HIV PREVENTION RESEARCH ON MEN WHO HAVE SEX ...
30
AIDS Education and Prevention, 32(1), 1–24, 2020 © 2020 The Guilford Press 1 HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW HIGA ET AL. HIV PREVENTION RESEARCH ON MEN WHO HAVE SEX WITH MEN: A SCOPING REVIEW OF SYSTEMATIC REVIEWS, 1988–2017 Darrel H. Higa, Nicole Crepaz, Christina M. McDonald, Adebukola Adegbite-Johnson, Julia B. DeLuca, Emiko Kamitani, Theresa Ann Sipe, and the Prevention Research Synthesis (PRS) Project In the United States, men who have sex with men (MSM) are dispro- portionately affected by HIV. To identify research gaps and inform HIV prevention for MSM, we conducted a scoping review of systematic reviews using CDC’s Prevention Research Synthesis database. Eligibility criteria comprised English-language systematic reviews focused on HIV preven- tion for MSM, published during 1988–2017, and included at least one U.S. primary study. We coded data type, subpopulations, topics, and key find- ings. To assess study quality, we used the Assessment of Multiple Systematic Reviews (AMSTAR). Among 129 relevant systematic reviews, study quality was high or moderate for 63%. Most common topics were sexual behavior and disease vulnerability. The most frequently mentioned MSM subgroups were HIV-positive, Black or African American, and young. Research gaps include Hispanic/Latino MSM, pre-exposure prophylaxis (PrEP), treatment as prevention, social determinants of health, health disparities, syndemics, and protective factors for sexual health. Keywords: gay men, systematic review, HIV In the United States (U.S.), men who have sex with men (MSM) continue to be disproportionately affected by HIV infection. Although MSM are estimated to com- prise 3.9% of the U.S. adult male population and 2% of the overall U.S. population (Purcell et al., 2012), they represented 72% of persons living with diagnosed HIV infection at year-end 2016 and 67% of new HIV diagnoses in 2017 (Centers for Disease Control and Prevention [CDC], 2018). Black or African American (hereafter Supplemental materials are available online. Darrel H. Higa, PhD, Nicole Crepaz, PhD, Christina M. McDonald, MPH, Julia B. DeLuca, MLS, Emiko Kamitani, PhD, and Theresa Ann Sipe, PhD, are affiliated with the Centers for Disease Control and Pre- vention, Division of HIV/AIDS Prevention, Atlanta, Georgia. Adebukola Adegbite-Johnson, MPH, is affiliated with ICF International, Atlanta, Georgia. The authors would like to thank Marie Morgan for editing the manuscript. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. The authors did not receive any funding for this study. Address correspondence to Darrel H. Higa, 1600 Clifton Rd., NE, Mail Stop US8-5, Atlanta, GA 30329. E-mail: [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of HIV PREVENTION RESEARCH ON MEN WHO HAVE SEX ...

AIDS Education and Prevention, 32(1), 1–24, 2020 © 2020 The Guilford Press
1
HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEWHIGA ET AL.
HIV PREVENTION RESEARCH ON MEN WHO HAVE SEX WITH MEN: A SCOPING REVIEW OF SYSTEMATIC REVIEWS, 1988–2017 Darrel H. Higa, Nicole Crepaz, Christina M. McDonald, Adebukola Adegbite-Johnson, Julia B. DeLuca, Emiko Kamitani, Theresa Ann Sipe, and the Prevention Research Synthesis (PRS) Project
In the United States, men who have sex with men (MSM) are dispro-portionately affected by HIV. To identify research gaps and inform HIV prevention for MSM, we conducted a scoping review of systematic reviews using CDC’s Prevention Research Synthesis database. Eligibility criteria comprised English-language systematic reviews focused on HIV preven-tion for MSM, published during 1988–2017, and included at least one U.S. primary study. We coded data type, subpopulations, topics, and key find-ings. To assess study quality, we used the Assessment of Multiple Systematic Reviews (AMSTAR). Among 129 relevant systematic reviews, study quality was high or moderate for 63%. Most common topics were sexual behavior and disease vulnerability. The most frequently mentioned MSM subgroups were HIV-positive, Black or African American, and young. Research gaps include Hispanic/Latino MSM, pre-exposure prophylaxis (PrEP), treatment as prevention, social determinants of health, health disparities, syndemics, and protective factors for sexual health.
Keywords: gay men, systematic review, HIV
In the United States (U.S.), men who have sex with men (MSM) continue to be disproportionately affected by HIV infection. Although MSM are estimated to com-prise 3.9% of the U.S. adult male population and 2% of the overall U.S. population (Purcell et al., 2012), they represented 72% of persons living with diagnosed HIV infection at year-end 2016 and 67% of new HIV diagnoses in 2017 (Centers for Disease Control and Prevention [CDC], 2018). Black or African American (hereafter
Supplemental materials are available online.
Darrel H. Higa, PhD, Nicole Crepaz, PhD, Christina M. McDonald, MPH, Julia B. DeLuca, MLS, Emiko Kamitani, PhD, and Theresa Ann Sipe, PhD, are affiliated with the Centers for Disease Control and Pre-vention, Division of HIV/AIDS Prevention, Atlanta, Georgia. Adebukola Adegbite-Johnson, MPH, is affiliated with ICF International, Atlanta, Georgia.The authors would like to thank Marie Morgan for editing the manuscript.The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.The authors did not receive any funding for this study. Address correspondence to Darrel H. Higa, 1600 Clifton Rd., NE, Mail Stop US8-5, Atlanta, GA 30329. E-mail: [email protected]

2 HIGA ET AL.
referred to as Black) MSM, Hispanic/Latino MSM, young MSM, and MSM living in the Southeast are members of the subgroups most vulnerable to new HIV infections (CDC, 2018).
Much research has been conducted to better understand how HIV has affected MSM and on intervention strategies. One perspective (Mansergh & Higa, 2011) characterizes the HIV prevention research literature on MSM as comprising four major periods: epidemic emergence (1981–1985), understanding behavior and change (1986–1995), chronic disease management (1996–2009), and moving for-ward (2010 and beyond). In the earliest period, prevention research consisted mostly of how HIV was transmitted and the ensuing effects for those infected. The next ten years focused on identifying behavioral risk factors for acquiring HIV, examining how MSM were living and coping with HIV/AIDS, exploring how HIV testing in-fluenced risk behavior, and investigating how HIV/AIDS was affecting diverse MSM populations. HIV prevention researchers also began to conduct behavioral interven-tion studies with MSM paralleling the historic reductions in sexual risk behavior among MSM.
The introduction of highly active antiretroviral therapy (HAART) in 1996 marks the beginning of the third period and transformed HIV infection from a life-threatening illness to managing a chronic disease. The release of the U.S. National HIV/AIDS Strategy in 2010 (Office of National AIDS Policy, 2010) marked the re-cent era that emphasizes increasing HIV care access and viral suppression among persons with HIV and reducing HIV-related health disparities. As more evidence shows that early and consistent ART treatment of persons with HIV and pre-expo-sure prophylaxis (PrEP) taken by HIV-negative persons prevent HIV transmission and infection, these biomedical approaches have become primary prevention strate-gies (Office of National AIDS Policy, 2015). With the expansion of HIV treatment during the post-ART era that spans across the third and fourth periods, prevention challenges such as engagement in HIV care, viral suppression, PrEP uptake, and seroadaptive strategies (e.g., serosorting) have emerged. Understanding sexual risk behaviors within the context of social determinants of health may also be important to address health disparities among MSM (Mansergh & Higa, 2011).
As the body of HIV prevention research literature has accumulated, researchers have conducted systematic reviews to synthesize the large volume of primary studies on MSM and identify evidence to guide HIV prevention efforts. More recently, re-searchers have conducted overviews of systematic reviews to summarize the growing evidence in the synthesized research. An overview of reviews is useful for analyzing what is known about the research area, making recommendations for programs, identifying research gaps, and offering directions for future research (Ortega, Lo-pez-Briz, & Fraga-Fuentes, 2016). Because an overview-of-reviews approach uses existing systematic reviews that have identified relevant studies and extracted data, conducting an overview may be more efficient and feasible than undertaking a sys-tematic review of primary studies (Tsagris & Fragkos, 2016). In the HIV prevention research literature, we found only one overview of reviews exclusively focused on MSM to date. This overview of reviews found strong, consistent evidence for the ef-fectiveness of group- and community-level interventions to reduce condomless anal sex and increase condom use, but inconsistent evidence for effectiveness of individ-ual-level interventions (Lorimer et al., 2013).
An overview of reviews that aims to map key concepts or topics underpinning a research area is a type of scoping review (Arksey & O’Malley, 2005). Scoping reviews highlight the area of interest in terms of volume, nature and characteristics

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 3
of research studies using rigorous and transparent methods (Arksey & O’Malley, 2005). They are particularly beneficial when the body of literature is large, complex or heterogeneous (Peters et al., 2015).
As the HIV prevention field approaches its fifth decade, a scoping review that systematically maps the synthesized HIV literature on MSM is timely for examining the accumulated evidence of HIV research on MSM in the US. We conducted a scop-ing review of HIV prevention literature on MSM to identify commonalities among the reviews, provide an overall picture of the quality of these reviews, and identify research gaps to inform future research and prevention efforts for this population.
METHODS
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analy-ses Extension for Scoping Reviews (PRISMA-ScR) to report this review (Tricco et al., 2018). A comprehensive search of the CDC’s HIV/AIDS Prevention Research Syn-thesis (PRS) Project database was performed to identify systematic reviews focused on MSM (1988–August 14, 2017; Lyles, Crepaz, Herbst, & Kay, 2006). By mid-August 2017, the PRS database contained approximately 87,000 records related to prevention research on HIV/AIDS or sexually transmitted infections (STIs). The PRS database consists of automated and manual searches that retrieve primary studies and systematic reviews. Online searches are implemented annually using the follow-ing databases: MEDLINE (OVID), EMBASE (OVID), CINAHL (EBSCO host), Psyc INFO (OVID), CAB Global Health (OVID), and Sociological Abstracts (ProQuest; DeLuca et al., 2008; Appendix A [Contact the author for Appendix A]). Each auto-mated search was developed in the MEDLINE (OVID) database by cross-referencing indexing and keyword terms using Boolean terms (no language limits). The manual search of the PRS database includes a quarterly manual search of 52 journals (PRS website: https://www.cdc.gov/hiv/dhap/prb/prs/index.html), publication alerts, and references from relevant articles. The initial search was conducted on March 28, 2015; updates were conducted on October 18, 2016, and August 14, 2017. For this review, a librarian used MSM key words and index terms to search the PRS data-base. (For the complete PRS database query, see Appendix A [Contact the author for Appendix A].)
Qualitative systematic reviews and meta-analyses of HIV prevention research were included if the reviews (a) contained at least one literature search element (e.g., search years, database searched, search terms given), (b) included a systematic syn-thesis of findings (Higgins & Green, 2011), (c) exclusively focused on MSM, (d) were published during 1988–August 14, 2017, (e) were written in English, and (f) contained at least one U.S. primary study. Reviews that included different popula-tions such as heterosexual men and MSM for example, but reported stratified data for MSM, were excluded.
We used Distiller SR software, a data management tool for systematic reviews (Evidence Partners, Ottawa, Canada), to screen and code reviews to determine eli-gibility and collect data on synthesis method used (i.e., meta-analysis or not), data type (i.e., intervention, correlational, prevalence, descriptive), number of primary studies, topics (e.g., sexual behavior, substance use, health disparities), and subpopu-lations (e.g., race/ethnicity, age, HIV status). Categories of data type, major topics, and subpopulations were not mutually exclusive. For data type, we coded reviews as including intervention data if the study synthesized findings from prevention in-

4 HIGA ET AL.
terventions for MSM. We coded reviews as correlational if association data were reported or key findings qualitatively suggested relationships between variables. We categorized reviews prevalence/incidence if they reported estimates of disease preva-lence/incidence, the size of MSM subpopulations or percentages of MSM engaging in behaviors. We coded reviews that narratively examined a topic in depth as descrip-tive. Topics and subpopulations were coded using the primary focus of reports. Key findings from each review were abstracted to flesh out themes within topics. When possible, we synthesized key findings within each topic using a thematic approach adapted from Mendelsohn et al. (Mendelsohn et al., 2015). Data were analyzed in SPSS Version 21 (IBM Corporation, 2011 ).
To assess review quality, we used the Assessment of Multiple Systematic Review (AMSTAR) tool (Shea, Grimshaw, et al., 2007) (for AMSTAR questions, see Appen-dix B [Contact the author for Appendix B]). The psychometric properties of the AM-STAR are well-established and reported (Shea, Bouter et al., 2007; Shea et al., 2009). Total scores (0 –11) were calculated by counting the number of Yes responses. Higher scores indicate better quality of the review; each review was classified as: high qual-ity (8–11 points), moderate (5–7 points), or low (0–4 points; Flodgren et al., 2011).
Screening, data abstraction, and review quality assessments were conducted by pairs of trained coders who independently coded each eligible review. The weighted inter-rater reliability (Cohen’s kappa [K]) for data abstraction was calculated as K = .68, and for AMSTAR coding as K = .46. Discrepancies were resolved by discussion until consensus was reached.
FIGURE 1. Flow chart showing number of reviews identified, reasons for exclusion, and total number of included systematic reviews and meta-analyses.

