Increasing readiness to decide and strengthening behavioral intentions: Evaluating the impact of a...
9
E-Health Increasing readiness to decide and strengthening behavioral intentions: Evaluating the impact of a web-based patient decision aid for breast cancer treatment options (BresDex: www.bresdex.com) §,§§ Stephanie Sivell a, *, Adrian Edwards b , Antony S.R. Manstead c , Malcolm W.R. Reed d , Lisa Caldon d , Karen Collins e , Alison Clements f , Glyn Elwyn b , on behalf of the BresDex group a Marie Curie Palliative Care Research Centre, Wales Cancer Trials Unit, School of Medicine, Cardiff University, Cardiff, UK b Cochrane Institute of Primary Care and Public Health, School of Medicine, Cardiff University, Cardiff, UK c School of Psychology, Cardiff University, Cardiff, UK d Department of Oncology, Faculty of Medicine, Dentistry and Health, University of Sheffield, Sheffield, UK e Centre for Health and Social Care Research, Sheffield Hallam University, Sheffield, UK f Department of Primary Care Health Sciences, University of Oxford, Oxford, UK 1. Introduction Little is known about how decision aids are used by patients or the effect they have on the process of deliberating and decision- making. In this paper we report on the use of an online decision aid (BresDex: www.bresdex.com) by women who are newly diagnosed with breast cancer and who have a choice of surgery; we also report how use of the decision aid influenced women’s knowledge, deliberation, surgery intentions and choices. Decision aids are designed to support the health-related decision-making of patients, by providing a personalized perspec- tive on the available options and their related outcomes [1]. They are of particular benefit in supporting preference-sensitive decisions such as those faced by women newly diagnosed with early invasive breast cancer (Stage I and II) who are typically offered the choice between mastectomy or breast conservation surgery (BCS) with radiotherapy as their primary surgical treatment [1,2]. Survival rates following the two surgery options are equivalent [3] and there are many factors known to influence the surgery choices of women in this situation, e.g., [4–16]. Decision aids exist to support women facing surgery for early breast cancer and have been reported to improve knowledge, Patient Education and Counseling 88 (2012) 209–217 A R T I C L E I N F O Article history: Received 6 September 2011 Received in revised form 18 January 2012 Accepted 27 March 2012 Keywords: Decision aids Decision support interventions Theory of Planned Behavior Common Sense Model of Illness Representations Online evaluation A B S T R A C T Objectives: To undertake a quantitative evaluation of a theory-based, interactive online decision aid (BresDex) to support women choosing surgery for early breast cancer (Stage I and II), based on observations of its use in practice. Methods: Observational cohort study. Website log-files collected data on the use of BresDex. Online questionnaires assessed knowledge about breast cancer and treatment options, degree to which women were deliberating about their options, and surgery intentions, pre- and post-BresDex. Results: Readiness to make a decision significantly increased after using BresDex (p < .001), although there was no significant improvement in knowledge. Participants that were ‘less ready’ to make a decision before using BresDex, spent a longer time using BresDex (p < .05). Significant associations between surgery intentions and choices were observed (p < .001), with the majority of participants going on to have BCS. Greater length of time spent on BresDex was associated with stronger intentions to have BCS (p < .05). Conclusion: The use of BresDex appears to facilitate readiness to make a decision for surgery, helping to strengthen surgery intentions. Practice implications: BresDex may prove a useful adjunct to the support provided by the clinical team for women facing surgery for early breast cancer. ß 2012 Elsevier Ireland Ltd. All rights reserved. § Ethical approval for the study was granted by the Multi-Centre Research Ethics Committee for Wales. Research governance was granted by Cardiff and Vales NHS Trust (now Cardiff and Vale University Health Board), Sheffield University Teaching Hospitals NHS Trust, Newcastle upon Tyne Hospitals NHS Foundation Trust and Velindre NHS Trust. §§ I confirm all patient/personal identifiers have been removed or disguised so the patient/person(s) described are not identifiable and cannot be identified through the details of the story. * Corresponding author at: Marie Curie Palliative Care Research Centre, Wales Cancer Trials Unit, School of Medicine, Cardiff University, Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, UK. Tel.: +44 029 2068 7198; fax: +44 029 2068 7501. E-mail address: [email protected] (S. Sivell). Contents lists available at SciVerse ScienceDirect Patient Education and Counseling jo ur n al h o mep ag e: w ww .elsevier .co m /loc ate/p ated u co u 0738-3991/$ – see front matter ß 2012 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.pec.2012.03.012
Transcript of Increasing readiness to decide and strengthening behavioral intentions: Evaluating the impact of a...

Patient Education and Counseling 88 (2012) 209–217
E-Health
Increasing readiness to decide and strengthening behavioral intentions:Evaluating the impact of a web-based patient decision aid for breast cancertreatment options (BresDex: www.bresdex.com)§,§§
Stephanie Sivell a,*, Adrian Edwards b, Antony S.R. Manstead c, Malcolm W.R. Reed d, Lisa Caldon d,Karen Collins e, Alison Clements f, Glyn Elwyn b,
on behalf of the BresDex groupa Marie Curie Palliative Care Research Centre, Wales Cancer Trials Unit, School of Medicine, Cardiff University, Cardiff, UKb Cochrane Institute of Primary Care and Public Health, School of Medicine, Cardiff University, Cardiff, UKc School of Psychology, Cardiff University, Cardiff, UKd Department of Oncology, Faculty of Medicine, Dentistry and Health, University of Sheffield, Sheffield, UKe Centre for Health and Social Care Research, Sheffield Hallam University, Sheffield, UKf Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
A R T I C L E I N F O
Article history:
Received 6 September 2011
Received in revised form 18 January 2012
Accepted 27 March 2012
Keywords:
Decision aids
Decision support interventions
Theory of Planned Behavior
Common Sense Model of Illness
Representations
Online evaluation
A B S T R A C T
Objectives: To undertake a quantitative evaluation of a theory-based, interactive online decision aid
(BresDex) to support women choosing surgery for early breast cancer (Stage I and II), based on
observations of its use in practice.
Methods: Observational cohort study. Website log-files collected data on the use of BresDex. Online
questionnaires assessed knowledge about breast cancer and treatment options, degree to which women
were deliberating about their options, and surgery intentions, pre- and post-BresDex.
Results: Readiness to make a decision significantly increased after using BresDex (p < .001), although there
was no significant improvement in knowledge. Participants that were ‘less ready’ to make a decision before
using BresDex, spent a longer time using BresDex (p < .05). Significant associations between surgery
intentions and choices were observed (p < .001), with the majority of participants going on to have BCS.
Greater length of time spent on BresDex was associated with stronger intentions to have BCS (p < .05).
Conclusion: The use of BresDex appears to facilitate readiness to make a decision for surgery, helping to
strengthen surgery intentions.
Practice implications: BresDex may prove a useful adjunct to the support provided by the clinical team
for women facing surgery for early breast cancer.
� 2012 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Patient Education and Counseling
jo ur n al h o mep ag e: w ww .e lsev ier . co m / loc ate /p ated u co u
1. Introduction
Little is known about how decision aids are used by patients orthe effect they have on the process of deliberating and decision-making. In this paper we report on the use of an online decision aid
§ Ethical approval for the study was granted by the Multi-Centre Research Ethics
Committee for Wales. Research governance was granted by Cardiff and Vales NHS
Trust (now Cardiff and Vale University Health Board), Sheffield University Teaching
Hospitals NHS Trust, Newcastle upon Tyne Hospitals NHS Foundation Trust and
Velindre NHS Trust.§§ I confirm all patient/personal identifiers have been removed or disguised so the
patient/person(s) described are not identifiable and cannot be identified through
the details of the story.
* Corresponding author at: Marie Curie Palliative Care Research Centre, Wales
Cancer Trials Unit, School of Medicine, Cardiff University, Neuadd Meirionnydd,
Heath Park, Cardiff, CF14 4YS, UK. Tel.: +44 029 2068 7198; fax: +44 029 2068 7501.
E-mail address: [email protected] (S. Sivell).
0738-3991/$ – see front matter � 2012 Elsevier Ireland Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.pec.2012.03.012
(BresDex: www.bresdex.com) by women who are newlydiagnosed with breast cancer and who have a choice of surgery;we also report how use of the decision aid influenced women’sknowledge, deliberation, surgery intentions and choices.
Decision aids are designed to support the health-relateddecision-making of patients, by providing a personalized perspec-tive on the available options and their related outcomes [1]. Theyare of particular benefit in supporting preference-sensitivedecisions such as those faced by women newly diagnosed withearly invasive breast cancer (Stage I and II) who are typicallyoffered the choice between mastectomy or breast conservationsurgery (BCS) with radiotherapy as their primary surgicaltreatment [1,2]. Survival rates following the two surgery optionsare equivalent [3] and there are many factors known to influencethe surgery choices of women in this situation, e.g., [4–16].Decision aids exist to support women facing surgery for earlybreast cancer and have been reported to improve knowledge,

S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217210
increase satisfaction with decision-making and lead to lowerdecisional conflict [1,2,17]. A systematic review reported womenusing these decision aids to be 20% more likely to choose BCScompared with those who do not [2]. However, a cohort study ofwomen using a DVD-based decision aid reported an increase inpreferences for mastectomy, with approximately one-third of thesample choosing to have mastectomy [17]. What we do not know,however, is how these decision aids are used by women who have achoice of surgery for breast cancer or what effect they have on thequality of their decisions.
Determining the quality of preference-sensitive decisions isdifficult and cannot be ascertained by the choice that is made [18].One approach is to look at whether patients are making decisionsbased on informed choices, that is a choice ‘‘based on relevantknowledge, consistent with the decision-makers’ values andbehaviorally implemented’’ [19]. If a patient has made an informedchoice, it would be expected that they would have high levels ofrelevant knowledge and a high concordance between theirtreatment preferences and choices [20]. Decision aids are reportedto lead to informed choices, by facilitating patients to participate indecision-making about their healthcare and make choices that areconsistent with their values [1]. Other approaches to determine thequality of preference-sensitive decisions have been suggested,including focusing on the quality of the decision-making processitself [21–23]. Deliberation requires patients to realize andunderstand the decision to be made, along with the availableoptions and their consequences, before they can consider theirpreferences; decision aids can support this process [21]. However,few studies have evaluated which components of decision aids areaccessed and used by patients [5,24]. Molenaar et al. [5] examinedthe types of information selected in a CD-ROM for women choosingsurgery for early breast cancer. Treatment related information wasselected more than other types of information, with age, educationand decision style factors associated with information selected.Many decision aids are now web-based, which provides theopportunity to collect data about uninstructed use of theseinterventions through the use of web-log data which record howpatients use the intervention, the pages they access and the timespent on each page [24–27]. It is also possible to correlate this usewith relevant outcomes for a more detailed evaluation of howdecision aids support their intended audience. Joseph-Williams et al.explored the relationship between the web-log data of a PSA testdecision-aid, reporting a significant positive association betweenincreased usage and knowledge, and significant negative associa-tions between increased usage and less favorable attitudes towardsPSA testing and reduced intention to undergo PSA testing [24].
BresDex is an online, interactive decision aid designed tosupport the surgical decision-making of women diagnosed withearly breast cancer in the UK. It is both theory guided and evidence-based [28]. An extended version of the Theory of Planned Behavior(TPB) [29,30] and the Common Sense Model of Illness Representa-tions (CSM) [31] were used to inform the content of BresDex [28].According to the TPB, behavior (e.g., choosing to undergo BCS ormastectomy) is predicted by behavioral intentions, which in turnare predicted by attitudes towards the behavior, subjective norm
(how significant others expect one to behave) and perceived
behavioral control (in the present case, how easy or difficult it is tomake the decision). The TPB has been extended to includeanticipated regret (the regret one anticipates experiencing afterengaging in the behavior), which has been shown to enhance theTPB’s power to predict intentions in situations such as the onefaced by women in the present context [32]. The CSM provides aframework for understanding how cognitive representations ofbreast cancer influence the choice of mastectomy or BCS as part of acoping strategy for dealing with the threat of breast cancer. TheCSM proposes that this occurs in three stages until the individual
perceives her coping strategies to be successful, thereby reaching astate of equilibrium: (i) interpretation of the problem; (ii)identification and development of action plan/coping strategies;(iii) appraisal of coping strategies [31]. According to the CSM,individuals generate cognitive representations of their illnessstructured around 5 key areas: consequences (beliefs concerningthe impact of breast cancer and/or the treatment on quality of lifeor functional capacity); cure/controllability (perceptions of treat-ment); identity (symptoms of breast cancer and relation to thetreatment options); cause (perceptions of the causal factors ofbreast cancer); and timeline (perceptions about the duration ofbreast cancer and the treatment options). The way in whichBresDex was developed has been reported elsewhere [33].
Initial usability evaluation and field-testing using qualitativemethods in a small study sample [28] found BresDex to be aneffective support to decision-making as an adjunct to the carereceived from the clinical team. In the present paper we report amore extensive, quantitative evaluation of BresDex, based onobservations of its use in practice by women choosing surgery forearly breast cancer. Our objectives were to:
i. examine uninstructed use of BresDex, in particular whichcomponents were accessed and the length of time spent usingeach component;
ii. assess users’ knowledge of breast cancer and their surgicaloptions before and after using BresDex;
iii. assess the users’ readiness to decide (or ‘deliberation’) onsurgery, both before and after using BresDex;
iv. observe the intentions and surgical choices of BresDex users;v. examine the association between users’ (a) uninstructed use of
BresDex and (b) knowledge, deliberation, changes in surgeryintentions and surgery choices.
Our hypotheses were as follows:
i. knowledge about breast cancer and the potential surgicaltreatment options would increase after using BresDex;
ii. improvements in knowledge would be positively correlatedwith the length of time spent on BresDex;
iii. users would feel more ready to make a decision after usingBresDex;
iv. increase in readiness to make a decision would be positivelycorrelated with the length of time spent on BresDex;
v. surgery intentions would become more clear-cut after usingBresDex;
vi. an increase in clarity of intentions would be positivelycorrelated with the length of time spent on BresDex.
2. Methods
2.1. Study design
This was an observational cohort study of the use of BresDex bywomen newly diagnosed with early breast cancer and eligible for achoice of surgical procedures as their primary therapeutictreatment. Women were invited to use BresDex while theyconsidered their options for surgery. Online questionnaires werecompleted before and after accessing BresDex.
2.2. Participant recruitment
Women newly diagnosed with breast cancer were identified bymultidisciplinary breast teams in Cardiff, Sheffield and Newcastleupon Tyne in the UK between December 2009 and October 2010.Exclusion criteria were: (i) any conditions or illness that would

S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217 211
preclude completion of questionnaires about breast cancer; and(ii) conditions precluding the ability to give informed consent toparticipate in the study. Eligible women were identified by theirbreast care teams; specialist breast care nurses gave these womena study information pack containing an information sheet and aunique password to log on to BresDex. Participants consented totake part in the study online.
2.3. Data collection and analysis
Website log-files collected data on participants’ use of BresDex,i.e., which pages were accessed and for how long. The onlinequestionnaires assessed knowledge about breast cancer andtreatment options, readiness to make a decision about surgeryand surgery intentions. Demographic information was alsocollected. Prior to surgery, participants completed questionnairesbefore and after accessing BresDex. On completion of the pre-BresDex questionnaire, participants were free to explore the
Table 1Theory guided design of BresDex.
Theoretical construct Related content
Extended
TPB
Attitudes � Information on surgical treatment options, i
* Survival rates and recurrence rates;
* Risks and side-effects;
* Treatment durations and recovery period
* Potential impact of surgery on psychosoc
� Cosmetic outcome of surgical treatment opt
� Information on possible further treatment, i
* Risks and side-effects;
* Treatment durations and recovery period
Anticipated Regret � Information on outcomes of surgical and po
including:
* Short, medium and long-term effects;
* Cosmetic outcomes;
* Psychosocial outcomes.
Subjective Norms � Structured guidance/decision-making suppo
* Consideration of the views of significant
* Information on what contemporaries cho
Perceived Behavioral
Control
� Structured guidance/decision-making suppo
* facility to state treatment intentions;
* facility to declare decision-making prefer
* consideration of the views of significant o
* information on what contemporaries cho
CSM Cause � Information on the causal and risk factors fo
Identity � Information on the types of breast cancer
Timeline � Information on outcomes of surgical and po
including:
* Survival rates and recurrence rates;
* Short, medium and long-term effects;
* Treatment durations and recovery period
Cure/Controllability � Information on survival and recurrence rate
options
Consequences � Information on outcomes of surgical and po
including:
* Survival rates and recurrence rates;
* Risks and side-effects;
* Treatment durations and recovery period
* Potential impact of surgery on psychosoc
* Short, medium and long-term effects;
* Cosmetic outcomes;
* Psychosocial outcomes.
website at their own pace, and to access as many areas of the site inwhatever order they wished. When participants felt that they hadfinished using the website, they were asked to complete the post-BresDex questionnaire which they could access either via a buttonpresent on every web-page, or via a link provided in an email ifthey registered their email address. A reminder email with URL linkwas sent to those participants who did not start the post-BresDexquestionnaire within two days of completing the first question-naire. Breast care nurses also reminded participants about thestudy by phone or during a home visit, where they handed them areminder postcard including the URL address and the participant’sunique login ID.
2.3.1. Measures
Website log-files (web-logs). Web-logs provided data on thecomponents of BresDex accessed by users, the length of timespent on BresDex overall, and the length of time spent on each
BresDex component
ncluding: � Your Surgery Options section
;
ial outcomes.
ions � Patient Photos
ncluding: � Information on Further Treatment section
.
ssible further treatment, � Video clips of enacted patient experiences
� Patient Photos
rt, including: � Health professional video clips (Home Page)
others; � Video clips of enacted patient experiences
ose in a similar situation.
rt, including: � Weighing It Up (interactive decision support
functionality)
� It’s Your Choice sectionences;
thers;
ose in a similar situation.
r breast cancer � What is Breast Cancer? Section, specifically the
following sub-sections:
* What causes breast cancer?
* What are the risk factors for breast cancer?
* What can reduce the risk of breast cancer?
� General background information: About the
Breast and Breast Cancer
ssible further treatment, � Your Surgery Options section Information on
Further Treatment section
.
s of surgical treatment � Surgery Options Comparison Table
ssible further treatment, � Your Surgery Options section (including
Surgery Options Comparison Table)
� Information on Further Treatment section
� Health professional video clips (Home Page)
; � Video clips of enacted patient experiences
ial outcomes � Patient Photos

Table 2Participant characteristics.
N = 54
Referral Route Screening 23 (42.6%)
Symptomatic 26 (48.1%)
Missing 5 (9.3%)
Age Mean 53.28 years
range 29–80 years
Education Left School before 16
(no formal qualifications)
12 (22.2%)
Left school at 16 (GCSE, GSE,
O Levels or equivalent)
14 (25.9%)
Left School at 18 (A Levels
or equivalent)
2 (3.7%)
College certificate or diploma 11 (20.4%)
University degree or other 15 (27.8%)
1 or more blood relatives diagnosed with breast cancer 22 (40.7%)
(1 unsure)
Surgery Breast Conservation 44 (81.5%)
Mastectomy 10 (18.5%)
No Visits to BresDex 1 28 (51.9%)
2 20 (37.0%)
3 3 (5.6%)
4 1 (1.9%)
5 2 (3.7%)
S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217212
component of BresDex. Components of BresDex were defined bythe sections/pages of BresDex pertaining to the relevant theoreticalconstructs of the extended TPB and the CSM (see Table 1).
Demographic information. Participants were asked to report theirdate of birth, the highest level of education they had attained, andthe date on which they were told they had breast cancer.
Knowledge. Ten true/false items, adapted from the Knowledgescale used by Chen et al. [34], were used to assess knowledge aboutbreast cancer and treatment options (see Appendix 1). A totalknowledge score was calculated by summing the correctresponses; higher scores indicated greater knowledge levels. Aknowledge change score was calculated by subtracting the pre-BresDex Knowledge score from its post-BresDex equivalent.
Deliberation process. A new scale (DelibeRATE) was used to assessthe extent to which participants were thinking about their decision[35]. The scale comprises 9 items scored on a 7-point scale withendpoints labeled ‘strongly disagree’ and ‘strongly agree’ (seeAppendix 1). Scores were summed and rescaled to a 0–100 scale; thehigher the score, the readier were women to make a decision aboutwhich surgery to choose. Reliability analyses showed high internalconsistency, with a Cronbach’s alpha of .945 (pre-BresDex) and .960(post-BresDex). A DelibeRATE change score was calculated bysubtracting the pre-BresDex DelibeRATE score from its post-BresDex equivalent.
Surgery intentions. Two items directly assessed participants’intentions to choose to have BCS and mastectomy. Each itemmeasured surgery intentions on a 7-point scale ranging from �3 (Idefinitely do not intend to choose a lumpectomy/mastectomy) to+3 (I definitely do intend to choose a lumpectomy/mastectomy)(see Appendix 1). Correlation coefficients were calculated for thepre-BresDex and the post-BresDex intentions items. Statisticallysignificant negative correlations at the 0.01 level (2-tailed)between the two intention measures were found, both pre- andpost-BresDex (�.837 and �.780, respectively).
Differential scores were calculated by subtracting intentions formastectomy from intentions for BCS, both pre- and post-BresDex; thepre-BresDex score was then subtracted from the post-BresDex scoreto calculate a change in intentions score. Scores ranged from �6 to +6;a negative score reflects a change in intentions in the direction ofmastectomy and a positive score reflects a change in intentions in thedirection of BCS, with a score of zero indicating no change inintentions.
Surgery choices. The clinical breast team notified the research teamof the type of surgery participants went on to have.
2.3.2. Data analysis
Data analyses were carried out using PASW 18 for Windows[36]. Descriptive statistics of the web-log data were used toexamine participants’ use of the site. Descriptive statistics werealso derived for knowledge scores, DelibeRATE scores, surgeryintentions and actual surgery choices. McNemar’s chi-squareexamined the change in having a preference and not having apreference for BCS and mastectomy, pre- and post-BresDex. T-testswere calculated to examine the relationship between surgeryintentions and surgery choices. One-way, within-subjects analysesof variance (ANOVAs) examined change in knowledge scores,DelibeRATE scores and surgery intentions over time (i.e., beforeand after use of BresDex). Correlations between the web-log dataand knowledge scores, DelibeRATE scores and surgery intentions(including changes in scores) were calculated using Pearson’scorrelation coefficient, at a significance level of p = 0.05.
3. Results
3.1. Participant characteristics
From 160 eligible women, 144 were handed a study pack, ofwhom 52.4% (n = 74) logged onto the BresDex site. Just under 95%(n = 70) of those who logged on consented to take part in the study,the majority of whom participated in the study before theirsurgery, in accordance with the protocol (n = 62, 88.6%). Dataanalysis was restricted to these 62 women.
The web-log data were examined for potential outliers. Eightwomen were excluded, leaving a total sample of 54 participants.Reasons for exclusion were: logging on but failing to use BresDex atall (n = 3); missing web-log data (n = 1); unusually extendedperiods of time spent on particular BresDex sections, suggestingthe web-page was left open but not used (n = 4). The analysesreported below are based on users’ first visit to BresDex.
Participants were aged between 29 and 80 years (mean53.3 years), with just under half the sample educated to collegelevel or higher (48.2%). Over 80% of participants went on to haveBCS (n = 44) (see Table 2).
3.2. Use of BresDex
Over 80% of participants visited BresDex either once or twice,with the total number of visits ranging from one to five (see Table2). The length of time spent on BresDex ranged from 55 s toapproximately 1 h and 27 min (mean � 24 min; med-ian � 21 min). Table 3 details the length of time spent on eachof the theory-derived components. Table 4 shows the number ofparticipants who accessed each section of BresDex and the numberof photos and videos accessed by participants.
3.3. Knowledge
Mean knowledge scores are shown in Table 5. Knowledgescores were high both pre- (mean = 8.28) and post-BresDex(mean = 8.51). Although scores increased after using BresDex,the increase was not significant (F(1,44) = 1.68, p = .202).
3.4. Deliberation
Mean DelibeRATE scores are shown in Table 5. There was a highlysignificant increase in DelibeRATE scores from pre- (mean = 65.88)

Table 3Time spent on BresDex.
Mean Median Standard deviation Minimum Maximum
BresDex: total time spent overall 00:24:26 00:21:40 00:18:31.188 00:00:55 01:27:43
Extended TPB Components Attitudes: surgical treatment options 00:02:26 00:00:00 00:06:40.901 00:00:00 00:42:21
Attitudes: cosmetic outcome 00:05:01 00:03:45 00:05:47.572 00:00:00 00:28:30
Attitudes: further treatment 00:02:30 00:01:15 00:02:56.046 00:00:00 00:08:59
Anticipated Regret 00:09:55 00:08:11 00:08:46.548 00:00:00 00:44:21
Subjective Norms 00:04:53 00:03:25 00:06:14.766 00:00:00 00:31:56
Perceived Behavioral Control 00:04:53 00:03:25 00:06:14.766 00:00:00 00:31:56
CSM Components Cause 00:01:09 00:00:00 00:01:36.337 00:00:00 00:05:07
Identity 00:00:51 00:00:00 00:02:15.259 00:00:00 00:15:24
Timeline 00:04:56 00:02:19 00:08:02.093 00:00:00 00:50:24
Cure/Controllability 00:02:16 00:01:45 00:02:19.542 00:00:00 00:13:05
Consequences 00:17:08 00:13:06 00:15:46.359 00:00:00 01:37:36
S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217 213
to post-BresDex (mean = 76.57) (F(1,45) = 637.31, p < 0.001), indi-cating greater readiness to make a decision after using BresDex.
3.5. Surgery intentions and surgery choices
Mean intentions scores are shown in Table 5. There was a non-significant increase in intentions to choose BCS (F(1,42) = 1.64,p = .208) and a non-significant decrease in intentions to choosemastectomy (F(1,42) = 0.75, p = .391). Participants who went on tohave BCS had significantly stronger intentions to choose BCS both pre-BresDex (t(52) = 5.95, p < .001) and post-BresDex (t(41) = 8.47,p < .001). Likewise, participants who went on to have mastectomyhad significantly stronger intentions to choose mastectomy both pre-BresDex (t(52) = �5.83, p < .001) and post-BresDex (t(41) = �5.07,p < .001).
The number of women with no preferences for surgery (i.e.,with scores of zero), halved from pre-to post-BresDex for both BCS(n = 10 vs. n = 5) and mastectomy (n = 12 vs. n = 6) (see Table 6).According to McNemar’s test this reduction in the number ofwomen with no preferences was not statistically significant, eitherfor intentions to choose BCS (p = .453) or for intentions to choosemastectomy (p = .754).
Table 4Sections and elements of BresDex accessed by participants.
Sections of BresDex accessed by participants at least once No. Participants
(n = 54)
It’s Your Choice section 28 (51.9%)
Lumpectomy and Radiotherapy
(in Your Surgery Options section)
17 (31.5%)
Mastectomy and Reconstruction
(in Your Surgery Options section)
12 (22.2%)
Axillary Surgery (in Further Treatment section) 32 (59.3%)
Chemotherapy (in Further Treatment section) 24 (44.4%)
About the Breast and Breast Cancer section 26 (48.1%)
What’s Next? 36 (66.7%)
Lumpectomy photos page 38 (70.4%)
Mastectomy photos page 32 (59.3%)
Reconstruction photos page 27 (50%)
Weighing It Up (interactive decision
support functionality)
26 (48.1%)
Forum 0 (0%)
Glossary 19 (35.2%)
No. videos accessed by participants Mean (sd)
Total no. Health professional video clips (n = 4) 1.30 (1.73)
Total no. Video clips of enacted
patient experiences (n = 18)
3.70 (4.15)
No. photos accessed by participants Mean (sd)
Total no. lumpectomy photos (n = 3) 1.48 (1.26)
Total no. mastectomy photos (n = 5) 1.15 (1.27)
Total no. reconstruction photos (n = 13) 1.94 (2.97)
3.6. Correlation between outcomes and use of BresDex
3.6.1. Knowledge and use of BresDex
There were no significant correlations between knowledgescores and time spent on BresDex.
3.6.2. Deliberation and use of BresDex
Significant negative correlations were observed between pre-BresDex DelibeRATE scores and (a) total time spent on BresDex(r = �.324, p < .05), (b) time spent on the Anticipated Regretcomponent (r = �.336, p < .05), (c) time spent on the SubjectiveNorms component (r = �.304, p < .05), (d) time spenton the PerceivedBehavioral Control component (r = �.304, p < .05), and (e) time spenton the Consequences component (r = �.281, p < .05). The lower thepre-BresDex DelibeRATE score (i.e., the less ready women were tomake a decision before using BresDex), the longer they spent on thetool as a whole and on these components in particular.
3.6.3. Surgery intentions and use of BresDex
Significant positive correlations were observed betweenchanges in intention to choose BCS and (a) time spent on theAttitudes to Cosmetic Outcome component (r = .306, p < .05), and(b) time spent on the Anticipated Regret component (r = .310,p < .05). The longer women spent on the Cosmetic Outcome andAnticipated Regret components, the more their intentions changedin the direction of BCS.
Table 5Mean scores for knowledge, DelibeRATE and surgery intentions.
Pre-BresDex
Mean
(sd)
Post-BresDex
Mean
(sd)
Change scorea
Mean
(sd)
Knowledge 8.28 8.51 0.20
(1.07) (1.01) (1.04)
n = 54 n = 45 n = 45
DelibeRATE 65.88 76.57 12.36*
(26.80) (23.55) (19.37)
n = 54 n = 46 n = 46
Intentions to have BCS 1.43 1.49 0.33
(1.91) (2.04) (1.21)
n = 54 n = 43 n = 43
Intentions to have mastectomy �1.02 �.91 �0.21
(2.00) (2.17) (1.58)
n = 54 n = 43 n = 43
Intentions differential scores 2.44 2.40 0.53
(3.77) (3.95) (2.42)
n = 54 n = 43 n = 43
a Change scores reported are not the exact difference between pre- and post-
BresDex scores due to the smaller number of participants who had available data
post-BresDex.* p < 0.001.

Table 6Surgery intentions pre- and post-BresDex.
Intentions Post-BresDex Total
Do not intend to have No Preference Do intend to have
Intentions Pre-BresDex BCS Do not intend to havea 5 1 0 6No preferenceb 1 5 4 10Do intend to havec 0 1 26 27
Mastectomy Do not intend to havea 18 3 1 22No Preferenceb 6 6 0 12Do intend to havec 0 1 8 9
a Do not intend to have = scores �3 through to �1.b No preference = 0.c Do intend to have = scores 1 through to 3.
S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217214
4. Discussion and conclusion
4.1. Discussion
Readiness to make a decision significantly increased after usingBresDex but there was no significant improvement in knowledgeabout breast cancer and the treatment options (for which scoreswere high both pre- and post-BresDex). The less ready participantswere to make a decision before using BresDex, the longer theyspent on BresDex overall and in particular on the componentsrelating to the theoretical constructs of Anticipated Regret,Subjective Norms, Perceived Behavioral Control (all extendedTPB constructs) and consequences (a CSM construct). Surgeryintentions changed from pre- to post-BresDex among those whodid not have a clear preference for surgery. Most participants wenton to have BCS, with a significant association between intentionsand actual surgery choices. The longer participants spent on theBresDex components relating to the theoretical constructs ofAttitudes to Cosmetic Outcome (extended TPB) and AnticipatedRegret (extended TPB), the more intentions for BCS strengthened.
The finding that knowledge scores did not improve runscontrary to our hypotheses; findings from other evaluations ofdecision aids report a significant increase in knowledge [1,2]. Thislack of improvement may reflect the items included in theknowledge measure. It is possible that the knowledge question-naire we used was not valid; we adapted this scale from a studythat used it on low-income, medically underserved womenapproximately 6 months after being diagnosed with breast cancer.However, we chose this particular questionnaire because itincluded adequate content for our purposes, in that all questionsare relevant to the treatment options available to them with regardto both the decision in question (i.e., whether or not to have BCS ormastectomy) and other relevant treatment and related factors. Itwas also brief enough not to add too great a burden on ourparticipants, bearing in mind that this was not the only set ofquestions we wanted them to answer. Knowledge scores werealready high prior to using BresDex, leaving little scope forimprovement. This may be the result of the information womenhad already received as part of the care provided by their clinicalteam. Women were invited to use BresDex after receivinginformation from their clinician about the available treatmentoptions. Women were also able to use BresDex and take part in thestudy until their actual surgery. During that time they may wellhave read further literature on breast cancer and discussed theiroptions with their specialist breast care nurse, thereby improvingtheir knowledge before using BresDex. Breast cancer also has ahigh media profile [37], resulting in relatively high generalawareness of the issues and outcomes.
BresDex appears to have been used most by those women whofelt less ready to make a decision; these women spent more timeon the site. BresDex appeared to enhance women’s readiness tomake a decision regarding which surgery to have, with DelibeRATE
scores significantly increasing after using BresDex. We are notaware of other studies that have examined patients’ readiness tomake a decision after using a decision aid and are therefore unableto discuss this finding in the context of the wider literature.However, one interpretation is that those participants who felt lessready to make a decision used BresDex as an additional source ofsupport when considering their options, in particular seekinginformation on the consequences of their decision, such as survivaland cancer recurrence [5,8], how they would feel about this in thefuture [10] and what experts (i.e., surgeons) would recommendand suggest [5,7], reflecting the significantly greater amount oftime they spent on these components of BresDex.
The high degree of concordance between surgery intentionsand surgery choices, along with the high knowledge scores,indicates that participants were making informed choices,consistent with their preferences [20]. The results also showed astrengthening in surgery intentions, with intentions changing inthe direction of BCS after using BresDex. This supports the findingsof other evaluation studies which showed that use of decision aidsleads to more conservative treatment choices, including BCS forearly breast cancer [2]. Women who spent longer on the cosmeticoutcome component of BresDex showed an increase in strength ofintentions to choose BCS. There is evidence that concerns aboutpost-surgery appearance influence women’s surgery choices, withsome studies reporting that patients opting for BCS place a greateremphasis on these factors [5,11,12,17].
4.1.1. Strengths and limitations of the study
Few studies have evaluated how patients actually use decisionaids, and this is a key strength of the present study. Using web-logdata to examine which components were accessed by theparticipants, and for how long, and then correlating thesemeasures with other outcome measures helps to provide a morein-depth examination of how this decision aid works. We areaware of only two other studies that have considered whichcomponents of decision aids are used by patients [5,24], and onlyone of these used web-log data in this way [24]. Furthermore, weare not aware of any other decision aid evaluation studies that haveattempted to examine the effects on the decision-making processitself, which is argued to a more appropriate indicator of the qualityof decision-making [18,22,23]. However, it needs to be acknowl-edged that DelibeRATE is a new scale that has not yet been validated,and that caution therefore needs to be exercised when interpretingthese results. Furthermore, ours was not a randomized studyand we are therefore unable to determine whether non-BresDexusers would also show an increase in DelibeRATE scores.However, it is worth noting that this study was intended toexplore how BresDex would be used in practice, as part of theprocess of developing the decision aid. For the same reason wedid not include outcome measures such as satisfaction with theintervention. A more extensive future evaluation of BresDexcould explore these issues.

S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217 215
4.2. Conclusion
The use of BresDex enhances readiness to make a decisionabout surgery and appears to help make women’s intentionsfor type of surgery clearer. Further work is neededcomparing women who use BresDex with women who do notuse the decision aid and to explore in greater depth thefactors that determine women’s surgery intentions andchoices.
4.3. Practice implications
This study demonstrates the usefulness of an online decisionaid in supporting women choosing surgery for early breast cancer.
Appendix 1. Questionnaire items
Demographic Information (Pre-BresDex Onl y)
DOB What is your date of birth? (DD MM YY)EDUC Your le vel of education: please clic k on the highest
level att ained o Left s chool
o Left school
o Left s chool
o Coll ege cer
o University
o Other (free
DIAG When were you told you had breast cancer? (the actual date if poss ible) (DD MM YY)
DelibeRATE (Pre-and Post-BresDex)
Please click on the number that match es wit h you r agree ment or d istatements below.
D1 I understand the o ptions avail able to me Strongly disagree
D2 I know enough about each op tion to help me decide Strongly disagree
D3 I know about t he advantages and disadvantages of each option Strongly disagree
D4 I know how I feel abo ut each option Strongly disagree
D5 I can imagine what it would feel li ke to live with each option Strongly disagree
D6 I can judge which option is bett er for me Strongly disagree
D7 I can judge which option is worse for me Strongly disagree
D8 I feel I’ve given the opti ons available to me enoug h thought Strongly disagree
D9 Even though it may be difficult, I am able to make a choice Strongly disagree
Knowledge (Pre-and Post-Br esDex)
The decision aid could prove a useful adjunct to the supportprovided by the clinical team.
Acknowledgements
The BresDex group also includes TJ Day, Dr Anne Donald, DrRhodri Evans, Prof Julietta Patnick, and Ms Veronica Rogers. We arealso indebted to the late Dr Joan Austoker for her work in the earlystages of the BresDex project. We would also like to acknowledgeand thank all the women who participated in the study, and theparticipating clinical breast care teams in Cardiff, Sheffield andNewcastle upon Tyne for their help in identifying and recruiting thenewly diagnosed sample. This work is supported by funds fromCancer Research UK (C6475/A7053).
before age 1 6 ( no formal qualification s)
at 16 (GSE, CSE, O levels or equivalent)
at 18 ( A levels or equivalent)
tificate or diploma
degree or higher
text)_____ ___ ________________ ___
sagree ment w ith the
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
1 2 3 4 5 6 7 Strong ly agree
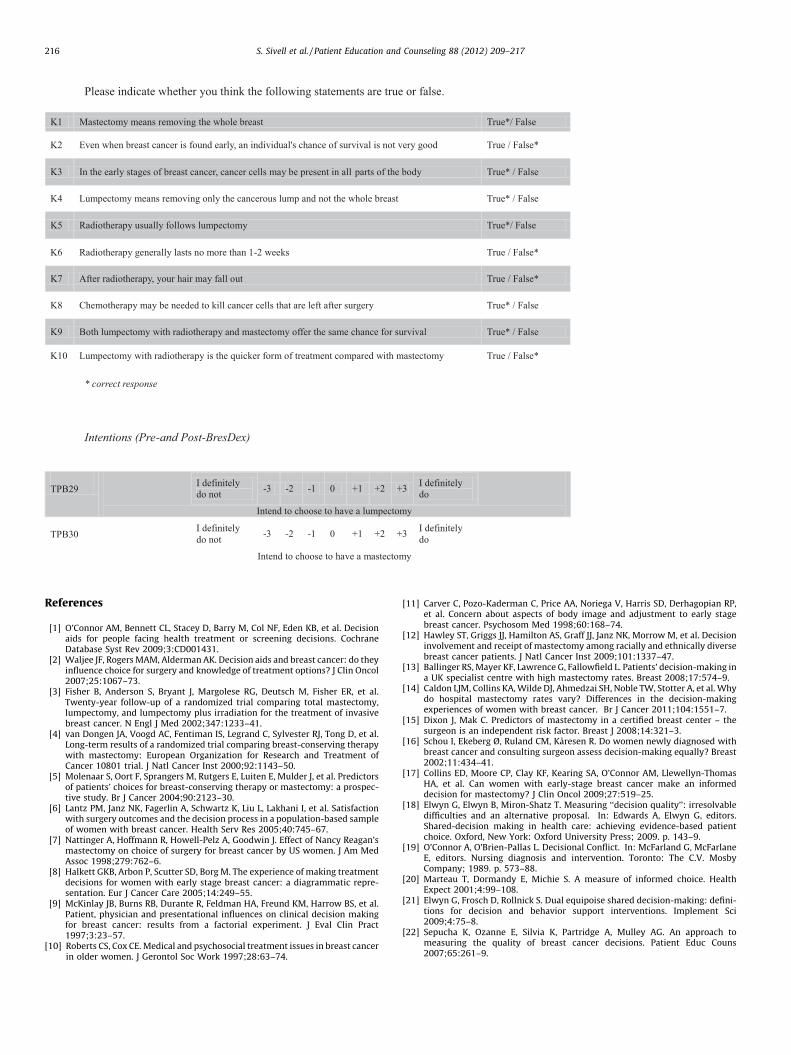
Please indicate whether you think the following stat ements are tr ue or false.
K1 Mastectomy means removing the whole breast True*/ Fa lse
K2 Even when breast cancer is foun d early, an individual's chance of survival i s not very good True / Fals e*
K3 In the early stages of breast cancer, cancer cell s may be present i n all parts of the bo dy True* / Fa lse
K4 Lumpectomy means removing only the cancerous lump and not t he who le breast True* / Fa lse
K5 Radiotherapy usually foll ows lumpectomy True*/ Fa lse
K6 Radiotherapy generally las ts no more than 1-2 weeks True / Fals e*
K7 Afte r r adiotherapy, your hai r may fall out True / Fals e*
K8 Chemotherapy may be needed to kill cancer cell s that are left after surgery True* / Fa lse
K9 Both lumpectomy with radiotherapy and mastectomy off er the same chance for survival True* / Fa lse
K10 Lumpectomy with r adiotherapy is the q uicker form of treatment compared with mastectomy True / Fals e*
* corr ect r espo nse
Intentions (Pre-and Po st-BresD ex)
TPB29 I definite ly do not -3 -2 -1 0 +1 +2 +3 I definite ly
do
Inte nd to choo se to have a lumpectomy
TPB30 I definite ly do not -3 -2 -1 0 +1 +2 +3 I definite ly
do
Inte nd to choose to have a mastectomy
S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217216
References
[1] O’Connor AM, Bennett CL, Stacey D, Barry M, Col NF, Eden KB, et al. Decisionaids for people facing health treatment or screening decisions. CochraneDatabase Syst Rev 2009;3:CD001431.
[2] Waljee JF, Rogers MAM, Alderman AK. Decision aids and breast cancer: do theyinfluence choice for surgery and knowledge of treatment options? J Clin Oncol2007;25:1067–73.
[3] Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al.Twenty-year follow-up of a randomized trial comparing total mastectomy,lumpectomy, and lumpectomy plus irradiation for the treatment of invasivebreast cancer. N Engl J Med 2002;347:1233–41.
[4] van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, et al.Long-term results of a randomized trial comparing breast-conserving therapywith mastectomy: European Organization for Research and Treatment ofCancer 10801 trial. J Natl Cancer Inst 2000;92:1143–50.
[5] Molenaar S, Oort F, Sprangers M, Rutgers E, Luiten E, Mulder J, et al. Predictorsof patients’ choices for breast-conserving therapy or mastectomy: a prospec-tive study. Br J Cancer 2004;90:2123–30.
[6] Lantz PM, Janz NK, Fagerlin A, Schwartz K, Liu L, Lakhani I, et al. Satisfactionwith surgery outcomes and the decision process in a population-based sampleof women with breast cancer. Health Serv Res 2005;40:745–67.
[7] Nattinger A, Hoffmann R, Howell-Pelz A, Goodwin J. Effect of Nancy Reagan’smastectomy on choice of surgery for breast cancer by US women. J Am MedAssoc 1998;279:762–6.
[8] Halkett GKB, Arbon P, Scutter SD, Borg M. The experience of making treatmentdecisions for women with early stage breast cancer: a diagrammatic repre-sentation. Eur J Cancer Care 2005;14:249–55.
[9] McKinlay JB, Burns RB, Durante R, Feldman HA, Freund KM, Harrow BS, et al.Patient, physician and presentational influences on clinical decision makingfor breast cancer: results from a factorial experiment. J Eval Clin Pract1997;3:23–57.
[10] Roberts CS, Cox CE. Medical and psychosocial treatment issues in breast cancerin older women. J Gerontol Soc Work 1997;28:63–74.
[11] Carver C, Pozo-Kaderman C, Price AA, Noriega V, Harris SD, Derhagopian RP,et al. Concern about aspects of body image and adjustment to early stagebreast cancer. Psychosom Med 1998;60:168–74.
[12] Hawley ST, Griggs JJ, Hamilton AS, Graff JJ, Janz NK, Morrow M, et al. Decisioninvolvement and receipt of mastectomy among racially and ethnically diversebreast cancer patients. J Natl Cancer Inst 2009;101:1337–47.
[13] Ballinger RS, Mayer KF, Lawrence G, Fallowfield L. Patients’ decision-making ina UK specialist centre with high mastectomy rates. Breast 2008;17:574–9.
[14] Caldon LJM, Collins KA, Wilde DJ, Ahmedzai SH, Noble TW, Stotter A, et al. Whydo hospital mastectomy rates vary? Differences in the decision-makingexperiences of women with breast cancer. Br J Cancer 2011;104:1551–7.
[15] Dixon J, Mak C. Predictors of mastectomy in a certified breast center – thesurgeon is an independent risk factor. Breast J 2008;14:321–3.
[16] Schou I, Ekeberg Ø, Ruland CM, Karesen R. Do women newly diagnosed withbreast cancer and consulting surgeon assess decision-making equally? Breast2002;11:434–41.
[17] Collins ED, Moore CP, Clay KF, Kearing SA, O’Connor AM, Llewellyn-ThomasHA, et al. Can women with early-stage breast cancer make an informeddecision for mastectomy? J Clin Oncol 2009;27:519–25.
[18] Elwyn G, Elwyn B, Miron-Shatz T. Measuring ‘‘decision quality’’: irresolvabledifficulties and an alternative proposal. In: Edwards A, Elwyn G, editors.Shared-decision making in health care: achieving evidence-based patientchoice. Oxford, New York: Oxford University Press; 2009. p. 143–9.
[19] O’Connor A, O’Brien-Pallas L. Decisional Conflict. In: McFarland G, McFarlaneE, editors. Nursing diagnosis and intervention. Toronto: The C.V. MosbyCompany; 1989. p. 573–88.
[20] Marteau T, Dormandy E, Michie S. A measure of informed choice. HealthExpect 2001;4:99–108.
[21] Elwyn G, Frosch D, Rollnick S. Dual equipoise shared decision-making: defini-tions for decision and behavior support interventions. Implement Sci2009;4:75–8.
[22] Sepucha K, Ozanne E, Silvia K, Partridge A, Mulley AG. An approach tomeasuring the quality of breast cancer decisions. Patient Educ Couns2007;65:261–9.

S. Sivell et al. / Patient Education and Counseling 88 (2012) 209–217 217
[23] Ubel P. Beyond knowledge: figuring out how to help people make ‘‘good’’decisions. In: Shafir E, editor. The behavioral foundations of policy. Princeton:Princeton University and Russell Sage Foundation Presses; 2009.
[24] Joseph-Williams N, Evans R, Edwards A, Newcombe RG, Wright P, Grol R,et al. Supporting informed decision making online in 20 minutes: anobservational web-log study of a PSA test decision aid. J Med InternetRes 2010;12:e15.
[25] Ivory M, Hearst M. Improving web site design. IEEE Internet Comput2002;6:56–63.
[26] Ivory M, Hearst M. The state of the art in automating usability evaluation ofuser interfaces. ACM Comput Survey 2001;33:470–516.
[27] Catledge L, Pitkow J. Characterising browsing strategies in the World WideWeb. Comput Netw ISDN Syst 1995;27:1065–73.
[28] Sivell S, Marsh W, Edwards A, Manstead ASR, Clements A, Elwyn G, et al.Theory-based design and field-testing of an intervention to support womenchoosing surgery for breast cancer: BresDex. Patient Educ Couns 2011 [May13, Epub ahead of print].
[29] Ajzen I. From intentions to actions: a theory of planned behavior. In: Kuhl J,Beckman J, editors. Action-control: from cognition to behavior. Heidelberg:Spring; 1985. p. 11–39.
[30] Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process1991;50:179–211.
[31] Leventhal H, Meyer D, Nerenz D. The common-sense model of illness repre-sentation danger. In: Rachman S, editor. Medical psychology, vol. 2. New York:Pergamon Press; 1980. p. 7–30.
[32] Abraham C, Sheeran P. Acting on intentions: the role of anticipated regret. J SocPsychol 2003;42:495–511.
[33] Elwyn G, Kreuwel I, Durand M-A, Joseph-Williams N, Sivell S, Evans R, et al.How to develop web-based decision support interventions for patients: aprocess map. Patient Educ Couns 2011;82:260–5.
[34] Chen JY, Diamant AL, Thind A, Maly RC. Determinants of breast cancerknowledge among newly diagnosed, low-income, medically underservedwomen with breast cancer. Cancer 2008;112:1153–61.
[35] Elwyn G, Sivell S, Edwards A, Miron-Shatz T, Montori V. Measuring ‘‘readinessto decide’’: using the DelibeRATE scale in an online evaluation of a decisionsupport tool for women facing breast cancer surgery options (BresDex). In: 6thInternational Shared Decision Making Conference. 2011. p. 34.
[36] PASW Statistics 18, Rel. 18.0.0. Chicago: SPSS Inc; 2009.[37] Williamson JML, Skinner CI, Hocken DB. Death and illness as depicted in the
media. Int J Clin Pract 2011;65:547–51.