
Integration of POC test card into a regional pharmacovigilance ...
60
1 Integration of POC test card into a regional pharmacovigilance system University of Notre Dame Marya Liberman Award Number: AID-OAA-F-15-00050
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Integration of POC test card into a regional pharmacovigilance ...

1
Integration of POC test card into a regional pharmacovigilance system University of Notre Dame Marya Liberman Award Number: AID-OAA-F-15-00050

2
DISCLAIMER This publication was produced at the request of the United States Agency for International Development. It was prepared independently by The University of Notre Dame and Dr. Marya Liberman. The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.

3
Integration of Paper Test Cards into a Pharmacovigilance System in Kenya
Location: Notre Dame, IN and Eldoret, Kenya 15-Month Period (09/15/2015 – 12/14/2016) Funding from USAID: $124,032 (100K direct)
Technical POC Marya Lieberman Professor, Department of Chemistry and Biochemistry University of Notre Dame Notre Dame IN 46556 USA +011.574.631.4665 phone +011.574.631.6652 fax [email protected] Website: https://padproject.nd.edu/
Administrative POC Tina Chandler Grants Program Manager 940 Grace Hall University of Notre Dame Notre Dame IN 46556 USA +011 (574) 631-6984 [email protected]

2
Table of Contents
Table of Contents .......................................................................................................................... 2
Deliverable #6 ............................................................................................................................... 4 DIV phase 1: Overview of project .......................................................................................................... 4 DIV phase 1: Lessons Learned ................................................................................................................. 4 DIV phase 1: Table of implementation activities and challenges ............................................................. 5 DIV phase 1: Final KPI Dashboard (as of August 31, 2018) ...................................................................... 5 DIV Phase 1: $741,000 in follow-on funding obtained ............................................................................. 6 DIV phase 1: Dissemination through scientific publications .................................................................... 6 DIV phase 1: Media coverage ................................................................................................................ 7 DIV phase 1: Timeline ............................................................................................................................. 8 Follow-on: The health impact of bad quality medicines is serious and would be easy to mitigate through more efficient post-market surveillance. PADs can help deliver this outcome. ......................... 9 Follow-on: Scale Strategy Plan ............................................................................................................. 10 Follow-on: Action plan ........................................................................................................................ 11 Follow-on: Cost and time projection .................................................................................................... 12 Follow-on: metrics for success .............................................................................................................. 12 Follow-on: Partners for PAD implementation ...................................................................................... 13 Follow-on: Investor presentation is attached as a Powerpoint file ....................................................... 14
Previous deliverables (#1-5) ........................................................................................................ 15 Milestones ........................................................................................................................................... 15 Deliverable #5 ...................................................................................................................................... 17
Dashboard for Q4 progress, 30 May 2017 ................................................................................................ 17 Summary of progress ................................................................................................................................ 17
Deliverable #4 ...................................................................................................................................... 20 Dashboard ................................................................................................................................................. 20 Summary: We are protecting patients from bad quality amoxicillin and amoxi-clav ............................. 21 Media dossier ............................................................................................................................................ 23 Commercialization update: 3 companies vying to license PAD patent ................................................... 23 Other activities .......................................................................................................................................... 23 PAD fabrication and transmittal to Kenyan and Ugandan partners is ahead of schedule ....................... 24 Computer image analysis app is behind schedule; here is the plan to get it back on track .................... 24 Sample collection in Kenya is on target .................................................................................................... 25 HPLC analyses conducted in US and Kenya are getting back on track with aid of DPAL program ........... 25
Deliverable #3: ..................................................................................................................................... 27 Dashboard for Q2 progress, 15 June, 2016............................................................................................... 27 Status update on PAD fabrication and transmittal to Kenyan and Ugandan partners ............................. 28 Sample collection and analysis in Kenya is on target ............................................................................... 29 HPLC capabilities (expect six methods to be validated) ........................................................................... 29

3
HPLC Assays behind schedule ................................................................................................................... 30 Plans for phone interface of computer image analysis (app vs online, front end & back end, database) 30 Information flow to KPPB .......................................................................................................................... 30 Updated strategic scaling plan. ................................................................................................................. 33
Deliverable #2 ...................................................................................................................................... 34 Dashboard ................................................................................................................................................. 34 PAD fabrication and transmittal to Kenyan and Ugandan partners ......................................................... 34 Report on methods and progress of sample collection and analysis in Kenya ......................................... 35 Kenyan HPLC capabilities .......................................................................................................................... 35 HPLC Assays Completed ............................................................................................................................ 36 Information flow to KPPB .......................................................................................................................... 37 Media Impact ............................................................................................................................................ 37
Deliverable #1 ...................................................................................................................................... 38 Updates to project implementation and scaling plan .............................................................................. 38 Grant USAID staff access to the US-Kenya databases which will be used to track sample collection and PAD analyses. ............................................................................................................................................ 40 Updates on hiring key staff and finalizing required partnerships............................................................. 40
Appendices .................................................................................................................................. 42 A. Selected media reports .................................................................................................................... 42 B. CVs of co-workers ............................................................................................................................ 46
B.1. Sonak Pastakia ................................................................................................................................... 46 B. 2. Mercy Maina ..................................................................................................................................... 51
C. Investor Presentation (1 page info sheet) ......................................................................................... 58
4
Deliverable #6
DIV phase 1: Overview of project WHO estimates that 1 in every 10 pharmaceuticals sold in low- and middle-income countries are substandard or falsified—which means that about 10% of the $300 billion USD spent to purchase pharmaceuticals in these countries is being wasted on bad quality medicines. We tested implementation of a new field screening tool for detecting bad quality medicines. Pharmacists in Kenya collected medicine samples and tested them with an inexpensive paper analytical device (the PAD). Then they sent the samples to the University of Notre Dame for HPLC assay. Working together, we identified multiple batches of amoxicillin and doxycycline adulterated with talcum powder, falsified paracetamol, and substandard losartan, all of which was reported to the Kenyan authorities and WHO within 2 months of detection. This process was faster than typical postmarket surveillance (PMS) operations in Kenya, which typically take 2-3 years to complete. By the time PMS is complete, bad quality products have all been sold to patients, so it is harder for the authorities to follow up with regulatory or legal action. Our results show that fast testing with PADs could make it easier to catch the people who manufacture and distribute bad quality medicines.
DIV phase 1: Lessons Learned
• Using a combination of PADs and HPLC, we discovered a small number of manufacturers whose products were consistently substandard. Removing just these manufacturers would greatly improve the quality of drugs in the Kenyan market.
• We can implement PADs within existing DRA procedures. Our current project in Tanzania (funded by MSH) involved training twenty of the 56 regional drug inspectors employed by TFDA. In under 3 months, the TFDA inspectors analyzed over 3,000 blinded samples with PADs with an accuracy of 93%.
• Computer image analysis will allow more users to participate in field screening of pharmaceuticals. We obtained internal funding from U. Notre Dame to train a neural network to read PADs and create a cell phone app. With an accuracy of 96% on the TFDA data set, this app is now being field tested in Malawi, Kenya, and Bangladesh.
5
DIV phase 1: Table of implementation activities and challenges Activity Implementation summary Challenges
Deliver 2400 PADs This activity was completed in full. Availability of fabrication equipment.
Collect 1200 medicine samples This activity was completed in full. Logistics of transporting samples
Analyze all samples with PADs
This activity was completed in full. Depending on the type of medicine, 5-15% failed PAD testing.
Reading PADs by eye required a lot of training and user support.
Validate 16 HPLC methods
11 methods were validated in the grant period.
Combination drugs were hard to validate on the HPLC.
Analyze 320 samples of the medicines
We analyzed over 700 medicine samples. Getting samples to analysis before they expired
Identify good and bad quality products
Found amoxicillin adulterated with talc, substandard losartan, doxycycline adulterated with talc, moldy acetaminophen, and falsified acetaminophen
A range of other characterization techniques were needed to identify fillers and degradation products.
Interactions with Kenyan regulatory authorities
Dr. V. Rakuomi assigned as focal point. Four product reports have been filed with PPB, and two with the WHO.
Strikes, contested elections, and turnover slowed response from the regulatory agency.
Reporting to DIV This is the last of six deliverables sent to DIV.
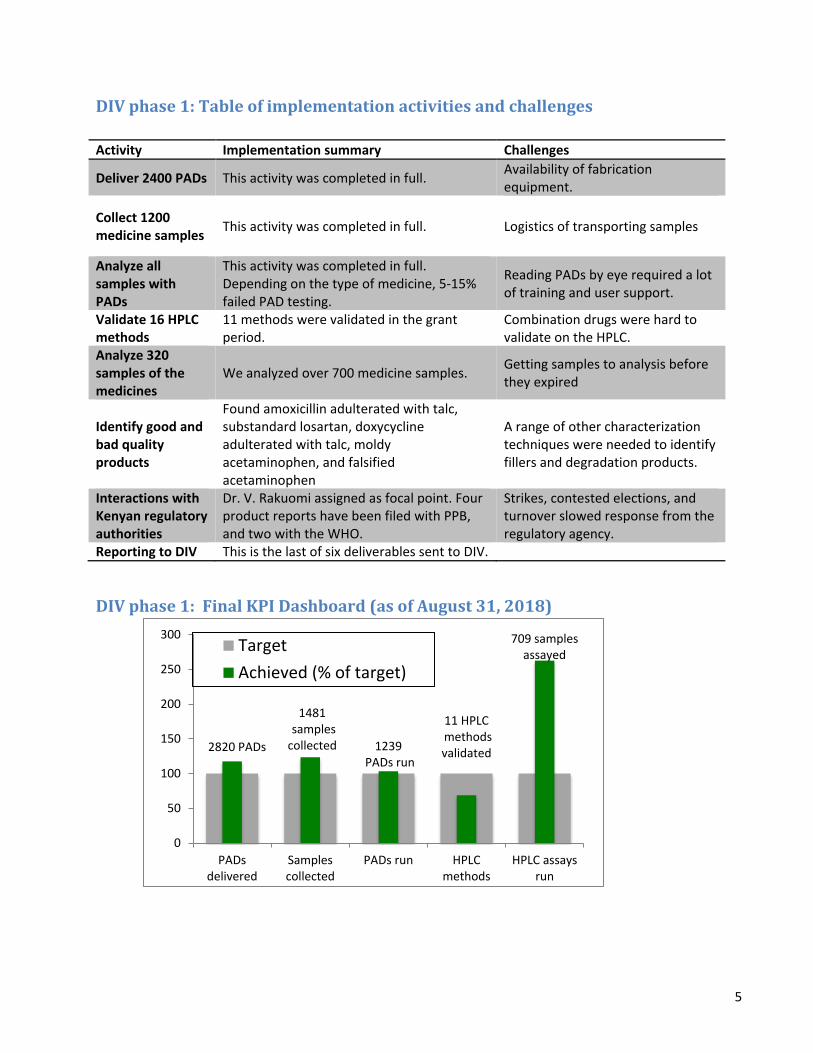
DIV phase 1: Final KPI Dashboard (as of August 31, 2018)
2820 PADs
1481samples
collected 1239PADs run
11 HPLCmethods validated
709 samples assayed
0
50
100
150
200
250
300
PADsdelivered
Samplescollected
PADs run HPLCmethods
HPLC assaysrun
TargetAchieved (% of target)

6
DIV Phase 1: $741,000 in follow-on funding obtained
• $250K USD to collaborator Ayenew Ashenef through Ethiopian Ministry of Science and Technology 2016-2020 for PAD technology transfer and pharmaceutical screening (UND is a subawardee)
• $10K USD from Clinical Translational Science Initiative (NIH money) for pilot project in Malawi to test antibiotic quality
• $54K USD from Walther Cancer Center 2017-2019 for testing chemotherapy drug quality in Ethiopia and Kenya.
• $86K USD from MSH for Operational Research in Tanzania and Kenya 2018-2019 • $316K USD from NSF EAGER/Illicit Supply Chains: In 2018 I obtained NSF funding with
operations engineer Karen Smilowitz at Northwestern University to study the problem of bad quality pharmaceuticals from the standpoint of illicit supply networks. Both of these collaborations will contribute to our capacity to identify vulnerable points in the distribution and sale of bad quality pharmaceutical products.
• $25K USD from University of Notre Dame: Internal support for development of PAD image analysis program and Blockchain-based shared lab notebook in 2018-2019.
DIV phase 1: Dissemination through scientific publications
• Case Study Report: Substandard Cisplatin from Addis Ababa, Ethiopia. M. Smith, M. Lieberman, A. Ashenf, and H. Gerba, 2019, manuscript in review.
• Lab on Paper: Assay of Beta-Lactam Pharmaceuticals by Redox Titration. N. M. Myers, M.W. Maina, P. M. Were, R. Karwa, S. D. Pastakia, J. C. Sharp, J. L. Luther, A. W. Cooper, S. L. Bliese, N. Oberhof, D. Aldulaimi and M. Lieberman, Anal. Methods, 2019, accepted mss, DOI: 10.1039/C9AY01547G.
• Detection of Degraded, Adulterated, and Falsified Ceftriaxone Using Paper Analytical Devices, Sarah L. Bliese, Mercy Wangechi Maina, Phelix Makoto Were and Marya Lieberman, 2019, Analytical Methods, accepted mss, DOI: 10.1039/C9AY01489F
• Paper Analytic Device to Detect the Presence of Four Chemotherapy Drugs, Madeline Smith, Ayenew Ashenef, and Marya Lieberman, 2018, Journal of Global Oncology, 4:1-10, DOI: https://doi.org/10.1200/JGO.18.00198
• Identification of substandard and counterfeit antimalarial pharmaceuticals chloroquine, doxycycline, and primaquine using surface-enhanced Raman scattering. Tackman EC, Trujillo MJ, Lockwood T-L E, Merga G., Lieberman M, and Camden JP. Anal. Methods, 2018,10, 4718-4722
• Amoxicillin Quality and Selling Practices in Urban Pharmacies and Drug Stores of Blantyre, Malawi. Chikowe, Ibrahim; Bliese, Sarah L.*; Lucas, Samuel; and Lieberman, Marya. Am J Trop Med Hyg. 2018 99(1) 233-238. DOI: 10.4269/ajtmh.18-0003
• Ensuring Patient-Centered Access to Cardiovascular Disease Medicines in Low-Income and Middle-Income Countries Through Health-System Strengthening, Dan N. Tran, Benson Njuguna, Timothy Mercer, Imran Manji, Lydia Fischer, Marya Lieberman, Sonak D. Pastakia, Cardiology Clinics, 2017 35(1) 125-134, ISSN 0733-8651, doi:10.1016/j.ccl.2016.08.008

