Initial Assessment of Urinary and Faecal Incontinence in Adult ...
82
331 Committee 5 Initial Assessment of Urinary and Faecal Incontinence in Adult Male and Female Patients Chairman D. STASKIN (USA) Co-Chairman C. KELLEHER (U.K) Members K. AVERY (U.K), R. BOSCH (N.L), N. COTTERILL (U.K), K. COYNE (USA), A. EMMANUEL (U.K), M. YOSHIDA (JAPAN) Consultant Z. KOPP (USA)
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Initial Assessment of Urinary and Faecal Incontinence in Adult ...

331
Committee 5
Initial Assessment of Urinary and Faecal Incontinence in Adult
Male and Female Patients
Chairman
D. STASKIN (USA)
Co-Chairman
C. KELLEHER (U.K)
Members
K. AVERY (U.K),
R. BOSCH (N.L),
N. COTTERILL (U.K),
K. COYNE (USA),
A. EMMANUEL (U.K),
M. YOSHIDA (JAPAN)
Consultant
Z. KOPP (USA)

332
REFERENCES
5B - E. RECOMMENDATIONS FORRESEARCH
5B - D. PATIENT REPORTEDOUTCOME (PRO)
QUESTIONNAIRES TO ASSESSTHE IMPACT OF URINARY
INCONTINENCE, OAB AND LOWERURINARY TRACT SYMPTOMS
5B - C. INTERNATIONALCONSULTATION ON
INCONTINENCE MODULARQUESTIONNAIRE (ICIQ):
WHAT IS THE ICIQ?
5B - B. RECOMMENDED PROQUESTIONNAIRES
5B - A. THE MEASUREMENT OFPATIENT-REPORTED OUTCOMES
(PROS) OF INCONTINENCE,OTHER LOWER URINARY TRACT
SYMPTOMS, AND BOWELPROBLEMS
INTRODUCTION
REFERENCES
I. FAECAL INCONTINENCEASSESSMENT
5A - B. INITIAL ASSESSMENT OFFAECAL INCONTINENCE
V. THE MALE PATIENT
IV. THE FEMALE PATIENT
III. THE UTILITY OF POST-VOIDINGRESIDUAL [PVR] URINE VOLUMEDETERMINATION IN THE INITIALASSESSMENT OF INCONTINENT
PATIENTS
II. URINALYSIS IN THE EVALUATIONOF THE PATIENT WITH LUTS AND UI
I. LOWER URINARY TRACTSYMPTOMS
5A - A. INITIAL ASSESSMENT OFURINARY INCONTINENCE INADULT MALE AND FEMALE
PATIENTS
CONTENTS
Committee 5 B
Patient-Reported Outcome Assessment
CONTENTS
Committee 5 A
Initial Assessment of Urinary and FaecalIncontinence in Adult Male and Female Patients

333
Organization of this committee report
Urinary (UI) and faecal incontinence (FI) are a concernfor individuals of all ages and both sexes. This reportreviews the “initial assessment” of urinary and faecalincontinence – and in addition, reviews the availableoutcome measures for symptom assessment andquality of life for these disorders. Therefore, the reportis divided into 2 major sections: 5A-A initial assessmentof urinary incontinence (UI) in adult male and femalepatients, 5A-B initial assessment faecal incontinence(FI) and 5B outcome measures. The initial assess-ments for the conditions of incontinence in paediatric,neurogenic, and geriatric patients and for patientswith pelvic pain are presented in the specificCommittee reports pertaining to these sub-groupsand conditions.
For the purpose of this report, the ‘initial assessment’represents the components of the history, physicalexamination, laboratory tests, and basic office testingto:
1. Establish a presumptive or condition specificdiagnosis, and exclude underlying organ-specificrelated or unrelated conditions that would requireintervention.
2. Assess the level of bother and desire forintervention from information obtained from thepatient or caregiver.
3. Institute empiric or disease specific primary therapybased on the risk and benefit of the untreatedcondition, the nature of the intervention and thealternative therapies.
4. Prompt the recommendation of additional morecomplex testing or specialist referral.
Within the initial assessment of UI, various sub-populations / subgroups are recognized because ofthe differences within patient groups or theinterrelationship between the conditions. The sub-sections in this report should be utilized in conjunctionwith other population or condition specific CommitteeReports of the Consultation and the final recom-mendations of the Consultation which are presentedin simplified form along with treatment algorithms inthe Management Recommendations. These sub-groups include patients with lower urinary tractsymptoms (LUTS) without incontinence and with pelvicpain. The requirements of specific sub-populationsnegate the ability to recommend a ‘universal’ initialevaluation. Pelvic organ prolapse in the female andprostatic obstruction in the male require uniquelydifferent approaches to lower urinary tract dysfunction.Congenital and maturational issues in the paediatricsubgroup and the effects of ageing on the lower urinarytract and medical co-morbidities in the geriatric grouppresent unique challenges. Specific risks for combinedstorage and emptying abnormalities and upper urinarytract deterioration in the neurogenic bladder populationdemand a more involved initial evaluation.
This committee report is evidence based and utilizesthe ICUD - EBM grades. A search of the availableliterature in English obtained from Medline© andPubmed© up to June 2008 by the individual committeemembers utilized multiple search terms related toassessment (eg., ‘urinary incontinence’, ‘faecalincontinence’, ‘lower urinary tract symptoms’, ‘vaginalprolapse’, and terminology related to ‘outcomeassessments’ and ‘quality of life measures’).
5A- A. INITIAL ASSESSMENT OFURINARY INCONTINENCE INADULT MALE AND FEMALE
PATIENTS
INTRODUCTION
Committee 5 A
Initial Assessment of Urinary and Faecal Incontinence in Adult
Male and Female Patients D. STASKIN, C.KELLEHER,
R.BOSCH, K.COYNE, N. COTTERILL, A. EMMANUEL, M.YOSHIDA, Z. KOPP

334
Purpose of the initial assessment
The initial assessment must consider the degree ofbother, and the costs of further evaluation, balancedagainst the consequences of a failure to diagnose anunderlying condition, the risk and benefits of conser-vative management or pharmacological therapy andthe need for an accurate diagnosis before morecomplex intervention or empiric therapy. The burdenof these conditions and the availability of resourcesto different patients, physicians, and health caresystems require that primary intervention strategiesbe formulated, when available from evidence basedfindings and decisions emanating from the initialevaluation. As will be noted, especially in thiscommittee report, the amount and sophistication of theliterature that contributes to the levels of evidencethat are available for determining the grades ofrecommendation in the area of “initial assessment”may often rely on expert opinion of the panel.
Of note, LUTS cannot be used to make a definitivediagnosis of a specific lower urinary tract condition orlower urinary tract disease (LUTD), as these symptomsmay suggest and indicate pathologies such as urinaryinfection or more serious underlying conditions. Basiclaboratory tests, such as testing for urinary or faecalinfection or blood, and appropriate screening formalignancy should be considered before the decisionis made to choose therapy for incontinence.
Concomitant pathology may affect urinary or faecalproduction as co-morbid contributory issues, byaffecting fluid balance or renal function (dietary oralimentary function) and may need to be addressed.The physician should elicit neurological symptomsand signs that may indicate alterations in the controlof the lower urinary tract / bowel function or thecognitive, motivational, physical, and environmentalfactors that determine the ability to perform toiletingfunctions effectively.
Symptoms are either volunteered by, or elicited from,the individual or may be described by the individual’scaregiver. The International Continence Society (ICS)has classified lower urinary tract symptoms (LUTS)into storage, voiding, and post-micturition symptoms[1]. The National Institutes of Health (NIH) recommendsimilar (but not identical) standards of terminology inpelvic floor disorders[2]. Although an accurateurological history will not establish a definitive diagnosisit will ultimately guide investigation and treatment [1].
The following section summarises the definitions ofsymptoms described by the International ContinenceSociety [1].NIH definitions are given (in italics and inparentheses) where they differ from ICS terminology.
1. STORAGE SYMPTOMS
OVERACTIVE BLADDER (OAB) - Urgency with or withouturgency incontinence usually with frequency andnocturia in the absence of an underlying metabolic orpathological condition.
URINARY INCONTINENCE (UI) is the complaint of anyinvoluntary leakage of urine. In each specificcircumstance, urinary incontinence should be furtherdescribed by specifying relevant factors such as type,frequency, severity, precipitating factors, social impact,effect on hygiene and quality of life, the measuresused to contain the leakage (wearing of protection,number and type of pads and change of underwearor outer clothes) and whether or not the individualseeks or desires help because of urinary incontinence.Urinary leakage may need to be distinguished fromperspiration or vaginal discharge.
STRESS URINARY INCONTINENCE (SUI) is the complaintof involuntary leakage on effort or exertion, or onsneezing or coughing (NIH – the patient’s or caregiver’sstatement of involuntary loss of urine during physicalexertion).
URGENCY URINARY INCONTINENCE (UUI) is the complaintof involuntary leakage accompanied by or immediatelypreceded by urgency. Urge incontinence can presentin different symptomatic forms; for example, asfrequent small losses between micturition or as acatastrophic leak with complete bladder emptying.Information should be sought on triggering eventssuch as cold, running water and ‘latch key’incontinence.
MIXED URINARY INCONTINENCE (MUI) is the complaint ofinvoluntary leakage associated with urgency and alsowith exertion, effort, sneezing or coughing.
CONTINUOUS URINARY INCONTINENCE is the complaint ofcontinuous leakage.
OTHER TYPES OF URINARY INCONTINENCE may besituational, for example the report of incontinenceduring sexual intercourse. Coital incontinence mayoccur during arousal, on penetration, throughoutintercourse, or specifically at orgasm; althoughurodynamic stress incontinence is the most commonurodynamic finding in each of these situations, detrusoroveractivity is found more often when leakage isrestricted to orgasm [3].
URGENCY is the complaint of a sudden compellingdesire to pass urine which is difficult to defer (NIH –the statement that the patient feels a strong need topass urine for fear of leakage).
INCREASED DAYTIME FREQUENCY is the complaint ofvoiding too often by day (NIH - the statement that thepatient voids eight or more times in 24 hours).
Increased daytime frequency may arise in thepresence of a normal bladder capacity when there is
I. LOWER URINARY TRACTSYMPTOMS

335
excessive fluid intake, or when bladder capacity isrestricted secondary to detrusor overactivity, impairedbladder compliance, or increased bladder sensation.
NOCTURIA is the complaint that the individual has towake at night one or more times to void (NIH - thestatement that the patient wakes from sleep to passurine). The term ‘night time frequency’ differs from thatfor nocturia, as it includes voids that occur after theindividual has gone to bed, but before he/she hasgone to sleep, and voids which occur in the earlymorning which prevent the individual from gettingback to sleep as he/she wishes. These voids beforeand after sleep may need to be considered in researchstudies. If this definition were used then an adapteddefinition of daytime frequency is required. Nocturiamay arise for similar reasons to daytime frequency,but may also occur due to an increase in fluid outputdue to other physiological abnormalities resulting in‘nocturnal polyuria’. (see Bladder diaries below).
NOCTURNAL ENURESIS is the complaint of loss of urineoccurring during sleep. Enquiry should includeprevious childhood nocturnal enuresis as delayedbladder control in childhood is associated with detrusoroveractivity in adulthood.
BLADDER SENSATION may be categorised as:
NORMAL: the individual is aware of bladder filling andincreasing sensation towards capacity.
INCREASED: the individual feels an early and persistentdesire to void.
REDUCED: the individual is aware of bladder filling butdoes not feel a definite desire to void.
ABSENT: the individual reports no sensation of bladderfilling or desire to void.
NON-SPECIFIC: the individual reports no specific bladdersensation but may perceive bladder filling as abdominalfullness, vegetative symptoms, or spasticity. Thesesymptoms are most frequently seen in neurologicalpatients, particularly those with spinal cord trauma ormalformation.
2. VOIDING SYMPTOMS
Voiding symptoms may occur in situations of overactiveoutlet, or under active detrusor[1]. The former may besecondary to outlet obstruction from urogenitalprolapse, urethral stricture or following previous bladderneck surgery. Detrusor atonia or hypotonia is howevermuch more common in the female, and may ariseidiopathically, or secondarily to over distension afterparturition or surgery, in peripheral neuropathy due todiabetes mellitus, and in other neurological conditions.Women with prolapse may require to digitate vaginallyto initiate or complete voiding.
SLOW STREAM is the individual’s perception of reducedurine flow, usually compared to previous performanceor in comparison to others.
INTERMITTENT STREAM (INTERMITTENCY) is when theindividual describes urine flow which stops and starts,on one or more occasions, during micturition.
HESITANCY is when an individual describes difficulty ininitiating micturition resulting in a delay in the onsetof voiding after the individual is ready to pass urine.
STRAINING to void describes the muscular effort usedto initiate, maintain or improve the urinary stream.
TERMINAL DRIBBLE is the term used when an individualdescribes a prolonged final part of micturition, whenthe flow has slowed to a trickle.
POST-MICTURITION SYMPTOMS
Post micturition symptoms are experiencedimmediately after micturition.
FEELING OF INCOMPLETE EMPTYING is a self-explanatoryterm for a feeling experienced by the individual afterpassing urine.
POST MICTURITION DRIBBLE is the term used when anindividual describes the involuntary loss of urineimmediately after he or she has finished passing urine,usually after leaving the toilet in men, or after risingfrom the toilet in women.
3. MEASURING THE FREQUENCY ANDSEVERITY OF LOWER URINARY TRACTSYMPTOMS
The frequency-volume chart or micturition diary recordsa patient’s voiding pattern during normal daily activities.In some women it may be therapeutic as it providesthem with insight into their bladder behaviour [4]. TheICS has described three different forms of diary,namely the micturition time chart which records thetiming of voids in twenty four hours; the frequencyvolume chart (FVC) which also includes the volumesvoided , and the bladder diary which in additionincludes incontinence episodes, pad usage, fluid
intake, degree of urgency and degree of incontinence.1
However, increasing either the complexity of the diaryor duration of recording is associated with poorercompliance [5]. The optimum duration of recordingdepends on the clinical context and the purpose of themeasurement. A properly performed 1-day FVC, whichincludes the first morning void the following day, is areasonable tool to gain insight into voiding habitsduring normal daily routine.
However, a 3-day FVC or diary is recommended foraccurate assessment of lower urinary tract symptomsand for confirming a consistent clinical pattern in day-to-day practice. Although never completely diagnostic,several different diary patterns have been describedwhich may characterise normal and abnormalstates[6]. For atypical clinical scenarios, a 7-day FVCor diary should be used. Equally, a 7-day diary hasbeen recom-mended for clinical research, [7] however,of note, most pharmacological studies now employ a

336
three day diary as a standard for improved patientcompliance (see Committee Report Pharmacologyfor further recommendations.
The following measurements can be abstracted fromfrequency volume charts and bladder diaries:
DAYTIME FREQUENCY is the number of voids recordedduring waking hours and includes the last void beforesleep and the first void after waking and rising in themorning.
NOCTURIA is the number of voids recorded during anight’s sleep; each void is preceded and followed bysleep.
NIGHT-TIME FREQUENCY is the number of voids recordedfrom the time the individual goes to bed with theintention of going to sleep, to the time the individualwakes with the intention of rising.
24-HOUR FREQUENCY is the total number of daytimevoids and episodes of nocturia during a specified 24hours period.
24-HOUR PRODUCTION is measured by collecting allurine for 24 hours; this is usually commenced after thefirst void produced after rising in the morning and iscompleted by including the first void on rising thefollowing morning.
POLYURIA is defined as the measured production ofmore than 2.8 litres of urine in 24 hours in adults. Itmay be useful to look at output over shorter timeframes.
NOCTURNAL URINE VOLUME is defined as the total volumeof urine passed between the time the individual goesto bed with the intention of sleeping and the time ofwaking with the intention of rising. Therefore, itexcludes the last void before going to bed but includesthe first void after rising in the morning.
NOCTURNAL POLYURIA is present when an increasedproportion of the 24-hour output occurs at night(normally during the 8 hours whilst the patient is inbed). The night time urine output excludes the lastvoid before sleep but includes the first void of themorning. The normal range of nocturnal urineproduction differs with age and the normal rangesremain to be defined. Therefore, nocturnal polyuriais present when greater than 20% (young adults) to33% (over 65 years) is produced at night. Hence theprecise definition is dependent on age.
AVERAGE VOLUME VOIDED is the mean volume of urinepassed in each void. This is calculated by dividing totalvoided volume by number of voids.
NORMALISED MICTURITION FREQUENCY is a moremeaningful way of expressing voided volume. Thisis defined as the number of micturitions required topass 1 litre of urine, and is calculated by dividing 1000
ml by average volume voided. This is a more specificmeasure of bladder function than micturition frequency,since it takes into account behavioural, dietary andpharmacological factors that affect urine volume.
MAXIMUM VOIDED VOLUME is the largest volume of urinevoided during a single micturition and is determinedeither from the frequency/volume chart or bladderdiary.
INCONTINENCE EPISODE FREQUENCY is the number ofepisodes of accidental urine leakage that occur overa specified period (e.g. 24 hours).
URGENCY is the complaint of a sudden compellingdesire to pass urine, which is difficult to defer, andwhich leads to a fear of incontinence. The impact ofthis symptom may be derived from a bladder diary byrecording episodes of urgency, episodes of urgencyleading to incontinence and severity of urgency (e.g.using a daily visual analogue scale).
PAD USAGE is the number of pads used over a specifiedperiod (e.g. 24 hours).
Recommendations
1. Lower Urinary Tract Symptoms (LUTS) cannotbe used to make a definitive diagnosis; theymay also indicate pathologies other than LowerUrinary Tract Disease (LUTD). Specific to thisreport, LUTS may include Overactive Bladder(OAB) a syndrome which may be associatedwith urgency incontinence (OAB-wet) or withoutincontinence (OAB-dry). Likewise, bowelsymptoms should prompt consideration and asappropriate, an evaluation for other similarsymptom based pathology. (Level 5 - Grade D)
2. Urinary and faecal incontinence should bedescribed by specifying relevant factors such astype, frequency, severity, precipitating factors,social impact, effect on hygiene and quality oflife, the measures used to contain the leakageand whether or not the individual seeks ordesires help. (Level 5 - Grade D)
3. Urinary incontinence should be categorized bysymptoms into urgency incontinence, stressincontinence or mixed incontinence andconservative (non-invasive) therapies may thenbe started based on this classification to treatthe most troublesome component, or eithercomponent of the incontinence. (Level 5 - GradeD) More sophisticated testing (eg. urodynamicstudies) is not required prior to the institution ofconservative therapy (see indications forurodynamics in the Committee Report onUrodynamic Studies). (Level 3 - Grade C)

337
Future research
1. Standardisation of the ‘definition of symptoms’ andthe ‘measurements of symptom frequency, severityand bother’ are essential for patient care andresearch. Continued research into the appropriatescales and metrics should be accompanied by asignificant attempt to establish best practiceguidelines for their use and a consensus on theadoption of universal standards.
2. Recognition and resolution of the differences incommon language usage and scientific utilisationof terms should continue (e.g. common use of‘urge to void’ and the ‘desire to void’ versus the ICSterminology of “urgency”). In addition, continuedresearch into the development of accuratemeasures to objectify subjective symptoms suchas “urgency”. This would include resolution of thedifferences in the ICS and NIH definitions (inaddition to other regulatory agencies) is essentialfor communicating data with respect to patientcare, research, and treatment outcomes.
3. Further development and standardisation ofsymptom assessment tools (questionnaires) toimprove the diagnostic accuracy of lower urinarytract symptoms. (Refer to section 2 of thiscommittee’s report)
4. Further validation of the accuracy of specificcomponents of the history and physical findings toestablish an accurate diagnosis and initiate non-invasive conservative or pharmacological therapy.In addition, to further identify components thatwould indicate the need for more invasive testing,complex therapeutic interventions, and indicationsfor referral.
“The urinalysis is a fundamental test that should beperformed in all urological patients. Although in manyinstances a simple dipstick urinalysis provides thenecessary information, a complete urinalysis includesboth chemical and microscopic analysis” [8].
In relation to urinary incontinence, dipstick urinalysisis not a diagnostic test, but a screening test, importantin order to detect haematuria, glucosuria, pyuria andbacteriuria. Haematuria can indicate importantpathology such as urothelial carcinoma in situ, leadingto lower urinary tract storage symptoms includingincontinence [9]. Glucosuria is relevant, as a potentialindicator of diabetes mellitus. This can causesymptoms via several mechanisms including polyuriasecondary to osmotic diuresis, peripheral autonomicneuropathy affecting bladder innervation leading toimpaired bladder emptying and chronic urinaryretention and finally due to increased risk of urinarytract infection (UTI), directly related to the glucosuriaand as a sequel to impaired bladder emptying.
Pyuria and bacteriuria, detected from urinary dipstickleukocyte esterase and nitrite tests respectively, areimportant signs of urinary tract infection. The specificityand sensitivity of these latter tests for UTI is increasedwhen used together compared to either individual test[10,11]. Even in the absence of controlled studies,there is general expert consensus that the benefits ofurinalysis clearly outweigh the costs involved, althoughthe use of urinalysis should always be associatedwith prognostic significance [12]. A positive dipstickurinalysis will prompt formal urine microscopy andculture to detect UTI prior to antibiotic treatment and/orthe use of additional tests such as endoscopy andurinary tract imaging. In the evaluation of urinaryincontinence and lower urinary tract symptoms, thevalue of urinalysis can be illustrated by the findingthat 60% of women with stable bladder will developdetrusor overactivity at the time of UTI.
The importance of urinalysis in the basic assessmentof patients with urinary incontinence and lower urinarytract symptoms is not dependent on gender, age oraetiology. Indeed, it has been recommended in theevaluation of geriatric patients including nursing homeresidents who are incontinent, [13,14] in peri- andpostmenopausal women, [15] and in older women
II. URINALYSIS IN THE EVALUATIONOF THE PATIENT WITH LUTS AND UI
4. A bladder diary is recommended in order todocument and communicate the frequency ofvoids and incontinence episodes experiencedby the patient - as well as additional metrics.Additional information as appropriate mayinclude volume of intake, voided volume, and /or symptoms such as urgency or discomfort.Additional metrics may be added for researchpurposes such as degree of urgency or timefrom urgency to toileting. A bladder diary isrecommended for a minimum of 3 days foraccuracy (Level 3 - Grade C) as the idealduration is not clear (Level 4). The committeeacknowledges the difficulty with patientcompliance and acknowledges some value ofshorter periods for patient compliance. (Level5 - Grade D).
5. Referral to a specialist is recommended forhematuria (visible or microscopic), urinary tractinfection (persistent or recurrent), prolapse(symptomatic or below the introitus) , obstructionor retention (symptoms or findings of palpablebladder, hydronephrosis or obstructive renalinsufficiency), suspected neurological disease,mass (urethral, bladder or pelvic - benign ormalignant), fistula (urinary or bowel), faecalincontinence, a history of prior pelvic surgery orradiation (incontinence, oncologic) (Level 5 -Grade D).

338
reporting urinary incontinence [16]. In the latter context,it has been suggested that significant urine samplescan even be obtained from disposable diapers inelderly incontinent women [17].
A Norwegian survey of general practitioners’management of female urinary incontinence suggestedthat urinalysis is the most frequently performed test(73%) and is far more frequent than gynaecologicalexamination (54%) [18]. Another survey proposedthat urinalysis is one of the three-part assessment ofurinary incontinence together with patient history andphysical examination [19].
The clinical relevance of asymptomatic bacteriuria(without pyuria) and pyuria (without bacteriuria) in theelderly is controversial, as eradication of bacteruriaappeared to have no effect on resolution ofincontinence, and many suggest thtat it does notdeserve any treatment. [20,21].
Recommendation
Future research
1. Determine the role of urinalysis as a screeningtest in various incontinent populations, specificallythe elderly patient with acute or establishedincontinence in combination with asymptomaticbacteruria. Specifically, to determine the relevanceof asymptomatic bacteriuria without pyuria, andpyuria without bacteriuria, in elderly patients. (seeGeriatric Committee Report).
2. Determine the prognostic significance of urinalysisresults and the impact of therapy the outcome oftreatment of urinary incontinence.
The PVR is the volume of urine remaining in thebladder following a representative void. PVRmeasurement can be accomplished within a fewminutes of voiding either by catheterisation or bycalculation of bladder volume using a portableultrasound scanner. Several studies have comparedvolumes measured with portable ultrasound scannersversus catheterisation and found portable scannersto be 85-94% accurate [22,23]. A study has imagedthe bladder volume after catheterisation and foundthat the volume of urine remaining in the bladder aftercatheterisation accounted for most of the differencebetween the two measurements [22]. Bimanualpalpation cannot reliably estimate the post-voidresidual urine volume [24].
Since PVR may vary, one measurement of PVR maynot be sufficient [25]. PVR should probably bemeasured several times to increase its reliability.Griffiths et al found a significant variability in PVRmeasurement depending on the time of the day, withthe greatest volume occurring in the morning [26]. Anon-representative PVR is particularly common if thepatient’s bladder is not full enough to yield an urge tovoid.
An increased PVR alone is not necessarily problem,but if combined with high pressures it can lead toupper tract problems. If related to UTI’s, PVR mayneed to be treated since UTI’s may not be eradicatedin the presence of an infected residual. A significantPVR also decreases the functional bladder capacityand contributes to urgency/frequency, urgeincontinence and nocturia. However, a Scandinavianstudy in nursing home residents found that an elevatedPVR was not associated with bacteruria and incon-tinence [27].
Review of the literature does not show an evidence-based specific maximum PVR that is considerednormal, nor is there a minimal PVR that is consideredabnormal. The amount of residual urine that precludestreatment by various therapies has also not beendetermined. The AHCPR guidelines state that, ingeneral, a PVR less than 50 ml is considered adequatebladder emptying and over 200 ml is consideredinadequate emptying (expert opinion of the panelmembers) [28].
III. THE UTILITY OF POST-VOIDINGRESIDUAL [PVR] URINE VOLUMEDETERMINATION IN THE INITIALASSESSMENT OF INCONTINENT
PATIENTS
1. It is considered standard to perform a urinalysiseither by using a dipstick test or examining thespun sediment. (Level 5 - Grade D)
2. If a dipstick test is used, it is recommended thata “multiproperty” strip that includes fields forhaematuria, glucose, leukocyte esterase andnitrite tests be chosen. (Level 5 - Grade D)Dipstick is not as accurate as urine culture,being specific for infection but not sensitive.(Level 2 - Grade C)
3. Additional tests available on urine dipstick strips,such a protein, bilirubin, ketones and pH, maybe helpful in the broader medical managementof patients. However, they are not essential inthe context of evaluation of the patient withurinary incontinence or lower urinary tractsymptoms. (Level 5 - Grade D)

339
“Normal values” of PVR have been determined inseveral groups of non-incontinent and incontinentwomen. Gehrich et al studied 96 women (mean age60 ± 11 yrs) that were seen in a well-women clinic.These women had no history of incontinence,retention, symptomatic prolapse or neurologicdisorders. Most (97%) had a minor (asymptomatic)degree of prolapse, 80% was post-menopausal and30% had had a hysterectomy. The median PVR was19 ml (range 0-145 ml; mean 24 ± 29 ml); only 5% hadPVR > 100 ml. Only, age > 65 yrs was associated withhigher PVR [29]. Tseng et al studied 107 women withurodynamic stress incontinence. They found a meanPVR of 62.5 ml by bladder scan and 38.5 ml bycatheterization. Only 15.9% had a PVR greater than100 ml. The PVR determined by bladder scan offereda sensitivity of 64.7% and a specificity of 94.3% indetecting PVR greater than 100 ml [30]. Haylen et alstudying women with lower urinary tract dysfunctionfound that 81% had a PVR of less than 30 ml Postvoidresidual volumes higher than this level are significantlyassociated with increasing age, higher grades ofprolapse, and an increased prevalence of recurrentUTIs. [31]. Fitzgerald et al studied women with urgency,frequency and urge incontinence: 10% had an elevatedPVR of > 100ml. In these women with OAB, thefollowing independent risk factors of increased PVRwere found: vaginal prolapse, symptoms of voidingdifficulty and abscence of stress-incontinence [32].Lukacz et al found that only 11% of women with pelvicfloor disorders had an elevated PVR [33]. Wu andBaguley studied 319 consecutive patients (196 women,123 men) in a subacute general, but predominantlygeriatric, rehabilitation unit. 22 had been admittedwith catheter and were excluded. Of the 297“asymptomatic” patients, 21.5% had PVR volumesof 150 mL or more. Patients with elevated PVR (>150 ml) were significantly more likely to have a urinarytract infection at admission and have urinaryincontinence on discharge [34]. Milleman et alretrospectively reviewed 201 women (mean age 55;range 20-90) who presented with complaints of urinaryfrequency, urgency and /or urge incontinence. 19% hadan elevated PVR of more than 100 ml (mean 211 ml;range 100-997 ml). On multivariate analysis thefollowing independent predictors of raised PVR wereidentified: age > 55 yrs [OR 3.71], prior incontinencesurgery [OR 4.32], a history of multiple sclerosis [OR15.32] and pelvic organ prolapse grade 2 or greater[OR 3.61] [35].
In summary, an elevated PVR > 100 ml was found in5% of women visiting a well-women clinic, in 10- 19%of women with OAB, in 11% of women with pelvicfloor disorders and in 15.9% of women withurodynamic SUI.
Does a significant PVR have an impact on the outcomeof treatment in patients with incontinence? Nager etal studied the predictive value of urodynamic measures
on stress continence outcomes after surgery for stressurinary incontinence. They found that urodynamicmeasures do not predict outcomes. However, sincewomen with PVR > 150 ml were excluded in thisstudy, one can only conclude that PVR volumes <150 ml did not have an adverse impact on stresscontinence outcome [36].
POST VIOIDING RESIDUAL URINE IN THEMALE PATIENT
PVR measurement is especially recommended inmen with suggestive of bladder outlet obstruction(BOO). PVR can be measured within a few minutesof voiding by catheterization to confirm that the bladderis empty [37] or by ultrasonography [38]. The AHCPRguidelines state that, in general, a PVR less than50ml is considered adequate bladder emptying andover 200ml is considered inadequate emptying. Morerecently, a dedicated ultrasound system has beendeveloped for automatic measurement of PVR, therebyimproving the accuracy over catheterization [39] whichhas been largely abandoned in clinical practice.International Consultation on BPH defined a rangeof 50 to 100 ml as the lower threshold to defineabnormal PVR [40]. Both the AUA and the EAUguidelines suggest a threshold of 300 ml to identifypatients at risk of unfavorable outcome following LUTS/ BPO treatment [41,42].
There is no consensus about the relation betweenPVR and UTI in the male patient. Although the negativerole of large residuals has been reported, the evidenceis controversial. Large residual urine volume has beenconsidered a bad prognostic factor for diseaseprogression. However, in the standard patients, renalfailure, acute retention and UTIs are uncommon in menwith large, chronic residuals [43]. No factors areavailable to identify patients, with significant residualurine, who are at risk for progression [44].
Therefore, on the basis of these trials, untreated LUTSmay place the male patient at risk for potential clinicaldeterioration. Thus, periodical measurements of PVRare recommended in such patients.
Recommendations
1. Female patients who present with storage specificsymptoms, with normal sensation and nocomplaints of decreased bladder emptying, andno anatomical, neurological, organ-specific, orco-morbid risk factors for retention may beassessed for bladder emptying by history andphysical examination alone, depending on thepotential morbidity of the failure to diagnose andthe nature of the intended therapy. (Grade B).
2. A palpable bladder on physical exam is anindication for referral to a specialist (Grade D).

340
Summary of recommendations
Varying degrees of decreased bladder emptying orurinary retention may be a cause of LUTS that areassociated with symptoms of decreased urinarystorage.
The decision to perform a PVR in disease specificsub-groups of patients (eg., male patients with bladderoutlet obstruction, in neurogenic patients whodemonstrate combined disorders of storage andemptying, and preoperatively in female patients beingconsidered for incontinence surgery) should be basedon an association of the condition with poor bladderemptying (Grade D), whereas in individual patients thisdecision may be based on symptoms or physicalfindings. (Grade C)
Future Research
1. Development of more specific indications for PVRtesting for diagnosis and prior to instituting therapybased on history, physical examination, and diseasespecific findings.
2. Further development of low cost, minimally invasive,and accurate means of measurement of PVR thatdo not require catheterisation.
3 Continued research in subsets of patients isrequired to determine the need for PVR assessmentand the correlation between elevated PVR andtreatment outcome, generally, to determine theeffect of varying levels of PVR on the outcomes ofobservational, conservative, pharmacological andsurgical interventions, and more specifically, thefemale patient prior to surgeries that increase outletresistance, the male patient with bladder outletobstruction where medications that can potentiallydecrease bladder contractility are considered, andthe patient with elevated residual urine whereintermittent catheterization is not practical andwhere recurrent urinary tract infections anddecreased functional bladder capacity are potentialcomplicating factors.
1. GENERAL MEDICAL HISTORY
The general history should include questions relevantto precipitating and aggravating factors of urinaryloss, time of onset and duration of symptoms, anddegree of bother. Acute symptoms may be furtherdefined by documenting patterns of fluid intake andoutput, acute infection, recent surgery or trauma.Chronic symptoms may be further defined by elicitinga history of congenital abnormalities, neurologicaldisease, relevant surgery or general health. Informationmust be obtained on medications with known orpossible effects on the lower urinary tract. The generalhistory should also include assessment of menstrual,obstetric, sexual and bowel function. The reader isreferred to the report of the Committee on Epide-miology for risk specific risk factors to be consideredduring the medical history and to the second sectionof this report for recommendations for disease specificquestionnaires.
2. URINARY SYMPTOMS
Women with urinary incontinence may have had thecondition for many years before presenting; they areoften embarrassed in disclosing their condition and arelikely to have undertaken significant adaptations to theirlifestyle to ameliorate their symptoms [45]. Inestablishing the history the opportunity should betaken not only to describe symptoms, but also theirprogression, impact on lifestyle and possible riskfactors. Multiple symptoms are commonly reported,[46] and during the history it is important to define themost troublesome symptoms and the patient’sexpectations from treatment.
Section 2 of this Committee Report presents acomplete review and evaluation of questionnairesthat are applicable for clinical and research use inevaluating patient symptoms. Structured conditionspecific questionnaires may be used, [47]and maybe either clinician or self-administered. Questionnairesmay facilitate disclosure of embarrassing symptoms,ensure that symptoms are not omitted, and standardiseinformation thereby aiding audit and research.
3. CORRELATION OF SYMPTOMS AND SIGNS WITH SOPHISTICATED TESTING
Harvey & Versi evaluated the symptom and sign ofstress incontinence in predicting the presence ofurodynamic stress incontinence, using the results ofa MEDLINE search for ‘urinary incontinence’,‘urodynamic’ or ‘urodynamics’ [48]. Of 42 articlesevaluated,12 yielded analysable data. The isolatedsymptom of stress incontinence had a positivepredictive value (PPV) of 56% for the diagnosis ofpure urodynamic stress incontinence (USI) and 79%for USI with other abnormalities. The PPV for stress
IV. THE FEMALE PATIENT3. Residual urine determination by bladder scan ispreferable to catheterisation due to the increasedmorbidity associated with instrumentation.(Grade D).
4. Due to the increased possibility of bladder outletobstruction due to prostatic obstruction isincreased in the male patient, the threshold forinvestigating residual urine in the male issignificantly lower (Grade D).
5. A PVR should be performed in patients wheredecreased bladder emptying is suspected,especially if treatments that decrease bladdercontractility or increase outlet resistance arebeing considered. (Grade D)

341
incontinence with other symptoms was 77% for USIwith or without other abnormalities. A positive coughtest had a PPV of 55% for the diagnosis of pure USIand 91% for USI with other abnormalities. Theyconcluded that in isolation, either symptom or signwere poor predictors of USI, although in combinationprediction may be more promising [48].
Horbach reviewed the literature regarding the reliabilityof stress symptoms in predicting USI; PPV valuesranged from 64% to 90% [49]. Summitt et al reportedthat 53% to 71% of women with detrusor overactivity(DO) gave similar histories to those with pure USI[50].The PPV of a history of pure urge incontinencemay be as low as 37%, [51] and overactive bladdersymptoms (OAB) only 54%, [52] in the diagnosis ofDO. It is however of interest to note that in a secondaryanalysis of data from a drug study in patients withpredominant stress incontinence, the main determinantof concurrent urge symptoms was not thepathophysiological condition present (i.e. the presenceof concurrent detrusor overactivity) but the severity ofincontinence [53].
Martin et al, have reported a systematic review ofmethods of assessing urinary incontinence.(54) Froman electronic search of MEDLINE, EMBASE andCINAHL between 1966 and 2002 they identified 6009individual papers; only 197 were relevant, and of these121 reached the standards required of their report.Only a limited number could be combined andsynthesised, although they were able to concludethat a large proportion of women with urodynamicstress incontinence can be correctly diagnosed inprimary care from clinical history alone (sensitivity0.92; specificity 0.56). The value of validated scalesand pad tests could not be determined from theavailable data. The urinary diary appears to be themost cost effective of tests that might be usedalongside clinical history within the primary care setting(sensitivity 0.88; specificity 0.82) [54].
Holroyd-Leduc performed a systematic reviewconcerning the most accurate way to determine thetype of urinary incontinence during an officeassessment was performed incorporating a reviewof the literature form 1966-July 2007. The authorsfound that “In women, simple questions modestlyhelped diagnose stress urinary incontinence but aremore helpful in diagnosing urge urinary incontinence.They concluded that a positive bladder stress testmay help diagnose stress urinary incontinence,however, a negative test is not as useful. Also, asystematic assessment combining the history, physicalexamination, and results of bedside tests to establisha clinical diagnosis appears to be of modest value indiagnosing stress urinary incontinence. In addition, asystematic assessment is less helpful in diagnosingurge urinary incontinence They concluded that “themost helpful component for diagnosing urge urinaryincontinence is a history of urine loss associated with
urgency. A bladder stress test may be helpful fordiagnosing stress urinary incontinence [55].
The reader is referred to the report of the Committeeon Sophisticated Testing - Urodyamics for specificindications for complex testing
4. OTHER SYMPTOMS OF PELVIC FLOOR DYSFUNCTION IN THE FEMALE PATIEINT
a) Prolapse symptoms
The feeling of a lump (“something coming down”),low backache, heaviness, dragging sensation, or theneed to digitally replace the prolapse in order todefaecate or micturate, are amongst the symptomswomen may describe who have a prolapse. Prolapsesymptoms may be associated with urinary storage oremptying symptoms. Outlet symptoms as diverse asgenuine or occult stress incontinence or obstruction,and bladder overactivity or underactivity may have acommon aetiology, exist as a cause or effect, or co-exist with lower urinary tract dysfunction.
b) Bowel symptoms
In addition to urinary complaints, women may havesymptoms relating to bowel function, sexual function,and pelvic organ prolapse (POP). Jackson et al.evaluated 247 women with either UI or POP. Thirtyone percent of women with UI and 7% with POP hadconcurrent anal incontinence (AI) [56]. In a reportfrom Sweden, 62% of 21 consecutive womenundergoing a Burch colposuspension for urodynamicstress urinary incontinence had concurrent faecalincontinence [57]. In a Norwegian study of womenpresenting with a complaint of urinary incontinence(UI), 38% of the women were found to have significantprolapse and 19% reported faecal incontinence [58].All these aspects of the pelvic floor and pelvic floorfunction must be included to plan a comprehensivetreatment strategy.
c) Symptoms associated with sexualdysfunction
Dyspareunia, vaginal dryness and coital incontinenceare amongst the symptoms women may describeduring or after intercourse. These various symptomsare reported by one third to two thirds of women withstress incontinence, and 68% report their sex life tobe spoilt by their urinary symptoms [59]. Symptomsof sexual dysfunction should be described as fully aspossible; it is helpful to define urine leakage asoccurring during arousal, on penetration, duringintercourse, or at orgasm (vide supra) [3].
5. PHYSICAL EXAMINATION
a) General examination
There are few data linking bladder, bowel, or sexualfunction to variations in examination findings of womenseeking routine gynaecological care. Similarly data on

342
women with complaints of urinary incontinence donot include detailed, specific information about theirpelvic examinations.
Physical examination is essential in the assessmentof all women with lower urinary tract dysfunction.Height and weight should be recorded so that bodymass index can be calculated (Kg/M2); this hasrecently been shown to be a significant risk factor forincontinence [59].
Neurological examination should be performed, withattention to the sacral neuronal pathways. Assessmentof gait, abduction and dorsiflexion of the toes (S3)and sensory innervation to the labia minora (L1-L2),sole and lateral aspect of the foot (S1), posterioraspects of the thigh (S2), and perineum (S3) andcutaneous sacral reflexes (bulbo-cavernosus andanal reflexes) may be assessed. A rectal examinationwill provide a subjective assessment of resting andvoluntary anal tone (S2-S4). For patients with possibleneurogenic lower urinary tract dysfunction, a moreextensive neurological examination is needed (videinfra).
The agitated patient with urgency and frequency mighthave a behavioural cause and those who are clinicallydepressed have a less successful response to surgicaltreatment for stress urinary incontinence. A mini-mental state assessment will assess cognitive function,and is particularly helpful in the elderly (vide infra).Restriction in mobility may lead to functionalincontinence and a lack of hand dexterity may precludeself-catheterisation and the use of prostheticcontinence devices.
b) Abdominal examination
Scars from previous surgery should be noted.Increased abdominal striae may be found inassociation with other markers of abnormal collagenmetabolism, and are more likely in patients withprolapse and stress incontinence [60].
An attempt should be made to palpate the kidneys,particularly where a voiding dysfunction or neurogenicbladder dysfunction are suspected. A distendedbladder may be identified by abdominal palpation orby suprapubic percussion. In one study designed tolook at the clinical utility of basic assessment in elderlywomen, palpable enlargement indicated a post-voidresidual volume of at least 300ml [61].
c) Perineal/genital inspection
Inspection of the vulva and perineum allows adescription of the skin and, for example, the presenceof any abnormal anatomical features, of atrophy orexcoriation, and erythema due to incontinence and thewearing of pads.
The patient should be asked to cough and strain todemonstrate stress urinary incontinence and to
observe urethral length, position, and mobility, andreflex contraction of the external anal sphincter.Howard and associates tested vesical neck descentduring cough and Valsalva manoeuvre [62]. Theyfound incontinent women have similar vesical neckmobility with both manoeuvres, whereas continentwomen have less vesical neck descent with a coughthan with Valsalva.
The clinical sign of urinary incontinence is definedas urine leakage seen during examination; this maybe urethral or extra-urethral.
Stress urinary incontinence is the observation ofinvoluntary leakage from the urethra, synchronouswith exertion/effort, or sneezing or coughing. If stressurinary incontinence is suspected, provocative stresstesting (direct visualization) can be performed byhaving the individual relax and then cough vigorouslywhile the examiner observes for urine loss from theurethra. Optimally these tests should be done whenthe patient’s bladder is full, but they should not beperformed when the patient has a precipitant urge tovoid. The test is usually performed initially in thelithotomy position, although if no leakage is observed,it should be repeated in the standing position, sincethe yield is increased when the test is repeated in theupright position. Coughing may induce a detrusorcontraction, hence the sign of stress incontinencemay only be a reliable indication of urodynamic stressincontinence when leakage occurs synchronouslywith the first cough and stops at the end of that cough.It has however been shown that following an increasein intra-abdominal pressure, and the immediate fall inurethral closure pressure, there follows a ‘refractoryperiod’ of several seconds during which the urethramaintains a lower pressure than at rest [63]. Theextent of pressure loss, and the time to recovery areboth less in stress continent then stress incontinentwomen [64]. If further increases in intra-abdominalpressure occur during this time, stress leakage ismore likely to be demonstrated after a series of coughsthan following a single cough.
Bonney’s original stress test was performed todemonstrate urinary leakage during coughing [65].Subsequent modifications of the test require supportof the urethra-vesical junction during coughing inwomen who leak during a stress test. Thesemodifications are not reliable in selecting a surgicalprocedure or in predicting cure.
Extra-urethral incontinence is defined as theobservation of urine leakage through channels otherthan the urethra. This may result from congenitalabnormality such as ectopic ureteric opening, or fromurogenital fistula.
d) Urethro-vesical junction (bladder neck)mobility
Urethro-vesical junction (bladder neck) mobility should

343
be assessed in all women with urinary incontinence.It is generally felt that women with urodynamicincontinence fall into several categories based onassessment of urethral support and urethral function.The choice of therapy may be affected by theassessment of bladder neck mobility [66]. One methodof assessing bladder neck mobility is by visualinspection. When the patient is in lithotomy position,the urethral meatus is horizontal to the floor in awoman with good bladder neck support. When sheincreases intra-abdominal pressure you can observefor posterior rotation of the anterior vagina anddeflection of the meatus toward the ceiling, both signsof some loss of support. You may ask her to contractthe pelvic muscles to determine if urethral supportimproves with muscle contraction, a sign pelvic floortraining may be therapeutic.
The cotton swab or Q-tip test is a simple out-patientprocedure to quantify bladder neck mobility [66]. Asterile, lubricated cotton or Dacron swab (Q-tip) isinserted into the urethra until it lies just within theurethra-vesical junction. Using a goniometer, the anglecircumscribed by the distal end of the swab ismeasured relative to the horizontal while the womanis performing a maximum Valsalva effort. Urethro-vesical junction hypermobility is defined by a maximumstrain axis exceeding +30 degrees from the horizontal.
There are no published reports about the reproducibilityof the cotton swab test for measuring bladder neckhypermobility, despite its widespread clinical applicationin the evaluation and management of women withurinary incontinence. The validity of this test fordiagnosing stress urinary incontinence was notsystematically evaluated until 15 years after itsintroduction. At that time, investigators found that asizable minority of women with the urodynamicdiagnosis of stress incontinence did not have a positivecotton swab test result [66] (considered a strainingangle >30°) and that many women with a positivecotton swab test result did not have stress urinaryincontinence on urodynamic testing. The test was notable to distinguish women with stress incontinencefrom continent control subjects [67,68], or womenwith stress incontinence from those with other urologicdisorders [69].The cotton swab test is now usedprimarily to assess results of incontinence surgery orto determine whether the degree of urethralhypermobility may influence treatment outcomes.Although the test is simple to perform, the insertionof the small cotton swab may be uncomfortable forsome women. Investigators have explored othermethods to assess hypermobility, including the POP-Q anatomic evaluation system and ultrasonography.In one study, the correlation coefficient between thecotton swab straining angle and point Aa (the urethro-vesical junction) on the POP-Q system was 0.47 [70].However, the cotton swab test was positive in 95% ofpatients with stage II prolapse at point Aa and in 100%
of patients with stages III and IV prolapse at point Aa,which suggests that the test may be unnecessary inpatients with stage II or greater prolapse at point Aa.A study evaluating the use of a urinary catheter toassess urethral hypermobility used the Q-tip test forcomparison in women with urinary incontinence andpelvic organ prolapse. Results of the study showedreduced angles of excursion from resting to Valsalvamanoeuvre using a catheter [71].
Ultrasonography can be used to measure the anglebetween the urethra and an axis corresponding tothe pubic symphysis, the urethra, the bladder base,and the position of the internal urethral meatus. Othertests to document bladder neck mobility are used,including bead-chain cystourethrography, andvideocystourethrography. The report of the Committeeon Imaging of the urinary tract addresses the placeof these techniques.
A comparison study was conducted to assess theinterobserver reliability of the Q-tip test, the Sensor-Qtrade mark test and ultrasonographic measurementof urethral mobility in women. 90 women took part inthe study; and underwent one method of theassessment by two different clinicians. The correlationcoefficient of the Q-tip test, the Sensor-Qtrade marktest and the ultrasonographic measurement was 0.83,0.92 and 0.43, respectively. The Sensor-Qtrade markand Q-tip test showed a higher inter-observer reliabilityfor the evaluation of urethral mobility compared toultrasound assessment [71,72].
The Q-tip test has been used in a number of studiesevaluating changes in urethrovescial junctionhypermobility and efficacy of surgical treatment ofstress incontinence including mid-urethral tapes,vaginal wall sling procedures and Burch colposu-spension [73-80]. A study investigating factorsassociated with severity of stress incontinence inwomen found that reduced urethral mobility using theQ-tip test was associated with greater severity ofurinary incontinence [81].
Correlation of Q-tip test and urethroscopic imaging ofthe f bladder neck was assessed in stress incontinentwomen. After the Q-tip test, patients underwent anurethroscopy; at bladder capacity the patient wasasked to strain and opening or closing of the bladderneck was noted. An abnormal Q-tip test duringValsalva (> 30°) was observed in 80% of patients. Theauthors suggest that a Q-tip test could diagnosebladder neck opening with a sensitivity of 91% anda specificity of 35% [82]. The correlation between thestraining Q-tip angle and anterior vaginal wall prolapseassessed using the POP-Q system has beeninvestigated in a number of studies. Noblett et alassessed the correlation between urethral mobilityand anterior wall prolapse, in order to determinewhether the Q-tip test was necessary in patients withstage 0/1 prolapse graded using the POP-Q system.

