Impact of a Designed In-Service Training Program on Nurse ...
115
Impact of a Designed In-Service Training Program on Nurse Midwives Knowledge, Attitude and Practices at Management Toward Postpartum Hemorrhage Khartoum Hospitals, Khartoum state, Sudan (2010) Asha Mohamed Elsofi Abd Elgalil Diploma in Nursing Khartoum Nursing College (1965) M.Sc,in Community Health,Faculty of Medicine University of Gezira (1998) A Thesis Submitted to the University of Gezira in Fulfillment of the Requirements for the Award of the Degree of Doctor of Philosophy in Community Health Primary Health Care and Health Education Centre Faculty of Medicine .. January, 2014
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Impact of a Designed In-Service Training Program on Nurse ...

Impact of a Designed In-Service Training Program on
Nurse Midwives Knowledge, Attitude and Practices
at Management Toward Postpartum Hemorrhage
Khartoum Hospitals, Khartoum state, Sudan (2010)
Asha Mohamed Elsofi Abd Elgalil
Diploma in Nursing Khartoum Nursing College (1965)
M.Sc,in Community Health,Faculty of Medicine
University of Gezira (1998)
A Thesis
Submitted to the University of Gezira in Fulfillment of the
Requirements for the Award of the Degree of Doctor of
Philosophy
in
Community Health
Primary Health Care and Health Education Centre
Faculty of Medicine
..
January, 2014

Impact of a Designed In-Service Training Program on
Nurse Midwives Knowledge, Attitude and Practices
at Management Toward Postpartum Hemorrhage
Khartoum Hospitals, Khartoum state, Sudan (2010)
Asha Mohamed Elsofi Abd Elgalil
Supervision Commi ee
Name Posi on Signature
Prof. Magda Elhadi Ahmed Yousif Main Supervisor ………………………
Prof. Mohamed Ahmed Abd Elgadir Co-supervisor ………………………
Date :January, 2014
I

Impact of a Designed In-Service Training Program on
Nurse Midwives Knowledge, Attitude and Practices
at Management Toward Postpartum Hemorrhage
Khartoum Hospitals, Khartoum state, Sudan (2010)
Asha Mohamed Elsofi Abd Elgalil
Examina on Commi ee:
Name Posi on Signature
Prof. Magda Elhadi Ahmed Yousif Chair Person ………………………
Prof.Yousif Abd Elhameed Alsisi External Examiner ………………………
Dr. Sumia Kalaf Alla Abderheem Internal Examiner ………………………..
Date of Examina on: 13 /1/ 2014
II

DEDICATION
All Praise is to God, the Almighty, by whose Grace and Mercy I have completed
this work. I would like to dedicate this thesis to my parents and my family who have shown me
unconditional love and support throughout my life. It was through their example that
I learned to strive toward my goals, and I will be forever grateful . To whoever stays wakeful to take care of humanity.
To whoever feels the other's suffering and tries to mitigate these sufferings. To
every nurse, midwife and health visitor who selected the way of sacrifice as
his/her own way and method. To those who grant endlessly in taking care of a child and a mother
To all these people: I dedicate this modest work, for the purpose of offering
better nursing services.
Asha Mohammad AI-Sofi
iv iii

ACKNOWLEDGMENTS I would like to express my gratitude to my supervisor Dr. Magda Elhadi Ahmed Yousif Professor
community medicine, faculty of medicine university of Gezera, for her invaluable advice, guidance,
unlimited help, patience and support. I would like also to thank my co-supervisor Professor Mohammed Ahmed Abdel Gadir Professor of
Obstetrics and Gynecology Ribat University for his great and valuable assistance, advice and his
useful suggestions. I also express my utmost gratitude and thanks to Dr Abdalmageed Osman Associate Professor,
Community Medicine International University of Africa, Sudan for his great help, patience and
support. My thanks also extends to Dr Hassan Eltegani, University of Ribat, researcher in strategic centre,
who helped with his advice and support.
My special thanks to my colleague Fatma Elbatoul and Lila Adam Sister Midwives for their great
help and their co-operation and patience, especially in data collection.
I would like to thank Dr Nahid Abdelazim, Head of the Departments of Community, Ribat
University, Faculty of Nursing and Dr Sohir Abdelsatar for their encouragement and help and their
contribution to the workshops. I would like to acknowledge the help and cooperation of the nurse midwives who participated in
this study.
Thanks also to the University of Ribat for providing their facilities which have been invaluable
to the study.
My thanks also extends to the Ministry of Health, Hospital Directors and Nursing Directors of
Obstetrics and Gynecology of Omdurman, Ribat and Khartoum North Hospital for their help and
support. Also thanks to everyone who contributed in this research. Great thanks to my family and friends for their support and patience during the entire period of
study.
Special thanks to my grand daughter Duaa who helped me refine my computer skills and English.
iv v

Service Training Program on Nurse Midwives Knowledge, Impact of a Designed In-at
Khartoum Management Attitude and Practices Toward Postpartum Hemorrhage
Hospitals, Khartoum state, Sudan (2010)
Asha Mohamed El-sofi Abd-Elgalil
ABSTRACT The risk of maternal death represents one of the greatest inequities in global health. Women in developing
countries are more than 40 times as likely to die in childbirth than women in developed countries (1 in 61 women
i developing countries versus 1 in 2800 in developed countries). The WHO states that 529000 women die from
complications relating to pregnancy and childbirth every year, PPH accounts for 34%. 31% of women die in
Africa.In Sudan, PPH accounts for 1107 deaths per 100,000 of maternal deaths. No information or studies were
done to evaluate the impact of in-service training programs on nurse midwives’ practices in Sudan. This hospital
based study was conducted at Khartoum state in three teaching hospitals which included six Midwifery
departments in order to evaluate the effect of in-service training program on nurse midwives’knowledge,attitude
and skills during process of labor to manage and prevent PPH. Adesigned in-service training program was
developed ,implemented and assessed.A total number of 100 nurse midwives selected from six midwifery
department randomly. Sample design chosen was cluster sample.The midwives were enrolled and randomized in
case and control group.Midwives in the case group received the training program.The KAP questionnaire was
administered to both case and control group,pre-trainig and at final follow-up to assess the knowledge,attitude and
practice regarding PPH.Official permission was obtained from hospitals’ directorates and verbal consent by the
participant.The study was implemented in three phases:preperatory phase,intervention phase and post intervention
phase and follow-up.An instructured questionnaire was used to assess the knowledge and an observational check
list was used to assess skills and practices in implementation of AMTSL, application of universal
precaution,estimation of blood loss and use of utero-tonic drugs.TOT training progrm implemented for six seniour
midwives ,two from each hospital,to participate in the training program and to carry on future in-service training
progrm in their respective hospitals. At the end of the study ,the KAP score of test group improved significantly.
Regarding knowledge,the overall mean scores(±sd) increased from 27.72 ±6.16 pre-intervention to 52.2 ±3.68
afte follow-up (P-value <0.005).Regarding skills and attitude ,the results showed a significant difference with ( P-
valu <0.005). The study showed that the impact of a designed in-service program was effective and nurse
midwives could be an important elements in management and prevention of PPH.The study concluded that in-
service trainin programe was very effective in improving NMS skills and Knowledge, Also the study
recommended review of th cruculm to include (AMTSL) and ultrasongram training coarses .Their attitudes were
fairly appropriate.Resources Needed for practice should alwayes be made available and improvement of
environment and review of salaries is very essential.
viv

فيت قاباللت الممرضاك اسلوو سةرممات ، معلوما علي لخدمھء اثناا یبرلتدا تأثیر
م(2013).ملخرطوا بوالیة لتعلیمیھت المستشفیاا فيدة لوالا مابعد نزیف معالجة
لجلیلا عبد لصوفيا محمد عائشة
ول لدا فيت المھا،ا عالمیًا لصحةل امجا فيت الختالالا كبرا منًا حددة وابالوال تتعلقب السبات المھات افیاو خطر یشكل
كل فيه حدة "وافاو لمتقدمةول الدا فيت المھاا منه مر "40" یذیدل بمعددة بالوال تتعلقت فیاو بنسبةت معرضا لنامیةا
529,000ان ضحاو لعالمیةا لصحةا منظمة تقریر، لمتقدمةول الدا فية فاو حالة 2800 في 1 مقابلام" 61
ریقیافا فيث تحد 31% منھا34% نسبة یشكلدة لوالا مابعد نزیفدة ،لوالت امضاعفاب باسبام عا كلث تحدة فاو حالة
توجد ال 2009. حیةدة الو حالة 000 ,100كل فية فاو حالة 1107 ليا صلتت والمھات افیاو نسبةدان لسوا في.
سةرالده اذھ جریت. ا لممرضةا لقابلةا سةرمما في لخدمةء اثناا یبرلتدا بآثر تتعلقت معلوما بتقویم قامتي خرت اسادرا
بھا تعملدة الف وغر ستة عليي تحتوم لخرطوا بوالیة تعلیمیةت امستشفی ثالثةد عد منت معلوما عليت ستندا لتيوا
دة لوالا بعد نزیفوث حد حالة في لممرضةا لقابلةواداء ا سةرمما علي یبرلتدا تأثیري مد لتقویم، ممرضة قابلة 110د عد
تقویمھ تمو نفذو لخدمةء اثناا یبرلتدا برنامجاد عدا تم،خليالتدا لتصمیما سةرالده اذھ ستخدمت.ا منھ لوقایةوا لنزیفرء الد
cluster لعینةدة . االم وقساا ستةد عد من ئیًااعشو نرھختیاإ تم ممرضة قابلة مائةد لعد
علیھا لبرنامجا تنفیذ تم لتي( والمتابعھي والبعدوا لقبليا لتدخل)ا مجموعة ئیًااعشو مجموعتین ليا لتقسیما عملیة جریتا
ك لسلوت والمعلوماا لتقویمه الخیرا لمتابعھا فيو ليوالا لمرحلةا في یبرلتدا فیھا تم لتيوا control لضبطا مجموعھو
ت كارلمشاا من یةھشفا فقھامو ليا باالضافھت لمستشفیاراء امد من سمیةت رنااذو خذا علي لباحثةا حرصت.سةرلمماوا
ن الستبیاا طریق عنت لقابالا لكل لمعرفية القاعدا خط تقویم :يھ حلامر ثالثة علي سةرالدت انفذ. لبرنامجا في
فيدة لوالء اثنارات المھاا لتقویم لتحققا قائمة طریق عن لمالحظةا ليا باإلضافھت ، لمعلوماا لتقویم
متابعھ ليا باالضافھ لنزیفس اقیاق طر عن، لوقائیةت االحتیاطاا تطبیق، لثالثةا لمرحلةا في لفاعلا لتدخلا سةرمما
قابلة سستر ثالثةد لعد یومینة لمد عمل شھور في بینرمد یبرتد تم. رحملا لعضلة لقابضةا یةدوالء اعطاوا بھرلوا عمل
كةرلمشاا ليا باالضافھ قعھنامو في لخدمةء اثناا یبرلتدا متابعھ منھف لھد،ا لمعدا لبرنامجا بنفست صحیاات ئرزا ثالثةو
بقیمةرات لمھات والمعلوماا في تحسنت لمستھدفةا لمجموعھان ا سةرالدت اظھر. ا لعمليا یبرلتدا في
0.005 من قلل احتماا بقیمةك ) لسلوا تغییر في كبیر تحسن سةرالدا نتائجت ظھرا كما. 0.005 >) من قلل )احتماا
كمادة . لوالء اثنارات المھاا تطبیقت ولمعلومادة ایاز في فعالیتھ ثبتا یبرلتدا برنامجان ليا سةرالدا خلصت >.)
ك لسلوا تغیرو بالنفس لثقةا ليا باالضافھ 100%ر حضو بنسبة كانت كةرلمشاوا علملتا فيت ساارلدا غبةر سةرالدا ثبتتا
لعملا ببیئةء لرضام اعد ليا باالضافھت لمستھلكاات والمعدا في نقص نالكان ھ سةرالدا ضحت.او الحسنا ليا
.لعملا بیئة تحسینو لمطلوبھارد الموا توفیر في لنظرا من البد علیھ،
vi

TABLE OF CONTENTS
Items Page No.
Declaration iii
Dedication iv
Acknowledgment v
Abstract (English+ Arabic) vi
Table of content vii
List of tables viii
List of figures ix
List of abbreviations x
Chapter One:
Introduction 1
1.1 Background
1
1.2 Problem identification and justification
1-3
1.3 Objectives
4
General objectives
4
Specific objectives
4
Chapter Two:
Literature Review 5-7
2.1 Background
2.2 History of midwifery in Sudan 7-9
2.3 In-service training 10
2.4 Definition 10
2.5 Pathophysiology 10-12
2.6 Frequency 12
2.7 Mortality, Morbidity 12
2.8 Etiology and risk factors 13-15
2.9 Clinical manifestation 15
2.10 Diagnosis 16
2.11 Complication 16-17
2.12 Management 17-20
2.13 Surgical management 20-21
2.14 Management of the third stage of labor 22-24
2.15 Prevention of post Partum Hemorrhage 24-26
2.16 Nursing Management-Responsibilities and rights 28-30
2.17 Safe environment for birth 30-33
2.18 Immediate care for newborn 33-35
2.19 Previous studies 35-42
vii

Chapter three:
Methodology 43
3.1 Study design 43
3.2 Study area and setting 44
3.3 The study population 44
3.4 Inclusion criteria 44
3.5 Exclusion criteria 44
3.6 Sampling 44-45
3.7 Data collection technique and tool 46
3.8 Phases of the study 46-50
3.9 Data analysis 50
3.10 Ethics 50
3.11 Validity of instruments 50
3.12Reliability 50
3.13 Implication of study results 50
3.14 Limitations 51
3.15 Expected results 51
Chapter Four:
Results and Discussion
Results 52-81
Socio-demographic data of the respondents 52
Knowledge of nurse midwives about post partum hemorrhage. 53-59
Attitude of Nurse Midwives 61-63
Skills of nurse midwives 63-73
Discussion 82-92
Chapter Five:
Conclusion and Recommendation 93
Conclusion
Recommendations 94
References 95-98
Appendices
1-Sample of structural interview questionnaire
2-Sample of observation check list
3-Learning packages of the training
4-Tables of final results
5-Booklet for training program
6- Blood loss estimation Pictures
7-Protocol to follow in case of emergency
viiivii

LIST OF TABLES
Tables Page No.
Table 4.1-Sociodemographic data of the respondent 52
Table 4.2- knowledge of the study group about PPH (definition and types) 53
Table 4.3 -Knowledge of the study group about PPH (Causes) 54
Table 4.4 -Knowledge about risk factors, signs and symptoms and 55
investigations of PPH
Table 4.5 -Knowledge of nurse midwives about complications of PPH 56
Table4.6 - Knowledge of nurse midwives about utertonic drugs 57
Table4.7- Knowledge of the study group about the principles of infection 58
prevention
Table 4.8 -Physiology and changes of the genital tract 59
Table 4.9- Evaluation of the study group about the working environment 60
and supplies
Table 4.10 (a)-Communication skills 61
Table 4.10 (b) -Harmful customs practiced during labor 62
Table 4.11 -Abdominal examination skills 62
Table 4.12 -The practice of nurse midwives towards Laboratory 64
investigations 65
Table 4.13- Skills of nurse midwives in episiotomy, area and time
Table 4.14(a) -Management before placental delivery 66
Table 4.14(b)- Skills of the nurse midwives during placental delivery 67
Table 4.15 Skills of nurse midwives after placental delivery and assessment 68
for uterine contraction and management 69
Table 4.16 -Skills of nurse midwives towards blood loss estimation
Table 4.17 -Prevention of PPH 70
Table 4.18-Management and nursing care of nurse midwives in the third 72-73
stage of labor 74
Table 4.19 -level of education of study group compared by (KAP) 75
viii
ix

LIST OF FIGURES
Figures Page No.
Figure 4.1 attitude of nurse midwives towards infection prevention 63
Figure 4.2 The use of protective barriers pre and post intervention 71
Fig.(4.3) years of experience compared with KAP 76-77
Figure(4.4) knowledge ,skills and attitude of the trainees pre, post and 79
follow-up
Figure 4. 5 Analysis of pre and post intervention compared different 80-81
between case and control group in KAP
ixx

List of Abbrevia on
PPH Post Partum Hemorrhage
APH An Par tum He mo r rhage
MMR Maternal mortality rate
KAP Knowledge, A tute,Prac ce
AMTSL Ac ve ma nageme nt of the thi rd stage of labor
PMTSL Physiologic management of the third stage of labor
CCT Controlled cord trac on
NMS Nurse Midwives
SBA Skilled Birth A endant
TBA Tradi onal Bi rth A endant
ANMS Auxiliary Nurse Midwives
ACNM American college nurse midwives
I.C.M Interna onal conf eder a on of mid wi v es
FIGO Interna onal conf eder a on of Gynecol ogy and Obs t etr ics.
NS Na onal St a s cs
SPSS Sta s cal Package f or Soci al Sci ences
EMTSL Expected Management of the Third Stage of Labor
POPPHI Preven on of Pos t Par tum He mo r rhage Ini a ve
PPPH Preven on of Pos t Par tum He mo r rhage
DIC Disseminated Intravascular Coagula on
FHR Fetal Heart Rate
PE/E Pre Eclampsia /Eclampsia
MCHIP Maternal and Child Health Integrated Program
TOT Training Of Trainers
WHO World Health Organiza on
USAID United States Agency for Interna onal Devel opme nt

FMOH Federal Ministry of Health
SMOH State Ministry of Health
GOSS Government of South Sudan
HCOs Health Care Organiza ons
AAFP American Academy of Family Physician
ICD Informed Choice and Disclosure
TMA Tennessee Midwives Associa on
ACOG American College of Obstetrician and Gynecologists
OSHA Occupa onal Saf et y and He al th Or gani za on
CDC Centre of Disease Control
GBS Group Beta Strep
RRs Rela ve Ri sk
IU Interna onal Uni ts
CIs Confidence Int er val s
RPOC Retained Products of Concep on
HBLSS Home Based Life Saving Skill Support
HELLP Haemolysis Elevated Liver Enzyme Low Platelets
Four Ts Tone,Trauma,Tissue,Thrombin
ECG Electro Cardio Gram
FBC Full Blood Count
CBC Complete Blood Count
GTT Glucose Tolerance Test
HIV Human Immunodefici ency Vi rus
AVPU Alert, Voice ,Pain, Unresponsive

PKU Phenyl ketonuria
HSV(1) Herpes Simplex Virus 1
HSV(2) Herpes Simplex Virus 2
NASG non-pneuma c an -shock garmen t
UPs Universal precau on
CEMACH confiden al Enqui r y i nto Mat ernal and Chi l
dHea l t h HBV Hepa s B Vir us
ivx

CHAPTER ONE
INTRODUCTION
1.1 Back ground Postpartum hemorrhage (PPH) is defined as excessive vaginal bleeding (blood loss than 500ml)
within 24 hours after delivery. Any amount of bleeding causes a change for the worst in the
woman’s condition i.e. low systolic blood pressure, increased heart rate, a decrease in red blood cells
(heamatocrit) and signs of shock.
(Mosby’s Medical Dictionary, 2009)
In caesarean births, the average blood loss rises to 800 -1000ml. There is a great risk of
hemorrhage in the first 24 hours after birth, called primary postpartum hemorrhage.
A secondary hemorrhage occurs after the first 24 hours of birth (JANICE M, 2007) in the majority
of cases, the cause of hemorrhage is uterine atony, retained placental fragments (possibly including a
placenta accrete), ruptured uterus, cervical lacerations, uterine inversion or clotting disorders.
(Tintinalli JE, 2004) .
1.2 problem Identification and Justification Worldwide PPH is an unpredictable and rapid cause of maternal death two –thirds of women with
PPH having no identifiable risk factor.70-90%of immediate PPH is attributed to uterine a tony
(ACOG,2006).
In developed countries the direct pregnancy – related maternal mortality rate in the United
States is approximately 7-10women per 100,000 live births. National statistics suggest that
approximately 8% of these deaths are caused by PPH. (ACOG, 2006) In industrialized countries, PPH usually ranks in the top three causes of maternal mortality, (along with embolism and hypertension). result of problems during and immediately after
the third stage of labor. (John R, 2012).
In the developing world several countries have maternal mortality rates in excess of 1000
women per 100,000 live births, and the world health organization statistics in the developing
countries PPH is the leading direct cause of maternal death and is a suggest that 25% of maternal
deaths are due to PPH, accounting for more than 100,000maternal deaths per year.
1

The most recent survey from the American college of Obstetricians and Gynecologists places the
estimate at 140,000 maternal deaths per year or 1 woman every 4 minutes(WHO,2005).
In Sudan PPH accounts for 1107 deaths per 100.000 of maternal deaths or one woman every
minute. (M.Hassan,2006)
Efforts by the save motherhood initiative and the world health organization(WHO), such as making
pregnancy safer and creating strategies to meet the united nations millennium development goals ,
are supporting worldwide activities to reduce maternal mortality. Previous studies have shown that PPH causes up to 60% of all maternal deaths in
developing countries, PPH also causes considerable suffering for women and their
families and creates major demands on health systems. (Berg, CJ,1996). The risk of maternal death from childbirth represents one of the greatest inequities in global health,
women in developing countries are more than 40 time morelikely to die in childbirth than women in
developed countries (1 in 61 women in developing countries versus 1 in 2800 in developed
countries).
Even within developing countries there is a striking differential risk of maternal death for women
who did not have access to basic essential care compared to those who did. (Rashmi B,2011).
In the developed world, PPH is a largely preventable and manageable condition; however mortality from PPH remains high despite international efforts. Efforts such as the save
motherhood initiative and (WHO) to make pregnancy safer and strategies to meet the United
Nations millennium development goals are supporting worldwide activities to reduce maternal
mortality. However, despite these efforts hundreds of thousands of women die due to complications
in pregnancy. Half of these maternal eaths occur within 24 hours of childbirth (Beck,D 2004). Since PPH is largely preventable and manageable condition nurse midwives is in a key position to
disseminate knowledge, and provide proper. Management for mothers with PPH.
Fortunately Research shows that using simple low cost intervention can help avoid most of these
tragic outcomes. Current evidence indicates prevention and active management of the third stage of
labor, and the use of specific uterotonic drugs, are new strategies to prevent and manage PPH in
developing countries. Community based use of Misoprostol, oxytocin and the balloon condom
catheter to treat intractable uterine bleeding can reduce the incidence of PPH by up to 60%. (Derman
RJ, 2006).
Bar the increase of maternal mortality rates, no studies were done to evaluate midwives management
in PPH.
2

