Breastfeeding and Substance Use: Evidence-based Practices ...
Upload
independentCategory
view
0download
0
http://jhl.sagepub.com/Journal of Human Lactation
http://jhl.sagepub.com/content/27/3/250The online version of this article can be found at:
DOI: 10.1177/0890334411402998
2011 27: 250J Hum LactPippa L. Craig, Jennifer Knight, Elizabeth Comino, Vana Webster, Lisa Jackson Pulver and Elizabeth Harris
Initiation and Duration of Breastfeeding in an Aboriginal Community in South Western Sydney
Published by:
http://www.sagepublications.com
On behalf of:
International Lactation Consultant Association
can be found at:Journal of Human LactationAdditional services and information for
http://jhl.sagepub.com/cgi/alertsEmail Alerts:
http://jhl.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jhl.sagepub.com/content/27/3/250.refs.htmlCitations:
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Original Research
Journal of Human Lactation27(3) 250 –261© The Author(s) 2011Reprints and permission: http://www. sagepub.com/journalsPermissions.navDOI: 10.1177/0890334411402998http://jhl.sagepub.com
Initiation and Duration of Breastfeeding in an Aboriginal Community in South Western Sydney
Pippa L. Craig, PhD, MHPEd, BSc, Dip NutrDiet,1 Jennifer Knight, PhD, BA,1 Elizabeth Comino, PhD, MPH, BVSc, BSc,2 Vana Webster, BSc,2 Lisa Jackson Pulver, PhD, MPH,1 and Elizabeth Harris, MPH, BA, DipEd, DipSocWork2
Abstract
The Gudaga Study is a prospective, longitudinal birth cohort study of Australian urban Aboriginal children. Mothers of Aboriginal infants were recruited using a survey of all mothers admitted to the maternity ward of an outer urban hospital in Sydney. These data established initiation rates among Gudaga infants and those of non-Aboriginal infants born locally (64.7% and 75.2%, respectively) and factors associated with breastfeeding. Older (relative risk, 1.24; confidence interval, 1.01-1.44), more educated (relative risk, 1.30; confidence interval, 1.11-1.48) mothers who intended to breastfeed (relative risk, 2.22; confidence interval, 2.12-2.3) were more likely to breastfeed. Smokers (relative risk, 0.72) and mothers of Aboriginal infants (relative risk, 0.78) were less likely to initiate breastfeeding. Breastfeeding rates for Gudaga infants dropped rapidly, with 26.3% breastfeeding at 2 months. Local health services providers can benefit from such information as they target relevant prenatal, perinatal, and postnatal services for Aboriginal mothers and their infants.
Keywords
Aboriginal; Australia; breastfeeding initiation; breastfeeding duration
There is substantial evidence for the nutritional and health benefits of breastfeeding,1 including protection against aller-gic diseases, gastrointestinal infection, and respiratory and ear infections.1-8 There is also evidence that breast milk has a posi-tive effect on cognitive development and provides immune protection.6,9 Compared with no breastfeeding, fully breast-fed infants had less illness and fewer doctor’s visits; the higher the proportion of feeds from human milk the lower the incidence of infection,1,3 with even some breastfeeding being advantageous.10 There is now mounting evidence of long-term benefits of breastfeeding on noncommunicable dis-ease risk factors.11-13
National and international organizations strongly recom-mend exclusive breastfeeding until 6 months of age.4,6,14-16 Australia recently released a National Breastfeeding Strat-egy17 that recommends initiation rate in excess of 90%, with 80% of mothers still breastfeeding at 6 months.6 However, initiation and duration of breastfeeding in Australia remain below the stated goals,18 with 87% ever breastfed, 54% breastfed at 6 months, and only 16% still exclusively breast-feeding at 6 months in the state of New South Wales (NSW).19 Similar results were found in other recent Australian studies.20,21
Within the Australian Aboriginal population, breastfeed-ing rates differ between reports, between states, and between
geographic locations. Higher breastfeeding initiation rates were found among Aboriginal women in rural and remote communities than in urban settings.2,22-24 The Perth (Western Australia) Aboriginal Breastfeeding Study25 reported higher rates of breastfeeding at discharge among Aboriginal (89.4%) than among non-Aboriginal (83.8%) mothers. However, at the national level, when compared to non-Aboriginal infants, fewer Aboriginal infants were breastfed (79% compared with 88% of non-Aboriginal infants) and for a shorter time.26
During the 1990s studies on breastfeeding habits in Western Australia9,27,28 identified factors predicting initiation, dura-tion, and reasons for stopping breastfeeding. The authors con-cluded that psychological factors (attitudes of partner and maternal grandmother, mother’s decision to breastfeed) were
Received for publication September 14, 2010; Accepted for publication February 7, 2011.
1University of New South Wales, Australia; Gudaga Project2Centre for Health Equity Training Research & Evaluation; Gudaga Project.
Corresponding Author:Pippa L. Craig, Visiting Fellow, Muru Marri Indigenous Health Unit, School of Public Health & Community Medicine, University of New South Wales, NSW, 2052, AustraliaE-mail: [email protected].
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 251
more important than were sociodemographic and biomedical factors.27,28 These studies have served as a useful model for subsequent Australian studies.
Although some of the variation may be owing to method-ological differences, these previous studies suggest that local factors affect initiation and duration of breastfeeding among Aboriginal infants, particularly in urban populations.
Gudaga StudyThe Gudaga Study is a prospective, longitudinal birth cohort study describing the health, development, and health service use of Aboriginal children from birth to 5 years in South Western (SW) Sydney in the state of NSW. It is the first study of its kind to be conducted on the east coast of Australia and provides a unique opportunity to describe the breastfeeding practices of mothers of Aboriginal infants living in an urban setting.
This research explores the initiation rates of breastfeeding among Gudaga infants compared with those of other infants born locally, the factors associated with initiation of breast-feeding and with breastfeeding at 2 to 3 weeks, and the dura-tion of breastfeeding among Gudaga infants.
MethodsThe study comprises 2 sections, the first on breastfeeding initiation and the second concerned with duration of breastfeeding.