344
Results of this study suggested that the POP-Q systemwas highly predictive of urethral hypermobility; thepositive and negative predictive values were 82%and 94% respectively [83].
A retrospective analysis conducted by Larrieux et alalso concluded that descent at point Aa is a strongpredictor of urethrovesical junction mobility, howeverurethral length did not affect the correlation betweenQ-tip angle and point Aa [84]. Zyczynski et alinvestigated the correlation between POP-Q gradedanterior vaginal wall prolapse and Q-tip test findingsin urinary incontinent women. The study showed thaton clinical examination, one third of the studyparticipants with urethral hypermobility by Q-tip testhad a well supported urethrovescial junction. Theresults of this study suggested that clinicians whodetermine urethral mobility by watching descent ofthe distal anterior vagina during Valsalva manoeuvremay underestimate the true incidence of urethralhypermobility [85].Mattison et al and Rosencrantz etal conducted retrospective reviews of a clinicaldatabase in order to determine the correlation betweenPOP-Q evaluation of anterior vaginal wall prolapse andthe straining Q-tip angle [86]. Mattison et al found thecorrelation between q-tip straining angle and pointAa was 0.54 (P<0.001). Rosencratz found correlationvalues between 0.26 and 0.78. Both studies concludedthat urethral hypermobility could not be predicted fromPOP-Q measurement alone [87].The Q-tip has notbeen shown to be predictive of Valsalva leak pointpressures in women with urethral hypermobility andstress urinary incontinence [88].
e) Vaginal examination
Presently there are few scientific data documentingthe parameters of a normal pelvic examination inwomen of various ages and with various obstetricalhistories. The components of the examination havenot been universally agreed upon. It seems intuitivethe examination should include an assessment of thebony architecture, pelvic floor muscle tone and musclemass, connective tissue support, the epithelial liningof the vagina, the size, location, and mobility of theuterus, the adnexal structures, and innervation of thepelvic floor structures.
It is important to establish the oestrogen status asoestrogen receptors are present within the lowerurinary tract [89], and are shown to influence cellproliferation [90]. Women with oestrogen deficiencymay complain of urgency and frequency and recurrenturinary tract infections may develop because of lossof urethral mucosal coaptation. In women ofreproductive age symptoms may vary with themenstrual cycle [91].
The well oestrogenised vagina has a thickenedepithelium, with transverse rugae in its lower two-thirds. The poorly-oestrogenised vagina has a thinnedepithelium with loss of transverse rugae [92]. A number
of authors have shown that vaginal pH levels aregenerally 5 or less in women with no infection and otherdefinitive signs of good oestrogen effect. The use ofa pH indicator paper may help you evaluate theoestrogen status in women with no vaginal infection[93]. The appearance of vaginal secretions maysuggest a vaginal infection; urine within the vaginasuggests genitourinary fistula, hypospadias or ectopicureter.
Bimanual examination is performed to determine thesize of the uterus and of the ovaries. Some womenhave co-existent pelvic disease which may requireattention in addition to the urinary incontinence. Whenhysterectomy or oophorectomy is indicated, there isno adverse effect on surgical success with acolposuspension procedure. Pelvic masses are rarelythe cause of urinary incontinence, and rarely doeshysterectomy by itself relieve incontinence.
Urethral diverticula are occasionally congenital butmost are acquired. They may have either a simple orcomplex sacculation. Many patients with urethraldiverticula are asymptomatic and need no treatment.Symptomatic patients report recurrent cystitis,frequency, dysuria, dyspareunia, urinary incontinenceand voiding difficulties. On clinical examination a sub-urethral mass may be palpable; the urethra is usuallytender; and, if the sacculation communicates with theurethra, it may be possible to express a purulentexudate from the urethra. Occasionally, a stone maydevelop within the diverticulum [94]
6. PELVIC ORGAN PROLAPSE
The anterior, superior, and posterior segments of thevagina should be examined for pelvic organ prolapse.The examiner may use a mirror to demonstrate thefindings to the patient; she can then confirm that theexaminer has identified the extent of prolapse thatshe experiences. If the patient indicates that shenormally has a greater amount of prolapse that youpresently see, provocative manoeuvres which normallyare associated with her symptoms may be undertaken,and the examination repeated while the patient isstanding.
Several systems for the description and classificationof prolapse have been described. This may bequantified descriptively as slight, moderate, marked[95], or first, second and third degree, or objectivelyusing the Baden and Walker halfway method [96], orthe International Continence Society Pelvic OrganProlapse Quantification (ICS POP-Q) [97], or modifiedPOP-Q [98]. In the latter, utilizing the introitus as thethreshold, six specific vaginal sites and the vaginallength are assessed using centimetres of measure-ment from the introitus. In addition, the lengths of thegenital hiatus and perineal body are measured incentimetres. Figure 1 demonstrates the summarydiagram of this quantitative system.

345
A simplified technique for use of the POP-Q systemwas evaluated for inter-examiner agreement and inter-system association with the standard POP-Q examin 48 subjects. The four areas examined are theanterior and posterior vaginal walls, the apex/cuff,and the cervix. In a patient who is post-hysterectomy,only three measurements are taken: the anterior andposterior vaginal walls and the cuff scar/apex. Kappastatistics (0.86) revealed good agreement betweenexaminers using the simplified POP-Q system. Inter-system agreement was evaluated using Kendall’stau-b statistic (0.90) also indicating good agreementbetween the two classification systems [99].
The pelvic organ prolapse quantification index (POP-Q-I) has been proposed for use in the research setting,as it provides a continuous variable rather thancategorical variables. The POP-Q was modified suchthat points Aa, Ab, C, Bp, and Ap are measured. PointD is used only for the identification of patients withcervical hyperplasia. Genital hiatus, perineal body,and total vaginal length are not assessed. The POP-Q-I has not undergone rigorous validation [100,101].
The original POP-Q system has been used extensivelyin research settings for the assessment of short-andlong-term outcomes of pelvic floor surgeries [102 - 105]including the use of mesh [106-120], laparoscopicsurgery [121-123].
robotic assisted vault suspension [124], sexualdysfunction associated with pelvic organ prolapse,[125- 128], and also in community-based prevalencestudies and selected patient populations with pelvicorgan prolapse [129-138].
The POP-Q has been used in the validation of theBrazilian version of the vaginal symptoms module ofthe ICIQ, [139] and for an interviewer-administeredpelvic floor symptoms questionnaire [140].
A novel speculum has been designed to facilitate useof the POP-Q system. The top and bottom blades ofthe speculum are adjustable and are marked incentimeters from the tip to the base of the blade.[141] Figure 2.
POP-Q definitions ICS report - simplified
Pelvic organ prolapse is defined as the descent ofone or more of anterior vaginal wall, posterior vaginalwall, and apex of the vagina (cervix/uterus) or vault(cuff) after hysterectomy.
Anterior vaginal wall prolapse is defined as descentof the anterior vagina so that the urethra-vesicaljunction (a point 3cm proximal to the external urinarymeatus) or any anterior point proximal to this is lessthan 3cm above the plane of the hymen.
The well-supported anterior vaginal wall should notcross the longitudinal axis of the vaginal canal.Hypermobility of the urethra-vesical junction isdemonstrated by having the patient perform a
maximum Valsalva effort. In women with hypermobilitythe increase in intra-abdominal pressure causesdescent of the urethra-vesical junction (bladder neck).On vaginal examination there may be loss of thetransverse crease between the lower and middlethirds of the anterior vaginal wall and descent of theanterior vaginal wall. Anterolateral protrusion into thevaginal canal may represent unilateral or bilateraldetachment of the pubocervical fascia along theanterolateral vagina sulcus from its attachment to thearcus tendineus fascia pelvis (white line). Centralprotrusions of the anterior vaginal wall may representdefects in the pubocervical fascia below the trigoneand base of the bladder. Advanced prolapse of theupper anterior vaginal wall may obstruct a well-supported bladder neck.
Prolapse of the apical segment of the vagina isdefined as any descent of the vaginal cuff scar (afterhysterectomy) or cervix, below a point which is 2cmless than the total vaginal length above the plane ofthe hymen. Descent of the cervix or of the vaginalapex following hysterectomy, below the level of theischial spines is evidence of a defective vaginalsuspension mechanism. In some women, theintravaginal portion of the cervix may becomeelongated and cause the cervix to extend into thelower vaginal canal, simulating prolapse; howeverthe fundus may have good support. In other womenthe uterus may prolapse fully outside the hymen asuterine procidentia. Following hysterectomy the vaginalcuff may be well supported or may prolapse fullyoutside the hymen along with other vaginal segments.
Posterior vaginal wall prolapse is defined as anydescent of the posterior vaginal wall so that a midlinepoint on the posterior vaginal wall 3cm above thelevel of the hymen or any posterior point proximal tothis, less than 3cm above the plane of the hymen.The well-supported posterior vaginal wall should notcross the longitudinal axis of the vaginal canal.Posterior protrusions into the vaginal canal are mostcommonly caused by defects in the recto-vaginalfascia allowing protrusions of the small bowel(enterocoele) and/or rectum (rectocele). Normally,the anterior vaginal wall lies upon the posterior vaginalwall. Therefore, protrusions of the posterior vaginal wallcan affect the function of the urethra and bladderwhich lie upon the anterior vaginal wall. For example,distal loss of support in the posterior segment mayresult in a bulge which compresses the urethra andaffects voiding.
As with most new systems, clinicians and researchershave mixed opinions regarding this system. Excellentinter- and intra-observer reliability has beenestablished, although patient position may affectreproducibility in that the degree of pelvic organprolapse was higher when women were examined ina birthing chair at a 45° angle rather than in dorsallithotomy. This system has been widely adopted for

346
Figure 1 : ICS POP-Q. Six sites (points Aa, Ba, C, D, Bp, and Ap), genital hiatus (gh), perineal body (pb), andtotal vaginal length (tvl)used for pelvic organ support quantitation.
Figure 2 : Speculum with adjustable blades and scale markings designed to allow easier assessment ofpelvic organ prolapse using the POP-Q system. (Diokno AC, Borodulin G. A new vaginal speculum forpelvic organ prolapse quantification (POPQ). Int Urogynecol J Pelvic Floor Dysfunct. 2005 Sep-

347
pelvic organ prolapse researchers. In addition tocollecting specific centimetre measures, an ordinalstage (0-IV) can be assigned.
Absence of prolapse is categorised as stage 0 support;prolapse can be staged from stage I to stage IV. Theclinical utility of such a classification might bequestioned, since clearly some degree of descent isthe norm especially in a parous population. In a studyof 477 women attending for annual gynaecologicalexamination, Swift et al found that the average numberof positive responses to a 7-question prolapsequestionnaire was 0.27 in patients with stage 0prolapse, 0.55 for stage I, 0.77 for stage II, and 2.1for stage III. They concluded that women with prolapsewith the leading edge beyond the hymenal ring hada significantly increased likelihood of having symptoms.In a general population of Swedish women ages 20-59, the prevalence of prolapse was found to be 31%,whereas only 2% of all women had a prolapse thatreached the introitus. It might seem more reasonabletherefore to define prolapse not on the basis of anyfinding greater than stage 0, but on the basis of findingswith a significant likelihood of being associated withsymptoms.
Urinary incontinence and pelvic organ prolapse areseparate clinical entities which often coexist. Significantprotrusions of the vagina can obstruct voiding anddefecation. Surgical repair of one pelvic support defectwithout repair of concurrent asymptomatic pelvicsupport defects appears to predispose to accentuationof unrepaired defects and new symptoms. Womenwith pelvic organ prolapse may have to reduce theirprolapse in order to void. Women with pelvic organprolapse and a large PVR should be evaluated forvoiding phase dysfunction (e.g., outlet obstruction,detrusor hypotonia).
Although anatomy can be measured and assessedaccurately, reproducibly and reliably, the relationshipof these anatomic findings with functional abnormalitiesis not well understood. For example, supportabnormalities in the anterior vaginal wall are commonin vaginally parous women; however, stress urinaryincontinence is not always associated with thisanatomic alteration. Likewise, distal posterior vaginalwall support abnormalities may exist with or withoutdefecation abnormalities. The important relationshipsbetween anatomy and function are one of the mostpressing research needs in the field of physicalexamination for women with pelvic organ prolapse.
Other important research needs include the develop-ment of clinically relevant ordinal staging that moreappropriately separates meaningful prolapse fromanatomic changes following vaginal delivery. Suchrevised staging would allow a meaningful dialog aboutthe appropriate surgical indications for pelvic organprolapse and development of clinically relevantanatomic outcome measures.
7. RECTAL EXAMINATION
Digital rectal examination allows the description ofobserved and palpable anatomical abnormalities andis the easiest method of assessing pelvic floor musclefunction in children and men. In addition, rectalexamination is essential in children with urinaryincontinence to rule out faecal impaction. In all womena digital rectal examination is also performed to assesssphincter tone (both resting and active) and to detectfaecal impaction or a rectal mass.
8. ADDITIONAL BASIC EVALUATION
a) Pad tests
The objective of pad testing is to quantify the volumeof urine lost by weighing a perineal pad before andafter some type of leakage provocation. This testhas also been used in an attempt to distinguishcontinent from incontinent women. Pad tests can bedivided into short-term tests, usually performed understandardized office conditions, and long-term tests,usually performed at home for 24–48 hours. Pad testsare generally performed with a full bladder or with afixed known volume of saline instilled bladder beforebeginning the series of exercises. A pad weight gain>1 g is considered positive for a 1-hour test, and a padweight gain >4 g is positive for a 24-hour test. Thereis wide variation in the pad weight gain in incontinentwomen participating in clinical trials. Although somestudies have found high test-retest correlations in padtests [142,143]. other studies have reported low inter-subject and intra-subject reliability [144,148]. Traditionalpad testing may be negative in women with mildleakage; an alternative “paper towel test” was shownto be a simple and reliable measure of cough-relatedurine loss typical of mild stress incontinence. (149)Long-term tests are more reproducible. The correlationcoefficient between total leakage during two 24-hourpad tests is good, at 0.66 [150] and 0.82 [151] andincreased to 0.90 in one study in which two 48-hourperiods were compared. There was no correlationbetween the leakage volume found in the 48-hourtest and a standard 1-hour test.
b) Dye testing
When it has proved impossible to confirm a patient’scomplaint of urinary leakage, it may be appropriate toseek to confirm firstly that the reported discharge isin fact urinary, secondly that the leakage is extra-urethral rather than urethral, and thirdly to establishthe site of leakage. Although other imaging techniquesundoubtedly have a role in this regard, carefullyconducted dye studies should be considered.Excessive vaginal discharge or the drainage of serumfrom a pelvic haematoma postoperatively may simulatea urinary fistula. If the fluid is in sufficient quantity tobe collected, biochemical analysis of its urea contentin comparison to that of urine and serum will confirmits origin. Phenazopyridine may be used orally (200mg

348
tds), or indigo carmine intravenously, to stain the urineand hence confirm the presence of a fistula. Theidentification of the site of a fistula is best carried outby the instillation of coloured dye (methylene blue orindigo carmine) into the bladder via catheter with thepatient in the lithotomy position. The traditional ‘threeswab test’ has its limitations and is not recommended;the examination is best carried out with directinspection; multiple fistulae may be located in thisway. It is important to be alert for leakage aroundthe catheter, which may spill back into the vaginacreating the impression of a fistula. It is also importantto ensure that adequate distension of the bladderoccurs as some fistulae do not leak at small volumes;conversely, some fistulae with an oblique track throughthe bladder wall may leak at small volumes, but notat capacity. If leakage of clear fluid continues after dyeinstillation a ureteric fistula is likely, and this is mosteasily confirmed by a ‘two dye test’, using Phenazo-pyridine to stain the renal urine, and methylene blueto stain bladder contents[152]
c) Pelvic floor muscle strength
Pelvic floor muscle function: can be qualitativelydefined by the tone at rest and the strength of avoluntary or reflex contraction as strong, weak orabsent or by a validated grading system (e.g. Oxford1-5). A pelvic muscle contraction may be assessedby visual inspection, by palpation, electromyographyor perineometry. Factors to be assessed includestrength, duration, displacement and repeatability.
The continence mechanisms imply that integrity ofthe levator ani and external urethral sphincter isnecessary to maintain continence [153]. It is thereforeimportant to test the contractility of these muscles.Once the patient understands how to contract thepelvic floor muscles correctly, the evaluation is carriedout during a maximum contraction [154].
STRENGTH is defined as the maximum force or tensiongenerated by a muscle or muscle group [155]. Itreflects the power, endurance and functional statusof the muscle.
WEAKNESS is defined as failure to generate theexpected force.
FATIGUE is defined as failure to maintain the expectedforce with continued or repeated contraction [156].
When considering methods/devices used to measurepelvic muscle strength, cost and availability should berecognized as important factors. Four methods ofassessment are considered here: observation, digitalpalpation, perineometry and cotton swab (Q-tip)testing.
Observation - This qualitative measure can detect anin-drawing of the anus, lifting of the posterior vaginalwall and narrowing of the vaginal introitus (females);an in-drawing of the anus and slight lifting of the penis(males).
• Advantages: Suitable for both sexes and all agegroups, where an internal evaluation may be in-appropriate. Inexpensive. Able to detect reflexcontraction with cough, and bulbo-cavernosusreflex. Observe accessory muscle activity.
• Disadvantages: Subjective. Cannot distinguishright and left sides independently. Generallyobserving activity of the superficial perinealmuscles, and assuming levatores are respondingin a like manner. Difficult to observe when thepatient is standing.
Digital palpation - Palpation of the right and leftlevator ani, per vaginam. Palpation of the perinealbody.
• Advantages: Suitable for both sexes. Inexpensive.Able to differentiate right from left. Quantitative -using modified Oxford scale or other systems[157,158]. Able to measure strength and endurance.Can detect reflex contraction with cough andpatient’s ability to hold contraction during a cough.Can be used when the patient is standing.
• Disadvantages: Subjective. Not sensitive.
Perineometer - Manometric measure of change in avaginal/anal pressure probe. Sensitivity depends onthe device.
• Advantages: Relatively inexpensive. Able tomeasure strength and endurance. Quantitative.Can be used when the patient is standing.
• Disadvantages: Unable to distinguish right fromleft. Pressure changes may be caused by increasein intra-abdominal pressure, due to co-contractionof the abdominal muscles. No ‘Gold Standard’device; different results with different probe sizesand materials [159].
Cotton swab (Q-tip) test Downward, posteriormovement of stem (measured on a goniometer) isdependent on the strength of the contraction of thepubo-coccygeus muscles, and mobility of the urethra[160].
• Advantages: Inexpensive. Can measure strengthand endurance.
• Disadvantages: Lacks sensitivity and specificity.Invasive. Females only.
The information learned from assessment of pelvicfloor muscle strength has the following practicalapplications:
1. The patient has good pelvic floor muscles that needskill training to help maintain continence. DeLanceyand associates have described ‘knack’ teaching[161,162].
2. The patient has weak muscles that are capable ofcontracting but need strength and skill training.

349
An effective exercise program should increaseresting tone (Type I fibres) as well as improve theability of fast twitch (Type II) fibres to respond toincreases in intra-abdominal pressure [163].
3. The patient has no perceptible contractions andneeds further evaluation (EMG, MRI, neuro-physiologic testing) or passive contraction therapyi.e., functional electro stimulation.
Recommendations
Future research
1. Correlation of symptoms and physical findings withurodynamic and colorectal investigations, and bothbasic and complex evaluations with treatmentoutcomes.
2. The development of a clinically relevant ordinalstaging that meaningfully separates significantfrom insignificant pelvic organ prolapse.
3. Impact of surgical interventions for incontinenceon pelvic organ support, and for pelvic organprolapse on continence mechanisms.
1. CHARACTERISTICS OF MALE INCONTINENCE?
In the male patients, lower urinary tract dysfunction,and obstruction from benign prostatic enlargementpresents a multi-factorial paradigm for symptomaetiology. Lower urinary tract symptoms (LUTS) inmen have a significant effect on quality of life (QOL),as compared with the unaffected general population.[163]. Several epidemiological reports demonstratedthat overactive bladder (OAB) syndrome also increasewith age in men [164,165]. Older age and highergrade of obstruction has been reported in men withbladder outlet obstruction and idiopathic detrusoroveractivity [166].
In the NOBLE study, a different sex-specific patternemerged for OAB with or without urge incontinence[165]. The prevalence of OAB with urge incontinencedisplays a steeper age-related increase among womenthan among men and the gender difference isstatistically significant. In women, OAB with urgeincontinence increased more than nine-fold from 2.0% in those 18-24 years of age to 19.1% among those65-74 years of age. In contrast, a substantial increasein prevalence of OAB with urge incontinence amongmen did not occur until 65 years of age, reaching8.2% for ages 65-74 years and 10.2% for those 75years and older. In men, OAB without urgeincontinence increased approximately three-fold, from8.5% below 45 years of age to 21.8% after 55 yearsof age, whereas OAB without urge incontinencegradually increased in women less than 44 years ofage and reached a plateau in women over the age of44 years.
‘Prevalence ratios for OAB with urge incontinenceand for OAB without incontinence were significantlyelevated for men who self-reported with a history ofprostate problems. Thus, the evaluation of men withsymptoms of OAB syndrome depends on theidentification and assessment of lower urinary tractobstruction that may be a cause (in part or in entirety)of the presenting symptoms.
The aetiology of obstructive symptoms may vary, frombenign prostatic hyperplasia (BPH), urethral stricture,primary bladder neck dysfunction, or abnormal voidingdynamics of detrusor. Chronic prostatic painsyndromes (e.g. non-bacterial chronic prostatitis) andother pelvic floor dysfunctions can also present with
V. THE MALE PATIENT
1. Although the value of individual urinary symptomsand symptom complexes in predicting theunderlying abnormality of lower urinary tractfunction is not high, a significant proportion ofwomen with stress incontinence can be correctlydiagnosed from basic evaluation only. GradeC
2. The frequency/volume chart or urinary diary isthe most effective additional test for usealongside basic evaluation in primary orsecondary care.Grade C
3. In assessing patients with urinary or faecalincontinence, the clinician should consider allaspects of pelvic floor dysfunction, i.e. urinary,bowel, prolapse, and sexual function. Grade D
4. Prolapse visible at the introitus or below may beassociated with symptoms (Level 3) Indescribing patients with pelvic organ prolapse,one of the several systems available forclassification and quantification of urethralhypermobility and pelvic prolapse should beemployed. The ICS recommends the POP-Q.(Grade D). In addition, an assessment of pelvicfloor identification and strength should beconsidered. Grade D

350
a component of symptoms compatible with OAB. Inyounger men, primary bladder neck dysfunction is acommon cause of LUTS, with or without pelvic pain[167]. Functional abnormalities of striated sphincterrelaxation may also occur in young men [168] Thecomplexity of the presenting symptoms and the variousdifferential diagnoses mandate a thorough basicassessment of the lower urinary tract in men to planoptimal therapeutic intervention.
Another important issue in male patients isincontinence after surgery or intervention for BPOand prostate cancer. A survey in England of 5276patients who had undergone TURP found that one-third of men (n=1759 men) who were continent beforesurgery reported some incontinence 3 months postTURP [169]. Recently many minimally invasive andsurgical techniques in management of BPO havebeen reported. A systematic review of the literatureshowed Urinary incontinence is more often seenfollowing TURP (1.4%). The rate of urinaryincontinence after other techniques are as follows:HIFU; 0.0%, ILCP: 0.1%, TUMT: 0.1%, TUNA: 0.0%,TUVP: 0.9%, VLAP: 0.2%, HoLEP: 1.2% [170].
It has been reported that after permanent prostatebrachytherapy, urinary incontinence was observed 0-19% [171]. After radical prostatectomy, Donnellan etal reported that 6 % of men were mildly incontinent,6 % were moderately incontinent and 4 % wereseverely incontinent at 1 year after surgery [172].Carson et al. reported that incontinence occurs in 0.5to 1.0% of all patients undergoing prostatectomy forbenign disease; high rates (5 to 30%) are associatedwith radical prostatectomy [173].
Although prostate-ctomy has a clinically significantbeneficial effect on LUTS with significant improvementsof AUA symptom index and flow rate, [174, 175] urinaryleakage can have a major impact on QOL. Greaterdegrees of urine loss are correlated with greater botherand more significant life-style changes [172]. AMedicare survey by Fowler showed that in 1072patients, more than half of the patients with urinaryleakage considered it to be a medium or large problem[176]. In spite of these findings, many investigatorshave been encouraged by overall patient satisfactionwith surgery and patients willingness to undergosurgery again, if faced with the same situation [176].
In the immediate postoperative period, stress andurge incontinence are common. This has beenattributed to varying degree of oedema and inflam-mation present in the healing prostatic urethra. Themajority of men achieve continence without invasiveintervention following total prostatectomy. Finalcontinence status should be measured using self-administrated disease specific instruments at 24months after operation [176]. And no factors (age,severity of LUTS, Gleason score, bilateral nervesparing surgery and estimated blood loss) were
identified that predicted early return of continence[172].
Post-prostatectomy incontinence may be caused bysphincter malfunction and/or bladder dysfunction.[177,178]. Urinary control in the adult male dependson integrity of both the internal and external sphincters.During TURP, the internal sphincter mechanism isvirtually destroyed, and in some cases, the externalsphincter is also damaged. Thus post-prostatectomystress incontinence may result.
In a recent study of patients undergoing radicalprostatectomy that specifically evaluated detrusordysfunction [179] de novo detrusor underactivity andimpaired or poor compliance, presumed to be aconsequence of bladder denervation, occurred in alimited proportion of patients (28.6% and 18.4%respectively), and this bladder dysfunction resolvedin the majority within 8 months. Detrusor underactivityand decreased bladder compliance are also pre-existing conditions in about 30% and 20% of patients.
The conditions relate to the presence of BOO, and theydo not appear to be influenced by prostatectomy.Persistent detrusor overactivity after obstruction reliefis probably related to concomitant sphincter deficiencyand stress urinary incontinence, which increaseafferent nerve activity of the proximal urethra andinduce involuntary detrusor contractions [180].
Obstruction after prostatectomy, resulting from ananastomotic stricture or residual prostatic tissue (postTUR-P), may also play an important role in thedevelopment of post-prostatectomy incontinence.Obstructing stricture often causes increase in post-voidresidual urine, resulting in the urinary leakage and/ora weak urinary stream. It has been reported that theanastomotic stricture treatment rates after radicalprostatectomy are 16% to 33% [181,182].
2. GENERAL MEDICAL HISTORY
The medical history should focus on the urinary tract,previous surgical and radiation therapy history, medicalcondition and symptoms that may cause to bladderdysfunction or polyuria, familial history of prostatediseases (BPH and cancer), and a review of sexualand bowel habits. Urinary incontinence is rare in menwithout a history of previous trauma or prostatic orpelvic surgery; therefore, neurogenic bladderdysfunction must be considered in men with no historyof surgery or trauma. A critical assessment of currentmedications is recommended to exclude the effectsof any pharmacological agents on lower urinary tractfunction.
In the evaluation of the patients with post-prostate-ctomy incontinence, an important aspect of the historyshould be a description of the type and severity ofincontinence and precipitating events, Severity maybe determined by the number of episodes per day, the

351
need for protection (e.g., pads, penile clamp, externalcatheter), and the impact of incontinence on activitiesof daily living. Bladder diaries and pad tests canquantify severity. The presence of other LUTS suchas OAB and decreased force of urinary stream shouldbe determined.
3. SYMPTOM ASSESSMENT
Diagnostic evaluation of men with LUTS depends onan initial estimation of subjective bother and objectivedata on bladder emptying. Because the occurrenceof LUTS does not necessarily indicate concomitantprostate enlargement and/or obstruction, specificmodalities should be used to ascertain the potentialfor the aetiologic role of these entities. A bladder diarymay be useful in almost all male patients, especiallyin those with OAB. Bladder diary completion by thepatient provides useful evidence about the normalurinary habits of the patient, including giving someestimate of bladder capacity and diurnal and nocturnalfrequency, urgency and incontinence. The dataobtained from frequency-volume chart provide a strongcorrelation to cystometric capacities and arereasonably immune to the effect of detrusor overactivityin men with LUTS [183]
A variety of symptom scores have been described toassess male patients with LUTS. In men, the AmericanUrological Association symptom score for BPH (AUA-7) is most commonly used in North America forassessment of subjective symptoms. However, equallyreproducible data can be obtained from theInternational Prostate Symptom Score (IPSS), theICSmale questionnaire (now renamed theICIQMLUTS, long and short forms, as part of the ICIQmodular questionnaire: www.iciq.net).
The IPSS has been the most widely used (in manycountries and languages), but neglects the symptomof urgency incontinence, a symptom that producessignificant bother. The ICIQMLUTS (ICSmale-SF) isslightly longer, but takes into account the symptom ofurgency incontinence, and in fact may be divided intovoiding and incontinence subscores. To date, it hasnot been as widely used as the IPSS, but may seemore widespread use as part of the ICIQ ModularQuestionnaire.
Among LUTS, urgency, nocturia, and hesitancy aremost bothersome, whereas weak stream, urgency,and frequency are the most prevalent in pooledpopulations being evaluated for BPH [184] Post-micturition dribbling is often provoked by an obstructingdisease such as BPH or urethral stricture but canalso be a symptom of a urethral diverticulum. Post-void residual urine volume and careful palpation of thegenitalia are recommended in these patients.
To determine the cause of post-prostatectomyincontinence, many studies have stressed the lack
of reliability of symptoms and emphasised theimportant role of urodynamic testing [185,186].Nevertheless, valuable information can be gainedfrom a careful history with regard to incontinence,especially when related to sphincter dysfunction. Thesymptom of stress incontinence is highly predictive ofthe presence of sphincter dysfunction. Chao and Mayofound that 67 of 71 men with post-prostatectomyincontinence secondary to sphincteric dysfunctioncomplained of the symptom of stress incontinence[187]. Similarly, Ficazzola and Nitti found 95% positivepredictive value and a 100 % negative predictive valuefor symptom of stress incontinence [177]. Urgeincontinence as a predictor of bladder dysfunctiondose not seem to be as valuable, and the presenceof bladder dysfunction cannot be determinedaccurately without urodynamic testing [177,187].
4. PHYSICAL EXAMINATION
A general physical examination with specific attentionto the presence or absence of a distended bladder,excoriation of the genitals secondary to urinaryincontinence, evidence of urethral discharge and afocused neurological examination is also highlyrecommended.
The assessment and treatment algorithm focuses onthe abdominal examination, digital rectal examination(DRE) and neurological testing of the perineum andlower extremities. In a patient suspected of neurogenicbladder, evaluation of perineal sensation and lowerextremity neuromuscular function, and anal sphinctertone, which is often decreased in neurogenic patients[188] is important. A focused neurogenic examinationshould also assess the patient’s general mental statusand ambulatory status. The examination should alsoinclude external genitalia, location of the urethralmeatus, retractability of the foreskin and evidence ofcongenital malformation. Abdominal palpation shouldbe performed to evaluate bladder distension, especiallyin elderly incontinent men, who may have overflowleakage due to obstruction. In patients suspected ofurinary retention, post-void residual volume (PVR)should be measured. The patients with incontinenceshould be asked to cough and to perform a Valsalvamanoeuvre so that the presence of stress incontinencecan be ascertained.
DRE should include palpation of the prostate to assesssize, symmetry and consistency of the gland and itsrelation to the pelvic sidewall and the rectum. Thelocally advanced prostatic cancer can also produceOAB-like symptoms. DRE may exclude prostaticcancer, although its specify and sensitivity is low [189]DRE tends to underestimate the true prostatic size:if the prostate feels large by DRE, it usually also isfound to be enlarged by ultrasound or othermeasurement technique [190, 191]. Prostate volumehas been recently associated with the risk of BPH

352
progression [192] and response to treatment [193].It has been reported that men with BPH with idiopathicdetrusor overactivity showed a significantly higherincidence (54%) of intravesical protrusion of theprostate [194]. This finding suggests that intravesicalprotrusion may in some way increase afferent impulsesfrom the prostate and alter the stability status of thebladder. Occasionally tumours of the anal canal canbe diagnosed while performing DRE of the prostate.
Incontinence combined with evacuation problems ina man often requires further investigation includingurodynamics. It may be helpful to ask these patientsto measure the voiding time for the first voided 100ml on several different occasions.
5. URINALYSIS AND URINE CYTOLOGY
Bladder cancer, carcinoma in situ of the bladder,urinary tract infections, urethral strictures, and bladderstones can cause OAB-like symptoms in aged men.Although haematuria or pyuria is not universallypresent in those conditions, urinalysis is important torule out these diseases. Urinalysis is not a single test,complete urinalysis includes physical, chemical, andmicroscopic examinations. Dipstick urinalysis iscertainly convenient but false-positive and falsenegative results may occur. It is considered aninexpensive diagnostic test able to identify patients withurinary tract infection as indicated by the presence ofleucocyte esterases and nitrites. A substantialproportion of older patients with chronic OAB-likesymptoms have significant bacteriuria, sometimesaccompanied by pyuria. In men, recent urinary tractinfections were associated with OAB without urgeincontinence (prevalence ration=2.9; 95% CI: 1.6-5.0) [165].
However, infection may exist in the absence of pyuriaand, in the elderly population, pyuria may develop inthe absence of urinary tract infection. Microscopichaematuria can be easily identified by dipstickingbecause of the presence of haemoglobin. Thedetection of haematuria is important because thecondition is associated with a 4-5% risk of diagnosingurological disorder or malignancy within 3 years.Because of the high prevalence of urinary tractinfection and the increase of LUTS in the presenceof urinary tract infection, all guidelines on themanagement of patients with LUTS suggestive ofBPO, and urinary incontinence, endorse the use ofurinalysis in primary care management [195,196].
Urine cytology is also recommended in male patientswith haematuria and a predominance of storagesymptoms, especially with a history of smoking orother factors, to aid in the diagnosis of bladdercarcinoma in situ and bladder cancer
6. MEASUREMENT OF THE SERUM CREATININE
Epidemiological studies in community dwelling men
have shown the absence of any association betweenBPO / BPE / BPO and chronic kidney disease [197]suggesting that screening for renal function is notjustified in male patients Recently, data from theMTOPS study showed that the risk of developing denovo renal failure in men with LUTS is low (less than1 %) suggesting that is not necessary to monitor renalfunction in patients with LUTS / BPO [197].
7. MEASUREMENT OF THE SERUM PROSTATE-SPECIFIC ANTIGEN (PSA)
In most patients, a normal DRE may be sufficient toexclude locally advanced cancer as a cause of LUTSor OAB. There is no consensus as to the measurementof prostate specific antigen (PSA) in patients withLUTS. The rationale for measuring PSA is twofold:to screen for prostate cancer [198] and to measure aparameter with prognostic value for the progressionof BPH and the response to treatment [192,193].Because prostatic cancer is one of the potential causesof LUTS or OAB in men, PSA (together with DRE) isa relatively sensitive way to exclude prostatic canceras a diagnosis [199,200].
However, it is important to understand that about 25%of men with BPH have a serum PSA greater than 4ng/ml. Because of the overlap between serum PSAvalues in men with BPH and those with clinicallylocalised prostate cancer, other parameters (PSAvelocity, free/total PSA ratio, complexed PSA andPSA density) will assist diagnostic specificity [201,202]. It has been suggested that a relationship betweeninitial PSA level and subsequent prostate cancerdetection with a stepwise increase in cancer detectionrate (from <1% to 58%) in patients with <1.0 ng/ml,1.1-2.5, 2.6-4.0, 4-1-10.0 and >10 ng/ml PSA valuein over 26.000 patients enrolled in a screeningprogramme [203]. In addition, Thompson reporteddata on prostate cancer prevalence from the prostatecancer prevention trial [204] confirming a stepwiseincrease in the risk of having a prostate cancer inpatients with serum PSA from 0.5 to 4.0 ng/ml butshowing the limitation of the current threshold of 4.0ng/ml. Change of PSA threshold from 4.0 to 2.0 ng/mlhas been proposed but currently no consensus exists[205]. PSA measurement is recommended in menwith LUTS and a life expectancy of over 10 years inwhom the diagnosis of prostate cancer would changethe management of patient’s symptoms.
It has been reported that the role of IPSS score in theassessment of BOO is questionable, and that thegrade of obstruction is more related to prostate volume,PVR, and Qmax [44]. It has been demonstrated thatmoderate-to-severe LUTS in men can result in urinaryretention. The incidence of retention in men withuntreated LUTS in community-based trials is 6.8 per1000 during longitudinal follow-up of 4 years [206]. Ifonly patients with moderate-to-severe symptoms areconsidered, the rate of retention increases to 25 per1000 [207] Moreover, in considering men with weak

353
urine flow, symptoms, and increased age, withouturodynamic evaluation, other parameters becomeindependently predictive of the development of acuteurinary retention. In a meta-analysis of predictors ofretention in pooled groups of placebo patients fromclinical trials of men with LUTS undergoing activeinterventions (4300 patients), Roehrborn et al. foundprostate-specific antigen and prostate volume to bestrong independent predictors of urinary retention andthe need for surgery in men with LUTS followed uplongitudinally in clinical trials [191,208].
Recently, Laniado et al (2004) [209] have also testedthe hypothesis that PSA level could be used to predictthe presence or absence of BOO, evaluated bypressure flow studies. In patients with LUTS, those witha PSA more than 4 ng/ml are significantly more likelyto have some degree of BOO. Conversely patients withPSA less than 2 ng/ml have a 33% risk of BOO.
Therefore, on the basis of these trials, untreated LUTSmay place the male patient at risk for potential clinicaldeterioration. Thus, periodical measurements of PVRare recommended in such patients.
Recommendations
Future research
1. Improve the understanding of the underlyingpathophysiology and contributory clinical factorsinvolved in the development and treatment ofdetrusor overactivity in the male patient, especiallyin differentiating the condition from female patients.
2. Development of simple, non-invasive, cost-effectivemethods to determine the contribution of bladderstorage and bladder emptying abnormalities inmale patients.
Basic assessment of faecal incontinence focuses ondetermining:
1. Type of incontinence
2. Functional limitations resulting from incontinence
3. Cause(s) of incontinence
1. HISTORY
History gathering requires particular tact in dealingwith this taboo symptom, but also a willingness to askdirect questions about the complaint. In taking ahistory, the necessary first step is to determine thenature of the incontinence being experienced by thepatient. True faecal incontinence must be differentiatedfrom conditions that cause seepage such as externalhaemorrhoids, fistulas, low rectal or anal tumours,and poor perineal hygiene.
Diagnostic administration of an enema may be usefulin this respect; retention of the enema suggests thatthe patient does not have clinically significant faecalincontinence. This serves to both clarify the patient’shistory, but also begins to suggest the anatomicaldeficit causing the incontinence (see below). The keyimportance of the history and examination is to identifyany conditions that are amenable to condition specificmanagement – these are cited in logical sequence inthe text below, and listed in the recommendation box.
a) Type of incontinence
• Flatus incontinence – incontinence of flatus due toinability to differentiate gas from solid or liquid
• Passive leakage – involuntary soiling of liquid orsolid stool without patient awareness
• Urge incontinence – inability to defer defaecationonce the urge is perceived, for long enough to finda toilet
The first two forms are primarily related to internalanal sphincter dysfunction, the latter form due toexternal anal sphincter dysfunction. (Grade B) [210].Soiling after defaecation is typically related to eithera defect in the internal sphincter or poor “snappingshut” of the external sphincter after voiding. (GradeC) [211]. It is also important to determine if theincontinence is for solid or only liquid stool; if for liquidstool, the possibility of a colonic cause of diarrhoeaneeds to be considered. (Grade B) [212].
I. FAECAL INCONTINENCEASSESSMENT
5A- B. INITIAL ASSESSMENT OFFAECAL INCONTINENCE
1. Male patients differ from female patients in thepresentation of LUTS. The incidence of OABwet is lower until the 7th decade. (Level 2)
2. Urinary stress incontinence is primarilyassociated with surgery of the prostate in malepatients. (Level 2)
3. Disorders of bladder emptying from benignprostatic enlargement should be consideredbefore treating male patients for OAB symptoms.(Level 2) ((Grade B).