Justification
Percentage of deliveries assisted by skilled midwives has become a proxy indicator for
reducing maternal mortality in developing countries; it was asserted that competence care in this
period is of high effect in decreasing mortality rate. Objectives of the study were to describe practice of nurse midwives regarding postpartum hemorrhage, and up grading nurse midwives knowledge and skills is argent to help in
reduce maternal mortality rate .
3

OBJECTIVES
1.3 General objective: To evaluate the impact of a designed in – service training on nurse midwives
Knowledge, Attitude and skills towards postpartum hemorrhage management at Khartoum state
hospitals.
Specific objectives:
1. To assess the nurse midwives knowledge,attitude and skills regarding postpartum
hemorrhage management.
2. To monitor nurse midwives practices towards PPH care.
3. To develop in-service training programs for nurse midwives regarding management of PPH
according to their needs.
4. To implement the designed training program for nurse midwives.
5. To evaluate the impact of training programs on the nurse midwives knowledge, skills and
practice.
4

CHAPTER TWO
LITREATURE REVIEW
2.1 Back ground
Post partum hemorrhage
The global maternal mortality ratio (MMR) of 400 per 100.000 live births results in an
estimated 529.000 maternal deaths annually. Most of these deaths occur in developing countries and
only about 1% in developed countries. Besides mortality data, the identification and accurate
documentation of “near-miss” morbidity is extremely important to assess the quality of health care
systems. It can suitably guide to adopt appropriate measures to reduce maternal mortality and
morbidity.
Post partum hemorrhage is an obstetrical emergency that can follow vaginal or cesarean
delivery; it is a major cause of maternal morbidity, and one of the top five causes of maternal
mortality in both high and low precipitant income countries, although the absolute risk of death is
much lower in high income countries 1 in100 000 versus 1 in 1000 births in low income countries.
(WHO Report2005) The risk of maternal death from childbirth represents one of the greatest
inequities in global health. Women in developing countries are more than 40 times likely to die in
childbirth than women in developed countries (1 in 61 women in developing countries versus 1in
2800 women in developed countries).(Henry A,primary PPH 2005) Even within developing
countries there is striking differential risk of maternal death for women who have access to basic
essential obstetrical care compared to those who do not.
Within a country, as poverty increases so does the proportion of women dying of maternal cause .More than 500,000 deaths per year globally, 98% in developing countries, mother dying every one
minute(M .Hassan 2006).
Obstetric hemorrhage is the world leading cause of maternal mortality, causing 24% of, or an
estimated 132,000, maternal deaths annually. Postpartum hemorrhage (PPH) is the most common
type of obstetric hemorrhage and accounts for the majority of the 14 million cases of obstetric
hemorrhage that occur each year (WHO Report 2005).
In the developed countries, PPH is a largely preventable and manageable condition. In
developing countries however, mortality from PPH remains high despite international efforts, while
data are limited, studies have shown that PPH causes up to 60% of all maternal deaths in developing
5

countries. (Lewis, G, 2007 2) For example,PPH accounts for 1107% of maternal deaths in Sudan ,(M Hassan 2006). South Sudan has one of the highest maternal mortality rates in the world at 2,054 to 100.000 live
birth(Gobbi, 2012).
PPH also causes considerable suffering for women and their families and creates major demands on
healthsystems.( Henry A,Birch MR,2005).
A recent study to the investigation of maternal deaths and their causes were retrospectively
reviewed and mortality index for each event was calculated in kassala hospital, eastern Sudan over a
two year period from January 2008 to December 2010 . There were 9578 deliveries, 205 near – miss
events and 40 maternal deaths. Maternal mortality ratios were ‘22.1 \1000, live birth and 432\
100\000 live births. Respectively hemorrhage accounted for the most common event ( 40.8 )
followed by infection. there is a high frequency of maternal morbidity and mortality at the level of
this facility, there for maternal health policy need to be concerned not only with averting the loss of
life, but also with preventing maternal-near miss events (hemorrhage , infection, hypertension ect.
Methods for preventing this event must be reviewed at all levels including primary level education
and training for midwives (Abdelaziem A Ali, 2011).
A retrospective study carried out at the Medani teaching hospital, Medani city, Sudan .Case
notes were reviewed for all the 877 women died during the period 1985-1999. All were followed for
at least six weeks after delivery so that deaths due to sequel of delivery and puerperium were also
included. Out of the total number of deliveries in that period (no= 44,655) 877 women died with a
rate of 1,966 per 100,000 . the period was divided into three periods of five years 1995 -1999. The
rate showed a decline each year ,being 2.661 per 100,000 during the first period ,the mortality rate
during second period was 2,021 per 100,000 and 1,363 per 100,000 during the last period . Sepsis
was the cause of death ,while malaria, hemorrhage and hypertensive disorders are the main
contributory factors. poor antenatal care ,poor intra natal care and poor provision of health services
add more to the problem .
The study highlighted the existence of a serious obstetrical problems which can be preventable,
research into the problem of malaria, sterilization, anesthesia, vascular accidents and indication for
cesarean section, management of hemorrhage together with social and medical improvement will
definitely reduce the maternal morbidity and mortality (Saudi Med. J 2003).
6

2.2 History of midwifery in Sudan In 20/s/ Sudanese Medical Services were established in 1912 and then it becomes the Sudanese
Ministry of Health in 1948. On the other hand Nursing Services were established on 1912 before the
medical school. On 1918 the Medical Assistant schools was established. The first Health Visitor’s
School was established in 1947. The first Midwifery School was established in Omdurman city in
1921, the first director of this school was (Miss ME. Wolff) .After many hard and inconceivable
difficulties, Miss Wolff developed and organized what became the midwifery services of the Sudan;
it took a long time to convince some old women to become midwives and to come in for training. At
that time the midwives of Sudan were untrained and old, very conservative and Ellet rate, in addition
the women resented any innovation which was not in accord with their customs. By 1924 it was
possible to train all the existing old midwives of both Omdurman and Khartoum. A training program
was started with very satisfactory results .The standard of midwifery has been raised to a higher
level at both cities. In 1930 Miss Wolff and her sisters started the first Antenatal clinic in Sudan; at
the midwifery training school which became very successful and popular. Since 1921, 624 midwives have been trained, of which 40 were trained nurses and 12 were health
visitors. The standard of training is gradually being raised as the younger and more educated women
come forward to join midwifery. Now there are four levels for training midwives in Sudan:
1. Village Midwives
2. Nurse Midwives
3. Assistant Health Visitors
4. Health Visitors.
5. Sister Midwives
6. Bsc midwifery (new program).
Village midwives: The level of education required for this cadre is intermediate school, to be nominated by the
community, must show interest, medically fit and her age not to b(e more than 30 years. Now there
are 27 schools in Sudan distributed in all states. The curriculum has been revised by an expert team,
supported by WHO .in accordance with the Sudan declaration for nursing, midwifery and
7

paramedical in 2001, the purpose of WHO .support was to provide save midwifery service to the
community. the village midwives trained to conduct antenatal care, labor ,and postnatal care, the total number of
the village midwives in northern states is12,863(Khartoum state Mof H,) The Nurse midwives: The basic education for this cadre was intermediate school , now after Sudan declaration is
secondary school ,to obtain the nursing certificate and have two years experience in teaching
hospitals midwifery departments, after passing special examination , can join the midwifery school
to be Trained for one year and then go back to work on hospitals midwifery departments as nurse
midwife, works in the obstetric emergency department, outpatient department ,antenatal wards ,
labor rooms , postnatal wards and gynecology wards. Job description conducts delivery, assists
obstetrician, provide postnatal care for patient with gynecological problems , care of neonate after
caesarian section , family planning and health education. The total number of nurse midwives in the fifteen northern state is 692 (FMof H statestic
department 2011). The assistant’s health visitors: This cadre is selected from among village midwives who is trained as assistant health visitors and
performs the roles of the health visitor in the rural areas in the absence of the health visitor. They
have to be trained for one year in the health visiting schools and after passing the final exam will be
assistant health visitors. The health visitors: This cadre to be selected from nurse midwives then attached to health visitors institute to be trained
for two years, graduating with diploma in midwifery , works in the community health centre as a
teacher in the midwifery schools, conducts ante natal care ,provides family planning, is educator
/counselor and disease prevention ,referral of complicated cases and do documentation. .
The health visitors and the nurse midwives are included in the government roll and get their salaries
and incentives from the Federal or state ministries of health.
The village midwives don’t get anything from the government, but recent there is a call nationwide
to pay the village midwives in appreciation of their work and a way to make them improve their
performance. There a response from River Nile and Sinnar states which employed some of the
assistant health visitors, Khartoum and Aljazeera States also employed some village midwive,(
FMOH nursing department 2010).
8

Sisters midwife: Graduated of high nursing college carrying either diploma or BSC in nursing , those who interested
in midwifery can join the high institute of midwifery for two years this instituted was established by
the WHO and Federal ministry of health in 1967, it grants post graduate diploma in midwifery.
Unfortunately this institute was closed in 1987 after graduating only 92 sisters’ midwives. Education of midwifery in UK: Midwives are practitioners in their own right in the United Kingdom, and take responsibility for the
antenatal, intrapartum and postnatal care of women, up until 28 days after the birth, or as required
thereafter. Midwives are the lead health care professional attending the majority of births, whether at
home or in a hospital (although most births in the UK occur in a hospital). There are two routes to
qualifying as a midwife. Most midwives now qualify via a direct entry course, which refers to a
three- or four-year course undertaken at university that leads to a degree in midwifery (diploma
courses in midwifery have been discontinued) and entitles them to apply for admission to the
register. Following completion of nurse training, a nurse may become a registered midwife by
completing an eighteen-month post-registration course (leading to a degree qualification); however,
this route is only available to adult branch nurses, and any child, mental health, or learning disability
branch nurse must complete the full three-year course to qualify as a midwife. Midwifery students
do not pay tuition fees and are eligible for financial support for additional while training(Royal
college of Midwives 2012). 2.3 In-Service Training Defined as an educational program for employees, provided by an employer and usually carried out
by a supervisor or specialist, designed to help employees become more productive and effective in
accomplishing a specific task or meeting the overall objectives of the organization. Usually in-
service training takes place after an employee begins work responsibilities, is done on the job for
short periods of time, and during a break in the employee's work schedule.(SIL
International,1999,Barker,2003).
Previously nurse –midwives weren’t properly trained after graduation in Sudan there was no proper
system of in-service training .Only short courses extending from three days to two weeks were held
in specific relevant areas such as infection control, family planning, antenatal care, neonatal care and
eradication of female circumcision . Recently, however the federal ministry of health has established
a centre for continuous training program in nursing and midwifery are taught(Dr.Rahim Hagaz
2011).
9

2.4 Definition Post partum hemorrhage is defined as excessive vaginal bleeding following delivery and is
described as primary and secondary.
Primary post partum hemorrhage (PPH) is loss of blood estimated to be more than 500 ml, from the
genital tract and greater than 1000 ml, in cesarean delivery within 24 hours of delivery( the most
common obstetric hemorrhage)(Mosby,s Medical dictionary ,2009). Mc Cormick etal stated that A more accurate definition of post partum hemorrhage is any blood loss
that causes a physiological change e.g. Low blood pressure, increased heart rate, decreased in red
blood cells that threatened the woman’s life.( Mc Cormick et al ,2009 ). Unfortunately waiting until there is a physical change would mean death for most women in
developing country settings, as immediate backup or emergency obstetric care is not
available.(Bouwmeester FW,2006).
The WHO stated 529,000 women died from complications related to pregnancy and child
birth a year. PPH accounts for of 34% and 31% of women dying from complications related to
pregnancy or childbirth in Africa and Asia. (FIGO,2003) Secondary PPH is defined as abnormal bleeding from the genital tract, from 24 hours after delivery
until 6 weeks post partum.
2.5 Pathophysiology Although most of the physiological processes in the third stage of labor remain unclear, they broadly
help to explain the etiology of a tonic postpartum hemorrhage. Uterine atony The most common cause of postpartum hemorrhage is uterine atony, i.e. failure of the uterus to
contract. Primary postpartum hemorrhage due to uterine atony occurs when the relaxed myometrium
fails to constrict these blood vessels, thereby allowing hemorrhage. Since up to one-fifth of maternal
cardiac output, or1000 ml/min, enters the uteroplacental circulation at term, postpartum hemorrhage
is capable of exsanguinations the mother within a short time. While uterine atony is responsible for 75–90% of primary postpartum hemorrhage. (Anderson, JM;
Etches, D., 2007).
Traumatic causes of primary postpartum hemorrhage (including obstetric lacerations, uterine
inversion and uterine rupture) comprise about 20% of all primary postpartum hemorrhage Failure of
the uterus to contract may be associated with retained placenta or placental fragments, either as
disrupted portions, or more rarely a succenturiate lobe.
10

The retained material acts as a physical block against strong uterine contraction, which is needed to
constrict placental blood vessels, but, in most cases, dysfunctional postpartum contraction is the
primary reason for placental retention. It is more likely for the placenta to be retained in cases of
atonic postpartum hemorrhage, and so the contraction failure often becomes self-perpetuating. (John
R Smith, 2011). The reasons for this contractile dysfunction are unknown. The exception is uterine fibroids, where the source of distension cannot be removed by uterine contraction, and must
therefore cause the atony. However, the uterus does not even have to be distended during the third
stage for contractile dysfunction to occur. Distension prior to delivery, which occurs with multiple
pregnancy and polyhydramnios, also affects the ability of the uterus to contract efficiently after
delivery, and is thus another risk factor for atonic postpartum hemorrhage. When postpartum
hemorrhage occurs following an antepartum hemorrhage, the scenario is particularly difficult since
there have been two episodes of blood loss. A rare but serious complication of abruption is
extravasation of blood into the myometrium, known as a Couvelaire uterus, which impairs the
physiological uterine contraction/retraction hemostatic process. However, the relationship between
the extravasation process and uterine dysfunction is not fully understood ( Diane M Fraser, 2003). The lower segment as an implantation site In both placenta previa and placenta accreta,the placental bed (and thus the postpartum bleeding site)
is in the lower segment. The presence of lower segment implantation makes hemorrhage and
placental retention much more likely. Although existing evidence is scanty, there are indications that the etiology of
pathological bleeding is inextricably linked with the anatomical and physiological
limitations of the lower segment. ( R.U. Khan and H. El-Refaey).
2.6 Frequency The exact incidence of PPH is difficult to determine. A reasonable Conesus is that 1-10% of
pregnancies are complicated by PPH, with the actual number in the range 2-4%.(Filippiv ,2005). 2.7 Mortality / Morbidity PPH can cause severe morbidity and mortality. According to CDC data , 17% of maternal mortality is due to hemorrhage .PPH is thought to be the
cause in one third to one half of these cases.
Possible complications include exposure to blood products, the need for surgical intervention and
the need for permanent sterilization to control bleeding. (ChitritY ,Obstet Gynecol Reprod
Biol2006).
11

Race Some study findings suggest that the incidence of PPH Asian and Hispanic women is increased
compared with that other women. Age PPH occurs in women of childbearing age.
History In addition to asking the standard questions about the prenatal period, request information about
previous episodes of PPH ,prior cesarean section, parity, and history of multiple fetuses or
polyhydraminous. Ascertain if the patient or family has a history of coagulation disorders or excessive bleeding with
surgical procedures or menses.
Obtain information about medications, with emphasis on medications for hypertension( calcium –
channel blockers) or heart disease ( e.g., digoxin , warfarin ). This information is important if the
coagulopathy develops and the patient requires transfusions. Determine if the placenta has already been delivered.(Dildy CA, 2002). In woman with excessive postpartum bleeding , simultaneously perform the physical examination
and resuscitation . Focus the examination on determining the cause of the bleeding. The patient may
not have the typical hemodynamic changes of shock early in the course of the hemorrhage due to
physiologic maternal hypervolemia. Occult PPH always is an important consideration when unstable
hemodynamic findings are present without evidence of excessive blood loss.Bimanual palpation of
the uterus may reveal bogginess, atony , or uterine enlargement , with a large amount of
accumulated blood. Palpation may also reveal hematomas in the perineum or pelvis. During suctioning , careful visual inspection of the cervix and vagina under good light may reveal
the presence and extent of lacerations.
Examine the placenta for missing portions, which suggest the possibility of retained placenta tissue.
Check for oozing from skin puncture sites or intravenous sites in patients with excessive bleeding as
this could indicate a coagulopathy (Price N, B.Lynch C 2005).
12

2.8 ETIOLOGY AND RISK FACTORS
Etiology Bleeding after delivery is controlled by a combination of (1) contraction of the myometrium, which
constricts the blood vessels supplying the placental bed, and local decidual haemostatic factors ,
including tissue factor, type – 1 plasminogen activator inhibitor and systemic coagulation factor ( eg,
platelet and circulating clotting factors ). Deficient contraction of the myometrium is manifested
clinically as uterine atony. Defective deicidal homeostasis is associated with inadequate
decidualization (eg.placenta accrete ) or bleeding diatheses (eg,factor deficiencies or
thrombocytopenia ). The major etiologies of and risk factor for PPH are descrieped below (Nichd
2004) Atony – the most common cause of PPH is uterine atony ( ie, lack of effective contraction of the
uterus after delivery) , which complicates 1 in 20 births and is responsible for at least 80 percent of
cases of PPH . An atonics uterus may be related to:-
o Over distension ( multiple gestation , polyhydramnios , macrosomia).
o Uterine infection .
o Drugs ( uterine relaxants) .
o "Uterine fatigue " after a prolonged or induced labor .
o Uterine in version.
o Retained placenta ( either a normally attached placenta or placenta accrete). If the uterus appears to be firmly contracted after delivery , then other etiologies of hemorrhage
should be considered . However , one should keep in mind that a focal area of the uterus can be
atonics, which is difficult to appreciate on physical examination , or the uterus may not be
maximally contracted . (Zahn CM,Yeomanser ,1990). Trauma – Trauma – related bleeding can be due to lacerations ( perineal vaginal , cervical
.uterine ) incisions ( hysterotomy,episiotomy or uterine rupture .Lacerations are more common after
instrumental delivery.(AAFP, 2007). Coagulation defects- Acquired and congenital bleeding diatheses may be associated with
thrombocytopenia and / or haemostatic defects .Acquired causes include severe preeclampsia ,
abruptio placenta , fetal demise , amniotic fluid embolism , and sepsis. Consumptive coagulopathy
may develop in women with severe hemorrhage. (AAFP, 2007).
13

Risk factors
Factors relating to the pregnancy:
o Antepartum hemorrhage in this pregnancy.
o Placenta praevia ( 15 x risk).
o Multiple pregnancy (5 x risk) .
o Pre-eclampsia or pregnancy-induced hypertension (4 x risk) .
o Null parity (3 x risk).
o Previous PPH (3 x risk).
o Asian ethnic origin (2 x risk).
o Maternal obesity (2 x risk).
Factors relating to delivery
o Emergency Caesarean section(CS) (9 x risk) Elective CS (4 x risk) – especially if > 3 repeat
procedures.
o Retained placenta (5 x risk).
o Mediolateral episiotomy (5 x risk).
o Operative vaginal delivery(2 x risk).
o Lab our of > 12 hours (2 x risk). (Magan EF,Evans S 2005)
o More than 4 kg baby (2X risk).
o Maternal pyrexia in lab our (2 x risk).
o Pre-existing maternal hemorrhagic conditions.
o Factor 8 deficiency – Hemophilia A carrier.
o Factor 9 deficiency – Hemophilia B carrier .
o Von Will brand’s disease
o Presentation.(Bais JM, Eskesm,2004). 2.9 Clinical manifestation: Common Signs and Symptoms
o Uncontrolled bleeding .
o Decreased Blood pressure.
o Increased Heart rate.
o Decreased in the red blood cell count ( hematocrit ).
o Swelling and pain in tissues in the vaginal and perinea area .
14

Symptoms Continuous bleeding , which fails to stop after delivery of the placenta – third stage.
Signs Loss of > 1000 ml may be accompanied by clinically apparent shock, i.e. tachycardia, hypotension.
(Houghton 2004).
Investigations
o Thorough examination of the lower genital tract. This may require
o theatre/ anesthesia.
o Ultra sound ,may be used if returned products of conception suspected (RPOC).
o FBC, clotting screen, cross match.
o Blood cultures .
o Hourly urine output.
o Continuous pulse/ blood pressure or central venous pressure monitoring.
o ECG, pulse oximetry.
o Associated diseases.
o Haemolysis,elevated liver enzyme and low platelets(HELLP).
2.10 Diagnosis Clinical Examination of Postpartum Hemorrhage: The doctors involved need to carefully but quickly make an assessment on the amount of blood loss
and to monitor vital signs including temperature, pulse, breathing and blood pressure until the
bleeding is controlled. Questions regarding the pregnancy, labor and delivery may be asked to assess for risk factors which
may help to identify the cause of bleeding.
While managing the blood loss, several key examinations need to be performed in an attempt to
identify the cause and control the hemorrhage.
These include:
o Examination of uterine size.
o Examination of the placenta for completeness.
o Examination of the birth canal for trauma .
Postpartum hemorrhage is diagnosed clinically when significant
blood loss (>500mL) is observed. (Virtual Medical Centre).
15

