
Fla. Bishops' speak on death penalty - St. Thomas University

Clin Chem Lab Med 2015; 53(2): 157–183
Review
Daniel M. Kobewka*, Paul E. Ronksley, Jennifer A. McKay, Alan J. Forster and Carl van Walraven
Influence of educational, audit and feedback, system based, and incentive and penalty interventions to reduce laboratory test utilization: a systematic review
DOI 10.1515/cclm-2014-0778Received July 29, 2014; accepted August 25, 2014; previously published online September 27, 2014
Abstract: Laboratory and radiographic tests are often ordered unnecessarily. This excess testing has financial costs and is a burden on patients. We performed a systematic review to determine the effectiveness interventions to reduce test utilization by physicians. The MEDLINE and EMBASE data-bases were searched for the years 1946 through to September 2013 for English articles that had themes of test utilization and cost containment or optimization. Bibliographies of included papers were scanned to identify other potentially
relevant studies. Our search resulted in 3236 articles of which 109 met the inclusion criteria of having an interven-tion aimed at reducing test utilization with results that could be expressed as a percent reduction in test use relative to the comparator. Each intervention was categorized into one or more non-exclusive category of education, audit and feed-back, system based, or incentive or penalty. A rating of study quality was also performed. The percent reductions in test use ranged from a 99.7% reduction to a 27.7% increase in test use. Each category of intervention was effective in reducing test utilization. Heterogeneity between interventions, poor study quality, and limited time horizons makes generaliza-tions difficult and calls into question the validity of results. Very few studies measure any patient safety or quality of care outcomes affected by reduced test use. There are numerous studies that use low investment strategies to reduce test uti-lization with one time changes in the ordering system. These low investment strategies are the most promising for achiev-able and durable reductions in inappropriate test use.
Keywords: audit and feedback; education; laboratory uti-lization; reducing; test use.
IntroductionHealthcare spending in has increased in both relative and absolute terms over the past several decades [1, 2]. This increase has been seen in many countries and will be unsustainable if the trend continues at the present rate [3]. Laboratory and radiographic testing is a promising target for reducing spending because many of the tests ordered by physicians are suspected to be unnecessary; in some studies, 95% of tests performed are inappropriate as judged by criteria of redundancy or their probability of adding value to patient care [4].
*Corresponding author: Dr. Daniel M. Kobewka, Departments of Medicine and Epidemiology and Community Medicine, Ottawa Hospital, Civic Campus, 1053 Carling Avenue, Ottawa, ON K1Y 4E9, Canada, E-mail: [email protected]; and Department of Medicine, The Ottawa Hospital, University of Ottawa, Ottawa, Ontario, Canada; and Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, Ontario, CanadaPaul E. Ronksley: Ottawa Hospital Research Institute, Department of Clinical Epidemiology, Ottawa, Ontario, CanadaJennifer A. McKay: Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, Ontario, CanadaAlan J. Forster: Department of Medicine, The Ottawa Hospital, University of Ottawa, Ottawa, Ontario, Canada; Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, Ontario, Canada; Ottawa Hospital Research Institute, Department of Clinical Epidemiology, Ottawa, Ontario, Canada; Performance Measurement, The Ottawa Hospital, Ottawa, Ontario, Canada; and Institute for Clinical Evaluative Sciences, Toronto, Ontario, CanadaCarl van Walraven: Department of Medicine, The Ottawa Hospital, University of Ottawa, Ottawa, Ontario, Canada; Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, Ontario, Canada; Ottawa Hospital Research Institute, Department of Clinical Epidemiology, Ottawa, Ontario, Canada; and Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada
UnauthenticatedDownload Date | 5/19/16 2:24 AM

158 Kobewka et al.: Systematic review of interventions to reduce test use
The perceived prevalence of inappropriate laboratory utilization has prompted many attempts to reduce test utilization. Several systematic and narrative reviews have been published on this topic [5–8]. The most recent review, published in 1998, used a behavioral framework to clas-sify interventions and found that targeting multiple behav-ioral factors was more successful than targeting a single factor [8]. However, this review only dichotomized study outcomes by statistical significance, making it difficult to understand the utility of these interventions. Other reviews used categories of education, audit and feedback or other but were unable to make generalizations about which strategy is most effective because of differences within each category of intervention, a wide range of effects, and lack of a common measure [5, 6]. To date, no review has quantitatively compared the influence of various interven-tions on test utilization reduction. In addition, previous reviews have not examined investments required to imple-ment these interventions. For these reasons, we performed a systematic review to determine the effectiveness of all interventions to reduce test utilization by physicians.
Methods
Data sources and searches
We performed a systematic review following a predeter-mined protocol in accordance with published guidelines for reporting of systematic reviews of randomized con-trolled trials [9]. We identified all potentially relevant articles published in English by searching Medline (1946 through September 2013) and Embase (1947 through Sep-tember 2013). Searches were enhanced by systematically scanning bibliographies of identified articles and relevant review articles as well as articles deemed by PubMed to be related to the included studies. To search electronic databases, we used the strategy recommended for sys-tematic reviews of interventional studies [10] and speci-fied two comprehensive search themes (Online-Appendix 1). Theme 1 identified relevant terms related to laboratory utilization. Theme 2 related to optimization and cost con-tainment. We then combined the two datasets using the Boolean operator ‘and’ and limited the intersection to human studies.
Study selection
Relevant articles were selected from the retrieved studies using a two-phase process. Abstracts were first reviewed
for eligibility by three researchers (DK, PR, JM). All abstracts reporting on the effect of an intervention on laboratory utilization were selected for full text review. This initial stage was intentionally liberal; we discarded only abstracts that clearly were not reporting inventions aimed at reducing test utilization. Full text articles were then assessed by one reviewer (DK) with verification by two reviewers (PR, JM) to determine if the study met the specified inclusion criteria. Inclusion criteria included: 1) study population had to include physicians; 2) the aim of the intervention was the modification of test utilization; 3) a comparator arm (either standard care or no intervention) was needed; and 4) the study had to quantify laboratory test utilization with and without the intervention so that a percent change could be calculated. All study designs were considered within this review.
Intervention classification
Interventions used to effect physician laboratory order-ing practices were categorized into one or more of the following non-exclusive categories:1. Educational interventions in which appropriate test
ordering (including the distribution of guidelines) was taught to physicians;
2. Audit and feedback interventions in which physicians were presented their test utilization compared to their previous utilization or peer utilization or the total costs of the tests they ordered;
3. System-based interventions involving one-time, permanent changes to test ordering processes including: order form modifications; computer order entry systems with rules disallowing test ordering in specific circumstances; and clinical decision support systems (CDSS) in which an interactive computer system forces physicians to integrate previous knowledge about the patient and/or the medical literature into the test ordering process; and
4. Incentive or penalty interventions in which physicians received rewards or punishments for certain test ordering practices. For each intervention, we also determined whether the targeted physicians were actively engaged during the intervention’s development [8].
Data extraction and quality assessment
For each study, we extracted information on publication year, country of origin, study design (randomized two-arm
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 159
trials, before and after studies, prospective cohort), the healthcare providers targeted and the tests targeted for reduction. We recorded characteristics of the study intervention(s) along with its duration. We assessed study quality using an adapted version of the Effective Practice and Organization of Care (EPOC) Cochrane guidelines for interventional studies [11]. In particular, we assessed whether: patients and providers were similar across inter-vention and comparator groups; a randomized control group was used within the study, there was sufficient detail to describe the intervention, there was risk of contamina-tion between the intervention and comparator groups, and whether a time-series analysis was performed. Lastly, we assessed whether studies measured any patient safety outcome that could be affected by reducing test utilization.
Statistical analysis
The unit of analysis was the intervention, with some studies having more than one intervention. The effective-ness of interventions was summarized using the percent relative reduction in test volume for the intervention group relative to the comparator group. This was calculated as:
−(# of tests in comparator group) (# of tests in interventiongroup)(# of tests in comparator group)
Given the variability in the types of interventions, duration of interventions, targeted tests, and patient populations, we did not conduct a meta-analysis. Instead, a descriptive analysis of the relative reductions was per-formed using medians and inter-quartile ranges (IQR) to summarize effects across the various intervention types. We also documented when these reductions in a particu-lar study were statistically significant. Results were strati-fied by categories of interventions (educational, system based, audit/feedback and incentive and penalty) and were visualized using box plots. Stratifications were then conducted by additional interventional factors within each category and by measures of study quality and sta-tistical significance. The effect of physician involvement was also measured across interventions. Finally sensitiv-ity analyses were conducted to assess the effect of inter-ventions that targeted four or more tests.
In order to highlight the interventions with the best return on investment we included a narrative review of interventions with the largest reductions in test utilization as well as the most effective system-based interventions tar-geting four or more tests. All analyses were performed using Stata version 13.0 (Stata Corp., College Station, TX, USA).
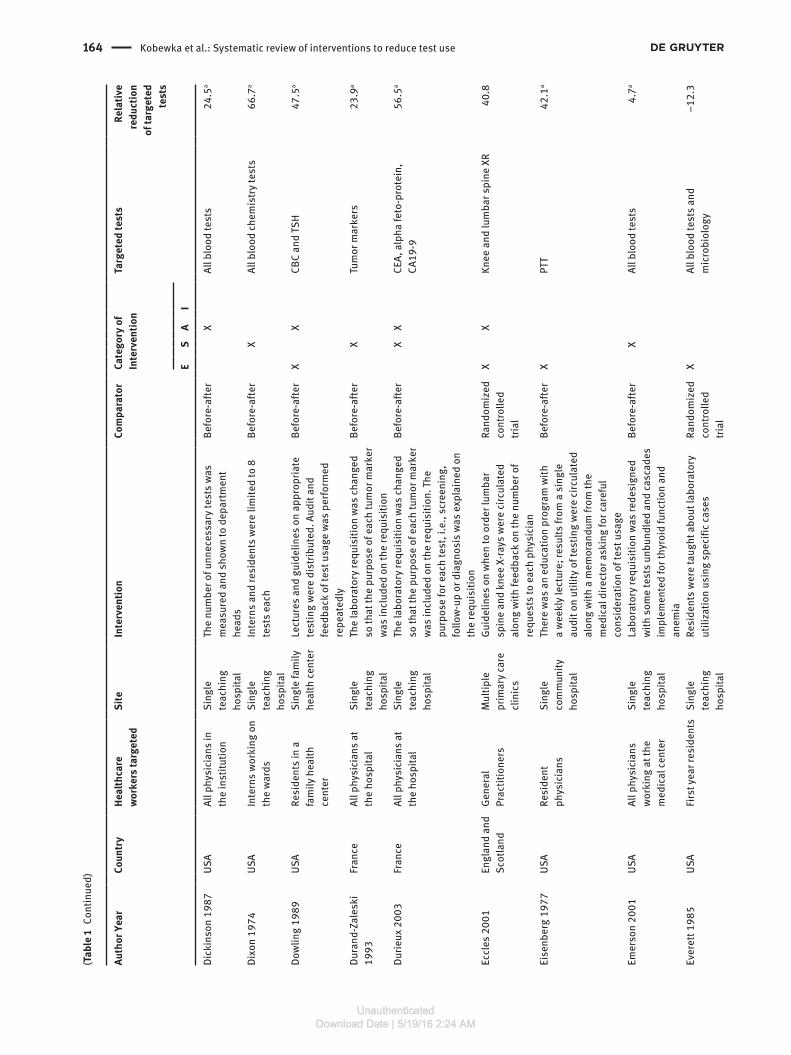
ResultsOur search generated 3236 unique citations. Following the initial screening and full-text review, 109 unique studies that included 119 interventions were included in the sys-tematic review (Figure 1) [12–121]. Study characteristics and brief descriptions of each intervention are shown in Table 1. Ninety-three studies (85.3%) used before-after designs, 2 (1.8%) were non-randomized prospective trials, and 14 (12.8%) were randomized controlled trials. Studies were published between 1974 and 2013 with 61 studies (56.0%) performed in North America, 27 (24.8%) in Europe, 11 (10.1%) Australasia, and 10 (9.2%) in other regions. Studies used very limited time horizons with only 15 of 109 studies (13.8%) measuring intervention effects beyond 1 year.
Study quality
Study quality is summarized in Online-Appendix 2. Of the 109 studies, 14 (12.8%) had a randomized design and 37 (33.9%) provided evidence that patients were similar between groups. Time-series analysis was performed in only 11 (10.1%) studies. Interventions were described
adequately to be reproducible in 88 (80.7%) studies. Test utilization was reported with the patient or the encoun-ter as the unit of analysis in 79/109 (72.5%) studies with the rest using the physician or the group of physicians working that location as the unit of analysis.
Intervention components
Of 119 interventions, 51 (42.9%) had an educational com-ponent, 54 (45.4%) had a system-based component, 41 (34.5%) had an audit feedback component, with only one (0.8%) using incentive or penalty. Physicians were involved in the development of interventions in only 17 (14.3%) interventions. Thirty-two (26.9%) interventions were multifaceted, being classified into more than one of the four main intervention categories. A measure of patient safety or quality of care was included in 13 (11.9%) studies.
Intervention effects
The percent relative reductions in laboratory utilization ranged from a +99.7% (a reduction in the test volumes)
UnauthenticatedDownload Date | 5/19/16 2:24 AM

160 Kobewka et al.: Systematic review of interventions to reduce test use
3236 citations (Medline: 1554; EMBASE: 1633) identified fromelectronic searches bibliography searching
272 studies that passed initialscreen and were retrieved forfurther scrutiny
109 studies includedin systematic review
49 relevant articles identifiedthrough bibliographic searchof included papers
163 studies excluded:- No intervention to reduce utilization- Did not report on outcomes of interest
2964 citations excluded (Studies did notreport on interventions related tolaboratory utilization, or did not containoriginal data)
Figure 1 Selection of articles in systematic review. The search was performed in September of 2013.
to –27.7% (an increase in test volume). Table 2 dis-plays the percent relative reductions in test volume for each intervention and their sub-categories. Interven-tions with an educational component had the highest median relative reduction in test volume at 34.5% (IQR 16.5–49.0) while audit feedback or system-based inter-ventions had a relative reduction of 22.0% (8.6–34.6) and 22.2% (3.6–68.3), respectively (Figure 2). The single incentive and penalty intervention had a 5.8% relative reduction.
