
Lopinavir/ritonavir population pharmacokinetics in neonates and infants
Upload
independentCategory
view
0download
0
C
Induction therapy with
trizivir plus efavirenz orlopinavir/ritonavir followed by trizivir alone in naiveHIV-1-infected adults
Josep Mallolasa, Judith Picha, Marıa Penarandab, Pere Domingoc,
Hernando Knobeld, Enric Pedrole, Felix Gutierrezf, Pilar Barrufetg,
Joaquin Peraireh, Miguel A. Asenjoa, Francesc Vidalh and
Josep M. Gatella
opyright © L
From the aHospitaMallorca, Spain, thBarcelona, Spain,hHospital Joan XX
Correspondence to
Tel: +34 93 2275Received: 21 June
ISS
Background: Induction-maintenance strategies were associated with a low responserate. We compared the virological response with two different induction regimens withtrizivir plus efavirenz or lopinavir/ritonavir.
Methods: A randomized, multicentre, open-label clinical trial with 209 antiretroviral-naive HIV-infected patients assigned to trizivir plus either efavirenz or lopinavir/ritonavir during 24–36 weeks. Patients reaching undetectable plasma viral loads duringinduction entered a 48-week maintenance on trizivir alone. The primary endpoint wasthe proportion of patients without treatment failure at 72 weeks using an intent to treat(ITT) analysis (switching equals failure).
Results: Patients were randomly assigned (efavirenz 104; lopinavir/ritonavir 105), and114 (55%) entered the maintenance phase (efavirenz 54; lopinavir/ritonavir 60).Baseline characteristics were balanced between groups. The response rate at 72 weekswas 31 and 43% (ITT analysis, P¼0.076) and 63 and 75% (on-treatment analysis,P¼0.172) in the efavirenz and lopinavir/ritonavir arms, respectively. Virological failureoccurred in 27 patients: six during induction (efavirenz, three; lopinavir/ritonavir, three;P¼1.0) and 21 during maintenance (efavirenz, 14; lopinavir/ritonavir, seven;P¼0.057). Thirty-four patients in the efavirenz arm switched treatment because ofadverse events compared with 25 in the lopinavir/ritonavir arm (P¼0.17).
Conclusion: Trizivir plus either efavirenz or lopinavir/ritonavir followed by mainten-ance with trizivir achieved a low but similar response at 72 weeks, with a highincidence of adverse events leading to drug discontinuation during the induction phasein both arms. The study showed a trend towards an increased virological failure rate inthe efavirenz arm during the maintenance phase.
� 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins
AIDS 2008, 22:377–384
Keywords: Induction-maintenance antiviral therapy, quadruple regimen, trizivir
Introduction
The introduction of HAART has resulted in dramaticreductions in HIV-1-associated mortality and morbidity
ippincott Williams & Wilkins. Unauth
l Clınic IDIBAPS, University of Barcelona, Barce cHospital de Sant Pau, Barcelona, Spain, the dHthe fHospital Universitario de Elche, Alicante, SIII-Universitat Rovira i Virgili, Tarragona, Spain.
Josep Mallolas, Infectious Diseases Service, Hos
574; fax: +34 93 4514438; e-mail: mallolas@cli2007; revised: 5 October 2007; accepted: 16 O
N 0269-9370 Q 2008 Wolters Kluwer He
[1,2]. Current recommendations support initiatingantiretroviral therapy (ART) with two nucleoside reversetranscriptase inhibitors plus a non-nucleoside reversetranscriptase inhibitor or a ritonavir-boosted protease
orized reproduction of this article is prohibited.
elona, Spain, the bHospital Son Dureta, Palma de Mallorca,ospital del Mar, Barcelona, Spain, the eHospital de Granollers,pain, the gHospital de Mataro, Barcelona, Spain, and the
pital Clınic-IDIBAPS, Villarroel 170, 08036 Barcelona, Spain.
nic.ub.esctober 2007.
alth | Lippincott Williams & Wilkins 377

Co
378 AIDS 2008, Vol 22 No 3
inhibitor. Although highly effective, HAART has beenassociated with significant short and long-term toxicities,including hyperlipidemia, insulin resistance, and fatredistribution syndromes, which may be associated withaccelerated atherosclerotic cardiovascular disease [3–6].Given these and other toxicities, interest has arisen inreducing prolonged exposure to antiretroviral agents. Thediscontinuation of ART in patients successfully treated forprolonged periods has, however, been associated withrapid virological rebound and decreasing CD4 cell counts[7,8], and CD4-driven intermittent ART has beenassociated with an increased incidence of opportunisticand non-opportunistic adverse clinical events [9].
Earlier studies have tested the concept of an induction-maintenance strategy with a suboptimal treatmentresponse [10–12]. In those trials, patients were treatedwith triple (two studies) or quadruple drug therapy for12–26 weeks, followed by simplification to monotherapyor dual combination therapy. Rebound rates ranged from22 to 31%, and were related to poor adherence, poorpharmacokinetic profiles, and baseline viral resistance.Despite these initial failures, interest in the induction-maintenance concept has persisted. Markowitz et al. [13]assessed this concept, using an induction phase withabacavir/lamivudine/zidovudine (trizivir) plus efavirenzfor 48 weeks and an additional 48 weeks of maintenancetherapy with trizivir alone in ART-naive patients,showing that the maintenance phase improved adherence,reduced fasting lipids and ART-associated adverse eventswhile maintaining virological control and the immuno-logical response. More recently, other induction-maintenance approaches have been reported that showedencouraging results [14–18].
Here, we describe an induction-maintenance strategy inwhich patients were randomly assigned to an inductionregimen that included a fixed-dose combination ofabacavir, lamivudine and zidovudine (trizivir) plus eitherefavirenz or lopinavir boosted with ritonavir (lopinavir/ritonavir) for 24–36 weeks, followed by maintenance withabacavir/lamivudine/zidovudine in those who reached anundetectable plasma viral load. We hypothesized that after24–36 weeks of treatment, the removal of one agent wouldresult in reduced toxicity while maintaining the antiviraland immunological benefits. Trizivir should be enough formaintenance therapy in suppressed patients withoutprevious archive mutations in the retrotranscriptase gene[19,20]. Moreover, we hypothesized that the utilization ofefavirenz or lopinavir/ritonavir in the induction phasewould be similar.
Methods
Study populationHIV-1-infected adults were eligible if they wereantiretroviral naive and had an HIV-1-RNA level above
pyright © Lippincott Williams & Wilkins. Unauthor
10 000 copies/ml. Exclusion criteria included the currentuse of experimental therapies, active opportunistic diseaserequiring parenteral treatment, and any contraindicationto study drugs. Female patients were excluded if theywere pregnant or breastfeeding.
Study designTrizefal was a randomized, open-label, 72-week studyconducted at 18 clinical sites in Spain. The duration of theinduction phase of the study was 24–36 weeks followedby a maintenance phase of 48 weeks for those reachingundetectable viral loads at the end of the induction phase.Enrollment took place between April 2003 and July 2004.
Patients were centrally randomly selected (1 : 1 ratio) toabacavir/lamivudine/zidovudine with either efavirenz orlopinavir/ritonavir. Randomization was stratified basedon an HIV-1-RNA level at study entry (baseline) of lessthan 100 000 copies/ml or 100 000 copies/ml or greater.During the 24–36-week induction period, all patientswere treated with the fixed-dose combination of abacavir(300 mg)/lamivudine (150 mg)/zidovudine (300 mg)(trizivir; GlaxoSmithKline, Greenford, Middlesex, UK)twice a day and with either efavirenz (600 mg, Sustiva;Bristol-Myers Squibb, New York, USA) once a day orlopinavir/ritonavir (Kaletra, Abbott, Abbott Park, Illinois,USA) three capsules � 133/33 mg twice a day. Patientswith HIV-1-RNA levels less than 50 copies/ml at week 24(or at week 36 if not reached at week 24) were eligible forsimplification into the 48-week maintenance phase withonly abacavir/lamivudine/zidovudine.
Screening evaluation included a clinical assessment andlaboratory evaluations: plasma HIV-1 RNA, T-lympho-cyte subsets, haematology, clinical chemistries, and thecollection of a plasma sample later analysed for viralresistance mutations. On-study evaluation includedclinical visits at baseline and weeks 4, 12, 24, 36, 48,64 and 72. HIV-1 RNAwas assessed at each visit using thelocal HIV-1 ultrasensitive assay. Clinical chemistries,haematology profiles, and T-cell subsets were performedat all visits. Fasting lipid profiles were also measured.Samples for possible viral resistance testing were collectedat baseline and at confirmation of virological failure.Safety was assessed through the reporting of adverseclinical events and abnormal laboratory values. Theseverity of adverse events was assessed by the investigatorusing the Division of AIDS toxicity grading scale [21].No substitutions were allowed for abacavir/lamivudine/zidovudine.
Adherence to therapy was not measured. Viral resistancetesting at baseline and at the time of virological failure wasattempted for all patients who met virological failurecriteria.
The protocol was reviewed and approved by the ethicscommittees of each of the participating sites and the
ized reproduction of this article is prohibited.

C
Induction-maintenance therapy in HIV patients Mallolas et al. 379
Spanish Medicines Agency. All patients provided writteninformed consent before entering the study.
AnalysesThe main study endpoint was the proportion of patientswithout treatment failure at 72 weeks using an intent totreat (ITT) analysis (switches and missing equals failure).Treatment failure was defined as virological failure, loss tofollow-up, discontinuation of study medication becauseof toxicity or any other reason, clinical disease progression(new Centers for Disease Control and Prevention grade Cevents), or death. Virological failure was defined as failureto suppress the HIV-1-RNA level to less than 50 copies/ml by week 24 or 36 or a confirmed HIV-1-RNA levelgreater than 200 copies/ml after suppression to less than50 copies/ml at any timepoint. Time to treatment failureor virological failure and proportions of patients withvirological failure at week 72 while on study medication(on-treatment analysis) were secondary endpoints. Othersecondary objectives included immunology, safety andtolerability, and the development of viral resistance.
A sample size of 220 patients provided 80% power todetect the superiority of any of the study arms based onproportions of patients with an HIV-1-RNA level lessthan 50 copies/ml at week 72 with a type 1 error rate of0.05, assuming a success rate of 80% in the most effectivetreatment group and a minimum detectable difference of20 percentage points.
Qualitative variables were described using frequency andpercentage and compared between groups by means ofFisher’s exact test. The proportion of patients with
opyright © Lippincott Williams & Wilkins. Unauth
Table 1. Baseline characteristics of patients included in the analysis.
EFV (n¼104)
Median age (IQR) 38.5 (32.5–43.9)Male sex, n (%) 79 (76)Behavioural risk for HIV infection, n (%)
Heterosexual 42 (40)Homosexual men 36 (34)Intravenous drug users 22 (21)Blood transfusion 2 (2)Unknown 2 (2)
Co-infection withHepatitis C virus 23 (22)Hepatitis B virus 3 (2)
Median baseline plasmaHIV-1-RNA level (IQR)Log10 copies/ml 5.15 (4.6–5.7)>100 000 copies/ml n (%) 62 (59)
Median baseline CD4Cell count (IQR) cell/ml 201 (109–293)<200 cells/ml, n (%) 54 (51)
Baseline CDC classification for HIV infection, n (%)Category A 57 (54)Category B 22 (21)Category C 25 (24)
CDC, Centers for Diseases Control and Prevention; EFV, efavirenz arm; IQ
virological failure and treatment failure was expressed bypercentage and 95% confidence intervals (CI). Quanti-tative characteristics were summarized using medianvalue and interquartile ranges (IQR), and the comparisonbetween groups was realized using the Wilcoxon ranksum test.
Time to failure was estimated using the Kaplan–Meiermethod and the Log-rank test was used to comparesurvivor functions between groups. All tests were two-sided with a confidence level of 95%. Statistical analyseswere performed using STATA (release 9; Stata Corpor-ation, College Station, Texas, USA).
Results
Patient dispositionA total of 220 patients were randomly assigned, but only209 were considered eligible and included in the analysis.The remaining 11 patients were excluded because 10withdrew consent and never started treatment and onewas randomly assigned twice.
Patients were predominantly male, with a median age of39 years (range 22–74), a median baseline HIV-1-RNAlevel of 159 500 copies/ml (IQR 42 600; 440 000) and amedian CD4 cell count of 202 cells/ml (IQR 104; 297).Table 1 shows the demographic characteristics of thepatients. Forty-five per cent (95/209 patients) did notreach the maintenance phase, primarily because ofadverse events (n¼ 58, 28%), and loss to follow-up
orized reproduction of this article is prohibited.
LPV/r (n¼105) Total (n¼209)
37.6 (32.4–43.1) 38.1 (32.4–43.5)89 (85) 168 (80)
48 (45) 90 (43)36 (34) 72 (34)19 (18) 41 (19)0 (0) 2 (1)2 (2) 4 (2)
26 (24) 49 (23)9 (8) 12 (5)
5.2 (4.6–5.6) 5.2 (4.6–5.6)61 (58) 123 (58)
205 (104–306) 202 (104–297)55 (52) 109 (52)
64 (60) 121 (57)18 (17) 40 (19)23 (21) 48 (22)
R, interquartile range; LPV/r, lopinavir/ritonavir arm.
Co
380 AIDS 2008, Vol 22 No 3
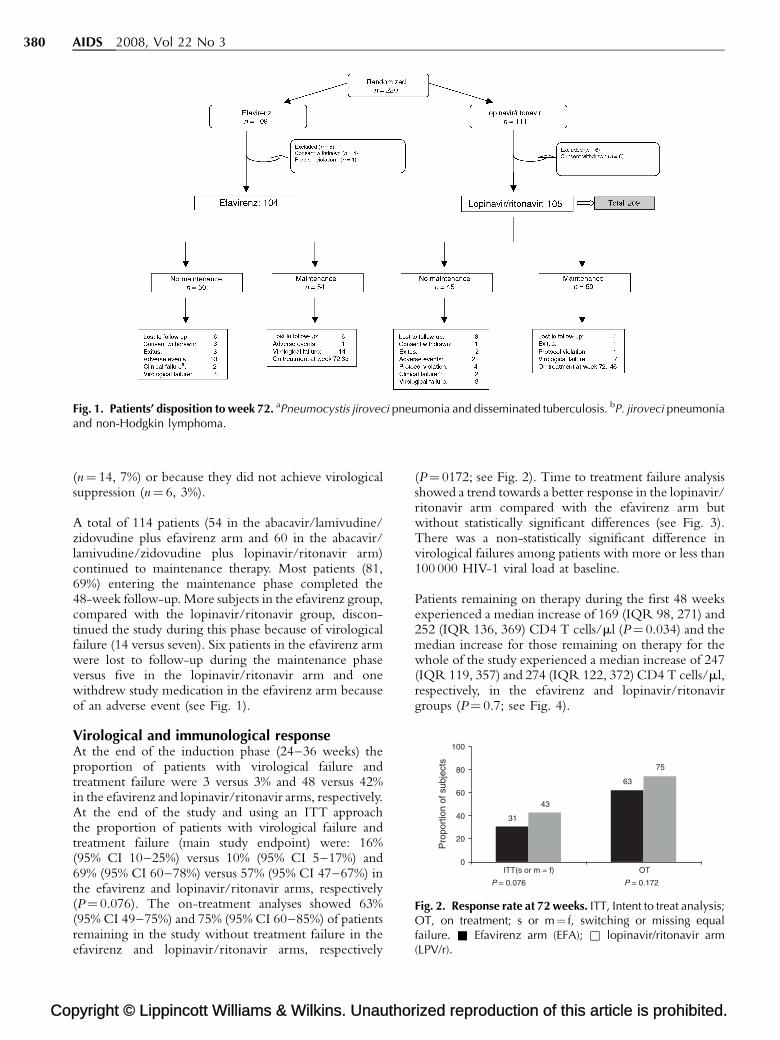
Fig. 1. Patients’ disposition to week 72. aPneumocystis jiroveci pneumonia and disseminated tuberculosis. bP. jiroveci pneumoniaand non-Hodgkin lymphoma.
31
63
43
75
0
20
40
60
80
100
ITT(s or m = f) OT
Pro
port
ion
of s
ubje
cts
P = 0.076 P = 0.172
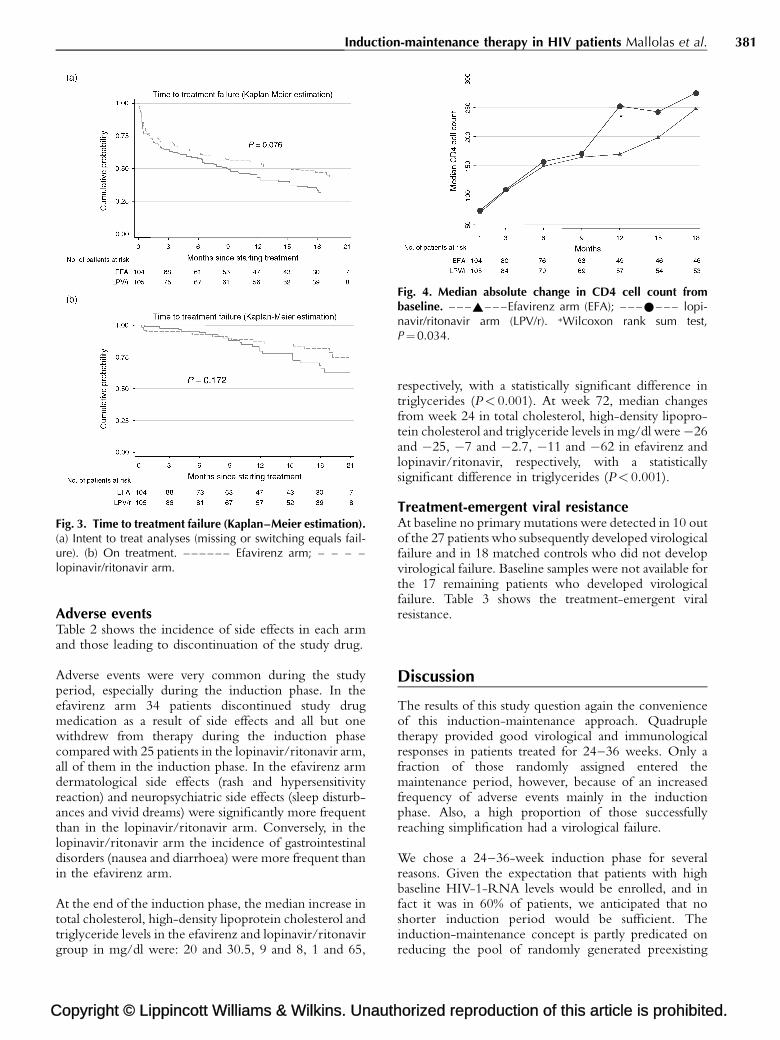
Fig. 2. Response rate at 72 weeks. ITT, Intent to treat analysis;OT, on treatment; s or m¼ f, switching or missing equalfailure. & Efavirenz arm (EFA); & lopinavir/ritonavir arm(LPV/r).
(n¼ 14, 7%) or because they did not achieve virologicalsuppression (n¼ 6, 3%).
A total of 114 patients (54 in the abacavir/lamivudine/zidovudine plus efavirenz arm and 60 in the abacavir/lamivudine/zidovudine plus lopinavir/ritonavir arm)continued to maintenance therapy. Most patients (81,69%) entering the maintenance phase completed the48-week follow-up. More subjects in the efavirenz group,compared with the lopinavir/ritonavir group, discon-tinued the study during this phase because of virologicalfailure (14 versus seven). Six patients in the efavirenz armwere lost to follow-up during the maintenance phaseversus five in the lopinavir/ritonavir arm and onewithdrew study medication in the efavirenz arm becauseof an adverse event (see Fig. 1).
Virological and immunological responseAt the end of the induction phase (24–36 weeks) theproportion of patients with virological failure andtreatment failure were 3 versus 3% and 48 versus 42%in the efavirenz and lopinavir/ritonavir arms, respectively.At the end of the study and using an ITT approachthe proportion of patients with virological failure andtreatment failure (main study endpoint) were: 16%(95% CI 10–25%) versus 10% (95% CI 5–17%) and69% (95% CI 60–78%) versus 57% (95% CI 47–67%) inthe efavirenz and lopinavir/ritonavir arms, respectively(P¼ 0.076). The on-treatment analyses showed 63%(95% CI 49–75%) and 75% (95% CI 60–85%) of patientsremaining in the study without treatment failure in theefavirenz and lopinavir/ritonavir arms, respectively
pyright © Lippincott Williams & Wilkins. Unauthor
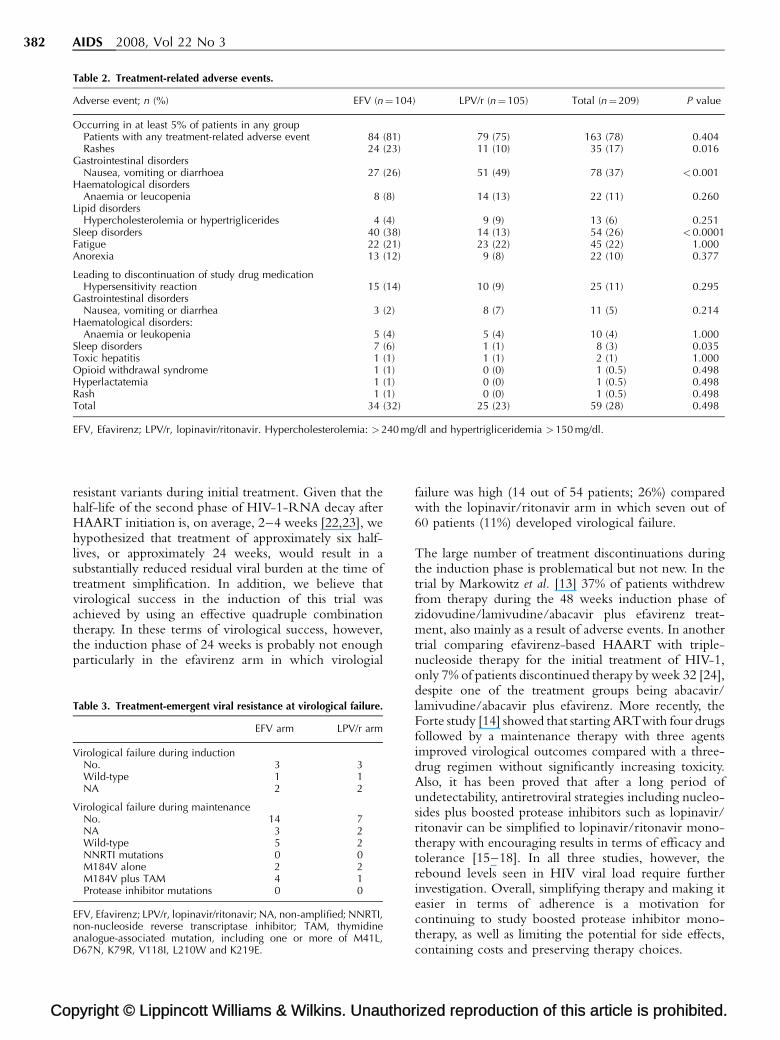
(P¼ 0172; see Fig. 2). Time to treatment failure analysisshowed a trend towards a better response in the lopinavir/ritonavir arm compared with the efavirenz arm butwithout statistically significant differences (see Fig. 3).There was a non-statistically significant difference invirological failures among patients with more or less than100 000 HIV-1 viral load at baseline.
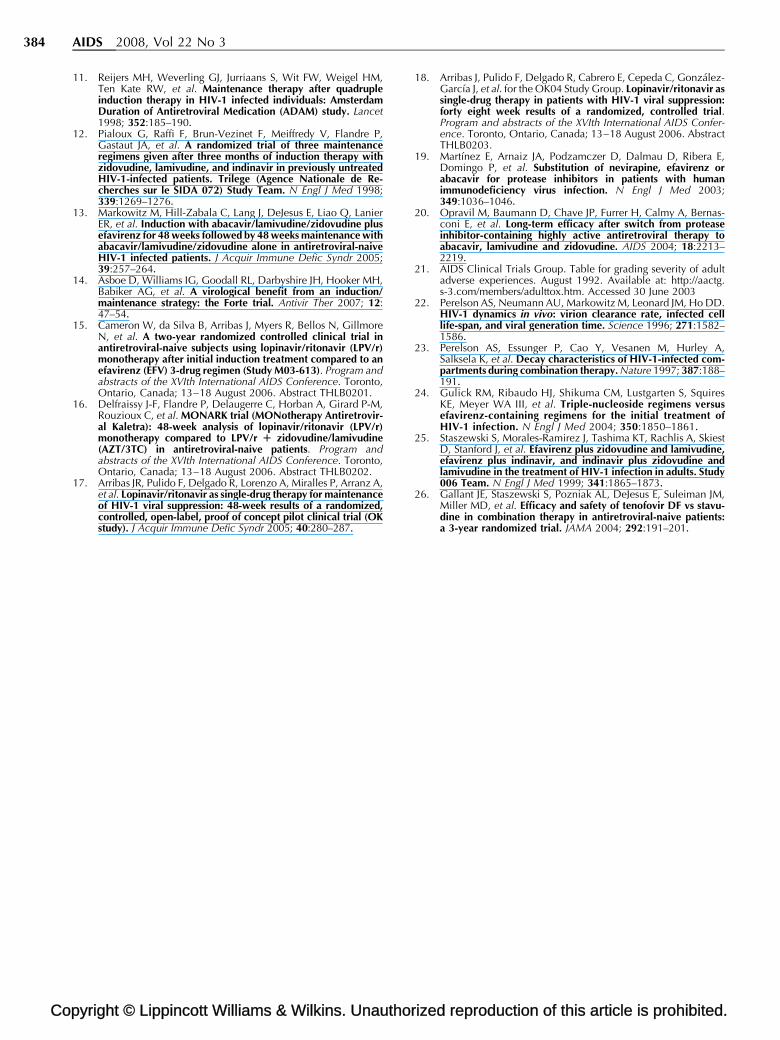
Patients remaining on therapy during the first 48 weeksexperienced a median increase of 169 (IQR 98, 271) and252 (IQR 136, 369) CD4 T cells/ml (P¼ 0.034) and themedian increase for those remaining on therapy for thewhole of the study experienced a median increase of 247(IQR 119, 357) and 274 (IQR 122, 372) CD4 T cells/ml,respectively, in the efavirenz and lopinavir/ritonavirgroups (P¼ 0.7; see Fig. 4).
ized reproduction of this article is prohibited.
C
Induction-maintenance therapy in HIV patients Mallolas et al. 381
Fig. 3. Time to treatment failure (Kaplan–Meier estimation).(a) Intent to treat analyses (missing or switching equals fail-ure). (b) On treatment. – – – – – – Efavirenz arm; – – – –lopinavir/ritonavir arm.
Fig. 4. Median absolute change in CD4 cell count frombaseline. – – –~– – –Efavirenz arm (EFA); – – –*– – – lopi-navir/ritonavir arm (LPV/r). �Wilcoxon rank sum test,P¼0.034.
Adverse eventsTable 2 shows the incidence of side effects in each armand those leading to discontinuation of the study drug.
Adverse events were very common during the studyperiod, especially during the induction phase. In theefavirenz arm 34 patients discontinued study drugmedication as a result of side effects and all but onewithdrew from therapy during the induction phasecompared with 25 patients in the lopinavir/ritonavir arm,all of them in the induction phase. In the efavirenz armdermatological side effects (rash and hypersensitivityreaction) and neuropsychiatric side effects (sleep disturb-ances and vivid dreams) were significantly more frequentthan in the lopinavir/ritonavir arm. Conversely, in thelopinavir/ritonavir arm the incidence of gastrointestinaldisorders (nausea and diarrhoea) were more frequent thanin the efavirenz arm.
At the end of the induction phase, the median increase intotal cholesterol, high-density lipoprotein cholesterol andtriglyceride levels in the efavirenz and lopinavir/ritonavirgroup in mg/dl were: 20 and 30.5, 9 and 8, 1 and 65,
opyright © Lippincott Williams & Wilkins. Unauth
respectively, with a statistically significant difference intriglycerides (P< 0.001). At week 72, median changesfrom week 24 in total cholesterol, high-density lipopro-tein cholesterol and triglyceride levels in mg/dl were�26and �25, �7 and �2.7, �11 and �62 in efavirenz andlopinavir/ritonavir, respectively, with a statisticallysignificant difference in triglycerides (P< 0.001).
Treatment-emergent viral resistanceAt baseline no primary mutations were detected in 10 outof the 27 patients who subsequently developed virologicalfailure and in 18 matched controls who did not developvirological failure. Baseline samples were not available forthe 17 remaining patients who developed virologicalfailure. Table 3 shows the treatment-emergent viralresistance.
Discussion
The results of this study question again the convenienceof this induction-maintenance approach. Quadrupletherapy provided good virological and immunologicalresponses in patients treated for 24–36 weeks. Only afraction of those randomly assigned entered themaintenance period, however, because of an increasedfrequency of adverse events mainly in the inductionphase. Also, a high proportion of those successfullyreaching simplification had a virological failure.
We chose a 24–36-week induction phase for severalreasons. Given the expectation that patients with highbaseline HIV-1-RNA levels would be enrolled, and infact it was in 60% of patients, we anticipated that noshorter induction period would be sufficient. Theinduction-maintenance concept is partly predicated onreducing the pool of randomly generated preexisting
orized reproduction of this article is prohibited.
Co
382 AIDS 2008, Vol 22 No 3
Table 2. Treatment-related adverse events.
Adverse event; n (%) EFV (n¼104) LPV/r (n¼105) Total (n¼209) P value
Occurring in at least 5% of patients in any groupPatients with any treatment-related adverse event 84 (81) 79 (75) 163 (78) 0.404Rashes 24 (23) 11 (10) 35 (17) 0.016
Gastrointestinal disordersNausea, vomiting or diarrhoea 27 (26) 51 (49) 78 (37) <0.001
Haematological disordersAnaemia or leucopenia 8 (8) 14 (13) 22 (11) 0.260
Lipid disordersHypercholesterolemia or hypertriglicerides 4 (4) 9 (9) 13 (6) 0.251
Sleep disorders 40 (38) 14 (13) 54 (26) <0.0001Fatigue 22 (21) 23 (22) 45 (22) 1.000Anorexia 13 (12) 9 (8) 22 (10) 0.377
Leading to discontinuation of study drug medicationHypersensitivity reaction 15 (14) 10 (9) 25 (11) 0.295
Gastrointestinal disordersNausea, vomiting or diarrhea 3 (2) 8 (7) 11 (5) 0.214
Haematological disorders:Anaemia or leukopenia 5 (4) 5 (4) 10 (4) 1.000
Sleep disorders 7 (6) 1 (1) 8 (3) 0.035Toxic hepatitis 1 (1) 1 (1) 2 (1) 1.000Opioid withdrawal syndrome 1 (1) 0 (0) 1 (0.5) 0.498Hyperlactatemia 1 (1) 0 (0) 1 (0.5) 0.498Rash 1 (1) 0 (0) 1 (0.5) 0.498Total 34 (32) 25 (23) 59 (28) 0.498
EFV, Efavirenz; LPV/r, lopinavir/ritonavir. Hypercholesterolemia: >240 mg/dl and hypertrigliceridemia >150 mg/dl.
resistant variants during initial treatment. Given that thehalf-life of the second phase of HIV-1-RNA decay afterHAART initiation is, on average, 2–4 weeks [22,23], wehypothesized that treatment of approximately six half-lives, or approximately 24 weeks, would result in asubstantially reduced residual viral burden at the time oftreatment simplification. In addition, we believe thatvirological success in the induction of this trial wasachieved by using an effective quadruple combinationtherapy. In these terms of virological success, however,the induction phase of 24 weeks is probably not enoughparticularly in the efavirenz arm in which virologial
pyright © Lippincott Williams & Wilkins. Unauthor
Table 3. Treatment-emergent viral resistance at virological failure.
EFV arm LPV/r arm
Virological failure during inductionNo. 3 3Wild-type 1 1NA 2 2
Virological failure during maintenanceNo. 14 7NA 3 2Wild-type 5 2NNRTI mutations 0 0M184V alone 2 2M184V plus TAM 4 1Protease inhibitor mutations 0 0
EFV, Efavirenz; LPV/r, lopinavir/ritonavir; NA, non-amplified; NNRTI,non-nucleoside reverse transcriptase inhibitor; TAM, thymidineanalogue-associated mutation, including one or more of M41L,D67N, K79R, V118I, L210W and K219E.
failure was high (14 out of 54 patients; 26%) comparedwith the lopinavir/ritonavir arm in which seven out of60 patients (11%) developed virological failure.
The large number of treatment discontinuations duringthe induction phase is problematical but not new. In thetrial by Markowitz et al. [13] 37% of patients withdrewfrom therapy during the 48 weeks induction phase ofzidovudine/lamivudine/abacavir plus efavirenz treat-ment, also mainly as a result of adverse events. In anothertrial comparing efavirenz-based HAART with triple-nucleoside therapy for the initial treatment of HIV-1,only 7% of patients discontinued therapy by week 32 [24],despite one of the treatment groups being abacavir/lamivudine/abacavir plus efavirenz. More recently, theForte study [14] showed that starting ARTwith four drugsfollowed by a maintenance therapy with three agentsimproved virological outcomes compared with a three-drug regimen without significantly increasing toxicity.Also, it has been proved that after a long period ofundetectability, antiretroviral strategies including nucleo-sides plus boosted protease inhibitors such as lopinavir/ritonavir can be simplified to lopinavir/ritonavir mono-therapy with encouraging results in terms of efficacy andtolerance [15–18]. In all three studies, however, therebound levels seen in HIV viral load require furtherinvestigation. Overall, simplifying therapy and making iteasier in terms of adherence is a motivation forcontinuing to study boosted protease inhibitor mono-therapy, as well as limiting the potential for side effects,containing costs and preserving therapy choices.
ized reproduction of this article is prohibited.

C
Induction-maintenance therapy in HIV patients Mallolas et al. 383
Our high discontinuation rate is difficult to explain. Thespecific four-drug regimens in this trial failed to improvethe initial response rate to antiviral therapy, in contrast toestablished three-drug regimens [24–26]. Response ratesin all strata of baseline HIV-1-RNA levels can beconsidered high and demonstrate the potency of bothfour-drug regimens with a low rate of virological failureduring induction. This good virological response in theinduction phase, however, does not accord with a goodtreatment success rate as shown in the ITT analyses as aresult of a high treatment drug discontinuation related tothe development of adverse events. This may not be thecase with future better tolerated agents such as raltegraviror maraviroc.
In assessing the results of this study, we must ask whatbenefits treatment simplification provided: in the shortterm, a reduction in treatment-related adverse events andalso an improvement in fasting lipid profiles. Further-more, in the face of the emergence of drug-resistant virus,treatment options in the three classes (nucleoside reversetranscriptase inhibitors, non-nucleoside reverse transcrip-tase inhibitors, protease inhibitors) remained available foruse in most of the patients who experienced virologicalfailure. It is important to note that during maintenancevirological failure and treatment-emergence drug resist-ance was more common in the efavirenz group than inthe lopinavir/ritonavir therapy group, although thedifference did not reach statistical significance.
This induction-maintenance approach is associated with ahigh rate of antiretroviral discontinuation as a result ofadverse events. Also, the rate of virological failure duringthe maintenance phase can be considered high, especiallyin the efavirenz arm. Therefore, we believe that currently itcan not be considered as a valid alternative for the manage-ment of treatment initiation in HIV-infected patients.
Acknowledgement
Other staff at the Clinical Trials Unit (Hospital clinic) whoconducted and analysed the study include: A. Cruceta, H.Agell, E. Aragon, S. Varea.
The other TRIFEZAL investigators were: Agathe Leon,Joan A. Arnaiz, Jose L. Blanco, Esteban Martınez, Jose M.Miro, Elisa De Lazzari, Cristina Gil, Tomas Pumarola,Hospital Clınic IDIBAPS, University of Barcelona,Barcelona; Melcior Riera, Hospital Son Dureta, Palmade Mallorca, Mallorca; Marıa Saumoy, Sergi Veloso,Consuelo Vilades, Hospital Joan XXIII-UniversitatRovira i Virgili, Tarragona; Mar Masia, Sergio Padilla,Hospital Universitario de Elche, Alicante; David Dalmau,Mutua de Terrassa, Barcelona; Esteve Ribera, HospitalVall Hebron, Barcelona; Antonio Ocampo, HospitalXeral-Cıes, Vigo; Miguel A. Muniaın, Hospital VirgenMacarena, Sevilla; Carlos Alonso-Villaverde, Hospital
opyright © Lippincott Williams & Wilkins. Unauth
Sant Joan de Reus, Tarragona; Vicente Estrada, HospitalClınico, Madrid; Jose R. Blanco, Hospital General de laRioja, Logrono; Josep Cucurull, Hospital de Figueres,Girona; Josep M. Llibre, Hospital de Calella, Barcelona;Jorge Carmena, Hospital Peset, Valencia; and Marıa J.Galindo, Hospital Clınico, Valencia.
The authors are indebted to the participants in the study.
Presented in part at the 8th International Congress onDrug Therapy in HIV Infection, Glasgow, November2006.
Clinical trial registry number: ISRCTN41611080.
Sponsorship: This study was partly supported by anunrestricted grant from GlaxoSmithKline and the RedTematica Cooperativa de Grupos de Investigacion enSida del Fondo de Investigacion Sanitaria (FIS), andgrant no. ISCIII-RETIC RD06/006 from the Instituto deSalud Carlos III, Madrid (Spain). J.M.M. was therecipient of a research grant from the Institut d’Investi-gacions Biomediques August Pi i Sunyer (IDIBAPS) andthe Conselleria de Salut de la Generalitat de Catalunya,Barcelona (Spain).
Conflicts of interest: None.
References
1. Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, GargalianosP, et al. Changing patterns of mortality across Europe inpatients infected with HIV-1. EuroSIDA Study Group. Lancet1998; 352:1725–1730.
2. Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J,Satten GA, et al. Declining morbidity and mortality amongpatients with advanced human immunodeficiency virus infec-tion. HIV Outpatient Study Investigators. N Engl J Med 1998;338:853–860.
3. Nolan D, Hammond E, Martin A, Taylor L, Herrmann S,McKinnon E, et al. Mitochondrial DNA depletion and morpho-logic changes in adipocytes associated with nucleoside reversetranscriptase inhibitor therapy. AIDS 2003; 17:1329–1338.
4. Carr A. Toxicity of antiretroviral therapy and implications fordrug development. Nat Rev Drug Discov 2003; 2:624–634.
5. Nolan D, Hammond E, James I, McKinnon E, Mallal S. Con-tribution of nucleoside-analogue reverse transcriptase inhibi-tor therapy to lipoatrophy from the population to the cellularlevel. Antivir Ther 2003; 8:617–626.
6. Bozkurt B. Cardiovascular toxicity with highly active antire-troviral therapy: review of clinical studies. Cardiovasc Toxicol2004; 4:243–260.
7. Davey RT Jr, Bhat N, Yoder C, Chun TW, Metcalf JA, Dewar R,et al. HIV-1 and T cell dynamics after interruption of highlyactive antiretroviral therapy (HAART) in patients with a historyof sustained viral suppression. Proc Natl Acad Sci U S A 1999;96:15109–15114.
8. Markowitz M, Jin X, Hurley A, Simon V, Ramratnam B, Louie M,et al. Discontinuation of antiretroviral therapy commencedearly during the course of human immunodeficiency virus type1 infection, with or without adjunctive vaccination. J Infect Dis2002; 186:634–643.
9. The Strategies for Management of Antiretroviral Therapy(SMART) Study Group. CD4R count-guided interruption ofantiretroviral treatment. N Engl J Med 2006; 355:2359–2361.
10. Havlir DV, Marschner IC, Hirsch MS, Collier AC, Tebas P,Bassett RL, et al. Maintenance antiretroviral therapies in HIVinfected patients with undetectable plasma HIV RNA aftertriple-drug therapy. AIDS Clinical Trials Group Study 343Team. N Engl J Med 1998; 339:1261–1268.
orized reproduction of this article is prohibited.
Co
384 AIDS 2008, Vol 22 No 3
11. Reijers MH, Weverling GJ, Jurriaans S, Wit FW, Weigel HM,Ten Kate RW, et al. Maintenance therapy after quadrupleinduction therapy in HIV-1 infected individuals: AmsterdamDuration of Antiretroviral Medication (ADAM) study. Lancet1998; 352:185–190.
12. Pialoux G, Raffi F, Brun-Vezinet F, Meiffredy V, Flandre P,Gastaut JA, et al. A randomized trial of three maintenanceregimens given after three months of induction therapy withzidovudine, lamivudine, and indinavir in previously untreatedHIV-1-infected patients. Trilege (Agence Nationale de Re-cherches sur le SIDA 072) Study Team. N Engl J Med 1998;339:1269–1276.
13. Markowitz M, Hill-Zabala C, Lang J, DeJesus E, Liao Q, LanierER, et al. Induction with abacavir/lamivudine/zidovudine plusefavirenz for 48 weeks followed by 48 weeks maintenance withabacavir/lamivudine/zidovudine alone in antiretroviral-naiveHIV-1 infected patients. J Acquir Immune Defic Syndr 2005;39:257–264.
14. Asboe D, Williams IG, Goodall RL, Darbyshire JH, Hooker MH,Babiker AG, et al. A virological benefit from an induction/maintenance strategy: the Forte trial. Antivir Ther 2007; 12:47–54.
15. Cameron W, da Silva B, Arribas J, Myers R, Bellos N, GillmoreN, et al. A two-year randomized controlled clinical trial inantiretroviral-naive subjects using lopinavir/ritonavir (LPV/r)monotherapy after initial induction treatment compared to anefavirenz (EFV) 3-drug regimen (Study M03-613). Program andabstracts of the XVIth International AIDS Conference. Toronto,Ontario, Canada; 13–18 August 2006. Abstract THLB0201.
16. Delfraissy J-F, Flandre P, Delaugerre C, Horban A, Girard P-M,Rouzioux C, et al. MONARK trial (MONotherapy Antiretrovir-al Kaletra): 48-week analysis of lopinavir/ritonavir (LPV/r)monotherapy compared to LPV/r R zidovudine/lamivudine(AZT/3TC) in antiretroviral-naive patients. Program andabstracts of the XVIth International AIDS Conference. Toronto,Ontario, Canada; 13–18 August 2006. Abstract THLB0202.
17. Arribas JR, Pulido F, Delgado R, Lorenzo A, Miralles P, Arranz A,et al. Lopinavir/ritonavir as single-drug therapy for maintenanceof HIV-1 viral suppression: 48-week results of a randomized,controlled, open-label, proof of concept pilot clinical trial (OKstudy). J Acquir Immune Defic Syndr 2005; 40:280–287.
pyright © Lippincott Williams & Wilkins. Unauthor
18. Arribas J, Pulido F, Delgado R, Cabrero E, Cepeda C, Gonzalez-Garcıa J, et al. for the OK04 Study Group. Lopinavir/ritonavir assingle-drug therapy in patients with HIV-1 viral suppression:forty eight week results of a randomized, controlled trial.Program and abstracts of the XVIth International AIDS Confer-ence. Toronto, Ontario, Canada; 13–18 August 2006. AbstractTHLB0203.
19. Martınez E, Arnaiz JA, Podzamczer D, Dalmau D, Ribera E,Domingo P, et al. Substitution of nevirapine, efavirenz orabacavir for protease inhibitors in patients with humanimmunodeficiency virus infection. N Engl J Med 2003;349:1036–1046.
20. Opravil M, Baumann D, Chave JP, Furrer H, Calmy A, Bernas-coni E, et al. Long-term efficacy after switch from proteaseinhibitor-containing highly active antiretroviral therapy toabacavir, lamivudine and zidovudine. AIDS 2004; 18:2213–2219.
21. AIDS Clinical Trials Group. Table for grading severity of adultadverse experiences. August 1992. Available at: http://aactg.s-3.com/members/adulttox.htm. Accessed 30 June 2003
22. Perelson AS, Neumann AU, Markowitz M, Leonard JM, Ho DD.HIV-1 dynamics in vivo: virion clearance rate, infected celllife-span, and viral generation time. Science 1996; 271:1582–1586.
23. Perelson AS, Essunger P, Cao Y, Vesanen M, Hurley A,Salksela K, et al. Decay characteristics of HIV-1-infected com-partments during combination therapy. Nature 1997; 387:188–191.
24. Gulick RM, Ribaudo HJ, Shikuma CM, Lustgarten S, SquiresKE, Meyer WA III, et al. Triple-nucleoside regimens versusefavirenz-containing regimens for the initial treatment ofHIV-1 infection. N Engl J Med 2004; 350:1850–1861.
25. Staszewski S, Morales-Ramirez J, Tashima KT, Rachlis A, SkiestD, Stanford J, et al. Efavirenz plus zidovudine and lamivudine,efavirenz plus indinavir, and indinavir plus zidovudine andlamivudine in the treatment of HIV-1 infection in adults. Study006 Team. N Engl J Med 1999; 341:1865–1873.
26. Gallant JE, Staszewski S, Pozniak AL, DeJesus E, Suleiman JM,Miller MD, et al. Efficacy and safety of tenofovir DF vs stavu-dine in combination therapy in antiretroviral-naive patients:a 3-year randomized trial. JAMA 2004; 292:191–201.
ized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN




















