
Striatal Sensitivity During Reward Processing in Attention-Deficit/Hyperactivity Disorder
Upload
independentCategory
view
2download
0
Behavioural Brain Research 130 (2002) 3–283
How specific is a deficit of executive functioning forAttention-Deficit/Hyperactivity Disorder?
Joseph A. Sergeant *, Hilde Geurts, Jaap OosterlaanKlinische Neuropsychologie, Vrije Uni�ersiteit, Van der Boechorststraat 1, 1081 BT Amsterdam, The Netherlands
Received 20 September 2000; accepted 13 August 2001
Abstract
A selective review of research in the executive functioning (EF) is given for attention deficit hyperactivity disorder (ADHD),oppositional defiant disorder (ODD), conduct disorder (CD), higher functioning autism (HFA) and Tourette syndrome. The reviewis restricted due to changes in the classification of the disorder in recent years and secondly the heterogeneity of EF is restrictedto five key areas of concern, inhibition, set shifting, working memory, planning, and fluency. The review makes clear that thereare strong differences between child psychopathological groups and controls on these EFs. However, future research will be neededto identify an EF deficit or profile, which is specific for these disorders. © 2002 Elsevier Science B.V. All rights reserved.
Keywords: Attention-deficit/hyperactivity disorder; Working memory; Inhibition; Attention; Planning; Stroop; Fluency; Higher functioningautism; Working memory; Tower of London; Stop-signal task
www.elsevier.com/locate/bbr
1. Introduction
In recent years, there has been an encouraging in-crease in interest from neuroscientists into the etiologyof attention deficit hyperactivity disorder (ADHD, [2]).This interest is expressed in a variety of reviews[9,104,128,130]. Five reasons exist for this enhancedresearch effort. Firstly, the phenotype of ADHD hasbecome more refined [127]. Secondly, structural mag-netic resonance imaging (MRI) has shown reducedwhite matter in basal ganglia structures in ADHDchildren compared with controls [33]. Thirdly, func-tional MRI (fMRI) studies with the primary pharmaco-logical tool for treating ADHD has shown thatneuropsychological dysfunctioning is reflected in neuralimaging differences between ADHD and control sub-jects [135]. Fourthly, quantitative cytochrome oxidasestudy of an animal model of ADHD has implicated aneural network involving both the anterior forebrain[89] and anterior accumbal interface [90]. Fifthly,molecular genetic research has offered a candidate gene,which has been successfully replicated by severalgroups, although the strength of that association isweak [27].
One of the primary models driving the research notedabove is neuropsychological functioning of ADHDchildren and specifically the frontal circuits involved inthe disorder [13,22,42]. Recently, the frontal hypothesishas become re-expressed as an executive functioning(EF) disorder [8,130]. The purpose of the current reviewis to evaluate the specificity of EF measures for ADHDwhen EF is contrasted with associated clinical groups,oppositional defiant disorder (ODD), conduct disorder(CD), higher functioning autism (HFA), Tourette syn-drome and learning disability (LD).
For this purpose, we selectively review EF studies ofADHD, in order to provide a more specific phenotypefor future molecular genetic research [94]. We restrictthis review for two reasons. The first is that diagnosis ofADHD [2] is based upon criteria which make it uncer-tain in how far results obtained from two previousclassifications which appeared in 1980 and 1987, respec-tively, can be directly translated into the current taxon-omy. Second we restrict ourselves to a major group ofneuropsychological tests and tasks, which have empiri-cal support for reflecting differing dimensions of EF[94]. There are 33 definitions of EF [32]. Therefore, areview of all of the operationalisations of these variousdefinitions cannot be met within current space limita-
* Corresponding author.E-mail address: [email protected] (J.A. Sergeant).
0166-4328/02/$ - see front matter © 2002 Elsevier Science B.V. All rights reserved.PII: S 0 1 6 6 -4328 (01 )00430 -2

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–284
tions. Among the EFs reviewed here are, inhibition; setshifting; working memory; planning; and fluency basedupon an empirical classification [94]. The neuropsycho-logical tests/tasks used here to review the literature arenot the entire possible battery of EF measures, but aselection which measures the common domains of EFnoted above.
This review will conclude that there is evidence of adeficit in some aspects of EF in ADHD children. Theresults are not always consistent within ADHD sam-ples, possibly reflecting sample differences within theADHD spectrum or paradigm differences betweenstudies. We will note that not all of these deficits arespecific to ADHD but occur in related childhood disor-ders. We will offer six methodological points to increasethe specificity of neuropsychological research. Hope-fully, this will encourage neuroscientists to appreciatethat they too will need to increase the specificity of thefunctions they measure.
1.1. Study of EF with neuropsychological tests/tasks
Neuropsychological tests have attained their validityfrom careful research on patients with neurologicaldisorder [60]. The primary dependent variables for testsare latency and accuracy. Tests are classically per-formed manually. The products latency and errors usu-ally fulfil psychometric criteria for test construction.Whereas a neuropsychological test reflects a wide vari-ety of processes (encoding, working memory, responseorganisation and strategy), the neuropsychological taskattempts to measure a particular process, such as, inhi-bition and not a variety of other processes. Neuropsy-chological tasks are performance challenges which seekto identify specific process deficiencies [120]. The taskdoes this by manipulating the process, for example,increasing or decreasing the inhibition demands in atask, such as, the stop-signal task [61]. Thus tasks areparametric [36] and employ the additive factor method[125]. Tasks are not constructed using psychometricprinciples but on the grounds of process purity [104].This is determined by the independence versus theinteraction of task variables. Two process which areadditive are said to be independent, two processeswhich interact are said to be common.
Given the multiple processes which may determineperformance on, say a working memory test (stimulusencoding, retrieval and response selection factors), neu-ropsychologists have recognised that process specificityrequires being able to account for the variance associ-ated with non-specific and specific processing. Twostrategies have been used. One is the control-task pro-cedure. Here a candidate neuropsychological process(set shifting) measured by a test such as the Wisconsincard sorting test is compared with performance on acontrol test (colour/form naming). Observed deficits in
the candidate compared with absence of deficit in thecontrol test is taken as evidence of a specific deficit[124]. The Stroop has this procedure built in such thatperformance on the ‘interference card’ (containingcolour names printed in opposite colours) is subtractedby the colour card (containing only colours).
A variation on this methodology to achieve processspecificity is regression analysis. For example, perfor-mance on an inhibition task is the primary variable ofinterest and is freed by partialing out variance associ-ated with intelligence [78]. Care needs to be taken inthis procedure that the control test is not so highlycorrelated with the candidate test that partialing outwill lead to loss of a true effect. However, when covari-ance analysis is applied and significant differences be-tween ADHD and comparison groups remain, one maybe confident in identifying a more or less specific EFdeficit.
A second area which is in need of greater specificityof research design is the comparison groups used instudies. For neuroscientists unfamiliar with ADHD as aclinical entity a few remarks may help in future designs.ADHD is recognised to contain three subgroups, theinattentive subtype; the hyperactive-impulsive subtypeand the combined subtype: inattentive, hyperactive,impulsive [2]. In contrast, hyperkinesis is only the com-bined subtype with both pervasiveness and early onset(around 3 years) of the disorder [54]. Both diagnosticsystems note that ADHD and hyperkinesis are highlyassociated with other disorders, but treat differently theassociation in their decision rules. ADHD may beassociated with other disorders (comorbidity) whereas,if the hyperkinesis may be explained by another disor-der, then that diagnosis is given.
For ADHD there are very strong associations withdisorders such as anxiety, depression, CD, Tourette’ssyndrome and ODD [3]. Furthermore, ADHD, particu-larly the inattentive symptoms, is associated with read-ing disability [139]. Thus without appropriatecomparison groups, studies with only a two-group com-parison will fail to provide specific effects. Screeningand exclusion for associated disorders has only recentlybecome standard practice in neuropsychological re-search of ADHD. For neuroscientists this point isimportant, since the specificity of the genotype willdepend upon both screening and comparison groups.Few molecular geneticists employ a multi-group designand, hence, rob themselves of specificity for the candi-date gene they are seeking.
Prior research has seldom employed comparison clin-ical groups other than normal controls. When meta-an-alytic methods have been used to compare ADHDchildren with other associated groups, such as ODDand CD, on a primary measure of EF, inhibition, it hasbeen found that ADHD and ODD/CD groups did notdiffer from one another [79]. This finding has been

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 5
recently confirmed with the stop-task in a recent largecomparison between ADHD and CD children [108].Put briefly, a common EF deficit exists between thesegroups. Nevertheless, it is unclear whether the commonEF deficit is generated by exactly the same brainnetworks.
The third area of discussion is the specificity ofneural networks leading to a given performance output.Attention has been drawn to neglect being present inADHD and it has been hypothesised that a prefrontalcircuit might be responsible for the disorder [46].SPECT reports indicated that ADHDs had hypoperfu-sion of striatal and frontal brain areas (about 10%lower than normal) and hyperperfusion of occipitalbrain areas [64,65]. It has been reported that ADHDmales had in the basal ganglia smaller right caudatevolumes while controls exhibited a right larger than leftasymmetry [21]. Another report indicated smaller leftcaudate areas in ADHD children, who also differedfrom controls by having larger left than right frontallobes [34]. The asymmetry of ADHD children for thecaudate has been replicated [118]. A third target locushas emerged with the finding that the volume of theposterior inferior cerebellar vermis lobules VIII–X issmaller in ADHD children than controls [12]. Conse-quently, the neural network involved in ADHD cannotbe confined only to the frontal lobes but must beextended to both the basal ganglia and cerebellum. Thisargues against the original localisation hypothesis at thefrontal lobes. Limitations in the resolution of pastfMRI magnets have not enabled a test to be conductedof the possible involvement of deep structures such asthe nucleus accumbens in such a putative circuit [89].
We have addressed three major reasons for determin-ing specificity in ADHD research. With the advance ofmolecular genetic studies in the field we provide here arecent example of the need to identify a specific neu-ropsychological phenotype in such research. A studyexamined the performance of ADHD children on neu-ropsychological tests designed to probe attentional net-works with neuroanatomical loci in D4-rich brainregions [127]. Two ADHD subgroups were employedthat were defined by the presence (7+ ) or absence(7− ) of the seven repeat allele. The overall ADHDgroup differed from the control group by being slowerand more variable in performance on all three atten-tional probes. However, the 7+ subgroup showednormal speed and variability, even though this groupmanifested the behavioural symptoms of ADHD to thesame degree as the 7− subgroup. The findings indi-cated that the cognitive deficit of ADHD measured bythese attentional probes is not due to the seven repeatallele. In order to identify a refined ADHD phenotype,we review a selective set of EF tests and tasks below fortheir specificity for ADHD in contrast to highly relateddisorders such as ODD, CD, HFA and LD.
1.2. ADHD and neuropsychological tests/tasks
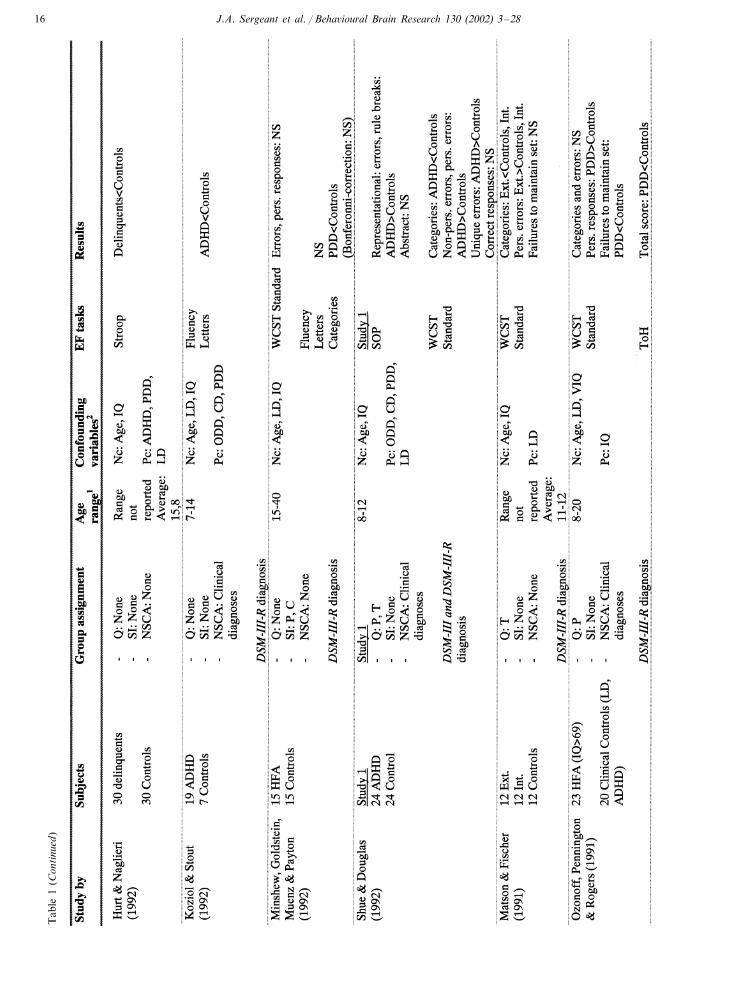
In Table 1, we present studies using EF tests andtasks and indicate the selection procedures which areused in the studies. The EF-tests are all widely usedmeasures across different disorders and are tests onwhich patients with frontal lesions perform poorer thannormal controls. The measures derived are significantly,but modestly associated with frontal lesions and be-havioural disturbance. Test validity has been estab-lished by the use of neuroimaging. All of the tests aresuitable for children aged 6–12 years and are frequentlyused in the literature.
1.2.1. Inhibition: stop task and Stroop
1.2.1.1. Stop task. The stop task was developed tomeasure response inhibition. The task requires childrento inhibit a motor response which is being executed.Briefly, the stop task requires fast and accurate execu-tion of a reaction time task, denoted as the primarytask. Occasionally, a stop signal is presented, whichrequires the child to inhibit the response to the primarytask. The major advantage of this paradigm is that it isbased on a well-developed mathematical model thatexplains performance on this task, known as the ‘racemodel’ [61]. In contrast to other measures of responseinhibition, the stop task enables one to investigatewhether poor response inhibition is due to a deficit inthe inhibitory process. By varying the timing of the stopsignal, the model allows estimation of the speed of theinhibitory process (stop signal reaction time; SSRT).
Studies using the stop task have been summarised ina quantitative meta-analysis [79]. Here we summarisethe results of that meta-analysis for SSRT, the maindependent variable in the stop task. In seven of eightstudies, children with ADHD were on average 103 msslower than normal control children. A medium com-bined effect size of d=0.64 was obtained, which trans-lated into 40% non-overlap between the two groupdistributions. Findings were similar across all studies.Four studies compared children with CD and normalcontrol children. SSRT was on average about 18 msslower in CD children than in normal controls. Theaverage effect size of d=0.51 equals Cohen’s thresholdfor a medium effect size. This effect size indicates 34%non-overlap between the SSRT distribution of the twogroups. However, findings varied across studies. Thecomparison between ADHD and CD was not signifi-cant. Furthermore, no SSRT differences were foundbetween children with comorbid ADHD+CD andADHD, nor between children with anxiety disordersand normal control children. To summarise, clear evi-dence was found for an inhibitory dysfunction inADHD, whereas for CD evidence for such a deficit wasless robust.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–286
Tab
le1
Stud
ies
Usi
ngT
heSt
opSi
gnal
Tas
k,T
heSt
roop
,T
heW
isco
nsin
Car
dSo
rtin
gT
est,
The
Self
Ord
ered
Poi
ntin
g,T
ower
Tas
ksan
dF
luen
cyin
Chi
ldre
nD
iagn
osed
wit
hA
DH
D,
CD
/OD
Dan
dP
DD

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 7
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–288
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 9
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2810
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 11
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2812
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 13
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2814
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 15
Tab
le1
(Con
tinu
ed)
J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2816
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 17
Tab
le1
(Con
tinu
ed)

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2818
Tab
le1
(Con
tinu
ed)
1A
gein
year
s.2T
hegr
oups
are
chec
ked
for
thes
edi
sord
ers,
ther
eis
aco
mpa
riso
ngr
oup
wit
hon
eof
the
diso
rder
sor
the
mea
nsof
the
grou
psar
the
sam
e.A
/D,
aggr
essi
on/d
efian
ce;
AD
D,
atte
ntio
nde
ficit
diso
rder
;A
DD
H,
atte
ntio
nde
ficit
diso
rder
,hy
pera
ctiv
esu
btyp
e;A
DH
D,
atte
ntio
nde
ficit
hype
ract
ivit
ydi
sord
er;
AW
,an
xiet
yw
ithd
raw
al;
C,
child
;C
A,
chro
nolo
gica
lag
em
atch
ed;
CD
,co
nduc
tdi
sord
er;
CT
,co
mbi
ned
subt
ype;
Dep
,de
pres
sion
;D
SM,
diag
nost
ican
dst
atis
tica
lm
anua
lof
men
tal
diso
rder
s;E
D,
emot
iona
ldi
sord
ers;
ED
,em
otio
nally
dist
urbe
d;E
xt.,
exte
rnal
ises
;H
,hy
pera
ctiv
ity;
HF
A,
high
func
tion
ing
child
ren
wit
hA
utis
m;
HF
C,
high
func
tion
ing
cont
rols
;H
2M,
hard
tom
anag
e;ID
/ED
,in
tra
dim
ensi
onal
/ext
radi
men
sion
al;
Int.
,in
tern
aliz
ers;
I/O
,in
atte
ntio
n/ov
erac
tivi
ty;I
Q,
inte
llige
nce
quot
ient
;IT
,in
atte
ntiv
esu
btyp
e;L
D,
lear
ning
disa
bled
;LD
A,
lear
ning
disa
bled
child
ren
wit
hA
utis
m;L
DC
,le
arni
ngdi
sabl
edco
ntro
ls;
MA
,m
enta
lag
e;M
D,
mat
hdi
sord
er;
Nc,
not
conf
ound
ing;
NS,
not
sign
ifica
nt;
NSC
A,
non
stan
dard
ised
clin
ical
asse
ssm
ent;
OC
D,
obse
ssiv
eco
mpu
lsiv
edi
sord
er;
OD
D,
oppo
siti
onal
defia
ntdi
sord
er;P
,par
ent;
Pc,
poss
ible
conf
ound
ing;
PD
D,p
erva
sive
deve
lopm
enta
ldis
orde
r;P
ers.
,per
seve
rati
ons
orpe
rsev
erat
ive;
PM
A,p
erfo
rman
cem
enta
lage
dm
atch
edco
ntro
ls;Q
,que
stio
nnai
res;
RD
,re
adin
gdi
sabi
litie
s;SA
,st
able
aggr
essi
ve;
SI,
(sem
i-)
stru
ctur
edin
terv
iew
sor
stan
dard
ised
obse
rvat
ion;
SLI,
spec
ific
lang
uage
impa
irm
ent;
SOM
GA
s,so
nsof
mul
ti-g
ener
atio
nal
alco
holic
s;SO
P,
self
orde
red
poin
ting
;SS
RT
,st
opsi
gnal
reac
tion
tim
e;T
,te
ache
r;T
oH,
Tow
erof
Han
oi;
ToL
,T
ower
ofL
ondo
n;T
S,T
oure
tte
synd
rom
e;U
S,un
stab
leag
gres
sive
;V
MA
,ve
rbal
men
tal
age
mat
ched
cont
rols
;W
CST
,W
isco
nsin
card
sort
ing
test
.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 19
Recent studies have replicated and extended the find-ing of impaired inhibitory control in ADHD [78,108].Note that two recent studies are not included in theTable 1 because these studies did not report SSRTfindings [14,102]. A recent study [78] showed thatADHD (combined type) is associated with poor in-hibitory control (as evidenced by slow SSRTs) evenwhen age, IQ, reading ability, and comorbid ODD/CDproblems were controlled. The same study demon-strated that girls are at least equally impaired in termsof response inhibition as compared with boys. Themeta-analytic finding of no difference between ADHDand CD with respect to the primary measure of inhibi-tion: SSRT has been recently replicated [98]. One studyshowed that autistic children were not impaired ininhibitory control in the stop task [87].
Research with structural MRI and inhibition taskssuggested involvement of frontostriatal circuitry inADHD [20]. This has been followed up with studiesusing fMRI. It has been shown that the stop taskactivates prefrontal and other brain regions [103]. Thisstudy showed that in ADHD adolescents there wasreduced activation of the right frontal cortex and theleft caudate nucleus. These findings support the ideathat both the frontal lobe and basal ganglia may medi-ate the inhibitory deficit in ADHD. Conflicting resultshave been obtained in a study which compared childrenwith ADHD and normal control children on the stoptask while recording their EEG [14]. That study sug-gested the involvement of posterior mechanisms. Itshould be noted that these two studies used an adapta-tion of the stop task and failed to replicate the findingof slow SSRT in ADHD children.
In summary, the stop-signal results suggest thatADHD and autistic children but not ODD/CD and LDchildren can be distinguished by this task and hence, aninhibition disorder is not specific to ADHD [8].
1.2.1.2. Stroop. The Stroop test [126] requires that thesubject read words which mean colours, such as red,yellow, green and blue. This is followed by a card inwhich only colours are printed and the subject has toname the colours. An interference card is used whichcontains colour words but now printed in a colourother than what the word means. It is thought tomeasure a variety of processes including attention andinhibition [68]. During the Stroop test there has beenobserved increased activity of the brain in de anteriorcingulate gyrus, frontal polar cortex, inferior parietallobe, thalamus and speech gyrus [19]. There has alsobeen observed during the Stroop increased activation ofthe right orbito– frontal and bilateral parietal lobes[10,17,131].
Ten studies reported Stroop interference deficits inADHD [9,18,42,48,67,69,114–117] and two did not[37,72]. Two studies examined the Stroop interference
score (corrected for reading and naming speed) andfound a significant ADHD group deficit [67,69]. In theADHD related groups, five studies have found forODD/CD a difference in interference with controls[38,52,58,66,67] and one study did not [137]. One studyof HFA failed to observe any difference [31].
Some studies have shown a group difference in thecolour and word conditions [116,118]. Thus, there isuncertainty whether only inhibition was measured inthe later neural imaging study but the results suggestthat the smaller caudate in ADHD subjects is related toStroop interference. There is also a clear interferenceeffect in the related-disorders ODD/CD. This is lessclear for the HFA group.
On balance there is evidence that the Stroop candifferentiate ADHD children from controls, but theprecise neuropsychological mechanism responsible forthis effect is currently unclear. Further, several clinicalgroups need to be employed in studies in order todetermine the specificity of the Stroop interference inADHD.
1.2.2. Set shifting: WCSTThe Wisconsin card sorting test (WCST; [40,45]) is
used traditionally as a test to tap set shifting. Fivepoints need to be noted with regards the WCST. First,the WCST does not always discriminate patients withfrontal lesions from normals or persons with lesions inother regions [101]. Second, the role of working mem-ory seems to be important in this test. The WCSTmeasures the following processes: conceptual problemsolving ability, use of feedback, the ability to modifyincorrect strategies, flexibility, and inhibition of prepo-tent but incorrect responses. Third, the problem solvingrules for reaching the goal must be extracted, andchange during the test without the subject’s knowledge.Subjects have to sort cards on three principles rein-forced by feedback [40]. Fourth, the computerised ver-sion differs from the traditional version, and autisticchildren tend to perform better on the computerisedrather than traditional version [83]. Fifth, the variablesreported for the WCST differ across studies, makingcomparisons between studies difficult. The main depen-dent variables are, the number of correctly identifiedcategories; perseverative responses (number of cardsthat the subject sorts by a previously correct category;despite negative feedback from the experimenter); per-severative errors; total amount of errors and the fail-ures to maintain set.
The WCST differentiates between ADHD childrenand controls (or from norms) in 17 out of 26 studies[9,18,35,41,42,48,55,59,63,71,97,100,115 – 117,124,136].It has been suggested that the significant comparisonsbetween ADHD and normals were confined to ayounger age group [9]. This cannot, however, be theonly explanation. Thirteen studies with HFA using the

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2820
WCST showed that 11 studies differentiated HFAs fromcontrols [11,23,50,74,83] (study 1 and 3), [84,86,91,99,129] and two did not [75,83] (study 2)]. One study [84]directly compared children with ADHD with autisticchildren. The autistic children performed poorer on theWCST than ADHD children [84]. The WCST can alsodifferentiate between CD and controls [29,55,66] andADHD with and without Tourette syndrome [44,110]with one failure to differentiate ADHD from ADHD+Tourette syndrome [24].
On balance, the WCST can differentiate betweenADHD and controls. It is possible that this may dependon age and the variable used. The WCST differentiatesHFA more consistently from normals and the effectappears to be greater than that for ADHD. This suggeststhat whichever process is being consistently measuredacross these studies it is indicative of a quantitative andnot a qualitative difference between HFA and ADHD.Again specificity of the subgroups of ADHD childrenused is difficult to assess from many publications. Littleresearch with the WCST has employed a neural imagingmodality and different clinical groups of interest, makingthis an urgent area of study.
1.2.3. Working memory: SOPFive functions for working memory have been pro-
posed, hindsight; forethought; anticipatory set; sense oftime; and self awareness [9]. Working memory is thecapacity to simultaneously store and manipulate infor-mation [5]. It is a computational mechanism [92] mea-sured by self-ordered sequencing tasks.
Performance on self-ordered sequencing tasks is dis-rupted after damage to the prefrontal cortex [26,95].Working memory tasks seems to be especially sensitiveto prefrontal damage [6]. The dorsolateral prefrontalcortex has been associated with working memory andself ordered pointing (SOP) task by imaging studies[7,82,96].
Working memory tasks tap several processes, workingmemory; inhibitory control, the ability to generate andperform a sequence of responses; and visuo-spatialabilities. It is important to differentiate between workingmemory deficiencies and, short term memory deficits.
In the SOP task [95], subjects are required to generate,organise and carry out a sequence of responses. On apage a number of different stimuli are printed. Theactual stimuli are the same on each page, but the spatialrelations differ. The subject has to point to one stimulusat a time and to point to each stimulus only once. Thesubject has to remember each time the stimuli whichshe/he has already pointed to and must point to a novelstimulus. The task is divided into different parts, eachpart containing an increasing number of stimuli—6, 8,10, and 12. No item is used in more than one list. Eachseries is repeated three times. There are four types of
SOP task in which the stimuli differ (concrete words,abstract words, concrete designs, and abstract designs).
The SOP has been employed in two studies comparingADHD children with controls and both show significantdifferences in performance to the disadvantage of theADHD group [74,138]. The performance of childrenwith ODD/CD is poorer compared with controls in twostudies [112,113]. Consequently, the specificity of theSOP for ADHD is currently unclear as also whetherthere is a quantitative difference between clinical groupsas well as a qualitative one. There is also urgentlyrequired research using the SOP with a neural imagingmodality in the clinical groups of interest.
1.3. Planning: towers
Planning is the ability to ‘look ahead’, to construct aplan, and to evaluate and monitor execution of a plan[39,60]. The attainment of a future goal is reachedthrough a sequence of intermediate steps which notalways directly lead to the future goal [8].
The tower tasks, Tower of Hanoi (ToH) and Towerof London (ToL) are used as measures of planning. Thetowers require subjects to plan, execute, monitor andrevise a sequence of moves. They are sensitive to bothprefrontal damage or dysfunction [51]. The performanceof patients with frontal lesions can also be explained interms of an inability to see or resolve goal-subgoalconflicts [39]. The rostrolateral (anterior) frontal cortexespecially seems to be involved in planning [7]. This PETstudy showed bilateral activation of the dorsolateralprefrontal cortex (BA 9/46); frontopolar (BA 10) andbilaterally at the occipito–parietal lobes.
The ToL [122] is derived from ToH and is a ball-trans-fer task. Requiring planning and working memory ca-pacity. Subjects have to plan a sequence of moves thattransforms an initial configuration of balls into a ‘tower’,in which balls are arranged on a designated peg. Lengthsfrom the three pegs differ. There are constraints: onlyone ball may be moved at a time, any ball not currentlymoved must remain on the peg, the number of movesallowed to solve the problem. The main dependentvariables are, mean numbers of extra moves taken;number of subjects solving at least half of the problemsperfectly and response latency.
Twelve relevant studies have been conducted using thetowers in the pathological groups of interest. Fivestudies differentiate ADHD from controls [1,55,93,136,138]. Two studies using ADHD children did not finda difference [48,84]. Five studies have been performedcomparing HFA with controls all show significant differ-ences between HFA and controls. One study comparedODD with controls and found a significant difference[43]. Two studies directly compared children withADHD with children with autism [84,86]. The autisticchildren performed poorer than the ADHD children andcontrols [11,50].

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 21
Clearly, the towers tasks need to be employed in amulti-clinical group comparison to establish their specifi-city, since they differentiate several clinical groups ofinterest from controls. There is, however, some supportfor the view that HFAs perform poorer than ADHDchildren in this type of planning task. Currently, there areno neural imaging studies available comparing the fourclinical groups of interest with one of the towers.
1.4. Fluency
In fluency tasks, the participant is required to generatesets of appropriate responses to a given set of stimulusconditions [133]. The tasks differ in the responses asubject is required to give. The main conditions are,letters; categories; and designs. Cognitive processes in-volved in fluency include processing speed, size of thevocabulary, semantic memory, working memory, inhibi-tion, and set maintenance. Patients with prefrontallesions perform poorer on fluency tasks, especially withpatients with right frontal lobe lesions [42,62,63].
Six studies compared ADHD children with controls onfluency tasks with letters and found poorer performancein ADHD compared with controls [41,42,55,63,97,111].Three studies did not find a difference [35,58,100]. Ninestudies used the fluency categories task, two found adifference, seven did not differentiate between ADHDand controls [9,42,58,63,97,100,136]. In four studies(using letters) of ODD/CD children, three reportedpoorer performance in the aggressive groups comparedwith controls [29,43,113] but one did not [132]. Only onestudy applied the category fluency task in ODD/CDchildren and found a difference [113]. In two studies ofautism, one used the letter version and differentiatedHFAs from controls [134] and one did not [74]. Threeapplied the category version [30,74,134]. These threestudies all differentiated autistics from controls. Onestudy found fewer responses in ADHD children thanchildren with ADHD and Tourette syndrome [111] andanother the reverse pattern [44].
Fluency seems to be dependent for its discriminatoryeffect upon which stimulus conditions are used. Lettersseem to differentiate better ADHD from controls. How-ever, these studies need to be qualified in that little isreported on control for LD and IQ. Again the ADHD-re-lated groups ODD/CD also perform poorer on the letterfluency task. Hence, the specificity of the test for ADHDis called into question. Categories have less discriminat-ing power between ADHD and controls but greatersuccess in differentiating HFAs from controls.
2. Discussion
In this paper, we have conducted a selective review of
EF measures in ADHD research, commencing from1990. We organise this discussion by summarising thefindings; we address six methodological issues which needto be addressed by the field and conclude with somegeneral remarks.
While the EF studies reviewed here indicate thatADHD children, adolescents and in some studies adultshave performance deficiencies in some EF tasks/tests, thepattern is not consistent between studies. There is evi-dence of an inhibitory deficit based on both the Stroopand the stop task. However, both measures are alsodeficient in other clinical groups such as ODD/CD. Thusthe findings with these two measures is not specific toADHD. On the other hand, there is evidence thatinhibition as measured by the stop task is not deficientin autism [87]. While the Stroop has often been shownto differentiate ADHD children from controls, the mech-anism responsible for this difference is currently uncer-tain and needs to be elucidated. The WCST is able todifferentiate HFA children from controls and there issome evidence that it can distinguish ADHD fromautistics [88]. This could be a possible starting point forfurther differentiation between the clinical groups ofinterest. The contrast between ADHD and controls usingthe WCST is less powerful: nearly a third of the studiesfailing to show a significant difference between these twogroups. Furthermore, a very large study with the WCSTcontrasted subgroups of ADHD children, ODD andreading disabled children found that perseverative errorsdid not differentiate ADHD subgroups nor ODD [55].Differentiation was obtained when non-perseverativeerrors were used. This finding argues against a cognitiveflexibility deficit in disruptive behaviour disorders, anessential feature of EF. The SOP has not been usedsufficiently to justify firm conclusions. Planning tasks asmeasured by the Towers differentiate HFAs from con-trols consistently. Differentiation of ADHD from con-trols is less consistent and there is a need for acomparison between all four clinical groups of interest.Fluency has produced in general a differentiation be-tween ADHD and controls. Here again is need a com-parison between the four clinical groups of interest.
Comparison between the clinical groups of interestusing neural imaging is sparse [33,53]. There are currentlyno studies which have used a neural imaging modalityin which all four groups (ADHD, ODD/CD, HFA andLD children) are compared with one another. This iscritical since there are both neuropsychological andneural imaging reports using the same paradigms andimplicating the same or related neural networks in thesegroups [33,38,77,130]. Furthermore, we did not locateneural imaging studies comparing these four groups ona variety of key EF measures such as: WCST, SOP, ToLand fluency.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2822
Scientific advancement in ADHD research will bedependent upon methodological improvement in atleast six areas. Rather than give a negative message tothe field, we feel that there is much to be accomplishedusing an EF approach to ADHD, for example, byshowing that the ADHD deficit is not confined tobottom-up processes but also to top-down processessuch as the effect of errors on one’s subsequent be-haviour [119]. Therefore, our comments are intended toenhance the potential impact that the EF approach mayhave for this syndrome (and others) in DevelopmentalNeuropsychology.
First, we have stressed the importance of comorbid-ity of ADHD with other disorders: ODD, CD, HFA,and LD, (see for the prior probabilities of this associa-tion, [3,123]. Whereas children in the CD group do notmeet criteria for ADHD, these children are likely toshow elevated levels of ADHD symptoms comparedwith normal children. The finding that CD was associ-ated with inhibitory deficits may, therefore, be due tothe presence of ADHD symptoms in this group. To ruleout this possibility, future studies using only a twogroup comparison (CD vs. controls) should control forthe presence of comorbid ADHD symptoms in CDchildren using statistical techniques. This point alsoapplies to other two-group comparisons. An equallyimportant issue to that of comorbidity is that of theneed to conduct research on subgroups of childrenwhich appear under the general diagnosis ADHD [72].This issue cannot for space reasons be addressed here.
Without proper assessment of these associations andeither their exclusion or statistical control, it is impossi-ble to know whether many current papers are specificto ADHD, the associated disorder or a combination ofboth. In addition to this point is needed not onlycontrol for IQ but also age. Children with ADHD havebeen shown to have a developmental delay of around 2years [106]. An important methodological improvementwould be to employ two control groups: age matchedand a younger age-group. This would enable one toestablish whether the observed group differences weredue only to the difference in a chronologically matchedgroup or were also shared by a younger control group,hence ruling out the developmental delay hypothesis.While there is discussion concerning matching for IQ orpartialing IQ out in an EF contrast [47], it is clearly astronger case when EF differences exist after account-ing for IQ differences between groups [25].
Second, many authors claim that the differences theyreport between ADHD and controls reflects a trueeffect for ADHD. This may be the case. However, theevidence to make that case is to show that the EFdifferences are specific to ADHD and not other clinicalgroups. This requires multiple clinical group compari-sons. For example, using set shifting tasks such as theWCST, there has been observed more perseverative
errors in HFAs than ADHD children [84]. This indi-cates two things, difficulties in cognitive flexibility arenot specific to ADHD and the degree of this deficit isless than in autistics. Likewise, assessment and inclu-sion of an appropriate learning disabled group willimprove the specificity of an EF difference betweenADHD and controls, as demonstrated in one largestudy [55].
Third, it has been recognised by leaders in the fieldthat measurement of EF is not an easy matter [15,16]and there are formidable measurement issues. Othershave addressed this issue with respect to tests such asthe Stroop [68] and indicated the plethora of processeswhich can account for the two dependent variables:latency and errors. Given the need for process specific-ity, there is a need to employ control tasks for thispurpose. This has seldom been done in EF research inADHD. A better approach is to employ well-definedparadigms, such as the stop task or a task-switchingparadigm [141] which enable measurement of specificcognitive processes. Alternatively, new computerparadigms based upon the WCST which distinguishbetween extra (between categories) and intra-dimen-sional (within categories) set shifting enable validationthrough neural imaging. For example, extra-dimen-sional shifting relative to intra-dimensional shifting hasbeen shown in a PET study [7] to activate the leftanterior PFC (BA 8 and 10), and the right dorsolateralprefrontal cortex (BA 9/46). Intra-dimensional set shift-ing activates the left-caudate nucleus. Using this distinc-tion, it has been shown that extra-dimensional shiftingdifferentiated ADHD children from controls [140]. Theimplication of this finding is that ADHD childrenexhibit a relative dysfunction in left anterior PFC andright dorsolateral PFC. Again, the specificity of thisfinding both in terms of clinical groups and neuralnetwork remains to be seen in future studies.
A related measurement problem is the face validity oftests. For example, the WCST is used in some researchto be a measure of set shifting and in others a measureof conceptual problem solving ability, use of feedback,the ability to modify incorrect strategies, flexibility, andinhibition of prepotent but incorrect responses. Itshould be noted that differences between groups havebeen found on the WCST but studies differ on whichdependent variable occurs. Specifically comparisonsbetween ADHD and control children are shown inTable 2.
From Table 2, it can be seen that perservative errorsand FTMS do a poor job in discriminating ADHDsfrom controls. These two critical variables seem tosuggest that cognitive flexibility may be disturbed inonly a subgroup of ADHD. Categories and total errorsare about equal. The only slight differentiation betweenADHD and controls is for non-perserverative errors.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 23
Table 2Studies reporting a comparison between ADHD and controls on dependent variables of the Wisconsin card sorting test (WCST)
Total errorsPerserverations NPerservative CategoriesFTMS
Difference 25 65 273No difference 3910
FTMS: failure to maintain a set (studies in Table 2: [4,18,35,41,42,44,48,56,61,93,97,100,110,116,117,124,136]).
One might question whether this variable is actuallyreflecting the fact that inaccuracy across a variety oftasks is characteristic of ADHD and not specific to theWCST. The argument that WCST might be bettersuited for discriminating younger than older ADHDsfrom controls has not been supported by a large study[55].
Clearly, the WCST may be measuring a variety ofprocesses and it is an empirical question which pro-cesses are being utilised in a given study. It wouldadvance the field when these processes would be distin-guished, preferably in a paradigm in which at least twoor more such as set shifting, flexibility and inhibitionare manipulated following the logic of the additivefactor method [121,125].
Another example of the issue face validity is theStroop. Many consider the Stroop as a measure ofinhibition [8,9,41,48,117] among others. Indeed, wehave placed the Stroop here under the heading ofinhibition. However, cognitive science, while not ex-cluding that possibility, has generated evidence thatthere are alternative processes which may account forthe Stroop interference effect [68]. We emphasise thispoint here in order to indicate that concepts such as‘inhibition’ may not be justified, when interpreting testresults such as the Stroop.
Fourth, a number of well-established task such as theToL have a myriad of dependent variables, decisiontime; execution time; total ToL errors; rule breaks;number of errors (to name a few). There is nothingwrong with using multiple dependent variables. Theissue here is that authors report some and not all of thedependent measures. Consequently, one cannot be sure,if the hypothesised process claimed to be measuredactually is being reported. Standardisation by editors ofreporting would greatly help the field. In addition,standardisation of the planning criterium/cut-off (some-times four sometimes five or another level) would en-sure that across studies the same level of task difficultywas employed and make studies comparable with oneanother.
Fifth, we propose that EF measures be used in thefield in which there is convergent evidence that the testor paradigm actually requires frontal functioning.While the EF concept is now treated as a psychologicalconstruct without necessarily implying frontal function-ing [32] others do employ tasks in which reports exist
for specific frontal functioning [16,140]. Advancementin the field would be made when bench mark tests ofEF were used with established activation patterns. Thiswould contrast with other tests/paradigms which couldbe shown to have widely distributed networks. Thesetests/paradigms, while less specific for frontal function-ing, might be more sensitive in detecting a loss ofgeneral cognitive control which might have clinicalrelevance.
Sixth, EF reports contain group (usually patient-con-trol) comparisons which are significant but with fewexceptions the effect size is not reported. This is notonly important for the researcher but also for theclinician in deciding whether to use a particular test foran assessment of a child. Often tests reported to havediscriminating effects between ADHD and controlsused in a single case (with ADHD) do not show adeficit. A variety of reasons for this is possible. Whatwe emphasise here is that such tests would be less oftenused if the clinician knew that the effect size wasmodest. Similarly, in addition to a group comparison,using symptom information as a dimension of ADHDa regression on to the dependent variables would en-hance insight into which clusters of ADHD (attention,hyperactivity and impulsivity) are contributing to theobserved finding.
The above proposals for methodological improve-ment in the field of EF and ADHD would enhance ourknowledge of the specificity of the function, the specifi-city of the disorder in a particular clinical group andguide both neural imaging and behavioural geneticstudies of a refined phenotype of ADHD. From theavailable results the following theoretical model is likelyto emerges.
When LD and IQ are controlled ADHD childrencompared with controls show a deficit in inhibition asmeasured by both the stop signal task and Stroop.Children with ODD/CD also exhibit this deficit. Thus,when inhibition is operationalised in this manner, com-mon inhibitory deficits appear with these disruptivebehaviour disorders. When, however, supervisory con-trol is required, there is evidence that ADHD childrenhave more difficulties than ODD children [25]. A keyissue to be clarified is why a working memory task(SOP) differentiates ODD/CD from controls followingcontrol for ADHD symptoms and general memory[111]. One possibility is that the relation between EF

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2824
and, on the one hand, ADHD and, on the other hand,ODD/CD reflects a developmental pattern of emergingdysfunction [74]. Hence, the relation between EF andADHD compared with ODD/CD may depend upon atwhich point in the developmental process these groupsof children are assessed. A second possibility is that therelation between EF and ADHD is dependent uponwhich ADHD subgroup one measures [9,55] or thegenetic subgroup studied [28,127]. Likewise, subtype ofaggression may have important effects upon whichaspect of EF is impaired [4,29,38,43,52,66,69,71,132]. Athird possibility is that the association of ODD/CDwith an inhibitory deficit reflects the ADHD symptoms,which are present in these disruptive groups rather thanaggression itself [108].
An intriguing difference emerges from this selectedreview concerning the absence of an inhibitory deficit inHFA in contrast to ADHD and aggressive disorders. Iffuture research could identify a deficit for HFA whichwas not present in ADHD, this would achieve thedouble dissociation which is required for neuropsycho-logical specificity between these two disorders [94].From the studies reviewed here, there would seem to besome indication that HFAs have greater deficits thanADHD children in set-shifting and planning. This mayprovide some of the necessary specificity for EF withrespect to the disorders reviewed here. Until this isachieved, EF specificity for ADHD remains to beestablished.
References
[1] Aman CJ, Roberts RJ, Pennington BF. A neuropsychologicalexamination of the underlying deficit in ADHD: the frontal vs.right parietal lobe theories. Devlopmental Psychology1998;34:956–69.
[2] American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 4th ed. Washington, DC: Author,1994.
[3] Angold A, Costello EJ, Erkanli A. Comorbidity. Journal ofChild Psychology and Psychiatry 1999;40:57–87.
[4] Aranowitz B, Liebowitz M, Hollander E, Fazzini E, Durlach-Misteli C, Frenkel M, Mosovich S, Garfinkel R, Saoud J,DelBene D, Cohen L, Jaeger A, Rubin AL. Neuropsychiatricand neuropsychological findings in conduct disorder and atten-tion-deficit hyperactivity disorder. Journal of Neuropsychiatryand Clinical Neurosciences 1994;6:245–9.
[5] Baddeley A. Working memory. Oxford: Clarendon, 1986.[6] Baddeley A, Della Sala S, Papagno C, Spinller H. Dual-task
performance in dysexecutive and nondysexecutive patients witha frontal lesion. Neuropsychology 1997;11(2):187–94.
[7] Baker SC, Rogers RD, Owen AM, Frith CD, Dolan RJ,Frackowiak RSJ, Robbins TW. Neural systems engaged byplanning: a PET study of the Tower of London task. Neuropsy-chologia 1996;34(6):515–26.
[8] Barkley RA. Behavioral inhibition, sustained attention, andexecutive functions: constructing a unifying theory of ADHD.Psychological Bulletin 1997;121:65–94.
[9] Barkley RA, Grodzinsky G, DuPaul G. Frontal lobe functionsin attention deficit disorder with and without hyperactivity: a
review and research report. Journal of Abnormal Child Psy-chology 1992;20:163–88.
[10] Bench CJ, Frith CD, Grasby PM, Friston KJ, Paulesu E,Frackowiak RSJ, Dolan RJ. Investigations of the functionalanatomy of attention using the Stroop test. Neuropsychologia1993;31:907–22.
[11] Bennetto L, Pennington BF, Rogers S. Intact and impairedmemory functions in autism. Child Development1996;67:1816–35.
[12] Berquin PC, Gied JN, Jacobsen LK, Hamburger SD, KrainAL, Rapoport JL, Castellanos FX. Cerebellum in attention-deficit hyperactivity disorder: a morphometric MRI study. Neu-rology 1998;50:1087–93.
[13] Boucagnani LL, Jones RW. Behaviors analogous to frontaldysfunction in children with attention deficit hyperactivity dis-order. Archives of Clinical Neuropsychology 1989;4:161–73.
[14] Brandeis D, van Leeuwen T, Rubia K, Vitacco D, Steger J,Pascual-Marqui L, Steinhausen HC. Neuroelectric mappingreveals precursor of stop failures in children with attentiondeficits. Behavioural Brain Research 1998;94:111–26.
[15] Burgess PW. Theory and methodology in executive function.In: Rabbitt P, editor. Methodology of frontal and executivefunction. Hove: England Psychology Press, 1997.
[16] Burgess PW, Veitch E, de Lacy Costello A, Shallice T. Thecognitive and neuroanatomical correlates of multitasking. Neu-ropsychologia 2000;38:848–63.
[17] Bush G, Whalen PJ, Rosen BR, Jenike MA, McInerney SC,Rauch SL. The counting Stroop: an interference task special-ized for functional neuroimaging—validation study with func-tional MRI. Human Brain Mapping 1998;6:270–82.
[18] Carter CS, Krener P, Chaderjian M, Northcutt C, Wolfe V.Asymmetrical visual-spatial attentional performance in ADHD:evidence for a right hemispheric deficit. Biological Psychiatry1995;37:788–97.
[19] Carter CS, Mintn M, Cohen JD. Interference and facilitationeffects during selective attention: an H2150 PET study ofStroop task performance. Neuroimage 1995;2:264–72.
[20] Casey BJ, Castellanos FX, Giedd JN, Marsh WL, HamburgerSD, Schubert AB, Vauss YC, Vaituzis CK, Dickstein DP,Sarfatti SE, Rapoport JL. Implication of right frontostriatalcircuitry in response inhibition and attention deficit/hyperactiv-ity disorder. Journal of American Academy of Child Adoles-cent Psychiatry 1997;36:374–83.
[21] Castellanos FX, Giedd JN, Eckburg P, Marsh WL, Vaituzis C,Kaysen D, Hamburger S, Hamburger S, Rapoport JL. Quanti-tative morphology of the caudate nucleus in attention deficithyperactivity disorder. American Journal of Psychiatry1994;151:1791–6.
[22] Chelune GJ, Fergusson W, Koon R, Dickey TO. Frontal lobedisinhibition in attention deficit disorder. Child Psychiatry andHuman Development 1986;16:221–34.
[23] Ciesielski KT, Harris RJ. Factors related to performance failureon executive tasks in autism. Child Neuropsychology 1997;3:1–12.
[24] Cirino PT, Chapieski ML, Massman PJ. Card sorting perfor-mance and ADHD symptomatology in children and adoles-cents with Tourette syndrome. Journal of Clinical andExperimental Neuropsychology 2000;22:245–56.
[25] Clark C, Prior M, Kinsella GJ. Do executive function deficitsdifferentiate between adolescents with ADHD and oppositionaldefiant/conduct disorder? A neuropsychological study using thesix elements test and Hayling sentence completion test. Journalof Abnormal Child Psychology 2000;28:403–14.
[26] Collins P, Roberts AC, Dias R, Everitt BJ, Robbins TW.Perseveration and strategy in a novel spatial self-ordered se-quencing task for nonhuman primates: effects of excitotoxiclesions and dopamine depletions of the prefrontal cortex. Jour-nal of Cognitive Neuroscience 1998;10:332–54.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 25
[27] Comings DE, Gade-Andavolu R, Gonzalez N, Wu S, Muhle-man D, Blake H, Dietz G, Saucier G, MacMurray JP. Com-parison of the role of dopamine, serotonin, and noradrenalinegenes in ADHD, ODD and conduct disorder: multivariateregression analysis of 20 genes. Clinical Genetics 2000;57:178–96.
[28] Daugherty TK, Quay HC, Ramos L. Response perseveration,inhibitory control, and central dopaminergic activity in child-hood behaviour disorders. Journal of Genetic Psychology1993;154:177–88.
[29] Dery M, Toupin J, Pauze R, Mercier H, Fortin L. Neuropsy-chological characteristics of adolescents with conduct disorder:association with attention-deficit-hyperactivity and aggression.Journal of Abnormal Child Psychology 1999;27:225–36.
[30] Dunn M, Gomes H, Sebastian M. Prototypicality of responsesof autistic, language disordered, and normal children in a wordfluency task. Child Neuropsychology 1996;2(2):99–108.
[31] Eskes GA, Bryson SE, McCormick TA. Comprehension ofconcrete and abstract words in autistic children. Journal ofAutism and Developmental Disorders 1990;20:61–73.
[32] Eslinger PJ. Conceptualizing, describing, and measuring com-ponents of executive function. In: Lyons GR, Krasnegor NA,editors. Attention, memory and executive function. Baltimore,MD: Brooks, 1996:367–95.
[33] Filipek PA. Neuroimaging in the developmental disorders: thestate of the science. Journal of Child Psychology Psychiatry1999;40:113–28.
[34] Filipek PA, Semrud-Clikeman M, Steingard RJ, Kennedy DN,Biederman J. Volumetric MRI analysis comparing attention-deficit hyperactivity disorder and normal controls. Journal ofChild Neurology 1997;48:589–601.
[35] Fischer M, Barkley RA, Edelbrock CS, Smallish L. The adoles-cent outcome of hyperactive children diagnosed by researchcriteria: II. Academic, attentional, and neuropsychologicalstatus. Journal of Consulting Clinical Psychology 1990;58:580–8.
[36] Frackowiak RSJ, Friston KJ, Frith CD, Dolan RJ, MaziottaJC. Human brain function. San Diego: Academic Press, 1997.
[37] Gaultney J-F, Kipp K, Weinstein JA, McNeill J. Inhibition andmental effort in attention deficit hyperactivity disorder. Journalof Developmental Physical Disabilities 1999;11:105–14.
[38] Giancola PR, Mezzich AC, Tarter RE. Executive cognitivefunctioning, temperament, and antisocial behavior in conduct-disordered adolescent females. Journal of Abnormal Psychol-ogy 1998;107:629–41.
[39] Goel V, Grafman J. Are frontal lobes implicated in ‘planning’functions? Interpreting data from the Tower of Hanoi. Neu-ropsychologia 1995;33:623–42.
[40] Grant DA, Berg EAA. A behavioural analysis of degree ofreinforcement and ease of shifting to new responses in a Weigel-type card-sorting problem. Journal of Experimental Psychology1948;38:404–11.
[41] Grodzinsky GM, Barkley RA. Predictive power of frontal lobetests in the diagnosis of attention deficit hyperactivity disorder.Clinical Neuropsychologist 1999;13:12–21.
[42] Grodzinsky GM, Diamond R. Frontal lobe functioning in boyswith attention deficit hyperactivity disorder. Journal of ClinicalPsychology 1992;45:427–46.
[43] Haggerty JC, Nevid JS, Moulton JL III. Anxiety and cognitiveperformance in adolescent women with disruptive behaviordisorders. Journal of Clinical Psychology 1998;54:1017–27.
[44] Harris EL, Schuerholz LJ, Singer HS, Reader MJ, Brown JE,Cox C, Mohr J, Chase CA, Denckla MB. Executive function inchildren with Tourette syndrome and/or attention deficit hyper-activity disorder. Journal of International NeuropsychologicalSociety 1995;1(6):511–6.
[45] Heaton RK. Wisconsin card sorting test manuel. Odessa, FL:Psychological Assessment Resource Inc, 1981.
[46] Heilman KM, Voeler KKS, Nadeau SE. A possible pathophys-iologic substrate of attention deficit hyperactivity disorder.Journal of Child Neurology 1991;6:S76–81.
[47] Hinshaw SP. Externalizing behavior problems and academicunderachievement in childhood and adolescence: causal rela-tionships and underlying mechanisms. Psychological Bulletin1992;111:127–55.
[48] Houghton S, Douglas G, West J, Whiting K, Wall M, Langs-ford S, Powell L, Carroll A. Differential patterns of executivefunction in children with attention-deficit hyperactivity disorderaccording to gender and subtype. Journal of Child Neurology1999;14:801–5.
[49] Hughes C, Dunn J, White A. Trick or treat?: Uneven under-standing of mind and emotion and executive dysfunction in‘Hard-to-manage’ pre-schoolers. Journal of Child PsychologyPsychiatry 1998;39:981–94.
[50] Hughes C, Russel J, Robbins TW. Evidence for executivedysfunction in autism. Neuropsychologia 1994;32:1–16.
[51] Humes GE, Welsh MC, Retzlaff P, Cookson N. Towers ofHanoi and London: reliability and validity of two executivefunction tasks. Psychological Assessment 1997;4:249–57.
[52] Hurt J, Naglieri JA. Performance of delinquent and nondelin-quent males on planning, attention simultaneous, and succes-sive cognitive processing tasks. Journal of Clinical Psychology1992;48:120–8.
[53] Hynd GW, Semrud-Clikeman M, Lorys AR, Novey ES, Eliop-ulos D. Brain morphology in developmental dyslexia and atten-tion deficit disorder/hyperactivity. Archives of Neurology1990;47:919–26.
[54] ICD-10 Classification of Mental and Behavioural Disorders:clinical descriptions and diagnostic guidelines 1992; Diagnosticcriteria for research 1993. World Health Organisation, Geneva.
[55] Klorman R, Hazel-Fernandez LA, Shaywitz SE, Fletcher JM,Marchione KE, Holahan JM, Stuebing KK, Shaywitz BA.Executive functioning deficits in attention deficit/hyperactivitydisorder are independent of oppositional defiant or readingdisorder. Journal of American Academy of Child AdolescentPsychiatry 1999;38:1148–55.
[56] Koziol LF, Stout CE. Use of a verbal fluence measure inunderstanding and evaluating ADHD as an executive functiondisorder. Perceptual Motor Skills 1992;75:1187–92.
[57] Krusch DA, Klorman R, Brumaghim JT, Fitzpatrick PA,Borgstedt AD, Strauss J. Slowing during and after errors inADD: methylphenidate slows reactions of children with atten-tion deficit disorder during and after an error. Journal ofAbnormal Child Psychology 1996;24:633–50.
[58] Kusche CA, Cook ET, Greenberg MT. Neuropsychologicaland cognitive functioning in children with anxiety, externaliz-ing, and comorbid psychopathology. Journal of Clinical ChildPsychology 1993;22:172–95.
[59] Lazar JW, Yitzchak F. Frontal systems dysfunction in childrenwith attention-deficit/hyperactivity disorder and learning dis-abilities. Journal of Neuropsychiatry Clinical Neurosciences1998;10:160–7.
[60] Lezak MD. Neuropsychological assessment, third ed. NewYork: Oxford University Press, 1995.
[61] Logan GD, Cowan WB. On the ability to inhibit thought andaction: a theory of an act of control. Psychological Review1984;91:295–327.
[62] Logan GD, Schachar R, Tannock R. Impulsivity and inhibitorycontrol. Psychological Science 1997;8:60–4.
[63] Loge DV, Staton DV, Beatty WW. Performance of childrenwith ADHD on tests sensitive to frontal lobe dysfunction.Journal of American Academy of Child Adolescent Psychiatry1990;29:540–5.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2826
[64] Lou HC, Henriksen L, Bruhn P. Focal cerebral hypoperfusionin children with dysphasia and/or attention deficit disorder.Archives of Neurology 1984;41:825–9.
[65] Lou HC, Henriksen L, Bruhn P, Borner H, Nielsen JB. Striataldysfunction in attention deficit and hyperkinetic disorder.Archives of Neurology 1989;46:48–52.
[66] Lueger RJ, Gill KJ. Frontal lobe cognitive dysfunction inconduct disorder adolescents. Journal of Clinical Psychology1990;46:696–706.
[67] Lufi D, Cohen A, Parish-Plass J. Identifying attention deficithyperactive disorder with the WISC-R and the Stroop colorand word test. Psychology in the Schools 1990;27:28–34.
[68] MacLeod CM. Half a century of research on the Stroop effect:an integrative review. Psychological Bulletin 1991;109:163–203.
[69] MacLeod D, Prior M. Attention deficits in adolescents withADHD and other clinical groups. Child Neuropsychology1996;21:1–10.
[70] Matson DE, Fischer M. A comparison of internalizers, extar-nalizers, and normals using the WISC-R and the Wisconsincard sorting test. Journal of Psychoeducational Assessment1991;9:140–51.
[71] McBurnett K, Harris SM, Swanson JM, Pfiffner LJ, Tamm J,Freeland D. Neuropsychological and psychophysiological dif-ferentiation of inattention/overactivity and aggression/defiancesymptom groups. Journal of Clinical Child Psychology1993;22:165–71.
[72] Milich R, Balentine AC, Lynam DR. ADHD combined typeand ADHD predominantly inattentive type are distinct andunrelated disorder. Clinical Psychology: Science and Practice2001;8:463–88.
[73] Miller DC, Kavcic V, Leslie JE. ERP changes induced bymethylphenidate in boys with attention-deficit hyperactivitydisorder. Journal of Attention Disorders 1996;1:95–113.
[74] Minshew NJ, Goldstein G, Muenz LR, Payton LR. Neuropsy-chological functioning in nonmentally retarded autistic individ-uals. Journal of Clinical and Experimental Neuropsychology1992;14:749–61.
[75] Minshew NJ, Goldstein G, Siegel DJ. Neuropsychologic func-tioning in autism: profile of a complex information processingdisorder. Journal of International Neuropsychological Society1997;3:303–16.
[76] Moffitt TE, Lynham DR, Silva PA. Neuropsychological testspredicting persistent male delinquency. Criminology1994;32:277–300.
[77] Moss HB, Talagala SL, Kirisci L. Phosphorous-31 magneticresonance brain spectroscopy of children at risk for a substanceuse disorder: preliminary results. Psychiatry Research NeuralImaging Section 1997;76:101–12.
[78] Nigg JT. The ADHD response-inhibition deficit as measured bythe stop task: replications with DSM-IV combined type, exten-sion, and qualification. Journal of Abnormal Psychology1999;27:393–402.
[79] Oosterlaan J, Logan GD, Sergeant JA. Response inhibition inAD/HD, CD, comorbid AD/HD+CD, anxious and controlchildren: a meta-analysis of studies with the stop task. Journalof Child Psychology and Psychiatry 1998;39:411–26.
[80] Oosterlaan J, Sergeant JA. Response inhibition and responsere-engagement in attention-deficit hyperactivity disorder, dis-ruptive, anxious and normal children. Behavioural Brain Re-search 1998a;94:33–43.
[81] Oosterlaan J, Sergeant JA. Effects of reward and response coston response inhibition in AD/HD, disruptive, anxious, andnormal children. Journal of Abnormal Child Psychology1998b;26:161–74.
[82] Owen AM, Evans AC, Petrides MP. Evidence for a two-stagemodel of spatial working memory processing within the lateral
frontal cortex: a positron emission tomography study. CerebralCortex 1996;6:31–8.
[83] Ozonoff S. Reliability and validity of the Wisconsin cardsorting test in studies of autism. Neuropsychology 1995;9:491–500.
[84] Ozonoff S, Jensen J. Brief report: specific executive functionprofiles in three neurodevelopmental disorders. Journal ofAutism and Developmental Disorders 1999;29:171–7.
[85] Ozonoff S, McEvoy RE. A longitudinal study of executivefunction and theory of mind development in autism. Develop-mental Psychopathology 1994;6:415–31.
[86] Ozonoff S, Pennington BF, Rogers SJ. Executive functiondeficits in high-functioning autistic individuals: relationship totheory of mind. Journal of Child Psychology and Psychiatry1991;32:1081–105.
[87] Ozonoff S, Strayer DL. Inhibitory function in nonretardedchildren with autism. Journal of Autism and DevelopmentalDisorders 1997;27:59–77.
[88] Ozonoff S, Strayer DL, McMahon W, Filloux F. Executivefunction abilities in autism and Tourette syndrome: an informa-tion processing approach. Journal of Child Psychology andPsychiatry 1994;35(6):1015–32.
[89] Papa M, Sergeant JA, Sadile AG. Reduced transduction mech-anisms in the anterior accumbal interface of an animal model ofthe attention-deficit hyperactivity disorder. Behavioural BrainResearch 1998;94:187–96.
[90] Papa M, Berger DF, Sagvolden T, Sergeant JA, Sadile AG. Aquantitative cytochrome oxidase mapping study, cross-regionaland neurobehavioural correlations in the anterior forebrain ofan animal model of attention deficit hyperactivity disorder.Behavioural Brain Research 1998;94:197–212.
[91] Pascualvaca DM, Fantie BD, Papageorgiou M, Mirsky AF.Attentional capacities in children with autism: is there a generaldeficit in shifting focus. Journal of Autism and DevelopmentalDisorders 1998;28:467–78.
[92] Pennington BF, Bennetto L, McAleer OK, Roberts RJ Jr.Executive functions and working memory: theoretical and mea-surement issues. In: Lyon GR, Krasnegor NA, editors. Atten-tion, memory and executive function. Baltimore: Paul H.Brookes, 1996:327–48.
[93] Pennington BF, Groissier D, Welsh MC. Contrasting cognitivedeficits in attention deficit hyperactivity disorder versus readingdisability. Developemental Psychology 1993;29:511–23.
[94] Pennington BF, Ozonoff S. Executive functions and develop-mental psychopathology. Journal of Child Psychology andPsychiatry 1996;37:51–87.
[95] Petrides M, Milner B. Deficits on subject-ordered tasks afterfrontal- and temporal-lobe lesions in man. Neuropsychologia1982;12:323–30.
[96] Petrides M, Alivisatos B, Evans AC, Meyer E. Dissociation ofhuman and mid-dorsolateral from posterior dorsolateral frontalcortex in memory processing. Proceedings of the NationalAcademy of Science of the United States of America1993;90:873–7.
[97] Pineda D, Ardila A, Rosselli M. Neuropsychological and be-havioural assessment of ADHD in seven- to 12-year-old chil-dren: a discriminant analysis. Journal of Learning Disabilities1999;32(2):159–73.
[98] Pliszka SR, Borcherding SH, Spratley K, Leon S, et al. Measur-ing inhibitory control in children. Journal of DevelopmentalBehavioural Paediatrics 1997;18:254–9.
[99] Prior MR, Hoffmann W. Neuropsychological testing of autisticchildren through an exploration with frontal lobe tests. Journalof Autism and Developmental Disorders 1990;20:581–90.
[100] Reader MJ, Harris EL, Schuerholz LJ, Denckla MB. Attentiondeficit hyperactivity disorder and executive dysfunction. Devel-opemental Neuropsychology 1994;10:493–512.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–28 27
[101] Reitan RM, Wolfson D. A selective and critical review ofneuropsychological deficits and the frontal lobes. Neuropsy-chology Review 1994;4:161–98.
[102] Rubia K, Oosterlaan J, Sergeant JA, Brandeis D, Leeuwen vanT. Response inhibition and response re-engagement in atten-tion-deficit/hyperactivity disorder, disruptive, anxious and nor-mal children. Behavioural Brain Research 1998;94:25–32.
[103] Rubia K, Overmeyer S, Taylor E, Brammer M, Williams SCR,Simmons A, Bullmore ET. Hypofrontality in Attention DeficitHyperactivity Disorder during higher-order motor control: Astudy with functional MRI. American Journal of Psychiatry1999;156:891–6.
[104] Sagvolden T, Sergeant JA. Attention-deficit hyperactivity disor-der: from brain dysfunctions to behaviour. Behavioural BrainResearch 1998;94:1–10.
[105] Sanders AF. Towards a model of stress and performance. ActaPsychologica 1983;53:61–97.
[106] Satterfield JH, Braley BW. Evoked potentials and brain matu-ration in hyperactive and normal children. Electroencephalog-raphy Clinical Neurophysiology 1977;43:43–51.
[107] Schachar R, Logan GD. Impulsivity and inhibitory control innormal development and childhood psychopathology. Devel-opemental Psychology 1990;26:710–20.
[108] Schachar R, Mota VL, Logan GD, Tannock R, Klim P.Confirmation of an inhibitory control deficit in attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psy-chology 2000;28:227–36.
[109] Schachar R, Tannock R, Mariott M, Logan G. Deficientinhibitory control in attention deficit hyperactivity disorder.Journal of Abnormal Child Psychology 1995;23:411–37.
[110] Schuerholz LJ, Baumgardner TL, Singer HS, Reiss AL,Denckla MB. Neuropsychological status of children withTourette’s syndrome with and without attention deficit hyperac-tivity disorder. Neurology 1996;46:958–65.
[111] Schuerholz LJ, Singer HS, Denckla MB. Gender study ofneuropsychological and neuromotor function in children withTourette syndrome with and without attention-deficit hyperac-tivity disorder. Journal of Child Neurology 1998;13:277–82.
[112] Seguin JR, Boulerice B, Harden PW, Tremblay RE, Pihl RO.Executive functions and physical aggression after controllingfor attention deficit hyperactivity disorder, general memory andIQ. Journal of Child Psychology and Psychiatry 1999;40:1197–208.
[113] Seguin JR, Pihl RO, Harden PW, Tremblay RE, Boulerice B.Cognitive and neuropsychological characteristics of physicallyaggressive boys. Journal of Abnormal Psychology1995;104:614–24.
[114] Seidman LL, Biederman J, Faraone SV, Milberger S, NormanD, Seiverd K, Benedict K, Guite J, Mick E, Kiely K. Effects offamily history and comorbidity on the neuropsychological per-formance of children with ADHD: preliminary findings. Jour-nal of American Academy of Child Adolescent Psychiatry1995;34:1015–24.
[115] Seidman LJ, Biederman J, Faraone SV, Weber W, Mennin D,Jones J. A pilot study of neuropsychological function in girlswith ADHD. Journal of American Academy of Child Adoles-cent Psychiatry 1997;36(3):336–72.
[116] Seidman LL, Biederman J, Faraone SV, Weber W, Oullette C.Towards defining a neuropsychology of attention deficit-hyper-activity disorder: performance of children and adolescents froma large clinically referred sample. Journal of Consulting ClinicalPsychology 1997;65:150–60.
[117] Seidman LJ, Biederman J, Monuteaux MC, Weber W, FaraoneSV. Neuropsychological functioning in nonreferred siblings ofchildren with attention deficit/hyperactivity disorder. Journal ofAbnormal Psychology 2000;109:252–65.
[118] Semrud-Clikeman M, Steingard RJ, Filipek P, Biederman J,
Bekken K, Renshaw PF. Using MRI to examine brain-behaviorrelationships in males with attention deficit hyperactivity disor-der. Journal of American Academy of Child Adolescent Psychi-atry 2000;39:477–84.
[119] Sergeant JA, van der Meere JJ. What happens after a hyperac-tive commits and error. Psychiatry Research 1988;28:157–64.
[120] Sergeant JA, van der Meere JJ. Additive factor methodologyapplied to psychopathology with special reference to hyperac-tivity. Acta Psychologica 1990;74:277–95.
[121] Sergeant JA, Oosterlaan J, van der Meere JJ. Informationprocessing and energetic factors in attention-deficit/hyperactiv-ity disorder. In: Quay HC, Hogan A, editors. Handbook ofdisruptive behavior disorders. New York: Plenum Press,1999:75–104.
[122] Shallice T. Specific impairments of planning. PhilosophicalTransactions of Royal Society of London B Biological Science1982;298:199–209.
[123] Shaywitz BA, Fletcher JM, Shaywitz SE. Defining and classify-ing learning disabilities and attention deficit/hyperactivity disor-der. Journal of Child Neurology 1995;10:S50–7.
[124] Shue KL, Douglas VI. Attention deficit hyperactivity disorderand the frontal lobe syndrome. Brain Cognition 1992;20:104.
[125] Sternberg S. Discovery of processing stages: extensions of don-ders’ method. In: Koster WG, editor. Attention and perfor-mance II. Amsterdam: Elsevier, 1969:276–315.
[126] Stroop JR. Studies of inference in serial verbal reactions. Jour-nal of Experimental Psychology 1935;18:643–62.
[127] Swanson J, Oosterlaan J, Murias M, Schuck S, Flodman P,Spence MA, Wasdell M, Ding YH-C, Smith M, Mann M,Carlson C, Kennedy JL, Sergeant JA, Leung P, Zhang YP,Sadeh A, Chen C, Whalen CK, Babb KA, Moyzis R, PosnerMI. Attention deficit/ hyperactivity disorder children with a7-repeat allele of the dopamine receptor D4 gene have extremebehavior but normal performance on critical neuropsychologi-cal tests of attention. Proceedings of the National Academy ofScience of the United States of America 2000;97:4754–9.
[128] Swanson JM, Sergeant JA, Taylor E, Sonuga-Barke EJS,Jensen PS, Cantwell DP. Attention-deficit hyperactivity disor-der and hyperkinetic disorder. Lancet 1998;351:429–33.
[129] Szatmari P, Tuff L, Finlayson MAJ, Bartolucci G. Asperger’ssyndrome and autism: neurocognitive aspects. Journal of Amer-ican Academy of Child Adolescent Psychiatry 1990;29:130–6.
[130] Tannock R. Attention deficit hyperactivity disorder. Journal ofChild Psychology and Psychiatry 1998;39:65–99.
[131] Taylor SF, Kornblum S, Lauber EJ, Minoshima S, KoeppeRA. Isolation of specific interference processing in the Strooptask: PET activation studies. Neuroimage 1997;6:81–92.
[132] Toupin J, Dery M, Pauze R, Mercier H, Fortin L. Cognitiveand familial contributions to conduct disorder in children.Journal of Child Psychology and Psychiatry 2000;4:333–44.
[133] Tranel D, Anderson SW, Benton A. Development of the con-cept of ‘executive function’ and its relationship to the frontallobes. In: Boller F, Grafman J, editors. Handbook neuropsy-chology. Amsterdam: Elsevier Science, 1994.
[134] Turner MA. Generating novel ideas: fluency performance inhigh-functioning and learning disabled individuals with autism.Journal of Child Psychology and Psychiatry 1999;40(2):189–201.
[135] Vaijdya CJ, Austin G, Kirkorian G, Ridlehuber HW, DesmondJE, Glover GH, Ganrieli JDE. Selective effects ofmethylphenidate in attention deficit hyperactivity disorder: afunctional magnetic resonance study. Proceedings of the Na-tional Academy of Science of the United States of America1998;95:14994–9.
[136] Weyandt LL, Willis WG. Executive functions in school-agedchildren: potential efficacy of tasks in discriminating clinicalgroups. Developemental Neuropsychology 1994;10(1):27–38.

J.A. Sergeant et al. / Beha�ioural Brain Research 130 (2002) 3–2828
[137] White JL, Moffitt TE, Caspi A, Jeglum Bartusch D, NeedlesDJ, Stouthamer-Loeber M. Measuring impulsivity and examin-ing its relationship to delinquency. Journal of Abnormal Psy-chology 1994;103(2):192–205.
[138] Wiers RW, Gunning WB, Sergeant JA. Is a mild deficit inexecutive functions in boys related to childhood ADHD or toparental multigenerational alcoholism? Journal of AbnormalChild Psychology 1998;26(6):415–30.
[139] Willcutt EG, Pennington BF, DeVries JC. Twin study ofthe etiology of comorbidity between reading disability andattention-deficit/hyperactivity disorder. American Journal of
Medical Genetics (Neuropsychology Genetics) 2000;96:293–301.
[140] Williams D, Stott CM, Goodyer IM, Sahakian BJ. Specificlanguage impairment with or without hyperactivity neuropsy-chological evidence for frontostriatal dysfunction. Developmen-tal Medicine and Child Neurology 2000;42(6):368–75.
[141] Wylie G, Allport A. Task switching and the measurement of‘switch costs’, Psychological Research; 63:212–33.
[142] Yeates KO, Bornstein RA. Attention deficit disorder and neu-ropsychological functioning in children with Tourette’s syn-drome. Neuropsychology 1994;8:65–74.
Copyright © 2022 FDOKUMEN




















