Hospital Admission and Community Treatment of Mental Disorders in England from 1998 to 2012
17
Admissions for Mental Disorders in England 1 Hospital Admission and Community Treatment of Mental Disorders in England from 1998 to 2012 Prof. B. H. Green 1 and Dr. E. C. Griffiths 2 1 Faculty of Health and Social Care, University of Chester, Chester, UK; 2 Department of Entomology, Gardner Hall, Derieux Place, North Carolina State University, Raleigh NC 27695, USA
-
Upload
manchester -
Category
Documents
-
view
1 -
download
0
Transcript of Hospital Admission and Community Treatment of Mental Disorders in England from 1998 to 2012
Admissions for Mental Disorders in England 1
Hospital Admission and Community Treatment of Mental Disorders in England from 1998 to 2012
Prof. B. H. Green1 and Dr. E. C. Griffiths2
1 Faculty of Health and Social Care, University of Chester, Chester, UK;
2 Department of Entomology, Gardner Hall, Derieux Place, North Carolina State University, Raleigh NC 27695, USA
Admissions for Mental Disorders in England 2
Abstract
Objective The number of psychiatric hospital beds in England has declined since the 1950s. Since the early 2000s mental health staff increasingly work in community treatment teams. We analysed recent trends in hospital and community treatment in England for eight mental health diagnoses. Method We obtained data from the UK Government Health and Social Care Information Centre covering the period 1998 to 2012. We analysed hospital admissions and length of stay for each diagnosis each year using linear regression. We studied associations among admissions, community treatment, and hospital bed availability each year using structural equation modeling. Results The number of mental health beds fell 39%, from 37000 in 1998 to 22300 in 2012.
Hospital admissions for five diagnoses declined significantly (depression, bipolar disorder, schizophrenia, dementia and Obsessive Compulsive Disorder, p<0.01 or p<0.001). The strongest decline for depression involved 1000 fewer admissions each year. Admissions for three disorders increased significantly (Post Traumatic Stress Disorder, eating disorders and alcohol-‐related disorders, p<0.01 or p<0.001). Alcohol-‐related admissions increased most strongly, by more than 1700 a year, and were significantly associated with increasing liver fibrosis and cirrhosis admissions (Pearson’s r=0.89, p<0.001) across the NHS, and the affordability of alcohol (Pearson’s r =0.76, p<0.01).
The median length of stay declined significantly for four diagnoses (p<0.001); the other four diagnoses did not change significantly. Depression had the steepest decline of almost one less day in hospital per admission per year.
Almost 300 more patients were sectioned under the Mental Health Act each year.
Community activity had relatively little effect on admissions, and its direct effect was not significantly different from zero. Years with more psychiatric beds had more admissions.
Conclusions Mental health bed numbers have declined significantly in England. Annual admissions and lengths of stay declined for a range of severe mental disorders including schizophrenia, bipolar disorder, and depression.
The fall in available beds can account for much of the decline in admissions. National reports of crisis team activity are not associated with declines in hospital admissions.
There may be significant needs, especially of depressive patients, not being met by secondary community services, such as 24-‐hour observation and care. This calls for policy review and further epidemiological study of morbidity, mortality and health needs associated with mental disorder in the community.
Admissions for Mental Disorders in England 3
Introduction
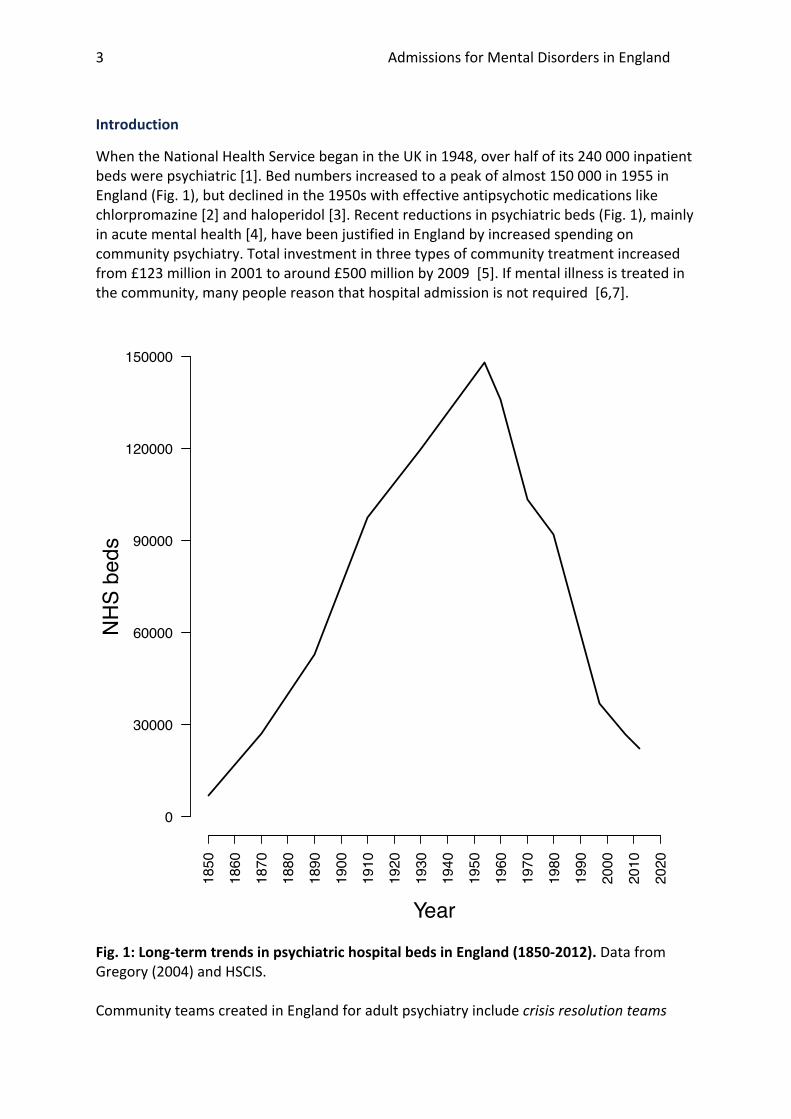
When the National Health Service began in the UK in 1948, over half of its 240 000 inpatient beds were psychiatric [1]. Bed numbers increased to a peak of almost 150 000 in 1955 in England (Fig. 1), but declined in the 1950s with effective antipsychotic medications like chlorpromazine [2] and haloperidol [3]. Recent reductions in psychiatric beds (Fig. 1), mainly in acute mental health [4], have been justified in England by increased spending on community psychiatry. Total investment in three types of community treatment increased from £123 million in 2001 to around £500 million by 2009 [5]. If mental illness is treated in the community, many people reason that hospital admission is not required [6,7].
Fig. 1: Long-‐term trends in psychiatric hospital beds in England (1850-‐2012). Data from Gregory (2004) and HSCIS. Community teams created in England for adult psychiatry include crisis resolution teams
1850
1860
1870
1880
1890
1900
1910
1920
1930
1940
1950
1960
1970
1980
1990
2000
2010
2020
0
30000
60000
90000
120000
150000
Year
NH
S be
ds

Admissions for Mental Disorders in England 4
who intervene and assess in emergencies, home treatment teams who visit patients’ homes, assertive outreach teams who engage with treatment resistant chronically ill patients, and early intervention teams who treat new cases of psychosis. Few countries manage psychiatric patients in exactly this way [8]. Precisely how recent shifts in mental health spending in England from hospital to community-‐based management have affected patient health and wellbeing is not clear and evaluations are preliminary [9]. This shift from hospital to community care occurred in other countries. Advances in psychopharmacology in the 1950s and 1960s and criticisms of asylums led to deinstitutionalization with widespread reduction in inpatient beds across Europe, and development of community-‐based treatments [10]. Psychiatric bed numbers also fell in the United States, down by 90% by 2002 from 525,000 in 1970 [11]. Studies appraising the policy of deinstitutionalization have reported that unintended reinstitutionalisation has occurred in many countries, with prisons now housing many mentally ill people. [12]. In England, spending on the ‘three key modernization services’ (assertive outreach, crisis resolution and home treatment and early intervention in psychosis) rose to £491 million by 2011/12. Although overall bed numbers have fallen, the 2011/12 spending on the remaining secure beds was over twice that spent on ‘modernization services’ at £1,056 million. National commissioner spending on all services was £5,496 million. The modernization services therefore represent about 9% of the total spend [5]. Whether this is adequate to treat the morbidity within the population is less clear, and would perhaps require a longitudinal population survey of mental health needs to have been running alongside the changes in service delivery. Some published studies report little advantage in community treatment over hospital admission. In the 1980s there were warnings that large-‐scale home treatment would burden patients' families and be less cost effective than hospital treatment [13]. Local assessment studies of the first years of community psychiatric team activity showed them treating hundreds of patients, but unchanged or even increased hospital referrals [14,15]. Studies finding modest reductions in hospital admission rates had a small sample size [16], or were short-‐term, e.g. a finding that hospital admission of crisis patients fell (OR 0.19) within an 8 week window [17]. Despite community treatment having expanded over decades in the UK to cover tens of thousands of patients, evaluations over longer timescales or wider geographic areas are rare. Psychiatric admissions were no different between health trusts with or without crisis teams [18]. Crisis or home treatment teams may offer insufficient treatment for older people [19, 20], uncooperative patients, or those at risk of self-‐neglect [21]. A recent systematic review of crisis intervention for severe mental illness found just six studies evaluating the effect of community crisis teams on 984 patients and judged their methodology to be “poor” [22]. These six studies excluded service users with alcohol or drug misuse or those in danger of harming themselves or others, and so are atypical of populations managed by community teams in England. Some studies report declines in admissions associated with early intervention [23] and crisis resolution [24], but others argue that community treatment does not reduce admissions [25, 26]. Studies on assertive outreach teams have found very little difference in primary outcomes (Inpatient bed use at 18 months) or other clinical or social outcome measures compared to standard treatment [27].
Admissions for Mental Disorders in England 5
The quality of hospital psychiatric treatment has also been criticised. Acute wards are reportedly poorly designed, poorly maintained and provide few activities, which leads to higher concentrations of bored, aggressive and challenging patients [28]. In a 2008 survey of 554 acute psychiatric wards, 23% were ‘weak’ on multiple factors, and nearly 20% were weak for safety [29]. Incidents on psychiatric wards have the capacity to damage patients and staff [30], with 1 in 10 nurses injured annually [31, 32]. We use annual, national-‐level data from 1998 to 2012 on the numbers of patients admitted and treated for various mental disorders (we chose eight ICD-‐10 diagnoses: schizophrenia, bipolar disorder, depression, post traumatic stress disorder (PTSD), obsessive compulsive disorder (OCD), eating disorders, alcohol misuse, and dementia) to examine whether the continued decline in inpatient beds and increase in community treatment were successful in terms of the following four hypotheses:
1. annual inpatient admissions would decline uniformly across diagnostic groups as community treatment prevented admission,
2. the length of hospital stay of admitted patients would decline as community treatment enabled earlier discharge,
3. annual compulsory patient detentions under the Mental Health Acts of 1983 and 2007 would also decline, as community teams prevented admissions, and
4. community team activity would be associated with greater declines in admissions than accounted for by continued declines in psychiatric beds.
Methods
We gathered data from 1998 to 2012 for admissions and median length of stay across NHS England from the UK Government Health and Social Care Information Centre. We analysed data on eight ICD-‐10 adult mental disorders derived from the annually published Health Episode Statistics spreadsheets on primary diagnoses of admissions, which give mean and median but no indication of variance. We use median length of stay because, unlike the mean, it is unaffected by outliers like patients with extremely long hospital stays. Admissions included beds in NHS hospitals and NHS-‐funded beds in independent hospitals. NHS mental health teams have been focused upon severe mental illness, though the term ‘severe mental illness’ is used inconsistently [33]. We chose to include the ‘severe’ diagnoses generally held to be within the remit of community teams such as schizophrenia (ICD-‐10 code F20), bipolar affective disorder (F31) and depression (we analysed depressive disorder F32 and recurrent depressive disorder F33). We also explored other disorders including eating disorders (F50), alcohol disorders (specifically F10 Mental and behavioural disorders due to use of alcohol), dementia (specifically we used F03 unspecified dementia, which represents the largest numerical ICD dementia grouping), and admissions for the ICD 10 code F43 (reaction to stress and adjustment disorders) as a representative grouping for PTSD and associated anxiety disorders. To assess community team activity we obtained data on the annual open records of community crisis teams in England from 2003 to 2010. National data for other types of
Admissions for Mental Disorders in England 6
community treatment team or for other years were unavailable. Data on mental disorder disorders treated by community teams were also unavailable. For earlier years when patients with severe mental illness were not treated in the community, activity level data were set to zero.
Community psychiatric services vary across the UK for instance in terms of how community teams and hospitalisations are managed. We analysed data at the national level to aggregate out this variability.
Annual numbers of available hospital beds and of Mental Health Act detentions were obtained from the UK Department of Health [34].
We analysed these data using statistical programming package R [35]. Trends in hospital admission, length of stay, and detentions between 1998-‐2012 were analysed using linear regression. We quote the gradient of the fitted line (β coefficient) and the p-‐values from a t-‐test. Further analyses of alcohol-‐related admissions use correlation; we quote Pearson’s r-‐statistic and its associated p-‐value. To test our fourth hypothesis that community team activity was significantly associated with hospital admissions we used structural equation modeling (SEM). Like multiple regression, SEM examines the covariances of variables in a proposed statistical model. SEM also allows indirect effects to be analysed, enabling us to test the direct effects of community team activity and available beds on hospital admissions, and the indirect effect of community team activity on bed numbers and, indirectly, on hospital admissions. Hospital admission was the total annual admissions for the eight diagnoses used above. We fitted the model by maximum likelihood using the R package lavaan [36]. Since our dataset is small we tested the significance of each path in the model using a parametric bootstrap and a two-‐tailed t-‐test. We scaled data to have covariances within an order of magnitude and report standardized coefficients so we can compare the association of community teams and available beds.
Admissions for Mental Disorders in England 7
Results Hypothesis 1: annual inpatient admissions would decline uniformly across diagnostic groups
Since 1998 the number of available psychiatric beds in England fell by 39% from 37,000 in 1998 to 22,268 in 2012 ([30], Fig. 1).
Annual hospital admissions declined between 1998 and 2012 for five diagnoses, and increased for three diagnoses (Fig. 2). All these trends were statistically significant (linear regression of admissions over time: all p<0.01 or p<0.001). The strongest decline was for depression with over 1000 fewer annual admissions (β=-‐1085; dementia β=-‐764; schizophrenia β=-‐468; Bipolar Disorder β=-‐159, Obsessive Compulsive Disorder β=-‐21). The strongest increase was for alcohol-‐related admissions with more than 1700 more per year (β=1764; Eating Disorders β=55; PTSD β=17).
Alcohol and cirrhosis
From 1998 to 2012 the number of admissions for overall alcohol-‐related psychiatric illness (F10) was significantly positively correlated with those admissions involving liver fibrosis and cirrhosis (Pearson’s r=0.89, p<0.001) throughout all beds in the NHS. The proportion of F10 alcohol admissions involving liver fibrosis or cirrhosis was unchanged between 1998 and 2012 with a mean of 0.103 (linear regression of proportion over time: β-‐coefficient<0.001, p>0.9). Alcohol-‐related admissions were significantly positively correlated with affordability of alcohol (r=0.76, p<0.01, n=12 1998-‐2010, data from HSCIS).
Admissions for Mental Disorders in England 8
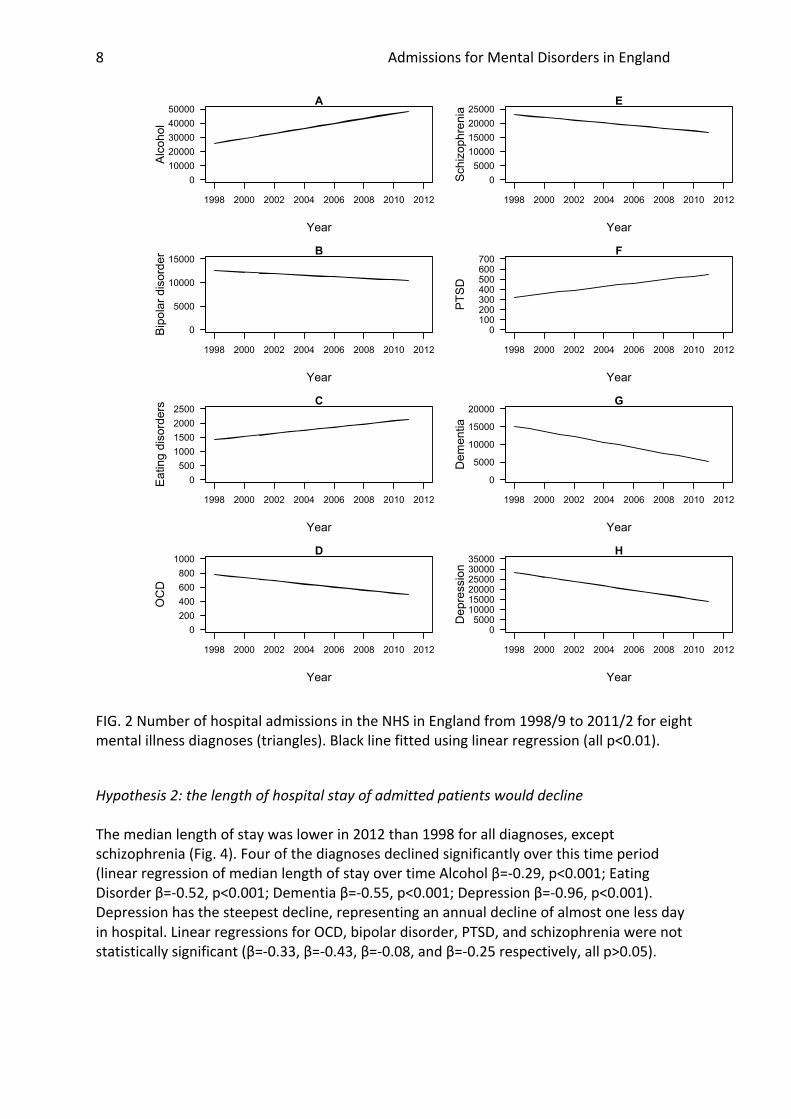
FIG. 2 Number of hospital admissions in the NHS in England from 1998/9 to 2011/2 for eight mental illness diagnoses (triangles). Black line fitted using linear regression (all p<0.01).
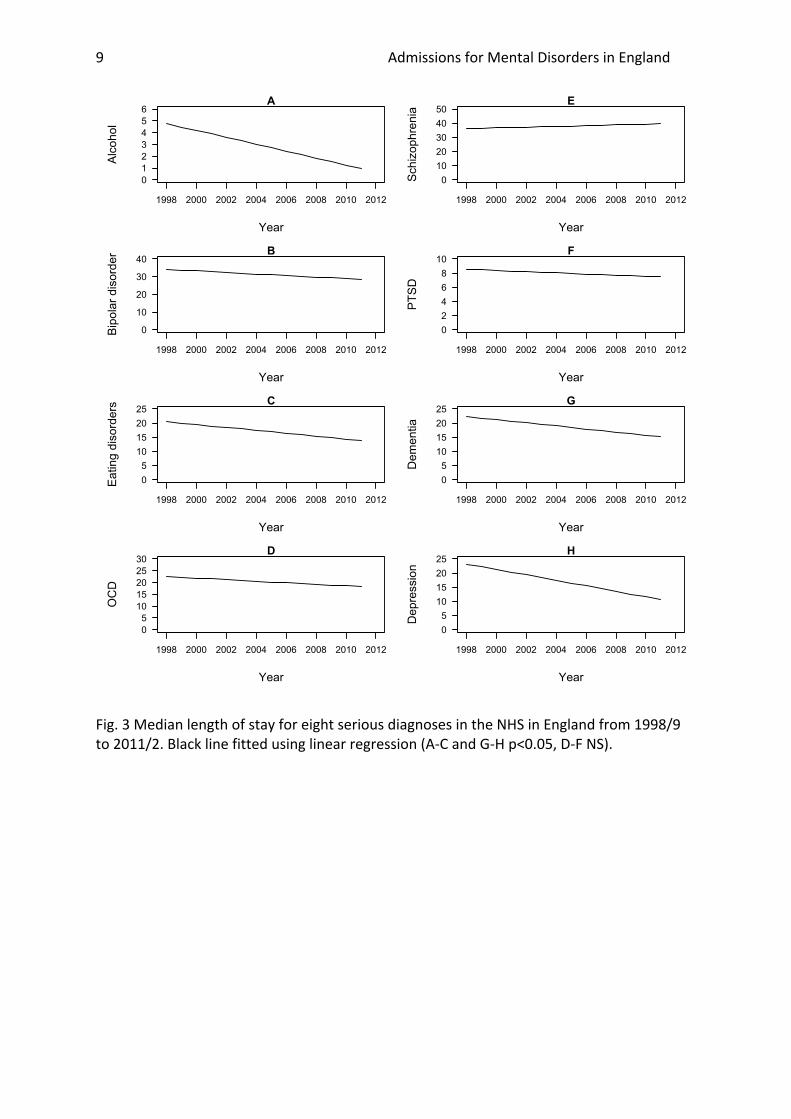
Hypothesis 2: the length of hospital stay of admitted patients would decline The median length of stay was lower in 2012 than 1998 for all diagnoses, except schizophrenia (Fig. 4). Four of the diagnoses declined significantly over this time period (linear regression of median length of stay over time Alcohol β=-‐0.29, p<0.001; Eating Disorder β=-‐0.52, p<0.001; Dementia β=-‐0.55, p<0.001; Depression β=-‐0.96, p<0.001). Depression has the steepest decline, representing an annual decline of almost one less day in hospital. Linear regressions for OCD, bipolar disorder, PTSD, and schizophrenia were not statistically significant (β=-‐0.33, β=-‐0.43, β=-‐0.08, and β=-‐0.25 respectively, all p>0.05).
1998 2000 2002 2004 2006 2008 2010 2012
01000020000300004000050000
A
Year
Alcohol
1998 2000 2002 2004 2006 2008 2010 2012
0
5000
10000
15000B
Year
Bip
olar
dis
orde
r
1998 2000 2002 2004 2006 2008 2010 2012
05001000150020002500
C
Year
Eat
ing
diso
rder
s
1998 2000 2002 2004 2006 2008 2010 2012
02004006008001000
D
Year
OCD
1998 2000 2002 2004 2006 2008 2010 2012
0500010000150002000025000
E
Year
Schizophrenia
1998 2000 2002 2004 2006 2008 2010 2012
0100200300400500600700
F
Year
PTSD
1998 2000 2002 2004 2006 2008 2010 2012
0
5000
10000
15000
20000G
Year
Dementia
1998 2000 2002 2004 2006 2008 2010 2012
05000100001500020000250003000035000
H
Year
Depression
Admissions for Mental Disorders in England 9
Fig. 3 Median length of stay for eight serious diagnoses in the NHS in England from 1998/9 to 2011/2. Black line fitted using linear regression (A-‐C and G-‐H p<0.05, D-‐F NS).
1998 2000 2002 2004 2006 2008 2010 2012
0123456
A
Year
Alcohol
1998 2000 2002 2004 2006 2008 2010 2012
0
10
20
30
40B
Year
Bip
olar
dis
orde
r
1998 2000 2002 2004 2006 2008 2010 2012
0510152025
C
Year
Eat
ing
diso
rder
s
1998 2000 2002 2004 2006 2008 2010 2012
051015202530
D
Year
OCD
1998 2000 2002 2004 2006 2008 2010 2012
01020304050
E
Year
Schizophrenia
1998 2000 2002 2004 2006 2008 2010 2012
0246810
F
Year
PTSD
1998 2000 2002 2004 2006 2008 2010 2012
0510152025
G
Year
Dementia
1998 2000 2002 2004 2006 2008 2010 2012
0510152025
H
Year
Depression
Admissions for Mental Disorders in England 10
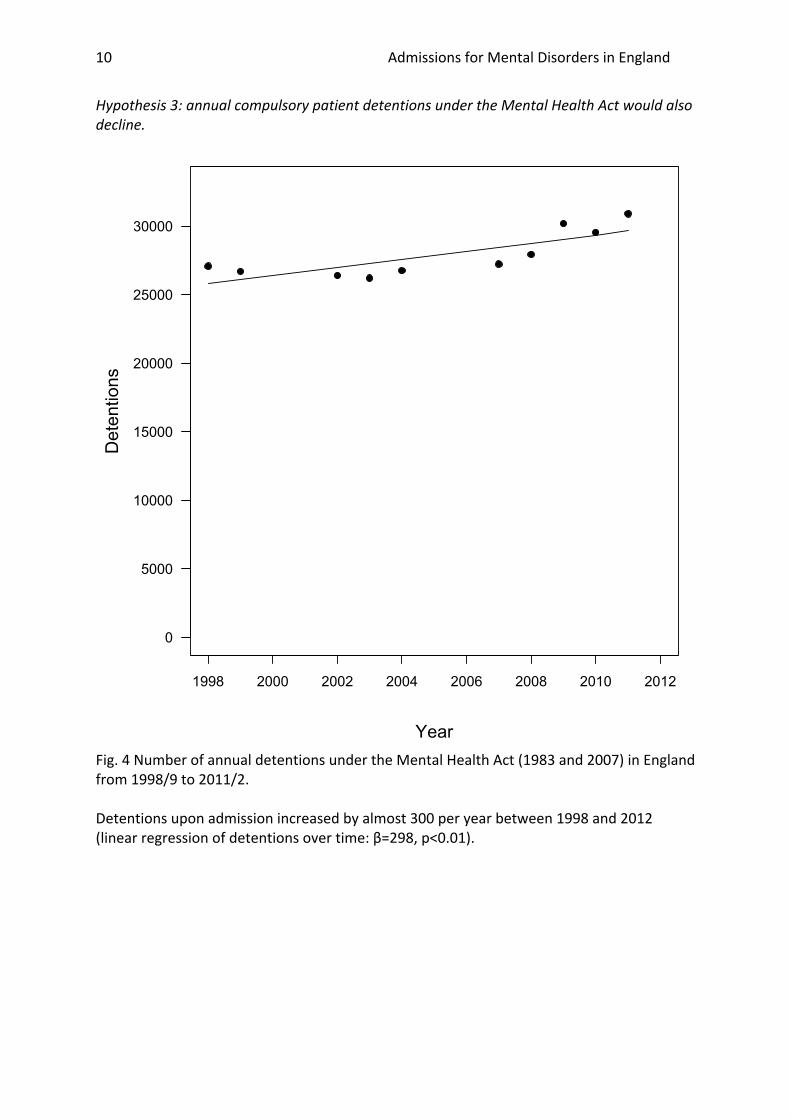
Hypothesis 3: annual compulsory patient detentions under the Mental Health Act would also decline.
Fig. 4 Number of annual detentions under the Mental Health Act (1983 and 2007) in England from 1998/9 to 2011/2. Detentions upon admission increased by almost 300 per year between 1998 and 2012 (linear regression of detentions over time: β=298, p<0.01).
1998 2000 2002 2004 2006 2008 2010 2012
0
5000
10000
15000
20000
25000
30000
Year
Detentions

Admissions for Mental Disorders in England 11
Hypothesis 4: community team activity would be associated with greater declines in admissions than accounted for by continued reductions in psychiatric beds Reported community team activity was not significantly associated with admissions and the confidence interval crossed zero, so this direct path was dropped from the model (coefficient=-‐0.121 p<0.001, bootstrapped 95% CI -‐0.35 to 0.42). The resulting model included a path from community team activity to hospital beds, and from hospital beds to hospital admissions. The resulting model had a good fit (X2=0.57, df=1, p=0.45, Tucker-‐Lewis Index=1.07, RMSEA=0.00). The number of mental health beds was significantly and positively associated with the number of severe psychiatric admissions (coefficient=0.683, p<0.001, bootstrapped 95% CI 0.37 to 1.06). Community team activity had a negative association with the number of beds (coefficient=-‐0.521 p<0.001, bootstrapped 95% CI -‐0.71 to -‐0.25). The same qualitative pattern was found for median length of stay (data not shown).

Admissions for Mental Disorders in England 12
Discussion
We used available national statistics to investigate trends in the admissions of various diagnoses against a background of ongoing closures of hospital beds and the introduction of community treatment teams. Hospital admissions and length of hospital stay declined for some but not all diagnoses tested. The number of detentions under the Mental Health Act increased. Nationally available figures for crisis resolution team activity do not account for the overall decline in hospital beds or admissions. Having rejected our four hypotheses that were based on assumptions that community teams were successful in reducing the need for hospital treatment, this suggests that an evaluation of the quality of different models of psychiatric treatment delivery is needed in England. We discuss our results in further detail below, including particular findings around the strong fall in admission and length of stay of depressed patients, and the increase in admissions for alcohol-‐related disorders.
The paper is based upon admissions across the NHS in various ICD-‐10 diagnostic categories. As the admission numbers involved represent thousands of individual patients and hence thousands of diagnostic decisions by many hundreds of clinicians this is more of a population study than a sampling exercise and we have assumed that variations in diagnostic practice between clinicians and over time are more or less evened out. Any individual errors in diagnosis would generally be subsumed within what is a very large, national dataset. This assumption is, of course, open to challenge, but we know of no papers indicating significant confounding factors in diagnostic practice over the time period of this study.
Annual admissions for different diagnoses
We hypothesised that successful introduction of community treatment would reduce admissions for all severe psychiatric diagnoses. While all trends were highly significant, some diagnoses increased over the study period.
The strongest decline in admissions was for depression. The role of community teams in this decline is doubtful. Depression admissions declined with a consistent rate (linear model fits well, Fig. 2H), started before community team deployment in 2002, and correlate strongly and positively with available psychiatric beds (Pearson’s r=0.94, p<0.001). The prevalence of depression in England is unlikely to have declined to explain the change in admissions for depression [40]. Our structural equation model indicated that the years with more community crisis assessments were those when fewer beds were available. These facts, and the data presented herein, indicate that depression admissions declined because of changes in mental health service primarily caused by declining bed numbers limiting admissions. Hospital admissions and median length of stay in hospital have both declined, and this then begs the question of whether community teams offer sufficient alternative treatment for severely depressed patients.
Psychiatric admissions of alcohol related disorders increased despite fewer beds being available. These admissions increased at a similar rate to physical liver disease, and were positively associated with alcohol affordability, adding to evidence that relaxed licensing

Admissions for Mental Disorders in England 13
laws and greater availability of cheap alcohol have increased mental illness [37]. We note that the UK National Institute for Health and Clinical Excellence (NICE) estimated that introducing a minimum price of £0.40 per unit of alcohol would yield savings of around 15 million pounds in the first year in terms of a reduction in alcohol related hospital admissions [38]. Increases in admissions for eating disorders and PTSD could be attributed to greater awareness of the diagnoses or, for PTSD, lengthy national involvement in military campaigns in Iraq and Afghanistan.
Admissions for schizophrenia and bipolar disorder declined slower than depression, suggesting a preferential admission for psychotic disorders in the context of diminishing national bed capacity. Declines in admissions for dementia may reflect a shift towards community teams, and the introduction of new drugs such as the acetylcholinesterase inhibitors [39].
Length of Stay
We hypothesised that the length of stay would decline with the introduction of community teams because they might enable more rapid discharge. Median length of stay for depression, which is not the focus of community teams, has declined. Median length of stay for schizophrenia, which is the core psychotic diagnosis treated by community teams was unchanged. This might indicate that diminished bed capacity and a pressure to admit psychotic disorders under compulsory detention are squeezing patients with depression out of hospital. Shorter lengths of stay for alcohol and dementia may reflect the trend toward community detoxifications and alternative treatment strategies (e.g. novel drugs and community teams for the elderly).
Compulsory admissions
We hypothesized that compulsory detentions would decline as community treatment, particularly assertive outreach teams, improved compliance and prevented the need for re-‐admission. However, compulsory detentions under the Mental Health Act (1983 and 2007) increased. In England, the Mental Health Act was amended in 2007. Hospital detention orders remained largely unchanged, but the introduction of community treatment orders to enforce treatment in the community could have been hypothesized to accelerate declines in the use of hospital detention orders. Public data available for the five years following this Act instead show hospital detentions increasing (Fig. 4).
Mental health system involving hospital beds and community treatment
Using an aggregated variable of national hospital admissions for each year we analysed the direct and indirect effects of crisis team activity and mental health beds Years with more psychiatric beds had more admissions. Recent years had fewer admissions and fewer beds consistent with a scarcity of beds squeezing admissions. Years with higher community team activity had no consistent direct association with admissions, but years with higher community team activity did have fewer hospital beds. This dataset gives suggests a constraint on mental health budgets with a tradeoff between hospital beds and community team activity, with bed availability having a stronger effect on admissions than community teams.
Opportunities for further study

Admissions for Mental Disorders in England 14
With limited availability of data on the activity of different community teams for different diagnoses in England, we could not directly compare hospital data on admission and length of stay for each diagnosis with community team activity. Indeed there are few data available for community treatment team activity in England. Published measures from HSCIS are not consistent between years, rarely cover the full range of community teams, and are not resolved by diagnosis. For a proper assessment of the effects of community care on national psychiatric epidemiology we need data on the prevalence and severity of various diagnoses, outcome measures like suicides and hospital admissions, and an assessment of unmet needs for treatment as might be occurring with depression. Our analyses raise other questions for further study, including the effects of recent restructuring of psychiatric treatment on service user and carer satisfaction, the pathways patients with different diagnoses take before hospital admission, the use of out-‐of-‐area and private sector admissions, and levels of morbidity, homicide and suicide in the community.
Conclusions
Publicly available data for the NHS in England reveal a complex picture of changes in admission practice for different mental disorders that are mainly a consequence of continuing reductions in the number of psychiatric inpatient beds and also coincide with the more recent introduction of community teams. The changes are not uniform across diagnoses and not closely associated with community team activity either directly or indirectly. Improvements in the published national data on community team activity, preferably by diagnostic category, gender and age group in a similar vein to NHS admission data would enable more hypotheses regarding the effects of community teams to be tested. A large scale, longitudinal epidemiological study into community psychiatric morbidity and mortality, to monitor service provision, treatment and unmet need is urgently required.
Acknowledgements We are grateful to Professor Ewan Wilkinson for helpful comments on an early draft of this paper. We are also indebted to the UK Government Health and Social Care Information Centre for their help in accessing data and with Freedom of Information Requests in relation to this research. References 1. Gregory, R. L. (Ed.) Oxford Companion to the Mind (2 Ed). Oxford, Oxford University Press, 2004. 2. Ban, T. A. Fifty years chlorpromazine: a historical perspective. Neuropsychiatr Dis Treat. 2007 August; 3(4): 495–500. 3. López-‐Munoz, F. & Alamo, C. The consolidation of neuroleptic therapy: Janssen, the discovery of haloperidol and its introduction into clinical practice. Brain Research Bulletin 2009; 79: 130–141.
Admissions for Mental Disorders in England 15
4. Goldberg D. Improved investment in mental health services: value for money? Br J Psychiatry 2008; 192(2): 88-‐91. 5. Mental Health Strategies 2011/2012 National Survey of Investment in Mental Health Services. London, Department of Health, 2012. 6. Lelliot, P, and Audini, B. Trends in the use of Part II of the Mental Health Act 1983 in seven English local authority areas. Brit. J. Psychiatry. 2003; 182: 68-‐70. 7. Glover G., Arts G., Babu, K. S. Crisis resolution/home treatment teams and psychiatric admission rates in England. British Journal of Psychiatry 2006; 189(5): pp.441-‐445. 8. World Health Organization, 2008 Policies and practices for mental health in Europe: meeting the challenges http://www.euro.who.int/__data/assets/pdf_file/0006/96450/E91732.pdf
9. Monzani, E, Erlicher A, Lora A, Lovaglio P, Vittadini, G. Does community care work? A model to evaluate the effectveness of mental health services. International Journal of Mental Health Systems 2008; 2:10. Accessed September 2008. http://www.ijmhs.com/content/2/1/10 10. Medeiros, H. McDaid, D. & Knapp, M. Shifting care from hospital to community in Europe: Economic challenges and opportunities. London, Personal Social Services Research Unit. London School of Economics and Political Science. (2008) 11. Sharfstein S.S. and Dickerson, F.B. Hospital Psychiatry For The Twenty-‐First Century. Health Affairs May/June 2009 vol. 28 no. 3 685-‐688. doi: 10.1377/hlthaff.28.3.685 12. Priebe, S., Badesconyi, A., Fioritti, A. Hansson, L., Kilian, R., Torres-‐Gonzales, F. Turner, T., Wiersma, D. Reinstitutionalisation in mental health care: comparison of data on service provision from six European countries. BMJ. 2005 January 15; 330(7483): 123–126. doi: 10.1136/bmj.38296.611215.AE 13. Goldie, 1983 The Mentally Ill in Contemporary Society/Home and Hospital Psychiatric Treatment/Mental Illness in the Community: the pathway to psychiatric care (Book). Sociology of Health & Illness 5.2: 233-‐234. 14. Wing J K & Hailey A M, Evaluating A Community Psychiatric Service: The Camberwell Register, 1964–71. 1972, London, Published for the Nuffield Provincial Hospitals Trust, by the Oxford University Press. 15. Jackson, G., Gater, R. Goldberg, D., Tantam, D, Loftus, L, Taylor, H. A new community mental health team based in primary care. A description of the service and its effect on service use in the first year. The British Journal of Psychiatry 1993; 162.3:375-‐384. 16. Craig, T.K.J. , Garety, P., Power, P., Rahaman, N., Colbert, S., Fornells-‐Ambrojo, M., Dunn, G. The Lambeth Early Onset (LEO) Team: randomised controlled trial of the effectiveness of specialised care for early psychosis. BMJ 2004; 329:1067 doi: http://dx.doi.org/10.1136/bmj.38246.594873.7C 17. Johnson, S., Nolan, F., Pilling, S., Sandor, A., Hoult, J., McKenzie, N., & Bebbington, P. Randomised controlled trial of acute mental health care by a crisis resolution team: the north Islington crisis study. BMJ 2005; 331(7517): 599.
Admissions for Mental Disorders in England 16
18. Jacobs, R. and Barrenho, E. Impact of crisis resolution and home treatment teams on psychiatric admissions in England. British Journal of Psychiatry 2010; 14: 1–6. doi: 10.1192/bjp.bp.110.079830 19. S. Toot, Devine, M., and Orrell, M. (2011) The effectiveness of crisis resolution/home treatment teams for older people with mental health problems: a systematic review and scoping exercise. Int J Geriatr Psychiatry 2011; 26: 1221–1230. 20. Carpenter, R.A., Falkenburg, J., White, T.P. and Tracy, D.K. Crisis teams: systematic review of their effectiveness in practice. The Psychiatrist 2013; 37:232-‐237. doi: 10.1192/pb.bp.112.039933 21. Cotton, M.A., Johnson, S., Bindman, J., Sandor, A., White, I.A., Thornicroft, G., Nolan, F., Pilling, S., Hoult, J., McKenzie, N., Bebbington, P. An investigation of factors associated with psychiatric hospital admission despite the presence of crisis resolution teams. BMC Psychiatry; 2007; 7:52. Accessed September 2008. http://www.biomedcentral.com/1471-‐244X/7/52 22. Murphy, S., Irving, C.B. Adams, C.E., Driver, R. Crisis intervention for people with severe mental illnesses. Cochrane Collaboration. 2012. DOI: 10.1002/14651858.CD001087.pub4 23. Dodgson, G., Crebbin, K., Pickering, C., Mitford, E., Brabban, A., & Paxton, R. Early intervention in psychosis service and psychiatric admissions. Psychiatric Bulletin 2008; 32(11): 413-‐416. 24. Barker, V., Taylor, M., Kader, I., Stewart, K., & Le Fevre, P. Impact of crisis resolution and home treatment services on user experience and admission to psychiatric hospital. The Psychiatrist 2011; 35(3): 106-‐110.
26. Tan, E., Higginbotham, A., McQueen, L., & Bhui, K. Crisis plans in a home treatment team before and after a quality improvement programme. The Psychiatrist 2012; 36(9): 331-‐334. 27. Burns, T., Rugkasa, J, Molodynski, A, Dawson, J, Yeles, K, Vazquez-‐Montes, M, Voysey, M, Sinclair, J, Priebe, S. Community Treatment Orders for patients with psychosis (OCTET): a randomised control trial, The Lancet 2013; Vol 381: 3
28. Killaspy, H., Bebbington, P., Blizard, R., Johnson, S., Nolan, F., and Pilling, S. The REACT study: randomised evaluation of assertive community treatment in north London. BMJ 1006; 332(7545): 815-‐820. doi: 10.1136/bmj.38773.518322.7C 29. Lelliott, P. Acute inpatient psychiatry in England. An old problem and a new priority. Epidemiologia e Psichiatria Sociale 2006; 15(2); 91-‐94. 30. Santry C. Inpatient mental health slammed as commissioners neglect services. Health Service Journal 2008. http://www.hsj.co.uk/news/inpatient-‐mental-‐health-‐slammed-‐as-‐commissioners-‐neglect-‐services/1739353.article#.UmfUURYZyHo Accessed October 2013. 31. Bowers, L, Simpson A, Eyres, S, Nijman, H, Hall, C, Grange, A, Phillips, L. Serious untoward incidents and their aftermath in acute inpatient psychiatry: the Tompkins Acute Ward Study. International Journal of Mental Health Nursing. 2006; 15(4); 226-‐234. 32. Bowers L, Nijman H. Aggressive behaviour on acute psychiatric wards: prevalence, severity and management. Journal of Advanced Nursing. 2007; 58(2): 140-‐149.
Admissions for Mental Disorders in England 17
33. Charlwood P, Mason A, Goldacre M, Cleary R, Wilkinson E (eds). Health Outcome Indicators: Severe Mental Illness. Report of a working group to the Department of Health. Oxford: National Centre for Health Outcomes Development, 1999. http://nchod.uhce.ox.ac.uk/mentalillness.pdf Accessed 17th August 2013. 34. Department of Health. 2012. Form KH03. Hospital Inpatient Activity Data DoH http://www.england.nhs.uk/statistics/statistical-‐work-‐areas/bed-‐availability-‐and-‐occupancy/bed-‐data-‐overnight/ Accessed September 26th 2013. 35. R Core Team (2013) R: A language and environment for statistical computing. Vienna, Austria. 36. Yves Rosseel, Daniel Oberski, Jarrett Byrnes, Leonard Vanbrabant, Victoria Savalei, Ed Merkle, Michael Hallquist, Mijke Rhemtulla, and Myrsini Katsikatsou. (2013) lavaan: Latent Variable Analysis. Version 0.5-‐12. 37. Herttua, K., Makela, P., Martikainen, P. Changes in alcohol-‐related mortality and its socioeconomic differences after a large reduction in alcohol prices: a natural experiment based on register data. American Journal of Epidemiology. 2008;168(10):1110-‐8. 38. NICE. Alcohol-‐use disorders: preventing harmful drinking. Costing report. Implementing NICE guidance. 2010. London, National Institute for Health and Clinical Excellence. 39. Fillit, H., and Hill, J. The economic benefits of acetylcholinesterase inhibitors for patients with Alzheimer disease and associated dementias. Alzheimer Disease & Associated Disorders. 2004; 18 Suppl 1:S24-‐9. 40. Spiers, N. Brugha, T S. Bebbington, P. McManus, S. Jenkins, R. Meltzer, H. Age and birth cohort differences in depression in repeated cross-‐sectional surveys in England: the National Psychiatric Morbidity Surveys, 1993 to 2007. Psychological Medicine. 2012; 42(10):2047-‐55.