Increase of body weight during the first year of intensive insulin treatment in type 2 diabetes:...
12
original article Diabetes, Obesity and Metabolism 13: 1008 – 1019, 2011. © 2011 Blackwell Publishing Ltd original article Increase of body weight during the first year of intensive insulin treatment in type 2 diabetes: systematic review and meta-analysis A. E. Pontiroli, L. Miele & A. Morabito Cattedra di Medicina Interna e Cattedra di Biometria, Dipartimento di Medicina, Chirurgia e Odontoiatria, Universit ` a degli Studi di Milano and Ospedale San Paolo, Milano, Italy Aim: This systematic review and meta-analysis was to evaluate the body weight increase and its clinical correlates, through direct weighted regressions, as well as the effect of different insulin regimens and insulin analogues, through meta-analysis. Methods: Appropriate methodology according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was adhered to. Forty-six randomized studies, published as full papers, reporting the effect of insulin treatment on change in body weight were identified, and used to identify predictors of weight change; studies were included in a meta-analysis to study the effect of different insulin regimens or insulin analogues on weight change. Results: Intensity of treatment [aim of study (fasting blood glucose, mg/dl), dose of insulin, final HbA1c, change of HbA1c and frequency of hypoglycaemia] was significantly associated with body weight increase, with small differences between basal versus twice-a-day and prandial regimen. At meta-analysis, body weight increase was lower with basal regimen than with twice-a-day regimen and than with a prandial regimen. Within all regimens, body weight increase was lower with detemir than with NPH, with no difference between glargine and NPH; only two studies directly compared detemir and glargine, indicating lower weight gain with the former insulin. Within twice-a-day regimens and within prandial regimens, comparison was between newer analogues and older drugs, with no significant difference in body weight increase. Conclusion: Body weight increase during the first year of insulin treatment is associated with the intensity of treatment; body weight increase also depends on the insulin regimen applied. Keywords: insulin, intensive insulin treatments, meta-analysis, oral antidiabetic drugs, randomized clinical trials, review, weighted regressions, weight gain Date submitted 9 March 2011; date of first decision 5 April 2011; date of final acceptance 1 June 2011 Introduction Usually, insulin treatment begins in type 2 diabetes because of poor metabolic control with oral antidiabetic drugs (OAD), alone or in combination, and in many instances, insulin starts as an add-on therapy to OAD. A recent meta-analysis [1] indicates that in insulin-naive patients, basal regimens, compared with other regimens, i.e. twice-a-day regimens or prandial regimens, induce a smaller increase of body weight and a lower frequency of hypoglycaemia, but have a smaller effect on glucose metabolism (HbA1c). In addition, detemir induces less weight gain than NPH [2], while there is conflict about the possible effect of glargine on body weight, in comparison with NPH; two meta-analysis aimed at evaluating safety and efficacy of newer analogues in comparison with NPH, appearing during the same period, considered different studies and had different conclusions, so that we have no firm conclusion [3,4]. Isolated reports and meta-analyses also indicate that long-acting Correspondence to: Antonio E. Pontiroli, Ospedale San Paolo, Via A di Rudin ` ı 8, 20142 Milano, Italy. E-mail: [email protected] analogues (glargine and detemir) induce less hypoglycaemia than NPH, with a metabolic control (HbA1c) that is not different from NPH [5 – 7]. Although there is an observed association between insulin use and body weight gain, a number of questions remain open; therefore, we performed a systematic review and meta-analysis of studies with intensive insulin treatments lasting up to 1 year, to give an answer to the following questions: (i) is the increase of body weight predictable, and which are the correlates; (ii) what is the difference among different regimens; and (iii) what is the difference among different analogues. Materials and Methods Search Strategy Eligible trials were randomized clinical trials (RCT), comparing different insulin treatments in type 2 diabetes, i.e. different insulins or insulin regimens, lasting 12–52 weeks, and published as full reports in english language. Measure of treatment effect was the difference between randomized groups in change in body weight. Only parallel studies, two to four arms each, and cross-over studies were considered. Since the
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Increase of body weight during the first year of intensive insulin treatment in type 2 diabetes:...

orig
inal
artic
le
Diabetes, Obesity and Metabolism 13: 1008–1019, 2011.© 2011 Blackwell Publishing Ltdoriginal article
Increase of body weight during the first year of intensiveinsulin treatment in type 2 diabetes: systematic reviewand meta-analysisA. E. Pontiroli, L. Miele & A. MorabitoCattedra di Medicina Interna e Cattedra di Biometria, Dipartimento di Medicina, Chirurgia e Odontoiatria, Universita degli Studi di Milano and Ospedale San Paolo, Milano, Italy
Aim: This systematic review and meta-analysis was to evaluate the body weight increase and its clinical correlates, through direct weightedregressions, as well as the effect of different insulin regimens and insulin analogues, through meta-analysis.Methods: Appropriate methodology according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statementwas adhered to. Forty-six randomized studies, published as full papers, reporting the effect of insulin treatment on change in body weight wereidentified, and used to identify predictors of weight change; studies were included in a meta-analysis to study the effect of different insulinregimens or insulin analogues on weight change.Results: Intensity of treatment [aim of study (fasting blood glucose, mg/dl), dose of insulin, final HbA1c, change of HbA1c and frequency ofhypoglycaemia] was significantly associated with body weight increase, with small differences between basal versus twice-a-day and prandialregimen. At meta-analysis, body weight increase was lower with basal regimen than with twice-a-day regimen and than with a prandialregimen. Within all regimens, body weight increase was lower with detemir than with NPH, with no difference between glargine and NPH; onlytwo studies directly compared detemir and glargine, indicating lower weight gain with the former insulin. Within twice-a-day regimens andwithin prandial regimens, comparison was between newer analogues and older drugs, with no significant difference in body weight increase.Conclusion: Body weight increase during the first year of insulin treatment is associated with the intensity of treatment; body weight increasealso depends on the insulin regimen applied.Keywords: insulin, intensive insulin treatments, meta-analysis, oral antidiabetic drugs, randomized clinical trials, review, weighted regressions,weight gain
Date submitted 9 March 2011; date of first decision 5 April 2011; date of final acceptance 1 June 2011
IntroductionUsually, insulin treatment begins in type 2 diabetes becauseof poor metabolic control with oral antidiabetic drugs (OAD),alone or in combination, and in many instances, insulin startsas an add-on therapy to OAD.
A recent meta-analysis [1] indicates that in insulin-naivepatients, basal regimens, compared with other regimens,i.e. twice-a-day regimens or prandial regimens, induce asmaller increase of body weight and a lower frequency ofhypoglycaemia, but have a smaller effect on glucose metabolism(HbA1c). In addition, detemir induces less weight gain thanNPH [2], while there is conflict about the possible effectof glargine on body weight, in comparison with NPH; twometa-analysis aimed at evaluating safety and efficacy of neweranalogues in comparison with NPH, appearing during thesame period, considered different studies and had differentconclusions, so that we have no firm conclusion [3,4]. Isolatedreports and meta-analyses also indicate that long-acting
Correspondence to: Antonio E. Pontiroli, Ospedale San Paolo, Via A di Rudinı 8, 20142Milano, Italy.E-mail: [email protected]
analogues (glargine and detemir) induce less hypoglycaemiathan NPH, with a metabolic control (HbA1c) that is notdifferent from NPH [5–7].
Although there is an observed association between insulinuse and body weight gain, a number of questions remain open;therefore, we performed a systematic review and meta-analysisof studies with intensive insulin treatments lasting up to 1 year,to give an answer to the following questions: (i) is the increaseof body weight predictable, and which are the correlates; (ii)what is the difference among different regimens; and (iii) whatis the difference among different analogues.
Materials and MethodsSearch Strategy
Eligible trials were randomized clinical trials (RCT), comparingdifferent insulin treatments in type 2 diabetes, i.e. differentinsulins or insulin regimens, lasting 12–52 weeks, andpublished as full reports in english language. Measure oftreatment effect was the difference between randomized groupsin change in body weight. Only parallel studies, two to fourarms each, and cross-over studies were considered. Since the

DIABETES, OBESITY AND METABOLISM original articleaim of the analysis was to compare insulins within themselves,and not with OAD or with placebo, only insulin-based armswere considered, i.e. placebo or OAD arms were not included.
Retrieval of RCTs was based on the The Cochrane Library,MEDLINE and EMBASE (until June 2010) using the termsdiabetes mellitus type 2, insulin, trials, treatment, body weightand limiting the search to randomized controlled clinical trialsand human studies. A manual search was also performed usingthe reference lists from articles, reviews, editorials and theproceedings of international congresses. When the results ofa single study were reported in more than one publication,only the most recent and complete data were included inthe meta-analysis. Decisions on which trials to include weretaken unblindly by the three authors (A. E. P, L. M. andA. M.). Disagreements were resolved by discussion. Excludedtrials were identified with the reason for exclusion. Forty-sixRCTs [8–53] fulfilled the inclusion criteria, all published as fullreports (Table 1).
Data Extraction
Data concerning trials, patient characteristics and treatmentoutcome were abstracted by the three authors (A. E. P., L.M. and A. M.) and discrepancies were resolved by discussion.In some studies there were three arms, with one test insulinand two comparators or two test insulins and one comparator;in such cases, the same study appears twice in figures. Thequality of reports was assessed using the parameters proposedby Jadad et al. [54], i.e. description of random allocation,blinding, clear and validated outcomes, description of dropoutsand withdrawals. Appropriate methodology according to thePreferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [55] was adhered to.
Statistical Analysis
Since studies were of different duration, increase of body weightwas calculated as kg/week. Regressions between the item ofinterest (kg/week), and clinical and methodologic variables[age, duration of diabetes, initial BMI, duration of study, doseof insulin, aim of the study (fasting blood glucose, mg/dl),baseline HbA1c, final HbA1c, change of HbA1c, frequency ofhypoglycaemia] were weighted by the inverse of variance ofsingle observations; weighted regressions were stratified by theinsulin regimen. Next, treatment outcome was expressed asstandardized mean difference (SMD, using mean and standarddeviation), with 95% confidence intervals (CIs) estimatedby a random-effects model according to Der Simonian andLaird [56]. Studies were grouped according to regimens(i.e. basal vs. twice-a-day, basal vs. prandial, twice-a-day vs.prandial), and, within each regimen, according to analogues(detemir and glargine vs. comparators, new combinations vs.older combinations). Heterogeneity was assessed through Qand I2 statistics for each comparison. A p value <0.05 wasconsidered indicative of statistically significant heterogeneity,and potential sources of heterogeneity were discussed whereappropriate. In each figure, vertical line (0) represents nodifference in the two treatment groups (SMD); squares andhorizontal lines represent the point estimates and associated
95% CI for each comparison; the diamonds represent thepooled effect size, with the center representing the pointestimate and the width representing the associated 95% CI.All statistical analyses were performed by stata 9 (StataCorporation, College Station, TX, USA).
ResultsThe PRISMA [55] flow diagram for systematic reviews ispresented in figure 1.
A total of 46 studies, including 14 250 patients (3166 withoutconcomitant administrations of OAD, 11 084 with OAD),treated for 12–52 weeks (mean 27.7 weeks), were consideredfor the study. All studies were similar as to age, durationof diabetes and for initial HbA1c (not shown); studies onlyincluded insulin-treated or insulin-naive patients.
The average (weighted) annualized increase in body weightwas 4.3 ± 2.74 kg (mean ± SD, range −2.76 to 14.7 kg, 95% CI4.32–4.38). We analysed the possible influence of concomitantOAD on insulin-associated weight gain; as a group, OADs werewithout effect; in almost all studies only one kind of OADwas employed (be it no treatment, sulfonylureas, metforminor combination therapy), and therefore no further comparisonwas possible.
Figure 2 shows that the dose of insulin, aim of the study(FBG, mg/dl), final HbA1c, but not baseline HbA1c, decreaseof HbA1c and frequency of hypoglycaemia were associatedwith increase in body weight. Figure 2 also shows that theincrease in body weight as a function of insulin dose wassignificantly lower with basal regimen than with twice-a-dayor with prandial regimen; in contrast, the increase in bodyweight as a function of change of HbA1c, and as a function offrequency of hypoglycaemia was similar with different insulinregimens.
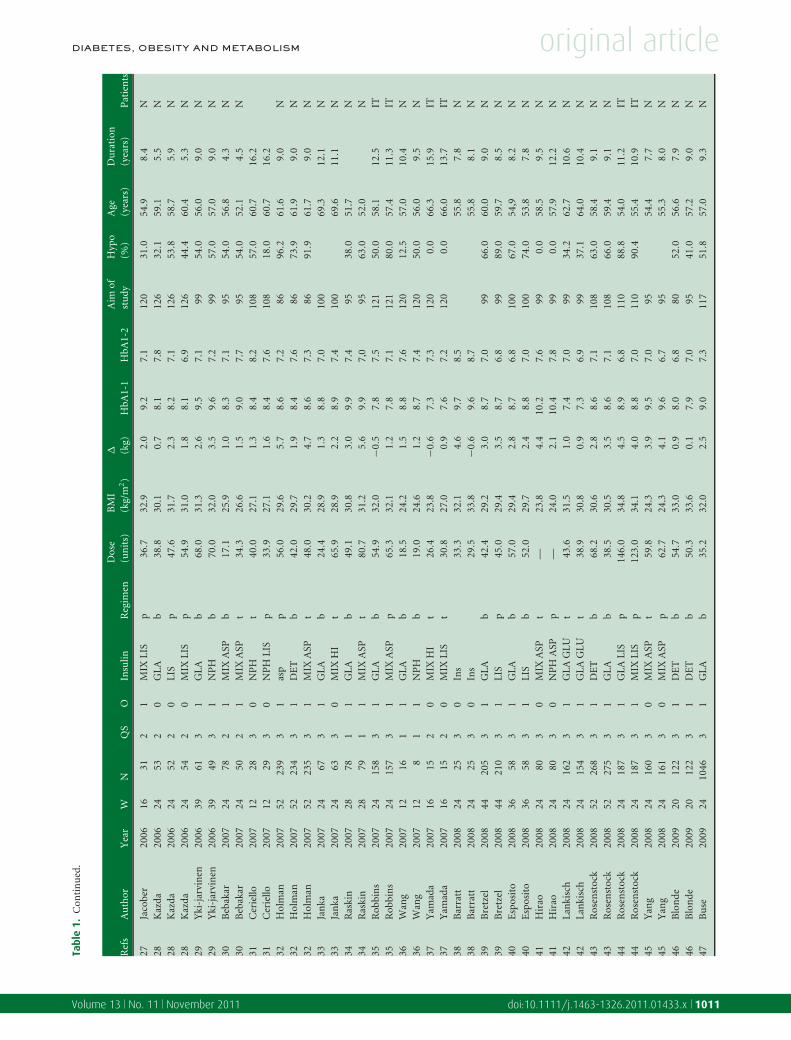
Comparison of different insulin regimens is shown infigure 3; panel a shows that the increase of body weight waslower with basal than with twice-a-day regimens (11 studies);panel b shows that the increase of body weight was lower withbasal than with prandial regimen (9 studies). Heterogeneitywas high, as indicated in panels a and b; heterogeneity was notreduced by stratifying studies by duration and aim of the study,dose of insulin and presence or absence of OAD; insulin doses,however, were significantly lower with basal regimens thanwith either twice-a-day (t = 4.904, p = 0.0005) or prandialregimens (t = 5.911, p = 0.0004). Comparison of twice-a-dayand prandial regimens yielded no difference in increase of bodyweight (8 studies, panel c). Annualized increase of body weightwas 3.1 ± 1.98 versus 5.3 ± 3.03 kg with basal versus twice-a-day regimen (p = 0.0141) and 3.6 ± 1.09 versus 6.4 ± 1.26 kgwith basal versus prandial regimen (p = 0.0054).
Within basal regimens, comparison was between neweranalogues (sorted by detemir or glargine) and older drugs,and showed no overall differences in weight gain. Figure 4(panel a) shows that increase of body weight was lower withdetemir than with NPH, with no other differences (five studies).However, this comparison is based on one single study [26].Within prandial regimens, comparison was between newer
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1009

original article DIABETES, OBESITY AND METABOLISM
Tabl
e1.
Stu
dies
con
side
red
inth
ere
view
.
Ref
sA
uth
orY
ear
WN
QS
OIn
sulin
Reg
imen
Dos
e(u
nit
s)B
MI
(kg/
m2)
� (kg)
HbA
1-1
HbA
1-2
Aim
ofst
udy
Hyp
o(%
)A
ge(y
ears
)D
ura
tion
(yea
rs)
Pat
ien
ts
8P
ater
son
1991
1619
20
HI
p44
.124
.72.
712
.09.
512
651
.35.
8N
8P
ater
son
1991
1616
20
LE
NT
Eb
26.7
22.7
0.3
12.5
10.7
126
59.0
5.3
N9
Lan
dste
t-H
al19
9516
412
1H
Ip
29.0
26.2
3.4
9.2
7.1
121
59.0
9.0
N9
Lan
dste
t-H
al19
9516
392
1N
PH
b26
.026
.21.
99.
17.
512
159
.09.