2.11 Complication
PPH is a major cause of maternal morbidity, with sequel such as shock, renal, failure , acute
respiratory distress syndrome , and disseminated Sheehan's syndrome ( ie , postpartum
hypopituitarism ) is a rare , but potentially life threatening , complication . The pituitary gland is
enlarged in pregnancy and prone to infarction from hypovolemic shock. . Damage to the pituitary can be mild or severe , and can affect the secretion of one , several , or all of
its hormones.Acommon presentation is failure to lactate and amenorrhea oligomenorrhea, but any of
the manifestations of hypopituitarism(eg , hypotension , hyponatraemia hypothyroidism ) can occur
anytime from the immediate postpartum period to years after delivery.If the patient remains
hypotensive after control of hemorrhage and volume replacement , she should be evaluated and
treated for adrenal insufficiency immediately ; evaluation of other hormonal deficiencies can be dip
erred until four to six weeks postpartum. Another rare , but life threatening , complication is abdominal compartment syndrome ( organ
dysfunction caused by intra abdominal hypertension ).
The diagnosis should be considered in patients with a tensely distended abdomen and progressive
oliguria who are developing multiorgan failure.
2.12 Management
Primary Postpartum Hemorrhage Principles of Care Consider the four T’s as the causes of Primary PPH . 1. Tone (Uterine atony). 2. Trauma (Genital trauma including damage to vulva, vagina, cervix
and uterus). 3. Tissue (Retained and invasive placenta). 4. Thrombin (coagulopathy) ( ACOG, 2009).
Management of a Primary Postpartum Hemorrhage All of these actions may occur simultaneously. • Call for help. • Rub up a contraction. • Ensure the woman is conscious, has a clear airway and is breathing and alert.
16

(AVPU score)
• Reassure the mother and her partner. • Check her pulse and blood pressure. • Lay down, with a head down tilt. • Give Oxygen by face-mask, 15 liters /min. • IV access with at least one Grey 16G cannula. • Take blood for Full Blood Count, baseline Clotting screen and Cross match .
Units
• Give IV Crystalloid ( e.g. Hartmann’s ) solution or normal saline. • Ensure bladder empty and Foley’s catheter inserted. Attach udometer bag to monitor hourly urine
output.
• Start vital signs chart to document maternal observations like respiratory rate, heart rate, blood
pressure, oxygen saturation and fluid balance chart.
• Commence Oxytocin infusion - 40 iu Oxytocin in 500mls Normal Saline 0.9% at 125mls per hour
(MOET 2007).
• Once bleeding is controlled, continue IV Oxytocin infusion and keep on labor ward for 4 hours
minimum and await FBC results.
• Ensure there is clear documentation of the sequence of events, plan of care and occurrence of
timely review.
• All entries to be signed and name printed. • All sanitary pads should be saved and weighed to measure the blood loss. This should continue
whilst the patient is being monitored for ongoing loss. Cumulative loss to be clearly documented in
the notes in this case.
TONE
• Expel clot from the vagina and uterine cavity with fundal massage . • Commence IV Syntocinon 40iu in 500ml Normal Saline @ 125ml/hr over 4hours. • IV or IM ergometrine 500mcg. • Rectal misoprostol 800mcg. • Bimanually compress the uterus external and internal. • Consider IM Carboprost 250mcv9ery 15 minutes to a maximum of 8 doses(2mg) (Malay Kmirdha
2007) .
17

Tissue
• Commence IV Syntocinon 40iu in 500ml Normal Saline at 125ml/hr over 4hours. • Deliver the placenta if not delivered – manually removal of placenta in case of retained placenta in
the room if epidural is dense enough. or take to theatre for manual removal of placenta if additional
analgesia required. • If placenta delivered check it is complete and clearly document in the notes. • Give Augmentin 1.2g IV (Habek D Vranjes M2006).
TRAUMA
• Check for obvious genital trauma. Ensure good lighting and visualize the cervix. • Visualize the apex, apply pressure to the bleeding point and suture in the room if it is easily
identified.
• Transfer to theatre if not. • Examine the anus, vulva, vagina and cervix under direct vision . • Consider laparotomy. • If the uterus is explored give IV 1.2g Augentin stat. Number of new and simpler techniques have emerged ,these techniques include :understanding the placental bed ,utrine
compression ,sutures, tamponade,utrine artery ligation,arterial embolization, and utero ovarian artery
anastomosis ligation. Community members or traditional birth attendants (TBA) can learn external Bimanual
compression,which in addition to stimulating contraction of the uterus ,places continous pressure on
the uterine veins and on the lower part of the uterus for reduction of further bleeding. (Suchismita
Roy. 2007). Thrombin • Risk factors for the development of coagulopathy include: pre-eclampsia complicate PPH due to
other causes (Tone, Tissue, Trauma)
• The diagnosis should be suspected when bleeding continues despite the presence of an empty, well
contracted uterus and in the absence of genital trauma. Ensure involvement of Anaesthetic team and
Haematologist. • Anticipate the need for and order blood components early; after transfusion of 6-8 red cell units
order 1 pool of platelets and 4 units of FFP. The Blood Transfusion Laboratory will permit this first
order of products to be issued empirically during a massive obstetric hemorrhage.
18

• If platelets are available in stock they can be issued in 10 minutes + transport time from lab to EGA. If no platelets in stock they will be ordered by the lab from the National Blood bank. • Further management will be determined on an individualized basis after liaison with the on call
hematology SpR and may include: FFP, platelets, and cryoprecipitate.
• If intractable bleeding, unresponsive to conventional blood product transfusion and surgical /
obstetric interventions, consider use of recombinant factor VIIa,only issued on after approval by
Consultant Hematologist. (Bouwmeester FW 2003).
2.13 Surgical management of intractable post-partum hemorrhage A patient who fails to respond to uterotonic agents and continues to bleed will quickly become
haemodynamically unstable and develop a cascade of clotting abnormalities.
The specter of maternal mortality can then only be prevented by initiating surgical homeostasis
sooner rather than later. The nature, timing and extent of these invasive interventions will depend on
the sophistication of the health facility which handles this medical crisis. The fate of such a woman
will therefore vary widely, depending not only on where she lives in the world but also on where she
lives in her own country. Traditionally, total abdominal hysterectomy provided the ultimate cure. The procedure is technically
different from hysterectomy for gynecological reasons. The main difference is identifying and
removing the lower uterine segment. This might be the curative part of the procedure and has to be
handled with care. The bladder has to be reflected, dissected and pushed inferiorly and laterally to
minimize the chances of bladder injury and ureteric injury. The boundaries of the lower uterine
segment are ill-defined and it can be difficult to identify the cervix. Often it can only be partially
removed. ( Basket TF 2002). Delaying the decision to carry out post-partum hysterectomy can be catastrophic because the patient
may deteriorate much further and faster than anticipated so that it becomes impossible later to carry
out what could have been a life-saving intervention. Hysterectomy should not be delayed until the patient is in extremes or while less definitive
procedures of which the surgeon has little experience are attempted.
Performing hysterectomy in a timely fashion is therefore a sign of maturity of the team looking after
the patient. The pressures to preserve fertility and avoid a hysterectomy can also be equally great
and several techniques have evolved in recent decades. Interventions to occlude the blood supply to the uterus or to tamponade the uterine cavity are
options to avoid inevitable hysterectomy. (J.Obstet and Gynaecol 2002, )
19

Ligation of the internal iliac arteries has been used but requires complex dissection of the lateral
pelvic wall. Vascular embolization procedures have become established and are less invasive
interventions with well documented curative effect. The technique involves inserting a catheter in
the femoral artery going into the large circulation and then to the uterine vessels. Embolization at
this point will at least lower the blood pressure around the uterus, These techniques require a
multidisciplinary approach and trained personnel who might not be available in many district
hospitals even in industrialized nations.(Rizvif,2004,). Within the last decade there has been renewed interest in new uterine tamponade procedures such as
balloon compression and other procedures, e.g. the B-Lynch suture.
The oldest form of tamponade, uterine packing, has a long history in obstetrics and was widely used
in the management of PPH before prostaglandin agents were an option or because of their expense.
A 20-m-long gauze pack has to be tightly inserted inside the uterus. For it to work, it must start at
the funds of the uterus otherwise bleeding will continue above the pack. The success of the
procedure is dependent on these points and this may become apparent some hours later. Anxieties
about the efficacy of the technique and its potential to act as a focus of infection and to cause
pressure necrosis on adjacent organs have led to alternative approaches such as the Sengstaken
balloon compression. Arulku maran and others described 14 cases of intractable PPH who avoided
surgery by the use of this balloon (Chong Ys,Arukumarans. 2004).It was first described in a case
series in 1997. Compared to hysterectomy or to vascular mobilization, the B-Lynch suture is a much
simpler procedure and its technique can be easily mastered. It does not require special training and is
illustrated in Figures.
Experience with this technique is promising but the evidence is limited to case reports. (H.Refaey,
Ch. Rodeck 2003) .
2.14 Management of the third stage of labor The third stage of labor commences with the completed delivery of the fetus and end with the
completed delivery of the placenta and its attached membranes. The clinician immediately
recognizes that from a practical perspective, the risk of complications continues for some period
after delivery of the placenta. For this reason many authorities have advocated a so-called fourth
stage of labor, which begins with the delivery of the placenta and lasts for an arbitrary period
afterward. The most commonly chosen duration is 1 hour; however, periods as long as 4 hours have
been suggested. The length of the third stage itself is usually 5-15 minutes. The absolute time limit
20

for delivery of the placenta, without evidence of significant bleeding, remains unclear. Periods
ranging from 30-60 minutes have been suggested.( Magann EF, Evanss,2005). There are two methods for managing the third stage of labor. One of these is the physiologic
("expectant") management in which oxytocin are not used; placenta is delivered by gravity and
maternal effort. The other one is the active management in which an uterotonic agent is
administered, after the cord is clamped, the placenta is delivered by controlled cord traction (CCT)
with counter-traction on the funds (upper part of the womb), uterine massage takes place after
delivery of the placenta as appropriate. (John R Smith 2012).
Active management of the third stage of labor (AMTSL) is an evidence-based, low-cost intervention
used to prevent postpartum hemorrhage. The Bristol 123 and Hinchingbrooke12 randomized control
trials provided conclusive evidence that active management of the third stage of labor (AMTSL)
significantly reduces postpartum hemorrhage, decreases blood loss , reduced postpartum anemia and
decreases the need for blood transfusions. (FIGO 2003). In response to the growing evidence supporting the use of active management of the third stage of
labor (AMTSL) for the prevention of PPH, the International Confederation of Midwives (ICM) and
the International Federation of Gynecology and Obstetrics (FIGO) issued a joint statement. The
November 2003 joint statement promotes AMTSL to save mother’s lives(ICM and FIGO 2003).
Every attendant at birth needs to have the knowledge, skills and critical judgment needed to carry
out active management of the third stage of labour and access to needed supplies and
equipment.ICM | FIGO joint statement has caused many discussions amongst midwives in the world . The different opinions of midwives in different part of the world ,made it clear that midwifery
skills do not need to be performed in the same standardized way .
The emphasis of (ICM and FIGO was still on promoting evidence Based interventions to prevent
PPH but nuances were made by saying that the intervention should be used properly and after
informed concent. This gave space to the different settings(low and high resources) and thus the
need for standardized interventions in which midwives do their work and even important , it gave
room to womens voices towards their care during child birth . Both ICM and FIGO endorse international recommendations that emphasize the provision of skilled
birth attendants and improved obstetric services as central to efforts to reduce maternal and neonatal
mortality. (Second ICM| FIGO 2006).
21

Three steps of AMTSL Active management of the third stage of labor consists of interventions designed to facilitate the
delivery of the placenta by increasing uterine contractions and to prevent PPH by averting uterine
atony.
The three components of AMTSL are: 1. Administration of a uterotonic agents; 2. Controlled cord traction; 3. Uterine massage after delivery of placenta, as appropriate. The third component – uterine massage - was not present in the Hinchinbrook randomized controlled trial 1998 ,but it was the ICM that took the initiative to add the uterine
massage so that the skilled birth attendants would stay alert on the late PPH. (ICM Recent evidence
on AMTSL 2006). Oxytocin is the uterotonic drug of choice. But in the second ICM/ FIGO Joint Statement, the two
key partners call upon national regulatory agencies and policy makers to approve misoprostol for
PPH prevention and treatment. (ICM |FIGO 2006). In a study conducted by the WHO `Stability of Injectable Oxytocic in Tropical Climates` there was, on average, no loss of potency of Oxytocin after twelve months refrigerated
storage, and about 14% loss after one year at 30°C in the dark (range 9-19%), No destabilizing
effect of light was found. (WHO report 2005).
Recent evidence on AMTSL Effectiveness of AMTSL in reducing the incidence of postpartum hemorrhage (PPH) and the need
for PPH treatment has been investigated by a number of large trials. The Hinchingbrooke12
randomized control trials provided evidence that AMTSL significantly reduces postpartum
hemorrhage, decreases blood loss, and decreases the need for blood transfusions. Findings from a
WHO multi-center study indicated that 10 IU oxytocin (intravenous or intramuscular) is preferable
to 600 microgram of oral misoprostol in the AMTSL in hospital settings where active management
is the norm. (International confederation of midwives 2006) Prognosis The confidential enquiry into maternal deaths for 2000 – 2002 reported 17 deaths related to obstetric hemorrhage in that triennium.This gives a rate of 8. 5 per million (Lewis, G 2007) .
22

2.15 Prevention of postpartum Hemorrhage Each year, hundreds of thousands of women and babies die or become disabled due to complications
of pregnancy and childbirth, hafe of these maternal deaths occur within 24 hours of childbirth .
postpartum hemorrhage (PPH) is the leading direct cause of maternal death in developing countries
and most often results from problems during and immediately after the third stage of labor. PPH is
an unpredictable and rapid cause of maternal death worldwide, with two thirds of women with PPH
having no identifiable risk factors, Seventy to ninety percent of immediate PPH is attributed to
uterine atony. Fortunately, research shows that simple, low cost interventions can help avoid most of these tragic
outcomes. Current evidence indicates active management of the third stage of labor (AMTSL)
(administration of uterotonic drugs, controlled cord traction, and fundal massage after delivery of the
placenta ) can reduce the incidence of postpartum hemorrhage by up to 60 percent.
Ongoing research in various settings continues to identify the best approaches for preventing and
managing postpartum bleeding and its complications. By developing national guidelines, training
skilled birth attendants, improving work environments of skilled providers, and supporting the
development of improved access to care, more women will have access to this lifesaving
intervention. (POPPHI, 2009) The primary intervention shown to reduce the incidence of PPH is active management of the third
stage of labor( AMTSL ).
Other preventive measures include reducing the incidence of prolong labor through the use of the
partograph and timely intervention , when needed, minimzing the trauma associated with
instrumental delivery, avoiding routine episiotomy, and detecting and treating anemia during
pregnancy. (Deborah Armbruster 2002).
Primary prevention of PPH is advocated at all levels of obstetric care. This implies active
management of the third stage of labor also at the first and most peripheral levels of obstetric care.
Active management includes the use of an oxytocic, early cord clamping and active delivery of the
placenta. The oxytocic drug of choice at this moment is oxytocin 5 IU given intramuscularly.
Women with hig.h-risk factors for PPH .(polyhydramnios, previous complications in third stage,
APH or multiple pregnancies)shoud be delivered in hospital .
Timely antepartum referral is necessary In these women,prevention and anticipatory management
includes the availability of intravenous treatment, as well as active management with an oxytocic.
Evidence for the effectiveness of active management of the third stage of labor in women at low risk
of PPH is not yet available. Whether women delivering at home with easy accessibility to hospital,
23

or those at low risk delivering in hospital, should be actively managed remains controversial, and
such an approach is not supported by us until a clinical trial in this particular group of women has
shown the effectiveness of the active management . The active management of the third stage of labor; prophylactic oxytocics should be routinely used
in the third stage of labor as they decrease the risk of PPH by 60% . (McCormick ML 2002).
WHO recommended oxytocin as the drug of choice. Within one minute of birth of the baby,
controlled cord traction to assist with prompt delivery of placenta and
massage the uterus after delivery of placenta. Though facility based service providers are the
primary users of AMTSL it can be practiced in community setting by appropriately trained health
service providers . The world Health Organization (WHO) recommends that AMTSL should be offered by skilled birth
attendants (SBA) to all women. (Midwifery, Org.nz 2006).
There are four strategies for implementing AMTSL ,the first strategy is uterotonic drug( oxytocin or misoprostol,) WHO recommended Oxytocin as the drug of choice ,In places,
where Oxytocin is unavailable, Misoprostol can be used as an alternative.
The second strategy : Controlled cord traction is the component of AMTSL for which clinical
training is required due to the potential risks of tearing of the cord from the placenta and inversion of
the uterus. This is why controlled cord traction should be practiced only by SBAs or health care
providers such as auxillary nurse
,midwives,community midwives,village midwives and health visitors who have acquired
appropriate skills and have been specially trained to competence. (Rogers J,WoodJ,1998).
Strategy : 3 – The use of uterotonic drug (Oxytocin or Misoprostol ) should become routine for all
postpartum women, particularly for women delivering in communities.
In Indonesia a study was completed on community –based distribution of Misoprostol in West Java
that proved the feasibility and acceptability of this
approach to PPH prevention. (Songhvi H et al 2004). Strategy – 4 : Uterine massage : In some setting there are no uterotonic, uterine massage may be the
only option women should be taught the value of uterine massage and how to evaluate if they are
bleeding too much. The international confederation of midwives and the international Federation of
Gynecology and Obstetrics(FIGO) recommended that when no uterotonic are available to either
skilled or non –skilled birth attendant, management of third stage of labor should include : waiting
for sign of separation of the placenta (cord lengthening, small blood loss, uterus firm and globular
24

on palpation at the umbilicus) encouraging maternal effort to bear down with contractions and if
necessary ,to encourage an upright position ,and uterine massage after the delivery of the placenta as
appropriate. Abdel-Aleem and colleagues conducted a randomized trial to determine the effectiveness of
intermittent uterine massage starting prior to the delivery of the placenta for 60 minutes to reduce
postpartum blood loss and the need for additional uterotonics. The trial showed that persistent
uterine massage reduced the amount of blood loss and the use of additional uterotonic. Massage
every 10minutes for one hour helped in prevention of PPH. (Abd Eleem H, 2006) Secondary postpartum Haemorrahage
This commonly presents in primary care as prolonged or excessive bleeding once the women has
returned home after delivery .
Assessment History: As above also extended labor, difficult third stage of labor , ragged placenta, primary PPH.
Examination: Systemic illness, fever, rigors, tachycardia, tissue visible within loss. Suprapubic area
may be tender, with elevated funds that feels boggy in retained products of conception (RPOC.s ) Investigation
FBC
Blood cultures are positive in 10 -30 %
Check MSU
High vaginal swab, also gonorrhea /Chlamydia
Ultrasound; may be used if RPOC suspected, although there may be difficulty distinguishing
between clot and products. RPOC are unlikely if a normal endometrial Stripe is seen.
Management of secondary postpartum Hemorrhage Speculum examination will allow visualization of cervix and lower genital tract to exclude
lacerations. if clot is visible within the cervical os , it may be removed with tissue forceps (though
few GPS regularly carry these ). Allowing the cervix to close . When antibiotics are clinically indicated, combination of ambicillin, (Clindamycin if penicillin –
allergic) and metronidazole is appropriate. In cases of
endomyometrtis (tender uterus) or overt sepsis, then the addition of gentamicin is
recommended.
25

If infection suspected combination of broad spectrum e.g. amoxicillin , gentamicin and
metronidazole , can be given . Patient may need to be referred if too unwell to tolerate oral
medication, Iv clindamycin and gentamicin tds until a febrile for greater than 24 hours. ( oral follow
up treatment is not required) .Use doxycycline if Chlamydia is suspected . if retained products of conception are suspected elective curettage with antibiotic cover may be
required .
Patient may require iron supplementation if Hb has fallen. Warn of the risk
of Constipation. Prognosis 90% of cases treated with antibiotics improve with in 48 -72 hours . if this is not the case, The
patient should be re- evaluated .
The confidential enquiry into maternal deathes for 2000-2002 seventeen deathes related to obstetric
haemorrage in the triennium 13. This gives a rate of 8.5 per million. ( Lewis, G (ed) 2007 2002).
2.16 Nursing management of postpartum
Haemorrhage Definition of midwifery care Midwifery care is the autonomous practice of giving care to women during pregnancy, labor, birth,
and the postpartum period, as well as care to the new born
infant. Midwifery care is provided in accordance with established standards, which promote safe and
competent care.
the midwife implements these standards though adherence to the Tennessee midwives, Association
(TMA practice Guidelines ). Competencies of midwives Evaluation of the childbearing woman is an on –going process, including risk screening to assess
and identify conditions, which may indicate a deviation from normaly. The identification of those
conditions may require physician involvement. In making this assessment, a Midwife relies on her /
his training, skill, and clinical judgment. This document is representative and not an exhaustive list
of the conditions that a Midwife may encounter. This document is not meant to replace the clinical
judgment or experience of the Midwife.
There may be variations based on agreements between individual midwives and their consulting
physicians. ( Obstet Gynecol2003).
26