7
DIV phase 1: Media coverage 2017 PBS Newshour segment 14 Dec 2017, https://www.pbs.org/newshour/show/fighting-the-public-health-threat-of-counterfeitdrugs Following a press conference at a 2016 ACS meeting, 67 news articles about use of PADs to detect falsified medicines appeared in 19 countries and 5 languages
BioScience, Chemical & Engineering News, DocCheck News, Fast Company, Lab Manager Magazine, Daz.Online, The Observer, Inside INdiana Business, Waspada Online, The Pharmaceutical Journal, Huntnews.id, suryaonline, VOA Indonesia, ORIGO, Newsbloggers.ch, Domain-b.com, Sound Cloud, International Business Times UK, Medindia, Mynahcare, Health Medicine Network, Israel Herald, Before It's News, International Travel News, Argentina Star, Orlando Echo, Buffalo Breeze, Afghanistan Sun, Herald Globe, Dublin News, The Africa News, Malaysia Sun, Paris Guardian, DuurzaamBedrijfsleven.nl, Nigeria Sun, Big News Network.com, Pressetext Austria, Wallstreet Online, South-South News, The Economic Times - Health World, What Is Said, Voice of America, Latest News & Headlines, Vocativ, Becker's Hospital Review, Technology Channels - Risiinfo, ScienceNewsline, The Hindu Business Line- Mobile, The Hindu Business Line, e! Science News, The Times Of India, Rediff.com, Daily Excelsior, The Statesman, Alphr.com, Business Today, IndiaToday.in, Latest News & Headlines, Electronic Specifier, The Economic Times - Indiatimes, Business Standard, Technology Networks, Phys.org, Health Medicine Network, Science Codex, Health Medicine Network, EurekAlert!
2015 BBC World News Health Check piece about Kenya PAD project and news article posted on BBC website, www.bbc.com/news/health-32938075 2015 Slate.fr article (French edition) discusses technologies for finding fake drugs: http://www.slate.fr/story/102983/mauvais-medicaments

8
DIV phase 1: Timeline
In US In Kenya
9
Follow-on: The health impact of bad quality medicines is serious and would be easy to mitigate through more efficient post-market surveillance. PADs can help deliver this outcome. In the US, amoxicillin is used for relatively minor infections, but in low and middle income countries, it is the first line treatment for childhood pneumonia. Its quality is a matter of life and death. The serious quality defects in amoxicillin that we observed in Kenya and in a small pilot project (funded by UND) in Bangladesh are responsible for many deaths. Over 2,000 children in Kenya and 9,000 children in Bangladesh who could have recovered if they had good quality medicine died, because they were given inactive or substandard amoxicillin. Most of these 11,000 deaths could have been avoided if post-market surveillance did not take so long to carry out. By identifying bad quality or fake products earlier, before they’d all been sold to patients, the regulatory system could remove them from their markets.
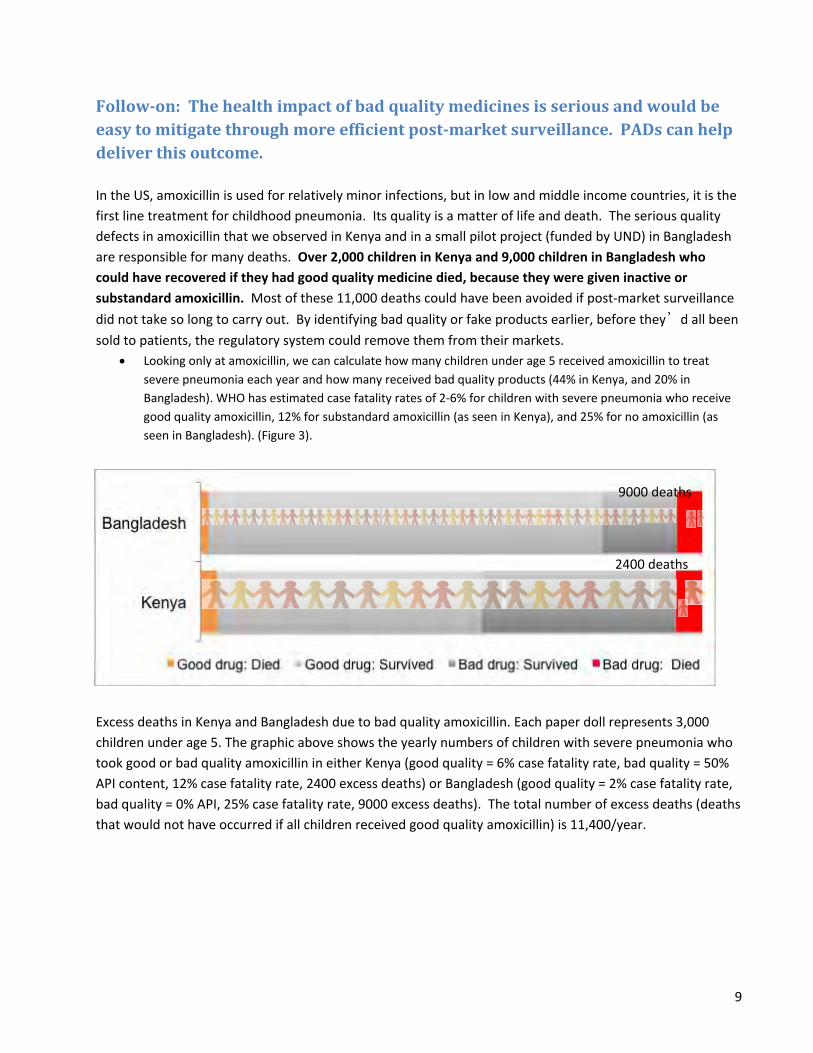
• Looking only at amoxicillin, we can calculate how many children under age 5 received amoxicillin to treat severe pneumonia each year and how many received bad quality products (44% in Kenya, and 20% in Bangladesh). WHO has estimated case fatality rates of 2-6% for children with severe pneumonia who receive good quality amoxicillin, 12% for substandard amoxicillin (as seen in Kenya), and 25% for no amoxicillin (as seen in Bangladesh). (Figure 3).
Excess deaths in Kenya and Bangladesh due to bad quality amoxicillin. Each paper doll represents 3,000 children under age 5. The graphic above shows the yearly numbers of children with severe pneumonia who took good or bad quality amoxicillin in either Kenya (good quality = 6% case fatality rate, bad quality = 50% API content, 12% case fatality rate, 2400 excess deaths) or Bangladesh (good quality = 2% case fatality rate, bad quality = 0% API, 25% case fatality rate, 9000 excess deaths). The total number of excess deaths (deaths that would not have occurred if all children received good quality amoxicillin) is 11,400/year.
9000 deaths
2400 deaths
10
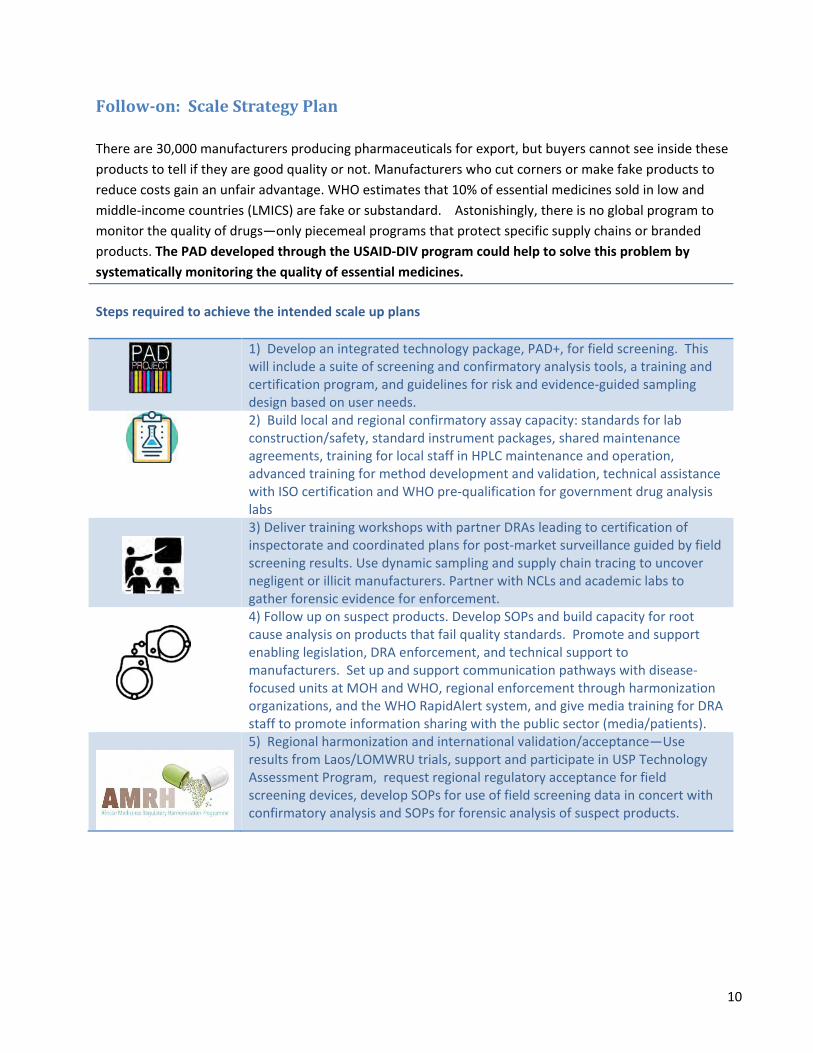
Follow-on: Scale Strategy Plan There are 30,000 manufacturers producing pharmaceuticals for export, but buyers cannot see inside these products to tell if they are good quality or not. Manufacturers who cut corners or make fake products to reduce costs gain an unfair advantage. WHO estimates that 10% of essential medicines sold in low and middle-income countries (LMICS) are fake or substandard. Astonishingly, there is no global program to monitor the quality of drugs—only piecemeal programs that protect specific supply chains or branded products. The PAD developed through the USAID-DIV program could help to solve this problem by systematically monitoring the quality of essential medicines. Steps required to achieve the intended scale up plans
1) Develop an integrated technology package, PAD+, for field screening. This will include a suite of screening and confirmatory analysis tools, a training and certification program, and guidelines for risk and evidence-guided sampling design based on user needs.
2) Build local and regional confirmatory assay capacity: standards for lab construction/safety, standard instrument packages, shared maintenance agreements, training for local staff in HPLC maintenance and operation, advanced training for method development and validation, technical assistance with ISO certification and WHO pre-qualification for government drug analysis labs
3) Deliver training workshops with partner DRAs leading to certification of inspectorate and coordinated plans for post-market surveillance guided by field screening results. Use dynamic sampling and supply chain tracing to uncover negligent or illicit manufacturers. Partner with NCLs and academic labs to gather forensic evidence for enforcement.
4) Follow up on suspect products. Develop SOPs and build capacity for root cause analysis on products that fail quality standards. Promote and support enabling legislation, DRA enforcement, and technical support to manufacturers. Set up and support communication pathways with disease-focused units at MOH and WHO, regional enforcement through harmonization organizations, and the WHO RapidAlert system, and give media training for DRA staff to promote information sharing with the public sector (media/patients).
5) Regional harmonization and international validation/acceptance—Use results from Laos/LOMWRU trials, support and participate in USP Technology Assessment Program, request regional regulatory acceptance for field screening devices, develop SOPs for use of field screening data in concert with confirmatory analysis and SOPs for forensic analysis of suspect products.
11
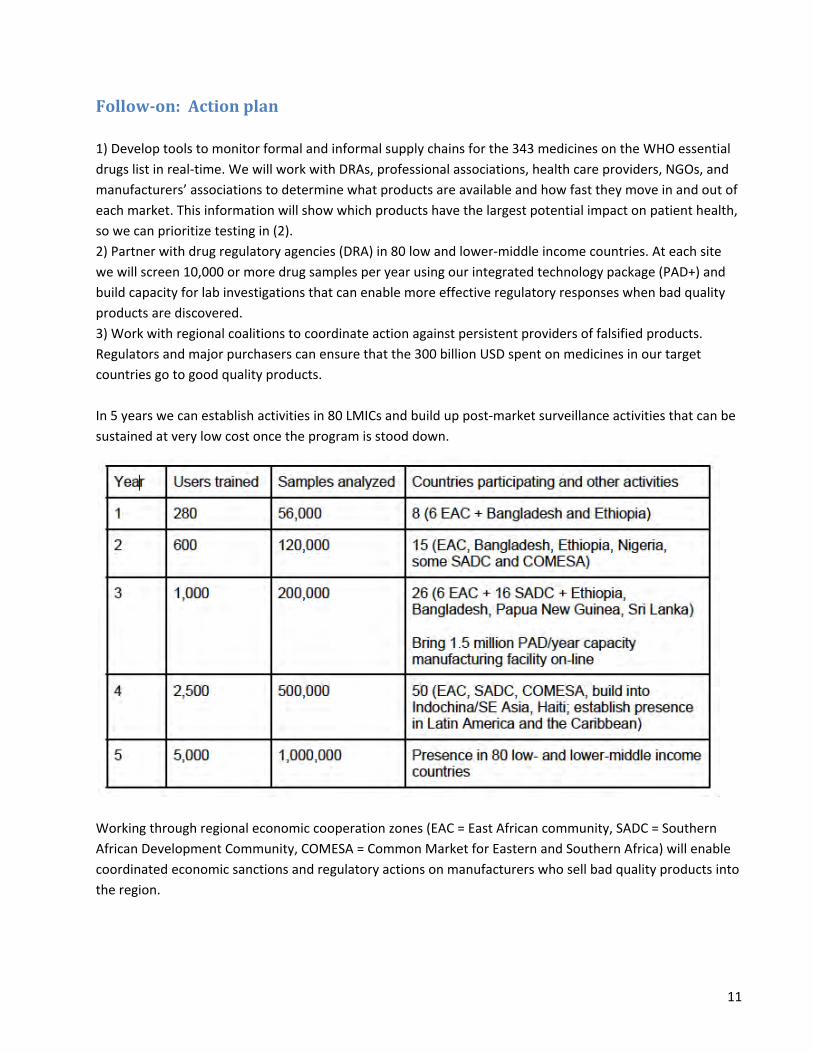
Follow-on: Action plan 1) Develop tools to monitor formal and informal supply chains for the 343 medicines on the WHO essential drugs list in real-time. We will work with DRAs, professional associations, health care providers, NGOs, and manufacturers’ associations to determine what products are available and how fast they move in and out of each market. This information will show which products have the largest potential impact on patient health, so we can prioritize testing in (2). 2) Partner with drug regulatory agencies (DRA) in 80 low and lower-middle income countries. At each site we will screen 10,000 or more drug samples per year using our integrated technology package (PAD+) and build capacity for lab investigations that can enable more effective regulatory responses when bad quality products are discovered. 3) Work with regional coalitions to coordinate action against persistent providers of falsified products. Regulators and major purchasers can ensure that the 300 billion USD spent on medicines in our target countries go to good quality products. In 5 years we can establish activities in 80 LMICs and build up post-market surveillance activities that can be sustained at very low cost once the program is stood down.
Working through regional economic cooperation zones (EAC = East African community, SADC = Southern African Development Community, COMESA = Common Market for Eastern and Southern Africa) will enable coordinated economic sanctions and regulatory actions on manufacturers who sell bad quality products into the region.