Initiation of BreastfeedingData collection. A total of 2100 mothers admitted to the
maternity ward of the recruitment hospital between October 2005 and May 2007 completed a brief survey. During the course of the survey, those mothers identifying either them-selves or their infants’ fathers as Aboriginal were invited to participate in the Gudaga Study (n = 159). Further informa-tion about the process of establishing the Gudaga birth cohort has been described elsewhere.29
For all mothers participating in the ward survey, routinely collected administrative data on antenatal care and obstetrics history were extracted from electronic medical records main-tained by the health service. Deterministic linkage, based on the mothers’ and infants’ medical record numbers and infant date of birth, successfully linked 2047 cases (97.5%). Of these, 1928 had complete information about feeding status at delivery and at discharge and have been included in the anal-ysis. More detail on the obstetrics data collection and the extraction process is available elsewhere.29
Study factors and outcome variables. Routinely collected data provided information on a number of variables potentially associated with rates of breastfeeding at hospital discharge. Study factors explored included demographic (Aboriginality
of infant, maternal age, marital status) and socioeco-nomic factors (Socio-economic Indexes for Areas [SEIFA] quintile of residence, maternal employment status before birth, maternal education level), maternal factors (smoking, late antenatal care, parity), psychosocial factors (intention to breastfeed, has help when first home from hospital, Edinburgh Depression Scale score), delivery factors (spon-taneity of labor, vaginal delivery, length of gestation, infant birth weight, admittance to special care nursery), and gen-der of infant.
For the purposes of this study, the variable “initiation of breastfeeding” included all those who breastfed at either delivery or discharge as recorded in routinely collected hos-pital data.
Statistical analysis. Data were analyzed using the Statistical Package for Social Sciences (SPSS for Windows version 17, SPSS Inc, Chicago, Illinois). Breastfeeding initiation among mothers of Aboriginal infants and mothers of non-Aboriginal infants was compared using a c2 test. Descriptive statistics using the linked data collection tables were used initially to identify frequency of study factors.
Unadjusted relative risk (RR) was calculated to examine factors associated with breastfeeding at discharge from hospi-tal. Variables with significant unadjusted RRs were included in a multivariate logistic regression analysis. As the outcome variable breastfeeding at discharge was not a rare event, the odds ratios and 95% confidence intervals from this analysis were adjusted to RR as outlined in Zhang and Yu (1998).30 Interaction effects between infant’s Aboriginality and mater-nal age, infant’s Aboriginality and antenatal smoking, and infant’s Aboriginality and most disadvantaged SEIFA (an index of relative socioeconomic disadvantage31) quintile were explored.
Duration of BreastfeedingData collection. Duration data were only collected for
Gudaga mothers for whom information on feeding practices in hospital and at discharge was available. This baseline infor-mation was not available for 4 of the 159 recruited Gudaga mothers. Additional information on breastfeeding duration was gathered from these mothers by questionnaire during home visits when their infants were 2 to 3 weeks, 6 months, and 12 months of age. If breastfeeding had ceased at a par-ticular data collection point, mothers were asked to report when this had occurred. These data were then used to con-struct breastfeeding duration rates. Reasons for choosing to breastfeed, not initiating breastfeeding, or stopping breast-feeding were explored in the 6-month survey.
Study factors and outcome variables. Routinely collected data provided information on a number of variables potentially associated with rates of breastfeeding duration. Study factors explored included demographic and socioeconomic fac-tors, maternal factors, psychosocial factors, and delivery
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

252 Journal of Human Lactation 27(3)
factors. Study factors examined to explore predictors of breastfeeding at 2 to 3 weeks for Gudaga mothers were the same as the predictors used in the initiation analysis, except:
• As all Gudaga infants were Aboriginal infants, mother’s Aboriginality status was used instead of infant’s Aboriginality status.
• Because of the smaller sample size, mothers’ age, SEIFA quintiles, and birth weight were converted to dichotomous variables.
• As only 4 Gudaga mothers indicated that they would not have help when first home from hospital, this variable was removed from the analysis.
The study used 3 outcome variables to explore duration of breastfeeding:
1. Feeding practices over time. Definitions adopted for the National Breastfeeding Strategy17 guided the breastfeeding questions for the Gudaga surveys (see Table 1).
2. Number of weeks breastfed was calculated from the reported length of time for which an infant was exclusively, predominantly, or partially breastfed. Survival graphs of these data, data from the whole state of NSW and from the South Western Sydney Area Health Service (the location of the Gudaga Study), were generated using Cox regression anal-yses.36 Gudaga mothers who were still breastfeed-ing when lost to follow-up before 12 months were included in the survival graph as censored par-ticipants at the last point they were known to be breastfeeding.
3. Exclusive, predominant, and partial breastfeeding at 2 to 3 weeks was used as the outcome measure for analyzing predictors of duration in the Gudaga mothers.
At the 6 months home visit, participating mothers were asked an open-ended question about their infant feeding practices. Those mothers who were still breastfeeding were asked the reason they chose to breastfeed their infants. Mothers who had initiated breastfeeding but who had stopped by 6 months were asked the reason they stopped breastfeeding, and those mothers who had never breastfed their infants were asked the reasons for choosing not to breastfeed. The open-ended responses were grouped into 2 broad categories: baby-centered reasons and mother-centered reasons. Using Binns’ classification method,32 responses referring to the infant were classified as baby-centered, whereas responses referring to the mother were classified as mother-centered.
Statistical analysis. Data were analyzed using the Statistical Package for Social Sciences (SPSS for Windows version 17; SPSS Inc). Univariate statistics were used to explore the associations between study factors and breastfeeding for the 100 women who initiated breastfeeding and participated in the Gudaga Study at the 2- to 3-week survey point.
Ethical ConsiderationsThe study was approved by the NSW Aboriginal Health and Medical Research Council and Sydney South West Area Health Service Human Research Ethics Committees. The research was undertaken in accordance with national guide-lines for research within indigenous communities.33,34 These strategies have been described in a previous article.35 Signed
Table 1. Definitions of Breastfeeding
Definitions of Breastfed Used in AustraliaaDefinitions of Breastfed Used in Gudaga Surveys
Exclusively breastfed
Only breast milk or expressed breast milk; no other liquids or solids with the exception of drops or syrups consisting of vitamin or mineral supplements or medicines
Only with breast milk (note: medicines, vitamin or mineral supplements allowed)
Fully breastfed Breast milk as main source of nourishment (includes exclusively breastfed plus predominantly breastfed categories)
As above but may have water or juice but no food-based fluidsPredominantly
breastfed Breast milk as predominant source of nourishment but may also receive
water, water-based drinks, fruit juice, oral rehydration solution, drops or syrups consisting of vitamin or mineral supplements or medicines, and ritual fluids (in limited quantities); all other food-based fluids are excluded, particularly nonhuman milk
Partial breastfeeding
Receives both breast milk and solid or semisolid (including any food or liquid including nonhuman milk)
Breast milk plus breast milk substitutes/nonhuman milk
Not breastfed Only breast milk substitutes Formula (bottle) feedingEver breastfed Has ever been put to the breast, if only once, and/or has received expressed
breast milkAny breastfeeding, no matter
how brief
aSee the Australian Health Ministers’ Conference (2009).17
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 253
informed consent (including permission to extract routinely collected hospital data) was obtained from all the mothers of Aboriginal infants participating in the Gudaga Study.
