
INEQUALITY IN UTILIZATION OF MATERNAL HEALTH CARE SERVICES AMONG TEENAGE MARRIED WOMEN IN UTTAR...
20
Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459 An international double – blind peer reviewed, refereed and Indexed Journal 70 INEQUALITY IN UTILIZATION OF MATERNAL HEALTH CARE SERVICES AMONG TEENAGE MARRIED WOMEN IN UTTAR PRADESH: EVIDENCES FORM NFHS-3 AMBARISH KUMAR RAI, PH. D. INTERNATIONAL INSTITUTE FOR POPULATION SCIENCES, MUMBAI, INDIA – 400088 BAL GOVIND CHAUHAN, M. PHIL. INTERNATIONAL INSTITUTE FOR POPULATION SCIENCES, MUMBAI, INDIA – 400088 ABSTRACT Objectives: Coupled with the largest number of maternal deaths, maternal care in India has received overriding importance due to early age at marriage and poor accessibility of maternal health services. This study examines the factors associated and assessed the economic inequality in utilization of maternal health care services (full ANC, Safe delivery and PNC) among teenage mothers in Uttar Pradesh. Methods: third wave of National Family Health Survey (2005–06) data was used for the study, Bi-variate analyses employed to determine the difference in proportion, and logistic regression to understand the effect of predictor variables on selected outcomes were applied, to access economic inequality, CI index have calculated. Results: significant differences have found in the utilization of maternal healthcare services by Birth order & birth interval, caste, wealth index and education. Teenage mothers from SC/ST, poorest quintile, Multiple birth orders & 24< months of interval, and no educated were less likely than their counterpart mothers. Economic inequality was highest in full ANC followed by PNC and safe delivery among teenage mothers. Conclusions: study found that all the previous programs related to utilization of maternal care services were being far from their target; although they are working but, not with the needed pace. Therefore, there is a need to introduce a new policy intervention in accordance with region wise which specially focuses on teenage mother and disadvantages mothers by improve the information-communication facilities. The government should ensure the local people participation to make efficient use of the opportunities available. Keywords: Full ANC, Safe Delivery, Postnatal Care, Teenage Mother, Economic-Inequality, CI Index, Logistic Regression,
Transcript of INEQUALITY IN UTILIZATION OF MATERNAL HEALTH CARE SERVICES AMONG TEENAGE MARRIED WOMEN IN UTTAR...

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
70
INEQUALITY IN UTILIZATION OF MATERNAL HEALTH CARE SERVICES
AMONG TEENAGE MARRIED WOMEN IN UTTAR PRADESH: EVIDENCES
FORM NFHS-3
AMBARISH KUMAR RAI, PH. D.
INTERNATIONAL INSTITUTE FOR POPULATION SCIENCES, MUMBAI,
INDIA – 400088
BAL GOVIND CHAUHAN, M. PHIL.
INTERNATIONAL INSTITUTE FOR POPULATION SCIENCES, MUMBAI,
INDIA – 400088
ABSTRACT
Objectives: Coupled with the largest number of maternal deaths, maternal
care in India has received overriding importance due to early age at marriage
and poor accessibility of maternal health services. This study examines the
factors associated and assessed the economic inequality in utilization of
maternal health care services (full ANC, Safe delivery and PNC) among
teenage mothers in Uttar Pradesh.
Methods: third wave of National Family Health Survey (2005–06) data was
used for the study, Bi-variate analyses employed to determine the difference
in proportion, and logistic regression to understand the effect of predictor
variables on selected outcomes were applied, to access economic inequality,
CI index have calculated.
Results: significant differences have found in the utilization of maternal
healthcare services by Birth order & birth interval, caste, wealth index and
education. Teenage mothers from SC/ST, poorest quintile, Multiple birth
orders & 24< months of interval, and no educated were less likely than their
counterpart mothers. Economic inequality was highest in full ANC followed
by PNC and safe delivery among teenage mothers.
Conclusions: study found that all the previous programs related to
utilization of maternal care services were being far from their target;
although they are working but, not with the needed pace. Therefore, there is
a need to introduce a new policy intervention in accordance with region wise
which specially focuses on teenage mother and disadvantages mothers by
improve the information-communication facilities. The government should
ensure the local people participation to make efficient use of the
opportunities available.
Keywords: Full ANC, Safe Delivery, Postnatal Care, Teenage Mother,
Economic-Inequality, CI Index, Logistic Regression,

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
71
Introduction
Pregnancy and its outcome as
childbearing are the most special
events in the women‟s life and their
families, hence, care of mother
during that partum period is the
necessary and effective
interventions for safer and
healthier outcome, and it is most
essentials if the mother is in
teenage stage. As a group, however,
teenagers have quite different
needs, in terms of reproductive
health services, from adults
mothers in different important
ways (1), but most of the developing
nations like India, it remains poorly
underserved. So, maternal health
care utilization became one of the
most important components of
MDGs during the ICPD 1994 with a
great emphasised on younger
mothers. In 2005, it was estimated
that about each second deaths
among mother only cause of
pregnancy related complications
over the worldwide (2, 3). The
„„greatest health divide in the world‟‟
is the gap of overall risk of death
caused by maternal causes
between develop and developing
nation. Globally, about four-fifth of
maternal death in women
contributed by haemorrhage,
sepsis, unsafe induced abortion,
hypertensive disorder of pregnancy
and obstructed labour and these
occurs only due to negotiate with
the needs of maternal care, but
these deaths are unjust and can be
prevented with some effective key
health interventions, like to insure
providing universal services of
maternal health care and assisted
safe delivery by health personnel (2,
4, 5).
In addition, the huge proportions
of the risk of maternal deaths were
not uniformly distributed across
globally, and it was more skewed
towards developing nations. In
2005, about 99% of total maternal
deaths occurred in the developing
world, and more drastically, 86% of
total maternal deaths of the world
concentrated in Sub-Saharan
Africa and South Asia alone.
In India, where the more than half
of the population (about 55%) lies
in reproductive (15-50 years) age
group (6), the importance of
maternal health services utilization
automatically gets a significant
attention because of the need of
health care for such a huge chunk
of the population. Utilization of
antenatal, natal and postnatal care
is important for reducing maternal
morbidity and mortality. India
contributed about one-fourth of
total maternal deaths across
worldwide and Uttar Pradesh have
the largest share of these all
maternal deaths (7). Uttar Pradesh,
one of the prime and highly
populous states of India, continues
to have one of highly reported
figure of maternal mortality ratio

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
72
i.e. 440 per 100, 000 live births and
still remains above the national
average (8). Uttar Pradesh,
however, is characterized by low
uptakes of maternal health
services, and it is one of the
deprived states of India in terms of
socio-economy and demographic
condition. Still there are a number
of health plans has executed
specially related to maternal health
care services, but that hasn't been
a change the expected scenario.
Earlier studies have underlined the
socioeconomic gradient in the
utilization of maternal health care
utilization among teenage mother
in the context of rural and urban
India (9, 10). About every second
mother, who was pregnant, only
able to seek any ANC care services
and even when they went for
services, it was the second
trimester with the sole purpose of
the confirmation of their pregnancy
in Uttar Pradesh. It is not so
surprisingly observation and so
common in Uttar Pradesh where
the utilization of maternal health
services is very low, and people are
not too much conscious about to
understand that pregnancy needs
any special attention (10).
Therefore, the extensive objective of
this study is to examine the
determinants and existing
inequality in utilization of maternal
health care services, in terms of,
full antenatal care, safe delivery
and postnatal care by wealth index
of the household in Uttar Pradesh.
Methods
Data
The present study utilizes data
from the third round of the
Demographic and Health Survey
(DHS), known as the National
Family Health Survey (NFHS),
carried out in India during 2005–
06. The NFHS is a large-scale,
multi-round survey conducted in a
representative sample of
households covering more than
99% of the population throughout
India. The main instrument for the
collection of the data in NFHS -3
was the set of structured
questionnaires. Information of the
maternal health care was from all
women who had given birth in the
five year preceding the survey. This
study considers only the most
recent live births and excludes
multiple births.
Outcome Variables
The term “Teenage Mother” refers
only to ever-married women who
have had the experience of
childbirth within 15–19 years of age
during the 5 years preceding the
survey date. The present study
measures three outcome variables:
Full Antenatal Care (Full ANC) has
been defines as at least three
antenatal care visits, consumed
90+ Iron Folic Acid (IFC) tablets

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
73
and took two or more tetanus-
toxoid injections.
Safe Delivery defined as either
institutional delivery or home
delivery assisted by doctor,
auxiliary nurse midwife, nurse,
midwife, lady health visitor or any
other health personnel.
Postnatal Care indicates whether
the women received any checkups
of her own health within 2 days (48
hrs.) after the delivery of child.
Exposure Variables
The explanatory variables included
in the analysis are: Maternal Age
(recoded <18 years and 18-19
years), Birth Order & Birth Interval,
Caste/Tribe, Religion, Place of
Residence, Educational Level,
Wealth Index, Women‟s Work
Status, Exposure to Mass Media
and Household Structure. Birth
order and interval were categorized
as, first birth order, birth order
second or third and interval < 24
months, and birth order second or
third and interval 24 and more
months. The place of residence
variable is categorized as urban
and rural. Caste/Tribe is
categorized as SC/ST, other
backward caste (OBC) and others.
Religion is categorized as Hindu
and non-Hindu. The economic
status of the households has been
captured in the wealth index which
has been categorized into poorest,
poor, middle, richer and richest.
Education of women is used as a
categorized variable with four
categories; No education, primary,
secondary and higher. Exposure to
mass media is categorized as
exposed and not exposed to any
means of mass media (newspaper,
radio, television and cinema).
Women‟s work status recoded as
not working, working, household
structure has been categorized as
nuclear, non-nuclear.
Analytical Approach
To identify factors associated with
selected maternal healthcare
utilization among adolescent
women, bivariate and multivariate
analyses were performed. Bivariate
analyses were performed to
examine the nature of association
between utilization of maternal
healthcare services by selected
socioeconomic and demographic
background characteristics.
Multivariate analyses used logistic
regression to investigate which
factors best explain and predict the
utilization of the health outcome.
Three outcome variables, namely
full antenatal care, safe delivery
and postnatal care (within 42 days
of delivery) were considered for the
multivariate analyses. The results
were presented by estimated odds
ratio with 95% confidence interval.
The appropriate sampling weight
has been supplemented to perform
the whole analysis. In order to
assess the economic inequality in

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
74
maternal health care services
utilization, concentration curve
have been employed. The analyses
were conducted using SPSS version
21.0.
Results
Background Characteristics of
Teenage Mothers
Table 1: The background
characteristics of teenage mothers,
who had at least one live birth
during last five years in Uttar
Pradesh, illustrated that nearly
one-third teenagers became the
mother before their legal age at
marriage (18 years), and nearly
17% have multiple births with
births interval of less than 24
months. 84 percent of them were
from rural, one-third belongs to
socially deprived classes (SCs &
STs) and less than one-fifth of them
were non-Hindu (Table 1). Three-
fifth teenage mothers belong to
poor wealth quintile and more than
25% were from non-nuclear family.
Half of this teenage mother hadn‟t
any type of media exposure, 57% of
them were illiterate, and only one-
fifth of them were secondary
educated. Five out of six teenage
mothers were reported do not have
any work while more than 75% of
them reported their spouses were
working but as an unskilled
worker. The surprising result has
found in the study was that about
84% of the teenage mother who has
child stated that they wanted the
child.
Table 1: percent distribution of women who had at least one live birth
during the last five year preceding the survey by background
characteristic in up, 2005-06
Background characteristics % n
Mother Age
<18 Years 30.77 187
18-19 Years 69.23 421
Birth Order & BI
Birth Order 1 67.09 407
Higher Order & < 24 Months BI 16.66 101
Higher Order & 24 < Months BI 16.26 99
Sex of the Child
Male 51.7 311
Female 48.93 297
Place of Residence
Urban 16.54 101
Rural 83.46 507

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
75
Caste/ Tribe
SC/ST 33.87 206
OBC 49.8 303
Others 16.34 99
Religion
Hindu 83.35 507
Non Hindu 16.65 101
Wealth Index
Poorest 26.58 162
Poor 30.42 185
Middle 21.19 129
Rich 14.3 87
Richest 7.5 46
Mother Education
No Education 56.26 342
Primary 15.48 94
Secondary 23.14 141
Higher 5.12 31
Father Education
No Education 25.99 156
Primary 11.79 71
Secondary 54.2 325
Higher 8.02 48
Working Status
Not Working 84.11 511
Working 15.89 96
Media exposure
No Exposure 51.27 312
Any Exposure 48.73 296
Wanted Last Child
Wanted 83.98 511
Unwanted 16.02 97
Household Structure
Nuclear 28.39 173
Non-Nuclear 71.61 435
Total 14.0 608
BI: Birth Interval, Higher Order: Birth Order more than one.

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
76
Prevalence and Differential in
Utilization of Maternal Health
Care Services
Birth order and interval, place of
residence, caste, wealth quintile,
education of women and her
spouses and media exposure
played an important role to
determine the level of maternal
health care services in teenage
mothers in Uttar Pradesh. Only 3%
of teenage mothers were able to
access the full antenatal care, less
than one-third went for safe
delivery and only every tenth
teenage mother were able to get
postnatal care after the childbirth
(Table 2). The result illustrate that
the teenage mothers of first parity
have higher chances (4.1% used
ANC, 38% safe delivery and 15%
used PNC) to go for maternal health
care services compared to those of
more than one parity. Those
mothers who had birth interval of
less than 24 month were less
accessible for full ANC (1.1%) than
those who had birth interval more
than 24 months (3.4%). Urban
teenage mothers were more
utilizing of maternal health care
services (7.7% ANC, 49% sage
delivery & 30% PNC) than rural
(2.7% ANC, 30% Safe delivery &
11% PNC).
Table 2: Percentage of women who had at least one live birth in their
teens (aged 15–19) during the last five years preceding the survey by
usage pattern of maternity and child health care services and by
background characteristics in Uttar Pradesh, 2005–06
Background
Characteristics
Full
ANC
Safe
Delivery PNC n
Age
<18 3.0 31.8 11.4 179
18-19 3.7 33.4 14.9 429
Birth Order & BI
Birth Order 1 4.1 38.4 15.4 401
Higher Order & < 24
month BI 1.1 23.2 13.3 106
Higher Order & 24< month
BI 3.4 20.5 8.1 100
Sex of the Child
Male - - 56.1 310
Female - - 41.5 297
Place of Residence

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
77
Urban 7.7 49.4 30.3 156
Rural 2.7 29.6 10.6 452
Caste/Tribe
SC/ST 1.6 23.3 10.3 195
OBC 4.1 34.8 12.7 309
Others 5.6 47.2 24.8 104
Religion
Hindu 3.9 33.7 13.9 482
Non- Hindu 1.2 29.0 13.6 126
Mother Education
No Education 1.0 22.0 8.0 335
Primary 4.7 38.0 17.9 95
Secondary 5.6 46.9 21.5 147
Higher 17.9 74.8 32.0 31
Paternal Education
No Education 0.7 22.3 8.8 157
Primary 3.2 23.7 8.1 73
Secondary 2.4 36.2 16.2 319
Higher 20.8 62.6 25.6 50
Wealth Index
Poorest 1.4 19.4 4.9 144
Poor 0.6 23.1 10.9 172
Middle 2.6 36.5 11.4 129
Rich 6.6 50 22.1 101
Richest 19.3 77.7 48.9 62
Mother Work Status
Not Working 3.7 33.7 15.0 517
Working 1.2 29.1 8.2 90
Media Exposure
No Exposure 0.7 27.0 9.0 299
Exposure 6.4 39.2 18.9 309
Wanted Last child
Wanted 3.3 32.2 13.6 513
Unwanted 4.6 36.8 15.0 95
Household Structure
Nuclear 2.6 21.6 8.6 180

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
78
Non-Nuclear 3.8 37.4 16.0 428
Total 3.5 32.9 13.8 608
BI: Birth Interval, Higher Order: Birth Order more than one
Social groups also had shown
uneven utilization of maternal
health care services among teenage
mothers. Only 1.6% of SCs/STs
teenage mothers received full ANC
while, in OBC and others group, it
was 4.1% and 5.6% respectively.
Less than one-fourth SC and STs
teenage mothers were used the safe
delivery services while, in OBCs,
and others social group mothers, it
was nearly 35% and 47%
respectively. The PNC services were
more accessible (25%) by other
caste mothers than SC/ST (10%)
and OBC group (13%) of teenage
mothers. There was a huge
disparity among different wealth
quintile teenage mothers for
accessing the maternal health
services. From poorest wealth
quintile, only about 1% of teenage
mothers accessed the ANC, 19%
went for safe delivery and 5% used
PNC services, while about one-fifth
mother used ANC, more than three-
fourth were accessed the safe
delivery and nearly every second
teenage mother get the postnatal
care from richest quintile of teenage
mothers. The mother who were
higher educated, nearly 18% of
them used antenatal care, about
three-fourth went for safe delivery
services and one-third woman
accessed the postnatal care, while
for not educated mother this
prevalence were 1%, 22% and 8%
respectively. An interesting result
had seen that the working teenage
women were less accessed the
maternal health care services than
their counterparts. Media exposed
teenage mothers were more
accessed the maternal health care
services (6.4% of ANC, 39% safe
delivery and 19% PNC) than their
counterparts mothers (1% ANC,
27% safe delivery & 9% PNC).
Figure 1: Concentration curves showing inequalities in Maternal Health
Care services by Wealth Quintile of Teenage Mothers in Uttar Pradesh,
2005-06

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
79
Economic Inequalities in Maternal Health Care Utilization
In order to assess the economic
inequality in Utilization of maternal
health care (full ANC, safe delivery
& PNC) services, concentration
indices (CI) and concentration
curves (CC) have employed (Figure
1). Findings indicate substantially
large, consistent and pro-rich
inequalities in the utilization of
these three indicators of maternal
healthcare services among teenage
mothers in Uttar Pradesh. The
magnitude of economic inequality
in utilization of full ANC was
highest (CI: 0.54) followed by PNC
(CI: 0.36) and lowest for safe
delivery (CI: 0.25) in Uttar Pradesh
during 2005-06. It indicates that
few numbers of the teenage mother
were able to access the ANC care
while, for safe delivery, most
women visited health facilities.
Probably it‟s only due to have any
type of pregnancy complication
rather than they aware.
Determinants of Maternal Health
Care Utilization
Birth order & birth interval, caste
of the teenage mother, wealth index
and education of the mother were
the most significant variables that
highly influenced the level of
utilization of maternal health care
services in teenage mothers, in
Uttar Pradesh (Table 3). The
results illustrate that the teenage
mothers, had birth interval of less
than 24 months, were less likely to
get the antenatal care, safe delivery
and PNC services than the teenage
mother of their reference category
mother. Rural mother were less
likely to use PNC services than
their counterparts (p=0.546 at 95%
of CI). Teenage mothers from OBC
and Others category were 40% and
80% more likely (p=1.405 (OBC) &
1.842 (others) at 95% CI) for using
the safe delivery services than
Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
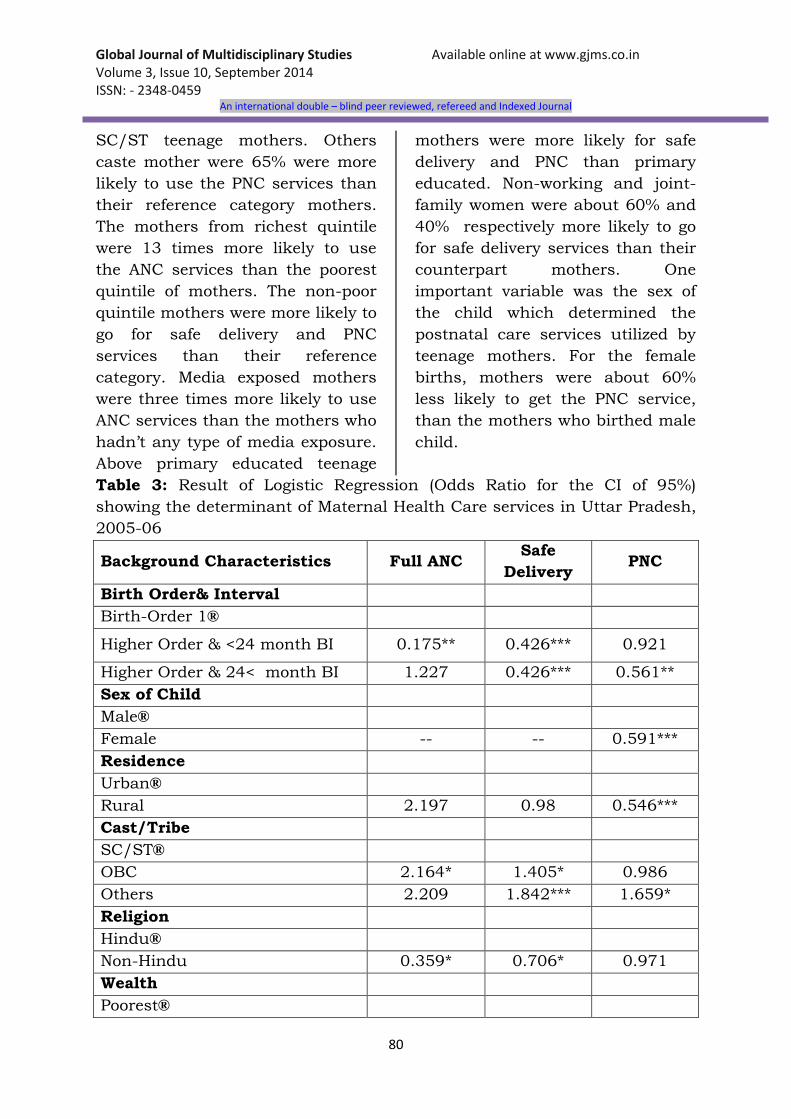
80
SC/ST teenage mothers. Others
caste mother were 65% were more
likely to use the PNC services than
their reference category mothers.
The mothers from richest quintile
were 13 times more likely to use
the ANC services than the poorest
quintile of mothers. The non-poor
quintile mothers were more likely to
go for safe delivery and PNC
services than their reference
category. Media exposed mothers
were three times more likely to use
ANC services than the mothers who
hadn‟t any type of media exposure.
Above primary educated teenage
mothers were more likely for safe
delivery and PNC than primary
educated. Non-working and joint-
family women were about 60% and
40% respectively more likely to go
for safe delivery services than their
counterpart mothers. One
important variable was the sex of
the child which determined the
postnatal care services utilized by
teenage mothers. For the female
births, mothers were about 60%
less likely to get the PNC service,
than the mothers who birthed male
child.
Table 3: Result of Logistic Regression (Odds Ratio for the CI of 95%)
showing the determinant of Maternal Health Care services in Uttar Pradesh,
2005-06
Background Characteristics Full ANC Safe
Delivery PNC
Birth Order& Interval
Birth-Order 1®
Higher Order & <24 month BI 0.175** 0.426*** 0.921
Higher Order & 24< month BI 1.227 0.426*** 0.561**
Sex of Child
Male®
Female -- -- 0.591***
Residence
Urban®
Rural 2.197 0.98 0.546***
Cast/Tribe
SC/ST®
OBC 2.164* 1.405* 0.986
Others 2.209 1.842*** 1.659*
Religion
Hindu®
Non-Hindu 0.359* 0.706* 0.971
Wealth
Poorest®

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
81
Poor 0.426 1.11 1.854
Middle 1.353 1.801*** 1.581
Rich 2.374 3.231*** 2.648**
Richest 13.424*** 8.245*** 6.543***
Media Exposure
No Exposure®
Exposure 3.563* 0.843 1.202
Mother Education
Primary®
Secondary 2.745 1.645** 1.971**
Middle 1.326 1.61*** 1.576**
Higher 0.954 3.953*** 1.688
Husband's Education
Primary®
Secondary 2.72 0.869 0.786
Middle 1.112 1.075 1.136
Higher 7.309** 1.722* 1.052
Work Status of Mother
Working®
Not working 0.963 1.631** 1.07
Child status
Wanted®
Unwanted 1.007 1.24 0.948
Household structure
Nuclear®
Non nuclear 0.53 1.396* 1.409*
®: Reference category; ***p<0.01; **p<0.05; *p<0.1 (at 95% of CI)
Abbreviation: BI: Birth Interval, Higher Order: Birth Order more than one,
CI: Confidence Interval
Reason for not delivering the
Birth in Health Facility
Women who did not deliver their
last child in a health facility were
asked about the reason for not
delivering in a health facility (11).
There seem to be several reasons.
The major reasons given (Figure 2),
it was found that, in Uttar Pradesh,
about 81% teenage mother
responded “not necessary” while,
for every fourth teenager, it was too
much costly. For 7% teenage
mothers, health facility was either
too far or not available, and a
similar number of teenage did not
go because their husband/family
did not allow them.

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
82
Figure 2: Percentage of women who had a live birth in the five year
preceding the survey by reason for not delivering the most recent live
birth in a health facility, india-2005-06
Note: Percentage is not 100 due to multiple responses by respondent
(n=455)
Discussion and Conclusion
Several numbers of governmental
and non-governmental organization
made their efforts to enhance the
level of maternal health care
services and made it more
accessible and effective in the last
decade. Early marriages of the girl
child and its negative impact on
their health have been seen widely
(12, 13), and, in most of the
developing countries, we found that
younger age mother were severe
threatening towards delivery
complications, which enhances the
chances of death of mother or poor
health of mothers (14, 15, 16).
Studies from developing countries
illustrate that women, for their first
delivery, are significantly more
likely to utilize the maternal
healthcare services (17, 18, 19).
Literature suggested that the
women having higher parity were
less likely to go for safe delivery by
health professionals (20), and the
same pattern has been seen a
study made in six developing
countries. Although it is not clearly
says why higher order younger age
mothers are less likely to utilize
safe delivery services (21), it may be
argue that the chances of the
higher number of parity exist to
those mothers only who were less

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
83
educated or from poor
socioeconomic stratum, so due to
lack of knowledge and due to time
and resource constraints, she does
not expose towards safe delivery
(22, 23, 24). Few other studies also
argued that lower parity women
tend to pay her full attention
towards seeking assistance by
health professionals during her
delivery due to her inexperience
with pregnancy and high risks for
women and child health (20, 25).
This study suggests the immediate
need for intense research to
understand the factors that being
obstacles in the path of utilization
of maternal healthcare services, in
higher birth order young age
mothers.
In teenage mothers, the utilization
of recommended ANC, safe delivery
and PNC services were higher in
urban than in rural areas. The
same finding has been seen that,
rural women give birth at home in
the absence of skilled care, in a
study conducted in eight other
West African countries, (26). The
urban teenage mothers have many
advantages over their counterparts,
like having higher levels of
knowledge due to media exposure,
more accessible towards services
and actively participation in health
promotion programs (27, 28). To
improve the level of maternal health
services a more comprehensive and
people participation based
approaches are needed in rural
population.
In the social groups, the difference
in healthcare service utilization
could be linked with the well
determine factors like social norms,
cultural beliefs and practices (29,
30). The study of Hausa community
has shown a number of negative
health experiences due to the
pregnancy on younger age of
mothers (29). Child marriage was
directly linked to the low level of
educational attainment and further
it associated with starting child
bearing at younger and high order
of births with narrow birth intervals
among young age mothers of the
Hausa/ Fulani/Kanuri social
groups and significantly influences
their healthcare utilization (31). So
this study underscore about
spreading awareness by
community-based interventions
that can change the behavior and
mentality of this underserved social
group about their specific health-
damaging cultural norms and
perceptions.
This study illustrates that the
utilization of ANC, safe delivery and
PNC services are significantly
associated with wealth quintile
status of teenage mothers. The
same finding has been seen in
previous widely available literature,
and one of the evidence from
African countries highlights the
significant economic inequality in
healthcare service utilization (32

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
84
33, 34). This may be due to the
poor are busy to earn their bread
and butter rather than to go for the
healthcare expenditure until unless
that is not severe while the people
from rich households can easily
affords and spend a higher
proportion of their own earning for
healthcare (35). Since teenage
mother has less exposure of
education and rare chances to
engage in earning, and hence there
may be chances to expand a
minimum for their good health
care. A community based approach
must be needed for utilization of
maternal health care services that
target the special group of poor and
especially teenage mothers. In
addition to providing reproductive
health information and services,
they also address a wide range of
needs including life skills, literacy,
vocational training, and livelihood
activities (36).
The findings of the study also
shows the significant positive
effects of the educational
attainment on maternal health
service utilization among teenage
mothers and are consistent with
other studies from developing
African countries (37, 38, 39) and
in India too (9, 10). Probably
educated women have better access
to health services and related
information along with improved
perceptions of the root causes of
disease and can utilize such
information optimally so for that
the positive association between
mother education and maternal
health service utilization has been
seen (31). Greater autonomy comes
only through the high attainment of
education in women, and that
helps to make decisions and have a
greater ability to use quality
healthcare inputs (19, 40).
The findings of this study confirm
that, along with mother‟s
education, there was a positive
effect of husband‟s education on
maternity care utilization has been
seen among teenage mothers of
Uttar Pradesh. Several studies have
been shown that male educational
attainment and his engagement in
women‟s health needs enhances
the chances of women‟s maternal
and reproductive healthcare
choices and their utilization (41,
42, 43, 44, 45, 46, 47, 48) and
support the same finding of this
study.
The effect of mass media exposure
on recommended ANC, safe delivery
and PNC services utilization are
positively associated and consistent
with previous studies (49, 50).
Existing studies clearly illustrated
that the mass media which is an
effective in information
dissemination, works to spread
awareness about healthcare
facilities that are available and
impetus inter-personnel
communication rapidly and that
could facilitate behavioral changes
(51). There is a need to broadcast

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
85
the educational programs through
electronic media and it also insure
that it could reach the teenage
mothers, along with to all those
belong to disadvantaged social
groups, and specifically, to the low
privileged teenage mothers living in
rural areas. One of the important
indicators, sex of child at birth,
illustrated that for male birth, large
number of teenage mother in Uttar
Pradesh, went for postnatal care
services compare to their counter
parts. The sex preference for child
birth is still high in State like Uttar
Pradesh, and similar result also
have been seen in the different
study (52, 53) which stated that,
due to strong desire of son
preference at births, mother as well
as child have been treated
accordingly, after the birth of child.
Implications for Policy and/or
Policy
The evidence of the study found
that all the previous programs
related to enhance the level of
utilization of maternal health care
services are far from their target;
although they are working but, not
with the needed pace. Therefore,
there is a need to adopt different
health policy intervention in
accordance with the urban and
rural area which specially focuses
on younger age mother and
socioeconomically disadvantages
mothers by improve the
information education
communication facilities with a
focus on rural area. The
government should collaborate and
co-operate with local level health
care agencies and ensure the local
people participation to make
efficient use of the opportunities
available. The need of the time is
weigh the available options and
stabilize up a weak health
infrastructure to minimize a
disaster as the road ahead is
uncertain, but definitely not short.
Acknowledgement
The authors acknowledge the editor
and anonymous reviewers whose
constructive suggestions helped
immensely to improve this paper.
References:
1.Siddiqi, N. U. (2010). Sexuality
and reproductive health: A socio
demographic study of
adolescents‟ perspective
regarding sexuality and
reproductive health done in
Karachi, LAP LAMBERT
Academic Publishing.
2.Pathak, P. K., Singh, A., &
Subramanian, S. V. (2010).
Economic inequalities in
maternal health care: prenatal
care and skilled birth
attendance in India, 1992–2006.
PLoS One, 5(10), e13593.
3.Ronsmans, C., & Graham, W. J.
(2006). Maternal mortality: who,
when, where, and why. The
Lancet, 368(9542), 1189-1200.

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
86
4.Freedman, L., Wirth M.,
Waldman R., Chowdhury M. &
Rosanfield A. (2003).
Background paper of the task
force on child health and
maternal health.
5.Freedman L.P., Graham W. J,
Brazier E, Smith J. M, Ensor T,
et al. (2007). Practical lessons
from global safe motherhood
initiatives: time for a new focus
on implementation. Lancet 370:
1383–91.
6.Census of India (2011). Office of
Registrar General and Census
commissioner of India, 2011
7.Gulati S.C., Sharma S. (2004).
Reproductive and child health
status in India: District level
analysis. Indian Journal of
Regional Sciences. Vol. 36(1), 7-
19.
8.Sample Registration System
(2011). Registrar General of
India.
9.Singh Lucky, R. K. Rai, P. K.
Singh (2011) Assessing the
utilization of maternal and child
health care among married
adolescent women: evidence
from India. Journal of Biosocial
Science, 44(1):1-26. DOI:
10.1017/S0021932011000472
10.Singh, P. K., Rajesh K. R.,
Manoj A., & Lucky S.
(2012)."Determinants of
Maternity Care Services
Utilization among Married
Adolescents in Rural India" PLoS
ONE 7.2, e31666
11.IIPS. (2007). National Health
Family Survey Report-3,
International Institute for
population Sciences and ORC
Macro International, Mumbai,
India.
12.Jain, S., & Kurz, K. (2007). New
insights on preventing child
marriage: A global analysis of
factors and programs.
Washington, DC: ICRW.
13.United Nations Children‟s Fund
(UNICEF). (2005). Early
marriage: A harmful traditional
practice. New York: USA.
14.Fatusi, A. O. & Hindin, M. J.
(2010). Adolescents and youth
in developing countries: Health
and development issues in
context. Journal of Adolescence,
33, 499–508.
15.Omar, K., Hasim, S.,
Muhammad, N. A., Jaffar, A.,
Hashim, S. M., & Siraj, H. H.
(2010). Adolescent pregnancy
outcomes and risk factors in
Malaysia. International Journal
of Gynecology & Obstetrics,
111(3), 220-223.
16.Rasheed, S., Abdelmonem, A., &
Amin, M. (2011). Adolescent
pregnancy in upper Egypt.
International Journal of
Gynecology & Obstetrics, 112(1),
21-24.
17.Stewart, K., & Sommerfelt, A. E.
(1991). Utilization of maternity
care services: A comparative
study using DHS data.
Proceedings of the Demographic
and Health Surveys World

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
87
Conference (Vol. III; pp. 1645–
1668). Washington, DC.
18.Akin, A., & Munevver, B. (1996).
Contraception, abortion and
maternal health services in
Turkey: Results of further
analysis of the 1993 Turkish
Demographic and Health
Survey. Calverton, MD: Ministry
of Health [Turkey] and Macro
International Inc.
19.Celik, Y., & Hotchkiss, D. R.
(2000). The socioeconomic
determinants of maternal health
care utilization in Turkey. Social
Science and Medicine, 50, 1797–
1806.
20.Bell, J., Curtis, S. L., & Alayon,
S. (2003). Trends in delivery
care in six countries. DHS
analytical studies: No 7.
Calverton, MD: ORC Macro.
21.Santhya, K. G., Jejeebhoy, S. J.,
& Ghosh, S. (2008). Early
marriage and sexual and
reproductive health risks:
Experiences of young women
and men in Andhra Pradesh
andMadhya Pradesh, India. New
Delhi, India: Population Council.
22.Wong, E. L., Popkin, B. M.,
Guilkey, D. K., & Akin, J. S.
(1987). Accessibility, quality of
care and prenatal use in the
Philippines. Social Science and
Medicine, 24, 927–944.
23.Elo, I. T. (1992). Utilization of
maternal health care services in
Peru: The role of women‟s
education. Health Transition
Review, 2, 49–69.
24.Bhatia, J. C., & Cleland, J.
(1995). Determinants of
maternal care in a region of
South India. Health Transition
Review, 5, 127–142.
25.Raj, A., Saggurti, N., Balaiah,
D., & Silverman, J. G. (2009).
Prevalence of child marriage and
its effect on fertility and fertility-
control outcomes of young
women in India: A cross
sectional, observational study.
Lancet, 373, 1883–1889.
26.Ronsmans, C., Etard, J.
F.,Walraven, G., Hoj, L.,
Dumont, A., Bernis, L., et al.
(2003). Maternal mortality and
access to obstetric services in
West Africa. Tropical Medicine
and International Health, 8,
940–948.
27.Ezeonwu, M. C. (2011).
Maternal birth outcomes:
Processes and challenges in
Anambra State, Nigeria. Health
Care for Women International,
32, 492–514.
28.Mekonnen, Y., & Mekonnen, A.
(2002). Utilization of maternal
health care services in Ethiopia.
Calverton, MD: ORC Macro.
29.Wall, L. L. (1998). Dead mothers
and injured wives: The social
context of maternal morbidity
and mortality among the Hausa
of Northern Nigeria. Studies in
Family Planning, 29, 341–359.
30.Babalola, S., & Fatusi, A.
(2009). Determinants of use of
maternal health services in
Nigeria-looking beyond

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
88
individual and household
factors. BMC Pregnancy and
Childbirth, 9, 43.
31.Antai, D. (2011). Inequalities in
under-5 mortality in Nigeria: Do
ethnicity and socioeconomic
position matter? Journal of
Epidemiology, 21, 13–20.
32.Rahman, M. H., Mosley, W. H.,
Ahmed, S., & Akhter, H. H.
(2007). Does service accessibility
reduce socioeconomic
differentials in maternal care
seeking? Evidence from rural
Bangladesh. Journal of Biosocial
Science, 40,19–33.
33.Nwogu, E. C. (2009). Utilization
of maternity care in Nigeria.
Global Journal of Pure and
Applied Sciences, 15. 439–437.
34.Ochako, R., Fotso, J., Ikamari,
L., & Khasakhala, A. (2011).
Utilization of maternal health
services among young women in
Kenya: Insights from the Kenya
Demographic and Health
Survey, 2003. BMC Pregnancy
and Childbirth, 11(1), 1.
35.Amin, R., Shah, N. M., &
Becker, S. (2010).
Socioeconomic factors
differentiating maternal and
child health-seeking behavior in
rural Bangladesh: A cross-
sectional analysis. International
Journal for Equity in Health,
9(9).
36.Rai, R. K., P. K. Singh, Lucky
Singh (2012). Utilization of
Maternal Health Care Services
among Married Adolescent
Women: Insights from the
Nigeria Demographic and Health
Survey, 2008. Women's Health
Issues 22-4 (2012). e407–e414
37.Magadi, M. A., Agwanda, A. O.,
& Obare, F. A. (2007). A
comparative analysis of the use
of maternal health services
between teenagers and older
mothers in sub-Saharan Africa:
Evidence from Demographic and
Health Surveys (DHS). Social
Science and Medicine, 64, 1311–
1325.
38.Ogunlesi, T. A. (2010). Maternal
socio-demographic factors and
the initiation and exclusivity of
breastfeeding in a Nigerian semi
urban setting. Maternal and
Child Health Journal, 14, 459–
465.
39.Ogunlesi, T. A., & Ogunlesi, F.
B. (2012). Family socio-
demographic factors and
maternal obstetric factors
influencing appropriate health-
care seeking behaviours for
newborn Jaundice in Sagamu,
Nigeria. Maternal and Child
Health Journal, 16, 677–684.
40.Mpembeni, R. N., Killewo, J. Z.,
Leshabari, M. T., Massawe, S.
N., Jahn, A., Mushi, D., &
Mwakipa, H. (2007). Use pattern
of maternal health services and
determinants of skilled care
during delivery in Southern
Tanzania: implications for
achievement of MDG-5 targets.
BMC pregnancy and childbirth,
7(1), 29.

Global Journal of Multidisciplinary Studies Available online at www.gjms.co.in Volume 3, Issue 10, September 2014 ISSN: - 2348-0459
An international double – blind peer reviewed, refereed and Indexed Journal
89
41.Agadjanian, V. (2002). Men‟s
talk about “women‟s matters:
Gender, communication, and
contraception in urban
Mozambique. Gender and
Society, 16, 194–215.
42.Mufune, P. (2009). The male
involvement programme and
men‟s sexual and reproductive
health in Northern Namibia.
Current Sociology, 57, 231–248.
43.Odimegwu, C. O., Adewuyi, A.
A., Odebiyi, T., Aina, B.,
Adesina, Y., Olatubara, O., et al.
(2005). Men‟s role in emergency
obstetric care in Osun State of
Nigeria. African Journal of
Reproductive Health, 9, 59–71.
44.Peacock, D., & Levack, A.
(2004). The men as partners
program in South Africa:
Reaching men to end gender-
based violence and promote
sexual and reproductive health.
International journal of Men‟s
Health, 3, 173–188.
45.Sternberg, P., & Hubley, J.
(2004). Evaluating men‟s
involvement as a strategy in
sexual and reproductive health
promotion. Health Promotion
International, 19, 389–396.
46.United Nations Agency for
International Development
(USAID). (2000). Involving men
in sexual and reproductive
health: An orientation guide.
Washington, DC: USAID,
Interagency Gender Working
Group.
47.United Nations Agency for
International Development
(USAID). (2003). Reaching men
to improve reproductive health
for all implementation guide.
Washington, DC: Interagency
Gender Working Group.
48.United Nations Agency for
International Development
(USAID). (2006). System
analyzing: Resources for
engaging men in sexual and
reproductive health.
Washington, DC: USAID, Inter
Agency Gender Working Group.
49.Bankole, A., & Wesstoff, C. F.
(1996). Mass media influences
on contraceptive behavior and
reproductive preferences. Paper
presented at the Annual Meeting
of the Population Association of
America, New Orleans, LA.
50.Retherford, R. D., & Mishra, V.
K. (1997). Media exposure
increases contraceptive use.
National Family Health Survey
Bulletin. Mumbai, India:
International Institute for
Population Sciences; and
Honolulu: East-West Center
Program on Population.
51.Valente, T. W., Poppe, P. R., &
Merritt, A. P. (1996). Mass-
media-generated inter personnel
communication as sources of
information about family
planning. Journal of Health
Communication, 1, 247–265.




