12
Follow-on: Cost and time projection Total project cost: $37.6 million/5 years to build a global PMS system. Cost of screening 8-10K samples and follow-up via confirmatory analysis are projected to average $200,000 per country. For each country we figure an average of 40 inspectors (DRA or NGO based) who each check 200 samples per year (8,000 per country). Costs include training/travel, capacity development to enable confirmatory analysis and effective regulatory followup, R&D to expand the capabilities of the PAD, and project management, financial administration, communications, and monitoring/evaluation/learning staff. In year 3, an additional $2 million is budgeted for developing a manufacturing facility with capacity of >1.5 million PADs per year.
Follow-on: metrics for success I have boxes in my lab full of fake medicines collected in Kenya, Bangladesh, and Ethiopia-- chemotherapy drugs with only 60% of the stated cisplatin content; “amoxicillin” capsules filled with chalk; doxycycline and amoxicillin that are adulterated with talcum powder. In five years, I want to drive all these products out of the market. The potential benefits are huge. WHO reported in 2017 that 10% of medicines sold in LMICs are substandard or falsified, and cause 200,000 excess malaria and pneumonia deaths each year in children under 5. 10% of the $300 billion yearly expenditures for pharmaceuticals in LMICs is essentially being wasted. When quality informs purchasing decisions, low quality products mysteriously vanish from the market. A major distributor in Kenya, MEDS, began testing each batch of medicine received from suppliers in their HPLC lab, rejecting products that failed assay. Within three years, the fraction of shipments that failed assay dropped from over 12% to under 3%. If we replace expensive HPLC with an integrated technology package based on PAD field screening and HPLC confirmatory analysis, the MEDs experience shows that the prevalence of bad quality products will drop below 3% after 3 years of continued monitoring. Based on WHO economic projections, this will save 140,000 lives and $21 billion per year. Metric #1: How many citizen scientists participate? How has the project empowered them to improve the health care system? Has the project improved governance and regulatory capacity? Metric #2: How many products are being screened, and what are the results of those tests? Are there “hot spots” of bad quality products? Metric #3: Are companies being held accountable for providing bad quality products? Are business models changing? How many lives are saved annually? Is AMR decreasing?
13
Follow-on: Partners for PAD implementation MTaPS: Notre Dame (and the PAD project in particular) is an academic partner for the 2018-2023 MTaPS program fielded by FHI 360. The focus of the MTaPS program is supply chain capacity development and operations. USP: Dr. Lieberman has an ongoing partnership with USP
• Support for the Distributed Pharmaceutical Analysis Laboratory (through free access to USP monographs and other technical support).
• USP Technology Assessment Program: External lab validation of pharmaceutical field screening tools
• USP PQM technical support and reference materials for HPLC and MS analyses. Management Sciences for Health (MSH): Funded operational research studies on PADs in Tanzania and Kenya in 2018-2019. FHI 360: detection of substandard products with PADs. Academic partners in developing countries and at NGOs who have had IRB or IREC-approved and funded research projects with Dr. Lieberman in the past 5 years:
• Prof. Ayenew Ashenef, Addis Ababa University, Ethiopia--$250,000 USD in funding through Ethiopian Ministry of Science and Technology 2016-2020 for PAD technology transfer
• Prof. Ibrahim Chikowe, University of Malawi, Malawi—Global Pilot Research grant through Indiana Clinical Translational Science Institute 2016-2017, USAID graduate fellowship 2017, NSF EAGER subaward 2019-2020, screening antibiotic quality
• Dr. Mercy Maina, Moi Teaching and Referral Hospital, Eldoret, Kenya; also Prof. Sonak Pastakia, Prof Rakhi Kharwa, AMPATH/Purdue University. Numerous awards since 2012 including USAID-DIV and Bill & Melinda Gates Foundation, screening antibiotic and NCD pharmaceutical quality.
• DRAs in Tanzania, Bangladesh, Malawi, Kenya, and Ethiopia • In 2017 I began a collaboration with health economist Sachiko Okuzawa at U. North Carolina Chapel
Hill to model the cost and impact of different post-market surveillance strategies. • In 2018 I received NSF funding with operations engineer Karen Smilowitz at Northwestern
University, to study illicit supply networks for fake medicines in Kenya, Malawi, and Bangladesh.

14
Follow-on: Investor presentation is attached as a Powerpoint file

15
Previous deliverables (#1-5)
Milestones Estimated Completion Date
Milestone (number and description)
Payment Amount ($)
Deliverable #1 Start date + 2 weeks Sept. 30, 2015
1
Updated project implementation and scaling plan
Grant USAID staff access to the US-Kenya databases which will be used to track sample collection and PAD analyses. Updates on key staff and finalizing required partnerships. Develop project assessment plan. Metrics will be reported in the form of Key Performance Indicator (KPI) dashboard for regular reporting. $30,000
Deliverable #2 March 1, 2016
2
Quarterly Report: Status update on PAD fabrication and transmittal to Kenyan and Ugandan partners Report on methods and progress of sample collection and analysis in Kenya Report on status of Kenyan HPLC capabilities
$30,000
Start date + 6 months
3
Quarterly Report on: Status update on PAD fabrication and transmittal Status of sample collection and analysis Report on HPLC analysis conducted in US and Kenya Develop and deliver plan for phone interface of computer image analysis Describe flow of information between project members, Kenyan PPB, Ugandan NDA, and WHO RapidAlert system and their response to information concerning poor quality drugs and knock offs. Updated strategic scaling plan. $25,000
Start date + 9 months
4
Quarterly Report: Status update on PAD fabrication and transmittal to Kenyan and Ugandan partners Status update on computer image analysis Status of sample collection in Kenya and Uganda Report on HPLC analyses conducted in US and Kenya $20,000
Start date + 12 months
5
Quarterly Report: Status update on PAD fabrication and transmittal to Kenyan and Ugandan partners Fabricate at least 600 PADs using new manufacturing process; $10,000

16
compare performance to wax-printed design report on phone interface for computer image analysis Status of sample collection Report on HPLC analysis conducted in US and Kenya Assess flow of information between project members, Kenyan PPB, Ugandan NDA, and WHO RapidAlert system. Report on dissemination of project results and actions taken by national medical regulators as result of project data
Start date + 15 months
6
This milestone requirement is considered fulfilled when the following actions have occurred and the deliverables and associated narrative have been submitted to the AOR for review and concurrence: Submit final KPI dashboard Submit completed final project report, including the following information: Summary of project implementation noting which activities occurred as planned and where the project experienced challenges. The final version of the scale strategy plan, previously submitted in draft form. This will include next steps required to achieve the intended scale up plans, including noting potential partners that are key to achieving next steps, commitments made by stakeholders and partners, and fundraising activities, and a final version of investor presentation. Supporting materials and documentation as appropriate. *Please note the AOR will provide further guidance for the final report during the project period of performance. $9,032
Total Award Request: $124,032

17
Deliverable #5
Dashboard for Q4 progress, 30 May 2017 Indicator Q1 progress/target Q2 progress/target Q3 progress/target Q4 progress/target PADs delivered 600/600 1200/1200 2300/1800 2820/2400 Samples collected426/300 640/600 972/900 1309/1200 PAD analyses uploaded 139/300 507/600 732/900 1051/1200
HPLC methods validated 7/3 7/6 8/9 9/15 HPLC assays 2/30 11/60 110/180 167/270 Information flow to KPPB 0/1 meeting 1 product reported Full report to PPB final report to PPB 1 product reported Impact 0 MOU from KPPB KPPB response to report See text KPPB response Status Updates to DIV team Q1 Q2 Q3 Q4 Media updates Media dossier
Summary of progress 1) No bottlenecks making or sending PADs to our partners: Location PADs transmitted PADS made on site Kenya/MTRH 180 100 Uganda/St Mary's 40 0 Malawi/UM 200 0 We sent 1100 PADs to MTRH in Q3, so the total number of PAD is actually well above our target. 2) Manufacturing prototyping will be shifted to Veripad Our commercialization partner Veripad LLC has been accepted into a prestigious accelerator program, the Mass Challenge Boston accelerator, for the June-Oct 2017 cohort. They plan to focus their 5 months in the accelerator on product design, using the 5,000 square-foot research and development lab, which provides the equipment and support needed to design, develop, and scale hardware solutions. 3) Status of sample collection in Kenya and Uganda (expect cumulative 1200 samples collected and analyzed by PADs) 1309 samples were collected and 1051 of them were analyzed by PADs, uploaded to our web site, and interpreted by our Kenyan partners. 4) Phone interface for computer image analysis is in beta testing now.
18
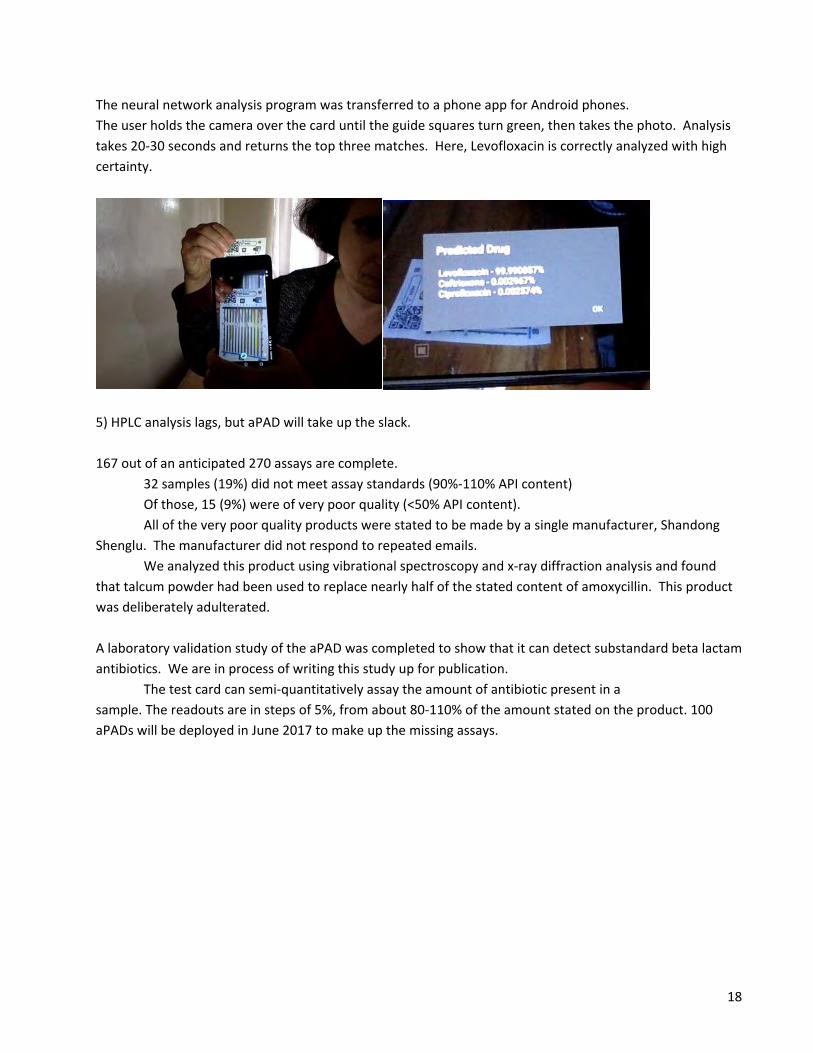
The neural network analysis program was transferred to a phone app for Android phones. The user holds the camera over the card until the guide squares turn green, then takes the photo. Analysis takes 20-30 seconds and returns the top three matches. Here, Levofloxacin is correctly analyzed with high certainty.
5) HPLC analysis lags, but aPAD will take up the slack. 167 out of an anticipated 270 assays are complete. 32 samples (19%) did not meet assay standards (90%-110% API content) Of those, 15 (9%) were of very poor quality (<50% API content). All of the very poor quality products were stated to be made by a single manufacturer, Shandong Shenglu. The manufacturer did not respond to repeated emails. We analyzed this product using vibrational spectroscopy and x-ray diffraction analysis and found that talcum powder had been used to replace nearly half of the stated content of amoxycillin. This product was deliberately adulterated. A laboratory validation study of the aPAD was completed to show that it can detect substandard beta lactam antibiotics. We are in process of writing this study up for publication. The test card can semi-quantitatively assay the amount of antibiotic present in a sample. The readouts are in steps of 5%, from about 80-110% of the amount stated on the product. 100 aPADs will be deployed in June 2017 to make up the missing assays.