0N
10M
akim
att
1999
5213
11
NP
Hb
41.0
27.9
3.8
10.5
7.6
108
54.0
>3
N10
Mak
imat
t19
9952
131
0N
PH
t78
.027
.87.
510
.27.
810
858
.0>
3N
11B
asty
r20
0012
412
1L
ISp
36.8
29.2
3.4
10.0
7.7
100
11.0
55.9
7.1
N11
Bas
tyr
2000
1250
21
NP
Hb
24.0
27.9
2.3
10.4
8.5
100
6.0
56.6
7.3
N12
Yki
-jar
vin
en20
0052
214
21
GL
Ab
23.0
29.3
2.6
9.1
8.3
121
34.0
59.0
10.0
N12
Yki
-jar
vin
en20
0052
208
21
NP
Hb
21.0
28.5
2.3
8.9
8.2
121
42.0
59.0
10.0
N13
Ros
enst
ock
2001
2825
92
0G
LA
b70
.030
.70.
38.
68.
012
161
.059
.513
.4IT
13R
osen
stoc
k20
0128
259
20
NP
Hb
70.0
30.4
1.4
8.5
8.0
121
67.0
59.2
14.1
IT14
Alt
un
tas
2003
2420
21
LIS
p—
31.8
2.4
9.4
6.7
105
53.8
5.2
N14
Alt
un
tas
2003
2420
20
NP
HH
Ip
—31
.33.
99.
67.
510
554
.510
.2N
14A
ltu
nta
s20
0324
202
0N
PH
LIS
p—
31.2
−0.6
10.1
7.4
105
54.8
6.1
N15
Frit
sch
e20
0324
236
31
GL
Ab
40.0
28.6
3.9
9.1
7.9
100
74.0
61.0
9.0
N15
Frit
sch
e20
0324
227
31
GL
Ab
39.0
28.7
3.7
9.1
8.1
100
68.0
60.0
8.2
N15
Frit
sch
e20
0324
232
31
NP
Hb
37.0
28.9
2.9
9.1
8.6
100
75.0
62.0
9.3
N16
Rid
dle
2003
2436
73
1G
LA
b47
.232
.53.
08.
67.
010
067
.055
.08.
4N
16R
iddl
e20
0324
389
31
NP
Hb
41.8
32.2
2.8
8.6
7.0
100
74.0
56.0
9.0
N17
Sarg
in20
0324
272
0N
PH
HI
p65
.531
.23.
79.
27.
813
955
.110
.8IT
17Sa
rgin
2003
2428
20
NP
HL
ISp
64.5
30.7
2.2
9.6
7.2
139
56.8
11.8
IT18
Steh
ouw
er20
0339
872
0M
IXH
It
35.8
29.7
4.7
9.4
8.3
9972
.457
.77.
6N
18St
ehou
wer
2003
3986
21
NP
Hb
44.0
29.8
3.8
9.4
8.9
9961
.657
.68.
1N
18St
ehou
wer
2003
3988
20
NP
Ht
46.8
29.2
5.4
9.4
8.3
9971
.658
.47.
9N
19H
endr
a20
0424
192
0N
PH
t49
.429
.14.
810
.09.
612
669
.47.
9N
19H
endr
a20
0424
192
0N
PH
LIS
p44
.029
.03.
09.
48.
412
668
.89.
9N
20M
alon
e20
0416
533
1G
LA
b53
.831
.71.
68.
77.
810
85.
455
.39.
8N
20M
alon
e20
0416
523
1M
IXL
ISt
54.9
30.1
2.3
8.7
7.4
108
3.3
54.5
8.1
N21
Ras
lova
2004
2219
52
0D
ET
ASP
p78
.029
.80.
58.
27.
510
834
.658
.313
.7IT
21R
aslo
va20
0422
199
20
NP
HH
Ip
63.2
28.7
1.1
8.1
7.5
108
36.1
58.2
14.5
IT22
Dou
ek20
0552
874
1M
IXH
It
61.0
30.9
6.3
9.7
8.2
126
82.0
58.0
9.0
N22
Dou
ek20
0552
884
0M
IXH
It
86.0
31.5
7.5
10.0
8.7
126
66.0
58.0
10.0
N23
Jan
ka20
0524
177
31
GL
Ab
28.2
29.5
1.4
8.9
7.2
100
61.0
60.9
9.9
N23
Jan
ka20
0524
187
30
MIX
HI
t64
.529
.62.
18.
87.
510
067
.060
.49.
9N
24M
alon
e20
0516
472
1G
LA
b27
.829
.60.
18.
58.
110
84.
359
.611
.9IT
24M
alon
e20
0516
502
1M
IXL
ISt
32.7
29.4
0.8
8.5
7.5
108
3.3
59.2
13.5
IT25
Ras
kin
2005
2811
62
1G
LA
b51
.031
.43.
59.
87.
410
016
.052
.38.
9N
25R
aski
n20
0528
117
21
MIX
ASP
t78
.031
.55.
49.
76.
910
043
.052
.69.
5N
26H
erm
anse
n20
0626
238
31
DE
Tb
65.0
29.0
1.1
8.6
6.8
108
64.0
61.3
9.6
N26
Her
man
sen
2006
2623
83
1N
PH
b44
.029
.02.
98.
56.
610
880
.060
.49.
8N
27Ja
cobe
r20
0616
292
1G
LA
b28
.032
.91.
59.
27.
312
045
.054
.98.
4N
1010 Pontiroli et al. Volume 13 No. 11 November 2011
DIABETES, OBESITY AND METABOLISM original articleTa
ble
1.C
onti
nu
ed.
Ref
sA
uth
orY
ear
WN
QS
OIn
sulin
Reg
imen
Dos
e(u
nit
s)B
MI
(kg/
m2)
� (kg)
HbA
1-1
HbA
1-2
Aim
ofst
udy
Hyp
o(%
)A
ge(y
ears
)D
ura
tion
(yea
rs)
Pat
ien
ts
27Ja
cobe
r20
0616
312
1M
IXL
ISp
36.7
32.9
2.0
9.2
7.1
120
31.0
54.9
8.4
N28
Kaz
da20
0624
532
0G
LA
b38
.830
.10.
78.
17.
812
632
.159
.15.
5N
28K
azda
2006
2452
20
LIS
p47
.631
.72.
38.
27.
112
653
.858
.75.
9N
28K
azda
2006
2454
20
MIX
LIS
p54
.931
.01.
88.
16.
912
644
.460
.45.
3N
29Y
ki-j
arvi
nen
2006
3961
31
GL
Ab
68.0
31.3
2.6
9.5
7.1
9954
.056
.09.
0N
29Y
ki-j
arvi
nen
2006
3949
31
NP
Hb
70.0
32.0
3.5
9.6
7.2
9957
.057
.09.
0N
30B
ebak
ar20
0724
782
1M
IXA
SPb
17.1
25.9
1.0
8.3
7.1
9554
.056
.84.
3N
30B
ebak
ar20
0724
502
1M
IXA
SPt
34.3
26.6
1.5
9.0
7.7
9554
.052
.14.
5N
31C
erie
llo20
0712
283
0N
PH
t40
.027
.11.
38.
48.
210
857
.060
.716
.231
Cer
iello
2007
1229
30
NP
HL
ISp
33. 9
27.1
1.6
8.4
7.6
108
18.0
60.7
16.2
32H
olm
an20
0752
239
31
asp
p56
.029
.65.
78.
67.
286
96.2
61.6
9.0
N32
Hol
man
2007
5223
43
1D
ET
b42
.029
.71.
98.
47.
686
73.9
61.9
9.0
N32
Hol
man
2007
5223
53
1M
IXA
SPt
48.0
30.2
4.7
8.6
7.3
8691
.961
.79.
0N
33Ja
nka
2007
2467
31
GL
Ab
24.4
28.9
1.3
8.8
7.0
100
69.3
12.1
N33
Jan
ka20
0724
633
0M
IXH
It
65.9
28.9
2.2
8.9
7.4
100
69.6
11.1
N34
Ras
kin
2007
2878
11
GL
Ab
49.1
30.8
3.0
9.9
7.4
9538
.051
.7N
34R
aski
n20
0728
791
1M
IXA
SPt
80.7
31.2
5.6
9.9
7,0
9563
.052
.0N
35R
obbi
ns
2007
2415
83
1G
LA
b54
.932
.0−0
.57.
87.
512
150
.058
.112
.5IT
35R
obbi
ns
2007
2415
73
1M
IXA
SPp
65.3
32.1
1.2
7.8
7.1
121
80.0
57.4
11. 3
IT36
Wan
g20
0712
161
1G
LA
b18
.524
.21.
58.
87.
612
012
.557
.010
.4N
36W
ang
2007
128
11
NP
Hb
19.0
24.6
1.2
8.7
7.4
120
50.0
56.0
9.5
N37
Yam
ada
2007
1615
20
MIX
HI
t26
.423
.8−0
.67.
37.
312
00.
066
.315
.9IT
37Y
amad
a20
0716
152
0M
IXL
ISt
30.8
27.0
0.9
7.6
7.2
120
0.0
66.0
13.7
IT38
Bar
ratt
2008
2425
30
Ins
33.3
32.1
4.6
9.7
8.5
55.8
7.8
N38
Bar
ratt
2008
2425
30
Ins
29.5
33.8
−0.6
9.6
8.7
55.8
8.1
N39
Bre
tzel
2008
4420
53
1G
LA
b42
.429
.23.
08.
77.
099
66.0
60.0
9.0
N39
Bre
tzel
2008
4421
03
1L
ISp
45.0
29.4
3.5
8.7
6.8
9989
.059
.78.
5N
40E
spos
ito
2008
3658
31
GL
Ab
57.0
29.4
2.8
8.7
6.8
100
67.0
54,9
8.2
N40
Esp
osit
o20
0836
583
1L
ISb
52.0
29.7
2.4
8.8
7.0
100
74.0
53.8
7.8
N41
Hir
ao20
0824
803
0M
IXA
SPt
—23
.84.
410
.27.
699
0.0
58.5
9.5
N41
Hir
ao20
0824
803
0N
PH
ASP
p—
24.0
2.1
10.4
7.8
990.
057
.912
.2N
42L
anki
sch
2008
2416
23
1G
LA
GL
Ut
43.6
31.5
1.0
7.4
7.0
9934
.262
.710
.6N
42L
anki
sch
2008
2415
43
1G
LA
GL
Ut
38.9
30.8
0.9
7.3
6.9
9937
.164
.010
.4N
43R
osen
stoc
k20
0852
268
31
DE
Tb
68.2
30.6
2.8
8.6
7.1
108
63.0
58.4
9.1
N43
Ros
enst
ock
2008
5227
53
1G
LA
b38
.530
.53.
58.
67.
110
866
.059
.49.
1N
44R
osen
stoc
k20
0824
187
31
GL
AL
ISp
146.
034
.84.
58.
96.
811
088
.854
.011
.2IT
44R
osen
stoc
k20
0824
187
31
MIX
LIS
p12
3.0
34.1
4.0
8.8
7.0
110
90.4
55.4
10.9
IT45
Yan
g20
0824
160
30
MIX
ASP
t59
.824
.33.
99.
57.
095
54.4
7 .7
N45
Yan
g20
0824
161
30
MIX
ASP
p62
.724
.34.
19.
66.
795
55.3
8.0
N46
Blo
nde
2009
2012
23
1D
ET
b54
.733
.00.
98.
06.
880
52.0
56.6
7.9
N46
Blo
nde
2009
2012
23
1D
ET
b50
.333
.60.
17.
97.
095
41.0
57.2
9.0
N47
Bu
se20
0924
1046
31
GL
Ab
35.2
32.0
2.5
9.0
7.3
117
51.8
57.0
9.3
N
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1011

original article DIABETES, OBESITY AND METABOLISM
Tabl
e1.
Con
tin
ued
.
Ref
sA
uth
orY
ear
WN
QS
OIn
sulin
Reg
imen
Dos
e(u
nit
s)B
MI
(kg/
m2)
� (kg)
HbA
1-1
HbA
1-2
Aim
ofst
udy
Hyp
o(%
)A
ge(y
ears
)D
ura
tion
(yea
rs)
Pat
ien
ts
47B
use
2009
2410
453
1M
IXL
ISt
41.8
32.0
3.6
9.1
7.2
117
57.1
57.0
9.7
N48
Lie
bl20
0926
537
30
DE
TA
SPp
80.9
31.0
2.4
8.5
7.0
9931
.960
.3>
0.5
48L
iebl
2009
2617
83
0M
IXA
SPt
57.8
30.6
2.1
8.4
7.2
9928
.061
.7>
0.5
49M
ilice
vic
2009
2468
30
MIX
LIS
t44
.128
.01.
49.
78.
412
158
.39.
1N
49M
ilice
vic
2009
2467
31
NP
Hb
21.0
27.9
1.2
9.6
9.2
121
56.4
9.2
N50
Wol
ffen
butt
el20
0924
222
31
GL
Ab
29.0
30.4
1.8
8.8
7.3
9964
.469
.911
.3N
50W
olff
enbu
ttel
2009
2425
83
1M
IXL
ISt
36.0
31.0
3.6
8.7
7.0
9968
.869
.412
.9N
51Fr
itsc
he
2010
5215
33
1G
LA
GL
Up
98.0
30.3
3.6
8.6
7.3
100
75.8
60.2
12.8
IT51
Frit
sch
e20
1052
157
31
MIX
t91
.329
.82.
28.
57.
710
073
.960
.912
.5IT
52H
eise
2010
2612
23
1G
LA
b30
.92.
28.
57.
090
62.1
10.7
N52
Hei
se20
1026
135
31
HI
p30
.71.
18.
66.
890
60.4
10.6
N53
Swin
nen
2010
2448
62
1D
ET
t76
.530
.60.
68.
77.
210
156
.258
.09.
7N
53Sw
inn
en20
1024
478
21
GL
Ab
43.5
29.7
1.4
8.7
7.2
101
55.9
58.7
10.1
N
Insu
lins:
HI,
hu
man
insu
lin;N
PH
,NP
Hin
sulin
;GL
A,g
larg
ine;
DE
T,d
etem
ir;A
SP,a
spar
t;L
IS,l
ispr
o;G
LU
,glu
lisin
e;M
IX,b
iph
asic
insu
lin.
For
each
stu
dy(r
ef),
auth
or,y
ear
ofpu
blic
atio
n,d
ura
tion
ofst
udy
inw
eeks
(W),
nu
mbe
rof
pati
ents
inea
char
m(N
),qu
alit
ysc
ore
(QS)
,pre
sen
ceor
abse
nce
ofor
alan
tidi
abet
icdr
ugs
(O),
nam
eof
insu
lin,
regi
men
ofad
min
istr
atio
n(b
,ba
sal,
once
-a-d
ayin
ject
ion
;t,
twic
e,tw
ice-
a-da
yin
sulin
inje
ctio
ns;
p,pr
andi
al,
thre
eto
fou
rin
ject
ion
s),
insu
lindo
se,
BM
I,in
crea
seof
body
wei
ght
(�kg
),ba
selin
ean
dfi
nal
HbA
1c(H
bA1-
1an
dH
bA1-
2,%
),ai
mof
stu
dy(f
asti
ng
bloo
dgl
uco
se,m
g/dl
),fr
equ
ency
ofh
ypog
lyca
emia
(hyp
o%
),ag
eof
pati
ents
(yea
rs),
dura
tion
ofdi
abet
es(y
ears
)an
dki
nd
ofpa
tien
ts(n
aive
,N;i
nsu
lintr
eate
d,IT
)ar
ein
dica
ted.
Dis
pers
ion
ofda
ta(S
D)
isn
otin
dica
ted.
Records identified throughdatabase searching(n = 170)
Additional records identified through other sources(n = 40)
Records after duplicate removed(n = 210)
Records screened(n = 210)
Records excluded(n = 109)
Full-text articles assessedfor eligibility
(n = 91)
Full-text articles excludedwith reasons
(n = 45)
Studies included inqualitative synthesis
(n = 46)
Studies included inquantitative synthesis
(meta-analysis)(n = 46)
Figure 1. Flowchart of clinical trials included in the systematic reviewand meta-analysis: reviews and meta-analyses were excluded first (recordsexcluded); studies or short duration, or without measures of dispersion ofincrease in body weight were excluded at a second step (full-text articlesexcluded with reasons).
analogues (NPH-LIS and DET-ASP) and older drugs (NPH-human insulin); figure 4 (panel b) shows no significant overallpreference, even if a difference in the increase in body weightin favor of NPH-LIS appeared in one study.
Panel c shows that in all studies, whatever the regimen and theshort-acting analogues, increase of body weight was lower withdetemir than with comparators (six studies). Heterogeneity washigh, and was not reduced by stratifying studies by durationand aim of the study, dose of insulin and presence or absenceof OAD; insulin doses were not different. Annualized increaseof body weight was 2.2 ± 1.11 versus 4.0 ± 1.1 kg with detemirversus comparators (p = 0.0012).
All studies with glargine, whatever the regimen, werecompared with other insulins. No difference in the increaseof body weight appeared (22 studies, panel d); a subanalysiswas performed by dividing studies by the number of insulininjections, and again no difference in the increase of bodyweight appeared (not shown). Annualized increase of bodyweight was 3.7 ± 2.72 versus 4.4 ± 2.71 kg with glargine versuscomparators (NS).
Within twice-a-day regimens, comparison was betweennewer analogues and older drugs; only a few studies considereddifferent insulins, while many others compared one insulinwith or without oral agents, and therefore were not includedin meta-analysis; no difference in the increase of body weightappeared (2 studies, not shown).
A direct comparison of detemir and glargine was the objectof two studies [44,53]; in the first study, detemir was associatedwith less weight gain when administered once daily, not whenadministered twice daily; in the second study, detemir was
1012 Pontiroli et al. Volume 13 No. 11 November 2011

DIABETES, OBESITY AND METABOLISM original article
Cha
nge
in b
ody
wei
ght (
kg/w
eek)
0 1 2 3 4
-.1
0.1
.2.3
-.1
0.1
.2.3
2 4 6 8 1 00 0 0 0 0 0
Decrease of HbA1c (%)Decrease of HbA1c (%)
Frequency of hypoglycaemia (%) Frequency of hypoglycaemia (%)
basal
twiceprandial
-.1
0.1
.2.3
2 4 6 8 1 00 0 0 0 0 0
-.1
0.1
.2.3
0 1 2 3 4
-.1
0.1
.2.3
7 8 9 1 0 1 1-.
10
.1.2
.38 0 1 0 0 1 2 0 1 4 0
Aim of the study (FBG mg/dl) Final HbA1c (%)-.
10
.1.2
.3
5 0 50 0 1 0 1 0
Dose of insulin (U/day)Dose of insulin (U/day)
basal
-.1
0.1
.2.3
5 0 50 0 1 0 1 0
twice
prandial
prandial
basal
twice
Figure 2. Weighted regression of change of body weight as a function of aim of the study (FBG, mg/dl), final HbA1c (%), insulin dose (U/day), change ofHbA1c (%) and frequency of hypoglycaemia (%); coefficients ± SE are indicated, together with r2 and p values. Regressions are also stratified by insulinregimen; basal regimen is the reference regression and coefficients of twice-a-day and prandial regimen are calculated as difference from basal regimen.
Regression of change of weight (kg/week) Regression by insulin regimen Coefficients ± SE r2 p
Aim of study (FBG, mg/dl) — −0.0028 ± 0.0005 0.2863 <0.0001Final HbA1c (%) — −0.0538 ± 0.005 0.5224 <0.0001Insulin dose (U/day) — 0.0017 ± 0.0004 0.1727 <0.0001
General (basal) −0.0017 ± 0.0007 0.4528 <0.0001Twice-a-day versus basal 0.0041 ± 0.0009 — <0.0001Prandial versus basal 0.0050 ± 0.0007 — <0.0001
Decrease of HbA1C (%) — 0.079 ± 0.0054 0.6869 <0.0001General (basal) 0.069 ± 0.0125 0.5876 <0.0001Twice-a-day versus basal 0.062 ± 0.029 — NSPrandial versus basal 0.025 ± 0.0248 — NS
Frequency of hypoglycaemia (%) — 0.0013 ± 0.0002 0.4655 <0.0001General (basal) 0.0016 ± 0.0003 0.4763 <0.0001Twice-a-day versus basal 0.002 ± 0.2287 — NSPrandial versus basal 0.0045 ± 0.0353 — NS
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1013

original article DIABETES, OBESITY AND METABOLISM
Overall (I-squared=89.1%, p=0.000)
MALONE (2005)
MILICEVIC (2009)
MALONE (2004)
BUSE (2009)
WOLFFENBUTTEL (2009)
MAKIMATT (1999)
RASKIN (2007)
RASKIN (2005)
SWINNEN (2010)
JANKA (2007)
IDStudy (a)
(b)
(c)
HOLMAN (2007)
JANKA (2005)
-0.26 (-0.60, 0.09)
-0.68 (-0.87, -0.50)
-0.18 (-0.39, 0.02)
-0.31 (-0.50, -0.12)
-0.30 (-0.70, 0.10)
-0.07 (-0.41, 0.27)
-0.17 (-0.56, 0.21)
-0.27 (-0.36,- 0.19)
-0.53 (-0.71, -0.34)
-0.79 (-1.59, 0.02)
-0.58 (-0.90, -0.26)
-0.41 (-0.67, -0.15)
0.26 (0.14, 0.39)
-0.26 (-0.60, 0.09)
SMD (95%CI)
-0.68 (-0.87, -0.50)
-0.18 (-0.39, 0.02)
0-2 -1 1 2
Overall (I-squared=87.9%, p=0.000)
KAZDA (2006)
JACOBER (2006)
ROBBINS (2007)
HOLMAN (2007)
IDStudy
LANDSTET-HALLIN (1995)
BASTYR (2000)
BRETZEL (2008)
KAZDA (2006)
PATERSON (1991)
HEISE (2010)
-0.46 (-0.74, -0.18)
-0.39 (-0.78, -0.01)
-1.01 (-1.55, -0.47)
-0.56 (-0.79, -0.34)
-0.86 (-1.05, -0.67)
-0.74 (-1.19, -0.29)
-0.41 (-0.83, 0.00)
-0.11 (-0.31, 0.08)
-0.30 (-0.68, 0.08)
-0.81 (-1.50, -0.11)
0.31 (0.07, 0.56)
-0.46 (-0.74, -0.18)
-0.39 (-0.78, -0.01)
-1.01 (-1.55, -0.47)
-0.56 (-0.79, -0.34)
SMD (95%CI)
-0.86 (-1.05, -0.67)
-0.74 (-1.19, -0.29)
-0.41 (-0.83, 0.00)
-0.11 (-0.31, 0.08)
-0.30 (-0.68, 0.08)
-0.81 (-1.50, -0.11)
0.31 (0.07, 0.56)
0-2 -1 1 2
Overall (I-squared=91.1%, p=0.000)
FRITSCHE (2010)
MIYASHITA (2008)
CERIELLO (2007)
HOLMAN (2007)
HIRAO (2008)
StudyID
YANG (2008)
LIEBL (2009)
HENDRA (2004)
-0.01 (-0.34, 0.32)
-0.33 (-0.55, -0.10)
0.00 (-0.60, 0.60)
-0.30 (-0.82, 0.23)
-0.23 (-0.41, -0.05)
0.52 (0.21, 0.84)
-0.80 (-1.03, -0.57)
-0.07 (-0.24, 0.10)
1.88 (1.10, 2.65)
-0.01 (-0.34, 0.32)
-0.33 (-0.55, -0.10)
0.00 (-0.60, 0.60)
-0.30 (-0.82, 0.23)
-0.23 (-0.41, -0.05)
0.52 (0.21, 0.84)
SMD (95%CI)
-0.80 (-1.03, -0.57)
-0.07 (-0.24, 0.10)
0-2 -1 1 2
favors basal
favors basal
SMD (95% CI)
SMD (95% CI)
SMD (95% CI)
Figure 3. Meta-analysis of different insulin regimens: (a) basal versus twice-a-day, (b) basal versus prandial and (c) twice-a-day versus prandial.
1014 Pontiroli et al. Volume 13 No. 11 November 2011
DIABETES, OBESITY AND METABOLISM original articleassociated with less weight gain; with only two studies, it wasnot possibile to perform a meta-analysis of detemir versusglargine.
DiscussionIn this article, we analysed data from 46 studies describingbody weight measurement in intensified insulin treatment in
type 2 diabetes in studies lasting up to 1 year. The main finding
was that intensity of treatment [aim of the study (fasting blood
glucose, mg/dl), dose of insulin, final HbA1c, change of HbA1c
and frequency of hypoglycaemia] was significantly associated
with body weight increase; an additional finding was that,
within different insulin regimens, the link between weight gain
and insulin dose depended on insulin regimen; in contrast, the
link between weight gain and change of HbA1c, and between
.
Overa (I-squared=99.4%, p=0.000)
WANG (2007)
RIDDLE (2003)
DET
FRITSCHE (2003)
ID
Study (a)
(b)
YKI (2006)
GLA
Subtotal (I-squared=94.9%, p=0.000)
HERMANSEN (2006)
FRITSCHE (2003)
Subtotal (I-squared=.%,p=.)
-0.40 (-1.60, 0.81)
0.24 (-0.61, 1.09)
1.00 (0.85, 1.15)
0.16 (-0.02, 0.35)
-0.06 (-0.43, 0.32)
0.31 (-0.15, 0.78)
-3.84 (-4.14, -3.54)
0.14 (-0.04, 0.32)
-3.84 (-4.14, -3.54)
-0.40 (-1.60, 0.81)
SMD (95%CI)
0.16 (-0.02, 0.35)
-0.06 (-0.43, 0.32)
0.31 (-0.15, 0.78)
0.14 (-0.04, 0.32)
-2 -1 0 1 2favors new
SMD (95% CI)
.
.
Overall (I-squared=55.6%, p=0.105)
DETASP
SARGIN (2003)
Subtotal (I-squared=.%,p=.)
ALTUNTAS (2003)
NPHLIS
RASLOVA (2004)
Subtotal (I-squared=0.0%, p=0.374)
ID
Study
-0.34 (-0.72, 0.04)
-0.74 (-1.28, -0.19)
-0.12 (-0.32, 0.07)
-0.36 (-0.99, 0.27)
-0.12 (-0.32, 0.07)
-0.57 (-0.99, -0.16)
-0.34 (-0.72, 0.04)
-0.74 (-1.28, -0.19)
SMD (95%CI)SMD (95%CI)
-0.12 (-0.32, 0.07)
-0.36 (-0.99, 0.27)
-0.12 (-0.32, 0.07)
-0.57 (-0.99, -0.16)
0-2 -1 0 1 2favors new
SMD (95% CI)
Figure 4. Meta-analysis of different insulin analogues: (a) new versus older analogues within basal regimens, (b) new versus older analogues withinprandial regimens, (c) detemir versus comparators and (d) glargine versus comparators.
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1015

original article DIABETES, OBESITY AND METABOLISM
Overall (I-squared=99.0%, p=0.000)
HERMANSEN (2006)
LIEBL (2009)
HOLMAN (2007)
HOLMAN (2007)
ROSENSTOCK (2008)
SWINNEN (2010)
RASLOVA (2004)
ID
Study (c)
(d)
-0.82 (-1.48, -0.16)
-3.84 (-4.14,-3.54)
0.07 (-0.10, 0.24)
-0.86 (-1.05, -0.67)
-0.68 (-0.87, -0.50)
-0.11 (-0.27, 0.06)
-0.26 (-0.39, -0.14)
-0.12 (-0.32, 0.07)
-0.82 (-1.48, -0.16)
-3.84 (-4.14,-3.54)
SMD (95%CI)SMD (95%CI)
0.07 (-0.10, 0.24)
-0.86 (-1.05, -0.67)
-0.68 (-0.87, -0.50)
-0.11 (-0.27, 0.06)
-0.26 (-0.39, -0.14)
-0.12 (-0.32, 0.07)
0-2 -1 0 1 2favors detemir
Overall (I-squared=93.7%, p=0.000)
JANKA (2005)
HEISE (2010)
FRITSCHE (2003)
RIDDLE (2003)
ROSENSTOCK (2008)
ESPOSITO (2008)
ROSENSTOCK (2008)
RASKIN (2007)
FRITSCHE (2010)
BUSE (2009)
ID
YKI (2006)
Study
RASKIN (2005)
JANKA (2007)
SWINNEN (2010)
BRETZEL (2008)
-0.10 (-0.28, 0.08)
-0.18 (-0.39, 0.02)
0.24 (-0.61, 1.09)
0.31 (0.07, 0.56)
0.14 (-0.04, 0.32)
1.00 (0.85, 1.15)
0.11 (-0.06, 0.27)
0.12 (-0.24, 0.48)
-0.53 (-0.71, -0.34)
0.12 (-0.09, 0.32)
-0.39 (-0.78, -0.01)
-0.58 (-0.90, -0.26)
-0.17 (-0.56, 0.21)
-0.56 (-0.79, -0.34)
0.33 (0.10, 0.55)
-0.27 (-0.36, -0.19)
-1.01 (-1.55, -0.47)
-0.06 (-0.43, 0.32)
-0.41 (-0.67, -0.15)
-0.26 (-0.60, 0.09)
-0.30 (-0.68, 0.08)
0.26 (0.14, 0.39)
-0.30 (-0.70, 0.10)
-0.11 (-0.31, 0.08)
-0.10 (-0.28, 0.08)
-0.18 (-0.39, 0.02)
0.31 (0.07, 0.56)
0.14 (-0.04, 0.32)
0.11 (-0.06, 0.27)
0.12 (-0.24, 0.48)
-0.53 (-0.71, -0.34)
0.12 (-0.09, 0.32)
-0.39 (-0.78, -0.01)
-0.58 (-0.90, -0.26)
-0.17 (-0.56, 0.21)
-0.56 (-0.79, -0.34)
0.33 (0.10, 0.55)
-0.27 (-0.36, -0.19)
SMD (95%CI)SMD (95%CI)
-1.01 (-1.55, -0.47)
-0.06 (-0.43, 0.32)
-0.41 (-0.67, -0.15)
-0.26 (-0.60, 0.09)
-0.30 (-0.68, 0.08)
0.26 (0.14, 0.39)
-0.30 (-0.70, 0.10)
-0.11 (-0.31, 0.08)
0-1.55 0 1.55
SMD (95% CI)
MALONE (2004)
MALONE (2005)
JACOBER (2006)KAZDA (2006)
ROBBINS (2007)
WANG (2007)
KAZDA (2006)
WOLFENBUTTEL (2009)
favors glargine
SMD (95% CI)
Figure 4. Continued.
weight gain and frequency of hypoglycaemia was not differentwith different insulin regimens. This finding is corroborated bythe fact that basal regimens are associated with a reduced effecton body weight [1].
There are few previous meta-analyses dealing with weightgain during insulin treatment, and only analysed differentregimens or different insulin analogues. For instance, Lassersononly analysed insulin regimens in insulin-naive patients [1],
1016 Pontiroli et al. Volume 13 No. 11 November 2011

DIABETES, OBESITY AND METABOLISM original articlewhile Bazzano [3] and Caballero [4] only analysed glargineversus comparators, and Philis-Tsimikas [2] only analyseddetemir versus comparators. The aim of this meta-analysiswas rather ambitious, i.e. to yield a full picture of increase inbody weight with different regimens and different analogues. Asimilar comprehensive analysis was published by Yki-Jarvinenin 2001 [57], but available insulins and regimens at that timewere quite different.
We meta-analysed different insulin regimens; as reportedin a few articles, we found that basal regimens, comparedwith twice-a-day and prandial regimens, are associated with areduced increase of body weight [1]. However, heterogeneitywas high, and could not be reduced by stratifying studies byduration and aim of the study, dose of insulin and presence orabsence of OAD; in addition, insulin doses were significantlylower with basal regimens than with either twice-a-day orprandial regimens. We should recall that no study was double-blind, and therefore a bias cannot be ruled out. The differencein basal versus other regimens seems to apply also to long-termstudies, as recently reported by Holman [58]; this supports thevalidity of results obtained at 1 year.
We also meta-analysed, within each regimen, various insulinformulations, and we found that, in general, newer analogueswere not better than older drugs in terms of weight gain, withthe exception of one study with detemir versus NPH [26], andone study with NPH-LIS versus NPH-regular insulin [17]. Thewithin twice-a-day regimen was made of too few studies (twostudies) to perform a meta-analysis.
One single meta-analysis on twice-a-day regimens waspublished [59], indicating that premixed insulin analoguesand premixed human insulin have a similar effect on weightgain. Unfortunately, most of the studies considered in thatmeta-analysis were of very short duration (4 weeks), or werenot randomized, or were in comparison with OADs. Therefore,no firm conclusion can be drawn on this topic.
A final meta-analysis was devoted to long-acting analogues,i.e. detemir and glargine, since these insulins can be usedalone or in various combinations. Compared with severalcomparators, detemir was associated with a lower increase ofbody weight. A subanalysis of studies based on the frequency ofassociated insulins was made impossible by the scant number ofstudies. However, heterogeneity was high, and was not reducedby stratifying studies by duration and aim of the study, doseof insulin and presence or absence of OAD; insulin doses werenot different. In contrast, glargine was similar to comparatorsin terms of increase in body weight; a subanalysis was madeconsidering the effects according to the number of insulininjections and again no difference was observed in terms ofincrease in body weight. A meta-analysis [60] focused on theeffect of long-acting insulin analogues on weight gain reachedsimilar conclusions, while other meta-analyses did not reporton weight gain [5–7].
There are limitations to this meta-analysis; first, we onlyincluded readily accessible published articles, while abstracts,proceedings or internal reports were not considered, being notnecessarily peer reviewed, and this might represent some biaslinked to publication policies. The second limitation is thatinsulin formulations and insulin combinations were several
(Table 1); in spite of this, multiple comparisons within singlestudies were only two [14,32], while in all remaining studiesonly two formulations/combinations at a time were compared.Another limitation is the paucity of studies directly comparingdetemir and glargine; as a matter of fact, we only found twostudies [44,53]; in the first study, detemir was associated withless weight gain than glargine when administered once daily,not when administered twice daily; in the second study, detemirwas associated with less weight gain than glargine; with onlytwo studies we did not think it was wise to state a differencebetween detemir and glargine. In a recent meta-analysis [61],similar conclusions were reached however based only on thefirst study. In adddition, as recently reported in a meta-analysison insulin analogues in type 1 diabetes [62], only 5 out of 49studies were double-blind, double-dummy; we could find onlyone double-blind study [22] out of 46 in type 2 diabetes, andopen-label studies are a possibile source of bias; in the future,more double-blind studies should by carried out. Finally, thestudies considered did not report, lasting up to 1 year, eventsor behaviour of long-term complications of diabetes.
In conclusion, increase in body weight seems an obligateeffect of intensified insulin treatment in type 2 diabetes, can bequantified in an average annual increase of 4.3 ± 2.74 kg (95%CI 4.32–4.38), and correlates with intensity of treatment. Basalregimens seem to yield a reduced increase in comparison withtwice-a-day or prandial regimens.
Conflict of InterestA. E. P. carried out design, data collection, analysis and writingof manuscript. L. M. conducted data collection, analysis andwrote the manuscript. A. M. did designing, data collection,analysis and manuscript writing.
A. E. P., L. M. and A. M. have no conflict of interests withthe contents of this article.
References1. Lasserson DS, Glasziou P, Perera R et al. Optimal insulin regimens in type
2 diabetes mellitus: systematic review and meta-analyses. Diabetologia2009; 52: 1990–2000.
2. Philis-Tsimikas A. An update on the use of insulin detemir, with a focuson type 2 diabetes (drug evaluation update). Expert Opin Pharmacother2008; 9: 2181–2195.
3. Bazzano LA, Lee LJ, Shi L et al. Safety and efficacy of glargine comparedwith NPH insulin for the treatment of type 2 diabetes: a meta-analysis ofrandomized controlled trials. Diabet Med 2008; 25: 924–932.
4. Caballero AE. Long-term benefits of insulin therapy and glycemic controlin overweight and obese adults with type 2 diabetes. J DiabetesComplications 2009; 23: 143–152.
5. Rosenstock J, Dailey G, Massi-Benedetti M et al. Reduced hypoglycemiarisk with insulin glargine: a meta-analysis comparing insulin glargine withhuman NPH insulin in type 2 diabetes. Diabetes Care 2005; 28: 950–955.
6. Duckworth W, Davis SN. Comparison of insulin glargine and NPH insulin inthe treatment of type 2 diabetes: a review of clinical studies. J DiabetesComplications 2007; 21: 196–204.
7. Horvath K, Jeitler K, Berghold A et al. Long-acting insulin analogues versusNPH insulin (human isophane insulin) for type 2 diabetes mellitus.Cochrane Database Syst Rev 2007; 2: CD005613.
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1017

original article DIABETES, OBESITY AND METABOLISM
8. Paterson KR, Wilson M, Kesson CM et al. Comparison of basal and prandialinsulin therapy in patients with secondary failure of sulphonylurea therapy.Diabetes Med 1991; 8: 40–43.
9. Landstedt-Hallin L, Adamson U, Arner P et al. Comparison of bedtime NPHor preprandial regular insulin combined with glibenclamide in secondarysulfonylurea failure. Diabetes Care 1995; 18: 1183–1186.
10. Makimattila S, Nikkila K, Yki-Jarvinen H. Causes of weight gain duringinsulin therapy with and without metformin in patients with Type IIdiabetes mellitus. Diabetologia 1999; 42: 406–412.
11. Bastyr EJ III, Stuart CA, Brodows RG, et al. Therapy focused on loweringpostprandial glucose, not fasting glucose, may be superior for loweringHbA1c. IOEZ Study Group. Diabetes Care 2000; 23: 1236–1241.
12. Yki-Jarvinen H, Dressler A, Ziemen M. Less nocturnal hypoglycemia andbetter post-dinner glucose control with bedtime insulin glargine comparedwith bedtime NPH insulin during insulin combination therapy in type2 diabetes. HOE 901/3002 Study Group. Diabetes Care 2000; 23:1130–1136.
13. Rosenstock J, Schwartz SL, Clark CM Jr, et al. Basal insulin therapy in type2 diabetes: 28-week comparison of insulin glargine (HOE 901) and NPHinsulin. Diabetes Care 2001; 24: 631–636.
14. Altuntas Y, Ozen B, Ozturk B et al. Comparison of additional metforminor NPH insulin to mealtime insulin lispro therapy with mealtime humaninsulin therapy in secondary OAD failure. Diabetes Obes Metab 2003; 5:371–378.
15. Fritsche A, Schweitzer MA, Haring HU. 4001 Study Group. Glimepiridecombined with morning insulin glargine, bedtime neutral protaminehagedorn insulin, or bedtime insulin glargine in patients with type 2diabetes. A randomized, controlled trial. Ann Intern Med 2003; 138:952–959.
16. Riddle MC, Rosenstock J, Gerich J. Insulin Glargine 4002 Study Investigators.The treat-to-target trial: randomized addition of glargine or human NPHinsulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003; 26:3080–3086.
17. Sargin H, Sargin M, Altuntas Y et al. Comparison of lunch and bedtimeNPH insulin plus mealtime insulin Lispro therapy with premeal regularinsulin plus bedtime NPH insulin therapy in type 2 diabetes. Diabetes ResClin Pract 2003; 62: 79–86.
18. Stehouwer MH, DeVries JH, Lumeij JA et al. Combined bedtime insulin–daytime sulphonylurea regimen compared with two different daily insulinregimens in type 2 diabetes: effects on HbA1c and hypoglycaemia rate–arandomised trial. Diabetes Metab Res Rev 2003; 19: 148–152.
19. Hendra TJ, Taylor CD. A randomised trial of insulin on well-being and carerstrain in elderly type 2 diabetic subjects. J Diabetes Complications 2004;18: 148–154.
20. Malone JK, Kerr LF, Campaigne BN et al. Lispro Mixture-Glargine StudyGroup. Combined therapy with insulin lispro Mix 75/25 plus metforminor insulin glargine plus metformin: a 16-week, randomized, open-label,crossover study in patients with type 2 diabetes beginning insulin therapy.Clin Ther 2004; 26: 2034–2044.
21. Raslova K, Bogoev M, Raz I et al. Insulin detemir and insulin aspart: apromising basal-bolus regimen for type 2 diabetes. Diabetes Res ClinPract 2004; 66: 193–201.
22. Douek IF, Allen SE, Ewings P et al. Metformin Trial Group. Continuingmetformin when starting insulin in patients with type 2 diabetes: adouble-blind randomized placebo-controlled trial. Diabetic Med 2005; 22:634–640.
23. Janka HU, Plewe G, Busch K. Combination of oral antidiabetic agents withbasal insulin versus premixed insulin alone in randomized elderly patientswith type 2 diabetes mellitus. J Am Geriatr Soc 2007; 55: 182–188.
24. Malone JK, Bai S, Campaigne BN et al. Twice-daily pre-mixed insulin ratherthan basal insulin therapy alone results in better overall glycaemic controlin patients with Type 2 diabetes. Diabetes Med 2005; 22: 374–381.
25. Raskin P, Allen E, Hollander P et al. INITIATE Study Group. Initiating insulintherapy in type 2 Diabetes: a comparison of biphasic and basal insulinanalogs. Diabetes Care 2005; 28: 260–265.
26. Hermansen K, Davies M, Derezinski T et al. A 26-week, randomized,parallel, treat-to-target trial comparing insulin detemir with NPH insulinas add-on therapy to oral glucose-lowering drugs in insulin-naive peoplewith type 2 diabetes. Diabetes Care 2006; 29: 1269–1274.
27. Jacober SJ, Scism-Bacon JL, Zagar AJ. A comparison of intensive mixturetherapy with basal insulin therapy in insulin-naıve patients with type 2diabetes receiving oral antidiabetes agents. Diabetes Obes Metab 2006;8: 448–455.
28. Kazda C, Hulstrunk H, Helsberg K et al. Prandial insulin substitution withinsulin lispro or insulin lispro mid mixture vs. basal therapy with insulinglargine: a randomized controlled trial in patients with type 2 diabetesbeginning insulin therapy. J Diabetes Complications 2006; 20: 145–152.
29. Yki-Jarvinen H, Kauppinen-Makelin R, Tiikkainen M et al. Insulin glargineor NPH combined with metformin in type 2 diabetes: the LANMET study.Diabetologia 2006; 49: 442–451.
30. Bebakar WM, Chow CC, Kadir KA et al. BIAsp-3021 study group. Addingbiphasic insulin aspart 30 once or twice daily is more efficacious thanoptimizing oral antidiabetic treatment in patients with type 2 diabetes.Diabetes Obes Metab 2007; 9: 724–732.
31. Ceriello A, Del Prato S, Bue-Valleskey J et al. Premeal insulin lispro plusbedtime NPH or twice-daily NPH in patients with type 2 diabetes: acutepostprandial and chronic effects on glycemic control and cardiovascularrisk factors. J Diabetes Complications 2007; 21: 20–27.
32. Holman RR, Thorne KI, Farmer AJ et al. 4-T Study Group. Addition ofbiphasic, prandial, or basal insulin to oral therapy in type 2 diabetes.N Engl J Med 2007; 357: 1716–1730.
33. Janka HU, Plewe G, Riddle MC et al. Comparison of basal insulin added tooral agents versus twice-daily premixed insulin as initial insulin therapyfor type 2 diabetes. Diabetes Care 2005; 28: 254–259.
34. Raskin PR, Hollander PA, Lewin A et al. on behalf of the INITIATE StudyGroup. Basal insulin or premix analogue therapy in type 2 diabetespatients. Eur J Intern Med 2007; 18: 56–62.
35. Robbins DC, Beisswenger PJ, Ceriello A et al. Mealtime 50/50 basal +prandial insulin analogue mixture with a basal insulin analogue, both plusmetformin, in the achievement of target HbA1c and pre- and postprandialblood glucose levels in patients with type 2 diabetes: a multinational,24-week, randomized, open-label, parallel-group comparison. Clin Ther2007; 29: 2349–2364.
36. Wang XL, Lu JM, Pan CY et al. Evaluation of the superiority of insulinglargine as basal insulin replacement by continuous glucose monitoringsystem. Diabetes Res Clin Pract 2007; 76: 30–36.
37. Yamada S, Watanabe M, Kitaoka A et al. Switching from premixed humaninsulin to premixed insulin lispro: a prospective study comparing theeffects on glucose control and quality of life. Intern Med 2007; 46:1513–1517.
38. Barratt R, Frost G, Millward DJ et al. A randomised controlled trialinvestigating the effect of an intensive lifestyle intervention v. standardcare in adults with type 2 diabetes immediately after initiating insulintherapy. Br J Nutr 2008; 99: 1025–1031.
39. Bretzel RG, Nuber U, Landgraf W et al. Once-daily basal insulin glargineversus thrice-daily prandial insulin lispro in people with type 2 diabeteson oral hypoglycaemic agents (APOLLO): an open randomised controlledtrial. Lancet 2008; 371: 1073–1084.
40. Esposito K, Ciotola M, Maiorino MI et al. Addition of neutral protaminelispro insulin or insulin glargine to oral type 2 diabetes regimens for
1018 Pontiroli et al. Volume 13 No. 11 November 2011

DIABETES, OBESITY AND METABOLISM original articlepatients with suboptimal glycemic control: a randomized trial. Ann InternMed 2008; 149: 531–539.
41. Hirao K, Arai K, Yamauchi M et al. Japan Diabetes Clinical Data Manage-ment Study Group. Six-month multicentric, open-label, randomized trialof twice-daily injections of biphasic insulin aspart 30 versus multiple dailyinjections of insulin aspart in Japanese type 2 diabetic patients (JDDM 11).Diabetes Res Clin Pract 2008; 79: 171–176.
42. Lankisch MR, Ferlinz KC, Leahy JL et al. Orals Plus Apidra and LANTUS(OPAL) study group. Introducing a simplified approach to insulin therapyin type 2 diabetes: a comparison of two single-dose regimens of insulinglulisine plus insulin glargine and oral antidiabetic drugs. Diabetes ObesMetab 2008; 10: 1178–1185.
43. Rosenstock J, Ahmann AJ, Colon G et al. Advancing insulin therapy in type2 diabetes previously treated with glargine plus oral agents: prandialpremixed (insulin lispro protamine suspension/lispro) versus basal/bolus(glargine/lispro) therapy. Diabetes Care 2008; 31: 20–25.
44. Rosenstock J, Davies M, Home PD et al. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine whenadministered as add-on to glucose-lowering drugs in insulin-naive peoplewith type 2 diabetes. Diabetologia 2008; 51: 408–416.
45. Yang W, Ji Q, Zhu D, Yang J et al. Biphasic insulin aspart 30 three timesdaily is more effective than a twice-daily regimen, without increasinghypoglycemia, in Chinese subjects with type 2 diabetes inadequatelycontrolled on oral antidiabetes drugs. Diabetes Care 2008; 31:852–856.
46. Blonde L, Merilainen M, Karwe V et al. TITRATE Study Group. Patient-directed titration for achieving glycaemic goals using a once-dailybasal insulin analogue: an assessment of two different fasting plasmaglucose targets - the TITRATE study. Diabetes Obes Metab 2009; 11:623–631.
47. Buse JB, Wolffenbuttel BH, Herman WH et al. DURAbility of basal versuslispro mix 75/25 insulin efficacy (DURABLE) trial 24-week results: safetyand efficacy of insulin lispro mix 75/25 versus insulin glargine added tooral antihyperglycemic drugs in patients with type 2 diabetes. DiabetesCare 2009; 32: 1007–1013.
48. Liebl A, Prager R, Binz K et al. PREFER Study Group. Comparison of insulinanalogue regimens in people with type 2 diabetes mellitus in the PREFERStudy: a randomized controlled trial. Diabetes Obes Metab 2009; 11:45–52.
49. Milicevic Z, Hancu N, Car N et al. Effect of two starting insulin regimensin patients with type II diabetes not controlled on a combination of oralantihyperglycemic medications. Exp Clin Endocrinol Diabetes 2009; 117:223–229.
50. Wolffenbuttel BH, Klaff LJ, Bhushan R et al. Initiating insulin therapy inelderly patients with Type 2 diabetes: efficacy and safety of lispro mix25 vs. basal insulin combined with oral glucose-lowering agents. DiabeticMed 2009; 26: 1147–1155.
51. Fritsche A, Larbig M, Owens D et al. GINGER study group. Comparisonbetween a basal-bolus and a premixed insulin regimen in individuals withtype 2 diabetes-results of the GINGER study. Diabetes Obes Metab 2010;12: 115–123.
52. Heise T, Mathieu C, Hey-Hadavi J et al. Glycemic control with preprandialversus basal insulin in patients with type 2 diabetes mellitus poorlycontrolled by oral antidiabetes agents. Diabetes Technol Ther 2010; 12:135–141.
53. Swinnen SG, Dain MP, Aronson R et al. A 24-week, randomized, treat-to-target trial comparing initiation of insulin glargine once-daily withinsulin detemir twice-daily in patients with type 2 diabetes inadequatelycontrolled on oral glucose-lowering drugs. Diabetes Care 2010; 33:1176–1178.
54. Jadad AR, Moore RA, Carroll D et al. Assessing the quality of reports ofrandomized clinical trials: is blinding necessary? Control Clin Trials 1996;17: 1–12.
55. Moher D, Liberati A, Tetzlaff J, Altman DG, Group PRISMA. Preferredreporting items for systematic reviews and meta-analyses: the PRISMAstatement. PLoS Med 2009; 6: e1000097.
56. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials1986; 7: 177–188.
57. Yki-Jarvinen H. Combination therapies with insulin in type 2 diabetes.Diabetes Care 2001; 24: 758–767.
58. Holman RR, Farmer AJ, Davies MJ et al. 4-T Study Group. Three-yearefficacy of complex insulin regimens in type 2 diabetes. N Engl J Med2009; 361: 1736–1747.
59. Qayyum R, Bolen S, Maruthur N et al. Systematic review: comparativeeffectiveness and safety of premixed insulin analogues in type 2 diabetes.Ann Intern Med 2008; 149: 549–559.
60. Monami M, Marchionni N, Mannucci E. Long-acting insulin analoguesversus NPH human insulin in type 2 diabetes: a meta-analysis. DiabetesRes Clin Pract 2008; 81: 184–189.
61. Waugh N, Cummins E, Royle P et al. Newer agents for blood glucosecontrol in type 2 diabetes: systematic review and economic evaluation.Health Technol Assess 2010; 14: 1–248.
62. Jacobsen IB, Henriksen JE, Hother-Nielsen O et al. Evidence-based insulintreatment in type 1 diabetes mellitus. Diabetes Res Clin Pract 2009; 86:1–10.
Volume 13 No. 11 November 2011 doi:10.1111/j.1463-1326.2011.01433.x 1019





![Intensive insulin therapy does not alter the inflammatory response in patients undergoing coronary artery bypass grafting: a randomized controlled trial [ISRCTN95608630]](https://static.fdokumen.com/doc/165x107/63353f6925325924170073d5/intensive-insulin-therapy-does-not-alter-the-inflammatory-response-in-patients-undergoing.jpg)