Improvement of Physical Health and Quality of Life of Alcohol-Dependent Individuals With Topiramate...
12
ORIGINAL INVESTIGATION Improvement of Physical Health and Quality of Life of Alcohol-Dependent Individuals With Topiramate Treatment US Multisite Randomized Controlled Trial Bankole A. Johnson, DSc, MD, PhD, MPhil, FRCPsych; Norman Rosenthal, MD; Julie A. Capece, BA; Frank Wiegand, MD; Lian Mao, PhD; Karen Beyers, MS; Amy McKay, PharmD; Nassima Ait-Daoud, MD; Giovanni Addolorato, MD; Raymond F. Anton, MD; Domenic A. Ciraulo, MD; Henry R. Kranzler, MD; Karl Mann, MD; Stephanie S. O’Malley, PhD; Robert M. Swift, MD, PhD; for the Topiramate for Alcoholism Advisory Board and the Topiramate for Alcoholism Study Group Background: Topiramate can improve drinking out- comes via a hypothesized mechanism of facilitating - aminobutyric acid function and inhibiting glutaminer- gic pathways in the corticomesolimbic system. We sought to determine whether topiramate’s antidrinking effects are bolstered by improvements in physical and psycho- social well-being. Methods: In a 17-site, 14-week, double-blind, random- ized controlled trial, we compared the effects of topira- mate (up to 300 mg/d) vs placebo on physical health, ob- sessional thoughts and compulsions about using alcohol, and psychosocial well-being among 371 alcohol- dependent subjects who received weekly adherence en- hancement therapy. Results: Topiramate was more efficacious than pla- cebo in reducing body mass index (calculated as weight in kilograms divided by height in meters squared) (mean difference, 1.08; 95% confidence interval [CI], 0.81- 1.34; P .001), all liver enzyme levels (P .01 for all com- parisons), plasma cholesterol level (mean difference, 13.30 mg/dL; 95% CI, 5.09-21.44 mg/dL; P =.002), and sys- tolic (mean difference, 9.70 mm Hg; 95% CI, 6.81- 12.60 mm Hg; P .001) and diastolic (mean difference, 6.74 mm Hg; 95% CI, 4.57-8.90 mm Hg; P .001) blood pressure to about prehypertension levels—effects that might lower the risk of fatty liver degeneration and cir- rhosis as well as cardiovascular disease. Topiramate com- pared with placebo significantly (P .05 for all compari- sons) decreased obsessional thoughts and compulsions about using alcohol, increased subjects’ psychosocial well- being, and improved some aspects of quality of life, thereby diminishing the risk of relapse and longer-term nega- tive outcomes. Paresthesia, taste perversion, anorexia, and difficulty with concentration were reported more fre- quently for topiramate than for placebo. Conclusion: Topiramate appears to be generally effec- tive at improving the drinking outcomes and physical and psychosocial well-being of alcoholic subjects. Trial Registration: clinicaltrials.gov Identifier: NCT00210925 Arch Intern Med. 2008;168(11):1188-1199 A LCOHOLISM IS A COMMON disease. 1 Notwithstand- ing the primary aberra- tion in drinking behavior, its extensive secondary physical and psychosocial consequences 2 are what make the burden of the disease so devastating. This realization is en- shrined in practice in that no commonly used diagnostic scheme for alcoholism or alcohol dependence includes a quantifi- cation of drinking behavior—only its physical and psychosocial sequelae. Epi- demiologically, these sequelae of alcohol- ism are manifested in the statistic that al- coholism as a risk factor ranks fifth on the global burden of disease. 3 Topiramate, a sulfamate-substituted fructopyranose derivative, has been shown to decrease the primary aberration of ex- cessive drinking by reducing the reinforc- ing effects of alcohol, 4 presumably through 2 pharmacologic mechanisms: the con- temporaneous facilitation of -aminobu- tyric acid function through a nonbenzo- diazepine site on the -aminobutyric acid–A receptor 5 and the antagonism of glutamate activity at -amino-3-hydroxy- 5-methylisoxazole-4-propionic acid and kainate receptors. 4 Indeed, the results of 2 recent clinical trials have demonstrated topiramate’s ef- ficacy at improving drinking outcomes. First, in a single-site, double-blind ran- Author Affiliations are listed at the end of this article. Group Information: The members of the Topiramate for Alcoholism Advisory Board and the Topiramate for Alcoholism Study Group are listed on page 1198. (REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM 1188 ©2008 American Medical Association. All rights reserved. Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Improvement of Physical Health and Quality of Life of Alcohol-Dependent Individuals With Topiramate...

ORIGINAL INVESTIGATION
Improvement of Physical Healthand Quality of Life of Alcohol-DependentIndividuals With Topiramate Treatment
US Multisite Randomized Controlled Trial
Bankole A. Johnson, DSc, MD, PhD, MPhil, FRCPsych; Norman Rosenthal, MD; Julie A. Capece, BA;Frank Wiegand, MD; Lian Mao, PhD; Karen Beyers, MS; Amy McKay, PharmD; Nassima Ait-Daoud, MD;Giovanni Addolorato, MD; Raymond F. Anton, MD; Domenic A. Ciraulo, MD; Henry R. Kranzler, MD;Karl Mann, MD; Stephanie S. O’Malley, PhD; Robert M. Swift, MD, PhD; for the Topiramate for AlcoholismAdvisory Board and the Topiramate for Alcoholism Study Group
Background: Topiramate can improve drinking out-comes via a hypothesized mechanism of facilitating �-aminobutyric acid function and inhibiting glutaminer-gic pathways in the corticomesolimbic system. We soughtto determine whether topiramate’s antidrinking effectsare bolstered by improvements in physical and psycho-social well-being.
Methods: In a 17-site, 14-week, double-blind, random-ized controlled trial, we compared the effects of topira-mate (up to 300 mg/d) vs placebo on physical health, ob-sessional thoughts and compulsions about using alcohol,and psychosocial well-being among 371 alcohol-dependent subjects who received weekly adherence en-hancement therapy.
Results: Topiramate was more efficacious than pla-cebo in reducing body mass index (calculated as weightin kilograms divided by height in meters squared) (meandifference, 1.08; 95% confidence interval [CI], 0.81-1.34; P� .001), all liver enzyme levels (P� .01 for all com-parisons), plasma cholesterol level (mean difference, 13.30mg/dL; 95% CI, 5.09-21.44 mg/dL; P=.002), and sys-
tolic (mean difference, 9.70 mm Hg; 95% CI, 6.81-12.60 mm Hg; P� .001) and diastolic (mean difference,6.74 mm Hg; 95% CI, 4.57-8.90 mm Hg; P� .001) bloodpressure to about prehypertension levels—effects thatmight lower the risk of fatty liver degeneration and cir-rhosis as well as cardiovascular disease. Topiramate com-pared with placebo significantly (P� .05 for all compari-sons) decreased obsessional thoughts and compulsionsabout using alcohol, increased subjects’ psychosocial well-being, and improved some aspects of quality of life, therebydiminishing the risk of relapse and longer-term nega-tive outcomes. Paresthesia, taste perversion, anorexia, anddifficulty with concentration were reported more fre-quently for topiramate than for placebo.
Conclusion: Topiramate appears to be generally effec-tive at improving the drinking outcomes and physical andpsychosocial well-being of alcoholic subjects.
Trial Registration: clinicaltrials.gov Identifier:NCT00210925
Arch Intern Med. 2008;168(11):1188-1199
A LCOHOLISM IS A COMMON
disease.1 Notwithstand-ing the primary aberra-tion in drinking behavior,its extensive secondary
physical and psychosocial consequences2
are what make the burden of the diseaseso devastating. This realization is en-shrined in practice in that no commonlyused diagnostic scheme for alcoholism oralcohol dependence includes a quantifi-cation of drinking behavior—only itsphysical and psychosocial sequelae. Epi-demiologically, these sequelae of alcohol-ism are manifested in the statistic that al-coholism as a risk factor ranks fifth on theglobal burden of disease.3
Topiramate, a sulfamate-substitutedfructopyranose derivative, has been shownto decrease the primary aberration of ex-cessive drinking by reducing the reinforc-ing effects of alcohol,4 presumably through2 pharmacologic mechanisms: the con-temporaneous facilitation of �-aminobu-tyric acid function through a nonbenzo-diazepine site on the �-aminobutyricacid–A receptor5 and the antagonism ofglutamate activity at �-amino-3-hydroxy-5-methylisoxazole-4-propionic acid andkainate receptors.4
Indeed, the results of 2 recent clinicaltrials have demonstrated topiramate’s ef-ficacy at improving drinking outcomes.First, in a single-site, double-blind ran-
Author Affiliations are listed atthe end of this article.Group Information: Themembers of the Topiramate forAlcoholism Advisory Board andthe Topiramate for AlcoholismStudy Group are listed onpage 1198.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1188
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

domized controlled trial, topiramate was shown to be moreefficacious than placebo at decreasing heavy drinking andpromoting abstinence from alcohol.6 Second, in a sub-sequent 17-site, double-blind randomized controlled trial,topiramate again was shown to improve drinking out-comes and promote abstinence.7 In both the single-siteand multisite trials, topiramate’s estimated therapeuticeffect size at reducing heavy drinking was in the me-dium range (0.61 and 0.52, respectively), and in the mul-tisite trial, the number of participants who would needto be treated with topiramate to have 1 additional suc-cess compared with placebo in reducing heavy drinkingdays was 3.4.8 Thus, topiramate appears to be a promis-ing medication for the treatment of alcohol dependence.
Nevertheless, to establish topiramate as being gener-ally effective for the treatment of alcohol dependencewould require a demonstration that it can reduce or at-tenuate the important physical and psychosocial conse-quences that are common among those with a pattern ofsevere, chronic, and pervasive alcohol consumption.
Physically, perhaps the best known sequelae of alco-hol dependence seen in general medical practice in-clude abnormalities of liver function (eg, elevated liverenzyme levels, fatty liver disease, and eventually liver cir-rhosis) and cardiovascular disease due to hypertensionand elevated cholesterol levels.9
Psychosocially, the sequelae of alcohol dependence in-clude persistent obsessional thoughts and compulsionsabout using alcohol that can maintain or provoke relapseto heavy drinking10 and increased social disenfranchise-ment due to reduced capability to maintain school, work,and interpersonal relationships. All of these sequelae of al-coholism contribute to decreased quality of life.11
Herein, we seek to determine whether topiramate isgenerally effective as a treatment for alcohol depen-dence that not only improves the “symptom” of drink-ing but also alleviates its important physical and psycho-social consequences.
METHODS
SUBJECTS
We enrolled 371 men and women who had been diagnosed ashaving alcohol dependence according to the Diagnostic and Sta-tistical Manual of Mental Disorders (Fourth Edition) (DSM-IV).12
Subjects were recruited across 17 sites in the United States be-tween January 27, 2004, and August 4, 2006, by newspaper,radio, and television advertisements.
We included male and female subjects between the ages of18 and 65 years who drank 35 or more (men) and 28 or more(women) standard drinks per week, as measured by the time-line follow-back method,13 during the 28-day period before thescreening visit to assess study eligibility and during the 7-dayperiod between the screening visit and randomization. One stan-dard drink was defined as 14.8 mL of absolute alcohol, equiva-lent to 295.7 mL of beer, 118.3 mL of wine, or 29.6 mL of 100-proof liquor. Also, subjects had to have negative results of urinetoxicologic screening for opioids, cocaine, amphetamines, an-tidepressants, propoxyphenes, and barbiturates at the time ofrandomization and before the beginning of the double-blindperiod in week 0. Participants with positive results of the urinedrug screening for tetrahydrocannabinol or benzodiazepines
in the week before randomization (week −1) could be en-rolled if they had negative results of urine drug screening onretesting 7 days later and met all other enrollment criteria. Ad-ditional inclusion criteria were as described previously.7
We excluded subjects who had a current Axis I psychiatricdiagnosis according to the DSM-IV other than alcohol, nico-tine, or caffeine dependence; had a history in the past 6 monthsof substance abuse or dependence, not including dependenceon alcohol, nicotine, or caffeine; had clinically significant al-cohol withdrawal symptoms (revised Clinical Institute With-drawal Assessment for Alcohol scale14 score �10); had mademore than 4 unsuccessful formal inpatient treatment attemptsto curb alcohol dependence; had clinically significant depres-sion, which was defined as a score of greater than 24 on theMontgomery-Asberg Depression Rating Scale15 or based on theimpression of a study physician; were receiving treatment foralcohol dependence other than Alcoholics Anonymous; had beencompelled to receive treatment for alcohol dependence to avoidimprisonment, parole, probation, or loss of employment; or werefrom the same household as another study participant. Addi-tional exclusion criteria were as described previously.7
Ethical approval for this study was provided by the insti-tutional review boards of all 17 participating sites.
ASSESSMENTS
At screening, the beginning of week −1 (approximately 7 daysbefore randomization), after obtaining written informed con-sent, we assessed participants on medical eligibility to meet thestudy inclusion criteria. Subjects returned for a separate visit atthe end of week −1 to complete the remainder of the screeningprocess, which included assessment of physical health as mea-sured by physical examination, electrocardiogram, vital signs (ie,blood pressure, pulse, and temperature), body mass index (BMI)(calculated as weight in kilograms divided by height in meterssquared), hematologic and biochemical screens (including plasmacholesterol), urine tests (including urine drug screen), and a urinepregnancy test for women of childbearing potential; and per-sonal and psychosocial harm from alcohol as measured by theAlcohol Use Disorders Identification Test.16 Subjects were not al-lowed to provide written informed consent unless they had a breathalcohol concentration less than 0.02 g%.
During the double-blind period from weeks 0 to 14, subjectswere assessed weekly on measures of vital signs (ie, blood pres-sure, pulse, and temperature) and BMI. At weeks 0, 4, 8, 12, and14, we assessed overall clinical improvement as measured by Clini-cal Global Impression scales for improvement and severity (CGI-Iand CGI-S, respectively)17; obsessional thoughts and compul-sions about using alcohol on the Obsessive Compulsive Drink-ing Scale (OCDS)18; and liver enzyme levels (alanine aminotrans-ferase, aspartate aminotransferase, and �-glutamyltransferase) toprovide an objective biochemical measure of alcohol consump-tion.19 Plasma �-glutamyltransferase level is well validated andaccepted widely as a biomarker of alcohol consumption. Our useof plasma �-glutamyltransferase as a biochemical measure of tran-sient alcohol consumption in this study also was designed to mir-ror what Johnson et al6 did in the previous single-site pharma-cotherapy trial of topiramate for treating alcohol dependence.Hematologic and biochemical screens, including urine preg-nancy tests, were repeated at weeks 0, 4, 8, 10, 12, and 14. Atweeks 0, 6, 10, and 14 we assessed the harmful consequences ofdrinking (Drinker Inventory of Consequences scale, Recent Con-sequences form [DrInC-2R]),20 general mood (Profile of MoodStates),21 sleep quality (Medical Outcomes Study Sleep scale),22
and quality of life (Quality of Life Enjoyment and SatisfactionQuestionnaire [Q-LES-Q]).23 Additional health and safety mea-sures included assessments of adverse events, concomitant medi-
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1189
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

cations, and breath alcohol concentration on a weekly basis anda second electrocardiogram and physical examination at the endof the trial. Subjects were not allowed to complete assess-ments during the double-blind period unless they had a breathalcohol concentration less than 0.02 g%.
PROCEDURES
Study procedures were as detailed previously.7 Briefly, sub-jects who continued to meet drinking eligibility criteria afterthe 7-day screening period were assigned at random in a 1:1ratio to receive topiramate or placebo. Study medication wasdispensed in double-blind fashion for the efficacy determina-tion period from the beginning of week 0 to the beginning ofweek 14. The medication dose was titrated from the begin-ning of week 0 to the beginning of week 6 and then main-tained until the beginning of week 14 (Table 1). All subjectshad to achieve a minimum topiramate dosage of 50 mg/d orthe placebo equivalent to remain in the trial. From weeks 14to 16, study medication was tapered as a safety precaution. Topi-ramate and matching placebo tablets were provided by Ortho-McNeil Janssen Scientific Affairs LLC (Raritan, New Jersey).
All subjects received Brief Behavioral Compliance Enhance-ment Treatment (BBCET) as their psychosocial treatment. TheBBCET program, a standardized, brief (delivered in about 15minutes) psychosocial adherence enhancement procedure, em-phasized that medication adherence is crucial to changing thedrinking behavior of alcohol-dependent individuals.24 Brief in-terventions,25 such as BBCET, have been shown to be benefi-cial in treating alcohol dependence. The BBCET program wasmodeled on the clinical management condition in the US Na-tional Institute of Mental Health collaborative depression trial,which was used as an adjunct to the medication condition forthat study.26 Also, it was used successfully as the psychosocialtreatment platform in the previous efficacy trial of topiramatefor the treatment of alcohol dependence.6 Trained clinicians de-livered manual-guided BBCET during each week of the double-blind period as described previously.7
OUTCOME AND SAFETY MEASURES
Outcome measures of physical health included liver functiontests (ie, plasma aspartate aminotransferase, alanine amino-transferase, and �-glutamyltransferase), hematologic and bio-chemical measures (including plasma cholesterol and bicar-bonate and urine pH levels), vital signs (ie, blood pressure, pulse,and temperature), and BMI.
Outcome measures of psychosocial function included ob-sessional thoughts and compulsions about using alcohol(OCDS), overall clinical improvement (CGI-I and CGI-S scales),
harmful consequences of drinking (DrInC-2R), quality of life(Q-LES-Q), general mood (Profile of Mood States), and sleepquality (Medical Outcomes Study Sleep scale).
Additionalhealthandsafetymeasures includedmeasurementsofadverseevents,concomitantmedications,withdrawalsymptoms,urine pregnancy tests, and physical examinations performed pe-riodically during the trial. An independent data monitoring com-mittee met periodically to ensure the safety of the study subjects.
STATISTICAL ANALYSIS PLAN
General Approaches
We managed the data according to the International Confer-ence on Harmonisation guidelines of good clinical practice. In-dividual plots were checked for unusual values and complete-ness. Efficacy values were validated as correct against case records.For all statistical tests, differences between the treatment groupswere accepted as significant if they achieved the 5% level with2-tailed tests. All efficacy analyses were conducted on the intent-to-treat population, which included all randomized subjects whoreturned for at least 1 double-blind visit and received at least 1dose of the study medication. All safety analyses were con-ducted on the evaluable-for-safety population, which includedall randomized subjects who took at least 1 dose of the studymedication. Data were analyzed with SAS statistical software, ver-sion 9.1 (SAS Institute Inc, Cary, North Carolina).27
The duration of the double-blind phase (ie, weeks 0 to 14)was calculated as the date of the first double-blind dose plus 1day to the date when the last double-blind dose of medicationwas taken but before the 2-week period during which the studymedication was tapered.
Analysis of the Outcome and Safety Measures
The null hypothesis of the study was that there would be no dif-ference between topiramate and placebo on target physical andpsychosocial outcome measures associated with alcohol depen-dence during the double-blind phase. The primary analytic ap-proach was to conduct inferential analysis on all randomized par-ticipants returning for at least 1 double-blind visit and receivingat least 1 medication dose. Unless stated otherwise, we ana-lyzed the difference between the treatment groups by means ofa repeated-measures mixed model (SAS PROC MIXED; SAS In-stitute Inc) with treatment, center, week, baseline measure of theoutcome variable, and treatment�week interaction as covari-ates. An unstructured covariance matrix was used to model thecorrelations between repeated measurements within subjects.Least-squares mean estimators and the 95% confidence inter-vals of the means were derived for each treatment group. Ninety-five percent confidence intervals also were calculated for the meandifference between treatment groups.
We used a fixed-sequence, multiple-testing procedure to con-trol for type 1 error when determining the earliest time point atwhich the difference between treatment groups on an outcomemeasure became significant statistically (based on the repeated-measures model) and was sustained for the subsequent timepoints. The basis of the procedure was to test the between-groups difference on the outcome measure at week 14 at the .05significance level (2-tailed). If there was a significant differenceat week 14, this procedure would be repeated for preceding weeksuntil a time point was reached at which there was no difference.A finding of no significant difference at week 14 would havestopped the comparison for the preceding weeks.
While all the outcome measures of physical health were ana-lyzed as outlined above, plasma �-glutamyltransferase was ex-amined as its incremental log ratio over time as done in the pre-vious study.6
Table 1. Topiramate Dose-Escalation Schedulea
Weeksb AM Dose PM DoseTotal DailyDose, mg
0-1 0 mg 1�25-mg tablet 251-2 1�25-mg tablet 1�25-mg tablet 502-3 2�25-mg tablets 2�25-mg tablets 1003-4 3�25-mg tablets 3�25-mg tablets 1504-5 1�100-mg tablet 1�100-mg tablet 2005-14 1�100-mg tablet 2�100-mg tablets 300
aAdapted from Table 1 in Johnson et al.7 The placebo and topiramategroups received the same number of tablets; placebo tablets were inactive.
bWeeks represent the beginning of one week to the beginning of the next.Study end was the beginning of week 14.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1190
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

Obsessional thoughts and compulsions about using alcohol,as assessed with the OCDS, was measured on the total score andon 4 subscale factors derived empirically by principal compo-nents analysis.28 These factors included Drinking Obsessions (ob-sessional thoughts related to drinking), Automaticity of Drink-ing (the extent to which drinking was controlled or uncontrolled),Interference Due to Drinking (the extent to which drinking in-terfered with work and social functioning and to which being pre-vented from drinking was distressing), and Alcohol Consump-tion (the quantity and frequency of drinking alcohol).
The differences between the topiramate and placebo groupson the ratings for overall clinical improvement (CGI-I andCGI-S) were analyzed with a Cochran-Mantel-Haenszel teststratified by sex and center using modified ridit scores. The CGI-Iwas scored on a 7-point scale ranging from 1 (“very much im-proved”) to 7 (“very much worse”) as a change from the base-line value at randomization and succeeding treatment weeks.The CGI-S is a 7-point scale ranging from 1 (reportedly absti-nent and not seeking alcohol or “not addicted”) to 7 (report-edly drinking more and constantly seeking alcohol or “ex-tremely severely addicted”) that was assessed during eachdouble-blind treatment week. On the CGI-S, an individual with-out a clinically significant addiction was defined as scoring either1 (reportedly abstinent and not seeking alcohol) or 2 (report-edly drinking less and occasionally seeking alcohol); individu-als with higher scores were considered to have a clinically sig-nificant severity of alcohol dependence.
We assessed treatment differences between topiramate and pla-cebo on DrInC-2R by means of the repeated-measures mixedmodel described earlier. The DrInC-2R was assessed on a 4-pointscale ranging from “never” to “daily or almost daily” (0 to 3 points,respectively). It was subdivided further into 6 subscales: Physi-cal Consequences (8 items; maximum score, 24), IntrapersonalConsequences (8 items; maximum score, 24), Social Responsi-bility Consequences (7 items; maximum score, 21), Interper-sonalConsequences (10 items;maximumscore,30), ImpulseCon-trol Consequences (12 items; maximum score, 36), and ControlItems (5 items; maximum score, 15), as well as a Total Conse-quences scale (45 items; maximum score, 135), which was thesum of all subscales other than the Control Items subscale. A lowerscore denoted a decreased adverse consequence of drinking ascompared with a higher score. The Control Items subscale wasthe sum of 5 reverse-scored validity items. Also, over the double-blind treatment period, we examined the correlation between de-creases in DrInC-2R score and percentage of heavy drinking daysmeasured by the timeline follow-back method.
The quality-of-life measure (Q-LES-Q) was categorized aslow and high scores. This categorization was based on the dif-ferent percentiles of the maximum possible scores, ranging fromthe 50th to the 90th. For each study week, if a subject had ascore higher than the given percentile of the maximum score,he or she was designated to have a high score; otherwise, it wasdetermined that the score was low. Pearlstein et al29 suggestedthat a score at the 70th percentile or higher represents a “nor-mal” quality of life. Because we observed that increasingly strin-gent cutoff points demonstrated the contrasts between the treat-ment groups more effectively, we chose the 90th percentile ofthe maximum score as the final discrimination criterion to per-form hypothesis testing. “High” scores were considered to beindicative of improvement. Thus, to analyze the Q-LES-Q, wecalculated the relative likelihood (odds ratios) of topiramatecompared with placebo to achieve the 90th percentile of im-provement in Q-LES-Q subscales at the end of the study usingthe generalized estimating equation method, which accountedfor the correlation of observations within individuals with au-toregressive structure as the correlation matrix, as imple-mented by the SAS PROC GENMOD software (SAS InstituteInc)—the same procedure used in the previous single-site trial.30
The Q-LES-Q was composed of 93 items, each containing re-sponses on a 5-point scale that ranged from 1 (“not at all ornever”) to 5 (“all the time”). Ninety-one of these items weregrouped into 8 summary scales. Five of the 8 summary scaleswere scored for all subjects: physical health (13 items; maxi-mum score, 65), subjective feelings (14 items; maximum score,70), leisure-time activities (6 items; maximum score, 30), so-cial relationships (11 items; maximum score, 55), and generalactivities (14 items; maximum score, 70). The 3 other sum-mary scales were scored only for subjects for whom the activi-ties were applicable: work (13 items; maximum score, 65), house-hold duties (10 items; maximum score, 50), and school/coursework (10 items; maximum score, 50). Two of the 93 items werescored separately as individual items: satisfaction with medi-cation, and overall life satisfaction and contentment.23
Themeasuresofgeneralmood(ProfileofMoodStates)andsleepquality (Medical Outcomes Study Sleep scale) were analyzed bythe general repeated-measures approach described earlier.
To assess the consistency of our statistical inferences to dif-ferent methods for handling missing data due to dropouts, wealso performed a sensitivity analysis that involved reanalyzingall the outcome data after imputing the missing values for drop-outs by means of the multiple imputation method. Multiple im-putation31,32 replaces each missing value with a set of plausiblevalues that represent the uncertainty about the right value toimpute. It draws a random sample of the missing values fromits distribution. The multiple imputed data sets are then ana-lyzed separately by standard procedures for complete data, andthe results are combined to produce the final inference. Thisprocess results in valid statistical inferences that properly re-flect the uncertainty due to missing values, eg, confidence in-tervals with the correct probability coverage. Multiple impu-tation inference involves 3 distinct phases: (1) the missing dataare filled in m times to generate m complete data sets, (2) them complete data sets are analyzed by standard statistical meth-ods, and (3) the results from the m complete data sets are com-bined to produce inferential results. For our application, wegenerated 10 complete data sets (m=5 is usually sufficient). Tocreate a monotone missing data pattern, intermittent missingvalues were imputed by means of the last-observation-carried-forward method. We then used the regression method for mono-tone missing data32 (SAS PROC MI, MONOTONE REG state-ment33) to impute the missing data due to dropouts. We thenperformed the statistical analyses on each complete data set andcombined the 10 analyses to arrive at the final results.
Cohen effect size34 estimates have been provided where ap-propriate for the outcomes.
RESULTS
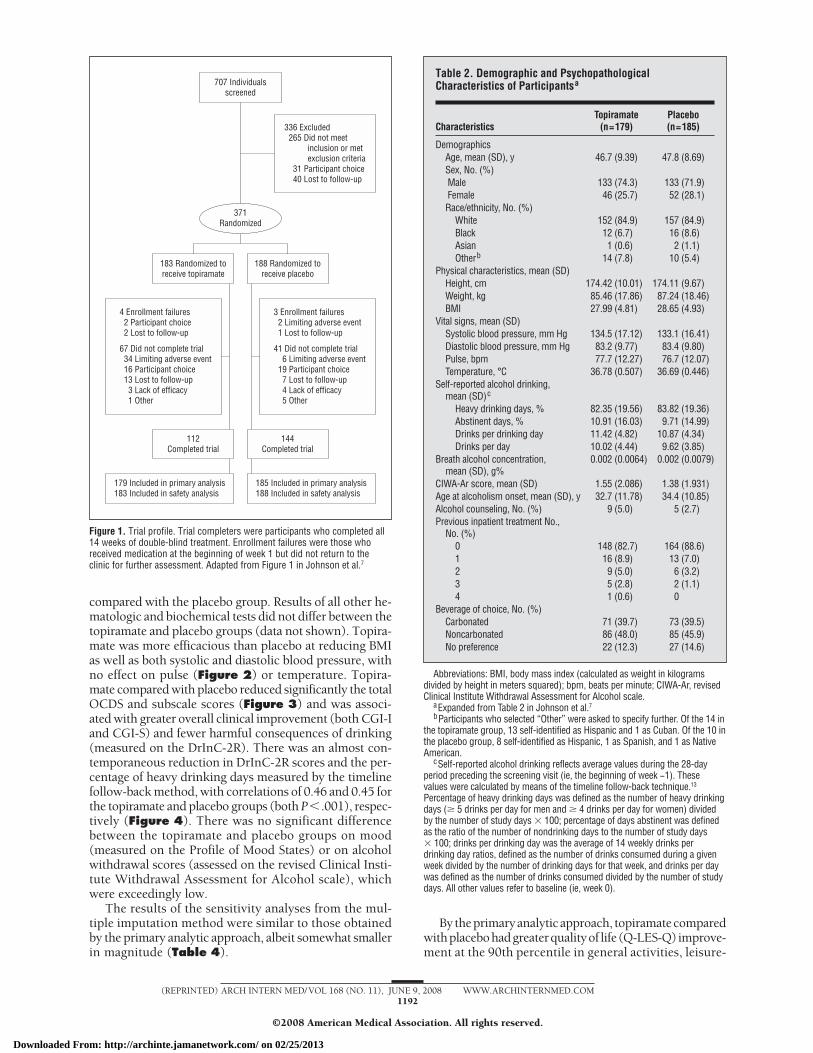
We assigned 183 subjects and 188 subjects (total N=371)at random into the topiramate and placebo groups, re-spectively (Figure 1). The subjects in the topiramateand placebo groups had similar baseline characteristics(Table 2).
By the primary analytic approach, topiramate was moreefficacious than placebo in decreasing all liver function testvalues, including the log plasma �-glutamyltransferase ra-tio, which is the objective marker of alcohol consumption(Table 3). Although plasma bicarbonate levels were sig-nificantly lower for the topiramate group than for the pla-cebo group, this did not require any medical intervention.Urine pH level did not differ significantly between the topi-ramate and placebo groups. There was a significant reduc-tion in plasma cholesterol level for the topiramate group
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1191
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
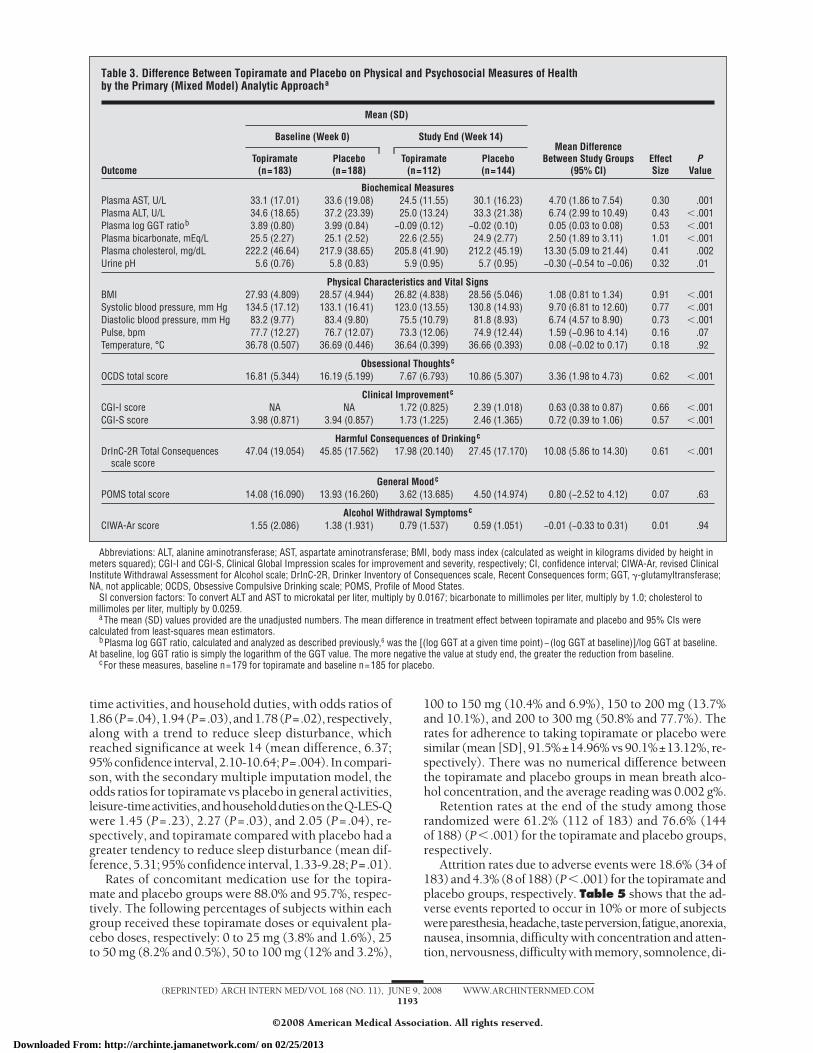
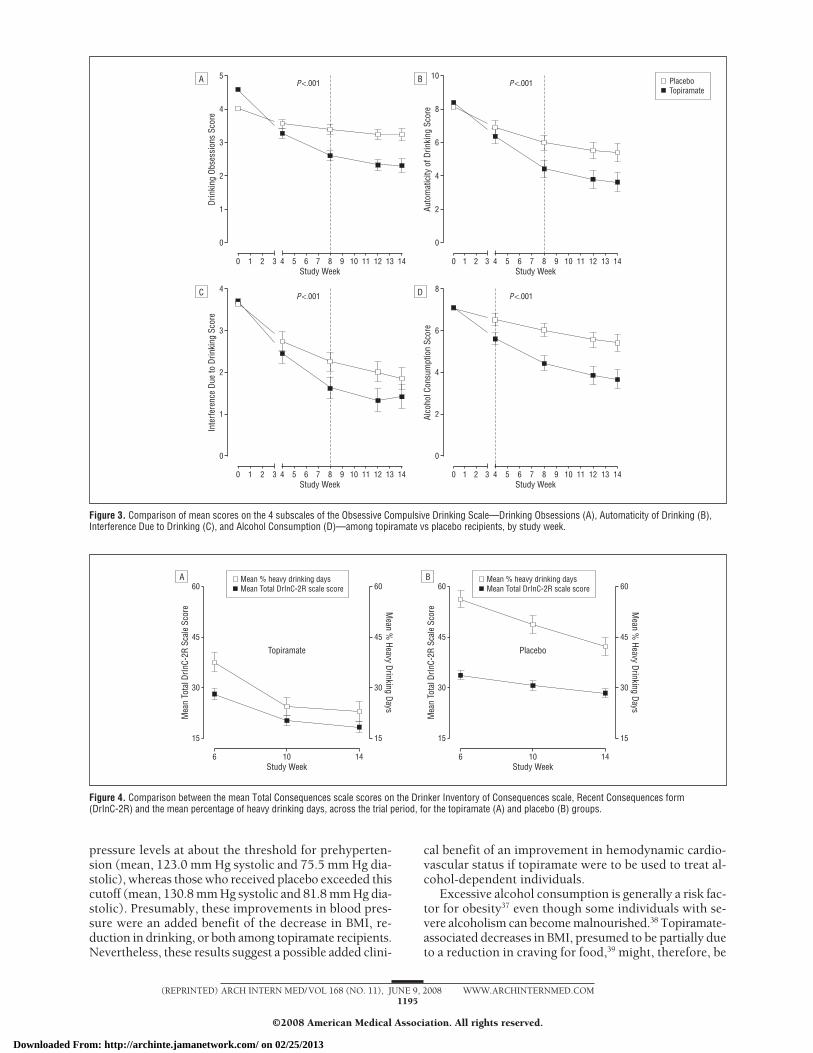
compared with the placebo group. Results of all other he-matologic and biochemical tests did not differ between thetopiramate and placebo groups (data not shown). Topira-mate was more efficacious than placebo at reducing BMIas well as both systolic and diastolic blood pressure, withno effect on pulse (Figure 2) or temperature. Topira-mate compared with placebo reduced significantly the totalOCDS and subscale scores (Figure 3) and was associ-ated with greater overall clinical improvement (both CGI-Iand CGI-S) and fewer harmful consequences of drinking(measured on the DrInC-2R). There was an almost con-temporaneous reduction in DrInC-2R scores and the per-centage of heavy drinking days measured by the timelinefollow-back method, with correlations of 0.46 and 0.45 forthe topiramate and placebo groups (both P�.001), respec-tively (Figure 4). There was no significant differencebetween the topiramate and placebo groups on mood(measured on the Profile of Mood States) or on alcoholwithdrawal scores (assessed on the revised Clinical Insti-tute Withdrawal Assessment for Alcohol scale), whichwere exceedingly low.
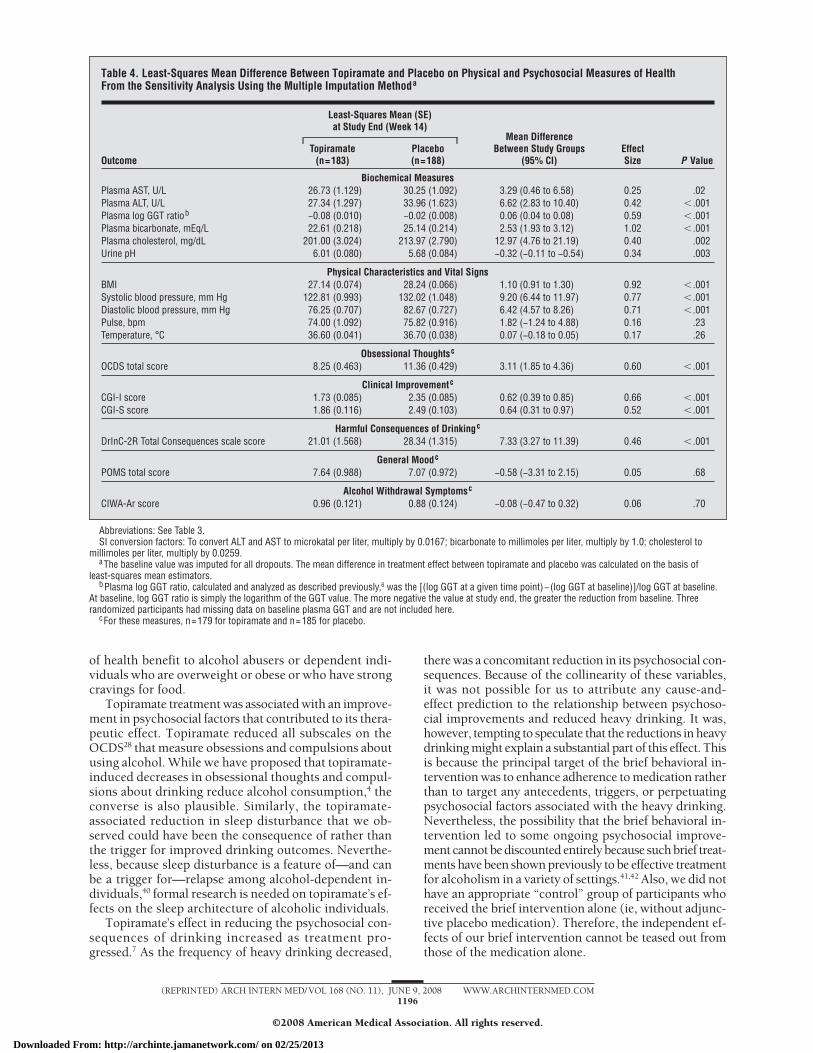
The results of the sensitivity analyses from the mul-tiple imputation method were similar to those obtainedby the primary analytic approach, albeit somewhat smallerin magnitude (Table 4).
By theprimaryanalyticapproach, topiramatecomparedwithplacebohadgreaterqualityof life(Q-LES-Q)improve-ment at the 90th percentile in general activities, leisure-
179 Included in primary analysis183 Included in safety analysis
185 Included in primary analysis188 Included in safety analysis
707 Individualsscreened
183 Randomized toreceive topiramate
188 Randomized toreceive placebo
112Completed trial
144Completed trial
336 Excluded0265 Did not meet000000inclusion or met000000exclusion criteria0031 Participant choice0040 Lost to follow-up
04 Enrollment failures002 Participant choice002 Lost to follow-up
067 Did not complete trial0034 Limiting adverse event0016 Participant choice0013 Lost to follow-up0003 Lack of efficacy0001 Other
03 Enrollment failures002 Limiting adverse event001 Lost to follow-up
041 Did not complete trial0006 Limiting adverse event0019 Participant choice0007 Lost to follow-up0004 Lack of efficacy0005 Other
371Randomized
Figure 1. Trial profile. Trial completers were participants who completed all14 weeks of double-blind treatment. Enrollment failures were those whoreceived medication at the beginning of week 1 but did not return to theclinic for further assessment. Adapted from Figure 1 in Johnson et al.7
Table 2. Demographic and PsychopathologicalCharacteristics of Participantsa
CharacteristicsTopiramate
(n=179)Placebo(n=185)
DemographicsAge, mean (SD), y 46.7 (9.39) 47.8 (8.69)Sex, No. (%)Male 133 (74.3) 133 (71.9)Female 46 (25.7) 52 (28.1)Race/ethnicity, No. (%)
White 152 (84.9) 157 (84.9)Black 12 (6.7) 16 (8.6)Asian 1 (0.6) 2 (1.1)Otherb 14 (7.8) 10 (5.4)
Physical characteristics, mean (SD)Height, cm 174.42 (10.01) 174.11 (9.67)Weight, kg 85.46 (17.86) 87.24 (18.46)BMI 27.99 (4.81) 28.65 (4.93)
Vital signs, mean (SD)Systolic blood pressure, mm Hg 134.5 (17.12) 133.1 (16.41)Diastolic blood pressure, mm Hg 83.2 (9.77) 83.4 (9.80)Pulse, bpm 77.7 (12.27) 76.7 (12.07)Temperature, °C 36.78 (0.507) 36.69 (0.446)
Self-reported alcohol drinking,mean (SD)c
Heavy drinking days, % 82.35 (19.56) 83.82 (19.36)Abstinent days, % 10.91 (16.03) 9.71 (14.99)Drinks per drinking day 11.42 (4.82) 10.87 (4.34)Drinks per day 10.02 (4.44) 9.62 (3.85)
Breath alcohol concentration,mean (SD), g%
0.002 (0.0064) 0.002 (0.0079)
CIWA-Ar score, mean (SD) 1.55 (2.086) 1.38 (1.931)Age at alcoholism onset, mean (SD), y 32.7 (11.78) 34.4 (10.85)Alcohol counseling, No. (%) 9 (5.0) 5 (2.7)Previous inpatient treatment No.,
No. (%)0 148 (82.7) 164 (88.6)1 16 (8.9) 13 (7.0)2 9 (5.0) 6 (3.2)3 5 (2.8) 2 (1.1)4 1 (0.6) 0
Beverage of choice, No. (%)Carbonated 71 (39.7) 73 (39.5)Noncarbonated 86 (48.0) 85 (45.9)No preference 22 (12.3) 27 (14.6)
Abbreviations: BMI, body mass index (calculated as weight in kilogramsdivided by height in meters squared); bpm, beats per minute; CIWA-Ar, revisedClinical Institute Withdrawal Assessment for Alcohol scale.
aExpanded from Table 2 in Johnson et al.7bParticipants who selected “Other” were asked to specify further. Of the 14 in
the topiramate group, 13 self-identified as Hispanic and 1 as Cuban. Of the 10 inthe placebo group, 8 self-identified as Hispanic, 1 as Spanish, and 1 as NativeAmerican.
cSelf-reported alcohol drinking reflects average values during the 28-dayperiod preceding the screening visit (ie, the beginning of week −1). Thesevalues were calculated by means of the timeline follow-back technique.13
Percentage of heavy drinking days was defined as the number of heavy drinkingdays (� 5 drinks per day for men and � 4 drinks per day for women) dividedby the number of study days � 100; percentage of days abstinent was definedas the ratio of the number of nondrinking days to the number of study days� 100; drinks per drinking day was the average of 14 weekly drinks perdrinking day ratios, defined as the number of drinks consumed during a givenweek divided by the number of drinking days for that week, and drinks per daywas defined as the number of drinks consumed divided by the number of studydays. All other values refer to baseline (ie, week 0).
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1192
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
time activities, and household duties, with odds ratios of1.86(P=.04),1.94(P=.03),and1.78(P=.02), respectively,along with a trend to reduce sleep disturbance, whichreached significance at week 14 (mean difference, 6.37;95%confidence interval,2.10-10.64;P=.004). Incompari-son, with the secondary multiple imputation model, theodds ratios for topiramate vs placebo in general activities,leisure-timeactivities,andhouseholddutiesontheQ-LES-Qwere 1.45 (P=.23), 2.27 (P=.03), and 2.05 (P=.04), re-spectively, and topiramate compared with placebo had agreater tendency to reduce sleep disturbance (mean dif-ference, 5.31; 95% confidence interval, 1.33-9.28; P=.01).
Rates of concomitant medication use for the topira-mate and placebo groups were 88.0% and 95.7%, respec-tively. The following percentages of subjects within eachgroup received these topiramate doses or equivalent pla-cebo doses, respectively: 0 to 25 mg (3.8% and 1.6%), 25to 50 mg (8.2% and 0.5%), 50 to 100 mg (12% and 3.2%),
100 to 150 mg (10.4% and 6.9%), 150 to 200 mg (13.7%and 10.1%), and 200 to 300 mg (50.8% and 77.7%). Therates for adherence to taking topiramate or placebo weresimilar (mean [SD], 91.5%±14.96% vs 90.1%±13.12%, re-spectively). There was no numerical difference betweenthe topiramate and placebo groups in mean breath alco-hol concentration, and the average reading was 0.002 g%.
Retention rates at the end of the study among thoserandomized were 61.2% (112 of 183) and 76.6% (144of 188) (P� .001) for the topiramate and placebo groups,respectively.
Attrition rates due to adverse events were 18.6% (34 of183) and 4.3% (8 of 188) (P� .001) for the topiramate andplacebo groups, respectively. Table 5 shows that the ad-verse events reported to occur in 10% or more of subjectswereparesthesia,headache,tasteperversion,fatigue,anorexia,nausea, insomnia, difficulty with concentration and atten-tion,nervousness,difficultywithmemory, somnolence,di-
Table 3. Difference Between Topiramate and Placebo on Physical and Psychosocial Measures of Healthby the Primary (Mixed Model) Analytic Approacha
Outcome
Mean (SD)
Mean DifferenceBetween Study Groups
(95% CI)EffectSize
PValue
Baseline (Week 0) Study End (Week 14)
Topiramate(n=183)
Placebo(n=188)
Topiramate(n=112)
Placebo(n=144)
Biochemical MeasuresPlasma AST, U/L 33.1 (17.01) 33.6 (19.08) 24.5 (11.55) 30.1 (16.23) 4.70 (1.86 to 7.54) 0.30 .001Plasma ALT, U/L 34.6 (18.65) 37.2 (23.39) 25.0 (13.24) 33.3 (21.38) 6.74 (2.99 to 10.49) 0.43 � .001Plasma log GGT ratiob 3.89 (0.80) 3.99 (0.84) −0.09 (0.12) −0.02 (0.10) 0.05 (0.03 to 0.08) 0.53 � .001Plasma bicarbonate, mEq/L 25.5 (2.27) 25.1 (2.52) 22.6 (2.55) 24.9 (2.77) 2.50 (1.89 to 3.11) 1.01 � .001Plasma cholesterol, mg/dL 222.2 (46.64) 217.9 (38.65) 205.8 (41.90) 212.2 (45.19) 13.30 (5.09 to 21.44) 0.41 .002Urine pH 5.6 (0.76) 5.8 (0.83) 5.9 (0.95) 5.7 (0.95) −0.30 (−0.54 to −0.06) 0.32 .01
Physical Characteristics and Vital SignsBMI 27.93 (4.809) 28.57 (4.944) 26.82 (4.838) 28.56 (5.046) 1.08 (0.81 to 1.34) 0.91 � .001Systolic blood pressure, mm Hg 134.5 (17.12) 133.1 (16.41) 123.0 (13.55) 130.8 (14.93) 9.70 (6.81 to 12.60) 0.77 � .001Diastolic blood pressure, mm Hg 83.2 (9.77) 83.4 (9.80) 75.5 (10.79) 81.8 (8.93) 6.74 (4.57 to 8.90) 0.73 � .001Pulse, bpm 77.7 (12.27) 76.7 (12.07) 73.3 (12.06) 74.9 (12.44) 1.59 (−0.96 to 4.14) 0.16 .07Temperature, °C 36.78 (0.507) 36.69 (0.446) 36.64 (0.399) 36.66 (0.393) 0.08 (−0.02 to 0.17) 0.18 .92
Obsessional Thoughtsc
OCDS total score 16.81 (5.344) 16.19 (5.199) 7.67 (6.793) 10.86 (5.307) 3.36 (1.98 to 4.73) 0.62 � .001
Clinical Improvementc
CGI-I score NA NA 1.72 (0.825) 2.39 (1.018) 0.63 (0.38 to 0.87) 0.66 � .001CGI-S score 3.98 (0.871) 3.94 (0.857) 1.73 (1.225) 2.46 (1.365) 0.72 (0.39 to 1.06) 0.57 � .001
Harmful Consequences of Drinkingc
DrInC-2R Total Consequencesscale score
47.04 (19.054) 45.85 (17.562) 17.98 (20.140) 27.45 (17.170) 10.08 (5.86 to 14.30) 0.61 � .001
General Moodc
POMS total score 14.08 (16.090) 13.93 (16.260) 3.62 (13.685) 4.50 (14.974) 0.80 (−2.52 to 4.12) 0.07 .63
Alcohol Withdrawal Symptomsc
CIWA-Ar score 1.55 (2.086) 1.38 (1.931) 0.79 (1.537) 0.59 (1.051) −0.01 (−0.33 to 0.31) 0.01 .94
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index (calculated as weight in kilograms divided by height inmeters squared); CGI-I and CGI-S, Clinical Global Impression scales for improvement and severity, respectively; CI, confidence interval; CIWA-Ar, revised ClinicalInstitute Withdrawal Assessment for Alcohol scale; DrInC-2R, Drinker Inventory of Consequences scale, Recent Consequences form; GGT, �-glutamyltransferase;NA, not applicable; OCDS, Obsessive Compulsive Drinking scale; POMS, Profile of Mood States.
SI conversion factors: To convert ALT and AST to microkatal per liter, multiply by 0.0167; bicarbonate to millimoles per liter, multiply by 1.0; cholesterol tomillimoles per liter, multiply by 0.0259.
aThe mean (SD) values provided are the unadjusted numbers. The mean difference in treatment effect between topiramate and placebo and 95% CIs werecalculated from least-squares mean estimators.
bPlasma log GGT ratio, calculated and analyzed as described previously,6 was the [(log GGT at a given time point)−(log GGT at baseline)]/log GGT at baseline.At baseline, log GGT ratio is simply the logarithm of the GGT value. The more negative the value at study end, the greater the reduction from baseline.
cFor these measures, baseline n=179 for topiramate and baseline n=185 for placebo.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1193
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
arrhea, sinusitis,dyspepsia, injury,dizziness, influenza-likesymptoms,pruritus, andmyalgia; all exceptheadache,nau-sea, sinusitis, dyspepsia, injury, influenza-like symptoms,and myalgia were more frequent for the topiramate groupthan for theplacebogroup.Four subjects ineach treatmentgroupexperiencedaseriousadverseevent. Inthetopiramategroup, 1 subject had myopia and another had cholelithia-sis.Also in the topiramategroup,1subjecthadconvulsionsand loss of consciousness; however, these could not be at-tributed to thestudymedication. Incontrast, in theplacebogroup, 1 subject died after a cardiac arrest associated withgastrointestinalbleedingandseizures.Theprecipitating in-cidentcouldnotbedetermined.Also,1 individualeachhadatibialplateaufracture,abnormallyelevated levelsof serumliver enzymes, and diverticulitis.
COMMENT
We have reported that topiramate was more efficaciousthan placebo at improving all self-reported drinking out-comes in a heterogeneous and geographically diverse popu-lation of alcohol-dependent individuals receiving weeklyBBCET during a 14-week period. Topiramate’s therapeu-tic effect on drinking outcomes appears to be the largestreported for a medication in a multisite alcoholism trial.7
Topiramate administration was associated with im-provements in physical health in the 3 domains of total
cholesterol level, hepatic function, and hemodynamic car-diovascular status.
Long-term heavy drinking has been associated withelevated lipid levels and the development of fatty liverdisease.35 Thus, topiramate’s ability to decrease choles-terol levels significantly—a feature that is perhaps re-lated to its complex effects on weight and metabolismas well as its direct effect to reduce heavy drinking—adds considerably to its general medical utility in treat-ing alcohol-dependent individuals.
Topiramate administration was associated with sig-nificant decreases in liver enzyme levels, probably dueto the reduction in heavy drinking. Taken together withthe lowered lipid levels and the consequent reduced riskof fatty liver degeneration, the propensity toward pro-gressive liver disease and eventual cirrhosis could, per-haps, be diminished if alcohol-dependent individuals weretreated with topiramate.
The average blood pressure readings in our subjectsdid not meet the diagnostic criterion for hypertension (ie,blood pressure of 140 mm Hg systolic and 90 mm Hgdiastolic).36 Nevertheless, they usually met the criterionfor prehypertension (ie, blood pressure of 120 mm Hgsystolic and 80 mm Hg diastolic), a level at which life-style modifications are required to prevent cardiovascu-lar disease.36 Therefore, it is of interest that, at the endof the study, the topiramate-treated group achieved blood
140
120
130
110
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
P < .001 P < .001
P = .02
Syst
olic
Blo
od P
ress
ure,
mm
Hg
A 90
75
85
80
70
65
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
Dias
tolic
Blo
od P
ress
ure,
mm
Hg
B
100
80
90
70
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
Puls
e, b
pm
C 30
27
28
29
26
25
1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
BMI
D
PlaceboTopiramate
Figure 2. Comparison of mean systolic blood pressure (A), diastolic blood pressure (B), pulse (C), and body mass index (BMI) (calculated as weight in kilogramsdivided by height in meters squared) (D) among topiramate vs placebo recipients, by study week.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1194
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
pressure levels at about the threshold for prehyperten-sion (mean, 123.0 mm Hg systolic and 75.5 mm Hg dia-stolic), whereas those who received placebo exceeded thiscutoff (mean, 130.8 mm Hg systolic and 81.8 mm Hg dia-stolic). Presumably, these improvements in blood pres-sure were an added benefit of the decrease in BMI, re-duction in drinking, or both among topiramate recipients.Nevertheless, these results suggest a possible added clini-
cal benefit of an improvement in hemodynamic cardio-vascular status if topiramate were to be used to treat al-cohol-dependent individuals.
Excessive alcohol consumption is generally a risk fac-tor for obesity37 even though some individuals with se-vere alcoholism can become malnourished.38 Topiramate-associated decreases in BMI, presumed to be partially dueto a reduction in craving for food,39 might, therefore, be
PlaceboTopiramate
5
3
4
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
P <.001 P <.001
Drin
king
Obs
essi
ons
Scor
e
A 10
4
8
6
2
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
Auto
mat
icity
of D
rinki
ng S
core
B
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
P <.001 P <.001
Inte
rfer
ence
Due
to D
rinki
ng S
core
C 8
4
6
2
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14Study Week
Alco
hol C
onsu
mpt
ion
Scor
e
D
Figure 3. Comparison of mean scores on the 4 subscales of the Obsessive Compulsive Drinking Scale—Drinking Obsessions (A), Automaticity of Drinking (B),Interference Due to Drinking (C), and Alcohol Consumption (D)—among topiramate vs placebo recipients, by study week.
60
30
45
15
6 10 14Study Week
Topiramate
Mea
n To
tal D
rInC-
2R S
cale
Sco
re Mean %
Heavy Drinking Days
A
45
30
15
60Mean % heavy drinking daysMean Total DrInC-2R scale score
Mean % heavy drinking daysMean Total DrInC-2R scale score60
30
45
15
6 10 14Study Week
Placebo
Mea
n To
tal D
rInC-
2R S
cale
Sco
re Mean %
Heavy Drinking Days
B
45
30
15
60
Figure 4. Comparison between the mean Total Consequences scale scores on the Drinker Inventory of Consequences scale, Recent Consequences form(DrInC-2R) and the mean percentage of heavy drinking days, across the trial period, for the topiramate (A) and placebo (B) groups.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1195
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013
of health benefit to alcohol abusers or dependent indi-viduals who are overweight or obese or who have strongcravings for food.
Topiramate treatment was associated with an improve-ment in psychosocial factors that contributed to its thera-peutic effect. Topiramate reduced all subscales on theOCDS28 that measure obsessions and compulsions aboutusing alcohol. While we have proposed that topiramate-induced decreases in obsessional thoughts and compul-sions about drinking reduce alcohol consumption,4 theconverse is also plausible. Similarly, the topiramate-associated reduction in sleep disturbance that we ob-served could have been the consequence of rather thanthe trigger for improved drinking outcomes. Neverthe-less, because sleep disturbance is a feature of—and canbe a trigger for—relapse among alcohol-dependent in-dividuals,40 formal research is needed on topiramate’s ef-fects on the sleep architecture of alcoholic individuals.
Topiramate’s effect in reducing the psychosocial con-sequences of drinking increased as treatment pro-gressed.7 As the frequency of heavy drinking decreased,
there was a concomitant reduction in its psychosocial con-sequences. Because of the collinearity of these variables,it was not possible for us to attribute any cause-and-effect prediction to the relationship between psychoso-cial improvements and reduced heavy drinking. It was,however, tempting to speculate that the reductions in heavydrinking might explain a substantial part of this effect. Thisis because the principal target of the brief behavioral in-tervention was to enhance adherence to medication ratherthan to target any antecedents, triggers, or perpetuatingpsychosocial factors associated with the heavy drinking.Nevertheless, the possibility that the brief behavioral in-tervention led to some ongoing psychosocial improve-ment cannot be discounted entirely because such brief treat-ments have been shown previously to be effective treatmentfor alcoholism in a variety of settings.41,42 Also, we did nothave an appropriate “control” group of participants whoreceived the brief intervention alone (ie, without adjunc-tive placebo medication). Therefore, the independent ef-fects of our brief intervention cannot be teased out fromthose of the medication alone.
Table 4. Least-Squares Mean Difference Between Topiramate and Placebo on Physical and Psychosocial Measures of HealthFrom the Sensitivity Analysis Using the Multiple Imputation Methoda
Outcome
Least-Squares Mean (SE)at Study End (Week 14)
Mean DifferenceBetween Study Groups
(95% CI)EffectSize P Value
Topiramate(n=183)
Placebo(n=188)
Biochemical MeasuresPlasma AST, U/L 26.73 (1.129) 30.25 (1.092) 3.29 (0.46 to 6.58) 0.25 .02Plasma ALT, U/L 27.34 (1.297) 33.96 (1.623) 6.62 (2.83 to 10.40) 0.42 � .001Plasma log GGT ratiob −0.08 (0.010) −0.02 (0.008) 0.06 (0.04 to 0.08) 0.59 � .001Plasma bicarbonate, mEq/L 22.61 (0.218) 25.14 (0.214) 2.53 (1.93 to 3.12) 1.02 � .001Plasma cholesterol, mg/dL 201.00 (3.024) 213.97 (2.790) 12.97 (4.76 to 21.19) 0.40 .002Urine pH 6.01 (0.080) 5.68 (0.084) −0.32 (−0.11 to −0.54) 0.34 .003
Physical Characteristics and Vital SignsBMI 27.14 (0.074) 28.24 (0.066) 1.10 (0.91 to 1.30) 0.92 � .001Systolic blood pressure, mm Hg 122.81 (0.993) 132.02 (1.048) 9.20 (6.44 to 11.97) 0.77 � .001Diastolic blood pressure, mm Hg 76.25 (0.707) 82.67 (0.727) 6.42 (4.57 to 8.26) 0.71 � .001Pulse, bpm 74.00 (1.092) 75.82 (0.916) 1.82 (−1.24 to 4.88) 0.16 .23Temperature, °C 36.60 (0.041) 36.70 (0.038) 0.07 (−0.18 to 0.05) 0.17 .26
Obsessional Thoughtsc
OCDS total score 8.25 (0.463) 11.36 (0.429) 3.11 (1.85 to 4.36) 0.60 � .001
Clinical Improvementc
CGI-I score 1.73 (0.085) 2.35 (0.085) 0.62 (0.39 to 0.85) 0.66 � .001CGI-S score 1.86 (0.116) 2.49 (0.103) 0.64 (0.31 to 0.97) 0.52 � .001
Harmful Consequences of Drinkingc
DrInC-2R Total Consequences scale score 21.01 (1.568) 28.34 (1.315) 7.33 (3.27 to 11.39) 0.46 � .001
General Moodc
POMS total score 7.64 (0.988) 7.07 (0.972) −0.58 (−3.31 to 2.15) 0.05 .68
Alcohol Withdrawal Symptomsc
CIWA-Ar score 0.96 (0.121) 0.88 (0.124) −0.08 (−0.47 to 0.32) 0.06 .70
Abbreviations: See Table 3.SI conversion factors: To convert ALT and AST to microkatal per liter, multiply by 0.0167; bicarbonate to millimoles per liter, multiply by 1.0; cholesterol to
millimoles per liter, multiply by 0.0259.aThe baseline value was imputed for all dropouts. The mean difference in treatment effect between topiramate and placebo was calculated on the basis of
least-squares mean estimators.bPlasma log GGT ratio, calculated and analyzed as described previously,6 was the [(log GGT at a given time point)−(log GGT at baseline)]/log GGT at baseline.
At baseline, log GGT ratio is simply the logarithm of the GGT value. The more negative the value at study end, the greater the reduction from baseline. Threerandomized participants had missing data on baseline plasma GGT and are not included here.
cFor these measures, n=179 for topiramate and n=185 for placebo.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1196
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

Topiramate had a significant effect in improving someaspects of quality of life at the end of the trial, includinggeneral and leisure-time activities and household du-ties. We found this to be an encouraging effect given therelatively short duration of the trial.
Recently, the authors of an influential review of theliterature suggested that harm reduction approaches mightbe as beneficial as abstinence-oriented strategies, espe-cially if treatments are directed to accommodate the needsand preferences of the individual or target popula-tions.43 Indeed, Johnson et al30 argued that a harm re-duction approach offers the potential to sustain “par-tial” remission from drinking, perhaps even over the longterm if therapeutically effective medication is taken con-tinuously. Not only does this allow for other psychoso-cial influences to bring about complete remission, but itprovides a framework for treating alcohol dependencein much the same way as any chronic relapsing disor-der, such as diabetes or hypertension. Further elucidat-ing the therapeutic benefit of long-term topiramate treat-ment on drinking behavior, and physical and psychosocialhealth, is, therefore, an important research goal.
We considered the possibility that the differential at-trition rate, greater for the topiramate group than for theplacebo group, might have an effect on outcome. Nev-ertheless, the consistency of the results between the pri-mary analytic approach (mixed model) and the sensitiv-ity analysis using the multiple imputation methodpresented herein, as well as information obtained by usingother modeling techniques reported elsewhere,7 sug-
gests that dropouts in this study were unlikely to be in-formative or affect the outcomes related to efficacy butwere more the direct result of adverse events.
The robustness of topiramate’s therapeutic efficacy wasevidenced by the similarity of the results obtained for theprimary and sensitivity analyses, and the effect sizes weretypically in the medium range or better on most out-comes for which there was an improvement in physicalor psychosocial health.
Our study had 4 limitations. First, while the pattern ofadverse events was similar to that found in our previousstudy,6 the more rapid titration was associated with de-creased study adherence. In that study, topiramate was ti-trated over an additional fortnight, and retention rates weresimilar between the topiramate and placebo groups. Weobserved that the clinical sites least familiar with topira-mate experienced more difficulties with retention, butcompletion rates among some experienced groups ap-proached 90% (data not shown). Therefore, an approachto more generalized use, especially among clinicians withless experience with topiramate, would be to propose aslower titration schedule, along with focused educationabout how best to manage emergent adverse events. Ofcourse, future studies elucidating the optimum topira-mate dose that balances efficacy, tolerability, and treat-ment adherence would be important, particularly withrespect to the transient cognitive effects—typically word-naming difficulties—that require careful management andappropriate reassurance. Second, it is plausible that cer-tain subtypes of alcoholic subjects might benefit the mostfrom topiramate treatment. Although we did not observea differential treatment response by age of problem drink-ing onset, subtype classifications that included genetics orother biomarkers might have provided additional infor-mation. Third, our study was not designed to examine topi-ramate’s posttreatment effects; thus, it remains unknownhow long these physical and psychosocial improvementswill be sustained. Nevertheless, even when a brief adher-ence enhancement intervention is coupled with effectivepharmacotherapy, there are important gains in physicaland psychosocial health during treatment. Fourth, our spe-cialists in this clinical trial treated alcohol-dependent in-dividuals who might be generally healthier and more mo-tivated to change than those in the community. Becausetopiramate pharmacotherapy can be paired with a brief in-tervention deliverable by nonspecialist health practition-ers, a next step, therefore, would be to examine its effi-cacy in community practice settings.
In summary, our findings demonstrate that topiramateappears to be a generally effective treatment for alcohol de-pendence because it improves not only the “symptom” ofdrinking but also its physical and psychosocial sequelae.
Accepted for Publication: December 30, 2007.Author Affiliations: Department of Psychiatry and Neu-robehavioral Sciences, University of Virginia, Charlottes-ville (Drs Johnson and Ait-Daoud); Ortho-McNeil Jans-sen Scientific Affairs LLC, Raritan, New Jersey (DrsRosenthal, Wiegand, Mao, and McKay and Mss Capece andBeyers); Institute of Internal Medicine, Catholic Univer-sity, Rome, Italy (Dr Addolorato); Department of Psychia-try and Behavioral Sciences, Medical University of South
Table 5. Adverse Events During TreatmentOccurring in 10% or More of Participantsa
Adverse Event
No. (%) of Participants
PValue
Topiramate(n=183)
Placebo(n=188)
Paresthesia 93 (50.8) 20 (10.6) � .001Headache 44 (24.0) 60 (31.9) .09Taste perversion 42 (23.0) 9 (4.8) � .001Fatigue 41 (22.4) 33 (17.6) .24Anorexia 36 (19.7) 13 (6.9) � .001Nausea 19 (10.4) 31 (16.5) .08Insomnia 35 (19.1) 30 (16.0) .42Difficulty with
concentration/attention27 (14.8) 6 (3.2) � .001
Nervousness 26 (14.2) 14 (7.4) .04Difficulty with memory 23 (12.6) 13 (6.9) .07Somnolence 22 (12.0) 19 (10.1) .56Diarrhea 22 (12.0) 16 (8.5) .27Sinusitis 15 (8.2) 26 (13.8) .08Dyspepsia 16 (8.7) 22 (11.7) .35Injury 8 (4.4) 22 (11.7) .01Dizziness 21 (11.5) 10 (5.3) .03Influenza-like symptoms 16 (8.7) 21 (11.2) .44Pruritus 19 (10.4) 2 (1.1) � .001Myalgia 14 (7.7) 19 (10.1) .41
a If a participant experienced more than 1 adverse event within a category,the participant is counted once under that category. Participants with morethan 1 occurrence of an adverse event are summarized under the mostrelated category. The World Health Organization Adverse ReactionsTerminology dictionary modified for topiramate (version 1992, third quarter)was used for coding. P values are from the �2 test. Adapted from Table 4 inJohnson et al.7
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1197
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

Carolina, Charleston (Dr Anton); Division of Psychiatry,Boston University, Boston, Massachusetts (Dr Ciraulo); De-partment of Psychiatry, University of Connecticut, Farm-ington (Dr Kranzler); Department of Addictive Behaviorand Addiction Medicine, University of Heidelberg, Mann-heim, Germany (Dr Mann); Department of Psychiatry, YaleUniversity, New Haven, Connecticut (Dr O’Malley); andDepartment of Psychiatry and Human Behavior, BrownUniversity, Providence, Rhode Island (Dr Swift).Correspondence: Bankole A. Johnson, DSc, MD, PhD,MPhil, FRCPsych, Department of Psychiatry and Neu-
robehavioral Sciences, University of Virginia, PO Box800623, Charlottesville, VA 22908-0623 ([email protected]).Author Contributions: Dr Johnson had full access to allof the data in the study and takes responsibility for the in-tegrity of the data and the accuracy of the data analysis.Drs Addolorato, Anton, Ciraulo, Kranzler, Mann, O’Malley,and Swift contributed equally as coauthors. Study conceptand design: Johnson, Rosenthal, Capece, and Beyers. Ac-quisition of data: Johnson, Capece, Wiegand, Beyers, McKay,Ait-Daoud, Anton, Ciraulo, Kranzler, O’Malley, and Swift.Analysis and interpretation of data: Johnson, Rosenthal,Capece, Wiegand, Mao, Ait-Daoud, Addolorato, Anton,Ciraulo, Kranzler, Mann, O’Malley, and Swift. Drafting ofthe manuscript: Johnson and Rosenthal. Critical revision ofthe manuscript for important intellectual content: Johnson,Rosenthal, Capece, Wiegand, Mao, Beyers, McKay, Ait-Daoud, Addolorato, Anton, Ciraulo, Kranzler, Mann,O’Malley, and Swift. Statistical analysis: Johnson, Wiegand,and Mao. Obtained funding: Johnson, Rosenthal, Capece,Wiegand, and McKay. Administrative, technical, or mate-rial support: Johnson, Rosenthal, Capece, Wiegand, Beyers,McKay, Ait-Daoud, Addolorato, Anton, Ciraulo, Kranzler,Mann, O’Malley, and Swift. Study supervision: Johnson,Rosenthal, Capece, Wiegand, McKay, and Ait-Daoud.Financial Disclosures: Dr Johnson has been a consul-tant for Ortho-McNeil Janssen Scientific Affairs LLC andis a consultant for Organon and TransOral Pharmaceuti-cals Inc. Drs Rosenthal, Wiegand, Mao, and McKay andMss Capece and Beyers are employees of Ortho-McNeilJanssen Scientific Affairs LLC. Dr Ait-Daoud has been aconsultant for Ortho-McNeil Janssen Scientific Affairs LLC.Dr Addolorato has been a consultant for Ortho-McNeilJanssen Scientific Affairs LLC and is a consultant for Or-ganon. Dr Anton has received consulting fees and hono-raria from Forest Laboratories and Alkermes Inc; consult-ing fees and grants from Bristol-Myers Squibb, Hythiam,and Pfizer; consulting fees, honoraria, and grants from Con-tral Pharma/Biotie Pharmaceuticals and Ortho-McNeil Jans-sen Scientific Affairs LLC; and consulting fees from Ast-raZeneca, Axis Shield, Cephalon, DrugAbuse Sciences,Sanofi-Aventis, Eli Lilly, and Solvay Pharmaceuticals. DrCiraulo has received consulting fees and clinical trial con-tracts from Janssen, Bristol-Myers Squibb, and Ortho-McNeil Janssen Scientific Affairs LLC; consulting fees fromCephalon; and clinical trial contracts from Alkermes Inc,AstraZeneca, Catalyst Pharmaceutical Partners, Drug-Abuse Sciences, Lipha, and UCB Pharma. Dr Kranzler hasserved as a consultant for and received research supportfrom Alkermes Inc, Ortho-McNeil Janssen Scientific Af-fairs LLC, Bristol-Myers Squibb, Forest Pharmaceuticals,and DrugAbuse Sciences, and served as a consultant forElbion, Sanofi-Aventis, and Solvay Pharmaceuticals. DrMann has received consulting fees and clinical trial con-tracts from Alkermes Inc, Janssen, Sanofi-Aventis, Pfizer,Lipha Pharmaceuticals, Ortho-McNeil Janssen ScientificAffairs LLC, and Forest Pharmaceuticals. Dr O’Malley hasserved as a consultant for and received medication sup-plies and/or clinical trial contracts from Alkermes Inc,GlaxoSmithKline, Ortho-McNeil Janssen Scientific Af-fairs LLC, and Pfizer; served as a consultant for Eli Lillyand Johnson & Johnson; received medication supplies or
Study Group and Advisory Board Members
Topiramate for Alcoholism Study Group:Participating Sites and Principal Investigators
(in Alphabetical Order)
Nassima Ait-Daoud, MD, University of Virginia, Char-lottesville; Robert M. Anthenelli, MD, University of Cin-cinnati, Cincinnati, Ohio; Raymond F. Anton, MD, Medi-cal University of South Carolina, Charleston; MarianneGuschwan, MD, New York Veterans Affairs Medical Cen-ter, New York, New York; Bankole A. Johnson, DSc, MD,PhD, MPhil, FRCPsych, The University of Texas HealthScience Center at San Antonio; Henry R. Kranzler, MD,University of Connecticut, Farmington; Sandra C.Lapham, MD, Behavioral Health Research Center of theSouthwest, Albuquerque, New Mexico; Francis Levin,MD, Columbia University, New York, New York; LanceLongo, MD, Aurora Sinai Medical Center, Milwaukee,Wisconsin; F. Gerard Moeller, MD, The University ofTexas Health Science Center at Houston; Stephanie S.O’Malley, PhD, Yale University, New Haven, Connecti-cut; Helen M. Pettinati, PhD, University of Pennsylva-nia, Philadelphia; Ihsan Salloum, MD, MPH, Universityof Pittsburgh, Pittsburgh, Pennsylvania; Ofra Sarid-Segal, MD, Boston University, Boston, Massachusetts;Robert M. Swift, MD, PhD, Brown University, Provi-dence, Rhode Island; Richard P. Trautman, MD, Uni-versity of Oklahoma, Oklahoma City; and Roger D. Weiss,MD, McLean Hospital, Belmont, Massachusetts.
Topiramate for Alcoholism Advisory Board(in Alphabetical Order)
Giovanni Addolorato, MD, Catholic University, Rome,Italy; Nassima Ait-Daoud, MD, University of Virginia,Charlottesville; Raymond F. Anton, MD, Medical Uni-versityof SouthCarolina,Charleston;DomenicA.Ciraulo,MD, Boston University, Boston, Massachusetts; Carlo C.DiClemente, PhD, University of Maryland, BaltimoreCounty, Baltimore; Scott E. Hemby, PhD, Wake ForestUniversity, Winston-Salem, North Carolina; EricHollander, MD, Mount Sinai School of Medicine, NewYork, New York; Bankole A. Johnson, DSc, MD, PhD,MPhil, FRCPsych, University of Virginia, Charlottes-ville; Falk Kiefer, MD, University Hospital of Hamburg,Hamburg, Germany; Henry R. Kranzler, MD, Universityof Connecticut, Farmington; Otto M. Lesch, MD, Medi-cal University of Vienna, Vienna, Austria; Robert J.Malcolm Jr, MD, Medical University of South Carolina,Charleston; Karl Mann, MD, University of Heidelberg,Mannheim, Germany; Stephanie S. O’Malley, PhD, YaleUniversity, New Haven, Connecticut; and Robert M. Swift,MD, PhD, Brown University, Providence, Rhode Island.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1198
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013

clinical trial contracts from Lipha Pharmaceuticals, Bristol-Myers Squibb, Sanofi-Aventis, and Mallinckrodt; and re-ceived travel reimbursement from Alkermes Inc. Dr Swifthas served as a consultant for and received grant fundingfrom Ortho-McNeil Janssen Scientific Affairs LLC andPfizer; served as a consultant and on speakers bureaus forCephalon and Forest Laboratories; served as a consultantfor Alkermes Inc, Organon, and TransOral Pharmaceuti-cals Inc; and received grant funding from US World Medsand Bristol-Myers Squibb.Funding/Support: Ortho-McNeil Janssen Scientific Af-fairs LLC provided the medication and funding for thisstudy.Role of the Sponsor: The sponsor was involved in all stagesfrom study design through interpretation of the results in-cluding critical review of the manuscript. Data were man-aged and analyzed by Ortho-McNeil Janssen Scientific Af-fairs LLC and PharmaNet Inc, a contract researchorganization, and were interpreted by authors of the studywith input from Ortho-McNeil Janssen Scientific AffairsLLC clinical and statistical staff. The entirety of the firstdraft was prepared by the lead author (Dr Johnson). Thedraft was reviewed by all of the authors, who discussed itas a group at a scheduled meeting of the Topiramate forAlcoholism Advisory Board (see box on page 1198) in NewYork, New York, on February 2, 2007. Amendments per-tained to style and presentation, and no changes were madeto the results or their interpretation from the initial draftor the results as presented at that meeting.Additional Contributions: We thank the staff at the par-ticipating sites for their skilled technical assistance, aswell as Robert H. Cormier Jr, BA, and ChamindiSeneviratne, MD, for their assistance with preparing thereport. Both Mr Cormier and Dr Seneviratne are em-ployed by the University of Virginia.
REFERENCES
1. Johnson BA. Epidemiology of alcoholism. In: Johnson BA, Ruiz P, Galanter M,eds. Handbook of Clinical Alcoholism Treatment. Baltimore, MD: Lippincott Wil-liams & Wilkins; 2003:2-9.
2. National Institute on Alcohol Abuse and Alcoholism. Alcohol Use and AlcoholUse Disorders in the United States: Main Findings from the 2001-2002 NationalEpidemiologic Survey on Alcohol and Related Conditions (NESARC)—U.S. Al-cohol Epidemiologic Data Reference Manual. Vol 8, No. 1. Bethesda, MD: Na-tional Institute on Alcohol Abuse and Alcoholism; 2006.
3. World Health Organization. The World Health Report 2002: Reducing Risks, Pro-moting Healthy Life. Geneva, Switzerland: World Health Organization; 2002.
4. Johnson BA. Recent advances in the development of treatments for alcohol andcocaine dependence. CNS Drugs. 2005;19(10):873-896.
5. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate modu-lates GABA-evoked currents in murine cortical neurons by a nonbenzodiazepinemechanism. Epilepsia. 2000;41(suppl 1):S17-S20.
6. Johnson BA, Ait-Daoud N, Bowden CL, et al. Oral topiramate for treatment ofalcohol dependence. Lancet. 2003;361(9370):1677-1685.
7. Johnson BA, Rosenthal N, Capece JA, et al. Topiramate for treating alcohol de-pendence: a randomized controlled trial. JAMA. 2007;298(14):1641-1651.
8. Johnson BA, Rosenthal N, Capece JA, et al. Topiramate for the treatment of alco-hol dependence: results of a multi-site trial. New Research poster presented at:160th Annual Meeting of the American Psychiatric Association; May 22, 2007; SanDiego, CA.
9. Cargiulo T. Understanding the health impact of alcohol dependence. Am J HealthSyst Pharm. 2007;64(5)(suppl 3):S5-S11.
10. Petrakis IL. A rational approach to the pharmacotherapy of alcohol dependence.J Clin Psychopharmacol. 2006;26(suppl 1):S3-S12.
11. Stewart SH, Hutson A, Connors GJ. Exploration of the relationship between drink-ing intensity and quality of life. Am J Addict. 2006;15(5):356-361.
12. American Psychiatric Association. Diagnostic and Statistical Manual of MentalDisorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
13. Sobell LC, Sobell MB. Timeline follow-back: a technique for assessing self-reported alcohol consumption. In: Litten RZ, Allen JP, eds. Measuring AlcoholConsumption: Psychosocial and Biochemical Methods. Totowa, NJ: Humana PressInc; 1992:41-72.
14. Sullivan JT, Sykora K, Schneiderman J, Naranjo CA, Sellers EM. Assessment ofalcohol withdrawal. Br J Addict. 1989;84(11):1353-1357.
15. Montgomery SA, Asberg M. A new depression scale designed to be sensitive tochange. Br J Psychiatry. 1979;134:382-389.
16. Bohn MJ, Babor TF, Kranzler HR. The Alcohol Use Disorders Identification Test(AUDIT). J Stud Alcohol. 1995;56(4):423-432.
17. National Institute of Mental Health. CGI: clinical global impressions. In: Guy W,Bonato RR, eds. Manual for the ECDEU Assessment Battery. 2nd rev ed. ChevyChase, MD: National Institute of Mental Health; 1970:12.1-12.6.
18. Anton RF, Moak DH, Latham P. The Obsessive Compulsive Drinking Scale. Al-cohol Clin Exp Res. 1995;19(1):92-99.
19. Conigrave KM, Degenhardt LJ, Whitfield JB, et al. CDT, GGT, and AST as mark-ers of alcohol use. Alcohol Clin Exp Res. 2002;26(3):332-339.
20. Miller WR, Tonigan JS, Longabaugh R. The drinker inventory of consequences(DrInC): an instrument for assessing adverse consequences of alcohol abuse.In: Mattson ME, Marshall LA, eds. Project MATCH Monograph Series. Vol 4. Rock-ville, MD: National Institutes of Health; 1995. NIH publication 95-3911.
21. McNair DM, Lorr M, Droppleman LF. Manual of the Profile of Mood States. SanDiego, CA: Educational & Industrial Testing Service; 1971.
22. Hays RD, Martin SA, Sesti AM, Spritzer KL. Psychometric properties of the Medi-cal Outcomes Study Sleep measure. Sleep Med. 2005;6(1):41-44.
23. Endicott J, Nee J, Harrison W, Blumenthal R. Quality of Life Enjoyment and Sat-isfaction Questionnaire. Psychopharmacol Bull. 1993;29(2):321-326.
24. Johnson BA, DiClemente CC, Ait-Daoud N, Stoks SM. Brief Behavioral Compli-ance Enhancement Treatment (BBCET) manual. In: Johnson BA, Ruiz P, Gal-anter M, eds. Handbook of Clinical Alcoholism Treatment. Baltimore, MD: Lip-pincott Williams & Wilkins; 2003:282-301.
25. Edwards G, Orford J, Egert S, et al. Alcoholism: a controlled trial of “treatment”and “advice.” J Stud Alcohol. 1977;38(5):1004-1031.
26. Fawcett J, Epstein P, Fiester SJ, Elkin I, Autry JH. Clinical management—imipramine/placebo administration manual: NIMH Treatment of Depression Col-laborative Research Program. Psychopharmacol Bull. 1987;23(2):309-324.
27. SAS Institute Inc. SAS version 9.1. Cary, NC: SAS Institute Inc; 2003.28. Bohn MJ, Barton BA, Barron KE. Psychometric properties and validity of the ob-
sessive-compulsive drinking scale. Alcohol Clin Exp Res. 1996;20(5):817-823.29. Pearlstein TB, Halbreich U, Batzar ED, et al. Psychosocial functioning in women
with premenstrual dysphoric disorder before and after treatment with sertralineor placebo. J Clin Psychiatry. 2000;61(2):101-109.
30. Johnson BA, Ait-Daoud N, Akhtar FZ, Ma JZ. Oral topiramate reduces the con-sequences of drinking and improves the quality of life of alcohol-dependentindividuals. Arch Gen Psychiatry. 2004;61(9):905-912.
31. Rubin DB. Inference and missing data. Biometrika. 1976;63(3):581-592.32. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York, NY: John
Wiley & Sons; 1987.33. SAS OnlineDoc, 9.1.3. Cary, NC: SAS Institute Inc; 2007.34. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale,
NJ: Lawrence Erlbaum Associates Inc; 1988.35. Lieber CS. Alcoholic fatty liver: its pathogenesis and mechanism of progression
to inflammation and fibrosis. Alcohol. 2004;34(1):9-19.36. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint Na-
tional Committee on Prevention, Detection, Evaluation, and Treatment of HighBlood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-2572.
37. Suter PM, Hasler E, Vetter W. Effects of alcohol on energy metabolism and bodyweight regulation. Nutr Rev. 1997;55(5):157-171.
38. Addolorato G, Capristo E, Greco AV, Stefanini GF, Gasbarrini G. Influence of chronicalcohol abuse on body weight and energy metabolism: is excess ethanol consump-tion a risk factor for obesity or malnutrition? J Intern Med. 1998;244(5):387-395.
39. Tata AL, Kockler DR. Topiramate for binge-eating disorder associated with obesity.Ann Pharmacother. 2006;40(11):1993-1997.
40. Crum RM, Ford DE, Storr CL, Chan YF. Association of sleep disturbance withchronicity and remission of alcohol dependence: data from a population-basedprospective study. Alcohol Clin Exp Res. 2004;28(10):1533-1540.
41. Wright S, Moran L, Meyrick M, O’Connor R, Touquet R. Intervention by an al-cohol health worker in an accident and emergency department. Alcohol Alcohol.1998;33(6):651-656.
42. Fleming MF, Mundt MP, French MT, Manwell LB, Stauffacher EA, Barry KL.Brief physician advice for problem drinkers: long-term efficacy and benefit-costanalysis. Alcohol Clin Exp Res. 2002;26(1):36-43.
43. Marlatt GA, Witkiewitz K. Harm reduction approaches to alcohol use: health pro-motion, prevention, and treatment. Addict Behav. 2002;27(6):867-886.
(REPRINTED) ARCH INTERN MED/ VOL 168 (NO. 11), JUNE 9, 2008 WWW.ARCHINTERNMED.COM1199
©2008 American Medical Association. All rights reserved.
Downloaded From: http://archinte.jamanetwork.com/ on 02/25/2013