19
6) Information flow between UND and Kenya PPB has been hampered by the lack of an MOU with the Kenyan PPB. Attempts were made to set up an MOU in 2012, working with Dr. Jayesh Pandit at the PPB. However, after the 2012/2013 elections he lost his position and the MOU fell through the cracks. This USAID project included a letter of support from Dr. Abwao, who was at the time working in pharmacovigilance, but he moved to a new position supervising clinical trials in 2015. I met with the Kenyan Minister of Health, Dr. Cleopa Mailu, at the World Health Assembly, along with three other health technology innovators. He brought two staff members, one of whom was Jackson Kioko, the Director of Medical Services, who is the new chair of the Pharmacy Board. Dr. Kioko had heard about the PAD project and was interested in further implementation. I learned that for the past two years the board membership has been in limbo due to a suit about how many members should be appointed from the Pharmaceutical Society of Kenya. As of March 15, the suit was settled, and the membership is: chairman Dr. Jackson Kioko, Dr. Kipkerich Chuma Koskei the Chief Pharmacist, Dr. Kisa Juma Ngeiywa Director of Veterinary Services, Dr. Alfred Rugendo Birichi, Dr. Mary Nthambi Kisingu, Dr. Rogers Atebe, Dr. Edith Wakori and Mr. Abdi Omar Jama. Through my Kenyan collaborator Prof. Gabriel Kigen, a meeting was arranged with Dr. Ronald Inyangala, whose title at PPB is Head, Quality Management Systems, Research and Development, and Christabel Khaemba, the Head of Post-Market Surveillance. Inyangala took me to visit Dr Fred Siyoi, the deputy Registrar at PPB. They suggested that I enter a formal request for an MOU and then work the details out with Christabel; I have begun that process. 7) Report on dissemination of project results and actions taken by national medical regulators as result of project data Mick Deats at the WHO RapidAlert system has requested samples of Caremox for evaluation at a forensic lab in Holland. 8) Contacts with other African regulatory agencies a) Ugandan FDA-- b) Malawi PMPB-- c) Ethiopian NIH--

20
Deliverable #4
Dashboard Indicator Q1 progress/target Q2 progress/target Q3 progress/target Q4 progress/target PADs delivered 600/600 1200/1200 2300/1800 600/ Samples collected426/300 640/600 972/900 300/ PAD analyses uploaded 139/300 507/600 732/900 300/
HPLC methods validated 7/3 7/6 8/9 3/ HPLC assays 2/30 11/60 110/180 /270 Information flow to KPPB 0/1 meeting 1 product reported See text final report 1 product reported Impact 0 MOU from KPPB KPPB response to report See text KPPB response Status Updates to DIV team Q1 Q2 Q3 Q4/ Media updates to DIV team Q1 Q2 Q3--Media dossier Q4/
21
Summary: We are protecting patients from bad quality amoxicillin and amoxi-clav We issued four reports about low-quality drugs to the KPPB, and it's natural to ask whether they have acted on these, and what the impact has been on the health of the 20 million Kenyans served by MTRH. Amoxicillin and amoxy-clav are used to treat ailments ranging from mild earaches, to acute respiratory infections and diarrhea, which are the first and third most common causes of death for young children in Kenya. Protecting patients from ineffective drugs can prevent mortality and morbidity from the underlying disease. If a child receives a bad antibiotic and their respiratory infection progresses, hospitalization may be necessary; the fatality rate among young children in Kenya hospitalized for pneumonia is 11%. The only national study on human use of antibiotics in Kenya dates from 2004 (Mitema and Kikuvi). It estimated use of antibiotics at roughly one course of treatment per person per year; this number is likely to have increased in the decade since the report was issued. About 1/3 of those antibiotics were beta lactam antibiotics, the kind we have focused on in this project, thus over the year of the project, more than 7 million Kenyans in the MTRH catchment area used a beta lactam antibiotic. Amoxicillin and amoxy-clav are among the most popular antibiotics. Given the 5-6% prevalence of the two main problem products in our sample pool, we estimate that 100,000 people per year in the MTRH catchment area have been using very bad quality amoxicillin and 120,000 people have been using very bad quality amoxyclav medicines each year. Our first two reports (2014 and 2015) focused on Bactoclav brand amoxicillin-clavulanic acid products stated to be made by MicroLabs Ltd, an Indian company.
• more than a third of the amoxy-clav samples collected across Western Kenya. • Tablets analyzed in 2013-2015 did not contain clavulanic acid, which renders the product ineffective. • We told KPPB that the cause of these quality problems might be from inadequate heat sealing on
the foil packages, a problem that would be easy for the manufacturer to remedy. • KPPB quarantined this product in 2015 after their own confirmatory testing showed the poor quality
of the product. • KPPB did not ban the product, but they discussed the quality problems with the manufacturer, and I
don't imagine that was a comfortable discussion for the manufacturer. • The product is still being sold in Kenya currently and makes up 26% of the 2016 sample collection. • None of the products we assayed in 2016 have shown quality problems. This suggests that the
intervention by the KPPB was effective. 120,000 people were protected from bad quality amoxy-clav. If just 1% would have experienced serious problems from their underlying infections, that's over 1,200 hospitalizations or deaths prevented. We also issued reports in 2015 and 2016 about amoxicillin capsules stated to be made by a Chinese contract manufacturer, Shangdong Shenglu, for a Kenyan wholesaler.
• 44% of the tablets collected in 2013-2015 were substandard. • In three packages of the product collected in 2016, the tablets contained less than half of the stated
amount of amoxicillin. • The product was adulterated with talcum powder • Adulteration and substandard amoxicillin content confirmed by WHO lab analysis

22
• The KPPB has requested the residual tablets from our assays in order to carry out their own confirmatory assays. This is the first step required for them to carry out a regulatory enforcement action.
If effective regulatory action is taken, more than 100,000 people will be protected by bad quality amoxicillin.

23
Media dossier 67 news articles about use of PADs to detect falsified medicines appeared in 2016, in 19 countries and 5 languages BioScience, C&E News, DocCheck News, Fast Company, Lab Manager Magazine, Daz.Online, The Observer, Inside INdiana Business, Waspada Online, The Pharmaceutical Journal, Huntnews.id, suryaonline, VOA Indonesia, ORIGO, Newsbloggers.ch, Domain-b.com, Sound Cloud, International Business Times UK, Medindia, Mynahcare, Health Medicine Network, Israel Herald, Before It's News, International Travel News, Argentina Star, Orlando Echo, Buffalo Breeze, Afghanistan Sun, Herald Globe, Dublin News, The Africa News, Malaysia Sun, Paris Guardian, DuurzaamBedrijfsleven.nl, Nigeria Sun, Big News Network.com, Pressetext Austria, Wallstreet Online, South-South News, The Economic Times - Health World, What Is Said, Voice of America, Latest News & Headlines, Vocativ, Becker's Hospital Review, Technology Channels - Risiinfo, ScienceNewsline, The Hindu Business Line- Mobile, The Hindu Business Line, e! Science News, The Times Of India, Rediff.com, Daily Excelsior, The Statesman, Alphr.com, Business Today, IndiaToday.in, Latest News & Headlines, Electronic Specifier, The Economic Times - Indiatimes, Business Standard, Technology Networks, Phys.org, Health Medicine Network, Science Codex, Health Medicine Network, EurekAlert!
Commercialization update: 3 companies vying to license PAD patent The utility patent for "Analytical Devices for the Detection of Low-Quality Pharmaceuticals", eg the PAD device and method of use (US Patent No. 9,354,181) was issued 31 May, 2016, to Toni Barstis, Patrick Flynn, and Marya Lieberman. The assignees are the University of Notre Dame and St Mary's College. Notre Dame is taking the lead on the tech transfer process, and is currently in discussions with three companies. Vuronxyx is a Boston tech company with whom I am working to develop a test card for illicit drugs. Mobility is an Indian start up company that is trying to get PADs included as a standard test method in Indian regulatory testing for pharmaceuticals. VeriPAD is a New York startup focusing on the African market. This company has developed its own proprietary PAD reader and is negotiating a license for the African PAD market. They have received over $50,000 in startup funding from winning two business plan competitions. The CEO and COO of the company have been in Nairobi for most of Q3, working with the Merck Accelerator program. They met with pharmacists, business people, and regulatory staff at KPPB to learn about the competitive market and business climate. My collaborators in Eldoret are working cooperatively with VeriPAD to test their software; a visit is scheduled for December 6, 2016, where PADs will be used to assess 277 real and fake formulations of four medicines. In an important advance, VeriPAD has reached an agreement with the National Quality Control Lab to test "genuine" fakes from their archived samples.
Other activities In July 2016, I met with Dr. Chepkwony, the director of the National Quality Control Laboratory in Nairobi, and exchanged information and testing results for an antiretroviral drug with his analytical
24
chemistry staff. We established a cordial relationship and Dr. Chepkwony has invited one of my students to visit his lab in June of 2017. I reported an amoxicillin product stated to be manufactured by Shangdong Shenglu (as a contract manufacturer for Kenyan company CarePlus) to the KPPB, AMPATH/MTRH, and NQCL. The product had less than 50% of the stated amoxicillin content in three different lot numbers of products. We are particularly concerned about this manufacturer because from our 2013-2015 samples, 44% of the amoxicillin stated to be manufactured by Shangdong Shenglu was substandard. We hope that a firm response from KPPB will prevent this company from sending such bad quality products to Kenya in future. VeriPAD, working with a mentor from Merck Pharmaceuticals, met multiple times with the Deputy Registrar at KPPB, and they agreed that PADs could be tested without going through the regulatory approval process as medical devices. Instead, a study will be carried out to see if the PADs can detect falsified medications from the NQCL archives. 83 samples will be studied, including analgesics, antibiotics, antihistamines, antimalarials, PDE-5 inhibitors, TB medications, and a worming medicine.
PAD fabrication and transmittal to Kenyan and Ugandan partners is ahead of schedule We mailed 500 finished PADs to Eldoret via FedEx in October, but they were held up for more than 3 weeks in customs. A second shipment of 600 PADs was hand-carried by an AMPATH staffer on Nov. 22. An additional 70 PADs were shipped to Doret Chang, a collaborator in Uganda. A very exciting advance was achieved in Q3: Local production of PADs at the AMPATH lab in Eldoret, Kenya. I brought supplies for 100 PADs, trained my two main Kenyan collaborators, and we made 20 PADs in an instruction session in late June, 2016. This brings the total number of PADs to 1190 for the quarter.
Computer image analysis app is behind schedule; here is the plan to get it back on track The analysis of the 600 Kenyan images requires the following processes: 1) Move images to the pad.crc.nd.edu server 2) Run scripts to enter the image data into the database so the the files can be accessed 3) Rectify the images using standard computer vision techniques 4) Move the Neural Network (NN) analysis code to the pad.crc.nd.edu server 5) Batch analyze the images The images were originally housed in a Dropbox folder, this folder has been attached to the server so that they can be copied to the desired location (1. completed). Our timescale for completing the image analysis is as follows: 1) Run database scripts (2. above), 3rd week in December 2016 2) Rectify images (3. above), 4th week in December 3) Install the NN software on pad.crc.nd.edu (4. above), 3rd week in December 4) Analysis of Kenyan images (5. above), 1st week in January 2017
25
Sample collection in Kenya is on target 332 samples were collected in Q3; the cumulative total is 972, so we are ahead of schedule. Acetaminophen - 30 samples Amoxicillin - 34 samples Amoxyclav – 20 samples Ampicillin – 20 samples Ciprofloxacin – 20 samples Azithromycin – 20 samples Cefuroxime – 20 samples Ceftriaxone – 20 samples Metformin – 24 samples Enalapril – 20 samples Anti-TB – 15 samples Albendazole – 20 samples Doxycycline – 22 samples Levofloxacin – 20 samples Lorsartan – 17samples Cephalexin – 10 samples Sample collection has begun in Malawi; a partner there is targeting 60 samples of beta lactam antibiotics and TB medications.
HPLC analyses conducted in US and Kenya are getting back on track with aid of DPAL program HPLC analysis was performed on 110 samples of beta lactam antibiotics. 14 failed, a 13% failure rate. Three of the samples were of very poor quality, with <50% of the stated API. Amoxicillin: 55 tested, 6 samples failed (<90% API), 3 of those samples very poor quality (<50% API for multiple tablets, all from one manufacturer stated to be Shandong Shenglu Pharmaceutical Co. Ltd.) Amoxy-clav: 35 tested, 5 samples failed (4 <90%, 1>120%). Notably, only one of the 12 Microlabs Bactoclav samples failed, and none were of very poor quality. Ampicillin: 20 tested, 3 samples failed (<90% API), no samples of very poor quality. We have developed a test card for beta lactam antibiotics which can quantify the active ingredients using a USP method without any instrumentation. Laboratory validation studies shows >95% sensitivity and 73-88%

26
specificity for detection of substandard amoxicillin or ampicillin. A publication is being prepared and we'll include it in the 4th quarter report.
27
Deliverable #3:
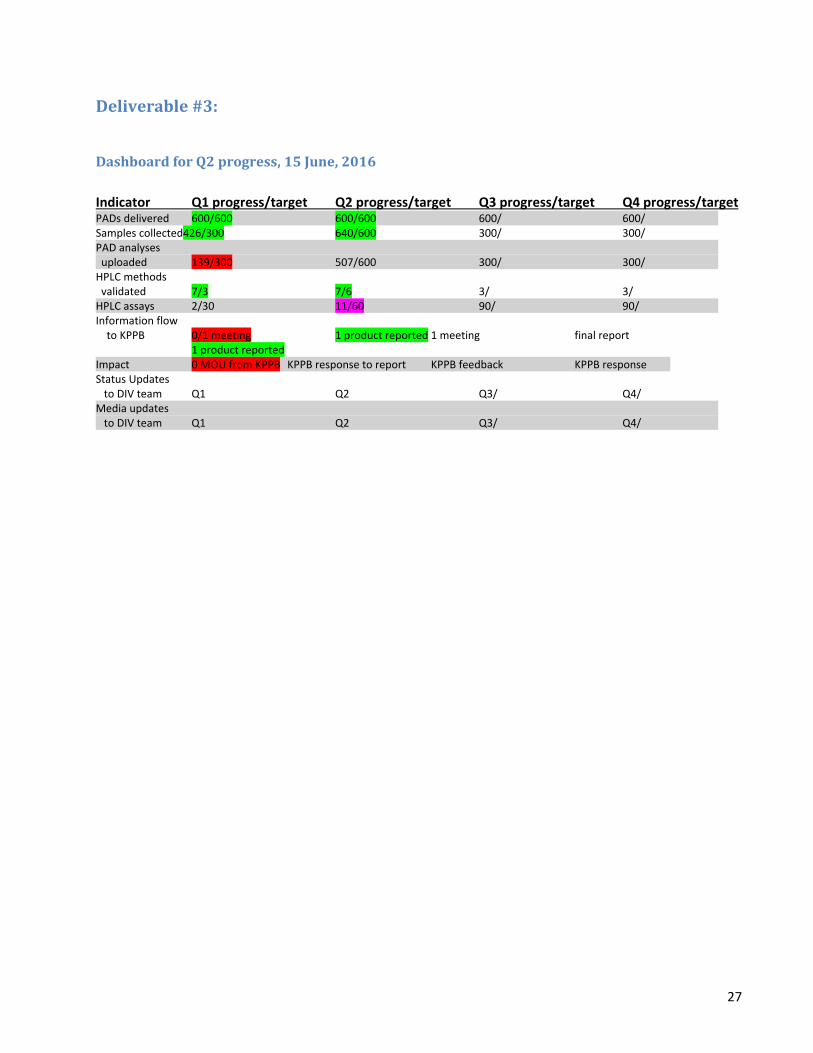
Dashboard for Q2 progress, 15 June, 2016 Indicator Q1 progress/target Q2 progress/target Q3 progress/target Q4 progress/target PADs delivered 600/600 600/600 600/ 600/ Samples collected426/300 640/600 300/ 300/ PAD analyses uploaded 139/300 507/600 300/ 300/
HPLC methods validated 7/3 7/6 3/ 3/ HPLC assays 2/30 11/60 90/ 90/ Information flow to KPPB 0/1 meeting 1 product reported 1 meeting final report 1 product reported Impact 0 MOU from KPPB KPPB response to report KPPB feedback KPPB response Status Updates to DIV team Q1 Q2 Q3/ Q4/ Media updates to DIV team Q1 Q2 Q3/ Q4/
28
Status update on PAD fabrication and transmittal to Kenyan and Ugandan partners 600 PADs delivered to MTRH (Eldoret, Kenya) on June 19. Delivery method: hand-carried by ML Prof. Chikowe and I received funding from the Indiana Clinical Translational Science Institute (CTSI) for a small prevalence study to be conducted in cooperation with the national drug monitoring agency. He will come to Eldoret in late June to learn how to conduct sampling and use the PADs for screening. 40 PADs will be mailed to Mr. Kamanda Godfrey, the head of the Ugandan Agroproduct Regulatory Agency. We will investigate the possibility of testing herbicides and pesticides, agricultural inputs which are often faked in Uganda. 100 PADs will be delivered to Bishoy Ghopal, from VeriPAD, a company recently formed to commercialize PADs in the developing world. VeriPAD won a $25,000 Social Impact Grand Prize in CUNY's Zahn Innovation Center Business Plan competition. This team took the 12-lane PAD and developed a mobile phone application to help interpret the PAD results. Da Wi Shin and Bishoy Ghopal will participate in the Zahn Center's summer accelerator program, and will travel to Kenya in June to see the lab at AMPATH and meet other potential customers.

29
Sample collection and analysis in Kenya is on target
Sample collection is ahead of schedule; we have a total of 640 products with complete metadata recorded in the dropbox database. PAD analysis and visual evaluation has caught up, with 507 "reads" recorded in the dropbox database. 53 products were flagged as suspicious. The PAD results suggest we should focus analysis on ampicillin, azithromycin, ceftriaxone, metformin, losartan, and amoxy-clav in the next quarter.
Sample Collected Q2
PAD analysis
Suspicious?
Acetaminophen 65 0 Amoxycillin 68 66 0 Amoxy-clav 40 40 5 Ampicillin 30 30 9 Ciprofloxacin 40 40 3 Cefuroxime Axetil 44 0 Azithromycin 43 41 8 Cephalixin 20 20 0 Ceftriaxone (injectable) 60 60 8 Metformin 41 41 7 Enalapril 39 39 2 Losartan 28 28 5 Levofloxacin 40 40 2 Doxycycline 33 32 1 RHZE (TB meds) 15 0 Albendazole 30 30 3 Sildenafil 4 0 Total 640 507 53
HPLC capabilities (expect six methods to be validated) We have demonstrated system suitability using the Waters 2695 at Notre Dame for analysis of 7 drugs: ampicillin, amoxycillin, amoxy-clav, acetaminophen, ceftriaxone, albendazole, and ciprofloxacin. In late June, we will import these methods to the Kenyan instruments, along with the necessary spreadsheets for record keeping. Question: should we work on assays for ARVs? If my Kenyan partners can receive primary reference standards through USP's donation program we can add these drugs to the roster. Prof. Gabriel Kigen, who is the Head of the Pharmacology department at Moi University, has begun developing a method for monitoring gemcitabine in patient samples. Gemcitabine is a chemotherapy agent in use at MTRH, but currently any patient samples have to be sent out for analysis at a lab in South Africa. Prof. Kigen received his PhD in the area of HPLC method development so this is going to be a good connection for capacity development. In early June he sent one of his students and Phelix Were to a 1 week HPLC training session in Nairobi. This is great as it shows he has some skin in the game. I will bring him some HPLC-grade gemcitabine in late June for method validation.
30
HPLC Assays behind schedule In Q2 we only did a handful of assays of DIV samples; the reason is that we were clearing a backlog of Gates samples before they hit their expiration dates. We will be working to get back on track in Q3. In Q3 we are focusing on developing HPLC capacity at MTRH and increasing our throughput of DIV HPLC samples at Notre Dame. Phelix Were and a lab tech in Dr. Kigen's group took a 1 week long HPLC training course in Nairobi from June 6-10, 2016, and I will work with Phelix June 19-29 to show system suitability and put assays for several antibiotics into practice. A refrigerator has been purchased and installed in the AMPATH lab for storing reference standards as well as some of the more thermally sensitive samples, and all the necessary reference standards will be in by June 19.
Plans for phone interface of computer image analysis (app vs online, front end & back end, database) We decided to use an Android phone application, rather than an online site. Our developer (UND Campus Research Computing) is using an LG-VS450PP phone (an inexpensive, unlockable model) running Android 4.4.2. This type of phone is available in Kenya. The CaffeNet version of our neural network was installed successfully and will undergo field testing June 19-29, 2016. The phone app is designed to:
• recognize a PAD card in the camera's field of view • automatically take the photo when the image is in focus and all fiducials are clear • perform the basic geometrical correction on the image • evaluate what substance best matches the PAD image results (using a database of 26 substances) • report to the user on the best match
In Q3 we will add the statistical confidence in the matches and upload the raw data and test result to a secure database. We have selected Open Science Framework as the database host; this program is free, provides up to 2GB storage with a base registration, and includes privacy and security controls.
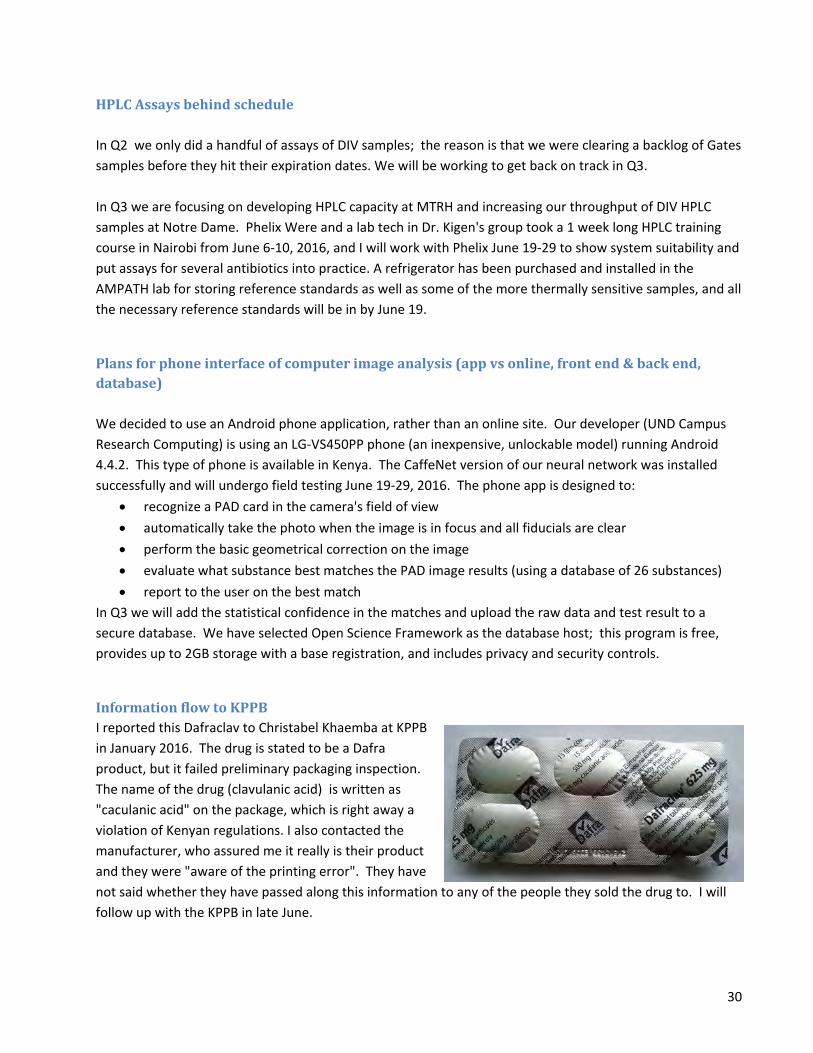
Information flow to KPPB I reported this Dafraclav to Christabel Khaemba at KPPB in January 2016. The drug is stated to be a Dafra product, but it failed preliminary packaging inspection. The name of the drug (clavulanic acid) is written as "caculanic acid" on the package, which is right away a violation of Kenyan regulations. I also contacted the manufacturer, who assured me it really is their product and they were "aware of the printing error". They have not said whether they have passed along this information to any of the people they sold the drug to. I will follow up with the KPPB in late June.

31
In May 2016, at the request of the AMPATH head pharmacist, I tested two brands of combination ARVs. These critical medicines both showed possible quality deficiencies. The products, manufactured by Aurobindo and by Hetero Labs, are stated to contain efavirenz (600 mg), lamivudine (300 mg), and tenofovir disoproxyl (300 mg).
Concerns: Tenofovir systematically low in all pills assayed. High degree of pill-to-pill heterogeneity. KPPB and PEPFAR program head were informed of these results in early June by AMPATH head pharmacist Breaking news: The Hetero Labs product just lost its PEPFAR status--see press release http://www.pepfar.gov/press/releases/258150.htm
Aurobindo Hetero Hetero Aurobindo
0
100
200
300
400
500
600
700
800
pill4
104A
pill5
104A
pill6
104A
pill4
104B
pill5
104B
pill6
104B
pill7
104
A 20
min
pill7
104
A
pill8
104
A
pill7
104
B
pill8
104
B
Efavirenz (mg) Lamivudine (mg) Tenofovir (mg)
Efavirenz 92%-110% of labeled API
content
Lamivudine and tenofovir
90%-110% of labeled API content
Error bars show LC error (replicate injections)
mg/
tabl
et

32
Samples were prepared by Mr. Nick Myers and run by Dr. Michelle Joyce. Aurobindo: EISA15005-A, Man 01/2015, Exp 12/2016 Hetero Labs: Batch No E151167, Man 8/2015, Exp 7/2018 Five Aurobindo pills and five Hetero pills were analyzed May 2016. All samples were within expiration date. Primary reference standards were donated by USP (Efavirenz lot G0L369, Lamivudine lot I0M388, Tenofovir lot G0M335; all current lots). Individual pills were ground in a mortar and 50 mg powder dissolved in 100 mL 1:1 methanol/water with 5 minutes sonication. For pill 7, 104A, we sonicated the powder for 5 minutes and filtered an aliquot for analysis; we continued sonicating the remaining powder for 20 minutes and filtered again for analysis. The two assay results were statistically indistinguishable. This suggests that the APIs are adequately extracted with 5 min sonication time. LC-MS was run in MRM mode using a triple quad mass spectrometer as the detector. Each drug was quantified by picking out the molecular ion, fragmenting it, and counting the main fragment ion; for Lamivudine we added in the intensity of the sodium adduct's main fragment. Calibration curves were generated from USP standards and each sample was diluted and analyzed in its linear range. 3 pills from each manufacturer (#4,5 and 6) were run on one LC column and 2 (#7, 8) on another column. Reproducibility of replicate injections ranged from 0.1-0.7% RSD. Instrument: Waters TQD triple quadrupole MS with Acquity UPLC Column: Waters UPLC BEH C18; 1.7 um particle; 2.1 x 150 mm Mobile Phases: A = Water with 0.1% formic acid B = Acetonitrile with 0.1% formic acid, Flow rate = 0.3 mL/min, Column Temp = 40⁰C Gradient: Time (min) %A %B 0 80 20 1 80 20 4 20 80 5 20 80 5.1 80 20 7 80 20 All samples were run in positive-ion mode. Multiple Reaction Monitoring (MRM) mode was used to detect each drug by the following transitions: Efavirenz m/z 316.0 → 168.2 Lamavudine m/z 230.2 → 112.1 + Lamavudine sodium adduct m/z 252.4 → 134.1 Tenofovir m/z 288.1 → 176.2
33
Updated strategic scaling plan. Our goal for the next phase of this project is to detect the "worst of the worst" medicines in East Africa through large scale screening with PADs. We want to screen in the private market, where hundreds of manufacturers vie to offer inexpensive generics. Conventional chemical analysis is too expensive for this initial screening --a WHO prequalified lab in Nairobi quoted us $430 per sample for analysis of amoxycillin--but drug regulatory agencies often will not act without conventional analytical evidence for quality problems. In view of the importance of quantitative data for detection of substandard products and for inspiring regulatory action, we plan to develop new capacity for quantitative assay of medications to go along with the increased level of screening. The next step is to dramatically scale up screening with PADs. We want to test more samples, from more types of medicines and veterinary products, in more locations across Eastern Africa. We also want to implement a cell-phone reader for the PADs and create new resources for confirmatory analysis. These activities will all help us to find the most efficient ways to discover and confirm poor quality human and animal medications. Scale up screening with PADs: We are currently testing medicines from 279 pharmacies in Western Kenya. We plan to scale up regionally, expanding to Nairobi and the Mombassa region, Malawi, and Uganda. These areas were selected based on expressions of interest from government agencies and academic or industrial partners. In addition to covert shopper collection, which is a gold standard sampling method, we will explore two novel sampling methodologies designed to take advantage of local knowledge. In order to facilitate screening with PADs, we will begin to explore local production of PADs at AMPATH in Q3 and Q4. The initial run of 100 PADs will undergo quality testing and some will be used at a workshop in London. Create new resources for confirmatory analysis: We hope to work with drug regulatory agencies in all the countries in which we test drugs, but realize that access to independent confirmatory analysis is a must-have. AMPATH/Moi University/MTRH is currently my main partner in Kenya. We are developing a pharmaceutical analysis laboratory which can perform confirmatory assays on a contract basis, thus ensuring sustainability of the instrumental facility. Capacity is currently low as we train pharmacists and pharmacologists from Moi University on the instruments. In order to make the HPLC lab sustainable, we plan to train the staff at the MEDS lab in Nairobi and at the USP Center for Pharmaceutical Advancement and Training (CePAT) in Ghana and obtain ISO certification for the lab, so it can be supported through recharge fees. Capacity to be built: 400 samples/year. Partners being sought: Gates, USP/CePAT. We are developing a secure web site to host confirmatory analysis data and metadata. The site will be based on Open Science Framework. It will allow different labs to enter their data and view each other's results. Results can be fed into reports that are easy to push to stakeholders such as regulatory agents.

34
Users can also drill down to see metadata, raw assay data and calculations for each result. This will allow transparency and scientific oversight over the assay process.
Deliverable #2
Dashboard Indicator Q1 progress/target Q2 progress/target Q3 progress/target Q4 progress/target PADs delivered 600/600 600/ 600/ 600/ Samples collected 426/300 300/ 300/ 300/ PAD analyses uploaded /300 300/ 300/ 300/
HPLC methods validated /3 3/ 3/ 3/ HPLC assays /30 60/ 90/ 90/ Information flow to KPPB 1 meeting midterm report 1 meeting final report Impact MOU from KPPB KPPB response to report KPPB feedback KPPB response Status Updates to DIV team Q1/ Q2/ Q3/ Q4/ Media updates to DIV team Q1/ Q2/ Q3/ Q4/
PAD fabrication and transmittal to Kenyan and Ugandan partners 600 PADs were delivered to MTRH (Eldoret, Kenya). Delivery method: 300 mailed to IU house (10 days transit time), 300 hand-carried by ML. In addition, we received numerous requests for PAD samples from potential users in Africa. 60 PADs were shipped by FedEx to Mr. Stephen Kigera, Mission for Essential Drugs and Supplies (MEDS), Nairobi, Kenya. This shipment broke all my speed records for Africa, arriving in just 3 days at the MEDS office. That's probably because MEDS is located just 20 minutes from the Nairobi airport. MEDS is an NGO that distributes quality-controlled pharmaceuticals to hospitals and clinics all over Kenya and some neighboring countries as well. They have their own quality control lab, which I visited in January. 40 PADs were shipped by FedEd to Prof. Ibrahim Chikowe, at the College of Medicine, University of Malawi. Prof. Chikowe and I submitted a proposal to the Indiana Clinical Translational Science Institute (CTSI) for a small prevalence study to be conducted in cooperation with the national drug monitoring agency. A separate proposal was submitted in partnership with the DMA to a small private foundation. I am awaiting a materials transfer agreement from the DMA before I ship them some PADs to trial. 20 PADs were shipped by regular US mail to Dr. Nawal Elhadi, the QA manager for the National Medical Supplies Fund in Khartoum, Sudan. This package broke the record for longest transit time, taking over 2 months to arrive at Dr. Elhadi's office. The National Medical Supplies Fund purchases and regulates

35
medications used in the public pharmaceutical supply chain in Sudan. Sudan is under a US Dept. of State Travel Warning due to the high risk of terrorism, kidnapping, and other crimes, so I don't plan to travel there. Instead, I will demonstrate the test cards via a video link. 20 PADs were shipped by Fed Ex to Prof Ikhlas Khan, at Ole Miss University, USA. Prof. Khan has an ongoing project to assess herbal medicines. These medicines are used all over the world and they are often adulterated with pharmaceuticals (eg, "male potency enhancers" which are pepped up with Viagra or weight loss products that contained amphetamines or other banned slimming drugs).
Report on methods and progress of sample collection and analysis in Kenya Sample collection is ahead of schedule with at least 426 products collected by 4 covert shoppers. 330 products have been run on the PADs, but visual analysis is behind schedule, with only 139 evaluations recorded in the dropbox database. 25 of the evaluated drugs were flagged as suspicious and all of these will go to the next stage of confirmatory analysis. The Kenyan team is awaiting an updated key for evaluating the many new drugs that are being sampled and run. We are almost done with the updated key but are waiting for one pharmaceutical, cefuroxime axetil, whose dosage form is very expensive when purchased as pure APIs. We are obtaining some samples of this dosage form from US sources. Acetaminophen: 41 samples tested, 41 interpreted, 2 suspicious Albendazole: will add to sample collection for Q2 Amoxycillin: 36 samples, 16 tested, 20 images on phone in US, 0 suspicious Amoxy-clav: 21 tested, 21 interpreted, 5 suspicious Ciprofloxacin: 20 tested, 20 interpreted, 3 suspicious Cefuroxime axetil: 22 tested, awaiting pharmaceutical standard Azithromycin: 21 tested, 21 interpreted, 6 suspicious Cefalexin: 10 tested, awaiting interpretation guidelines Ceftriazone, 42 tested, awaiting interpretation guidelines Metformin: 21 tested, awaiting interpretation guidelines Enalapril: 20 tested, awaiting interpretation guidelines Losartan: 16 tested, awaiting interpretation guidelines Levofloxacin: 20 tested, awaiting interpretation guidelines Ampicillin: 20 tested, 9 suspicious Doxycycline: 20 tested, awaiting interpretation guidelines RHZE: None collected. Will collect Global Fund samples from different clinics.
Kenyan HPLC capabilities Two Waters 2695 High Performance Liquid Chromatography instruments were set up in the AMPATH pharmacy office in May of 2015. One of these instruments was not working properly and was diagnosed with a degasser problem by Dr. Lieberman on her January visit; a new degasser costs over $3,000. We knew

36
that instrument maintenance and repair problems are typical roadblocks to implementation of scientific instrumentation in Africa, and we have planned out strategies to solve these problems.
1) We selected the Waters 2695 in part because it is easy to maintain and repair, with many modular components.
2) The Lieberman lab has a stock of four identical Waters 2695 instruments which were donated by Merck Pharmaceuticals.
3) We have the capability of making quick instructional videos and of providing live video assistance to the HPLC operators in Kenya. In this case, we pulled one of the degassers from a donated HPLC and replacing the seals and gaskets. The reconditioned degasser was hand-carried to Eldoret by a Purdue professor. It arrived at the AMPATH lab Feb. 23, and will be installed by Phelix and Mercy next week.
We have demonstrated system suitability using the Waters 2695 at Notre Dame for analysis of 7 drugs: ampicillin, amoxycillin, amoxy-clav, acetaminophen, ceftriaxone, albendazole, and ciprofloxacin. A quick test in Kenya in January with the functional Waters 2695 unit demonstrated linearity and good peak metrics for amoxicillin, and Phelix will begin running assays in Q2. Prof. Gabriel Kigen, who is the Head of the Pharmacology department at Moi University, has begun developing a method for monitoring gemcitabine in patient samples. Gemcitabine is a chemotherapy agent in use at MTRH, but currently any patient samples have to be sent out for analysis at a lab in South Africa. Prof. Kigen received his PhD in the area of HPLC method development so this is going to be a good connection for capacity development.
HPLC Assays Completed HPLC assays completed in Kenya: 2 amoxycillin (done in conjunction with the system suitability testing). Both assayed within the expected 90-120% API content. We have had problems with our pharmacopeia reference standards. One bottle of clavulanic acid was stored in a -80˚C freezer in another lab, and was thrown out during a cleanup of the freezer. One bottle of amoxicillin was used to test a new PAD design (a different, less expensive grade of amoxicillin should have been used for that test). A refrigerator/freezer has been purchased for storing reference standards as well as some of the more thermally sensitive samples. It is currently at MTRH and just needs to be installed in the lab. Reagent grade samples of the APIs will be purchased for use in PAD testing. Replacement standards were kindly donated by USP; a clavulanic acid standard was hand carried last week and is now at the lab. HPLC assays completed in the US: We are still analyzing a backlog of samples collected in 2014, as we have not yet received any of the Q1 samples from Kenya. In November I received a request from Maryam Hynds, who is the pharmaceutical inspector for the government of Barbados, to assess their national stockpile of Oseltamivir Phosphate (Tamiflu). Barbados was at the time having an outbreak of swine flu at a correctional facility, and the drug was long past its expiration date. We received standards and technical support from USP and were able to get samples from Barbados and complete this assay within 2 weeks. The assay results

37
showed that some of the material did not meet standards and the government of Barbados asked for help from PAHO, which has supplied a new stock of Tamiflu capsules to help control flu outbreaks.
Information flow to KPPB I reported one medication to Christabel Khaemba at KPPB in January 2016. The drug is stated to be a Dafra product, but it failed preliminary packaging inspection. The name of the drug (clavulanic acid) is written as "caculanic acid" on the package, which is right away a violation of Kenyan regulations. Christabel is checking the registration status on this product.
Media Impact The Nation, which is one of Kenya's largest newspapers, ran a piece on the project (see Media Appendix): http://www.nation.co.ke/news/Survey-reveals-poor-likely-to-buy-fake-drugs/-/1056/3071314/-/format/xhtml/-/alvhqf/-/index.html. That was good publicity for the hospital and my Kenyan colleagues. However, the Pharmacy and Poisons Board was not very pleased about the piece because it repeated a statistic that 30% of medicines in Kenya are low quality (that number actually originated at the PPB, by the

38
way). We are still dealing with the fallout. I will visit KPPB when I go to Kenya in late June and see if I can smooth some feathers down.
Deliverable #1
Updates to project implementation and scaling plan 1) Test card production: I have met with five different manufacturers (Hach, Biodot, LasX, DCN, and Lohmann Technologies) and and over the next quarter, will explore rotary die slitting and laser cutting for card assembly. I anticipate a trial reagent deposition run at Biodot in February 2016, which will fall into the Q2 update report. Neural network software to analyze test results has been developed in a desktop form. Over the next two quarters, I have arranged to work with a Campus Research Computing programmer who will migrate the image analysis software to an Android phone platform. This application is on the cutting edge of machine learning; we are applying for a Google Faculty research award to support expert knowledge-based neural net training and continual updating of the neural network database. I will provide updates for the progress of automated image analysis in Q1-Q4. 2) Educating and engaging health care workers and pharmacists: We will integrate paper test cards into a strong pharmacovigilance effort that is currently underway at AMPATH/MTRH. We hypothesize that low quality medications will be associated with particular adverse drug reactions (ADRs), such as failure to respond to treatment. We will educate medical caregivers and pharmacists to be alert for signs of fake TB and diabetes drugs and antibiotics, and train them to collect samples for analysis by the Pharmacovigilance (PV) group. A "drawer of shame" has been designated for these samples, and several products have already been collected, such as this imipenim/cilastatin injectable antibiotic (on right) which gave a dark brown solution instead of the clear solution expected. Based on prior rates of ADRs and the number of patients seen at these clinics, AMPATH/MTRH personnel expect to collect 100 samples of drugs implicated in ADRs and 30 control samples. I will report on the training of the clinicians and the "drawer of shame" in the Q2 and Q4 status updates.

39
3) Plans for postmarket surveillance After a three way discussion between MTRH, KPPB, and UND, we decided to increase the scope of the post-market surveillance in order to cover more pharmaceutical types. Eleven drugs, mostly antibiotics, were identified by MTRH and KPPB as being of particular concern in Kenya. Ninety samples of each drug will be collected via secret shoppers. We have already surveyed 279 pharmacies and small medicine shops in Western Kenya, and will choose sampling locations by random selection from this list. This number of samples was chosen to provide statistical power. The scale of testing necessary to detect a given prevalence of "bad" drugs can be estimated statistically.1 If the fraction of pharmaceuticals in a region that are very low quality is and one wishes to measure the prevalence to within ±u, the number of samples m that must be examined in order to estimate the prevalence with 95% confidence is given by:
(1) If the true prevalence of bad quality drugs is 15% and we want to measure that prevalence rate with an accuracy of at least ± 8%, we must test at least 80 samples of each of those 11 medications. 90 samples of each medication will be collected to allow a little margin for error. An additional four (mostly chronic care drugs) were selected for a preliminary survey of 20 samples each, and 130 drugs will be collected through interactions with clinicians at MTRH who are suspicious due to unusual patient reactions to medications. The numbers of drugs collected will be tracked on the KPI dashboard and the status updates will include a summary of information about the samples; the sample metadata will be posted to the project web site. 90 samples each of 1. Acetaminophen 2. Ampicillin 3.Amoxycillin 4.Amoxy/Clav 5. Ciprofloxacin 6. Azithromycin 7.Ceftriaxone 8. Cefuroxime 9. Levofloxacin 10.Doxyxycline 11. Metformin
1 Aitken CGG. Sampling—how big a sample? J Forensic Sci 1999;44(4):750–760.

40
20 samples each of: 12. Cephalexin 13. Enalapril 14. Losartan 15. RHZE 130 samples from Pharmacovigilence effort (the "drawer of shame")
Grant USAID staff access to the US-Kenya databases which will be used to track sample collection and PAD analyses. Done. A password for the pad.crc.nd.edu website has been sent to Samuel Bishop, the AOR for the award, and Duc Tran. Other staff will be added as needed. Currently this website houses PAD images from in-house testing.
Updates on hiring key staff and finalizing required partnerships. Staff deliverables include submitted resumes/CVs with associated roles and responsibilities; partnership deliverables include signed MOUs, as applicable See appendix A for CVs from Dr. Sonak Pastakia, Mercy Maina, and Phelix Were. Prof. Sonak Pastakia (PharmD, MPH, BCPS) is an assistant professor of pharmacy practice at Purdue University School of Pharmacy and the co-chair of AMPATH’s Chronic Disease Management Team. He spends 11 months of the year on site in Eldoret, supervising 20-30 pharmacy interns and 10 pharmacy students from the University of Nairobi pharmacy school. We have collaborated since 2011. Roles and responsibilities: supervise training of clinicians in falsified drug awareness and detection, oversee sample collection, responsible for managing flow of PAD and HPLC analysis and record keeping in Kenya, and liason to KPPB. AMPATH/MTRH Clinical Pharmacist Mercy Maina (B. Pharm) has been the lead investigator on several studies in Kenya including pharmacovigilance techniques and detection of substandard medication and is a member of the MTRH Pharmacovigilence team. Role and responsibilities: ensure that samples are properly stored and manage logistics of getting them to UND for HPLC analysis if necessary, develop and deliver training materials for clinicians on falsified drug awareness and detection, perform PAD and HPLC tests in Kenya and record results in online database, main "reader" for PADs in Kenya. AMPATH/MTRH Pharmacy Technician Phelix Were (D. Pharm) is the current coordinator for the PAD project through AMPATH. Roles and responsibilities: Train and manage "secret shoppers", manage paperwork for reimbursements for cost of purchases, intake of samples and entry of sample metadata, perform PAD and

41
HPLC tests and record results in online database, perform simple HPLC maintenance & QA/QC tasks and record in HPLC log book.

42
Appendices
A. Selected media reports

43

44

45

46
B. CVs of co-workers
B.1. Sonak Pastakia NAME: Pastakia, Sonak D eRA COMMONS USER NAME (credential, e.g., agency login): PASTAKIAS POSITION TITLE: Associate Professor of Pharmacy Practice EDUCATION/TRAINING
INSTITUTION AND LOCATION DEGREE (if applicable)
Completion Date MM/YYYY
FIELD OF STUDY
Temple University, Philadelphia, PA University of North Carolina Hospitals, Chapel Hill, NC Harvard University, Boston, MA
PharmD Residency MPH
2004 2006 2007
Clinical Pharmacy HIV/Infectious Disease International Health
A. Personal Statement Through my unique position as Associate Professor at Purdue University, I spend 10-11 months per year on site in Kenya where I fulfill a wide variety of roles including, a consultant for Abbott on delivering chronic disease care in rural markets, a founding member and a member of the board of directors of the Tumaini Street Youth Center, co-chair of the Academic Model Providing Access to Health Care (AMPATH) Pharmacy department, member of the AMPATH Cardiovascular/ Chronic Disease Management Working Group, and a lecturer at the Moi University School of Medicine. Through my past 8 years in Kenya, I have focused on implementing a wide variety of programs including a rural diabetes care program which currently serves over 5000 patients with diabetes and has screened over 20,000 people, a portabilized care system linked to microfinance groups which provides chronic disease management services, a pharmacy distribution system which provides antiretroviral medications to over 150,000 HIV-infected patients receiving care at 600 clinics throughout western Kenya, and an anticoagulation monitoring program which serves over 1500 patients and has a focus on rheumatic heart disease. These multifaceted roles have helped me develop a deep first hand understanding of the environment in LMICs. My past experiences make me well suited to lead the on the ground implementation of the care strategy proposed in this application. Revolving Fund Pharmacy - http://www.grandchallenges.ca/grantee-stars/0146-01/ Counterfeit Detection - http://www.nd.edu/fighting-for/2013/fighting-to-protect-the-sick/ Pastakia SD, Ogallo WM. Designed to fail, re-engineered to succeed. J Amer Pharm Assoc 2014, 54(4):85-89. Portabilized Group Care for Chronic Diseases- http://www.purdue.edu/globalaffairs/videos/index.html B. Positions and Honors 2004–2006 Clinical Instructor, University of North Carolina School of Pharmacy, Chapel Hill, NC 2006–2007 Adjunct Assistant Professor, Massachusetts College of Pharmacy, Boston, MA 2006–2007 Intern, Institute for Healthcare Improvement, Boston, MA 2007–2013 Assistant Professor, Purdue University College of Pharmacy 2007– Visiting Lecturer, Moi University School of Medicine 2007- Adjunct Assistant Professor, Indiana University School of Medicine 2007– Diabetes Clinical Pharmacist, Diabetes Clinic, Moi Teaching and Referral Hospital 2008– Department Co-Chair, Pharmacy Working Group, Academic Model Providing Access to Healthcare (AMPATH) Center, Eldoret, Kenya

47
2009– Department Co-Chair, Chronic Disease Management, Academic Model Providing Access to Healthcare (AMPATH) Center, Eldoret, Kenya 2012- Consultant, Abbott Fund 2012- Consultant, Abbott India 2013- Associate Professor, Purdue University College of Pharmacy Honors 2004 Eli Lilly Achievement Award for Highest Pharmacy School Grade Point Average 2004 McKesson Award for Superior Leadership and High Scholastic Aptitude 2005 UNC Residency Award for Resident Most Likely to Lend a Helping Hand 2009 Purdue University Service Learning Faculty Fellow 2010 American Society of Health Systems Best Practices Award-Implementation of Pharmacy Practice in a Rural, Resource-constrained setting 2010 American College of Clinical Pharmacists – New Clinical Practitioner of the Year Award 2010 American Association of Colleges of Pharmacy – Student Community Engaged Service Award 2012 Indiana Public Health Foundation Preventive Medicine and Public Health Award 2013 Runner-up, C. Peter Magrath Engagement Award 2013 Runner-up, Outreach and Engagement Scholarship 2013 Awardee, Purdue University Corps of Engagement Award ($5,000) 2014 Albert B Prescott Leadership Award ($1,000) – Phi Lambda Sigma and American Pharmacist’s Association Annual Award Certifications 2004 – Registered Pharmacist, State of North Carolina #17275 2005 – Board Certified Pharmacotherapy Specialist, American College of Clinical Pharmacy C. Contribution to Science Healthcare delivery in the developing world continues to face many challenges that limit access to care for patients. Our early work focused on identifying many of these barriers and describing the magnitude of these deficiencies in the healthcare system. As our research highlighted the disturbingly low availability of high quality services, we then set out to implement patient centric care services that were designed around the unique needs and barriers faced by patients in this setting. This included the creation of one of the largest anticoagulation monitoring services in the world with over 1700 patients enrolled, the creation of diabetes care infrastructure to support care delivery at rural health facilities throughout western Kenya, and the implementation of a novel microfinance linked group care delivery model for patients with hypertension and/or diabetes. It is within this last care delivery innovation that we were able demonstrate dramatically improved performance metrics highlighting the improved access and subsequent clinical outcomes observed when delivering patient centric services. Within this model, patients experienced a doubling in their linkage to care along with a four-fold reduction in blood pressure compared to the standard of care. We are currently implementing contextualized models of this for other diseases (as described in this proposal) and scaling it up in other countries and settings. I am responsible for the design, coordination, and expansion of all of these initiatives.

48
Park PH, Wambui CK, Pastakia SD, et al. Improving diabetes management and cardiovascular risk factors through peer-led self-management support groups in western Kenya. Diab Care 2015;38:e110-e111. Pastakia SD, Cheng SY, Kirui, et al. Dynamics, impact, and feasibility of Self-Monitoring of Blood Glucose in the Rural, Resource-Constrained Setting of Western Kenya. Clin Diab 2015. Pastakia SD, Ali SM, Kamano JH, Bloomfield J, et al. Screening for diabetes and hypertension in a rural low income setting in western Kenya utilizing home-based and community-based strategies. Globalization and Health 2013, 9; 1-9 PMID: 23680083 Manji I, Pastakia S, Do AN, Ouma MN, et al. “Performance Outcomes of a Pharmacist-Managed Anticoagulation Clinic in the Rural, Resource-constrained setting of Eldoret Kenya” Journal of Thrombosis and Haemostasis 2011;9:2215-2220 PMID: 21914124 Pastakia SD, Nyabundi J, Karwa R, et al. “Evolution of Diabetes Care Through Partnerships in a Rural Resource-Constrained Setting” Ann Pharmacother 2011:45;1-6. PMID: 21558485 Pastakia SD, Cheng SY, Kirui NK, Kamano JH. Dynamics, impact, and feasibility of self-monitoring of blood glucose in the rural, resource-constrained setting of western Kenya. Clin Diabetes. 2015;33(3):136-143. At the heart of many of the care delivery challenges seen in LMICs is the lack of a well-functioning supply chain and a patient focused pharmacy practice. In order to address this we have initiated multiple activities at all levels of the healthcare system. This includes the creation of a clinical pharmacy consultation service where Kenyan and North American pharmacists round on inpatients and provide timely recommendations to optimize care. In the outpatient setting we have focused our efforts on addressing all aspects of the supply chain. To address the limitations with availability, we have implemented revolving fund pharmacies at over 50 sites throughout western Kenya to ensure essential medication availability at public sector health facilities remains above 90% compared to the typical availability of only ~40-50%. We have also developed novel methods for pharmacovigilance by utilizing HIV infected peers to interview other patients. Through this method, there has been a six fold increase in the number of side effects reported. The dramatic improvement seen through this program has given rise to a peer led care delivery system which has been utilized to improve patient linkage to care, provide ongoing psychosocial support, and assist with medication refills. I have designed, supervised and helped lead all of the aforementioned activities. Pastakia SD, Vincent WR, Manji I, et al. “Clinical Pharmacy Consultations Provided by American and Kenyan Pharmacy Students During and Acute Care Advanced Pharmacy Practice Experience” American Journal of Pharmaceutical Education 2011;75(3): 42 PMID: 21655396 Schellhase EM, Miller M, Ogallo W, Pastakia SD. Pharmaceutical Care in Kenya: An Elective Course. American Journal of Pharmaceutical Education 2013, 77; Article 60 PMID: 23610478 Pastakia SD, Karwa R, Maina M. Reframing the focus of international health experiences. Pharmacy Times 2013, November issue. Crowe S, Manyara S, Pastakia SD (corresponding author). Lessons still needing to be learned. Currents in Pharmacy Teaching Learning 2015, 7:141-143. With the limited healthcare worker resources available in LMICs, our efforts have focused on training the next generation of global health leaders that are needed to manage these novel patient centric delivery models. From the outset of our program, training has been a central piece of all of our activities. I was responsible for designing our unique global health residency and was also the primary preceptor for the first class of residents. I have since shifted my focus to other program development efforts, but still continue to precept trainees within the residency program and students from the University of Nairobi and Purdue.