354
b) Functional status
After confirming the nature of faecal incontinence, itis necessary to determine the impact of the conditionon a patient’s lifestyle and quality of life. Thisassessment offers the opportunity to both empathisewith the patient and to understand the pertinentemotional and social factors in the manifestation ofsymptoms. The history should include:
• Need to wear tissues or pads in underwear –indication of severity. (Grade B) [213-215]
• Degree of soiling of tissues, pads or underwear.(Grade C) [213,215]
• Duration, frequency and timing of incontinenceepisodes – indication of severity. (Grade C)[213,216]
Ability to wear clothing of choice, eat food of choice,participate in work and social activity. (Grade C)[213,216]
Severity of faecal incontinence can be classified as:
• minor - if faecal seepage occurs less than once amonth,
• moderate - if there is incontinence to solids morethan once a month or liquids more than once aweek, and
• severe - if there is loss of control of solids severaltimes a week or liquids on a daily basis.
An alternative classification grades continence asfollows:
Grade 1: Complete
Grade 2: Incontinence of flatus
Grade 3: Incontinence of flatus and liquid stools
Grade 4: Incontinence of flatus, liquid stools, and solidstools.
c) Aetiology
A careful, thorough history and full physicalexamination are essential and will identify the majorityof causes of faecal incontinence. The history shouldinclude:
• Dietary history – in particular excess ingestion ofsorbitol and caffeine. (Grade C) [217]
• Medical history – particularly anti-anginals, anti-hypertensives which may reduce sphincter tone,and ferrous sulphate or antacids which mayprovoke diarrhoea. (Grade C) [214]
• Presence of benign anal disease – haemorrhoids,fistula, anal warts. (Grade B) [218]
• History of chronic straining – suggestive of rectalmucosal prolapse, an important cause of internalanal sphincter dysfunction. (Grade B) [219]
• Obstetric history – particularly with regard to: (GradeB) [220,221]
- number of vaginal deliveries
- need for forceps or Ventouse
- birth weights
- duration of second stage(s)
- episiotomy
• Perianal surgery history – particularly: (Grade B)[222]
• Anal fissure surgery (sphincterotomy or analstretch)
• Fistula surgery
• Low colonic resection surgery
• History of pelvic radiation – risk of radiation proctitis(causing heightened rectal contractions) andinternal anal sphincter radiation damage (GradeB) [223]
• Symptoms of other pelvic floor problems (urinaryincontinence and pelvic organ prolapse), whichhave similar risk factors should be elicited (GradeC) [224])
• Cognitive assessment in appropriate patients(Grade C) [225]
2. EXAMINATION
Examination is focussed towards the detection ofevidence of incontinence and identifying the cause ofincontinence.
a) Evidence of incontinence
Physical examination should include inspection ofunderclothing for soiling and staining by stool, pus, ormucus.
Perianal skin should be examined for irritation andexcoriation due to over-zealous hygiene. Perianalinspection should include attempts to identify thefollowing: (Grade B) [215,226,227]
• Perianal excoriation or erythema – suggestive ofchronic passive soiling
• A patulous anus or one which gapes on gentletraction of the anal verge
• A “keyhole” deformity of the anal canal – suggestinga persisting sphincter defect
b) Cause of incontinence
Inspection may reveal scars from previousepisiotomies or obstetric tears. Abnormalities at theanal verge from previous surgery or a gaping anussuggestive of marked loss of function may be present.Perianal inspection should identify: (Grade C) [215,226,227]

355
• Scars from previous surgery
• Perianal disease – prolapsing haemorrhoids, fistula,anal warts
• Absence of perineal body – suggestive of obstetrictrauma; at its worst this may manifest as a cloacaldeformity
• Inspection for sphincter asymmetry whilst patientcontracts sphincter – suggestive of regionalsphincter defect
• Function of the puborectalis muscle (palpable atthe anorectal junction) is assessed by asking thepatient to squeeze the sphincter at which time thepuborectalis should push the examiner’s fingeranteriorly.
Digital examination should identify: (Grade C)[210,226,227].
• Rectal content – if faecal impaction is present thiscould explain incontinence
• Resting tone – indicative of internal anal sphincterfunction
• Voluntary and involuntary squeeze pressure –indicative of external anal sphincter function andpotential function, respectively. The latter is elicitedmost commonly by asking the patient to coughwhile assessing sphincter tone – a cough causesa near-maximal external sphincter contraction(analogous to the guarding reflex in the bladder)
• Regional sphincter defects – detected asasymmetry
• A thickened sphincter – suggestive of chronicstraining and occult rectal mucosal prolapse
If suggested by earlier findings (history of straining,thickened sphincter), the patient should be asked tosit on a commode and attempt voiding – the perineumshould then be inspected for evidence of a rectalmucosal or full thickness prolapse (Grade C) [219]
Proctoscopy or rectosigmoidoscopy with a rigidinstrument is a bedside test of value in excludingpotentially treatable causes of faecal incontinence:
• Anal tumours or polyps
• Low rectal cancers or adenoma (Grade B) [228].
• Solitary rectal ulcer syndrome – a functionaldisorder of evacuation, in which repeated strainingat stool and rectal self-digitation results in anulcerated area of the anterior rectal wall (Grade)[229].
Vaginal examination using a Simms speculum mayshow a rectocele, cystocele and/or uterine prolapse,all of which may contribute to developing faecal
incontinence (Grade C) [230].
Physiological and complimentary radiological testsare used to confirm clinical suspicions and provideobjective data on the function of the anorectum. Pelvicfloor dysfunction is a complex problem and multipletests may be needed based on the initial findings andcomplexity of the planned intervention.
KEY RECOMMENDATIONS FAECALINCONTINENCE
• It is essential to perform a baseline assessmentcomprising:
- focussed medical history
- a general examination
- an anorectal examination
a cognitive assessment (when appropriate)
• The following conditions should be specificallyassessed for as they may be amenable to definitivetreatment:
- rectal prolapse or third-degree haemorrhoids
- faecal loading
- potentially treatable causes of diarrhoea (eginflammatory bowel disease and irritable bowelsyndrome, infection, adenomas)
- acute anal sphincter injury including obstetric andother trauma
- acute disc prolapse/cauda equina syndrome
Future research
• Development and validation of a digital (finger)instrument to assess anal sphincter function(analogous to the instrument in existence forurological assessment of pelvic floor musculature).
• Development of a psychometrically valid andreproducible instrument to assess quality of life infaecal incontinence.
1. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, UlmstenU, et al. Standardisation of terminology of lower urinary tractfunction: report from the Standardisation Sub-committee ofthe International Continence Society. Neurourology andUrodynamics 2002;21:167-178.
2. Weber AM, Abrams P, Brubaker L, Cundiff G, Davis G,Dmochowski RR, et al. The standardization of terminologyfor researchers in female pelvic floor disorders. InternationalUrogynecology Journal 2001;12(3):178-186.
3. Hilton P. Urinary incontinence during sexual intercourse: Acommon, but rarely volunteered, symptom. Brit J ObstetGynaecol 1988;95(4):377-381.
4. Burgio KL, Locher JL, Goode PS, Hardin JM, McDowell BJ,Dombrowski M, et al. Behavioral vs drug treatment for urgeurinary incontinence in older women: A randomized controlledtrial. J Am Med Assoc 1998;280(23):1995-2000.
5. Gordon D, Groutz A. Evaluation of female lower urinary tract
REFERENCES

356
symptoms:overview and update. Curr Op Obstet Gynaecol2001;13(5):521-527.
6. Abrams P. Urodynamics. London: Springer-Verlag; 1997.
7. Addla S, Adeyouju A, Neilson D. Assessment of reliability of1-day, 3-day and 7-day frequency volume charts. EuropeanUrology supplements 2004(2):30.
8. Gerber GS, Brendler CB. Evaluation of the urologic patient:history, physical examination, and urinalysis. In: Walsh PC,editor. Campbell’s Urology. 8 ed. Philadelphia: Saunders;2002. p. 83-110.
9. Khadra MH, Pickard RS, Charlton M, Powell PH, Neal DE.A prospective analysis of 1,930 patients with hematuria toevaluate current diagnostic practice. J Urol 2000;163(2):524-7.
10. Al-Daghistani HI, Abdel-Dayem M. Diagnostic value of variousurine tests in the Jordanian population with urinary tractinfection. Clin Chem Lab Med 2002;40(10):1048-51.
11. Semeniuk H, Church D. Evaluation of the leukocyte esteraseand nitrite urine dipstick screening tests for detection ofbacteriuria in women with suspected uncomplicated urinarytract infections. Journal of Clinical MIcrobiol 1999;37(9):3051-3052.
12. European Urinalysis Guidelines. Summary. Scand J ClinLab Invest 2000;60:1-96.
13. Ouslander JG. Geriatric urinary incontinence. Dis Mon1992;38(2):65-149.
14. Ouslander JG, Schnelle JF. Incontinence in the nursinghome. Ann Int Med 1995;122(6):438-449.
15. Young SB, Pingeton DM. A practical approach toperimenopausal and postmenopausal urinary incontinence.Obstet Gynecol Clin N Am 1994;21(2):357-379.
16. McIntosh LJ, Richardson DA. 30-minute evaluation ofincontinence in the older woman. Geriatrics 1994;49(2):35-8, 43-4.
17. Belmin J, Hervias Y, Avellano E, Oudart O, Durand I. Reliabilityof sampling urine from disposable diapers in elderlyincontinent women. J Am Geratr Soc 1993;41(11):1182-1186.
18. Sandvik H, Hunskaar S. General practitioners’ managementof female urinary incontinence. Medical records do not reflectpatients’ recall. Scand J Prim Health Care 1995;13(3):168-174.
19. Kennedy KL, Steidle CP, Letizia TM. Urinary incontinence:the basics. Ostomy Wound Manage 1995;41(7):16-22.
20. DuBeau CE, Resnick NM. Evaluation of the causes andseverity of geriatric incontinence. A critical appraisal. Urol ClinNorth Am 1991;18(2):243-256.
21. Ouslander JG, Schapira M, Schnelle JF, Fingold S. Pyuriaamong chronically incontinent but otherwise asymptomaticnursing home residents. J Am Geratr Soc 1996;44(4):420-423.
22. Goode PS, Locher JL, Bryant RL, Roth DL, Burgio KL.Measurement of postvoid residual urine with portabletransabdominal bladder ultrasound scanner and urethralcatheterization. Int Urogynecol J Pelvic Floor Dysfunct 2000;11: 296-300
23. Ouslander JG, Simmons S, Tuico E, Nigam JG, Fingold S,Bates-Jensen B, Schnelle JF. Use of a portable ultrasounddevice to measure post-void residual volume amongincontinent nursing home residents. J Am Geriatr Soc 1994;42: 1189-1192.
24. Nygaard IE. Postvoid residual volume cannot be accuratelyestimated by bimanual examination. Int Urogynecol J PelvicFloor Dysfunct 1996; 7: 74-6
25. Hall AF, Theofrastus JP, Cundiff GW, Harris RL, Hamilton LF,Swift SE et al. Interobserver and intraobserver reliability of
the proposed International Continence Society, Society ofGynecologic Surgeons and American Urogynecologic Society,pelvic organ prolapse classification system. Am J ObstetGynecol 1996; 175: 1467-1470
26. Griffiths DJ, Harrison G, Moore K, McCracken P: Variabilityof post-void residual urine volume in the elderly. Urol Res1996; 24: 23.
27. Barabas G, Mölstad S. No association between elevatedpost-void residual volume and bacteriuria in residents ofnursing homes. Scand J Prim Health Care 2005; 23: 52-56
28. Agency for Health Care Policy and Research. Clinical practiceguideline: urinary incontinence in adults. AHPCR Pub. No.96-0682. Rockville, MD: Dept of Health and Human Services(US), Agency for Health Care Policy and Research; 1996
29. Gehrich A, Stany MP, Fischer JR, Buller J, Zahn CM.Establishing a mean postvoid residual volume inasymptomatic perimenopausal and postmenopausal women.Obstet Gynecol 2007; 110: 827-832
30. Tseng LH, Liang CC, Chang YL, Lee SJ, Lloyd LK, Chen CK.Postvoid residual urine in women with stress incontinence.Neurourol Urodyn 2008; 27: 48-51
31. Haylen BT, Law MG, Frazer M. Urine flow rates and residualurine volumes in urogynecology patients. Int Urogynecol J1999; 10: 378-383
32. Fitzgerald MP, Jaffar J, Brubaker L. Risk factors for anelevated postvoid residual urine volume in women withsymptoms of urinary urgency, frequency and urgeincontinence. Int Urogynecol J Pelvic Floor Dysfunct 2001;12: 237-239.
33. Lukacz ES, Duhamel E, Menefee SA et al. Elevated postvoidresidual in women with pelvic floor disorders: prevalenceand associated risk factors. Int Urogynecol J Pelvic FloorDysfunct 2007; 18: 397-400
34. Wu J, Baguley IJ. Urinary retention in a general rehabilitationunit: prevalence, clinical outcome, and the role of screening.Arch Phys Med Rehabil 2005; 86: 1772-1777
35. Milleman M, Langenstroer P, Guralnick ML. Post-void residualurine volume in women with overactive bladder symptoms.J Urol 2004; 172(5 Pt 1): 1911-1914
36. Nager CW, FitzGerald M, Kraus SR, Chai TC, Zyczynski H,Sirls L, Lemack GE, Lloyd LK, Litman HJ, Stoddard AM,Baker J, Steers W, Urinary Incontinence Treatment Network.Urodynamic measures do not predict stress continenceoutcomes after surgery for stress urinary incontinence inselected women. J Urol 2008; 179: 1470-1474
37. Stoller, M. L. and Millard, R. J. The accuracy of a catheterizedresidual urine. J Urol. 1989; 141: 15-16.
38. Holmes, J. H. Ultrasonic studies of the bladder. J Urol. 1967;97: 654-663.
39. Marks, L. S., Dorey, F. J., Macairan, M. L., et al. Three-dimensional ultrasound device for rapid determination ofbladder volume. Urology.1997; 50: 341-348.
40. Abrams, P., Griffiths, D., Hoefner, K., Liao, L., Schafer, W.,Tubaro, A., and Zimmern, P. The Urodynamic assessmentof lower urinary tract symptoms. In: Benign ProstaticHyperplasia. Eds. Chatelain, C., Denis, L., Foo, K., Khoury,S., and McConnell, J. Health Publication Ltd., Plymouth,2001, pp:227-281.
41. AUA Practice Guidelines Committee. AUA guideline onmanagement of benign prostatic hyperplasia (2003). Chapter1: Diagnosis and treatment recommendations. J Urol. 2003;170: 530-547.
42. Madersbacher, S., Alivizatos, G., Nordling, J., et al. EAU2004 guidelines on assessment, therapy and follow-up of menwith lower urinary tract symptoms suggestive of benignprostatic obstruction (BPH guidelines). Eur.Urol. 2004; 46:547-554.

357
43 Bates, T. S., Sugiono, M., James, E. D., Stott, M. A., andPocock, R. D. Is the conservative management of chronicretention in men ever justified? BJU.Int. 2003; 92: 581-583.
44. Vesely S, Knutson T, Fall M, Damber JE, Dahlstrand C.Clinical diagnosis of bladder outlet obstruction in men withlower urinary tract symptoms: reliability of commonlymeasured parameters and the role of idiopathic detrusoroveractivity. Neurourol Urodyn 2003;22(4):301-305.
45. Norton PA, MacDonald LD, Sedgwick PM, Stanton SL.Distress and delay associated with urinary incontinence,frequency, and urgency in women. Brit Med J 1988;297:1187-1189.
46. Weidner AC, Myers ER, Visco AG, Cundiff GW, Bump RC.Which women with stress incontinence require urodynamicevaluation? American Journal of Obstetrics & Gynecology2001;184(2):20-27.
47. Donovan J, Badia X, Corcos J, Gotoh M, Kelleher C,Naughton M, et al. Symptom and quality of life assessment.In: Abrams P, Cardozo L, Khoury S, Wein A, editors.Incontinence; 2nd WHO International Consultation onIncontinence. Plymouth: Health Publications Ltd; 2002. p. 267-316.
48. Harvey MA, Versi E. Predictive value of clinical evaluationof stress urinary incontinence: A summary of the publishedliterature. International Urogynecology Journal 2001;12(1):31-37.
49. Horbach NS. Problems in the clinical diagnosis of stressincontinence. Journal of Reproductive Medicine for theObstetrician & Gynecologist 1990;35(8):751-757.
50. Summitt RL, Stovall TG, Bent AE, Ostergard DR. Urinaryincontinence: Correlation of history and brief office evaluationwith multichannel urodynamic testing. American Journal ofObstetrics & Gynecology 1992;166(6 I):1835-1844.
51. Young SB, Pingeton DM. Office assessment of female urinaryincontinence. Clin Obstet Gynecol 1999;42(2):249-266.
52. Digesu G, Khullar V, Cardozo L, Salvatore S. Overactivebladder symptoms: do we need urodynamics? NeurourolUrodyn 2003;22:105-108.
53. Bump RC, Norton PA, Zinner NR, Yalcin I. Mixed urinaryincontinence symptoms: urodynamic findings, incontinenceseverity, and treatment response. Obstetrics & Gynecology2003;102(1):76-83.
54. Martin J, Williams K, Abrams K, Assassa R, Turner D, SuttonA, et al. Systematic review and evaluation of methods ofassessing urinary incontinence. In: International ContinenceSociety (UK); 2004; Bournemouth; 2004. p. 31
55. Holroyd-Leduc J, Tannenbaum C, Thorpe H, etal. WhatType of Urinary incontinence Does This Woman Have?JAMA, 2008 299(12): 1446-1456
56. Jackson S, Weber A, Hull T, Mitchinson A, Walters M. Fecalincontinence in women with urinary incontinence and pelvicorgan prolapse. Obstet Gynecol 1997;89:423-427.
57. Kjølhede P, Noren B, Ryden G. Prediction of genital prolapseafter Burch colposuspension. Acta Obstet Gynecol Scand1996;76:849-854.
58. Seim A, Eriksen B, Hunskaar S. A study of female urinaryincontinence in general practice: demography, medicalhistory, and clinical finding. Scand J Urol Nephrol1996;30:465-471.
59. Hannestad YS, Rortveit G, Daltveit AK, Hunskaar S. Aresmoking and other lifestyle factors associated with femaleurinary incontinence? The Norwegian EPINCONT Study.Brit J Obstet Gynaecol 2003;110(3):247-254.
60. Norton PA. Pelvic floor disorders: the role of fascia andligaments. Clin Obstet Gynecol 1993;36(4):926-38.
61. Hilton P, Stanton SL. Algorithmic method for assessingurinary incontinence in elderly women. Brit Med J1981;282(6268):940-942.
62. Howard D, Miller JM, Delancey JO, Ashton-Miller JA.Differential effects of cough, valsalva, and continence statuson vesical neck movement. Obstet Gynecol 2000;95(4):535-540.
63. Hilton P. Urethral pressure measurement on stress: ananalysis of profiles obtained on coughing and straining.Neurourology & Urodynamics. Neurourol Urodyn 1983;2:55-62.
64. Hilton P, Stanton SL. Urethral pressure measurement bymicrotransducer: The results in symptom-free women andin those with genuine stress incontinence. Brit J ObstetGynaecol 1983;90(10):919-933.
65. Bonney V. On diurnal incontinence of urine in women. JObstet Gynaecol Brit Emp 1923;30:358-365.
66. Crystle CD, Charme LS, Copeland WE. Q-tip test in stressurinary incontinence. Obstetrics & Gynecology 1971;38(2):313-315.
67. Karram MM, Bhatia NN. The Q-tip test: Standardization ofthe technique and its interpretation in women with urinaryincontinence. Obstetrics & Gynecology 1988;71(6 I):807-811.
68. Fantl JA, Hurt WG, Bump RC, Dunn L, Choi S. Urethral axisand sphincteric function. American Journal of Obstetrics &Gynecology 1986;155(3):554-558.
69. Walters MD, Diaz K. Q-tip test: a study of continent andincontinent women. Obstetrics & Gynecology 1987;70(2):208-211.
70. Cogan SL, Weber AM, Hammel JP. Is urethral mobility reallybeing assessed by the pelvic organ prolapse quantification(POP-Q) system? Obstetrics & Gynecology 2002;99(3):473-476.
71. Weber Lebrun EE, Harmanli OH, Lidicker J, Dandolu V. Canwe use a catheter to do the q-tip test? Obstet Gynecol. 2007Dec;110(6):1297-300
72. Salvatore S, Serati M, Uccella S, Koelbl H, Artibani W,Cardozo L, Bolis P. Inter-observer reliability of three differentmethods of measuring urethrovesical mobility. Int UrogynecolJ Pelvic Floor Dysfunct. July 2008. (e pub)
73. Paick JS, Cho MC, Oh SJ, Kim SW, Ku JH. Is proximalurethral mobility important for transobturator tape procedurein management of female patients with stress urinaryincontinence? Urology. 2007 Aug;70(2):246-50
74. Metin A, Kayigil O, Ahmed SI, Atmaca AF. Is the efficacy ofin situ vaginal wall slings decreasing in the late follow-up?Int Urol Nephrol. 2008;40(1):51-5.
75. Giberti C, Gallo F, Cortese P, Schenone M. Transobturatortape for treatment of female stress urinary incontinence:objective and subjective results after a mean follow-up of twoyears. Urology. 2007 Apr;69(4):703-7.
76. Walsh LP, Zimmern PE, Pope N, Shariat SF; UrinaryIncontinence Treatment Network. Comparison of the Q-tiptest and voiding cystourethrogram to assess urethralhypermobility among women enrolled in a randomized clinicaltrial of surgery for stress urinary incontinence. J Urol. 2006Aug;176(2):646-9
77. Liapis A, Bakas P, Christopoulos P, Giner M, Creatsas G.Tension-free vaginal tape for elderly women with stressurinary incontinence. Int J Gynaecol Obstet. 2006Jan;92(1):48-51.
78. Segal JL, Vassallo BJ, Kleeman SD, Hungler M, KarramMM. The efficacy of the tension-free vaginal tape in thetreatment of five subtypes of stress urinary incontinence.Int Urogynecol J Pelvic Floor Dysfunct. 2006 Feb;17(2):120-4.
79. Long CY, Hsu SC, Chang Y, Chen YC, Su JH, Tsai EM. Theclinical and urodynamic effects of the tension free bladderneck sling procedure. Int Urogynecol J Pelvic Floor Dysfunct.2004 Sep-Oct;15(5):344-9. ]

358
80. Bai SW, Kwon JY, Chung da J, Park JH, Kim SK. Differencesin urodynamic study, perineal sonography and treatmentoutcome according to urethrovesical junction hypermobilityin stress urinary incontinence. J Obstet Gynaecol Res. 2006Apr;32(2):206-11.
81. [Richter HE, Burgio KL, Brubaker L, Moalli PA, Markland AD,Mallet V, Menefee SA, Johnson HW, Boreham MK, DandreoKJ, Stoddard AM; Urinary Incontinence Treatment Network.Factors associated with incontinence frequency in a surgicalcohort of stress incontinent women. Am J Obstet Gynecol.2005 Dec;193(6):2088-93.]
82. Thomakos N, Young RL, Daskalakis G. The Q-tip testcorrelation with urethroscopic findings in urinary stressincontinence. Int J Gynaecol Obstet. 2005 Dec;91(3):264-5.]
83. Noblett K, Lane FL, Driskill CS. Does pelvic organ prolapsequantification exam predict urethral mobility in stages 0 andI prolapse? Int Urogynecol J Pelvic Floor Dysfunct. 2005Jul-Aug;16(4):268-71.
84. Larrieux JR, Balgobin S. Effect of anatomic urethral lengthon the correlation between the Q-tip test and descent atpoint Aa of the POP-Q system. Int Urogynecol J Pelvic FloorDysfunct. 2008 Feb;19(2):273-6.
85. Zyczynski HM, Lloyd LK, Kenton K, Menefee S, BorehamM, Stoddard AM; Urinary Incontinence Treatment Network(UITN). Correlation of Q-tip values and point Aa in stress-incontinent women. Obstet Gynecol. 2007 Jul;110(1):39-43.
86. Mattison ME, Simsiman AJ, Menefee SA. Can urethralmobility be assessed using the pelvic organ prolapsequantification system? An analysis of the correlation betweenpoint Aa and Q-tip angle in varying stages of prolapse.Urology. 2006 Nov;68(5):1005-8.
87. Rosencrantz M, Menefee SA, Lukacz ES. The correlation ofurethral mobility and point Aa of the pelvic organ prolapsequantification system before and after surgery. Am J ObstetGynecol. 2006 Dec;195(6):1841-5.
88. Lemack GE, Xu Y, Brubaker L, Nager C, Chai T, Moalli P,Kraus SR, Kerr L, Sirls L, Stoddard A; for the UrinaryIncontinence Treatment Network. Clinical and demographicfactors associated with valsalva leak point pressure amongwomen undergoing burch bladder neck suspension orautologous rectus fascial sling procedures. Neurourol Urodyn.2007;26(3):392-6.
89. Blakeman PJ, Hilton P, Bulmer JN. Oestrogen andprogesterone receptor expression in the female lower urinarytract, with reference to oestrogen status. Brit J Urol Int2000;86(1):32-38.
90. Blakeman PJ, Hilton P, Bulmer JN. Cellular proliferation inthe female lower urinary tract with reference to oestrogenstatus. Brit J Obstet Gynaecol 2001;108(8):813-816.
91. Hextall A, Bidmead J, Cardozo L, Hooper R. The impact ofthe menstrual cycle on urinary symptoms and the results ofurodynamic investigation. Brit J Obstet Gynaecol2001;108(11):1193-1196.
92 Fantl JA, Cardozo L, McClish DK. Estrogen therapy in themanagement of urinary incontinence in postmenopausalwomen: a meta-analysis. First report of the Hormones andUrogenital Therapy Committee. Obstetrics & Gynecology1994;83(1):12-18.
93 Molander U, Milsom I, Ekelund P, Mellstrom D, Eriksson O.Effect of oral oestriol on vaginal flora and cytology andurogenital symptoms in the post-menopause. Maturitas1990;12(2):113-120.
94. Fortunato P, Schettini M, Gallucci M. Diverticula of the femaleurethra. British Journal of Urology 1997;80(4):628-632.
95. Porges R. A practical system of diagnosis and classificationof pelvic relaxations. Surgery, Gynecology & Obstetrics1963;117:761-773.
96. Baden WF, Walker TA. Physical diagnosis in the evaluationof vaginal relaxation. Clin Obstet Gynecol 1972;15(4):1055-1069.
97. Bump RC, Mattiasson A, Bo K, Brubaker LP, DeLancey JO,Klarskov P, et al. The standardization of terminology offemale pelvic organ prolapse and pelvic floor dysfunction.American Journal of Obstetrics & Gynecology1996;175(1):10-17.
98. Swift S. Current opinion on the classification and definitionof genital tract prolapse. Curr Opin Obstet Gynecol2002;14(5):503-7.
99. Swift S, Morris S, McKinnie V, Freeman R, Patri E, Scotti R,Dwyer P. Validation of a simplified technique for using thePOPQ pelvic organ prolapse classification system. IntUrogynecol J. 17;6 Nov 2006.
100. Lemos NLBM, Auge APF, Lunardelli JL, Frade AB, FradeCL, Oliveira AL, Ribeiro PAAG, Aoki T (2007) Optimizingpelvic organ prolapse research. Int Urogynecol J18(6):609–611.
101. Lemos NL, Auge AP, Lunardelli JL, Carramão Sda S, FariaAL, Aoki T.. Validation of the Pelvic Organ ProlapseQuantification Index (POP-Q-I): a novel interpretation ofthe POP-Q system for optimization of POP research. IntUrogynecol J Pelvic Floor Dysfunct. 2008 Jul;19(7):995-7]
102. Brubaker L, Nygaard I, Richter HE, Visco A, Weber AM,Cundiff GW, Fine P, Ghetti C, Brown MB.Two-year outcomesafter sacrocolpopexy with and without burch to preventstress urinary incontinence. Obstet Gynecol. 2008Jul;112(1):49-55.
103. Guiahi M, Kenton K, Brubaker L. Sacrocolpopexy withoutconcomitant posterior repair improves posterior compartmentdefects. Int Urogynecol J Pelvic Floor Dysfunct. 2008 May22.
104. Silva WA, Pauls RN, Segal JL, Rooney CM, Kleeman SD,Karram MM. Uterosacral ligament vault suspension: five-year outcomes. Obstet Gynecol. 2006 Aug;108(2):255-63
105. Vierhout ME, Stoutjesdijk J, Spruijt J. A comparison ofpreoperative and intraoperative evaluation of patientsundergoing pelvic reconstructive surgery for pelvic organprolapse using the Pelvic Organ Prolapse QuantificationSystem. Int Urogynecol J Pelvic Floor Dysfunct. 2006Jan;17(1):46-9.
106. Ross JW. Porcine dermal hammock for repair of anterior andposterior vaginal wall prolapse: 5-year outcome. J MinimInvasive Gynecol. 2008 Jul-Aug;15(4):459-65.
107. Lee HJ, Lee YS, Koo TB, Cho YL, Park IS. Laparoscopicmanagement of uterine prolapse with cystocele andrectocele using “Gynemesh PS”.J Laparoendosc Adv SurgTech A. 2008 Feb;18(1):93-8.
108. Altman D, Väyrynen T, Engh ME, Axelsen S, Falconer C;For the Nordic Transvaginal Mesh Group. Short-termoutcome after transvaginal mesh repair of pelvic organprolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2007 Dec12.
109. Carey M, Slack M, Higgs P, Wynn-Williams M, Cornish A.Vaginal surgery for pelvic organ prolapse using mesh anda vaginal support device. BJOG. 2008 Feb;115(3):391-7.
110. Ross JW. The use of a xenogenic barrier to prevent mesherosion with laparoscopic sacrocolpopexy. J Minim InvasiveGynecol. 2007 Jul-Aug;14(4):470-4.
111. Yau JL, Rahn DD, McIntire DD, Schaffer JI, Wai CY. Thenatural history of posterior vaginal wall support afterabdominal sacrocolpopexy with and without posteriorcolporrhaphy. Am J Obstet Gynecol. 2007 May;196(5):e45-7
112. Digesu GA, Salvatore S, Chaliha C, Athanasiou S, MilaniR, Khullar V. Do overactive bladder symptoms improveafter repair of anterior vaginal wall prolapse? Int UrogynecolJ Pelvic Floor Dysfunct. 2007 Dec;18(12):1439-43.

359
113. Diez-Itza I, Aizpitarte I, Becerro A. Risk factors for therecurrence of pelvic organ prolapse after vaginal surgery:a review at 5 years after surgery. Int Urogynecol J PelvicFloor Dysfunct. 2007 Nov;18(11):1317-24.
114. Robles JE, Rioja J, Saiz A, Brugarolas X, Rosell D, ZudaireJJ, Berian JM. Anterior compartment prolapse repair witha hybrid biosynthetic mesh implant technique.Int UrogynecolJ Pelvic Floor Dysfunct. 2007 Oct;18(10):1191-6.
115. Chaliha C, Khalid U, Campagna L, Digesu GA, Ajay B,Khullar V. SIS graft for anterior vaginal wall prolapse repair—a case-controlled study. Int Urogynecol J Pelvic FloorDysfunct. 2006 Sep;17(5):492-7.
116. Culligan PJ, Blackwell L, Goldsmith LJ, Graham CA, RogersA, Heit MH. A randomized controlled trial comparing fascialata and synthetic mesh for sacral colpopexy. ObstetGynecol. 2005 Jul;106(1):29-37.
117. Gandhi S, Goldberg RP, Kwon C, Koduri S, Beaumont JL,Abramov Y, Sand PK. A prospective randomized trial usingsolvent dehydrated fascia lata for the prevention of recurrentanterior vaginal wall prolapse. Am J Obstet Gynecol. 2005May;192(5):1649-54.
118. Groutz A, Chaikin DC, Theusen E, Blaivas JG. Use ofcadaveric solvent-dehydrated fascia lata for cystocelerepair—preliminary results. Urology. 2001 Aug;58(2):179-83.
119. Flynn MK, Webster GD, Amundsen CL. Abdominal sacralcolpopexy with allograft fascia lata: one-year outcomes.Am J Obstet Gynecol. 2005 May;192(5):1496-500.
120. Gregory WT, Otto LN, Bergstrom JO, Clark AL. Surgicaloutcome of abdominal sacrocolpopexy with synthetic meshversus abdominal sacrocolpopexy with cadaveric fascialata. Int Urogynecol J Pelvic Floor Dysfunct. 2005 Sep-Oct;16(5):369-74.
121. Sarlos D, Brandner S, Kots L, Gygax N, Schaer G.Laparoscopic sacrocolpopexy for uterine and post-hysterectomy prolapse: anatomical results, quality of life andperioperative outcome-a prospective study with 101 cases.Int Urogynecol J Pelvic Floor Dysfunct. 2008 Jun 7.
122. Schwartz M, Abbott KR, Glazerman L, Sobolewski C,Jarnagin B, Ailawadi R, Lucente V. Positive symptomimprovement with laparoscopic uterosacral ligament repairfor uterine or vaginal vault prolapse: interim results from anactive multicenter trial. J Minim Invasive Gynecol. 2007Sep-Oct;14(5):570-6
123. Medina C, Takacs P. Laparoscopic uterosacral uterinesuspension: a minimally invasive technique for treatingpelvic organ prolapse. J Minim Invasive Gynecol. 2006Sep-Oct;13(5):472-5.Daneshgari F, Kefer JC, Moore C,Kaouk J.
124. Robotic abdominal sacrocolpopexy/sacrouteropexy repairof advanced female pelvic organ prolaspe (POP): utilizingPOP-quantification-based staging and outcomes.BJU Int.2007 Oct;100(4):875-9.
125. Handa VL, Cundiff G, Chang HH, Helzlsouer KJ. Femalesexual function and pelvic floor disorders. Obstet Gynecol.2008 May;111(5):1045-52.
126. Novi JM, Bradley CS, Mahmoud NN, Morgan MA, Arya LA.Sexual function in women after rectocele repair with acellularporcine dermis graft vs site-specific rectovaginal fasciarepair. Int Urogynecol J Pelvic Floor Dysfunct. 2007Oct;18(10):1163-9.
127. Stoutjesdijk JA, Vierhout ME, Spruijt JW, Massolt ET. Doesvaginal reconstructive surgery with or without vaginalhysterectomy or trachelectomy improve sexual well being?A prospective follow-up study. Int Urogynecol J Pelvic FloorDysfunct. 2006 Feb;17(2):131-5.
128. Ozel B, White T, Urwitz-Lane R, Minaglia S. The impact of
pelvic organ prolapse on sexual function in women withurinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct.2006 Jan;17(1):14-7.
129. Trowbridge ER, Fultz NH, Patel DA, DeLancey JO, FennerDE. Distribution of pelvic organ support measures in apopulation-based sample of middle-aged, community-dwelling African American and white women in southeasternMichigan. Am J Obstet Gynecol. 2008 May;198(5):548.e1-6.
130. Bradley CS, Zimmerman MB, Wang Q, Nygaard IE;Women’s Health Initiative. Vaginal descent and pelvic floorsymptoms in postmenopausal women: a longitudinal study.Obstet Gynecol. 2008 May;111(5):1148-53.
131. Dietz HP, Lekskulchai O. Ultrasound assessment of pelvicorgan prolapse: the relationship between prolapse severityand symptoms. Ultrasound Obstet Gynecol. 2007Jun;29(6):688-91.
132. Bradley CS, Zimmerman MB, Qi Y, Nygaard IE. Naturalhistory of pelvic organ prolapse in postmenopausal women.Obstet Gynecol. 2007 Apr;109(4):848-54.
133. DeLancey JO, Morgan DM, Fenner DE, Kearney R, GuireK, Miller JM, Hussain H, Umek W, Hsu Y, Ashton-Miller JA.Comparison of levator ani muscle defects and function inwomen with and without pelvic organ prolapse. ObstetGynecol. 2007 Feb;109(2 Pt 1):295-302.
134. Buchsbaum GM, Duecy EE, Kerr LA, Huang LS, PerevichM, Guzick DS. Pelvic organ prolapse in nulliparous womenand their parous sisters. Obstet Gynecol. 2006 Dec; 108(6):1388-93.
135. Liang CC, Tseng LH, Horng SG, Lin IW, Chang SD.Correlation of pelvic organ prolapse quantification systemscores with obstetric parameters and lower urinary tractsymptoms in primiparae postpartum. Int Urogynecol J PelvicFloor Dysfunct. 2007 May;18(5):537-41.
136. Larsen WI, Yavorek T. Pelvic prolapse and urinaryincontinence in nulliparous college women in relation toparatrooper training. Int Urogynecol J Pelvic Floor Dysfunct.2007 Jul;18(7):769-71.
137. Kahn MA, Breitkopf CR, Valley MT, Woodman PJ, O’BoyleAL, Bland DI, Schaffer JI, Grady JJ, Swift SE. Pelvic OrganSupport Study (POSST) and bowel symptoms: straining atstool is associated with perineal and anterior vaginal descentin a general gynecologic population. Am J Obstet Gynecol.2005 May;192(5):1516-22.
138. Latini JM, Zimmerman MB, Kreder KJ Jr. Associationbetween valsalva and cough leak point pressures and pelvicorgan prolapse quantification in women with stressincontinence. J Urol. 2005 Apr;173(4):1219-22.
139. Tamanini JT, Almeida FG, Girotti ME, Riccetto CL, PalmaPC, Rios LA. The Portuguese validation of the InternationalConsultation on Incontinence Questionnaire-VaginalSymptoms (ICIQ-VS) for Brazilian women with pelvic organprolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2008 May28.
140. Baessler K, O’Neill SM, Maher CF, Battistutta D. Aninterviewer-administered validated female pelvic floorquestionnaire for community-based research. Menopause.2008 May 2.
141. Diokno AC, Borodulin G. A new vaginal speculum for pelvicorgan prolapse quantification (POPQ). Int Urogynecol JPelvic Floor Dysfunct. 2005 Sep-Oct;16(5):384-8.
142. Kinn AC, Larsson B. Pad test with fixed bladder volume inurinary stress incontinence. Acta Obstetricia et GynecologicaScandinavica 1987;66(4):369-371.
143. Fantl JA, Harkins SW, Wyman JF, Choi SC, Taylor JR. Fluidloss quantitation test in women with urinary incontinence:a test-retest analysis. Obstetrics & Gynecology 1987;70(5):739-743.

360
144. Sutherst J, Brown M, Shawer M. Assessing the severity ofurinary incontinence in women by weighing perineal pads.Lancet 1981;1(8230):1128-30.
145. Sutherst JR, Brown MC, Richmond D. Analysis of the patternof urine loss in women with incontinence as measured byweighing perineal pads. British Journal of Urology1986;58(3):273-278.
146. Lose G, Rosenkilde P, Gammelgaard J, Schroeder T. Pad-weighing test performed with standardized bladder volume.Urol 1988;32(1):78-80.
147. Kromann-Andersen B, Jakobsen H, Andersen JT. Pad-weighing tests: A literature survey on test accuracy andreproducibility. Neurourol Urodyn 1989;8(3):237-242.
148. Klarskov P, Hald T. Reproducibility and reliability of urinaryincontinence assessment with a 60 min test. Scand J UrolNephrol 1984;18(4):293-8.
149. Miller JM, Ashton-Miller JA, Delancey JO. Quantificationof cough-related urine loss using the paper towel test.Obstetrics & Gynecology 1998;91(5 Pt 1):705-709.
150. Victor A, Larsson G, Asbrink AS. A simple patient-administered test for objective quantitation of the symptomof urinary incontinence. Scand J Urol Nephrol1987;21(4):277-9.
151. Jorgensen L, Lose G, Thunedborg P. Diagnosis of mildstress incontinence in females: 24-hour pad weighing testversus the onw-hour test. Neurourol Urodyn 1987;6:165-166.
152. Raghavaiah N. Double-dye test to diagnose various typesof vaginal fistulas. J Urol 1974;112:811-812.
153. Gosling J. The structure of the bladder and urethra in relationto function. Urol Clin North Am 1979;6(1):31-38. muscleexercise performance after brief verbal instruction. AmericanJournal of Obstetrics & Gynecology 1991;165(2):322-327.
154. DiNubile NA. Strength training. Clin Sports Med 1991;10(1):33-62.
155. Edwards RH. Physiological analysis of skeletal muscleweakness and fatigue. Clin Sci Mol Med 1978;54(5):463-470.
156. Laycock J. Assessment and treatment of pelvic floordysfunction [PhD]: University of Bradford; 1992.
157. Brink CA, Sampselle CM, Wells TJ, Diokno AC, Gillis GL.A digital test for pelvic muscle strength in older women withurinary incontinence. Nurs Res 1989;38(4):196-199.
158. Laycock J, Sherlock R. Perineometers - do we need a “GoldStandard”? In: International Continence Society; 1995;Sydney, Australia; 1995. p. 144-145.
159. Schüssler B, Hesse U. Q-Tip Testing. In: Schüssler B,Laycock J, Norton P, Stanton S, editors. Pelvic Floor Re-education: Principles and Practice. London: Springer-Verlag;1994. p. 49-50.
160. Miller J, Ashton-Miller J, Carchidi L, DeLancey J. Does athree month pelvic muscle exercise intervention improve theeffectiveness of the knack in reducing cough-induced urineloss in a standing stress test? In: American UrogynecologicSociety; 1997; Tuscon, Ariz; 1997.
161. Perucchini D, DeLancey J, Miller J, Carchidi L, KrajewskiK, Ashton-Miller J. A levator ani precontraction significantlyreduces bladder neck descent during coughing in womenwith SUI. In: American Urogynecologic Society; 1997;Tuscon, Ariz; 1997.
162. McLennan MT, Bent AE. Supine empty stress test as apredictor of low valsalva leak point pressure. NeurourolUrodyn 1998;17(2):121-127
163. Welch G, Weinger K, Barry M. Quality-of-life im-pact oflower urinary tract symptom severity: results from the HealthProfessionals Follow up Study. Urol 2002;59:245-250.
164. Milsom I, Abrams P, Cardozo L, Roberts R, Thuroff J, WeinA. How widespread are the symptoms of an overactivebladder and how are they managed? A population-basedprevalence study. Brit J Urol Int 2001;87:760-766.
165. Stewart W, van Rooyen J, Cundiff G, Abrams P, Herzig A,Corey R, et al. Prevalence and burden of overactive bladderin the United States. World Journal of Urology 2003;20:327-336.
166. Knutson T, Edlund C, Fall M, Dahlstrand C. BPH withcoexisting overactive bladder-An everday urologicaldilemma. Neurourol Urodyn 2001;20:237-247.
167. Kaplan S, Te A, Jacobs B. Urodynamic evidenceof vesicalneck obstruction in men with misdiagnosed chronicnonbacterial prostatitis and the therapeutic role of endoscopicincision of the bladder neck. J Urol 1994;152:2063-2065.
168. Yalla S, Gabilondo F, Blunt K, Fam B, Castello A, KaufmanJ. Functional striated sphincter component at the bladderneck: clinical implications. J Urol 1977;118(3):408-411.
169. Emberton M, Neal DE, Black N, Fordham M, Harrison M,McBrien MP, et al. The effect of prostatectomy on symptomseverity and quality of life. British Journal of Urology1996;77(2):233-247.
170. De La Rosette, J., Baba S., Baldani G., Elhilali S., GravasR., Muschter R., Naito S., Netto N.R. New minimally invasiveand surgical developments in the management of BPO.Male lower urinary tract dysfunction. Evaluation andmanagement. Eds: MaConnel J. et al., Health PublicationLtd., Plymouth, pp197-233, 2006
171. Stone N.N., Stock R.G. Complications following permanentprostate brachytherapy. Eur. Urol: 2002; 41: 427-433
172. Donnellan SM, Duncan HJ, MacGregor RJ, Russell JM.Prospective assessment of incontinence after radicalretropubic prostatectomy: objective and subjective analysis.Urol 1997;49(2):225-230.
173. Carlson KV, Nitti VW. Prevention and management ofincontinence following radical prostatectomy. Urol Clin NorthAm 2001;28(3):595-612.
174. Lepor H, Kaci L. The impact of open radical retropubicprostatectomy on continence and lower urinary tractsymptoms: a prospective assessment using validated self-administered outcome instruments. J Urol 2004;171(3):1216-1219.
175. Masters JG, Rice ML. Improvement in urinary symptomsafter radical prostatectomy: a prospective evaluation of flowrates and symptom scores. Brit J Urol Int 2003;91(9):795-797.
176. Fowler FJ, Jr., Barry MJ, Lu-Yao G, Wasson J, Roman A,Wennberg J. Effect of radical prostatectomy for prostatecancer on patient quality of life: results from a Medicaresurvey. Urol 1995;45(6):1007-1013.
177. Ficazzola MA, Nitti VW. The etiology of post-radicalprostatectomy incontinence and correlation of symptoms withurodynamic findings. J Urol 1998;160(4):1317-1320.
178. Groutz A, Blaivas JG, Chaikin DC, Weiss JP, VerhaarenM. The pathophysiology of post-radical prostatectomyincontinence: a clinical and video urodynamic study. J Urol2000;163(6):1767-1770.
179. Giannantoni A, Mearini E, Di Stasi SM, Mearini L, Bini V,Pizzirusso G, et al. Assessment of bladder and urethralsphincter function before and after radical retropubicprostatectomy. J Urol 2004;171(4):1563-1566.
180. Jung SY, Fraser MO, Ozawa H, Yokoyama O, YoshiyamaM, De Groat WC, et al. Urethral afferent nerve activityaffects the micturition reflex; implication for the relationshipbetween stress incontinence and detrusor instability. J Urol1999;162(1):204-212.