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 5
RESULTS
We identified 397 reviews as potentially relevant (Figure 1). A total of 129 qualita-tive systematic reviews (n = 86) and meta-analyses (n = 43) published 1995 to 2017 met eligibility criteria. (For the study characteristics of included reviews, see Appen-dix C [contact the author for Appendix C].)
REVIEW QUALITYThe overall mean review quality score for all reviews was 5.4 (moderate); cate-
gorized scores were high (25/129, 20%), moderate (54/129, 43%), and low (48/129, 37%). (For AMSTAR total scores, see Appendix C; for individual scores, by ques-tion, and mean quality score, see Appendix D [contact the Author for Appendix D].)
OVERALL CHARACTERISTICS Of the 129 reviews, 93 (72%) comprised studies from the U.S. and other coun-
tries; 36 (28%) comprised only U.S.-based studies. The most common type of data was correlational (54/129, 42%), followed by intervention data (32/129, 25%), prevalence data (31/129, 24%), and descriptive data (22/129, 17%). Findings of 71 reviews (54%) concerned one or more MSM subpopulations: HIV-positive (21/71, 16%), Black (16/71, 12%), HIV-negative (12/71, 9%), young (11/71; 8%), sub-stance user (11/71, 8%), venues or the Internet to meet sex partners (10/71, 8%), MSM of color (3/71, 2%), Latino/Hispanic (n = 2/71, 2%), MSM with childhood sexual abuse histories (2/71, 2%), MSM who had sex with women (2/71, 2%), older (1/71, 1%), Asian and Pacific Islander (API) (1/71, 1%), and MSM couples (1/71, 1%).
TOPICS We mapped 129 reviews into 15 topics (Table S1, in the Supplemental Materi-
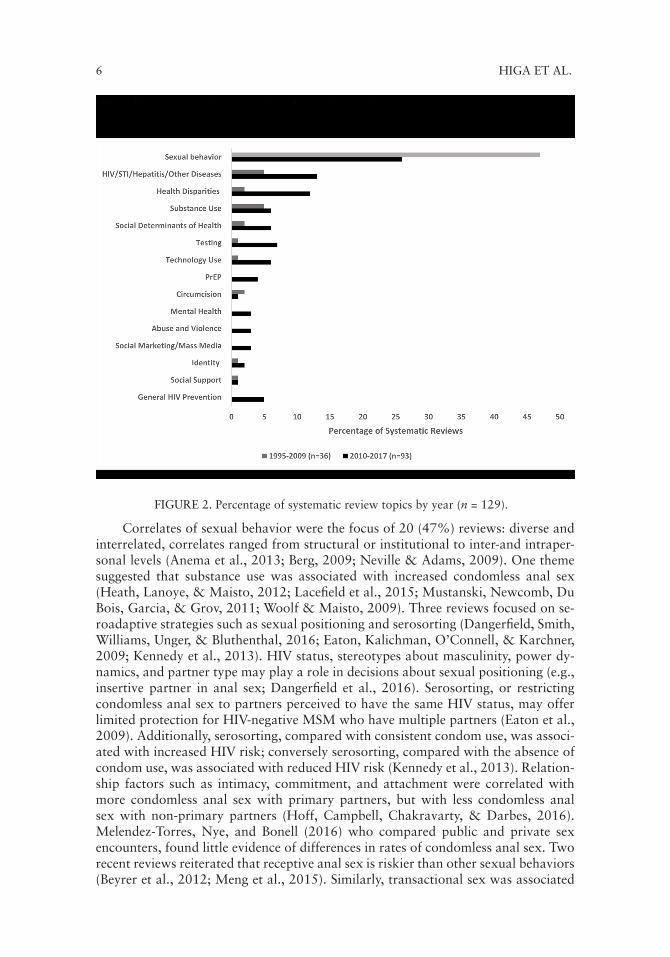
als). The most common topic was sexual behavior followed by disease vulnerability to HIV/STI/hepatitis/other diseases. Less frequently covered topics included PrEP, health disparities, substance use, social determinants of health, testing for HIV/STI/hepatitis/other diseases, technology use, general HIV prevention mental health, abuse and violence, social marketing/mass media, identity, and social support. Fig-ure 2 presents systematic review topics by publication time periods. The percentage of reviews focusing on sexual behavior was larger in earlier years (1995–2009) com-pared to later years (2010–2017). Other than disease vulnerability to HIV/STI/hepa-titis/other disease-related topics, less frequently covered topics appeared in more recent reviews than older reviews. The results for the topics, which are not mutually exclusive, are presented below.
SEXUAL BEHAVIOR Of 129 reviews, 43 (33%) focused primarily on sexual behavior; mean qual-
ity was moderate; 17 (40%) were meta-analyses (Andrew et al., 2016; Berg, Ross, & Tikkanen, 2011; Crepaz et al., 2009; Friedman et al., 2014; Herbst et al., 2005, 2007; Johnson et al., 2002, 2005, 2009; Johnson, Hedges, & Diaz, 2002; Ken-nedy et al., 2013; Lacefield, Negy, Schrader, & Kuhlman, 2015; Melendez-Torres & Bonell, 2014; Meng et al., 2015; Oldenburg, Perez-Brumer, Reisner, & Mimiaga, 2015; Purcell et al., 2012; Ye et al., 2014). The most common MSM subpopulations were young (5/43, 12%), HIV-positive (5/43, 12%), substance users (4/43, 9%), and Internet or venue users for meeting sex partners (3/43, 7%).
6 HIGA ET AL.
FIGURE 2. Percentage of systematic review topics by year (n = 129).
Correlates of sexual behavior were the focus of 20 (47%) reviews: diverse and interrelated, correlates ranged from structural or institutional to inter-and intraper-sonal levels (Anema et al., 2013; Berg, 2009; Neville & Adams, 2009). One theme suggested that substance use was associated with increased condomless anal sex (Heath, Lanoye, & Maisto, 2012; Lacefield et al., 2015; Mustanski, Newcomb, Du Bois, Garcia, & Grov, 2011; Woolf & Maisto, 2009). Three reviews focused on se-roadaptive strategies such as sexual positioning and serosorting (Dangerfield, Smith, Williams, Unger, & Bluthenthal, 2016; Eaton, Kalichman, O’Connell, & Karchner, 2009; Kennedy et al., 2013). HIV status, stereotypes about masculinity, power dy-namics, and partner type may play a role in decisions about sexual positioning (e.g., insertive partner in anal sex; Dangerfield et al., 2016). Serosorting, or restricting condomless anal sex to partners perceived to have the same HIV status, may offer limited protection for HIV-negative MSM who have multiple partners (Eaton et al., 2009). Additionally, serosorting, compared with consistent condom use, was associ-ated with increased HIV risk; conversely serosorting, compared with the absence of condom use, was associated with reduced HIV risk (Kennedy et al., 2013). Relation-ship factors such as intimacy, commitment, and attachment were correlated with more condomless anal sex with primary partners, but with less condomless anal sex with non-primary partners (Hoff, Campbell, Chakravarty, & Darbes, 2016). Melendez-Torres, Nye, and Bonell (2016) who compared public and private sex encounters, found little evidence of differences in rates of condomless anal sex. Two recent reviews reiterated that receptive anal sex is riskier than other sexual behaviors (Beyrer et al., 2012; Meng et al., 2015). Similarly, transactional sex was associated

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 7
with increased HIV prevalence for MSM (Oldenburg et al., 2015). Finally, three re-views suggested that individual and interpersonal factors (e.g., intention to use con-doms, perception of behavioral control, recognition of at-risk status, commitment to safer sex, and number of supportive peers; Andrew et al., 2016; Flowers, Sheeran, Beail, & Smith, 1997; McKechnie, Bavinton, & Zablotska, 2013) may be associated with safer sexual practices (Andrew et al., 2016; Flowers et al., 1997; McKechnie et al., 2013). The remaining review found a positive association between increased condom use and free or reduced-cost condoms (Ubrihien, Davies, & Driscoll, 2016).
By category, 17 (40%) reviews contained intervention-related data. A major theme for this group of reviews suggested that behavioral interventions in gener-al reduced sexual risk behavior or increased protective behaviors (Carrico, Zepf, Meanley, Batchelder, & Stall, 2016; Herbst et al., 2005, 2007; Johnson et al., 2002, 2005, 2009; Lorimer et al., 2013; Maulsby et al., 2013). Three meta-analytic re-views estimated that behavioral interventions reduced condomless anal sex 21% to 27% (Johnson et al., 2002, 2005, Johnson, Hedges, & Diaz, 2002). Peer-led inter-ventions reduced condomless anal sex with any sexual partners, but efficacy varied by study design (Ye et al., 2014). Specifically, quasi-experimental designs and serial cross-sectional intervention studies (but not randomized controlled trials or pre-post intervention studies) found a statistically significant reduction in condomless anal sex (Ye et al., 2014). Other intervention strategies such as motivational interviewing and cognitive behavioral techniques demonstrated some effectiveness for condom-less anal sex reduction, but not significantly more than other strategies (e.g., group therapy, contingency management, information) or assessment alone (e.g., no or minimal treatment; Berg et al., 2011; Melendez-Torres & Bonell, 2014). Similarly, Rees et al. (2004) suggested that counseling and risk-contextualizing workshops had no effect on condomless anal sex. Two reviews suggested that theory-grounded interventions may be important in intervention effectiveness (Lorimer et al., 2013; Neumann, Herbst, & Guenther-Grey, 2010). One descriptive review (Hergenrather, Emmanuel, Durant, & Rhodes, 2016) found that condomless anal sex, HIV risk behavior, condom use, HIV testing, safer sex, and HIV prevention communication were the most common studied outcomes in intervention studies. Another review suggested a lack of behavioral and biomedical interventions specifically for young MSM (Mustanski et al., 2011).
Six reviews (14%) estimated population sizes for MSM or the prevalence of sexual behaviors practiced by MSM. Estimates of the MSM population suggested that 2% of the U.S. population are MSM (Purcell et al., 2012) and 1% are MSM who have sex with women (Friedman et al., 2014). One review on the prevalence of sexual behaviors showed high levels of condomless anal sex (over 40%) among HIV-positive MSM (van Kesteren, Hospers, & Kok, 2007) and condomless anal sex with HIV-negative or unknown-status partners was estimated as 26% (Crepaz et al., 2009). Frankis and Flowers (2005) found that 10% of MSM reported serodiscor-dant condomless anal sex in public sex environments (PSEs). One review indicated variations among MSM populations with some groups reporting more sex risk be-haviors such as young MSM in North America (Oldenburg et al., 2016). Men aged 25–30 years may have the highest risk of seroconverting since they are more likely to sexually partner with men over 30 than their younger peers (Mansergh & Marks, 1998).
Three reviews (7%) contained descriptive data and suggest the importance of various factors (e.g., physical settings, sex partners, survival needs) that influence sexual behavior. One review described sexual behavior within the contexts of PSEs,

8 HIGA ET AL.
serosorting, and sex work (Rees et al., 2004). Frankis and Flowers (2009) suggested that nonverbal communication is the norm in public sex environments (i.e., specific, codified behaviors indicate sexual interest). Ronn, White, Hughes, and Ward (2014) suggested that serosorting is less premeditated and more context driven. The risk of violence was identified as an issue for MSM who engaged in sex work (Rees et al., 2004).
DISEASE VULNERABILITYOf the 129 reviews, 18 (14%; mean quality, moderate) examined disease vul-
nerability to HIV, STI, hepatitis, and other diseases. Of the 18, four were meta-analyses (Ghisla, Scherrer, Nicca, Braun, & Fehr, 2017; Hagan, Jordan, Neurer, & Cleland, 2015; Oldenburg et al., 2016; Ronn & Ward, 2011). The most commonly reported subpopulations were HIV-positive MSM (4/18, 22%) and HIV-negative MSM (3/18, 17%).
Eleven reviews contained correlational data that examined factors associated with HIV infection and other diseases affecting MSM. The findings from this group of reviews suggested a link between various STIs and HIV (Bonell, Hickson, Beau-mont, & Weatherburn, 2008; Cooper & Barber, 2014; Ronn et al., 2014), but evi-dence of a causal relationship was insufficient (Bonell, Weatherburn, & Hickson, 2000). Moreover, the association of STIs and HIV infection may not apply to API MSM (Wei, Raymond, et al., 2011). This review also suggested that low HIV preva-lence was not related to factors such as condomless anal sex, substance use, HIV testing, and use of HIV prevention services for API MSM. Although studies pub-lished in 2004 and 2005 provided some evidence of increased risk of prostate cancer among HIV-positive MSM, compared with HIV-negative MSM, studies published in 2010, 2013, and 2014 found no difference or less risk (Rosser et al., 2016). The possible link between MSM blood donors and transfusion transmissible infections was examined in one review (De Buck, Dieltjens, Compernolle, & Vandekerckhove, 2015). Traumatic sex and sex while under the influence of methamphetamines were associated with hepatitis C (HCV) infection for HIV-positive MSM (Hagan et al., 2015). Reviews also examined relationships between increased HIV infection and factors other than individual risk behaviors. For example, disproportionately high HIV rates among young Black and Hispanic/Latino MSM may be related to unrec-ognized HIV infection, social/sexual networks, and childhood sexual abuse (Feld-man, 2010). HIV infection rates are lower in countries whose penal codes contain protective language for sexual minorities, including MSM (Oldenburg et al., 2016).
Of the 18 reviews, eight reported the prevalence of diseases affecting MSM or specific MSM subgroups. A major theme highlights the vulnerability of MSM to certain STIs such as syphilis (Abara, Hess, Neblett Fanfair, Bernstein, & Paz-Bailey, 2016), intestinal parasites (Abdolrasouli, McMillan, & Ackers, 2009), human pap-illomavirus (HPV; Machalek, Grulich, Grulich, Templeton, & Poynten, 2012), and HIV (Grulich & Kaldor, 2008). A review using modeling methods projected that 60% of Black MSM would be HIV-positive by age 40, based on recent incidence estimates of 4.16% per year (Matthews et al., 2016). For HIV-positive MSM, HCV incidence was estimated as 6.3 per 1,000 person-years (Ghisla et al., 2017); the HCV seroconversion rate was 5.3 per 1000 person-years (Hagan et al., 2015). The likeli-hood of HIV infection among MSM with lymphogranuloma venereum (LGV) was eight times the likelihood among MSM with non-LGV chlamydia infection (Ronn & Ward, 2011). Two descriptive reviews identified research gaps for some STIs (e.g.,

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 9
genital warts) and other diseases affecting MSM (e.g., prostate cancer; Nadarzynski, Smith, Richardson, Jones, & Llewellyn, 2014; Rosser et al., 2016).
HEALTH DISPARITIES Sixteen reviews (11%; mean quality, moderate) highlighted HIV-related health
disparities. Ten (67%) were meta-analyses (Friedman et al., 2014; Ghisla et al., 2017; Jin, Matthews, & Grulich, 2016; King et al., 2016; Machalek, Poynten et al., 2012; Millett, Flores, Peterson, & Bakeman, 2007; Millett, Jeffries et al., 2012; Millett, Peterson et al., 2012; Purcell et al., 2012; Yaphe et al., 2012). The most-often studied subpopulations were Black MSM (7/16, 44%) and HIV-positive MSM (7/16, 44%). Fifteen reviews (94%) contained prevalence data. The general theme highlighted health-related disparities for MSM, particularly Black MSM and HIV-positive MSM. For example, MSM, compared with other groups, bear a greater bur-den of HIV, syphilis, and HPV (Brown et al., 2012; Purcell et al., 2012). Childhood sexual abuse is also more prevalent among MSM than among heterosexual men (Schafer, Gupta, & Dillingham, 2013). Black MSM, compared with other MSM or other populations, are more likely to be HIV-positive and to report an STI (Millett et al., 2007; Millett, Jeffries, et al., 2012; Millett, Peterson, et al., 2012; Millett, Pe-terson, Wolitski, & Stall, 2006; Walsh, Bertozzi-Villa, & Schneider, 2015). Greater numbers of HIV-positive MSM, compared with HIV-negative MSM, are affected by HCV, HPV, and syphilis (Abara et al., 2016; Ghisla et al., 2017; Jin et al., 2016; King et al., 2016; Machalek, Poynten, et al., 2012). Moreover, MSM who have sex with women, compared with men who have sex only with women, are five times more likely to be HIV-positive (Friedman et al., 2014). The lone correlational review suggested that HIV disparities for Black versus White MSM may be explained by a higher prevalence of STI, greater number of undiagnosed HIV infections, less access to care and treatment, and less use of ART (Maulsby et al., 2014).
SUBSTANCE USE Substance use, including alcohol, was a focus or an outcome of interest for 11
reviews (8%; mean quality, moderate). Two were meta-analyses (Berg et al., 2011; Vu, Maher, & Zablotska, 2015). The most frequently studied subpopulation was MSM who self-identified as substance users (9/11, 82%). No review specifically focused on opioid use among MSM.
Of the 11 substance use–related reviews, seven included correlational data. The evidence suggests that the likelihood of engaging in high risk sex increases with the use of alcohol, particularly binge drinking, and drugs, particularly methamphet-amines (crystal meth; Drumright, Patterson, & Strathdee, 2006; Heath et al., 2012; Rajasingham et al., 2012; Vosburgh, Mansergh, Sullivan, & Purcell, 2012; Woolf & Maisto, 2009). Methamphetamine use may also be associated with increased HIV infection (Vu et al., 2015). Evidence suggests a link between nitrate use (e.g., poppers) and increased high-risk sex (Drumright et al., 2006), but the evidence of a link between nitrate use and HIV-related Kaposi’s sarcoma (Haverkos & Drotman, 1995) is inconclusive.
Three substance-use related reviews contained intervention-related data (Berg et al., 2011; Rajasingham et al., 2012; Wray et al., 2016): two suggested preliminary support for motivational interviewing in reducing alcohol use (Berg et al., 2011; Wray et al., 2016); the third reported inconsistent results for treating crystal meth addiction (Rajasingham et al., 2012). The two descriptive reviews suggested that

10 HIGA ET AL.
recreational drug use at circuit parties and clubs was a common practice (Romanelli & Smith, 2004; Weidel, Provencio-Vasquez, & Grossman, 2008).
SOCIAL DETERMINANTS OF HEALTH Social determinants of health were the focus of eight reviews (8/129, 6%; mean
quality, low), one of which was a meta-analysis (Millett, Jeffries, et al., 2012). Five reviews examined social determinants of health among Blacks (Dillon & Basu, 2014; Levy et al., 2014; Millett, Jeffries, et al., 2012; Nelson, Walker, DuBois, & Giwa, 2014; Wilson et al., 2016). Although the type of data varied, four were descriptive (Dillon & Basu, 2014; Kuszelewicz & Lloyd, 1995; Levy et al., 2014; Smit et al., 2012). A central theme suggests that MSM and MSM of color in particular experi-ence multiple forms of oppression, stigma, and discrimination and that these barri-ers may interfere with accessing and using HIV prevention services (Dillon & Basu, 2014; Kuszelewicz & Lloyd, 1995; Levy et al., 2014; Smit et al., 2012).
Two reviews provided intervention data: one found that only three interven-tions for Black MSM addressed social determinants of health such as racism and religious oppression (Nelson et al., 2014); the other recommended multilevel in-terventions for reducing stigma for Black MSM (Wilson et al., 2016). Two reviews were correlational: one reported that HIV-positive MSM may not engage in HIV services because of factors such as stigma, health literacy, poverty, and insurance gaps (Natale & Moxley, 2009); the other suggested that the disproportionate inci-dence of HIV among Black MSM may be partially rooted in social inequalities and insufficient funding (Millett, Jeffries, et al., 2012).
TESTING FOR HIV, STI, AND OTHER DISEASESEight reviews (6%; mean quality, moderate) focused on testing for HIV, STIs,
and other diseases (e.g., anal cancer). One was a meta-analysis (Noble, Jones, Bowles, DiNenno, & Tregear, 2017). Seven reviews did not focus on a specific MSM subpopulation. Identification of a common theme among the eight reviews was dif-ficult. Two intervention-focused reviews that examined the acceptance of HIV or STI testing found multiple strategies may be effective. Rapid tests, opt-out testing, and intensive peer counseling can increase HIV testing (Lorenc, Marrero-Guillamón, Aggleton, et al., 2011) while clinic-based interventions such as provider alerts may increase STI testing (Zou, Fairley, Guy, & Chen, 2012). Of the four reviews that included descriptive data, two suggested that fear of a positive test result was a ma-jor reason for not testing (Flowers & Church, 2002; Lorenc, Marrero-Guillamón, Llewellyn, et al., 2011), one reported that few HIV guidelines recommended digital-rectal exams for anal cancer screening (Ong, Chen, Grulich, & Fairley, 2014), and one suggested that annual screening for pharyngeal gonorrhea can miss this diag-nosis given its short duration of infection compared to chlamydia and rectal gon-orrhea (Chow et al., 2016). Of the two prevalence-related reviews, one suggested that persistent high rates of STI among MSM may be due to a disconnect between screening recommendations for STI and actual screening (Lutz, 2015); the other found that 85% of Internet-using MSM had tested for HIV (Noble et al., 2017). The latter review also provided correlational data and found that age >30 years, college education, drug use, and self-identification as gay were associated with HIV testing.
TECHNOLOGY USESeven (5%; mean quality, moderate) reviews centered on technology use in HIV
prevention and how MSM incorporated technology (e.g., the Internet) in their sexual

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 11
behaviors. Four were meta-analyses (Lewnard & Berrang-Ford, 2014; Liau, Millett, & Marks, 2006; Yang, Zhang, Dong, Jin, & Han, 2014; Zou & Fan, 2017). Five re-views focused on MSM who used venues or the Internet to meet sex partners. Three reviews contained correlational data and findings were mixed. Two reviews sug-gested increased sexual risk for MSM who used the Internet (Lewnard & Berrang-Ford, 2014) or a geospatial networking app (Zou & Fan, 2017); the other found no clear evidence for the relationship (Melendez-Torres, Nye, & Bonell, 2015). Two prevalence reviews suggested that condomless anal sex was more prevalent among MSM who were recruited or sought partners online than among those who did not report either behavior (Liau et al., 2006; Yang et al., 2014). The single review with intervention data concluded that eHealth interventions may reduce sexual risk and increase HIV testing (Schnall, Travers, Rojas, & Carballo-Diéguez, 2014). Finally, the only descriptive review highlighted that MSM use the Internet for multiple sexu-al purposes (Grov, Breslow, Newcomb, Rosenberger, & Bauermeister, 2014).
PRE-EXPOSURE PROPHYLAXIS (PREP)Four (3%) reviews focused on PrEP use to prevent HIV infection (Holt, 2014;
Kojima, Davey, & Klausner, 2016; Scholl, 2016; Zablotska, 2016); mean quality was low. One was a meta-analysis (Kojima et al., 2016). The reviews were too het-erogeneous to summarize although the overall tone of the more recent reviews em-phasized the issues associated with study methods used the limitations of PrEP. For example, although the meta-analysis reported an increase in STIs among MSM tak-ing PrEP (Kojima et al., 2016), this finding was later questioned because of concerns regarding data analysis (Harawa et al., 2017; Kojima et al., 2016). Another review concluded that PrEP alone cannot reduce HIV diagnoses to zero and thus eliminate HIV transmission by the year 2030 (Zablotska, 2016). Finally, PrEP access may also be limited because of barriers such as stigma and low awareness of PrEP (Holt, 2014; Scholl, 2016).
CIRCUMCISIONThree (3%) reviews examined circumcision for MSM (Fankem, Wiysonge, &
Hankins, 2008; Millett, Flores, Marks, Reed, & Herbst, 2008; Wiysonge et al., 2011); mean quality, high. All were meta-analyses (Fankem et al., 2008; Millett et al., 2008; Wiysonge et al., 2011) and contained correlational data; none were focused on an MSM subpopulation. Two reviews that included U.S.- and non-U.S.-based studies suggested that the evidence regarding circumcision and prevention of HIV acquisition is insufficient; however, the insertive anal sex partner may be at lower risk for HIV (Millett et al., 2008; Wiysonge et al., 2011). The third review, which included only two U.S.-based studies, found similar results of circumcision associated with less acquisition of HIV (Fankem et al., 2008); however, the author did not distinguish between insertive and receptive anal sex.
MENTAL HEALTHThree reviews (2%; Lassiter & Parsons, 2016; Newcomb & Mustanski, 2011;
Woodward, Banks, Marks, & Pantalone, 2016) were broadly categorized as mental health; mean quality, moderate. All included correlational data. One (Newcomb & Mustanski, 2011) was a meta-analysis, and one also reported descriptive data (Woodward et al., 2016).
The heterogeneity of topics—religion/spirituality, resiliency, and internalized homophobia—made it difficult to synthesize the findings into a major theme. Las-

12 HIGA ET AL.
siter and Parsons (2016) suggested that religion and spirituality have mixed effects on depression and substance use; Newcomb and Mustanski (2011) found that high-risk sexual behavior was associated with high levels of internalized homophobia, but this relationship was moderated by a year of data collection (i.e., the correlation decreased over time). Finally, Woodward and colleagues (2016) offered a taxonomy of resiliency-related resources and suggested that resilience resources may be associ-ated with lower HIV risk.
ABUSE AND VIOLENCE Three reviews (2%; mean quality, moderate) synthesized primary studies related
to abuse or violence. Two were meta-analyses (Buller, Devries, Howard, & Bacchus, 2014; Lloyd & Operario, 2012). Two reviews focused on MSM with histories of childhood sexual abuse (Lloyd & Operario, 2012; Schafer et al., 2013). The major theme from this group of reports suggested that experiencing abuse or violence can be a factor in HIV infection and other health outcomes.
SOCIAL MARKETING/MASS MEDIA CAMPAIGNSThree reviews (2%, mean quality, high; French, Bonell, Wellings, & Weath-
erburn, 2014; Neville, Adams, & Holdershaw, 2014; Wei, Herrick, et al., 2011) focused on interventions related to social marketing or mass media. One was a meta-analysis (Wei, Herrick, et al., 2011). The summary evidence suggested that market-ing campaigns are associated with increases in HIV testing (French et al., 2014; Wei, Herrick, et al., 2011), but not STI testing (Wei, Herrick, et al., 2011). There is in-consistent evidence for the effect of social marketing campaigns on sexual behaviors (French et al., 2014; Neville et al., 2014). French et al. (2014; high study quality, n = 4 primary studies published 1990–2011), found no rigorous evidence of interven-tion effects on sexual behavior. Neville et al. (2014; moderate study quality, n = 11 primary studies and systematic reviews published 2007–2013) concluded that social marketing campaigns resulted in increased condom use.
IDENTITY Three (2%) systematic reviews touched on aspects related to identity, or percep-
tions of self (e.g., labeling self as gay or Black) in relation to HIV prevention and sexual behavior; mean quality was low. One review (Millett, Malebranche, Mason, & Spikes, 2005) was focused on Black MSM. The reviews were too heterogeneous to identify a major theme. Zeglin et al. (2015) suggested that embracing masculine norms may be related to sex risk behaviors such as low condom use and partner concurrency. Millet et al. (2005) found that Black MSM were more likely than other racial groups to identify as bisexual. Brennan, Bauer, Bradley, and Tran (2017) sug-gested that sexual orientation tends to be defined as behavioral in disease-focused research (e.g., MSM), but defined as an identity (e.g., gay) for other research topics.
SOCIAL SUPPORTTwo descriptive systematic reviews (1%) were broadly categorized as social
support (Hall, 1999; Phillips, Peterson, Binson, Hidalgo, & Magnus, 2011); mean quality was low. One focused on young Black MSM (Phillips et al., 2011). These reviews suggested that social support such as having a peer network (Hall, 1999) or a social structure such as the house/ball community (Phillips et al., 2011) may be important in preventing HIV among MSM.

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 13
GENERAL HIV PREVENTIONFour (3%) of the reviews discussed HIV prevention interventions in general
and did not fit into previously described categories. All were descriptive system-atic reviews and mean quality was moderate. These reviews focused on gaps in the intervention research literature (e.g., the lack of interventions for MSM in general compared with other populations (Higa et al., 2013) and for specific MSM subpopu-lations such as young MSM (Harper & Riplinger, 2013). Another gap, or need, is for a comprehensive approach that includes behavioral, biomedical, and structural interventions (Sullivan et al., 2012). One review (Wao, Aluoch, Odondi, Tenge, & Iznaga, 2016) found that knowledge and cost of HIV prevention interventions are barriers to acceptance of interventions by MSM.
DISCUSSION
To our knowledge, this is the first scoping overview of reviews that broadly exam-ines the HIV prevention research literature on MSM. Our review of 129 qualitative systematic reviews and meta-analyses shows that the most frequently mentioned MSM subgroups were HIV-positive, Black, and young; the most common topics were sexual behavior and disease vulnerability. Limited synthesized literature was found on Hispanic/Latino MSM. Understudied topics include PrEP, syndemics of mental health, substance use, and abuse/violence, health disparities, social determi-nants of health, testing for HIV, STI, and other diseases, technology use, mass media/social marketing, identity, and health-protective factors such as social support. The mean review quality when grouped by topics was mostly moderate. Below, we focus on select research gaps relevant for current HIV prevention efforts for MSM in the U.S. and offer potential directions for future research to address those research gaps.
RESEARCH GAPSA noticeable research gap is the lack of synthesized research on Hispanic/Latino
MSM. The incidence of HIV among Hispanic/Latino MSM is increasing (Singh, Song, Johnson, McCray, & Hall, 2018) and there is evidence of high rates of con-domless anal sex and stimulant use among the foreign-born members of this group (Lewis & Wilson, 2017). Thus, synthesis of the HIV prevention literature is urgently needed for Hispanic/Latino MSM to reduce new HIV infections in this population. A recent review not included in this review reported mixed findings for behavioral interventions for reducing condomless anal sex and increasing HIV testing among Hispanic/Latino MSM (Pérez, Santamaria, & Operario, 2018), The review also found that some cultural elements (e.g., bilingual recruitment) were included as in-tervention components, but others (e.g., machismo) were lacking.
Another research gap—the lack of systematic reviews on treatment as preven-tion—may reflect a time lag in the published research literature corresponding to the recent shift from a behavioral to a biomedical approach. Synthesizing publications related to HIV-positive MSM and the HIV care continuum, particularly publications that examine barriers and facilitators, will be beneficial for designing interventions and prevention programs, and laying the groundwork for future research. An en-couraging example is a systematic review suggesting that mobile health interventions show acceptability, feasibility, and preliminary efficacy for increasing intentions to use ART, self-reported adherence, and viral suppression (Muessig, LeGrand, Hor-vath, Bauermeister, & Hightow-Weidman, 2017).

14 HIGA ET AL.
The synthesized PrEP literature on MSM is nascent and difficult to summarize. As the PrEP research literature accumulates and matures, more rigorously conducted reviews will be important. Evidence of effectiveness of behavioral and structural in-terventions for PrEP uptake, use, and adherence will be needed as we try to end the HIV epidemic in the next 10 years. Community perspectives and innovative strate-gies will also be helpful in this endeavor. For example, a systematic review not in-cluded in our review analyzed the published research literature and online social me-dia posts to identify barriers and facilitators for PrEP use among MSM (Hannaford et al., 2017 ). The authors suggested that traditional research approaches may miss important factors for designing and implementing PrEP-related interventions and offer less concrete and nuanced information than newer online approaches. Further-more, both peer-reviewed articles and online published messages or posts identified barriers such as cost and lack of PrEP-related knowledge; online posts described facilitators such as culturally competent providers and online ordering and delivery of PrEP.
In this review, we found that substance use, abuse/violence, and other mental health conditions often associated with HIV risk were less frequently synthesized as major topics. Although the association between substance use and increased sexual risk behavior was a consistent finding, the evidence for interventions that reduced substance use was limited (Carrico et al., 2016; Melendez-Torres & Bonell, 2014). Bourne and Weatherburn (2017) argue that a robust understanding of how and why substance-use patterns emerge is key for developing interventions to reduce substance abuse among MSM (Bourne & Weatherburn, 2017). Race, Lea, Murphy, and Pienaar (2017) suggest a broader harm-reduction approach—ideally, one that includes decriminalization and destigmatizing of substances.
Mental health was not a common focus and warrants more attention. MSM report more depression, anxiety, panic, and alcohol and drug dependency compared with heterosexual men (Cochran & Mays, 2009). Moreover, sexual compulsivity and depression have been linked to HIV infection and sexual risk behavior for MSM (Parsons, Grov, & Golub, 2012). Syndemic approaches that acknowledge the role of social context and the interaction of co-existing diseases (Carnes, 2016) may be useful. Also, the addition of treatment for mental health issues in sexual reduction strategies and the examination of mental health in relation to HIV care outcomes and PrEP are equally important.
The lack of reviews on health disparities indicate a research gap in this area. The persistence of HIV disparities for Black MSM compared with other racial groups of MSM (CDC, 2017) demonstrates the need for systematic reviews to identify con-tributing factors for health disparities for this population. Investigating and inter-vening on structural levels that influence individual decisions and behaviors (Millett, Peterson, et al., 2012) may be central to reducing health disparities for Black MSM.
Social determinants of health may also merit further investigation given the relatively few reviews and the growing awareness that structural factors influence health outcomes. Factors such as societal homo-negativity (Berg, 2009), racism (Nelson et al., 2014), cultural values (Wei, Raymond, et al., 2011), and masculinity ideology (Zeglin, 2015) have been found to inform sexual behaviors of MSM. Trans-national migration may be an HIV risk factor for foreign-born MSM who report high levels of substance use and condomless anal sex (Lewis & Wilson, 2017). For HIV-positive MSM, social stigma, poverty, and insurance gaps may hinder access to HIV care (Natale & Moxley, 2009). Structural interventions focused on how a

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 15
person’s external environment affects risk or behavioral choices (Sipe et al., 2017) may be a necessary component in beginning to address social determinants of health.
Although we found relatively few reviews on testing for HIV and other diseases, we found encouraging evidence that mass media campaigns and new testing tech-nologies may increase HIV testing among MSM. A recent meta-analysis not included in our review found that peer-led interventions increased HIV testing among MSM (Shangani et al., 2017). Because learning one’s HIV status is a critical step toward initiating ART or PrEP, it is important that researchers continue to synthesize the research on interventions intended to increase HIV testing among MSM not previ-ously tested, and to conduct reviews on advances in testing technologies. A recent re-view not included in our review suggests that interventions in which the distribution of free HIV self-test kits was coupled with comprehensive support for the self-testing process addressed more barriers than did the distribution of free self-tests alone (Le-Grand, Muessig, Horvath, Rosengren, & Hightow-Weidman, 2017).
Technology use was understudied, but we found some overlap with sexual be-havior and to a lesser extent with HIV testing. Grov asserts that MSM have adapted to technological advances and use the Internet for various sexual purposes, includ-ing finding sex partners, dating, cybersex, pornography, and sex work (Grov et al., 2014). Technology-based interventions may be a cost-effective way to reach greater numbers of MSM and can be used in various functions for HIV prevention such as information dissemination, self-assessment, appointment and adherence remind-ers, access to prevention tools (e.g., condoms, HIV self-test kits), delivering preven-tion interventions, and referrals to services (Sullivan, Jones, Kishore, & Stephenson, 2015). Interventions that have been integrated into technology-based environments have demonstrated some evidence of reducing sex risk (Schnall et al., 2014) and are increasingly being incorporated into interventions for improving HIV care outcomes (Tanner et al., 2018) and improving use of PrEP (Liu et al., 2014; Mitchell et al., 2018; Refugio et al., 2019).
Finally, it may be beneficial to expand the research synthesis literature by con-ducting reviews that focus on health-protective factors for MSM. Synthesizing top-ics such as the influence of religion/spirituality and resilience on risk behaviors may indicate the emergence of a more holistic approach to HIV prevention for MSM. Moreover, exploring topics such as social support, reduction of experienced and internalized stigma, and other protective factors such as feeling part of a community may be beneficial because these factors may reduce HIV risk (Hart et al., 2017) and have a role in increasing access to HIV care, treatment, and prevention.
LIMITATIONS First, to narrow the scope, we excluded reviews focused on mixed populations
with MSM data as a subgroup. Including stratified data on MSM from mixed-popu-lation studies might have provided a more comprehensive picture of the HIV preven-tion research literature on MSM. Second, the probable overlap of primary studies among the included systematic reviews may be overstating some of the conclusions from this effort. Third, reliance on the synthesized findings of reviews may exclude important research findings from primary studies. Fourth, the weighted kappa for AMSTAR before coder pairs resolved discrepancies was low. We addressed this issue by discussing and resolving discrepancies and reaching agreement for final review quality scores. Finally, in our summary of intervention-related findings, we focused more on what worked than on what did not.

16 HIGA ET AL.
CONCLUSIONS Our findings indicate that the synthesized research literature focuses more on
sexual behavior and disease vulnerability, and less on biomedical approaches which have become the core of current HIV prevention efforts to end the epidemic. We also found a lack of synthesized research on Hispanic/Latino MSM. We suggest that fu-ture research on HIV prevention for MSM address gaps identified in the synthesized research literature that support the federal initiative of Ending the HIV Epidemic (EHE) in the U.S. Promising research areas most EHE-relevant for MSM include PrEP-related behavioral interventions, and interventions that increase HIV testing and engagement in HIV care. A better understanding of how to intervene on social determinants of health may help with reducing HIV and health disparities for all MSM, and in particular, MSM of color. Incorporating technology in interventions, addressing substance use and mental health issues, and promoting protective factors may also be crucial for HIV prevention among MSM. Finally, the HIV prevention research literature on MSM must continue to evolve to meet new challenges in the fifth decade of HIV and to ultimately end the epidemic among this population.
REFERENCES
Abara, W. E., Hess, K. L., Neblett Fanfair, R., Ber-nstein, K. T., & Paz-Bailey, G. (2016). Syph-ilis trends among men who have sex with men in the United States and Western Eu-rope: A systematic review of trend studies published between 2004 and 2015. PLoS One, 11, e0159309.
Abdolrasouli, A., McMillan, A., & Ackers, J. P. (2009). Sexual transmission of intestinal parasites in men who have sex with men. Sexual Health, 6, 185–194.
Andrew, B., Mullan, B. A., de Wit, J. B., Monds, L. A., Todd, J., & Kothe, E. J. (2016). Does the theory of planned behavior explain condom use behaviour among men who have sex with men? A meta-analytic review of the literature. AIDS and Behavior, 20, 2834–2844.
Anema, A., Marshall, B. D., Stevenson, B., Gurm, J., Montaner, G., Small, W., . . . Hogg, R. S. (2013). Intergenerational sex as a risk fac-tor for HIV among young men who have sex with men: A scoping review. Current HIV/AIDS Reports, 10, 398–407.
Arksey, H., & O’Malley, L. (2005). Scoping stud-ies: Towards a methodological framework. International Journal of Social Research Methodology, 8, 19–32.
Berg, R. (2009). Barebacking: A review of the lit-erature. Archives of Sexual Behavior, 38, 754–764.
Berg, R., Ross, M., & Tikkanen, R. (2011). The effectiveness of MI4MSM: How useful is motivational interviewing as an HIV risk prevention program for men who have sex with men? A systematic review. AIDS Edu-cation and Prevention, 23, 533–549.
Beyrer, C., Baral, S. D., Van Griensven, F., Goodreau, S. M., Chariyalertsak, S., Wirtz, A. L., & Brookmeyer, R. (2012). Global epidemiology of HIV infection in men who have sex with men. Lancet, 380, 367–377.
Bonell, C., Hickson, F., Beaumont, M., & Weath-erburn, P. (2008). Sexually transmitted in-fections as risk factors for HIV infection among MSMs: Systematic review [letter]. Sexually Transmitted Diseases, 35, 209–209.
Bonell, C., Weatherburn, P., & Hickson, F. (2000). Sexually transmitted infection as a risk fac-tor for homosexual HIV transmission: A systematic review of epidemiological stud-ies. International Journal of STD & AIDS, 11, 697–700.
Bourne, A., & Weatherburn, P. (2017). Substance use among men who have sex with men: Patterns, motivations, impacts and inter-vention development need. Sexually Trans-mitted Infections, 93, 342–346.
Brennan, D. J., Bauer, G. R., Bradley, K., & Tran, O. V. (2017). Methods used and topics ad-dressed in quantitative health research on gay, bisexual and other men who have sex with men: A systematic review of the litera-ture. Journal of Homosexuality, 18, 1–20.
Brown, B., Davtyan, M., Galea, J., Chow, E., Leon, S., & Klausner, J. D. (2012). The role of hu-man papillomavirus in human immunode-ficiency virus acquisition in men who have sex with men: A review of the literature. Viruses, 4, 3851–3858.
Buller, A., Devries, K., Howard, L., & Bacchus, L. (2014). Associations between intimate partner violence and health among men who have sex with men: A systematic re-

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 17
view and meta-analysis. PLoS Medicine, 11, e1001609.
Carnes, N. (2016). Gay men and men who have sex with men: Intersectionality and syn-demics. In E. R. Wright & N. Carnes (Eds.), Understanding the HIV/AIDS epidemic in the United States: The role of syndemics in the production of health disparities (pp. 43–69). New York, NY: Springer.
Carrico, A. W., Zepf, R., Meanley, S., Batchelder, A., & Stall, R. (2016). When the party is over: A systematic review of behavioral in-terventions for substance-using men who have sex with men. Journal of Acquired Im-mune Deficiency Syndromes, 73, 299–306.
Centers for Disease Control and Prevention. (2017). Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas, 2015. HIV Surveillance Supplemental Report 2017; 22 (No. 2). Retrieved from http://www.cdc.gov/hiv/li-brary/reports/hiv-surveillance.html
Centers for Disease Control and Prevention. (2018). HIV Surveillance Report, 2017. Retrieved from http://www.cdc.gov/hiv/li-brary/reports/hiv-surveillance.html
Chow, E. P., Camilleri, S., Ward, C., Huffam, S., Chen, M. Y., Bradshaw, C. S., & Fairley, C. K. (2016). Duration of gonorrhoea and chlamydia infection at the pharynx and rec-tum among men who have sex with men: A systematic review. Sexual Health, 13, 199–204.
Cochran, S. D., & Mays, V. M. (2009). Burden of psychiatric morbidity among lesbian, gay, and bisexual individuals in the California Quality of Life Survey. Journal of Abnor-mal Psychology, 118, 647–658. https://doi.org/10.1037/a0016501
Cooper, F., & Barber, T. (2014). ‘Gay bowel syn-drome’: Relic or real (and returning) phe-nomenon? Current Opinion in Infectious Diseases, 27, 84–89.
Crepaz, N., Marks, G., Liau, A., Mullins, M. M., Aupont, L. W., Marshall, K. J., . . . Wolitski, R. J. (2009). Prevalence of unprotected anal intercourse among HIV-diagnosed MSM in the United States: A meta-analysis. AIDS, 23, 1617–1629.
Dangerfield, D. T., Smith, L. R., Williams, J., Un-ger, J., & Bluthenthal, R. (2016). Sexual positioning among men who have sex with men: A narrative review. Archives of Sexual Behavior, 46, 869–884.
De Buck, E., Dieltjens, T., Compernolle, V., & Vandekerckhove, P. (2015). Is having sex with other men a risk factor for transfu-sion-transmissible infections in male blood donors in Western countries? A systematic review. PLoS One, 10, e0122523.
DeLuca, J., Mullins, M., Lyles, C., Crepaz, N., Kay, L., & Thadiparthi, S. (2008). Developing a comprehensive search strategy for evidence based systematic reviews. Evidence Based Library and Information Practice, 3, 3–32.
Dillon, P. J., & Basu, A. (2014). HIV/AIDS and minority men who have sex with men: A meta-ethnographic synthesis of qualita-tive research. Health Communication, 29, 182–192.
Drumright, L., Patterson, T., & Strathdee, S. (2006). Club drugs as causal risk factors for HIV acquisition among men who have sex with men: A review. Substance Use & Mis-use, 41, 1551–1601.
Eaton, L., Kalichman, S., O’Connell, D., & Karch-ner, W. (2009). A strategy for selecting sexual partners believed to pose little/no risks for HIV: Serosorting and its implica-tions for HIV transmission. AIDS Care, 21, 1279–1288.
Fankem, S., Wiysonge, C., & Hankins, C. (2008). Male circumcision and the risk of HIV infection in men who have sex with men. International Journal of Epidemiology, 37, 353–355.
Feldman, M. B. (2010). A critical literature review to identify possible causes of higher rates of HIV infection among young Black and La-tino men who have sex with men. Journal of the National Medical Association, 102, 1206–1221.
Fish, J., Papaloukas, P., Jaspal, R., & Williamson, I. (2016). Equality in sexual health promo-tion: A systematic review of effective in-terventions for Black and minority ethnic men who have sex with men. BMC Public Health, 16, 810.811–810.818.
Flodgren, G., Eccles, M. P., Shepperd, S., Scott, A., Parmelli, E., & Beyer, F. R. (2011). An over-view of reviews evaluating the effectiveness of financial incentives in changing health-care professional behaviours and patient outcomes. Cochrane Database of System-atic Reviews, 2011, CD009255. https://doi.org/10.1002/14651858.CD009255
Flowers, P., & Church, S. (2002). To test or not? HIV antibody testing amongst gay men. Culture, Health & Sexuality, 4, 43–65.
Flowers, P., Sheeran, P., Beail, N., & Smith, J. A. (1997). The role of psychosocial factors in HIV risk-reduction among gay and bisexual men: A quantitative review. Psychology & Health, 12, 197–230.
Frankis, J., & Flowers, P. (2005). Men who have sex with men (MSM) in public sex environ-ments (PSEs): A systematic review of quan-titative literature. AIDS Care, 17, 273–288.
Frankis, J., & Flowers, P. (2009). Public sexual cultures: A systematic review of qualitative research investigating men’s sexual behav-

18 HIGA ET AL.
iors with men in public spaces. Journal of Homosexuality, 56, 861–893.
French, R., Bonell, C., Wellings, K., & Weather-burn, P. (2014). An exploratory review of HIV prevention mass media campaigns tar-geting men who have sex with men. BMC Public Health, 14, 616.611–616.617.
Friedman, M., Wei, C., Klem, M., Silvestre, A., Markovic, N., & Stall, R. (2014). HIV infection and sexual risk among men who have sex with men and women (MSMW): A systematic review and meta-analysis. PLoS One, 9, e87139.
Ghisla, V., Scherrer, A. U., Nicca, D., Braun, D. L., & Fehr, J. S. (2017). Incidence of hepatitis C in HIV positive and negative men who have sex with men 2000–2016: A system-atic review and meta-analysis. Infection, 45, 309–321.
Grov, C., Breslow, A. S., Newcomb, M. E., Rosen-berger, J. G., & Bauermeister, J. A. (2014). Gay and bisexual men’s use of the Internet: Research from the 1990s through 2013. Journal of Sex Research, 51, 390–409.
Grulich, A. E., & Kaldor, J. M. (2008). Trends in HIV incidence in homosexual men in devel-oped countries. Sexual Health, 5, 113–118.
Hagan, H., Jordan, A. E., Neurer, J., & Cleland, C. M. (2015). Incidence of sexually transmit-ted hepatitis C virus infection in HIV-posi-tive men who have sex with men. AIDS, 29, 2335–2345.
Hall, V. P. (1999). The relationship between social support and health in gay men with HIV/AIDS: An integrative review. Journal of the Association of Nurses in AIDS Care, 10, 74–86.
Hannaford, A., Lipshie-Williams, M., Starrels, J. L., Arnsten, J. H., Rizzuto, J., Cohen, P., . . . Patel, V. V. (2018). The use of online posts to identify barriers to and facilitators of HIV pre-exposure prophylaxis (PrEP) among men who have sex with men: A comparison to a systematic review of the peer-reviewed literature. AIDS and Behav-ior, 22, 1080–1095.
Harawa, N., Holloway, I., Leibowitz, A., Weiss, R., Gildner, J., Landovitz, R., . . . Shoptaw, S. (2017). Serious concerns regarding a me-ta-analysis of preexposure prophlaxis use and STI acquisition. AIDS, 31, 739–743.
Harper, G. W., & Riplinger, A. J. (2013). HIV pre-vention interventions for adolescents and young adults: What about the needs of gay and bisexual males? AIDS and Behavior, 17, 1082–1095.
Hart, T., Noor, S., Adam, B., Vernon, J., Bren-nan, D., Gardner, S., . . . Myers, T. (2017). Number of psychosocial strengths predicts reduced HIV sexual risk behaviors above and beyond syndemic problems among gay
and bisexual men AIDS and Behavior, 21, 3035–3046.
Haverkos, H. W., & Drotman, D. P. (1995). Mea-suring inhalant nitrite exposure in gay men: Implications for elucidating the etiology of AIDS-related Kaposi’s sarcoma. Genetica, 95, 157–164.
Heath, J., Lanoye, A., & Maisto, S. A. (2012). The role of alcohol and substance use in risky sexual behavior among older men who have sex with men: A review and critique of the current literature. AIDS and Behavior, 16, 578–589.
Herbst, J. H., Beeker, C., Mathew, A., McNally, T., Passin, W. F., Kay, L. S., . . . Johnson, R. L. (2007). The effectiveness of individual-, group-, and community-level HIV behav-ioral risk-reduction interventions for adult men who have sex with men: A systematic review. American Journal of Preventive Medicine, 32(4 Suppl. 1), S38–S67.
Herbst, J. H., Sherba, R. T., Crepaz, N., DeLuca, J. B., Zohrabyan, L., Stall, R. D., & Lyles, C. M. (2005). A meta-analytic review of HIV behavioral interventions for reducing sexual risk behavior of men who have sex with men. Journal of Acquired Immune De-ficiency Syndromes, 39, 228–241.
Hergenrather, K. C., Emmanuel, D., Durant, S., & Rhodes, S. D. (2016). Enhancing HIV prevention among young men who have sex with men: A systematic review of HIV behavioral interventions for young gay and bisexual men. AIDS Education and Preven-tion, 28, 252–271.
Higa, D. H., Crepaz, N., Marshall, K. J., Kay, L., Vosburgh, H. W., Spikes, P., . . . Pur-cell, D. W. (2013). A systematic review to identify challenges of demonstrating ef-ficacy of HIV behavioral interventions for gay, bisexual, and other men who have sex with men (MSM). AIDS and Behavior, 17, 1231–1244.
Higgins, J., & Green, S. (2011). Cochrane hand-book for systematic reviews of interven-tions version 5.1.0. Retrieved from www.handbook.cochrane.org
Hoff, C., Campbell, C., Chakravarty, D., & Darbes, L. (2016). Relationship-based pre-dictors of sexual risk for HIV among MSM couples: A systematic review of the litera-ture. AIDS and Behavior, 20, 2873–2892.
Holt, M. (2014). HIV pre-exposure prophylaxis and treatment as prevention: A review of awareness and acceptability among men who have sex with men in the Asia-Pacific region and the Americas. Sexual Health, 11, 166–170.
IBM Corporation. (2011 ). IBM SPSS Statistics for Windows (Version 21.0.) [Computer soft-ware]. Armonk, NY: IBM Corp.

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 19
Jin, F., Matthews, G. V., & Grulich, A. E. (2016). Sexual transmission of hepatitis C virus among gay and bisexual men: A systematic review. Sexual Health, 14, 28–41.
Johnson, W. D., Diaz, R. M., Flanders, W. D., Goodman, M., Hill, A. N., Holtgrave, D., . . . McClellan, W. M. (2009). Behavioral in-terventions to reduce risk for sexual trans-mission of HIV among men who have sex with men. Cochrane Database of System-atic Reviews, 2009, CD001230. https://doi.org/10.1002/14651858.CD001230.pub2
Johnson, W. D., Hedges, L. V., & Diaz, R. M. (2002). Interventions to modify sexual risk behaviors for preventing HIV in-fection in men who have sex with men. Cochrane Database of Systematic Re-views, 2002(4), CD001230. https://doi.org/10.1002/14651858.CD001230
Johnson, W. D., Hedges, L. V., Ramirez, G., Semaan, S., Norman, L. R., Sogolow, E., . . . Diaz, R. M. (2002). HIV prevention re-search for men who have sex with men: A systematic review and meta-analysis. Jour-nal of Acquired Immune Deficiency Syn-dromes, 30(Suppl 1), S118–S129.
Johnson, W. D., Holtgrave, D. R., McClellan, W. M., Flanders, W. D., Hill, A. N., & Good-man, M. (2005). HIV intervention research for men who have sex with men: A 7-year update. AIDS Education and Prevention, 17, 568–589.
Kennedy, C. E., Bernard, L. J., Muessig, K. E., Konda, K. A., Akl, E. A., Lo, Y. R., . . . O’Reilly, K. R. (2013). Serosorting and HIV/STI infection among HIV-negative MSM and transgender people: A systematic review and meta-analysis to inform WHO guidelines. Journal of Sexually Transmitted Diseases, 2013, 583627.
King, E., Oomeer, S., Gilson, R., Copas, A., Bed-dows, S., Soldan, K., . . . Sonnenberg, P. (2016). Oral human papillomavirus in-fection in men who have sex with men: A systematic review and meta-analysis. PLoS One, 11, e0157976.
Kojima, N., Davey, D. J., & Klausner, J. D. (2016). Pre-exposure prophylaxis for HIV infection and new sexually transmitted infections among men who have sex with men. AIDS, 30, 2251–2252.
Kuszelewicz, M., & Lloyd, G. A. (1995). Lesbians and gays of color and HIV/AIDS: A litera-ture review, 1988–1993. In G. A. Lloyd & M. A. Kuszelewicz (Eds.), HIV disease: Lesbians, gays and the social services (pp. 107–119). New York, NY: Haworth Press.
Lacefield, K., Negy, C., Schrader, R. M., & Kuhl-man, C. (2015). Comparing psychosocial correlates of condomless anal sex in HIV-diagnosed and HIV-nondiagnosed men who have sex with men: A series of meta-
analyses of studies from 1993–2013. LGBT Health, 2, 200–220.
Lassiter, J. M., & Parsons, J. T. (2016). Religion and spirituality’s influences on HIV syn-demics among MSM: A systematic review and conceptual model. AIDS and Behavior, 20, 461–472.
LeGrand, S., Muessig, K., Horvath, K., Rosengren, A., & Hightow-Weidman, L. (2017). Us-ing technology to support HIV self-testing among MSM. Current Opinion HIV/AIDS, 12, 425–431.
Levy, M. E., Wilton, L., Phillips, G., II, Glick, S. N., Kuo, I., Brewer, R. A., . . . Magnus, M. (2014). Understanding structural barriers to accessing HIV testing and prevention ser-vices among Black men who have sex with men (BMSM) in the United States. AIDS and Behavior, 18, 972–996.
Lewis, N., & Wilson, K. (2017). HIV risk behav-iors among immigrant and ethnic minority gay and bisexual men in North America and Europe: A systematic review. Social Sci-ence and Medicine, 179, 115–128.
Lewnard, J. A., & Berrang-Ford, L. (2014). In-ternet-based partner selection and risk for unprotected anal intercourse in sexual en-counters among men who have sex with men: A meta-analysis of observational stud-ies. Sexually Transmitted Infections, 90, 290–296.
Liau, A., Millett, G., & Marks, G. (2006). Meta-analytic examination of online sex-seeking and sexual risk behavior among men who have sex with men. Sexually Transmitted Diseases, 33, 576–584.
Liu, Y., Qian, H. Z., Ruan, Y., Yin, L., Ma, J., Da-hiya, K., . . . Vermund, S. H. (2014). Alcohol use among Chinese men who have sex with men: An epidemiological survey and meta-analysis. BioMed Research International, 2014, 414381.414381–414381.414311.
Lloyd, S., & Operario, D. (2012). HIV risk among men who have sex with men who have ex-perienced childhood sexual abuse: System-atic review and meta-analysis. AIDS Educa-tion and Prevention, 24, 228–241.
Lorenc, T., Marrero-Guillamón, I., Aggleton, P., Cooper, C., Llewellyn, A., Lehmann, A., & Lindsay, C. (2011). Promoting the uptake of HIV testing among men who have sex with men: Systematic review of effective-ness and cost-effectiveness. Sexually Trans-mitted Infections, 87, 272–278.
Lorenc, T., Marrero-Guillamón, I., Llewellyn, A., Aggleton, P., Cooper, C., Lehmann, A., & Lindsay, C. (2011). HIV testing among men who have sex with men (MSM): Systematic review of qualitative evidence. Health Edu-cation Research, 26, 834–846.
Lorimer, K., Kidd, L., Lawrence, M., McPherson, K., Cayless, S., & Cornish, F. (2013). Sys-

20 HIGA ET AL.
tematic review of reviews of behavioural HIV prevention interventions among men who have sex with men. AIDS Care, 25, 133–150.
Lutz, A. R. (2015). Screening for asymptomatic ex-tragenital gonorrhea and chlamydia in men who have sex with men: Significance, rec-ommendations, and options for overcoming barriers to testing. LGBT Health, 2, 27–34.
Lyles, C. M., Crepaz, N., Herbst, J. H., & Kay, L. S. (2006). Evidence-based HIV behav-ioral prevention from the perspective of the CDC’s HIV/AIDS Prevention Research Syn-thesis Team. AIDS Education and Preven-tion, 18(Suppl. A), 21–31.
Machalek, D. A., Grulich, A. E., Grulich, A. E., Templeton, D. J., & Poynten, I. M. (2012). The epidemiology and natural history of anal human papillomavirus infection in men who have sex with men. Sexual Health, 9, 527–537.
Machalek, D. A., Poynten, M., Jin, F., Fairley, C. K., Farnsworth, A., Garland, S. M., . . . Grulich, A. E. (2012). Anal human papillo-mavirus infection and associated neoplastic lesions in men who have sex with men: A systematic review and meta-analysis. Lan-cet Oncology, 13, 487–500.
Mansergh, G., & Higa, D. H. (2011). HIV/AIDS in lesbian, gay, bisexual, and transgender communities. In J. C. Hall, B. J. Hall, & C. J. Cockerell (Eds.), HIV/AIDS in the post-HAART era. Shelton, CT: People’s Medical Publishing House—USA.
Mansergh, G., & Marks, G. (1998). Age and risk of HIV infection in men who have sex with men. AIDS, 12, 1119–1128.
Matthews, D. D., Herrick, A., Coulter, R. W., Friedman, M. R., Mills, T. C., Eaton, L. A., . . . Stall, R. D. (2016). Running backwards: Consequences of current HIV incidence rates for the next generation of Black MSM in the United States. AIDS and Behavior, 20, 7–16.
Maulsby, C., Millett, G., Lindsey, K., Kelley, R., Johnson, K., Montoya, D., & Holtgrave, D. (2013). A systematic review of HIV interventions for Black men who have sex with men (MSM). BMC Public Health, 13, 625.621–625.613.
Maulsby, C., Millett, G., Lindsey, K., Kelley, R., Johnson, K., Montoya, D., & Holtgrave, D. (2014). HIV among Black men who have sex with men (MSM) in the United States: A review of the literature. AIDS and Behav-ior, 18, 10–25.
McKechnie, M. L., Bavinton, B. R., & Zablotska, I. B. (2013). Understanding of norms re-garding sexual practices among gay men: Literature review. AIDS and Behavior, 17, 1245–1254.
Melendez-Torres, G., & Bonell, C. (2014). Sys-tematic review of cognitive behavioural interventions for HIV risk reduction in sub-stance-using men who have sex with men. International Journal of STD & AIDS, 25, 627–635.
Melendez-Torres, G., Nye, E., & Bonell, C. (2015). Internet sex-seeking is inconsistently linked with sexual risk in men who have sex with men: Systematic review of within-subjects comparisons. Sexual Health, 12, 183–187.
Melendez-Torres, G., Nye, E., & Bonell, C. (2016). Is location of sex associated with sexual risk behaviour in men who have sex with men? Systematic review of within-subjects stud-ies. AIDS and Behavior, 20, 1219–1227.
Melendez-Torres, G. J., & Bourne, A. (2016). Il-licit drug use and its association with sexual risk behaviour among MSM: More ques-tions than answers? Current Opinion in Infectious Diseases, 29, 58–63.
Mendelsohn, J., Calzavara, L., Daftary, A., Mi-tra, S., Pidutti, J., Allman, D., . . . Myers, T. (2015). A scoping review and thematic analysis of social and behavioral research among HIV-serodiscordant couples in high-income settings. BMC Public Health, 15, 241–259.
Meng, X., Zou, H., Fan, S., Zheng, B., Zhang, L., Dai, X., . . . Lu, B. (2015). Relative risk for HIV infection among men who have sex with men engaging in different roles in anal sex: A systematic review and meta-analysis on global data. AIDS and Behavior, 19, 882–889.
Millett, G., Flores, S., Marks, G., Reed, J., & Herbst, J. (2008). Circumcision status and risk of HIV and sexually transmitted infec-tions among men who have sex with men: A meta-analysis. JAMA Journal of the Ameri-can Medical Association, 300, 1674–1684.
Millett, G., Flores, S., Peterson, J., & Bakeman, R. (2007). Explaining disparities in HIV infec-tion among Black and white men who have sex with men: A meta-analysis of HIV risk behaviors. AIDS, 21, 2083–2091.
Millett, G., Jeffries, W., Peterson, J., Malebranche, D., Lane, T., Flores, S., . . . Heilig, C. (2012). Common roots: A contextual re-view of HIV epidemics in Black men who have sex with men across the African dias-pora. Lancet, 380(9839), 411–423.
Millett, G., Malebranche, D., Mason, B., & Spikes, P. (2005). Focusing “down low”: Bisexual Black men, HIV risk and heterosexual transmission. Journal of the National Medi-cal Association, 97(Suppl. 7), S52–S59.
Millett, G., Peterson, J., Flores, S., Hart, T., Jef-fries, W., Wilson, P., . . . Remis, R. (2012). Comparisons of disparities and risks of HIV infection in Black and other men who have sex with men in Canada, UK, and

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 21
USA: A meta-analysis. Lancet, 380(9839), 341–348.
Millett, G., Peterson, J., Wolitski, R., & Stall, R. (2006). Greater risk for HIV infection of Black men who have sex with men: A criti-cal literature review. American Journal of Public Health, 96, 1007–1019.
Mitchell, J. T., LeGrand, S., Hightow-Weidman, L. B., McKellar, M. S., Kashuba, A. D., Cottrell, M., . . . McClernon, F. J. (2018). Smartphone-based contingency manage-ment intervention to improve pre-exposure prophylaxis adherence: Pilot trial. JMIR Mhealth and Uhealth, 6, e10456.
Muessig, K., LeGrand, S., Horvath, K., Bauermeis-ter, J., & Hightow-Weidman, L. (2017). Re-cent mobile health interventions to support medication adherence among HIV-positive MSM. Current Opinion in HIV and AIDS, 12, 432–441.
Mustanski, B., Newcomb, M. E., Du Bois, S. N., Garcia, S. C., & Grov, C. (2011). HIV in young men who have sex with men: A re-view of epidemiology, risk and protective factors, and interventions. Journal of Sex Research, 48, 218–253.
Nadarzynski, T., Smith, H., Richardson, D., Jones, C. J., & Llewellyn, C. D. (2014). Human papillomavirus and vaccine-related percep-tions among men who have sex with men: A systematic review. Sexually Transmitted Infections, 90, 515–523.
Natale, A. P., & Moxley, D. P. (2009). Service en-gagement with high-risk men who have sex with men: Challenges and implications for social work practice. Social Work in Health Care, 48, 38–56.
Nelson, L., Walker, J., DuBois, S., & Giwa, S. (2014). Your blues ain’t like mine: Consid-ering integrative antiracism in HIV preven-tion research with Black men who have sex with men in Canada and the United States. Nursing Inquiry, 21, 270–282.
Neumann, M. S., Herbst, J. H., & Guenther-Grey, C. A. (2010). Developing HIV behavioral interventions for men who have sex with men: Comparing experiences from the United States and Australia. In D. A. Feld-man (Ed.), AIDS, culture, and gay men (pp. 184–212). Gainesville: University Press of Florida.
Neville, S., & Adams, J. (2009). Condom use in men who have sex with men: A literature review. Contemporary Nurse, 33, 130–139.
Neville, S., Adams, J., & Holdershaw, J. (2014). Social marketing campaigns that promote condom use among MSM: A literature re-view. Nursing Praxis in New Zealand, 30, 5–16.
Newcomb, M. E., & Mustanski, B. (2011). Mod-erators of the relationship between internal-ized homophobia and risky sexual behavior
in men who have sex with men: A meta-analysis. Archives of Sexual Behavior, 40, 189–199.
Noble, M., Jones, A. M., Bowles, K., DiNenno, E. A., & Tregear, S. J. (2017). HIV testing among internet-using MSM in the United States: Systematic review. AIDS and Behav-ior, 21, 561–575.
Office of National AIDS Policy. (2010). National HIV/AIDS Strategy for the United States. Washington, DC: Author. Retrieved from https://obamawhitehouse.archives.gov/sites/default/files/uploads/NHAS.pdf
Office of National AIDS Policy. (2015). National HIV/AIDS strategy for the United States: Updated to 2020. Washington, DC: Author.
Oldenburg, C. E., Perez-Brumer, A. G., Reisner, S. L., Mayer, K. H., Mimiaga, M. J., Hatzen-buehler, M. L., & Barnighausen, T. (2016). Human rights protections and HIV preva-lence among MSM who sell sex: Cross-country comparisons from a systematic review and meta-analysis. Global Public Health, 15, 1–12.
Oldenburg, C. E., Perez-Brumer, A. G., Reisner, S. L., & Mimiaga, M. J. (2015). Transactional sex and the HIV epidemic among men who have sex with men (MSM): Results from a systematic review and meta-analysis. AIDS and Behavior, 19, 2177–2183.
Ong, J. J., Chen, M., Grulich, A. E., & Fairley, C. K. (2014). Regional and national guideline recommendations for digital ano-rectal examination as a means for anal cancer screening in HIV positive men who have sex with men: A systematic review. BMC Cancer, 14, 557.551–557.557.
Ortega, A., Lopez-Briz, E., & Fraga-Fuentes, M. D. (2016). From qualitative reviews to um-brella reviews. In G. Biondi-Zoccai (Ed.), Umbrella reviews: Evidence synthesis with overview of reviews and meta-epidemio-logic studies (pp. 21–41). New York, NY: Springer.
Parsons, J., Grov, C., & Golub, S. (2012). Sexual compulsivity, co-occurring psychosocial health problems, and HIV risk among gay and bisexual men: further evidence of a syn-demic. American Journal of Public Health, 102, 156–162.
Pérez, A., Santamaria, E. K., & Operario, D. (2018). A systematic review of behavioral interventions to reduce condomless sex and increase HIV testing for Latino MSM. Jour-nal of Immigrant and Minority Health, 20, 1261–1276.
Peters, M., Godfrey, C., Khalil, H., McInerney, P., Parker, D., & Soares, C. (2015). Guidance for conducting systematic scoping reviews. International Journal of Evidence-Based Healthcare, 13, 141–146.

22 HIGA ET AL.
Phillips, G., Peterson, J., Binson, D., Hidalgo, J., & Magnus, M. (2011). House/ball culture and adolescent African-American transgender persons and men who have sex with men: A synthesis of the literature. AIDS Care, 23, 515–520.
Punyacharoensin, N., Edmunds, W. J., De Angelis, D., & White, R. G. (2011). Mathematical models for the study of HIV spread and control amongst men who have sex with men. European Journal of Epidemiology, 26, 695–709.
Purcell, D. W., Johnson, C. H., Lansky, A., Prejean, J., Stein, R., Denning, P., . . . Crepaz, N. (2012). Estimating the population size of men who have sex with men in the United States to obtain HIV and syphilis rates. Open AIDS Journal, 6(Suppl. 1), 98–107.
Race, K., Lea, T., Murphy, D., & Pienaar, K. (2017). The future of drugs: recreational drug use and sexual health among gay and other men who have sex with men. Sexual Health, 14, 42–50.
Rajasingham, R., Mimiaga, M. J., White, J. M., Pinkston, M. M., Baden, R. P., & Mitty, J. A. (2012). A systematic review of behav-ioral and treatment outcome studies among HIV-infected men who have sex with men who abuse crystal methamphetamine. AIDS Patient Care and STDs, 26, 36–52.
Rees, R., Kavanagh, J., Burchett, H., Shepherd, J., Brunton, G., Harden, A., . . . Oakley, A. (2004). HIV health promotion and men who have sex with men (MSM): A system-atic review of research relevant to the de-velopment and implementation ofeffective and appropriate interventions. London, UK: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London.
Refugio, O. N., Kimble, M. M., Silva, C. L., Lykens, J. E., Bannister, C., & Klausner, J. D. (2019). PrEPTECH: A telehealth-based initiation program for human immuno-deficiency virus pre-exposure prophylaxis in young men of color who have sex with men—A pilot study of feasibility. Journal of Acquired Immune Deficiency Syndromes, 80, 40–45.
Rhodes, S. D., & Yee, L. J. (2007). Using hepatitis A and B vaccination as a paradigm for ef-fective HIV vaccine delivery. Sexual Health, 4, 121–127.
Romanelli, F., & Smith, K. M. (2004). Recreation-al use of sildenafil by HIV-positive and -neg-ative homosexual/bisexual males. Annals of Pharmacotherapy, 38, 1024–1030.
Ronn, M., White, P. J., Hughes, G., & Ward, H. (2014). Developing a conceptual frame-work of seroadaptive behaviors in HIV-diagnosed men who have sex with men.
Journal of Infectious Diseases, 210(Suppl. 2), S586–S593.
Ronn, M. M., & Ward, H. (2011). The association between lymphogranuloma venereum and HIV among men who have sex with men: Systematic review and meta-analysis. BMC Infectious Diseases, 11, 70.71-70.78.
Rosser, B. R. S., Merengwa, E., Capistrant, B. D., Iantaffi, A., Kilian, G., Kohli, N., . . . West, W. (2016). Prostate cancer in gay, bisexual, and other men who have sex with men: A review. LGBT Health, 3, 32–41.
Schafer, K. R., Gupta, S., & Dillingham, R. (2013). HIV-infected men who have sex with men and histories of childhood sexual abuse: Im-plications for health and prevention. Jour-nal of the Association of Nurses in AIDS Care, 24, 288–298.
Schnall, R., Travers, J., Rojas, M., & Carballo-Diéguez, A. (2014). eHealth interventions for HIV prevention in high-risk men who have sex with men: A systematic review. Journal of Medical Internet Research, 16, e134.131–e134.110.
Scholl, E. (2016). Improving outpatient imple-mentation of preexposure prophylaxis in men who have sex with men. Journal of the American Association of Nurse Practitio-ners, 28, 446–452.
Shangani, S., Escudero, D., Kirwa, K., Harrison, A., Marshall, B., & Operario, D. (2017). Effectiveness of peer-led interventions to increase HIV testing among men who have sex with men: A systematic review and me-ta-analysis AIDS Care, 29, 1003–1013.
Shea, B., Bouter, L., Peterson, J., Boers, M., An-dersson, N., Ortiz, Z., . . . Grimshaw, S. (2007). External validation of a measure-ment tool to assess systematic reviews (AM-STAR). PLoS One, 2, e1350.
Shea, B., Grimshaw, J., Wells, G., Bouter, L., Kristanjansson, E., Grimshaw, J., . . . Boers, M. (2009). AMSTAR is a reliable and valid measurement tool to assess the methodolog-ical quality of systematic reviews. Journal of Clinical Epidemiology, 62, 1013–1020.
Shea, B. J., Grimshaw, J. M., Wells, G. A., Boers, M., Andersson, N., Hamel, C., . . . Bouter, L. M. (2007). Development of AMSTAR: A measurement tool to assess the method-ological quality of systematic reviews. BMC Medical Research Methodology, 7, 10. https://doi.org/10.1186/1471-2288-7-10
Singh, S., Song, R., Johnson, A. S., McCray, E., & Hall, H. I. (2018). HIV incidence, HIV prevalence, and undiagnosed HIV infec-tions in men who have sex with men, Unit-ed States. Annals of Internal Medicine, 168, 684–694.
Sipe, T., Barham, T., Johnson, W., Joseph, H., Tun-gol-Ashmon, M., & O’Leary, A. (2017). Structural interventions in HIV prevention:

HIV PREVENTION RESEARCH ON MSM: SCOPING REVIEW 23
A taxonomy and descriptive systematic re-view. AIDS and Behavior, 21, 3366–3430.
Smit, P. J., Brady, M., Carter, M., Fernandes, R., Lamore, L., Meulbroek, M., . . . Thompson, M. (2012). HIV-related stigma within com-munities of gay men: A literature review. AIDS Care, 24, 405–412.
Sullivan, P., Jones, J., Kishore, N., & Stephenson, R. (2015). The roles of technology in pri-mary HIV prevention for men who have sex with men. Current HIV/AIDS Reports, 12, 481–488.
Sullivan, P. S., Carballo-Dieguez, A., Coates, T., Goodreau, S. M., McGowan, I., Sanders, E. J., . . . Sanchez, J. (2012). Successes and challenges of HIV prevention in men who have sex with men. Lancet, 380(9839), 388–399.
Tanner, A. E., Song, E. Y., Mann-Jackson, L., Alonzo, J., Schafer, K., Ware, S., . . . Rhodes, S. D. (2018). Preliminary impact of the weCare social media intervention to support health for young men who have sex with men and transgender women with HIV. AIDS Patient Care and STDs, 32, 450–458.
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoan, H., Levac, D., . . . Straus, S. E. (2018). PRISMA extension for scoping re-views (PRISMA-ScR): Checklist and expla-nation. Annals of Internal Medicine, 169, 467–473.
Tsagris, M., & Fragkos, K. C. (2016). Umbrella reviews, overviews of reviews, and meta-ep-idemiologic studies: similarities and differ-ences. In G. Biondi-Zoccai (Ed.), Umbrella reviews: Evidence synthesis with overviews of reviews and meta-epidmiologic studies (pp. 43–54). New York, NY: Springer.
Ubrihien, A., Davies, S. C., & Driscoll, T. (2016). Is cost a structural barrier preventing men who have sex with men accessing condoms? A systematic review. AIDS Care, 28, 1473–1480.
van Kesteren, N. M., Hospers, H. J., & Kok, G. (2007). Sexual risk behavior among HIV-positive men who have sex with men: A literature review. Patient Education and Counseling, 65, 5–20.
Vosburgh, H. W., Mansergh, G., Sullivan, P. S., & Purcell, D. W. (2012). A review of the literature on event-level substance use and sexual risk behavior among men who have sex with men. AIDS and Behavior, 16, 1394–1410.
Vu, N. T., Maher, L., & Zablotska, I. (2015). Am-phetamine-type stimulants and HIV infec-tion among men who have sex with men: Implications on HIV research and preven-tion from a systematic review and meta-analysis. Journal of the International AIDS Society, 18, 19273.19271–19273.19214.
Walsh, T., Bertozzi-Villa, C., & Schneider, J. A. (2015). Systematic review of racial dispari-ties in human papillomavirus-associated anal dysplasia and anal cancer among men who have sex with men. American Journal of Public Health, 105, e34–e35.
Wao, H., Aluoch, M., Odondi, G. O., Tenge, E., & Iznaga, T. (2016). MSM’s versus health care providers’ perceptions of barriers to uptake of HIV/AIDS-related interventions: Systematic review and meta-synthesis of qualitative and quantitative evidence. In-ternational Journal of Sexual Health, 28, 151–162.
Wei, C., Herrick, A., Raymond, H. F., Anglemyer, A., Gerbase, A., & Noar, S. M. (2011). Social marketing interventions to increase HIV/STI testing uptake among men who have sex with men and male-to-female transgender women. Cochrane Database of Systematic Reviews, 2011(9), CD009337. ht tps : / /do i .org /10.1002/14651858.CD009337
Wei, C., Raymond, H. F., Wong, F. Y., Silvestre, A. J., Friedman, M. S., Documét, P., . . . Stall, R. (2011). Lower HIV prevalence among Asian/Pacific Islander men who have sex with men: A critical review for possible rea-sons. AIDS and Behavior, 15, 535–549.
Weidel, J., Provencio-Vasquez, E., & Grossman, J. (2008). Sex and drugs: High-risk behav-iors at circuit parties. American Journal of Men’s Health, 2, 344–352.
Wilson, P., Valera, P., Martos, A., Wittlin, N., Mu-noz-Laboy, M., & Parker, R. (2016). Con-tributions of qualitative research in inform-ing HIV/AIDS interventions targeting Black MSM in the United States. Journal of Sex Research, 53, 642–654.
Wiysonge, C. S., Kongnyuy, E. J., Shey, M., Muula, A. S., Navti, O. B., Akl, E. A., & Lo, Y. R. (2011). Male circumcision for preven-tion of homosexual acquisition of HIV in men. Cochrane Database of Systematic Reviews, 2011(6), CD007496. https://doi.org/10.1002/14651858.CD007496.pub2
Woodward, E. N., Banks, R. J., Marks, A. K., & Pantalone, D. W. (2016). Identifying resil-ience resources for HIV prevention among sexual minority men: A systematic review. AIDS and Behavior, 10, 2860–2873.
Woolf, S. E., & Maisto, S. A. (2009). Alcohol use and risk of HIV infection among men who have sex with men. AIDS and Behavior, 13, 757–782.
Wray, T. B., Grin, B., Dorfman, L., Glynn, T. R., Kahler, C. W., Marshall, B. D., . . . Oper-ario, D. (2016). Systematic review of inter-ventions to reduce problematic alcohol use in men who have sex with men. Drug and Alcohol Review, 35, 148–157.

24 HIGA ET AL.
Yang, Z., Zhang, S., Dong, Z., Jin, M., & Han, J. (2014). Prevalence of unprotected anal intercourse in men who have sex with men recruited online versus offline: A meta-analysis. BMC Public Health, 14, 508.501–508.509.
Yaphe, S., Bozinoff, N., Kyle, R., Shivkumar, S., Pai, N. P., & Klein, M. (2012). Incidence of acute hepatitis C virus infection among men who have sex with men with and without HIV infection: A systematic review. Sexu-ally Transmitted Infections, 88, 558–564.
Ye, S., Yin, L., Amico, R., Simoni, J., Vermund, S., Ruan, Y., . . . Qian, H. Z. (2014). Efficacy of peer-led interventions to reduce unpro-tected anal intercourse among men who have sex with men: A meta-analysis. PLoS One, 9, e90788.
Zablotska, I. B. (2016). Likely impact of pre-exposure prophylaxis on HIV epidemics among men who have sex with men. Sexual Health, 14, 97–105.
Zeglin, R. J. (2015). Assessing the role of mascu-linity in the transmission of HIV: A system-
atic review to inform HIV risk reduction counseling interventions for men who have sex with men. Archives of Sexual Behavior, 44, 1979–1990.
Zou, H., Fairley, C. K., Guy, R., & Chen, M. Y. (2012). The efficacy of clinic-based inter-ventions aimed at increasing screening for bacterial sexually transmitted infections among men who have sex with men: A sys-tematic review. Sexually Transmitted Dis-eases, 39, 382–387.
Zou, H., Fairley, C. K., Hocking, J. S., Garland, S. M., Grulich, A. E., & Chen, M. Y. (2012). The prevalence of anal human papilloma-virus among young HIV negative men who have sex with men. BMC Infectious Dis-eases, 12, 341.341–341.344.
Zou, H., & Fan, S. (2017). Characteristics of men who have sex with men who use smart-phone geosocial networking applications and implications for HIV interventions: A systematic review and meta-analysis. Ar-chives of Sexual Behavior, 46, 885–894.

SUPPLEMENTAL MATERIALS
Table S1. Study Characteristics, Most Common Men Who Have Sex With Men (MSM) Subpopulations, and Major Themes by Topic Areas (N = 129)
Topic, Number of reviews, References
Number of Meta-Analyses n (%)
Includes only US-based primary studies n (%)
Intervention Data n (%)
Correlational Data n (%)
Prevalence Data n (%)
Descriptive Data n (%)
Averaged AMSTARa
Score and Rating
Most Common MSMb Sub-Population(s)
Major Themes
Sexual Behavior
(n = 43)
Andrew et al., 2016; Anema et al., 2013; Berg, 2009, 2011; Beyrer et al., 2012; Carrico et al., 2016; Crepaz et al., 2009; Dangerfield et al., 2016; Eaton et al., 2009; Fish, Papaloukas, Jaspal, & Williamson, 2016; Flowers et al., 1997; Frankis & Flowers, 2005, 2009; Friedman et al., 2014; Heath et al., 2012; Herbst et al., 2005, 2007; Hergenrather et al., 2016; Hoff et al., 2016;
17 (40) 9 (21) 17 (40) 20 (47) 6 (14) 3 (7) 6.1 Moderate
Young MSM
HIV-positive MSM
Substance-using MSM
MSM who use technology or venues to meet sex partners
Diverse and interrelated factors related to sexual behavior, but more correlates of condomless anal sex have been examined than correlates of protected sex
Substance use is a consistent correlate of condomless anal sex.
Behavioral interventions are efficacious in reducing sexual risk and increasing protective behaviors, but may not be effective for reducing HIV infection.
Designing interventions based on theory may enhance effectiveness.
Population estimates of MSM and MSM who have sex with women comprise small percentages of the U.S. population.
Prevalence of high-risk behavior may be more common among younger MSM and Internet/app-using MSM than other subpopulations.
Important to contextualize MSM sexual behavior.
HIV PREVENTION RESEARCH ON MSM S1

Johnson et al., 2002, 2005, 2007, 2009; Kennedy et al., 2013; Lacefield et al., 2015; Lorimer et al., 2013; Mansergh & Marks, 1998; Maulsby et al., 2013; McKechnie et al., 2013; Melendez-Torres & Bonell, 2014; Melendez-Torres & Bourne, 2016; Mendelsohn et al., 2015; Mustanski et al., 2011; Neumann et al., 2010; Neville & Adams, 2009; Oldenburg et al., 2015; Purcell et al., 2012; Rees et al., 2004; Ronn et al., 2014; Ubrihien et al., 2016; van Kesteren et al., 2007; Woolf & Maisto, 2009; Ye et al., 2014
Disease Vulnerability
4 (22) 4 (22) 0 11 (61) 8 (44) 2 (11) 4.7 Moderate
HIV-positive MSM Some evidence suggests syphilis and HIV
increasing for MSM
S2 HIGA ET AL.

(n = 18)
Abara et al., 2016; Abdolrasouli et al., 2009; Bonell et al., 2000, 2008; Cooper & Barber, 2014; De Buck et al., 2015; Feldman, 2010; Ghisla et al., 2017; Grulich & Kaldor, 2008; Hagan et al., 2015; Machalek, Grulich, et al., 2012; Matthews et al., 2016; Nadarzynski et al., 2014; Oldenburg et al., 2016; Rhodes & Yee, 2007; Ronn & Ward, 2011; Rosser et al., 2016; Wei, Raymond, et al., 2011
HIV-negative MSM
Young MSM
MSM are vulnerable to intestinal parasites, human papillomavirus (HPV), lymphogranuloma venereum (LGV)
Incident Hepatitis C (HCV) predominantly affects HIV-positive MSM.
Herpes simplex virus (HSV) and protective language in the penal code for MSM associated with HIV infection
Prostate cancer and HPV among MSM are understudied.
Health Disparities
(n = 14)
Abara et al., 2016; Brown et al., 2012; Friedman et al., 2014; Ghisla et al., 2017; Machalek, Poynten, et al., 2012; Maulsby
8 (57) 7 (50) 0 (0) 2 (14) 13 (93) 0 (0) 4.9 Moderate
Black or African American MSM
HIV-positive MSM
MSM bear a greater burden of HIV and some STI compared to non-MSM groups.
Black or African American MSM bear more HIV and STI burden than other racial/ethnic groups.
HIV-positive MSM bear more STI burden than HIV-negative MSM.
HIV PREVENTION RESEARCH ON MSM S3

et al., 2014; Millett et al., 2006, 2007; Millett, Jeffries, et al., 2012; Millett, Peterson, et al., 2012; Purcell et al., 2012; Schafer et al., 2013; Walsh, Bertozzi-Villa, & Schneider, 2015; Yaphe et al., 2012 Substance Use
(n = 11)
Berg et al., 2011; Drumright et al., 2006; Haverkos & Drotman, 1995; Heath et al., 2012; Rajasingham et al., 2012; Romanelli & Smith, 2004; Vosburgh et al., 2012; Vu et al., 2015; Weidel et al., 2008; Woolf & Maisto, 2009; Wray et al., 2016
2 (18) 2 (18) 3 (27) 7 (64) 0 (0) 2 (18) 4.9 Moderate
MSM who use substances
Some evidence of consistent associations found between substance use and increased sexual risk behavior.
Preliminary support for motivational interviewing for reducing alcohol use.
Social Determinants of Health
(n = 8)
Dillon & Basu, 2014;
1 (13) 5 (63) 2 (25) 2 (25) 0 (0) 4 (50) 4.3 Low
Black or African American MSM
MSM in general and MSM of color experience multiple forms of oppression, stigma, and discrimination that interfere with using HIV prevention services.
Few HIV prevention interventions for MSM address social determinants of health.
S4 HIGA ET AL.

Kuszelewicz & Lloyd, 1995; Levy et al., 2014; Millett et al., 2012; Natale & Moxley, 2009; Nelson et al., 2014; Smit et al., 2012; Wilson et al., 2016 Testing for HIV, STI, Hepatitis and other Diseases
(n = 8)
Chow et al., 2016; Flowers & Church, 2002; Lorenc, Marrero-Guillamón, Aggleton, et al., 2011; Lorenc, Marrero-Guillamón, Llewellyn, et al., 2011; Lutz, 2015; Noble et al., 2017; Ong et al., 2014; Zou, Fairley, Guy, et al., 2012
1 (13) 1 (13) 2 (25) 1 (13) 2 (25) 4 (50) 5.6 Moderate
None Strategies such as rapid tests, opt-out testing, and peer counseling may increase HIV testing while clinic-based interventions may increase STI screening.
Reasons for not testing included fear of a positive test result.
Technology Use
(n = 7)
Grov et al., 2014; Lewnard & Berrang-Ford, 2014; Liau et al., 2006; Melendez-Torres et al.,
4 (57) 0 (0) 1 (14) 3 (43) 2 (29) 1 (14) 6.4 Moderate
MSM who use technology or venues to meet sex partners
Some evidence for increased sexual risk for MSM using the Internet or mobile apps compared to MSM who do not use from between-person comparisons, but evidence less clear from within-person comparisons.
Some evidence for efficacy of eHealth interventions for HIV prevention.
HIV PREVENTION RESEARCH ON MSM S5

Social Marketing/ Mass Media Campaigns
(n = 3)
French et al., 2014; Neville et al., 2014; Wei, Herrick, et al., 2011
1 (33) 0 (0) 3 (100) 0 (0) 0 (0) 0 (0) 8.0 High
None Mass media campaigns may be effective for increasing HIV testing.
Conflicting evidence on effects of mass media campaigns on sexual behavior.
Identity
(n = 3)
Brennan, Bauer, Bradley, & Tran, 2017; Millett et al., 2005; Zeglin, 2015
0 (0) 2 (67) 0 (0) 1 (33) 1 (33) 1 (33) 3.3 Low
None Identities and their intersections (e.g., sexual, masculine, racial) may play an important role in sexual behaviors and HIV prevention.
Social Support
(n = 2)
Hall, 1999; Phillips et al., 2011
0 (0) 2 (100) 0 (0) 0 (0) 0 (0) 2 (100) 4.0 Low
Young Black MSM
Peers may be important resources for MSM.
The house/ball community may play a vital role in providing a social structure to young MSM of color.
General HIV Prevention
(n = 4)
Harper & Riplinger, 2013; Higa et al., 2013; Sullivan et al., 2012; Wao et al., 2016
0 (0) 2 (50) 4 (100) 0 (0) 0 (0) 0 (0) 5.0 Moderate
None Few interventions for MSM compared to other populations and for specific populations such as young MSM.
A combination of behavioral, biomedical and structural approaches may be necessary to decrease new HIV infections among MSM.
aAMSTAR: A measurement Tool to Assess Systematic reviews [high quality (8–11 points), moderate (5–7 points), and low (0–4 points)]. Scores were rounded up if .5 or higher.
bMen who have sex with men
HIV PREVENTION RESEARCH ON MSM S7