The sensations generated by receptors in the muscles, tendons,and joints that inform us of our skeletal movement.
Korsakoff’s syndrome A brain disorder characterized by serious memorydisturbances. The most common cause is extreme and chronic alcohol use.
latent content In psychoanalytic interpretation, the anxiety-inducing wishesand concerns that a dream or behavior expresses in disguised form; usuallycontrasted with manifest content.
latent learning Learning that occurs without a corresponding change in behavior.
lateral fissure The deep indentation that runs horizontally across eachhemosphere of the brain and separates the frontal lobe (above the fissure)from the temporal lobe (below).
lateral geniculate nucleus (LGN) An important neural way station on thepath from the eye to the brain; ganglion neurons on the retina send theirsignals to the lateral geniculate nucleus; from there, other neurons carry thesignal to the visual cortex in the occipital lobe.
lateral inhibition The pattern of interaction among neurons in the visualsystem in which activity in one neuron inhibits adjacent neurons’ responses.
lateralization Functional differences between the two cerebral hemispheres.E.g., in most right-handers, the left hemisphere is specialized for language,while the right hemisphere is better at some visual and spatial tasks.
PGLOSSARYO G11
law of effect Thorndike’s theory that a response followed by a reward will bestrengthened, whereas a response followed by no reward (or by punishment)will be weakened.
learned helplessness A condition of passivity apparently created by exposureto inescapable aversive events. This condition inhibits or prevents learning inlater situations in which escape or avoidance is possible.
learning model The hypothesis that mental disorders result from some formof faulty learning.
learning theorists Researchers who argued that most learning can be under-stood in terms of a small number of principles that apply to all organisms andall situations.
lens The portion of the eye that bends light rays and thus can focus an imageon the retina.
leptin A chemical produced by the adipose cells that seems to signal thatplenty of fat is stored and that no more fat is needed. This signal may dimin-ish eating.
LGN See lateral geniculate nucleus.
life data Data about a person concerning concrete, real-world outcomes.
lifetime prevalence The percentage of people in a certain population whowill have a given disorder at any point in their lives.
liking The pleasure that follows receipt of a reward.
limbic system A group of interconnected structures (including the hypothal-amus, the amygdala, and others) that are crucial for emotion, motivation, andmany aspects of learning and memory.
linear perspective A cue for distance based on the fact that parallel linesseem to converge as they get farther away from the viewer.
literature review A summary of research findings on a particular topic; liter-ature reviews are available in scientific journals.
lock-and-key model The theory that neurotransmitter molecules will affectthe postsynaptic membrane only if their shape fits into that of certain synap-tic receptor molecules.
long-term memory The vast memory depository containing all of an indi-vidual’s knowledge and beliefs—including all those not in use at any giventime.
long-term potentiation (LTP) A long-lasting increase in a neuron’s responseto specific inputs, caused by repeated stimulation. See also activity dependence.
longitudinal fissure The front-to-back cleavage dividing the left and righthemispheres of the brain.
loss aversion The strong tendency to regard losses as considerably moreimportant than gains of comparable magnitude—and, with this, a tendency totake steps (including risky steps) to avoid possible loss.
LTP See long-term potentiation.
M See mean.
Mach bands The accentuated edges between two adjacent regions that differin brightness. This sharpening is maximal at the borders, where the distancebetween the two regions is smallest and the contrast most striking.
magnetic resonance imaging See MRI.
magno cells Ganglion cells that, because of their sensitivity to brightnesschanges, are particularly suited to perceiving motion and depth. See alsoparvo cells.
maintenance rehearsal Mechanical repetition of material without thinkingabout its meaning or patterns.
mania A state characterized by racing thoughts, pressured speech, irritabilityor euphoria, and impaired judgment. See also bipolar disorder.
manifest content In psychoanalytic interpretation, the visible, surfacecontent of a dream or behavior. This content is hypothesized to be a means ofdisguising the latent content, to protect against the anxiety associated withthe latent content.
manualized therapy A form of therapy, often used in research, in which amanual describes a set course of therapy, indicating what steps the therapistshould take, what instructions to offer, and so on.
mastery orientation A learning orientation characterized by a focus on gain-ing new knowledge or abilities and improving.
maximum variation sampling A strategy of deliberately seeking out forstudy the unusual or extreme cases.
mean (M) A measure of central tendency computed by calculating the sum ofall the observations, then dividing by the number of observations.
means-end analysis A problem-solving strategy in which you continuallyevaluate the difference between your current state and your goal, and considerhow to use your resources to reduce the difference.
measure of central tendency A single number intended to summarize anentire distribution of experimental results. Two commonly used measures ofcentral tendency are the mean and the median.
median A measure of central tendency taken by putting the data values inorder and finding the value that divides the distribution in half.
medulla The lower part of the brain stem that controls respiration, circula-tion, and balance.
memory consolidation The biological process through which memories aretransformed from a transient and fragile status to a more permanent androbust state; according to most researchers, consolidation occurs over thecourse of several hours.
memory trace The physical record in the nervous system that preserves amemory.
mental images Mental representations that resemble the objects they repre-sent by directly reflecting the perceptual qualities of the thing represented.
mental maps An internal representation of the spatial layout of a scene.
mental representations Contents in the mind that stand for some object,event, or state of affairs.
mental set The perspective that a person takes and the assumptions hemakes in approaching a problem.
mere presence effect Changes in a person’s behavior due to another person’spresence.
meta-analysis A statistical technique for combining the results of manystudies on a particular topic, even when the studies used different data collec-tion methods.
method of loci A mnemonic technique that requires the learner to visualizeeach of the items she wants to remember in a different spatial location (locus).Recall requires that each location be mentally inspected for the item placedthere.
midbrain The portion of the brain between hindbrain and forebrain that isinvolved in arousal, the sleep-wake cycle, and auditory and visual targeting.

G12 PGLOSSARYO
middle ear An antechamber to the inner ear; it amplifies the sound-produced vibrations of the eardrum and transfers them to the cochlea. See alsocochlea.
midlife transition A period of time proposed by many authors in which indi-viduals reappraise what they have done with their lives thus far and mayreevaluate their marriage and career.
mind-body problem The difficulty in understanding how the mind andbody influence each other—so that physical events can cause mental events,and so that mental events can cause physical ones.
mirror neurons Neurons that fire whenever an animal performs an action,such as stretching out its arm or reaching toward a target, and also wheneverthe animal watches another performing the same action.
misinformation effect The result of a procedure in which, after an experi-ence, people are exposed to questions or suggestions that misrepresent whathappened. The term refers to people’s tendency to include the misinformationas part of their recall of the original experience.
miss One of the four possible outcomes in a detection task. A response indi-cating that a signal is not present when it actually is. See also correct negative.
mixed states A pattern sometimes observed with bipolar disorder in whichthe person displays a combination of manic and depressive symptoms.
mnemonics Deliberate techniques people use to memorize new materials.
monocular depth cues Features of the visual stimulus that indicate distanceeven if the stimulus is viewed with only one eye.
monogamy A mating pattern in which one male and one female form anenduring reproductive partnership.
monozygotic (MZ) twins Twins that develop from a single fertilized egg thatthen splits in half. These twins are genetically identical. See also dizygotic (DZ)twins.
mood disorders A group of disorders distinguished primarily by changes inpositive and negative affective state.
mood stabilizers Medications that treat bipolar disorder, such as lithium.
moods Affective responses that are typically longer-lasting than emotions,and less likely to have a specific object.
morbid obesity The level of obesity at which someone’s health is genuinelyat risk, usually defined as a BMI over 40.
morpheme The smallest significant unit of meaning in a word (e.g., theword boys has two morphemes, boy and -s).
motion detectors Cells in the visual cortex that are sensitive to an imagemoving in a particular direction across the retina.
motion parallax A depth cue based on the fact that, as an observer moves,the retinal images of nearby objects move more rapidly than do the retinalimages of objects farther away.
motivated social cognition Thinking about the social world in ways that serve anemotional need, such as when people hold beliefs that help them feel less anxious.
motivational-enhancement therapy A brief, nonconfrontational, client-centered therapy designed to change specific problematic behaviors such asalcohol or drug use.
MRI (magnetic resonance imaging) A neuroimaging technique that documentsthe effects of strong magnetic pulses on the molecules that make up brain tissue.A computer then assembles this information into a picture of brain structure.
MS See multiple sclerosis.
multi-unit recording A procedure that uses microelectrodes to simultane-ously record the activity of individual cells in the nervous system.
multicausal model A conception of how mental disorders arise that empha-sizes the roles played by many different factors.
multiple intelligences In Howard Gardner’s theory, the six essential, inde-pendent mental capacities (linguistic, logical-mathematical, spatial, musical,bodily-kinesthetic, and personal intelligence).
multiple sclerosis (MS) A progressive neurological disease wherein theimmune system mistakenly destroys the myelin sheaths that comprise thebrain’s white matter, producing manifestations such as numbness, blindness,and paralysis.
mutations Errors in the replication of DNA.
myelin A fatty substance that makes up some types of glial cells; these cellswrap around the axon of some neurons, providing an insulating myelinsheath around these neurons. See also myelin sheath, nodes of Ranvier.
myelin sheath The series of fatty wrappers, formed by special glial cells, thatsurrounds the axon of a neuron that communicates over a long distance in thenervous system; the sheath helps speed the propagation of action potentialsalong the axon. See also nodes of Ranvier.
MZ twins See monozygotic (MZ) twins.
narcissistic personality disorder A personality disorder characterized bygrandiosity, lack of empathy, and a need for the attention and admiration ofothers.
national character The idea that people in different cultures have differentpersonalities.
natural selection The mechanism that drives biological evolution. It refers tothe greater likelihood of successful reproduction for organisms whose attrib-utes are advantageous in a given environment.
naturalistic fallacy The (mistaken) idea that anything “natural” must be“good.”
negative afterimage In color vision, the persistence of an image that pos-sesses the hue complementary to that of the stimulus (e.g., seeing a yellowafterimage after staring at a blue lamp) due to the operation of opponentprocesses.
negative cognitive schema According to Aaron Beck, the core cognitive com-ponent of depression, consisting of an individual’s automatic negative inter-pretations concerning himself, his future, and the world. See also explanatorystyle.
neglect syndrome The result of certain right parietal lobe lesions that leave apatient completely inattentive to stimuli to her left, including the left side ofher own body.
neural correlates of consciousness Specific brain states that seem tocorrespond to the content of someone’s conscious experience.
neural synchrony A pattern of firing in the nervous system in which neu-rons in different brain areas fire at the same rate and at the same time; thisseems to be a cue within the nervous system that links processing in distinctareas.
neural tube The tubular structure formed early in the embryonic stage fromwhich the central nervous system (brain and spinal cord) develops.
neurodevelopmental disorder A disorder that stems from early brainabnormalities.
PGLOSSARYO G13
neurogenesis The process through which the nervous system grows anddevelops, which includes cellular signaling, differentiation, migration andproliferation.
neuroimaging techniques Methods that permit noninvasive study anddepiction of brain structure or function. See also CT scan, MRI, functional MRIscan, PET scan.
neuron A specialized cell in the nervous system that accumulates and trans-mits information.
neuropeptide Y (NPY) A chemical found widely in the brain and periphery.In the brain, it acts as a neurotransmitter; when administered at sites in andnear the hypothalamus, it is a potent elicitor of eating.
neuropsychology The study of brain-damaged individuals with the aim oflearning how brain function makes psychological processes possible.
neuroscience A multidisciplinary field—drawing on psychology, biology,and chemistry—focused on learning how the nervous system functions.
neurotransmitters Chemicals released by one neuron (usually the presynap-tic neuron), which trigger a response in another neuron (usually the postsy-naptic neuron); the chief means of communication among neurons.
niche construction The process in which organisms, through their ownbehaviors, alter the environment and create their own circumstances.
nociceptors Receptors in the skin that give rise to the sense of pain; theyrespond to various forms of tissue damage and to temperature extremes.
node In network-based models of mental representation, a “meeting place”for the various connections associated with a particular topic.
nodes of Ranvier The gaps between the glial-cell wrappers that form themyelin sheath surrounding many kinds of axons. The nodes help speed thepropagation of action potentials along the axon. See also myelin, myelin sheath.
nonfluent aphasia Speech disorder in which the main difficulty is in speechproduction, often involving damage to Broca’s area in the frontal lobe.
norm of reciprocity The social standard that suggests that a favor must berepaid.
normative influence A reason for conformity based on people’s desire to beliked (or not appear foolish).
NPY See neuropeptide Y.
nucleus accumbens A dopamine-rich area in the forebrain that is critical inthe physiology of reward.
obedience A change in behavior in response to an instruction or commandfrom another person.
object permanence The conviction that an object exists even when it is outof sight. Piaget believed infants didn’t develop this level of understandinguntil the age of at least eight months.
object relations A school of psychodynamic thought that emphasizes thereal (as opposed to fantasized) relations an individual has with others.
observational learning The process of watching how others behave andlearning from their example.
obsessions Recurrent unwanted or disturbing thoughts. See also compul-sions, obsessive-compulsive disorder.
obsessive-compulsive disorder (OCD) A disorder whose symptoms areobsessions and compulsions, which seem to serve as defenses against anxiety.
obsessive-compulsive personality disorder A personality disorder charac-terized by a preoccupation with orderliness, perfection, and control.
occipital lobe The rearmost area of each cerebral hemisphere; includes tissuecrucial for processing visual information.
OCD See obsessive-compulsive disorder.
odorants Airborne molecules that can produce a response in the olfactoryreceptor neurons in the epithelial tissue of the nasal cavity.
Oedipus complex In psychoanalytic theory, a general term for the cluster ofimpulses and conflicts hypothesized to occur during the phallic phase, ataround age five. In boys, a fantasized form of intense, possessive sexual love isdirected at the mother, which is soon followed by hatred for and fear of thefather. As the fear mounts, the sexual feelings are pushed underground andthe boy identifies with the father. An equivalent process is hypothesized ingirls and is called the Electra complex.
olfactory epithelium A mucous membrane at the top of the nasal cavity; con-tains the olfactory receptor neurons that respond to airborne molecules calledodorants.
one-trial learning In classical conditioning, the establishment of a condi-tioned response after only one pairing of the conditioned stimulus and theunconditioned stimulus.
operant In Skinner’s system, an instrumental response that is defined by itseffect (the way it operates) on the environment. See instrumental conditioning.
operant conditioning See instrumental conditioning.
operational definition A definition that translates the variable we want toassess into a specific procedure or measurement.
opponent-process theory A theory of color vision that proposes three pairsof color antagonists: red-green, blue-yellow, and white-black. Excitation ofneurons sensitive to one member of a pair automatically inhibits neurons sen-sitive to the other member.
optic flow The phenomenon wherein an object’s retinal image enlarges as weapproach the object and shrinks as we retreat from it. The visual system usesoptic flow as a depth cue.
optic nerve The bundle of fibers that proceeds from each retina to the brain.
oral stage In psychoanalytic theory, the earliest stage of psychosexual devel-opment during which the primary source of bodily pleasure is stimulation ofthe mouth and lips, as in sucking at the breast.
orienting The tendency of an organism to shift its attention and sensory sur-faces (e.g., by moving the eyes or turning the ears) to inspect a stimulus.
ought self The concept that each person holds of the self that she should be.
out-group homogeneity effect The tendency for a member of a group (the in-group) to view members of another group (the out-group) as “all alike”or less varied than members of his or her own group.
outcome expectations A set of beliefs, drawn from experience, about whatthe consequences (rewards or punishments) of certain actions are likely to be.
outer ear The external structures of the ear; these include the pinna, theauditory canal, and the outer surface of the eardrum.
oval window The membrane separating the middle ear from the inner ear.
p-value The probability of getting a particular data pattern purely byaccident.
pain matrix A distributed network of brain regions, including the thalamusand anterior cingulate cortex, thought to respond to many types of pain.
G14 PGLOSSARYO
panic attack A sudden episode of terrifying bodily symptoms such as laboredbreathing, choking, dizziness, tingling hands and feet, sweating, trembling,heart palpitations, and chest pain.
panic disorder An anxiety disorder characterized by repeated or disablingpanic attacks. See also anxiety disorders, panic attack.
papillae Structures on the tongue that contain the taste buds, which in turncontain taste receptors.
paranoid personality disorder A personality disorder characterized by wide-spread suspiciousness and mistrust of others.
parasympathetic branch The division of the autonomic nervous system thatrestores the body’s normal resting state and conserves energy.
parietal lobe The area in each cerebral hemisphere that lies between thefrontal and occipital lobes; includes tissue crucial for receiving informationfrom the skin senses.
parsing The perceptual process of determining which parts of a figure belongtogether as aspects of a whole.
partial reinforcement A learning condition in which only some of the organ-ism’s responses are reinforced.
parvo cells Ganglion cells that, because of their sensitivity to differences inhue, are particularly suited to perceiving color and form. See also magno cells.
pattern theory The proposal that different sensory qualities are encoded byspecific patterns of firing among the relevant neurons.
payoff matrix The pattern of benefits and costs associated with certain typesof responses.
peer review A procedure that provides the main “quality control” within thescientific community; in this procedure, other investigators (presumably thepeers of the initial study’s authors) evaluate the methods and interpretation ofthe data in a paper that has been submitted for publication.
penis envy In psychoanalytic theory, the wish for a penis that is assumed toensue normally in females as part of the Electra complex.
perceptual constancy The accurate perception of certain attributes of a dis-tal object, such as its shape, size, and brightness, despite changes in the prox-imal stimulus caused by variations in our viewing circumstances.
perceptual sensitivity An organism’s ability to detect a signal.
performance orientation A learning orientation characterized by a focus onpresenting oneself well and appearing intelligent to others.
period A measure of how much time elapses between one crest of a wave(e.g., a sound wave) and the next.
peripheral nervous system (PNS) The afferent and efferent nerves that extendfrom the brain and spinal cord to connect them with the organs and muscles.
peripheral route to persuasion The process involved in attitude changewhen someone relies on superficial factors, such as the appearance orcharisma of the person presenting the argument.
permissive parents One of the four types of parents; they set few explicit dosand don’ts for their children, and try not to assert their authority.
perseveration The tendency to repeat a response inappropriately; often aresult of deficits in executive control caused by prefrontal lesions.
personal constructs The dimensions used by a person to organize his or herexperience.
personal myths The personal narratives or stories that provide a person witha sense of direction and meaning.
personality disorders Relatively stable, pervasive patterns of behavior andinner experience that are culturally discrepant and lead to distress or impair-ment; noted on Axis II of the DSM.
personality paradox The idea that people seem to behave much less consis-tently than a trait conception would predict.
PET (positron emission tomography) scan A technique for examining brainfunction by observing the amount of metabolic activity in different brain regions.
phallic stage In psychoanalytic theory, the stage of psychosexual develop-ment during which the child begins to regard his or her genitals as a majorsource of gratification.
phenomenology The study of individuals’ own unique, first-person,conscious experience.
phenotype The overt characteristics and behaviors of an organism. See alsogenotype.
phenylketonuria (PKU) A condition in which a person lacks the gene thatenables him to metabolize the anino acid phenylalanine. If detected early, thiscondition can be treated by means of a special diet. If not detected early, it cancause a severe form of retardation.
pheromones Biologically produced odorants that convey information toother members of the species.
phobia An anxiety disorder characterized by an intense and, at least on thesurface, irrational fear.
phoneme The smallest significant unit of sound in a language. Alphabeticcharacters roughly correspond to phonemes (e.g., apt, tap, and pat are all madeup of the same phonemes).
photopigment A chemical in the photoreceptors that changes its form inresponse to light, producing an electrical change that signals to the nervoussystem that light is present.
photoreceptor A light-sensitive cell located on the retina that converts lightenergy into neural impulses.
phrase structure description A tree diagram or labeled bracketing thatshows the hierarchical structure of a sentence.
physiological data Data about a person derived from measurement of bio-logical structures and processes.
pictorial cues Patterns that can be represented on a flat surface in order tocreate a sense of a three-dimensional object or scene.
PKU See phenylketonuria.
place theory A proposal about pitch perception stating that regions of thebasilar membrane respond to particular sound frequencies, and the nervoussystem interprets the excitation from different basilar regions as differentpitches.
placebo A chemically inert substance that produces real medical benefitsbecause the patient believes it will help her.
pleasure principle One of two major principles that Freud held governedpsychological life. This principle is thought to characterize the id, which seeksto reduce tensions generated by biological urges. See also reality principle.
pluralistic ignorance A type of misunderstanding that occurs when mem-bers of a group don’t realize that the other members share their perception(often, their uncertainty about how to react to a situation). As a result, eachmember wrongly interprets the others’ inaction as reflecting their betterunderstanding of the situation.
PNS See peripheral nervous system.
PGLOSSARYO G15
point prevalence The percentage of people in a given population who have agiven disorder at any particular point in time.
polygamy Any mating system in which a member of one sex mates with sev-eral members of the opposite sex.
polygenic inheritance A pattern in which many genes all influence a singletrait.
pons The upper part of the brain stem that coordinates facial sensations andmuscular actions and regulates sleep and arousal.
population The entire group about which the investigator wants to drawconclusions. See also sample.
position constancy The capacity to perceive an object as having anunchanging location in space, even though changes in the viewer’s positioncause a change in the spatial position of the retinal image cast by the object.
positive psychology A research movement that emphasizes factors that makepeople psychologically healthy, happy, or able to cope well with their lifecircumstances.
positron emission tomography scan See PET (positron emission tomogra-phy) scan.
possible selves Self-schemas for whom one may be in the future; theseinclude the ideal self and the ought self.
post-traumatic stress disorder (PTSD) A chronic, sometimes lifelong disor-der that may follow a traumatic experience. Symptoms include dissociation,recurrent nightmares, flashbacks, and sleep disturbances.
postconventional reasoning According to Kohlberg, the fifth and sixth stagesof moral reasoning, which are focused on ideals and broad moral principles.
posthypnotic amnesia The situation a hypnotist can produce by instructinga person to forget certain events that took place during his or her hypnosis.
posthypnotic instructions Various directions given to a person under hyp-nosis, telling the person specifically how he or she should behave after thehypnosis is done.
postsynaptic neuron The cell receiving a neural message at the synapse.
power of the situation The notion that our behavior often depends more onthe setting we are in than on who we are in terms of traits.
practical intelligence The ability to solve everyday problems through skilledreasoning that relies on tacit knowledge.
preconventional reasoning According to Kohlberg, the first and second stages ofmoral reasoning,which are focused on getting rewards and avoiding punishments.
predicate verb phrase The verb phrase immediately descending from theroot of the sentence tree. In simple English sentences, this verb phrase usuallyexpresses the action or state of the agent or actor.
predictive validity An assessment of whether a test measures what it’sintended to measure, based on whether the test score correlates with anotherrelevant criterion measured later.
prefrontal area The frontmost portion of the frontal lobes, involved in work-ing memory, strategy formation, and response inhibition.
prejudice A negative attitude toward another person based on that person’sgroup membership.
preoperational period In Piaget’s theory, the period from about ages 2 to 7,in which a child can think representationally, but can’t yet relate these repre-sentations to each other or take a point of view other than her own.
preparation The first of Wallas’s four stages of problem solving. In his the-ory, this is the stage in which the person works on the problem but makes lit-tle progress. See also incubation, illumination, verification.
prepared learning Learning that occurs without extensive training becauseof an evolved predisposition to the behavior.
presynaptic facilitation A process, documented in studies of Aplysia, thatunderlies many kinds of learning. It occurs when learning results in anincreased release of neurotransmitter into the synapse.
presynaptic neuron The cell that releases a neurotransmitter across thesynaptic gap.
prevalence For a particular illness or condition, the number of active cases ina population at any point in time.
prevention focus An orientation to avoid doing harm thought to arise whenwe compare our actual self to our ought self.
primacy effect In free recall, the tendency to recall the first items on the listmore readily than those in the middle. See also recency effect.
primary attachment figure The main person with whom an infant forms astrong, enduring, emotional bond.
primary reinforcers Stimuli that serve as reinforcers because of their imme-diate biological significance; e.g., food, water, or escape from the scent of apredator.
primary sexual characteristics Bodily structures directly related toreproduction.
primary somatosensory projection area Areas of the cortex that are the ini-tial “receiving stations” for sensory information.
priming The process through which a detector or portion of the nervous sys-tem is prepared for an upcoming input, making it easier for the participant torecognize that input.
procedural knowledge Knowledge of how to do something, such as riding abike; expressed in behaviors rather than in words.
progesterone A female sex hormone that dominates the latter phase of thefemale cycle during which the uterine walls thicken to receive the embryo.
prognosis The forecast of how a situation (including an illness) will improveor fail to improve in the future.
projection A mechanism of defense in which various forbidden thoughts andimpulses are attributed to another person rather than the self.
projection areas Areas in which the brain tissue seems to form a “map” ofsensory information.
promotion focus An orientation to actively pursue valued goals thought toarise when we compare our actual self to our ideal self.
propagation The spread of the action potential down an axon, caused bysuccessive changes in electrical charge along the length of the axon’s mem-brane.
proposition (1) A statement relating a subject and a claim about that subject.(2) A predicate-argument structure. In a sentence, the verb is the predicatedact or state and the noun phrases are its arguments, playing various semanticroles.
prosopagnosia The inability to recognize faces; this disorder is usually pro-duced by lesions in the parietal lobes.
prototype The typical or most familiar example of a category (e.g., a robin isa prototypical bird for many Americans but an auk might be the prototype forLaplanders). See also prototype theory.
G16 PGLOSSARYO
prototype theory A theory in which concepts and word meanings are formedaround average or typical values. Some prototype theories comprise featurerepresentations, but without the necessary and sufficient conditions ofdefinitional theory, but some are exemplar representations. In both cases,centrality in the category is measured by closeness to an ideal or average.See also prototype.
proximal stimulus The energies from the outside world that directly reachour sense organs. See also distal stimulus.
proximate cause The influences within an organism’s lifetime that led to itsparticular traits or behaviors.
proximity In perception, the closeness of two figures. The closer togetherthey are, the more we tend to group them together perceptually.
psychoanalysis A theory of human personality development formulated byFreud, based on assertions about unconscious conflict and early psychosexualdevelopment; also the method of therapy that draws heavily on this theory.
psychodynamic approaches Approaches to personality and/or therapy thatare derived from psychoanalytic theory, which asserts that clinical symptomsarise from unconscious conflicts rooted in childhood.
psychogenic hypothesis The hypothesis that mental disorders result frompsychological causes.
psychogenic symptoms Symptoms believed to result from some psychologi-cal cause rather than from tissue damage.
psychological intensity The magnitude of a stimulus as it is perceived, ratherthan in terms of its physical attributes.
psychometric approach to intelligence An attempt to understand thenature of intelligence by studying the pattern of results obtained on intelli-gence tests.
psychopathology The study of mental disorders, or a term for the mentaldisorder itself.
psychopathy See antisocial personality disorder.
psychophysics An approach to perception that relates the characteristics ofphysical stimuli to the sensory experiences they produce.
psychosis Loss of contact with reality, most often evidenced as delusions orhallucinations.
psychosurgery Neurosurgery performed to alleviate manifestations of men-tal disorders that cannot be alleviated using psychotherapy, medication, orother standard treatments.
psychotropic drugs Medications that control, or at least moderate, the man-ifestations of some mental disorders.
PTSD See post-traumatic stress disorder.
puberty The period of physical and sexual maturation in which the child’sbody begins to assume develop into its adult form.
quasi-experiment A comparison that relies on already-existing groups (i.e., groups the experimenter did not create).
r See correlation coefficient.
random assignment In an experimental design, the random placement ofparticipants in either the experimental or control groups, ensuring that thegroups are matched at the outset of the experiment.
random sampling A procedure in which every member of the population hasan equal chance of being picked to participate in a study.
randomized clinical trial (RCT) A procedure for evaluating the outcome oftherapy, usually involving random assignment of participants to one or moretreatment groups or a no-treatment control group.
ratio schedule A pattern of delivering reinforcements only after a certainnumber of responses.
rational emotive behavioral therapy A form of cognitive therapy associatedwith Albert Ellis, in which the therapist actively challenges the patient’s irra-tional beliefs.
rationalization A mechanism of defense by means of which unacceptablethoughts or impulses are reinterpreted in more acceptable and, thus, lessanxiety-arousing terms.
RCT See randomized clinical trial.
reaction formation A mechanism of defense in which a forbidden impulse isturned into its opposite.
reality principle One of two major principles that Freud held governed psycho-logical life. This principle is thought to characterize the ego, which is satisfied byfinding strategies that work in the real world. See also pleasure principle.
reasoning The process of figuring out the implications of particular beliefs.
recall A type of retrieval that requires you to produce an item from memoryin response to a cue or question. See also recognition, recollection.
recency effect In free recall, the tendency to recall items at the end of the listmore readily than those in the middle. See also primacy effect.
receptive field For a particular cell in the visual system, the pattern of retinalstimulation that most effectively causes the cell to fire. For some cells, thispattern is defined solely in terms of a retinal location; for others, the mosteffective input has a particular shape, color, or direction of motion.
recessive A term for a gene that directs the development of a particular char-acteristic only if the corresponding gene on the other chromosome matchesit—i.e., is the same allele.
recognition A type of retrieval that requires you to judge whether you haveencountered a stimulus previously. See also recall, recollection.
recollection Recall of the context in which a certain stimulus wasencountered. See also recall.
reconditioning In classical conditioning, the presentation of further reinforcedconditioning trials after a conditioned response (CR) has been extinguished.
reflex A simple, stereotyped reaction in response to a stimulus (e.g., flexing alimb in withdrawing from pain).
refractory period The time after an action potential during which a neuron’scell membrane is unprepared for the next action potential.
reinforcement schedule See schedule of reinforcement.
reinforcer A stimulus delivered after a response that makes the responsemore likely in the future.
reliability The degree of consistency with which a test measures a trait orattribute. See also test-retest reliability.
REM rebound The tendency to spend more time in REM sleep if deprived ofit on previous nights. REM rebound often occurs during withdrawal fromdrugs that suppress REM sleep (e.g., barbiturates or alcohol).
REM sleep Sleep characterized by rapid eye movements, EEG patterns simi-lar to wakefulness, speeded heart rate and respiration, near-paralysis of skele-tal muscles, and highly visual dreams.
PGLOSSARYO G17
repetition priming An increase in the likelihood that an item will be identi-fied, recognized, or recalled; caused by recent exposure to that item, which mayoccur without explicit awareness.
repetitive transcranial magnetic stimulation (rTMS) An emerging biomed-ical treatment for depression that involves applying rapid pulses of magneticstimulation to the brain from a coil held near the scalp.
replication A repetition of an experiment that yields the same results.
representativeness heuristic A strategy for judging whether an individual,object, or event belongs in a certain category based on how typical of the cat-egory it seems to be.
repression In psychoanalytic theory, a mechanism of defense by means ofwhich thoughts, impulses, or memories that give rise to anxiety are pushed outof consciousness.
resistance In psychoanalysis, a term describing the patient’s failure to asso-ciate freely and say whatever enters her head.
response rate The number of responses per unit of time; one way to measureof the strength of an operant response.
resting potential The voltage difference between the inside and the outsideof a neuronal membrane when the neuron is not firing.
restructuring A reorganization of a problem that can facilitate its solution; acharacteristic of creative thought.
retention interval The time that elapses between learning and retrieval.
retinal image The image of an object that is projected on the retina. Its sizeincreases with the size of that object and decreases with the object’s distancefrom the eye.
retrieval The process of searching for a memory and finding it.
retrieval cue A hint or signal that helps one to recall a memory.
retrieval failure The inability to access a memory, often due to poor encod-ing; an alternative to erasure as an explanation for forgetting.
retrieval paths The mental connections linking one idea to the next thatpeople use to locate a bit of information in memory.
retrograde amnesia A memory deficit, often suffered after a head injury,in which the patient loses memory for events that occurred before the injury.See also anterograde amnesia.
reversible figure A visual pattern that easily allows more than one interpre-tation, in some cases changing the specification of figure and ground, in othercases changing the perceived organization in depth.
rhodopsin The photopigment used in the rods within the retina.
risky shift A pattern in which a group appears more willing to take chancesor to take an extreme stance than any individual members would have been ontheir own.
rods Photoreceptors in the retina that respond to lower light intensities andgive rise to achromatic (colorless) sensations. See also cones.
romantic love An emotional state characterized by idealization of thebeloved, obsessive thoughts of this person, and turbulent feelings. See alsocompanionate love.
Romeo-and-Juliet effect The intensification of romantic love that can occurwhen the couple’s parents oppose relationship.
rooting reflex In an infant, the sucking elicited by stroking applied on oraround the lips; the reflex aids breast-feeding.
rules of syntax (or grammar) The regular principles governing how wordscan be assembled into sentences.
rTMS See repetitive transcranial magnetic stimulation.
sample The subset of the population that the investigator studies in order tolearn about the population at large. See also population.
satisfice In decision making, seeking a satisfactory option rather than spend-ing more time and effort to locate and select the ideal option.
saturation A perceived dimension of visual stimuli that describes the“strength” of a color—the extent to which it appears rich or pale (e.g., lightpink versus hot pink).
savant syndrome A syndrome in a developmentally disabled person who hassome remarkable talent that contrasts with his low level of general intelligence.
scatter plot A graph depicting the relationship between two variables, inwhich each axis represents one variable; often used to graph correlation data.
Schachter-Singer theory of emotion The theory that emotional experienceresults from the interpretation of bodily responses in the context of situa-tional cues.
schedule of reinforcement The rules about how often and under what con-ditions a response will be reinforced. See also interval schedule, ratio schedule.
schema An individual’s mental representation that summarizes her knowl-edge about a certain type of event or situation.
schizoid personality disorder A personality disorder characterized by astriking detachment from others.
schizophrenia A group of severe mental disorders characterized by at leastsome of the following: marked disturbance of thought, withdrawal, inappro-priate or flat emotions, delusions, and hallucinations.
schizotypal personality disorder A personality disorder characterized bydiscomfort with close relationships, cognitive or perceptual distortions, andodd behavior.
SD See standard deviation.
second-order conditioning A form of learning in which a neutral stimulus isfirst made meaningful through classical conditioning. Then, that stimulus(the CS) is paired with a new, neutral stimulus until the new stimulus alsoelicits the conditioned response.
secondary sexual characteristics Bodily structures that change with sexualmaturity but are not directly related to reproduction.
secure base According to John Bowlby, the relationship in which the childfeels safe and protected.
selection task A task used in research on reasoning, in which participants arepresented with four cards (each showing one side) and a rule about whatappears on each side of them. Participants must decide which cards to turnover to determine whether the rule has been followed.
selective serotonin reuptake inhibitors (SSRIs) Medications such asProzac, Zoloft, and Paxil that increase serotonin turnover in the brain and findwide use as treatments for depression, obsessive-compulsive disorder, panicdisorder, and many other disorders.
self-actualization According to Abraham Maslow and some other adherentsof the humanistic approach to personality, the full realization of one’spotential. See also hierarchy of needs.
G18 PGLOSSARYO
self-control The ability to pursue a goal while adequately managing internalconflicts about it, or to delay pursuing a goal because of other considerationsor constraints.
self-efficacy The sense a person has about what things he can plausiblyaccomplish.
self-esteem The relative balance of positive and negative judgments aboutoneself.
self-fulfilling prophecies Beliefs about how a person will behave that actu-ally make the expected behavior more likely.
self-handicapping A self-protective strategy of arranges for an obstacle toone’s own performance, so that failure can be attributed to the obstacle insteadof one’s own limitations.
Self-Monitoring Scale A personality measure that seeks to determine thedegree to which a person alters or adjusts their behavior in order to act appro-priately in new circumstances.
self-perception theory The theory that we know our own attitudes and feel-ings only by observing our own behaviors and deciding what probably causedthem, just as we do when trying to understand others.
self-report data Data supplied by the research participant describing herself(usually, ratings of attitudes or moods, or tallies of behavior), rather than thatcollected by the experimenter.
self-schema An organized body of knowledge about the self and that shapesone’s behaviors, perceptions, and emotions.
self theory Carl Rogers’s theory of personality, which emphasizes the indi-vidual’s active attempts to satisfy his needs in a manner that is consistent withhis self-concept.
semantic feature A basic semantic category or concept that cannot bedecomposed into smaller or less inclusive categories. According to severalstrict theories (e.g., Hume, 1739), the basic features are all sensory-perceptual.
semantic memory Memory for facts (including word meanings); these mem-ories are not tied to any specific time or place.
semantic role The part that each phrase plays in the “who did what towhom” drama described by a sentence. One word takes the role of being thecause of the action, another, its effect, and so on.
semicircular canals Structures in the inner ear that contain the receptors forthe vestibular sense.
semistructured interview An interview in which questions are posed in astandardized yet flexible way.
sensation seeking A predisposition to seek novel experiences, look for thrillsand adventure, and be highly susceptible to boredom.
sensitive period An early period during the development of an organismwhen it is particularly responsive to environmental stimulation. Outside ofthis period, the same environmental events have less impact and may yieldimperfect learning even after lengthy exposure and practice.
sensorimotor period In Piaget’s theory, the period of cognitive developmentfrom birth to about 2 years, in which the child has not yet achieved object per-manence.
sensory adaptation The process by which the sensitivity to a stimulusdeclines if the stimulus is presented for an extended period of time.
sensory coding The process through which the nervous system repre-sents the qualities of the incoming stimulus—whether auditory or visual,for example, or whether a red light or a green one, a sour taste or a sweettaste.
sensory memory A type of memory included in early stage models, preserv-ing sensory in “raw” form. Iconic memory holds onto visual inputs; echoicmemory holds onto auditory inputs.
sensory projection area See primary somatosensory projection area.
sensory quality A distinguishing attribute of a stimulus (e.g., brightness,hue, or pitch).
separation anxiety A pattern of emotions and behaviors that reflect a child’sfear when her mother (or other caregiver) leaves the room; usually observed inchildren 6 to 8 months of age.
set point A general term for the level at which negative feedback tries tomaintain stability.
shallow processing An approach to memorization that involves focusing onthe superficial characteristics of the stimulus, such as the sound of a word orthe typeface in which it’s printed.
shape constancy The tendency to perceive objects as retaining their shapesdespite changes in our angle of regard that produce changes in the image pro-jected on the retina.
shaping The process of eliciting a desired response by rewarding behaviorsthat are increasingly similar to that response.
short-term memory See stage theory of memory.
signal-detection theory The theory that perceiving or not perceiving a stim-ulus is actually a judgment about whether a momentary sensory experience isdue to background noise alone or to the background noise plus a signal.
signs In psychopathology, what the clinician observes about a patient’s phys-ical or mental condition. See also symptoms.
similarity In perception, a principle by which we tend to group like figures,especially by color and orientation.
simple reaction time A measurement of how quickly someone can respondto a stimulus.
simultaneous color contrast The effect produced because any region in thevisual field tends to induce its complementary color in adjoining areas.For example, a gray patch will tend to look bluish if surrounded by yellow andyellowish if surrounded by blue.
sine waves Waves (e.g., sound waves or light waves) that correspond to theplot of the trigonometric sine function.
single-cell recording A procedure of monitoring the moment-by-momentelectrical activity of an individual cell in the nervous system.
situational attributions Explanations of someone’s behavior in terms of thecircumstances rather than aspects of the person.
size constancy The tendency to perceive objects as retaining their size,despite the increase or decrease in the size of the image projected on the retinacaused by moving closer to or farther from the objects. See also unconsciousinference.
skin senses The group of senses, including pressure, warmth, cold, and pain,through which we gain information about our immediate surroundings.
slow-wave sleep A term used for both Stage 3 and Stage 4 sleep; character-ized by slow, rolling eye movements, low cortical arousal, and slowed heart rateand respiration.
smooth muscles The nonstriated muscles controlled by the autonomic nerv-ous system. Smooth muscles constrict the blood vessels to help regulate bloodpressure, and they line many internal organs.
PGLOSSARYO G19
social facilitation The tendency to perform simple or well-practiced tasksbetter in the presence of others than alone.
social inhibition The tendency to perform complex or difficult tasks morepoorly in the presence of others.
social loafing A pattern in which people working together on a task generateless total effort than they would have if they had each worked alone.
social referencing A process of using others’ facial expressions as a cue aboutthe situation.
sociometric data Data that describe how individuals in a group interact.
sociopathy See antisocial personality disorder.
somatic nervous system (SNS) The division of the peripheral nervoussystem that controls the skeletal muscles and transmits sensory information.
somatogenic hypothesis The hypothesis that mental disorders result fromorganic (bodily) causes.
somatosensory area See primary somatosensory projection area.
sound waves Successive pressure variations in the air that vary in amplitudeand wavelength.
species general Pertaining to all organisms in a species.
species specific Pertaining to just one species.
Specific Language Impairment (SLI) A syndrome of unknown etiology inwhich the course of development of a first language is unusually protracteddespite otherwise normally developing cognitive functions. The languageproblems may eventually diminish or disappear but sometimes persistthroughout life.
specific phobias Any of the disorders characterized by extreme and irrationalfear of a particular object or situation.
specificity theory The proposal that different sensory qualities are signaledby different quality-specific neurons. This theory is correct in only a few cases(e.g., pain)
spontaneous recovery The reappearance of an extinguished response after aperiod in which no further conditioning trials have been presented.
spreading activation The process through which activity in one node in anetwork flows outward to other nodes through associative links.
SSRIs See selective serotonin reuptake inhibitors.
stage theory of memory An approach to memory that proposes a short-termmemory store, which holds small amounts of information for fairly short inter-vals, and a long-term memory store, which can hold vast amounts of informationfor extended periods. According to the theory, information can be transferred tolong-term memory only if it has first been in short-term memory.
stages of psychosexual development The sequence of four developmentalstages from infancy through the attainment of adult sexuality that is consid-ered universal in psychoanalytic theory: the oral stage, the anal stage, the phal-lic stage, and the genital stage.
standard deviation (SD) A measure of the variability of a data set, calculatedas the square root of the variance (V).
Stanford Prison Experiment Philip Zimbardo’s study of the effect of roleson behavior. Participants were randomly assigned to play either prisoners orguards in a mock prison. The study was ended early because of the “guards’”role-induced cruelty.
states Temporary patterns of thought, feeling, or behavior.
statistical significance A calculation central to inferential statistics thatdescribes the likelihood that the results of a study happened by chance.
stem cells Cells that are found in early stages of an organism’s developmentand are the precursors for all the other cells; stem cells have not begun to spe-cialize or differentiate.
stereotype threat A mechanism through which a person’s performance isinfluenced by her perception that her score may confirm stereotypes about hergroup.
stereotypes Schemas that are often negative and are used to categorize com-plex groups of people.
stimulants Drugs that have activating or excitatory effects on brain or bodilyfunctions.
stimulus generalization The tendency for stimuli similar to those usedduring learning to elicit a reaction similar to the learned response.
strange situation An experimental procedure for assessing attachment, inwhich the child is allowed to explore an unfamiliar room with the motherpresent before the mother leaves for a few minutes, and then returns.
stress disorders Anxiety disorders that develop after experiencing a trau-matic stressor.
Stroop effect A marked decrease in the speed of naming the colors of ink inwhich various color names are printed when the color words themselves don’tmatch the ink colors. An effect of the automatization of reading.
subject noun phrase The noun phrase immediately descending from theroot of the sentence tree. In simple English sentences, this noun phrase usu-ally plays the semantic role of actor or agent of the action.
subjective contours Perceived contours that do not exist physically. We tendto complete figures that have gaps in them by perceiving a contour as contin-uing along its original path.
subordinates Concepts that are less abstract or more particular than basic-level concepts (e.g., poodle, soup spoon). See also basic level, superordinates.
subroutines In problem solving, specific procedures for solving familiar,well-defined problems.
subsyndromal disorder An instance of a mental disorder in which someonedoes show symptoms, but not at a level of intensity, frequency, or duration thatwould justify a formal diagnosis.
successive approximations A learner’s responses during instrumental con-ditioning that are rewarded for being increasingly similar to the desiredresponse. See also shaping.
sucking reflex An infantile reflex in which an infant sucks on whatever isplaced in his mouth.
superego In Freud’s theory, reaction patterns that emerge from within theego, represent the internalized rules of society, and come to control the ego bypunishment with guilt. See also ego, id.
superordinates Concepts that are more abstract or inclusive than basic-levelconcepts (e.g., animal, utensil). See also basic level, subordinates.
supertasters People who are extremely sensitive to certain tastes, probablybecause they have more papillae than other people do.
suppression A form of emotion regulation that involves inhibiting emotion-expressive behavior.
syllogism A logic problem containing two premises and a conclusion; the syl-logism is valid if the conclusion follows logically from the premises.

G20 PGLOSSARYO
symbolic representation A mental representation that stands for some con-tent without sharing any characteristics with the thing it represents. See alsoanalogical representation.
sympathetic branch The division of the autonomic nervous system thatmobilizes the organism for physical exertion
symptoms In psychopathology, what the patient reports about his physicalor mental condition. See also signs.
synapse The small gap between two adjacent neurons, consisting of thepresynaptic and postsynaptic neurons’ membranes and the space betweenthem.
synaptic reuptake The presynaptic neuron’s process of reabsorbing its ownneurotransmitters after signaling so that they can be released again the nexttime the neuron fires.
synaptic vesicles Tiny sacs within a presynaptic membrane that contain theneurotransmitter; when the presynaptic neuron fires, some of these vesiclesburst and eject their contents into the synaptic gap.
syntax See rules of syntax (or grammar).
System 1 In dual-process models of judgment, the fast, efficient, but some-times faulty type of thinking.
System 2 In dual-process models of judgment, the slower, more effortful, andmore accurate type of reasoning.
tabula rasa Latin for “blank slate”; a reference to the idea that people areborn without innate knowledge—so that all knowledge must be gained fromexperience.
tacit knowledge Practical “how-to” knowledge accumulated from everydayexperience.
tangible support Social support focused on practical or material needs.
tastants Molecules that can trigger a response by the neural receptors withinthe sense of taste.
taste aversion learning A form of learning in which an organism learns toavoid a taste after just one pairing of that taste with illness.
temperament A person’s characteristic level of reactivity and energy; oftenthought to be constitutional.
temporal lobe The areas in each cerebral hemisphere lying below the tem-ples; includes tissue crucial for hearing and many aspects of language use.
teratogens Environmental factors that can disrupt healthy neural develop-ment. These include lead, alcohol, and cigarette smoke.
test-retest reliability An assessment of whether a test is consistent in whatit measures, determined by asking whether the test results on one occasion arecorrelated with the results from the same test (or a close variant on it) onanother occasion.
testable hypothesis A prediction that has been formulated specificallyenough so that it is clear what observations would confirm the prediction andwhat observations would challenge it.
testosterone The principal male sex hormone in mammals.
texture gradient A depth cue based on changes in surface texture thatdepend on how far away the observer is.
thalamus The part of the brain that serves as a major relay and integrationcenter for sensory information.
that’s-not-all technique A sales method that starts with a modest offer, thenimproves on it. The improvement seems to require reciprocation, which oftentakes the form of purchasing the item.
theory of mind The set of interrelated concepts we use to make sense of ourown thoughts, feelings, and behaviors, as well as those of others.
therapeutic alliance The relationship between therapist and patient thathelps many patients feel hopeful and supported.
thermoregulation The process by which organisms maintain a constantbody temperature.
third-variable problem The possibility that two correlated variables may bechanging together only due to the operation of a third variable.
timbre The quality of a sound apart from its pitch or loudness; timbreenables us to distinguish a clarinet from an oboe, or one person’s voice fromanother.
tip-of-the-tongue (TOT) effect The condition in which one remains on theverge of retrieving a word or name but continues to be unsuccessful.
TMS See transcranial magnetic stimulation.
token economy A behavioral therapy technique based on operant condition-ing in which patients’ positive behaviors are reinforced with tokens that theycan exchange for desirable items.
tonotopic map A map organized on the basis of tone.
TOT effect See tip-of-the-tongue (TOT) effect.
traits Relatively stable patterns of thought, feeling, or behavior that charac-terize an individual.
transcranial magnetic stimulation (TMS) The technique of applyingrepeated magnetic stimulation at the surface of the skull to temporarily stim-ulate or disable a target brain region.
transduction The process through which a physical stimulus is convertedinto a signal within the nervous system.
transection Surgical cutting of a nerve tract or brain region, performed tofunctionally isolate the regions on either side.
transference A patient’s tendency to respond to the analyst or therapist inways that re-create her responses to major figures in her life.
tree diagram A geometric representation of the structure of a sentence. Itsnodes are labeled with phrase- (e.g., noun phrase) and word-class (e.g., adjec-tive) category names, and the descending branches indicate relationshipsamong these categories.
trichromatic color vision The principle underlying human color vision.Color vision occurs through the operation of three sets of cones, each maxi-mally sensitive to a different wavelength of light.
ultimate cause The reasons why, over many years of evolution, a particulartrait or behavior helped members of a population to survive and reproduce.
unconditioned response (UR) A response elicited by an unconditionedstimulus without prior training. See also conditioned response (CR),conditioned stimulus (CS), unconditioned stimulus (US).
unconditioned stimulus (US) A stimulus that reliably triggers a particularresponse without prior training. See also conditioned response (CR),conditioned stimulus (CS), unconditioned response (UR).
unconscious inference A process postulated by Hermann von Helmholtz toexplain certain perceptual phenomena such as size constancy. For example, an
PGLOSSARYO G21
object is perceived to be at a certain distance and this is unconsciously takeninto account in assessing its retinal image size, with the result that size con-stancy is maintained. See also size constancy.
UR See unconditioned response.
US See unconditioned stimulus.
vagal nerve stimulation An emerging biomedical treatment for depressionthat involves electrically stimulating the vagus nerve with a small battery-powered implant.
validity The extent to which a method or procedure measures what it is sup-posed to measure. See also construct validity, external validity, internal validity,predictive validity.
variability The degree to which scores in a frequency distribution departfrom the central value.
variable Any characteristic whose values can change.
verification The last of Wallas’s four stages of problem solving. In his theory,this is the stage in which the person confirms that the ideas that emerged inthe illumination stage actually solve the problem. See also illumination, incu-bation, preparation.
vestibular senses The sensations generated by receptors in the semicircularcanals of the inner ear that inform us about the head’s orientation andmovements.
vicarious conditioning A form of learning in which the learner acquires aconditioned response merely by observing another participant being condi-tioned.
visible spectrum The range of wavelengths that our visual system canrespond to; extends from about 400 (the wavelength usually perceived as thecolor violet) to 750 nanometers (the wavelength usually perceived as the colorreddish orange).
visual agnosia The inability to recognize a visual stimulus despite the abilityto see and describe it.
visual perspective A depth cue in which—due to the principles of optics—parallel lines appear to converge as they recede into the distance, and objectscast smaller images if they are farther away from the viewer.
visual search A task in which participants are asked to determine whether aspecified target is present within a field of stimuli.
wait-list control In randomized clinical trials, a control condition in whichpatients receive delayed treatment rather than no treatment. Before beingtreated, they are compared to patients treated earlier.
wanting An organism’s motivation to obtain a reward.
wavelength The distance between the crests of two successive waves and themajor determinant of pitch (for sound) and hue (for light).
Weber fraction In Weber’s law, the fraction given by the change in stimulusintensity (D I) divided by the standard intensity (I) required to produce a just-noticeable difference: D I/I & C.
Weber’s law The observation that the size of the difference threshold is pro-portional to the intensity of the standard stimulus.
well-defined problem A problem for which there’s a clear-cut way ofdeciding whether a proposed solution is correct.
Wernicke’s area A brain area in the temporal lobe and adjacent to the audi-tory projection area, damage to which leads to deficits in understanding wordmeaning. See also aphasia, fluent aphasia.
“what” system The visual pathway leading from the visual cortex to the tem-poral lobe; especially involved in identifying objects.
“where” system The visual pathway leading from the visual cortex to theparietal lobe; especially involved in locating objects in space and coordinatingmovements.
white matter Whitish-appearing brain tissue that is composed of myelinatedaxons.
Whorfian hypothesis The proposal that the language one speaks determinesor heavily influences the thoughts one can think or the saliency of differentcategories of thought.
withdrawal A consequence of drug dependence that occurs when the drug iswithheld, such that the person feels strong drug cravings and psychologicaland medical distress.
withdrawn-rejected The social status of children who are not respected orliked by peers and become anxious as a result.
within-subject comparisons Within a study, comparing the data about eachparticipant in one situation to data about the same participant in anothersituation.
working memory A term describing the status of thoughts in memory thatare currently activated.
Young-Helmholtz theory A theory of color vision holding that each of thethree receptor types (short-wave, medium-wave, and long-wave) gives rise tothe experience of one basic color (blue, green, or red).
zone of proximal development The range of accomplishments that arebeyond what the child can do on her own, but that she can achieve with helpor guidance.
zygote The fertilized egg, formed by the union of sperm and egg.

This page intentionally left blank
N1
Abbott, F. V., 697Abel, T., 296Abelson, J. L., 703Aber, J. L., 630Abi-Darham, A., 664Abrahams, D., 535Abrams, D. B., 249Abramson, L. Y., 657Abudara, V., 90Abukmeil, S. S., 665Acebo, C., 238Ackerman, P. L., 436Adams, C. M., 489Adams, D. B., 481Adams, Margie, 155Adams, M. D., 54Adams, M. J., 308Adamson, L. B., 563Addis, M. E., 682, 708Adelson, E. H., 204, 207Adler, N. T., 479, 480Adler, T. F., 453Adolphs, R., 9, 329, 331Adorno, T. W., 523Affleck, G., 711Aggarwal, A., 149Aggleton, J. P., 323, 329Agyei, Y., 484Ahem, F., 72Ahn, H., 711Ahn, W., 357Ainsworth, M. D. S., 565, 614Akhtar, N., 402Aksan, N., 576Alam, D., 703Alanko, L. O., 238Albano, A., 705Albaum, G., 5Albers, P., 665
Albright, T. D., 177Albucher, R. C., 703Alderton, D. L., 452Alexander, K. W., 330Alexander, R., 79Alhakami, A., 353Alkire, M., 233Allan, L. G., 278Allen, C., 357Allen, V. L., 522Allison, J., 284Allopenna, P., 382Alloy, L. B., 657Allport, F. H., 528Allport, G. W., 593Alsobrook, J. P., 650Altmann, E. M., 318Altmann, G., 394, 396Amabile, T. M., 372, 510Amato, P. R., 571Ambadar, Z., 320, 331, 332Ambady, N., 453, 456American Medical Association, 477American Psychiatric Association, 477American Psychological Association, 477American Psychological Association
Presidential Task Force onEvidence-Based Practice, 706
Ames, D., 696Anas, A., 336Anderson, A. K., 497Anderson, C., 290Anderson, I. M., 475, 477Anderson, J. R., 346Anderson, M. C., 612Andersson, M., 78Andreasen, N. C., 649, 650, 655, 659,
661, 665, 671, 701Angleitner, A., 599
Angold, A., 570Annus, A. M., 643Antonuccio, D. O., 668Apfel, M., 456Arabinell, L., 421Aram, J. D., 530Archibald, A. B., 578Archimedes, 372, 372Arcona, A. P., 668Arendt, Hannah, 523Arias, B., 58, 655Ariely, D., 364, 620Armitage, R., 239Armstrong, S., 389Armstrong, S. L., 388Arnason, U., 64Arnau, R., 430Arndt, J., 619Arnett, J. J., 581Arnold, L. E., 668Arnold, M., 320, 331, 332Arnsten, J. H., 251Aro, H., 574Aron, A. P., 538Aronson, E., 515, 516, 535Aronson, J., 456Arrigo, J. M., 331Asch, S. E., 520, 520, 521, 522Ashbrook, E. F., 406Asher, E. J., 446Asher, S. J., 573Ashton, M., 439Ashwin, E., 549Aslin, R. N., 400, 551Assanand, S., 467Astrup, A., 473Atkinson, J. W., 486Atkinson, L., 566Atkinson, R. C., 245, 304
Atran, S., 389Auyeung, B., 549Awh, E., 122Axel, R., 149
Baars, B. J., 232Babinsky, R., 9Babula, T., 430Bachman, H. J., 568Bachrach, L. L., 696Bachtold, D., 699Back, M. D., 535Bacon, M. K., 602Baddeley, A. D., 315, 318, 329Baer, L., 701Baguley, T., 314Bagwell, C. L., 572, 573Bahrick, H. P., 330Bahrick, L., 330Bailey, C., 318Bailey, J. M., 484Bailey, M., 484Baillargeon, R., 558, 560Bajpai, S., 64Bakalar, J. B., 252Bakeman, R., 563Baker, J. H., 73Baker, M., 390Baker, N., 629Bakermans-Kranenburg, M., 566Baldwin, D. A., 400Ball, S. A., 686Ball, T. M., 343Ballenger, J. C., 699Balster, R. L., 664Baltes, P. B., 583Banaji, M. R., 512Bancroft, J., 481Bandi Rao, S., 400
Name Index
N2 PNAME INDEXO
Bandura, A., 290, 623, 690Banich, M., 435Banks, C., 530Banks, W. P., 231Bannerman, H. A., 706Bantick, R. A., 696Barban, L., 671Barber, J. P., 704, 711Barcklay, J. R., 317Bargh, J., 225Bargh, J. A., 368, 512Barkley, R. A., 668Barlow, D. H., 647, 648, 711Barnes, M. F., 78, 482Barnes, V. A., 247Barnet, R. C., 274Barnier, A. J., 245Baron-Cohen, S., 549, 667Barrett, H. C., 369Barrett, L. F., 493, 496Barrouillet, P., 434Barry, H. I., 602Barselou, I. W., 388Bartell, P., 238Barth, H., 559Bartholomew, K., 614Bartlett, F. C., 321Bartlett, J. R., 701Bartlett, M. Y., 79Bartol, C. R., 600Bartoshuk, L. M., 151, 152Bates, E., 386, 396Bates, J., 567, 573Bates, T. C., 433Bateson, G., 665Batson, C. D., 533Battle, Y. L., 663Baudonniere, P. -M., 572Baumeister, R. F., 36, 476, 481, 483Baumrind, D., 44, 569, 575, 581Baup, N., 703Bayer, E., 470Baynard, M. D., 236Beach, F. A., 76Bear, M. F., 121Beauchamp, G., 151Bebeau, M., 575Bechara, A., 438Beck, A. T., 641, 653, 657, 691, 692Beckers, T., 275Becklen, R., 211Bédard, J., 373Beech, J. S., 128Beecher, M. D., 291Beedle, D., 703Beehner, J., 414Beers, M., 438Beethoven, Ludwig van, 372Begg, I., 336, 370Behrmann, M., 344Beier, M. E., 436Beitman, B. D., 692Belin, D., 601Bell, A. P., 483Bell, S. M., 565Bellugi, U., 410
Bem, D. J., 517Benbow, C., 452Benbow, C. P., 452Bendixen, L., 366Benet-Martínez, V., 598Bengel, D., 58Ben Hamida, S., 290, 651Benjet, C., 576Bennett, C., 530Bennett, R., 530Benson, H., 707Benson, K., 711Berens, M. S., 408Bergbower, K., 627Bergen, J. R., 204Bergen, S. E., 73Berger, S., 330Bergin, A. E., 711Berglas, S., 627Berglund, P., 649, 682Bergman, T., 414Bergson, C., 664Berkeley, George, 135, 135, 260Berkeley, M. A., 204Berman, J. S., 710Bermant, G., 481Bernard, V. W., 526Bernardo, M., 702Berndt, T. J., 572, 574, 582Bernstein, D., 325Bernstein, D. A., 477Bernstein, D. M., 320, 332Berntsen, D., 330Berrettini, W. H., 655Berridge, K. C., 490Berry, D. T. R., 642Berscheid, E., 535, 536, 537, 539Bersoff, D. M., 534Berthomier, P., 238Bertoncini, J., 398Besner, D., 368Bessenoff, G. R., 535Betancourt, T. S., 658Bever, T., 392Bhardwaj, R. D., 127Bialystok, E., 409, 584Biederman, Irving, 191Biello, S.M., 251Bigelow, B., 582Bihrle, A., 410Bijl, R. V., 644Billings, F. J., 320Binder, E. B., 650, 713Binet, A., 426, 426, 427, 441Birmaher, B., 705Birnbaum, M., 360Bitterman, M. E., 295Bittigau, P., 549Björk-Eriksson, T., 127Bjorklund, D. F., 35, 78, 475, 483Björklund, L., 128Black, D. N., 700Black, D. W., 649, 650, 655, 661, 665,
671, 701Black, J. B., 321Blackwell, L., 624
Blair, H., 312Blair, I., 322Blair, N. J., 275Blake, R., 230Blanchette, I., 370Blandon-Gitlin, I., 332Blankenship, S. E., 372Blascovich, J., 456Blatt, S. J., 682Blehar, M. C., 565, 614Bleuler, M., 638Blier, P., 697Blin, O., 650Bliss, E. L., 671Bliss, T. V. P., 297Block, J., 595, 613Block, J. H., 613Block, N., 233, 256Blois, W. O., 325Bloom, B. S., 486Bloom, P., 396, 401Blumberg, S. J., 361Bodenhausen, G. V., 237, 370, 456Bodkin, J. A., 330Bogen, J. E., 117Boget, T., 702Bogg, T., 598Bohus, M., 693Bolland, S. W., 334Bolles, R. C., 291, 294Bollini, A., 661, 663Bolnick, D. I., 63Bolton, P., 658Bond, M., 613Bond, R., 510, 522Bonnet, M. H., 236Boodoo, G., 455Book, A. S., 476Boone, A. L., 36Bootzin, R. R., 238Bordone, Paris, 136Boring, E. G., 197Borkenau, P., 599Born, J., 238Bornstein, M. H., 551Bornstein, R. F., 642Bortz, R., 238Both, S., 482Botvinick, M. M., 435Bouchard, C., 471Bouchard, T. J., 599, 603Bouchard, T. J., Jr., 444, 455, 472Bourdon, K. H., 645Bouret, S. G., 468Bouton, M. E., 274Bowen, M., 694Bower, G. H., 284, 311, 321Bower, J. M., 115Bowerman, M., 417Bowker, A., 574Bowmaker, J. K., 169Boyd, J. H., 645Brabeck, M., 575Brackett, M. A., 438, 439Bradley, G. W., 626Bradley, R., 708
Bradley, R. G., 650Bradshaw, J. L., 124Braffman, W., 245Brailowsky, S., 698Brainerd, C., 322Brambrilla, P., 656Brandone, A. C., 560Brannan, S. K., 656, 703Brannon, E., 559Bransford, J. D., 309, 310, 317Braswell, L., 690Brauer, M., 530Brawman-Mintzer, O., 699Brechbühl, J., 150Breedlove, S. M., 476, 480, 549Brendgen, M., 574Brennan, K. A., 614Brennen, T., 314Brenner, L., 362Breslau, N., 644Bretherton, I., 566Breuer, A., 252Breuer, J., 606Brewer, J., 309Brewer, N., 325Brewer, W. F., 321Brewin, C. R., 330Brickman, J. S., 656, 703Brickman, P., 620Bridgeman, B., 206, 453Bridges, M., 571Bridges, P., 701Bright, J., 314Britton, W. B., 331Broadbent, D. E., 304Brobeck, J. R., 465Broca, Pierre-Paul, 123Brody, G. H., 570Brody, N., 438, 452, 454Broillet, M.-C., 150Bronfenbrenner, U., 442Brooks, K., 373Brooks-Gunn, J., 448, 578Brown, A., 313Brown, B. B., 582Brown, C. M., 383Brown, E., 324Brown, G., 58Brown, G. K., 641Brown, H. E., 313Brown, M. W., 323Brown, N., 12Brown, P., 395Brown, R., 313, 329, 385, 403, 405, 453Brown, S. A., 249Brown, T., 650Browning, P., 435Bruce, C., 177Bruce, V., 314Bruck, M., 320, 321Brunell-Neuleib, S., 642Bruner, J. S., 510Bryant, G. A., 79Bryant, J., 482Brzustoski, P., 456Buchanan, D. R., 535
PNAME INDEXO N3
Buchanan, G. M., 628Buchanan, T. W., 9, 329, 331, 498Buchholz, B. A., 127Buchtel, E., 602Buckley, M., 435Buckner, R., 309, 330, 334Budson, A., 330Bugnyar, T., 290Bukowski, W., 573, 574Bull, R. H. C., 321Buller, D. J., 79, 483Bullock, T. H., 92Bullock, W. A., 600Bundesen, C., 122Bunting, M., 214Burch, R. L., 80Burger, J. M., 517, 525, 527Burgess, C. A., 325Burgess, E. W., 537Burgess, M. F., 325Burke, D. M., 313Burke, M. J., 696Burns, D. D., 691Burris, K. D., 664Burrows, L., 512Burt, B. D., 481Burt, S. A., 668Burton, M. J., 470Bushman, B., 290Bushman, B. J., 290, 475, 476, 477Bushnell, M., 148Buss, A. H., 6, 567, 599Buss, D. M., 78, 79, 482, 483Butcher, J. N., 641Butler, L. D., 670Butler, R. A., 284Buzsáki, G., 196
Cabeza, R., 124, 329, 498Cable, C., 283Cacioppo, J. T., 352, 514Cahill, L., 9, 325Cahoon, L., 337Caldi, S., 560Call, J., 414Calleja, M., 65Callero, P. L., 534Cameron, J., 286Camos, V., 434Campbell, F. A., 446Campbell, J., 536Campbell, J. B., 600Campbell, J. D., 520Campbell, V. L., 642Campfield, L. A., 468Canal, I., 65Cannon, T. D., 663Cannon, Walter B., 474Cannon, W. B., 494Cantor, N., 439, 510Caramazza, A., 328, 386Carbone, M., 430Cardno, A. G., 661Carelli, R. M., 490Carey, B., 333
Carey, D. B., 194Carey, S., 396, 402Carlsmith, J. M., 515, 516Carlson, E. B., 671Carlson, J., 454Carlson, M., 392Carlsson, A., 664Carnagey, N. L., 290Carney, D., 439Carney, S., 701Carothers, A., 452Carpenter, D., 482Carpenter, P. A., 396Carrier, B., 148Carroll, C., 534Carroll, J., 432Carroll, J. B., 431Carroll, L., 386Carskadon, M. A., 238Carstensen, L., 587Carter, C. S., 435Carter-Saltzman, L., 454, 455Cartwright, R. D., 239, 240Carulli-Rabinowitz, V., 562Caruso, D. R., 438Casey, K., 148Cash, S., 235Caspi, A., 58, 539, 598, 655, 656Cassel, E., 477Cassidy, J., 573Cassidy, K., 403Castellani, A. M., 694Castle, J., 499, 572Catalán, R., 58Catanese, K. R., 481Catrambone, R., 370Cattell, R. B., 593Cavalli-Svorza, L., 454Cavoto, B. R., 283Cavoto, K. K., 283Ceci, S., 320, 332, 437, 446, 447Ceci, S. J., 442Cederbork, A.-C., 331Centerwall, B. J., 477Cernoch, J. M., 150Chageux, J.-P., 256Cervone, D., 597Cervone, J. C., 536Cesario, J., 512Chabris, C. F., 211Chaffin, R., 453Chaiken, S., 514, 515Chalmers, D., 233Chambless, D. L., 706, 712Chang, S.-J., 360Charman, S. D., 325Charman, T., 667Chartrand, T., 517Chase, W. G., 307, 373, 374Chastain, R. L., 454Chavda, S., 122Chen, M., 318, 512Chen, S., 386Cheney, D. L., 414Cheng, P. W., 357
Chentsova-Dutton, Y., 658Cherrier, M. M., 453Cherry, E. C., 214Cheryan, S., 456Chess, S., 567, 599Cheung, F. M., 595Chevrier, J., 197Chi, M., 373Chi, M. T. H., 373, 374Chiat, S., 667Chilcoat, H. D., 644Child, I. L., 602Chiles, C., 522Chitajallu, R., 92Chiu, C. Y., 510, 511Choi, S., 417Chomsky, N., 383, 383, 391, 400Chouinard, C., 699Christensen, S., 122Christian, K., 568Christian, V., 410Christiansen, B. A., 249Chrobak, Q. M., 13, 320, 332Chrysikou, E., 369Chua, S. E., 665Cialdini, R. B., 526, 527, 538Cianciolo, A. T., 438Cichon, S., 662Cillessen, A. H. N., 573Cipolotti, L., 313Cirelli, C., 238Cizkova, D., 128Clark, A. E., 620Clark, C. L., 614Clark, D. M., 651Clark, E. V., 403Clark, H. H., 395Clark, L. A., 485, 671, 672Clark, R. A., 486Clark, R. E., 296Clasen, D., 582Clausen, J., 574Clayton, A. H., 698Cleeremans, A., 231, 232Clements, M. T., 64Clifford, C. A., 666Cloitre, M., 712Coates, D., 620Coe, W. C., 245Cogoi, S., 398Cohen, A., 210Cohen, D., 477Cohen, G., 330, 456, 583Cohen, G. L., 618Cohen, J., 3Cohen, J. D., 435, 578Cohen, M., 566Cohen-Kettenis, P., 453Coie, J., 573, 574Colby, A., 575Colcombe, S., 585Cole, M., 568Cole, P. M., 493Cole, S., 55Cole, S. R., 568
Cole, S. W., 659Coles, R., 579Coley, J., 389Collette, F., 238Collins, A., 532Collins, N. L., 566Collins, W., 581Collins, W. A., 572Coman, A., 13Compton, F. N., 570Compton, S. N., 705Conduct Problems Prevention Research
Group, The, 573Conel, J. L., 550Connolly, A., 389Connolly, M. B., 704Connor, R., 533Connors, B. W., 121Connors, E., 324Conway, A. R., 214, 434Conway, M. A., 313, 329, 330Cook, R. G., 283Cook, R. S., 417Cooke, D. J., 672Cooney, J. W., 232Cooper, F. S., 382Cooper, L. N., 64Cooper, Z., 692Coppola, M., 407Cordes, S., 559Corkin, S., 333Corley, R., 445, 599Correll, J., 512Corrigan, P. W., 644Cosmides, L., 79, 357, 497Costa, P. T., 593, 594, 595Costello, E. J., 570Costello, N., 600Côté, S., 438Coughlin, J. F., 582Courchesne, E., 667Cousins, S. D., 618Couvillon, P., 295Couzin, J., 473, 699Cowan, C. P., 585Cowan, N., 214Cowan, P. A., 585Cowan, R., 439Coward, T. R., 520Cox, C. B., 485Cox, D., 389Cox, J. R., 357Coy, K., 581Coyle, J. T., 664Crabbe, J. C., 255Crago, M. B., 410Craig, I. W., 58Craighead, L. W., 689Craighead, W. E., 689Craighero, L., 290Craik, F. I., 309Craik, F. I. M., 309, 314, 583, 584Crain, S., 394Craske, M. G., 688Crawford, M., 453
N4 PNAME INDEXO
Crawley, A., 563Crick, F., 232Crisafi, M., 402Cristol, A. H., 712Crits-Christoph, L. S., 712Crits-Christoph, P., 686, 704, 709Croft, C., 572Crosby, R., 711Cross, S. E., 598Crossman, A. M., 320Crow, T. J., 663Crowder, R. G., 319Crowe, D. H., 626Crowley, M., 533Crowley, W. F., 453Crowther, S., 533Crutchfield, R. S., 520Csernansky, J. G., 697Csibra, G., 66, 196Csikszentmihalyi, M., 372, 620Cuc, A., 330Cucciare, M., 324Culver, C., 117Cummings, E. M., 564, 571Cummings, J. L., 124Cummins, D., 357, 370, 374Curie, Marie, 371Curtis, G. C., 703Curtis, M. A., 127Curtiss, S., 405, 406Cusato, B., 294Cusi, A., 497Cutrona, C. E., 656Cutting, J., 659, 660Czeisler, C. A., 237
Dabbs, J. M., 476Dadds, M. R., 694Dafters, R. I., 251Dahlstrom, W. G., 641Daley, T. C., 447Dallas, M., 335Dallenbach, K. M., 319Dalley, J. W., 601Daly, M., 79, 80, 81Damasio, A., 256Damasio, A. R., 122, 195, 312, 438Damasio, H., 122, 195, 312, 438D’Ambrosio, L. A., 582Damon, W., 618Daneman, M., 434Daniels, D., 603Dannon, P., 108Danthiir, V., 433Darley, J., 3, 533Dar-Nimrod, I., 456Dartnall, H. J. A., 169Darwin, C., 61, 68, 491Darwin, Charles, 279, 371, 372, 399Daskalakis, Z. J., 108Davachi, L., 323Davidson, J. M., 480, 481Davidson, R. J., 247, 496Davies, G. M., 321Davies, K. G., 701Davies, P., 571
Davis, D., 324, 663Davis, D. D., 692Davis, D. E., 476Davis, D. M., 663Davis, G., 196Davis, G. C., 644Davis, H., 247Davis, H. P., 312Davis, J. M., 696Davis, K., 405Davis, K. E., 539Davis, M., 266, 646Davis, M. K., 711Davis, P. H., 670Davison, G. C., 688Davison, L., 534Daw, N. W., 90Dawes, R. M., 142Deakin, J. F., 696Deary, I. J., 427, 428, 433Deary, J., 452DeCasper, A. J., 551DeCesare, K., 527Deci, E. L., 286, 616Deecke, L., 121Deese, J., 322Deffenbacher, K., 324DeFries, J. C., 445, 599deGeus, E., 445Degirmencioglu, S. M., 574De Grada, E. D., 531de Groot, A. D., 373Dehaene, S., 256, 441Dehghani, N., 235De Houwer, J., 275Deiber, M., 126Dell, G. L., 395Delorme, A., 197Delton, A., 79Dement, W. C., 237, 239, 240Demetrikopoulos, M. K., 476Demler, O., 649Demonet, J. F., 124Demos, K. E., 617DeMulder, E., 566Denham, S., 566Dennett, D., 232Dennis, S., 334Denny, B. T., 617deOrtiz, S., 312de Renzi, E., 122Dermer, M., 536DeRosier, M., 574De Rougemont, D., 540Derr, G., 428Derrick, B. E., 297DeRubeis, R. J., 705de Sanchez, M., 446Descartes, René, 86, 87, 87Desimone, R., 177, 196Desmond, A., 59Desmond, J., 309Desmurget, M., 231D’Esposito, M., 125, 435Dess, N. K., 372DeSteno, D., 79, 498
Detterman, D. K., 433Detweiler, J. B., 622Deutsch, G., 117Deutsch, J. A., 468Deutsch, M., 520De Valois, R. L., 172Devanand, D. P., 701, 702Devane, W. A., 252Deveaux, T. C., 650Devlin, B., 442DeYoe, E. A., 193Dhaliwal, H., 122Diamond, A., 558Diamond, J., 669Diaz-Loving, R., 595Di Blas, L., 595Dickens, W. T., 447, 454Diefenbach, D. L., 644Diener, E., 529, 620Digney, A. L., 433Dijksterhuis, A., 372Diller, L. H., 668Dinges, D. F., 236DiNubila, J. A., 403Dion, K., 535Dion, K. K., 540Dion, K. L., 540Dobbins, I., 323Dobbs, D., 649Doctora, J. D., 627Dodds, R. A., 372Dodge, K., 573Dohm, F. A., 669Dohrenwend, B. P., 652, 658, 665Dolan, S. L., 708, 711Dold, G., 126Domhoff, G., 240Domhoff, G. W., 240Domjan, M., 275, 278, 291, 292, 294Donahue, E. M., 593Donaldson, D., 334Donlea, J. M., 238D’Onofrio, B., 72, 449Dorfman, J. H., 663Dorn, L. D., 578Doss, A., 711Dossje, B., 618Douglas, A. B., 325Douglas, R. M., 297Dove, H., 551Dovidio, J. F., 516Dow, S., 4Dowd, S. M., 703Downey, G., 574Downing, L. L., 529Downs, D. L., 486Dragoin, W. B., 293Draguhn, A., 196Draijer, N., 649Draper, S. J., 468Draper, T., 573Drevets, W. C., 656Driscoll, R., 539Dubanoski, J., 595Duckworth, A. L., 486Dudai, Y., 329
Duffy, J. F., 237Duffy, V. B., 152Duke, P., 573Dumay, N., 238Dunbar, K., 370Duncan, B. L., 704Duncan, G., 148, 448Duncan, J., 122, 125, 432, 435Duncan, M., 252Dunham, H. W., 665Dunkle, M., 366Dunn, E., 225Dunn, J., 573Dunner, D. L., 654Dunning, D., 594, 618Dunphy, D. C., 582Dupoux, E., 396Durik, A. M., 486Durrant, C., 58, 657Dutton, D. G., 538Dweck, C. S., 486, 510, 511, 624Dykema, J., 627Dysarz, F. A., 252
Eagly, A. H., 483, 514, 515, 533, 535Eaves, L., 58Ebbinghaus, Hermann, 318Eberhard, K. M., 394Ebert, J. E. J., 362Eccles, J. S., 453Edwards, J., 520Edwards, M., 206Efron, R., 118Eftekhari-Sanjani, H., 452Egeland, B., 566Egertova, M., 252Eglin, M., 210Egloff, B., 535Egner, T., 435Eibl-Eibesfeldt, I., 491Eicher, S., 582Eimas, P. D., 399Eimer, M., 230Einstein, G. O., 325Eisenberg, A. R., 569Eisenberg, N., 573Eisenberger, R., 286Eisner, D. A., 684Ekman, P., 67, 68, 491, 492, 493Elbert, T., 126Elicker, J., 566Elkin, I., 712Ellemers, N., 618Elliot, R., 712Elliott, M. A., 196Elliott, R., 687Ellis, A., 453, 690Elovainio, M., 602Elphick, M. R., 252Emery, G., 691, 692Emmelkamp, P. M., 688Emmelkamp, P. M. G., 687Endler, N. S., 520, 596Engel, A. K., 232Engle, R. W., 125, 434, 435Englund, B. R., 566
PNAME INDEXO N5
Englund, M., 566Enns, J. T., 187Epstein, A. N., 468Epstein, H. T., 551Epstein, M. P., 650Epstein, W., 385Ericsson, K. A., 307Eriksen, W., 446Erikson, E. H., 579, 580, 582Eriksson, P. S., 126Eron, L. D., 477Erpenbeck, D., 64Eskenazi, J., 43Espinosa, M. P., 447Etkin, A., 650Evangelista, F., 5Evans, F. J., 244Evans, J. S. B. T., 356Everaerd, W., 482Everitt, B. J., 601Everson, C. A., 236Eyer, D. E., 565Eysenck, H. J., 433, 706
Fabes, R. A., 573Fabrigar, L. R., 515Fagot, B. I., 566Fairburn, C. G., 692, 712Fairey, P. J., 520Fañanás, L., 58Fanselow, M. S., 296, 297Fantauzzo, C., 499Farah, M., 122, 191, 195, 448Farah, M. J., 125, 435Faraone, S. V., 662Farinacci, S., 336Faris, R. E. L., 665Farley, F., 581Faw, G. D., 689Fawcett, J., 705Fazio, R., 334Fechner, Gustav Theodor, 139Feder, H. H., 480Feeney, A., 356Feeney, B. C., 566Feiman, R., 497Fein, D., 667Feinberg, T. E., 122Feingold, A., 535, 604Feinman, J. A., 654Feirtag, M., 88Feldman, H., 406Fellenius, J., 646Feltovich, P. J., 374Feng, J., 454Ference, R., 531Ferguson, J. M., 698Ferguson, M. J., 368Fernald, A., 396, 403Fernandes, K. J., 403Feshbach, S., 290Festinger, L., 516, 521, 529Ffytche, D. H., 600Fiddick, L., 79Fields, W., 415
Fifer, W. P., 551Fingerhut, A. W., 585Fink, B., 481Fink, D., 127Fink, M., 701Finucane, M. L., 353Fischer, E. F., 540Fischer, J., 414Fischer, Q. S., 90Fisher, C., 403Fisher, E. D., 117Fisher, R. P., 314, 324Fisher, S., 241Fiske, A. P., 510Fiske, D. W., 593Fiske, S. T., 508Fitzgerald, P. B., 108Fivush, R., 569Flaum, M., 659, 665Flavell, J. H., 554Flavell, R. A., 549Fleeson, W., 596Fleishman, M., 696Flinker, A., 149Flint, J., 58, 657Florida, R., 603Florio, C. M., 642Flynn, J. R., 447, 454Foa, E. B., 649Fodor, J. A., 386, 387, 388Foley, H., 323Foley, P. P., 452Follette, W., 687Fonagy, P., 711, 6722Fong, G., 353Fong, G. T., 618Fong, G. W., 489Fontaine, D., 703Ford, C. S., 76Forman, E., 571Forman, E. M., 711Forzi, M., 595Fothergill, L., 102Foucault, M., 679Foulkes, D., 239Fountain, S., 108Fourier, Joseph, 155Fox, H. C., 427Fox, N., 572Fox, N. A., 601Frackowiak, R. S. J., 124Fraley, R., 567Francis, E. L., 657Frank, E., 712Frank, J. B., 704Frank, J. D., 704Frankforter, T. L., 686Franklin, M., 481Franklin, S., 232Franklin, T., 251Franks, J. J., 317Fraser, S., 442Fraser, S. C., 517Frazier, L., 392Freedheim, D. K., 692
Freedman, J. L., 517Freeman, A., 692Freeman, R., 669Freiburger, K. L., 283Freisen, C., 117Freitas, A., 574Fremouw, W. J., 655Freud, S., 606, 607, 609, 610, 611Freund, A. M., 583Frey, D., 355Freyd, J., 332Friedman, H. S., 493Friedman, M. I., 467, 472, 473Friedman, M. J., 649Friedman, R., 707Friedman-Hill, S., 210Fries, P., 196Friesen, W. V., 67, 492, 493Frijda, N., 453Frith, C., 230Frome, P. M., 453Fromkin, V., 405Frost, P., 481Frye, D., 408, 558Fthenaki, K., 313Fujimoto, W. Y., 473Fulker, D. W., 445, 599Fulkerson, J., 711Furtado, E., 572
Gabbay, P., 332Gabrieli, J., 330Gabrieli, J. D. E., 309Gaertner, S. L., 516Gaeth, G., 360Gaeth, G. J., 5Gage, Phineas, 107Galanter, E., 138Galati, D., 491Galef, B. G., 290Galileo Galilei, 86, 87Galinsky, A. D., 372Gallagher, A., 452Gallistel, C. R., 287, 294, 421, 559Gallo, V., 92Gallup, G. G., Jr., 80Ganaway, G. K., 671Gangestad, S., 598Garb, H. N., 642Garber, J., 653Garcia, J., 292, 456Garcia, O., 698Gard, D. E., 660Gardner, C. O., 73Gardner, H., 439Gardos, P. S., 482Garnsey, S. M., 392Garrigan, P., 186Garske, J. P., 711Gaskell, M. G., 238Gastó, C., 58Gathercole, S. E., 434Gazzaniga, M., 122, 334Gazzaniga, M. S., 117, 121, 232Ge, H., 312
Ge, X., 570Geary, D., 452Geary, D. C., 35, 475Gebhard, P., 484Geddes, J., 701Geis, G., 533Geisler, J. M., 64Gekoski, M., 562Gelernter, J., 650Gelman, R., 403, 559Gene (patient), 328Gentner, D., 369, 370, 387, 388Genz, K., 549Georgellis, Y., 620Geraerts, E., 320, 331, 332Geren, J., 412Gerg, S., 72Gergely, G., 66German, T. P., 369Germans Gard, M., 660Gershoff, E., 576Gershon, A., 108Gershon, S., 655Gersons, B. P. R., 649Gervain, J., 398Geschwind, N., 123Gewirtz, J. C., 266Ghazanfar, A. A., 414Ghera, M. M., 601Giaume, C., 90Gibb, R., 125Gibbs, W. W., 468Gibson, E., 395, 396Gibson, J. J., 202Gick, M. L., 370Gigante, R. A., 671Gigerenzer, G., 353, 357Gilbert, A., 148Gilbert, D., 361, 362, 364Gilbert, D. T., 353, 620Gilbert, J., 582Gilbert, J. J., 63Gilbert, S. J., 125, 435Gilbertson, L. G., 63Gilbertson, M. W., 662Gilbertson, T., 151Gilestro, G., 238Gilhooly, K., 356Gillham, J., 628Gilligan, Carol, 574Gilliland, K., 600Gilovich, T., 355, 618Gil-Verona, J. A., 702Gingerich, P. D., 63Gitlin, M. J., 701Giurfa, M., 283Gladis, L., 704Glaser, J., 222Glaser, R., 374Glass, G. V., 711Glass, R. M., 702Glauberman, N., 442Gleitman, H., 287, 388, 392, 399, 400,
403, 409Gleitman, L., 392, 409
N6 PNAME INDEXO
Gleitman, L. R., 388, 389, 395, 399, 400,403, 406, 408, 410, 416, 420, 421
Glick, I. D., 696Gliner, M. D., 530Glover, G., 309Gobet, F., 374Goddard, G. V., 297Godden, D. R., 315Goedert, M., 585Goff, D. C., 664Goggin, J., 330Gold, A. R., 481Gold, P., 325Goldberg, E. M., 665Goldberg, L. R., 593, 598Goldenthal, P., 68Goldfried, M. R., 688, 692Goldin, P. R., 650Golding, L. R., 655Goldin-Meadow, S., 406, 407Goldman, M. S., 249Goldman-Rakic, P., 124, 233, 558Goldman-Rakic, P. S., 664Goldstein, E. B., 158Goldstone, R. L., 387, 388Golinkoff, R., 403Gombrich, E. H., 215Gomez, R., 313Gomez, R. L., 238Gonzalez, R., 652Goodale, M. A., 194, 195, 224Goodman, G. S., 330Goodwin, F. K., 656, 658Gooley, J. J., 234Gooren, L., 453Gopnik, A., 561Gopnik, M., 410Gordon, H., 446Gordon, P., 401Gordon, R. D., 326Gorelick, D. A., 664Goren, A., 535Gorman, J. M., 711, 712Gösele, U., 713Gosling, S. D., 523, 602Gosling, S. P., 593Gottesman, I. I., 72, 449, 661Gottestam, K., 587Gottfredson, L. S., 425, 428, 438, 454Gotts, S. J., 196Gotzche, P. C., 707Gould, J. L., 287Gould, S. J., 442Gourevitch, M. N., 251Graaf, R. de, 644Graber, J. A., 578Grabowecky, M., 210Grabowski, H. G., 706Grabski, W., 497Graf, P., 335Grafman, J., 126Graham, C. A., 482Graham, C. H., 174Graham, J. R., 641Graham, J. W., 255Graham, L. M., 357
Grahame, N. J., 274Grammer, K., 481Grant, V. W., 540Grasby, P. M., 696Gray, J. A., 600Gray, W. D., 318Green, M. F., 660Green, R., 483Green, R. L., 446Green, S., 414Green, S. K., 535Greenberg, B. D., 58Greenberg, D., 12Greenberg, D. L., 330Greenberg, J., 619Greenberg, L. S., 687, 712Greenberg, R. P., 241Greenblatt, B. J., 698Greene, D., 285Greene, J., 3Greenfield, P. M., 441, 447Greenwald, A., 43Greenwald, A. G., 512Gregg, P. A., 618Gregoriou, G. G., 196Greischar, L. L., 247Greischer, Grewal, D., 438Grice, H. P., 395Griffin, G., 252Griggs, R. A., 357Grigorenko, E., 437Grigorenko, E. L., 454Grimes, K. E., 663Grimshaw, J., 390Grinspoon, L., 252Grodner, D., 395Grodzinsky, Y., 124Groop, L. C., 473Gross, C. G., 177Gross, J. J., 491, 493, 498, 499, 587, 630Grotzer, T. A., 353, 446Grove, W. M., 642Gruber, A. J., 252Gruber, S. A., 656Grudnik, J. L., 433Gruenberg, A. M., 662Grunhaus, L., 108Gudjonsson, G. H., 8Guesbeck, N. R., 467Guinn, J., 617Gur, R. C., 452Guroff, J. J., 671Gursky, J. T., 698Gutiérrez, B., 58Guttmann, N., 282Guyer, M. J., 332
Habib, M., 124Hackett, G., 549Hackman, A., 651Hackman, D., 448Haddad, P., 698Haddad, R., 149Haden, C., 569Hadjiyannakis, K., 656Hadley, S. W., 711
Hagel, R., 481Hagen, D. W., 63Hager, J. L., 291Haggard, P., 230, 231Hagoort, P., 383Haidt, J., 3, 620Haier, R., 433Halari, R., 453Haley, A., 72, 448, 449Halgren, E., 235Hall, C., 535Hall, C. S., 240Hall, D. G., 403Hall, L., 330Hallmark, R., 642Halpern, D., 452, 453Hamada, W. C., 595Hamani, C., 702, 703Hamann, S., 329, 331Hambrick, D. Z., 436Hamburg, D. A., 481Hamill, R., 352Hammersmith, S. K., 483Hampson, E., 453Haney, C., 530Hansen, N. B., 711Hanus, L., 252Harackiewicz, J. M., 486Harber, K. D., 513Hardt, O., 313Hare, R. D., 672Harkins, S., 528Harley, T. A., 313Harlow, H. F., 475, 563, 571Harlow, M. K., 571Harrigan, M., 703Harris, C. R., 79Harris, G. W., 480Harris, J. R., 572, 580Harris, M. J., 513Harris, P. L., 554Harris, T., 58Harris, Z., 391Harrison, F., 465Harrison, J. A., 672Harsch, N., 12Hart, C., 252, 573Hart, D., 618Hart, S. D., 672Harter, S., 618Hartmann, H., 613Hartrup, W., 572Hartshorne, H., 596Harvey, L. O., Jr., 197Harvey, O. J., 515Harvey, P. D., 661Harwood, R. L., 534Haselton, M., 79Hasher, L., 237Hasselmo, M. E., 312, 331Hastie, R., 322Hatfield, E., 537, 539Hatten, M. E., 548Hauer, B., 320, 331, 332Hauri, P., 235Hauser, M. D., 414
Hawkins, R. D., 297Hawley, C. W., 600Hawley, K., 711Haxby, J. V., 194Hay, P., 701Hayes, J., 373Hayes, M. E. B., 446Hayne, H., 322Haynes, J. D., 230Haynes, O., 499Haynes, R. B., 706Hayward, W. G., 418Hazel, T., 128Hazelrigg, M., 709Heath, C., 594Heatherton, T. F., 617Heckers, S., 665Heckman, J. J., 446Heider, F., 417, 507Heien, M. L. A. V., 490Heils, A., 58Heimberg, R. G., 646Heine, S., 456Heine, S. J., 602, 618, 625Heingartner, A., 528Held, J. D., 452Hellstrom, K., 646Helmholtz, Hermann von, 158, 158, 169,
197, 202Hemphill, J. F., 672Hen, R., 127Henderlong, J., 286Henderson, H. A., 601Henderson, J. M., 209Henderson, V. K., 570Hendry, D. P., 284Henry, P. J., 437Herbener, E. S., 539Herdt, G., 483Hering, Ewald, 172Herman, E. M., 528Herman, L., 415Hermann, D., 44Herness, M., 151Herrell, R., 58Herrnstein, R. J., 283, 442, 446Hertel, P., 9, 438Hertz, Heinrich, 154Hertzog, C., 583Hespos, S. J., 418Hess, E. H., 564Hetherington, E. M., 571Hettema, J. M., 650Heuer, F., 329Heuer, S. K., 535Hewer, A., 575Hezlett, S. A., 427Hier, D. B., 453Higbee, K. L., 311Higgins, E. T., 512, 617Higgins, J., 689Higgins, R., 627Hilgard, E. R., 245, 246, 671Hilgard, J. R., 245Hill, A. L., 439Hill, C. T., 537
PNAME INDEXO N7
Hill, N. M., 409Hiller, J. B., 642, 656Hillery, J. M., 528Hillis, A., 386Hilts, P. J., 333Hineline, P. N., 294Hines, M., 453, 484Hinshaw, S. P., 644, 668Hinton, G. E., 190Hintzman, D. L., 317Hirsch, S. R., 663Hirschfeld, R. M. A., 656Hirsh-Pasek, K., 403, 409Hirst, W., 13, 330Hitch, G. J., 318H.M. (patient), 333Hoberman, H., 711Hobson, J. A., 236, 238Hobson, R. P., 667Hochman, K., 661, 663Hoda, H., 435Hodge, C. N., 535Hodges, B., 521Hodges, E. V. E., 573Hodges, H., 128Hoefnagel-Hohle, M., 412Hoffman, L. T., 446Hoffman, M. L., 576Hoffrage, U., 353Hofstede, G., 602Hogarty, G. E., 692Holden, C., 650, 654Holland, J. H., 353Holland, P., 275Hollander, E., 698Hollerman, J. R., 489Hollingshead, A. B., 665Hollis, K. L., 275Hollister, L. E., 697Hollon, S. D., 692, 697, 705, 712Holm, K. H., 128Holmes, D., 612Holtzman, P. S., 666Holway, A. F., 197Holyoak, K. F., 353Holyoak, K. J., 357, 370Holzberg, A. D., 618Hommer, D., 489Honarvar, S., 296Hong, H., 510, 511Honzik, C. H., 287Hood, W. R., 515Hooley, J. M., 656, 666Horan, W. P., 660Horn, J. L., 432Horowitz, J. L., 653Horowitz, L. M., 614Horowitz, T. S., 189Horvath, J. A., 437Hovland, C. I., 515Howard, K. I., 712Howe, M., 322Howes, C., 570, 572Howlett, A. C., 252Hrobjartsson, A., 707
Hsia, Y., 174Hsu, A. Y. C., 587Hsu, L. K. G., 669Hu, R. J., 696Hubble, M. A., 704Hubel, D., 175Hudetz, A., 233Hudson, J. I., 330, 671Huesmann, L. R., 477Hug, K., 357Hugart, J. A., 283Hughes, C., 573Hughes, J., 102Hughes, J. D., 334Hume, D., 386, 386Humphreys, M. S., 334Hunt, E., 432, 433, 454Hunt, P. J., 528Hunt, W. A., 496Hunter, J. E., 427, 535Hupbach, A., 313Hurley, R. A., 700Hurvich, L. M., 172Husband, T., 320Huston, L., 566Huston, T. L., 533Hutchinson, R. R., 475Huttenlocher, J., 402Hwang, W., 683Hyde, J., 452, 453Hyde, J. S., 604Hyman, I., 320Hyman, S. E., 644, 659, 713Hymel, S., 574Hymphreys, G., 122Hyson, D., 566
Iacono, W. G., 444, 668Ibanez, V., 126Ide, E., 625Iglowstein, I., 237Ikonomidou, C., 549Infante, J. R., 247Insabella, G. M., 571Inzlicht, M., 514Irion, A., 319Isacson, O., 128Isham, E. A., 231Ishimaru, M. J., 549Ising, M., 713Ito, T. A., 512Ivry, R., 117, 122Iyengar, S., 362, 626Izard, C., 499Izard, C. E., 68, 491, 492Izard, V., 441Izpisúa-Belmonte, J. C., 65
Jaafari, N., 703Jablensky, A., 659Jackendoff, R., 256, 386, 390Jackson, L. A., 535Jacobs, W. J., 331Jacobsen, F. M., 698Jacobsen, L. K., 665
Jacoby, L. L., 335Jacoby, R., 442James, L., 313James, L. E., 313James, W., 220, 463, 494, 616Jameson, Dorothea, 172Jamison, K. R., 653, 654, 658Jang, K. L., 599, 671Janicek, P. G., 701, 703Janis, I., 531Janke, A., 64Jankowiak, W. R., 540Janoff-Bullman, R., 620Janowsky, J. S., 453Janssen, E., 482January, D., 421Javitt, D. C., 664Jelicic, M., 320, 331, 332Jencks, C., 454, 455Jenett, A., 283Jenike, M. A., 701Jenkins, J. G., 319Jenni, O. G., 237, 238Jensen, A. R., 433, 454Jensen, M., 245Jensen, P. S., 668Jerabek, P. A., 656, 703Jeziorski, M., 369Jin, R., 649Jobe, J., 318Johansson, B., 72Johe, K., 128John, O. P., 593, 594Johns, M., 514Johnson, A. M., 484Johnson, C., 682Johnson, J., 412Johnson, M. H., 196, 562Johnson, M. K., 310, 333Johnson, M. R., 252Johnson, R. D., 529Johnson, S. L., 654, 655, 656, 692, 698Johnson, S. M., 353Johnson, S. P., 558Johnson, V. E., 481Johnson, W., 452, 453Johnston, J. C., 368Johnston, R., 68Johnston, V. S., 481Johnstone, T., 490Joiner, T., 657Joint Statement on the Impact of
Entertainment Violence onChildren: Congressional PublicHealth Summit, 477
Jokela, M., 602Jones, B. P., 665Jones, E. E., 507, 626, 627Jones, G. V., 308Jones, P. B., 660Jones, S., 402Jooste, P., 238Jordan, K., 573Jorgensen, B. W., 536Josephs, R. A., 249
Joshi, A. K., 391Joslyn, S. L., 612Jost, J. T., 523Jouvet, M., 235Joy, L. A., 477Judd, C. M., 530Judd, L. L., 711Judy, B., 575Jung, C. G., 611Junque, C., 702Jusczyk, P. W., 399Jussim, L., 513Just, M. A., 396
Kaczala, C. M., 453Kaemmer, B., 641Kagan, J., 599, 601Kahan, J. P., 626Kahana-Kalman, R., 562Kahn, I., 309, 323Kahneman, D., 350, 352, 360Kakinohana, O., 128Kako, E., 415, 421Kalat, J. W., 291Kalish, H. I., 282Kamide, Y., 394Kamin, Leon, 274Kamin, L. J., 442Kaminski, J., 414Kaminsky, H., 575Kampmann, K. M., 254Kanagawa, C., 598Kanaya, T., 332, 447Kandel, D. B., 536Kandel, E. R., 296Kane, J. M., 696Kane, M. J., 125, 434, 435Kant, Immanuel, 136, 136Kanwisher, N., 229, 559Kaplan, H., 551Kapur, S., 313, 696Karasawa, M., 510Karau, S. J., 528Karch, S., 146Karkowski, L. M., 662Kashiwayanagi, M., 151Kasser, T., 483Kassin, S. M., 8Katz, J. J., 386Kauffman, T., 126Kaufman, A. S., 454Kaufman, J. C., 437Kay, P., 415, 417Kaye, W., 669Kazdin, A. E., 576, 689, 711Kean, M., 388Keane, T. M., 649Keating, D., 581Keefe, K., 582Keel, P. K., 670Keeler, G., 570Kegeles, L. S., 664Kegl, J., 407Keil, F. L., 389Keith, B., 571
N8 PNAME INDEXO
Keizer, K., 519Keller, M. B., 653Kelley, H. H., 507Kelley, M. W., 617Kellman, P. J., 186, 558Kelsoe, J. R., 655Keltikangas-Jarvinen, L., 602Kendall, P. C., 690Kendler, K. S., 73, 650, 655, 662Kenrick, D., 79Kenrick, D. T., 538Kentle, R. L., 593Kepler, Franz, 86Keren, G., 5, 353Kerr, M. E., 694Kessler, R. C., 644, 645, 646, 647, 648,
649, 652, 653, 654Kestler, L., 661, 663Kety, S. S., 655, 662Keverne, E. B., 150Khan, R., 149Kihlstrom, J. F., 222, 246, 439, 612, 670Kilham, W., 525, 526Killeen, P. R., 246Kilstrom, J. F., 332Kim, A., 453, 456Kim, C.-Y., 230Kim, J. A., 278Kim, J. K., 333Kim, W.-Y., 127Kimball, M. M., 477Kimberg, D. Y., 125, 435King, C. E., 63King, J. E., 593King-Casas, B., 672Kingsley, P., 252Kingstone, A., 117Kinney, D., 582Kinoshita, S., 334Kinsbourne, M., 233Kinsey, A., 484Kinzler, K. D., 396Kirkpatrick-Steger, K., 283Kirsch, I., 245Kita, S., 407Kitano, J., 63Kitayama, S., 508, 625Kivimaki, M., 602Klaey, M., 150Klaiman, C., 439Klauer, K. C., 356Klein, D. C., 289Kleinman, A., 658Kleitman, N., 240Klerman, G., 685Klerman, G. L., 697Klima, E. S., 406Kluender, K., 207Kluft, R. P., 670Klump, K. L., 670Knaack, A., 576Knickmeyer, R., 549Knight, J., 536Knight, R. T., 210Knutson, B., 489Koch, C., 223, 229, 230, 232, 549
Kochanska, G., 576Kochenderfer, B., 573Koekoek, S., 297Koelling, R. A., 292Koestner, R., 286, 642Koh, E. S., 663Koh, P. O., 664Kohn, A., 285Kohn, M. L., 665Kolb, B., 89, 115, 125, 548, 551Kolers, P., 336Kondziolka, D., 128Koops, W., 561Kopta, S. M., 712Korn, J. H., 44Kornhuber, H. H., 121Kosslyn, S. M., 343, 344, 345Kosterlitz, H., 102Kotrschal, K., 290Kotter, R., 116Kotz, K., 430Koulakoff, A., 90Kounts, S. L., 534Koutstaal, W., 309Kovacs, A., 409Kovelman, I., 408Kovera, M. B., 531Kraemer, H. C., 669Krahn, L. E., 698Kral, P. A., 293Kramer, A., 583Kramer, A. F., 585Kramer, P. D., 697Kranzler, J. H., 433Krashen, S., 405Krasnow, A. D., 708Krasuski, J., 703Krause, M., 294Krause, M. S., 712Kraut, M. A., 584Kraut, R., 68Kreiman, G., 223Kring, A. M., 660Krueger, R. F., 668, 673Kruglanski, A. W., 531Kruschke, J. K., 275Ksir, C., 252Kuan, D. Y., 549Kucharova, K., 128Kuhl, B., 612Kuhn, D., 581Kuhn, I. F., 402Kulik, J., 329Kumari, V., 600, 680Kuncel, N., 598Kuncel, N. R., 427, 428Kunda, Z., 353, 618Kurihara, K., 151
Laan, E., 482LaBar, K. S., 329, 498Laboratory of Comparative Human
Cognition, 568Labov, W., 383, 396Ladd, G., 573Ladefoged, P., 381
Ladouceur, C. D., 656LaFarge, L., 610Lagaipa, J., 582Lagerspetz, K. R., 477Laible, D., 576Laibson, D. I., 578Laird, R., 573Lalonde, J. K., 671Lam, A. G., 682Lamb, H. R., 696Lamb, M., 331, 562Lamb, M. E., 565Lamberg, L., 696Lambert, M. J., 711Lampert, C., 669Landau, B., 389, 402, 403, 408, 410, 418Landis, C., 496Lane, M., 682Lane, N. M., 403Lane, S. D., 252Laney, C., 320Lang, B., 561Lang, P. J., 646Langeland, W., 649Langer, E. J., 625Langlois, J. H., 573Lapid, H., 149Largo, R. H., 237La Rosa, J., 595Larsen, B., 121Larsen, R. J., 79Larson, R., 577Laruelle, M., 664Lassen, N. A., 121Lassiter, G. D., 374Latané, B., 528, 533Lattal, K. M., 296Lau, H. C., 231Lau, R. R., 627Laughlin, J. E., 434Laureys, S., 229Laursen, B., 581Lawrence, A. D., 496Lawrence, K. Q., 311Lawrie, S. M., 665Lazareva, O. F., 283Lazarus, A. A., 692Lazarus, R. S., 493Lea, S. E. G., 283Leary, M. R., 485, 486Lebedev, M., 106Lebolt, A., 574Le Bon, G., 529Leckman, J. F., 650Leclercq, Y., 238LeDoux, J., 312LeDoux, J. E., 116Lee, A., 667Lee, D., 652Lee, D. H., 497Lee, P., 12LeFever, G. B., 668Leggett, E. L., 624Lehman, D., 353, 358Lehman, D. R., 467, 625Lehmann, R., 117
Lehner, T., 58Leibowitz, H., 197Leibowitz, S. F., 469Leiman, A. K., 480, 549Leiman, A. L., 476Lempert, R. O., 353Lenneberg, E. H., 410Lennox, B. R., 660Lenton, A., 322Lenzenweger, M. F., 661Leon, A. C., 712Leonard, H. L., 648Lépine, R., 434Lepper, M., 362, 626Lepper, M. R., 285, 286, 355, 530LeRoith, D., 105Lesch, K. P., 58, 650Lettvin, J. Y., 174Leung, C., 625Leung, K., 595Levelt, W. J. M., 382Levenson, R. W., 491, 494Levi, D., 207Levin, I., 5, 360Levine, B., 125, 435Levine, C., 575Levine, J. M., 522, 530Levine, L., 452Levine, L. J., 497Levine, M., 532, 533Levine, P., 668Levinson, S. C., 419Levitsky, D. A., 467Levy, A., 566Levy, B. J., 612Levy, J., 118Levy, W. B., 297Lewis, C., 353, 453Lewis, D. O., 671Lewis, G., 58, 657Lewis, M., 671Lewontin, R. C., 451Li, P., 386, 420, 421Li, P. W., 54Liang, K. -Y., 58Liberman, A. M., 382, 515Liberzon, I., 496Libet, B., 230Lichter, D. G., 124Lichtner, P., 713Lidow, M. S., 664Lietaer, G., 687, 712Liker, J., 437Lilienfeld, S. O., 642, 671, 711Lindberg, S., 453Lindenberg, S., 519Lindenberger, U., 583Linder, D. E., 538Lindsay, D. S., 320, 331, 332Lindskold, S., 530Lindzey, G., 454Linehan, M. M., 693Linn, M., 452, 453Liotti, M., 656Lipetz, M. E., 539Lippa, Y., 388
PNAME INDEXO N9
Lipton, J. S., 559Lisanby, S. H., 702Lisman, J., 296Liu, W., 650Livesley, W. J., 599, 671, 672Livingstone, K., 668Livson, N., 574Lobaugh, N. J., 233Lock, T. G., 325Locke, John, 134, 135, 260, 389, 400Loehlin, J. C., 454, 599Loewenstein, G., 578Loftus, E., 325Loftus, E. F., 320, 324, 332Logothetis, N. K., 230Logrip, M. L., 409Lohman, D., 433Lohrenz, T., 672Lollis, S. P., 572Lomax-Bream, L., 672Lomo, T., 297London, P., 534Longo, L. C., 535Lopes, P. N., 438Lord, C., 355Lord, C. G., 530Lorenz, K., 475, 564Lovaas, O. I., 689Love, J., 570Loveland, D. H., 283Lowell, E. L., 486Lowry, D., 311Lozano, A. M., 702, 703Lu, C. H., 65Lubinski, D., 428, 448, 452Luborsky, L., 712Lucas, R. E., 620Lucca-Irizarry, N., 618Luginbuhl, J. E. R., 626Luk, C.-H., 149Lundregan, T., 324Luo, D., 433Luo, Y., 560Luria, A. R., 440Lüthgens, C., 355Lutz, A., 247Lydiard, R. B., 699Lykken, D. T., 444, 599Lynch, T. R., 693Lynn, R., 442, 452Lynn, S. J., 325Lyubomirsky, S., 620, 652
Ma, V., 618Maass, A., 510McAdams, D. P., 617, 642Macagno, F., 398MacArthur, R., 206McCabe, A., 569McCarrell, N. S., 317McCarter, L., 491McCauley, C. R., 586McClearn, G. E., 72McClelland, D. C., 486, 642McClelland, J. L., 190McClelland, P., 442
McClintock, M., 150, 483McClintock, M. K., 150, 479McClure, S. M., 578Maccoby, E. E., 569, 572, 602McConkey, K. M., 245, 246McCowan, B., 414McCrae, R. R., 593, 594, 595, 602McCrink, K., 559McCullogh, W. S., 174McDaniel, M. A., 325McDermott, K., 322MacDonald, A. W., 249MacDonald, M. C., 392, 396MacDonald, T. K., 249McDougal, W., 463McEachin, J. J., 689McEwan, S. R., 433McEwan, T., 324McEwen, B. S., 480McFall, R. M., 142, 682Macfarlane, A., 150McGaugh, J., 9McGaugh, J. L., 9, 312, 313, 315, 331McGee, A. W., 90McGeoch, J. A., 319McGhee, D. E., 512McGinnis, S., 656McGrath, J., 663McGraw, A. P., 353McGregor, G. P., 468McGue, M., 444, 472, 599, 668McGuffin, P., 655Machin, D., 663Machin, S., 452McIntosh, A. R., 233Mack, A., 212McKenna, P. J., 665Mackie, K., 252McLachlan, D. R., 325McLaughlin, T., 689McLean, J., 284McLean, J. E., 454MacLean, P., 116McManus, F., 651McNally, D., 330, 331McNally, R., 332McNaughton, B. L., 297McNeeley, H. E., 702, 703McNeill, D., 313MacNichol, E. F., Jr., 169Macphail, E. M., 296Macrae, C. N., 617Madden, E. C., 402Maddux, J. E., 623Maffei, M., 468Magdalin, W., 468Magen, E., 630Magnuson, D., 596Magoun, H. W., 465Maguire, A. M., 334Maguire, E., 126Maguire, M. C., 573Mahalik, J. R., 682Mahboubi, M., 435Mahli, G. S., 701Mahon, B. Z., 328
Mahoney, M. J., 689Mahurin, R. K., 656, 703Mai, N., 122Maia, T. V., 231, 232Maier, S. F., 289, 325Main, M., 566Makhijani, M. G., 535Malcolm, G. L., 209Maldonado, J. R., 670Malkin, C., 562Mallet, L., 703Malone, M. J., 573Manderscheid, R., 696Mandisodza, A., 535Mandler, G., 335, 396Mangun, G., 117, 122Manier, D., 13Manly, T., 122Mann, L., 525, 526Mannetti, L., 531Manning, R., 532Manns, J. R., 296Mansouri, F., 435Mantell, D. M., 525Maquet, P., 242Mar, A., 601Marañon, G., 496March, J. S., 648Marcus, G. F., 391, 400, 403, 404, 410Marder, S. R., 696Marino, L., 283, 414Markman, E. M., 400, 402Markon, K. E., 673Markowitsch, H. J., 9Markowitz, J. C., 685, 697, 712Marks, S., 410Markus, H. R., 508, 598Marler, P. R., 295, 412Marsala, S., 128Marsella, A. J., 595, 649Marshall, G. D., 496Marshall, N. L., 570Marshall, P. J., 601Marshall-Goodell, B. S., 514Marslen-Wilson, W., 396Marslen-Wilson, W. D., 333Martin, C. E., 484Martin, D. J., 711Martin, J. A., 569Martin, L., 416Martin, M., 308Martin, M. F., 670Martin, P., 663, 665Martinez, J. L., 297Martinez, M., 446Martino, S., 686Martis, B., 703Maslow, A. H., 485, 615Massey, C., 395Massimini, M., 233Master, A., 456Masters, W. H., 481Mather, M., 587Matin, L., 206Matsukura, M., 122Matsumoto, D., 67, 493
Matt, G. E., 709Matthews, G., 439Mattia, J. I., 709Maturan, H. R., 174Maunsell, J. H. R., 194Mauskopf, J., 706Mauss, I. B., 491May, C. P., 237May, M. A., 596Mayberg, H. S., 656, 702, 703Mayer, J. D., 438Mayes, A. R., 313Mayhan, W. G., 102Meachem, J., 284Medin, D. I., 389Medin, D. L., 387, 388Medley, F., 660Mednick, S., 238Meehl, P. E., 638Meeter, M., 312Mehandran, R., 663Mehler, J., 382, 398, 399, 409Mellers, B., 353, 360Melnyk, L., 321Meltzer, H. Y., 656Meltzoff, A. N., 290, 562Melvin, L. S., 252Melzack, R., 148Mendoza-Denton, R., 597Mennella, J. A., 152Menozzi, P., 454Menzel, R., 283Mercer, K. B., 650Merckelbach, H., 320, 331, 332Merikangas, K. R., 649Mervis, C. B., 402Merzenich, M., 126Mesquita, B., 493Metcalfe, J., 371Meyer, B. U., 117Meyer, D. E., 347, 373Meyer, N., 116Meyer-Lindenberg, A., 672Meyerowitz, J. A., 618Micallef, J., 650Michael, R. P., 150, 480Michela, J. L., 507Miklowitz, D. J., 654, 655, 656, 692, 694,
698Mikulincer, M., 614Milazzo-Sayre, L. J., 696Milgram, S., 44, 524, 526Miller, Arthur, 355Miller, D. T., 255, 534, 626Miller, E. M., 433Miller, G., 90, 92, 237, 657, 658, 682, 703Miller, G. A., 305Miller, I. J., 152Miller, J., 62Miller, J. G., 510, 534Miller, L. K., 439Miller, L. S., 477, 663Miller, N., 324Miller, N. E., 469Miller, R. L., 521, 711Miller, R. R., 274, 275
N10 PNAME INDEXO
Miller, S. D., 704Miller, T. E., 573Miller, W. R., 289, 686Mills, B., 322Milner, A. D., 194, 224Milner, B., 124, 333Mineka, S., 290, 294, 651Minsky, M., 228Minuchin, S., 694Mischel, H. N., 629Mischel, W., 510, 596, 597, 624, 628,
629, 630Miselis, R. R., 468Mishkin, M., 194Mishler, E. G., 666Mistlberger, R. E., 233Mita, T. H., 536Mitchell, D., 238Mitchell, J., 323, 566, 711Miyake, A., 396Modrek, S., 668Moen, P., 442Modahl, C., 667Moffat, S., 453Moffitt, T. E., 58, 655Moghaddam, F., 522Mohamed, F., 80Mohyde, M., 582Molden, D. C., 624Molinari, L., 237Moloney, D. P., 603Monahan, J., 142Mondin, G. W., 7111Monroe, S. M., 656Montagu, A., 442Montague, D., 562Montague, P., 672Montgomery, S. A., 698Moody, M., 711Moore, B., 629Moore, J., 59Moore, M. K., 290Moorhead, G., 531Moos, R. H., 481Mora, F., 470, 695Moran, T. J., 575Moray, M., 582Moray, N., 214Moreland, R. L., 530, 536Moreno, C., 654Morewedge, C., 240Morewedge, C. K., 361Morgan, B., 102Morgan, C. P., 530Morgan, J. L., 382, 399Morgan, M. J., 251Morgan, R. F., 446Morris, A. S., 578Morris, E. K., 320Morris, H., 102Morris, P. G., 660Morrison, F. J., 568Morrison, S. L., 665Morse, H. M., 595Morse, R., 446Moscovici, S., 355, 530
Moscovitch, M., 313, 325Moser, M. B., 125, 297Mosher, D. L., 482Moskovitch, M., 4Mosnaim, A. D., 647Motohashi, K., 148Mottolese, C., 231Mouihate, A., 252Mounts, N. S., 574Mozel, M., 150Mullen, M. K., 569Müller, H. J., 196Müller, Johannes, 143Mulrow, C. D., 697Munafo, M. R., 58, 657Munnich, E., 418Mural, R. J., 54Murphy, B. C., 573Murphy, F. C., 496Murphy, G. L., 387Murray, C., 428Murray, C. A., 442Murray, S. R., 696Murray, T. H., 44Murre, J. M. J., 312Musch, J., 356Mussell, M., 711Myers, B., 325Myers, E. W., 54Myers, T., 80Mynatt, C. R., 355
Nadel, L., 238, 313, 331Nader, K., 312Nagel, T., 256Naigles, L. G., 403Nakagawa, S., 493Nakamura, J., 372Nakayama, K., 229Nappa, R., 403Narvaez, D., 575Nash, M. R., 245, 246Nasser, M., 670Nathan, P. E., 708, 711, 712National Research Council and Institute
for Medicine, 571Naumer, B., 356Nauta, W. J. H., 88Navarro, A. M., 709Nazzi, T., 398Neale, M. C., 484, 650, 655, 662Neck, C. P., 531Needham, D., 370Neimeyer, G., 539Neisser, U., 12, 211, 330, 442, 446, 447,
449, 455Nelson, C. A., 572Nelson, E. S., 575Nelson, K., 569Nemeth, C., 522Neria, Y., 656Nespor, M., 382, 399Nettelbeck, T., 439Neumann, C., 447Newcomb, A. F., 572, 573, 574Newcomb, T., 529
Newcombe, F., 195Newcombe, N., 453Newcombe, N. S., 2002Newell, A., 366Newell, L., 573Newman, E. A., 92Newport, E. L., 400, 406, 410, 412, 413Nezworski, M. T., 642Nich, C., 686NICHD Early Child Care Research
Network, 570Nichols, K. E., 601Nicholson, R. A., 710Nickens, S., 453Nickerson, R. A., 308Nickerson, R. S., 446Nicolelis, M., 106Nida, S. A., 533Nieberding, R., 642Nilsson, M., 64Nimmo-Smith, I., 496Nisbett, R., 358Nisbett, R. E., 224, 225, 226, 285, 352,
353, 357, 440, 477, 507, 508, 596Nitsch, K., 317Nobler, M. S., 701, 702Nolen-Hoeksema, S., 628, 652Noll, J., 432Nopoulos, P., 659, 665Norbury, H. M., 419Norcross, J. C., 692, 711Norenzayan, A., 534, 602Norman, D. A., 304Norman, W. T., 593Norton, M. I., 240Noseck, B. A., 523Nosek, B. A., 512Novak, M. A., 571Novick, J. M., 410Novotny, C., 708Noyes, R., 650Nurnberger, J. I., 655Nyberg, L., 124Nystrom, L., 3
Oakes, M. A., 612Oberman, L. M., 667Obhi, S., 231Ochsner, K. N., 493, 499, 612O’Connor, T. G., 572Odbert, H. S., 593Odiorne, J. M., 474Oesterman, K., 35, 476Ofshe, R., 332Ohlsson, S., 373Öhman, A., 290, 294, 646, 651Okamoto, S., 62Okasha, A., 636Okasha, T., 636Olff, M., 649Olfson, M., 682, 697Oliva, P., 330Oliver, L. M., 357Ollendick, T. H., 706, 712Olsen, J., 573Olsen, S., 573
Olson, A., 122Olson, D. J., 295Olson, E. A., 325Olson, M., 334Omoto, A. M., 534O’Neal, J., 659Ones, D. S., 427Oomen, A., 561Opie, M., 386Orbach, Y., 331Ordóñez, L., 360Orne, M. T., 244Ortmann, J., 655Orwoll, E. S., 453Osherson, A., 670Osherson, D. N., 388Osler, S., 317Ost, L. G., 646Oster, H., 491Ottenberg, P., 526Oviatt, S. K., 453Owens, E., 566Ozer, E. J., 598Özyürek, A., 407
Pacifici, R., 251Packer, D. J., 531Palmer, S. E., 186Pals, J. L., 617Panksepp, J., 668Pantev, C., 126Panyavin, I. S., 80Panzarella, R., 524Papafragou, A., 395, 403, 416, 421Paradiso, M. A., 121Paris, J., 671Park, B. G., 660Park, C., 627Park, M., 628Parker, E. S., 313Parker, G., 663Parker, J., 573, 574Parson, L. M., 115Parsons, J. E., 453Pascual-Leone, A., 126Pashler, H., 368, 372Pasupathi, M., 587Patnoe, S., 516Pattee, L., 574Patterson, B. W., 245Patterson, D., 245Pauls, D. L., 650Paulus, M. P., 711Pavlov, Ivan Petrovich, 263–64, 263Payne, D. G., 325Payne, J. D., 331Peabody, D., 595Peace, K. A., 330Peake, P. K., 629Pearce, J. M., 274Pearlmutter, N. J., 392, 396Pearson, J., 656Pedersen, N., 72Pederson, E., 419Pekkarinen, T., 452Pemberton, M., 663
PNAME INDEXO N11
Peña, M., 382, 398Penfield, Wilder, 119–20Pennebaker, J. W., 16Pennisi, E., 478Penton-Voak, I. S., 481Pepino, M. Y., 152Pepitone, A., 529Peplau, L. A., 537, 585Pepperberg, I., 415Perani, D., 413Perczel, M., 655Perkins, D. N., 353, 446Perls, F. S., 687Perner, J., 561Perrett, D. I., 481Perrott, D. A., 370Perry, D. G., 573Pertwee, R. G., 252Peskin, H., 574Petersen, S., 334Peterson, C., 569, 619, 621, 625, 627, 628,
657Petitto, L., 408, 415Petitto, L. A., 415Petrides, G., 701Petrides, M., 124Petrill, S., 72Petrill, S. A., 433Petry, N. M., 711Pettigrew, T. F., 516Pettit, G., 573Petty, R. E., 352, 514, 515Peyser, S., 702Pezdek, K., 12, 331, 332Pham, D. L., 584Phan, K. L., 496Phelps, E., 330Phelps, E. A., 497Philips, M. F., 128Phillips, M., 454, 455Phillips, M. L., 656Phillips, P. E. M., 490Piacentini, J., 705Piaget, Jean, 553, 554Piazza, A., 454Pica, P., 441Pickering, S. J., 434Picoult, E., 206Pierce, W. D., 286Pierro, A., 531Pike, K. M., 669Pilgrim, C., 574Piliavin, J. A., 534Pilkonis, P. A., 682, 712Pillard, R. C., 484Pinckert, S., 517Pincus, H., 705Pincus, J. H., 671Pinel, E. C., 361Pinel, J. P. J., 467Pinker, S., 79, 256, 403, 404, 410, 415Pinto, S., 468Pipe, M.-E., 331Pittenger, C., 296Pittinsky, T. L., 453, 456Pitts, W. H., 174
Pizarro, D. A., 497Plaks, J., 512Planetta, P., 231Platek, S. M., 80Plaud, J. J., 687Plomin, R., 6, 444, 445, 449, 567, 599,
603Pogue-Geile, M. F., 660Poincaré, Henri, 372Politi, F., 510Pollack, M. H., 646Polosan, M., 703Pomeroy, W. B., 484Pope, H. G., 252, 330Pope, H. G., Jr., 671Porter, R., 150Porter, R. H., 150Porter, S., 330Posner, M. I., 209Post, R. M., 671Posternak, M. A., 709Posthuma, D., 445Potter, J., 602Poulos, A. M., 296, 297Pratkanis, A., 43Pratt, J., 454Premack, A., 283Premack, D., 283, 284, 560Prentice, D. A., 255Prescott, C. A., 650Preskhorn, S. H., 696Price, D., 148Price, J., 573, 574Principe, G., 332Prochaska, J. O., 711Proffitt, J. S., 389Provine, W. B., 56Prudic, J., 702Puerto, A., 468Purdie-Vaughns, V., 456Putnam, E. W., 671Putnam, F. W., 671Putnam, P., 499Pütz, B., 713Pyszczynski, T., 619
Quine, W., 400Quinn, D., 456Quirk, G., 312Qunisey, V. L., 476
Rachlin, H., 294Rae, C., 433Rae, D. S., 645Rafal, R. D., 122, 210Raines, D., 80Rainville, P., 148Rajah, M. N., 233Rajaram, S., 4, 323Rakic, P., 127, 549, 551Ramachandran, V. S., 667Ramanan, N., 238Ramey, C. T., 446Rami-Gonzalez, L., 702Ramón y Cajal, Santiago, 126Ramsay, D. S., 275
Ranganath, C., 323Ranson, S. W., 465Rapaport, M. H., 711Rapoport, J. L., 648Rasch, B., 238Rasmussen, S. A., 650Rasmussen, T., 120Ratcliff, G., 195Ratey, J., 682Rauch, S. L., 601Rauner, S., 527Raven, B. H., 541Ravussin, E., 471, 473Rawlings, N. B., 247Rawlings, Rayias, M., 499Ray, O., 252Raymaekers, L., 320, 331, 332Rayner, K., 209, 392Reber, A. S., 537Reber, E., 618Recanzone, G., 126Redelmeier, D. A., 364Redl, F., 526Redlich, F. C., 665Reed, D. R., 152Reed, M., 527Rees, G., 223, 230Reese, E., 569Reeves, A. G., 117Reeves, L., 374Regier, D. A., 646, 647Regier, T., 417Reichenberg, A., 661Reid, D. H., 689Reid, V. M., 559Reilly, K., 231Reisberg, D., 9, 214, 325, 329, 438Reiss, D., 283, 414Reisser, B. J., 344Remington, G., 696Ren, K., 312Renfrew, J. W., 475Rensink, R. A., 212Rentfrow, P. J., 602, 617Rescorla, R. A., 269, 271, 274Resick, P. A., 649Resnick, S. M., 584Ressler, K. J., 703Rest, J., 575Rest, J. R., 575Retzlaff, P., 244Reveley, A. M., 666Reveley, M. A., 666Reyna, V., 322, 581Reynolds, C. R., 454Reynolds, J. H., 196Reynolds, K., 334Rhines, H., 576Ribot, T., 313Ricard, M., 247Ricci-Bitti, P. E., 491Richard, N., 231Richards, J. M., 499Richardson, W. S., 706Rickard, T. C., 238Rickels, K., 648, 699
Rieffe, C., 561Riemann, R., 599Rigler, D., 405Rigler, M., 405Rimmer, D. W., 237Rinck, M., 308Rincon, C., 574Rincón-Limas, D. E., 65Rips, L. J., 388Risch, N., 58, 657Risen, J. L., 361Risse, G., 333Rizzolatti, G., 290Robbins, S., 266Robbins, S. J., 267Robbins, T. W., 601Roberts, B. W., 598Roberts, R. D., 433, 438, 439Robertson, I. H., 122Robertson, L. C., 210Robertson, T., 79Robins, L. N., 646, 647Robins, R. W., 491Robinson, T. E., 125, 490Rochat, P., 563Rock, Irvin, 212Rockstroh, B., 126Rodin, J., 625Rodriguez, M. L., 628, 630Rodríguez-Esteban, C., 65Roediger, H., 322, 336Roediger, H. L., III, 311Rogers, C., 616Rogers, C. R., 616, 686Rogers, N. L., 236Rogers, T. B., 617Rogoff, B., 568Roland, P. E., 121Rollnick, S., 686Rolls, E. T., 470Romanes, G. J., 279Romano, J., 711Roper, T. J., 294Rorie, A. E., 196Rosch, E. H., 387, 388, 401Rosen, W. D., 563Rosenbaum, M., 468Rosenberg, W., 706Rosenfield, D., 626Rosenstein, M. J., 696Rosenthal, D., 638, 655, 661Rosenthal, R., 513, 642Rosenzweig, M. R., 476, 480, 481, 549Roser, M., 232Ross, C. A., 670, 671Ross, H. S., 572Ross, J., 311Ross, L., 352, 509, 510, 530Ross, M., 350, 355, 626Rossetti, A., 235Roth, A., 711Roth, J., 105Roth, K. A., 549Roth, W. T., 650Rothbart, M. K., 209, 567, 599Rothbaum, F., 540
N12 PNAME INDEXO
Rothman, A. J., 622Rottenstreich, Y., 362Rottman, L., 535Rouach, N., 90Rovee-Collier, C., 562Rozin, E., 153Rozin, P., 4, 291, 575, 586Rozolis, J., 527Rubenstein, J. L. R., 549Rubin, H., 573, 574Rubin, J. Z., 541Rubin, K., 574Rubin, L., 537Ruggiero, M., 533Rujescu, D., 662Rumelhart, D. E., 190Rush, A. J., 691, 692Rushton, J. P., 454Russek, M., 467Russell, D., 627Russell, J. A., 492Russo, E., 252Ruthruff, E., 368Rutter, M., 655Ryan, C. M. E., 283Ryan, R. M., 286, 616Ryff, C. D., 622Rynn, M. A., 648
Sabini, J., 509Sabo, H., 410Sabol, S. Z., 58Sachs, G. S., 698Sackeim, H., 701Sackeim, H. A., 702Sackett, D. L., 706Sackett, P., 455Sacks, O., 122Sadato, N., 126Sadler, H., 534Saffran, J. R., 400Sagher, O., 703St. Clair, D., 663St. Jacques, P., 329Saitoh, O., 667Salamero, M., 702Salovey, P., 79, 438, 622Salthouse, T. A., 432, 583, 584, 585Salyakina, D., 713Samuels, C., 325Sanders, W. J., 63Sanderson, C. J., 672Sanislow, C. A., III, 682Sanitioso, R., 618Santi, A., 124Santini, E., 312Saper, C. B., 234Sapolsky, R. M., 475, 476Satir, V., 694Saunders, S. M., 712Savage-Rumbaugh, E. S., 415Savin, H. B., 44Savin-Williams, R. C., 484Savoie, T., 663Savova, V., 391Sawa, A., 663, 664
Sawamoto, K., 128Sawyer, K., 372Saxe, G., 568Scantlebury, J., 231Scarr, S., 454, 455, 603Schaal, B., 150Schachter, F., 604Schachter, S., 224, 496Schacter, D. L., 309, 323, 328, 332, 335,
670Schafe, G., 312Scharfman, H., 127Scheffler, R. M., 668Scheid, P., 121Scher, C. D., 651Scherer, K. R., 490, 491Schiefelbein, V. L., 578Schildkraut, J. J., 655Schimel, J., 619Schmader, T., 514Schmidt, C., 238Schmidt, Hunter, 427Schmidt, M., 566Schmidt, V., 713Schmitt, D. P., 79, 483Schmukle, S. C., 535Schnedler, R., 534Schneider, B., 566Schneider, D. J., 510Schneider, T., 655Schoeneman, T. J., 618Schooler, J., 332, 373Schooler, J. W., 320, 331, 332, 585Schork, N. J., 650Schorr, A., 490Schraw, G., 366Schreiber, J., 5Schreiber, N., 324Schreiner, C., 126Schroeder, H. E., 530Schuengel, C., 566Schul, Y., 609Schull, J., 291Schulman, P., 628Schulsinger, F., 655Schultz, R. T., 439Schultz, W., 489Schulze, R., 433Schulz-Hardt, S., 355Schunk, D. H., 623Schvaneveldt, R. W., 347Schwartz, B., 266, 272, 313, 620, 626Schwartz, C. E., 601Schwartz, D., 573Schwartz, E., 586Schwartz, J. L. K., 512Schwartz, S., 242Schwarz, N., 360Schwarzer, R., 623Schweitzer, E., 699Scott, E., 62Scott, F. J., 667Scott, L. A., 656Scullin, M. H., 320, 447Sedikides, C., 618Sedivy, J. C., 394
Segal, N. L., 444, 472, 599, 603Segal, Z., 656Segall, D. O., 452Segerstrom, S. C., 622Seidenberg, M. S., 392, 413Sekerina, I., 409Selfridge, O. G., 189Seligman, M. E., 628Seligman, M. E. P., 272, 288, 289, 291,
293, 486, 621, 651, 657, 711Seminowicz, D., 702, 703Semmelroth, J., 79Semmler, C., 325Senghas, A., 406, 407Senko, C., 486Sereno, A. B., 194Serpell, R., 440, 441Sethi, A., 630Seyfarth, R. M., 414Shackelford, T. K., 78, 483Shader, R. I., 698Shadish, W. R., 709Shaffer, D., 454Shafir, E., 363Shafto, C., 412Shah, A. M., 626Shalinsky, M. H., 408Shallice, T., 125, 435Shanab, M. E., 525Shankweiler, D. P., 382Shannon, B. J., 309Shannonhouse, R., 680Shapiro, C. M., 238Shariff, A. F., 534Sharma, Y. S., 483Sharp, C., 672Shaver, P. R., 614Shaw, B. F., 691, 692Shaw, D., 566Shaw, P. J., 238Shea, D. L., 452Shea, M., 672Shear, M. K., 712Sheehan, P. W., 245Sherburne, L., 290Sheridan, J. F., 236Sherif, C. W., 515Sherif, M., 515, 519Sherman, J. W., 535Sherrill, J. T., 705Shettleworth, S. J., 294, 295Shi, R., 382Shibuya, H., 122Shieles, A., 433Shiffrin, R. M., 304, 388Shih, M., 453, 456Shiloach, J., 105Shin, L. M., 601Shiner, R. N., 598Shipley, E. F., 402Shipley, T. F., 186, 399Shoda, Y., 597, 624, 628, 629, 630Shors, T., 127Short, K. R., 558Shulman, S., 566Sicoly, F., 350, 626
Siegal, M., 559Siegel, A., 476Siegel, J. M., 238Siegel, S., 278Siegle, G., 709Siegle, G. J., 705Siegler, R. S., 579Siepmann, M., 509Sigelman, C. K., 573Sigman, M. D., 447Silberman, E. K., 671Silverman, P., 244Simerly, R. B., 468Simon, H. A., 363, 366, 373, 374Simoncelli, E. P., 207Simons, D. J., 211, 212Simonson, I., 363Simpson, E. L., 575Sims, E. A., 473Singer, B., 712Singer, J., 496Singh, M., 332Sinha, D., 440Siqueland, E. R., 399Siqueland, L., 704Sirigu, A., 231Sitarenios, G., 438Skinhøj, E., 121Skinner, B. F., 281, 281Sloane, R. B., 712Slobin, D. I., 410Sloman, S. A., 352Slovic, P., 353Smit, F., 644Smith, A., 318Smith, A. J., 663Smith, B., 150Smith, B. H., 63Smith, E. E., 387, 388Smith, F. J., 468Smith, G. T., 643Smith, J. R., 448Smith, L., 402Smith, L. B., 400Smith, M., 536Smith, M. C., 573Smith, M. L., 709, 710, 711, 712Smith, P., 150Smith, P. B., 510, 522Smith, S. M., 316, 372Smith, T., 689Smith, T. J., 209Smith, T. W., 102Snedeker, J., 392, 403, 412Snider, W., 127Snow, C., 412Snow, R. E., 431Snyder, C. R., 627Snyder, D. K., 694Snyder, M., 534, 598Snyder, M. L., 626Snyder, S. H., 663, 664Soares, J. J., 294Soja, N. N., 402Sokolowska, M., 278Solomon, J., 566
PNAME INDEXO N13
Solomon, S., 619Sommerville, R., 3Song, H., 419Sood, S., 362Sorkhabi, N., 581Sox, H. C., Jr., 706Spalding, K. L., 127Spangenberg, E., 43Spanier, C., 712Spanos, N. P., 325, 245, 671Sparrow, S. S., 666Spearman, C., 430–31Spears, R., 618Spelke, E., 559Spelke, E. S., 396, 402, 418, 441, 453, 558Spence, I., 454Spencer, S. J., 456Sperber, D., 395, 560Spiegel, D., 670Spiegel, K., 236Spiering, M., 482Spijker, J., 644Spillane, N. S., 643Spillantini, M. G., 585Spinath, F. M., 445, 449, 599Spitz, C. J., 481Spitz, H. H., 513Spivey-Knowlton, M. J., 394Spratling, M. W., 196Springer, S. P., 117Spuhler, J. M., 454Squire, L. R., 296, 312Srinivasan, M. V., 283Srivastava, S., 593, 594Sroufe, L. A., 566Stake, J., 453Stanhope, N., 330Stanley, B. G., 468Stanovich, K. E., 352, 353Stanton, D., 148Staples, F. R., 712Stark, D. E., 439Stark, H. A., 335Stark, L., 206Starr, J. M., 427Starzyk, K. B., 476Staudinger, U. M., 583Steblay, N., 325Stecker, D., 403Steedman, M., 394, 396Steele, C., 453Steele, C. M., 249, 456Steer, R. A., 641Stefansson, H., 662Steg, L., 519Stegge, H., 561Stein, J., 509Stein, M. B., 650, 651Steinberg, L., 572, 574, 578, 581Steinmetz, J. L., 510Stejskal, W. J., 642Stephan, W. G., 626Stern, J. A., 245Stern, K., 150Sternberg, R., 454
Sternberg, R. J., 372, 437, 438, 440, 441,537
Sterpenich, V., 238Stevens, J., 206Stevens, L., 626Stevens, S. S., 154Stevenson, L. A., 252Steward, O., 297Steward, W. T., 622Stewart, M. O., 692, 712Stich, F., 711Stickgold, R., 238, 240Stip, E., 700Stokoe, W. C., Jr., 406Stolz, J. A., 368Stoolmiller, M., 570Straus, S. E., 706Striano, T., 559, 563Stricker, E. M., 467, 469Striegel-Moore, R. H., 669Strittmatter, S. M., 90Strober, M., 669, 670Stroemer, R. P., 128Stroop, J. R., 267, 267Strosberg, R., 402Strunk, D., 692, 712Strupp, H. H., 711Stuart, S. P., 708, 711Stuber, G. D., 490Studdert-Kennedy, M., 382Sturgill, W., 324Stuss, D. T., 125, 435Sue, S., 682, 683Suga, S., 510Sugden, K., 58Sugrue, K., 322Sullivan, P. F., 655, 662Sullivan, R., 150Sulloway, F. J., 604Suls, J. M., 521, 594Sundet, J., 446Supalla, T., 406Super, C. M., 551Sur, M., 549Surian, L., 560Susman, E. J., 578Susskind, J. M., 497Sutcliffe, J. S., 667Sutton, J., 290Swann, W. B., 617Swearingen, L., 566Swedo, S. E., 648Swender, P., 150Swets, J. A., 142, 446Swica, Y., 671Swingley, D., 403Szathmari, A., 231Szatmari, P., 666Szymanski, K., 529
Taber, K. H., 700Tagiuri, R., 510Taipale, V., 574Takata, T., 625Tambor, E. S., 486Tambs, K., 446
Tandon, R., 696Tanenhaus, M. K., 391, 392, 394, 396Tangney, J., 290Tangney, J. P., 36Tannock, R., 668Tarbox, S., 660Tardif, C., 566Tarr, M. J., 183, 418Tassinary, L. G., 514Taub, E., 126Taylor, A., 58Taylor, K., 549Taylor, M., 561Taylor, S. F., 496, 703Taylor, W. S., 670Tekell, J. L., 656, 703Tellegen, A., 245, 444, 472, 599, 603Tellegen, A. M., 641Tenenbaum, J., 400Tennen, H., 711Terdal, S. K., 486ter Keurs, M., 383Terracciano, A., 593, 602Terry, R., 573Terwogt, M. M., 561Tesser, A., 520, 536Teuber, H. L., 333Thagard, P. R., 353Thara, R., 683Thase, M., 656Thase, M. E., 697, 698, 712Theodor, J. M., 64Theoret, H., 126Thesen, T., 235Thewissen, J. G. M., 64Thioux, M., 439Thomas, A., 567, 599Thomas, J., 575Thompson, B., 430Thompson, D. M., 317Thompson, L. A., 433Thompson, R. A., 566, 567, 576Thompson, W. L., 344Thompson-Brenner, H., 708–9Thompson-Schill, S. L., 410Thomsen, D. K., 330Thomson, J., 80Thorndike, Edward L., 279–80, 279, 281Thornton, K. M., 628Thornton, N., 628Tierney, A. J., 700Tietjen, A. M., 575Timberlake, W., 284Tiwari, B. N., 64Todorov, A., 535Tolin, D. F., 649Tolman, Edward C., 287, 287Tomasello, M., 66, 396, 402, 415Tomkins, S. S., 491Tong, F., 229Tononi, G., 232, 233Tooby, J., 79, 497Torgerson, S., 655Torrey, E. F., 663, 666Toth, L. A., 236Tourangeau, R., 318
Townsend, J. P., 667Trabert, W., 650Tracy, J. L., 491Tranel, D., 195Treat, T. A., 142Treiber, F., 247Treisman, A. M., 188, 210Tremblay, L., 489Treyens, J. C., 321Treynor, W., 652Triandis, H. C., 440, 508Trimble, J. E., 255Triplett, N., 527Tropp, L. R., 516Trueswell, J., 392Trueswell, J. C., 391, 392, 396, 409, 410Trueswell, J. T., 403Trull, T. J., 673Trzesniewski, K., 624Tsai, J., 587Tsai, J. L., 658Tsang, B. Y. P., 540Tsuang, M. T., 662, 666Tuholski, S. W., 434Tulving, E., 309, 317, 323, 328, 335Tunoni, G., 238Tuomi, T., 473Tupes, E. C., 593Turati, C., 562Turkheimer, E., 72, 448, 449, 603Turner, J. A., 515Turner, T. J., 321Tversky, A., 350, 352, 360, 363, 388Tweney, R. D., 355Tyack, P., 414Tzeng, O., 386
Uhlenhuth, E. H., 699Ul-Haq, M., 63Umino, M., 148Undie, A. S., 664Ungerleider, L. G., 194Urbani, P., 252Urberg, K. A., 574Urushihara, K., 275Uyeyama, R., 415
Vaidya, R. S., 628Vaillant, C. O., 613Vaillant, G. E., 613Valenstein, E. S., 107, 124, 700Valenzuela, M., 566Van Cauter, E., 236Vandell, D. L., 572Van de Poll, N., 453van der Lely, H. K., 410Vandewalle, G., 238Van Essen, D. C., 193Van Goozen, S., 453Van Hoesen, G. W., 122van Horn, D., 686van IJzendoorn, M., 566Vanous, S., 324Van Putten, T., 696van Sickle, M., 252Varner, J. L., 489
N14 PNAME INDEXO
Vasudevan, P., 696Vaughan, C., 237, 240Vaughan, J. T., 229Vaultin, R. G., 204Veizovic, T., 128Vela, E., 316Venter, J. C., 54Verkhratsky, A., 92Vernon, P., 439Vernon, P. A., 433, 599Vigorito, J., 399Vijayan, S., 400Vinokur, A. D., 609Vishton, P. M., 400Visser, B., 439Vitaro, F., 574Vitevitch, M. S., 212Vogel, P. J., 117Vogel, S., 117Vohs, K. D., 481, 483Volkmar, F. R., 666Vollenbergh, W. A. M., 644Voltaire, 604Von Cramon, D., 122Vondra, J., 566Von Koenigswald, W., 63Voon, V., 702, 703Vouloumanos, A., 403Vul, E., 372Vuong, Q. C., 183Vygotsky, L., 568
Waddington, J. L., 663Wager, T. D., 496, 650Wagner, A., 323Wagner, A. D., 309, 323Wagner, A. R., 274Wagner, R., 438Wagner, R. K., 437Wakefield, B. M., 320Waldron, M., 72, 448, 449, 603Walker, E., 661, 663Walker, L. J., 575Walker, M. P., 238Walker-Andrews, A., 562Walkup, J. T., 705Wall, P., 148Wall, S., 565, 614Wallace, G., 656Wallace, J., 655Wallace, P., 150Wallace, R. L., 63Wallas, G., 372Waller, N. G., 671Wallin, P., 537Walsh, J. K., 237Walster, E., 515, 535, 536, 537Walster, E. H., 537Walton, K., 598Wampold, B. E., 710, 711, 712Wang, C. M., 235Wang, M. L., 468Wang, P. S., 682Ward, L. M., 211Ward, T. B., 372Warren, S. L., 566Wason, P. C., 355, 357
Wasserman, B. H., 80Wasserman, E. A., 266, 283Waterhouse, L., 667Waters, E., 564, 565, 614Watkins, C. E., 642Watkins, M., 430Watson, D., 485Watson, John B., 623Watson, J. S., 288Watson, W. P., 128Waugh, N. C., 304Waxler, N. E., 666Waxman, S. R., 419Webb, W., 239Webb, W. B., 236Weber, A., 311Weber, E. H., 138Wechsler, D., 427Wechsler, H., 249Weeks, R. D., 701Wegener, D. T., 515Wegner, D. M., 230Weibe, D., 370Weinberg, M. S., 483Weinberg, R. A., 455Weinberger, J., 642Weingartner, H., 313Weisberg, R. W., 369, 374Weiskrantz, L., 223Weisler, R. H., 706Weiss, L. H., 581Weiss, W., 515Weiss, Y., 207Weissman, M., 685Weissman, M. M., 685Weisz, J. R., 711Weldon, M. S., 13Welham, J., 663Well, G. L., 325Wellman, H., 562Wellman, H. M., 560, 561Wels, K. B., 711Welter, M. -L., 703Wender, P. H., 655Wenk, G., 325Werebe, M. G., 572Werker, J. F., 399Wernicke, Carl, 123Wertheimer, M., 186, 204Wesner, K., 656West, R. F., 352, 353West, S. G., 534Westcott, H. L., 321Westen, D., 79, 614, 642, 708Wethington, E., 442, 586Whaley, S. E., 447Whalley, L. J., 427Wheatley, T. P., 361Whipple, K., 712Whishaw, I. Q., 89, 115, 548, 551Whisman, M. A., 694White, B., 515White, D. J., 290White, J., 647, 648Whiteman, M. C., 427Whitney, G., 534Whitworth, L. A., 573
Whorf, B., 416Widaman, K. F., 449Widiger, T. A., 672, 673Wiebe, R. P., 598Wienbruch, C., 126Wiesel, Torsten, 175Wiesenthal, D. L., 520Wightman, R. M., 490Wilcoxin, H., 293Wiley, J. L., 252Wilhelm, F. H., 491, 650Wilhelm, O., 433Willadsen-Jensen, E. C., 512Willecke, K., 90Williams, C., 453Williams, G., 77Williams, K. D., 528Williams, L. A., 498Williams, R., 689Williams, S. C., 600Williams, W., 442Williams, W. M., 437, 446Willingham, B., 67Willis, S. L., 585Wilson, D., 396Wilson, D. H., 117Wilson, D. W., 533Wilson, E. O., 79Wilson, G. T., 249, 669, 712Wilson, K. S., 570Wilson, M., 80, 81Wilson, P. G., 689Wilson, R., 583Wilson, S., 430, 577Wilson, T., 225Wilson, T. D., 225, 226, 352, 361Wimmer, H., 561Winter, D. G., 642Wirshing, W. C., 696Wisco, B. E., 652Wise, R., 124Witherspoon, D., 335Wittchen, H.-U., 653Wittgenstein, L., 388Wixted, J. T., 312, 319Wochnik, G. M., 713Woiciechowsky, C., 117Wolf, M. E., 649Wolfe, J., 207Wolfe, J. M., 188Wolford, G., 626Wollen, K. A., 311Wolpe, J., 651, 687Wong, S., 672Wood, J. M., 642Wood, N., 214Wood, W., 483Woods, S. C., 275Woodward, A. L., 560Woody, E., 574Woolf, N. J., 125, 296, 297Woolf, S. H., 706World Federation for Mental Health, 668Wozniak, D. F., 549Wright, C. I., 601Wright, R. D., 211Wrzesniewski, A., 586
Wu, X., 573Wurtman, R. J., 234Wyland, C. L., 617Wynn, K., 559
Xu, F., 400, 418Xu, M., 663
Yahya, K. A., 525Yalom, I. D., 481Yan, L., 473Yang, S.-Y., 440Yang, Y., 90, 322Yaniv, I., 373Yarmey, A., 314Yeager, C. A., 671Yeung, W. J., 448Yi, S., 569Yoder, C., 44Yonelinas, A., 334Yoo, S. H., 493Yorkston, N. J., 712Young, K., 652Young, R., 439Young, Thomas, 169Youngstedt, S. D., 238Yu, C., 400Yurgelin-Todd, D., 252 Yurgelin-Todd, D. A., 656
Zabrack, M. L., 477Zahs, K. R., 92Zajonc, R. B., 528, 536Zakriski, A., 574Zaragoza, M. S., 13, 320, 332Zarkin, G. A., 706Zarzo, M., 148Zavalloni, M., 530Zeanah, C., 572Zeidner, M., 439Zelazo, P. D., 408, 558Zentall, R., 290Zentall, T. R., 283Zevin, J. D., 413Zhang, H., 650Zhang, S., 283Zhao, Z., 309Zhdanova, I. V., 234Zhong, C., 372Zhou, H., 196Zigmond, M. J., 469Zihl, J., 122Zillman, D., 482Zimbardo, P. G., 44, 529, 530Zimmer, C., 445Zimmerman, M., 709Zinbarg, R., 651Zonderman, A. B., 584Zucker, K. J., 484Zuckerman, M., 599, 600, 604Zukowski, A., 410Zumbahlen, M., 563Zuroff, D. C., 682Zweig-Frank, H., 671
S1
Page numbers in italics refer to illustrations.
abnormal psychology, see psychopathologyabsolute threshold, 137, 138Abu Ghraib prison, 505–6, 530accents, in language, 396accommodation, 554–55, 555acetylcholine (ACh), 100achromatic sensations, 164action potential, of neurons, 92–96, 94, 95, 96,
96, 99, 100, 296–97activation-synthesis hypothesis, 241, 242, 243active perception, 214actual selves, 617, 617acuity, visual, 164acupuncture, 245, 246acute stress disorder, 649Adams, Margie, 155adaptation, 620
sensory, 144–45, 145, 178addiction, classical conditioning and, 276–78addiction, drug, 253–54A-delta fibers, 147adipose cells, 468, 469, 501Adler, Alfred, 578adolescence, 576–82, 589
cognitive development in, 578–79, 589delay of gratification and competence by,
629–230, 629, 633depression in, 653development of self-identity in, 580identity and, 581–82logical reasoning in, 579menstrual cycle and, 577
parent and peer relationships during, 581–82,581
physical development in, 557–58, 557puberty in, 577, 577, 589socioemotional development in, 579–82stress of, 581
adoption studies, 412, 445, 445, 455, 655adrenal glands, 105, 474adulthood, 582–87, 583, 589
changes in intellectual performance in, 583–84changes in well-being in, 586–87cognitive changes in, 583–85crystallized intelligence and, 583–84, 589fluid intelligence and, 583–84, 589midlife transition and, 586, 587physical and sensorimotor changes in, 582, 582sensory decline and, 583socioemotional development in, 585–87, 589stages of, 585–86and transition to senescence, 586–87
affective disorders, 652see also mood disorders
affective forecasting, 276, 360–61, 364affective neuroscience, 496, 503afferent nerves, 113afferent neurons, 89, 90African Americans, IQ scores of, 450–51aggression, 24, 26, 27, 27, 28–29, 30, 33, 33, 34,
473–78, 502biological factors of, 476cultural and cognitive aspects of, 476–78, 502“fight or flight” response and, 474–75gender differences in, 25, 475–76hormones and, 475–76individual differences in, 476–77, 476
limiting of, 477–78morality and, 478physical, 35, 475–76physiological aspects of, 474–76predation and, 475sexual, 482social, 36, 476, 476societal influences on, 477, 502TV violence and, 477, 477
aggressive-rejected children, 574aging:
adulthood and, 582–87, 583exercise and, 585sensory decline of, 583see also adulthood
agnosias, 122, 131associative, 192visual, 174, 191–92, 194–95
agonists, 101–3, 130agoraphobia, 646–47agreeableness, 593
gender differences and, 604, 604Ainsworth, Mary, 565, 614alcohol, alcoholism, 257, 654, 698–99
addiction to, 253daily consumption of, 21–22as depressant, 248, 249drunk driving and, 249mental disorders and, 635
Alcoholics Anonymous, 693Alexander, Richard, 79Alexander the Great, 485Alice in Wonderland (Carroll), 712, 712alleles, 57, 61, 69, 81, 82, 133all-or-none law, 96
Subject Index
S2 PSUBJECT INDEXO
alpha rhythm, 234, 235, 247, 257altruism, 613
bystander effect and, 532–33helping and, 532self-interest and, 534
Alzheimer’s disease, 107, 127, 128, 129, 325, 584–85amacrine cells, 162Amala (wild girl), 405American Psychiatric Association, 639, 642American Psychological Association, 43American Sign Language (ASL), 406, 413, 413, 423amnesia, 471
anterograde, 233, 333, 333, 339dissociative, 670, 671, 675retrograde, 312–13, 313, 338
amphetamines, 250, 251, 664amplitude, of sound waves, 154, 154amygdala, 8–9, 9, 10, 18, 116, 228, 242, 488, 496,
498, 499, 601, 601, 650, 656, 667anagrams, 366, 371analgesics, 248analogical representations, 343, 343, 376analogies, 369–70, 374, 377anal stage, 609–10analytic intelligence, 437–38anandamide, 252, 257androgens, 484anecdotal evidence, 25anhedonia, 660animals, animal behavior:
communication in, 413–15, 414sexuality in, 70–71
anorexia nervosa, 636, 668–69, 669A-not-B effect, 554, 554, 558, 588antagonists, 101–3, 130anterior cingulate cortex, 148, 435, 488, 650anterograde amnesia, 223, 333, 333, 339antidepressants, 248, 696–98, 701, 705, 714
atypical, 697side effects of, 698
antipsychotics, 664, 675, 695–96, 714antisocial personality disorder, 672anxiety, 608, 698–99
depression and, 653Freud on, 610–11, 632medication for, 698–99, 714neo-Freudian view of, 613punishment and, 576
anxiety disorders, 636, 640, 644–52, 674, 692,705, 712
biological factors for, 650genetic risk factors for, 650, 652psychological risk factors for, 651roots of, 650–52
anxiety hierarchy, 688anxiolytics, 698, 714anxious/avoidant children, 588, 614anxious/resistant children, 588, 614aphasia, 107, 123, 131, 410, 423Aplysia (mollusk), 296
apparent movement, 204, 204, 205, 208, 217apraxia, 121, 131archetypes, 611, 611Archimedes, 372, 372Arendt, Hannah, 523, 524Aristotle, 146, 531, 540arousal:
personality and, 600romantic love and, 537–38, 538sexual, 264, 482
Asch, Solomon, 520–21, 520ASL (American Sign Language), 406, 413, 413, 423aspirin, 245, 246assessment:
clinical, 640of mental disorders, 640–42psychological, 674structured interview in, 674vs. diagnosis, 643
assimilation, 554–55, 555association areas, 118, 121associations:
empiricist view of, 136learning and, 260, 269in network model, 346–47, 346predispositions to specific, 291–94
associative links, 346, 376asylums, see mental hospitalsAs You Like It (Shakespeare), 546attachment:
Bowlby’s theory of, 563–65, 588child care and, 570–71, 570, 589childhood differences in, 565–67comfort and, 563–64, 564, 588culture and biology and, 571–72face-to-face interaction and, 588imprinting and, 564–65lack of, 571–72, 572object relations and, 613–14, 632patterns of, 588–89secure, 566–67, 567secure base in, 564, 564, 588separation anxiety and, 563
attention:age-related decline of, 584consciousness and, 232emotional memories and, 11limits of, 213–14, 213memory acquisition and, 305–8, 309, 324,
435–36in perception, 208–12, 212, 217working memory and, 434
attentional state, 400–401attention-deficit/hyperactivity disorder (ADHD),
250, 636, 667–68, 667, 675, 699, 714attitudes, 514–19, 514, 542
advertisements and, 515change in, 515–16intergroup contact and, 516, 518persuasion and, 515
psychological definition of, 514stability of, 518–19, 518
attraction, 534–37homogamy and, 537proximity and, 535–36, 535, 543similarity and, 536–37, 536, 543
attractiveness, physical, 535attribution, 507–10
casual, 507, 510challenges to, 508culture and, 508–9dispositional, 507, 509, 510, 541fundamental attribution error and, 509–10,
509, 541internal, 627situational, 507, 509, 510, 541
attributional style, 625, 626–28, 627attributional-style questionnaire (ASQ), 627atypical antidepressants, 697atypical antipsychotic drugs, 696audition, see hearingauditory canal, 156, 157auditory nerve, 143, 157, 158auditory ossicles, 156, 157auditory projection area, 119, 120, 123, 126auditory receptors, 156–57, 157authoritarian parents, 569, 589authoritarian personalities, 523, 542authoritative parents, 569–70, 581, 589autism, 666–67, 666, 675, 689autobiographical memory, 329autokinetic effect, 519automaticity, 367–68autonomic nervous system (ANS), 113, 131,
464–65, 474, 502, 650parasympathetic branch of, 113, 114, 464, 501sympathetic branch of, 113, 114, 464, 474–75,
497, 499autosomes, 54availability heuristic, 348–50, 351, 376avoidant personality, 672axons, 88–89, 88, 91, 99, 105, 109, 127, 162axon terminals, 90, 98
presynaptic, 100
Baldwin, Alec and Billy, 604Bandura, Albert, 623, 631Bard, Philip, 494Bartlett, Frederic, 321basic-level words, 401–2, 422basilar membrane, 156, 157, 158, 159Basinger, Kim, 673, 673Baumrind, Diana, 569Beck, Aaron, 691–92
cognitive theory of depression of, 657, 674, 714Beck Depression Inventory, 641Beethoven, Ludwig van, 372, 635befriending, 474, 474behavior:
biology and, 599
PSUBJECT INDEXO S3
compensatory, 669consciousness and, 221consistency in, 595–97evolution and, 66, 79expressions and, 66–69genetic influence on, 79hormonal changes and, 480instrumental (operant) conditioning and, 281,
299natural selection and, 59–60niche construction and, 66sexual, 478–85see also social behavior
behavioral contrast, 285–86, 299behavioral data, 597behaviorism, 623behavior modification, 281, 283–85, 284, 287,
687–90, 714vs. acquired knowledge, 287–89
behavior therapy, 687–90, 687, 714belongingness, 291–94Bem, Daryl, 517benzodiazepines, 248, 249, 698–99Berkeley, George, 135, 135, 260Bernard, Claude, 463–64Bernard, Luther, 463beta-blockers, 698beta rhythm, 234–35, 235between-subject comparisons, 41bias, confirmation, 354–55, 355, 376, 530–31
see also prejudice; stereotypesbidirectional activation, 189–90, 190Biederman, Irving, 191Big Five, 591, 593–98, 599, 602, 604, 605, 632bilingualism, 408–10
cognitive flexibility of, 409crib, 408executive control and, 409rate of learning and, 408–9
binding problem, 195–96, 210, 216Binet, Alfred, 426, 426, 428, 458binge eating, 669binocular cues, 200binocular disparity, 200, 200, 203binocular rivalry, 229, 230biological constraints, on conditioning, 291–94biology, biological factors:
behavior and, 599depression and, 638in learning, 291–94in personality, 598–601, 599, 632in psychopathology, 638–39race and, 442see also brain; nervous system; neurons; specific
organsbiomedical factors, psychopathology and, 638–39biomedical treatments, 694–703
for psychopathology, 694–703, 714
biopsychosocial perspective, of psychopathology,638–39, 674
bipolar cells, 162, 163bipolar disorder, 58, 635–36, 653–55, 674, 677–78,
692, 698medication for, 698suicide and, 654–55
bisexuality, 484“black box” warning, 699, 700Bleuler, Eugen, 658blindsight, 223blind spot, 163, 164, 164blocking effect, 274–75, 298blood-brain barrier, 102blood circulation, 130blood-injury-injection phobia, 645–46bloodletting, 694blood-oxygenation-level-dependent signal
(BOLD), 111bloodstream, communication through, 103–5bodily-kinesthetic intelligence, 439Body Mass Index (BMI), 471, 471, 473body temperature, 464–66, 465, 478“Bonnie Earl O’Murray,” 182borderline personality disorder, 672, 693Bordoni, Paris, 136bottom-up processing, 189–90, 190Bowlby, John, 566–67, 613–14Bowlby’s theory of attachment, 563–65, 588brain:
activity of, 3, 3, 6, 8–9, 9, 65, 229–31, 230, 233,234, 238, 241–43, 242, 247, 248, 309, 345,433, 488, 488, 650, 656
amygdala of, 116antipsychotics and, 695–96autism and, 667blood-brain barrier of, 102chemical signals of, 97consciousness and, 227–29, 228decision making and, 4–6depression and, 703development of, 57, 90, 550EEG and, 109ERP and, 109executive control in, 435, 435of fruit flies, 238gray matter in, 91, 91hemispheres of, 116–18, 120hippocampus of, 116imaging, 2lateralization of, 116–18, 117lesions of, 106–7, 106localization of function in, 131major structures of, 87–94, 115manipulation of, 106–7maturation of, 588meditation and, 247–48, 248, 257mental disorders and, 680mental retardation and, 57
morality and, 2–3, 3, 4nervous system and, 85–131neuroimaging of, 110–11parts of, see specific partsplasticity of function in, 125–28, 296–97prenatal development of, 547psychotherapy and function of, 700–701recording electrical activity of, 109, 109schizophrenia and development of, 661–63schizophrenia and structural defects in,
664–65, 665structure of, 9, 112, 126subcortical structures of, 89, 116THC and, 252in visualization, 344visual processing in, 192–95, 193white matter in, 91, 91
brain damage, 85–86, 106–8, 121–25, 124, 130agnosias and, 95, 122, 131amnesias and, 313, 333to amygdala, 9, 10aphasias and, 123apraxias and, 121, 131consciousness and, 229, 256effects of, 106–9episodic memory and, 328to frontal lobe, 124–25goal maintenance and, 435of H.M., 333, 333to hypothalamus, 469memory loss and, 4neglect syndrome caused by, 122neuroimaging and, 112of Phineas Gage, 26–27, 107, 107to prefrontal cortex, 124repair of, 127–28, 128unconscious functioning and, 223–24vision and, 376
brain stem, 114, 115breeding, 61, 63, 75, 77Breuer, Joseph, 606brightness, 161, 164
amplification of, 165of color, 168, 168of light, 161, 164, 165, 166perceived, 166physical, 166
brightness contrast, 165–68, 165, 166Broca’s area, 123, 123Brunn Natural History Society, 56Brunn Society’s Proceedings, 56Buddhism, 247bulimia nervosa, 668, 669–70, 669, 699, 712Bush, George W., 12, 12, 128BuSpar, 699Buss, David, 78bystander effect, 532–33, 533, 543
caffeine, 250, 250, 251
S4 PSUBJECT INDEXO
Callahan, Katie, 133–34cannabinoid (CB) receptors, 252Cannon, Walter B., 474–75, 494–95Cannon-Bard theory of emotion, 494, 496, 502CAP (Colorado Adoption Project), 445, 445Carolina Abecedarian Project, 446Carstensen, Laura, 587case markers, 390case studies, 48
use of, 26, 26, 47catatonic schizophrenia, 660, 661CAT (computerized axial tomography) scan, 110,
110Cattel, Raymond, 593–94caudate nucleus, 650causal ambiguity, 36–38, 38causal attribution, 507, 510Ceausescu, Nicolae, 571–72Celexa, 697cell body (soma), 88–89cells:
blood and, 103development of, 548gene expression and, 54–55nuclei and, 53, 53proteins and, 53see also neurons; specific types of cells
central nervous system (CNS), 90, 112–13, 113, 127central route to persuasion, 515, 542cerebellum, 115, 115, 146, 667cerebral cortex 85, 115, 118–25, 127, 234
projection areas of, 118–19structure of, 118–21
cerebral hemispheres, 118, 120cerebrospinal fluid, 113C fibers, 148Challenger Space Shuttle, 12, 531character strengths, 621, 621Charcot, Jean, 606child care, 570–71, 570, 589childhood, 550–76childhood socialization, 589child memory, 568child-rearing patterns, culture and, 571–72children, 550–76
aggression of, 24, 25anxious/avoidant, 588, 614anxious/resistant, 588, 614brain maturation in, 588cognitive development in, 552–62, 588concrete operational period of, 588conscience and, 576, 589differences among, 565–67disorganized, 614false-belief tasks and, 561, 561, 588gratification delay by, 629–30, 629, 633growth of language in, 396–404, 422–23isolated, 405–6memories of, 14memorizing and, 403–4
numerical reasoning and, 588object permanence and, 588playing and, 5–7, 24preoperational period of, 588reflexes of, 588securely attached, 588, 614sensitivity to foreign languages of, 399sensorimotor period of, 588socioemotional development in, 562–76, 588temperament in, 6, 567, 567, 589understanding of beliefs and, 561understanding of preference and, 561wild, 405, 405
chimpanzees, language in, 414choice reaction time, 433Chomsky, Noam, 383, 383chromosomes, 53, 53, 54, 55, 56, 57, 61, 82Chu, John, 591–92chunking, 306–7, 338, 373–74Churchill, Winston, 635Cialdini, Robert, 526cingulate cortex, 496circadian rhythms, 233, 234, 239Clark, Chris, 677–78Clark’s nutcracker, 294–95, 294classical conditioning, 259, 267, 276–78, 337
addiction and, 276–78attitude formation and, 514biological constraints on, 291–94compensatory reactions to, 276–78extinction in, 266–68, 278generalization and discrimination in, 268–69,
278, 298major phenomena of, 263–78Pavlov’s findings on, 263–78reconditioning in, 266–67spontaneous recovery in, 267surprise in, 273–75
classification scheme, 493claustrophobia, 651client-centered therapies, 686, 686, 714clinical interviews, 640–41clinical utility, 709Clinton, Bill, 673Clozaril, 696Coca-Cola, 251cocaine, 103, 250, 251, 253–55cochlea, 156–58, 157, 159cochlear implants, 158, 158cocktail party effect, 213codeine, 148cognition:
cognitive dissonance and, 516, 516crowd behavior and, 529–30cultural influences on, 568, 568social, see social cognitionsocial-cognitive theories of personality, 622–31,
633cognitive-affective personality system (CAPS), 624cognitive behavior therapy, see cognitive therapy
cognitive consistency, 518cognitive control, 661cognitive deficits, depression and, 653cognitive development:
concrete operations in, 552, 553, 556conservation in, 555–56, 556cultural and social influences on, 568, 568formal operations in, 552, 553infant dissociation and, 554numerical skills in, 558–59, 568, 568object permanence in, 553–54, 553, 555, 558occlusion in, 557–58, 557preoperational period in, 552, 553, 555–56schemas in, 554–55sensorimotor period in, 552–55, 553social and cultural influences on, 568social cognition in infancy and, 559–62space and objects in infancy and, 557–58
cognitive dissonance, 516, 516, 517, 542cognitive reappraisal, 498–99, 499, 500, 503cognitive restructuring, 691cognitive theory of depression, 657cognitive therapy, 684, 690–92, 705, 712, 714cognitive unconscious, 222–23,
256collective unconscious, 611, 632collectivistic cultures, 508–9, 509, 510, 511, 541,
542, 543, 581, 618, 619, 627conformity and, 522love in, 540
color:achromatic, 168brightness of, 168, 168chromatic, 168, 168language and perception of, 417perception of, 168
Colorado Adoption Project (CAP), 445, 445color blindness, 165, 173–74, 173color vision:
color mixing and, 171, 171complementary hues in, 170–71neural basis of, 169–74opponent-process theory of, 172, 172, 179Young-Helmholtz theory of, 169
comfort, 563–64, 564, 588commissures, 117commitment, 537, 543
emotional vs. sexual, 79–80communication:
animal, 413–15, 414conversational patterns in, 568–69see also language
communicative intent, 400comorbidity, 650, 709, 715companionate love, 539, 539, 543, 585comparative method, 475compensation, 500compensatory behavior, 669compensatory response, 276competence, cultural, 682–83, 714
PSUBJECT INDEXO S5
competencies, self-regulatory plans and, 625–26,633
complementary hues, 170–71complex waves, 155, 155compliance, 526–27, 542
reciprocity and, 526–27that’s-not-all technique and, 527, 542
compulsions, 648computerized axial tomography (CAT) scan, 110,
110computerized tomography (CT) scan, 100concepts, 346conciliatory signals, 478, 478concordance rate, 650concrete operations, 552, 553, 556, 578, 588, 589conditional statements, 291conditioned reflex, 263–69conditioned reinforcement, 282–85conditioned reinforcer, 284–85, 299conditioned responses, 263–78, 267, 268, 274, 298conditioned stimulus, 268, 273, 274conditioning:
biological constraints on, 291–94classical, see classical conditioningcontiguity in, 270contingency in, 270–71, 287–89extinction in, 266–68, 267, 278generalization and discrimination in, 268–69,
278, 282–83, 298instrumental (operant), see instrumental
conditioningPavlovian, 651second-order, 265vicarious, 290, 651
cones, 162, 163, 163, 170day vision served by, 164pattern of response of, 169–70, 169in trichromatic vision, 169visual pigments in, 164–65
confederates, 496confirmation bias, 25, 354–55, 355, 356, 376,
530–31conflict, and defense, 608–9conformity, 519–22, 521, 542
causes of, 520–21culture and, 522minority influence vs., 522, 522psychological distance and, 525
conjunction search, 209conscience, 576, 589
parent-child relationships and, 576punishment and, 576
conscientiousness, 593conscious level, 607consciousness, 219–57
automatic processes and, 226, 226behavior and, 221brain activity and, 229–31, 230brain areas needed for, 228–29, 228
cognitive unconscious and, 222–23, 256dreams and, see dreams, dreamingdrug-induced changes in, 248–55executive control and, 226–27“free will” and, 230–31, 231, 257function of, 226–27, 231global workspace hypothesis and, 231–33, 257honest reporting and, 220–21, 221hypnosis and, 243–46implicit memory and, 223ineffable experiences of, 221introspection and functions of, 220–27, 256inverted spectrum in, 221, 221meditation and, 247–48memory and, 223, 224mind-body problem of, 227–28, 255, 256neural basis for, 227–33, 256–57neural correlates of, 229–31, 257perception and, 222, 224readiness potential and, 231, 231religious states of, 247–48sleep and, see sleeptranslating thoughts into words and,
220–22two aspects of, 228–29, 229unconscious attributions and, 224–25unconscious functioning and, 223–24varieties of, 233–55
conservation, failure of, 555–56, 556consistency, cultural differences in, 598consolidation, 498constancy, perceptual, 196–99, 196
brightness and, 196of position, 205of shape, 196, 196, 198of size, 196, 197, 198
construals, 632construct validity, 24contact comfort, 563–64, 564, 588content morphemes, 382–83, 422context reinstatement, 315–16, 316, 339contingency management, 689contralateral control, 119, 120, 131contrast effects, 165–68, 165, 166control, 625–26, 626, 633control groups, 38–40, 44, 48conventional reasoning, 574conversational inference, 395conversational patterns, 568–69conversion disorder (hysteria), 606, 637, 643Copland, Aaron, 484copulation, 481cornea, 162, 162corpus callosum, 117, 117correlation coefficient, 31, 32correlations, correlational studies, 31–33, 37–38, 37,
48, 112, 427–28, 458, 459causation and, 3reliability and, 32–33
twin studies and, 70see also statistics
correspondence problem, 207–8, 207cortex:
development of, 550parallel processing and visual, 192–94structure of, 115, 131
cortical reorganization, 126Cosmides, Leda, 357counterirritation, 148counting, 559couples therapy, 694, 694Creedence Clearwater Revival, 181crib bilingualism, 408critical thinking, 375Crow, Sheryl, 673crowd behavior, bystander effect and, 532–33, 533Crucible, The (Miller), 355crystallized intelligence, 432, 459, 583–84, 589CT (computerized tomography) scan, 100cultural competence, 682–83, 714culturally appropriate therapy, 682culture:
childhood socialization and, 589collectivistic, 543, 627conformity and collectivistic, 522conversational patterns and, 568–69depression and, 657–58, 658individualistic, 543 love in, 540influence of, on cognition, 568intelligence and, 440–41, 450–51language learning and, 396, 422love in collectivistic, 540mate choice and, 78moral reasoning and, 575parenting and, 571–72perception shaped by language in, 417–21personality and, 602–3personality trait taxonomy and, 595, 632psychotherapy and, 714romantic love and, 539–40, 540, 543slow pace of human growth and, 550, 550
Curie, Marie, 371
d-amphetamine, 250Darkness Visible (Styron), 652–53Darley, John, 532Darwin, Charles, 52, 59, 61, 64, 68, 81, 278–79, 371,
372, 380, 491on evolution, 59–61, 278–79
data:collecting of, 25, 25, 26correlations in, 31–33demand characteristics’ influence on, 28descriptive statistics and, 28, 29frequency distribution and, 29, 30, 30means and variability of, 29–31scatter plots and, 31, 31standard deviation and, 30
S6 PSUBJECT INDEXO
data (cont.)testing differences and, 34–36variability and, 30, 34working with, 28–36
data-driven processing, 189–90, 190day vision, 164deafness, language learning and, 406debriefing, 44decibels, 154decision criteria, 140decision making, 4–6, 341, 348, 358–64, 376–77
affective forecasting in, 360–61, 364, 376excessive options in, 361–63, 361, 376framing effects and, 5, 5, 359–61, 360, 364in groups, 530–31influences on, 5, 6justifications of decisions in, 364loss aversion in, 360morals and, 2–3predictions of outcomes and, 361, 363, 364, 376,
377process of, 364, 377reason-based choices of, 363–64, 363satisfice and, 363, 364, 377
declarative knowledge, 334deductive reasoning, 354, 356deep brain stimulation (DBS), 702, 702, 714deep processing, 309, 338defense, conflict and, 608–9defense mechanisms, 608–9, 612–13, 613, 632definitional theory of word meaning, 386–87, 386dehumanization, of victims, 526, 542deindividuation, 529–30, 529, 542deinstitutionalization, 696, 696, 714delta-9–tetrahydrocannabinol (THC), 251, 252delta rhythm, 235, 235delusions, 659–60, 674
depression and, 653of reference, 660
demand characteristics, 27–28dendrites, 88–89, 88, 90, 92
spines, 125, 130, 297dependent personality disorder, 672dependent variables, 24, 24, 33, 35, 36, 39, 42, 48depolarization, 95depressants, 248–49, 257depression, 37, 636, 638, 652–53, 652, 669, 673,
674, 677, 691–92, 701, 703, 707anxiety and, 653bipolar disorder and, 653–55childhood, 653cognitive deficits and, 653cognitive theory of, 657culture and, 657–58, 658delusions and, 653electroconvulsive therapy for, 701–2, 701genetic components of, 638genetic factors of, 655helplessness and hopelessness and, 657learned helplessness and, 289
major, 652medication for, 103, 696–98, 701, 714neurochemical malfunction and, 656obsessive-compulsive disorder and, 648predictors for, 628social support vs., 657socioeconomic status and, 658stress and, 656–57subsyndromal, 711suicide and, 654–55war and, 657–58, 658
Depression and Bipolar Support Alliance, 678deprivation, social, 571–72, 572depth cues, 200, 202, 203depth perception:
binocular disparity, 200, 200, 203monocular cues for, 200–202, 203through motion, 202pictorial cues for, 201, 201redundancy in, 203
Descartes, René, 86, 227–28, 228, 379on reflexes, 87, 96
descriptive statistics, 28, 29desensitization, 688despair, integrity versus, 586, 589detectors:
activation and inhibition of, 189–90, 190complex, 174feature, 174–75, 182, 191, 209motion, 204
development, 545–89adult, 582–87childhood, 550–76after childhood, 589cognitive, 552–62conversational patterns and, 568–69fluid and crystallized intelligence throughout,
432, 459genetic transmission and, 54, 55–56as growth, 546–50growth of brain throughout, 550human physical, 546–50language learning throughout, 343–45, 396, 411of manual skills, 550–51, 551of memory, 568milestones of, 552newborn’s capacities and, 550–51of personal identity, 581–82Piaget’s stages of, 552–56prenatal, 546–49, 547proximal, 568psychosexual, Freud’s theories of, 609–10, 632representational thought in, 555sexual, 589social cognition and, 559–62spatial knowledge and, 557–58see also cognitive development; social
developmentdevelopmental disorders, 666–68, 675
attention-deficit/hyperactivity disorder(ADHD), 250, 636, 667–68, 667, 675, 699,714
autism, 666–67, 666, 675, 689dhat, Indian illness, 643diabetes, 473diagnosis, assessment vs., 643Diagnostic and Statistical Manual of Mental Disorders
(DSM-IV-TR), 639, 640, 643, 650, 668,669, 674
dialectical behavior therapy (DBT), 692–93Diana, Princess of Wales, 669diathesis-stress models, 638, 638, 674difference threshold, 137–39, 178diffusion of responsibility, 532, 533, 543digital representations, see symbolic
representationsDimensional Change Card Sorting Task, 408–9dimples, 57, 57directed thinking, 348direction specific cells, 204disengaged parents, 570, 589dishabituation, 261, 298disorders:
of action, 121of language, 123–24of memory, 333mental, see mental disordersof perception, 122of planning and social cognition, 124–25
disorganized children, 614disorganized schizophrenia, 660, 660displacement, 609, 632display rules, 492–93, 500dispositional attribution, 507, 509, 510, 541dissociation, 649, 670–71
in infant cognition, 554dissociative amnesia, 670, 671, 675dissociative fugue, 670, 671, 675dissociative identity disorder (multiple personality
disorder), 658n, 670–71, 671, 675distal stimulus, 135, 135distance, psychological, 525, 542distance cues, 136, 197
see also depth cuesdistance perception, 200–203divorce, domestic conflict and, 571Dix, Dorothea, 679–80dizygotic twins, see fraternal twinsDNA (deoxyribonucleic acid), 52–53, 53, 54, 82
mutations in, 61paternity testing of, 80, 80
doctrine of specific nerve energies (specificitytheory), 144
dodo bird verdict, 712–13, 712, 715dominant genes, 57dopamine (DA), 100, 103, 490, 600, 655, 695–96,
697dopamine hypothesis, 644, 664double-blind design, 28, 28, 43
PSUBJECT INDEXO S7
downward drift, 665dreams, dreaming, 239–43, 239
activation-synthesis hypothesis of, 241, 242,243
brain activity during, 238, 241–43, 242consciousness and, 229emotions within, 240Freudian view of, 241, 241Freud’s theories on, 611, 632interpretation of, 240–41, 241latent content of, 241, 611, 632manifest content of, 241, 611, 632reasons for, 240–43reports of, 239–40themes in, 240
drive, 464, 485–90, 500–501, 502drive-reduction, 464, 485, 487DRM paradigm, 322, 322, 339drugs, 248–55, 257, 325
abuse of, 654addiction to, 253–54, 257agonists vs. antagonists, 101–3conditioning and use of, 276–78, 277depressants, 248–49difference among people and, 254–55“gateway,” 252genetics and, 255hallucinogens, 251, 252–53mental disorders and, 635mind-altering, 257in nervous system, 101–3psychoactive drugs, 699psychotropic, 683, 714side effects, 249, 251, 251stimulants, 250–51tolerance for, 249, 253withdrawal from, 249, 250, 253–54see also medication
drug therapy, 710DSM-IV-TR (Diagnostic and Statistical Manual of
Mental Disorders), 639, 643, 640, 650, 668,669
dual-center theory, 469dual-process systems, 353dual-process theories, 352–54, 376duplex theory of vision, 164Dweck, Carol, 624
ear, 145–46, 146, 156, 157eardrum, 133, 157, 159eating, 466–73, 466, 501–2
cognitive control over, 471control signals for, 468–69cultural influences on, 470, 471disorders, 668–70, 669memory and, 471physiological aspects of, 467–70poverty and, 471social influences on, 470, 470, 502
Ebbinghaus, Hermann, 318Eber papyrus, 636eclecticism, 692–93ecstasy (MDMA), 250ECT (electroconvulsive therapy), 701–2, 701, 703,
714ectotherms, 464EEG (electroencephalogram), 109, 111, 234–35, 235,
247–48, 248, 257efferent nerves, 113efferent neurons, 89, 90Effexor, 697efficacy, 709, 714
utility vs., 708–9egg cells, 55–56, 56, 69–70, 70, 546, 588ego, 607–8, 611, 612–13, 632ego identity, 580, 589ego psychology, 612–13, 632Egyptian art, 215, 215Eichmann, Adolf, 523–24, 524eight ages of man, Erikson on, 580, 580, 5898–stage model, 579Einstein, Albert, 440Electra complex, 610, 612, 632electroconvulsive therapy (ECT), 701–2, 701, 703,
714electroencephalogram (EEG), 109, 111, 131, 234–35,
235, 247–48, 248, 257electroencephalography (EEG), 111electromagnetic spectrum, 161Ellis, Albert, 690–91, 692, 714Ellsworth, Phoebe, 341embryo, 480, 546, 547, 548, 588emotion, 490–500, 493, 502–3
behavioral aspects of, 491–93Cannon-Bard theory of, 494, 496, 502cognitive reappraisal and, 498–99, 499, 500,
503cultural perspective of, 491, 493, 494dimensions of, 493, 493display rules of, 492–93, 492, 500, 502experiential aspects of, 493facets of, 490–96facial expressions and, 491–93, 499, 502functions of, 497–98James-Lange theory of, 494, 495–96, 502of jealousy, 79–80of love, 537–40memory and, 329–32, 497–98models of, 495mood vs., 491motivation and, 461–503perception of, 492perceptual effects of, 497, 497physiological aspects of, 494–96regulation of, 498–500Schachter-Singer theory of, 496, 502, 538in sleep, 240–41, 241suppression of, 498–99, 503
emotional experience, 493emotional intelligence, 438–39, 459emotional memory, 9
active interpretation of, 11, 18children and, 14cognitive influences on, 11–12, 14cultural setting of, 13–14, 13developmental perspective on, 14–15disorders of, 15–16, 15evolutionary basis for, 9–11genetic heritage and, 9–11, 17neural basis of, 8–9painful, 15–16PTSD and, 16, 18recorded information in, 11sharing of, 12–13social influences on, 12–13, 14survival advantage to, 10as unreliable, 12, 13
emotional support, 486, 502empirical claims, 46empirically supported treatments (EST), 706, 714empiricism, 135–36empty chair technique, 687encoding of memories, 303–4, 309
context of, 315–16retrieval and, 315–16
encoding specificity, 317, 339endocrine glands, 104, 130
functions of, 104endocrine system, 103–4, 130endorphins, 102, 102, 148, 490endotherms, 464, 501entity view, 624–25, 625environment:
external, 463–64intelligence and, 445–48, 446, 450–51internal, 463–64, 501IQ and, 445–48language learning and, 404–10, 423prenatal, 548vs. genetics, 446–47, 450–51, 602–3
environment of evolutionary adaptiveness (EEA),73
epilepsy, 119, 701epinephrine (adrenaline), 103, 474, 495, 496episodic memory, 328–29, 331, 339, 583, 661Erikson, Erik, 579, 582, 585–86
on eight ages of man, 580, 580, 589ERP (event-related potential), 109estrogen, 479, 480estrus cycle, 479, 481, 502ethics, in scientific research, 14, 43–45, 48–49,
106–7, 128, 289neuphoria, 102, 103European Americans, IQ scores of, 450event-related potential (ERP), 109evolution, 51–83, 481, 483, 497
adaptive specializations of, 294–95
S8 PSUBJECT INDEXO
evolution (cont.)of behavior and genetics, 65–81broken-wing display and, 62, 62Darwin’s theory of, 59–61, 278–79EEA and, 73emotional remembering and, 9–11, 10finches and, 59, 65fossils and, 63, 63genes and, 61–62of intelligence, 73–75learning and, 294–95of mating patterns, 75–81natural selection and, 58–65proximate causes and, 58sexual behavior and, 479as “survival of the fittest,” 61–62ultimate causes and, 58unity of life and, 64–65, 65
evolutionary psychology, 77excitation threshold, of neurons, 93, 106excitement phase, of sexual response, 481, 502executive control, 124, 226–27, 409, 434–36, 435,
436exercise, 585exogenous agents, 102expectations, surprise and, 273, 274, 298experiential therapies, 687, 712experimental groups, 39, 40, 48experimental manipulation, 39, 40, 41, 47, 48experimental studies, 38–43, 108
animals in, 65, 106, 106groups of, 38, 40, 48internal validity of, 41–42manipulation of, 41, 47quasi-, 36, 44random assignment in, 41, 47replication of, 42scientific process and, 42signal-detection, 140, 140see also research methods
experts, 367explanatory style, 657, 674explicit memory, 327, 328, 334, 336, 337, 339exposure therapy, 267–77, 688, 688, 714Expression of the Emotions in Man and Animals
(Darwin), 68expression rules, 658external environment, 463–64external validity, 27, 27, 47, 48extinction procedures, 267, 688extraversion, 593, 594, 599, 600, 632extrinsic rewards, 489eye, 162–63, 162
see also visioneye movements, 209, 211
in motion perception, 205–6, 205eyewitness testimony, false memories in, 11, 320,
320, 324, 324, 325Eysenck, Hans, 593, 600, 706
facial expressions, 491–93, 492, 499facial recognition, 562, 562facilitation, social, 528, 542factor analysis, 430, 458false-belief tests, 561, 561, 588false memories:
in eyewitness testimony, 11, 320, 320hypnosis and, 324–25leading questions and, 320–21recovery of repressed memories and, 331–32schemas and, 321source confusion and, 256–57
familiarity, 322–24, 323, 339, 536, 536family environment, and schizophrenia, 665–66family resemblance structure, 388, 388family therapy, 694, 714fear conditioning, 10, 10feature detectors, 174–75, 182, 191, 209feature nets, 188–91, 189, 216features, 182–83
geons and, 191, 191hidden figures and, 184parsing and, 185
Fechner, Gustav Theodor, 139Fechner’s law, 139, 178feelings:
conscience and, 576see also emotion
Festinger, Leon, 516–17fetal alcohol syndrome, 549, 549fetal stage, 548fetus, 548, 588fidelity, emotional vs. sexual, 79–80figure, in form perception, 185figures, impossible, 188Fillmore, Kaye, 21–22finches, 59, 65firstborns, 604, 604, 632Fischer, Bobby, 620Fisher, Carrie, 653fixed-interval (FI) schedule, 286, 287fixed-ratio (FR) schedule, 286, 286flashbulb memories, 329–30, 329, 339flow states, 620fluid intelligence, 432, 459, 583–84, 589Flynn effect, 447, 447fMRI (functional magnetic resonance imaging), 2,
3, 9, 48, 112, 230, 230, 4999folk theories, 389follicles, 479–80Food and Drug Administration (FDA), U.S., 108,
128, 699, 700, 702foot-in-the-door technique, 517–18forebrain, 115
see also cortexforgetting, 318–19forgetting curve, 318, 318formal operational period, 578, 589formal operations, 552, 553
form perception:Biederman’s model of, 191figure and ground in, 186–88, 187nervous system and, 192of partially occluded figures, 183variability of stimuli and, 183, 835visual processing in, 192
fossils, 63, 63Fourier, Joseph, 155–56fovea, 162, 163, 163, 164, 165Fox, Michael J., 128fragment-completion tasks, 335framing effects, 5, 5, 359–61, 360, 363, 364Franklin, Eileen, 332Franklin, George, Sr., 332fraternal (dizygotic) twins, 70–71, 70, 71, 73, 444,
444, 448, 484, 599, 650, 652, 655free association, 606free recall, 304, 304frequency, light, see wavelengths, of lightfrequency, sound, 154, 154, 158, 159frequency distributions, 30frequency estimates, 349frequency theory, 158Freud, Sigmund, 17, 222, 241, 241, 614, 674, 680,
684–85, 687, 712, 714on adolescence, 632case studies of, 26on dreams, 611, 632on mythology, 611, 612psychoanalysis and, 606–15, 606, 632, 687psychopathology of everyday life and, 610–11on slips of the tongue, 610–11, 611on stages of psychosexual development,
609–10, 632Freudian slips, 610–11, 611friendships, 572–74, 589frontal cortex, 489frontal lobe, 119, 124, 700functional magnetic resonance imaging (fMRI), 2,
3, 9, 111, 111, 112, 230, 230, 489function morphemes, 382–83, 391–92, 422fundamental attribution error, 509–10, 509, 541fusiform face area (FFA), 229, 230, 499
g (general intelligence), 431–32, 431, 433, 435, 458–59GABA (gamma-amino butyric acid), 100, 698Gage, Phineas, 26–27, 107, 107, 124Galapagos Islands, 59Gale, Crystal, 181Galileo Galilei, 86, 87gamma-amino butyric acid (GABA), 100, 698ganglion cells, 162, 163–64, 192
see also magno cells; parvo cellsgarden path, 392–93, 422Gardner, Howard, on multiple intelligences,
439–40gate control theory, 148gender:
agreeableness differences of, 604, 604
PSUBJECT INDEXO S9
autism and, 666development of, 589genetic determination of, 43, 54intelligence differences of, 452–54moral reasoning and, 574–75, 589personality and, 604stereotypes of, 453suicide and, 655see also sex, sexuality
general intelligence (g), 431–32, 431, 433, 435,458–59
generalization gradient, 268, 268, 282, 282generalized anxiety disorder, 647–48, 698general paresis, 637generativity versus stagnation, 586, 589generic knowledge and memory, 268, 321genes, genetics, 51–83
alleles and, 57, 61, 69, 81anorexia nervosa and, 669attention-deficit/hyperactivity disorder
(ADHA) and, 668bulimia nervosa and, 670codominance in, 57, 82concordance rate and, 650depression and, 638development and, 548dimples and, 57, 57DNA and, 52–53dominance in, 57, 82drug dependence and, 255earlobes and, 74–75, 75emotional remembering and, 9–11, 17environment vs., 446–47, 450–51, 602–3evolution and, 61–62evolution of behavior and, 65–81gender determination and, 54gene expression and, 54–55, 79genes and, 53–54gene transmission and, 55–56genome and, 54, 61, 64, 69, 70, 73, 74, 75, 81genotype of, 55, 57, 66, 70, 73, 81, 82, 443–45,
484incomplete dominance in, 57, 82of intelligence, 69–75, 71intelligence and, 443–45, 444, 450, 454interactions among, 56–58IQ and, 443–45learning capacity and, 445malfunctioning, 57mental disorders and, 647–48, 655, 661–63,
662, 674pattern of, 58, 81personality traits and, 598–601phenotype of, 55, 57, 61, 65, 72, 73, 81polygenic inheritance and, 58recessive, 82SES and IQ interaction with, 447–48set point and, 620sexual orientation and, 484
survival of, 62taste and, 133, 152
genetic survival, 79–80Genghis Khan, 301–2geniculate nucleus, 163Genie, 405–6genital stage, 609genome, human, 55, 61, 64, 69, 70, 73, 74, 75, 81,
548, 588genotype, 55, 57, 66, 70, 73, 81, 82, 443–45, 484Genovese, Kitty, 532, 532geons, 191, 191, 216Gestalt psychology, 184–85, 186Gestalt therapy, 686, 714gestural language, 406–7, 407ghost sickness, Native American, 643Gilligan, Carol, on moral reasoning, 574–75glia, 548glial cells, 90–92, 90, 130global workspace hypothesis, 231–33, 257glomeruli, 149, 149, 178glove anesthesia, 606, 606glucoreceptors, 468, 469, 501glucose, 467–68glutamates, schizophrenia and transmission
dysfunction of, 664, 675glycogen, 467goal maintenance, 435goal neglect, 435goal state, in problem solving, 365–66, 377good continuation, 186, 186Good Samaritan, 533Good Samaritan, The (Bassano), 534grasp reflex, 551, 551, 588gratification, delay of, 629–30, 629, 633ground, in form perception, 186–88group dynamics, 527–31
deindividuation in, 529–30, 542mere presence effects and, 527–28, 527, 542
group inhibition, 533group polarization, 530–31, 542group therapy, 693–94, 693, 714groupthink, 531, 531, 542growth, developmental, 546–50, 550guilt, survival, 649
habituation, 259, 261–62, 298habituation procedures, 557, 588hair cells, as auditory receptors, 134, 157Haldol, 696hallucinations, 660, 674hallucinogens, 251, 252–53, 257halo effect, 535Harlow, Harry, 563Harman, Sabrina, 505Harper’s Weekly, 182Harvard College, 613Hawn, Goldie, 389hearing (audition), 118, 143, 153–60
absolute threshold of, 138decline of, 583frequency theory in, 158language in absence of, 406, 407loss of, 158nervous system and, 158–59place theory in, 158sound as stimulus for, 153–60, 153tonotopic map and, 159–60, 160transduction in, 156–58Weber fraction for, 139
Helmholtz, Hermann von, 158, 158, 169on unconscious inference, 197–98
helping, 532, 534, 543costs of, 533–34
helplessness, learned, see learned helplessnessHering, Ewald, 172heritability, intelligence and, 71–73, 75, 448–50,
450, 451heritability ratio (H), 72, 73, 83, 448–50, 459heroin, 102, 253, 254, 276–78, 277Herrnstein, Richard J., 442hertz, 154, 155Hertz, Heinrich, 154heterosexuality, 483–85heterozygous, 57heuristics, 348, 349–52, 376
availability, 348–49, 376judgment, 348representativeness, 348–49
hierarchical conception, of intelligence, 431–32,431, 458–59
hierarchy of needs, 487, 487, 502, 615Higgins, E. Tory, 617Hilgard, Ernest, 246Hinduism, 247hippocampus, 9, 9, 116, 126, 223, 309histrionic personality disorder, 672H.M., 26, 333, 333homelessness, 696, 696homeostasis, 464, 464, 474, 478, 501
internal, 276homogamy, 537homosexuality, 483–85homozygous, 57Horemhab offering wine to Annubis, 215horizontal cells, 162hormonal cycles, 479–80hormones, 103–5, 234, 238, 453, 475–76, 479
aggression and, 502changing of, 480prenatal, 484, 549secretion of, 104sexuality and, 481
horse racing, predicting outcome of, 437hospitals, mental, 679, 679, 696, 696Hubel, David, 175, 175hue, 168, 168, 169hue pairs, 172, 172
S10 PSUBJECT INDEXO
humanistic approach to personality, 615–22,632–33
humanistic-experiential therapies, 705, 714human racial groups, 450–51human sexual response cycle, 481, 481, 502Hume, David, 386hunger, 466–73, 478, 501–2
control signals for feeding and, 468–69cultural and cognitive aspects of, 470–71physiological aspects of, 467–70
Huntington’s disease, 325Hurvich, Leo, 172Huxley, Thomas Henry, 61hyperactivity, and attention-deficit disorder
(ADHD), 250, 636, 667–68, 667, 675, 699,714
hypnagogic imagery, 234hypnosis, 243–46, 244, 246, 257, 325, 339, 671
memory and, 244–45, 324–25hypnotic age regression, 244, 245hypnotic analgesia, 245, 257hypomania, 653hypothalamus, 104, 116, 228, 233, 234, 465, 466,
468, 470, 479, 480, 501control centers of, 469
hypothesis, 42confirmation of, 45testable, 48
hysteria (conversion disorder), 606, 637, 643
ICD-10 (International Classification of DiseaseSystem), 642
id, 607–8, 613, 632ideal self, 617, 617identical (monozygotic) twins, 70–71, 70, 71, 73,
444, 444, 448, 472, 472, 484, 599, 599, 603,632, 650, 652, 655, 665
identity:confusion, 580, 589ego, 580, 589negative, 580, 589role confusion vs., 589self-, 580
ill-defined problem, 365illogical interpretations, 215illusions:
brightness, 199perception and, 198–99, 199
illusory conjunctions, 210images, symbols and, 343imitation, 563immigration policy, intelligence testing and, 442,
442immune system, 96
sleep deprivation and, 236Implicit Association Test (IAT), 512implicit memory, 223, 327, 334, 335, 336–37, 339, 583implicit theories of personality, 510–11, 542impossible figures, 187, 187, 214–15imprinting, 564–65, 565
impulsive-control disorder, 640incidental learning, 338incremental view, 624–25, 625incubation, in problem solving, 372indentity versus role confusion, 579independent variables, 24, 36, 39individualistic cultures, 508–9, 508, 510–11, 541,
543, 581, 619love in, 540
induced motion, 206–7, 217infancy and childhood, see childreninference, unconscious, 197–98inferential statistics, 28, 33–34inferotemporal cortex, 194, 194influence:
informational, 520, 542minority, 522, 522normative, 521, 542social, 519–31, 542
influenza virus, 662informant data, 594informational influence, 520, 542informed consent, 44inhibited temperament, 601, 601, 632inhibition:
group, 533social, 528, 542
initial state, in problem solving, 365, 366, 377inner ear, 156, 157insomnia, 237inspection time, 433, 459instincts, 463, 463, 501instrumental (operant) conditioning, 259, 278–79
attitude formation and, 514behavior modification and, 281, 283–85, 284,
299, 714biological constraints on, 294contingency in, 287–89generalization and discrimination in, 282–84major phenomena of, 281–86reinforcement (reward) in, 281–86, 689response rate in, 212schedules of reinforcement in, 286, 299shaping in, 283–84successive approximations in, 283
insufficient justification, 517insula, 650integrity versus despair, 586, 589intellectual functioning, 436intelligence, 66, 425–59
age and, 73analytic, 437–38beliefs about, 625, 625beyond IQ, 436–41, 459building blocks of, 432–36comparisons among relatives of, 69–71creative, 459crystallized, 583–84cultural context of, 440–41, 450cultural influences of gender, 453
emotional, 438–39environmental influence on, 71environment and, 445–48, 446, 450–51evolution of, 73–75executive control and, 434–36fluid, 583–84fluid and crystallized, 432, 459gender differences of, 452–54general (g), 431–32, 431, 458–59genetic factors in, 443–45, 444, 450genetics of, 69–75, 71group differences in, 450–56heritability and, 71–73, 75, 448–50hierarchical model of, 431–32, 431, 458–59hormones and, 453intellectual functioning and, 436IQ and, 425–26, 426, 431, 432linguistic, 439mental speed and, 433mental tests and, 458nature vs. nurture problems and, 443and notion of multiple intelligences, 459political issues of, 442poverty and, 447, 455practical, 437–38, 437, 459psychometric approach to, 428–32, 429, 458racial differences of, 454–55roots of, 441–56, 459SES and, 447–48, 455and social factors on gender, 453talent vs., 440testing of, see intelligence testingand theory of multiple intelligences, 439–40types of, 439–40working memory and attention in, 434working-memory capacity (WMC) and, 434,
459intelligence quotient (IQ), as measure, 425–26,
426, 431, 432, 454, 513development of, 426, 427–28, 428, 433, 441–42,
446–48, 458, 459environment and, 445–48genetics and, 443–45, 447–48group differences in, 450–56nutrition and, 447poverty and, 447tests, 425–26
intelligence testing, 70, 425, 427, 431, 433, 454–55,457 458
in adults, 427in children, 426in cultural context, 440–41, 440political issues in, 441–42, 442psychometric approach and, 458by U.S. Army, 442see also intelligence; mental testing
intentional learning, 303interdependent cultures, 618interference, 319, 319intergroup contact, 516, 518
PSUBJECT INDEXO S11
internal environment, 463–64, 473, 501internal homeostasis, 276internal validity, 34, 41–42internal working model, 566–67International Classification of Disease System
(ICD-10), 642interneurons, 89interpersonal intelligence, 439interpersonal therapy (IPT), 685, 712interposition, 201, 217Interpretation of Dreams (Freud), 241interpretations, illogical, 215inter-rater reliability, 32intimacy, 537, 543
isolation vs., 585, 586, 589intrapersonal intelligence, 439intrinsically rewarding, 489, 620intrinsic motivation, 285–86, 299introspection, 256
cognitive unconscious and, 222–23communication of, 225functions of consciousness and, 220–27honest reporting and, 220–21, 221mistaken, 225–26translating thoughts into words and, 220–22
introversion, 600, 632intrusion:
memory, 319–25semantic memory and, 322
intrusion errors, 319, 321, 339intuition, vs. reasoning, 352inverted spectrum, 221, 221in vivo desensitization, 688, 688ion channels, 94ion pump, 94IPT (interpersonal therapy), 685IQ, as measure, see intelligence quotient (IQ), as
measureiris, 138, 162Isabelle (code name), 405isolated children, 405–6, 423isolation, intimacy versus, 585, 586, 589Iyengar, Sheena, 626
Jamadi, Manadel al-, 505James, William, 220, 463, 494, 616, 616James-Lange theory of emotion, 494, 495–96,
502Jameson, Dorothea, 172Jamison, Kay Redfield, 653–54jealousy, 79–80Jefferson, Thomas, 615, 615jet lag, 234J.S., 86judgment, 348–54, 376
heuristics, 348–49, 376moral, 574–75reasoning and, 358training and, 358
Jung, Carl, on collective unconscious, 611, 611justification:
of effort, 516–17, 516, 517insufficient, 517
just-noticeable difference (jnd), 137, 178
Kahneman, Daniel, 348–49, 349Kamala (wild girl), 405Kant, Immanuel, 136, 136Kanzi (chimpanzee), 414Kelley, Harold, 507–8Kelly, George, 624Kennedy, John F., 329Kepler, Franz, 86kinesthesis, 145
Weber fraction for, 139King, Coretta Scott, 522King, Martin Luther, Jr., 522Kinsey, Alfred, 485Kluver-Bucy syndrome, 9knowledge:
declarative, 334expert, 367fluid vs. crystallized intelligence and, 432, 459perception and, 215procedural, 334tacit, 438
knowledge acquired, vs. behavior modification,287–89
knowledge-driven processing, 189–90, 190Knowles, Beyoncé, 440Kohlberg, Lawrence, on stages of moral reasoning,
574–75, 575, 589Korsakoff’s syndrome, 333Kraepelin, Emil, 637, 637Krafft-Ebbing, Richard von, 637
labeling, of mental illnesses, pros and cons, 644Lake Washington, 63–64, 64Lamb, Fred and Don, 599Lamictal, 678Lange, Carl, 494language, 379–423
accents and, 396adult, progression to, 403–4, 423ambiguity in, 391basic-level words and, 401–2, 422basic units of, 380–85bilingualism and, 408–10building blocks of, 397–98, 422child, 401–3, 422–23color perception and, 417combining definitional and prototype theories
of, 388–89, 389, 422comprehension of, 395–96cultural perceptions and, 417–21and definitional theory of word meaning,
386–87, 386, 422disorders of, 123–24
environment and growth of, 404–10, 423foreign, 399frequency sensitivity in infants, 399–400, 422gestural, 406–7, 407, 423hierarchical nature of, 380–81, 381, 422late exposure to, 405–6, 413, 423learning and, 396–404, 422–23meaning conveyed by, 385–96, 422without models, 406–7, 423morphemes and words in, 314–17, 422in nonhumans, 413–15, 414, 423phrases and sentences in, 383–85, 389–91,
390, 393, 395, 422phrase structure organization in, 384–85, 384,
385, 422prototype theory of meaning of, 387–88, 422rhythm of, 381–82, 398–99rules of syntax in, 383, 422and second-language learning, 412–13, 412sensitive period hypothesis of, 410–15, 411, 423social origins in learning of, 396, 396social origins of word learning in, 400–401without sound, 406, 423sound units in, 380–82, 399of spatial position and direction, 417–21, 418,
419spatial thinking and Tzeltal, 419–21stages of development and growth of,
396–404, 422subordinates and, 403, 422superordinates and, 403, 422syntax rules of, 391thought and, 415–21, 423understanding, 391–96see also sign language
larynx, 381Latané, Bibb, 532latent content, of dreams, 611, 632latent learning, 287, 299lateral geniculate nucleus, 163, 241–42, 242lateral hypothalamus, 469lateral inhibition, 166, 167lateralization, 116–18, 117Law and Order: Criminal Intent, 7law of effect, 278–81, 280, 299leading questions, 320–21learned helplessness, 299
depression and, 289learning, 259–99
associative, 273biological constraints on, 291–94brain activity during, 309classical conditioning in, 259empiricist view of, 136evolution and, 294–95incidental, 338intentional, 303language and, 262, 396–404, 406–7, 422–23latent, 287
S12 PSUBJECT INDEXO
learning (cont.)memory and, 309, 311–12method of loci and, 311neural basis for, 296–97new, 318–19observational, 289–90, 299, 477, 514–15operant conditioning in, 259prenatal, 548prepared, 294, 294in progression to adult language, 403–4punishment and, 287of second language, 412–13, 412slow pace of human growth and, 550social origins of, 400–401social origins of language learning, 396, 396species similarities and, 295–96theory, 260–61, 298varieties of, 291–96
learning capacity, genetic factors in, 445learning curve, 265, 265, 279, 279learning theorists, 261Le Bon, Gustave, 529left neglect (neglect syndrome), 122, 122lens, of eye, 162, 162Leonardo da Vinci, 485Lepper, Mark, 626leptin, 468–69, 468, 469, 472, 501Lexapro, 697life data, 613lifetime prevalence, 640light:
amplitude of, 161brightness of, 161, 164, 165, 166, 168, 179frequency of waves of, 161perceived color and, 164, 168, 179visible spectrum of, 161, 168, 169wavelengths of, 161, 168, 168, 169, 169
liking, 489, 490, 502limbic system, 116, 116, 242, 656, 702linear perspective, 202, 202, 203, 217Linehan, Marsha, 692–93linguistic intelligence, 439lithium, 677lithium carbonate, 698liver, role of, 467–68, 469loafing, social, 528–29, 542lobotomy, side effects of, 700localization of function, in brain, 131lock-and-key model, 101, 101, 130Locke, John, 134, 135, 260Loewi, Otto, 97logic, formal, 356logical-mathematical intelligence, 439logical reasoning, 579long-term memory:
active engagement and, 307–8storage capacity of, 304, 338transfer into, 304understanding and, 308–10
long-term potentiation (LTP), of neurons, 297,297, 299
loss aversion, 360love, 537–40
companionate, 539, 539, 543, 585individualistic cultures and, 540passionate, 585romantic, 537–39, 538, 543
LSD (lysergic acid diethylamide; “acid”), 252
McCabe, Clint, 461McDougal, William, 463Mach bands, 165–66, 166, 167, 179Madden, John, 673magnetic resonance image (MRI), 83–84, 110, 110,
111magno cells, 192, 216maintenance rehearsal, 308, 338major depression, 652, 653majorities, 522Malthus, Thomas, 59mania, 654, 677, 698, 701manic-depressive illness, see bipolar disordermanifest content, of dreams, 611, 632Manning, Peyton, 440manualized therapy, 708, 715manual skills, 551marijuana (Cannabis sativa; Cannabis indica),
251–52, 254, 257Maslow, Abraham, 485, 487, 487, 488, 502, 615–16,
615, 620, 622mastery orientation, 486matchstick problem, 366, 371mating, 83
choosing a mate and, 77–78, 482–83, 482commitment and, 79–80courtship and, 77, 77different expectations of sexes and, 76economic status and, 78, 78emotional vs. sexual commitment in, 79–80evolution of, 75–81females and, 77males and, 77mate selection and, 83mating systems and, 75–76monogamy and, 75paternity and, 80–81pheromones and, 150polyandry and, 75polygamy and, 75–76polygyny and, 75, 76reproduction and, see reproductionself-promotion and, 77, 77sexual behavior and, 479
Mayer-Salovey-Caruso Emotional Intelligence Test(MSCEIT), 438–39, 438
MDMA (ecstasy), 250means-end analysis, 366medial prefrontal cortex, 496, 617
medication:antianxiety, 698–99, 714antidepressant, 103, 696–98, 714antipsychotic, 102, 664, 675, 695–96, 714atypical antidepressants, 697evaluating of, 699–700psychotropic drugs as, 695see also drugs
meditation, 247–48, 248, 257medulla, 114, 115melatonin, 234Memento, 303memorizing, 403–4memory, 301–39
acquisition of, 302–12, 338anterograde amnesia and, 223assessment of, 326–27attention and, 11, 11, 305–8, 324, 435–36autobiographical, 329brain damage and loss of, 4, 313, 333of children, 14, 568chunking in, 306–7, 373–74consciousness and, 224consolidation, 312context and, 315–16context reinstatement and, 315–16, 316, 339development of, 568dissociation of, 331distortions of, 331–32DRM paradigm and, 322, 322, 339eating and, 471ECT and damage to, 702emotional, see emotional memoryemotional remembering and, 329–32emotion and, 497–98encoding of, see encoding of memoriesepisodic, 328–29, 331, 339, 583, 661explicit, 327, 328, 334, 336, 337, 339failure of, see memory failurefalse, 324–25, 326familiarity and, 322–24, 323, 339feeling of hunger and, 4flashbulb, 329–30, 329, 339games of, 303generic knowledge and, 321hypnosis and, 244–45, 324–25, 325, 339implicit, 223, 327, 334, 335, 336–37, 339, 583improvement of, 324–25interacting images and, 311, 311intrusions in, 319–25intrusions and overwriting in, 339learning and, 309, 311–12long-term, 304, 307–12, 338loss of, 328maintenance rehearsal and, 308method of loci and, 311misinformation effect and, 320–21mnemonics and connections in, 310–11, 311non-interacting images and, 311, 311primacy effects in, 304–5, 304, 305, 338
PSUBJECT INDEXO S13
procedural, 334, 335, 339recall and, 303, 319, 322, 336recency effects in, 304–5, 304, 305recoding in, 306–7recognition and, 303recollection and, 308, 314, 322–23, 339, 498recovered, 332, 332rehearsal, 305, 306–7repression of, 331–32, 339retrieval, see retrieval, memoryschemas and, 321, 339selective, 25semantic, 328, 583short-term, see working memorystage theory of, 304storage, 245, 302–3storage capacity, 304storage of, 338as supplemented, 11–12thinking and, 373–74, 374trauma and, 330–32, 330types of, 327–37, 327as unreliable, 5, 11–12, 25witnesses and testimony and, 320, 320, 324,
325working, see working memorysee also false memories
memory failure, 583decay as, 318–19forgetting in, 318–19interference and, 319, 319retention intervals and, 318–19retrieval failure in, 338–39
memory span, 304memory trace, 303, 312, 338menarche, 577Mendel, Gregor, 56–57, 56menopause, 586menstruation, 480, 481, 577mental disorders, 636–52, 673
alcohol consumption and, 635anxiety, 644–52, 674assessment of, 640–42biological factors of, 680biomedical treatments, 694–703biomedical treatments for, 680, 702–3causal models of, 674clinical interviews, 640–41cognitive-behavioral approaches to treatment
of, 690–92, 714comorbidity and, 650cultural considerations in treatment for,
682–83current treatments for, 680–83defined, 639–40dissociative, 670–71, 675drug use and, 635early conceptions of, 637, 674early treatments of, 694–95, 695
evaluating treatments of, 705–13genetic factors in, 647–48, 655, 661–63, 662,
674humanistic approaches to treatment of,
685–87medication for, 680, 695–700, 714misdiagnosis of, 677modern conceptions of, 638–39, 674mood, 652–58, 674multicausal models of, 638–39nonpharmalogical treatments for, 700–703,
700overprescribed medication for, 699, 699past treatments for, 678–80, 679psychodynamic approaches to treatment of,
684–85as psychological illness, 638–39psychological risk factors for, 656–57psychological treatments for, 680, 683–94psychotherapy for, 714schizophrenia, 644, 674–75signs of, 641, 674social support for, 639, 652, 681stress, 649, 674subsyndromal, 673, 682, 711–12symptoms of, 640–41treatment of, 677–715treatment providers for, 681–82, 681treatment recipients for, 682see also psychopathology
mental exercise, 585mental hospitals, 679, 679, 696, 696mental images, imagery, 343–45, 345, 376mental representations, 342, 376, 588, 617mental retardation:
autism and, 667, 675PKU and, 449
mental rotation, 452, 452mental sets, 368–69, 377mental speed, 433mental testing, 458
see also intelligence testingmere presence effects, 527–28, 527, 542mescaline, 251, 252Mesmer, Franz, 243–44, 244meta-analysis, 42, 709–10, 713, 715methamphetamine, 250, 251method of loci, 309, 311methodological eclecticism, 46–47methylenedioxymethamphetamine (MDMA;
ecstasy), 250, 251midbrain, 115, 115middle age, 582middle ear, 156midlife transition (midlife crisis), 586, 587Milgram, Stanley, studies of, 524–26, 524, 542Miller, Arthur, 355mind-body connection, 228, 228mind-body problem, 227–28, 255, 256
Minnesota Multiphasic Personality Inventory(MMPI), 641–42, 642
minorities, 522mirror neurons, 290, 290Mischel, Walter, 596, 624, 628, 630misinformation effect, 320–21, 339mixed states, depression and mania as, 653MMPI (Minnesota Multiphasic Personality
Inventory), 641–42, 642mnemonics, 302, 310–11, 311, 338modeling, as behavior therapy, 690, 690, 714mondegreen, 181–82monoamine oxidase (MAO) inhibitors, 696–97,
697monocular depth cues, 200–202, 203monocular distance cues, 217monogamy, 75, 79–80monosodium glutamate (MSG), 151monozygotic twins, see identical twinsmood disorders, 652–58, 674
explanatory style, 657negative cognitive schema and, 567risk factors for, 656–57roots of, 655–58
moods, 491mood stabilizers, 698moral development:
conscience and, 576, 589prosocial behavior and, 589
morality, 2–3, 4making decisions and, 2, 3
moral judgment, 574–76moral reasoning, 574–76, 575, 589morbid obesity, 471, 473morphemes, 382–83, 391, 399, 406, 422morphine, 102, 148, 245, 246motion detectors, 204, 208motion parallax, 202, 203, 217motion perception, 202, 203–8, 204, 205, 217motivated social cognition, 523motivation, motives, 485–90, 502
diversity of, 487–90, 502drive and, 464drive-based, 500–501emotion and, 461–503hierarchy of needs and, 487, 487, 502motivational states, 462–64, 501motive to achieve, 486, 486, 502motive to belong, 485–86, 485, 502
motivational-enhancement therapy, 686motor areas, 118motor cortex, 242motor neurons, 89motor projection area, primary, 119, 119, 121MRI (magnetic resonance imaging), 83–84, 110,
110, 111MSCEIT (Mayer-Salovey-Caruso Emotional
Intelligence Test), 438–39, 438MSG (monosodium glutamate), 151
S14 PSUBJECT INDEXO
Müller, Johannes, 143–44multicausal model of mental disorders, 674multimodal therapy, 693, 705multiple intelligences, 439–40, 459multiple personality disorder (dissociative identity
disorder), 658n, 670–71, 671, 675women and, 670
multiple sclerosis (MS), 96, 107multi-unit recording, 105Murray, Charles, 442muscular action, 119–20, 119musical intelligence, 439mutations, in DNA, 61myelin, 88, 91, 91, 96My Fair Lady, 397myths, psychoanalytic theory of, 611–12, 612
Nagel, Thomas, 256narcissistic personality, 672Nardil, 696national character, 602, 632National Highway Traffic Safety Administration,
249National Science Foundation, 452Native Americans, 440naturalistic fallacy, 60, 60, 82naturalistic intelligence, 439natural selection, 10, 58–65, 64, 66, 69, 73, 74, 76,
77, 79, 81, 82, 152, 278, 280–81, 475, 478,483, 651
nature vs. nurture, problems with, 443Navratilova, Martina, 485Nazi Germany, 523, 526, 526Nebuchadnezzar, King of Babylon, 636, 636Necker cube, 187, 187needs, hierarchy of, 615negative afterimage, 171, 171negative cognitive schema, 657, 674negative identity, 580, 589negative symptoms, 660–61, 674neglect syndrome (left neglect), 122, 122neocortex, see cortexnerve cells, interaction between, 88–89, 113nerve impulses, 88–89nervous system:
adolescent changes of, 578architecture of, 112–18, 131autonomic (ANS), 113, 133, 131, 464–65, 474,
501, 502, 650brain and, 85–130central (CNS), 90, 112–13, 113, 127chemical signals of, 97, 103communication of, 103, 195–96communication within, 91–103, 113contralateral quality of, 119, 120, 131depressant drugs and, 248development of, 549effect of drugs on, 101–3endocrine system and, 103–4form perception and, 192
functional specialization of, 112hearing and, 158–59memory traces in, 303pattern coding and, 170peripheral, 112–13, 113, 127PGO waves of, 242plasticity of, 125–28pre-natal development of, 547–48repairing damage to, 127–28, 127role of neurotransmitters in, 130senses and, 142sleep and, 238–39, 241–42, 242somatic, 113, 113stimulant drugs and, 250structure of, 88–92, 112–18, 113study of, 85–131sympathetic, 474–75, 497, 499
neural correlates, 229–31, 257neural plasticity, 125–28, 296neural synchrony, 195–96neural tube, 547neurochemical malfunction, 656neurodevelopmental disorder, 663, 675neurogenesis, 127neuroimaging, 110–11, 344
see also CT scan, fMRIneuroleptics, see antipsychoticsneurons, 88, 88, 105, 195
afferent, 90chemical signals between, 92communication among, 92, 109, 232development of, 548efferent, 90electrical activity of, 92–95electrical signals within, 92, 109excitation threshold of, 99firing synchrony of, 195–96function of, 88–89interaction among, 88–89, 296–97learning and function of, 296–97mirror, 290, 290motor, 89new, 126–27parts of, see specific partspostsynaptic, 98–99potentiation of, 297presynaptic, 98–99, 100projection, 89protomaps and, 549recording from, 105in sensory coding, 143sleep deprivation and, 238sound frequency and, 158structure of, 88–89, 99, 130, 189types of, 89workspace, 232
neuropeptide-Y (NPY), 468–69, 472neuropsychology, 107–8neuroscience, 88, 192–96, 216
affective, 496, 503
neuroscience approach, see perception,neuroscience approach
neurosis, 643neurosurgery, 700neuroticism, 593, 599, 602neurotransmission, 148neurotransmitters, 98–99, 100, 103, 104, 105, 130,
252, 257depression and, 655–56effect of drugs on, 101–3, 697, 697, 698lock-and-key model of, 101, 130in schizophrenics, 664in sensation seeking personalities, 600
newborns, 550–51, 562, 562New Freedom Commission on Mental Health, 673New Guinea, 67Newton, Isaac, 87, 635Nicaragua, deaf children in, 407, 407niche construction, 66night vision, 164nine-dot problem, 366, 3719/11 terrorist attack, 12, 12, 13–14, 329, 329, 518–19,
534No Child Left Behind (NCLB), 452nociceptors, 147–48nodes, 346–48, 376nodes of Ranvier, 88, 91, 91, 95non-primary areas (association areas), 121norepinephrine (NE), 100, 103, 105, 474, 655, 697,
697normative influence, 521, 542norm of reciprocity, 526, 542noun phrases, 384, 384novocaine, 250NPY (neuropeptide-Y), 468–69, 472nucleus accumbens, 489, 490
Obama, Barack, 128obedience, 523–26, 523, 542
psychological distance and, 525obesity, 37, 81–82, 471–73, 501–2, 692
environmental factors and, 473genetic roots of, 472–73morbid, 471, 473twin studies of, 472, 472
object permanence, 553–54, 553, 555, 558, 588object relations, and attachment theory, 613–14,
632objects, and space in infancy, 557–58observational learning, 289–90, 299, 477, 514–15observational studies, 36–38, 47
see also case studies; correlations, correlationalstudies
observations, 22–28behavior changes during, 27–28clinical, 107–8
obsessive-compulsive disorder (OCD), 648, 648,650, 672, 674, 701
occipital cortex, 118, 242, 242occipital lobe, 86, 120
PSUBJECT INDEXO S15
occlusion, 557–58, 557OCD (obsessive compulsive disorder), 650odorants, 149, 149, 151Oedipus complex, 609–10, 609, 612, 612, 632olfactory bulbs, 149, 149, 178olfactory epithelium, 148, 151, 178one-trial learning, 292On the Origin of Species (Darwin), 59openness to experience, 593operant conditioning, see instrumental
conditioningoperants, 281, 299operations:
cognitive, 555concrete, 556
opponent-process theory, 172, 172, 179optic chiasm, 163optic flow, 202optic nerve, 143, 143, 162, 163, 163, 234optimism, 621oral stage, 609–10orbitofrontal cortex, 650orgasm phase, of sexual response, 481, 502orphans:
lack of attachment and, 571–72, 572, 589Romanian, 571–72, 572, 589
ossicles, auditory, 156, 157, 159ought self, 617, 617outcome expectations, 623, 633outcome research, 706–7outer ear, 156out-group homogeneity effect, 512ova, 479, 480oval window, 156, 157, 159ovaries, 479overregularization errors, 404, 422ovulation, 481
pain:avoidance of, 487–88matrix, 488, 502reduction of, 245–46, 246sensation of, 139, 147–48, 178Weber fraction for, 139
panic attacks, 646–47, 647panic disorder, 646–47, 675, 698papillae, 151, 151, 152, 178parahippocampal place area (PPA), 229–30, 230parallel processing, visual cortex and, 192–94paranoid personality, 672parasympathetic activation, 465parasympathetic branch of the autonomic nervous
system, 113, 114, 464, 501parenting, 589
authoritarian parents and, 569, 589authoritative parents and, 569–70, 581, 589conscience and, 576disengaged parents and, 570, 589paternal bonding and, 565
permissive parents and, 569, 589paresis, 680paresis, general, 637parietal cortex, 194, 194, 210, 309parietal lobe, 86, 120, 436parieto-frontal integration theory (P-FIT), 436,
436Parkinson’s disease, 107, 127, 128parsing, 184–86, 185
perceptual, 184–86partial retrieval, 313–14parvo cells, 192, 216passion, 537, 543passionate love, 585paternity, 80–81, 80pattern coding, 145, 170pattern theory, 144, 144, 178Pauley, John, 673Pavlov, Ivan Petrovich, 263–64, 263
on classical conditioning, 263–78, 297, 651Pavlovian conditioning, 651Paxil, 103, 697payoff matrix, 141PCP (phencyclidine; “angel dust”), 252, 664Pearl Harbor, 518Peek, Kim, 440peer relationships, 572–74, 589penis envy, 610perception, 181–217
active, 136, 187, 196, 214attention and, 208–12, 212binding problem in, 195–96blindsight and, 223closure principle and, 186of color, 168consciousness and, 222, 224of constancy, 196–99of depth, 200–203detectors of, 188, 189, 208distance, 200–203features and, 182–83good continuation and, 186, 186hallucinogens and, 232illogical interpretations and, 215illusions and, 198–99, 199illusory conjunctions and, 210impossible figures and, 187, 187, 214–15knowledge and, 215language and, 417mis-, 181–82, 208of movement, 203–8nervous system and, 192network models of, 188–92, 216neuroscience approach to, 192–96neuroscience of vision in, 216organization of, 183–88parallel processing and, 192–94parsing in, 184–86, 185passive, 135–36
perceptual constancy and, 196–99, 216person, see person perceptionpriming for, 211proximity and, 186, 186reversible figures and, 186, 187selection in, 208–12similarity principle and, 186, 186simplicity principle and, 186social, 511of speech in infants, 397–99, 399subjective contours and, 186, 187theory of self-, 517unconscious inference in, 197, 222visual, 189, 231visual pathway and, 192–95
perceptual constancy, 196–99, 216perceptual effects, 497, 497perceptual learning, 336, 339perceptual sensitivity, 140perceptual system, 188performance orientation, 486peripheral nervous system, 112–13, 113, 127
see also autonomic nervous system; somaticnervous system
peripheral route to persuasion, 515, 515, 542Perls, Fritz, 686, 714permissive parents, 569, 589Perry, Tyler, 389perseveration, 124, 435personal consistency, 625personal constructs, 624personal contact, loss of in schizophrenia, 660–61personality, 591–633
authoritarian, 523, 542between-family differences in, 599, 603–4, 632Big Five dimensions in, 598, 599, 602, 604,
632biological makeup and, 598–601, 599, 632character strengths and, 621, 621childhood delay and adolescent competence of,
633and consistency of behavior, 595–97control and, 625–26, 626, 633culture and, 602–3, 632dimensions of, 593–94, 632disorders of, 671–72, 674–75, 692, 693firstborns and, 604, 604, 632gender and, 604genes and environment in, 599, 602–3hierarchy of, 594humanistic approach to, 615–22, 632–33implicit theories of, 510–11, 541methods of assessment of, 641–42national character and, 602, 632need for multiple approaches to, 632–33obedience and, 523paradox, 596, 632physiological arousal and, 600positive traits and, 621–22
S16 PSUBJECT INDEXO
personality (cont.)psychodynamic approach to, 605–15, 632psychodynamic perspective of, 605self and, 616–19self-control and, 625–26, 628–30, 628, 633self-monitoring of, 597, 598, 632social-cognitive approach to, 622–31, 632, 633social roles and, 596, 618taxonomy of traits of, 592–605, 632trait approach to, 592–93, 632traits vs. situations, 596, 632within-family differences in, 603–4, 632
personality paradox, 596, 632personality tests, 641–42personal myths, 617person perception, 510–14
implicit theories of personality and, 510–11, 541prejudice and, 511stereotypes and, 511–14
perspective, biopsychosocial, 639persuasion:
central route to, 542foot-in-the-door technique and, 517–18insufficient justification and, 517peripheral route to, 515, 542
persuasion, self, 516–18Peterson, Christopher, 621PET scan (positron emission tomography), 110–11,
656PGO waves, 242phallic stage, 609–10, 632pharmacological treatments, 695–700Phelps, Michael, 673, 673phenotype, 55, 57, 61, 65, 72, 73, 81, 82, 443phenylketonuria (PKU), 57, 449–50, 449pheromones, 150, 178Phillipa (brain damage victim), 85phobias, 645–46, 650, 651, 673, 674, 687–88,
690, 711, 712social, 646, 650specific, 645–46, 645, 674
phonemes, 381–82, 422phonetic distinctions, 398, 398photopigment, 164–65, 169photoreceptors, 162, 162, 163, 164phrases, 383–85, 422phrase structure organization, 384–85, 384, 385physical attractiveness, 535physical development, 546–50
before birth, 546–50after birth, 550–51senses and, 550–51
physical exercise, 585Piaget, Jean, 587, 588
case studies of, 26, 26stages of development of, 552–56, 553
pictorial cues, 201, 201piloerection, 474, 474pineal gland, 228, 228, 234Pinel, Philippe, 679
pitch, 154, 158pituitary gland, 103, 479PKU (phenylketonuria), 57, 449–50, 449placebo, 43, 43, 224–25, 246placebo effects, 43, 705, 707–8, 715placenta, 547place theory, 158plasticity, 125–28, 131plateau phase, of sexual response, 481, 502play:
across cultures, 6, 7across species, 7, 7aggression during, 24, 27, 27, 28biological influences on, 6–7sexual differentiation of, 5, 6
pleasure, pursuit of, 488–90, 489pleasure principle, 607pluralistic ignorance, 532, 543Poincaré, Henri, 372point prevalence, 640Pollock, Jackson, 620polyandry, 75polygamy, 75–76, 83polygenic inheritance, 58polygyny, 75, 76pons, 114–15, 115, 241–42, 242position constancy, 205positive psychology, 619–22, 633positive symptoms, 659–60, 674positive traits, 621–22positron emission tomography (PET) scan, 110–11,
656possible selves, 617postconventional reasoning, 574–75posterior parietal cortex, 194posthypnotic amnesia, 245posthypnotic instructions, 245postsynaptic neuron, 98–99post-traumatic stress disorder (PTSD), 15, 18, 331,
649, 649, 650, 651–52, 658medications for, 698
potentiation, of neurons, 297actively dependent potentiation, 297
poverty:eating and, 471intelligence and, 447, 455
PPA (parahippocampal place area), 229–30,230
practical intelligence, 437–38, 437, 459prayer mandala, 247, 247preconscious level, 607preconventional reasoning, 574–75predicate, sentence, 389–90, 422predictive validity, 427prefrontal cortex (PFC), 124, 233, 243, 309, 435,
435, 558, 589pregnancy, 480prejudice, 511, 515, 542
intergroup contact and, 516, 518see also bias; stereotypes
prenatal development, 546–49, 547, 588teratogens and, 549, 588
prenatal environment, 548, 588prenatal hormones, 484prenatal learning, 548preoperational period, 552, 553, 555–56, 588prepared learning, 294, 294pressure, sensation of, Weber fraction for, 139presynaptic axon terminals, 100presynaptic facilitation, 228, 296, 299presynaptic neurons, 98–99, 100prevention focus, self and, 617primacy effects, 304–5, 304, 305–6, 306, 338primary attachment figure, 613–14primary reinforcers, 284primary sexual characteristics, 577, 589priming, 210priming effects, 211, 335–36, 347–48Principia Mathematica (Newton), 87problem solving, 348, 365–75, 366, 377
analogies for, 369–70, 374, 377automaticity in, 367–68creative thinking in, 371–73experts and, 367, 377goal state of, 365–66hierarchical structure of, 366, 377ill-defined problems in, 365initial state of, 365–66means-end analysis in, 366memory chunks and, 373–74obstacles to, 368–70organization in, 365–75, 367, 373–74restructuring in, 371, 372, 377subproblems in, 366, 367well-defined problem in, 365
procedural knowledge, 268, 334procedural learning, 335procedural memory, 334, 335, 339progesterone, 480, 480projection, 609, 613, 632, 642projection areas, 118–19projection neurons, 89projective tests, 642promotion focus, self and, 617propagation, 95propositions, 346–48, 347, 376, 389–90, 422, 423propylthiouracil (PROP), 152prosopagnosia, 122protective factors, psychopathology, 638proteins, 53, 54, 55, 66protomaps, 549prototype theory of meaning, 387–88proximal stimulus, 135, 135, 151proximate causes, 58, 73, 75proximity, 186, 186, 535–36, 535, 543Prozac, 103, 677, 697psilocybin, 252psychiatric hospitals, see mental hospitalspsychoactive drugs, 699psychoanalysis, 684, 712, 714
PSUBJECT INDEXO S17
classic, 687, 714critiques of Freudian theory of, 632free association in, 606Freud on, 606–12, 632origins of, 606–7repression in, 606, 608–9, 613, 632resistance in, 606
psychodynamic approach, personality and,605–15, 632
psychodynamic models, 638–39psychodynamic perspective, 605psychodynamic therapies, 693, 705psychogenic symptoms, 606psycholinguists, 392psychological distance, 331, 525, 542psychological intensity, 143psychological treatments, of mental disorders,
680, 683–94psychology:
abnormal, see mental disorders;psychopathology
definition of, 1dichotomies of, 17–18diverse methods and perspectives of, 8–16multiple perspectives of, 16–17, 17positive, 619–22, 633science of, see research methodsscientific methods of, 18–19thematic concerns of, 16see also specific subject entries
psychometric approach, 428–32, 429, 458psychopathology, 498, 628, 635–73, 702
biomedical factors and, 638biomedical treatments for, 694–703, 714as demonic possession, 637diathesis-stress models in, 638, 638of everyday life, 610–11multicausal models in, 638–39see also mental disorders
psychophysics, 136–42, 178psychosexual development, stages of, 609–10, 632psychosis, 659
medication for, 102psychosurgery, 700–701, 714psychotherapy, 684, 685, 692, 705, 706, 709, 710
behavior therapy, 687–90, 687, 714classic psychoanalysis, 687, 714cognitive therapy, 690–92, 714common factors in, 704–5culture and, 714psychodynamic therapy, 714spontaneous recovery rate in, 707
psychotropic drugs, 683, 695, 714PTSD, see post-traumatic stress disorderpuberty, 483, 577, 589, 669punishment:
avoidance learning and, 287physical, 576reward and, 576
self-, 576pupil, 162, 162pupillary dilation, 474purgatives, 694puzzle boxes, 279, 279, 281p-value, 34–35
quasi-experiment, 36
race, intelligence comparisons in, 454–55racial-ethnic groups, 450Rain Man, 440Ramu (wild boy), 405random assignment, 21, 41, 47, 48, 707
in observational studies, 40randomized clinical trials (RCT), 707, 713, 715random sampling, 26, 48rational emotive behavioral therapy, 690, 714rationalization, 609, 632Raven’s Progressive Matrices, 427, 427, 433, 441, 455ray-tumor problem, 369–70, 370reaction formation, 609, 613, 632reaction time, 433readiness potential, 231, 231Reagan, Ronald, 128reality principle, 608reappraisal, cognitive, 489–99, 499, 500, 503reasoning, 348, 354–58, 376
choices based on, 363–64, 363conditional statements and, 291confirmation bias in, 354–55, 355, 376conventional, 574–75deductive, 354, 356, 375effect of education on, 353errors in, 356extrapolating from observations in, 351faulty logic in, 355–56frequency estimates in, 349heuristics in, 349–52, 351intuition vs., 352judgment and, 358logical, 579moral, 574–76, 575, 589numerical, 588postconventional, 574–75preconventional, 574–75selection task and, 356–57, 356, 357survival advantage of, 357syllogism and, 355–56training and, 358validity and, 355
recall, memory, 303, 319, 322, 336recency effects, 304–5, 304, 305, 338receptive fields, 175, 176receptors:
for color vision, 169–70molecular, 101neuronal, 99, 125visual, 163–65; see also cones; rods
recessive genes, 57reciprocity:
compliance and, 526–27norm of, 526, 542
recollection, 314, 322–23, 339, 498memory and, 308
red-green color blindness, 173, 174redundancy, in depth perception, 203Reeve, Christopher, 127, 127referencing, social, 521, 542, 563, 563, 589reflexes, 87
brain and physiology of, 96–97conditioned and unconditioned, 263–69Descartes’ theory of, 87grasp, 551, 551, 588rooting, 551, 588sucking, 551, 551, 588in vision, 209
refractory period, 95rehearsal, memory, 264, 305, 306–7reinforcement, in conditioning, 281–86, 299, 690
fixed-interval (FI) schedule, 286, 287fixed-ratio (FR) schedule, 286, 286partial, 286, 299punishment and, 287variable-interval (VI) schedule, 287variable-ratio (VR) schedule, 286
reinforcers, 284–85rejection, vs. friendship, 573–74, 589relationship effects, 704, 704, 715relationship therapy, 714relative size, as depth cue, 202reliability:
correlations and, 32–33inter-rater, 32–33, 33memories and, 5, 11–12, 25test, 458test-retest, 32, 458validity and, 427
religious states, of consciousness, 247–48REM sleep, 235–36, 235, 237, 238, 239, 243, 257repetition priming, 335repetitive transcranial magnetic stimulation
(rTMS), 703, 703, 714representations:
mental, 555, 556symbolic, 346–48
representativeness heuristic, 348–49, 350–52, 351,376
repressed memories, 331–32, 339repression, 606, 608–9, 613, 632reproduction, 56, 61, 67, 74, 75, 77
sexual advertising and, 70–71research methods, 18–19, 21–49
collection and evaluation of data in, 25construct validity in, 24data collecting and, 25, 25defining the question in, 23–24double-blind design and, 28, 28
S18 PSUBJECT INDEXO
research methods (cont.)effect size and, 34ethics in, 43–45, 48–49, 289nexperiments and, 36, 38–43explicit measures and, 512implicit measures and, 512maximum variation sampling, 26observational studies in, 36–38observations and, 22–28operational definitions in, 24outside the lab, 45–46, 45testable hypotheses and, 23–24, 23testing differences and, 31–36working with data and, 28–36
resilience, 621resistance, 606resolution phase, of sexual response, 481, 502respiratory system, 88response control, 280, 280responses, to stimuli:
conditioned, 263–78, 298unconditioned, 198–202, 298
resting potential, of neurons, 93, 94, 98restructuring, in problem solving, 377retention interval, 318, 339reticular activating system, 229reticular formation, 228retina, 135, 162, 163, 163, 164, 165, 196
color receptors in, 169, 169, 172, 172ganglion cells in, 192; see also magno cells;
parvo cellsin perception of movement, 204, 205
retinal image, 145, 162, 197–98, 197, 198, 205, 206retinal motion, 204retrieval, memory, 302–3, 310–11, 313–16, 338,
372–73context reinstatement and, 315–16, 338cues for, 310–11, 314–16, 338–39encoding and, 315–16failure, 338partial, 313–14paths, 310, 314, 339
retrograde amnesia, 312–13, 313, 338reversible figures, 187, 187rewards:
intrinsic vs. extrinsic, 285and punishment, 576
rhodopsin, 164–65rhythm, 381–82, 398Ribot’s law, 313Rico (comprehending dog), 414risk factors, psychopathology, 638–39risky shift, 530Risperdal, 696Ritalin, in attention-deficit/hyperactivity disorder,
667–68rods, 162, 163, 163
night vision served by, 164visual pigment in, 164–65as visual receptors, 164
Rogers, Carl, 616, 619, 622, 631, 686, 686, 714romantic love, 537–39, 538, 540, 543Romeo-and-Juliet effect, 538–39, 538Roosevelt, Eleanor, 615, 615rooting reflex, 551, 588Rorschach inkblot technique, 643Rozin, Paul, 462Ruffini endings, 147, 147rules, expression, 658Rush, Benjamin, 694
sample selection, 25–26satisfice, 363, 364, 377saturation, color, 168, 169Saul, King of Judea, 636savant syndrome, 439, 459scatter plots, 31, 31Schachter-Singer theory of emotion, 496, 502, 538schedules of reinforcement, 286, 299schemas, 321, 339
cognitive, 554–55, 657, 674schematic knowledge, 510, 511schizoid personality disorder, 672schizophrenia, 58, 103, 636, 644, 658–66, 673,
674–75, 692, 701behavioral disorder in, 660brain defects and, 664–65, 665brain development and, 661–63catatonic, 660, 661cognitive symptoms of, 661cultural sensitive treatment for, 683disorganized, 660, 660disorganized speech in, 660electroconvulsive therapy (ECT) for, 701–2, 701family environment and, 665–66glutamate transmission dysfunction and, 664,
675hallucinations in, 660heredity and, 661–63, 662homelessness and, 696, 696medication for treatment of, 103, 695–96negative symptoms of, 660–61neurotransmitter malfunctioning in, 664painting by sufferers of, 659personal contact loss in, 660–61positive symptoms of, 659–60precursors of, 663, 663, 675prenatal environment and, 675prenatal factors of, 663signs and symptoms of, 659–61, 674social and psychological environment and,
665–66social realities of treating, 695–96socioeconomic status and, 665, 665, 675structural defects in, 664–65viral infection and, 662–63
schizotypal personality disorder, 672Scholastic Aptitude Test (SAT), 452scientific method, see research methodsScream, The (Munch), 647
secondary sexual characteristics, 577, 589second-order conditioning, 265–66, 266, 298secure attachment, 566–67, 567secure base, 564, 566, 588securely attached children, 588, 614segmentation, 382selection, perceptual:
central, 209–11eye movements and, 209, 211in hearing, 213through orientation, 209in vision, 209–11
selection task, 356–57, 356, 357selective serotonin reuptake inhibitors (SSRIs),
697, 699, 700, 714self, 616–19
actual, 617, 617culture and, 618–19in humanistic psychology, 616ideal, 617, 617ought, 617, 617possible, 617theory, 616, 633
self-actualization, 487, 615–16, 615, 622, 632self-concept, 616self-consistency, 598self-control, 36, 500, 625–26, 628–30, 628self-descriptions, 618–19, 619self-efficacy, 623, 633self-enhancement, 617–18self-esteem, 476, 486, 617–18, 618, 619, 633self-fulfilling prophecies, 513, 541self-handicapping, 627self-identity, 580self-interest, altruism and, 534self-monitoring scale, 597, 598, 632self-perception theory, 517self-promotion, 619self-punishment, 576self-regulation, 499, 578, 630self-regulatory plans, competencies and, 625–26,
633self-report data, 594self-schema, 616–17, 616, 618, 633self theory, 616, 633Seligman, Martin, 289, 621, 657semantic features, 386, 422semantic memory, 328, 583semantic roles, 389–90semistructured interview, 640senescence, 587sensation, 133–79
detection and, 137detection and decision of, 139–42detection for complex forms and, 176–77empiricist view of, 136genetics and, 133, 152hearing as, 129–36kinesthesis and, 145of pain, 147–48, 178
PSUBJECT INDEXO S19
sensory adaptation and, 144–47, 145sensory thresholds and, 137–39of skin, 146–47, 147, 178of smell, 148–50, 178supertasting and, 133–34, 152of taste, 151–53, 151, 178vestibular, 143, 145–46, 178vision as, 160–77see also senses; sensory processes
sensation seeking, 476sensation seeking personalities, 600, 600, 632senses, 142–53
kinesthesis, 139, 145pain, 139, 147–48, 178pressure, 139see also hearing (audition); skin senses; smell;
taste; visionsensitive period hypothesis, 410–15, 411, 423sensorimotor capacities, of newborns, 550–51sensorimotor period, 552–55, 553, 588sensory adaptation, 144–45, 145, 178sensory areas, 118sensory coding, 143–44
for psychological intensity, 143, 178sensory perception, 96–97, 118, 119
see also perceptionsensory processes, 133–79
active perceiver in, 136, 168, 214coding in, 143–44decision and detection in, 139–40, 140, 141empiricist view of, 136, 178hearing as, 153–60, 178–79intensity of sensation in, 137–39passive perceiver in, 135–36pattern theory of, 144perceptual sensitivity in, 140psychological intensity in, 143, 178quality in, 143–44, 178signal-detection in, 140–42, 140, 141, 178specificity theory of, 144, 178transduction in, 143, 156–58vision in, 160–77, 179
sensory projection areas, primary, 118–19, 119, 120sentences, 383–85, 422
meanings of, 389–91, 390, 393, 394phrase structure description of, 383–85, 384,
385predicates of, 389, 422
separation anxiety, 563Seroquel, 696serotonin (5HT), 100, 655, 697, 697serotonin transporter gene, 57–58Serzone, 697set point, 467, 501, 620sex, sexuality, 83, 478–85, 502
and advertising for a mate, 70–71animal, 70–71attraction and, 483cultural and cognitive aspects of, 482–83, 502
estrus cycle and, 479, 481, 502hormones and, 481human response cycle of, 481, 481, 502mate choice and, 78, 482–83, 482physiological aspects of, 479–81situational determinants of, 482see also gender
sexual abuse, repressed memories of, 331sexual aggression, 482sexual arousal, 482sexual development, 589sexual orientation, 483–85, 483
attraction and, 483genetic influence on, 484
sexual reproduction, 56, 66shading, as depth cue, 203Shakespeare, William, 79, 538, 546shallow processing, 309, 338shape constancy, 196, 196, 198shape perception, 174
see also form perceptionshaping, 283–84shared-problem groups, 693Shaver, Phillip, 493shenjing shauiro, Chinese illness, 643Sherif, Muzafer, 519–20shock treatment, see electroconvulsive therapyshort-term memory, see working memoryside effects:
of drug treatment, 698, 699of lobotomy, 700
sight, see visionsignal-detection analysis, 141–42, 141
medicine and, 141–42, 141signal-detection theory, 140–42, 178
analysis, 141–42, 141implications of, 141–42procedures, 140–41
sign language, American Sign Language (ASL),406, 413, 413, 423
signs, see symptoms and signssimilarity, 536–37, 536, 543
principle of, 185, 186simple reaction time, 433simultaneous color contrast, 170, 171sine wave, 154, 154single-case experiments, see case studiessingle-cell recording, 105, 130situational attributions, 507, 509, 510, 541size constancy, 196, 196, 198Skinner, B. F., 17
on operant behavior, 281, 281Skinner box, 281, 281skin senses, 143, 146–47, 147, 178
absolute threshold of touch and, 138sleep, 229, 233–43
alpha rhythm of, 234, 235beta rhythm of, 234–35, 235brain activity during, 233, 234–35
circadian rhythm of, 233, 239delta rhythm of, 235, 235deprivation of, 236–38, 236, 238, 239dreams and, see dreams, dreamingfunction of, 238–39, 239hypnagogic imagery of, 234insomnia and, 237lateral geniculate nucleus and, 241–42, 242need for, 236–38, 237neural communication during, 233paradoxical, 235paralysis of, 235REM, 235–36, 235, 237, 238, 239, 243, 257slow-wave, 235, 235, 236, 237, 238, 239, 257spindles of, 235stages of, 234–35wake cycles and, 234–36
slippery slope, 526slow-wave sleep, 235, 235, 236, 237, 238, 239, 257smell, 148–50, 149, 178
absolute threshold of, 138communication based on, 150decline in, 583flavor and, 149–50menstrual synchrony and, 150pheromones and, 150sensation of, Weber fraction for, 139
smiling, 67–69, 83biological roots of, 67crow’s feet and, 68, 68expressive, 68, 68origins of, 67–68, 69polite, 68, 68as species general, 68–69
smooth muscles, 113“Snow White and the Seven Dwarfs,” 612Snyder, Mark, 597social aggression, 36, 476, 476social animal, man as, 531social behavior, 7–8
brain damage affecting, 124–25conformity in, 519–22false confessions and, 7helping in, 532obedience in, 523–26, 523police interrogations and, 7–8, 7
social class, and schizophrenia, 665social cognition, 506–19, 541–42
attribution, 507–10, 541cognitive dissonance and, 516, 516development and, 559–62disorders of, 124–25motivated, 523person perception and, 510–14
social-cognitive approach to personality, 622–31,633
social-cognitive approach to psychology, origins of,623–25, 633
social contact, 486
S20 PSUBJECT INDEXO
social development:attachment in, 588–89childhood socialization and, 589conscience and, 576, 589day care and, 570–71, 570differences in attachment and, 565–67domestic conflict and divorce, and, 571face-to-face interaction in, 588friendships in, 572–74, 589Kohlberg’s stages of moral reasoning in,
574–75, 575, 589maternal separation and, 571parenting and, 589peer relationships in, 572–74, 589sexual development and, 589social referencing in, 563, 563, 588
social exclusion, 488, 488social facilitation, 528, 542social influence, 519–31, 542
group dynamics as, 527–31vs. depression, 658
social inhibition, 528, 542social intelligence, 439socialization, 589social loafing, 528–29, 542social perception, 511social phobia, 646, 650social pressure, 520social psychology, 505–43
attribution and, 507–10collectivistic cultures and, 508–9, 509, 510, 511,
541individualistic cultures and, 508–9, 509,
510–11, 541social cognition and, 506–19
social referencing, 521, 542, 563, 563, 588social relations, attractiveness and, 535social roles, 596, 618social support, 639, 652sociobiology, 79socioeconomic status:
depression and, 658genetics and IQ interaction with, 447–48intelligence and, 447–48, 455low, 72, 83schizophrenia and, 665, 665, 675
socioemotional development, adolescence and, 579socioemotional-selectivity theory, 587, 589sociometric data, 573soma (cell body), 88–89somatic nervous system (SNS), 113somatogenic hypothesis, 637, 674somatosensory cortex, 148somatosensory projection areas, 119, 120, 120, 126,
232sound:
amplitude and loudness of, 154, 154, 178decibels of, 154frequency and pitch of, 154, 154, 158, 179hertz as measure of, 154, 155
timbre of, 158units of, 380–82, 381, 399–400, 422
sound waves, 153–60, 154space, and objects in infancy, 557–58spatial intelligence, 439spatial knowledge, 557–58spatial thinking, 417–21, 418, 419, 557–58
Tzeltal language and, 419–21Spearman, Charles, 430–31species general, 67, 68, 83species specific, 67, 83specificity coding, 147specificity theory (doctrine of specific nerve
energies), 144, 178specific language impairment, 410, 423speech:
disorders of, 123–24infant’s perception of, 397–99, 399rate of, 382sound patterns in, 382see also language
speed, cultural differences and, 440spermarche, 577sperm cells, 55–56, 56, 70, 77, 479, 546split-personality disorder, 658nspontaneous improvement, 707spontaneous recovery, 267, 298, 714stage theory of memory, 304stagnation, generativity versus, 586, 589Stanford Prison Experiment, 530, 530, 542states, personality, 592statistical significance, 34statistics:
correlation in, 37–38, 427–28, 459descriptive, 28, 29inferential, 28, 33–34, 48meta-analysis and, 42p-value and, 34–35variance and, 72
Stein, Gertrude, 485Stelazine, 696stem cells, 127–28
embryonic, 128neural, 127–28
stereotypes, 511–14, 541effects of, 513–14explicit vs. implicit assumptions in, 512group exposure and, 511–12origins and measurement of, 511–13prejudice and, 511see also bias; prejudice
stereotype threat, 455–56, 513, 542Sternberg, Robert, on intelligence, 425, 437sticklebacks, 63–64, 64stimulants:
drug, 250–51, 257see also specific stimulants
stimuli, 142, 144–45, 151, 152, 181, 187, 188, 192, 207,223, 229, 232, 234, 239
conditioned, 263–69, 294, 298
as conditioned reinforcers, 282–85discriminative, 282distal, 135, 135, 178habituation and response to, 261–62as inhibitors, 269perception and variability of, 183, 183proximal, 135, 135, 178for sound, 153–60stimulus generalization, 268, 282–83, 282, 298transduction of, 143unconditioned, 263–69, 294, 298
Strange Situation procedure, 565–66, 566, 588,630
stress, 674depression and, 656–57dissociation and, 671vocal, 382
stress disorders, 649, 674strong situations, 596, 597Stroop effect, 367, 367Structured Clinical Interview for DSM Disorders
(SCID), 640structured interview, in assessment, 674Styron, William, 652–53subcortical structures, 116, 116subgenual cingulate cortex, 656, 702subjective contours, 184, 186, 187subjective experience, 221subordinates, 402, 422subproblems, 366, 367, 377subroutines, 367, 368, 377subsyndromal conditions, 673, 682, 711–12successive approximations, 283, 299sucking reflex, 551, 551, 588suicide, 654–55, 674, 699
bipolar disorder and, 654–55depression and, 654–55ECT vs., 702gender and, 655
superego, 607–8, 611, 613, 632Superman, 127, 127superordinates, 402, 422supertasting, 133–34, 152suppression, 498–99, 503surprise, in classical conditioning, 273–75survival, genetic, 79–80survival guilt, 649Sybil, 671syllables, 382, 399–400syllogisms, 355–56, 355, 376symbolic elements, 346–48symbolic representations, 343, 343, 346–48, 376symbols, images and, 343sympathetic activation, 464–65, 474, 474sympathetic branch of the autonomic nervous
system, 113, 114, 464, 474–75, 497, 499symptoms and signs:
of mental disorders, 640–41, 674negative, 660–61, 674positive, 659–60, 674
PSUBJECT INDEXO S21
of schizophrenia, 659–61synapses, 96–100, 99, 100, 130, 296–97
communication between, 97communications across, 97mechanism of, 97–100, 98, 99, 101vesicles of, 98, 100
synaptic gap, 99synaptic reuptake, 100, 101–3, 130, 697synchrony, neural, 195–96syntax, rules of, 324–25, 383, 390, 391, 414, 422syphilis, 637systematic desensitization, 688
tabula rasa, 135tacit knowledge, 438talent, intelligence vs., 440talking cures, see psychotherapytangible support, 486, 502Taoism, 247task model, 434–36tastants, 151taste, 151–53, 152
absolute threshold of, 138age and, 151genetics and, 133, 152papillae and, 151, 151, 152, 178as sensation, Weber fraction for, 139supertasting and, 133–34, 152
taste aversion, learned, 152, 292–94, 292, 293, 299TAT (Thematic Apperception Test), 642, 642temperament, 6, 599, 632
among children, 567, 567, 589inhibited, 601, 601, 632
temperature, body, 464–66, 465, 478temporal cortex, 118, 194temporal lobe, 86, 120temptation, 577tending, 474, 474tension-reduction, 485teratogens, 549, 588testable hypothesis, 23–24, 23testosterone, 453, 476, 502test-retest reliability, 32, 458tests, testing:
culture and, 440–41, 440false-belief, 561, 561Implicit Association Test (IAT), 512intelligence, see intelligence testingMayer-Salovey-Caruso Emotional Intelligence
Test (MSCEIT), 438–39, 438mental, see mental testingpersonality, 641–42projective, 642Raven’s Progressive Matrices, 427, 427, 433, 441,
455reliability and validity of, 427, 458stereotypes and, 457, 512Thematic Apperception Test (TAT), 642, 642
Wechsler Adult Intelligence Scale (WAIS), 427,427, 458
Wechsler Intelligence Scale for Children(WISC), 426
see also statisticstexture gradients, 202, 202, 203thalamus, 115, 115, 116, 163–64, 163, 228, 229, 257,
488, 548, 700that’s-not-all technique, 527, 542THC (tetrahydrocannabinol), 251, 252Thematic Apperception Test (TAT), 642, 642theory of mind, 545, 560–61, 562, 588therapeutic alliance, 704, 715thermal stimulation, 488, 488thermoregulation, 464–66, 473, 478, 501thinking, 341–77
creative, 371–73critical, 375directed, 348dual-process theories of, 352–54in groups, 530–31heurisitics and, 348–49, 376illumination and, 372images and symbols in, 343incubation and, 372judgment in, 348–54, 376language and, 415–21, 423mental representations, 342, 376preparation and, 372problem-organization and, 365–69problem solving and, 365–75, 377problem-solving obstacles and, 368–70problem-solving process of, 365–75reasoning and decision making in, 341, 354–58,
376–77spatial, see spatial thinkingsymbolic, 346–48symbolic elements and, 346–48types of, 353verification and, 372
third-variable problem, 37, 38, 40, 48Thorazine, 696Thorndike, Edward L., 279
on learning, 278–80, 279, 280, 281, 297threat, 473–78, 478, 502
cultural and cognitive aspects of, 476–78“fight or flight” response and, 474–75physiological aspects of, 474–76
Three Faces of Eve, The, 671, 671“thrifty gene” hypothesis, 473timbre, 158tip-of-the-tongue (TOT) effect, 313–14, 338Toastmasters, 693Tofranil, 696token economies, 689, 714Tolman, Edward, C., 287, 287tone, 382Tong et al. procedure, 230tonotopic map, 159–60, 160
Tooby, John, 357top-down processing, 189–90, 190touch, see skin sensestrait approach, personality and, 592–93, 632traits, personality, 592–93, 632
and biology, 598–601, 599cultural taxonomy differences in, 595, 632taxonomy of, 632vs. situations, 596, 632
tranquilizers, see anxiolyticstranquilizers, major, see antipsychoticstranscranial magnetic stimulation (TMS), 108–9,
108, 112, 131, 345transduction, 89
of stimuli, 143, 156–58transference, 684, 687, 714traumatic events, 330–32, 330tree diagram, 384, 384, 422trephining, 694, 694trichromatic vision, 169tricyclic antidepressants, 696Triplett, Norman, 527Turing, Alan, 485Turner, Amanda, 591–92Tversky, Amos, 348–49, 349twins:
fraternal, 70–71, 70, 71, 73, 444, 444, 448, 484,599, 650, 652, 655
identical, 70–71, 70, 71, 73, 444, 444, 448, 472,472, 484, 599, 599, 603, 632, 650, 652, 655,665
twin studies, 6, 69–71, 70, 71, 73, 444, 444, 448,472, 472, 484, 599, 599, 603, 632, 650, 655,661–62, 665
Tzeltal (language), 419–21
ultimate causes, 58, 73, 74, 75umami, 151umbilical cord, 547unconditional positive regard, 633unconditioned reflex, 263–69unconditioned response, 263–69, 276–78, 298unconditioned stimulus, 268, 273, 274unconscious, 607, 607, 611unconscious attributions, 224–25unconscious conflict, 608–9unconscious functioning, brain damage and,
223–24unconscious inference, 197–98, 216, 222unconscious processes, 226, 226understanding, language, 391–96unique colors, 168, 168uterus, 480utility:
clinical, 709efficacy vs., 708–9
vagal nerve stimulation, 702, 714vagus nerve, 97, 702
S22 PSUBJECT INDEXO
Vaillant, George, 613validity, test, 33, 458
reliability and, 427, 458Valium, 248Van Gogh, Vincent, 635variability, statistical, 30, 30, 34, 452variable-interval (VI) schedule, 287variable-ratio (VR) schedule, 286variables, 22, 31, 55vasoconstriction, 465–66vasodilation, 465–66, 474, 501Venezuelan Intelligence Project, 446ventromedial hypothalamus, 469, 469verb phrases, 384, 384vestibular sense, 143, 145–46, 146, 178vicarious conditioning, 290, 651vicarious reinforcement, 690victims, dehumanization of, 526, 542View-Master, 201viral encephalitis, 86virtual reality displays, 689visceral reactions, 494, 496visible spectrum, 161, 161, 168, 169vision, 105, 118, 139, 144, 160–77, 231
absolute threshold of, 138acuity of, 164analysis of complex shapes in, 174brightness contrast in, 165, 166change in stimuli for, 165of color, 168–74color blindness in, 173–74complex form detectors in, 174contrast effects in, 165, 165, 166day, 164decline of, 583feature detectors in, 174–75, 182, 191, 209language learning in absence of, 407–8, 408lateral geniculate nucleus and, 241–42, 242lateral inhibition in, 179light as stimulus for, 161, 162, 179night, 164partial views and, 183photopigment in, 164–65, 169receptive fields of, 175, 176shape perception, 174, 179visual pathway and, 163see also depth perception; form perception;
motion perceptionvisual agnosia, 174, 191–92, 194–95visual cortex, 120, 126, 192–94, 193, 195, 204, 205,
208, 221, 223, 232, 345, 549
“what” and “where” systems of, 194–95, 194,216
visual imagery, 345visual pathway, 192–95visual pigments, 165visual projection area, 119, 120
see also visual cortexvisual receptors, 163–65
see also cones; rodsvisual search, 188, 188visual search task, 183, 209, 216visual stimuli, 223visual system, 145, 146, 175, 188, 189, 229visuospatial ability, 452, 453vocal tract, human, 381Voltaire, 604
WAIS (Wechsler Adult Intelligence Scale), 427,427, 430, 458
wait-list control, 708Wallace, Mike, 673Wallas, Graham, 272wanting, 489, 490, 502war, depression and, 657–58, 658water jar problem, 368, 368Watson, John B., 623wavelengths, of light, 161, 168, 168, 169, 169weak situations, 596, 597Weber, E. H., 138Weber fraction (Weber’s law), 138, 139, 139, 178Wechsler Adult Intelligence Scale (WAIS), 427,
427, 430, 458Wechsler Intelligence Scale for Children (WISC),
426Wellbutrin, 697, 706–7well-defined problem, 365Wernicke’s area, 123, 123“what” and “where” systems, 194–95, 194, 216whole objects, 402–3Whorf, Benjamin, 416, 421Whorfian hypothesis, 416, 421, 423Wiesel, Torsten, 175, 175wild children, 405, 405Wilde, Oscar, 485Williams syndrome, 410, 411will power, 628Wilson, Edward O., 79, 80–81Winehouse, Amy, 635–36WISC (Wechsler Intelligence Scale for Children),
426Wisconsin Card-Sorting Task, 124
wish fulfillment, 611withdrawn-rejected children, 574within-subject comparisons, 40–41, 48witnesses and testimony, 320, 320, 324, 325Wittgenstein, Ludwig, 485wolf children, 405, 405women, intelligence of men vs., 452–54Woolf, Virginia, 635words, word meanings, 386–88, 389
classes of, 403combining definitional and prototype theories
of, 388–89definitional theory of, 386–87family resemblance structure of, 388, 388in folk theories, 389growth of, 400–403learning, 402–4prototype theory of, 387–88semantic features of, 386, 422
working memory, 207, 232, 307, 338, 435–36, 583,584
active process of, 306–7attention and, 434expanding capacity of, 306–7intelligence and, 434as loading platform, 304storage capacity of, 304work in, 306–7
working-memory capacity (WMC), 434, 435, 459working models, 614workspace neurons, 232World Health Organization, 471, 657, 682World Trade Center attack, 12, 12, 13–14, 329, 329,
518–19, 534Wright, Sylvia, 182
Xanax, 248X-chromosomes, 54X rays, 110
Y-chromosomes, 54Young, Thomas, 169Young-Helmholtz theory, 169
Zajonc, Robert, 341, 528Zimbardo prison study, 530, 530Zoloft, 103, 697zolpidem, 248zone of proximal development, 568











































































![Bob Dylan in China, America in Bob Dylan: Visions of Social Beatitude and Critique [Chinese translation]](https://static.fdokumen.com/doc/165x107/6331ca78576b626f850d1a9c/bob-dylan-in-china-america-in-bob-dylan-visions-of-social-beatitude-and-critique.jpg)