Thirty-three (27.7%) of the interventions targeted three or fewer tests, while 86 (72.3%) targeted four or more tests. The median relative reduction for interventions that tar-geted three or fewer tests was 40.2% (IQR 23.7–52.8) while that targeting four or more tests was 18.8% (IQR 8.2–28.5) (Figure 3). Thirty interventions (25.2%) used multiple interventions; these multifaceted interventions had larger reductions in test use with a median relative reduc-tion in test volume of 32.7% (IQR 15.1–47.5) versus 21.4% (IQR 9.5–33.3) for interventions that were classified into a single category. Interventions for which physicians were engaged during the intervention development had similar median relative reductions as interventions without phy-sician input.
Finally, we found important differences in the rela-tive reductions across quality indicators (Table 3). Most notably, the effect of interventions was less if a study reported a reduction in test utilization per patient rather than reduction per institution or physician group and studies with a concurrent control group had smaller reductions. Unexpectedly there were larger relative reduc-tions in studies that had a risk of contamination between the experimental and control groups.
Interventions with the largest effects
We found extensive heterogeneity in the components that made up each intervention, how interventions were imple-mented, the study setting, and the tests that were targeted for reduction. Meaningful generalizations across interven-tion types is therefore difficult; so the interventions with the largest relative reductions in test volume are described here (Table 1). The studies by Froom et al. and Lewand-rowski et al. attained the largest relative reductions with both targeting a single test. Froom et al. changed labo-ratory policy so that urine microscopy was done only if specifically requested by the physician; this resulted in
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 161
Tabl
e 1
Stud
y ch
arac
teris
tics
and
desc
riptio
n of
inte
rven
tions
.
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Amuk
ele
2011
US
A
Phys
icia
ns
wor
king
in
surg
ery,
he
mat
olog
y, a
nd
inte
rnal
med
icin
e
Si
ngle
te
achi
ng
hosp
ital
Th
e or
der f
orm
was
mod
ified
with
som
e te
sts
bein
g bu
ndle
d an
d ot
hers
bei
ng
unbu
ndle
d. P
hysi
cian
s w
ho w
ere
high
us
ers
wer
e ed
ucat
ed a
bout
coag
ulat
ion
test
s an
d an
alg
orith
m w
as d
istri
bute
d
Be
fore
-afte
r
X
X
PT, P
TT, T
T an
d fib
rinog
en
77.8
Arch
amba
ult
2011
US
A
All p
hysi
cian
s
Sing
le
teac
hing
ho
spita
l
ES
R te
stin
g w
as n
o lo
nger
per
form
ed
Befo
re-a
fter
X
ESR
and
CRP
47
.5
Atta
li 20
06
Isra
el
Resi
dent
ph
ysic
ians
Si
ngle
te
achi
ng
hosp
ital
Ed
ucat
iona
l lec
ture
abo
ut e
xces
sive
an
d in
appr
opria
te te
stin
g; te
sts
wer
e un
bund
led
on th
e re
ques
t for
m; a
sen
ior
phys
icia
n ga
ve fe
edba
ck a
bout
ord
erin
g pr
actic
es
Be
fore
-afte
r
X
X
X
Al
l blo
od te
sts
34
.5a
Bara
zzon
i 200
2
Switz
erla
nd
All p
hysi
cian
s se
eing
pat
ient
s pr
e-op
erat
ivel
y fo
r ele
ctiv
e pr
oced
ures
6
com
mun
ity
hosp
itals
w
ith s
urge
ry
faci
litie
s
Al
l sta
keho
lder
s w
ere
invo
lved
in
a gu
idel
ine
crea
tion
proc
ess.
The
guid
elin
es w
ere
then
ado
pted
as
hosp
ital
polic
y
Be
fore
-afte
r
X
Al
l pre
-ope
rativ
e te
sts
26
.1a
Bare
ford
199
0
USA
Al
l med
ical
sta
ff:
cons
ulta
nts
and
juni
or h
ouse
sta
ff
Si
ngle
co
mm
unity
ho
spita
l
M
onth
ly u
sage
sta
tem
ents
wer
e di
strib
uted
to p
hysi
cian
s. G
uide
lines
on
app
ropr
iate
test
ing
wer
e di
strib
uted
an
d so
me
test
s w
ere
canc
eled
if
inap
prop
riate
Be
fore
-afte
r
X
X
X
CB
C, E
SR a
nd P
T
62.1
Baric
chi 2
012
Ita
ly
Gene
ral
prac
titio
ners
4
prim
ary
care
clin
ics
Te
stin
g al
gorit
hms
for 7
com
mon
clin
ical
sc
enar
ios
wer
e de
velo
ped.
Phy
sici
ans
wer
e th
en e
duca
ted
abou
t the
alg
orith
ms
and
told
to u
se th
em
Be
fore
-afte
r
X
X
All b
lood
test
s
4.7
Barie
199
5
USA
Al
l med
ical
sta
ff in
th
e IC
U
Sing
le
teac
hing
ho
spita
l
Te
stin
g pa
thw
ays
wer
e in
trodu
ced
and
audi
t and
feed
back
was
don
e m
onth
ly
Befo
re-a
fter
X
X
Al
l blo
od te
sts
and
ches
t ra
diog
raph
s
34.6
Bate
s 19
99
USA
Al
l phy
sici
ans
Si
ngle
te
achi
ng
hosp
ital
De
finiti
ons
of a
redu
ndan
t tes
t wer
e cr
eate
d. Th
e co
mpu
ter o
rder
ent
ry
syst
em cr
eate
d re
min
ders
whe
n te
sts
wer
e or
dere
d th
at w
ere
redu
ndan
t
Ra
ndom
ized
tri
al
X
El
ectro
lyte
s, u
rinal
ysis
, di
goxi
n, to
bram
ycin
, am
inop
hylin
e, va
ncom
ycin
, an
d ge
ntam
ycin
leve
ls,
urin
e, sp
utum
and
stoo
l cu
lture
s, C
lost
ridiu
m d
iffic
ile
test
ing,
fibr
in sp
lit p
rodu
cts
0.
1
UnauthenticatedDownload Date | 5/19/16 2:24 AM

162 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Bate
s 19
97
USA
Al
l phy
sici
ans
Si
ngle
te
achi
ng
hosp
ital
Co
sts
wer
e di
spla
yed
for e
ach
test
that
w
as o
rder
ed.
Be
fore
-afte
r
X
Al
l blo
od te
sts
and
the
35
mos
t com
mon
radi
olog
ic
test
s
4.
1
Bere
nhol
tz 2
001
US
A
Phys
icia
ns
wor
king
in a
su
rgic
al IC
U
Si
ngle
te
achi
ng
hosp
ital
Cl
inic
al p
athw
ays
wer
e cr
eate
d fo
r va
rious
sur
gica
l pro
blem
s. A
ppro
pria
te
labo
rato
ry te
stin
g w
as s
ugge
sted
by
the
path
way
Be
fore
-afte
r
X
Al
l lab
orat
orie
s in
clud
ed in
th
e pa
thw
ay
–6.8
Berw
ick
1986
US
A
35 in
tern
ists
Si
ngle
hea
lth
man
agem
ent
orga
niza
tion
Do
ctor
s m
et to
dis
cuss
the
use
of
part
icul
ar te
sts
and
jour
nal a
rtic
les
wer
e di
strib
uted
on
the
use
of th
ese
test
sCl
inic
ians
rece
ived
indi
vidu
aliz
ed
feed
back
on
thei
r rat
es o
f tes
t ord
erin
g co
mpa
red
to th
eir p
eers
and
thei
r ran
k re
lativ
e to
thei
r pee
rsPh
ysic
ians
wer
e ra
nked
by
the
prop
ortio
n of
test
s th
ey o
rder
ed th
at
wer
e ab
norm
al. E
ach
phys
icia
n w
as th
en
give
n th
eir r
ank
Be
fore
-afte
r
Befo
re-a
fter
Befo
re-a
fter
X X X
ESR,
T4, s
erum
glu
cose
, he
tero
phile
ant
ibod
y te
stin
g, A
NA, S
LE
prep
arat
ion,
RF,
liver
en
zym
es, c
hole
ster
ol
leve
ls, r
adio
grap
hs o
f pe
riphe
ral b
ones
and
ch
est,
ECGs
0.
2
14.2
a
–4.1
Boon
-Fal
leur
19
95
Belg
ium
Ph
ysic
ians
w
orki
ng o
n liv
er a
tra
nspl
ant u
nit
Pe
diat
ric li
ver
unit
A
rule
bas
ed d
ecis
ion
supp
ort
appl
icat
ion
deci
ded
on th
e ne
xt d
ay’s
la
bora
tory
test
s ba
sed
on p
revi
ous
resu
lts
Be
fore
-afte
r
X
Al
l blo
od te
sts
24
.9
Buck
ingh
am
1994
Sc
otla
nd
All p
hysi
cian
s
All h
ospi
tals
in
a s
ingl
e ci
ty
Ju
stifi
catio
n fo
r tes
ts o
rder
ed h
ad to
be
give
n. S
peci
fics
on h
ow th
is w
as d
one
are
not g
iven
Be
fore
-afte
r
X
Al
l bio
chem
ical
blo
od te
sts
1.
4
Bunt
ing
2004
Ca
nada
20
0 ph
ysic
ians
w
ho o
rder
ed th
e m
ost t
ests
in 1
997
Si
ngle
pr
ovin
ce
Feed
back
on
test
usa
ge w
as g
iven
four
tim
es o
ver a
2-y
ear p
erio
d
Rand
omiz
ed
cont
rolle
d tri
al
X
All b
lood
test
s
7.8a
Burn
ett 1
991
Au
stra
lia
All p
hysi
cian
s re
ques
ting
bloo
d w
ork
from
a s
ingl
e m
edic
al la
bora
tory
Si
ngle
priv
ate
med
ical
la
bora
tory
Al
l lab
orat
ory
test
s w
ere
unbu
ndle
d so
th
ey h
ad to
be
orde
red
indi
vidu
ally
Be
fore
-afte
r
X
Al
l blo
od te
sts
18
.8a
Cald
eron
-M
arga
lit 2
005
Is
rael
Al
l phy
sici
ans
Si
ngle
te
achi
ng
hosp
ital
Se
vera
l int
erve
ntio
ns in
clud
ing
man
dato
ry co
nsul
tatio
n pr
ior t
o or
derin
g,
educ
atio
n, re
stric
tion
or e
limin
atio
n of
va
rious
test
s
Be
fore
-afte
r
X
X
All b
lood
test
s
19.0
a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 163
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Cars
on 1
995
US
A
All p
hysi
cian
s
Sing
le
teac
hing
ho
spita
l
An
alg
orith
m th
at a
utom
atic
ally
re
stric
ted
fibrin
deg
rada
tion
prod
uct
test
ing
and
inst
ead
used
D-d
imer
test
ing
for s
uspe
cted
DIC
Be
fore
-afte
r
X
D-
Dim
er a
nd fi
brin
de
grad
atio
n pr
oduc
ts
48.3
a
Cart
er 2
002
US
A
Phys
icia
ns
send
ing
spec
imen
s to
the
lab
Si
ngle
te
achi
ng
hosp
ital
Al
l tes
t req
uest
s w
ere
revi
ewed
by
a m
ore
seni
or p
hysi
cian
Be
fore
-afte
r
X
Al
l lab
orat
orie
s th
at
cost
> $7
5 US
D
23.0
Chen
200
3
USA
Al
l Phy
sici
ans
orde
ring
sele
cted
te
sts
Si
ngle
te
achi
ng
hosp
ital
A
rem
inde
r on
the
half-
life
of v
ario
us
anti-
epile
ptic
dru
gs w
as s
how
n on
th
e co
mpu
ter w
hen
repe
at le
vels
wer
e re
ques
ted
in a
sho
rt tim
e pe
riod
Be
fore
-afte
r
X
X
Anti
epile
ptic
dru
g le
vels
23
.4a
Chu
2012
Au
stra
lia
Med
ical
stu
dent
s an
d re
side
nts
Si
ngle
te
achi
ng
hosp
ital
Se
lect
ed te
sts
wer
e re
stric
ted
and
requ
ired
a se
nior
sta
ff m
embe
r to
sign
off
on th
em p
rior t
o be
ing
orde
red
Be
fore
-afte
r
X
Co
agul
atio
n te
sts,
thyr
oid
func
tion
test
s, E
SR a
nd
d-di
mer
7.
5a
Chu
1996
US
A
Phys
icia
ns ta
king
ca
re o
f tra
uma
patie
nts
Si
ngle
te
achi
ng
hosp
ital
A
liber
al a
dmis
sion
alg
orith
m w
ith
exte
nsiv
e te
stin
g w
as co
mpa
red
to
phys
icia
ns o
nly
orde
ring
test
s th
ey
thou
ght n
eces
sary
Be
fore
-afte
r
X
He
mat
olog
y, ch
emis
try
and
coag
ulat
ion
prof
ile,
urin
alys
is, b
lood
gas
, blo
od
alco
hol l
evel
, typ
e an
d sc
reen
68
.3
Cohe
n 19
82
USA
Al
l phy
sici
ans
wor
king
on
the
teac
hing
uni
ts
4
clin
ical
te
achi
ng
units
at
a si
ngle
te
achi
ng
hosp
ital
Th
e co
st o
f all
imag
ing
test
s or
dere
d w
ere
give
n to
eac
h te
am w
eekl
y
The
cost
of a
ll bl
ood
test
s or
dere
d w
ere
give
n to
eac
h te
am w
eekl
y
Ra
ndom
ized
co
ntro
lled
trial
Rand
omiz
ed
cont
rolle
d tri
al
X X
CXR,
CT
scan
s, U
S an
d liv
er
scan
sAl
l blo
od te
sts
12
.9
24.7
a
Da
vido
ff 19
89
USA
24
med
ical
in
tern
s en
terin
g a
univ
ersi
ty tr
aini
ng
prog
ram
Si
ngle
te
achi
ng
hosp
ital
Le
ctur
es o
n pr
obab
ility
and
test
ch
arac
teris
tics
wer
e co
mpa
red
to
plac
ebo
lect
ures
on
econ
omic
s an
d co
st
cont
rol
Ra
ndom
ized
co
ntro
lled
trial
X
All b
lood
test
s
16.5
a
Dets
ky 1
986
Ca
nada
Al
l atte
ndin
g ph
ysic
ians
20
teac
hing
ho
spita
ls
in a
sin
gle
prov
ince
Re
side
nts
and
inte
rns
wen
t on
strik
e fo
r 7
days
in 1
980
Be
fore
-afte
r
X
Al
l blo
od te
sts
8.