ResultsInitiation of Breastfeeding
Among the mothers of Aboriginal infants, 64.7% (n = 112) initiated breastfeeding compared with 75.2% (n = 1319) of mothers of non-Aboriginal infants born at the recruitment hospital (χ2
1 = 8.9, P = .003).Factors associated with breastfeeding at discharge from hospital.
Factors that were associated with breastfeeding among all the infants born at recruitment hospital are reported in Table 2. The univariate analysis identified a number of sociodemo-graphic and psychosocial factors that were significantly associated with breastfeeding. Age, being married or in a de facto relationship, SEIFA index, previous employment, edu-cation, and intention to breastfeed were positively associated; Aboriginality, smoking, late commencement of antenatal care, multiparity, and having help when first home from hospital were negatively associated with breastfeeding. Many of the sociodemographic factors dropped out of the equation during the multiple logistic regression analysis, leaving 3 indepen-dent risk factors predicting increased likelihood to breastfeed at discharge: mothers older than 25 years, those who had completed 10 years of education, and intention to breast-feed. Two risk factors predicting decreased likelihood to breastfeed at discharge were still significant: being a mother of an Aboriginal infant antenatally.
We observed a significant interaction between infant Aboriginality and maternal antenatal smoking. These results indicated that smoking had less of an impact on breastfeed-ing behavior for mothers of Aboriginal infants than for moth-ers of non-Aboriginal infants.
Duration of BreastfeedingFeeding practices of the Gudaga infants over time are found in Table 3. Twenty mothers (12.9%) who initiated breast-feeding in hospital were no longer breastfeeding when dis-charged. By 2 to 3 weeks after birth, a further 22 mothers had ceased breastfeeding. By 6 months, about 15% of mothers who initiated breastfeeding continued to breastfeed their infants fully or partially.
Overall, the median duration of breastfeeding among the 72 mothers who were feeding at discharge (and were not lost to follow-up before stopping breastfeeding) was 8 weeks. Duration of breastfeeding for Gudaga infants as well as for infants in NSW and in SW Sydney is found in Figure 1. The immediate drop among the Gudaga mothers is a reflection of the low initiation rates of mothers of Aboriginal infants described above. Among Gudaga mothers who initiated, there
is a substantial drop in breastfeeding within the first 2 weeks (approximately 18% of mothers giving up in this time period). Up until 2 months, these mothers continue to stop breastfeeding at a greater rate than both comparison groups. After this point, the Gudaga mothers show a similar pattern to the NSW and South Western Sydney Area Health Service mothers.
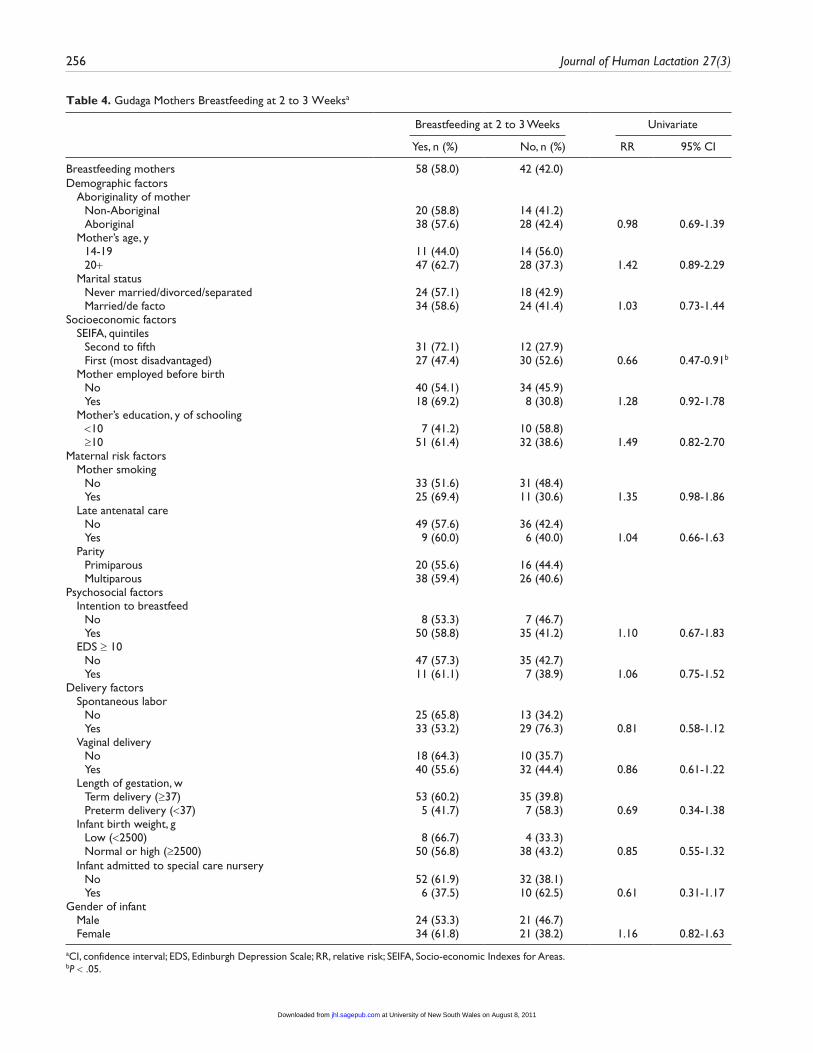
Factors that predict breastfeeding at 2 to 3 weeks. Table 4 lists the univariate associations for factors that may have influenced breastfeeding of Gudaga infants at the 2- to 3-week data collection point for mothers who initiated breastfeeding. Residing in a suburb in the most disadvan-taged SEIFA quintile decreased likelihood to breastfeed at 2 to 3 weeks.
Reasons for and against breastfeeding. At the 6-month inter-view, the Gudaga mothers were asked why they chose to, or not to, breastfeed their infants. The majority of responses from the 13 mothers who were breastfeeding at this time were mother-centered, reflecting confidence in the mother’s ability to breastfeed and a commitment to its benefits (Table 5). Most commonly cited reasons for not breastfeeding were mother-centered, with mothers stating they had formula fed their previous children and/or had experienced breast or feed-ing problems.