Midwife and client responsibilities and rights The informed choice and Disclosure ( ICD ) . The midwife is required to have on file, assigned statement that each client has read and understood.
Midwifes; informed choice and Disclosure (ICD) agreement. The ICD should be written or
translated in language understandable to the client. There must be a place on the form for the client
to attest that she understands the content, by signing her full name.
The ICD disclosures, to a prospective client, information regarding the Midwife’s practice. The ICD includes information regarding the Midwife’s responsibilities and rights as well as the
client’s responsibilities and rights .each Midwife may broaden the agreement to include additional
information reflecting details of the midwife’s practice. The ICD shares information regarding the responsibilities and rights of the midwife. It includes
information including, but not limited to:
1- Philosophy of practice and care. 2- Benefits and risk of out- of- hospital birth .
3- Training and education .
4- Years of experience. 5- Participation in peer review . 6- Information regarding the Midwife’s emergency care plan and collaborating or consulting
physician .
7- Care/ equipment provided; 8- Information regarding a clients right to giving informed consent prior to any procedure and / or
administration of any prescribed medication to mother or newborn , risks, benefits, options and
alternatives . 9- Acceptance/ refusal of Midwives recommended care. the client ,s decision to refuse/ decline
recommended care will be made in writing, signed by the client , and kept in client’s records.
10- Information regarding client conditions/ concerns for which a midwife may need to consult with
a physician, refer client to a physician, and /or transfer client out of midwife’s care to physician’s
care.
27

and client responsibilities and rights The informed choice and disclosure (ICD ) agreement, continued . 1- midwife’s expectations of the clients , responsibilities and the midwife’s right to discontinue care ; 2- legal requirements, i.e. TN mandated newborn screening for inborn errors of metabolism(
PKU)eye prophylaxis, reporting of communicable diseases ,and registration of birth and death
certificates . 3- financial information. 4- midwife’s current legal status. 5- grievance processes for client complaints regarding care. 6- Process to access copies of the client’s midwifery records. The midwife will give a copy of the
ICD to the client and keep a copy of the ICD agreement statement in the client, s records (ICD
Agreement 19-2006).
Midwifery Record Keeping The midwife: A. documents completely and accurately the client's history, physical exam, laboratory test results,
prenatal visits, consultation reports, referrals , labor and birth care postpartum care/ visits,and
neonatal evaluations at the time midwifery services are delivered and when reports are received . B. facilitates clients' access to their own records . C. maintains the confidentiality of client records. D. Retains records for a minimum of five years . E. Completes / files all state required reports/ certificates in timely manner .
PRACTICE PROTOCOLS Practice protocols based on TMA practice Guidelines will be avaialable for each potential client to
review. 2.17 SAFE ENVIRONMENT FOR BIRTH
The midwife: A. Asesses the birth setting for freedom from environmental hazard. B. Brings own equipment to birth setting. C. Promptly responds to client's needs. D.Practices universal precautions established by Occupational Safety and Health Adminstration
(OSHA).guidelines regarding equipment, examinations, and procedures. PRENATAL CARE
28

During prenatal care , the client shall be seen by the Midwife or other appropriate health care
provider at least once every four weeks until 30 weeks gestation, once every two weeks from 30
until 36 weeks gestation , and weekly after 36 weeks gestation , or as appropriate ( Sullivan
EA,2005 jun). Initial prenatal Visit 1/ History/assessment of general health.
2/ History/assessment of obstetric status. 3/ History/assessment of psychosocial status. 4/ Physical Exam to include, but not limited to:. height, weight , blood pressure, pulse,breasts , to
include teaching on self exam.
abdomen ,to include fundal height ; fetal heart tones , fetal lie and presentation.
Estimation of gestational age by physical findings .
Assessment of varicosities, edema and reflexes .
laboratory Tests.
The client will be offered the following laboratory tests to include but
not limited to:
a. hemoglobin and or hematocrit or CBC . b. gross urinalysis for protein and glucose . c. Syphilis serology . d. Blood group , Rh type , and antibody screen. e. Hepatitis B surface antigen . f. Rubella screen . g. Genetic screening tests. h. Gonorrhea test , if at risk . i. Chlamydia test , if at risk. j. HIV test if at risk.
B. on – going prenatal care. 1. Assessment of general health. 2. Assessment of psychosocial health. 3. Nutritional counseling. 4. Physical Exam to include, but not limited to:
a. blood pressure;
29

b. pulse optionac. weight , abdomen , to include fundal height , fetal heart tones fetal lie and
presentation . e. estimation of gestational age by physical findings ; f. assessment of varicosities , edema and reflexes .
5. Laboratory Tests. The client will be offered the following
laboratory tests to include but not limited to:
a. hemoglobin , hematocrit , or CBC by 28 and or after 32 weeks . b. gross urinalysis for protein and glucose at each visit . c. Glucose Tolerance Test ( GTT) , IF indicated ; d. Group Beta Strep (GBS)culture(s),according to CDC Guidelines ; e Herpes (HSV 1 and /or HSV 2) cultures(s), if indicated.
INTRAPARTUM CARE: During labor, the Midwife shall monitor and support the natural process of labor and birth, assessing
mother and baby throughout the birthing process:
1.Assess and monitor fetal well – being . While in attendance, assess FHR. a. 1st Stage of labor ; at least once every hour, or as indicated . b. 2nd Stage of labor ; at least every 10 minutes, or as indicated . 2. Assess and monitor maternal well- being While in attendance, assess vital signs at least every 4
hours, or as indicated .
3. Monitor the progress of labor. 4. Monitor membrane status for relative fluid volume, odor of amniotic fluid. 5. Assist in birth of baby. 6. Inspections of placenta and membranes . 7. Manage any problems in accordance with the guidelines cited elsewhere in this document. 8. Whenever vaginal examination. Are performed to assess the progress of labor, they will be kept
to a minimum to reduce the risk of infection . Attention will be directed toward aseptic technique
Assess cervical dilatation ,effacement, station, and position during each exam and document in,
client's chart.
30

POSTPARTAL CARE: After the birth of the baby, the Midwife shall assess, monitor , and support the mother during the
immediate postpartum period until the mother is in stable condition and during the on-going
postpartum period.
Immediate postpartum care Overall maternal well- being ,Bleeding and Vital signs. Abdomen including fundal height and
firmness .
Bowel/bladder function .
Perineal exam and assessment .
Suture firest or second degree laceration(s)/episiotomy, as indicated . Facilitation of maternal- infant bonding and family adjustment Concerns of the mother. (virtual
medical centre2005)
2. 18 Immediate care for the newborn:- Health assessments of the new baby begin immediately. One of the first checks is the Apgar test to
evaluate the condition of the newborn at one minute and five minutes after birth. The physician and
nurses will evaluate the following signs and assign a point value:
Activity; muscle tone
Pulse rate
Grimace; reflex irritability
Appearance; skin color
Respiration A score of 7 to 10 is considered normal. A score of 4 to 6 may indicate that the baby needs some
resuscitation measures (oxygen) and careful monitoring. A score of 3 or below indicates that the
baby requires immediate resuscitation and lifesaving techniques.
Physical examination of the newborn in the delivery room: A brief, physical examination is performed to check for obvious signs that the baby is healthy. Other
necessary procedures will be done over the next few minutes and hours.
measurement of the temperature, heart rate, and respiratory rate
measurement of weight, length, and head circumference - these measurements help
determine if a baby's weight and measurements are normal for the number of weeks of
31
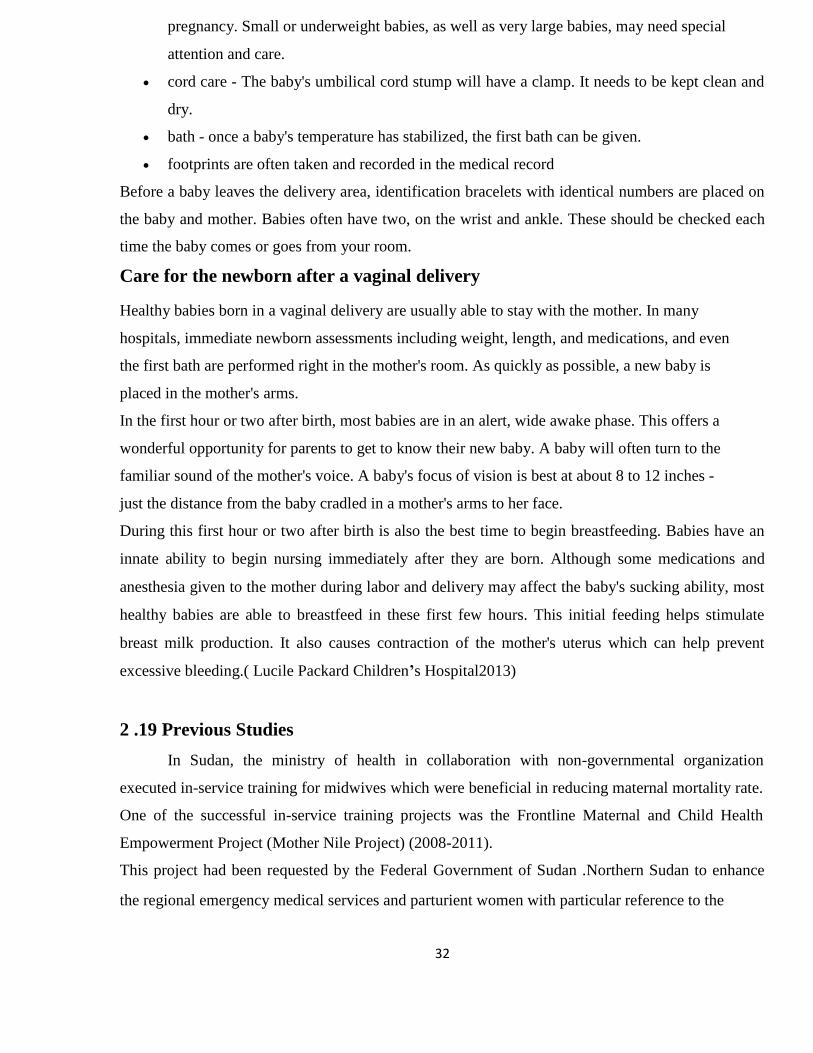
pregnancy. Small or underweight babies, as well as very large babies, may need special
attention and care.
cord care - The baby's umbilical cord stump will have a clamp. It needs to be kept clean and
dry.
bath - once a baby's temperature has stabilized, the first bath can be given.
footprints are often taken and recorded in the medical record Before a baby leaves the delivery area, identification bracelets with identical numbers are placed on
the baby and mother. Babies often have two, on the wrist and ankle. These should be checked each
time the baby comes or goes from your room. Care for the newborn after a vaginal delivery Healthy babies born in a vaginal delivery are usually able to stay with the mother. In many
hospitals, immediate newborn assessments including weight, length, and medications, and even
the first bath are performed right in the mother's room. As quickly as possible, a new baby is
placed in the mother's arms.
In the first hour or two after birth, most babies are in an alert, wide awake phase. This offers a
wonderful opportunity for parents to get to know their new baby. A baby will often turn to the
familiar sound of the mother's voice. A baby's focus of vision is best at about 8 to 12 inches -
just the distance from the baby cradled in a mother's arms to her face.
During this first hour or two after birth is also the best time to begin breastfeeding. Babies have an
innate ability to begin nursing immediately after they are born. Although some medications and
anesthesia given to the mother during labor and delivery may affect the baby's sucking ability, most
healthy babies are able to breastfeed in these first few hours. This initial feeding helps stimulate
breast milk production. It also causes contraction of the mother's uterus which can help prevent
excessive bleeding.( Lucile Packard Children’s Hospital2013)
2 .19 Previous Studies
In Sudan, the ministry of health in collaboration with non-governmental organization
executed in-service training for midwives which were beneficial in reducing maternal mortality rate.
One of the successful in-service training projects was the Frontline Maternal and Child Health
Empowerment Project (Mother Nile Project) (2008-2011).
This project had been requested by the Federal Government of Sudan .Northern Sudan to enhance
the regional emergency medical services and parturient women with particular reference to the
32

hardware services .In response to this request,JICA carried out the project ,the period (2008-2011)
aiming to decrease the infant mortality rate and maternity mortality ratio in Northern Sudan. To achieve this goal, the Project has been endeavoring to enhance the capabilities of the federal and
state health administrations and village midwives who are active on the frontlines of health services
in the communities; strengthen the network among village midwives and the network on the state
level and build a framework providing mothers and children in the communities with the quality and
continuing care services. A study review which conducted in February 2010, had put forward some recommendations for
enhancing and institutionalizing the support systems of FMOH and SMOH to village midwives; and
standardizing the engagements (the Sinnar Model) in the Sinnar State, the pilot state of the Project,
to introduce to other states.
Following the review, the project team set about training of trainers (TOT) for in-service training of
village midwives in five states including the threeDarfurStates.
The Project has realized empowerment of village midwives in both material and psychological terms
by carrying out in-service training; strengthening the relationships between health professionals and
village midwives; strengthening the support system including additional instructions and individual counseling, and
upgrading tools consumable goods necessary for delivery and care of pregnant women. It has also
demonstrated that empowerment of village midwives has certain effects on improvement in the
quality of maternal and child health services in the regional health sector.
A survey on the effect of training carried out in line with the Project has clarified that part of the
maternal and child health services provided by village
midwives has in fact improved. Also, Confirmed improvement in knowledge and practical skills of
village midwives about infection prevention, referrals system due to in-service training.
The study recommended the provision of midwives with in-service training and to prepare
guidelines for a set of teaching materials for the 7-day in-service training .In addition to, Continued
commitment to training and strengthening the capabilities of health visitors, nurse midwives and
assistant health visitors who are supervisors of village midwives.
Another in-service midwifery training program that aims to improve maternity services, lower
maternal mortality rates and empower women in South Sudan, had developed by Academics and
midwives at the University of Southampton. South Sudan has one of the highest maternal mortality rates in the world at 2,054 to 100,000 live
births. The majority of current maternity services, including deliveries, are provided by about 2,500
33

women who have had between two weeks and eighteen months midwifery training. There are 12
midwives across South Sudan that are recognized as ‘registered midwives’, the majority of whom
are from neighboring African countries. The University of Southampton was appointed by the United Nations Population Fund (UNFPA) to
design a comprehensive and standardized national in-service midwifery training program for the
newly developed Ministry of Health, Government of South Sudan (GOSS) (Gobbi,M. et al 2012). The program’s aim was to strengthen midwifery education in line with the United Nations’
Millennium Development Goal targets of reducing maternal mortality and ensuring universal access
to reproductive health services by 2015. Many midwifery staff in South Sudan has lower literacy
skills so it was a challenge to write a program that would be understandable and able to be taught.
Therefore, the team developed new ways of teaching, through methods such as picture cards and
color codes. The program is designed to be appropriate to the South Sudan local needs and
enhancing what is available to ensure all women have access to a standardized service. The completed training program had been developed, implemented and benefit many midwives in
South Sudan. (Gobbi,M. et al 2012) .
Teaching Guatemala midwives about postpartum hemorrhage study by Garcia K, Morrison FB, and
Savirin C 2012) evaluated the effect of a culturally sensitive teaching unit on traditional midwives'
knowledge of nursing interventions to prevent and treat postpartum hemorrhage (PPH).Sixteen
midwives participated in a 1-day training program at a Refuge International Health Clinic in the
remote town of Sarstun, Guatemala. The quasi experimental study used a one-group, pre test-post
test design.
Researchers used a PPH Behavioral Checklist from the American College of Nurse Midwives
(ACNM) to assess and compare knowledge of PPH interventions before and after the PPH teaching.
The final analysis included 13 traditional midwives as the subjects. The culturally sensitive teaching
improved traditional midwives' knowledge and skills about nursing interventions to manage PPH
(pretest M = 1.385/8, post test M = 4.846/8). The results of this pilot project suggest a culturally
sensitive oral teaching in the primary language of the participants positively affects traditional
midwives' knowledge and skills to manage PPH. Future training should be presented in a similar
format to meet the needs of illiterate audiences in resource-poor settings. Another study to assess the effectiveness of active management of third-stage labor in reducing PPH
had been done in Vietnam by Tsu VD, Mai TT, Nguyen YH, Luu HT(2006).The study was
undertaken to meet the need of the Ministry of Health to have local evidence on the effectiveness of
active management of third-stage labor (AMTSL) in reducing the incidence of postpartum
34

hemorrhage (PPH) > or = 500 mL and the need for PPH treatment.Using a quasi-experimental
design, AMTSL was introduced for all births attended by government midwives (at home,
community, and district levels) in one district while standard practice without AMTSL was
continued in three neighboring districts (with a 1:2 ratio of participants). Oxytocin (10 IU) was
administered either by standard disposable syringe and needle or by a prefilled ,single-use injection
device. Postpartum blood loss was estimated using standard containers . other outcome measures included the duration of third stage, the need for additional treatments, and
final maternal condition. A total of 3607 women participated (1236 in the intervention district and
2371 in the comparison districts). Multivariate logistic regression was used to control for age, parity, place of delivery, and first-stage
oxytocin augmentation.
The results found that AMTSL was associated with reduced risks for prolonged third stage beyond
30 minutes, supplemental oxytocin, and bimanual compression. When cases with first stage oxytocin
augmentation were excluded, AMTSL was associated with a 34 percent reduction in PPH incidence
5. Although a WHO multicenter trial concluded that, in hospital settings, oxytocin is preferable to
misoprostol in AMTSL, in home births without a skilled attendant, misoprostol may be the only
technology available to control PPH. The safety and efficacy of misoprostol as an alternative to
oxytocin is now well documented. International Confederation of Midwives, International Federation ofGynecology and
Obstetrics2006 evaluated the effectiveness of AMTSL in reducing the incidence of postpartum
hemorrhage through a study done in a university teaching hospital in England. It demonstrated that
giving misoprostol to women immediately after childbirth resulted in significantly lower rates of
PPH than when the third stage of labor was managed only through controlled cord traction and
rubbing the uterus. Studies also found that 18 percent of women would experience PPH if the
placenta were delivered on its own, 2.7 percent if oxytocin were used, and 3.6 percent if misoprostol
were used .
A recent study from India provided evidence that oral misoprostol was associated with about 50
percent reduction (from 12.0 percent to 6.4 percent) in the rate of acute postpartum hemorrhage and
mean blood loss. The WHO recommends that AMTSL should be practiced by skilled midwives. Another study by (Angeline Fujioka and Jeffrey Smith March 2011) in the Prevention and
Management of Postpartum Hemorrhage for nurse midwives revealed that Maternal mortality
persists at exceedingly high rates—with the World Health Organization (WHO) reporting a maternal
mortality ratio (MMR) of 290 maternal deaths per 100,000 live births in developing nations. (WHO
35

2010). Consequently, reducing maternal mortality is a global development priority for donors and a
global program priority for the United States Agency for International Development (USAID) and
the Maternal and Child Health Integrated Program (MCHIP) as part of USAID efforts to support
achievement of Millennium Development Goals 4 and 5. MCHIP is focused on advancing the
uptake of evidenced-based, high-impact interventions appropriate for low-resource settings in which
postpartum hemorrhage (PPH) and pre-eclampsia/eclampsia (PE/E) are of major concern. Further,
MCHIP supports USAID and other donor programs to scale-up these interventions with the overall
goal of reducing maternal mortality in the 30 priority countries with the highest mortality rates by
2013, a shared goal of USAID’s Maternal Health Results Pathway. Programs to reduce mortality
from PPH are in place in many countries around the world. a database on PPH-reduction activities
was using developed in 2010 with input from multiple partners (based on, and some, initial work
done by PATH and the Prevention of Postpartum Hemorrhage Initiative (POPPHI). A further update and analysis of that database is presented for 31 countries worldwide in the regions
of Africa, Asia and Latin America. The 21 African countries are: Angola, Democratic Republic of
the Congo (DRC), Ethiopia, Equatorial Guinea (E. Guinea), Ghana, Guinea,Kenya, Liberia,
Madagascar, Malawi, Mali, Mozambique, Nigeria,Rwanda, Senegal, South Sudan, Tanzania,
Uganda, Zambia, Zanzibar and Zimbabwe. Afghanistan Bangladesh India,Indonesia and Nepal are
the five Asian countries. The five Latin American countries are Bolivia, Guatemala, Honduras,
Nicaragua and Paraguay. one of five themes across all 31countries was : Education and training in AMTSL. The outcomes was that the majority (94%) of countries stated that AMTSL is currently included in
education and training components through service delivery guidelines, pre-service education and
in-service training for skilled birth attendants (SBAs). One hundred percent of LAC countries have
AMTSL in all three training components.
Zimbabwe does not currently have AMTSL in its service delivery guidelines, although the regarding
AMTSL integration with education and training components. Guidelines are under revision to
include AMTSL. Zimbabwe does have partial in-service training in AMTSL but not for all cadres of
SBAs.
In India, the government is working with MCHIP to include AMTSL in pre service education at
schools for Auxiliary Nurse Midwives (ANMs). In DRC, training materials have been developed,
and training has begun for teachers on AMTSL. However, AMTSL is not yet integrated with the
pre-service education system in DRC. Angola and Madagascar did not provide additional
information.
36

policies and education guidelines to reduce PPH and PE/E and actual services delivered. Multiple,
creative approaches are needed—and are being implemented—to address this gap between policy
and practice. Possible approaches include quality improvement initiatives, change management strategies and
health approaches.
Nurses in Low Resource Settings Save Mothers’ Lives With Non-pneumatic Anti-Shock Garment
was a recent study done by Farah, K. et al ,( ) which presents results from six referral hospitals: two
in Egypt (Cairo and Assuit) and four in Nigeria (Southern and Northern Nigeria). These locations
represent an array of settings from the well-resourced urban areas of Cairo to the limited resourced
rural areas of Northern Nigeria. The Purpose was to discuss the role of nurses and nurse-midwives in preventing and treating
postpartum hemorrhage (PPH) from uterine atony in developing countries and examine the role of a
new device, the Non-pneumatic Anti-Shock Garment (NASG), in improving the outcomes for these
patients.
In this sub analysis of a larger pre intervention phase/intervention phase study of 1,442 women with
obstetric hemorrhage, postpartum women with hypovolemic shock (N = 578) from uterine atony
(.750 mL blood loss; systolic blood pressure <100 mm Hg and/or pulse >100 beats per minute) were
enrolled in two referral facilities in Egypt and four referral facilities in Nigeria. The study had two
temporal phases: a pre intervention phase and an NASG-intervention phase. Women with
hemorrhage and shock in both phases were treated with the same evidence-based protocols for
management of hypovolemic shock and hemorrhage, but women in the NASG-intervention phase
also received the NASG.Relative risks (RRs) with 95% confidence intervals (CIs) were estimated
for primary outcomes—measured blood loss, incidence of emergency hysterectomy and mortality. The result showed that women in the NASG-intervention phase had significantly better outcomes,
50% lower blood loss, reduced rates of hysterectomy (8.9% vs. 4%), and mortality decreased from
8.5% to 2.3% (RR = 0.27, 95% CI: 0.12-0.60). In low-resource settings nurses have few resources with which to stabilize women with severe PPH.
With training nurses and nurse-midwives can stabilize hemorrhaging women with the NASG, a low-
technology first-aid device that shows promise for reducing blood loss, rates of hysterectomy, and
mortality.
Another study by Mobasherizadeh S,et al ,2009 about Injury resulting from contaminated sharp
devices among health care workers (HCWs)which can lead to dangerous infections such as human
immunodeficiency virus, hepatitis B virus and hepatitis C virus among people.the objective was to
37

study cases of injuries by sharp devices before and after the implementation of intervention methods
among 87 HCWs in Sadi Hospital in Iran.The study revealed that In the first phase of the study in
2003, 55.2% of those injured had been injured by sharp devices. After intervention in 2004, this
percentage was reduced to 19.5% (p < 0.05). At the beginning of the study, 26.4% of the injured had
been injured by sharp devices more than twice, and at the end of the study this number was reduced
to 2.3% (p < 0.05). Also, injuries resulting from recapping were 45.8% at the beginning of the study,
which was reduced to 5.9% at the end (p < 0.05). With regard to this study and other studies carried out in other countries, a large number of injuries
by contaminated sharp devices can be prevented by implementing suitable educational programs
regarding disposal of sharp devices. Jane Bott in 1999 highlighted the importance of Prevention of occupational infection for
midwives.Universal precaution (UP) is now a common concept and guidelines have been developed
to enable all health-care workers to reduce their risk of occupational exposure to HIV and other
body fluid and blood-borne infections. However, issues surrounding implementation of UP into
midwifery practice are complex.The research findings highlight the need for effective education,
well-publicized guidelines and a conducive work environment. Role models within the practice area
appear to facilitate successful adoption of UP by midwives within the practice areas. In addition to
providing equipment, managers need to review the effectiveness of the equipment, and introduce
safer devices, as they become available. The findings suggest that a democratic management style,
with an emphasis on team working, is more suited to the successful implementation of UP. Staff
development needs may be identified during Individual Performance Review (IPR). Aprevious study by Patel,A etal,2006 that estimating postpartum hemorrhage blood loss was
performed with 123 women delivered at the District Hospital, Belgaum, India.The objective was to
compare visual estimation of postpartum blood loss with estimation using a specifically designed
blood collection drape and the drape estimate with a measurement of blood loss by
photospectrometry. . The women were randomized to visual or drape estimation of blood loss. A
subsample of 10 drape estimates was compared with photospectrometry results. Results: The visual
estimate of blood loss was 33% less than the drape estimate. The interclass correlation of the drape
estimate to photospectrometry measurement was 0.92. Conclusion: Drape estimation of blood loss is
more accurate than visual estimation and may have particular utility in the developing world. Prompt
detection of postpartum hemorrhage may reduce maternal morbidity and mortality in low-resource
settings.
38