3a
UnauthenticatedDownload Date | 5/19/16 2:24 AM
164 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Dick
inso
n 19
87
USA
Al
l phy
sici
ans
in
the
inst
itutio
n
Sing
le
teac
hing
ho
spita
l
Th
e nu
mbe
r of u
nnec
essa
ry te
sts
was
m
easu
red
and
show
n to
dep
artm
ent
head
s
Be
fore
-afte
r
X
Al
l blo
od te
sts
24
.5a
Dixo
n 19
74
USA
In
tern
s w
orki
ng o
n th
e w
ards
Si
ngle
te
achi
ng
hosp
ital
In
tern
s an
d re
side
nts
wer
e lim
ited
to 8
te
sts
each
Be
fore
-afte
r
X
Al
l blo
od ch
emis
try te
sts
66
.7a
Dow
ling
1989
US
A
Resi
dent
s in
a
fam
ily h
ealth
ce
nter
Si
ngle
fam
ily
heal
th ce
nter
Le
ctur
es a
nd g
uide
lines
on
appr
opria
te
test
ing
wer
e di
strib
uted
. Aud
it an
d fe
edba
ck o
f tes
t usa
ge w
as p
erfo
rmed
re
peat
edly
Be
fore
-afte
r
X
X
CBC
and
TSH
47
.5a
Dura
nd-Z
ales
ki
1993
Fr
ance
Al
l phy
sici
ans
at
the
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
Th
e la
bora
tory
requ
isiti
on w
as ch
ange
d so
that
the
purp
ose
of e
ach
tum
or m
arke
r w
as in
clud
ed o
n th
e re
quis
ition
Be
fore
-afte
r
X
Tu
mor
mar
kers
23
.9a
Durie
ux 2
003
Fr
ance
Al
l phy
sici
ans
at
the
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
Th
e la
bora
tory
requ
isiti
on w
as ch
ange
d so
that
the
purp
ose
of e
ach
tum
or m
arke
r w
as in
clud
ed o
n th
e re
quis
ition
. The
pu
rpos
e fo
r eac
h te
st, i
.e.,
scre
enin
g,
follo
w-u
p or
dia
gnos
is w
as e
xpla
ined
on
the
requ
isiti
on
Be
fore
-afte
r
X
X
CEA,
alp
ha fe
to-p
rote
in,
CA19
-9
56.5
a
Eccl
es 2
001
En
glan
d an
d Sc
otla
nd
Gene
ral
Prac
titio
ners
M
ultip
le
prim
ary
care
cl
inic
s
Gu
idel
ines
on
whe
n to
ord
er lu
mba
r sp
ine
and
knee
X-ra
ys w
ere
circ
ulat
ed
alon
g w
ith fe
edba
ck o
n th
e nu
mbe
r of
requ
ests
to e
ach
phys
icia
n
Ra
ndom
ized
co
ntro
lled
trial
X
X
Kn
ee a
nd lu
mba
r spi
ne X
R
40.8
Eise
nber
g 19
77
USA
Re
side
nt
phys
icia
ns
Sing
le
com
mun
ity
hosp
ital
Th
ere
was
an
educ
atio
n pr
ogra
m w
ith
a w
eekl
y le
ctur
e; re
sults
from
a s
ingl
e au
dit o
n ut
ility
of t
estin
g w
ere
circ
ulat
ed
alon
g w
ith a
mem
oran
dum
from
the
med
ical
dire
ctor
ask
ing
for c
aref
ul
cons
ider
atio
n of
test
usa
ge
Be
fore
-afte
r
X
PT
T
42.1
a
Emer
son
2001
US
A
All p
hysi
cian
s w
orki
ng a
t the
m
edic
al ce
nter
Si
ngle
te
achi
ng
hosp
ital
La
bora
tory
requ
isiti
on w
as re
desi
gned
w
ith s
ome
test
s un
bund
led
and
casc
ades
im
plem
ente
d fo
r thy
roid
func
tion
and
anem
ia
Be
fore
-afte
r
X
Al
l blo
od te
sts
4.
7a
Ever
ett 1
985
US
A
Firs
t yea
r res
iden
ts
Sing
le
teac
hing
ho
spita
l
Re
side
nts
wer
e ta
ught
abo
ut la
bora
tory
ut
iliza
tion
usin
g sp
ecifi
c cas
es
Rand
omiz
ed
cont
rolle
d tri
al
X
All b
lood
test
s an
d m
icro
biol
ogy
–1
2.3
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 165
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Ever
ett 1
983
US
A
Firs
t yea
r res
iden
ts
train
ing
in in
tern
al
med
icin
e
Si
ngle
te
achi
ng
hosp
ital
Au
dit a
nd fe
edba
ck o
f cos
ts w
as
perfo
rmed
wee
kly,
cost
edu
catio
n ne
ws
lette
rs w
ere
dist
ribut
ed a
nd co
sts
of
test
s w
ere
put i
n pa
tient
char
ts. T
here
w
ere
one-
on-o
ne m
eetin
gs o
f fac
ulty
with
re
side
nts
to d
iscu
ss co
sts
Ra
ndom
ized
co
ntro
lled
trial
X
X
Al
l blo
od te
sts
15
.1a
Feld
kam
p 19
96
USA
Al
l phy
sici
ans
in
heal
th ce
nter
Si
ngle
te
achi
ng
hosp
ital a
nd
22 s
atel
lite
clin
ics
Al
gorit
hms
wer
e de
velo
ped
for t
hyro
id
func
tion
test
ing
and
impl
emen
ted
by th
e la
bora
tory
Be
fore
-afte
r
X
Th
yroi
d fu
nctio
n te
stin
g
21.6
Feld
man
201
3
USA
Al
l pro
vide
rs w
ho
orde
r lab
orat
ory
test
s th
roug
h a
com
pute
rized
or
der e
ntry
sys
tem
Si
ngle
te
achi
ng
hosp
ital
Co
st o
f eac
h te
st w
as d
ispl
ayed
whe
n it
was
ord
ered
Ra
ndom
ized
co
ntro
lled
trial
X
X
61
dia
gnos
tic b
lood
test
s
8.6a
Fine
gan
2005
Ca
nada
Al
l phy
sici
an
train
ees
in a
ho
spita
l
Si
ngle
te
achi
ng
hosp
ital
Ea
ch a
nest
hetis
t sel
ecte
d te
sts
to
be p
erfo
rmed
pre
oper
ativ
ely
at th
eir
disc
retio
n. Th
e co
mpa
rato
r was
sur
gery
sp
ecifi
c pro
toco
ls th
at w
ere
bein
g us
ed
Be
fore
-afte
r
All b
lood
test
s
3.6
Fong
200
8
Aust
ralia
Al
l phy
sici
ans
wor
king
in th
e em
erge
ncy
room
Si
ngle
te
achi
ng
hosp
ital
A
clin
ical
dec
isio
n ru
le w
as u
sed
inst
ead
of p
hysi
cian
dis
cret
ion
Be
fore
-afte
r
X
CT
hea
d
–27.
7a
Fow
kes
1986
Un
ited
King
dom
Al
l res
iden
ts
wor
king
on
the
med
ical
uni
t
Si
ngle
te
achi
ng
hosp
ital
A
guid
elin
e on
test
ing
was
dis
tribu
ted
and
wee
kly
mee
tings
wer
e he
ld w
ith
med
ical
sta
ff to
dis
cuss
thei
r use
of t
ests
in
the
prev
ious
wee
k
No
n-ra
ndom
ized
co
ntro
lled
trial
X
X
Al
l blo
od te
sts
63
.4a
Frie
dman
201
0
USA
Ph
ysic
ians
taki
ng
care
of c
hild
ren
post
pro
cedu
re
Si
ngle
te
achi
ng
hosp
ital
A
set o
f sta
ndar
d as
sess
men
t and
m
anag
emen
t pla
ns w
ere
deve
lope
d an
d im
plem
ente
d af
ter c
erta
in p
roce
dure
s
Be
fore
-afte
r
X
Al
l blo
od te
sts
and
imag
ing
15
.6
Froo
m 2
012
Is
rael
Al
l phy
sici
ans
Re
gion
al
labo
rato
ry
serv
ing
a si
ngle
Hea
lth
Man
agem
ent
Orga
niza
tion
Ur
ine
mic
rosc
opy
was
no
long
er d
one
auto
mat
ical
ly in
stea
d th
e ph
ysic
ian
had
to s
peci
fical
ly re
ques
t it
Be
fore
-afte
r
X
Ur
ine
for d
ip a
nd
mic
rosc
opy
99
.7a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

166 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Gam
a 19
91
Unite
d Ki
ngdo
m
Gene
ral i
nter
nist
s
Sing
le
com
mun
ity
hosp
ital
Da
ta o
n pe
rson
al a
nd p
eer e
xpen
ditu
re
of la
bora
tory
reso
urce
s w
as g
iven
to
phys
icia
ns m
onth
ly fo
r 12
mon
ths
Ra
ndom
ized
co
ntro
lled
trial
X
Clin
ical
chem
istry
24
.6a
Gam
a 19
92
Unite
d Ki
ngdo
m
Phys
icia
ns ta
king
ca
re o
f inp
atie
nts
Si
ngle
co
mm
unity
ho
spita
l
Da
ta o
n pe
rson
al a
nd p
eer c
linic
al
chem
istry
exp
endi
ture
per
pat
ient
was
pr
ovid
ed to
phy
sici
ans
mon
thly
for 1
2 m
onth
s
Be
fore
-afte
r
X
Cl
inic
al ch
emis
try a
nd
hem
atol
ogy
27
.0a
Godd
ard
2011
Ire
land
Al
l phy
sici
ans
wor
king
in th
e IC
U
Sing
le
teac
hing
ho
spita
l
Al
l rec
urrin
g or
ders
for b
lood
wor
k w
ere
disc
ontin
ued;
inst
ead
each
test
had
to b
e or
dere
d as
a s
ingl
e oc
curr
ence
Be
fore
-afte
r
CBC,
ure
a, e
lect
roly
tes,
co
agul
atio
n, L
FTs,
m
agne
sium
, Ca,
PO4
, al
bum
in, C
RP
33
.1
Gold
en 1
987
US
A
All p
hysi
cian
s
Outp
atie
nt
depa
rtmen
t of
a s
ingl
e te
achi
ng
hosp
ital
Th
e co
st o
f tes
ts b
illed
to th
e pa
tient
was
ch
ange
d so
that
ord
erin
g in
divi
dual
test
s w
as ch
eape
r tha
n or
derin
g th
e w
hole
pa
nel
Be
fore
-afte
r
X
Al
l blo
od ch
emis
try te
st
33.5
a
Gortm
aker
198
8
USA
Al
l phy
sici
ans
wor
king
in th
e ho
spita
l
Si
ngle
co
mm
unity
ho
spita
l
Ni
ne s
taff
mee
tings
wer
e he
ld to
dis
cuss
co
st is
sues
. Dat
a on
exc
ess
usag
e w
as s
ent t
o al
l doc
tors
. All
phys
icia
ns
reac
hed
a co
nsen
sus
on w
hen
each
test
w
as co
nsid
ered
inap
prop
riate
Be
fore
-afte
r
X
BU
N, C
BC, c
hem
istry
pr
ofile
, CK,
crea
tinin
e,
elec
troly
tes,
fast
ing
and
rand
om b
lood
sug
ar,
hem
atoc
rit, P
T, S
GOT,
ur
inal
ysis
14
.0a
Griv
ell 1
981
Au
stra
lia
All p
hysi
cian
s ca
ring
for
inpa
tient
s
Si
ngle
te
achi
ng
hosp
ital
Ph
ysic
ians
rece
ived
a re
port
ever
y 4
wee
ks o
n th
e ty
pe a
nd n
umbe
r of t
ests
or
dere
d. P
hysi
cian
s w
ere
also
sho
wn
whe
re th
ey ra
nk in
com
paris
on to
thei
r pe
ers
Be
fore
-afte
r
X
Al
l blo
od te
sts
0.
0
Groo
pman
199
2
USA
Al
l med
ical
st
aff o
rder
ing
labo
rato
ries
in
the
ER
Si
ngle
te
achi
ng
hosp
ital
Te
sts
wer
e ta
ken
off t
he s
tand
ard
requ
isiti
on a
nd h
ad to
be
writ
ten
in b
y ha
nd
Be
fore
-afte
r
X
PT
/PTT
61
.6a
Gros
s 19
88
USA
Al
l phy
sici
ans
taki
ng ca
re o
f in
patie
nts
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
on
whe
n to
ord
er b
lood
cu
lture
s w
ere
dist
ribut
ed
Befo
re-a
fter
X
Bloo
d cu
lture
s
75.0
a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 167
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Hasc
hke-
Bech
er
2009
Au
stria
No
doc
tors
wer
e ta
rget
ed, i
t was
a
labo
rato
ry
inte
rven
tion
Si
ngle
te
achi
ng
hosp
ital
A
deci
sion
rule
was
crea
ted
to d
eter
min
e w
hen
the
labo
rato
ry w
ould
pro
cess
liq
uor d
iagn
ostic
s
Be
fore
-afte
r
X
Li
quor
dia
gnos
tics
28
.6a
Hutto
n 20
09
Unite
d Ki
ngdo
m
All e
mer
genc
y ro
om a
nd m
edic
al
unit
phys
icia
ns
Si
ngle
te
achi
ng
hosp
ital
Re
ques
ts fo
r CRP
from
the
ER h
ad to
be
app
rove
d by
a s
enio
r phy
sici
an.
Juni
or s
taff
wer
e to
ld to
lim
it CR
P us
e.