49
Pastakia SD, Njuguna B, Le P, Brock TB. To Address Emerging Infections, we must invest in enduring systems: The kinetics and dynamics of Health Systems Strengthening. Clin Pharmacol Ther 2015. Schellhase EM, Miller M, Ogallo W, Pastakia SD. Pharmaceutical Care in Kenya: An Elective Course. American Journal of Pharmaceutical Education 2013, 77; Article 60 PMID: 23610478 Pastakia SD, Vincent WR, Manji I, et al. “Clinical Pharmacy Consultations Provided by American and Kenyan Pharmacy Students During and Acute Care Advanced Pharmacy Practice Experience” American Journal of Pharmaceutical Education 2011;75(3): 42 PMID: 21655396 Complete List of Published Work in MyBibliography: http://www.ncbi.nlm.nih.gov/sites/myncbi/sonak.pastakia.1/bibliography/48313789/public/?sort=date&direction=ascending. D. Research Support Ongoing Research Support R01 HL125487-01A1 Vedanthan (PI) 04/1/2015 – 1/31/2016 NIH Bridging Income Generation with Group Integrated Care (BIGPIC) The goal of this research program is to assess the differences in outcomes between microfinance linked group care to standard care methodologies utilized to treat chronic diseases in Kenya. I am responsible for the overarching design and on the on the ground implementation of this project. Role: Co-Investigator 623-A-00-08-00003-00 Einterz (PI) 09/30/2012 – 09/30/2017 USAID AMPATH, controlling and preventing HIV/AIDS in Western Kenya This program is tasked with increasing treatment of HIV-infected patients in 55 clinical sites and one national referral hospital affiliated with the Indiana University-Moi University collaboration throughout Western Kenya. I help to lead the delivery of pharmacy services to the patients receiving care within this program. Role: Investigator [no number] Pastakia (PI) 7/1/2015 – 9/31/2018 Medical Research Council (MRC) (UK) Ethnic Specific Risk Stratification in Early Pregnancy for Identifying Mothers at Risk of Gestational Diabetes Mellitus (GDM) in Kenya and India This multi-country research program is designed to investigate methods for the earlier identification of GDM amongst pregnant mothers in low- and middle- income countries. This collaborative effort works with investigators from the University of Warwick in the UK and Dr. Mohan’s Diabetes Specialities Centre in India. I lead the Kenyan implementation of this effort and am responsible for the design, implementation, and coordination of all study related activities. Role: PI [no number] Pastakia (PI) 8/1/2014 – 9/31/2015 Celgene

50
Creation of a Pharmacy Information Management System and Enhancement of Physical Security The purpose of this project is to develop a customized electronic pharmacy management system to facilitate greater tracking, organization, transparency, integration, and research of pharmacy records. This project will also be used to implement security features to enhance security of medication supplies. Role: PI [no number] Pastakia (PI) 6/1/2013 – 9/31/2015 Lilly Endowment Medication Safety Fund Countrywide Scale-up of Paper-based Analytical Devices to Detect Counterfeit Medication Products The goal of this research program is to demonstrate the scalability of our novel counterfeit detection devices in a rural resource-constrained setting. We hope to illustrate that this highly effective device can be incorporated into a government based pharmacovigilance program to minimize the patient exposure to substandard medications. I am involved with the overarching design and coordination of this effort. Role: PI

51
B. 2. Mercy Maina Mercy Wangechi Maina (BPharm) P.O BOX 9424- 30100, Eldoret – Kenya Cell Phone Number: +254 720 281 275 Email: [email protected] Career Objective To advance health care locally and internationally through research, mentorship and the establishment of programs that address global health challenges. Current goal Improve patient care in resource limited settings through the practice of evidence- based medicine, research and precepting of students. Education background May 2014 – Jun 2014: Summer course: Clinical and Translational Writing Brown University, USA. Sept 2013 – Sept 2015: Masters in Global Health: Non communicable diseases University of Edinburgh, United Kingdom. Online Distance Learning Program. Jul 2011- Jun 2012: Global Health Pharmacy Residency Exchange Program Purdue University College of pharmacy, Moi Teaching and Referral Hospital (MTRH) and Academic Model Providing Access to Healthcare (AMPATH) Oct 2005-Nov 2009: Bachelor degree of Pharmacy, College of Pharmacy, University of Nairobi Work Experience Jul 2012 to present: Pharmacist, Pharmacovigilance, Moi Teaching and Referral Hospital – Academic Model Providing Access to Healthcare, Eldoret, Kenya Responsibilities Project coordinator for Antiretroviral Therapy (ART) pharmacovigilance studies Project coordinator for the Paper Analytical Device study Carrying out continuous education on adverse drug reaction monitoring Student precepting
52
Jul 2011 to Jun 2012: Resident, Global Pharmacy Residency Exchange Program, Moi Teaching and Referral Hospital - Academic Model Providing Access to Healthcare, Eldoret, Kenya Responsibilities: Assistant project coordinator for pharmacovigilance studies Student precepting Carrying out in-patient ward rounds Carrying out continuous medical education on various topics Dispensary and health center supervisory visits May 2011 to Jun 2011: Pharmacist, Kerugoya District Hospital, Kerugoya, Kenya. Responsibilities: Administrative pharmacy report writing Pharmacy consultancy services HIV clinic management Drug Procurement and Inventory control Apr 2011 to May 2011: Pharmacist, Kimbimbi Sub- District Hospital, Mwea, Kenya. Responsibilities: Pharmacy consultancy services Drug procurement and inventory control HIV Patient Support Centre management Sept 2010 to Mar 2011: Pharmacist Intern, Moi Teaching and Referral Hospital, Eldoret, Kenya Jun 2010 to Aug 2010: Pharmacist Intern, Laboratory and Allied Limited, Nairobi, Kenya. Feb 2010 to May 2010: Pharmacist Intern, Transwide Pharmaceuticals Limited, Nairobi, Kenya Residency experience May 2012 – Jul 2012: Ambulatory care I rotation: Anticoagulation and Primary Health Care. Preceptor: Imran Manji, Bpharm Apr 2012: USA residency experience rotation Preceptor: Monica Miller, PharmD, MS Ellen Shellhause, PharmD Mar 2012: Research month Preceptor: Rakhi Karwa, PharmD, BCPS Feb 2012: Ambulatory care II rotation (Chronic disease management) Preceptor: Sonak Pastakia, PharmD, MPH, BCPS Jan 2012: Pharmacy management rotation (AMPATH pharmacy)

53
Preceptor: Dr. Beatrice Jakait, Bpharm Dec 2011: Adult Internal Medicine ward coverage and research Preceptor: Dr. Gilbert Koech, Bpharm Nov 2011: Drug information center rotation Preceptor: Dr Celia Chema, BPharm Oct 2011: Maternal Health rotation (Riley Mother and Baby Hospital) Preceptor: Dr. Mercy Nabwire, BPharm Aug 2012 – Sept 2011: Adult and pediatric internal medicine (Nyayo wards) Preceptor: Dr. Gilbert Koech, Bpharm Teaching Experience Oct 2012: Facilitator for training on the pharmacovigilance study protocol, tools, and procedures. Jul 2012- present: Preceptor of Purdue – Kenya Global health pharmacy residents. Jul 2011- Oct 2012: Precepting of 40 of the 4th year Purdue University, College of Pharmacy students and 12 University of Nairobi students. Research Work Sept 2013 - present: Title: Assessment of the Tenofovir-related renal impairment in AMPATH. Jul 2012- present: Title: Impact of the Global Health pharmacy residency program. Dec 2011 – Jul 2013: Title: Building off the HIV platform: Extension of pharmacovigilance to the Tuberculosis population. Sept 2011- Jan 2012: Title: Assessment of the completeness of the indication for treatment change documentation at AMPATH center. Oct 2011 - present: Title: Optimization and validation of Paper Analytical Devices for rapid screening of antibiotics and artemisinin combination therapy tablets in Kenya. Jul 2011 – Dec 2013: Title: Pharmacovigilance in a Resource- constrained setting: Approaches to Targeted Spontaneous Reporting for Suspected Adverse Drug Reactions to antiretrovirals. Feb 2011 – May 2012: Title: Describing the effect of rifampicin in patients on concurrent warfarin therapy in western Kenya: a case series. Feb 2009 – Nov 2009: Title: The antibacterial and antifungal properties of Kenyan bee Propolis. Feb 2009: Title: A literature study on the common side effects of Anti retroviral drugs (ARVs) Grants July 2015: “Mobile HIV care & microfinance groups to improve HIV treatment outcomes in Kenya” R01 submitted to NIH. (awaiting response)

54
Jan 2015: “Integration of paper test cards in to pharmacovigilance system in Kenya” submitted to USAID Development Innovation Ventures. (pre-qualification stage) Oct 2014: “Collaboration of Students and HIV Peer Counselors to Promote Patient Education” submitted for the Purdue Service Learning Grant (Received) Mar 2013: “Expansion of the application of portable counterfeit and adherence detection in resource constrained settings” submitted to Lilly Seed Grant Fund. (Received) May 2012: “Establishing a drug information center in a resource constrained setting” submitted to Celgene Pharmaceutical, USA. (Received) April 2012: “Paper Analytical Device: a simple solution to counterfeit drugs” submitted to the Rising Stars Grand Challenges, Canada. Presentations Nov 2013: “Use of Paper Analytical Devices in Screening of Substandard drugs” at Hilton Hotel, Addis Ababa, Ethiopia. Nov 2013: “Pharmacovigilance in a Resource-Limited Setting: Approaches to Targeted Spontaneous Reporting for Suspected Adverse Drug Reactions to Antiretroviral Treatment” at Starling Hotel, Geneva, Switzerland. Aug 2013: “Clinical Pharmacy Internship Program at MTRH” at the University of Nairobi, College of Pharmacy. Aug 2012: “Global Health Pharmacy Residency Program and its impact: Concept adoption” during the 2012 Hospital Pharmacists Association of Kenya (HOPAK) symposium at Laico Regency, Nairobi. Aug 2012: “MTRH Internship Program” at the University of Nairobi, College of Pharmacy. Jun 2012: “Establishment of a Global Health Pharmacy Residency Program in Eldoret, Kenya” during the 2012 Annual Pharmaceutical Society of Kenya Symposium at White Sands Hotel, Mombasa. Apr 2012: “Descriptive evaluation of the effect of rifampicin in patients on concurrent warfarin therapy” at Great Lakes Conference in Purdue University, USA. Apr 2012: “Global Health Residency Program and Pharmacovigilance” at Celgene, New Jersey, USA. Feb 2012: “Tuberculosis” video presentation for Purdue University, College of Pharmacy. Aug 2011: “Hospital Internship program at MTRH” at University of Nairobi, College of Pharmacy. Mar 2011: “Safe Use of medication in Pregnancy” at Riley Mother and Baby Hospital, MTRH. Dec 2010: “Seizures in Pediatrics” at AMPATH main pharmacy, AMPATH center. Nov 2010: “Gestational Diabetes” at AMPATH main pharmacy, AMPATH center. Publications July 2015: Meeting the Public Health Needs of Underserved Patients in Western Kenya by Creating the Next Generation of Global Health Pharmacy Leaders. Monica Miller, Rakhi Karwa, Ellen Schellhase, Sonak Pastakia, Susie Crowe, Imran Manji, Beatrice Jakait and Mercy Maina. Published in American College of Clinical Pharmacy (submitted and awaiting publication) Nov 2013: Reframing the Focus of International Health Experiences. Sonak Patakia, Rakhi Karwa and Mercy Maina. Published in Pharmacy Times Health System Edition.

55
Sept 2013: Describing the profile of patients on concurrent rifampin and warfarin therapy in western Kenya: a case series. Maina MW ; Pastakia SD ; Manji I ; Kirui N ; Kirwa C ; Karwa R . Published in Drugs in R & D. Poster Paper Analytical Devices for Rapid Screening of Substandard or Falsified Medications in Western Kenya (American Society of Tropical Medicine and Health Poster Nov 2013) Mercy Maina, Sonak Pastakia, Rakhi Karwa, Celia Ngetich, Beatrice Jakait, Phelix Were, Emalee Kernisan, Emily Mediate, Nicholas Myers, Abigail Weaver and Marya Lieberman Paper Analytical Devices for the screening of substandard medications in western Kenya Mercy W. Maina, Abigail Weaver, Nick Myers, Celia Chema, Phelix Were, Rakhi Karwa, Sonak Pasakia and Marya Lieberman (American Society of Tropical Medicine and Health Poster Nov 2014) Professional Affiliations Jun 2012 - present: Member of the Hospital Pharmacists Association of Kenya. Nov 2011- present: Affiliate Instructor of pharmacy practice, Purdue University-College of Pharmacy Nov 2011- present: Member of Pharmaceutical Society of Kenya (PSK) Jul 2011- present: Registered pharmacist, Pharmacy and Poisons Board (PPB) Honors and Awards Feb 2014: Forgarty scholarship award Aug 2013: Commonwealth Scholarship Award Mar 2013: Corps Engagement award from Purdue University CURRICULUM VITAE PERSONAL DETAILS NAME : Phelix Makoto Were DATE OF BIRTH : 24th Sept.1986 GENDER : Male NATIONALITY : Kenyan ID: NUMBER : 24590943 LANGUAGE : Swahili, English CONTACT : +254723731239 EMAIL : [email protected] EDUCATIONAL BACKGROUND 1992-2000 Ebubaka Primary School 2001-2004 St. Kizito’s Secondary School

56
PROFESSIONAL BACKGROUND January 2006; - Modia Driving School – PASS (Class B, C & E) May 2006- November 2009:- Eldoret Polytechnic. Diploma in Pharmaceutical Technology. December 2009; - Computer packages – PASS March 2010; - Pharmacy and Poisons Board professional examinations Level One – PASS January 2011 – December 2011; - Mt. Kenya University Diploma in Business Management - Purchasing and Supplies. April 2011 – Pharmacy and Poisons Board professional examinations Level Two – Pass Enrolled by the Pharmacy and Poisons Board - Registration No. 3842 January 2014 (Ongoing) – Mt. Kenya University Bachelors in Business Management OTHER QUALIFICATION NASCOP: AMPATH TRAINING INSTITUTE Training on Comprehensive Care of HIV Infected Patient with Special Emphasis on Antiretroviral Therapy CITI: INDIANA UNIVERSITY – INDIANAPOLIS (ONLINE). -Training on Research Ethics Education -Biomedical Research, Stage 1 -Biomedical Responsible Conduct of Research, Basic Course -Good Clinical Practice, Stage 1 -Social/Behavioral Research, Stage 1 -Social and Behavioral Responsible Conduct of Research, Basic Course WORKING EXPERIENCE December 2004 – December 2005: Aldo Pharmaceuticals Ltd. : Pharmacy assistant. June 2008 – October 2008: Moi Teaching and Referral Hospital. : Attachment as a pharmaceutical technology student. May 2010 – Aug 2010 – Moi Teaching and Referral Hospital : Ampath/USAID programme – Intern of Pharmacy & Poisons Board August 2010 – December 2010 – Aldo Pharmaceuticals Ltd : Intern of Pharmacy and Poisons Board December 2010 – January 2011; Kainvestor Holdings : Research Assistant. August 2011 to June 2011; - Malibu Group of Companies : Eltons (City Centre) Pharmacy Ltd : Pharmaceutical Technologist In-Charge

57
July 2012 to date: - Ampath/USAID – Pharmacovigilance (PAD Project) : Project Coordinator. PERSONAL PROFILE: Team player, good interpersonal and communication skills, able to work well with people of various background and endowments. Able to work in a challenging environment, creative and offering room for career progression. Able to work within tight schedules and with minimum supervision and deliver results within short deadlines. An honest, smart and highly self-motivated individual with a high sense of responsibility. Ability to work and organize groups to focus positively in daily endeavors regardless of the challenge. Able to work independently with minimum supervision and goal oriented.

58
C. Investor Presentation (1 page info sheet)




