361
181. Hu JC, Gold KF, Pashos CL, Mehta SS, Litwin MS. Temporaltrends in radical prostatectomy complications from 1991to 1998. J Urol 2003;169(4):1443-1448.
182. Stanford JL, Feng Z, Hamilton AS, Gilliland FD, StephensonRA, Eley JW, et al. Urinary and sexual function after radicalprostatectomy for clinically localized prostate cancer: theProstate Cancer Outcomes Study. J Am Med Assoc2000;283(3):354-360.
183. van Venrooij GE, Eckhardt MD, Gisolf KW, Boon TA. Datafrom frequency-volume charts versus filling cystometricestimated capacities and prevalence of instability in men withlower urinary tract symptoms suggestive of benign prostatichyperplasia. Neurourol Urodyn 2002;21(2):106-111.
184. Eckhardt MD, van Venrooij GE, van Melick HH, Boon TA.Prevalence and bothersomeness of lower urinary tractsymptoms in benign prostatic hyperplasia and their impacton well-being. J Urol 2001;166(2):563-568.
185. Hammerer P, Huland H. Urodynamic evaluation of changesin urinary control after radical retropubic prostatectomy. JUrol 1997;157(1):233-236.
186. Winters JC, Appell RA, Rackley RR. Urodynamic findingsin postprostatectomy incontinence. Neurourol Urodyn1998;17(5):493-498.
187. Chao R, Mayo ME. Incontinence after radical prostatectomy:detrusor or sphincter causes. J Urol 1995;154(1):16-18.
188. Agarwal, P. and Rosenberg, M. L. Neurological evaluationof urinary incontinence in the female patient. Neurologist.2003; 9: 110-117.
189. Chodak, G. W., Keller, P., and Schoenberg, H. Routinescreening for prostate cancer using the digital rectalexamination. Prog.Clin.Biol.Res. 1988; 269: 87-98.
190. Roehrborn C, Girman C, Rhodes T, Hanson K, Collins G,Sech S, et al. Correlation between prostate size extimatedby digital rectal examination and measured by transrectalultrasound. Urol 1997;49:548-557.
191 Roehrborn C, Sech S, Montoya J, Rhodes T, Girman C.Interexamner reliability and validity of a three dimensionalmodel to asses prostate volume by digital examination.Urol 2001;57:1087-1092.
192. McConnell J, Roehrborn C, Bautista OM, et al. The long termeffects of doxazosin, finasteride and combination therapyon the clinical progression of benign prostatic hyperplasia.NEJM 2003; 349:2387-2398
193 Boyle, P., Gould, A. L., and Roehrborn, C. G. Prostatevolume predicts outcome of treatment of benign prostatichyperplasia with finasteride: meta-analysis of randomizedclinical trials. Urology. 1996; 48: 398-405
194. Tong YC, Lin YM, Yang WH, Tzai TS, Lin JS. Correlation oftransrectal ultrasonographic findings of the prostate with theoccurrence of detrusor instability in patients with benignprostatic hyperplasia. Urol Int 1995;55(3):154-157.
195. Gerber, G. S., Goldfischer, E. R., Karrison, T. G., and Bales,G. T. Serum creatinine measurements in men with lowerurinary tract symptoms secondary to benign prostatichyperplasia. Urology. 1997; 49: 697-702.
196. Roehrborn, C. G., Bartsch, G., Kirby, Ret al. Guidelines forthe diagnosis and treatment of benign prostatic hyperplasia:a comparative, international overview. Urology. 2001; 58:642-650.
197 Rule, A. D., Jacobson, D. J., Roberts, R. O., Girman, C. J.,et al. The association between benign prostatic hyperplasiaand chronic kidney disease in community-dwelling men.Kidney Int. 2005; 67: 2376-2382.
198. Noel, G. Prostate-specific antigen (PSA) best practice policy.American Urological Association (AUA). Oncology (Huntingt).2000; 14: 267-8, 280.
199. Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino
PT, Flanigan RC, et al. Comparison of digital rectalexamination and serum prostate specific antigen in theearly detection of prostate cancer: results of a multicenterclinical trial of 6,630 men. J Urol 1994;151(5):1283-1290.
200. Carvalhal GF, Smith DS, Mager DE, Ramos C, Catalona WJ.Digital rectal examination for detecting prostate cancer atprostate specific antigen levels of 4 ng./ml. or less. J Urol1999;161(3):835-839.
201. Polascik TJ, Oesterling JE, Partin AW. Prostate specificantigen: a decade of discovery—what we have learnedand where we are going. J Urol 1999;162(2):293-306.
202. Mikolajczyk SD, Marks LS, Partin AW, Rittenhouse HG.Free prostate-specific antigen in serum is becoming morecomplex. Urol 2002;59(6):797-802.
203. Antenor, J. A., Han, M., Roehl, K. A., Nadler, R. B., andCatalona, W. J. Relationship between initial prostate specificantigen level and subsequent prostate cancer detection ina longitudinal screening study. J Urol. 2004; 172: 90-93.
204. Thompson, I. M., Pauler, D. K., Goodman, P. J., et al.Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter. N.Engl.J Med.2004; 350: 2239-2246.
205. Wilson, S. S. and Crawford, E. D. Screening for prostatecancer: current recommendations. Urol Clin.North Am.2004; 31: 219-226.
206. Jacobsen SJ, Girman CJ, Guess HA, Oesterling JE, LieberMM. New diagnostic and treatment guidelines for benignprostatic hyperplasia. Potential impact in the United States.Arch Intern Med 1995;155(5):477-481.
207. Barry MJ, Fowler FJ, Jr., Bin L, Pitts JC, 3rd, Harris CJ,Mulley AG, Jr. The natural history of patients with benignprostatic hyperplasia as diagnosed by North Americanurologists. J Urol 1997;157(1):10-14.
208. Roehrborn CG, Boyle P, Bergner D, Gray T, Gittelman M,Shown T, et al. Serum prostate-specific antigen and prostatevolume predict long-term changes in symptoms and flowrate: results of a four-year, randomized trial comparingfinasteride versus placebo. PLESS Study Group. Urol1999;54(4):662-669.
209. Laniado, M. E., Ockrim, J. L., Marronaro, A., et al. Serumprostate- specific antigen to predict the presence of bladderoutlet obstruction in men with urinary symptoms. BJU.Int.2004; 94: 1283-1286.
210. Engel AF, Kamm MA, Bartram CI, Nicholls RJ. Relationshipof symptoms in faecal incontinence to specific sphincterabnormalities. Int J Colorectal Disease 1995;10(3):152-155.
211. Wall LL. The muscles of the pelvic floor. Clin Obstet Gynecol1993;36(4):910-925.
212. Hill J, Corson RJ, Brandon H, Redford J, Faragher EB, KiffES. History and examination in the assessment of patientswith idiopathic fecal incontinence. Dis Colon Rectum1994;37(5):473-477.
213. Soffer EE, Hull T. Fecal incontinence: a practical approachto evaluation and treatment. American Journal ofGastroenterology 2000;95(8):1873-1880.
214. Jorge JM, Wexner SD. Etiology and management of fecalincontinence. Dis Colon Rectum 1993;36(1):77-97.
215. Cooper ZR, Rose S. Fecal incontinence: a clinical approach.Mt Sinai J Med 2000;67(2):96-105.
216. Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospectivecomparison of faecal incontinence grading systems. Gut1999;44(1):77-80.
217. Bliss DZ, McLaughlin J, Jung HJ, Lowry A, Savik K, JensenL. Comparison of the nutritional composition of diets ofpersons with fecal incontinence and that of age- and gender-

362
matched controls. J Wound Ostomy Continence Nurs2000;27(2):90-1, 93-7.
218. Holzheimer RG. Hemorrhoidectomy: indications and risks.Eur J Med Res 2004;9(1):18-36.
219. Parmentier H, Damon H, Henry L, Barth X, Mellier G, MionF. Frequency of anal incontinence and results of pelvicviscerography in 291 women with pelvic organ prolapse.Gastroenterol Clin Biol 2004;28(3):226-230.
220. Sultan AH, Kamm MA, Talbot IC, Nicholls RJ, Bartram CI.Anal endosonography for identifying external sphincterdefects confirmed histologically. Br J Surg 1994;81(3):463-5.
221. Snooks SJ, Swash M, Mathers SE, Henry MM. Effect ofvaginal delivery on the pelvic floor: a 5-year follow-up. BritJ Surg 1990;77(12):1358-1360.
222. Kamm MA. Faecal incontinence. Brit Med J 2003;327(7427):1299-1300.
223. Kushwaha RS, Hayne D, Vaizey CJ, Wrightham E, PayneH, Boulos PB. Physiologic changes of the anorectum afterpelvic radiotherapy for the treatment of prostate and bladdercancer. Dis Colon Rectum 2003;46(9):1182-1188.
224. Jackson SL, Weber AM, Hull TL, Mitchinson AR, Walters MDObstet Gynecol 1997; 89: 423-427
225. Maloney A, Cafiero J Gerontol Nurs. 1999 Jun;25( 6): 47-52
226. Hallan RI, Marzouk DE, Waldron DJ, Womack NR, WilliamsNS. Comparison of digital and manometric assessment ofanal sphincter function. Brit J Surg 1989;76(9):973-975.
227. Kaushal JN, Goldner F. Validation of the digital rectalexamination as an estimate of anal sphincter squeezepressure. American Journal of Gastroenterology1991;86(7):886-887.
228. Henry MM. Pathogenesis and management of fecalincontinence in the adult. Gastroenterol Clin North Am1987;16(1):35-45.
229. Vaizey CJ, van den Bogaerde JB, Emmanuel AV, TalbotIC, Nicholls RJ, Kamm MA. Solitary rectal ulcer syndrome.Brit J Surg 1998;85(12):1617-1623.
230. Soligo et al Am J Obstet Gynecol. 2006 Jul;195(1):50-5.

363
In the first three International Consultations onIncontinence reports, the impact of incontinence onquality of life (QoL) and methods of measuring thesefactors were described with questionnaire recom-mendations for use in research and clinical practice[1, 2]. This triennial update is a departure from previousreports in that the scope of this chapter encompassesnot only quality of life, but all patient-reported outcomes(PRO); and will also include a review of screeningtools, not just outcome measures. Additionally, thischapter will extend and update the prior literaturereviews of PROs, broaden the review to include lowerurinary tract (LUTS) and bowel incontinence outcomesmeasures, and provide recommendations forquestionnaire selection for use in clinical practice andresearch. In addition, this summary will review thepurpose and content of the ICI questionnaire (ICIQ)modules. Given the burgeoning literature in this area,a complete review of all studies with PROs will not beprovided, but rather PRO highlights will be included.
The expansion in scope of this review to include alltypes of patient reported outcomes (PRO) is animportant step in recognising the inherent conceptualdifferences of various PROs each with differentassessment goals. A PRO is an objective assessmentof the patient’s subjective experience and can includeaspects of the patient’s health. PROs measure differentaspects of disease and therapeutic impact such as:symptom frequency or symptom bother, health-relatedquality of life (HRQL), treatment satisfaction, or workproductivity measures (Figure 1). An essentialcomponent of selecting a PRO for use is to ensure thatthe selected PRO is consistent with the objective ofthe study or clinical purpose. For example, if the goalis to assess treatment satisfaction, then a treatmentsatisfaction measure should be incorporated into thestudy design or as a clinical outcome. The matchingof appropriate PRO selection with one’s desired
outcomes is critical to success when assessing PRO’sand will be reviewed further in this chapter.
Ultimately, the last decade has been one of tremen-dous growth in the area of PROs with influences fromscientific and regulatory communities. As such, the ICIwill endeavour to continually update the recom-mendations it offers on the basis of emerging data andpublished evidence based on the sound and rigidrecommendations of the previous three reviews.
A number of different electronic databases weresearched, limited to adults over the age of 18 yearsand human studies from January 2004 to June 2008,including Pub-Med, Medline, PsychInfo, theLOCATORplus database for books, serial titles andaudiovisuals, the Cochrane Library for randomisedcontrolled trials, and the NLM Gateway database.The following keywords were used separately and/or
LITERATURE SEARCH STRATEGY
INTRODUCTION
Committee 5 B
Patient-Reported OutcomeAssessment
Figure 1 : Patient-Reported Outcomes AssessmentAreas. Burke L, Evidence Review Branch DDMAC,FDA; DIA Workshop on pharmacoeconomic andQuality of Life Labeling and Marketing Claims NewOrleans October 3, 2000

364
in combination: “urinary incontinence”, “urinarysymptoms”, “urgency”, “overactive bladder”, “stressincontinence”, “incontinence”, “questionnaire”,“epidemiology”, “prostate”, “prolapse”, “fecal”, “faecal”,“bowel”, “anal” and “quality of life”, “sexual” and “healthutilities”. Questionnaires identified in previous ICIreports were also searched in PubMed and Medline.
Incontinence and other lower urinary tract symptoms(LUTS) as well as bowel problems and their impacton patients and their lives can be assessed in anumber of ways. Traditionally, the clinical history hasbeen used to gain a summary view of the symptomsexperienced by patients and in some cases the impacton their lives. Increasingly however, patient-completedmethods of measuring incontinence and LUTS arebeing used, including voiding diaries and question-naires.
Patient self-completed questionnaires or patientreported outcomes (PROs) represent the mostimportant clinical review of symptom impact andtreatment benefit from a patient perspective. PROsprovide a method for the standardised collection ofdata, or an objective assessment of a subjective
phenomenon, from patients relating to incontinence,other LUTS, and bowel problems. Clinicians’ assess-ments of patients’ outcomes have often been shownto underestimate the degree of bother perceived bypatients, and to focus on issues of lesser importanceto patients [3-6].
PRO questionnaires can be used to record thepresence and severity of urinary symptoms includingincontinence, as well as the impact of symptoms oneveryday activities and health-related quality of life(HRQL). To ensure that the results obtained withPROs are clinically useful, data must be gatheredusing valid and reliable instruments. Questionnairedesign and development is not a simple process.Developing such instruments requires a multistep,structured process that incorporates cognitivepsychology, psychometric theory, and patient andclinician input. The process begins by determiningthe intent and purpose of the PRO and culminates instudies that demonstrate the measure’s validity,reliability, and responsiveness. The specific stepsrequired for developing a PRO questionnaire areoutlined in the following section and are showndiagrammatically in Figure 2.
The development of a PRO is a rigorous, scientificprocess to provide confidence that the PRO ismeasuring what it is intended to measure, that it doesthis reliably, and is appropriate for use in the patient
I. PRO QUESTIONNAIREDEVELOPMENT AND VALIDATION5B- A. THE MEASUREMENT OF
PATIENT-REPORTEDOUTCOMES (PROS) OF
INCONTINENCE, OTHER LOWERURINARY TRACT SYMPTOMS,
AND BOWEL PROBLEMS
Figure 2 : The development of a patient reported outcome is a multistep process. Food & Drug Administration(3). Guidance for industry - patient-reported outcome measures: Use in medical product development tosupport labeling claims. Silver Spring, MD: FDA; February 2006.

365
or population group under investigation. The finalinstrument must have demonstrated validity andreliability in the intended target population. PROsneed to be developed with patient and clinician inputand have the psychometric, or measurement,properties of the PRO evaluated to determine that itis a valid outcome meaure. To be a useful measure-ment tool, a PRO instrument must also be easy toadminister, reliable, and valid. Only PROs that haveundergone this process and have published validationdata are discussed in this chapter.
1. DETERMINING QUESTIONNAIRE INTENT AND PURPOSE
The first task in developing a PRO measure is todetermine why the instrument is needed. Given thecurrent number of disease-specific questionnairesavailable in the field of incontinence and related pelvicdisorders, a new PRO measure must fill a need thathas not already been met by an existing instrument.Once the need for the measure is recognised, itspurpose and clinical usefulness need to be consideredbecause the purpose dictates the validation designprocess. For example, a symptom- and a treatment-satisfaction measure would be developed andvalidated differently because the outcome is different.
The development stage would focus on the outcomeof interest (eg, symptoms patients experience andthe significance of each symptom, or what issuespatients consider when determining how satisfiedthey are with treatment) with the items derived directlyrelating to the outcome of interest. Validation effortswould include designing a study focused on theoutcome of interest with the appropriate patientinclusion/exclusion criteria to enhance generalisabilitywhile maintaining internal consistency and providingopportunities to test—at a minimum—reliability andconstruct validity.
2. DEVELOPING THE ITEMS
Designing a clinically useful PRO measure involvesmore than just developing a series of questions. Inaddition to clinician input and literature review,questionnaire items should be generated from patientinput. This is obtained through focus groups or one-on-one interviews to provide qualitative data on issuespertinent to patients and to identify the words patientsuse to describe their symptoms or disease impact.Focus groups and one-to-one interviews should becarefully planned to address the goals of thequestionnaire being developed. For example, if ameasure is intended to assess symptom bother,interview questions should pertain to the patient’ssymptom experience. Importantly, rather than usingclinical terminology which patients may notcomprehend, the words used during the focus groupsor interviews should be common to patients. Afteritems are generated, the newly drafted questionnaire
should be reviewed by other patients and experts toensure its readability and content validity.
An alternative approach to questionnaire developmentis to adapt an existing measure to meet the needs ofthe desired questionnaire. Although no patient inputis required at the outset when adapting an existinginstrument, patients need to be involved after thequestionnaire is adapted to ensure that the revisedmeasure is pertinent to the population of interest.Also, the adapted questionnaire must be validatedon its own in the target population; the validity of theoriginal questionnaire does not apply to an adaptedmeasure.
For newly developed and adapted questionnaires,think-out-loud interviews or cognitive debriefinginterviews should be used to ascertain the correctnessand validity of the revised questionnaire. In a think-out-loud interview, patients are asked to review aquestion and describe what they are thinking as theycognitively process the question; the patients thinkout loud about what the question means to them. Fora cognitive debriefing approach, patients review andrespond to the questionnaire items, then areinterviewed about what each item meant to them asthey completed the questionnaire. Both approachesprovide information about what patients consider whenresponding to each question.
3. DETERMINING THE MODE OFADMINISTRATION OF A QUESTIONNAIRE
Once items have been generated, the mode ofadministration must be considered. Will the measurebe completed by the patient (ie, self-administered) oradministered by an interviewer (ie, interviewer-administered)? How the questionnaire will becompleted needs to be determined before thevalidation stage because mode of administration canaffect patient responses. For highly personal or intimatequestions, a self-administered questionnaire isrecommended to avoid response bias. Questionnairesthat are self-administered are preferable to interviewer-administered questionnaires because the datacollection burden is reduced and patients are morelikely to provide unbiased information on self-administered questionnaires. Importantly, if aquestionnaire has been validated for a particular modeof administration, this does not make the questionnairevalid for all modes of administration. Each mode ofadministration should be validated separately.
4. QUESTIONNAIRES’ PSYCHOMETRIC PROPERTIES
All PRO measures must demonstrate reliability, validity,and responsiveness, which are described in detailbelow. This can be accomplished in several ways:
1. Perform a stand-alone cross-sectional study tovalidate the questionnaire in the patient populationfor which it was designed;

366
2. Administer the untested questionnaire in a clinicaltrial and use the baseline data to performpsychometric validation (the end-of-study data canalso be used to evaluate responsiveness); or
3. Perform a stand-alone longitudinal study with anintervention to determine the instrument’spsychometric performance and responsiveness ina non-clinical trial setting.
The following psychometric properties must be testedfor and demonstrated in a validated questionnaire.
Reliability refers to the ability of a measure to producesimilar results when assessments are repeated (ie, isthe measure reproducible?) [4, 5]. Reliability is criticalto ensure that change detected by the measure isdue to the treatment or intervention and not due tomeasurement error [6]. One measure of reliability isthe questionnaire’s internal consistency, whichindicates how well individual items within the samedomain (or subscale) correlate [7]. Cronbach’s alphacoefficient is used to assess internal consistencyreliability, with higher alphas indicating greatercorrelation [6]. Typically, Cronbach’s alpha should begreater than 0.70 to indicate good internal consistencyreliability [6, 7]. If the item-to-total alpha is less than0.20, the question should be removed or rewritten[4].
Test-retest reliability, or reproducibility, indicateshow well results can be reproduced with repeatedtesting. To assess test-retest reliability, the samepatient completes the questionnaire more than once,at baseline and again after a period of time duringwhich the impact of symptoms is unlikely to change(e.g., a few days or weeks) [4, 6, 7]. The Pearsoncorrelation coefficient and intraclass correlationcoefficient are used to demonstrate reproducibility.For group data, a Pearson correlation coefficient oran intraclass correlation coefficient of at least 0.70demonstrate good test-retest reliability [6, 7].
Interrater reliability indicates how well scorescorrelate when a measure is administered by differentinterviewers or when multiple observers rate the samephenomenon [7]. Demonstration of interrater reliabilityis not necessary for self-administered questionnairesbut is necessary for instruments based on observerratings or using multiple interviewers. A correlation of0.80 or higher between raters indicates good interraterreliability [7].
Validity refers to the ability of an instrument to measurewhat it was intended to measure [4, 6, 7]. A measureshould be validated for each specific condition oroutcome for which it will be used. For example ameasure designed to assess stress incontinencewould not be valid for OAB unless it were specificallyvalidated in patients with OAB symptoms.
Content validity, convergent validity, discriminant
validity and criterion validity typically are required tovalidate a questionnaire [7]. Content, or face, validityis a qualitative assessment of whether the question-naire captures the range of the concept it is intendedto measure [6, 7]. For example, does a measure ofsymptom severity capture all the symptoms thatpatients with a particular condition have, and if so, isthe measure capturing the items in a mannermeaningful to patients? To obtain content validity,patients and clinical experts review the measure andjudge whether the questions are clear, unambiguous,and comprehensive [4].
Convergent validity is a quantitative assessment ofwhether the questionnaire measures the theoreticalconstruct it was intended to measure [4, 6]. Convergentvalidity indicates whether a questionnaire has strongerrelationships with similar concepts or variables.Stronger relationships should be seen with the mostclosely related constructs and weaker relationshipsseen with less-related constructs [6]. Discriminantvalidity indicates whether the questionnaire candifferentiate between known patient groups (eg, thosewith mild, moderate, or severe disease) [6];. generally,measures that are highly discriminative are also highlyresponsive.
Criterion validity reflects the correlation betweenthe new questionnaire and an accepted reference,or gold standard [6, 7]. One difficulty in establishingcriterion validity is that a gold-standard measure mightnot be available [6, 7]. When criterion validity can beestablished with an existing measure, the correlationshould be 0.40 to 0.70; correlations approaching 1.0indicate that the new questionnaire may be too similarto the gold-standard measure and therefore redundant[7].
Responsiveness indicates whether the measure candetect change in a patient’s condition [5].An importantaspect of responsiveness is determining not onlywhether the measure detects change but whether thechange is meaningful to the patient. This can be doneby determining the minimal important difference(MID) of the measure. The MID is the smallest changein a PRO questionnaire score that would be consideredmeaningful or important to a patient [6, 8-10]. Atreatment that is statistically significantly better thananother may not necessarily have made a meaningfuldifference to the patient; the MID indicates whetherthe treatment made such a difference from a patientperspective [8-10].
Unfortunately, there is no scientific test for MID as itis an iterative process that involves two methodologiesto determine the MID of a questionnaire: an anchor-based approach and a distribution-based approach [11,12]. With the anchor-based approach, the MID isdetermined by comparing the measure to othermeasures (or “anchors”) that have clinical relevance[12], such as a global measure of well-being or

367
perception of treatment benefit [10]. With the distribution-based approach, the MID is determined by the statisticaldistributions of the data [12], using analyses such aseffect size, one-half standard deviation, and standarderror of measurement [10, 13].
5. LINGUISTIC AND CULTURAL VALIDATION
Increasingly, PRO questionnaires are required to beused in a number of different populations and settings,however, questionnaires and their psychometricproperties are not necessarily transferable [13, 14].A measure that is valid and reliable for a particularlanguage and culture may not prove so when used ina different population. Linguistic and cultural adaptationof a questionnaire can occur during the developmentphase before validation, or it can be done after thequestionnaire is validated in the language in which itwas initially developed, with the latter being the morecommon approach. Ensuring the linguistic and culturalvalidity of a questionnaire is especially important formeasures used in multinational clinical trials [14].
The principal steps in adapting a measure for differentlanguages and cultures are as follows:
1. two forward translations of the original instrumentinto the new language;
2. quality-control procedures that may include abackward translation (translating the instrumentback into the original language) (15);
3. adjudication of all translated versions;
4. discussion by an expert panel to ensure clarity ofthe translated questionnaire; and
5. testing the translated instrument in monolingual orbilingual patients to ensure that it measures thesame concepts as the original instrument [4, 7,14, 15].
However, if a backward translation of the measuredoes not produce a semantically equivalent instrument,then the instrument may need to be developed in thetarget language, rather than just translated [15].
After cultural and linguistic validation, PROs shouldalso be psychometrically validated within the targetlanguage. Thus, reliability, validity, and responsivenessneed to be assessed with each language translationto confirm the same measurement properties arepresent in the translated language(s) to ensurepsychometric equivalence. If psychometric equivalenceis not present (e,g, not achieving similar or betterresults in new language translation), the cultural andlinguistic translations need to be re-evaluated andperhaps a new instrument may need to be developed.
The ICIQ questionnaires and many of the otherquestionnaires discussed in this chapter have multiplelinguistically validated versions making them useful forInternational implementation. It is also important to notethat the step after linquistic validation, demonstratingpsychometric equivalence, should also be demons-
trated to ensure that the PRO performs equivalentlyin different languages and cultures.
6. REGULATORY OVERSIGHT
As clinicians and scientists have begun to appreciateand accept PROs as appropriate outcome measures,regulatory authorities have issued guidance documentson current best practices in the development andimplementation of PRO in clinical trial settings [3, 16].For PROs to be acceptable outcome measures forregulatory authorities, documentation of measurementproperties must be present as well as evidence ofinclusion of the patient perspective and understandingof the PRO and a cohesive conceptual frameworkthat stipulates how the PRO is related to theintervention. While PROs within this document mayhave a “recommended” status, they may not meet allof the required regulatory guidelines and may requireadditional validation work either from a qualitative orquantitative perspective. It is strongly suggested thatregulatory authorities be contacted early in the processof selecting a PRO for clinical trials to ensure regulatoryacceptance of the PRO.
7. QUESTIONNAIRE DEVELOPMENT - A CONCLUSION
Patient self-completed questionnaires are the mostsuitable method for assessing the patient’s perspectiveof their lower urinary tract, vaginal and bowelsymptopms [17]. Questionnaires may be long anddetailed for use in research, but need to be short andeasy to use to be relevant for clinical practice. Inaddition to being valid and reliable, they need to beeasy to complete, and, if they are being used tomeasure outcome, sensitive to change. Developinga new questionnaire and testing it thoroughly takesa great deal of time and is only necessary if there isnot an existing instrument available.
There are many questionnaires currently availablefor use and these have been reviewed and describedwith recommendations from the Committee for theiruse in the last three ICI reports.
The major purpose of the ICI has been to provide adefinitive international review and consultative opinionregarding the recommended measures to assesspatient reported outcomes within the area of urinaryincontinence and LUTS. To this end since the FirstConsultation, the ICI has worked to develop a modularformat for the various patient reported outcomesincluding health related quality of life (HRQL) allowingclinicians and researchers to select internationallyrecommended questionnaires for the assessment oftheir patients in both clinical practice and clinical trials.In this the fourth ICI review, the ICIQ modularquestionnaires (supported by the InternationalConsultation) are presented in detail and their useevaluated. Whilst some of the modular questionnairesare still currently under full evaluation their content andformat are presented within this chapter.

368
A detailed review of recommended questionnaireswas provided in the First Consultation chapter [18].At the Second Consultation, the Committee developedstandardised grades of recommendation forquestionnaires which attempted to reflect the OxfordCentre for Evidence Based Medicine’s Levels ofEvidence. These were applied to evaluate question-naires concerned with urinary incontinence [19]. Atthe Third Consultation, these grades were revisedand updated to take into account the increasingnumbers of published questionnaires concerned withLUTS and incontinence, and also broadening of thefield to include pelvic organ prolapse (POP) and faecalincontinence (FI) as well as LUTS and urinaryincontinence (UI).
At the Second and Third Consultations, the Committeedevised three grades of recommendation [19] (Table1).
• Questionnaires were ‘highly recommended’ andgiven a Grade A if the Committee found “Publisheddata indicating that the questionnaire is valid,reliable and responsive to change followingstandard psychometric testing. Evidence must bepublished on all three aspects and questionnairesmust be relevant for use with persons withincontinence.”
• Questionnaires were “recommended” and givena Grade B if the Committee found “Published dataindicating that the questionnaire is valid and reliablefollowing standard psychometric testing. Evidencemust be published on two of the three main aspects(usually validity and reliability).”
• Questionnaires were considered to have “potential”and given Grade C if the Committee found“Published data (including abstracts) indicating
that the questionnaire is valid or reliable orresponsive to change following standardpsychometric testing.”
The Committee decided that evidence published inabstracts or posters could be used to indicate adeveloping questionnaire’s potential, but was notsufficiently peer-reviewed to provide the basis for astronger recommendation.
This current Fourth Consultation represents adeparture from the recommendation scheme of the lastreview. In this fourth review questionnaires will still begraded A, B, or C as outlined above. However therecommendation will be to preferably utilisequestionnaires from the ICIQ modules described indetail below. Many, but not all, of these questionnairesare Grade A questionnaires by previously stipulatedcriteria. Within the description of the ICIQ modulesbelow the grade assigned to each module is indicated.
Should none of the modular questionnaires be deemedappropriate for specific research or clinical purposes,ICI’s recommendation is to use a Grade A question-naire as previously recommended and where nosuitable instrument exists a Grade B or C question-naire.
For UI and UI/LUTS, the Committee examined thequality of the psychometric evidence. Only wherepublished data were scientifically sound was the label‘with rigour’ allowed. Where the Committee hadconcerns about the quality of evidence, this is notedin the descriptions of the questionnaires below. TheCommittee considered that the number of high qualityquestionnaires means that there are now sufficientquestionnaires for most purposes and it is notnecessary to encourage the development of newquestionnaires, except for particular patient groups(see below). As for the last Consultation, it is expectedthat by the next Consultation, Grade Anewquestionnaires will either be promoted to Grade Abecause of further high quality publications or relegatedto Grade B if further development does not occur.
The Committee felt that the development ofquestionnaires in the areas of pelvic organ prolapse(POP) and faecal incontinence (FI) was at a muchearlier level. This necessitated a slightly different setof grades of recommendation so that researchers are
GRADES OF RECOMMENDATION FORQUESTIONNAIRES 2008
5B - B. RECOMMENDED PROQUESTIONNAIRES
Table 1. Criteria for recommendation of questionnaires for UI and UI/LUTS at the Fourth Consultation 2008
Grade of recommendation Evidence required (published)
Recommended (Grade A) Validity, reliability and responsiveness established with rigour in several data sets
Recommended (Grade Anew) Validity, reliability and responsiveness indicated with rigour in one data set
(Grade B) Validity, reliability and responsiveness indicated but not with rigour. Validity and reliability established with rigour in several data sets. To be used if suitable questionnaires not available in ICIQ modular format or Grade A or Grade A new

369
encouraged to continue to work to producequestionnaires with the highest levels of evidence(see Table 2).
The ICIQ modular questionnaire was developed tomeet the need for a universally applicable standardguide for the selection of questionnaires for use inclinical practice and clinical research [18, 19]. Thedecision to develop standard questionnaire moduleswas taken by the Committee after the first ICI meetingin 1998, and resulted in the development of the ICIQcore questionnaire discussed in this section. It wasrecognised at that time that there were many goodvalidated questionnaires each developed for a specificpurpose and each subtly different. Although developersof the questionnaires were familiar with their contentand use, the increasing number of questionnairesmade appropriate selection difficult and limited theability to compare similar clinical and research datadue to different data collection methods.
An international advisory board was established tocontinue the development of the modular ICIquestionnaire outside the limits imposed by triennialconvening of the ICI Committee. Early discussionswith the advisory board resulted in the decision toexpand the concept to include wider urinary symptoms,bowel symptoms and vaginal symptoms. The advisoryboard consisted of clinicians and researchers withexperience in the design and use of questionnairesrepresenting the major societies involved in theassessment and research of lower genital tract, lower
urinary tract and bowel function. The members of theadvisory board of the ICI can be seen on the ICIQwebsite at www.iciq.net. The ICIQ modular question-naire was then established.
The ICIQ’s objective is to provide internationalconsensus on the use of patient completedquestionnaires for the assessment of lower pelvicsymptoms and their impact on patient’s lives. Threeaims underpin the ICIQ in order to achieve clarityover questionnaire use:
• To recommend high quality self-completionquestionnaires according to evidence of validationas stipulated by the three prior ICI Committees;
• To promote wider use of questionnaires tostandardise assessment of lower urinary tract andpelvic dysfunction and its impact on patients’s lives,in order to;
• Facilitate communication in different patient settingsand different patient groups both in clinical practiceand wider clinical research.
The ICIQ recognised that many high quality publishedquestionnaires already existed and, with permissionfrom the authors, those instruments were adoptedinto the modular project. It was not possible to adoptall available questionnaires and where more than oneoption existed the most appropriate questionnaire forthe purpose was included. Where high qualityquestionnaires were not available, the need to developa new questionnaire/s was acknowledged. Collabo-rative efforts to develop new questionnaires arewelcome and encouraged.
The ICIQ’s international nature requires thatlinguistically validated translations are available. Morethan 50 language versions of various modules havebeen validated to date, conducted according toestablished protocol.
Thirteen ICIQ modules/questionnaires are currentlyavailable for use, with further modules in development(discussed in detail below). Clinicians or researchersare able to select module(s) to meet the particularrequirements of their study or clinical practice. In orderto simplify this selection process, modules have beencategorised as shown in Table 3. It must be stressedthat although multiple questionnaires can and probablyshould be used they must be used in the format inwhich they were originally designed and thequestionnaires cannot be merged together.
In this chapter questionnaires forming part of the ICIQmodular format are referred to as those preferred forusage. Although many of the modules are Grade Aquestionnaires, others are still under various phasesof development and are graded appropriately.
I. AIMS AND OBJECTIVES
5B - C. INTERNATIONALCONSULTATION ON
INCONTINENCE MODULARQUESTIONNAIRE (ICIQ):
WHAT IS THE ICIQ?
Table 2. Criteria for recommedation of questionnairesfor POP and FI at the Fourth Consultation 2008
Grade of recommendation Evidence required (published)
Recommended (Grade A) Validity, reliability and responsiveness established with rigour.
(Grade B) Validity and reliability established with rigour, or validity, reliability andresponsiveness indicated.
With potential (Grade C) Early development – further work required and encouraged

370
RE
CO
MM
EN
DE
DM
OD
UL
ES
RE
CO
MM
EN
DE
D A
DD
-ON
MO
DU
LE
SC
ON
DIT
ION
Co
re M
od
ule
s(s
ymp
tom
ass
essm
ent)
OP
TIO
NA
L M
OD
UL
ES
HR
QL
Gen
eric
HR
QL
Sex
ual
Mat
ters
Po
st-
Tre
atm
ent
Uri
nar
y sy
mp
tom
sM
ales
: IC
IQ-M
LUT
SF
emal
es:
ICIQ
-FLU
TS
Mal
es: I
CIQ
-MLU
TS
LF
Fem
ales
: IC
IQ-F
LUT
S L
FIC
IQ-L
UT
Sqo
lS
F-1
2M
ales
: IC
IQ-M
LUT
Sse
xF
emal
es: I
CIQ
-FLU
TS
sex
Vag
inal
sym
pto
ms
and
sexu
al m
atte
rsIC
IQ-V
SIC
IQ-V
Sqo
l*S
F-1
2
Bo
wel
sym
pto
ms
and
qu
alit
y o
f lif
eIC
IQ-B
SF
-12
Mal
es: I
CIQ
-Bse
x*F
emal
es: I
CIQ
-Bse
x*
Uri
nar
y In
con
tin
ence
ICIQ
-UI S
hort
For
mIC
IQ-U
I LF
*IC
IQ-L
UT
Sqo
lS
F-1
2M
ales
: IC
IQ-M
LUT
Sse
xF
emal
es: I
CIQ
-FLU
TS
sex
CO
ND
ITIO
NB
) S
pec
ific
pat
ien
t g
rou
ps
HR
QL
Gen
eric
HR
QL
Sex
ual
Mat
ters
No
ctu
ria
ICIQ
-NIC
IQ-N
qol
SF
-12
Mal
es: I
CIQ
-MLU
TS
sex
Fem
ales
: IC
IQ-F
LUT
Sse
x
Ove
ract
ive
Bla
dd
erIC
IQ-O
AB
ICIQ
-OA
Bqo
lS
F-1
2M
ales
: IC
IQ-M
LUT
Sse
xF
emal
es: I
CIQ
-FLU
TS
sex
Neu
rog
enic
ICIQ
-Spi
nal C
ord
Dis
ease
*S
F-1
2
Lo
ng
-ter
m c
ath
eter
use
rsIC
IQ-L
TC
*S
F-1
2
Ch
ildre
nIC
IQ-C
LUT
S*
ICIQ
-CLU
TS
qol*
ICIQ
-S
atis
fact
ion*
Gra
y: In
dev
elo
pm
ent;
bla
ck:
Gra
de
A o
r A
(N
ew)
Tab
le 3
. T
he
ICIQ
Mo
du
lar
Str
uct
ure

371
Questionnaires that are in early stages of developmentand have yet to reach Grade C are described as “indevelopment”. Where an ICIQ module is not availableit is recommended that a Grade A or B or C question-naire is used.
1. CORE MODULES
Questionnaires to assess the core symptoms of lowerpelvic dysfunction:
• Lower urinary tract symptoms (male and femalespecific versions).
• Urinary incontinence (male and female applicableversion).
• Vaginal symptoms (female version only).
• Bowel symptoms including incontinence (male andfemale applicable version).
Each module is intended for the comprehensive yetsuccinct measurement of symptoms and associated‘bother’. The bother item attached to each symptomenables the individual to indicate areas that causethe greatest negative impact on HRQL as perceivedby them. This can be a more sensitive indicator oftreatment goals than frequency of symptoms alone.
2. SPECIFIC PATIENT GROUPS
Questionnaires to assess specific conditions orsymptom complexes such as nocturia and overactivebladder are contained in this section. This categoryalso includes specific patient groups, for example,children. These instruments contain only questionitems characteristic of the symptom complex or havebeen developed specifically for use in a diverse groupmaking the items/questionnaire only utilisable in thatpopulation.
• Nocturia (male and female applicable version).
• Overactive bladder (male and female applicableversion).
• Patients with spinal cord disease.
• Patients using long term catheters.
• Lower urinary tract symptoms in children.
Bother items are again included for all except thechildren’s questionnaire.
1. CORE MODULES
These questionnaires incorporate modules for
assessment of health-related quality of life (HRQL) andsexual matters and are recommended to be completedalongside symptom evaluations. The core symptommodules described above contain bother itemsindicating impact on quality of life directly related tosymptoms. The HRQL questionnaires recommendedhere cover specific issues that are a consequence ofsymptoms, such as limitations on activities and impacton relationships.
• HRQL associated with lower urinary tract symptoms(male and female applicable version).
• HRQL associated with vaginal symptoms (femaleversion only).
• HRQL associated with bowel symptoms (male andfemale applicable version).
• Sexual matters associated with lower urinary tractsymptoms (male and female specific versions).
• Sexual matters associated with vaginal symptomsare included in the symptom questionnaire as theissues were considered too intrinsically linked toseparate for evaluation.
Bother sub-items are again included to provide moredetailed information about impact on quality of lifethan frequency of impact alone. The assessment ofsymptoms in combination with quality of life enablesa more thorough and detailed evaluation of thepatient’s experience [20,21]. Given the nature of lowerpelvic dysfunction, sexual matters can also be affectedand questionnaires are available to evaluate thiswhere appropriate.
2. SPECIFIC PATIENT GROUPS
In the same manner as the symptom modules, HRQLmodules are available for specific symptom complexes:
• HRQL associated with nocturia (male and femaleapplicable version).
• HRQL associated with overactive bladder (male andfemale applicable version).
This category includes lengthier questionnaires formore exploratory evaluation of the core symptoms oflower pelvic dysfunction. Whilst these questionnairesare suitable for use in clinical practice, they have notbeen shortened for clinical efficiency and are thereforemore widely used in research studies where explora-tion of broader associated symptoms may be desired.
• Lower urinary tract symptoms (male and femalespecific versions).
• Urinary incontinence (male and female applicableversion).
IV. OPTIONAL MODULES
III. ICIQ HEALTH-RELATED QUALITYOF LIFE AND SEXUAL FUNCTION
MODULES
II. ICIQ SYMPTOM AND BOTHERMODULES

372
The ICIQ module for post-treatment satisfaction is inthe early stages of development. Assessment of apatient’s satisfaction with treatment (behavioural,surgical or medication) provides information ontreatment impact on their condition and life andincludes their perception of effectiveness, tolerabilityand convenience. It is not yet clear if satisfactionfollowing treatment can be characterised by a set ofcommon question items that are applicable to alldisorders of the lower urinary tract and pelvic floor. Aswith HRQL, there are generic and disease specificquestionnaires that assess satisfaction. Ongoingstudies will provide further evidence on which to makesuggestions regarding post treatment evaluation butit is likely that this will encompass both generic andcondition specific measures. Ultimately, the develop-ment of post treatment modules will also rely on advicefrom regulatory authorities (eg FDA) to ensure thatmeasures capture a recognised multidimensionalityof satisfaction.
The ICIQ recommends the use of a ‘core’, ‘symptom-specific’,or ‘add-on’ modules that match the intendedpurpose of a study. Whilst this may necessitate the useof a module from each section, there is no requirementto do so. The characteristics of each module is summa-rised below, although more extensive information canbe found on the project website, www.iciq.net.
Tables 4, 5 a,b,c
The ICIQ modular questionnaire has attractedconsiderable attention from both clinicians andresearchers worldwide since its structure was finalisedin 2004. More than 500 requests for use of the variousmodules have been documented and over 40published studies were identified up to April 2008,with the majority originating from Europe, particularlythe UK.
The most widely applied module is the ICIQ-UI ShortForm, particularly to evaluate female urinary
incontinence, though a handful of studies evaluatingseverity of incontinence in men resulting fromprostatectomy for cancer or treatment for bladderoutlet obstruction related to benign prostatic enlar-gement have been reported [31, 32]. Most studiesrelate to epidemiological research, including preva-lence surveys of urinary incontinence or lower urinarytract symptoms [33, 34]; and outcomes research,including prospective and randomised clinical trials oftreatments including surgery [35], drug therapies [36]and conservative treatments [37]. For example, arecent placebo-controlled randomised trial found thatduloxetine significantly reduced ICIQ scores in womenwith mixed urinary incontinence[36].
Reports on further validation and translations of theICIQ and related educational projects have also beenpublished. A recent study conducted by Franco, Leeand Fynes [38], for example, compared variousvalidated subjective measures of urinary incontinenceseverity to the one hour pad test in women andreported that only the ICIQ correlated significantlywith this clinical variable, thereby recommending itsuse in routine clinical practice as an alternative to padtests. Encouraging relationships between the ICIQand other urodynamic parameters have also beenreported [39].
The ICIQ has also been applied to hospital and generalpractice settings, and has been adopted in nationalguidelines for the management of urinary incontinencein primary care by the Scottish IntercollegiateGuidelines Network (www.sign.ac.uk/pdf/sign79.pdf)and in a primary care resource pack by the BritishSociety of Urogynaecology.
The ICIQ modular questionnaire project (www.iciq.net)provides a series of standardised questionnaires forthe patient reported assessment of lower pelvicdysfunction symptoms and their impact on patientslives. The ICIQ provides clarity over the selection ofquestionnaires by recommending only those withevidence of high quality and robust psychometricvalidation including validity, reliability and sensitivityto change. This assurance provides the user withconfidence in the results obtained, which is importantin clinical practice and research where treatmentdecisions or trial outcomes depend on this evidence.Increasing awareness of the ICIQ aims to promoteincreased use of standardised questionnaires, therebyfacilitating communication between clinicians andresearchers and enable more widespread compa-risons between different treatments and patient groupsworldwide.
IX. CONCLUSION
VIII. ICIQ QUESTIONNAIREIMPLEMENTATION
VII. ICIQ MODULES
VI. GUIDANCE FOR USE OF THE ICIQ
V. POST-TREATMENT MODULE

373
Nam
e/G
rad
eP
urp
ose
Ava
ilab
ility
Do
mai
ns
Item
sA
vaila
ble
Tra
nsl
atio
ns
ICIQ
-FLU
TS
(BF
LUT
S-S
F [2
2])
Gra
de
A
Com
preh
ensi
ve a
sses
smen
t of
fem
ale
low
eru
rin
ary
trac
t sy
mp
tom
s an
d as
soci
ated
both
er.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[22]
.
Fill
ing.
Voi
ding
.In
cont
inen
ce.
1219
ICIQ
-FLU
TS
Lon
gF
orm
(B
FLU
TS
[23]
) G
rad
e A
Det
aile
d as
sess
men
t of f
emal
e lo
wer
uri
nar
y tr
act
sym
pto
ms
and
asso
ciat
edbo
ther
.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[22,
23].
Var
ied
low
er u
rinar
y tr
act
sym
ptom
s.18
7
ICIQ
-FLU
TS
sex
(BF
LUT
S[2
3])
Gra
de A
Ass
essm
ent o
f fe
mal
e se
xual
mat
ters
asso
ciat
ed w
ith u
rin
ary
sym
pto
ms
and
rela
ted
both
er.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[23]
.
Pai
n an
d le
akag
e w
ith s
exua
lin
terc
ours
e.O
vera
ll in
terf
eren
ce.
418
ICIQ
-LU
TS
qol
(Kin
g’s
Hea
lthQ
uest
ionn
aire
[24]
) G
rad
e A
Det
aile
d as
sess
men
t of H
RQ
L is
sues
asso
ciat
ed w
ith u
rin
ary
sym
pto
ms
and
rela
ted
both
er in
bot
h m
en a
nd w
omen
.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[24]
.
Life
res
tric
tions
.E
mot
iona
l asp
ects
.P
reve
ntiv
e m
easu
res.
2245
ICIQ
-MLU
TS
(IC
Sm
aleS
F[2
5])
Gra
de
A
Com
preh
ensi
ve a
sses
smen
t of
mal
e lo
wer
uri
nar
y tr
act
sym
pto
ms
and
asso
ciat
edbo
ther
.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
.
Voi
ding
.In
cont
inen
ce.
Indi
vidu
al it
ems
eval
uatin
gfr
eque
ncy
and
noct
uria
.
1326
ICIQ
-MLU
TS
Long
For
m(I
CS
mal
e[2
6,27
])G
rad
e A
Det
aile
d as
sess
men
t of m
ale
low
er u
rin
ary
trac
t sy
mp
tom
s an
d as
soci
ated
bot
her.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[26,
27].
Var
ied
low
er u
rinar
y tr
act
sym
ptom
s.23
29
ICIQ
-MLU
TS
sex
(IC
Sm
ale[
27])
Gra
de
A
Ass
essm
ent o
f m
ale
sexu
al m
atte
rsas
soci
ated
with
uri
nar
y sy
mp
tom
s an
dre
late
d bo
ther
.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[26,
27].
Ere
ctio
n an
d ej
acul
atio
nis
sues
.O
vera
ll in
terf
eren
ce.
424
ICIQ
-Nqo
l(N
-QoL
[28]
)G
rad
e A
Det
aile
d as
sess
men
t of H
RQ
L is
sues
asso
ciat
ed w
ith n
oct
uri
a.
Ava
ilabl
e fo
r us
e.P
ublis
hed
evid
ence
of v
alid
ity,
relia
bilit
y an
d re
spon
sive
ness
[28]
.
Issu
es a
ssoc
iate
d w
ith s
leep
dist
urba
nce.
Life
res
tric
tions
.P
reve
ntiv
e m
easu
res.
1327
Tab
le 4
. IC
IQ M
od
ule
Des
crip
tio
n

374
Nam
e/G
rad
eP
urp
ose
Ava
ilab
ility
Do
mai
ns
Item
sA
vaila
ble
Tra
nsl
atio
ns
ICIQ
-N(I
CS
mal
eSF
/B
FLU
TS
-SF
[22,
25])
Gra
de
B
Com
preh
ensi
ve a
sses
smen
t of s
ympt
oms
ofn
oct
uri
a a
nd a
ssoc
iate
d bo
ther
.A
vaila
ble
for
use.
Evi
denc
e of
val
idity
, rel
iabi
lity
and
resp
onsi
vene
ss [2
2,25
,27]
.
Fre
quen
cy.
Noc
turia
.
230
ICIQ
-OA
B(I
CS
mal
eSF
/B
FLU
TS
-SF
[22,
25])
Gra
de
A
Com
preh
ensi
ve a
sses
smen
t of s
ympt
oms
ofo
vera
ctiv
e b
lad
der
and
ass
ocia
ted
both
er.
Ava
ilabl
e fo
r us
e.
Evi
denc
e of
val
idity
, rel
iabi
lity
and
resp
onsi
vene
ss [2
2,25
,27]
.R
esp
on
sive
nes
s n
ot
dem
on
stra
ted
in O
AB
pat
ien
ts
Fre
quen
cy.
Noc
turia
.
Urg
ency
.
Urg
ency
inco
ntin
ence
.
422
ICIQ
-OA
Bqo
l(O
AB
-q [
29])
Gra
de
A
Det
aile
d as
sess
men
t of h
ealt
h-r
elat
edq
ual
ity
of
life
issu
es a
ssoc
iate
d w
itho
vera
ctiv
e b
lad
der
.
Ava
ilabl
e fo
r us
e.
Pub
lishe
d ev
iden
ce o
f val
idity
,re
liabi
lity
and
resp
onsi
vene
ss [2
9].
Cop
ing,
Con
cern
/Wor
ry
Sle
ep
Soc
ial I
nter
actio
n
2550
+
ICIQ
-UI S
hort
For
m [1
8] (
ICIQ
)G
rad
e A
Com
preh
ensi
ve a
sses
smen
t of m
ale/
fem
ale
uri
nar
y in
con
tin
ence
.A
vaila
ble
for
use.
Pub
lishe
d ev
iden
ce o
f val
idity
,re
liabi
lity
and
sens
itivi
ty to
cha
nge1 .
Urin
ary
inco
ntin
ence
incl
udin
gite
ms
on fr
eque
ncy
and
amou
nt o
f lea
kage
and
ove
rall
inte
rfer
ence
.
A s
elf-
diag
nost
ic it
em in
vite
sre
spon
dent
s to
indi
cate
the
perc
eive
d ca
use
ofin
cont
inen
ce.
432
ICIQ
-VS
[30]
Gra
de
A
Com
preh
ensi
ve a
sses
smen
t of v
agin
alsy
mp
tom
s an
d as
soci
ated
bot
her.
Ava
ilabl
e fo
r us
e.
Pub
lishe
d ev
iden
ce o
f val
idity
,re
liabi
lity
and
resp
onsi
vene
ss [3
0].
Vag
inal
sym
ptom
s.
Sex
ual m
atte
rs.
Qua
lity
of li
fe.
142
Tab
le 4
. IC
IQ M
od
ule
Des
crip
tio
n (
con
tin
ued
)

375
Nam
e / G
rad
eP
urp
ose
Cu
rren
t S
tatu
sD
evel
op
men
t M
eth
od
olg
yD
om
ain
sIt
ems
ICIQ
-B
Gra
de C
Com
preh
ensi
veas
sess
men
t of
mal
e/fe
mal
e b
ow
elsy
mp
tom
s, , p
redo
min
antly
inco
ntin
ence
, and
asso
ciat
ed b
othe
r.
New
ly d
evel
oped
; tes
ting
com
plet
ed;
awai
ting
publ
icat
ion
Item
s ge
nera
ted
by c
linic
al e
xper
ts a
nd p
atie
nts
with
ana
l inc
ontin
ence
[12]
.
Ext
ensi
ve c
onte
nt v
alid
ity te
stin
g w
ith p
oten
tial
resp
onde
nts
and
clin
ical
exp
erts
. Psy
chom
etric
test
ing
perf
orm
ed; a
wai
ting
publ
icat
ion
Bow
el p
atte
rn.
Bow
el c
ontr
ol.
Qua
lity
of li
fe.
21
ICIQ
-CLU
TS
Gra
de C
Ass
essm
ent o
f urin
ary
sym
ptom
s in
ch
ildre
n.
Crit
erio
n va
lidity
test
ing
is c
urre
ntly
ongo
ing
in th
e U
K, I
taly
and
Ger
man
y by
way
of c
ompa
rison
sw
ith c
linic
al fl
ow te
sts
to e
valu
ate
the
abili
ty o
f the
que
stio
nnai
re to
ref
lect
clin
ical
find
ings
.
The
dra
ft in
stru
men
t has
bee
n pr
epar
ed th
roug
hqu
alita
tive
inte
rvie
ws
with
chi
ldre
n an
d th
eir
pare
nts/
care
give
rs in
com
bina
tion
with
clin
ical
expe
rts
in th
e fie
ld to
est
ablis
h th
e cl
inic
al a
reas
of im
port
ance
and
the
pert
inen
t iss
ues
for
thos
ew
ith th
e sy
mpt
oms.
Dom
ains
to b
e de
term
ined
;
Que
stio
ns o
n ur
inar
y sy
mpt
om,
bedw
ettin
g an
d in
cont
inen
ce
ICIQ
-LT
C
Gra
de C
Ass
essm
ent o
f urin
ary
sym
ptom
s an
d im
pact
on
qual
ity o
f life
ass
ocia
ted
with
lon
g t
erm
cath
eter
isat
ion
and
rela
ted
both
er.
Con
tent
val
idity
test
ing
and
full
psyc
hom
etric
val
idat
ion
are
unde
rway
.
Thi
s dr
aft q
uest
ionn
aire
has
bee
n pr
epar
ed in
colla
bora
tion
with
clin
ical
exp
erts
in th
is a
rea
and
patie
nts
who
man
age
thei
r ur
inar
y sy
mpt
oms
thro
ugh
long
term
cat
hete
risat
ion.
Dom
ains
to b
e de
term
ined
;Q
uest
ions
to b
e as
sess
ed:
leak
age,
blo
ckag
e, b
ladd
er s
tone
s,in
fect
ions
;cop
ing
stra
tegi
es; s
ocia
lfu
nctio
ning
; at
titud
es; a
nd b
ody
imag
e.
Tab
le 5
a. I
CIQ
Des
crip
tio
n o
f M
od
ule
s in
Dev
elo
pm
ent

376
Tab
le 5
b.
ICIQ
Des
crip
tio
n o
f M
od
ule
s in
Dev
elo
pm
ent
Nam
e/G
rad
eP
urp
ose
Cu
rren
t S
tatu
sD
evel
op
men
t M
eth
od
olg
yD
om
ain
sIt
ems
ICIQ
-Spi
nal c
ord
dise
ase
Inde
velo
pmen
t
Ass
essm
ent o
f urin
ary
sym
ptom
s an
d im
pact
on q
ualit
y of
life
asso
ciat
ed w
ithsp
ecif
ic m
anag
emen
td
evic
es a
nd r
elat
edbo
ther
.
Con
tent
val
idity
test
ing
and
full
psyc
hom
etric
val
idat
ion
are
due
toco
mm
ence
.
Thi
s dr
aft q
uest
ionn
aire
has
bee
npr
epar
ed in
col
labo
ratio
n w
ithcl
inic
al e
xper
ts in
this
are
a an
dpa
tient
s w
ho m
anag
e th
eir
urin
ary
sym
ptom
s w
ith v
aryi
ng d
evic
es.
Pat
ient
s w
ith s
pina
l cor
d di
seas
eof
var
ying
cau
ses
part
icip
ated
inqu
alita
tive
inte
rvie
ws
to e
xplo
reth
e ef
fect
s an
d im
pact
on
qual
ityof
life
ass
ocia
ted
with
the
devi
ces
used
to m
anag
e th
eir
blad
der
sym
ptom
s.
lQu
estio
n s
rega
rdin
g th
efo
llow
ing
will
be
ask e
d: B
ladd
eran
d b
owel
func
tion,
iss u
es a
s soc
iate
d w
ith s
pec i
ficm
an ag
emen
t dev
ices
, s ex
ual
mat
ters
, and
life
styl
ein
terfe
re nc
e.
ICIQ
-UI L
ong
For
mD
etai
led
asse
ssm
ent o
fp
erce
ived
cau
ses
of
uri
nar
y in
con
tin
ence
.
Con
tent
v al
idity
test
ing
ha s
been
com
plet
edpr
e pa
ring
the
d ev
elop
men
tal I
CIQ
-UI L
on g
For
m fo
r fu
ll p
sych
om et
ric v
alid
a tio
n.In
terv
iew
s w
ith p
oten
tial r
espo
nd en
ts h
ave
con
firm
ed th
at th
e qu
estio
n na
ire is
app
licab
le a
nd a
ppro
p ria
te fo
r a d
etai
led
ass e
ssm
en t o
f u rin
ary
inco
n tin
enc e
sym
ptom
s. V
alid
atio
n is
und
erw
ay.
Thi
s dr
aft q
uest
ionn
aire
has
bee
npr
epar
ed in
col
labo
ratio
n w
ithcl
inic
al e
xper
ts in
this
are
a an
dpa
tient
s w
ith s
ympt
oms
of u
rinar
yin
cont
inen
ce. P
atie
nts
with
urin
ary
inco
ntin
ence
par
ticip
ated
inqu
alita
tive
inte
rvie
ws
to e
xplo
reth
e ca
use
of th
eir
sym
ptom
s an
dth
e is
sues
of i
mpo
rtan
ce r
elat
edto
this
.
For
eac
h pe
rcei
ved
caus
e of
inco
ntin
ence
, e.g
. phy
sica
lac
tivity
, urg
ency
rel
ated
,no
ctur
nal l
eaka
ge, t
he d
egre
eof
bot
her
and
amou
nt o
fle
akag
e ar
e ev
alua
ted.
Tab
le 5
c: I
CIQ
Des
crip
tio
n o
f M
od
ule
s in
Dev
elo
pm
ent
Nam
e/G
rad
eP
urp
ose
Cu
rren
t S
tatu
sD
evel
op
men
t M
eth
od
olg
yD
om
ain
sIt
ems
ICIQ
-VS
qol (
Inde
velo
pmen
t)D
etai
led
asse
ssm
ent o
fH
RQ
L is
sues
asso
ciat
ed w
ith v
agin
alsy
mp
tom
s an
d re
late
dbo
ther
.
Con
tent
val
idity
test
ing
has
been
com
plet
ed p
repa
ring
the
deve
lopm
enta
l IC
IQ-V
Sqo
l.In
terv
iew
s w
ith p
oten
tial
resp
onde
nts
have
con
firm
ed th
atth
e qu
estio
nnai
re is
app
licab
lean
d ap
prop
riate
for
asse
ssm
ent
of th
e ef
fect
s of
vag
inal
sym
ptom
s, c
aptu
ring
all a
spec
tsof
rel
evan
ce. P
syho
met
ricva
lidat
ion
is u
nder
way
.
Thi
s dr
aft q
uest
ionn
aire
has
bee
n pr
epar
edin
col
labo
ratio
n w
ith c
linic
al e
xper
ts in
this
area
and
wom
en w
ith v
agin
al s
ympt
oms.
Pat
ient
s w
ith v
agin
al s
ympt
oms
of v
aryi
ngca
use
part
icip
ated
in q
ualit
ativ
e in
terv
iew
sto
exp
lore
the
effe
cts
and
impa
ct o
n qu
ality
of li
fe a
ssoc
iate
d w
ith th
eir
sym
ptom
s.
Dom
ains
to b
e de
term
ined
.Q
uest
ions
reg
ardi
ng th
efo
llow
ing
will
be
aske
d: l
ifere
stric
tions
and
em
otio
nal
aspe
cts.

377
There are a variety of PRO measures available for usein clinical practice and research that assess a rangeof concepts (e.g. HRQL, patient satisfaction, symptombother, etc). This section and table series provides anoverview and assessment of those measures.Importantly, clinical practitioners and researchersneed to clearly determine their clinical and researchobjectives before selecting a PRO as it is theseobjectives and the target patient population that willhelp determine which validated PRO is appropriate touse. Tables 6 to 10 provide a brief overview of allcurrent PRO measures for urinary incontinence andLUTS, their purpose, psychometric properties,translation availability, and recommended ICI grade.
Certainly an area which has rapidly grown with PROmeasures is that of urinary incontinence and LUTS andHRQL assessments (Table 6). The literaturesupporting HRQL assessments was reviewed and aGrade A to C recommendation assigned. Please note,as instrument development and validation is anongoing process, the tables below contain publicationsprior to July 2008. As additional work may have beenperformed on an instrument, it is always prudent toconduct a further literature search and/or contact theinstrument developer prior to selecting an outcomemeasure for your clinical practice or study.
One trend that has become more apparent since theprevious Consultations is the modification of moreestablished urinary incontinence questionnaires for usein selected patient groups (e.g., pelvic organ prolapse;males; different cultural/language groups). When usinga questionnaire in a patient group other than the groupin which it was initially developed, cognitive debriefingswith the new patient population should be held toreview the applicability of the questionnaire to thenew patient group. Several of the main questionnairesto be discussed below have now had modified versionspublished in the literature. The Committee’s view isthat although it may be appropriate to modifyestablished questionnaires for use with somepopulations, it is advisable to keep such modificationsto a minimum, and to use the original versionswhenever possible. Any modifications of establishedquestionnaires may result in changes (sometimessubstantial) in the psychometric performance of theinstrument, and thus all modified instruments shouldbe subjected to the same psychometric testing as
that employed in developing a completely newinstrument. Specifically, modified instruments shouldreport information regarding the instrument’s constructvalidity, reliability, and test-retest reliability, at aminimum, and sensitivity to change, in interventionstudies.
For some of the more widely used instruments listedbelow, several modified, shortened versions havebeen published. Information regarding the modifiedversions is provided under the original source versionsof the questionnaires, but the modified versions areevaluated and graded separately, based on theavailable information regarding their psychometricproperties and performance.
1. BFLUTS AND BFLUTS-SF
The long form of BFLUTS [23, 26] was developed foruse with women, following the pattern established forthe questionnaire developed for the ICS-’BPH’ study.The questionnaire covers the occurrence andbothersomeness of symptoms relating to incontinenceand other lower urinary tract symptoms [23, 26]. Ithas shown good levels of validity and reliability andhas been increasingly used in epidemiological andoutcome studies [40-45]. Validity, reliability andresponsiveness have been demonstrated, and ascored short form has been produced, which is nowthe recommended version [22].
2. DAN-PSS
This questionnaire was designed in Denmark tomeasure the degree to which men are bothered byurinary symptoms [46, 47]. A composite score isachieved by the multiplication of the ‘symptom’ by the‘bother’ score, with a total range of 0 to 108 [46, 47].A computer version of this questionnaire has beenvalidated and patients seemed to appreciated morethis new version than the paper version [48]. It isprimarily a questionnaire for the assessment of theoccurrence and bothersomeness of a wide range ofLUTS in men.
3. ICSMALE AND ICSMALE SF
The ICSmale questionnaire contains 22 questions on20 urinary symptoms, and, for most questions, thedegree of problem that the symptom causes [26]. Ithas exhibited acceptable levels of validity, reliabilityand sensitivity to change following a range oftreatments including surgery, minimally invasivetherapies and drug treatments [26, 27, 49]. This longversion has been largely replaced now by a scoredshort-form – ICSmaleSF [25]. A modified form ofICSmale has been used to assess LUTS andincontinence in prostate cancer [50]. It also continues
I. HEALTH-RELATED QUALITY OFLIFE MEASURES
5B - D. PATIENT REPORTEDOUTCOME (PRO)
QUESTIONNAIRES TO ASSESSTHE IMPACT OF URINARYINCONTINENCE, OAB ANDLOWER URINARY TRACT
SYMPTOMS

378
Tab
le 6
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– H
RQ
L
Rel
iab
ility
Val
idit
y
PR
O N
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
met
ric
Val
idat
ion
inO
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
esB
FL
UT
S (B
risto
lF
emal
e Lo
wer
Urin
ary
Tra
ctS
ympt
oms
Que
stio
nnai
re).
Cur
rent
ly th
e IC
IQ-
FLU
TS
(IC
IQ-F
emal
eLo
wer
Urin
ary
Tra
ctS
ympt
oms)
[23]
Gra
de
A
To
asse
ss fe
mal
eLU
TS
, par
ticul
arly
urin
ary
inco
ntin
ence
,m
easu
re im
pact
on
qual
ity o
f life
and
eval
uate
trea
tmen
tou
tcom
eW
omen
,in
cont
inen
ce√
√√
√B
FLU
TS
Tra
nsla
ted
in 1
0 La
ngua
ges.
http
://w
ww
.iciq
.net
/ICIQ
.FLU
TS
.htm
l
Co
nti
life®
(Q
ualit
y of
Life
Ass
essm
ent
Que
stio
nnai
reC
once
rnin
g U
rinar
yIn
cont
inen
ce)[
102]
Gra
de
B
To
asse
ss th
e im
pact
of u
rinar
yin
cont
inen
ce o
nqu
ality
of l
ife.
Orig
inal
ly d
evel
oped
in F
renc
h an
dde
sign
ed fo
r w
omen
with
UI
(urg
e, s
tres
san
d m
ixed
UI)
Wom
en, S
UI
√√
√√
Con
tilife
Tra
nsla
ted
in 1
1 La
ngua
ges.
http
://pr
oqol
id.o
rg/in
stru
men
ts/q
ualit
y_of
_life
_ass
essm
ent_
ques
tionn
aire
_con
cern
ing_
urin
ary_
inco
ntin
ence
_con
tilife
_rD
AN
-PS
S-1
(D
anis
hP
rost
atic
Sym
ptom
Sco
re)[
46]
Gra
de
A
To
eval
uate
mal
esw
ith L
UT
S s
ugge
stiv
eof
unc
ompl
icat
edB
PH
Men
, BP
H√
√√
√
DA
N-P
SS
-1 tr
ansl
ated
in 9
lang
uage
sht
tp://
proq
olid
.org
/inst
rum
ents
/dan
ish_
pros
tatic
_sym
ptom
_sco
re_d
an_p
ss_1
EP
IQ (
Epi
dem
iolo
gyof
Pro
laps
e an
dIn
cont
inen
ceQ
uest
ionn
aire
)[10
3]G
rad
e B
Dev
elop
ed a
ndva
lidat
ed in
Eng
lish
and
Spa
nish
toas
sess
the
pres
ence
or a
bsen
ce o
f AI,
OA
B, S
UI,
and
pelv
icor
gan
prol
apse
infe
mal
e po
pula
tion
Wom
en,
PF
D√
√√
√√
√T
rans
late
d in
Eng
lish
and
Spa
nish
IBS
(In
cont
inen
ceB
othe
rsom
eS
cale
)[10
4]G
rad
e C
One
item
ques
tionn
aire
toas
sess
the
qual
ity o
flif
e in
wom
en w
ithur
inar
y in
cont
inen
ce.
Wom
en,U
IN
one
Fou
ndIC
IQ-U
I Sh
ort
Fo
rm(I
nter
natio
nal
Con
sulta
tion
onIn
cont
inen
ceQ
uest
ionn
aire
-U
rinar
y In
cont
inen
ceS
hort
For
m (
ICIQ
-UI
Sho
rt F
orm
)[18
,25]
Gra
de
A
To
asse
ss th
esy
mpt
oms
and
impa
ctof
urin
ary
inco
ntin
ence
incl
inic
al p
ract
ice
and
rese
arch
Men
and
Wom
en,
Urin
ary
Sym
ptom
s√
√√
√√
(8 w
eeks
)√
ICIQ
-UI S
F T
rans
late
d in
38
Lang
uage
sht
tp://
proq
olid
.org
/inst
rum
ents
/inte
rnat
iona
l_co
nsul
tatio
n_on
_inc
ontin
ence
_que
stio
nnai
re_u
rinar
y_in
cont
inen
ce_s
hort
_fo
rm_i
ciq_
ui_s
hort
_for
m

379
Tab
le 6
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,O
AB
an
d L
UT
S P
RO
Mea
sure
s –
HR
QL
(co
nti
nu
ed)
Rel
iab
ility
Val
idit
y
RO
Nam
e / G
rad
eP
urp
ose
of
To
ol
Po
pu
lati
on
Sam
ple
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
-m
etri
cV
alid
atio
nin
Oth
erL
ang
uag
esA
vaila
ble
Lan
gu
ages
ICS
mal
e (I
CIQ
-M
LUT
S)
(Int
erna
tiona
lC
ontin
ence
Soc
iety
-M
ale)
[18,
25,2
6]G
rad
e A
To
prov
ide
a th
orou
ghev
alua
tion
of th
eoc
curr
ence
and
both
erso
men
ess
oflo
wer
urin
ary
trac
tsy
mpt
oms
and
thei
rim
pact
on
the
lives
of
men
with
ben
ign
pros
tatic
dis
ease
Men
with
LUT
S a
ndpo
ssib
leB
PH
√√
√√
√
icsm
ale
Tra
nsla
ted
in 1
1La
ngua
ges.
http
://pr
oqol
id.o
rg/in
stru
men
ts/
icsm
ale_
icsm
ale
ICS
Qo
L(I
nter
natio
nal
Con
tinen
ce S
ocie
ty-
Ben
ign
Pro
stat
icH
yper
plas
ia s
tudy
qual
ity-o
f-lif
e)[1
05]
Gra
de
A
To
asse
ss im
pact
of
low
er u
rinar
y tr
act
sym
ptom
s on
the
lives
of m
en w
ithLU
TS
Men
with
LUT
S a
ndpo
ssib
leB
PH
√√
√√
√
ICS
QoL
Tra
nsla
ted
in 1
1La
ngua
ges
http
://pr
oqol
id.
org/
inst
rum
ents
/inte
rnat
iona
l_co
ntin
ence
_soc
iety
_ben
ign_
pros
tatic
_hyp
erpl
asia
_stu
dy_
qual
ity_o
f_lif
e_ic
sqol
__1
IIQ (
Inco
ntin
ence
Impa
ctQ
uest
ionn
aire
)[64
]G
rad
e A
Dev
elop
ed to
desc
ribe
the
seve
rity
of in
cont
inen
ce in
apo
pula
tionU
sed
toas
sess
the
impa
ct o
fur
inar
y in
cont
inen
ceon
HR
QL.
Prim
arily
been
eva
luat
ed in
patie
nts
with
str
ess
inco
ntin
ence
.W
omen
, UI,
SU
I√
√√
√ (1
2W
eeks
)√
Ava
ilabl
e in
Eng
lish
and
Tur
kish
IIQ-7
( In
cont
inen
ceIm
pact
Que
stio
nnai
re-
shor
t for
m)[
101]
Gra
de
A
Use
d to
ass
ess
the
impa
ct o
f urin
ary
inco
ntin
ence
on
HR
QL
*val
idat
ion
stud
y on
men
afte
rra
dica
lpr
osta
tect
om
y w
ho h
adU
I√
√√
√A
vaila
ble
in E
nglis
h an
dT
urki
sh
IOQ
(In
cont
inen
ceO
utco
me
Que
stio
nnai
re)[
106]
Gra
de
C
Dev
elop
ed fo
ras
sess
ing
HR
QL
afte
rsu
rger
y fo
r st
ress
urin
ary
inco
ntin
ence
Wom
en S
UI
√√
√N
one
Fou
ndI-
QO
L (I
CIQ
-Uiq
ol)
(Urin
ary
Inco
ntin
ence
-S
peci
fic Q
ualit
y of
Life
Inst
rum
ent)
[75,
107]
Gra
de
A
To
asse
ss q
ualit
y of
life
of w
omen
with
urin
ary
inco
ntin
ence
Men
, UI
√√
√
I-Q
OL
Tra
nsla
ted
in 3
5La
ngua
ges
http
://pr
oqol
id.
org/
inst
rum
ents
/urin
ary_
inco
ntin
ence
_spe
cific
_qua
lity_
of_
life_
inst
rum
ent_
i_qo
l

380
Tab
le 6
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– H
RQ
L(c
on
tin
ued
)
35
PR
O N
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lS
amp
lest
ency
rete
stte
nt
rio
ncu
rren
tim
inan
tD
ura
tio
n)
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
KH
Q (
ICIQ
-LU
TS
qol)
(Kin
g’s
Hea
lthQ
uest
ionn
aire
)[2
4,10
8]G
rad
e A
To
asse
ss th
e im
pact
of lo
wer
urin
ary
trac
tsy
mpt
oms
incl
udin
gur
inar
y in
cont
inen
ceon
hea
lth r
elat
edqu
ality
of l
ife.
Dev
elop
ed in
a c
linic
alpe
rspe
ctiv
e to
eval
uate
inco
ntin
ence
in w
omen
.
Men
and
Wom
en,
OA
B√
√√
√√
√√
(12
Wee
ks)
√
KH
Q T
rans
late
d in
45
Lang
uage
s. h
ttp://
proq
olid
.or
g/in
stru
men
ts/k
ing_
s_he
alth
_que
stio
nnai
re_k
hq
LIS
(Le
ices
ter
Impa
ctS
cale
) [9
0]
A c
ondi
tion
spec
ific
qual
ity o
f life
mea
sure
for
mal
es a
nd fe
mal
esw
ith u
rinar
y st
orag
esy
mpt
oms
of u
rgen
cy,
freq
uenc
y, n
octu
riaan
d in
cont
inen
ce.
Was
orig
inal
lyde
velo
ped
for
wom
enw
ith in
cont
inen
ceon
ly.
men
and
wom
en,
LUT
S√
√√
√
√
N
one
Fou
nd
MU
DI (
Mal
eU
roge
nita
l Dis
tres
sIn
vent
ory)
[109
,110
]G
rad
e C
To
addr
ess
the
dim
ensi
on o
f phy
sica
lhe
alth
, foc
usin
g on
both
er fr
om m
ultip
lesy
mpt
oms
asso
ciat
edw
ith u
rinar
yin
cont
inen
ce in
men
.C
reat
ed b
y el
imin
atin
gfo
ur g
ende
r sp
ecifi
cite
ms
from
UD
I and
IIQ.
Men
with
LUT
Sfo
llow
ing
ara
dica
lpr
osta
tect
om
y fo
rpr
osta
teca
ncer
√√
√N
one
Fou
nd
MU
SIQ
(M
ale
Urin
ary
Sym
ptom
Impa
ctQ
uest
ionn
aire
)[10
9,11
0]G
rad
e C
To
capt
ure
men
tal/p
sych
olog
ical
heal
th, s
ocia
l hea
lth,
and
glob
alpe
rcep
tions
of
func
tion
and
wel
l-be
ing
in m
en w
ithur
inar
y in
cont
inen
ce.
Cre
ated
by
elim
inat
ing
four
gen
der
spec
ific
item
s fr
om U
DI a
ndIIQ
.M
en, U
I√
√√
Non
e F
ound
N-Q
oL
( IC
IQ-N
qol
(Noc
turia
Qua
lity
ofLi
feQ
uest
ionn
aire
)[28
]G
rad
e A
To
asse
ss th
e im
pact
of n
octu
ria o
n th
equ
ality
of l
ife o
fpa
tient
sM
en a
ndW
omen
√√
√√
√√
N-Q
ol T
rans
late
d in
17
Lang
uage
sw
ww
. pro
luts
sh.c
om
OA
B-q
SF
(OA
B-q
Sho
rt F
orm
)[29
]G
rad
e A
A s
hort
ened
ver
sion
of
the
OA
B-q
to e
valu
ate
both
con
tinen
t and
inco
ntin
ent s
ympt
oms
of O
AB
and
thei
rim
pact
on
HR
QL
Men
and
Wom
enO
AB
√√
√√
√ (
12W
eeks
)√
OA
B-q
SF
Tra
nsla
ted
in 4
0La
ngua
ges
ww
w.p
rolu
tssh
.com
Rel
iab
ility
Val
idit
y
RO
Nam
e / G
rad
eP
urp
ose
of
To
ol
Po
pu
lati
on
Sam
ple
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
-m
etri
cV
alid
atio
nin
Oth
erL
ang
uag
esA
vaila
ble
Lan
gu
ages

381
Tab
le 6
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,O
AB
an
d L
UT
S P
RO
Mea
sure
s –
HR
QL
(co
nti
nu
ed)
Rel
iab
ility
Val
idit
y
PR
O N
ame
/ Gra
de
Pu
rpo
se o
f T
oo
l
Po
pu
la-
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-t
ent
Cri
te-
rio
nC
on
-cu
rren
tD
iscr
-im
inan
t
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
met
ric
Val
idat
ion
inO
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
OA
B-q
(IC
IQ-
OA
Bqo
l)(O
vera
ctiv
e B
ladd
erQ
uest
ionn
aire
) [2
9]G
rad
e A
To
eval
uate
bot
h co
ntin
ent a
ndin
cont
inen
t sym
ptom
s of
OA
Ban
d th
eir
impa
ct o
n H
RQ
L.D
evel
oped
from
focu
s gr
oups
of
men
and
wom
en, c
linic
ian
opin
ion,
and
a th
orou
ghlit
erat
ure
revi
ew
Con
tinen
tan
din
cont
inen
tO
AB
√√
√√
√√
(12
Wee
ks)
√
OA
B-q
Tra
nsla
ted
in 4
1La
ngua
ges
ww
w.p
rolu
tssh
.com
PR
AF
AB
(Pro
tect
ion,
Am
ount
,F
requ
ency
,A
djus
tmen
t, B
ody
imag
e )
[111
-113
]G
rad
e A
5 ite
m q
uest
ionn
aire
wid
ely
used
in th
e N
ethe
rland
s b
yph
ysio
ther
apis
ts a
ndre
sear
cher
s u
sed
to e
valu
ate
trea
tmen
t effe
cts
for
UI i
nw
omen
Wom
en,
UI
√√
√√
√√
Eng
lish,
Ara
bic
and
Dut
ch
IHI (
Urin
ary
Inco
ntin
ence
Han
dica
p In
vent
ory)
[114
]G
rad
e C
To
iden
tify
diffi
culti
es p
atie
nts
may
be
expe
rienc
ing
beca
use
ofth
eir
inco
ntin
ence
Eld
erly
wom
en, U
Idu
e to
detr
usor
inst
abili
ty√
Non
e F
ound
UIS
S (
Urin
ary
Inco
ntin
ence
Sev
erity
Sco
re)
[115
]G
rad
e A
Des
igne
d by
the
Fin
nish
Gyn
ecol
ogic
al S
ocie
ty’s
urog
ynec
olog
ic w
orki
ng g
roup
toas
sess
sym
ptom
sev
erity
and
impa
ct o
f urin
ary
inco
ntin
ence
on e
very
day
life
Wom
en,
UI
√√
√√
√N
one
Fou
nd
UQ
(U
rgen
cyQ
uest
ionn
aire
)[1
16,1
17]
Gra
de
B
To
asse
ss th
e se
verit
y an
dim
pact
of u
rinar
y ur
genc
ysy
mpt
oms
on h
ealth
-rel
ated
qual
ity o
f lif
e. V
AS
sca
le is
use
dto
mea
sure
the
impa
ct o
fur
inar
y ur
genc
y o
n ov
eral
lqu
ality
of
life,
the
seve
rity
ofur
genc
y th
e in
tens
ity o
fur
genc
y a
nd t
he d
isco
mfo
rtex
perie
nced
in
conj
unct
ion
with
urge
ncy.
Wom
en,
OA
B√
√√
√ (1
0 D
ays)
Non
e F
ound
Uro
life (
BP
HQ
oL9)
(Ben
ign
Pro
stat
icH
yper
trop
hy H
ealth
-R
elat
ed Q
ualit
y of
Life
Que
stio
nnai
re)
[118
)G
rad
e A
To
ass
ess
the
impa
ct o
f B
PH
and
its tr
eatm
ent
on t
he q
ualit
yof
life
of p
atie
nts
Men
, BP
H√
√√
√√
√
UR
OLI
FE
TM
/BP
HQ
oL9
Tra
nsla
ted
in 1
1La
ngua
ges
http
://pr
oqol
id.o
rg/in
stru
men
ts/b
enig
n_pr
osta
tic_h
yper
trop
hy_h
ealth
_re
late
d_qu
ality
_of_
life_
ques
tionn
aire
_uro
life_
sup_
tm_s
up_b
phqo
l9Y
IPS
(Y
ork
Inco
ntin
ence
perc
eptio
ns s
cale
)[5
8]G
rad
e C
To
mea
sure
the
psyc
hosc
ocia
las
pect
s of
urin
ary
inco
ntin
ence
Wom
en U
I√
√√
√N
one
foun
d

382
to be used to assess LUTS in men [51] and minimallyinvasive therapies and drug treatments [52-55]. It isprimarily a questionnaire for the assessment of theoccurrence and bothersomeness of a wide range ofLUTS in men.
The scored short-form – ICSmaleSF, [25] wasdeveloped from the longer ICSmale questionnaire toassess LUTS in men.61 The short form has two majorscored sections: ICSmaleVS (voiding subscore)containing five questions (hesitancy, straining, reducedstream, intermittency, incomplete emptying), andICSmaleIS (incontinence subscore) containing sixquestions(urge, stress, unpredictable and nocturnalincontinence, urgency, postmicturition dribble).(25)The scores are obtained by simple addition. Theauthors indicate that questions to assess nocturia,frequency and impact on quality of life should beadded to provide full data, but these questions shouldnot be included in the score as they are separateconstructs [25]. The ICSmaleSF has been used instudies focusing on prostate cancer [56, 57] and onLUTS [51] as well as minimally invasive therapiesand drug treatments [52, 53].
4. INCONTINENCE IMPACT QUESTIONNAIRE (IIQ) AND IIQ-7
This questionnaire was developed to assess thepsychosocial impact of urinary incontinence in womenand consists of 30 items (24 on the degree to whichincontinence affects activities and 6 on the feelingsengendered) [58-60]. Scores are obtained overall orfor four subscales determined by factor and clusteranalyses: physical activity, travel, social relationships,and emotional health. The IIQ has been found to haveacceptable levels of reliability and validity across arange of studies [61-67]. The IIQ has also beenproduced in a short form comprising 7 items, alsowith evidence of validity and reliability [67, 68].Responsiveness of the IIQ has been assessed inseveral intervention studies [69-74].
5. I-QOL
This questionnaire was designed to be used in clinicaltrials to measure the impact of incontinence on menand women [75]. Psychometric information ontranslated versions of the I-QOL have been reportedfor French, Spanish, Swedish, German, Korean andThai language versions [76-78]. Other cultural andlinguistic adaptations are available but have not beenvalidated. In all countries, the use of three subscales,and an overall summary score was confirmed to beuseful.
6. KING’S HEALTH QUESTIONNAIRE (KHQ)
The King’s Health Questionnaire (KHQ) consists ofthree parts. The first section contains two questionsmeasuring general health and overall health relatedto urinary symptoms. The second section includes
19 questions divided into seven domains of quality oflife: incontinence impact, role limitations, physicallimitations, social limitations, personal relationships,emotions, sleep and energy, severity coping measures,general health perception, and symptom severity. Thethird section of the questionnaire comprises 11questions measuring the bother or impact of urinarysymptoms. The KHQ has demonstrated reliability andvalidity in men and women [24] [79-81] is availablein 37 languages [82-84]. Sensitivity to change hasbeen shown successfully in clinical trials where it hasbeen used to assess the HRQL improvement followingtreatment for patients with OAB, USI and mixedincontinence symptoms [79, 85-88]. A minimallyimportant difference has been derived to establishclinically meaningful interpretations of the KHQ scoresand a QALY measure has been derived from KHQscoring [89].
7. LEICESTER IMPACT SCALE (LIS)
The LIS is a condition-specific HRQL measure formen and women assessing the symptoms of urgency,frequency, nocturia, and incontinence. It is aninterviewer-administered tool so it is not a true PROas interviewer administration can introduce potentialbias into the patient responses. The LIS does haveutility in the clinical and research settings [90].
8. OVERACTIVE BLADDER SYMPTOM ANDHEALTH-RELATED QUALITY OF LIFE (OAB-Q) AND OAB-Q SF
The OAB-q is a 33-item questionnaire developed toassess the Symptom Bother (8 items) and HRQLimpact of OAB (25 items; 4 domains: Coping,Concern/Worry, Sleep, and Social Interaction.). It hasdemonstrated reliability, validity, responsiveness inmultiple clinical studies of men and women. (91) Aminimally important difference has been derived [91,92] to establish clinically meaningful interpretationsof the OAB-q scores and a QALY measure has beenderived from OAB-q scoring [93]. The 19-item short-form (OAB-q SF) is a six-item symptom bother scaleand 13-item HRQL scale that is a single score whichhas also demonstrated reliability, validity, andresponsiveness to change [94].
The OAB-q was the basis for the OAB-V8 AwarenessTool to screen for symptoms of OAB [95] and hasbeen used in a Parkinson disease patient population[96].
9. UROGENITAL DISTRESS INVENTORY (UDI)AND UDI-6
This questionnaire was developed in the US withwomen to assess the degree to which symptomsassociated with incontinence are troubling [59]. Itcontains 19 lower urinary tract symptoms and hasbeen shown to have high levels of validity, reliabilityand responsiveness in a community-dwelling popu-

383
lation of women with incontinence, (59) women over60 years, [97] women in two regions of Scotland [64].Responsiveness to changes in clinical status as aresult of treatment have been reported in a numberof areas: cadaveric fascia lata sling for stressincontinence, [72] comparing abdominal and vaginalprolapse surgery, [98] and the use of a simple urethralocclusive device [99].
A short-form version of the UDI (UDI-6 short form)has been shown to be valid and reliable in older adultmales and females, [100, 101] with demonstratedresponsiveness to resonstructuve pelvic surgery, [69]tension-free vaginal tape, [71, 73] and imipramine [74]
A number of other questionnaires noted in Table 6have been developed to assess symptoms or health-related quality of life impact of LUTS and/or UI,however they do not reach the highest level of gradingbecause they do not have the full complement ofpsychometric evaluation or robust data, or are lessrelevant for the assessment of UI than the question-naires reported above. Each is referenced in the tableshould further information be needed.
Patient satisfaction is the subjective, individualevaluation of treatment effectiveness and/or the serviceprovided by the healthcare system. Measures ofsatisfaction can include evaluation of accessi-bility/convenience, availability of resources, continuityof care, efficacy, finances, humaneness, informationgathering and giving processes, pleasantness ofsurroundings and perceived quality/competence ofhealth care personnel [119]. At its most basic level,satisfaction is a comprehensive evaluation of severaldimensions of health care based on patient expecta-tions and provider and treatment performance. As anoutcomes measure, patient satisfaction allows healthcare providers to assess the appropriateness oftreatment according to patient expectations. In chronicdiseases, where patients must live with treatment,patient satisfaction may be the distinguishing outcomeamong treatments with comparable efficacy [120].
Two patient satisfaction methods of promise withGrade B criteria are the BSW and OAB-S. Generallyresponsiveness cannot be assessed as there is nobaseline assessment of patient satisfaction withtreatment as no treatment has been given. Table 7below presents a summary of satisfaction instrumentsidentified in UI, OAB and other LUTS.
1. BENEFIT, SATISFACTION, AND WILLIN-GNESS (BSW) QUESTIONNAIRE
This 3-item questionnaire is designed to assess
treatment benefit, patient satisfaction with treatment,and patient willingness to continue treatment. TheBSW questionnaire was validated using data fromthree 12-week placebo-controlled trials of tolterodinein patients with OAB [121]. In this validation study,correlations were seen between patient-reportedtreatment satisfaction and improvements in the OAB-q, the KHQ, and micturition variables.
2. THE OVERACTIVE BLADDER TREATMENTSATISFACTION QUESTIONNAIRE (OAB-S)
The OAB-S is a 5 domain questionnaire whichevaluates control expectations, impact on daily livingwith OAB, OAB control, fulfillment of OAB medicationtolerability and satisfaction with control. Internalreliability coefficients were good (Cronbach’s alpha0.76-0.96), and test retest reliability has beenestablished (reliability coefficients 0.72-0.87) [122,123]. Cultural and linguistic differences wereconsidered early in the development process, andthe OAB-S is available in over sixteen languages[124].
In order to improve the detection of incontinence,OAB and other LUTS, several screening tools havebeen developed (Table 8). These tools help patientsself-describe symptoms and facilitate diagnosis ofLUTS by the clinician. Only the B-SAQ has beendesigned to screen for general lower urinary tractsymptoms (LUTS) rather than solely symptoms ofone condition. The majority of patients with LUTShave mixed urinary symptoms, and therefore aquestionnaire which can detect more than onesymptom complex may be more functional as ascreening tool in clinical practice than a highly specificquestionnaire. The Leiscester Impact Scale (LIS),OAB-V8, OAB-SS and QUID are all GradeA, short,simple to understand and complete, and easy tointerpret, however the LIS is interviewer, not patientadministered. Importantly, with screeners, responsi-veness is not assessed, however the sensitivity andspecificity of each tool is critical.
1. LEICESTER URINARY SYMPTOM QUESTIONNAIRE (LUSQ)
The LUSQ is a 10-item, interviewer-administeredquestionnaire developed to assess storage LUTS. Asan interviewer-administered tool, it is not a true PRObut is mentioned here as it may be useful in clinicalpractice and research when it is necessary or preferredto use interviewer administrative tools. The LUSQassesses the presence and severity of incontinence,urgency, frequency and nocturia, and the tool can beused for both male and female patients [127].
2. OAB-V8/OAB AWARENESS TOOL
The OAB-V8/OAB Awareness tool has been adapted
IV. SCREENING TOOLS
III. PATIENT SATISFACTION
II. OTHER UI/LUTS QUESTIONNAIRES

384
Tab
le 7
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– P
atie
nt
Sat
isfa
ctio
n
Rel
iab
ility
Val
idit
y
PR
O N
ame
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
-m
etri
cV
alid
atio
n in
Oth
erL
ang
uag
esA
vaila
ble
Lan
gu
ages
BS
W (
Ben
efit,
Sat
isfa
ctio
n w
ithtr
eatm
ent,
and
Will
ingn
ess)
[121
]G
rad
e B
To
capt
ure
patie
nts'
perc
eive
d be
nefit
,sa
tisfa
ctio
n w
ithtr
eatm
ent,
and
the
will
ingn
ess
toco
ntin
ue tr
eatm
ent
Men
and
Wom
en,
OA
B√
√√
ww
w.p
rolu
tssh
.com
EP
I (E
stim
ated
Per
cent
Impr
ovem
ent)
[125
]G
rad
e C
One
item
ques
tionn
aire
to g
ain
a pa
tient
'sim
prov
emen
t in
ape
rcen
t sca
leW
omen
,U
I,SU
I, M
UI
√√
(2-4
Wee
ks)
Non
e F
ound
GP
I (G
loba
lP
erce
ptio
n of
Impr
ovem
ent)
[125
]G
rad
e C
One
item
ques
tionn
aire
toas
sess
pat
ient
'sim
prov
emen
tW
omen
,U
I,SU
I, M
UI
√N
one
Fou
nd
OA
B-S
(O
vera
ctiv
eB
ladd
er S
atis
fact
ion
Que
stio
nnai
re)[
122,
123]
Gra
de
B
To
asse
ss p
atie
nts’
satis
fact
ion
with
OA
Btr
eatm
ent i
nclu
ding
/or
not m
edic
atio
n. T
hepr
e-m
edic
atio
nm
odul
e is
des
igne
d to
asse
ss th
e pa
tient
’sex
pect
atio
ns w
ithtr
eatm
ent a
nd im
pact
of O
AB
on
patie
nt’s
day
to d
ay li
fe
Men
and
Wom
en,
OA
B√
√√
√√
Non
e F
ound
/thou
gh m
entio
ned
in li
tera
ture
PS
Q (
Pat
ient
Sat
isfa
ctio
nQ
uest
ion)
[125
]G
rad
e C
One
item
ques
tionn
aire
use
d to
mea
sure
how
satis
fied
a su
bjec
tw
as w
ith a
pro
gram
Wom
en,
UI,S
UI,
MU
I√
Non
e F
ound
TB
S (T
reat
men
tB
enef
it S
cale
)[12
6]
A s
ingl
e-ite
m s
cale
used
to a
sses
s th
epa
tient
-rep
orte
dbe
nefit
s of
trea
tmen
tof
OA
B
Men
and
Wom
en,
OA
B√
√√
TB
S is
ava
ilabl
e in
oth
erla
ngua
ges

385
Tab
le 8
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– S
cree
ner
s
Rel
iab
ility
Val
idit
y
PR
O N
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cri-
min
ant
Sen
siti
vity
/sp
ecif
icit
y
Val
idat
ion
in O
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
esB
-SA
Q (
Bla
dder
Sel
f-A
sses
smen
tQ
uest
ionn
aire
) or
Bla
dder
Con
trol
Sel
f-A
sses
smen
tQ
uest
ionn
aire
(BC
SQ
) [1
29]
Gra
de
A
A s
cree
ning
tool
for
the
pres
ence
of
both
erso
me
LUT
S in
Wom
enW
omen
√√
√√
√√
√
B-S
AQ
Q T
rans
late
d in
14
Ava
ilabl
eht
tp://
ww
w.m
api-
rese
arch
.fr/i_
03_l
ist_
urol
.htm
ISQ
(In
cont
inen
ceS
cree
ning
Que
stio
nnai
re)
[130
]G
rad
e C
5 ite
m q
uest
ionn
aire
deve
lope
d to
scr
een
for
inco
ntin
ence
inw
omen
Wom
en, U
I√
√√
Non
e F
ound
LU
SQ
(T
he L
eice
ster
Urin
ary
Sym
ptom
Que
stio
nnai
re)
[127
]G
rad
e A
A c
ondi
tion-
spec
ific
scre
ener
of s
tora
geLU
TS
( ur
genc
y,fr
eque
ncy,
noc
turia
and
inco
ntin
ence
).W
as o
rigin
ally
deve
lope
d fo
r w
omen
with
inco
ntin
ence
only
.
Men
and
Wom
en,
LUT
S√
√√
√N
one
Fou
nd
ME
SA
(M
edic
al,
Epi
dem
iolo
gica
l, an
dS
ocia
l Asp
ects
of
Agi
ng Q
uest
ionn
aire
)[1
31]
Gra
de
C
A 1
5 ite
m s
cree
ning
tool
for
urin
ary
inco
ntin
ence
infe
mal
e pe
lvic
med
icin
e an
dre
cons
truc
tive
surg
ery
patie
nts
Wom
en, U
I√
√
Tra
nsla
ted
in E
nglis
h an
d S
pani
shht
tp://
ww
w.n
cbi.n
lm.n
ih.g
ov/p
ubm
ed/1
7576
498?
ordi
nalp
os=
2&ito
ol=
Ent
rezS
yste
m2.
PE
ntre
z.P
ubm
ed.P
ubm
ed_R
esul
tsP
anel
.Pub
med
_RV
Doc
Sum
OA
B-S
S (O
vera
ctiv
eB
ladd
er S
ympt
omS
core
) [1
32]
Gra
de
A
A 7
item
ques
tionn
aire
valid
ated
to m
easu
reov
eral
l sym
ptom
seve
rity
due
to th
efo
ur in
dex
sym
ptom
sof
OA
B
Men
and
Wom
en,
LUT
S w
ithor
with
out
OA
B√
√√
√√
Non
e F
ound
OA
B-V
8 (O
AB
Aw
aren
ess
Too
l) [9
5]G
rad
e A
An
8-ite
m s
cree
ning
tool
for
use
in a
prim
ary
care
set
ting
to id
entif
y pa
tient
sw
ho m
ay h
ave
OA
B
Men
and
Wom
en,
OA
B√
√√
√O
AB
-V8
is T
rans
late
d in
32
Lang
uage
sht
tp://
ww
w.o
abq.
com
/tran
slat
ions
.htm
l
PU
F p
atie
nt s
ympt
omsc
ale
(Pel
vic
Pai
n,U
rgen
cy, a
ndF
requ
ency
) [1
33]
Gra
de
C
To
eval
uate
of
patie
nts
with
susp
ecte
d IC
/PB
S
Wom
en a
ndW
omen
,IC
/PB
S√
√
PU
F a
vaila
ble
in E
nglis
h an
d S
pani
shht
tp://
ww
w.n
cbi.n
lm.n
ih.g
ov/p
ubm
ed/1
5833
505?
ordi
nalp
os=
3&ito
ol=
Ent
rezS
yste
m2.
PE
ntre
z.P
ubm
ed.P
ubm
ed_R
esul
tsP
anel
.Pub
med
_RV
Doc
Sum