A study by Suellen Miller in 2008 concluded that the non-pneumatic anti-shock garment (NASG) is
a first-aid device that reverses hypovolaemic shock and decreases obstetric hemorrhage and could
reduce maternal mortality rate in lower resource settings. It is a simple, relatively inexpensive,
lightweight, reusable compression suit, comprising ve neoprene segments that close tightly with
Velcro around the legs, pelvis, and abdomen. The abdominal segment incorporates a small foam
pressure ball to supply uterine compression . The entire garment, when tightly applied by one
person, supplies 20–40mmHg circumferential pressure. This lower body circumferential
counterpressure shunts blood from the lower extremities and abdominal area to the essential core
organs: heart,lungs, and brain. Within minutes of application, women suffering from shock have
been seen to regain consciousness and normalise their vital signs.
39

CHAPTER THREE
METHODOLOGY
3.1 The study design: This was an interventional prospective case control (NRCT) non randomized control trial hospital
based study. This intervention study was carried out to evaluate the Impact of a Designed In- service
Training program on Nurse Midwives Knowledge, attitude and practices toward postpartum
haemorrahage mangement and nursing care during the third stage of labor.
Variables such as social status, educational level, experience, knowledge, attitude and practices were
assessed. 3.2 Study area and Setting
3.2.1 Study area This study was carried out in Khartoum state which is the national capital and one of the 17th State
of Sudan, area of 20.140 km2 and the population according to 2003 census, of 5, 352, 000, and
estimated to be 6,203,000 in 2007 (which is 1/6 of Sudan population) Sudan population according to
2008 33,419,625.
The people of Sudan are different ethnic groups, from all parts of other states. The state is divided in
to seven localities. Most of the health Institutes belong to Khartoum state government; others belong
to federal government and some are private sectors,“No of private Hospitals 185”."State Hospitals
are 366 .”
(CBS, 2007).
3.2.2 Setting The Study was carried out in six midwifery departments in three teaching hospitals which were
selected randomly from Khartoum State teaching hospitals.The hospitals were Omdurman Maternity
Hospital, Khartoum North Teaching Hospitals and Alribat University Hospital.Each hospital
consisted of two midwifery departments, public and private sector.The private sectors are Sahroon
Midwifery Department, Bahry private Midwifery Department and Omdurman private Midwifery
Department.
40

3.3 The study population
The nurse midwives who work in the six midwifery departments, the total number of them was
"110 in 2010 ".The level of education midwives who completed basic Nursing education for three
years and had experience of at least two years and then studied midwifery for one year and
experience for two years in the labor Rooms. 3.4 Inclusion criteria
Certified nurse midwives, who are regularly working in the labor rooms in midwifery department,
with two or more years of experience. Who agreed to participate. 3.5 Exclusion criteria
Other types of midwives, "Sister midwives, village midwives and traditional midwives .
3.6 Sampling The target population included 100 nurse midwives who works in the six midwifery department
labor room from the three selected teaching Hospitals in Khartoum state. 3.6.1 Sample Size
The population of this study was midwives who completed their midwifery programme. The total
number was 110 from six midwifery department in three main teaching hospitals which were
selected randomly; Omdurman midwifery hospital (Number of midwives 52 ) in both midwifery
department, Khartoum North Teaching Hospital in both department of midwifery (number of
midwives 30), Ribat Hospital and Sahroon midwifery department ( No of midwives 28). Sample size
was calculated using the computerized program for standardized sample size using a degree of
confidence 95%.
Accordingly the sample size was found as follows:
Hospitals No of midwives Sample size
Omdurman Maternity Hospital 52 46
Khartoum North Hospital 30 28
Ribat University Hospital 28 26
Total 110 100
41

Half of the midwives (50%) was decided to be trained as interventional group (case), who had been
chosen randomly from the public sector in the three teaching hospitals.The other half (control
group) had been chosen randomely from the NMs who were working in the private midwifery
department(Sahroon labor room, Bahry labor room and Omdurman labor room). The program was designed to measure the effect of training on the interventional group compared
with the control group.
The number of midwives who trained (interventional group) were as follows
Hospitals Sample size Interventional group
1- Omdurman Maternity Hospital 46 23
2- Khartoum North Hospital 28 14
3- Ribat University Hospitals 26 13
Total 100 50
3.6.2 Sample design Given study objectives and structure of the population out lined above the appropriate sample design
chosen was a cluster sampling from each of the six area of midwifery department. 3.6.4 Selection procedures of the study subject
Midwives divided in to two groups, one group is subject to the study (intervention group), the other
was a control group NMs whom working in Sahroon labor room, Bahry labor room and Omudorman
labor room (no 50) Assessment of the intervention group was done by pre and post and follow up
survey , then the result of the two groups was compared (intervention vs control), the result of
intervention is measured by comparing the two groups. 3.7 Data collection technique and tools
Technique used a standardized close ended written questionnaire through a direct interview with the
nurse midwives themselves, and an observation checklist. Data collection tools were designed by
the researcher ,adapted from Prevention of postpartum Hemorrhage initiative (POPPHI) facilitator’s
Guide (Metcafe,G.;Armbruster,D.,2007).
42

3.7.1 Data collection tools Data were collected using structure interview questionnaire prepared by the researcher from the
reviewed literature, information included questionnaire identification data, participant demographic
characteristics, knowledge about PPH, universal precautions, uterotonic drugs, prevention and early
detection of PPH and behaviour of the midwives towards mother. An observational checklist used
pre intervention and post intervention to assess the nurse midwives skills and practice in caring for
the patient in the third stage of labour, episiotomy, estimation of blood loss and assessment of the
implemention of the steps of AMSTL and the principles of infection prevention. 3.8 Phases of the study
3.8.1:Pre intervention phase composed of the
following: 3.8.1.1 Preparatory phase: In this phase the following was done: - Before conduction of the study a written letter explaining the aim of the study was directed from
university of Gezira to the directors of the Hospitals , the directors of the Hospitals agreed and
informed head departments of obstetric and labor room authorities and the matrons of the Hospitals
in order to obtain their permission to collect the necessary data.
An agreement to participate in the study was taken from nurse midwives after explaining the
purpose of the study for each of them. “Verbal agreement”.
- Tools were designed
- Data collector teams were trained and participated in the pilot study. They were 6, 3 of them
are sister midwives (qualifications postgraduate midwifery diploma from the high institute of
midwifery) and 3 are health visitors (qualifications diploma in midwifery). A sister midwife
and health visitor from the three public sectors in teaching hospitals, one from each of the six
midwifery department. A pilot study was carried out to ensure validity of the tools and to test
the work of the data collector who trained for TOT, done on a sample of fifteen nurse
Midwives, five from each hospital, the aim was to test the feasibility and legibility of the
study. Instruments according to the result obtained, some questions were restructured to give
the most accurate answers or response.
- Education programs for nurse midwives, theoretical and practical, were developed.
43

Training of Trainers (TOT) It was decided before implementation of the educational program to select three sisters midwives
and three health visitors, one from each midifery department of the selected teaching
Hospitals,Omdurman midwifery Hospital , Alribat university Hospital and Khartoum north teaching
Hospital. The purpose of the training this leading group was to train other nurses midwives and to
carry in the future the continous training programe in their respective Hospitals . In adition to this
they participated in the practical training of the participant (interventional group in the labor room
and skill lab. The team who consisted of six midwives were trained for two dayes theoritical and practical. The
programe was designed to improve the knowledge, skills and practice in an important issues and
new strategies to prevent postpartum Haemorrhage by impleminting (AMTSL),use of uterotonic
drugs ,universal precautions, review of episiotomy , attitude towards mothers and communication
skills and the new method of how to estimate blood loss . Training done by the researcher and two sisters midwives from Aribat nursing college demonstration
done in the skill lab and labor room in Alribat university Hospital.
The second training package run by obstetricion from Khartoum north Hospital it was about steps of
( AMTSL) and Physiological management of the third stage of labor ,evidence to support why is it
important . Another lecture was about uterotonic drugs given by a pharmasist from Sahroon Hospital . The
session followed by discussion about the essential care during the third stage of labor and discussed
the importance of the communication skills and Attitude and support for mothers during labor.
3.8. 1.2 Education programs for nurse midwives Instructors and trainers were chosen. The programe was designed by the researcher and adapted from Prevention of Postpartum
Heamorrage Initiative(POPPHI) Prevention of PPH AMTSL training packages(POPPHI 2007).It
aimed to improve the nurse Midwives knowledge, skills and practice in management and preventing
the occurrence of (PPH) by implementing (AMTSL) during the third stage of labor. Four learning
packages was prepared and distributed after the training implementation for the intervention group
in a form of notes.
44

3.8.2 Intervention phase Education and training programs for five days was implemented for nurse midwives for the
intervention group only , included three lectures for six hours followed by discussion.
Demonstration for skills done on the skills Lab at Alribat Nursing College for six hours in which
application of steps of active management of third stage of labor (AMTSL), universal infection
control ,precaution,skills of episiotomy ,ways of estimation of blood loss,uses of utertonic drugs and
placenta inspection using a simultaneous models for obstetric delivery. Two days practical training
in the clinical area organized to practice in the real situation labor room in their place of work,
training done by the researcher and TOT team used check list . It was a group work , then individual
work , it took six hours per day.In the fifth day midwives divided into three groups , (group work
three different topic divided between them). ANNEX Session 1 Sudden postpartum bleeding in the third stage of labor. a) Identify postpartum hemorrhage b) The role of nurse midwives and Responsibilities. c) Emergency management and nursing care.
Session 2 Prevention and management of “PPH” by implementing Active management of the third stage of
labor. Session 3 Management and nursing care of the massive obstetric hemorrhage in the labor room.
Teaching and training was done according to the following schedule : The training was run by three lecturers according to the prepared learning packages (4 packages) .
The first one was given by the Researcher, it was about the magnitude of the problem,
factors that contribute to “PPH”. Another two session consisted of the prevention strategies during
antenatal , during labor and after delivery of the placenta.
The second package Run by obstetrician from Khartoum north teaching hospital, associate
professor, and the package consisted of describe structure and function of the uterus during the third
stage of labor. Also the anatomy of the genital tract. Another session define AMTSL and “physiological MTSL” and compare between Them. The
discussion was about evidence to support “AMTSL” and Explain why it can save life.
The third training package was about uterotonic drugs given by a pharmacist from ALRibat
University Hospital, teaching and training was done according to the following schedule:The
45

session identified the uterotonic drugs, dosage, route of administration, side effect and cautions for
uterotonic drugs used for “AMTSL”. list of danger and improper use of the drugs ,essential uses and
contraindications.
The fourth package :training was demonstration in the skill lab at ALRibat Nursing College
and in labor room in the clinical area by the Researcher and TOT team. Demonstrated the steps of
“AMTSL” using the check list in the labor room also demonstrated the essential care during the
third stage of labor important point discussed about precaution for the provider and the mother.
Performed and practice the skills of nursing care for the mother and the newborn after labor and
follow up for two hours and inspection of the perineum tear and laceration. The total No. of “50”
nurse midwives were trained.
3.8.3 Post Intervention Monitoring
After training programe finished immediate post test was carried out.
Monitoring and supervision was carried out after six month to assess implementation of
“AMTSL” by the Researcher and the TOT team in each of the selected Hospitals.
Observation done in the morning shift and evening nightshift (midwives were working in
two shifts only).
Workshop for one day was done for the intervention group after six months from the
previous educational programme in order to strengthen the skills learnt in the original
training program, in particular in the new skills they had not previously known.
A follow up meeting for one day was done six month after the one day work shop to enables
midwives to share experiences, to report successes, review progress and discuss problems
related to practice.
Protocol and guide lines for the midwives to follow in the labor room was the outcome of the
meeting.
Post intervention data was collected (using check list) after a final six months to assess
application of “AMTSL” and the principles of infection prevention and Nursing
management Practice and skills of nursing care for mother and the newborn after labor by the
same data collector. 3.9 Data analysis The statistical package for social sciences (SPSS) was used, frequency distribution, intra group cross
tabulation and inter group comparison, the results were displayed in figures and tables.
46

3.10 Ethics Permission was obtained from health authorities and from hospitals directors, consents were taken
verbally from participants. Confidentiality was insured. 3.11 Validity of instruments The instruments were pre tested in the pilot study before data collection.
3.12 Reliability Test/re-test of the research instruments were done before the actual administration of the
questionnaire and check list. The aim was to test the feasibility and legibility of the study.
The pre test,post test and follow up at interval. Period, This result confirmed that the instrument
was suitable for the study. The result showed improvement on knowledge 27.7±6.16 to 47.9±4.4 to
52.2±3.6 .skills and attitude .showed significant (P-value with <0.005) 3.13 Implications of study results On management and preventing PPH, this Result is considered as the first base line data
(implementing) “AMTSL” by nurses midwives, a protocol for nurse midwives to follow is now
Recommended.Guidelines will be distributed to the midwifery departments in Khartoum State
hospitals. This also highlighted the importance of in-service training in order to maintain the
standards of care since the nurse midwives are the first carers the patients will encounter during their
stay.
3.14 Limitations
Lack of supplies.
Limitations of facilities.
Not funded.
The groups of NMs are the same qualification and midwifery education. half of them are
attached to private midwifery department and this might effect the result.
3.15 Expected results
As a result of in-service training the expected improvement to the practice of nurse midwives
is theefold, the knowledge of the NMS with regards to( AMTSL), the skills of the NMS with regard
to how tomanage and actively prevent (PPH) and the (NMS) attitude towards the patient, namely
treating the patient with respect and maintaining their dignity through out labor.
47

CHAPTER FOUR
RESULTS AND DISSCUSION
RESULTS
4.1 – Socio-demographic data of the respondents The study was carried out in Khartoum state with 50 respondents in three teaching hospitals’
midwifery departments. The majority (42) of the midwives were married (85.7%) and have children
(86.7%), family income revenue midst (80%). Apart from their midwifery certificate, their highest
educational qualification was intermediate school (68%), high school or secondary school was 32%.
They were mainly certified nurse midwives with their years in current occupation experience being
more than 21 years in obstetrics and gynecology units (53.1%). The majority of the respondents
were over the age of 33 (95.9%). Table 4.1: Socio demographic data of the respondents (n,50)
Question no. Socio demographic Frequency Percentage
1 – Social Status
Married 42 85.7%
Celibate 1 2%
Other 6 12%
Total 49 100%
Have children 39 86.7%
Do not have children 6 13.3%
Total 45 100%
2 – Educational Level
Intermediate school 34 68%
High/Secondary school 16 32.%
Total 50 100%
3 – Years in Current Occupational Experience
More than 21 years 26 53.1%
Less than 17 years 23 46.9%
Total 49 100%
4 – Age
More than 33 years 47 95.9%
Less than 32 years 2 4.1%
Total 49 100%
5-Previous in-service training
Yes 19 38%
No 31 62%
48

4.2 Knowledge of nurse widwives about postpartum haemorrhage
Analysis of the structure of the interview questionnaire about the correct definition is very weak, in
pre-training only 6% mentioned the correct answer, which improved after the training programme
post to (98%).
Their knowledge with regard to the types, the majority of them knew primary PPH (92%). Only
(8%) of the midwives mentioned the most correct answers but this improved in post training to
(86%).(4% ) did not know the types.
Table 4.2 – Knowledge of the study group about PPH (n,50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
PPH is described by/as:
Primary and secondary 36 72% 44 88% 48 96%
PPH Primary PPH is the 36 72% 46 92% 50 100%
loss of more than 500
ml of blood within 24
hrs and 800 – 1000ml
in the case of a
caesarean section
Any amount of 30 60% 41 82% 49 98% bleeding causes a
change for the worse in
the woman’s condition
The bleeding causes a 15 30% 44 88% 50 100% low systolic blood
pressure, increasing
heart rate
All of the above 3 6% 20 40% 49 98%
Types of PPH:
Primary PPH occurs 46 92% 47 94% 50 100% during 24hrs of
delivery
Secondary PPH can 28 56% 49 98% 48 96% occur from 24hrs to 6
weeks
Both the above are 4 8% 33 66% 43 86%
correct
Can occur after 6 10 20% 24 48% 22 44%
weeks
Unknown 2 4% 1 2% 5 10%
49

4.3 – Knowledge of the study group about PPH :
Analysis of the structured questionnaire with regard to causes showed 78% of the nurse midwives
knew multiple gestation, polyhydraminous and placenta previa and this increased post training to
100%. Knowledge abou uterine atony and drugs which relax uterine muscle was poor (14% - 36%)
and this improved in both after training to 84% - 94%. Less than half (48%) of the nurse midwives
knew that trauma is one of the causes, but post training this improved to 94%.
Table 4.3 Knowledge of the study group about PPH causes (n,50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Causes of PPH:
Multiple 39 78% 47 94% 50 100%
gestation,
polyhydraminous
Uterine atony 7 14% 22 44% 42 84%
Drugs (uterine 18 36% 34 68% 47 94%
relaxants
Uterine inversion 30 60% 41 82% 47 94%
Placenta previa 39 78% 43 86% 47 94%
(retained or
adherent)
Trauma 24 48% 43 86% 47 94%
50

4.4 – Knowledge about risk factors, signs and symptoms and investigations of
PPH
Their knowledge with regards to risk factors was poor, in blood coalgulation (10%), infections and
baby > 2kg (14%). Half of them knew trauma, infection and null parity was less than half 48%. 90%
of the nurse midwives knew that placenta previa is a risk factor.
Analysis of the signs and symptoms showed that 80% of them knew decreased BP, uncontrollable
bleeding (62%) and signs of shock (56%). Only (10% )knew about the decrease in red blood cells
and (32%) mentioned a loss of blood more than 1000cc. (Table 4.4)
Analysis of the investigations showed that most of the nurse midwives knew the essential
investigations – blood grouping, cross matching and clotting screen (92%). This improved to 94%
post training. Only 6% of the nurse midwives knew that an ECG is one of the essential
investigations and 4% only mentioned the liver enzymes. Knowledge was poor, but improved post
training to 86% (Table 4.4).
Table 4.4 – Knowledge of the study group about risk factors, common signs and symptoms
and investigations. (Average scores when n=50)
Pre (mean) Post (mean) Follow up (mean)
Frequen Percentag Frequen Percentag Frequen Percentag
cy e cy e cy e
Risk Factors 22.5 45.1% 34.2 68.4% 42.8 85.6%
Common signs and symptoms 24.8 49.7% 41.8 83.7% 45.8 91.7%
Investigations 27.4 54.8% 35.6 71.2% 44.6 89.2%
51

4.5 Knowledge of nurse midwives about complications of PPH
Knowledge about the complications of PPH was that (92%) of them knew shock and (82%) knew
about hypotension. However, knowledge about other complications was poor as only (18%) knew
renal failure, (30%) respiratory failure and (36%) knew disseminated intravascular coagulation.
Table 4.5 Knowledge of nurse midwives about complications of PPH
Pre Post Follow up
Frequen Percentag Frequenc Percentag Frequen Percentag
cy e y e cy e
Complications:
Shock 46 92% 48 96% 48 96%
Renal failure 9 18% 33 66% 34 68%
Acute respiratory distres 15 30% 37 74% 46 92%
syndrome
Hypotension 41 82% 47 94% 50 100%
Disseminated intravascular 18 36% 36 72% 46 92%
coagulation
52

4.6 – Knowledge of nurse midwives about utertonic drugs (no.50)
Analysis of the structured interview questionnaire showed that most of the nurse midwives knew
about oxytocin drugs (70%) and this improved post training to (76%). The knowledge with regards
to misoprostol was poor (26%) but improved to (96%) post training. Knowledge about drugs which
increase the risk of PPH was very poor – only (10%) knew. This improved after training to (80%).
Concerning the exact time to give uterotonic drugs, only (26%) knew and this improved after
training to (96%).
Table 4.6 Knowledge of nurse midwives about utertonic drugs
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Oxytocin 5-10 units 35 70% 36 72% 38 76%
Ergometrine and 32 64% 46 92% 48 96%
oxytocin
Misoprostol oral or rectal 13 26% 40 80% 47 94%
Anaesthesia with ether 5 10.2% 26 52% 40 80% and halothane increase
the risk of PPH Uterotonic given after 13 26.5% 40 80% 48 96%
shoulder delivery
53

4.7 – Knowledge of the study group about the principles of infection prevention
(safe labour (no, 50))
Most of the nurse midwives knew that the equipment should be sterilised by autoclaves (81.6%).
This number increased after training and (77.6%) mentioned that sterilisation means the destruction
of microorganisms and spores and this number was (96%) post training. (61%) of the nurse
midwives used disposable needles for suturing once and this increased post training to (96%). Less
than a third of the nurse midwives (30.6%) used a separate set for each delivery and this improved
after training to (90%). (38%) used disinfectants to clean the equipment and floors but only a third
of the nurse midwives (30.6%) mentioned that boiling achieves a high level of disinfection and post
training this was (62%). (34.7%) only knew that disinfection means killing all microorganisms
except spores and this improved post training to (82%).
Table 4.7 Knowledge of the study group about the principles of infection prevention
Correct Response
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Do you use a separate set 15 30.6% 35 70% 45 90%
for each delivery?
Equipment should be 40 81.6% 46 92% 47 94%
sterilised by autoclave Do you use disinfectant to 19 38.8% 36 72% 44 88%
clean the equipment and
floors?
Do you use disposable 30 61.2% 47 94% 48 96%
needles for suturing once?
Sterilisation means killing 38 77.6% 47 94% 48 96% all types of micro-
organisms and spores
Disinfection means 17 34.7% 34 68% 41 82% killing all microbes
except spores
Boiling for 20 minutes 15 30.6% 24 48% 31 62% achieves a high level of
disinfection
54

4.8 – Physiology and changes of the genital tract
Knowledge of the nurse midwives about the physiology of the genital tract was only (14.2% ) but
increased after training to (96%). Knowledge about the physiological changes in the third stage of
labour was very weak (8.2%). After training this number was (98%) .
Table 4.8 – Physiology of the genital tract (no, 50)
Correct Response
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Do you know the 7 14.3% 47 94% 48 96% physiology of the genital
tract?
Do you know the 4 8.2% 45 90% 49 98% importance of the third
stage of labour and its
physiological changes?
55

4.9 – Evaluation of the study group about the working environment and supplies
It seems that nurse midwives are not satisfied by the work environment since less that half (43.5%)
indictated this to be true and even post training this number further decreased to 24%. A satisfactory
opinion of the quantity of supplies and equipment provided to carry out work was only 26% and this
further decreased post trainng once their knowledge of the required equipment had increased and
their dissatisfation reflected a poor number of only 20% who thought the equipment provided was
adequate.
Table 4.9 Evaluation of supplies and work environment (n,50)
Correct Response
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Do you think there are 12 24% 10 20% 10 20% adequate supplies
provided for work?
Do you think the work 20 43% 12 24% 10 20% environment is generally
suitable for effective
work?
4.10 Attitude of nurse midwives towards mothers
Analysis of elements on communication skills towards mothers showed that nurse midwives did not
introduce themselves or ask for permission to begin work (4.1%) in both items. Also it was noted
that the nurse midwives did not smile at the patients (10.2%) but this increased post training to
(74%) of the nurse midwives who did. (75%) of the nurse midwives greeted the patients but only
(14.3% )explained the procedures to the patient. [See table 4.10 (a)]
Analysis of the harmful customs practiced during labour showed that (75.5%) of the nurse midwives
increased the rate of oxytocin to hasten labour but after training this decreased to (26%). (38.8%) of
the respondents administered rough or painful massages on the mother’s abdomen in order to
56

increase contractions but post training this decreased to (16%). (32.7%) encouraged pushing before
the cervix is fully dilated but this also decreased after training to (20%). The use of fundal pressure
to hasten labour was (18.4%) and this did not change post training. [See table 4.10 (b)]
Analysis of the interventional relationship between the mothers and the nurse midwives showed that
only (12%) communicated with the mother in a humane and respectful way and this increased after
training to( 88%). Only (2%) provided proper nursing care to both the mothers and the newborn but
this showed improvement post training (84%). It was noted that (14.3%) of the nurse midwives were
harsh and tough in their attitude and handling of the mothers and this unfortunately did not change
after training. A small percentage (10.2%) were noted to have pinched or hit the mother both pre and
post training. Only (10.2%) of the nurse midwives reassured the mother and this attitude improved
after training to (88%). [See table 4.10 (a)
Table 4.10 (a) – Communication skills
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Introduced her self 2 4.1% 37 75.5% 46 92%
Explained the procedure 7 14.3% 21 42.9% 42 84%
Took permission to carry 2 4.1% 30 61.2% 41 82%
out procedure
Greeted the patient 37 75.5% 48 98% 49 98%
Smiled and thanked the 5 10.2% 22 44.9% 37 74%
patient
Table 4.10 (b) – Harmful customs practiced during labour
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Giving oxytocin I.V and 37 75.5% 21 42% 13 26%
increase the rate Administering rough 19 38.8% 8 16% 9 18%
massages on the abdomen Encouraging pushing 16 32.7% 10 20% 12 24% before the cervix is fully
dilated(sweeping) Using fundal pressure to 9 18.4% 4 8% 10 20%
hasten labour
57

Table 4.10 (c) – The interventional relationship between midwives and mothers
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Communicate in a 6 12.2% 35 70% 44 88% humane and respectful
way
Reassure and support the 5 10.2% 38 76% 44 88%
mother
Provide proper nursing 1 2% 24 48% 42 84% care to both mother and
newborn
Harsh and tough attitude 7 14.3% 9 18% 9 18%
with mothers
Mild physical abuse (ie 5 10.2% 6 12% 6 12% pinching and smacking
their legs)
Figure 4.1 Principles of infection prevention
It was note that attitudes towards handwashing before and after performing any nursing procedure
compared with post intervention, improved from (51%) to (100%). The use of protective barriers eg
sterile gloves for vaginal examination was good (85.7%) and improved to (100%) after training.
(71.4%) used sterile gloves to insert cannulas and this improved to (96%) post training. Only (8.2%)
wore masks and (12.2%) wore plastic aprons whilst attending to childbirth. Both improved post
training to (88%) and (84%) respectively. Diposing of sharp instruments after use in a safe box was
very poor, but improved post training to (62%).
58

120% 100%
80%
60%
40%
Pre
20%
Post
Follow up
0%
Figure 4.1 attitude of nurse midwives towards infection prevention
4.11 – Skills of nurse midwives in taking obstetric history Analysis of the observation checklist pre intervention compared with post intervention in history
taking and abdominal examination. Analysis of taking information about social and family history
pre intervention was weak (4.1% and 26.5%). This improved post training to (86%). Most of the
nurse midwives knew the importance of taking menstrual and obstetric history 95%). It appeared
that taking history of present pregnancies was weak (36%) and this improved post training to (90%).
Analysis of the skills of the study group about general examinations was very poor – only (8.2%)
examined the mothers properly. After training (48%) examined mothers properly. Skills in
abdominal examinations showed that nurse midwives concentrated on the height of the fundus,
foetal position (93.9%) and foetal heart (79.6%) but only (16.3%) inspected deep vein thrombosis
and only (24%) inspected external genitalia and varicose veins. This improved post training. Only
(20.4%) palpated the liver, speen and kidney and post training this was (48%).
59

Table 4.11 – Abdominal examination skills
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage Shape of the 32 65% 34 69.4% 41 82%
abdomen
Signs of pregnancy 34 69.4% 41 83.7% 45 90%
Liver, speen and 10 20.4% 26 53.1% 24 48%
kidney palpation
Height of the fundus 34 69.4% 40 81.6% 48 96%
Foetal position 46 93.9% 48 98% 50 100%
Foetal heart 39 79.6% 48 98% 50 100%
Inspection of 12 24.5% 42 85.7% 48 96% external genitalia
and varicos veins Deep vein 8 16.3% 34 69.4% 44 88%
thrombosis
inspection Vaginal 14 28.6% 27 55.1% 39 78%
examination
Pelvic measurement 2 4.1% 10 20.4% 32 64%
General 4 8.2% 29 59.2% 24 48% examination from
head to toe
4.12 – The practice of nurse midwives towards investigations The majority of nurse midwives examined the urine general (91.8%) and 89.8% checked
haemoglobin and (75.5%) of the nurse midwives made sure the blood groups and cross matching
was taken and the results prepared. None of the nurse midwives mentioned AIDs screening and
Hepatitis B (VHB) but post training awareness increased to (66%).
60

Table 4.12 The practice of nurse midwives towards Laboratory investigations
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Urine general 45 91.8% 47 95.9% 50 100%
Urine for glucose 40 81.6% 48 98% 50 100%
Urine for albumen and 28 57.1% 45 91.8% 49 98%
acetone
Blood haemoglobin 44 89.8% 47 95.9% 50 100%
Blood group and cross 37 75.5% 45 91.8% 49 98%
matching
AIDs screening 0 0% 11 22.4% 25 50%
Hepatitis B (VHB) 0 0% 14 28.6% 33 66%
4.13 The practice of nurse midwives in the labour room
Only (55%) of nurse midwives used sterile scissors for episiotomy pre training but post training this
increased to (100%). (67% )of them preferred mediolateral incision for episiotomy to right or left
and this increased post training to (96%). Half of them did stitches according to the depth and post
training this was (90%). About the exact time to do episiotomy (59.2%) performed it during the birth
process, post training the percentage decreased to (20%). (46.9%) performed it the correct way
during the crowning of the head and this improved post training to (98%). Performing 15 minutes
before delivery of the head was done by only (10%) and this practice decreased to (6%).
61

Table 4.13 – Skills of nurse midwives in episiotomy, area and time
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Made with sterile 27 55.1% 50 100% 50 100%
scissors
Made in the area 11 22.4% 12 24% 10 20% between vagina and
rectum
Diagonal incision 4 8.2% 9 18% 20 4% across midline
between vagina and
anus
Mediolateral incision 33 67.3% 36 72% 48 96%
to right or left Done during birth 29 59.2% 23 46% 10 20%
process 15 minutes before 5 10.2% 4 8% 3 6%
delivery of the head
During crowning of 23 46.9% 46 92% 49 98%
the head
The incision was 24 94% 41 82% 45 90% stitched according to
depth
4.14 (a) Management of nurse midwives before placental delivery Less than half of the nurse midwives made sure that the bladder was empty (42%) . (59.2%)
inspected the birth canal, perineum and cervix for lacerations and this improved post training to
(96%). (71.4%) checked the amount of blood loss and gave oxytocin properly. Only (16.3%) took
the vital signs but post training this was (86%). [See table 4.14(a)]
62

Table 4.14(a) – Management before placental delivery (no, 50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage Made sure the bladder is 21 42% 42 84% 49 98%
empty Careful inspection of 29 59.2% 44 88% 48 96%
birth canal
Observe and measure 35 71.4% 43 86% 46 92%
blood loss
Take vital signs 8 16.3% 27 54% 43 86%
Give oxytocin (10 units) 35 71.4% 25 50% 43 86%
4.14 (b) Skills of nurse midwives during placental delivery
Only (14.3%) read the time before placental delivery and (77.6%) clamped the umbilical cord near
the perineum, (77.5%) prepared oxytocin injections before delivery but only 26% applied CCT but
this improved post training to (88%). Only (32.7%) examined the maternal side of the placenta and
post training this was also (88%). Only (2%) of nurse midwives weighed the placenta and after
training this was still a percentage of less than half (40%). Most of the nurse midwives waited for
signs of separation (79.6%). 64.3% supported the placenta with both hands.[ See table 4.14(b)]
Table 4.14(b) – Skills of the nurse midwives during placental delivery
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Reading the time before 7 14.3% 16 32% 34 68%
placental delivery
Clamping the umbilical 38 77.6% 47 94% 45 90%
cord near perineum
Applying CCT 13 26.5% 40 80% 44 88%
Preparing oxytocin 37 75.5% 37 74% 47 94%
injections
Supporting placenta 31 63.3% 44 88% 47 94%
with both hands Waiting for signs of 39 79.6% 47 94% 50 100%
separation
Examining the maternal 16 32.7% 27 54% 44 88%
side of the placenta
Weighing the placenta 1 2% 11 22% 20 40%
63

4.15 Skills of nurse midwives after placental delivery and assessment for uterine
contraction and management
(83.7%) of the nurse midwives inspected the placenta carefully and ensured that the uterine muscle
was well contracted. Less than half (46%) checked the vagina and cervix for lacerations and this
improved post training to (98%) . Taking the vital signs was very poor - only (28.6%) did. (71.4%)
massaged the uterus immediately after placental delivery, manual exploration and reinspection of the
genital tract was done by the majority of the nurse midwives (89.8%). It was noted that nurse
midwives did not encourage breast feeding (12%) but this increased after training to (82%).
Table 4.15 Skills of nurse midwives after placental delivery and assessment for uterine
contraction and management (n,50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage Careful inspection of 41 83.7% 48 96% 50 100%
the placenta Ensure the uterus 41 83.7% 48 96% 50 100%
muscle is contracted Ensure there are no 23 46% 44 88% 49 98% vaginal or cervical
lacerations
Take vital signs 14 28.6% 37 70% 48 96%
Manual exploration and 44 89.8% 48 96% 48 96% reinspection of the
genital tract
Massage the uterus 35 71.4% 45 90% 49 98% immediately after
placental delivery
Encourage 6 12.2% 22 44% 41 82%
breastfeeding
64

4.16 Skills of the study group about the estimation of blood loss
(30%) of the nurse midwives used a measured plastic bag and this practice improved post training
by the use of a urine bag to estimate blood loss to(74%). (68%) of them weighed pads before and
after bleeding and this percentage increased post training to (100%). Only (16%) used a large kidney
dish but they were not measure. All the nurse midwives had not previously heard of estimation of
blood loss by the new method which was to spill a known quantity of coloured liquid (to represent
the blood) over a linen and then to measure the surface area covered by the liquid to give the nurse
midwives a standard to compare patients’ blood loss with and therefore estimate the actual amount
of blood loss effectively or drape estimation.
Table 4.16 – Skills of nurse midwives towards blood loss estimation (n,50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Put under a measured 15 30% 37 74% 44 88%
plastic bag
Weigh the pads before 34 68% 49 98% 50 100%
and after bleeding Put in a measured 8 16% 41 82% 46 92%
kidney dish
Estimation by the 0 0% 10 20.4% 29 58% amount of blood
covering the surface
area
Drape estimation of 0 0 11 22.4% 12 24%
blood loss
65

Figure 4.2 Applications of the universal precautions pre and post intervention Analysis of the observational checklist of the use of protective barriers pre intervention compared
with post intervention increased – handwashing from (76%) increase post training to (94%).
Wearing gloves, gowns and masks in an appropriate way was (59%) and (90%) after training. Only
(46%) of the midwives properly sterilised the equipment and post training this increased to (92%).
Only (20.4%) of the participants prevented splashes and contamination but after training this was
(86%). Reprocessing of the equipment to prevent contamination was poor (10%) but improved to
(70%) post training. Managing with sharp instruments was also poor (4%) but improved after
training to (74%).
100% 90% 80% 70% 60% 50% 40% 30% 20% 10%
Pre
Post
0%
Handwashing Wearing Preven ng Proper Steps of Handling and protec ve splashes sterilisa on processing the disposal of barriers instruments sharps
Figure 4.2 The use of protective barriers pre and post intervention
66

4.17 Prevention of PPH by Active Management of the Third Stage of Labour Analysis about AMTSL of early cord clamping and active delivery of placenta was( 79.6%) pre
training and increased post training to (96%). The practice of controlled cord traction was poor
(22.4%) and improved after training to (86%). Most of the nurse midwives practiced uterine
massages after placental delivery if appropriate (71.4%) and this increase post training to (94%).
(36.7%) of the participants only gave uterotonic drugs in time and in a proper way after the delivery
of the interior shoulder. The majority of them did not give oxytocin at an appropriate time or way
(63.3%). Other preventative measures to reduce the incidents of prolonged labour were (62%), minimising
trauma (54%) and avoiding routine episiotomy was (55%) pre training. But after training this
increased to (96%). (79.6%) of the nurse midwives agreed that training skilled birth attendants
would decrease the maternal mortality rate and prevent PPH. If anaemia is treated early, this can
also be counted as a preventative measure against PPH. Concerning the development of national
guidelines, most of the nurse midwives agreed this would serve as protection for both mothers and
midwives post training.
67

Table 4.17 Prevention of PPH(n,50)
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Prevention of PPH by AMTSL
Early cord 39 79.6% 50 100% 48 96% clamping and
active delivery
Controlled cord 11 22.4% 48 96% 43 86%
traction
Uterine massage 35 71.4% 29 58% 47 94% after placental
delivery Administration of 18 36.7% 32 64% 34 68% uterotonic drugs
as appropriate
until the delivery
of the shoulders
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage
Other preventative measures
Avoiding routine 27 55.1% 47 94% 48 96%
episiotomy
Reducing 31 62% 46 92% 44 88% incidents of
prolonged labour
Minimising 27 54% 41 82% 33 66% trauma associated
with instrumental
delivery
Treating anaemia 15 30% 26 53.1% 33 66%
early
Training skilled 39 79.6% 48 96% 48 96%
birth attendants Developing 20 40% 35 71.4% 42 84%
national guidlines
68

4.18 Management and nursing care in case of complications in the third stage of
labour Most of the nurse midwives (87.8%) inserted intravenous lines immediately and this improved post
training to (94%). (67.3%) gave oxytocin as ordered but only (49%) prepared oxygen, after training
this was (92%). (63.3%) called the emergency team when required and only (14.3%) of the nurse
midwives evaluated and measured blood loss but this improved post training to (90%). In addition,
(14.2%) prepared the results of blood tests and this improved post training to (84%). Only (20.4%)
took the vital signs and evaluated the patients condition but post training this was (90%). It was also
noted that they did not use misoprosol orally or rectally and was only used by (4%) of the nurse
midwives.
Table 4.18– Management and nursing care of nurse midwives in the third stage of labour
Pre Post Follow up
Frequency Percentage Frequency Percentage Frequency Percentage Call for 31 63.3% 48 96% 47 94%
emergency
team
Evaluate and 7 14.3% 25 50% 37 74% measure the
blood loss
Insert IV line 43 87.8% 49 98% 47 94%
Prepare oxygen 24 49% 39 79% 46 92%
Evalute the 10 20.4% 36 72% 45 90% patients
condition and
take vitals sign Prepare the 7 14.3% 25 50% 42 84%
results of the
blood tests
Make sure 5 10.2% 18 36% 30 60%
blood is ready
Give oxytocin 33 67.3% 39 78% 48 96%
as ordered
Give IV fluids 26 53.1% 40 80% 48 96%
Misoprostol 2 4.1% 20 40% 29 58% used rectally or
orally
69

Table 4.19 level of education of study group compared by (KAP): Results showed that 68% of NMs level of education was intermediate school,32% was high
seconadry school.Analysis showed that the level of education of NMs had no significant impact on
KAP (P.> 0.05). Table 4.19 level of education of study group compared by knowledge
Knowledge
Level of education Pre Post Follow up
Mean±SD Mean±SD Mean±SD
Intermediate 27.65±5.43 47.79±4.22 52.53±3.45
2 7 7
High secondary 27.87±7.67 48.19±5.01 51.5±4.147
6
Table 4.19 level of education of study group compared by skills
Skills
Level of education Pre Post Follow up
Mean±SD Mean±SD Mean±SD
Intermediate 54.73±6.8 81.94±9.9 99.79±7.5
6 4 3
High secondary 60.94±7.5 85.31±6.1 95.63±6.7
8 3
Table 4.19 level of education of study group compared by attitude
Attitude
Level of education Pre Post Follow up
Mean±SD Mean±SD Mean±SD
Intermediate 6.32±2.3 8.68±2.2 14.94±1.7
6 7
High secondary 6.19±2.5 8.44±1.5 15.13±2.5
4
70

Figure 4.3-Years of experience compared with KAP: Results showed that 52% of NMs experience was more than 21 years and 22% of their work
experience from12-16 years.
Results showed that experience doesnot affect the outcome of training,was not significant in KAP
(P.<0.05).
Fig.(4.3) years of experience compared with knowledge
71

Fig.(4.3) years of experience compared with skills
Fig.(4.3) years of experience compared with attitude
72

Figure 4.4-the level of knowledge ,skills and attitude of the trainees pre,post and
follow-up (final results): Results showed that knowledge of NMs pre-training was (27.72%) improved post to (47.92%) and
to (52.2%) in follow-up.
Regarding skills pre results was (56.76%),this improved post to( 82.92%).In post monitoring follow-
up analysis was (98.35%).
Attitude showed that NMs changed their attitude positively,pre was (6.28%), post (8.60%) and in
follow-up was (15%).
Figure(4.4) knowledge of the trainees pre,post and follow-up Figure(4.4) skills of the trainees pre,post and follow-up
73

Figure(4.4) attitude of the trainees pre,post and follow-up
Figure 4.5-Analysis of pre and post intervention compared different between
control and case group in KAP: Pre intervention,control group results in knowledge of NMs was (22.38%). In post training results
was 22.92%). Analysis of case group pre was 27.72%) in knowledge , this improved post training to
(47.92%). Analysis of observational check list pre intervention skills of control group was (56.4) the post
intervention was 55.66,with (9.30)
Analysis of observational check list of pre intervention of the case group compared with post ,skills
pre was (56.76%).this improved post to (82.92%) with( t=9.03) and (P.<0.0005).
Attitude of control group pre was (5.84%).this increased post training to (6.26%) .Compared with
case group results pre was (6.28%) improved post training to (8.6%) with t=1.99 .P.value showed
significant different between control and cases (<0.005).
74

22.72
Figure 4.5 Analysis of pre and post intervention compared different between case and control
group in knowledge
Figure 4.5 Analysis of pre and post intervention compared different between case and control
group in skills
75

Figure (4.5) Analysis of pre/post intervention compared the difference between control and
case group in attitude
76

DISCUSSION
Worldwide PPH is an unpredictable and rapid cause of maternal death.Two thirds of women with
PPH having no identifible risk factors.70-90% of immediate PPH is due to uterine atony.In
developing countries several countries have maternal mortality rate in excess of 1000 women per
100,000 life birth,PPH is the leading direct cause of maternal deaths(25%).PPH has anegative
impact on mother’s quality of life due to its complications. Percentages of delivery assisted by
skilled midwives have become aproxy indicator for reducing maternal mortality rate in developing
countries.It was asserted that competence care is of high effect in decreasing maternal mortality rate.
This study targeted in-service training of nurse midwives.The main objective was to evaluate the
practice of nurse midwives regarding PPH, and up grading their knowledge ,attitude and skills
through adesigned in-service training program in prevention and management.Atotal of 100 nurse
midwives were enrolled in this study. In-service training is an important element for nurse midwives especially in developing countries
such as Sudan,where there is a limited resources and lack of an organized system,besides shortage of
health cadre specifically nurses and midwives.Level of education in Sudan was primary,intermediate
and after Sudan declartaion it raised to secondary school.Now there are four levels for trainig
medwifery,one of them is nurse midwive.In this study it is clear that level of education the majority
were intermediate school(68%) and (32%) high secondary school.The mean age was 33 years(Table
4.1) which will also support the chances of success for in-service training.The level of education and
age are very important factors of improving the kowledge and skills of the trainees.
Recent studies in the United Kindom about career profile (Royal Collegue of Midwives, 2012)
stated that as midwives are the lead health care professional attending the majority of birthes,the
level of education should be raised.There are two routes only to raise the level of education;a
university degree in midwifery or in- job training.The college suggested eighteen months
registeration course.In Sudan,it is difficult now to up grade the educational level of the in-job MWs
with the university career.So the study selected an in-job training.
It was clear that previously midwives were not trained properly after graduation.There was no
proper system of in-service training ,only limited courses (Table 4.1).
77

Recently the federal ministery of health has established acenter for on-job training program,short
courses held in specific relevant areas.It seems that they realised the importance of the in-sevice
training for all health workers.Still,the contents of the courses need more effort to be improved. This is supported by one of the successful in-service training project (Mother Nile Projet 2008-
2011).The federal ministery of health excuted in-sevice training program for midwives aiming to
decrease the materanal mortality rate (MMR) in Northern Sudan.After implementation of the
program the outcome of the training confirmed improvement in knowledge and practical skills of
midwives .It also has showed that empowerment of midwives has certain effect on improvement in
the quality of maternal and child health services.
This study recommened provision of midwives with in –service training,to and strenghtening the
capabilities of health visitors and nurse midwives who are supervisor to village midwives.
Previous studies by ( Garcia K. etal 2012) teaching guatemala midwifes about post partum
heamorrahge evaluated the effects of in-service training on PPH.16 MWs participated in the training
program. The researchers used the checklist to assess and compare knowledge of post partum
hemorrhage interventions before and after post partum hemorrhage teaching, knowledge and skills
improved (pretest M =1.385\8), post test (M=4.846\8) In general the knowledge of nurse midwives about post partum hemorrahge has improved after
training.Their knowledge about definition of PPH was only (6%)but this improved to (98%) post
training.Also,only (8% ) knew the types of PPH ,this has improved to (86%) post training.(Table
4.2)
The knowledge of the nurse midwives (NMs) about the causes was good except about uterine atony
and uterine drugs relaxant was poor. (Table 4.3)
It is known that the knowledge about these items are very essential in controlling PPH.Knowledge
was improved post training and specifically on the above mentioned information about uterine atony
improved from (14%) to (84%).While improvement of uterine relaxant drugs from (36%) to (94%). Another recent study done by (Farah kausar etal,2010) midwives in low resource settings save
`mothers lives` with NON-pneumatic Antic Shock garment. The purpose of this was to discuss the
role of nurses and nurse midwives in preventing and treating post partum hemorrhage from uterine
atony in deveolping countries and examine the role of the new device , (NASG) in improving the
outcome for patients. The study phases , pre intervention and intervention phase of 1442 women
with obstetric hemorrhage, post partum women with hypovolemic shock.(N=578) from uterine atony
(750 ml blood loss;systolic blood pressure <100mm Hg , pulse > 100) enrolled in two referral
facilities in Egypt and four in Nigeria a pre intervention phase and NON pneumatic Anti shock
78

garment.(NASG) intervention phase, women with hemorrhage and shock in both phases were
treated with the same evidence based protocol for management of hypovolemic shock and
hemorrhage, but women in the (NASG)- intervention also received the (NASG).relative risks (RRS)
with 95% confidence intervals were estimated.For primary outcomes measured blood loss,incidence
of emergency, hysterectomy and mortality. The results showed women in the (NASG)- intervention phase had significantly better
outcomes(50% ) lower blood loss, reduced rate of hysterectomy (8.5% to 2.3% RR=0.27, 95% Ci;
0.12-0.6 ). This study showed that in low –resource setting nurse midwives with simple training can stablize
hemorrhaging women with the (NASG) which, is a simple low technology first aid device,in-
expensive,light weight and reusable compression suit , shows promise for reducing blood loss, rates
of hysterectomy ,and mortality.
The nurse midwives knowledge about risk factors, sign and symptom and the necessary
investigation genarally was good except about some risk factors , blood coagulation pre was 10%
improved to 80% , most of them knew the routine investigation except the investigation about liver
enzymes and ECG was 6% improved post training (table 4.4). The study showed that most of NMs
knew about PPH complications except renal failure it was (18%) improved post to 68%) (table 4.5).
The knowledge of nurse midwives about utertonic drugs showed that 70% knew about oxytocin, but
knowledge with regards to other drugs which increase the risk of postpartum hemorrhage was poor
only 10% pre but increased to 80% post training ,about Misoprostol their knowledge pre was 26%
improved post to 94% (table 4.6).It is well known that knowledge about uterotonic drugs is very
essential for midwives to know the uses,dose,side effect and its contraindications.
Previous study done in a university teaching hospital in England by international confideration of
midwives and interanational federation of Gyneocology and Obestetric (FIGO 2006) evaluated the
effectiveness of Misoprestol and reducing incidence of PPH.Demonistrated that giving Misoprostol
to women immediately after child birth resulted in significantly lower rates of PPH, found that
(18%) of women would experience PPH if the placenta where delivered on its own, (2.7%) if
Oxytocin where used and (3.6%) if Misoprostol were used.
Recent study from India by (Kennedy,EH. 2004) provided evidence that oral Misoprostol was
associated with about (50%) reduction (from 12% to 6.4%)in the rate of acute PPH and mean blood
loss. Previous study by (Mc Cormick ML,2002) concluded that the AMTSL and prophlactic Oxytocins
should be routinely used in the third stage of labor as they decrease risk of PPH by (60%).
79

The knowledge of the study group about the principals of infection prevention (Table 4.7).In this
study the impact of knowledge ,attitude and practical skills with universal precautions generaly was
good except about using separate set for each delivery was (30%) and in using sterile needles with
handle for suituring was (61%) which was not satisfactory in these important items,but this
improved post training. About application of universal precaution Pre/Post intervention , performance of nurse midwives
showed positive improvement (Fig.2). Application of UPs during the process of labor pre compaired
with post –intervention ,proper handling and disposal of sharps was poor only (4%) but improved
post training to (74%) . It seems that NMs had a problem on processing instruments to prevent
contamination, was10% improved to (70%) .Only (20%) of them prevent splashes but this improved
post training to (86%).
A previous study by ( Mobasher Izadeh etal ,2005) concluded that a large number of injuries by
contaminated sharps devices can be prevented by implementing educational programe regarding
disposal of sharps.Study showed that cases of injeries by sharp devices before and after the
implementation of intervention programe reduced from (55.2 to 19.5% ) (<0.05) .It seems that
application of universal precaution (UPs) and infection prevention is not a matter of knowledge and
practice only , but also related to adequate supplies, suitable environment to carry out work in a
proper way for effective out comes, and this what exactly mentioned by nurse midwives (table 4.9).
90% of NMs were not satisfied by the work environment , they mentioned inadequate supplies even
drugs needed in the labor rooms in addition to shortage of staff and low income salaries. This is
supported by a previous study by (Grellier 2000) who concluded that knowledge obtained within
midwivery education may not found its way to be translated into clinical practice especially in
developing countries . Another study by ( Maclean, 2003) who showed the importance of the three (Es) Education ,the
Effectiveness of skilled birth Attendant (SBA) and the Environment in which she works and practice
.(Tables 4.7, , 4.9 ). Knowledge of NMs about the physiology of the gental tract was very poor only 14% and about the
physiological changes was 8%, this improved post training , it seems the cruculm of NMs devist in
anatomy and physiology although it is important.( table 4.8). Skills of NMs in history taking and abdominal examination was poor in pre test , history taking is
skill which needs a continous training and supportive supervision,physical and abdominal
examination is very essential in child birth management, unfortunately the pre test showed poor
skills regards general examination from head to toe only (8.2%) examined mothers properly, after
80

training improved but still less than half (48%) applied it . From disscussion, NMs related this to over work due to shortage of midwives that is why they were concentrating on the essential
procedure showed in table (4.11). Skills of NMs concerning abdominal examination was good
except in examining the liver, spleen and kidney palpation ,only (20%) done this and inspection of
deep vien thromposis done by (16%) but improved post from (16%-88%)(Table 4.11). They
considered these procedure must be done by doctors ,but it is very essential for midwives to inspect
for the above mentioned item, plus varicose viens inspection which was also done by (24%). Results
showed that NMs concentrating in abdominal examination in fetal lie (93%), fetal heart sound done
by (79.6 %) and in gestational age , presenting part which was very good, all these improved post
training ,(Table 4.11). No related studies was traced to compare. (Table 4.4 ) showed that all the essential investigations are usually done before delivery with the
exceptions of Hepatitis B and HIV (Both are 0%). This percentage improved post training to (66%
and 50% respectively) unfortunatly NMs did not encourraged to suggest or discuss treatment with
doctors it seems that there is a lack of team work.Team work is very essential as highlighted in
previous study by (Jane Bott, 1999) the need for effective education, well publicized guidelines,
providing equipment , with an emphasis on team working are more suited to the success of work .
The skills of NMs on episiotomy,assessment of uterine contraction and placental delivery were very
essential and important procedures because most of the problems and complication occur in the third
stage of labor, this study concentrated in these items in details in the training programe ,theoratical
and practical (table 4. 13) and (table 4.14 a- 4.14 b ).Skills of NMs in placental delivery before,
during and after delivery table(4.15). A previous study by (Gloria Metacalfe 2007) Concluded in her study that simple ,low cost
intervention programe for NMs can help avoid most of these tragic complications, as PPH is an
unpredictable and rapid cause of maternal death world wide with two thirds of women having no
identifiable risk-factors, (70-90%) due to uterine atony .On going researches in various setting
approaches for preventing and managing PPH bleeding and its complications , by training skilled
birth Attendents (SBA). And improving work environment of skilled providers, supporting the
development of improved access to care ,more women will have access to this life saving
intervention. Another study by (Maclean,2003) showed the importance and the effect of training programmes for
skilled attendants at birth, mentioned the need for the strong infrastructure, effective NMs supported
by the education and a healthy environment in which they practice. In this study, the skills and
practices of NMs in the labor room on episiotomy generally improved but specifically with regards
81

to using sterile scissors, from (55%-100%) and also on the exact time to do episiotomy - during
crowning of head, from (46%-98%) post training. This is mentioned in previous studies by (Deborah
Armbruster, 2002)one of the preventative measures in reducing PPH is avoiding routine episiotomy
before the exact time. Generally the skills of NMs about management before, during and after placental delivery improved,
(Table 4.14-4.15), except for reading the time before placental delivery, which was (14.3%) and
improved post to (68%). However, the percentage of the MWs who showed improvement remains
unsatisfactory. The importance of this issue has been discussed in study by (Magann EF,et al,2005)
which showed that the risk of complications continues for some period after delivery and this is the
reason why authorities called for the fourth stage of labor. The length of the third stage of labor is
usually 5-15 minutes and this is the absolute time limit for the delivery of the placenta.
On assessment of uterine contractions and management after placental delivery, skills were
generally good and improved post in all procedures between (82%-100%) (Table 4.15). Taking the
vital signs,which is essential in monitoring the patient’s condition,was improved from (28%) pre
training, to (96%)post training.
It was very clear from the results that NMs did not encourage breast feeding as it was done by only
(12%) (Table 4.15). It is known that breast feeding has important role in uterine contraction, in
addition to providing new babies with immunity and a maternal connection. This study showed that there is a problem with the methods used to estimate blood loss, only (16%)
of them knew about the new methods such as the drape estimation of the blood loss, measured
kidney dish and standard container.(68%) of the NMs kept and weighed pads before and after
bleeding and this improved post to (100%) (Table 4.16).Training MWs about the methods of
estimation blood loss is highly needed, as PPH is mainly defined by the estimation of the blood
loss(>500 ml). As MWs in the first line of care givers, it is essential to train them to save mothers’
lives, as mentioned in study by (Bouwmeester FW,2006). It concluded that unfortunately until there
is a physical change it would mean death for most women in developing country settings, as
immediate back up or emergency obestetric care is not available. A previous study was done by (A.Patel,et al,2006) about Drape estimation vs visual assessment for
estimating PPH. The objective of the study was to compare visual estimation of post partum blood
loss with an estimation using specifically designed blood collection Drapes. The Drape estimate was
a measurement of blood loss by photospectrometry.The study was randomised controlled with (123)
women delivered at district hospitasl in India.The women were randomised to visual or Drape
82

estimation of blood loss. A sub-sample of (10) drape estimates was compared with photo-
spectrometry results.The visual estimates of the blood was (33%) less than the Drape estimate and
the correlation of drape estimate to photospectrometry was (0.92). Drape estimation is more accurate
than visual estimation and has particular utility in the developing world since it is simple and easy to
use. It is well known that prevention is better than cures, so it is essential for NMs to know methods of
prevention of PPH. Fortunately previous studies about AMTSL by (FIGO,2003) showed that simple
low cost intervention can help most of these tragic outcomes and current evidence indicates
AMTSL, administration of uterotonic drugs, controlled cord traction(CCT) and fundal massage after
delivery of placenta can reduce the incidence of PPH by up to 60%.This study showed that NMs
were very willing to learn and practice the new methods for prevention by AMTSL as a primary
prevention of PPH is advocated at all levels of obestetric care - this emphasis is on AMTSL in most
developing countries.
Skills and practices of NMs on steps of AMTSL was generally good, except for CCT - only (22%)
did this appropriately but this improved to (86%) post training. Administration of uterotonic drugs in
a proper way and in time was practiced by (36.7%) and this improved post training to (68%)(Table
4.17) However, the percentages are not satisfactory because uterotonic drugs are essential for uterine
contraction. In previous a study by (Songhai H et al,2004), it concluded that in Indonesia, a study
was completed in the community-based distribution of Misoprostol in West Java and it proved the
feasibility and acceptibility of this approach to PPH prevention. Another study by (FIGO and international council of midwives (ICM), 2003), provided conclusive
evidence that AMTSL signinficantly reduces PPH by up to (60%) and decreases blood loss, reduces
post partum anaemia and decreases the need for blood transfusion. Recently, evidence of the
importance of the AMTSL in reducing the incidence of PPH has been proved in a number of large
trials (The Hinching brooke 12 randomized control trials). However, it is not included in NMs
curriculum in Sudan, although it has recently started to be practiced by doctors.
WHO recommended through facility-based providers who are the primary users of AMTSL, that it
can be practiced and offered by Skilled Birth Attendants(SBA).This WHO report was agreed by
(Midwifery Organization , 2006). Another study by (Angeline Fujiok and Jeffrey Smith,2011) in the prevention and management of
PPH for NMs revealed that maternal mortality rates were exceedingly high (WHO report ,2010).
Maternal mortality rates (MMR) was 290 maternal deaths per 100,000 live births in developing
countries. Reducing (MMR) is a global development priority for donors(USAID) focused on
83

evidence –based high impact intervention for the low resource setting in which PPH is of major
concern.The goal of the study was to reduce MMR in thirty one priority countries with the highest
rates, by (2013) worldwide. In the region of Africa,there were twenty one countries, South Sudan
included and the other ten countries were from Asia and Latin America. The African countries program had been done for education and training in AMTSL.The outcomes
(94%) stated that AMTSL was included in education and in-service training for SBA. In India the
government included AMTSL in pre-service education at schools for Auxiliary nurse
midwives(ANMW). Although the level of education of NMs in Sudan is higher than most of these
countries, it has still not yet been implemented.This is was agreed by (96%) of NMs (Table4.17),
that training them about AMTSL is crucial because it is one of the preventive measures for PPH.
Also, they agreed in developing national guidelines for management. Management and nursing care
in the case of complications in PPH, improved generally in giving care and especially in the
estimation of blood loss, from (14%-74%) (Table 4.18). This study showed that nurse midwives have a moderate attitude and behaviour towards mothers in
the labor room.The percentages of the NMs that smile, thank patients and display positive facial
emotions was low(10%), and only (4%) introduced themselves to patients or took permission to
carry out procedures. This trait is not limited or specific to NMs and it must be noted that this
characteristic is intrinsically linked in Sudanese culture and is present in all professions, NMs
included.(table 4.10).
With regards to the harmful practices that were used by NMs to speed up the birthing process, it was
found that (75.5%) of the NMs increased the rate of the Oxytocin to fasten labor and this practice is
very serious because it can lead to ruptured uterus. Fortunatly practiced this habit decreased post
training to (26%). Also, it was found that between (38%-18%) of NMs performed these negative
customs. Indeed it was actions such as punching the abdomen, encouraging pushing or sweeping
before the cervix was fully dilated and use of fundal pressure. These harmful practices, especially
sweeping the cervix is very painful and can cause oedema and delay labor. Fortunately all these
negative practices decreased post training, except for the fundal pressure which increased in follow-
up (Table 4.10 b). It was noticed that the attitude of NMs towards hand washing before and after any nursing
procedure compared with post, improved from (51%-100%). The use of protective barriers was
poor, also in disposing of sharps in a saftey box was only (6%) pre (Figure 4. 2). Irregular supplies of resources and limited equipment as mentioned by NMs in (Table 4 .9).may be
an important factor besides attitude.
84

No previous studies describe the attitude and behaviour of health care workers. The level of education doesnot affect the NMs knowledge ,attitude and skills,it was not significant
(P>.0.05)( table 4.19 ).This results is possible due to the different cruculum and quality of primary
and secondary school where the NMs studied.The level of education should not be a constrain for in-
service training of NMs.
Aprevious study done by FMOH (The mother Nile Project 2008) set an in-service training for
village midwives aimed to decrease (MMR) and to empower the village midwives practice.The
outcome of the in-service training confirmed improvement in KAP.It was a succesful project
although the level of education was primary school.
Regarding years of experience ,it doesnot affect the outcome of the training, experience was not
signinficant when comparing it with KAP (p.value>0.05) (figure 4.3). This could be due to lack of
in-service training and age.Results showed an improvement in young age group (2-6 and 7-11 years
of experience),as young age is better in understanding and concentration than old age.No similar
comparison was traced in previous studies. The overall knowledge ,skills and attitude of the study group was improved. Improvement was
highly significant (p. value<0.0005) (figure 4.4).
The in-service trainig succeded due to the availability of all training resources (trained
personnel,materials,budget and management).It is here to mention the trainees have high desire
,demand and interest in training. Aprevious study done by (Jane Bott,1999) highlighted that for
effective education and training we need publicized guidelines ,a conducive work environment in
addition to providing equipment.Managers need to review the effectiveness of equipment.The
findings suggest ademogratic management style,with an emphasis on team working which is more
suitable for the sucessful of work. The analysis of KAP of NMs that was comparing the case group with control group pre and post
showed a highly significant difference between control and case (P.value <0.0005) (figure 4.5).
It is well known that in-service training up grade the knowledge and practical skills.This trainig
program designed to help NMs become more productive and effective in specific tasks especially
skills in the third stage of labor to prevent PPH complications. There were many element that helped in the success of the program. Firstly,the NMs in the study
group had showed an interest in improving their KAP.Secondly ,the availability of the training
resources.Finally,the personnel who implemented the program were welltrained which reflected in
an efficient training.No similar comparison was traced in previous studies.
85

CHAPTER FIVE
CONCLUSIONS AND RECOMMENDATION
5.1CONCLUSIONS The main results showed that the training programme was effec ve i ni mpr ovi ng nur s es mid wi v es
knowledge and skills.
A tude t owar ds mot her s was not sa sfactory pre- tr aini ng but, i mpro ved post traini ng.
The sudy revealed that simple,low cost interven on pr ogramme can hel p i n r educi ng PPH
complica ons .
With such programme if fine tuned and imp l eme nt ed in PPH ma nageme nt coul d definit ely have
immense impact of the proffessi on of Mi dwi fer y. Nurse midwives showed interest and ac ve par cipa on on t r aini ng program,t h is proved by t he
full a endence on bot h ac vi es t heor a cal andpr ac cal .
Educa on and trai ni ng in Ac ve man agemen t in t he t hir ds tage of labor (AMTS L) was effec ve
and nurse midwives skills was exellent in implemen ng the steps of (AMT SL) .
86

5.2 RECOMMENDATIONS Education and training in Active Management in the third stage of labor (AMTSL ) to be included in
the cruculum .
Upgrading the nurse midwives cruculum to include coarses in ultrasound gram . Continuation of in- service training programe and effective training and refresher coarses to be held
regularly .
Resources needed for safe practice should be available at all time . Improvement of environment and review of salaries for midwives is very essential Empourment of nursemidwives to prescribe uterotonic drugs and adminster it in case of emergency . Application of universal precaution should be implemented to midwives under supervision of a
trained specialized team so as to grantee the sustainabilty of the program .
Providing the appropriate protective measures to enable (NMS) safe practice for both mothers and
midwives .
Promotion of safe delivery requires , more qualified midwives to correct the shortage .
Quidelines and protocol should be agreed and practice in labor rooms.
87

REFERNCES Abdel-Aleem, H.;Hofmeyr, G.J.;Shokry M.;EL-Sonoosy,E. (2006). Brief Communication :
Uterine Massage and Postpartum Blood Loss. International Journal of Gynecology and
Obstetrics (93): 238-239.Assiut University. Ali,A.A.;Khojali,A.;Adam,G.K. (2011).Maternal near-miss in a rural hospital in Sudan. Biomed
central(BMC) pregnancy and childbirth(11),48.
American Family Physician(2007).Causes of Post Partum Heamorrage,The four T’s. (75)(6).
American family physician(2007).Coagulation disorders,a rare cause of PPH. American Family
Physician (Vol.75),No.6)pp. 880.
Anderson, JM; Etches, D. (2007).The four T’s mnemonic device for causes of PPH.(75)(6)
pp.876.
Api,M.;Api,O.; Yayla,M. (2005). Fertility after B-Lynch suture and hypogastric artery ligation.
Fertil Steril(84)(2):509.
Bais, JM ; Eskesm (2004).Post partum heamorrage in nulliparous women:Incidence and risk
factors in low and high risk women.Obestet gynecol report Biol (115)(2):166-72.
Beck,D. (2004).Primary postpartum Hemorrhage, National college des Gynecologists et
Obstetriciens, France. French national Agency for accreditation and Evaluation in Health care
guidelines Department.
Bott,J. (1999). Prevention of occupational infection. British Journal of Midwifery (7)(11):
671-675.
Bouwmeester, F.W.; Jonkhoff, A.R.;Verheijen, R.H. (2003).Successful treatment of life –
threatening postpartum hemorrhage with recombinant activated factorV11.Obstet Gynecol
(101)(6):1174-1176.
CEMACH(2007) - Why mothers die; Confidential enquiry into maternal deathes in the UK
confidential enquiry into maternal and child Health Executive Summary ;(2000-2002).
Chauhan,SP ; Martin,JN (2003).Maternal and Perinatal complications with uterine rupture in
142,075 patients who attempted vaginal birth after cesarean delivery. Obstet Gynecol
(189)(2):408-417.
Chitrit Y, Zafy S, Pelage JP,et al (2005).Amenorrhea due to partial uterine necrosis after uterine
artery embolization for control of refractory postpartum haemorrhage.Eur J obstet Gynecol
Reprod Biol(127)(1): 140-142.
Chong,YS;Chua,S;Arulkumaran,S.(2004).Does the route of adminstration of Misoprostol make
adifference?.The uterotonic effect and side effects of Misoprostol given different route after
vaginal delivery.Eur.Obstet Gynecol Reprod Biol (113)(2):191-198.
Combs, CA; Murphy, EL. ;Laros, R .K. (1991). Factors Associated With Postpartum
Hemorrhage With Vaginal Birth.Obstetrics & Gynecology (77)(1):69-76. Deborah, A.; Malay, K. M. (2002).Prevention of PPH in low resource setting. International
Journal of Gynecology and Obstetrics (77):267-275. Dehbashi,S.; Honarvar,.M; Fardi, F.H.(2004). Manual removal or spontaneous placental delivery
and postcesarean endometritis and bleeding.Int j Gynaecol Obstet.(86)(1):12-15.
Diane,M.(2003).Causes of postpartum heamorrage.University of Nottingham UK. Dildy,GA.(2002).Postpartum hemorrage:new mangement options.Clinic obestetric and
gynacology.(45)(2):330-344. Filippi,V. (2005).Maternity wards or emergency obstetric room?Incidence of near miss events in
african hospitals. Acta Obstet Gynecol (84)(1):11-6.
French, L.(2003) prevention and treatment of postpartum endometritis. CurrWomans Health
Rep(3)(4): 274-9.
88

French,L.M.; Smaill,F.M.(2004).Antibiotic regimens for endometrities after delivery. Cochrane Database Syst Rev (18)(4): CD001067.
Gobbi,M. ; Foss,M. ;Cullen,J. (2012). Improving maternal mortality in South Sudan University
of Southhampton U.K.For the newly government of south Sudan(GOSS) supported by UNFPA.
Grellier,R. (2000). 'Everyone is scared of it inside so they start being a bit irrational'.(16)(1):56-
67.
Habek D, Vranjes M,Bobic VukovicM, et al(2006).Successful term pregnancy after B-Lynch
compression Suture in a previous pregnancy on account of massive primary postpartum
hemorrhage . Fetal Diagn Ther.(21)(5) :475-6.abstract. Henry, A.; Birch, M.R.; Sullivan, E.A .; (2005). Primary postpartum haemorrhage in an Australian
tertiary hospital: a case control study. Aust NZJ Obstet Gynaecol.(45)(3): 233-6. International
Federation of Gynecology and Obstetrics (FIGO)(2003).The November 2003 Joint statement,promotes AMTSL to save mother’s lives.ICM and FIGO. JANICE M. ANDERSON(2007). Prevention and Management of Postpartum Hemorrhage. Physician. 2007 Mar 15;75(6):875-882.
John,R.;Chelow,D.(2012).Management of the third stage of labor. Medscape. Feb2013
Kennedy,EH.(2004).Acute postpartum hemorrage in India.National institute of child health and
human development(NICHID).Study November 17,2004.last updated December 2008.
Lewis, G. (2007). The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving
Mothers’ Lives: reviewing maternal deaths to make motherhood safer- 2003-2005. The Seventh
Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London:
CEMACH.
Lucile Packard Children’s Hospital (2013). Care of the Baby in the Delivery Room
online.Available from:
http://www.lpch.org/DiseaseHealthInfo/HealthLibrary/pregnant/care.html
Magann EF, Evans S, Hutchinson M,et al ( 2005).Postpartum haemorrhage after vaginal birth:
an analysis of risk factors. South Med j.(98)(4):419-22 .
Magann EF,Evans S, Hutchinson M, et al ( 2005 ).postpartum haemorrhage after cesarean
delivery : an analysis of risk factors. South Med jJ (98) (7):681-685.
Magann,EF.;Evans,S(2005).The length of the third stage and the risk of PPH.Obstet and gynecol
(105):190-193.
MC Cormic,ML.;Sanghri,HC(2002).Aveting maternal death and disability;preventing PPH in
low resource setting.International Journal of Gynacology and Obstetric2002.(77):267-275.
Metcafe,G.;Armbruster,D.(2007).Prevention of PPH initiative(POPPH) office of
health,infectious diseases and nutrition,Bureau for Global Health,US Agency for international
Development.
Minino AM,Heron MP,Murphy SL,Kochanek KD, et al (2007).National Vital statistic
Reports:Deaths 2004.US Department of Health and Human Services and centre for disease
control and prevention p.120. Mobasherizadeh,S.et al (2009).Interventionstudy of needle stick injury in Iran.Saudi Med J.,(30)(12):1616. Mosby’s Medical Dictionary(2009).Post Partum Heamorrage definition.8
th Edition
2009. Elservier. Mutashmi,H(2006).United nation fund of population on a ctivities (UNFPA).Maternal
mortality:reality and challenges.
Patel,A. (2006).Drape estimation vs. visual assessment for estimating PPH.International Journal
og Gynecology and Obstetric (93):220-224.
Pelage, J.P.; Le Dref,O.; Mateo,J.; et al (1998). Life threatening primary postpartum
haemorrhage: treatment with emergency selective arterial embolization Radiology. (208)(2) :
359 -62 .
89
Am Fam

POPPHI (2009). Prevention of Postpartum Hemorrhage: Implementing Active Management of
the Third Stage of Labor (AMTSL). Facilitator’s Guide: Training of AMTSL mentors. Seattle:
PATH; 2009 POPPHI (2009). Prevention of PPH AMTSL Training Package. Available
from: http://pphprevention.org/AMTSLlearningmaterials.
Price N,B-Lynch C (2005). Technical description of the B-lynch brace suture for treatment of
massive postpartum hemorrhage and review of published cases.Int J Fertil Womans Med.
(50)(4): 148 63.
Rashmi,B and Vanita,J (2011).The impact of postpartum heamorrage in near-mis morbidity and
mortality in developing countries.European clinics in obstetric and gynacology.(2)(3) “161-
169”.
Rizvi,F ;Mackey,R (2004).Successfull Reduction of Massive PPH by use of guidelines and staff
education. BJOG (111)(5):495-8.
Royal college of Midwives 2012.Career profile:Education of Midwifery in UK.
Royal college Obstetricians and Gynaecologists 2009.prevention and management of postpartum
haemorrhage.
Saad,E. ;Farouk,H. (2003).Maternal Mortality in A teaching hospital in Sudan.Saudi Medical
Journal .(24)(4)) “369-372”.
Sanghvi,H.;Wiknjosastro,G.;Ghanpong,G.(2004).Prevention of postpartum hemorrhage
study, West Java, Indonesia. JHPIEGO.
Seror,J.;Allouche,C, Elhaik, S.(2005) Use of Sengstaken-Blakemore tube in massive postpartum
haemorrhage : a series of 17 cases . Acta obstet Gynecol Scand. (84)(7) :660-664.
Silver RM, Landon MB,Rouse DJ, et al (2005): Maternal morbidity associated with multiple
repeat cesarean deliveries. Obestet Gynecol.(107)(6): 1226-32 .
Soriano D, Dulitzki M,Schiff E, et al (1996).A prospective cohort study of oxytocin Plus
ergometrine compared with oxytocin alone for prevention of postpartum haemorrhage. Br J
Obstet Gynaecol.(103)(11):1068-73.
Statistic Department in Ministery of Health (2011).Map of midwifery work force in 15 Northern
states. Khartoum state.
TENNESSEE MIDWIVES’ ASSOCIATION (TMA) PRACTICE
GUIDELINES © TMA, Adopted 01/22/2001.
The American Heritage Medical Dictionary(2007).By Houghton Mifflin 2004
company.published by Houghton Mifflin company.All right reseved.
Tintinalli JE, 2004.Clinical practice Guidelines of Postpartum Heamorrage.Ballarat Health
Service.
Tran SH,Caughey AB, Musci TJ(2003). Meconium-stained amniotic fluid is associated with
puerperal infections .Amj Obstet Gynecol.(189)(3) 746-50.
USAID (2007). Prevention of PPH : implementing AMTSL, ,POPPHI project by the office of
health, infectious diseases and nutrition,Bureau for Global health,USAID.
Verre M, BossioF, Mammone A,et al (2006). Use of recombinant activated factor V11 in case of
severe postpartum haemorrhage . Minerva Ginecol. (58)(1): 81-84.
Virtual Medical Centre (2005). Diagnosis of postpartum heamorrage online.
Available from:http://www.virtualmedicalcentre.com/diseases/postpartum-haemorrhage-
pph/676#How_is_it_diagnosed
World Health Organization(WHO)(2005).World health report:Make every mother and child
count.Accessed september10,2008.
Zahn,CM;Yeomans,ER.(1990).Postpartum hemorrage:Placenta accreta,Uterine inversion
and puerperal hematomas.Clinic obstetric and gynecol(33)(3): 422-431.
90

APPENDICES 91

Knowledge of nurse midwives about post partum heamorrage
(The study Group) 2010
Ques onar e:
No. Item Yes No To some extent
Q1 Defini on: PPH i s des cri bed by/ as:
1. Primarty and secondary PPH
2. Primary PPH is the loss of more than
500ml of blood wiyhin 24 hrs and 800-
1000 ml in case of caeesarean sec on.
3. Any amount of bleeding causes change
for the worse in women’s condi on.
4. The bleeding causes a low systolic blood
pressure,increased heart rate,decreased
in red blood cells,signs of shock.
5. All of the above is true.
Q2 Types of PPH:
1. Primary PPH occurs during 24hrs od
delivery.
2. Secondary PPH can occur from 24hrs -6
weeks.
3. A and B are correct.
4. Can occur a er 6 we eks.
5. Not known.
Q3 Causes of PPH:
1. Uterine atony.
2. Mul pl e gesta on, pol yhydrami o us .
3. Uterine infec on.
4. Drugs(uterine relaxants).
5. Uterine inversion.
6. Placenta previa(retained or adherent)
7. Trauma.
Q4 Risk factors:
1. Antepartum heamorrage.
2. Placenta previa.

3. Mul pl e pr egnances .
4. Pre-eclampsia or pregnancy induced
hypertension.
5. Previous PPH.
6. Emergency caearean sec on.
7. Null parity.
8. Infec ons .
9. Trauma.
10 baby > 2kg.
11 Blood coagula on.
Q5 The common signs and symptoms:
1. Uncontrollable bleeding.
2. Decreased blood pressure.
3. Increased heart rate.
4. Decrease in red blood cells.
5. Loss of blood > 1000 cc.
6. Signs of shock.
Q6 The necessary inves ga ons :
1. Blood grouping and cross matching.
2. Haemoglobin,clo ng screen.
3. Urine output hourly.
4. ECG.
5. Liver enzymes and low platelets.
6. TPR and BP monitoring.
7. Checking lacera on of per neal cer vi x.
Q7 Complica ons :
1. Shock.
2. Renal failure.
3. Acute respiratory distress syndrome.
4. Hypotension.
5. Disseminated intravascular coagula on
Q9 Uterotonic drugs used in labor:
Oxytocin 5-10 units.
Ergometrine and Oxytocin.
Misoprostol.
Q10 Was uterotonic drugs given a er
shoulder delivery.

Q11 Did anaesthesia with ether or halothane
increase the risk of PPH.
Q12 Principals of infec on pr even on:
9. Do use separate set for each delivery.
10. Equipment should be steriliazed by
autoclaves.
11. Do you use disinfectant for cleaning
equipments and floor .
12. Types:Detol/stavelon.
14. Using disposable needles for suturing
once only.
15. Steriliza on me ans ki lling of al l types of
micro organism.
16. Disinfec ons me ans k i lling a l l mi cro
organisms except spores.
17. Boiling for 20 minutes is the way for
achieving disinfec on.
Q13 Physiology of genital tract:
1. Do you know the physiology of the
genital tract?
2. Do you know the importance of the
third stage of labor and it’s physiological
changes?
Q14 Do you think there are adequate
supplies to carry out your work?
Q15 Do you think the work environment is
generaly suitable for the effec ve
implementa on f or t he m i dwi fer y
procedure?
If not,explain the reasons?
Q16 What ini al car e is recomme nded in the event of eme r gency PPH?

A tute of nur s e mid wi v es towar ds mot her s
No. Item Yes No To some extent
Q1 Communica on ski lls:
1. Introduce her self.
2. Explain the procedure.
3. Take permission to carry out procedur.
4. Greated mother , say hello.
5. Smile and thanks the pa ent .
Q2 Harmful customs prac ce dur ing
labor:
1. Giving oxytocin I.M and increase the rate.
2. Providing herbal remedies to increase
contac on. Rough ma ssage.
3. Encourage bushing before the cervix is
fully dilated or sweeping.
4. Use fundal pressure to hasten labor.
Q3 Interven onal rel a ons hi p bet wee n
midwives and mothers:
1. Communicate in a humane way.
2. Reassure and support the mother.
3. Provide proper nursing care to mother
and new born.
4. Verbal abuse(Harsh and tough ).
5. Physical abuse(binsh and hit).

Q4 Principles of infec on pr even on:
1. Do you wash your hands before you
perform any nursing procedure?
2. Do you wash your hands a er any nur si ng
procedure?
3. Do you use sterile gloves for PV
examina ons ?
4. Do you use gloves during the
decontamina ons of the del iver y set ?
5. Do you use sterile gloves when inser ng
acannula?
6. Do you wear aplas c a pr on w h i le
a endi ng to chi ldbi rth?
7. Do you wear amask?
8. Do you dispose offs har p i ns trume nt s
a er us e ,in the sa ey box?

Impact of a designed in-service training program on nurse midwives knowledge, a tude and prac ces t owar d s post part umhe mor r hage mana gement at
Khartoum state midwifery hospitals.
2010
An observa on check list (1)
Informa on for research pur pos e.
NO ITEM Done Not To some
Done extend
Q2 History taking:
1. Age
2. Occupa on
3. Educa on
4. Address
Q3 Social Life :
1. Income.
2. Family member.
Q4 Family history:
1. Common disease.
2. Any gene c di sease.
3. Hypertension.
4. DM.
5. Heart disease.
6. TB.
Q5 Menstrual :
1. Last menstrual period (LMP).
2. Expected date of delivery
(EDD).
3. Any disorders or irregulari es .
4. Menarche.

Q6 Obstetetric :
1. Gravidity. 2. Parity. 3. Abor ons . 4. Complica ons for mo t her
or baby.
Q7 History of present pregnancy:
1. Any signs of diseases
2. Antepartum hemorrhage
3. Twins
4. Caesarian sec on
5. Baby > 2 KG
Q8 General Examina on :
Head, ears, eyes, nose Mouth and
throat, neck, palpa on of thyroi d
gland.
Observa on of ski n and Ha i r.
Q9 Abdominal Examina on:
1. Shape of the abdomen.
2. Signs of pregnancy. 3. Liver, spleen and kidney
palpa on. 4. Height of the fundus. 5. Fetal lie. 6. Fetal heart. 7. Inspec on of exter nal genet al
ia and varicose veins. 8. Deep vein thrombosis
inspec on.
9. Vaginal examina on. 10. Pelvic measurement.
Laboratory Inves ga on : 1. Urine general.
Q10 2. Urine for glucose. 3. Urine for albumen and acetone. 4. Blood hemoglobin. 5. Blood group and
cross matching. 6. Screening AIDs. 7. Hepa s B ( VHB) .

ميحرلا رلامحن هللا مسب
Impact of a designed in-service training program on the nurse
Midwives knowledge, a tude and prac ces t owar d s post part um
hemorrhage management at Khartoum state midwifery hospitals.
2010
An observa on check list 2: (labor room )
NO ITEM Done Not To some
Done extend
Q11 Episiotomy : -
1. Made with sterile scissors.
2. Made in the area between vagina and rectum.
3. Diagonal incision across the midline between
the vagina and anal.
4. Mediolateral incision to right or le .
5. The incision s tches accor di ng to the dept h.
6. Done during the birth process.
7. Before the delivery of the head (15min.).
8. During crowning of the head
Q12 Management before placental delivery :-
1. Make sure bladder is empty.
2. Careful inspec on of bi rth canal , per ineum
and cervical lacera on.
3. Observe and measure the amount of blood
loss and explora on of ut er ine cavi ty.
4. Take vital signs.
5. Give oxytocin 5-10 units a er int er ior shoul der
delivery.
Q13 1. Skills of nurse midwives during Delivery of
the placenta :-
2. Reading the me bef or e del iver y of pl acent a.
3. Clamping the umbilical cord near the
perineum.
4. Applying control cord trac on (CCT) .
5. Preparing Oxytocin injec on.
6. Suppor ng pl acent a wi th bot h hands .
7. Wai ng for si gns of separ a on.
8. Examining the maternal side of the placenta.
9. Weigh the placenta.

Q14 Assessment for uterine contrac on a er placental delivery:-
1. Careful inspec on of the pl acent a. 2. Ensure the uterus muscle is contracted. 3. Manual explora on and re- inspec on of the
geni tract. 4. Massaging the uterus immediately a er Pl acent
a Delivery.
5. Uterine assessment for lacera on.
6. Take the vital signs.
7. Encourage breast feeding.
Q15 Principles of infec on pr even on : -
1. Hand washing before wearing sterile gloves.
2. Wearing gloves, gown and mask in an appropria
way.
3. Prevent splashes and contamina on.
4. Steriliza on of equi pme nt done pr oper ly.
5. Steps of processing instruments to prevent
contamina on.
6. Proper handling and disposal of sharps.
Q16 Ac ve ma nageme nt of the thi rd stage
of labor (AMTSL):-
Preven on of (PPH) :-
1. Early cord clamping and ac ve del iver y of placenta.
2. Controlled cord trac on.
3. Uterine massage a er del iver y of pl acent a.
4. Administra on of ut er ot oni c drugs approp
un l del iver y of the shoul der .
5. Avoiding rou ne epi si ot omy .
2

6. Reducing incidence of prolonged labor.
7. Minimizing trauma associated with
instrumental delivery.
8. Training skilled birth a endant s.
9. Developing na onal qui d lines .
Q17 Management and nursing care in case of
complica on in
the third stage of labor:
1. Call for emergency team.
2. Evaluate and measure the amount of blood l
3. Insert I.V vein line.
4. Prepare oxygen.
5. Evaluate the pa ent condi on and t ake t he vit
signs.
6. Prepare results of blood tests.
7. Make sure blood is ready.
8. Give Oxytocin as ordered.
9. Give I.V flui ds .
10. Misoprostol used rectally or orally.
Q18 Skills of the nurse midwives towards
es ma on of blood l oss :
1. Put in a measured plas c bag.
2. Weigh pads before and a er bl eedi ng.
3. Put in a measured kidney dish.
4. Drape es ma on of blood l oss .
5. Covering surface area standard container.
3