
Influence of silane heat treatment on bond strength of resin cement to a feldspathic ceramic
6
Dental Materials Journal 2011; 30(3): 392–397 INTRODUCTION Ceramics are often the materials of choice for aesthetic restorations in dentistry due to their high resistance to abrasion, compression, chemical stability, biocompatibility, favorable aesthetic features, translucence and fluorescence 1) . Among several types of ceramics, feldspathic ceramic is commonly used in the fabrication of indirect restorations such as laminates, inlays, onlays or overlays. Feldspathic ceramics are composed of two minerals: quartz and feldspath. The feldspath is linked to some metallic oxides forming the glass phase while the quartz comprises a crystalline phase 1) . The effectiveness of partial ceramic restorations is linked to adequate cementation procedures that are dependent on some factors such as composition of ceramic materials, surface conditioning methods and cement agents 2,3) . The surface conditioning of ceramics vary between ceramic types depending on their chemical composition 4) . The feldspathic ceramics are classified as acid sensitive materials that suffer from surface degradation by hydrofluoric acid gel (HF). HF application creates a topography favoring micro-mechanical retention 5-8) due to selective dissolution of glass matrix that is identified as retentive micro-pores, fissures and grooves on the conditioned ceramic surface 4,8-11) . The cementation process of a prosthetic restoration is the final step of operative treatment after a series of procedures. For adhesive cementation of glassy matrix ceramics, after etching with HF, it is recommended to use silane coupling agent, a monomer with reactive organic radicals and hydro-soluble monovalent group 12,13) . Silane coupling agents promote bonding between inorganic phase of ceramic and organic phase of bonding agent applied on the ceramic surface by siloxane bond 12,13) . In addition, silane increases the surface energy of ceramic substrates and improves cement damping. These events consequently promote microscopic interactions between both parts. Silane performance could be improved by heat treatment procedure. Heat treatment of silane results in the elimination of alcohol, water and other by-products of the ceramic surface 14-16) . In addition, heat treatment helps to complete the condensation reaction between silicate and silane providing formation of covalent bonds between the silane-ceramic interface, which in turn becomes more effective and stable 14-16) . Therefore, it could be anticipated that this stable silane reaction may eliminate the use of hazardous HF acid gel during the cementation phase. Resin cements exhibit low solubility in the oral environment, and adhere effectively to different substrates when compared to other luting agents 17) . Resin cements that are suitable for glass ceramics are usually composed of bis-phenol glycidyl methacrylate (bis-GMA) or urethane dimethacrylate (UEDMA) matrix in combination with other monomers with lower molecular weight such as triethyleneglycol dimethacrylate (TEGDMA). An annexation of hydrophilic functional groups, HEMA and 4-META, changes the organic composition of resin cements enabling adhesion to dental tissues. Such materials are basically composites with adequate viscosity for cementation that may be chemically, photo or dual polymerized. The resin cement Panavia F2.0 (Kuraray, Japan) contains phosphate Influence of silane heat treatment on bond strength of resin cement to a feldspathic ceramic Rodrigo Furtado de CARVALHO 1 , Maria Elizabeth Marques Nogueira MARTINS 2 , José Renato Cavalcanti de QUEIROZ 2 , Fabíola Pessoa Pereira LEITE 2 and Mutlu ÖZCAN 3 1 Federal University of Juiz de Fora, Faculty of Dentistry, Rua Jose Lourenco Kelme, Campus University, Bairro São Pedro 36036-900, Juiz de Fora, MG, Brazil 2 Federal University of Juiz de Fora, Faculty of Dentistry, Department of Restorative Dentistry, Rua Jose Lourenco Kelme, Campus University, Bairro São Pedro 36036-900, Juiz de Fora, MG, Brazil 3 University of Zürich, Dental Materials Unit, Center for Dental and Oral Medicine, Clinic for Fixed and Removable Prosthodontics and Dental Materials Science, Plattenstrasse 11, CH-8032 Zürich, Switzerland Corresponding author, Rodrigo Furtado de CARVALHO; E-mail: [email protected] This study evaluated the influence of heat treatment (HT) of the silane on the microtensile bond strength of resin cement to a feldspathic ceramic. Ceramic (VITA VM7) and composite blocks (N=32) were divided into four groups (n=6 for bond test, n=2 for SEM) at random and subject to following sequence of conditioning: G1: HF 9.6%+Silane+Panavia F2.0, G2: HF 9.6%+Silane+HT+Panavia F2.0, G3: Silane+HT+Panavia F2.0, and G4: Silane+Panavia F2.0. HT was performed in an oven (100°C, 2 minutes). G1 (17.6±2.3 MPa) and G2 (19±3.2 MPa) showed significantly higher mean bond strength than those of G3 (9.1±2.8 MPa) and G4 (10.9±1.8 MPa). SEM analysis showed exclusively mixed failures. Silane HT did not increase the bond strength. Keywords: Adhesion, Cementation, Ceramics, Microtensile strength, Thermal treatment Received Aug 25, 2010: Accepted Feb 23, 2011 doi:10.4012/dmj.2010-137 JOI JST.JSTAGE/dmj/2010-137
Transcript of Influence of silane heat treatment on bond strength of resin cement to a feldspathic ceramic

Dental Materials Journal 2011; 30(3): 392–397
INTRODUCTION
Ceramics are often the materials of choice for aesthetic restorations in dentistry due to their high resistance to abrasion, compression, chemical stability, biocompatibility, favorable aesthetic features, translucence and fluorescence1).
Among several types of ceramics, feldspathic ceramic is commonly used in the fabrication of indirect restorations such as laminates, inlays, onlays or overlays. Feldspathic ceramics are composed of two minerals: quartz and feldspath. The feldspath is linked to some metallic oxides forming the glass phase while the quartz comprises a crystalline phase1).
The effectiveness of partial ceramic restorations is linked to adequate cementation procedures that are dependent on some factors such as composition of ceramic materials, surface conditioning methods and cement agents2,3). The surface conditioning of ceramics vary between ceramic types depending on their chemical composition4). The feldspathic ceramics are classified as acid sensitive materials that suffer from surface degradation by hydrofluoric acid gel (HF). HF application creates a topography favoring micro-mechanical retention5-8) due to selective dissolution of glass matrix that is identified as retentive micro-pores, fissures and grooves on the conditioned ceramic surface4,8-11).
The cementation process of a prosthetic restoration is the final step of operative treatment after a series of procedures. For adhesive cementation of glassy matrix ceramics, after etching with HF, it is recommended to use silane coupling agent, a monomer with reactive organic radicals and hydro-soluble monovalent group12,13).
Silane coupling agents promote bonding between inorganic phase of ceramic and organic phase of bonding agent applied on the ceramic surface by siloxane bond12,13). In addition, silane increases the surface energy of ceramic substrates and improves cement damping. These events consequently promote microscopic interactions between both parts.
Silane performance could be improved by heat treatment procedure. Heat treatment of silane results in the elimination of alcohol, water and other by-products of the ceramic surface14-16). In addition, heat treatment helps to complete the condensation reaction between silicate and silane providing formation of covalent bonds between the silane-ceramic interface, which in turn becomes more effective and stable14-16). Therefore, it could be anticipated that this stable silane reaction may eliminate the use of hazardous HF acid gel during the cementation phase.
Resin cements exhibit low solubility in the oral environment, and adhere effectively to different substrates when compared to other luting agents17). Resin cements that are suitable for glass ceramics are usually composed of bis-phenol glycidyl methacrylate (bis-GMA) or urethane dimethacrylate (UEDMA) matrix in combination with other monomers with lower molecular weight such as triethyleneglycol dimethacrylate (TEGDMA). An annexation of hydrophilic functional groups, HEMA and 4-META, changes the organic composition of resin cements enabling adhesion to dental tissues. Such materials are basically composites with adequate viscosity for cementation that may be chemically, photo or dual polymerized. The resin cement Panavia F2.0 (Kuraray, Japan) contains phosphate
Influence of silane heat treatment on bond strength of resin cement to a feldspathic ceramicRodrigo Furtado de CARVALHO1, Maria Elizabeth Marques Nogueira MARTINS2, José Renato Cavalcanti de QUEIROZ2, Fabíola Pessoa Pereira LEITE2 and Mutlu ÖZCAN3
1Federal University of Juiz de Fora, Faculty of Dentistry, Rua Jose Lourenco Kelme, Campus University, Bairro São Pedro 36036-900, Juiz de Fora, MG, Brazil2Federal University of Juiz de Fora, Faculty of Dentistry, Department of Restorative Dentistry, Rua Jose Lourenco Kelme, Campus University, Bairro São Pedro 36036-900, Juiz de Fora, MG, Brazil3University of Zürich, Dental Materials Unit, Center for Dental and Oral Medicine, Clinic for Fixed and Removable Prosthodontics and Dental Materials Science, Plattenstrasse 11, CH-8032 Zürich, SwitzerlandCorresponding author, Rodrigo Furtado de CARVALHO; E-mail: [email protected]
This study evaluated the influence of heat treatment (HT) of the silane on the microtensile bond strength of resin cement to a feldspathic ceramic. Ceramic (VITA VM7) and composite blocks (N=32) were divided into four groups (n=6 for bond test, n=2 for SEM) at random and subject to following sequence of conditioning: G1: HF 9.6%+Silane+Panavia F2.0, G2: HF 9.6%+Silane+HT+Panavia F2.0, G3: Silane+HT+Panavia F2.0, and G4: Silane+Panavia F2.0. HT was performed in an oven (100°C, 2 minutes). G1 (17.6±2.3 MPa) and G2 (19±3.2 MPa) showed significantly higher mean bond strength than those of G3 (9.1±2.8 MPa) and G4 (10.9±1.8 MPa). SEM analysis showed exclusively mixed failures. Silane HT did not increase the bond strength.
Keywords: Adhesion, Cementation, Ceramics, Microtensile strength, Thermal treatment
Received Aug 25, 2010: Accepted Feb 23, 2011doi:10.4012/dmj.2010-137 JOI JST.JSTAGE/dmj/2010-137

Dent Mater J 2011; 30(3): 392–397 393
monomer in its composition being capable of adhering to oxides and at the same time providing adequate adhesion between the cement and the restorative material.
The choice of standardized tests focusing on adhesive joint strength is essential to evaluate the bond strength of different materials18). Among different testing methods, the conventional tensile test yields to non-uniform force distribution at the adhesive area. Also, in tensile bond tests the exact parallel alignment of the test specimens is difficult19). While the pull-out test creates the concentration of tension in the substrate having no effect in the adhesive area13,20), microtensile test allows the distribution of tension in the adhesive area18,21-25).
The aim of this present study was to evaluate the influence of heat treatment of silane coupling agent on the microtensile bond strength of phosphate monomer based resin cement to feldspathic ceramic.
MATERIALS AND METHODS
Ceramic specimen preparationThe brands, manufacturers, chemical compositions and batch numbers of the materials used in this study are listed in Table 1.
Initially, a standard acrylic resin with dimensions of 6 mm×8 mm×8 mm was made. From this acrylic, ceramic blocks were obtained measuring the same size for all groups. The pattern of acrylic resin was molded with a dense mass of the heavy part of polysiloxane (Elite HD, Zhermach, Badia Polesine, Italy). The powder (VITA VM7 Dentin 5M2) and modeling liquid (Modeling for Liquid Vita VM7, VITA Zahnfabrik, Bad Säckingen, Germany) were mixed according to the manufacturer’s
instructions. The ceramic slurry was placed in small portions using a spatula, condensed inside the silicon impression and vibrated manually until completing the entire space of this impression. The excess fluid was removed with soft absorbent paper. Then, the ceramic block was removed from the tray. Finally, 32 blocks of ceramic were obtained from a single impression. The blocks were sintered on the refractory base in the furnace (Vacumat, VITA Zahnfabrik) following the firing cycles recommended by the manufacturer. Considering that the contraction after sintering of ceramics is around 20%, post-sintering blocks had approximate dimensions of 4.8 mm×6.4 mm×6.4 mm. The internal surfaces of each block have undergone a radiographic evaluation in order to observe possible faults within the body. In case of such defects, the specimens were excluded from the study and new ones were made. Subsequently, the ceramic excess was removed with diamond discs at low speed. The bond surface was ground finished using silicone carbide abrasives of 600, 800, 1000, 1200 grit in sequence under water. Then the specimens were ultrasonically cleaned in distilled water for 5 minutes.
Impressions were made from each ceramic block. After the impression material (Elite HD) was set, ceramic blocks were removed from the mold. Microhybrid resin composite (W3D MASTER, Wilcos of Brazil Ind., RJ, Brazil) was placed in increments of 2 mm. Each increment was photo polymerized for 40 seconds (Ultraled, Ultradent®, UT, USA) until the mold was filled, resulting in a block of composite (4.8 mm×6.4 mm×6.4 mm) for each ceramic block. As a result, the bonding surface of the composite resin blocks had the same area as the surfaces of ceramic blocks. The ceramic blocks were again ultrasonically cleaned as described above.
Brands Manufacturer Chemical composition Batch number
W3D MASTER Wilcos of Brazil, Rio de Jeneiro, Brazil
Methacrylate-based monomers 23.7 w%, silica, silicate glass and fluoride containing fillers 75.6 w%, polymerization catalysts 0.6 w%, inorganic pigments 0.1 w%
002051
Vita VM7 Vita Zahnfabrik, Bad Säckingen, Germany
Silicaoxide, aluminiumoxide, lanthanumoxide, magnesium oxide, zincoxide, potassiumoxide, inorganic pigments
11040
Porcelain Conditioner
Dentsply, Petrópolis, RJ, Brazil
9.6% Hydrofluoric acid 11040
Clearfil Ceramic Primer
Kuraray Medical Inc., Tokyo, Japan
3-Methacryloxypropyl trimethoxy silane, MDP, ethanol
61182
Panavia F2.0 Kuraray Medical Inc., Tokyo, Japan
Silanated barium glass, silanated silica, surface treated sodium fluoride, bis-phenol polyethoxy dimetacrylate, MDP, hydrophobic dimethacrylate, hydrophilic dimethacrylate, benzoyl peroxide, sodium aromatic sulfinate, N,N-diethanol p-toluidine, photo-initiator
61187
Table 1 The brands, manufacturers, chemical compositions and batch numbers of the materials used in this study.

Dent Mater J 2011; 30(3): 392–397394
Adhesion protocolThe ceramic blocks were then randomly divided into four groups (n=6) and conditioned as follows:
In Groups 1 and 2, the ceramic blocks were conditioned with HF acid gel (Porcelain Conditioner, Dentsply, Rio de Jeneiro, Brazil) for 20 seconds, rinsed with water spray for 60 seconds, and ultrasonically cleaned in distilled water for 4 minutes. They were then dried with air spray for 30 seconds. In Group 1, silane was applied on the bonding surface of each ceramic block (Clearfil Ceramic Primer, Kuraray Medical Inc., Okayama, Japan) and dried completely with air spray.
In Group 2, after silane application, heat treatment was achieved in a furnace (EDG, Sao Paulo, Brazil) at 100°C for 2 minutes.
In Group 3 and 4, on the ceramic surfaces no HF etching but only silanization was performed. In Group 3 silane layer was heat-treated but in Group 4 no heat treatment was applied.
Subsequently, resin cement (Panavia F2.0, Kuraray Medical Inc., Tokyo, Japan) was adhered onto the conditioned ceramic surface, according to the manufacturers instructions. The ceramic and the composite block were aligned perpendicular. After the cement was placed on the conditioned surface, vertical load of 750 g was applied for 10 minutes. The excess of cement was removed, margins of the blocks were photo-polymerized for 40 seconds at each site (Ultra LED, Ultradent, UT) and an oxygen inhibiting gel was applied at the margins. The ceramic-cement-resin assembly was then washed with air-water spray and kept in distilled water at 37°C for seven days prior to specimen preparation for microtensile bond strength test.
Microtensile bond strength testInitially, the ceramic-cement-composite resin assembly was fixed with cyanoacrylate adhesive (Super Bonder Gel, Loctite Ltd., São Paulo, Brazil) on cylindrical metallic base of the cutting machine. The calibration of the machine was repeated for each new specimen. Bar specimens were obtained by cutting the assembly using steel diamond discs (Microdont, São Paulo, Brazil) at low speed under water-cooling. The external sections of 1 mm were eliminated due to possible excess cement. The blocks were turned 90° and fixed again on the metallic base. From each block, 9 transversal sections were obtained and from those sections bar specimens with a length of ±8 mm and adhesive area of ±1 mm² were obtained.
Bonding area of each bar specimen was measured
before the tests using a digital caliper (Starret Industry Commerce Ltd., Sao Paulo, Brazil) with an accuracy of 100 µm. The bar specimens were fixed to the alignment device with one drop of cyanoacrylate glue (Super Bonder Gel) on the composite and one on the ceramic part of the bar specimen. It was made sure that the adhesive interface was free of the glue. The tensile forces were applied at a cross-head speed of 1 mm/min until debonding in the Universal Testing Machine (Model DL 1000, EMIC, Systems and Equipments Ltd., São José dos Pinhais, Brazil).
After the tests, failure types were analyzed using an optical microscope (Zeiss MC 80 DX, Jena, Germany) at ×50 magnification. Failure classification was as follows: adhesive between the cement and ceramic (adhesive zone), cohesive in the ceramic or cohesive in the resin block. Specimens were further evaluated under Scanning Electron Microscopy (SEM) (Jeol-JSM-T330A, Tokyo, Japan).
Furthermore, on additional eight ceramic blocks chemical analysis was performed using X-ray Energy Dispersive Spectrometry (EDS) (Jeol-JSM-T330A) at low vacuum level of 40 Pa pressure using the secondary electron mode (20 KV of acceleration, working distance: 15 mm).
Statistical analysisStatistical analysis was performed using SPSS 11.0 software for Windows (SPSS Inc., Chicago, IL, USA). Bond strength data (MPa) were submitted to two-way analysis of variance (2-way ANOVA) with the bond strength as the dependent variable and the heat treatment and etching as independent variables. Due to significant differences between groups, multiple comparisons were made using Tukey’s tests. P values less than 0.05 were considered to be statistically significant in all tests.
RESULTS
During cutting procedures, 0, 0, 5, 3 pre-test failures were experienced for Groups 1, 2, 3 and 4. These were considered as 0 MPa.
Groups 1 and 2, where the ceramic surfaces were etched with HF gel, showed significantly higher mean bond strength (17.6±2.3 and 19±3.2, respectively) than those of Groups 3 and 4 where the ceramics were only silanized (9.1±2.8, 10.9±1.8, respectively) (p<0.05) (Table 2). Heat treatment of silane did not increase the results neither in the HF etched nor in the non-etched groups
Groups Mean (SD) Minimum Maximum1 17.6 (2.3)a 13.72 20.392 19.0 (3.2)a 13.98 22.403 9.1 (2.8)b 6.31 12.594 10.9 (1.8)b 7.37 13.63
*The same superscripted letters indicate no significant differences (Tukey’s test, =0.05).
Table 2 The mean (±standard deviations-SD) microtensile bond strength (MPa) values for the experimental groups.
Dent Mater J 2011; 30(3): 392–397 395
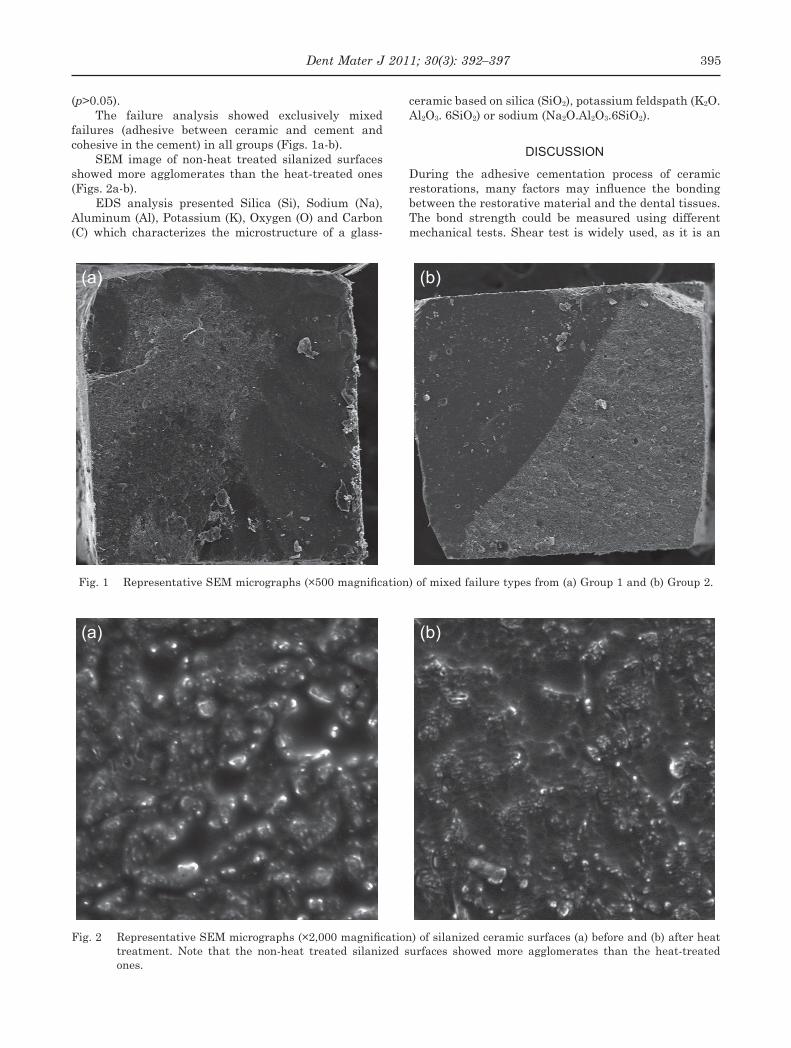
(p>0.05).The failure analysis showed exclusively mixed
failures (adhesive between ceramic and cement and cohesive in the cement) in all groups (Figs. 1a-b).
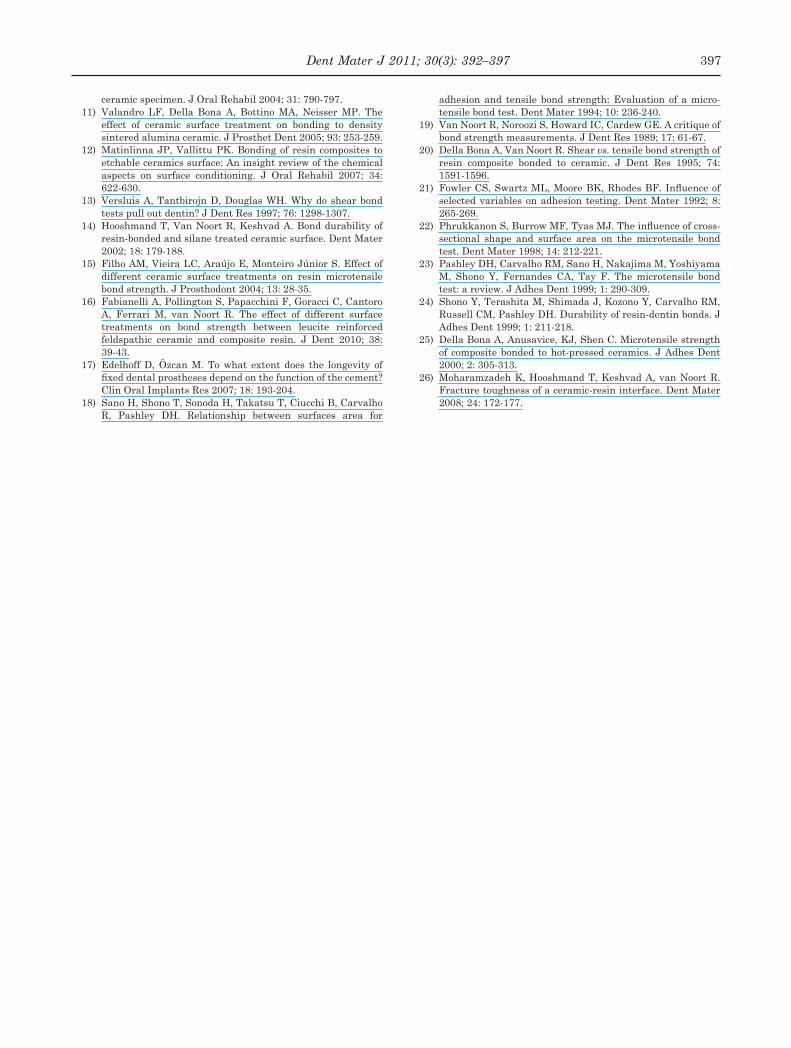
SEM image of non-heat treated silanized surfaces showed more agglomerates than the heat-treated ones (Figs. 2a-b).
EDS analysis presented Silica (Si), Sodium (Na), Aluminum (Al), Potassium (K), Oxygen (O) and Carbon (C) which characterizes the microstructure of a glass-
ceramic based on silica (SiO2), potassium feldspath (K2O. Al2O3. 6SiO2) or sodium (Na2O.Al2O3.6SiO2).
DISCUSSION
During the adhesive cementation process of ceramic restorations, many factors may influence the bonding between the restorative material and the dental tissues. The bond strength could be measured using different mechanical tests. Shear test is widely used, as it is an
Fig. 1 Representative SEM micrographs (×500 magnification) of mixed failure types from (a) Group 1 and (b) Group 2.
Fig. 2 Representative SEM micrographs (×2,000 magnification) of silanized ceramic surfaces (a) before and (b) after heat treatment. Note that the non-heat treated silanized surfaces showed more agglomerates than the heat-treated ones.
(a) (b)
(a) (b)

Dent Mater J 2011; 30(3): 392–397396
easy method to perform. However, shear test is not considered as an ideal mechanical test since it often yields to cohesive failures in the substrate19). The high incidence of cohesive failures of the substrate is related to non-uniform stress distribution at the adhesive joint that undergo shear stresses requiring more forces from the substrate than the adhesive interface itself. On the other hand, conventional tensile tests have some limitations due to the difficulty of aligning the specimens in the universal testing machine, which in turn distributes the stresses uneven at the adhesive interface25). The choice of the microtensile test in this study was because of its reliability in testing adhesion to dental tissues or and ceramics as opposed to the other methods2,13). Alignment of the bar specimens are also of importance in this test. Therefore, an alignment device was adapted for parallel placement of the specimens during testing.
The results of this study showed no additional effect of silane heat treatment on the mean bond strength. Thus, the hypothesis was rejected. These findings did not corroborate with the studies of Hooshmand et al.14) and Moharamzadeh et al.26). This may be explained by the differences in the test method used. While Hooshmand et al.14) used the conventional tensile test, in the study of Moharamzadeh et al.26) shear test was used.
The heat treatment of silane in fact eliminates the water, alcohol and other by-products from the ceramic surface. In addition, it helps to complete the condensation reaction between silica and silane promoting the formation of a covalent bond in the silane-ceramic interface, making it more effective and resistant3). Silane heat treatment could be achieved in different ways. In previous studies, hot air application at 100°C for 1 minute16), hot air application at 50°C for 15 seconds16) and heat treatment in furnace at 100°C for 2 minutes26) have been tried. As a result of a series of preliminary experiments for standardization, in this study, heat treatment was performed in the oven at 100°C for 2 minutes. The results of this study also did not corroborate with the results of Fabianelli et al.16), where also microtensile test was employed. Although the test method was the same in that study, silane heat treatment was performed with hot air at 100°C for only 1 minute. Therefore, prolonged duration and heat application mode seems to affect the results yielding to discrepancy between the results of different studies. Future studies should try to standardize the heat application on silane.
The durable bonding between ceramic and resin cement that is achieved through surface conditioning appeared to be an important factor in the longevity of the restorations17). The commonly applied surface conditioning feldspathic ceramic is HF acid etching followed by silane application7-9). The hydrofluoric acid reacts selectively with the silica present on the microstructure of ceramic forming hexafluorsilica. As a result of this reaction, the ceramic surface becomes irregular and porous increasing the surface area and facilitating the penetration of the bonding agent into the microretentions of ceramic surface conditioned by acid.
In this study, the major gain in bond strength was due to the HF etching as observed in Groups 1 and 2. In the groups where no HF etching was performed the mean bond strength was almost 50% less. These findings indicate the importance of etching prior to silane application that was clearly more important than the silane heat treatment. On the other hand, the use of silane has a great importance for the adhesive cementation technique11,22). As it is considered an organic-functional molecule, it promotes chemical adhesion between the inorganic substratum and organic polymers. It should also be noted that in this study an MDP containing resin cement was used. Silane reaction may differ with other resin cements containing methacrylate monomers.
Besides microtensile bond strength results, the SEM findings showed that heat treatment seemed to promote better damping, absorption of the silane yielding to greater contact and infiltration of the bonding agent into the porosities of the etched ceramic.
The microtensile bond strength data must be coupled with the failure types. Failure analysis showed exclusively mixed failures. No cohesive failures in the ceramic substrate were observed. Previous studies also reported higher incidence of mixed or adhesive failures compared to other test methods where more cohesive failures of the substrate was observed5,26).
According to results of this study, it may be possible to conclude that the heat treatment of silane does not improve the bond strength of the cement, Panavia F2.0, tested in this study.
REFERENCES1) Gomes EA, Assunção WG, Rocha EP, Santos PH. Ceramic in
dentistry: current situation. Cerâmica 2008; 54: 319-325.2) Della Bona A, Anusavice KJ. Microstructure, composition,
and etching topography of dental ceramics. Int J Prosthodont 2002; 15: 159-167.
3) Matinlinna JP, Lassila LV, Özcan M, Yli-Urpo A, Vallittu PK. An introduction to silanes and their clinical applications in dentistry. Int J Prosthodont 2004; 17: 155-164.
4) Özcan M, Vallittu PK. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent Mater 2003; 19: 725-731.
5) Aida M, Hayakawa T, Mizukawa K. Adhesion of composite to porcelain with various surface conditions. J Prosthet Dent 1995; 73: 464-470.
6) Brentel AS, Özcan M, Valandro LF, Alarça LG, Amaral R, Bottino MA. Microtensile bond strength of resin cement to feldpathic ceramic after different etching and silanization regimens in dry and aged conditions. Dent Mater 2007; 23: 1323-1331.
7) Ayad MF, Fahmy NZ, Rosenstiel SF. Effect of surface treatment on roughness and bond strength of a heat-pressed ceramic. J Prosthet Dent 2008; 99: 123-130.
8) Chen JH, Matsumura H, Atsuta M. Effect of different etching periods on the bond strength of a composite resin to a machinable porcelain. J Dent 1998; 28: 53-58.
9) Canay S, Hersek N, Ertan A. Effect of different acid treatments on a porcelain surface. J Oral Rehabil 2001; 28: 95-101.
10) Saraçoglu C, Cura C, Çötert HS. Effect of various surface treatment methods on the bond strength of the heat-pressed
Dent Mater J 2011; 30(3): 392–397 397
ceramic specimen. J Oral Rehabil 2004; 31: 790-797.11) Valandro LF, Della Bona A, Bottino MA, Neisser MP. The
effect of ceramic surface treatment on bonding to density sintered alumina ceramic. J Prosthet Dent 2005; 93: 253-259.
12) Matinlinna JP, Vallittu PK. Bonding of resin composites to etchable ceramics surface: An insight review of the chemical aspects on surface conditioning. J Oral Rehabil 2007; 34: 622-630.
13) Versluis A, Tantbirojn D, Douglas WH. Why do shear bond tests pull out dentin? J Dent Res 1997; 76: 1298-1307.
14) Hooshmand T, Van Noort R, Keshvad A. Bond durability of resin-bonded and silane treated ceramic surface. Dent Mater 2002; 18: 179-188.
15) Filho AM, Vieira LC, Araújo E, Monteiro Júnior S. Effect of different ceramic surface treatments on resin microtensile bond strength. J Prosthodont 2004; 13: 28-35.
16) Fabianelli A, Pollington S, Papacchini F, Goracci C, Cantoro A, Ferrari M, van Noort R. The effect of different surface treatments on bond strength between leucite reinforced feldspathic ceramic and composite resin. J Dent 2010; 38: 39-43.
17) Edelhoff D, Özcan M. To what extent does the longevity of fixed dental prostheses depend on the function of the cement? Clin Oral Implants Res 2007; 18: 193-204.
18) Sano H, Shono T, Sonoda H, Takatsu T, Ciucchi B, Carvalho R, Pashley DH. Relationship between surfaces area for
adhesion and tensile bond strength: Evaluation of a micro-tensile bond test. Dent Mater 1994; 10: 236-240.
19) Van Noort R, Noroozi S, Howard IC, Cardew GE. A critique of bond strength measurements. J Dent Res 1989; 17: 61-67.
20) Della Bona A, Van Noort R. Shear vs. tensile bond strength of resin composite bonded to ceramic. J Dent Res 1995; 74: 1591-1596.
21) Fowler CS, Swartz ML, Moore BK, Rhodes BF. Influence of selected variables on adhesion testing. Dent Mater 1992; 8: 265-269.
22) Phrukkanon S, Burrow MF, Tyas MJ. The influence of cross-sectional shape and surface area on the microtensile bond test. Dent Mater 1998; 14: 212-221.
23) Pashley DH, Carvalho RM, Sano H, Nakajima M, Yoshiyama M, Shono Y, Fernandes CA, Tay F. The microtensile bond test: a review. J Adhes Dent 1999; 1: 290-309.
24) Shono Y, Terashita M, Shimada J, Kozono Y, Carvalho RM, Russell CM, Pashley DH. Durability of resin-dentin bonds. J Adhes Dent 1999; 1: 211-218.
25) Della Bona A, Anusavice, KJ, Shen C. Microtensile strength of composite bonded to hot-pressed ceramics. J Adhes Dent 2000; 2: 305-313.
26) Moharamzadeh K, Hooshmand T, Keshvad A, van Noort R. Fracture toughness of a ceramic-resin interface. Dent Mater 2008; 24: 172-177.




















