
Identifying research priorities to be addressed in the area of suicide prevention
82
Identifying research priorities to be addressed in the area of suicide prevention Final Report Jane Pirkis, Jo Robinson, Karolina Krysinska, Sara Niner, Tony Jorm, Michael Dudley, Emily Schindeler, Diego De Leo and Susy Harrigan 31 October 2006
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Identifying research priorities to be addressed in the area of suicide prevention

Identifying research priorities to be addressed in the area of suicide
prevention
Final Report
Jane Pirkis, Jo Robinson, Karolina Krysinska, Sara Niner, Tony Jorm, Michael Dudley, Emily Schindeler, Diego De Leo
and Susy Harrigan
31 October 2006
1
Table of contents
Executive summary ...........................................................................................................2
Chapter 1: Background and methodological overview.................................................9
Chapter 2: Review of published literature (Study 1)...................................................13
Chapter 3: Review of funded grants (Study 2) .............................................................22
Chapter 4: Web-based questionnaire (Study 3) ...........................................................29
Chapter 5: Focus groups (Study 4)................................................................................42
Chapter 7: Discussion and conclusions.......................................................................48
References........................................................................................................................55
Acknowledgements .........................................................................................................56
Appendix A: List of peer-reviewed journal articles in which suicide or suicidal behaviour was the primary focus ..................................................................................57
Appendix B: List of funded grants.................................................................................70
Appendix C: Questionnaire ............................................................................................72
2
Executive summary
Background Consistent with the evidence-based approach of the National Suicide Prevention Strategy, the National Advisory Council for Suicide Prevention has recommended the development of a national suicide prevention research agenda and options to encourage further research in the field. The current project aimed to identify current priorities in suicide prevention research, as evidenced by the kinds of research that have been funded and published in recent times. It also aimed to identify future priorities, by considering the gaps in existing research, and by consulting with stakeholders in the field.
Method The project comprised four studies which, taken together, permitted an examination of current and future priorities in suicide prevention research. Current priorities were examined via:
• An analysis of extent and nature of current research, as assessed by examination of abstracts of peer-reviewed journal articles on suicide prevention research published during the life of the National Suicide Prevention Strategy (1999-2006 inclusive).
• An analysis of extent and nature of current research, as assessed by
examination of summaries of grants funded by the National Health and Medical Research Council (NHMRC), the Australian Rotary Health Research Fund (ARHRF) and the Australian Research Council (ARC) during the life of the National Suicide Prevention Strategy.
Future priorities were examined via:
• Broad analysis of 231 stakeholders’ views on future priorities, elicited via a web-based questionnaire. Stakeholders were selected on the basis of their membership of 11 groups with a known interest in suicide prevention research.
• Detailed analysis of 28 stakeholders’ views on future priorities, elicited via three
focus groups. Stakeholders were purposively sampled, and known to have an interest in suicide prevention research.
Key findings Current investment and outputs During the life of the National Suicide Prevention Strategy, 263 journal articles have been published in the peer-reviewed literature that qualify as research where suicide is the primary focus. During the same period, 36 grants have been funded to the tune of $5,839,341 for projects or fellowships in the area of suicide prevention. Although these figures are not insignificant, they do not seem to be commensurate with the high individual, societal and economic burden of suicide and suicidal behaviours.
3
Priorities for type of research The profiles of published literature and funded grants differed in terms of the type of research they involved. The majority of research in the published literature was epidemiological, with a focus on descriptive analyses of rates. By contrast, the studies funded through the grants most commonly assessed the efficacy of interventions, particularly indicated interventions aimed at individuals who are already manifesting suicidal thoughts or behaviours. The majority of questionnaire respondents identified intervention studies as the highest priority for future suicide prevention research, calling for further work on indicated interventions and, to a lesser extent, selective and universal intervention. Their views were supported and expanded upon by focus group participants, who stressed that in future suicide prevention research efforts, priority should be given to evaluating the efficacy of specific interventions. They also stressed the importance of evaluations of suicide prevention policies, programs and services, which to date have received less attention. They felt that the epidemiological profile of suicidal individuals has been explored, at least with respect to rates and individual-level risk factors, and that intervention and evaluation research should focus on groups identified as having particularly high levels of risk. Most saw limited value in continuing to explore individual-level risk factors ad infinitum, and felt that the time has come to move on to considering wider societal influences on suicide and individual-level protective factors, and to do so from a multi-disciplinary perspective. Priorities for suicidal behaviour In the international suicidology literature, there is a recognition that suicidal behaviours occur on a gradient, from suicidal ideation to attempted suicide to completed suicide, and there has been a consequent acknowledgement that it is important for prevention to focus on the full spectrum of suicidality. It may be appropriate, therefore that where a particular suicidal behaviour was examined in the published journal articles and funded grants, and equal amount of research effort was found for completed and attempted suicide. Although completed suicide is regarded as the more extreme manifestation of suicidality, suicide attempts are more prevalent and may affect different populations.1 From the perspective of questionnaire respondents, this division of emphasis would seem to be appropriate, in the sense that although respondents from most groups suggested that attempted suicide should be given priority in future research, people involved in funding suicide prevention research recommended that completed suicide should be addressed. Focus group participants did not comment explicitly on the relative emphases that should be given to particular suicidal behaviours. Priorities for suicide method Few of the retrieved journal articles reported on research into specific methods of suicide, and none of the funded grants supported method-specific research. This may be appropriate in the sense that much of the research effort has focussed on understanding suicidal behaviours in general, rather than on examining particular means. Having said this, reducing access to means has been acknowledged internationally as one promising way of preventing suicide,2 so it would be desirable to augment the current knowledge base with some more detailed analyses of method-specific issues. Focus group participants did not comment directly on the suicide methods which should be given priority, but questionnaire respondents emphasised two suicide methods of interest: poisoning by drugs and hanging. The methods of choice may reflect the particular perspectives of the respondent groups. For example, the clinicians (i.e., psychiatrists, GPs and psychologists) were among those most inclined to endorse
4
poisoning by drugs as a research priority, which may reflect the fact that they commonly see people who have overdosed. Alternatively, the methods chosen may be related to how commonly they occur, as evidenced by the fact that hanging is the most common method of suicide in Australia.3 Priorities for target groups Young people emerged as the most commonly-researched target group in both the review of published literature and the review of funded grants. Other major target groups of interest in both cases were people who have attempted suicide or deliberately self-harmed and people with mental health problems. Stakeholders were divided about the target groups who should receive greatest attention in future suicide prevention research. The majority of questionnaire respondents endorsed young people and people with mental health problems. Focus group respondents mentioned a range of groups, with men and older people standing out. It is worth examining the relative emphasis on these target groups, and to consider ways of prioritising the suicide prevention research effort in this regard. As one focus group participant noted, there is a need to develop objective criteria against which to make these judgements. There is an argument, for example, that those groups who are acknowledged as having particularly high levels of suicide risk (e.g., people who have attempted suicide and people with mental health problems) should remain on the research radar, and that groups (e.g., adult men) for whom suicide rates are on the rise may warrant renewed attention. Priorities for settings Certain settings took precedence in the research published in peer-reviewed literature and funded through grants. Other health service settings received particular emphasis, and communities, mental health service settings, emergency departments, schools and prisons were also afforded attention. Questionnaire respondents held various views about where the priority should lie in terms of future setting-specific suicide prevention research. Although communities was the response most commonly endorsed by the greatest number of groups, primary care settings and mental health service settings were also given prominence. Focus group respondents did not comment directly on the settings in which future suicide prevention research should be conducted, although they emphasised the importance of critically examining the response of the health and community service systems.
Recommendations Some of the findings from the current project are unequivocal, and point clearly to specific recommendations about the direction the development of a national postgraduate scholarships and/or national research grants program should take. Other findings are more mixed and/or reflect the project’s limitations, and require that additional information be sought before clear direction can be given. The following recommendations reflect the nature of these findings: Recommendation 1: Priority should be given to funding studies that evaluate interventions It is clear from the data that priority should be given to funding studies about interventions. Although these studies have been the subject of a relatively high proportion of funded grants, relatively few published papers have emanated from these
5
grants, and stakeholders stress that discovering efficacious interventions to prevent suicide should be the ‘main game’. A systematic review of the international literature on suicide prevention strategies by Mann and colleagues found only two interventions which showed any evidence of reducing suicide rates (educating physicians about depression and restricting access to lethal means), and concluded that all other interventions require further testing.2 Australian research should build on international studies, and should pay heed to any contextual factors that might make a given intervention more or less likely to work in the local setting. Given the dearth of knowledge on which interventions might be efficacious, it would seem reasonable for attention to be paid to studies that assess of the efficacy of the full spectrum of suicide prevention interventions (universal, selective and indicated) and/or evaluate suicide prevention policies, programs and services. This research should be scientifically sound, and should employ appropriate methodologies to allow given interventions to be tested in the most rigorous manner possible. For example, it should explicitly test the theory or logic underpinning given interventions, and should pay heed to questions of sample size, use of appropriate comparison groups, and use of suitable outcome measures. The research should represent a balance of priority-driven and investigator-driven research, and should involve thorough evaluations of government-funded programs and projects, as well as purpose-designed evaluations of specific interventions. Recommendation 2: A content-based literature review should be commissioned to determine what is known and what is not known about suicide prevention in the Australian context A content-based review of the scientific literature should be commissioned to provide a picture of what is known and what is not known about suicide prevention in the Australian context. The review should summarise what the literature says about the epidemiology of completed and attempted suicide for key target groups, and about interventions that show promise for suicide prevention for each of these groups. The review should use as its starting point the literature identified in Study 1. Additional reports and journal articles in progress should be sought from the principal investigators of the funded grants identified in Study 2. The review should not be limited to the Australian literature, however, as there has been considerable international investment in suicide prevention research. While it is reasonable that the Australian literature will provide the best summary of the epidemiology of completed and attempted suicide in this country, a fuller picture of current knowledge with regard to interventions will come from a broader examination of studies from overseas. In particular, the literature review should draw on existing review papers that summarise what is known about what works and what doesn’t work in suicide prevention, such as the above-mentioned systematic review by Mann and colleagues.2 Recommendation 3: Funding for epidemiological studies should be provided only in circumstances where new knowledge will be gleaned It is clear that much emphasis has already been given to epidemiological studies, particularly those concerning rates and risk factors. Stakeholders argued that sufficient work has been done in this area, and that the focus should shift elsewhere. To a large extent, this seems reasonable. At the very least, funding for future epidemiological studies should be awarded only when they demonstrate innovation and make a novel contribution to knowledge. This does not necessarily mean that new studies must be commissioned; there may be a place for funding secondary analysis of existing data, or systematic reviews and meta-analyses that bring together the findings of a number of studies in a comparable way.
6
Recommendation 4: Criteria should be developed to assess the significance of suicide among particular target groups, in order to prioritise the research attention that should be paid to each group The current study was unable to prioritise particular groups in terms of warranting research attention. Take, for example, the target group of young people. Young people were the target group investigated in the majority of published journal articles and the majority of funded grants, but survey respondents and focus group participants were divided as to whether they should continue to receive research attention. Some felt that they had received sufficient attention, particularly since the youth suicide rate is now declining; others felt that there is still ‘unfinished business’ with respect to research into what prompts young people to choose suicide as an option and what interventions may prove most successful with this group. What is needed is more objective information about the significance of suicide among this group, relative to other groups, some of which may have been available to the current project had a formal content review of the published literature and/or recourse to routinely-collected suicide data been within its remit. In addition to the subjective views of importance put forward by stakeholders, epidemiological (and, for that matter, economic) measures of importance are required. Such measures need to be readily comparable across groups, and might include group-specific rates, indices of relative risk, indices of population attributable risk, and measures of burden (e.g., disability adjusted life years). This is consistent with the international and Australian literature on priority-setting in public health research, which emphasises significance as a key criterion.4 5 It is recommended that a study be commissioned that objectively assesses the relative importance of completed suicide and attempted suicide as public health issues among particular target groups. This could be commissioned as part of the content-based literature review proposed in Recommendation 2. In line with Recommendation 3, this study should re-examine existing epidemiological data wherever possible (e.g., by synthesising the findings of the epidemiological studies examined in the content-based review), and should complement this with the most up-to-date statistics on completed suicide and attempted suicide as necessary. The study should pay heed to issues of comparability between estimates for particular groups. For example, it should note the likelihood that estimates of rates of attempted suicide will be lower in registration studies (which enumerate presentations to emergency departments or admissions to hospital for medically-serious suicide attempts) than in population-based surveys (which rely on self-report).6 The presentation of a range of estimates and sensitivity analyses may be necessary to improve the comparability of data across groups. Recommendation 5: Criteria should be developed to assess the significance of suicide in particular settings, in order to prioritise the research attention that should be paid to each setting The current study was unable to prioritise particular settings in terms of warranting research attention. Existing research had been conducted in a range of settings, and stakeholders held convergent views about where future priorities should lie. Again, more objective information is needed to shed light on the relative emphasis that should be given to different settings. Some of this information would flow from the study of the relative significance of completed suicide and attempted suicide for different target groups (see Recommendation 4), in the sense that some target groups are associated with particular settings. So, for example, if people with mental health problems emerged as a group to whom research priority should be given, it would make sense to consider mental health service settings as a key setting of interest. Other guidance in this regard may be gained by considering settings in which interventions occur which, although not
7
yet proven in terms of their efficacy, show promise. This information could be drawn out in the content-based literature review, proposed under Recommendation 2. Recommendation 6: Studies of completed suicide and attempted suicide should both receive research funding The current balanced emphasis on both completed suicide and attempted suicide would seem to be appropriate, given that stakeholders give weight to both. As noted, prevention efforts should cover the full spectrum of suicidality, particularly since a previous suicide attempt is one of the strongest predictors of completed suicide.1 For this reason, it is recommended that the intervention studies proposed in Recommendation 1 not be limited to those addressing completed suicide, but also include those addressing attempted suicide (and, to a lesser extent, suicidal ideation). Similarly, it is recommended that the criteria to be developed under Recommendations 4 and 5 address the significance of both completed suicide and attempted suicide for various target groups and in a range of settings. Recommendation 7: Method-specific studies should be given funding support, and criteria should be developed against which to judge whether a given suicide method warrants particular research attention On the whole, the generalist approach to suicide prevention research would appear to be appropriate, since lessons about suicide and its prevention will often not be method-specific. Focus group participants did not raise method-specific research as an issue, but, when directly asked, questionnaire respondents emphasised the need to pursue research into poisoning by drugs and hanging as priorities. There is certainly an argument for some research attention to be directed towards particular methods, and for criteria to be developed that ranks them in terms of their significance. Such criteria might be based on the relative rate at which they occur (derived from the content review of the epidemiological literature proposed in Recommendation 2 and a thorough examination of routinely-collected statistics). Alternatively, criteria might be based on the feasibility of targeting an intervention towards particular methods (e.g., reducing access to paracetamol via repackaging efforts, as was done in the United Kingdom7). Recommendation 8: Multi-disciplinary research that employs a range of methodologies should be encouraged On the whole, the generalist approach to suicide prevention research would appear to be appropriate, since lessons about suicide and its prevention will often not be method-specific. Focus group participants did not raise method-specific research as an issue, but, when directly asked, questionnaire respondents emphasised the need to pursue research into poisoning by drugs and hanging as priorities. There is certainly an argument for some research attention to be directed towards particular methods, and for criteria to be developed that ranks them in terms of their significance. Such criteria might be based on the relative rate at which they occur, and/or trends in relative rates over time (derived from the content review of the epidemiological literature proposed in Recommendation 2 and a thorough examination of routinely-collected statistics). Alternatively, criteria might be based on the feasibility of targeting an intervention towards particular methods (e.g., reducing access to paracetamol via repackaging efforts, as was done in the United Kingdom7). Recommendation 9: Research findings should be communicated as widely as possible, in order to maximise their influence on policy and practice Certain contractual ‘deliverables’ should be tied to future suicide prevention research funding, in order to maximise ‘knowledge transfer’. These deliverables should include peer-reviewed journal articles, but also less traditional communications that ensure that

8
findings are reported in meaningful ways to a range of stakeholders. The latter might include reports for a range of audiences, community presentations and media releases.
Conclusions The current report presents a picture of the status quo with regard to suicide prevention research, identifying some areas where there are clear gaps and others where relatively greater efforts have been made. Interpreting these findings in a manner that can inform the proposed research agenda is not simple, and is not just a matter of giving weight to previously under-emphasised areas and reducing the attention paid to previously well-covered areas. The findings from the web-based questionnaire and the focus groups enable these results to be assessed through the lens of what stakeholders view as priorities. Other factors should also be taken into account in formulating future priorities, but the findings may assist in re-directing Australian suicide prevention research endeavours to help fill internationally-identified gaps in knowledge about what works and what does not work in suicide prevention.

9
Chapter 1: Background and methodological overview
Background Australia’s National Suicide Prevention Strategy began in 1999, consolidating and building on the achievements of its predecessor, the National Youth Suicide Prevention Strategy. The National Suicide Prevention Strategy has been operationalised through the Living Is For Everyone (LIFE) Framework,8-10 which provides strategic direction to governments, communities and businesses regarding priority areas for action. From the outset, the strategic national approach taken in Australia has sought to draw on the best available evidence. Under the National Youth Suicide Prevention Strategy, funding was made available for a three-part literature review that examined the research evidence regarding the epidemiology of suicide, and risk factors and interventions for suicide.11 This work then provided direction for the National Suicide Prevention Strategy. Under the National Suicide Prevention Strategy, the reliance on sound evidence to guide practice has continued. One of the six action areas of the LIFE Framework is progressing the evidence base for suicide prevention and good practice. This quest for knowledge regarding the most effective means of addressing suicide permeates the other five action areas of the LIFE Framework, which relate to activities, services and partnerships designed to reduce risk factors and heighten protective factors among particular individuals and groups. The National Advisory Council for Suicide Preventiona was established to provide strategic advice to government on suicide prevention and related matters, and to oversee the National Suicide Prevention Strategy. Within this remit, and consistent with the evidence-based thrust of the LIFE Framework8-10 and the National Suicide Prevention Strategy, the National Advisory Council for Suicide Prevention has recommended the development of a national research agenda and options to encourage further research in the field. The project described in the current report represents Stage 1 of the development of such an agenda, and involves four studies which identify what suicide prevention research is currently being undertaken in Australia and the gaps which exist.b
Four studies for identifying current and future priorities in suicide prevention research The project comprised four studies which, taken together, permitted an examination of current and future priorities in suicide prevention research. Current priorities were examined via reviews of literature published and grants funded during the period 1999-2006 inclusive (i.e., the duration of the National Suicide Prevention Strategy). Future priorities were assessed in terms of stakeholders’ views, elicited via a web-based questionnaire and a series of focus groups. With the exception of the focus groups, the methodology for each of these components drew on that used by Jorm and colleagues in a previous project which examined research priorities in mental health.12-14 Table 1
a The National Advisory Council for Suicide Prevention comprises a Board, a Community and
Expert Advisory Forum, and a Suicide Prevention Advisory Committee in each jurisdiction. b Stage 2 involves the development of a national postgraduate scholarships and/or national
research grants program, and is not addressed here since it will form the subject of a separate tender process.

10
summarises the method employed in each of the four studies, and additional detail is provided in Chapters 2-5. Table 1: Summary of studies
CURRENT PRIORITIES IN SUICIDE PREVENTION RESEARCH
FUTURE PRIORITIES IN SUICIDE PREVENTION RESEARCH
Study 1: Review of published literature Study 3: Web-based questionnaire
Analysis of extent and nature of current research, as assessed by examination of abstracts of peer-reviewed journal articles on suicide prevention research published during the period 1999-2006 inclusive.
Analysis of stakeholders’ views on future priorities, elicited via a web-based questionnaire. Stakeholders were selected on the basis of their membership of 11 groups with a known interest in suicide prevention research
Study 2: Review of funded grants Study 4: Focus groups
Analysis of extent and nature of current research, as assessed by examination of summaries of grants funded by key granting bodies during the period 1999-2006 inclusive.
Analysis of stakeholders’ views on future priorities, elicited via three focus groups. Stakeholders were purposively sampled, and known to have an interest in suicide prevention research.
Defining ‘suicide prevention research’ ‘Suicide prevention research’ was defined relatively broadly, drawing on the definition of mental health research used by Jorm and colleagues in their earlier project.12-14 Specifically, ‘suicide prevention research’ was defined as
‘... [involving] activities which collect new data or carry out some novel analysis of existing data, and which pertain to suicide prevention but may not necessarily involve evaluation of suicide prevention initiatives.’
For the purposes of the current project, research relating to euthanasia was excluded from the above definition.
A framework for examining current and future priorities The reviews of published literature and funded grants and the web-based questionnaire were conducted within a comprehensive framework which enabled current and future priorities to be examined in a systematic manner. The focus groups also reflected this framework, although the discussion within the focus groups was more wide-ranging. The framework was developed in an iterative fashion, drawing on preliminary inspection of the abstracts of published journal articles and summaries of funded grants, and on discussion arising from the focus groups. The framework permitted different elements of suicide prevention research to be considered within various classifications, namely research type, suicidal behaviour, suicide method, target group and setting. The sub-categories within the framework are summarised in Table 2.

11
Table 2: Framework for examining current and future priorities in suicide prevention research
Research type
a. Assessment studies d. Evaluation of policies/programs/services
• Assessment/classification of suicide risk (including development/validation of risk assessment tools)
• Policy evaluation
• Assessment studies – Other • Program evaluation
b. Epidemiological studies • Services evaluation
• Rates (including comparisons of rates) • Evaluation of policies/programs/services - Other
• Risk factors e. Biological research
• Protective factors • Neurobiology (including brain anatomy and physiology)
• Epidemiological studies – Other • Genetics
c. Intervention studies • Biological research – Other
• General intervention issues and methods f. Social science
• Practice guidelines • Sociology
• Efficacy of universal interventions • History
• Efficacy of selective interventions • Literature
• Efficacy of indicated interventions • Media studies
• Intervention studies - Other • Social science – Other
g. Other
h. Not specified / unknown
Suicidal behaviour
a. Completed suicide d. Other
b. Attempted suicide e. Not specified / unknown
c. Suicidal ideation
Suicide method
a. Poisoning by drugs f. Jumping from a high place
b. Poisoning by other g. Jumping or lying before a moving object
c. Hanging h. Other
d. Firearms i. Not specified / unknown
e. Drowning
Target group
a. Young people (aged 24 or less) j. People with physical health problems
b. Adults (aged 25-64) k. People with substance use problems
c. Older people (aged 65 or more) l. People who have attempted suicide
d. Indigenous people m. Offenders
e. People from culturally and linguistically diverse backgrounds n. Men
f. People in rural and remote areas o. Women
g. People bereaved by suicide p. Veterans
h. People who are gay, lesbian, bisexual or transgender q. Other
i. People with mental health problems r. Not specified / unknown
Setting
a. Communities g. Emergency departments
b. Schools h. Mental health service settings
c. Tertiary institutions i. Other health service settings
d. Prisons j. Other
e. Workplaces k. Not specified / unknown
f. Primary care settings
These classifications and the categories within them are largely self-explanatory, with a few possible exceptions. Specifically, it is worth commenting on Research type. The identified types were deliberately designed to be as inclusive as possible, and to recognise that suicide prevention research occurs not only in medical and psychiatric domains, but also in the social sciences. It is also worth providing definitions for universal, selective and indicated interventions, referred to under intervention studies. Universal interventions target whole populations, with the aim of favourably shifting risk and protective factors across the whole population. Selective interventions target population subgroups with particular risk factors for suicide who are not yet exhibiting suicidal thoughts or behaviours. Indicated interventions are designed for people who are already beginning to exhibit suicidal thoughts or behaviours. The application of the framework can be explained by the example of target group. With regard to current priorities, each journal abstract and grant summary was coded in terms

12
of the target group that was the focus of the research, in order to determine whether particular target groups had been given greater or lesser priority in the past seven years. Similarly, questionnaire respondents were asked to make ratings as to the target group(s) which should be given highest priority. The framework therefore enabled comparisons to be made between the status quo and stakeholder-identified future priorities.
Structure of the current report The remainder of this report describes the project in detail. As noted above, Chapters 2-5 provide methodological information about each of the four studies. These chapters also highlight the key findings from each of the four studies. Chapter 6 synthesises these findings, comparing and contrasting current research priorities in suicide prevention with those which stakeholders view as important for future work. Based on these findings, Chapter 6 also makes recommendations for the national research agenda.

13
Chapter 2: Review of published literature (Study 1)
Method As noted in Chapter 1, the review of published literature analysed the extent and nature of current research by examining the abstracts of peer-reviewed journal articles on suicide prevention research published during the period 1999-2006 inclusive. The abstract identification and retrieval process is described in more detail below, as is the way in which the abstracts were coded. The approach to data analysis is also described. Abstract identification and management A decision was made at the outset to restrict the review to literature published in peer-reviewed journals, on the grounds that this was the most systematic way to identify current research. Time and resources did not permit a comprehensive search of other sources, such as reports in the ‘grey’ literature or student theses. Letters, reports, conference abstracts, book chapters, news items, magazine articles and newsletters were also beyond the scope of the review. The decision to focus on peer-reviewed journal articles is consistent with the approach taken by Jorm and colleagues in their earlier study,12-14 and affords some check on the quality of the research included in the review. Searches of the following databases were conducted from their respective years of inception to May or June 2006: Medline; PsychInfo; CINAHL; AUSTInfo; ISI Web of Science (including the Social Science Citation Index and the Arts and Humanities Index). The following search terms were used in this process: suicid* OR parasuicid* OR deliberate self harm OR deliberate self-harm OR suicid* attempt* AND Australia. Consistent with the definition of suicide prevention research provided in Chapter 1, articles were excluded from the review if they pertained to euthanasia (or assisted suicide). Articles were also excluded they did not include a full abstract; did not involve primary research, a systematic or narrative review or an evidence-based commentary; and/or did not have a first author with an Australian address or were not conducted in Australia. All abstracts were downloaded or manually entered into an Endnote database. Abstract classification Abstracts were initially categorised by:
• Publication focus (suicide primary focus, suicide secondary focus, other focus, not specified / unknown);
• Year of publication;
• Publication type (primary research, review, evidence-based commentary, not
specified / unknown);
• Type of data (qualitative, quantitative, other, not specified / unknown); and
• Research design (descriptive, analytical, other, not specified /unknown).

14
These categories are self-explanatory, with the possible exception of Publication focus and Research design. Publication focus is perhaps best explained by example. An abstract reporting on an epidemiological study of the rates of suicide among young people would have been classified as having suicide or suicidal behaviour as its primary focus. By contrast, an abstract pertaining to an intervention study of cancer among older people in which suicidality was listed as one of many outcome variables would have been classified as having suicide or suicidal behaviour as its secondary focus. Research design was categorised according to definitions provided by Hennekens and Buring.15 Descriptive studies were defined as those which profiled characteristics of suicide or suicidal behaviour in relation to particular individuals or groups, with no point of comparison. By contrast, analytical studies were defined as those which explicitly made comparisons between different groups in terms of risk and/or protective factors (i.e., exposure variables) and suicide or suicidal behaviour (i.e., outcome variables). Following the initial categorisation of abstracts, further categorisation took place according to the framework outlined in Chapter 1. As noted, this framework enabled each abstract to be categorised according to the following classifications:
• Research type (assessment studies; epidemiological studies; intervention studies; evaluation of policies/programs/services; biological research; social science studies; other; not specified / unknown);
• Suicidal behaviour (completed suicide; attempted suicide; suicidal ideation; other;
not specified / unknown);
• Suicide method (poisioning by drugs; poisoning by other; hanging; firearms; drowning; jumping from a high place; jumping or lying before a moving object; other; not specified / unknown);
• Target group (young people; adults; older people; Indigenous people; people
from culturally and linguistically diverse backgrounds; people in rural and remote areas; people bereaved by suicide; people who are gay, lesbian, bisexual or transgender; people with mental health problems; people with physical health problems; people with substance use problems; people who have attempted suicide; offenders; men; women; veterans; other; not specified / unknown); and
• Setting (communities; schools; tertiary institutions; prisons; workplaces; primary
care settings; emergency departments; mental health service settings; other health service settings; other; not specified / unknown).
In most cases, a single category was selected within each classification and coded as 1 (with the alternative, non-endorsed categories being coded as 0). For example, most studies about older people did not involve any other target group, so these abstracts would have received a score of 1 for older people and 0 for all other target groups. In some cases, however, an abstract covered more than one category within a given classification. To avoid double-counting, the alternatives were weighted so that they summed to 1. Continuing with the example of target groups, if an abstract described a study dealing with rural youth, young people and people in rural and remote areas were both given a weight of 0.50. Similarly, if an abstract described a study focusing on people with co-morbid mental health problems and substance use problems who had attempted suicide, all three relevant target group categories were given weights of 0.33. Each abstract was examined and classified according to the above categories by a single team member (Jo Robinson), in consultation with the team leader (Jane Pirkis) wherever necessary.

15
Data management and analysis Data on each abstract were entered into a purpose-designed Access database and subsequently imported into SPSS for analysis. Simple weighted frequencies and percentages were calculated for each category.
Results Overview In total, 373 abstracts were retrieved and reviewed. As noted, consideration was given to each abstract’s focus, in terms of whether suicide or suicidal behaviour constituted the primary focus of the research, or whether it was more secondary in focus. In 263 (71%) of the 373 abstracts, suicide or suicidal behaviour was rated as being the primary focus of the reported research. The remainder of this chapter focuses on the 263 abstracts with suicide or suicidal behaviour as their primary focus, on the grounds that these provide the most representative picture of the priority that has been given to suicide prevention research in the past seven years. A full list of these 263 abstracts is available at Appendix A. Year of publication Year of publication was available for 262 abstracts. Forty four of these were published in 1999, 44 in 2000, 35 in 2001, 40 in 2002, 36 in 2003, 18 in 2004, 32 in 2005 and 13 in 2006. Figure 1 provides a graphical representation of these data on year of publication, excluding the data for the 2006 year because abstracts were only available for the first four months of that year. The trendline in Figure 1 indicates that there has been an overall decline in abstracts published over the course of the National Suicide Prevention Strategy. Figure 1: Abstracts for which suicide or suicidal behaviour is the primary focus (n=262), by year of publication
44 44
35
40
36
18
32
0
5
10
15
20
25
30
35
40
45
50
1999 2000 2001 2002 2003 2004 2005
Perc
en
tag
e

16
Publication type Publication type could be determined for 251 of the 263 abstracts. Figure 2 profiles the abstracts by publication type. The majority (72%) constituted primary research. A further 18% involved systematic or narrative reviews, and 10% were classified as evidence-based commentaries, which drew on expert opinion or evidence from selected studies (e.g., case studies), but did not constitute comprehensive reviews. Figure 2: Abstracts for which suicide or suicidal behaviour is the primary focus (n=251), by publication type
0
10
20
30
40
50
60
70
80
Primary research Review Evidence-based commentary
Weig
hte
d p
erc
en
tag
e
Type of data The type of data reported in the given research could be ascertained for 164 abstracts. Figure 3 summarises the broad type of data reported in each of these. The vast majority (90%) reported on quantitative data, while only 10% described qualitative data.

17
Figure 3: Abstracts for which suicide or suicidal behaviour is the primary focus (n=164), by type of data
0
10
20
30
40
50
60
70
80
90
100
Quantitative Qualitative Other
Weig
hte
d p
erc
en
tag
e
Research design Information on research design was available for 203 abstracts. As Figure 4 shows, 54% employed descriptive designs, with no point of comparison. Forty six per cent utilised analytical designs where they explicitly made comparisons between different groups in terms of various exposure variables and suicidal outcomes. Figure 4: Abstracts for which suicide or suicidal behaviour is the primary focus (n=203), by research design
40
42
44
46
48
50
52
54
56
Descriptive Analytical
Weig
hte
d p
erc
en
tag
e
18
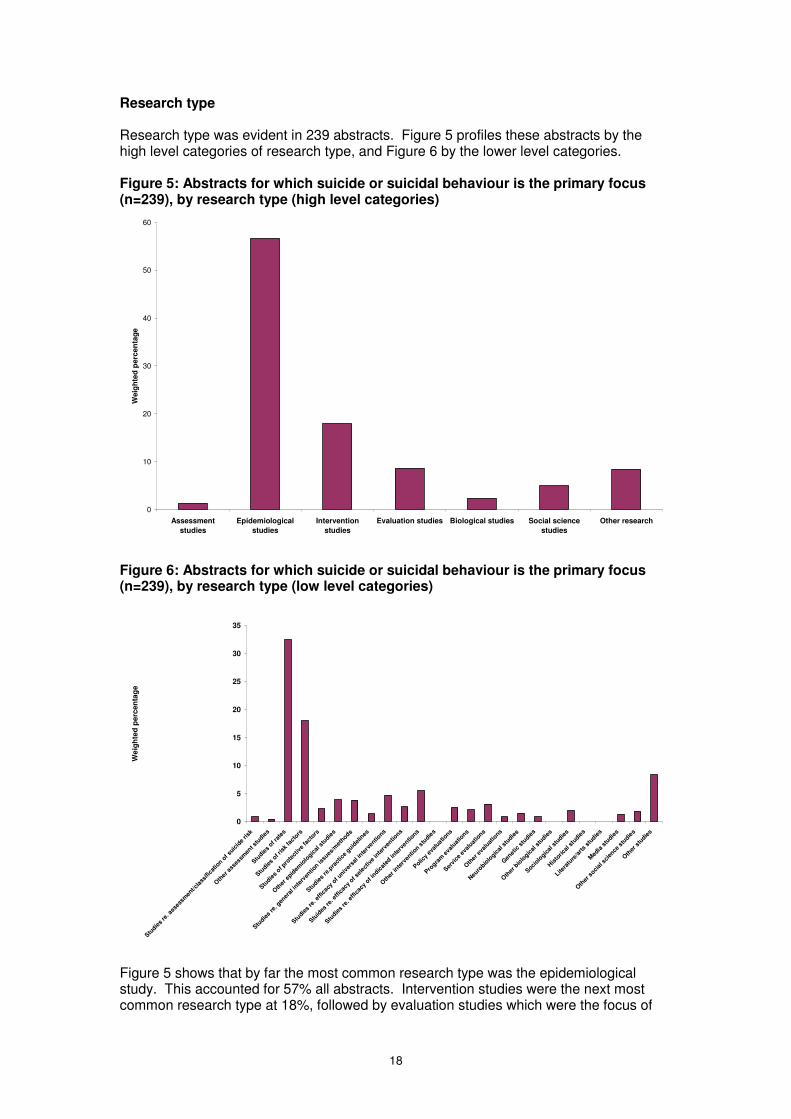
Research type Research type was evident in 239 abstracts. Figure 5 profiles these abstracts by the high level categories of research type, and Figure 6 by the lower level categories. Figure 5: Abstracts for which suicide or suicidal behaviour is the primary focus (n=239), by research type (high level categories)
0
10
20
30
40
50
60
Assessment
studies
Epidemiological
studies
Intervention
studies
Evaluation studies Biological studies Social science
studies
Other research
Weig
hte
d p
erc
en
tag
e
Figure 6: Abstracts for which suicide or suicidal behaviour is the primary focus (n=239), by research type (low level categories)
0
5
10
15
20
25
30
35
Studie
s re
. ass
essm
ent/c
lass
ifica
tion o
f suic
ide
risk
Oth
er ass
essm
ent s
tudie
s
Studie
s of r
ates
Studie
s of r
isk
fact
ors
Studie
s of p
rote
ctiv
e fa
ctors
Oth
er e
pidem
iolo
gical
stu
dies
Studie
s re
. gen
eral
inte
rven
tion is
sues
/met
hods
Studie
s re
.pra
ctic
e guid
elin
es
Studie
s re
. effi
cacy
of u
niver
sal i
nterv
entions
Stuid
es re
. effi
cacy
of s
elect
ive
inte
rven
tions
Studie
s re
. effi
cacy
of i
ndicat
ed in
terv
entio
ns
Oth
er in
terv
entio
n stu
dies
Policy
eval
uations
Progra
m e
valu
ations
Servi
ce e
valu
atio
ns
Oth
er e
valu
atio
ns
Neu
robio
logic
al s
tudie
s
Gen
etic
stu
dies
Oth
er bio
logic
al s
tudie
s
Sociolo
gical
stu
dies
His
toric
al s
tudie
s
Litera
ture
/arts s
tudie
s
Med
ia s
tudie
s
Oth
er s
ocial
sci
ence
stu
dies
Oth
er s
tudie
s
We
igh
ted
perc
en
tag
e
Figure 5 shows that by far the most common research type was the epidemiological study. This accounted for 57% all abstracts. Intervention studies were the next most common research type at 18%, followed by evaluation studies which were the focus of

19
9% of abstracts. Figure 6 shows that epidemiological studies of rates were the most popular, accounting for 32% of abstracts. These were followed by epidemiological studies of risk factors, which made up a further 18%. Suicidal behaviour Figure 7 provides a breakdown of the suicidal behaviour of interest in the 240 abstracts for which this could be identified. Forty two per cent of all abstracts focused on completed suicide, 37% on attempted suicide and 20% on suicidal ideation. A further 1% focused on some other kind of suicidal behaviour, most notably suicide plans and threats of suicide. Figure 7: Abstracts for which suicide or suicidal behaviour is the primary focus (n=240), by suicidal behaviour
0
5
10
15
20
25
30
35
40
45
Completed suicide Attempted suicide or deliberate
self-harm
Suicidal ideation Other
Weig
hte
d p
erc
en
tag
e
Suicide method Only 38 abstracts focused on a particular suicide method, with most presenting more general research about suicide. Figure 8 presents the suicide method of interest across these 38 abstracts. Poisoning by drugs was the most common method represented in these abstracts, accounting for 54% of them. This was followed by firearms and hanging, accounting for a further 12% and 10%, respectively.

20
Figure 8: Abstracts for which suicide or suicidal behaviour is the primary focus (n=38), by suicide method
0
10
20
30
40
50
60
Poisoning by
drugs
Poisoning by
other
Hanging Firearms Drowning Jumping from
high place
Jumping/lying
before moving
object
Other method
Weig
hte
d p
erc
en
tag
e
Target group It was possible to identify a target group of interest in 209 abstracts, and Figure 9 shows the resultant breakdown. Collectively, greatest emphasis has been given to young people (28%), followed by people who have attempted suicide / deliberately self-harmed (18%) and people with mental health problems (11%). Figure 9: Abstracts for which suicide or suicidal behaviour is the primary focus (n=209), by target group
0
5
10
15
20
25
30
Young peo
ple (a
ged 2
4 or l
ess)
Adults
(aged
25-
64)
Old
er p
eople
(aged
65+
)
Indig
enous
people
People
from
cultu
rally
/linguis
tical
ly d
iver
se b
ackg
rounds
People
in ru
ral/r
emote
are
as
People
bere
aved b
y su
icid
e
People
who a
re g
ay/le
sbia
n/bis
exual
/tran
sgen
der
People
with
men
tal h
ealth
pro
blem
s
People
with
phys
ical
hea
lth p
roble
ms
People
with
subst
ance
use
pro
blem
s
People
who h
ave
attem
pted s
uicid
e/del
iber
atel
y se
lf-har
med
Offe
nders
Men
Wom
en
Veter
ans
Oth
er ta
rget
gro
up
Weig
hte
d p
erc
en
tag
e
21
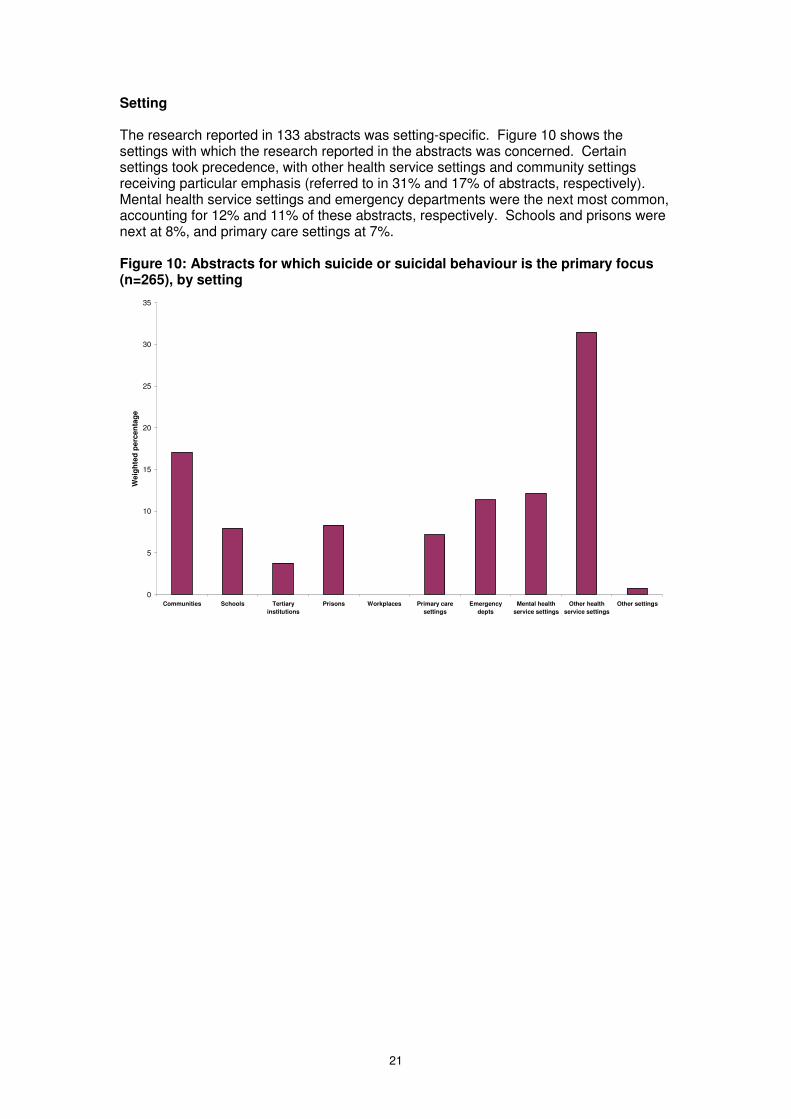
Setting The research reported in 133 abstracts was setting-specific. Figure 10 shows the settings with which the research reported in the abstracts was concerned. Certain settings took precedence, with other health service settings and community settings receiving particular emphasis (referred to in 31% and 17% of abstracts, respectively). Mental health service settings and emergency departments were the next most common, accounting for 12% and 11% of these abstracts, respectively. Schools and prisons were next at 8%, and primary care settings at 7%. Figure 10: Abstracts for which suicide or suicidal behaviour is the primary focus (n=265), by setting
0
5
10
15
20
25
30
35
Communities Schools Tertiary
institutions
Prisons Workplaces Primary care
settings
Emergency
depts
Mental health
service settings
Other health
service settings
Other settings
Weig
hte
d p
erc
en
tag
e

22
Chapter 3: Review of funded grants (Study 2)
Method As noted in Chapter 1, the review of funded grants analysed the extent and nature of current research by examining grants provided for suicide prevention research during the period 1999-2006 inclusive. The grant identification and retrieval process is described in more detail below, as is the way in which the grants were coded. The approach to data analysis is also described. Identification of information about funded grants The review included grants provided for projects and fellowships by the following key Australian academic funding bodies: the National Health and Medical Research Council (NHMRC), the Australian Rotary Health Research Fund (ARHRF) and the Australian Research Council (ARC). Each of these funding bodies was contacted by one member of the research team (Jo Robinson), who explained the purpose of the review and requested the required information. The amount of information available varied according to the organisation, as did the format of this information:
• The NHMRC provided an Excel spreadsheet detailing all grants which they classified as pertaining to suicide prevention between 1999 and 2006.
• The ARHRF provided summaries of all grants funded between 2000 (the year
they began funding mental health grants) and 2006 via their information booklet. These were examined by Jo Robinson who identified all those that appeared to relate to suicide and requested hard copies of the summaries of these grants.
• The ARC provided an Excel spreadsheet of all grants which they classified as
pertaining to suicide prevention between 1999 and 2006. Table 3 provides a summary of the information available on each of the grants, broken down by funding body. It shows that the ARHRF and the ARC were able to provide additional information over and above that provided by the NHMRC, in the form of abstracts or summaries. Table 3: Information available on suicide prevention research grants, by funding body
NHMRC ARHRF ARC
Funding years 1999-2006 2000-2006 1999-2006
Grant type � � �
Chief investigator � � �
Project/fellowship title � � �
Administering institution � � �
State/territory � � �
Start year � � �
Duration � � �
Amount of funding per year � � �
Total funding � � �
Abstract/summary � �

23
Coding the grants Grants were initially categorised by:
• Year of initial funding;
• Funding (amount per year and total); Beyond this, grants were classified in the same way as the abstracts described in Chapter 2, using the framework outlined in Chapter 1. This enabled each grant to be categorised according to the following classifications:
• Research type (assessment studies; epidemiological studies; intervention studies; evaluation of policies/programs/services; biological research; social science studies; other; not specified / unknown);
• Suicidal behaviour (completed suicide; attempted suicide; suicidal ideation; other;
not specified / unknown);
• Suicide method (poisioning by drugs; poisoning by other; hanging; firearms; drowning; jumping from a high place; jumping or lying before a moving object; other; not specified / unknown);
• Target group (young people; adults; older people; Indigenous people; people
from culturally and linguistically diverse backgrounds; people in rural and remote areas; people bereaved by suicide; people who are gay, lesbian, bisexual or transgender; people with mental health problems; people with physical health problems; people with substance use problems; people who have attempted suicide; offenders; men; women; veterans; other; not specified / unknown); and
• Setting (communities; schools; tertiary institutions; prisons; workplaces; primary
care settings; emergency departments; mental health service settings; other health service settings; other; not specified / unknown).
As with the coding of the abstracts described in Chapter 2, in the case of most grants, a single category was selected within each classification and coded as 1 (with the alternative, non-endorsed categories being coded as 0). In some cases, however, an abstract covered more than one category within a given classification. To avoid double-counting, the alternatives were weighted so that they summed to 1. Each grant was examined and classified according to the above categories by a single team member (Jo Robinson), in consultation with the team leader (Jane Pirkis) wherever necessary. Data management and analysis Data provided by the funding bodies and generated during the course of coding the grants were entered into an Excel spreadsheet and subsequently imported into SPSS for analysis. Simple weighted frequencies and percentages were calculated for each category.
Results Overview In total, 36 grants were provided for research into suicide or suicidal behaviour between 1999 and 2006. Thirty four (94%) of these grants were for projects and two (6%) were
24
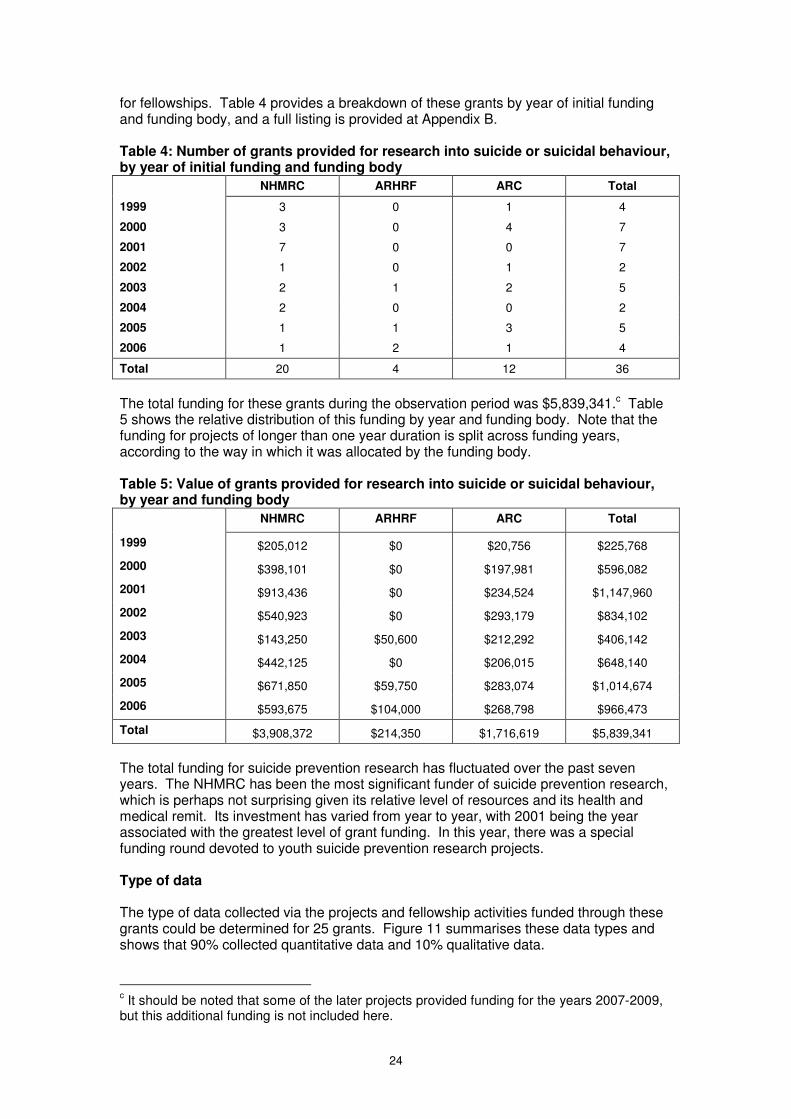
for fellowships. Table 4 provides a breakdown of these grants by year of initial funding and funding body, and a full listing is provided at Appendix B. Table 4: Number of grants provided for research into suicide or suicidal behaviour, by year of initial funding and funding body
NHMRC ARHRF ARC Total
1999 3 0 1 4
2000 3 0 4 7
2001 7 0 0 7
2002 1 0 1 2
2003 2 1 2 5
2004 2 0 0 2
2005 1 1 3 5
2006 1 2 1 4
Total 20 4 12 36
The total funding for these grants during the observation period was $5,839,341.c Table 5 shows the relative distribution of this funding by year and funding body. Note that the funding for projects of longer than one year duration is split across funding years, according to the way in which it was allocated by the funding body. Table 5: Value of grants provided for research into suicide or suicidal behaviour, by year and funding body
NHMRC ARHRF ARC Total
1999 $205,012 $0 $20,756 $225,768
2000 $398,101 $0 $197,981 $596,082
2001 $913,436 $0 $234,524 $1,147,960
2002 $540,923 $0 $293,179 $834,102
2003 $143,250 $50,600 $212,292 $406,142
2004 $442,125 $0 $206,015 $648,140
2005 $671,850 $59,750 $283,074 $1,014,674
2006 $593,675 $104,000 $268,798 $966,473
Total $3,908,372 $214,350 $1,716,619 $5,839,341
The total funding for suicide prevention research has fluctuated over the past seven years. The NHMRC has been the most significant funder of suicide prevention research, which is perhaps not surprising given its relative level of resources and its health and medical remit. Its investment has varied from year to year, with 2001 being the year associated with the greatest level of grant funding. In this year, there was a special funding round devoted to youth suicide prevention research projects. Type of data The type of data collected via the projects and fellowship activities funded through these grants could be determined for 25 grants. Figure 11 summarises these data types and shows that 90% collected quantitative data and 10% qualitative data.
c It should be noted that some of the later projects provided funding for the years 2007-2009,
but this additional funding is not included here.

25
Figure 11: Grants provided for suicide prevention research (n=25), by type of data
0
10
20
30
40
50
60
70
80
90
100
Quantitative data Qualitative data
Weig
hte
d p
erc
en
tag
e
Research design Information on research design was available for 23 grants. As Figure 12 shows, 39% employed descriptive designs, with no point of comparison. Sixty one per cent utilised analytical designs where they explicitly made comparisons between different groups in terms of various exposure variables and suicidal outcomes. Figure 12: Grants provided for suicide prevention research (n=23), by research design
0
10
20
30
40
50
60
70
Descriptive Analytical
Weig
hte
d p
erc
en
tag
e

26
Research type Research type could be ascertained for 32 grants. Figure 13 profiles these grants by the high level categories of research type, and Figure 14 by the lower level categories. Figure 13: Grants provided for suicide prevention research (n=32), by research type (high level categories)
0
10
20
30
40
50
60
Assessment
studies
Epidemiological
studies
Intervention
studies
Evaluation studies Biological studies Social science
studies
Other research
Weig
hte
d p
erc
en
tag
e
Figure 14: Grants provided for suicide prevention research (n=32), by research type (lower level categories)
0
5
10
15
20
25
30
Studie
s re
. ass
essm
ent/c
lass
ifica
tion o
f suic
ide
risk
Oth
er ass
essm
ent s
tudie
s
Studie
s of r
ates
Studie
s of r
isk
fact
ors
Studie
s of p
rote
ctiv
e fa
ctors
Oth
er e
pidem
iolo
gical
stu
dies
Studie
s re
. gen
eral
inte
rven
tion is
sues
/met
hods
Studie
s re
.pra
ctic
e guid
elin
es
Studie
s re
. effi
cacy
of u
niver
sal i
nterv
entions
Stuid
es re
. effi
cacy
of s
elect
ive
inte
rven
tions
Studie
s re
. effi
cacy
of i
ndicat
ed in
terv
entio
ns
Oth
er in
terv
entio
n stu
dies
Policy
eval
uations
Progra
m e
valu
ations
Servi
ce e
valu
atio
ns
Oth
er e
valu
atio
ns
Neu
robio
logic
al s
tudie
s
Gen
etic
stu
dies
Oth
er bio
logic
al s
tudie
s
Sociolo
gical
stu
dies
His
toric
al s
tudie
s
Litera
ture
/arts s
tudie
s
Med
ia s
tudie
s
Oth
er s
ocial
sci
ence
stu
dies
Oth
er s
tudie
s
We
igh
ted
perc
en
tag
e
Figure 13 shows that just over half (52%) of the grants funded intervention studies. Epidemiological studies were the next most common research type, accounting for 22% of all grants. Figure 14 shows that one quarter (25%) of all grants have involved funding for studies of the efficacy of indicated interventions, and 14% for studies of the efficacy of
27
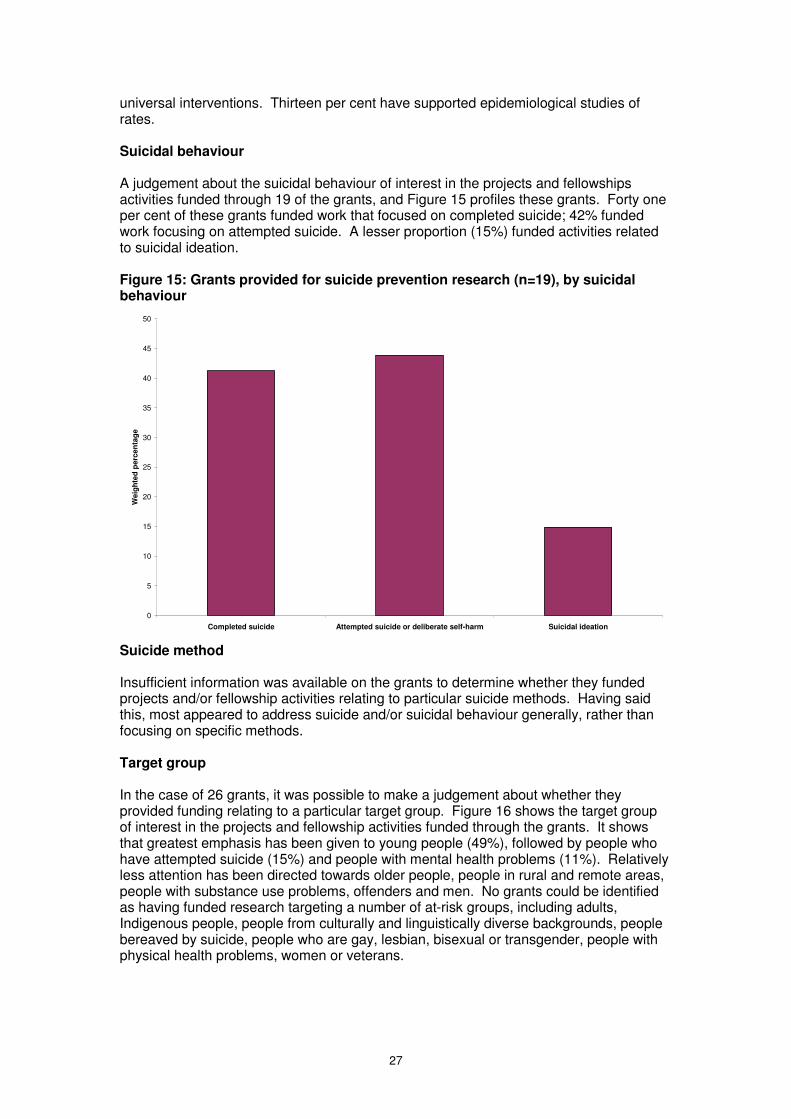
universal interventions. Thirteen per cent have supported epidemiological studies of rates. Suicidal behaviour A judgement about the suicidal behaviour of interest in the projects and fellowships activities funded through 19 of the grants, and Figure 15 profiles these grants. Forty one per cent of these grants funded work that focused on completed suicide; 42% funded work focusing on attempted suicide. A lesser proportion (15%) funded activities related to suicidal ideation. Figure 15: Grants provided for suicide prevention research (n=19), by suicidal behaviour
0
5
10
15
20
25
30
35
40
45
50
Completed suicide Attempted suicide or deliberate self-harm Suicidal ideation
Weig
hte
d p
erc
en
tag
e
Suicide method Insufficient information was available on the grants to determine whether they funded projects and/or fellowship activities relating to particular suicide methods. Having said this, most appeared to address suicide and/or suicidal behaviour generally, rather than focusing on specific methods. Target group In the case of 26 grants, it was possible to make a judgement about whether they provided funding relating to a particular target group. Figure 16 shows the target group of interest in the projects and fellowship activities funded through the grants. It shows that greatest emphasis has been given to young people (49%), followed by people who have attempted suicide (15%) and people with mental health problems (11%). Relatively less attention has been directed towards older people, people in rural and remote areas, people with substance use problems, offenders and men. No grants could be identified as having funded research targeting a number of at-risk groups, including adults, Indigenous people, people from culturally and linguistically diverse backgrounds, people bereaved by suicide, people who are gay, lesbian, bisexual or transgender, people with physical health problems, women or veterans.

28
Figure 16: Grants provided for suicide prevention research (n=26), by target group
0
10
20
30
40
50
60
Young peo
ple (a
ged 2
4 or l
ess)
Adults
(aged
25-
64)
Old
er p
eople
(aged
65+
)
Indig
enous
people
People
from
cultu
rally
/linguis
tical
ly d
iver
se b
ackg
rounds
People
in ru
ral/r
emote
are
as
People
bere
aved b
y su
icid
e
People
who a
re g
ay/le
sbia
n/bis
exual
/tran
sgen
der
People
with
men
tal h
ealth
pro
blem
s
People
with
phys
ical
hea
lth p
roble
ms
People
with
subst
ance
use
pro
blem
s
People
who h
ave
attem
pted s
uicid
e/del
iber
atel
y se
lf-har
med
Offe
nders
Men
Wom
en
Veter
ans
Oth
er ta
rget
gro
up
Weig
hte
d p
erc
en
tag
e
Setting For 20 grants, no setting was specified; Figure 17 shows the settings associated with the remaining 16 grants. Certain settings took precedence in these grants. Twenty five per cent were concerned with other health service settings, and 19% each with communities, schools and mental health service settings. Prisons, primary care settings and emergency departments each accounted for a further 6% of these grants. Tertiary institutions and workplaces were not the subject of any grants. Figure 17: Grants provided for suicide prevention research (n=16), by setting
0
5
10
15
20
25
30
Communities Schools Tertiary
institutions
Prisons Workplaces Primary care
settings
Emergency
depts
Mental health
service settings
Other health
service settings
Other settings
Weig
hte
d p
erc
en
tag
e

29
Chapter 4: Web-based questionnaire (Study 3)
Method As noted in Chapter 1, the web-based survey was designed to elicit stakeholders’ views on future priorities. Stakeholders were selected on the basis of their membership of groups with a known interest in suicide prevention research. More detail is provided below with regard to the sampling and recruitment strategy, the nature and conduct of the survey, and the data analysis strategy. Information on the response rate is also presented. Sampling and recruitment strategy Stakeholders were sampled from 11 groups known to conduct suicide prevention research, use suicide prevention research (in clinical practice or in policy-making/planning activities), fund suicide prevention research and/or provide advocacy for people who have been affected by suicide. Table 6 profiles the members of these groups according to their major role in relation to suicide prevention research. It is acknowledged that some groups may include members with overlapping functions (e.g., Suicide Prevention Australia is primarily an advocacy and awareness-raising organisation targeted at people who have been affected by suicide, but includes suicide prevention researchers among its membership. Table 6: Respondent groups and their major role in relation to suicide prevention research
Members’ role in relation to suicide prevention research
Group
People who conduct suicide prevention research Researchers
Psychiatrists
GPs
People who use suicide prevention research (in clinical practice)
Psychologists
Members of the National Advisory Council on Suicide Prevention (NACSP)
Members of the National Mental Health Standing Committee (NMHCS)
People who use suicide prevention research (in policy-making/planning activities)
Officers responsible for state/territory co-ordination re. the LIFE Framework
Members of the National Health and Medical Research Council (NHMRC) Youth Suicide Working Committee (YSWC)
People involved in funding suicide prevention research
Members of the Australian Rotary Health Research Fund (ARHRF) Research Committee
Members of the Australian Mental Health Consumer Network (AMHCN)
People who have been affected by suicide
Members of Suicide Prevention Australia (SPA)
The sampling frames for the different groups were identified and approached in various ways, depending on the nature and operation of the group, and their requirements with regard to confidentiality of members. In the case of groups with fewer than 200 members, the whole group was invited to participate in the survey; in all other cases, a random selection of 200 members was invited. The majority of groups were invited to

30
participate by email and given a web-link for the questionnaire; a minority were mailed a paper-based copy of the questionnaire and invited to return it in a reply-paid envelope as an alternative to completing the questionnaire online. Groups which were invited to participate via email were sent reminders; groups receiving their invitation via mail-out were not sent reminders. Table 7 details the sampling and recruitment strategy for each of the 11 groups. Each potential respondent was given an identifier that corresponded with the group from which they had been recruited. Those who were invited to complete the web-based version of the questionnaire were also given a group-based password. No individuals were identified in this process, but this process enabled the number of respondents from any given group to be monitored.
31
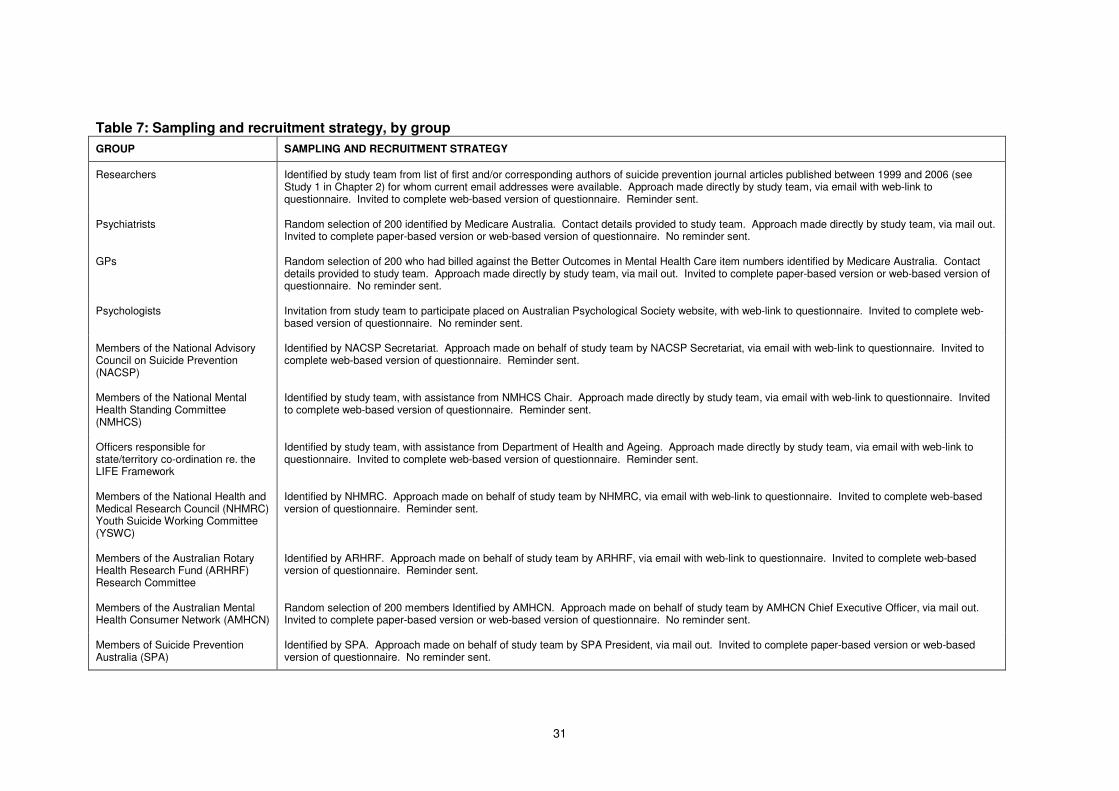
Table 7: Sampling and recruitment strategy, by group
GROUP SAMPLING AND RECRUITMENT STRATEGY
Researchers Identified by study team from list of first and/or corresponding authors of suicide prevention journal articles published between 1999 and 2006 (see Study 1 in Chapter 2) for whom current email addresses were available. Approach made directly by study team, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Psychiatrists Random selection of 200 identified by Medicare Australia. Contact details provided to study team. Approach made directly by study team, via mail out. Invited to complete paper-based version or web-based version of questionnaire. No reminder sent.
GPs Random selection of 200 who had billed against the Better Outcomes in Mental Health Care item numbers identified by Medicare Australia. Contact details provided to study team. Approach made directly by study team, via mail out. Invited to complete paper-based version or web-based version of questionnaire. No reminder sent.
Psychologists Invitation from study team to participate placed on Australian Psychological Society website, with web-link to questionnaire. Invited to complete web-based version of questionnaire. No reminder sent.
Members of the National Advisory Council on Suicide Prevention (NACSP)
Identified by NACSP Secretariat. Approach made on behalf of study team by NACSP Secretariat, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Members of the National Mental Health Standing Committee (NMHCS)
Identified by study team, with assistance from NMHCS Chair. Approach made directly by study team, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Officers responsible for state/territory co-ordination re. the LIFE Framework
Identified by study team, with assistance from Department of Health and Ageing. Approach made directly by study team, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Members of the National Health and Medical Research Council (NHMRC) Youth Suicide Working Committee (YSWC)
Identified by NHMRC. Approach made on behalf of study team by NHMRC, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Members of the Australian Rotary Health Research Fund (ARHRF) Research Committee
Identified by ARHRF. Approach made on behalf of study team by ARHRF, via email with web-link to questionnaire. Invited to complete web-based version of questionnaire. Reminder sent.
Members of the Australian Mental Health Consumer Network (AMHCN)
Random selection of 200 members Identified by AMHCN. Approach made on behalf of study team by AMHCN Chief Executive Officer, via mail out. Invited to complete paper-based version or web-based version of questionnaire. No reminder sent.
Members of Suicide Prevention Australia (SPA)
Identified by SPA. Approach made on behalf of study team by SPA President, via mail out. Invited to complete paper-based version or web-based version of questionnaire. No reminder sent.

32
Questionnaire content The questionnaire assessed stakeholders views with regard to research priorities in suicide prevention according to the framework outlined in Chapter 1. Specifically, the questionnaire asked stakeholders to consider each of the following classifications, and rate the categories within a given classification in terms of priority.
• Research type (assessment studies; epidemiological studies; intervention studies; evaluation of policies/programs/services; biological research; social science studies; other);
• Suicidal behaviour (completed suicide; attempted suicide; suicidal ideation;
other);
• Suicide method (poisioning by drugs; poisoning by other; hanging; firearms; drowning; jumping from a high place; jumping or lying before a moving object; other);
• Target group (young people; adults; older people; Indigenous people; people
from culturally and linguistically diverse backgrounds; people in rural and remote areas; people bereaved by suicide; people who are gay, lesbian, bisexual or transgender; people with mental health problems; people with physical health problems; people with substance use problems; people who have attempted suicide; offenders; men; women; veterans; other); and
• Setting (communities; schools; tertiary institutions; prisons; workplaces; primary
care settings; emergency departments; mental health service settings; other health service settings; other).
The questionnaire also profiled respondents in terms of such characteristics as their interest in suicide prevention research and their affiliations. As noted above, the questionnaire was primarily web-based, but paper-based versions were made available where necessary. The paper-based version of the questionnaire is provided at Appendix C. Data management and analysis Data from the paper-based versions of the questionnaire were consolidated with data from the web-based questionnaire application, and all data were downloaded into an Excel spreadsheet and subsequently imported into SPSS for analysis. Simple frequencies and percentages were calculated for each category. Response rate and sample characteristics The questionnaire was completed by a total of 231 respondents. As noted above, a given individual may have completed the questionnaire as a member of one group but may also have been affiliated with several other groups. Because each individual would only have been expected to complete the questionnaire once, regardless of how many groups he or she belonged to, calculating group-based response rates on the basis of the primary group would be likely to underestimate the true response rate for each group. For this reason, Table 8 presents response rates for each primary group with and without additionally indicated affiliations.

33
Table 8: Response rates, by primary group and affiliations
PRIMARY GROUP
Psychiatrists GPs Psychologistsa
Researchers NACSP
Members NMHSC
Members LIFE
Coordinators AMHCN
Members SPA
Members
NHMRC YSWC
Members
ARHRF Research
Committee Members
(200) (200) (N/A) (151) (14) (17) (7) (200) (118) (6) (12)
AFFILIATIONS
Researchers 14 3 9 47 1 0 0 1 3 2 1
Psychiatrists 40 0 0 0 0 0 0 1 1 1 0
GPs 0 30 1 1 0 0 0 0 0 0 0
Psychologists 0 0 32 2 0 0 0 0 0 0 0
NACSP Members 0 1 0 0 4 0 0 0 0 0 0
NMHSC Members 1 0 1 0 0 7 0 0 0 0 0
LIFE Coordinators 0 0 0 0 1 0 5 0 0 1 0
NHMRC YSWC Members 0 0 0 1 0 0 0 0 1 1 0
ARHRF RC Members 2 0 2 3 0 0 0 0 1 0 6
AMHCN Members 0 0 0 0 0 0 0 16 1 1 0
SPA Members 1 1 10 11 1 0 0 1 43 0 0
Total GROUP 40 30 32 47 4 7 5 16 43 1 6
Response rate GROUP 20% 15% (N/A) 31% 29% 41% 71% 8% 36% 17% 50%
Total GROUP + AFFILIATIONS 58 35 55 65 7 7 5 19 50 6 7
Response rate GROUP + AFFILIATIONS 29% 18% (N/A) 43% 50% 41% 71% 10% 42% 100% 58%
a. Denominator not calculable because invitation to complete questionnaire was posted on the Australian Psychological Society website and potential users of the site could not be accurately estimated.

34
For example, 43 individuals completed the questionnaire as SPA members, but an additional 7 who completed the questionnaire as members of some other group also indicated that they were SPA members, bringing the total to 50. The total number of SPA members who were approached to complete the survey was 118, so the former figure yields a response rate of 36% and the latter one of 42%. Overall, the response rate ranged from a lower limit of 8% for AMHCN members to an upper limit of 100% for NHMRC YSWC members. Some caution should be exercised in the case of the upper estimates for psychiatrists, GPs, researchers and AMHCN members, since respondents from a different primary group indicating an affiliation with any of these groups may not have received the original invitation via these groups (i.e., may not have been in the relevant denominator). For this reason, the upper limit of the range for these groups should be regarded as indicative only. Twenty per cent of respondents conducted suicide prevention research; 53% used it; 15% were involved in funding it; and 38% had been affected by suicide.
Results To avoid double-counting, results are presented for each primary group only, without the addition of affiliations. Primary group members are aggregated by their role in relation to suicide prevention research, to cater for the low number of respondents in some primary groups. Research type Tables 9 and 10 show the research types rated by the various stakeholder groups as the highest priority for future suicide prevention research. The majority of stakeholder groups most commonly identified intervention studies as the highest priority, giving greatest emphasis to indicated interventions, followed by selective and universal interventions. The next most commonly identified research type was the epidemiological study, and in particular studies of protective factors and risk factors.
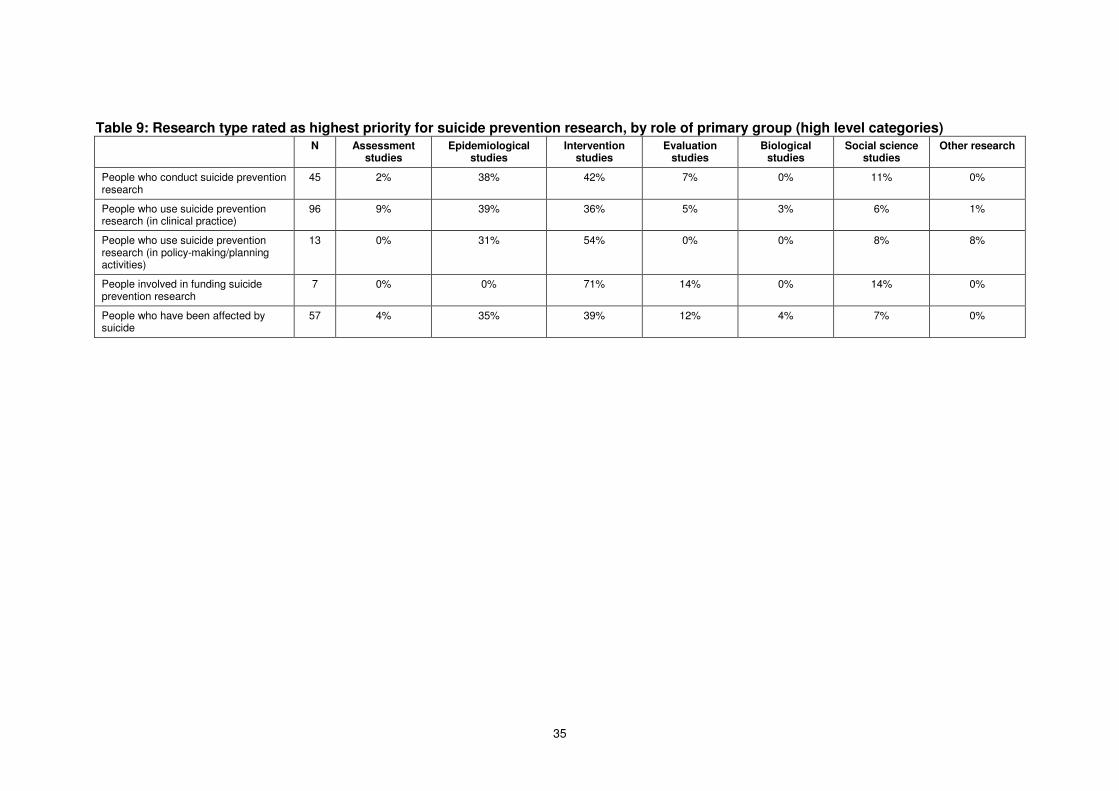
35
Table 9: Research type rated as highest priority for suicide prevention research, by role of primary group (high level categories) N Assessment
studies Epidemiological
studies Intervention
studies Evaluation
studies Biological
studies Social science
studies Other research
People who conduct suicide prevention research
45 2% 38% 42% 7% 0% 11% 0%
People who use suicide prevention research (in clinical practice)
96 9% 39% 36% 5% 3% 6% 1%
People who use suicide prevention research (in policy-making/planning activities)
13 0% 31% 54% 0% 0% 8% 8%
People involved in funding suicide prevention research
7 0% 0% 71% 14% 0% 14% 0%
People who have been affected by suicide
57 4% 35% 39% 12% 4% 7% 0%

36
Table 10: Research type rated as highest priority for suicide prevention research, by role of primary group (lower level categories)
N
Stu
die
s r
e. assessm
en
t o
f su
icid
e r
isk
Stu
die
s o
f ra
tes
Stu
die
s o
f ri
sk f
acto
rs
Stu
die
s o
f p
rote
cti
ve f
acto
rs
Stu
die
s r
e. g
en
era
l in
terv
en
tio
n i
ssu
es/m
eth
od
s
Stu
die
s r
e. p
racti
ce g
uid
elin
es
Stu
die
s r
e. eff
icacy o
f u
niv
ers
al in
terv
en
tio
ns
Stu
die
s r
e. eff
icacy o
f sele
cti
ve i
nte
rven
tio
ns
Stu
die
s r
e. eff
icacy o
f in
dic
ate
d in
terv
en
tio
ns
Po
licy e
valu
ati
on
s
Pro
gra
m e
valu
ati
on
s
Serv
ice e
valu
ati
on
s
Neu
rob
iolo
gic
al stu
die
s
Gen
eti
c s
tud
ies
So
cio
log
ical stu
die
s
His
tori
cal stu
die
s
Oth
er
People who conduct suicide prevention research
45 2% 0% 18% 20% 9% 0% 11% 16% 7% 0% 7% 0% 0% 0% 7% 4% 0%
People who use suicide prevention research (in clinical practice)
96 9% 0% 21% 18% 3% 1% 13% 8% 11% 1% 2% 2% 2% 1% 4% 2% 1%
People who use suicide prevention research (in policy-making/planning activities)
13 0% 0% 15% 15% 23% 0% 0% 0% 31% 0% 0% 0% 0% 0% 8% 0% 8%
People involved in funding suicide prevention research
7 0% 0% 0% 0% 0% 0% 0% 14% 57% 0% 14% 0% 0% 0% 0% 14% 0%
People who have been affected by suicide
57 4% 5% 16% 14% 7% 2% 7% 5% 18% 2% 7% 4% 0% 4% 5% 2% 0%
37
Suicidal behaviour Attempted suicide or deliberate self-harm was regarded as the highest priority for suicide prevention research by the majority of stakeholder groups (see Table 11). The exception was people involved in funding suicide prevention research, who indicated that completed suicide should be given precedence. Suicide method Table 12 shows the priority ratings given to various methods of suicide, by group. Poisoning by drugs was regarded at the method warranting the greatest attention in terms of suicide prevention research by people who conduct suicide prevention research, people who use suicide prevention research in clinical practice and people who have been affected by suicide. By contrast, people who use suicide prevention research in policy-making/planning activities and people involved in funding suicide prevention research emphasised hanging. Target group Table 13 profiles the ratings given to particular target groups in terms of the research effort that they should be afforded. Young people most commonly received the highest rating from people who conduct suicide prevention research, people who use suicide prevention research in clinical practice and people who have been affected by suicide. People with mental health problems were given prominence by people involved in funding suicide prevention research and people who use suicide prevention research in policy-making/planning activities. The latter group also endorsed men as a target group deserving of priority. Setting Table 14 shows the ratings given to different settings by the 11 groups. Most commonly, the highest rating was given to communities (by people who conduct suicide prevention research, people who use suicide prevention research in clinical practice and people who have been affected by suicide). People who use suicide prevention research in policy-making/planning activities viewed primary care settings as most important. People involved in funding suicide prevention research most commonly endorsed mental health service settings as the setting of highest priority.
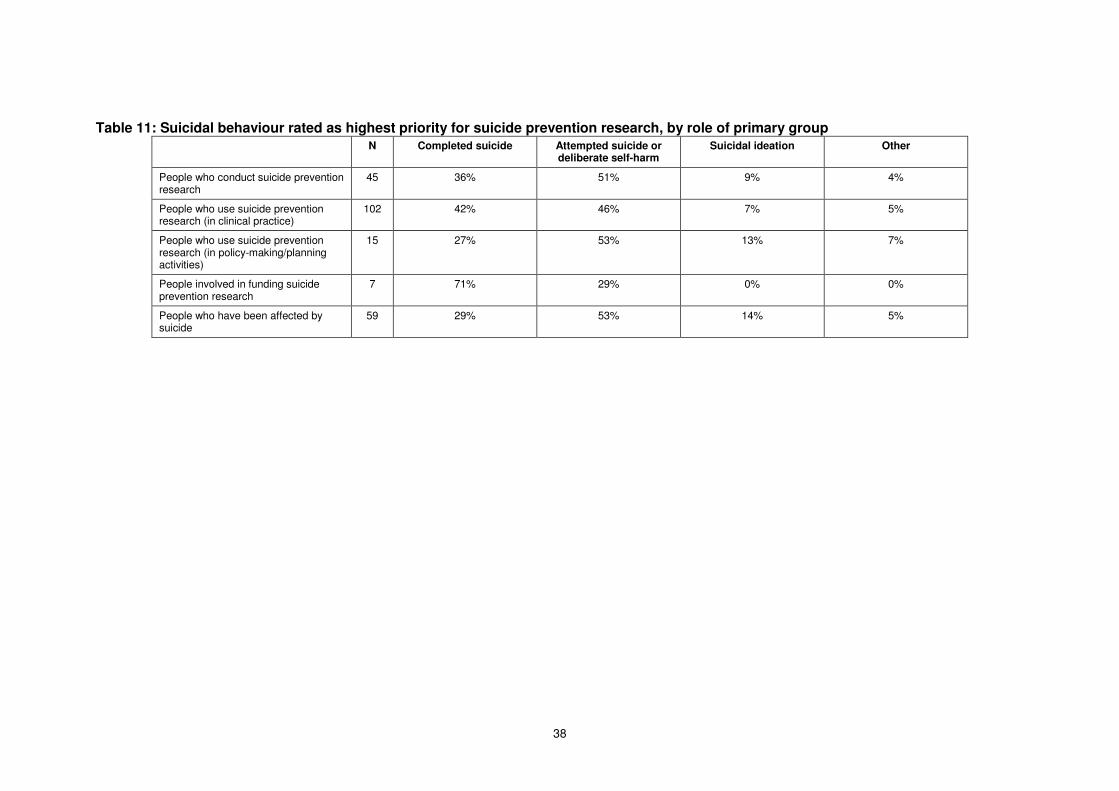
38
Table 11: Suicidal behaviour rated as highest priority for suicide prevention research, by role of primary group N Completed suicide Attempted suicide or
deliberate self-harm Suicidal ideation Other
People who conduct suicide prevention research
45 36% 51% 9% 4%
People who use suicide prevention research (in clinical practice)
102 42% 46% 7% 5%
People who use suicide prevention research (in policy-making/planning activities)
15 27% 53% 13% 7%
People involved in funding suicide prevention research
7 71% 29% 0% 0%
People who have been affected by suicide
59 29% 53% 14% 5%
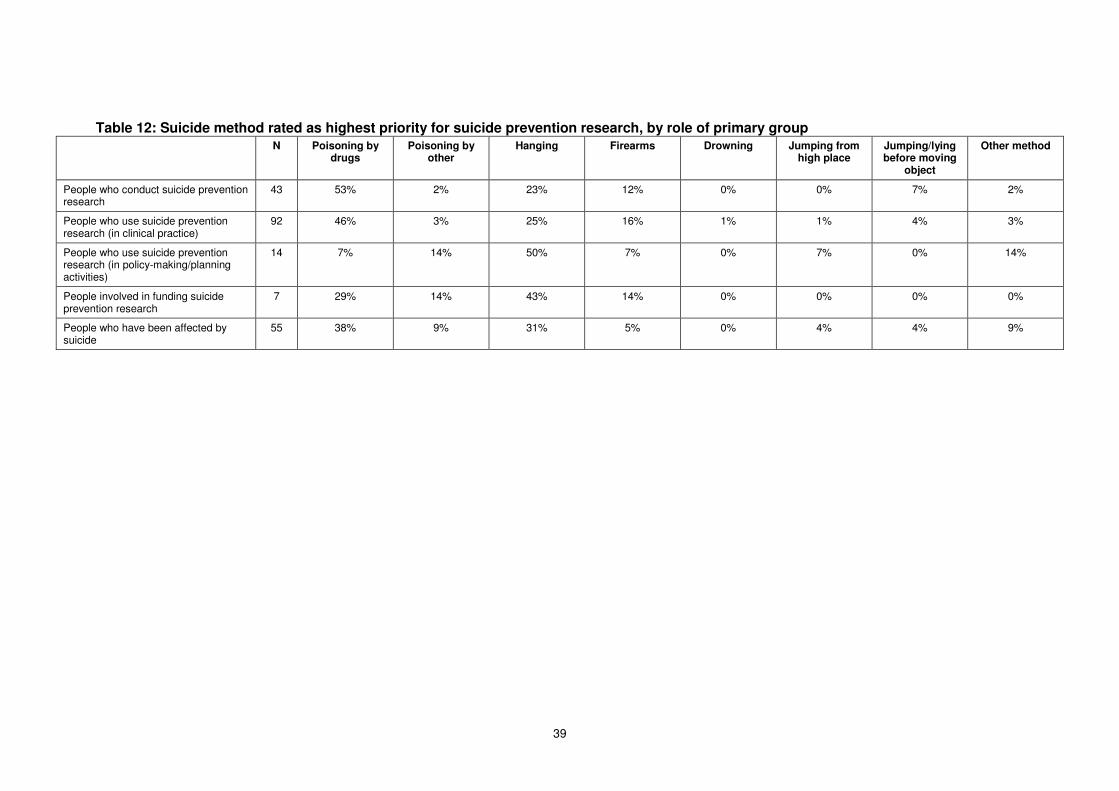
39
Table 12: Suicide method rated as highest priority for suicide prevention research, by role of primary group N Poisoning by
drugs Poisoning by
other Hanging Firearms Drowning Jumping from
high place Jumping/lying before moving
object
Other method
People who conduct suicide prevention research
43 53% 2% 23% 12% 0% 0% 7% 2%
People who use suicide prevention research (in clinical practice)
92 46% 3% 25% 16% 1% 1% 4% 3%
People who use suicide prevention research (in policy-making/planning activities)
14 7% 14% 50% 7% 0% 7% 0% 14%
People involved in funding suicide prevention research
7 29% 14% 43% 14% 0% 0% 0% 0%
People who have been affected by suicide
55 38% 9% 31% 5% 0% 4% 4% 9%

40
Table 13: Target group rated as highest priority for suicide prevention research, by role of primary group
N
Yo
un
g p
eo
ple
Ad
ult
s (
ag
ed
25-6
4)
Old
er
peo
ple
(ag
ed
65+
)
Ind
igen
ou
s p
eo
ple
Peo
ple
fro
m c
ult
ura
lly o
r li
ng
uis
ticall
y d
ivers
e
backg
rou
nd
s
Peo
ple
in
ru
ral
an
d r
em
ote
are
as
Peo
ple
bere
aved
by s
uic
ide
Peo
ple
wh
o a
re g
ay, le
sb
ian
, b
isexu
al o
r tr
an
sg
en
der
Peo
ple
wit
h m
en
tal h
ealt
h
pro
ble
ms
Peo
ple
wit
h s
ub
sta
nce u
se
pro
ble
ms
Peo
ple
wh
o h
ave a
ttem
pte
d
su
icid
e o
r self
-harm
ed
Men
Oth
er
targ
et
gro
up
People who conduct suicide prevention research
45 31% 13% 4% 11% 2% 0% 0% 4% 13% 2% 11% 4% 2%
People who use suicide prevention research (in clinical practice)
97 51% 7% 1% 8% 1% 1% 1% 2% 11% 1% 14% 0% 1%
People who use suicide prevention research (in policy-making/planning activities)
13 8% 8% 0% 15% 0% 0% 0% 0% 23% 0% 15% 23% 8%
People involved in funding suicide prevention research
7 14% 14% 0% 0% 0% 0% 0% 0% 43% 0% 29% 0% 0%
People who have been affected by suicide
58 33% 17% 2% 9% 0% 0% 2% 2% 9% 3% 16% 7% 2%
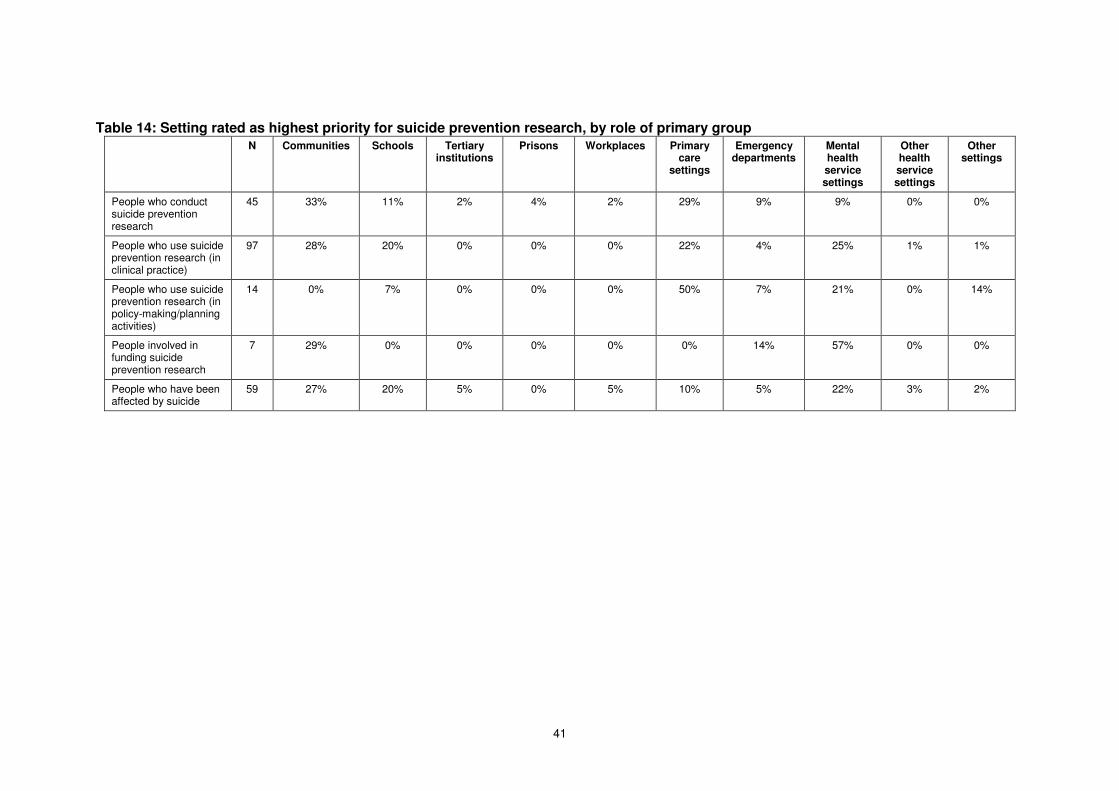
41
Table 14: Setting rated as highest priority for suicide prevention research, by role of primary group N Communities Schools Tertiary
institutions Prisons Workplaces Primary
care settings
Emergency departments
Mental health service settings
Other health service settings
Other settings
People who conduct suicide prevention research
45 33% 11% 2% 4% 2% 29% 9% 9% 0% 0%
People who use suicide prevention research (in clinical practice)
97 28% 20% 0% 0% 0% 22% 4% 25% 1% 1%
People who use suicide prevention research (in policy-making/planning activities)
14 0% 7% 0% 0% 0% 50% 7% 21% 0% 14%
People involved in funding suicide prevention research
7 29% 0% 0% 0% 0% 0% 14% 57% 0% 0%
People who have been affected by suicide
59 27% 20% 5% 0% 5% 10% 5% 22% 3% 2%
42
Chapter 5: Focus groups (Study 4)
Method Three focus groups were conducted. The first took place in at the University of Melbourne’s School of Population Health in Melbourne on 31 July 2006, the second was conducted at the South East Health Service Offices in Sydney on 1 August 2006, and the third was run at the Australian Institute for Suicide Research and Prevention in Brisbane on 9 August 2006. Participants for each focus group were purposively sampled in a manner that ensured representation from people who conduct suicide prevention research, people who use suicide prevention research, people who are involved in funding suicide prevention research, and people who have been affected by suicide. Seven participants attended the Melbourne focus group, 11 attended the Sydney focus group and 10 attended the Brisbane focus group. Participants in each focus group were asked to consider the priority given to suicide prevention research to date, and then to discuss whether this emphasis should change in the future. The discussion was guided by a facilitator, using the following prompts:
• I’d like to start by asking you to think about our current level of knowledge about suicide prevention. What do we know?
• What don’t we know? • Thinking now about Australian suicide prevention research, what kind of research
has taken priority in the last seven years (i.e., the duration of the National Suicide Prevention Strategy)?
• Can you comment on the overall quality of Australian suicide prevention research?
• Bearing in mind your responses to the earlier questions, what do you think should be the future priorities for suicide prevention research in Australia?
• What factors do you think should influence future priorities for suicide prevention research in Australia?
The Melbourne focus group was facilitated by Jane Pirkis, the Sydney focus group was co-facilitated by Michael Dudley and Sara Niner, and the Brisbane focus group was facilitated by Emily Schindeler. Sara Niner managed and recorded all three focus groups, took extensive notes at the time, and transcribed salient parts of the recordings later. Karolina Krysinska assisted Sara Niner at the Brisbane focus group. Qualitative data generated from the focus groups were analysed for themes. Sara Niner conducted the analysis, consulting with Jane Pirkis on matters of interpretation.
Results Although perspectives, experiences and views of focus group participants varied, several recurring themes emerged. These are summarised below. Evaluating the efficacy of interventions The most commonly raised issue across all three focus groups was the need for greater emphasis on the evaluation of interventions. Various participants observed that good epidemiological data exist on rates of suicide among particular population groups, and a reasonable amount of research has been conducted on risk and (to a lesser extent) protective factors, but that research into the efficacy of given interventions has been relatively neglected to date. Many felt that research resources should now be targeted
43
towards evaluating the gamut of potential suicide prevention interventions. As one participant put it, ‘Efficacy is a major issue.’ The majority of participants believed that suicide prevention interventions have been at best under-evaluated and at worst unevaluated. Some felt that no evaluation had occurred, others felt that not enough had occurred, and still others felt that that which had occurred had been ad hoc and/or inefficient. Several commented that interventions and programs were designed using flimsy evidence, based on anecdotes and personal opinions. One participant summed this up in the following way: ‘The system does have some theories about how it could prevent suicide, such as how to manage discharged patients from emergency departments, but none of these care models are well researched or evaluated … If we look at assertive follow-up, case care etc, it’s done with good intention but no-one knows the effectiveness of it.’ Several participants articulated the view that funding for intervention programs should explicitly include a budget for evaluation and knowledge development. One noted that this would require education on the evaluation process for service providers. Some participants suggested specific intervention activities that required evaluation. These straddled the spectrum of interventions from mental health promotion (e.g., activities for strengthening resilience among young people), through primary and secondary prevention (e.g., early intervention and assertive follow-up with people presenting to mental health teams following suicide attempts), to treatment (e.g., cognitive behavioural therapy) and postvention (e.g., support groups for people who have attempted suicide and people who have been bereaved by suicide). In particular, there was consensus that interventions that seemed to show promise should be critically examined, such as ‘the intervention programs that have resulted in a turnaround of young male suicides since 1997.’ In a similar vein, several participants suggested that evaluation efforts should concentrate on people who have survived a suicide attempt. One participant, for example, said the following: ‘Focus on those who have survived and what worked for them and what intervention helped at that time.’ Another made a similar but more specific comment, suggesting that ‘We need details of the therapeutic alliance. What is the variable for the person to survive?’ Some participants argued that evaluative evidence is particularly lacking for interventions with specific subgroups. Indigenous communities are a case in point. One participant noted, ‘From the Aboriginal perspective, there must be more work done in remote Aboriginal communities where suicide has been a big concern and issue. They have no consultants or counsellors. How did the community cope with suicide and what successful mechanisms did they put in place to recover from it? Have they been able to stop others from doing the same? We need to find this out and develop a model to transfer this knowledge to other situations. We need real statistics and information on causes and effects on the groups of interventions. We often only have assumptions.’ Critically examining the response of the health and community service systems Beyond specific interventions, there was a view that critical examination of the service delivery system was needed. Many participants were critical of the current health system, claiming that they were ill-equipped to assess and manage people who presented with suicidal thoughts or behaviours. One participant cited GPs as an example, noting deficiencies in their ability to deal with suicidality: ‘My GP couldn’t tell after 11 years [of suicide attempts] … I got treatment for myself … he didn’t notice the scars on my hands.’ Another participant spoke of difficulties for clinicians in the public and private mental health sectors: ‘The quality of risk assessment in the public sector is ordinary/limited. Many are afraid to ask a question that they fear the answer to. People
44
in the private sector are terrified to ask because what do they do with the answer? No beds are available anyway, so what do you do? … Maybe the question is what has to be put into place for them to feel safer to ask the questions.’ Several participants felt that the solution to these problems lay in research into structured clinical assessment processes, clinical guidelines, risk management tools and professional judgement processes. Mention was frequently made of the fact that many people who die by suicide receive services from different health and community services in the months, weeks and even days before death, often in relation to prior suicidal thoughts or behaviours. Participants noted that co-ordination between different sectors is sub-optimal, and that better communication between services might prevent some people ‘falling through the gaps.’ Several participants recommended that research to map these gaps could be useful in addressing them. Specifically, suggestions included research into the linkages between police and mental health services, between drug and alcohol services and mental health services, and between community services and clinical services. Some participants stressed that a significant proportion of people who complete, attempt or consider suicide do not seek help, raising issues about the accessibility of services that warrant research attention. Some commented that it would be short-sighted to focus the entire research effort on those who do present to health and community services, making comments like: ‘In all this we are still focusing on those people who present rather than on those people who don’t present. The shocking question is: Why do people kill themselves? Is it factors outside the mental health system, way beyond clinical presentations to broader reasons? We need to have a systematic look at these issues.’ Several participants suggested that investigating the trajectory of suicidal behaviour via longitudinal methods may assist in this regard, because it might tease out where in the continuum people decide to act on suicidal ideation and why people choose to seek help or not to seek help. This in turn might provide clues about ways in which the health and community service systems can be optimally responsive. A focus on high risk groups Some participants felt that sufficient was known about high risk groups, at least in terms of their epidemiology. The majority, however, expressed the view that particular groups should still take precedence in terms of the suicide prevention research effort. Men stood out as one such high risk group. Some participants felt that young male suicide has received significant attention, and that the reversal of their previously high suicide rate might mean that other groups should warrant research attention. Others argued, however, that young male suicide has not decreased among lower socio-economic groups, and that these groups should maintain research priority. Still others mentioned different sub-groups of men, including older men, male prisoners and ex-prisoners, rural men, unemployed men, men in traditional male occupations and workplaces (e.g., builders, truck drivers), war veterans, recently separated men and men with relationship problems, and men with histories of sexual abuse. Several noted that many men do not seek help, and those who do are often not well served by services. One participant described this in the following way: ‘Men don’t access services because the services are disrespectful of men and the circumstances in which they might come to seek help.’ Older people were another commonly mentioned group. Many participants felt that older people had been marginalised and had been paid insufficient attention in suicide prevention research. For this reason, a number of participants felt that older people should become the new priority in suicide prevention research. Specific suggestions for the research focus among this group included identifying reasons for their high suicide
45
rates, evaluating interventions that work for older people, and examining the blurring between euthanasia and suicide among the elderly. A number of other specific groups were mentioned by at least one participant as requiring research attention. These included people detained in or recently released from immigration centres, people in Indigenous communities, members of the stolen generation, people who have experienced domestic violence, children in the juvenile justice system, children of recently-separated parents, people with drug and alcohol problems, people exhibiting suicidal behaviours (e.g., those presenting to emergency departments having deliberately self-harmed), people who have been bereaved by suicide and/or have a family history of suicide, people with mental health problems (particularly those who have been recently discharged from mental health services) and crisis line callers. There was an acknowledgement that individual participants would ‘lobby’ for a focus on the high risk groups with whom they were most familiar, which led to discussion of how to develop more objective criteria for selecting particular groups of interest. One participant questioned how decisions are and should be made, asking others to consider why some groups have received more research attention than others. He questioned whether high group-specific suicide rates have made the difference, or whether other factors, such as perceived attractiveness or vulnerability, might have had an influence. Balancing individual risk factors with societal, environmental, cultural and political influences on suicide Most participants acknowledged that there are some clear individual-level risk factors for suicide, such as mental illness. However, several participants argued that there are also broader societal, environmental, cultural and political influences on suicide that to date have been under-researched. Some attributed this to the largely bio-medical paradigm within which they perceived current suicide prevention research to be occurring. Participants expressed this notion in different ways, using different examples. One mentioned suicide by those in or recently released from detention centres, suggesting that the political situation would need to be taken into account in researching appropriate and effective suicide prevention interventions for this group. Others talked about job insecurity, unemployment, rurality and low socio-economic status, recommending that anthropological and sociological issues must be addressed in understanding these factors and their impact on suicide. Still others mentioned cultural factors, suggesting, for example, that more research attention needs to be devoted to stigma and how this may impact on suicidality. One participant summed up the need to examine the influence that these factors can have on human lives in the following way: ‘[We must] look at people’s quality of life and the telltale signs [of despair].’ Consideration of protective factors Many participants felt that if individual-level variables were to continue to be considered, the traditional examination of risk factors should give way to a greater consideration of protective factors. Several participants heavily emphasised that a much deeper understanding is needed of people’s capacity for resilience, hope and optimism. They felt that if these constructs were better understood, society would be better equipped to prevent suicide. Suggestions included looking at different levels of resilience in different communities, and examining why individuals in similar circumstances respond to traumatic and challenging events with different levels of optimism. One participant put this succinctly, claiming ‘Research should be looking at what are the pathways to hope (and despair) in our society.’

46
Methodological and related issues A number of participants commented on the overall direction suicide prevention research to date, making suggestions about how different methodological approaches could improve the knowledge base. Participants saw the value in real-world research, and advocated conducting rigorous evaluations alongside funded service delivery projects in a way that could provide evidence of effectiveness. One participant summed up the strength of this approach in the following way: ‘Operational and applied research is more important than that done under artificial conditions.’ A strong, recurring theme, however, was that deeper, more detailed and longer term research provided better quality and more useful information. Most felt that the research and evaluation efforts that sat alongside short term pilot project were insufficient to contribute to evidence about what works and what does not work, and concluded that there should be ‘no more pilots!’ A number commented that it would be more useful to have fewer projects funded to a greater degree, with strong evaluation components built in. One participant who had just completed a rigorous evaluation as part of a tailored service delivery project noted that, ‘if we had stopped at 12-18 months we would have had nothing, only ideas, not hard evidence.’ Several participants commented on the need to involve people in meaningful ways in any research into suicide prevention. This point was summed up in the following way by one participant: ‘Participate with people so they understand what we are doing and why we are doing it with them.’ There was seen to be an educative element to this approach, in that it could empower those involved in the research to become effective community agents in the area of suicide prevention. This was seen to be especially important for particular groups, such as people in remote Indigenous communities with few resources. Multi-disciplinary research was also emphasised. This occurred in the context of several participants noting that suicide is not simply a medical problem, but also a social problem, and commenting that this therefore required the involvement of anthropologists and sociologists as part of research teams. A few participants made mention of the fact that secondary analyses of existing data could complement the kind of primary research described above. Specific examples of routinely-collected datasets that could inform questions related to suicide prevention included coronial data and data from telephone help lines. Several participants noted that irrespective of whether research used primary or secondary data sources, it needed to emphasise the Australian context. Several examples were cited where Australia-specific studies are required, including studies of community structure and interventions to improve social cohesion, studies of male behaviour (including reticence with communication and help-seeking) in the Australian culture, and studies of differing protective factors in multi-cultural Australia. Some participants advocated a large-scale longitudinal study that followed a large cohort from infancy to adulthood, examining risk and protective factors for suicide. Utilising research findings Many participants indicated that research findings are not used optimally by relevant stakeholders. Some felt that researchers could do more to translate their findings into practice. One, for example, observed that research not only required recommendations but also action statements and commitments by researchers to follow them up. Others noted that researchers could do more to disseminate their findings in meaningful ways to communities, policy-makers, planners, clinicians and other practitioners, non-government

47
representatives, other researchers, and those who use health and mental health services. On a related note, a number of participants talked about the need to raise the profile of suicide as a public health issue and suggested that the media has a role to play here. In part, this role involves disseminating research findings (e.g., about risk and protective factors and about interventions that show promise). The role may be broader than this, however, and could involve reducing stigma, changing culture and encouraging help-seeking behaviour. Participants acknowledged the need to conduct media campaigns and related activities with caution, given the strong evidence that reporting of suicide can lead to copycat behaviours. They suggested that media activities themselves would need to be closely evaluated. Developing a framework for suicide prevention that could guide suicide prevention research Several participants drew together the above themes in a call for a cohesive framework for suicide prevention that could guide suicide prevention research. A number felt that the approach to date had been somewhat ad hoc, and that more strategic directions were necessary, contrasting the current approach to suicide prevention with that used to tackle the road toll. One participant summarised the idea in the following way: ‘We need a framework against which we place criteria – macro-level for the whole population, such as education at a young age about resilience and protective factors, and then at the micro-level, training about intervention that can help us identify risk factors.’

48
Chapter 7: Discussion and conclusions
Synthesising the findings from the four studies The findings from the current project are complex, but an attempt is made here to draw together the results of the four different studies in an effort to inform the national suicide prevention research agenda. Current investment and outputs During the life of the National Suicide Prevention Strategy, 263 journal articles have been published in the peer-reviewed literature that qualify as research where suicide is the primary focus. During the same period, 36 grants have been funded to the tune of $5,839,341 for projects or fellowships in the area of suicide prevention. Although these figures are not insignificant, they do not seem to be commensurate with the high individual, societal and economic burden of suicide and suicidal behaviours. Priorities for type of research The profiles of published literature and funded grants differed in terms of the type of research they involved. The majority of research in the published literature was epidemiological, with a focus on descriptive analyses of rates. By contrast, the studies funded through the grants most commonly assessed the efficacy of interventions, particularly indicated interventions aimed at individuals who are already manifesting suicidal thoughts or behaviours. The different emphases identified through the two reviews is perhaps not surprising, given their varying scopes. The review of published literature was restricted to articles published in peer-reviewed journals, but was not limited to studies funded by academic granting bodies and would therefore have been likely to include research funded through other sources. By contrast, the current review was, by design, limited to research funded by the three key granting bodies in Australia. Such granting bodies tend to favour investigator-driven intervention studies, particularly those where the intervention itself is relatively cheap, specifically targeted, and lends itself to relatively rigorous evaluation designs (e.g., where participants can be randomised and where outcomes can be readily measured). They are less likely to fund information-gathering or scoping exercises, such as descriptive epidemiological studies. The latter types of studies are more likely to be funded by health departments, and are more likely to be funded in a priority-driven fashion. It is worth considering how these findings sit with the views of stakeholders elicited from the web-based questionnaire and the focus groups. The majority of questionnaire respondents identified intervention studies as the highest priority for future suicide prevention research, calling for further work on indicated interventions and, to a lesser extent, selective and universal intervention. Their views were supported and expanded upon by focus group participants, who stressed that in future suicide prevention research efforts, priority should be given to evaluating the efficacy of specific interventions. They also stressed the importance of evaluations of suicide prevention policies, programs and services, which to date have received less attention. They felt that the epidemiological profile of suicidal individuals has been explored, at least with respect to rates and individual-level risk factors, and that intervention and evaluation research should focus on groups identified as having particularly high levels of risk. Most saw limited value in continuing to explore individual-level risk factors ad infinitum, and felt that the time has come to move on to considering wider societal influences on suicide and individual-level protective factors, and to do so from a multi-disciplinary perspective.

49
Priorities for suicidal behaviour In the international suicidology literature, there is a recognition that suicidal behaviours occur on a gradient, from suicidal ideation to attempted suicide to completed suicide, and there has been a consequent acknowledgement that it is important for prevention to focus on the full spectrum of suicidality. It may be appropriate, therefore that where a particular suicidal behaviour was examined in the published journal articles and funded grants, and equal amount of research effort was found for completed and attempted suicide. Although completed suicide is regarded as the more extreme manifestation of suicidality, suicide attempts are more prevalent and may affect different populations.1 From the perspective of questionnaire respondents, this division of emphasis would seem to be appropriate, in the sense that although respondents from most groups suggested that attempted suicide should be given priority in future research, people involved in funding suicide prevention research recommended that completed suicide should be addressed. Focus group participants did not comment explicitly on the relative emphases that should be given to particular suicidal behaviours. Priorities for suicide method Few of the retrieved journal articles reported on research into specific methods of suicide, and none of the funded grants supported method-specific research. This may be appropriate in the sense that much of the research effort has focussed on understanding suicidal behaviours in general, rather than on examining particular means. Having said this, reducing access to means has been acknowledged internationally as one promising way of preventing suicide,2 so it would be desirable to augment the current knowledge base with some more detailed analyses of method-specific issues. Focus group participants did not comment directly on the suicide methods which should be given priority, but questionnaire respondents emphasised two suicide methods of interest: poisoning by drugs and hanging. The methods of choice may reflect the particular perspectives of the respondent groups. For example, the clinicians (i.e., psychiatrists, GPs and psychologists) were among those most inclined to endorse poisoning by drugs as a research priority, which may reflect the fact that they commonly see people who have overdosed. Alternatively, the methods chosen may be related to how commonly they occur, as evidenced by the fact that hanging is the most common method of suicide in Australia.3 Priorities for target groups Young people emerged as the most commonly-researched target group in both the review of published literature and the review of funded grants. Other major target groups of interest in both cases were people who have attempted suicide or deliberately self-harmed and people with mental health problems. Stakeholders were divided about the target groups who should receive greatest attention in future suicide prevention research. The majority of questionnaire respondents endorsed young people and people with mental health problems. Focus group respondents mentioned a range of groups, with men and older people standing out. It is worth examining the relative emphasis on these target groups, and to consider ways of prioritising the suicide prevention research effort in this regard. As one focus group participant noted, there is a need to develop objective criteria against which to make these judgements. There is an argument, for example, that those groups who are acknowledged as having particularly high levels of suicide risk (e.g., people who have attempted suicide and people with mental health problems) should remain on the

50
research radar, and that groups (e.g., adult men) for whom suicide rates are on the rise may warrant renewed attention. Priorities for settings Certain settings took precedence in the research published in peer-reviewed literature and funded through grants. Other health service settings received particular emphasis, and communities, mental health service settings, emergency departments, schools and prisons were also afforded attention. Questionnaire respondents held various views about where the priority should lie in terms of future setting-specific suicide prevention research. Although communities was the response most commonly endorsed by the greatest number of groups, primary care settings and mental health service settings were also given prominence. Focus group respondents did not comment directly on the settings in which future suicide prevention research should be conducted, although they emphasised the importance of critically examining the response of the health and community service systems.
Project limitations Several caveats should be borne in mind in interpreting the above findings. Assessing current priorities The reviews of published literature and funded grants were extensive, covering the seven years of the National Suicide Prevention Strategy. The reviews were limited to articles published in peer-reviewed journal articles and grants funded by Australia’s key competitive granting bodies. It is acknowledged that this strategy would have missed research funded by governments or other bodies and reported in the ‘grey’ literature, but it was considered defensible because it provided a non-arbitrary sampling frame and afforded some check on the quality of the research included in the review. It was beyond the scope of the reviews to retrieve full journal articles or complete grant proposals, and instead they relied on abstracts and summaries, respectively. In the main, this précis information was sufficient to make judgements according to the framework for examining current priorities in suicide prevention research, but it is acknowledged that in some instances detail was lacking. Assessing future priorities The examination of future priorities relied solely on stakeholders’ views of where ongoing effort should be placed. This is certainly one legitimate way of gauging future priorities, but desirably others should also be drawn upon. In their earlier study of research priorities in mental health, Jorm and colleagues12-14 examined the current distribution of research into a range of mental disorders against standards of prevalence, burden and health system costs, as well as stakeholder-perceived priority areas. It was not possible to use the former standards in the current project, because suicide was considered in isolation, with no other comparators. Nonetheless, stakeholder views should be regarded as one information source only, and other relevant factors should be taken into account in assessing future priorities. Stakeholders were selected in a manner designed to ensure that they were representative of people who conduct, use and are involved in funding suicide prevention research, and people who have been affected by suicide. However, the questionnaire response rates varied by group, and the purposive sampling strategy used to recruit focus group participants relied on the project team’s knowledge of people and organisations with an interest in suicide prevention. In addition, stakeholders had varying

51
degrees of knowledge about what is happening (and should be happening) in suicide prevention research in Australia. For these reasons, some caution should be exercised in generalising the views of questionnaire respondents and focus group participants to other stakeholders.
Recommendations Some of the findings from the current project are unequivocal, and point clearly to specific recommendations about the direction the development of a national postgraduate scholarships and/or national research grants program should take. Other findings are more mixed and/or reflect the project’s limitations, and require that additional information be sought before clear direction can be given. The following recommendations reflect the nature of these findings: Recommendation 1: Priority should be given to funding studies that evaluate interventions It is clear from the data that priority should be given to funding studies about interventions. Although these studies have been the subject of a relatively high proportion of funded grants, relatively few published papers have emanated from these grants, and stakeholders stress that discovering efficacious interventions to prevent suicide should be the ‘main game’. A systematic review of the international literature on suicide prevention strategies by Mann and colleagues found only two interventions which showed any evidence of reducing suicide rates (educating physicians about depression and restricting access to lethal means), and concluded that all other interventions require further testing.2 Australian research should build on international studies, and should pay heed to any contextual factors that might make a given intervention more or less likely to work in the local setting. Given the dearth of knowledge on which interventions might be efficacious, it would seem reasonable for attention to be paid to studies that assess of the efficacy of the full spectrum of suicide prevention interventions (universal, selective and indicated) and/or evaluate suicide prevention policies, programs and services. This research should be scientifically sound, and should employ appropriate methodologies to allow given interventions to be tested in the most rigorous manner possible. For example, it should explicitly test the theory or logic underpinning given interventions, and should pay heed to questions of sample size, use of appropriate comparison groups, and use of suitable outcome measures. The research should represent a balance of priority-driven and investigator-driven research, and should involve thorough evaluations of government-funded programs and projects, as well as purpose-designed evaluations of specific interventions. Recommendation 2: A content-based literature review should be commissioned to determine what is known and what is not known about suicide prevention in the Australian context A content-based review of the scientific literature should be commissioned to provide a picture of what is known and what is not known about suicide prevention in the Australian context. The review should summarise what the literature says about the epidemiology of completed and attempted suicide for key target groups, and about interventions that show promise for suicide prevention for each of these groups. The review should use as its starting point the literature identified in Study 1. Additional reports and journal articles in progress should be sought from the principal investigators of the funded grants identified in Study 2. The review should not be limited to the Australian literature, however, as there has been considerable international investment in suicide prevention research. While it is reasonable that the Australian literature will provide the best

52
summary of the epidemiology of completed and attempted suicide in this country, a fuller picture of current knowledge with regard to interventions will come from a broader examination of studies from overseas. In particular, the literature review should draw on existing review papers that summarise what is known about what works and what doesn’t work in suicide prevention, such as the above-mentioned systematic review by Mann and colleagues.2 Recommendation 3: Funding for epidemiological studies should be provided only in circumstances where new knowledge will be gleaned It is clear that much emphasis has already been given to epidemiological studies, particularly those concerning rates and risk factors. Stakeholders argued that sufficient work has been done in this area, and that the focus should shift elsewhere. To a large extent, this seems reasonable. At the very least, funding for future epidemiological studies should be awarded only when they demonstrate innovation and make a novel contribution to knowledge. This does not necessarily mean that new studies must be commissioned; there may be a place for funding secondary analysis of existing data, or systematic reviews and meta-analyses that bring together the findings of a number of studies in a comparable way. Recommendation 4: Criteria should be developed to assess the significance of suicide among particular target groups, in order to prioritise the research attention that should be paid to each group The current study was unable to prioritise particular groups in terms of warranting research attention. Take, for example, the target group of young people. Young people were the target group investigated in the majority of published journal articles and the majority of funded grants, but survey respondents and focus group participants were divided as to whether they should continue to receive research attention. Some felt that they had received sufficient attention, particularly since the youth suicide rate is now declining; others felt that there is still ‘unfinished business’ with respect to research into what prompts young people to choose suicide as an option and what interventions may prove most successful with this group. What is needed is more objective information about the significance of suicide among this group, relative to other groups, some of which may have been available to the current project had a formal content review of the published literature and/or recourse to routinely-collected suicide data been within its remit. In addition to the subjective views of importance put forward by stakeholders, epidemiological (and, for that matter, economic) measures of importance are required. Such measures need to be readily comparable across groups, and might include group-specific rates, indices of relative risk, indices of population attributable risk, and measures of burden (e.g., disability adjusted life years). This is consistent with the international and Australian literature on priority-setting in public health research, which emphasises significance as a key criterion.4 5 It is recommended that a study be commissioned that objectively assesses the relative importance of completed suicide and attempted suicide as public health issues among particular target groups. This could be commissioned as part of the content-based literature review proposed in Recommendation 2. In line with Recommendation 3, this study should re-examine existing epidemiological data wherever possible (e.g., by synthesising the findings of the epidemiological studies examined in the content-based review), and should complement this with the most up-to-date statistics on completed suicide and attempted suicide as necessary. The study should pay heed to issues of comparability between estimates for particular groups. For example, it should note the likelihood that estimates of rates of attempted suicide will be lower in registration studies (which enumerate presentations to emergency departments or admissions to hospital for
53
medically-serious suicide attempts) than in population-based surveys (which rely on self-report).6 The presentation of a range of estimates and sensitivity analyses may be necessary to improve the comparability of data across groups. Recommendation 5: Criteria should be developed to assess the significance of suicide in particular settings, in order to prioritise the research attention that should be paid to each setting The current study was unable to prioritise particular settings in terms of warranting research attention. Existing research had been conducted in a range of settings, and stakeholders held convergent views about where future priorities should lie. Again, more objective information is needed to shed light on the relative emphasis that should be given to different settings. Some of this information would flow from the study of the relative significance of completed suicide and attempted suicide for different target groups (see Recommendation 4), in the sense that some target groups are associated with particular settings. So, for example, if people with mental health problems emerged as a group to whom research priority should be given, it would make sense to consider mental health service settings as a key setting of interest. Other guidance in this regard may be gained by considering settings in which interventions occur which, although not yet proven in terms of their efficacy, show promise. This information could be drawn out in the content-based literature review, proposed under Recommendation 2. Recommendation 6: Studies of completed suicide and attempted suicide should both receive research funding The current balanced emphasis on both completed suicide and attempted suicide would seem to be appropriate, given that stakeholders give weight to both. As noted, prevention efforts should cover the full spectrum of suicidality, particularly since a previous suicide attempt is one of the strongest predictors of completed suicide.1 For this reason, it is recommended that the intervention studies proposed in Recommendation 1 not be limited to those addressing completed suicide, but also include those addressing attempted suicide (and, to a lesser extent, suicidal ideation). Similarly, it is recommended that the criteria to be developed under Recommendations 4 and 5 address the significance of both completed suicide and attempted suicide for various target groups and in a range of settings. Recommendation 7: Method-specific studies should be given funding support, and criteria should be developed against which to judge whether a given suicide method warrants particular research attention On the whole, the generalist approach to suicide prevention research would appear to be appropriate, since lessons about suicide and its prevention will often not be method-specific. Focus group participants did not raise method-specific research as an issue, but, when directly asked, questionnaire respondents emphasised the need to pursue research into poisoning by drugs and hanging as priorities. There is certainly an argument for some research attention to be directed towards particular methods, and for criteria to be developed that ranks them in terms of their significance. Such criteria might be based on the relative rate at which they occur, and/or trends in relative rates over time (derived from the content review of the epidemiological literature proposed in Recommendation 2 and a thorough examination of routinely-collected statistics). Alternatively, criteria might be based on the feasibility of targeting an intervention towards particular methods (e.g., reducing access to paracetamol via repackaging efforts, as was done in the United Kingdom7).

54
Recommendation 8: Multi-disciplinary research that employs a range of methodologies should be encouraged As noted, the majority of suicide prevention research that has been conducted to date has been epidemiological and relatively uni-disciplinary. Multi-disciplinary research that broadens this perspective by should be encouraged through innovative funding mechanisms, as should include research that combines quantitative and qualitative data. In the context of emphasising research into suicide prevention interventions as suggested in Recommendation 1, this might translate into supporting diverse study teams to measure intervention recipients’ quantitative outcomes (e.g., repeat suicide attempts) and to explore their qualitative experiences of the benefits and disadvantages of the intervention. Depending on the intervention and the research questions being investigated, these study teams might include clinicians, community development experts, epidemiologists, program evaluators, health economists, sociologists and anthropologists. Recommendation 9: Research findings should be communicated as widely as possible, in order to maximise their influence on policy and practice Certain contractual ‘deliverables’ should be tied to future suicide prevention research funding, in order to maximise ‘knowledge transfer’. These deliverables should include peer-reviewed journal articles, but also less traditional communications that ensure that findings are reported in meaningful ways to a range of stakeholders. The latter might include reports for a range of audiences, community presentations and media releases.
Conclusions The current report presents a picture of the status quo with regard to suicide prevention research, identifying some areas where there are clear gaps and others where relatively greater efforts have been made. Interpreting these findings in a manner that can inform the proposed research agenda is not simple, and is not just a matter of giving weight to previously under-emphasised areas and reducing the attention paid to previously well-covered areas. The findings from the web-based questionnaire and the focus groups enable these results to be assessed through the lens of what stakeholders view as priorities. Other factors should also be taken into account in formulating future priorities, but the findings may assist in re-directing Australian suicide prevention research endeavours to help fill internationally-identified gaps in knowledge about what works and what does not work in suicide prevention.

55
References 1. Suicides and medically serious attempted suicides: Two populations or one?
Suicide Prevention Australia 8th National Conference; 2001; Sydney. 2. Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, et al. Suicide
prevention strategies: A systematic review. Journal of the American Medical Association 2005;294(16):2064-2074.
3. Australian Bureau of Statistics. Suicides: Recent Trends, Australia (Cat. No. 3309.0.55.001). Canberra: Australian Bureau of Statistics, 2004.
4. World Health Organization. Investing in Health Research and Development: Report of the Ad Hoc Committee on Health Research Relating to Future Intervention Options. Geneva: World Health Organization, 1996.
5. Carson N, Ansari Z, Hart W. Priority setting in public health and health services research. Australian Health Review 2000;23(3):46-57.
6. Welch SS. A review of the literature on the epidemiology of parasuicide in the general population. Psychiatric Services 2000;52(3):368-375.
7. Hawton K, Simkin S, Deeks J, Cooper J, Johnston A, Waters K, et al. UK legislation on analgesic packs: Before and after study of long term effect on poisonings. British Medical Journal 2004;329(7474):1076.
8. Commonwealth Department of Health and Aged Care. LIFE: Learnings About Suicide. Canberra: Commonwealth of Australia, 2000.
9. Commonwealth Department of Health and Aged Care. LIFE: Areas for Action. Canberra: Commonwealth of Australia, 2000.
10. Commonwealth Department of Health and Aged Care. LIFE: Building Partnerships. Canberra: Commonwealth of Australia, 2000.
11. Commonwealth Department of Health and Aged Care. Setting the Evidence-based Research Agenda for Australia (A Literature Review). Canberra: Commonwealth of Australia, 1999.
12. Jorm A, Griffiths K, Christensen H, Medway J. Research Priorities in Mental Health. Canberra: Mental Health and Special Programs Branch, Commonwealth Department of Health and Ageing, 2002.
13. Jorm AF, Griffiths KM, Christensen H, Medway J. Research priorities in mental health. Part 1: An evaluation of the current research effort against the criteria of disease burden and health system costs. Australian and New Zealand Journal of Psychiatry 2002;36:322-326.
14. Griffiths KM, Jorm AF, Christensen H, Medway J, Dear KBG. Research priorities in mental health. Part 2: An evaluation of the current research effort against stakeholders’ priorities. Australian and New Zealand Journal of Psychiatry 2002;36:327-339.
15. Hennekens CH, Buring JE. Epidemiology in Medicine. Boston: Little, Brown and Co., 1987.

56
Acknowledgements The authors would like to thank the 231 questionnaire respondents and 28 focus group participants for sharing their views on suicide prevention research. They would also like to thank several of the staff from Strategic Data Pty Ltd – David Jones-Ellis for developing the Access database for coding abstracts from peer-reviewed journal articles, Gayle Main and Adam Clarke for developing and maintaining the web-based questionnaire, and Malvina Tsecoutanis for entering data from the paper-based version of the questionnaire.

57
Appendix A: List of peer-reviewed journal articles in which suicide or suicidal behaviour was the primary focus 1. Boyce P, Oakley-Browne MA, Hatcher S. The problem of deliberate self-harm.
Current Opinion in Psychiatry 2001;14(2):107-111. 2. Acres JG, McKelvey RS, Pfaff JJ. Training general practitioners to recognise and
respond to psychological distress and suicidal ideation in young people. Medical Journal of Australia 2001;174(5):222-226.
3. Allen F. Suicide: What is to be done? Australian Psychologist 2000;35(1):29-31. 4. Allison S, Roeger L, Martin G, Keeves J. Gender differences in the relationship
between depression and suicidal ideation in young adolescents. Australian and New Zealand Journal of Psychiatry 2001;35(4):498-503.
5. Aoun S. Deliberate self-harm in rural Western Australia: Results of an intervention study. Australian and New Zealand Journal of Mental Health Nursing 1999;8(2):65-73.
6. Aoun S, Johnson L. A consumer's perspective of a suicide intervention programme. Australian and New Zealand Journal of Mental Health Nursing 2001;10(2):97-104.
7. Balit CR, Isbister GK, Peat J, Dawson AH, Whyte IM. Paracetamol recall: A natural experiment influencing analgesic poisoning. Medical Journal of Australia 2002;176(4):162-164.
8. Balit CR, Lynch CN, Isbister GK. Bupropion poisoning: A case study. Medical Journal of Australia 2003;178(2):61-63.
9. Barber JG. Relative misery and youth suicide. Australian and New Zealand Journal of Psychiatry 2001;35(1):49-57.
10. Barnes J. Murder followed by suicide in Australia 1973-1992: A research note. Journal of Sociology 2000;36(1):1-11.
11. Beckinsale P, Martin G, Clark S. Sexual abuse and suicidal issues in Australian young people. Australian Family Physician 2000;28(12):1298-1303.
12. Beckinsale P, Martin G, Clark S. Youth sucide issues in general practice. Australian Family Physician 2001;30(4):391-394.
13. Bell D. Ethical issues in the prevention of suicide in prison. Australian and New Zealand Journal of Psychiatry 1999;33(5):723-728.
14. Bergen HA, Martin G, Richardson AS, Allison S, Roeger L. Sexual abuse and suicidal behavior: A model constructed from a large community sample of adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 2003;42(11):1301-1309.
15. Berk M, Dodd S. Are treatment emergent suicidality and decreased response to antidepressants in younger patients due to bipolar disorder being misdiagnosed as unipolar depression? Medical Hypotheses 2005;65(1):39-43.
16. Berk M, Dodd S, Henry M. The effect of macroeconomic variables on suicide. Psychological Medicine 2006;36(2):181-189.
17. Blair-West GW, Mellsop GW. Major depression: Does a gender-based down-rating of suicide risk challenge its diagnostic validity? Australian and New Zealand Journal of Psychiatry 2001;35(3):322-328.
18. Blashki G, Pirkis J, Morgan H, Ciechomski L. Managing depression and suicide risk in men presenting to primary care physicians. Primary Care: Clinics in Office Practice 2006;33(1):211-221.
19. Boddy G. Young people at Risk Program. Youth Suicide Prevention Bulletin 1999;3:38-49.
20. Borges G. A case-crossover study of acute alcohol use and suicide attempt. Journal of Studies on Alcohol 2004;65(6):708-714.
21. Bourke L. Toward understanding youth suicide in an Australian rural community. Social Science and Medicine 2003;57(12):2355-2365.
58
22. Brett A. Murder-parasuicide: A case series in Western Australia. Psychiatry, Psychology and Law 2002;9(1):96-99.
23. Brown G. 'Here for life' youth sexuality project: An overview of some early results. Youth Suicide Prevention Bulletin 1999;3:28-31.
24. Brown R. Self harm and suicide risk for same-sex attracted young people: A family perspective. Australian e-Journal for the Advancement of Mental Health 2002;1(1).
25. Burgess P, Pirkis J, Morton J, Croke E. Lessons from a comprehensive clinical audit of users of psychiatric services who committed suicide. Psychiatric Services 2000;51(12):1555-1560.
26. Burgess P, Pirkis J, Jolley D, Whiteford H, Saxena S. Do nations' mental health policies, programs and legislation influence their suicide rates? An ecological study of 100 countries. Australian and New Zealand Journal of Psychiatry 2004;38(11-12):933-939.
27. Burns J, Patton G. Preventive interventions for youth suicide: A risk factor-based approach. Australian and New Zealand Journal of Psychiatry 2000;34(3):388-407.
28. Burns J, Dudley M, Hazell P, Patton G. Clinical management of deliberate self-harm in young people: The need for evidence-based approaches to reduce repetition. Australian and New Zealand Journal of Psychiatry 2005;39(3):121-128.
29. Byard RW, Knight D, James RA, Gilbert J. Murder-suicides involving children: A 29-year study. American Journal of Forensic Medicine and Pathology 1999;20(4):323-327.
30. Byard RW, Houldsworth G, James RA, Gilbert JD. Characteristic features of suicidal drownings: A 20-year study. American Journal of Forensic Medicine and Pathology 2001;22(2):134-138.
31. Byard RW, Gilbert JD. Cervical fracture, decapitation, and vehicle-assisted suicide. Journal of Forensic Sciences 2002;47(2):392-394.
32. Byard RW, Hanson KA, Gilbert J, James RA, Nadeau J, Blackbourne B, et al. Death due to electrocution in childhood and early adolescence. Journal of Paediatric and Child Health 2003;39(1):46-48.
33. Caldwell TM, Jorm AF, Dear KBG. Suicide and mental health in rural, remote and metropolitan areas in Australia. Medical Journal of Australia 2004;181(7):S10-S14.
34. Cantor CH, Neulinger K, De Leo D. Australian suicide trends 1964-1997: Youth and beyond? Medical Journal of Australia 1999;171(3):137-141.
35. Cantor C, Baume P. Suicide prevention: A public health approach. Australian and New Zealand Journal of Mental Health Nursing 1999;8(2):45-50.
36. Cantor CH, Hickey PA, De Leo D. Seasonal variation in suicide in a predominantly Caucasian tropical/subtropical region of Australia. Psychopathology 2000;33(6):303-306.
37. Cantor C, Neulinger K. The epidemiology of suicide and attempted suicide among young Australians. Australian and New Zealand Journal of Psychiatry 2000;34(3):370-387.
38. Cantor C, McTaggart P, De Leo D. Misclassification of suicide: The contribution of opiates. Psychopathology 2001;34(3):140-146.
39. Capp K, Deane FP, Lambert G. Suicide prevention in Aboriginal communities: Application of community gatekeeper training. Australian and New Zealand Journal of Public Health 2001;25(4):315-321.
40. Carr-Gregg M. Suicide, schools and young people: Tackling the youth suicide industry. Youth Studies Australia 2003;22(3):32-35.
41. Carr-Gregg M. Cutting out self harm. Australian Doctor 2006;39. 42. Carter G, Whyte I, Ball K, Carter NT, Dawson AH, Carr VJ, et al. Repetition of
deliberate self-poisoning in an Australian hospital-treated population. Medical Journal of Australia 1999;170(7):307-311.
59
43. Carter GL, Clover KA, Bryant JL, Whyte IM. Can the Edinburgh Risk of Repetition Scale predict repetition of deliberate self-poisoning in an Australian clinical setting? Suicide and Life-Threatening Behavior 2002;32(3):230-239.
44. Carter GL, Issakidis C, Clover K. Correlates of youth suicide attempters in Australian community and clinical samples. Australian and New Zealand Journal of Psychiatry 2003;37(3):286-293.
45. Carter G, Reith DM, Whyte IM, McPherson M. Repeated self-poisoning: Increasing severity of self-harm as a predictor of subsequent suicide. British Journal of Psychiatry 2005;186:253-257.
46. Carter GL, Lewin TJ, Stoney C, Whyte IM, Bryant JL. Clinical management for hospital-treated deliberate self-poisoning: Comparisons between patients with major depression and borderline personality disorder. Australian and New Zealand Journal of Psychiatry 2005;39(4):266-273.
47. Carter G, Reith DM, Whyte IM, McPherson M. Non-suicidal deaths following hospital-treated self-poisoning. Australian and New Zealand Journal of Psychiatry 2005;39(1-2):101-107.
48. Carter G, Clover K, Whyte I, Dawson AH, D'Este C. Postcards from the Edge project: Randomised controlled trial of an intervention using postcards to reduce repetition of hospital treated deliberate self poisoning. British Medical Journal 2005;331(7520):No pagination.
49. Carter GL, Safranko I, Lewin TJ, Whyte IM, Bryant JL. Psychiatric hospitalization after deliberate self-poisoning. Suicide and Life-Threatening Behavior 2006;36(2):213-222.
50. Chatterton R, McTaggart P, Baume P, Harrison K. Suicides in an Australian inpatient environment. Journal of Psychosocial Nursing and Mental Health Services 1999;37(6):34-40.
51. Ciesielski H, Belperio D. Analysis of system mechanism in relation to suicide, intervention and prevention. Mental Health in Australia 1999;9(1):98-100.
52. Clarke DM. Autonomy, rationality and the wish to die. Journal of Medical Ethics 1999;25(6):457-462.
53. Cleary M, Jordan R, Horsfall J, Mazoudier P, Delaney J. Suicidal patients and special observation. Journal of Psychiatric and Mental Health Nursing 1999;6(6):461-467.
54. Clover K, Carter GL, Whyte IM. Posttraumatic stress disorder among deliberate self-poisoning patients. Journal of Traumatic Stress 2004;17(6):509-517.
55. Coman M, Meyer AD, Cameron PA. Jumping from the Westgate Bridge, Melbourne. Medical Journal of Australia 2000;172(2):67-69.
56. Corcos CD, Lewin RD. The use of "safe cells" in the management of suicidal and violent prisoners. Australasian Psychiatry 2001;9(1):47-50.
57. Crawford J, Zielinski MA, Fisher LJ, Sutherland GR, Goldney RD. Is there a relationship between Wolfram syndrome carrier status and suicide? American Journal of Medical Genetics 2002;114(3):343-346.
58. Darke S, Ross J. The relationship between suicide and heroin overdose among methadone maintenance patients in Sydney, Australia. Addiction 2001;96(10):1443-1453.
59. Darke S, Ross J, Lynskey M. The relationship of conduct disorder to attempted suicide and drug use history among methadone maintenance patients. Drug and Alcohol Review 2003;22(1):21-25.
60. Darke S, Ross J, Lynskey M, Teesson M. Attempted suicide among entrants to three treatment modalities for heroin dependence in the Australian Treatment Outcome Study (ATOS): prevalence and risk factors. Drug and Alcohol Dependence 2004;73(1):1-10.
61. Darke S, Williamson A, Ross J, Teesson M. Attempted suicide among heroin users: 12-month outcomes from the Australian Treatment Outcome Study (ATOS). Drug and Alcohol Dependence 2005;78(2):177-186.
62. Davidson JA. Presentation of near-hanging to an emergency department in the Northern Territory. Emergency Medicine 2003;15(1):28-31.
60
63. De Leo D, Hickey PA, Meneghel G, Cantor CH. Blindness, fear of sight loss, and suicide. Psychosomatics 1999;40(4):339-344.
64. De Leo D, Padoani W, Scocco P, Lie D, Bille-Brahe U, Arensman E, et al. Attempted and completed suicide in older subjects: Results from the WHO/EURO Multicentre study of suicidal behaviour. International Journal of Geriatric Psychiatry 2001;16(3):300-310.
65. De Leo D, Evans R, Neulinger K. Hanging, firearm, and non-domestic gas suicides among males: A comparative study. Australian and New Zealand Journal of Psychiatry 2002;36(2):183-189.
66. De Leo D, Dwyer J, Firman D, Neulinger K. Trends in hanging and firearm suicide rates in Australia: Substitution of method? Suicide and Life-Threatening Behavior 2003;33(2):151-164.
67. De Leo D, Spathonis K. Culture, society and suicide. Australian Mosaic 2003;4:27-30.
68. De Leo D, Heller TS. Who are the kids who self harm? An Australian self-report school survey. Medical Journal of Australia 2004;181(3):140-144.
69. De Leo D, Cerin E, Spathonis K, Burgis S. Lifetime risk of suicide ideation and attempts in an Australian community: Prevalence, suicidal process, and help-seeking behaviour. Journal of Affective Disorders 2005;86(2-3):215-224.
70. De Leo D, Burgis S, Bertolote JM, Kerkhof A, Bille-Brahe U. Definitions of suicidal behavior: Lessons learned from the WHO/EURO Multicentre Study. Crisis 2006;27(1):4-15.
71. de Moore GM, Robertson AR. Suicide attempts by firearms and by leaping from heights: A comparative study of survivors. American Journal of Psychiatry 1999;156(9):1425-1431.
72. de Moore GM. The suicide of Thomas Wentworth Wills. Medical Journal of Australia 1999;171(11-12):656-658.
73. Deane FP, Wilson CJ, Ciarrochi J. Suicidal ideation and help-negation: Not just hopelessness or prior help. Journal of Clinical Psychology 2001;57(7):901-914.
74. Dear GE, Thomson DM, Hills AM. Self-harm in prison: Manipulators can also be suicide attempters. Criminal Justice and Behavior 2000;27(2):160-175.
75. Dear GE. Functional and dysfunctional impulsivity, depression, and suicidal ideation in a prison population. Journal of Psychology 2000;134(1):77-80.
76. Dear GE, Slattery JL, Hillan RJ. Evaluations of the quality of coping reported by prisoners who have self-harmed and those who have not. Suicide and Life-Threatening Behavior 2001;31(4):442-450.
77. Dear GE, Thomson DM, Hall GJ, Howells K. Non-fatal self-harm in Western Australian prisons: Who, where, when and why. Australian and New Zealand Journal of Criminology 2001;34(1):47-66.
78. Dear GE, Thomson DM, Hall G, Howells K. Self-harm in Western Australian prisons: Differences between prisoners who have self-harmed and those who have not. Australian and New Zealand Journal of Criminology 2001;34(3):277-292.
79. Di Ciero J. Peer survivors of adolescent suicide. Health Education of Australia 1999:30-32.
80. Donald M, Dower J, Lucke J, Raphael B. Prevalence of adverse life events, depression and suicidal thoughts and behaviour among a community sample of young people aged 15-24 years. Australian and New Zealand Journal of Public Health 2001;25(5):426-432.
81. Donald M, Dower J, Correa-Velez I, Jones M. Risk and protective factors for medically serious suicide attempts: a comparison of hospital-based with population-based samples of young adults. Australian and New Zealand Journal of Psychiatry 2006;40(1):87-96.
82. Dudley M, Beard J, Clarke AR, Knowles M, Buss R. Effectiveness of a 'Green Card' intervention for patients engaging in deliberate self-harm. Archives of Suicide Research 2003;7(2):175-181.

61
83. Eccleston L, Sorbello L. The RUSH program - Real understanding of self-help: A suicide and self-harm prevention initiative within a prison setting. Australian Psychologist 2002;37(3):237-244.
84. Eckersley R, Dear K. Cultural correlates of youth suicide. Social Science and Medicine 2002;55(11):1891-1904.
85. Einfeld SL, Beard J, Tobin M, Buss R, Dudley M, Clarke AR, et al. Evidence-based practice for young people who self harm: Can it be sustained and does it improve outcomes? Australian Health Review 2002;25(4):178-178.
86. Einfeld S, Tobin M, Beard J, Evans E, Buss R, Dudley M. Sustaining evidence-based practice for young people who self harm: A 4-year follow-up. Australian Health Review 2004;27(2):94-99.
87. Elliott-Farrelly T. Indigenous suicide in the United States of America, Canada and New Zealand: Part one. Aboriginal and Islander Health Worker Journal 2004;28(4):21-25.
88. Elliott-Farrelly T. Australian Aboriginal suicide: The need for an Aboriginal suicidology? Australian e-Journal for the Advancement of Mental Health 2004;3(3):1-8.
89. Elliott-Farrelly T. An overview of Australian Aboriginal suicide: Part one. Aboriginal and Islander Health Worker Journal 2005;29(1):11-15.
90. Elliott-Farrelly T. An overview of Australian Aboriginal suicide: Part two. Aboriginal and Islander Health Worker Journal 2005;29(1):24-28.
91. English V, Mussell R, Sheather J, Sommerville A. Ethics briefings. Journal of Medical Ethics 2005;31(1):61-62.
92. Farrow TL. Owning their expertise: Why nurses use 'no suicide contracts' rather than their own assessments. International Journal of Mental Health Nursing 2002;11(4):214-219.
93. Fulde G. Another 'deliberate self-harm': Attempting suicide by overdose. Medicine Today 2000;1(2):109-110.
94. Fulde G, Preisz P. A new approach to overdose management. Current Therapeutics 2001;42(3):71-74.
95. Fullagar S. Wasted lives: The social dynamics of shame and youth suicide. Journal of Sociology 2003;39(3):291-307.
96. Gair S, Camilleri P. Attempting suicide and help-seeking behaviours: Using stories from young people to inform social work practice. Australian Social Work 2003;56(2):83-93.
97. Giskes R. Suicide in Queensland: An update on recent trends and strategies. Queensland Parliamentary Library Research Brief 2005;8.
98. Gladstone GL, Mitchell PB, Parker G, Wilhelm K, Austin MP, Eyers K. Indicators of suicide over 10 years in a specialist mood disorders unit sample. Journal of Clinical Psychiatry 2001;62(12):945-+.
99. Gladstone GL, Parker GB, Mitchell PB, Malhi GS, Wilhelm K, Austin MP. Implications of childhood trauma for depressed women: An analysis of pathways from childhood sexual abuse to deliberate self-harm and revictimization. American Journal of Psychiatry 2004;161(8):1417-1425.
100. Goldney RD, Wilson D, Dal Grande E, Fisher LJ, McFarlane AC. Suicidal ideation in a random community sample: Attributable risk due to depression and psychosocial and traumatic events. Australian and New Zealand Journal of Psychiatry 2000;34(1):98-106.
101. Goldney R. A South Australian coronial inquiry into suicide and homicide. Australasian Psychiatry 2000;8(2):142-146.
102. Goldney RD, Fisher LJ, Wilson DH, Cheok F. Suicidal ideation and health-related quality of life in the community. Medical Journal of Australia 2001;175(10):546-549.
103. Goldney RD, Fisher LJ, Wilson DH, Cheok F. Mental health literacy of those with major depression and suicidal ideation: An impediment to help seeking. Suicide and Life-Threatening Behavior 2002;32(4):394-403.

62
104. Goldney R. A global view of suicidal behaviour. Emergency Medicine 2002;14(1):24-34.
105. Goldney RD. A novel integrated knowledge explanation of factors leading to suicide. New Ideas in Psychology 2003;21(2):141-146.
106. Goldney RD, Dal Grande E, Fisher LJ, Wilson D. Population attributable risk of major depression for suicidal ideation in a random and representative community sample. Journal of Affective Disorders 2003;74(3):267-272.
107. Goldney R. Management of suicidal behaviour. Australian and New Zealand Journal of Psychiatry 2005;39(10):948-949.
108. Graham A, Reser J, Scuderi C, Zubrick SR, Smith M, Turley B. Suicide: An Australian Psychological Society discussion paper. Australian Psychologist 2000;35(1):1-28.
109. Hall WD, Mant A, Mitchell PB, Rendle VA, Hickie IB, McManus P. Association between antidepressant prescribing and suicide in Australia, 1991-2000: Trend analysis. British Medical Journal 2003;326(7397):1008-1011.
110. Hamilton TK, Schweitzer RD. The cost of being perfect: Perfectionism and suicide ideation in university students. Australian and New Zealand Journal of Psychiatry 2000;34(5):829-835.
111. Harrison JE, Steenkemp M. Suicide in Australia: Trends an data for 1998. Australian Injury Prevention Bulletin 2000;23:1-14.
112. Hassan R. Is suicide a disease? Medical Journal of Australia 2001;175(10):554-555.
113. Hay PJ, Denson LA, van Hoof M, Blumenfeld N. The neuropsychiatry of carbon monoxide poisoning in attempted suicide: A prospective controlled study. Journal of Psychosomatic Research 2002;53(2):699-708.
114. Hazell P, Hazell T, Waring T, Sly K. A survey of suicide prevention curricula taught in Australian universities. Australian and New Zealand Journal of Psychiatry 1999;33(2):253-259.
115. Hazell P. Establishment and evaluation of a clinical pathway for young suicide attempters and ideators. Australasian Psychiatry 2003;11(1):54-58.
116. Heale P, Dietze P, Fry C. Intentional overdose among heroin overdose survivors. Journal of Urban Health-Bulletin of the New York Academy of Medicine 2003;80(2):230-237.
117. Herdson PB, Dellar GG, McFawn P, Fuderer EM, Tait R. Third time lucky: An unusual suicide. Medicine, Science and the Law 1999;39(3):262-265.
118. Herdson PB. Shotgun suicide with a difference. Medical Journal of Australia 2000;173(11-12):604-605.
119. Hitchman P. Organophosphate overdose: A case study. Australasian Journal of Emergency Care 1999;6(1):28-29.
120. Hopes LM, Williams A. Depression, self-defeating, and self-destructive behaviors as predictors of suicide ideation in males and females. Psychological Reports 1999;84(1):63-66.
121. Horgan D. Practical management of the suicidal patient. Australian Family Physician 2002;31(9):819-822.
122. Howard J, Lennings CJ, Copeland J. Suicidal behaviour in a young offender population. Crisis 2003;24(3):98-104.
123. Howells K, Hall G. The management of suicide and self-harm in prisons: Recommendations for good practice. Australian Psychologist 1999;34(3):157-165.
124. Hunter E, Harvey D. Indigenous suicide in Australia, New Zealand, Canada and the United States. Emergency Medicine 2002;14(1):14-23.
125. Isbister GK, Balit CR. Bupropion overdose: QTc prolongation and its clinical significance. Annals of Pharmacotherapy 2003;37(7-8):999-1002.
126. Jaworski K. Suicide and gender: Reading suicide through Butler's notion of performativity. Journal of Australian Studies 2003;76:137-146.

63
127. Johnson GR, Krug EG, Potter LB. Suicide among adolescents and young adults: A cross-national comparison of 34 countries. Suicide and Life-Threatening Behavior 2000;30(1):74-82.
128. Jones R, Lennings C, Ward PB, Neville M, Howard J, Mackdacy EA. Descriptions of youth who self harm: The MacKay-Mooranbah Youth Suicide Prevention Project. Journal of Applied Health Behaviour 1999;1(2):23-30.
129. Judd F, Jackson H, Fraser C, Murray G, Robins G, Komiti A. Understanding suicide in Australian farmers. Social Psychiatry and Psychiatric Epidemiology 2006;41(1):1-10.
130. Judd F, Cooper A-M, Fraser C, Davis J. Rural suicide-people or place effects? Australian and New Zealand Journal of Psychiatry 2006;40(3):208-216.
131. Jureidini JN, Tonkin A. Suicide and antidepressants in children. Australian Prescriber 2005;28(5):110-111.
132. King R, Nurcombe B, Bickman L, Hides L, Reid W. Telephone counselling for adolescent suicide prevention: Changes in suicidality and mental state from beginning to end of a counselling session. Suicide and Life-Threatening Behavior 2003;33(4):400-411.
133. Kisley SR, Lawrence D, Preston NJ. The effect of recalling paracetamol on hospital admissions for poisoning in Western Australia. Medical Journal of Australia 2003;178(2):72-74.
134. Kissane M, McLaren S. Sense of belonging as a predictor of reasons for living in older adults. Death Studies 2006;30(3):243-258.
135. Klinger J. Suicide among seniors. Australasian Journal on Ageing 1999;18(3):114-118.
136. Komiti A, Judd F, Grech P, Mijch A, Hoy J, Lloyd JH, et al. Suicidal behaviour in people with HIV/AIDS: a review. Australian and New Zealand Journal of Psychiatry 2001;35(6):747-757.
137. Kosky RJ, Dundas P. Death by hanging: Implications for prevention of an important method of youth suicide. Australian and New Zealand Journal of Psychiatry 2000;34(5):836-841.
138. Kosky R. Perspectives in suicidology: Families, mental illness, and suicide. Suicide and Life-Threatening Behavior 2000;30(1):1-7.
139. Krysinska K, Heller TS, De Leo D. Suicide and deliberate self-harm in personality disorders. Current Opinion in Psychiatry 2006;19(1):95-101.
140. Kuipers P, Lancaster A. Developing a suicide prevention strategy based on the perspectives of people with brain injuries. Journal of Head Trauma Rehabilitation 2000;15(6):1275-1284.
141. Lambert G, Reid C, Kaye D, Jennings G, Esler M. Increased suicide rate in the middle-aged and its association with hours of sunlight. American Journal of Psychiatry 2003;160(4):793-795.
142. Lawrence DM, Holman CDJ. Suicide rates in psychiatric in-patients: An application of record linkage to mental health research. Australian and New Zealand Journal of Public Health 1999;23(5):468-470.
143. Lawrence D, Almeida OP, Hulse GK, Jablensky AV, Holman CDJ. Suicide and attempted suicide among older adults in Western Australia. Psychological Medicine 2000;30(4):813-821.
144. Lawrence D, D'Arcy C, Holman J, Jablensky AV, Fuller SA, Stoney AJ. Increasing rates of suicide in Western Australian psychiatric patients: A record linkage study. Acta Psychiatrica Scandinavica 2001;104(6):443-451.
145. Lorensini S, Bates G. Relationship difficulties and unemployment in attempted suicide in an Australian regional center. Psychological Reports 2002;90(3):923-929.
146. Lynskey M, Degenhardt L, Hall W. Cohort trends in youth suicide in Australia 1964-1997. Australian and New Zealand Journal of Psychiatry 2000;34(3):408-412.
147. Maccallum F, Blaszczynski A. Pathological gambling and suicidality: An analysis of severity and lethality. Suicide and Life-Threatening Behavior 2003;33(1):88-98.

64
148. Magin P, Pond D, Smith W. Isotretinoin, depression and suicide: A review of the evidence. British Journal of General Practice 2005;55(511):134-138.
149. Magin P, Adams J, Heading G, Pond D, Smith W. Patients' perceptions of isotretinoin, depression and suicide: a qualitative study. Aust Fam Physician 2005;34(9):795-797.
150. Maine S, Shute R, Martin G. Educating parents about youth suicide: Knowledge, response to suicidal statements, attitudes, and intention to help. Suicide and Life-Threatening Behavior 2001;31(3):320-332.
151. Maple M. Parental bereavement and youth suicide: An assessment of the literature. Australian Social Work 2005;58(2):179-187.
152. Martin G, Bergen HA, Richardson AS, Roeger L, Allison S. Sexual abuse and suicidality: Gender differences in a large community sample of adolescents. Child Abuse and Neglect 2004;28(5):491-503.
153. Martin G, Richardson AS, Bergen HA, Roeger L, Allison S. Perceived academic performance, self-esteem and locus of control as indicators of need for assessment of adolescent suicide risk: Implications for teachers. Journal of Adolescence 2005;28(1):75-87.
154. Mathy RM. Suicidality and sexual orientation in five continents: Asia, Australia, Europe, North America and South America. International Journal of Sexuality and Gender Studies 2002;7(2-3):215-225.
155. Mayer P. Development, gender equality, and suicide rates. Psychological Reports 2000;87(2):367-372.
156. McAlister M. Multiple meanings of self harm: A critical review. International Journal of Mental Health Nursing 2003;12(3):177-185.
157. McAlister M. Self-harm in the emergency setting: Understanding and responding. Contemporary Nurse 2003;15(1-2):130-139.
158. McAllister M, Creedy D, Moyle W, Farrugia C. Nurses' attitudes towards clients who self-harm. Journal of Advanced Nursing 2002;40(5):578-586.
159. McAllister M, Creedy D, Moyle W, Farrugia C. Study of Queensland emergency department nurses' actions and formal and informal procedures for clients who self harm. International Journal of Nursing Practice 2002;8(4):184-190.
160. McKenzie K. Youth suicide: What can we do? LAMP 1999;56(5):12-17. 161. McLaren S, Hopes LM. Rural-urban differences in reasons for living. Australian
and New Zealand Journal of Psychiatry 2002;36(5):688-692. 162. Mitchell P. A content analysis: First national stocktake of youth suicide prevention
activities. Youth Suicide Prevention Bulletin 1999;2:2-7. 163. Mitchell P. Primary prevention of youth suicide in Australia: First national
stocktake of youth suicide prevention activities. Youth Suicide Prevention Bulletin 1999;2:12-19.
164. Mitchell P. Community development approaches to preventing youth suicide: First national stocktake of youth suicide prevention activities. Youth Suicide Prevention Bulletin 1999;3:2-13.
165. Mitchell P. Talk, be loud and be heard. Youth Suicide Prevention Bulletin 1999;3:32-35.
166. Mitchell P. Yarrabah: A success story in community empowerment. Youth Suicide Prevention Bulletin 2000;4:16-23.
167. Mitchell P. Valuing young lives: The National Youth Suicide Prevention Strategy and its evaluation. Family Matters 2000;57:54-61.
168. Morrell S, Taylor R, Slaytor E, Ford P. Urban and rural suicide differentials in migrants and the Australian-born, New South Wales, Australia 1985-1994. Social Science and Medicine 1999;49(1):81-91.
169. Morrell S, Page A, Taylor R. Birth cohort effects in New South Wales suicide, 1865-1998. Acta Psychiatrica Scandinavica 2002;106(5):365-372.
170. Mullen PE. The autogenic (self-generated) massacre. Behavioral Sciences and the Law 2004;22(3):311-323.
65
171. Nicholls N, Butler CD, Hanigan I. Inter-annual rainfall variations and suicide in New South Wales, Australia, 1964-2001. International Journal of Biometeorology 2006;50(3):139-143.
172. Nirui M, Chenoweth L. The response of healthcare services to people at risk of suicide: A qualitative study. Australian and New Zealand Journal of Psychiatry 1999;33(3):361-371.
173. Page A, Morrell S, Taylor R. Suicide and political regime in New South Wales and Australia during the 20th century. Journal of Epidemiology and Community Health 2002;56(10):766-772.
174. Page AN, Fragar LJ. Suicide in Australian farming, 1988-1997. Australian and New Zealand Journal of Psychiatry 2002;36(1):81-85.
175. Page A, Morrell S, Taylor R. Suicide differentials in Australian males and females by various measures of socio-economic status, 1994-98. Australian and New Zealand Journal of Public Health 2002;26(4):318-324.
176. Parker R, Ben-Tovim DI. A study of factors affecting suicide in Aboriginal and 'other' populations in the Top End of the Northern Territory through an audit of coronial records. Australian and New Zealand Journal of Psychiatry 2002;36(3):404-410.
177. Parker G, Malhi G, Mitchell P, Kotze B, Wilhelm K, Parker K. Self-harming in depressed patients: Pattern analysis. Australian and New Zealand Journal of Psychiatry 2005;39(10):899-906.
178. Patterson I, Pegg S. Nothing to do: The relationship between 'leisure boredom' and alcohol and drug addiction: Is there a link to youth suicide in rural Australia? Youth Studies Australia 1999;18(2):24-28.
179. Pearce K, Rickwood D, Beaton S. Preliminary evaluation of a university-based suicide intervention project: Impact on participants. Australian e-Journal for the Advancement of Mental Health 2003;2(1):11p.
180. Penrose-Wall J. Can you put a price tag on fostering an evaluation culture in mental health and youth health services? Youth Suicide Prevention Bulletin 1999;3:14-17.
181. Pfaff JJ, Acres J, Wilson M. The role of general practitioners in parasuicide: A Western Australia perspective. Archives of Suicide Research 1999;5(3):207-214.
182. Pfaff JJ, Acres JG, McKelvey RS. Training general practitioners to recognise and respond to psychological distress and suicidal ideation in young people. Medical Journal of Australia 2001;174(5):222-226.
183. Pfaff JJ, Almeida OP. Identifying suicidal ideation among older adults in a general practice setting. Journal of Affective Disorders 2004;83(1):73-77.
184. Pfaff JJ, Almeida OP. Detecting suicidal ideation in older patients: Identifying risk factors within the general practice setting. British Journal of General Practice 2005;55(513):269-273.
185. Pirkis J, Burgess P, Jolley D. Suicide attempts by psychiatric patients in acute inpatient, long-stay inpatient and community care. Social Psychiatry and Psychiatric Epidemiology 1999;34(12):634-644.
186. Pirkis J, Burgess P, Dunt D. Suicidal ideation and suicide attempts among Australian adults. Crisis 2000;21(1):16-25.
187. Pirkis JE, Burgess PM, Meadows GN, Dunt DR. Suicidal ideation and suicide attempts as predictors of mental health service use. Medical Journal of Australia 2001;175(10):542-545.
188. Pirkis J, Burgess P, Meadows G, Dunt D. Self-reported needs for care among persons who have suicidal ideation or who have attempted suicide. Psychiatric Services 2001;52(3):381-383.
189. Pirkis J, Francis C, Blood RW, Burgess P, Morley B, Stewart A, et al. Reporting of suicide in the Australian media. Australian and New Zealand Journal of Psychiatry 2002;36(2):190-197.
190. Pirkis J, Burgess P, Jolley D. Suicide among psychiatric patients: A case-control study. Australian and New Zealand Journal of Psychiatry 2002;36(1):86-91.

66
191. Pirkis JE, Irwin CE, Brindis CD, Sawyer MG, Friestad C, Biehl M, et al. Receipt of psychological or emotional counseling by suicidal adolescents. Pediatrics 2003;111(4).
192. Pirkis JE, Burgess PM, Francis C, Blood RW, Jolley DJ. The relationship between media reporting of suicide and actual suicide in Australia. Social Science and Medicine 2006;62(11):2874-2886.
193. Plunkett A, O'Toole B, Swanston H, Oates RK, Shrimpton S, Parkinson P. Suicide risk following child sexual abuse. Ambulatory Pediatrics 2001;1(5):262-266.
194. Power PJR, Bell RJ, Mills R, Herrman-Doig T, Davern M, Henry L, et al. Suicide prevention in first episode psychosis: The development of a randomised controlled trial of cognitive therapy for acutely suicidal patients with early psychosis. Australian and New Zealand Journal of Psychiatry 2003;37(4):414-420.
195. Pritchard C, Baldwin DS. Elderly suicide rates in Asian and English-speaking countries. Acta Psychiatrica Scandinavica 2002;105(4):271-275.
196. Procter NG. Mental health promotion and suicide prevention for people released from immigration. Synergy 2003;1:17.
197. Procter NG. Parasuicide, self-harm and suicide in Aboriginal people in rural Australia: A review of the literature with implications for mental health nursing practice. International Journal of Nursing Practice 2005;11(5):237-241.
198. Proctor NG. Emergency mental health nursing for self-harming refugees and asylum seekers. International Journal of Mental Health Nursing 2005;14(3):196-201.
199. Pullen L, Gow K. University students elaborate on what young persons 'at risk of suicide' need from listeners. Journal of Applied Health Behaviour 2000;2(1):32-39.
200. Putnins AL. Correlates and predictors of self-reported suicide attempts among incarcerated youths. International Journal of Offender Therapy and Comparative Criminology 2005;49(2):143-157.
201. Radford AJ, Brice GA, Harris R, Van der Byl M, Monten H, McNeece-Neeson M, et al. The 'Easy Street' Myth: Self harm among Aboriginal and non-Aboriginal female sole parents in urban state housing. Australian and New Zealand Journal of Public Health 1999;23(1):77-85.
202. Ranson D. Suicide and the media. Journal of Law and Medicine 2001;9(1):18-19. 203. Rigby K, Slee P. Suicidal ideation among adolescent school children,
involvement in bully-victim problems, and perceived social support. Suicide and Life-Threatening Behavior 1999;29(2):119-130.
204. Robson A, Silburn SR. Building healthy lives: Partnerships to promote Aboriginal child health and wellbeing and family and community resilience. Auseinetter 2002(15):4-6.
205. Rock D, Greenberg DM, Hallmayer JF. Increasing seasonality of suicide in Australia 1970-1999. Psychiatry Research 2003;120(1):43-51.
206. Rock DJ, Greenberg DM, Hallmayer JF. Impact of case fatality on the seasonality of suicidal behaviour. Psychiatry Research 2005;137(1-2):21-27.
207. Rock D, Greenberg D, Hallmayer J. Season-of-birth as a risk factor for the seasonality of suicidal behaviour. European Archives of Psychiatry and Clinical Neuroscience 2006;256(2):98-105.
208. Routley V, Ashby K, Lough J. Adult poisoning overview: Victoria. Hazard 1999;39:1-17.
209. Rowling L, Holland J. Grief and school communities: The impact of social context, a comparison between Australia and England. Death Studies 2000;24(1):35-50.
210. Royal Australian and New Zealand College of Psychiatrists. Australian and New Zealand clinical practice guidelines for the management of adult deliberate self-harm. Australian and New Zealand Journal of Psychiatry 2004;38(11-12):868-884.

67
211. Royal Australian and New Zealand College of Psychiatrists. Summary Australian and New Zealand clinical practice guidelines for the management of adult deliberate self-harm. Australasian Psychiatry 2003;11(2):150-155.
212. Russell D, Judd F. Why are men killing themselves? A look at the evidence. Australian Family Physician 1999;28(8):791-795.
213. Ruzicka LT, Choi CY, Sadkowsky K. Medical disorders of suicides in Australia: Analysis using a multiple-cause-of-death approach. Social Science and Medicine 2005;61(2):333-341.
214. Rycroft P. Touching the heart and soul of therapy: Surviving client suicide. Women and Therapy 2005;28(1):83-94.
215. Salter A, Pielage P. Emergency departments have a role to play in the prevention of suicide. Emergency Med 2000;12(3):198-203.
216. Sawyer M, Whaites L. Addressing suicidal behaviour in adolescents. Current Therapeutics 2002;43(3):21-24.
217. Schweitzer RD, McLean J, Cvetkovich L, Rose D. Methods and consequences of suicide attempts among Australian students. Australian and New Zealand Journal of Psychiatry 2000;34(1):17-172.
218. Scocco P, Meneghel G, Caon F, Dello Buono M, De Leo D. Death ideation and its correlates: Survey of an over-65-year-old population. Journal of Nervous and Mental Disease 2001;189(4):210-218.
219. Scouller KM, Smith DI. Prevention of youth suicide: How well informed are the potential gatekeepers of adolescents in distress? Suicide and Life-Threatening Behavior 2002;32(1):67-79.
220. Serafino S, Somerford P, Codde JP. Hospitalisation as a consequence of deliberate self-harm in Western Australia, 1981-1998. Epidemiology Occasional Papers 2000;11:1-100.
221. Silburn SR. Frameworks for conceptualising youth suicide prevention. Youth Suicide Prevention Bulletin 1999;2:21-24.
222. Simpson G, Tate R. Suicidality after traumatic brain injury: Demographic, injury and clinical correlates. Psychological Medicine 2002;32(4):687-697.
223. Simpson G, Winstanley J, Bertapelle T. Suicide prevention training after traumatic brain injury: Evaluation of a staff training workshop. Journal of Head Trauma Rehabilitation 2003;18(5):445-456.
224. Simpson G, Tate R. Clinical features of suicide attempts after traumatic brain injury. Journal of Nervous and Mental Disease 2005;193(10):680-685.
225. Singh B, Jenkins R. Suicide prevention strategies: An international perspective. International Review of Psychiatry 2000;12(1):7-14.
226. Slaven J, Kisely S. The Esperance primary prevention of suicide project. Australian and New Zealand Journal of Psychiatry 2002;36(5):617-621.
227. Slaven J, Kisely S. Staff perceptions of care for deliberate self-harm patients in rural Western Australia: A qualitative study. Australian Journal of Rural Health 2002;20(5):233-238.
228. Smith DI, Scoullar KM. How well informed are Australian general practitioners about adolescent suicide? Implications for primary prevention. International Journal of Psychiatry in Medicine 2001;31(2):169-182.
229. Smith D, Fisher LJ, Goldney R. Do suicidal ideation and behaviour influence duration of psychiatric hospitalization. International Journal of Mental Health Nursing 2002;11(4):220-224.
230. Snowdon J, Baume P. A study of suicides of older people in Sydney. International Journal of Geriatric Psychiatry 2002;17(3):261-269.
231. Sparke C. Suicide in young men. Australian Doctor 1999;24:31-32. 232. Starling J, Rey JM, Simpson JM. Depressive symptoms and suicidal behaviour:
Changes with time in an adolescent clinic cohort. Australian and New Zealand Journal of Psychiatry 2004;38(9):732-737.
233. Steel Z, McDonald B. Suicide in immigrants born in non-English speaking countries: The latest research. Synergy 2000;15:38-41.
68
234. Stevens A. Paracetamol recall: A natural experiment influencing analgesic poisoning. Medical Journal of Australia 2002;176(11):562: author reply 562-563.
235. Swanston SP, Roberts LJ, Chapman MD. Are anaesthetists prone to suicide? A review of rates and risk factors. Anaesthetic Intensive Care 2003;31(4):434-445.
236. Taylor R, Page A, Morrell S, Carter G, Harrison J. Socio-economic differentials in mental disorders and suicide attempts in Australia. British Journal of Psychiatry 2004;185:486-493.
237. Taylor R, Page A, Morrell S, Harrison J, Carter G. Mental health and socio-economic variations in Australian suicide. Social Science and Medicine 2005;61(7):1551-1559.
238. Taylor R, Page A, Morrell S, Harrison J, Carter G. Social and psychiatric influences on urban-rural differentials in Australian suicide. Suicide and Life-Threatening Behavior 2005;35(3):277-290.
239. Taz C. Aboriginal, Maori and Inuit youth suicide: Avenues to alleviation? Australian Aboriginal Studies 2004;2:15-25.
240. Teasdale TW. 17% of people with traumatic brain injury attempted suicide. Evidence-Based Mental Health 2003;6(1):11.
241. Thacore VR, Varma SL. A study of suicides in Ballarat, Victoria, Australia. Crisis 2000;21(1):26-30.
242. Ticehurst S, Carter GL, Clover KA, Whyte IM, Raymond J, Fryer J. Elderly patients with deliberate self-poisoning treated in an Australian general hospital. International Psychogeriatrics 2002;14(1):97-105.
243. To TP, Tierney JP, Hopwood MJ. Serotonergic and dopaminergic agents facilitate rehabilitation following hypoxic brain injury. Australian Journal of Hospital Pharmacy 2000;30(5):202-205.
244. Tobin M, Clarke AR, Buss R, Einfeld SL, Beard J, Dudley M, et al. From efficacy to effectiveness: Managing organisation change to improve health services for young people with deliberate self harm behaviour. Australian Health Review 2001;24(2):143-151.
245. Toumbourou JW, Gregg ME. Impact of an empowerment-based parent education program on the reduction of youth suicide risk factors. Journal of Adolescent Health 2002;31(3):277-285.
246. Trimble L, Jackson K, Harvey D. Client suicidal behaviour: Impact, interventions, and implications for psychologists. Australian Psychologist 2000;35(3):227-232.
247. Tucker P. Substance abuse and suicidality. Australasian Psychiatry 1999;7(1):23-24.
248. Vajda J, Steinbeck K. Factors associated with repeat suicide attempts among adolescents. Australian and New Zealand Journal of Psychiatry 2000;34(3):437-445.
249. Vanderhorst RK, McLaren S. Social relationships as predictors of depression and suicidal ideation in older adults. Aging and Mental Health 2005;9(6):517-525.
250. Venamore J. Q and A: Suicide of a colleague. LAMP 1999;56(5):23. 251. Verberne TJP. A developmental model of vulnerability to suicide: Consistency
with some recurrent findings. Psychological Reports 2001;89(2):217-226. 252. Vivekananda K. Integrating models for understanding self injury. Psychotherapy
Australia 2000;7(1):18-25. 253. Wallace KL, Pegg S. Self-inflicted burn injuries: An 11-year retrospective study.
Journal of Burn Care and Rehabilitation 1999;20(2):191-194. 254. Wand T. Duty of care in the emergency department. International Journal of
Mental Health Nursing 2004;132(2):135-139. 255. Wastell CA, Shaw TA. Trainee teachers' opinions about suicide. British Journal of
Guidance and Counselling 1999;27(4):555-565. 256. Webb D. Bridging the spirituality gap. Australian e-Journal for the Advancement
of Mental Health 2005;4(1):90. 257. West B. Crime, suicide, and the anti-hero: 'Waltzing Matilda' in Australia (Popular
song). Journal of Popular Culture 2001;35(3):127-141.

69
258. Wilhelm K, Schnieden V, Kotze B. Selecting your options: A pilot study of short interventions with patients who deliberately self harm. Australasian Psychiatry 2000;8(4):349-354.
259. Wilkins R. Elderly suicide: An overview. Australasian Journal of Emergency Care 2000;7(3):26-32.
260. Wilkinson D, Gunnell D. Youth suicide trends in Australian metropolitan and non-metropolitan areas, 1988-1997. Australian and New Zealand Journal of Psychiatry 2000;34(5):822-828.
261. Wilkinson D, Gunnell D. Comparison of trends in method-specific suicide rates in Australia and England and Wales, 1968-97. Australian and New Zealand Journal of Public Health 2000;24(2):153-157.
262. Wright S, Martin G. Suicide prevention training: A workshop. Youth Studies Australia 2000;19(2):39-42.
263. Zickler P. Twin study links marijuana abuse, suicide, and depression. NIDA Notes 2005;20(2):12.
70
Appendix B: List of funded grants
National Health and Medical Research Council 1. Almeida OP. Reducing depression and suicide amongst older Australians: A
clustered randomised clinical trial in primary health care, 2005. 2. Chanen AM. Indicated prevention of borderline personality disorder in young
people, 1999. 3. Deane F. Help seeking and the responses of young men to intervention services,
2001. 4. De Leo D. Suicide ideation, attempts, help-seeking behaviour and compliance
within the Gold Coast District, 2002. 5. Einfeld SL. Evidence based practice for young people who self harm: Can it be
sustained and does it improve outcome? A 2-year follow-up, 2001. 6. Goldney RD. Possible role of the Wolfram syndrome gene in suicide, 2001. 7. Meares RA. Borderline personality disorder: A randomised controlled trial to
evaluate patient outcome after psychodynamic intervention, 2003. 8. Patton G. Population based prevention of adolescent depression and suicidal
behaviour: A randomised controlled trial, 1999. 9. Patton G. Scoping study for an Australian longitudinal, prospective adolescent
cohort study, 2001. 10. Pettigrew JD. Neural rhythms and bipolar disorder, 2001. 11. Pirkis J. Preventing suicidal behaviours: Ecological studies of systemic protective
factors, 2004. 12. Roberts CM. Prevention of anxiety and depression in children: Development and
evaluation of a universal life skills program, 2000. 13. Sheffield JK. Increasing resilience and reducing risk for depression in
adolescents: Universal controlled trial, 2001. 14. Shochet I. Reducing risk and increasing protection for adolescent depression and
suicide: A large scale RCT of RAP, 2001. 15. Simpson GK. A clinical trial of the effectiveness of a psychological treatment in
reducing hopelessness and suicide ideation after trauma, 2006. 16. Sitharthan T. A controlled trial of opportunistic intervention to reduce suicide risk
among alcohol and other substance misusers, 2003. 17. Taylor R. Case-control studies of completed and attempted suicide in young
people in New South Wales, 2004. 18. Taylor R. National trends in suicide by age, gender, geography, socio-economic
and migrant status, and mental health, 2000. 19. Tobin, M. Evidence based practice for young people who self harm: Can it be
sustained and does it improve outcomes? 1999. 20. Viet FCM. Mortality in young offenders who have had custodial sentences, 2000.
Australian Rotary Health Research Fund 1. Dadds M. A randomized controlled trial of a family intervention program for young
people with suicidal behaviour, 2006. 2. Jorm A. Development of mental health first aid standards, 2005. 3. Pirkis J. The impact of media reporting of suicide on actual suicidal behaviour,
2003. 4. Yung A. Suicide prevention amongst help-seeking adolescents: An intervention
study, 2006.
71
Australian Research Council 1. Blood RW. Communicating risk: Journalistic news values, and medical, health
professional and lay discourses on suicide and mental illness, 2003. 2. De Leo D. An investigation into suicidal behaviours by males during the process
of marital and de facto separation, 2005. 3. De Leo D. Preventing suicide: A psychological autopsy study of the last contact
with a health professional before suicide, 2005. 4. Homel RJ. The contribution of youth development programs in preventing youth
crime, drug and alcohol misuse, and suicide, 2005. 5. Investigator(s) not listed. Understanding serious self-harm and risk-taking
behaviour: A study of attempted suicide in Western Sydney, 1999. 6. Investigator(s) not listed. Identity, sexuality and youth suicide: A socio-cultural
analysis of urban and regional communities, 2000. 7. Investigator(s) not listed. The political economy of violent death in India, 2000. 8. Investigator(s) not listed. The effectiveness of student welfare professional
development as a strategy for whole school student welfare, health promotion and suicide prevention, 2000.
9. Investigator(s) not listed. A school, family and rural community partnership to reduce suicide risk in same sex attracted young people, 2000.
10. Jalland P. The social and cultural history of death and bereavement in Australia and England, 1914-1980, 2003.
11. Joubert LB. Suicide prevention and management of deliberate self-harm: Randomised controlled trial of an assertive engagement, brief psychotherapy and community linkage model, 2006.
12. Simpson LE. The development and evaluation of an online support system for mental health workers in rural, remote and regional areas, 2002.

72
Appendix C: Questionnaire
73
National Survey of Suicide Prevention Research Priorities Australia has limited resources to put into suicide prevention research. Although it would be good if all types of research could be fully supported, in practice some priorities must be set. The purpose of this questionnaire is to find out what you think are the most important priorities. In a number of questions, you are asked to rate the priority which should be given to various areas of research as VERY LOW, LOW, MEDIUM, HIGH or VERY HIGH. When making these ratings, please use the full range if possible. It will not help in setting priorities if you give the same rating to all areas. In making your ratings, please remember that you are rating priorities for Australian suicide prevention research, rather than priorities for suicide prevention research worldwide.
1a. Rate the following suicidal behaviours and thoughts in terms of how high a priority they should be for Australian suicide prevention research [Tick one response per row]
Very low Low Medium High Very high
Completed suicide
Attempted suicide or deliberate self harm
Suicidal thoughts
Other suicidal behaviours (please specify) ______________________________________________________
1b. Of the above suicidal behaviours and thoughts, which do you think should be given the highest priority? [Tick one response only]
Completed suicide
Attempted suicide or deliberate self harm
Suicidal thoughts
Other suicidal behaviours (as specified in Q1a)
74
2a. Rate the following target groups in terms of how high a priority they should be for Australian suicide prevention research [Tick one response per row]
Very low Low Medium High Very high
Young people (aged 24 or less)
Adults (aged 25-64)
Older people (aged 65 or more)
Indigenous people
People from culturally and linguistically diverse backgrounds
People in rural and remote areas
People bereaved by suicide
People who are gay, lesbian, bisexual or transgender
People with mental health problems
People with physical health problems
People with substance use problems
People who have attempted suicide or deliberately self-harmed
Offenders
Men
Women
Veterans
Other target group (please specify) _____________________________________________________
75
2b. Of the above target groups, which do you think should be given the highest priority? [Tick one response only]
Young people (aged 24 or less)
Adults (aged 25-64)
Older people (aged 65 or more)
Indigenous people
People from culturally and linguistically diverse backgrounds
People in rural and remote areas
People bereaved by suicide
People who are gay, lesbian, bisexual or transgender
People with mental health problems
People with physical health problems
People with substance use problems
People who have attempted suicide or deliberately self-harmed
Offenders
Men
Women
Veterans
Other target group (as specified in Q2a)

76
3a. Suicide prevention activities can be carried out in various settings. Rate the following settings in terms of how high a priority they should be for suicide prevention research [Tick one response per row]
Very low Low Medium High Very high
Communities
Schools
Tertiary institutions
Prisons
Workplaces
Primary care settings (e.g., general practice)
Emergency departments
Mental health service settings
Other health service settings
Other settings (please specify) _____________________________________________________
3b. Of the above settings, which do you think should be given the highest priority? [Tick one response only]
Communities
Schools
Tertiary institutions
Prisons
Workplaces
Primary care settings (e.g., general practice)
Emergency departments
Mental health service settings
Other health service settings
Other settings (as specified in Q3a)
77
4a. Rate the following methods of suicide in terms of how high a priority they should be for suicide prevention research [Tick one response per row]
Very low Low Medium High Very high
Poisoning by drugs
Poisoning by other (includes poisoning by other gases and vapours, such as motor vehicle exhaust)
Hanging (includes strangulation and suffocation)
Firearms (includes explosives)
Drowning
Jumping from a high place
Jumping or lying before a moving object
Other method (please specify) ______________________________________________________
4b. Of the above methods of suicide, which do you think should be given the highest priority? [Tick one response only]
Poisoning by drugs
Poisoning by other (includes poisoning by other gases and vapours, such as motor vehicle exhaust)
Hanging (includes strangulation and suffocation)
Firearms (includes explosives)
Drowning
Jumping from a high place
Jumping or lying before a moving object
Other method (as specified in Q4a)
78
5a. Rate the following types of studies in terms of how high a priority they should be for Australian suicide prevention research [Tick one response per row]
Very low Low Medium High Very high
Studies about assessment or classification of suicide risk (including studies of the development or validation of risk assessment tools)
Studies of rates of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of risk factors for completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of protective factors for completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies considering general intervention issues and approaches in suicide prevention
Studies of practice guidelines
Studies of the efficacy of universal interventions (i.e., interventions targeting whole populations, with the aim of favourably shifting risk and protective factors across the whole population)
Studies of the efficacy of selective interventions (i.e., interventions targeting population subgroups with particular risk factors for suicide who are not yet exhibiting suicidal thoughts or behaviours)
Studies of the efficacy of indicated interventions (i.e., interventions designed for people who are already beginning to exhibit suicidal thoughts or behaviours)
Evaluations of suicide prevention policies
Evaluations of suicide prevention programs
Evaluations of services (e.g., health and/or community services)
Neurobiological studies, including studies of brain anatomy and physiology and their relationship to completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Genetic studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Sociological studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of the history of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts in literature or the arts
Studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts in the media
Other studies on completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts (please specify) ______________________________________________________

79
5b. Of the above types of studies, which do you think should be given the highest priority? [Tick one response only]
Studies about assessment or classification of suicide risk (including studies of the development or validation of risk assessment tools)
Studies of rates of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of risk factors for completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of protective factors for completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies considering general intervention issues and approaches in suicide prevention
Studies of practice guidelines
Studies of the efficacy of universal interventions (i.e., interventions targeting whole populations, with the aim of favourably shifting risk and protective factors across the whole population)
Studies of the efficacy of selective interventions (i.e., interventions targeting population subgroups with particular risk factors for suicide who are not yet exhibiting suicidal thoughts or behaviours)
Studies of the efficacy of indicated interventions (i.e., interventions designed for people who are already beginning to exhibit suicidal thoughts or behaviours)
Evaluations of suicide prevention policies
Evaluations of suicide prevention programs
Evaluations of services (e.g., health and/or community services)
Neurobiological studies, including studies of brain anatomy and physiology and their relationship to completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Genetic studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Sociological studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of the history of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts
Studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts in literature or the arts
Studies of completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts in the media
Other studies on completed suicide, attempted suicide or deliberate self harm, and/or suicidal thoughts (as specified in Q5a)

80
Finally, here are a few questions about yourself 6. What is your age? [Tick one response only]
Under 20
20-29
30-39
40-49
50-59
60-69
70 or over
7. What is your gender? [Tick one response only]
Male
Female
8. Which of the following statements describe your interest in suicide prevention research? [Tick all that apply]
I conduct suicide prevention research
I use suicide prevention research (e.g., in clinical work or in policy-making/planning)
I have been involved in decision-making regarding funding of suicide prevention research
I have been affected by suicide
Other (please specify) _______________________________________________________

81
9. People were invited to complete this survey because of their affiliation with various groups. Which of the following statements describe the group(s) you belong to? [Tick all that apply]
I am a psychiatrist
I am a general practitioner
I am a psychologist
I am a mental health nurse
I am a suicide prevention researcher
I am a member of the National Advisory Council on Suicide Prevention (NACSP)
I am a member of the Mental Health Standing Committee (MHSC)
I am an officer responsible for state/territory co-ordination under the Living is For Everyone (LIFE) Framework
I am a member of Suicide Prevention Australia (SPA)
I am a member of the Australian Mental Health Consumer Network (AMHCN)
I am or was a member of the National Health and Medical Research Council’s (NHMRC) Public Health Grant Review Panel and Psychiatry/Psychology Grant Review Panel, or the Panel responsible for projects funded under the Suicide Initiative
I am or was a member of the Australian Rotary Health Research Fund’s (ARHRF) Research Committee
10. Any additional comments?
THANK YOU FOR TAKING THE TIME TO COMPLETE THIS QUESTIONNAIRE. We do not anticipate that anyone completing the questionnaire should have experienced any adverse effects. However, if you are experiencing stress, anxiety or depression as a result of issues raised by the questionnaire, you may wish to contact Lifeline on 13 11 14. Alternatively, you can contact Dr Michael Dudley from Suicide Prevention Australia on (02) 9382 4347 or Professor Diego De Leo from the Australian Institute for Suicide Research and Prevention on (07) 3735 3382. Dr Dudley and Professor De Leo are both members of the study team, and are both qualified psychiatrists with considerable clinical experience.




