386
Tab
le 8
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce a
nd
LU
TS
PR
O M
easu
res
– S
cree
ner
s (c
on
tin
ued
)
Rel
iab
ility
Val
idit
y
PR
O N
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Sen
siti
vity
/sp
ecif
icit
y
Val
idat
ion
in O
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
QU
ID (
Que
stio
nnai
refo
r U
rinar
yIn
cont
inen
ceD
iagn
osis
)[12
8]G
rad
e A
6 ite
m q
uest
ionn
aire
used
to d
iagn
ose
stre
ss a
nd/o
r ur
gety
pes
of u
rinar
yin
cont
inen
ceW
omen
, UI
and
SU
I√
√√
√√
Non
e F
ound
3IQ
(T
hree
Inco
ntin
ence
Que
stio
nsQ
uest
ionn
aire
) [1
34]
Gra
de
C
A th
ree
item
ques
tionn
aire
use
d to
clas
sify
urg
e an
dst
ress
inco
ntin
ence
Wom
en, U
I
Psy
chom
etric
eval
uatio
n no
tre
port
ed√
UI (
Urin
ary
Inco
ntin
ence
Sco
re)
[135
]G
rad
e C
Dev
elop
ed in
Ger
man
used
to a
sses
UI
Wom
en, U
I√
Ava
ilabl
e in
Ger
man
US
P (
Urin
ary
Sym
ptom
Pro
file)
[139
]G
rad
e B
To
asse
ss u
rinar
ysy
mpt
oms
in m
ale
and
fem
ale
with
stre
ss, u
rge,
freq
uenc
y or
urin
ary
obst
ruct
ive
sym
ptom
sfo
r us
e in
clin
ical
prac
tice
toco
mpl
emen
t clin
ical
mea
sure
s an
ddi
agno
sis
Men
and
Wom
enst
ress
UI,
urge
UI,
freq
uenc
y,lo
w s
trea
m,
com
bine
dsy
mpt
oms
√√
√√
Non
e F
ound
I-P
SS
(In
tern
atio
nal
Pro
stat
e S
ympt
omS
core
) [1
37]
Gra
de
B
8- it
em q
uest
ionn
aire
used
to c
aptu
re th
ese
verit
y of
urin
ary
sym
ptom
s re
late
d to
beni
gn p
rost
atic
hype
rpla
sia.
Orig
inal
lyde
velo
ped
from
the
Am
eric
an U
rolo
gica
lA
ssoc
iatio
n S
ympt
omIn
dex.
Men
√√
√√
√
I-P
SS
tran
slat
ed in
to 4
0 la
ngua
ges
http
://pr
oqol
id.o
rg/in
stru
men
ts/in
tern
atio
nal
_pro
stat
e_sy
mpt
om_s
core
_i_p
ss

387
from the OAB-q questionnaire; which is a 33 itemquestionnaire which assess symptom bother andHRQL impact of OAB [29]. The OAB-V8 is an 8-itemquestionnaire, which evaluates the symptoms ofoveractive bladder; namely urinary frequency, nocturia,urgency and urge incontinence. Responses are gradedon a 6 point Likert scale. Patients with an overall scoreof eight or more are directed to seek medical advice.This questionnaire is validated for use by men andwomen [98].
3. OAB-SS
The OAB-SS is a validated A 7-item questionnairevalidated to measure overall symptom severity due tothe four index symptoms of OAB. It quantifies allsymptoms of OAB in men and women. The OAB-SSincludes a detailed evaluation of the urgency symptom.Responses are graded on a 5 point Likert scale.
4. QUESTIONNAIRE FOR URINARYINCONTINENCE DIAGNOSIS(QUID)
The QUID is a 6-item patient admisitered questionnairedeveloped to idenitify and differentiate stress vs urgeincontinence. There are 3 items each related to stressand urge incontinence. Scoring is 0 (not at all) to 5 (allthe time) for each response. The tool was developedfor use with females [128].
Measures that can be used to assess how botheredpatients are by urinary symptoms are included inTable 9. The Patient Perception of Bladder Condition[138] and the Urogenital Distress Inventory are the onlyGrade A recommend instrument. There are severalGrade B and C measures which assess bother forincontinence and LUTS.
1. PATIENT PERCEPTION OF BLADDER CONDITION (PPBC)
The PPBC is a single item questionnaire designed torapidly assess patients’ perception of their bladdercondition [138].
The questionnaire asks patients to choose one of 6statements that best describes their present bladdercondition. The scale was validated during two large12-week clinical studies evaluating the efficacy andtolerability of Tolterodine in patients with OAB. Patientstaking part in the studies completed the PPBC, OAB-q, KHQ and bladder diaries. Baseline and week 12data was used for statistical analysis. PPBC scoreswere well correlated with OAB-q questionnaire scoresand bladder diary variables. Correlations of the KHQand PPBC were significant for all KHQ domains withthe exception of the general health perception domain.The scale was found to be responsive to change in
OAB symptoms and to have discriminant validity asreflected in the OAB-q, KHQ score and bladder diarychanges. The PPBC has also shown to have good testretest reliability [117]. This scale has been widelyused in studies evaluating the use of drug therapy inpatients with OAB [139-141].
2. UROGENITAL DISTRESS INVENTORY (UDI-6)
The UDI-6 is a six item questionnaire which assessesthe presence and bother of 6 lower urinary tractsymptoms [101]. The UDI-6 assesses types ofincontinence, frequency, difficulty emptying bladder andpain/discomfort in the lower abdomen/genitalia. Theresponse options are 0-3. The instrument hasdemonstrated validity, reliability and responsiveness[142].
Several instruments have been developed specificallyto assess urinary urgency, which is defined by theInternational Continence Society as “the complaintof a sudden compelling desire to pass urine which isdifficult to defer “[147]. Urgency is the principlesymptom of OAB [148], and, as such, assessing theeffect of treatment on this symptom and its impact onHRQL is important. With any measure designed toevaluate urgency, patients must be able to distinguishbetween the normal desire to urinate (urge) and thedifficult-to-postpone need to urinate (urgency) [149,150]. Wording thus becomes critical in the developmentof urgency assessment measures. Chapple and Wein[151] make a case for describing urgency as a“compelling desire to void in which patients fearleakage of urine” as a means of distinguishing thisabnormal sensation from the normal need to void.However, some patients may have a sensation ofurgency without fear of leakage, further complicatingattempts to define urgency. Importantly, with some ofthese scales, patients have the option of indicating thatthey experienced UUI (an event) rather than thestrongest feeling of urgency (a sensation) itself. Insuch cases, patients who have severe urgency, butnot UUI, do not have an option for endorsing thehighest (worst) value, because they are not incontinent.Urgency severity scales that include a UUI responseoption thus may be less useful than those that do notbecause such scales are trying to measure 2 thingsat once, both urgency and UUI.
Several instruments have been developed to assessurinay urgency these are summarized in Table 10.Given no urgency measures have a Grade A rating,a brief summary of each urgency measure is presentedbelow.
Urgency Perception Scale was designed for use inclinical trials to evaluate patient-perceived urgency
VI. ASSESSING THE IMPACT OFURGENCY
V. ASSESSING SYMPTOM BOTHERAND OVERALL BOTHER

388
Tab
le 9
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– S
ymp
tom
Bo
ther
Rel
iab
ility
Val
idit
y
PR
ON
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
C
on
si-
sten
cyT
est-
rete
stC
on
-te
nt
Cri
te-
rio
nC
on
-cu
rren
tD
iscr
-im
inan
t
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
-m
etri
cV
alid
atio
nin
Oth
erL
ang
uag
esA
vaila
ble
Lan
gu
ages
PG
I-I a
nd
PG
I-S
(Pat
ient
Glo
bal
Impr
essi
on o
fS
ever
ity a
nd o
fIm
prov
emen
t)[1
43]
Gra
de
C
Tw
o si
ngle
-que
stio
n gl
obal
inde
xes
to m
easu
re s
ympt
ombo
ther
rel
ated
to u
rinar
yin
cont
inen
ceW
omen
,S
UI
√√
(12
Wee
ks)
Non
e F
ound
PO
SQ
(P
rimar
yO
AB
Sym
ptom
Que
stio
nnai
re)
[117
]G
rad
e C
To
asse
ss w
hich
sym
ptom
of
OA
B is
the
mos
t bot
hers
ome
topa
tient
s
Men
and
Wom
en,
OA
B√
√N
one
Fou
nd
PP
BC
(P
atie
ntP
erce
ptio
n of
Bla
dder
Con
ditio
n)[1
38]
Gra
de
A
To
asse
ss p
atie
nts’
sub
ject
ive
impr
essi
on o
f the
ir cu
rren
tur
inar
y pr
oble
ms.
Dev
elop
ed fo
rpa
tient
s w
ith u
rinar
y pr
oble
ms
asa
glob
al a
sses
smen
t of b
ladd
erco
nditi
on a
nd is
rec
omm
ende
das
a g
loba
l out
com
e m
easu
re fo
rur
inar
y in
cont
inen
ce b
y th
eE
urop
ean
Med
icin
e E
valu
atio
nA
ssoc
iatio
nM
en a
ndW
omen
√√
√√
PP
BC
is tr
ansl
ated
in 2
2 La
ngua
ges
ww
w.p
rolu
tssh
.com
SP
I (S
ympt
omP
robl
emIn
dex)
[144
]G
rad
e B
To
mea
sure
how
trou
bles
ome
the
patie
nts
find
thei
r ur
inar
ysy
mpt
oms
Mal
e, B
PH
√√
√√
SP
I is
tran
slat
ed in
19
lang
uage
sht
tp://
proq
olid
.org
/inst
rum
ents
/sy
mpt
om_p
robl
em_i
ndex
_spi
SS
I an
d S
II(S
ympt
omS
ever
ity In
dex
and
Sym
ptom
Impa
ct In
dex
for
stre
ssin
cont
inen
ce in
wom
en)[
145]
Gra
de
C
To
mea
sure
str
ess
inco
ntin
ence
seve
rity
and
impa
ct o
rbo
ther
som
e of
sym
ptom
s. T
his
ques
tionn
aire
was
dev
elop
edan
d ad
min
iste
red
to w
omen
unde
rgoi
ng s
tres
s in
cont
inen
cesu
rger
yW
omen
,S
UI
√√
√√
SS
I and
SII
tran
slat
ed in
5 la
ngua
ges
http
://pr
oqol
id.o
rg/in
stru
men
ts/s
ympt
om
_sev
erity
_ind
ex_a
nd_s
ympt
om_i
mpa
ct_i
ndex
_for
_str
ess_
inco
ntin
ence
_in
_wom
en_s
si_a
nd_s
ii
UI-
4 (U
rinar
yIn
cont
inen
ce -
4Q
uest
ionn
aire
[146
]G
rad
e C
To
asse
s ho
w p
atie
nts
are
both
ered
by
urin
ary
inco
ntin
ence
Wom
en, U
I√
Ava
ilabl
e on
ly in
Spa
nish
http
://w
ww
.ncb
i.nlm
.nih
.gov
/pub
med
/10
4886
09?o
rdin
alpo
s=3&
itool
=E
ntre
zS
yste
m2.
PE
ntre
z.P
ubm
ed.P
ubm
ed_
Res
ults
Pan
el.P
ubm
ed_R
VD
ocS
um

389
[152]. This instrument consists of a single questionasking patients to describe their typical experiencewhen they feel the need to urinate. The 3 possibleresponses are “I am usually not able to hold urine,”“I am usually able to hold urine until I reach the toiletif I go immediately,” and “I am usually able to finishwhat I am doing before going to the toilet.” [152]. Thisscale was validated in a clinical trial evaluating theefficacy of tolterodine in treating OAB symptoms;[152] however, its limited responsiveness maypreclude its usefulness in clinical practice [153].
Indevus Urgency Severity Scale asks patients to ratetheir level of urgency on a 4-point scale, from 0 (nourgency) to 4 (extreme urgency discomfort that abruptlystops all activity/tasks) [154]. The scale has beenvalidated in a clinical trial of trospium in patients withOAB, [154] but Chapple et al [153] question whetherthis scale actually measures urgency or just the normalurge to void.
Urinary Sensation Scale is a 5-point scale rangingfrom 1 (no urgency; can continue activities until it isconvenient to use the bathroom) to 5 (urge incon-tinence; extreme urgency discomfort, cannot holdurine and have a wetting accident before arriving atthe bathroom) [155]. The content validity of this scalewas established through a physician survey and patientinterviews [155].
Urgency Rating Scale, recommended by theEuropean Medicines Evaluation Agency, consists ofa 5-point rating scale to be rated with every void,ranging from 1 (no urgency; I felt no need to emptymy bladder but did so for other reasons) to 5 (urgeincontinence; I leaked before arriving at the toilet)[16].This scale was used in a tolterodine clinical trial,in which responses on this scale were used to calculatesum urgency, a measure that accounts for changesin both urgency and frequency [156].
Many women present with vaginal symptoms andpelvic organ prolapse (POP) is frequently implicated.A traditional clinical history is usually used in an effortto assess the symptoms experienced by the patientand a thorough clinician will try to gain insight intohow these symptoms are impacting on the patient’slife. A detailed description of the clinical techniques ofpelvic floor assessment are described in anotherchapter in this book. However, symptoms do notalways correlate with objective examination findings.Indeed the clinical assessment itself can beinconsistent, depending upon the position of thepatient, whether they have been standing for a
VII. QUESTIONNAIRES TO ASSESSSYMPTOMS AND HEALTH RELATED
QUALITY OF LIFE IMPACT OF PELVICORGAN PROLAPSE
Tab
le 9
. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– S
ymp
tom
Bo
ther
(co
nti
nu
ed)
Rel
iab
ility
Val
idit
y
PR
ON
ame
/ Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
met
ric
Val
idat
ion
inO
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
UD
I (U
roge
nita
lD
istr
ess
Inve
ntor
y)[6
4]G
rad
e B
To
asse
s sy
mpt
om b
othe
rre
late
d to
urin
ary
inco
ntin
ence
.U
DI i
s m
eant
to c
ompl
emen
tth
e IIQ
, was
dev
elop
ed a
t the
sam
e tim
e as
the
IIQ.
Wom
en, U
I,S
UI
√√
√√
√√
Ava
ilabl
e in
3 la
ngua
ges
(Eng
lish,
Ital
ian
and
Ara
bic)
UD
I-6
(Uro
geni
tal
Dis
tres
s In
vent
ory
-6)
[142
]G
rad
e A
To
asse
ss L
UT
S b
othe
r,in
clud
ing
inco
ntin
ence
, in
wom
en.
Wom
en√
√√
√√
Ava
ilabl
e in
3 la
ngua
ges
(Eng
lish,
Tur
kish
and
Ara
bic)

390
Tab
le 1
0. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
B a
nd
LU
TS
PR
O M
easu
res
– U
rgen
cy
Rel
iab
ility
Val
idit
y
PR
ON
ame/
Gra
de
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
me-
tric
Val
idat
ion
in O
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
IUS
S (
Inde
vus
Urg
ency
Sev
erity
)[1
57]
Gra
de
A
Use
d to
qua
ntify
the
leve
lof
urg
ency
ass
ocia
ted
with
eac
h to
ilet v
oid
asm
easu
red
durin
gst
anda
rd v
oidi
ng d
iarie
s.
OA
B w
ithur
genc
yin
cont
inen
ce,
men
and
wom
en√
√√
√√
(12
Wee
ks)
Non
e F
ound
SU
IQ(S
tres
s/U
rge
Inco
ntin
ence
Que
stio
nnai
re)
[158
]G
rad
e C
Tw
o ite
m q
uest
ionn
aire
used
to d
iffer
entia
tebe
twee
n sy
mpt
oms
ofst
ress
and
urg
e ur
inar
yin
cont
inen
ceW
omen
, UI
√√
Non
e F
ound
UD
I (U
roge
nita
lD
istr
ess
Inve
ntor
y)[6
4]G
rad
e B
To
asse
s sy
mpt
ombo
ther
rel
ated
to u
rinar
yin
cont
inen
ce. U
DI i
sm
eant
to c
ompl
emen
t the
IIQ, w
as d
evel
oped
at t
hesa
me
time
as th
e IIQ
.W
omen
, UI,
SU
I√
√√
√√
√A
vaila
ble
in 3
lang
uage
s(E
nglis
h, It
alia
n an
d A
rabi
c)
UP
S (
Urg
ency
Per
cept
ion
Sco
re)[
159]
Gra
de
C
self-
repo
rt 5
item
OA
Bqu
estio
nnai
re u
sed
for
grad
ing
the
urge
to v
oid
and
asse
ssin
g th
e re
ason
why
indi
vidu
als
usua
llyvo
idM
en a
ndW
omen
√√
√√
Non
e F
ound
Non
e F
ound
UP
S (
Urg
ency
Per
cept
ion
Sca
le)
[152
]G
rad
e B
To
asse
ss th
e se
verit
y of
urge
ncy
– w
heth
er o
r no
tur
genc
y, th
e su
dden
and
com
pelli
ng d
esire
tour
inat
e sh
ould
hav
e a
seve
rity
mea
sure
isde
bate
d. T
he U
PS
was
desi
gned
for
use
incl
inic
al tr
ials
to e
valu
ate
patie
nt p
erce
ived
urge
ncy
OA
B(d
oubl
e-bl
ind)
, men
and
wom
en√
√√
Non
e F
ound
UR
IS-2
4 (U
rge
Impa
ct S
cale
)[1
60]
Gra
de
C
To
asse
ss o
f the
impa
ctof
the
mos
t com
mon
form
of U
I in
olde
r pe
rson
sO
lder
pers
ons,
UI
√√
√√
Non
e F
ound
UR
S (
Urg
ency
Rat
ing
Sca
le)
[161
]G
rad
e C
5-po
int s
cale
to b
e us
edco
ncur
rent
ly w
ith v
oidi
ngdi
arie
s to
mea
sure
the
leve
l of u
rgen
cyas
soci
ated
with
eac
hm
ictu
riatio
n. A
dvoc
ated
by th
e E
ME
A C
PM
PP
sych
omet
ric e
valu
atio
n no
t rep
orte
dN
one
Fou
nd

391
prolonged time or have just used a pessary or tampon.While there is a little research defining the associationbetween specific symptoms and support defects [164-166], measuring subjective outcome after treatmentis problematic. Unlike lower urinary tract dysfunction,where increasingly patient-completed methods suchas diaries and questionnaires are being used tomeasure outcome, there are fewer such instrumentsavailable for POP. Clinician based history isinconsistent, disease impact may not be assessed,leading questions can be asked and patients may beunwilling to volunteer symptoms, particularly aftersurgical intervention, for fear of appearing ungratefulor a nuisance. Consequently, despite the highlyprevalent nature of this condition we have little ideahow intervention, which is frequently surgical, alterssymptoms and HRQL. As for incontinence, question-naires to assess symptoms and HRQL impact of pelvicorgan prolapse would be highly desirable.
For POP, the Committee examined the quality of thepsychometric evidence and only where publisheddata were scientifically sound was the label ‘withrigour’ allowed. The Committee noted that this is adeveloping area with few questionnaires currentlyreaching the highest levels of evidence. Thus threegrades of recommendation were established (Table11).
1. GRADE A
a) Pelvic Floor Distress Inventory (PFDI) andPFIQ (Pelvic Floor Impact Questionnaire)
This questionnaire is an adaptation of the well-established UDI with the aim of developing acomprehensive condition specific instrument to assessimpact from pelvic organ prolapse and other aspectsof colorectal-anal dysfunction, as well as LUTS [167].
Tab
le 1
0. S
um
mar
y o
f U
rin
ary
Inco
nti
nen
ce,
OA
Ban
d L
UT
S P
RO
Mea
sure
s –
Urg
ency
(co
nti
nu
ed)
Rel
iab
ility
Val
idit
y
PR
O N
ame
Pu
rpo
se o
f T
oo
lP
op
ula
tio
nS
amp
le
Inte
rnal
Co
nsi
-st
ency
Tes
t-re
test
Co
n-
ten
tC
rite
-ri
on
Co
n-
curr
ent
Dis
cr-
imin
ant
Res
po
nsi
ve-n
ess
(Tre
atm
ent
Du
rati
on
)
Psy
cho
met
ric
Val
idat
ion
inO
ther
Lan
gu
ages
Ava
ilab
le L
ang
uag
es
US
S (
Urin
ary
Sen
satio
n S
cale
)[1
62]
Gra
de
C
To
asse
ss th
e im
pact
of
urge
ncy
with
pat
ient
sw
ith O
AB
Uro
logi
sts
orur
ogyn
ecol
o-gi
sts,
Sur
vey
resp
onde
nts
with
OA
Bsy
mpt
oms
N/A
√N
/AN
/AN
/AN
/AN
one
Fou
nd
UU
Sca
le (
10-I
tem
Sca
le to
Mea
sure
Urin
ary
Urg
ency
)[1
63]
Gra
de
B
10 it
em q
uest
ionn
aire
use
to m
easu
re u
rinar
yur
genc
yM
en a
ndW
omen
√√
√N
ON
EN
one
Fou
nd
Table 11. Criteria for recommendation of question-naires for POP at the Fourth Consultation
Grade of recommendation Evidence required (published)
Recommended (Grade A) Validity, reliability and responsiveness established with rigour.
(Grade B) Validity and reliabilityestablished with rigour, or validity, reliability and responsiveness indicated.
With potential (Grade C) Early development –further work requiredand encouraged

392
The PFDI retains the 19 original items of the UDI,and adds 9 items related to lower urinary tractsymptoms that are common in women with pelvicfloor disorders. The three original subscales of theUDI are retained (i.e., obstructive, irritative/discomfort,and stress). Psychometric testing included internalreliability (PFDI Cronbach’s alpha 0.88, PFIQ 0.98),1 week test-retest (interclass correlation coefficientPFDI 0.87, PFIQ 0.86).
Both correlated with stage of prolapse (Spearmancorrelation coefficient for pelvic organ prolapse distressinventory and impact questionnaire 0.32 p<0.01, 0.33p<0.01). Respon-siveness has not yet been tested.
PFIQ is an adaptation of the IIQ to assess quality oflife impact in women with pelvic floor disorders. Itcontains items included in the original IIQ and newitems related to other pelvic floor disorders. PFIQ has3 scales including 92 items: IIQ (30 items), Colorectal-anal impact Questionnaire (CRAIQ) (31 items) andPelvic Organ Prolapse impact Questionnaire (POPIQ)(31 items).
Each scale includes 4 domains of travel, social,emotional and physical activity. The psychometricproperties of the PFIQ were evaluated in 100 femalepatients with pelvic floor dysf-unction [167].
The PFIQ showed good validity; each of IIQ, CRAIQand POPIQ revealed significant correlation withincontinence episode and number of pad use perweek, faecal incontinence per week and stage ofprolapse, respectively. Internal consistency wasexcellent (Cronbach alpha 0.98) and test-retestreproducibility was high (overall ICC 0.86 rangingfrom 0.69 to 0.92). A French language version hasbeen produced [168].Responsiveness has not yetbeen evaluated.
Responsiveness of the PFDI and PFIQ was tested inwomen with pelvic organ prolapse undergoing surgicaland conservative management with vaginal pessaries.Women undergoing surgical treatment for prolapsereported significantly greater improvement in allsubscales of the PDFI and PFIQ than those patientstreated with pessaries.
The PFDI was found to be more responsive to changethan the PFIQ [169]. French and Spanish versions ofboth the PFIQ and PFDI have been produced [170,171]. Long forms of the PFDI and PFIQ have alsobeen validated for telephone administration [172].
Short forms of the PFDI and PFIQ questionnaireshave been developed. Reliability, validity andresposiveness were tested in a populatin of patientsbefore and 3-6 months after pelvic floor surgery. Theshort form of the PFIQ and PFDI correlated well withthe long form versions of the questionnaires (r=0.88-0.94) [173] (Table 12).
Table 12. Recommended questionnaires for theevaluation of symptoms and quality of life impact ofpelvic organ prolapse
Grade A New (recommended)
Pelvic Floor Distress Inventory (PFDI) [167]
Pelvic Floor Impact Questionnaire (PFIQ) [167]
Grade B
The electronic Personal Assessment Questionnaire –Pelvic Floor (ePAQ-PF) [174]
Grade C (with potential)
P-QOL/St. Mary’s Questionnaire [175]
Pelvic Floor Dysfunction Questionnaire [176]
Danish Prolapse Questionnaire [164]
2. GRADE B
• e-PAQ Electronic Pelvic Floor SymptomsQuestionnaire
The electronic Personal Assessment Questionnaire– Pelvic Floor (ePAQ-PF) is an interactivecomputerised system that comprehensively measurespelvic floor symptoms and their impact on HRQL inwomen. It comprises a maximum of 124 items in 4dimensions (Urinary, Bowel, Vaginal & Sexual) andincludes 19 scored domains:
The original 14 domain version underwent psycho-metric testing in primary and secondary care, whereit was found to be valid, reliable and acceptable(Radley et al 2006) [177]. Since this initial validationstudy, a further 5 domains have been added including:Irritable Bowel, Dyspareunia, Vaginal Capacity, UrinaryVoiding and General Sex Life [178]. Each domain isscored on a scale of zero (best possible health) to 100(worst possible health) and the symptom domainsalso each provide a 4-point scale. Recent tests ofdata quality on this version of ePAQ-PF supportedthe 19 domain structure of the instrument and itsreliability and validity (Jones et al, 2008) [179]. Theresponsiveness of the instrument has also beendemonstrated [177].
3. GRADE C
Several other questionnaires of Grade C level orbelow have been developed in the area of POP. Ifthe validation of these instruments progress they maybe useful for researchers. These include:
• P-QOL/St Mary’s Questionnaire [175] [180] -PelvicFloor Dysfunction Questionnaire [176]
• -Danish prolapse questionnaire [164]
• Pelvic symptom inventory and quality of lifequestionnaire [181,182]

393
• Pelvic floor questionnaire [183]
• Sheffield prolapse symptom questionnaire [178]
• ICIQ-Vaginal Symptoms (In development). [30],[184].
A range of questionnaires have been developed toidentify the severity of faecal incontinence (FI) and itsinfluence on HRQL. Despite the large number, onlya few are in regular use in research practice, and fewservices routinely use them in clinical assessment. Dueto the close overlap between faecal incontinence andother pelvic floor disorders (in particular urinaryincontinence), some of those questionnaires used forother pelvic disorders also include items to coverfaecal incontinence. For similar reasons, items relatingto faecal incontinence have often been included inquestionnaires addressing general gastro-intestinaland colo-rectal function, as well as condition specificinstruments in such areas as irritable bowel syndromeand inflammatory bowel disease, conditions whichare commonplace in colorectal practice as well as inother specialties dealing with pelvic floor disorders[185, 186]. It is also important to remember that thenormal range of bowel function is broad, that bowelfunction may be highly variable within individualswithout significant pathology. Consequently instru-ments in this field are likely to lack a degree ofsensitivity or specificity for the specific bowel disorderssuch as IBS, IBD evacuation disorder and constipation.
Anal incontinence and bowel evacuation are intrin-sically related to pelvic floor function and it may beinappropriate to consider bowel function purely interms of continence and constipation. Evacuatorydysfunction may result from a variety of underlyingpathologies including outlet obstruction, slow transitor other mechanical, pharmacological, metabolic,endocrine and neurogenic abnormalities [187]. Analincontinence occurs in both sexes, but is morecommon in women than men [188]. Symptoms areconsidered crucial to diagnosis as specific symptomsare thought to reflect the underlying pathophy-siology[189]. Thus, urgency (the inability to defer defecation)and urgency incontinence are thought to indicate lossof voluntary control due to impaired external analsphincter function, whereas passive incontinence isthought to indicate impairment of the smooth muscleof the internal sphincter.
For FI, the Committee examined the quality of thepsychometric evidence and noted that this is a
developing area with questionnaires currently reachingthe highest level of evidence. A FI outcomes measureis currently in development by the ICIQ (Table 3). Acommonly used score for FI (Wexner), for example,does not appear to have published data related to itspsychometric properties and thus while it is usedwidely cannot be recommended by the committee.The grades of recommendation are as outlined inprevious sections (Tables 13,14).
Table 13. Criteria for recommendation of question-naires for faecal incontinence
Grade of recommendation Evidence required (published)
(Grade A) Validity, reliability and responsiveness established with rigour.
(Grade B) Validity and reliability established with rigour, or validity, reliability and responsiveness indicated.
With potential (Grade C) Early development – further work required and encouraged
Table 14. Recommended questionnaires for the eva-luation of symptoms and quality of life impact offaecal incontinence
Grade A
None
Grade B
Faecal Incontinence Quality of Life Scale [190]
Manchester Health Questionnaire [191]
Birmingham Bowel and Urinary SymptomsQuestionnaire (BBUS-Q) [192, 193]
Grade C (with potential)
Wexner score [194]
St Mark’s score [195]
Faecal Incontinence Survey [196]
Elderly Bowel Symptoms Questionnaire [197]
Postpartum Flatal and Faecal Incontinence Quality ofLife Scale [198]
Bowel Disease Questionnaire [199]
Gastrointestinal Quality of Life Index [200]
VIII. QUESTIONNAIRES TO ASSESSSYMPTOMS AND HRQL IMPACT OF
FAECAL INCONTINENCE

394
1. GRADE A
No questionnaires are currently available at this level.
2. GRADE B
a) Faecal Incontinence Quality of Life Scale
The 29-item Faecal Incontinence Quality of Life Scaledeveloped and tested by Rockwood et al measuresimpact of anal incontinence over four scales of HRQL;Lifestyle (10 items), Coping/behaviour (9 items),Depression/Self perception (7 items) and Embar-rassment (3 items) [190]. The instrument was designedto measure the effect on quality of life of treatment forindividuals with faecal incontinence. A panel of colo-rectal surgeons and researchers generated the items.Psychometric properties were tested in 118 patientswith faecal incontinence and 72 controls.
The question-naire showed good discriminant validity,with significant differences between patients withfaecal incontinence and those with other gastro-intestinal disorders. There were also significantcorrelations with selected subscales of the SF-36.Test-retest reliability at a mean interval of 8 days wassatisfactory, with correlations for the 4 scales of 0.8 -0.96. Internal consistency of the 4 scales was >0.7.The instrument does not measure physical symptomseverity and has not been tested in asymptomaticcontrols, but appears to offer a valid and reliablemeasure of the impact of faecal incontinence on qualityof life in men and women with this condition [190].However, in order to demonstrate discriminant validity,the researchers deemed it necessary to modify thequestionnaire for use in controls. Its use in anunscreened population is as yet unreported, and noresponsiveness data have yet been produced.
b) Manchester Health Questionnaire
This questionnaire consists of items adapted fromthe King’s Health Questionnaire [191]. It uses thesame basic structure and format but items have a 5-point response scale (rather than the 4-point scale inthe KHQ). It includes items in the 8 domains of HRQLas well as a symptom severity scale. Face validitywas assessed by interview with 15 patients with faecalincontinence. Test-retest reliability was measured(Pearson correlation > 0.8 in all 9 domains).
The questionnaire was posted to 236 women withfaecal incontinence, of which 159 returned completedquestionnaires. 121 performed test-retest at a meaninterval of 20 days. Cronbach’s alpha was > 0.7 in alldomains tested, indicated adequate internalconsistency.
Convergent validity was assessed by comparisonwith responses in the SF-36, which showed significantcorrelations between domains of the 2 instruments.Data relating to women without faecal incontinenceor unscreened women are not yet available. The
questionnaire’s sensitivity to change is also not yetestablished.
c) Birmingham Bowel and Urinary SymptomsQuestionnaire (BBUS-Q)
This is a 22-item questionnaire developed to evaluatesymptoms of both bowel and urinary dysfunction inwomen which has a published scoring manual [192,193]. Items were generated by a panel of cliniciansand scientists and following review of existinginstruments in the literature. The instrument was testedin the gynaecology departments of three hospitals, aurogynaecology clinic, a functional bowel clinic anda general practice. A total of 630 women completedthe questionnaire; 379 women awaiting hysterectomy,45 women following hysterectomy 65 women referredwith functional bowel and/or urinary symptoms and 141asymptomatic controls.
The content, construct and criterion validity, internalconsistency, reliability and responsiveness of thequestionnaire were measured. Low levels of missingdata, peer and patient reports supported face andcontent validity.
Factor analysis showed a clinically relevant four-factorstructure: Constipation, Evacuatory function, Analincontinence and Urinary symptoms with low contentreplication able to distinguish between patient groups,indicating good internal structure. Comparison withclinical, anorectal physiological, videoproctographic,transit time and urodynamic test results supportedthe instrument’s criterion validity. Key domain questionanalysis and Cronbach's alphas showed internalconsistency. Kappa values and limits of agreementdemonstrated good test-retest reliability. Someresponsiveness data have been produced.
The authors recommended the questionnaire for useas both a research tool and as a useful clinicalmeasure. This questionnaire also forms a core elementin an electronic pelvic floor symptoms assessmentquestionnaire (e-PAQ) (see above).
3. QUESTIONNAIRES WITH POTENTIAL[GRADE C]
There are several questionnaires on faecalincontinence which have not yet reached Grade Cstatus. They may undergo further development andbe of use in future research:• Wexner score [194]• St. Mark’s score [195]• Faecal incontinence survey [184,185,190,196,
201, 202]• Elderly Bowel Symptom Questionnaire (EBSQ)
[197]. • Postpartum Flatal and Faecal Incontinence Quality
of life Scale [198].• Bowel Disease Questionnaire [199]
• Gastro-intestinal Quality of Life index (GIQLI) [200]
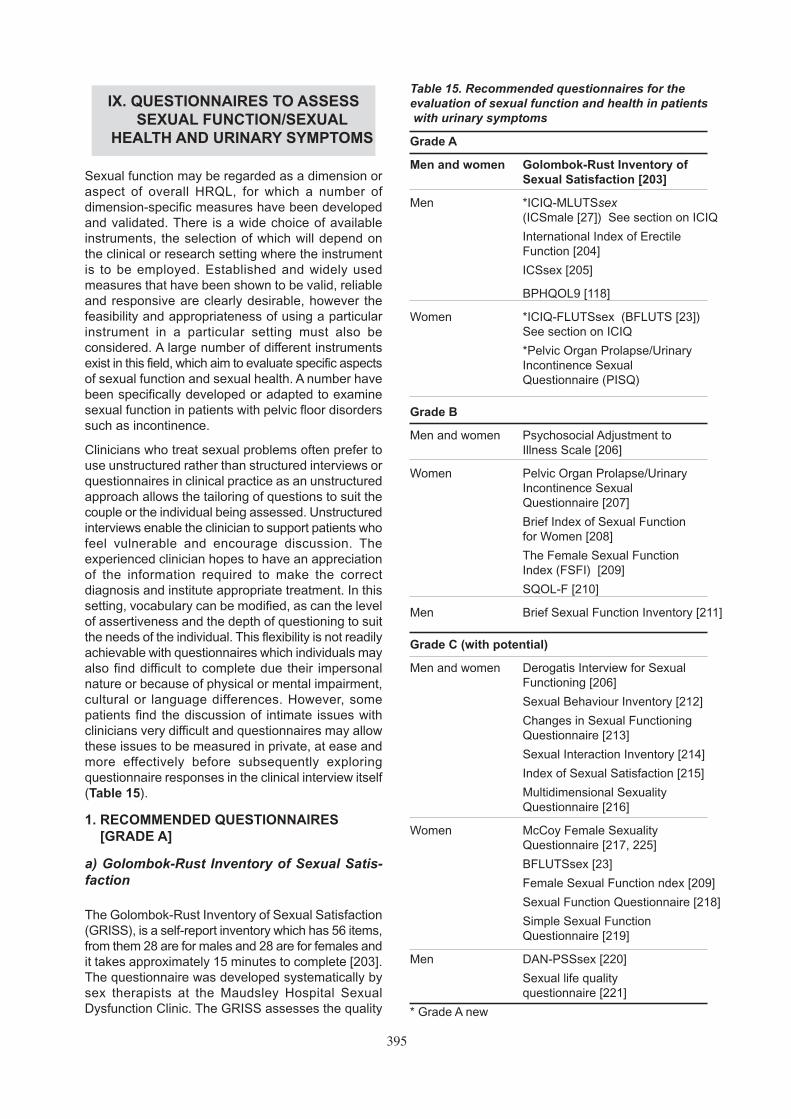
395
Sexual function may be regarded as a dimension oraspect of overall HRQL, for which a number ofdimension-specific measures have been developedand validated. There is a wide choice of availableinstruments, the selection of which will depend onthe clinical or research setting where the instrumentis to be employed. Established and widely usedmeasures that have been shown to be valid, reliableand responsive are clearly desirable, however thefeasibility and appropriateness of using a particularinstrument in a particular setting must also beconsidered. A large number of different instrumentsexist in this field, which aim to evaluate specific aspectsof sexual function and sexual health. A number havebeen specifically developed or adapted to examinesexual function in patients with pelvic floor disorderssuch as incontinence.
Clinicians who treat sexual problems often prefer touse unstructured rather than structured interviews orquestionnaires in clinical practice as an unstructuredapproach allows the tailoring of questions to suit thecouple or the individual being assessed. Unstructuredinterviews enable the clinician to support patients whofeel vulnerable and encourage discussion. Theexperienced clinician hopes to have an appreciationof the information required to make the correctdiagnosis and institute appropriate treatment. In thissetting, vocabulary can be modified, as can the levelof assertiveness and the depth of questioning to suitthe needs of the individual. This flexibility is not readilyachievable with questionnaires which individuals mayalso find difficult to complete due their impersonalnature or because of physical or mental impairment,cultural or language differences. However, somepatients find the discussion of intimate issues withclinicians very difficult and questionnaires may allowthese issues to be measured in private, at ease andmore effectively before subsequently exploringquestionnaire responses in the clinical interview itself(Table 15).
1. RECOMMENDED QUESTIONNAIRES [GRADE A]
a) Golombok-Rust Inventory of Sexual Satis-faction
The Golombok-Rust Inventory of Sexual Satisfaction(GRISS), is a self-report inventory which has 56 items,from them 28 are for males and 28 are for females andit takes approximately 15 minutes to complete [203].The questionnaire was developed systematically bysex therapists at the Maudsley Hospital SexualDysfunction Clinic. The GRISS assesses the quality
IX. QUESTIONNAIRES TO ASSESSSEXUAL FUNCTION/SEXUAL
HEALTH AND URINARY SYMPTOMS
Table 15. Recommended questionnaires for theevaluation of sexual function and health in patientswith urinary symptoms
Grade A
Men and women Golombok-Rust Inventory of Sexual Satisfaction [203]
Men *ICIQ-MLUTSsex(ICSmale [27]) See section on ICIQ
International Index of Erectile Function [204]
ICSsex [205]
BPHQOL9 [118]
Women *ICIQ-FLUTSsex (BFLUTS [23]) See section on ICIQ
*Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ)
Grade B
Men and women Psychosocial Adjustment to Illness Scale [206]
Women Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire [207]
Brief Index of Sexual Function for Women [208]
The Female Sexual Function Index (FSFI) [209]
SQOL-F [210]
Men Brief Sexual Function Inventory [211]
Grade C (with potential)
Men and women Derogatis Interview for Sexual Functioning [206]
Sexual Behaviour Inventory [212]
Changes in Sexual Functioning Questionnaire [213]
Sexual Interaction Inventory [214]
Index of Sexual Satisfaction [215]
Multidimensional Sexuality Questionnaire [216]
Women McCoy Female Sexuality Questionnaire [217, 225]
BFLUTSsex [23]
Female Sexual Function ndex [209]
Sexual Function Questionnaire [218]
Simple Sexual Function Questionnaire [219]
Men DAN-PSSsex [220]
Sexual life quality questionnaire [221]
* Grade A new

396
of a sexual relationship in a heterosexual couple andan individual’s functioning within it. This questionnaireis designed for people who are currently in arelationship. There are 12 domain scores, 5 of whichare female specific, 5 male specific and 2 non-genderspecific. The 5 female specific domains are:Anorgasmia, Vaginismus, Avoidance, Nonsexualityand Dissatisfaction. The 2 non-gender specificdomains are: Frequency of sexual contact and Non-communication. The questionnaire was validated ona clinical sample recruited from sexual dysfunctionclinics throughout the UK, consisting of 68 men and63 women, and a control group of 29 men and 30women randomly selected from primary careattendees. Split half reliability was 0.94 for the femalescale and 0.87 for the male overall scale. Averageinternal consistency of subscales was 0.74.
Both the overall female and male scores were foundto discriminate well between clinical and non-clinicalsamples and scores on subscales successfullydiscriminated specific diagnostic groups. There wasalso a significant correlation between therapists’ ratingsof severity and scores on the questionnaire.Responsiveness was assessed by comparing changein the questionnaire scores with rated improvementsby sex therapists. Correlations were moderate butstatistically significant (0.54 for males and 0.43 forfemales, p<.005 and p<.01 respectively). Test-retestreliability was assessed in 41 couples receiving eithermarital or sex therapy. A further two subscales applyto both males and females and cover infrequencyand non-communication. An additional 2 items eachfor males and females contribute to the overall scoresbut are not included in the subscales. The GRISShas been used by Hunt & Moss (1996) in a smallstudy exploring the relationship of unwanted sexualexperience to detrusor instability and sexualdysfunction [222]. High levels of sexual dysfunctionwere found in incontinent subjects compared to otherclinical groups. The GRISS is not applicable tohomosexual couples or people without a partner, butdoes provide an otherwise comprehensive, effectiveand well-used questionnaire.
b) ICIQ-MLUTSsex (ICSsex)
This forms one of the modules of the ICIQ modularquestionnaire (see above) [205]. It consists of 4 items:to what extent sex life has been spoilt by urinarysymptoms, ability to have erections, ability to ejaculate,and pain or discomfort on ejaculation. As with theother ICS questionnaires each item has an additionalpart to each item concerning the amount of bother thesymptom causes i.e. how much of a problem is thisfor you? It has been used in both clinic and communitysamples to assess the relationship between urinarysymptoms and sexual function, [205] and to showthat urinary symptoms most frequently associatedwith sexual dysfunction were those related toincontinence [223]. It has also been used in a
randomised trial of treatments for LUTS to investigatesexual side effects [224]. Aspects of reliability, validityand responsiveness have been tested and found tobe satisfactory.
c) International Index of Erectile Function (IIEF)
The international index of erectile function (IIEF) is a15-item self-administered questionnaire. It wasdesigned to assess erectile function and is culturallyand linguistically validated in at least 10 languages foruse in multinational clinical trials.213 It was initiallyvalidated in 351 patients with erectile dysfunction(ED) and found to have a high degree of internalconsistence (Crohnbach’s alpha > 0.85) and sensitivityto change with treatment. The questionnaire wasculturally and linguistically validated in the followinglanguages: Danish, Dutch, English (American,Australian and British), Finnish, French, German,Italian, Norwegian, Spanish and Swedish. The final 15-item instrument addresses five different domains ofsexual function: erectile function, orgasmic function,sexual desire, intercourse satisfaction and overallsatisfaction. The IIEF has a high degree of internalconsistence. Test-retest repeatability was high for thedomains of erectile function and intercoursesatisfaction and moderately high for the other domains.Discriminant validity was good for most domains(except the sexual desire domain). Construct validitywas good and all five domains showed a high degreeof sensitivity to change. An abridged 5-item versionof the questionnaire has also been developed (IIEF-5) [225]. Of the 5 items, 4 are from the erectile functiondomain and one addresses sexual intercoursesatisfaction. The main difference between the 5- andthe 15-item version is that the former asks patients toself-assess erectile function and satisfaction over thepast 6 months while the latter refers to a time frameof 4 weeks. It has been used recently in a multinationalsurvey of male ageing [220].
d) BPH QOL9
The QOL9 is a short form of the QOL20, a question-naire previously validated in French for men withLUTS related to BPH [118]. The short form wasdeveloped using a large-scale cohort study of 7093men with BPH who received alfuzosin for 3 months.The items were reduced by identifying questions thatcontributed most to establishing the global score andthat reflected the structure of the questionnaire onprincipal components analysis. The final, 9-itemquestionnaire consists of 3 items concerning generalwell being, 3 items assessing BPH interferences withactivities, and 3 items pertaining to patients’perceptions of their sexual life. The sexual functiondomain covered sexual desire, erectile function andsatisfaction with sex life. The QOL9 was validated intwo studies, a longitudinal study of alfuzosin, havinga sample size of 4259, and a smaller cross-sectionalstudy of men having symptomatic BPH (n=48), or no

397
symptoms of BPH (n=42), and a group of youngermen (n=23). Feasibility and acceptability of thequestionnaire were assessed by completion ratesthat exceeded 85%. Principal components analysisconfirmed the three-factor structure. Discriminantvalidity was measured by comparing cases and non-cases. On the sexual function domain cases scored10.5, non-cases 15.2 and young men 26.3. The moststrongly discriminating question between cases andnon-cases was satisfaction with sex life. There wasalso a good correlation between symptom severityand the total QOL9 score. Internal consistency of theoverall scale was fair with Cronbachs alpha of 0.79for patients with BPH and 0.85 for the control groups.Test-retest reliability was good for the total score butmoderate for the sexual function subscale (ICC =0.69 - 0.88) with the reliability of the erection itemhaving an ICC of 0.53. After treatment the effect sizeof the change in the sexual function domain was linkedto age and initial symptoms severity but had a meanof 0.02 and 0.55 for patients treated in each of the twostudies.
e) ICIQ-FLUTSsex (BFLUTSsex)
This forms one of the modules of the ICIQ modularquestionnaire (see above) The questionnaire contains4 questions related to sexual function: pain ordiscomfort due to dry vagina, whether sex life hasbeen spoilt by urinary symptoms, pain on sexualintercourse, and leakage on intercourse [23]. Inaddition to each of these items the respondent isasked how much of a problem this is for them. It hasbeen used to assess sexual function after hormonereplacement therapy [226] and pelvic floor muscletraining [40]. There are 18 linguistic translationsavailable and there is published evidence of validity,reliability and sensitivity to change..
f) Pelvic Organ Prolapse/Urinary IncontinenceSexual Questionnaire (PISQ)
Rogers and colleagues in the United States havereported the development and validation of a measureof sexual function in women with urinary incontinenceor pelvic organ prolapse [207]. The scale consists of31 items spread across 3 domains: behavioural/emotive, physical, and partner-related. The measurehas been found to have acceptable convergent anddivergent validity and to be able to discriminatebetween women with and without urinary incontinenceor pelvic organ prolapse [207, 227]. Test-retest rangedfrom 0.56 to 0.93, showing some variability in themoderate to high reliability ranges [228]. The internalconsistency of the total measure and thebehavioural/emotive, physical and partner-relateddomains was .85, .86, .77, and .43, respectively [228].Sensitivity of the PISQ-31 has now been assessed inseveral studies.
A short form version of the questionnaire PISQ-12
has also been developed by the same team ofresearchers [229]. All subsets regression analyseswith r > 0.92 identified 12 items, across all threedomains, that were the most highly predictive of thePISQ-31 scores. Construct validity of the PISQ-12was examined through correlations with the long formof the questionnaire PISQ-31 (r=0.75-0.95), the SexualHistory Form -12, and the IIQ-7. Correlations of thePISQ-12 with these latter measures were similar tothose found for the PISQ-31.
The PISQ-12 scores were lower in those patients withpoorer sexual functioning and more depressivesymptoms. Test-retest reliability was moderate to high.Internal consistency reliability was stated as havingbeen done, although the values were not reported inthe article. Sensitivity of the PISQ-12 was notassessed.
An initial validation of a Spanish version of the PISQ-31 was reported for 34 bilingual patients of Mexican,Central or South American, Puerto Rican and Cubanorigins living in the United States [230]. Goodagreement between the Spanish and English versionswas achieved for 30 of the 31 items. The three-factorstructure of the original measure was validated in thissample of participants [227, 231-239].
2. RECOMMENDED QUESTIONNAIRES [GRADE B]
a) The Female Sexual Function Index (FSFI)
The Female Sexual Function Index (FSFI) [209] is a19-item self-report questionnaire for measuring femalesexual function and takes approximately fifteenminutes to complete. It provides five domains of sexualfunction, which have been confirmed using factoranalysis they include: Desire, Lubrication, Orgasm,Arousal, Pain and Satisfaction. An overall total scoreis also provided. The FSFI was developed using asample of 131 female controls (between the age of21-68) and 128 females who met Diagnostic andStatistical Manual of Mental Disorders (DSM-IV;American Psychiatric Association, 1994) criteria forFemale Arousal Disorder (FSAD). The age of theparticipants was matched [21-69]. Norms are availablefor both groups (controls and FSAD) at the individualitems level, the domains level, and the full-scalescores.
The FSFI discriminated reliably between women witharousal disorder (FSAD) and a control group on eachof the domains of sexual function as well as on thefull-scale score. FSFI data were also compared withresults from the Locke-Wallace Marital Adjustmenttest (1959), Correlations between the two weregenerally modest in magnitude, with the strongestobserved for the satisfaction domain of the FSFI.Internal consistency and test-retest reliability of theFSFI have been established. Test retest reliability ofthe scale was assessed in women with multiple

398
sclerosis with associated urinary and sexual symptoms[240].
Further cross validation studies were carried out todevelop cut-off scores for potential classification offemale sexual dysfunction [241, 242].
The FSFI was used in a study to investigate theprevalence of sexual dysfunction in women withchronic pelvic pain and with the [243] Female sexualdistress score (FSDS) to investigate sexual outcomesin women with LUTS who were successfully treatedwith sacral neuromodulation. A 60% increase in theFSFI overall score or 50% increase in FSDS score wasregarded as significant improvement [244]. The FSFIhas been used in a study of pelvic floor muscle trainingfor women with pelvic floor disorders and a study ofsexual function in women with symptomatic pelvicorgan prolapse who were treated with pessaries [233,245].
The Italian version of the FSFI has been used as ascreening tool for sexual dysfunction in healthy womenattending annual gynaecological health checks [246]The impact of LUTS and urinary incontinence onfemale sexual dysfunction was investigated over a 3year period in women undergoing urodynamic studiesusing the FSFI [247]. The Malay translation has alsobeen validated [248].
b) The Psychosocial Adjustment to Illness Scale(PAIS)
The Psychosocial Adjustment to Illness Scale (PAIS)was designed to assess the psychological and socialadjustment of male and female medical patients to theirillness and is in an interview or self-report format(PAIS and PAIS-SR) [206]. It contains a sexualrelationships domain consisting of 6 items assessingthe quality of interpersonal sexual relationships, sexualinterest, frequency of sexual activity, sexualsatisfaction, sexual dysfunction and interpersonalsexual conflict. Validation was carried out on groupsof patients having renal dialysis, lung cancer, cardiacproblems, breast cancer, and Hodgkin’s disease.Internal consistency of the sexual relationships domainranged from 0.8 to 0.93 in these different clinicalgroups. Factor analysis confirmed the subscalestructure. All 6 items in the sexual relationships domainhad very marked loadings on this dimension, with noappreciable loadings from other items. Convergentvalidity was assessed by comparing the scale to theGlobal Adjustment To Illness Scale (r-0.46), the SCL-90R (r=0.13), Affect Balance Scale (r=0.42), and thePatients Attitudes, Information and Expectancies Scale(r=0.40). Discriminant validity was assessed bycomparing patients screened positive and negative forlung cancer. There were differences in the meanscores between the two groups which approachedsignificance (t=1.53, p<0.10) [206]. 14 The PAIS hasbeen used to investigate the impact of different types
of urinary incontinence on sexual function [249] in asample of 200 patients referred for urodynamicassessment. Compared to patients with Urodynamicstress incontinence USI, patients having detrusoroveractivity DO were significantly impaired on all itemsof the sexual relationships subscale, apart from the‘sexual satisfaction’ item. Some aspects of validationwere also carried out in a small study of 29 patientswho had been treated successfully for penile cancer[250]. Internal consistency of the sexual relationshipsscales was good having Cronbach alpha of 0.83.Convergent and discriminant validity was shown insignificant correlations with well-being scales but notwith social scales. In addition, patients who had hadthe most radical treatments in terms of partial or totalpenectomy scored lower on the sexual relationshipsscale as did older patients (mean age 63 years)compared to younger patients (mean age 41 years),whereas having a mental disorder showed nocorrelation with sexual relationship scores.
c) The Brief Index of Sexual Function for Women(BISF-W)
The Brief Index of Sexual Function for Women (BISF-W) is a 22-item self-completed questionnaire thattakes 15-20 minutes to complete [208] It is designedto assess current levels of female sexual function andsatisfaction. It was originally validated in a sample of269 sexually active women age 20-73, and used a 3-factor scoring system (Interest/desire, Sexual activity,Sexual satisfaction) with acceptable test-retestreliability. A new quantitative scoring algorithm wasdeveloped to facilitate the use of the BISF-W in clinicaltrials, providing an overall composite score for sexualfunction and 7 domain scores; Thought/desire, Arousal,Frequency of sexual activity, Receptivity/initiation,Relationship satisfaction, Pleasure/orgasm, andProblems affecting sexual function. Norms for thecomposite score and for each of the seven dimensionscores are available, derived from a sample of 225healthy women (age 20-55) [251]. Comparing thesescores with those of 104 surgically menopausal,sexually active women who reported impaired sexualfunction (age 20-55), the instrument showed gooddiscriminant validity between women with and withoutsexual complaints in each of the 7 sexuality domains.In a placebo-controlled study, the BISF-W wassensitive to detecting differences between treatmentgroups in two of the 7 sexuality domains and on theoverall composite BSIF-W score.
d) Brief Sexual Function Inventory
This 22-item questionnaire concerning male sexualfunction was designed for clinical and researchpurposes in urological settings [211]. Items weregenerated from the literature to produce a 50-itemquestionnaire which was then reduced down to 22items in a series of pilot studies prior to the finalvalidation study. The questionnaire comprises of 5

399
subscales: Libido, Erectile function, Ejaculation,Assessment of significance of each domain andOverall satisfaction. Validation was carried out on asample of 74 men with sexual dysfunction and 60general medical patients. Mean age was 55 and 45years respectively. The study describes developmentof individual subscales down to a final questionnaireof 11 items based on measures of internal consistencyand test-retest reliability. Internal consistency of thesubscales ranged from 0.62 to 0.95 and ICC’s from0.79 to 0.89 for test-retest reliability.
All subscales except the drive and ejaculationsubscales discriminated between patients beingtreated for sexual dysfunction and general medicalpatients, but it was not expected that drive would bereduced in patients experiencing sexual dysfunctionand ejaculation did not appear to be an importantissue for patients.
e) Sexual quality of life-female questionnaire(SQOL-F)
This questionnaire was developed to assess theimpact of sexual dysfunction on womens’ quality of life.Responsiveness to change has not been established[210]. The content validity of the SQOL-F, sexualfunction questionnaire (SFQ) and PISQ were furtherassessed in a postal study of women with OAB andurinary incontinence in the United States, and theSQOL-F was rated most relevant and understandableamong this group of women [252].
3. QUESTIONNAIRES WITH POTENTIAL[GRADE C]
Several questionnaires that have potential and arecurrently under development or in need of furtherdevelopment. With further validations these instrumentcould provide additional resources to research:
• The Derogatis Interview for Sexual Functioning(DISF) [206]
• Sexual Behaviour Inventory (SBI) [212, 223]
• The Changes in Sexual Functioning Questionnaire(CSFQ) [213]
• Index of Sexual Satisfaction (ISS) [215]
• Multidimensional Sexuality Questionnaire (MSQ)[216, 223].
• The Sexual Interaction Inventory (SII) [214]
• McCoy Female Sexuality Questionnaire (MFSQ)[217]
• Simple Sexual Function Questionnaire [219, 219,253]
• Sexual function questionnaire [218]
• DAN-PSSsex [220]
• Sexual life quality questionnaire (SLQQ) [221]
a) Other measures of sexual function
Many of the questionnaires assessing the psychosocialimpact of LUTS and/or UI contain one or two questionsrelated to sexual function. The majority of these arediscussed above, either as symptom questionnairesor general quality of life questionnaires. Questionnairescontaining just one question tend to focus on a generalassessment of the overall impact of urinary symptomson sexual functioning. The Kings Health questionnaire,[24] the Incontinence Impact Questionnaire [59] andthe I-QOL [75] are recommended by the Committeefor use for UI/LUTS. However, when considering thesexual items it must be borne in mind that validationof the sexual items was not always carried out ormade explicit. But the questions relating to sexualfunction in each of the questionnaires are very similarand judgements on validity can be made by comparingquestions and psychometric data between question-naires as well as considering the psychometricproperties of the scales as a whole. If more in-depthinformation is required concerning sexual function,the questionnaires recommended for this aspectshould be used (see above).
There are other general measures of sexual function,such as the Watts Sexual Function Questionnaire.[254] and Medical Outcomes Study (MOS) SexualFunctioning Scale [255]. There are also questionnairesthat have been designed for sexual dysfunction specificto particular diseases, such as Radiumhemmets Scaleof Sexual Function, [256] Sexual AdjustmentQuestionnaire (SAQ), [257] and Prostate-targetedHealth Related Quality of Life [258].
A small number of questionnaires have producedinitial validation but without publications during thereporting period: Effect of Urinary Incontinence onSexuality Questionnaire (EISQ), [259] and Effects ofurinary incontinence on sexual activity [260].
Most studies and questionnaires have been developedfor use with members of the general population orurology/gynaecology patients with incontinence orPOP. However, some specific patient groups mayexperience particular problems with incontinence (forexample, children, frail elderly or those who areseverely disabled), which may require independentinvestigation and potentially the development of morespecific measures or the addition of a new subset ofitems on already developed instruments. TheCommittee advises that researchers should useexisting highly recommended or recommendedquestionnaires if possible as this aids comparisonand to reduce the increasing proliferation ofquestionnaires. Many of the questionnaires developed
X. QUESTIONNAIRES FOR SPECIFICPATIENT GROUPS

400
below for particular conditions (e.g. prostate cancer)pre-dated the development of highly recommendedquestionnaires, and highly recommended question-naires should be used preferentially.
a) Older people
Urinary incontinence symptoms play an influentialrole on the overall HRQL in older people (>65) andcauses a significant decrease in HRQL, as severeas that of many chronic disease states. Since theelderly commonly have a number of associatedcomorbid conditions, it may be difficult to measurethe impact of urinary incontinence with generic HRQLmeasures. The use of incontinence specific tools tomeasure patient-reported outcomes in the elderly,therefore, is of considerable importance.
Validated incontinence-specific PRO questionnaires,such as IIQ, I-QOL or KHQ, are used for clinical trialsor research on urinary incontinence including elderlypeople, but their validity has not been specificallyassessed in this age group. Okamura, assessedsymptoms and HRQL in older people (men andwomen) with lower urinary tract symptoms includingincontinence, using the KHQ and IPSS. Theydemonstrated that symptoms and HRQL in the elderlywith LUTS could be assessed by IPSS and KHQ andthat urinary incontinence appeared to be moreassociated with a decreased HRQL in elderly women[80].
On the other hand, there are a variety of factorsaffecting older people, including physical, social,mental, economic or environmental conditions, whichare different from those of the young. In frail elderlypeople with dementia or physical impairment, it maybe difficult to assess the impact of urinary incontinencealone. Questionnaires specifically developed for theelderly may be of great importance in this respect.However, there is little relating to the development orvalidation of particular questionnaires for older peoplewith urinary incontinence. Two questionnaires dealingwith older people were found and are described below.No questionnaires dealing with patient outcomesspecifically for frail older incontinent people werefound.
1. THE URGE IMPACT SCALE (URIS) [GRADE B]
The Urge Impact Scale (URIS) was designed andtested specifically for older persons with urgencyincontinence. The URIS was developed and validatedby DuBeau et al. (1999) [261] and included 32 items,reduced to 24 items (URIS-24). The URIS-24 waspsychometrically assessed for validity and reliabilityin community-dwelling older (>65y) men and womenwith urge incontinence,. Cronbach alpha was 0.84for the URIS-32 and 0.94 for the URIS-24. Inassessment of test-retest reliability, interclasscoefficient (ICC) was 0.88. The URIS-24 had modestbut nearly significant correlation with the number of
urgency incontinence episodes (rho=-0.39, p=0.05).Factor analysis revealed 3 component structurescorresponding to physiological burden, perception ofpersonal control and self-concept. There was noanalysis for responsiveness. They showed that theURIS-24 is an internally consistent, highly reproducibletool for the assessment of the QOL impact of urgencyincontinence on older persons.
2. SWEDISH QUESTIONNAIRE [GRADE C]
A questionnaire survey was conducted among menand women aged over 75 years in Sweden [262]. Thequestionnaire was developed specifically for the studyalthough many questions had been used in a previousepidemiological survey [263]. The questionnaireachieved an admirable 62% response rate, but nodetails were published describing the psychometricproperties of the questionnaire or the method of itsconstruction.
There still remains a gap in the assessment of PROsfor frail older adults by other than subjective means.Many of the commonly used measures have beenused for older people as part of pharmaceuticalcompany studies but it is not known whether these arerelevant to the needs of the frail elderly or that theyrespond in a similar fashion when used in youngerpopulations.
b) Children
Some questionnaires have been developed specificallyto address issues for children, particularly enuresis.See Chapter (Children) and section on ICIQ modularquestionnaire.
c) Spinal cord injured/neurologically damaged
Individuals who have a spinal cord injury or areneurologically damaged can experience particulardifficulties with incontinence and the use of variousdevices. It would be useful to investigate whetherGrade A questionnaires, developed for people withoutneurological damage, can be used in this group, orwhether additional modules or instruments arerequired. This is an area where a small number ofquestionnaires are being developed with the Qualiveenbeing a notable exception (Also see section on theICIQ questionnaire and below).
QUALIVEEN: QUALITY OF LIFE RELATED TO URINARY
PROBLEMS IN SPINAL CORD INJURY [GRADE A]
The Qualiveen was developed to evaluate the specificimpact of urinary dysfunction on the quality of life ofspinal cord injury patients in France [264]. The initialitems were developed following patient interviews,and were then assessed for validity and reliability in281 spinal cord injury patients with urinary difficulties.The Qualiveen contains 30 items and has demons-trated good reliability and validity [264]. Furthervalidation of the Qualiveen has occurred in multiple

401
sclerosis patients [265] and it has been translatedand validated into English [266], German [267], andPortuguese [268]. The Qualiveen has demonstratedresponsiveness in multiple sclerosis patients and hasa suggested MID of 0.5 [269].
d) Prostate/bladder cancer
Many PRO questionnaires are available forassessment in this area: Post-radical prostatectomyquestionnaire, [270, 271] Cancer RehabilitationEvaluation System - Short Form (CARES-SF), [272]Prostate Cancer Treatment Outcome Questionnaire(PCTO-Q), [273] PROSQOLI, [274] ModifiedSouthwest Oncology Group (SWOG), [275] FunctionalAssessment of Cancer Therapy - (FACT-G), Bladderform (FACT-B) and Prostate form (FACT-P), [276]Functional Assessment of Cancer Therapy VandervietCystectomy Index (FACT-VCI), [277] EORTCmetastatic prostate cancer, [273] Changes in UrinaryFunction, [257] Prostate-targeted Health RelatedQuality of Life [258]. While it is beyond the scope ofthis chapter to review and recommend PROs in thisarea, the principles and guidelines discussed hereinapply to selecting a PRO related to prostate andbladder cancer.
e) Lower urinary tract symptoms/benignprostate disease
Many questionnaires have been developed to assessLUTS and benign prostate disease, however mostdo not contain a full evaluation of UI. Perhaps themost widely known urology PRO is the AUA SymptomIndex, [137] I-PSS (International Prostate SymptomScore) [137, 278].The IPSS has been utilitized interna-tionally to assess symptoms of prostate disease withdocumented reliability, validity and responsiveness.Additional PRO measures for BPH are as follows:Patient-completed modification of the Boyarsky [279]BPH Impact Index, [144] and BPH Health-related QoLsurvey [280].
The previous sections have provided an overview ofPRO measures with evidence of reliability, validity,and responsiveness. But, how does a researcherchoose which instruments are most appropriate for aparticular research study and/or clinical assessment?The following section provides general guidelines foruse in conducting PRO assessments in clinical trialsor other research investigations related to urinary orfaecal incontinence.
As there are many available PROs, it is of utmostimportance to select the PRO measure that is relevantand applicable to one’s desired outcome. If an
intervention is designed to reduce symptom bother,then a relevant PRO would be a symptom bothermeasure. Multiple PROs can be included in a researchstudy, however the designation of the PRO as aprimary or secondary endpoint must be . In addition,issues of staff and participant burden, time constraints,and resources should be considered in the selectionof a PRO measure.
1. SELECTING PRO MEASURES FOR RESEARCH STUDIES
a) Study Design
There are several protocol concerns that must betaken into account when using PRO measures inresearch studies, including the length of the study,the frequency of contact with the study participants,the timing of clinical assessments, the complexity ofthe trial design, the number of participants enrolled,and participant and staff burden. The goal of the PROinvestigation is to "fit" the PRO measures to theprotocol without compromising either the studyobjective or design. For example, if the study designis complex with frequent participant contacts andmultiple clinical measures, it may be necessary tokeep the PRO measures at a minimum or to reducethe number of times the PRO is assessed (e.g.baseline and end of study rather than during allparticipant contacts) to minimise participant and staffburden.
At the same time, however, PROs must be viewed asan important variable in the overall trial design andcannot be devalued in the data collection process.Consequently, PRO measures cannot be altered orreduced to accommodate study design as suchalterations may yield potentially less reliable measuresor may seriously diminish the integrity of the overallstudy design and yield useless information. Having welldeveloped research goals and questions regardingPROs will help to guide you in the selection ofmeasures for a study. The goal is to develop aconceptually adequate, yet practical PRO batterygiven the study population, the specific intervention,and the study design.
The frequency with which PRO will need to beassessed in a research study will depend upon thenature of the condition or intervention beinginvestigated and the expected effects (both positiveand negative) of treatment. At a minimum, as with allmeasurements collected in a research study, abaseline and end of study assessment should becompleted. In addition, other PRO assessments shouldbe timed to match expected changes in functioningdue to either the intervention or the condition or thedisease itself. Timing follow-up assessments tocoincide with typical patient follow-up visits, ifappropriate, may also reduce the costs involved infollow-up PRO and symptom assessments.
XI. SELECTING PRO MEASURES FORCLINICAL TRIALS AND CLINICAL
PRACTICE

402
b) Study Population
It is crucial to specify key population demographicsthat could influence the choice of instruments, therelevant dimensions of PRO to be assessed, and themode of administration. Thus, age range, gender,educational level, the language(s) spoken, and culturaldiversity should be carefully considered prior toselecting PRO measures. For example, a cohort ofpatients over the age of 70 may have more visionproblems than middle-aged persons, making self-administered questionnaires potentially inadvisable.Ethnically diverse groups also require measures thathave been validated across different cultures and/orlanguages.
In clinical trials, it is also as important to consider howthe disease or condition will progress and affect theoutcomes of patients in the control group as it is tounderstand the effects of the study treatment. Forexample, in patients with incontinence assigned to aplacebo-control arm of a study, one might expect asymptom to worsen and thus have an effect on dailyfunctioning. The point is to select PRO measures thatare sufficiently sensitive to detect changes in boththe treated and the control group patients. Use of thesame measures for both groups will ensure anunbiased and comparable assessment.
c) Intervention
There are three major factors related to the interventionthat are relevant to PRO assessment, and thereforerequire careful consideration: 1) the positive andadverse effects of treatment; 2) the time course ofthe effects; and 3) the possible synergism of thetreatment with existing medications and conditions. Itis crucial to understand how a proposed treatmentcan affect patient outcomes in both positive andnegative ways. For example, some drug therapiesmay relieve LUTS but produce side effects like drymouth or sexual dysfunction.
In addition, the time course of an intervention's effectson PROs is also critical both in terms of the selectionof measures and the timing of when PRO measuresare administered to study participants. For example,in a trial comparing coronary artery bypass graft(CABG) surgery to angioplasty, an assessment ofPRO one week post-intervention might lead to aninterpretation that the surgical arm was more negativethan angioplasty for PRO since the individuals in thisarm of the trial would still be suffering the effects ofthe surgical procedure (for instance, sore musclesand surgical site discomfort) which could overwhelmany benefits associated with CABG. However, at sixmonths post-intervention, the benefits of CABG surgerysuch as, relief from angina, might be more profoundthan the benefits received from angioplasty. Thus,when PRO is assessed could influence how oneinterprets the benefits (or negative effects) of theinterventions.
Finally, it is important to have a clear understandingof the current medications the patient population islikely to be taking prior to randomisation to the studytreatment, and how these medications might interactwith the trial intervention, (either a pharmacologicalor behavioural intervention), to influence patientoutcomes.
There are two types of PRO measures: generic andcondition-specific. Generic measures are designedto assess outcomes in a broad range of populations(e.g., both healthy as well as ill individuals). Theseinstruments are generally multidimensional, andassess at least the physical, social and emotionaldimensions of life. An example of this type of instrumentis the Medical Outcomes Study SF-36 Health StatusProfile. [281]. A second type of measure is condition-specific (e.g., instruments designed to assess theimpact of specific diseases, conditions, age groups,or ethnic groups). Condition-specific measures can besimilar to generic instruments in that they assessmultiple outcome dimensions, but condition-specificmeaures also include items more specific to theparticular condition or population being studied.Examples of frequently used condition specificinstruments include the Incontinence ImpactQuestionnaire, the King’s Health Questionnaire, andthe OAB-q (described above).
In general, the growing trend has been to includecondition-specific outcome measures in clinical trialsdue to their enhanced sensitivity to change and theneed to minimise participant burden. Importantly, thetype of instruments selected for inclusion in a researchstudy will depend on the goals of the intervention andthe specific research questions to be addressed. Inpractice, clinical trials that include PROs usuallyincorporate a combination of PRO measures mostrelevant to the study population and intervention, ifapplicable, being mindful of resource constraints andstaff and participant burden.
1. QUALITY-ADJUSTED LIFE YEAR (QALY)
Increasingly HRQL outcome measures are being usedin the development of quality-adjusted life year (QALY)measures. A QALY is a universal health outcomemeasure applicable to all individuals and all diseases,which combines gains or losses in both life quantity(mortality) and life quality (morbidity) and enablescomparisons across diseases and programs. QALYsare widely used for cost-utility analysis [282]. In thepast decades, economic evaluation has beenincreasingly important for the decision maker to decidewhich treatment or intervention is more cost-effective,in order to allocate limited healthcare resourcessoundly. Economic evaluation aims to compareinterventions in terms of their costs and benefits,
XII. TYPES OF PRO MEASURES

403
including their patient outcome impact. Health benefitscan be quantified as QALYs (pronounced “qualies”),which has become a standard measure and is nowrecommended in most of health economics guidelinesas the method of choice [283]. The economic chaptercontains additional information regarding QALYs, asdo the following references: [284, 285].
2. SUMMARY
In summary, some general points to consider inselecting PRO measures for lower urinary tract andpelvic floor disorder studies:
• Ensure that the PRO research questions and studyendpoints are clearly defined. Determine the PROsthat are most crucial to assess and which are mostlikely to be affected by a particular condition and/orits treatment.
• Make good use of prior literature searches inidentifying past research in the area(s) of interest,as well as in identifying the types of PRO measuresother researchers have used in past work. Thisinformation can provide valuable information onhow particular outcome measures have performedin previous populations, as well as provideadditional information to assist in defining researchquestions/issues regarding the PRO componentsof any given study.
• Consider the characteristics of the population inselecting measures. For example, are the studysubjects to be children or older adults, well educatedvs. those with limited education, or persons withlow literacy? Ensure that the mode of data collectionis appropriate for use with the study population.Furthermore, do not assume that an instrumentvalidated for use with Caucasian, middle-classindividuals in the U.S. will be appropriate for usein other countries, and/or those of a lower socio-economic status or of different educationalbackgrounds. This chapter has indicated, wherepossible, the extent to which specific PROmeasures have been validated, and used reliablywith different populations.
• Use the questionnaires recommended in thischapter whenever possible. Do not “reinvent thewheel.” Developing new PROs is a time-consumingand complicated process. If a new scale needs tobe developed, ensure that the guidelines proposedby the FDA and EMEA on developing PROs arefollowed and that the appropriate expertise inquestionnaire development and psychometrics isavailable to your research team in order to guidethe questionnaire development process.
• Know the strengths and weaknesses of differenttypes of PRO measures. In general, genericmeasures are useful in providing information onmultiple patient outcome dimensions that can becompared across different populations. They may
lack sensitivity, however, in addressing concernsof specific patient populations (e.g., OAB, UI, faecalincontinence). Condition-specific instruments, incontrast, do address areas of function more specificto the condition, and tend to be more responsiveto changes in clinic status, due to their increasedspecificity in addressing the conditions of theirpatient populations. Weaknesses of condition-specific instruments, however, are that they areoften not appropriate for use with multiplepopulations, and cannot be used to make directcomparisons across different patient groups.
• Know how to score your selected PRO measuresand how to interpret the scores. Specifically, ensurethat the scoring method of a measure providesyou with the information you need to answer yourresearch question?
• Pilot testing of PRO measures with participants/patients similar to those in the target patientpopulation who will be assessed in a researchinvestigation is always advisable. Adjustments canthen be made in the protocol, if necessary, prior tothe initiation of the study.
• Finally, train and certify your staff to administerPRO measures using either patient interview and/orself-administration techniques, depending on themethod to be used in the study. The administrationprocess needs to be standardised and completelysimilarly across all participants.
The following recommendations were unanimous:
1. The selection of a PRO questionnaire must reflectstudy purpose and objectives
2. Grade A recommended questionnaires should beused in all clinical trials evaluating treatments
3. The inclusion of the ICIQ modules is preferredin all studies to standardise outcome assessment
4. Continued PRO development, refinement, anduse should accurately and adequately report onthe methods, samples, statistical analyses andpsychometric properties of questionnaires inscientific journals (i.e. validity, reliability andresponsiveness), so the quality of each studycan be assessed Researchers are encouragedto use existing questionnaires and refine forspecific populations when needed (e.g. frailelderly, children)
5. Researchers are encouranged to collaboratewith the ICIq project on the development andrefinement of modules and translations.
5B - F. RECOMMENDATIONS FORRESEARCH

404
1. Donovan JL NM, Gotoh M, et al. Symptom and quality of lifeassessment. . In: Abrams P KS, Wein AJ, editor. Incontinence:Plymouth: Health Publication Ltd; 1999. p. 295-332.
2. Donovan JL BX, Corcos J, et al. Symptoms and quality oflife assessment. In: Abraims P CL, Koury S, Wein A, editor.Incontinence: Plymouth: Health Publication Ltd; 2002. p.267-316.
3. Food & Drug Administration (FDA). Guidance for indsutry- patient-reported outcome measures: Use in medical productdevelopment to support labeling claims.: Silver Spring, MD:FDA; February 2006.
4. Jenkinson C, Lawrence K, McWhinnie D, Gordon J. Sensitivityto change of health status measures in a randomizedcontrolled trial: comparison of the COOP charts and the SF-36. Qual Life Res. 1995 Feb;4(1):47-52.
5. Murawski MM, Miederhoff PA. On the generalizability ofstatistical expressions of health related quality of lifeinstrument responsiveness: a data synthesis. Qual Life Res.1998 Jan;7(1):11-22.
6. Kazis LE, Anderson JJ, Meenan RF. Effect sizes forinterpreting changes in health status. Med Care. 1989Mar;27(3 Suppl):S178-89.
7. Guyatt GH, Juniper EF, Walter SD, Griffith LE, GoldsteinRS. Interpreting treatment effects in randomised trials. Bmj.1998 Feb 28;316(7132):690-3.
8. Jaeschke R, Singer J, Guyatt GH. Measurement of healthstatus. Ascertaining the minimal clinically important difference.Control Clin Trials. 1989 Dec;10(4):407-15.
9. Naughton MJ SS. Assessment of health-related quality of life.In: CD F, editor. Fundamentals of Clinical Trials: St. Louis:Mosby Press; 1996. p. 185.
10. World H. Definition of Health: Geneva:WHO; 1978.
11. Gill TM, Feinstein AR. A critical appraisal of the quality ofquality-of-life measurements. Jama. 1994 Aug 24-31;272(8):619-26.
12. McGee HM, O'Boyle CA, Hickey A, O'Malley K, Joyce CR.Assessing the quality of life of the individual: the SEIQoL witha healthy and a gastroenterology unit population. PsycholMed. 1991 Aug;21(3):749-59.
13. Witjes WP, de la Rosette JJ, Donovan JL, et al. TheInternational Continence Society "Benign ProstaticHyperplasia" Study: international differences in lower urinarytract symptoms and related bother. J Urol. 1997Apr;157(4):1295-300.
14. Guess HA, Chute CG, Garraway WM, et al. Similar levelsof urological symptoms have similar impact on Scottish andAmerican men--although Scots report less symptoms. JUrol. 1993 Nov;150(5 Pt 2):1701-5.
15. Herdman M, Fox-Rushby J, Badia X. A model of equivalencein the cultural adaptation of HRQoL instruments: theuniversalist approach. Qual Life Res. 1998 May;7(4):323-35.
16. European Agency for the Evaluation of Medicinal ProductsCfPMP. Note for guidance on the clinical investigation ofmedicinal productsfor the treatment of urinary incontinence.: London; December 2002. Report No.: Report No.:CPMP/EWP/18/01.
17. Aaronson NK. Quality of life assessment in clinical trials:methodologic issues. Control Clin Trials. 1989 Dec;10(4Suppl):195S-208S.
18. Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, AbramsP. ICIQ: a brief and robust measure for evaluating thesymptoms and impact of urinary incontinence. NeurourolUrodyn. 2004;23(4):322-30.
19. Abrams P, Avery K, Gardener N, Donovan J. The InternationalConsultation on Incontinence Modular Questionnaire:www.iciq.net. J Urol. 2006 Mar;175(3 Pt 1):1063-6; discussion6.
20. Abrams P, Artibani W, Gajewski JB, Hussain I. Assessmentof treatment outcomes in patients with overactive bladder:importance of objective and subjective measures. Urology.2006 Aug;68(2 Suppl):17-28.
21. Fairclough DL. Patient reported outcomes as endpoints inmedical research. Stat Methods Med Res. 2004Apr;13(2):115-38.
22. Brookes ST, Donovan JL, Wright M, Jackson S, Abrams P.A scored form of the Bristol Female Lower Urinary TractSymptoms questionnaire: data from a randomized controlledtrial of surgery for women with stress incontinence. Am JObstet Gynecol. 2004 Jul;191(1):73-82.
23. Jackson S, Donovan J, Brookes S, Eckford S, SwithinbankL, Abrams P. The Bristol Female Lower Urinary TractSymptoms questionnaire: development and psychometrictesting. Br J Urol. 1996 Jun;77(6):805-12.
24. Kelleher CJ, Cardozo LD, Khullar V, Salvatore S. A newquestionnaire to assess the quality of life of urinary incontinentwomen. Br J Obstet Gynaecol. 1997 Dec;104(12):1374-9.
25. Donovan JL, Peters TJ, Abrams P, Brookes ST, de aa RosetteJJ, Schafer W. Scoring the short form ICSmaleSFquestionnaire. International Continence Society. J Urol. 2000Dec;164(6):1948-55.
26. Donovan JL, Abrams P, Peters TJ, et al. The ICS-'BPH'Study: the psychometric validity and reliability of the ICSmalequestionnaire. Br J Urol. 1996 Apr;77(4):554-62.
27. Donovan JL, Brookes ST, de la Rosette JJ, et al. Theresponsiveness of the ICSmale questionnaire to outcome:evidence from the ICS-'BPH' study. BJU Int. 1999Feb;83(3):243-8.
28. Abraham L, Hareendran A, Mills IW, et al. Development andvalidation of a quality-of-life measure for men with nocturia.Urology. 2004 Mar;63(3):481-6.
29. Coyne K, Revicki D, Hunt T, et al. Psychometric validationof an overactive bladder symptom and health-related qualityof life questionnaire: the OAB-q. Qual Life Res. 2002Sep;11(6):563-74.
30. Price N, Jackson SR, Avery K, Brookes ST, Abrams P.Development and psychometric evaluation of the ICIQ VaginalSymptoms Questionnaire: the ICIQ-VS. Bjog. 2006Jun;113(6):700-12.
31. Romano SV, Metrebian SE, Vaz F, et al. An adjustable malesling for treating urinary incontinence after prostatectomy:a phase III multicentre trial. BJU Int. 2006 Mar;97(3):533-9.
32. Suardi N, Scattoni V, Briganti A, et al. Nerve-sparing radicalretropubic prostatectomy in patients previously submittedto holmium laser enucleation of the prostate for bladderoutlet obstruction due to benign prostatic enlargement. EurUrol. 2008 Jun;53(6):1180-5.
33. Araki I, Beppu M, Kajiwara M, et al. Prevalence and impacton generic quality of life of urinary incontinence in Japaneseworking women: assessment by ICI questionnaire and SF-36 Health Survey. Urology. 2005 Jul;66(1):88-93.
34. Cetinel B, Demirkesen O, Tarcan T, et al. Hidden femaleurinary incontinence in urology and obstetrics and gynecologyoutpatient clinics in Turkey: what are the determinants ofbothersome urinary incontinence and help-seeking behavior?Int Urogynecol J Pelvic Floor Dysfunct. 2007 Jun;18(6):659-64.
35. Meschia M, Bertozzi R, Pifarotti P, et al. Peri-operativemorbidity and early results of a randomised trial comparingTVT and TVT-O. Int Urogynecol J Pelvic Floor Dysfunct.2007 Nov;18(11):1257-61.
REFERENCES

405
36. Bent AE, Gousse AE, Hendrix SL, et al. Duloxetine comparedwith placebo for the treatment of women with mixed urinaryincontinence. Neurourol Urodyn. 2008;27(3):212-21.
37. Suzuki T, Yasuda K, Yamanishi T, et al. Randomized, double-blind, sham-controlled evaluation of the effect of functionalcontinuous magnetic stimulation in patients with urgencyincontinence. Neurourol Urodyn. 2007;26(6):767-72.
38. Franco AV, Lee F, Fynes MM. Is there an alternative to padtests? Correlation of subjective variables of severity of urinaryloss to the 1-h pad test in women with stress urinaryincontinence. BJU Int. 2008 Aug 5;102(5):586-90.
39. Seckiner I, Yesilli C, Mungan NA, Aykanat A, Akduman B.Correlations between the ICIQ-SF score and urodynamicfindings. Neurourol Urodyn. 2007;26(4):492-4.
40. Bo K, Talseth T, Vinsnes A. Randomized controlled trial onthe effect of pelvic floor muscle training on quality of life andsexual problems in genuine stress incontinent women. ActaObstet Gynecol Scand. 2000 Jul;79(7):598-603.
41. Sung MS, Hong JY, Choi YH, Baik SH, Yoon H. FES-biofeedback versus intensive pelvic floor muscle exercise forthe prevention and treatment of genuine stress incontinence.J Korean Med Sci. 2000 Jun;15(3):303-8.
42. Swithinbank LV, Abrams P. The impact of urinary incontinenceon the quality of life of women. World J Urol. 1999Aug;17(4):225-9.
43. Swithinbank LV, Donovan JL, du Heaume JC, et al. Urinarysymptoms and incontinence in women: relationships betweenoccurrence, age, and perceived impact. Br J Gen Pract.1999 Nov;49(448):897-900.
44. Swithinbank LV, Donovan JL, Rogers CA, Abrams P.Nocturnal incontinence in women: a hidden problem. J Urol.2000 Sep;164(3 Pt 1):764-6.
45. Temml C, Haidinger G, Schmidbauer J, Schatzl G,Madersbacher S. Urinary incontinence in both sexes:prevalence rates and impact on quality of life and sexual life.Neurourol Urodyn. 2000;19(3):259-71.
46. Hansen BJ, Flyger H, Brasso K, et al. Validation of the self-administered Danish Prostatic Symptom Score (DAN-PSS-1) system for use in benign prostatic hyperplasia. Br J Urol.1995 Oct;76(4):451-8.
47. Meyhoff HH, Hald T, Nordling J, Andersen JT, Bilde T, WalterS. A new patient weighted symptom score system (DAN-PSS-1). Clinical assessment of indications and outcomes oftransurethral prostatectomy for uncomplicated benignprostatic hyperplasia. Scand J Urol Nephrol. 1993;27(4):493-9.
48. Flyger HL, Kallestrup EB, Mortensen SO. Validation of acomputer version of the patient-administered Danish prostaticsymptom score questionnaire. Scand J Urol Nephrol. 2001Jun;35(3):196-9.
49. Abrams P, Donovan JL, de la Rosette JJ, Schafer W.International Continence Society "Benign ProstaticHyperplasia" Study: background, aims, and methodology.Neurourol Urodyn. 1997;16(2):79-91.
50. Olsson LE, Salomon L, Nadu A, et al. Prospective patient-reported continence after laparoscopic radical prostatectomy.Urology. 2001 Oct;58(4):570-2.
51. Bertaccini A, Vassallo F, Martino F, et al. Symptoms,bothersomeness and quality of life in patients with LUTSsuggestive of BPH. Eur Urol. 2001;40 Suppl 1:13-8.
52. Gacci M, Bartoletti R, Figlioli S, et al. Urinary symptoms,quality of life and sexual function in patients with benignprostatic hypertrophy before and after prostatectomy: aprospective study. BJU Int. 2003 Feb;91(3):196-200.
53. Joshi HB, Newns N, Stainthorpe A, MacDonagh RP, KeeleyFX, Jr., Timoney AG. Ureteral stent symptom questionnaire:
development and validation of a multidimensional quality oflife measure. J Urol. 2003 Mar;169(3):1060-4.
54. Joshi HB, Okeke A, Newns N, Keeley FX, Jr., Timoney AG.Characterization of urinary symptoms in patients with ureteralstents. Urology. 2002 Apr;59(4):511-6.
55. Joshi HB, Stainthorpe A, MacDonagh RP, Keeley FX, Jr.,Timoney AG, Barry MJ. Indwelling ureteral stents: evaluationof symptoms, quality of life and utility. J Urol. 2003Mar;169(3):1065-9; discussion 9.
56. Foley CL, Bott SR, Thomas K, Parkinson MC, Kirby RS. Alarge prostate at radical retropubic prostatectomy does notadversely affect cancer control, continence or potency rates.BJU Int. 2003 Sep;92(4):370-4.
57. Hara I, Kawabata G, Miyake H, et al. Comparison of qualityof life following laparoscopic and open prostatectomy forprostate cancer. J Urol. 2003 Jun;169(6):2045-8.
58. Lee PS, Reid DW, Saltmarche A, Linton L. Measuring thepsychosocial impact of urinary incontinence: the YorkIncontinence Perceptions Scale (YIPS). J Am Geriatr Soc.1995 Nov;43(11):1275-8.
59. Shumaker SA, Wyman JF, Uebersax JS, McClish D, FantlJA. Health-related quality of life measures for women withurinary incontinence: the Incontinence Impact Questionnaireand the Urogenital Distress Inventory. Continence Programin Women (CPW) Research Group. Qual Life Res. 1994Oct;3(5):291-306.
60. Wyman JF, Harkins SW, Choi SC, Taylor JR, Fantl JA.Psychosocial impact of urinary incontinence in women.Obstet Gynecol. 1987 Sep;70(3 Pt 1):378-81.
61. Corcos J, Behlouli H, Beaulieu S. Identifying cut-off scoreswith neural networks for interpretation of the incontinenceimpact questionnaire. Neurourol Urodyn. 2002;21(3):198-203.
62. Dmochowski RR, Sand PK, Zinner NR, Gittelman MC, DavilaGW, Sanders SW. Comparative efficacy and safety oftransdermal oxybutynin and oral tolterodine versus placeboin previously treated patients with urge and mixed urinaryincontinence. Urology. 2003 Aug;62(2):237-42.
63. Dowd T, Kolcaba K, Steiner R. Correlations among measuresof bladder function and comfort. J Nurs Meas. 2002 Spring-Summer;10(1):27-38.
64. Hagen S, Hanley J, Capewell A. Test-retest reliability, validity,and sensitivity to change of the urogenital distress inventoryand the incontinence impact questionnaire. Neurourol Urodyn.2002;21(6):534-9.
65. Sander P, Thyssen HH, Lose G, Andersen JT. [The effect ofa vaginal device on urinary leakage and quality of life ofwomen with stress urinary incontinence]. Ugeskr Laeger.2000 May 22;162(21):3038-41.
66. Tibaek S, Jensen R, Lindskov G, Jensen M. Can quality oflife be improved by pelvic floor muscle training in women withurinary incontinence after ischemic stroke? A randomised,controlled and blinded study. Int Urogynecol J Pelvic FloorDysfunct. 2004 Mar-Apr;15(2):117-23; discussion 23.
67. Yu HJ, Wong WY, Chen J, Chie WC. Quality of life impactand treatment seeking of Chinese women with urinaryincontinence. Qual Life Res. 2003 May;12(3):327-33.
68. Blanc E, Hermieu JF, Ravery V, Moulinier F, Delmas V,Boccon-Gibod L. [Value of the use of a questionnaire in theevaluation of incontinence surgery]. Prog Urol. 1999Feb;9(1):88-94.
69. FitzGerald MP, Kenton K, Shott S, Brubaker L.Responsiveness of quality of life measurements to changeafter reconstructive pelvic surgery. Am J Obstet Gynecol. 2001Jul;185(1):20-4.
70. O'Connor RC, Kuznetsov DD, Patel RV, Galocy RM,

406
Steinberg GD, Bales GT. Artificial urinary sphincter placementin men after cystectomy with orthotopic ileal neobladder:continence, complications, and quality of life. Urology. 2002Apr;59(4):542-5.
71. Pang MW, Chan LW, Yip SK. One-year urodynamic outcomeand quality of life in patients with concomitant tension-freevaginal tape during pelvic floor reconstruction surgery forgenitourinary prolapse and urodynamic stress incontinence.Int Urogynecol J Pelvic Floor Dysfunct. 2003 Oct;14(4):256-60; discussion 9-60.
72. Richter HE, Burgio KL, Holley RL, et al. Cadaveric fascia latasling for stress urinary incontinence: a prospective quality-of-life analysis. Am J Obstet Gynecol. 2003 Dec;189(6):1590-5; discussion 5-6.
73. Vassallo BJ, Kleeman SD, Segal JL, Walsh P, Karram MM.Tension-free vaginal tape: a quality-of-life assessment. ObstetGynecol. 2002 Sep;100(3):518-24.
74. Woodman PJ, Misko CA, Fischer JR. The use of short-formquality of life questionnaires to measure the impact ofimipramine on women with urge incontinence. Int UrogynecolJ Pelvic Floor Dysfunct. 2001;12(5):312-5; discussion 5-6.
75. Wagner TH, Patrick DL, Bavendam TG, Martin ML, BueschingDP. Quality of life of persons with urinary incontinence:development of a new measure. Urology. 1996 Jan;47(1):67-71; discussion -2.
76. Chaisaeng S, Santingamkun A, Opanuraks J, RatchanonS, Bunyaratavej C. IQOL: translation & reliability for use withurinary incontinence patients in Thailand. J Med Assoc Thai.2006 Sep;89 Suppl 3:S33-9.
77. Oh SJ PH, Lim SH, Hong SK, Kim SW, Kim HH, Paick JS.Translation and linguistic validation of Korean version of theIncontinence quality of life(I-QoL) instrument. J KoreanContinence Soc. December 2002 6(2):10-23.
78. Patrick DL, Martin ML, Bushnell DM, Yalcin I, Wagner TH,Buesching DP. Quality of life of women with urinaryincontinence: further development of the incontinence qualityof life instrument (I-QOL). Urology. 1999 Jan;53(1):71-6.
79. Badia L CD, Conejero S. Validity of the King's Healthquestionnaire in the assessment of quality of life of patientswith urinary incontinence. The King's Group. Med Clin (Barc)2000 May 6;114(17):647-52.
80. Okamura K, Usami T, Nagahama K, Maruyama S, Mizuta E."Quality of life" assessment of urination in elderly Japanesemen and women with some medical problems usingInternational Prostate Symptom Score and King's HealthQuestionnaire. Eur Urol. 2002 Apr;41(4):411-9.
81. Yip SK, Chan A, Pang S, et al. The impact of urodynamicstress incontinence and detrusor overactivity on maritalrelationship and sexual function. Am J Obstet Gynecol. 2003May;188(5):1244-8.
82. Homma YAT, Yoshida M, et al. Validation of Japanese versionof QOL questionnaire for urinary incontinence. Journal ofNBS. 2002;13:247-2.
83. Homma Y GM, Ando T, Fukuhara S. Development of theJapanese version of QOL questionnaires for urinaryincontinence. Jpn J NBS. 1999;10:225-36.
84. Tamanini JT, D'Ancona CA, Botega NJ, Rodrigues Netto N,Jr. [Validation of the Portuguese version of the King's HealthQuestionnaire for urinary incontinent women]. Rev SaudePublica. 2003 Apr;37(2):203-11.
85. Liu JF, Wang QZ, Hou J. Surgical treatment for cancer of theoesophagus and gastric cardia in Hebei, China. Br J Surg.2004 Jan;91(1):90-8.
86. Plachta Z, Adamiak A, Jankiewicz K, Skorupski P, RechbergerT. [Quality of life after mid-urethra polypropylene tape slingsurgery (IVS, TVT) in female stress urinary incontinence].Ginekol Pol. 2003 Sep;74(9):986-91.
87. Rufford J, Hextall A, Cardozo L, Khullar V. A double-blindplacebo-controlled trial on the effects of 25 mg estradiolimplants on the urge syndrome in postmenopausal women.Int Urogynecol J Pelvic Floor Dysfunct. 2003 Jun;14(2):78-83.
88. Wang AC, Wang YY, Chen MC. Single-blind, randomized trialof pelvic floor muscle training, biofeedback-assisted pelvicfloor muscle training, and electrical stimulation in themanagement of overactive bladder. Urology. 2004Jan;63(1):61-6.
89. Kelleher CJ, Pleil AM, Reese PR, Burgess SM, Brodish PH.How much is enough and who says so? The case of heKing's Health Questionnaire and overactive bladder. BritishJournal of Gynaecology. 2004;111:605-12.
90. Shaw C, Matthews RJ, Perry SI, et al. Validity and reliabilityof a questionnaire to measure the impact of lower urinary tractsymptoms on quality of life: the Leicester Impact Scale.Neurourol Urodyn. 2004;23(3):229-36.
91. Coyne KS, Matza LS, Thompson C, Jumadilova Z, BavendamT. The responsiveness of the OAB-q among OAB patientsubgroups. Neurourol Urodyn. 2007;26(2):196-203.
92. Coyne KS, Matza LS, Thompson CL, Kopp ZS, Khullar V.Determining the importance of change in the overactivebladder questionnaire. J Urol. 2006 Aug;176(2):627-32;discussion 32.
93. Yang Y, Brazier J, Tsuchiya A, Coyne K. Estimating aPreference-Based Single Index from the Overactive BladderQuestionnaire. Value Health. 2008 Jul 18.
94. Coyne K, Lai JS, Zyczynski T, Kopp Z, Avery K, Abrams P.An overactive bladder symptom and quality-of-life short form:development of the overactive bladder questionnaire (OAB-q) short form (SF). ICS. Paris, France; 2004.
95. Coyne KS, Zyczynski T, Margolis MK, Elinoff V, Roberts RG.Validation of an overactive bladder awareness tool for usein primary care settings. Adv Ther. 2005 Jul-Aug;22(4):381-94.
96. Palleschi G, Pastore AL, Stocchi F, et al. Correlation betweenthe Overactive Bladder questionnaire (OAB-q) andurodynamic data of Parkinson disease patients affected byneurogenic detrusor overactivity during antimuscarinictreatment. Clin Neuropharmacol. 2006 Jul-Aug;29(4):220-9.
97. Robinson D, Pearce KF, Preisser JS, Dugan E, Suggs PK,Cohen SJ. Relationship between patient reports of urinaryincontinence symptoms and quality of life measures. ObstetGynecol. 1998 Feb;91(2):224-8.
98. Roovers JP, van der Vaart CH, van der Bom JG, van LeeuwenJH, Scholten PC, Heintz AP. A randomised controlled trialcomparing abdominal and vaginal prolapse surgery: effectson urogenital function. Bjog. 2004 Jan;111(1):50-6.
99. Simons AM, Dowell CJ, Bryant CM, Prashar S, Moore KH.Use of the Dowell Bryant Incontinence Cost Index as a post-treatment outcome measure after non-surgical therapy.Neurourol Urodyn. 2001;20(1):85-93.
100. Dugan E, Cohen SJ, Robinson D, et al. The quality of lifeof older adults with urinary incontinence: determining genericand condition-specific predictors. Qual Life Res. 1998May;7(4):337-44.
101. Uebersax JS, Wyman JF, Shumaker SA, McClish DK, FantlJA. Short forms to assess life quality and symptom distressfor urinary incontinence in women: the Incontinence ImpactQuestionnaire and the Urogenital Distress Inventory.Continence Program for Women Research Group. NeurourolUrodyn. 1995;14(2):131-9.
102. Amarenco G, Arnould B, Carita P, Haab F, Labat JJ, RichardF. European psychometric validation of the CONTILIFE: aQuality of Life questionnaire for urinary incontinence. EurUrol. 2003 Apr;43(4):391-404.