At this same interview, those mothers who had switched from breastfeeding to formula feeding were asked their rea-sons (Table 6). The majority of reasons for switching were mother-centered, with low milk production, anxiety over milk supply, and a range of breast and feeding problems the most commonly cited reasons. Many of the reasons for switching were similar to those given by mothers not initiating breast-feeding at birth: difficulties with breastfeeding, convenience/ease, and smoking.
DiscussionThis study has confirmed that more educated mothers of Australian Aboriginal infants in an outer urban environment were more likely to breastfeed. To this, it has added that intending to breastfeed and having confidence in their ability to do so are even more important. Conversely, younger, less educated mothers who smoked and did not intend to breast-feed were less likely to do so.
Initiation of BreastfeedingReported initiation of breastfeeding rates of 64.7% (Aborigi-nal infants) and 75.2% (non-Aboriginal infants) were well below the Australian targets of more than 90%6 and below the rates reported in other studies among Australian Aboriginal communities of between 84.5% and 89.4%.2,23,25 Although some of these differences can be explained by the inclusion of some mothers from rural and remote communities (noted for higher breastfeeding rates) in the Western Australian
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

254 Journal of Human Lactation 27(3)
Table 2. Mothers Breastfeeding at Discharge From the Recruitment Hospital (Corrected)a
Breastfeeding at Discharge Univariate Multivariate
Yes, n (%) No, n (%) RR 95% CI RR 95% CI
Total breastfeeding at discharge 1368 (71.0) 560 (29.0)Demographic factors Aboriginality of infant
Non-Aboriginal 1276 (72.7) 479 (27.3) Aboriginal 92 (53.2) 81 (46.8) 0.73 0.63-0.84d 0.78 0.62-0.93c
Mother’s age, y 14-19 69 (52.7) 62 (47.3) 20-24 271 (65.3) 144 (34.7) 1.24 1.03-1.48b 1.14 0.91-1.35 25-29 432 (72.4) 165 (27.6) 1.37 1.16–1.63d 1.24 1.01-1.44b
≥30 596 (75.9) 189 (24.1) 1.44 1.22-1.70d 1.30 1.07-1.49b
Marital status Never married/divorced/separated 198 (57.1) 149 (42.9) Married/de facto 1170 (74.0) 411 (26.0) 1.30 1.18-1.43d 1.06 0.93-1.18
Socioeconomic factors SEIFA, quintile
Fifth 146 (82.0) 32 (18.0) Fourth 235 (79.1) 62 (20.9) 0.97 0.88-1.06 1.03 0.93-1.1 Third 228 (73.8) 81 (26.2) 0.90 0.82-0.99b 0.98 0.87-1.06 Second 323 (70.7) 134 (29.3) 0.86 0.79-0.94c 0.98 0.88-1.06 First (most disadvantaged) 436 (63.5) 251 (36.5) 0.77 0.71-0.84d 0.98 0.88-1.06
Mother employed before birth No 708 (65.0) 382 (35.0) Yes 660 (78.8) 178 (21.2) 1.21 1.15-1.28d 1.05 0.95-1.14
Mother’s education, y of schooling <10 93 (46.5) 107 (53.5) ≥10 1275 (73.8) 453 (26.2) 1.59 1.36-1.85d 1.30 1.11-1.48c
Maternal risk factors Mother smoking
No 1168 (75.7) 375 (24.3) Yes 200 (51.9) 185 (48.1) 0.69 0.62-0.76d 0.72 0.62-0.82d
Late antenatal care No 1167 (72.4) 445 (27.6) >20 weeks’ gestation 201 (63.6) 115 (36.4) 0.88 0.80-0.96c 0.97 0.88-1.01
Parity Primiparous 515 (74.6) 175 (25.4)
Multiparous 853 (68.9) 385 (31.1) 0.92 0.87-0.98c 0.94 0.86-1.02Psychosocial factors Intention to breastfeed
No 209 (37.8) 344 (62.2) Yes 1158 (84.3) 216 (15.7) 2.23 2.00-2.49d 2.22 2.12-2.3d
Has help when first home No/not sure 55 (85.9) 9 (14.1) Yes 1313 (70.4) 551 (29.6) 0.82 0.74-0.91b 0.86 0.65-1.00
EDS ≥ 10 No 1157 (71.0) 472 (29.0) Yes 211 (70.6) 88 (29.4) 0.99 0.92-1.08
Interaction Aboriginality of infant by smoking 1.38 1.05-1.62b
Delivery factors Spontaneous labor
No 617 (70.0) 265 (30.0) Yes 751 (71.8) 295 (28.2) 1.03 0.97-1.09
Vaginal delivery No 420 (71.3) 169 (28.6) Yes 947 (70.8) 391 (29.2) 0.98 0.92-1.04
(continued)
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 255
Table 2. (continued)
Breastfeeding at Discharge Univariate Multivariate
Yes, n (%) No, n (%) RR 95% CI RR 95% CI
Length of gestation, w Term delivery (≥37) 1307 (71.1) 28 (31.5) Preterm delivery (<37) 61 (68.5) 532 (28.9) 0.96 0.90-1.20
Infant birth weight, g Low (<2500) 56 (75.7) 18 (24.3) 1.07 0.94-1.22 Normal (≥2500-3999) 1125 (70.5) 470 (29.5) High (≥4000) 187 (72.2) 72 (27.8) 1.02 0.94-1.11
Infant admitted to special care nursery No 1205 (71.2) 488 (28.8) Yes 163 (69.4) 72 (30.6) 0.97 0.89-1.07
Gender of infant Male 724 (72.9) 269 (27.1) Female 644 (68.9) 291 (31.1) 0.94 0.89-1.00
aCI, confidence interval; EDS, Edinburgh Depression Scale; RR, relative risk; SEIFA, Socio-economic Indexes for Areas.bP < .05.cP < .01.dP < .001.
