How transformation in the management of hematologic cancer ...
57
How transformation in the management of hematologic cancer will impact the invasive fungal disease ecosystem Dimitrios P. Kontoyiannis MD, ScD, PhD (Hon), FACP, FIDSA, FAAM, FECMM, FAAAS Texas 4000 Distinguished Endowed Professor Deputy Head-Research, Division of Internal Medicine 29° ECCMID 21-24 April 2018 Madrid, Spain ESCMID eLibrary © by author
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of How transformation in the management of hematologic cancer ...

How transformation in the management of hematologic cancer will impact the invasive fungal disease ecosystem
Dimitrios P. Kontoyiannis MD, ScD, PhD (Hon), FACP, FIDSA, FAAM, FECMM, FAAAS
Texas 4000 Distinguished Endowed ProfessorDeputy Head-Research, Division of Internal Medicine
29° ECCMID 21-24 April 2018Madrid, Spain
ESCMID eLibrary
©
by author

Disclosures
Research support and/or honoraria* from:
Merck, Inc
Astellas, Inc
Cidara, Inc
Amplyx, Inc
Last 12 months ESCMID eLibrary
©
by author

Major events in the supportive care of patients with hematological cancer pertaining to mycology
1960’s 1970s 1980’s 2000 2018
Platelet transfusionsDecreased death from bleeding
Autopsy studies(NCI) showing IFIs as a cause of death
Recognition of neutropenia and infection risk
Invasive candidiasis major threat(wave 1)
Decades of newantifungal agents(broad-spectrum triazoles,echinocandins)
Introduction of fluconazole advances in allogeneic HSCT, GvHD, CMV as IFI risk factors
Anti-StaphpenicillinsReduced mortality from S. aureus
Empirical therapy for Gram negative rods->Decreased mortality in neutropenic patients
1990’s
Azole-resistant Candida and invasive aspergillosis(wave 2)
2010
Complex epidemiology, antifungal resistant yeast and molds(wave 3)
Era of targeted therapies for hematological malignancies, immunotherapy improvements in allogeneic HSCT and availability
?
Major events in supportive care of patients with hematologic cancer-pertaining to mycology
ESCMID eLibrary
©
by author

Annual number of HSCTs in USA by transplant type
Reduction of transplant-relatedmorbidity and mortality (reduced-Intensity conditioning, PBSC)
Improved control of CMV
Expanded donor pools(Haplo-HSCT)
GVHD biomarkers? Targeted immunosuppression
Targeted therapies forGVHD, graft vs- tumor effect
Microbiome?Source: CIBMTR
Improved control of CMV and fungal diseases
Major advances:
ESCMID eLibrary
©
by author

Increasing treatment options for hematologic malignancies
ESCMID eLibrary
©
by author

AMLPrognostic relevance of integrated genomic profiling
an explosion of new drugs
under testing
Patel JP et al. N Engl J Med. 2012;366:1079-1089.
Gene Overall Frequency, %
FLT3 (ITD, TKD) 37 (30, 7)
NPM1 29
DNMT3A 23
NRAS 10
CEBPα 9
TET2 8
WT1 8
IDH2 8
IDH1 7
KIT 6
RUNX1 5
MLL-PTD 5
ASXL1 3
PHF6 3
KRAS 2
PTEN 2
TP53 2
HRAS 0
EZH2 0 ESCMID eLibrary
©
by author

New therapies for AML
…for many populations,
including those at high risk or defined by
molecular abnormalities
Novel cytotoxic agents (CPX-351, vosaroxin)
Emerging/next-generation HMAs
(SGI-110; CC-486; ASTX727)
Targeted therapies
(FLT3i, IDHi, Bcl-2, SINE, HDAC)
Immune checkpoint inhibitors
(Nivolumab, Pembrolizumab)
Novel antibodies
(Gemtuzumab, IMGN 33 and 123,
AMG-330, Xmab-CD33/CD123)
AML with actionable mutations, molecular, or
high-risk features (eg, age)
Combination therapy with HMAs for older patients
ESCMID eLibrary
©
by author

A new era for drug toxicity and interactions of azoles with targeted therapies?
ABL1 CEBPA HRAS MYD88 SF3B1
ASXL1 CSF3R IDH1 NOTCH1 SMC1A
ATRX CUX1 IDH2 NPM1 SMC3
BCOR DNMT3A IKZF1 NRAS SRFS2
BCORL1 ETV6/TEL JAK2 PDGFRA STAG2
BRAF EZH2 JAK3 PHF6 TET2
CALR FBXW7 KDM6A PTEN TP53
CBL FLT3 KIT PTPN11 U2AF1
CBLB GATA1 KRAS RAD21 WT1
CBLC GATA2 MLL RUNX1 ZRSR2
CDKN2A GNAS MPL SETBP1
AG120
AG221
Idasanutinib
Decitabine
Sorafenib
Midstaurin
Quizartinib
ASP2215
Azacitidine
Decitabine
Vemurafenib
Cobimetinib
Cobimetinib
TKI
PONATINIB
Slide: Cristina Papayannidis, M.D.
58% of new therapies in Phase I-III clinical trials have relative or absolute contraindications for triazole prophylaxis of CYP 3A4, QTc prolongation) ESCMID eLibrary
©
by author

Immune-based approaches for AML
ESCMID eLibrary
©
by author

CAR-T cell treatments for AML and ALL
Ideal antigen: CD33, CD123, TIM3, CLEC12… others?
Off target activation of macro/monocytes: CRS, prolonged cytopenia
CARTox guidelines (Nature Reviews Clin Oncol 2017)
ESCMID eLibrary
©
by author

How do new therapies affect the risk for fungal disease?
ESCMID eLibrary
©
by author

The Good:
Epigenetic therapy in MDS
Hypo-methylating agents: azacitidine, decitabine
Equivalent to best supportive care and low-dose ARA-C in high-risk disease;superior in low-risk diseaseNature Reviews Clin Oncol 2010 ESCMID eLibrary
©
by author

Do all patients with MDS need antifungal prophylaxis?
Impact of epigenetic therapeutics on the management of AML/MDS
274/948 courses (28%) associated with grade 4 neutropenia (< 0.5x109/L for >10 days)• 12% associated with febrile neutropenic episode• Only 4 invasive fungal infection documented• Incidence: 0.42% per treatment cycle, 3.3% among
patients with grade 4 neutropenia
Fenaux et al. J Clin Oncol 2010;28:562-569.
Pomares H et al. Mycoses 2016; 59: 516–519. ESCMID eLibrary
©
by author

The bad…
Chamilos G, Lionakis MS, Kontoyiannis DP. Clin Infect Dis 2018; 66: 140–148. ESCMID eLibrary
©
by author

Ibrutinib: a “game-changing drug” in B-cell malignancies
(accelerated FDA Approval in 2013)
Byrd et al., J Clin Oncol, 2014, 32:3039-3048
Burger JA et al. N Engl J Med 2015;373:2425-2437
RESONATE-2 (CLL, frontline ibrutinib)
4 year follow up: only 12% of patients
D/C due to AEs (AF, bleeding, infection) ESCMID eLibrary
©
by author

Uncommon opportunistic infections in lymphoma patients treated with ibrutinib
39% IA
5% PCP
ESCMID eLibrary
©
by author
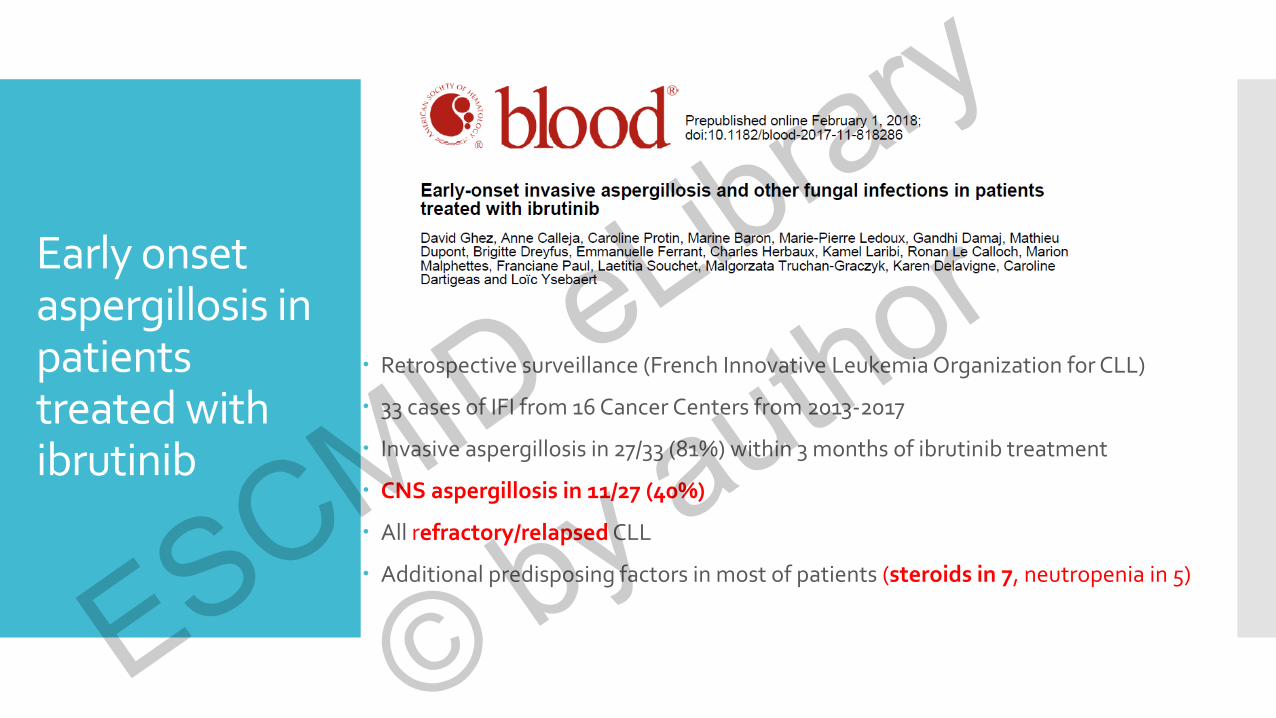
Early onset aspergillosis in patients treated with ibrutinib
Retrospective surveillance (French Innovative Leukemia Organization for CLL)
33 cases of IFI from 16 Cancer Centers from 2013-2017
Invasive aspergillosis in 27/33 (81%) within 3 months of ibrutinib treatment
CNS aspergillosis in 11/27 (40%)
All refractory/relapsed CLL
Additional predisposing factors in most of patients (steroids in 7, neutropenia in 5)
ESCMID eLibrary
©
by author

Increased susceptibility of mice for of IA with pharmacological or genetic ablation of BTK
Increased susceptibility of mice for of IA upon pharmacological of genetic ablation of BTK
Stadler N et al., Haematologica 2017 102:e191-194 Lionakis MS et al., Cancer Cell 2017 31, 833-843 ESCMID eLibrary
©
by author

Is ibrutinib associated with increased risk of cerebral aspergillosis?
Type of IA Time after
treatment
Age/Sex Type of
Cancer
Status of
Malignancy
Concomitant
steroids
Outcome Ref
CNS 1 month N/A CLL PD Yes Dead Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
Lungs 6 wks 62/M CLL PD No Alive Arthus et al.
CNS, lungs 2 wks 76/F PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 2 wks 65/M PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 3 months 87/F PCNSL Active Yes Dead Lionakis et al.
Lungs 4 months 60/M PCNSL Active Yes Alive Lionakis et al.
Lungs 2 months 53/M PCNSL Active Yes Alive Lionakis et al.
Lungs 1 month 64/M PCNSL Active Yes Alive Lionakis et al.
CNS, lungs 2 wks 49/M PCNSL Active Yes Alive Lionakis et al.
Sinusitis, CNS 3 wks 75/F CLL PD No Alive Baron et al.
CNS, lungs 2 months 76/NA CLL PD No Dead Jain et al.
Lungs 7 months 67/M CLL N/A No Dead Kreiniz et al.
Chamilos G et al. Clin Infect Dis. 2018 Jan 6;66(1):140-148
CNS aspergillosis in 9/14 (64%)
ESCMID eLibrary
©
by author

Is ibrutinib associated with increased risk of early aspergillosis?
Type of IA Time after
treatment
Age/Sex Type of
Cancer
Status of
Malignancy
Concomitant
steroids
Outcome Ref
CNS 1 month N/A CLL PD Yes Dead Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
Lungs 6 wks 62/M CLL PD No Alive Arthus et al.
CNS, lungs 2 wks 76/F PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 2 wks 65/M PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 3 months 87/F PCNSL Active Yes Dead Lionakis et al.
Lungs 4 months 60/M PCNSL Active Yes Alive Lionakis et al.
Lungs 2 months 53/M PCNSL Active Yes Alive Lionakis et al.
Lungs 1 month 64/M PCNSL Active Yes Alive Lionakis et al.
CNS, lungs 2 wks 49/M PCNSL Active Yes Alive Lionakis et al.
Sinusitis, CNS 3 wks 75/F CLL PD No Alive Baron et al.
CNS, lungs 2 months 76/NA CLL PD No Dead Jain et al.
Lungs 7 months 67/M CLL N/A No Dead Kreiniz et al.
IA within the first 4
months (> 93%)
Chamilos G et al. Clin Infect Dis. 2018 Jan 6;66(1):140-148 ESCMID eLibrary
©
by author

Does pre-existing brain pathology exacerbate ibrutinib-associated aspergillosis?
Chamilos G et al. Clin Infect Dis. 2018 Jan 6;66(1):140-148
Type of IA Time after
treatment
Age/Sex Type of
Cancer
Status of
Malignancy
Concomitant
steroids
Outcome Ref
CNS 1 month N/A CLL PD Yes Dead Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
Lungs 6 wks 62/M CLL PD No Alive Arthus et al.
CNS, lungs 2 wks 76/F PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 2 wks 65/M PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 3 months 87/F PCNSL Active Yes Dead Lionakis et al.
Lungs 4 months 60/M PCNSL Active Yes Alive Lionakis et al.
Lungs 2 months 53/M PCNSL Active Yes Alive Lionakis et al.
Lungs 1 month 64/M PCNSL Active Yes Alive Lionakis et al.
CNS, lungs 2 wks 49/M PCNSL Active Yes Alive Lionakis et al.
Sinusitis, CNS 3 wks 75/F CLL PD No Alive Baron et al.
CNS, lungs 2 months 76/NA CLL PD No Dead Jain et al.
Lungs 7 months 67/M CLL N/A No Dead Kreiniz et al.
45% of cases of CNS aspergillosis
in pts with brain pathology
ESCMID eLibrary
©
by author

Is ibrutinib the only risk factor?
Type of IA Time after
treatment
Age/Sex Type of
Cancer
Status of
Malignancy
Concomitant
steroids
Outcome Ref
CNS 1 month N/A CLL PD Yes Dead Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
Lungs 6 wks 62/M CLL PD No Alive Arthus et al.
CNS, lungs 2 wks 76/F PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 2 wks 65/M PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 3 months 87/F PCNSL Active Yes Dead Lionakis et al.
Lungs 4 months 60/M PCNSL Active Yes Alive Lionakis et al.
Lungs 2 months 53/M PCNSL Active Yes Alive Lionakis et al.
Lungs 1 month 64/M PCNSL Active Yes Alive Lionakis et al.
CNS, lungs 2 wks 49/M PCNSL Active Yes Alive Lionakis et al.
Sinusitis, CNS 3 wks 75/F CLL PD No Alive Baron et al.
CNS, lungs 2 months 76/NA CLL PD No Dead Jain et al.
Lungs 7 months 67/M CLL N/A No Dead Kreiniz et al.
Refractory of relapsed malignancy
in 100% of patients
ESCMID eLibrary
©
by author

Is ibrutinib the only risk factor?
Type of IA Time after
treatment
Age/Sex Type of
Cancer
Status of
Malignancy
Concomitant
steroids
Outcome Ref
CNS 1 month N/A CLL PD Yes Dead Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
CNS 2 month N/A CLL PD Yes Alive Ruchlemer et al.
Lungs 6 wks 62/M CLL PD No Alive Arthus et al.
CNS, lungs 2 wks 76/F PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 2 wks 65/M PCNSL Active Yes Dead Lionakis et al.
CNS, lungs 3 months 87/F PCNSL Active Yes Dead Lionakis et al.
Lungs 4 months 60/M PCNSL Active Yes Alive Lionakis et al.
Lungs 2 months 53/M PCNSL Active Yes Alive Lionakis et al.
Lungs 1 month 64/M PCNSL Active Yes Alive Lionakis et al.
CNS, lungs 2 wks 49/M PCNSL Active Yes Alive Lionakis et al.
Sinusitis, CNS 3 wks 75/F CLL PD No Alive Baron et al.
CNS, lungs 2 months 76/NA CLL PD No Dead Jain et al.
Lungs 7 months 67/M CLL N/A No Dead Kreiniz et al.
71% of patients also
received corticosteroids
ESCMID eLibrary
©
by author

How will targeted therapies for malignant and autoimmune diseases affect the epidemiology of IFI?
A surge of therapies with SMKIs targeting antifungal immune signaling pathways
BTK inhibitors
PI3K inhibitors
Syk inhibitors
NOX inhibitors
MAPK inhibitors
JAK/STAT inhibitors
Additional IA cases associated with biological therapies
TNF inhibitors
eculizumab
Chamilos G, Lionakis MS, Kontoyiannis DP. Clin Infect Dis 2018; 66: 140–148. ESCMID eLibrary
©
by author

Other SMKIs are associated invasive aspergillosis: the sorafenib story
Type of IFI Sites of
infection
Type of cancer Age/Sex Concomitant
corticosteroids
Comorbiditie
s
Subacute invasive
aspergillosis*
lung Hepatocellular
carcinoma
64/M No DM, Asthma
Invasive
aspergillosis
pneumonia Thyroid cancer N/A Yes N/A
Invasive
aspergillosis
pneumonia Salivary gland
carcinoma
N/A No N/A
Talaromyces
marneffei infection
disseminated AML 67/M No N/A
*Bazaz R & DW Denning, Clin Infect Dis 2018 Jan 23Chamilos G, Lionakis MS, Kontoyiannis DP, Clin Infect Dis 2018 ESCMID eLibrary
©
by author

Checkpoint inhibitors-good, bad or ugly?
ESCMID eLibrary
©
by author

Check point inhibitors: A revolution in modern oncology
DiesendruckY & Benhar Drug Res Updates 2017
Schematic representation of immune checkpoint blockade by targeted mAbs. A ‘Two signal model' of T cell
activation. Antigen-presenting cells (APC) display tumor specific antigens on their surface by MHC-II molecules,
recognized by T cell receptor (TCR). A second signal, mediated by CD28 binding to B7 costimulatory molecules (such as
CD80 or CD86) is required for full activation. CTLA-4 is up-regulated shortly after T-cell activation, down-regulating the
immune response to maintain tolerance. PD-1 is expressed by tumor infiltrating lymphocytes (TILs) after antigen
exposure, and its interaction with its ligands results in T cells inhibition in the tumor microenvironment. B. Antibodies
targeting these immune checkpoints, such as ipilimumab (anti CTLA-4) or nivolumab (anti PD-1) block the inhibitory
signal, thus markedly enhancing the immune response to the tumor. ESCMID eLibrary
©
by author

FDA approval of checkpoint inhibitors
20+ approvals in 3 years
Cancer type/Therapy
Ipilimumab
(YEVROY)
(CTLA-4i)
Pembrolizumab
(KEYTRUDA)
(PD-1i)
Nivolumab
(OPTIVO)
(PD-1i)
Atezolizumab
(TECENTRIQ)
(PD-L1i)
Avelumab
(BAVENCIO)
(PD-L1i)
Durvalumab
(IMFINZI)
(PD-L1i)
Metastatic melanoma 2011 2014, 2015
2014,
2015
(Nivo + IPI)
Squamous cell lung cancer
(NSCLC)2015
Non-squamous non-
small cell lung cancer
(NSCLC)
2017
Non-small cell lung cancer
(NSCLC)2015, 2016 2015 2016
Renal cell cancer 2015
Squamous cell carcinoma
of the head and neck
(SCCHN)
2016 2016
Urothelial carcinoma 2017 2017 2016 2017 2017
Hodgkin lymphoma 2016
Colorectal cancer 2017
Merkel cell carcinoma 2017 ESCMID eLibrary
©
by author
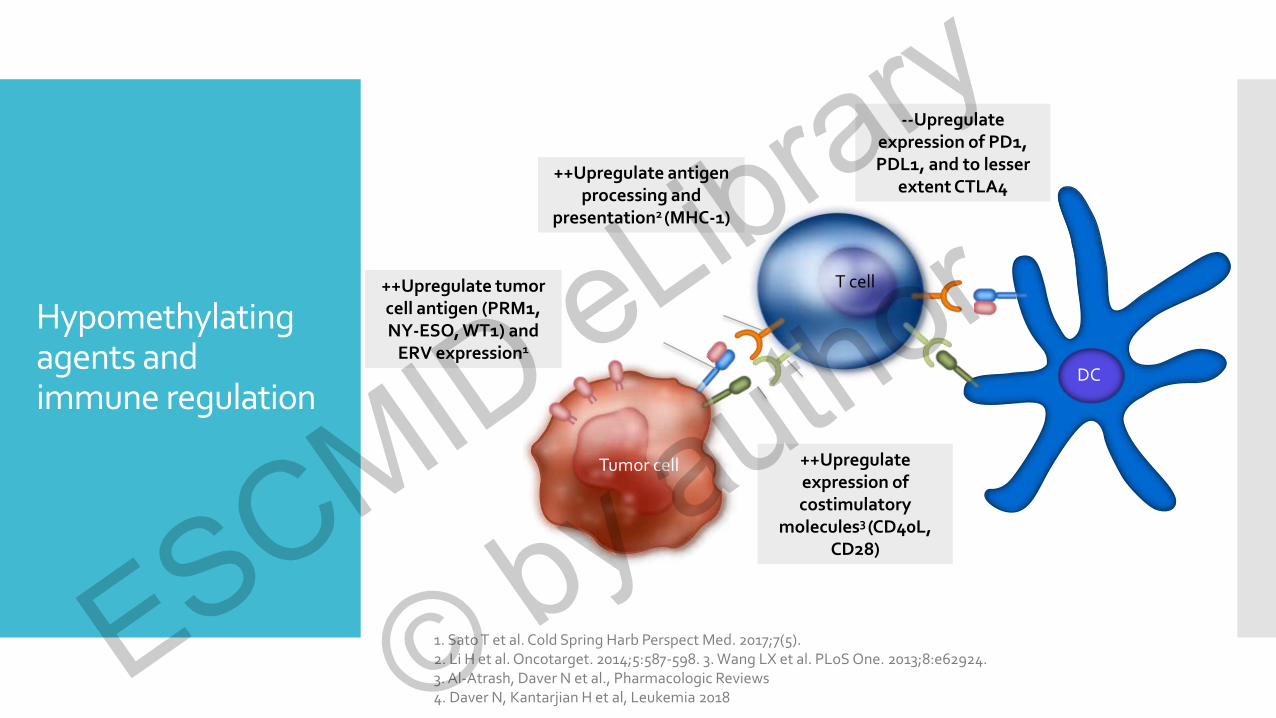
Hypomethylating agents and immune regulation
T cell
Tumor cell
TCR++Upregulate tumor cell antigen (PRM1, NY-ESO, WT1) and
ERV expression1
++Upregulate antigen processing and
presentation2 (MHC-1)
CD28
CD80/86
++Upregulate expression of costimulatory
molecules3 (CD40L, CD28)
Tumor antigen
Antigen bound to MHC class I
--Upregulate expression of PD1, PDL1, and to lesser
extent CTLA4
1. Sato T et al. Cold Spring Harb Perspect Med. 2017;7(5). 2. Li H et al. Oncotarget. 2014;5:587-598. 3. Wang LX et al. PLoS One. 2013;8:e62924. 3. Al-Atrash, Daver N et al., Pharmacologic Reviews4. Daver N, Kantarjian H et al, Leukemia 2018 ESCMID eLibrary
©
by author

AZA+Nivo in Relapsed AML
OS (censored for SCT) by response (N = 70): 33%
Slide courtesy N Daver, MD ESCMID eLibrary
©
by author
Growing literature that CPI can enhance T-cell mediated antifungal activity
Spec, A, Shindo, Y, Burnham, CA et al. T cells from patients with Candida sepsis display a suppressive immunophenotype. Crit Care. 2016; 20: 15
Krummey, SM, Floyd, TL, Liu, D, Wagener, ME, Song, M, and Ford, ML. Candida-elicited murine Th17 cells express high Ctla-4 compared with Th1 cells and are resistant to costimulation blockade. J Immunol. 2014; 192: 2495–2504
Chang, KC, Burnham, CA, Compton, SM et al. Blockade of the negative co-stimulatory molecules PD-1 and CTLA-4 improves survival in primary and secondary fungal sepsis. CritCare. 2013; 17: R85
Barrios, CS, Johnson, BD, Henderson, JD Jr, Fink, JN, Kelly, KJ, and Kurup, VP. Enhanced expression of CTLA-4 and concurrent downregulation of CD28 on lung cells of mice exposed to Aspergillus antigen. J Allergy Clin Immunol. 2005; 115: pS258
Campanelli, AP, Martins, GA, Souto, JT et al. Fas-Fas ligand (CD95-CD95L) and cytotoxic T lymphocyte antigen-4 engagement mediate T cell unresponsiveness in patients with paracoccidioidomycosis. J Infect Dis. 2003; 187: 1496–1505
McGaha, T and Murphy, JW. CTLA-4 down-regulates the protective anticryptococcal cell-mediated immune response. Infect Immun. 2000; 68: 4624–4630
Grimaldi, D, Pradier, O, Hotchkiss, RS, and Vincent, JL. Nivolumab plus interferon-γ in the treatment of intractable mucormycosis. Lancet Infect Dis. 2017; 17: 18
Lázár-Molnár, E, Gácser, A, Freeman, GJ, Almo, SC, Nathenson, SG, and Nosanchuk, JD. The PD-1/PD-L costimulatory pathway critically affects host resistance to the pathogenic fungus Histoplasma capsulatum. Proc Natl Acad Sci USA. 2008; 105: 2658–2663
. Stephen-Victor E, Karnam A, Fontaine T, et al. Aspergillus fumigatus Cell Wall α-(1,3)-Glucan Stimulates Regulatory T-Cell Polarization by Inducing PD-L1 Expression on Human Dendritic Cells. J Infect Dis. 2017 5;216(10):1281-1294
Daver N, Kontoyiannis DP. Checkpoint inhibitors and aspergillosis in AML: the double hit hypothesis. Daver N, Kontoyiannis DP .Lancet Oncol. 2017 ;18(12):1571 ESCMID eLibrary
©
by author

Survival differences between non treatment nasally infected immunosuppressed mice
(control) vs. PD-1 treatment of infected mice
Robinson P… Kontoyiannis DP. Unpublished
0 2 4 6 8
0
2 0
4 0
6 0
8 0
1 0 0
D a y (s )
Pe
rc
en
t s
urv
iva
l
C o n tro l M ic e n = 1 5
P D -1 T M T M ic e n = 2 0
P value 0.0301
ESCMID eLibrary
©
by author

Checkpoint inhibitor therapy is associated with frequent, pleiotropic, immune-related adverse effects
Treatment: long termglucocorticosteroidsand TNF inhibition(Infliximab) for
GC-refractory cases
Postow MA et al. NEJM 2018 ESCMID eLibrary
©
by author

Opportunistic infections in patients treatedfor immune related adverse effects during checkpoint inhibitor therapy
Retrospective study of 740 patients with melanoma at MSKCC (2010-2014) who received immune checkpoint blockers.
Serious infection occurred in 54 patients (7.3%) Fungal infection in 6 ( PJP in 3, IPA in 2)
Average time to infection: 135d, 805 within 6 months
Risk factors for serious infections: corticosteroids (odds ratio [OR], 7.71; and use of infliximab (OR, 4.74)
Use of a combination of ipilimumab and nivolumab was associated with increased risk of serious infection, whereas use of pembrolizumab was inversely associated
Del Castillo M et al. CID 2016, Kyi C et al. J immunother Cancer 2014, Arriola E et al. OncoImmunology 2015, Uslu U et al. J Immunother 2015, ESCMID eLibrary
©
by author

Some future questions-1How we evaluate best IFI epidemiology in the new era?
RCTs excluded cancer patients with active infections!
How study the full range of CPI effects on the immune
system?
Human studies vs murine studies
Best treatment strategies of IFIs developing post CPI-immune AEs, or in the setting of restarting or changing CPIs
Natural history of IFIs in hematology patients receiving various CPIs
Synergy of CPIs with antifungals that have adjunct immuno-potentiating action (e.g., echinocandins)
CPIs and IRIS-like manifestations in patients with IFIS
35
Some interesting future questions
ESCMID eLibrary
©
by author

What else is out there?
Novel biomarkersInnovative imagingImmunogenetics
New drugs
ESCMID eLibrary
©
by author

Point of care diagnostics
Lateral-Flow Technology
Immunochromatographic assays into POC diagnostic assays
Murine monoclonal antibody, JF5 IgG3Binds to an extracellular
glycoprotein antigen secreted during growth of Aspergillus
Distinguishes between hyphaeand conidia
A. Brightfield B. Epifluroescence
Convincingclinical
validation
As GM, LFD
sensitivity is reduced
by mold-active
antifungals
Thornton C, et al. Clin Vaccine Immunol 2008, Hoenigl M et al. Mycoses 2018 ESCMID eLibrary
©
by author

Diagnosing invasive molds by breath?
In Vitro volatile metabolite profiles of molds
Fungal cultures inoculated in parallel with matched media controls
Adsorption/concentration onto a sorbent bed
Thermal Desorption
Gas Chromatography-Tandem Mass Spectrometry
Koo S, et al. Clin Infect Dis 2014, Koshy S et al. ID week 2017, abst 1776 ESCMID eLibrary
©
by author
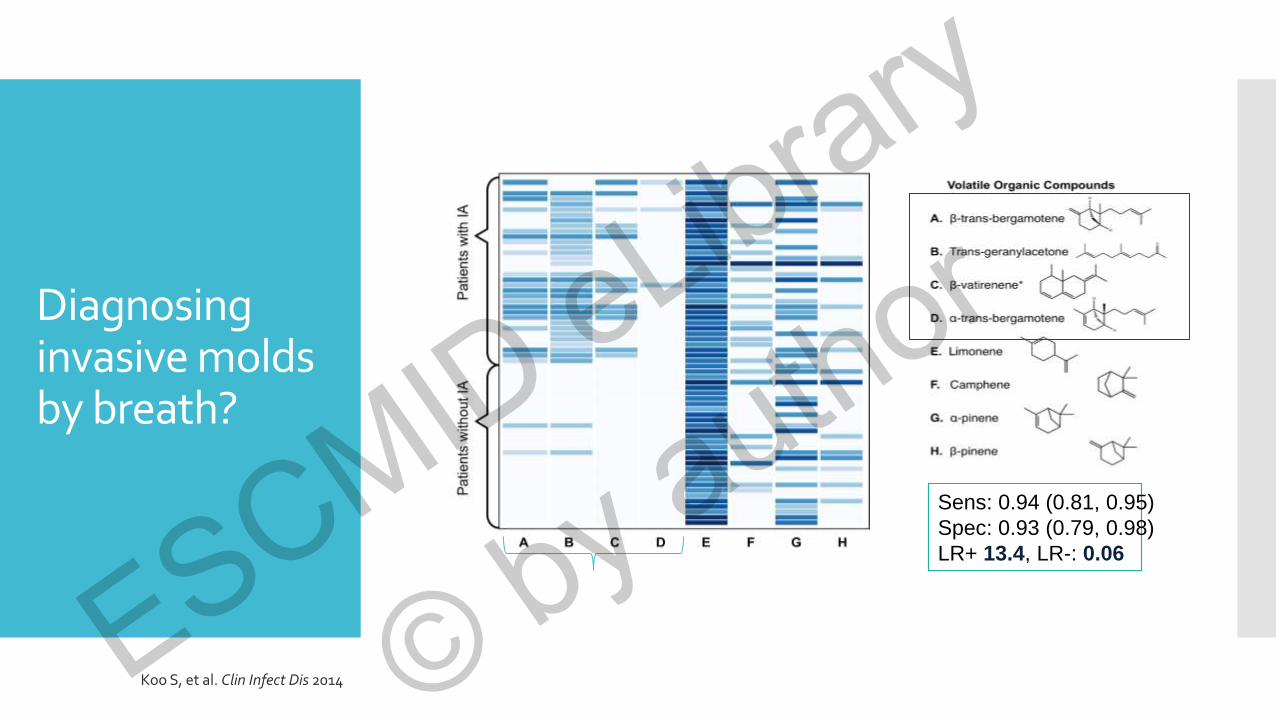
Diagnosing invasive molds by breath?
Sens: 0.94 (0.81, 0.95)
Spec: 0.93 (0.79, 0.98)
LR+ 13.4, LR-: 0.06
Koo S, et al. Clin Infect Dis 2014 ESCMID eLibrary
©
by author

Diagnosing invasive mold disease by urine samples?
Urinary Excreted Galactomannan-like Antigens for IA
Novel IgM MAb476 that recongizes GM-like (Galf) antigens
Antigenuria a clinically relevant target
Guinea pigs
Clinical samples
Detection with lateral flow device
POC diagnostic
Urine GM/
Urine creatinine
ratio to diagnose
IA
Reischies FM et al.
JCM 2016
Dufresne SF, et al. PLoS ONE. 2012;7:e42736. ESCMID eLibrary
©
by author

41
Radiolabeled Ga or Zn-labeled siderophore uptake in PET
Gliotoxin and methylated gliotoxin detection
Detection of Aspergillus siderophores in serum as secondary metabolites
Nuclear magnetic resonance metabolomics
Other metabolite-based diagnostic tools for aspergillosis
Savelieff MG, Pappalardo L. PLoS Pathog. 2017 ESCMID eLibrary
©
by author

Improved CT imaging of invasive mold disease?
CT pulmonary angiography for IMD:
A good idea from Switzerland, refined in Italy
14 cases
Histological documentation of lesions in 8 cases
Vessel occlusion sign (VOS) observed in 4/5 histologically-documented mould disease cases (80%)
1 false negative: mucormycosis
No VOS in 9/9 patients with non-fungal causes of infection
Sonnet S et al. AJR 2005;184:746-751 ESCMID eLibrary
©
by author

Specific PET imaging for invasive mold disease
Rolle AM et al. PNAS 2016, Davies G et al. Theragnostics 2017
Future targeting of invasive fungal disease? Immuno PET and targeting antibodies
Previous proof of
concept
Gamma-imaging
with-labeled
cyclic peptide
targeted to A.
fumigatus hyphae
in a mouse model of
IPA
Yang Z, Kontoyiannis
DP et al
Nucl Med Biol 2009
Regular PET/CT.
Chamilos G..
Kontoyiannis DP.
Med Myc 2008
mAB JF5 is the basis of Aspergillus LFA
Hyphal-specific->good for monitoring of response?
Long half life->single injection
Humanized version of Ab (hJF5) to enter clinical trials in 2018! ESCMID eLibrary
©
by author

Engineering
specificity
of Dectin-1 on CAR
T cells as a new
platform
for treatment
Naïve T cells Dectin-1 expressing
T cells
Kumaresan PR, ….Kontoyiannis DP, Cooper LJ. PNAS 2014.
POSA loading in CAR-T cells?
ESCMID eLibrary
©
by author

Current estimate of IFI risk based on underlying disease: crude and “qualitative”
Chronic granulomatous disease
Allogeneic HSCT with graft versus host disease
AML/MDS treated with remission-induction chemotherapy
Lung or heart transplantation
Small-bowel transplantation
Liver transplantation
Allogeneic HSCT without graft versus host disease
Acute myeloblastic leukemia during consolidation phase
Acute lymphoblastic leukemia
Heart transplantation
Chronic lymphocytic leukemia
Myelodysplastic syndrome
Multiple myeloma
COPD with acute exacerbation
AIDS
Non-Hodgkin’s lymphoma
Autologous HSCT
Kidney transplantation
Solid tumor
Autoimmune disorder
HIGH RISK
INTERMEDIATERISK
LOWRISK
Herbrecht et al. Ann NY Acad Sci 2012;1272:23-30. ESCMID eLibrary
©
by author

BoScore2018: Individualized prediction of risk for invasive mold disease
Risk of invasive mold disease within 60 days of admission
No Yes
No Yes
No Yes
No Yes
No Yes
No Yes
No Yes
Uncontrolled malignancy
High-risk chemotherapy
High-dose corticosteroids
Lymphopenia < 50/mm
CMV disease or viremia
PMN< 100 /mm3 > 10 days
Previous history of mould disease
0 1 2 3 4 5 6 7 8 9 10 11Score
1 5 10 20 30 40 50 60 70 80
Probability (%) of developing
invasive mold disease within
60 days
0 5 10 15 20 25 30 35 40 45Total score
Stanzani M… Kontoyiannis DP, Lewis RE. 2018 submitted ESCMID eLibrary
©
by author

Immunogenetics
Why do “similar” patients have different attack rates of and IFI (and outcome)?
Differences in exposure and virulence of offending fungus?
Host genetic differences in immunity (e.g., pattern recognition receptors such as Toll-like receptors (TLRs) and the C-type lectin receptors (CLRs) and/or pharmacology?
Lionakis MS & Levitz SM. Annu Rev Immunol 2017 ESCMID eLibrary
©
by author

The challenge with genetic studies
“Locating, from scratch, the gene related to a disease is like trying to find a burned-out light bulb in a house located somewhere between the East and West coasts without knowing the state, much less the town or street the house is on”
Francis S. Collins, Quoted in Philip Elmer-Dewitt, et al.
'The Genetic Revolution', Time magazine (17 Jan 1994), 46-53 ESCMID eLibrary
©
by author
Genetic polymorphisms and risk stratification:
maturation but not maturity!
Solution: Well designed large prospective whole-genome association studies (IA seems to be a polygenic disease)
Incorporation of fungal genetics, microbiome and/or mycobiome
Incorporation of validated clinical risk models and specific imaging diagnostics
ESCMID eLibrary
©
by author

Antifungals in the pipeline
Improved echinocandin-like drugs?- CD-101, rezafungin (Cidara)
- SCY-078 (Scynexis)
Improved triazole-like drugs?- VT-1161, VT-1129, VT-1598 (Viamet)
Novel mechanisms- F901318 (F2G)
- APX001 (Amplyx)
- VL-2397 (Vical)
ESCMID eLibrary
©
by author

Full• New mechanisms of activity• Activity for resistant pathogens• IV and oral formulations• Few or no drug-drug interactions• Favorable safety profiles• Interesting future for combination therapy (new mechanisms)?
Empty• Small biotechs
• Crowded field for clinical trials of uncommon infections
• Proof of principle: clinical efficacy for new mechanisms of action
• Unknown toxicity, resistance potential
ESCMID eLibrary
©
by author

Future questions
How we evaluate best epidemiology in the new era?
How to study new antineoplastic effects on the immune system?
How the new biomarkers perform according to disease severity?
How biomarkers/imaging helps us on when to stop therapy?
What is the relevance of the in vitro resistance of fungi ?
What is a cost effective risk stratification? Clinical score cards?
Immunogenetics?
Pharmacogenetics?
Combinations?
Should we invest more to the idea of Theragnostics?
How we incorporate new antifungals to a congested scene of existing antifungals?
ESCMID eLibrary
©
by author

The future?
Golconde, 1953Renè MagritteMenil Collection, Houston,TX
Dutch Proverbs, 1559Pieter Bruegel the ElderGemäldegalerie, Staatliche Museen, Berlin
Manage patients in groups?
Manage patients as individuals?
ESCMID eLibrary
©
by author

Acknowledgements
UT M.D. Anderson Cancer CenterKontoyiannis Group
Michail Lionakis, MDG Chamilos , MDNathan Albert, B.ScGregory Lamaris, MDRonen-Ben Ami, MDGeorge Pongas, MDSarah Georgiadou, MDAnne-Pauline Bellanger , PharmDElena Barbu, PhDMarisa Gomes, MDSetareh Davoudi, MDFazal Shirazi, PhDAndreas Kyvernitakis, MDMinas Economides, MDKumar Kumaresan, PhDSang Taek Heo, MDLuke Jung, MDS Aitken, PharmDFrank Tverdek, PharmDYing Jiang, MSN Raman, PhDS Wuster, MD, PhDE Magira, MD
The University of HoustonCollege of Pharmacy
Russell E Lewis, Pharm.DRandy Prince, Pharm DN Beyda, PharmD
Non-MDACC CollaboratorsThomas J Walsh, MD, Cornell UniversityAshraf Ibrahim, PhD, UCLAAntony Mikos, PhD, Rice UniversityD Perlin, PhD, Rutgers University Nir Osherov, PhD, Tel Aviv UniversityG Chamilos, MD Univ of CreteN Sipsas, MD, Univ of Athens
MDACC CollaboratorsSam Shelburne, MD, PhDJeff Tarrrand, MDEdith Marom, MDKaty Rezvani, MD, PhDS Bose, MDN Daver, MDKaleigh Marx, PharmD Caitlin Early, PharmDA Dippo, PharmDG Einsenhoffer, PhD ESCMID eLibrary
©
by author

Special gratitude to my friends
especiallyGeorge Samonis, MDRussell E Lewis,
PharmD
Thank you to my patients and to all my colleagues in ID, Leukemia, SCT services at MDACC
ESCMID eLibrary
©
by author

And above all
My family
ESCMID eLibrary
©
by author

See you at the next meeting!
Thank you!
(and see you
In Athens!)
For more information:
WWW.ICHS.ORG
ESCMID eLibrary
©
by author