407
103. Lukacz ES, Lawrence JM, Buckwalter JG, Burchette RJ,Nager CW, Luber KM. Epidemiology of prolapse andincontinence questionnaire: validation of a new epidemiologicsurvey. Int Urogynecol J Pelvic Floor Dysfunct. 2005 Jul-Aug;16(4):272-84.
104. Abdel-Fattah M, Ramsay I, Barrington JW. A simple visualanalogue scale to assess the quality of life in women withurinary incontinence. Eur J Obstet Gynecol Reprod Biol.2007 Jul;133(1):86-9.
105. Donovan JL, Kay HE, Peters TJ, et al. Using the ICSOoLto measure the impact of lower urinary tract symptoms onquality of life: evidence from the ICS-'BPH' Study.International Continence Society--Benign ProstaticHyperplasia. Br J Urol. 1997 Nov;80(5):712-21.
106. Bjelic-Radisic V, Dorfer M, Tamussino K, et al. TheIncontinence Outcome Questionnaire: an instrument forassessing patient-reported outcomes after surgery for stressurinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct.2007 Oct;18(10):1139-49.
107. Bushnell DM, Martin ML, Summers KH, Svihra J, Lionis C,Patrick DL. Quality of life of women with urinary incontinence:cross-cultural performance of 15 language versions of theI-QOL. Qual Life Res. 2005 Oct;14(8):1901-13.
108. Reese PR, Pleil AM, Okano GJ, Kelleher CJ. Multinationalstudy of reliability and validity of the King's HealthQuestionnaire in patients with overactive bladder. Qual LifeRes. 2003 Jun;12(4):427-42.
109. Robinson JP, Avi-Itzhak T, McCorkle R. Psychometricproperties of the Male Urogenital Distress Inventory (MUDI)and Male Urinary Symptom Impact Questionnaire (MUSIQ)in patients following radical prostatectomy. Urol Nurs. 2007Dec;27(6):512-8.
110. Robinson JP, Shea JA. Development and testing of ameasure of health-related quality of life for men with urinaryincontinence. J Am Geriatr Soc. 2002 May;50(5):935-45.
111. Hendriks EJ, Bernards AT, Berghmans BC, de Bie RA. Thepsychometric properties of the PRAFAB-questionnaire: abrief assessment questionnaire to evaluate severity ofurinary incontinence in women. Neurourol Urodyn.2007;26(7):998-1007.
112. Hendriks EJ, Bernards AT, de Bie RA, de Vet HC. Theminimal important change of the PRAFAB questionnaire inwomen with stress urinary incontinence: results from aprospective cohort study. Neurourol Urodyn. 2008;27(5):379-87.
113. Hendriks EJ, Bernards AT, Staal JB, de Vet HC, de Bie RA.Factorial validity and internal consistency of the PRAFABquestionnaire in women with stress urinary incontinence.BMC Urol. 2008;8:1.
114. Rai GS, Kiniors M, Wientjes H. Urinary incontinencehandicap inventory. Arch Gerontol Geriatr. 1994 Jul-Aug;19(1):7-10.
115. Stach-Lempinen B, Kujansuu E, Laippala P, Metsanoja R.Visual analogue scale, urinary incontinence severity scoreand 15 D--psychometric testing of three different health-related quality-of-life instruments for urinary incontinentwomen. Scand J Urol Nephrol. 2001 Dec;35(6):476-83.
116. Coyne KS ML, Versi E. Urinary Urgency: Can “Gotta Go”Be Measured? 10th Annual Conference of the InternationalSociety for Quality of Life Research. Prague, CzechRepublic: Quality of Life Research; 2003. p. 828.
117. Matza LS, Thompson CL, Krasnow J, Brewster-Jordan J,Zyczynski T, Coyne KS. Test-retest reliability of fourquestionnaires for patients with overactive bladder: theoveractive bladder questionnaire (OAB-q), patient perceptionof bladder condition (PPBC), urgency questionnaire (UQ),and the primary OAB symptom questionnaire (POSQ).Neurourol Urodyn. 2005;24(3):215-25.
118. Lukacs B, Comet D, Grange JC, Thibault P. Constructionand validation of a short-form benign prostatic hypertrophyhealth-related quality-of-life questionnaire. BPH Group inGeneral Practice. Br J Urol. 1997 Nov;80(5):722-30.
119. Krowinski W, Steiber S. Measuring patient satisfacion. 2nded: American Hospital Publishing; 1996.
120. Weaver M, Patrick DL, Markson LE, Martin D, Frederic I,Berger M. Issues in the measurement of satisfaction withtreatment. Am J Manag Care. 1997 Apr;3(4):579-94.
121. Pleil AM, Coyne KS, Reese PR, Jumadilova Z, Rovner ES,Kelleher CJ. The validation of patient-rated globalassessments of treatment benefit, satisfaction, andwillingness to continue--the BSW. Value Health. 2005 Nov-Dec;8 Suppl 1:S25-34.
122. Piault E, Evans CJ, Espindle D, Kopp Z, Brubaker L, AbramsP. Development and validation of the Overactive BladderSatisfaction (OAB-S) Questionnaire. Neurourol Urodyn.2008;27(3):179-90.
123. Piault E EC, Marcucci G, Kopp Z, Brubaker L and AbramsP. Patient satisfaction: international development,translatability assessment and linguistic validation of theOAB-S, an overactive bladder treatment satisfactionquestionnaire. ISPOR 8th Annual European Congress.Florence, Italy: Value in Health; 2005. p. A88.
124. Conway K AC, Uzun V, Kopp Z and Coyne K. Linguisticvalidation of the overactive bladder questionnaire (OAB-q),OAB-q SF and the overactive bladder-validated 8 (OABV8) screening questionnaire for this condition in Europe, Asia,North America, and South America. 30th Annual Meetingof the International Urogynecological Association (IUGA).Copenhagen, Denmark: Int Urogynecol J; 2005. p. S103-4.
125. Burgio KL, Goode PS, Richter HE, Locher JL, Roth DL.Global ratings of patient satisfaction and perceptions ofimprovement with treatment for urinary incontinence:validation of three global patient ratings. Neurourol Urodyn.2006;25(5):411-7.
126. Colman S, Chapple C, Nitti V, Haag-Molkenteller C, HastedtC, Massow U. Validation of treatment benefit scale forassessing subjective outcomes in treatment of overactivebladder. Urology. 2008 Oct;72(4):803-7.
127. Shaw C, Matthews RJ, Perry SI, et al. Validity and reliabilityof an interviewer-administered questionnaire to measure theseverity of lower urinary tract symptoms of storageabnormality: the Leicester Urinary Symptom Questionnaire.BJU Int. 2002 Aug;90(3):205-15.
128. Bradley CS, Rovner ES, Morgan MA, et al. A newquestionnaire for urinary incontinence diagnosis in women:development and testing. Am J Obstet Gynecol. 2005Jan;192(1):66-73.
129. Basra R, Artibani W, Cardozo L, et al. Design and validationof a new screening instrument for lower urinary tractdysfunction: the bladder control self-assessmentquestionnaire (B-SAQ). Eur Urol. 2007 Jul;52(1):230-7.
130. Gunthorpe W, Brown W, Redman S. The development andevaluation of an incontinence screening questionnaire forfemale primary care. Neurourol Urodyn. 2000;19(5):595-607.
131. Diokno AC, Brock BM, Brown MB, Herzog AR. Prevalenceof urinary incontinence and other urological symptoms inthe noninstitutionalized elderly. J Urol. 1986 Nov;136(5):1022-5.
132. Blaivas JG, Panagopoulos G, Weiss JP, Somaroo C.Validation of the overactive bladder symptom score. J Urol.2007 Aug;178(2):543-7; discussion 7.
133. Parsons CL, Dell J, Stanford EJ, et al. Increased prevalenceof interstitial cystitis: previously unrecognized urologic andgynecologic cases identified using a new symptomquestionnaire and intravesical potassium sensitivity. Urology.2002 Oct;60(4):573-8.

408
134. Brown JS, Bradley CS, Subak LL, et al. The sensitivity andspecificity of a simple test to distinguish between urge andstress urinary incontinence. Annals of internal medicine.2006 May 16;144(10):715-23.
135. Gaudenz R. [A questionnaire with a new urge-score andstress-score for the evaluation of female urinary incontinence(author's transl)]. Geburtshilfe Frauenheilkd. 1979Sep;39(9):784-92.
136. Haab F, Richard F, Amarenco G, et al. Comprehensiveevaluation of bladder and urethral dysfunction symptoms:development and psychometric validation of the UrinarySymptom Profile (USP) questionnaire. Urology. 2008Apr;71(4):646-56.
137. Barry MJ, Fowler FJ, Jr., O'Leary MP, et al. The AmericanUrological Association symptom index for benign prostatichyperplasia. The Measurement Committee of the AmericanUrological Association. J Urol. 1992 Nov;148(5):1549-57;discussion 64.
138. Coyne KS, Matza LS, Kopp Z, Abrams P. The validation ofthe patient perception of bladder condition (PPBC): a single-item global measure for patients with overactive bladder. EurUrol. 2006 Jun;49(6):1079-86.
139. Capo JP, Jr., Laramee C, Lucente V, Fakhoury A, Forero-Schwanhaeuser S. Solifenacin treatment for overactivebladder in Hispanic patients: patient-reported symptombother and quality of life outcomes from the VESIcare Open-Label Trial. Int J Clin Pract. 2008 Jan;62(1):39-46.
140. Chapple C, DuBeau C, Ebinger U, Rekeda L, Viegas A.Darifenacin treatment of patients >or= 65 years withoveractive bladder: results of a randomized, controlled, 12-week trial. Curr Med Res Opin. 2007 Oct;23(10):2347-58.
141. Staskin DR, Rosenberg MT, Dahl NV, Polishuk PV, ZinnerNR. Effects of oxybutynin transdermal system on health-related quality of life and safety in men with overactivebladder and prostate conditions. Int J Clin Pract. 2008Jan;62(1):27-38.
142. Lemack GE, Zimmern PE. Predictability of urodynamicfindings based on the Urogenital Distress Inventory-6questionnaire. Urology. 1999 Sep;54(3):461-6.
143. Yalcin I, Bump RC. Validation of two global impressionquestionnaires for incontinence. Am J Obstet Gynecol.2003 Jul;189(1):98-101.
144. Barry MJ, Fowler FJ, Jr., O'Leary MP, Bruskewitz RC,Holtgrewe HL, Mebust WK. Measuring disease-specifichealth status in men with benign prostatic hyperplasia.Measurement Committee of The American UrologicalAssociation. Med Care. 1995 Apr;33(4 Suppl):AS145-55.
145. Black N, Griffiths J, Pope C. Development of a symptomseverity index and a symptom impact index for stressincontinence in women. Neurourol Urodyn. 1996;15(6):630-40.
146. Badia Llach X CDD, Perales Cabañas L, Pena Outeriño JM,Martínez-Agulló E, Conejero Sugrañés J, Arañó Beltrán P,Marqués Queimadelos A, Roset Gamisans M, PeruleroEscobar N. [The development and preliminary validation ofthe IU-4 questionnaire for the clinical classification of urinaryincontinence]. Actas Urol Esp. 1999;23(7):565-72.
147. Abrams P, Cardozo L, Fall M, et al. The standardisation ofterminology in lower urinary tract function: report from thestandardisation sub-committee of the InternationalContinence Society. Urology. 2003 Jan;61(1):37-49.
148. Brubaker L. Urgency: the cornerstone symptom of overactivebladder. Urology. 2004 Dec;64(6 Suppl 1):12-6.
149. Staskin DR. The urge to define urgency: a review of threeapproaches. Current urology reports. 2004 Dec;5(6):413-5.
150. Brubaker L. Urinary urgency and frequency: what should
a clinician do? Obstetrics and gynecology. 2005Mar;105(3):661-7.
151. Chapple CR, Wein AJ. The urgency of the problem and theproblem of urgency in the overactive bladder. BJU Int. 2005Feb;95(3):274-5.
152. Cardozo L, Coyne KS, Versi E. Validation of the urgencyperception scale. BJU Int. 2005 Mar;95(4):591-6.
153. Chapple CR, Artibani W, Cardozo LD, et al. The role ofurinary urgency and its measurement in the overactivebladder symptom syndrome: current concepts and futureprospects. BJU Int. 2005 Feb;95(3):335-40.
154. Bowden A CS, Sabounjian L, Sandage B, Schwiderski U andZayed H. Psychometric validation of an Urgency SeverityScale (IUSS) for patients with overactive bladder. 33rdAnnual Meeting of the International Continence Society.Florence, Italy: Neurourology and Urodynamics; 2003. p.531-2.
155. Brewster JL GZ, Green H, Jumadilova Z, Coyne K.Establishing the Content Validity Of The Urinary SensationScale (USS). International Society For Pharmacoeconomicsand Outcomes Research. Washington, DC: Value in Health;2005. p. 418-9.
156. Coyne KS ML, Thompson C, et al. A comparison of threeapproaches to analyze urinary urgency as a treatmentoutcome. 35th Annual Meeting of the InternationalContinence Society. Montreal, Canada; 2005.
157. Nixon A, Colman S, Sabounjian L, et al. A validated patientreported measure of urinary urgency severity in overactivebladder for use in clinical trials. J Urol. 2005 Aug;174(2):604-7.
158. Bent AE, Gousse AE, Hendrix SL, et al. Validation of a two-item quantitative questionnaire for the triage of women withurinary incontinence. Obstet Gynecol. 2005 Oct;106(4):767-73.
159. Blaivas JG, Panagopoulos G, Weiss JP, Somaroo C, ChaikinDC. The urgency perception score: validation and test-retest. J Urol. 2007 Jan;177(1):199-202.
160. DuBeau CE, Kiely DK, Resnick NM. Quality of life impactof urge incontinence in older persons: a new measure andconceptual structure. J Am Geriatr Soc. 1999 Aug;47(8):989-94.
161. European Agency for the Evaluation of Medicinal ProductsCfPMP. Note for Guidance on the Clinical Investigation ofMedicinal Products for the Treatment of Urinary Incontinencein Women. November 2001.
162. Coyne KS, Tubaro A, Brubaker L, Bavendam T. Developmentand validation of patient-reported outcomes measures foroveractive bladder: a review of concepts. Urology. 2006Aug;68(2 Suppl):9-16.
163. Al-Buheissi S, Khasriya R, Maraj BH, Malone-Lee J. Asimple validated scale to measure urgency. J Urol. 2008Mar;179(3):1000-5; discussion 5.
164. Mouritsen L, Larsen JP. Symptoms, bother and POPQ inwomen referred with pelvic organ prolapse. Int UrogynecolJ Pelvic Floor Dysfunct. 2003 Jun;14(2):122-7.
165. Swift SE, Tate SB, Nicholas J. Correlation of symptomswith degree of pelvic organ support in a general populationof women: what is pelvic organ prolapse? Am J ObstetGynecol. 2003 Aug;189(2):372-7; discussion 7-9.
166. Weber AM, Walters MD, Ballard LA, Booher DL, PiedmonteMR. Posterior vaginal prolapse and bowel function. Am JObstet Gynecol. 1998 Dec;179(6 Pt 1):1446-9; discussion9-50.
167. Barber MD, Kuchibhatla MN, Pieper CF, Bump RC.Psychometric evaluation of 2 comprehensive condition-specific quality of life instruments for women with pelvic
409
floor disorders. Am J Obstet Gynecol. 2001 Dec;185(6):1388-95.
168. de Tayrac R C-LA, Fernandez D, Fernandez H. Quality oflife instruments for women with pelvic organ prolapse. JGynecol Obstet Biol Reprod (Paris). 2003;32(6):503-23.
169. Barber MD, Walters MD, Cundiff GW. Responsiveness ofthe Pelvic Floor Distress Inventory (PFDI) and Pelvic FloorImpact Questionnaire (PFIQ) in women undergoing vaginalsurgery and pessary treatment for pelvic organ prolapse.Am J Obstet Gynecol. 2006 May;194(5):1492-8.
170. de Tayrac R, Deval B, Fernandez H, Mares P. [Developmentof a linguistically validated French version of two short-form, condition-specific quality of life questionnaires forwomen with pelvic floor disorders (PFDI-20 and PFIQ-7)].J Gynecol Obstet Biol Reprod (Paris). 2007 Dec;36(8):738-48.
171. Young AE, Fine PM, McCrery R, et al. Spanish languagetranslation of pelvic floor disorders instruments. IntUrogynecol J Pelvic Floor Dysfunct. 2007 Oct;18(10):1171-8.
172. Geller EJ, Barbee ER, Wu JM, Loomis MJ, Visco AG.Validation of telephone administration of 2 condition-specificquality-of-life questionnaires. Am J Obstet Gynecol. 2007Dec;197(6):632 e1-4.
173. Barber MD, Walters MD, Bump RC. Short forms of twocondition-specific quality-of-life questionnaires for womenwith pelvic floor disorders (PFDI-20 and PFIQ-7). Am JObstet Gynecol. 2005 Jul;193(1):103-13.
174. Radley SCJ, G. L. Kubwalo, B. E. Stevens, V. Leathard, A.Tanguy, E. Feasibility and acceptability of electronicinterviewing in urogynaecology. International UrogynecologyJournal. 2003;14(SUPP/1):239
175. Digesu GA, Santamato S, Khullar V, et al. Validation of anItalian version of the prolapse quality of life questionnaire.Eur J Obstet Gynecol Reprod Biol. 2003 Feb 10;106(2):184-92.
176. Ellerkmann RM, Cundiff GW, Melick CF, Nihira MA, LefflerK, Bent AE. Correlation of symptoms with location andseverity of pelvic organ prolapse. Am J Obstet Gynecol.2001 Dec;185(6):1332-7; discussion 7-8.
177. Radley SC, Jones GL, Tanguy EA, Stevens VG, Nelson C,Mathers NJ. Computer interviewing in urogynaecology:concept, development and psychometric testing of anelectronic pelvic floor assessment questionnaire in primaryand secondary care. Bjog. 2006 Feb;113(2):231-8.
178. Fernando RJ, Thakar R, Sultan AH, Shah SM, Jones PW.Effect of vaginal pessaries on symptoms associated withpelvic organ prolapse. Obstet Gynecol. 2006 Jul;108(1):93-9.
179. Jones GL, Radley SC, Lumb J, Jha S. Electronic pelvicfloor symptoms assessment: tests of data quality of ePAQ-PF. Int Urogynecol J Pelvic Floor Dysfunct. 2008Oct;19(10):1337-47.
180. Digesu GA, Khullar V, Cardozo L, Robinson D. Inter-observerreliability of digital vaginal examination using a four-gradescale in different patient positions. Int Urogynecol J PelvicFloor Dysfunct. 2008 Sep;19(9):1303-7.
181. Kobashi KC GE, Govier F, Hadley R, Luber K, Nitti V, et al.Development of a validated quality of life instrument forpatients with pelvic prolapse. In: Urol J, editor. AmericanUrological Association 95th Annual Meeting; 2000; Atlanta,Georgia; 2000. p. 76.
182. Carey M, Slack M, Higgs P, Wynn-Williams M, Cornish A.Vaginal surgery for pelvic organ prolapse using mesh anda vaginal support device. Bjog. 2008 Feb;115(3):391-7.
183. Baessler K, O'Neill SM, Maher CF, Battistutta D. Aninterviewer-administered validated female pelvic floor
questionnaire for community-based research. Menopause.2008 Sep-Oct;15(5):973-7.
184. Tamanini JT, Almeida FG, Girotti ME, Riccetto CL, PalmaPC, Rios LA. The Portuguese validation of the InternationalConsultation on Incontinence Questionnaire-VaginalSymptoms (ICIQ-VS) for Brazilian women with pelvic organprolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2008Oct;19(10):1385-91.
185. Mann CH, Radley SC, Begum G, et al. Constipation, faecalincontinence and urinary symptoms in women awaitinghysterectomy. J Obstet Gynaecol. 2000 Sep;20(5):530-2.
186. Radley S, Keighley MR, Radley SC, Mann CH. Boweldysfunction following hysterectomy. Br J Obstet Gynaecol.1999 Nov;106(11):1120-5.
187. Ramsch KD. Experiences with GCP in the pharmaceuticalindustry [corrected]. Methods Find Exp Clin Pharmacol.1993 May;15(4):237-40.
188. Henry DA, Johnston A, Dobson A, Duggan J. Fatal pepticulcer complications and the use of non-steroidal anti-inflammatory drugs, aspirin, and corticosteroids. Britishmedical journal (Clinical research ed. 1987 Nov14;295(6608):1227-9.
189. Engel AF, Kamm MA, Bartram CI, Nicholls RJ. Relationshipof symptoms in faecal incontinence to specific sphincterabnormalities. Int J Colorectal Dis. 1995;10(3):152-5.
190. Rockwood TH, Church JM, Fleshman JW, et al. FecalIncontinence Quality of Life Scale: quality of life instrumentfor patients with fecal incontinence. Diseases of the colonand rectum. 2000 Jan;43(1):9-16; discussion -7.
191. Bug GJ, Kiff ES, Hosker G. A new condition-specific health-related quality of life questionnaire for the assessment ofwomen with anal incontinence. Bjog. 2001 Oct;108(10):1057-67.
192. Hiller L, Bradshaw HD, Radley SC, Radley S. A scoringsystem for the assessment of bowel and lower urinary tractsymptoms in women. Bjog. 2002 Apr;109(4):424-30.
193. Hiller L, Radley S, Mann CH, et al. Development andvalidation of a questionnaire for the assessment of boweland lower urinary tract symptoms in women. Bjog. 2002Apr;109(4):413-23.
194. Jorge JM WS. Etiology and management of fecalincontinence. Dis Colon Rectum 1993;36(1):77-97.
195. Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospectivecomparison of faecal incontinence grading systems. Gut.1999 Jan;44(1):77-80.
196. Reilly WT, Talley NJ, Pemberton JH, Zinsmeister AR.Validation of a questionnaire to assess fecal incontinenceand associated risk factors: Fecal IncontinenceQuestionnaire. Dis Colon Rectum. 2000 Feb;43(2):146-53;discussion 53-4.
197. O'Keefe EA, Talley NJ, Tangalos EG, Zinsmeister AR. Abowel symptom questionnaire for the elderly. J Gerontol.1992 Jul;47(4):M116-21.
198. Cockell SJ, Oates-Johnson T, Gilmour DT, Vallis TM, TurnbullGK. Postpartum flatal and Fecal Incontinence Quality-of-LifeScale: a disease- and population-specific measure. QualHealth Res. 2003 Oct;13(8):1132-44.
199. Osterberg A, Graf W, Karlbom U, Pahlman L. Evaluation ofa questionnaire in the assessment of patients with faecalincontinence and constipation. Scand J Gastroenterol. 1996Jun;31(6):575-80.
200. Eypasch E, Williams JI, Wood-Dauphinee S, et al.Gastrointestinal Quality of Life Index: development, validationand application of a new instrument. Br J Surg. 1995Feb;82(2):216-22.
201. Borrie MJ, Davidson HA. Incontinence in institutions: costsand contributing factors. Cmaj. 1992 Aug 1;147(3):322-8.

410
202. Sandler RS. Epidemiology of irritable bowel syndrome in theUnited States. Gastroenterology. 1990 Aug;99(2):409-15.
203. Rust J, Golombok S. The Golombok-Rust Inventory ofSexual Satisfaction (GRISS). Br J Clin Psychol. 1985 Feb;24( Pt 1):63-4.
204. Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J,Mishra A. The international index of erectile function (IIEF):a multidimensional scale for assessment of erectiledysfunction. Urology. 1997 Jun;49(6):822-30.
205. Frankel SJ, Donovan JL, Peters TI, et al. Sexual dysfunctionin men with lower urinary tract symptoms. J Clin Epidemiol.1998 Aug;51(8):677-85.
206. Derogatis LR. The psychosocial adjustment to illness scale(PAIS). J Psychosom Res. 1986;30(1):77-91.
207. Lowe FC, Fagelman E. Phytotherapy in the treatment ofbenign prostatic hyperplasia. Curr Opin Urol. 1998Jan;8(1):27-9.
208. Taylor JF, Rosen RC, Leiblum SR. Self-report assessmentof female sexual function: psychometric evaluation of theBrief Index of Sexual Functioning for Women. Arch SexBehav. 1994 Dec;23(6):627-43.
209. Rosen R, Brown C, Heiman J, et al. The Female SexualFunction Index (FSFI): a multidimensional self-reportinstrument for the assessment of female sexual function.J Sex Marital Ther. 2000 Apr-Jun;26(2):191-208.
210. Symonds T, Boolell M, Quirk F. Development of aquestionnaire on sexual quality of life in women. Journal ofsex & marital therapy. 2005 Oct-Dec;31(5):385-97.
211. O'Leary MP, Fowler FJ, Lenderking WR, et al. A brief malesexual function inventory for urology. Urology. 1995Nov;46(5):697-706.
212. Trudel G, Ravart M, Matte B. The use of the multiaxialdiagnostic system for sexual dysfunctions in the assessmentof hypoactive sexual desire. J Sex Marital Ther. 1993Summer;19(2):123-30.
213. Clayton AH, McGarvey EL, Clavet GJ. The Changes inSexual Functioning Questionnaire (CSFQ): development,reliability, and validity. Psychopharmacol Bull.1997;33(4):731-45.
214. LoPiccolo J, Steger JC. The sexual interaction inventory:a new instrument for assessment of sexual dysfunction.Arch Sex Behav. 1974 Nov;3(6):585-95.
215. Hudson W. Index of sexual satisfaction. The clinicalmeasurement package: a field manual. Chicago: DorseyPress 1982. p. 190-1.
216. Adamson AS, Francis JL, Witherow RO, Snell ME. Urinarytissue factor levels in prostatic carcinoma: a potential markerof metastatic spread? Br J Urol. 1993 May;71(5):587-92.
217. McCoy N. The McCoy Female Sexuality QuestionnaireQuality of Life Research. 2000;9(Supplement 6):739-45.
218. Giberti C, Rovida S. Transvaginal bone-anchored syntheticsling for the treatment of stress urinary incontinence: anoutcomes analysis. Urology. 2000 Dec 20;56(6):956-61.
219. Walters MD, Taylor S, Schoenfeld LS. Psychosexual studyof women with detrusor instability. Obstet Gynecol. 1990Jan;75(1):22-6.
220. Rosen R, Altwein J, Boyle P, et al. Lower urinary tractsymptoms and male sexual dysfunction: the multinationalsurvey of the aging male (MSAM-7). Eur Urol. 2003Dec;44(6):637-49.
221. Woodward JM, Hass SL, Woodward PJ. Reliability andvalidity of the sexual life quality questionnaire (SLQQ). QualLife Res. 2002 Jun;11(4):365-77.
222. Hunt J MJ. Unwanted sexual experience and female urinaryincontinence. Br J Health Psychol 1996;1:91–4.
223. Tubaro A, Polito M, Giambroni L, Famulari C, Gange E,Ostardo E. Sexual function in patients with LUTS suggestiveof BPH. Eur Urol. 2001;40 Suppl 1:19-22.
224. Brookes ST, Donovan JL, Peters TJ, Abrams P, Neal DE.Sexual dysfunction in men after treatment for lower urinarytract symptoms: evidence from randomised controlled trial.Bmj. 2002 May 4;324(7345):1059-61.
225. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM.Development and evaluation of an abridged, 5-item versionof the International Index of Erectile Function (IIEF-5) as adiagnostic tool for erectile dysfunction. Int J Impot Res.1999 Dec;11(6):319-26.
226. Jackson S, Shepherd A, Brookes S, Abrams P. The effectof oestrogen supplementation on post-menopausal urinarystress incontinence: a double-blind placebo-controlled trial.Br J Obstet Gynaecol. 1999 Jul;106(7):711-8.
227. Rogers GR, Villarreal A, Kammerer-Doak D, Qualls C.Sexual function in women with and without urinaryincontinence and/or pelvic organ prolapse. Int UrogynecolJ Pelvic Floor Dysfunct. 2001;12(6):361-5.
228. Rogers RG, Kammerer-Doak D, Villarreal A, Coates K,Qualls C. A new instrument to measure sexual function inwomen with urinary incontinence or pelvic organ prolapse.Am J Obstet Gynecol. 2001 Mar;184(4):552-8.
229. Rogers RG, Coates KW, Kammerer-Doak D, Khalsa S,Qualls C. A short form of the Pelvic Organ Prolapse/UrinaryIncontinence Sexual Questionnaire (PISQ-12). IntUrogynecol J Pelvic Floor Dysfunct. 2003 Aug;14(3):164-8; discussion 8.
230. Romero AA, Hardart A, Kobak W, Qualls C, Rogers R.Validation of a Spanish version of the Pelvic Organ ProlapseIncontinence Sexual Questionnaire. Obstet Gynecol. 2003Nov;102(5 Pt 1):1000-5.
231. Botros SM, Abramov Y, Miller JJ, et al. Effect of parity onsexual function: an identical twin study. Obstet Gynecol.2006 Apr;107(4):765-70.
232. Brubaker L, Handa VL, Bradley CS, et al. Sexual function6 months after first delivery. Obstet Gynecol. 2008May;111(5):1040-4.
233. Brubaker L, Shott S, Tomezsko J, Goldberg RP. Pelvic floorfitness using lay instructors. Obstet Gynecol. 2008Jun;111(6):1298-304.
234. Jha S, Moran P, Greenham H, Ford C. Sexual functionfollowing surgery for urodynamic stress incontinence. IntUrogynecol J Pelvic Floor Dysfunct. 2007 Aug;18(8):845-50.
235. Komesu YM, Rogers RG, Kammerer-Doak DN, Barber MD,Olsen AL. Posterior repair and sexual function. Am J ObstetGynecol. 2007 Jul;197(1):101 e1-6.
236. Melin I, Falconer C, Rossner S, Altman D. Sexual functionin obese women: impact of lower urinary tract dysfunction.Int J Obes (Lond). 2008 Aug;32(8):1312-8.
237. Murphy M, van Raalte H, Mercurio E, Haff R, Wiseman B,Lucente VR. Incontinence-related quality of life and sexualfunction following the tension-free vaginal tape versus the"inside-out" tension-free vaginal tape obturator. IntUrogynecol J Pelvic Floor Dysfunct. 2008 Apr;19(4):481-7.
238. Rogers RG, Kammerer-Doak D, Darrow A, et al. Doessexual function change after surgery for stress urinaryincontinence and/or pelvic organ prolapse? A multicenterprospective study. Am J Obstet Gynecol. 2006 Nov;195(5):e1-4.
239. Sentilhes L, Berthier A, Sergent F, Verspyck E, DescampsP, Marpeau L. Sexual function in women before and aftertransvaginal mesh repair for pelvic organ prolapse. IntUrogynecol J Pelvic Floor Dysfunct. 2008 Jun;19(6):763-72.

411
240. Borello-France D, Dusi J, O'Leary M, et al. Test-retestreliability of the Urge-Urinary Distress Inventory and FemaleSexual Function Index in women with multiple sclerosis.Urol Nurs. 2008 Feb;28(1):30-5.
241. ter Kuile MM, Brauer M, Laan E. The Female SexualFunction Index (FSFI) and the Female Sexual DistressScale (FSDS): psychometric properties within a Dutchpopulation. J Sex Marital Ther. 2006 Jul-Sep;32(4):289-304.
242. Witting K, Santtila P, Jern P, et al. Evaluation of the femalesexual function index in a population based sample fromFinland. Arch Sex Behav. 2008 Dec;37(6):912-24.
243. Verit FF, Verit A, Yeni E. The prevalence of sexual dysfunctionand associated risk factors in women with chronic pelvic pain:a cross-sectional study. Arch Gynecol Obstet. 2006Aug;274(5):297-302.
244. Lombardi G, Mondaini N, Macchiarella A, Cilotti A, PopoloGD. Clinical female sexual outcome after sacralneuromodulation implant for lower urinary tract symptom(LUTS). J Sex Med. 2008 Jun;5(6):1411-7.
245. Kuhn A, Bapst D, Stadlmayr W, Vits K, Mueller MD. Sexualand organ function in patients with symptomatic prolapse:are pessaries helpful? Fertil Steril. 2008 Apr 12.
246. Nappi RE, Albani F, Vaccaro P, et al. Use of the Italiantranslation of the Female Sexual Function Index (FSFI) inroutine gynecological practice. Gynecol Endocrinol. 2008Apr;24(4):214-9.
247. Cohen BL, Barboglio P, Gousse A. The impact of lowerurinary tract symptoms and urinary incontinence on femalesexual dysfunction using a validated instrument. J Sex Med.2008 Jun;5(6):1418-23.
248. Sidi H, Abdullah N, Puteh SE, Midin M. The Female SexualFunction Index (FSFI): validation of the Malay version. Thejournal of sexual medicine. 2007 Nov;4(6):1642-54.
249. Kelleher CJ CL, Wise BG, Cutner A. The impact of urinaryincontinence on sexual function. Neurourology andUrodynamics. 1992;11(4):359-60.
250. Opjordsmoen S, Fossa SD. Quality of life in patients treatedfor penile cancer. A follow-up study. Br J Urol. 1994Nov;74(5):652-7.
251. Mazer NA, Leiblum SR, Rosen RC. The brief index of sexualfunctioning for women (BISF-W): a new scoring algorithmand comparison of normative and surgically menopausalpopulations. Menopause (New York, NY. 2000 Sep-Oct;7(5):350-63.
252. Coyne KS, Margolis MK, Brewster-Jordan J, SutherlandSE, Bavendam T, Rogers RG. Evaluating the impact ofoveractive bladder on sexual health in women: what isrelevant? The journal of sexual medicine. 2007 Jan;4(1):124-36.
253. Plouffe L, Jr. Screening for sexual problems through asimple questionnaire. Am J Obstet Gynecol. 1985 Jan15;151(2):166-9.
254. Watts RJ. Sexual functioning, health beliefs, and compliancewith high blood pressure medications. Nurs Res. 1982 Sep-Oct;31(5):278-83.
255. Stewart A WJ. Measuring functioning and well-being : themedical outcomes study approach Durham: Duke UniversityPress; 1992.
256. Helgason Á. Prostate Cancer Treatment and Quality of Life- a Three Level Epidemiological Approach Stockholm:Karolinska Institute; 1997.
257. Watkins-Bruner D, Scott C, Lawton C, et al. RTOG's firstquality of life study--RTOG 90-20: a phase II trial of externalbeam radiation with etanidazole for locally advanced prostatecancer. Int J Radiat Oncol Biol Phys. 1995 Nov 1;33(4):901-6.
258. Litwin MS, Hays RD, Fink A, et al. Quality-of-life outcomesin men treated for localized prostate cancer. Jama. 1995 Jan11;273(2):129-35.
259. Komatsu H, Kojima M, Suzuki K, et al. [Development of aquestionnaire to measure the effect of urinary incontinenceon female sexuality: a reliability and validity study]. KangoKenkyu. 1996;29(5):386-98.
260. Clark A, Romm J. Effect of urinary incontinence on sexualactivity in women. J Reprod Med. 1993 Sep;38(9):679-83.
261. DuBeau CE, Levy B, Mangione CM, Resnick NM. Theimpact of urge urinary incontinence on quality of life:importance of patients' perspective and explanatory style.Journal of the American Geriatrics Society. 1998Jun;46(6):683-92.
262. Kitagawa M FH, Fukuta K, Aso Y. A randomized studycomparing holmium laser resection of the prostate totransurethral resection of the prostate. BJU Int 1997;Suppl80:209.
263. Hellstrom L, Ekelund P, Milsom I, Mellstrom D. Theprevalence of urinary incontinence and use of incontinenceaids in 85-year-old men and women. Age Ageing. 1990Nov;19(6):383-9.
264. Costa P, Perrouin-Verbe B, Colvez A, et al. Quality of lifein spinal cord injury patients with urinary difficulties.Development and validation of qualiveen. Eur Urol. 2001Jan;39(1):107-13.
265. Bonniaud V, Bryant D, Parratte B, Gallien P, Guyatt G.Qualiveen: a urinary disorder-specific instrument for use inclinical trials in multiple sclerosis. Arch Phys Med Rehabil.2006 Dec;87(12):1661-3.
266. Bonniaud V, Jackowski D, Parratte B, et al. Quality of lifein multiple sclerosis patients with urinary disorders:discriminative validation of the English version of Qualiveen.Qual Life Res. 2005 Mar;14(2):425-31.
267. Pannek J, Mark R, Stohrer M, Schurch B. [Quality of life inGerman-speaking patients with spinal cord injuries andbladder dysfunctions. Validation of the German version ofthe Qualiveen questionnaire]. Urologe A. 2007Oct;46(10):1416-21.
268. D'Ancona CA, Tamanini JT, Botega N, et al. Quality of lifeof neurogenic patients: translation and validation of thePortuguese version of Qualiveen. Int Urol Nephrol; 2008June 5 [Epub ahead of print].
269. Bonniaud V, Bryant D, Parratte B, Guyatt G. Qualiveen, aurinary-disorder specific instrument: 0.5 corresponds to theminimal important difference. J Clin Epidemiol. 2008May;61(5):505-10.
270. Fowler FJ, Jr., Barry MJ, Lu-Yao G, Roman A, Wasson J,Wennberg JE. Patient-reported complications and follow-up treatment after radical prostatectomy. The NationalMedicare Experience: 1988-1990 (updated June 1993).Urology. 1993 Dec;42(6):622-9.
271. Fowler FJ, Jr., Barry MJ, Lu-Yao G, Wasson J, Roman A,Wennberg J. Effect of radical prostatectomy for prostatecancer on patient quality of life: results from a Medicaresurvey. Urology. 1995 Jun;45(6):1007-13; discussion 13-5.
272. Schag CA, Ganz PA, Heinrich RL. CAncer RehabilitationEvaluation System--short form (CARES-SF). A cancerspecific rehabilitation and quality of life instrument. Cancer.1991 Sep 15;68(6):1406-13.
273. da Silva F RE, Costa T, Denis L. Quality of life in patientswtih prostatic cancer. Cancer. 1993;71(3):113-1142.
274. Stockler MR, Osoba D, Goodwin P, Corey P, Tannock IF.Responsiveness to change in health-related quality of lifein a randomized clinical trial: a comparison of the ProstateCancer Specific Quality of Life Instrument (PROSQOLI)with analogous scales from the EORTC QLQ-C30 and a trial

412
specific module. European Organization for Research andTreatment of Cancer. J Clin Epidemiol. 1998 Feb;51(2):137-45.
275. Clark JA, Inui TS, Silliman RA, et al. Patients' perceptionsof quality of life after treatment for early prostate cancer. JClin Oncol. 2003 Oct 15;21(20):3777-84.
276. Cella D. Manual of the Functional Assessment of ChronicIllness Therapy (FACIT) Measurement System. Version 4ed. Evanston IL: Center on Outcomes, Research andEducation (CORE), Evanston Northwestern Healthcare andNorthwestern University; 1997.
277. Cookson MS, Dutta SC, Chang SS, Clark T, Smith JA, Jr.,Wells N. Health related quality of life in patients treatedwith radical cystectomy and urinary diversion for urothelialcarcinoma of the bladder: development and validation of anew disease specific questionnaire. The Journal of urology.2003 Nov;170(5):1926-30.
278. Cockett AT, Aso Y, Chatelain C, et al. . The internationalconsultation on benign prostatic hyperplasia (BPH). Paris;1991.
279. Boyarsky S, Jones G, Paulson DF, Prout GR, Jr. A newlook at bladder neck obstruction by the food and drugadministration regulators: guide lines for investigation ofbenign prostatic hypertrophy. Transactions of the AmericanAssociation of Genito-Urinary Surgeons. 1976;68:29-32.
280. Epstein RS, Deverka PA, Chute CG, et al. Urinary symptomand quality of life questions indicative of obstructive benignprostatic hyperplasia. Results of a pilot study. Urology.1991;38(1 Suppl):20-6.
281. Ware JE, Jr., Kosinski M, Bayliss MS, McHorney CA, RogersWH, Raczek A. Comparison of methods for the scoring andstatistical analysis of SF-36 health profile and summarymeasures: summary of results from the Medical OutcomesStudy. Med Care. 1995 Apr;33(4 Suppl):AS264-79.
282. Berger M, et al. Health care cost, quality and outcomes.ISPOR Book of Terms; 2003. p. 195-97.
283. Ingolf G, Joanna C, Jackie B. Quality-Adjusted Life-Year LackQuality in Pediatric Care: A Critical Reiew of PublishedCost-Utility Studies in Child Health. Pediatrics.2005;115(5):e600.
284. Karen B, Magnus J. Incorporating quality of life changes intoeconomic evaluations of health care: an overview. HealthPolicy. 1996;36:155-66.
285. Rasanen P, Roine E, Sintonen H, Semberg-Konttinen V,Ryynanen OP, Roine R. Use of quality-adjusted life yearsfor the estimation of effectiveness of health care: A systematicliterature review. Int J Technol Assess Health Care. 2006Spring;22(2):235-41.