Last
ly re
peat
test
ing
with
in 2
4 h
was
di
sallo
wed
Be
fore
-afte
r
X
X
CRP
85
.0a
Jelin
ek 1
990
Au
stra
lia
All p
hysi
cian
s
Sing
le
teac
hing
ho
spita
l
Gu
idel
ines
on
whe
n ab
dom
inal
film
s co
uld
be o
rder
ed w
ere
circ
ulat
ed a
nd
all r
eque
sts
had
to b
e ru
n by
a s
enio
r ph
ysic
ian
Be
fore
-afte
r
X
X
Abdo
min
al p
lain
film
s
52.2
Kelly
199
8
Aust
ralia
Al
l phy
sici
ans
in
the
ER
Sing
le
com
mun
ity
hosp
ital
Gu
idel
ines
on
who
sho
uld
rece
ive
a bl
ood
cultu
re w
ere
dist
ribut
ed
Befo
re-a
fter
X
Bloo
d cu
lture
s
53.0
Kum
wila
isak
20
08
USA
Al
l phy
sici
ans
wor
king
in th
e su
rgic
al IC
U
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
rega
rdin
g w
hen
certa
in b
lood
te
sts
shou
ld b
e us
ed w
ere
intro
duce
d at
a
staf
f mee
ting
and
sent
out
by
emai
l. A
sess
ion
was
repe
ated
for n
ew re
side
nts
ever
y m
onth
Be
fore
-afte
r
X
Al
l blo
od te
sts
20
.8a
Laro
cque
199
4
Cana
da
Surg
eons
and
su
rgic
al h
ouse
st
aff
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
on
whi
ch te
sts
wer
e ap
prop
riate
for d
iffer
ent m
edic
al
cond
ition
s w
ere
post
ed o
n th
e w
ards
and
di
strib
uted
as
pock
et ca
rds
Be
fore
-afte
r
X
Pr
e-op
scr
eeni
ng te
sts
incl
udin
g bl
ood
wor
k, C
XR
and
ECGs
10
.1a
Levi
ck 2
013
US
A
Clin
icia
ns o
rder
ing
the
BNP
test
A
heal
th
netw
ork
incl
udin
g 2
hosp
itals
an
d se
vera
l co
mm
unity
he
alth
ce
nter
s
Co
mpu
ter o
rder
ent
ry s
yste
m d
ispl
ayed
a
war
ning
whe
n a
repe
at B
NP w
as b
eing
or
dere
d
Be
fore
-afte
r
X
BN
P
22.2
a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

168 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Lew
andr
owsk
i 19
94
USA
Al
l phy
sici
ans
wor
king
at t
he
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
A
guid
elin
e on
app
ropr
iate
test
ing
was
dev
elop
ed. A
ll re
ques
ts w
ere
then
re
view
ed b
y la
bora
tory
sta
ff an
d th
e or
derin
g ph
ysic
ian
was
cont
acte
d if
the
requ
est w
as n
ot in
acc
orda
nce
with
the
guid
elin
e
Be
fore
-afte
r
X
X
LD-is
ozym
es
99.6
Man
cuso
199
9
USA
Al
l phy
sici
ans
at
the
hosp
ital
Si
ngle
sp
ecia
lized
or
thop
edic
su
rger
y ho
spita
l
Gu
idel
ines
wer
e pu
blis
hed
sugg
estin
g se
lect
ive
test
ord
erin
g pr
eope
rativ
ely
Be
fore
-afte
r
X
Pr
e-op
erat
ive
bloo
d w
ork,
EC
G, C
XR,
30
.0a
Mar
tin 1
980
US
A
Resi
dent
s an
d m
edic
al s
tude
nts
Si
ngle
te
achi
ng
hosp
ital
Th
ere
was
a 1
h le
ctur
e on
labo
rato
ry
cost
s. M
oney
was
giv
en to
the
resi
dent
s if
thei
r lab
orat
ory
use
decr
ease
d
No
n-ra
ndom
ized
co
ntro
lled
trial
X
X
Al
l rad
iolo
gic a
nd b
lood
te
sts
5.
8a
Ther
e w
as a
1-h
lect
ure
on la
bora
tory
co
sts.
Sen
ior p
hysi
cian
s th
en m
et w
eekl
y w
ith re
side
nts,
they
revi
ewed
case
s an
d su
gges
ted
chan
ges
in te
st o
rder
ing
prac
tices
.
X
X
–1
7.8a
Mar
ton
1985
US
A
Resi
dent
s an
d m
edic
al s
tude
nts
Si
ngle
te
achi
ng
hosp
ital
A
man
ual a
bout
ratio
nal t
est o
rder
ing
was
giv
en to
the
train
ees
Ra
ndom
ized
co
ntro
lled
trial
X
All b
lood
test
s
18.2
Feed
back
on
labo
rato
ry u
sage
and
cost
s in
curr
ed w
as s
how
n to
trai
nees
alo
ng
with
thei
r usa
ge co
mpa
red
with
pee
rs
X
33.3
A m
anua
l abo
ut ra
tiona
l tes
t ord
erin
g w
as g
iven
to th
e tra
inee
s. Th
ey a
lso
rece
ived
feed
back
on
labo
rato
ry u
sage
, co
sts
incu
rred
and
thei
r usa
ge co
mpa
red
with
pee
rs
X
X
40
.9a
May
200
6
USA
Al
l doc
s w
orki
ng
on in
patie
nt
serv
ice
Si
ngle
te
achi
ng
hosp
ital
Du
plic
ate
orde
rs w
ere
dele
ted
and
all
bloo
d w
ork
orde
rs e
xpire
d in
24
h. B
lood
w
ork
wou
ld o
nly
be d
raw
n ev
ery
4, 6
or
12 h
. Fut
ure
orde
rs co
uld
only
be
for a
si
ngle
occ
urre
nce
Be
fore
-afte
r
X
Al
l blo
od te
sts
11
.5a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 169
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Meh
ari 1
997
Ne
w
Zeal
and
Ph
ysic
ians
w
orki
ng in
ICU
Si
ngle
te
achi
ng
hosp
ital
A
guid
elin
e w
as p
lace
d on
eac
h pa
tient
s ch
art s
tatin
g w
hen
it is
app
ropr
iate
to d
o ea
ch te
st
Be
fore
-afte
r
X
CB
C, co
agul
atio
n te
sts,
Cr
, Na,
K, u
rea,
calc
ium
, gl
ucos
e, M
g, P
O4, A
BGs
21
.2
Men
g 20
06
Cana
da
All p
hysi
cian
s
3 te
achi
ng
hosp
itals
A
polic
y w
as cr
eate
d re
gard
ing
who
is
allo
wed
to o
rder
trop
onin
test
ing
and
how
man
y re
peat
s ca
n be
ord
ered
Be
fore
-afte
r
X
Tn
I
2.9
Mer
lani
200
1
Switz
erla
nd
Doct
ors
resi
dent
s an
d nu
rses
w
orki
ng in
the
inte
nsiv
e ca
re u
nit
Sing
le
teac
hing
ho
spita
l
A
guid
elin
e on
whe
n ar
teria
l blo
od g
ases
ca
n be
don
e w
as ci
rcul
ated
Be
fore
-afte
r
X
X
ABG
41
.5a
Mey
er 2
010
US
A
Gyne
colo
gic
onco
logi
sts
and
othe
r phy
sici
ans
Si
ngle
te
achi
ng
hosp
ital
A
mul
tidis
cipl
inar
y te
am cr
eate
d a
guid
elin
e an
d th
en cr
eate
d a
com
mun
icat
ion
plan
to d
isse
min
ate
it
Be
fore
-afte
r
X
Pa
p te
sts
31
.2a
Miy
akis
200
6
Gree
ce
All p
hysi
cian
s w
orki
ng a
t the
ho
spita
l
Si
ngle
te
achi
ng
hosp
ital
Th
e re
sults
of a
n au
dit o
n te
st u
se w
ere
pres
ente
d al
ong
with
stra
tegi
es fo
r re
duci
ng u
tiliz
atio
n
Be
fore
-afte
r
X
X
25 la
bora
torie
s he
mat
olog
y an
d ch
emis
try te
sts
13
.5a
Mor
ris 1
992
US
A
All p
hysi
cian
s w
orki
ng a
t the
ho
spita
l
Si
ngle
te
achi
ng
hosp
ital
On
ly o
ne s
tool
sam
ple
for p
aras
ites
was
ac
cept
ed b
y th
e la
bora
tory
inst
ead
of
thre
e
Be
fore
-afte
r
X
St
ool f
or o
va a
nd p
aras
ite
33.3
Mut
imer
199
2
Unite
d Ki
ngdo
m
All p
hysi
cian
s w
orki
ng in
the
liver
uni
t
Li
ver u
nit
at a
sin
gle
teac
hing
ho
spita
l
La
bora
tory
test
s to
be
orde
red
for t
he
next
day
wer
e de
term
ined
by
prot
ocol
ba
sed
on p
atie
nt ch
arac
teris
tics
and
prev
ious
test
ing
Be
fore
-afte
r
X
He
mat
olog
y, b
ioch
emis
try,
imm
unol
ogy,
mic
robi
olog
y an
d cr
oss
mat
chin
g
9.
3a
Nard
ella
199
5
USA
An
esth
etis
ts a
nd
surg
eons
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
abo
ut a
ppro
pria
te p
re-
oper
ativ
e te
stin
g w
ere
dist
ribut
ed a
nd
disc
usse
d at
sta
ff m
eetin
gs
Be
fore
-afte
r
X
CB
C, P
T, P
TT, b
leed
ing
time,
BU
N, C
r, Gl
ucos
e AL
T AS
T,
elec
troly
tes
61
.8a
Neils
on 2
004
US
A
Resi
dent
s,
phys
icia
ns a
nd
nurs
e pr
actit
ione
rs
who
use
d co
mpu
ter o
rder
en
try
Si
ngle
te
achi
ng
hosp
ital
Re
curr
ing
test
s ha
d to
be
conf
irmed
da
ily, m
any
test
s w
ere
limite
d to
a s
ingl
e oc
curr
ence
and
pre
viou
s re
sults
wer
e di
spla
yed
whe
n or
derin
g te
sts
Be
fore
-afte
r
X
Al
l blo
od te
sts
and
imag
ing
64
.2a
Nels
on 1
978
US
A
All p
hysi
cian
s w
ho w
ork
at th
e ho
spita
l
Si
ngle
co
mm
unity
ho
spita
l
Th
ere
was
a 2
0-m
in g
rand
roun
ds
pres
enta
tion
on B
12 te
stin
g.
Sugg
estio
ns w
ere
give
n on
whe
n to
ord
er
this
test
Be
fore
-afte
r
X
B1
2 an
d fo
late
45
.3
UnauthenticatedDownload Date | 5/19/16 2:24 AM

170 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Nigh
tinga
le 1
994
Unite
d Ki
ngdo
m
Resi
dent
s w
orki
ng
on th
e liv
er u
nit
Li
ver u
nit
at a
sin
gle
teac
hing
ho
spita
l
A
com
pute
rized
pro
toco
l was
crea
ted
that
su
gges
ted
test
s fo
r the
nex
t day
bas
ed
on cu
rren
t lab
orat
ory
valu
es a
nd p
atie
nt
char
acte
ristic
s
Be
fore
-afte
r
X
Al
l blo
od te
sts
23
.7
Nire
l 201
1
Isra
el
All p
hysi
cian
s w
orki
ng in
the
heal
th s
yste
m
Pr
imar
y ca
re
clin
ics
An
onl
ine
med
ical
reco
rd w
as in
trodu
ced
so th
at o
ld la
bora
tory
test
s co
uld
be
acce
ssed
Be
fore
-afte
r
X
Al
l blo
od te
sts
3.
6a
An o
nlin
e m
edic
al re
cord
was
intro
duce
d so
that
old
radi
olog
y te
sts
coul
d be
ac
cess
ed
Be
fore
-afte
r
X
Al
l rad
iolo
gy te
sts
12
.3
Page
ler 2
013
US
A
Phys
icia
ns
wor
king
in
pedi
atric
ICU
Si
ngle
te
achi
ng
hosp
ital
A
rule
pre
vent
ing
repe
atin
g te
stin
g w
as
crea
ted
in th
e co
mpu
ter o
rder
ent
ry
syst
em. I
t had
to b
e ov
errid
den
to o
rder
re
peat
test
ing
Be
fore
-afte
r
X
CB
C, ch
emis
try a
nd
coag
ulat
ion
37
.7a
Page
ler 2
009
US
A
Not r
epor
ted
Si
ngle
te
achi
ng
hosp
ital
Re
curr
ing
orde
rs fo
r CXR
wer
e no
long
er
allo
wed
and
inst
ead
had
to b
e re
-ord
ered
da
ily
Be
fore
-afte
r
X
Ch
est X
R
10.0
Pate
l 200
5
Unite
d Ki
ngdo
m
All p
hysi
cian
s w
orki
ng in
the
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
Ur
ine
was
not
cultu
red
if th
e ur
inal
ysis
w
as n
orm
al
Befo
re-a
fter
X
Urin
e cu
lture
4.
0
Pilo
n 19
97
Cana
da
Phys
icia
ns a
nd
nurs
es w
orki
ng in
th
e IC
U
Si
ngle
te
achi
ng
hosp
ital
A
guid
elin
e ab
out w
hen
ABGs
sho
uld
be u
sed
was
crea
ted.
It w
as d
istri
bute
d on
poc
ket c
ards
and
taug
ht d
urin
g ed
ucat
ion
sess
ions
Be
fore
-afte
r
X
AB
Gs
36.7
a
Pop
1989
Ne
ther
land
Ge
nera
l pr
actit
ione
rs
All p
hysi
cian
s us
ing
the
sam
e la
bora
tory
in
one
city
Tw
o tim
es p
er y
ear p
hysi
cian
s w
ere
give
n a
repo
rt of
test
s th
ey h
ad o
rder
ed a
nd
whe
ther
they
wer
e ap
prop
riate
or n
ot.
Phys
icia
ns w
ere
also
info
rmed
of t
heir
redu
ndan
t tes
ts
Be
fore
-afte
r
X
BU
N, C
r, liv
er e
nzym
es,
WBC
, Hgb
, ESR
, glu
cose
36
.2
Pow
er 1
999
Au
stra
lia
Surg
ical
Res
iden
ts
in p
re-o
p cl
inic
Si
ngle
te
achi
ng
hosp
ital
Pu
blis
hed
guid
elin
es o
n te
st o
rder
ing
wer
e di
strib
uted
. A m
axim
um n
umbe
r of
test
s pe
r pat
ient
was
inst
itute
d an
d te
st
orde
ring
was
revi
ewed
by
a co
nsul
tant
Be
fore
-afte
r
X
X
X
CB
C, co
agul
atio
n te
sts,
ur
ea, L
FTs,
CXR
, ECG
37
.1
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 171
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Pow
les
2009
Un
ited
King
dom
Al
l phy
sici
ans
in re
gion
usi
ng
the
univ
ersi
ty
labo
rato
ry fo
r PSA
te
stin
g
Si
ngle
te
achi
ng
hosp
ital
Pr
osta
te-s
peci
fic a
ntig
en w
as ta
ken
off
the
requ
est f
orm
and
had
to b
e w
ritte
n in
by
hand
Be
fore
-afte
r
X
PS
A
17.3
a
Prat
200
9
Fran
ce
All p
hysi
cian
s w
orki
ng in
ICU
Si
ngle
te
achi
ng
hosp
ital
A
guid
elin
e w
as cr
eate
d on
whe
n to
pe
rform
eac
h of
the
com
mon
blo
od te
sts.
Th
e co
st o
f eac
h te
st w
as a
lso
show
n on
th
e gu
idel
ine.
Teac
hing
was
don
e on
how
to
redu
ce te
st u
tiliz
atio
n
Be
fore
-afte
r
X
CX
R an
d da
ily ro
utin
e BW
49
.0a
Pysh
er 1
999
US
A
All p
hysi
cian
s or
derin
g te
sts
at
this
labo
rato
ry
Si
ngle
te
achi
ng
hosp
ital
Pr
edef
ined
chem
istry
pan
els
wer
e el
imin
ated
from
the
requ
isiti
on fo
rms.
In
stea
d ea
ch te
st h
ad to
be
orde
red
sepa
rate
ly
Be
fore
-afte
r
X
Al
l blo
od ch
emis
try te
sts
32
.7a
Ram
oska
199
8
USA
Ph
ysic
ians
and
re
side
nts
wor
king
in
the
emer
genc
y de
partm
ent
Si
ngle
te
achi
ng
hosp
ital
Gr
aphs
of l
abor
ator
y ut
iliza
tion
and
cost
s of
labo
rato
ry te
sts
at th
e ho
spita
l was
di
spla
yed
on a
bul
letin
boa
rd
Be
fore
-afte
r
X
Al
l blo
od te
sts
17
.8a
Ratn
aike
199
3
Aust
ralia
Al
l phy
sici
ans
wor
king
in th
e ca
rdia
c car
e un
it
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
wer
e cr
eate
d by
the
hosp
ital
and
issu
ed to
the
card
iolo
gy u
nit.
No
furt
her d
etai
ls a
bout
the
guid
elin
es w
ere
give
n
Be
fore
-afte
r
X
Al
l blo
od te
sts
57
.2
Rhyn
e 19
79
USA
Fa
mily
doc
tors
Th
e fa
mily
m
edic
ine
prog
ram
as
soci
ated
w
ith o
ne
univ
ersi
ty
A
char
t aud
it of
test
ord
erin
g w
as d
one
and
the
resu
lts w
ere
pres
ente
d to
m
edic
al s
taff
Be
fore
-afte
r
X
X
Thyr
oid
func
tion
test
s
36.4
a
Robe
rts
1993
Ca
nada
Al
l phy
sici
ans
wor
king
at t
he
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
Se
rum
osm
olal
ity w
as re
mov
ed fr
om
the
requ
isiti
on a
nd b
lood
coun
t di
ffere
ntia
l was
not
don
e if
whi
te ce
ll co
unt w
as n
orm
al. A
pro
toco
l was
use
d to
det
erm
ine
whe
n el
ectro
lyte
s sh
ould
be
chec
ked.
Dai
ly C
XRs
wer
e no
long
er
allo
wed
Be
fore
-afte
r
X
X
Bloo
d ga
ses,
ser
um
osm
olal
ity, C
BC, N
a, K
, gl
ucos
e, C
XR, a
nd E
CG
18
.1a
UnauthenticatedDownload Date | 5/19/16 2:24 AM

172 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Rose
nblo
om
2005
US
A
All p
hysi
cian
s w
orki
ng o
n se
lect
ed in
patie
nt
units
Si
ngle
te
achi
ng
hosp
ital
M
agne
sium
coul
d on
ly b
e or
dere
d on
ce w
ith n
o re
curr
ence
and
a s
cree
n di
spla
ying
old
resu
lts a
nd e
duca
tion
on
whe
n m
agne
sium
sho
uld
be ch
ecke
d ha
d to
be
view
ed b
efor
e th
e or
der c
ould
be
ente
red
Be
fore
-afte
r
X
X
Mag
nesi
um
55.2
a
Sant
os 2
012
Br
azil
Al
l res
iden
ts
and
phys
icia
ns
wor
king
at t
he
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
A
mee
ting
was
hel
d to
dis
cuss
evi
denc
e fo
r cer
tain
test
s an
d th
e co
sts
of
the
test
s. P
atte
rns
of te
stin
g an
d ap
prop
riate
ness
of v
ario
us te
sts
was
di
scus
sed
Be
fore
-afte
r
X
CR
P
48.4
Segu
in 2
002
Fr
ance
Al
l phy
sici
ans
wor
king
in IC
U
Sing
le
teac
hing
ho
spita
l
Co
sts
for e
ach
test
was
sho
wn
on th
e or
der f
orm
Be
fore
-afte
r
X
El
ectro
lyte
s, C
BC, A
BG,
LFTs
, coa
gula
tion
pane
l, CX
R
18
.9
Shal
ev 2
009
Is
rael
Al
l prim
ary
care
ph
ysic
ians
in
Isra
el
Si
ngle
hea
lth
serv
ice
prov
ider
27
test
s w
ere
rem
oved
from
the
requ
isiti
on a
nd 2
wer
e ad
ded
Be
fore
-afte
r
X
Al
l blo
od te
st
4.3a
Sorit
a 20
11
USA
Re
side
nts
train
ing
in m
edic
ine
and
surg
ery
Si
ngle
te
achi
ng
hosp
ital
Th
ere
was
a 1
h te
achi
ng s
essi
on
rega
rdin
g w
hen
to o
rder
STA
T bl
ood
test
s an
d re
sults
of a
n au
dit w
ere
pres
ente
d.
The
high
est u
sers
of S
TAT
test
s w
ere
give
n in
divi
dual
feed
back
Be
fore
-afte
r
X
X
All s
tat l
abor
ator
y te
sts
21
.0a
Spra
y 20
12
USA
Ph
ysic
ians
taki
ng
care
of i
npat
ient
s
Sing
le
com
mun
ity
hosp
ital
An
ele
ctro
nic p
roto
col f
or e
lect
roly
te
repl
acem
ent a
nd re
test
ing
was
inst
itute
d
Befo
re-a
fter
X
Mag
nesi
um, p
hosp
horo
us
and
ioni
zed
calc
ium
32
.0a
Staf
ford
200
3
USA
11
7 pr
imar
y ca
re
prov
ider
s
Prim
ary
care
pr
actic
es
affil
iate
d w
ith a
sin
gle
teac
hing
ho
spita
l
Au
dits
of i
ndiv
idua
l and
gro
up E
CG
usag
es p
atte
rns
wer
e m
aile
d to
ph
ysic
ians
Be
fore
-afte
r
X
EC
G
28.3
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 173
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Suco
v 19
98
USA
Al
l phy
sici
ans
wor
king
in th
e ho
spita
l
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
wer
e cr
eate
d re
gard
ing
wha
t te
sts
to o
rder
for w
hich
pat
ient
gro
ups.
Th
e gu
idel
ine
was
then
rolle
d ou
t with
a
serie
s of
edu
catio
nal s
essi
ons.
Eac
h de
partm
ent r
ecei
ved
feed
back
on
its
orde
ring
prac
tices
but
ther
e w
as n
o in
divi
dual
feed
back
Be
fore
-afte
r
X
X
All b
lood
test
s
22.0
a
Suss
man
198
4
USA
Al
l phy
sici
ans
wor
king
in th
e ho
spita
l
Si
ngle
te
achi
ng
hosp
ital
Al
l rec
urrin
g or
ders
wer
e el
imin
ated
Be
fore
-afte
r
X
CB
C, e
lect
roly
tes,
CXR
, ch
emis
try p
anel
, FBG
, el
ectro
card
iogr
am, P
T
20
.8
Thom
pson
198
3
USA
Al
l phy
sici
ans
part
of th
e he
alth
pla
n
Sing
le p
re-
paid
hea
lth
plan
A
reco
mm
enda
tion
was
mad
e ag
ains
t sc
reen
ing
heal
thy
adul
ts w
ith b
lood
test
s an
d CX
R. A
n ed
ucat
iona
l cam
paig
n w
as
then
impl
emen
ted
Be
fore
-afte
r
X
Al
l blo
od ch
emis
try te
sts
and
CXR
60
.0a
Tier
ney
1987
US
A
Resi
dent
s an
d st
aff w
orki
ng in
th
e cl
inic
Si
ngle
un
iver
sity
as
soci
ated
ge
nera
l m
edic
ine
clin
ic
Al
l pre
viou
s re
sults
for a
test
wer
e sh
own
whe
n us
ing
the
com
pute
r ord
er e
ntry
sy
stem
. An
optio
n to
canc
el th
e cu
rren
t te
st w
as th
en a
vaila
ble
Ra
ndom
ized
co
ntro
lled
trial
X
All l
abor
ator
y an
d im
agin
g an
d EC
Gs
8.9a
Tier
ney
1990
US
A
Phys
icia
ns
wor
king
in th
e cl
inic
Si
ngle
un
iver
sity
as
soci
ated
ge
nera
l m
edic
ine
clin
ic
Co
st to
the
patie
nt o
f ord
erin
g ea
ch
test
s w
as d
ispl
ayed
bef
ore
the
orde
r is
conf
irmed
Ra
ndom
ized
co
ntro
lled
trial
X
All b
lood
test
s
17.6
a
Toub
ert 2
000
Fr
ance
Al
l phy
sici
ans
in
the
hosp
ital
Si
ngle
te
achi
ng
hosp
ital
Ed
ucat
iona
l mat
eria
l on
thyr
oid
dise
ase
was
dis
tribu
ted.
Phy
sici
ans
wer
e to
ld
that
any
test
oth
er th
an TS
H re
quire
d ju
stifi
catio
n. Te
sts
wer
e st
ill p
roce
ssed
ev
en if
no
just
ifica
tion
was
pro
vide
d
Be
fore
-afte
r
X
TS
H, T
3, T
4,
39.6
van
Wijk
200
1
Neth
erla
nds
GPs
wor
king
in
prac
tices
with
el
ectro
nic m
edic
al
reco
rds
Si
ngle
hea
lth
regi
on
Com
pute
rized
dec
isio
n su
ppor
t su
gges
ted
appr
opria
te te
sts
base
d on
ba
sic c
linic
al in
form
atio
n
Ra
ndom
ized
co
ntro
lled
trial
X
All b
lood
test
s
20.3
a
UnauthenticatedDownload Date | 5/19/16 2:24 AM
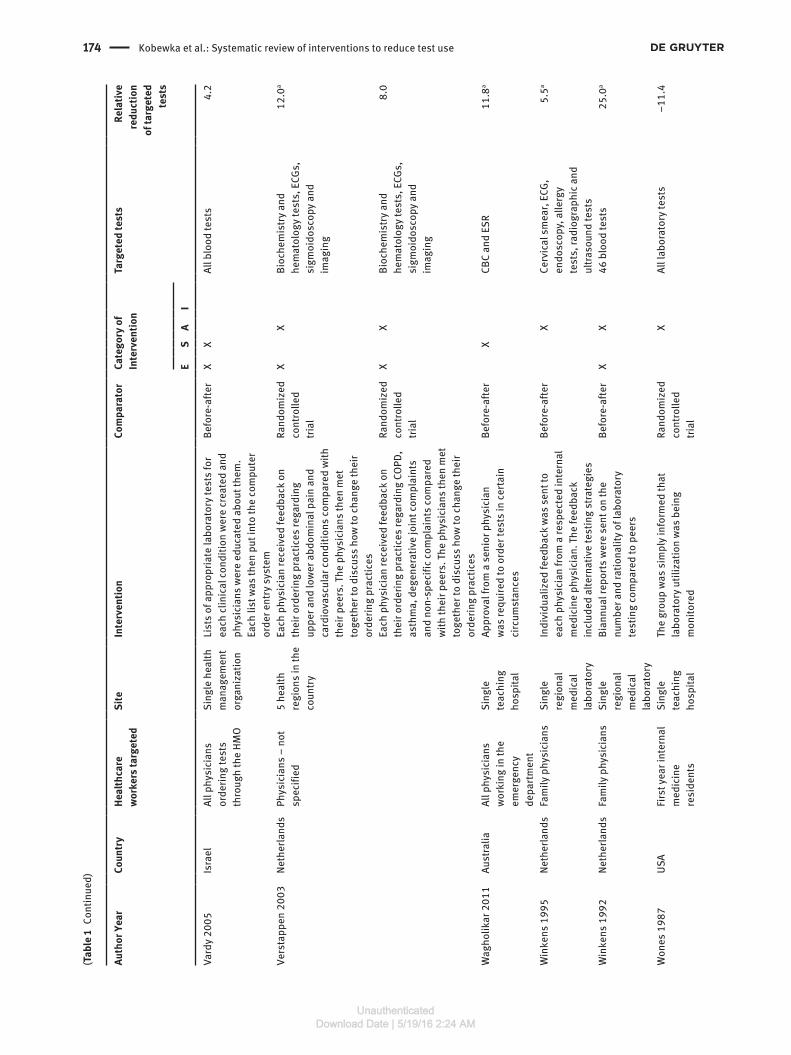
174 Kobewka et al.: Systematic review of interventions to reduce test use
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
Vard
y 20
05
Isra
el
All p
hysi
cian
s or
derin
g te
sts
thro
ugh
the
HMO
Si
ngle
hea
lth
man
agem
ent
orga
niza
tion
Li
sts
of a
ppro
pria
te la
bora
tory
test
s fo
r ea
ch cl
inic
al co
nditi
on w
ere
crea
ted
and
phys
icia
ns w
ere
educ
ated
abo
ut th
em.
Each
list
was
then
put
into
the
com
pute
r or
der e
ntry
sys
tem
Be
fore
-afte
r
X
X
All b
lood
test
s
4.2
Vers
tapp
en 2
003
Ne
ther
land
s Ph
ysic
ians
– n
ot
spec
ified
5
heal
th
regi
ons
in th
e co
untry
Ea
ch p
hysi
cian
rece
ived
feed
back
on
thei
r ord
erin
g pr
actic
es re
gard
ing
uppe
r and
low
er a
bdom
inal
pai
n an
d ca
rdio
vasc
ular
cond
ition
s co
mpa
red
with
th
eir p
eers
. The
phy
sici
ans
then
met
to
geth
er to
dis
cuss
how
to ch
ange
thei
r or
derin
g pr
actic
es
Ra
ndom
ized
co
ntro
lled
trial
X
X
Bi
oche
mis
try a
nd
hem
atol
ogy
test
s, E
CGs,
si
gmoi
dosc
opy
and
imag
ing
12
.0a
Each
phy
sici
an re
ceiv
ed fe
edba
ck o
n th
eir o
rder
ing
prac
tices
rega
rdin
g CO
PD,
asth
ma,
deg
ener
ativ
e jo
int c
ompl
aint
s an
d no
n-sp
ecifi
c com
plai
nts
com
pare
d w
ith th
eir p
eers
. The
phy
sici
ans
then
met
to
geth
er to
dis
cuss
how
to ch
ange
thei
r or
derin
g pr
actic
es
Ra
ndom
ized
co
ntro
lled
trial
X
X
Bi
oche
mis
try a
nd
hem
atol
ogy
test
s, E
CGs,
si
gmoi
dosc
opy
and
imag
ing
8.
0
Wag
holik
ar 2
011
Au
stra
lia
All p
hysi
cian
s w
orki
ng in
the
emer
genc
y de
partm
ent
Si
ngle
te
achi
ng
hosp
ital
Ap
prov
al fr
om a
sen
ior p
hysi
cian
w
as re
quire
d to
ord
er te
sts
in ce
rtain
ci
rcum
stan
ces
Be
fore
-afte
r
X
CB
C an
d ES
R
11.8
a
Win
kens
199
5
Neth
erla
nds
Fam
ily p
hysi
cian
s
Sing
le
regi
onal
m
edic
al
labo
rato
ry
In
divi
dual
ized
feed
back
was
sen
t to
each
phy
sici
an fr
om a
resp
ecte
d in
tern
al
med
icin
e ph
ysic
ian.
The
feed
back
in
clud
ed a
ltern
ativ
e te
stin
g st
rate
gies
Be
fore
-afte
r
X
Ce
rvic
al s
mea
r, EC
G,
endo
scop
y, a
llerg
y te
sts,
radi
ogra
phic
and
ul
traso
und
test
s
5.
5a
Win
kens
199
2
Neth
erla
nds
Fam
ily p
hysi
cian
s
Sing
le
regi
onal
m
edic
al
labo
rato
ry
Bi
annu
al re
port
s w
ere
sent
on
the
num
ber a
nd ra
tiona
lity
of la
bora
tory
te
stin
g co
mpa
red
to p
eers
Be
fore
-afte
r
X
X
46 b
lood
test
s
25.0
a
Won
es 1
987
US
A
Firs
t yea
r int
erna
l m
edic
ine
resi
dent
s
Si
ngle
te
achi
ng
hosp
ital
Th
e gr
oup
was
sim
ply
info
rmed
that
la
bora
tory
util
izat
ion
was
bei
ng
mon
itore
d
Ra
ndom
ized
co
ntro
lled
trial
X
All l
abor
ator
y te
sts
–1
1.4
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 175
(Tab
le 1
Cont
inue
d)
Auth
or Y
ear
Co
untr
y
Heal
thca
re
wor
kers
targ
eted
Si
te
Inte
rven
tion
Co
mpa
rato
r
Cate
gory
of
Inte
rven
tion
Ta
rget
ed te
sts
Re
lativ
e re
duct
ion
of ta
rget
ed
test
s
E
S
A
I
This
gro
up re
ceiv
ed in
divi
dual
feed
back
on
labo
rato
ry u
sage
and
cost
s ev
ery
2 w
eeks
X
Al
l lab
orat
ory
test
s
–13.
15
This
gro
up re
ceiv
ed in
divi
dual
feed
back
on
labo
rato
ry u
sage
and
cost
s ev
ery
2 w
eeks
alo
ng w
ith g
roup
dat
a fo
r co
mpa
rison
X
Al
l lab
orat
ory
test
s
–7.2
7
Zaat
199
2
Neth
erla
nds
Gene
ral
Prac
titio
ners
Tw
o he
alth
re
gion
s
The
labo
rato
ry re
quis
ition
was
mod
ified
so
that
it o
nly
had
15 te
sts
on it
. All
othe
r te
sts
had
to b
e w
ritte
n in
Be
fore
-afte
r
X
Al
l hem
atol
ogic
al a
nd
chem
istry
test
s
18.2
a
Zaid
i 199
9
USA
Al
l phy
sici
ans
send
ing
sam
ples
to
the
hosp
ital l
ab
Si
ngle
te
achi
ng
hosp
ital
Gu
idel
ines
wer
e cr
eate
d fro
m lo
cal d
ata
and
shar
ed w
ith a
ll m
edic
al s
taff.
Afte
r th
is a
ll sa
mpl
es n
ot m
eetin
g th
e cr
iteria
w
ere
reje
cted
Be
fore
-afte
r
X
X
Stoo
l cul
ture
30
.9
Zia
2013
US
A
All P
hysi
cian
s at
th
e ho
spita
l
Sing
le
teac
hing
ho
spita
l
Th
e te
st w
as re
mov
ed fr
om th
e la
bora
tory
re
quis
ition
but
coul
d st
ill b
e or
dere
d if
writ
ten
in b
y ha
nd
Be
fore
-afte
r
X
Se
rum
pro
tein
el
ectro
phor
esis
and
im
mun
ofix
atio
n
29
.6
a Deno
tes
stud
ies
in w
hich
a te
st o
f sta
tistic
al s
igni
fican
ce w
as p
erfo
rmed
and
foun
d to
be
sign
ifica
nt b
y th
e st
udie
s’ a
utho
rs. A
, Aud
it an
d fe
edba
ck; E
, Edu
catio
nal;
I, In
cent
ive
or p
enal
ty;
S, S
yste
m-b
ased
.
UnauthenticatedDownload Date | 5/19/16 2:24 AM

176 Kobewka et al.: Systematic review of interventions to reduce test use
Figure 2 Box plots of relative reductions in laboratory utilization stratified by intervention type.1) Interventions with an educational component; 2) Interventions classified as educational only; 3) Interventions classified as educational only that use distribution of a guideline to educate; 4) Interventions with a system-based component; 5) Interventions classified as system-based only; 6) Interventions classified as system-based only that used a clinical decision support tool; 7) Interventions with an audit and feedback component; 8) Interventions classified as audit and feedback only; 9) Interventions classified as audit and feedback only that use cost information display.
Table 2 Percent relative reductions in test utilization by intervention type.a
Number of interventions
Median RR (IQR)
Minimum RR
Maximum RR
Educational interventions 51 34.5 (16.5–49.0) –12.3 99.6 –Δ between intervention and control statistically significant 33 31.2 (18.1–47.5) 4.7 85.0 –Δ between intervention and control statistically insignificant 18 38.3 (8.0–53.0) –12.3 99.6Exclusively education intervention 22 30.6 (16.5–48.5) –12.3 75.0Exclusively guideline distribution 13 30.0 (20.8–53.0) 4.7 99.6
System-based interventions 54 22.2 (3.6–68.3) 0.1 99.7 –Δ between intervention and control statistically significant 36 19.6 (10.4–36.1) 3.6 99.7 –Δ between intervention and control statistically insignificant 18 24.8 (10.0–37.1) 0.1 77.8Exclusively system-based intervention 37 21.6 (10.0–32.7) 0.1 99.7Exclusively clinical decision support 10 22.8 (9.3–23.9) 4.7 85.0
Audit feedback interventions 41 22.0 (8.6–34.6) –13.1 99.6 –Δ between intervention and control statistically significant 24 23.2 (13.8–34.5) 5.5 63.4 –Δ between intervention and control statistically insignificant 17 18.9 (0–36.2) –13.1 99.6Exclusively audit and feedback intervention 20 18.4 (2.1–24.8) –13.1 36.2Exclusively cost display 12 18.4 (2.1–28.8) 5.5 99.6
Physicians targeted were involved in creating and implementing the intervention 17 23.0 (8.0–39.6) 3.6 99.6Physicians targeted were not involved in creating and implementing the intervention
103 22.2 (10.1–36.7) –27.7 99.7
aCategories of interventions are not mutually exclusive unless stated.
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 177
Figure 3 Box plots of relative reductions in laboratory utilization stratified by intervention type among interventions targeting four or more tests.1) Interventions with an educational component; 2) Interventions classified as educational only; 3) Interventions classified as educational only that use distribution of a guideline to educate; 4) Interventions with a system-based component; 5) Interventions classified as system-based only; 6) Interventions classified as system-based only that used a clinical decision support tool; 7) Interventions with an audit and feedback component; 8) Interventions classified as audit and feedback only; 9) Interventions classified as audit and feedback only that use cost information display.
Table 3 General descriptions of study quality (n = 109).
Number of studies
Median relative reduction (IQR)
Where patients similar between groups? Yes 37 19.0 (8.6–37.7) No 72 24.8 (14.0–41.5)Were those ordering the tests similar between groups? Yes 103 23.8 (11.9–40.2) No 6 11.7 (4.2–25.0)Was there a concurrent control group? Yes 27 16.5 (5.8–27.0) No 82 24.9 (14.0–47.5)Was the intervention described adequately enough to be replicated? Yes 88 23.5 (12.4–38.6) No 21 20.8 (4.7–36.7)Was there a risk of contamination between experimental and control groups? Yes 89 24.9 (13.5–40.8) No 20 15.8 (4.8–29.6)Were the results reported per patient instead of per institution or per physician? Yes 79 19.9 (9.1–35.4) No 30 33.4 (23.4–48.3)Was a time-series analysis conducted? Yes 11 26.1 (14.0–55.2) No 98 23.5 (10.1–37.1)
a 99.7% reduction in test use [53]. Lewandrowski et al. distributed guidelines stating when it was appropriate to order LD-isozymes with a laboratory physician notifying the ordering physician when the LD-isozyme request was not compliant with the guideline [69]. This combination of education and feedback led to a 99.6% reduction in LD-isozymes being ordered. The two largest relative reduc-tions among interventions that targeted four or more tests were by Chu et al. and Dixon et al. Chu et al. used a pro-tocol driven algorithm for admitting trauma patients and found a 68.3% reduction in the number of tests ordered per patient [33]. Dixon et al. limited the number of tests that interns could order to eight per patient per day, result-ing in a 66.7% reduction in the number of tests ordered per patient [38].
The most successful interventions targeting four or more tests that were purely system based were the study by Chu et al, discussed above, and a study by Neilson et al. Neilson et al. sequentially implemented a number of system-based interventions using a computerized order entry system including: the display of previous labora-tory results to physicians ordering tests; the prevention of recurring orders in various circumstances; and the unbun-dling of tests so that each component had to be ordered
UnauthenticatedDownload Date | 5/19/16 2:24 AM

178 Kobewka et al.: Systematic review of interventions to reduce test use
individually [82]. This package of interventions resulted in a 64.2% relative reduction in the tests targeted.
DiscussionWe summarized 109 studies evaluating the effect of inter-ventions aimed at reducing test utilization by calculating relative reductions to compare interventions. We found that all intervention categories (including education, system based, audit feedback, and incentive penalty) can reduce test utilization. Even though educational interven-tions had the largest relative reduction in test utilization, the inter-quartile ranges were large and overlapping. The greatest difference in our stratified analysis was between interventions that targeted less than four tests, which had much larger relative reductions than interventions that targeted four or more tests. Consistent with past reviews, we found that interventions using multiple strategies were more effective [8]. Even though all intervention types seem to be effective, we found a large range of effects and much heterogeneity between studies. Many studies did not use appropriate statistical techniques and follow-up was often short. These shortcomings call into question the sustainability and generalizability of many interventions in our review.
Sustainability
Although interventions with an educational component had the greatest median relative reductions, their long-term sustainability is questionable. The resources needed to perpetuate educational strategies (i.e., lectures or indi-vidual teaching sessions) are significant and probably need to be continuous to maintain an effect, especially in teaching hospitals where ordering physicians are con-stantly changing. Even in studies where the educational strategy was low effort (i.e., the distribution of a guide-line), multiple reminders and repeated meetings were necessary to maintain the change in behavior [89, 97, 106, 111]. There was only one purely educational intervention that reported results from > 1 year after the intervention began but this study did not use time series analysis to determine if utilization returned to baseline during this time [70]. With all but one purely educational interven-tions having a time horizon of < 1 year there is no evidence in our review that educational strategies have long-term sustainability. In contrast there are several examples of system-based interventions which by definition require
few resources to maintain, that are shown to maintain their effect for > 1 year [14, 47, 53]. The ratio of resource input to test reduction is not measured in the included studies but is an important consideration when deciding to implement a particular intervention.
Generalizability
Many of the interventions have questionable generaliz-ability. There is a wide range of relative reductions among included studies due to heterogeneity at every level. There are differences in how an invention type is implemented, who is target by the intervention, and the pre-existing ordering practices among the targeted physicians. Due to the heterogeneity, similar results cannot be expected even if an intervention is perfectly replicated. Some of the large reductions ( > 70%) suggest that anomalous ordering is being targeted which further calls into question the gen-eralizability of results. Lastly many of the studies target physicians in training who would likely respond differ-ently than physicians in independent practice.
Quality
The quality of included studies was poor. As expected studies with lower quality had higher relative reductions suggesting that poor quality studies were over estimating the effects of interventions. Surprisingly, very few of the before and after studies used time-series analysis or auto-correlation to analyze results, bringing into question the validity of results.
Limitations
This review has several limitations. Our search strategy used only studies published in English ignoring poten-tially important studies published in other languages and only searched two databases. Another limitation is that the heterogeneity between interventions makes generalizations about effective strategies difficult. Despite this weakness the relative reduction does tell us which interventions were associated with the largest reductions. This allows these successes to be examined to see if they are applicable to other settings. This review is broad in scope and therefore does not allow detailed examination of particular intervention types to find the elements that lead to success. Reviews of particu-lar types of interventions have been done and explore
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 179
these factors closely [122–124]. Lastly, our use of rela-tive reductions leaves out absolute reduction and cost savings information that may be important to decision makers.
ConclusionsOur review found that research into interventions to reduce test utilization is ongoing and many strategies can be successful. There are many examples of low investment interventions that work, especially when they target tests that have a high rate of inappropriate use. Due to questionable validity and generalizability of these results, this review should be used as a refer-ence for finding high quality studies with large relative reductions that apply to a setting of interest. Future research needs to determine how low input strategies using computerized order entry can be used to imple-ment system changes, audit and feedback, and educa-tion. Database monitoring should be developed so that institutions know when anomalous test use is occurring and which physicians are deviating from the mean. This will allow for targeting of interventions to where they will have the greatest effect. Lastly, further studies in this field must monitor for adverse events caused by reduced testing.
Author contributions: All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission.Financial support: None declared.Employment or leadership: None declared.Honorarium: None declared.Competing interests: The funding organization(s) played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
References1. National Health Expenditure trends, 1975 to 2013. Ottawa, ON:
Canadian Institute for Health Information, 2013.2. Health at a Glance 2013: OECD Indicators. Paris: OECD Publish-
ing, 2013.3. Qaseem A, Alguire P, Dallas P, Feinberg LE, Fitzgerald FT,
Horwitch C, et al. Appropriate use of screening and diagnostic tests to foster high-value, cost-conscious care. Ann Intern Med 2012;156:147–9.
4. van Walraven C, Naylor CD. Do we know what inappropriate laboratory utilization is? A systematic review of laboratory clini-cal audits. J Am Med Assoc 1998;280:9.
5. Grossman RM. A review of physician cost-containment strate-gies for laboratory testing. Med Care 1983;21:783–802.
6. Axt-Adam P, van der Wouden JC, van der Does E. Influencing behavior of physicians ordering laboratory tests: a literature study. Med Care 1993;31:784–94.
7. Young DW. Improving laboratory usage: a review. Postgrad Med 1988;64:283–9.
8. Solomon DH, Hashimoto H, Daltroy L, Liang MH. Techniques to improve physicians’ use of diagnostic tests: a new conceptual framework. J Am Med Assoc 1998;280:2020–7.
9. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Br Med J 2009;339:b2535.
10. Egger M, Smith GD, Altman DG. Principles of and procedures for systematic reviews. Systematic Reviews in Health Care: meta analysis in context, 2nd ed. London: BMJ Publishing Group, 2008:23–42.
11. Cochrane Effective Practice and Organization of Care Review Group. Data collection checklist. Ottawa: Institute of Population Health, University of Ottawa, 2002.
12. Al AM, Zidan A, Hamza AA, Al-Suwaidi R. Evaluation of laboratory investigations in accident and emergency depart-ment, Salmaniya Medical Complex. Bahrain Med Bull 2002;24:95–7.
13. Amukele TK, Baird GS, Chandler WL. Reducing the use of coagu-lation test panels. Blood Coagul Fibrinolysis 2011;22:688–95.
14. Archambault AJ, Arkin CF, Skelton T, Abel G, Gawoski J. Blood (ASH Annual Meeting Abstracts) 2011;118:Abstract 4774.
15. Attali M, Barel Y, Somin M, Beilinson N, Shankman M, Acker-man A, et al. A cost-effective method for reducing the volume of laboratory tests in a university-associated teaching hospital. Mt Sinai J Med 2006;73:787–94.
16. Barazzoni F, Grilli R, Amicosante AM, Brescianini S, Marca MA, Baggi M, et al. Impact of end user involvement in implementing guidelines on routine pre-operative tests. Int J Qual Health Care 2002;14:321–7.
17. Bareford D, Hayling A. Inappropriate use of laboratory services: long term combined approach to modify request patterns. Br Med J 1990;301:1305–7.
18. Baricchi R, Zini M, Nibali MG, Vezzosi W, Insegnante V, Manfuso C, et al. Using pathology-specific laboratory profiles in clinical pathology to reduce inappropriate test requesting: two com-pleted audit cycles. BMC Health Serv Res 2012;12:187.
19. Barie PS, Hydo LJ. Lessons learned: durability and progress of a program for ancillary cost reduction in surgical critical care. J Trauma 1997;43:590–6.
20. Bates DW, Kuperman GJ, Jha A, Teich JM, Orav EJ, Ma’luf N, et al. Does the computerized display of charges affect inpatient ancil-lary test utilization? Arch Intern Med 1997;157:2501–8.
21. Bates DW, Kuperman GJ, Rittenberg E, Teich JM, Fiskio J, Ma’luf N, et al. A randomized trial of a computer-based intervention to reduce utilization of redundant laboratory tests. Am J Med 1999;106:144–50.
22. Berenholtz S, Pronovost P, Lipsett P, Dawson P, Dorman T. Assessing the effectiveness of critical pathways on reducing resource utilization in the surgical intensive care unit. Intens Care Med 2001;27:1029–36.
UnauthenticatedDownload Date | 5/19/16 2:24 AM
180 Kobewka et al.: Systematic review of interventions to reduce test use
23. Berwick DM, Coltin KL. Feedback reduces test use in a health maintenance organization. J Am Med Assoc 1986;255:1450–4.
24. Boon-Falleur L, Sokal E, Peters M, Ketelslegers JM. A rule-based decision support application for laboratory investigations man-agement. Proc Annu Symp Comput Appl Med Care 1995;314–8.
25. Buckingham K, Russell I, Ross I, Gibson P, Paterson N. The effect of allowing clinical discretion in ordering biochemical tests. Evaluation by complementary methods. Int J Technol Assess 1994;10:695–700.
26. Bunting PS, Van Walraven C. Effect of a controlled feedback intervention on laboratory test ordering by community physi-cians. Clin Chem 2004;50:321–6.
27. Burnett L, Chesher D, Burnett JR. Optimizing the availability of ‘stat’ laboratory tests using Shewhart ‘C’ control charts. Ann Clin Biochem 2002;39:140–4.
28. Calderon-Margalit R, Mor-Yosef S, Mayer M, Adler B, Shapira SC. An administrative intervention to improve the utilization of laboratory tests within a university hospital. Int J Qual Health Care 2005;17:243–8.
29. Carson K, Murillo P, Runge A, Vogel DG, Baum LG. A test-ordering algorithm can reduce laboratory test use. Lab Med 1995;26:277–81.
30. Carter E, Bennett BD. Reference test review by pathology house staff: a cost-containment strategy for the clinical laboratory. Clin Leader Manag Rev 2002;16:3–6.
31. Chen P, Tanasijevic MJ, Schoenenberger RA, Fiskio J, Kuperman GJ, Bates DW. A computer-based intervention for improving the appropriateness of antiepileptic drug level monitoring. Am J Clin Pathol 2003;119:432–8.
32. Chu K, Wagholikar A, Greenslade J. Reducing laboratory test ordering by limiting the range of tests that may be requested by interns and residents on pathology request forms. Emerg Med Australas 2012;24:21.
33. Chu UB, Clevenger FW, Imami ER, Lampard SD, Frykberg ER, Tepas JJ. The impact of selective laboratory evaluation on utiliza-tion of laboratory resources and patient care in a level-I trauma center. Am J Surg 1996;172:558–3.
34. Cohen DI, Jones P, Littenberg B, Neuhauser D. Does cost infor-mation availability reduce physician test usage? A randomized clinical trial with unexpected findings. Med Care 1982;20: 286–92.
35. Davidoff F, Goodspeed R, Clive J. Changing test ordering behavior. A randomized controlled trial comparing probabil-istic reasoning with cost-containment education. Med Care 1989;27:45–58.
36. Detsky AS, McLaughlin JR, Abrams HB, L’Abbe K, Markel FM. Do interns and residents order more tests than attending staff? Results of a house staff strike. Med Care 1986;24: 526–34.
37. Dickinson JC. From process to policy: a generic prescription for test over-utilization in the emergency department. Fam Pract Res J 1987;7:12–21.
38. Dixon RH, Laszlo J. Utilization of clinical chemistry services by medical house-staff. Arch Intern Med 1974;134:1064–7.
39. Dowling PT, Alfonsi G, Brown MI, Culpepper L. An education program to reduce unnecessary laboratory tests by residents. Acad Med 1989;64:410–2.
40. Durand-Zaleski I, Rymer JC, Roudot-Thoraval F, Revuz J, Rosa J. Reducing unnecessary laboratory use with new test request form: example of tumour markers. Lancet 1993;342:150–3.
41. Durieux P, Ravaud P, Porcher R, Fulla Y, Manet C-S, Chaussade S. Long-term impact of a restrictive laboratory test ordering form on tumor marker prescriptions. Int J Technol Assess Health Care 2003;19:106–13.
42. Eccles M, Steen N, Grimshaw J, Thomas L, McNamee P, Soutter J, et al. Effect of audit and feedback, and reminder messages on primary-care radiology referrals: a randomised trial. Lancet 2001;357:1406–9.
43. Eisenberg JM. An educational program to modify laboratory use by house staff. J Med Educ 1977;52:578–81.
44. Emerson JF, Emerson SS. The impact of requisition design on laboratory utilization. Am J Clin Pathol 2001;116:879–84.
45. Everett GD. Impact of supervision by medical teachers and in-patient test control programmes on the out-patient test utiliza-tion of residents. Med Educ 1985;19:138–42.
46. Everett GD, deBlois CS, Chang PF, Holets T. Effect of cost educa-tion, cost audits, and faculty chart review on the use of labora-tory services. Arch Intern Med 1983;143:942–4.
47. Feldkamp CS, Carey JL. An algorithmic approach to thyroid func-tion testing in a managed care setting: 3-Year experience. Am J Clin Pathol 1996;105:11–6.
48. Feldman LS, Shihab HM, Thiemann D, Yeh HC, Ardolino M, Mandell S, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med 2013;173:903–8.
49. Finegan BA, Rashiq S, McAlister FA, O’Connor P. Selective order-ing of preoperative investigations by anesthesiologists reduces the number and cost of tests. Can J Anaesth 2005;52:575–80.
50. Fong BW. Common diagnostic tests: use and interpretation. Hawaii Med J 1989;48:7–9.
51. Fowkes FG, Hall R, Jones JH, Scanlon MF, Elder GH, Hobbs DR, et al. Trial of strategy for reducing the use of laboratory tests. Br Med J 1986;292:883–5.
52. Friedman KG, Rathod RH, Farias M, Graham D, Powell AJ, Fulton DR, et al. Resource utilization after introduction of a standard-ized clinical assessment and management plan. Congenit Heart Dis 2010;5:374–81.
53. Froom P, Barak M. Cessation of dipstick urinalysis reflex testing and physician ordering behavior. Am J Clin Pathol 2012;137:486–9.
54. Gama R, Nightingale PG, Broughton PM, Peters M, Bradby GV, Berg J, et al. Feedback of laboratory usage and cost data to clinicians: does it alter requesting behaviour? Ann Clin Biochem 1991;28(Pt 2):143–9.
55. Gama R, Nightingale PG, Broughton PM, Peters M, Ratcliffe JG, Bradby GV, et al. Modifying the request behaviour of clinicians. J Clin Pathol 1992;45:248–9.
56. Goddard K, Austin SJ. Appropriate regulation of routine labora-tory testing can reduce the costs associated with patient stay in intensive care. Crit Care 2011;15:S47–8.
57. Golden WE, Pappas AA, Lavender RC. Financial unbun-dling reduces outpatient laboratory use. Arch Intern Med 1987;147:1045–8.
58. Gortmaker SL, Bickford AF, Mathewson HO, Dumbaugh K, Tirrell PC. A successful experiment to reduce unneces-sary laboratory use in a community hospital. Med Care 1988;26:631–42.
59. Grivell AR, Forgie HJ, Fraser CG, Berry MN. Effect of feedback to clinical staff of information on clinical biochemistry requesting patterns. Clin Chem 1981;27:1717–20.
UnauthenticatedDownload Date | 5/19/16 2:24 AM

Kobewka et al.: Systematic review of interventions to reduce test use 181
60. Groopman DS, Powers RD. Effect of ‘standard order’ deletion on emergency department coagulation profile use. Ann Emerg Med 1992;21:524–7.
61. Gross PA, Van Antwerpen CL, Hess WA, Reilly KA. Use and abuse of blood cultures: program to limit use. Am J Infect Control 1988;16:114–7.
62. Haschke-Becher E, Totzke U, Afazel S, Johansson T, Schwarz M, Ladurner G, et al. Clinical decision rules for the use of liquor diagnostics in hospitalized neurology patients reduced costs without affecting clinical outcomes. Int J Technol Assess Health Care 2009;25:208–13.
63. Hutton HD, Drummond HS, Fryer AA. The rise and fall of C-reac-tive protein: managing demand within clinical biochemistry. Ann Clin Biochem 2009;46:155–8.
64. Jelinek GA, Banham ND. Reducing the use of plain abdominal radiographs in an emergency department. Arch Emerg Med 1990;7:241–5.
65. Kelly AM. Rationalising the ordering of blood cultures. Aust Health Rev 1998;21:245–50.
66. Kumwilaisak K, Noto A, Schmidt UH, Beck CI, Crimi C, Lewand-rowski K, et al. Effect of laboratory testing guidelines on the utilization of tests and order entries in a surgical intensive care unit. Crit Care Med 2008;36:2993–9.
67. Larocque BJ, Maykut RJ. Implementation of guidelines for preoperative laboratory investigations in patients scheduled to undergo elective surgery. Can J Surg 1994;37:397–401.
68. Levick DL, Stern G, Meyerhoefer CD, Levick A, Pucklavage D. Reducing unnecessary testing in a CPOE system through implementation of a targeted CDS intervention. BMC Med Inform Decis 2013;13:43.
69. Lewandrowski K, Bailey E, Dhanak E, Laposata M, Flood J. Mandatory laboratory consultation: how one hospital’s program reduced overuse of cardiac tests. Lab Med 1994;25:460–3.
70. Mancuso CA. Impact of new guidelines on physicians’ ordering of preoperative tests. J Gen Intern Med 1999;14:166–72.
71. Martin AR, Wolf MA, Thibodeau LA, Dzau V, Braunwald E. A trial of two strategies to modify the test-ordering behavior of medi-cal residents. N Engl J Med 1980;303:1330–6.
72. Marton KI, Tul V, Sox HC. Modifying test-ordering behavior in the outpatient medical clinic. A controlled trial of two educational interventions. Arch Intern Med 1985;145:816–21.
73. May TA, Clancy M, Critchfield J, Ebeling F, Enriquez A, Gallagher C, et al. Reducing unnecessary inpatient laboratory testing in a teaching hospital. Am J Clin Pathol 2006;126:200–6.
74. Mehari SM, Havill JH, Montgomery C. A written guideline imple-mentation can lead to reductions in laboratory testing in an intensive care unit. Anaesth Intensive Care 1997;25:33–7.
75. Meng QH, Zhu S, Booth C, Stevens L, Bertsch B, Qureshi M, et al. Impact of the cardiac troponin testing algorithm on exces-sive and inappropriate troponin test requests. Am J Clin Pathol 2006;126:195–9.
76. Merlani P, Garnerin P, Diby M, Ferring M, Ricou B. Quality improvement report: linking guideline to regular feedback to increase appropriate requests for clinical tests: blood gas analysis in intensive care. Br Med J 2001;323:620–4.
77. Meyer L, Schmeler K, Wallbillich J, Urbauer D, Soliman P, Frumo-vitz M, et al. Clinical practice guidelines decrease unnecessary Pap tests in survivors of gynecologic malignancies. Gynecol Oncol 2011;120:S30–1.
78. Miyakis S, Karamanof G, Liontos M, Mountokalakis TD. Factors contributing to inappropriate ordering of tests in an academic
medical department and the effect of an educational feedback strategy. Postgrad Med 2006;82:823–9.
79. Morris AJ, Wilson ML, Reller LB. Application of rejection criteria for stool ovum and parasite examinations. J Clin Microbiol 1992;30:3213–6.
80. Mutimer D, McCauley B, Nightingale P, Ryan M, Peters M, Neuberger J. Computerised protocols for laboratory investiga-tion and their effect on use of medical time and resources. J Clin Pathol 1992;45:572–4.
81. Nardella A, Pechet L, Snyder LM. Continuous improvement, quality control, and cost containment in clinical laboratory testing: effects of establishing and implementing guidelines for preoperative tests. Arch Pathol Lab Med 1995;119:518–22.
82. Neilson EG, Johnson KB, Rosenbloom ST, Dupont WD, Talbert D, Giuse DA, et al. The impact of peer management on test-order-ing behavior. Ann Intern Med 2004;141:196–204.
83. Nelson III RB. Teaching technologic restraint. An evaluation of a single session. Eval Health Prof 1978;1:21–8.
84. Nightingale PG, Peters M, Mutimer D, Neuberger JM. Effects of a computerised protocol management system on ordering of clini-cal tests. Qual Health Care 1994;3:23–8.
85. Nirel N, Rosen B, Sharon A, Samuel H, Cohen AD. The impact of an integrated hospital-community medical information system on quality of care and medical service utilisation in primary-care clinics. Inform Health Soc Ca 2011;36:63–74.
86. Pageler N, Longhurst C, Shin A, Adams E, Widen E, Barth R, et al. Using computerized provider order entry (CPOE) to promote sus-tained optimization of diagnostic radiologic service utilization. Crit Care Med 2009;37:A363.
87. Pageler NM, Franzon D, Longhurst CA, Wood M, Shin AY, Adams ES, et al. Embedding time-limited laboratory orders within com-puterized provider order entry reduces laboratory utilization. Pediatr Crit Care Med 2013;14:413–9.
88. Patel HD, Livsey SA, Swann RA, Bukhari SS. Can urine dipstick testing for urinary tract infection at point of care reduce labora-tory workload? J Clin Pathol 2005;58:951–4.
89. Pilon CS, Leathley M, London R, McLean S, Phang PT, Priestley R, et al. Practice guideline for arterial blood gas measurement in the intensive care unit decreases num-bers and increases appropriateness of tests. Crit Care Med 1997;25:1308–13.
90. Pop P, Winkens RA. A diagnostic centre for general practitioners: results of individual feedback on diagnostic actions. J R Coll Gen Pract 1989;39:507–8.
91. Power LM, Thackray NM. Reduction of preoperative investigations with the introduction of an anaesthetist-led preoperative assessment clinic. Anaesth Intensive Care 1999;27:481–8.
92. Powles L, Green J, Taylor E. Can redesigning a laboratory request form reduce the number of inappropriate PSA requests without compromising clinical outcome. Urology 2009;74:S148.
93. Prat G, Lefevre M, Nowak E, Tonnelier J-M, Renault A, L’Her E, et al. Impact of clinical guidelines to improve appropriateness of laboratory tests and chest radiographs. Intens Care Med 2009;35:1047–53.
94. Pysher TJ, Bach PR, Lowichik A, Petersen MD, Shields LH. Chemistry test ordering patterns after elimination of predefined multitest chemistry panels in a children’s hospital. Pediatr Dev Pathol 1999;2:446–53.
95. Ramoska EA. Information sharing can reduce laboratory use by emergency physicians. Am J Emerg Med 1998;16:34–6.
UnauthenticatedDownload Date | 5/19/16 2:24 AM

182 Kobewka et al.: Systematic review of interventions to reduce test use
96. Ratnaike S, Hunt D, Eilermann LJ, Hazen R, Deam D. The inves-tigation of chest pain: audit and intervention. Med J Australia 1993;159:666–71.
97. Rhyne RL, Gehlbach SH. Effects of an educational feedback strategy on physician utilization of thyroid function panels. J Fam Practice 1979;8:1003–7.
98. Roberts DE, Bell DD, Ostryzniuk T, Dobson K, Oppenheimer L, Martens D, et al. Eliminating needless testing in intensive care – an information-based team management approach. Crit Care Med 1993;21:1452–8.
99. Rosenbloom ST, Chiu K-W, Byrne DW, Talbert DA, Neilson EG, Miller RA. Interventions to regulate ordering of serum magne-sium levels: report of an unintended consequence of decision support. J Am Med Informat Assoc 2005;12:546–53.
100. Santos IS, Bensenor IM, Machado JB, Fedeli LM, Lotufo PA. Intervention to reduce C-reactive protein determination requests for acute infections at an emergency department. Emerg Med J 2012;29:965–8.
101. Seguin P, Bleichner J, Grolier J, Guillou Y, Malledant Y. Effects of price information on test ordering in an intensive care unit. Intens Care Med 2002;28:332–5.
102. Shalev V, Chodick G, Heymann AD. Format change of a labora-tory test order form affects physician behavior. Int J Med Inform 2009;78:639–44.
103. Sorita A, Steinberg D, Leitman M, Luhan P, Burger A, Sivaprasad L. Impact of targeted individual feedback on pro-vider patterns of stat laboratory test ordering frequency. J Hosp Med 2011;6:S135–6.
104. Spray J, Brackbill M, Baker P. Evaluation of effect of electronic decision tree electrolyte replacement protocol on number of electrolyte labs ordered for patients in critical care. Crit Care Med 2012;40:248.
105. Stafford RS. Feedback intervention to reduce routine electrocardiogram use in primary care. Am Heart J 2003;145:979–85.
106. Sucov A, Bazarian JJ, deLahunta EA, Spillane L. Test ordering guidelines can alter ordering patterns in an academic emer-gency department. J Emerg Med 1999;17:391–7.
107. Sussman E, Goodwin P, Rosen H. Administrative change and diagnostic test use: the effect of eliminating standing orders. Med Care 1984;22:569–72.
108. Thompson RS, Kirz HL, Gold RA. Changes in physician behavior and cost savings associated with organizational recommen-dations on the use of ‘routine’ chest X rays and multichannel blood tests. Prev Med 1983;12:385–96.
109. Tierney WM, McDonald CJ, Hui SL, Martin DK. Computer predic-tions of abnormal test results. Effects on outpatient testing. J Am Med Assoc 1988;259:1194–8.
110. Tierney WM, Miller ME, McDonald CJ. The effect on test order-ing of informing physicians of the charges for outpatient diagnostic tests. N Engl J Med 1990;322:1499–504.
111. Toubert ME, Chevret S, Cassinat B, Schlageter MH, Beressi JP, Rain JD. From guidelines to hospital practice: reducing inap-
propriate ordering of thyroid hormone and antibody tests. Eur J Endocrinol 2000;142:605–10.
112. van Wijk MA, van dL, Mosseveld M, Bohnen AM, van Bemmel JH. Assessment of decision support for blood test ordering in pri-mary care. a randomized trial. Ann Intern Med 2001;134:274–81.
113. Vardy DA, Simon T, Limoni Y, Kuperman O, Rabzon I, Cohen A, et al. The impact of structured laboratory routines in computer-ized medical records in a primary care service setting. J Med Syst 2005;29:619–26.
114. Verstappen WH, van der Weijden T, Sijbrandij J, Smeele I, Hermsen J, Grimshaw J, et al. Effect of a practice-based strat-egy on test ordering performance of primary care physicians: a randomized trial. J Am Med Assoc 2003;289:2407–12.
115. Wagholikar A, O’Dwyer J, Hansen D, Chu K. Observing effective-ness of pathology ordering controls in emergency depart-ments. Stud Health Tech Informat 2011;168:172–8.
116. Winkens RA, Pop P, Bugter-Maessen A, Grol RP, Kester AD, Beusmans GH, et al. Randomised controlled trial of routine individual feedback to improve rationality and reduce numbers of test requests. Lancet 1995;345:498–502.
117. Winkens RA, Pop P, Grol RP, Kester AD, Knottnerus JA. Effect of feedback on test ordering behaviour of general practitioners. Br Med J 1992;304:1093–6.
118. Wones RG. Failure of low-cost audits with feedback to reduce laboratory test utilization. Med Care 1987;25:78–82.
119. Zaat JO. Attempts to change test ordering behavior in laborato-ries. Ann Clin Biochem 1992;17:8–14.
120. Zaidi AK, Macone A, Goldmann AD. Impact of simple screening criteria on utilization of low-yield bacterial stool cultures in a Children’s Hospital. Pediatrics 1999;103: 1189–92.
121. Zia HM, Singh G. Optimization of utilization of serum protein analysis: role of the electronic medical record in promoting consultation by pathology. Am J Clin Pathol 2013;139:793–7.
122. Roshanov PS, You JJ, Dhaliwal J, Koff D, Mackay JA, Weise-Kelly L, et al. Can computerized clinical decision support systems improve practitioners’ diagnostic test ordering behavior? A decision-maker-researcher partnership systematic review. Implement Sci 2011;6:88.
123. Buntinx F, Winkens R, Grol R, Knottnerus JA. Influencing diagnostic and preventive performance in ambulatory care by feedback and reminders. A review. Fam Pract Res J 1993;10:219–28.
124. Ivers N, Jamtvedt G, Flottorp S, Young JM, Odgaard-Jensen J, French SD, et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev 2012;6:CD000259.
Supplemental Material: The online version of this article (DOI: 10.1515/cclm-2014-0778) offers supplementary material, available to authorized users.
UnauthenticatedDownload Date | 5/19/16 2:24 AM
Kobewka et al.: Systematic review of interventions to reduce test use 183
Daniel Kobewka MD, FRCPC is a Master’s of science student and general internist at the Ottawa Hospital. He received his MD from the University of Alberta and completed his training in General Internal Medicine at the University of Ottawa. His research interests include quality improvement and end-of-life care.
Paul Ronksley PhD is a post-doctoral fellow in the department of clinical epidemiology at the Ottawa Hospital Research Institute. He received his PhD in Epidemiology from the University of Calgary and is currently funded by a CIHR post-doctoral fellowship award. His research interests are in chronic disease epidemiology and the use of administrative and population-based survey data to study access to care and health care utilization for patients with multi-morbidity.
Jennifer McKay is a Master’s student in the Epidemiology program at the University of Ottawa. Jennifer’s research interests are quality of care, health economics and the funding dynamics of the health care system.
Alan J. Forster MD, FRCPC, MSc is a general internist and Chief Quality and Performance Officer at the Ottawa Hospital. He is a Professor of Medicine at the University of Ottawa and Senior Sci-entist in the Clinical Epidemiology Program at the Ottawa Hospital Research Institute. His research focuses on patient safety and quality improvement. He has received several prestigious awards recognizing his work within the field of health services research, including a Career Scientist Award with the Ontario Ministry of Health and Long-Term Care and an Early Research Award and Ontario Research Fund grant from the Ontario Government’s Min-istry of Research and Innovation. He has performed seminal work evaluating the incidence of adverse events following discharge from hospital.
Carl van Walraven MD, FRCPC, MSc is a Senior Scientist with the Ottawa Hospital Research Institute (OHRI) and is the Site Director for the Institute for Clinical Evaluative Sciences uOttawa Site. He is a general internist at the Ottawa Hospital and is a Professor in the Faculties of Medicine and Epidemiology and Community Medicine at the University of Ottawa. Carl’s research focuses on quality improvement, continuity of care, and administrative database research. He has over 150 publications in peer-reviewed journals. Carl has also been the recipient of several prestigious awards recognizing his work within the field of health services research, including the Ontario Ministry of Health Career Scientist Award and the Premier Research Excellence Award.
UnauthenticatedDownload Date | 5/19/16 2:24 AM
Copyright © 2022 FDOKUMEN




