Table 3. Feeding Practices Among Gudaga Infants (n = 155) Over Time
Discharge 2-3 Weeks 6 Months 12 Months
Infants exclusively breastfed (only breast)83 (53.5%)
14 (9.0%)Infants fully breastfed (may have dummy or water/juice) 19 (12.3%) 7 (4.5%) 1 (0.6%)Infants partially breastfed (in addition to formula feeding) 25 (16.1%) 8 (5.2%) 2 (1.3%)No longer breastfeeding 20 (12.9%) 42 (27.1%) 75 (48.4%) 86 (55.5%)Lost to follow-up 3 (1.9%) 13 (8.4%) 14 (9.0%)Never breastfed 52 (33.5%) 52 (33.5%) 52 (33.5%) 52 (33.5%)
0 4 8 12 16 20 24 28 32 36 40 44 48 520
20
40
60
80
100
Gudaga mothers
NSWb mothers35
SWSAHSa mothers35
Weeks
Perc
ent s
urvi
val
Figure 1. Breastfeeding duration among Gudaga mothers compared with rates for the SW Sydney area and all NSW infants.aMothers of children born in a South West (SW) Sydney Area Health Service region of the state of New South Wales (NSW).bMothers of children born in the state of NSW.
cohorts,23,25 it does not explain the lower rates compared with other urban Aboriginal communities.2
South Western Sydney is an area of disadvantage, and lower rates of breastfeeding have been reported among
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from
256 Journal of Human Lactation 27(3)
Table 4. Gudaga Mothers Breastfeeding at 2 to 3 Weeksa
Breastfeeding at 2 to 3 Weeks Univariate
Yes, n (%) No, n (%) RR 95% CI
Breastfeeding mothers 58 (58.0) 42 (42.0)Demographic factors Aboriginality of mother
Non-Aboriginal 20 (58.8) 14 (41.2) Aboriginal 38 (57.6) 28 (42.4) 0.98 0.69-1.39
Mother’s age, y 14-19 11 (44.0) 14 (56.0) 20+ 47 (62.7) 28 (37.3) 1.42 0.89-2.29
Marital status Never married/divorced/separated 24 (57.1) 18 (42.9) Married/de facto 34 (58.6) 24 (41.4) 1.03 0.73-1.44
Socioeconomic factors SEIFA, quintiles
Second to fifth 31 (72.1) 12 (27.9) First (most disadvantaged) 27 (47.4) 30 (52.6) 0.66 0.47-0.91b
Mother employed before birth No 40 (54.1) 34 (45.9) Yes 18 (69.2) 8 (30.8) 1.28 0.92-1.78
Mother’s education, y of schooling <10 7 (41.2) 10 (58.8) ≥10 51 (61.4) 32 (38.6) 1.49 0.82-2.70
Maternal risk factors Mother smoking
No 33 (51.6) 31 (48.4) Yes 25 (69.4) 11 (30.6) 1.35 0.98-1.86
Late antenatal care No 49 (57.6) 36 (42.4) Yes 9 (60.0) 6 (40.0) 1.04 0.66-1.63
Parity Primiparous 20 (55.6) 16 (44.4) Multiparous 38 (59.4) 26 (40.6)
Psychosocial factors Intention to breastfeed
No 8 (53.3) 7 (46.7) Yes 50 (58.8) 35 (41.2) 1.10 0.67-1.83
EDS ≥ 10 No 47 (57.3) 35 (42.7) Yes 11 (61.1) 7 (38.9) 1.06 0.75-1.52
Delivery factors Spontaneous labor
No 25 (65.8) 13 (34.2) Yes 33 (53.2) 29 (76.3) 0.81 0.58-1.12
Vaginal delivery No 18 (64.3) 10 (35.7) Yes 40 (55.6) 32 (44.4) 0.86 0.61-1.22
Length of gestation, w Term delivery (≥37) 53 (60.2) 35 (39.8) Preterm delivery (<37) 5 (41.7) 7 (58.3) 0.69 0.34-1.38
Infant birth weight, g Low (<2500) 8 (66.7) 4 (33.3) Normal or high (≥2500) 50 (56.8) 38 (43.2) 0.85 0.55-1.32
Infant admitted to special care nursery No 52 (61.9) 32 (38.1) Yes 6 (37.5) 10 (62.5) 0.61 0.31-1.17
Gender of infant Male 24 (53.3) 21 (46.7) Female 34 (61.8) 21 (38.2) 1.16 0.82-1.63
aCI, confidence interval; EDS, Edinburgh Depression Scale; RR, relative risk; SEIFA, Socio-economic Indexes for Areas.bP < .05.
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 257
Table 5. Reasons for Initiating Breastfeeding or Feeding Infant Formula From Birth
n %a
Reasons for breastfeeding (n = 13) Healthier for baby 6 46.1 Mother’s personal preference 6 46.1 Convenience/ease 5 38.5 Cost 4 30.8 Breastfed previous children 4 30.8 Breastfeeding is natural 2 15.4Reasons for not breastfeeding (n = 46) Breast- or feeding-related problems 13 28.3 Bottle-fed previous children 11 23.9 Personal preference 9 19.6 Found breastfeeding difficult/hard/frustrating 6 13.0 Convenience/ease 6 13.0 Mother uncomfortable/embarrassed to breastfeed 4 8.7 Mother’s health 2 4.3 Lack of support 1 2.2 Mother smoking 1 2.2 Concern over quantity of milk 1 2.2 Mother perceived baby to be too big to breastfeed 1 2.2 Infant health reasons 1 2.2
aPercentages may add up to more than 100 as some respondents gave multiple responses.
Table 6. Reasons for Terminating Breastfeeding (n = 54)
n %a
Stopped producing milk 14 25.9Anxiety over milk supply 13 24.1Breast- or feeding-related problems 12 22.2Infant health reasons 6 11.1Maternal tiredness or health/stress problems 6 11.1Convenience/ease 4 7.4Return to work 3 5.6Found breastfeeding difficult/hard/frustrating 3 5.6Mother smoking 1 1.9
aPercentages may add up to more than 100 as some respondents gave multiple responses.
women from lower socioeconomic status,37 although in our population it was mother’s age and education that remained important (Table 2). Although some of the Gudaga mothers were from disadvantaged backgrounds (Table 4 shows those in the lowest SEIFA quintile as less likely to continue with breastfeeding), this by no means applied to all in the Gudaga cohort.
Our study confirmed the association between a number of socioeconomic factors and the initiation of breastfeeding: an indication of a community at risk. The fact that younger, less educated mothers who smoked were less likely to breastfeed has been found previously.27,32,38
The association between smoking and breastfeeding rates differed between Aboriginal and non-Aboriginal mothers and was consistent with the findings of the Perth Aboriginal Breastfeeding Study.39 Smoking may not be as important a consideration when Aboriginal women decide to breastfeed than with other women. On the contrary, Glover et al identi-fied smoking as a significant barrier to breastfeeding among Maori in New Zealand.7
Given the significance of intention to breastfeed, it is inter-esting to consider whether this factor is amenable to influence. Presence of a supportive partner; attitude of maternal grand-mother, friends, and members of the extended family towards breastfeeding; together with prenatal class attendance and professional support have all been found to be significant potential drivers for developing a positive attitude towards breastfeeding.7,32,38 Lack of adequate antenatal/postnatal support services, lack of trained staff (such as lactation con-sultants), and lack of knowledge about where to go or whom to call when breastfeeding problems arise have been identi-fied previously as issues for the Aboriginal community in SW Sydney.40
Duration of BreastfeedingIt was only possible to undertake a meaningful analysis of the factors associated with breastfeeding in the early stages of follow-up due to the rapid decrease in breastfeeding rates.
Approximately 20% of those who initiated breastfeeding were no longer doing so after 2 weeks, and a further 20% had ceased by 4 weeks. It took another 4 weeks before the next 20% stopped breastfeeding. By comparison, of the 85% of the Aboriginal mothers in metropolitan Melbourne who com-menced breastfeeding, less than 10% stopped within the first week, with a further 6% stopping within 4 weeks. Only 15% of Gudaga infants were still being breastfed at 6 months, compared with 32% of the Melbourne infants.2 These differ-ences are supported by data from the Western Australian Aboriginal Child Health Survey23 and nationally.22 A rapid decline in breastfeeding rates was also evident for other SW Sydney infants when compared with infants across the state of NSW (Figure 1). Routinely collected data of breastfeed-ing rates in SW Sydney at first visit (mean age, 2 weeks), although not directly comparable with our results, found that nearly 60% of infants were breastfed,41 compared with approx-imately 40% of the Gudaga infants at the 2- to 3-week visit. However, these researchers explored only sociodemographic and biomedical factors, and it may be that psychological fac-tors are more important.27,28
No Gudaga infants were exclusively breastfed at 6 months compared with 15% at 5 months in South East Queensland and 16% at 6 months in NSW.19,20 New Zealand authors were concerned that only 10% of Maori mothers were exclusively breastfeeding by 6 months,7 yet our results were far lower.
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

258 Journal of Human Lactation 27(3)
This is of particular concern in this population, given the nutri-tional, immunological, psychological, and economic benefits of breastfeeding.
The rapid decrease in breastfeeding rates suggests either a lack of commitment or lack of support to assist new mothers with any early difficulties with breastfeeding. New mothers are seldom aware of the type and extent of problems likely to face women attempting to breastfeed.32 Inadequate support and lack of awareness of where to find assistance have already been noted.40 Practical advice on breastfeeding is readily avail-able in Australia,42-44 but mothers need to be aware of these organizations and to be proactive in seeking advice. More-over, not all Aboriginal families in SW Sydney have easy access to a telephone.45 Mothers engaging late with antenatal services may receive insufficient information and advice on breastfeeding or feel unnecessarily pressured to breastfeed without adequately exploring the benefits and barriers for themselves. An urban-based New Zealand study of Maori mothers and their extended families cited inadequate antena-tal education and support, lack of culturally appropriate educa-tion material, dissatisfaction with lactation advice in hospital, and lack of culturally relevant breastfeeding support as bar-riers to breastfeeding.7
Reasons for BreastfeedingOur results showed that reasons for breastfeeding were expressed in terms of benefits (such as cost and health of baby), confidence, and commitment. On the other hand, reasons given for terminating breastfeeding or not choosing to breastfeed were expressed as anxiety, indifference, or lower priority. Reasons volunteered for terminating breastfeeding by 2 to 3 weeks indicated commonly encountered problems such as how to facilitate breast attachment and increase milk supply (difficulties often encountered during early stages of breast-feeding38,43), implying a lack of readily available support when most needed. By the time the infants reached 6 months, most of the reasons given for terminating breastfeeding or not breastfeeding were due to lack of interest from either infants or their mothers or a preference for the bottle (infant formula), with fewer attributed to feeding problems. This suggests that the first few weeks after birth are a critical time for making an impact on duration of breastfeeding.46
Strengths and Limitations of the StudyThe strengths of this study were its longitudinal nature and the availability of a comparison group of mothers and their infants regarding breastfeeding initiation. The 2001 NSW Child Health Survey was used as a source for the duration of breast-feeding in Figure 1. The 2004 survey, although providing more recent data, was based on larger, amalgamated health areas that were less comparable than the more localized SW Sydney data used in the 2001 survey.
The study was limited by the extent and format of the data routinely collected by the health services. We were unable to explore the finer details about breastfeeding commencement and cessation at hospital and the type of feeding (eg, comple-mentary) in hospital due to inconsistencies in the hospital data. Whether a mother has ever breastfed her infant is critically important information for longitudinal tracking of the breast-feeding experience. It has been recommended that breast-feeding questions assess breastfeeding exclusivity during the in-hospital stay of the mothers in preference to using the term at discharge.47 Such data would be invaluable for assessing efforts made by hospitals to provide lactation support and promote breastfeeding and for monitoring progress towards improving breastfeeding practices in Australia.
There is no doubt that we did not identify all the relevant factors that influence whether a Gudaga mother initiated or continued to breastfeed. Asking mothers directly about their choice went some way towards addressing this deficit. Lim-iting these questions to the 6-month interview was necessi-tated by the fact that the breastfeeding questions were among many others posed to mothers about care of their children at each interview.
Promoting Breastfeeding of Aboriginal Infants in Outer Metropolitan SydneyIt was the intention to breastfeed and mother’s age and years of schooling that proved to be the most significant factors associated with initiating breastfeeding for Gudaga mothers, whereas those in the lowest SEIFA quintile were less likely to continue. Although this finding is not surprising, a number of aspects of this study suggest a response specifically targeting this population.
Interventions that promote the initiation and duration of breastfeeding include developing skills among mothers; ensuring that the health services enable and facilitate breast-feeding, in particular by providing guidance in hospital; and ensuring continued postnatal support.48 To be effective, this education and support should be face-to-face, intensive, and long-term. Peer support is particularly effective when offered in addition to, rather than as a substitute for, professional support.48 A randomized control trial demonstrated a signifi-cant effect on both initiation and duration could be achieved by providing lactation and postnatal breastfeeding support.5
Families First, an early intervention and prevention program in the state of NSW, offers a home visit to every family with a new baby within 2 weeks of the birth.49 Although a positive start, it may be necessary to provide more assistance to these new mothers through the early stages of breastfeeding. The majority (86%) of the Gudaga mothers still breastfeeding at the 2- to 3-week visit intended to breastfeed. One can only speculate that more may have persevered past these ini-tial, sometimes challenging weeks if practical and culturally appropriate support had been available. The lower rate of
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 259
breastfeeding among non-Aboriginal infants born at the hospital supports this conjecture.
Successful approaches in rural areas may provide some new directions. The Strong Women, Strong Infants, Strong Culture Program in Northern Australia is a community-based intervention in which senior Aboriginal women supported younger women during pregnancy.50 Senior Aboriginal women hold positions of respect in Aboriginal communities, know community members well, and are able to provide support when asked.
Younger mothers in the community who have successfully breastfed are also likely to be known to the pregnant women and can act as role models and engage prospective mothers earlier in their pregnancies. Promoting and supporting breast-feeding across the prenatal, perinatal, and postnatal contin-uum may help maintain breastfeeding levels. Resolve and reinforcement are required to overcome early hurdles and persist with breastfeeding.7 Providing culturally appropriate and practical information at an earlier stage gives pregnant women the opportunity to consider the benefits of breastfeed-ing for both baby and mother and to explore ways to address the barriers. Community members are in the best position to offer continuing support, providing additional professional assistance is also available as required.
Pertinent advice and support from trusted sources, deliv-ered in a culturally appropriate and timely manner, were criti-cal to Maori women and their extended families in New Zealand. Aboriginal mothers are no more likely to access mainstream breastfeeding support organizations than were their Maori sisters,40 given that Aboriginal women access antenatal care later and less frequently than do other women.22 The Maori mothers acknowledged that there is “a lot to learn” about successful breastfeeding and that “you need to start early.”7 Culturally appropriate advice and guidelines before, during, and after birth are as relevant for Aboriginal mothers in SW Sydney.
ConclusionThis study provides ample evidence on the need for raising initiation and duration rates of breastfeeding among mothers of urban Aboriginal infants. Success will require a systematic and sustained approach. Our findings indicate that interven-tions should begin early and aim to build supportive networks to target relevant prenatal, perinatal, and postnatal services in the Aboriginal community in SW Sydney.
AcknowledgmentThe authors gratefully acknowledge the Tharawal people of SW Syd-ney and extend thanks for their encouragement and enthusiastic sup-port of this research. We also thank the mothers who participated in this project, for without their willingness to be involved this study would not be possible. The support of the Tharawal Aboriginal Corpo-ration, Sydney South West Area Health Service, the University of New
South Wales, and the NSW Aboriginal Health and Medical Research Council is also acknowledged. Funding to support the research was received from the National Health and Medical Research Council. The Gudaga research team comprises A/Prof Elizabeth Comino, Dr Pippa Craig, Elizabeth Harris, Prof Mark Harris, Prof Richard Henry, A/Prof Dennis McDermott, Alison Derrett, Prof Lisa Jackson Pulver, Dr Bin Jalaludin, Brendon Kelaher, Dr Jenny McDonald, Sharon Nicholson, Darryl Wright, Dr Jennifer Knight (project manager), Cheryl Jane Anderson, and Kelly Hampton (project officers).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Financial Disclosure/Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Funding to support the research was received from the National Health and Medical Research Council, Australia. No support was received from any commercial organizations.
References
1. Lawrence RM, Pane CA. Human breast milk: current concepts of immunology and infectious diseases. Curr Probl Pediatr Adolesc Health Care. 2007;37:7-36.
2. Holmes W, Phillips J, Thorpe L. Initiation rate and duration of breast-feeding in the Melbourne Aboriginal community. Austr N Z J Public Health. 1997;21:500-503.
3. Raisler J, Alexander C, O’Campo P. Breastfeeding and infant illness: a dose-response relationship? Am J Public Health. 1999;89:25-30.
4. US Department of Health and Human Services. HHS Blueprint for Action on Breastfeeding. Washington, DC: US Department of Health and Human Services; 2000.
5. Kramer MS, Chalmers B, Hodnett ED, et al, for the PROBIT Study Group. Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA. 2001;285:413-420.
6. National Health and Medical Research Council. Food for Health: Dietary Guidelines for Children and Adolescents in Australia. Canberra, Australia: Commonwealth of Australia; 2003.
7. Glover M, Waldon J, Manaena-Biddle H, Holdaway M, Cunningham C. Barriers to best outcomes in breastfeeding for Maori: mothers’ perceptions, Whanau perceptions, and services. J Hum Lact. 2009;25:307-316.
8. Kramer MS, Kakuma R. Optimal duration of exclusive breast-feeding. Cochrane Database Syst Rev. 2002;1:CD003517. Available at: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD003517/frame.html.
9. Oddy WH, Scott JA, Graham KI, Binns CW. Breastfeeding influences on growth and health at one year of age. Breastfeed Rev. 2006;14:15-23.
10. A warm chain for breastfeeding. Lancet. 1994;344:1239-1241.11. Krebs NF, Jacobson MS, Baker RD, et al. Prevention of pediat-
ric overweight and obesity. Pediatrics. 2003;112:424-430.
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

260 Journal of Human Lactation 27(3)
12. Gillman MW, Rifas-Shiman SL, Camargo CA, et al. Risk of overweight among adolescents who were breastfed as infants. JAMA. 2001;285:2461-2467.
13. Horta BL, Bahl R, Martines JC, Victoria CG. Evidence on the Long-term Effects of Breastfeeding: Systematic Reviews and Meta-Analyses. Geneva, Switzerland: Department of Child and Adolescent Health and Development, World Health Organiza-tion; 2007.
14. World Health Organization. The Optimal Duration of Exclu-sive Breastfeeding. A Systematic Review. Geneva, Switzerland: World Health Organization; 2002. Available at: www.who .int/nutrition/publications/optimal_duraton_of_exc_bfeeding _review_eng.pdf.
15. Canadian Paediatric Society, Dietitians of Canada and Health. Nutrition for Healthy Term Infants. Ottawa, Canada: Minister for Public Works and Government Services; 2005.
16. Department of Health. Infant Feeding Recommendation. London, England: Department of Health; 2003. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/ PublicationsPolicy andGuidance/DH_4097197.
17. Australian Health Ministers’ Conference. The Australian National Breastfeeding Strategy 2010-2015. Canberra, Australia: Australian Government Department of Health and Ageing; 2009.
18. Australian Institute of Health and Welfare. A Picture of Australia’s Children. Cat. no. PHE58. Canberra, Australia: Australian Institute of Health and Welfare; 2005.
19. Garden F, Hector D, Eyeson-Annan M, Webb K. Breastfeed-ing in New South Wales: Population Health Survey 2003-2004. Sydney, Australia: NSW Centre for Public Health Nutrition, University of Sydney, and Population Health Division, NSW Health Department; 2007.
20. Paul E, Johnston S, Walker J, Stanton R, Bibo M. Infant Nutrition Project 2006-2007: Measurement of Exclusive Breastfeeding. Brisbane, Australia: Queensland Health; 2007.
21. Australian Institute of Family Studies. Growing up in Australia: the longitudinal study of Australian children: 2006-07 annual report. Available at: http://www.aifs.gov.au/growingup/pubs/ar/ar200607/breastfeeding.htm.
22. Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework 2006 Report: Detailed Analysis. AIHW cat. no. IHW 20. Canberra, Australia: Australian Institute of Health and Welfare; 2007.
23. Zubrick SR, Lawrence DM, Silburn SR, et al. The Western Australian Aboriginal Child Health Survey: The Health of Aborig-inal Children and Young People. Perth, Western Australia: Telethon Institute for Child Health Research; 2004.
24. Eades SJ, Read AW, Bibbulung Gnarneep Team. Infant care practices in a metropolitan Aboriginal population. J Paediatr Child Health. 1999;35:541-544.
25. Binns C, Gilchrist G, Gracey M, Zhang M, Scott J, Lee A. Factors associated with the initiation of breast-feeding by Aboriginal mothers in Perth. Public Health Nutr. 2004;7:857-861.
26. Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework 2008 Report:
Detailed Analyses. Cat. no. IHW 22. Canberra, Australia: Australian Institute of Health and Welfare; 2009.
27. Scott JA, Aitkin I, Binns CW, Aroni RA. Factors associated with the duration of breastfeeding amongst women in Perth, Australia. Acta Paediatr. 1999;88:416-421.
28. Scott JA, Binns CW, Graham KI, Oddy WH. Temporal changes in the determinants of breastfeeding initiation. Birth. 2006;33: 37-45.
29. Comino E, Craig P, Harris E, et al. The Gudaga Study: estab-lishing an Aboriginal birth cohort study in an urban community. Austr N Z J Public Health. 2010l;34(suppl 1): S9-S17.
30. Zhang J, Yu KF. What’s the relative risk? A method of cor-recting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280:1690-1691.
31. Australian Bureau of Statistics. Information paper: an introduc-tion to Socio-economic Indexes for Areas (SEIFA), 2006. Avail-able at: http://www.abs.gov.au/ausstats/[email protected]/mf/2039.0/. Accessed April 14, 2009.
32. Binns C, Scott J. Breastfeeding: reasons for starting, reasons for stopping and problems along the way. Breastfeed Rev. 2002;10:13-19.
33. National Health and Medical Research Council. The NHMRC Roadmap: A Strategic Framework for Improving Aboriginal and Torres Strait Islander Health Through Research. Canberra, Australia: Commonwealth of Australia; 2002.
34. National Health and Medical Research Council. Values and Eth-ics: Guidelines for Ethical Conduct in Aboriginal and Torres Strait Islander Health Research. Canberra, Australia: Commonwealth of Australia; 2003.
35. Knight J, Comino E, Harris E, Jackson Pulver L, Craig P. Indigenous research: a commitment to walking the talk: the Gudaga Study: an Australian case study. J Bioeth Inq. 2009;6: 467-476.
36. Centre for Epidemiology and Research, NSW Department of Health. New South Wales child health survey 2001. N S W Public Health Bull. 2002;13:S-4.
37. Dubois L, Girard M. Social inequalities in infant feeding dur-ing the first year of life: the Longitudinal Study of Child Devel-opment in Quebec (LSCDQ 1998–2002). Public Health Nutr. 2003;6:773-783.
38. Giugliani ESJ, Ciaffa WT, Vogelhut J, Witter FR, Perman JA. Breastfeeding support from different sources on mothers’ deci-sions to breastfeed. J Hum Lact. 1994;10:157-161.
39. Gilchrist G, Woods B, Binns CW, Scott JA, Gracey M, Smith H. Aboriginal mothers, breastfeeding and smoking. Aust N Z J Public Health. 2004;28:255-258.
40. Jackson Pulver LR, Sullivan E, Craig P. Report of the Healthy for Life Project Coordination Team: Phase One Healthy for Life, South Western Sydney Area Health Service (Western Zone). Sydney, Australia: Muru Marri Indigenous Health Unit, School of Public Health and Community Medicine, University of NSW; 2006.
41. Yeoh BH, Eastwood J, Phung Ha, Woolfenden S. Factors influ-encing breastfeeding rates in south-western Sydney. J Paediatr Child Health. 2007;43:249-255.
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from

Craig et al. 261
42. Australian Breastfeeding Association. Australian Breastfeeding Association homepage. Available at: http://www.breastfeeding .asn.au.
43. Karitane. Karitane homepage. Available at: http://www.karitane .au/services/karitaneathome.php.
44. Tresillian Family Care Centres. Tresillian Family Care Centres homepage. Available at: http://www.tresillian.net/home.html.
45. Australian Institute of Aboriginal and Torres Strait Islander Studies, Research School of Social Sciences, Australian National University. Aboriginal Health in South West Sydney: Report of the Tharawal Aboriginal Family Environment and Health Survey. Sydney, Australia: Tharawal Aboriginal Corpo-ration, Campbelltown, NSW; 1994.
46. Kervin BE, Kemp L, Jackson Pulver L. Types and timing of breastfeeding support and its impact on mothers’ behaviours. J Paediatr Child Health. 2010;46:85-91.
47. Chapman DJ, Merewood A, Armah RA, Perez-Escamilla R. Breastfeeding status on US birth certificates: where do we go from here? Pediatrics. 2008;122:e1159-e1163. Available at: www.pediatrics.org. Accessed January 12, 2009.
48. Hector D, King L, Webb K. Overview of Recent Reviews of Interventions to Promote and Support Breastfeeding. State of Food and Nutrition in NSW Series. Sydney, Australia: NSW Centre for Public Health Nutrition and NSW Depart-ment of Health; 2004. Available at: www.cphn.biochem .usyd.edu.au.
49. NSW Health. Integrated Primary and Community Health Policy 2007-2012. Sydney, Australia: NSW Department of Health; 2006.
50. Tursan d’Espaignet E, Measey ML, Carnegie MA, Mackerras D. Monitoring the “Strong Women, Strong Babies, Strong Cul-ture Program”: the first eight years. J Paediatr Child Health. 2003;39:668-672.
at University of New South Wales on August 8, 2011jhl.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN