HNA Medical Intake Forms - Hijama Nation
28
ACCREDITED HIGHER DIPLOMA IN HIJAMA CUPPING THERAPY (DIP.HCT) E: [email protected] | W: WWW.HIJAMACERTIFICATION.COM COPYRIGHT © 20112019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED HNA Medical Intake Forms PRINTABLE TEMPLATES FOR HNA CERTIFIED HIJAMA PRACTITIONERS
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of HNA Medical Intake Forms - Hijama Nation
ACCREDITED HIGHER DIPLOMA IN HIJAMA CUPPING THERAPY (DIP.HCT) E: [email protected] | W: WWW.HIJAMACERTIFICATION.COM
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
HNA Medical Intake Forms PRINTABLE TEMPLATES FOR HNA CERTIFIED HIJAMA PRACTITIONERS

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
2
CONTENTS
Introduction 3
PRINTABLE TEMPLATES
Standard Holistic Medical History (Short Form) 6
Premium Holistic Medical History (Long Form) 12
Allergies Form 19
Female Medical History Intake Form 20
Male Medical History Intake Form 22
Pre-‐Treatment Care Form 24
Post-‐Treatment Care Form 26
Session Review Form 28
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
3
INTRODUCTION
HNA have designed customized medical forms to suit different circumstances. These are templates which all students and graduates can use. They can be copied, edited or amended. They do not need to be redesigned for content as we have covered most areas comprehensively. But you can add your own logo and images and so on. In this template pack, you will find the following items:
Standard Holistic Medical History Form
This is a standard intake medical history form to be completed for all standard Client’s at the start of the first appointment with you.
Premium Holistic Medical History Form
This is the longer version of the form which is designed for Practitioners who are offering a premium Holistic Hijama Coaching service to their Clients. This will give you a detailed background of the Client’s lifestyle and help you to coach them professionally and efficiently in the long term.
Allergies Form
This form should be completed at the start of the first appointment with you, alongside the standard, generic, holistic medical history intake form.
Female Medical History Intake Form
This is a supplementary medical form to be completed for female Clients at the start of the first appointment with you after you finish the standard medical history intake form. It covers areas such as fertility and women’s issues.
Male Medical History Intake Form
This is a supplementary medical form to be completed for male Clients at the start of the first appointment with you after you finish the standard medical history intake form. It covers areas such as fertility and women’s issues.
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
4
Pre-‐Treatment Form
Give this information to the Client before each appointment in writing and verbally.
Post Treatment Form
Give this information at the end of every appointment.
Session Review Form
Complete this form at the end of each appointment.
If Students have any new ideas or require more forms for various circumstances, please email us at [email protected]. We will be happy to design new templates and add them to the course accordingly.

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
5
PRINTABLE MEDICAL HISTORY
INTAKE FORM TEMPLATES
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
6
STANDARD HOLISTIC MEDICAL HISTORY FORM
HAVE YOU EATEN ANY FOOD IN THE LAST 2-‐3 HOURS? MEDICATIONS ARE YOU DIABETIC? ARE YOU ANEMIC? IF SO, ARE YOU TAKING MEDICATION FOR IT? ARE YOU PREGNANT? HOW MANY WEEKS? DO YOU HAVE ANY SEIZURE DISORDERS? DO YOU HAVE ANY ALLERGIES TO OILS? Name: DOB: Age: Address: Tel. Number-‐Home: Mobile: Work: Email address: Emergency contact Name: Tel: Relationship: Blood Sugar Level: Blood pressure: Height: Weight : Blood Type: Ph level: MEDICAL HISTORY Any diseases or illnesses & Current medications? Do you have any bleeding disorders? Do you have any metal plates, metal rods, or pacers in your body? Do you have any disabilities/special needs? Do you have any hereditary/genetic diseases? Do you have any problems with your heart? Do you have a heart stent? Have you had any recent surgery? Do you have any scars/disfiguration on your body? Do you have allergies/skin conditions/hair growth issues? Do you have mercury tooth fillings? Are you taking any herbal or homeopathic remedies? Are you taking any supplements, vitamins or minerals? Are you taking any Hormone treatments? Are you taking any Hormonal replacement therapy? Are you taking any steroids? Do you take drugs? Type? Do you smoke? How much? Do you use a Nicotine patch, nicotine replacement treatment or Vape Therapy?
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
7
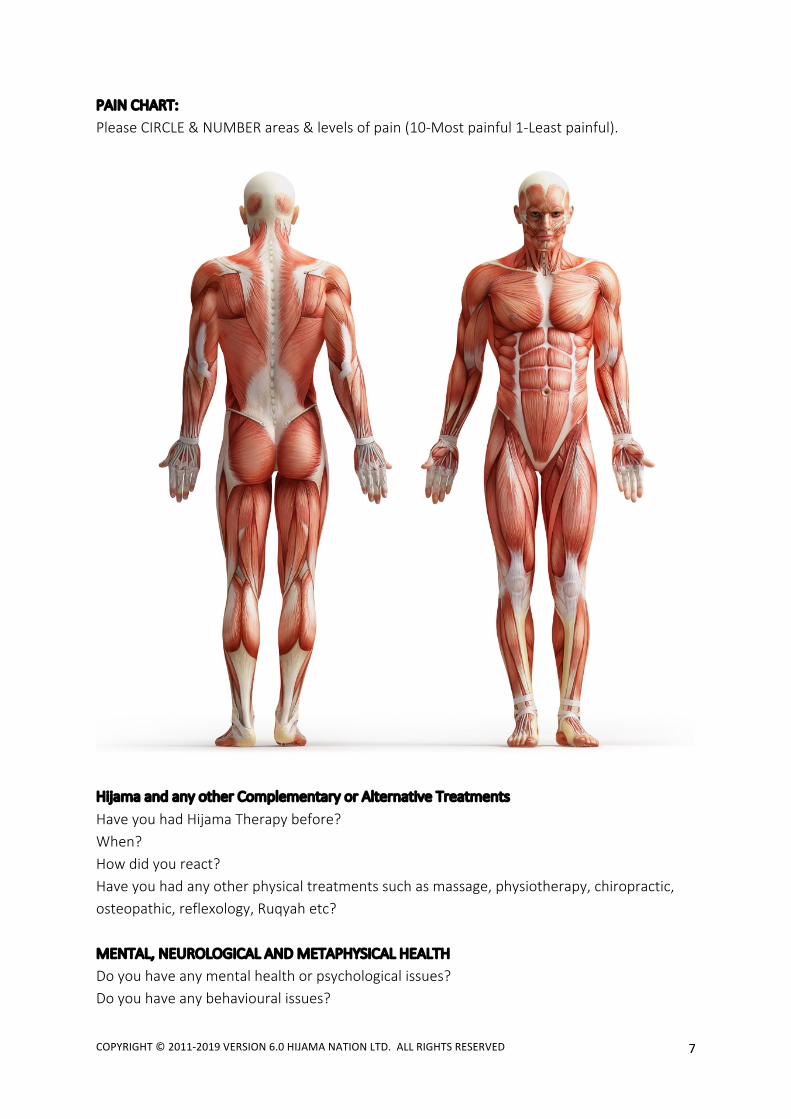
PAIN CHART: Please CIRCLE & NUMBER areas & levels of pain (10-‐Most painful 1-‐Least painful).
Hijama and any other Complementary or Alternative Treatments Have you had Hijama Therapy before? When? How did you react? Have you had any other physical treatments such as massage, physiotherapy, chiropractic, osteopathic, reflexology, Ruqyah etc? MENTAL, NEUROLOGICAL AND METAPHYSICAL HEALTH Do you have any mental health or psychological issues? Do you have any behavioural issues?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
8
Are you aware of any metaphysical issues such as Jinn, Black Magic, Evil eye? Do you follow a religion? Which one? Do you pray/meditate? Current family unit: Number of Children? Who lives in your household? Current stress levels? Please describe in detail and mark from 1-‐10. (10 is most stressful). Emotional Mental Physical Are you a Student? F/T or P/T? Education and qualifications? Are you employed? Job and Title: F/T OR P/T? Describe your workspace/environment DIET & NUTRITION Describe your daily diet/food intake: How often do you eat in a day? What do you eat daily? Breakfast? Lunch? Dinner? Snacks? Do you eat a balanced diet?
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
9
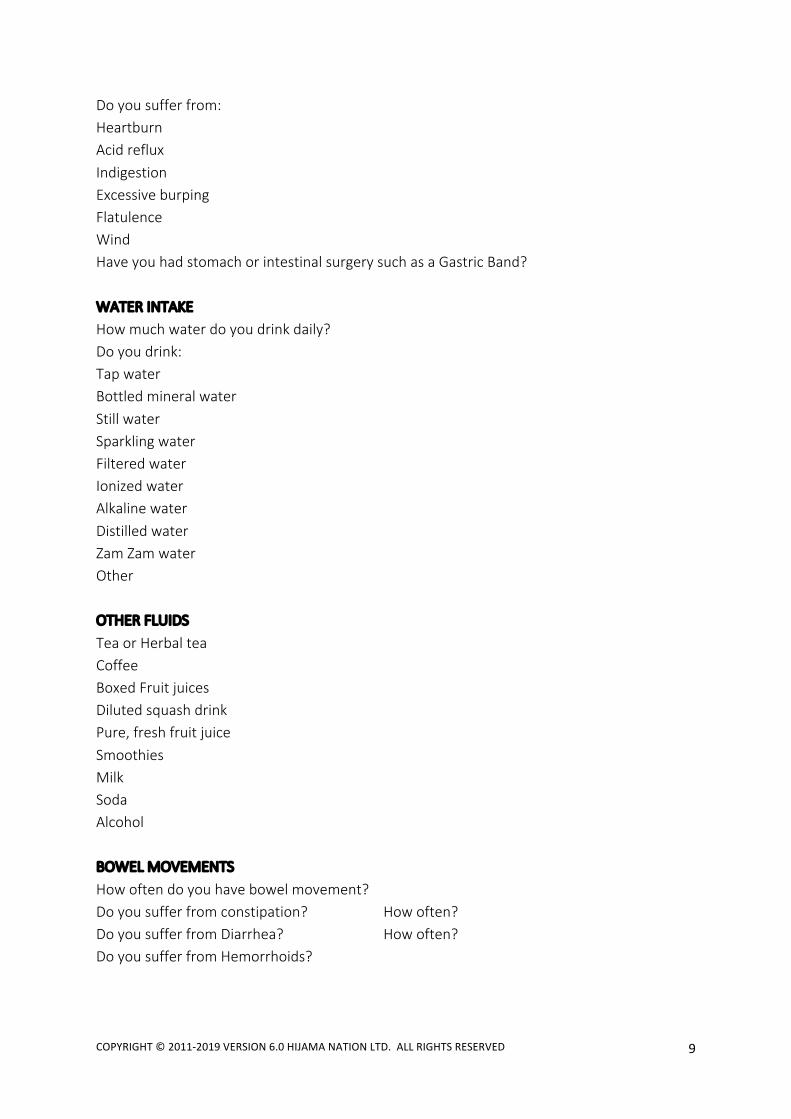
Do you suffer from: Heartburn Acid reflux Indigestion Excessive burping Flatulence Wind Have you had stomach or intestinal surgery such as a Gastric Band? WATER INTAKE How much water do you drink daily? Do you drink: Tap water Bottled mineral water Still water Sparkling water Filtered water Ionized water Alkaline water Distilled water Zam Zam water Other OTHER FLUIDS Tea or Herbal tea Coffee Boxed Fruit juices Diluted squash drink Pure, fresh fruit juice Smoothies Milk Soda Alcohol BOWEL MOVEMENTS How often do you have bowel movement? Do you suffer from constipation? How often? Do you suffer from Diarrhea? How often? Do you suffer from Hemorrhoids?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
10
SLEEP Bed time? Describe your sleeping patterns/habits? What time do you usually eat your last meal before sleeping? What time do you usually wake up? Quality of sleep-‐deep and restful? Restless, Agitated, erratic, disturbed? Do you sleep walk? Do you sleep talk? Do you clench your teeth? Do you grind your teeth? Do you wet the bed? Do you watch TV, use a phone, ipad, tablet, computer or any other electronic devices before sleep? EXERCISE How much exercise do you do? What kinds of exercise do you do?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
11
CONTRAINDICATIONS: Various stages of Pregnancy IVF Treatment PRECAUTIONS:
• Diabetes • Epilepsy, fits or seizures and/or metaphysical issues • Cuts/abrasions • Skin Diseases/ disorders • High/Low Blood Pressure • Thrombosis/Embolism • Early and late stages of pregnancy • Contagious diseases • Blood Borne Pathogens • Post-‐operation of an organ transplant • Recent Injuries/surgery • Bleeding disorders & being on blood thinners
o The CHP has fully explained the Hijama procedure, contraindications, outcomes, after
effects and post care instructions of the HCT procedure to me, shown me the equipment and I understand the process of HCT.
o I understand it is my responsibility to inform my CHP of any changes in my medical condition or medications and agree to do so at the start of any Hijama sessions.
o I give permission to the CHP to safely and professionally perform Dry and Hijama Wet
Cupping on my body, create several, small, shallow incisions by breaking the skin barrier with a size 15, single use, sterile blade or with a diabetic needle and lancet within the circle of the Hijama site. Also, to clean me up, sanitize and seal me with oil.
o I understand that the CHP cannot be held responsible or liable for any
contraindications, negative after effects, side effects, injuries, accidents or other liabilities after the HCT treatment.
CHP Name: CHP Signature: Date:
Client Name: Client Signature: Date:
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
12
PREMIUM HOLISTIC MEDICAL HISTORY FORM
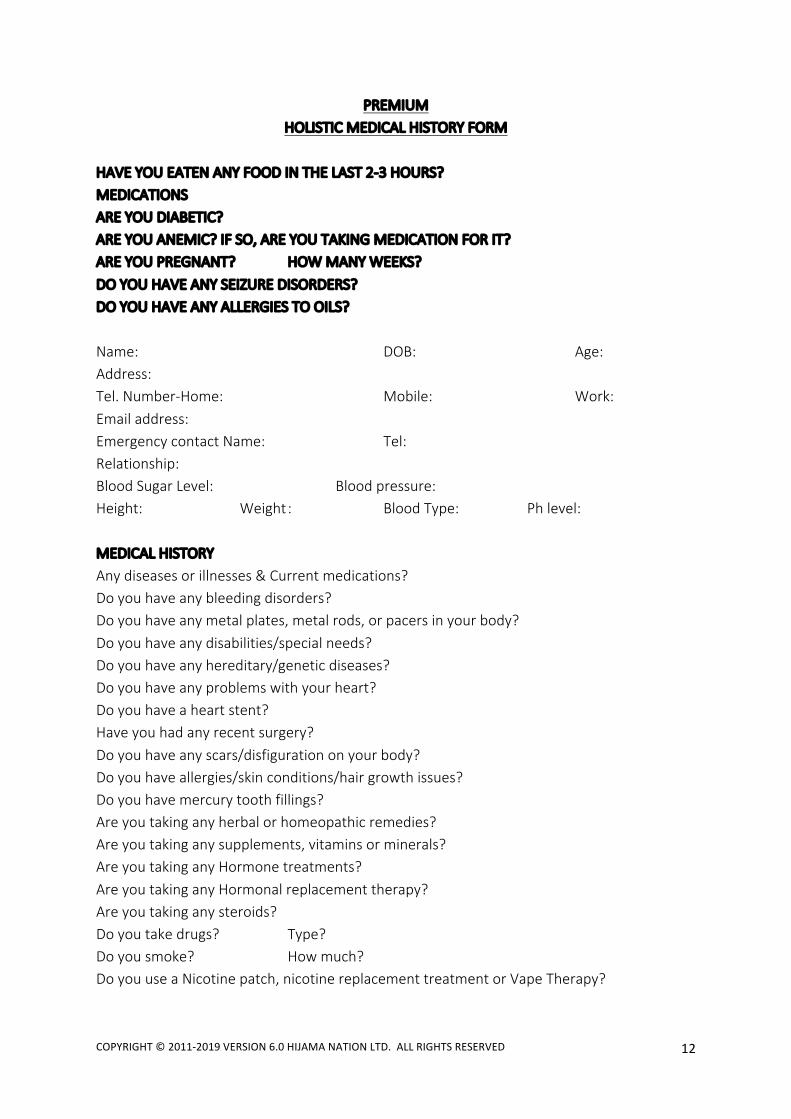
HAVE YOU EATEN ANY FOOD IN THE LAST 2-‐3 HOURS? MEDICATIONS ARE YOU DIABETIC? ARE YOU ANEMIC? IF SO, ARE YOU TAKING MEDICATION FOR IT? ARE YOU PREGNANT? HOW MANY WEEKS? DO YOU HAVE ANY SEIZURE DISORDERS? DO YOU HAVE ANY ALLERGIES TO OILS? Name: DOB: Age: Address: Tel. Number-‐Home: Mobile: Work: Email address: Emergency contact Name: Tel: Relationship: Blood Sugar Level: Blood pressure: Height: Weight : Blood Type: Ph level: MEDICAL HISTORY Any diseases or illnesses & Current medications? Do you have any bleeding disorders? Do you have any metal plates, metal rods, or pacers in your body? Do you have any disabilities/special needs? Do you have any hereditary/genetic diseases? Do you have any problems with your heart? Do you have a heart stent? Have you had any recent surgery? Do you have any scars/disfiguration on your body? Do you have allergies/skin conditions/hair growth issues? Do you have mercury tooth fillings? Are you taking any herbal or homeopathic remedies? Are you taking any supplements, vitamins or minerals? Are you taking any Hormone treatments? Are you taking any Hormonal replacement therapy? Are you taking any steroids? Do you take drugs? Type? Do you smoke? How much? Do you use a Nicotine patch, nicotine replacement treatment or Vape Therapy?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
13
PAIN CHART: Please CIRCLE & NUMBER areas & levels of pain (10-‐Most painful 1-‐Least painful).
Hijama and any other Complementary or Alternative Treatments Have you had Hijama Therapy before? When? How did you react? Have you had any other physical treatments such as massage, physiotherapy, chiropractic, osteopathic, reflexology, Ruqyah etc? MENTAL, NEUROLOGICAL AND METAPHYSICAL HEALTH Do you have any mental health or psychological issues? Do you have any behavioural issues?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
14
Are you aware of any metaphysical issues such as Jinn, Black Magic, Evil eye? Do you follow a religion? Which one? Do you pray/meditate? Current family unit: Married Married (Polygynus) Single/Never married Single/Divorced Single/Widowed Single/Separated Number of Children? Biological Miscarriages Deceased after birth Stillborn Fostered Adopted Step-‐children Who lives in your household? Current stress levels? Please describe in detail and mark from 1-‐10. (10 is most stressful). Emotional Mental Physical Are you a Student? F/T or P/T? Education and qualifications? Are you employed? F/T OR P/T? Job and Title: Describe your workspace/environment
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
15
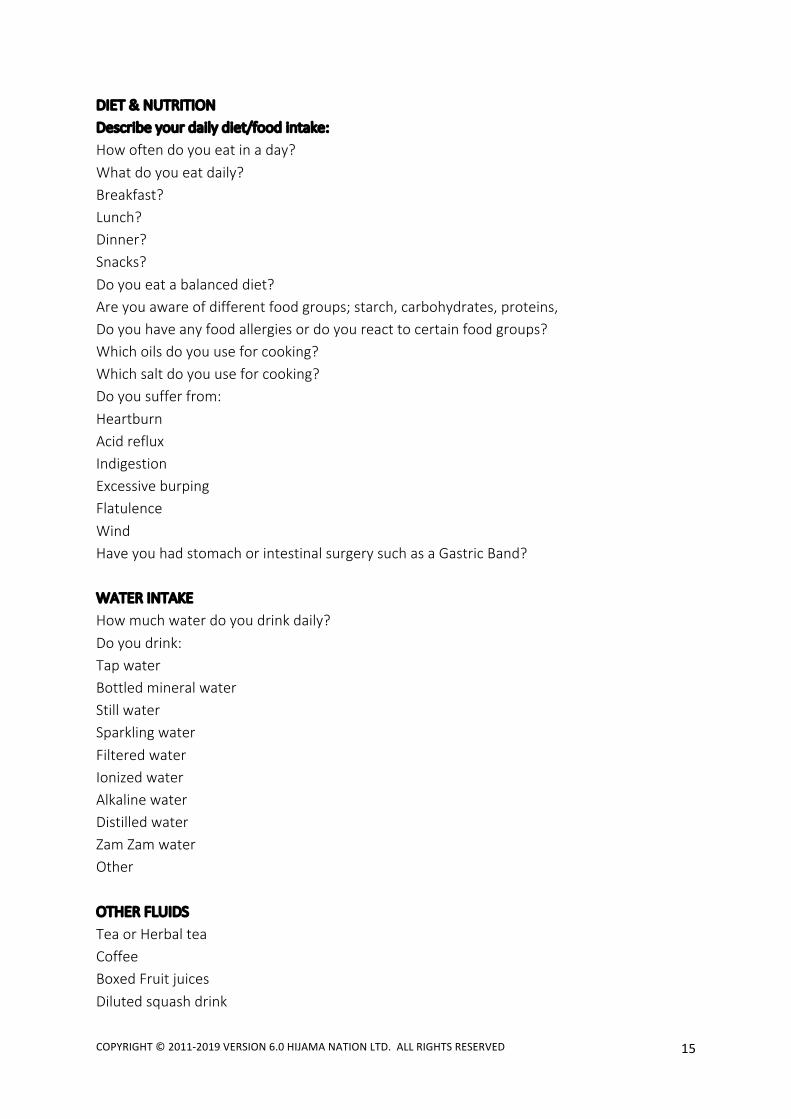
DIET & NUTRITION Describe your daily diet/food intake: How often do you eat in a day? What do you eat daily? Breakfast? Lunch? Dinner? Snacks? Do you eat a balanced diet? Are you aware of different food groups; starch, carbohydrates, proteins, Do you have any food allergies or do you react to certain food groups? Which oils do you use for cooking? Which salt do you use for cooking? Do you suffer from: Heartburn Acid reflux Indigestion Excessive burping Flatulence Wind Have you had stomach or intestinal surgery such as a Gastric Band? WATER INTAKE How much water do you drink daily? Do you drink: Tap water Bottled mineral water Still water Sparkling water Filtered water Ionized water Alkaline water Distilled water Zam Zam water Other OTHER FLUIDS Tea or Herbal tea Coffee Boxed Fruit juices Diluted squash drink
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
16
Pure, fresh fruit juice Smoothies Milk Soda Alcohol URINATION How often do you urinate daily? Usual colour of urine Any burning or discomfort? Describe your urination problems: BOWEL MOVEMENTS How often do you have bowel movement daily? Do you have to strain or experience pain or bleeding? Describe your stool-‐hard, soft, runny? Do you suffer from constipation? How often? Do you suffer from Diarrhea? How often? Do you suffer from Hemorrhoids? EYESIGHT Is your eyesight: Normal Near-‐sighted Far-‐sighted Do you wear glasses? Contact lenses? Any other eye conditions? HEAD CONDITIONS Migraines? How often? Which Kind? Headaches? How often? Location? HAIR Do you suffer from hair loss and where? Do you suffer from excessive hair growth and where? Do you have any hormonal issues? Do you have any autoimmune conditions? Are you undergoing any hair related surgery, laser treatment or any other procedures.
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
17
SLEEP Bed time? Describe your sleeping patterns/habits? What time do you usually eat your last meal before sleeping? What time do you usually wake up? Quality of sleep-‐deep and restful? Restless, Agitated, erratic, disturbed? Do you sleep walk? Do you sleep talk? Do you clench your teeth? Do you grind your teeth? Do you wet the bed? Do you watch TV, use a phone, ipad, tablet, computer or any other electronic devices before sleep? STRUCTURAL OR MUSCULAR ISSUES Describe posture-‐poor, good, excellent. Do you have any spinal, neck, knee or ankle issues? Do you suffer from any swelling, inflammation or water retention anywhere? Do you carry heavy bags or weights in your shoulders or back? Do you carry children on your hips, on one side? Are you flatfooted? Do you have a collapsed arch in either or both feet? Do you use computers a lot? Do you suffer from Repetitive Work Syndrome/carpal tunnel? Do you exercise? Type? How often? Do you stretch? Do you suffer from Sciatica? EXERCISE How much exercise do you do? What kinds of exercise do you do? ENVIRONMENT Are you aware of any damp or mould in your home? Are you exposed to a lot of dust, pollen, cold or wet weather? How much air or dust pollution are you exposed to? Do you use a dishwasher? What type of clothes washing detergent do you use? Do you use soaps, shampoos and other cosmetic chemicals?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
18
CONTRAINDICATIONS: Various stages of Pregnancy IVF Treatment PRECAUTIONS:
• Diabetes • Epilepsy, fits or seizures and/or metaphysical issues • Cuts/abrasions • Skin Diseases/ disorders • High/Low Blood Pressure • Thrombosis/Embolism • Early and late stages of pregnancy • Contagious diseases • Blood Borne Pathogens • Post-‐operation of an organ transplant • Recent Injuries/surgery • Bleeding disorders & being on blood thinners
o The CHP has fully explained the Hijama procedure, contraindications, outcomes, after
effects and post care instructions of the HCT procedure to me, shown me the equipment and I understand the process of HCT.
o I understand it is my responsibility to inform my CHP of any changes in my medical condition or medications and agree to do so at the start of any Hijama sessions.
o I give permission to the CHP to safely and professionally perform Dry and Hijama Wet
Cupping on my body, create several, small, shallow incisions by breaking the skin barrier with a size 15, single use, sterile blade or with a diabetic needle and lancet within the circle of the Hijama site. Also, to clean me up, sanitize and seal me with oil.
o I understand that the CHP cannot be held responsible or liable for any
contraindications, negative after effects, side effects, injuries, accidents or other liabilities after the HCT treatment.
CHP Name: CHP Signature: Date:
Client Name: Client Signature: Date:
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
19
ALLERGIES FORM
I CONFIRM THAT, TO THE BEST OF MY KNOWLEDGE:
I DO NOT HAVE ALLERGIES.
I DO HAVE ALLERGIES TO:………………………………………………………..................................................
SPECIFICALLY, I AM/AM NOT ALLERGIC OR TO:
o OLIVE OIL o COCONUT OIL o BLACK SEED OIL o LATEX o ALCOHOL WIPES o HONEY o DATES o ANY FRUITS o OTHER
I CONFIRM THAT, TO THE BEST OF MY KNOWLEDGE:
I DO HAVE A BAD REACTION TO:…………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………
Name:
Signature:
Date:
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
20
FEMALE MEDICAL HISTORY FORM Are you pregnant now? How many weeks? Are you on your period today? Do you wear make up? How Much? How often? Do you use nail polish or wear fake nails? Do you use any other beauty and cosmetic chemicals/lotions etc? How much? How often? Do you use skin bleach? Do you use hair bleach or hair dye? REPRODUCTIVE & SEXUAL HEALTH Describe your Menstrual cycle When was your last period? Do you have any other issues with your uterus, fallopian tubes or ovaries? Have you had a hysterectomy or any other major surgeries on your reproductive or sexual organs? Do you have any hormonal issues? Are you pre-‐menopausal, menopausal or post-‐menopausal? Are you undergoing Hormone Replacement Therapy (HRT)? Number of previous pregnancies? Live births? Miscarriages? Abortions? Stillborn births? Deceased after birth? C-‐Sections? Describe previous labour and deliveries: Are you currently nursing? When was the last time you had a bra fitting? Do you know if you are wearing the correct size? Do you use deodorant? (OPTIONAL) FERTILITY Are you taking contraceptives? Which kind? Are you in a Polygynous marriage? How often do you engage in (halal) sexual intercourse with your spouse? Are you fertile now? Have you been fertile in the past? If no, have you and/or your spouse had the relevant fertility tests?
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
21
What were the results? Do you know your ovulation cycle? How often do you engage in (halal) sexual intercourse with your spouse? Are you undergoing any medical or fertility treatment? Are you undergoing IVF treatment? If yes: For how long? Which stage of the cycle are you at? How many cycles have you undergone?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
22
MALE MEDICAL HISTORY FORM Do you use any other beauty and cosmetic chemicals/lotions etc? How much? How often? Do you use deodorant? Do you use perfume or after-‐shave? Do you use skin bleach? Do you use hair bleach or hair dye? REPRODUCTIVE AND SEXUAL HEALTH Do you have any known spinal issues? Have you had any recent injuries to your spine or reproductive organs? Have you had any recent surgeries on your spine reproductive organs? Do you exercise? Do you take steroids? Do you take testosterone supplements? Do you take any other supplements? Do you have any of the following issues? Sperm production problems • Chromosomal or genetic causes • Undescended testes (failure of the testes to descend at birth) • Infections • Torsion (twisting of the testis in scrotum) • Varicocele (varicose veins of the testes) Blockage of sperm transport & Sexual Problems • Infections • Prostate-‐related problems • Absence of vas deferens • Vasectomy • Retrograde and premature ejaculation • Failure of ejaculation • Erectile dysfunction • Infrequent intercourse • Spinal cord injury • Prostate surgery • Damage to nerves Hormonal problems
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
23
• Pituitary tumours • Congenital lack of LH/FSH (pituitary problem from birth) • Anabolic (androgenic) steroid abuse Sperm antibodies • Vasectomy • Injury or infection in the epididymis (OPTIONAL) FERTILITY Are you using contraceptives? Which kind? Are you in a Polygynous marriage? How often do you engage in (halal) sexual intercourse with your spouse? Are you fertile now? Have you been fertile in the past? If no, have you and/or your spouse had the relevant fertility tests? What were the results? Are you undergoing any medical or fertility treatment with your spouse? Are you undergoing IVF treatment with your spouse? If yes: For how long? Which stage of the cycle are you at? How many cycles have you undergone?

COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
24
PRE-‐TREATMENT CARE INSTRUCTIONS DO NOT stop or reduce medication without their Doctors permission. Do not to eat 2-‐3 hours before the appointment time If you are taking medication which needs to be taken with or after food, please wait and take your medication immediately after the Hijama session with food to avoid any negative after effects such as low blood pressure or low blood sugar such as:
• Dizziness or lightheadedness • Fainting (syncope) • Blurred vision • Nausea • Fatigue • Lack of concentration • Shock
Please do the following before your Hijama session:
• Perform ritual bathing and ablution before the session as is Sunnah. • Make intention and pray for healing and cleansing on a physical and metaphysical
level. • Bring two large towels. • Bring water and a snack/meal. • Children should be accompanied by a responsible adult, with written consent from
both parents for the child. • Inform us of any known metaphysical issues. • Inform us of pregnancy, menstrual cycle, anemia, diabetes, blood pressure issues and
seizures beforehand.
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
25
OPTIONAL PRE-‐TREATMENT CARE
• Hot shower or hot bath soak.
• Foot soak
• A massage.
• A few minutes on a vibration machine
• A brisk walk or quick jog Possible rare reactions to be aware of are:
• Dizziness or light headedness-‐Can be due to low blood pressure, low blood sugar, anemia or metaphysical issues
• Nausea or vomiting • Shaking or seizures • Blackout or fainting • Plasma and blisters • Weakness or tiredness • Skin colouration on Hijama cupping sites
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
26
POST-‐TREATMENT CARE INSTRUCTIONS
• Drink plain or honey water after Hijama • Eat dates or fruit immediately after a Hijama treatment. Eat a solid, healthy, balanced
home after Hijama treatment. • You may be extra hungry over the next few days, so eat as much you can or need to.
Eat a balanced and healthy diet. • Do not eat red meat for 24 hours. • Do not eat dairy food for 24 hours. • Skin colouration and incisions will heal in 2-‐10 days. • You can have a quick shower rinse. But do not use soap, shampoo or chemicals. • Do NOT soak in a bath tub or go swimming for 24 hours after Wet Cupping. • You MUST rest after a session. Do NOT physically over exert yourself, do exercise,
chores etc at all. You can sleep if you need to after Hijama. • Do NOT engage in marital relations for 24 hours after any type of cupping. • Do regular, moderate light exercise after 24 hours and make this a regular routine. • Try to relax, pray, and think positive thoughts. Keep a daily journal and make notes of
your progress. Over the next few days, you may notice changes in your;
• Bowel and Urinary habits • Sleep Patterns • Mood swings/emotional levels • Appetite • Vision
You may experience;
• Skin breakouts • Tiredness and feeling drained or low on energy • General weakness • Excessive flatulence • Excessive release of bodily fluids such as, phlegm, mucus, sweat, urine, spots of
pimples, pus, tears (crying). • More energy
These are nothing to be concerned about. This process is called a “Healing Crisis” and means that your body has reacted to the Hijama and is now detoxifying itself. It is simply your body getting used to the massive shifts in energy after treatments. Your body will now be dealing with and adjusting to huge changes in your physical, mental, emotional and spiritual state.
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
27
Your body has just been kick-‐started in to a different zone and forced to get out of its usual state of pain/sickness/discomfort. You will feel better after a few sessions and your body will become more balanced.
POSSIBLE AFTER EFFECTS
• Healing Crisis and detox
• Increased hunger
• Increased energy
• Increased sleepiness or tiredness.
• Increased bowel movements or urination.
• Better metabolism.
• Better sleep quality
• Better mood and relaxation
• Pain relief and increased mobility
• General improvement in well being
• Increase or changes in any metaphysical activity
• Skin colouration on Hijama cupping points-‐may last for 2-‐10 days.
COPYRIGHT © 2011-‐2019 VERSION 6.0 HIJAMA NATION LTD. ALL RIGHTS RESERVED
28
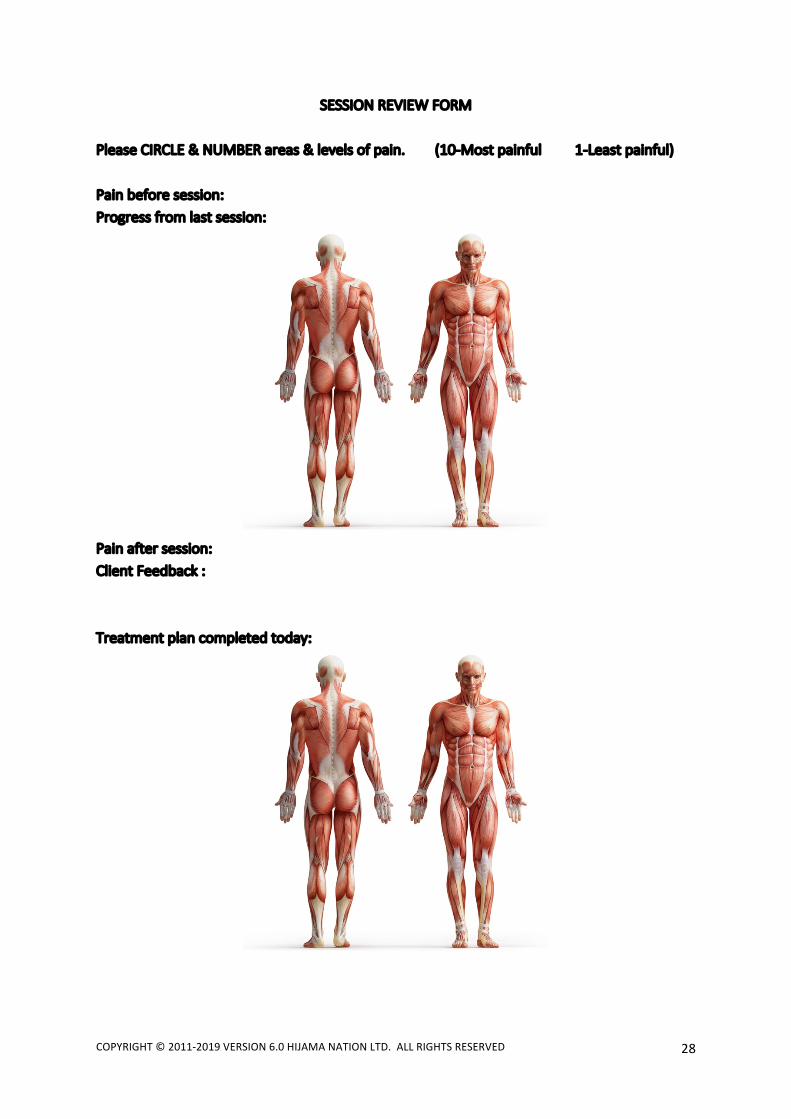
SESSION REVIEW FORM Please CIRCLE & NUMBER areas & levels of pain. (10-‐Most painful 1-‐Least painful) Pain before session: Progress from last session:
Pain after session: Client Feedback : Treatment plan completed today: